A CASE STUDY OF KAWAALA HEALTH CENTRE IV IN ...
43
AN INVESTIGATION INTO THE CONTINUED CASES OF LOST TO FOLLOW-UP TB PATIENTS: A CASE STUDY OF KAWAALA HEALTH CENTRE IV IN KAMPALA, UGANDA. BY NAB WIRE SARAH B5W14403411431DU SUPERVISOR: MR.OMUYA RONALD A RESEARCH REPORT SUBMITTED TO THE COLLEGE OF HUMANITIES AND SOCIAL SCIENCES IN PARTIAL FULFILLMENT FOR THE REQUIREMENTS OF THE AWARD OF THE DEGREE OF BACHELOR OF SOCIAL WORK AND SOCIAL ADMINISTRATION OF KAMPALA INTERNATIONAL UNIVERSTY SEPTEMBER, 2017
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of A CASE STUDY OF KAWAALA HEALTH CENTRE IV IN ...
AN INVESTIGATION INTO THE CONTINUED CASES OF LOST TO FOLLOW-UP
TB PATIENTS: A CASE STUDY OF KAWAALA HEALTH CENTRE IV IN
KAMPALA, UGANDA.
BY
NABWIRE SARAH
B5W14403411431DU
SUPERVISOR: MR.OMUYA RONALD
A RESEARCH REPORT SUBMITTED TO THE COLLEGE OF HUMANITIES AND
SOCIAL SCIENCES IN PARTIAL FULFILLMENT FOR THE REQUIREMENTS OF
THE AWARD OF THE DEGREE OF BACHELOR OF SOCIAL WORK AND
SOCIAL ADMINISTRATION OF KAMPALA
INTERNATIONAL UNIVERSTY
SEPTEMBER, 2017
DECLARATION
I Nabwire Sarah declare to the best of my knowledge that this report is a result of my
effort from Kawaala HCIV and it has never been submitted to any university for any
ward.
1
APPROVAL
This is to affirm that this study titled “An investigation into the continued cases of Lost to
follow-up: a case study of Kawaala Health Centre IV, Kampala”. Has been done under
my supervision and is now ready for submission.
Signature
MR. OMUYA RONALD
(SUPERVISOR)
Date .~

DEDICATION
I dedicate this piece of work to my family ; thank you for your unending love, Francis my
brother for your continued efforts and encouragement, thanks a lot it has kept me moving,
to my friends; Morgan, Rachael, Sam, thank you for your care and comfort and to Denis
that I love you so much.
111
ACKNOWLEDGMENTS
This piece of work would not have been complete without the efforts of many people to
whom I am very grateful; however a few of these deserve special recognition.
First , I would like to extend my heartfelt gratitude to my siblings, the Wanderas of
Naguru for your moral support to me through all my life , thank you, it has made me get
this far in my education.
I extend my sincere thanks to my supervisor Mr. Omuya ,for his helpfiil guidance, you’ve
always encouraged me to dig deeper as well as carry out more research and I hope this
will soon be a success. To the entire KIU staff that has been of great help during my
whole stay at the University.
Lastly, to my work mates and classmates for the encouragement and support they gave
me throughout our stay at KIU.
Also, I wish to make special mention of the staff at Kawaala Health Centre IV for the
help they gave me during my study visits there.
God bless you all.
iv

LIST OF ACRONYMS AND ABBREVIATIONS
FA Field Assistants
GOU Government of Uganda
HCIV Health Centre Four
HIV Human Immunodeficiency Virus
KCCA Kampala City Council Authority
LTFU Lost to Follow-up
MDG Millennium Development Goals
MDR-TB Multi-Drug Resistant Tuberculosis
NTLP National Tuberculosis and Leprosy Program
NTP National Tuberculosis Program
PBC Pulmonary Bacteriologically Confirmed
PCD Pulmonary Clinically Confirmed
SDG Sustainable Development Goals
TB Tuberculosis
WHO World Health Organization
v
TABLE OF CONTENTS
DECLARATION.
APPROVAL
DEDICATION
ACKNOWLEDGMENTS iv
LIST OF ACRONYMS AND ABBREVIATIONS v
TABLE OF CONTENTS
ABSTRACT ~aii
CHAPTER ONE 1
INTRODUCTION 1
1.0 Introduction 1
1.1 Background 1
1 .2Problem statement 4
1.3 Objectives of the Study 4
1.3.1 General Objective 4
1.3.2 Specific Objectives of the Study 5
1.4 Research Questions 5
1.5 Significance of the study 5
1.6 Scope of the study 6
CHAPTER TWO 8
LITERATURE REVIEW 8
2.0 Introduction 8
2.1 Definition of Lost to Follow-up 8
2.2 GOU Interventions in TB Treatment 9
2.3Background factors associated with Lost to Follow-ups during TB treatment 12
vi
CHAPTER THREE .15
METHODOLOGY 15
3.0 Introduction 15
3.1 Research Design 15
3.2AreaofStudy 15
3.3 Study population 16
3.4. Sample Size 16
3.5 Data Collection Methods and Instruments 16
3.6 Data Quality Control 16
3.7 Procedure 16
3.8 Data Analysis 17
3.9 Limitationsof the Study 17
3.10 Ethical Considerations 18
CHAPTER FOUR 19
PRESENTATION OF THE FINDINGS 19
4.1 Characteristics of Patients 19
CHAPTER FIVE 23
DISCUSSION OF THE FINDINGS 23
REFERENCES 30
APPENDIX I 33
RESEARCH BUDGET 33
APPENDIX II 34
TIME FRAMEWORK 34
vii
ABSTRACT
This study was conducted to establish the extent to which background factors have
perpetuated the cases of lost to follow-up in the Tuberculosis treatment despite the
government of Uganda intervention to providing universal free treatment and care for
patients in all public health facilities. Patients’ lack of motivation to complete treatment
and rehabilitation remains a challenge. The study was conducted as a across sectional
investigation through the review and analysis of registers of all 298 patients that were
enrolled on TB treatment from January to December 2016 at Kawaala HCIV. A
univariate analysis of the data was done using measures of central tendency.
Demographic variables were compared using the Chi-square tests. The study established
more males (62.4%) contracted Tuberculosis and more HIV positive patients (55.1%)
contracted the disease as an opportunistic co- infection. Although a higher percentage of
(63.2%) of TB patients was cured, the study further established that (5.4%) was still
worryingly high and this occurrence was more commonly among patients of 15 years and
more (93.3%). This study concluded that there is a clear co-relation between background
factors and Lost To Follow-Upamong TB patients and therefore recommends that further
interventions in TB treatment should specifically target these but also make aim for other
possible variables like mass sensitization and education, community linkages efforts play
a central role in attaining desired TB treatment success targets.
viii
CHAPTER ONE
INTRODUCTION
1.0 Introduction
The study investigated the background factors influencing the increasing cases of Lost to
follow-up(LTFU) in the treatment and care of Tuberculosis (TB) in Uganda despite the
availability of free treatment and care for TB patients in all public health facilities across
the country.
