
1,6)Fucosyltransferase expression is an independent prognostic factor for disease-free survival in...
11
Original contribution α(1,6)Fucosyltransferase expression is an independent prognostic factor for disease-free survival in colorectal carcinoma ☆ L. Muinelo-Romay PhD a , S. Villar-Portela PhD a , E. Cuevas Alvarez MD, PhD b , E. Gil-Martín PhD a,1 , Almudena Fernández-Briera PhD a, ⁎ ,1 a Department of Biochemistry, Genetics and Immunology, Faculty of Biology, University of Vigo, Spain b Pathology Service, University Complex Hospital of Ourense, Spain Received 22 November 2010; revised 23 January 2011; accepted 28 January 2011 Keywords: Colorectal cancer; Glycosylation; Core-fucosylation; α(1,6)Fucosyltransferase; Tumor biomarker; Prognostic factor Abstract We previously reported that α(1,6)fucosyltransferase (Enzyme class 2.4.1.68) activity and expression are increased in colorectal cancer, suggesting a role for this enzyme in tumor development and progression. However, the possible impact of α(1,6)fucosyltransferase activity or expression on clinical outcomes in colorectal cancer patients has never been studied. Thus, the present study was conducted to determine the value of α(1,6)fucosyltransferase as a prognostic factor for colorectal cancer. α(1,6)Fucosyltransferase expression was analyzed using immunohistochemistry in 141 colorectal tumors, and α(1,6)fucosyltransferase activity was determined in 39 tumors. A complete standardized follow-up of patients was documented until the end of the observation period of 5 years or patient death. Univariate analysis demonstrated the absence of a correlation between enzyme activity and disease evolution. However, in patients with moderate or strong α(1,6)fucosyltransferase expression, a significant decrease in the overall (P = .04) and disease-free (P = .03) survival rates was observed. In addition, when local and distant disease recurrence were considered separately, enzyme expression was found to correlate with local tumor recurrences (P = .01). Furthermore, multivariate analysis showed that α(1,6)fucosyltransferase expression has independent value for predicting tumor recurrences and, specifically, local recurrences. These findings suggest that α(1,6) fucosyltransferase expression may be a good indicator of poor prognosis in colorectal cancer and, therefore, a helpful tool to choose the most effective treatment. © 2011 Elsevier Inc. All rights reserved. 1. Introduction Colorectal carcinoma (CRC) is one of the most frequent tumors in the Western world. Despite the fact that survival rates have improved over the last decades, nearly one half of patients with CRC develop local recurrences or distant metastasis after surgery [1,2]. Therefore, the identification of new biomolecules implicated in tumor progression could ☆ This project was partially supported by the “Xunta de Galicia” Grant INCITE08PXIB310249PR. ⁎ Corresponding author. Almudena Fernández-Briera, Department of Biochemistry, Genetics and Immunology, Faculty of Biology, University of Vigo, Campus As Lagoas-Marcosende, 36310, Vigo, Spain. E-mail address: [email protected] (A. Fernández-Briera). 1 These authors contributed equally to this work. www.elsevier.com/locate/humpath 0046-8177/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.humpath.2011.01.021 Human Pathology (2011) 42, 1740–1750
Transcript of 1,6)Fucosyltransferase expression is an independent prognostic factor for disease-free survival in...

www.elsevier.com/locate/humpath
Human Pathology (2011) 42, 1740–1750
Original contribution
α(1,6)Fucosyltransferase expression is an independentprognostic factor for disease-free survival incolorectal carcinoma☆
L. Muinelo-Romay PhDa, S. Villar-Portela PhDa, E. Cuevas Alvarez MD, PhDb,E. Gil-Martín PhDa,1, Almudena Fernández-Briera PhDa,⁎,1
aDepartment of Biochemistry, Genetics and Immunology, Faculty of Biology, University of Vigo, SpainbPathology Service, University Complex Hospital of Ourense, Spain
Received 22 November 2010; revised 23 January 2011; accepted 28 January 2011
IN
BV
0d
Keywords:Colorectal cancer;Glycosylation;Core-fucosylation;α(1,6)Fucosyltransferase;Tumor biomarker;Prognostic factor
Abstract We previously reported that α(1,6)fucosyltransferase (Enzyme class 2.4.1.68) activity andexpression are increased in colorectal cancer, suggesting a role for this enzyme in tumor developmentand progression. However, the possible impact of α(1,6)fucosyltransferase activity or expression onclinical outcomes in colorectal cancer patients has never been studied. Thus, the present study wasconducted to determine the value of α(1,6)fucosyltransferase as a prognostic factor for colorectalcancer. α(1,6)Fucosyltransferase expression was analyzed using immunohistochemistry in 141colorectal tumors, and α(1,6)fucosyltransferase activity was determined in 39 tumors. A completestandardized follow-up of patients was documented until the end of the observation period of 5 years orpatient death. Univariate analysis demonstrated the absence of a correlation between enzyme activityand disease evolution. However, in patients with moderate or strong α(1,6)fucosyltransferaseexpression, a significant decrease in the overall (P = .04) and disease-free (P = .03) survival rateswas observed. In addition, when local and distant disease recurrence were considered separately,enzyme expression was found to correlate with local tumor recurrences (P = .01). Furthermore,multivariate analysis showed that α(1,6)fucosyltransferase expression has independent value forpredicting tumor recurrences and, specifically, local recurrences. These findings suggest that α(1,6)fucosyltransferase expression may be a good indicator of poor prognosis in colorectal cancer and,therefore, a helpful tool to choose the most effective treatment.© 2011 Elsevier Inc. All rights reserved.
☆ This project was partially supported by the “Xunta de Galicia” GrantCITE08PXIB310249PR.⁎ Corresponding author. Almudena Fernández-Briera, Department of
iochemistry, Genetics and Immunology, Faculty of Biology, University ofigo, Campus As Lagoas-Marcosende, 36310, Vigo, Spain.E-mail address: [email protected] (A. Fernández-Briera).1 These authors contributed equally to this work.
046-8177/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.humpath.2011.01.021
1. Introduction
Colorectal carcinoma (CRC) is one of the most frequenttumors in the Western world. Despite the fact that survivalrates have improved over the last decades, nearly one half ofpatients with CRC develop local recurrences or distantmetastasis after surgery [1,2]. Therefore, the identification ofnew biomolecules implicated in tumor progression could

1741α(1,6)FT expression is a prognostic factor for CRC
be helpful for recognizing patients at high risk for relapse andto select adequate postoperative therapy.
We have previously reported that α(1,6)fucosyltransferase[α(1,6)FT (Enzyme class 2.4.1.68)] activity and expression isincreased in CRC, suggesting a role for this enzyme in tumordevelopment and progression [3]. Similar results have beendescribed for other human malignant processes, such ashepatocellular carcinoma [4,5], thyroid papillary carcinoma[6], and ovarian adenocarcinoma [7]. The α(1,6)FT enzymecatalyzes the transfer of fucose from guanosine diphosphate(GDP)–fucose to the innermost GlcNAc of hybrid andcomplex N-linked oligosaccharides via an α(1,6)linkage,resulting in core-fucosylated glycoproteins [8]. This catalyticactivity constitutes a form of posttranslational modification,because itmodulates the steric conformational properties of thecore-fucosylated glucide antenna and, consequently, the actionof other FTs on carbohydrate side chains and the biologicalfunction of resulting glycoproteins [9]. In support of this,several studies have demonstrated an important role for α(1,6)fucosylation in regulating the activity of proteins stronglyimplicated in tumor growth (eg, epidermal growth factorreceptor [EGFR], transforming growth factor receptor β1[TGFR-β1], and vascular endothelial growth factor receptor 2[VEGFR-2]) [10-12] and tumor dissemination (E-cadherin[13,14], α3β1, and α5β1 integrins [5,15]). Interestingly,inhibition of these proteins is currently a therapeutic strategyagainst several different neoplasias [16,17]. Consequently, theresponse of tumor cells to these new treatments could bepartially regulated by the action of the α(1,6)FT enzyme [18].
