
A Healthy Start in Life - full document - CiteSeerX
240
a healthy start in life a nutrition manual for health professionals 2008
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of A Healthy Start in Life - full document - CiteSeerX
a healthy start
in life
a nutrition manual for health professionals
2008
b A HEALTHY START IN LIFE INTRODUCTION
First published by Queensland Health, 1997
First revised 1999 Revised 2008
Second edition Copyright © Queensland Health 2008
Copyright protects this publication. However Queensland health has no objection to this material being reproduced with acknowledgement, except for commercial purposes or where the material is being modified. Requests and enquiries concerning reproduction rights should be directed to the Principal Project Officer - Intellectual Property
Queensland Health GPO Box 48 BRISBANE QLD 4001
ISBN: 978-1-921021-83-1
Property of Queensland Health
Designed by VC Graphics
cA HEALTHY START IN LIFE INTRODUCTION
AcknowledgementsMany people have provided time, expertise, feedback and support throughout the development of this resource. This project would not have been possible without funding from Golden Casket and project management provided by Southern Area Population Health Public Health Units Nutrition Team.
The steering committee: Lyza Norton, Barbara Radcliffe, Doug Shelton, Peta Patterson and Jacqui Kaye.
The reference group which included Public Health Nutritionists, Child Health Nurses, Paediatric Dietitians, Midwives, Lactation Consultants and other health professionals.
Authors: Jacqui Kaye, Peta Patterson, Susan Croaker, Lyza Norton and Fiona Lewis.
Reviewers: Helen Vidgen, Michelle Harrison, Sue Wellings, Jillian Dymock, Penny Beatty, Vicki Attenborough, Liz Good, Judy Wilcox, Jan Branch, Amanda Allen, Renee Watts, Barbara Radcliffe, Doug Shelton, Helen Clifford, Peter Smith and the Australian Breastfeeding Association.
The health professionals involved in the focus groups
Southern Area Population Health Units
Southern Area Child and Youth Health Clinical Network
Gold Coast Health Service District Librarians
Mater Misericordiae Public Hospital Department of Nutrition and Dietetics
Royal Children’s Hospital Health Service District Department of Nutrition and Dietetics and Community Child Health Service
Golden Casket
Australian Breastfeeding Association
Australasian Society of Clinical Immunology and Allergy
This manual is on the Queensland Health Internet site at www.health.qld.gov.au
d A HEALTHY START IN LIFE INTRODUCTION
ContentsAcknowledgements cGlossary i
1.0 Introduction 11.1 Abbreviations 21.2 Symbols 21.3 Communicating with clients 31.4 Key documents 4
The Dietary Guidelines for Children and Adolescents in Australia 5The Australian Guide to Healthy Eating 8
The Aboriginal and Torres Strait Islander Guide to Healthy Eating 91.5 Food groups 10
Bread, cereal, rice, pasta, noodles 11Vegetables, legumes 11Fruit 11Milk, yoghurt, cheese 12Meat, fish, poultry, eggs, nuts, legumes 12Extra foods 13Putting it all together 13
1.6 Nutrient reference values 14For infants and children 14Energy 14Protein 14Fat 15Carbohydrate 15Iron 15Zinc 16Calcium 17Folate/folic acid 18Vitamin B12 19Vitamin B6 19Vitamin C 20
1.7 Physical activity 21Benefits 21Barriers 21Physical activity recommendations 21Strategies to promote physical activity 22Family activities 22Sport and recreation resources 22Useful websites and resources 23
1.8 Culturally and Linguistically Diverse (CALD) Communities 24Cultural competence in early life 24How culturally competent is your health service? 24How to go about cultural competence 24Multicultural profile of Queensland 25Vulnerable migrants: refugee and asylum seeker 25Females: special considerations 25Working with interpreters 26Communication style 26Religion 27Case studies: an African woman new to Australia 28Nutritional risks identified 28Useful websites and resources 29References 30
1.9 Aboriginal and Torres Strait Islander nutrition 31Current health and nutritional status 31Recommendations from the Dietary Guidelines for Australians 32Protocols for engaging with Aboriginal and Torres Strait Islander communities 32Antenatal nutrition 33Breastfeeding 34Useful websites and resources 37
eA HEALTHY START IN LIFE INTRODUCTION
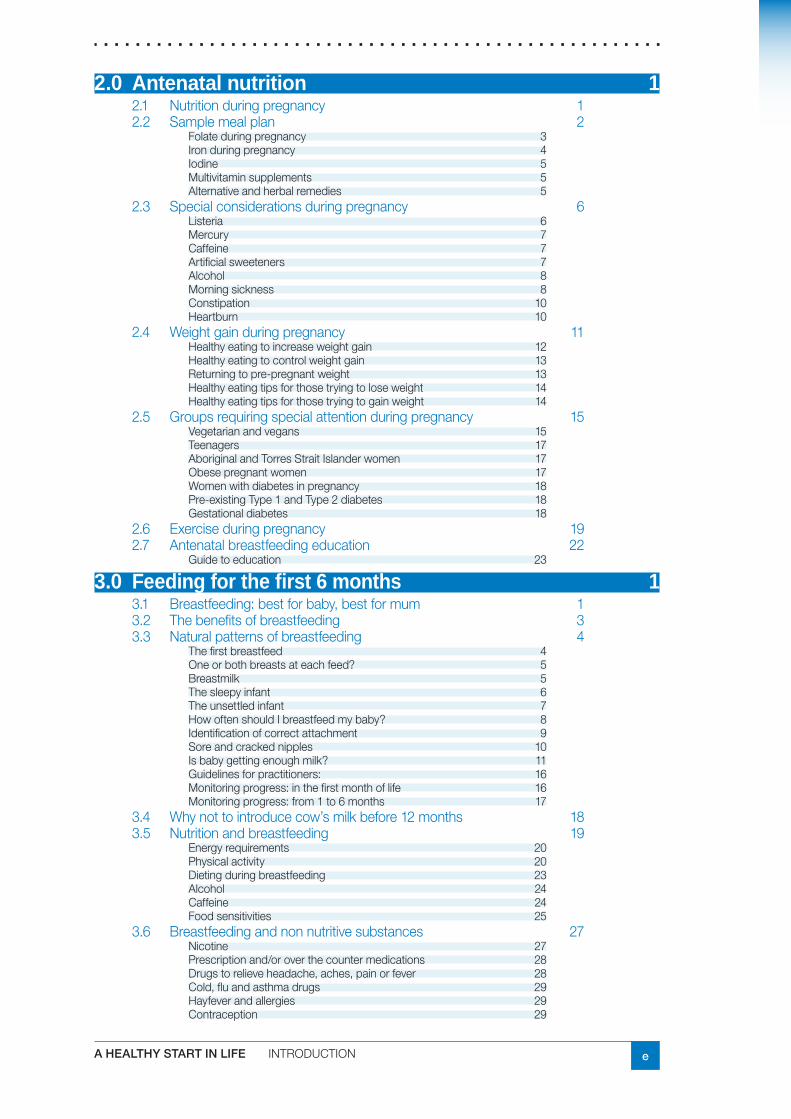
2.0 Antenatal nutrition 12.1 Nutrition during pregnancy 12.2 Sample meal plan 2
Folate during pregnancy 3Iron during pregnancy 4Iodine 5Multivitamin supplements 5Alternative and herbal remedies 5
2.3 Special considerations during pregnancy 6Listeria 6Mercury 7Caffeine 7Artificial sweeteners 7Alcohol 8Morning sickness 8Constipation 10Heartburn 10
2.4 Weight gain during pregnancy 11Healthy eating to increase weight gain 12Healthy eating to control weight gain 13Returning to pre-pregnant weight 13Healthy eating tips for those trying to lose weight 14Healthy eating tips for those trying to gain weight 14
2.5 Groups requiring special attention during pregnancy 15Vegetarian and vegans 15Teenagers 17Aboriginal and Torres Strait Islander women 17Obese pregnant women 17Women with diabetes in pregnancy 18Pre-existing Type 1 and Type 2 diabetes 18Gestational diabetes 18
2.6 Exercise during pregnancy 192.7 Antenatal breastfeeding education 22
Guide to education 23
3.0 Feeding for the first 6 months 13.1 Breastfeeding: best for baby, best for mum 13.2 The benefits of breastfeeding 33.3 Natural patterns of breastfeeding 4
The first breastfeed 4One or both breasts at each feed? 5Breastmilk 5The sleepy infant 6The unsettled infant 7How often should I breastfeed my baby? 8Identification of correct attachment 9Sore and cracked nipples 10Is baby getting enough milk? 11Guidelines for practitioners: 16Monitoring progress: in the first month of life 16Monitoring progress: from 1 to 6 months 17
3.4 Why not to introduce cow’s milk before 12 months 183.5 Nutrition and breastfeeding 19
Energy requirements 20Physical activity 20Dieting during breastfeeding 23Alcohol 24Caffeine 24Food sensitivities 25
3.6 Breastfeeding and non nutritive substances 27Nicotine 27Prescription and/or over the counter medications 28Drugs to relieve headache, aches, pain or fever 28Cold, flu and asthma drugs 29Hayfever and allergies 29Contraception 29
f A HEALTHY START IN LIFE INTRODUCTION
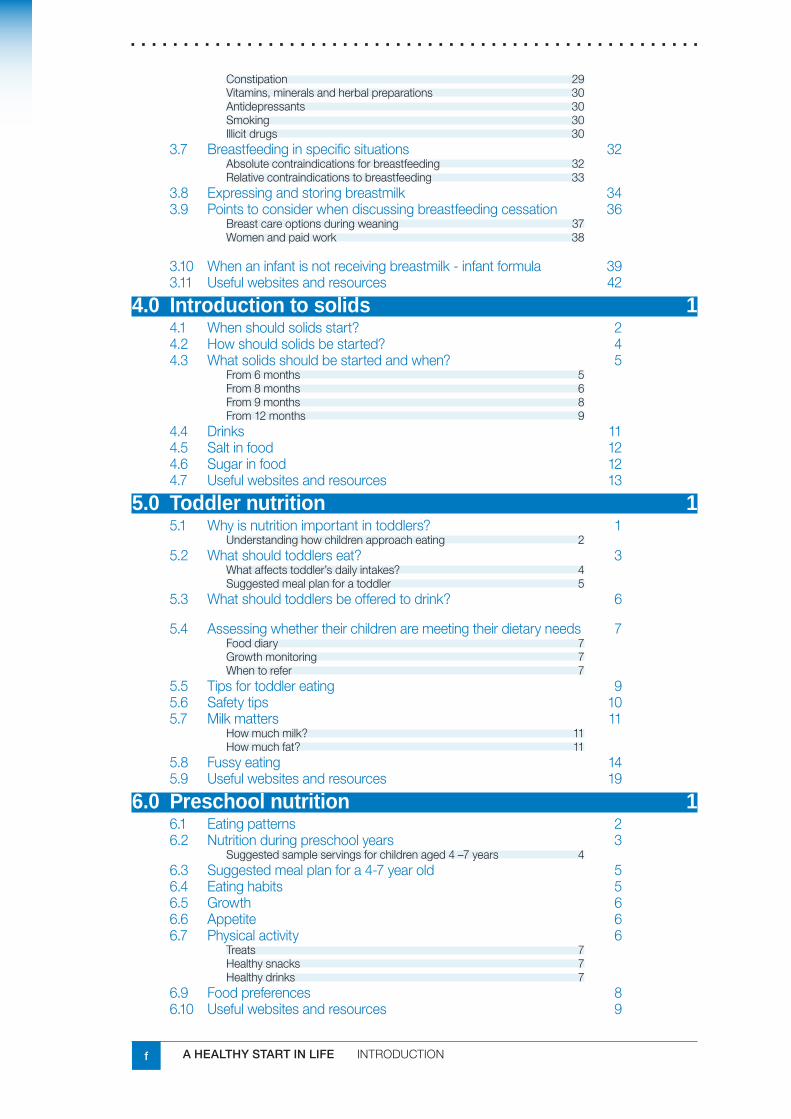
Constipation 29Vitamins, minerals and herbal preparations 30Antidepressants 30Smoking 30Illicit drugs 30
3.7 Breastfeeding in specific situations 32Absolute contraindications for breastfeeding 32Relative contraindications to breastfeeding 33
3.8 Expressing and storing breastmilk 343.9 Points to consider when discussing breastfeeding cessation 36
Breast care options during weaning 37Women and paid work 38
3.10 When an infant is not receiving breastmilk - infant formula 393.11 Useful websites and resources 42
4.0 Introduction to solids 14.1 When should solids start? 24.2 How should solids be started? 44.3 What solids should be started and when? 5
From 6 months 5From 8 months 6From 9 months 8From 12 months 9
4.4 Drinks 114.5 Salt in food 124.6 Sugar in food 124.7 Useful websites and resources 13
5.0 Toddler nutrition 15.1 Why is nutrition important in toddlers? 1
Understanding how children approach eating 25.2 What should toddlers eat? 3
What affects toddler’s daily intakes? 4Suggested meal plan for a toddler 5
5.3 What should toddlers be offered to drink? 6
5.4 Assessing whether their children are meeting their dietary needs 7Food diary 7Growth monitoring 7When to refer 7
5.5 Tips for toddler eating 95.6 Safety tips 105.7 Milk matters 11
How much milk? 11How much fat? 11
5.8 Fussy eating 145.9 Useful websites and resources 19
6.0 Preschool nutrition 16.1 Eating patterns 26.2 Nutrition during preschool years 3
Suggested sample servings for children aged 4 –7 years 46.3 Suggested meal plan for a 4-7 year old 56.4 Eating habits 56.5 Growth 66.6 Appetite 66.7 Physical activity 6
Treats 7Healthy snacks 7Healthy drinks 7
6.9 Food preferences 86.10 Useful websites and resources 9
gA HEALTHY START IN LIFE INTRODUCTION
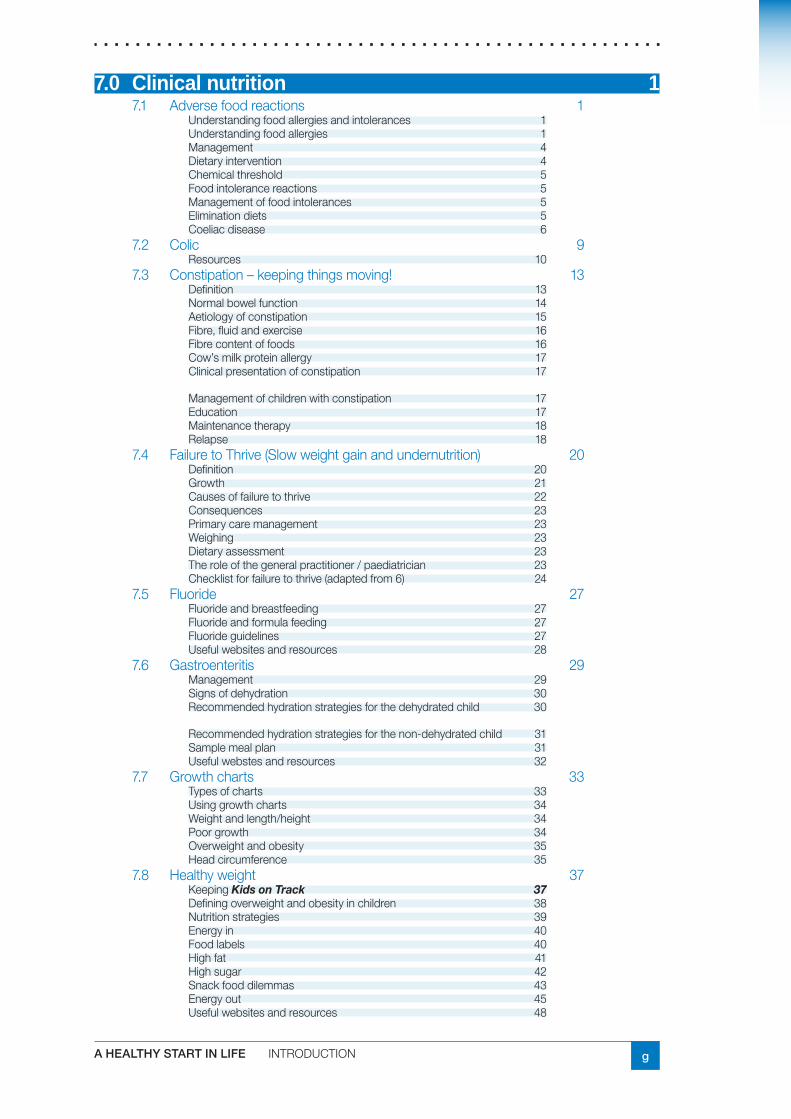
7.0 Clinical nutrition 17.1 Adverse food reactions 1
Understanding food allergies and intolerances 1Understanding food allergies 1Management 4Dietary intervention 4Chemical threshold 5Food intolerance reactions 5Management of food intolerances 5Elimination diets 5Coeliac disease 6
7.2 Colic 9Resources 10
7.3 Constipation – keeping things moving! 13Definition 13Normal bowel function 14Aetiology of constipation 15Fibre, fluid and exercise 16Fibre content of foods 16Cow’s milk protein allergy 17Clinical presentation of constipation 17
Management of children with constipation 17Education 17Maintenance therapy 18Relapse 18
7.4 Failure to Thrive (Slow weight gain and undernutrition) 20Definition 20Growth 21Causes of failure to thrive 22Consequences 23Primary care management 23Weighing 23Dietary assessment 23The role of the general practitioner / paediatrician 23Checklist for failure to thrive (adapted from 6) 24
7.5 Fluoride 27Fluoride and breastfeeding 27Fluoride and formula feeding 27Fluoride guidelines 27Useful websites and resources 28
7.6 Gastroenteritis 29Management 29Signs of dehydration 30Recommended hydration strategies for the dehydrated child 30
Recommended hydration strategies for the non-dehydrated child 31Sample meal plan 31Useful webstes and resources 32
7.7 Growth charts 33Types of charts 33Using growth charts 34Weight and length/height 34Poor growth 34Overweight and obesity 35Head circumference 35
7.8 Healthy weight 37Keeping Kids on Track 37Defining overweight and obesity in children 38Nutrition strategies 39Energy in 40Food labels 40High fat 41High sugar 42Snack food dilemmas 43Energy out 45Useful websites and resources 48
h A HEALTHY START IN LIFE INTRODUCTION
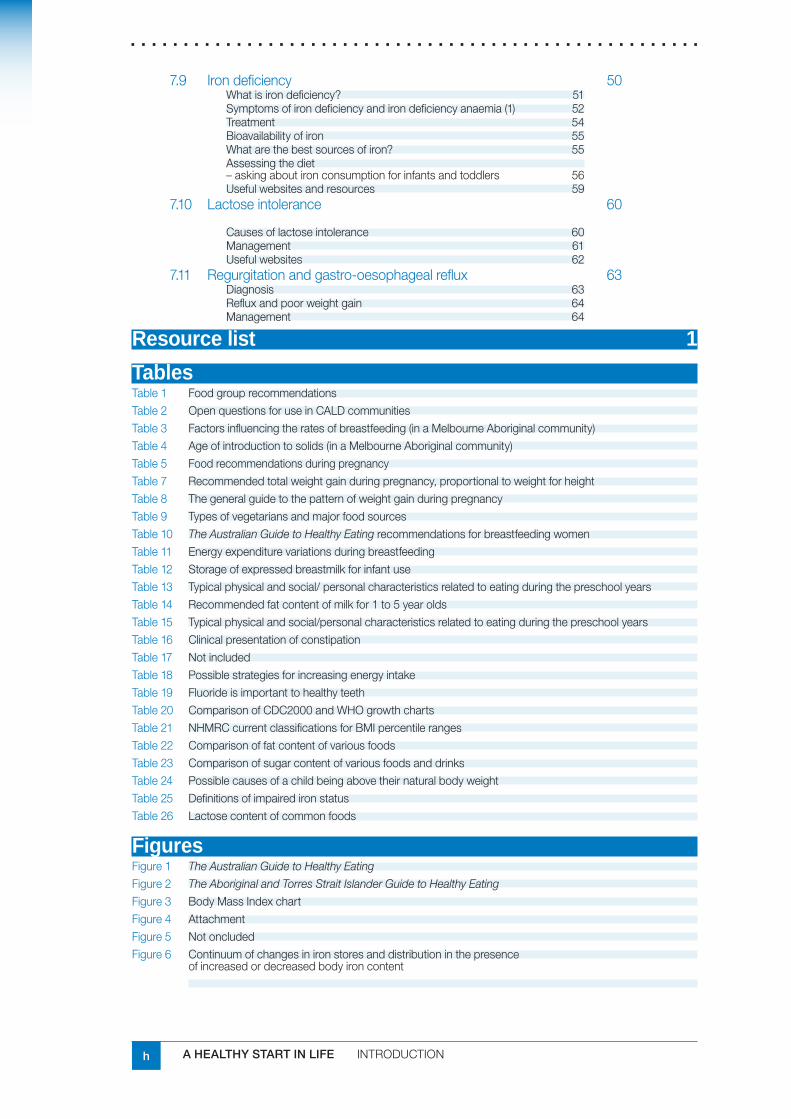
7.9 Iron deficiency 50What is iron deficiency? 51Symptoms of iron deficiency and iron deficiency anaemia (1) 52Treatment 54Bioavailability of iron 55What are the best sources of iron? 55Assessing the diet – asking about iron consumption for infants and toddlers 56Useful websites and resources 59
7.10 Lactose intolerance 60
Causes of lactose intolerance 60Management 61Useful websites 62
7.11 Regurgitation and gastro-oesophageal reflux 63Diagnosis 63Reflux and poor weight gain 64Management 64
Resource list 1
TablesTable 1 Food group recommendationsTable 2 Open questions for use in CALD communitiesTable 3 Factors influencing the rates of breastfeeding (in a Melbourne Aboriginal community)Table 4 Age of introduction to solids (in a Melbourne Aboriginal community)Table 5 Food recommendations during pregnancyTable 7 Recommended total weight gain during pregnancy, proportional to weight for heightTable 8 The general guide to the pattern of weight gain during pregnancyTable 9 Types of vegetarians and major food sourcesTable 10 The Australian Guide to Healthy Eating recommendations for breastfeeding women Table 11 Energy expenditure variations during breastfeedingTable 12 Storage of expressed breastmilk for infant use Table 13 Typical physical and social/ personal characteristics related to eating during the preschool yearsTable 14 Recommended fat content of milk for 1 to 5 year oldsTable 15 Typical physical and social/personal characteristics related to eating during the preschool yearsTable 16 Clinical presentation of constipationTable 17 Not includedTable 18 Possible strategies for increasing energy intakeTable 19 Fluoride is important to healthy teethTable 20 Comparison of CDC2000 and WHO growth chartsTable 21 NHMRC current classifications for BMI percentile rangesTable 22 Comparison of fat content of various foodsTable 23 Comparison of sugar content of various foods and drinksTable 24 Possible causes of a child being above their natural body weight Table 25 Definitions of impaired iron statusTable 26 Lactose content of common foods
FiguresFigure 1 The Australian Guide to Healthy Eating
Figure 2 The Aboriginal and Torres Strait Islander Guide to Healthy Eating
Figure 3 Body Mass Index chartFigure 4 AttachmentFigure 5 Not oncludedFigure 6 Continuum of changes in iron stores and distribution in the presence
of increased or decreased body iron content
iA HEALTHY START IN LIFE INTRODUCTION
GlossaryGrowth The acquisition of tissue and the consequent
increase in body size.
Development The increased ability of the body to function physically and intellectually. Physical and intellectual development proceed at different rates in different individuals.
Breastfeedingduration The total length of time during which an infant receives any breastmilk at all - from initiation until breastfeeding has ceased.
Breastmilksubstitute Any food being marketed or otherwise represented as a partial or total replacement for breastmilk, whether or not it is suitable for that purpose. In Australia, this term is considered inappropriate because it implies an equivalence to breastmilk. The term infant formula is used throughout this document, although it is acknowledged that other foods and fluids are used in place of breastmilk. Infant formula is the term used in Australia New Zealand Food Standards Code, volume 2.
Complementaryfood Any food - manufactured or locally prepared - suitable as a complement to breastmilk or infant formula, when either becomes insufficient to satisfy the nutritional requirements of the infant. Such food is also commonly called weaning food or breastmilk supplement. In this document the following working definition is used any nutrient-containing foods or liquids (other than breastmilk) given to infants who are breastfeeding.
Complementaryfeeding The infant or child is receiving both breastmilk and nutrient-containing foods, which includes any food or liquid containing non-human milk.
Caregivers Those who provide care to the infant/child.
Exclusivebreastfeeding An infant receives only breastmilk from his or her mother or a wet nurse, or in the form of expressed breastmilk, and no other liquids or solids apart from drops or syrups containing vitamins, mineral supplements or medicines.
Fullybreastfed This term embraces the WHO indicators of ‘exclusive’ breastfeeding and ‘predominant’ breastfeeding. It refers to infants who are receiving almost all of their nutrients from breastmilk but take some other liquids such as water, water-based drinks, oral rehydration solutions, ritual fluids, and drops or syrups. It excludes any food-based fluids.
j A HEALTHY START IN LIFE INTRODUCTION
Infant A child aged less than 12 months.
Infantformula An infant formula product represented as a breastmilk substitute for infants and which satisfies the nutritional requirements of infants aged up to 4 to 6 months. Australia New Zealand Food Standards (volume 4 to 6)
Preschoolchild A child aged from 3 to 5 years of age.
Solidfoods Any nutrient-containing foods (semi-solid or solid) for example, dilute infant cereals. Excludes breastmilk and breastmilk substitutes, fruit and vegetable juices, sugar water, and so on.
Supplementaryfeed Fluids or foods dissolved in fluids given to completely replace a breastfeed. The distinction between complementary feeds and supplementary feeds is important there seems to be a great deal of confusion among health professionals.
Toddler A child aged from 1 to 2 years.
Weaning The period during which an infant is introduced to breastmilk substitutes or solid foods, or both, with the intention of ceasing breastfeeding. (This term should be used with care in the literature, weaning, weaning foods and weaned are used in different ways).
Weaned The infant or child no longer receives any breastmilk.
Youngchild A child aged less than 5 years.
6months Is defined as the end of the first 6 months of life (180 days), when the infant is 26 weeks old as opposed to the start of the 6th month of life, that is at 21-22 weeks of age. For pre term infants this means 6 months corrected age.
1A HEALTHY START IN LIFE INTRODUCTION
1.0 Introduction
Thismanualcoversthenutritionneedsofpregnantandlactatingwomen,andalsothatofinfantsandchildren,frombirthto6years.Ithasbeendevelopedforusebycommunityandchildhealthnursesandmayextendtootherhealthprofessionals.
A healthy start in life waslastreviewedin1999.Thisrevisionwasinitiatedtoupdatethenutritioninformationavailabletochildhealthprofessionals.GoldenCasketprovidedfundingtoSouthernAreaPopulationHealthUnitstoundertakethisreview.
Thismanualcoversawidevarietyofnutritionissues.Itisintendedtobeusedasaresourcemanualtoclarify,instructandsupplementthebaselevelofknowledgeofcommunityandchildhealthnursesandotherhealthprofessionals.
Ithasbeendevelopedinconsultationwithchildhealthnursesanddietitian/nutritioniststhroughoutQueensland,andshouldthereforeprovideinformationfromabroadperspective.
Theinformationpresentedinthismanualassumesthereisavariedbaselinelevelofnutritionknowledgeamongsthealthprofessionals.Itaimstosupplementthisknowledge,providingaconsistentandreliablesourceofnutritioninformationacrossQueensland.Italsoincludesavailableparentresourcestoaidinclienteducation.
Whileallpregnantwomen,mothers,infantsandfamiliesareentitledtoappropriateandaccessibleantenatal,birthingandpostnatalcareandsupport,somepopulationgroupsarelesslikelytoaccesshealthservicesduringtheantenatalperiodand/ortobreastfeed.Theseinclude:womenfromlowsocioeconomicgroups;AboriginalandTorresStraitIslanderwomen,particularlyinurbanareas;womenfromculturallyandlinguisticallydiversebackgrounds,particularlyAsianwomen;youngwomen;andobesewomen.
SpecificcoverageofculturalandlinguisticallydiversepopulationsandAboriginalandTorresStraitIslanderpeoplehasbeenincludedinthismanualtoenablepractitionerstoaddressspecificconcernsfromthesepopulations.
Therearemanypeoplewhomightconsiderthemselvesexpertsinfeedingbabiesandyoungchildren.Thesemayincludegrandparents,parents-in-law,friends,workmates,brothersandsisterswhohavehadababy.Whilstvaluable,advicefromallanglesoftenmakesfeedingyoungchildrenmorecomplicatedandconfusingforparentsit’simportanttorecognisethatwhiletherearegeneralguidelinestohelpnewparents,allbabiesandyoungchildrenareindividualswiththeirowngrowthrates,activityanddevelopmentthatmayinfluencetheirappetiteandfoodpreferences.
2 A HEALTHY START IN LIFE INTRODUCTION
1.1 AbbreviationsBMI BodyMassIndex
FSANZ FoodStandardsAustraliaandNewZealand
NHMRC NationalHealthandMedicalResearchCouncil
RDI RecommendedDietaryIntake
NVR NutrientReferenceValue
kg kilogram
g gram
mg milligram
ug microgram
ml millilitres
L litre
Tbsp tablespoon
wt weight(kg)
ht height(cm/m)
kJ kilojoules
cm centimetres
m metres
1.2 Symbols
Parenthandouts
Webresource
Professionaldevelopmentresource
RecommendationsfromtheDietary Guidelines for Children and Adolescents in Australia
3A HEALTHY START IN LIFE INTRODUCTION
1.3 Communicating with clientsSomeofthetechniquesyoumayusetofindoutwhatinformationamotherneedsandtohelphermakethebestuseofthisinformationarelistedbelow.
Listening
Listeningwellletstheparent/caregiverexplainthesituationastheyseeit.Bodylanguageandnonverbalcommunicationisalsoimportant.
Showingyouunderstand
Useyourownwordstoexplainwhatyouhaveheard.Thisletsyoucheckwiththeparent/caregiverthatyouhaveunderstoodwhatshehassaid.
Askingaboutwhathasbeentriedalready
Beforeyouoffersuggestionsaskwhattheparent/caregiverhasalreadytried.Thisgivesyouabetterpictureofthesituationandhelpstoidentifywhatmightwork.
Askingaboutpreviousadvice
Everyoneseemstobeanexpertonpregnancyandbabies.Parent/caregiverscangetveryconfusediftheyarebeinggivenconflictingadvice.Itisimportanttoknowwhattheparent/caregiverhasbeentoldbeforeyouofferyourowninformationandsuggestions.Becarefulnottoputdowntheadvicegivenbyanyoneelse.
Offeringsuggestions
Itisourjobtoofferideasaboutwhatshecoulddo.Itisuptotheparent/caregivertodecidewhatwillworkbestinhersituationandwhatsheisabletodo.
Helpingbelievetheycandoit
Itisimportantnotonlytogiveinformationandmakesuggestionsbutalsotoprovidetheskillsneeded.
Identifyingsupport
Somewillneedmoresupportthanothers.Talktotheparent/caregiveraboutwhatsupporttheywouldlikeandwhocouldprovideit.Givereferralstootherstafforagenciesifappropriate.
Summarising
Attheendofasessiongooverthemainpointsofyourdiscussion.
4 A HEALTHY START IN LIFE INTRODUCTION
Client education action checklist
What information, knowledge or skill does the client already have?✔✔
Explore previous experiences … Have you seen this before? … Have you ✔✔heard about? …
What does the client want and need to know?✔✔
Base your information/client education on the priorities set by the client.✔✔
Work from known to the unknown: from simple to complex.✔✔
Get client’s attention.✔✔
Clarify what you want to do.✔✔
Present content using appropriate strategies.✔✔
Adjust the content so it is relevant to the client and their experiences.✔✔
Get feedback from client of their understanding of the content.✔✔
Reinforce learning (praise, acknowledgement and more praise).✔✔
What take away material/information is available?✔✔
Summarise what you have covered.✔✔
Document client education.✔✔
1.4 Key documentsThekeynutritionguidingdocumentsusedinthisresourceare:
Dietary Guidelines for Children and Adolescents in Australia✔■
Australian Guide to Healthy Eating✔■
Nutrient Reference Values (including RDIs) ✔■
NationalBreastfeedingStrategy
NationalPhysicalActivityGuidelines
ReportoftheChiefHealthOfficerQueensland,2006
Clinicalpracticeguidelinesusedinthisdocumentinclude:
NHMRC Clinical practice guidelines for the management of overweight and obesity ✔■
in children
NHMRC Child health screening guidelines✔■
WHO Infant and young child feeding: standard recommendations for the European ✔■
Union
Specific Clinical Practice guidelines are available at www.mja.com.au✔■
Queensland Health Optimal Infant Feeding: evidence based guidelines 2003-2008
Queensland Health: Enhanced Child Health Model of Care for Community Health Services (0-12 years)
Infant and Child Nutrition in Queensland 2003 www.health.qld.gov.au/healthieryou/food_nutrition.asp
5A HEALTHY START IN LIFE INTRODUCTION
The Dietary Guidelines for Children and Adolescents in Australia
TheDietaryGuidelinesforAustraliansarethebestguidetofood,nutritionandhealth.The Dietary Guidelines for Children and Adolescents in Australiahighlightthegroupsoffoodsandlifestylepatternsthatfostergoodnutritionandhealth.Thelatesteditionavailablewasrevisedin2003.
TheDietaryGuidelinesgiveevidencebasedprinciplesforhealthyeatingandapplytothetotaldiet.Theyarenotrankedinorderofimportanceandshouldbeconsideredintheirentiretyie.notjustindividualguidelinesinisolation.
TheDietaryGuidelinesincorporateThe Australian Guide to Health Eating.
TheNHRMCDietary Guidelines for Children and Adolescentsincorporatingthe infant feeding guidelines for health workersprovideacomprehensiveoverviewofappropriatefoodchoicesforinfantsandchildrenatvariousdevelopmentalstagesandtherisksassociatedwiththeintroductionofinappropriatefoods.Healthworkersshouldrefertothesedocumentsforguidancewhenadvisingpregnantwomen,mothers,familiesandcarersaboutinfantnutrition.
Forcopiesofthe Dietary Guidelines for Children and AdolescentsinAustralia contact:
PopulationHealthPublicationsOfficer CommonwealthDepartmentofHealthandAgeing 1800020103
Email: [email protected]
Web: www.nhmrc.gov.au/publications/synopses/dietsyn.htm
Summarydocument www.population.health.wa.gov.au/Promotion/resources/Infant%20Feeding%20Guidelines.pdf
6 A HEALTHY START IN LIFE INTRODUCTION
7A HEALTHY START IN LIFE INTRODUCTION
8 A HEALTHY START IN LIFE INTRODUCTION
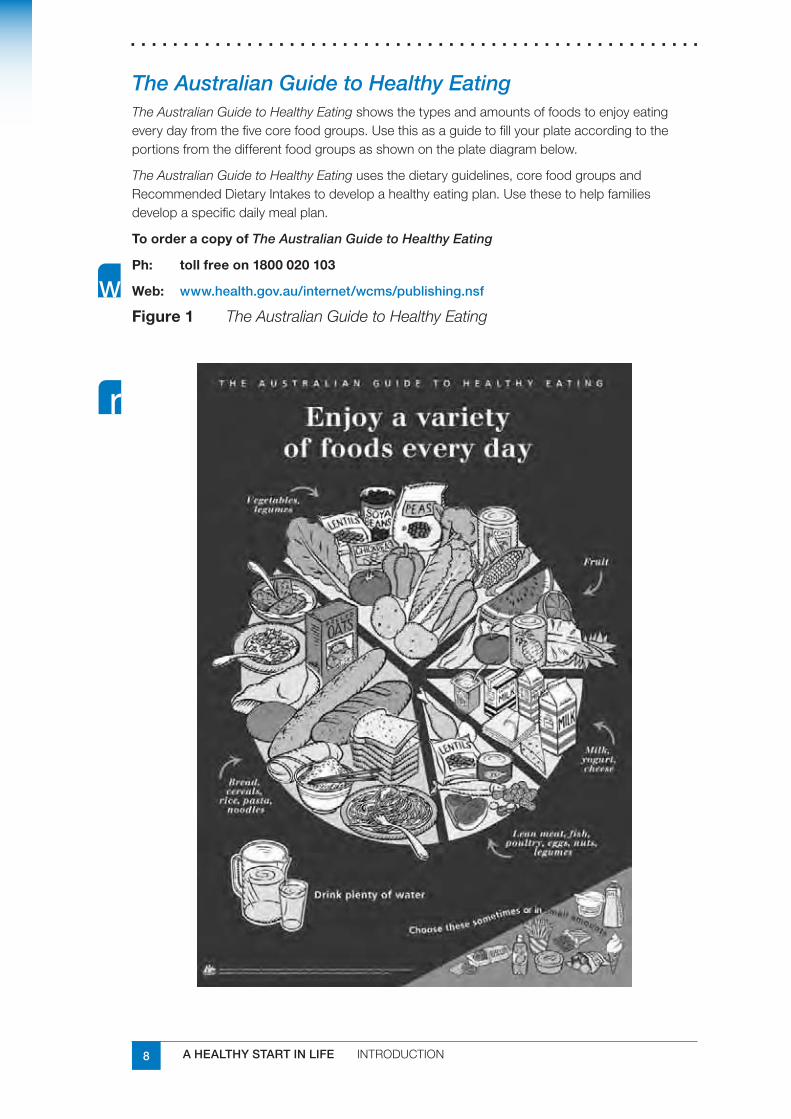
The Australian Guide to Healthy EatingThe Australian Guide to Healthy Eatingshowsthetypesandamountsoffoodstoenjoyeatingeverydayfromthefivecorefoodgroups.Usethisasaguidetofillyourplateaccordingtotheportionsfromthedifferentfoodgroupsasshownontheplatediagrambelow.
The Australian Guide to Healthy Eatingusesthedietaryguidelines,corefoodgroupsandRecommendedDietaryIntakestodevelopahealthyeatingplan.Usethesetohelpfamiliesdevelopaspecificdailymealplan.
ToorderacopyofThe Australian Guide to Healthy Eating
Ph: tollfreeon1800020103
Web: www.health.gov.au/internet/wcms/publishing.nsf
Figure1 The Australian Guide to Healthy Eating
9A HEALTHY START IN LIFE INTRODUCTION
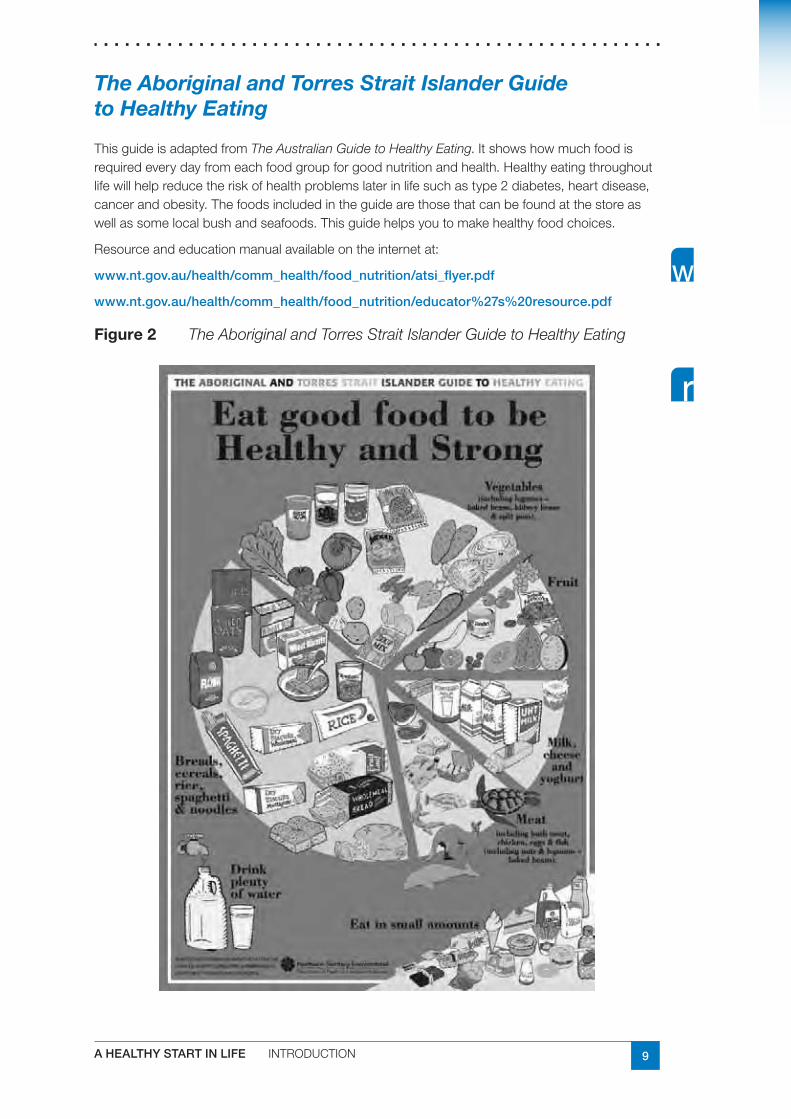
The Aboriginal and Torres Strait Islander Guide to Healthy Eating
ThisguideisadaptedfromThe Australian Guide to Healthy Eating.Itshowshowmuchfoodisrequiredeverydayfromeachfoodgroupforgoodnutritionandhealth.Healthyeatingthroughoutlifewillhelpreducetheriskofhealthproblemslaterinlifesuchastype2diabetes,heartdisease,cancerandobesity.Thefoodsincludedintheguidearethosethatcanbefoundatthestoreaswellassomelocalbushandseafoods.Thisguidehelpsyoutomakehealthyfoodchoices.
Resourceandeducationmanualavailableontheinternetat:
www.nt.gov.au/health/comm_health/food_nutrition/atsi_flyer.pdf
www.nt.gov.au/health/comm_health/food_nutrition/educator%27s%20resource.pdf
Figure2 The Aboriginal and Torres Strait Islander Guide to Healthy Eating
10 A HEALTHY START IN LIFE INTRODUCTION
1.5 Food groupsAnumberoffoodselectionguideshavebeendevelopedinAustraliaoverthelast50years,includingtheFiveFoodGroupsmodelandtheHealthyEatingPyramid.ThecorefoodgroupsmodelwasendorsedbytheNHMRCin1994.ThemainuseoftheCoreFoodGroupswastoprovideascientificbasisforthedevelopmentofuptodatenutritioneducationtools.ThishasseenthereplacementoftheFiveFoodGroupsmodelwiththeAustralian Guide to Healthy Eating.
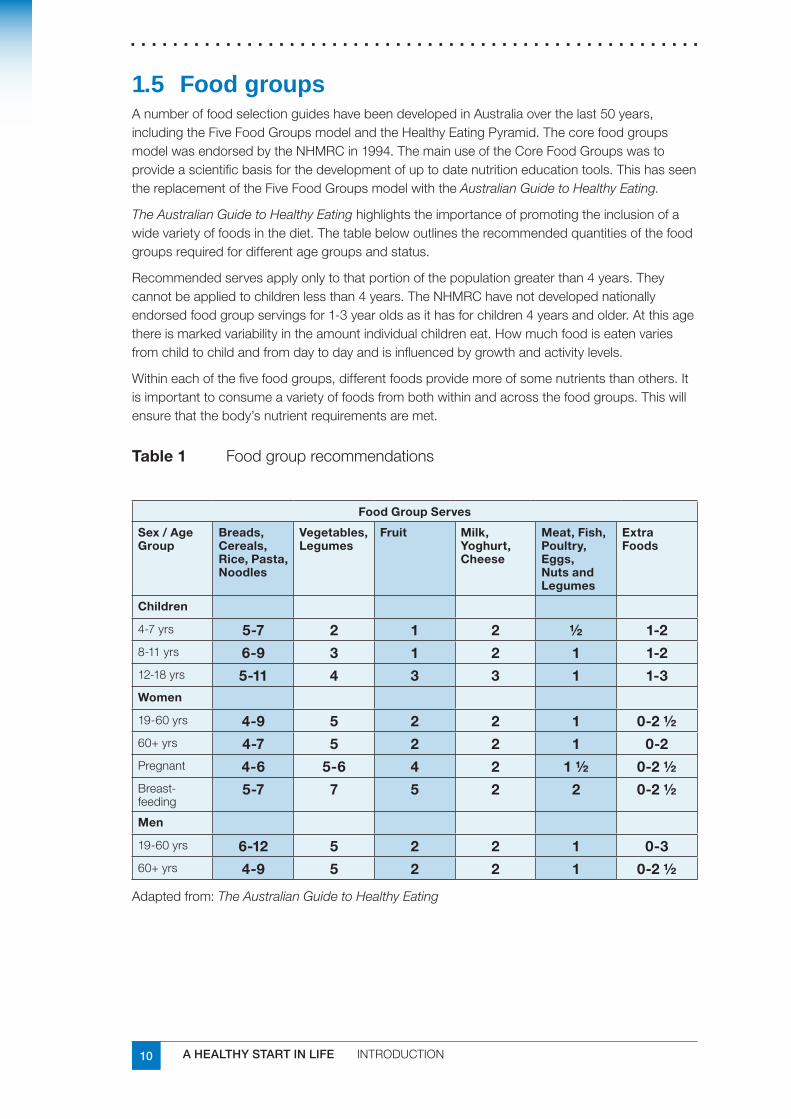
The Australian Guide to Healthy Eatinghighlightstheimportanceofpromotingtheinclusionofawidevarietyoffoodsinthediet.Thetablebelowoutlinestherecommendedquantitiesofthefoodgroupsrequiredfordifferentagegroupsandstatus.
Recommendedservesapplyonlytothatportionofthepopulationgreaterthan4years.Theycannotbeappliedtochildrenlessthan4years.TheNHMRChavenotdevelopednationallyendorsedfoodgroupservingsfor1-3yearoldsasithasforchildren4yearsandolder.Atthisagethereismarkedvariabilityintheamountindividualchildreneat.Howmuchfoodiseatenvariesfromchildtochildandfromdaytodayandisinfluencedbygrowthandactivitylevels.
Withineachofthefivefoodgroups,differentfoodsprovidemoreofsomenutrientsthanothers.Itisimportanttoconsumeavarietyoffoodsfrombothwithinandacrossthefoodgroups.Thiswillensurethatthebody’snutrientrequirementsaremet.
Table1 Foodgrouprecommendations
FoodGroupServes
Sex/AgeGroup
Breads,Cereals,Rice,Pasta,Noodles
Vegetables,Legumes
Fruit Milk,Yoghurt,Cheese
Meat,Fish,Poultry,Eggs,NutsandLegumes
ExtraFoods
Children
4-7yrs 5-7 2 1 2 ½ 1-28-11yrs 6-9 3 1 2 1 1-212-18yrs 5-11 4 3 3 1 1-3Women
19-60yrs 4-9 5 2 2 1 0-2½60+yrs 4-7 5 2 2 1 0-2Pregnant 4-6 5-6 4 2 1½ 0-2½Breast-feeding
5-7 7 5 2 2 0-2½
Men
19-60yrs 6-12 5 2 2 1 0-360+yrs 4-9 5 2 2 1 0-2½
Adaptedfrom:The Australian Guide to Healthy Eating
11A HEALTHY START IN LIFE INTRODUCTION
Bread,cereal,rice,pasta,noodlesWhy?
Thenutrientsprovidedbythefoodsinthisgroupincludecarbohydrates,protein,fibreandawiderangeofvitaminsandmineralsincludingfolate,thiamin,riboflavin,niacinandiron.Wholemealorwholegrainvarietiesprovidemorefibre,vitaminsandminerals.Somefoodsinthisgroupmayhavefibre,vitaminsandmineralsaddedduringprocessing.
What?
Asampleserveofbread,cereal,rice,pasta,noodlesis:
2slicesbread
1mediumbreadroll
1cupcookedrice,pasta,noodles
1cupporridge,11/3cupsbreakfastcerealflakes½cupmuesli
Vegetables,legumesWhy?
Vegetablesandlegumesareagoodsourceofvitamins,minerals,dietaryfibreandcarbohydrate.
capsicum,broccoli,cauliflower,cabbageandtomatoesarehighinvitaminC✔■
darkgreenvegetablesegspinach,broccoli,andorangevegetablesegcarrotsand✔■
pumpkinarehighinvitaminA
greenvegetables,driedpeas,beansandlentilsareagoodsourceoffolate✔■
What?
Asampleserveofvegetables,legumesis:
75gor½cupcookedvegetables
75gor½cupcookeddriedbeans,peasorlentils
1cupsaladvegetables
1potato
FruitWhy?
Fruit isagoodsourceofvitamins,includingvitaminCandfolate.Italsoprovidescarbohydratesinparticularnaturalsugarsandfibre,especiallyintheedibleskins.Juicesbelongtothisgroup,buttheyhaveamuchlowerfibrecontentthanfreshfruit.
What?
Asampleserveoffruitis:
1mediumpiece,egapple,banana,orange,pear
2smallpieces,egapricots,kiwifruit,plums
1cupdicedpiecesorcannedfruit
½cupjuice
driedfruit,eg4driedapricothalves,1½tablespoonssultanas
12 A HEALTHY START IN LIFE INTRODUCTION
Milk,yoghurt,cheeseWhy?
Milk,yoghurtandfirmcheesesarethethreeimportantfoodsinthisgroup.
Thefoodsinthisgroupareanexcellentsourceofcalcium;veryfewotherfoodsintheAustraliandietcontainasmuchofthisimportantnutrient.Thesefoodsarealsoagoodsourceofprotein,riboflavinandvitaminB12.
Themilk,yoghurt,cheesegroupcanincreasethefatcontentofyourdietifyouchoosefullcreamproducts.Formostpeople,2yearsandover,thebestchoicesarereducedfatmilk,yoghurtandcheese.Forchildrenunder2yearsofage,fullcreamvarietiesarerecommendedbecauseoftheirhighenergyneeds.
What?
Asampleserveofmilk,yoghurt,cheeseis:
250ml(1cup)fresh,long-lifeorreconstituteddriedmilk
½cupevaporatedmilk
40g(2slices)cheese
200g(1smallcarton)yoghurt
250ml(1cup)custard
Meat,fish,poultry,eggs,nuts,legumesWhy?
Thereisawidevarietyoffoodsinthisgroup.Itconsistsofallkindsofmeat,poultry,fish,eggs,nutsandnutpastessuchaspeanutbutter,legumes,andsomeseedssuchassunflowerandsesameseeds.
Thefoodsinthisgroupareagoodsourceofprotein,iron,niacinandvitaminB12.Withinthisgroup,redmeatsareaparticularlygoodsourceofironandalsozinc.Theironinanimalfoodsismoreeasilyabsorbedbythebodythantheironinplantfoods.Redmeatshouldbeeaten3to4timesaweek,orhighironreplacementfoodswillberequired.Thisisespeciallytrueforgirls,women,vegetariansandathletes.
What?
Asampleserveofmeat,fish,poultry,eggs,nuts,legumesis:
65-100gcookedmeat,chicken
½cupleanmince
2smallchops
2slicesroastmeat
½cupcooked(dried)beans,lentils,chickpeas,splitpeas,orcannedbeans
80-120gcookedfishfillet
2smalleggs
1/3cuppeanutsoralmonds¼cupsunflowerseedsorsesameseeds

13A HEALTHY START IN LIFE INTRODUCTION
ExtrafoodsWhy?
Somefoodsdonotfitintothefivefoodgroups.Theyarenotessentialtoprovidethenutrientsthebodyneedsandsomecontaintoomuchaddedfat,saltandsugars.Thesefoodsarelikelytocontributelargeamountsofenergy.However,theycanaddtotheenjoymentofeatingahealthydiet.
What?
Asampleserveofextrafoodsistheamountoffoodthatprovides600kJ.
Someexamplesare:
1(40g)doughnut
4(35g)plainsweetbiscuits
1slice(40g)plaincake
½smallbar(25g)chocolate
2tablespoons(40g)cream,mayonnaise
1tablespoon(20g)butter,margarine,oil
200mlwine(2standarddrinks)
60mlspirits(2standarddrinks)
600mllightbeer(1½standarddrinks)
400mlregularbeer(1½standarddrinks)
1can(375ml)softdrink
1/3(60g)meatpieorpastie
12(60g)hotchips
1½scoops(50gscoop)icecream
PuttingitalltogetherPeople’sneedforenergy,carbohydrates,fatsandprotein,vitaminsandmineralsvariesdependingontheirageandsexandisalteredwhenpregnantorbreastfeeding.Thesequantitiesrepresenttheminimumamountsoffoodwhichneedtobeconsumedinordertomeettherequirementsforahealthydiet.
14 A HEALTHY START IN LIFE INTRODUCTION
1.6 Nutrient reference values www.nhmrc.gov.au/publications/synopses/_files/n35.pdf
NH&MRChasrecentlydevelopedNutrient Reference Values for Australia and New Zealand(2005).ItreplacestheRDIsystem.NutrientReferenceValuesinclude:
RDI:RecommendedDietaryIntake
Theaveragedailyintakethatissufficienttomeetthenutrientrequirementsofnearlyall(97-98%)healthyindividualsinaparticularlifestageorgendergroup.
AI:AdequateIntakeusedwhenRDIcannotbedetermined
Theaveragedailynutrientintakelevelbasedonobservedorexperimentally-determinedapproximationsofnutrientintakebyagroupofapparentlyhealthypeoplethatareassumedtobeadequate.
EER:EstimatedEnergyRequirement
Theaveragedietaryenergyintakethatispredictedtomaintainenergybalanceinahealthyadultorchild.
UL:UpperLevelofIntake
Highestaveragedailynutrientintakelevellikelytopostnoadversehealtheffectstoalmostallindividuals.Thismaybeofinteresttothosepeopletakingsupplements.
ForinfantsandchildrenAswithpregnancy,certainnutrientshavebeenidentifiedasbeingparticularlyimportantforinfantsandchildrenduringtheirgrowingyears.
EnergyThelargestgrowthspurtisseeninthefirstyearofaninfant’slife.Duringthistimenutritionalneedsarehigh.Howeverbetweentheagesof1-5yearschildrenstillcontinuetohavehighnutritionalneedsdespiteaslowergrowthrate.Thisslowergrowthratecanbereflectedinalessreliableappetite.Achild’srateofgrowthisoftenanindicatorofdietaryadequacy.
ProteinProteinisessentialforgrowth,repair,andmaintenanceandimportantlymustbeprovidedinquantitiesappropriatetothegrowthperiod.Proteinrichfoodsincludemeat,fish,poultry,eggs,nuts,legumes,milk,yoghurtandcheese.
0-12months AI10g/day
1-3yrs RDI14g/day
4-8yrs RDI20g/day
15A HEALTHY START IN LIFE INTRODUCTION
FatFatisanimportantsourceofenergyandfatsolublevitaminsintheinfantandchild’sdietandshouldbeprovidedinadequateamounts.Fatsprovidenotonlyenergy,butalsoasourceofessentialfattyacids,necessaryforgrowthanddevelopment,particularlyofthespineandbrain.
0-6months AI31g/day✔■
7-12months AI30g/day✔■
1-8yrs norecommendationfortotalfat✔■
Fatrequirementsofinfantsandchildren
From6monthsto2yearsofageinfantsshouldbereceivingatleast40%ofenergyintakefromfat.Skimmilkandreducedfatmilksshouldnotbeusedinchildrenlessthan2yearsofage.
From2-5yearsofageagradualincreaseinproportionofenergyfromcarbohydratewilloccurandfatintakeshouldprovide35-40%ofenergy.
From5-14yearsofage35%ofenergyshouldbeprovidedfromfat.
Growthanddevelopmentshouldbemonitoredandcheckedagainstacceptedpercentilegrowthtrends.
CarbohydrateCarbohydrateprovidesenergytocells,particularlythebrain.Carbohydraterichfoodsincludebreads,cereals,rice,pasta,noodles,fruit,somevegetables,milkandyoghurt.
0-12months AI60g/day✔■
1-8yrs norecommendationforcarbohydrateintake(45-65%oftotalenergy✔■
predominantlyfromlowenergydensityand/orlowglycaemicindexfoods)
Iron0-6months AI0.2mg/day✔■
7-12months RDI11mg/day✔■
1-3yrs RDI9mg/day✔■
4-8yrs RDI10mg/day✔■
Ironisimportantforthetransportifoxygenintheblood.Twoformsofironexistinfood:haemandnonhaem.Haemiron(foundinmeat,fishandpoultry)iswellabsorbed.Nonhaemironispresentincerealsandvegetablesandisnotaswellabsorbed.ThepresenceofvitaminCandheamironincreasestheabsorptionofnonheamiron.
Haemironsources
Foodtypeironcontent(mg)
Lean beef (~100 g) 3.0
Lean lamb (~100 g) 2.8
Chicken (~100 g) 0.6/0.7
Fish (~100 g) 0.5
Egg (55-60 g) ~0.9-1.3
Liver (~100 g) ~10-11
Kidney (50 g) 5.7
16 A HEALTHY START IN LIFE INTRODUCTION
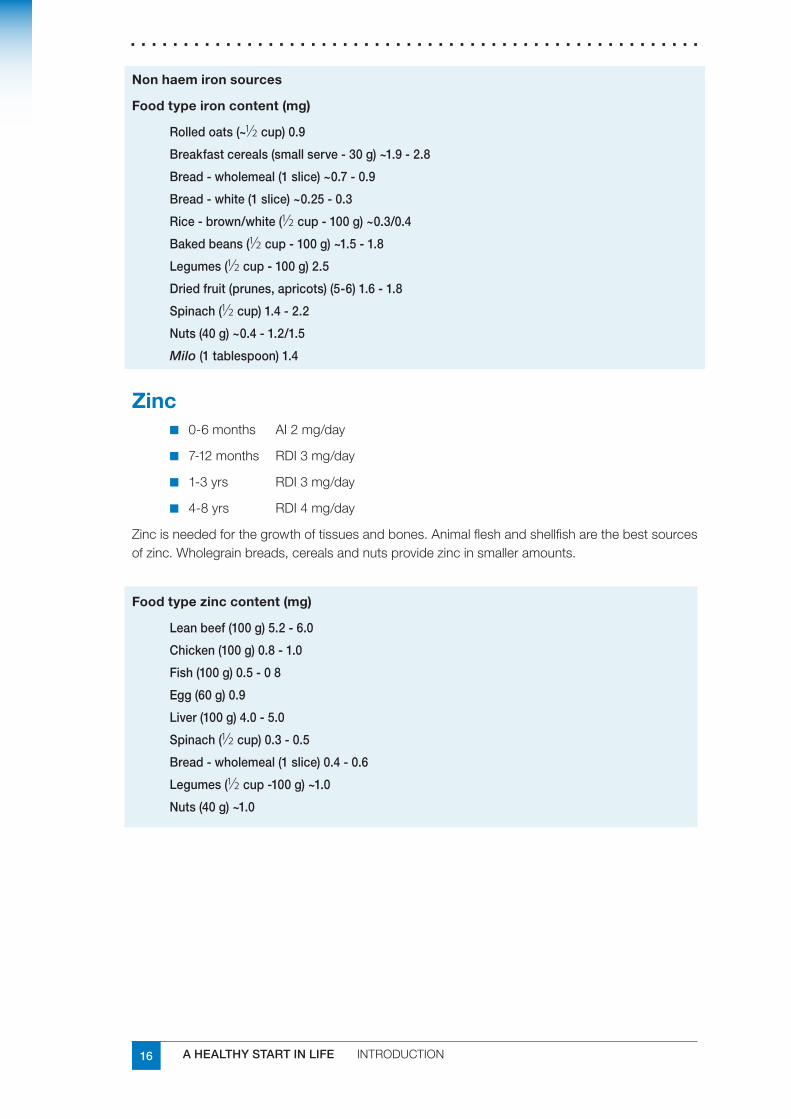
Nonhaemironsources
Foodtypeironcontent(mg)
Rolled oats (~1⁄2 cup) 0.9
Breakfast cereals (small serve - 30 g) ~1.9 - 2.8
Bread - wholemeal (1 slice) ~0.7 - 0.9
Bread - white (1 slice) ~0.25 - 0.3
Rice - brown/white (1⁄2 cup - 100 g) ~0.3/0.4
Baked beans (1⁄2 cup - 100 g) ~1.5 - 1.8
Legumes (1⁄2 cup - 100 g) 2.5
Dried fruit (prunes, apricots) (5-6) 1.6 - 1.8
Spinach (1⁄2 cup) 1.4 - 2.2
Nuts (40 g) ~0.4 - 1.2/1.5
Milo (1 tablespoon) 1.4
Zinc0-6months AI2mg/day✔■
7-12months RDI3mg/day✔■
1-3yrs RDI3mg/day✔■
4-8yrs RDI4mg/day✔■
Zincisneededforthegrowthoftissuesandbones.Animalfleshandshellfisharethebestsourcesofzinc.Wholegrainbreads,cerealsandnutsprovidezincinsmalleramounts.
Foodtypezinccontent(mg)
Lean beef (100 g) 5.2 - 6.0
Chicken (100 g) 0.8 - 1.0
Fish (100 g) 0.5 - 0 8
Egg (60 g) 0.9
Liver (100 g) 4.0 - 5.0
Spinach (1⁄2 cup) 0.3 - 0.5
Bread - wholemeal (1 slice) 0.4 - 0.6
Legumes (1⁄2 cup -100 g) ~1.0
Nuts (40 g) ~1.0
17A HEALTHY START IN LIFE INTRODUCTION
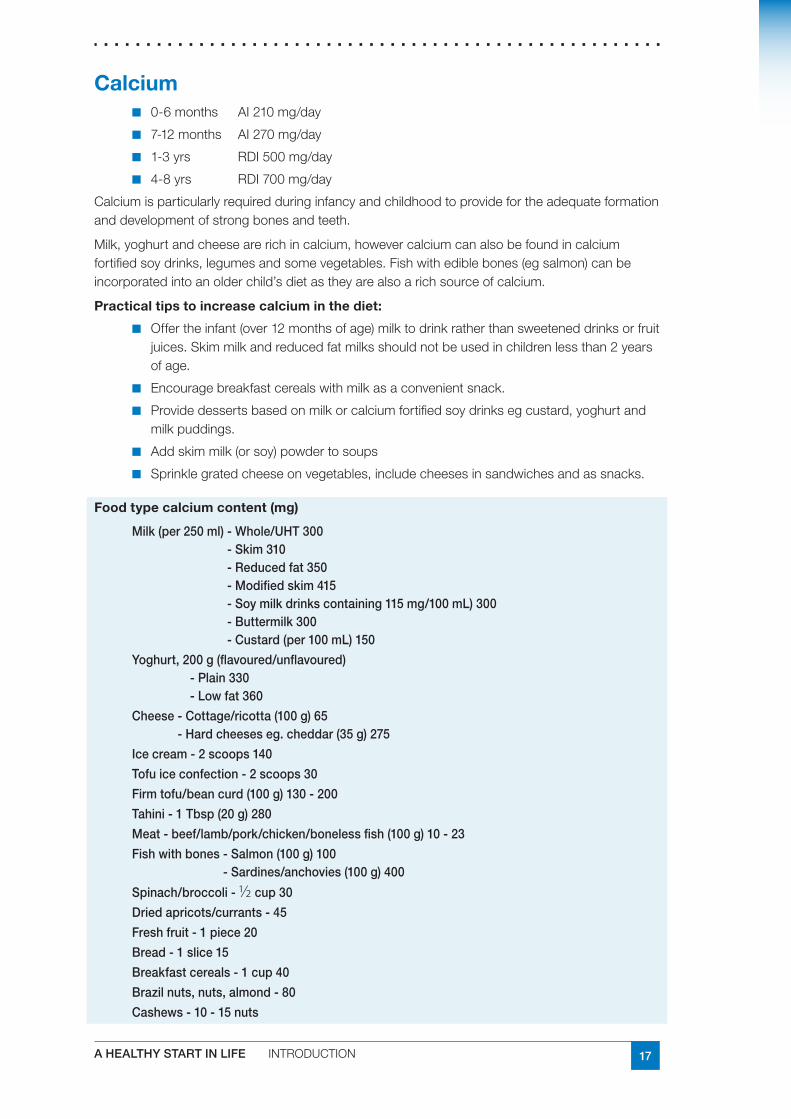
Calcium0-6months AI210mg/day✔■
7-12months AI270mg/day✔■
1-3yrs RDI500mg/day✔■
4-8yrs RDI700mg/day✔■
Calciumisparticularlyrequiredduringinfancyandchildhoodtoprovidefortheadequateformationanddevelopmentofstrongbonesandteeth.
Milk,yoghurtandcheesearerichincalcium,howevercalciumcanalsobefoundincalciumfortifiedsoydrinks,legumesandsomevegetables.Fishwithediblebones(egsalmon)canbeincorporatedintoanolderchild’sdietastheyarealsoarichsourceofcalcium.
Practicaltipstoincreasecalciuminthediet:
Offertheinfant(over12monthsofage)milktodrinkratherthansweeteneddrinksorfruit✔■
juices.Skimmilkandreducedfatmilksshouldnotbeusedinchildrenlessthan2yearsofage.
Encouragebreakfastcerealswithmilkasaconvenientsnack.✔■
Providedessertsbasedonmilkorcalciumfortifiedsoydrinksegcustard,yoghurtand✔■
milkpuddings.
Addskimmilk(orsoy)powdertosoups✔■
Sprinklegratedcheeseonvegetables,includecheesesinsandwichesandassnacks.✔■
Foodtypecalciumcontent(mg)
Milk (per 250 ml) - Whole/UHT 300 - Skim 310 - Reduced fat 350 - Modified skim 415 - Soy milk drinks containing 115 mg/100 mL) 300 - Buttermilk 300 - Custard (per 100 mL) 150
Yoghurt, 200 g (flavoured/unflavoured) - Plain 330
- Low fat 360
Cheese - Cottage/ricotta (100 g) 65 - Hard cheeses eg. cheddar (35 g) 275
Ice cream - 2 scoops 140
Tofu ice confection - 2 scoops 30
Firm tofu/bean curd (100 g) 130 - 200
Tahini - 1 Tbsp (20 g) 280
Meat - beef/lamb/pork/chicken/boneless fish (100 g) 10 - 23
Fish with bones - Salmon (100 g) 100 - Sardines/anchovies (100 g) 400
Spinach/broccoli - 1⁄2 cup 30
Dried apricots/currants - 45
Fresh fruit - 1 piece 20
Bread - 1 slice 15
Breakfast cereals - 1 cup 40
Brazil nuts, nuts, almond - 80
Cashews - 10 - 15 nuts
18 A HEALTHY START IN LIFE INTRODUCTION
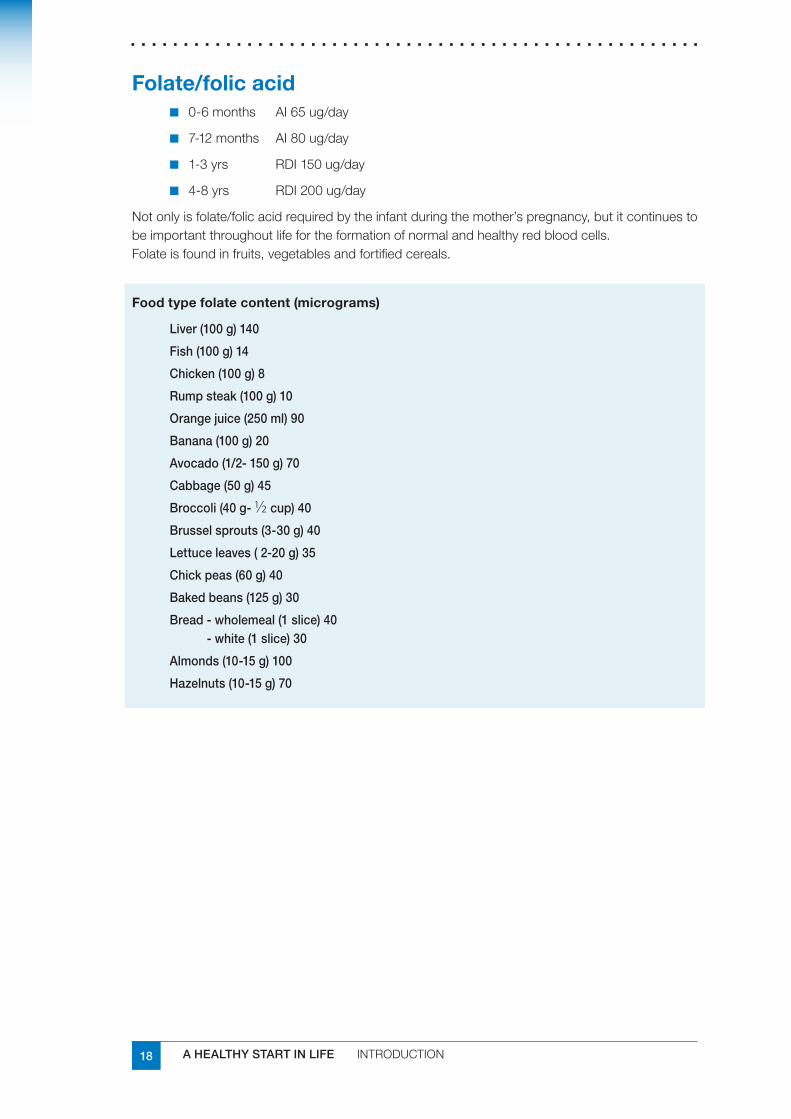
Folate/folicacid0-6months AI65ug/day✔■
7-12months AI80ug/day✔■
1-3yrs RDI150ug/day✔■
4-8yrs RDI200ug/day✔■
Notonlyisfolate/folicacidrequiredbytheinfantduringthemother’spregnancy,butitcontinuestobeimportantthroughoutlifefortheformationofnormalandhealthyredbloodcells.Folateisfoundinfruits,vegetablesandfortifiedcereals.
Foodtypefolatecontent(micrograms)
Liver (100 g) 140
Fish (100 g) 14
Chicken (100 g) 8
Rump steak (100 g) 10
Orange juice (250 ml) 90
Banana (100 g) 20
Avocado (1/2- 150 g) 70
Cabbage (50 g) 45
Broccoli (40 g- 1⁄2 cup) 40
Brussel sprouts (3-30 g) 40
Lettuce leaves ( 2-20 g) 35
Chick peas (60 g) 40
Baked beans (125 g) 30
Bread - wholemeal (1 slice) 40 - white (1 slice) 30
Almonds (10-15 g) 100
Hazelnuts (10-15 g) 70
19A HEALTHY START IN LIFE INTRODUCTION
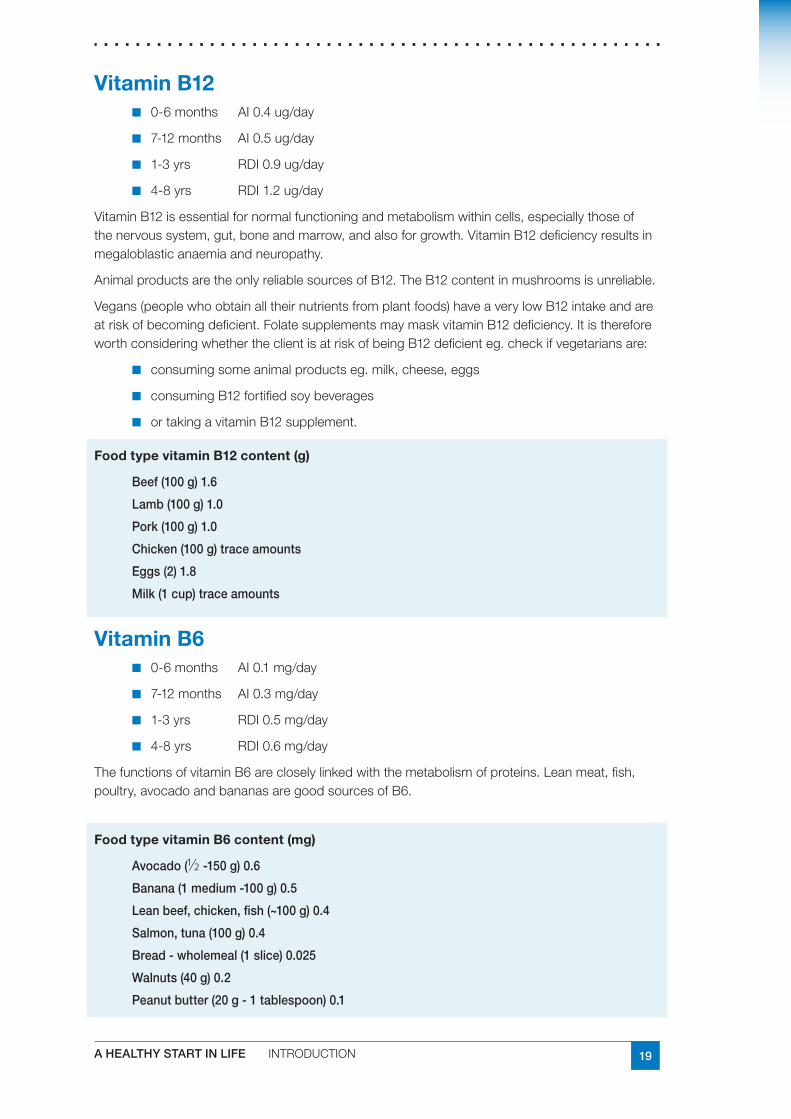
VitaminB120-6months AI0.4ug/day✔■
7-12months AI0.5ug/day✔■
1-3yrs RDI0.9ug/day✔■
4-8yrs RDI1.2ug/day✔■
VitaminB12isessentialfornormalfunctioningandmetabolismwithincells,especiallythoseofthenervoussystem,gut,boneandmarrow,andalsoforgrowth.VitaminB12deficiencyresultsinmegaloblasticanaemiaandneuropathy.
AnimalproductsaretheonlyreliablesourcesofB12.TheB12contentinmushroomsisunreliable.
Vegans(peoplewhoobtainalltheirnutrientsfromplantfoods)haveaverylowB12intakeandareatriskofbecomingdeficient.FolatesupplementsmaymaskvitaminB12deficiency.ItisthereforeworthconsideringwhethertheclientisatriskofbeingB12deficienteg.checkifvegetariansare:
consumingsomeanimalproductseg.milk,cheese,eggs✔■
consumingB12fortifiedsoybeverages✔■
ortakingavitaminB12supplement.✔■
FoodtypevitaminB12content(g)
Beef (100 g) 1.6
Lamb (100 g) 1.0
Pork (100 g) 1.0
Chicken (100 g) trace amounts
Eggs (2) 1.8
Milk (1 cup) trace amounts
VitaminB60-6months AI0.1mg/day✔■
7-12months AI0.3mg/day✔■
1-3yrs RDI0.5mg/day✔■
4-8yrs RDI0.6mg/day✔■
ThefunctionsofvitaminB6arecloselylinkedwiththemetabolismofproteins.Leanmeat,fish,poultry,avocadoandbananasaregoodsourcesofB6.
