Colorectal Disease - AECP
113
Colorectal Disease Volume 19 Supplement 3 September 2017 Pelvic Floor Soc / ACPGBI / ESCP Graded Practice Recommendations on Chronic Constipation
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Colorectal Disease - AECP

Colorectal Disease
Volume 19 Supplement 3 September 2017
Pelvic Floor Soc / ACPGBI / ESCP Graded Practice Recommendations on Chronic
Constipation

Contents
1. Editorial Surgery for constipation: systematic review and clinical guidance 3–4
2. Surgery for constipation: systematic review and clinical guidance Paper 1: Introduction & Methods 5–16
3. Surgery for constipation: systematic review and practice recommendations Results I: Colonic resection 17–36
4. Surgery for constipation: systematic review and practice recommendations Results II: Hitching procedures for the rectum (rectal suspension) 37–48
5. Surgery for constipation: systematic review and practice recommendations Results III: Rectal wall excisional procedures (Rectal Excision) 49–72
6. Surgery for constipation: systematic review and practice recommendations Results IV: Recto-vaginal reinforcement procedures 73–91
7. Surgery for constipation: systematic review and practice recommendations Results V: Sacral Nerve Stimulation 92–100
8. Surgery for constipation: systematic review and practice recommendations Graded practice and future research recommendations 101–113

Surgery for constipation: systematic review and clinicalguidance
The surgical treatment of functional and pelvic floor dis-
orders has often been a “Cinderella” subject, both in
terms of the health care and academic agendas. Histori-
cally this status may have been in part be due to the com-
plexities of the treatment of such conditions, due to their
multidisciplinary nature, cutting across three main surgi-
cal specialties (coloproctology, urology & gynaecology),
as well as necessitating input from colleagues in medical,
nursing, physiotherapy, radiology and clinical physiology
specialties. It does, however, in no way reflect the preva-
lence of the disorders or their burden on both the indi-
vidual or society as a whole. Not surprisingly this
problem has led to wide variation in clinical practice and a
degree of uncertainty among those who fund or reim-
burse healthcare as to exactly what constitutes acceptable
evidence based surgical care, resulting in some declining
to fund some treatments at all. As multidisciplinary work-
ing has become the norm within modern health care sys-
tems, its application to functional and pelvic floor
disorders has changed resource provision and led to a
renewed interest in their aetiology and treatment strate-
gies resulting in a profound transformation of academic
endeavour in the field.
The two decades since Horton’s polemic editorial
regarding the “comic opera” of surgical research [1], has
generated a focus on the performance and publication of
the gold standard of intervention assessment, the ran-
domised controlled trial. More complex to perform in
the setting of surgery, compared with pharmaceutical
studies for example, the past decade alone has seen several
high quality multicentre studies investigating surgical
interventions within the field of functional and pelvic
floor disorders, but mainly related to faecal incontinence
and rectal prolapse [2–5]. Despite the high prevalence
and demand on health care resources, surgical treatments
for chronic constipation have not received the same in-
depth assessment, with placebo controlled trials of novel
pharmaceutical agents predominating.
The UK National Institute for Health Research
(NIHR) have funded the investigation of three types of
non-drug therapies for chronic constipation (bowel
retraining, anal irrigation & laparoscopic ventral mesh
rectopexy for internal rectal prolapse - see www.blizard.
qmul.ac.uk/capacity.html). As a prelude to these well
designed but complex studies, the CapaCiTY Working
Group, along with a broad consensus group derived
from the ACPGBI affiliated Pelvic Floor Society and
ESCP have seized the opportunity to assess the litera-
ture available on the surgical treatment of chronic
constipation. The aim has clearly been to try and make
sense of a confusing array of procedures described
across a plethora of manuscripts and to provide a rigor-
ous assessment of the quality of the currently available
literature. In addition, the team have endeavoured to
make a series of graded practice recommendations in
order to facilitate the often challenging decision making
relating to the care of such patients. The intention is
help optimise patient outcome, minimise harm and
reduce unjustifiable variation in practice. Unfortunately,
there is no similar national body in the USA although
the American Society of Colon and Rectal Surgeons
publishes practice parameters on a variety of topics.
This series of seven papers collates for the first time the
evidence for five key areas of surgical practice relating to
the treatment of chronic constipation: colonic resection,
rectal suspension, rectal wall excision, reinforcement of the
rectovaginal septum and sacral nerve stimulation. The series
starts with an introductory paper that gives a detailed over-
view of the general methods used, search results and study
characteristics. Subsequently, each of the five areas of surgi-
cal practice has its own detailed systematic review (and
where appropriate meta-analysis) with summary evidence
statements. The final paper is a synopsis of graded practice
recommendations and crucially, recommendations for
future research. Here the authors have been open and shar-
ing suggestions for alternative appropriate study designs
when randomised trials are unfeasible. For some of the
more uncommon procedures multicentre international col-
laborative prospective cohort studies using the paradigms
exemplified in previous ESCP studies may be more infor-
mative [6]. We endorse the authors recommendations of
appropriate outcomes reporting via core outcome data sets
(http://www.comet-initiative.org/) and that the evalua-
tion of future innovations should adhere to the principles
of the IDEAL collaboration (http://www.ideal-collabora
tion.net/). There remains, however, the issue of health
economic impact and what treatments will ultimately be
funded. All healthcare systems face financial challenges and
increasingly cost effectiveness is important in the decision-
making process for healthcare funders. There remains
much to be investigated and little work has, as yet, been
directed at the assessment of surgical interventions in this
context. Determining and delivering a high quality research
agenda that answers the needs of patients, healthcare provi-
ders and healthcare funder alike will be welcomed by all.
The focus on quality of surgical outcome, procedural
safety and patient reported outcomes in this series of seven
papers is to be commended. The quotidian dilemmas
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 3–4 3
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Editorial doi:10.1111/codi.13809

within coloproctology practice have been expertly sum-
marised and sensible recommendations with reasonable
consensus made. We would encourage their widespread
use by multidisciplinary teams in the formation of their
treatment pathways / algorithms. There remain, however,
some questions that have not been addressed because they
are beyond the scope of such a clearly defined review topic
and they relate to the more global management controver-
sies that pervade and area of our specialty that can be both
simultaneously rewarding and frustrating.
Many of the studies included in this series of manu-
scripts highlight the issue of complex interventions having
favourable outcomes in patients who are often
euphemistically described as being “carefully selected”.
This nebulous term rarely relates to judiciously described
preoperative evaluation protocols and results defined a
priori that mandate consideration of certain operative
interventions. How should such patients be investigated
when debate remains regarding the interpretation of some
investigations such as defaecating proctography [7] and
the expense of others (e.g. wireless motility capsule)
severely limits widespread dissemination [8]?
While non-operative management strategies form the
mainstay of therapy, by what criteria should patients
progress through increasingly invasive treatment
options? The association of functional gastrointestinal
and pelvic floor disorders with psychological diagnoses
is increasingly recognised and the influence on treat-
ment outcomes being defined [9]. How psychological
factors are accounted for in the decision to progress
through step wise pathways of care that ultimately lead
to operative intervention in many of the reported series
is opaque and yet may have a profound impact on the
consultation between patient and surgeon. It is reassur-
ing to note that in this series of papers the consensus
was towards mandating psychological evaluation in all
those considering colectomy and should only be per-
formed in centres with access to appropriate specialist
services.
Finally, what is the course of action when catastrophe
strikes? The operations described within this series,
including colectomy and ileorectal anastomosis, STARR,
ventral mesh rectopexy and others all have something to
offer the right patient with the right pathology when
appropriately counselled and operated upon by the right
surgeon. Despite optimal circumstances each of these
operations is associated with some of the most devastating
complications, including anastomotic leak, rectovaginal
fistulae, intractable pelvic pain and worse. They are thank-
fully rare but do occur and how these situations should be
managed needs clarifying. In such circumstances the role
of a stoma as an active positive choice, rather than being a
sign of failure, should be considered.
The heuristics used by surgeons when evaluating
what interventions to offer patients with functional gas-
trointestinal and pelvic floor disorders have not been
studied, unlike in rectal cancer patients. It may be that
the perceived risk benefit ratio in a benign disease
(where propensity for risk-taking tends to be lower) has
had a negative impact on the utilisation of some opera-
tions (e.g. STARR, TranSTARR) when on a prima facie
basis, the evidence may point to benefit. Surgeons may
not be the most evidence based practitioners within the
broader medical fraternity, but they are rarely abject
fools. The core principle of the management of patients
with these conditions remains primum non nocere.
Hopefully, the impressive authoritative comprehensive
compendium published by Professor Knowles and his
colleagues will help us achieve that goal.
Neil J Smart* and Steven Wexner†*Royal Devon & Exeter Hospital & Honorary Senior Lecturer, University of
Exeter Medical School, Exeter, UK and †Digestive Disease Center, Depart-ment of Colorectal Surgery, Cleveland Clinic Florida, Weston, Florida, USA
References
1 Horton R. Surgical research or comic opera: questions, but
few answers. Lancet 1996; 347: 984–5.
2 Knowles CH, Horrocks EJ, Bremner SA et al., CONFI-
DeNT study group. Percutaneous tibial nerve stimulation
versus sham electrical stimulation for the treatment of faecal
incontinence in adults (CONFIDeNT): a double-blind, mul-
ticentre, pragmatic, parallel-group, randomised controlled
trial. Lancet 2015; 386: 1640–8.
3 Graf W, Mellgren A, Matzel KE, Hull T, Johansson C,
Bernstein M, NASHA Dx Study Group. Efficacy of dextra-
nomer in stabilised hyaluronic acid for treatment of faecal
incontinence: a randomised, sham-controlled trial. Lancet
2011; 377: 997–1003.
4 Morris OJ, Smith S, Draganic B. Comparison of bulking
agents in the treatment of fecal incontinence: a prospective
randomized clinical trial. Tech Coloproctol 2013; 17: 517–23.
5 Senapati A, Gray RG, Middleton LJ et al. PROSPER: a ran-
domised comparison of surgical treatments for rectal pro-
lapse. Colorectal Dis 2013 Jul; 15: 858–68.
6 2015 European Society of Coloproctology collaborating
group. The relationship between method of anastomosis and
anastomotic failure after right hemicolectomy and ileo-caecal
resection: an international snapshot audit. Colorectal Dis
2017, https://doi.org/10.1111/codi.13646.
7 Palit S, Bhan C, Lunniss PJ et al. Evacuation proctography: a rea-
ppraisal of normal variability. Colorectal Dis 2014; 16: 538–46.
8 Rao SS, Meduri K. What is necessary to diagnose constipa-
tion? Best Pract Res Clin Gastroenterol 2011; 25: 127–40.
9 Nehra V, Bruce BK, Rath-Harvey DM, Pemberton JH,
Camilleri M. Psychological disorders in patients with evacua-
tion disorders and constipation in a tertiary practice. Am J
Gastroenterol 2000; 95: 1755–8.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 3–44
Editorial

