A Paired, Double-Blind, Randomized Comparison of a Moisturizing Durable Barrier Cream to 10%...
6
Clinical Investigation: Breast Cancer A Paired, Double-Blind, Randomized Comparison of a Moisturizing Durable Barrier Cream to 10% Glycerine Cream in the Prophylactic Management of Postmastectomy Irradiation Skin Care: Trans Tasman Radiation Oncology Group (TROG) 04.01 Peter H. Graham, FRANZCR,* Natalie Plant, MHSc,* Jennifer L. Graham, MN,* Lois Browne, PhD,* Martin Borg, FRANZCR, y Anne Capp, FRANZCR, z Geoff P. Delaney, MD, x Jennifer Harvey, FRANZCR, jj Lisbeth Kenny, FRANZCR, { Michael Francis, FRANZCR, # and Yvonne Zissiadis, FRANZCR** *Cancer Care Centre, St. George Hospital, Kogarah, New South Wales, Australia; y Department of Radiation Oncology, Royal Adelaide Hospital; z Department of Radiation Oncology, Mater Hospital, Newcastle, New South Wales, Australia; x Cancer Care Centre, Liverpool Hospital, Liverpool, New South Wales, Australia; jj Mater Hospital, South Brisbane, Queensland, Australia; { Royal Brisbane Hospital, Herston; # Andrew Love Cancer Centre, Geelong; and **Department of Radiation Oncology, Royal Perth Hospital, Perth, Australia Received Sep 14, 2012, and in revised form Dec 7, 2012. Accepted for publication Dec 11, 2012 Summary This study used a double- blind, randomized, intra- patient, paired design to test the hypothesis that an acrylate terpolymer alcohol-free barrier film reduces the degree of radiation skin reac- tion compared with the 10% glycerine cream most commonly used for this purpose in Australia. No significant difference was found using this rigorous trial Purpose: A previous, unblinded study demonstrated that an alcohol-free barrier film containing an acrylate terpolymer (ATP) was effective in reducing skin reactions compared with a 10% glycerine cream (sorbolene). The different appearances of these products precluded a blinded comparison. To test the acrylate terpolymer principle in a double-blinded manner required the use of an alternative cream formulation, a moisturizing durable barrier cream (MDBC); the study was conducted by the Trans Tasman Radiation Oncology Group (TROG) as protocol 04.01. Methods and Materials: A total of 333 patients were randomized; 1 patient was ineligible and 14 patients withdrew or had less than 7 weeks’ observations, leaving 318 for analysis. The chest wall was divided into medial and lateral compartments, and patients were randomized to have MDBC applied daily to the medial or lateral compartment and sorbolene to the other compart- ment. Weekly observations, photographs, and symptom scores (pain and pruritus) were collected to week 12 or resolution of skin reactions if earlier. Skin dose was confirmed by centrally cali- brated thermoluminescent dosimeters. Results: Rates of medial and lateral compartment Common Toxicity Criteria (CTC), version 3, greater than or equal to grade 3 skin reactions were 23% and 41%, but rates by skin care product Reprint requests to: Peter H. Graham, FRANZCR, Cancer Care Centre, St George Hospital, Short St, Kogarah 2217, Australia. Tel: (61) 2-9113- 3934; E-mail: [email protected] Conflict of interest: 3M supplied creams for study use to the coordi- nating trial center. Otherwise the conduct and analysis of the study was independent of 3M. There are no other potential conflicts of interest to declare. AcknowledgmentdData management support was provided by the Cancer Council NSW Clinical Trials Network. Int J Radiation Oncol Biol Phys, Vol. 86, No. 1, pp. 45e50, 2013 0360-3016/$ - see front matter Ó 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ijrobp.2012.12.009 Radiation Oncology International Journal of biology physics www.redjournal.org
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A Paired, Double-Blind, Randomized Comparison of a Moisturizing Durable Barrier Cream to 10%...

