
A between-patient disinfection method to control water line contamination and biofilm inside dental...
8
A between-patient disinfection method to control water line contamination and biofilm inside dental units L. Montebugnoli a, *, S. Chersoni a , C. Prati a , G. Dolci b a Department of Oral Science, University of Bologna, Via S. Vitale 59, 40125 Bologna, Italy b University of Rome “La Sapienza”, Rome, Italy Received 28 July 2003; accepted 16 December 2003 KEYWORDS Biofilm(s); Dental unit; Cross-contamination; Disinfection; Heterotrophs; Infection control Summary The aim of the present study was to evaluate the efficacy of a between-patient disinfection procedures to maintain low bacterial counts in dental unit water line (DUWL) effluents, and control dental water line biofilms. Six dental units already in use, that had never been cleaned, were monitored for three weeks. During the first week only baseline contamination levels were assessed with no treatment of the system. In the second week lines were flushed with water for 30 s before treating each patient. During the third week, a disinfection procedure with 0.26% peracetic acid, followed by a water flush, was implemented before treating each patient. DUWL samples were collected both at the beginning and at the end of 216 dental procedures (72 during each period), plated on R2A agar and incubated at room temperature for seven days to obtain total bacterial counts in colony forming units per millilitre. To assess biofilm control, nine dental units (five never used and four old dental units with established biofilm) were used for 30 days in routine dental practice undergoing five between-patient DUWL disinfecting cycles every day. Water line samples were removed at baseline and at the end of the study and examined by scanning electron microscopy to determine the presence or absence of biofilms. A significant difference ðP , 0:01Þ in mean DUWL bacterial counts was found between the three sets of observations. Biofilms were not present in any of the new dental units and a demonstrable reduction in the biofilms from the four dental units with previous presence of established biofilms was observed at the end of the study. In this study, a between-patient disinfection procedure consisting of flushing DUWL with peracetic acid with use of water was efficacious in the control of both microbial contamination of dental treatment water and dental water line biofilms. Q 2004 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved. 0195-6701/$ - see front matter Q 2004 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jhin.2004.01.015 Journal of Hospital Infection (2004) 56, 297–304 www.elsevierhealth.com/journals/jhin *Corresponding author. Tel.: þ 39-51-278006; fax: þ39-51- 225208. E-mail address: [email protected]
Transcript of A between-patient disinfection method to control water line contamination and biofilm inside dental...

A between-patient disinfection method to controlwater line contamination and biofilm inside dentalunits
L. Montebugnolia,*, S. Chersonia, C. Pratia, G. Dolcib
aDepartment of Oral Science, University of Bologna, Via S. Vitale 59, 40125 Bologna, ItalybUniversity of Rome “La Sapienza”, Rome, Italy
Received 28 July 2003; accepted 16 December 2003
KEYWORDSBiofilm(s); Dental unit;
Cross-contamination;
Disinfection;
Heterotrophs; Infection
control
Summary The aim of the present study was to evaluate the efficacy of abetween-patient disinfection procedures to maintain low bacterial counts indental unit water line (DUWL) effluents, and control dental water linebiofilms. Six dental units already in use, that had never been cleaned, weremonitored for three weeks. During the first week only baseline contaminationlevels were assessed with no treatment of the system. In the second weeklines were flushed with water for 30 s before treating each patient. During thethird week, a disinfection procedure with 0.26% peracetic acid, followed by awater flush, was implemented before treating each patient. DUWL sampleswere collected both at the beginning and at the end of 216 dental procedures(72 during each period), plated on R2A agar and incubated at roomtemperature for seven days to obtain total bacterial counts in colony formingunits per millilitre. To assess biofilm control, nine dental units (five neverused and four old dental units with established biofilm) were used for 30 daysin routine dental practice undergoing five between-patient DUWL disinfectingcycles every day. Water line samples were removed at baseline and at the endof the study and examined by scanning electron microscopy to determine thepresence or absence of biofilms. A significant difference ðP , 0:01Þ in meanDUWL bacterial counts was found between the three sets of observations.Biofilms were not present in any of the new dental units and a demonstrablereduction in the biofilms from the four dental units with previous presence ofestablished biofilms was observed at the end of the study. In this study, abetween-patient disinfection procedure consisting of flushing DUWL withperacetic acid with use of water was efficacious in the control of bothmicrobial contamination of dental treatment water and dental water linebiofilms.Q 2004 The Hospital Infection Society. Published by Elsevier Ltd. All rightsreserved.
0195-6701/$ - see front matter Q 2004 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.jhin.2004.01.015
Journal of Hospital Infection (2004) 56, 297–304
www.elsevierhealth.com/journals/jhin
*Corresponding author. Tel.: þ39-51-278006; fax: þ39-51-225208.