FoodtypevitaminB6content(mg)
Avocado (1⁄2 -150 g) 0.6
Banana (1 medium -100 g) 0.5
Lean beef, chicken, fish (~100 g) 0.4
Salmon, tuna (100 g) 0.4
Bread - wholemeal (1 slice) 0.025
Walnuts (40 g) 0.2
Peanut butter (20 g - 1 tablespoon) 0.1
20 A HEALTHY START IN LIFE INTRODUCTION
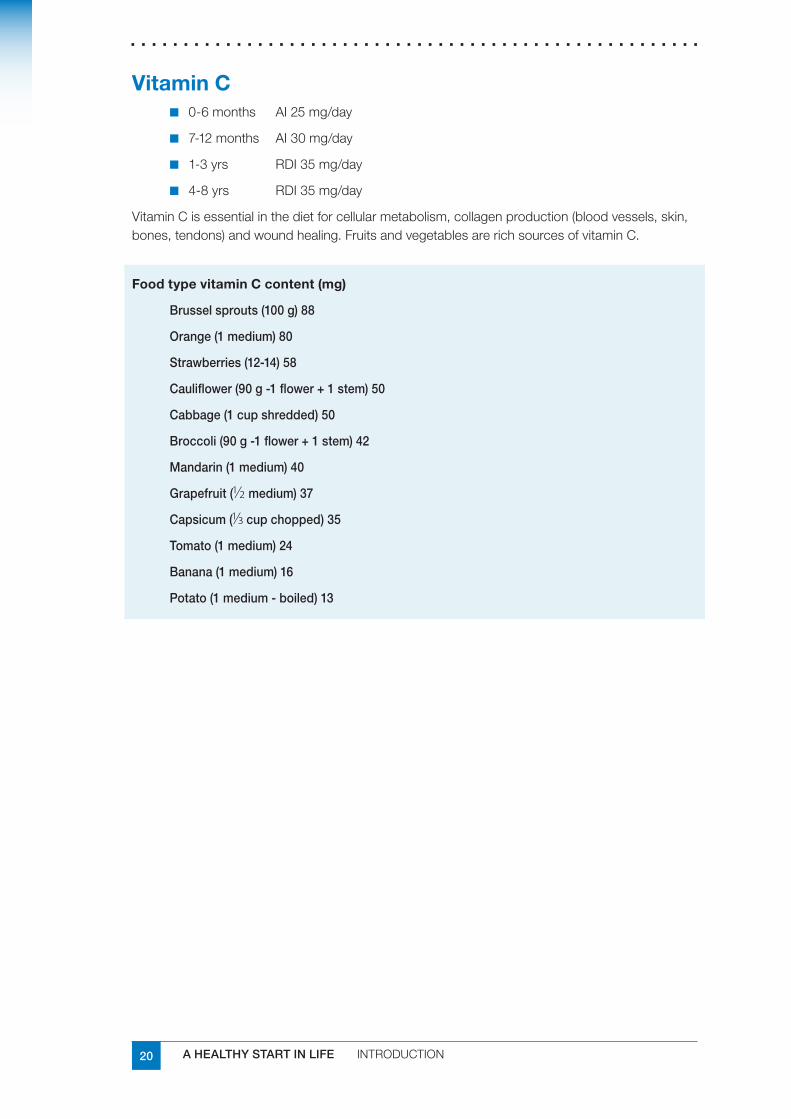
VitaminC0-6months AI25mg/day✔■
7-12months AI30mg/day✔■
1-3yrs RDI35mg/day✔■
4-8yrs RDI35mg/day✔■
VitaminCisessentialinthedietforcellularmetabolism,collagenproduction(bloodvessels,skin,bones,tendons)andwoundhealing.FruitsandvegetablesarerichsourcesofvitaminC.
FoodtypevitaminCcontent(mg)
Brussel sprouts (100 g) 88
Orange (1 medium) 80
Strawberries (12-14) 58
Cauliflower (90 g -1 flower + 1 stem) 50
Cabbage (1 cup shredded) 50
Broccoli (90 g -1 flower + 1 stem) 42
Mandarin (1 medium) 40
Grapefruit (1⁄2 medium) 37
Capsicum (1/3 cup chopped) 35
Tomato (1 medium) 24
Banana (1 medium) 16
Potato (1 medium - boiled) 13
21A HEALTHY START IN LIFE INTRODUCTION
1.7 Physical activityPhysicalactivityisanormalandessentialcomponentofeverydaylifeforinfantsandchildren.Itisimportantforgrowth,developmentofskillsandessentialinmaintainingahealthyweight.
BenefitsImprovedmovementskillsandcoordination.✔■
Cardiovascularfitness.✔■
Strongerbones.✔■
Weightcontrol.✔■
Socialenjoymentandskillssuchasturntaking,cooperation,winingandloosing.✔■
Improvedmentalhealth.✔■
Betterschoolperformance.✔■
BarriersTherearemanysuggestedreasonswhyphysicalactivitylevelsmaynotbeoptimised.Activitiessuchastelevision,videos,computergamesandtheinternetarepartofachild’slifebutlimitsshouldbeplacedonthesetoensuresufficientphysicalactivityoccurs.Thesearethemainreasonbehindinsufficientphysicalactivity.
Otherbarriersinclude:
theuseofmotorisedtransportinplaceofwalkingorriding✔■
insufficientcommunityfacilitiesforoutdoorplay✔■
busyfamilylife✔■
safetyconcerns✔■
peerinfluences✔■
costconcerns✔■
Alltheseperceivedbarrierscanbeovercomeanditisimportanttodiscusssolutionsoralternativestoensureadequatephysicalactivity.
PhysicalactivityrecommendationsTheAustralianGovernmenthasrecentlydevelopedPhysical Activity Recommendations for Children and Young People.
Children and young people should participate in at least 60 minutes (and up to several 1hours) of moderate to vigorous intensity—physical activity every day.
Children and young people should not spend more than 2 hours a day using electronic 2media for entertainment (eg computer games, Internet, TV) particularly during daylight hours.
Therecommendationsareintendedtoidentifytheminimumlevelofphysicalactivityrequiredforgoodhealthinchildrenandyoungpeoplefrom5–18yearsofage.
www.health.gov.au/internet/wcms/publishing.nsf/Content/phd-physical-activity-kids-pdf-cnt.htm/$FILE/kids_phys.pdf
www.health.gov.au/internet/wcms/publishing.nsf/Content/phd-physical-activity-youth-pdf-cnt.htm/$FILE/youth_phys.pdf
22 A HEALTHY START IN LIFE INTRODUCTION
StrategiestopromotephysicalactivityManagethetimechildrenspendinfrontoftelevision,watchingvideos,ontheinternet✔■
andplayingcomputergames.
Ensureenjoyableactivitiesareavailableasanalternativetosedentaryrecreation.✔■
Consideractivetransport.✔■
Beaphysicallyactiveadultandapositiverolemodel.✔■
FamilyactivitiesRolemodellinganactivelifestyleforchildrenisveryimportantandhasaninfluenceoverthechild’sphysicalactivitylevel.Whileitisappropriateforchildrentobeinvolvedinorganisedsports,physicalactivitycanalsobeafamilyactivity.
Playcricket,soccer,frisbeeorbarefootlawnbowlsinthebackyard.✔■
Showkidssomeoftheactivegamesyouplayedasakidlikehopscotch,quoits,✔■
skippinggames,hide-and-seekortiggy.
Getabasketballornetballhoopfortheyard.✔■
Flyakite.✔■
Joinneighboursatthelocalparkforafungameoffooty,cricketorsoftball.✔■
Exploretheneighbourhoodonabike.✔■
Goonapicnicorawalktogether.✔■
SportandrecreationresourcesMove Baby Move
Abookletdesignedtohelpparentsandearlychildhoodcarersincorporatesafe,activemovementintotheirbaby’sdailyroutines.
www.sportrec.qld.gov.au/school_community/active_baby.cfm
Active Alphabet
Aresourcedesignedespeciallyforparents,carersandtheirtoddlerstousetogethertolearnbasicactivemovementskillswhilealsolearningimportanthealthmessages
www.sportrec.qld.gov.au/school_community/active_toddler.cfm
Let’s Get Moving
Afunresourceforpreschoolchildren(3-6yearolds)tolearnbasicmovementskillsandimportanthealthmessageswhiletheirparents,carersorteacherslearnallabouttheimportanceofmovementfortheirpreschooler.
www.sportrec.qld.gov.au/school_community/active_preschooler.cfm
23A HEALTHY START IN LIFE INTRODUCTION
UsefulwebsitesandresourcesWebsites
EatWellBeActive
www.eatwellbeactive.qld.gov.au/eatwellbeactive/default.asp
BuildingaHealth,ActiveAustralia
www.healthyactive.gov.au/getmoving
AustralianSportsCommission
www.ausport.gov.au/
RaisingChildrenNetwork
raisingchildren.net.au/
SportandRecreationQueensland
www.sportrec.qld.gov.au
ActiveAte
education.qld.gov.au/schools/healthy/active-ate/
Parenthandouts
www.eatwellbeactive.qld.gov.au/eatwellbeactive/documents/fact/tips_for_children_fact_sheet.pdf
www.eatwellbeactive.qld.gov.au/eatwellbeactive/documents/fact/tips_for_families_fact_sheet.pdf
www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=301&id=1977
Books
Parentscanchecktheirlocallibrariesforbooks/CDs/DVDspromotingphysicalactivity.
FitKIDSbyMaryGalvinMD,StevenA.DowshenMD,andNeilIzenberg
MD,DorlingKingsleyLtd,London,2004
Fit KidsbyLisaCurry,aHarperCollinsbook,publishedbyCurryKennyPromotions,2000,Sydney
“501 TV Free Activities for KidsbyDiHodges,publishedbyHinklerBooksPty.Ltd.,2000,Dingley,Victoria
ReferencesQueenslandHealth:1. Kids on Track program Parent Manual(2006)GoldCoastHealthServiceDistrict
Department Health and Ageing Physical Activity Guidelines for Children and Young People2. (2005)
NHMRC (2003) Dietary Guidelines for Children and Adolescents in Australia3.
PediatricsVol117No5May2006pp1834-1842ActiveHealthyLiving:Preventionof4.ChildhoodObesityThroughIncreasedPhysicalActivity
24 A HEALTHY START IN LIFE INTRODUCTION
1.8 Culturally and Linguistically Diverse (CALD) Communities
Culturalcompetenceinearlylife
Howculturallycompetentisyourhealthservice?Dowomenofavarietyofculturesuseyourhealthservice?✔■
Isyourclientprofilerepresentativeofyourpopulationwithrespecttoculturaldiversity?✔■
Doyouhaveeducationmaterialsusinggraphicsforclientsilliterateintheirfirstlanguage✔■
andyourcollectionoftranslatededucationalmaterialsarewellusedforliterateclients.
Yourserviceunderstandshowtodeliverculturallyappropriatesupportandadvice.✔■
Australiaisamulticulturalsociety;however,mainstreamparentingpracticesarebasedonAnglo-Australianvaluesandideals.Parentsandcarerscanfeelconflictedbetweentheadvicetheyreceivefromhealthprofessionalsandadvicefromtheirownparents(1).
Inallcountrieswomenadapttheirfeedingpracticestotheirowncircumstancesandtheenvironmenttheylivein.Womenadapttotheirinfant’sneeds,andinfantsadapttotheirmothers’availability(2).
Parentingpracticesareculturalphenomenathatsuchchangeandarereinventedovertimeandplace.Therefore,culturalcompetencerequirescontinuedlearningandnotresortingtosimplisticstereotypes.
HowtogoaboutculturalcompetenceAttend cultural awareness - training and begin to understand the cultural lens you view your 1work with other people through. A realisation of your own biases and prejudices toward other cultural groups.
Identify culturally diversity in your region i.e. what languages do the people speak, what 2religions and faiths are practiced, have they migrated from rural or metropolitan regions?
Meet with other health professionals experienced with working with other cultural groups, 3undertake training in how to use an interpreter in your health service.
Next, identify what skills you need to develop, such as explorative communication 4techniques to illicit information. As you become more culturally competent your knowledge deepens, this can be facilitated through cultural encounters, and these connections with your communities can enhance partnerships and participation, but may only be achieved with a desire or willingness to understand others.
Finally, cultural competency encourages the creation of culturally safe environments to 5promote equitable health outcomes. Share your learnings with other health professionals, advocate for improved service delivery for people from culturally and linguistically diverse backgrounds.
25A HEALTHY START IN LIFE INTRODUCTION
MulticulturalprofileofQueenslandQueenslandisaculturallydiversestate.In2001oftheQueenslandpopulation:
17%werebornoverseas✔■
ofthese9%camefromanon-Englishspeakingcountryregardlessofthelengthof✔■
timespentinAustralia,femaleswerelesslikelythanmalestospeakonlyEnglishathome.
themostpopularlanguagesspokenwereItalian,Cantonese,Mandarin,Vietnamese,✔■
German,SouthSlavicandGreek.
216differentcountriesrepresented✔■
Morethan130differentlanguagesspoken✔■
Morethandifferentfaithspractised✔■
MigrationtoQueenslandhasoccurredoverdifferentperiodsoftimewithethnicgroupsarrivingunderarangeofbusiness,skill,familyreunionandhumanitarianimmigrationprograms.Since2001,therehasbeenincreasingmigrationfromAsian,PacificIslandercountriesandrefugeesfromMiddleEasternandAfricancountries(4).
Vulnerablemigrants:refugeeandasylumseekerPeoplefromculturallyandlinguisticallydiversebackgrounds(CALDB)areparticularlyvulnerableasthegreaterthedifferencesbetweencountryoforiginandAustralia,thegreaterarethedifficultiesinintegrationandsettlement.
Migrationcategoriesarefundamentaltothewaypeopleadapttotheirnewenvironments.Thereisanimportantdistinctiontobemadebetweenhumanitarianandnon-humanitarianimmigrants.Since1991,Australia’sHumanitarianProgramhasfocusedonpeoplefromtheformerYugoslavia,theMiddleEastandtheHornofAfrica.Itiswelldocumentedthatrefugeesfromtheseregionsarelikelytohavesufferedextremehardshipduetoconflictandwarintheircountryoforigin.Theymayhavespentconsiderabletimeinprisonsand/orrefugeecampswithlimitedaccesstobasichumanservices,suchaswater,foodandadequateprotectionfromtheelements.Asaconsequenceoftherefugeeexperience,manynewarrivalsareinpoorphysicalhealthandmaysufferpsychologicalproblemsthattendtopersistlongaftertheirarrival(3)
Females:specialconsiderationsTherearealsogenderdifferencesinthesettlementexperienceofmaleandfemalemigrants,withwomenbeingmorevulnerabletosettlementandadjustmentproblems.FemaleimmigrantsandrefugeesgenerallyhavepoorerEnglishproficiencythanmenandaremorelikelytoimmigrateasdependentsratherthanintheirownright.Comparedwithmen,womenaremorelikelytohavelimitedeconomicmeansandcanbesubjectedtotraditionalfamilyconstraintsonbehaviour.Separationfromfamilyandkin-basedsocialsupportsystemsisaparticularlyimportantfactorforwomen.
Unfavourableemploymentandhousingcircumstances,prejudiceanddiscriminationinthelabourmarketandinthecommunityalsohavedisproportionateimpactsonwomen(5).Anunderstandingofsettlementandtheprocessofadaptationiscrucialtoanyoneworkingwithimmigrantsandrefugees.
26 A HEALTHY START IN LIFE INTRODUCTION
Workingwithinterpreters
CommunicationstyleCulturaldifferencesinlearningstylesbetween,aswellaswithin,groupswillinfluencethebestwaytocommunicate:
determinethemostappropriatecommunicationmethodeitherlanguageorliteracyor✔■
both;notesomemigrantgroups,andparticularlywomenmaybeilliterateintheirfirstlanguage,thereforetranslationofresourceswillnothelp
alwaysaskifaninterpreterisrequired,refertoQueenslandHealthLanguageServices✔■
Policy.Somegroupsmaypreferdidacticstyle,whileothersmaylearnbetterthroughdiscussionandsharinginformationandexperiencesandsomemaypreferaninteractiveapproach
becomefamiliarwiththeformsofaddress,rulesofpoliteness,the‘yes’syndrome,non-✔■
verbalbehaviour,acceptanceoftouchingandpersonalspaceoftheculturalgrouptoassistyourcommunicationprocess
this information can often be sought from organisations such as Ethnic Communities ✔■
Council of Queensland, Transcultural Mental Health Unit, and Multicultural Affairs Queensland Training Unit or from www.ethnomed.org
CreateacomfortablecrossculturalinteractionandusetheLEARNguidelinesfor✔■
negotiatingaculturallysensitivetreatmentplan(6). L:Listenwithsympathyandunderstandingtoaclient’sperceptionofaproblem
E:ExplainyourperceptionsoftheproblemA:AcknowledgeanddiscussdifferencesandsimilaritiesR:Recommendtreatmentthatisrelevant,conciseandpracticalN:Negotiateagreement
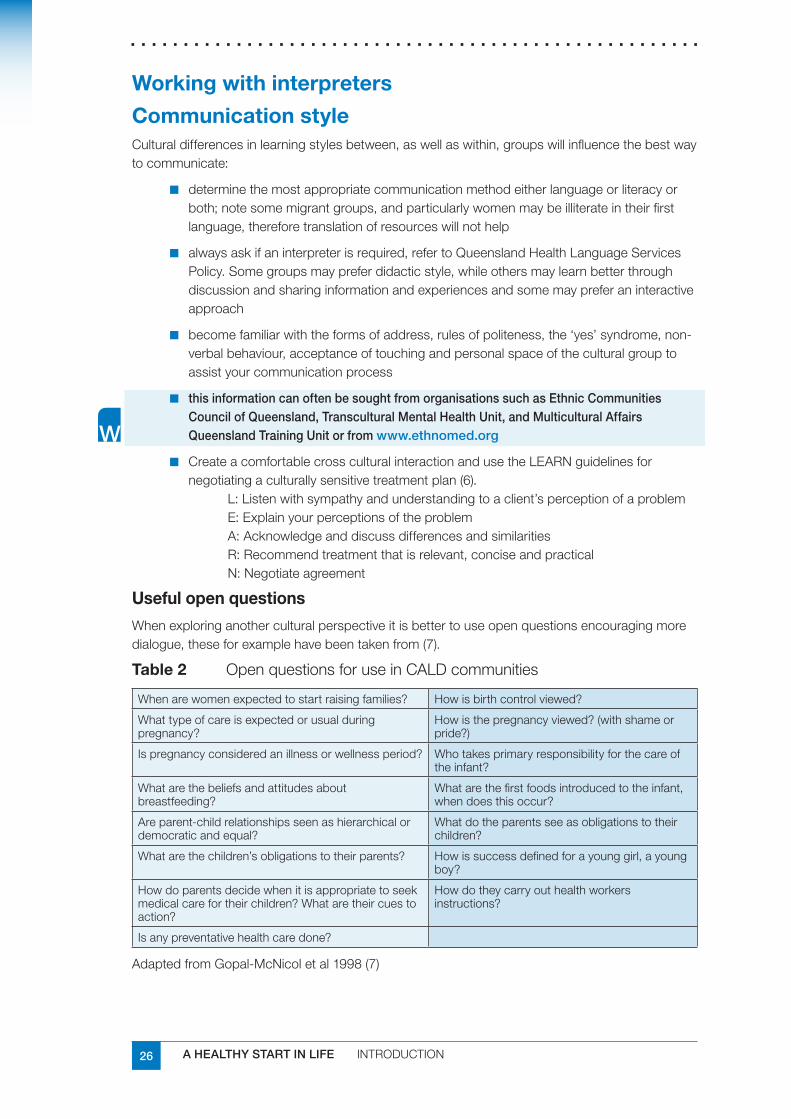
Usefulopenquestions
Whenexploringanotherculturalperspectiveitisbettertouseopenquestionsencouragingmoredialogue,theseforexamplehavebeentakenfrom(7).
Table2 OpenquestionsforuseinCALDcommunities
Whenarewomenexpectedtostartraisingfamilies? Howisbirthcontrolviewed?
Whattypeofcareisexpectedorusualduringpregnancy?
Howisthepregnancyviewed?(withshameorpride?)
Ispregnancyconsideredanillnessorwellnessperiod? Whotakesprimaryresponsibilityforthecareoftheinfant?
Whatarethebeliefsandattitudesaboutbreastfeeding?
Whatarethefirstfoodsintroducedtotheinfant,whendoesthisoccur?
Areparent-childrelationshipsseenashierarchicalordemocraticandequal?
Whatdotheparentsseeasobligationstotheirchildren?
Whatarethechildren’sobligationstotheirparents? Howissuccessdefinedforayounggirl,ayoungboy?
Howdoparentsdecidewhenitisappropriatetoseekmedicalcarefortheirchildren?Whataretheircuestoaction?
Howdotheycarryouthealthworkersinstructions?
Isanypreventativehealthcaredone?
AdaptedfromGopal-McNicoletal1998(7)
27A HEALTHY START IN LIFE INTRODUCTION
Nutritionalrisks
Whenworkingwithpeoplefromrefugeebackground,itisimportanttonotetheymayhavesub-optimalnutrition,nutritionaldeficiencies(eg.iron,folate,VitaminD),undetectednutritionalproblemssuchaspoororalhealth,limitedexposuretodietandlifestylehealthpromotionmessages,problemsassociatedwithinadequatewaterintake(eg.headaches/constipation),reducedornoappetiteandgrowthanddevelopmentalproblemsinchildrenduetopastdeprivation.
Encouragewomenofchildbearingagetotakeafolatesupplement✔■
StresstheimportanceofdrinkingwaterandthesafesupplyinAustralia.✔■
Discussstrategiesforrebuildingappetite,forbothadultsandchildren.✔■
Checkfornutritionaldeficiencies,VitaminDisnotuncommonespeciallypeoplewho✔■
aredark-skinned,veiledandthoseforwhomthebodyhaslittleexposuretothesunbecauseofthestyleofclothing.
Promoteexclusivebreast-feedingforatleastthefirst6months,asnewarrivalsdonot✔■
seeAustralianwomenbreastfeedingsoregularly,somebelieveyouarenotallowedtobreastfeedinAustralia(8).
Beawaresomepeoplemayhavelimitedunderstandingofbasicdietaryprinciples,✔■
shoppingandcookingskillsandrequireassistance.
Supportnewarrivalstore-establishhealthyfoodandlifestyleroutines.Muchofthe✔■
healthyfoodinAustraliaisunfamiliartopeoplefromCALDbcommunities,particularlyinhowtoprepareit.Anappropriate,safeandhealthyfoodforchildren’sschoollunchboxisasignificantissueforparents.
Demonstrateaninterestin,andrespectof,people’straditionalfoodsandassociated✔■
rituals.Forexample,peanutbutterandhalvaareeatenby‘tenthousandsofchildren’inthetreatmentofmalnutritionfrom6monthsofage(9).
ReligionWhenworkingwithpeoplefrommigrantbackground,theinfluenceofreligionislikelytohaveasignificantimpactoneatinghabits,ritualsassociatedwithpregnancy,breastfeedingandchildrearing.ForexampleIslamicbeliefsandpracticesraiseimportantissuesinrelationtotheprovisionofhealthservices.ManyMuslimparentswanttobeabletocontinueobservingandpracticingtheirreligionwhentheyareinhospital,forexample,byhavingaquietplacetoprayandbyeatinghalal food(10).HealthworkersneedtounderstandtheinfluenceIslamcanhaveonshapingnewparents’needsforantenatalandpostnatalservices.InsensitivitytotheseissuescanadverselyaffectMuslimwomen’suseofmaternitycare.
28 A HEALTHY START IN LIFE INTRODUCTION
Casestudies:anAfricanwomannewtoAustraliaAyen,whenIfirstmetherwasamotheroftwoyoungchildrenaged6yrsand18months,andninemonthspregnantandcomplainedoftiredness.AyenwasanAcholispeakingSudanesewhohadaverygoodunderstandingofEnglish.Shehadworkedasanurseintherefugeecamp,butherqualificationswerenotrecognisedinAustralia.AyenwasmarriedtoGorengandrequiredhispermissiontoleavethehouse.GorengandAyenleasedamotorcarnecessaryforGorengtogainwork,thisexpenseandtheirrentedhomeleftlittlemoneyforfood,clothingandpersonalneeds.Ayensaidsheregularlyonlyhadonly$50topurchasefoodforherfamilyoffourandsoontobefive.Ayen,avegetarian,wouldoftenmissmealsallowingsufficientfoodforherhusband.DuringherpregnancyAyenaskedifshecouldeatthedirt,geophagiaiscommoninAfrica.Ayenunderstoodtheneedtovisitthedoctorregularlyduringherpregnancy,butwouldoftenmisstheappointments.Itiscustomaryjustbeforethebirthofhernewchild,thatayounggirlofabout18yearsisorganisedtostaywithsoontobemumsbythewomenintheircommunity.Thisgirlwouldlearnthewaysofearlyinfantcareandcarefortheyoungergirls,howeverAyenalthoughSudanesedidnothavemanyofher‘tribe’tohelpherout.Onarrivalathomefromhospital,Ayenconstantlycarriedtheinfantorrestedinbedwithhimandwouldbreastfeedondemand,theinfantwasrarelywithouthismother.Ayenbreastfedhernewbornforapproximately2months,beforedecidinghershedidnothaveenoughgoodqualitymilkandstartedcomplementingwithformula.Ataround5monthstheinfantwaseatingatypeofporridge,meatandsomevegetables.
Thechildwhowas18months,wouldconstantlyguzzlefromabottleofmilk,heappearedchubbyandhappy,butheateverylittleofthefamilymeal.Theyounggirlwhowasattendingprimaryschoolwouldaskhermothertobuybrightlycolouredpacketsofbiscuitsandpoppersforschoollunch,becauseshesaidtheAustralianchildrentookthoseintheirlunchbox.
NutritionalrisksidentifiedAyenhaslimitedsupportfromthecommunityduetoherlanguagedifferenceasmost✔■
oftheSudaneseareDinkaspeakers.ThislackofsupportforhouseholdchoresandshoppingpossiblycontributetoAyenbeingtired.Sudanesemengenerallydonotassistwiththecookingorotherhouseholdchores.
Ayenhadlimitedfinancestopurchasesufficienthealthyfoodforherfamilyoffour.✔■
Avegetariandietneedstobewellbalancedtoensureadequateprotein,ironandzinc.ThemultiplepregnanciesandlifeinrefugeecampmaymeanAyenisanaemic.
Ayenisunfamiliarwiththefoodstopackinherdaughter’slunchboxanddoesnotusea✔■
waterbottlethatcouldbefrozenovernightfortemperaturecontrolofthelunchfoodortoprovideahealthierfluidthancordial.
Achildof18monthsofageshouldbedrinkingmilkfromacup(ifnotbreastfed)and✔■
haveupto2cupsperdayallowingtheconsumptionofotherfoods(andtextures)providingessentialmicronutrientsnotfoundinmilk.Thislinkprovidesacolourfulbrochure“Teach your baby to drink from a cup”in4languages.www.mhcs.health.nsw.gov.au/mhcs/topics/Infant_and_Child_Feeding.html
Theyounginfantismissingtheopportunitytoreceiveexclusivelybreastmilkforthefirst✔■
6monthsofhislife,mostlyduetofactorsthatcanbecontrolled.
29A HEALTHY START IN LIFE INTRODUCTION
UsefulwebsitesandresourcesGoodFoodforNewArrivals:
www.asetts.org.au/nutrition.htm
ThisWesternAustralianwebsiteprovidesavarietyofresourcesforuseinschoolandcommunitysettings,manysuitableforlowliterateaudiencethatmaybedownloadedorordered.ResourcesavailablespecificallyforSudaneseonanaemia,appetiteandhealthylunchboxes.
NourishingNewCommunities:
www.health.qld.gov.au/multicultural/health_workers/support_tools.asp
ThisQueenslandwebsiteprovidesresourcesforuseinbothschoolandcommunitysettingswithfamiliesandstudents.Resourcesinclude,culturallyappropriateshoppinglistsandmenuplansformajorrefugeegroups,healthylunchboxresourcesincludingdrinkingwaterpromotion.
NSWMulticulturalHealthCommunicationService:
ThisNewSouthWaleswebsiteprovidesnumerousresourcesforhealthprofessionals.
www.mhcs.health.nsw.gov.au/
VictorianHealthTranslations
TranslatedhealthinformationonthisVictorianwebsiteprovidesnumerousresourcesforhealthprofessionals.
www.mhcs.health.nsw.gov.au/
30 A HEALTHY START IN LIFE INTRODUCTION
ReferencesChalmers,S.2006.1. Culture, Health and Parenting in Everyday Life.UniversityofWesternSydney.NSW.
Small,M.1997.2. Our babies, ourselves.NaturalHistory,Oct.,pp.42-51.
Ackerman,L.1997.3. Health Problems of Refugees.JAmericanBoardFamilyPractice10(5)pp337-348.
ABS,2001.CensusofPopulationandHousing4.
WoodenM.,HoltonR.,&SloanJ.,(1994)5. Australian Immigration: ASurvey of the Issues,AGPS:Canberra.
Berlin&Fowkes,19836.
Gopaul-McNicol,S.&Brice-Baker,J.1998.7. Cross-Cultural Practice, Assessment, Treatment and Training.JohnWiley&Sons:USApp39-41
GoodFoodforNewArrivals,2007.8. Breastfeeding in Africa and Australia.NewsletterVol3,Issue7April2007.AssistingTortureandTraumaSurvivors.WesternAustralia.www.asetts.org.au/nutrition.htmAccessedApril11th,2007.
Patel,M.,etal.2005.9. Supplemental feeding with ready-to-use therapeutic food in Malawian children at risk of malnutrition.JHealthPopulationNutrition,Dec23(4)pp351-7.www.bioline.org.br/request?hn05047AccessedApril11th,2007.
Balarajan,R.,Raleigh,V.S.,1995,10. Ethnicity and Health, DepartmentofHealth.HMSO,London.
AWorldofFood,Amanualtoassistintheprovisionofculturallyappropriatemealsfor11.olderpeople,1995.www.culturaldiversity.com.au/Resources/ServiceProviderResources/FoodServices/tabid/88/Default.aspx AccessedApril11th,2007.
Davidson,N.,etal.12. An issue of access: Delivering equitable health care for newly arrived refugee children in Australia.J.Paediatr.ChildHealth,40,pp569-575.
DiversityFigures.MulticulturalAffairsQueensland,CommunityEngagementDivision,13.DepartmentofthePremierandCabinetandtheOfficeofEconomicandStatisticalResearch,QueenslandTreasury
www.multicultural.qld.gov.au14. AccessedApril10th,2007.
EasingtheTransition,Aresourceguideforhealthandsettlementworkerssupporting15.thoserecentlyarrivedinAustraliatomaintainahealthydietandlifestyle,2000.VictorianFoundationforSurvivorsofTortureInc.
Gopalkrishnan,N.2005.16. Cultural Diversity and Civic Participation in Queensland,CentreforMulticulturalandCommunityDevelopment
UniversityoftheSunshineCoast.SippyDowns,Queensland.17.
Munns,C.etal.2006.18. Prevention and treatment of infant and childhood vitamin D deficiency in Australia and New Zealand: a consensus statement.MedicalJournalofAustralia,185,5,pp268–272.
NHMRC,2006.19. Cultural Competency in Health. A guide for policy, partnerships and participation.Canberra.ACT.www.nhmrc.gov.au/publications/synopses/hp25syn.htmAccessedApril11th,2007.
Renzaho,A.M.N.,&Burns,C.2006.20. Post-migration food habits of sub-Saharan African migrants in Victoria: A cross sectional study.Nutrition&Dietetics,63,pp91-102.
Sivagnanam,R.2004.21. Experiences of Maternity Services: Muslim Women’s Perspectives, MaternityAlliance,NHS.UK
31A HEALTHY START IN LIFE INTRODUCTION
1.9 Aboriginal and Torres Strait Islander nutritionCurrenthealthandnutritionalstatus“Queenslandishometo27%ofthenationalIndigenouspopulation…numericallyQueenslandhasthesecondlargestIndigenouspopulation”(1)inAustralia,behindNewSouthWales.IndigenousQueenslandersincludebothAboriginalandTorresStraitIslanderpeoples,twoculturallydistinctIndigenousgroups.
AboriginalandTorresStraitIslanders’viewsofhealthtendtobecomprehensiveandholisticandemphasisesocial,emotionalandculturalwell-being.Traditionally,theymakelittledistinctionbetweenthewellbeingoftheindividualandthewellbeingofthecommunity.
Anexampleofthisistheconceptofhealth;Aboriginallanguagesdonotcontainexpressionsforhealth(2).SicknessorinjuryinanindividualAboriginalpersonislikelytobeinterpretedinrelationtoitseffectontheperson’sabilitytofulfilsocialandothercommunitycommitments.
Secondlythemethodsofacquisitionofhealthknowledgeneedtobeunderstood.“AboriginalandTorresStraitIslanderpeoples,likemanyotherIndigenouspeoples,haveculturally-specificwaysofknowingabouthealth:storiesfromoraltradition,authoritativeknowledgeofelders,spiritualknowledge,commonsensemodelsofillnessandhealth,andknowingoneself”(2).
Thirdly,amongAboriginalandTorresStraitIslanderpeoples,personalidentityisdefinedintermsofkinshipandotherrelationshipswithpeople,communitiesandnature,especiallyland.
Health is not just the physical wellbeing of the individual but the social, emotional and cultural wellbeing of the whole community. This is a whole-of-life view and it also includes the cyclical concept of life-death-life (2).
Alltheavailableevidencesuggeststhat,traditionally,IndigenousAustralianswerefitandhealthy(3)andlivedinharmonywiththeenvironment.Withthetransitionofatraditionalhuntergathererlifestyletoasettledwesternisedexistence,AboriginalandTorresStraitIslanderpeople’sdiethasgenerallychangedfromavaried,nutrient-densediettoanenergy-densedietthatishighinfatandrefinedsugars(3).
TheissuesfacingtheIndigenouspeopleofAustraliaarewelldocumented,withconsistentevidenceinthepastdecadeshowinghealthdisparitiesincreasing.Indigenouslifeexpectancyis15-20yearslessthanthatofnon-IndigenousAustralians.InfantmortalityisthreetimeshigherinIndigenousinfantswhencomparedtonon-Indigenousdata(5).Additionally,AboriginalandTorresStraitIslanderchildrenarealmostfivetimesmorelikelytodiebeforetheageoffiveasnonIndigenouschildren(4).
“The statistics of infant and perinatal mortality are our babies and children who die in our arms…. The statistics of shortened life expectancy are our mothers and fathers, uncles aunties and elders who live diminished lives and die before their gifts of knowledge and experience are passed on” (4).
Goodmaternalnutritionandadequatenutritionduringinfancyarefundamentaltotheachievementandmaintenanceofhealththroughoutthelifecycleandassistsinpreventingchronicdiseasessuchasdiabetesandcardiovasculardisease.
Lowbirthweight,failuretothriveandinappropriatechildgrowthareseriousconcernsinIndigenousAustraliancommunities(3).Severalcausalfactorsareimplicatedincludingmaternalillhealth,smokingandmalnutrition(6).
AboriginalandTorresStraitIslanderpeoplearelesslikelytoeatadietconsistentwiththedietaryguidelinesandmorelikelytosufferfrombothovernutritionandundernutrition.Theimpactofpastpoliciesandpractices,economicdisadvantageandthe‘introduced’dietaremajorcausesofpoorhealthoutcomes(7).
32 A HEALTHY START IN LIFE INTRODUCTION
RecommendationsfromtheDietary Guidelines for Australians
Choosestoreboughtfoodthataremostliketraditionalbushfoods✔■
Enjoytraditionalbushfoodswheneverpossible✔■
Encourage the whole family to include a variety of nutritious foods.
Use the Aboriginal and Torres Strait Islander Guide to Healthy Eating as a resource.
ProtocolsforengagingwithAboriginalandTorresStraitIslandercommunities(8)KIndlyadaptedfromProtocolsforconsultationandnegotiationwithAboriginalpeople(8)
EachAboriginalandTorresStraitIslandercommunityhastheirownlocalprotocols.Theseshouldbeadheredtowhenyouareseekingtoengagewithindividualpeopleorgroupswithinthecommunity.Therearesomebroadguidelineswhichmayassistwhenseekingtoconsultforthefirsttime.
Hints-general
beopen,honestandsincereandtakeagenuineinterestinpeople✔■
genuinerespectforlocalbeliefs,opinionsandlifestyleisessential✔■
beawarethatinsomecommunitiessomepeoplemaynotbecomfortablewithdirect✔■
eyecontactandyouwillneedtomodifyyourbehaviouraccordingly
itisimportantthatyouallowplentyoftimetodevelopthecontextofyour✔■
communicationtoensurethereisanunderstandingofwhatyouwanttodiscuss
Hints-Communication
speakclearly,withoutusingjargon,acronymsortechnicalterms✔■
hintsandinvitationstovolunteerinformationarepreferredtodirectquestioning✔■
speakinamoderatetone;avoidtryingtobeforcefulorspeakingloudly✔■
inadialoguewithanAboriginalandTorresStraitIslanderperson:✔■
listencarefullywithoutinterruptionuntiltheotherpersonhasfinishedspeakingthismay✔■
takesometime—beattentiveandpatient
whenreplying,paraphrasewhathasbeensaidtoclarifytheotherspeaker’smeaning✔■
andtoindicatethatyouarelisteningandunderstandwhathasbeensaid
respectandlearntobecomecomfortablewithsilencesincommunication,particularly✔■
whenseekingorsharinginformationofasensitivenature
recognisethetendencyofAboriginalandTorresStraitIslanderpeopletosay‘yes’in✔■
answertoadirectquestion
recognisethepartplayedbynon-verbalcommunicationandbodylanguagein✔■
AboriginalandTorresStraitIslandercommunicationBeawareofyourownbodylanguageandnon-verbalcommunicationandbesuretolook,aswellaslistenforaresponse
33A HEALTHY START IN LIFE INTRODUCTION
Hints-genderissues
Recognisethatinsomecommunitiestherearemattersthataredesignatedas‘men’s✔■
business’and‘women’sbusiness’.Seekadvicefromakeycommunitymemberbeforediscussingsuchsensitivematters.Likewise,sensitiveissuesshouldonlybeapproachedbymembersofthesamegender.
Hints-talkingtofamilies
Wherepossible,speaktomembersofyourowngenderastheremaybeprotocolsfor✔■
communicationwiththeoppositesex.
Worktowardsbuildingrelationshipsanddon’texpectpeopletoacceptyouimmediately.✔■
Beconsciousofverbalandnon-verbalcuesbeforeintroducingthepurposeofyourvisit,✔■
especiallywhendiscussingmattersofasensitivenature.
Takealocalcommunitymemberwithyouonyourfirstvisit,oraskforakeycommunity✔■
membertointroduceyou.
Trytobeopen-mindedandflexibleinyourcommunication.✔■
AntenatalnutritionComparedwithotherAustralianmothers,Aboriginalmothersaretwiceaslikelytogivebirthtolowbirthweightbabies(13).LowbirthweightisalsoanissueamongTorresStraitIslanderpeopleyetinlowerproportionsthanAboriginalpeople.
Anaemiaiscommonforanumberofreasonseg.poornutrition,multiplepregnancies.✔■
Folicaciddeficiencyiscommonlyseenamongthisgroup.✔■
Increasedincidenceofinfantmortality.✔■
Increasedincidenceofmultiplepregnancies.StudiesshowAboriginalwomenhave✔■
higherfertilityrates.Multiplepregnanciesdonotallowsufficienttimeforthemothers’nutrientstorestobereplenishedbetweeneachpregnancy.Multiplepregnanciesalsoencourageanincreaseinweight.Witheachpregnancy,weightincreasessincethereisashortenedtimetoreturntoprepregnancyweight.
Highincidenceofteenagepregnancies.✔■
Lactoferrinconcentrationsarereducedinthebreastmilkofmalnourishedmothers.✔■
Lactoferrinisanironbindingproteinwithantibacterialproperties,andreduced✔■
concentrationsmayrenderinfantsmoresusceptibletoinfection
Theincidenceofoverweightishighinthisgroupduetohighintakesoffoodswhichare✔■
highinfat,sugarandsalt(suchastakeawaysandconveniencefoods).Inisolatedareasaccesstoaffordablefreshfoodsisoftenlimited.
LackofcookingfacilitiescanimpactonthenutritionalintakeofIndigenouspeople.✔■
ItisessentialtodiscusswithAboriginalandTorresStraitIslanderwomenandtheir✔■
families,waysofensuringgoodnutritionduringpregnancy.
34 A HEALTHY START IN LIFE INTRODUCTION
RefertoGrowing Strongtopics
healthymums✔■
pregnancyissues✔■
keepingfoodsafe✔■
howtobreastfeed✔■
expressingbreastmilk✔■
diabetesduringpregnancy*✔■
alcohol,tobaccoandotherdrugsduringpregnancyandbreastfeeding*✔■
physicalactivityduringandafterpregnancy*✔■
youngmums*✔■
howdadscanhelp*✔■
howgrandparentscanhelp*✔■
*Topicsincludedintheupdatein2007
Breastfeeding“Breastfeedingisassociatedwithareducedinfantandchildmortalityandisincreasinglyrecognisedasfundamentalforlongtermhealth”(9).Thenutritionalandimmunologicaleffectsofprolongedbreastfeedingareparticularlyimportantincommunitieswithahighprevalenceofinfectiousdiseases(3,6).
DurationofbreastfeedingNationalbreastfeedingdataforIndigenousAustraliansislimited.The1995NationalHealthSurveyfoundthatIndigenousmothersbreastfedlongerthannon-Indigenousmothers(3).Traditionally,Aboriginalmothersbreast-fedtheirbabiesexclusivelyandfrequentlyforatleast6months,andcontinuedtobreastfeedforupto4years(10).
However,IndigenousAustralianshavelowerbreastfeedinglevelsthannon-IndigenousAustralians,exceptwheremoretraditionallifestyleshavebeenmaintained.“InQueensland,70.5%ofIndigenousmalesand69.7%ofIndigenousfemalesundertheageof13hadbeenbreastfedasaninfant”(9).
InaBrisbanestudyitwasnotedthatalthough59%ofIndigenousmothersinitiatedbreastfeeding,only25%werestillbreastfeedingby6months(6).AnotherstudyinMelbournefound‘mostmotherswhostarttobreastfeedplantodosoforatleast6months,soitislikelythatthosewhostoppedsoonerhadencounteredproblems…womensaidthatmostwouldwanttobreastfeedforatleastayear(10)(Table1).
Furthermore,astudyinWesternAustraliafoundAboriginal“mothersunderstoodthebenefitsofbreastfeedingbutneededsupportandassistancetoenablethemtoinitiateandcontinuebreastfeedingforanoptimalperiodoftime”(7).
WhatyoucandoFocusgroupdiscussionswithAboriginalpeopleinMelbourneidentifiedthatmostAboriginalwomenwantedandexpectedtobreastfeed.Theyperceivedtheircommunityassupportiveofbreastfeeding,thoughtheyoftenlackedpeopletoturntoforadviceandsupport(9,10)
You,asahealthprofessionalcanprovideinvaluableassistancetonewmotherswhentheystartbreastfeeding.Itisimportanttoprovideculturallyappropriate,factualinformation,sympatheticsupportandincludedemonstrationsofpracticalskills.ItisimportanttoensureAboriginalandTorresStraitIslanderfamiliesareawareof,andarecomfortableaccessingculturallyappropriatesupportserviceswithintheircommunityforcontinuedsupport.
35A HEALTHY START IN LIFE INTRODUCTION
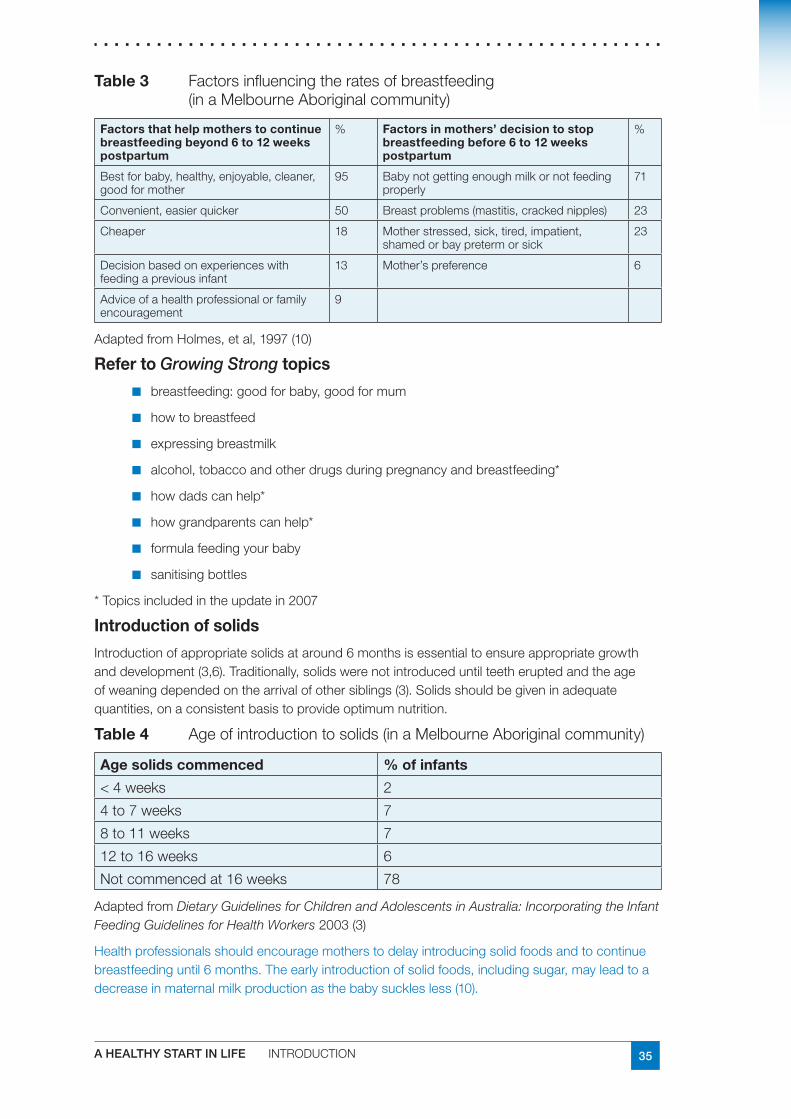
Table3 Factorsinfluencingtheratesofbreastfeeding(inaMelbourneAboriginalcommunity)
Factorsthathelpmotherstocontinuebreastfeedingbeyond6to12weekspostpartum
% Factorsinmothers’decisiontostopbreastfeedingbefore6to12weekspostpartum
%
Bestforbaby,healthy,enjoyable,cleaner,goodformother
95 Babynotgettingenoughmilkornotfeedingproperly
71
Convenient,easierquicker 50 Breastproblems(mastitis,crackednipples) 23
Cheaper 18 Motherstressed,sick,tired,impatient,shamedorbaypretermorsick
23
Decisionbasedonexperienceswithfeedingapreviousinfant
13 Mother’spreference 6
Adviceofahealthprofessionalorfamilyencouragement
9
AdaptedfromHolmes,etal,1997(10)
RefertoGrowing Strongtopics
breastfeeding:goodforbaby,goodformum✔■
howtobreastfeed✔■
expressingbreastmilk✔■
alcohol,tobaccoandotherdrugsduringpregnancyandbreastfeeding*✔■
howdadscanhelp*✔■
howgrandparentscanhelp*✔■
formulafeedingyourbaby✔■
sanitisingbottles✔■
*Topicsincludedintheupdatein2007
Introductionofsolids
Introductionofappropriatesolidsataround6monthsisessentialtoensureappropriategrowthanddevelopment(3,6).Traditionally,solidswerenotintroduceduntilteetheruptedandtheageofweaningdependedonthearrivalofothersiblings(3).Solidsshouldbegiveninadequatequantities,onaconsistentbasistoprovideoptimumnutrition.
Table4 Ageofintroductiontosolids(inaMelbourneAboriginalcommunity)
Agesolidscommenced %ofinfants
<4weeks 2
4to7weeks 7
8to11weeks 7
12to16weeks 6
Notcommencedat16weeks 78
AdaptedfromDietary Guidelines for Children and Adolescents in Australia: Incorporating the Infant Feeding Guidelines for Health Workers2003(3)
Healthprofessionalsshouldencouragemotherstodelayintroducingsolidfoodsandtocontinuebreastfeedinguntil6months.Theearlyintroductionofsolidfoods,includingsugar,mayleadtoadecreaseinmaternalmilkproductionasthebabysucklesless(10).
36 A HEALTHY START IN LIFE INTRODUCTION
RefertoGrowing Strongtopics
startingsolids✔■
ironrichfoods✔■
drinksforbabies*✔■
*Topicsincludedintheupdatein2007
Growth
Dietary Guidelines for Children and Adolescents in Australia Recommendations
Ensurethegrowthofyoungchildrenischeckedregularly
13percentofIndigenousbabiesborninAustraliaareoflowbirthweight(4)
Normalgrowthresultsfromthecombinedeffectsoffavourablegeneticandenvironmentalinfluences…whenthesefactorsarecompromised,growthofthefoetus,infantandyoungchildislikelytobeinadequate(9).
Forgrowthassessment,refertogrowthchartsection.
GrowthfalteringamongstAboriginalinfantsaftertheageoffourto6monthshasbeenconsistentlynoted(3,6).Relativelypoorgrowthhasbeenshowntopersistinolderchildren,althoughoverweightandobesityarebecomingincreasingconcerns,particularlyamongTorresStraitIslanderchildren(6).
DiarrhoealandrespiratoryinfectionsinAboriginalandTorresStraitIslanderinfantshavethemostsignificantimpactongrowth(5).
Childrenhaveanin-builthungeralertandsatietymechanism,sotheyknowwhentheyarehungryandwhentheyarefull,andtheyeataccordingly.Ahealthychildwillneverstarveitself,soencourageparentstotrusttheirchildtoeatenough.AtraditionalpracticeamongAboriginalpeopleistowaituntilachilddemandsfoodbeforebreastfeedingorgivingotherfoods.Thistraditionwillnotadverselyaffectawellnourishedchild.
However,lackofhungerandapathyarecommonresultsofmildmalnutrition.Hence,childrenwhohaveevenmildgrowthfailuremaynotbeveryhungryandneedtobeencouragedtoeat.Theywouldbedisadvantagediftheirmotherswaitedforsignsofhungerbeforefeedingthem(9).
RefertoToddlersection
RefertoGrowthchartsection
RefertoGrowingStrongtopics
growthspurts*✔■
overweightandobesityinchildren*✔■
healthyfoodforage1–4years*✔■
healthydrinksforage1–4years*✔■
healthyfoodideasfortoddlers*✔■
37A HEALTHY START IN LIFE INTRODUCTION
Lactoseintolerance
Lactoseintoleranceaftertheageofthreetofiveyearsmaybeproblematicinsomeareasorindividuals(3,11)andmayaffectconsumptionoflactosecontainingfoods.
AsmallstudyinWesternAustraliafound70%ofchildrenagedbetween6and14werefoundtobelactosemalabsorbers(12).
RefertoLactoseIntolerancesection
Irondeficiency
StudiesinNewSouthWalesandtheTopEndoftheNorthernTerritoryshowedtherateofanaemiainAboriginalchildrentobemuchhigherthaninnon-Aboriginalchildren(9).Irondeficiencymayremainmoreofaproblemamongstchildren,particularlyinurbanareas,whencomparedtocommunitiesinremoteareas,whereironintakemaybehighduetoamoretraditionalmeatbaseddiet(9).
RefertoGrowingStrongtopics
ironrichfoods✔■
UsefulwebsitesandresourcesNHMRC Dietary Guidelines for Children and Adolescents in Australia
National Aboriginal and Torres Strait Islander Nutrition Strategy and Action Plan 2000-2010.
Nutrition in Aboriginal and Torres Strait Islander Peoples: An Information Paper NHMRC, 2000
Close the Gap: Solutions to the Indigenous Health Crisis facing Australia. A policy Briefing paper from the national Aboriginal Community Controlled Health Organisation and OXFAM Australia, 2007
Professionaldevelopmenttools
Communicatingpositively:AguidetoappropriateAboriginalTerminology.NewSouthWalesHealth,2004
www.health.nsw.gov.au
ProtocolsforconsultationandnegotiationwithAboriginalpeople
DepartmentofAboriginalandTorresStraitIslanderPolicyandDevelopment2000,PublishedbyQueenslandGovernment,Brisbane
www.qld.gov.au/indigenous/ www.datsip.qld.gov.au/resources/cultures.cfm
Healthyjarjumsmakehealthyfoodchoices
ThisprogramisaimedatteachingyoungAboriginalandTorresStraitIslanderchildrenaboutfoodsthataregoodfortheirbodies,sothattheymayimprovetheirqualityoflifethroughbetternutrition.Theprogramisdesignedtoguideandassisteducatorsbypresentingsuggestedactivities,lessonsandresources.
www.health.qld.gov.au/eatwellbeactive/documents/jarjum_notice.pdf
38 A HEALTHY START IN LIFE INTRODUCTION
Indigenoustraditionalgames
Traditionalgamesprovidetheopportunitytolearnabout,appreciateandexperienceaspectsofAboriginalculture.Theyalsoprovideessentialtraininginsocialinteraction.Itispossibletoincludetraditionalgamesinclassroomlessons,outdooreducationandadventureactivities,physicaleducationclassesandsporteducationactivities.www.health.qld.gov.au/eatwellbeactive/documents/jarjum_notice.pdf.
OneTalk
Queensland Health’s Aborignal and Torres Strait Islander Community Engagement Manual,2005.
Parenthandouts
The Aboriginal and Torres Strait Islander Guide to Healthy Eating
Thisguideshowshowmuchfoodisrequiredeverydayfromeachfoodgroupforgoodnutritionandhealth.Thefoodsincludedintheguidearethosethatcanbefoundatthestoreaswellassomelocalbushandseafoods.Thisguidehelpsyoutomakehealthyfoodchoiceswww.health.qld.gov.au/eatwellbeactive/documents/atsig_the_brochure.pdf www.health.qld.gov.au/eatwellbeactive
AnoteonGrowing Strong
TheGrowing StrongresourceshavebeendevelopedtohelpstafftalkwithIndigenousfamiliesaboutnutritionformothers,babiesandyoungchildren.Informationispresentedintwoforms:abookusingstraightforwardlanguageandplentyofillustrations,andamanualwithmoredetailedbackground.
Growing Strongresourcesprovideinformationabouteatingwellduringpregnancyaswellasofferingsuggestionsfordealingwithsomecommonfoodandnutritionelatedproblems.Informationisalsoprovidedaboutcommonbreastfeedingissuesincludinghowtoknowwhenababygetsenoughbreastmilkandcorrectpositioningandattachment. Growing Strongresourcesarecurrentlybeingupdated.Topicsincludedintheupdatein2007asdenotedwithanasterisk(*).
FormoreinformationaboutGrowingStrongcontact:
NutritionPromotionOfficer(IndigenousHealth)NorthernAreaHealthServicePublicHealthNutritionTeamPOBox1103CairnsQLD4870Ph (07)40503600Fax (07)40503662
NutritionPromotionOfficer(IndigenousHealth)CentralAreaHealthServicePublicHealthNutritionTeamPOBox946RockhamptonQLD4700Ph (07)49207383Fax (07)49206865
IndigenousNutritionPromotionOfficerBrisbaneSouthsidePopulationHealthUnitPOBox333ArcherfieldQLD4108Ph (07)30009148Fax (07)30009121

39A HEALTHY START IN LIFE INTRODUCTION
ReferencesTheIndigenousPopulationofQueensland.PlanningInformationandForecastingUnit1.PlanningServices.Brisbane,August2000
TheNationalAboriginalHealthStrategy,1989,AGPS2.
Dietary Guidelines for Children and Adolescents in Australia: Incorporating the Infant 3.Feeding Guidelines for Health Workers,NHMRC,Canberra2003.
ClosetheGap:SolutionstotheIndigenousHealthCrisisfacingAustralia.ApolicyBriefing4.paperfromthenationalAboriginalCommunityControlledHealthOrganisationandOXFAMAustralia
NationalAboriginalandTorresStraitIslanderNutritionStrategyandActionPlan5.2000-2010.
QueenslandPublicHealthForum(2002).6. Eat Well Queensland 2002–2012: Smart Eating for a Healthier State.Brisbane,QueenslandPublicHealthForum.
EadesS.,TheBibbulungGnarneepTeam‘BreastfeedingAmongUrbanAboriginal7.WomeninWesternAustralia’AboriginalandIslanderHealthWorkerJournal24(3)2000pp9-14
DepartmentofAboriginalandTorresStraitIslanderPolicyandDevelopment2000,8.ProtocolsforconsultationandnegotiationwithAboriginalpeople,PublishedbyQueenslandGovernment,Brisbane.
NutritioninAboriginalandTorresStraitIslanderPeoples:AnInformationPaperNHMRC,9.2000
HolmesW.,PhillipsJ.,ThorpeL.,Initiationrateanddurationofbreastfeedinginthe10.MelbourneAboriginalcommunity.AustralianandNewZealandJournalofPublicHealth1997:21(5)pp500-3
ButtenshawR.,SheridanJ.,TyeV.,MillerO.,CarseldineJ.,BattistuttaD.,GaffenyP/.11.LawrenceG.,LactoseMalabsorptionanditstemporalstabilityinAboriginalChildren.Proc.NutAust(1990)15pp228
BrandJ.C.,Darnton-HillI.,GraceyM.S.,SpargoR.M.,LactoseMalabsorptioninAustralian12.AboriginalChildrenAmJClinNutr1985;41:620-622
JohnstonT.,CooryM.,InformationCircular,EpidemiologyServicesUnit,Health13.InformationBranch.Trendsinperinatalmortality,birthweightandgestationalageamongAboriginalandTorresStraitIslander,andnonIndigenousbabiesinQueensland.
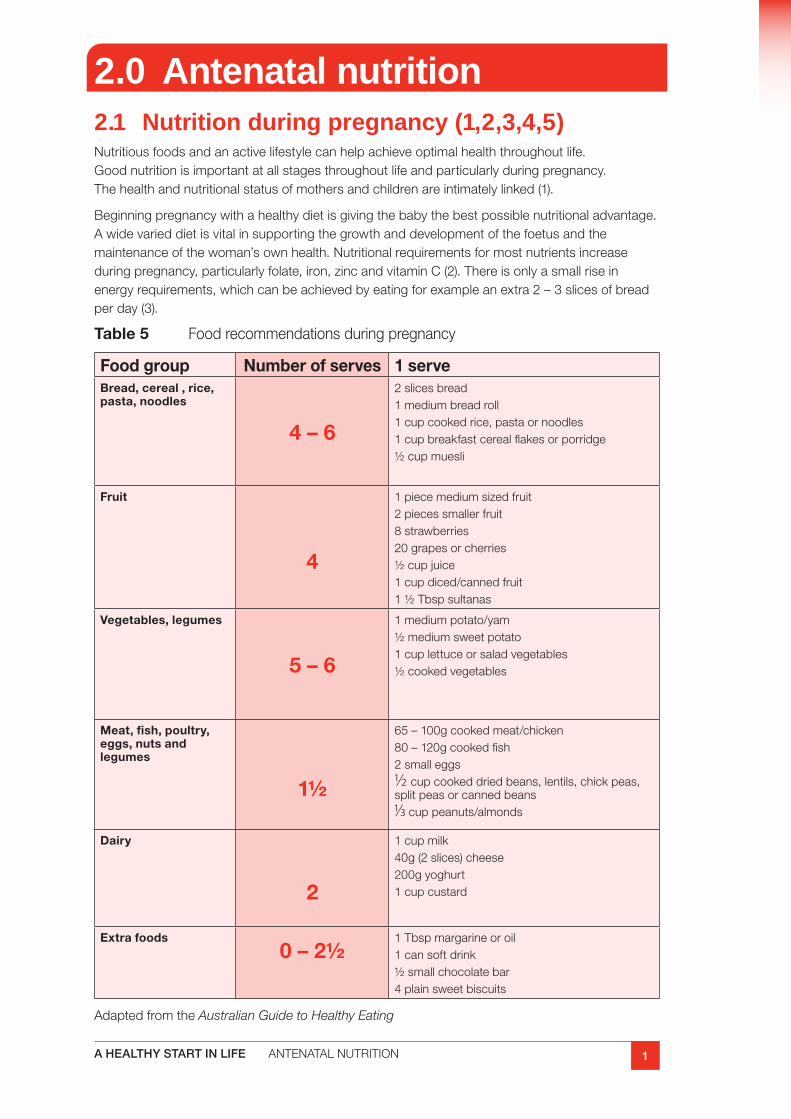
1A HEALTHY START IN LIFE ANTENATALNUTRITION
2.0 Antenatal nutrition2.1 Nutrition during pregnancy (1,2,3,4,5)Nutritiousfoodsandanactivelifestylecanhelpachieveoptimalhealththroughoutlife.Goodnutritionisimportantatallstagesthroughoutlifeandparticularlyduringpregnancy.Thehealthandnutritionalstatusofmothersandchildrenareintimatelylinked(1).
Beginningpregnancywithahealthydietisgivingthebabythebestpossiblenutritionaladvantage.Awidevarieddietisvitalinsupportingthegrowthanddevelopmentofthefoetusandthemaintenanceofthewoman’sownhealth.Nutritionalrequirementsformostnutrientsincreaseduringpregnancy,particularlyfolate,iron,zincandvitaminC(2).Thereisonlyasmallriseinenergyrequirements,whichcanbeachievedbyeatingforexampleanextra2–3slicesofbreadperday(3).
Table 5 Foodrecommendationsduringpregnancy
Food group Number of serves 1 serveBread, cereal , rice, pasta, noodles
4 – 6
2slicesbread1mediumbreadroll1cupcookedrice,pastaornoodles1cupbreakfastcerealflakesorporridge½cupmuesli
Fruit
4
1piecemediumsizedfruit2piecessmallerfruit8strawberries20grapesorcherries½cupjuice1cupdiced/cannedfruit1½Tbspsultanas
Vegetables, legumes
5 – 6
1mediumpotato/yam½mediumsweetpotato1cuplettuceorsaladvegetables½cookedvegetables
Meat, fish, poultry, eggs, nuts and legumes
1½
65–100gcookedmeat/chicken80–120gcookedfish2smalleggs1/2 cupcookeddriedbeans,lentils,chickpeas,splitpeasorcannedbeans1/3cuppeanuts/almonds
Dairy
2
1cupmilk40g(2slices)cheese200gyoghurt1cupcustard
Extra foods0 – 2½
1Tbspmargarineoroil1cansoftdrink½smallchocolatebar4plainsweetbiscuits
Adaptedfromthe Australian Guide to Healthy Eating
2 A HEALTHY START IN LIFE ANTENATALNUTRITION
2.2 Sample meal planThe following examples illustrate how the Australian Guide to Healthy Eating can be incorporated into a daily meal plan to meet minimum nutritional requirements.
Breakfast
1cupbreakfastcerealflakes/1cupporridge
Milk(250ml)
1cupstrawberries/1freshorange/½grapefruit
Morning tea
2ricecakes/1slicetoastwith1slicecheeseandtomato
Lunch
Salmon/eggortuna/andsaladbreadroll
1piecefreshfruit
Afternoon tea
1scone
½cupfruitjuice
Dinner
1smallsteak(100g)withmixedvegetables(total1½cups)
1smallpotato
1cupfruitsaladwith2Tbspyoghurt
Supper
2slicesraisintoast,scrapemargarine
Parenthandoutsavailableat
qheps.health.qld.gov.au/ahwac/content/home_nemo.htm
3A HEALTHY START IN LIFE ANTENATALNUTRITION
Folate during pregnancyFolateisaBgroupvitaminneededforhealthygrowthanddevelopment.Itsrequirementsareincreasedduringpregnancyfornormalgrowthoftheunbornbaby.Adequatefolateintakehelpstopreventneuraltubedefectsinthebaby,suchasspinabifida(2).
Thevitaminisknownasfolatewhenitisfoundnaturallyinfoodandasfolicacidwhenitisaddedtofoodorusedindietarysupplements(4).
Therecommendedintakeofdietaryfolateforpregnantwomenis600µg/daythroughoutpregnancy.However,toreducethelikelihoodofneuraltubedefectsinthebaby,itisrecommendedthatwomenconsumeanadditional400µg/dayfolicacidthroughasupplementorintheformoffortifiedfoodsforatleast1monthbeforeand3monthsafterconceptioninadditiontoconsumingfoodfolatefromavarieddiet(2).
Itisdifficulttogetenoughfolatefromnaturalsourcesalonetoreducetheriskofneuraltubedefectsinpregnancy.Folicacidsupplementsareavailableoverthecounter.Womenwhohaveafamilyhistoryofneuraltubedefectslikespinabifidarequiremedicaladvicebeforebecomingpregnant(4)astheymayneedevenhigheramountsoffolicacid.
Goodsourcesoffolateincludeleafyvegetables,wholegrains,fortifiedcereals,peas,nuts,avocadosandyeastextracts(egMarmite, Promite, Vegemite etc).
Forfurtherinformationandparenthandouts:
www.foodstandards.gov.au/foodmatters/pregnancyandfood.cfm
Checkdiet contains rich sources of folate before and during pregnancy✔✔
advise women to take folate supplements for 1 month before conception ✔✔and during the first trimester of pregnancy
if dietary intake is poor, consider continuing folate supplement after ✔✔the first trimester
folic acid intakes should not exceed 800 – 1000 µg/day.✔✔
4 A HEALTHY START IN LIFE ANTENATALNUTRITION
Iron during pregnancyIronisacomponentofhaemoglobin,thecomponentofbloodwhichcarriesoxygenaroundthebody.Thepeakironrequirementinpregnancyoccursthroughoutthesecondandthirdtrimesters.Thisistosupporttheexpansionofthematernalredbloodcellmass,thegrowingfoetusandtheplacenta.Alackofironmayresultinanaemia.Womenwhosedietpriortopregnancywaslowiniron,mayhavelowironstores.Thisincreasestheirriskofdevelopingirondeficiencyanaemiaduringpregnancy.Dietaryironisusedbythegrowingbabyfirst,leavingthemother’sstoresdepletedifherintakeisinadequate.Lowironlevelsinearlypregnancyhavebeenlinkedtoprematurebirthandlowbirthweight.
TheRDIforironinpregnancyis27mg/day(5).Amixeddietofanimalandplantfoodscanhelpyouachieveyourironintake.AbsorptionofironisbetterfromanimalfoodscomparedtoplantsourcesandtherecommendeddietaryintakesarebasedonamixedWesterndiet.
Therearetwotypesofironinfood:ironfromanimalfoods(calledhaemiron)andironfromplantfoods(callednon-haemiron).
Haemironistakenupbythebodyabout10timesbetterthannon-haemiron.Meatsarethebestsourceofiron.Theredderthemeat,thehigheritisiniron.Thismeansbeefandlambarehigherinironthanpork,chickenorfish.Colouredfleshfish,suchastunaandmulletarehigherinironthanreeffish,suchasbarramundi.
Non-haemironisfoundinsomeplantfoodssuchas:
wholegrainandironfortifiedbreadsandcerealsfoods,eg.breakfastcereal✔■
withaddediron
legumes,eg.kidneybeans,bakedbeans✔■
greenleafyvegetables,eg.spinachandbroccoli✔■
nutsanddriedfruit.✔■
Rememberthatironfromthesefoodsisnottakenupbythebodyaswellasironfromanimalfoods.Youwillneedtoeatmoreofthesefoodsiftheyareyouronlyironsource.
AddingaglassoffruitjuiceorotherfoodsrichinvitaminC(suchastomato,broccoliorcapsicum)toamealwillincreasetheamountofironthebodyabsorbs.Incontrast,tea,coffeeandunprocessedbrancaninhibitironabsorption.
Indicators of iron deficiency
Ironstatusisdeterminedbymeasuringbloodlevelsofhaemoglobin,serumferritinandserumtransferrin.Serumferritinisthebestindicatorofironstores.Lowserumferritinlevelsindicatedepletedironstores.Haemoglobinisnotasensitiveindicatorofironstatus,withlevelsdecreasingoftenonlywhenferritinstoresareseverelydepleted.Inaddition,haemoglobinlevelsdecreaseduringthethirdtrimesterofpregnancyduetohaemodilutioneffects.Ferritinlevelsremainunchangedduringthistime.Serumtransferrintransportsironintheblood.Transferrinvaluesincreasewithirondeficiencyanddecreasewithironoverload.Ironintakeshouldbeincreasedwhenserumferritinlevelsarelow.Ideallythedietshouldbeexaminedforadequateironintake.Ifthedietappearstoprovideadequateirondespitelowferritinlevels,supplementsmaybeconsidered.
5A HEALTHY START IN LIFE ANTENATALNUTRITION
Checkif serum ferritin levels are low, iron intake needs to be increased✔✔
iron supplements may cause constipation. Constipation may be minimised ✔✔by consuming adequate intakes of dietary fibre and fluid. Foods from the meat/meat alternatives group provide the best sources of iron. Vegetarians need to consume vitamin C rich foods with meals to increase iron vabsorption and eat a good variety of non-haem iron sources.
IodineTheRDIforiodineinpregnancyis220ug/day(5).Iodinedeficiencyinpregnancycanaffectgrowthanddevelopmentintheunbornchild,increasethechanceofmiscarriageandhaveseriousimplicationsforintellectualdevelopment.Iodinecanbefoundindairyproductsiemilkandyoghurt,breadbakedwithiodisedsaltandsaltwaterfish.Itisveryimportantformotherstoconsumesufficientiodinefromthetimeofconception,justasitisforthemorewell-knownnutrientsofironandfolate(5).
Multivitamin supplementsApartfromtherecommendedfolatesupplement,itisbesttoobtainnutrientsfromahealthydiet.MultivitaminsnotdesignedforpregnancyarenotrecommendedastherearedangersassociatedwithexcessivedosesofnutrientssuchasVitaminsA,DandB6(2).
Alternative and herbal remediesMostherbalandhomeopathicremedieshavenotbeentestedtodeterminetheirsafetyduringpregnancy.Manyherbalpreparationshaveadrug-likeeffectandshouldbeusedwiththesamecautionaswithotherdrugsduringpregnancy.Herbalpreparationsshouldbeavoidedduringthefirsttrimester.TheNationalPrescribingService(NPS)Medicineslinecanprovideinformationregardingalternativetreatmentsinpregnancy,phone1300888763.
Patienthandoutsavailableat
qheps.health.qld.gov.au/ahwac/content/home_nemo.htm
6 A HEALTHY START IN LIFE ANTENATALNUTRITION
2.3 Special considerations during pregnancyListeriaListeriaarebacteriacarriedinsomefoodsthatcancauseaninfectioncalledlisteriosis.Thebacteriacommonlyinhabitsoil,water,plantsandsewerage.Theinfectionmaycausefewornosymptomsinhealthypeople,includingpregnantwomen.However,theriskoftransmissionfromtheinfectedpregnantwomantoherunbornchildishigher.Infectionofthefoetuscanleadtomiscarriage,stillbirth,prematurebirthorsevereillnessinnewbornbabies(2).
Thebestwaystoavoidlisteriainfectionsincludehygienicpreparation,storingandhandlingoffood.Foodsshouldbeeatenfresh,orthoroughlycooked,orwellwashedifeatenraw(fruitandvegetables).Leftoverscanbeeateniftheyhavebeenrefrigeratedimmediatelyandstoredforlessthan24hours.
Thefoodsmostlikelytocarrythebacteria,increasetheriskofinfectionandthereforeshouldbeavoided,include:
softandsemisoftcheeses,eg.brie,camembert,ricotta,blue,fetta✔■
softserveicecream✔■
unpasteuriseddairyproducts✔■
pate✔■
chilledseafood✔■
salads-fruit/vegetable,eg.prepared,prepackaged,smorgasbord/saladbars✔■
coldmeats,includingchicken,eg.deli,sandwichbars,andpackagedready-to-eat.✔■
Healthy tips
always wash hands before preparing or serving food and after handling ✔✔animals or visiting the toilet
animals can carry the toxoplasmosis parasite which can cause disease in ✔✔humans so keep them out of the kitchen; avoid touching faeces and wear rubber gloves under garden gloves
wash cookware and utensils well after use ✔✔
store raw foods down low in the fridge and check fridge temperature ✔✔regularly
foods and leftovers that belong in the fridge should always be refrigerated ✔✔as soon as possible
thaw frozen meats in the fridge ✔✔
once cooked, pasta and rice should be stored in the fridge ✔✔
look for ‘best before’ and ‘use by’ dates on packaged foods.✔✔
Forfurtherinformation:
www.foodstandards.gov.au/foodmatters/pregnancyandfood.cfm
7A HEALTHY START IN LIFE ANTENATALNUTRITION
MercuryFishisasafeandimportantpartoftheAustraliandiet.Itcontainsanexcellentsourceofprotein,islowinsaturatedfat,highinomega3fishoilsandisanexcellentsourceofiodine.Therehasbeensomeconcernregardingthelevelofmercuryinfish,specificallyaccumulationofmercuryinfishthatarehigherupthefoodchain.
Food Standards Australia and New Zealand(FSANZ)advisespregnantwomen,andwomenplanningpregnancy,toeatavarietyoffishaspartofahealthydiet.However,pregnantwomenshouldlimittheirintakeofcertaintypesoffish.
Table 6. Recommendationsoffishconsumptionduringpregnancy
Pregnantwomenandwomenplanningpregnancy(1serve=150g)
1serveper fortnight ofshark(flake)orbillfish(swordfish/broadbillandmarlin)andNOotherfishthatfortnight
OR
1serveperweek oforangeroughy(deepseaperch)orcatfishandNOotherfishthatweek
OR
2–3servesperweekofanyotherfishandseafoodnotlistedabove
AdaptedfromFood Standards Australia and New Zealand
Forfurtherinformation:
www.foodstandards.gov.au/foodmatters/pregnancyandfood.cfm
CaffeineCaffeineisachemicalfoundinmanyfoodsanddrinks,includingcoffee,teaandcola.Itaffectsthenervoussystemandcancauseirritability,nervousnessandsleeplessness.Duringpregnancyittakeslongertobreakdowncaffeine.
Whilehavinglargeamountsofcaffeinedoesnotappeartocausebirthdefects,drinkinghighamountsofcaffeinemaymakeitmoredifficulttobecomepregnantandmayincreasetheriskofmiscarriage.
Itisbesttolimitthedailyamountofcaffeineto:
2cupsofcoffee,or✔■
4cupsoftea,or✔■
4cupsofcoladrink,or✔■
lessthan1cupofcolaorenergydrinksthatcontainextracaffeine,or✔■
decaffeinatedvarietiesareanoptionwhichcontainslittlecaffeinehoweversafelevelsof✔■
decaffeinatedproductsforpregnantwomenareunknown.
(ReproducedwiththepermissionofCommonwealthDepartmentofHealthandAgeing)
Artificial sweetenersTheuseofonlysomeartificialsweetenersisconsideredtobesafeduringpregnancy.FSANZhaslistedaspartame(marketedinfoodproductsasEqual, Hermesetas and Nutrasweet)andsucralose(Splenda)assafetouseduringpregnancy(2).
8 A HEALTHY START IN LIFE ANTENATALNUTRITION
AlcoholDuringpregnancyalcoholcrossestheplacentaandcanleadtophysical,growthandmentalproblemsinsomebabies.Babiesaffectedbyalcoholtendtohavelowbirthweights.Theymayalsohavephysicalandbehaviourproblemsatbirthandthroughoutchildhood.(2)
Therearenoknownsafelevelsofalcoholconsumptioninpregnancy.Therefore,itisbesttoavoiddrinkingalcoholduringpregnancyasmuchaspossible.
The Australian National Health and Medical Research Council (NHMRC) has made the following recommendations for women who are pregnant or planning a pregnancy:
Women may consider not drinking alcohol at all
It is most important not to become intoxicated
Women who choose to drink should have less than 7 standard drinks per week
Women should have at least 2 alcohol free days a week
On any 1 day no more than 2 standard drinks should be consumed. These drinks should be spread over at least 2 hours.
Drinkinglargerquantitiesatanyonetimemayaffectthedevelopingfoetalbrain.
1standarddrinkisequalto:✔■
100mlwine✔■
1‘pot’ofbeer(285ml)✔■
1can/stubbie(375ml)lowalcoholbeer✔■
1nipofspirits(30ml)✔■
60mlfortifiedwine(portorsherry).✔■
Checkalcohol consumption is reduced to nil where possible. If alcohol is consumed, ✔✔the intake should not exceed more than 2 standard drinks per day.
Morning sicknessMorningsicknessisacommonsymptomofearlypregnancyand,inmanycases,goesawaybytheendofthefirsttrimester.Itiscausedbychangesinhormonesduringpregnancyandmaymakeeatingdifficult.Althoughitiscalled‘morningsickness’,nausea(withorwithoutvomiting)canhappenatanytimeoftheday.Asmallnumberofwomenexperienceseverevomitingwhichcanleadtodehydrationandelectrolyteimbalances.Suchwomenrequiremedicalassistanceandpossiblyhospitaladmissionforcorrection.Inothercases,frequentandprolongednausea/vomitingcanleadtoaninadequateenergyintakewhichresultsinweightloss.Thisweightlossusuallyceasesoncenauseareducesandappetiteimproves.
