
A phase II multicenter study of ipilimumab with or without dacarbazine in chemotherapy-naïve...
10
PHASE II STUDIES A phase II multicenter study of ipilimumab with or without dacarbazine in chemotherapy-naïve patients with advanced melanoma Evan M. Hersh & Steven J. O’Day & John Powderly & Khuda D. Khan & Anna C. Pavlick & Lee D. Cranmer & Wolfram E. Samlowski & Geoffrey M. Nichol & Michael J. Yellin & Jeffrey S. Weber Received: 23 October 2009 / Accepted: 11 December 2009 # Springer Science+Business Media, LLC 2010 Summary Objective: Ipilimumab is a fully human, anti– cytotoxic T-lymphocyte antigen-4 (CTLA-4) monoclonal antibody that has demonstrated antitumor activity in advanced melanoma. We evaluated the safety and efficacy of ipilimumab alone and in combination with dacarbazine (DTIC) in patients with unresectable, metastatic melanoma. Methods: Chemotherapy-naïve patients were randomized in this multicenter, phase II study to receive ipilimumab at 3 mg/kg every 4 weeks for four doses either alone or with up to six 5-day courses of DTIC at 250 mg/m 2 /day. The primary efficacy endpoint was objective response rate. Results: Seventy-two patients were treated per-protocol (ipilimumab plus DTIC, n =35; ipilimumab, n =37). The objective response rate was 14.3% (95% CI, 4.8–30.3) with ipilimumab plus DTIC and was 5.4% (95% CI, 0.7–18.2) with ipilimumab alone. At a median follow-up of 20.9 and 16.4 months for ipilimumab plus DTIC (n =32) and ipilimu- mab alone (n =32), respectively, median overall survival was 14.3 months (95% CI, 10.2–18.8) and 11.4 months (95% CI, 6.1–15.6); 12-month, 24-month, and 36-month survival rates were 62%, 24% and 20% for the ipilimumab plus DTIC group and were 45%, 21% and 9% for the ipilimumab alone E. M. Hersh (*) : L. D. Cranmer Arizona Cancer Center, University of Arizona, 1515 North Campbell Avenue, Tucson, AZ 85724, USA e-mail: [email protected] S. J. O’Day The Angeles Clinic and Research Institute, 2001 Santa Monica Blvd, Suite 560W, Santa Monica, CA 90404, USA J. Powderly Carolina Bio-Oncology Institute, Cancer Therapy & Research Center, 9801 W. Kincey Ave, Suite 145, Huntersville, NC 28078, USA K. D. Khan St. Francis Hospital & Health Centers, 8111 S. Emerson Ave, Indianapolis, IN 46237, USA A. C. Pavlick New York University Medical Center, 160 East 34th Street, New York, NY 10016, USA W. E. Samlowski Nevada Cancer Institute, One Breakthrough Way, Las Vegas, NV 89135, USA G. M. Nichol : M. J. Yellin Medarex, Inc, 707 State Road, Princeton, NJ 08540, USA J. S. Weber H. Lee Moffitt Cancer Center and Research Institute, 12902 Magnolia Drive, Tampa, FL 33612, USA Present Address: K. D. Khan Elizabethtown Hematology & Oncology, 1107 Woodland Drive, Elizabethtown, KY 42701, USA Invest New Drugs DOI 10.1007/s10637-009-9376-8
Transcript of A phase II multicenter study of ipilimumab with or without dacarbazine in chemotherapy-naïve...

PHASE II STUDIES
A phase II multicenter study of ipilimumab
with or without dacarbazine in chemotherapy-naïve
patients with advanced melanoma
Evan M. Hersh & Steven J. O’Day & John Powderly & Khuda D. Khan &
Anna C. Pavlick & Lee D. Cranmer & Wolfram E. Samlowski & Geoffrey M. Nichol &
Michael J. Yellin & Jeffrey S. Weber
Received: 23 October 2009 /Accepted: 11 December 2009# Springer Science+Business Media, LLC 2010
Summary Objective: Ipilimumab is a fully human, anti–
cytotoxic T-lymphocyte antigen-4 (CTLA-4) monoclonal
antibody that has demonstrated antitumor activity in
advanced melanoma. We evaluated the safety and efficacy
of ipilimumab alone and in combination with dacarbazine
(DTIC) in patients with unresectable, metastatic melanoma.
Methods: Chemotherapy-naïve patients were randomized in
this multicenter, phase II study to receive ipilimumab at
3 mg/kg every 4 weeks for four doses either alone or with
up to six 5-day courses of DTIC at 250 mg/m2/day. The
primary efficacy endpoint was objective response rate.
Results: Seventy-two patients were treated per-protocol
(ipilimumab plus DTIC, n=35; ipilimumab, n=37). The
objective response rate was 14.3% (95% CI, 4.8–30.3) with
ipilimumab plus DTIC and was 5.4% (95%CI, 0.7–18.2) with
ipilimumab alone. At a median follow-up of 20.9 and
16.4 months for ipilimumab plus DTIC (n=32) and ipilimu-
mab alone (n=32), respectively, median overall survival was
14.3 months (95% CI, 10.2–18.8) and 11.4 months (95% CI,
6.1–15.6); 12-month, 24-month, and 36-month survival rates
were 62%, 24% and 20% for the ipilimumab plus DTIC
group and were 45%, 21% and 9% for the ipilimumab alone
E. M. Hersh (*) : L. D. Cranmer
Arizona Cancer Center, University of Arizona,
1515 North Campbell Avenue,
Tucson, AZ 85724, USA
e-mail: [email protected]
S. J. O’Day
The Angeles Clinic and Research Institute,
2001 Santa Monica Blvd, Suite 560W,
Santa Monica, CA 90404, USA
J. Powderly
Carolina Bio-Oncology Institute,
Cancer Therapy & Research Center,
9801 W. Kincey Ave, Suite 145,
Huntersville, NC 28078, USA
K. D. Khan
St. Francis Hospital & Health Centers,
8111 S. Emerson Ave,
Indianapolis, IN 46237, USA
A. C. Pavlick
New York University Medical Center,
160 East 34th Street,
New York, NY 10016, USA
W. E. Samlowski
Nevada Cancer Institute, One Breakthrough Way,
Las Vegas, NV 89135, USA
G. M. Nichol :M. J. Yellin
Medarex, Inc,
707 State Road,
Princeton, NJ 08540, USA
J. S. Weber
H. Lee Moffitt Cancer Center and Research Institute,
12902 Magnolia Drive,
Tampa, FL 33612, USA
Present Address:
K. D. Khan
Elizabethtown Hematology & Oncology,
1107 Woodland Drive,
Elizabethtown, KY 42701, USA
Invest New Drugs
DOI 10.1007/s10637-009-9376-8

group, respectively. Immune-related adverse events were, in
general, medically manageable and occurred in 65.7% of
patients in the combination group versus 53.8% in the
monotherapy group, with 17.1% and 7.7% ≥grade 3,
respectively. Conclusion: Ipilimumab therapy resulted in
clinically meaningful responses in advanced melanoma
patients, and the results support further investigations of
ipilimumab in combination with DTIC.
Keywords Metastatic melanoma . Ipilimumab . CTLA-4 .