E-mail address: [email protected]

Introduction
It has been known for more than 30 years thattreatment water, delivered by dental units duringroutine practice of dentistry, is highly contami-nated by numerous species of pathogenic and non-pathogenic micro-organisms. The organisms enterdental units from the mains water source, or couldbe retracted into the dental unit water lines(DUWLs) from the oral cavity of patients duringroutine dental care,1–3 These heterotrophic bac-teria persist in DUWLs as a multispecies biofilm onthe lumenal surface, contaminating the dental unitwater system. In 1996 the American Dental Associ-ation established a goal for treatment water tocontain no more than 200 cfu/mL of heterotrophicunfiltered output.4 Several methods have beensuggested through which the DUWL contaminationby heterotrophic mesophilic organisms may be keptunder this limit including flushing protocols andchemical treatment.5,6
Of the chemicals now available, peracetic acidhas a rapid and broad-spectrum biocidal activitythat could be useful in controlling DUWL contami-nation between patient treatments,7,8 but, asdelivered, it has a series of side effects limiting itsuse in dentistry.9 –11 However, a new chemicalformulation (tetraacetylethylenediamine (TAED)in association with persalt) has been recentlyproposed as a non-hazardous means of generatingperacetic acid in situ. This form of peracetic aciddoes not have the same side effects as pre-formedperacetic. acid.12,13
The aim of this study was to evaluate the efficacyof peracetic acid in controlling heterotrophicbacterial contamination when used betweenpatient treatments and compare the results withthose achieved through pure mechanical flushingwith mains water, or in the absence of anytreatment. An additional aim was to evaluate itslong-term efficacy in controlling DUWL biofilms.
Method and materials
To study the control of dental treatment watercontamination, six dental units (Castellini Logos,Castellini S.p.A., Bologna, Italy) that had been inuse for over one year were selected. These unitswere directly connected to mains water as a sourcefor irrigation. None of these units had been treatedto remove biofilm or reduce planktonic bacterialcontamination. During the first week all unitsreceived no treatment (control), during the secondweek mechanical flushing with mains water for 30 s
before each dental procedure (flushing) wasimplemented. During the third week a disinfectingcycle (disinfection) was initiated with each dentalunit before dental treatment session. The disinfec-tion cycle consisted of an automated procedure bya device integral to each dental unit (Autosteril,designed by Castellini S.p.A., Bologna, Italy) pro-grammed to flush the disinfectant solution (con-tained in a built-in talk) through the water systemand purge with water. The Autosteril procedureconsisted of purging the residual dental treatmentwater loading the system with Ster4spray (manu-factured by Farmed S.p.A and distributed byCastellini S.p.A., Bologna, Italy) for 5 min ofcontact, purging the chemical and finally flushingwith water. Ster4spray is a fine powder containing abinary active system (TAED and sodium perborate),which is activated by dissolving in water at atemperature above 35 8C to from peracetyl ions atpH 8, equivalent to 0.26% in peracetic acid,ensuring a stable concentration for up to 24 h.The active ingredient is completely biodegradableand degrades to acetic acid, oxygen and water.13
Each dental unit was used for 12 dental pro-cedures (requiring the use of the high-speed hand-piece) every week for a total of 36 procedures. Thenumber of dental procedures per day and per weekwas standardized between and within dental units.The total number of dental procedures during thethree periods was 216 (72 each for control, flushand disinfection periods). An external evaluatorobserved and audited the time for each dentalprocedure and that of the handpiece use. Watersamples were collected from the high-speed hand-piece lines of each dental unit at the beginning andat the end of each dental procedure for a total of432 samples.
Each sample was processed to evaluate the totalnumber of heterotrophic micro-organisms. Twomillilitres of water from each unit were collectedin a sterile tube with filter-sterilized sodiumthiosulphate at a final concentration of 18 mg/Lto oppose the growth-inhibiting effects of residualchlorine. Samples were plated on R2A Agar (Difco,Becton Dickinson, Le Pont de Claix, France) within3 h of collection and incubated at room tempera-ture (22–24 8C) for seven days and the total numberof heterotrophic micro-organisms counted. Allabsolute counts were converted to log10 values tonormalize data. A one-way analysis of variance(ANOVA) was used to study differences betweenheterotrophic plate counts values, length of thedental session and duration of handpiece usage forthe three periods. After fitting a general linearmodel, multiple regression ANOVA for repeatedmeasures with split-plot design was used to
L. Montebugnoli et al.298
evaluate differences between dental units, pro-cedures (control, flush and disinfection periods)time (colony forming units per millilitre at thebeginning and at the end of dental treatmentsregardless of the decontaminating procedureadopted) and the interaction of decontaminatingprocedure multiplied by the time; the post hoc testapplied was Bonferroni t-test for multiple-compari-sons at a ¼ 0:05:
To evaluate biofilm removal, nine CastelliniLogos dental units (five new dental units and fourin use for 2, 3, 24 and 48 months) were used. Alldental units were supplied by mains water and wereused in routine dental practice for 30 days duringwhich they were subjected to repeated between-patient DUWL disinfection cycles with Ster4spray(approximately 5 cycles/day). The disinfectioncycle was identical to the protocol stated earlier.A 10 nm section of the water line tubing connectedto the high-speed handpiece was removed fromeach dental unit at baseline and at the end of thestudy period, fixed in 3% glutaraldehyde in a 0.2 Msodium cacodylate buffer, treated with increasingconcentration of ethyl alcohol (05–95 and finally100%), desiccated overnight using hexamethyldisi-lazane following the method of Perdigao et al.,14
mounted on a stud, coated with 10 nm gold andviewed using scanning electron microscopy (SEM;Jeol 5400, Jeol Japan, operating at 5 and 10 kV atmagnification ranging £ 500–5000. Biofilm wasquantified using the following criteria: (1) exten-sion (% surface covered by biofilm at £ 500), (2)matrix thickness (microns), and (3) number ofvisible bacteria per 500 mm2 at £ 5000).
