99m Tc-Doxycycline hyclate: a new radiolabeled antibiotic for bacterial infection imaging
Upload
independentCategory
view
2download
0
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Abstract. The aim of this study was to evaluate the use-fulness of 99mTc-tetrofosmin single-photon emission to-mography (SPET) in the detection of both primary breastcancer and axillary lymph node metastasis. We studied192 consecutive patients in whom primary breast cancerwas suspected on the basis of mammography and/orphysical examination. After intravenous injection of740 MBq 99mTc-tetrofosmin, both planar and SPETscintimammography was performed in all patients usinga rectangular dual-head gamma camera equipped withlow-energy, high-resolution, parallel-hole collimators. In175 patients with breast cancer at histology, the per-lesion overall sensitivity of SPET and planar imaging forthe detection of breast cancer was 95.8% and 75.9%(P<0.0005), respectively. The sensitivity of SPET andplanar imaging was, respectively, 96.5% and 79.5% inpalpable (P<0.0005) and 90% and 45% in non-palpablelesions (P<0.01). With regard to lesion size, the sensitiv-ity of SPET and planar imaging was, respectively, 90.5%and 45.2% in lesions ≤10 mm (P<0.0005), 95.3% and81.4% in lesions of 11–20 mm (P<0.005), 100% and84.6% in lesions of 21–30 mm (P<0.05) and 100% and95.8% in lesions >30 mm (P>0.05). In the remaining 17 patients with benign mammary lesions at histology,per-lesion overall specificity of SPET and planar imag-ing was 76.2% and 85.7% (P>0.05), respectively. Nei-ther SPET nor planar imaging showed false-positive re-sults in non-palpable lesions or in those ≤10 mm. In 173 breast cancer patients submitted to axillary lymphnode dissection (ALND), per-axilla overall sensitivity ofSPET and planar imaging in the detection of axillarylymph node metastasis was 93% and 52.3% (P<0.0005),respectively. The sensitivity of SPET and planar imagingwas, respectively, 100% and 82.6% in palpable nodes(P>0.05), 90.5% and 41.3% in non-palpable nodes
(P<0.0005), 92.8% and 35.7% in the presence of ≤3nodes (P<0.0005) and 93.2% and 68.2% in the presenceof >3 nodes (P<0.005). The specificity of SPET and pla-nar imaging was 91% and 100% (P<0.05), respectively.99mTc-tetrofosmin SPET appears to be a reliable methodfor the detection of both primary BC and axillary lymphnode metastasis, and its diagnostic accuracy exceeds thatof 99mTc-tetrofosmin planar scintimammography. Theuse of SPET is particularly important in the identifica-tion of small non-palpable primary carcinomas andmetastatic axillae with ≤3 non-palpable lymph nodes.More extensive use of SPET appears warranted in themanagement of breast cancer patients.
Keywords: 99mTc-tetrofosmin – SPET – Breast cancer –Axillary lymph node metastasis
Eur J Nucl Med (2001) 28:1781–1794DOI 10.1007/s00259-001-0657-5
Introduction
Mammography combined with clinical examination rep-resents the method of choice both in the screening and inthe diagnosis of primary breast cancer, demonstratinghigh sensitivity even in the detection of small non-palpa-ble lesions. However, mammography can also yieldfalse-negative results in some cases [1]; in addition, it ischaracterised by low specificity and a low positive pre-dictive value [2]. Ultrasonography and magnetic reso-nance imaging can slightly increase the sensitivity ofmammography in some conditions, but both have a lowspecificity.
Scintimammography with the cationic lipophilic on-cotropic radiotracers 99mTc-methoxyisobutylisonitrile(MIBI) and 99mTc-tetrofosmin, and positron emission to-mography (PET) with 2-[18F]fluoro-2-deoxy-D-glucose(FDG), have proved useful methods for the detection of
Giuseppe Madeddu (✉ )Department of Nuclear Medicine, University of Sassari, Viale San Pietro, 8, 07100 Sassari, Italye-mail: [email protected].: +39-079-228342, Fax: +39-079-228208
Original article
99mTc-tetrofosmin SPET in the detection of both primary breast cancer and axillary lymph node metastasisAngela Spanu1, Giuseppe Dettori2, Susanna Nuvoli1, Alberto Porcu2, Antonio Falchi1, Pierina Cottu2, Maria E. Solinas1, Antonio M. Scanu2, Francesca Chessa1, Giuseppe Madeddu1
1 Department of Nuclear Medicine, University of Sassari, Viale San Pietro, 8, 07100 Sassari, Italy2 Department of Surgery, University of Sassari, Sassari, Italy
Received 9 June and in revised form 31 August 2001 / Published online: 1 November 2001© Springer-Verlag 2001

primary breast cancer and the differentiation of malig-nant from benign mammary lesions [3, 4, 5, 6, 7, 8, 9,10, 11, 12]. However, scintimammography is conven-tionally performed with the planar acquisition method,which has a low sensitivity in lesions <10 mm [13, 14,15, 16, 17]. The sensitivity of SPET has been reported tobe higher than that of planar imaging by some authors inthe small number of cases studied comparatively [18, 19,20, 21], but these findings have not been confirmed byothers [22, 23].
FDG-PET has proved a highly sensitive method forthe detection of primary breast cancer, but only smallcase studies have been reported and these have been lim-ited to palpable and large lesions [9, 10]. FDG-PET hasalso shown high sensitivity and specificity in axillarylymph node staging [24, 25, 26], but until now its usehas been limited. Scintimammography has likewise beendemonstrated to be useful for axillary lymph node detec-tion [5, 27]. The few studies to have compared SPET andplanar studies for this purpose have shown the former tobe more effective, particularly in non-palpable nodes andin the presence of a small number of metastases [21, 28].Recently, lymphatic mapping combined with radioguid-ed biopsy of the sentinel node in breast cancer hasproved useful to determine the axillary lymph node sta-tus [29, 30, 31]. However, to date axillary lymph nodedissection (ALND) remains the method of choice for thedetection of lymph node metastases.
The limited use of SPET in scintimammography andthe sparse and sometimes conflicting comparative dataon planar and SPET acquisition prompted us to performfurther evaluations. We thus investigated, in a largegroup of breast cancer patients, whether the use of SPETcould provide additional pre-operative information ascompared with conventional planar imaging, thereby im-proving the accuracy of scintimammography in both thediagnosis of primary breast cancer and axillary lymphnode staging. In our series we used 99mTc-tetrofosmin asa cationic lipophilic tumour-seeking radiotracer. We pre-ferred tetrofosmin to MIBI because of its more favour-able pharmacokinetics: its faster and greater clearancefrom the lungs and liver allow a higher target to back-ground ratio [32].
Materials and methods
Patients. One hundred and ninety-two consecutive patients (190females and 2 males), aged 32–83 years (mean 57.7±10.9 years),in whom primary breast cancer was suspected on the basis ofmammography and/or clinical examination were enrolled in thisstudy. All patients had previously undergone clinical examinationand mammography, and in some cases also ultrasonography. Twoof the patients had already undergone contralateral mastectomyand ALND for infiltrating ductal carcinomas 9 and 12 years previ-ously.