Immune therapy . Dacarbazine
Introduction
The incidence rates of melanoma have been increasing for
at least 30 years in western populations, and the number of
cases worldwide has doubled in the past 20 years [1, 2]. In
2009, it is estimated that a total of 68,700 new cases of
melanoma will be diagnosed in the United States, with an
estimated 8,650 deaths [2]. Approximately 20% of cases
are diagnosed as invasive, and while overall 5-year survival
rates for melanoma have improved during the past 30 years,
the survival rate for patients diagnosed with metastatic
disease remains poor [2]. A recent meta-analysis of phase II
trials involving treatment-naïve and previously treated
patients with stage IV melanoma showed a median overall
survival (OS) of 6.2 months and a 1-year survival rate of
25.5% [3]. More recent trials with patients having good
prognostic factors [e.g., normal serum lactate dehydrogenase
(LDH) levels] have demonstrated longer survival times. For
example, a median OS of 9.7 months was shown in a recent
phase III trial involving chemotherapy-naïve patients with
advanced melanoma and normal LDH levels who received
dacarbazine (DTIC at 1,000 mg/m2) in the control group [4].
Only three agents are currently approved for the treatment
of metastatic melanoma in the United States: DTIC, hydroxy-
urea, and high-dose bolus interleukin-2 (IL-2). Single-agent
fotemustine (a nitrosourea) is also available in Europe. None
of these agents has demonstrated the ability to improve overall
survival (OS) in a randomized, phase III trial against a control,
whether used alone or as part of a combination regimen [5].
High-dose bolus IL-2 is effective mainly in a small subset of
highly selected patients with metastatic melanoma, and was
approved in the United States on the basis of durable objective
responses in 6% of patients [5, 6]. At present, it is the only
therapy that offers the possibility of a ‘cure’. However, high-
dose bolus IL-2 can result in serious and toxic side effects,
limiting its use to a small number of centers that specialize in
this type of therapy. Thus, there remains a great unmet
medical need for the treatment of advanced melanoma.
A novel approach to immunotherapy involves aug-
mentation of cell-mediated immunity by blocking key
checkpoint molecules [7]. One such target is cytotoxic T-
lymphocyte antigen-4 (CTLA-4), which is expressed on
the surface of activated T cells and functions to counteract
co-stimulatory signals mediated by CD28, thus limiting
natural anti-cancer immunity [8]. Ipilimumab (Bristol-
Myers Squibb, Princeton, NJ) is a fully human, monoclo-
nal antibody that inhibits binding of CTLA-4 to its natural
ligands (CD80 or CD86), thereby abrogating T-cell
suppression and enhancing antitumor immune responses
[9–12]. Results of phase I/II studies in previously treated
patients with metastatic melanoma show that ipilimumab
induces antitumor responses when administered as mono-
therapy [13–17], and when combined with vaccine [18,
19] or IL-2 [20]. A dose-escalation trial with ipilimumab
alone demonstrated a dose-effect trend with response rates
of 0%, 4.2%, and 11.1% at 0.3 mg/kg, 3 mg/kg, and
10 mg/kg, respectively (P=.0015) [21]. Importantly,
ipilimumab is capable of inducing durable responses in
some patients (ongoing for ≥1 year) [16, 19, 22].
This study was conducted in order to begin to
evaluate the efficacy and safety of ipilimumab in
combination with DTIC in patients with chemotherapy-
naïve metastatic melanoma. An ipilimumab dose of
3 mg/kg was chosen for this combination study based
on the efficacy and safety data that was available when
this study was initiated. Subsequently, a dose of 10 mg/
kg was shown to provide a good benefit-to-risk ratio for
ipilimumab monotherapy in previously treated patients
with advanced melanoma, although ipilimumab at 3 mg/
kg also induces objective responses in these patients
[21]. In this report, we present results from the first study
of ipilimumab in combination with DTIC for patients with
advanced melanoma. The results of a follow-up study to
assess the long-term survival of patients participating in
this trial are also reported herein.
Patients and methods
This was a phase II, randomized, multicenter, open-label study
(MDX010-08; ClinicalTrials.gov identifier: NCT00050102)
in which patients received multiple doses of ipilimumab alone
or in combination with DTIC. Enrollment started in September
of 2002 and ended in August of 2004.
Patient selection
Eligible patients were ≥18 years of age, with a histologic
diagnosis of unresectable metastatic melanoma and progres-
sive disease defined by Response Evaluation Criteria in Solid
Tumors (RECIST) [23], ≥1 measurable lesion, and life
expectancy ≥12 weeks. Patients were required to have
Invest New Drugs

discontinued any other melanoma therapy ≥4 weeks before
enrollment, and were excluded if they had received previous
chemotherapy, vaccine immunotherapy, or an anti-CTLA-4
antibody. Signed informed consent was also required.
Exclusion criteria included any other prior malignancy;
history or clinical evidence of autoimmune disease; treatment
with an immunosuppressive drug, melanoma vaccine, anti-
CTLA-4 antibody, or chemotherapy within the past 5 years
(except for regional chemotherapy); active infection requiring
therapy; chronic active hepatitis B or C virus infection, or
human immunodeficiency virus reactivity.
Crossover patients included all those who initially
received ipilimumab alone and then received ipilimumab
plus DTIC following disease progression (n=13). For the
crossover phase, patients must have met all inclusion and
exclusion criteria (with the exception of prior anti-CTLA-4
antibody administration). Patients were administered all
baseline tests and procedures prior to entering the crossover
phase; a complete medical history including all treatments
received between the end of ipilimumab monotherapy and
the initiation of the crossover phase were recorded.
Treatment schema
Patients were randomly assigned to receive ipilimumab at
3 mg/kg every 4 weeks for four doses, either alone or in
combination with DTIC at 250 mg/m2 for five consecutive
days every 3 weeks (maximum of six cycles). Patients who
progressed on monotherapy could cross over and receive
combination therapy. The study was designed and con-
ducted in accordance with the principles of Good Clinical
Practice. The protocol was approved by the institutional
review board (IRB) or independent ethics committee at
each study site. A separate follow-up study (MDX010–028)
to assess the OS of patients participating in this study was
conducted. IRB approval was obtained to collect the date of
death from patients who died subsequent to completing
study MDX010-08.
The primary objectives of this study were to assess the
safety and activity (objective response rate; ORR) of
ipilimumab alone and in combination with DTIC. Second-
ary objectives included evaluations of response duration,
stable disease (SD), lymphocyte subpopulations, and the
pharmacokinetic profile of ipilimumab with and without
DTIC. ORR was determined by investigator assessment of
target and non-target lesions using RECIST; to be assessed as
complete or partial response (CR or PR), changes in tumor
measurements had to be confirmed by repeat assessments no
less than 4 weeks after the criteria for response were first met.
Adverse events (AEs), serious AEs (SAEs), and immune-
related AEs (irAEs) were coded according to the Medical
Dictionary for Regulatory Affairs, and severities were graded
using Common Toxicity Criteria version 2.0. Severe events
were defined as those ≥grade 3. Survival was determined in a
separate study (MDX010-28).