Results
No significant differences between the three groupswere detected with reference to duration (inminutes) of dental treatment sessions (control33.7 ^ 12.4, flush 30.9 ^ 11.4, and disinfection32.0 ^ 13.8, F ¼ 0:84; P . 0:05). The duration ofuse of handpiece in minutes also showed nosignificant difference within each dental session(control 5.9 ^ 1.9, flush 6.2 ^ 2.0, and disinfection5.5 ^ 2.4, F ¼ 1:12; P . 0:05). Multiple regressionANOVA showed significant differences in the log10
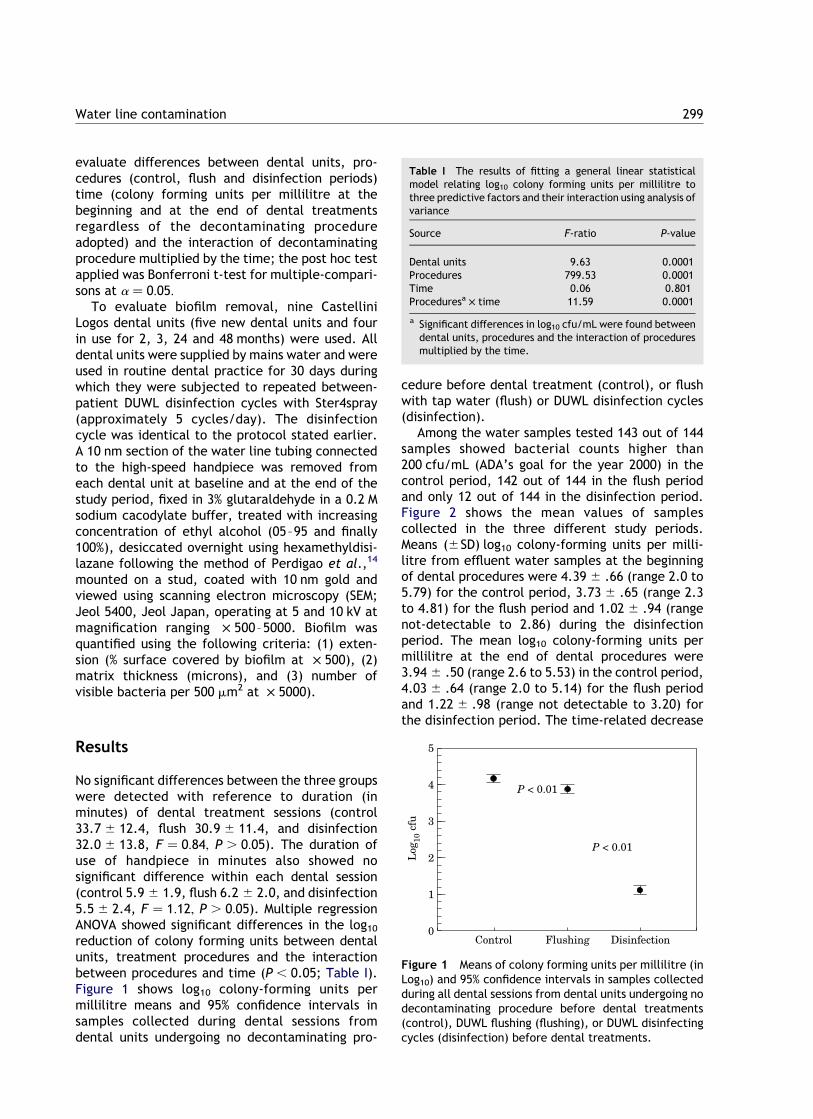
reduction of colony forming units between dentalunits, treatment procedures and the interactionbetween procedures and time (P , 0.05; Table I).Figure 1 shows log10 colony-forming units permillilitre means and 95% confidence intervals insamples collected during dental sessions fromdental units undergoing no decontaminating pro-
cedure before dental treatment (control), or flushwith tap water (flush) or DUWL disinfection cycles(disinfection).