Checkadequate energy intake to prevent weight loss✔✔
if morning sickness persists with vomiting more than twice daily for more ✔✔than 2 days, medical intervention should be sought as hospitalisation may be required. Ensure adequate fluid replacement to avoid dehydration.
Patienthandoutsavailableat
qheps.health.qld.gov.au/ahwac/content/nemo_review.htm
Thefollowingpagecanbeusedasaparenthandout.
9A HEALTHY START IN LIFE ANTENATALNUTRITION
Morning sickness
Morningsicknessdoesnotusuallycauseanyproblemsfortheunbornbaby.Somefoodandeatingsuggestionsthatmayhelpmanagesymptomsofmorningsicknessornauseainclude:
eatsmallermealsmoreoften.missingmealscanmakenauseaworse✔■
avoidlargedrinks.havefrequentsmalldrinksbetweenmeals✔■
limitfatty,spicyandfriedfoods✔■
foodhasastrongerodourorsmellwhenitisheated,whichmaymake✔■
nauseaworse.ifpossible,haveotherpeoplehelpwithcooking,orprepareyourfoodattimesofthedaywhenyoufeelbetter
tryeatingadrybiscuitbeforeyougetoutofbedinthemorning✔■
eatahealthysnackbeforeyougotobedatnight.thismightincludefruit✔■
(fresh,tinned,dried),crackerswithhardcheeseoryoghurt
avoidfoodsiftheirtaste,smellorappearancemakeyoufeelsick✔■
ifvomiting,itisimportanttodrinkenoughfluids.Itmaybeeasiertohave✔■
lotsofsmalldrinksthantotryanddrinkalargeamountinonego.Tryavarietyoffluidssuchaswater,fruitjuice,lemonadeandclearsoups.Sometimesitcanbehelpfultotrycrushedice,slushies,iceblocksorevensuckonfrozenfruitsuchasgrapesororangesegments.
Note: Thestomachacidsinvomitingcansoftenteethenamel.Itisbestnottouseatoothbrushtocleantheteethstraightaftervomitingasthismaydamagethem.Haveadrinkofwatertocleanyourmouth.
10 A HEALTHY START IN LIFE ANTENATALNUTRITION
ConstipationConstipationiscommoninpregnancyforthefollowingreasons:
Intestinalmuscleappearstolosetone,makingitdifficultforfoodtopassthrough:✔■
thebabyinlatterpregnancy,placespressureontheintestine,exacerbatingtheproblem✔■
ironsupplementationmaycauseconstipationinsomewomen.✔■
Constipationcanbeminimisedbyensuring:adequateexercise✔■
highfibreintake✔■
adequatefluidintake(1.5–2Lperday).✔■
Checkensure adequate fibre intake by eating fruit, vegetables and wholemeal/✔✔wholegrain breads and cereals
ensure adequate fluid intake (ie. 1.5 l/day)✔✔
regular activity ✔✔
regular use of laxatives is not recommended.✔✔
Parenthandoutsavailableathttp://qheps.health.qld.gov.au/ahwac/content/nemo_review.htm
HeartburnHeartburnoccursforanumberofreasonsincluding:
Relaxationoftheoesophagealmusclesduringpregnancy(underhormonalinfluences)✔■
allowsacidtorunintotheoesophagus,andpressurefromthegrowingbabyonthestomachcausesabackflowofacid.Somesuggestionsforreliefofheartburninclude:
Eatsmallermealsfrequently✔■
Chewfoodwell✔■
Avoidfattyandspicyfoodswhichmayirritatethecondition✔■
Drinkfluidsseparatelytomeals✔■
Snackondrybiscuitsortoast✔■
Sippingmilkmayeaseheartburntemporarily✔■
Relaxwhileeating✔■
Avoidlyingdownorbendingoverdirectlyaftermeals✔■
Don’tsmoke✔■
Avoidalcohol✔■
Careneedstobetakentoensurenoneofthefoodgroupsareomittedfromthediet,✔■
sincethiscanreducethenutritionaladequacyofthediet
Someantacidsaresafetotakeduringpregnancy,butmayinhibitironabsorption.✔■
Recommenduseundermedicalsupervision.
Parenthandoutsavailable
qheps.health.qld.gov.au/ahwac/content/nemo_review.htmwww.foodstandards.gov.au/foodmatters/pregnancyandfood.cfm
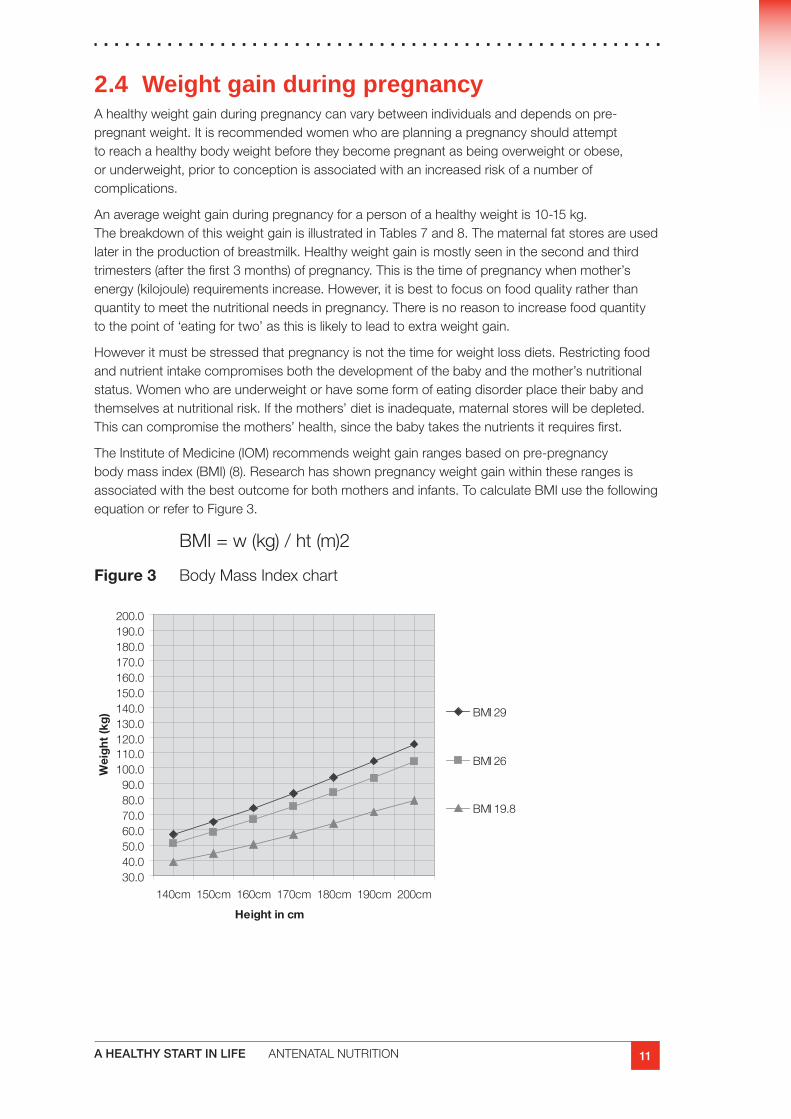
11A HEALTHY START IN LIFE ANTENATALNUTRITION
2.4 Weight gain during pregnancyAhealthyweightgainduringpregnancycanvarybetweenindividualsanddependsonpre-pregnantweight.Itisrecommendedwomenwhoareplanningapregnancyshouldattempttoreachahealthybodyweightbeforetheybecomepregnantasbeingoverweightorobese,orunderweight,priortoconceptionisassociatedwithanincreasedriskofanumberofcomplications.
Anaverageweightgainduringpregnancyforapersonofahealthyweightis10-15kg.ThebreakdownofthisweightgainisillustratedinTables7and8.Thematernalfatstoresareusedlaterintheproductionofbreastmilk.Healthyweightgainismostlyseeninthesecondandthirdtrimesters(afterthefirst3months)ofpregnancy.Thisisthetimeofpregnancywhenmother’senergy(kilojoule)requirementsincrease.However,itisbesttofocusonfoodqualityratherthanquantitytomeetthenutritionalneedsinpregnancy.Thereisnoreasontoincreasefoodquantitytothepointof‘eatingfortwo’asthisislikelytoleadtoextraweightgain.
Howeveritmustbestressedthatpregnancyisnotthetimeforweightlossdiets.Restrictingfoodandnutrientintakecompromisesboththedevelopmentofthebabyandthemother’snutritionalstatus.Womenwhoareunderweightorhavesomeformofeatingdisorderplacetheirbabyandthemselvesatnutritionalrisk.Ifthemothers’dietisinadequate,maternalstoreswillbedepleted.Thiscancompromisethemothers’health,sincethebabytakesthenutrientsitrequiresfirst.
TheInstituteofMedicine(IOM)recommendsweightgainrangesbasedonpre-pregnancybodymassindex(BMI)(8).Researchhasshownpregnancyweightgainwithintheserangesisassociatedwiththebestoutcomeforbothmothersandinfants.TocalculateBMIusethefollowingequationorrefertoFigure3.
BMI=w(kg)/ht(m)2
Figure 3 BodyMassIndexchart
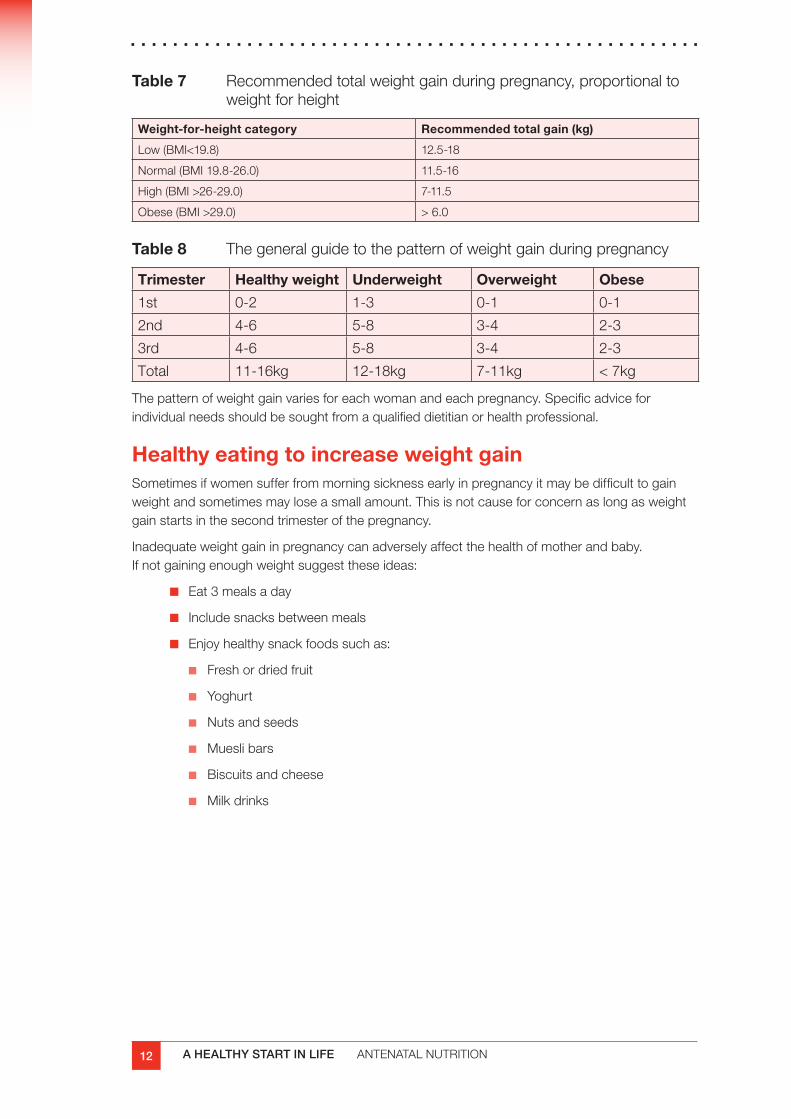
12 A HEALTHY START IN LIFE ANTENATALNUTRITION
Table 7 Recommendedtotalweightgainduringpregnancy,proportionaltoweightforheight
Weight-for-height category Recommended total gain (kg)
Low(BMI<19.8) 12.5-18
Normal(BMI19.8-26.0) 11.5-16
High(BMI>26-29.0) 7-11.5
Obese(BMI>29.0) >6.0
Table 8 Thegeneralguidetothepatternofweightgainduringpregnancy
Trimester Healthy weight Underweight Overweight Obese
1st 0-2 1-3 0-1 0-1
2nd 4-6 5-8 3-4 2-3
3rd 4-6 5-8 3-4 2-3
Total 11-16kg 12-18kg 7-11kg <7kg
Thepatternofweightgainvariesforeachwomanandeachpregnancy.Specificadviceforindividualneedsshouldbesoughtfromaqualifieddietitianorhealthprofessional.
Healthy eating to increase weight gain Sometimesifwomensufferfrommorningsicknessearlyinpregnancyitmaybedifficulttogainweightandsometimesmayloseasmallamount.Thisisnotcauseforconcernaslongasweightgainstartsinthesecondtrimesterofthepregnancy.
Inadequateweightgaininpregnancycanadverselyaffectthehealthofmotherandbaby.Ifnotgainingenoughweightsuggesttheseideas:
Eat3mealsaday✔■
Includesnacksbetweenmeals✔■
Enjoyhealthysnackfoodssuchas:✔■
Freshordriedfruit✔■
Yoghurt✔■
Nutsandseeds✔■
Mueslibars✔■
Biscuitsandcheese✔■
Milkdrinks✔■
13A HEALTHY START IN LIFE ANTENATALNUTRITION
Healthy eating to control weight gain Pregnancyisnotatimeforstrictdieting.However,excessiveweightgainduringpregnancycancauseproblemswithhighbloodpressure,gestationaldiabetesforthemother,alargeforgestationalagebabyanddeliverycomplications.Ifmotherisoverweightitisimportantcontrolweightgaininpregnancy.
Limit the amount of fat eaten
Limitintakeofbiscuitsandcakes✔■
Limitintakeofchipsandcrisps✔■
Reducetheamountoffatusedincooking✔■
Chooselowfatdairyproductsincludingmilk,yoghurt,andcheese✔■
Avoidcreamandsourcream✔■
Trimallthefatoffmeatbeforecooking✔■
Removetheskinfromchicken✔■
Limithighfattake-awayfoods✔■
Limit high sugar foods
Drinkwaternotsoftdrinkorcordial✔■
Use“diet”orlowjouleproducts✔■
Limitfruitjuicestoonceaday,thesearehighinsugar✔■
Limitchocolates,lolliesandsweets✔■
Limitintakeofdesserts✔■
Minimisesnacking✔■
Increasephysicalactivity✔■
Checkweight loss is not recommended during pregnancy✔✔
weight gain education provided based on pre-pregnant BMI.✔✔
Returning to pre-pregnant weight Manywomenareconcernedaboutweightgainedduringpregnancyandarekeentoreturntotheirpre-pregnancyweightassoonaspossibleaftertheirbabyisborn.Itisimportanttorememberthatawoman’snutritionalrequirementsremainincreasedwhilebreastfeeding.Itisessentialthatintakeisnotrestrictedtoapointwherenutritionalrequirementsarenotmet.
Womenwhogainexcessiveweightduringpregnancyareatriskofpostpartumweightretention(9).Thegreatestamountofweightlossoccursinthefirst3monthsafterbirthandthencontinuesataslowandsteadyrateuntil6monthsafterbirth(9).
14 A HEALTHY START IN LIFE ANTENATALNUTRITION
Healthy eating tips for those trying to lose weightExercisingisagoodwayofstimulatingweightloss.Notonlydoesithavephysicalbenefitseg.weightlossandimprovedgeneralhealth,butalsopsychologicalbenefitsforthemother.Theexerciseneednotbevigorous.Infact,regularwalkingisaverygoodformofactivity.Encouragemotherstoexerciseregularly-atleast5timesaweekfor30minutesatatime.
Frequentbreastfeedingcanbebeneficialforweightlossandincreaseswiththelengthofthelactationcourse.
Theextraenergyrequiredtobreastfeedcanoftenbesignificant.Thesurplusfatstoreslaiddownduringpregnancy(ie.aroundhips)canbeusedtomeettheseadditionalenergyneeds.
Encouragemotherstoeatregularmeals.Skippingmealscanresultinsnackingbetweenmeals.Itcanalsoslowdownthebody’smetabolism,makingitmoredifficulttoloseweight.
Avoidchoosingfoodswithahighfatcontentiechooseleancutsofmeat,skinlesschickenandfish;choosecookingmethodsthatuseminimalfat;chooselowfatproductswherepossible;uselessmargarine,butter,oil;avoidcakes,biscuits,chocolates,lollies,cordialsandsoftdrinks.
Healthy eating tips for those trying to gain weightSomewomenalsolosealotofweightwhiletheyarebreastfeedingandfinditdifficulttomaintainanacceptableweight.ThisisNOTanindicationthatbreastfeedingshouldstop.Thefollowinglistsgivesomeideasforgainingandmaintainingweight.
Don’tskipmeals.✔■
Havethreemainmealsandthreebetweenmealsnacks.✔■
Keepeasytopreparenutritioussnacksonhandegcrackersandcheese,freshfruit,✔■
yoghurt,nuts,seeds,driedfruit,cannedbeans,flavouredmilk,fruitsmoothies,breakfastcerealsandmilk.
Prepareapackedlunchorvarietyofsnackstohaveinacontainerbesideyouwhen✔■
babyfeeds.
Prepareandfreezemealsinadvancewhenpossible(oraskyourfriends/familytohelp).✔■
Checkif client is experiencing problems returning to healthy weight range ✔✔recommend consultation with a dietitian/ nutritionist.
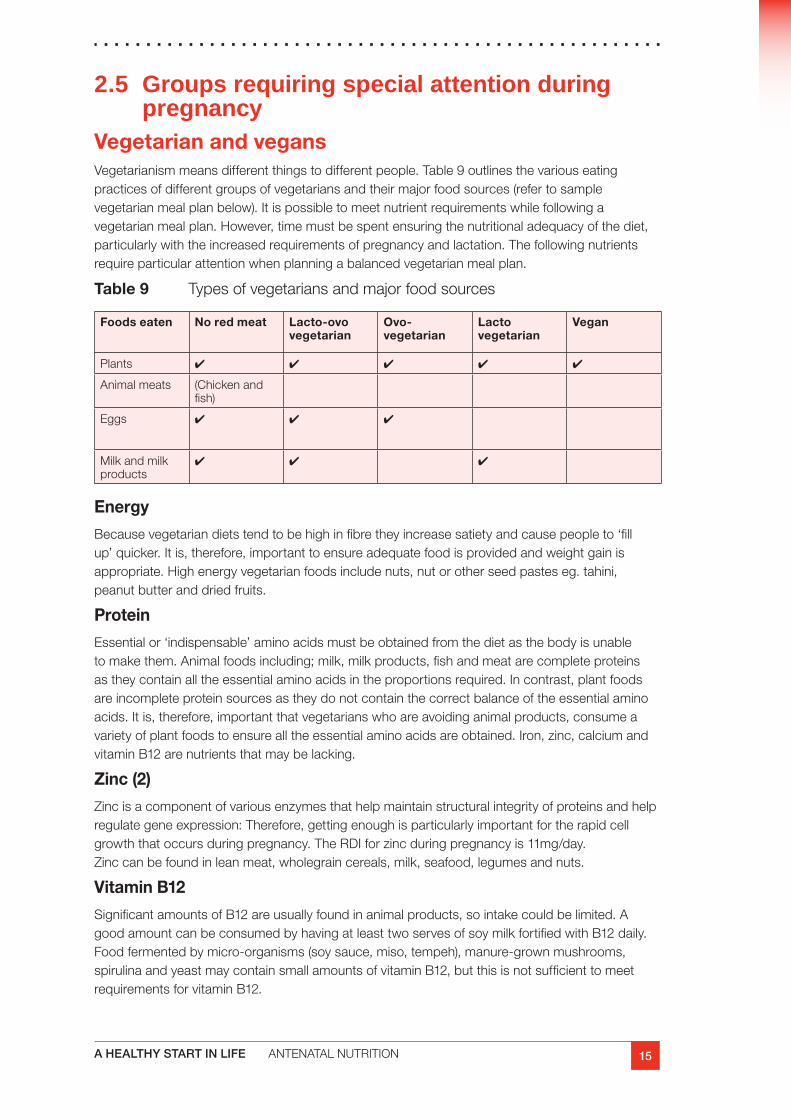
15A HEALTHY START IN LIFE ANTENATALNUTRITION
2.5 Groups requiring special attention during pregnancy
Vegetarian and vegansVegetarianismmeansdifferentthingstodifferentpeople.Table9outlinesthevariouseatingpracticesofdifferentgroupsofvegetariansandtheirmajorfoodsources(refertosamplevegetarianmealplanbelow).Itispossibletomeetnutrientrequirementswhilefollowingavegetarianmealplan.However,timemustbespentensuringthenutritionaladequacyofthediet,particularlywiththeincreasedrequirementsofpregnancyandlactation.Thefollowingnutrientsrequireparticularattentionwhenplanningabalancedvegetarianmealplan.
Table 9 Typesofvegetariansandmajorfoodsources
Foods eaten No red meat Lacto-ovo vegetarian
Ovo- vegetarian
Lacto vegetarian
Vegan
Plants ✔ ✔ ✔ ✔ ✔
Animalmeats (Chickenandfish)
Eggs ✔ ✔ ✔
Milkandmilkproducts
✔ ✔ ✔
Energy
Becausevegetariandietstendtobehighinfibretheyincreasesatietyandcausepeopleto‘fillup’quicker.Itis,therefore,importanttoensureadequatefoodisprovidedandweightgainisappropriate.Highenergyvegetarianfoodsincludenuts,nutorotherseedpasteseg.tahini,peanutbutteranddriedfruits.
Protein
Essentialor‘indispensable’aminoacidsmustbeobtainedfromthedietasthebodyisunabletomakethem.Animalfoodsincluding;milk,milkproducts,fishandmeatarecompleteproteinsastheycontainalltheessentialaminoacidsintheproportionsrequired.Incontrast,plantfoodsareincompleteproteinsourcesastheydonotcontainthecorrectbalanceoftheessentialaminoacids.Itis,therefore,importantthatvegetarianswhoareavoidinganimalproducts,consumeavarietyofplantfoodstoensurealltheessentialaminoacidsareobtained.Iron,zinc,calciumandvitaminB12arenutrientsthatmaybelacking.
Zinc (2)
Zincisacomponentofvariousenzymesthathelpmaintainstructuralintegrityofproteinsandhelpregulategeneexpression:Therefore,gettingenoughisparticularlyimportantfortherapidcellgrowththatoccursduringpregnancy.TheRDIforzincduringpregnancyis11mg/day.Zinccanbefoundinleanmeat,wholegraincereals,milk,seafood,legumesandnuts.
Vitamin B12
SignificantamountsofB12areusuallyfoundinanimalproducts,sointakecouldbelimited.AgoodamountcanbeconsumedbyhavingatleasttwoservesofsoymilkfortifiedwithB12daily.Foodfermentedbymicro-organisms(soysauce,miso,tempeh),manure-grownmushrooms,spirulinaandyeastmaycontainsmallamountsofvitaminB12,butthisisnotsufficienttomeetrequirementsforvitaminB12.
16 A HEALTHY START IN LIFE ANTENATALNUTRITION
A sample vegetarian meal plan:
Breakfast
½cupmueslior2wheatbiscuits
Milk
1slicewholemealtoastwithpeanutbutter
1orange
Morning tea
2wholemealcrackerswithtomatoandcheese
Freshfruit
Lunch
Wholemealroll,1-2cupsofsaladwithanavocado
Milkand2tspMilo
Afternoon tea
½cupalmondsand4Tbspraisins
Dinner
1cupkidneybeans
2-3cupsservesvegetablesincludingbroccoli
Fruityoghurt
Supper
2slicesofraisintoastwithmargarine
Soybeverage,fortifiedwithcalciumandvitaminB12couldreplacemilkinveganmealplans
Check
foods from the meat, fish, poultry, eggs, nuts, legumes groups and iron ✔✔fortified cereals should be consumed each day for adequate iron and zinc intake. Soy beverages should be fortified with calcium (containing at least 115mg per 100mL) and B12
ensure sufficient energy is consumed and appropriate weight gained ✔✔
consider supplementation with a multivitamin (which includes iron, zinc, ✔✔calcium and B12) if needs are not being met
refer to dietitian for individual assessment and advice. ✔✔
17A HEALTHY START IN LIFE ANTENATALNUTRITION
TeenagersThenutrientrequirementsofpregnantteenagersareincreased.Notonlymusttheyeattoprovidethenutrientsrequiredforthepregnancy,butalsotoprovidefortheirowngrowthanddevelopmentduringpuberty.Pregnantteenagersshouldbetreatedasaseparategroup.TherearespecificRDIsforpregnantteenagersbetween14-18years.Girlswithalowgynaecologicalage(differencebetweenageofmenarcheandageatconception)requireadditionalnourishmentastheyareoftenstillgrowing.Eveniftheyhavestoppedgrowing,teenagegirlswithalowgynaecologicalagearelikelytohaveinadequatenutrientstores,becauseittakesabout2yearstobuildupstoresaftermenarch(10).
Itisimportanttoensureteenagemothershaveanappropriateweightgainduringpregnancy.Pregnantadolescentsareatriskofbothinadequateandexcessiveweightgain(11).Theyareatriskforadverseoutcomesincludinglowbirthweight,pretermdelivery,anaemia,andexcessivepostpartumweightretentionduetoacombinationofphysiological,socioeconomic,andbehaviouralfactors(11).Itisworthbearinginmindthatatthistimeinateenager’slife,thereareanumberofotherfactorswhichimpactontheireatingpatterns,forexample:peerpressure,socialsupports,lackofshoppingandcookingskillsandafearofgainingweightandbecoming“fat”.
Aboriginal and Torres Strait Islander womenSeeAboriginalandTorresStraitIslandersection
Obese pregnant womenMaternaloverweightandobesityisnowanimportantissueinaboutonethirdofallpregnanciesintheAustraliancontext(13).Increasedmaternalbodymassindex(BMI)atconceptionisassociatedwitharangeofadversematernal,obstetricandneonataloutcomes.Hypertensivedisordersofpregnancy,impairedglucosemetabolism,gestationaldiabetes,hyperlipidemia,caesareansectiondelivery,prolongedmaternalhospitalization,foetalandneonataldeath,birthdefectsandneonatalintensivecareadmissionareallconsequencesofmaternalobesity(13,14,15).
Overweightandobesityhasbeenassociatedwithreducedinitiationanddurationofbreastfeeding(16,17).Thecausesforthismaybemultifactorial.Factorstoconsiderinpoorlactationperformanceinclude:
Socio-culturalfactors,suchasconcernaboutbodyshape,lowselfesteemandpoor✔■
mentalhealth(16)
Physicalfactorsforexample,womenwithlargebreastsmayhavemechanicaldifficulties✔■
withbreastfeeding(16)
Physiologicalfactorssuchasreducedprolactinresponsetosuckling(18)✔■
Check
overweight and obese women identified as high risk during pregnancy✔✔
advice about appropriate weight gain✔✔
oral glucose tolerance test (OGTT) taken 24 – 28 weeks gestation✔✔
targeted for post partum lactation consultant assistance with ✔✔breastfeeding.
18 A HEALTHY START IN LIFE ANTENATALNUTRITION
Women with diabetes in pregnancy
Pre-existing Type 1 and Type 2 diabetesWomenwithpreexistingdiabetescanhaveahealthyandsuccessfulpregnancy.Howevertheyneedclosemonitoringbyateamincludinganobstetrician,endocrinologist(orphysicianexperiencedindiabetescareduringpregnancy),diabeteseducatoranddietitiantoensurethediabetesiswellmanagedduringthepregnancy.
Womenwithpre-existingdiabeteshaveahigherriskofinfants:
havingabirthdefect;✔■
beingbornprematurely;✔■
havingalowbirthweightorbeingmacrosomic;✔■
havingdangerouslylowbloodsugarlevelsafterbirth.✔■
Itisimportantthatwomencontroltheirbloodsugarlevelsbeforebecomingpregnantandthroughoutthepregnancytominimisetheserisks.
Gestational diabetesInsomewomenduringpregnancytheirabilitytoutiliseglucosebecomesimpaired.Thehormonesproducedbytheplacentacauseinsulinresistance.Ifthebodyisunabletomeettheincreasedneedforinsulingestationaldiabetesdevelopusuallyaroundthe24th–28thweekofgestation.
Gestational diabetes is more likely to occur in (19):
Women over 30 years of age✔■
Women with a family history of Type 2 diabetes✔■
Women who are overweight✔■
Aboriginal and Torres Strait Islander women✔■
Certain ethnic groups are also at increased risk: Indian, Chinese, Polynesian/Melanesian, ✔■
Vietnamese, Middle Eastern
Women who have had gestational diabetes during previous pregnancies✔■
Women who have had difficulty carrying a pregnancy to term.✔■
GestationaldiabetesisdiagnosedafteraGlucoseChallengeTest(GCT)whichisascreeningtest.IfthisisabnormalanOralGlucoseToleranceTest(OGTT)isnecessary.
Ifgestationaldiabetesisuntreatedthereisincreasedriskofalargeforgestationalagebaby,deliverycomplicationsandlowbloodsugarlevelsofthebabyatbirth.
There are four basic components to treatment of gestational diabetes: dietary modifications, physical activity, medications and monitoring blood glucose levels.
These women should be referred to a dietitian for individualised nutritional advice. The most important points are for regular carbohydrate distribution and low glycemic index (GI) diet.
After the birth of the baby, the mother’s blood sugar levels should return to normal and an OGTT at around 6 weeks post partum should be done to confirm this.
Women who develop gestational diabetes are at increased risk of developing Type 2 diabetes later in life with a 30% – 50% chance of developing it within 15 years after pregnancy (19).
19A HEALTHY START IN LIFE ANTENATALNUTRITION
2.6 Exercise during pregnancy (20,21,22)Regularexerciseduringpregnancyisinmostcases,safeforbothmotherandbaby.Womenshouldbeencouragedtoinitiateorcontinueexerciseduringthistimetoobtainthehealthbenefitsassociatedwithsuchactivities.
Adoctor,physiotherapistorexercisephysiologistcanprovideindividualadviceforwomenaboutexerciseduringpregnancy.
Benefits of exercising regularly throughout pregnancy include:
resistancetofatigue✔■
reducedbackpain,constipation,bloatingandswelling✔■
improvedposture✔■
improvedweightcontrol✔■
stressrelief✔■
improvedsleep✔■
preparationforphysicaldemandsoflabour✔■
fasterrecuperationafterlabour✔■
fasterreturntopre-pregnancyfitnessandhealthyweight.✔■
Body changes during pregnancy
Hormonesproducedduringpregnancy,suchasrelaxin,softentheligamentsthatsupportjoints,resultinginjointsbeingmoremobileandincreasingtheriskofjointinjury.
Extraabdominalweightshiftsthebody’scentreofgravity,placingstressonthepelvisandlowerbackjoints,andcanaffectbalance.
Pregnancyincreasesrestingheartrate.
General exercise suggestions
Aimfor4to5exercisesessionsperweek.✔■
Don’ttrytoexercisetoofarbeyondcurrentfitnesslevel.✔■
Warmupandcooldownforaround10minutes.✔■
Trytoexerciseonsoftsurfaces,suchasgrassorcarpet.✔■
Avoidexercisinginthemiddleofthedayorhothumidconditions—takecarenotto✔■
overheat.
Maintainamoderateintensity—keepheartratebelow140beatsperminute.✔■
Restfrequently,particularlyiffeelingbreathless.✔■
Wearasupportivebraandfootwear.✔■
Wherecool,loosefittingclothing.✔■
Changepositionsslowlyandgradually.✔■
20 A HEALTHY START IN LIFE ANTENATALNUTRITION
Suggested activitiesWater activities✔■
Walking ✔■
Swimming✔■
Yoga✔■
Dancing✔■
Pilates✔■
Pregnancy exercise classes✔■
Cycling on a stationary bike✔■
Exercises to avoidContactsportsorthoseactivitieswherethereispotentialforlossofbalancethatcould✔■
resultintraumatobaby.
Exercisinginwaterwherethetemperatureisgreaterthan32ºC.✔■
Activitiesthatinvolvejolting,jarringorrapidchangesofdirection,particularlyinthelatter✔■
stagesofpregnancy.
After16weeksavoidactivitiesinvolvinglyingflatonback—theweightoftheuterusand✔■
babycompressthemainarterybacktotheheart.Thiscanlowerbloodpressureandresultinfeelingsofdizzinessandlightheadedness.
Scubadiving-babiesarenotprotectedfromdecompressionsickness.✔■
Don’texercisewhenill.✔■
Conditions requiring medical supervision while exercising in pregnancy
Cardiacdisease✔■
Restrictivelungdisease✔■
Persistentbleedinginthesecondandthirdtrimesters✔■
Pre-eclampsiaorpregnancy-inducedhypertension✔■
Pretermlabour(previous/present)✔■
Intrauterinegrowthrestriction✔■
Cervicalweakness/cerclage✔■
Placentapraeviaafter26weeks✔■
Pretermprelabourruptureofmembranes✔■
Heavysmoker(morethan20cigarettesaday)✔■
Orthopaediclimitations✔■
Poorlycontrolledhypertension✔■
Extremelysedentarylifestyle✔■
Unevaluatedmaternalcardiacarrhythmia✔■
Chronicbronchitis✔■
Multiplegestation(individualisedandmedicallysupervised)✔■
Poorlycontrolledthyroiddisease✔■
Malnutritionoreatingdisorder✔■
Poorlycontrolleddiabetesmellitus✔■
Poorlycontrolledseizures✔■
Anaemia.✔■
21A HEALTHY START IN LIFE ANTENATALNUTRITION
Warning signs to cease exercise
Excessiveshortnessofbreath✔■
Chestpainorpalpitations✔■
Pre-syncopeordizziness✔■
Painfuluterinecontractionsorpretermlabour✔■
Leakageofamnioticfluid✔■
Vaginalbleeding✔■
Excessivefatigue✔■
Abdominalpain,particularlyinbackorpubicarea✔■
Pelvicgirdlepain✔■
Reducedfetalmovement✔■
Dyspnoeabeforeexertion✔■
Headache✔■
Muscleweakness✔■
Calfpainorswelling✔■
Medicaladviceshouldbesoughtifanyoftheabovesymptomsoccur.
Pelvicfloorexerciseshouldbedonebefore,duringandafterpregnancy.
Careshouldbetakenwithbacksupport.
Wheneverchangingposition,bendingandlifting:
tightenabdominalmuscles-particularlythetransverseabdominalmusclewhichformsa✔■
naturalcorsetinthelowerpartoftheabdomen
tightenpelvicfloormuscles✔■
uselegmuscles.✔■
Informationsheetcanbefoundat:
www.betterhealth.vic.gov.au
Check
women have no contraindications to exercise✔✔
advise of benefits of exercising in pregnancy✔✔
inform of criteria to cease exercise.✔✔
22 A HEALTHY START IN LIFE ANTENATALNUTRITION
2.7 Antenatal breastfeeding education Healthprofessionalsoftenleavediscussionofbreastfeedinguntillaterinthepregnancy.Researchdemonstratesthattheearlierinthepregnancyadecisiontobreastfeedismadethemorelikelythebreastfeedingwillbesuccessful(23).Thedecisionisusuallymadebeforepregnancyandisbasedonlifeexperiences,beliefsandattitudesoffamilyandotherstobreastfeeding(24).
Antenatal education should include:
importance of exclusive breastfeeding for the first 6 months ✔■
(including the nutritional and protective benefits)
basic breastfeeding management✔■
coping with minor problems (23). ✔■
Mothersshouldbeencouragedtobecomefamiliarandcomfortablewithhandlingtheirbreasts(23).
Virtuallyeverymothercanbreastfeed,butforsomeitisnotsoeasyandlearningandpatiencearenecessary(23).
Benefits of breastfeeding for mother
Helpsuterusreturntopre-pregnantstatefaster✔■
Canhelpwithweightlossafterbaby✔■
Reduceslikelihoodofovarianandpremenopausalbreastcancer✔■
LessenslikelihoodofmotherswithgestationaldiabetesdevelopingType2diabetes(24).✔■
Formula feeding increases the risk of baby developing:
Infectionsanddiseasessuchasurinarytractinfections,gastrointestinalinfections(eg.✔■
diarrhoea)andrespiratoryillnesses(eg.asthma)andsomechildhoodcancers
Allergiesandfoodintolerancessuchascoeliacdisease✔■
Obesity,diabetesandheartdiseaselaterinlife.✔■
Benefits of breastfeeding to the community
Reducedhealthcarecostsfromillnessandchronicdiseaseprevention✔■
Reducedecologicaldamagefromproduction,packaging,anddisposalofbreastmilk✔■
substitutesandcontainers.Italsosavesfoodresources,fuelandenergy.
23A HEALTHY START IN LIFE ANTENATALNUTRITION
Guide to educationEarly pregnancy
Ask questions ‘how do you plan to feed your baby?’•✔
Importance of decision about feeding choice•✔
Assess knowledge and perceptions regarding breastfeeding•✔
Reasons mothers choose•✔
Explore and identify concerns and feelings •✔
Acknowledge and validate feelings•✔
Educate using targeted messages to address individual concerns•✔
Benefits of breastfeeding (infant, mother, community)•✔
Risks of formula-feeding•✔
Ease of breastfeeding, difficulties that may be encountered•✔
Breastfeeding with modesty•✔
Family involvement•✔
Lack of dietary restrictions and lifestyle changes•✔
Feasibility with employment•✔
Availability of people to assist•✔
Identify breastfeeding resource network (family and friends, health care providers and •✔
mother-to-mother support groups).
Later in pregnancy
Practical skills on how to breastfeed•✔
Possible difficulties and how to overcome these•✔
Importance of skin-to-skin contact and rooming in•✔
More information can be found on the following sites
HowdoIstartbreastfeeding?www.health.qld.gov.au/phs/documents/cyhu/28099.pdf
BreastfeedingGettingStartedwww.health.qld.gov.au/phs/documents/cyhu/28098.pdf
Antenatal checklist
education on healthy eating and special considerations in pregnancy ✔✔provided
calculate pre-pregnant BMI - provide education on appropriate ✔✔weight gain
breastfeeding education provided✔✔
glucose screen for gestational diabetes at 24-28 weeks gestation.✔✔
24 A HEALTHY START IN LIFE ANTENATALNUTRITION
ReferencesWHO.1. Global strategy for infant and young child feeding.Geneva:WorldHealthOrganisation;2003.
AustralianGovernmentDepartmentofHealthandAgeing.(2006).Healthyeatingat2.variouslifestages:pregnantwomen.[Accessed2007May8].www.healthyactive.gov.au/internet/healthyactive/publishing.nsf/Content/pregnant-women.
WHO.3. Healthy eating during pregnancy and breastfeeding.Geneva:WorldHealthOrganisation;2001.
FSANZ.(2005).Folicacidandpregnancyadviceforwomen.[Accessed2007May4.8].www.foodstandards.gov.au/_srcfiles/FSANZ%20Folic%20Acid.pdfhttp://www.foodstandards.gov.au/_srcfiles/FSANZ%20Folic%20Acid.pdf
NationalHealthandMedicalResearchCouncil.5. Nutrient reference values for Australia and New Zealand:CommonwealthofAustralia;2006.
AndersonJ.,6. IodineEssencearticleVol43,No2March2007
FoodStandardsAustralia&NewZealand,2005FoodandPregnancy.[online]7. www.foodstandards.gov.au/foodmatters/pregnancyandfood.cfmMarch2007.
InstituteofMedicine.(1990)8. Nutrition during pregnancy, weight gain and nutritional supplements. Report of the Subcommittee on Nutritional Status and Weight Gain during Pregnancy, Subcommittee on Dietary intake and Nutrient Supplements during Pregnancy and Lactation, Food and Nutrition Board.Washington,DC:NationalAcademyPress:1-233.
CrowellDT.(1995)Weightchangeinthepostpartumperiod:areviewoftheliterature.9.JournalofNurseMidwifery;40:418-23.
JobJ,CapraS,AshS.(1995)Nutritionalassessmentofpregnantteenagersattendinga10.metropolitanpublicmaternityhospitalinBrisbane.1.NutritionalIntakes.AustralianJournalofNutritionandDietetics,Vol52,No.2:76-82.
NeilsenJ,GittelsohnJ,AnlikerJ,O’BrienK.(2006)InterventionstoImproveDietand11.WeightGainamongPregnantAdolescentsandRecommendationsforFutureResearch.JournaloftheAmericanDieteticAssociation;106:1825-1840.
SIGNAL:12. National Aboriginal and Torres Strait Islander Nutrition Strategy and Action Plan 2000 – 2010.NationalAboriginalandTorresStraitIslanderNutritionWorkingParty
CallawayLK,P.J.,ChangAM,McIntyreHD,13. The impact and prevalence of overweight and obesity in an Australian obstetric population.MedJAust,2005.
25A HEALTHY START IN LIFE ANTENATALNUTRITION
Cnattingius,S.,etal.,14. Prepregnancy weight and the risk of adverse pregnancy outcomes.NEnglJMed,1998.338(3):p.147-52.
KingJ.(2006)MaternalObesity,metabolism,andPregnancyOutcomes15.
DonathSM,AmirLH.(2000)Doesmaternalobesityadverselyaffectbreastfeeding16.initiationandduration?BreastfeedingReview;8(3):29-33
LoveladyCA.(2005)Ismaternalobesityacauseofpoorlactationperformance?Nutrition17.Reviews;63,10:352-355.
RasmussenKM,KjolhedeCL.(2004)Prepregnantoverweightandobesitydiminishthe18.prolactinresponsestosucklinginthefirstweekpostpartum.Pediatrics;113:1388-9
DiabetesAustralia.(2004)GestationalDiabetes.DiabetesAustralia.19.
RoyalCollegeofObstetriciansandGynaecologists.(2006)ExerciseinPregnancy20.(StatementNo.4).
BetterHealthChannel2006.PregnancyandExerciseFactsheet.[online]21.www.betterhealth.vic.gov.au.March2007.
AmericanCollegeofObstetriciansandGynaecologists.(2003)ExerciseDuringPregnancy22.PatientEducation.[online]www.acog/publications/patient_education/bp119.cfm?printerFriendly=yes.March2007.
NationalHealthandMedicalResearchCouncil.(2003)23. Food for Health. Dietary Guidelines for Children and Adolescents in Australia incorporating the Infant Feeding Guidelines for Health Workers.CommonwealthofAustralia,Canberra.
BrodribbW.(2004)BreastfeedingManagement.Thirdedition.AustralianBreastfeeding24.Association.
QueenslandHealth(2005)ChildandYouthHealthFactsheetsBreastfeeding:25.bestforbaby,bestforyou.[online]www.health.qld.gov.au/child&youth/factsheets
RiordanJ.(2005)26. Breastfeeding and Human Lactation.Thirdedition.JonesandBartlettPublishersInc.
1A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.0 Feeding for the first 6 months3.1 Breastfeeding: best for baby, best for mum
“Breastfeeding is an unequalled way of providing ideal food for the healthy growth and development of infants.... with important implications for the health of mothers” (1).
Thissectionofisnotabouthowtobreastfeed,northeanatomyofthebreast.Therearemanyprofessionalresourcesyoucanreferto,includingtheAustralianBreastfeedingAssociation(refertokeydocumentssection)whoprovidereviewsandsummariesofavailableresourcesforbothyourprofessionaldevelopmentandparentinformation.
In Australia, it is recommended that infants be exclusively breastfed until 6 months of age. It is further recommended infants continue breastfeeding until 12 months of age – and beyond if both mother and infant wish (2).
Wehaveapproachedthissectionfromthestancethatbreastmilkisthesolefood(andnormalnutrition)forthefirst6monthsoflifeandtobeusedcomplementarilyuntilatleast12monthsofage.
Almostallmothersarecapableofbreastfeedingtheirinfants.Outcomesaremuchimprovedwherethemotherhasthesupportandencouragementoftheinfant’sfather,otherfamilymembers,thehospital,andthecommunity.Manymothers–perhapsthemajority–encountersomedifficultieswithbreastfeedingbut,withsupportandencouragementfromhealthprofessionalsandcommunityorganisations,theycannearlyalwayscontinuetobreastfeed.Further,mostmotherscancontinuebreastfeedingiftheychoosetoreturntopaidworkorstudy.
Allhealthworkershaveanobligationtopromotebreastfeedinginthecommunityandtoensurebestpracticeinbreastfeedingisfollowed.Incomparisonwithsomeothercountries,Australia’sbreastfeedingrecordisgood,butitisimportantforthehealthofthenation’smothersandinfantsthatinitiationratesandthedurationofbreastfeedingbeincreased.
In2003,mostQueenslandchildren(92%)under5yearshadbeenbreastfedatsomepoint.ThisisinlinewiththeNHMRCobjectiveofbreastfeedinginitiationrateinexcessof90%(2).At6monthsofage,therateofbreastfeedinghadfallento57%(3,4).ItisanAustralianobjectivetohave80percentofinfantsbeingbreastfedattheageof6months(2).
Approximatelythreeinfivemothers(60%)surveyedintheQueensland Infant Nutrition Survey, 2003,“whohadeverbreastfedtheirchildsoughthelporsupportwithbreastfeedingafterleavinghospital.Thesemothersusuallywenttoatleasttwodifferentsourcesofsupportandadvice.Themainsourcewasfamilyandfriends,followedcloselybythelocalcommunityorchildhealthcentre”(3).
We want to ensure parents are making informed decisions. Breastfeeding and bottle feeding with artificial infant milks are not comparable.
Womenneedinformationaboutwhybreastfeedingisnormalandabouttheproblemsassociatedwithinfantformula,sotheycanmakeaninformeddecisionaboutfeedingmethod(7).
Inthischapteryouwillfindsomepracticaladvice,toolsandfurtherresourcesforyoutoincorporateintoyourdailypracticetoencourage,supportandpromoteexclusivebreastfeedinguntil6monthsofageandcontinuedbreastfeedingalongwithcomplementaryfoodsuntilbeyondtheinfant’sfirstbirthday.
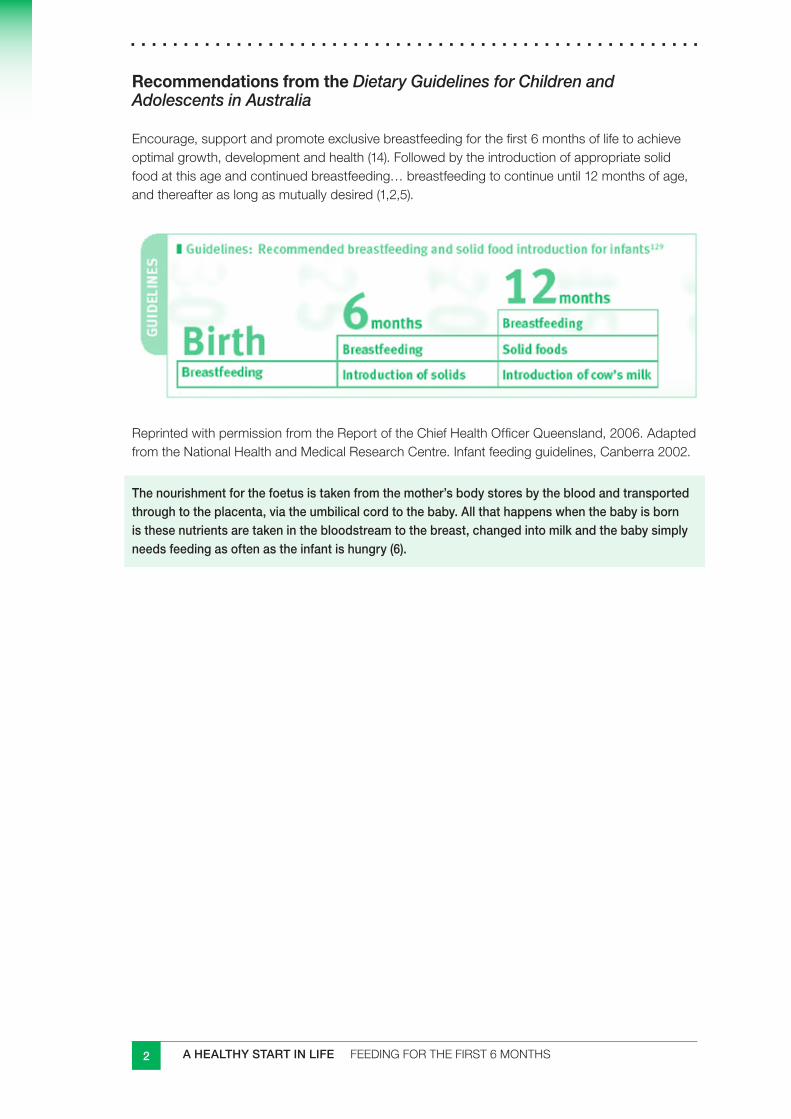
2 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Encourage,supportandpromoteexclusivebreastfeedingforthefirst6monthsoflifetoachieveoptimalgrowth,developmentandhealth(14).Followedbytheintroductionofappropriatesolidfoodatthisageandcontinuedbreastfeeding…breastfeedingtocontinueuntil12monthsofage,andthereafteraslongasmutuallydesired(1,2,5).
ReprintedwithpermissionfromtheReportoftheChiefHealthOfficerQueensland,2006.AdaptedfromtheNationalHealthandMedicalResearchCentre.Infantfeedingguidelines,Canberra2002.
The nourishment for the foetus is taken from the mother’s body stores by the blood and transported through to the placenta, via the umbilical cord to the baby. All that happens when the baby is born is these nutrients are taken in the bloodstream to the breast, changed into milk and the baby simply needs feeding as often as the infant is hungry (6).
3A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.2 The benefits of breastfeeding (2,5,9,10,11)
Baby
Breastmilkisdynamicandliving.Itconstantlychangesinitsnutrientcompositionto■■
meettheneedsofthebabythroughoutdifferenttimesoffeeding.
Breastfeedingprotectsagainstgastrointestinaland(toalesserextent)respiratory■■
infection,andtheprotectiveeffectisenhancedwiththegreaterdurationandexclusivityofbreastfeeding(9).
Prolongedandexclusivebreastfeedinghasbeenassociatedwithareducedriskofthe■■
suddeninfantdeathsyndrome(SIDS)(9).
Breastfeedingreducesthelikelihoodoflaterdiseasesandhealthrisksincludingobesity,■■
diabetes,heartdisease(10),Crohnsdiseaseandlymphoma(9).
Breastmilkisreadywhenyourbabyneedsit.■■
Breastmilkishygienic.■■
Babiesdigestbreastmilkeasily.■■
Breastmilkcontainsalotofnaturalsubstancesthathelpababy’sdevelopmentand■■
growth.
Mother
Breastfeedinghelpsinthephysicalrecoveryfromchildbirth.■■
Breastfeedinghelpsthemotherinweightstabilisationafterpregnancyandchildbirth.■■
Breastfeedingmaypossiblyalsoreducetheriskofsomecancers,suchasbreastor■■
ovariancancer(9,10).
Bondinghappensbetweenthemotherandbabyduringbreastfeeding.■■
Breastmilkisinexpensiveanddoesnotneedtobeprepared.■■
Increasedfertilitycontrol(5).■■
Reductionintheriskofmotherswithahistoryofgestationaldiabetesdeveloping■■
Type2diabetes(5).
Possibleprotectionagainstosteoporosis(9).■■
Parenthandoutcanbefoundat
www.health.qld.gov.au/child&youth/factsheets/
4 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.3 Natural patterns of breastfeedingThe first breastfeed
Studies have shown that mothers who feed or have skin contact with their babies in the first 2 hours after birth are more likely to breastfeed for longer than those who do not (7).
Ideallyuninterruptedskin-to-skincontactshouldbemaintainedfollowingbirth.Thiswillincreasethechanceoftheinfantattachingcorrectlyatthefirstfeed(7).Manyinfantsarenotreadytofeeddirectlyfollowingdelivery.Theinfantisoftenquietandalertduringthefirst20minutesorso,thenspontaneouslybeginstheinstinctiveprefeedbehaviour,orientatingitselftothebreastandpreparingtofeed(7).
Iftheinfantisleftskin-to-skin,proneonmother’sabdomenfollowingbirth,theinfantwillgraduallycrawltothebreast,findthenipple,attachandbegintosuckleunaided,usuallywithin70-90minutes(7).
Asuccessfulfirstbreastfeedhasanumberofpositiveeffects(2)
Itbuildsthemother’sconfidenceinherabilitytobreastfeed.■■
Theinfantstartstoreceivetheimmunologicalbenefitsofcolostrum.■■
Theinfant’sdigestionandbowelfunctionarestimulated.■■
Correctsuckingatthebreastatthisstagemayavertlatersuckingdifficulties.■■
Thebondingandattachmentbetweenmotherandinfantareenhanced.■■
Unlessthereisamedicalreason,motherandinfantshouldremaintogetherforatleastthefirsthourafterbirth,priortoweighingandbathingtoallowtheinfanttofollowtheirinstinctivebehaviours.Thereaftermotherandinfantshouldroom-intogether,sobreastfeedingbeginsandproceedsaccordingtotheinfant’sneeds–withoutrestrictiononthenumberandlengthoffeeds(2).Thisalsoensurestheinfantreceivescolostrumearlytopreventorreduceearlyweightloss;stimulatesthepassageofmeconium,reducingtheriskofneonataljaundice;andconfersimmunologicalprotectiontotheinfant(7).
Colostrum
Colostrum,whichisproducedinthebreastduringlatepregnancyandforthefirst30to40hoursafterbirth,isyellowishandthickerthanmaturemilk(2).Colostrumprovidesallthenutrients,includingwater,requiredbytheneonate(2).Itishighinprotein,andsodium,andlowinlactose(7).Italsocontainslactoferrin,immunoglobulinA,enzymes,maternalantibodies,livingcells—leukocytes,neutrophilsandmacrophages—andnon-pathogenicbacteriaandprebiotics,whichhelptocolonisethegutofthenewbornandlimitthegrowthofpathogenicbacteriaandvirusesandtoprotectagainstillness(2).
Initiationofbreastfeedingintroducesthewiderangeofnormalcyexperiencedbyindividualwomenthroughouttheirfeedingpractices.Feedswithinthefirst48hours,produceonlyasmallamountofcolostrum(aslittleashalfateaspoon).Anywherefrom2-4daysafterbirth,supplywillriseto500-800mlofmilkperday(6)
5A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Exclusive breastfeeding ensures an infant receives the full nutritional and protective benefits of colostrum and breastmilk (2).
Informationcanbefoundatwww.health.qld.gov.au/phs/documents/cyhu/28099.pdf
Furtherinformationonbabyledattachmentcanbefoundatwww.breastfeeding.asn.au,orcontactthebreastfeedinghelpline.
One or both breasts at each feed?Asageneralrule,thebabyshouldbeallowedtofinishfeedingfromthefirstbreastbeforeswitchingtotheotherbreast.Thisallowsthebabytoreceivethehigher-fatmilkasthebreastempties(7).
Whilethemajorityofbabieswillindicatetheyhavefinishedthefirstsidebycomingoffthebreastspontaneously,otherswillstayonthebreast,withoutactivelysuckingorswallowing.Ifthisisoccurring,themothershouldbeencouragedtoswaptothesecondsideafter20-30minutes(7).
Evenwhenthemotherinitiatesswappingsides,therearesomebabieswho:
havedampbutnotwetnappies■■
cryconstantlybutsleepwithinaminuteortwoofthebreastbeingoffered■■
sleepforlongperiods,especiallyovernight■■
havepoorweightgains.■■
Thesebabiesneedtobeswappedonesidetotheothermorefrequently,assoonastheswallowingintervalslengthenorafter5minutesofactivefeeding.Theinfantwillgetarushofmilkastheinfantswapsfrombreasttobreastandwillbeinclinedtosuckmoreefficiently.
Someinfantswhocomeoffthebreastspontaneouslyonlyneedtofeedfromonebreastatsomeorallfeeds…Occasionally,ifamotherhasanabundantmilksupplyfeedingfromjustonebreastateachfeedmaysettleanupset,cryinginfant(7).Iftheinfantisonlytakingonebreastateachfeed,ensuretheotherbreastisofferedfirstthenexttime(7).
If milk withdrawal has not started within 3 days post-partum, the changes in milk composition with lactogenesis are reversed and the likelihood of the establishment of successful breastfeeding declines (2).
Breastmilk
Breastmilk is constantly changing – throughout lactation and throughout the feed (2).
Humanmilkuniquelyadaptstothechangingneedsoftheinfantduringthecourseoflactation.Itrequiresacomplexcombinationandinterplayofhormones,togetherwithaninfantwhoinitiatesandmaintainslactation,andamotherresponsivetoherinfantneeds(7).
Thecompositionofthefirstsecretionafterbirthgraduallychangesaslactationisestablishedandproductionofmilkbeginsinthebreasttissue.Milkcomesinabout48to72hoursafterbirth.By7to14daysafterbirth,lactationshouldbeestablishedandthetransitionfromcolostrumtomaturemilkshouldbeunderway.
6 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Colostrumandbreastmilkcanvarygreatlyincolourandconsistency.Thecolourisirrelevanttothequalityofthemilk(8).
Thecolourofcolostrumvariesfromcleartopaleyellowtobrightorange.Maturebreastmilkvariesfromcreamytoopalescent.Vitaminsupplementsandsomefoodstakenbythemothercanalterthecolourofmilk(8).
Thepresenceofbloodmaycauseredtopinkishbrownor“rusty”discolourationofbreastmilk.Smallamountsofbloodincolostrummaybeduetoducthyperplasia–anextragrowthofcellsinmilkductsduringpregnancy,whichcausesbleedingwhendislodgedasthemilkbeginstoflow.Itisusuallyofnosignificanceandwilldisappearinafewdays(8).
Traumatothemother’snippleisthemostcommoncauseofblood-stainedmilk.Itisimportanttoestablishthecauseofblood-stainingandtreatit.However,itwillcausenoharmtotheinfant(8)althoughitmaycausevomitingiftherearesignificantamountsofbloodinthestomach.
Therateofmilkproductionisregulatedtomatchtheamountofmilkremovedfromeachbreastateachbreastfeedie.SUPPLY=DEMAND.Unrestrictedfeeding,bothdayandnight,isanimportantfactorinsuccessfullyestablishingbreastfeedingandresultsinadequatemilkproduction.
Additionally,theanatomyofthebreastvariesgreatlybetweenwomen.Somewomencanstoreuptosixtimesmoremilkthanotherwomen.Womenwithlargestoragecapacityhavemoreflexibilityinfeedingfrequency,whereaswomenwithasmallerstoragecapacityneedtofeedfairlyevenlyandfrequentlythroughoutthe24-hourday.
Other variances include rate of milk flow, nature of mouth-breast positioning … Advice should be tailored for individual differences (2).
The sleepy infantAftertheinitialalertperiodfollowingbirth,someinfantsbecomeverysleepyforthenext24hoursorso.Theinfantmaybeaffectedbyalonglabour,ormedicationsgivenduringlabour.
Skin-to-skincontactisbestpracticefollowingbirth.Thiscanassistwiththeinstinctivebehavioursofbothmothersandinfantsandlessenthechanceoffeedingdifficultiesinthedaysahead.
Thefirst72hoursareveryimportantforthestimulationofbreastmilk.Iftheinfanthasfedwellatleastonceinthefirstdayfollowingbirththereisnocauseforconcern.Duringthedaytime,iftheinfantdoesnotaskforafeedafterabout5hours,rousetheinfantandputhim/heronthebreast(2).
Anumberofstrategiescanbeusedtorouseaninfant:(2,12)
skin-to-skincontact,allowingtheinfanttofeedwhenready■■
changingthenappy■■
expressingalittlecolostrumandgivingitbyateaspoon,syringeorcupcangivethe■■
infantthe‘taste’andtheinfantwillthenwanttostartsuckingfromthebreast
unwrappingtheinfant,talkingtotheinfant,gentlystrokelegs,tummy,cheeksandlips■■
cuddlingtheinfant■■
7A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Mostinfantssoonrecoverfromtheinitialsleepyperiodandbegintoseekfeedsfrequently.Thiscanbeverytiringforthemother,butthemidwifecanprepareherforthisandreassureheraboutthebenefitsofearlyfrequentfeeding.Thisgivestheinfantcolostrum,stimulatesfullmilkproduction,andreducesthechanceofbreastengorgement(2).
Iftheinfantdoesnottakethebreastinspiteofalleffortsandisotherwisewell,itisessentialtoexpressthecolostrumandfeeditbyteaspoon,syringeorcup(2).Refertolactationconsultant.
Parenthandoutat:www.health.qld.gov.au/child&youth/factsheets/default.asp
The unsettled infant (2)
Infants cry for many reasons. This is the infant’s most powerful means of communication.
Itisnormalforinfantstohaveatleastoneunsettledperiodperday.Itusuallyoccursintheeveningbutcanhappenatanytime.Duringthesetimes,theinfantmaywanttofeedfrequently.Thisoftencausesmotherstobeworriedabouttheirmilksupplybutitisrarelythecauseoftheproblem.Reassurethemotherhermilkproductioniscontinuousovera24hourperiod,andtherateofproductionvariesaccordingtothefullnessofthebreast(2).
Thesefrequentfeeds‘putintheorder’forthenextdayandshouldbewelcomedastheywillensurecontinuedmilksupply.Bottlesofinfantformulaarenotneededintheseinstancesandcanaffectthemother’smilksupply.
Regurgitationiscommonandmayoccurinabout40%ofinfantsunder3months.Mostinfantswithregurgitationorrefluxarehealthyandgrowwell.Itisonlyaproblemifitiscausingtheinfantgreatdistressand/orinsufficientmilkisstayingdowntoenabletheinfanttogrow.
By6-10months,astheinfantspendsmoretimeduringthedayinanuprightposition,theconditionusuallysettles.Breastfeedingisnotthecauseanddoesnotmaketheconditionanyworse.Infact,itisusuallyworsewithartificialfeeds.Inthosecaseswhenitisaproblemmanagementtechniquesmayhelp.Inseverecasesmedicalinterventionmaybenecessary.
Parenthandoutat:www.health.qld.gov.au/child&youth/factsheets/default.asp
ABABooklet:Gastro-oesophagealRefluxandtheBreastfedBabywww.mothersdirect.com.au/prod790.htm
Breastfeeding does not cause colic or reflux. Bottles and dummies may cause confusion in the infant when breastfeeding is established. If these products are to be used they should be introduced after 1 to 2 months and be used infrequently.
8 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Summary
Some new infants may need to be woken to feed. You can help infants wake up to feed by:■■
placing them skin-to-skin on their mother’s chest■■
changing their nappy■■
unwrapping the infant■■
stroking their legs, tummy, lips and cheeks■■
encouraging mums to cuddle them■■
Most infants have at least one unsettled period a day often in the afternoon/evening – ■■
when they need to feed more often and be cuddled more.
Regular evening feeds stimulate the production of milk supply for the next day.■■
Swapping a breastfeed for a bottle of artificial infant milk can upset the milk supply.■■
Many infants regurgitate their milk, and this usually settles by 6-10 months.■■
Breastfeeding does not cause colic or reflux.■■
How often should I breastfeed my baby? (7, 2, 12)
Theinfantwillvaryitsfeedsaccordingtohisorherneedsandtherateofmilktransfer.Allowingthebabyunrestrictedaccesstothebreastintheearlydaysensuresregulardrainageandstimulationofthebreast.Thisinturnenablesthemothertoestablishhermilksupplyaccordingtotheinfant’sneeds,conditionstheletdownreflexandminimisesvenousengorgement(7).
Duringthefirstfewdaysafterbirth,babiesvaryconsiderablyinhowoftentheyneedtobefed.Somebabieswillwanttobefedevery1or2hours,andthen,asthemilkcomesin,willincreasetheintervalsbetweenfeeds.Othersappeartobequitesleepyatfirst,feedingevery4hoursorso,andthenreducingtimeintervalbetweenfeedsastheybecomemorewakeful(7).
Each breastfeeding dyad will develop a feeding pattern that fits with the mother’s storage capacity and the infant’s appetite (7).
Adherencetoastrictfeedingschedulemaycauseamothertobeanxiousandillatease....andheranxietyislikelytoinhibitherletdownreflex(7).
Infantsneedtofeedoften,especiallyintheearlyweeks.Theycanhavearound8-12in■■
24hours,notnecessarilyevenlyspaced.
Theinfantwillvarythefeedsaccordingtohis/herneedsandtherateofmilktransfer.■■
Also,‘demandfeeding’allowsinfantstoletmothersknowtheirneeds.
Infantswillknowwhentheyarehungrysofeedingcanbedonetosuittheinfant’s■■
needs.Infantsmaybecomeunsettledandwanttofeedmoreoftenfromtimetotime.
Feedingtimesvaryfromfeedtofeedandinfanttoinfant.Asinfantsgetolderand■■
areabletosuckmoreefficiently,theyoftenhaveshorterfeedsandmaysleeplongerbetweensomefeedsorbeawakeandcontent.
Breastmilkiseasilydigested,andmostbabieswantandneedtobefedmore■■
frequentlythan3to4hourly,especiallyasthegastricemptyingtimeofhumanmilkisapproximately90minutes(7).
9A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Itisfinetogiveinfantsanextrafeedor‘top-up’tosettlehim/herwhenneeded.■■
Encouragemumstoletaninfantfeedaslongastheinfantwantsto.Someinfantswill■■
havearestatthebreastandthenstartsuckingagain,lettheinfantdecidewhentocomeoff.
Ifaninfantisfeedinglongerthan30to45minutes,theremaybesomeproblemswithattachment.Refertolactationconsultant,orAustralianBreastfeedingAssociationHelpline.
For how long should an infant breastfeed? (10)
Breastmilkgivestheinfantallthenutrientsrequirementsforaroundthefirst6monthsoflife.Afterthistimebabiesneedsolidfoodinadditiontobreastmilk.QueenslandHealth,theNationalHealthandMedicalResearchCouncilrecommendsbreastfeedingiscontinueduntiltheinfantis12monthsold,andthenforaslongasmutuallydesired.
Check: tips to share with mums
Feed when your baby asks for it, as all babies have different feeding ■✔requirements.
Breastmilk is easily digested, so baby may feed often.■✔
As baby grows and sucks more, she/he may have shorter feeds and sleep ■✔longer between feeds.
Identification of correct attachment
47% of mothers who have ever breastfed said they experienced problems with breastfeeding: the problem most commonly experienced was attachment, 30.7% (3)
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Pay particular attention to the importance of correct attachment and positioning when breastfeeding. Effective, rapid management of any breastfeeding difficulties is important to extend the duration of breastfeeding.
Indicatorsforcorrectattachment
Breastfeedingshouldnotbepainful.Mostwomenexperiencenipplesensitivityand■■
tendernessinthefirstfewdaysandthisisnormal,butpainisnot.
Ifthecheeksarebeingsuckedinoryoucanheara‘clicking’,infantisnotattached■■
properly.
Ifmumreportsithurtswheninfantsucksoryoususpectpoorattachment,advisemum■■
toputherfingerininfant’smouthtobreakthesuctionandtryagain.Justpullinginfantoffwillhurt.
Swallowingcanbeseen/heard.■■
Infantlookscomfortable,relaxedandnottenseorfrowning.■■
Afterfeeding,mum’snippleswillappearslightlylongerbutshouldnotlooksquashed,■■
flattened,whiteorridged.
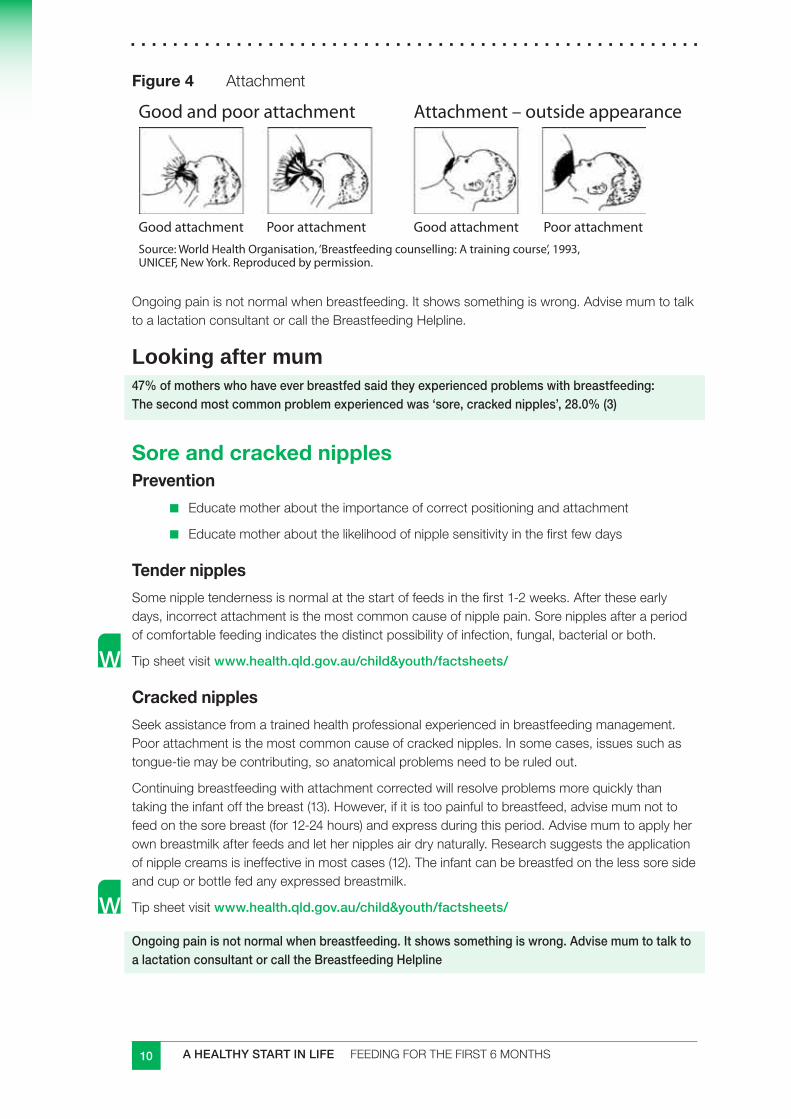
10 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Figure 4 Attachment
Good and poor attachment Attachment – outside appearance
Good attachment Poor attachment Good attachment Poor attachmentSource: World Health Organisation, ‘Breastfeeding counselling: A training course’, 1993, UNICEF, New York. Reproduced by permission.
Ongoingpainisnotnormalwhenbreastfeeding.Itshowssomethingiswrong.AdvisemumtotalktoalactationconsultantorcalltheBreastfeedingHelpline.
Looking after mum47% of mothers who have ever breastfed said they experienced problems with breastfeeding: The second most common problem experienced was ‘sore, cracked nipples’, 28.0% (3)
Sore and cracked nipplesPrevention
Educatemotherabouttheimportanceofcorrectpositioningandattachment■■
Educatemotheraboutthelikelihoodofnipplesensitivityinthefirstfewdays■■
Tender nipples
Somenippletendernessisnormalatthestartoffeedsinthefirst1-2weeks.Aftertheseearlydays,incorrectattachmentisthemostcommoncauseofnipplepain.Sorenipplesafteraperiodofcomfortablefeedingindicatesthedistinctpossibilityofinfection,fungal,bacterialorboth.
Tipsheetvisitwww.health.qld.gov.au/child&youth/factsheets/
Cracked nipples
Seekassistancefromatrainedhealthprofessionalexperiencedinbreastfeedingmanagement.Poorattachmentisthemostcommoncauseofcrackednipples.Insomecases,issuessuchastongue-tiemaybecontributing,soanatomicalproblemsneedtoberuledout.
Continuingbreastfeedingwithattachmentcorrectedwillresolveproblemsmorequicklythantakingtheinfantoffthebreast(13).However,ifitistoopainfultobreastfeed,advisemumnottofeedonthesorebreast(for12-24hours)andexpressduringthisperiod.Advisemumtoapplyherownbreastmilkafterfeedsandlethernipplesairdrynaturally.Researchsuggeststheapplicationofnipplecreamsisineffectiveinmostcases(12).Theinfantcanbebreastfedonthelesssoresideandcuporbottlefedanyexpressedbreastmilk.
Tipsheetvisitwww.health.qld.gov.au/child&youth/factsheets/
Ongoing pain is not normal when breastfeeding. It shows something is wrong. Advise mum to talk to a lactation consultant or call the Breastfeeding Helpline
11A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Is baby getting enough milk?Changes in milk supply
Amothermayperceivehermilksupplyaslowforthefollowingreasons(7):
aninfantisfussyanddoesnotsettleafterfeeds.Theinfantmaycrymorethanthe■■
parentexpects
theinfanthaslowweightgains,especiallyoverashortperiodoftime■■
afterinitialfullnessandengorgement,thebreastssettledownandbecomesofter,■■
asthemilksupplyadjuststotheinfant’sneeds
theinfantrequiresalotofcomfortsucking■■
expressedbreastmilklooksdifferenttocow’smilk(orcouldjust‘lookdifferent’)■■
theinfantkeepsturninghisorherheadandopeningmouth,asifwantingtosuck.■■
thisisthe‘rootingreflex’,presentfrombirthto3or4monthsofage(2)
themothermaynotbeabletoexpressmuchmilk.Itmustberememberedthatthe■■
abilitytoexpressisnotareflectionofhowmuchmilktheinfanttakes(2).
CheckAll infants, regardless of how they are fed, require careful monitoring of growth and ■✔development, with appropriate interventions undertaken when clinically indicated (9).
Ifthefully-breastfedinfantshowstwoormoreofthesignsbelowtheinfantismostlikelyhavingenoughmilk.
Atleast5to7heavily-wetdisposablenappies(or6to8verywetclothnappies)in■■
24hoursprovidednootherfluidsorsolidsarebeinggiven.
Averyyounginfantwillusuallyhavetwoormoresoftbowelmovementsadayfor■■
severalweeks.Anolderinfantmayhavefewerthanthis.
Smallquantitiesofstrong,darkurineorformedbowelmotionsindicatethattheinfantis■■
inneedofmorebreastmilk.
Goodskincolourandmuscletone.■■
Theinfantisalertandreasonablycontentedanddoesnotconstantlywanttofeed.She■■
willprobablywakefornightfeeds.Afewinfantssleepthroughthenightatanearlyage,whilemostwillwakeoneormoretimesduringthenightforquitesometime.
Someweightgainandgrowthinlengthandheadcircumference.Recordthisinthe■■
infant’sPersonalHealthRecord.
KindlyadaptedfromAustralianBreastfeedingAssociationwww.breastfeeding.asn.au
ChildHealthFactsheetavailableat:www.health.qld.gov.au/phs/documents/cyhu/28100.pdf
Unless medically indicated, there is no need to supplement breastmilk with other foods or fluids (15).
Studies suggest that partially breastfed and formula fed infants consume 20% more calories than do exclusively breastfed infants. Excessive weight during the first 4-6 months of life is associated with future risk of overweight in babies who are not exclusively breastfed (15).
12 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Prompting questions
Here are some prompting questions and responses you can use when talking with mums (adapted from the Dietary Guidelines for Children and Adolescents in Australia)
Is your infant losing or gaining weight and growing in length■■ ?
Assure mums that the overall rate of growth is the most important factor and a ■■
judgement is best made only after a series of measures.
It is often assumed infant’s weight gain will be steady; however it is not uncommon for a ■■
breastfed infant’s gain to be erratic – large one week and small the next. It is important to look at the overall trend for a month or so, rather than week by week. This is often reassuring to the mother who has an otherwise healthy infant. (7)
Does your infant have 6 to 8 wet cloth nappies or at least 5 heavily wet disposable ■■
nappies per day?