Surgery for constipation: systematic review and clinicalguidance
Paper 1: Introduction & Methods
C. H. Knowles*, U. Grossi*, E. J. Horrocks*, D. Pares†, P. F. Vollebregt*, M. Chapman‡,S. R. Brown§, M. Mercer-Jones¶, A. B. Williams**, R. J. Hooper††, N. Stevens††, J. Mason‡‡,on behalf of the NIHR CapaCiTY working group§§ and The Pelvic floor Society¶¶*National Bowel Research Centre, Blizard Institute, Queen Mary University London, London, UK, †Hospital Germans Tr�ıas i Pujol, Barcelona, Spain,
‡Good Hope Hospital, Heart of England NHS Trust, Birmingham, UK, §Sheffield Teaching Hospitals, Sheffield, UK, ¶Queen Elizabeth Hospital,
Gateshead NHS Trust, Gateshead, UK, **Guy’s and St Thomas’ NHS Foundation Trust, London, UK, ††Pragmatic Clinical Trials Unit, Blizard Institute,
Queen Mary University of London, London, UK, ‡‡University of Warwick, Coventry, UK, §§National Institute for Health Research: Chronic
Constipation Treatment Pathway, UK, and ¶¶Affiliate section of the Association of Coloproctology of Great Britain and Ireland, London, UK
Abstract
Aim This manuscript provides the introduction and
detailed methodology used in subsequent reviews to
assess the outcomes of surgical interventions with the
primary intent of treating chronic constipation in adults
and to develop recommendations for practice.
Method PRISMA guidance was adhered to throughout.
A literature search was performed in public databases
between January 1960 and February 2016. Studies that
fulfilled strictly-defined PICOS (patients, interventions,
controls, outcome, and study design) criteria were
included. The process involved two groups of partici-
pants: (i): ‘a clinical guidance group’ of 18 UK experts
(including junior support) who performed the system-
atic reviews and produced summary evidence statements
(SES) based strictly on data synthesis in each review.
The same group then produced prototype graded prac-
tice recommendations (GPRs) based on coalescence of
SES and expert opinion; (ii): a European Consensus
group of 18 ESCP (European Society of Coloproctol-
ogy) nominated experts from nine European countries
evaluated the appropriateness of each prototype GPR
based on published RAND/UCLA methodology.
Results An overview of the search results is provided in
this manuscript. A total of 156 studies from 307 full
text articles (from 2551 initially screened records) were
included, providing data on procedures characterized
by: (i) colonic resection (n = 40); (ii) rectal suspension
(n = 18); (iii) rectal wall excision (n = 44); (iv) recto-
vaginal septum reinforcement (n = 47); (v) sacral nerve
stimulation (n = 7). The overall quality of evidence was
poor with 113/156 (72.4%) studies providing only
Oxford level IV evidence. The best evidence was
extracted for rectal excisional procedures, where the
majority of studies were Oxford level I or II. The five
subsequent reviews provide a total of 99 SES (reflecting
perioperative variables, efficacy, harms and prognostic
variables) that contributed to 100 prototype GPRs cov-
ering patient selection, procedural considerations and
patient counselling. The final manuscript details the
85/100 GPRs that were deemed appropriate by Euro-
pean Consensus (remaining 15 were all uncertain) and
future research recommendations.
Conclusion This manuscript and the following 6 papers
suggest that the evidence base for surgical management
of chronic constipation is currently poor although some
expert consensus exists on best practice. Further studies
are required to inform future commissioning of treat-
ments and of research funding.
Keywords Constipation, surgery, obstructed defaecation
Introduction
Constipation is common in adults and children with up
to 20% of the population reporting symptoms
depending on the definition used (2–28% adults; 0.7–30% children) [1–3]. Chronic constipation (CC), usu-
ally defined as more than 6 months of symptoms, is less
common but results in 0.5 million UK GP consulta-
tions per annum. A proportion of the population suffer
symptoms that are both chronic and more disabling
(probably about 0.4% population) [4]. Such patients,
Correspondence to: Prof. Charles H. Knowles, NBRC, 1st Floor Abernethy
Building, 2 Newark St, London E1 2AT, UK.
E-mail: [email protected]
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–16 5
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13774