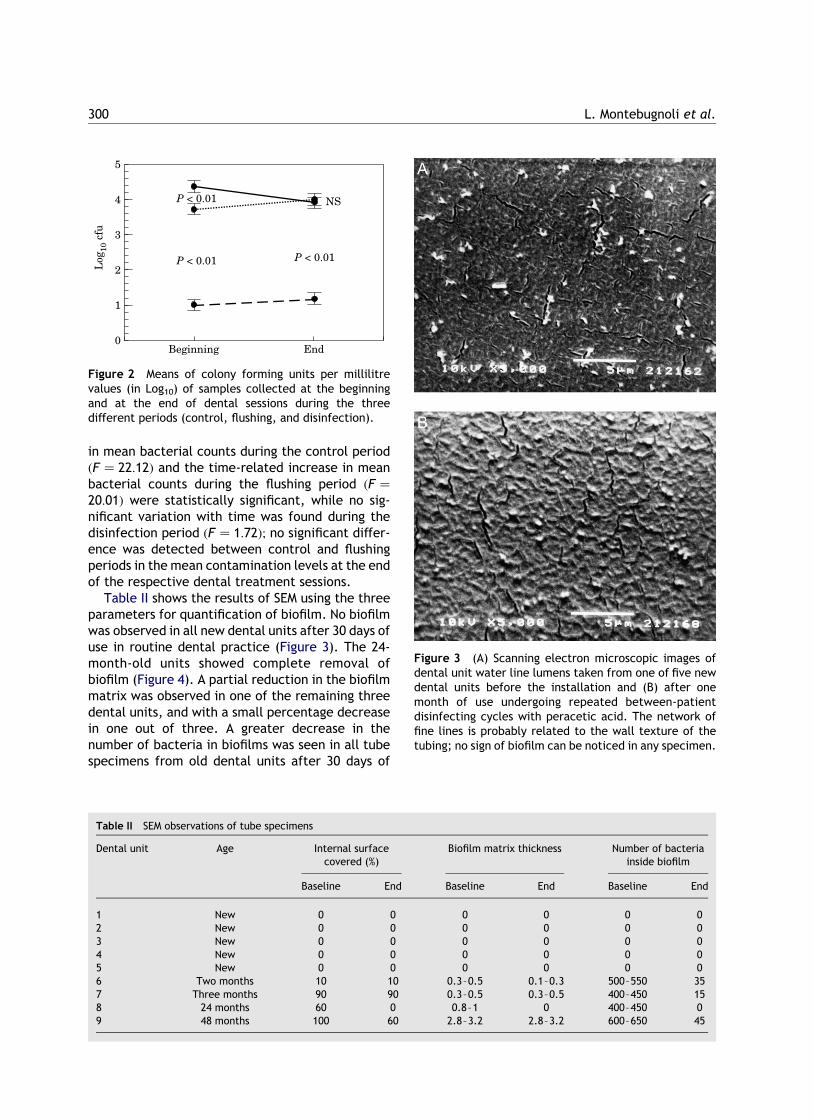
Among the water samples tested 143 out of 144samples showed bacterial counts higher than200 cfu/mL (ADA’s goal for the year 2000) in thecontrol period, 142 out of 144 in the flush periodand only 12 out of 144 in the disinfection period.Figure 2 shows the mean values of samplescollected in the three different study periods.Means (^SD) log10 colony-forming units per milli-litre from effluent water samples at the beginningof dental procedures were 4.39 ^ .66 (range 2.0 to5.79) for the control period, 3.73 ^ .65 (range 2.3to 4.81) for the flush period and 1.02 ^ .94 (rangenot-detectable to 2.86) during the disinfectionperiod. The mean log10 colony-forming units permillilitre at the end of dental procedures were3.94 ^ .50 (range 2.6 to 5.53) in the control period,4.03 ^ .64 (range 2.0 to 5.14) for the flush periodand 1.22 ^ .98 (range not detectable to 3.20) forthe disinfection period. The time-related decrease
Table I The results of fitting a general linear statisticalmodel relating log10 colony forming units per millilitre tothree predictive factors and their interaction using analysis ofvariance
Source F-ratio P-value
Dental units 9.63 0.0001Procedures 799.53 0.0001Time 0.06 0.801Proceduresa £ time 11.59 0.0001
a Significant differences in log10 cfu/mL were found betweendental units, procedures and the interaction of proceduresmultiplied by the time.
Figure 1 Means of colony forming units per millilitre (inLog10) and 95% confidence intervals in samples collectedduring all dental sessions from dental units undergoing nodecontaminating procedure before dental treatments(control), DUWL flushing (flushing), or DUWL disinfectingcycles (disinfection) before dental treatments.