The mammographic findings were classified as follows: highlysuggestive of malignancy in the presence of features of breast can-
cer (i.e. dominant or spiculated opacity with or without microcal-cification, irregular border of the opacity in fatty breast), suspi-cious in the presence of indirect diagnostic signs for breast cancer(i.e. microcalcification without mass, focal architectural distor-tions, asymmetrical breasts), indeterminate in the presence of highbreast density and negative in the absence of any abnormalities.
In total, in the 192 patients, 210 lesions were suspected to becancerous: 173 lesions (159 palpable and 14 non-palpable) werehighly suggestive of malignancy on mammography and 27 (20palpable and 7 non-palpable) had suspicious abnormalities, whilemammography was negative in seven palpable lesions and indeter-minate for dense breast in the remaining three palpable lesions. Ahypoechoic nodule was ascertained on ultrasonography in each le-sion that was negative on mammography and positive at clinicalexamination.
Twenty-nine patients had presented axillary lymph node en-largement at clinical examination on the same side as the breast le-sion: two of these had been submitted to lymph node biopsy 15days before our first observation, and metastases from breast can-cer had been ascertained at histology.
All patients underwent planar and SPET scintimammographywith 99mTc-tetrofosmin (Myoview, Amersham International),which we have used routinely since 1995. Written informed pa-tient consent was always obtained before scintigraphy.
99mTc-tetrofosmin scintimammography protocol. Radiolabellingand quality control procedures with respect to the tracer were car-ried out according to the manufacturer’s instructions. Labelling ef-ficiency always exceeded 95%. In all patients, 740 MBq of 99mTc-tetrofosmin was injected in the arm contralateral to the mammarylesion; when bilateral disease was suspected, the radiotracer wasinjected in a pedal vein. Ten minutes later, planar imaging wasperformed, followed by SPET, using a rectangular, large field ofview, dual-head gamma camera (Elscint, Helix) equipped withlow-energy, high-resolution, parallel-hole collimators. A 10%window and a 140-keV photopeak were selected. Planar imageswere acquired in both anterior and lateral views, with a 256×256matrix size, an acquisition time of 600 s per view and a zoom fac-tor ranging from 1 to 1.3 according to the individual patient.
First the anterior planar view was acquired in the supine posi-tion with the arms raised above the head and with the chest, bothbreasts and the axillae included in the field of view. Not having aspecial cushion or table for the prone lateral view, we obtainedplanar lateral images with the patient in lateral recumbency, withthe arms flexed at the elbows and raised above the head and withthe knees also flexed to maintain balance. The detector was posi-tioned below and as close as possible to the table, including the in-volved breast and the corresponding axilla in the field of view.This projection permitted the necessary separation of the mamma-ry gland, including its deep structures, from the elevated activityderiving from the heart and the liver. In addition, like other au-thors [5], we used a lead shield between the breasts to minimisethe counts from the contralateral breast. The shield was positionedso that it completely covered the contralateral breast, which waspulled away laterally, and fixed to the chest in a stable position us-ing adhesive tape.
SPET images were acquired over 360° (180° per head) in thesupine position with the same zoom factor as used for the anteriorplanar view, and with a 64×64 matrix size, a 3° angular step andan acquisition time of 30 s/frame. The body contouring systemwas always used in order to ensure the minimum distance betweenthe patient and the collimator. Before reconstruction, SPET imag-es were normalised to correct for misalignments and radiation
1782
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001

time decay. Reconstruction was performed with the back-projec-tion filter method (with a count-optimised Metz filter) without at-tenuation correction, including both breasts and axillae in the re-construction region of interest, to obtain transaxial, coronal andsagittal slices. A separate reconstruction of each axilla, using thesame filter but a zoom factor of 2, was also performed.
Data analysis. Planar and SPET images of both breasts and axillaewere independently evaluated by two experienced nuclear medi-cine physicians (A.S. and G.M.) who were blinded to the clinicalfindings, to data from all the other diagnostic imaging proceduresand to the final histopathological diagnoses. However, the site ofinjection was known to the observers (and thus, indirectly the af-fected breast) in order to avoid false-positive interpretations in theaxillary region on the same side as the site of injection possiblycaused by radiotracer extravasation.
Scintigraphy was considered positive for breast or axillarylymph node involvement when one or more focal area of increaseduptake was identified in the breast or in the axilla as comparedwith the surrounding normal tissues.
Particular care was taken in the evaluation of the axillary later-al planar view; only the deeply located focal areas of increased up-take were considered positive, i.e. non-specific uptake in, for ex-ample, skin folds and thyroid and muscular structures, was exclud-ed. Similar care was taken to distinguish the axillary cavity fromsurrounding muscular structures in SPET images.
Interobserver variability was extremely low; disagreement wasobserved in only four cases in the qualitative analysis of SPET im-ages (in one case at the level of the breast and in three cases at thelevel of the axilla) and was resolved by consensus. The scinti-graphic results obtained by SPET were compared with those ob-tained by planar imaging, and both were compared with the otherdiagnostic imaging data and subsequently related to the histopath-ological findings obtained from surgical samples.
Histopathological diagnosis. Histopathological diagnosis was ob-tained in all 192 patients. Tumour size analysis was performed ac-cording to the largest dimension. Breast surgical specimens werefixed in 10% buffered formalin and stained with haematoxylin andeosin. Surgical cancer specimens were evaluated for tumour histo-logical type and grading. Further immunohistochemical analysiswas performed on malignant breast specimens, including oestro-gen and progesterone receptor status and proliferation index(MIB-1).
The lymph nodes excised at ALND in breast cancer patientswere submitted to histopathological analysis by haematoxylin andeosin. They were fixed in 10% buffered formalin and then embed-ded in paraffin. Lymph nodes <5 mm were buffered and embeddedintact, those between 5 and 10 mm were halved and those >10 mmwere cut into slices of about 5 mm. Four-µm-thick sections werestained with haematoxylin and eosin for microscopic evaluation.The lymph nodes were also stained immunohistochemically withCAM 5.2 when the haematoxylin and eosin method gave doubtfulresults.
Statistical analysis. 99mTc-tetrofosmin planar and SPET imageswere classified as true positive, true negative, false positive orfalse negative, considering histology as the “gold standard”. Sen-sitivity, specificity and accuracy for the detection of both primarybreast cancer and axillary lymph node metastasis were calculatedon this basis.
McNemar’s test was used to assess the statistical significanceof the differences between the sensitivity and specificity of SPET
and planar scintimammography for the detection of primary breastcancer and axillary lymph node metastasis. The statistical signifi-cance of the differences between the sensitivity of the two proce-dures was calculated taking into account overall primary breastcarcinomas and overall metastatic axillae. The differences werealso calculated after subdividing the carcinomas according to pal-pability (palpable vs non-palpable) and size (≤10 mm, 11–20 mm,21–30 mm, >30 mm) and subdividing the axillary lymph node me-tastases according to palpability (palpable vs non-palpable) andnumber of involved nodes (≤3 and >3).
The χ2 test or Fisher exact test, when appropriate, was used toassess the statistical significance of differences in the sensitivity ofeach procedure after subdividing the carcinomas according to pal-pability (palpable vs non-palpable) and size (≤10 mm, >10 mm)and subdividing the axillary lymph node metastases according topalpability (palpable vs non-palpable) and number of involvednodes (≤3 and >3).