who are predominantly female [5], are usually referred
to secondary care with many progressing to tertiary spe-
cialist investigation. Patient dissatisfaction is high in this
group; nearly 80% feel that laxative therapy is unsatisfac-
tory [6] and the effect of symptoms on measured QOL
is significant [7]. CC consumes significant healthcare
resources. In the US in 2012, a primary complaint of
constipation was responsible for 3.2 million physician
visits resulting in (direct and indirect) costs of $1.7 bil-
lion [8]. In the UK, it is estimated 10% of district nurs-
ing time is spent on bowel control [9] and the annual
spend on laxatives exceeds £117 m, with 18.3 million
prescriptions in 2014 of which 91% were for stimulant
and osmotic laxatives (Health and Social Care Informa-
tion Centre) [10].
The act of defaecation is dependent on the coordi-
nated functions of the colon, rectum and anus. Consid-
ering the complexity of neuromuscular (sensory and
motor) functions required to achieve planned, con-
scious, and effective defaecation [11], it is no surprise
that disturbances to perceived ‘normal’ function occur
commonly at all stages of life. Clinically, such problems
commonly lead to symptoms of obstructed defaecation
e.g. straining; incomplete, unsuccessful or painful evacu-
ation; bowel infrequency; abdominal pain and bloating.
After exclusion of secondary causes (obstructing colonic
lesions, neurological, metabolic and endocrine disor-
ders), the pathophysiology of CC can broadly be
divided into problems of colonic contractile activity
(and thus stool transit) and problems allied to rectal
emptying (evacuation disorder). A combination of clini-
cal expertise and specialist radio-physiological investiga-
tions can determine which patients have slow colonic
transit, evacuation disorder, both (in whom transit is
usually characterized by a left-sided delay) or neither
(no abnormality found with current tests) [12]. Evacua-
tion disorders can be further subdivided into those with
a structurally significant pelvic floor abnormality (usually
as a consequence of pelvic floor weakness or injury) e.g.
rectocoele or internal prolapse (intussusception), and
those characterized by a dynamic failure of evacuation
without structural abnormality: most commonly termed
‘functional defaecation disorder (FDD) [13]’ (Fig. 1).
The management of CC is a major problem due to
its high prevalence and lack of widespread specialist
expertise. In general, a step-wise approach is under-
taken, with first line conservative treatment such as life-
style advice and laxatives (primary care) followed by
nurse-led bowel re-training programs, sometimes
including focused biofeedback and psychosocial support
(secondary/tertiary care). Although these treatments
may improve symptoms in more than half of patients
[14], patients with intractable symptoms and impaired
QOL may subsequently be offered a range of surgical
interventions.
Surgical decision-making is greatly influenced by local
expertise, commissioning or reimbursement, and per-
sonal enthusiasm for particular interventions. While
robust diagnosis of specific pathophysiologies combined
with multidisciplinary team discussion may help direct
surgery, in the absence of an agreed pathway to stratify
patients, there is a current large and difficult-to-justify
variation in surgical practice that continues to risk inade-
quately-informed and potentially harmful interventions
being offered. The need to reduce such variations in prac-
tice, based on available evidence, has been a recurrent
theme of recent national specialty group discussions (e.g.
ACPGBI) with various initiatives proposed. As part of the
Chronic Constipation Treatment PathwaY (CapaCiTY)
programme funded by National Institute of Health
Research (NIHR), a multi-disciplinary working group
was convened in July 2014 to address this need. This
group of medical and nursing experts included members
of The Pelvic Floor Society and urogynaecology expertise
derived from the International Continence Society (ICS).
As a prelude to developing new evidence from trials
within the CapaCiTY programme, it was agreed that the
current surgical evidence base would benefit from coales-
cence in the form of systematic review and graded prac-
tice recommendations. This paper and the accompanying
subsequent six papers address this aim.
Methods
Systematic review
Protocol and registrationThe authors developed the protocol for review, detail-
ing pre-specified methods of the analysis and eligibility
for the review in accord with 2009 PRISMA guidance
[15] using also the new reporting elements derived
from the 2016 harms checklist [16]. While the protocol
was not registered, a description of the NIHR Capa-
CITY programme is available in the public domain
(http://www.isrctn.com/ISRCTN11747152) and has
been presented nationally (DDF meeting, London
2015; National Pelvic Floor Meeting, Manchester
2015).
Eligibility criteria
Study characteristics
Study characteristics were defined using the PICOS
framework. Search term definitions were inclusive, pro-
moting a sensitive search of studies reporting surgical
interventions for chronic constipation.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–166
Surgery for constipation C. H. Knowles et al.
Population: The review aimed to identify studies of
patients undergoing surgical interventions with the pri-
mary intent of treating chronic constipation. The defini-
tion of chronic constipation is neither straightforward
nor uniformly applied [17]. On this basis, all common
terms encompassing problematic defecation were used
(see search strategy syntax: Appendix I). However, sev-
eral pelvic floor procedures may be performed com-
monly for non-chronic constipation indications.
Examples include pelvic organ prolapse syndromes
where the physical prolapse or other organ dysfunctions
of the vagina or bladder are the main motivation for
surgery. While such patients invariably also have some
degree of defaecatory problems, and their perioperative
data could still be used to inform procedural safety,
these patients may phenotypically differ at baseline and
in response to surgical intervention even if the interven-
tion itself is identical or at least similar. Cochrane
reviews such as ‘surgical repair of pelvic organ prolapse
in women’ [18] and of surgical management of external
rectal prolapse [19] include some RCTs where defaeca-
tory symptoms are recorded as a secondary outcome or
as a complication but not as a primary presenting com-
plaint of the population studied. Thus these were ineli-
gible for inclusion. Similarly, for colonic excisional
procedures, patients with the very rare diagnoses of
adult Hirschsprung disease or idiopathic megacolon-
megarectum [20] were considered distinct from chronic
constipation and thus not included. Some studies
reported outcomes on two populations, only one of
which was eligible e.g. internal and external rectal pro-
lapse. Where such data could not be separated by
population, the study was also deemed ineligible for
inclusion.
A minimum population sample of 20 patients was
imposed for eligibility. This threshold was taken to
exclude case reports and small case series that often
reported a single surgeon’s personal experience or early
experience of experimental procedures.
Intervention: Surgical procedures for chronic consti-
pation are subject to heterogeneous descriptions. On
this basis, an iterative approach was taken by cross refer-
encing e.g. with textbook reference lists to ensure that
all terms in common usage were incorporated in the
eventual search strategy. These included some genuine
procedural variations but also multiple small changes in
syntax for the same procedure e.g. ‘stapled transanal
rectal resection’ vs ‘stapled transanal rectum resection’.
A decision was taken by the review team that results
would be grouped by five main approaches to surgically
treating chronic constipation: (i) colonic resection, (ii)
hitching procedures of the rectum (rectal suspension);
(iii) excisional procedures of the rectal wall (rectal exci-
sion); (iv) reinforcement of the rectovaginal septum
(RV reinforcement); and (v) sacral nerve stimulation
(SNS). This approach was taken because initial review
(Oct 2014) determined that other procedures either
lacked sufficient evidence for review. The first major
exclusion on this basis were stomas leading to intestinal
discontinuity or for the purpose of administering bowel
irrigation (continence enema). It is acknowledged that
in the real world many patients have stomas either
deliberately or as an eventual outcome of other surgery.
Figure 1 Schematic of pathophysiology
of chronic constipation.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–16 7
C. H. Knowles et al. Surgery for constipation

However, eligible studies were sparse after application
of inclusion criteria and markedly heterogeneous
between and within studies (patients and techniques).
Other procedures were excluded if still considered
experimental e.g. colonic exclusion procedures [21].
Comparisons: Studies were eligible regardless of
whether they were retrospective or prospective in
design, controlled or uncontrolled. Only a minority of
studies reported more than one procedure or more than
one population.
Outcomes: Studies were broadly eligible if they pro-
vided extractable data on benefit (treatment efficacy),
risk (harms) or both. For efficacy, inclusion necessitated
the acceptance of the huge disparity in quality of out-
comes reporting that are well acknowledged in the liter-
ature [14], with a heavy reliance on estimates of global
patient satisfaction with the procedure (an indirect
measure of the patients own judgement of their post-
operative state compared to their pre-operative state).
Studies of physiological and anatomical outcomes alone
were excluded since these are generally regarded as a
poor surrogate of efficacy in this patient population
[22]. Because the outcomes of surgical interventions for
chronic constipation are known to exhibit a ‘honey-
moon period’ in the months immediately following sur-
gery, a minimum (mean or median) follow up of
12 months was applied for eligibility. It is acknowl-
edged that enforcement of this criteria excluded some
level I studies. Several studies reported the outcomes of
more than one procedure. Where such data could not
be separated by procedure, these were not included
(often resulting in study ineligibility).
Report characteristicsYear of publication: Any publication date was eligible as
covered by database search from 1960 to the date of
final search (22nd February 2016).
Language: Due to the large number of studies
retrieved, it was decided to include only studies with
full text in the English language. While the numbers of
foreign language studies were small, these have been
detailed for the reader in ‘reasons for exclusion’ at the
full-text stage (rather than at the abstract screening
stage). There is reasonable evidence to suggest that
searching only in English does not have an adverse
effect on the quality of systematic reviews [23].
Type of study: Only peer-reviewed publications
reporting primary data were eligible. Thus reviews, edi-
torials, letters and other forms of secondary expert
opinion were excluded at the screening stage. Only full
manuscripts were eligible thus conference abstracts and
proceedings were also excluded. No constraint was
imposed based on level of evidence. This decision was
taken in the knowledge that the vast majority of data
would be extracted from case series rather than higher
quality study types.
Information sourcesThe senior author (CK) performed a comprehensive
search of the literature on 22nd February 2016 using
PubMed and Evidence Based Medicine reviews (includ-
ing the Cochrane database of systematic reviews and the
Cochrane central register of controlled trials). A prelim-
inary search in 2014 had determined that Embase and
Web of Science led to almost 2000 duplicate records
with no additional yield. Search terms used a sensitive
combination of population, intervention and report
terms. A keyword and hand search was used within rele-
vant Cochrane systematic reviews. The specific search
terms are listed in Appendix I.
Study selectionScreening was performed at the abstract level by the
senior author (CK), excluding studies not meeting eligi-
bility criteria where this could be readily determined
from the abstract alone. Full-text copies of all remaining
English language studies were obtained and assessed by
reviewers, who were un-blinded to the names of studies,
authors, institutions or publications. Disagreement
regarding inclusion was resolved by the senior author
(CK). Duplicate data sets generated from the same
cohort of patients were excluded with the larger popula-
tion size and longer follow-up cohort included at the
expense of earlier reports from the same cohort. In
instances of doubt, authors from the relevant institu-
tions were contacted to confirm or refute any repetition
of results (performed on three occasions).
Search results were cross-referenced to bibliographies
from other sources (previous reviews and book chap-
ters). Care was taken that any studies missed by the
original search met the strict inclusion criteria and did
not circumnavigate the carefully-defined search strategy
especially in relation to population terms.
Data collection processOutcome data were extracted by the junior authorship
team (UG, EJH, DP, PFV) paired with one senior
author for each procedure: colonic resections (CK); rec-
tal hitching procedures (SB); rectovaginal septum rein-
forcement (ABW); rectal wall excision (MM-J); sacral
nerve stimulation (SP). Data were extracted to a stan-
dardized template (Microsoft Excel spreadsheet) includ-
ing study characteristics and outcome data (see below).
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–168
Surgery for constipation C. H. Knowles et al.