International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Clinical Investigation: Breast Cancer
A Paired, Double-Blind, Randomized Comparisonof a Moisturizing Durable Barrier Cream to 10%Glycerine Cream in the Prophylactic Managementof Postmastectomy Irradiation Skin Care: Trans TasmanRadiation Oncology Group (TROG) 04.01Peter H. Graham, FRANZCR,* Natalie Plant, MHSc,* Jennifer L. Graham, MN,*Lois Browne, PhD,* Martin Borg, FRANZCR,y Anne Capp, FRANZCR,z
Geoff P. Delaney, MD,x Jennifer Harvey, FRANZCR,jj Lisbeth Kenny, FRANZCR,{
Michael Francis, FRANZCR,# and Yvonne Zissiadis, FRANZCR**
*Cancer Care Centre, St. George Hospital, Kogarah, New South Wales, Australia; yDepartment of Radiation Oncology,Royal Adelaide Hospital; zDepartment of Radiation Oncology, Mater Hospital, Newcastle, New South Wales, Australia;xCancer Care Centre, Liverpool Hospital, Liverpool, New South Wales, Australia; jjMater Hospital, South Brisbane,Queensland, Australia; {Royal Brisbane Hospital, Herston; #Andrew Love Cancer Centre, Geelong; and **Department ofRadiation Oncology, Royal Perth Hospital, Perth, Australia
Received Sep 14, 2012, and in revised form Dec 7, 2012. Accepted for publication Dec 11, 2012
Summary
This study used a double-blind, randomized, intra-patient, paired design to testthe hypothesis that an acrylateterpolymer alcohol-freebarrier film reduces thedegree of radiation skin reac-tion compared with the 10%glycerine cream mostcommonly used for thispurpose in Australia. Nosignificant difference wasfound using this rigorous trial
Reprint requests to: Peter H. Graham, FRAN
St George Hospital, Short St, Kogarah 2217, A
3934; E-mail: [email protected]
Conflict of interest: 3M supplied creams fo
nating trial center. Otherwise the conduct and
Int J Radiation Oncol Biol Phys, Vol. 86, No. 1
0360-3016/$ - see front matter � 2013 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2012.12.009
Purpose: A previous, unblinded study demonstrated that an alcohol-free barrier film containingan acrylate terpolymer (ATP) was effective in reducing skin reactions compared with a 10%glycerine cream (sorbolene). The different appearances of these products precluded a blindedcomparison. To test the acrylate terpolymer principle in a double-blinded manner requiredthe use of an alternative cream formulation, a moisturizing durable barrier cream (MDBC);the study was conducted by the Trans Tasman Radiation Oncology Group (TROG) as protocol04.01.Methods and Materials: A total of 333 patients were randomized; 1 patient was ineligible and14 patients withdrew or had less than 7 weeks’ observations, leaving 318 for analysis. The chestwall was divided into medial and lateral compartments, and patients were randomized to haveMDBC applied daily to the medial or lateral compartment and sorbolene to the other compart-ment. Weekly observations, photographs, and symptom scores (pain and pruritus) were collectedto week 12 or resolution of skin reactions if earlier. Skin dose was confirmed by centrally cali-brated thermoluminescent dosimeters.Results: Rates of medial and lateral compartment Common Toxicity Criteria (CTC), version 3,greater than or equal to grade 3 skin reactions were 23% and 41%, but rates by skin care product
ZCR, Cancer Care Centre,
ustralia. Tel: (61) 2-9113-
.gov.au
r study use to the coordi-
analysis of the study was
independent of 3M. There are no other potential conflicts of interest to
declare.
AcknowledgmentdData management support was provided by the Cancer
Council NSW Clinical Trials Network.
, pp. 45e50, 2013
r Inc. All rights reserved.

Graham et al. International Journal of Radiation Oncology � Biology � Physics46
design, towhich few skin care
products are subjected. Moistdesquamation remainscommon in post-mastectomypatients, and other skin careproducts should be evaluatedin this way.were identical at 32%. There was no significant difference between MDBC and sorbolene in theprimary endpoint of peak skin reactions or secondary endpoints of area-under-the-curve skinreaction scores.Conclusions: The MDBC did not reduce the peak skin reaction compared to sorbolene. It ispossible that this is related to the difference in the formulation of the cream compared withthe film formulation. Skin dosimetry verification and double blinding are essential for radiationskin care comparative studies. � 2013 Elsevier Inc.