Pharmacokinetics
Plasma ipilimumab concentrations obtained during screening,
30 min before infusion of study drug, 120 min post-infusion,
on days 29, 57, 85, 113, 141, and 169, and every 3 months
during the follow-up phase were determined by quantitative
enzyme-linked immunosorbent assay. The parameters AUC,
Cmax and T1/2 could not be determined due to the limited
number of samples collected.
Lymphocyte subpopulations
Two-color flow cytometry analysis was conducted on periph-
eral blood samples obtained from each patient drawn before
and 14 days after each administration of ipilimumab as
described previously [20]. Specific parameters included
analysis of CD3+, CD4+, CD8+, CD4+CD25+, CD8+
CD25+, CD4+HLA-DR+, and CD8+HLA-DR+ lymphocyte
subpopulations.
Statistics
The sample size was based on the primary objective of
evaluating the safety and activity of ipilimumab alone or in
combination with DTIC. By Fisher’s exact test, a sample
size of 23 evaluable patients in each group was required to
provide 80% power to detect treatment differences (objec-
tive response rate) in a one-sided test at the 0.05
significance level. For quantitative parameters (continuous
variables), descriptive statistics included mean, standard
deviation, minimum, median, and maximum. For qualita-
tive parameters (categorical variables), descriptive statistics
included frequency and percentage. The 95% confidence
intervals (CIs) for response and disease control rate were
calculated for each treatment group. Duration of response,
time to response, and duration of stable disease were
analyzed using parametric and non-parametric statistics. OS
was determined using the Kaplan–Meier product limit
method. The crossover patients were analyzed according
to the treatment group to which they were originally
randomized, i.e., ipilimumab monotherapy.
Results
Patient disposition and demographics
Figure 1 shows the treatment schema and the patients in each
treatment category. Seventy-six patients were randomized to
Invest New Drugs
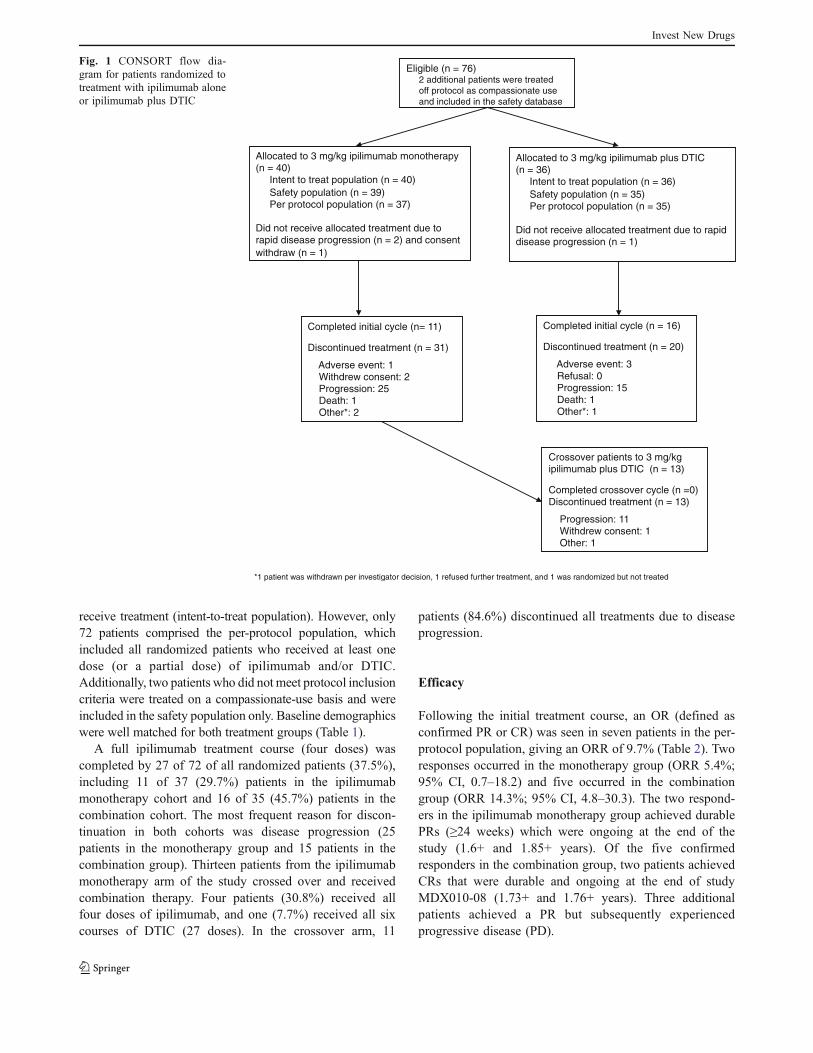
receive treatment (intent-to-treat population). However, only
72 patients comprised the per-protocol population, which
included all randomized patients who received at least one
dose (or a partial dose) of ipilimumab and/or DTIC.
Additionally, two patients who did not meet protocol inclusion
criteria were treated on a compassionate-use basis and were
included in the safety population only. Baseline demographics
were well matched for both treatment groups (Table 1).
A full ipilimumab treatment course (four doses) was
completed by 27 of 72 of all randomized patients (37.5%),
including 11 of 37 (29.7%) patients in the ipilimumab
monotherapy cohort and 16 of 35 (45.7%) patients in the
combination cohort. The most frequent reason for discon-
tinuation in both cohorts was disease progression (25
patients in the monotherapy group and 15 patients in the
combination group). Thirteen patients from the ipilimumab
monotherapy arm of the study crossed over and received
combination therapy. Four patients (30.8%) received all
four doses of ipilimumab, and one (7.7%) received all six
courses of DTIC (27 doses). In the crossover arm, 11
patients (84.6%) discontinued all treatments due to disease
progression.
Efficacy
Following the initial treatment course, an OR (defined as
confirmed PR or CR) was seen in seven patients in the per-
protocol population, giving an ORR of 9.7% (Table 2). Two
responses occurred in the monotherapy group (ORR 5.4%;
95% CI, 0.7–18.2) and five occurred in the combination
group (ORR 14.3%; 95% CI, 4.8–30.3). The two respond-
ers in the ipilimumab monotherapy group achieved durable
PRs (≥24 weeks) which were ongoing at the end of the
study (1.6+ and 1.85+ years). Of the five confirmed
responders in the combination group, two patients achieved
CRs that were durable and ongoing at the end of study
MDX010-08 (1.73+ and 1.76+ years). Three additional
patients achieved a PR but subsequently experienced
progressive disease (PD).