This is typical in a breastfed infant. ■■
Are you concerned with bowel motions? (refer to constipation section)■■
Breastfed infants are rarely constipated, so a dirty nappy can occur after each ■■
feed. Typical breastfed infants’ bowel motions are a loose, mustard yellow but can sometimes be green or orange. None of these changes are a problem in a healthy breastfed infant. As the infant gets older, dirty nappies can occur less frequently. It is important to discuss this with families
Is infant’s urge to suck being met in another way?■■
Breasts respond to frequent stimulation by producing more milk. Check if infant is ■■
sucking on a dummy or a bottle, as the infant won’t feed as much and mum’s milk supply will decrease. Complementary bottles should be completely avoided.
Do you have any concerns with the changes in your daily life? ■■
Changes after having an infant are normal…
Infants can’t tell the time! In the first months of life infants don’t always become hungry ■■
at the same time each day.
Encourage mums not to feed on a rigid schedule – feed according to need.■■
Encourage mums to create a flexible, evolving routine that meets both her and her ■■
infant’s needs.
Concerns with breast size or changes?■■
Breast size has no relationship to milk production.■■
Breasts may soften once mum’s body has settled into breastfeeding. This does not ■■
necessarily mean a low supply. The milk supply has settled to the infant’s needs. Hard breasts are engorged and this is not the normal state, just common in the early days.
Changes in feeding patterns?■■
The infant will want to feed more often from time to time and this is quite normal.■■
How often the infant needs to feed and how long they take to feed differs a lot from one ■■
infant to the next.
The more mums feed, the more milk they make.■■
13A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Not able to express much breastmilk?■■
This is not a reflection of how much milk the infant actually takes.■■
It possibly just means that the let-down reflex is not working when mum expresses.■■
Is mum eating a nutritious diet■■ ?
The ■■ Australian Guide to Healthy Eating provides recommendations on mum’s intake. Help mum to follow the serving recommendations and limit extra foods.
Is mum drinking plenty of water? ■■
Suggest drinking a glass of water each time she breastfeeds.■■
Is mum getting as much rest as possible? ■■
Encourage mum to look at feeding time as rest time.■■
She may like to lie down to feed for some feeds at home.■■
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Ifapacifier(dummy)isused,itshouldnotbeintroduceduntilafter1to2monthsandbeusedinfrequently.
Earlyuseofdummiesandbottles,especiallybeforethefirstbreastfeed,caninterferewiththenaturalprocessesofbreastfeeding,reducingtheinfant’ssuckingcapacityandthestimulationofthemother’sbreasts(2).
Dummy use is associated with lower exclusivity and duration of breastfeeding (16).
Risksassociatedwiththeuseofapacifierandthenon-nutritivesuckinghabititpromotesinclude:
failureofbreastfeeding■■
dentaldeformities■■
recurrentacuteotitismedia■■
riskofaccidents■■
latexallergy■■
toothdecay■■
oralulcers■■
sleepdisorders(17).■■
Breastsrespondtofrequentstimulationbyproducingmoremilk.Ifinfantissuckingonadummyorabottle,theinfantwon’tbreastfeedasmuchandmum’smilksupplywilldecrease.Complementarybottlesshouldbecompletelyavoided(2).
Remember: supply = demand
14 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Monitoring an infant’s progress
Checkinfant’sgrowthregularlyandmakesureitisrecordedonthegrowthchartinthe■■
PersonalHealthRecordbook.Ajudgementoninfant’sgrowthisbestmadeonlyafteraseriesofmeasures.Itisimportanttoassessweightgainonafourweekaverage(2).
A one-off unusual measure is not usually cause for concern if infant is content and healthy. ■■
Check the accuracy of measurements, use the same scales all the time and always weigh without clothes (12).
Normal ranges of infant weight gain
Anumberoffactorsinfluencegrowthininfancyincluding(7):
intrauterineenvironment■■
birthsize■■
sex■■
parentalstature■■
feedingmode.■■
Infantsloseweightshortlyaftertheyareborn,uptoabout10%(7).Theystarttoregainthisweightbyday4-6andshouldhaveregainedtheirbirthweightby2weeks(2).
Birth–3months:gain150to200gperweek■■
Age3to6months:gain100to150gperweek■■
Age6to12month:gain70to90gperweek■■
Itisoftenassumedinfant’sweightgainwillbesteady;howeveritiscommonforabreastfedinfant’sgaintobeerratic–largeoneweekandsmallthenext(7).Afterthefirst2weeksthereshouldbesomeweightgainonaregular(butnotnecessarilyweekly)basisusuallyaveragingatleast500g(7)to600g(2)permonth.Infantsusuallydoubletheirbirthweightbytheageof6months;tripletheirbirthweightby1yearofage.(2)
Weight gain is only one aspect to consider. Positive support of the mother and clinical observations of the infant are equally important.
Patterns of weight gain in breastfed infants are different from those of infant-formula-fed ones. They should not be compared. (7)
Growth charts
Growthchartsareusefultomonitorinfantgrowth,butshouldnotbethesoledeterminantoftheneedfortheintroductionofcomplementaryfeeding…;theyarenotanindicationofthereadinessforcomplementaryfoods(15).RefertoGrowthChartsection.
15A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
CheckFeeding patterns■✔
Feedingondemand.■■
Lengthoffeedsvariable(if>1/2houronfirstbreast,checkattachment).■■
Urine output, after infant is 3 or 4 days old■✔
Clothnappiessoakedwithpaleorcolourlessurine6ormoretimesperday.■■
Veryheavydisposalnappiesatleast5timesperday.■■
Bowel actions■✔
Breastfedinfantsarerarelyconstipated,soadirtynappycanoccuraftereachfeed.■■
Typicalbreastfedinfants’bowelmotionsareloose,mustardyellowbutcan■■
sometimesbegreenororange.
Asyourinfantgetsolder,dirtynappiescanoccurlessfrequently.■■
Growth ■✔
Thefactthatyourinfant’sgrowthfollowsthegeneralpatternorcurveofthegraphis■■
themostimportantthing.
(adaptedfrom2,12,14)
If the infant’s growth appears to be faltering, check for other indicators of wellbeing, and if there seems to be insufficient milk, efforts should be made to increase the milk supply in the first instance (5).
16 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Guidelines for practitioners:Approximately 3 in 5 mothers (60%) surveyed in the Infant Nutrition Survey who had ever breastfed their child sought help or support with breastfeeding after leaving hospital. These mothers usually went to at least two different sources of support and advice. The main source was family and friends, followed by the local community or child health centre (3)
Monitoring progress: in the first month of lifeAdapted from Global Strategy for Infant and Young Child Feeding, WHO (14)
Mothers should be visited or otherwise communicated within 48 hours of discharge to check 1 exclusive breastfeeding is progressing satisfactorily. Most problems identified at this stage can be easily solved. Difficult problems should be referred to a lactation consultant. The longer the first visit is delayed the more difficult it is to solve any problems that might have arisen.
During this visit observe a breastfeed to: 2
ensure correct position and attachmenta.
confirm good milk transferb.
reassure mum.. knowledge and practice of breastfeeding should be reinforced.c.
Breastfeeding problems such as sore nipples and breast engorgement do not require the 3 discontinuation of breastfeeding and short-term interruption is rarely needed (see www.health.qld.gov.au/child&youth/factsheets/default.asp : common breastfeeding concerns, or refer mums to their Child Health Information booklet).
Mothers perceiving infant crying and frequent feeding as breastmilk insufficiency need 4 explanation, reassurance and support. These episodes are normal; they are a regulating mechanism of milk removal and milk synthesis to meet the evolving needs of the infant.
If a child fails to follow a growth curve check the effectiveness of breastfeeding and correct 5 feeding technique if necessary. Weight gain should always be calculated from the lowest post-partum weight, not from birth weight.
If growth is above 956 th centile, or below 5th centile, or crosses these centiles, (2) or should growth faltering persist further investigation is required. Remember, though, that 5% of normal infants will be above the 95th percentile and another 5% will be below the 5th.
17A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Monitoring progress: from 1 to 6 monthsAdapted from Global Strategy for Infant and Young Child Feeding, WHO (14)
If exclusive breastfeeding is well established, there is no need to supplement breastmilk with 1 other food or fluids
Mothers should be advised to check growth, by arranging infant checks monthly. 2
Mothers should be advised to continue breastfeeding on demand3
At around 6 months, most infants will show an interest in complementary foods as well as 4 breastfeeds. Provided infants are in good health parents should be advised to observe their infant’s feeding behaviour and respond appropriately (ie never force infants to eat).
Growth charts are useful to monitor infant growth, but should not be the sole determinant of 5 the need for the introduction of complementary feeding.
To facilitate mothers in the paid workforce, a breastfeeding supportive workplace as well as 6 family and/or social support is helpful. Access to ongoing expert support, and information on expression, safe handling and storage of breastmilk is also required
Exclusively breastfeeding mothers who use the Lactation Amenorrhoea Method (LAM) 7 of birth control have a high rate of protection from unwanted pregnancy until her infant is 6 months old. After this, other contraceptive methods are required. Progestin-only contraceptives are highly effective and usually have no inhibitory effect on lactation, however, combination contraceptives appear to be associated with a decline in milk production (see section on medications for further information). Occasionally, a mother might find progestin-only contraceptives affect lactation, especially if begun very early following the birth.
18 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.4 Why not to introduce cow’s milk before 12 months (2)
Cow’smilkasacompletefeedisnotsuitableforinfantsunder12monthsofageforanumberofreasons.
Composition
Breastmilkisalivingtissuethatincludesmanyspecies-specificcompounds(2).Becausecow’smilkisintendedforcalves,whichhaveamuchhighergrowthvelocitythaninfants,thecontentofnutrientsessentialforgrowth,likeproteinandsomemineralsaremuchhigher(typically2-3times)thaninhumanmilk(18)andtoohighforhumaninfants.
Thecompositionofcow’smilkisnotidealforinfants.Comparedwithbreastmilk■■
andinfantformula,cow’smilkcontainshigherlevelsofprotein,sodium,potassium,phosphorousandcalciumandlowerlevelsofiron,vitaminCandlinoleicacid,addingtothedifficultyofprovidingabalanceddietforolderinfants(2,18,19).
Thehigherlevelsofprotein,sodiumandpotassiumincow’smilkhavebeenassociated■■
withanincreaseinrenalsoluteload(2,18)thatmightcausedehydrationandhypernatremiaduringillness(18).
Thehighphosphorousandcalciumcontentofcow’smilkmaydecreasethe■■
bioavailabilityofironfromotherdietarysourcessuchasinfantcereals.
Thefatincow’smilkismuchharderforinfantstodigestduetothewayfatsare■■
hydrolysed.Longchainpolyunsaturatesaredeficientincow’smilk.Theseareessentialforaninfant’snervoussystemdevelopmentandvisualfunction(20).
Iron
Cow’smilkisapoorsourceofironandtheironitdoescontainispoorlyabsorbed:■■
50%ofironfrombreastmilkisabsorbedcomparedwith10%incow’smilk.
Introducingcow’smilkbefore12monthsofagepredisposesaninfanttoirondeficiency■■
atanagewhentheirironstoresbecomedepleted.
Cow’smilkthathasnotbeenheattreatedcancausegastro-intestinalbleeding(26),■■
exacerbatingtheproblemofirondeficiency(2).
Health consequences
Earlyintroductionofcow’smilkmaybeassociatedirondeficiency.■■
Avoidingcow’smilkduringthefirst12monthsoftheinfant’slifewillhelpprotectagainst■■
thedevelopmentofcow’smilkallergy(2).
Earlyintroductionofcow’smilkhasbeenlinkedtoanincreasedriskofdeveloping■■
asthmaortype1diabetes(5).
‘Milkaholics’
Ayoungchildconsumingeitheronelitreofcow’smilkoranequivalentformulamilk■■
productismeetingasmuchastwothirdsofhisorherenergyrequirementsfromthissource,leavingverylittleappetiteforothermorevariedhealthyfoods(2).
19A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Breastfeeding and allergies
Exclusivebreastfeedingatleast6months,andpreferablylongerisrecommended.■■
Ifbreastfeedingisdiscontinuedforanyreason,seekprofessionaladvice:hydrolysed■■
proteinformulamayberecommended.
Soymilkandgoat’smilkformulasdonotreduceallergies,andshouldnotbeusedasan■■
alternativetocow’smilkformulas.
Maternaldietaryrestrictionsduringbreastfeedingarenotrecommendedforprevention■■
(21)
Ifaninfantisbreastfeedingandshowingsignsofallergies,refertolocalgeneral■■
practitionerorpaediatrician.
3.5 Nutrition and breastfeeding Healthyeatingisimportantforallmothers.Itisimportantforthemothertoeatadequatelyforherownnutritionneedsaswellasprovidingforthenutritionalneedsofherinfant.Withrigoroushoursandconstantdemandsthatneedimmediateattention,breastfeedingisafull-timejob.Andaswithanyrolethatisphysicallyandemotionallychallenging,mothersneedtoregularlyrefueltokeeptheirenergylevelshigh.
Unlessextremelymalnourished,virtuallyallmotherscanproduceadequateamountsofbreastmilk.Whenthebreastfeedingmotherisundernourished,itissafer,easier,andlessexpensivetogivehermorefoodthantoexposetheinfanttotherisksassociatedwithbreastmilksubstitutes(22).
Lactationplaceshighdemandsonmaternalstoresofenergyandprotein.Thesestoresneedtobeestablished,conserved,andreplenished(22).
Breastfeedingcanaffectthemother’snutritionalstatus,dependingonthemother’sdiet.Theenergy,protein,andothernutrientsinbreastmilkcomefromthemother’sdietorfromherownbodystores.Whenwomendonotgetenoughenergyandnutrientsintheirdiets,repeated,closely-spacedcyclesofpregnancyandlactationcanreducetheirenergyandnutrientreserves,aprocessknownasmaternaldepletion(22).
Breastfeedingmothershaveanincreasedrequirementformostnutrientscomparedtomotherswhodonotbreastfeed,asmanyvitaminsandmineralsinabreastfeedingmother’sdietaretransferredintothebreastmilk.
Abreastfeedingmothershouldeatregularnutritiousmealsandsnackstomeettheextraenergy(kilojoules)neededformakingbreastmilkandfeeding.Consumingavarietyoffoodseachdayisimportantinmeetingboththemother’sandinfant’snutritionalneeds.
Utilise the Australian Guide to Healthy Eating as a guide for mother’s intake.
20 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Energy requirementsTheenergyneedsofabreastfeedingmotherareincreasedbecauseofmilkproduction.Infact,theenergyrequirementsforbreastfeedingmothersare,onaverage,2000kJ(445kCal)perdaymorethanthatofausualadultwoman’sdailyenergyneeds.Theseenergyrequirementsarebasedonfullbreastfeedinginthefirst6monthsandpartialbreastfeedingafterthattime.
Whileitisnormal(andexpected)thatmothersputonweightwhilepregnant,itisnotrecommendedthatmothersfollowastrictweightlossdietafterchildbirth.Breastfeedingnaturallyallowsforgradualweightloss.Ifweightisgainedafterbirth,itismostlikelymumiseatingtoomuchfood,orchoosingfoodshighinenergy(kilojoules).
Becausethereisindividualvariationinmilkproduction,levelsofphysicalactivityandweightlossduringlactation,itisdifficulttomakeanexclusiverecommendationonenergyneedsduringbreastfeeding.
Forindividualisedadvice,refertoadietitian.
Physical activityRegular,moderatephysicalactivityisgoodforhealth.Itappearsmostbreastfeedingwomencanparticipateinexercisewithoutaffectingtheirlactation.
Itisbesttocombineexercisewithbalancedeatingandadequatenutrition.Itisalsoimportanttodrinkplentyoffluidswhenbreastfeedingandexercising.
Forindividualnutrientrequirementssuchasthosedescribedbelow,theNutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakesprovidesanaveragenutrientintakerequirementforindividualsandavaluethatwouldmeettheneedsofmostindividualsinthepopulation.Becauseitisdifficulttoassessanindividual’sexactrequirementforaparticularnutrient,youmightliketoaimfortheupperfiguretomaximisethecertaintythatasufficientamountofthenutrientisobtainedfromfood.
For health professionals
Formoreinformationgotowww.nhmrc.gov.au/publications/_files/n35.pdf
TheinformationinthisnextsectioniskindlyadaptedfromtheHealthyActivewebsite.ItisbasedontheNutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes,theDietary Guidelines for Children and Adolescents in Australia,andThe Australian Guide to Healthy Eating.Theserecommendationsareforhealthywomenwithstandardisedweight,heightandestimatedenergyrequirementsandmaynotmeetthespecificnutritionalrequirementsofindividuals.
Specificadviceforindividualneedsshouldbesoughtfromaqualifieddietitian.
Parenthandoutscanbefoundatwww.qheps.health.qld.gov.au/ahwac/content/home_nemo.htm
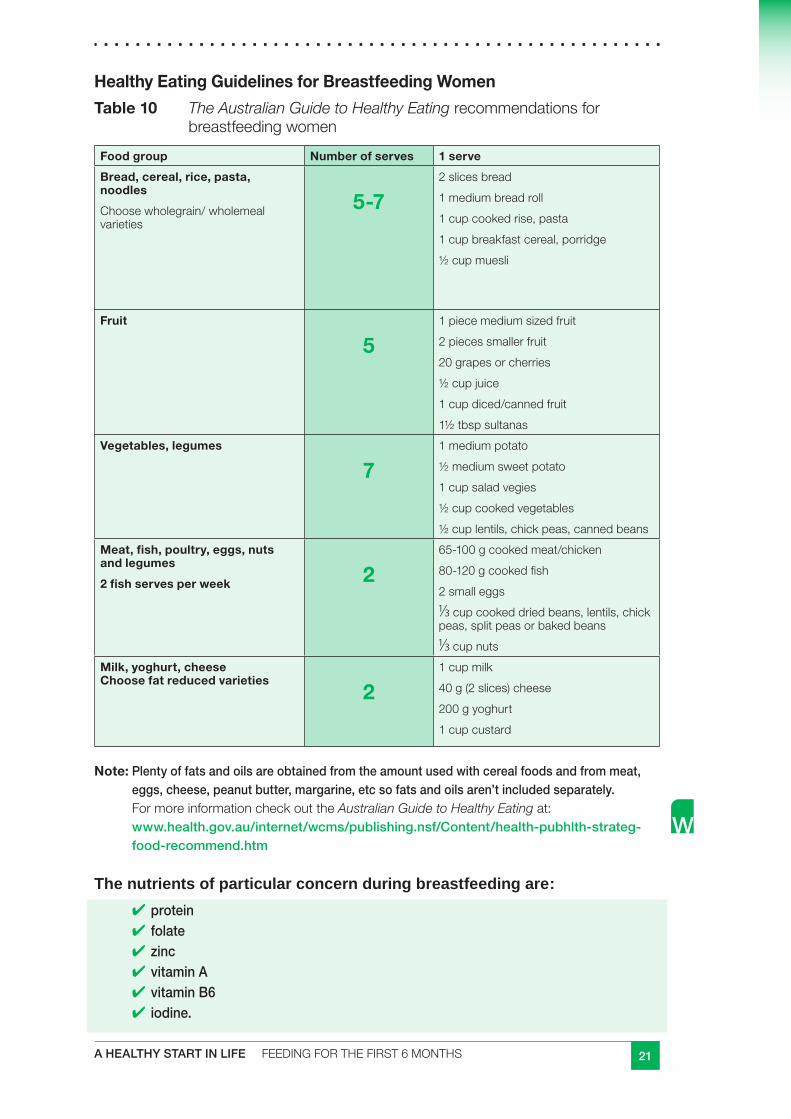
21A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Healthy Eating Guidelines for Breastfeeding Women
Table 10 The Australian Guide to Healthy Eatingrecommendationsforbreastfeedingwomen
Food group Number of serves 1 serve
Bread, cereal, rice, pasta, noodles
Choosewholegrain/wholemealvarieties
5-72slicesbread
1mediumbreadroll
1cupcookedrise,pasta
1cupbreakfastcereal,porridge
½cupmuesli
Fruit
51piecemediumsizedfruit
2piecessmallerfruit
20grapesorcherries
½cupjuice
1cupdiced/cannedfruit
1½tbspsultanas
Vegetables, legumes
71mediumpotato
½mediumsweetpotato
1cupsaladvegies
½cupcookedvegetables
½cuplentils,chickpeas,cannedbeans
Meat, fish, poultry, eggs, nuts and legumes
2 fish serves per week 265-100gcookedmeat/chicken
80-120gcookedfish
2smalleggs
1/3cupcookeddriedbeans,lentils,chickpeas,splitpeasorbakedbeans
1/3cupnutsMilk, yoghurt, cheese Choose fat reduced varieties
21cupmilk
40g(2slices)cheese
200gyoghurt
1cupcustard
Note: Plenty of fats and oils are obtained from the amount used with cereal foods and from meat, eggs, cheese, peanut butter, margarine, etc so fats and oils aren’t included separately. FormoreinformationcheckouttheAustralian Guide to Healthy Eatingat:www.health.gov.au/internet/wcms/publishing.nsf/Content/health-pubhlth-strateg-food-recommend.htm
The nutrients of particular concern during breastfeeding are:
protein■✔
folate ■✔
zinc ■✔
vitamin A ■✔
vitamin B6■✔
iodine.■✔
22 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Protein
Abreastfeedingmotherneedsadditionaldietaryproteintobuildtheproteininherbreastmilk.Proteinisvitalforthegrowth,maintenanceandrepairofcells.TheRDIforproteinduringbreastfeedingis67g/day.Proteinisfoundinawiderangeoffoodssuchasmeat(includingfishandpoultry),eggs,dairy,legumes(suchasbeans,pulsesandsoyproducts)andnuts.Smalleramountsofproteinarefoundingrain-basedfoodssuchasbreadandpasta.
Folate
FolateisaBvitamin,neededforhealthygrowthanddevelopment.TheRDIforbreastfeedingmothersis500µg/day.Folatecanbefoundinleafyvegetables,wholegrains,beans,peas,peanuts,avocadoandyeastextract(egPromite, Vegemite, Marmiteetc).
Zinc
Zincisacomponentofvariousenzymesthathelpmaintainstructuralintegrityofproteinsandhelpregulategeneexpression.Breastfeedingmothersrequire12mg/day.Zinccanbefoundinleanmeat,wholegraincereals,milk,seafood,legumesandnuts.
Vitamin A
VitaminAisvitalfornormalgrowthandhelpsprovideresistancetoinfections.Breastfeedingmothersrequire1,100µg/day.VitaminAcanbefoundinmilk,cheese,eggs,fattyfish,yellow-orangevegetablesandfruitssuchascarrots,pumpkin,mango,apricots,andother(dark-green)vegetablessuchasspinachandbroccoli.
Vitamin B6
VitaminB6isimportantforthemetabolismofproteinandtheformationofredbloodcells.Breastfeedingmothersrequire2mg/day.VitaminB6canbefoundinmuscleandorganmeat,poultry,fish,wholegrains,brusselsprouts,greenpeasandbeans.
Iodine
Iodineisavitalnutrientforthethyroidglandtomakethyroidhormones,andtheseareessentialfornormaldevelopmentofthebrainandnervoussystem.Iodinecontentinbreastmilkreflectsthemother’sintake,soifthisislow,theamounttransferredtothebabywillalsobelow.Untilaninfantcaneatweaningfoodscontainingiodine,theinfantreliesentirelyonsuppliesofthisnutrientfromhismother,acrosstheplacentaandthenthroughbreastmilk(23).TheRDIforiodineduringbreastfeedingis270µg/day.
Water (fluids)
Breastfeedingmothersshoulddrinkanadditional700ml/day(atleast)abovenon-lactatingrequirementstoreplacethefluidlostthroughbreastfeeding.Thisequalstoatotalof9cupsdaily,andcanbeintheformofwater,milk,soup,juiceandotherdrinks(avoidalcoholandlimitcaffeine-containingfluids,suchascoffee,teaandcola).However,purewatershouldbeeveryone’smaindrink.
Apracticalideayoucanadvisemumistohaveadrinkatthetimeofeachbreastfeed,aswellasdrinkingregularlythroughoutothertimesoftheday.
23A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Dieting during breastfeeding
Breastfeedinghelpsmotherstoshapeup.Weightlossdietsarenotrecommendedduringbreastfeeding.Advisemothersonafewofthesestrategiestoensuretheyaremaximisingtheirnutrientintake,whilstdecreasingextras.
Don’tskipmeals.■■
Limitfoodshighinfatandsugarsuchaslollies,chocolate,softdrinks,cakes,sweet■■
biscuits,chipsandfattytakeaways.
Usehealthycookingmethodssuchassteam,boil,microwave,andgrillorstirfry.■■
Trimfatfrommeatsandavoidchickenskin.■■
Dosomegentleexercisesuchastakingyourbabyforawalk-consultaphysiotherapist.■■
Parenthandout
qheps.health.qld.gov.au/ahwac/content/home_nemo.htm
Excess weight loss and breastfeeding
Encouragethemothertocontinuebreastfeeding.Helpthemtofindwaystoeatmore.Somesuggestions:
don’tskipmeals■■
havethreemainmealsandthreebetweenmealsnacks■■
keepeasytopreparenutritioussnacksonhandegcrackersandcheese,freshfruit,■■
yoghurt,nuts,seeds,driedfruit,cannedbeans,flavouredmilk,fruitsmoothies,breakfastcerealsandmilk
prepareapackedlunchorvarietyofsnackstohaveinacontainerbesideyouwhen■■
babyfeeds
prepareandfreezemealsinadvancewhenpossible(oraskyourfriends/familytohelp).■■
When the breastfeeding mother is undernourished, it is safer, easier and less expensive to give her more food than to expose an infant under 6 months of age to the risks associated with feeding infant formula or other foods (22)
Parenthandout
qheps.health.qld.gov.au/ahwac/content/home_nemo.htm
24 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Foods that may adversely affect a breastfed infant
Somefoodsthatbreastfeedingmotherseatordrinkcanaffecttheinfant:
alcohol■■
caffeine■■
anyfoodsthatarenotpartofhernormaldiet,egforsome,spicyfoods■■
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Encouragebreastfeedingmothersnottodrinkalcohol.
AlcoholThelevelofalcoholinbreastmilkisvirtuallythesameasamother’sbloodalcohollevel.Evenifonestandarddrinkisingested,asmallquantityofethanolpassesintothebreastmilkandissubsequentlytakenbythesucklinginfantifshefeedstheinfantwhileintoxicated(2).Astheliverremovesthealcoholfromtheblood,thealcoholalsoleavesthemilk.
It is advised not to drink any alcohol when breastfeeding an infant, especially in the first 3 months because it is not clear what negative effects alcohol has on the infant’s rapidly-developing brain.
Additionally, mothersalsoreportalowertolerancetoalcoholwhilstbreastfeeding(24).Anintoxicatedmothershouldnotbreastfeed.Highintakesofalcoholmayaffectthemother’sabilitytolookafterherinfantandincreasesherriskofdevelopingdepression.Largequantitiesofalcoholhavealsobeenseentodisplacegoodnutrition.
Ifmothersdodrink,advisethemtolimittheamountandtakeitjustafterfeeding.Thiswillallowaloweralcohollevelinthebreastmilkbythetimeofthenextfeed(25).
CaffeineSomebreastfeedingmothersreportthattheirinfantisunsettled,irritable,orevenconstipatediftheydrinklargevolumesofcoffee,strongtea,highenergydrinksorcola.However,thereappearstobeindividualvariationinhowmuchcaffeineisfoundinbreastmilkafterhavingahighcaffeinedrink.
Peaklevelsofcaffeinearefoundinbreastmilkapproximately60minutesafteringestion.Newbornsmetabolisecaffeineveryslowly,thehalflifeofcaffeinebeing80hoursinanewborncomparedto2.6hoursina6monthold(24).
Caffeinecanalsoaffectthenutrientmakeupofbreastmilk.Theironlevelsinthebreastmilkofawomanwhodrinksmorethan3cupsofcoffeeadayduringpregnancyandtheearlyphasesofbreastfeeding,areone-thirdlessthanthatofamotherwhodoesnotdrinkcoffee.
Duringbreastfeeding,caffeineconsumptionshouldbelimitedto2to4cupsofcoffee,teaorcolaperday(25).
25A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Just how much caffeine is in that drink or food?
Coffee■■
80to350mgcaffeinepercup,dependingonthetypeofbeansandhowitis■■
prepared
Instant coffee■■
60to100mgcaffeinepercup■■
Decaffeinated coffee■■
2to4mgcaffeinepercup■■
Tea■■
8to90mgcaffeinepercup■■
Energy drinks and coffee flavoured milks■■
upto130mgcaffeineper250mlserve(alsohighinsugar)■■
Cola drinks■■
35mgcaffeineper250mlserve(alsohighinsugar)■■
Cocoa and chocolate drink■■
10to70mgcaffeinepercup■■
Chocolate bars■■
20to60mgcaffeineper200gbar(alsohighinsugarandfat).■■
Additionally,themothershouldbewarnedthatcigarettesmokingcompoundstheeffectsofcaffeineinbreastfedinfants(24).
Formoreinformationaboutthecaffeinecontentinfoodanddrink:
www.foodstandards.gov.au/whatsinfood/caffeine/
www.breastfeeding.asn.au/bfinfo/drugs.html
Food sensitivities Somebreastfedinfantsmaygetupsetorunsettlediftheirmotherseatalotofrichorspicyfoods,orparticularfruitsorvegetables.Ifabreastfeedingmumissuspiciousafoodbeingconsumedisaffectingtheinfant,advisehertostopeatingitforafewdays.Iftheinfantsettlesdown,advisemumtointroducethefoodagaintoseehowitaffectstheinfant.Itmaybehelpfultoavoidthatfoodiftheinfantbecomesunsettledagain. Itisadvisabletospeakwithadietitianornutritionistforfurtheradviceifavoidanceofseveraldifferentfoodsseemstobenecessary.
Guidelinesforpregnantandbreastfeedingvegetariansandveganscanalsobefoundat
www.qheps.health.qld.gov.au/ahwac/content/home_nemo.htm
26 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Sample meal plan for a breastfeeding woman
Breakfast
Wholegraintoast,thinscrapeofmargarineandvegemite/jam/honeyTuboflowfatyoghurt(200g)withpieceoffruit
OR
Bowlofwholegraincerealand1cuplowfatmilkand1cupcannedfruitinnaturaljuiceApieceoffruitorasmallglassoforangejuice
Morning tea
Carrotandcelerystickswithlowfatdip/salsa
Lunch
2-4slicesofbread/breadroll/lavashbread100gleanham/turkeywithmustard/cranberrysauce/2smalleggsSaladeg.lettuce,tomato,beetroot,cucumber
Apieceoffruit
OR
Tinoftunaorsalmonstirredthrough1cupcookedpastaSidesalad
Apieceoffruit
OR
Smalltinbakedbeanson2slicestoastandabanana/apple/orange/2apricotsorplums
Afternoon tea
Bananasmoothie-madewith1cupofmilk,honey,banana
Handfulofsultanas
Dinner
100gleanmeat/chicken/fish/lamb/porkwith2cupsofavarietyofvegetableseg.grilledsteakorfishwithmashedpotato,peas,carrots,broccoli;curriedmeatwithsweetpotato,eggplant,carrots,chickpeas;stirfriedchickenwithcapsicum,ginger,garlic,beansprouts,snowpeas,carrots
Pastasaucewithtinnedtomato,mushrooms,capsicum,zucchiniandpastaorrice
Supper
2piecesofraisintoastwithbananaandhoney
Aglassofwater
Parenthandout:Formenuideasvisitwww.eatwellbeactive.qld.gov.au/eatwellbeactive/eatwelltips/menu_plan.asp
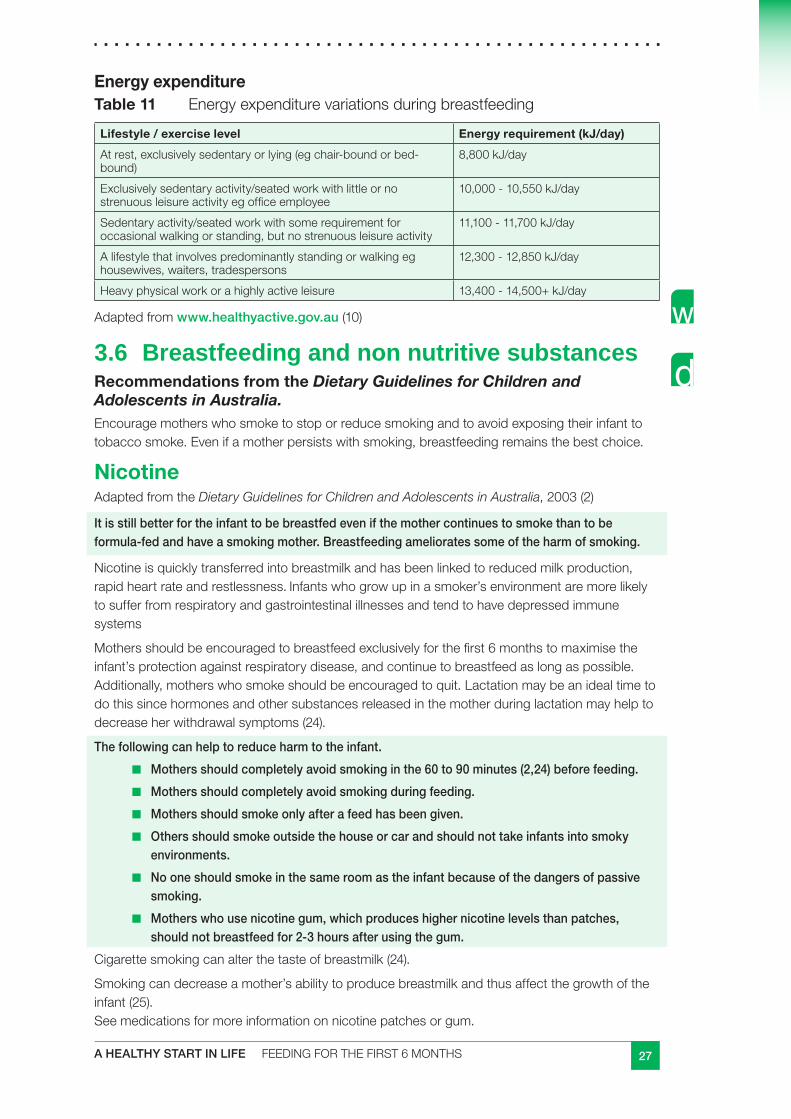
27A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Energy expenditureTable 11 Energyexpenditurevariationsduringbreastfeeding
Lifestyle / exercise level Energy requirement (kJ/day)
Atrest,exclusivelysedentaryorlying(egchair-boundorbed-bound)
8,800kJ/day
Exclusivelysedentaryactivity/seatedworkwithlittleornostrenuousleisureactivityegofficeemployee
10,000-10,550kJ/day
Sedentaryactivity/seatedworkwithsomerequirementforoccasionalwalkingorstanding,butnostrenuousleisureactivity
11,100-11,700kJ/day
Alifestylethatinvolvespredominantlystandingorwalkingeghousewives,waiters,tradespersons
12,300-12,850kJ/day
Heavyphysicalworkorahighlyactiveleisure 13,400-14,500+kJ/day
Adaptedfromwww.healthyactive.gov.au(10)
3.6 Breastfeeding and non nutritive substancesRecommendations from the Dietary Guidelines for Children and Adolescents in Australia. Encouragemotherswhosmoketostoporreducesmokingandtoavoidexposingtheirinfanttotobaccosmoke.Evenifamotherpersistswithsmoking,breastfeedingremainsthebestchoice.
NicotineAdaptedfromtheDietary Guidelines for Children and Adolescents in Australia,2003(2)
It is still better for the infant to be breastfed even if the mother continues to smoke than to be formula-fed and have a smoking mother. Breastfeeding ameliorates some of the harm of smoking.
Nicotineisquicklytransferredintobreastmilkandhasbeenlinkedtoreducedmilkproduction,rapidheartrateandrestlessness.Infantswhogrowupinasmoker’senvironmentaremorelikelytosufferfromrespiratoryandgastrointestinalillnessesandtendtohavedepressedimmunesystems
Mothersshouldbeencouragedtobreastfeedexclusivelyforthefirst6monthstomaximisetheinfant’sprotectionagainstrespiratorydisease,andcontinuetobreastfeedaslongaspossible.Additionally,motherswhosmokeshouldbeencouragedtoquit.Lactationmaybeanidealtimetodothissincehormonesandothersubstancesreleasedinthemotherduringlactationmayhelptodecreaseherwithdrawalsymptoms(24).
The following can help to reduce harm to the infant.
Mothers should completely avoid smoking in the 60 to 90 minutes (2,24) before feeding.■■
Mothers should completely avoid smoking during feeding. ■■
Mothers should smoke only after a feed has been given. ■■
Others should smoke outside the house or car and should not take infants into smoky ■■
environments.
No one should smoke in the same room as the infant because of the dangers of passive ■■
smoking.
Mothers who use nicotine gum, which produces higher nicotine levels than patches, ■■
should not breastfeed for 2-3 hours after using the gum.
Cigarettesmokingcanalterthetasteofbreastmilk(24).
Smokingcandecreaseamother’sabilitytoproducebreastmilkandthusaffectthegrowthoftheinfant(25). Seemedicationsformoreinformationonnicotinepatchesorgum.
28 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Prescription and/or over the counter medicationsAdaptedfromChildHealthfactsheets(12)
Most prescription drugs are compatible with breastfeeding, but each case should be specifically assessed.
Human breastmilk is undoubtedly the most important food an infant can have. It is so important that breastfeeding should only be discontinued if there is strong evidence that a drug taken by the mother will harm the infant.
Choose the right medication
Motherswhoarebreastfeedingshouldnotbegivenamedicationunlessthereisconvincingevidencethatitwillreallyhelpthemother’sconditionatthetime.Aworseningillnesscanhaveagreateraffectonamother’sbreastfeedingabilitythansomemedicaltreatments.Ifthereisarangeofsuitabledrugsavailable,yourdoctororpharmacistshouldchoosethedrugthatistheabsolutesafest,basedonevidence.
Exposure in the womb
Infantsareexposedtomoremedicationinthewombthanthroughbreastfeeding.
Ifmumhasbeentakingmedicationsduringpregnancy–forexample,drugstocontrolepilepsy–theinfantwillalreadyhavebeenexposedtomoredrugsinthewombthanthroughbreastmilk.
Drugstakenbyabreastfeedingmothermaypassintothemilkthroughthemother’sbloodstream,usuallyinverysmallamounts.Theextenttowhichthishappensdependsonanumberoffactors,includingthenatureofthedrugconcerned,thefatcontentofthebreastmilkandthedruglevelinthemother’sbody.Generally,themajorityofmedicationsdonotneedtobeavoidedwhenbreastfeeding.Whenbreastfeedingmumsdoneedmedication,however,advisethemtofeedtheirinfantjustbeforethenextdoseisduetoreducetheinfant’sexposuretothedrug.
Somedrugsmaybecontraindicatedduringbreastfeeding,butthisisacomplexsubject.Advicefromthegeneralpractitionerorpharmacistshouldbesought(2).For more information contact the Royal Women’s Hospital Obstetric Drug Information Service on (07) 3253 7300.
Usethisfactsheetasareadyreferencetoworkoutwhichcommondrugsaresafetotake.www.health.qld.gov.au/child&youth/factsheets/
AlsoseeWorldHealthOrganisation‘BreastfeedingandMaternalMedication’(2002)
Drugs to relieve headache, aches, pain or feverParacetamol,whentakenasdirected,isquitesafetotakewhilebreastfeeding.CommonbrandnamesforparacetamolincludePanadol, Dymadon and Panamax.Aspirin(includingDisprin, Aspro and Solprin)issafetotakeforpainoccasionally,butnotregularly.Moreseverepaincanbetreatedwithstrongerproducts,suchasparacetamol-codeinecombinations.Theseinclude Panadeine, Dymadon Co and Codalgin.Forperiodormuscularpain,taketheabovedrugs.Aswell,anti-inflammatorydrugssuchasibuprofen(Nurofen, Actoprofen)andnaproxen(Naprogesic, Naprosyn)areveryeffective,butshouldbetakeninlowdosesforshortperiodsoftimeonly.Creamsandspraysavailableformuscleachesandpainsaresafetouse.Ponstan and Indocidarebestavoidedbybreastfeedingmothers.
29A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Cold, flu and asthma drugsBreastfeedingmothersshouldtrytoavoidcoldandflutabletscontainingpseudoephedrine,suchasSudafed and Demazin.Pseudoephedrinecansometimescausebreastfeedinginfantstobecomeirritableandrestless.Pseudoephedrinecanalsocauseasignificantreductioninmilkvolume.
Trynasalspraydecongestantsinstead,likeSinex and Otrivin.Lozengesandgarglesaresafeforsorethroats,thoughitisbesttoavoidgarglescontainingpovidone-iodine,suchasfoundinViraban, Betadine, Minidine and Viodine.
Mostcoughmixturesaresafe,butavoidproductscontainingpseudoephedrine.
Asthmatreatmentshouldbethesameforbreastfeedingwomenasforthosewhoarenotbreastfeeding,andisquitesafe.
Hayfever and allergiesTherearesomeantihistaminesonthemarketthatdonotcausesleepiness,andofthose,ioratadine(Claratyne)isthesafestforbreastfeedingmotherstouse.Terfenadine(Teldane)andastemizle (Hismanal) haveoccasionallybeenknowntocauserestlessnessandirritabilityinbreastfedinfants,sotheyarebestavoided.Mostoftheolderantihistaminesmaycausedrowsinessasasideeffect.Howevertheyaresafetousewhilebreastfeedingandincludedexchlorphenirimine (Polaramine)andpheniramine (Avil).
Nasalsprayssuchasbudesonide (Rhinocort) andbeclomethasone(Aldecin and Beconase) arequitesafeandmaybeprescribedforbreastfeedingmothersbytheirdoctor.
ContraceptionIfbreastfeedingmotherswanttotakethecontraceptivepillwhilebreastfeeding,themini-pillonlyshouldbeprescribed.CommonbrandnamesincludeMicrolut, Microval and Micronor.
Otherpills–like Nordette, Microgynon, Triphasil and Tranquilar–shouldnotbetaken.Thesescontainahormone,oestrogen,whichcandecreasemilksupply.
Themorning-afterpill(Postinor-2)isquitesafeforemergencycontraception.
Depot Provera and Depot Ralovera(boththree-monthlyinjectablecontraceptives)areexcretedintobreastmilkinverylowamounts,andarealsosafeforuse.Theyshouldbegivenaboutsixweeksafterthebirth.
Notethatoccasionally,progesterone-onlycontraceptivescanalsoaffectmilksupplyorcauseinfantfussiness.Whenothercauseshavebeenruledout,thisshouldbeconsidered.
ConstipationThesafestlaxativestousearefibre-basedproducts,suchasMetamucil and Fybogel,followedbydocusate(Coloxyl).Largedosesofsennaasfoundin Senokot, Coloxyl with Senna, and Nulax) orbisacodyl(Durolax)cancausediarrhoeainthebreastfedinfant.
30 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Vitamins, minerals and herbal preparations Somevitaminandmineralsupplementsaresafetouseduringthebreastfeedingperiod.
Infact,B-groupvitaminsmaybeparticularlybeneficialtomotherslackingenergy.Andeveningprimroseoilissafetotakewhilebreastfeeding.Beaware,though,thatnaturaldrugslikeherbalpreparationsmaybenatural,buttheymaynotnecessarilybeharmless.Manyherbaldrugscontainchemicalsubstancesthatmaybedangeroustotheinfantandnumerouspoisoningshavebeenreportedinthepast.
So,ifbreastfeedingmotherswanttotakeherbalsupplements,advicefromthegeneralpractitionerorpharmacistshouldbesought.Atalltimes,donotusemorethantherecommendedstandarddoseofherbalproducts,andusesingleingredientproductsratherthancombinationproductsofunknownherbs.
AntidepressantsAntidepressantdrugsareofmanydifferentformsandhavedifferentpharmacologicaleffectsinthebody.Moreover,theycanexertdifferenteffectsindifferentwomen.
Theextentofbreastmilkpassageofantidepressantdrugsalsodifferswithdrugtypeandmother.
Antidepressantsareexcretedinsmallamountsinthebreastmilkanditiscurrentlyunknownwhatlongtermeffectsthismighthaveontheinfant.Thereforeitisrecommendedthatantidepressantsbeusedwithcautionduringbreastfeeding.Thereshouldbediscussionwithbothmedicalpractitionerandpharmacistbeforetakingthesemedications.
TheABAbookletPostnatal Depression and Breastfeedingcontainsvaluableinformationforparentsandhealthprofessionalsaboutdepression,anti-depressantsandbreastfeeding.
SmokingIfbreastfeedingmothersaresmoking,encouragethemtostopordecreasesmokingasmuchaspossible.Nicotinepatchesorgumusedtoquitsmokingissaferthancontinuedsmoking,aslongasyoudonotsmokeaswell.
Motherswhousenicotinegum,whichproducedhighernicotinelevelsthanpatches,shouldnotbreastfeedfor2-3hoursafterusingthegum.
Illicit drugs
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Encourage mothers to… avoid illicit drugs.
Illegal drugs like heroin or marijuana, or prescription drugs like morphine, methadone or oxycodone – can lead to the infant being excessively drowsy and feeding poorly (12).
Prolonged exposure to these drugs can also result in both the mother and the infant becoming dependent on the drugs (12).
31A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Marijuana
Theuseofmarijuanaorexposinginfantstosidestreamsmokeduringbothpregnancyandlactationisdiscouraged.Itisknownthattheactivecomponentofmarijuanaisfatsolubleandshowsaneightfoldaccumulationinbreastmilkcomparedtoplasma(26).
Infantsexposedtomarijuanathroughbreastmilkoftenexhibitsignsofsedation,weaknessandpoorfeedingpatterns.Marijuanausemayalsodecreasemilkproductionandthelongtermeffectsonaninfant’srapidlydevelopingbrainareunknown(26).Ifpossibleitisbesttoavoidusingmarijuanawhilstbreastfeeding(24,27).
Heroin, methadone
Theactivecomponentsofmethadoneandheroin,likemarijuana,areknowntobefatsolubleandconcentrateinthebreastmilk.Heroinusecanresultinlowbirthweightinfants,whocanexperiencebreathingdifficultiesandinfections(27).Ideallyitisbesttorestrictsuchsubstancesduringpregnancyandwhenbreastfeeding.Howeverifthemotherdoesuseheroin,itisnotadvisableforhertostopusingheroinsuddenly.Thiswillresultinthemotherandtheinfantexperiencingwithdrawal.Itisrecommendedthatthemothergoesonamethadoneprogramasthiswillhelpcontrolthemother’sgeneralhealth.Womenwhoareonamethadoneprogramexperiencefewercomplicationsduringchildbirthandpregnancythanthosewhouseheroin.Heroinandmethadonecrossthroughthebreastmilkhowevertheriskofcomplicationsfortheinfantisreducedwithmethadoneuse(27).Itisnotrecommendedtobreastfeedwhilstusingheroin.
Cocaine
Cocaineishighlylipidsolubleandreadilycrossesbiologicalmembranesandshouldnotbeusedduringpregnancyorbreastfeeding(28).Cocainemaycauseprematurelabourandstillbirth,reducethebloodsupplytotheinfantduringpregnancyandincreasetheheartrateofthemotherandinfant(27).Itisrecommendedthatmothersstopusingcocaineearlyinthepregnancy.Cocaineincreasesirritabilityandcancausecocaineintoxication.Itisthereforenotrecommendedwhilebreastfeeding(27).
Amphetamines
Amphetaminesaremembersofaclassofdrugsknownasstimulantsthatincludescaffeine,cocaine,andnicotine.Stimulantshavethecommonpropertyofincreasingactivityinthecentralnervoussystem(29).
Amphetamineaccumulatesinbreastmilk,causingirritabilityandpoorsleeppatterns.Therefore,amphetamineshouldnotbeusedduringpregnancyandlactation(29).
Parenthandoutfoundat
www.rwh.org.au/emplibrary/wads/PregAmphet.pdf
www.rwh.org.au/wads/health-info.cfm?doc_id=3844
32 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.7 Breastfeeding in specific situationsAdaptedfromDietary Guidelines for Children and Adolescents in Australia,2003(2)
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Atpresent,breastfeedingiscontraindicatedwhenamotherisknowntobeHIVpositive(researchintothepossiblebenefitsofantiretroviraldrugsiscontinuing).
There are very few situations for which breastfeeding is contraindicated. Even mothers who have serious conditions are able to breastfeed successfully; among these conditions are:
type 1 diabetes■■
type 2 diabetes■■
gestational diabetes■■
multiple sclerosis■■
systemic lupus erythematosis■■
hypothyroidism■■
hypertension■■
crohn’s disease and ulcerative colitis■■
phenylketonuria■■
cystic fibrosis■■
fibrocystic disease.■■
Absolute contraindications for breastfeedingCurrentlytheNHMRCDietary Guidelines for Children and Adolescents in Australialistthefollowingcontraindicationsforbreastfeeding(2).
Activetuberculosisthathasnotyetbeentreated.Anycontactwiththeinfant,including■■
breastfeeding,isnotpermitteduntilthemotherhasfinishedtwoweeksoftreatment.Theinfantisusuallyprescribedprophylactictreatment.Lactationisinitiatedandmaintainedbyexpressingbreastmilkuntilcontactisapproved.
Brucellosis(undulantfever)which,liketuberculosis,canpassfromthemother’sbloodto■■
thebreastmilk.
Recentlyacquiredmaternalsyphiliswithanunaffectedinfant.Mother–infantcontact■■
andbreastfeedingcanbeginafter24hoursoftherapy,providedtherearenolesionsaroundthebreastsornipples.Iftherearelesionsaroundthebreastsornipples,feedingmaybeginorresumeoncetreatmentiscompleteandthelesionsarehealed.
Breastcancerdetectedduringpregnancy.■■
33A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
HIVinfection.InAustralia,womenwhoareHIVpositiveareadvisednottobreastfeed.■■
Transmissionofthehumanimmunodeficiencyvirusthroughbreastfeedingiswelldocumented.TheUSCentersforDiseaseControlandPreventionadvisewomenwithHIVinfectionnottobreastfeed(2)TheNHMRCandtheAmericanAcademyofPediatricshaveissuedstatementsinsupportofthisposition.Othercountriesmayhavedifferentpolicies.Fordevelopingcountries,theWHOandotherUNagenciescurrentlyrecommendexclusivebreastfeedingbyHIV-positivemothersuntil6monthsofageandthentransfertoothermethodsofbreastfeeding.Useofretroviraldrugsassistsinreducingmother-to-infanttransmission.Itisestimatedthattherateofmother-to-infanttransmissionduringbreastfeedingis10–20%,butallthestudiesarefraughtwithproblemsofdefinitionofexclusivebreastfeeding(2).
Raremetabolicdisordersofinfantssuchasgalactosaemiaandmaplesyrupurine■■
disease,whichseverelylimitorrenderimpossibletheinfant’suseofcertainmilkcomponents.Incasesofphenylketonuria,partialbreastfeedingmaybepossible,providedthereiscarefulmonitoringbyapaediatricianandadietitianwithexpertiseinmetabolicdisease.
HepatitisBinfection,althoughbreastfeedingmaybeginorresumeoncetheinfanthas■■
beenimmunised.
Relative contraindications to breastfeedingCurrentlytheNHMRCDietary Guidelines for Children and Adolescents in Australialistthefollowingconditionsthatmayneedtobeconsideredontheirmeritsbeforeuseofinfantformulaisadvised.
Maternalmedications.Mostdrugsareexcretedintothebreastmilkbutusuallyin■■
concentrationslessthan1–2%ofthematernaldose,whichrarelyposesadangertotheinfant.Somedrugsmaybecontraindicatedduringbreastfeeding,butthisisacomplexsubjectandadvicegivenmaydependonfactorssuchasthedrugdose,thedurationoftreatment,andthenatureoftheillness.Theadviceofthegeneralpractitionerwhoprescribedthemedicationorthepharmacistatthenearestwomen’sorchildren’shospitalshouldbesoughtifthereisanydoubt.
HepatitisC.ThereisasyetnoevidencethathepatitisCistransmittedthrough■■
breastmilk.
Specificillnessesintheinfant.Breastfeedingcancontinueinalmostallcircumstances.■■
Maternalillnessandmalignancy,dependingonthemother’shealthandthemedications■■
used.
Maternalpsychiatricillnessifthereisdefinitedangertotheinfant.Apsychiatrist’sadvice■■
shouldbesought.
34 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.8 Expressing and storing breastmilkParenthandoutatwww.health.qld.gov.au/child&youth/factsheets/default.asp
CheckStorage tips (2,13)
Verylittlespecialhandlingofamother’smilkisnecessary.Sinceitisalreadysterilewhenitcomesfromthebreast,expressedbreastmilkissafertousethanpreparedinfantformula.Itcanbestoredinglassorplasticcontainers,includingsealableplasticbags.Freshlyexpressedmilkcanbechilledintherefrigeratorandaddedtofrozenmilkinthefreezer.
Thefollowingisasimpleguideformothersstoringexpressedbreastmilkathome.
Washhandsthoroughlywithsoapandwater.■■
Refrigerateorfreezemilkafterexpressing.■■
Usefreshmilkwheneverpossible.■■
Freezemilkthatwillnotbeusedwithintwodays.■■
Usetheoldestmilkfirst;datethecontaineratthetimeofcollection.■■
Refrigerator
Breastmilkisbestusedwhenfresh.Amothershouldtrytoprovidefreshbreastmilkdailyforherinfant;ifthisisnotpossible,themilkcanbestoredinarefrigeratororfreezerincleanplasticcontainers.
Breastmilkrefrigeratedat4°Cfor48hourssufferslittlelossofnutrients,orimmunologicalpropertiesandthebacterialcountisactuallyreduced.Breastmilkcanbestoredupto5daysinthefridge.
Chillfreshlyexpressedbreastmilkbeforeaddingtocoldorfrozenmilk.
Freezer
Neverrefreezeorreheatbreastmilk.
Donotthaworwarmbreastmilkinthemicrowave.
Thawbreastmilkbyeitherplacingitincoolorwarmwater(2).
Whenfreezingbreastmilk,leavesomespaceatthetopofcontainer(itexpandsasitfreezes).
Freezeinsmallamountstoavoidunnecessarywastage,eg.50ml.
Fatinbreastmilkwillseparateandrisetothetop–gentlyswirltoremixtheseparatedfat.
Transport
Transportbreastmilkinacoolerwithanicebrickandplaceitintherefrigerator(orthefreezerifitisfrozen)immediatelywhenyouarrive.
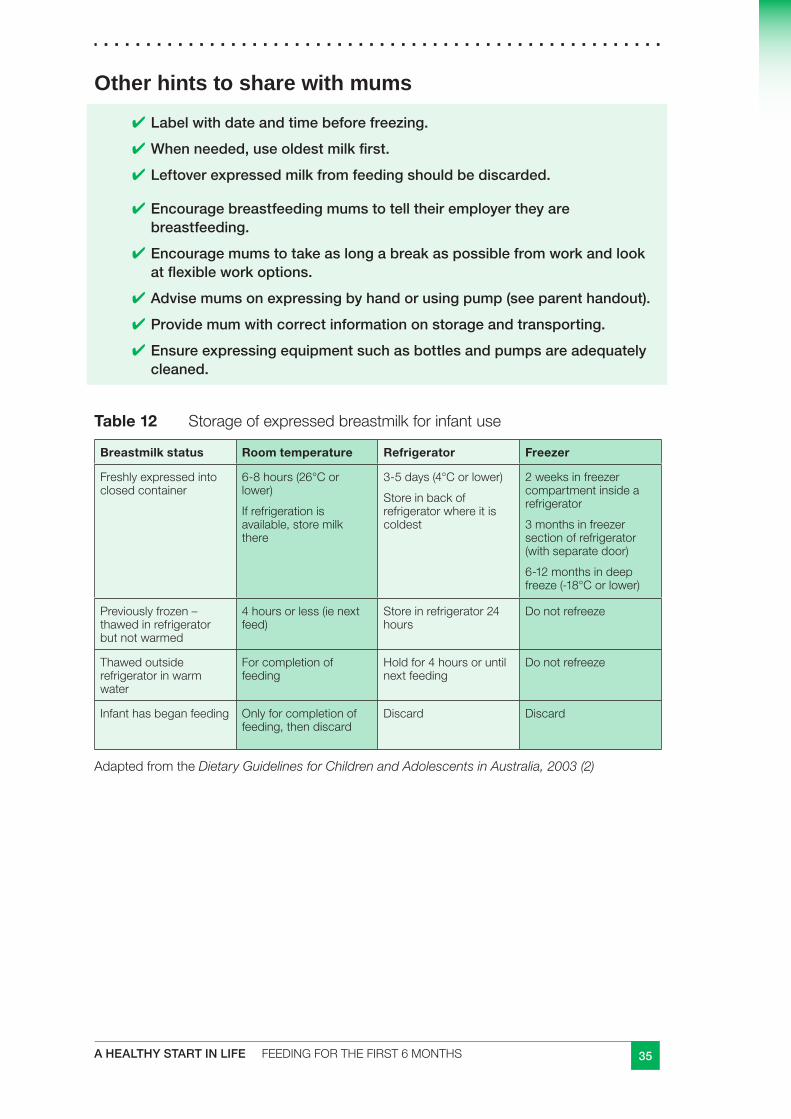
35A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Other hints to share with mums
Label with date and time before freezing.■✔
When needed, use oldest milk first.■✔
Leftover expressed milk from feeding should be discarded.■✔
Encourage breastfeeding mums to tell their employer they are ■✔breastfeeding.
Encourage mums to take as long a break as possible from work and look ■✔at flexible work options.
Advise mums on expressing by hand or using pump (see parent handout).■✔
Provide mum with correct information on storage and transporting. ■✔
Ensure expressing equipment such as bottles and pumps are adequately ■✔cleaned.
Table 12 Storageofexpressedbreastmilkforinfantuse
Breastmilk status Room temperature Refrigerator Freezer
Freshlyexpressedintoclosedcontainer
6-8hours(26°Corlower)
Ifrefrigerationisavailable,storemilkthere
3-5days(4°Corlower)
Storeinbackofrefrigeratorwhereitiscoldest
2weeksinfreezercompartmentinsidearefrigerator
3monthsinfreezersectionofrefrigerator(withseparatedoor)
6-12monthsindeepfreeze(-18°Corlower)
Previouslyfrozen–thawedinrefrigeratorbutnotwarmed
4hoursorless(ienextfeed)
Storeinrefrigerator24hours
Donotrefreeze
Thawedoutsiderefrigeratorinwarmwater
Forcompletionoffeeding
Holdfor4hoursoruntilnextfeeding
Donotrefreeze
Infanthasbeganfeeding Onlyforcompletionoffeeding,thendiscard
Discard Discard
AdaptedfromtheDietary Guidelines for Children and Adolescents in Australia, 2003 (2)
36 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.9 Points to consider when discussing breastfeeding cessation
The most common reasons given by Queensland mothers for breastfeeding cessation was ‘no milk or not enough milk’ (29.6%) (3)
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Encourage, support and promote exclusive breastfeeding for the first 6 months of life.
Breastmilk gives the infant all the nutrients it needs for around the first 6 months of life. After this time infants need solid food in addition to breastmilk. Queensland Health, the National Health and Medical Research Council and the World Health Organization all recommend that breastfeeding continues until the infant is 12 months old and for as long after as suits both mother and infant.
Amother’sdecisiontoceasebreastfeedingmaybeinfluencedbymanyfactorsincludingherexperienceofbreastfeeding.Themostcommonreasonsgivenbymothersforbreastfeedingcessationwas‘nomilkornotenoughmilk’(29.6%),followedby‘childoldenoughtostop’(16%)and‘childselfweaned’(16%)(3).
See‘Ismyinfantgettingenoughmilk?’section
Parenthandoutswww.health.qld.gov.au/child&youth/factsheets
Support from family and friends is a really important part of establishing and continuing breastfeeding (12)
Astheirinfantgetsolder,mothersmayexperiencesomeproblems.Theyarenotsignsaninfantisreadytowean(12).
Low supply
Checkbreastfeedingmumsarefeedingondemand.Explaintheconceptsupply=demand.Refertothesectionandparenthandout‘Ismyinfantgettingenoughmilk’.IfmotherdoeshavealowsupplyprovideherwithinformationonhowtoincreasehermilksupplyandrefertoABAHelplineand/orlactationconsultant.
Teeth
Teethmayinitiallymakethefeedfeeldifferentbutshouldnotcauseanydiscomfort.Bitingmayoccuratthisstagewhentheinfantisgettingusedtoandtestingouther/hisnewteeth.Whenthisoccurs,advisemumstotemporarilyremovetheirinfantfromthebreastandreturnthemwhentheyarereadytofeed.Theinfantwillsoonlearnnottobiteatfeedingtime.
Distractions
Astheinfantgetsolderandmoreinterestedinandawareoftheworldaroundit,theinfantmayfrequentlycomeoffduringafeedtohavealookaround.AdvisemumtotemporarilyfeedinaquietroomwithfewerdistractionsorturnofftheTVduringfeeds.Thisstagetoopasses.
37A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Breast refusal
Infantscansometimesrefusethebreast–thiscanbeone-offorrepeatedandismostoftentemporary.Causescanbeinfantrelated(eg.acold,distractions,teething)ormotherrelated(eg.hormonalchanges,medications,changeinperfume).Trytofindanddealwiththeunderlyingproblem.Ifrefusalcontinues,referraltoanAustralianBreastfeedingAssociationcounsellororlactationconsultantmayberequired.
Return of menstrual cycle
Duetothechangeinmum’shormones,theinfantmaybeabitfussierwithfeeding,howeverthiswillpassafterthefirstfewdaysofthecycle.
Breast care options during weaning (8)Thereareseveralwaystomanagebreastsduringsuddenweaning.Alloptionsshouldbediscussedwiththemothertoallowhertomakeaninformeddecisionregardinghowshewillcareforherbreasts.Thedegreeanddurationofbreastrefillingdependsontheamountofmilkbeingproducedbeforeweaningcommences.Themajorityofbreastdiscomfortshouldresolvewithin72hours.
Ideallyallinfantsshouldbeweanedslowly.Thatis,breastfeedsshouldgraduallybereplacedwithothermilkfeeds.
Somemothershavetoweansuddenlyeg,maternalillness,althoughthisisseldomnecessary,andmedicationsincompatibletobreastfeeding.Propercareofthebreastsisimportanttominimisediscomfortduringthistime.
Breast care options during sudden weaning
Express for comfort only, until lactation diminishes.■■
Express breasts fully twice a day and then once a day as lactation diminishes. ■■
Express in between times for comfort only.
Women with a large milk supply may find option two more comfortable. ■■
It is important to discuss contraception with mums during and after weaning as the ■■
contraceptive effect of breastfeeding will cease once weaning begins.
38 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Women and paid work (2)Returningtopaidworkcanhaveasignificantimpactontheexperienceofbreastfeedingandiscommonlycitedasareasonforceasingtobreastfeed.Amongthefactorsthathavelimitedmothers’abilitytocontinuebreastfeedingare:
Lackofinformationthatbreastfeedingandworkingarecompatibleandpracticalways■■
onhowtodoit.
Lackofsocietalvalueinbreastfeeding.■■
Therelativebrevityofmaternityleave,(returningtoworkcommencesbeforelactationis■■
fullyestablished).
Inflexiblehoursofwork.■■
Lackofpaidbreastfeeding(orpumping)breakswhileatwork.■■
Untilrecently,therightsofawomaninpaidemploymenttobreastfeedherinfanthavebeenneglected;increasingly,though,thesocialenvironmentinAustraliaisallowingmothersthechoiceofworkingandbreastfeedingandthisisbeingrecognisedinemploymentcontracts.ThebookletBalancing Breastfeeding and Work outlinesthebenefitsofpromotingbreastfeeding—foremployers,mothersandinfants.
Healthworkersneedtobewellinformedandpositivewhenadvisingparentsaboutcombiningbreastfeedingandpaidwork.Whenitisnotpossibleforthemothertogotoherinfantduringworkinghours,severaloptionsareavailable:
replacingbreastfeedsduringworkhourswithexpressedbreastmilkfedfromacupora■■
bottle
forinfantsaged6monthsandover,replacingbreastfeedsduringworkhourswithfood■■
fromaspoonandwaterfromacup
replacingbreastfeedsduringworkhourswithinfantformulafedfromacuporabottle.■■
Healthworkersneedtobeawarethatbreastfeedingandformulafeedingcanbecombined:usingformuladoesnotmeanthemotherhastoceasebreastfeeding.Whenformulaisusedduringworkinghours,breastfeedingcanstillcontinuebeforeandafterworkandduringweekends.Acombinationofbothexpressedbreastmilkandformulacanbegiventoaninfantwhenthereisnotenoughexpressedmilk.
CheckouttheQueenslandHealthWorkandBreastfeedingsiteqheps.health.qld.gov.au/breastfeeding/home.htm
39A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.10 When an infant is not receiving breastmilk - infant formula
Formula is widely used and introduced early. Twenty three percent (23%) of all children aged less than 5 years, commenced formula before the age of 4 weeks (4).
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Parentsshouldbeinformedofthebenefitsofbreastfeedingandoftherisksofnot■■
breastfeedingwhenachangefrombreastfeedingisbeingconsidered.
Ifcomplementaryfeedingisconsideredinhospital,themother’sinformedconsent■■
shouldbeobtained.
Ifforanyreasonbreastmilkisdiscontinuedbefore12monthsofage,acommercialinfant■■
formulashouldbeused–insteadofcow’smilk–asthemainsourceofmilk.
Usesoy-basedorotherspecialformulasonlyforinfantswhocannottakedairy-based■■
productsorbecauseofspecificmedical,culturalorreligiousreasons.
Specialtyformulasareindicatedonlyforinfantswithdetectedorsuspectedpathology:■■
theadviceofahealthcareprofessionalshouldbesought.
Itisnotappropriatetousenutritionallyincompletealternatemilksasthesolesourceof■■
nutritionforinfants.
Parenthandoutat
www.health.qld.gov.au/child&youth/factsheets/default.asp
Ifaninfantisnotbreastfedorispartiallybreastfed,thecommercialinfantformulasarethemostacceptablealternativetobreastmilkuntil12monthsofage(2).
Ifbreastfeedingisnotpossible,theuseofaninfantformulawithaddedvitamins,minerals,protein,fatandcarbohydrateisrecommended.Cow’smilkbasedformulaissuitableformostinfantsandisrecommendedoverformulasmadefromsoyorgoat’smilk.Itisnotrecommendedthatinfantformulabechangedregularly.Thereislittleevidencethatchangingformulawillhelpanunsettledinfant.Specialisedformulasshouldonlybeusedwerethereisadiagnosedindicateduseandshouldbedonesoinconsultationwithadietitianormedicalofficer(8).
Regularunmodifiedcow’sorgoat’smilkisnotsuitableforinfantsandshouldneverbeusedinthefirst12months(2).
Soymilkandgoat’smilkformulasdonotreduceallergies,andshouldnotbeusedasanalternativetocow’smilkformulas(2).
40 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Dietary Guidelines for Children and Adolescents in Australia recommendation:
Ifyourinfantisformulafed,pleaseseekadviceonformulafromyourdoctor,childhealthnurseordietitian.Itisrecommendedtokeepyourinfantonformulauntil12monthsofage.
Whenaninfantformulaisused,theinstructionsforpreparationmustbefollowedexactly.
Tips for families
Getting started
Boil water for 5 minutes.■✔
Let it cool.■✔
Use the instructions on the can to make the formula just right for infant. ■✔Too strong and it will hurt the kidneys; too weak and your infant won’t grow well. Measure the formula carefully, using the scoop from the container. Level with a knife. Take care not to mix up scoops from other containers.
Refrigerate made-up milk if not using immediately.■✔
Only keep made-up formula in the fridge for 24 hours.■✔
Only put formula and water in the bottle. Do not add cereal, sugar, cordial ■✔or anything else.
Do not use a bottle to give soft drink, tea or cordial. These are not good ■✔drinks for an infant and will greatly increase their chance of getting tooth decay.
Hold your infant close when feeding. Do not leave your infant alone to drink ■✔the bottle.
Do not put your infant to bed with a bottle containing anything other than ■✔water.
Sterilising bottles
Bottles can be sterilised using boiling, steaming or chemical methods.■✔
Use sterilising chemicals or commercial steamers according to the ■✔manufacturers’ instructions.
Boiling method
Wash hands.■✔
Wash teats and bottles in hot, soapy water using a bottle brush and rinse ■✔well.
Place equipment in a saucepan of cold water.■✔
Bring to the boil and boil for five minutes, turn off and allow to cool.■✔
Store sterilised equipment in a clean, covered container.■✔
Sterilised equipment can be stored in the refrigerator for up to 24 hours.■✔
41A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
How much milk?
Bottlefedinfantsshouldbefedondemand.Eachinfantisdifferentandneedsvaryfromdaytoday.
As a guide:
5days-3months 150ml/kgbodyweight/day
3-6months 120ml/kgbodyweight/day
6-12months 100ml/kgbodyweight/day
Itisimportantthatinfantformulaismadeupaccordingtothedirectionsandisnottoo■■
dilutedoroverconcentrated.
Avoidusingthemicrowaveforheatingbottles.Microwavesdonotheatliquidsevenly.■■
Hotspotscanformandburntheinfant’smouth.
Itmaytakeawhiletosettleintoafeedingroutinethatsuitsbothcaregiversandinfants.■■
Theinfantmaywanttobefedasoftenasevery3hoursduringtheday.Anexactroutine■■
doesnotneedtobefollowed.Whentheinfantsleepsthroughanightfeed,itmeanstheynolongerneedit.Donotwaketheinfanttofeedit.Feedingtimemaylast
20to30minutes.
How to feed
Seat yourself comfortably and hold the infant in your arms while giving the bottle. ■■
Hold the bottle tilted, with the neck and teat filled with formula.■■
If the infant does not firmly grip the teat, gently press under their chin with your thumb and ■■
slightly withdraw the teat to encourage sucking.
This method will help prevent the infant from swallowing air, which can cause wind pain.■■
Check the bottle flow. When the bottle is upside down, the milk should drop at a steady ■■
flow from the teat. Sometimes the teat gets clogged when a powdered formula is used. Check teats often.
Even when fed properly, an infant swallows some air. Burping them helps get rid of it. Hold ■■
the infant upright over your shoulder or upright on your lap with your hand supporting under the chin. Pat or rub the mid back gently until they burp. Do this halfway through the feed and again at the end.
Some infants need to be burped more often. However, if the infant is feeding happily, don’t ■■
stop until they are ready!
Watch for signs that your infant has had enough.■■
Remember
If breastfeeding isn’t possible, feed your infant with infant formula.■■
Talk to a doctor or child health nurse before you start bottle-feeding.■■
Follow the instructions on the can to make the formula just right for your infant.■■
Sterilise bottles by boiling, steaming or using special chemicals.■■
Wash your hands before you prepare a bottle.■■
Feed your infant on demand.■■
Hold your infant while they’re drinking their bottle.■■
42 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
3.11 Useful websites and resourcesBaby friendly hospital initiative (BFHI)
Developed by WHO/UNICEF to encourage health care practices that support breastfeeding while addressing those known to interfere with breastfeeding. The Ten Steps to Successful Breastfeeding, which are outlined in the BFHI and which have been shown to positively influence breastfeeding outcomes, are as follows.
Have a written breastfeeding policy that is routinely communicated to all health care staff.1
Train all health care staff in skills necessary to implement this policy.2
Inform all pregnant women about the advantages and management of breastfeeding.3
Help mothers initiate breastfeeding within a half-hour of birth.4
Show mothers how to breastfeed, and how to maintain lactation even if they should be 5 separated from their infants.
Give newborn infants no food or drink other than breastmilk, unless medically indicated.6
Practice rooming-in - allow mothers and infants to remain together - 24 hours a day.7
Encourage breastfeeding on demand.8
Give no artificial teats or pacifiers (also called dummies or soothers) to breastfeeding 9 infants.
Foster the establishment of breastfeeding support groups and refer mothers to them on 10 discharge from the hospital or clinic.
Formoreinformation:Tel.1300360480or www.acmi.org.au or www.UNICEF.org
TheWHOInternational Code of Marketing of Breast-milk Substitutes and the Marketing in Australia of Infant Formulas: Manufacturers and Importers Agreement providethebasisforcontrolofthemarketingofinfantformulainAustralia
The MAIF Agreement
TheMAIFAgreementistheMarketinginAustraliaofInfantFormulas:ManufacturersandImporters(MAIF)Agreement1992(30).
TheMAIFagreementisAustralia’sresponsetobecomingasignatorytotheWorldHealthOrganisation’sInternationalCodeofMarketingofBreast-milkSubstitutes(WHOcode)(30).
BoththeWHOCodeandtheMAIFAgreementareintendedtoprotectinfanthealthbyprotectingandpromotingbreastfeeding,andensuringtheproperuseofInfantformulaswhentheyareneeded(31).
TheMAIFagreementappliesonlytomanufacturersandimportersofinfantformulaanddoesnotincluderetailersorothermilkproducts,foods,beveragesorfeedingbottlesandteats.

43A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Interpretation and implementation of the WHO Code in Australia (2)
TheWHOCodehasbeenimplementedinAustraliathroughtheMAIFAgreement.
Followingisasummaryofthemainpointscoveredbythesedocuments.
TherestrictionsintheCodeapplytoinfantformulaandotherproductsmarketedor■■
representedasinfantformulasandtofeedingbottlesandteats.Responsibilitiesareoutlinedforcompaniesthatmanufacture,marketordistributetheseproducts,aswellasforhealthworkersandthehealthcaresystem.
Educationalmaterialsproducedbycompaniesforparentsshouldbeunbiasedand■■
consistent;theyshouldincludeallthefacts,describeallthehazards,andavoidreferencetoaspecificproduct.Distributionofmaterialsshouldbeonlythroughthehealthcaresystem,notthroughretailoutlets.
Companiesarenotpermittedtopromotetheirproductstothegeneralpublic,either■■
directlyorthroughretailoutlets.Companiesmaynotgivesamplesorgiftstoparents.Health workers may not give samples to parents.
Healthworkersshouldconsiderthemessageaboutinfantfeedingthattheiractionsand■■
theirhealthcarefacilitygivestomothers.Thereshouldbenodisplayordistributionofproductsorofcompanymaterialsthatrefertoaproductorencourageartificialfeeding.
Marketingpersonnel—eveniftheyarehealthprofessionals—shouldhavenocontact■■
withparentsandshouldnotperformanyeducationalorhealthcarefunctions.
Companiesmayprovidescientificandfactualinformationabouttheirproductsdirectlyto■■
healthworkersthroughmeetingsormaterials.
Companiesmaynotoffer,andhealthworkersmaynotaccept,giftsorother■■
inducementsthatmightinfluenceahealthworker’sproductrecommendationstoparentsortheirhealthcarefacility.Studygrantsmaybeacceptedinsomecircumstances,buttheymustbedisclosed.
AllproductswithinthescopeoftheCodemustconformtostandardsforquality,■■
compositionandlabelling.
IndependentlyofmeasurestakentoimplementtheCode,companiesandhealth■■
workersshouldtakestepstoconformtotheprinciplesandaimoftheCodeandtomonitortheirownpractices.
Modifiedfromwww.health.gov.au/pubhlth/strateg/brfeed/index.htm
TheinfantformulamanufacturershavevoluntarilysignedontotheMAIFAgreementintheinterestofhealthanddevelopmentofinfantsinAustralia.OrganisationsinvolvedintheMAIFAgreementinclude:
HeinzWattiesAustralasia■■
NestleAustraliaLimited■■
NutriciaAustraliaPtyLtd■■
WyethAustralia■■
AbbottAustralasia(10)■■
Despitethisvoluntaryagreement,breachestotheagreementhaveandcontinuetooccur.
44 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Non-governmentorganisations,individualsandprofessionalgroupshavearesponsibilitytomonitorandreportcomplianceornon-compliancewiththeCode(31). Forinformationonhowtodothis,contact
APMAIFSecretariatDepartmentofHealthandAgeingMailDropPoint15GPOBox9848ACT2601Phone(02)62895181
Website(healthprofessionals): www.health.gov.au/internet/wcms/publishing.nsf/content/health-pubhlth-strateg-foodpolicy-apmaif.htm
Key state and national documents for health workers
NationalHealthandMedicalResearchCouncil:DietaryGuidelinesforChildrenandAdolescentsinAustralia,incorporatingtheInfantFeedingGuidelinesforHealthWorkers,Canberra2003.