The study was carried out at one Kampala Capital City Authority (KCCA) Health Centre
(HC) IV called Kawaala HC IV.
This chapter presents the background of the study, statement of the problem, objectives
of the study, research questions, scope of the study and significance of the findings.
Li Background
TB is a bacterial disease which in humans is caused by an organism called
Mycobäcterium tuberculosis and the bacteria usually infects the lungs. But in some
individuals the TB germ can also affect all other parts of the body except the hair and
nails. When people with lung TB cough, sneeze, spit, or even talk, they propel the TB
germs into the air. A healthy person needs to inhale only a few of these germs to become
infected; making the disease airborne.
The signs and symptoms depend on which area of the body has been infected. These
signs may include: coughing that lasts two or more weeks, coughing out blood stained
sputum, chest pain or pain with breathing or coughing, noticeable weight loss, fatigue,
fever, excessive sweating especially at night lasting for 2 weeks or longer, loss of
appetite, poor weight gain among children, history of contact with a TB patient among
children etc.
TB can be treated and cured. The World Health Organization (WHO) Global TB report
of 2016 states that TB treatment averted 49 million deaths globally between 2000 and
2015.
The testing and treatment services are free in all public health facilities. The patients that
have started treatment are expected to take their medicines continuously for a period of
six months and then be reviewed after for response to the prescribed drug.
Although there have been globally concerted efforts to provide free Tuberculosis (TB)
treatment services in public health facilities, TB remains a major global health problem
causing~ill-health and death among millions of people each year and ranks as the second
leading cause of death from an infectious disease worldwide, after Human
Immunodeficiency Virus (HIV).
According to World Health Organization Global TB Report (2014) there were 8.7 million
new cases and 1.4 million deaths in 2013 and almost one million deaths among HIV
positive TB patients. According to WHO (2016) important diagnostic and treatment gaps
persist. Globally there was a 4.3 Million gap between incident and notified cases, with
India, Indonesia and Nigeria accounting for almost half of this gap.
2
Sendagire et al (2012) argues that retaining patients on TB treatment is .a major challenge
in many countries. Interruption of treatment has been associated with failure and death.
Levels of defaulting of up to 26% have been reported in Africa. Defaulting levels tend to
be especially high in urban areas. In Uganda, an estimated 14% of the new smear-positive
patients defaulted from treatment in 2006, while in Kampala city, where a quarter of the
notified TB cases in Uganda are registered, defaulting levels are around 20%.
Owing to the fact that there are gaps in the universal TB treatment and care interventions,
a number of patients have abandoned or failed to complete the treatment course. A
patient who has had treatment for at least one month but then discontinues it for two
months or more is referred to as Lost to follow-up. Stopping treatment too soon or
skipping doses can allow the bacteria that are still alive to become resistant to the
prescribed drugs, leading to a TB strain that is much more dangerous and difficult to
treat. The NTLP Annual Report 2015-2016 on TB Treatment Outcomes states that of the
26, 632 new Pulmonary Bacteriologically Confirmed (PBC) cases notified in 2014/2015,
79% were successfully treated (51% cured), 5% died, and 1% failed while 11% were lost
to follow up, which is over twice high the WHO target of 5%.
It is under this background that the researcher was interested in finding out the
background factors associated with the increasing numbers of TB patients abandoning
treatment, yet at all public health facilities in Uganda TB treatment and care is free.
3
1.2Problem statement
The Government of Uganda (GOU) has intensified its efforts in the fight against TB.
Namagembe (2017) states thatl 12 health facilities in over 60 districts across the country
are equipped with the Genexpert TB machine. This intervention is far more effective than
the smears that are on the other hand also more widely spread across the whole country.
However, despite these and other interventions ( for example, early diagnosis and DOT
[Kirenga et al,20 14]) intended to rid the population of the highly fatal TB, patients have
also increasingly abandoned treatment and care; contributing to the high prevalence of
the disease: 36 cases for every 100,000 among children only (2016 National TB
Prevalence Survey).
This has therefore prompted the researcher to carry out a study intended to investigate the
background factors contributing to the increasing LTFU cases yet there is free treatment
and management of TB in all health facilities across the country. This will help to inform
the government of Uganda in planning relevant interventions in order to achieve the
World Health Organization’s (WHO) goal of eliminating TB as a public health threat by
2035.
1.3 Objectives of the Study
1.3.1 General Objective
This study sought to investigate the contributory background factors associated with non
adherence to TB treatment despite the availability of free universal treatment in all public
health facilities in Uganda.
4
1.3.2 Specific Objectives of the Study
i. Determine the proportion of patients regarded as lost to follow up abandoning
treatment at Kawaala HCIV.
ii. Describe the background factors associated to cases of Lost to Follow Up during
TB treatment at Kawaala Health Centre IV.
1.4 Research Questions
i. What proportion of patients on TB treatment in Kawaala HCIV is lost to
follow-up?
ii. What are the background factors associated to cases of lost to follow-up during
TB treatment?
1.5 Sighificance of the study
The findings of the study will be of the following significance:
Health authorities in Uganda and the world at large will get to ascertain the relationship
between background factors and lost to follow-up in TB treatment and thereby design
interventions that are more relevant to patient characteristics.
Health workers at different health facilities managing TB will get to understand how
and the need to retain patients on TB treatment until declared cured or complete for TB
treatment.
5
All health facilities involved in the management and treatment of TB will use the findings
of this study to improve their information systems and data management so as to
accurately record and report the LTFU cases to improve health interventions.
Other researchers will use the finding of this study as baseline data for their studies and
also as a basis for further research to influence TB treatment and management policy.
1.6 Scope of the study
The study was conducted on the background factors influenced by the increasing cases of
Lost to Follow-Up in the treatment and management of TB. It was conducted in one of
the Kampala Capital City Authority clinics called Kawala HC IV. The study was
conducted between May and August 2017.The researcher used a quantitative research
design. In particular, a cross-sectional design with TB patients for the entire population
o120 1 6’n the treatment register who were initiated on TB treatment was considered.
6
1.7 Definition of Key terms
Lost to follow-up: A patient who has had treatment for at least one month but then
discontinues it for two months or more.
TB: TB is a bacterial disease which in humans is caused by an
organism called Mycobacterium tuberculosis and the bacteria
usually infects the lungs.