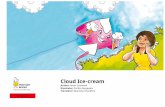
Fig. 1. Skin products presentation, with figures illustratingapplication areas.
Introduction
Few studies have demonstrated significant differences in acuteradiation skin reactions when comparing different skin care proto-cols or products. A previous unblinded study demonstrated that analcohol-free barrier film (AFBF) (3M Cavilon No Sting BarrierFilm) containing an acrylate terpolymer (ATP) applied as a surfaceprotectant was effective in reducing skin reaction and symptomscompared with a 10% glycerine cream (sorbolene), and reduced therate of moist desquamation from 46% to 33% (1). The differentappearances of these products precluded a blinded comparison. Totest the ATP principle in a double-blinded manner required the useof a cream formulation. The investigators approached the manu-facturer of the AFBF, and a moisturizing durable barrier cream(MDBC) (3MCavilon Durable Barrier Cream), was made availableto the investigators and tested against sorbolene by the Trans Tas-man Radiation Oncology Group (TROG) as protocol 04.01 inwomen receiving post-mastectomy radiation therapy.
Methods and Materials
Eligibility criteria included planned radiation therapy dose of atleast 45 Gy in 25 fractions post total mastectomy, age �18 years,European Cooperative Oncology Group (ECOG) performancestatus 0-2, ability to consent, and ability to attend weekly for up to6 weeks after treatment completion. Patients were ineligible ifthey had previous radiation therapy to the chest wall, clinicallyevident cutaneous involvement by malignancy, were pregnant, orhad known allergy to the skin care products.
The trial was conducted by the Trans Tasman RadiationOncology Group (TROG) with 12 participating centers, clinicaltrials registry identifier NCT00193908. Product supplied by themanufacturer was repackaged at the trial coordinating center intocontainers labeled for medial or lateral application. All analysiswas conducted by TROG independently of 3M. All participatinghospitals required ethics approval. Signed informed consent wasobtained from all patients.
Patients were randomized to receive MDBC to the medial orlateral side and sorbolene to the other side. If the internalmammary chain (IMC) was treated, this skin area was included inthe medial compartment. The paired nature of the data controlledfor systematic differences in reactions across the chest wall areaand the influence of other patient and treatment factors. Creamsets were prepared for each allocation and supplied to patientswith instructions and a diagram. Patients were instructed to applythe separate creams daily to each half of the area on the chest wallreceiving radiation therapy and to continue until 2 weeks afterradiation completion. The protocol did not specify the time of dayfor cream application but did recommend nurse application orsupervision on treatment days to help ensure or verify compliance,
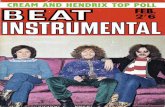
which typically occurred after radiation therapy sessions. In theevent of moist desquamation, a hydrocolloid dressing was rec-ommended. Product containers were labeled with a diagramillustrating the correct region for application. Application wascommenced at start of radiation therapy until 2 weeks after radi-ation therapy was completed or until skin reaction ceased. Bolusapplication was at the treating physician’s discretion. All patientswere treated with photons to the chest wall. If a boost wasprescribed, it had to be evenly split over the skin assessment areas.Thermoluminescent dosimeter (TLD) measurements were per-formed twice during the course of radiation with 2 TLDs per skincompartment. Additional TLDs measurements were performed inthe IMC area if treated. TLDs were centrally calibrated. Figures 1and 2 illustrate cream presentations and instructions along withdemarcation of medial and lateral areas for assessment, withindication of TLD measurement placements (M1, M2, L1, L2).
Stratification was by treatment center to accommodate varia-tions in inter-center radiation prescription practices and bolustechniques. Randomization sequences for strata were generated byand maintained by staff at The St. George Cancer Centre ClinicalTrials Unit independently of trial investigators. Randomizationwas based on random block sequences. After consent, randomi-zation was by telephone call to the independent center. Patientsand treating physicians/nurses were blinded to the supply of creamproducts in de-identified containers. Blinding was maintaineduntil after completion of analysis by the trial statistician. In thecase of an adverse reaction to topical creams, both products wereceased.

