
Myocardial viability index in chronic coronary artery disease: technetium-99m-methoxy isobutyl...
9
show significant redistribution (1 ). Recent studies, how ever, demonstrated that delayed @Tc-MIBIredistribution may be observed in a model of transient myocardial isch emia (3) or under conditions of sustained low coronary flow (4). Furthermore, it has also been reported that myocardial uptake and retention of 99mTc@MIBI are dependent on both cell viability and regional blood flow and that tissue viability is required for @Tc-MIBIredistribution (5—9). Clinical studies evaluated the phenomenon of @Tc MIBI redistribution after stress injection in patients with CAD (10,11). The occurrenceof 99mTcMIBIredistribution after rest injection and its clinical implications have not yet been widely evaluated. Preliminary results reported by Dil sizian et al. recently suggested that @Tc-MIBIredistribu tion imaging following tracer injection at rest can detect viable myocardium using standard imaging protocols (12). Furthermore,these authors suggestthat detectionof viable myocardium may be enhanced with @Tc-MIBIcardiac imaging if an additional redistribution image is acquired after tracer injection at rest (12 ). It is still uncertain, how ever, whether 99mTcMIBI redistribution after rest injection is predictive of improved ventricular function after coro nary revascularization. The purpose of this study was to evaluate whether an additional redistribution image after rest @mTc@MIBI injec tion enhances detection of viable myocardium and predicts functional recovery after coronary revascularization in pa tients with chronic coronary artery disease (CAD). MATERIALSAND METhODS Patients We prospectivelystudied31 patients(29men, 2 women;mean age 55 ±10yr) with angiographically documented CAD and with left ventricular dysfunction (Tables 1 and 2). Seven patients had significant stenosis of all three major coronary vessels, 11 had significant stenosis of two major coronary vessels and 13 had significant stenosis of only one major coronary vessel. The mean left ventricular ejection fraction (LVEF) by resting equilibrium radionuclide angiography was 39% ±9%. All patients had a previous myocardial infarction that was documented clinically and by electrocardiography. No patient, however, had an acute myo cardial infarction within 6 mo of the study. The majority of patients The purpose of this study was to evaluatewhether an additional redistribution image after a rest @‘@Tc-MlBl injection enhances detection of viable myocardium and predicts functional recovery aftercoronaryrevascularizationin patientswith chroniccoronary artery disease (CAD). Methods: Thirty-one patients (29 men, mean age 55 ±10 yr) with proven CAD and left ventricular (LV) dysfunction (ejection fraction 39% ±9%) underwent resting @â€oeTc-MlBI tomography with initial (1 hr) and delayed (5 hr) images. Within 1 wk of MIBI imaging, all patients underwent rest-redistribution 201fl imaging. Eight patients also underwent two-dimensional echocardiography before and 5 ±3 mo after coronary revascularization.Results: On the initial @ images, 302 myocardial segments were normal, 183 showed moderate and 197 severe reduction of tracer uptake. Of these 197 segments,47 (24%) demonstrated increasedtracer uptake (1O% versusinitia@on delayedimages(from43% ±8% to 60% ±8%, p<O.OO1) and were considered as showing @9@c- MIBI redistribution. These 47 segments were observed in 20 (65%) patients in whom 201fl images detected viable myocar dium in the same segments. In the eight patients studied before and after revasculanzation,83% of segmentswith @â€oeTc-MlBI redistribution and abnormal LV function showed functional re covetyafterrevascularization, while96%of segmentswithout @â€oeTc-MlBI redistribution did not show functional recovery. Conclusion: Resting @°‘Tc-MlBI redistribution frequently oc curs in patients with chronic CAD. Acquisition of @‘@Tc-MlBl redistribution images enhancesdetection of viable myocardium and predicts functional recovery after revascularization. Key Words: technetium-99m-sestamibi; left ventriculardys function; functional recovery;thallium-201 J NucI Med 1995;36:1953-1960 echnetium-99m-methoxy isobutyl isonitrile (MIBI) is a cardiac perfusion agent that initially distributes in the myo cardium proportional to coronary blood flow, similar to 2O1@ (1,2). It has been suggested that 99mTc@MIBI does not ReCeiVedJan. 1, 1995; revision accepted Jul. 14, 1995 For correspondenceor repnntscontact Simone Maurea,MD, via RaffaeleDe Cesare7, 80132 Napoli, Italy. Technetium-99m-MIBI Redistribution• Maurea et al. 1953 Myocardial Viability Index in Chronic Coronary Artery Disease : Technetium-99m-Methoxy Isobutyl Isonitrile Redistribution Simone Maurea, Alberto Cuocolo, Andrea Soricelli, Luisa Castelli, Fiorenzo Squame, Massimo Imbriaco, Nicola De Luca, Bruno Trimarco and Marco Salvatore Nuclear Medicine Department, CNR Nuclear Medicine Center and Medical Clinic, University Federico II; and National Cancer Institute, Naples, Italy by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from
Transcript of Myocardial viability index in chronic coronary artery disease: technetium-99m-methoxy isobutyl...

show significant redistribution (1 ). Recent studies, however, demonstrated that delayed @Tc-MIBIredistributionmay be observed in a model of transient myocardial ischemia (3) or under conditions of sustained low coronary flow(4). Furthermore, it has also been reported that myocardialuptake and retention of 99mTc@MIBIare dependent on bothcell viability and regional blood flow and that tissue viabilityis required for @Tc-MIBIredistribution (5—9).
Clinical studies evaluated the phenomenon of @TcMIBI redistributionafter stress injection in patients withCAD (10,11). The occurrenceof 99mTcMIBIredistributionafter rest injection and its clinical implications have not yetbeen widely evaluated. Preliminary results reported by Dilsizian et al. recently suggested that @Tc-MIBIredistribution imaging following tracer injection at rest can detectviable myocardium using standard imaging protocols (12).Furthermore,these authorssuggestthat detectionofviablemyocardium may be enhanced with @Tc-MIBIcardiacimaging if an additional redistribution image is acquiredafter tracer injection at rest (12 ). It is still uncertain, however, whether 99mTcMIBI redistribution after rest injectionis predictive of improved ventricular function after coronary revascularization.
The purpose of this study was to evaluate whether anadditional redistribution image after rest @mTc@MIBIinjection enhances detection of viable myocardium and predictsfunctional recovery after coronary revascularization in patients with chronic coronary artery disease (CAD).