HC IV This is a mini hospital that serves a county or a parliamentary
constituency. It should have a senior doctor and other doctors, a
ward for men, women and children besides having an operating
theatre for carrying out emergency operations.
BACKGROUND: The conditions that form the setting within which something is
experienced OR information essential to understanding of a
problem or situation.
7
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
By examining related works of other researchers and scholars, this chapter will highlight
the definition of LTFU, establish the already existing knowledge and literature about the
variables of LTFU patients on TB treatment, and the GOU intervention of providing them
free treatment to combat the vice. It will also establish the proportion of LTFU patients in
the selected KCCA clinic of Kawaala HCIV in Kampala as well as describing the
background reasons surrounding their defaulting on the free TB treatment.
2.1 Definition of Lost to Follow-up
In clinical medicine, a person who has not returned for continued care or evaluation (e.g.
because of death, disability, relocation, or drop-out) is a Lost to follow-up (Medical
Dictionary, 2009).
Lost to follow -up is a TB patient who starts treatment for one month or more and whose
treatment is then interrupted for 2 consecutive months or more (WHO, 2007).
Lost to follow-up has also been defined as patients who at one point in time were actively
participating in a clinical research trial, but have become lost (either by error in a
computer tracking system or by being unreachable) at the point of follow-up in the trial
(Wikipedia).
8
A defaulter is a patient who had documented discontinuation of anti-TB treatment for
two or more consecutive months due to reasons other than physician’ s advice. (Elbireer,
Guwatudde, Mudiope, Ssekandi, and Manabe ,201 1).
It should be noted that the various scholars on LTFU do not differ at all. Their conclusion
is that LTFU may in some instances be only as result of error on part of the health
facility, but on the whole it is largely a patient-driven occurrence.
2.2 GOU Interventions in TB Treatment
The GOU in its efforts to totally eradicate TB in the country ratified the Millennium
Development Goals (MDGs) and their successors; the Sustainable Development Goals
(SDGs).Of particular interest is MDG and SDG number 6. According to the Revised
National strategic plan 2015/16 report; Case holding among drug susceptible TB cases
has remained a challenge in the country. For example, of the 2014/15 new
bacteriologically confirmed cohort, only 79% were successfully treated (51% cured and
28% treatment completed) while 21% had unfavorable outcomes (5% died, 1% failed,
4% wei’e not evaluated, and 11% were lost to follow up).
The chronic nature of TB demands that two or more kinds of drugs are taken for periods
ranging between 6 and 12 months, depending on the treatment regimen. Because of this,
motivation to complete treatment fluctuates in intensity, and loss of follow up may be
considered at many stages during treatment. Thus the most difficult task in TB control is
to persuade patients to take their drugs regularly and for the required duration
(Nakanwagi et al, 2010).
9
A study carried out that included 331 retreatment patients (68% males), with a median
age of 36 years, 93 (2 8%) of whom were relapse smear-positive, 21(6%) treatment after
failure, 159 (48%) return after loss to follow-up, 26 (8%) relapse smear-negative and 32
(10%) relapse cases with no smear performed. This clearly shows that the dropout rate is
higher than the recommended WHO target of 5% in LTFU.
Owing to the fact that many national and international efforts are exerted against T.B
prevention and control but still the patients are failing to complete their treatment to be
declared cured or completed treatment. The internationally accepted WHO strategy for
TB control, the DOTS program was implemented since 1997 Nevertheless; coverage of
DOTS service is still minimal and has made little progress on treatment adherence in
some resource- meager countries such as Uganda meanwhile in Nairobi too in
2006,Nairobi had the highest notification rate at 652/100000 among the TB control
regions, further the highest defaulter rate (out of control), Bernard N Mature etal.
Meanwhile the NTLP Annual Report 2015-2016 on TB Treatment Outcomes: Of the 26,
632 new PBC cases notified in 2014/2015, 79% were successfully treated (51% cured),
5% died, and 1% failed while 11% were lost to follow up which is twice high the WHO
target of 5%. The unfavorable outcomes could be due to poor recording and reporting,
inadequate engagement of families as well as communities in providing treatment support
to patients.
It is therefore important to note that the problem of lost to follow up actually exists and
there is need to address it(Sendagire etal, 2012).
10

Retaining patients on TB treatment is a major challenge in many countries. Interruption
of treatment has been associated with failure and death. Levels of defaulting of up to 26%
have been reported in Africa. Defaulting levels tend to be especially high in urban areas.
In Uganda, an estimated 14% of the new smear-positive patients defaulted from treatment
in 2006, while in Kampala city, where a quarter of the notified TB cases in Uganda are
registered, defaulting levels are around 20 %( Sendagire, Ibid).
Non-compliant patients were more likely to be workers. This was attributed to the fact
that the travelling time for an employed patient represents a time absent from work.
Coupled with the fact that some employers may not take kindly to the frequent long
periods during which TB patients need to attend health facilities for treatment, means that
long-term treatments such as that for TB may pose huge problems for such individuals. In
the present study, the possible explanation for non-compliance among employed patients
could be because they belonged to lower socio-economic strata and they were the sole
bread earning members of their family. These factors may put a lot of stress on them, to
the extent that as soon as they begin to feel better, they will choose to return to work to
continue to provide for their families (O’Boyle et al, 2013)
It is upon this background that the researcher decided to look at these background factors
associated with the phenomenon and came up with information as well as
recommendations to the challenge; hence the study.
11
2.3Background factors associated with Lost to Follow-ups during TB treatment
This study documents some of the background factors associated with an increased risk
of loss to follow-up and treatment non-compliance which may include sex, age,
geographical location, type of patient, type of TB, type of treatment regimen and HIV
status. According to Gopi et al(nd) age affects adherence to TB medication where old age
increases the risk of loss to follow(1). It was shown that the default rate among cases
diagnosed at health facility was significantly higher in the older age group of 45 years or
more compared to that of 15-44 years of age.
Gopi et al (nd) continues to emphasize the relationship between sex and loss to follow-
up. Looking at the survey component done at the health facility which indicated that the
default rates among males and females were 17.0% and 8.4% respectively and the
difference was statistically significant (p<O.0 1). However, the survey component canied
out in the community showed a difference by sex where the default rates among males
and females were 24.4% and 17.6%.
A study carried out in Southwest of Ethiopia among tuberculosis patients at Jimma
University hospital also showed no significant differences in terms of gender and age for
patients who were classified as Lost To Follow-Up. In the same study it was concluded
that HIV negative TB patients were more prone to loss to follow-up as opposed to HIV
positive TB patients. Indeed being HIV positive appeared to be associated with lost to
follow-up in the univariate but not in the multivariate analysis (Akesa, 2015).