The results were considered significant when P was <0.05.
Results
Histopathological Findings
All 192 patients underwent surgery within 1 week ofscintigraphy. Benign mammary lesions were ascertainedin 17 cases at histology, while cancer was diagnosed in175 cases. Of the patients with benign mammary lesions,15 had unilateral unifocal disease while two had bilateraldisease; one of the latter patients had one lesion in eachbreast, while the other had two lesions in each breast.
One hundred and sixty-seven of the 175 breast cancerpatients had unilateral disease (unifocal in 160 cases andbifocal in seven cases), while eight had bilateral disease.Of the 167 patients with unilateral disease, 119 under-went mastectomy and 48 quadrantectomy; moreover,ALND was performed in all 167 cases with the excep-tion of one patient considered too elderly.
The remaining eight breast cancer patients with bilat-eral disease had one lesion in each breast, except for onewho had two lesions in one breast and one in the contra-
1783
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Table 1. Histological results in respect of 191 malignant and 21benign breast tumours
Histology No.
Malignant tumours 191Infiltrating ductal 167Ductal carcinoma in situ (DCIS) 4Infiltrating lobular 14Infiltrating mucinous 4Medullary 1Invasive papillary 1
Benign tumours 21Fibroadenoma 8Sclerosing adenosis 8Fibrocystic disease 4Chronic mastitis 1

1784
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Tab
le2.
SP
ET
and
pla
nar
brea
st im
agin
g re
sult
s, m
amm
ogra
phic
fin
ding
sa, l
esio
n pa
lpab
ilit
y, le
sion
siz
e an
d hi
stop
atho
logy
in th
e 17
5 pa
tien
ts w
ith
191
prim
ary
brea
st c
arci
nom
as
Fin
ding
sN
o. o
f le
sion
s (n
=19
1)P
alpa
ble
(n=
171)
Non
-pal
pabl
e (n
=20
)P
atho
logi
cal l
esio
n si
ze
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
≤10
mm
(n=
42)
11–2
0m
m (
n=86
)21
–30
mm
(n=
39)
>30
mm
(n=
24)
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
Tru
e po
siti
ve18
314
518
616
513
616
818
918
3819
3782
7086
3933
3924
2324
Sen
siti
vity
95.8
%*
75.9
%97
.4%
96.5
%*
79.5
%98
.2%
90%
+45
%90
%90
.5%
*45
.2%
88.1
%95
.3%
**
81.4
%10
0%10
0%+
+84
.6%
100%
100%
95.8
%10
0%In
filt
rati
ng d
ucta
l16
213
316
314
712
514
815
815
3216
3176
6778
3532
3519
1819
Duc
tal c
arci
nom
a in
sit
u3
23
11
12
12
32
3In
filt
rati
ng lo
bula
r13
814
138
142
12
53
63
13
33
3In
filt
rati
ng m
ucin
ous
32
42
23
11
11
12
22
Med
ulla
ry1
11
11
1In
vasi
ve p
apil
lary
11
11
11
Fal
se n
egat
ive
846
36
351
211
24
233
416
61
Infi
ltra
ting
duc
tal
534
24
261
18
13
192
211
31
Duc
tal c
arci
nom
a in
sit
u1
21
12
11
21
Infi
ltra
ting
lobu
lar
16
16
11
32
Infi
ltra
ting
muc
inou
s1
21
11
11
1M
edul
lary
11
1In
vasi
ve p
apil
lary
11
1
Mx,
Mam
mog
raph
y*P
<0.
0005
com
pare
d w
ith
the
corr
espo
ndin
g pl
anar
val
ues
in r
espe
ct o
f al
l ca
rcin
omas
,pa
lpab
le
carc
inom
as
and
carc
inom
as
mea
suri
ng ≤1
0m
m
(McN
emar
’s
test
re
sult
s);
**P
<0.
005
com
pare
d w
ith
the
corr
espo
ndin
g pl
anar
val
ues
in r
espe
ct o
f ca
rcin
omas
mea
suri
ng 1
1–20
mm
(M
cNem
ar’s
tes
t re
sult
s);
+P
<0.
01 c
ompa
red
wit
h th
e co
rres
pond
-in
g pl
anar
va
lues
in
re
spec
t of
no
n-pa
lpab
le
carc
inom
as
(McN
emar
’s
test
re
sult
s);
++P
<0.
05 c
ompa
red
wit
h th
e co
rres
pond
ing
plan
ar v
alue
s in
res
pect
of
carc
inom
as m
ea-
suri
ng 2
1–30
mm
(M
cNem
ar’s
test
res
ults
)a T
wo
inde
term
inat
e m
amm
ogra
phic
fin
ding
s ar
e no
t in
clud
ed i
n th
e ta
ble;
the
y co
rre-
spon
ded
to 2
pal
pabl
e 10
mm
inf
iltr
atin
g du
ctal
car
cino
mas
pos
itiv
e on
SP
ET
and
neg
a-ti
ve o
n pl
anar
imag
ing

Tab
le3.
SP
ET
and
pla
nar
brea
st im
agin
g re
sult
s, m
amm
ogra
phic
fin
ding
sa, l
esio
n pa
lpab
ilit
y, le
sion
siz
e an
d hi
stop
atho
logy
in th
e 17
pat
ient
s w
ith
21 b
enig
n m
amm
ary
lesi
ons
Fin
ding
sN
o. o
f le
sion
s (n
=21
)P
alpa
ble
(n=
18)
Non
-pal
pabl
e (n
=3)
Pat
holo
gica
l les
ion
size
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
≤10
mm
(n=
8)11
–20
mm
(n=
11)
21–3
0m
m (
n=0)
>30
mm
(n=
2)
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
SP
ET
Pla
nar
Mx
Tru
e ne
gati
ve16
186
1315
63
38
84
810
2F
ibro
aden
oma
66
23
32
33
44
12
21
Scl
eros
ing
aden
osis
68
26
82
33
23
5F
ibro
cyst
ic d
isea
se4
42
44
21
11
33
1
Fal
se p
osit
ive
53
145
311
33
31
92
22
Fib
road
enom
a2
26
22
33
31
12
11
1S
cler
osin
g ad
enos
is2
52
52
5F
ibro
cyst
ic d
isea
se2
22
Chr
onic
mas
titi
s1
11
11
11
11
Mx,
Mam
mog
raph
yaO
ne i
ndet
erm
inat
e m
amm
ogra
phic
fin
ding
is
not
incl
uded
in
the
tabl
e; i
t co
rres
pond
ed t
o a
palp
able
scl
eros
ing
aden
osis
of
<10
mm
tha
t w
as n
egat
ive
on b
oth
SP
ET
and
pla
nar
imag
ing
1785
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
lateral breast. Four of these eight patients underwent bothmastectomy (bilateral in three cases and unilateral in one)and ALND (bilateral in two cases and unilateral in two),while two were submitted to both quadrantectomy andALND, bilaterally in one case. The patient with three car-cinomas underwent both mastectomy and ALND on theside with two carcinomas and only quadrantectomy in thebreast with one carcinoma. The eighth patient was con-sidered inoperable and underwent chemotherapy.