MATERIALSAND METhODS
PatientsWe prospectivelystudied31 patients (29men, 2 women;mean
age 55 ±10yr) with angiographically documented CAD and withleft ventricular dysfunction (Tables 1 and 2). Seven patients hadsignificant stenosis of all three major coronary vessels, 11 hadsignificant stenosis of two major coronary vessels and 13 hadsignificant stenosis of only one major coronary vessel. The meanleft ventricular ejection fraction (LVEF) by resting equilibriumradionuclide angiography was 39% ±9%. All patients had aprevious myocardial infarction that was documented clinicallyandby electrocardiography. No patient, however, had an acute myocardial infarction within 6 mo of the study. The majority of patients
The purposeof this study was to evaluatewhetheran additionalredistribution image after a rest @‘@Tc-MlBlinjectionenhancesdetection of viable myocardium and predicts functional recoveryaftercoronaryrevascularizationin patientswith chroniccoronaryartery disease (CAD). Methods: Thirty-one patients (29 men,mean age 55 ±10 yr) with proven CAD and left ventricular (LV)dysfunction (ejection fraction 39% ±9%) underwent resting
@“Tc-MlBItomography with initial (1 hr) and delayed (5 hr)images. Within 1 wk of MIBI imaging, all patients underwentrest-redistribution201fl imaging. Eight patients also underwenttwo-dimensional echocardiography before and 5 ±3 mo aftercoronary revascularization.Results: On the initial@images, 302 myocardial segments were normal, 183 showedmoderate and 197 severe reduction of tracer uptake. Of these197 segments,47 (24%)demonstrated increasedtracer uptake(1O% versusinitia@on delayedimages(from43% ±8% to60% ±8%, p<O.OO1)and were consideredas showing @9@c-MIBI redistribution. These 47 segments were observed in 20(65%) patients in whom 201fl images detected viable myocardium in the same segments. In the eight patientsstudied beforeand after revasculanzation,83% of segments with @“Tc-MlBIredistribution and abnormal LV function showed functional recovetyafterrevascularization,while96% of segmentswithout
@“Tc-MlBIredistribution did not show functional recovery.Conclusion: Resting @°‘Tc-MlBIredistribution frequently occurs in patients with chronic CAD. Acquisition of @‘@Tc-MlBlredistributionimagesenhancesdetection of viable myocardiumand predicts functional recoveryafter revascularization.
Key Words: technetium-99m-sestamibi;left ventriculardysfunction; functional recovery;thallium-201
J NucI Med 1995;36:1953-1960
echnetium-99m-methoxy isobutyl isonitrile (MIBI) is acardiac perfusion agent that initially distributes in the myocardium proportional to coronary blood flow, similar to2O1@ (1,2). It has been suggested that 99mTc@MIBI does not
ReCeiVedJan. 1, 1995; revision accepted Jul. 14, 1995Forcorrespondenceor repnntscontact SimoneMaurea,MD,via RaffaeleDe
Cesare7, 80132 Napoli, Italy.
Technetium-99m-MIBIRedistribution•Maureaet al. 1953
Myocardial Viability Index in Chronic CoronaryArtery Disease : Technetium-99m-MethoxyIsobutyl Isonitrile RedistributionSimone Maurea, Alberto Cuocolo, Andrea Soricelli, Luisa Castelli, Fiorenzo Squame, Massimo Imbriaco,Nicola De Luca, Bruno Trimarco and Marco Salvatore
Nuclear Medicine Department, CNR Nuclear Medicine Center and Medical Clinic, University Federico II; and National CancerInstitute, Naples, Italy
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

TABLE IPatientCharacteristics
position. A 20% symmetric energy window centered on the 140-keV peak was used. All projection images were stored on magneticdisk in a 64 x 64 word matrix. Each projection image was corrected for nonuniformity, with a 120-millioncount image obtainedweekly from a uniform 57Cflood source. The mechanical center ofrotation was determined from the projection data to align thedetector data with respect to the reconstruction matrix (14). Theraw data were initially smoothed with a nine-point weighted average algorithm. Filtered backprojection was then performed with alow-resolution Butterworth filter with a cutoff frequency of 0.5cycles/pixel, order 5.0, to reconstruct transverse axial tomogramsof 6.2-mm thickness per slice, which encompassed the entire heart.Sagittal and oblique tomograms parallel to the long-axisand shortaxis of the left ventricle were then extracted from the filteredtransaxial tomograms by performing coordinate transformationwith the appropriate interpolation (14). No attenuation or scattercorrection was applied.
Thallium-201ImagingAll patients underwent rest-redistribution 2°'Tlmyocardial to
mography. Patients were ambulatory and remained in the restingcondition for 30 mm before thallium administration. After anovernight fast, 201Tl(111 MBq) was intravenously injected at rest.Initial and delayed images were acquired 15 mm and 4 hr afterinjection. During the time between the initial and delayed images,all patients were ambulatory and remained in the fasting state. A3-day interval separated the thallium from [email protected] acquisition was performed with the same gamma camera,matrix and computer system used for the 99mTc@MIBIstudies. Thephotopeak was centered on the 68-keV with a 20% window.
EchocardiographyDuring the same week of 99mTc@MIBIand 201T1imaging, all
patients underwent echocardiographic studies. A phased-arraysector scanner with a 2.5 MHz transducer was used. Two-dimensional images of the left ventricle were obtained at rest with thepatient lying in the left lateral decubitus position using multipleimaging sections, including the parasternal long- and short-axesand apical two- and four-chamber views. Images were recorded onvideotape for analysis. In the eight patients studied before andafter coronary revascularization, two sequential echocardiographicstudies were performed. The first evaluation (baseline) was performed during the same week of 99mTc@MIBIand 201Tlstudies.The second evaluation (follow-up) was performed an average of 5± 3 mo aftercoronary revascularization.No patientreceived
beta-blockers or inotropic drugs during the follow-up evaluation.
DataAnalysisIn each patient, correspondinginitialand delayed99mTc@MIBI
and rest-redistribution 201Tltomographic images were evaluatedfor direct comparison, as previously described (13). For eachstudy, tomograms were divided into 22 myocardial segments (Fig.1). Regional 99mTcMIBI and 2°'Tluptake were quantitativelyanalyzed. In each tomogram, the myocardial region with the maximum counts was considered as the normal reference region.Technetium-99m-MIBI and 201T1uptake in all other segmentswere then expressed as the percentage of the activity measured inthe reference region.