Completed initial cycle (n= 11)
Discontinued treatment (n = 31)
Adverse event: 1 Withdrew consent: 2 Progression: 25 Death: 1 Other*: 2
Completed initial cycle (n = 16)
Discontinued treatment (n = 20)
Adverse event: 3 Refusal: 0 Progression: 15 Death: 1 Other*: 1
Crossover patients to 3 mg/kg ipilimumab plus DTIC (n = 13)
Completed crossover cycle (n =0) Discontinued treatment (n = 13)
Progression: 11 Withdrew consent: 1 Other: 1
Allocated to 3 mg/kg ipilimumab monotherapy (n = 40) Intent to treat population (n = 40)
Safety population (n = 39) Per protocol population (n = 37)
Did not receive allocated treatment due to rapid disease progression (n = 2) and consent
withdraw (n = 1)
Allocated to 3 mg/kg ipilimumab plus DTIC (n = 36) Intent to treat population (n = 36)
Safety population (n = 35) Per protocol population (n = 35)
Did not receive allocated treatment due to rapid disease progression (n = 1)
Eligible (n = 76) 2 additional patients were treated
off protocol as compassionate use
and included in the safety database
*1 patient was withdrawn per investigator decision, 1 refused further treatment, and 1 was randomized but not treated
Fig. 1 CONSORT flow dia-
gram for patients randomized to
treatment with ipilimumab alone
or ipilimumab plus DTIC
Invest New Drugs
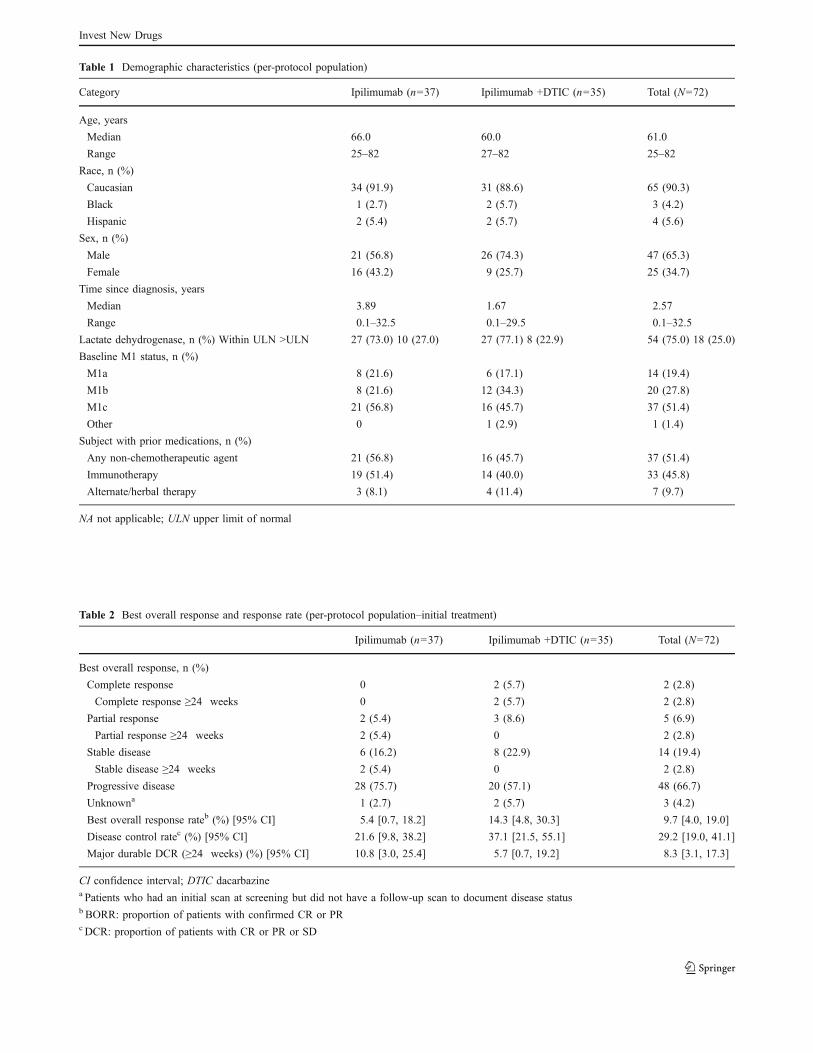
Table 1 Demographic characteristics (per-protocol population)
Category Ipilimumab (n=37) Ipilimumab +DTIC (n=35) Total (N=72)
Age, years
Median 66.0 60.0 61.0
Range 25–82 27–82 25–82
Race, n (%)
Caucasian 34 (91.9) 31 (88.6) 65 (90.3)
Black 1 (2.7) 2 (5.7) 3 (4.2)
Hispanic 2 (5.4) 2 (5.7) 4 (5.6)
Sex, n (%)
Male 21 (56.8) 26 (74.3) 47 (65.3)
Female 16 (43.2) 9 (25.7) 25 (34.7)
Time since diagnosis, years
Median 3.89 1.67 2.57
Range 0.1–32.5 0.1–29.5 0.1–32.5
Lactate dehydrogenase, n (%) Within ULN >ULN 27 (73.0) 10 (27.0) 27 (77.1) 8 (22.9) 54 (75.0) 18 (25.0)
Baseline M1 status, n (%)
M1a 8 (21.6) 6 (17.1) 14 (19.4)
M1b 8 (21.6) 12 (34.3) 20 (27.8)
M1c 21 (56.8) 16 (45.7) 37 (51.4)
Other 0 1 (2.9) 1 (1.4)
Subject with prior medications, n (%)
Any non-chemotherapeutic agent 21 (56.8) 16 (45.7) 37 (51.4)
Immunotherapy 19 (51.4) 14 (40.0) 33 (45.8)
Alternate/herbal therapy 3 (8.1) 4 (11.4) 7 (9.7)
NA not applicable; ULN upper limit of normal
Table 2 Best overall response and response rate (per-protocol population–initial treatment)
Ipilimumab (n=37) Ipilimumab +DTIC (n=35) Total (N=72)
Best overall response, n (%)
Complete response 0 2 (5.7) 2 (2.8)
Complete response ≥24 weeks 0 2 (5.7) 2 (2.8)
Partial response 2 (5.4) 3 (8.6) 5 (6.9)
Partial response ≥24 weeks 2 (5.4) 0 2 (2.8)
Stable disease 6 (16.2) 8 (22.9) 14 (19.4)
Stable disease ≥24 weeks 2 (5.4) 0 2 (2.8)
Progressive disease 28 (75.7) 20 (57.1) 48 (66.7)
Unknowna 1 (2.7) 2 (5.7) 3 (4.2)
Best overall response rateb (%) [95% CI] 5.4 [0.7, 18.2] 14.3 [4.8, 30.3] 9.7 [4.0, 19.0]
Disease control ratec (%) [95% CI] 21.6 [9.8, 38.2] 37.1 [21.5, 55.1] 29.2 [19.0, 41.1]
Major durable DCR (≥24 weeks) (%) [95% CI] 10.8 [3.0, 25.4] 5.7 [0.7, 19.2] 8.3 [3.1, 17.3]
CI confidence interval; DTIC dacarbazinea Patients who had an initial scan at screening but did not have a follow-up scan to document disease statusbBORR: proportion of patients with confirmed CR or PRcDCR: proportion of patients with CR or PR or SD
Invest New Drugs
Fourteen patients (eight who received ipilimumab +DTIC
and six who received ipilimumab alone) achieved SD. The
duration of SD ranged from ~1 month to 15+ months. The
disease control rate (DCR; CR + PR + SD/N) was 37.1%
(95% CI, 21.5–55.1; n=13) in the ipilimumab plus DTIC
group and 21.6% (95% CI, 9.8–38.2; n=8) in the ipilimumab
group. Six of these 21 patients (four who received
ipilimumab +DTIC and two who received ipilimumab alone)
achieved disease control that lasted ≥24 weeks (Table 2).
There were no statistically significant differences between
the treatment groups for either ORR or DCR.