For each procedure, one reviewer extracted the data
and one verified content.
Data itemsA full list of data fields is included in Table 1 (with
annotation). These followed the PICOS framework with
outcomes broadly divided into those assessing harms
(intra- and perioperative complications and long-term
adverse outcomes), and those assessing efficacy: global
success ratings and functional outcomes (organized into
validated symptom, QOL scoring instruments and indi-
vidual symptoms). For perioperative complications,
some consideration was given to classifying complica-
tions by established systems e.g. Clavien-Dindo however
inconsistencies in reporting made this unfeasible. Data
were not collected in relation to cost effectiveness which
was deemed to fall outside the remit of the process
aims. To simplify data extraction and presentation, for
ordinal data, summary statistics were extracted as mean
or median (with SD when provided).
Individual study quality and risk of biasThe methodological quality of all individual included
studies was assessed by the senior author (CK) and classi-
fied in accord with Oxford CEBM levels of evidence defi-
nitions for ‘therapy or harm’ [16]. The following rules
were applied accepting that distinguishing study designs
can be problematic for observational studies [24]:
1 A study was deemed prospective if this was categori-
cally stated or if patients were ‘enrolled’ or ‘re-
cruited’ to a study that systematically recorded pre-
and post-operative data. All other studies were
assumed to be retrospective.
2 A cohort study was defined as one designed to address a
clear stated aim or hypothesis using specified analytical
methods. In general, these included a comparison
group related either to the relative efficacy of more than
one specified procedure or to patient selection where a
specified baseline ‘risk factor’ was analysed in relation to
relative success or failure of the intervention.
3 A case series was defined as a report of observations
based on clinical practice. Such studies may generate
hypotheses by post-hoc case comparisons.
4 For randomized trials and cohort studies, Cochrane
risk of bias tools were applied [http://ohg.cochrane.
org/sites/ohg.cochrane.org/files/uploads/Risk%20of
%20bias%20assessment%20tool.pdf] and used to dis-
tinguish between high and low quality RCTs
(Oxford level 1b or level 2b) and high and low qual-
ity cohort studies (Oxford level 2b or level 4). Case
control studies were assessed using the National
Institutes of Health (NIH) quality assessment tool
[http://www.nhlbi.nih.gov/health-pro/guidelines/
in-develop/cardiovascular-risk-reduction/tools/case-
control] (Oxford level 3b or 4).
Further sub-analysis of the quality of observational
studies (e.g. compliance with STROBE, Newcastle-Ottawa
or MINORS) was not undertaken as it was felt that this
would add little to the overall assessment of quality.
Summary measuresResults were tabulated by outcome and described with
appropriate summary statistics (percentages, means and
ranges). For very rare events, the aggregate number and
denominator were reported. Quantitative data synthesis
was performed for key outcomes using meta-analysis in
STATA SE v14. Pooled proportions and means were
estimated, permitting exploration of heterogeneity and
bias. Where continuous measures failed to report mea-
sures of variance these were approximated as range/4.
Random effect meta-analytic models were estimated to
characterise rates of events and heterogeneity between
studies, with sub-grouping by procedure. Where studies
did not provide data in a useful summary form, available
data were tabulated but not included in the meta-analy-
sis. Results were presented as aggregate means with
confidence intervals and graphically displayed within
Forest plots. For pooled studies, the I2 value (reflecting
intra-group heterogeneity) was reported and interpreted in
accord with published guidance where 0–40% = hetero-
geneity might not be important, 30–60% = moderate
heterogeneity, 50–70% substantial heterogeneity and
75–100% = considerable heterogeneity [25]. The mag-
nitude and direction of effect, and strength of evidence
P-value from the chi-squared test, were used to inter-
pret the importance of heterogeneity.
Evidence within reviews was predominantly provided
by observational cohort data with relatively few experi-
mental studies (trials) identified. Consequently, the
reviews analyse all studies as individual cohorts, by pro-
cedure, to achieve inclusion and consistency; pooled
findings are compared with the findings of individual
trials. Where several trials were identified within a
review (e.g. rectal excision procedures) meta-analyses
was performed with sub-grouping by procedure and by
evidence grade. Findings by evidence grade were
reported only when they deviated qualitatively from the
overall pooled summary. Given the nature and reporting
of data, study-level meta-regression was not attempted.
Risk of bias across studiesPublication bias was assessed for outcomes where meta-
analysis was performed. Other limited analysis was per-
formed based on study size, design and publication date
where this contributed to interpretation. Subgroup analy-
sis was explored for the main procedural variations.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–16 9
C. H. Knowles et al. Surgery for constipation

Funding statementThis review was funded by the NIHR Programme
Grant for Applied Research Programme (Ref: RP-PG-
0612-20001) who had no role in study design, data
collection, analysis, interpretation, writing of the report
or the decision to submit the paper.
Clinical guidance development
AimsThe process had three main aims:
1 Development of summary evidence statements;
2 Development of graded practice recommendations;
3 Development of summary research recommenda-
tions.
Development of summary evidence statementsSummary evidence statements were produced by the
Clinical Guidance Group (CGG). This group was con-
vened in summer 2014. A final list of participants was
selected primarily from colorectal surgeons, gastroen-
terologists, urogynaecologists and specialist nurses with
a strong interest in functional colorectal and pelvic floor
disorders. This group included all senior authors of the
Table 1 Data field for systematic review.
Data extract Description Notes
Study characteristics
First author Text(num) With citation number
Year publication Text To 2016
Number of pts Number Ordinal integer
Follow up Months Mean or median as documented in study (integer)
Study design Text abbreviation As Oxford CEBM levels of evidence
Evidence grade IA–IV As Oxford CEBM levels of evidence
Population
Disease Text abbreviation As supplied key
Sex ratio Female:male Ratio not simplified
Age Years (integer) Mean or median as supplied (range)
Intervention
Operation (s) Text abbreviation As supplied key
Op duration Minutes Mean (integer)
Length of stay Days Mean to 1 decimal place
Outcomes
Harms
Perioperative
Total cx Percentage % to 1 decimal place
Infective cx Percentage % to 1 decimal place
Bleeding cx Percentage % to 1 decimal place
Proc specific cx Percentage As per specific procedure: % to 1 decimal place
Mortality Percentage % to 1 decimal place
Repeat intervention Percentage Generally procedure specific for complications
or poor functional outcome
Mortality rate Number Absolute number over reported denominator
Adverse long-term symptoms Percentage Some procedural specificity: Includes re-operation
rate where relevant
Efficacy
Global success rating Scale Very commonly employed: % patients with good or
excellent outcomes unless specified
Symptom scores Count Several variably validated summative scoring instruments:
pre and post or post only as available: mean + SD
Individual symptoms Percentage Some procedural specificity: pre and post or post
only as available
QOL measures Count or scale Few instruments used: pre and post or post only as
available: mean + SD
Cx, complications.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–1610
Surgery for constipation C. H. Knowles et al.

five reviews and associated junior investigators. Method-
ological expertise was provided by Professor James
Mason (University of Warwick), and NHS Specialised
Services stakeholder representation by Mr Mark Chap-
man. A series of meetings followed (Bristol, November
2014; London, June 2015; Manchester, November
2015; and Edinburgh, July 2016) at which the evolving
summary evidence statements (from reviews) were even-
tually ratified and prototype clinical practice recommen-
dations drafted.
The CGG used ‘focus group’ methodology to gain
consensus by in silico and face to face meetings. The num-
ber of participants (> 12), and four rounds of written revi-
sions fulfilled the basic criteria required for a guideline
decision group (National Institute for Health and Clinical
Excellence, April 2007) and allowed a sufficiently reliable
process at an acceptable cost in terms of travel, expenses
etc. The heterogeneity of the group (specialty, nationality,
expertise) was deemed desirable to be representative of a
range of stakeholders. Agreement was defined without
‘weighting’ of any participant’s views, although some par-
ticipants contributed more than others to the process.
Using the synthesis of the evidence base the group
drafted statements of evidence based on best evidence
available (which varied significantly by procedure). The
clinical guidance group discussed, revised and graded
summary statements of evidence level using the Oxford
2009 CEBM system (http://www.cebm.net/oxford-ce
ntre-evidence-based-medicine-levels-evidence-march-2009)
(Table 2) based on the review of evidence. For clarity,
roman numerals (I–IV) were used to denote summary
levels of evidence for graded evidence in contrast to
Arabic numerals for individual studies, e.g. 1a, 2b etc.
Summary levels could apply either positively or nega-
tively to each procedure. Care was taken to avoid any
contamination of expert opinion into statements, these
thus solely reflecting summated evidence from system-
atic review. Some language used in summary evidence
statements was deliberately chosen to reflect use of
pooled data. Thus the term ‘typical’ or ‘typically’ specif-
ically denotes that data for the event in question have
been derived from random effects analysis.
Development of graded practice recommendations(GPRs)This had two main stages: (i) development of ‘prototype’
GPRs by the Clinical Guidance Group, and (ii) develop-
ment of a final GPR list by a European Consensus group.
This approach, including the methodology used
(RAND/UCLA – see below) is established and has been
used previously in the coloproctology field [26].
Development of prototype GPRs: After a common
understanding of the evidence was established, group
discussion balanced clinical experience and evidence sum-
maries to arrive at shared judgements about recommen-
dations for care, thus deriving relevant recommendations
for decision making in clinical practice. Group processes
risk personal bias based on ‘eminence’ or ‘eloquence’ if
led and supported ineffectively: adequate methodological
support in the use of evidence and dialectic was provided
to support the process to ensure a balance of views as well
as to promote generalizability and impact. This stage
embodied summary evidence statements (from each
review), data from some excluded level I studies (e.g.
RCTs that were excluded for short follow up or pub-
lished after the review date) (a further search was run by
CK on 03.10.16 for the date range 22.02.16 to 03.10.16
including original terms and ‘clinical trial’) and expert
opinion derived from the decision group and selected
prior published guidance documents (Oxford 5) (Fig. 2).
Final grading followed Oxford CEBM recommenda-
tions (A–D) [27] [Table 3]. As with levels of evidence
the grades of evidence could apply either positively or
negatively to the procedure.
Development of final GPRs: The European Consensus
group comprised a panel of European experts (colorectal
and pelvic floor surgeons) nominated by the European
Society of Coloproctology (ESCP). Twenty experts were
invited from 10 European countries of whom 18 partici-
pated from nine countries (Appendix II).
Consensus methodology was derived from the
RAND/UCLA Appropriateness Method (Prepared for
Directorate General XII, European Commission 2001)
[28]. Prototype Graded Practice Recommendations
(derived from the clinical guidance group) were pre-
sented (on a spreadsheet) for each procedure under three
subheadings: ‘patient selection’, ‘procedural considera-
tions’ and ‘patient counselling’. For each, a number of
GPRs were listed, each with associated levels of evidence
and grade of prototype recommendation. For each, con-
sensus panellists were asked ‘Does this recommendation
lead to an expected health benefit that exceeds the
expected negative consequences of its introduction?’
Examples of health benefits in this context could be
improved surgical outcome, improved patient experience,
improved functional capacity etc.; the negative conse-
quences could include increased morbidity, anxiety, pain,
time lost from work, denial of an investigation or treat-
ment. Panellists were asked to base their judgement on
clinical grounds only, i.e. exclusive of financial cost [29].
Responses to each listed recommendation used a lin-
ear analogue scale of 1–9 to assess views on the benefit-
to-harm ratio. Using this scale, a score of 1–3 indicated
that they expected the harms of introducing the recom-
mendation to greatly outweigh the expected benefits
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–16 11
C. H. Knowles et al. Surgery for constipation