To assess the normal range for quantitativedata analysis,agroup of 14 age-matched normal volunteers (13 men, 1 woman)with no evidence of cardiovascular or pulmonary disease was alsostudied. In these subjects, clinical examination, echocardiogramsand stress electrocardiograms were normal. A myocardial segment
Patientno.SexAge (yr)LVEF(%)Site
ofmyocardialinfarctionStableangina1M6242PosterolateralYes2M6224Inferior,
anteriorYes3M4449AnteroseptalYes4M6338AnteriorYes5M5744InferiorYes6M6742InferiorYes7M6039InferolateralYes8M4935Anteroseptal,
inferoapicalNo9M6939InferolateralYes10M4634AnteriorYes1
1M6348InferolateralYes12M4828AnteriorYes13M4341AnteroseptalYes14M6142Inferior,
anteriorYes15M4048AnteroseptalYes16M6331Anteroseptal,
inferiorYes17M5430InferolateralYes18M6647AnteroapicalYes19M5849InferiorYes20M6548AnteriorYes21M6130AntenorYes22M6849AnteriorYes23M5036AnteroseptalYes24M5748Anteroseptal,
apicalYes25M3823AnteriorNo26M3226Anterior,
infenorNo27M4220AnteriorYes28M5349AnteriorYes29M4744AnterolateralYes30F5746InferiorYes31F6544AnteriorYes
LVEF= leftventricularejectionfraction.
(n = 28) were symptomatic with episodes of stable angina requiring antianginal treatment, while three patients were asymptomatic.All patients, however, underwent radionuclide studies after withdrawal of all medications. Eight of the 31 patients were alsostudied after coronary revascularization, coronary artery bypassgraft in six and percutaneous transluminal coronary angioplasty intwo. In these patients, none had clinical evidence of perioperativeor postangioplastymyocardialinfarctionor restenosis.Informedconsent, as part of the protocol approved by the InstitutionalClinical Research Subpanel on Human Studies at our University,was obtained from all patients.
Technetium-99m-MIBI ImagingAfter an overnight fast, all patients underwent rest-redistribu
tion 99mTc@MIBImyocardial tomography. Patients were ambulatory and remained in the resting condition for 30 mm beforeintravenous injection of @mTc@MIBI(740 MBq). Initial imageswere acquired I hr after tracer administration. Delayed imageswere then taken 5 hr later.
SPED' was performed as previouslydescribed (13) using arotating large field of view gamma camera equipped with a lowenergy, all-purpose, parallel-hole collimator and connected with adedicated computer system. Briefly, 32 projections (40 sec/projection) were obtained over a semicircular 180°arch, which extendedfrom the 30°right anterior oblique to the left posterior oblique
1954 The Journal of Nuclear Medicine •Vol. 36 •No. 11 •November 1995
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

Patientno.Coronary
arterystenosis(50%)Site
ofwallmotionabnormalitiesSite
of Segmentswith @‘@‘Tc-MlBlredistribution1LAD,
LCx, PDALateralLateral, inferoseptal,apical(n=4)2LAD,PDAInferior, apicalInferoseptal, anteroseptal(n =2)3LAD,LCxSeptal, apicalAnteroseptal, apical,infenor(n -8)4LAD,
LCx, PDASeptal, lateral,apicalInferoseptal, inferolateral,apical(n=3)5PDAlnferolateraiInferolateral,septal(n =5)6LAD,
PDAInferiorNone7LAD,LCxSeptal, inferoapical,
lateralApical(n =1)8LADInferoapicalApical
(n =1)9LAD,LCx, PDASeptal, posterolateralInferoseptal (n=1)10LAD,
PDAAnteroapicalInferolateral, anterior(n =2)11LAD, PDASeptal, inferolateralLateral (n=1)12LCxAnteroseptal,
apicalAnteroseptal, inferolateral(n =5)13LAD,LCxSeptalNone14LAD,
LCx,PDAlnferoapicalInferolateral (n =1)15LADSeptalNone16LAD,
LCx, PDAAnteroseptal, apicalApical (n =1)17LAD,PDAlnferoapicalNone18LADAnterior,
apicalNone19PDAInferoapicalNone20LAD,
LCxAnteroseptalNone21LADAnteroapical,inferiorAnteroseptal, apical(n =4)22LAD,
LCx,PDASeptalNone23LADSeptalNone24LADApicalNone25LADAnterior,
inferoapicalInferoseptal (n —1)26LAD,LCxAnterior, inferior,apicalNone27LADAnterior,
apicalSeptal (n=1)28LCx,PDASeptalInferoseptal (n =1)29LADAnteroseptalInferoseptal,
inferolateral(n =3)30LAD,LCx,PDAInferoapical, septalInferolateral (n =1)31LADAnteroseptal,
apicalApical (n =1)LAD
—left antenordescendingartery;LCx = leftcircumflex artery;PDA= posteriordescendingartery.
TABLE 2Angiographic Data, Site of Left VentricularDysfunctionand Technetium-99m-MlBl Redistributionon Delayed Imaging
was considered abnormal if initial 99mTc@MIBI or 201Tl uptake was
>2 s.d. below the mean observed in the same region for age- andsex-matched normal volunteers. On initial 99mTc@MIBIimages,segments with abnormal uptake were subgrouped on the basis of
FIGURE I . Diagramofstandardsegmentationschemeusedforregionalquantitativeanalysisof @Tc-MlBland 201fluptake.
severity of reduction in tracer activity: moderate (50% of peakactivity) and severe (<50% of peak) defects, as previously re
ported (12,15,16). On the basis of previous reproducibility measurements performed by other authors and in our laboratory(12,17),a segmentwith reducedactivityon initial @mTc@MIBIor201Tlimages was considered reversible if the activity increased
10% on delayed 99mTcMIBI or 2o―flimages, respectively. Altematively, a segment with reduced activity on initial 99mTc@MIBIor 201T1imageswasconsideredirreversibleif the activitydid notincrease 10% or increased 10% but remained <50% on delayed 99mTcMIBI or 201'flimages, respectively. Thallium-201 irreversible defects were divided on the basis of severity of reductionin tracer activity: moderate (50% of peak activity) and severe
(<50% of peak) defects,as previouslyreported(12,17).Echocardiographic images were interpreted by two experienced
observers who were unaware of clinical, radionuclide and angiographic findings. A third investigator blindly reviewed the echocardiograms when the first two observers did not agree. Regionalleft ventricular function was assessed according to the recommendations of the American Society of Echocardiography (18,19).Segmental left ventricular wall motion was graded as: 1, normal; 2,hypokinetic; 3, akinetic; and 4, dyskinetic. The echocardiographic
Vertical Horizontal
1955Technetium-99m-MIBIRedistribution•Maureaet al.