In addition, increased expression levels of α(1,6)fucosy-lated glycoproteins, coupled with an enhancement of α(1,6)FT activity, have been described in a wide variety of humantumors, suggesting their potential usefulness as biomarkers.The most representative case is the α(1,6)fucosylatedα-fetoprotein, which is used as a specific tumor markerfor hepatocellular carcinoma, whereas other unusually core-fucosylated serum glycoproteins, such as haptoglobin orGp73, have recently been proposed as potential diagnosticmarkers for this malignancy [19,20].
Although many studies have reported an associationbetween altered α(1,6)FT status [3,6,21] or its catalyticproducts [13,22] and the clinicopathologic parameters ofadvanced and aggressive tumors, to our knowledge, theinfluence of α(1,6)FT on tumor progression remainsunknown. In fact, only one recent report has analyzed theprognostic value of α(1,6)FT activity for predicting theresponse of metastatic breast cancer patients treated withthe anti-EGFR antibody, trastuzumab, with negative results[18]. In this context, the present study was undertaken toassess the possible impact of α(1,6)FT activity andexpression on clinical outcomes (local recurrence, distantmetastasis, disease-free, and overall survival rates) ofcuratively CRC resected patients, in an attempt to clarifythe real value of α(1,6)FT as a prognostic factor for thismalignant tumor and, therefore, its utility in helping to selectthe most effective treatment strategy.
2. Materials and methods
2.1. Patients and specimens
A total of 141 tumor colorectal tissue samples wereobtained from CRC patients who underwent curativesurgery (1995-2004) at the University Complex Hospitalof Ourense (Ourense, Spain), after receiving approval fromthe appropriate local institutional review board (ComitéÉtico de Investigación Clínica de Galicia, Spain). Sixty-onewomen and 80 men were included in the present study,with a mean age at diagnosis of 71.65 ± 0.77 years. Patientswith metastasis at the time of surgery or who died within30 days postoperation were excluded from this study. Forall 141 patients, α(1,6)FT expression was determined byimmunohistochemistry, whereas α(1,6)FT activity wasmeasured for 39 cases. Specimens used for immunohisto-chemical analysis were fixed in formalin (10%) andembedded in paraffin (60°C). Specimens used for α(1,6)FT assays were washed with ice-cold saline buffer andstored frozen at −85°C until use. Tumors were macroscop-ically and microscopically examined to determine theirlocation, size, and growth, as well as the histologic type andtumor staging based on Dukes [23] and TNM [24]classifications, respectively. For all analyzed patients, acomplete standardized follow-up was documented until theend of the observation period (60 months) or patient death.Follow-up information included local and distant metastasis(determined by x-ray, computed tomography scan, orendoscopy biopsy), as well as patient death.
2.2. Immunohistochemistry
Immunohistochemistry was performed as previouslydescribed [3,6]. Tissue sections (2-3 μm) were deparaffi-nized in xylene and rehydrated in a graded ethanol series(100°, 96°, and 70°). To quench endogenous peroxidaseactivity, sections were incubated with 0.5% (vol/vol)hydrogen peroxide in methanol. After rinsing withphosphate-buffered saline (PBS), bovine serum was appliedto block nonspecific binding of the antibody. Sections werethen incubated with primary antibody (dilution 1:40,antihuman α(1,6)FT, 15C6; Fujirebio Corp, Tokyo,Japan) at 4°C overnight. After rinsing with PBS, sectionswere incubated with secondary antibody bound to horse-radish peroxidase; horseradish peroxidase activity wasvisualized by incubating with 3,3-diaminobenzidine. Final-ly, after a wash in water, sections were counterstained withhematoxylin, dehydrated in a graded ethanol series (70°,96°, and 100°), washed in xylene, and mounted on aglass slide.
Negative controls were performed using PBS instead ofprimary antibody. Semiquantitative staining analysis wasperformed by a pathologist from the University ComplexHospital of Ourense (Ourense, Spain). The immunostaining

Fig. 1 Immunohistochemical analysis of α(1,6)FT expression inhealthy (A) and cancerous (B) colorectal mucosa. The signal wasclearly located in the cytoplasm of the epithelial cells.
1742 L. Muinelo-Romay et al.
expression pattern was classified as follows: 0, no staining;1, weak, less than 10% staining; 2, moderate, 10% to 50%,and 3, strong, more than 50% of the tissue was stained.
2.3. Determination of α(1,6)FT activity
2.3.1. Preparation of samples for enzyme activity assaysColorectal tissues were homogenized in 6 volumes of
0.01 mol/L Tris-HCl buffer (pH 7.4), containing 0.25 mol/Lsucrose. The homogenate was centrifuged for 10 minutes at500×g, at 4°C. The resulting supernatant was centrifuged at33 000×g for 60 minutes, at 4°C. Subsequently, the pelletwas resuspended in 1.5 mL of 0.01 mol/L Tris -HCl buffer(pH 7.4) and centrifuged at 145 000×g for 45 minutes, at4°C. The final pellet, containing the total cell membranefraction, was resuspended in 300 μL of 0.01 mol/L Tris-HClbuffer (pH 7.4) and stored at −20°C until use in enzymaticassays. Total protein content in the final membranepreparation was determined using the Bicinchoninic acidassay, with bovine serum albumin as a standard.
2.3.2. Enzyme activity assaysStandard α(1,6)FT activity assays were performed as
previously described [3], using 100 μmol/L donor substrate[0.5 μmol/L GDP-L-[14C]-fucose (Amersham BioscienceEurope GMBH, Uppsala, Sweden; 270-283 mCi/mmol),99.5 μmol/L GDP-L-fucose] and 0.32 mg acceptor substrate(asialoagalactofetuin). The radioactivity incorporated in theproteins was measured in a Wallac 1409-12 scintillatorsystem (Pegasus Scientific Inc., Rockville, MD, USA), usingEcoscint H as a scintillation counting mixture (NationalDiagnostics, Atlanta, GA, USA). Enzyme activity wasexpressed as microunits per milligram of protein = picomolesof fucose incorporated in asialoagalactofetuin per minute permilligram of protein.
2.4. Statistical analyses
Statistical analyses were performed using SPSS, version15.00, for Windows XP (SPSS, Chicago, IL, USA). χ2
and Fisher exact probability tests were used to evaluate thedifferences between categorical data. For continuous data,we used the Mann-Whitney U test and the Kruskal-Wallistest. Survival time was calculated as the number of monthspostsurgery to the final event (local recurrence, distantmetastasis, or death). Data from patients who were alivewithout recurrence at the end of the 60 months ofevaluation were censored. Survival curves were calculatedby the Kaplan-Meier method, and the significance ofdifferences was estimated by the log-rank test. Finally,multivariate analysis was performed using Cox regressionmodel. Results were considered statistically significantwhen P b .05.