12

In a survey done in 2007 at the Infectious Diseases Institute clinic (IDI), an urban HIV
clinic in Kampala Uganda by Sawsaw, Osman Abdalla, results indicated that the annual
default ,rate from TB treatment was at 30% and a number of health facility-specific
factors and individual characteristics were found to be associated with TB treatment
default like; long waiting time in the treatment Centre, lack of health education, conduct
of clinic staff, running out of drugs and fear of side effects of anti-TB treatment etc.
Another case control-study carried out in Brazilian Amazon, by Malucia dasilva etal,
retorted that; treatment default is influenced by a number of factors: lack of knowledge
about the disease, distance from the health post, partial or complete regression of
symptoms in the first two months of treatment, the side effects associated with the
medication, male gender, age, the use of toxic substances and hospitalization during
treatment pre-existing pulmonary disease, previous default, TB/HIV co-infection,
absence of supervised treatment and poor quality of patient care at the Health Unit.
Furthermore a study carried out by USAID in Gulu District referral hospital in Northern
Uganda reported that with an average of 80 patients every quarter diagnosed with active
TB and initiated on treatment, the quarterly treatment completion rate from January to
September was reported to range from 18.3% to 27.7% and several factors contributed to
poor out comes in reaching the national target for completion of TB treatment. The TB
clinic, staffed primarily by nurses and nursing assistants. In addition to the human
resource limitation, the patient information system including the TB registers and patient
13
held-cards was often inaccurate or incomplete. The patient information system also
lacked contact information for proactive client follow-up and this is the reason why the
problem of lost to follow-up is still a challenge because there is no way of tracking those
clients that fail to return for routine clinical review.
The Uganda Radio Network (URN) is an independent Ugandan subscription
based news agency headquartered in Kampala. In April 2014, it released a report which
expressed concern on the alarming rate of TB patients defaulting on treatment in
Kitgum District. The report cited that in Lagoro sub county 53 of the 60 registered
tuberculosis patients had defaulted on treatment and disappeared without trace.
14
CHAPTER THREE.
METHODOLOGy
3.0 Introduction
This chapter presents a detailed description of the research design that was adopted for
the study, the study area, study population, sample size, data collection methods, tools,
and limitations of the study among others.
3.1 Research Design
This was a cross sectional study which collected secondary data from the TB treatment
register of Kawaala Health Center IV to determine the proportion of Lost To Follow-Up
and the background characteristics that determine Lost To Follow-Up.
3.2 Area of Study
The study was carried out in Kampala Capital City Authority (KCCA), specifically in the
HC IV of Kawaala. KCCA is located in Buganda region, in the central part of the
Uganda. Kawaala Health Center IV is located in the Rubaga Municipality of KCCA on
Kawaala Village.
This particular health center was chosen for the study due to the fact that it is located an
urban area and so more likely to have high TB incidences and prevalence due to
congestion of people. Kawaala is among the health centers that are located in areas which
are predominantly inhabited by people of lower socio-economic standing and such people
are more susceptible to defaulting on treatments owing to the fact that they are
preoccupied with achieving basic daily necessities of life like food and shelter.
15
3.3 Study population
The population of the study comprised of all patients that were initiated on TB treatment
for the year 2016.
3.4. Sample Size
A total of all the patients diagnosed TB positive in the year 2016 were considered in this
study.
3.5 Data Collection Methods and Instruments
This was a retrospective study that focused on the review of documents, in specific the
TB treatment registers. The study of documents method was used because of its ability to
cover the whole span of a year that the researcher intended to investigate since all the
patient information during that period was contained in the documents.
3.6 Data Quality Control
There was a regular cross checking, inspection and scrutinizing of information on the
research instruments at the end of the day of data collection by the researcher to ensure
accuracy, relevance, completeness, consistency and uniformity of the data. Double entry
of data and data cleaning was conducted before data analysis.
3.7 Procedure
Upon approval of the research proposal, the researcher got an introductory letter from the
Head of Department College of humanities and social sciences, Faculty of Applied
16
psychology Kampala International University. This letter was presented to the facility
inhcargeat Kawaala HC IV. This was done so as to seek permission to carry out the study
at the facility. After seeking permission, the researcher was then given access to the
treatment register and all the fields were entered in a database using Redcap.
3.8 Data Analysis
The researcher conducted a multivariate analysis. Continuous data was analyzed using
measures of central tendency (mean and median) with standard deviations and
interquartile ranges respectively. The researcher summarized the categorical data using
percentages. Data was presented using tables. For categorical variables, Chi-square test
was used to make any comparisons as required.
3.9 Limitations of the Study
The study should have been conducted in all public health facilities across the country
that are involved in the management and treatment of TB however, the time and financial
constraints that the researcher met in the whole research process dictated a selection of
one clinic that represents both rural and urban. The researcher not only had to meet the
full cost of the study, but also the period of four months that the researcher was allowed
to develop a proposal, collect and analyze data and compile and submit a report was not
sufficient for a more comprehensive study. Also, the localization of the study to just one
health facility may limit the generalization of the findings but the researcher feels that
those findings will be representative enough to influence TB management and treatment
across Uganda and the world over.
17
3.10 Ethical Considerations
Permission was sought from the facility incharge at Kawaala HCIV before data
collection. The researcher ensured confidentiality of all participants’ information by
assigning identification numbers rather than using their names and stored the information
with a password that was kept strictly confidential and used only by the researcher.
18
CHAPTER FOUR.