Eighteen carcinomas were located in the internal low-er quadrants, 12 in the left and six in the right; such sitesare generally difficult to investigate by scintigraphy.
In total, 212 mammary lesions were ascertained, twomore than had been suspected pre-operatively. One hun-dred and ninety-one were primary carcinomas and 21 were benign lesions. Table 1 reports the histologicalresults. According to the TNM classification, the patho-logical stages of the carcinomas were: Tis in 4 cases, T1ain 4 cases, T1b in 34 cases, T1c in 86 cases and T2 in theremaining 63 cases. Forty-two carcinomas were≤10 mm, 86 from 11 to 20 mm, 39 from 21 to 30 mmand 24 >30 mm. Eight benign mammary lesions were≤10 mm and 13 were >10 mm (11 were from 11 to20 mm and 2 were >30 mm).
A total of 173 patients were also submitted to ALND:176 axillae were examined histologically and metastaseswere ascertained in 86. According to the TNM classifi-cation, the pathological stages of the axillae were: N0 in90 cases, N1a in 1 case, N1b in 72 cases and N2 in the re-maining 13 cases. Nineteen metastatic axillae each hadone metastatic node, 23 had two or three, while the re-maining 44 had more than three.
99mTc-tetrofosmin breast imaging
The results of both SPET and planar breast imaging inthe 175 patients with 191 primary breast carcinomas arereported in Table 2, which also includes results relatingto mammography, lesion palpability, size and histologi-cal type. The statistical differences in sensitivity (overallsensitivity, sensitivity according to tumour palpabilityand sensitivity according to tumour size) between SPETand planar imaging in breast cancer detection are also re-ported in Table 2. The difference in sensitivity betweenSPET and planar imaging was significant, except for le-sions >30 mm. However, the difference in sensitivity be-tween SPET and planar imaging was statistically signifi-cant when all 149 lesions >10 mm were considered(97.3% vs 84.6%; P<0.0005). There was no statisticallysignificant difference in the sensitivity of SPET for thedetection of palpable (96.5%) versus non-palpable (90%)carcinomas, or for the detection of the 149 lesions>10 mm (97.3%) versus the 42 lesions ≤10 mm (90.5%).By contrast, the sensitivity of planar imaging differedsignificantly in these groups (79.5% vs 45% and 84.6%vs 45.2%; P<0.005 and P<0.0005, respectively).

1786
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Fig. 1A–E. Patient with a proven non-palpable 8 mm infiltratingductal carcinoma in the lower external quadrant of the left breast.99mTc-tetrofosmin planar scintimammography is negative in bothanterior (A) and lateral (B) views; SPET shows a focal area of in-creased uptake corresponding to the carcinoma (single arrow) inboth coronal (C) and sagittal (D) views. Mammography in the me-diolateral oblique projection demonstrates a nodular spiculatedopacity with microcalcifications (E)
Figure 1 shows a true-positive SPET finding in a pa-tient with non-palpable (8 mm) breast carcinoma thatwas negative on planar imaging.
One hundred and sixty-five of the 183 SPET-positivecarcinomas were highly suggestive of malignancy onmammography, while 14 carcinomas showed suspiciousabnormalities. In two cases of palpable 10 mm infiltrat-ing ductal carcinomas, mammography was negative inone case and indeterminate for dense breast in the other;in the latter case a hypoechoic nodule was ascertained at
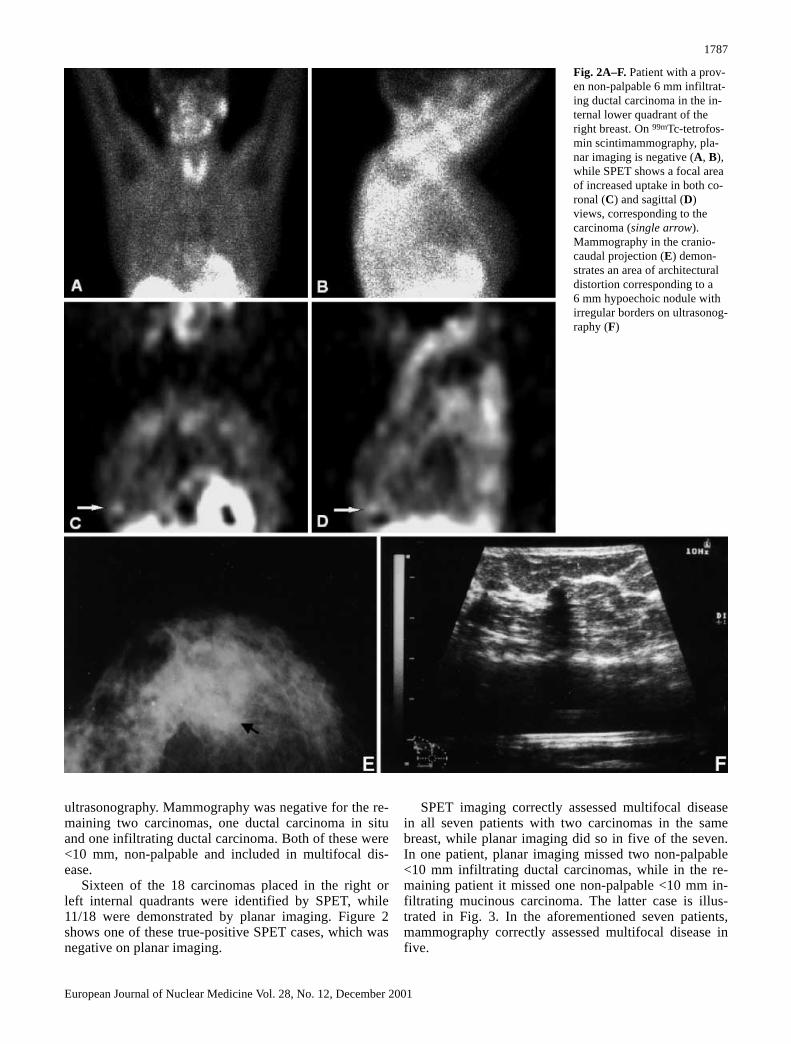
ultrasonography. Mammography was negative for the re-maining two carcinomas, one ductal carcinoma in situand one infiltrating ductal carcinoma. Both of these were<10 mm, non-palpable and included in multifocal dis-ease.
Sixteen of the 18 carcinomas placed in the right orleft internal quadrants were identified by SPET, while11/18 were demonstrated by planar imaging. Figure 2shows one of these true-positive SPET cases, which wasnegative on planar imaging.
SPET imaging correctly assessed multifocal diseasein all seven patients with two carcinomas in the samebreast, while planar imaging did so in five of the seven.In one patient, planar imaging missed two non-palpable<10 mm infiltrating ductal carcinomas, while in the re-maining patient it missed one non-palpable <10 mm in-filtrating mucinous carcinoma. The latter case is illus-trated in Fig. 3. In the aforementioned seven patients,mammography correctly assessed multifocal disease infive.
