20 Operative Management of Anomalies in Males
8
20.1 Introduction Anorectal malformations (ARM) represent a wide spectrum of defects. e terms low, intermediate, and high are arbitrary and not very useful in therapeutic or prognostic terms. Within the group of ARM tra- ditionally referred to as high, there are defects with different therapeutic and prognostic implications. For instance, retroprostatic fistula and rectobladderneck fistula were both considered high, yet the first can be repaired with a posterior sagittal approach alone, but the second also requires an abdominal approach. e prognosis for each type is completely different. ere- fore, anatomic descriptions of the malformations are more useful clinically (Table 20.1). In the past, many surgical techniques to repair ARM have been described. ese included endorectal dissection [1–3], anterior perineal approach to a rec- tourethral fistula [4], and many different types of ano- plasties [5]. However, most pediatric surgeons now use the posterior sagittal approach to repair these malformations with or without laparotomy or lapa- roscopy. e debate recently has been centered more on the possibility of performing these operations pri- marily without a protective colostomy and using lapa- roscopy if an abdominal component is needed [6–8]. Contents 20.1 Introduction . . . 295 20.2 Posterior Sagittal Approach . . . 295 20.3 Repair of Specific Defects in Boys . . . 296 20.3.1 Rectoperineal Fistulas . . . 296 20.3.2 Rectourethral Fistulas . . . 297 20.3.3 Rectobladderneck Fistula . . . 300 20.3.4 Imperforate Anus Without Fistula . . . 301 20.3.5 Rectal Atresia and Stenosis . . . 301 20.4 Postoperative Management and Colostomy Closure . . . 301 20.4.1 Evaluation of Results . . . 302 References . . . 302 20.2 Posterior Sagittal Approach e patient is placed in the prone position with the pelvis elevated. e use of an electrical stimulator to elicit muscle contraction during the operation is very helpful. is contraction serves as a guide to keep the incision precisely in the midline, leaving equal amounts of muscle on either side. e length of the incision varies with the type of defect and can be ex- tended to achieve the necessary exposure to effect a satisfactory repair. us, a perineal fistula requires a minimal posterior sagittal incision (2 cm), whereas higher defects may require a full posterior sagittal incision that runs from the middle portion of the sa- crum towards the base of the scrotum in the male. e incision includes the skin, subcutaneous tissue, para- sagittal fibers, muscle complex, and levator muscles (Fig. 20.1). In simple defects (perineal), the incision includes the parasagittal fibers and the muscle com- 20 Operative Management of Anomalies in Males Marc A. Levitt and Alberto Peña Table 20.1 Classification of anomalies (according to Peña [14], with permission) Males Cutaneous (perineal fistula) Rectourethral fistula Bulbar Prostatic Rectobladderneck fistula Imperforate anus without fistula Rectal atresia Females Cutaneous (perineal fistula) Vestibular fistula Imperforate anus without fistula Rectal atresia Cloaca Complex malformations
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of 20 Operative Management of Anomalies in Males
295
20.1 Introduction
Anorectal malformations (ARM) represent a wide spectrum of defects. The terms low, intermediate, and high are arbitrary and not very useful in therapeutic or prognostic terms. Within the group of ARM tra-ditionally referred to as high, there are defects with different therapeutic and prognostic implications. For instance, retroprostatic fistula and rectobladderneck fistula were both considered high, yet the first can be repaired with a posterior sagittal approach alone, but the second also requires an abdominal approach. The prognosis for each type is completely different. There-fore, anatomic descriptions of the malformations are more useful clinically (Table 20.1).
In the past, many surgical techniques to repair ARM have been described. These included endorectal dissection [1–3], anterior perineal approach to a rec-tourethral fistula [4], and many different types of ano-plasties [5]. However, most pediatric surgeons now use the posterior sagittal approach to repair these malformations with or without laparotomy or lapa-roscopy. The debate recently has been centered more on the possibility of performing these operations pri-marily without a protective colostomy and using lapa-roscopy if an abdominal component is needed [6–8].