Short@ 12(:\rL@@ (iir@1dAxis@ 10 9
Apical Mid-ventricular Basal
LongAxis
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from
results were directly compared with those of @mTc@MIBIand201Tl,as previouslydescribed(20). In the eight patients studiedbefore and after coronary revascularization, a myocardial segmentwas considered as showing functional recovery when the regionalwall motion score was abnormal at baseline and improved at leastone echocardiographic grade during the follow-up study, as previously reported (21). Conversely, a myocardial segment was considered as showing no functional recovery when regional wallmotion score was severely impaired at baseline (grade 3 or 4) anddid not change during follow-up (21).
Statistical AnalysisData are expressedas mean ±1 s.d. Differencesin the mean
values were assessed by Student's t-test for unpaired data withBonferroni correction for multiple groups comparison, or Student's t test for paired data, as appropriate. Bonferroni correctionestablishes that the p value for each comparison should be multiplied by the total number of comparisons undertaken (22). TheSpearman correlation coefficient (p) was used to assess the relationships between wall motion score and tracer uptake. Linearregression was used to evaluate the relationship between LVEFand the number of myocardial segments showing reversible @“@TcMIBIdefects.Chisquareanalysiswasusedto assessdifferencesbetween proportions. Probability values <0.05 were consideredsignificant.
RESULTS
Technetium-99m-MIBIA total of 682 myocardialsegments were analyzed. On
initial 99mTcMIBI images, 302 (44%) segments had normaltracer uptake, 183 (27%) showed moderate and 197 (29%)severe reduction of tracer uptake.
Myocardial segments with moderate reduction of @TcMIBI uptake on the initial images were observed in all 31patients (range 3—10segments/patient, mean 5.9 ±1.9). Ofthe 183 segments with moderate reduction of @Tc-MIBIuptake on initial images, 51 (28%) were reversible on delayed images, showing significant increased tracer uptake(from 61% ±7% to 78% ±10% ofpeak activity, p<O.OOl).Moderate reversible wmTc@MIBIdefects on delayed imageswere observed in 23 (74%) patients (range 1—5segments/patient, mean 2.2 ±1.2). The remaining 132 (72%) segments with moderate reduction of @mTc@MIBIuptake oninitial images were irreversible on delayed images, showingno significant change in tracer uptake (from 63% ±6% to58% ±9% of peakactivity).
Myocardial segments with severe reduction of @TcMIBI uptake on initial images were observed in all 31patients (range 1—14segments/patient, mean 6.4 ±3.6). Ofthe 197 segments with severe reduction of 9@Tc-MIBIuptake on initial images, 47 (24%) were reversible on delayed images, showing significant increased tracer uptake(from 43% ±8% to 60% ±8% of peak activity, p<O.OOl)(Fig. 2). Severe reversible wmTc@MIBIdefects on delayedimages were observed in 20 (65%) patients (range 1—8segments/patient, mean 2.3 ±1.9) (Table 2). The remaining 150 (76%) segments with severe reduction of 99mTc..MIBI uptake on the initial images were irreversible ondelayed images, showing no significant change in tracer
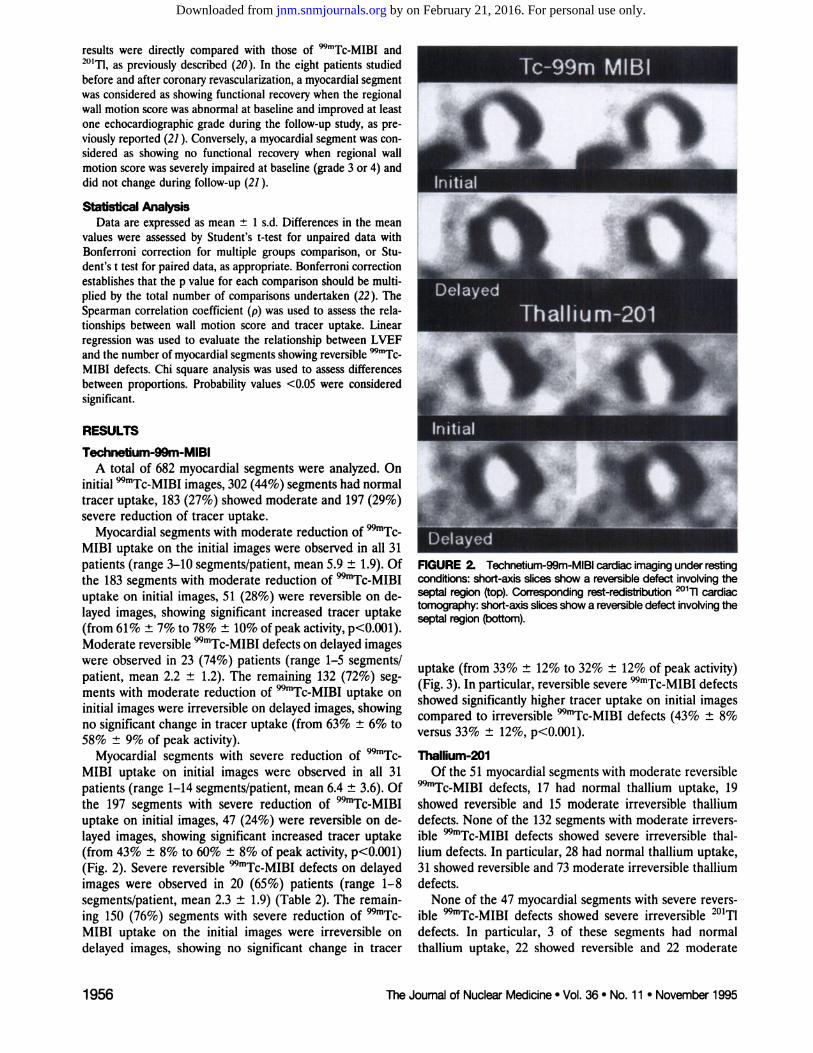
FIGURE 2@ Technetium-99m-MIBIcardiacimagingunderrestingconditions:short-axisslicesshowa reversibledefectinvolvingtheseptal region (top). Corresponding rest-redistribution 201fl @@Jiactomography:short-axisslicesshowa reversibledefectinvolvingtheseptal region (bottom).
uptake (from 33% ±12% to 32% ±12% of peak activity)(Fig. 3). In particular, reversible severe wmTc@MIBIdefectsshowed significantly higher tracer uptake on initial imagescompared to irreversible wmTc@MIBIdefects (43% ±8%versus 33% ±12%, p<O.OOl).