and a score of 7–9 that the expected benefits greatly
outweighed the expected harms. A middle rating of 4–6could mean either that the harms and benefits were
considered about equal or that the panellist was unable
to make a judgement for the recommendation. Panel-
lists were asked to try and provide a response for all
listed recommendations.
Responses were analysed in accordance with the first
phase of RAND/UCLA guidance, with each recom-
mendation classified as ‘appropriate,’ ‘uncertain’ or
‘inappropriate’ according to the panellists’ median score
and the level of disagreement. Indications with median
scores in the 1–3 range were classified as inappropriate,
those in the 4–6 range as uncertain, and those in the 7–9 range as appropriate. All indications rated ‘with dis-
agreement,’ whatever the median, were classified as
uncertain. ‘Disagreement’ here basically implied a lack
of consensus, either because of polarisation or spread
over the entire scale (defined for a sample of 18 pan-
elists as > 5 rating the indication outside the 3-point
region [1–9,28]). Further phases of consensus followingdiscussion to reduce variation were not conducted.
Summary research recommendationsOne of the initial drivers for this process (NIHR Capa-
CiTY) was the need to define the main evidence needed
for future surgical trials of patients with CC. During
the development of this guidance, some trials have com-
menced patient recruitment such as CapaCiTY study 3
(RCT of laparoscopic ventral rectopexy). There is how-
ever still a great need to define research questions that
could inform future UK and international commission-
ing of research funding. Research recommendations
Table 2 (a) Oxford CEBM (2009) summary levels of evidence and (b) grades of recommendation.
(a) Summary level
of evidence Type of studies
Evidence
included specific
to review
Notes specific to review
exclusions
I High quality RCT
All or none study
Oxford 1b,
1c*
1a (SR RCTs) excluded since no
secondary research included in
systematic review
II Poor quality RCT
Individual high quality
cohort study
Ecological study
Oxford 2b
2c*
2a (SR cohort studies) excluded
since no secondary research
included in systematic review
III Individual high quality
case-control study
Oxford 3b* 3a (SR case-control studies)
excluded since no secondary
research included in systematic
review
IV Case series and poor
quality cohort and
case-control studies
Oxford 4 The majority of studies included
in systematic review
V Expert opinion, bench
research
Oxford 5 Excluded in systematic review
(b) Grades of recommendation Evidence required
A Consistent level 1 studies
B Consistent level 2 or 3 studies or extrapolations from level 1 studies
C Level 4 studies or extrapolations from level 2 or 3 studies
D Troublingly inconsistent or inconclusive studies of any level (I–IV)
N Recommendation based on clinical understanding in the absence of evidence†
*No studies of these designs found by search for any procedure.
†But where a recommendation was considered necessary to highlight the absence of evidence for an important practice point.
Figure 2 Schematic showing process of transition from sum-
mary evidence statements to graded practice recommendations.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–1612
Surgery for constipation C. H. Knowles et al.

have been attributed a priority (high, medium or low)
based on the expert opinion of the current working
group and may help inform discussion about future
funding priorities.
Presentation of results
In view of the large scale of the systematic review and
prototype guidance process, results have been presented
as a series of separate manuscripts:
1 Overview of search results and study characteristics
(this manuscript);
2 Systematic review results and summary evidence
statements for colonic resection;
3 Systematic review results and summary evidence state-
ments for procedures characterized by rectal suspension;
4 Systematic review results and summary evidence state-
ments for procedures characterized by rectal wall excision;
5 Systematic review results and summary evidence
statements for procedures characterized by rectovagi-
nal septum reinforcement;
6 Systematic review results and summary evidence
statements for sacral nerve stimulation;
7 Coalescence of systematic review data, summary of graded
practice recommendations and research recommendations.
The main conclusions of this process were presented
at the Pelvic Floor Society Meeting in Cardiff, January
2017.
Overview of search results
Study selectionFigure 3 (PRISMA flow diagram) shows the results of
population and intervention term searches with reasons
for exclusion of studies at the full text review stage.
Table 3 Reviewed studies by main procedure type and evi-
dence level.
Procedure
Number of reviewed studies
by evidence level
1b 2b 3b 4 Total
Colonic resection 0 1 0 39 40
Rectal suspension procedures 0 2 0 16 18
Rectal excisional procedures 3 26 0 18 47
RV Reinforcement procedures 1 10 0 33 44
Sacral nerve stimulation 0 0 0 7 7
ALL 4 39 0 113 156
Figure 3 PRISMA diagram showing all review results.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–16 13
C. H. Knowles et al. Surgery for constipation

Study characteristicsTable 3 gives information on the overall study charac-
teristics and by procedure. Detailed data on individual
reviewed studies are provided by procedure type in the
accompanying papers. It can readily be noted that the
overall quality of evidence was poor with 113/156
(72.4%) providing only level IV evidence. The best evi-
dence to date exists for rectal excisional procedures
where the majority of studies where level I or II. This is
discussed further in the final graded practice recommen-
dations and research recommendations paper.
Acknowledgements
We would like to acknowledge the following people in
relation to the NIHR CapaCiTY working group: Mr Ste-
ven Brown, Sheffield Teaching Hospitals NHS Founda-
tion Trust; Mr Kenneth Campbell, The University of
Dundee, NHS Education for Scotland; Mr Mark Chap-
man, Heart of England NHS Trust; Mr Andrew Clarke,
Poole Hospital NHS Foundation Trust; Mr Neil Cruick-
shank, Sandwell and West Birmingham Hospitals NHS
Trust; Mr Anthony Dixon, University of Bristol, Bristol,
UK; Dr Christopher Emmett, County Durham and Dar-
lington NHS Foundation Trust; Mr Ugo Grossi, Queen
Mary University of London; Dr Richard Hooper, PCTU,
Queen Mary University of London; Miss Emma Hor-
rocks, University Hospital Southampton NHS Founda-
tion Trust; Professor Charles Knowles, Queen Mary
University of London; Mr Jon Lacy-Colson, Shrewsbury
and Telford Hospital NHS Trust; Mr Ian Lindsey,
Oxford University Hospitals NHS Trust; Professor James
Mason, University of Warwick, Coventry; Mr Mark Mer-
cer-Jones, Gateshead Health NHS Foundation Trust; Mr
Andrew Miller, University Hospitals of Leicester NHS
Trust; Mr David Pares, Hospital Germans Trias i Pujol,
Barcelona, Spain; Miss Sophie Pilkington, University
Hospital Southampton NHS Foundation Trust; Mr Neil
Smart, Royal Devon & Exeter NHS Foundation Trust;
Ms Natasha Stevens, PCTU, Queen Mary University of
London; Professor Douglas Tincello, University Hospi-
tals of Leicester NHS Trust; Miss Karen Telford, South
Manchester NHS Foundation Trust; Mr Paul Vollebregt,
Queen Mary University of London; Mr Andrew Wil-
liams, Guy’s and Thomas’ NHS Foundation Trust; Pro-
fessor Yan Yiannakou, County Durham and Darlington
NHS Foundation Trust.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opinions
expressed in this report are those of the authors and are
not those of the PGfAR Programme, NIHR, the UK
National Health Service, or the UK Department of Health.
Conflicts of interest
All authors have no conflict of interest in relation to
the content of the manuscript. In the last 2 years,
C.H. Knowles has received speaker fees and consul-
tancy payments from Medtronic Inc., S. Brown has
received speaker fees and consultancy payments from
Allergan. M. Mercer-Jones has received fees as a pre-
ceptor for Medtronic Inc. and A.B. Williams has
received speaker fees and consultancy payments from
Medtronic Inc., and acts as a non-payed consultant for
Cook Medical. M. Chapman has received funding to
attend courses from Medtronic Inc.
References
1 Stewart WF, Liberman JN, Sandler RS et al. Epidemiology of
constipation (EPOC) study in the United States: relation of
clinical subtypes to sociodemographic features. Am J Gastroen-
terol 1999; 94: 3530–40.
2 van den Berg MM, Benninga MA, Di Lorenzo C. Epidemi-
ology of childhood constipation: a systematic review. Am J
Gastroenterol 2006; 101: 2401–9.
3 Suares NC, Ford AC. Prevalence of, and risk factors for,
chronic idiopathic constipation in the community: system-
atic review and meta-analysis. Am J Gastroenterol 2011;
106: 1582–91; quiz 1581, 1592.
4 Shafe AC, Lee S, Dalrymple JS, Whorwell PJ. The LUCK
study: Laxative Usage in patients with GP-diagnosed Con-
stipation in the UK, within the general population and in
pregnancy. An epidemiological study using the General
Practice Research Database (GPRD). Therap Adv Gastroen-
terol 2011; 4: 343–63.
5 Knowles CH, Scott SM, Rayner C et al. Idiopathic slow-
transit constipation: an almost exclusively female disorder.
Dis Colon Rectum 2003; 46: 1716–7.
6 Wald A, Scarpignato C, Mueller-Lissner S et al. A multina-
tional survey of prevalence and patterns of laxative use
among adults with self-defined constipation. Aliment Phar-
macol Ther 2008; 28: 917–30.
7 Irvine EJ, Ferrazzi S, Pare P, Thompson WG, Rance L.
Health-related quality of life in functional GI disorders:
focus on constipation and resource utilization. Am J Gas-
troenterol 2002; 97: 1986–93.
8 Peery AF, Dellon ES, Lund J et al. Burden of gastrointesti-
nal disease in the United States: 2012 update. Gastroen-
terology 2012; 143: 1179–87.e1–3.
9 Poulton BTS. The nursing cost of constipation. Primary
Health Care 1999; 9: 17–22.
10 H.a.S.C.I.C. Prescription Cost Analysis: England 2014. Pre-
scribing & Medicines Team, Health and Social Care Infor-
mation Centre, 2015.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–1614
Surgery for constipation C. H. Knowles et al.