Contents
20.1 Introduction . . . 29520.2 Posterior Sagittal Approach . . . 29520.3 Repair of Specific Defects in Boys . . . 29620.3.1 Rectoperineal Fistulas . . . 29620.3.2 Rectourethral Fistulas . . . 29720.3.3 Rectobladderneck Fistula . . . 30020.3.4 Imperforate Anus Without Fistula . . . 30120.3.5 Rectal Atresia and Stenosis . . . 30120.4 Postoperative Management
and Colostomy Closure . . . 30120.4.1 Evaluation of Results . . . 302
References . . . 302
20.2 Posterior Sagittal Approach
The patient is placed in the prone position with the pelvis elevated. The use of an electrical stimulator to elicit muscle contraction during the operation is very helpful. This contraction serves as a guide to keep the incision precisely in the midline, leaving equal amounts of muscle on either side. The length of the incision varies with the type of defect and can be ex-tended to achieve the necessary exposure to effect a satisfactory repair. Thus, a perineal fistula requires a minimal posterior sagittal incision (2 cm), whereas higher defects may require a full posterior sagittal incision that runs from the middle portion of the sa-crum towards the base of the scrotum in the male. The incision includes the skin, subcutaneous tissue, para-sagittal fibers, muscle complex, and levator muscles (Fig. 20.1). In simple defects (perineal), the incision includes the parasagittal fibers and the muscle com-
20 Operative Management of Anomalies in MalesMarc A. Levitt and Alberto Peña
Table 20.1 Classification of anomalies (according to Peña [14], with permission)
Males
Cutaneous (perineal fistula)
Rectourethral fistula
Bulbar
Prostatic
Rectobladderneck fistula
Imperforate anus without fistula
Rectal atresia
Females
Cutaneous (perineal fistula)
Vestibular fistula
Imperforate anus without fistula
Rectal atresia
Cloaca
Complex malformations

Marc A. Levitt and Alberto Peña296
plex, and it is not usually necessary to expose the le-vator ani muscle. Once the sphincter mechanism has been divided, the next most important step of the op-eration is the separation of the rectum from the uro-genital structures, which represents the most delicate part of the procedure. Any kind of blind maneuver exposes the patient to a serious injury during this part of the operation [9].
About 90% of defects in boys can be repaired via the posterior sagittal approach alone without an ab-dominal component [10]. Each case has individual anatomical characteristics that mandate technical modifications. An example is the size discrepancy fre-quently seen between an ectatic rectum and the space available for pull-through. If the discrepancy is sig-nificant, the surgeon must tailor the rectum to fit. The number of rectums that need tapering is decreasing, probably because patients are receiving better colos-tomies, and the babies are undergoing the main repair earlier in life so that the distalrectosignoid does not have time to dilate.
A posterior sagittal approach should never be at-tempted without a technically adequate high-pressure distal colostogram to determine the exact position of the rectum and the fistula [11]. Attempting the repair without this important information significantly in-creases the risk of nerve damage, damage to the semi-nal vesicles, prostate, urethra, ureters, bladder neck, and bladder denervation [9].
20.3 Repair of Specific Defects in Boys
20.3.1 Rectoperineal Fistulas
Rectoperineal fistula is what traditionally was known as a low defect. The rectum is located within most of
the sphincter mechanism. Only the lowest part of the rectum is anteriorly mislocated (Fig. 20.2). Some-times the fistula does not open into the perineum, but rather follows a subepithelial midline tract, opening somewhere along the midline perineal raphe, scro-tum, or even at the base of the penis. The diagnosis is established by perineal inspection. No further in-vestigations are required. Most of the time, the anal fistula opening is abnormally narrow (stenosis). The terms “covered anus,” “anal membrane,” and “anteri-orly mislocated anus,” as well as “bucket-handle mal-formations” refer to different external manifestations of perineal fistulas. We prefer the term “rectoperineal fistula” as this is most descriptive. The opening is not an anus as it is not a normal anal canal and is not sur-rounded by sphincter. The term “fistula” therefore is more accurate.