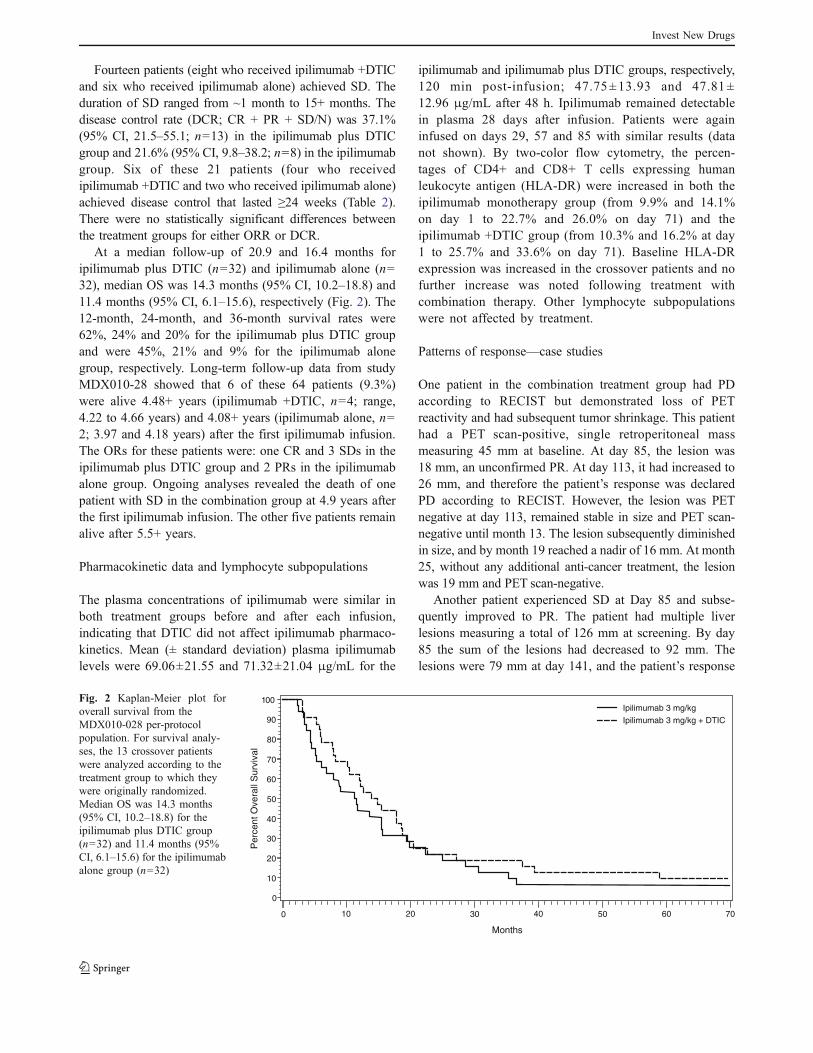
At a median follow-up of 20.9 and 16.4 months for
ipilimumab plus DTIC (n=32) and ipilimumab alone (n=
32), median OS was 14.3 months (95% CI, 10.2–18.8) and
11.4 months (95% CI, 6.1–15.6), respectively (Fig. 2). The
12-month, 24-month, and 36-month survival rates were
62%, 24% and 20% for the ipilimumab plus DTIC group
and were 45%, 21% and 9% for the ipilimumab alone
group, respectively. Long-term follow-up data from study
MDX010-28 showed that 6 of these 64 patients (9.3%)
were alive 4.48+ years (ipilimumab +DTIC, n=4; range,
4.22 to 4.66 years) and 4.08+ years (ipilimumab alone, n=
2; 3.97 and 4.18 years) after the first ipilimumab infusion.
The ORs for these patients were: one CR and 3 SDs in the
ipilimumab plus DTIC group and 2 PRs in the ipilimumab
alone group. Ongoing analyses revealed the death of one
patient with SD in the combination group at 4.9 years after
the first ipilimumab infusion. The other five patients remain
alive after 5.5+ years.
Pharmacokinetic data and lymphocyte subpopulations
The plasma concentrations of ipilimumab were similar in
both treatment groups before and after each infusion,
indicating that DTIC did not affect ipilimumab pharmaco-
kinetics. Mean (± standard deviation) plasma ipilimumab
levels were 69.06±21.55 and 71.32±21.04 μg/mL for the
ipilimumab and ipilimumab plus DTIC groups, respectively,
120 min post-infusion; 47.75±13.93 and 47.81±
12.96 μg/mL after 48 h. Ipilimumab remained detectable
in plasma 28 days after infusion. Patients were again
infused on days 29, 57 and 85 with similar results (data
not shown). By two-color flow cytometry, the percen-
tages of CD4+ and CD8+ T cells expressing human
leukocyte antigen (HLA-DR) were increased in both the
ipilimumab monotherapy group (from 9.9% and 14.1%
on day 1 to 22.7% and 26.0% on day 71) and the
ipilimumab +DTIC group (from 10.3% and 16.2% at day
1 to 25.7% and 33.6% on day 71). Baseline HLA-DR
expression was increased in the crossover patients and no
further increase was noted following treatment with
combination therapy. Other lymphocyte subpopulations
were not affected by treatment.
Patterns of response—case studies
One patient in the combination treatment group had PD
according to RECIST but demonstrated loss of PET
reactivity and had subsequent tumor shrinkage. This patient
had a PET scan-positive, single retroperitoneal mass
measuring 45 mm at baseline. At day 85, the lesion was
18 mm, an unconfirmed PR. At day 113, it had increased to
26 mm, and therefore the patient’s response was declared
PD according to RECIST. However, the lesion was PET
negative at day 113, remained stable in size and PET scan-
negative until month 13. The lesion subsequently diminished
in size, and by month 19 reached a nadir of 16 mm. At month
25, without any additional anti-cancer treatment, the lesion
was 19 mm and PET scan-negative.
Another patient experienced SD at Day 85 and subse-
quently improved to PR. The patient had multiple liver
lesions measuring a total of 126 mm at screening. By day
85 the sum of the lesions had decreased to 92 mm. The
lesions were 79 mm at day 141, and the patient’s response
Pe
rce
nt
Ove
rall
Su
rviv
al
0
10
20
30
40
50
60
70
80
90
100
Months
0 10 20 30 40 50 60 70
Ipilimumab 3 mg/kg
Ipilimumab 3 mg/kg + DTIC
Fig. 2 Kaplan-Meier plot for
overall survival from the
MDX010-028 per-protocol
population. For survival analy-
ses, the 13 crossover patients
were analyzed according to the
treatment group to which they
were originally randomized.
Median OS was 14.3 months
(95% CI, 10.2–18.8) for the
ipilimumab plus DTIC group
(n=32) and 11.4 months (95%
CI, 6.1–15.6) for the ipilimumab
alone group (n=32)
Invest New Drugs

was considered PR. The sum of the lesions had reached a
nadir of 50 mm at the last study visit at month 25.