Water line contamination 299
in mean bacterial counts during the control periodðF ¼ 22:12Þ and the time-related increase in meanbacterial counts during the flushing period ðF ¼
20:01Þ were statistically significant, while no sig-nificant variation with time was found during thedisinfection period ðF ¼ 1:72Þ; no significant differ-ence was detected between control and flushingperiods in the mean contamination levels at the endof the respective dental treatment sessions.
Table II shows the results of SEM using the threeparameters for quantification of biofilm. No biofilmwas observed in all new dental units after 30 days ofuse in routine dental practice (Figure 3). The 24-month-old units showed complete removal ofbiofilm (Figure 4). A partial reduction in the biofilmmatrix was observed in one of the remaining threedental units, and with a small percentage decreasein one out of three. A greater decrease in thenumber of bacteria in biofilms was seen in all tubespecimens from old dental units after 30 days of
Figure 2 Means of colony forming units per millilitrevalues (in Log10) of samples collected at the beginningand at the end of dental sessions during the threedifferent periods (control, flushing, and disinfection).
Table II SEM observations of tube specimens
Dental unit Age Internal surfacecovered (%)
Biofilm matrix thickness Number of bacteriainside biofilm
Baseline End Baseline End Baseline End
1 New 0 0 0 0 0 02 New 0 0 0 0 0 03 New 0 0 0 0 0 04 New 0 0 0 0 0 05 New 0 0 0 0 0 06 Two months 10 10 0.3–0.5 0.1–0.3 500–550 357 Three months 90 90 0.3–0.5 0.3–0.5 400–450 158 24 months 60 0 0.8–1 0 400–450 09 48 months 100 60 2.8–3.2 2.8–3.2 600–650 45
Figure 3 (A) Scanning electron microscopic images ofdental unit water line lumens taken from one of five newdental units before the installation and (B) after onemonth of use undergoing repeated between-patientdisinfecting cycles with peracetic acid. The network offine lines is probably related to the wall texture of thetubing; no sign of biofilm can be noticed in any specimen.
L. Montebugnoli et al.300
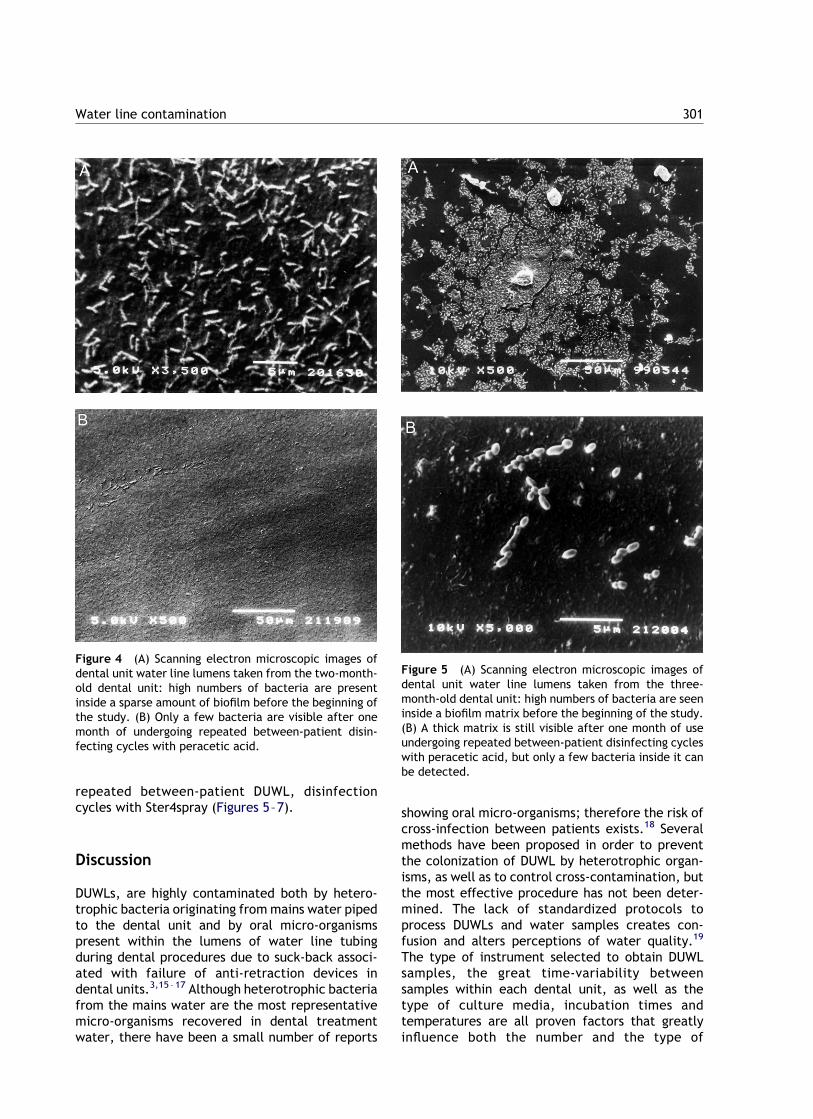
repeated between-patient DUWL, disinfectioncycles with Ster4spray (Figures 5–7).