1787
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Fig. 2A–F. Patient with a prov-en non-palpable 6 mm infiltrat-ing ductal carcinoma in the in-ternal lower quadrant of theright breast. On 99mTc-tetrofos-min scintimammography, pla-nar imaging is negative (A, B),while SPET shows a focal areaof increased uptake in both co-ronal (C) and sagittal (D)views, corresponding to thecarcinoma (single arrow).Mammography in the cranio-caudal projection (E) demon-strates an area of architecturaldistortion corresponding to a6 mm hypoechoic nodule withirregular borders on ultrasonog-raphy (F)

In the eight patients with bilateral multifocal disease,SPET imaging correctly assessed all lesions with the ex-ception of one palpable 20 mm infiltrating ductal carci-noma located in the right external upper quadrant whichwas highly suggestive of malignancy on mammography.Planar imaging also gave a false-negative result for thislesion and in addition missed one lesion in each of twoother patients. Mammography correctly assessed multi-focal disease in all eight cases.
In total, SPET missed 8/191 carcinomas, includingone of the above-mentioned cases with bilateral multifo-cal disease. Of the remaining seven carcinomas, two(one infiltrating mucinous and one infiltrating lobular)were located in the internal lower quadrants. Mammog-raphy was highly suggestive of malignancy in four ofthese seven carcinomas, showed suspicious abnormali-ties in two and was indeterminate for dense breast in theremaining case.
All eight carcinomas that were false negative onSPET were also false negative on planar imaging, whichmissed a further 38 malignancies (including the caseswith unilateral and bilateral multifocal disease) locatedin different mammary quadrants.
Table 3 reports the results relating to the remaining 17 patients with 21 benign mammary lesions.
The overall specificity of SPET and planar imagingwas 76.2% and 85.7%, respectively; this difference wasnot statistically significant.
The specificity of SPET was 72.2% in palpable le-sions and 61.5% in those >10 mm; comparative figures
1788
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Fig. 3A–D. Patient with proven multifocal disease with two infil-trating mucinous carcinomas in the left breast. On 99mTc-tetrofos-min scintimammography, both planar (A, B) and SPET (C) imag-ing identified the palpable 35 mm carcinoma in the left externalquadrant (single arrow). Only SPET demonstrated the other non-palpable 8 mm carcinoma, adjacent to the other lesion but sited ina more internal position, as shown in the coronal (C) view (doublearrows). Mammography in the craniocaudal projection (D) dem-onstrates a large nodular opacity with shaded and poorly definedborders and a smaller opacity in a more internal position
for planar imaging were 83.3% and 76.9%, respectively.Both SPET and planar imaging were true negative in100% of non-palpable and lesions ≤10 mm.
Six of the 16 benign lesions that were negative onSPET were also negative on mammography, while ultra-sonography identified a hypoechoic nodule correspond-ing to each lesion. In the other ten lesions, mammogra-phy was indeterminate for dense breast in one lesion,highly suggestive of malignancy in two and suspicious inthe remaining seven.
Mammography was highly suggestive of malignancyin one of the five lesions that were false positive onSPET (a 20 mm palpable fibroadenoma), and showedsuspicious abnormalities in the remaining four. Planarimaging was false positive in three of these five cases.
The accuracy of SPET and planar imaging in the de-tection of breast cancer in the 192 patients was 93.9%and 76.9%, respectively.
99mTc-Tetrofosmin axillary imaging
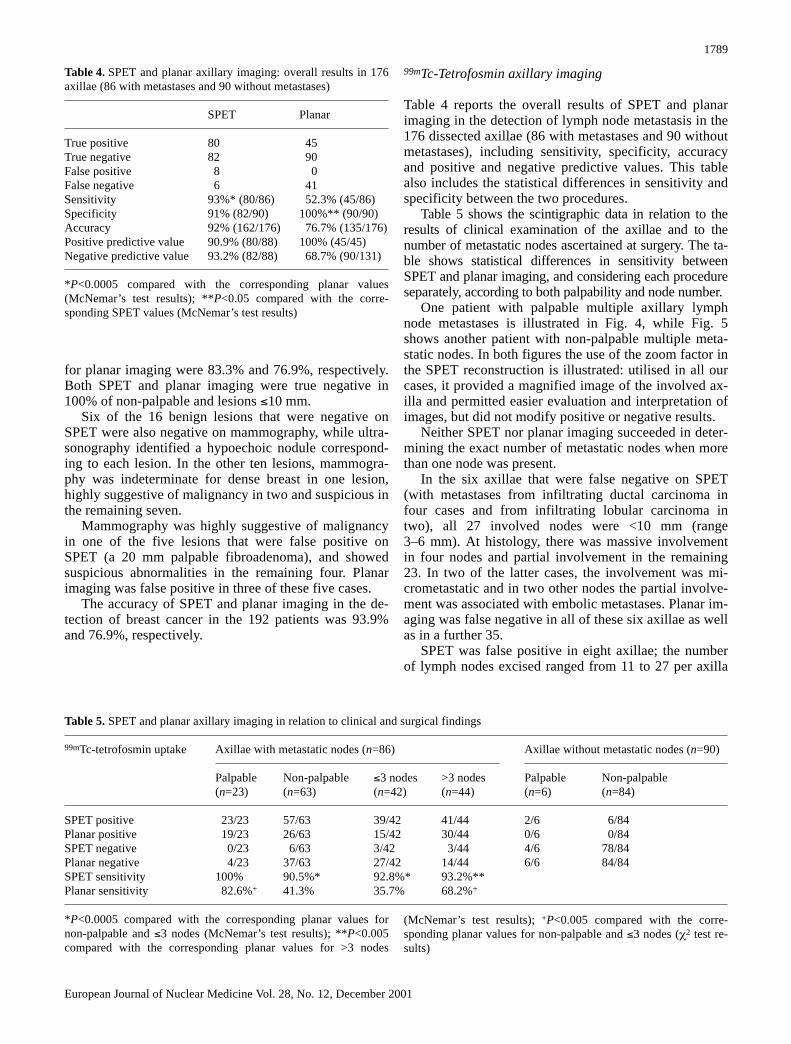
Table 4 reports the overall results of SPET and planarimaging in the detection of lymph node metastasis in the176 dissected axillae (86 with metastases and 90 withoutmetastases), including sensitivity, specificity, accuracyand positive and negative predictive values. This tablealso includes the statistical differences in sensitivity andspecificity between the two procedures.
Table 5 shows the scintigraphic data in relation to theresults of clinical examination of the axillae and to thenumber of metastatic nodes ascertained at surgery. The ta-ble shows statistical differences in sensitivity betweenSPET and planar imaging, and considering each procedureseparately, according to both palpability and node number.
One patient with palpable multiple axillary lymphnode metastases is illustrated in Fig. 4, while Fig. 5shows another patient with non-palpable multiple meta-static nodes. In both figures the use of the zoom factor inthe SPET reconstruction is illustrated: utilised in all ourcases, it provided a magnified image of the involved ax-illa and permitted easier evaluation and interpretation ofimages, but did not modify positive or negative results.
Neither SPET nor planar imaging succeeded in deter-mining the exact number of metastatic nodes when morethan one node was present.