Thallium-201Of the 51 myocardialsegmentswithmoderate reversible
@“@Tc-MIBIdefects, 17 had normal thallium uptake, 19showed reversible and 15 moderate irreversible thalliumdefects. None of the 132 segments with moderate irreversible 99mTcMIBI defects showed severe irreversible thalhum defects. In particular, 28 had normal thallium uptake,31 showed reversible and 73 moderate irreversible thalliumdefects.
None of the 47 myocardial segments with severe reversible 99mTcMIBI defects showed severe irreversible 201'fldefects. In particular, 3 of these segments had normalthallium uptake, 22 showed reversible and 22 moderate
1956 The Journal of Nuclear Medicine •Vol. 36 •No. 11 •November 1995
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

80
60[__P<O.OO1
@
II—p<O.O1—@
:i:40200——
*G@p 1 = normalwallmotion;Group2 = hypokine@csegments;Group3 = segmentswithakinesiaordySldneSia.
tp < 0.001versusGroup1;*p .<0.001versusGroupsland2.
Initial Delayed
To.99mMIBI
Inhial Delayed
Thalllurn-201
FIGURE4. Technetium-99m-MIBIand @°@11uptake(expressedas percentage of peak activity) in myocardial segments with severereduction of initial @Tc-MlBluptake and increased tracer uptakeon delayed images. ns = nonsignificant.
3 and in Group 2 segments compared to those of Group 3(Table3). Similarly,initialand delayed99mTc..MIBIuptakewere significantly higher (p<O.OOl) in Group 1 segmentscompared with those of Groups 2 and 3 and in Group 2segments compared to those of Group 3 (Table 3). Asignificant relationship (p<O.OOl) between wall motionscore and initial (p = —0.45)and delayed (p = —0.41)thallium uptake was observed. Similarly, a significant relationship (p<O.OOl) between wall motion score and initial(p = —0.50)and delayed (p = —0.47)w@@@Tc@MIBIuptakewas found. No significant relationship was observed between LVEF and the number of myocardial segmentsshowing moderate and/or severe reversible @Tc-MIBIdefects.
Follow-up after Coronaty RevascularizationIn the eight patients studied before and after coronary
revascularization, 33 (19%) myocardial segments with wallmotion abnormalities showed moderate reduction of @“@TcMIBI uptake on initial images. Of these 33 segments, 13were reversible and 20 did not change on delayed @TcMIBI images. Moderate reversible99mTc@MIBIdefects on
FIGURE 3. Technetium-99m-MIBIcardiac tomography underrestingconditions:short-axisslicesshowa largeirreversibledefectinvoMngthe septaland inferiorregions(top).Correspondingrestredistribution201@flcardiactomography:short-axisslices show alarge irreversibledefect involvingthe septal and inferiorregions(bottom).
irreversible thallium defects (Fig. 2). On the other hand,the majority (80%) of myocardial segments with severeirreversible 99mTcMIBI defects showed severe irreversible201T1defects (Fig. 3).
In the 47 myocardial segments with severe reversible99mTcMIBI defects, initial 99mTc@MIBIuptake was significantly lower (p<O.OOl) compared to both initial and delayed thallium uptake (Fig. 4). On the other hand, in thesesegments delayed wmTc@MIBI uptake was significantlyhigher (p<O.Ol) compared to initial thallium uptake, butnot different from delayed thallium uptake (Fig. 4).
Relation with Left Ventricular FunctionOf the total 682 myocardialsegments, 332 (49%) showed
normal wall motion (Group 1) on echocardiographic images, 160 (23%) were hypokinetic (Group 2) and 190 (28%)were akinetic or dyskinetic (Group 3). Initial and delayedthallium uptake were significantly higher (p<O.OO1) forGroup 1 in segments compared with those of Groups 2 and
TABLE aInitialand Delayed Techrietium-99m-MIBI and Thallium-201
Uptake in Myocardial Segments@
Group1 Group2 Group3
Myocardialsegments(no.)Initial @9@c-MIBIuptake(%)Delayed @‘Tc-MlBluptake(%)Initial@°@Tluptake(%)Delayed201@fluptake(%)
332 160 19089±13 6O±llt 38±16@87±14 62±l4t 39±18@88±14 65±l4t 42±20@87±15 67±l4t 45±21*
1957Technetium-99m-MIBIRedistribution•Maureaet al.
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

comparative studies between 99mTcMIBI scintigraphy andmetabolic imaging with [‘8F]fluorodeoxyglucose showedthat 99mTcMIBI myocardial uptake on conventional 1-hrimaging is mainly related to regional coronary blood flowrather than tissue viability (15,31). Experimental studies,however, have shown that myocardial retention of wmTc@MIBI depends not only on coronaryblood flow but also oncellular viability (5,6). Furthermore, recent clinical reportssuggest that quantitative analysis of resting wmTc@MIBImay enhance differentiation between viable myocardiumfrom necrotic tissue in patients with chronic ischemic leftventricular dysfunction (12,32).
Technetium-99m-MIBI RedistributionThe occurrence of wmTc@MIBIredistribution has been
previously demonstrated in a model of transient ischemiaor under conditions of sustained reduced coronary bloodflow (3,4). In particular, Li et al. showed that normalizationof @mTc@MIBIdefects in ischemic regions is progressiveover time and that such redistribution is detectable ontomographic images and also confirmed by serial myocardial biopsies (3). Sinusas et al. recently demonstrated that99mTcMIBI redistributes in the presence of severe coronary artery stenosis, as documented by gamma well counting techniques and by high-resolution postmortem gammacamera imaging of myocardial slices (4). In clinical studies,there are conflicting data on @mTc@MIBIredistributionafter stress imaging. Taillefer et al. (10) described a decrease in @Tc-MIBIdefect size after exercise with serialplanar imaging between 1 hr and 3 hr following stressinjection. On the other hand, Villanueva-Meyer et at. (11)recently reported no change in defect size between 1 and 4hr after stress @“@Tc-MIBIinjection using quantitative tomographic imaging. Dilsizian et at. recently described redistribution of @Tc-MIBIafter rest injection in a smallnumber of patients with chronic CAD and severe left yentncular dysfunction (12). Its clinical utility, however, hasnot yet gained wide application.