The operation is performed in the prone position with the pelvis elevated. Multiple 6-0 silk stitches are placed in the fistula orifice. An incision, usually about 2 cm, is created dividing the entire sphincter mecha-nism located posterior to the fistula. The sphincter is
Fig. 20.1 Posterior sagittal incision. Separation of the parasagittal fibers and exposure of the muscle complex ([15], with permission)
Fig. 20.2 Perineal fistula ([15], with permission)

29720 Operative Management of Anomalies in Males
divided and the posterior rectal wall is identified by its characteristic whitish appearance. Dissection of the rectum begins laterally, which makes dissection of the anterior rectal wall easier to visualize.
Dissection of the anterior rectal wall is the most critical because even when these patients have a low malformation, the rectum is still intimately attached to the urethra. The most common, and feared com-plication in these operations involves injury to the urethra. The patient must have a Foley catheter in place. To avoid a urethral injury, the surgeon must be meticulous during the dissection of the anterior rectal wall, and must keep in mind that the common wall has no plane of dissection and two walls must be cre-ated out of one.
These patients have an excellent functional prog-nosis in terms of bowel control. However, they suf-fer from the highest incidence of constipation. When the problem of constipation is not treated properly, chronic fecal impaction and overflow pseudoinconti-nence can occur.
20.3.2 Rectourethral Fistulas
Imperforate anus with rectourethral fistula is the most frequent defect in male patients [10]. The fistula may be located at the lower part of the urethra (bul-bar urethra; Fig. 20.3) or the upper urethra (prostatic urethra) (Fig. 20.4). Immediately above the fistula site, the rectum and urethra share a common wall, an anatomic fact with significant technical and surgi-cal implications. The rectum is usually distended and surrounded laterally and posteriorly by the levator ani muscle. Between the rectum and the perineal skin, a portion of striated voluntary muscle, called the mus-cle complex, is present. Contraction of these muscle
fibers elevates the skin of the anal dimple. At the level of the skin, a group of voluntary muscle fibers, called parasagittal fibers, are located on both sides of the midline.
Lower urethral (bulbar) fistulas are usually associ-ated with good-quality muscles, a well-developed sa-crum, a prominent midline groove, and a prominent anal dimple. Higher urethral (prostatic) fistulas are more frequently associated with poor-quality muscles, an abnormally developed sacrum, a flat perineum with a poor midline groove, and a barely visible anal dimple. Of course, exceptions to these rules exist.
A Foley catheter is inserted through the urethra. About 20% of the time, this catheter goes into the rectum rather than the bladder. Under these circum-stances, the surgeon can attempt catheterizing again using a catheter guide, or can relocate the catheter into the bladder under direct visualization during the operation. The incision is performed as previously described (Fig. 20.1); the parasagittal fibers, muscle complex, and levator muscle fibers are completely di-vided. Sometimes, the coccyx can be split in the mid-line with a cautery, particularly in those cases of rec-toprostatic fistula in which the surgeon requires more exposure in the upper part of the incision. The higher the malformation, the deeper the levator muscle is located. When the entire sphincter mechanism has been divided, the surgeon expects to find the rectum.
It is at this point in the operation that the impor-tance of a good high-pressure distal colostogram can-not be overstated. If the radiologic image shows the presence of a rectourethral bulbar fistula, the surgeon can expect that the rectum will be found just below the levator, and there is no way to injure the urinary tract because the rectum extends all the way down to the area of the bulbar urethra. On the other hand, if the preoperative image of the distal colostogram
Fig. 20.3 Rectourethrobulbar fistula ([15], with permission) Fig. 20.4 Rectourethroprostatic fistula ([15], with permission)

Marc A. Levitt and Alberto Peña298
shows a rectoprostatic fistula, the surgeon must be particularly careful and look for the rectum near the coccyx. Looking for the rectum lower than that ex-poses the patient to the risk of urinary tract injury. Also, if the high-pressure distal colostogram discloses the presence of a rectobladder-neck fistula, the sur-geon should not even look for the rectum posterior sagittally because it is not there, and during a blind search, injury to the genitourinary tract could occur. In patients with rectourethrobulbar fistula, the rec-tum actually bulges through the incision when one completes division of the entire sphincter mechanism (Fig. 20.5).
Silk stitches are placed in the posterior rectal wall on both sides of the midline. The rectum is opened in the midline and the incised distally, exactly in the midline, down to the fistula site. Temporary silk stitches are placed on the edges of the opened poste-rior rectal wall. When the fistula site is visualized, a final silk stitch is placed in the fistula orifice itself.