PRESENTATION OF THE FINDINGS
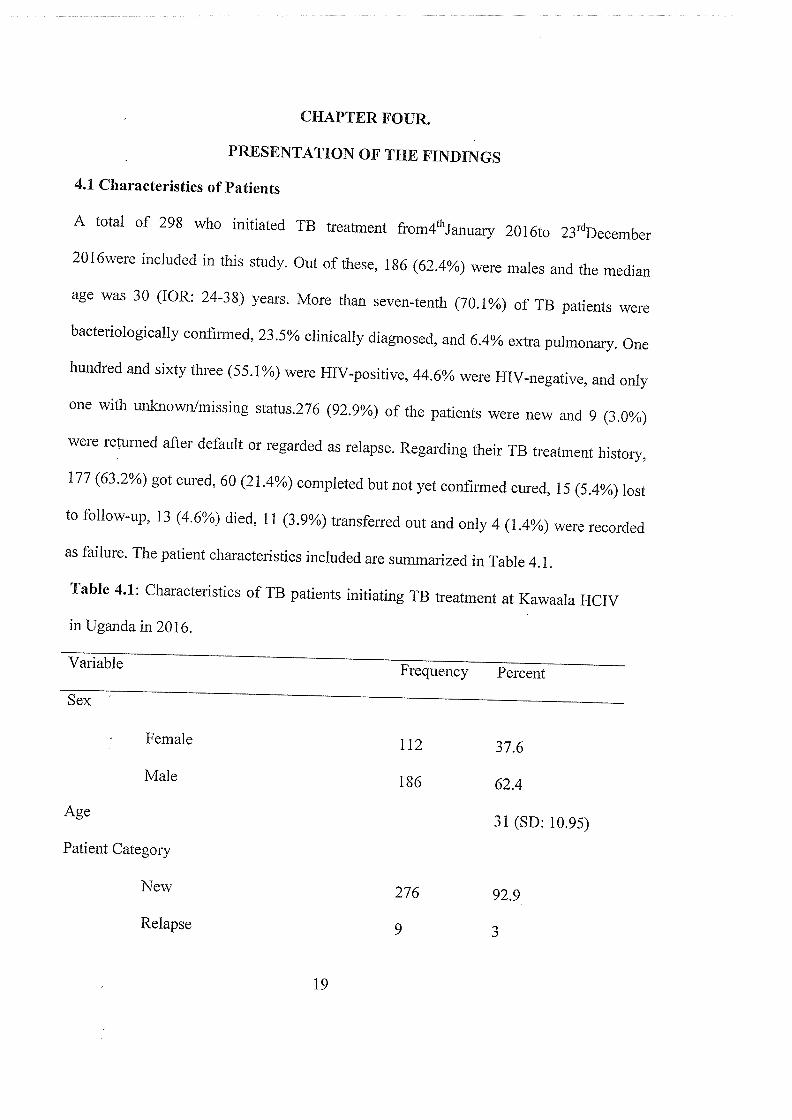
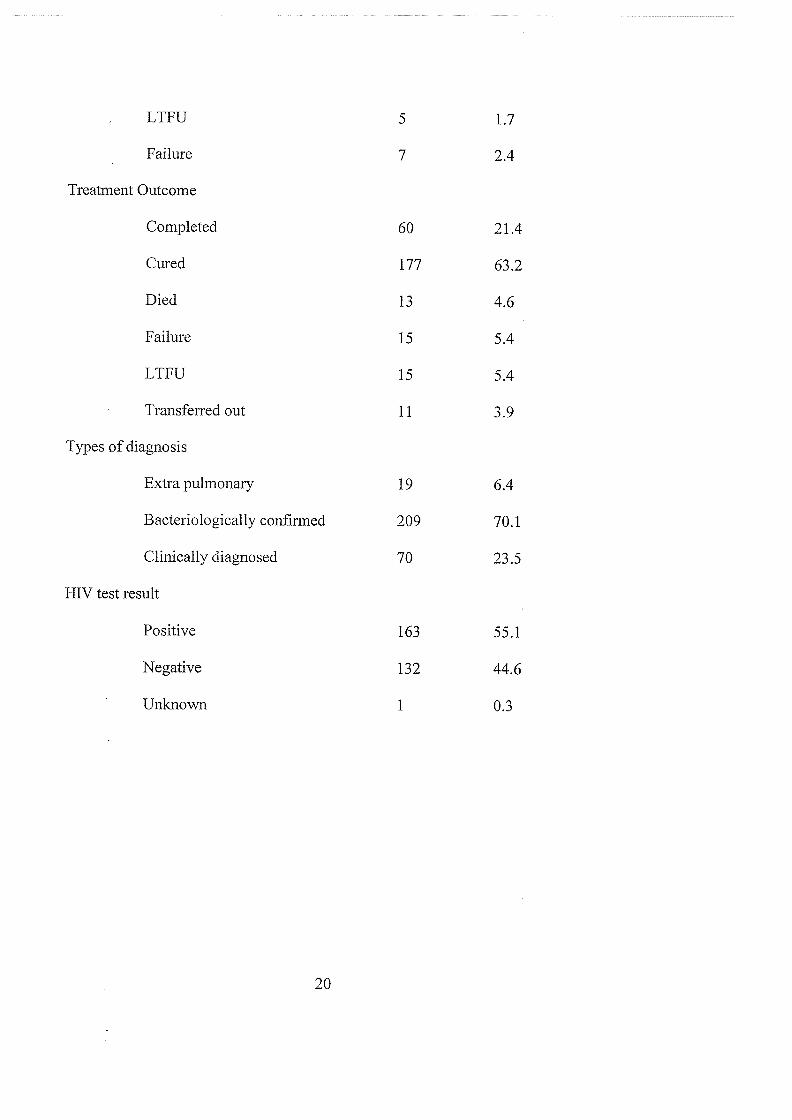
4.1 Characteristics of Patients
A total of 298 who initiated TB treatment from4thJanuary 201 6to 23’~December
2Ol6were included in this study. Out of these, 186 (62.4%) were males and the median
age was 30 (IOR: 24-3 8) years. More than seven-tenth (70.1%) of TB patients were
bacteriologically confirmed, 23.5% clinically diagnosed, and 6.4% extra pulmonary. One
hundred and sixty three (55.1%) were HIV-positive, 44.6% were HIV-negative, and only
one with unknownlmissing status.276 (92.9%) of the patients were new and 9 (3.0%)
were returned after default or regarded as relapse. Regarding their TB treatment history,
177(63.2%) got cured, 60(21.4%) completed but not yet confirmed cured, 15 (5.4%) lost
to follow-up, 13 (4.6%) died, 11(3.9%) transferred out and only 4 (1.4%) were recorded
as failure. The patient characteristics included are summarized in Table 4.1.
Table 4.1: Characteristics of TB patients initiating TB treatment at Kawaala HCIV
in Uganda in 2016.
Variable Frequency Percent
Sex’
Female 112 37.6
Male 186 62.4
Age 31 (SD: 10.95)
Patient Category
New 276 92.9
Relapse 9 3
19
LTFU 5 1.7
Failure 7 2.4
Treatment Outcome
Completed 60 21.4
Cured 177 63.2
Died 13 4.6
Failure 15 5.4
LTFU 15 5.4
Transferred out 11 3.9
Types of diagnosis
Extra pulmonary 19 6.4
Bacteriologically confirmed 209 70.1
Clinically diagnosed 70 23.5
HIV test result
Positive 163 55.1
Negative 132 44.6
Unknown 1 0.3
20

4.2 Loss to Follow-Up (LTFU) during Treatment
All TB’ patients were supposed to start treatment and follow treatment until they were
declared as cured or completed as was also in a study carried out in Nairobi province Of
the 298 TB patients followed, the minimum follow-up time was one month and the
maximum was eight months. Fifteen patients (5.4%) were lost to follow-up of their
treatment. With regard to timing of LTFU, 3 were lost to follow-up during the first two
months of treatment. This was also reported by Bernard Mature etal in a case control
study; Factors associated with Default from Treatment among TB patients in Nairobi
Province where results showed that of the 945 Defaulters 22.7 %( 215) and 20.4 %( 193)
abandoned treatment within the first and second months (Intensive phase) of treatment
respectively. 7 during the next 3-4 months, and 5 after four months of TB treatment
initiation. Time until LTFU treatment among tuberculosis patients ranged from 14 days
to 120 days.