In the six axillae that were false negative on SPET(with metastases from infiltrating ductal carcinoma infour cases and from infiltrating lobular carcinoma intwo), all 27 involved nodes were <10 mm (range3–6 mm). At histology, there was massive involvementin four nodes and partial involvement in the remaining23. In two of the latter cases, the involvement was mi-crometastatic and in two other nodes the partial involve-ment was associated with embolic metastases. Planar im-aging was false negative in all of these six axillae as wellas in a further 35.
SPET was false positive in eight axillae; the numberof lymph nodes excised ranged from 11 to 27 per axilla
1789
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Table 4. SPET and planar axillary imaging: overall results in 176axillae (86 with metastases and 90 without metastases)
SPET Planar
True positive 80 45True negative 82 90False positive 8 0False negative 6 41Sensitivity 93%* (80/86) 52.3% (45/86)Specificity 91% (82/90) 100%** (90/90)Accuracy 92% (162/176) 76.7% (135/176)Positive predictive value 90.9% (80/88) 100% (45/45)Negative predictive value 93.2% (82/88) 68.7% (90/131)
*P<0.0005 compared with the corresponding planar values(McNemar’s test results); **P<0.05 compared with the corre-sponding SPET values (McNemar’s test results)
Table 5. SPET and planar axillary imaging in relation to clinical and surgical findings
99mTc-tetrofosmin uptake Axillae with metastatic nodes (n=86) Axillae without metastatic nodes (n=90)
Palpable Non-palpable ≤3 nodes >3 nodes Palpable Non-palpable(n=23) (n=63) (n=42) (n=44) (n=6) (n=84)
SPET positive 23/23 57/63 39/42 41/44 2/6 6/84Planar positive 19/23 26/63 15/42 30/44 0/6 0/84SPET negative 0/23 6/63 3/42 3/44 4/6 78/84Planar negative 4/23 37/63 27/42 14/44 6/6 84/84SPET sensitivity 100% 90.5%* 92.8%* 93.2%**Planar sensitivity 82.6%+ 41.3% 35.7% 68.2%+
*P<0.0005 compared with the corresponding planar values fornon-palpable and ≤3 nodes (McNemar’s test results); **P<0.005compared with the corresponding planar values for >3 nodes
(McNemar’s test results); +P<0.005 compared with the corre-sponding planar values for non-palpable and ≤3 nodes (χ2 test re-sults)

1790
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Fig. 4A–E. Patient with a proven non-palpable 8 mm infiltrating ductal carcinoma in the rightexternal upper quadrant and with ipsilateral multiple palpable axillary lymph node metastases(four metastatic nodes were ascertained at histology). On 99mTc-tetrofosmin scintimammography,both planar (A, B) and SPET (C) imaging show an irregular focal area of increased uptake in theright axillary cavity (single arrow) corresponding to the metastatic nodes. Neither acquisitionmethod determined the exact number of nodes. Magnified imaging of the involved axilla, by re-construction of the SPET image with a zoom factor of 2 (D), does not modify the data. Moreover,the primary carcinoma is visible in the planar lateral (B) view (double arrows). Mammography inthe mediolateral oblique projection (E) demonstrates a nodular spiculated opacity in the rightbreast and multiple opacities in the ipsilateral axillary cavity

1791
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Fig. 5A–E. Patient with a proven palpable infiltratingductal carcinoma in the left areolar region and withipsilateral multiple non-palpable axillary lymph nodemetastases. On 99mTc-tetrofosmin scintimammogra-phy, only SPET shows a focal area of increased traceruptake (double arrows) in the involved axilla. Coro-nal SPET views both with a normal reconstruction(C) and with a zoom factor of 2 (D) are shown. SPETdid not determine the exact number of nodes (fournodes were ascertained at histology). As can be seen,the primary lesion is visible in planar views (A, B),being indicated by a single arrow. Mammography inthe craniocaudal projection (E) demonstrates a nodu-lar opacity with shaded borders

and histopathological findings showed a non-specific in-flammatory reaction for each node. Planar imaging wastrue negative in these eight axillae, as it was in all othercases without metastases.
Discussion
The data of the present study, which was performed in alarge series of pre-operative breast cancer patients, con-firm the usefulness of 99mTc-tetrofosmin scintimammog-raphy both in the diagnosis of primary cancer and in ax-illary lymph node staging. Moreover, the comparativeevaluation of SPET and planar acquisitions emphasisedthe greater effectiveness of SPET. We found a particular-ly marked difference in sensitivity in non-palpable pri-mary carcinomas and those ≤10 mm, the two categoriesthat are most difficult to detect and to discriminate frombenign lesions using conventional diagnostic procedures.Planar imaging missed more than 50% of these lesions,whereas SPET missed less than 10%. Moreover, planarimaging was never positive in carcinomas that were neg-ative on SPET. These results suggest that the use ofSPET must be preferred in small non-palpable carcino-mas. However, there does seem to be a role for planarimaging in the detection of palpable carcinomas>10 mm, even though, in the present study, its sensitivityin the latter was slightly lower than that of SPET.
SPET, rather than planar imaging, should be used toassess multifocal disease prior to surgery, since in ourstudy it ascertained all cases except one, including all le-sions ≤10 mm. By comparison, planar imaging identified66.7% and mammography, 86.7%. SPET also identifiedfour small lesions which were missed by mammography(including two in cases of multifocal disease), while pla-nar imaging identified only one. This result would seemto demonstrate that in certain conditions SPET couldalso be a complementary tool to mammography in breastcancer detection.
On the other hand, SPET failed to identify eight pri-mary lesions, of which seven were highly suggestive orsuspected of malignancy on mammography, while onlyone was indeterminate. Only four of these eight lesionswere ≤10 mm, suggesting that, besides size, other factorssuch as histological type, tumour cellularity and viabili-ty, and the site may limit the sensitivity of scintimam-mography. For example, two palpable lesions of >10 mmthat were negative on SPET were non-ductal carcinomas,one being an infiltrating lobular carcinoma and the other,an infiltrating mucinous carcinoma. The latter type of le-sion is generally characterised by low cellularity and aslow growth rate. In addition, both of these lesions werelocated in the left internal lower quadrant. This locationcan be difficult to study by means of scintigraphy withcationic lipophilic tracers; however, in our cases SPETidentified all lesions in the lower quadrants except forthese two, while planar imaging detected 61% of such le-
sions. It should also be noted that the expression of P-glycoprotein or other multidrug resistance factors wasnot measured in the eight carcinomas that were falsenegative on scintimammography, and their over-expres-sion therefore could not be excluded.
The overall specificity values of SPET and planar im-aging obtained in this study were similar to those report-ed by others [33]. Both SPET and planar imagingshowed higher specificity (76.2% and 85.7%, respective-ly) than mammography (30%, but excluding the indeter-minate cases). Our data demonstrate that SPET, as wellas planar imaging, can improve the low specificity ofmammography. The low specificity of mammographythat we observed is concordant with observations by oth-er authors [4, 14].
The difference in overall specificity between planarand SPET imaging was not statistically significant. How-ever, this result could have been affected by the lowprevalence of benign lesions in our patients, all of whomwere selected for surgery on the basis of suspicion ofbreast cancer. Our data obviously need to be confirmedby studying a larger number of lesions.