CommonwealthDepartmentofHealthandAgedCare,NationalBreastfeedingStrategy1996-2001,Canberra
QueenslandHealth:OptimalInfantNutrition:EvidenceBasedGuidelines2003-2008,Brisbane
QueenslandHealth:InfantandChildNutritioninQueensland2003.Brisbane2005
QueenslandHealth:TheHealthofQueenslander2006,ReportoftheChiefHealthOfficerQueensland,Brisbane
QueenslandHealth:GrowingStrong:feedingyouandyourbaby,PublicHealthServices,QueenslandHealth2003
Further professional development reading
BreastfeedingManagement,3rdedition.WendyBrodribb.LigarePty,Ltd,RiverwoodNSW
RamsayD.T.,KentJ.C.,HartmanR.A.,andHartmannP.E.Anatomy of the lactating human breast redefined with ultrasound imaging JournalAnatomy(2005)206pp525-
WorldHealthOrganization:BreastfeedingandMaternalMedication,2002
www.who.int/child-adolescent-health/publications/NUTRITION/BF_MM.htm
ThomasHale:MedicationsandMothersMilk2006,12thed
Parent resources
QueenslandHealth:Childhealthinformationfactsheetswww.health.qld.gov.au/child&youth/factsheets/
QueenslandHealth:ChildHealthInformation:yourguidetothefirst12months
QueenslandHealth:GrowingStrong:feedingyouandyourinfant,PublicHealthServices,QueenslandHealth2003
ArangeofparentresourcesarealsoavailableforpurchasefromtheAustralianBreastfeedingAssociation
45A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Booklets
Eachbookletdealswithspecifictopicsrelatedtobreastfeeding.DrawingoncurrentmedicalandtechnicalinformationandthevastcounsellingexperienceoftheAustralianBreastfeedingAssociationcounsellors,theseeasytoreadbookletscontainpracticalsuggestionsandreflectAustralianBreastfeedingAssociationpoliciesonthemanagementoflactation.Theyvaryinsize,upto36pages.www.breastfeeding.asn.au
Posters
Books
VideoandDVDs
Multilingualresources
Lactationaids
Lactationeducationaids
A note on Growing Strong: feeding you and your baby
TheGrowing StrongresourceshavebeendevelopedtohelpstafftalkwithIndigenousfamiliesaboutnutritionformothers,infantsandyoungchildren.Informationispresentedintwoforms:abookusingstraightforwardlanguageandplentyofillustrations,andamanualwithmoredetailedbackgroundinformation.Growing Strongresourcesprovideinformationabouteatingwellduringpregnancyaswellasofferingsuggestionsfordealingwithsomecommonfoodandnutritionrelatedproblems.Informationisalsoprovidedaboutcommonbreastfeedingissuesincludinghowtoknowwhenababygetsenoughbreastmilkandcorrectpositioningandattachment.
FormoreinformationaboutGrowing Strongcontact:
NutritionPromotionOfficer(IndigenousHealth)NorthernAreaHealthServicePublicHealthNutritionTeamPOBox1103CairnsQLD4870Ph40503600Fax40503662
NutritionPromotionOfficer(IndigenousHealth)CentralAreaHealthServicePublicHealthNutritionTeamPOBox946RockhamptonQLD4700Ph49207383Fax49206865
IndigenousNutritionPromotionOfficerBrisbaneSouthsidePopulationHealthUnitPOBox333ArcherfieldQLD4108Ph30009148Fax30009121
46 A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
A note on the Australian Breastfeeding Association:
TheAustralianBreastfeedingAssociation(ABA)isAustralia’sleadingsourceofbreastfeedinginformationandsupporttoallsectorsofthecommunity.ABAissupportedbyhealthauthoritiesandspecialistsininfantandchildhealthandnutrition.ABAoperatesa7-dayBreastfeedingHelpline,wherecallerscancontactvolunteerbreastfeedingcounsellorstoassistthemwithbreastfeedingissues.ABAprovidesanelectricbreastpumphireserviceaswellasmother-to-mothersupportthroughmorethan75Queenslandgroups.ABA’sMelbourne-basedLactationResourceCentrespecialisesinprovidingcomprehensiveinformationandresourcesonallaspectsofhumanlactation.Studymodulesandthelatestresearcharticlesonbreastfeedingareavailableforafee.
Formoreinformation:ABAQueenslandBranchOffice(07)38446488,7-dayBreastfeedingHelplineStatewidecontactnumbers,(07)38448166or(07)38448977orwww.breastfeeding.asn.au(21)
ReferencesGlobalStrategyforInfantandYoungChildFeeding,WHO2003.[online]1.
NationalHealthandMedicalResearchCouncil:2. Dietary Guidelines for Children and Adolescents in Australia incorporatingthe Infant Feeding Guidelines for Health Workers,Canberra2003.
QueenslandHealth:InfantandChildNutritioninQueensland2003.Brisbane20053.
QueenslandHealth.4. The Health of Queenslanders 2006.ReportoftheChiefHealthOfficer,Queensland,QueenslandHealth.Brisbane2006.
QueenslandHealth:OptimalInfantNutrition:EvidenceBasedGuidelines2003-2008,5.Brisbane.
CoxS.(2005)6. Breastfeeding with confidence.
BrodribbW.(2004)7. Breastfeeding Management.Thirdedition.AustralianBreastfeedingAssociation.
QueenslandHealth,ChildHealthNursesManual,draftSept20068.
KramerMS,KakumaR.Optimaldurationofexclusivebreastfeeding.TheCochrane9.databaseofsystematicreviews.UpdatedNov2004
AustralianGovernmentDeptHealthandAging2006HealthyEatingatVariousLifestages:10.PregnantWomen.[online]www.healthyactive.gov.au/internet/healthyactive/publishing.nsf/Content/pregnant-women.March2007.
QueenslandHealth,ChildHealthRecord.11.
ChildHealthfactsheets[onlineMarch2007]www.health.qld.gov.au/phs/documents/12.cyhu/28101.pdf
AustralianBreastfeedingAssociation,Breastfeedingconfidence:ABAparenthandout13.
47A HEALTHY START IN LIFE FEEDINGFORTHEFIRST6MONTHS
Infantandyoungchildfeeding:standardrecommendationsfortheEuropeanUnion200614.[online]
ilca.org/liasion/Infant-andYoungChildFeeding/EUPolicy06English.pdf15.
DietaryrecommendationsforChildrenandAdolescents:AGuideforPractitioners,16.Paedatrics2006:117;544-559
CallaghanA,KendallG,LockC,MahonyA,PayneJ,VerrierL,Associationbetween17.pacifieruseandbreast-feeding,suddeninfantdeathsyndrome,infectionanddentalmalocclusionIntJEvidBasedHealthc.2005.3:147-167
VallenasC,SavageF.Evidenceforthetenstepstosuccessfulbreastfeeding.Geneva:18.WorldHealthOrganisation,1998
FleischerK.,Cow’smilkinComplementaryFeeding.PaeadtricsVol106,No5,19.SupplmenetNov2000pp1302-1303
TheUseofCow’sMilkinInfancy.PaedatircsVol89No6June1992pp1105-110920.
Tuckertalk: The Family Nutrition Education Manual.21. DepartmentofHealthandCommunityServices,Tasmania.2004
PrescottS.L.,TangM.,(2004)TheAustralasianSocietyofClinicalImmunologyandAllergy22.positionstatement:Allergypreventioninchildren.[online]10thAprilwww.allergy.org.au/pospapers/Allergy_prevention.htm
www.aed.org/ToolsandPublications/upload/FAQMatNutEng.pdf23. [online]27thApril
AndersonJ.,24. IodineEssencearticleVol43,No2March2007
Breastfeedingandtheuseofrecreationaldrugs–alcohol,caffeine,nicotineand25.marijuana,BreastfeedingReview19986(2):27-30
WHOHealthyeatingduringPregnancyandBreastfeeding200126.
HaleT.(1998).MedicationsandMother’sMilk.PharmasoftMedicalPublishing,Amarillo,27.Texas.
Holmes,D.(1998).Alcohol,OtherDrugsandPregnancy.DepartmentofHuman28.Services,Victoria.
Minchin,M.K.(1991)SmokingandBreastfeeding:AnOverview.JournalofHuman29.Lactation,7(4),183-188.
corp.aadac.com/other_drugs/the_basics_about_other_drugs/amphetamines_beyond_30.abcs.asp[online]27thApril
TheMAIFagreement:whatisitandwhatdoesitmeanforyou?[online]31.
www.health.gov.au/internet/wcms/Publishing.nfs/Content/health-pubhlth-strateg-32.foodpolicy-apmaif.htm
MarketingArtificialBabyMilkinAustralia:McGuireE.,HotTopic:LactationResource33.CentreNo23,November2006.
1A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
4.0 Introduction to solidsTheintroductionofsolidsisanessentiallearningexperienceforboththeinfantandfamily.Itisthetimewhenaninfant’seatingandhealthhabitsbegintobeestablished.Theoverallobjectiveofintroducingsolidsistograduallymoveaninfantfrombreastmilkonlyat6monthstoeatingafullrangeofhealthyfamilyfoodsby12months.
Firstattemptsateatingmaybeslowandawkward.Allinfantsdevelopatdifferentratesandsodotheirfeedingpractices,appetite,etc.Caregiversshouldlearntorespondtotheinfant’scueswithpatiencesothatfeedingskillsdevelopoverafewmonths.
Itisimportanttounderstandthattheroleofthecaregiveristochoosethetypeoffood,provideandmakethefood,andit’stheinfant’sroletodecideiftheywanttoeatandhowmuch.
Introductionofsolidshelpswiththebeginningsofspeech,teethandjawdevelopment.
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia (1)
The transition to solid foods
Introducesolidfoodataround6months,tomeettheinfant’sincreasingnutritionaland■■
developmentalneeds.
Startwithlow-allergenicfoodssuchassingle-grainbabycereals;followthiswith■■
vegetablesandfruitsandthenmeats.Addonlyonefoodatatimeandwaitseveraldaysbeforeintroducinganewfood.
Topreventirondeficiency,ironcontainingfoodssuchasiron-fortifiedcerealsare■■
recommendedasthefirstfoods,followedlaterbyfoodscontainingmeatsandotheriron-richfoods.
Alternate milk recommendations
Usebreastmilkorinfantformulauntilthebabyis12months.■■
Pasteurisedwholecow’smilkmaybeintroducedtoachild’sdietataround12monthsof■■
ageandbecontinuedthroughoutthesecondyearoflife–and,ofcourse,beyond.Itisanexcellentsourceofprotein,calciumandothernutrients.
Reducedfatmilks(skimmilkandmilkwith1or2%fat)arenotrecommendedinthefirst■■
2yearsoflife.
Soy(exceptsoyformulawherespecificallyindicated),riceandothervegetarian■■
beverages—whetherornottheyarefortified—areinappropriatealternativestobreastmilk,formulaorpasteurisedwholecow’smilkinthefirst2yearsoflife.
Other fluids in infant feeding
Boilwaterthatistobefedtotheinfantuntil12months.■■
Limittheinfant’sfruitjuiceintake,toavoidinterferingwiththeirintakeofbreastmilkor■■
infantformula.
Donotuseherbalteas,softdrinksorotherbeverages.■■
2 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
4.1 When should solids start?Breastmilkorinfantformulaprovideallthenutrientsrequiredbyaninfantforthefirst6monthsoflifeandcontinuetobeanimportantnutritionalsourceuntil12monthsandbeyond(1,2,3).Ataround6monthstheinfant’sironandzincstoresbegintofallandenergyneedsstarttoincrease.Theinfantshouldalsobeshowingdevelopmentalsignsconsistentwithareadinesstoeat.
Aninfantisreadytoeatwhen:(4)
Theinfanthasgoodheadcontrolandcansitwithsupport.■■
Themouthopenseasilyasthespoontouchesthelipsorfoodapproaches.■■
Reducedtonguethrustreflex—thetonguedoesnotprotrudeasstronglyasfoodenters■■
themouth.
Theinfantcanswallowinsteadofjustbeingabletosuck.■■
Foodstaysinthemouthandismovedtothebackofthemouthandswallowed.■■
Theinfantisinterestedintheworldaroundthem,especiallythecaregiverseating.■■
Itisimportanttonotehoweverthateitherearly(before6months)ordelayedintroduction(after6months)ofsolidscanbedisadvantageousfortheinfantforthefollowingreasons.
Early introduction of solids (1, 5, 6)
Earlyintroductionofsolidscandisplacenutrient-densebreastmilkorformula.Thiscanresultininadequatenutrientsandenergyforgrowth.Insomeinfants,earlyintroductionofsolidsmayencourageoverfeedingandobesityiflargeamountsofsolidsareeateninadditiontousualamountsofbreastmilkorformula.Givingotherfoodsandfluidscanleadtoareductioninthemother’sbreastmilksupply.
Sinceayounginfant’sdigestiveandimmunesystemisnotfullydeveloped,theinfantisplacedatahigherriskofallergyandintolerance.Breastmilkhelpsprotectagainstallergyandisrecommendedasthesolesourceofnutritionforthefirst6months.
Salivaryamylasesarepresentat4months,butpancreaticamylaseswhichareresponsiblefordigestionofcarbohydratesareabsentuntil3months,andremaininadequateuntil6months,thusaffectingdigestion.
Theearlyexposureofinfantstomicrobialpathogenspotentiallycontaminatingcomplementaryfoodsandfluidsputsthematincreasedriskofdiarrhoealdiseases.
Before6monthsofage,thekidneyisnotabletocopewiththeincreasedsoluteloadcausedbysolidfoodsandmayresultinoverloadandanexcessofsodiumintheblood.
Thereisanearlierreturntofertilityformothers,becausedecreasedsucklingreducestheperiodduringwhichovulationissuppressed.
Thecommonreasonsgivenbymothersforstartingsolidsearlyinclude:itwillhelpthebabygainweight,itwillhelpthemsleepthrough,andtheyseemedreadyforsolids.
Nobenefitshavebeenidentifiedfromintroducingsolidfoodsbeforetheageof6months.
3A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
Delayed introduction of solids (1, 5, 6, 7)
Breastmilkorformulaalonemaynotprovideenoughenergyandnutrientsandmayleadtogrowthfalteringandmalnutrition.
Nutrientrequirementschangefrom6months.Theironandzincstorespresentatbirthhavebeguntodecreaseandneedtobemetbyconsumingavarietyoffoods.
Delayedintroductionofsolidscanslowdowndevelopmentalprogress.Theintroductionofsolidsisimportantforjawandmuscledevelopmentandalsoforintellectualstimulation.
Growthcanbeaffectediftheamountofbreastmilkorformulaprovideddecreasesandthereisnoresultingincreaseinfoodprovided.
Texture transition guide
Itisimportantthatinfantsgettherightsortoffoodtexturesattheappropriatetimessothattheiroralmusclesareexercisedappropriately,andthattheygetplentyofpracticesothattheycanmoveontothenexttypeoftexture.
Childrenwhohavedifficultyinprogressingoftenstayeitheronapureedorsoftdietorskipsomeofthetransitions.Thereareanumberofpossiblecausesforchildrennotprogressingwiththeirtransitionofsolids.Theseinclude:
childrenwhohavehadpreviousdifficultywithlumpyorchewyfoodsandmaybe■■
reluctanttotryagain
childrenwhohavedifficultybreakingdownthelumpyorchewyfood■■
childrenwhohavedifficultyusingtheirtonguetomovethelumpsintheirmouth■■
Childrenwhoareunabletoprogressthroughthetextureswillprobablyexperiencelimitedfoodchoicesand,therefore,maylimittheirconsumptionofessentialnutrients.Forsomechildrentheremayalsobealinkbetweendifficultyinprogressingthroughfoodtextures,anddelaysintheirspeechandlanguagedevelopment.
Developmental stages
Birth
Atthisstagethetonguetakesupmostofthespaceinthemouth.Thisallowssufficient■■
suckingtooccurwithsimpleforwardbackwardmovementsofthetongue.
4 – 7 months
Improvedmotorfunction,egheadandneckcontrol,handmovements.■■
Thereisgrowthofthemouthgivingthetonguemoreroomtomoveandassistthebaby■■
togaincontrol.
‘Inandout’movementscharacteristicofthefirstfewmonthsaregraduallyreplacedby■■
‘upanddown’movementsofthetongue.
Feedingbecomesvoluntarywiththetonguemoving‘upanddown’inthemouth.■■
Earlymunchingpatternofthejawcanbeseenwhenfedpureedsolids.■■
Increasedstrengthofsuck.■■
Movementofgagreflexfrommidtoposteriorthirdoftongue.■■
Earlycupdrinkingcanbeintroducedatthisstage.■■
4 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
7 – 12 months
Handtomouthcoordinationimprovestofacilitateselffeeding.■■
Babystartstoclearspoonwithlips.■■
Experimentationwithsoundswhenhands,fingersorotherobjectsareintheirmouths.■■
Developmentof‘upanddown’andlateraltonguemovementsinpreparationfor■■
chewing.
Lipcontrolimproveswhilechewingtopreventspillageoffood.■■
Jawmovementsarecharacterisedby‘upanddown’movements,whichiscalledthe■■
munchingpattern.
12 – 24 months
Begintoselffeedwhichisveryimportantfortactileandmotordevelopment.■■
Atthisstagethechildiseatingwiththefamilyandthemainformofdrinking■■
isfromthecup.
Rotarychewingmovementandimprovedjawstability.■■
Foodsaremovedefficientlyaroundthemouth,spillageisuncommon.■■
Chewingandthelipsealarewelldevelopedsothatfoodandliquidarenotlostfrom■■
themouth.
Please refer to parent handout
Fun not Fuss with FoodFactsheet1Importance of Nutrition
Growing Strong Starting Solidsbrochure
4.2 How should solids be started?Initially,theintroductionofsolidsmaybeslowanduncoordinated,butwithpatience,persistenceandtime,theinfantwilldevelopskills.Breastmilkorinfantformulashouldcontinuetobetheprimarymilksourceforthefirst12monthsoflife.Thequantityofbreastmilkorinfantformulaconsumedwilldecreaseasthevarietyandquantityofotherfoodsincreases.
Chooseatimewhentheinfantishappyandthecaregiveriscalm.■■
Provideasecuredsittingorslightlyreclinedposition,egonthelap.■■
Offerabouthalfateaspoon,withsmoothedges,ofsolidsAFTERabreastorformula■■
feed.
Startwithofferingsolidsonceadayandgraduallybuildupto3timesadayover■■
2months.
2−3mealsperdayforinfantsaged6−8months(8).■■
3−4mealsperdayforinfantsaged9–11monthsandchildren12−24months.■■
Introduceonesinglefoodatatime,onenewfoodevery3-4days.■■
5A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
Typically8–10exposuresareneeded,withclearincreasesinfoodacceptance■■
appearingafter12–15exposures(5)
Oncesinglefoodshavebeenintroducedsuccessfully,starttooffermixedmeals,■■
egricecereal,mincedmeatandvegetables.
Donotaddsugar,honeyorsalttofoods.■■
Donotputthespoonorfoodinadult’smouthbeforeit’sgiventotheinfant–thispasses■■
inbacteriathatcancausetoothdecay.
Ifanyoftheinfant’srelativesareallergictoafood,waituntil12monthstointroduceit■■
andwait5–6daysbeforeintroducingthenextfood.
Theuseofcommercialfoodsmaydelaytheinfant’sacceptanceofthefamily’snormal■■
dietandrepresentsanunnecessaryfinancialburden.
4.3 What solids should be started and when?From 6 monthsWhenstartingsolidfooditneedstobewarm,sloppy,smoothintextureandmildintaste.Itisimportantfortheinfanttolearnthedifferencebetweenliquidandsolidfoods,thereforesolidsshouldnotbeprovidedinabottle.
What
Continuetobreastfeedondemandorformulafeed(about5–6bottlesof200mleach).■■
Givesolidsafterbreastmilkorformulafeeds.■■
Singlegrainironenrichedbabycereal,egironfortifiedricecereal.Mixwithbreastmilkor■■
formulatoasmoothpaste.Cerealswithwheatarenotsuitableatthisstage.
Vegetablesthatcanbecookedandfinelymashed/sieved,skinsremoved.■■
Forexamplepotato,sweetpotato,pumpkin,carrot,zucchini,peas,andlegumes.
Fruitthathasbeenpureedandsieved,skinsandseedsremoved.■■
Forexample,softcookedapple,pear,peach,apricot,banana,avocado,pawpaw.
Meatsthathavebeencooked,pureedandsieved.■■
Forexample,beef,lamb,pork,chicken,legumes.
Cooledboiledwatercanbeofferedfromacupwithaspout.■■
Texture
Smooth,pureed(useablender,foodprocessororsieve).Semiliquidatfirst,thenmorepastelike.
How much
Startwith½teaspoonandbuildupto2–4tablespoons.
6 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
TipsBystartingvegetablesfirstinfantsaremorelikelytoenjoythetastenowandlaterinlife.■■
Followwithfruit,andoncetheinfantiseatingavarietyofvegetablesandfruitstarttointroducemeats.
Foodspreparedinthehomewithfreshingredientsaredesirablebecausefreshfoods:■■
allowtheinfanttobeintroducedtoasinglefoodtasteatatime,■■
increasethevarietyoffoodsthatcanbeoffered,■■
canbemoreeconomicaland■■
assisttheinfantinbecomingfamiliarwithnormalfamilyfoods.■■
Commerciallypreparedbabyfoodsareanutritiousalternative.Ifreliedontotally,they■■
restrictaninfantfromexperiencingotherfoodtastes,astheyoftencontainfoodsinamixedformwhicharesimilarintasteandtexture.
Itisoftenusefultopreparebatchesoffoodwhichcanbefrozenasicecubesforlater■■
useandsealedinsidelabelledplasticbags.Theydefrostquicklyoverhotwater.Thefoodshouldbestirredwelltoevenoutthetemperatureandtestedbeforegivingtothebaby.Discardanyfoodleftoverfromameal.Itisbesttodiscardpreparedfrozenfoodsafter3–4months.Ifthefoodsarestoredintherefrigerator,theyshouldbediscardedafter1day.
Preparefoodwithoutaddingsalt.Itisbesttoallowaninfanttodeveloptasteswith■■
unseasonedfoods.
Oncetheinfanthasteeth,brushteethtwiceadayusingacleansoftclothorsmallsoft■■
toothbrushandathinsmearoflowdosefluoridetoothpaste.
Continuetocheckgrowthregularly.Refertogrowthchartsection.■■
Please refer to parent handout
ChildandYouthHealthFactSheetFeeding from 6 months.
From 8 monthsTheinfantshouldbeeatingpureedmeats,babyricecereal,pureedfruitandvegetableswithcontinuedbreastmilkorformula.
What
Continuebreastfeedingondemandorformulafeeding(90-100ml/kgbodyweight/day).■■
Givesolidsbeforebreastmilkorformulafeeds.
Addmixedinfantcereals,oats,barley,rye,semolina,ricepasta,wheatflakedbiscuits■■
andrusks.
Vegetables–allsortscookedandmashedwithsoftlumps.■■
Fruit–allkindswithskinandseedsremoved.■■
Meat–continueasat6monthsbutaddinfish(freshortinnedunsaltedwaterpacked)■■
andeggyolks.
Cooledboiledwaterfromacupwithaspout.■■
7A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
Texture
Mashed,somelumpscanbetolerated.Stoppureeing.Importanttoencouragetexturetransition–ifthisisdelayeditcanleadtofussyeatingastheinfantgetsolder.
How much
2tablespoonsto½cup
Buildupto3timesaday
Sample menu
Breakfast
Babycereal(3-4tablespoons)mixedwithbreastmilk,formulaorwater
Mashedfruit2tablespoons)
Breastmilkorinfantformula
Mid morning
Breastmilkorinfantformula
Lunch
Strained(blended)meat(2tablespoons)
Strained(blended)vegetables(2tablespoons)
Breastmilkorinfantformula
Mid afternoon
Breastmilkorinfantformula
Dinner
Strained(blended)meatorfish(2tablespoons)
Mashedvegetables(2tablespoons)
Strained(blended)fruit(2tablespoons)
Breastmilkorinfantformula
Checkgradually change the texture from smooth puree, to mashed with a fork, ■✔to mashed with lumps
the infant is the only one who knows when they have had enough■✔
this period can be quit messy, but this is normal■✔
sugar and salt should not be added to solids■✔
check the infant’s growth regularly ■✔Refer to growth chart section
Please refer to parent handout
ChildandYouthHealthFactSheetFeeding from 8 months.
8 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
From 9 monthsTheinfantshouldbeeatingmeatandfish,cereals,fruitandvegetablesaswellasbreastmilkorinfantformula.By9–12months,finemotorcontrolandpincergripshouldhavedeveloped.Aninfantshouldbeeatingthesamefoodsastherestofthefamilyandbeingencouragedtoexperimentwithfingerfoodsandselffeeding.
What
Continuebreastfeedingondemand,ifformulafed(90–100ml/kgbodyweight/day)■■
iearound600–800ml/day.
Cereals–continuewithinfantcerealforiron,whiteorwholemealbreadandtoast.■■
Vegetables–includeallvegetables,includingsomeraw.■■
Fruit–includeall,removetoughskinsandlargeseeds,softfruitsgiveninpieces.■■
Meat–removeallskin,gristleandbonesfrommeat.■■
Dairy–fullfatdairyproducts,egyoghurt,custard,gratedcheeseandcottagecheese.■■
Pasteurisedcow’smilkinthepreparationofmainmealsanddesserts.Milkshouldnotbeprovidedasadrinkuntil12months.
Cooledboiledwaterfromacupwithaspout.■■
Texture
Piecesorchopped–fingerfood.
How much
3mealsadaywithsomesnacks,about1½cupsateachmeal.
TipsThe change in texture is very important for jaw and speech development.■✔
Finger foods are popular and the infant should start to self feed.■✔
Lollies, soft drinks, cordials or other sweetened foods are not ■✔recommended. They can displace other important nutrients, interfere with appetite, cause diarrhoea and lead to tooth decay.
It is best to leave hard foods such as popcorn, corn chips, hard lollies ■✔and some hard raw fruit and vegetables until four years of age to avoid choking.
Please refer to parent handout
ChildandYouthHealthFactSheetFeeding from 9 months.
9A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
From 12 monthsThechildshouldbeeatingawidevarietyoffamilyfoods.Sweet,salty,processedorfattyfoodsshouldbeavoided.
What
Foodstoinclude
Fullcreamcow’smilk■■
Wholeegg■■
Peanutbutter■■
Unboiledwater■■
Texture
Familyfoods–somefoodswillneedtobecutintosmallpieces.
How much
Continuedbreastfeedingisrecommended.Breastmilkstillprovidesimportantnutrients■■
intothechild’ssecondyearoflife.
After12monthsinfantformulacanbereplacedwithcow’smilk.Noneedforinfant■■
follow-onformula.
Givesolidsbeforefluids.■■
3mealsadayandsnacks.Thisisdependantonage,growthandactivitylevels.■■
TheNationalHealthandMedicalResearchCouncilhavenotdevelopednationallyendorsedfoodgroupservingsfor1-3yearoldsasithasforchildrenfouryearsandolder.Atthisagethereismarkedvariabilityinhowmuchindividualchildreneat.Howmuchfoodiseatenvariesfromchildtochildandfromdaytodayandisinfluencedbygrowthandactivitylevels.
Ensurethatthechildhasfoodsfromallfivecorefoodgroupsandhasavarietyoffoodsfromwithineachfoodgroup.Theemphasisisonhealthyfamilyfoodsandhavinganenvironmentaroundeatingthatencourageshealthyfoodbehaviours.Intakecanbemonitoredbyassessingthechild’sgrowthanddevelopment.
Thefollowingsamplemenuisaguideonly.
10 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
Sample menuBreakfast
Cerealmadewithmilk
Toastwithspread
Fruit
Breastfeed/milkdrink
Morning tea
Toastorcrackerswithspread
Drinkofmilk
Fruit
Lunch
Meat/chicken/fish/egg/legumes
Vegetables(raworcooked)
Bread
Afternoon tea
Yoghurt
Pikeletorfruitbread
Fruit
Dinner
Meat/chicken/fish/egg/legumes
Vegetables(raworcooked)
Rice/pasta/noodles
Avoidhoneyforinfantslessthenoneyearofage.TheorganismthatcausesinfantbotulismhasbeenfoundinsomehoneysinAustralia.Theinfant’sgutatthisagedoesnothaveenoughresistancetoprovideadequateprotectionfromthesebacteriawhichproducesalethaltoxin.Itshould,therefore,beexcludedfromthedietuntilafter1yearofage(5).
Please refer to parent handoutChildandYouthHealthFactSheetFeeding from 12 months.
ChildandYouthHealthFactSheetSolids Table.
ChildandYouthHealthFactSheetRecipes for Babies.
Fun not Fuss with FoodFactSheet2Is this Normal?
Allergies
Ifthereisafamilyhistoryofallergytrytodelaythecommonlyallergenicfoodsuntil12monthsespeciallywherethereisastrongfamilyhistoryofpreviousreactionsincaregiversorsiblings.
Foodsshouldneverberestrictedinchildrenunnecessarilyasgrowthandhealthmaybeaffected.Ifinanydoubtthegeneralpractitionershouldbeconsulted.Areferraltoapaediatriciananddietitiancanthenbearranged.
Refertosectiononallergies.
Pleaserefertoparenthandout
ChildandYouthHealthFactSheetFood Allergies.
11A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
4.4 DrinksWateristhefluidofchoice.Itneedstobecleanandboiledforinfantslessthan12monthsofage.Itisgoodtoencouragechildrentoacceptthetasteofwaterfromanearlyageandtoconsumeappropriateamounts.Waterisessential,notonlytoensuretheinfant/childremainswellhydrated,butalsotoassistinmaintainingregularbowelactivity.Breastmilkis87%water,soexclusivelybreastfeedinfantswhoarebreastfedondemandwillgenerallyreceiveadequatefluid.Nonbreastfedinfantsneedatleast400–500ml/dayextrafluidfromothersourceswhencomplementaryfoodsaregiven,aswellasinfantformula,andupto1200ml/dayinahotclimate.
Fruitjuices,softdrinksandcordialsshouldbeavoided.Theycontainsugarswhich,becauseoftheiraciditycancausedentalcariesanderosionoftheteethandmayreplacetheamountofbreastmilkorformulaconsumedandmayalsoinitiateapreferenceforsweettastes.Thesedrinksarealsoveryhighinenergy;whileprovidinglimitedsatietytheycontributeasignificantamountofenergytothediet.Theseshouldneverbegiveninabottle.In2003,15%ofchildreninQueensland,lessthan1yearofage,hadbeengivensweetdrinksregularly(9).
Teaisnotsuitableforinfantsandyoungchildren.Teacontainstanninsandothercompoundsthatbindironandreduceitsbioavailability.Herbaldrinks/preparationsarenotsuitableforinfantsandyoungchildren.Infantsarepotentiallymorevulnerablethanadultstothepharmacologicaleffectsofthechemicalsubstancesinherbaldrinks.Thereisalackofdataonthesafetyofherbalteasforinfants.
Milkremainsanimportantdrinkthroughoutchildhoodandassuch,consumptionofadequateamountsshouldbeencouraged.Includeupto500ml/dayonly.
Aninfantorchildshouldbeencouragedtodrinkfromacupbyabout6months.
Parenthandout
Growing Strong Healthy Drinks for Babies
NSWHealthTeach your baby to drink from a cup.
CheckTry not to expect too much. Infants and children have small appetites and ■✔stomach capacities.
Allow an infant to exert some independence. Do not force an infant or child ■✔to finish everything on the plate.
Turn a blind eye to the mess produced as a result of the feeding attempts.■✔
A relaxed and comfortable atmosphere during meals will facilitate good ■✔eating practices, as well as providing an opportunity for social interaction and cognitive development.
It is normal for an infant’s stools to change in colour and consistency as ■✔solids are introduced. Refer to constipation section for more information.
Vegetarian diets in infants can be concerning due to the high risk of ■✔nutritional deficiencies, malnutrition, growth retardation and delayed psychomotor development. Infants should be referred to a paediatric dietitian or paediatrician to assess the adequacy of the diet and appropriate growth.
12 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
4.5 Salt in foodDietarysaltisaninorganiccompoundconsistingofsodiumandchlorideions.Itisfoundnaturallyinmanyfoods,butitisalsoaddedtomanyfoodsbecauseofitspreservativeandflavouringcharacteristics.
Recommendedintakeforsodium(1)
0–6months 140–280mgperday
7–12months 320–580mgperday
1–3yearolds 460–1730mgperday
1000mgsodiumiscontainedinabout3gofcommonsalt,orjustoverhalfateaspoon.
Toachievethisintake,infantsandchildrenshouldconsumefreshfood,foodsnormallyprocessedwithoutsalt,andlowsaltornoaddedsalt,andavoidaddingsalttofood(10).
Forinfants,ingestionoffoodshighinsodiumcanleadtodeathbecausethekidneysarenotfullydevelopeduntilmanymonthsafterbirth.Thisisanotherreasonwhysolidsshouldnotbeintroduceduntil6monthsofage.ThenewfoodstandardscodeforAustraliaandNewZealandstipulatesthetotalamountofsodiumallowedinfoodsforinfantsisamaximumof100mg/100ginflours,pastaandreadytoeatfoods.However,inbiscuitsitis300mg/100gand350mg/100gtoteethingrusks.Incomparison,thesodiumcontentofbreastmilkis18mg/100g.
Food Standards Australia New Zealanddefinesalowsaltfoodasafoodwithasodiumconcentrationofupto12mg/100g.
4.6 Sugar in foodManyfoodsintheAustraliandietcontainnaturallyoccurringsugars.Inotherfoods,sugarsmaybeaddedduringprocessingtoincreasethefood’spalatabilityandacceptabilityandsometimestoaddbulk.Sugarsprovideareadilyabsorbedsourceofenergyandhaveanimportantroleassweetenersandflavourenhancers.
Thepresenceofhighamountofsugarscandilutethenutrientdensityofthediet,anddietshighinaddedsugarhavebeenassociatedwithdevelopmentofobesityanddentalcaries.
Tastebudsdetectfourprimarytastequalities:sweet,bitter,saltandsour.Children’spreferenceforamajorityoffoodsareinfluencedbylearningandexperience,theydevelopapreferenceinrelationtothefrequencyandexposuretoparticulartastes.Theonlyinnatepreferenceisforsweet,andevennewborninfantswillavidlyconsumesweetsubstancesifgiventhem.Itisthereforeimportantnottointroducesugarinanyconcentratedformuntiltheinfanthasachancetoexperienceanddevelopatasteforotherflavours,especiallyfruitsandvegetables(5).
Parenthandout
Foodlabelposter
http://www.foodstandards.gov.au/_srcfiles/final%20FSANZPosterV2.pdf
13A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
4.7 Useful websites and resourcesQueensland
ChildHealthFactSheetswww.health.qld.gov.au/child&youth/factsheets/
CommunityChildHealthwww.health.qld.gov.au/cchs/nutrition.asp
GrowingStrong:feedingyouandyourbabymanualwww.health.qld.gov.au
FunnotFusswithFood
OrderformfornonQHstaff■■
www.health.qld.gov.au/phs/Documents/sphun/27967.pdf
OrderformforQHstaff■■
qheps.health.qld.gov.au/PHS/Documents/sphun/27966.pdf
Fact Sheets
qheps.health.qld.gov.au/PHS/Documents/sphun/27484.pdf
RoyalChildren’sHospitalHealthServiceDistrictDepartmentofNutritionandDietetics–Infantandtoddlerfeedingguide-ParentInformation(2004).HardcopiesavailablefromNutritionandDieteticDepartmentph0736368571.
RoyalChildren’sHospitalHealthServiceDistrict–CommunityChildHealthService:TimetoEat–baby’sfirstfoods(2004).Heathpromotionandpreventionissues,educationdocumentservicescchs106,secondedition.Ph0732508530officermanagerprimarycareprogramcost$104.60includingGSTpluspostage.
RoyalChildren’sHospitalHealthServiceDistrict–CommunityChildHealthService:FirstSteps
qheps.health.qld.gov.au/rch/cchs/Resources/first_steps.pdf
New South Wales
Teachyourbabytodrinkfromacup.
www.mhcs.health.nsw.gov.au
South Australia
Foodsforbabies(solids)
www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=302&id=1487
Foodsforbabies(solids)questionsandanswers
www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=302&id=1927
Nutritiontopics
www.cyh.com/HealthTopics/HealthTopicCategories.aspx?p=302
Tasmania
TuckerTalkManual(2003).DepartmentofHealthandHumanServicesTasmania.Ph0362227222
14 A HEALTHY START IN LIFE INTRODUCTIONTOSOLIDS
National
RaisingChildrenNetwork
www.raisingchildren.net.au/nutrition/babies_nutrition.html
NHMRC
www.health.gov.au/nhmrc/publications
Hillis,AandStone,P(2003).BreastBottleBowl.HarperCollinsPublishers
International
WHO
http://www.who.int/child-adolescent-health/NUTRITION/infant.htm
InternationalAssociationofInfantFoodManufactures
www.ifm.net/sitemap.htm
EllynSatter
http://www.ellynsatter.com/index.htm
ReferencesNationalHealthandMedicalResearchCouncil.1. Dietary Guidelines for Children and Adolescents in Australia: Infant Feeding Guidelines for Health Workers,Canberra2003
QueenslandHealth(2003).OptimalInfantNutrition:EvidenceBasedGuidelines2.2003-2008,
WHO(2002).GlobalStrategyforInfantandYoungChildFeeding.Geneva:WorldHealth3.Organization.
QueenslandHealth(2005).ChildandYouthHealthFactsheets[online]4.www.health.qld.gov.au/child&youth/factsheets
Infantandyoungchildfeeding:standardrecommendationsfortheEuropeanUnion20065.[online]http://ilca.org/liasion/Infant-and-YoungChildFeeding/EUPolicy06English.pdf
Children,women’sandyouthhealthservice,SAgovernment.Foodsforbabies–howand6.whentostart[online]www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=302&id=1487
BrownKH.(2000).WHO/UNICEFReviewoncomplementaryfeedingandsuggestions7.forfutureresearch:WHO/UNICEFguidelinesoncomplementaryfeeding.Pediatrics106(5):1290
WHO(2001).ComplementaryFeedingSummaryofguidingprincipals.Geneva8.[online]http://www.who.int/child-adolescent-health/New_Publications/NUTRITION/Complementary_Feeding.pdf
QueenslandHealth.InfantandChildNutritioninQueensland2003.[online]9.http://www.health.qld.gov.au/hic/epidemiology/nutrition_report2005.pdf
McCarronDA.(2000)Thedietaryguidelineforsodium:shouldweshakeitup?Yes!10.AmJClinNutr71:1013-19
1A HEALTHY START IN LIFE TODDLERNUTRITION
5.0 Toddler nutrition5.1 Why is nutrition important in toddlers?Thetoddleryearsofachild’slife,thatistheagesbetween1and3,presentanexcitingandbusytimeforchildrenastheybegintoexplorelifeindependently.Itisatimewhenchildrenarelearningeatingbehaviours,skills,knowledgeandattituderelatingtofood(1);auniqueperiod,whichinstilsattitudesandpracticesthatcanformthebasisforlifelonghealth-promotingeatingpatterns(1,2,3).
Theseyearsforcaregiverscanbequitedaunting.Toddlersareexploringtheirindependence,whilst“forcaregiversitisthetimetoteachtheirchildtoeatwiththefamilyandtryawidevarietyoffoodsandtastes”(3).“Thetimebetween18monthsand3yearscanbedifficultforbothadultsandchildrenalike.Thisistheperiodwheninfantsbegintorecognisethemselvesasseparatefromtheadultsintheirlife...Theyenterintopowerstruggleswiththeiradultcaregiver;atthesametime,theyarefearfulofnewexperiences.Thesebehavioursareparticularlyevidentinfeedingsituations”(4).
Anenormousshiftoccursinthevarietyofaninfant’sdietfromtheperiodof6to12months.Bythetimeachildis12monthsold,therelianceonthebreastorformulaasthesolefoodsourcehasdecreased,andthetoddlershouldbeeatingavarietyoffamilyfoods,aswellselffeedingandlearningtodrinkfromacup.Healthyeatingisimportant-it“providestheenergyandnutrientsneededforgrowthanddevelopment;itdevelopsasenseoftasteandanacceptanceandenjoymentofdifferentfoods”(5).
Poornutritioninchildrencanleadtocommonchildhoodnutritionproblemssuchasconstipationandirondeficiencyanaemia(seerespectivesections).Also,ifinadequatefoodisconsumed,childrendonothaveenoughenergytoexplore,discoverandlearnastheyshould.Inadditiontheymaynotprogressoptimallyinthelongterm,inareassuchasmotordevelopment(movement,motorskills),physicaldevelopment(heightandmuscledevelopment)andcognitivedevelopment(5).Developinghealthyeatinghabitsinchildhoodcanreducetheriskofnutritionrelatedchronicdiseaseinlaterlife(8).
So,let’stakeitbacktobasics.Thischapterexploresthe‘parent-childfeedingrelationship,’(3,4,5,7,8)recognisingtheimportanceofboththeparentandchildinthecomplexprocessofeatingandmealtimes,particularlyinthecontextoffussyeating.
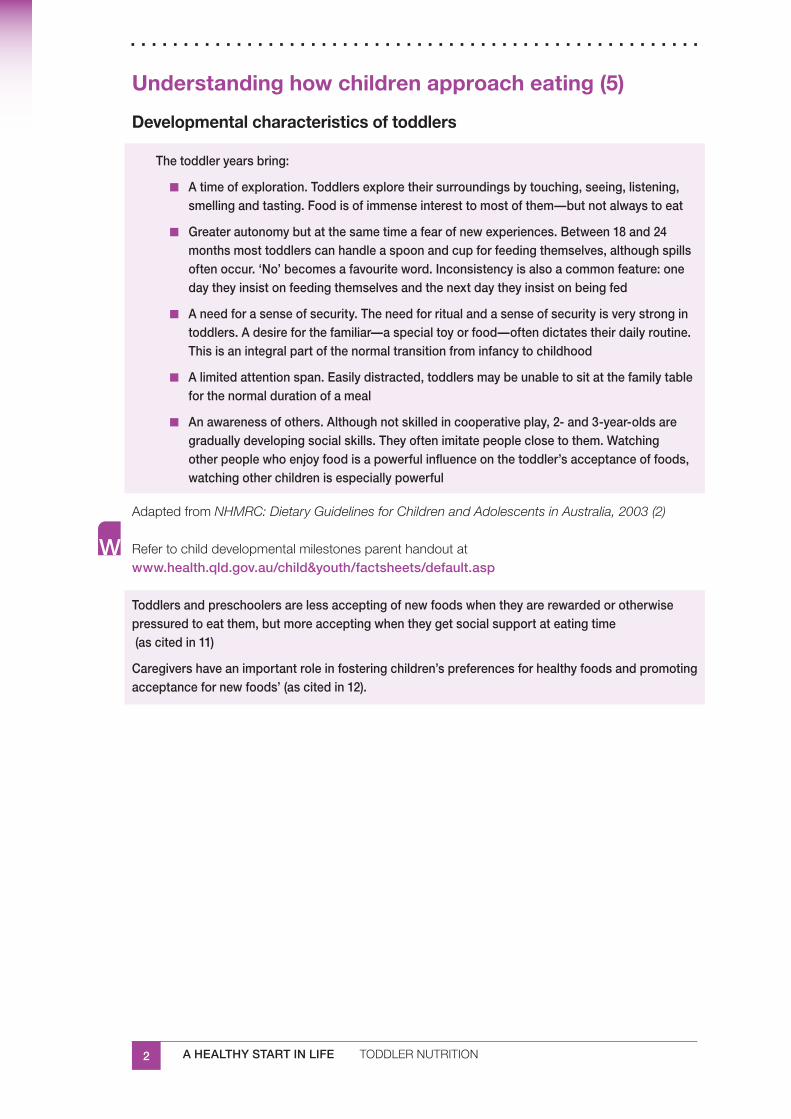
2 A HEALTHY START IN LIFE TODDLERNUTRITION
Understanding how children approach eating (5)
Developmental characteristics of toddlers
The toddler years bring:
A time of exploration. Toddlers explore their surroundings by touching, seeing, listening, ■■
smelling and tasting. Food is of immense interest to most of them—but not always to eat
Greater autonomy but at the same time a fear of new experiences. Between 18 and 24 ■■
months most toddlers can handle a spoon and cup for feeding themselves, although spills often occur. ‘No’ becomes a favourite word. Inconsistency is also a common feature: one day they insist on feeding themselves and the next day they insist on being fed
A need for a sense of security. The need for ritual and a sense of security is very strong in ■■
toddlers. A desire for the familiar—a special toy or food—often dictates their daily routine. This is an integral part of the normal transition from infancy to childhood
A limited attention span. Easily distracted, toddlers may be unable to sit at the family table ■■
for the normal duration of a meal
An awareness of others. Although not skilled in cooperative play, 2- and 3-year-olds are ■■
gradually developing social skills. They often imitate people close to them. Watching other people who enjoy food is a powerful influence on the toddler’s acceptance of foods, watching other children is especially powerful
AdaptedfromNHMRC: Dietary Guidelines for Children and Adolescents in Australia, 2003 (2)
Refertochilddevelopmentalmilestonesparenthandoutatwww.health.qld.gov.au/child&youth/factsheets/default.asp
Toddlers and preschoolers are less accepting of new foods when they are rewarded or otherwise pressured to eat them, but more accepting when they get social support at eating time (as cited in 11)
Caregivers have an important role in fostering children’s preferences for healthy foods and promoting acceptance for new foods’ (as cited in 12).
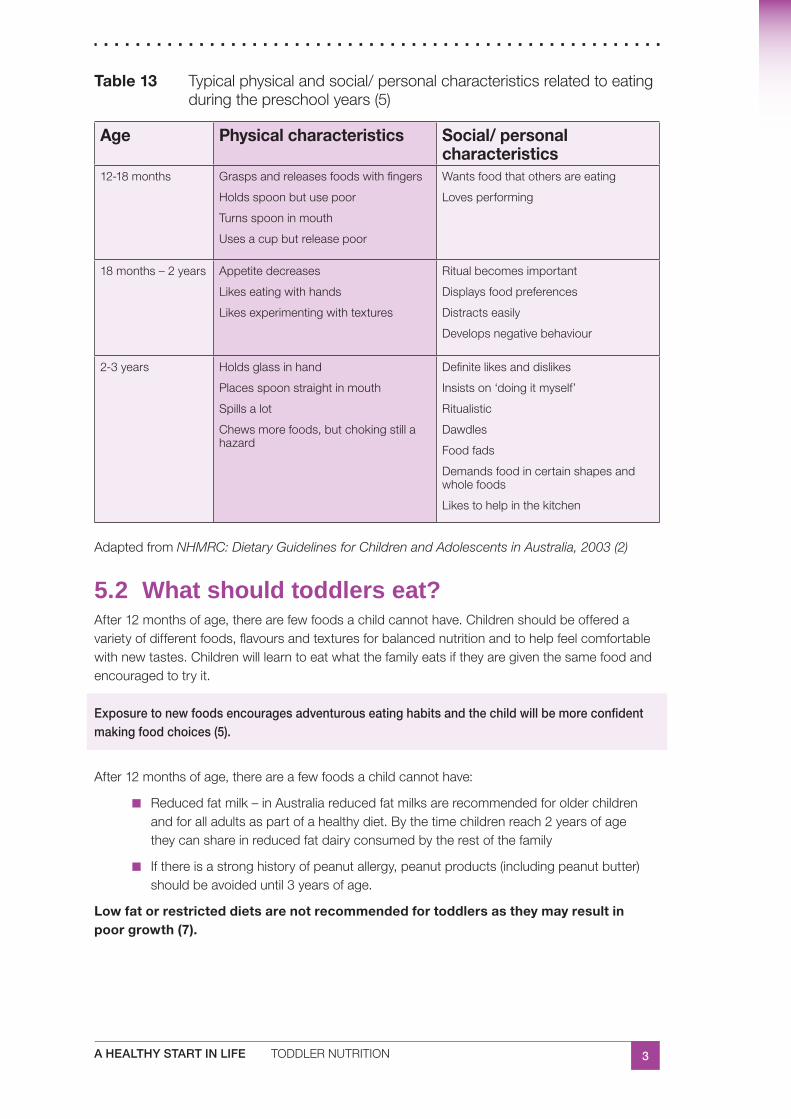
3A HEALTHY START IN LIFE TODDLERNUTRITION
Table 13 Typicalphysicalandsocial/personalcharacteristicsrelatedtoeatingduringthepreschoolyears(5)
Age Physical characteristics Social/ personal characteristics
12-18months Graspsandreleasesfoodswithfingers
Holdsspoonbutusepoor
Turnsspooninmouth
Usesacupbutreleasepoor
Wantsfoodthatothersareeating
Lovesperforming
18months–2years Appetitedecreases
Likeseatingwithhands
Likesexperimentingwithtextures
Ritualbecomesimportant
Displaysfoodpreferences
Distractseasily
Developsnegativebehaviour
2-3years Holdsglassinhand
Placesspoonstraightinmouth
Spillsalot
Chewsmorefoods,butchokingstillahazard
Definitelikesanddislikes
Insistson‘doingitmyself’
Ritualistic
Dawdles
Foodfads
Demandsfoodincertainshapesandwholefoods
Likestohelpinthekitchen
AdaptedfromNHMRC: Dietary Guidelines for Children and Adolescents in Australia, 2003 (2)
5.2 What should toddlers eat?After12monthsofage,therearefewfoodsachildcannothave.Childrenshouldbeofferedavarietyofdifferentfoods,flavoursandtexturesforbalancednutritionandtohelpfeelcomfortablewithnewtastes.Childrenwilllearntoeatwhatthefamilyeatsiftheyaregiventhesamefoodandencouragedtotryit.
Exposure to new foods encourages adventurous eating habits and the child will be more confident making food choices (5).
After12monthsofage,thereareafewfoodsachildcannothave:
Reducedfatmilk–inAustraliareducedfatmilksarerecommendedforolderchildren■■
andforalladultsaspartofahealthydiet.Bythetimechildrenreach2yearsofagetheycanshareinreducedfatdairyconsumedbytherestofthefamily
Ifthereisastronghistoryofpeanutallergy,peanutproducts(includingpeanutbutter)■■
shouldbeavoideduntil3yearsofage.
Low fat or restricted diets are not recommended for toddlers as they may result in poor growth (7).
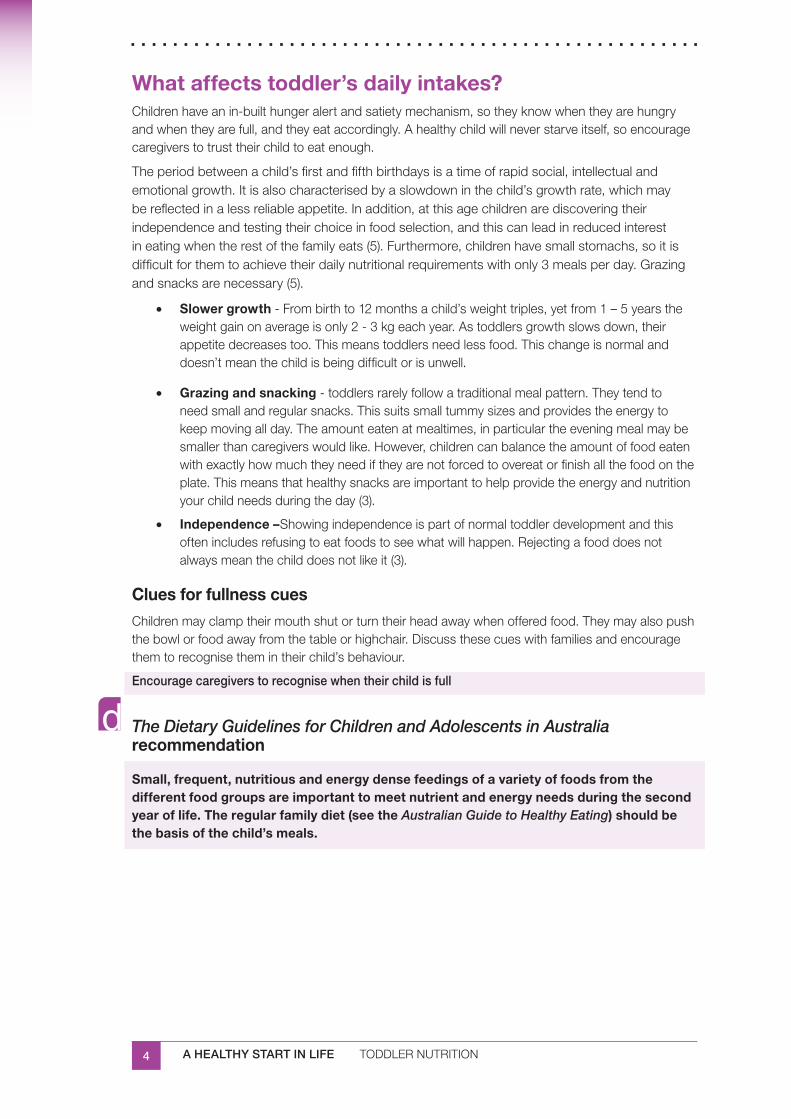
4 A HEALTHY START IN LIFE TODDLERNUTRITION
What affects toddler’s daily intakes?Childrenhaveanin-builthungeralertandsatietymechanism,sotheyknowwhentheyarehungryandwhentheyarefull,andtheyeataccordingly.Ahealthychildwillneverstarveitself,soencouragecaregiverstotrusttheirchildtoeatenough.
Theperiodbetweenachild’sfirstandfifthbirthdaysisatimeofrapidsocial,intellectualandemotionalgrowth.Itisalsocharacterisedbyaslowdowninthechild’sgrowthrate,whichmaybereflectedinalessreliableappetite.Inaddition,atthisagechildrenarediscoveringtheirindependenceandtestingtheirchoiceinfoodselection,andthiscanleadinreducedinterestineatingwhentherestofthefamilyeats(5).Furthermore,childrenhavesmallstomachs,soitisdifficultforthemtoachievetheirdailynutritionalrequirementswithonly3mealsperday.Grazingandsnacksarenecessary(5).
Slower growth• -Frombirthto12monthsachild’sweighttriples,yetfrom1–5yearstheweightgainonaverageisonly2-3kgeachyear.Astoddlersgrowthslowsdown,theirappetitedecreasestoo.Thismeanstoddlersneedlessfood.Thischangeisnormalanddoesn’tmeanthechildisbeingdifficultorisunwell.
Grazing and snacking• -toddlersrarelyfollowatraditionalmealpattern.Theytendtoneedsmallandregularsnacks.Thissuitssmalltummysizesandprovidestheenergytokeepmovingallday.Theamounteatenatmealtimes,inparticulartheeveningmealmaybesmallerthancaregiverswouldlike.However,childrencanbalancetheamountoffoodeatenwithexactlyhowmuchtheyneediftheyarenotforcedtoovereatorfinishallthefoodontheplate.Thismeansthathealthysnacksareimportanttohelpprovidetheenergyandnutritionyourchildneedsduringtheday(3).
Independence –• Showingindependenceispartofnormaltoddlerdevelopmentandthisoftenincludesrefusingtoeatfoodstoseewhatwillhappen.Rejectingafooddoesnotalwaysmeanthechilddoesnotlikeit(3).
Clues for fullness cuesChildrenmayclamptheirmouthshutorturntheirheadawaywhenofferedfood.Theymayalsopushthebowlorfoodawayfromthetableorhighchair.Discussthesecueswithfamiliesandencouragethemtorecognisethemintheirchild’sbehaviour.
Encourage caregivers to recognise when their child is full
The Dietary Guidelines for Children and Adolescents in Australia recommendation
Small, frequent, nutritious and energy dense feedings of a variety of foods from the different food groups are important to meet nutrient and energy needs during the second year of life. The regular family diet (see the Australian Guide to Healthy Eating) should be the basis of the child’s meals.
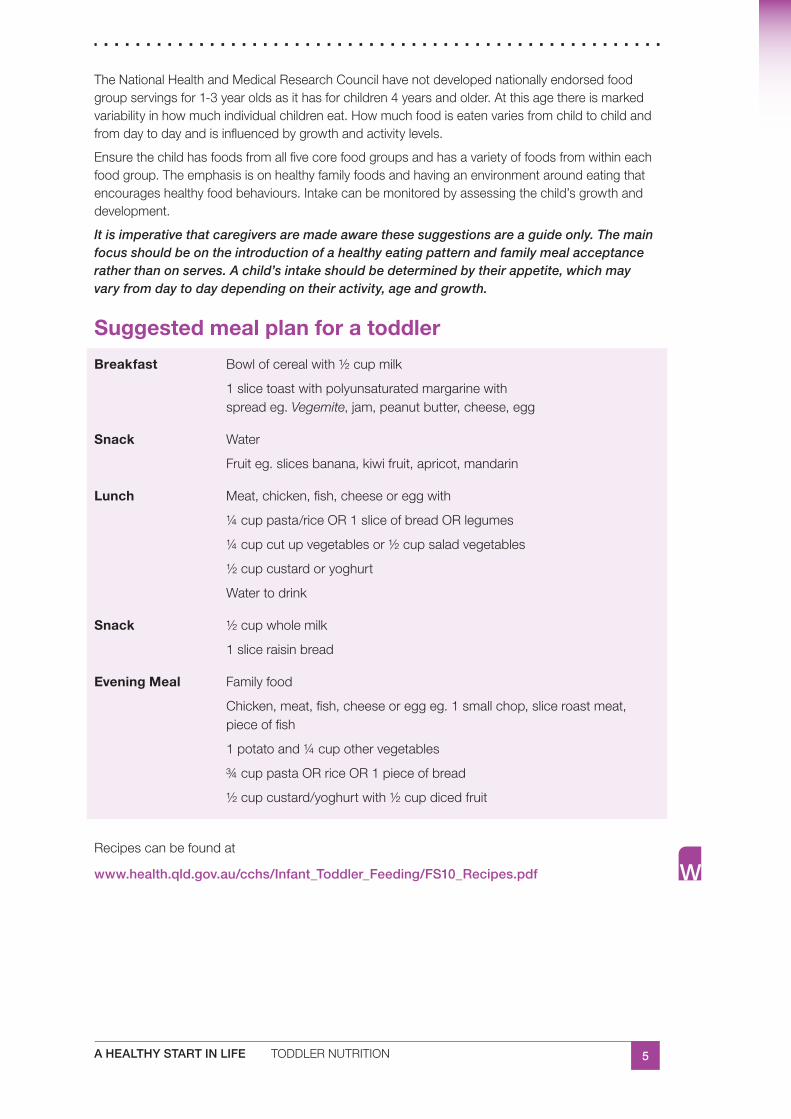
5A HEALTHY START IN LIFE TODDLERNUTRITION
TheNationalHealthandMedicalResearchCouncilhavenotdevelopednationallyendorsedfoodgroupservingsfor1-3yearoldsasithasforchildren4yearsandolder.Atthisagethereismarkedvariabilityinhowmuchindividualchildreneat.Howmuchfoodiseatenvariesfromchildtochildandfromdaytodayandisinfluencedbygrowthandactivitylevels.
Ensurethechildhasfoodsfromallfivecorefoodgroupsandhasavarietyoffoodsfromwithineachfoodgroup.Theemphasisisonhealthyfamilyfoodsandhavinganenvironmentaroundeatingthatencourageshealthyfoodbehaviours.Intakecanbemonitoredbyassessingthechild’sgrowthanddevelopment.
It is imperative that caregivers are made aware these suggestions are a guide only. The main focus should be on the introduction of a healthy eating pattern and family meal acceptance rather than on serves. A child’s intake should be determined by their appetite, which may vary from day to day depending on their activity, age and growth.
Suggested meal plan for a toddler
Breakfast Bowlofcerealwith½cupmilk
1slicetoastwithpolyunsaturatedmargarinewithspreadeg.Vegemite,jam,peanutbutter,cheese,egg
Snack Water
Fruiteg.slicesbanana,kiwifruit,apricot,mandarin
Lunch Meat,chicken,fish,cheeseoreggwith
¼cuppasta/riceOR1sliceofbreadORlegumes
¼cupcutupvegetablesor½cupsaladvegetables
½cupcustardoryoghurt
Watertodrink
Snack ½cupwholemilk
1sliceraisinbread
Evening Meal Familyfood
Chicken,meat,fish,cheeseoreggeg.1smallchop,sliceroastmeat,pieceoffish
1potatoand¼cupothervegetables
¾cuppastaORriceOR1pieceofbread
½cupcustard/yoghurtwith½cupdicedfruit
Recipescanbefoundat
www.health.qld.gov.au/cchs/Infant_Toddler_Feeding/FS10_Recipes.pdf
6 A HEALTHY START IN LIFE TODDLERNUTRITION
Extra foods
Thesearefoodsthatdonotfitintothefivefoodgroups.Theyarenotessentialtoprovidethenutrientsthebodyneeds.NOmorethanoneextrafoodperdayisrecommendedfor1-3yearolds.
Some examples are:
1(40g)donut
4plainsweetbiscuits
1(40g)slicecake
1tablespoonbutter,margarine,oil
1(375mL)softdrink
1smallpacket(30g)potatocrisps
12hotchips
1½scoopsoficecream
60gjamandhoney(1tablespoon)
25g(1funsizeorhalfaregular)chocolatebar
5.3 What should toddlers be offered to drink?
Water is the best drink for children.
Fluidrequirementsdependonbodysize.IntheAustralianclimateveryyoungchildrenareatparticularriskofdehydration.Achild’sfluidneedsarebestmetbywater,thenmilk.
Avoid fruit juices, cordials and soft drinks.
Excessiveconsumptionoffruitjuiceandsoftdrinksshouldbediscouraged:theseliquidshaveahighsugarandenergycontent,whichmaydisplaceothernutrientsinthedietandcontributetodentalcaries.
Earlychildhoodcaries,arecognisedproblemininfantsandtoddlers,ischaracterisedbyextensiveandrapidtoothdecay.Prolongedsessionsofbottlefeedingandliquidscontainingsucrosearetwopotentiallycariogenicpractices.
Toddlersshouldbeofferedalldrinksinacup.Somechildrenmayfillupondrinks,particularlysweetoneslikejuiceandmilk,thisleaveslittleroomforsolidfood,whilstprovidinglimitednutrients
Encouragecaregiversto:
offer1to3glasses(200ml)ofmilkonlyperday(dependingonotherdairyfoods■■
consumed),andwateratothertimes
givefoodbeforedrinksatmealtimes,particularlyforsmallandpickyeater■■
understandwhyjuiceandsweeteneddrinksareunnecessary■■
Foraparenthandout‘teaching my child to drink from a cup’,www.health.nsw.gov.au/mhcs/publication_pdfs/7845/AHS-7845-ENG.pdf
7A HEALTHY START IN LIFE TODDLERNUTRITION
5.4 Assessing whether their children are meeting their dietary needs
The focus in feeding should not be on getting food into the child…Instead the focus should be on the feeding relationship and on the achievable goal of helping the child learn eating skills and positive eating behaviours (8)
Caregiversoftenappeartobemoreconcernedwiththeamountoffoodconsumedratherthanthetypeoffoodofferedoreventhefeedingenvironment(4).Butobviouslyabalancebetweentheamount,typeandvarietyoffoodsisnecessary.Thenutritionalqualityofthedietisimportanttoensurethatthechildreceivesthelevelsofnutrientsspecifiedintherecommendeddietaryintakes(1,9)
Food diaryAtooltoassesstoddlerintakeisafooddiary.Encouragecaregiverstokeeparecord(afooddiary,seeparenthandout)ofeverythingtheirchildateovera2to4weekperiod.
Instructthemto:
includeallmealsandsnacksinandoutsidethehome■■
includeanybehaviourthataccompanieseating■■
after2to4weeks,checkallfoodgroupsarecoveredinthesufficientamounts■■
lookforanyareasinthedietthatneedattentionandanylinkstofussybehaviour.■■
Growth monitoringEncouragecaregiverstohaveregularvisitstothechildhealthcentresoweightandheightcanbecontinuouslymonitored.Forassessmentofgrowthandinterpretationofgrowthcharts,refertogrowthchartssection.
When to referNo healthy child has ever starved from refusing food. If the child is growing normally, and is busy and active, reassure families their child is getting enough.
Pleasenote,somemedicalconditionsresultindecreasedappetite(eg.irondeficiencyanaemia).Itisimportanttheunderlyingmedicalconditioniscorrected.Supplements(suchasvitaminsandminerals)shouldonlybeprescribedbasedonclinicalfindings.Intheseinstancesreferralisessential.
CheckEncourage families to seek a referral to a paediatrician or dietitian if they have:
concerns about child’s growth■✔
the child is unwell, tired and not eating■✔
mealtimes are causing a lot of stress and anxiety (3)■✔
“Infants are currently exposed to a wide variety of ‘kid’ foods that tend to be high in fat and sugar, including excess juice, juice-based sweetened beverages, French fries and nutrient poor snacks. Usual food intakes of infants and young children may exceed estimated energy requirements… for children aged 1 to 4 years; intakes exceed requirements by 20 to 35%” (12)
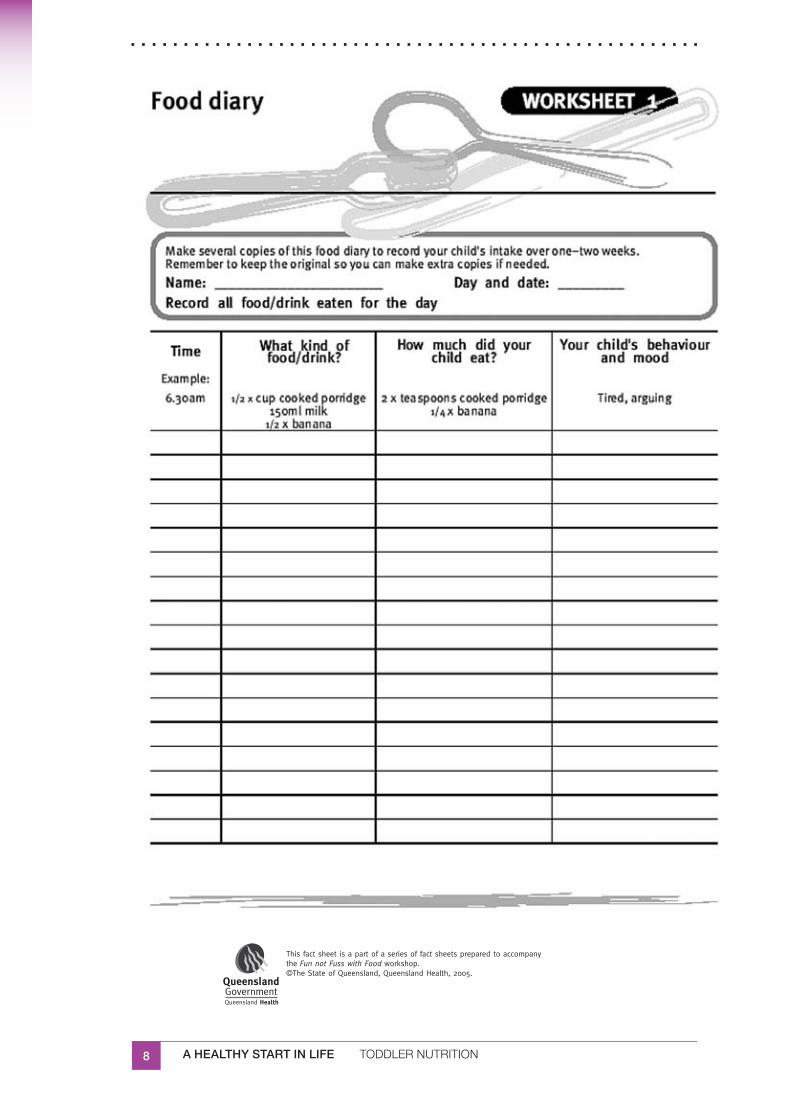
8 A HEALTHY START IN LIFE TODDLERNUTRITION
9A HEALTHY START IN LIFE TODDLERNUTRITION
5.5 Tips for toddler eating (3, 8)
Children do not need special foods. By this age they should be eating the same sort of meals as the rest of the family.
Toddlersshouldbeeatingandenjoyinghealthymealsandmealtimeswiththerestof■■
thefamily.Asmuchaspossible,offer‘familymeals’.
Toddlersappetiteandfoodintakecanvarydaily■■
Toddlersneedsmallmealsandregularsnacks.Regularmealandsnacktimes,with■■
adequatetimesetaside:20-30minutesformealtimesand10-20minutesforsnackshelps!
Encouragecaregiverstolettheirchildidentifywhentheyarefull,insteadofforcinga■■
childtofinishallfoodontheplate
Thisisagreattimeforlearningandexploring.Newfoodsmayberejectedatfirst,infact■■
somefoodswon’tbewellaccepteduntiltasted10-20times.
Dishing up:
Serveanewfoodwithafavouritefood.■■
Serveanamountyouknowyourchildcanfinish.■■
Givesolidsfirst-beforefluids.■■
Offerdrinksinacup■■
Donotaddsugarandsalttobasicfoods■■
Mealtimes should be relaxed and fun
Thisisatimeforlearningthesocialskillsofeatingasafamilyandlearningcourtesyat■■
themealtable.
EncouragecaregiverstoavoiddistractionssuchasTV,toysandgames.■■
Keepmealtimesascalmandrelaxedaspossible.Avoidfamilyargumentsatmealtimes!■■
Giveplentyofpositiveencouragement.Donotbribechildrenwithfood.■■
10 A HEALTHY START IN LIFE TODDLERNUTRITION
5.6 Safety tips
Chewing tips for kidsThere are a few safety issues with small children that need to be addressed. Firstly, children under 4 years have not fully developed their chewing skills so extra care is required with hard foods such as popcorn, nuts, fruit and raw vegetables.
How to help toddlers chewEncourage caregivers to serve food in bite-size pieces.■✔
Encourage children to bite through food. Start with soft foods such as ■✔bananas, tinned fruit, macaroni, and progress to apples, raw carrot, dried fruit and meat.
As each food is mastered, try a new one.■✔
Encourage caregivers to praise their toddler as they attempts chewy food.■✔
Role model behaviour: there are always opportunities for familles and ■✔friends to show children how to take small bites. Move the food to the side of the mouth and chew (4).
Some tips to prevent chokingYoung children should always be supervised when eating.■✔
Encourage caregivers to make a rule that eating is to be a sit down activity, ■✔to prevent accidents with food or unintentional swallowing of large pieces of food.
Try role modelling sitting and eating, so that your child will learn that eating ■✔is a sit-down activity for all family members.
It is best to leave hard foods such as popcorn, corn chips, hard lollies and ■✔hard, raw fruit or vegetables until the child is 4 years of age as they may cause choking.
For safety reasons never give whole nuts under 5 years — always use ■✔paste.
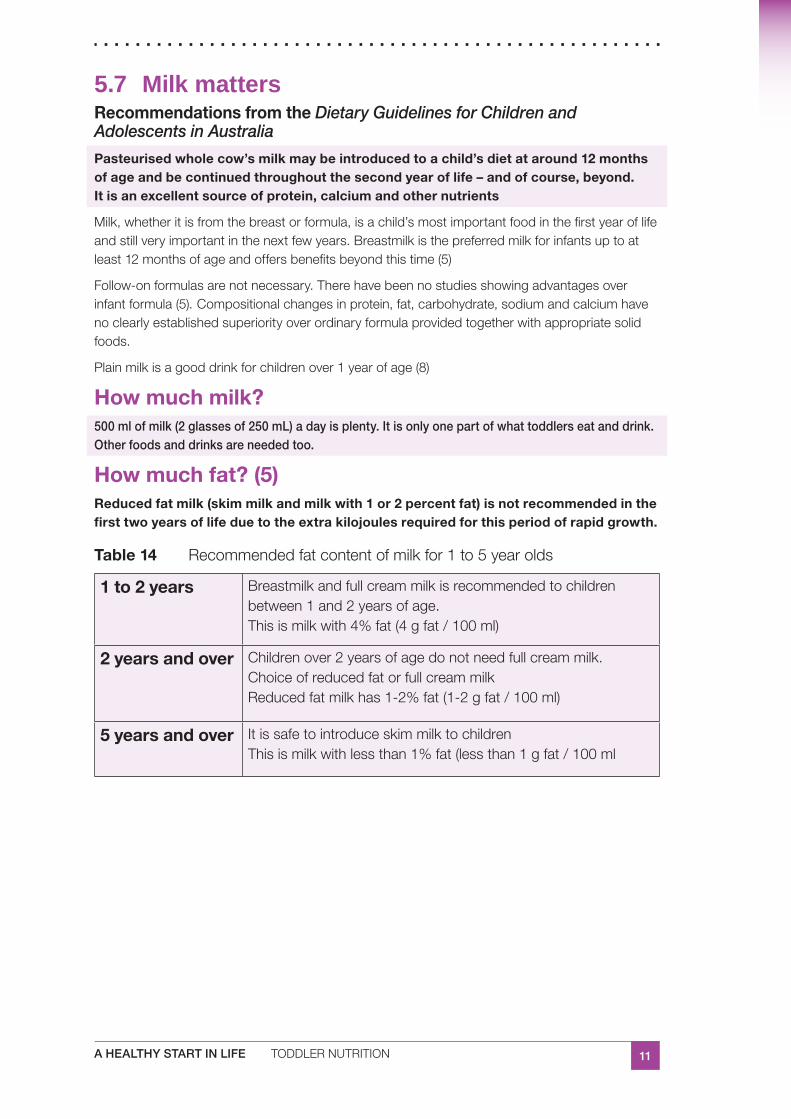
11A HEALTHY START IN LIFE TODDLERNUTRITION
5.7 Milk mattersRecommendations from the Dietary Guidelines for Children and Adolescents in Australia
Pasteurised whole cow’s milk may be introduced to a child’s diet at around 12 months of age and be continued throughout the second year of life – and of course, beyond. It is an excellent source of protein, calcium and other nutrients
Milk,whetheritisfromthebreastorformula,isachild’smostimportantfoodinthefirstyearoflifeandstillveryimportantinthenextfewyears.Breastmilkisthepreferredmilkforinfantsuptoatleast12monthsofageandoffersbenefitsbeyondthistime(5)
Follow-onformulasarenotnecessary.Therehavebeennostudiesshowingadvantagesoverinfantformula(5). Compositionalchangesinprotein,fat,carbohydrate,sodiumandcalciumhavenoclearlyestablishedsuperiorityoverordinaryformulaprovidedtogetherwithappropriatesolidfoods.
Plainmilkisagooddrinkforchildrenover1yearofage(8)
How much milk?500 ml of milk (2 glasses of 250 mL) a day is plenty. It is only one part of what toddlers eat and drink. Other foods and drinks are needed too.
How much fat? (5)Reduced fat milk (skim milk and milk with 1 or 2 percent fat) is not recommended in the first two years of life due to the extra kilojoules required for this period of rapid growth.