The results of the present study show the occurrence of@Tc-MIBIredistribution after rest injection in patients
with chronic ischemic left ventricular dysfunction, suggesting that acquisition of delayed images after resting @TcMIBI injection may enhance the detection of severely hypoperfused but still viable myocardium. We focused ouranalysis on the clinical significance of @“@Tc-MIBIredistribution in myocardial segments with severe reduction oftracer uptake on initial images, in whom the presence ofviable tissue is in question. In particular, 24% of segmentswith severe reduction of @Tc-MIBIuptake on initial images showed a significant increase in tracer uptake ondelayed images. Our results with earlier data of Dilsizian etat. in a group of patients with chronic CAD (12). Theseauthors described @mTc@MIBIredistribution in 38% ofmyocardial segments with irreversible defects on stress-rest
@Tc-MIBIimaging (12). Furthermore, our results confirm the experimental evidence of resting @Tc-MIBIredistribution in a model of sustained coronary low flow (4).
FiGURE 5. Flowdiagramshowswall motionaftercoronaryrevascularization in asynergic segments with severe redUCtiOnof
@Tc-MIBluptakeon initial imagesand reversibleor irreversibledefects on delayed images.
delayed images were observed in seven of these patients(range 0—4segments/patient, mean 2.1 ±1.4). The majority of segments with moderate reversible @Tc-MIBIdefects (85%) showed functional recovery after revascularization. Furthermore, 41 (23%) segments with wall motionabnormalities showed severe reduction of @“@Tc-MIBIuptake on initial images. Of these 41 segments, 18 werereversible and 23 did not change on delayed @mTc@MIBIimages. Severe reversible @mTc@MIBIdefects on delayedimages were observed in all these patients (range 1—8segments/patient, mean 3.1 ±2.6). The majority (83%) ofsegments with severe reversible @Tc-MIBIdefectsshowed functional recovery after revascularization (Fig. 5).Conversely, the majority (96%) of segments with severeirreversible @“@Tc-MIBIdefects did not show improved wallmotion after revascularization (p<O.OOlversus severe reversible defects) (Fig. 5). In these patients, LVEF significantly (p<O.Ol) improved after revascularization (from42% ±7% at baseline to 47% ±7% after revascularization).
DISCUSSION
Our results agree with those of Dilsizian et al. (12) anddemonstrate that in patients with chronic CAD and leftventricular dysfunction @mTc@MIBIredistribution on delayed images occurs in 24% to 38% of myocardial segmentswith severe reduction of tracer uptake at rest. Delayed
@Tc-MIBIimaging improves the differentiation betweenischemic but still viable myocardium from fibrotic tissue inregions with severe reduction of resting @Tc-MIBIuptake. Furthermore, @mTc@MIBIredistribution is predictiveof functional recovery following coronary revascularization.
Technetium-99m-MIBI Identificationof Myocardial Viability
Previous clinical studies demonstrated that severe reduction of 99mTcMIBI uptake underestimates the presence ofviable myocardium in patients with chronic CAD and leftventricular dysfunction (12,15,16,23—31). In particular,
1958 The Journal of Nuclear Medicine •Vol. 36 •No. 11 •November 1995
41 Initial_____ Tc-99mMIBIAsynergic5e@ments
with Severe Reduction of Uptake__ , __18 23 Delayed
_____ _____ Tc-99mMIBIReveraible lffever@e
I Unchanged Wall Motion After
0 Improved Revasculanzation
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

In our study, the occurrence of 99mTc@MIBIredistributionon delayed images in myocardial segments with severereduction of 99mTcMIBI uptake on initial images was observed in 65% of the patients. This finding may be clinicallyrelevant since it demonstrates that @Tc-MIBIredistribution may occur in a substantial number of patients withchronic ischemic left ventricular dysfunction.
Comparison with Thallium-201 ImagingThe results of rest-redistribution 201'flcardiac imaging in
myocardial segments with 99mTc@MIBIredistribution support the hypothesis that these regions may contain hypoperfused but viable myocardium. In particular, each segmentshowed evidence of myocardial viability according to thathum imaging criteria. In myocardial segments with severereversible 99mTcMIBI defects, initial 99mTc@MIBIuptakewas significantly lower compared to both initial and delayedthallium uptake. A possible explanation for this findingcould be that only segments with severe reduction of initial99mTcMIBI uptake and increased tracer activity on delayedimages were included in the analysis. Moreover, none ofthese segments showed severe irreversible thallium defects.On the other hand, delayed wmTc@MIBIuptake was significantly higher compared to initial thallium uptake but notdifferent compared to delayed thallium uptake. These datacorrelate with previous comparative studies between 201'fland 99mTc@MIBIcardiac imaging (26—29).Furthermore,Dilsizian et al. recently reported concordant results between resting 99mTcMIBI redistribution and 201'fl reinjection imaging studies (12). These findings suggest that resting @Tc-MIBI redistribution imaging identifies thepresence of hypoperfused but viable myocardium in patients with chronic ischemic left ventricular dysfunction.Thus, it may have important clinical implications.
Follow-up after Coronary RevascularizationAlthough thallium uptake is usually considered an accu
rate marker of myocardial viability in patients with chronicCAD (33—40),the definite gold standardfor the presenceof viable tissue in such patients is functional recovery aftercoronary revascularization (41). In the present study, weevaluated whether resting 9@Tc-MIBI redistribution is predictive of improved left ventricular function after coronaryrevascularization and, thus, of myocardial viability. Ourresults obtained after revascularization support the hypothesis that 99mTcMIBI redistribution reflects the presence ofviable myocardium. In fact, the majority of segments withseverely impaired ventricular function and increased @TcMIBI uptake on delayed images showed improved wallmotion after revascularization. Conversely, the majority ofakinetic segments with no change on delayed @Tc-MIBIimages did not show functional recovery after coronaryrevascularization. Furthermore, a significant improvementof global LVEF was observed after coronary revascularization. Therefore, these findings demonstrate that delayedredistribution cardiac imaging after resting @mTc@MIBIinjection can detect severely hypoperfused but still viablemyocardium as well as predict reversibility of severe re
gional wall motion abnormalities after coronary revascularization in patients with chronic ischemic left ventriculardysfunction.
StudyUmitationsTwo potential limitations of this study deserve comment.