3. Results
3.1. Association of α(1,6)FT activity andimmunohistochemical expression withclinicopathologic parameters
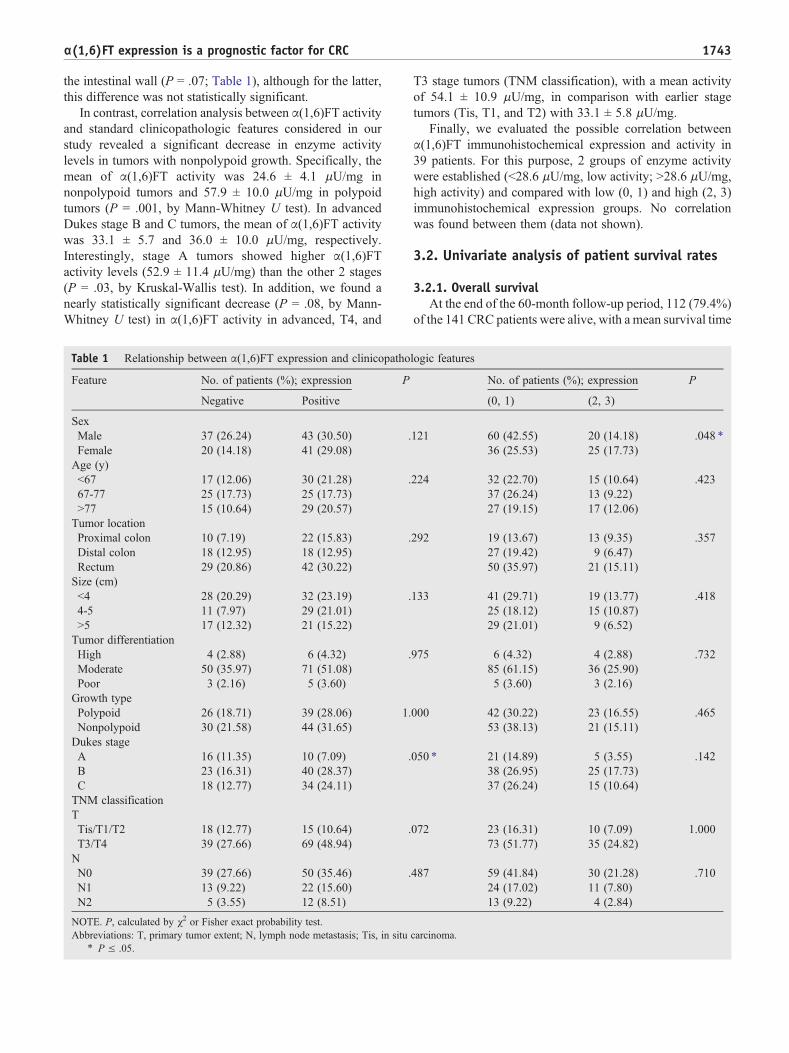
Expression of α(1,6)FT, as evidenced by immunohisto-chemical brown staining clearly located in the cytoplasm ofepithelial cells (Fig. 1), was observed in 84 (59.57%) of the141 CRC patients analyzed. Of these, the intensity ofstaining, and therefore α(1,6)FT expression, was weak in38 (26.9%) cases, moderate in 31 (22%) cases, and strong in15 (10.67%) cases. After correlation analysis (Table 1), nostatistically significant differences between α(1,6)FT expres-sion and clinicopathologic features such as age, tumor size,localization, pattern growth, differentiation, or lymph nodeinfiltration were found. Nevertheless, the percentage of caseswith moderate (2) or strong (3) α(1,6)FT expression washigher in women than in men (P = .05). In addition, α(1,6)FTexpression was more frequent in patients with advancedDukes stage (P = .05) tumors or higher infiltration rates into
1743α(1,6)FT expression is a prognostic factor for CRC
the intestinal wall (P = .07; Table 1), although for the latter,this difference was not statistically significant.
In contrast, correlation analysis between α(1,6)FT activityand standard clinicopathologic features considered in ourstudy revealed a significant decrease in enzyme activitylevels in tumors with nonpolypoid growth. Specifically, themean of α(1,6)FT activity was 24.6 ± 4.1 μU/mg innonpolypoid tumors and 57.9 ± 10.0 μU/mg in polypoidtumors (P = .001, by Mann-Whitney U test). In advancedDukes stage B and C tumors, the mean of α(1,6)FT activitywas 33.1 ± 5.7 and 36.0 ± 10.0 μU/mg, respectively.Interestingly, stage A tumors showed higher α(1,6)FTactivity levels (52.9 ± 11.4 μU/mg) than the other 2 stages(P = .03, by Kruskal-Wallis test). In addition, we found anearly statistically significant decrease (P = .08, by Mann-Whitney U test) in α(1,6)FT activity in advanced, T4, and
Table 1 Relationship between α(1,6)FT expression and clinicopatho
Feature No. of patients (%); expression P
Negative Positive
SexMale 37 (26.24) 43 (30.50) .Female 20 (14.18) 41 (29.08)Age (y)b67 17 (12.06) 30 (21.28) .67-77 25 (17.73) 25 (17.73)N77 15 (10.64) 29 (20.57)Tumor locationProximal colon 10 (7.19) 22 (15.83) .Distal colon 18 (12.95) 18 (12.95)Rectum 29 (20.86) 42 (30.22)Size (cm)b4 28 (20.29) 32 (23.19) .4-5 11 (7.97) 29 (21.01)N5 17 (12.32) 21 (15.22)Tumor differentiationHigh 4 (2.88) 6 (4.32) .Moderate 50 (35.97) 71 (51.08)Poor 3 (2.16) 5 (3.60)Growth typePolypoid 26 (18.71) 39 (28.06) 1.Nonpolypoid 30 (21.58) 44 (31.65)Dukes stageA 16 (11.35) 10 (7.09) .B 23 (16.31) 40 (28.37)C 18 (12.77) 34 (24.11)TNM classificationTTis/T1/T2 18 (12.77) 15 (10.64) .T3/T4 39 (27.66) 69 (48.94)NN0 39 (27.66) 50 (35.46) .N1 13 (9.22) 22 (15.60)N2 5 (3.55) 12 (8.51)
NOTE. P, calculated by χ2 or Fisher exact probability test.Abbreviations: T, primary tumor extent; N, lymph node metastasis; Tis, in situ
⁎ P ≤ .05.
T3 stage tumors (TNM classification), with a mean activityof 54.1 ± 10.9 μU/mg, in comparison with earlier stagetumors (Tis, T1, and T2) with 33.1 ± 5.8 μU/mg.
Finally, we evaluated the possible correlation betweenα(1,6)FT immunohistochemical expression and activity in39 patients. For this purpose, 2 groups of enzyme activitywere established (b28.6 μU/mg, low activity; N28.6 μU/mg,high activity) and compared with low (0, 1) and high (2, 3)immunohistochemical expression groups. No correlationwas found between them (data not shown).