Table 14 Recommendedfatcontentofmilkfor1to5yearolds
1 to 2 years Breastmilkandfullcreammilkisrecommendedtochildrenbetween1and2yearsofage.Thisismilkwith4%fat(4gfat/100ml)
2 years and over Childrenover2yearsofagedonotneedfullcreammilk.ChoiceofreducedfatorfullcreammilkReducedfatmilkhas1-2%fat(1-2gfat/100ml)
5 years and over ItissafetointroduceskimmilktochildrenThisismilkwithlessthan1%fat(lessthan1gfat/100ml
12 A HEALTHY START IN LIFE TODDLERNUTRITION
Milks
Homogenised and pasteurised milk:
ismilksoldfromrefrigerationattheshops■■
hasbeenhomogenised(ie.mixedthroughandmadeintouniformconsistency)andthen■■
pasteurised(heatedtokillanygermsthatcouldcauseillnesses,suchastuberculosis)It is safest for young children to drink milk that has been treated in both these ways
Long life and UHT milk:
hasbeenpartiallysterilisedbyheatingitforashorttime,around1-2seconds,ata■■
temperatureexceeding135ºC,whichisthetemperaturerequiredtokillsporesinmilk,butmaintainnutritientprofile
hasthesamefoodvaluesasordinarymilk,ithasjustbeentreateddifferentlysoitlasts■■
longer
Untreated cow’s milk:
iscow’smilkthatcomesstraightfromthefarm■■
■■ requires boiling before it is given to toddlers
needstobestirredasitcools,tomixinthefat■■
Low lactose milk:
■■ Used when indicated (ie lactose intolerance), under the guidance of a suitable health professional
refertolactoseintolerancesection■■
Goat’s milk:
goatandsheepmilkshaveoverallnutrientprofilessimilartocow’smilk■■
goat’smilkmustbepasteurisedorboiled,asitcancontaingermsthatcouldmakea■■
youngchildveryill
goat’smilkcomposition,whencomparedtocow’smilkis:■■
higherinprotein,potassiumandchloridecontributestoincreasedrenalsoluteload■■
andriskofdehydration,particularlyininfants
containsinadequateamountsoffolicacidandvitaminB12■■
verylowinVitaminC,vitaminb6andvitaminD■■
itisverylowiniron(7)■■
itspopularitycomesinpartfromunsubstantiatedclaimsthatitislessallergenicand■■
moredigestiblethancow’smilk(7)
Parenthandoutavailable
www.cyh.com

13A HEALTHY START IN LIFE TODDLERNUTRITION
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Soy (except soy formula where specifically indicated), rice and other vegetarian beverages – whether or not they are fortified - are inappropriate alternatives to breastmilk, formula or pasteurised whole cow’s milk in the first 2 years of life.
Soy milk
■■ full fat fortified soy beverages are suitable for use after 2 years of age as part of a mixed diet
infantsandchildrenmedicallyrequiringasoymilkshouldcontinuetouseasoyinfant■■
formulaforthefirst12monthsandpossibly2years.Afterthistimeafortifiedsoymilkshouldbeusedwithacalciumcontentgreaterthan100mg/100mlmilk(7)
Rice milk
■■ not a suitable substitute for breastmilk or cow’s milk for young children (8)
ricemilkismadefromfilteredwater,riceflour,oilandseasalt.Itmayalsohaveadded■■
calcium(7)
toddlerscouldhaveanoccasionaldrinkofricemilk,aslongasitdoesn’ttaketheplace■■
ofothermilksintheirdiet(8)
comparedtocow’smilkandsoymilk,ricemilkishigherincarbohydrates,lowerin■■
proteinandnaturallylowerinfat.Ithasanaturallysweetertasteduetothehighercarbohydratecontent(7).
Coconut milk
■■ not an infant food and certainly cannot be used to replace other milks
doesn’tprovidethesamenourishmentasnormalmilks■■
containsalotoffatandlittleelseofvaluetothediet■■
canbeusedoccasionallyinmeals■■
Condensed milk
■■ not an infant food and certainly cannot be used to replace other milks
doesn’tprovidethenourishmentofnormalmilks■■
ishighinsugarandfat■■
Check
Encourage breastfeeding to 12 months and beyond, as long as mutually ■✔desired
Full cream cow’s milk until 2 years of age■✔
From 2 years onwards■✔
Reduced fat milks can be introduced■■
Soy, rice and other vegetarian beverages can be introduced■■
Milk is limited to 2 glasses of 250ml per day from 12 months onwards■✔
14 A HEALTHY START IN LIFE TODDLERNUTRITION
5.8 Fussy eating
‘Fussy eating’ is common among toddlers and often worries caregivers. Usually it is a stage in normal development, but it can be aggravated by parental response. When growth and development are normal and a variety of foods are offered to the child, simple reassurance from the child’s caregivers may be all that is needed. (5)
Manycaregiversworryabouttheirchild’seatingatsomestage,particularlyinyoungerchildrenwhenfoodintakeandappetiteappeartochangedaily(3).Workwithcaregiverstounderstandtheprinciplesbehindfussingeating,anddevelopsomestrategieswiththemtotacklefussyeating.UsetheparenthandoutsincludedinthissectionfromFun not Fuss with Food.
Parent-child feeding relationship (2, 8)
Theparent–childfeedingrelationshiprecognisestheimportanceofboththeparentandchildinthecomplexprocessofeatingandmealtimes.Feedingrequiresadivisionofresponsibilitybetweenparentandchild.Theparentisresponsibleforwhatthechildisofferedtoeat,thechildisresponsibleforhowmuch(2,7,8,10,11).
Breastfeeding is an example of the parent-child feeding relationship ‘caregivers must provide an appropriate feed….. but they must allow the infant to regulate the amounts’
Caregivers decide what to feed their child and when:
choosing,preparingandpresentingawidevarietyoffoods■■
continuingtoofferfoodswithoutafuss,evenwhentheyarerejected■■
avoiding‘junk’foodsandsweetdrinks,whichmayreducetheirappetitefor‘healthier’■■
options
providingfoodsinwaysthatchildrencaneasilyhandle(egcutintosmallpieces)■■
providingmealsandsnacksatregulartimes■■
caregivershavingmealsandsnackswithchildrenwheneverpossible■■
settingrulesaboutbehaviouratthemealtableandstickingtothem■■
Children decide whether to eat and how much to eat
rememberchildreneatwhentheyarehungryanddonostarvethemselves■■
Remindcaregiverstoavoidfeelingtheneedtoencouragetheirchildtoeatalittlemore,eveniftheyhaveleftmostoftheirmeal.Thechildwillnotstarve!Whencaregiverstrytocontrolwhether theirchildeatsandhow muchiseaten,theyareprovidingopportunitiesforfussingandtantrums(7).
15A HEALTHY START IN LIFE TODDLERNUTRITION
‘Parking foods’ (5)
‘Parking’ a new food, that is, placing the new food on the plate with no expectations that the food will be eaten, is a concept to discuss with caregivers. Research suggests that some children need to be offered new foods up to 30 times before they will accept them.
‘Parkingfoods’provideschildrentheopportunitytobecomefamiliarwithcolour,textureandsmellsevenbeforeattemptingtotastethenewfood.
Encouragecaregiverstoallowtoddlerstotouch,smellormanipulatethenewfoods.Ifcaregiversareconcernedtheirchilddevelopsasuddenpreferenceforonlyalimitedrangeoffoods,thisisnormal.Encouragecaregiverstocontinuetoofferavarietyoffoodsateachmealandthechild’srangeoffoodseatenshouldincreaseagainwithtime.
Foodrefusalisnotnecessarilyaboutthechilddislikingthetasteofthefood.Mostchildrenacceptmostfoodseventually.
Caregiver development
Whendiscussingfussyeatingitisessentialtobemindfulofhowcaregiversareapproachingthesituation,andhowtheyarefeeling.Adultsreceiveavarietyofmessagesregardingtheirroleinthefeedingsituation(4)...Andoftenadultsreceiveconflictinginformation.Bombardedwithahostofexpectations,caregiversandcaregiverscanbecomeeasilyconfusedandunsure.Limitednutritionknowledgeandfoodpreparationskillsmaynegativelyaffectcaregiversabilitiestofeedchildrenappropriately(4).
Itistheresponsibilityofthehealthworkerstoassistcaregiversinrecognisingthebiological,physicalandsocialenvironmentsassociatedwithfeedingpreschoolersandtoenablecaregiverstodeveloppersonalfeedingandfoodselectionstrategieswithoutunwarrantedfeelingsofguilt(4).
UseFun not Fuss with Foodhandoutsasatooltodiscussfeedingandfoodselectionstrategies.
UseMy child won’t… handoutandFussy eating checklistastoolsforcaregiveradvice.
16 A HEALTHY START IN LIFE TODDLERNUTRITION
My child won’t ... AdaptedfromFun not Fuss with Food,2004(5)
Won’t eat vegetables■■ –considertheflavours,aretheytoostrong,wouldyoueatthem?Tryrawvegetableswithhealthydips,oraddtootherfoodsthattheyenjoysuchaspizza,rissolesandspaghettibolognaise.Youmayhavemoresuccessifyouletyourchildhelptopreparethevegetables.Allowyourchildtoexperimentwithvegetables.Atastedoesnotalwaysleadtoaswallow.The‘onebite’policyisalsoagoodtechniqueandthechildwilleventuallyrealisethatthevegetableisactuallyedible.
Won’t drink water■■ –encouragewaterandmakesureitiseasytoaccess,serveitcoldwithinterestingicecubeshapesadded.Leavethecordialinthebackofthecupboardoronthesupermarketshelf.Ascaregiversyouneedtorolemodelwaterdrinkingyourself.Evidencesuggeststhatcaregiverswhodrinkwateraremorelikelytohavechildrenwhodrinkwater.
Won’t drink milk ■■ –tryotherdairyfoodssuchascheesesandyoghurt.Childrenusuallylikesoftcheesesandflavouredyoghurts(usuallywithoutthefruitbits).YoucanalsomakeflavouredmilkwithMilo, Actavite or Ovaltineandsmoothieswithmilkandfruitoryoghurt.
Won’t eat meat■■ –Somecutsofmeatmaybetootoughordryforchildrentochewproperly.Youcantrysoftercutssuchasminceorthinlyslicedmeatinsandwiches.Otherfoodscantaketheplaceofmeat,soincludeeggs,peanutpaste,nutsorcombinationsoflegumesandgrainssuchasbakedbeansontoast,hommoswithpitabread,orkidneybeantacosortortillas.
Trytoperseverewhenofferingnewfoodstoyourchild.Becomfortablewiththeconcept■■
ofparkingthenewfood
Eats too much at snack times■■ –snacktimesaremealtimesforchildren.Ensuresnacksarenutritious,soservefruitsorvegetableswithwholegrainbreadsorcrackers.Snacktimessuchasafternoonteamaybewhenyourchildisattheirhungriest.Youcanserveasmallmeal(equivalentofadinner)atthistimeifitisconvenient.
17A HEALTHY START IN LIFE TODDLERNUTRITION
Fussy eating checklistTakeamomenttothinkaboutWHYyourchildmayberefusingameal
Checkrecent snacks:■■ havetheseprovidedthechildwithenoughenergy?
drinks:■■ didtheyhaveadrinkrecently,whichmayhavefilledthemup?
family situation:■■ whatisthefamilydoing–areyousinglingoutthechildforaspecialmeal?
activity:■■ whatactivityweretheydoing–wasitnewandinterestingorafavouritethatishardtodragthemawayfrom?
time:■■ isthisnormaltimeforameal?
illness:■■ isyourchildill?
Remember
it’sOKforachild’sfoodintaketovary.Childrenareverygoodatjudgingtheirhunger■■
andfullnesssigns
includeavarietyoffoodstoensureyourchildisreceivingallthenutrientsheorshe■■
needs
achild’sintakewillincreaseduringgrowthorasactivitylevelsincrease■■
childrentendtoeatlessiftheyaretired■■
childrenneedtoenjoyfoodandeating■■
childrenshouldnotbepressuredabouthowmuchorhowlittletheyeat■■
don’tuselollies,chocolates,biscuits,milkordessertsasbribesorrewards■■
Notes:
18 A HEALTHY START IN LIFE TODDLERNUTRITION
CheckCaregivers understand types and amounts of food and drinks suitable for ■✔toddlers
Checkfivefoodgroupsandextras.Discusschokingissues■■
Toddler is being allowed to determine when they are hungry and when they ■✔are full
Question:whatsignsdoesyourchildshowwhentheyarehungry?■■
Question:whatsignsdoesyourchildshowwhentheyarefull?■■
Toddler is consuming a wide variety of ‘family foods’■✔
Question:Tellmeaboutthefoodyourchildiseatingattheirmainmeal
Toddler is drinking from a cup■✔
Checkwithtoddler:Canyoushowmehowyoudrink?■■
Checkcontentofcup/bottle■■
Waterisofferedasadrink■■
Appropriate milk and appropriate amount of milk■✔
Checktoddlerisconsuming1-3glassesofmilk/day■■
19A HEALTHY START IN LIFE TODDLERNUTRITION
5.9 Useful websites and resourcesKey state and national documents for health workers
Dietary Guidelines for Children and Adolescents in Australia and Infant Feeding Guidelines for Health Workers
OptimalInfantNutrition:evidencebasedguidelines
InfantandChildNutritioninQueensland2003
ReportoftheChiefHealthOfficerQueensland,2006
Further professional development reading:
Parent handouts
ChildHealthInformationFactSheetswww.health.qld.gov.au/child&youth/factsheets/
Guidelinesfortoddlerswww.health.qld.gov.au/cchs/Infant_Toddler_Feeding/FS8_Guidelines_Todd.pdf
Recipefactsheetwww.health.qld.gov.au/cchs/Infant_Toddler_Feeding/FS10_Recipes.pdf
Guidelinesforfussyeaterswww.health.qld.gov.au/cchs/Infant_Toddler_Feeding/FussyEaters.pdf
Parent books
JennyO’Dea.Doublebay,2005.Positive Foods For Kids; Healthy Food, Healthy Children, Healthy Life.
Yummy! Every Caregivers Nutrition Bible,JaneClarke,2006
Video / DVD
Websites
www.health.vic.gov.au/nutrition/child_nutrition/eat.htm
A note on Fun not Fuss with Food
Fun not Fuss with Food wasdevelopedin2000byamultidisciplinaryteamofhealthprofessionalsattheGoldCoastHealthServiceDistrict,andisnowdistributednationallythroughPopulationHealthServices.
Itisasinglesession,two-and-a-half-hourworkshopthatcoversnutritionforchildrenandbehaviouralmanagementstrategies.Theworkshopaimstoincreasethecapacityofcaregiverswithchildrenaged2–10yearsinmanagingtheirchild’sproblemeatingandmealtimebehaviours.Thereisarangeofresourcestosupporthealthprofessionals(childhealthnurses,childpsychologist/earlyinterventionspecialists,andnutritionists/dietitians)todelivertheworkshop.Theseincludeafacilitator’smanual,facilitator’sguide(video/DVD),andparentresources.Thispackagecanbeorderedfromqheps.health.qld.gov.au/PHS/Documents/sphun/27966.pdf
Someparenthandoutsareincludedinthemanual.Andcanalsobeaccessedat qheps.health.qld.gov.au/ahwac/docs/nutrition/fun_not_fuss.pdf
20 A HEALTHY START IN LIFE TODDLERNUTRITION
References:QueenslandPublicHealthForum(2002).1. Eat Well Queensland 2002–2012: Smart Eating for a Healthier State.Brisbane,QueenslandPublicHealthForum.
Dietary Guidelines for Children and Adolescents in Australia incorporating the Infant 2.Feeding Guidelines for Health Workers,NHMRC,Canberra2003.
DepartmentofHumanServices(DHS),PublicHealthDivision.‘What’stheretoeat?Food3.&Nutrition,Melbourne[online]www.health.vic.gov.au/nutrition/downloads/whatstoeat/29thMarch2007
Sigman-GrantM.,Feedingpreschoolers:balancingnutritionalanddevelopmentalneeds.4.NutrToday1992;27:13-17
QueenslandHealth;5. Fun not Fuss with Food.Brisbane2004.
QueenslandHealth:6. Infant and Child Nutrition in Queensland 2003.QueenslandHealth.Brisbane2005
CommunityPopulationandRuralHealth(2003).7. Tuckertalk (child nutrition)fullyrevised.Tasmania,
SatterE.,TheFeedingRelationship.ZerotothreeJournal,June19928.
QueenslandHealth:Child&youthhealthfactsheets:Brisbane[online]9.www.health.qld.gov.au/child&youth/factsheets/13thMarch2007
EvansMorris,S.&DunnKlein,M.2000,10. Pre-feeding Skills: A Comprehensive Resource for Mealtime Development(2ndEdition),TherapySkillBuilders,SanAntonia.
SouthAustraliaChildandyouthhealth–healthtopics-milkfortoddlers[online]11.
DietaryrecommendationsforChildrenandAdolescents:AGuideforPractitioners,12.Paedatrics2006:117;544-559
1A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.0 Preschool nutrition
Theyearsbetweenachild’s2ndand5thbirthdaysrepresentaperiodofrapidsocial,intellectualandemotionalgrowth.Atthesametime,overallphysicalgrowthisdeceleratingwhilemotorskillsarebeingfine-tuned.Preschoolersarebusyexploringtheenvironment(1).Theyhavetestedtheirindependenceandarenowreadytolearn.
Preschoolershavetwocommonpreferences.Firstly,theyhaveapreferenceforroutineindailylife.Mostchildrenneedsomestructureandroutinetotheirday.Generally,theyprefermealsandsnacksatregulartimes,asgovernedbythefamily’slifestyle.
Secondly,theyhaveapreferenceforsimplicity.Manychildrenmaylikesimplyprepared,mildtastingfoodsthattheycaneasilyidentify.Theypreferfoodstheycanmanage,forexample,cut-upvegetablestheycaneatwiththeirfingersandsoupstheycandrinkfromacup(1).
Inthepreschoolyears,foodtakesonmorecomplexmeanings.Preschoolershaveanassociationwithfoodofmorethaneating.Foodshavespecificmeaningsdeterminedbyachild’sassociationswiththem.Forexample,sweetsmaymeanarewardforgoodbehaviourinthesupermarket.Additionally,caregiversshouldbeawarethatearlyimpressionsassociatedwithvarioususesoffood,affectfood-relatedattitudesandpracticesthatcanlastthroughoutlife(1).
Foodpreferencescannowbeinfluenced;parentsandfriendsaswellastelevisionadvertisingwillaffectfoodconsumed.
Acceptance of new foods, new textures and new tastes takes time and patience. Caregivers should be encouraged to maintain their responsibility to provide preschoolers with adequate amounts of a variety of nutritious foods and allow the children to select the amounts needed from these foods (1).
2 A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.1 Eating patternsOncechildrencommencechildcare,kindergartenorschool,lifetakesonanewroutine.Aregularintakeoffoodisneededthroughoutthedaytokeepchildrenactiveandtohelptheirconcentrationwhilelearning.
Somechildreninthisagegrouparestillfussy,soencourageparentstoofferawidevarietyoffoodsandregularmealsandsnacks,andallowchildrentoeattoappetitewithoutforceorarguments(3).
Developmental characteristics of preschoolers (2)
Generallyinpreschoolersthereis:
progressive acquisition of new skills. Preschoolers are striving for independence and ■■
gaining competence in such activities as tying their shoelaces, brushing their teeth and pouring milk. A preschooler’s oral motor development and manual dexterity should be considered, so that foods of appropriate texture, consistency and ease of eating are chosen for them
energy. Sitting still for more than a few minutes might be difficult. Preschoolers need ■■
plenty of time for active play and opportunities to develop gross motor coordination
more effective communication. Language is important. Peers become increasingly ■■
important. Most preschoolers enjoy sharing food with friends and carers
a keen curiosity. ‘Why’ has usually replaced ‘no’ as the favourite spoken word. The kitchen ■■
provides an opportunity for experiments, crafts, and participation in food preparation
comfort with the familiar but willingness to try new challenges. Food fads are common at ■■
this time. Preschoolers might insist on having a particular food prepared in a particular way for several days then, once it has been experienced to the full, become infatuated with another food. This has been called ‘fussiness’, but it is actually characteristic of normal development. Although variety may be limited while the fad persists, the preschooler is gradually expanding their food choices.
Preschoolers showed significant levels of nutrition knowledge…. They were able to identify foods of higher nutrient density as being ones to use to make their doll ‘grow bigger and stronger’ (1).
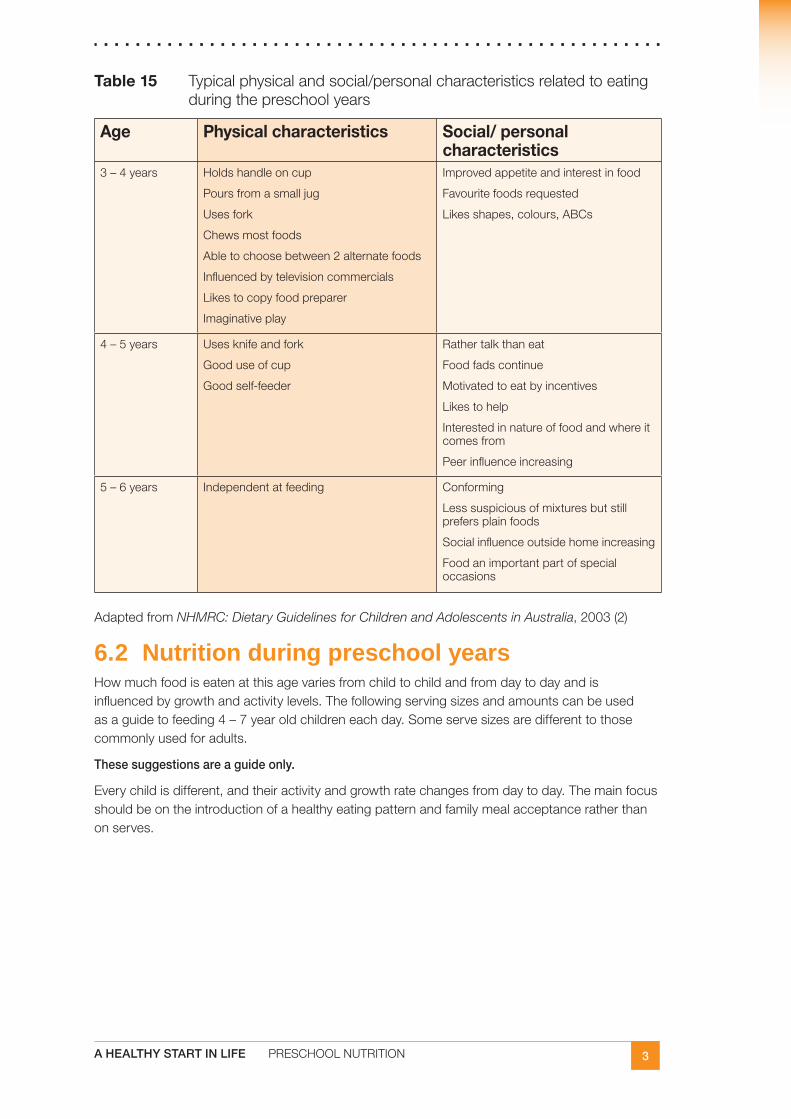
3A HEALTHY START IN LIFE PRESCHOOLNUTRITION
Table 15 Typicalphysicalandsocial/personalcharacteristicsrelatedtoeatingduringthepreschoolyears
Age Physical characteristics Social/ personal characteristics
3–4years Holdshandleoncup
Poursfromasmalljug
Usesfork
Chewsmostfoods
Abletochoosebetween2alternatefoods
Influencedbytelevisioncommercials
Likestocopyfoodpreparer
Imaginativeplay
Improvedappetiteandinterestinfood
Favouritefoodsrequested
Likesshapes,colours,ABCs
4–5years Usesknifeandfork
Gooduseofcup
Goodself-feeder
Rathertalkthaneat
Foodfadscontinue
Motivatedtoeatbyincentives
Likestohelp
Interestedinnatureoffoodandwhereitcomesfrom
Peerinfluenceincreasing
5–6years Independentatfeeding Conforming
Lesssuspiciousofmixturesbutstillprefersplainfoods
Socialinfluenceoutsidehomeincreasing
Foodanimportantpartofspecialoccasions
AdaptedfromNHMRC: Dietary Guidelines for Children and Adolescents in Australia,2003(2)
6.2 Nutrition during preschool yearsHowmuchfoodiseatenatthisagevariesfromchildtochildandfromdaytodayandisinfluencedbygrowthandactivitylevels.Thefollowingservingsizesandamountscanbeusedasaguidetofeeding4–7yearoldchildreneachday.Someservesizesaredifferenttothosecommonlyusedforadults.
These suggestions are a guide only.
Everychildisdifferent,andtheiractivityandgrowthratechangesfromdaytoday.Themainfocusshouldbeontheintroductionofahealthyeatingpatternandfamilymealacceptanceratherthanonserves.
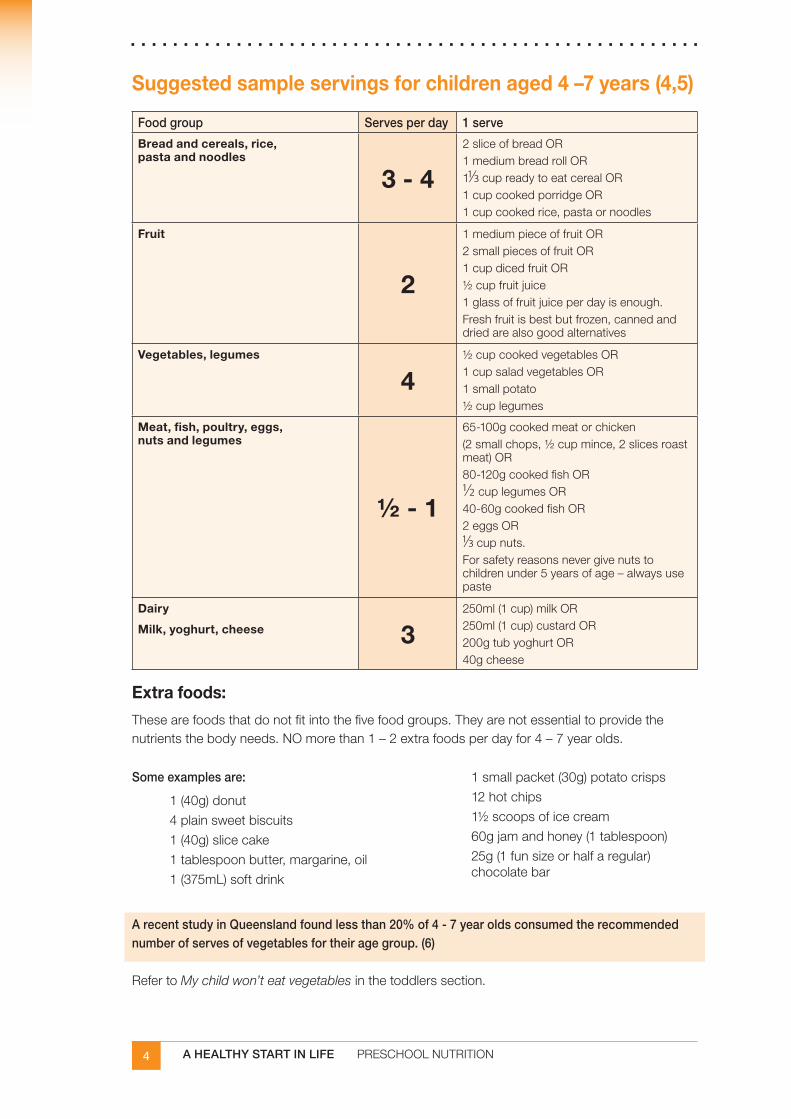
4 A HEALTHY START IN LIFE PRESCHOOLNUTRITION
Suggested sample servings for children aged 4 –7 years (4,5)
Food group Serves per day 1 serve
Bread and cereals, rice, pasta and noodles
3 - 4
2sliceofbreadOR1mediumbreadrollOR11/3cupreadytoeatcerealOR1cupcookedporridgeOR1cupcookedrice,pastaornoodles
Fruit
2
1mediumpieceoffruitOR2smallpiecesoffruitOR1cupdicedfruitOR½cupfruitjuice1glassoffruitjuiceperdayisenough.Freshfruitisbestbutfrozen,cannedanddriedarealsogoodalternatives
Vegetables, legumes
4½cupcookedvegetablesOR1cupsaladvegetablesOR1smallpotato½cuplegumes
Meat, fish, poultry, eggs, nuts and legumes
½ - 1
65-100gcookedmeatorchicken(2smallchops,½cupmince,2slicesroastmeat)OR80-120gcookedfishOR1/2cuplegumesOR40-60gcookedfishOR2eggsOR1/3cupnuts.Forsafetyreasonsnevergivenutstochildrenunder5yearsofage–alwaysusepaste
Dairy
Milk, yoghurt, cheese 3250ml(1cup)milkOR250ml(1cup)custardOR200gtubyoghurtOR40gcheese
Extra foods:
Thesearefoodsthatdonotfitintothefivefoodgroups.Theyarenotessentialtoprovidethenutrientsthebodyneeds.NOmorethan1–2extrafoodsperdayfor4–7yearolds.
Some examples are:
1(40g)donut
4plainsweetbiscuits
1(40g)slicecake
1tablespoonbutter,margarine,oil
1(375mL)softdrink
1smallpacket(30g)potatocrisps
12hotchips
1½scoopsoficecream
60gjamandhoney(1tablespoon)
25g(1funsizeorhalfaregular)chocolatebar
A recent study in Queensland found less than 20% of 4 - 7 year olds consumed the recommended number of serves of vegetables for their age group. (6)
RefertoMy child won’t eat vegetablesinthetoddlerssection.
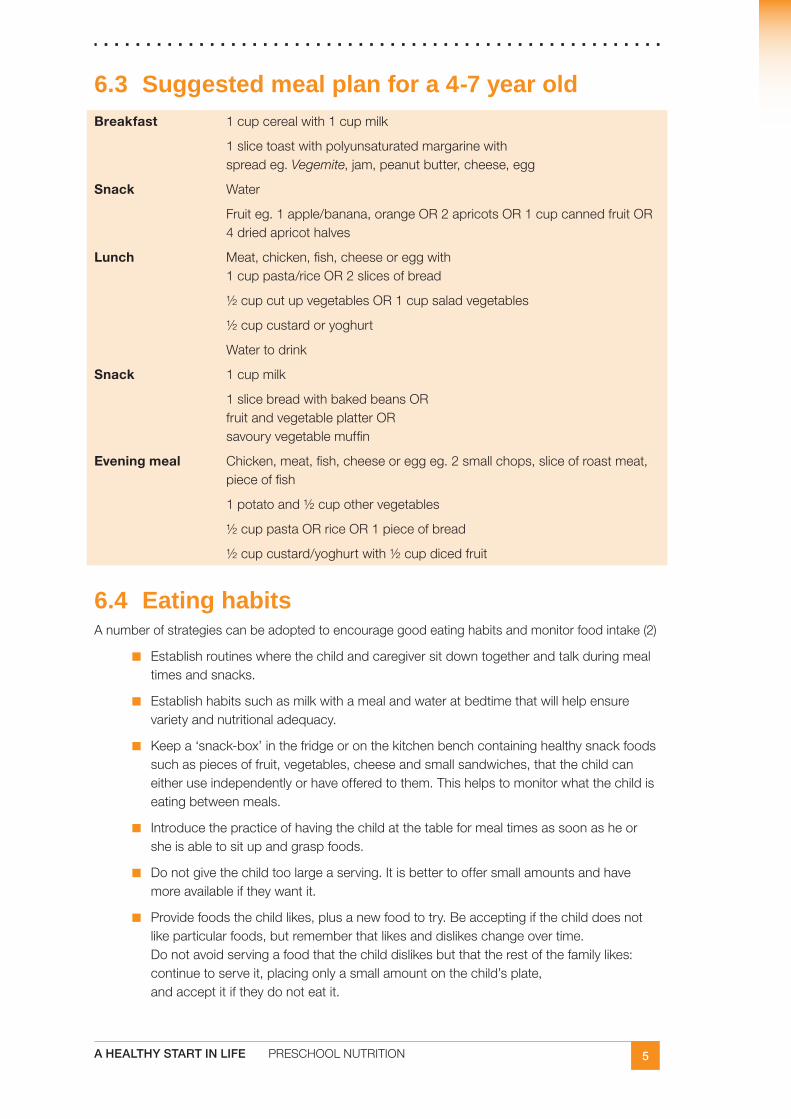
5A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.3 Suggested meal plan for a 4-7 year oldBreakfast 1cupcerealwith1cupmilk
1slicetoastwithpolyunsaturatedmargarinewithspreadeg.Vegemite,jam,peanutbutter,cheese,egg
Snack Water
Fruiteg.1apple/banana,orangeOR2apricotsOR1cupcannedfruitOR4driedapricothalves
Lunch Meat,chicken,fish,cheeseoreggwith1cuppasta/riceOR2slicesofbread
½cupcutupvegetablesOR1cupsaladvegetables
½cupcustardoryoghurt
Watertodrink
Snack 1cupmilk
1slicebreadwithbakedbeansORfruitandvegetableplatterORsavouryvegetablemuffin
Evening meal Chicken,meat,fish,cheeseoreggeg.2smallchops,sliceofroastmeat,pieceoffish
1potatoand½cupothervegetables
½cuppastaORriceOR1pieceofbread
½cupcustard/yoghurtwith½cupdicedfruit
6.4 Eating habits Anumberofstrategiescanbeadoptedtoencouragegoodeatinghabitsandmonitorfoodintake(2)
Establishroutineswherethechildandcaregiversitdowntogetherandtalkduringmeal■■
timesandsnacks.
Establishhabitssuchasmilkwithamealandwateratbedtimethatwillhelpensure■■
varietyandnutritionaladequacy.
Keepa‘snack-box’inthefridgeoronthekitchenbenchcontaininghealthysnackfoods■■
suchaspiecesoffruit,vegetables,cheeseandsmallsandwiches,thatthechildcaneitheruseindependentlyorhaveofferedtothem.Thishelpstomonitorwhatthechildiseatingbetweenmeals.
Introducethepracticeofhavingthechildatthetableformealtimesassoonasheor■■
sheisabletositupandgraspfoods.
Donotgivethechildtoolargeaserving.Itisbettertooffersmallamountsandhave■■
moreavailableiftheywantit.
Providefoodsthechildlikes,plusanewfoodtotry.Beacceptingifthechilddoesnot■■
likeparticularfoods,butrememberthatlikesanddislikeschangeovertime.Donotavoidservingafoodthatthechilddislikesbutthattherestofthefamilylikes:continuetoserveit,placingonlyasmallamountonthechild’splate,andacceptitiftheydonoteatit.
6 A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.5 Growth (1,3)Childrengrowatasteadyrateduringthekindergartenandearlyschoolyears.‘Thisslowergrowthrateisreflectedinadecreaseinappetiteandlessinterestinfood.Paradoxically,whileparentsworrythattheirpreschoolermaynotbeeatingenough,theincidenceofchildhoodobesitycontinuestorise’(1).Strict or low fat diets are not recommended because children’s energy and nutrient needs are high.Forparentswhoareconcernedaboutexcessiveweightgain,agoodapproachtodiscusswiththemisto:
develophealthyeatinghabitsforthewholefamily■■
encourageregularphysicalactivitiesforeveryone■■
limittelevisiontime.■■
Seeobesitysectionforfurtherdiscussion
6.6 Appetite (2,3)Thereisconsiderablevariationinchildren’sappetite,fluctuatingfromdaytoday,■■
dependingontheirrateofgrowthandlevelofphysicalactivity.
Childrenareabletodecidehowmuchfoodtheyneedifallowedtoeattoappetite,■■
encourageparentstoallowthis.
Childrencommonlyeatsmallamountsoffoods,frequently,duetotheirsmallstomach■■
capacity.
Manyparentsfindtheirchildreneatbetteratcertaintimesoftheday.■■
Forcingchildrento‘cleantheplate’orgivingsweetsasrewardsmayleadtoproblemsof■■
overeatinglateron.
Tiredness and irritability can prevent children from eating, especially at the evening meal (1)
6.7 Physical activity Childrenshouldbeencouragedtobephysicallyactivefromayoungage.Physicalactivityhelpschildrenfeelgoodandencouragesahealthyappetite.Encourageparentstopromoteafamilysettingthat:
playsgamesinthebackyard■■
goesforawalkinthepark■■
learnstoswim■■
participatesinkindergartenandschoolactivities■■
watcheslesstelevision■■
FormoreideascheckoutEat Well, Be Activewebsiteat
www.health.qld.gov.au/eatwellbeactive/funideas/active_fun.asp
www.health.qld.gov.au/eatwellbeactive/beactivetips/tips_for_families.asp
7A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.8 Packing lunches for kindergarten Ifchildrenareawayfromhomefor8hours,theyshouldeatabouthalfofthefoodneededfortheday.Therestshouldbeeatenatbreakfastandattheeveningmeal(7).
Treats Bythisagechildrencaneatindependentlyandenjoythesocialaspectsofeating.Havingfriendsmeanseatingoutofhomemore,andtheoccasionalmealatafastfoodrestaurantorpartyfilledwithhighenergyandfatsnacksdoesnoharmifgoodnutritioniscontinuedmostdays.
Parenthandoutcanbefoundat
www.health.qld.gov.au/cchs/Gen_Nutrition_Activity/lunches.pdf
Healthy snacks Parenthandoutcanbefoundat
www.health.qld.gov.au/cchs/Gen_Nutrition_Activity/lunches.pdf
Healthy drinks Anadequateintakeoffluidsisimportantatallages.Childrenshouldbeencouragedtodrinkasmuchwateraspossible,inpreferencetootherfluids.Milkisagoodsourceoffluid,animportantsourceofcalciumand,becauseithasahighproteincontent,ithasagreatersatiatingeffectthanotherdrinks.1-3glassesof250mlofmilkaday(dependingonotherdairyconsumption)isenough.
Sweet drinks such as juice, soft drink or cordial are unnecessary in a child’s diet.
8 A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.9 Food preferencesChildren’s eating is not only influenced by family life but also by other children and messages from television. Children can learn to make healthy food and lifestyle choices if given help from parents and carers (3).
Parents and peers
Parentalinfluencesonfoodpatternsarecriticalinthedevelopmentoffoodpreferences(1,6)
parental pressure■■ ,evenifitispositive,canaffectachild’sfoodacceptance(1).
Usingfoodsas■■ rewardsorpresentingthempairedwithadultattentionincreasesachild’spreferenceforthatfood.
frequency■■ withwhichchildrenseeaparticularfood(1).Itisimportantchildrenarepresentednewfoodsfrequently;continuedexposurepromotesacceptance.
role modelling:■■ whenchildrenobserveadultsconsumingafood,itismorelikelythechildrenmayconsumethefood(1)
Peerinfluencecanalsoaffectchildren’sfoodpreferencesastheyage(1).
Children should like to eat and enjoy food, not see food as threatening or as a reward (9).
Television advertising
Inadditiontoitseffectsonphysicalactivity,televisionexposeschildrentonumerousfoodadvertisements.Publichealthexpertsandnutritioneducatorshaveexpressedconcernthatmanyofthefoodadvertisementsontelevisiondirectedatchildrenareforanarrowrangeofproductsthatarehighinfats,sugarsand/orsaltandlowindietaryfibre(2).
Therehasbeenincreasingevidencethattelevisioncommercialsinfluenceschildfoodpreferences.AnAmericanstudyfoundtelevisioncommercialswereimportantinfluencesonthetypesoffoodchildrenasktheirparentstobuyandthefoodstheybuyforthemselves(1).
Sweetenedbreakfastcereals,candy,desserts,low-nutrientbeverages,andsaltysnackfoodsweretheproductsmostcommonlyadvertisedtochildrenandarealsotheitemsmostfrequentlyrequestedofparents.KraakandPelletier(2)suggestthatbuildingchildren’sandteenagers’skillsinprocessingconsumerinformationisonestrategy—whencombinedwithparentalguidanceandenvironmentalsupport(includinggovernment–industrypartnerships)—thatcanhelpyoungconsumersmake‘healthful’dietarychoicesbeforeundesirabledietarybehaviourshavedeveloped.
Check
Food tips for growing children (3):
a variety of foods should be offered every day■✔
encourage healthy eating for everyone in the family■✔
let children decide if they are full or hungry■✔
offer healthy snacks between meals■✔
encourage children to help prepare meals■✔
encourage water rather than sweet drinks■✔
encourage family mealtimes and activities to be enjoyed together■✔
9A HEALTHY START IN LIFE PRESCHOOLNUTRITION
6.10 Useful websites and resourcesKey state and national documents for health workers
Dietary Guidelines for Children and Adolescents in AustraliaandInfantFeedingGuidelinesforHealthWorkers
OptimalInfantNutrition:evidence-basedguidelines
InfantandChildNutritioninQueensland2003
ReportoftheChiefHealthOfficerQueensland,2006
Further professional development reading
Parent handouts
ChildHealthInformationFactSheets www.health.qld.gov.au/child&youth/factsheets/
Parenthandoutforlunchboxandsnackideas
‘Greatlunchandsnackideasforhungrykids’(seebrochure):ToordercontactQueenslandHealthPublicationsGPOBox48BrisbaneQLD4001Phone(07)32341053Fax(07)32340659
www.health.qld.gov.au/cchs/Gen_Nutrition_Activity/lunches.pdf
A note on Fun not Fuss with Food
Fun not Fuss with Food wasdevelopedin2000byamultidisciplinaryteamofhealthprofessionalsattheGoldCoastHealthServiceDistrict,andisnowdistributednationallythroughPopulationHealthServices.
Itisasinglesession,two-and-a-half-hourworkshopthatcoversnutritionforchildrenandbehaviouralmanagementstrategies.Theworkshopaimstoincreasethecapacityofparentswithchildrenaged2–10yearsinmanagingtheirchild’sproblemeatingandmealtimebehaviours.Thereisarangeofresourcestosupporthealthprofessionals(childhealthnurses,childpsychologists/earlyinterventionspecialists,andnutritionists/dietitians)todelivertheworkshop.Theseincludeafacilitator’smanual,facilitator’sguide(video/DVD),andparentresources.Thispackagecanbeorderedfromqheps.health.qld.gov.au/PHS/Documents/sphun/27966.pdf
Someparenthandoutsareincludedinthemanualandcanalsobeaccessedat qheps.health.qld.gov.au/ahwac/docs/nutrition/fun_not_fuss.pdf
10 A HEALTHY START IN LIFE PRESCHOOLNUTRITION
ReferencesSigman-GrantM.Feedingpreschoolers:balancingnutritionalanddevelopmentalneeds.1.NutrToday1992;27:13-17.
Dietary Guidelines for Children and Adolescents in Australia incorporating the Infant 2.Feeding Guidelines for Health Workers, NHMRC,Canberra2003.
VicHealth.What’stheretoeat?Foodandnutrition:Part2.Melbourne.3.
QueenslandHealth.4. Fun not Fuss with Food.Brisbane2004.
QueenslandHealth:Child&youthhealthfactsheets:Brisbane[online]5.www.health.qld.gov.au/child&youth/factsheets/13thMarch2007
QueenslandHealth.InfantandChildNutritioninQueensland2003.QueenslandHealth.6.Brisbane2005.
QueenslandHealth.WhatisBetterFood?Brisbane2002.7.
GrayG.Afferentsignalsregulatingfoodintake8. .ProcNutSoc2000;59:373-84.
KlesgesRC.,SteinRJ.,EckRJ.,IsbellTR.,KlesgesLM.Parentalinfluenceonfood9.selectioninyoungchildrenanditsrelationshipstochildhoodobesity.AmericanJournalofClinicalNutrition53(4)859-64,1991April.
1A HEALTHY START IN LIFE CLINICALNUTRITION
7.0 Clinical nutrition7.1 Adverse food reactions Foodallergiesandintolerancesareexamplesofadversefoodreactionsanddescribeadversereactionstofoods.Regardlessofwhetherclassifiedaseitheranallergyorintolerance,dietarymanagementshouldbehandledbyaqualifieddietitian/nutritionist(inconjunctionwithanallergistinthecaseoffoodallergies),sinceselfimposedrestrictionsmayleadtonutritionaldeficiencies.Theareaoffoodallergiesandintolerancesisnotatallclear-cut.Accuratediagnosisisessential,andthisusuallyrequiresareferralfromaGeneralPractitionertoanAllergist.
Understanding food allergies and intolerancesThissectioniskindlyadaptedfromFriendly Food,RoyalPrinceAlfredHospitalAllergyUnit.
Understandingthedifferencebetweenintoleranceandothertypesoffoodreactionisanimportantstartingpointbecausetheapproachtodealingwiththemisquitedifferent.Unlikeallergiesandcoeliacdisease,whichareimmunereactionstofoodproteins,intolerancesdon’tinvolvetheimmunesystematall.Theyaretriggeredbyfoodchemicalswhichcausereactionsbyirritatingnerveendingsindifferentpartsofthebody,ratherinthewaythatcertaindrugscancauseside-effectsinsensitivepeople(2).
Thechemicalsinvolvedinfoodintolerancesarefoundinmanydifferentfoods,sotheapproachinvolvesidentifyingthemandreducingyourintakeofgroups of foods,allofwhichcontainthesameoffendingsubstances.Bycontrastproteinallergensareuniquetoeachfood(forexample,egg,milkandpeanut),anddealingwithafoodallergyinvolvesidentifyingandavoidingalltracesofthat particular food. Similarlygluten,theproteininvolvedincoeliacdisease,isonlyfoundincertaingrains(wheat,barley,rye)andtheireliminationisthebasisofagluten-freediet(2).
If food allergy is suspected, refer patient to an allergist or immunologist for assessment.
Understanding food allergiesAfoodallergyisanabnormalimmunereactiontoafoodthatisharmlessformostpeople.Antibodiesagainstthefoodareproducedsothatwhentheallergicindividualeatsthefood,histamineandotherdefensivechemicalsarereleasedcausinginflammation.Thesechemicalstriggerallergicsymptomsthatcanaffecttherespiratorysystem,gastrointestinaltract,skinorcardiovascularsystem(5).
Arathershortlistoffoodsaccountsfor85-90%ofsignificantreactions,althoughanyfoodcanprovokeareaction.Foodsresponsibleforthemajorityofsignificantfoodallergyininfants,childrenandadultsareasfollows:
infants:cow’smilk,soy■■
children:cow’smilk,egg,peanut,soy,wheat,treenuts(walnuts,hazelnutsetc),fish,■■
shellfish
adults:peanut,treenuts,fish,shellfish(9)■■
Fortunately,mostchildrengrowoutoftheireggandmilkallergiesbeforetheyreachschoolage,orduringtheearlyschoolyears,butallergiestonutsandseafoodscanpersist.Wheatandsoycancauseallergies,buttheytendtobemildandtransient(2).
2 A HEALTHY START IN LIFE CLINICALNUTRITION
Common food allergens (2, 3, 5)
Peanutandothernuts■■
Egg■■
Milk■■
Seafood■■
Sesame■■
Wheat■■
Soy■■
Children born into atopic families are more likely to develop allergic diseases (50-80% risk) compared to those with no family history of atopy (20% risk) The risk appears to be higher if both parents are allergic.. and if the mother (rather than the father) has allergic disease (8)
Symptoms usually begin in the first 2 years of life, often after the first known exposure to the food… It is estimated that up to 6% of children under 3 years of age are affected by food allergies (3).
Formoreinformation,thehandoutsbelowcanbeaccessedattheRoyalPrinceAlfredHospitalwebsite:www.cs.nsw.gov.au/rpa/Allergy/default.htm
Egg Allergy■■
Frequently Asked Questions about Food Allergies (includes Advice for Schools)■■
Latex Allergy■■
Milk Allergy■■
Peanut Allergy■■
Food Allergy Prevention■■
Upper Airway■■
Wheat Allergy■■
Food allergy reactions (2)
Foodallergyreactionsvaryinseverity,dependingonhowsensitivethepersonisandhowmuchofthefoodthey’veeaten.
Foodallergyismainlyaproblemofinfants,toddlersandyoungchildren.Over90%ofcasesareassociatedwithatopiceczema-anintenselyitchychronicskinrashaffectingtheface,arms,legs,andotherpartsofthebody(2).
Moreseverereactionsareusuallyobviousandoccurconsistently,everytimethepersonhasthefood.Contactwiththemouthandtonguecancauseanimmediateburningsensation,withhivesandrednessaroundthefaceandifthefoodisswallowed,animmediatefeelingofbeingunwellcanbefollowedbyvomiting,crampsanddiarrhoea.Theface,mouthandeyescanswelldramatically,andhivesonthebodycanjoinintolarge,rapidlyspreadingwelts(2).
Themostseveretypeofreaction–anaphylaxis-canprogressrapidlywithbreathingdifficulty(fromswellingofthethroatorsevereasthma),allergicshockandcollapse,andcanbelife-threateningifnottreatedimmediatelywithadrenaline(epinephrine)byinjection.Inthemostsensitivepeoplewithafoodallergy,tinyamountsofthefood(pin-headsized)canbeenoughtoprovokeaseverereaction(2).
3A HEALTHY START IN LIFE CLINICALNUTRITION
Minimising the risk of allergy in high-risk infants (1, 8)
Pregnancy
Do not smoke during pregnancy, and provide a smoke-free environment for your child after ■■
birth.
Dietary restrictions in pregnancy are not recommended.■■
Breastfeeding, formula feeding
Exclusively breastfeed your child for at least 6 months, and preferably longer.■■
If breastfeeding is discontinued for any reason, seek professional advice: hydrolysed ■■
protein formula may be recommended.
Soy milk and goat’s milk formulas do not reduce allergies, and should not be used as an ■■
alternative to cow’s milk formulas.
Maternal dietary restrictions during breastfeeding are not recommended for prevention (8)■■
If an infant is breastfeeding and showing signs of allergies, refer to local general ■■
practitioner or specialist (eg paediatrician, allergist).
Introducing solids
Solid foods should not be introduced until about 6 months of age.■■
Start with low-allergenic foods such as rice and rice based cereals, followed by vegetables ■■
(eg. potato, pumpkin) and fruits (pear, apple, banana), then meats.
Add only one food at a time. Wait several days (ideally 5 to 10 days) before introducing a ■■
new food.
4 A HEALTHY START IN LIFE CLINICALNUTRITION
ManagementDietary Guidelines for Children and Adolescents in Australia recommendation
Encourageexclusivebreastfeedingfor6monthstodecreasetheriskofallergyininfantswithapositivefamilyhistory.
Ifthereisastrongfamilyhistoryofallergy,delayintroducingsomeorallofthehighlyallergenicfoodsduringthefirstyear;amongthesefoodsarecow’smilkandotherdairyproducts,soy,eggs,nuts,peanutsandfish.
Itisbesttocontinueavoidingeggs,nutsandshellfishuntiltheageof3years.
Whenfoodchoicesarerestricted,theadviceofadietitianshouldbesoughttoensurethatthedietaryintakecontinuestomeetnutrientandenergyneeds.
BestPracticemanagementisessential;refertopaediatricianoranallergist.
Dietary interventionThemainprincipleoffoodallergymanagementisavoidanceoftheoffendingantigen.Anincorrectdiagnosisislikelytoresultinunnecessarydietaryrestrictions,which,ifprolonged,mayadverselyaffectthechild’snutritionalstatusandgrowth.Forpatientsrequiringprolongedrestrictivediets,aformaldieteticevaluationisrecommendedtoensurethatnutritionalrequirementsaremet(3).
Food Intolerances
Foodintolerancesareanadversereactiontoafoodorsubstancethatdoesnotinvolvetheimmunesystem(5).Foodintolerancereactionscanbetriggeredbyarangeofnaturalsubstancesoradditivespresentinmanydifferentfoods.
Somepeoplearebornwithasensitiveconstitutionandreactmorereadilytofoodchemicalsthanothers.Thetendencyisprobablyinherited,butenvironmentaltriggerscanbringonsymptomsatanyagebyalteringthewaythebodyreactstofoodchemicals.Thesetriggersmayinclude:
asuddenchangeofdiet■■
abadfoodordrugreaction■■
anastyviralinfection;forexample,gastroenteritisorglandularfever(2).■■
Natural food chemicals
Naturalchemicalsarefoundinthefoodsweeat.Foodiscomposedofprotein,carbohydrate,fatandvariousnutrientsaswellasanumberofnatural‘chemicals’.Thesenaturallyoccurringmoleculesoftenaddflavourandsmelltofood.Sometimestheywilltriggersymptomsinunluckyindividuals.Thesechemicalsinclude(6):
salicylates■■
amines■■
glutamate.■■
Thesenaturalsubstancesaretheonescommontomanydifferentfoods,andthereforeconsumedingreatestquantityinthedailydiet.Asarule,thetastierafoodis,thericherit’slikelytobeinnaturalchemicals.
It is important to realise that reactions to these substances are not due to allergy, and so allergy testing is of little use in helping us to decide what to avoid (6).
5A HEALTHY START IN LIFE CLINICALNUTRITION
Chemical threshold Thesmallamountsofnaturalchemicalspresentinaparticularfoodmaynotbeenoughtocauseareactionstraightaway.However,becauseonesubstancemaybecommontomanydifferentfoodsitcanaccumulateinthebody,causingareactionwhenthethresholdisfinallyexceeded(2).
Food intolerance reactions (2)Symptomstriggeredbyfoodchemicalintolerancesvaryfrompersontoperson.Commononesinclude:
recurrenthivesandswellings■■
headaches■■
sinustrouble■■
mouthulcers■■
nausea■■
stomachpains■■
bowelirritation.■■
Somepeoplefeelvaguelyunwell,withflu-likeachesandpains,orgetunusuallytired,run-downormoody,oftenfornoapparentreason.
Management of food intolerances Thechemicalsinvolvedinfoodintolerancesarefoundinmanydifferentfoods,sotheapproachinvolvesidentifyingthemandreducingtheintakeof groups of foods,allofwhichcontainthesameoffendingsubstances(2).
Elimination dietsOnceadiagnosisismade,thehistorymayhelpidentifytheroleofdietaryorotherfactorsinmakingsymptomsworse.Theonlyreliablewaytosortoutwhetherdietisplayingaroleisbypeoplebeingplacedonatemporaryeliminationdietunder the supervision of a skilled dietitian and medical practitioner.Ifthediethelps,thisisfollowedbychallengesundercontrolledconditionstoidentifydietarytriggerssothattheycanbeavoidedinthefuture(6).
Itisimportanttoemphasiseeliminationdietsmustonlybeundertakenforashortterm,understrictmedicalsupervisionandonlyforverygoodreasons.Prolongedrestricteddietscanleadtoproblemswithnutrition,particularlyinchildren(6).
Refertoadietitian.
Parenthandoutcanbefoundat
www.medeserv.com.au/ascia/aer/infobulletins/food_intolerence.htm
6 A HEALTHY START IN LIFE CLINICALNUTRITION
Coeliac diseaseThissectioniskindlyadaptedfromFriendly Food,RoyalPrinceAlfredHospitalAllergyUnit.
Coeliacdiseaseiscausedbyanimmunereactiontogluten,aproteinfoundinwheat,barleyandrye.Thereactioncausesinflammationanddamagetotheliningofthesmallbowel,whichimpairsitsabilitytoabsorbnutrients.Typicalsymptomsincludemouthulcers,fatigue,bloating,crampsanddiarrhoea,butsomepeoplehavenosymptomsatall,andinotherstheonlycluemaybeanaemia(duetoironorfolicaciddeficiency)oranunusualchronicskinrash(dermatitis
herpetiformis). Coeliacdiseaseshouldnotbeconfusedwithwheatallergy,whichrarelyoccursbeyondinfancy,orthestomachandbowelirritationthatglutencansometimescauseinpeoplewithchemicalintolerances.
Screeningbloodtestsareavailable,butdefinitediagnosisrequiresasmallbowelbiopsy.Thesetestscanbecomenegativeafterafewweeksofglutenavoidance.Untreatedcoeliacdiseasecarriesalong-termriskofnutritionaldeficiency,osteoporosisand/orbowelmalignancy.Currently,alife-longgluten-freedietistheonlyknowntreatment.
Useful websites and resourcesDietary Guidelines for Children and Adolescents in Australia
Clinical guidelines
KatrinaJAllen,DavidJHill,RalfGHeine.FoodAllergyinChildhood.MJA185(7)394-400.
www.mjw.public/issues/182_09_020505/pre10874_fm.html
SusanLPrescottandMimiLKTang(2005).TheAustralasianSocietyofClinicalImmunologyandAllergypositionstatement:summaryofallergypreventioninchildrenMJA182(9)464-467.www.mja.com.au/public/issues/185_07_021006/all10609_fm.pdf
Parent books, DVDs
Friendly Food(MurdochBooks)byAnneSwain,VelenciaSoutterandRobertLoblay,RoyalPrinceAlfredHospitalAllergyUnit.
Orderformcanbefoundatwww.cs.nsw.gov.au/rpa/Allergy/default.htm
“DealingwithFoodAllergy”DVDandbooklet–availablefromRoyalPrinceAlfredHospital.
Parenthandoutsregardingfoodallergyandintolerancecanbefoundat www.foodauthority.nsw.gov.au/consumer/c-allergies.htmlincludingtranslatedinformationsheetsineightdifferentlanguages.
7A HEALTHY START IN LIFE CLINICALNUTRITION
A note on the Australasian Society of Clinical Immunology and Allergy (ASCIA)
ASCIAisaprofessionalnonprofitorganisation,comprisedpredominantlyofClinicalImmunologists,AllergySpecialistsandImmunologyScientists.ThemainrolesofASCIAareto:promotethehigheststandardsofscientificandmedicalpracticeandeducationamongstitsmembers…..andtocoordinateeducationprogrammesforitsmembers,otherhealthprofessionalsandthepublic.
Contact information:
ExecutiveOfficerTheAustralasianSocietyofClinicalImmunologyandAllergy(ASCIA)POBox450BalgowlahNSW2093
Email: [email protected]
Website: www.allergy.org.au
Patienteducationresourcescanbefoundatwww.allergy.org.au/aer/infobulletins/index.htm
A note on the Royal Prince Alfred Hospital (RPAH)
TheRPAHAllergyUnitisattachedtotheDepartmentofClinicalImmunology,RoyalPrinceAlfredHospital(RPAH),andisaffiliatedwiththeDisciplineofMedicineattheUniversityofSydney.ThestaffattheAllergyUnitarecommittedtoexcellenceinclinicalcare,researchandteaching,andactasacentreofnationalexpertiseprovidinginformationandresourcematerialsforhealthcareprovidersaswellasthewidercommunity.
Contact information:
Email: [email protected]
Website: www.cs.nsw.gov.au/rpa/Allergy/default.htm
8 A HEALTHY START IN LIFE CLINICALNUTRITION
ReferencesDietaryGuidelinesforChildrenandAdolescentsinAustraliaincorporatingtheInfant1.FeedingGuidelinesforHealthWorkers,NHMRC,Canberra2003.
FriendlyFood(MurdochBooks)byAnneSwain,VelenciaSoutterandRobertLoblay,2.RoyalPrinceAlfredHospitalAllergyUnit.
AllenKJ.,HillDJ.,HeineRG.,(2006)FoodAllergyinChildhood.MJAPracticeEssentials3.185(7)394-400
FoodAllergyPrevention;RPA4.www.cs.nsw.gov.au/rpa/Allergy/default.htm[online]5thApril,2007
NSWFoodAuthority:FoodAllergiesandsIntolerancesFactSheet:25thAugust2005.5.[online4thApril]www.foodauthority.nsw.gov.au
www.medeserv.com.au/ascia/aer/infobulletins/food_intolerence.htm6. [online10thApril]
BischoffS.,CroweS.E.,(2005)GastrointestinalFoodAllergy:NewInsightsInto7.PathophysiologyandClinicalPerspectives.Gastroenterology2005;128:1089-1113
SusanLPrescottandMimiLKTang(2005)TheAustralasianSocietyofClinical8.ImmunologyandAllergypositionstatement:summaryofallergypreventioninchildrenMJA182(9)464-467
AmericanGastroenterologicalAssociationmedicalpositionstatement:guidelinesforthe9.evaluationoffoodallergies,Gastroenterology2001Mar;120(4)1023-5
PrescottS.L.,TangM.,(2004)TheAustralasianSocietyofClinicalImmunologyandAllergy10.positionstatement:Allergypreventioninchildren.[online]10thAprilwww.allergy.org.au/pospapers/Allergy_prevention.htm
9A HEALTHY START IN LIFE CLINICALNUTRITION
7.2 ColicTheword‘colicky’isusedtodescribeafussybabywhoisotherwiseahealthy,growinginfantyoungerthan4months.Whethercolicexistsasaseparateentityorasasymptomofamaternalproblemisoftendebated.
InarecentAustralianstudy60%ofparentsreportedthattheirbabieshadsufferedfromcolic.Eventhoughcoliciscommoniscanbeverydistressingfortheparentsandotherfamilymembers.Inconsolable,unexplainedandincessantcryinginaseeminglyhealthyinfantgivesrisetotired,frustratedandconcernedparents(1).
Normal patterns of crying
Allinfants,whetherornottheyhavecolic,crymoreduringthefirst3monthsoflifethanatanyothertime.Onestudydescribescryingpatterns–cryinglastedapproximately2hoursperdayat2weeksofage,increasedtoapeakof3hoursadayat6weeks,andgraduallydecreasedtoabout1hourby3monthsofage.Thehypothesesforthesefindingswerethattheaccumulatedexcitementcausedbyenvironmentalstimuliduringthedaywasdischargedintheformofcryingduringlateafternoonandevening(2).
Mostofthefeaturesofcryingininfantswithcolicalsooccurinnormalinfantsbutwithlessfrequencyandshorterduration.
AcommonlyusedcriterionfordefiningcolicistheWessel’sruleofthrees,whichstatesthatinfantilecolicinvolvescryinglastingforatleast3hoursaday,foratleast3daysinanyweek,foratleast3weeksinthefirst3or4monthsoflife.
Therehavebeenmanyarticlesandresearchreportspublished,yetstilllittleisknownaboutthecauseorwhattodoaboutit.Somestudiessuggestcoliccanbecausedbyfoodallergies,gastrointestinalproblems,environmentalandbehaviouralfactors.Otherssuggestthatitisnormalforinfantstofussandhaveincreasinglylongerboutsofcryingfrombirthtoabout6weeks,afterwhichthecryingdecreases.
Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
Changesindietsandrestrictionsonindividualfoodshavehadaverylimitedsuccessinthetreatmentofcolic.Ensuredietarymodificationorpharmacologicalinterventionissafeanddoesnotresultinnutritionaldeficiencies.
Tips for practice
Providereassurancethattheinfantishealthy.■■
Athoroughexaminationandhistoryshouldbeconducedtoeliminateotherpossible■■
physiologicalproblems.
Establishiftheinfantiscryingforotherreasonssuchashunger,temperature,boredom.■■
Establishtheinfant’sdiet,indicationsofreflux,sleepingpatterns,bowelandurination■■
patterns.
Askaboutthegeneralwellbeingoftheparentsandthesocialsituationoftheinfant.■■
10 A HEALTHY START IN LIFE CLINICALNUTRITION
Resourceswww.raisingchildren.net.au/articles/colic:_what_to_do.html/context/255
www.raisingchildren.net.au/articles/colic:_what_is_it.html
www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=304&id=1735
www.gut.nsw.edu.au/pcinfo1.htm
www.gut.nsw.edu.au/free1.htm
www.healthinsite.gov.au/
www.healthinsite.gov.au/topics/Colic
ReferencesJBI2004,TheEffectivenessofInterventionsforInfantColic,1. Best Practice8(2)1-6.www.joannabriggs.edu.au/pdf/BPIScolic.pdf
TurnerT.L.,(2006)Clinicalfeaturesandaetiologyofcolic:[online]18thApril2007,2.www.uptodateonline.com/utd/content/topic.do?topicKey=behaviour/2155

11A HEALTHY START IN LIFE CLINICALNUTRITION
Intentionally blank

12 A HEALTHY START IN LIFE CLINICALNUTRITION
Intentionally blank
13A HEALTHY START IN LIFE CLINICALNUTRITION
7.3 Constipation – keeping things moving!Recommendations from the Dietary Guidelines for Children and Adolescents in Australia
To avoid unnecessary intervention, parents need to be educated about the wide variation in normal bowel function in infants (particularly those who are breastfed) and toddlers.
Therehavebeensomerecentchangesinthewayconstipationisbeingmanaged.Thissectionwillgiveyouanoverviewofmanagementplans,andprovidesomedetailedadviceonwhenreferralsarenecessary.
Anormalpatternofstoolevacuationisthoughttobeasignofhealthinchildrenofallages.Especiallyduringthefirstmonthsoflife,parentspaycloseattentiontothefrequencyandthecharacteristicsoftheirchildren’sdefecation.Anydeviationfromwhatisthoughtbyanyfamilymembertobenormalforchildrenmaytriggeracalltothenurseoravisittothepaediatrician(4).
Stoolconsistencyandfrequencycanbeveryvariableininfantsandchildren.Healthybreastorformulafedinfantsmaypassstoolsasregularlyasaftereveryfeedorasseldomasonceaweek.Aslongasthestoolsaresoftandeasilypassedandtheinfantiscontinuingtogrowappropriately,thereisgenerallynocauseforconcern.Somefoodswillchangestoolstoadifferentcolour,forexample,spinachmaycausedarkgreenstoolsorbeetrootmaycauseareddishcolour.
Chronic constipation is a source of anxiety for parents who worry that a serious disease may be causing the symptoms (4).
Constipationinchildhoodiscommon,withareportedprevalencerangingfrom0.3–28%.Faecalsoilingoccursin1–3%ofchildrenaged4–7years(2).
Symptoms persist beyond puberty in about 30% of children with constipation and soiling (2)
DefinitionAninfantorchildisconsideredconstipatedifthereispainassociatedwithpassingstoolsandthestoolsarehardordry.Infrequencyisinsufficientgroundsuponwhichtomakeadiagnosisofconstipation.However,thereisgeneralacceptancethatitisabnormaltohave
stoolfrequencyoflessthan3timesperweek,■■
hardpainfuldefecation■■
periodicpassageofverylargeamountsofstoolatleastonceevery7–30days■■
orapalpableabdominalorrectalmassonphysicalexamination(2).■■
14 A HEALTHY START IN LIFE CLINICALNUTRITION
Normal bowel functionWhatisstrikingisthevarianceofnormalfrequencyofbowelmovements,particularlyininfants;breastfedbabies0–3monthsold,rangefrom5–40bowelmovementsperweek(4).
Normal bowel function (1, 2, 3)
Firstbowelactionconsistsofmeconium,whichisgreenish-black■■
24–48hoursmeconiumchanges;browntransitionalstools■■
Breastfed:■■
3■■ rdor4thday,mustardcoloured
Mayalsobegreenororange■■
Milkcurdsmaybepresent■■
6weeksto3months-numberofbowelmotionsdecrease;intervalsofseveraldaysor■■
morearecommon
Babiesolderthan2monthsmaynormallyhaveinfrequentstools,sometimesupto■■
1–2weeksapart(1)
Formulafedbabiespassfewerstools,onceadayoreverysecondday,khakicoloured■■
andplasticinelikeconsistency
Meconiumispassedwithinthefirst24hoursinabout87%ofinfantsandwithin48hoursby99%;thisisnotinfluencedbywhethertheinfantisreceivingbreastmilkorformula(2).
Subsequently,however,themethodoffeedinghasasignificantimpactonstoolfrequency,colourandconsistency.Breast-fedinfantspasssofter,uniformlyyellowstoolsupto5timesaday.Thisismorefrequentthaninbottle-fedinfants.However,breast-fedinfantsmayoccasionallyhavenobowelactionsfor3daysormore,whichisrareinbottle-fedinfants.Withinthefirstfewweeksoflife,64%ofbreast-fed,butonly30%ofbottle-fed,infantsarehavingmorethan3bowelactionsaday(2).
Stoolfrequencyreducesprogressivelywithage,sothatby16weeksofagebothbreastfedandbottlefedinfantsarepassingonaverage2stoolsaday.
Hard, dry motions are more likely to occur after formula or solids are introduced (1).
Pleasenote:continuedpassageofmeconiuminthefirstcoupleofmonthsmaybeasignofinadequatemilkintakeandmaybethefirstsignofanunderfedbaby(1).SeeFailuretoThrivesection.
15A HEALTHY START IN LIFE CLINICALNUTRITION
Aetiology of constipationThe aetiology of constipation and soiling is multifactorial.
Functional constipation (2,4)
Constipationwithoutobjectiveevidenceofapathologicalcondition.Itismostcommonlycausedbypainfulbowelmovementswithresultantvoluntarywithholdingoffaecesbyachildwhowantstoavoidunpleasantdefecation(seeBox2).Withholdingfaecescanleadtoprolongedfaecalstasisinthecolon,withreabsorptionoffluidsandanincreaseinsizeandconsistencyofthestools.
Up to 63% of children with constipation and faecal soiling will have a history of painful defecation beginning before 3 years of age and secondary withholding behaviour (2).
Events leading to painful defecation (4)
toilettraining■■
changesinroutineordiet■■
stressfulevents■■
intercurrentillness■■
unavailabilityoftoilets■■
thechild’spostponingdefecationbecauseheorsheistoobusy.■■
Recognising the signs to prevent functional constipation: ‘withholding’
Thepassageoflargehardstoolsthatpainfullystretchtheanusmayfrightenthechild,resultinginafearfuldeterminationtoavoidalldefecation.Suchchildrenrespondtotheurgetodefecateby(2,4):
contractingtheiranalsphincterandglutealmuscles,attemptingtowithholdstool■■
risingontheirtoesandrockingbackandforthwhilestiffeningtheirbuttocksandlegs■■
wrigglingorfidgeting■■
assumingunusualpostures■■
crossingtheirthighs■■
walkingontiptoestoclenchtheirbuttocks■■
performingtheseactionsoftenwhilehidinginacorner■■
Often parents believe this behaviour is the child attempting to defecate (4)
Eventuallytherectumhabituatestothestimulusoftheenlargingfaecalmass,andtheurgetodefecatesubsides.Withtime,suchretentivebehaviourbecomesanautomaticreaction.Astherectalwallstretches,faecalsoilingmayoccur(4),duringspontaneousrelaxationofsphincters(2)angeringtheparentsandfrighteningthechild.Afterseveraldayswithoutabowelmovementirritability,abdominaldistension,cramps,anddecreasedoralintakemayresult(4).
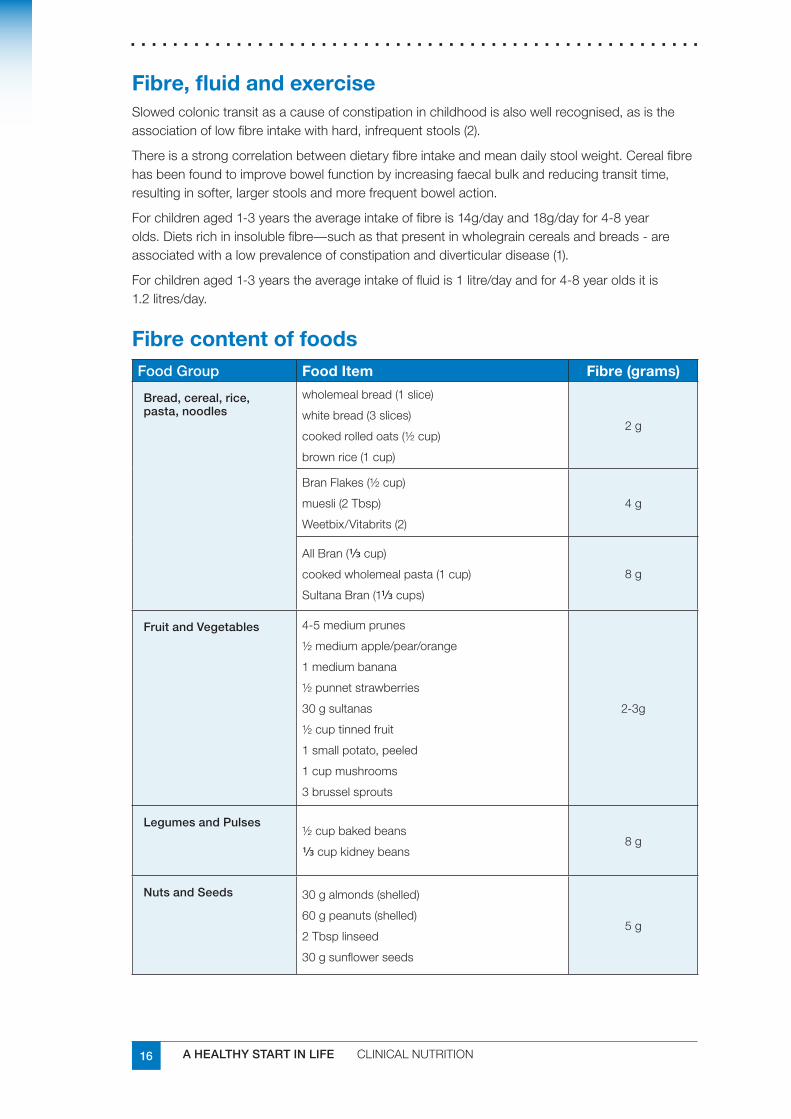
16 A HEALTHY START IN LIFE CLINICALNUTRITION
Fibre, fluid and exerciseSlowedcolonictransitasacauseofconstipationinchildhoodisalsowellrecognised,asistheassociationoflowfibreintakewithhard,infrequentstools(2).
Thereisastrongcorrelationbetweendietaryfibreintakeandmeandailystoolweight.Cerealfibrehasbeenfoundtoimprovebowelfunctionbyincreasingfaecalbulkandreducingtransittime,resultinginsofter,largerstoolsandmorefrequentbowelaction.
Forchildrenaged1-3yearstheaverageintakeoffibreis14g/dayand18g/dayfor4-8yearolds.Dietsrichininsolublefibre—suchasthatpresentinwholegraincerealsandbreads-areassociatedwithalowprevalenceofconstipationanddiverticulardisease(1).
Forchildrenaged1-3yearstheaverageintakeoffluidis1litre/dayandfor4-8yearoldsitis1.2litres/day.
Fibre content of foodsFood Group Food Item Fibre (grams)
Bread, cereal, rice, pasta, noodles
wholemealbread(1slice)
whitebread(3slices)
cookedrolledoats(½cup)
brownrice(1cup)
2g
BranFlakes(½cup)
muesli(2Tbsp)
Weetbix/Vitabrits(2)
4g
AllBran(≈cup)
cookedwholemealpasta(1cup)
SultanaBran(1≈cups)
8g
Fruit and Vegetables 4-5mediumprunes
½mediumapple/pear/orange
1mediumbanana
½punnetstrawberries
30gsultanas
½cuptinnedfruit
1smallpotato,peeled
1cupmushrooms
3brusselsprouts
2-3g
Legumes and Pulses½cupbakedbeans
≈cupkidneybeans8g
Nuts and Seeds 30galmonds(shelled)
60gpeanuts(shelled)
2Tbsplinseed
30gsunflowerseeds
5g
17A HEALTHY START IN LIFE CLINICALNUTRITION
Cow’s milk protein allergyIthasrecentlybeenrecognisedthatoneofthemanifestationsofthespectrumofcow’smilkproteinallergyinearlychildhoodisconstipation(2).
Inonestudythe“relationshipbetweencow’smilkproteinintoleranceandchronicconstipationwasobserved.In28%ofthechildren,constipationdisappearedduringtheCMP-freedietandreappearedafterthechallenge”(5).
Theseresultssuggestcow’smilkproteinintolerancemustbeconsideredinthedifferentialdiagnosisofchronicconstipation’(5).‘Inchildrenunresponsivetoconventionalmedicalandbehaviouralmanagement,considerationmaybegiventoatime-limitedtrialofcow’smilk-freediet(6).
Inchildrenbetween1–4yearsofage,ahistoryofallergy,analfissureorabdominaldiscomfortmaysuggestallergytocow’smilkprotein,justifyinga2weektrialofrestrictionofcow’smilkprotein(2).
Refer to dietitian
Clinical presentation of constipationTable 16 Clinicalpresentationofconstipation(2)
First week of life Delayedpassageofmeconiumbeyondthefirst48hours,suggestseitherananatomicalobstruction,suchasanalatresiaorstenosis,orHirschsprung’sdisease
Before introducing solids
Formulafedinfantspassharderstools
Maypresentwithdifficultpassageofhardstools,occasionallyafissure
Breastfedinfantsunlikelytopresentwithhardstools,butstoolsmaybeinfrequent.Breastmilkissogoodthereisnothingtowaste(1)
Introducing solids Commonforbothbreastandbottlefedinfantstochangebowelfunctioning.Constipationmayfirstpresenthere
Toilet training Maybeassociatedwithdevelopmentofwithholdingbehaviourandfunctionalfaecalretention
AdaptedfromCatto-Smithetal(2005)(2)
Exclusively breastfed infants are rarely constipated. Many breastfed infants show signs of discomfort or distress before passing a motion: this is a normal response to body sensations they are not used to. It does not indicate pain or constipation (1)
Management of children with constipation Evidence Based Practice tip: A combination of behavioural therapy and laxatives is more effective than behavioural therapy used alone (2).