The false-positive lesions observed by SPET and pla-nar imaging, all of which were palpable and >10 mm insize (including two >30 mm), were also false positive onmammography. Tracer accumulation in these cases wasdue to hyperproliferative and inflammatory benign le-sions, both of which have been reported to cause highuptake in other studies performed with 99mTc-tetrofosminor 99mTc-MIBI [3, 4, 6, 7, 8]. Reconstruction artefactscould be excluded in the five false-positive lesions, threeof which were also false positive on planar imaging.
Both SPET and planar imaging achieved 100% speci-ficity in non-palpable lesions and in lesions ≤10 mm.Planar imaging showed higher specificity than SPET inlarger lesions (76.9% vs 61.5%). However, in our casesSPET showed a higher overall accuracy than planar im-aging (93.9% vs 76.9%). SPET also showed high sensi-tivity and specificity in the study of axillary lymph nodestatus: it determined the correct staging in 92% of pa-tients, while planar imaging did so in only 76.7%. More-over, SPET identified all metastatic axillae with palpablenodes and more than 90% with non-palpable nodes. Inthe 7% of metastatic axillae that it missed, all nodeswere ≤6 mm, and they typically showed partial tumourinvolvement. SPET thus demonstrated a significantlyhigher sensitivity than planar imaging, which missed47.7% of metastatic axillae, most of which had ≤3 nodes.
The significantly higher sensitivity of SPET was asso-ciated with a significantly lower specificity in comparisonwith planar imaging. However, the lower number of false-negative results and the higher accuracy of SPET whencompared with planar imaging indicate SPET to be thepreferred procedure in axillary lymph node staging. Thus,SPET could play a more important role than planar imag-ing in the management of breast cancer patients. In partic-ular, our data seem to suggest that 99mTc-tetrofosmin
1792
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001

SPET could be proposed as one of the most useful non-in-vasive procedures for the selection of patients who shouldundergo ALND, since it correctly evaluated axillarylymph node status in a very high percentage of cases inour study. However, the fact that 8% of our patients werenot correctly staged by SPET precludes the use of SPETas the only reference procedure for ALND. Our data needto be confirmed in a far greater number of cases beforeSPET can be assigned a definitive role in axillary lymphnode staging. A comparative evaluation of SPET and oth-er procedures, such as the minimally invasive radioguidedsentinel node biopsy method, could also be useful.
In the present study, neither SPET nor planar imagingwas able to determine the exact number of multiplemetastatic nodes per axilla; such data could have givenmore useful prognostic information. We partiallyachieved this goal in a previous study, also employing99mTc-tetrofosmin, by using an acquisition method, pin-hole SPET, with higher resolution than conventionalSPET and planar imaging [34]. In that study only thepinhole SPET procedure correctly detected the numberof multiple lymph nodes when it was ≤3. It was conse-quently able to correctly differentiate 88.67% of patientswith ≤3 nodes from those with >3 nodes. This is of prog-nostic significance in that it is accepted by many authorsthat patients with ≤3 axillary metastatic nodes survivelonger than those with >3 [35, 36].
Finally, in the present study, SPET permitted a usefulcomparative evaluation of cross-sectional images be-tween the two mammary regions as well as between theaxillary cavities. Moreover, in our experience, SPET issimple to perform, saves time and is well tolerated; wealso obtained very high quality images by using a dual-head gamma camera and our own acquisition/processingprotocol. 99mTc-tetrofosmin proved a suitable tumour-seeking agent for breast cancer since it accumulated inapproximately 96% of primary lesions and in 93% ofmetastatic axillae.
In conclusion, SPET acquisition improves the diag-nostic accuracy of 99mTc-tetrofosmin planar scintimam-mography. We found that SPET has a particularly impor-tant role in the detection of non-palpable primary breastcarcinomas measuring ≤10 mm and metastatic axillaewith involvement of ≤3 non-palpable lymph nodes. Wesuggest that SPET should be more extensively used inthe management of breast cancer patients.
Acknowledgement. This study was supported in part by a grantfrom the Public Health Service of the Sardinia Region, Italy.
References
1. Bird RE, Wallace TW, Yankaskas BC. Analysis of cancersmissed at screening mammography. Radiology 1992; 184:613–617.
2. Kopans DB. The positive predictive value of mammography.AJR 1992; 158:521–526.
3. Khalkhali I, Cutrone J, Mena I, Diggles L, Venegas R, VargasH, Jackson B, Klein S. Technetium-99m-sestamibi scintimam-mography of breast lesions: clinical and pathological follow-up. J Nucl Med 1995; 36:1784–1789.
4. Palmedo H, Grünwald F, Bender H, Schomburg A, MallmannP, Krebs D, Biersack HJ. Scintimammography with techne-tium-99m methoxyisobutile: comparison with mammographyand magnetic resonance imaging. Eur J Nucl Med 1996;23:940–946.
5. Mansi L, Rambaldi PF, Procaccini E, Di Gregorio F, Laprovitera A, Pecori B, Del Vecchio W. Scintimammographywith technetium-99m tetrofosmin in the diagnosis of breastcancer and lymph node metastases. Eur J Nucl Med 1996; 23:932–939.
6. Lind P, Umschaden HW, Forsthuber E, Oman J, KerschbaumerK, Gallowitsch HJ, Mikosch P, Kresnik E, Molnar M, GomezI. Scintimammography using Tc-99m tetrofosmin. Acta MedAustriaca 1997; 24:50–54.
7. Adalet I, Demirkol MO, Müslümanoðlu M, Bozfakioðlu Y,Cantez S. 99Tcm-tetrofosmin scintigraphy in the evaluation ofpalpable breast masses. Nucl Med Commun 1997; 18:118–121.
8. Fenlon HM, Phelan N, Tierney S, Gorey T, Ennis JT. Tc-99mtetrofosmin scintigraphy as an adjunct to plain-film mammog-raphy in palpable breast lesions. Clin Radiol 1998; 53:17–24.
9. Wahl RL, Cody R, Hutchins GD, Mudgett E. Primary andmetastatic breast carcinoma: initial clinical evaluation withPET with the radiolabeled glucose analog 2-[18F]-fluoro-deoxy-2-D-glucose (FDG). Radiology 1991; 179:765–770.
10. Adler LP, Crowe JP, Al-Kaisi NK, Sunshine JL. Evaluation ofbreast masses and axillary lymph nodes with (18F) 2-deoxy-2-fluoro-D-glucose PET. Radiology 1993; 187:743–750.
11. Dehdashti F, Mortimer JE, Siegel BA, Griffeth LK, BonaseraTJ, Fusselman MJ, Detert DD, Cutler PD, KatzenellenbogenJA, Welch MJ. Positron tomographic assessment of estrogenreceptors in breast cancer: comparison with FDG-PET and invitro receptor assays. J Nucl Med 1995; 36:1776–1784.
12. Avril N, Dose J, Janicke DF, Bense S, Ziegler S, LaubenbacherC, Romer W, Pache H, Herz M, Allgayer B, Nathrath W,Graeff H, Schwaiger M. Metabolic characterization of breasttumors with positron emission tomography using 18F fluorode-oxyglucose. J Clin Oncol 1996; 14:1848–1857.