The anterior rectal wall above the fistula is a thin structure. It is actually a common wall with no plane of separation between the urinary tract and the rec-
tum. Therefore, a plane of separation must be created in that common wall. For this, multiple 6-0 silk trac-tion stitches are placed in the rectal mucosa immedi-ately above the fistula site. The rectum is then sepa-rated from the urethra, creating a submucosal plane for approximately 5–10 mm above the fistula site (Fig. 20.6). This dissection is the source of the most serious complications during this repair. Creating a lateral plan first makes the anterior dissection easier.
The rectum is covered by a thin fascia that must be completely removed to be sure that one is work-ing as close as possible to the rectal wall, to avoid denervation and injury to neighboring structures and to insure mobilization. Once the rectum is fully separated, a circumferential perirectal dissection is performed to gain enough rectal length to reach the perineum. In cases of rectourethrobulbar fistula, the dissection is rather minimal because only a short gap exists between the rectum and the perineum. In cases of rectoprostatic fistulas, the perirectal dissection is significant.
During this dissection, uniform traction is ap-plied on the multiple silk stitches that were originally placed on the rectal edges and on the mucosa above the fistula. Uniform traction shows the rectal wall and identifies bands and vessels that hold the rectum in the pelvis. These bands must be carefully separated from the rectal wall and cauterized because they are vessels that tend to retract into the pelvis. The dissec-tion should be performed as close as possible to the rectal wall without injuring the wall itself. Injury to the rectal wall can disrupt the intramural blood sup-ply, upon which the pulled-through rectum depends.
The bands that are divided around the rectum are actually vessels and nerves. One would think that this denervation would provoke dysmotility, which leads to the problem of constipation in these patients. Thus, patients with higher malformations (which require
Fig. 20.5 Dividing the muscle complex and levator muscle. The rectum is exposed ([15], with permission)
Fig. 20.6 A, B Separation of the rectum from the urethra. C The rec-tum is completely separated ([15], with permission)
29920 Operative Management of Anomalies in Males
more dissection) would be expected to suffer from more severe constipation. However, the opposite is true in that patients with lower defects suffer more severe constipation than patients with higher defects [10]. The explanation for the observed dysmotility re-mains elusive [12].
The circumferential dissection of the rectum con-tinues until the surgeon feels that enough length has been gained to allow a tension-free rectoperineal anastomosis. At this point, the size of the rectum can be evaluated and compared with the available space. If necessary, the rectum can be tapered, removing part of the posterior wall. In such cases, the rectal wall is reconstructed with two layers of interrupted long-lasting absorbable stitches.
The anterior rectal wall is frequently damaged to some degree as a consequence of the mucosal sepa-ration between rectum and urethra. To reinforce this wall, both smooth muscle layers can be stitched to-gether with interrupted 5-0 long-lasting absorbable stitches. The urethral fistula is sutured with the same material. The rectal tapering should never be per-formed anteriorly as this would leave a rectal suture line in front of the urethral fistula repair, and may lead to a recurrent fistula.
The limits of the sphincter mechanism are deter-mined electrically and marked with temporary silk stitches at the skin level. Those limits are sometimes easily visible without electrical stimulation in patients with a good sphincter mechanism. The limits of the sphincter are represented by the crossing of the mus-cle complex (the voluntary muscle structure that runs from the levator all the way down to the skin paral-lel to the direction of the rectum) with the parasagit-
tal fibers (which run perpendicular and lateral to the muscle complex and parallel to the posterior sagittal incision.).