EducationBothparentandchildneedtounderstandthatconstipationandfaecalsoilingarecommon,andarelikelytoimprovewithageandsimpletherapies.Theeasiestwaytoexplainsoilingistoemphasisethelossofconsciousawarenessoftheneedtodefecatethatcomeswithchronicrectaldistensionwithfaeces(2).Theemphasison‘keepingtherectumempty’islikelytoalleviateblame,andimprovecooperationandcompliance(2)
18 A HEALTHY START IN LIFE CLINICALNUTRITION
Maintenance therapy (2)Establishingaregulartoiletingregime,generallyabout2to3timesperdayfor■■
5-10minutesatatimeaftermeals.
Ensureappropriatetoiletingpostureandcomfortablefootsupportwithfeetflat.■■
Ifdietaryfibreisdeficient,itshouldthenbeoptimised.Dietarychangesareunlikelytobe■■
helpfulifthemainmechanismofconstipationiswithholdingbehaviour.
Adiaryishelpful,andcanbelinkedtoarewardchart.Encourageparentstorecord■■
toiletingfrequency,successfulpassageofstoolinthetoilet,soilingfreedays,dailymedicationsandepisodesofsoiling.
Stool reimpaction is less likely to occur if stools are being passed daily (2).
When to refer
Referralofachildforspecialistadviceshouldbeconsideredwhen:
impaction is suspected – referral to general practitioner, hospital or paediatrician1
symptoms of constipation do not respond to treatment in general practice after 3-6 months2
there is frequent soiling and distress3
in doubt about the cause of the symptoms4
the condition is interfering with the child’s schooling or social relationships5
Relapse
A significant proportion (30-50%) of children will relapse after being successfully treated for constipation (2)
Longtermrelapseismorefrequentinchildrenunder4yearsattheonsetofsymptomsandinwhomthereisahistoryoffaecalsoilingassociatedwithconstipation(2).
Initialreviewshouldbeafter1-2weeks,thenmonthly,andeventuallyat3monthlyintervals.Maintenancetherapyandfollowupshouldbecontinuedforatleast6–24months.Atrialofweaningfromtheuseoflaxativesshouldbeattemptedat6monthlyintervals(2).Itisimperativetostresstocaregiverstheimportanceoflongtermmaintenancetherapy,includingtheuseoflaxatives.
19A HEALTHY START IN LIFE CLINICALNUTRITION
ReferencesDietary Guidelines for Children and Adolescents in Australia incorporating the Infant 1.Feeding Guidelines for Health Workers,NHMRC,Canberra2003.
Catto-SmithAG.,(2005).Constipationandtoiletissuesinchildren.MJAPractice2.essentials–Pediatrics182(5)242-246
Breastfeeding management,3. AustralianBreastfeedingAssociation.3rdedition(2004).WendyBrodbirbb.Ligare
BakerSS,LiptakGS,CollettiRB.,CroffieJM.,DiLorenzeC.,EctorW.,NurkoS(1999)4.ConstipationinInfantsandChildren:EvaluationandTreatment.Journalofpaediatricgastroenterologyvol29(5)pp612-626
DaherS.,TahanS.,SoleD.,NapitzCK.,PatricioFRS.,Fagundes-NetoU.,MorrisMB.5.Cowsmilkintoleranceandchronicconstipationinchildren.PaedatricAllergyImmunology2001:12:339-342
2006.ClinicalPracticeGuideline:EvaluationandTreatmentofConstipationinChildren:6.SummaryofUpdatedRecommendationoftheNorthAmericanSocietyforPaediatricGastroenterology,HepatologyandNutrition.JournalofGastroenterologyandNutrition43:405-407
20 A HEALTHY START IN LIFE CLINICALNUTRITION
7.4 Failure to Thrive (Slow weight gain and undernutrition)
Failure to Thrive (FTT) has been recognised as more of a clinical description of growth failure in infants and children, rather than a stand alone diagnosis. FTT continues to be used as a blanket term for children, especially infants with perceived growth abnormalities (1). Now it is accepted that FTT has a predominantly nutritional cause, it has been suggested slow weight gain or undernutrition are reasonable alternate terms.
Themostseriousconsequencesofaninappropriatefoodintakeininfancyandearlychildhoodareunderweightandfailuretothrive.InAustralia,inrecentyears,concernabouttheprevalenceofunderweightandfailuretothriveininfancyandchildhoodhaslargelyfocusedonIndigenouscommunities,wheretheaetiologyoftheproblemrestsinacomplexmixofsocialandeconomicfactors(2).
Failuretothriveamongothersectionsofthecommunityisalsomostcommonlyaresultofpsychosocialfactors,includingpoorlivingconditions(2).
Theliteratureprovidesevidencethatfromtimetotimecasesoffailuretothrivealsooccurinmoreaffluentsectionsofthecommunityasaconsequenceofparentsinappropriatelyrestrictingthedietaryintakeofyoungchildrenbecauseoffearsaboutobesityandatherosclerosisorthedevelopmentof‘unhealthy’dietaryhabits.Suchcasesare,however,relativelyrarecomparedwiththeproblemofdietaryrestrictioninolderchildrenandadolescents(2).
Although it is now accepted that FTT has a predominantly nutritional cause, the implication of an association with emotional and physical deprivation persists (3).
There are a number of causes of failure to thrive and referral to a medical practitioner is recommended. If undernutrition is diagnosed, a dietitian/nutritionist will help in the management of this problem.
DefinitionFailuretothriveisaconditioncharacterisedbyfailure of expected growth(usuallyweight)(3,4,5).Onsetoftenoccurswithinweeksofbirthandwithhindsightgrowthfalteringisclearlyevidentongrowthchartsby6months.Failuretothriveoftenpersistsuptotheageof5years(5).
Currently,therearenonationallyorinternationallystandardisedguidelinesfordiagnosingFTT.Instudiesreviewed,chronicpoorweightgainisthemostcommonlyusedfeaturefordiagnosisfailuretothrive.Chronicpoorweightgainincludesgrowthdeviationfromtheexpectedweightpercentiles,atrend,whichmayalsobereflectedintheheightpercentiles(6).
Chronicpoorweightgainmayinclude:
inadequateweightgain■■
staticweight■■
intermittentperiodsofpoorgrowth.■■
Anadequateassessmentmustbebasedonaseriesofaccuratemeasurementsofboth length and weight.Longtermlengthandweightchangesaredesirable(refertogrowthchartsection).Head circumference shouldalsobemonitored(7).
21A HEALTHY START IN LIFE CLINICALNUTRITION
GrowthNormal growth (1)
Growth and development represent the end product of a multitude if factors both intrinsic and extrinsic to the infant or child. Normal growth is as much dependant on the genome of a particular individual as it is the external environment in which the individual thrives. Therefore, regular routine monitoring of growth indexes represents one of the most important responsibilities facing health professionals.
Althoughnewbornsizeisdependantonintrauterinefactors,growthduringinfancyislargelynutritionallydriven.Thereistransitionfromthenutritionbasedgrowthofinfancytothegrowthhormonedependantchildhoodphase.
Factitious failure to thrive (1)
Normalgrowthishighlyvariable.Somephysiologicaladjustmentssuchasconstitutionalgrowthdelay,familialshortstatureandintrauterinegrowthretardationdonotrepresenttruefailuretothriveorpaediatricundernutrition.
Familial short stature:■■
infantshaveadecreasedgrowthvelocitybetween6and18monthspfage■■
graduallytheseinfantswillfallintoanew,geneticallypredetermined,percentile■■
afterthisdecelerationofgrowth,theyhavenormalgrowthratealongtheirnew■■
centiles
characteristicsincludenormalbirthweightandlength,butfrequentlyafamilyhistory■■
ofshortstature
infantswithnormalshortstaturehavenormalskeletalmaturation■■
Constitutional growth delay: ■■
decelerationingrowthvelocitythatoccursbefore2yearsofage,andcanbegin■■
before6monthsofage
alsoadecreaseinweightforlengthcausedbyslowgainingofweight■■
decelerationofgrowthusuallyendsby3yearsofage,followedbynormalisationof■■
growthrate,albeitbelowthe3rdcentile
familyhistoryofgrowthdelaycharacterisedbyfeaturessuchasdelayedpubertyor■■
menarcheinaparent
boysaremorecommonlyaffectedthangirls■■
increasedgrowthpotentialduringchildhood■■
22 A HEALTHY START IN LIFE CLINICALNUTRITION
Intrauterine growth retardation (IUGR):■■
infantswhoaresmallfortheirgestationalage,andtendtohaveglobalgrowth■■
retardation
catchupgrowthusuallyoccursbefore2yearsofage■■
thoseinfantsthatfailtodisplaycatchupgrowth,typicallyremainedsmall,and■■
growthproceedsveryslowly
28%to70%arebelievedtobeconstitutionallysmall,displayingtheirgenetic■■
predisposition,withtheremainderoftheinfantsexpressingIUGRcausedbyunderlyingpathologicalprocesses,andoverlappingproblemssuchasmalnutritionorsubstanceabusearerecognisedcontributors
itisimportanttorealise,byassessmentofgrowthindexes,growthrateandhistory■■
thatiugrinfantsmaybegrowingnormallywhilenotachievingcatchupgrowth
Causes of failure to thrive (3)“Traditionally,FTThasbeensubdividedintoorganicornon-organicinnature.Studieshavefound5% or less have major organicdiseases,mostlydiagnosablefromothersignsandsymptoms”(5).
Abuse and neglect■■ –Twostudieshavefoundthatbetween5-10%ofchildrenwithFTThavebeenregisteredforabuseorneglect.“However,thestudyofSkuseandcolleaguesfoundthatchildrenwithFTTwerefourtimesmorelikelytobeabusedthancontrols”(3).
Emotional■■ –doesnotappeartobestronglylinkedtoFTT(3,5)
Undernutrition■■ –MostchildrenwithFTThavebeenfoundtobesubstantiallyunderweightforheight
“Simply,thereareinadequatecaloriesforgrowthanddevelopment.Theundernourishedstateoccurseitherby,oracombinationof(1)
inadequatesupplyofcalories■■
impairedorexcessiveutilisationofcalories”■■
“It might seem puzzling that a healthy child in a loving affluent home can become undernourished. This is less so when one recognises the high energy needs of infants: approximately three times those of adults (for each kg body weight)” (3).
The fastest decline in weight gain occurs in the early weeks of life, when energy needs are the highest and the highest proportion is required for growth.
Catchupgrowthmaythennotoccurforsometime,ifsubsequentintakeismerelysufficientforimmediateneeds.Awiderangeandcombinationoffactorsmaycontributetoeitherthedeclineorthefailureforcatchup.Forexample,attheageof14months,childrenwithFTThavearelativelydelayedprogressionontosolidfoods,poorerappetitesandeatamorenarrowrangeoffoods(3).
23A HEALTHY START IN LIFE CLINICALNUTRITION
Consequences (1,3)Growth–thenaturalhistoryofFTTisgradualimprovement■■
Cognition–evidencesuggeststhatalthoughFTTprobablyinfluencesdevelopmentin■■
theshortterm,apermanent effect on head circumference and brain growth is possible.
Primary care managementAhomevisitmightrevealobviousdietaryissuesandthisinputaloneoftenresultsinimprovement.Itiscrucialthatparentsaretoldatanearlystageandinsimpletermsthatundernutritionisthelikelycause,whileemphasisingwhatacommonphenomenonitis.
WeighingRoutineweightmonitoringatbirth,at6-8weeksandat8-12monthsaspartofroutineclinicalcare(3,5).Weightmonitoring(particularlyifconductedfrequently)canleadtoparentanxietyifababyisseennottobegainingweightfastenoughortoofast…(5)
Dietary assessment
“ A fifth of the children showed an improvement in their growth pattern immediately after dietary advice” (3).
Thepurposeoftheassessmentistoidentifypotentialareasfortailoredintervention,nottodiagnosedietaryinsufficiency.
AfirmgraspoftheenergybalanceequationisessentialforthesuccessfulmanagementofFTT.Howevermuchfoodachildappearstobeconsuming,iftheyareunderweightforheightandfailingtogainweightattheexpectedrate,orfailingtocatchup,theyarenotconsumingsufficientfortheirneedsandadviceonenergyenhancementisrequired(3).
ToddlerswithFTToftenhavealowintakeofimmature,lowenergyfoods,withahighfluidintake.Thustheaimofmanagementistoexpeditetheirprogressionontomoreenergydensesolidfoods.Liquidsupplementsortubefeedingmerelydelaythis,whereashospitaladmissionexposeschildrentotheriskofinfectionandfurtherdisruptiontoroutines.Thedramaticgainsthatcanbemadeathomeinresponsetoadviceandsupportaloneareoftennotappreciated(3).
The role of the general practitioner / paediatrician Ifmedicalcausesaresuspected,investigationsshouldbeundertaken.Mosttestsareundertakentoexcludepathologyratherthantoarriveatadiagnosis.
Improvement in growth should be evident approximately 1-3 months following initiation of treatment (5) SeeTable18onfollowingpage.
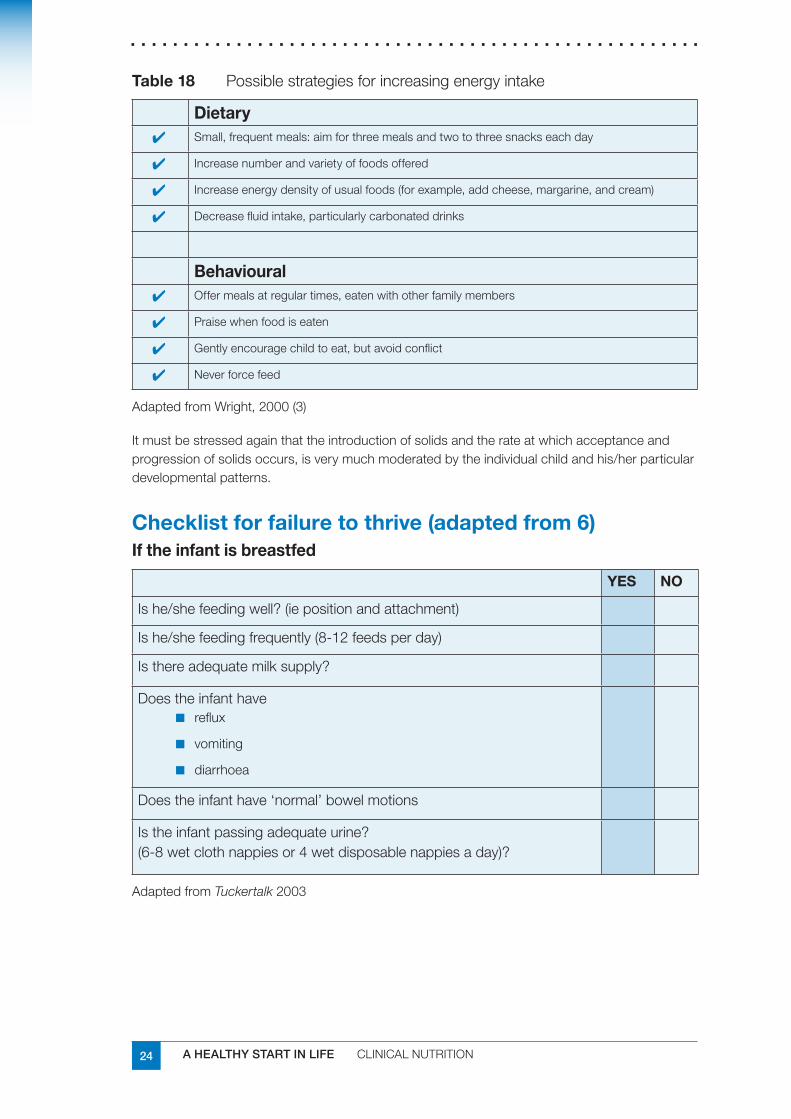
24 A HEALTHY START IN LIFE CLINICALNUTRITION
Table 18 Possiblestrategiesforincreasingenergyintake
Dietary ■✔ Small,frequentmeals:aimforthreemealsandtwotothreesnackseachday
■✔ Increasenumberandvarietyoffoodsoffered
■✔ Increaseenergydensityofusualfoods(forexample,addcheese,margarine,andcream)
■✔ Decreasefluidintake,particularlycarbonateddrinks
Behavioural ■✔ Offermealsatregulartimes,eatenwithotherfamilymembers
■✔ Praisewhenfoodiseaten
■✔ Gentlyencouragechildtoeat,butavoidconflict
■✔ Neverforcefeed
AdaptedfromWright,2000(3)
Itmustbestressedagainthattheintroductionofsolidsandtherateatwhichacceptanceandprogressionofsolidsoccurs,isverymuchmoderatedbytheindividualchildandhis/herparticulardevelopmentalpatterns.
Checklist for failure to thrive (adapted from 6)If the infant is breastfed
YES NO
Ishe/shefeedingwell?(iepositionandattachment)
Ishe/shefeedingfrequently(8-12feedsperday)
Isthereadequatemilksupply?
Doestheinfanthavereflux■■
vomiting■■
diarrhoea■■
Doestheinfanthave‘normal’bowelmotions
Istheinfantpassingadequateurine?(6-8wetclothnappiesor4wetdisposablenappiesaday)?
AdaptedfromTuckertalk2003
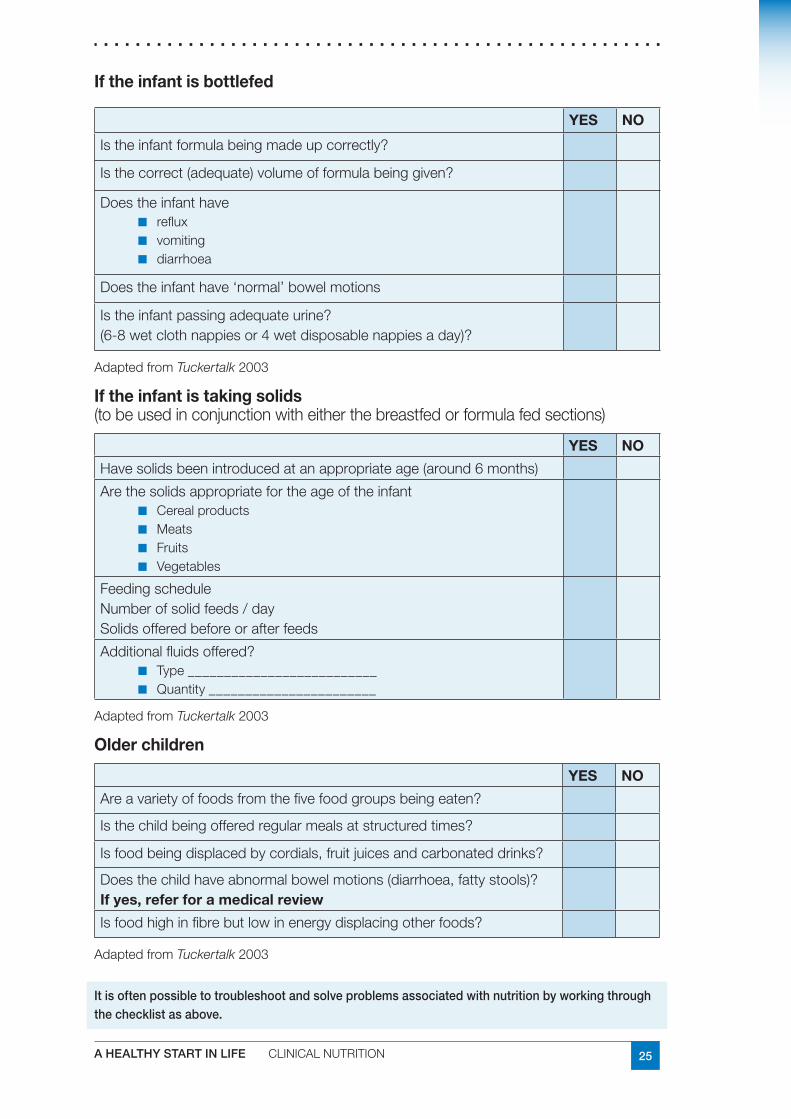
25A HEALTHY START IN LIFE CLINICALNUTRITION
If the infant is bottlefed
YES NO
Istheinfantformulabeingmadeupcorrectly?
Isthecorrect(adequate)volumeofformulabeinggiven?
Doestheinfanthavereflux■■
vomiting■■
diarrhoea■■
Doestheinfanthave‘normal’bowelmotions
Istheinfantpassingadequateurine?(6-8wetclothnappiesor4wetdisposablenappiesaday)?
AdaptedfromTuckertalk2003
If the infant is taking solids (tobeusedinconjunctionwitheitherthebreastfedorformulafedsections)
YES NO
Havesolidsbeenintroducedatanappropriateage(around6months)
ArethesolidsappropriatefortheageoftheinfantCerealproducts■■
Meats■■
Fruits■■
Vegetables■■
FeedingscheduleNumberofsolidfeeds/daySolidsofferedbeforeorafterfeeds
Additionalfluidsoffered?Type__________________________■■
Quantity_______________________■■
AdaptedfromTuckertalk2003
Older children
YES NO
Areavarietyoffoodsfromthefivefoodgroupsbeingeaten?
Isthechildbeingofferedregularmealsatstructuredtimes?
Isfoodbeingdisplacedbycordials,fruitjuicesandcarbonateddrinks?
Doesthechildhaveabnormalbowelmotions(diarrhoea,fattystools)?If yes, refer for a medical review
Isfoodhighinfibrebutlowinenergydisplacingotherfoods?
AdaptedfromTuckertalk2003
It is often possible to troubleshoot and solve problems associated with nutrition by working through the checklist as above.
26 A HEALTHY START IN LIFE CLINICALNUTRITION
Tips for practice:
If an infant or child is not experiencing any difficulties with any of the previous checklist points and there is no medical reason for the failure to thrive according to medical examinations, but is still not gaining weight, it may simply be that the infant requires more food.
Thisisaspecialsituationandrequiresadditionalthought.Extraenergycanbeaddedbyofferingahighenergy/highproteinmealplanusingtherecommendationsinthenextsection.
If unsure refer to dietitian for assessment and advice.
ReferencesJolleyC.D.,FailuretoThriveCurrProblPediatrAdolescHealthCare2003;33:183-2061.
Dietary Guidelines for Children and Adolescents in Australia incorporating the Infant 2.Feeding Guidelines for Health Workers,NHMRC,Canberra2003
WrightC.M.,Identificationandmanagementoffailuretothrive:acommunityperspective.3.ArchDisChild2000:82:5-9
OlsenE.M.,2006FailuretoThrive:StillaProblemofDefinition.ClinicalPaediatrics45:1-64.
ChildHealthScreeningandSurveillance:2002AcriticalReviewoftheevidence.NHMRC5.[online]13thApril2007www.nhmrc.gov.au/publications/synopses/_files/ch42.pdf
CommunityPopulationandRuralHealth(2003).6. Tuckertalk (child nutrition) fully revised.Tasmania,
ShawV.,LawsonM.,ClinicalPaediatricDietetics,1994.BlackwellSciences,London7.
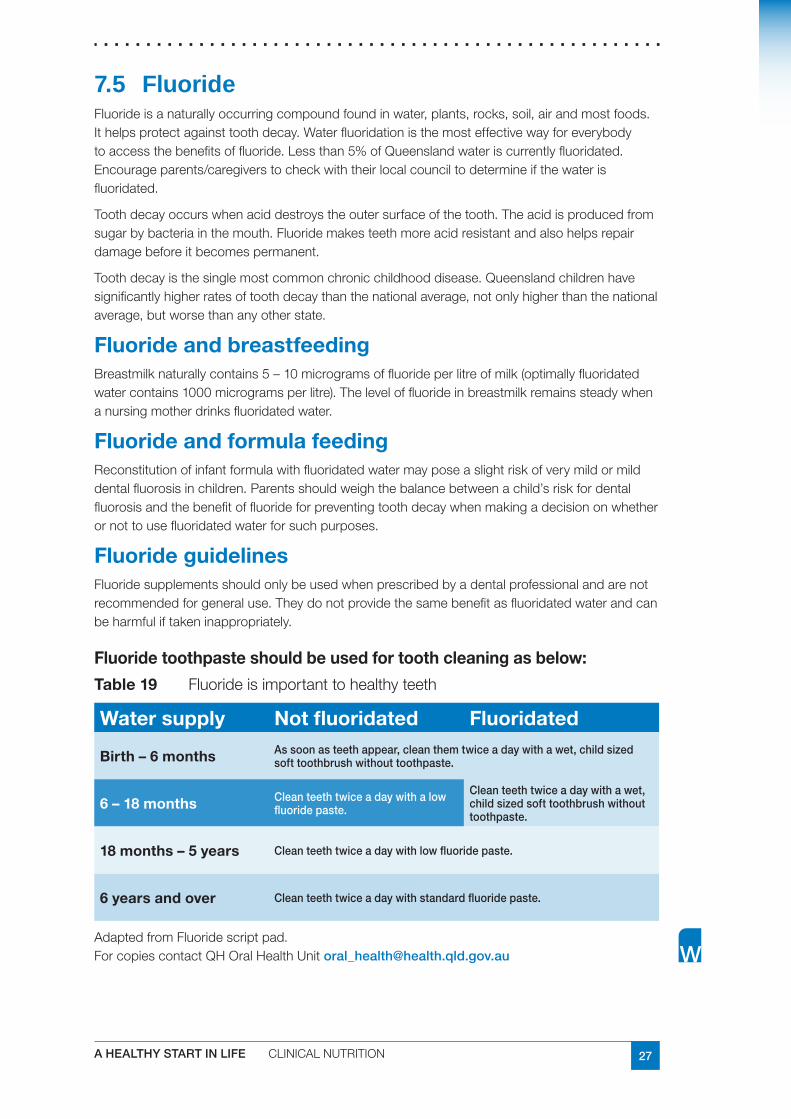
27A HEALTHY START IN LIFE CLINICALNUTRITION
7.5 FluorideFluorideisanaturallyoccurringcompoundfoundinwater,plants,rocks,soil,airandmostfoods.Ithelpsprotectagainsttoothdecay.Waterfluoridationisthemosteffectivewayforeverybodytoaccessthebenefitsoffluoride.Lessthan5%ofQueenslandwateriscurrentlyfluoridated.Encourageparents/caregiverstocheckwiththeirlocalcounciltodetermineifthewaterisfluoridated.
Toothdecayoccurswhenaciddestroystheoutersurfaceofthetooth.Theacidisproducedfromsugarbybacteriainthemouth.Fluoridemakesteethmoreacidresistantandalsohelpsrepairdamagebeforeitbecomespermanent.
Toothdecayisthesinglemostcommonchronicchildhooddisease.Queenslandchildrenhavesignificantlyhigherratesoftoothdecaythanthenationalaverage,notonlyhigherthanthenationalaverage,butworsethananyotherstate.
Fluoride and breastfeedingBreastmilknaturallycontains5–10microgramsoffluorideperlitreofmilk(optimallyfluoridatedwatercontains1000microgramsperlitre).Theleveloffluorideinbreastmilkremainssteadywhenanursingmotherdrinksfluoridatedwater.
Fluoride and formula feeding Reconstitutionofinfantformulawithfluoridatedwatermayposeaslightriskofverymildormilddentalfluorosisinchildren.Parentsshouldweighthebalancebetweenachild’sriskfordentalfluorosisandthebenefitoffluorideforpreventingtoothdecaywhenmakingadecisiononwhetherornottousefluoridatedwaterforsuchpurposes.
Fluoride guidelinesFluoridesupplementsshouldonlybeusedwhenprescribedbyadentalprofessionalandarenotrecommendedforgeneraluse.Theydonotprovidethesamebenefitasfluoridatedwaterandcanbeharmfuliftakeninappropriately.
Fluoride toothpaste should be used for tooth cleaning as below:
Table 19 Fluorideisimportanttohealthyteeth
Water supply Not fluoridated Fluoridated
Birth – 6 months As soon as teeth appear, clean them twice a day with a wet, child sized soft toothbrush without toothpaste.
6 – 18 months Clean teeth twice a day with a low fluoride paste.
Clean teeth twice a day with a wet, child sized soft toothbrush without toothpaste.
18 months – 5 years Clean teeth twice a day with low fluoride paste.
6 years and over Clean teeth twice a day with standard fluoride paste.
AdaptedfromFluoridescriptpad.ForcopiescontactQHOralHealthUnit [email protected]
28 A HEALTHY START IN LIFE CLINICALNUTRITION
Useful websites and resourcesTakingcareofyourbaby’steeth–childhealthfactsheetwww.health.qld.gov.au/phs/documents/cyhu/28096.pdf,
QHWaterFluoridationQuestionsandAnswerswww.health.qld.gov.au/oralhealth/documents/30265.pdf
InformationBulletinforcommunity.FluoridationofwatersuppliesandyourHealth,QueenslandHealth:OralHealthUnit,2005
www.health.qld.gov.au/phs/documents/ohu/30268.pdf
QueenslandHealth.Waterfluoridation:helpsprotectteeththroughoutlife
QueenslandHealth:OralHealthUnit,2005www.health.qld.gov.au/oralhealth/documents/31293.pdf
QueenslandHealthWaterfluoridation:informationforhealthprofessionals.QueenslandHealth:OralHealthUnit,2005www.health.qld.gov.au/fluoride/health_professionals.pdf.
QHfluoridefactsheetwww.health.qld.gov.au/phs/Documents/ohu/21922.pdf.
ThehealthofQueenslandersCHOreport2006www.health.qld.gov.au/cho_report/documents/32048.pdf
29A HEALTHY START IN LIFE CLINICALNUTRITION
7.6 GastroenteritisGastroenteritisisthetermusedtodescribeacute,infectivediarrhoeaandiscommonlycausedbypathogenssuchasviruses,bacteriaandparasites.Themostcommoncauseofgastroenteritisinchildrenlessthan2yearsisRotavirus;however,itisrarelyseenininfantslessthan6monthsofage.Aninfantorchildwithgastroenteritismostoftenpresentswithvomitinganddiarrhoea.Diarrhoeaisdefinedasanincreaseinthefrequency,fluidityandvolumeofstools.Thegastrointestinallossofwaterandelectrolytesaccompanyingthisisthemostcommoncauseofdehydrationininfantsandchildren.Themorewateryandfrequentthediarrhoea,thegreatertheriskofdehydration(particularlyifvomitingisalsoassociated).
ManagementAchildwhohasdiarrhoeaand/orvomitingisatriskofdehydrationandshouldbeseenbyadoctor.Donotgivemedicinestostopvomitingordiarrhoea.
Solely breastfed
Continue breastfeeding (there is no need to cease feeding).■■
Ensure fluid and electrolyte losses are recovered by either:■■
Increasing the frequency of breast feeds■■
Offering additional clear fluids such as cooled, boiled water between feeds■■
Formulafed
Continue normal strength formula feeds.■■
Ensure adequate hydration/rehydration by offering extra clear fluids.■■
If formula feeding has been stopped reintroduce formula after 24 hours.■■
Solids
Reintroduce food within 24 hours even if diarrhoea has not settled.■■
Ensure adequate hydration/rehydration by offering extra clear fluids.■■
Suitable foods include bread, potatoes, rice, noodles, vegetables, plain meats, fish and ■■
eggs.
Consult a doctor if one or more of the following applies:
theinfantislessthan6monthsofage■■
diarrhoeaisprofuseeg8–10waterystools■■
diarrhoeaorvomitinglastslongerthan24hours■■
theinfantorchildisvomitingandcannotkeepfluidsdown,willnotdrink,orhasnot■■
passedurinein4–6hours
thereisstomachpainorbloodinthediarrhoea■■
thereisapersistenthighfever>39.5■■ oC.
30 A HEALTHY START IN LIFE CLINICALNUTRITION
It is essential, when treating gastroenteritis to:
Ensurethattheinfant/childremainshydratedbycorrectingandpreventingfurtherlossesoffluidsandelectrolytes.
Reintroducefoodsassoonaspossibleinordertopreventprolongednutritionaldeficit.
Researchhasshownthatrefeeding,soonerratherthanlater,reducesthedurationofdiarrhoealdisease.
Signs of dehydration (1)Mild –5%bodyweightloss,thirsty,alert,restless,otherwisenormal
Moderate–6–9%bodyweightloss,thirsty,restless,lethargicbutirritable,rapidpulsenormalbloodpressure,sunkeneyes,sunkenfontanelle,drymucousmembranes,absenttears,pinchedskinretractsslowly,decreasedurineoutput
Severe–10%ormorebodyweightloss,drowsy,limp,cold,sweatycyanoticlimbs,comatose,rapidfeeblepulse,lowbloodpressure,sunkeneyesandfontanelle,verydrymucousmembranes,pinchedskinretractsslowly,nourineoutput.
Recommended hydration strategies for the dehydrated child
If a child is dehydrated medical attention should be sought.
Oral Rehydration Solution (ORS):
Arethebestcleardrinksforbabies(ofanyage)andchildrenwithgastroenteritisbecause:
theyhavetherightamountsofsugar,saltandwatertobeeasilyabsorbedinthegut■■
mustbemadeexactlyaccordingtodirectionsinthepackage■■
include■■ Gastrolyte, Gastrolyte-R, Pedialyte, Repalyte (New Formulation) and Hydralyte**(iceblocks)
availablefromchemistsinAustralia.Alwaysaskthepharmacistwhichonewouldbe■■
best
thesesolutionsarethefluidofchoicefortreatingdehydration.Theabsorptionofglucose■■
andsodiumislinkedtogetherandactsasapump,promotingtheabsorptionofwater.Theysupplyfluid,glucose,andhelpcorrectelectrolyteimbalances.ItisbesttoprovideORSinsmall,frequentdoses10–20mlevery10minutes
reviewchildafter24hoursforrehydrationstatus.■■
Please refer to:
QueenslandHealth,SouthernZonepaediatricsparentinformation–gastroenteritisinchildrenqheps.health.qld.gov.au/twmba/Pdf/SZ_gastro_fact.pdf
31A HEALTHY START IN LIFE CLINICALNUTRITION
Recommended hydration strategies for the non-dehydrated child
Usual maintenance fluids per hour is on a sliding scale:
First10kg4ml/kg/hr.Next10kg2ml/kg/hr.
Everykgover20-1ml/kg/hr.
Forexample-fora30kgchild(40ml+20ml+10ml)=70mlperhour.
Givesmallamountsfrequently.
Full strengthfruitjuice,lemonade,cordialandsportsdrinksshouldnotbeused.Thehighsugarcontentdrawswaterintothebowelandcanmakediarrhoeaworse.
Donotgivelowjouledrinks.
Dilution rates for fluids for use in non-dehydrated children
Cordial15mlin235mlwater
Softdrinks(notlowjoule)50mlsoftdrinkin200mlwater
Unsweetenedfruitjuice50mlfruitjuicein200mlwater
ORSreconstitutedasdirected
Sample meal planBreakfast
Cereal
Applejuice
WhitetoastwithscrapeofmargarineandVegemite
Lunch
1slicewhitebreadwithVegemite
Tinned/stewedfruit
Jelly
Dinner
Leanmeat
Mashedpotato(nobutterormilkadded)
Mashedpumpkin(nobutterormilkadded)
Gravy
Tinned/stewedfruit
Jelly
AdaptedfromWestmeadChildren’sHospital,2004(2)
32 A HEALTHY START IN LIFE CLINICALNUTRITION
Useful webstes and resourcesFact sheets
Whenyourchildissick–childhealthfactsheet[accessed2007April27]www.health.qld.gov.au/child&youth/factsheets/
GastrofactsheetCYHSA[accessed2007April27]www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=303&id=1845#6
GastrofactsheetChildren’sHospitalWestmead[accessed2007April27]www.chw.edu.au/parents/factsheets/gastroj.htm
Websites
AustralianGastroenterologyInstitutewebsite[accessed2007April27]
www.gesa.org.au/
ReferencesDepartmentofHealthandHumanServices.1. TuckerTalk Manual:keepingabreastofnutrition.Tasmania;2003.
WestmeadChildren’sHospital;JamesFairfaxInstituteofPaediatricNutrition.2. The feeding guide: a handbook on the nutritional composition of infant formula.Sydney:WestmeadChildren’sHospital;2001.
DepartmentofNutritionandDietetics;MaterChildren’sHospital.Gastrochildren’s3.guidelines.Brisbane.
GutFoundation.4. Diarrhoea in children.Randwick,Sydney:TheFoundation.
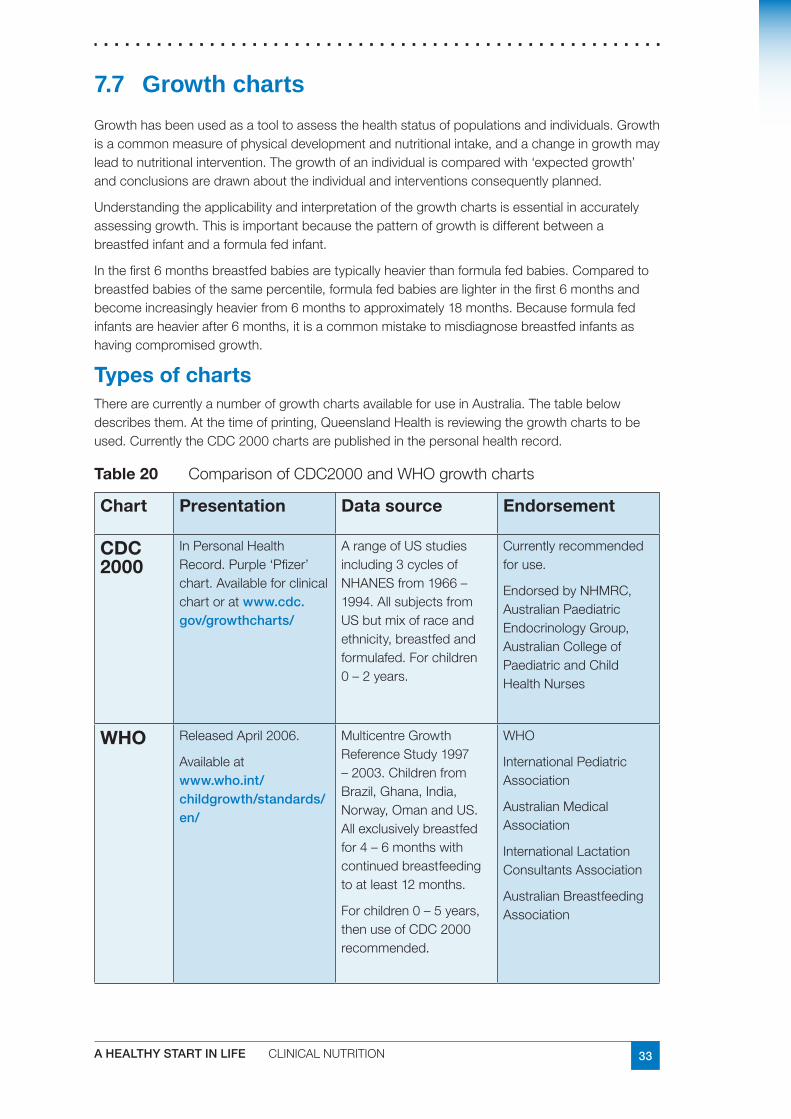
33A HEALTHY START IN LIFE CLINICALNUTRITION
7.7 Growth charts
Growthhasbeenusedasatooltoassessthehealthstatusofpopulationsandindividuals.Growthisacommonmeasureofphysicaldevelopmentandnutritionalintake,andachangeingrowthmayleadtonutritionalintervention.Thegrowthofanindividualiscomparedwith‘expectedgrowth’andconclusionsaredrawnabouttheindividualandinterventionsconsequentlyplanned.
Understandingtheapplicabilityandinterpretationofthegrowthchartsisessentialinaccuratelyassessinggrowth.Thisisimportantbecausethepatternofgrowthisdifferentbetweenabreastfedinfantandaformulafedinfant.
Inthefirst6monthsbreastfedbabiesaretypicallyheavierthanformulafedbabies.Comparedtobreastfedbabiesofthesamepercentile,formulafedbabiesarelighterinthefirst6monthsandbecomeincreasinglyheavierfrom6monthstoapproximately18months.Becauseformulafedinfantsareheavierafter6months,itisacommonmistaketomisdiagnosebreastfedinfantsashavingcompromisedgrowth.
Types of chartsTherearecurrentlyanumberofgrowthchartsavailableforuseinAustralia.Thetablebelowdescribesthem.Atthetimeofprinting,QueenslandHealthisreviewingthegrowthchartstobeused.CurrentlytheCDC2000chartsarepublishedinthepersonalhealthrecord.
Table 20 ComparisonofCDC2000andWHOgrowthcharts
Chart Presentation Data source Endorsement
CDC 2000
InPersonalHealthRecord.Purple‘Pfizer’chart.Availableforclinicalchartoratwww.cdc.gov/growthcharts/
ArangeofUSstudiesincluding3cyclesofNHANESfrom1966–1994.AllsubjectsfromUSbutmixofraceandethnicity,breastfedandformulafed.Forchildren0–2years.
Currentlyrecommendedforuse.
EndorsedbyNHMRC,AustralianPaediatricEndocrinologyGroup,AustralianCollegeofPaediatricandChildHealthNurses
WHO ReleasedApril2006.
Availableatwww.who.int/childgrowth/standards/en/
MulticentreGrowthReferenceStudy1997–2003.ChildrenfromBrazil,Ghana,India,Norway,OmanandUS.Allexclusivelybreastfedfor4–6monthswithcontinuedbreastfeedingtoatleast12months.
Forchildren0–5years,thenuseofCDC2000recommended.
WHO
InternationalPediatricAssociation
AustralianMedicalAssociation
InternationalLactationConsultantsAssociation
AustralianBreastfeedingAssociation
34 A HEALTHY START IN LIFE CLINICALNUTRITION
Using growth chartsRegular and consistent growth monitoring is more important than the chart used.
Thepatternofgrowthismoreimportantthanasingleplot.Itshouldfollowthelineofthe■■
curve,irrespectiveofitscentile.
Growthmeasurementsmustbeaccuratelyrecordedonthegrowthchart.■■
Referchildrenwho,overaseriesofreadingsarenotfollowingtheshapeofthecurve.■■
Notethedifferenceinpatternsofgrowthbetweenbreastfedandformulafedinfants.
Ensurethecorrectstaturechartisused.‘Length’referstoachildlyingdown.■■
‘Height’referstoachildstandingup.Thesevalueswilldiffer.
Whentakingweightmeasurements,ensurethesamescalesareusedwherever■■
possible,theyareroutinelycalibratedandtheinfantiswearingminimalclothing.
Encourageparents/caregiverstounderstandandinterpretgrowthcharts.■■
Allowanceforgestationalageismadeforchildrenbornunder37weeks.Generallythe■■
allowanceshouldbemadeuntilthechildis2yearsofageandupto5yearsofageforextremeprematurity,forexample,lessthan28weeks.
Forexample,ifaninfantbornat32weeksgestationvisitstheChildHealthCentreat■■
8weeksofagetheweightwillbeplottedattheageof40weeksgestation.
Weight and length/heightLength/heightisamandatorycomponentofthegrowthassessment;weightismeaninglessunlessacorrespondinglength/heightisdonesimultaneously.
Action
Forinfantsunder12monthsofage,actionwillberequirediftheweightdiffersby2percentilelinesorgreatercomparedtothelength.
Poor growthWhilethereisnostandard‘cutoff’fordefiningshortortallstature,traditionallyithasbeenrecommendedthatchildrenfallingbelowthe3rdcentilebereferredforfurtherassessment.
FTTisoftendefinedasanabsoluteweightcriterion,forexample,adropbelowthe3rdcentileforweightorthe5thcentileorwhengrowthdeviatesfromanestablishedgrowthcurvefor3consecutivemonths.Thisapproachislikelytoidentifyfalsepositives,forexample,naturallysmallchildren,whilemissingnaturallytallchildrenwithaFTTissue.Ajudgementshouldbemadeaccordingtoafallonacentilechartoveraperiodoftime/visitsorwherechildren’sweightis2centilelinesless,comparedwiththeirheight.
NB: Weightgainsininfantsareoftenstep-wiseratherthanaconstantprocess;thereforethetrendovertimeismoreimportantthanindividualweights.
35A HEALTHY START IN LIFE CLINICALNUTRITION
Overweight and obesityChildren less than 2 years
Youngchildrenwhoseweightisgreaterby2centilelinesormorecomparedtotheirlengthmayrequireinterventionandreferral.
Children over 2 years
BMI
TodeterminewhetheranolderchildisoverweightorobeseitisnecessarytocalculateBodyMassIndex(BMI)andplottheresultonanappropriateBMIpercentilechartforthechild’sageandsex.
Calculation of BMI
BMI = weight (kg) height (m)2
For example :
A2yearoldchildwhowas87cmtallandweighed13kgwouldhaveaBMIof17
BMI=13/(0.87x0.87kg/m2)
BMI=17
Thiswouldputthechildjustabovethe50thpercentileforBMI.
AchildisoverweightiftheirBMIisatorabovethe85thpercentile.Suchachildrequiresinterventionandreferral.
AchildisobeseiftheirBMIisatorabovethe95thpercentile.Suchachildrequiresinterventionandreferral.
Itisimportanttonotethatdiscussionofchildren’sweightandassociatedfoodandactivitypatternscanbeasensitiveissue.Carersshouldunderstandthatthegrowthchartisascreeningtool.Itisintendedtobeaguideofwhentotakesmallstepstomakechangesandwhentoseekfurtherguidancefromadoctororadietitian.
Head circumferenceThechildshouldbeseenbyamedicalofficeriftheheadcircumferenceis:
abovethe95thpercentile■■
belowthe5thpercentile■■
crossingthepercentilelines,eitherupwardordownwards,aftermeasurementontwo■■
separateoccasions
smallanteriorfontanelle■■
anteriorfontanellenotclosed.■■
Closureoftheanteriorfontanelleisvariablebutusuallycompleteby18months.
Anysuspectedsmallanteriorfontanellewithbossingofsutures,orsplitandseparatedsuturesoranteriorfontanellethatisnotclosedby2yearsshouldbeseenbyamedicalofficer.
36 A HEALTHY START IN LIFE CLINICALNUTRITION
ReferencesCDCGrowthCharts1.www.cdc.gov/growthcharts
WHOGrowthStandards2.www.who.int/childgrowth/standards/en/
VictorianHealthDepartment3.www.health.vic.gov.au/childhealthrecord/growth_details/index.htm
NHMRC“ClinicalPracticeGuidelinesfortheManagementofOverweightandObesityin4.ChildrenandAdolescents”and“OverweightandObesityinAdultsandinChildrenandAdolescents:AGuideforGeneralPractitioners”.www.dhac.gov.au/internet/wcms/Publishing.nsf/Content/obesityguidelines-guidelines-children.htm
NHMRC“ChildHealthScreeningandSurveillance:Acriticalreviewoftheevidence”5.(2002)www.nhmrc.gov.au/publications/synopses/_files/ch42.pdf
Foranthropometrytechniquestandards:6.depts.washington.edu/growth/module5/text/page5a.htm
Standardmethodsforthecollectionandcollationofanthropometricdatainchildren.7.PSWDavies,RRoodveldtandGMarks(2001)CommonwealthofAustralia
OlsenEM.Failuretothrive:stillaproblemofdefinition.ClinPediatr(Phila).2006Jan-Feb;8.45(1):1-6.
BatchelorJA.Hasrecognitionoffailuretothrivechanged?ChildCareHealthDev.19969.Jul;22(4):235-240.
37A HEALTHY START IN LIFE CLINICALNUTRITION
7.8 Healthy weightKeeping Kids on TrackThewirysun-bronzedAussieisbecomingafigureofthepast.Wearebecominganationoffatcouchpotatoes.Obesityisbringinguslifelonghealthproblems.Alifestylediseaserequiresalifestylesolution.Fortunately,thisiswithinthecapabilitiesofallAustralians(1).
Thischapterexplorestoolsyoucanuseinyourpracticetohelpcombattherisingepidemicofchildhoodobesity.
OverweightandobesityisalreadyaseriousprobleminQueensland.WhilerecentdataisnotavailableforQueensland,inAustraliabetween1985and1997thepopulationprevalenceofoverweightincreasedby60-70%,obesityincreased2-4fold(2).Theproblemhascontinuedtoworsen.Therearenowanestimated1.5millionyoungpeopleundertheageof18inAustraliawhoareoverweightorobese(3).
“New data indicates that an additional 1% of children in Australia are becoming overweight each year, which is amongst the highest rates of increase in the world” (4).
Childhoodoverweightisassociatedwithincreasedriskfactorsforheartdiseasesuchasraisedbloodpressure,bloodcholesterolandbloodsugar.OfgreatconcernistheappearanceofType2diabetesinadolescents—evenprimaryschoolchildren—withitspotentialforcomplicationssuchasheartdisease,stroke,limbamputation,kidneyfailureandblindness(3).
Themostsignificantlongtermconsequenceofobesityinchildhoodisitspersistenceintoadulthood.Overweightyoungpeoplehavea50%chanceofbeingoverweightadults,andperhapsnotsurprisinglychildrenofoverweightparentshavetwicetheriskofbeingoverweightthanthosewithhealthyweightparents.Obeseadultswhowereoverweightasadolescentshavehigherlevelsofweight-relatedillhealthandahigherriskofearlydeaththanthoseadultswhoonlybecameobeseinadulthood(3).
WHOhasidentifiedtheunderlyingcausesoftheglobalobesityepidemicas(5):
sedentary lifestyles ■■
high intake of energy-dense, micro-nutrient poor foods■■
heavy marketing of fast food outlets and energy-dense, micronutrient-poor foods and ■■
beverages
a high intake of sugar-sweetened drinks■■
large portion sizes■■
Obese children are at increased risk of:
hyperlipidemia■■
hypertension■■
abnormal glucose tolerance■■
psychosocial problems ■■
adult obesity (6)■■
38 A HEALTHY START IN LIFE CLINICALNUTRITION
The 1995 Australian Nutrition Survey indicated that children aged 4-7 years had excessively high fat intakes, one third ate no fruit and one fifth ate no vegetables on the day of the survey (2)
Onestudyfound“consensusamongstparentsthatobesitypreventionstrategiesneededtobeginearlyinachild’slife,longbeforetheyreachedtheschoolsetting.Parentsrecognizedthatbehaviorsareshapedearlyinlifeandwerelargelyalreadyentrenchedbythetimechildrenreachedschoolage”(8).
Defining overweight and obesity in children
An Australian expert working group identified body mass index (BMI) as the most appropriate clinical measure of excessive weight in children (9)
It is essential for height and weight to be accurately measured to determine if a child is overweight or obese. Visual assessment should be avoided.
About the BMI for children BMI = weight (kg)
height (m)2
AlthoughtheBMInumberiscalculatedthesamewayforchildrenandadults,thecriteriausedtointerpretthemeaningoftheBMInumberforchildrenandteensaredifferentfromthoseusedforadults.Forchildrenandteens,BMIage-andsex-specificpercentilesareusedfortworeasons:
theamountofbodyfatchangeswithage■■
theamountofbodyfatdiffersbetweengirlsandboys■■
TheCDCBMI-for-agegrowthchartstakeintoaccountthesedifferencesandallowtranslationofaBMInumberintoapercentileforachild’ssexandage.Foradults,ontheotherhand,BMIisinterpretedthroughcategoriesthatdonottakeintoaccountsexorage(11).
Table 21 NHMRCcurrentclassificationsforBMIpercentileranges(13)
Weight status category Percentile rangeOverweight 85thtolessthanthe95thpercentile
Obese Equaltoorgreaterthanthe95thpercentile
How is BMI calculated and interpreted for children and teens?
(adaptedfromCentersforDiseaseControlandPrevention)
CalculatingandinterpretingBMIinvolvesthefollowingsteps:
Before calculating BMI, obtain accurate height and weight measurements.1
Calculate the BMI; weight (kg) / [height (m)]2 2
Plot the BMI on the appropriate chart to determine the percentile 3
Review the calculated BMI-for-age percentile and results 4
Find the weight status category for the calculated BMI-for-age percentile as shown in BMI 5 table (see table 1). These categories are based on expert committee recommendations
ABMIcalculatorcanbefoundat apps.nccd.cdc.gov/dnpabmi/Calculator.aspx

39A HEALTHY START IN LIFE CLINICALNUTRITION
Nutrition strategiesFood language: everyday vs sometime foods
Thelanguageweusewhencommunicatingaboutfoodisveryimportant.Oftenwedescribehighcaloriefoodasverynegative.Wordslike“junk’/‘bad”canbeguiltinducingandmaybringupfeelingsofnegativityandfailure.Amorepositiveandhelpfulapproachistousetermssuchas“sometimes” foods and “everyday/always” foods.Thisdescribesfoodsmoreaccuratelyandprovidesabasisforlanguagearoundfoodchoices(1).Encourageparentstousethisformoflanguagewhendiscussingfoodchoiceswiththeirfamily.
Energy balance
Offeringasimpleconcepttoexplainenergyimbalanceasthecauseofoverweightisoftenignoredasmoreglamorous/novelideascapturepeople’sattentionandtheirmoney.Unfortunately,theseexplanationsareoftenscientificallyunfoundedandcauseconsiderablyconfusionbutdosellalotofbooks. Weallknowsomeonewhoisoverweight.Uponreflection,thispersonmaynotseemtoeatexcessively.Manychildrenweseeformanagementofobesityeatonlyslightly in excess oftheirdailyrequirements.
Sowhyisitthattheyareveryobesewhentheyonlyeatasmallamountofextracaloriesperday?Theanswerislikegettinginterestinabankaccount.Smallamountsovertimeadduptolargeamountsintheend.Forexample,imagineifsomeoneate2levelteaspoonsofextrafatperday(10g).Overayearthisaddsupto3.5kgofexcessweight(10gX365days).Keepthisupfor5yearsandallofasuddenyouhaveachildwhois17.5kgovertheirexpectedweight.Obesityresultsfromsmallamountsofexcessenergyeachday.Evenifchildrenleadveryactivelives,itiseasierforthemtocollectmoreenergythantheyexpendthroughexercise(1).
Sometimestheaimforchildrenistomaintaintheirweightsothatwhentheygrowtallertheywillthenbeinproportion.Howeverattimeslosingsomeexcessweightisnecessary.Thequalityoffoodweconsumecanhavealargeimpactonourweight.Itisimportanttounderstandthatthebuildingblocksoffood,fat,proteinandcarbohydrate containdifferentamountsofkilojoules(1).Theseare:
Fat: 37 kilojoules per gram ■■
Protein: 17 kilojoules per gram ■■
Carbohydrate: 16 kilojoules per gram ■■
Satisfying appetite
Researchhasshownthattheabovenutrientsdonotsatisfyourhungerinthesameway.Fattyfoodshaveonlyaweakeffectonsatisfyingourappetite.Incomparison,certaincarbohydratefoodshavebeenshowntohaveamoresatisfyingeffectontheappetite(1).Formoreinformation,contactyourlocaldietitian.
NB:Itisimportanttorememberthatchildrendoneedsomefatsintheirdietforgoodnutrition.
TheAustralian Guide to Healthy Eatinghasbeendevelopedtoprovidepeoplewithpracticalapplicationstoachievedailyenergybalances.Additionally,itmaximisestheamountofvitaminsandmineralsconsumed.Usethisasyourevidencebasedtoolwhenprovidingnutritioninformationtoparents.
40 A HEALTHY START IN LIFE CLINICALNUTRITION
Energy inPortion sizes
Itisimportanttoemphasisethecorrectportionsizeswhendiscussingwithparentshealthyeating.Portionsizeshavebeenincreasingoverthepastdecades,driveninpart,bycompaniesprofitingfromaperson‘upsizing’.Plates,bowlsandglassesarenowbigger,requiringmorefoodtofillthem.Snackfoodsareavailableinavarietyofincreasingsizes.UtiliseTheAustralianGuidetoHealthEatingasyourevidencebasedtooltoadviseparentsofcorrectportionsizes.
Every little bit extra contributes to energy in. Being more concise with portion sizes is a good place to start when looking at improving a child’s diet.
Energy dense foods
Manyfoodsarepre-packaged,readytoeatandloadedwithcaloriesforconvenienceandtaste.Compareyourselftosomeonewhomayhavelivedmanyyearsago.Theymighthavehadtoworkthefieldwithahorsedrawnplough,sowseedsbyhand,harvesttheseedswithascythe,threshtheseedsbyhand,milltheseedsintoflourandthenbaketheminawoodfiredoven.Theywouldalsohavetochopandtransportthewoodanddoothertasksintheirsparetime(1).
Thispersoncouldeat20loavesofcaloriedensebreadinadayandstillnotbecomeoverweightbecausetheyburnedmoreenergythantheyconsumed.Thisenergybalancehaschangedforusandproducedanepidemicofobesity.Wearenowpayingthepricefortheimbalancewithourhealth(1).
92% of children less than five years of age consume takeaway food regularly (6).
OnestudyfoundmanyAustralianchildren“weregenerallywellinformedaboutthehealthvalueofdifferentfoods,couldidentifythehealthyandunhealthyfoodspictured,andwereawareofthenutrientscontributingtotheirperceptionoffoodsbeingmoreorlesshealthy”(8).
“Parentsbelievedtheirchildrenknewwhichfoodswerehealthy,butsuspectedtheydidnotfullycomprehendtheconsequencesofeatingunhealthyfoods….Theypostulatedthattheinconsistentmessagesaboutunhealthyenergy-densefoods,includingattractivemarketingandadvertisingstrategies,confusedchildren”(8).
Parentsthemselves,althoughgenerallywellinformed,requestedmoreparenteducation…theydidnotfeelwellequippedtodistinguishbetweenmoreandlesshealthypre-packagedsnacksinlightofthehugearrayavailableandmarketedtochildren.“There’s so much deception in marketing, it’s hard to know which snacks are healthy”(8).
Food labels Bylaw,foodlabelsinAustraliamustcontainanutritioninformationpanelandaningredientslist.Youcanencouragefamiliestodotheirowninvestigatingwhentryingtoascertainwhetherfoodsareeverydayfoodsorsometimesfoods,byusingthefollowinginformationsheets.
Ingredient list
Thisliststheamountofingredientsbyweightindescendingorder(highesttolowest).Soifthefirstfewingredientslistedarefatorsugar(seebelowforothernamesforthese),thenitisoneofthemajoringredientsintheproductandthereforelikelytobehighinenergy.
Nutrition information panels
Allmanufacturedfoodsneedtocarryanutritioninformationpanel.Thisshowstheamountofenergy(inkilojoules),andnutrientcontentincludingprotein,totalfat,saturatedfat,carbohydrateandsugars,aswellasanyothernutrientthataclaimhasbeenmadeabout(eg:iron,calcium,fibre)inmeasurementsperserveandper100grams.
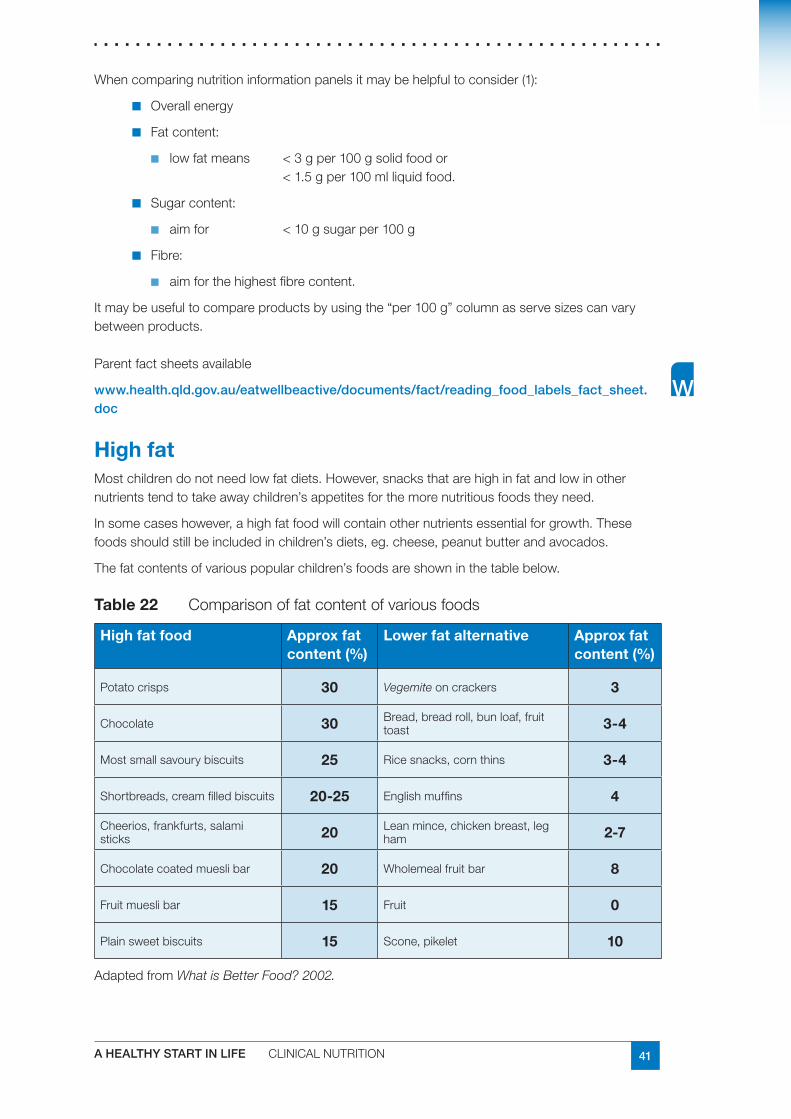
41A HEALTHY START IN LIFE CLINICALNUTRITION
Whencomparingnutritioninformationpanelsitmaybehelpfultoconsider(1):
Overallenergy■■
Fatcontent:■■
lowfatmeans <3gper100gsolidfoodor■■
<1.5gper100mlliquidfood.
Sugarcontent:■■
aimfor <10gsugarper100g■■
Fibre:■■
aimforthehighestfibrecontent.■■
Itmaybeusefultocompareproductsbyusingthe“per100g”columnasservesizescanvarybetweenproducts.
Parentfactsheetsavailable
www.health.qld.gov.au/eatwellbeactive/documents/fact/reading_food_labels_fact_sheet.doc
High fatMostchildrendonotneedlowfatdiets.However,snacksthatarehighinfatandlowinothernutrientstendtotakeawaychildren’sappetitesforthemorenutritiousfoodstheyneed.
Insomecaseshowever,ahighfatfoodwillcontainothernutrientsessentialforgrowth.Thesefoodsshouldstillbeincludedinchildren’sdiets,eg.cheese,peanutbutterandavocados.
Thefatcontentsofvariouspopularchildren’sfoodsareshowninthetablebelow.
Table 22 Comparisonoffatcontentofvariousfoods
High fat food Approx fat content (%)
Lower fat alternative Approx fat content (%)
Potatocrisps 30 Vegemiteoncrackers 3
Chocolate 30 Bread,breadroll,bunloaf,fruittoast 3-4
Mostsmallsavourybiscuits 25 Ricesnacks,cornthins 3-4
Shortbreads,creamfilledbiscuits 20-25 Englishmuffins 4
Cheerios,frankfurts,salamisticks 20 Leanmince,chickenbreast,leg
ham 2-7
Chocolatecoatedmueslibar 20 Wholemealfruitbar 8
Fruitmueslibar 15 Fruit 0
Plainsweetbiscuits 15 Scone,pikelet 10
AdaptedfromWhat is Better Food? 2002.
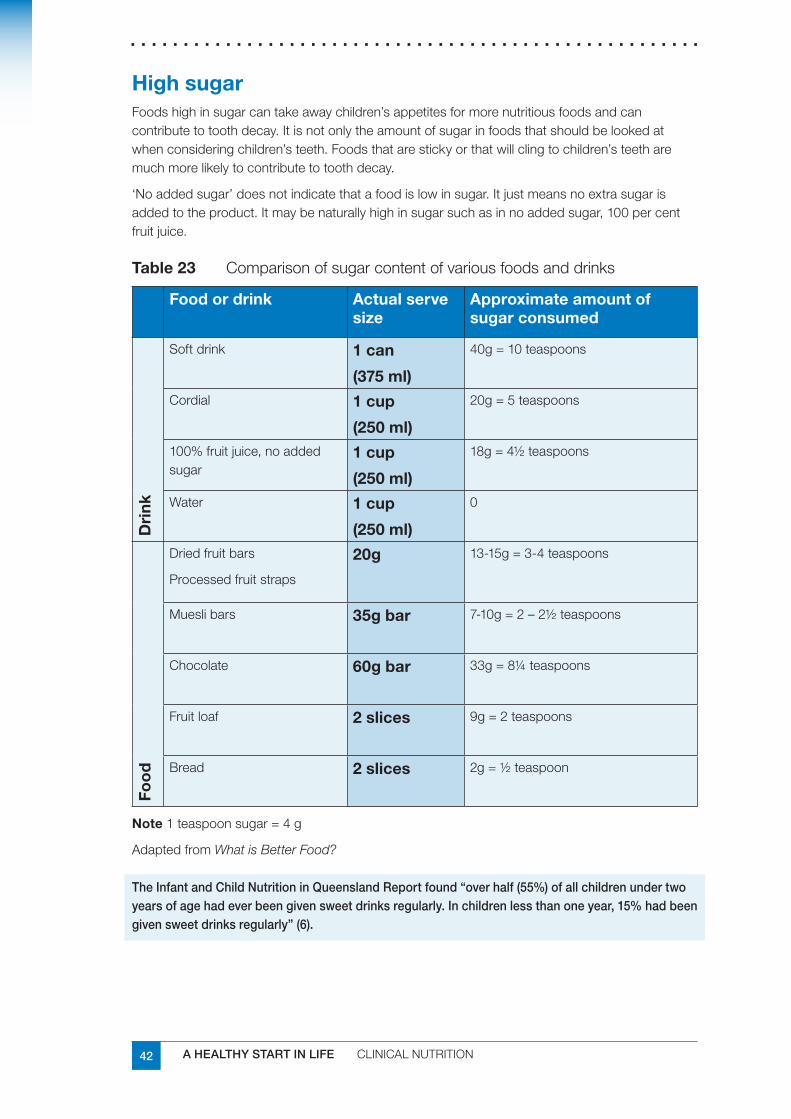
42 A HEALTHY START IN LIFE CLINICALNUTRITION
High sugarFoodshighinsugarcantakeawaychildren’sappetitesformorenutritiousfoodsandcancontributetotoothdecay.Itisnotonlytheamountofsugarinfoodsthatshouldbelookedatwhenconsideringchildren’steeth.Foodsthatarestickyorthatwillclingtochildren’steetharemuchmorelikelytocontributetotoothdecay.
‘Noaddedsugar’doesnotindicatethatafoodislowinsugar.Itjustmeansnoextrasugarisaddedtotheproduct.Itmaybenaturallyhighinsugarsuchasinnoaddedsugar,100percentfruitjuice.
Table 23 Comparisonofsugarcontentofvariousfoodsanddrinks
Food or drink Actual serve size
Approximate amount of sugar consumed
Dri
nk
Softdrink 1 can
(375 ml)
40g=10teaspoons
Cordial 1 cup
(250 ml)
20g=5teaspoons
100%fruitjuice,noaddedsugar
1 cup
(250 ml)
18g=4½teaspoons
Water 1 cup
(250 ml)
0
Foo
d
Driedfruitbars
Processedfruitstraps
20g 13-15g=3-4teaspoons
Mueslibars 35g bar 7-10g=2–2½teaspoons
Chocolate 60g bar 33g=8¼teaspoons
Fruitloaf 2 slices 9g=2teaspoons
Bread 2 slices 2g=½teaspoon
Note1teaspoonsugar=4g
AdaptedfromWhat is Better Food?
The Infant and Child Nutrition in Queensland Report found “over half (55%) of all children under two years of age had ever been given sweet drinks regularly. In children less than one year, 15% had been given sweet drinks regularly” (6).
43A HEALTHY START IN LIFE CLINICALNUTRITION
Snack food dilemmasAdaptedfromWhat is Better Food?
Belowissomenutritioninformationaboutfoodproductsthatoftenappearinlunchboxes,orusedassnacks.Wegenerallyknowthatfoodssuchaschocolateandpotatochipsarenotsuitabletoberegularlyincludedinchildren’slunchboxes.However,therearemanyfoodsthatchildrenbringwhereitishardertodecide.
Dried fruit bars and fruit straps
Thesedocontainsomedriedfruitbutaregenerallyveryhighinaddedsugar,lowinfibreandclingtochildren’steeth.Theyarenotcomparabletofreshfruit,despitetheadvertisingclaims.Theymayreducechildren’sfruitintake,takeawaytheirappetitesandcontributetotoothdecay.
Recommendation:Notrecommended.
Dried fruit
Driedfruitcontainssimilarnutrientlevelsandfibretofreshfruit.However,becausewaterhasbeenremoved,driedfruithasmoreconcentratedsugarandwillclingtoteeth.Driedfruitisrecommended,butisbesteatenjustpriortobrushingteethoratmealtimeswhenotherfoodsarebeingeaten.Givingdriedfruitaloneformorningteameansitwillremainonchildren’steethforsometimebeforeitisremovedbybrushingorbyeatingotherfoods.
Recommendation:Recommendedatmealtimesorwithotherfood.
Small oven baked savoury biscuits
Companiesarenowtargetingchildrenwiththesesnacksandareprovidingthesebiscuitsinsmall,convenientpackets.Manyparentsthinkthatsmallsavourybiscuitsareahealthieroptionthanpotatochipsfortheirchild.Howevertheyareoftenashighinfatandsaltasregularpotatochipsandcaneasilytakeawaychildren’sappetitesforthemorenutritiousfoodstheyneed.
Recommendation:Notrecommended.
Noodle snacks
Two-minuteareveryhighinfatasthenoodlesareusuallydeepfriedinoilpriortopackaging.Theflavouringisalsoveryhighinsalt.
Recommendation:Betteralternativesincludefat-freeAsianororientalnoodles.Theseareverytastywhenaddedtostirfrymeatandvegetables,ie.leftovers.Checktheingredientlistforfatoroil.
Muesli bars and breakfast bars
Mueslibarsarepopularwithchildrenandareoftenfoundinchildren’slunchboxes.Theyvaryinflavour,textureandnutritionalcontent.Ingeneral,chocolatecoatedorchocolatechipmueslibarsareveryhighinfatandsugar.Chewymueslibarsclingtochildren’steethandcancontributetotoothdecay.Snackbarsmadefromchildren’sbreakfastcerealsarealsoveryhighinsugarandwillclingtoteeth.
Recommendation:Chocolatecoated,chocolatechipandchewymueslibarsarenotrecommended.Children’sbreakfastcerealbarsshouldalsobelimited.Adultbreakfastcerealbarsareabetteralternative.Ifthesefoodsarebroughtalongtheyshouldbeeatenwithotherfoodsandteethbrushedaftereating.
44 A HEALTHY START IN LIFE CLINICALNUTRITION
Flavoured milk
Dairyfoodshavepropertiesthathelpprotectteethagainsttoothdecay.Flavouredmilkhasaddedsugarbutisstilldesirable,asitisanimportantsourceofcalcium.Somechildrenwillnotdrinkplainmilk.Childrenenjoythevarietythatflavouredmilkprovides.Itisimportantthatchildrenreceiveanadequatecalciumintakeanddrinkingmilkisoneoftheeasiestwaystoachievethis.
Recommendation:Allmilkisrecommended.
Fortoddlersover12monthsofageplain,fullcreammilkispreferredandforchildrentwo■■
tofiveyearsofagereducedfatmilks(1.5-2.5%fat)shouldbeused.
Skimmilk(lessthan0.5%fat)shouldnotbeuseduntilchildrenareoverfiveyears.Itis■■
finetohaveflavouredmilkoccasionally.
Makesuremilkconsumptiondoesnotexceedrecommendationsforage.■■
Flavoured dairy desserts
Yoghurtistheidealdairydessertforchildren.Itismoderateinsugarandfatandhighincalciumandprotein.Reducedfatvarietiesarerecommendedforchildrenoncetheyareovertwoyearsofage.Therearemanyflavoureddairydessertsmarketedforyoungchildren.Thesevaryintheirfat,sugarandcalciumcontents.Comparedtoyoghurt,dessertswhichhave‘mix-ins’are,ingeneral,muchhigherinsugarandsometimeshigherinfat.Thisisalsothecasewiththemajorityofchocolatemousseandcrèmecarameldesserts.Popularcustardbasedflavoureddessertsaregenerallyhigherinsugarthanyoghurtandtheyvaryintheircalciumcontent.Thesearenotabadchoiceifchildrenwillnoteatyoghurtandcanbeavaluablewayofimprovingcalciumintakes.
Recommendation:
encouragefullcreamflavouredorunflavouredyoghurtinpreferencetootherproducts■■
usethenutritionpanelofyoghurttocomparethevariousproductsthatappearin■■
children’slunchboxes
discourageyoghurtwithmix-inlolliesandhighfatdesserts,likechocolatemousse.■■
Cheese and biscuit snacks
Thesearepopularinchildren’slunchboxesandareagoodsourceofcalcium.Ratherthanthepre-packagedvarieties,wrappingupsomecrackersandasliceofcheeseinplasticwrapforthelunchboxreducescostandpackaging.
Recommendation:Recommended.
Biscuit and dip packs
Manydifferenttypesofbiscuitanddippacksexistforchildren.Somedipsarecheese-basedandareagoodsourceofcalcium.Thesweetflavoureddipsnackpacksareveryhighinsugar.
Recommendation:Cheeseorcheddardippacksarerecommendedbutsweetflavoureddipsnackpacksarebetterleftout.
Jam, honey or chocolate paste sandwiches
Thebreadisahealthychoicebutjam,honeyandchocolatepasteprovidesugarwithfewothernutrients.Childrenneedagoodsourceofironeachday.Thefillingonsandwichesisusuallytheeasiestwaytoprovidethis.
Recommendation:JamandhoneyareOKtohaveoccasionally,buttrytoencouragehighironfoodseg.roastmeat,chicken,ham,tuna,egg,peanutbutterorbakedbeans
45A HEALTHY START IN LIFE CLINICALNUTRITION
Energy outKids sport and technology
Energyexpenditurethroughphysicalactivityisanimportantpartoftheenergybalanceequationthatdeterminesbodyweight.Adecreaseinenergyexpenditurethroughdecreasedphysicalactivityislikelytobeoneofthemajorfactorscontributingtotheglobalepidemicofoverweightandobesity(5).Refertophysicalactivitysection.
Children aged 5-12 years spend an average of 2.5 hours per day watching television (2).
How much physical activity is sufficient for children?
New physical activity guidelines from the Department of Health and Ageing 2004 (4):
Children and youth should participate in at least 60 minutes (and up to several hours) of 1 moderate – to vigorous intensity physical activity every day
Children and youth should not spend more than 2 hours per day using electronic media for 2 entertainment (eg television, computer games, internet), particularly during daylight hours.
Physicalactivityhasdecreasedmarkedlyoverthelastcentury(especiallyinthelast20years).Theadventoftechnologyhasencouragedchildrentopursuemoresedentaryactivitiessuchasplayingvideogames,computers,VCRs,DVDs,CDs,andMP3s.Concernsaboutsafetyhavediscouragedparentsfromallowingtheirchildrentoplayunsupervisedinparks,streetsandneighbourhoods.Childrendon’trideorwalktoschool(1).
Young children spend more than 50% of their time in sedentary play (13).
Onestudyfoundsomechildrenviewanyamountofbodymovementconstitutedphysicalactivity;“playingpianoorcomputerisabithealthybecauseyou’removingyourfingers”(GradeTwo)(8).
Media and peer conformity
Peerpressureandwhatotherchildrenareeating/doingdirectlyimpactsuponourthinkingandexpectations.Advertisingcompanieshavebecomeverycunninginpromotingtheirproducts.Forexample,productplacementnowoccursinmovieswherecompanieswillpaytohavetheirbrandexclusivelyusedinamovie.Thisisasneakyandhiddenwaytopromoteandinfluencepeopletobuytheproduct(1).