3.2. Univariate analysis of patient survival rates
3.2.1. Overall survivalAt the end of the 60-month follow-up period, 112 (79.4%)
of the 141 CRC patients were alive, with a mean survival time
logic features
No. of patients (%); expression P
(0, 1) (2, 3)
121 60 (42.55) 20 (14.18) .048 ⁎
36 (25.53) 25 (17.73)
224 32 (22.70) 15 (10.64) .42337 (26.24) 13 (9.22)27 (19.15) 17 (12.06)
292 19 (13.67) 13 (9.35) .35727 (19.42) 9 (6.47)50 (35.97) 21 (15.11)
133 41 (29.71) 19 (13.77) .41825 (18.12) 15 (10.87)29 (21.01) 9 (6.52)
975 6 (4.32) 4 (2.88) .73285 (61.15) 36 (25.90)5 (3.60) 3 (2.16)
000 42 (30.22) 23 (16.55) .46553 (38.13) 21 (15.11)
050 ⁎ 21 (14.89) 5 (3.55) .14238 (26.95) 25 (17.73)37 (26.24) 15 (10.64)
072 23 (16.31) 10 (7.09) 1.00073 (51.77) 35 (24.82)
487 59 (41.84) 30 (21.28) .71024 (17.02) 11 (7.80)13 (9.22) 4 (2.84)
carcinoma.

Table 2 Univariate analysis with respect to overall and disease-free survival of CRC patients
Feature n Mean survival time (mo) Survival rate (%) P
Overallsurvival
Disease-freesurvival
Overallsurvival
Disease-freesurvival
Overallsurvival
Disease-freesurvival
SexMale 80 52.5 47.8 76.8 62.7 .791 .482Female 61 54.2 48.6 77.7 70.9Age (y)b67 47 55.2 45.7 84.3 61.4 .150 .34067-77 50 54.5 50.8 72.8 74.6N77 44 49.6 48.1 66.6 58.8Tumor locationProximal colon 32 49.1 42.3 73.5 48.7 .573 .052 ⁎
Distal colon 36 53.8 50.1 81.5 72.3Rectum 71 54.6 50.0 77.8 71.9Size (cm)b4 60 52.4 50.2 78.9 73.1 .913 .4754-5 40 53.0 45.3 74.2 61.2N5 38 54.4 49.0 78.4 67.6Tumor differentiationHigh 10 47.9 44.6 70.0 56.3 .568 .495Moderate 1211 53.7 48.4 77.7 67.0Poor 8 57.4 54.7 85.7 87.5Growth typePolypoid 65 54.0 49.0 76.5 70.1 .861 .406Nonpolypoid 74 52.4 47.1 76.9 62.4Dukes stageA 26 56.3 52.6 85.6 79.8 .185 .034 ⁎
B 63 53.9 50.8 80.7 71.9C 52 50.9 43.0 68.5 53.8TNM classificationTTis/T1/T2 33 52.7 51.1 74.8 76.7 .785 .217T3/T4 108 51.1 47.4 77.7 63.5NN0 89 54.6 51.3 82.3 74.0 .175 .002 ⁎
N1 35 50.1 46.4 66.1 63.8N2 17 52.7 36.6 74.8 35.3α(1.6)FT activity (μU/mg)b24.4 15 56.2 47.6 86.7 65.2 .363 .30824.3- 44.1 13 53.7 46.5 66.6 60.6N44.1 11 55.3 56.3 87.5 90.0α(1.6)FT expressionNegative 57 55.3 51.6 84.4 74.9 .130 .084Positive 84 51.8 45.9 72.4 60.8(0, 1) 96 54.6 51.0 82.1 71.4 .047 ⁎ .029 ⁎
(2. 3) 45 50.2 42.1 65.7 55.0
NOTE. P, calculated by log-rank test.Abbreviations: T, primary tumor extent; N, lymph node metastasis; Tis, in situ carcinoma.
⁎ P ≤ .05.
1744 L. Muinelo-Romay et al.
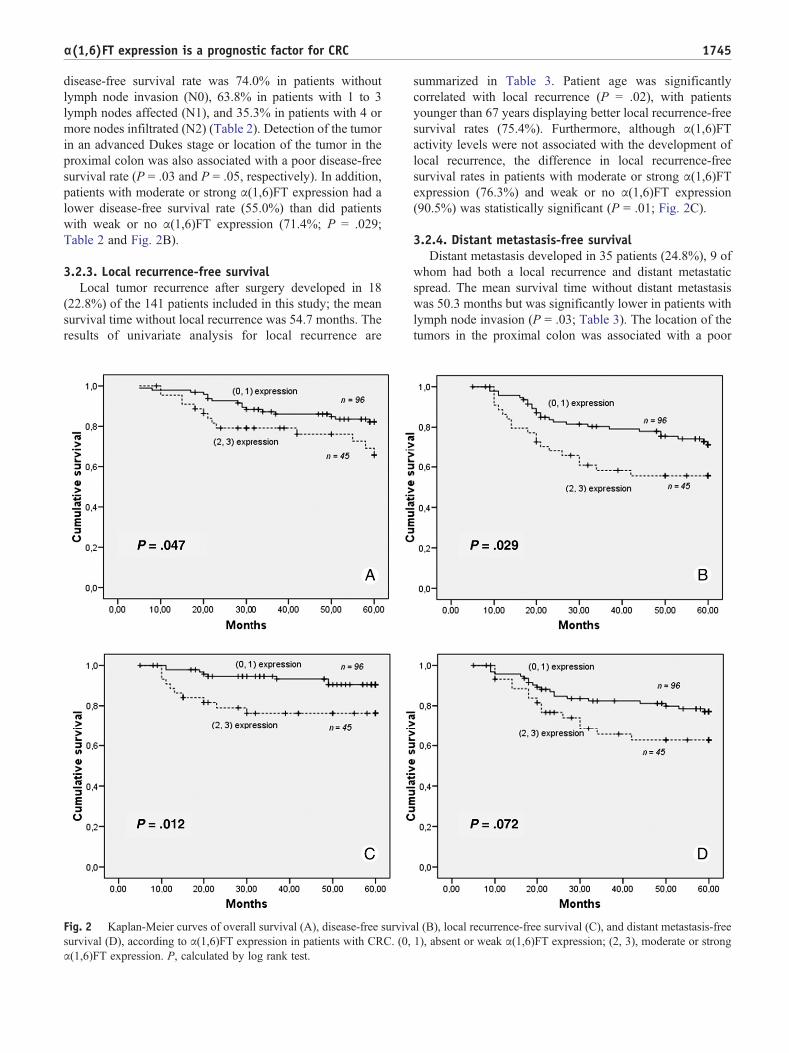
of 51.4 months. With the exception of α(1,6)FT expression,univariate analysis showed total independence between allvariables evaluated in the present study and overall patientsurvival rate. The presence of moderate or strong α(1,6)FTexpression significantly correlated with a fatal outcome inCRC patients (P = .047; Table 2 and Fig. 2A).
3.2.2. Disease-free survivalDuring follow-up evaluation period, 44 (31.2%) patients
had disease recurrence, and the overall mean disease-freesurvival time was 48.2 months. Interestingly, a clearcorrelation between lymph node infiltration and diseaserecurrence was found (P b .01; Table 2). Specifically, the
1745α(1,6)FT expression is a prognostic factor for CRC
disease-free survival rate was 74.0% in patients withoutlymph node invasion (N0), 63.8% in patients with 1 to 3lymph nodes affected (N1), and 35.3% in patients with 4 ormore nodes infiltrated (N2) (Table 2). Detection of the tumorin an advanced Dukes stage or location of the tumor in theproximal colon was also associated with a poor disease-freesurvival rate (P = .03 and P = .05, respectively). In addition,patients with moderate or strong α(1,6)FT expression had alower disease-free survival rate (55.0%) than did patientswith weak or no α(1,6)FT expression (71.4%; P = .029;Table 2 and Fig. 2B).