Fig. 2. Markup of post-mastectomy chest wall for study.Vertical mid-clavicular line divides medial and lateral creamapplication zones. M1, M2, L1, L2 indicate location of thermo-luminescent dosimeter (TLD) placements. In this case, the dottedlines indicate the superior and inferior extent of bolus that is to beapplied.
Table 1 Population and treatment characteristics
MDBC applied to me(n Z 161)
Patient baseline characteristicsAge, y Mean 56 (range 26-85Fitzpatrick1 skin typesn (%) 1-2, 3-4, 5-6
72, 81, 8(45, 50, 5)
Menopausal statusn (%) pre, post, other
26, 92, 43(16, 57, 27)
Body mass index Mean 28.4 (18-48)Treatment
Dose (Gy) Mean 49.8 (38-56)Fractions Mean 25 (19-28)Treatment regionsCWþSCFþAXþIMC,CWþSCFþAX, CWþSCFþIMC,CWþSCF, CW only n (%)
3, 29, 5, 93, 31(2, 18, 3, 58, 19)
Photon energy4, 6, 10, 18 n (%)
2, 132, 23, 4(1, 82, 14, 3)
Boost, n (%) 0 (0)Bolus applied, n (%) 153 (95)Bolus extent, n (%)Nil, parascar strip, full chest wall
8, 39, 114(5, 24, 71)
Bolus frequencyn (%) nil, daily, other
8, 87, 66(5, 54, 41)
TLD measured doses per fraction (Gy) Mean medially 2.06Mean laterally 2.09Mean IMC 1.77
Prior chemotherapy, n (%) 138 (86)Concurrent chemotherapy, n (%) 9 (6)Chemotherapy after, n (%) 15 (9)Hormones, n (%) 106 (66)
Abbreviations: AX Z axilla; CW Z chest wall; IMC Z internal mammar
clavicular fossa; TLD Z thermoluminescent dosimeter.
Volume 86 � Number 1 � 2013 TROG 04.01 skin care trial 47
The primary objective was to ascertain whether peak andoverall skin reactions may be reduced by the moisturizing durablebarrier cream compared with sorbolene. Patient outcomes werescored by weekly medical skin score using National CancerInstitute Common Terminology Criteria for Adverse Events(CTCAE), version 3.0, scores (2). Photographic audit of skinscores confirmed the pattern of reactions scored by clinicians (3).Primary outcomes were frequency of grade 3 or greater skinreaction during the course of treatment and mean area under thecurve (AUC) of the total skin reactions, which provided an inte-grated assessment of both degree and duration of skin reaction.Because the grading system excludes some forms of moistdesquamation from a grade 3 or greater score, and because thealcohol-free barrier film study was based on any moist desqua-mation that was considered to be a less subjective measure, moistdesquamation of any degree was also scored separately. Skin scoreassessments continued to week 12 or until resolution of skinreactions (whichever occurred first), and an assessment at week 12was mandatory. Patients also recorded weekly skin symptomscores for pruritus and discomfort using a Likert 5-point scalefrom 0 to 4. Patient skin types were classified according to theFitzpatrick system (4).