Inthesimplestterms,obesityresultsfromanimbalancebetweencalorieseatenandcaloriesexpendedthroughactivityandexercise.Television(andmediabehaviour)upsetsthisbalancethrough:
reducedmetabolicratewhenwatchingTVandothermediaactivities■■
reducedactivitybecauseofwhattheyarenotdoingwhilsttheyareinteractingwiththe■■
media(childrenwhowatchmoreTVdolesssport)
increasedfoodandcalorieconsumption(fromadvertisingandsnacking).■■
Children are vulnerable to food messages portrayed through television advertisements, with food advertising affecting the choices and amounts of foods consumed (17).
46 A HEALTHY START IN LIFE CLINICALNUTRITION
OneAustralianstudyfound“Confectionery’and‘fastfoodrestaurants’werethemostadvertisedfoodcategoriesduringchildren’sTVviewinghours.Confectioneryadvertisementswerethreetimesaslikely,andfastfoodrestaurantadvertisementstwiceaslikely,tobebroadcastduringchildren’sprogramsthanadults’programs(17).
“Foodsmostadvertisedduringchildren’sviewinghoursarenotthosefoodsthatcontributetoahealthydietforchildren.Confectioneryandfastfoodrestaurantadvertisingappearstotargetchildren’(17).
It is well recognized that childhood obesity is a worldwide problem. The heavy marketing of energy-dense, nutrient-poor foods influences food choices and contributes to the incidence of overweight and obesity in children (14).
Checkreduce TV viewing for children and set specific limits■✔
remove TVs from bedrooms■✔
limit mobile phone usage■✔
cease cable TV■✔
reduce computer time especially chat rooms, emails, videos, video games■✔
remove electronic toys■✔
reduce and limit dvd’s movies■✔
look for product placements in media with your children ie turn sound off ■✔and guess what products have been placed in TV-movies
AdaptedfromKids on Track, 2004
Meal time tipsuse smaller plates/ bowls■✔
do not over fill plate■✔
have water available with all meals■✔
allow children to leave food on their plates■✔
minimise distractions eg TV off■✔
encourage your children to eat slowly■✔
encourage mealtime conversation■✔
eat together as a family■✔
model all the above tips yourself during the meal■✔
try these during at least one meal per day■✔
a small amount of sugar and salt per day■✔
increase plant based unprocessed foods■✔
increase high fibre foods■✔
reduce family grazing between meals and limit it to fruit and water■✔
AdaptedfromKids on Track, 2004
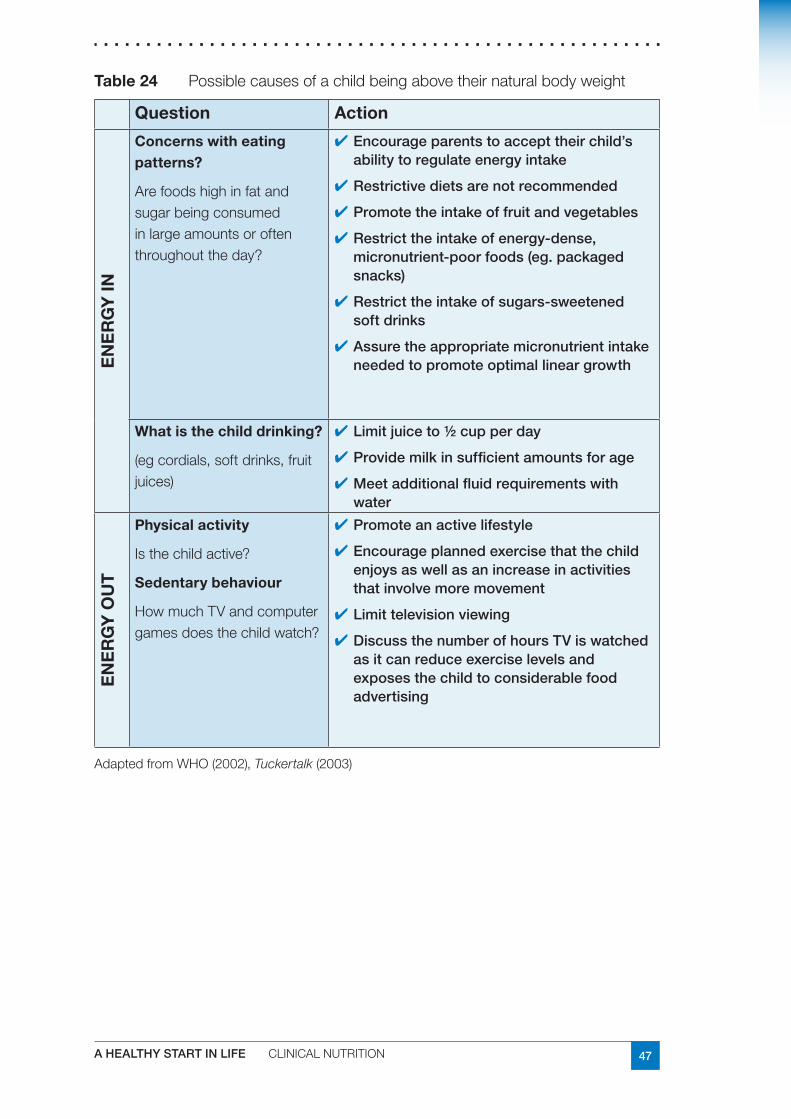
47A HEALTHY START IN LIFE CLINICALNUTRITION
Table 24 Possiblecausesofachildbeingabovetheirnaturalbodyweight
Question ActionE
NE
RG
Y IN
Concerns with eating patterns?
Arefoodshighinfatandsugarbeingconsumedinlargeamountsoroftenthroughouttheday?
Encourage parents to accept their child’s ■✔ability to regulate energy intake
Restrictive diets are not recommended■✔
Promote the intake of fruit and vegetables■✔
Restrict the intake of energy-dense, ■✔micronutrient-poor foods (eg. packaged snacks)
Restrict the intake of sugars-sweetened ■✔soft drinks
Assure the appropriate micronutrient intake ■✔needed to promote optimal linear growth
What is the child drinking?
(egcordials,softdrinks,fruitjuices)
Limit juice to ½ cup per day■✔
Provide milk in sufficient amounts for age ■✔
Meet additional fluid requirements with ■✔water
EN
ER
GY
OU
T
Physical activity
Isthechildactive?
Sedentary behaviour
HowmuchTVandcomputergamesdoesthechildwatch?
Promote an active lifestyle■✔
Encourage planned exercise that the child ■✔enjoys as well as an increase in activities that involve more movement
Limit television viewing■✔
Discuss the number of hours TV is watched ■✔as it can reduce exercise levels and exposes the child to considerable food advertising
AdaptedfromWHO(2002),Tuckertalk(2003)
48 A HEALTHY START IN LIFE CLINICALNUTRITION
Useful websites and resourcesFurther reading
The Queensland Strategic Policy Framework for Children’s and Young People’s Health 1.2002 – 2007.QueenslandHealth2002
Eat Well Queensland 2002-2012, Smart Eating for a Healthier State, Queensland Public 2.Health Forum.June2002
Eat Well, Be Active – Healthy Kids for Life: 2005-20083. .QueenslandGovernment2005
Healthy Weight 2008, the National Action Agenda for Children and Young People and 4.Their Families, Commonwealth of Australia.2003.
Queensland Health, Enhanced Child Health Model of Care for Community Health Services 5.(0-12 years)
Strategic Policy Framework for Aboriginal and Torres Strait Islander Children and Young 6.People’s Health 2005- 2010
Growth charts
CentresforDiseaseControlandPreventionwww.cdc.gov/
WorldHealthOrganisationwww.who.int/childgrowth/en/
Parent resources
Eat Well, Be Activewww.health.qld.gov.au/eatwellbeactive
A note on Kids on Track
Kids on Tracktargetschildrenthreetotenyearswhodonothaveanymedicalconditionsthatmightcauseoverweight.Itspurposeistoexaminetheeffectofagroupparentinterventiononthecourseandseverityofoverweight.Ithelpsparentsaddresstheirchildren’shealthproblemsviathreekeyareasofnutrition,physicalactivityandfamilybehaviourchange.Italsoinvestigatesifpositivehealthoutcomescanbemaintained.TheseprogramsarecurrentlybeingrunontheGoldandSunshineCoastsaswellasBayside.
Forfurtherinformationpleasecontact
TheReceptionistBundallCommunityChildHealthPOBox5699GCMCBundallQLD9726Phone:0755708553
49A HEALTHY START IN LIFE CLINICALNUTRITION
ReferencesQueenslandHealth:‘1. Kids on Track,’GoldCoast,2004
Booth,M.L.,Wake,M.,Armstrong,T.,Chey,T.,Hesketh,K.,&Mathur,S.(2001).The2.epidemiologyofoverweightandobesityamongAustralianchildrenandadolescents,1995-97.Australian and New Zealand Journal of Public Health,25(2),162-169.
CommonwealthofAustralia20033. Healthy Weight 2008, Australia’s Future,Canberra[online]29thAprilwww.healthyactive.gov.au/publications.htm
QueenslandGovernment.SmartStatehealthyweightforchildrenandyoungpeople.4.Eat well, be active – healthy kids for life.TheQueenslandGovernment’sfirstactionplan2005-2008.
JointWHO/FAOExpertConsultationonDiet,NutritionandthePreventionofChronic5.Diseases(2002:Geneva,Switzerland)Diet,nutritionandthepreventionofchronicdiseases:reportofajointWHO/FAOexpertconsultation,Geneva,28January--1February2002.[online]29thAprilwww.who.int/hpr/NPH/docs/who_fao_expert_report.pdf
QueenslandHealth:InfantandChildNutritioninQueensland20036.
Best Practice Dietetic Management of Overweight and Obese Children and Adolescents7. .AustralianCentreforEvidenceBasedNutritionandDietetics.TheJoannaBriggsInstitute[online]26thApril
Healthyeating,activityandobesityprevention:aqualitativestudyofparentandchild8.perceptionsinAustraliaK.HESKETH,E.WATERS,J.GREEN,L.SALMONandJ.WILLIAMSHealthPromotionInternational,2005,Vol.20No.1pp19-26
Batch,J.A.,&Baur,L.A.(2005).Managementandpreventionofobesityandits9.complicationsinchildrenandadolescents.MJA,182,130-135.
NationalHealthandMedicalResearchCouncil:10. Dietary Guidelines for Children and Adolescents in Australia incorporatingthe Infant Feeding Guidelines for Health Workers,Canberra2003.
CentresforDiseaseControlandPrevention11. www.cdc.gov/nccdphp/dnpa/bmi/childrens_BMI/about_childrens_BMI.htm[online]2ndMay,2007
QueenslandHealth:12. What is better food? Brisbane2002
Clinical Practice Guidelines for the Management of Overweight and Obesity in Children 13.and Adolescents,NHMRC.Canberra,2003
HowmuchfoodadvertisingisthereonAustraliantelevision?KathyChapman,Penny14.NicholasandRajahSupramaniam.HealthPromotionInternational200621(3):172-180;doi:10.1093/heapro/dal021
CommunityPopulationandRuralHealth15. Tuckertalk,Tasmania,2003
online[2ndMay]16. www.culturaldata.gov.au/publications/statistics_working_group/australias_culture_pamphlets/10_childrens_participation
NevilleL.,ThomasM.,BaumanT.,FoodadvertisingonAustraliantelevision:theextentof17.children’sexposureHealthPromotionInternational2005,Vol.20No.2.pp105-112
Borushek,A.18. Pocket calorie, fat & carbohydrate counter,2007,FamilyHealthPublications,WesternAustralia
50 A HEALTHY START IN LIFE CLINICALNUTRITION
7.9 Iron deficiencyIron deficiency is the most common nutritional deficiency in children and adults in both developed and developing countries (1)
ThosemostatriskofIrondeficiencyare:
childrenparticularlyagedbetween9-18months■■
womenofchildbearingage(1).■■
As many as 10% of Australian toddlers are iron deficient (2).
Irondeficiencyinchildhooddiffersinmanywaysfromthatinadults.Inchildren,themostlikelycauseisaninadequateamountofironinthediet,coupledwiththeextrarequirementforironbecauseofgrowth(2).
The effects of anaemia and iron deficiency on brain development in infancy and very early childhood are well documented: “infancy is the critical period for brain growth, and nutrient deficiencies during this time may affect psychomotor development and neurocognition” (3). “There is some disturbing evidence which suggests that the intellectual and psychomotor impairment caused by iron deficiency may not always be completely reversible when iron status is corrected” (as cited in 2).
For these reasons, the Australian Iron Status Advisory panel strongly believes that iron deficiency should be regarded as a serious illness in the first years of life’ (2)
Irondeficiencyiscommon,butitispreventableifsuitablefeedingchoicesaremade.Exclusivebreastfeedingtotheageof6monthswillensurethatbreastmilkisnotreplacedbyfoodoflowernutrientdensityandwillminimisetheriskofirondeficiency(8).Ifformulafeeding,itisimperativeparentsorcaregiverschooseanironfortifiedcow’smilkformula.
TheRDIforinfantsagedbetween7and12monthsis11mg/day;forchildren1-3yearsofage9mg/day,andchildrenaged4-8yearsis10mgperday.Pregnancyandbreastfeedingto27mg/dayand9-10mgperdayrespectively.
Animportantaspectofpreventioniseducatingparentsaboutthechangingdietaryneedsoftheirgrowingchildandthetypesoffoodsthatarerichinironorwhichencourageironabsorptionandalsothosethatrestrictironabsorption.
Informingparentsofthetwomostcommonfactorsassociatedwithirondeficiencymayalsobeausefulpreventativeactivity.Thesetwofactorsare(1)beingfedoncows’milkpriorto12monthsofage,and(2)continuingsolelyonmilk(eitherbreastorcows’milk)after12monthsofage,withouttheintroductionofsolids.
If unsure of iron intake – refer to a dietitian for assessment and advice.
The Dietary Guidelines for Children and Adolescents in Australia recommendations
Continue exclusive breastfeeding for about 6 months■■
Introduce complementary foods containing iron at about 6 months of age■■
Choose iron-containing formula for infants who are not breastfeed and for ■■
infants receiving formulas as well as breastmilk
Delay the introduction of whole cow’s milk until 12 months of age■■
Continue to offer iron-fortified and meat containing foods beyond ■■
12 months of age
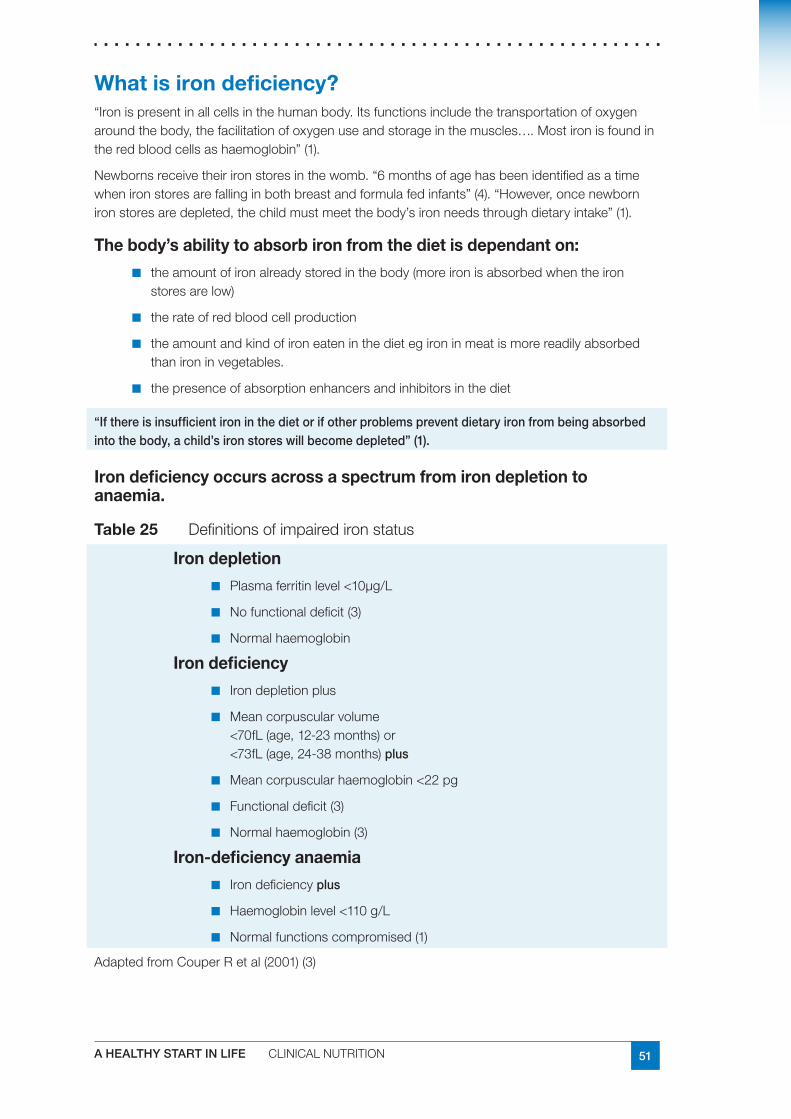
51A HEALTHY START IN LIFE CLINICALNUTRITION
What is iron deficiency?“Ironispresentinallcellsinthehumanbody.Itsfunctionsincludethetransportationofoxygenaroundthebody,thefacilitationofoxygenuseandstorageinthemuscles….Mostironisfoundintheredbloodcellsashaemoglobin”(1).
Newbornsreceivetheirironstoresinthewomb.“6monthsofagehasbeenidentifiedasatimewhenironstoresarefallinginbothbreastandformulafedinfants”(4).“However,oncenewbornironstoresaredepleted,thechildmustmeetthebody’sironneedsthroughdietaryintake”(1).
The body’s ability to absorb iron from the diet is dependant on:
theamountofironalreadystoredinthebody(moreironisabsorbedwhentheiron■■
storesarelow)
therateofredbloodcellproduction■■
theamountandkindofironeateninthedietegironinmeatismorereadilyabsorbed■■
thanironinvegetables.
thepresenceofabsorptionenhancersandinhibitorsinthediet■■
“If there is insufficient iron in the diet or if other problems prevent dietary iron from being absorbed into the body, a child’s iron stores will become depleted” (1).
Iron deficiency occurs across a spectrum from iron depletion to anaemia.
Table 25 Definitionsofimpairedironstatus
Iron depletion
Plasmaferritinlevel<10µg/L■■
Nofunctionaldeficit(3)■■
Normalhaemoglobin■■
Iron deficiency
Irondepletionplus■■
Meancorpuscularvolume■■
<70fL(age,12-23months)or<73fL(age,24-38months)plus
Meancorpuscularhaemoglobin<22pg■■
Functionaldeficit(3)■■
Normalhaemoglobin(3)■■
Iron-deficiency anaemia
Irondeficiency■■ plus
Haemoglobinlevel<110g/L■■
Normalfunctionscompromised(1)■■
AdaptedfromCouperRetal(2001)(3)
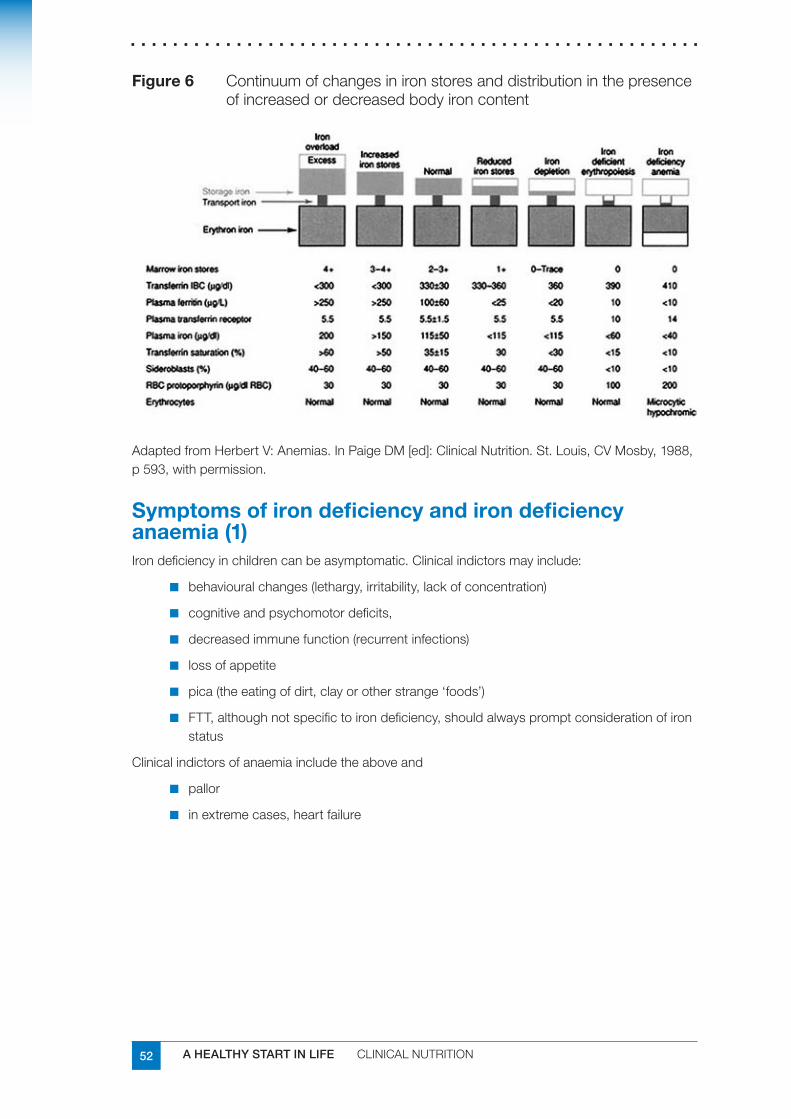
52 A HEALTHY START IN LIFE CLINICALNUTRITION
Figure 6 Continuumofchangesinironstoresanddistributioninthepresenceofincreasedordecreasedbodyironcontent
AdaptedfromHerbertV:Anemias.InPaigeDM[ed]:ClinicalNutrition.St.Louis,CVMosby,1988,p593,withpermission.
Symptoms of iron deficiency and iron deficiency anaemia (1)Irondeficiencyinchildrencanbeasymptomatic.Clinicalindictorsmayinclude:
behaviouralchanges(lethargy,irritability,lackofconcentration)■■
cognitiveandpsychomotordeficits,■■
decreasedimmunefunction(recurrentinfections)■■
lossofappetite■■
pica(theeatingofdirt,clayorotherstrange‘foods’)■■
FTT,althoughnotspecifictoirondeficiency,shouldalwayspromptconsiderationofiron■■
status
Clinicalindictorsofanaemiaincludetheaboveand
pallor■■
inextremecases,heartfailure■■
53A HEALTHY START IN LIFE CLINICALNUTRITION
What causes iron deficiency?
Infants
Theinfantyearisoneofrapidgrowth.Dietaryinadequaciesduringthisperiodplacetheinfantatriskofdevelopingirondeficiency.
Risk factors for iron deficiency:uncorrectedmaternalirondeficiencyduringpregnancy■■
prematurity,leadingtoinadequateaccumulationofironinthenewborn’sstores■■
agelessthan2years■■
introductionofcow’smilkasthemainsourcebefore12monthsofage■■
cow’smilkintakeexceeding600mlperday(6)■■
Common feeding practices contributing to iron deficiencyInfantsmaybedevelopingirondeficiencyifanyofthefollowingfeedingpracticesoccur(6):
useofcow’smilkinsteadofinfantformulaorbreastmilk,ininfantsunder12monthsofage■■
delayedintroductionofsolids■■
displacementofsolidfoodintakebymilk■■
prolongedbottlefeedingwithcow’smilk■■
lowmeatorhaemironintake■■
bottleuseinchildrenover12monthsofageencouragesexcessivefluidintakethatmay■■
displaceothermorenutritioussolidfoods
NB:Cow’smilknotonlyhasalowconcentrationofiron,buttheironispoorlyabsorbed(refertotoddlersection).
NHMRC states health professionals should be vigilant with their clients and assess iron status based on the above risk factors (6)
Recommendation: Commercial infant cereal is the preferred first solid food because it is iron fortified (6).
Rice cereal was the first food given to the majority (70%) of children in the findings in the Infant and Child Nutrition in Queensland Report, 2003 (7).
Toddlers and preschoolers Thesamebasicscenarioappliesinthesecondyearoflife.Themainproblemwithtoddlersistheoverrelianceonmilk:unfortunately,thislowironfoodendsupformingalargepartofthetotalfoodintake.Thesecommentsapplytoallformsofmilk,notjustcow’smilk.Goat’smilkisaparticularlypoorsourceofironandsoymilkisnotsatisfactoryeither(seetoddlersection).
Vegetarianism in infants and childrenAvegetariandietthatisadequateforadultsisnotnecessarilysuitableforinfantsandyoungchildren,whofaceconstraintssuchaslimitedstomachcapacityandhigherneedsfornutrientsperunitweight.Eachdietmustbeassessedseparatelyforitssuitabilityforchildren;iftheregimenisveryrestrictiveintermsofthetypeandamountofanimalproteinsconsumed,itisessentialtoplanadietcarefullysoastoavoiddeficiencies.
Ingeneral,lacto-vegetarianandlacto-ovovegetariandietsprovideadequatenutritioniftheyareproperlyplanned.Vegandietsposeariskifcareisnottakentoensurethatthedietprovidesadequateenergy,vitaminB12,proteinandiron(8).Referral to dietitian for assessment and advice
54 A HEALTHY START IN LIFE CLINICALNUTRITION
All ages:
Irondeficiencyresultsfromoneoracombinationoffactors,whichinclude:
inadequateoralintake■■
impairedabsorption■■
bloodloss–includingmenstrualbleeding■■
pregnancy(withoutadequateintake/oralsupplementation)■■
TreatmentAdietaryassessmentisthefirstcomponentofmanagement.Followingthis,thehealthprofessionalcanadviseparentsonwaystoincreasetheirchild’sconsumptionoffoodsrichinironandthosethatenhanceironabsorption,whilstdecreasingtheconsumptionoffoodsthathamperironabsorption.
Initiallychildrenmaybealsobeprescribedironsupplementstorepletetheirironstores(1).Parentsshouldbewarnedthatbowelmotionsareoftenblackandthatthisdoesnotdenoteillhealth.
Too much iron can be harmfulThebodystoresironveryefficiently,andtoomuchironcanbetoxic.
Haemochromatosisisaconditioncharacterisedbyexcessiveironstores(9)
Supplementation must never be given, unless under the supervision of a medical practitioner.
“ Once children become iron deficient, they become very restricted in the range of foods they will accept. Appetite and tolerance of new or previously discarded foods improves with iron repletion” (3).
Referral to general practitioner / paediatrician and dietitian
55A HEALTHY START IN LIFE CLINICALNUTRITION
Bioavailability of ironDietaryironcomesintwoforms:
Haem iron isfoundinfleshfoodssuchasredmeat,chickenandfish.
Non-haem iron isfoundinplantfoodssuchaswholegrainbreadsandcerealsandsomevegetables.
The body absorbs:Just under one quarter of the iron contained in animal foods. ■■
Less than one tenth of the iron from plant sources■■
What are the best sources of iron? (10)Foods which contain haem iron include:
leanredmeatssuchasbeef,lambandveal.■■
offalmeatssuchasliverandkidney.■■
chicken,pork(includingham),fishandshellfish.■■
pateorfishpaste.■■
Foods which contain non-haem iron include:Iron-fortifiedbreakfastcereals(checkthelabeltoseeifironisadded).■■
Wholemeal/wholegrainbreadsandcereals.■■
Driedpeas,beansandlegumeseg.lentils,bakedbeans,soybeans,kidneybeans,tofu.■■
Leafygreenvegetableseg.spinach,parsley,broccoli.■■
Eggs.■■
Driedfruit.■■
Peanutbutterandnuts(wholenutsarenotrecommendedforchildrenunder5).■■
Tahiniandhommus.■■
Dietary factors that boost iron absorption (9)Certainfoodsanddrinkshelpyourbodytoabsorbgreateramountsofiron,including:
VitaminC(foundinfruitsandvegetablessuchas:citrusfruits,redcapsicum,kiwifruit)■■
increaseironabsorptionfrombothhaemandnohaemironsources.
Dietary factors that reduce iron absorption (9)Certainfoodsanddrinksreduceyourbody’sabilitytoabsorbiron,including:
Tanninsfromtea,coffeeandwinereduceironabsorptionbybindingtotheironand■■
carryingitoutofthebody.
Thephytatesandfibresinwholegrainssuchasbrancanreducetheabsorptionofiron■■
andotherminerals.
Checkeat foods high in haem iron■✔
eat foods high in non-haem iron, and where possible combine with haem ■✔iron to help absorption
eat vitamin C rich foods (citrus and berry fruits, tomato, broccoli and ■✔capsicum) at each meal as this further increase iron absorption
56 A HEALTHY START IN LIFE CLINICALNUTRITION
Assessing the diet – asking about iron consumption for infants and toddlersAdaptedfromtheAustralianIronStatusAdvisoryPanel2,6
First year
Wasthechildbreastfedorformulafed(iron-fortified)?■■
Whatagedidyouceasebreastfeeding■■
Whatdrinksdidyouintroduce?(iron-fortifiedformulaorcow’smilk)?■■
Solids
Atwhatagedidyouintroducesolids?■■
Werethefoodsironfortified(orweresupplementsgiven)?■■
Whendidthechildstarttoeatredmeat,chickenandfish?Howmuch?■■
Current diet
Whatdoesyourchildeatnow?■■
Whataboutfleshfoods(redmeat,chicken,fish)andplantsourcesofiron(grains,■■
legumes).
HowmanyvitaminCrichfoodsareeatenatthesametime(eg.citrusfruits,cauliflower,■■
broccoli,strawberries,melon)?
Cow’s milk
Atwhatagedidyourchildstartoncow’smilkandhowmuchisconsumed?■■
Other fluids
Whataboutthevolumeofotherfluids-otheranimalmilks,juices,cordialsandsoft■■
drinks,teaandcoffee?(Tannininhibitsironabsorption,juicesdisplaceironrichfoodsfromthechild’sdiet)
57A HEALTHY START IN LIFE CLINICALNUTRITION
Suggestions to prevent or treat iron deficiency in pregnant and breastfeeding mums (4, 9) One and a half serves of meat, fish, poultry or alternatives each day are recommended in pregnancy and 2 during lactation. The Australian Guide to Healthy Eating recommends that red meat be eaten 3 to 4 times a week; less than this and high-iron replacement foods will be required.
Pregnancy
Eataniron-richdietduringpregnancy.Redmeatisthebestsourceofiron(seeantenatal■■
section).Chooseiron-fortifiedbreakfastcerealsandbreads.
Teststocheckforanaemiashouldbeconductedduringpregnancy.Ifyourdoctor■■
prescribesironsupplements,takethemaccordingtoinstructions.
Discussanysideeffectscausingconcernwithyourdoctor.Itisnormaltoseechanges■■
instools.
Breastfeeding
Whenbreastfeeding,ensureahealthydietisconsumed,withadequateamountsofiron■■
(seebreastfeedingsection)
Cutbackontheamountofteaandcoffeeyoudrink,especiallyaroundmealtimes,since■■
thetanninsinteaandcoffeebindtotheironandinterferewithabsorption.
Pregnancy / breastfeeding checklist
Mumincludesredmeat3-4timesaweek
Ironlevelshavebeencheckedwhilstpregnant,andmumisawareofherironstatus
Ifironsupplementisrequired,itistakenasdirected
Encouragefoodshighinnonhaemirontobeeatenwithhaemironfoods
EncouragefoodshighinvitaminCtobeconsumedwithironcontainingfoods
Limitintakeofteaandcoffee(around3aday)
Limitexcessiveintakeofbran
Ifmumisavegetarianrefertodietitian
Suggestions to prevent or treat iron deficiency in infants (4,9)
Introducing solids
Don’tgiveyourbabycow’smilkorotherfluidsthatmaydisplaceiron-richsolidfoods■■
before12monthsofage.
Startgivingyourbabypureedfoodswhentheyarearound6monthsofage.Fortified■■
babycerealmadewithiron-fortifiedformulaorbreastmilk,atfirstalongwithpureedvegetablesandfruit.Graduallyincludefinelymincedmeatatonemealtimefrom6monthsonwards.
58 A HEALTHY START IN LIFE CLINICALNUTRITION
Introducing solids with appropriate iron checklist (adapted from 4)
Babiesareexclusivelybreastfeduntil6monthsofage
Ifformulafed,ironfortifiedmilkformulaischosen
Ironfortifiedcerealshavebeenintroducedaround6months
Haemironfoods(egredmeat,chickenandfish)havebeenintroducedaround7months
Cow’smilkisdelayedasthemainmilkdrinkuntil12months
Onceavarietyoffoodshavebeenintroduced,vitaminCrichfoods(egcitrus,berries,tomatoesetc)areeatenwithhaemandnonhaemironfoods
Ifmotherand/orchildarevegetariansrefertodietitian
Suggestions to prevent or treat iron deficiency in toddlers and preschoolers (4,9)
meat,poultryandfishareimportantsourcesofironinyourchild’sdailydiet.includered■■
meat3to4timesperweek(8)
vitaminChelpsthebodytoabsorbmoreiron,somakesureyourchildhasplentyoffruit■■
andvegetables
watchyourchild’sfluidconsumption;lotsofmilkandjuicecantaketheedgeoffan■■
alreadysmallappetiteandthereforelimitintakeofironrichfoods
chronicdiarrhoeacandepleteyourchild’sironstores,whileintestinalparasitessuchas■■
wormscancauseirondeficiency.Referaltodoctorforpromptdiagnosisandtreatment.
Practical ways to increase iron in the diet for young children
includenutrientdensefingerfoodssuchasslicesofroastmeat,leftoverminimeatballs,■■
sandwicheswithcoldmeat,coldcookedsausages,coldplatterwithcookedmeatandrawvegetableswithadip
offermeatalternativesincludingdriedbeans,lentils,chickpeas,cannedbeans,fish,■■
eggsandsmallamountsofnutsandnutpastes.
includefoodsrichinvitaminclikeoranges,mandarins,berriesandtomatoes.■■
encourageyoungchildren,toddlersorfussyeaterstotrymincedmeats,fortified■■
breakfastcereals,eggsandsmoothnutpastes.
Iron in toddlers and children checklist (adapted from 4)
Smallportionsofavarietyoffoodsfromallfoodgroupsareofferedregularly
Toddlersconsumingupto600mlmilkperday(nomore)
Toddlerconsumingupto½cupofjuiceperday(nomore)
Highiron,nutrientdensefingerfoodsareencouraged
Ifconcernswithfussyeating,refertodietitian
Ifmotherand/orchildarevegetariansrefertodietitian
AdaptedfromTuckertalk,2003
59A HEALTHY START IN LIFE CLINICALNUTRITION
Useful websites and resourcesKey state and national documents for health workers:
Dietary Guidelines for Children and Adolescents in AustraliaandInfantFeedingGuidelinesforHealthWorkers
OptimalInfantNutrition:evidencebasedguidelines
InfantandChildNutritioninQueensland2003
NationalBreastfeedingStrategy
ReportoftheChiefHealthOfficerQueensland,2006
AustralianironStatusAdvisoryPanel
www.ironpanel.org.au/AIS/AISdocs/childdocs/Ccontents.html
Further professional development reading:
SandovalC.,JayaboseS.,EdenA.N.,(2004):Trendsindiagnosisandmanagementofirondeficiencyduringinfancyandearlychildhood.HaematologyOncolClinNAm18(2004)1423-1438
Parent handouts:
ChildHealthInformationFactSheetswww.health.qld.gov.au/child&youth/factsheets/
www.health.qld.gov.au/cchs/Gen_Nutrition_Activity/whyiron.PDF
BetterhealthChannel;VictorianGovernment
www.chw.edu.au/parents/factsheets/iron.htm
GrowingStrong:Feedingyouandyourbaby
ReferencesChildHealthScreeningandSurveillance:2002AcriticalReviewoftheevidence.NHMRC1.[online]13thApril2007www.nhmrc.gov.au/publications/synopses/_files/ch42.pdf
[onlineApril2007]2. www.ironpanel.org.au/AIS/AISdocs/childdocs/Ccontents.html
CouperR.,andSimmerK.3. Iron deficiency in children: Food for thought.MJA2001;174:162
Tuckertalk:TheFamilyNutritionEducationManual.DepartmentofHealthandCommunity4.Services,Tasmania.2004
CouperR.,andSimmerK.5. Iron deficiency in children: Food for thought.MJA2001;174:162
KruskeS.,NorbergM.,StewartL.,MillenL.2004.‘FeedingPracticesandIronDeficiency6.inChildrenunder2yearsofage:CentreforFamilyHealthandMidwifery,Sydney
QueenslandHealth:RosGabriel,GaylePollard,GhazalaSuleman,TerryCoyneandHelen7.Vidgen.InfantandChildNutritioninQueensland2003.QueenslandHealth.Brisbane2005.
NationalHealthandMedicalResearchCouncil:8. Dietary Guidelines for Children and Adolescents in Australia incorporatingthe Infant Feeding Guidelines for Health Workers,Canberrawww.health.gov.au/pubhlth/strateg/childnutirtion/index.htm
[onlineApril2007]9. www.betterhealthchannel.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Iron_explained?open
[onlineApril2007]10. www.chw.edu.au/parents/factsheets/iron.htm
60 A HEALTHY START IN LIFE CLINICALNUTRITION
7.10 Lactose intoleranceLactoseintoleranceisaconditionwhichresultsinaninabilitytodigestlactose.Lactoseisasugarfoundinmilk.Lactosemustbebrokendowninthebodyinthesmallintestinebyanenzymecalledlactase,intoitsindividualcomponents-glucoseandgalactose-beforeitcanbeabsorbed.Aninabilitytodigestlactoseduetoadecreasedorabsentlactaseactivitycanresultinsymptomsof:
diarrhoea■■
nausea■■
flatulence■■
abdominaldiscomfortanddistensionaftertheingestionoflactose■■
Dietarylactoseeliminationorclinicaltestsareavailabletodetectlactoseintoleranceanditisimportanttohavethiscorrectlydiagnosedbyadoctor.Thesetestscanincludenon-invasivehydrogenbreathtesting,stoolaciditytestorinvasiveintestinalbiopsydeterminationoflactaseconcentrations(1).
Lactoseintoleranceisadistinctentityfromcow’smilksensitivity,whichinvolvestheimmunesystemandcausesvaryingdegreesofinjurytotheintestinalsurface.Cow’smilkproteinintoleranceisreportedin2%-5%ofinfantswithinthefirst1to3monthsoflife,typicallyresolvesby1yearofage(1).
Frequentrunnystoolsdonotmeanabreastfedinfanthasdiarrhoeaorlactoseintolerance:theyaresimplyviewedadevidenceofsufficientmilk.Diarrhoeaentailsveryfrequentwaterystools(2).
Causes of lactose intolerance Congenital alactasia or hypolactasia
Thisconditionisseenininfantsfrombirthandresultsintheenzymelactaseeitherbeingabsentorpresentinlowlevels.Thisconditionisrare.
Primary lactose intolerance
Thisconditionresultsinanabsentorlowlactaseactivity.Itisrarebeforetheageof3years.DecreasedlactaseactivityisgeneticallyinheritedandismorecommonamongstnearEastandMediterranean,Asian,AfricanandNorthandSouthAmericanethnicgroups.Thisconditiongenerallypersiststhroughoutlifeandrequireslife-longadherencetoalowlactosediet,atalevelofrestrictionthateliminatessymptoms.
Secondary lactose intolerance
Thisisusuallyonlytemporaryandoccursasaresultofdamagetotheintestinalmucosa,forexample,coeliacdisease,inflammatoryboweldiseaseorgutsurgery.Itmayalsooccuraftergastroenteritis.Treatmentrequiresalowlactosediettobefollowedforashortperiodoftime.
Developmental lactase deficiency
Relativelactasedeficiencyobservedamongpreterminfantsoflessthan34weeksofgestation.
61A HEALTHY START IN LIFE CLINICALNUTRITION
ManagementBreastfed Infants
Lactoseisthesugarinallmammalianmilks,itisproducedinthebreastandisindependentofthemother’sconsumptionoflactose(3).Breastmilkcontainsaround7%lactose.
Itisuncommonforbreastfedinfantstoexhibitsignsofprimaryorsecondarylactoseintolerance.Breastmilkisusuallywelltolerateddespiteitcontaininglactose.Breastfedinfantsshouldbecontinuedonhumanmilkinallcases.
Ensuringtheinfant’scorrectattachmenttothebreastinordertoalloweffectivedrainageisimportant.Encouragingtheinfanttofinishsucklingonebreastbeforeofferingthesecondmayalsobehelpfulforinfantssufferingfromlactoseintolerance.Thisresultsintheinfantreceivingahigherfatfeedandtendstodelaygastricemptying.Italsoslowstherateatwhichlactoseispresentedtothesmallintestine.
Althoughlactosefreecow’smilkproteinbasedformulasarereadilyavailablenostudieshavedocumentedthattheseformulashaveanyclinicalimpactoninfantoutcomesmeasureincludingcolic,growthordevelopment(4).
Lactasedropsareanoptioninexpressedbreastmilk–butthesearenotalwayshelpful.
Inspecialcasesbreastfedinfantsmayberequiredtochangetoalowlactoseformula.Breastfeedingshouldonlybeceasedduetolactoseintoleranceafterreceivingmedicaladvice.
Formula fed Infants
Indevelopedcountriesenoughlactosedigestionandabsorptionarepreservedsothatlow-lactoseandlactosefreeformulashavenoclinicaladvantagescomparedwithstandardlactosecontainingformulas.Infantswithsecondarylactoseintoleranceshouldonlybegivenlactosefreeformulasforashortperiodoftimeasprescribedbyadoctor.
Note Althoughsoymilkformulaearelowinlactose,theyarenotthefeedofchoiceforthetreatmentoflactoseintolerance.Forinfants,acow’smilkbasedlowlactoseformulashouldberecommended.
Low lactose solids
Itisrareforyoungchildrenlessthan3yearsofagetohaveprimarylactoseintolerance.Lactoseintoleranceinthisagegroupusuallyexistsduetoaninjurytotheintestinalmucosa.Lowlactosedietsshouldusuallyonlyberequiredforshortperiodsoftime.
Forchildrenrequiringlongtermadherencetoalowlactosediet,advicefromadietitianshouldbesought.Itisimportantthatmealsremainbalancedandthatnutrientrequirementssuchascalciumaremet.Amoreextensivelistoflowlactosefoodscanthenbeprovided.
Childrenvaryintheleveloflactosetheycantolerateanditisoftennotnecessarytoeliminatealldairyfoodsfromthediet.Oftenlevelsoflactoseequivalenttotheamountin1glassofmilkaretoleratedeachday.Somemilkproductssuchasyoghurt,buttermilkandhardcheeses(eg.swiss,cheddar)containonlysmallamountsoflactoseandareusuallywelltolerated.
Itisimportanttotestachild’sleveloftoleranceandprovidethemaximumamountofdairyfoodpossibletoensureadequatecalciumintakes.Acalciumsupplementmayberequiredifintakesoflowlactosemilkorcalciumfortifiedsoymilkarelow.
Forsecondarylactoseintolerance,lowlactosefoodsandfluidsshouldbeprovidedfor1-4weeksdependingontheseverityofthesymptoms.Anormaldietshouldthenbegraduallyintroduced.
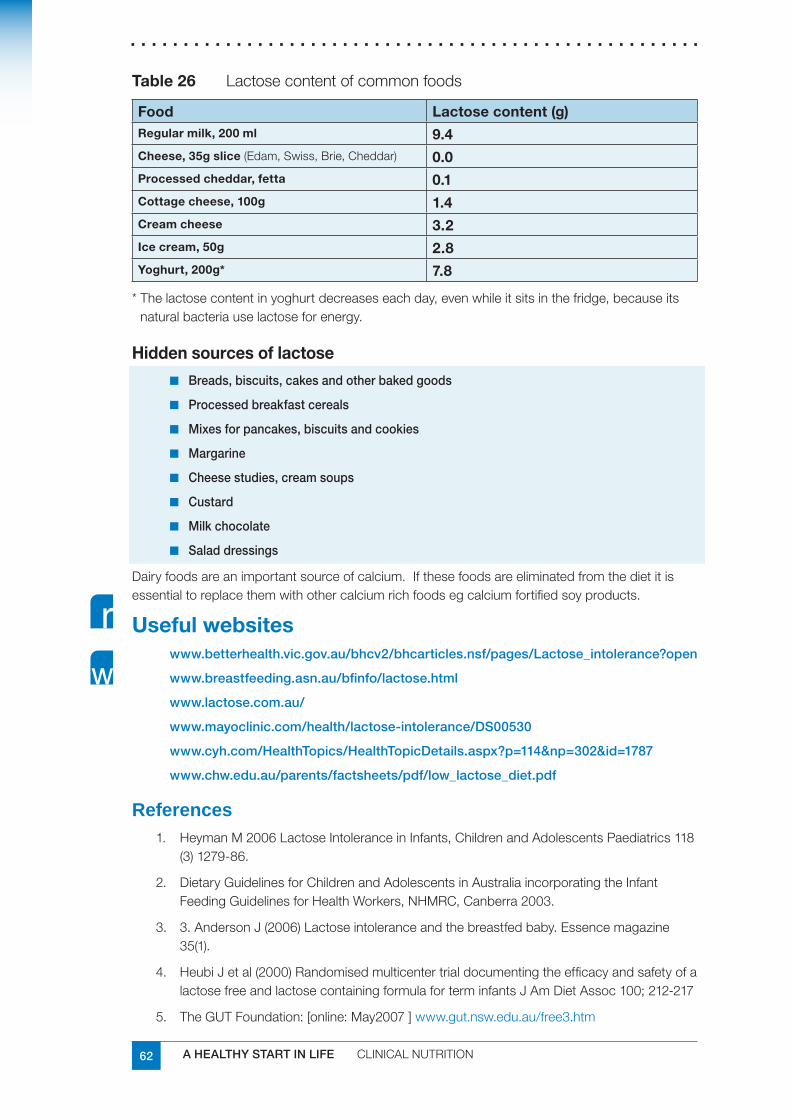
62 A HEALTHY START IN LIFE CLINICALNUTRITION
Table 26 Lactosecontentofcommonfoods
Food Lactose content (g)Regular milk, 200 ml 9.4Cheese, 35g slice(Edam,Swiss,Brie,Cheddar) 0.0Processed cheddar, fetta 0.1Cottage cheese, 100g 1.4Cream cheese 3.2Ice cream, 50g 2.8Yoghurt, 200g* 7.8
*Thelactosecontentinyoghurtdecreaseseachday,evenwhileitsitsinthefridge,becauseitsnaturalbacteriauselactoseforenergy.
Hidden sources of lactose
Breads, biscuits, cakes and other baked goods■■
Processed breakfast cereals■■
Mixes for pancakes, biscuits and cookies■■
Margarine■■
Cheese studies, cream soups■■
Custard■■
Milk chocolate■■
Salad dressings■■
Dairyfoodsareanimportantsourceofcalcium.Ifthesefoodsareeliminatedfromthedietitisessentialtoreplacethemwithothercalciumrichfoodsegcalciumfortifiedsoyproducts.
Useful websiteswww.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Lactose_intolerance?open
www.breastfeeding.asn.au/bfinfo/lactose.html
www.lactose.com.au/
www.mayoclinic.com/health/lactose-intolerance/DS00530
www.cyh.com/HealthTopics/HealthTopicDetails.aspx?p=114&np=302&id=1787
www.chw.edu.au/parents/factsheets/pdf/low_lactose_diet.pdf
ReferencesHeymanM2006LactoseIntoleranceinInfants,ChildrenandAdolescentsPaediatrics1181.(3)1279-86.
DietaryGuidelinesforChildrenandAdolescentsinAustraliaincorporatingtheInfant2.FeedingGuidelinesforHealthWorkers,NHMRC,Canberra2003.
3.AndersonJ(2006)Lactoseintoleranceandthebreastfedbaby.Essencemagazine3.35(1).
HeubiJetal(2000)Randomisedmulticentertrialdocumentingtheefficacyandsafetyofa4.lactosefreeandlactosecontainingformulaforterminfantsJAmDietAssoc100;212-217
TheGUTFoundation:[online:May2007]5. www.gut.nsw.edu.au/free3.htm
63A HEALTHY START IN LIFE CLINICALNUTRITION
7.11 Regurgitation and gastro-oesophageal refluxThepassageofgastriccontentsintotheoesophagusisanormalphysiologicalprocessthatoccursinhealthyinfantsandchildren.Infact,inhealthyinfants,gastricfluidsmayfrequentlyeruptintotheoesophagus,anywherefrom10to50timesaday(1).Many,butnotalloftheseepisodesresultinregurgitation.Regurgitationdescribesrefluxintotheoropharynx.Regurgitationismostfrequentlyreportedbetween1and3months(50%)toaround4months(61%).Bythetimetheinfantis10to12monthsold,only5%ofparentsstillreportitasaproblem(1).
Gastro-oesophagealreflux(GOR)isaconditionoffrequentregurgitationorvomiting,oftenbeginningbetween2and6weeksofage(2).
Thesymptomsinyounginfantsdifferfromthoseseeninolderchildrenandinclude:
excessivecrying■■
irritability■■
backarching■■
breastrefusal■■
feedingdifficulties(1,2)■■
Mostinfantswithregurgitationorrefluxremainhealthyandthrive,andthesymptomssettledownbetween6and10monthsofage,whentheinfantbeginstospendmoreofthedayinanuprightposture(2).Ifsevere,itcanleadtogastro-oesophageal reflux disease (GORD),whenrefluxleadstopathologicalconsequencessuchas,oesophagitis(inflammationoftheoesophagus)failuretothrive,recurrentaspiration(whichmaybeassociatedwithapnoea)andpneumonia.
Gastro-oesophageal reflux is significantly less common in breastfed infants than in those fed formula. This finding is unrelated to feed volume (2).
DiagnosisThediagnosisofgastro-oesophagealrefluxismadeonclinicalgrounds.Itisimportanttodetermineifsymptomsarecausedbyanunderlyingpathologicalcondition,orifthereisevidencerefluxiscausingsecondarycomplicationssuchasfailuretothrive.
Inmostcasesrefluxisuncomplicatedandlittleinterventionisrequired.
Investigationisrequiredonlywhencomplicationsarepresentoriftheinfantdoesnotrespondtosimplemanagementmeasures(2).
Some warning signs of underlying pathology (1)
Doestheinfanthave:
Biliousand/forcefulvomiting■■
Onsetofvomitingafter6months*■■
GIbleeding*■■
Constipation■■
Diarrhoea■■
Abdominaltenderness,distension■■
Fever■■
Lethargy■■
Failuretothrive*■■
*mayalsobeasymptomofGORD
Refer for medical intervention if the infant has one or more of these symptoms
64 A HEALTHY START IN LIFE CLINICALNUTRITION
Reflux and poor weight gainInfantswithrecurrentvomitingandpoorweightgainshouldundergoevaluationfortheadequacyofcaloricintakeandtheeffectivenessofswallowing.
PoorweightgaindespiteanadequateintakeofcaloriesshouldpromptevaluationforcausesofvomitingandweightlossotherthanGORD.
Referral to dietitian
ManagementReassurance
Themajorityofinfantswillhavephysiologicalregurgitationandwillsettlespontaneously.Providedtheinfantisthriving,noinvestigationorinterventionisrequired.Itisimportantnottolabelthesechildrenashavingaconditionsuchasgastro-oesophagealreflux(2).
Posture (2)
Placingtheinfantinamoreuprightfeedingpositioncanbehelpfulforregurgitation.■■
Keepingtheinfantuprightfor15to30minutesafterfeedingalsohelps;ababyslingis■■
usefulinthissetting.
Thebestpositionforreducingrefluxispronebut,becausethispositionhasbeen■■
associatedwithanincreasedincidenceofsuddeninfantdeathsyndrome,itisnotgenerallyrecommended.
Nootherlyingpositionhasbeenshowntobeeffective.■■
Food thickening
Whenbreastfeeding,liquid■■ Gavisconissometimeseffective,althoughitcancauseconstipation(2).
Recentlyinfantformulascontainingathickeningagent(ARformulas)havebecome■■
widelyavailable…..Theyshouldbeconsideredonlyforreducingregurgitation;theyarenotananti-refluxformula(2).
Thickeningsolidfeedswithricecerealcanassistinregurgitation.■■
If an infant is placed on a thickened feed or is using a thickener, this should only occur under appropriate medical supervision.
65A HEALTHY START IN LIFE CLINICALNUTRITION
Milk free diet
Somestudiesreportupto40%ofinfantswithGORhasacow’smilkproteinintolerance.Thisisimportanttoinvestigate,particularlyiftheinfanthaspoorweightgain,irritabilityandfeedingrefusal(3).
Referral to dietitian for assessment and advice
Drug therapy
Drug therapy should be given only under medical supervision.
Therearetwopossibletherapies:acidreductionanduseofprokineticagents.Atpresentthereisnodrugavailablethatistrulyanti-reflux(2).Inmostcasestheyarenotvaluabletreatmentofinfantswithregurgitation(1).
Outcome
Active medical management controls symptoms leading to:
50 % of children needing no further therapy beyond 8 to 10 months of age■■
30 % beyond 18 months of age. ■■
However, 17% of patients have ongoing symptoms or complications requiring anti-reflux surgery (2)
Surgical intervention
Surgicalinterventionisrestrictedtoinfantsforwhommedicalmanagementhasfailedand/orwhohavepotentiallylife-threateningcomplicationssuchasapnoeaoraspiration.Thisisrare.
ReferencesWinterH.S.(2007)GastroesophagealrefluxinInfants,1. www.uptodate.com/udt/content/topic.do?topicKey=pedigast/16818[online]18thApril,2007
DietaryGuidelinesforChildrenandAdolescentsinAustraliaincorporatingtheInfant2.FeedingGuidelinesforHealthWorkers,NHMRC,Canberra2003.
SalvatoreS.,VandenplasY.,(2002)Gastroesophagealrefluxandcow’smilkallergy:Is3.therealink?PedatricsNov2002.110(5):972
HuangR-C.,ForbesDA.,DaviesMW.,(2003)Feedthickenerfornewborninfantswith4.gastroesophagealreflux.CochraneReviewAbstracts
1A HEALTHY START IN LIFE RESOURCELIST
Resource listUseful phone numbers
Australian Breastfeeding Association Brisbane (07)38446488 7-dayBreastfeedingHelpline (07)38448166
13HEALTH 13432584
Lifeline 131114
Child Health Information Service Brisbane (07)38622333Freecall 1800177135
Kids Help Line 1800551800
Parentline 1300301300
Poisons Information Centre 131126
TravelSmart (07)32534006
Sport and Recreation Queensland 1300656191
Women’s Health Brisbane (07)38399988Freecall 1800017676
Useful websitesThefollowingwebsitescontainawiderangeofusefulinformationonhealth,nutrition,andphysicalactivity:
Australian Breastfeeding Association (ABA)TheAustralianBreastfeedingAssociationisAustralia’sleadingsourceofbreastfeedinginformationandsupporttoallsectorsofthecommunity.ABAissupportedbyhealthauthoritiesandspecialistsininfantandchildhealthandnutrition.ABAoperatesa7-dayBreastfeedingHelpline,wherecallerscancontactvolunteerbreastfeedingcounsellorstoassistthemwithbreastfeedingissues.ABAprovidesanelectricbreastpumphireserviceaswellasmother-to-mothersupportthroughmorethan75Queenslandgroups.
Website:www.breastfeeding.asn.au
2 A HEALTHY START IN LIFE RESOURCELIST
Australian Council for Health and Physical Education and Recreation (ACHPER) Queensland ACHPER Queenslandisanational,not-for-profitprofessionalassociationrepresentingpeoplewhoworkintheareasofhealtheducation,physicaleducation,recreation,sport,dance,communityfitnessormovementscience.ThemissionoftheCouncilistopromotehealthylifestylesforallAustraliansandtostudyandpromoteitsareasoffocus.TheACHPERQLDwebsiteincludesinformationabout:
events,suchastheACHPERQLDWomeninSportbreakfast■■
programs,suchasSchoolsNetwork■■
conferences,suchastheACHPERQLDStateHPEConference■■
resources,suchastheACHPERAdvocacyKit.■■
Website:www.achper.org.au/
Australian Dental Association Queensland (ADAQ)InQueensland,ADAQisregardedastherecognisedvoiceofdentistry.Witharound90percentofregistereddentistsanddentalspecialistsacrosstheprivateandpublicsectorsasmembers,theAssociationprovidesamosteffectiverepresentativebody.
ADAQstrivestopromotetheartandscienceofdentistry,torepresenttheprofessionandtoprovideserviceswhichpromotethehighestleveloforalhealthinthecommunity.
Website:www.ada.org.au/default.aspx
Australian Medical Association (AMA) QueenslandAMAQueenslandisthepeakmedicalbodyfordoctorsinQueenslandandiscommittedtobetteringpublichealthintheStatethrougharangeofdifferentinitiatives.OneoftheseisAMAQueensland’sKids GPcampaign,whichisaimedatprovidinganeffectivepublichealthcontributiontowardsthespirallingratesofoverweightandobesechildreninQueensland.FormoreinformationaboutAMAQueensland’sKids GPcampaignpleasevisitKids GPwebsite.
Website:www.kidsgp.com.au/
Australian Indigenous Health InfoNetTheAustralianIndigenousHealthInfoNetisaninnovativewebresourcethatmakesknowledgeandinformationonIndigenoushealtheasilyaccessibletoinformpracticeandpolicy.
Thewebresourceisa‘one-stopinfo-shop’forpeopleinterestedinimprovingthehealthofIndigenousAustralians.Weprovidequality,up-to-dateknowledgeandinformationaboutmanyaspectsofIndigenoushealth,andsupport‘yarningplaces’(electronicnetworks)thatencourageinformation-sharingandcollaborationamongpeopleworkinginhealthandrelatedsectors
Website:http://www.healthinfonet.ecu.edu.au/

3A HEALTHY START IN LIFE RESOURCELIST
Brisbane MarketsBrisbaneMarketsLimitedisinvolvedinarangeofactivitiestopromotehealthandnutrition,supportthefruitandvegetableindustryandinteractwithourlocalcommunity.
Theseinclude:
The■■ Queensland Kids Fresh-Net -acentralinformationandmaterialsresourceforschools
The■■ Fresh for Kids program-multifacetedprogramtoencourageschoolchildrentomakehealthyeatingchoices
Fresh Tastes ■■ -amultifacetedprogramtoprovidesupportandrewardexcellenceamongstindependentfruitandvegetableretailers
Localcommunityandschoolsponsorships■■
Sponsorshipof■■ Life Education Queensland
Website:www.brisbanemarkets.com.au/
The Cancer Council Queensland TheCancer Council Queenslandwasestablishedin1961andistheState’sforemostanti-cancerorganisation.Itisanindependent,community-basedcharityandisnotgovernmentfunded.TheCancerCouncilaimstoreducetheimpactofcancer-particularlythesufferingitcauses-andultimatelytoeliminatethedisease,byraisingfundstoadvancecancerresearch;improvecancertreatment;supportpeoplewithcancer,theirfamilyandfriends;andincreasecommunityawarenessofcancer,itspreventionandearlydetection.
Website:www.cancerqld.org.au/default.asp
The Coeliac Society of Australia TheStateSocietiesaimtogiveinformationandsupporttomedicallydiagnosedcoeliacsandtheirfamilies,sufferersofdermatitisherpetiformisandthosemedicallydiagnosedasrequiringaglutenfreediet.Adviceandinformationisgivenabouttheglutenfreediet,ingredients,wheretobuy,recipesandcooking,overseastravel,educationalmaterial,aswellasresearchinformation.SupportgroupshavebeensetupthroughouttheStatesandTerritorieswherememberscanmeettogivesupportandexchangeideasandinformation.
Website:qld.coeliacsociety.com.au
Diabetes Australia QueenslandDiabetes Australia - Queenslandisanot-for-profitorganisationdedicatedtoimprovingthelivesofpeoplewithdiabetes.DiabetesAustraliaQueenslandisamember-basedassociationandispartofthenationalorganisation,DiabetesAustraliaLtd.DiabetesAustraliaQueenslandwasformedin1968andcurrentlyhasover44,000members.Theorganisation’svisionisanAustraliancommunityfreefromdiabetesanditsimpacts.
Website: www.daq.org.au/
4 A HEALTHY START IN LIFE RESOURCELIST
Dietitians Association of Australia (DAA) DAAisthelargestprofessionalnutritionorganisationinAustraliawithover3000members.Accreditedpractisingdietitians(APDs)areuniversity-qualifiedprofessionalscommittedtoqualityserviceandtheDAACodeofProfessionalPractice.TheDAAwebsitegivespractical,up-to-dateinformationonnutritionandhealthyeatingandprovidesanonline‘findanAPD’service.
Website:www.daa.asn.au/
Eat Well Be ActiveTheEatWellBeActivewebsiteisagoldmineoffactsheets,downloads,information,recipesandadvice.
Website:www.health.qld.gov.au/eatwellbeactive/default.asp
Food Standards Australia and New ZealandFoodStandardsAustraliaNewZealand(FSANZ)isanindependentstatutoryagencyestablishedbytheFood Standards Australia New Zealand Act 1991.WorkingwithinanintegratedfoodregulatorysysteminvolvingthegovernmentsofAustraliaandtheNewZealandGovernments,wesetfoodstandardsforthetwocountries.FSANZispartoftheAustralianGovernment’sHealthandAgeingportfolio.
Theultimategoalis:Asafefoodsupplyandwell-informedconsumers.FSANZdevelopsfoodstandards,andjointcodesofpracticewithindustry,coveringthecontentandlabellingoffoodsoldinAustraliaandNewZealand.Inaddition,wedevelopAustralia-onlyfoodstandardsthataddressfoodsafetyissues–includingrequirementsforprimaryproduction-andmaximumresiduelimitsforagriculturalandveterinarydrugresidues.
Usingourskills,knowledge,andscientificcapabilities,wedevelopfoodstandardsforcomposition,labellingandcontaminants,includingmicrobiologicallimits,thatapplytoallfoodsproducedorimportedforsaleinAustraliaandNewZealand.
Website:www.foodstandards.gov.au
Formula for LifeFormulaforLifeisoneofAustralia’smostcomprehensivedietaryandanalysiswebsites.Inadditiontonutritioninformation,FormulaforLifealsogivesyoufreeaccesstomorethan140recipesandhealthyeatingtipsaswellaslifestyletips,informationonfoodgroups,nutrients,vitamins,minerals,vegetables,dietrelateddiseasesandmore.
ThesiteisconsistentwithcontemporaryAustralianstandardsandhasappliedrecognisedgovernmentagencystandards.However,givenrecentchangestotheNationalHealthandMedicalResearchCouncil’sNutrientReferenceValues(2006),nutrient-specificanalysismaynotprovideup-to-dateinformation.Thewebsiteisfreetouse.ItisdevelopedandsupportedbyQueenslandvegetablegrowersandGrowcom,Queensland’speakhorticulturebody.
Website:www.formulaforlife.com.au/
5A HEALTHY START IN LIFE RESOURCELIST
Gut FoundationTheGutFoundationprovidesprofessionalandpubliceducationandpromotesresearchintodigestivedisorderstoimprovegastrointestinalhealth.Informationprovidedexploresbotha)termsofunderstandingtheprocessofdigestionandabsorptionandb)howthatmightaffectthedevelopmentofsubsequentdiseases.
Thereisalsoinformationonhowtomanagecommonproblems,includingtheverycommonirritablebowelsyndromeanddyspepsia,togetherwithothermoreseriousdiseases,suchascolorectalcancer.websitefeaturesinteractivepresentationsonanatomy,endoscopy,colonoscopy,sigmoidoscopy,wirelessvideocapsuleendoscopy,etc.
Website:www.gut.nsw.edu.au/
The Heart FoundationTheHeartFoundation,Australia’sleadinghearthealthorganisation,hasdevelopedtheWalk of Life - for all walks of lifecampaignandabookletcalledLosing Weight the Healthy Way,witheasyandcleartipstohelpyouachieveandmaintainahealthyweightandahealthylifestyle.
TheHeartFoundationsaveslivesbyfundingworld-classresearch,guidelinesforhealthprofessionals,informingthepublicandassistingpeoplewithcardiovasculardisease.Asacharity,theHeartFoundationreliesondonationsandgiftsinwillstocontinueitslifesavingresearch,educationandhealthpromotionwork.
ForfurtherinformationvisitHeartFoundationorcall1300362787.
Website:www.heartfoundation.com.au/
International Lactation Consultants AssociationTheInternationalLactationConsultantAssociation(ILCA)istheprofessionalassociationforInternationalBoardCertifiedLactationConsultants(IBCLCs)andotherhealthcareprofessionalswhocareforbreastfeedingfamilies.
Thevisionisaworldwidenetworkoflactationprofessionals.Theirmissionistoadvancetheprofessionoflactationconsultingworldwidethroughleadership,advocacy,professionaldevelopment,andresearch.
Website:www.ilca.org/
Lactation Resource CentreAustralianBreastfeedingAssociation’sMelbourne-basedLactationResourceCentrespecialisesinprovidingcomprehensiveinformationandresourcesonallaspectsofhumanlactation.Studymodulesandthelatestresearcharticlesonbreastfeedingareavailableforafee.
Website:www.breastfeeding.asn.au/lrc/lrc.html
National Health and Medical Research Council (NHMRC)NHMRCisAustralia’speakbodyforsupportinghealthandmedicalresearch;fordevelopinghealthadvicefortheAustraliancommunity,healthprofessionalsandgovernments;andforprovidingadviceonethicalbehaviourinhealthcareandintheconductofhealthandmedicalresearch.ClinicalPraticePublicationsarealsoavailable.
Website:www.nhmrc.gov.au/
Nutritionpublicationswww.nhmrc.gov.au/publications/subjects/nutrition.htm
6 A HEALTHY START IN LIFE RESOURCELIST
Nutrition AustraliaNutritionAustralia(theregisteredbusinessnamefortheAustralianNutritionFoundationInc.)isanon-government,non-profitcommunity-basedorganisationthataimstoprovidescientificallybasednutritioninformationtoencourageallAustralianstoachieveoptimalhealththroughfoodvarietyandphysicalactivity.
Website:www.nutritionaustralia.com.au/
Queensland Divisions of General Practice (QDGP) TheQDGPisthepeakrepresentativebodyfordivisionsofgeneralpracticeinQueensland.QDGPpromotesthecentralroleofgeneralpracticeinprimaryhealthcarebyensuringthatkeystakeholdersandgeneralpracticeworktogetherinasupportedenvironment.
Establishedin1997andrepresenting18DivisionsinQueensland,QDGPaimstoinfluenceandimplementprimaryhealthcarereforminQueensland.
Website:www.qdgp.org.au/
Queensland Health: Health Information DirectoryTheHealthInformationDirectoryprovidesaccesstoonlinehealthandwellbeinginformation.Thefactsheetsandotherresourcesonthissiteareconstantlyexpandedandregularlyreviewed.
Website: www.health.qld.gov.au/healthtopics/result.asp?browseaz=N
Sport and Recreation New Zealand (SPARC) TheSPARCwebsiteisdedicatedtogettingNewZealandersmoving.Itfeaturessomegreatwaystohelppeoplegetmoreactive,includingtheOnlineActivator,whichhelpsindividualstochoosephysicalactivitiestosuittheirlifestyle;andActionPacksforKids,whichhasloadsoffunideastogetkidsactive.
Website:www.sparc.org.nz/getting-active
Sport and Recreation QueenslandSport,RecreationandRacingisproactivelyworkingtowardshelpingQueenslandersbecomemoreactive.
AstheleadagencyresponsibleforimplementingtheQueenslandGovernment’ssportandrecreationpolicies,weworkwithsportingorganisations,councils,schools,Indigenousorganisationsandthewidercommunitytoincreaseparticipation,developbetterskillsintheindustryandcreatebetterplacesandopportunitiesforsportandrecreation.
Website:www.sportrec.qld.gov.au/
7A HEALTHY START IN LIFE RESOURCELIST
Queensland Government programs10,000 Steps The10,000 Stepsprogramaimstoincreasetheday-to-dayactivityofQueenslandersandAustraliansbyencouragingtheaccumulationof‘incidental’physicalactivityaspartofeverydayliving.Theprogramusedthe10,000 Stepsperdaymessageasawaytohelppeopletoincreasetheiractivitylevels.
TheQueenslandGovernmentsupportedtheinitial10,000 StepsRockhamptonprojectandthenthefurtherdevelopmentofthe10,000 Stepsprogramand10,000 Steps websitesothatotherscanimplementprogramactivitiesandpromotephysicalactivityintheirlocalcommunities.Itisfreeforcommunitygroupsandorganisationstobecomearegisteredproviderof10,000 Stepsactivities.
The10,000 Stepswebsitehasarangeofphysicalactivityresourcesandinformation,includinganonlineSteplog,aworkplacechallenge,apedometerlibraryloanschemeandwalkwaysignage;plusinformationpackagesforGPsandotherhealthprofessionals.
Website:www.10000steps.org.au/
Easy StepsEasy Stepsisatoolkitforplanning,designingandpromotingsafewalkingisaresourcethathasbeenpreparedbyQueenslandTransporttoassistlocallocalgovernmentsthroughtheprovisionofarangeoftoolstohelpthemimprovewalkingenvironmentsinQueenslandthroughtheprovisionofthrougharangeoftools,informationandencouragement.Theseriesof Easy Stepsmodulesaredesignedtoassistcouncilmanagers,plannersandengineersplanfor,promoteandprovideforincreasedwalkinglevelsintheirlocalarea.
Website:www.transport.qld.gov.au/Home/Safety/Road/Pedestrians/Pedestrian_easy_steps
Go for 2&5® fruit and vegetable campaignQueenslandHealthlaunchedtheGo for 2&5® fruitandvegetablecampaigninOctober2005toincreaseawarenessoftheneedtoeatmorefruitandvegetables;andtoencourageallQueenslanderstoincreasetheirintakeoffruitandvegetablesby1serveperday.
The Australian Guide to Healthy Eating recommendseatingatleast5servesofvegetablesand2servesoffruitperday.Priortothecampaign,Queenslandadultswereonlyeating2.1servesofvegetablesand1.4servesoffruiteachday.
SincetheGo for 2&5®fruitandvegetablecampaignwasintroducedtherehavealreadybeenimprovementsinQueenslanders’intakeoffruitandvegetables.Phase1campaignresultsfromasurveyconductedin2006showsanincreaseinfruitintakeby0.1serveperpersonaday,andanincreaseinvegetableintakeby0.3perpersonperday.Thisamountstoanoverallreportedincreaseinconsumptionby0.4perpersonperserve,whichiswellonthewaytoachievingthecampaigntarget.
ThePhase1resultsshowthatthecreativeapproachusingthe‘VegeMan’characterhasbeensuccessfulinencouragingQueenslanderstoeatmorefruitandvegetableseveryday.Phase2ofthe4.5yearcampaignintroducedthecolourful‘DameEdna’characterandincludedthelaunchoftheGo for 2&5®websiteinAugust2006.
Thewebsiteincludesalargerangeofrecipeideasandhelpfulhintstoincludemoreservesoffruitandvegetableseveryday.
Website:www.qheps.health.qld.gov.au/gofor2and5/default.htm
8 A HEALTHY START IN LIFE RESOURCELIST
Growing Strong, feeding you and your baby resourcesGrowing StrongresourceshavebeendevelopedbyQueenslandHealthstafftoprovideevidence-basedinformationabouteatingwellduringpregnancyaswellassuggestionsfordealingwithsomecommonfoodandnutritionrelatedproblems.Informationisalsoprovidedaboutcommonbreastfeedingissuesincludinghowtoknowwhenababygetsenoughbreastmilkandcorrectpositioningandattachment.Theresourceshelptodispelmythsandmisinformationaboutfeedingyoungchildren.
CurrentlytheGrowing StrongresourcesaredesignedforhealthworkerstousewithAboriginalandTorresStraitIslanderfamilies.Factsheetsforcommunitymembersarecurrentlybeingdeveloped.
Website:www.health.qld.gov.auandsearch‘Growing Strong’
Healthy Food Access Basket (HFAB) SurveysHFABsurveysareconductedregularlytomonitorthecostandavailabilityoffoodthroughoutQueensland.Thesurveyassessesthevariabilityincostsandavailabilityofastandardbasketofbasichealthyfooditemsfromnearly100storesingeographicallocationsacrossQueensland.Thefoodsthatareinthestandardbasketrepresentcommonlyavailableandpopularfoods.
AstheHFABsurveyhasbeenrepeatedovertime,thelatestsurveyfindingscanbecomparedtosurveyfindingsfrompreviousyears.Reportsfromthe2000,2001and2004HFABsurveysareavailableontheQueenslandHealthwebsite.AreportfromthelatestHFABsurvey,conductedin2006,iscurrentlyunderpreparation.Thiswillbeavailablelaterin2007.
Website:www.health.qld.gov.auandsearch‘HealthyFoodAccessBasket’
Lighten Up to a Healthy Lifestyle ProgramLighten Up to a Healthy Lifestyle isagroup-basedhealthylifestylesupportprogramdeliveredbytrainedfacilitators(communityhealthnursesoralliedhealthprofessionals)inselectedcommunityhealthcentresin27HealthServiceDistrictsofQueenslandHealth.AllQueenslanderswhoareeitheroverweightoratriskofchronicdiseasesareeligibletoparticipateinthiscommunity-basedprogram.
Lighten Up to a Healthy Lifestyle doesnotfocusondietingorscales,butemphasisesmakinghealthyfoodchoices,beingphysicallyactive,settingrealisticgoals,modestweightloss,increasingselfesteemandmanagingstress.Theprogramissupportedbyaparticipantworkbookwhichincludessevenworkshopscoveringincreasingeverydayphysicalactivity,makingbetterfoodchoices,skillsinreadingfoodlabels,shoppingandadaptingrecipes,stressmanagementandproblem-solving.
ContactyourlocalCommunityHealthCentre(checktheWhitePages)tofindoutiftheprogramisavailableinyourarea.
ToordertheLighten Upworkbook,phone1800679778orvisittheQueensland Government Publicationswebsite,thenchoose‘Searchcatalogue’fromthemenuandenterLIGHTENUPthenSEARCH.
9A HEALTHY START IN LIFE RESOURCELIST
Smart Choices - healthy food and drink supply strategy for Queensland schoolsSmartChoices,amajorelementoftheSafeandHealthySchoolsinitiatives,isallaboutofferinghealthyfoodanddrinkchoicestostudentsinQueenslandschoolsettings.ItappliestoanyplaceoreventwherefoodanddrinkissuppliedinQueenslandstateschools,includingtuckshops,fundraising,vendingmachines,excursions,camps,classroomrewards,sportsdaysandcurriculumactivities.
SmartChoicesismandatoryforallQueenslandstateschoolsfromJanuary2007.
TheSmartChoiceswebsitecontainsaresourcepackageandtoolkitthathasbeendevelopedtohelpschoolsimplementthestrategy.
Website:www.education.qld.gov.au/schools/healthy/food-drink-strategy.html
TravelSmartTheTravelSmartprogramencouragesandsupportsvoluntarychangeinthebehaviourofindividualsandorganisationstoincreasetheuseofenvironmentally-friendlytransportsuchaswalking,cyclingandpublictransport.TravelSmartraisesawarenessthroughcampaigns,improvesaccesstoinformationandpromotesalternativestocaruse.SeetheTravelSmart websiteformoreinformation.
Website:www.transport.qld.gov.au/Home/General_information/Travelsmart/
A Healthy Start in Life ‐ a nutrition manual for health professionals
ORDER FORM
Your name: __________________________________________________ Position: __________________________________________________
Organisation: _________________________________________________ Address: __________________________________________________
_____________________________Postcode_____________ Telephone: ________________________ Fax: ___________________ Email: ___________________________________________________ Number of manuals required (maximum of 2) PLEASE FAX TO: Gold Coast Population Health Unit 5561 1851 Please note: Hard copies of the manual are only available for distribution within Queensland for health professionals only. If you are interstate please view the manual online at: www.health.qld.gov.au/healthieryou/healthystartinlife.asp




