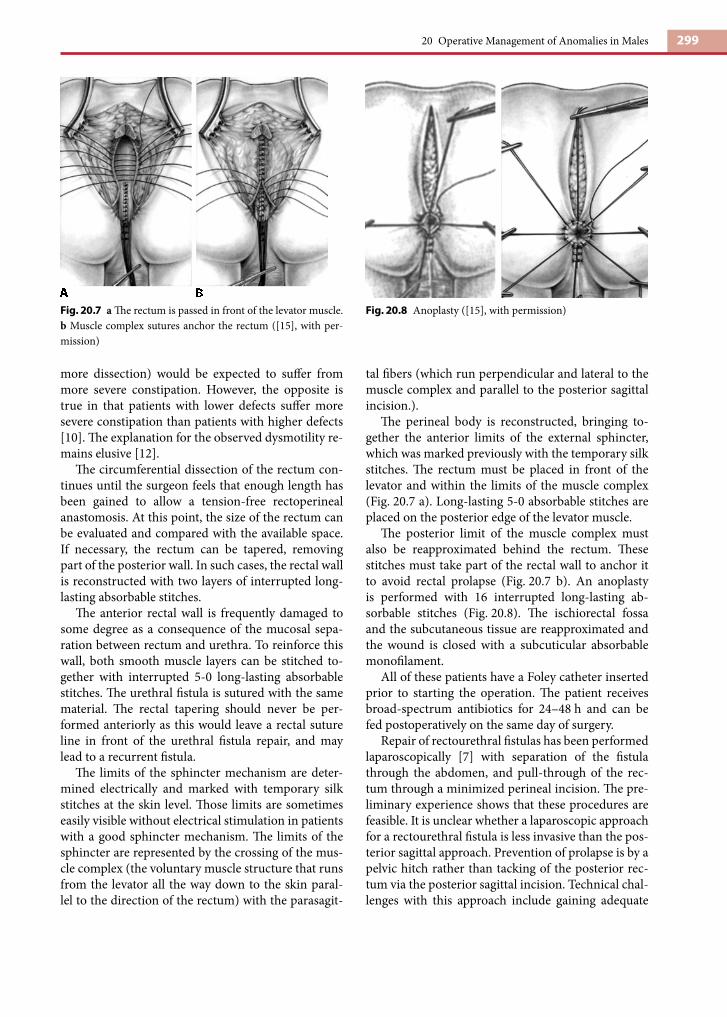
The perineal body is reconstructed, bringing to-gether the anterior limits of the external sphincter, which was marked previously with the temporary silk stitches. The rectum must be placed in front of the levator and within the limits of the muscle complex (Fig. 20.7 a). Long-lasting 5-0 absorbable stitches are placed on the posterior edge of the levator muscle.
The posterior limit of the muscle complex must also be reapproximated behind the rectum. These stitches must take part of the rectal wall to anchor it to avoid rectal prolapse (Fig. 20.7 b). An anoplasty is performed with 16 interrupted long-lasting ab-sorbable stitches (Fig. 20.8). The ischiorectal fossa and the subcutaneous tissue are reapproximated and the wound is closed with a subcuticular absorbable monofilament.
All of these patients have a Foley catheter inserted prior to starting the operation. The patient receives broad-spectrum antibiotics for 24–48 h and can be fed postoperatively on the same day of surgery.
Repair of rectourethral fistulas has been performed laparoscopically [7] with separation of the fistula through the abdomen, and pull-through of the rec-tum through a minimized perineal incision. The pre-liminary experience shows that these procedures are feasible. It is unclear whether a laparoscopic approach for a rectourethral fistula is less invasive than the pos-terior sagittal approach. Prevention of prolapse is by a pelvic hitch rather than tacking of the posterior rec-tum via the posterior sagittal incision. Technical chal-lenges with this approach include gaining adequate
Fig. 20.7 a The rectum is passed in front of the levator muscle. b Muscle complex sutures anchor the rectum ([15], with per-mission)
Fig. 20.8 Anoplasty ([15], with permission)

Marc A. Levitt and Alberto Peña300
rectal length, and tapering an ectatic rectum if neces-sary.
20.3.3 Rectobladderneck Fistula
In this defect, which affects 10% of males, the rectum opens at the bladder neck (Fig. 20.9). The patient has a poor prognosis because the levator ani muscle, mus-cle complex, and external sphincter are frequently poorly developed. Consistent with the caudal regres-sion, the sacrum and entire pelvis is often deformed and underdeveloped. The perineum is often flat, with evidence of poor muscle development.