The statistics also show 3.9%(l 1) patients as transferred out ;this doesn’t clearly show
their treatment outcomes from the clinics they were transferred to and in any case they
could also be lost because there was no proof of treatment continuation in the registers
for those patients that were transferred out. There’s a weak follow-up system for these
patients. Although the receiving health facilities are responsible for reporting patient
treatment outcomes to the referring facilities, this communication is failing.
21
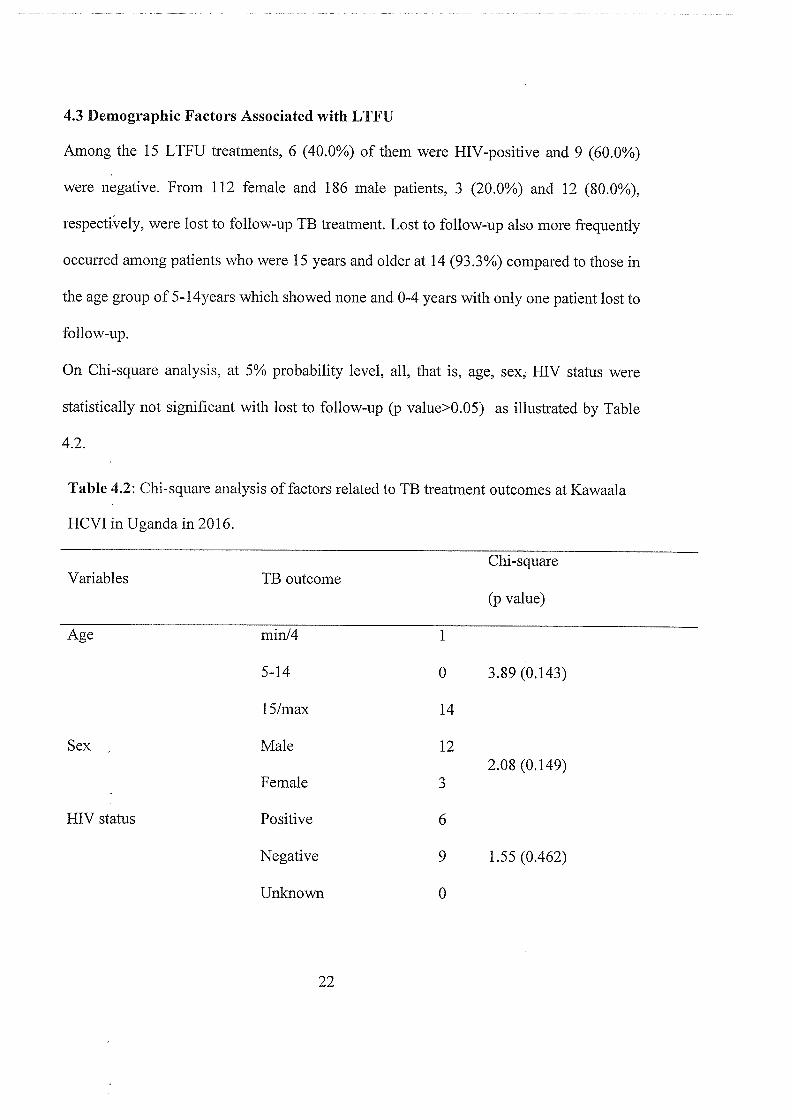
4.3 Demographic Factors Associated with LTFU
Among the 15 LTFU treatments, 6 (40.0%) of them were HIV-positive and 9 (60.0%)
were negative. From 112 female and 186 male patients, 3 (20.0%) and 12 (80.0%),
respectfvely, were lost to follow-up TB treatment. Lost to follow-up also more frequently
occurred among patients who were 15 years and older at 14 (93.3%) compared to those in
the age group of 5-l4years which showed none and 0-4 years with only one patient lost to
follow-up.
On Chi-square analysis, at 5% probability level, all, that is, age, sex, HIV status were
statistically not significant with lost to follow-up (p value>0.05) as illustrated by Table
4.2.
Table 4.2: Chi-square analysis of factors related to TB treatment outcomes at Kawaala
HCVI in Uganda in 2016.
Chi-squareVariables TB outcome
(p value)
Age min/4 1
5-14 0 3.89 (0.143)
15/max 14
Sex Male 122.08 (0.149)
Female 3
HIV status Positive 6
Negative 9 1.55 (0.462)
Unknown 0
22
CHAPTER FIVE.
DISCUSSION OF THE FINDINGS
The government of Uganda has intensified its efforts to fight against Tuberculosis and in
over 60 District across the country, Health facilities have been equipped with genexpert
machines for fast TB diagnosis so as patients are started on TB treatment immediately.
TB treatment and care is free in all public health facilities across the country. Despite the
government’s efforts to end TB infections with free treatment, many patients are failing
to adhere to the TB treatment. World Health Organization places high emphasis on
achieving high compliance levels than finding new cases. Non-compliance increases the
likelihood of developing multi-drug resistance TB (MDR-TB) and extreme-drug resistant
TB (XDR-TB). This will further increase the burden of a disease that is already very
great and increases the costs of its management.
This research was done so as to analyze the possible reasons for non-adherence to TB
treatment. It is a retrospective study that involved the review and analysis of documents.
During the study all TB treatment registers of the year 2016 were reviewed and data was
collected for analysis.
In this study, the researcher found out that, the total number of patients that were initiated
on TB treatment in 2016 was 298. Out of these 186(62.4%) were males, 112(37.6%) were
females with the median age of 30(IOR: 24-38) years. More than seven-tenth (70.1%)
were bacteriologically confirmed, 23.5% were clinically diagnosed and 6.4% had extra
pulmonary TB. 163(55.1%) were HIV-positive, 44.6% were HIV-negative and only one
had an unknown/missing status. 276 (92.9%) of the patients were new and 9 (3.0%) were
regarded as relapse.
23
Regarding their TB treatment history, 177 (63.2%) got cured, 60 (21.4%) completed but
were not yet confirmed cured, 15 (5.4%) lost to follow-up, 13 (4.6%) died, 11(3.9%)
transferred out and only 4 (1.4%) were recorded as failure.