11 Palit S, Lunniss PJ, Scott SM. The physiology of human
defecation. Dig Dis Sci 2012; 57: 1445–64.
12 Ragg J, McDonald R, Hompes R, Jones OM, Cunningham
C, Lindsey I. Isolated colonic inertia is not usually the cause
of chronic constipation. Colorectal Dis 2011; 13: 1299–302.
13 Bharucha AE, Wald A, Enck P, Rao S. Functional anorectal
disorders. Gastroenterology 2006; 130: 1510–8.
14 Woodward S, Norton C, Chiarelli P. Biofeedback for treat-
ment of chronic idiopathic constipation in adults. Cochrane
Database Syst Rev 2014; 3: CD008486.
15 Liberati A, Altman DG, Tetzlaff J et al. The PRISMA
statement for reporting systematic reviews and meta-ana-
lyses of studies that evaluate health care interventions:
explanation and elaboration. J Clin Epidemiol 2009; 62:
e1–34.
16 Zorzela L, Loke YK, Ioannidis JP et al. PRISMA harms
checklist: improving harms reporting in systematic reviews.
BMJ 2016; 352: i157.
17 Cook IJ, Talley NJ, Benninga MA, Rao SS, Scott SM.
Chronic constipation: overview and challenges. Neurogas-
troenterol Motil 2009; 21(Suppl 2): 1–8.
18 Maher C, Feiner B, Baessler K, Adams EJ, Hagen S, Glaz-
ener CM. Surgical management of pelvic organ prolapse in
women. Cochrane Database Syst Rev 2010; 4: CD004014.
19 Tou S, Brown SR, Nelson RL. Surgery for complete (full-
thickness) rectal prolapse in adults. Cochrane Database Syst
Rev 2015; 11: CD001758.
20 Gladman MA, Scott SM, Lunniss PJ, Williams NS. System-
atic review of surgical options for idiopathic megarectum
and megacolon. Ann Surg 2005; 241: 562–74.
21 Peng HY, Xu AZ. Colonic exclusion and combined ther-
apy for refractory constipation. World J Gastroenterol
2006; 12: 7864–8.
22 Knowles CH, Dinning PG, Pescatori M, Rintala R, Rosen
H. Surgical management of constipation. Neurogastroen-
terol Motil 2009; 21(Suppl 2): 62–71.
23 Moher D, Pham B, Lawson ML, Klassen TP. The inclusion
of reports of randomised trials published in languages other
than English in systematic reviews. Health Technol Assess
2003; 7: 1–90.
24 Dekkers OM, Egger M, Altman DG, Vandenbroucke JP.
Distinguishing case series from cohort studies. Ann Intern
Med 2012; 156(Pt 1): 37–40.
25 Higgins JPT, Green S. Cochrane Handbook for Systematic
Reviews of Interventions. The Cochrane Collaboration,
2011. http://handbook.cochrane.org
26 Juillerat P, Peytremann-Bridevaux I, Vader JP et al.
Appropriateness of colonoscopy in Europe (EPAGE II).
Presentation of methodology, general results, and analysis
of complications. Endoscopy 2009; 41: 240–6.
27 Evans C, Ong E, Jones OM, Cunningham C, Lindsey I.
Laparoscopic ventral rectopexy is effective for solitary rectal
ulcer syndrome when associated with rectal prolapse.
Colorectal Dis 2014; 16: O112–6.
28 Finch KBS, Bernstein SJ, Aguilar MD et al. The RAND/
UCLA Appropriateness Method User’s Manual. Santa Mon-
ica, CA, USA: Rand Europe, 2001.
29 Brook RH, Chassin MR, Fink A, Solomon DH, Kosecoff
J, Park RE. A method for the detailed assessment of the
appropriateness of medical technologies. Int J Technol Assess
Health Care 1986; 2: 53–63.
Appendix I: Search strategy
Population terms
“constipation”[All Fields] OR “obstructed defecation”[All
Fields] OR “colonic inertia”[All Fields] OR
“intussusception”[All Fields] OR “rectal prolapse”[All Fields]
OR “outlet obstruction”[All fields] OR “SRUS”[All Fields]
OR “solitary rectal”[All Fields] OR “defecation disorder”[All
Fields]) OR “impaired defecation”[All Fields] OR “rectal
emptying”[All Fields] OR “bowel dysfunction”[All Fields]
OR “bowel function”[All Fields] OR “defecography”[All
Fields] OR “defaecography”[All Fields] OR
“defecographic”[All Fields] OR “evacuation difficulty”[All
Fields] OR “evacuation disorder”[All Fields] OR
(“Constipation”[Mesh Terms]) NOT (“child”[MeSH
Terms]).
Intervention terms
“Delorme procedure”[All Fields] OR “delormes
procedure”[All Fields] OR “delorme’s procedure”[All Fields]
OR “sacral nerve stimulation”[All Fields] OR “sacral
neuromodulation”[All Fields] OR “neurostimulation”[All
Fields] OR “sacral nerve modulation”[All Fields] OR
“STARR”[All Fields] OR “stapled transanal resection”[All
Fields] OR “stapled transanal rectal resection” [All Fields]
OR “trans-STARR”[All Fields] OR “Stapled trans-anal rectal
resection”[All Fields] OR “rectopexy”[All Fields] OR
“sacrocolpopexy”[All Fields] OR “sacropexy”[All Fields] OR
“promontofixation”[All Fields] OR “colectomy”[All Fields]
OR “proctocolectomy”[All Fields] OR “ileorectal”[All Fields]
OR “cecorectal” [All Fields] OR “ileoproctostomy”[All
Fields] OR “cecoproctostomy”[All Fields] OR
“ileosigmoid”[All Fields] OR “rectocele repair”[All Fields]
OR “posterior repair”[All Fields] OR “colporrhaphy”[All
Fields] OR “rectovaginal septum reinforcement”[All Fields]
OR “anterior rectal wall repair”[All Fields] OR “surgical
repair of rectocele”[All Fields] OR (“transperineal mesh
repair”[All Fields] OR “transperineal repair”[All Fields] OR
“transvaginal repair”[All Fields] OR “transanal repair”[All
Fields] OR “endorectal repair”[All Fields] OR “transrectal
repair”[All Fields] OR “transanal longitudinal plication”[All
Fields] OR (“Constipation/surgery”[Mesh Terms])
Report terms
(hasabstract[text]) AND (“0001/01/01”[PDat]: “2016/02/
22”[PDat])
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–16 15
C. H. Knowles et al. Surgery for constipation

Appendix II: European reference group*
Name Institution
Donato Altomare Bari, Italy
Lars Boenicke Wuerzburg, Germany
Steen Buntzen Tromsø, Norway
Ken Campbell Dundee, UK
Peter Christensen Aarhus, Denmark
Andre D’Hoore Leuven, Belgium
Eloy Espin Barcelona, Spain
David Jayne Leeds, UK
Oliver Jones Oxford, UK
Jens-Christian Knapp Stavanger, Norway
Soren Laurberg Aarhus, Denmark
Paul Lehur Nantes, France
Klaus Matzel Erlangen, Germany
Ronan O’Connell Dublin, Ireland
Michel Prud’homme N̂ımes, France
Carlo Ratto Rome, Italy
Mario Trompetto Turin, Italy
Caroline Vaizey London, UK
*Derived from European Society of Coloproctology.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 5–1616
Surgery for constipation C. H. Knowles et al.