For this repair, a total body preparation is per-formed; the sterile field includes the entire lower part of the patient’s body. The initial incision is posterior sagittal. All of the muscle structures are divided in the midline. The channel for the rectum, which lies just under the coccyx, is created bluntly. This poste-rior sagittal incision can be created with the child in supine position and the legs lifted up. At this point, laparoscopy represents an excellent minimally inva-sive alternative to a laparotomy.
These patients have the rectum connected to the bladder neck, located approximately 2 cm below the peritoneal reflection. Interestingly, the higher the malformation, the shorter the common wall between the rectum and the urinary tract. This means that the rectum in this group of defects opens in a perpen-
dicular fashion into the bladder neck, which makes its dissection much easier. The laparoscopic approach provides an excellent view of the peritoneal reflection, and one can also see the ureters and the vas deferens, which tend to run in the direction of the bladder neck. During the dissection of the rectum, therefore, these structures must be kept under direct view to prevent damage to them. The serosa that covers the most dis-tal part of the rectum should be divided, creating a plane of dissection around the rectum; it is this plane that is used to continue the dissection distally. The rectum rapidly narrows down, and this is where the fistula should be ligated.
At this point the surgeon must gain adequate length for the rectum to reach the perineum. The vessels that supply the distal rectum must be meticulously di-vided. Laparoscopically, or through a laparotomy, the space in the retroperitoneum for pull-through of the rectum is visualized (Fig. 20.10). An instrument or trocar from the perineum can be introduced to grab the rectum and pull it down. This allows the surgeon to see from above the tension lines that represent the vessels that it must be divided until the rectum reaches the perineum.
Tapering of the rectum, if that is required, is dif-ficult with a laparoscopic approach, and mobilization of a very high rectum is technically challenging. In addition, passage of the trocar from perineum into the pelvis must be done carefully to avoid injury to the bladder neck and ureters.
Fig. 20.9 Rectobladderneck fistula ([15], with permission) Fig. 20.10 A Abdominal approach for high defects (rectoblad-der-neck fistula). The rectum has been separated from the blad-der neck. The presacral rubber tube is identified. B The rectum is anchored to the rubber tube to guide the pull-through ([15], with permission)

30120 Operative Management of Anomalies in Males
20.3.4 Imperforate Anus Without Fistula
Most patients with this unusual defect have a well-developed sacrum and good muscles, and thus they have good prognosis for bowel function. The rectum ends approximately 2 cm from the perineal skin. Even though the patient has no communication between rectum and urethra, these two structures are sepa-rated only by a thin, common wall, which is an im-portant anatomic detail with technical implications. About half of the patients with no fistula also have Down’s syndrome and more than 90% of the patients with Down’s syndrome and imperforate anus suffer from this specific defect, hinting at a chromosomal link [13]. The fact that these patients have Down’s syndrome does not seem to interfere with the good prognosis in terms of bowel control.
In these cases, the blind end of the rectum is usually located at the level of the bulbar urethra. The rectum must be carefully separated from the urethra, because both structures share a common wall even though no fistula is present. The rest of the repair must be per-formed as described for the rectourethral fistula.
20.3.5 Rectal Atresia and Stenosis
This is an extremely unusual defect that occurs in only 1% of male patients, occurring in 1% of our cases, in which the lumen of the rectum may be atretic or ste-notic. The upper pouch is dilated and the lower por-tion is a small anal canal in the normal location. The narrow area starts at a depth of approximately 1–2 cm. These two structures may be separated by a thin mem-brane or by a dense portion of fibrous tissue. Patients with this defect have all the necessary elements to be continent and have an excellent functional prognosis. Because they have a well-developed anal canal, they have normal sensation in the anorectum. They also have almost normal voluntary sphincters.
The approach to these malformations is also via a posterior sagittal incision. The upper rectal pouch is open, as well as the short distal anal canal. An end-to-end anastomosis is performed under direct visu-alization, followed by a meticulous reconstruction of the sphincter mechanism posterior to the rectum (see Chap. 12)..