Statistical assumptions were based on outcomes of the previousalcohol-free barrier film trial and allowed for an anticipated lower
dial MDBC applied to lateral(n Z 157) Total (n Z 318)
) Mean 55 (range 33-89) Mean 55 (range 26-89)54, 96, 7(34, 61, 5)
126, 177, 15(40, 55, 5)
34, 88, 35(22, 56, 22)
60, 180, 78(19, 57, 24)
Mean 28.4 (18-44) Mean 28.4 (18-48)
Mean 49.7 (40-54) Mean 49.8 (38-56)Mean 25 (20-27) Mean 25 (19-28)
4, 34, 3, 81, 35(2, 22, 2, 52, 22)
7, 63, 8, 174, 66(2, 20, 2, 55, 21)
0, 129, 24, 4(0, 82, 15, 3)
2, 261, 47, 8(1, 82, 15, 2)
3 (2) 3 (1)152 (97) 305 (96)5, 26, 126(3, 17, 80)
13, 65, 240(4, 21, 75)
5, 87, 65(3, 56, 41)
13, 174, 131(4, 55, 41)
Mean medially 2.06Mean laterally 2.09Mean IMC 1.82
Mean medially 2.06Mean laterally 2.09Mean IMC 1.80
136 (87) 274 (86)12 (8) 21 (7)20 (13) 35 (11)100 (64) 206 (65)
y chain; MDBC Z moisturizing durable barrier cream; SCF Z supra-

Table 2 Skin reaction results summary (unpaired)
Compartment Product
Skin reaction graden (%) Any moist desquamation
n (%) AUC (mean)1 2 3 4
Lateral MDBC 4 (2) 95 (61) 55 (35) 3 (2) 101 (64) 12.3Sorbolene 10 (6) 78 (49) 70 (43) 3 (2) 115 (71) 12.2
Medial MDBC 16 (10) 100 (62) 44 (27) 1 (1) 74 (46) 11.3Sorbolene 13 (8) 115 (73) 28 (18) 1 (1) 63 (40) 11.2
Abbreviations: AUC Z area under the curve; MDBC Z moisturizing durable barrier cream.
Graham et al. International Journal of Radiation Oncology � Biology � Physics48
rate of bolus application. Sample size was determined by primaryendpoint dichotomous analysis. If the frequency of grade 3 orgreater skin reaction was 35% for sorbolene and 25% for MDBC,the minimum sample size was 160, maximum 394, and midpoint277 total. The recommended sample size was therefore 300. Asimilar sample size of 264 was required if determined by mean areaunder the curve (AUC) of the total skin reaction with sorbolene as 9and the mean AUC of the total skin reaction with MDBC as 8.Statistical analysis for primary endpoints were paired comparisonby the McNemar test for grade 3 or greater skin comparison andpaired t test for AUC. Analyses for eligible patients with sufficientobservations were by intention to treat irrespective of compliance.The total trial recruitment was increased to more than 300 inresponse to monitoring of ineligibility/insufficient observationsrates. After the planned analysis results indicating that the statis-tical assumption that cream effect does not differ by side may nothold, a random effects model was examined.
Results
A total of 333 patients were randomized and completion ofplanned radiation therapy and assessment of skin scores wasachieved for 94% and 96% respectively in the 2 arms of the study.Data for analysis was available for 318 patients. The trial openedin March 2004 and closed to recruitment in June 2007. Patientbaseline parameters and treatments received are summarized inTable 1. Fifteen patients had internal mammary node treatment, ofwhom 9 had electrons used as a component of this treatment.
Table 2 presents a summary of unpaired results by treatmentarea and skin care product applied. Skin reactions differed moreby compartment than by product and were worse in the lateralcompartment. Table 3 presents the summary of paired results fordichotomous skin reactions grade 3 or greater. By the McNemarc2 test there was no significant difference between treatmentgroups. Table 4 summarizes the AUC scores. By paired t test therewas no significant difference between treatment groups. Table 5summarizes compliance during the first 8 weeks from study
Table 3 Results summary for grade 3 or greater skin reaction(paired)
MDBC skinreaction
Sorbolene skin reaction
P (McNemar’s c2)No Yes Total
No 173 42 215 .01 (.91)Yes 43 60 103Total 216 102 318
Abbreviation: MDBC Z moisturizing durable barrier cream.
initiation, with the primary reason provided when not fullycompliant. Overall there was no difference in compliance. Thelarge majority of patients who were partially compliant used theirallocated cream in correct locations but applied the cream morefrequently. A smaller proportion of partially compliant patientsapplied an additional cream in the allocated area. Table 6summarizes patient symptomatic skin scores. Again, reactionsdiffer more by compartment than product, with greater pruritus inthe medial compartment and pain symptoms in the lateralcompartment of the chest wall but no significant difference byproduct. There was no difference in measured skin dose bytreatment product but lateral compartment doses were higher(Table 1). Measured skin doses were higher in areas that devel-oped grade 3 to 4 skin reaction with means of 2.12 Gy (95%confidence interval Z 2.10-2.15) versus 2.05 Gy (95% confidenceinterval Z 2.03-2.08) in grade 1 to 2 areas (PZ.001).