3.2.3. Local recurrence-free survivalLocal tumor recurrence after surgery developed in 18
(22.8%) of the 141 patients included in this study; the meansurvival time without local recurrence was 54.7 months. Theresults of univariate analysis for local recurrence are
Fig. 2 Kaplan-Meier curves of overall survival (A), disease-free survivsurvival (D), according to α(1,6)FT expression in patients with CRC. (0,α(1,6)FT expression. P, calculated by log rank test.
summarized in Table 3. Patient age was significantlycorrelated with local recurrence (P = .02), with patientsyounger than 67 years displaying better local recurrence-freesurvival rates (75.4%). Furthermore, although α(1,6)FTactivity levels were not associated with the development oflocal recurrence, the difference in local recurrence-freesurvival rates in patients with moderate or strong α(1,6)FTexpression (76.3%) and weak or no α(1,6)FT expression(90.5%) was statistically significant (P = .01; Fig. 2C).
3.2.4. Distant metastasis-free survivalDistant metastasis developed in 35 patients (24.8%), 9 of
whom had both a local recurrence and distant metastaticspread. The mean survival time without distant metastasiswas 50.3 months but was significantly lower in patients withlymph node invasion (P = .03; Table 3). The location of thetumors in the proximal colon was associated with a poor
al (B), local recurrence-free survival (C), and distant metastasis-free1), absent or weak α(1,6)FT expression; (2, 3), moderate or strong
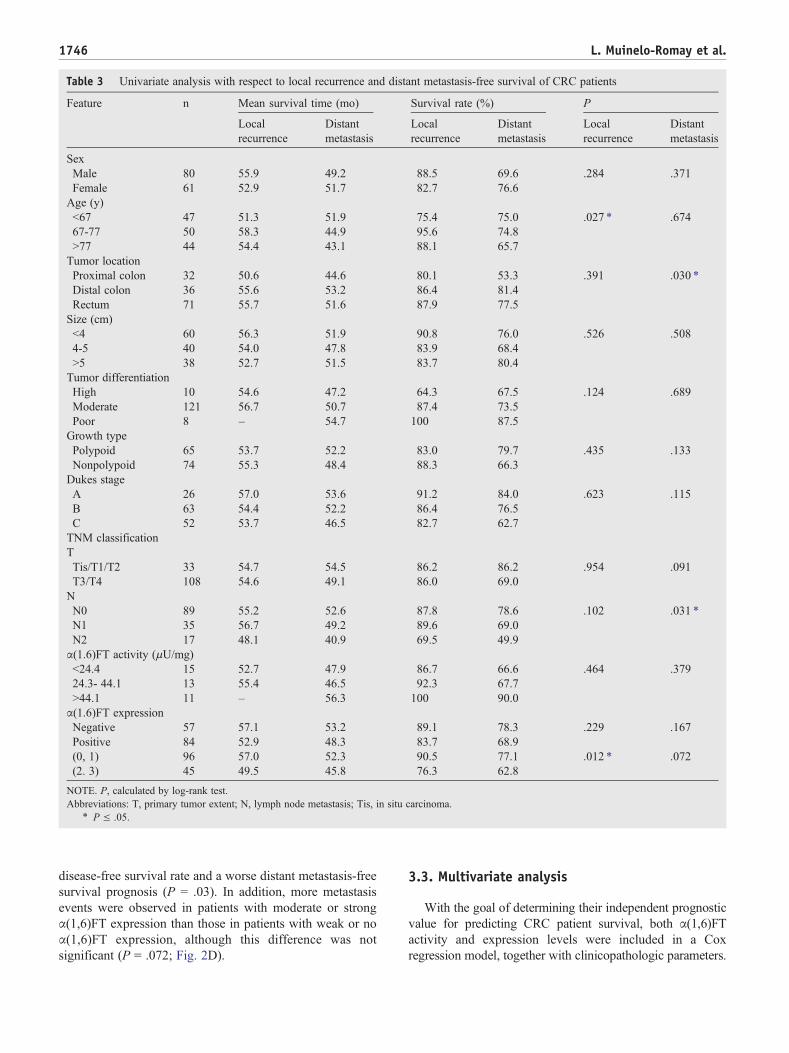
Table 3 Univariate analysis with respect to local recurrence and distant metastasis-free survival of CRC patients
Feature n Mean survival time (mo) Survival rate (%) P
Localrecurrence
Distantmetastasis
Localrecurrence
Distantmetastasis
Localrecurrence
Distantmetastasis
SexMale 80 55.9 49.2 88.5 69.6 .284 .371Female 61 52.9 51.7 82.7 76.6Age (y)b67 47 51.3 51.9 75.4 75.0 .027 ⁎ .67467-77 50 58.3 44.9 95.6 74.8N77 44 54.4 43.1 88.1 65.7Tumor locationProximal colon 32 50.6 44.6 80.1 53.3 .391 .030 ⁎
Distal colon 36 55.6 53.2 86.4 81.4Rectum 71 55.7 51.6 87.9 77.5Size (cm)b4 60 56.3 51.9 90.8 76.0 .526 .5084-5 40 54.0 47.8 83.9 68.4N5 38 52.7 51.5 83.7 80.4Tumor differentiationHigh 10 54.6 47.2 64.3 67.5 .124 .689Moderate 121 56.7 50.7 87.4 73.5Poor 8 – 54.7 100 87.5Growth typePolypoid 65 53.7 52.2 83.0 79.7 .435 .133Nonpolypoid 74 55.3 48.4 88.3 66.3Dukes stageA 26 57.0 53.6 91.2 84.0 .623 .115B 63 54.4 52.2 86.4 76.5C 52 53.7 46.5 82.7 62.7TNM classificationTTis/T1/T2 33 54.7 54.5 86.2 86.2 .954 .091T3/T4 108 54.6 49.1 86.0 69.0NN0 89 55.2 52.6 87.8 78.6 .102 .031 ⁎
N1 35 56.7 49.2 89.6 69.0N2 17 48.1 40.9 69.5 49.9α(1.6)FT activity (μU/mg)b24.4 15 52.7 47.9 86.7 66.6 .464 .37924.3- 44.1 13 55.4 46.5 92.3 67.7N44.1 11 – 56.3 100 90.0α(1.6)FT expressionNegative 57 57.1 53.2 89.1 78.3 .229 .167Positive 84 52.9 48.3 83.7 68.9(0, 1) 96 57.0 52.3 90.5 77.1 .012 ⁎ .072(2. 3) 45 49.5 45.8 76.3 62.8
NOTE. P, calculated by log-rank test.Abbreviations: T, primary tumor extent; N, lymph node metastasis; Tis, in situ carcinoma.
⁎ P ≤ .05.
1746 L. Muinelo-Romay et al.
disease-free survival rate and a worse distant metastasis-freesurvival prognosis (P = .03). In addition, more metastasisevents were observed in patients with moderate or strongα(1,6)FT expression than those in patients with weak or noα(1,6)FT expression, although this difference was notsignificant (P = .072; Fig. 2D).
3.3. Multivariate analysis
With the goal of determining their independent prognosticvalue for predicting CRC patient survival, both α(1,6)FTactivity and expression levels were included in a Coxregression model, together with clinicopathologic parameters.