Adverse events
Sixty of the 74 patients (81%) in the safety population
reported ≥1 treatment-related AEs, with nausea and fatigue
being the most frequent (Table 3). AEs of grade 3 or higher
occurred in 12.8% of patients in the monotherapy group
and in 22.9% of patients in the combination therapy group,
while the rate was 15.4% during crossover treatment. No
infusion reactions occurred during or immediately after
ipilimumab administration. One patient (2.6%) from the
ipilimumab monotherapy group discontinued treatment due
to colitis, and 3 of 35 patients (8.6%) from the combination
therapy group discontinued treatment due to recurrent
gastrointestinal bleeds/inflammatory colitis, low-grade con-
stitutional symptoms (e.g., fatigue, malaise, sweats, muscle
weakness), and grade 3 liver enzyme elevation. Severe
(≥grade 3) and SAEs (most commonly anemia, tachycardia,
abdominal pain, colitis, fatigue, dehydration, pain in
extremity, and dyspnea) were generally medically manage-
able and reversible without known sequelae.
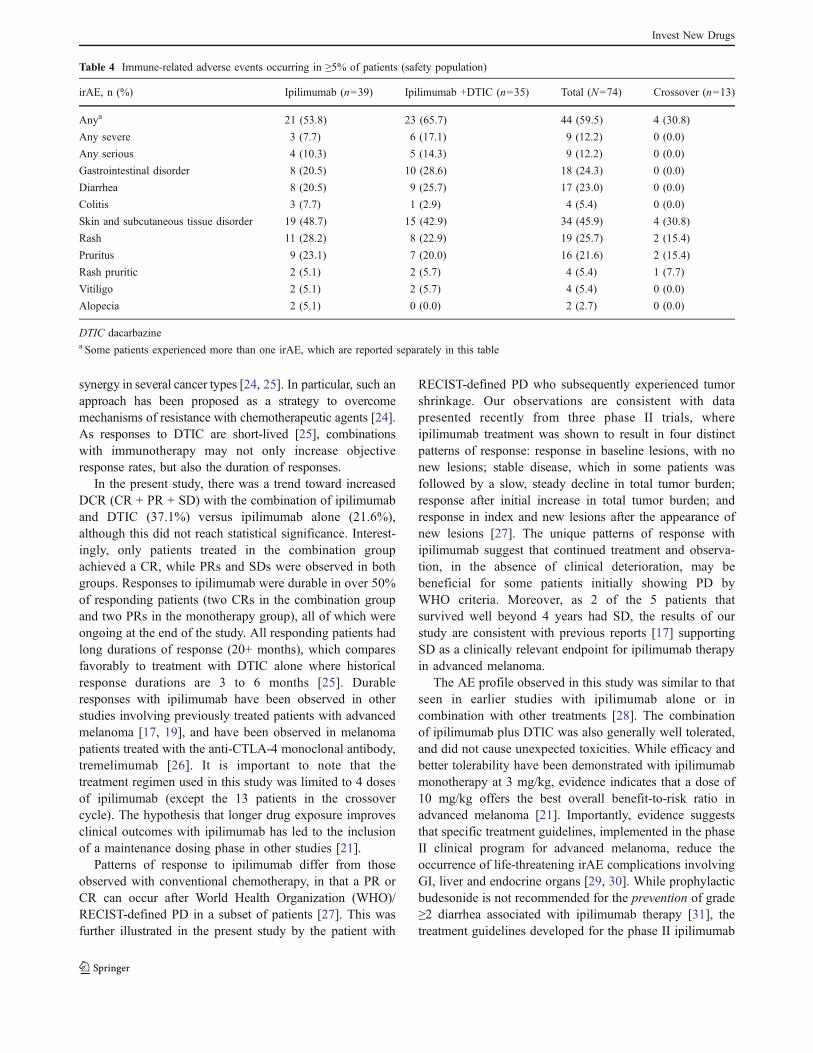
IrAEs of any grade occurred in 65.7% of patients in the
ipilimumab plus DTIC cohort (Table 4); 17.1% (6/35) were
severe (patients experienced either elevated ALT, elevated
AST, generalized rash and pruritis, rash, or multi-organ
failure, and one patient had colitis, GI hemorrhage,
hematochezia, rectal bleeding, and autoimmune vasculi-
tis);14.3% (5/35) were serious/ongoing (grade 2 adrenal
insufficiency, grade 3 elevated AST leading to study drug
discontinuation, grade 3 generalized rash and pruritis, or
grade 4 multi-organ failure, and one patient experienced
grade 2 diarrhea, grade 3 rectal bleeding, grade 4 colitis,
and grade 4 autoimmune vasculitis). In the ipilimumab
group, 53.8% of patients experienced an irAE of any grade
(Table 4); 7.7% (3/39) were severe (two patients experi-
enced colitis and one patient experienced rash); 10.3% (4/
39) were serious/ongoing (two patients had grade 3 colitis,
one patient had grade 2 diarrhea, and one patient had grade
2 diarrhea as well as grade 2 colitis). After crossover,
30.8% of patients experienced ≥1 irAE, none being severe
or serious.
Severe and serious irAEs were, in general, medically
manageable and reversible without known sequelae. One
exception was a patient from the ipilimumab plus DTIC
group who, after the fourth dose of ipilimumab, developed
grade 4 steroid-refractory colitis requiring colectomy with
ileostomy. The patient subsequently died from infectious
complications, including disseminated aspergillosis. This
death was not considered directly related to study treatment.
One patient in the monotherapy group died with pulmonary
embolus/sepsis (Day 108) that was considered related to
ipilimumab treatment, and one patient in the combination
group died from acute multiorgan failure shortly after the
third treatment cycle (Day 59) that was considered possibly
related to both ipilimumab and DTIC.
Discussion
The strategy of combining various antineoplastic therapies
is based on the proposal that agents with different
mechanisms of action and non-overlapping toxicity profiles
can potentially have an additive or even a synergistic effect
while maintaining a manageable safety profile. It has been
hypothesized that combining chemotherapy with immuno-
therapy allows the neoantigens released upon cytotoxic
drug-induced tumor cell death to be more readily recog-
nized by a potentiated immune system [7]. There is
currently a great deal of interest in using combinations of
chemotherapy and immunotherapy for a potential therapeutic
Table 3 Treatment-related adverse events by preferred term and severity reported in ≥10% of patients (safety population)
Ipilimumab (n=39) Ipilimumab +DTIC (n=35) Total (N=74) Crossover (n=13)
AE, n (%) Grade 1/2 Grade 3/4 Grade 1/2 Grade 3/4 Grade 1/2 Grade 3/4 Grade 1/2 Grade 3/4
Any 24 (61.5) 5 (12.8) 23 (65.7) 8 (22.9) 47 (63.5) 13 (17.6) 7 (53.8) 2 (15.4)
Nausea 11(28.2) 0 (0) 19 (54.3) 1 (2.9) 30 (40.5) 1 (1.4) 3 (23.1) 0 (0)
Fatigue 10 (25.6) 0 (0) 15 (42.9) 2 (5.7) 25 (33.8) 2 (2.7) 4 (30.8) 2 (15.4)
Rash 10 (25.6) 1 (2.6) 7 (20.0) 1 (2.9) 17 (22.9) 2 (2.7) 2 (15.4) 0 (0)
Chills 9 (23.1) 0 (0) 8 (22.9) 0 (0) 17 (23.0) 0 (0) 1 (7.7) 0 (0)
Pruritus 9 (23.1) 0 (0) 7 (20.0) 0 (0) 16 (21.6) 0 (0) 1 (7.7) 0 (0)
Anorexia 5 (12.8) 0 (0) 10 (28.6) 0 (0) 15 (20.3) 0 (0) 1 (7.7) 0 (0)
Diarrhea 8 (20.5) 0 (0) 9 (25.7) 0 (0) 17 (23.0) 0 (0) 0 (0) 0 (0)
Pyrexia 4 (10.3) 0 (0) 6 (17.1) 1 (2.9) 10 (13.5) 1 (1.4) 0 (0) 0 (0)
DTIC dacarbazine
Invest New Drugs
synergy in several cancer types [24, 25]. In particular, such an
approach has been proposed as a strategy to overcome
mechanisms of resistance with chemotherapeutic agents [24].