In view of the primary analysis finding, an exploratory randomeffects analysis was performed. The analysis indicated that treat-ment was not significant but that side was, and that there wasa significant interaction between side and treatment. Medial andlateral effects analyzed separately show opposite treatment effects,with medial being significant and lateral being nonsignificant(Table 7).
Discussion
Randomized controlled studies of prophylactic skin care productshave generally been negative. These have included comparisons ofcorticosteroids, hyaluronic acid, Trolamine (Biafine), aloe vera,ascorbic acid, aqueous cream, and sucralfate to placebo or delayedtopical intervention (5-12). Positive comparisons between activeinterventions have included sucralfate over base cream, cortico-steroid over emollient, calendula over trolamine, anionicphospholipid-based cream over aloe vera, and alcohol-free barrierfilm over sorbolene (1, 13-16). Many of these were small or didnot control for factors such as actual skin dose, skin areas irra-diated, skin types, or use of radiosensitizers such as cytotoxicagents other than the intervention to explain the results. Theevidence-based standard of care remains unclear, but routine useof some form of topical cream remains common in Australia.
Table 4 Results summary for skin reaction area under thecurve (paired)
Cream applied Mean AUC Range P (paired t test)
MDBC (n Z 318) 11.77 2-21 .44 (.66)Sorbolene (n Z 318) 11.70 2-23
Abbreviation: MDBC Z moisturizing durable barrier cream.

Table 5 Compliance with skin care allocations at each weekly assessment, first 8 weeks
Compliance, %
MDBC applied to medialn Z 1288
MDBC applied to lateraln Z 1256
Total weekly assessmentsn Z 2544
Medial (full, partial, non) 67, 22, 11 66, 27, 7 66, 25, 9Lateral (full, partial, non) 66, 23, 11 65, 27, 8 65, 25, 10
Primary reason if partial or noncompliance (medial) %
MDBC Sorbolene
Partialn Z 625
Nonn Z 235
Partialn Z 288
Nonn Z 143
Partialn Z 337
Nonn Z 92
>2 weeks post radiation 0 4 0 10 0 6Forgot 2 1 2 5 2 3Confused site <1 1 1 1 1 1Discomfort/irritation 1 29 0 0 <1 18More frequently applied 67 0 74 0 71 0Additional cream applied 30 53 21 65 25 58Other or withdrawn or no assessment 0 12 2 19 1 14
Primary reason if partial or noncompliance (lateral), %
Sorbolene MDBC
Partialn Z 637
Nonn Z 245
Partialn Z 301
Nonn Z 142
Partialn Z 336
Nonn Z 103
>2 Weeks post radiation 0 5 0 9 0 7Forgot 2 1 3 5 3 2Confused site 0 1 <1 1 <1 1Discomfort/irritation 1 0 0 0 <1 0More frequently applied 64 0 72 0 68 0Additional cream applied 31 86 24 66 27 78Other or withdrawn or no assessment 2 7 1 19 2 12
Abbreviations: MDBC Z moisturizing durable barrier cream; Non Z noncompliance; Partial Z partial compliance.
Volume 86 � Number 1 � 2013 TROG 04.01 skin care trial 49
The mechanisms hypothesized to explain the potential benefitof the alcohol-free barrier film were prolongation of skin surfaceintegrity by preventing normal wear, thus allowing sufficientrepopulation by epidermal stem cells to avoid moist desqua-mation, maintaining a scaffold for cell migration and also bymaintaining skin hydration, considered important to optimizeskin injury repair (17, 18). Encouraged by the results of theinitial study using the alcohol-free barrier film that did controlfor multiple extraneous factors by the paired randomized design,the investigators sought to verify the findings in a double-blindstudy. In addition to an acrylate terpolymer that provides thesurface barrier, the MDBC contains emollients and dimethicone,which might be expected to make the skin more comfortable bycountering ablation of intrinsic glandular function (19). Itseemed reasonable that this could provide the beneficial
Table 6 Patient skin symptom scores summary (unpaired)
Compartment Product Pruritus >2, n (%) Pain >2, n (%)
Lateral MDBC 33/157 (21) 67/157 (43)Lateral Sorbolene 35/161 (22) 67/161 (42)Medial MDBC 56/161 (35) 55/161 (34)Medial Sorbolene 51/157 (32) 44/157 (28)
Abbreviation: MDBC Z moisturizing durable barrier cream.