13. Scopinaro F, Schillaci O, Ussof W, Nordling K, Capoferro R,De Vincentis G, Danieli R, Ierardi M, Picardi V, Tavolaro R,Colella AC. A three center study on the diagnostic accuracy of99mTc-MIBI scintimammography. Anticancer Res 1997;17:1631–1634.
14. Palmedo H, Biersack HJ, Lastoria S, Maublant J, Prats E,Stegner HE, Bourgeois P, Hustinx R, Hilson AJW, Bischof-Delaloye A. Scintimammography with technetium-99m-me-thoxyisobutylisonitrile: results of a prospective Europeanmulticentre trial. Eur J Nucl Med 1998; 25:375–385.
15. Mekhmandarov S, Sandbank J, Cohen M, Lelcuk S, Lubin E.Technetium-99m-MIBI scintimammography in palpable andnonpalpable breast lesions. J Nucl Med 1998; 39:86–91.
16. Howarth D, Sillar R, Clark D, Lan L. Technetium-99m ses-tamibi scintimammography: the influence of histopathologicalcharacteristics, lesion size and the presence of carcinoma insitu in the detection of breast carcinoma. Eur J Nucl Med1999; 26:1475–1481.
17. Tofani A, Sciuto R, Semprebene A, Festa A, Pasqualoni R, Giunta S, Mottolese M, Benevolo M, Botti C, Maini CL.99Tcm-MIBI scintimammography in 300 consecutive patients:
1793
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001

factor that may affect accuracy. Nucl Med Commun 1999;20:1113–1121.
18. Becherer A, Helbich T, Staudenherz A, Jakesz R, Kubista E,Lehner R, Rudas M, Teleky B, Kletter K, Leitha T. The diag-nostic value of planar and SPECT scintimammography in dif-ferent age groups. Nucl Med Commun 1997; 18:710–718.
19. Helbich TH, Becherer A, Trattnig S, Leitha T, Kelkar P, Sei-fert M, Gnant M, Staudenherz A, Rudas M, Wolf G, MostbeckGH. Differentiation of benign and malignant breast lesions:MR imaging versus Tc-99m sestaMIBI scintimammography.Radiology 1997; 202:421–429.
20. Schillaci O, Scopinaro F, Danieli R, Tavolaro R, Picardi V,Cannas P, Colella AC. 99Tcm-sestamibi scintimammography inpatients with suspicious breast lesions: comparison of SPECTand planar images in the detection of primary tumours and ax-illary lymph node involvement. Nucl Med Commun 1997;18:839–845.
21. Spanu A, Dettori G, Meloni G, Chiaramida P, Bagella C, Porcu A, Solinas ME, Cottu P, Falchi A, Solinas P, MadedduG. Tc-99m tetrofosmin (T) scan in the diagnosis and staging ofprimary breast cancer: role of SPECT [abstract]. Eur J NuclMed 1998; 25 Suppl:1041P.
22. Palmedo H, Schomburg A, Grünwald F, Mallmann P, Krebs D,Biersack HJ. Technetium-99-MIBI scintimammography forsuspicious breast lesions. J Nucl Med 1996; 37:626–630.
23. Nagaraj N, Waxman A, Ashok G, Khan S, Memsic L, YadegarJ, Phillips E. Comparison of SPECT and planar Tc-99m ses-tamibi (MIBI) imaging in patients with carcinoma of thebreast [abstract]. J Nucl Med 1994; 35 Suppl:229P.
24. Utech CI, Young CS, Winter PF. Prospective evaluation of flu-orine-18 fluorodeoxyglucose positron emission tomography inbreast cancer for staging of the axilla related to surgery andimmunocytochemistry. Eur J Nucl Med 1996; 23:1588–1593.
25. Crippa F, Agresti R, Seregni E, Greco M, Pascali C, Bogni A,Chiesa C, De Sanctis V, Delledonne V, Salvatori B, LeutnerM, Bombardieri E. Prospective evaluation of fluorine-18-FDGPET in presurgical staging of the axilla in breast cancer. JNucl Med 1998; 39:4–8.
26. Smith IC, Ogston KN, Whitford P, Smith FW, Sharp P, NortonM, Miller ID, Ah-See AK, Heys SD, Jibril JA, Eremin O.Staging of the axilla in breast cancer: accurate in vivo assess-ment using positron emission tomography with 2-(fluorine-18)-fluoro-2-deoxy-D-glucose. Ann Surg 1998; 228:220–227.
27. Taillefer R, Robidoux A, Turpin S, Lambert R, Cantin J, Lèveillè J. Metastatic axillary lymph node technetium-99m-MIBI imaging in primary breast cancer. J Nucl Med 1998;39:459–464.
28. Schillaci O, Scopinaro F, Danieli R, Tavolaro R, Cannas P, Picardi V, Centi Colella A. Technetium-99m sestamibi imag-ing in the detection of axillary lymph node involvement in pa-tients with breast cancer. Anticancer Res 1997; 17:1607–1610.
29. Veronesi U, Paganelli G, Galimberti V, Viale G, Zurridda S,Bedoni M, Costa A, de Cicco C, Geraghty JG, Luini A, Sacchini V, Veronesi P. Sentinel node biopsy to avoid axillarydissection in breast cancer with clinically negative lymphnodes. Lancet 1997; 349:1864–1887.
30. Borgstein PJ, Pijpers R, Comans, van Diest PJ, Boom RP,Meijer S. Sentinel lymph node biopsy in breast cancer: guide-lines and pitfalls of lymphoscintigraphy and gamma probe de-tection. J Am Coll Surg 1998; 186:275–283.
31. Keshtgar MRS, Ell PJ. Sentinel lymph node detection and im-aging. Eur J Nucl Med 1999; 26:57–67.
32. Higley B, Smith FW, Gemmel HG, Das Gupta P, GvozdanovicDV, Graham D, Hinge D, Davidson J, Lahiri A. Technetium-99m-1,2-bis[bis(2-ethoxyethyl) phosphino] ethane: humanbiodistribution, dosimetry and safety of a new myocardial per-fusion imaging agent. J Nucl Med 1993; 34:30–38.
33. Obwegeser R, Berghammer P, Rodrigues M, Granegger S, Hohlagschwandtener H, Kucera H, Singer C, Berger A, Kubista E, Sinzinger H. A head-to-head comparison betweentechnetium-99m-tetrofosmin and technetium-99m-MIBI scin-tigraphy to evaluate suspicious breast lesions. Eur J Nucl Med1999; 26:1553–1559.
34. Spanu A, Dettori G, Chiaramida P, Cottu P, Falchi A, Porcu A,Solinas ME, Nuvoli S, Madeddu G. The role of 99mTc-tetrofos-min pinhole-SPECT in breast cancer axillary lymph node stag-ing. Cancer Biother Radiopharm 2000; 15:81–91.
35. Fisher B, Slack N, Katrych D. Ten-year follow up results ofpatients with carcinoma of the breast in a cooperative clinicaltrial evaluating surgical adjuvant chemotherapy. Surg GynecolObstet 1975; 140:528.
36. Carter C, Allen C, Henson D. Relation of tumor size, lymphnode status, and survival in 24,740 breast cancer cases. Can-cer 1989; 63:181.
1794
European Journal of Nuclear Medicine Vol. 28, No. 12, December 2001
Copyright © 2022 FDOKUMEN