Table 4 Multivariate analysis of CRC patient survival
Feature Disease recurrence Local recurrence Distant metastasis
RR (95% CI) P RR (95% CI) P RR (95% CI) P
NN0 1 1N1 1.8 (0.86-3.94) 1.8 (0.79-4.35)N2 3.9 (1.85-8.51) .002 ⁎ NS 3.5 (1.48-8.63) .027 ⁎
α(1,6)FT expression(0, 1) 1 1(2, 3) 1.9 (1.02-3.78) .041 ⁎ 3.6 (1.35-9.78) .010 ⁎ NS
Abbreviations: RR, relative risk; CI, confidence interval; NS, not statistically significant; N, lymph node metastasis.⁎ P ≤ .05, calculated by Cox regression analysis.
1747α(1,6)FT expression is a prognostic factor for CRC
No independent prognostic factors were identified for theprediction of overall survival. However, both lymph nodestatus and α(1,6)FT expression levels displayed independentprognostic value for predicting tumor recurrence, taking intoconsideration both local recurrence and distant metastasis(Table 4). In particular, the presence of tumor infiltration in 4 ormore lymph nodes increased the relative risk of diseaserecurrence 3.9-fold [95% confidence interval (CI), 1.85-8.51;P = .002), whereas moderate or strong α(1,6)FT expressionincreased the relative risk of disease recurrence 1.9-fold (95%CI, 1.02-3.78; P = .04). For local recurrence, only α(1,6)FTexpression levels showed true prognostic utility, with in-creased α(1,6)FT expression levels associated with a 3.6-foldincreased risk for local recurrence (95% CI, 1.35-9.78; P =.01). Finally, in the present study, lymph node infiltration wasthe only independent prognostic factor able to predictmetastasis development in CRC patients and was associatedwith a 3.5-fold increased risk for distant metastasis (95% CI,1.48-8.63; P = .02; Table 4).
4. Discussion
During neoplastic transformation, numerous changes inthe composition and structure of cell-surface glycoproteinsare frequently observed [25]. Accumulating evidencesuggests that many of these alterations are influenced bythe production of extensive fucosylated sugar chains [22]. Infact, altered levels of α(1,6)FT activity and expression havebeen described in a variety of human tumors and arenormally associated with an advanced disease stage [3-5].
In a previous study, we demonstrated that increasedα(1,6)FT activity and expression are associated with alteredα(1,6)fucosylation in human CRC as a result of malignanttransformation [3]. In support of this, elevated α(1,6)FTmessenger RNA levels were also reported in humancolorectal tumor tissues and colon cell lines [6,26]. Withrespect to the role of α(1,6)FT in tumor malignancy, weobserved a close association between α(1,6)FT activity orexpression levels and colorectal tumor aggressiveness [3].However, the impact of α(1,6)FT on CRC patient outcome
has never been analyzed, and therefore, its prognostic valuefor CRC or other tumor types remains unknown. In thiscontext, we conducted the present study to determinepossible correlations between α(1,6)FT activity and expres-sion, and CRC progression.
In agreement with our previous results, α(1,6)FT activitylevels in tumor tissues analyzed in the present studydecreased progressively with the degree of tumor infiltrationinto the intestinal wall. Consistent with these results,increased α(1,6)FT activity was observed in polypoidtumors, which are more localized and less invasive thannonpolypoid tumors. In contrast, the percentage of cases withpositive α(1,6)FT immunohistochemical staining was higherin advanced stage tumors than early stage tumors. In fact, thisabsence of a correlation between α(1,6)FT expression andactivity has been previously described [27,28] and has beenproposed to be due to a posttranslational modification oralternative enzyme activation mechanism that modulates thelevels of active catalytic protein [28].
Interestingly, α(1,6)FT expression was found to be less inmen than in women. Consistent with this finding, thedecrease in biantennary core-fucosylated structures reportedfor patients older than 40 to 50 years occurs earlier in womenthan in men [29]. Most patients included in the present studywere older than 40 to 50 years; and no differences in α(1,6)FT status were observed among the 3 age groups considered.In our opinion, sex-associated α(1,6)FT expression differ-ences could be influenced by sex hormone balance. Severalstudies have described modulation of estrogen and proges-terone levels in colorectal epithelium homeostasis [30,31].Consequently, the glycosylation dynamics of colorectal cellscould be also influenced by these hormone modulators. Inany case, despite this hypothetical correlation between sexand α(1,6)FT status, the possible clinical utility of α(1,6)FTis not invalidated, assuming the determination of appropriatenormality reference intervals for each sex.
With respect to the prognostic value of the standardclinicopathologic features included in the present study, asexpected, the presence of lymph node invasion correlatedwith more aggressive tumor progression at the 5-year follow-up in terms of disease-free survival and, specifically, with the

1748 L. Muinelo-Romay et al.
appearance of distant metastasis. The predictive power oflymph node metastasis for cancer evolution is wellestablished in the literature, and the lymphatic system isconsidered the main pathway by which cancer cellsdisseminate [32]. In agreement with this, tumors in anadvanced Dukes stage were associated with poor disease-freesurvival rates. However, remarkably, overall survival rateswere observed to be independent of the clinicopathologicvariables analyzed. Considering that metastasis is the majorcause of death in cancer patients with solid tumors, acorrelation between lymph node infiltration and overallsurvival rates for CRC patients was expected. Nevertheless,in older populations such as the one included in the presentstudy, it is frequently difficult to identify with precisioncancer-related deaths, because most patients present withsynergistic pathologies. Thus, we consider disease-freesurvival rates more informative about CRC progressionthan overall survival rates.
The anatomical location of the primary tumor was foundto correlate with CRC disease progression. Specifically,tumors localized to the proximal colon (right and transversecolon) presented poor rates of disease-free survival. Conse-quently, in terms of metastasis development, tumorslocalized to the distal colon and rectum are associated withbetter outcomes. Traditionally, rectum lesions correlate withunfavorable prognoses after surgery, because of the difficultyof removing these tumors per se. However, right colontumors are usually detected in an advanced stage, becausesymptoms typically present later than in left colon tumors,and thus, they are frequently more aggressive [33]. Inaddition, the group of patients older than 67 years analyzed inour study had a higher rate of local disease recurrence.Although some studies of colon and rectum tumors havedescribed a rapid downhill course, characteristic of youngcancer patients, others reported the contrary [34,35].
Interestingly, the present study demonstrates the useful ofα(1,6)FT expression levels for predicting CRC recurrenceafter the surgical resection. Specifically, patients withmoderate or strong α(1,6)FT expression had lower disease-free survival rates than did patients with weak or no α(1,6)FTexpression. The negative influence of α(1,6)FT expressionwas also observed for local recurrence after curative surgery,with less aggressive tumor progression in patients with lowimmunohistochemical α(1,6)FT levels. The same trend wasobserved between distant metastasis and α(1,6)FT expres-sion, although a nonstatistically significant association wasfound between both variables. In addition, α(1,6)FTexpression was the only factor in this study that correlatedwith overall CRC survival rates. Therefore, for the first time,α(1,6)FT tissue expression has been correlated with thesurvival of cancer patients. To the best of our knowledge,only one previous study has analyzed the utility of plasmaα(1,6)FT activity levels for predicting clinical outcomes.This study of breast cancer patients [18] indicated a lack ofcorrelation between plasma α(1,6)FT activity and theresponse of metastatic breast tumors to treatment with
trastuzumab, a potent anticancer agent used against tyrosinekinase-type cell receptor HER2 overexpressing tumors [36].α(1,6)Fucosylation of EGFR regulates its intracellularsignaling pathway and sensitivity to EGFR tyrosine kinaseinhibitors. However, in the aforementioned study, plasmaα(1,6)FT catalytic levels seemed to be irrelevant forpredicting patient response to treatment [18].