properties of the film formulation but could still be compared ina blinded fashion to the usual topical cream products. Theproduct is very similar in appearance to the most common skincare product in Australia, known as sorbolene. Sorbolenegenerically refers to a group of skin creams comprising a mix ofoils and water. The oils are generally mineral, such as paraffinand other petrochemical by-products. Products sold as sorboleneon the Australian market generally comprise 10% glycerine(1,2,3 trihydroxy propane, a trihydric alcohol, commonlyreferred to as glycerine or glycerol, also propylene glycol).Although the MDBC formulation used in this study contains anacrylate terpolymer, it was only after analysis of this study wascompleted that the manufacturer advised the investigators that itis a different acrylate terpolymer from that in the AFBF used inthe previous trial.
Table 7 Grade 3 or greater skin reaction (by side separately)
Compartment
Grade 3-4, n (%)
OR (95% CI) PSorbolene MDBC
Lateral 73/161 (45) 58/157 (37) 1.42 (0.9-2.2) .129Medial 29/157 (18) 45/161 (28) 0.58 (0.34-0.99) .047
Abbreviations: CI Z confidence interval; MDBC Z moisturizing
durable barrier cream; OR Z odds ratio.

Graham et al. International Journal of Radiation Oncology � Biology � Physics50
The results of this study do not support a reduction in radi-ation skin reaction attributable to moisturizing durable barriercream compared with sorbolene. The higher rates of skin reac-tion in the lateral compartment are consistent with the previousstudy, as is the apparently greater effect in the unpaired analysisof the MDBC in that compartment; but there is no good expla-nation for why this effect was reversed in the medial compart-ment. The logical explanation for the result of the exploratoryrandom effects analysis of this matched pair design, whichavoids confounding by other factors, is simple type I error, withchance statistical significance. This emphasizes the requirementfor well-designed appropriately powered and controlled studiesfor skin care protocols, of which there have been very few. Itremains likely that the film formulation does indeed reduce skinreactions, as shown in the previous study, and that the differentformulation required to undertake a double-blind study does notprovide the same effect. In the original study, the film accu-mulated on the skin, and application was less frequent in themedial compartment to avoid excessive accumulation. In thisstudy, no clinically detectable accumulation of product occurredon the skin, suggesting that the cream application daily does notoffer the same surface protection effect or that more frequentapplication might be required. Although the largest group ofpartially compliant patients were deemed partially compliantbecause they applied creams more frequently, overall this formof partial compliance comprised only 17% of weekly assess-ments and would be unlikely to have exerted sufficient effect ifincreased frequency of application was required as a matter ofroutine to achieve the desired action. In a study using the sameproduct for a different indication with a positive outcome,application was twice daily (20). It may simply be that the creamformulation does not achieve the desired effect in this populationbecause of significant differences in formulation and ingredients.
References
1. Graham P, Browne L, Capp A, et al. A randomized, paired comparison
of No-Sting Barrier Film versus sorbolene cream (10% glycerine) skin
care during post-mastectomy irradiation. Int J Radiat Oncol Biol Phys
2004;58:241-246.
2. Trotti A, Colevas AD, Setser A, et al. CTCVE v3.0: development of
a comprehensive grading system for the adverse effects of cancer
treatment. Semin Radiat Oncol 2003; 13:176-181.
3. Graham PH, Plant NA, Graham JL, et al. Digital photography as
source documentation of skin toxicity: an analysis from the
Trans Tasman Radiation Oncology Group (TROG) 04.01 Post-
Mastectomy Radiation Skin Care Trial. J Med Im Radiat Oncol
2012;56:458-463.
4. Freedberg ID, Eisen AZ, Wolff K, et al., editors. Fitzpatrick’s Derma-
tology in General Medicine. 5th ed. New York: McGraw-Hill; 1999.