Of all patients initiating first-line TB treatment during 2016,15(5.4%) were lost to
follow-up. This is a lower rate documented compared to the NTLP Annual Report 2015-
2016 on TB Treatment Outcomes which documented an 11% lost to follow-up. This
result is also not consistent with the one documented in the sub-Saharan Africa (18%) by
a systematic review and meta-analysis by MacPherson et al (2014). This is due to the
population considered for this study where only one KCCA clinic was considered but this
was documented under the study limitations. It might also be due to the massive rollout
of household contact investigation programs and this being one of the clinics that is
currently participating in the program. The 5.4% of lost to follow-up rate was slightly
higher than the WHO recommended target of less than 5% nationally(WHO,2014)
despite the extensive expansion of services and the massive rollout of contact
investigation programs. This calls for more comprehensive approaches to reduce Lost to
Follow-Up among TB patients by targeting those risk factors for treatment interruptions.
Previous studies have identified wide ranges of factors associated with loss to follow-up
treatment among TB patient including age, sex, HIV status and others. In the current
study the researcher identified that, the same factors mentioned are associated with Lost
to Follow-Up.
24
In view of the first objective, the research established that, of the 15 who were LTFU, 3
patients were female and the 12 patients were male composing the biggest percentage of
LTFU.
In view of the second objective that was to find out the background factors associated
with the cases of LTFU. The research established that of the 15 who were lost to follow-
up, 6 of them were HIV-positive and of the positives 4 patients were males clearly
showing that more men do not adhere to treatment than women and this could be because
men have poor health seeking behaviors than women and also them being HIV-positive,
they were challenged by the number of drugs they had to take, it was hard for them to
take drugs for both disease and as a result many had their treatment interrupted.
Conclusion
This study investigated the continued cases of lost to follow-up in Tuberculosis treatment
and care, taking Kawaala Health Centre IV as a case study. This was in relation to the
persistence of the situation in which TB patients failed to adhere to treatment and care yet
this was readily and universally available at all public health facilities across the country
and also provided free of charge. The study specifically sought to determine the
proportion of patients regarded as LTFU and also describe the background factors leading
to the increasingly persistent cases of LTFU during TB treatment.
The study established that cases of LTFU appeared from as early as 13 days into
treatment to 548 days and these accounted for up to 5.4 %of those patients that enrolled
for treatment and care. The study further established that LTFU was an occurrence
25
majorly among patients that were 15 years or older (93.3%), non-existent among those
between 5 and 14 years, and only 2.98% among those between 0 and 4 years. Further
still, the study established that LTFU occurred more frequently among HIV-positive
patients (at 55.1%) and generally the phenomenon occurred more frequently among men
at (80.0%). Finally, the 5.4%LTFU incidence was lower than the regional and global
incidenèe of 11% though very significantly high for an urban health Centre because poor
adherence to treatment means that patients remain infectious for longer and are more
likely to relapse or emerge to drug resistant tuberculosis which may increase the cost of
treatment. In view of these findings, the study concludes thus:
LTFU was an occurrence not exclusive to a specific section of the population, in other
words all those enrolling for TB treatment were likely to abandon treatment in case any
one or a combination of the background factors leading to the situation was present.
The background factors that led to the existence of LTFU in TB treatment were majorly
demographic, including age, sex, HIV status and socio-economic status. These
notwithstanding, there were several other factors that had not been given consideration by
this particular study yet they too had a bearing on the phenomenon. Among these was the
inadequate treatment support, non-aggressive mass education about TB, the kind of TB
that a patient was suffering from and the length of time taken by each visit to a health
facility.
26
Recommendations
The researcher has argued that interventions to combat LTFU must be designed in view
of demographic factors of patients generally because the phenomenon is not exclusively
borne of one particular background factor but by a combination of all depending on the
patient and their circumstances.
The study has also shown patients begin to abandon treatment as early as the second
week of enrolment. Also the study established that the incidence of LTFU in Uganda was
commendably lower than the regional and global incidence. It is against this background
that the recommendations below are made. Despite its limitations, this study should be
relevant in the total eradication of LTFU cases in TB treatment and care. Basing
generalizations on the findings of this study, the researcher recommends that:
Interventions to address the issue of LTFU should be designed to address the background
factors leading to the persistence of the phenomenon. The aforesaid background factors
include the core demographic variables like age and sex. Also, these interventions should
address the extraneous factors like socio- economic background of the patients,
knowledge on duration of treatment.
The health authorities in Uganda should address the fact that the national LTFU
incidence is far lower than the regional and global. The low incidence depicts a situation
of logistical limitations confounding the findings of this and any other study because the
circumstances of TB treatment and care are still incomplete in themselves. In other
words, chances are that many TB positive patients are going undetected, thereby
27

rendering all other efforts to combat the disease irrelevant because of it being a highly
contagious airborne malady.
Treatment support for the patients and mass-sensitization, (prior attendance to a TB
health education session, awareness campaigns that TB is curable as other diseases)
should be intensified in order to motivate those patients already enrolled for treatment to
complete their treatment schedules and also encourage the community, To void future
infections and re-infections by equipping them with information necessary to undertake
informed decisions in relation to the disease.
With the findings of the study indicating that more HIV-positive patients (55.1%) were
again the LTFU in TB treatment, health authorities should design joint clinics for both
TB and HIV/AIDS treatment and care because in the current arrangement the two clinics
are attended separately; hence increasing the likelihood of the patient missing this clinic
or the o~her or both.
Areas for Further Research
The conundrum of LTFU despite free universal TB treatment can be addressed better if
further research is done on more effective mass sensitization and the role of educational
institutions in the fight against TB. Also, the medicines that are given to both TB and
HIV patients need further research into so that more combined drugs treating the co
infections are developed because currently these patients are given medicines for each
disease separately, which makes taking them inconveniencing.
28
Statistically more men were found to be lost to follow-up than women; further research
should be carried out to establish why more men fail to adhere to treatment than women
so that interventions brought rid this vice.
29
REFERENCES
~cess~ GM, etal Survival Analysis ofLoss to Follow-Up Treatment among Tuberculosis
Patients at Jimma University Specialized Hospital, Jimma, Southwest Ethiopia.
Bryman, A(2008 ). Social research methods. 3~C~ Edition. New York, Oxford University
Press.
CDC (2005) Guideline for preventing the transmission of n2ycobacterium Tuberculosis
in health care settings.
Communication strategyfor TB/HIV Collaboration in Uganda. March 2006.
Community Contribution to TB care: Practice and policy.