Surgery for constipation: systematic review and practicerecommendations
Results I: Colonic resection
C. H. Knowles*, U. Grossi*, M. Chapman†, J. Mason‡, on behalf of the NIHR CapaCiTY working
group§ and Pelvic floor Society¶*National Bowel Research Centre, Blizard Institute, Queen Mary University London, London, UK, †Good Hope Hospital, Heart of England NHS Trust,
Birmingham, UK, ‡University of Warwick, Coventry, UK, §National Institute for Health Research: Chronic Constipation Treatment Pathway, and
¶Affiliate section of the Association of Coloproctology of Great Britain and Ireland
Abstract
Aim To assess the outcomes of colectomy in adults
with chronic constipation (CC).
Method Standardised methods and reporting of bene-
fits and harms were used for all CapaCiTY reviews that
closely adhered to PRISMA 2016 guidance. Main con-
clusions were presented as summary evidence statements
(SES) with a summative Oxford Centre for Evidence-
Based Medicine (2009) level.
Results Forty articles were identified, providing data on
outcomes in 2045 patients. Evidence was derived
almost exclusively from observational studies, the major-
ity of which concerned colectomy and ileorectal anasto-
mosis (CIRA) rather than other procedural variations.
Average length of stay (LOS) ranged between 7–15 days. Although inconsistent, laparoscopic surgery
may be associated with longer mean operating times
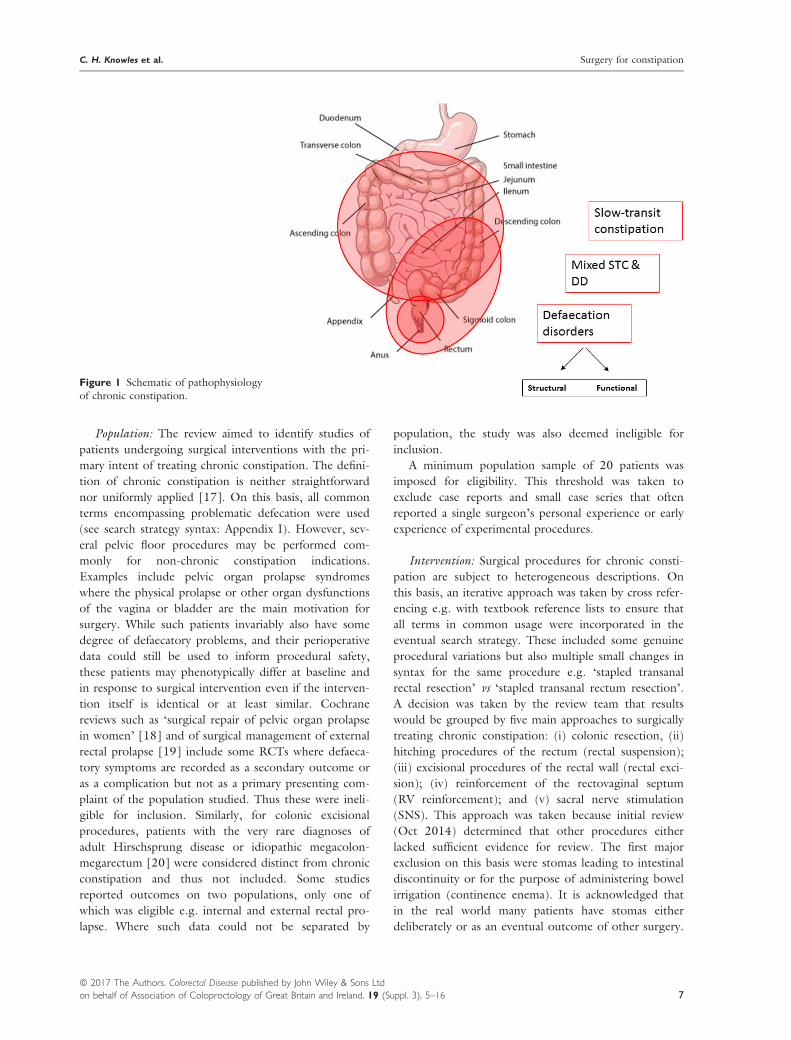
(210 vs 167 min) and modest decreases in LOS (10–8 days). Complications occurred in approximately 24%
of patients. Six (0.4%) procedure-related deaths were
observed. Recurrent episodes of small bowel obstruc-
tion occurred in about 15% (95%CI: 10–21%) of
patients in the long-term, with significant burden of re-
hospitalisation and frequent recourse to surgery. Most
patients reported a satisfactory or good outcome after
colectomy but negative long-term functional outcomes
persist in a minority of patients. The influence of resec-
tion extent, anastomotic configuration and method of
access on complication rates remains uncertain. Avail-
able evidence weakly supports selection of patients with
an isolated slow-transit phenotype.
Conclusion Colectomy for CC may benefit some
patients but at the cost of substantial short- and long-
term morbidity. Current evidence is insufficient to
guide patient or procedural selection.
Keywords Constipation, colectomy, ileorectal, slow-
transit
Introduction
Background and procedural variations
The concept of resection of the colon to treat constipa-
tion originates more than a century ago [1]. Modern
surgical approaches mostly continue in the historical
practice of removing the whole colon with anastomosis
of the terminal ileum to the upper rectum (or very dis-
tal sigmoid) usually at the level of the sacral promon-
tory. Usually termed colectomy and ileorectal
anastomosis (CIRA), the procedure is also sometimes
described as colectomy with ileoproctostomy. Total
colectomy is not favoured by all surgeons and other less
radical colonic resections may also be employed. The
simplest variation is to perform a subtotal colectomy
and ileosigmoid anastomosis (SCISA) but an increas-
ingly popular choice is subtotal colectomy with sparing
of the caecum and thence caecorectal anastomosis
(SCCRA). Since this is not a common procedure in
routine colorectal surgical practice, it merits some back-
ground description. First described by Ogilvie (1931),
retention of the ileocaecal junction has the theoretical
advantage of preservation of absorptive functions (bile,
vitamin B12 and electrolytes) and thus perhaps reduced
diarrhoea. No standard technique exists for creating a
CRA. The general principle involves colonic mobiliza-
tion followed by ligation of all vascular pedicles except
the ileocolic branches. In the technique proposed by
Correspondence to: Prof. C. H. Knowles, NBRC, 1st Floor Abernethy Building, 2
Newark St, London E1 2AT, UK.
E-mail: [email protected]
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 17
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13779

Lillehei and Wangensteen (1955) a 180° rotation of the
remaining mesentery from the right to the left is per-
formed to place the caecum in the left iliac fossa, with
apex cephalad. During the rotation the remaining meso-
colon passes over the aorta, and it is sutured to the
mesorectum and to the third portion of the duodenum
to avoid internal hernia or intestinal obstruction, which
may complicate such technique. Deloyers (1963) pro-
posed a variation of this technique in which there is a
craniocaudal rotation of the caecum to allow a pelvic
isoperistaltic CRA (IPSCCRA) but this required a retro-
ileal tunnel and 180° torsion of the vascular pedicle
which may result in ischemia or venous stasis. These dif-
ficulties have in part be mitigated by development of an
antiperistaltic end-to-end caecorectal anastomosis (at-
tributed to Sarli [2]) (APSCCRA) which avoids the vas-
cular problems due to the torsion of the pedicle,
obviates the need to tailor the caecum and lowers the
risk of intestinal obstruction due to the rotation of the
mesocolon in front of the aorta.
Scope
Procedures considered beyond the scope of systematic
review [1–18] were:1 Total colonic and rectal excision (proctocolectomy).
These procedures have been variously employed for
chronic constipation with or without ileal pouch
formation in small numbers of patients and usually as
a salvage after failed colectomy;
2 Subtotal colectomy and modification of the rectal reser-
voir (modified Duhamel procedure; Jinling procedure);
3 Colonic exclusion and ileorectal anastomosis i.e.
without resection.
Previous reviews
Narrative reviews focused on the outcome of colectomy
for constipation have been published in 1996 [10],
1999 [11], and 2006 [12]. No previous systematic
review was identified.
Summary of search results and study quality
The search yielded a total of 85 manuscripts for full
text review (Fig. 1). From these, 40 articles published
between 1988 and 2015 contributed to the systematic
review, providing data on outcomes in a total of 2045
patients (range 20–144 patients per study) based on
39 defined patient cohorts (Table 1). A US nationwide
dataset derived from hospital episode statistics was also
included covering 2377 procedures coded as colectomy
for constipation indications [19]. Specific exclusions
after full-text review (and after exclusion of non-Eng-
lish language publications: n = 10) included 27 studies
where the population sample was confirmed to be less
Figure 1 PRISMA diagram.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3618
Surgery for constipation C. H. Knowles et al.