The goal of the present study was to define the clinicalusefulness of α(1,6)FT status as a prognostic factor in A, B,and C stage tumors, independently of the adjuvant therapyused. The results of multivariate analysis revealed that α(1,6)FT immunohistochemical expression in colorectal tumors isan independent predictor of tumor recurrence, even more sothan the most conventional clinicopathologic factors. Hence,the relative risk of disease reappearance was doubled inpatients with moderate or strong α(1,6)FT expression,whereas the relative risk of local recurrence in this groupof patients was increased 3.6-fold. Moreover, based onunivariate analysis, the only clinicopathologic factor usefulfor predicting disease recurrence in this study (specifically,distant metastasis development) was lymph node infiltration,as expected. Based on our results, the evaluation of α(1,6)FTimmunohistochemical expression in colorectal tumors addsimportant prognostic information about cancer recurrenceand could help specialists select the appropriate treatmentstrategy to prevent CRC progression.
A molecular explanation for the correlation betweenα(1,6)FT expression and CRC disease outcome should bedefined in future studies. In fact, it is well known thatmolecular determinants of proximal and distant tumorrecurrences are quite different, with local recurrencesessentially occurring as a result of the presence oftreatment-resistant tumor cells, which maintain their unre-strained proliferative dynamics. Several studies have dem-onstrated that core-fucosylation regulates the biologicalfunction of numerous molecules implicated in cell prolifer-ation, differentiation, and apoptosis. In addition to the α(1,6)FT-mediated modulation of EGFR function mentionedabove, other receptors, such as TGFβ-R or VEGFR, alsomust be core-fucosylated to activate their respectiveintracellular signaling pathways. Moreover, some recentreports have shown that α(1,6)fucosylation of E-cadherinmodulates the processing of its oligosaccharide antennae, aswell as the turnover of this adhesion molecule and,consequently, cell-cell interactions in tumor cells [13,14].These E-cadherin–mediated adhesions could also modulatetyrosine kinase or Wnt signaling receptors, both of which up-regulate the signaling pathways in different types of tumors[37,38]. In particular, β-catenin/Wnt plays an important rolein the control of colon epithelium homeostasis [39]. In thismolecular context, we propose that high α(1,6)FT levels incolorectal cancer cells could be decisive in maintaining itsproliferative status and in modulating its response to differentchemotherapy agents.
However, for distant metastases development, cancercells must dissociate from the original tumor and migrate via

1749α(1,6)FT expression is a prognostic factor for CRC
blood vessels or the lymph system to colonize specific targetorgans. Distant metastasis is a multistep process in whichadhesive interactions play a critical role. In turn, α(1,6)fucosylation of different adhesion molecules, such asadhesins or integrins, modifies their functional activity andmay be a relevant factor for determining the acquisition of amigratory phenotype by epithelial tumor cells. For example,core-fucosylation is a prerequisite for neural cell adhesionmolecule (NCAM) polysialylation [40]. Furthermore, ex-pression of the polysialylated form of NCAM has beendemonstrated in some malignant tumors, allowing prostatespecific antigen (PSA) positive cancer cells to detach fromthe primary tumor by attenuating the adhesive properties ofNCAM and, consequently, by increasing the metastaticpotential of tumor cells [41-43]. Interestingly, a study of lungcancer cells demonstrated that E-cadherin is core-fucosy-lated in highly metastatic cells, whereas this type ofglycosylation is absent in low metastatic cells. These authorsproposed that core-fucosylation on E-cadherin inhibits cell-cell aggregation and promotes matrix metallopeptidases 9and 2 (MMP 9 and MMP 2) activity, contributing to lung cellmigration and invasiveness [13]. Likewise, other moleculesimplicated in cell-extracellular matrix interactions and cancercell invasiveness, such as α3β1 or α5β1 integrins, are α(1,6)fucosylated in their active form [5,15,44]. Probably, the highα(1,6)FT expression observed in colon cancer cells promotescell interactions mediated by these integrins and, therefore,facilitates tumor progression. In summary, the present studyhas demonstrated, for the first time, that α(1,6)FT expressionmay be a good prognostic factor for predicting colorectalcancer progression after surgery. The role of α(1,6)FT intumor cell aggressiveness may be explained by its effects onthe activity of several molecules strongly implicated incritical malignancy processes, including cell proliferationand dissemination. Although further, multicentric studieswill be required to validate the use of α(1,6)FT immunohis-tochemical expression for the therapeutic management ofCRC, our findings suggest that α(1,6)FT and its core-fucosylated products could be promising tumor markers andtherapeutic targets for this pathology.
Acknowledgments
The members of the Pathology Service of the UniversityComplex Hospital of Ourense (Ourense, Spain) have played avery important role in the immunohistochemical evaluationused in this study, and this kind collaboration is acknowledged.
References
[1] Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics, 1998.CA Cancer J Clin 1998;48:6-29.
[2] Benson AL. Epidemiology, disease progression, and economic burdenof colorectal cancer. J Manag Care Pharm 2007;13:5-18.
[3] Muinelo-Romay L, Vazquez-Martin C, Villar-Portela S, et al.Expression and enzyme activity of alpha(1,6)fucosyltransferase inhuman colorectal cancer. Int J Cancer 2008;123:641-6.
[4] Hutchinson WL, Du MQ, Johnson PJ, Williams R. Fucosyltrans-ferases: differential plasma and tissue alterations in hepatocellularcarcinoma and cirrhosis. Hepatology 1991;13:683-8.
[5] Miyoshi E, Noda K, Ko JH, et al. Overexpression of alpha1-6fucosyltransferase in hepatoma cells suppresses intrahepatic metastasisafter splenic injection in athymic mice. Cancer Res 1999;59:2237-43.
[6] Ito Y, Miyauchi A, Yoshida H, et al. Expression of alpha1,6-fucosyltransferase (FUT8) in papillary carcinoma of the thyroid: itslinkage to biological aggressiveness and anaplastic transformation.Cancer Lett 2003;200:167-72.
[7] Takahashi T, Ikeda Y, Miyoshi E, et al. alpha1,6fucosyltransferase ishighly and specifically expressed in human ovarian serous adenocar-cinomas. Int J Cancer 2000;88:914-9.
[8] Longmore GD, Schachter H. Product-identification and substrate-specificity studies of the GDP-L-fucose:2-acetamido-2-deoxy-beta-D-glucoside (FUC goes to Asn-linked GlcNAc) 6-alpha-L-fucosyltrans-ferase in a Golgi-rich fraction from porcine liver. Carbohydr Res1982;100:365-92.
[9] Stubbs HJ, Lih JJ, Gustafson TL, Rice KG. Influence of corefucosylation on the flexibility of a biantennary N-linked oligosaccha-ride. Biochemistry 1996;35:937-47.
[10] Wang X, Fukuda T, Li W, et al. Requirement of Fut8 for theexpression of vascular endothelial growth factor receptor-2: a newmechanism for the emphysema-like changes observed in Fut8-deficient mice. J Biochem 2009;145:643-51.