Elbireer 5, etal (2011). Tuberculosis treatment default among HIV-TB co-infected
patients in urban Uganda. In tropical medicine and international health vol.1 6.No
8(nd) Blackwell punishers limited.
Esther Achen, HIV Clinic, HIV in charge and HIV teams, TuesdayNov-20 12. Improving
TB.
Farlex and Partners (2009). Medical dictionary
Gawatudde etal (2003) Burden ofTB in Kampala.
Gawatudde etal (2010) TB in Household contacts.
Gopi PG, etal. Failure to InitiateTtreatrnent for Tuberculosis patients diagnosed in a
community survey and at health facilities under a DOTS programme in a District
of South India. Short Communication. Indian J Tuberc [Internet]. [cited 2017 Oct
9]; Available from: http ://medind.nic.iniibr/tos/j3/ibrtosi3p 153 .pdf
Kirenga, JB (2014) treatment outcome of new Tuberculosis patients hospitalized in
Kampala, Uganda: A prospective cohort study.
30
Kombo,D.K and Tromp; D.L.A(2006)Proposal and thesis writing: An introduction.
Nairobi. Pauline Publications Africa
MacPherson P, Houben RM, Glynn JR, Corbett EL, Kranzer K. Pre-treatment loss to
follow-up in tuberculosis patients in low- and lower-middle-income countries
and high-burden countries: a systematic review and meta-analysis. Bull World
Health Organisation
Ministry of health manual of the National Tuberculosis and Leprosy. Programme; 2nd
Edition(20 10)
Nakanwagi, A etal( 2010) Characteristics and treatment out comes of Tuberculosis
Retreatment cases in Three Regional Referral Hospitals, Uganda
National Communication strategy for Tuberculosis control. National Tuberculosis and
Leprosy prograinme and Health promotion and Education Division. October
(2015).
New vision newspaper for 7th July-20 17
NTLP Annual report for2Ol4-2015 on TB treatment out come
Obuku etal
Oso,W.Y &Onen.D(2005)A general guide to writing research proposal and report
.Kisumu. Options Press and publishers.
Scientific writing by Jennifer Peat.
Sizomu.A, Brucker,M and Muwonge Moses(2014). Family planning in Uganda: A
review ofNational and Districtpolicies and Budgets, Kampala.DSW
Ssendagire, I etal (2012) urban movement and alcohol intake strongly predict defaulting
from Tuberculosis treatment
31
Stop TB Initiative (2010) Treatment ofTuberculosis guidelines: WHO.
Treatment completion rates: Experience from Gulu Regional Referral Hospital,
Uganda.
Uganda National TB guidelines for Tuberculosis Infection control in health care
facilities, Congregate settings and Households (2011)
WHO report (2007) Global TB Report.
WHO Treatment Guidelines; Treatment oftuberculosis Guidelines ~ Edition.
WHO. Definitions and reporting framework for tuberculosis — 2013 revision. 2014
[cited 2017 Oct 10]
32
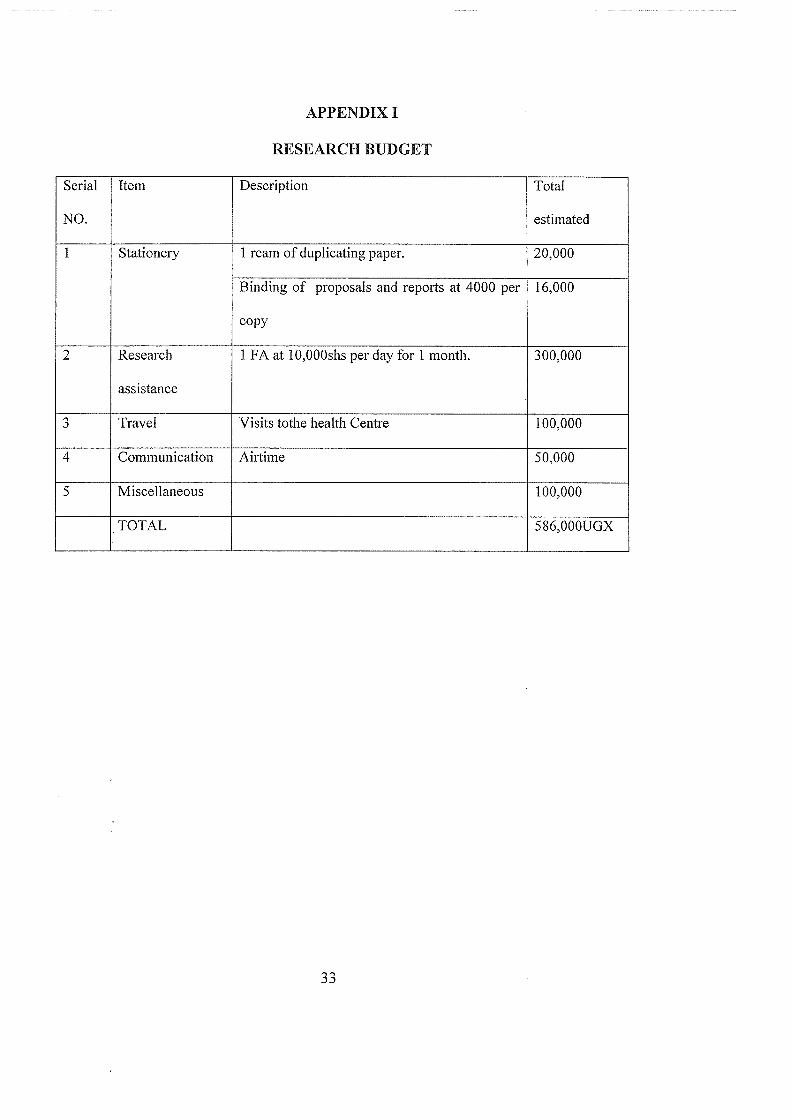
APPENDIX I
RESEARCH BUDGET
Serial Item Description Total
NO. estimated
1 Stationery 1 ream of duplicating paper. 20,000
Binding of proposals and reports at 4000 per 16,000
copy
2 Research 1 FA at 10,000shs per day for 1 month. 300,000
assistance
3 Travel Visits tothe health Centre 100,000
4 Communication Airtime 50,000
5 Miscellaneous 100,000
TOTAL 586,000UGX
ii

APPENDIX II
TIME FRAMEWORK
Phase/Activity Time(Weeks) Dates
Development, Writing and Presentation of Proposal 4 April-i 5th to May~2Oth~20 17
Development and pretesting of instruments 1 ~2nt~9th -May-20 17
Data collection 4 June-i to June-30~-20 17
Data organization analysis and interpretation 4 July lstto July-31 st.20 17
Report writing and submission of final copy 3 August 1st to August~3 1st -2017
34