Discussion
DUWLs, are highly contaminated both by hetero-trophic bacteria originating from mains water pipedto the dental unit and by oral micro-organismspresent within the lumens of water line tubingduring dental procedures due to suck-back associ-ated with failure of anti-retraction devices indental units.3,15 –17 Although heterotrophic bacteriafrom the mains water are the most representativemicro-organisms recovered in dental treatmentwater, there have been a small number of reports
showing oral micro-organisms; therefore the risk ofcross-infection between patients exists.18 Severalmethods have been proposed in order to preventthe colonization of DUWL by heterotrophic organ-isms, as well as to control cross-contamination, butthe most effective procedure has not been deter-mined. The lack of standardized protocols toprocess DUWLs and water samples creates con-fusion and alters perceptions of water quality.19
The type of instrument selected to obtain DUWLsamples, the great time-variability betweensamples within each dental unit, as well as thetype of culture media, incubation times andtemperatures are all proven factors that greatlyinfluence both the number and the type of
Figure 4 (A) Scanning electron microscopic images ofdental unit water line lumens taken from the two-month-old dental unit: high numbers of bacteria are presentinside a sparse amount of biofilm before the beginning ofthe study. (B) Only a few bacteria are visible after onemonth of undergoing repeated between-patient disin-fecting cycles with peracetic acid.
Figure 5 (A) Scanning electron microscopic images ofdental unit water line lumens taken from the three-month-old dental unit: high numbers of bacteria are seeninside a biofilm matrix before the beginning of the study.(B) A thick matrix is still visible after one month of useundergoing repeated between-patient disinfecting cycleswith peracetic acid, but only a few bacteria inside it canbe detected.
Water line contamination 301

organisms recovered from a DUWL sample. As suchthey affect the evaluation of the efficacy of adisinfecting procedure, and when comparing differ-ent decontaminating procedures.20,21
This study was designed using the ‘worst-casescenario’ approach to testing the efficacy of thedecontamination protocols. High-speed handpiecetubing has the smallest bores, which have highestpotential for contamination.19 We measured con-tamination in each dental unit multiple times overeach period to establish its mean contaminationvalue, and applied the three different decontami-nating procedures on the same dental units. Finallyan appropriate cultural medium/method wasselected.22 –24
This study has confirmed that DUWLs are highlycontamined if they have been in use over a period of
time without being subjected to methods of biofilmand treatment water contamination control. Therehave been no studies in the past demonstratingbetween-patient methods of chemical treatment tocontrol both heterotrophic mesophilic organisms inmains water, and also those organisms originatingfrom patients. Between-patient treatmentaddresses contamination from the mains watersource, as well as potential cross-contaminationbetween patients by oral microbes. The amount ofcontamination varied significantly from one dentalunit to another. Although the rate of contaminationappeared to decrease with every procedure per-formed within a day as a consequence of flushingwater, less than 1% of samples reached levels below200 cfu/mL.4 Flushing of DUWLs for 30 s beforeeach patient provided significantly lower mean
Figure 6 (A) Scanning electron microscopic images ofdental unit water line lumens taken from the 24-month-old dental unit: a well established biofilm with bacteriainside can be detected before the beginning of the study.(B) No sign of biofilm after one month of undergoingrepeated between-patient disinfecting cycles with per-acetic acid.
Figure 7 (A) Scanning electron microscopic images ofdental unit water line lumens taken from the 48-month-old dental unit: a strongly established biofilm is detect-able before the beginning of the study. (B) A thick matrixis still visible after one month of undergoing repeatedbetween-patient disinfecting cycles with peracetic acid,but only a few bacteria can be detected.
L. Montebugnoli et al.302

bacterial counts during the early phase in spite ofover 98% of samples reaching counts higher than200 cfu/mL. However, DUWL contaminationincreased with time, possibly due to detachmentof micro-organisms from the biofilm, reaching meanvalues equivalent to those obtained in absence ofany decontaminating procedure.
These results are similar to data from theliterature demonstrating that mechanical flushingalone is not efficacious in controlling microbialcontamination.25,26 Conversely interesting resultshave been recently obtained by disinfecting waterlines with peracetic acid left standing in DUWLs for5 min before each dental procedure.27 In thepresent study all dental units showed adequatecontrol of treatment water contamination both atthe beginning and at the end of tile procedures. Themean colony-forming units per millilitre valueswere well below the ADA standard, with onlyabout 9% being greater than 200 cfu/mL.