5. Schmuth M, Wimmer MA, Hofer S, et al. Topical corticosteroid
therapy for acute radiation dermatitis: a prospective, double-blind,
randomized trial. Br J Dermatol 2002;146:983-991.
6. Liguori V, Guillemin C, Pesce GF, et al. Double-blind, randomized,
clinical study comparing hyaluronic acid cream to placebo in patients
treated with radiotherapy. Radiother Oncol 1997;42:155-161.
7. Fenig E, Brenner B, Katz A, et al. Topical Biafin and Lipderm for the
prevention of radiation dermatitis: a randomized prospective trial.
Oncol Rep 2001;8:305-309.
8. Fisher J, Scott C, Stevens R, et al. Randomized phase III study
comparing best supportive care to Biafine as a prophylactic agent for
radiation induced skin toxicity for women undergoing breast irradia-
tion: Radiation Therapy Oncology Group (RTOG) 97-13. Int J Radiat
Oncol Biol Phys 2000;48:1307-1310.
9. Elliott EA, Wright JR, Swann S, et al. Phase III trial of an emulsion
containing Trolamine for the prevention of radiation dermatitis in
patients with advanced squamous cell cancer of the head and neck:
results of the Radiation Therapy Oncology Group trial 99-13. J Clin
Oncol 2006;24:2092-2097.
10. Williams MS, Burk M, Loprinzi CL, et al. Phase III double-blind
evaluation of an aloe vera gel as a prophylactic agent for radiation-
induced skin toxicity. Int J Radiat Oncol Biol Phys 1996;36(Suppl
1):345-349.
11. Halperin EC, Gaspar L, George S, et al. A double-blind, randomised
prospective trial to evaluate topical vitamin C solution for the
prevention of radiation dermatitis. Int J Radiat Oncol Biol Phys 1993;
26:413-416.
12. Wells M, MacMillan M, Raab G, et al. Does aqueous or sucralfate
cream affect the severity of erythematous radiation skin reactions? A
randomised controlled trial. Radiother Oncol 2004;73:153-162.
13. Maiche A, Isokangas OP, Grohn P. Skin protection by sucralfate
cream during electron beam therapy. Acta Oncologica 1994;33:201-
203.
14. Bostrom A, Lindman H, Swartling C, et al. Potent corticosteroid
cream (mometasone furoate) significantly reduces acute radiation
dermatitis: results from a double-blind randomized study. Radiother
Oncol 2001;59:257-265.
15. Pommier P, Gomez F, Sunyach MP, et al. Phase III randomized trial of
calendula officinalis compared with Trolamine for the prevention of
acute dermatitis during irradiation for breast cancer. J Clin Oncol
2004;22:1447-1453.
16. Merchant TE, Bosley C, Smith J, et al. A phase III trial comparing
anionic phospholipid-based cream and aloe vera-based gel in the
prevention of radiation dermatitis in pediatric patients. Radiat Oncol
2007;2:45.
17. Grove GL, Leydon JL. Comparison of the skin protectant properties
of various film-forming products. Available at: http://multimedia.
3m.com/mws/mediawebserver?mwsIdZ66666UF6EVsSyXTtmxM2Nx
T2EVtQEVs6EVs6EVs6E666666-&fnZ70-2008-6035-4.pdf. Accessed
August 14, 2012.
18. Visscher M, Hoath SB, Conroy E, et al. Effect of semipermeable
membranes on skin barrier repair following tape stripping. Arch
Dermatol Res 2001;293:491-499.
19. Morris WJ, Dische S, Mott G. A pilot study of a method of estimating
the number of functional eccrine sweat glands in irradiated human
skin. Radiother Oncol 1992;25:49-55.
20. Frocillo CA. Improving resident care through the use of a barrier
cream with durable properties. Available at: http://multimedia.3m.
com/mws/mediawebserver?mwsIdZ66666UF6EVsSyXTt48T6Nxf2
EVtQEVs6EVs6EVs6E666666-&fnZ70-2009-5984-2.pdf. Accessed
August 14, 2012.