20.4 Postoperative Management and Colostomy Closure
In male patients with rectourethral fistulas, the Foley catheter remains in for 7 days. If the catheter comes out accidentally before that, patients usually void without any problem and do not require catheter replacement. Intravenous antibiotics are adminis-tered for 48 h. Antibiotic ointment is applied to the perineum for 7 days. Most patients usually go home after 2 days, or after 3–4 days if the abdomen was en-tered.Two weeks after the repair anal dilatations are started. A dilator that fits snugly into the anus is passed twice daily by the parents. Every week, the size of the dila-tor is increased, until the rectum reaches the desired size, which depends on the patient’s age (Table 20.2). Once this desired size is reached, the colostomy may be closed. The frequency of dilatation may be reduced once the dilator goes in easily with no resistance ac-cording to the following protocol: once a day for 1 month, every 3rd day for 1 month, twice a week for 1 month, once a week for 1 month, and once a month for 3 months. Nonmanageable, severe strictures are seen in cases in which the dilatation program was not carried out as indicated or when the blood sup-ply of the distal rectum was damaged during the pull-through.
After the colostomy is closed, the patient usually has multiple bowel movements and may develop per-ineal excoriation. A constipating diet may be helpful in the treatment of this problem. After several weeks, the number of bowel movements decreases and most patients then start to have constipation. After 3 months, the patient develops a more regular bowel movement pattern. A patient who has one to three bowel movements per day, remains clean between bowel movements, and shows evidence of a feeling or pushing during bowel movements, has a good bowel movement pattern and is usually able to potty train. A
Table 20.2 Size of dilator according to age ([14], with permis-sion)
Age Hegar dilator (no.)
1–4 months 12
4–12 months 13
8–12 months 14
1–3 years 15
3–12 years 16
>12 years 17
302
patient with multiple bowel movements or one who passes stool constantly without showing any signs of sensation or pushing usually has a poor functional prognosis.
20.4.1 Evaluation of Results
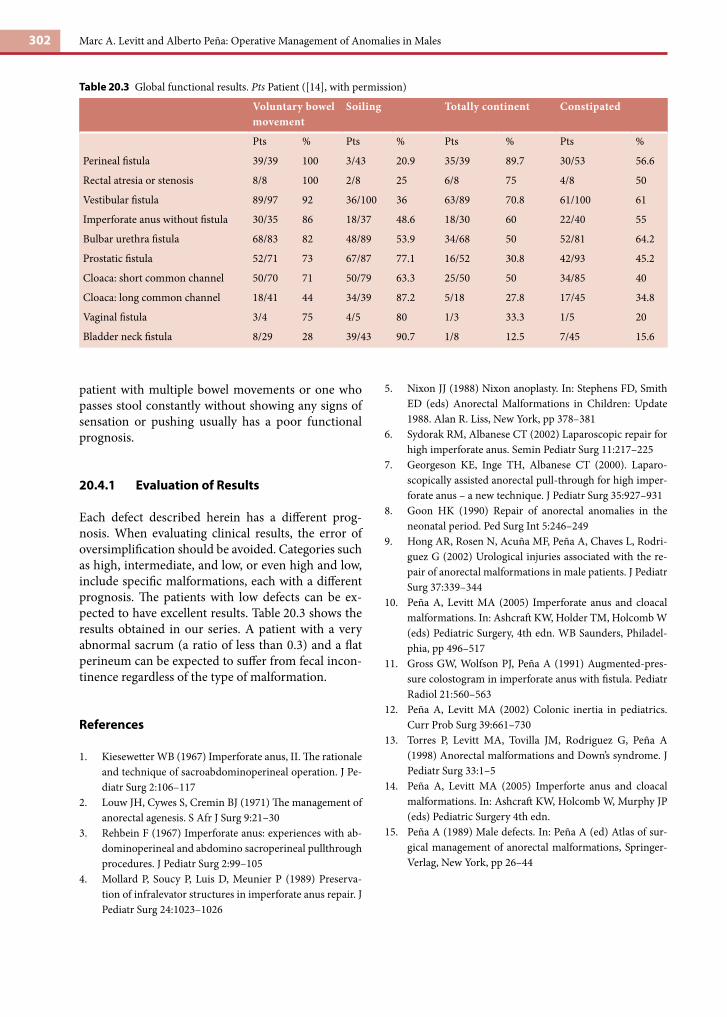
Each defect described herein has a different prog-nosis. When evaluating clinical results, the error of oversimplification should be avoided. Categories such as high, intermediate, and low, or even high and low, include specific malformations, each with a different prognosis. The patients with low defects can be ex-pected to have excellent results. Table 20.3 shows the results obtained in our series. A patient with a very abnormal sacrum (a ratio of less than 0.3) and a flat perineum can be expected to suffer from fecal incon-tinence regardless of the type of malformation.