SEM analysis of specimens treated with Stersprayshowed no formation of biofilm in the new units,and a decrease in the number of bacteria in thebiofilm samples of the older units with previouslyestablished biofilms. These data are in agreementwith other studies, which adopted different treat-ment procedures.28 –30 The use of chemicals intro-duced into water systems either continuously orintermittently to control DUWL contamination andbiofilm inside dental units has been proposed.31,32
Continuous treatment has involved several chemi-cal agents including chlorine compounds,33 chlor-hexidine gluconate,34 hydrogen peroxide,35
povidone– iodine36 and commercial mouthrinses.37,38 Although continuous treatment withlow-grade disinfectants offers a lower potentialfor recolonization of water lines, it may damageequipment, affect the healthcare worker or inter-fere with any dental materials.39,40 Furthermore,all the above-mentioned agents possess low bioci-dal activity when used at lower concentrations anddo not deal with micro-organisms sucked backduring dental procedures.3 Although DUWL decon-tamination and inhibition of biofilm formation havebeen achieved by overnight or pre-working treat-ments with chemical solutions, these procedurescannot ensure the control of micro-organismssucked back during dental treatment.41 –43
TAED with a peroxygen source at near neutral pHis claimed to provide a non-hazardous means ofgenerating peracetic acid in situ. It is quite simpleto prepare, has low inventory costs and low cost ofworking solution (about $7/L; $1/cycle); further itis non-damaging to instruments and is completelywashed out from DUWL after 5 min contact.
Preliminary data from a previous study con-
firmed the relevant biocidal in vitro activity of thetest formulation, and data from the present studyunderline its efficacy in controlling heterotrophicDUML contamination during dental practice andbiofilm formation inside DUWLs.12,27 Unlike pre-formed peracetic acid, glutaraldehyde or chlorine,solutions of TAED activated peroxide release noirritating fumes or unpleasant odours. In addition,TAED is traditionally formulated with a persalt toform solid, concentrated products with a long shelflife. In an attempt to control cross-contaminationbetween patients, the test formulation could bevery useful in dental units that incorporate auto-mated devices to disinfect DUWLs with minimaleffort from the dental staff.
References
1. Molinari JA. Dental infection control at the year 2000. J AmDent Assoc 1999;130:1291—1298.
2. Smith AJ, Hood J, Bagg J. Water, water everywhere but not adrop to drink? Br Dent J 1999;186:12—14.
3. Walker JT, Bradshaw DJ, Bennett AM. Microbial biofilmformation and contamination of denial unit water systems ingeneral dental practice. Appl Environ Microbiol 2000;66:3363—3367.
4. Shearer BG. Biofilm and the dental office. J Am Dent Assoc1996;127:181—189.
5. US Department of Health and Human Services. Rec-ommended infection control practices for dentistry. MMWR1993;42:RR-8.
6. Meiller TF, Depaola LG, Kelley JI. Dental unit waterlines:biofilms, disinfection and recurrence. J Am Dent Assoc 1999;130:65—72.
7. Rutala WA, Weber DJ. Disinfection of endoscopes: review ofnew chemical sterilants used for high-level disinfection.Infect Control Hosp Epidemiol 1999;20:69—76.
8. Morin P. Identification of the bacteriological contaminationof a water treatment line used for haemodialysis and itsdisinfection. J Hosp Infect 2000;45:218—224.
9. Griffiths PA, Babb JR, Fraise AP. Mycobactericidal activity ofselected disinfectants using quantitative suspension test.J Hosp Infect 1999;41:111—121.
10. Middleton AM, Chadwick MV, Gaya H. Disinfection ofbronchoscopes, contaminated in vitro with Mycobacteriumtuberculosis, Mycobacterium avium-intracellulare andMycobacterium chelonae in sputum, using stabilized, buf-fered peracetic acid solution (Nu-Cidex). J Hosp Infect 1997;37:137—143.
11. Stanley P. Destruction of a glutaraldehyde-resistant myco-bacterium by a peroxygen disinfectant. Am J Infect Control1998;26:185.
12. Montebugnoli L, Vasconi L, Dolei G. Evaluation of a newchemical formulation for a rapid cold sterilization of dentalinstrument. J Dent Res 2000;79:3399.
13. Davis DM, Deary ME. Kinetics of the hydrolysis andperhydrolysis of tetraacetylethylenediamine, a peroxidebleach activator. J Chem Soc Perkin Trans 1991;2:15491—15552.
14. Perdigao J, Lambrechts P, Van Meerbeek B. Morphologicalfield emission—SEM study of the effect of six phosphoric acid
Water line contamination 303

etching agents on human dentin. Dent Mater 1996;12:262—271.
15. Montebugnoli L, Dolci G. Effectiveness of two devicesdesigned to prevent fluid retraction in a high-speed hand-piece. J Prosthet Dent 2000;84:225—228.
16. Putnins EE, Di Giovanni D, Bhullar AS. Dental unit water linecontamination and its possible implications during period-ontal surgery. J Periodontol 2001;372:393—400.
17. Berlutti F, Testarelli L, Vaia F, De Luca MD, Dolei G. Efficacyof anti-retraction devices in preventing bacterial contami-nation of dental unit water lines. J Dent 2003;31:105—110.