First, follow-up evaluation after coronary revascularizationwas obtained in a limited number of the patients in whomresting @Tc-MIBIredistribution was observed. Althoughour data need confirmation in larger series of patients, thefollow-up results of the present study confirm and may beconsidered representative of the enhanced detection ofviable myocardium by resting @“@Tc-MIBIcardiac imagingusing delayed acquisition. Second, since there are no established criteria in the literature to assess the severity of
@‘Tc-MIBIdefects, the selection of the threshold value forseverely reduced @Tc-MIBI uptake was chosen arbitrarily. The same threshold, however, has been used inprevious studies (12,15,16).
CONCLUSION
Resting @Tc-MIBIredistribution frequently occurs inpatients with chronic CAD and left ventricular dysfunction.Acquisition of delayed @Tc-MIBIimages enhances thedifferentiation between severely hypoperfused, but still viable myocardium from fibrotic tissue in such patients. Thepresence of @Tc-MIBIredistribution may be predictive offunctional recovery after coronary revascularization. Therefore, our results suggest that resting @‘@Tc-MIBIcardiacimaging should be delayed when assessing myocardial viability in patients with chronic CAD.
REFERENCES
1. Okada RD, Glover D, Gaffney 1, Williams S. Myocardial kinetics of technetium-9@-hexakis-2-methoxy-2-methylpropyl-isonitrile. Circulation 1988;77:491—498.
2.CanbyRC,SilberS,PohostGM.RelationsofthemyocardialimagingagentsTc-99m MIBI and 11-201 to myocardial blood flow in a canine model ofmyocardial ischemic insult. Circulation 1990;81:289—296.
3. Li OS,SolotA, FrankIL, WagnerHN, BeckerLC.Myocardialredistribution of technetium-99m methoxy isobutyl isonitrile (sestamibi). I Nuci Med1990;31:1069—1076.
4. Sinusas AJ, Bergin JD, Edwards NC, et al. Redistribution of Tc-99m sestamibi and 11-201 in the presence of a severe coronary artery stenosis. Circul@ztion1994;89:2332—2341.
5. BeanlandsRSB,Dawood F, Wen WH, Ctal. Are the kinetics of technetium99m-methoxyisobutyl isonitrile affected by cell metabolism and viability?Circulation 1990;82:1802—1814.
6. Freeman I, Grunwald AM, Hoory 5, Bodenheimer MM. Effect of coronaiyocclusion and myocardialviability on myocardial activity of technetium-99m-sestamibi. I Nuci Med 1991;32:292—299.
7. Glover DK, Okada RD. Myocardial technetium-99m sestamibi kinetics afterreperfusion in a canine model. Am Heart I 1993;125:657—666.
8. BelIer GA, Glover DK, Edwards NC, Ruiz M, Simanis JP, Watson DD.Technetium-99m-sestamibi uptake and retention during myocardial ischemia and reperfusion. Circulation 1993;87:2033-2042.
9. Merhi J, Arsenault A, Latour JG. Time course of technetium-99m-sestamibimyocardial distribution in dogs with a permanent or transient coronaiyocclusion. EurI Nuci Med 1994;21:481—487.
10. Taillefer R, Primeau M, Costi P, Lambert R, Leveille J, Latour Y. Technetium-99m-sestamibi myocardial perfusion imaging in detection of coronaryarteiy disease: comparison between initial (1-hour) and delayed (3-hour)postexercise. I Nuci Med 1991;32:1961—1965.
11. Villanueva-Meyer J, Mena I, Diggles L, Narahara KA. Assessment of myocardial perfusion defect size after early and delayed SPECF imaging with
1959Technetium-99m-MIBIRedistribution•Maureaet aI.
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

technetium-99m-hexakis 2-methoxyisobutyl isonitrile after stress. I Nuc! Med1993;34:187—192.
12. Dilsizian V, Arrighi JA, Diodati JG, et al. Myocardial viability in patientswith chronic coronary artery disease. Comparison of @“Tc-sestamibiwiththallium reinjection and [‘8F]fluorodeoxyglucose.Circulation 1994;89:578—587.
13. Cuocolo A, Soricelli A, Pace L, et al. Adenosine technetium-99m methoxyisobutyl isonitrile myocardial tomography in patients with coronary arterydisease: comparison with exercise. 1 NucI Med 1994;35:l11O—1115.
14. Borrello JA, Clinthorne NH, Rogers WL, Thrall JH, Keyes JW. Obliqueangle tomography: a reconstructing algorithm for transaxial tomographicdata. I Nuci Med 1981;22:471—473.
15. Sawada SG, Aliman KC, Muzik 0, et al. Positron emission tomographydetects evidence of viability in rest technetium-99m sestamibi defects. JAmCoil Cardiol 1994;23:92—98.
16. Rocco TP, Dilsizian V, Strauss HW, Boucher CA. Technetium-99m isonitrile myocardial uptake at rest. II. Relation to clinical markers of potentialviability. JAm Coil Cardiol 1989;14:1678—1684.
17. Maurea S, Cuocolo A, Soricelli A, et al. Enhanced detection of viablemyocardium by technetium-99m methoxy isobutyl isonitrile tomography after nitrates administration in patients with chronic coronary artery disease. JNuciMed 1945;36:1945—1952.
18. Henry WL, De Maria A, Feigenbaum H, et al. Report of the AmericanSociety of Echocardiography Committee on nomenclature and standards:Identification of Myocardial Wall Segments. American Society of Echocardiography, November 1982, North Carolina: Duke University Medical Center.
19. Shiller NB, Shah PM, Crawford M, et at. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Twodimensional Echocardiograms: recommendations for quantitation of the leftventricle by two-dimensional echocardiography. JAm Soc Echo 1989;2:358—367.
20. PozzoliMMA,FiorettiPM,SalustriA, ReijisAEM,RoelandtJRTC.Exercisc echocardiography and technetium-99m MIBI single-photon emissioncomputed tomography in the detection of coronary artery disease. Am ICardiol 1991;67:350—355.
21. Marzullo P, Parodi 0, Reisenhofer B, et al. Value of rest thallium-201/technetium-99m sestamibi scans and dobutamine echocardiography for detecting myocardial viability. Am I Cardiol 1993;71:166—172.
22.MatthewsDE,FarewellV. Dataanalysis.A formaldiscussionof multiplecomparisons. In: Using and understanding medical statistics. Basel: Karger S;1985:169—172.
23. Cuocolo A, Pace L, Ricciardetli B, Chiariello M, Trimarco B, Salvatore M.Identification of viable myocardium in patients with chronic coronary arterydisease: comparison of thallium-201 scintigraphy with reinjection and technetium-99m-methoxyisobutyl isonitrile. I NucI Med 1992;33:505—511.