References
1. Kiesewetter WB (1967) Imperforate anus, II. The rationale and technique of sacroabdominoperineal operation. J Pe-diatr Surg 2:106–117
2. Louw JH, Cywes S, Cremin BJ (1971) The management of anorectal agenesis. S Afr J Surg 9:21–30
3. Rehbein F (1967) Imperforate anus: experiences with ab-dominoperineal and abdomino sacroperineal pullthrough procedures. J Pediatr Surg 2:99–105
4. Mollard P, Soucy P, Luis D, Meunier P (1989) Preserva-tion of infralevator structures in imperforate anus repair. J Pediatr Surg 24:1023–1026
5. Nixon JJ (1988) Nixon anoplasty. In: Stephens FD, Smith ED (eds) Anorectal Malformations in Children: Update 1988. Alan R. Liss, New York, pp 378–381
6. Sydorak RM, Albanese CT (2002) Laparoscopic repair for high imperforate anus. Semin Pediatr Surg 11:217–225
7. Georgeson KE, Inge TH, Albanese CT (2000). Laparo-scopically assisted anorectal pull-through for high imper-forate anus – a new technique. J Pediatr Surg 35:927–931
8. Goon HK (1990) Repair of anorectal anomalies in the neonatal period. Ped Surg Int 5:246–249
9. Hong AR, Rosen N, Acuña MF, Peña A, Chaves L, Rodri-guez G (2002) Urological injuries associated with the re-pair of anorectal malformations in male patients. J Pediatr Surg 37:339–344
10. Peña A, Levitt MA (2005) Imperforate anus and cloacal malformations. In: Ashcraft KW, Holder TM, Holcomb W (eds) Pediatric Surgery, 4th edn. WB Saunders, Philadel-phia, pp 496–517
11. Gross GW, Wolfson PJ, Peña A (1991) Augmented-pres-sure colostogram in imperforate anus with fistula. Pediatr Radiol 21:560–563
12. Peña A, Levitt MA (2002) Colonic inertia in pediatrics. Curr Prob Surg 39:661–730
13. Torres P, Levitt MA, Tovilla JM, Rodriguez G, Peña A (1998) Anorectal malformations and Down’s syndrome. J Pediatr Surg 33:1–5
14. Peña A, Levitt MA (2005) Imperforte anus and cloacal malformations. In: Ashcraft KW, Holcomb W, Murphy JP (eds) Pediatric Surgery 4th edn.
15. Peña A (1989) Male defects. In: Peña A (ed) Atlas of sur-gical management of anorectal malformations, Springer-Verlag, New York, pp 26–44
Table 20.3 Global functional results. Pts Patient ([14], with permission)
Voluntary bowel movement
Soiling Totally continent Constipated
Pts % Pts % Pts % Pts %
Perineal fistula 39/39 100 3/43 20.9 35/39 89.7 30/53 56.6
Rectal atresia or stenosis 8/8 100 2/8 25 6/8 75 4/8 50
Vestibular fistula 89/97 92 36/100 36 63/89 70.8 61/100 61
Imperforate anus without fistula 30/35 86 18/37 48.6 18/30 60 22/40 55
Bulbar urethra fistula 68/83 82 48/89 53.9 34/68 50 52/81 64.2
Prostatic fistula 52/71 73 67/87 77.1 16/52 30.8 42/93 45.2
Cloaca: short common channel 50/70 71 50/79 63.3 25/50 50 34/85 40
Cloaca: long common channel 18/41 44 34/39 87.2 5/18 27.8 17/45 34.8
Vaginal fistula 3/4 75 4/5 80 1/3 33.3 1/5 20
Bladder neck fistula 8/29 28 39/43 90.7 1/8 12.5 7/45 15.6
Marc A. Levitt and Alberto Peña: Operative Management of Anomalies in Males