As responses to DTIC are short-lived [25], combinations
with immunotherapy may not only increase objective
response rates, but also the duration of responses.
In the present study, there was a trend toward increased
DCR (CR + PR + SD) with the combination of ipilimumab
and DTIC (37.1%) versus ipilimumab alone (21.6%),
although this did not reach statistical significance. Interest-
ingly, only patients treated in the combination group
achieved a CR, while PRs and SDs were observed in both
groups. Responses to ipilimumab were durable in over 50%
of responding patients (two CRs in the combination group
and two PRs in the monotherapy group), all of which were
ongoing at the end of the study. All responding patients had
long durations of response (20+ months), which compares
favorably to treatment with DTIC alone where historical
response durations are 3 to 6 months [25]. Durable
responses with ipilimumab have been observed in other
studies involving previously treated patients with advanced
melanoma [17, 19], and have been observed in melanoma
patients treated with the anti-CTLA-4 monoclonal antibody,
tremelimumab [26]. It is important to note that the
treatment regimen used in this study was limited to 4 doses
of ipilimumab (except the 13 patients in the crossover
cycle). The hypothesis that longer drug exposure improves
clinical outcomes with ipilimumab has led to the inclusion
of a maintenance dosing phase in other studies [21].
Patterns of response to ipilimumab differ from those
observed with conventional chemotherapy, in that a PR or
CR can occur after World Health Organization (WHO)/
RECIST-defined PD in a subset of patients [27]. This was
further illustrated in the present study by the patient with
RECIST-defined PD who subsequently experienced tumor
shrinkage. Our observations are consistent with data
presented recently from three phase II trials, where
ipilimumab treatment was shown to result in four distinct
patterns of response: response in baseline lesions, with no
new lesions; stable disease, which in some patients was
followed by a slow, steady decline in total tumor burden;
response after initial increase in total tumor burden; and
response in index and new lesions after the appearance of
new lesions [27]. The unique patterns of response with
ipilimumab suggest that continued treatment and observa-
tion, in the absence of clinical deterioration, may be
beneficial for some patients initially showing PD by
WHO criteria. Moreover, as 2 of the 5 patients that
survived well beyond 4 years had SD, the results of our
study are consistent with previous reports [17] supporting
SD as a clinically relevant endpoint for ipilimumab therapy
in advanced melanoma.
The AE profile observed in this study was similar to that
seen in earlier studies with ipilimumab alone or in
combination with other treatments [28]. The combination
of ipilimumab plus DTIC was also generally well tolerated,
and did not cause unexpected toxicities. While efficacy and
better tolerability have been demonstrated with ipilimumab
monotherapy at 3 mg/kg, evidence indicates that a dose of
10 mg/kg offers the best overall benefit-to-risk ratio in
advanced melanoma [21]. Importantly, evidence suggests
that specific treatment guidelines, implemented in the phase
II clinical program for advanced melanoma, reduce the
occurrence of life-threatening irAE complications involving
GI, liver and endocrine organs [29, 30]. While prophylactic
budesonide is not recommended for the prevention of grade
≥2 diarrhea associated with ipilimumab therapy [31], the
treatment guidelines developed for the phase II ipilimumab
Table 4 Immune-related adverse events occurring in ≥5% of patients (safety population)
irAE, n (%) Ipilimumab (n=39) Ipilimumab +DTIC (n=35) Total (N=74) Crossover (n=13)
Anya 21 (53.8) 23 (65.7) 44 (59.5) 4 (30.8)
Any severe 3 (7.7) 6 (17.1) 9 (12.2) 0 (0.0)
Any serious 4 (10.3) 5 (14.3) 9 (12.2) 0 (0.0)
Gastrointestinal disorder 8 (20.5) 10 (28.6) 18 (24.3) 0 (0.0)
Diarrhea 8 (20.5) 9 (25.7) 17 (23.0) 0 (0.0)
Colitis 3 (7.7) 1 (2.9) 4 (5.4) 0 (0.0)
Skin and subcutaneous tissue disorder 19 (48.7) 15 (42.9) 34 (45.9) 4 (30.8)
Rash 11 (28.2) 8 (22.9) 19 (25.7) 2 (15.4)
Pruritus 9 (23.1) 7 (20.0) 16 (21.6) 2 (15.4)
Rash pruritic 2 (5.1) 2 (5.7) 4 (5.4) 1 (7.7)
Vitiligo 2 (5.1) 2 (5.7) 4 (5.4) 0 (0.0)
Alopecia 2 (5.1) 0 (0.0) 2 (2.7) 0 (0.0)
DTIC dacarbazinea Some patients experienced more than one irAE, which are reported separately in this table
Invest New Drugs

clinical trial program recommend the use of budesonide for
grade 2 diarrhea and high-dose steroids for grade 3–4
diarrhea once they appear [29, 30].
The results of the present study show that ipilimumab
causes an increase in the percentage of activated T cells in
the periphery, suggesting an immune response, although
this study was not powered to detect such differences
between the ipilimumab alone and ipilimumab plus DTIC
groups. We demonstrate in this study that ipilimumab at a
dose of 3 mg/kg produces durable objective responses and
long-term survival in some patients, with a trend toward
better efficacy in the combination group. These results
support further investigations of ipilimumab and DTIC for
the treatment of chemotherapy-naïve advanced melanoma.
In the dose-ranging phase II trial, CA184-022, ipilimumab
alone at 10 mg/kg produced greater response rates (p=
0.0015), a better pharmacokinetic profile, higher absolute
lymphocyte counts, and numerically greater survival than at
3 mg/kg in patients with pretreated advanced melanoma
[21]. This study evaluated ipilimumab at 10 mg/kg given
every 3 weeks for 4 doses (induction), followed by the
same dose given every 12 weeks beginning at week 24 in
eligible patients (maintenance). Using the same dosing
schedule as in study CA184-022 [21] and treatment
guidelines for the management of irAEs [29, 30], the safety
and efficacy of ipilimumab at 10 mg/kg in combination
with DTIC at 850 mg/m2 are being evaluated in a
randomized phase III trial in chemotherapy-naive patients
with advanced melanoma [32].
Acknowledgments The authors thank Steven A. Fischkoff (currently
at Palatin Technologies, Cranbury, NJ) for technical assistance and
Georgia Brockway for assistance in preparing and reviewing the data.
Writing and editorial support was provided by StemScientific, funded by
Bristol-Myers Squibb Co.