24. Marzullo P, Sambuceti G, Parodi 0. The role ofsestamibi scintigraphy in theradioisotopic assessment of myocardial viability. I Nucl Med 1992;33:1925—1930.
25. Altehoefer C, Kaiser Hi, Dorr R, et al. Ruorine-18-deoxyglucose PET for
assessment of viable myocardium in perfusion defects in Tc-99m-MIBISPED':a comparativestudyin patientswithcoronaryarterydisease.EurINucI Med 1992;19:334-342.
26. Dondi M, Tartagni F, Fallani F, et al. A comparison of rest sestamibi andrest-redistribution thallium single photon emission tomography: possibleimplications for myocardial viability detection in infarcted patients. Eur INucIMed 1993;20:26—31.
27. Maurea 5, Cuocolo A, Pace L, et al. Rest-injected thallium-201 redistribution and resting technetium-99m methoxy isobutyl isonitrile uptake in coronary artery disease: relation to the severity of coronary artery stenosis. EurI Nuci Med 1993;20:502—510.
28. Cuocolo A, Maurea S, Pace L, et al. Resting technetium-99m-methoxyisobutyl isonitrile cardiac imaging in chronic coronary artery disease: cornparison with rest-redistribution thallium-201 scintigraphy. Eur I Nuci Med1993;20:1186—1192.
29. Maurea S, Cuocolo A, Pace L, Ct al. Left ventricular dysfunction in coronaryartery disease: comparison between rest-redistribution thalliurn-201 andresting technetium-99m-methoxy isobutyl isonitrile cardiac imaging. I NucICardiol 1994;1:65—71.
30. Maurea S, Cuocolo A, Nicolai E, Salvatore M. Improved detection of viablemyocardium by thallium-201 reinjection in chronic coronary artery disease:comparison with technetium-99m-MIBI imaging I NucI Med 1994;35:621—624.
31. Altehoefer C, vom Dahi i, Biedermann M, et al. Significance of defectseverity in technetium-99m-MIBI SPEC!' at rest to assess myocardial viability: comparison with fluorine-18-FDG PET. I NuclMed 1994;35:569—574.
32. Udelson JE, Coleman PS, Metherall i, et al. Predicting recovery of severeregional ventricular dysfunction. Comparison of resting scintigraphy with11-201 and Tc-99m sestamibi. Circulation 1994;89:2552—2561.
33. Bonow RO, Dilsizian V, Cuocolo A, Bacharach SL. Identification of viablemyocardium in patients with chronic coronary artery disease and left yentricular dysfunction. Comparison of thallium scintigraphy with reinjectionand PET imaging with 8F-fluorodeoxyglucose. Circulation 1991;83:26—37.
34. Dilsizian V, Perrone-Filardi P, Arrighi iA, et al. Concordance and discordance between stress-redistribution-reinjection and rest-redistribution thathum imaging for assessing viable myocardium. Comparison with metabolicactivity by positron emission tomography. Circulation 1993;88:941—952.
35. Kiat H, Berman DS, Maddahi i, et at. Late reversibility of tomographicmyocardial thallium-201 defects. An accurate marker of myocardial viability.JAm Coil Cardiol 1988;12:1456—1463.
36. Kayden DS, Sigal 5, Soufer R, Mattera i, Zaret BL, Wackers Fl. Thallium201 for assessment of myocardial viability: quantitative comparison of 24-hour redistribution imaging with imaging after reinjection at rest. I Am CoilCardiol 1991;18:1480—1486.
37. Dilsizian V, Smeltzer WR, Freedman NMT, Dextras R, Bonow RO. ThaIhum reinjection after stress-redistribution imaging. Does 24-hour delayedimaging after reinjection enhance detection of viable myocardium? Circula.fion1991;83:1247—1255.
38. Mori 1, Minamiji K, Kurogane H, Ogawa K, Yoshida Y. Rest-injectedthallium-201 imaging for assessing viability of severe asynergic regions. INucI Med 1991;32:1718—1724.
39. Ragosta M, BelIer GA, Watson DD, Kaul S, Gimple LW. Quantitativeplanar rest-redistribution 11-201 imaging in detection of myocardial viabilityand prediction of improvement in left ventricular function after coronarybypass surgery in patients with severely depressed left ventricular function.Circulation 1993;87:1630—1641.
40. Altehoefer C, vom Dahl i, Buell U, Uebis R, Kleinhans E, Hanrath P.Comparison of thalliurn-201 single-photon emission tomography after restinjection and fluorodeoxyglucose positron emission tomography for assessment of myocardial viability in patients with chronic coronary artery disease.Eurl Nucl Med 1994;21:37—45.
41. BraunwaldE, RutherfordiD. Reversibleischemicleftventriculardysfunction: evidence for “hibernating―myocardium. I Am Coil Cardiol 1986;8:1467—1470.
1960 The Journal of Nuclear Medicine •Vol. 36 •No. 11 •November 1995
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from

1995;36:1953-1960.J Nucl Med. Bruno Trimarco and Marco SalvatoreSimone Maurea, Alberto Cuocolo, Andrea Soricelli, Luisa Castelli, Fiorenzo Squame, Massimo Imbriaco, Nicola De Luca, Technetium-99m-Methoxy Isobutyl Isonitrile RedistributionMyocardial Viability Index in Chronic Coronary Artery Disease:
http://jnm.snmjournals.org/content/36/11/1953This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1995 SNMMI; all rights reserved.
by on February 21, 2016. For personal use only. jnm.snmjournals.org Downloaded from




![Noninvasive Molecular Imaging of MYC mRNA Expression in Human Breast Cancer Xenografts with a [ 99m Tc]Peptide−Peptide Nucleic Acid−Peptide Chimera](https://static.fdokumen.com/doc/165x107/63214cddbc33ec48b20e4a4a/noninvasive-molecular-imaging-of-myc-mrna-expression-in-human-breast-cancer-xenografts.jpg)




![Novel S1P 1 Receptor Agonists - Part 2: From Bicyclo[3.1.0]hexane-Fused Thiophenes to Isobutyl Substituted Thiophenes](https://static.fdokumen.com/doc/165x107/633790042d5148431a056390/novel-s1p-1-receptor-agonists-part-2-from-bicyclo310hexane-fused-thiophenes.jpg)