[11] Wang X, Gu J, Ihara H, et al. Core fucosylation regulates epidermalgrowth factor receptor–mediated intracellular signaling. J Biol Chem2006;281:2572-7.
[12] Wang X, Inoue S, Gu J, et al. Dysregulation of TGF-beta1 receptoractivation leads to abnormal lung development and emphysema-likephenotype in core fucose–deficient mice. Proc Natl Acad Sci U S A2005;102:15791-6.
[13] Geng F, Shi BZ, Yuan YF, Wu XZ. The expression of core fucosylatedE-cadherin in cancer cells and lung cancer patients: prognosticimplications. Cell Res 2004;14:423-33.
[14] Osumi D, Takahashi M, Miyoshi E, et al. Core fucosylation of E-cadherin enhances cell-cell adhesion in human colon carcinoma WiDrcells. Cancer Sci 2009;100:888-95.
[15] Zhao Y, Itoh S, Wang X, et al. Deletion of core fucosylation onalpha3beta1 integrin down-regulates its functions. J Biol Chem 2006;281:38343-50.
[16] Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety oftrastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol 2002;20:719-26.
[17] Hurley J, Doliny P, Reis I, et al. Docetaxel, cisplatin, and trastuzumabas primary systemic therapy for human epidermal growth factorreceptor 2-positive locally advanced breast cancer. J Clin Oncol2006;24:1831-8.
[18] Matsumoto K, Shimizu C, Arao T, et al. Identification of predictivebiomarkers for response to trastuzumab using plasma FUCA activityand N-glycan identified by MALDI-TOF-MS. J Proteome Res 2009;8:457-62.
[19] Ang IL, Poon TC, Lai PB, et al. Study of serum haptoglobin and itsglycoforms in the diagnosis of hepatocellular carcinoma: a glycopro-teomic approach. J Proteome Res 2006;5:2691-700.
[20] Comunale MA, Lowman M, Long RE, et al. Proteomic analysis ofserum associated fucosylated glycoproteins in the development ofprimary hepatocellular carcinoma. J Proteome Res 2006;5:308-15.
[21] Mita Y, Aoyagi Y, Suda T, Asakura H. Plasma fucosyltransferaseactivity in patients with hepatocellular carcinoma, with specialreference to correlation with fucosylated species of alpha-fetoprotein.J Hepatol 2000;32:946-54.
[22] Yamashiki N, Seki T, Wakabayashi M, et al. Usefulness of Lensculinaris agglutinin A–reactive fraction of alpha-fetoprotein (AFP-L3)
1750 L. Muinelo-Romay et al.
as a marker of distant metastasis from hepatocellular carcinoma. OncolRep 1999;6:1229-32.
[23] Dukes CE. The classification of cancer of rectum. J Pathol Bacteriol1932;35:323-32.
[24] Sobin LH, Wittekind CH. TNM classification of malignant tumours,6th ed. New York: Wiley-Liss; 2002. p. 1-15, 66-9.
[25] Hakomori S. Aberrant glycosylation in tumours and tumour-associatedcarbohydrate antigens. Adv Cancer Res 1989;52:257-331.
[26] Kemmner W, Roefzaad C, Haensch W, Schlag PM. Glycosyltransfer-ase expression in human colonic tissue examined by oligonucleotidearrays. Biochim Biophys Acta 2003;1621:272-9.
[27] Miyoshi E, Uozumi N, Noda K, et al. Expression of alpha1-6fucosyltransferase in rat tissues and human cancer cell lines. Int JCancer 1997;72:1117-21.
[28] Noda K, Miyoshi E, Uozumi N, et al. High expression of alpha-1-6fucosyltransferase during rat hepatocarcinogenesis. Int J Cancer1998;75:444-50.
[29] Vanhooren V, Desmyter L, Liu XE, et al.N-glycomic changes in serumproteins during human aging. Rejuvenation Res 2007;10:521a-31a.
[30] Meggouh F, Lointier P, Saez S. Sex steroid and 1,25-dihydroxyvita-min D3 receptors in human colorectal adenocarcinoma and normalmucosa. Cancer Res 1991;51:1227-33.
[31] Castiglione F, Taddei A, Degl'Innocenti DR, et al. Expression ofestrogen receptor beta in colon cancer progression. Diagn Mol Pathol2008;17:231-6.
[32] Compton C, Fenoglio-Preiser CM, Pettigrew N, Fielding LP.American Joint Committee on Cancer Prognostic Factors ConsensusConference: Colorectal Working Group. Cancer 2000;88:1739-57.
[33] Wray CM, Ziogas A, Hinojosa MW, et al. Tumour subsite locationwithin the colon is prognostic for survival after colon cancer diagnosis.Dis Colon Rectum 2009;52:1359-66.
[34] Svendsen LB, Sorensen C, Kjersgaard P, Meisner S, Kjaergaard J. Theinfluence of age upon the survival after curative operation forcolorectal cancer. Int J Colorectal Dis 1989;4:123-7.
[35] McMillan DC, McArdle CS. The impact of young age on cancer-specific and non–cancer-related survival after surgery for colorectalcancer: 10-year follow-up. Br J Cancer 2009;101:557-60.
[36] Spector NL, Blackwell KL. Understanding the mechanisms behindtrastuzumab therapy for human epidermal growth factor receptor2–positive breast cancer. J Clin Oncol 2009;27:5838-47.
[37] Nelson WJ, Nusse R. Convergence of Wnt, beta-catenin, and cadherinpathways. Science 2004;303:1483-7.
[38] Hu P, Shi B, Geng F, et al. E-cadherin core fucosylation regulatesnuclear beta-catenin accumulation in lung cancer cells. Glycoconj J2008;25:843-50.
[39] Kobayashi M, Honma T, Matsuda Y, et al. Nuclear translocation ofbeta-catenin in colorectal cancer. Br J Cancer 2000;82:1689-93.
[40] Kojima N, Tachida Y, Yoshida Y, Tsuji S. Characterization of mouseST8Sia II (STX) as a neural cell adhesion molecule–specific polysialicacid synthase. Requirement of core alpha1,6-linked fucose and apolypeptide chain for polysialylation. J Biol Chem 1996;271:19457-63.
[41] Gluer S, Schelp C, Gerardy-Schahn R, von Schweinitz D.Polysialylated neural cell adhesion molecule as a marker fordifferential diagnosis in pediatric tumours. J Pediatr Surg 1998;33:1516-20.
[42] Miyahara R, Tanaka F, Nakagawa T, et al. Expression of neural celladhesion molecules (polysialylated form of neural cell adhesionmolecule and L1-cell adhesion molecule) on resected small cell lungcancer specimens: in relation to proliferation state. J Surg Oncol2001;77:49-54.
[43] Fernandez-Briera A, Garcia-Parceiro I, Cuevas E, Gil-Martin E.Effect of human colorectal carcinogenesis on the neural cell adhesionmolecule expression and polysialylation. Oncology 2010;78:196-204.
[44] Wang H, Fu W, Im JH, et al. Tumour cell alpha3beta1 integrin andvascular laminin-5 mediate pulmonary arrest and metastasis. J CellBiol 2004;164:935-41.










![The jet-cooled S 0→S 1 excitation spectrum of 1,6-epoxy-[10]annulene](https://static.fdokumen.com/doc/165x107/631e1beedc32ad07f3076a22/the-jet-cooled-s-0s-1-excitation-spectrum-of-16-epoxy-10annulene.jpg)