18. Mills S. The dental unit water controversy: defusing themyths, defining the solutions. J Am Dent Assoc 2000;131:1427—1450.
19. Noce L, DiGiovanni D, Putnins EF. An evaluation of samplingand laboratory procedures for determination of hetero-trophic plate counts in dental unit waterlines. J Can DentAssoc 2000;66:262—272.
20. Barbeau J, Tanguay R, Faucher E, Avezard C, Trudel L, CoteL. Multiparametric analysis of water line contamination ofdental units. Appl Environ Microbiol 1996;62:3954—3959.
21. Zanetti F, Stampi S, DeLuea G, et al. Water characteristicsassociated with the occurrence of Legionella pneumophilain dental units. Eur J Oral Sci 2000;108:22—28.
22. Williams HN, Kelley J, Folineo D. Assessing microbialcontamination in clean water dental units and compliancewith disinfection protocol. J Am Dent Assoc 1994;125:1205—1211.
23. Karpay RI, Plamondon TJ, Mills SE. Validation of an in-officedental unit monitoring technique. J Am Dent Assoc 1998;129:207—211.
24. Williams HN, Quinby H, Romberg E. Evaluation and use of alow nutrient medium and reduced incubation temperatureto study bacterial contamination in the water supply ofdental units. Can J Microbiol 1994;40:127—131.
25. Williams HN, Baer ML, Kelley JL. Contribution of biofilmbacteria to the contamination of the dental unit watersupply. J Am Dent Assoc 1995;126:1255—1260.
26. Santiago JI, Huntington MK, Johnston MA. Microbial con-tamination of dental unit water lines: short and long-termeffects of flushing. Gen Dent 1994;45:528—535.
27. Montebugnoli L, Dolci G. A new chemical formulation forcontrol of dental unit water line contamination: an ‘in vitro’and clinical study. BMC Oral Health 2002;2:1—4.
28. Kim PJ, Cederberg RA, Puttaiah R. A pilot study of 2 methodsfor control of dental unit biofilms. Quintessence Int 2000;31:41—48.
29. Wirthlin MR, Marshall GW. Evaluation of ultrasonic scalingunit water line contamination after use of chlorine dioxidemouthrinse lavage. J Periodontol 2001;72:401—410.
30. Meiller TF, Kelley JI, Baqui AA, et al. Laboratory evaluationof anti-biofilm agents for use in dental unit water lines. J ClinDent 2001;12:97—103.
31. Fayle SA, Pollard MA. Decontamination of dental unit watersystem: a review of current recommendations. Br Dent J1996;181:369—372.
32. Marais JT, Brozel VS. Electro-chemically activated water indental unit water lines. Br Dent J 1999;187:154—158.
33. Karpay RI, Plamondon TJ, Mills SE. Combining periodic andcontinuous sodium hypochlorite treatment to control bio-films in dental unit water systems. J Am Dent Assoc 1999;130:957—965.
34. Blake GC. The incidence and control of infection in dentalspray reservoirs. Br Dent J 1963;115:413—420.
35. Kellet M, Holbrook WP. Bacterial contamination of dentalhandpieces. J Dent 1980;8:249—253.
36. Mills SE, Lauderdale PW, Mayhew RB. Reduction of microbialcontamination in dental units with povidone—iodine 10%.J Am Dent Assoc 1986;113:280—284.
37. Meiller T, Baqui A, DePaola I, Overholser CD. Disinfection ofdental unit water lines using Listerine antiseptic. J Dent Res1995;74:153.
38. Eleazer PD, Schuster GS, Weathers DR. A chemical treat-ment, regimen to reduce bacterial contamination in dentalwaterlines. J Am Dent Assoc 1997;128:617—623.
39. Bull RJ, Birnbaum LS, Cantor KP. Water chlorination:essential process of cancer hazard? Fundam Appl Toxicol1995;28:155—166.
40. Roberts HW, Karpay RI, Mills SE. Dental unit water lineantimicrobial agents’ effect on dentin bond strength. J AmDent Assoc 2000;131:179—183.
41. Waslker JT, Bradshaw DJ, Fulford MR, Marsh PD. Micro-biological evaluation of a range of disinfectant product tocontrol mixed-species biofilm contamination in a laboratorymodel of a dental unit water system. Appl Environ Microbiol2003;69:3327—3332.
42. Smith AJ, McHugh S, Aitken I, Hood J. Evaluation of theefficacy of Alpron disinfectant for dental unit water lines. BrDent J 2003;194:64—65.
43. Tuttlebee CM, O’Donnelll MJ, Keane CT, et al. Effectivecontrol of dental chair unit waterline biofilm and markedreduction of bacterial contamination of output water usingtwo peroxide-based disinfectants. J Hosp Infect 2002;52:192—205.
L. Montebugnoli et al.304




