References
1. Lens MB, Dawes M (2004) Global perspectives of contemporary
epidemiological trends of cutaneous malignant melanoma. Br J
Dermatol 150:179–185
2. Cancer Facts & Figures (2009) American cancer society, Atlanta,
GA, USA. http://www.cancer.org/downloads/STT/2009CAFFfinal
secured.pdf Accessed August 31st, 2009
3. Korn EL, Liu PY, Lee SJ et al (2008) Meta-analysis of phase II
cooperative group trials in metastatic stage IV melanoma to
determine progression-free and overall survival benchmarks for
future phase II trials. J Clin Oncol 26:527–534
4. Bedikian AY, Millward M, Pehamberger H et al (2006) Bcl-2
antisense (oblimersen sodium) plus dacarbazine in patients with
advanced melanoma: the oblimersen melanoma study group. J
Clin Oncol 24:4738–4745
5. Agarwala SS (2009) Current systemic therapy for metastatic
melanoma. Expert Rev Anticancer Ther 9:587–595
6. Petrella T, Quirt I, Verma S, Haynes AE, Charette M, Bak K,
Melanoma Disease Site Group of Cancer Care Ontario’s Program
in Evidence-based Care (2007) Single-agent interleukin-2 in the
treatment of metastatic melanoma: a systematic review. Cancer
Treat Rev 33:484–496
7. Peggs KS, Segal NH, Allison JP (2007) Targeting immunosup-
portive cancer therapies: accentuate the positive, eliminate the
negative. Cancer Cell 12:192–199
8. Melero I, Hervas-Stubbs S, Glennie M, Pardoll DM, Chen L
(2007) Immunostimulatory monoclonal antibodies for cancer
therapy. Nat Rev Cancer 7:95–106
9. Morse MA (2005) Technology evaluation: Ipilimumab, Medarex/
Bristol-Myers Squibb. Curr Opin Mol Ther 7:588–597
10. Cranmer LD, Hersh E (2007) The role of the CTLA4 blockade in
the treatment of malignant melanoma. Cancer Invest 25:613–631
11. Fong L, Small EJ (2008) Anti–cytotoxic T-lymphocyte antigen-4
antibody: the first in an emerging class of immunomodulatory
antibodies for cancer treatment. J Clin Oncol 26:5275–5283
12. Ridolfi L, Ridolfi R (2009) Anti-CTLA-4 therapy in melanoma:
role of ipilimumab (MDX-010). Expert Rev Dermatol 4:199–210
13. Hodi FS, Mihm MC, Soiffer RJ et al (2003) Biologic activity of
cytotoxic T lymphocyte-associated antigen 4 antibody blockade in
previously vaccinated metastatic melanoma and ovarian carcino-
ma patients. Proc Natl Acad Sci USA 100:4712–4717
14. Langer LF, Clay TM, Morse MA (2007) Update on anti-CTLA-4
antibodies in clinical trials. Expert Opin Biol Ther 7:1245–1256
15. Margolin K (2008) Moving forward with immunotherapy: the
rationale for anti-CTLA-4 therapy in melanoma. Comm Oncol
5:367–374
16. O’Day SJ, Ibrahim R, DePril V et al (2008) Efficacy and safety of
ipilimumab induction and maintenance dosing in patients with
advanced melanoma who progressed on one or more prior
therapies. J Clin Oncol 26(19s):abstract 9021
17. Weber JS, O’Day S, Urba W et al (2008) Phase I/II study of
ipilimumab for patients with metastatic melanoma. J Clin Oncol
26:5950–5956
18. Phan GQ, Yang JC, Sherry RM et al (2003) Cancer regression and
autoimmunity induced by cytotoxic T lymphocyte-associated
antigen 4 blockade in patients with metastatic melanoma. Proc
Natl Acad Sci USA 100:8372–8377
19. Attia P, Phan GQ, Maker AVet al (2005) Autoimmunity correlates
with tumor regression in patients with metastatic melanoma
treated with anti-cytotoxic T-lymphocyte antigen-4. J Clin Oncol
23:6043–6053
20. Maker AV, Phan GQ, Attia P et al (2005) Tumor regression and
autoimmunity in patients treated with cytotoxic T lymphocyte-
associated antigen 4 blockade and interleukin 2: a phase I/II study.
Ann Surg Oncol 12:1005–1016
21. Wolchok JD, Neyns B, Linette G et al (2009) Ipilimumab
monotherapy in patients with pretreated advanced melanoma: a
randomised, double-blind, multicentre, phase 2, dose-ranging
study. Lancet Oncol; in press
22. Urba WJ, Weber JS, O’Day SJ et al (2008) Long-term survival of
patients with advanced melanoma who received ipilimumab
administered at 10mg/kg every 3weeks for 4 doses (induction
dosing). J Clin Oncol 26(19s):abstract 3018
23. Therasse P, Arbuck SG, Eisenhauer EA et al (2000) New
guidelines to evaluate the response to treatment in solid tumors.
J Natl Cancer Inst 92:205–216
24. Lake RA, Robinson BW (2005) Immunotherapy and chemother-
apy–a practical partnership. Nat Rev Cancer 5:397–405
25. Zigler M, Villares GJ, Lev DC, Melnikova VO, Bar-Eli M (2008)
Tumor immunotherapy in melanoma: strategies for overcoming
mechanisms of resistance and escape. Am J Clin Dermatol 9:307–311
26. Ribas A, Camacho LH, Lopez Berestein G et al (2005) Antitumor
activity in melanoma and anti-self responses in a phase I trial with
the anti-cytotoxic T lymphocyte-associated antigen 4 monoclonal
antibody CP-675, 206. J Clin Oncol 23:8968–8977
Invest New Drugs

27. Wolchok JD, Hoos A, O’Day S et al (2009) Guidelines for the
evaluation of immune therapy activity in solid tumors:
immune-related response criteria. Clin Cancer Res 15:7412–
7420
28. Weber J (2009) Ipilimumab: controversies in its development,
utility and autoimmune adverse events. Cancer Immunol Immun-
other 58:823–830
29. Lin R, Yellin MJ, Lowy I, Safferman A, Chin K, Ibrahim R
(2008) An analysis of the effectiveness of specific guidelines for
the management of ipilimumab-mediated diarrhea/colitis: preven-
tion of gastrointestinal perforation and/or colectomy. J Clin Oncol
26(19s):abstract 9063
30. Weber J (2007) Review: Anti–CTLA-4 antibody ipilimumab: case
studies of clinical response and immune-related adverse events.
Oncologist 12:864–872
31. Weber J, Thompson JA, Hamid O et al (2009) A randomized,
double-blind, placebo-controlled, phase II study comparing the
tolerability and efficacy of ipilimumab administered with or
without prophylactic budesonide in patients with unresectable
stage III or IV melanoma. Clin Cancer Res 15:5591–5598
32. ClinicalTrials.gov. Dacarbazine and ipilimumab vs. dacarbazine
with placebo in untreated, unresectable stage III or IV melanoma.
www.clinicaltrials.gov/ct/show/NCT00324155 Accessed September
3rd, 2009
Invest New Drugs


















![[Distribution of blaOXA genes in Acinetobacter baumannii strains: a multicenter study]](https://static.fdokumen.com/doc/165x107/6337b5c66f78ac31240eb601/distribution-of-blaoxa-genes-in-acinetobacter-baumannii-strains-a-multicenter.jpg)