than 20 patients, four studies of out of scope proce-
dures, one study where data were considered duplicate
[13], one where outcomes could not be segregated by
eligible procedure [14], and one where data for multi-
ple clinical indications for colectomy were merged
[15].
Table 1 All studies included in systematic review.
Author Year Centre Country Total N FU* Design Level†
Kamm [23] 1988 St Marks, London UK 44 > 12 RCS IV
Vasilevsky [24] 1988 Mayo Clinic, MN USA 52 46 RCS IV
Yoshioka & Keighley [25] 1989 Birmingham UK 40 36 RCS IV
Pemberton [26] 1991 Mayo Clinic, MN USA 36 36 PCS IV
Piccirillo [27] 1995 Cleveland Clinic, FL USA 54 27 RCS IV
Redmond [21] 1995 John Hopkins, Baltimore USA 34 90 PCH IIB
de Graaf [28] 1996 Rotterdam Netherlands 42 46 PCH IV
Lubowski [29] 1996 Sydney Australia 52 42 RCS IV
Platell [30] 1996 Perth Australia 96 60 RCS IV
Pluta [31] 1996 Alberta Canada 24 65 RCS IV
Ghosh [32] 1996 Edinburgh UK 21 96 RCS IV
Nyam [33] 1997 Singapore Singapore 74 56 PCH IV
Ho [34] 1997 Singapore Singapore 24 24 RCH IV
You [35] 1998 Taiwan China 40 24 PCS IV
Bernini [36] 1998 Mayo Clinic, MN USA 106 78 RCH IV
Hasegawa [37] 1999 Birmingham UK 61 84 RCH IV
Fan [38] 2000 Taiwan China 24 23 RCS IV
Pikarsky [39] 2001 Cleveland Clinic, FL USA 62 105 RCH IV
Pikarsky [40] 2001 Cleveland Clinic, FL USA 30 60 PCS IV
Webster & Dayton [41] 2001 Cancun Mexico 50 12 RCS IV
Mollen [42] 2001 Bennekom Netherlands 21 62 PCS IV
Nylund [43] 2001 Goteburg Sweden 40 132 PCS IV
Lundin [44] 2002 Uppsala Sweden 28 50 PCS IV
Fitzharris [45] 2003 Mayo Clinic, MN USA 75 47 RCS IV
Hassan [46] 2006 Mayo Clinic, MN USA 104 68 RCH IV
Marchesi [47] 2007 Parma Italy 23 72 PCS IV
Zutshi [48] 2007 Cleveland Clinic, OH USA 69 130 RCS IV
Feng [22] 2008 Zheijang China 79 47 RCH IIB
Hsiao [49] 2008 Taiwan China 44 12 PCS IV
Jiang [50] 2008 Whuhan China 37 48 RCH IV
Pinedo [51] 2009 Santiago Chile 20 25 RCS IV
Riss [52] 2009 Vienna Austria 20 84 RCS IV
Sohn [53] 2011 Soeul Korea 37 41 RCS IV
Xu LS [20] 2012 Harbin China 64 32‡ RCT IIB
Marchesi [54] 2012 Parma Italy 30 12 CCS IV
Wang [55] 2013 Zheijang China 124 12 RCH IV
Reshef [56] 2013 Cleveland Clinic, OH USA 144 43 RCH IV
Li [57] 2014 Chongqing China 72 64§ RCH IV
Sun [58] 2015 Shanghai China 48 36 RCH IV
Total 2045 47¶ –
Dudekula [19] 2015 US nationwide sample USA 2377** 12 RCH IV
RCS, retrospective cohort study; PCS, prospective cohort study; RCT, randomised controlled trial; CCS, case control study.
*Mean follow up in months.†Oxford CEBM [16].‡Only 4 days blinded.§For CIRA but 32 months for APSCCRA.¶Median value of follow up.
**181 for state sample and 56 with 12 months pre & post-intervention.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 19
C. H. Knowles et al. Surgery for constipation

The general quality of studies was poor due to inade-
quate description of methods. The 40 included studies
comprised: a single poor quality randomized trial (uncertain
or high risk of bias in most domains) [20] (Oxford level
IIB); one good quality prospective [21] and one retrospec-
tive cohort study [22] (level IIB); and 37 level IV studies
(comprising 14 poor quality cohort studies, i.e. ‘case com-
parison studies’; one poor quality case-control study with
non-consecutive controls; eight prospective case series; and
14 retrospective case series). A general problem was the lack
of prospectively defined follow up intervals. Patient follow
up ranged from 12 months to 11 years (median
47 months) but this clearly varied greatly for individual
patients within studies without defined follow up periods.
Eleven studies derived from US centres, 11 from European
centres, nine from Chinese centres with the remaining nine
spilt across five countries.
Perioperative data
Perioperative data were reported by 37 studies
(Table 2). Reporting of procedure duration was incon-
sistent but mean procedural duration ranged from
approximately 2–4 h. Within this variation were trends
of shorter operating times for open vs laparoscopic pro-
cedures (e.g. colectomy and ileorectal anastomosis
(CIRA), median open: 167 min vs median laparoscopic:
210 min), as well as for subtotal procedures: median
135 min. The average length of stay (LOS) reported
was 10.4 days, ranging from 7.0 to 15.5 days duration.
However laparoscopic procedures consistently reported
shorter lengths of stay e.g. the median LOS for open
CIRA was 10.6 days compared to 8.1 days for laparo-
scopic CIRA. This evidence is supported by individual
cohort comparisons [34,55] and in the single RCT
where mean LOS was reduced from 9.7 to 7.6 days
with laparoscopy [20].
Summary evidence statements: perioperative data
1 Length of stay after colectomy for constipation is 7–15 days, even in the modern era (level IV).
2 Laparoscopic surgery may be associated with longer
operating times and modest decreases in length of
stay (from 10 to 8 days), however there is consider-
able variation between studies (level IV).
Harms
Perioperative complications
Presented meta-analyses showed considerable hetero-
geneity of complications, not explained by procedure
or age of publication. The attentiveness to harm
recording and the duration of recording were inconsis-
tent and studies limited only to laparoscopic procedures
are characterized by small numbers limiting scope for
comparison with open procedures and no adjustment
has been attempted for potential differences in the
populations recruited into individual studies. Conse-
quently estimates of harm provided are necessarily ten-
tative.
Surgical morbidity remains a concern for all types of
colectomy with total complication rates. A random
effects meta-analysis estimated total complications to be
24.4% (95%CI: 17.8–31.7%); I2 = 88.1% (Fig. 2),
although findings were heterogeneous including indi-
vidual study rates from 7% to 54% (Table 2). Aside
from the incidence of anastomotic leaks and other
more general complications (high even in some recent
series from expert centres [56] and including six fatali-
ties in 1568 patients: 0.4%) the incidence of prolonged
post-operative ileus (POI) and early adhesional small
bowel obstruction (SBO) are known to be dispropor-
tionally high for patients undergoing colectomy for
slow-transit constipation when compared to other indi-
cations [17].
A random effects meta-analysis estimated early post-
op POI/SBO to be 9.7% (95%CI: 5.7–14.6%);I2 = 87.9% (Fig. 3), although findings were heteroge-
neous including individual study rates from 0% to 33%.
Current findings are inconclusive as to whether laparo-
scopic or open surgery are safer: there is some sugges-
tion however that the POI rate is lower in newer
studies. Rates of further surgical intervention for POI in
the perioperative period were similarly heterogeneous:
2.7% (95%CI: 1.0–5.0%) I2 = 64.3%, including study
rates from 0% to 15%.
These data have been put into a broader context by
the recent (2015) US national database study of 2377
colectomies for constipation between 1998–2011 [19],
providing 60% of all subjects within the review. This
study based on registered health episodes re-affirms a
high rate of perioperative complications in a national
sample (42.7% patients during index hospitalisation 30-
day period), with the main contribution (27%) coming
from “intestinal obstruction, ileus, nausea & vomit-
ing”.
Long-term adverse outcomes
Long-term rates of SBO reported by studies were
heterogeneous: 15.2%, (95%CI: 10.2–20.9%)I2 = 85.5%, including study rates from 0% to 71%
(Table 3; Fig. 4a). Re-operation rates (principally for
SBO but also other severe ongoing functional
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3620
Surgery for constipation C. H. Knowles et al.

Table 2 Perioperative data by procedure.
Author Year N Time LOS Bleed Inf Total cx POI* Re-op Leak Mort
(a) Open colectomy and ileorectal anastomosis
Pemberton [26] 1991 36 NR 12.0 NR 8.3 22.2 13.0 0 0 0
Piccirillo [27] 1995 54 NR 7.0 NR NR NR 3.7 6 0 0
Redmond† [21] 1995 37 NR 12.1 NR NR 24 NR NR 0 0
Lubowski [29] 1996 52 NR NR NR NR NR NR NR 1.9 0
Pluta [31] 1996 24 NR NR 4.2 12.5 25 4.2 0 0 0
Ghosh [32] 1996 21 NR NR NR NR NR NR NR NK 0
Nyam [33] 1997 74 NR NR NR 9.0 NR 12.0 0 0 0
Ho [34] 1997 17 ‡ 10.6 NR 12.0 23.0 13.0 13.0 0 0
Bernini [36] 1998 106 NR NR NR NR NR 23.0 14.1 0 0
Fan [38] 2000 24 NR 10.0 NR NR NR NR 0 0 0
Pikarsky [40] 2001 30 NR NR NR NR NR NR NR 0 0
Webster & Dayton§ [41] 2001 55 NR 10.0 NR NR 42.0 32.0 NR 4.0 0
Mollen [42] 2001 21 NR NR NR NR 33.0 19.0 9.5 0 0
Nylund [43] 2001 40 NR NR 5.0 7.5 20.0 5.0 5.0 0 0
Fitzharris [45] 2003 75 NR NR NR NR NR NR NR 7 0.9
Hassan [46] 2006 65 NR NR NR NR NR NR NR 0 0
Jiang [50] 2008 21 140 15.5 NR 5.0 NR NR NR 0 0
Sohn [53] 2011 37 203 12.0 NR 5.4 13.5 10.8 2.7 2.7 0
Xu [20] 2012 32 145 9.7 NR NR NR 0 3.1 0 0
Wang [55] 2013 68 190 11.0 0 7.4 8.8 1.5 0 0 0
Li F [57] 2014 40 NR NR 1.25 2.5 32.5 15.0 7.5 2.5 0
(b) Series including open and laparoscopic colectomy and ileorectal anastomosis
Zutshi [48] 2007 69 NR 10.0 1.4 7.2 17.4 16.0 1.4 1.4 0
Riss [52] 2009 20 190 10.5 5.0 35.0 45.0 5.0 15.0 5.0 15.0
Reshef† [56] 2013 144 NR 7.8 3.5 17.0 54.0 26.0 14.0 6.9 1.0
Dudekula [19] 2015 2377 NR 8.0 NR NR 42.7 27.0¶ NR NR NR
(c) Laparoscopic colectomy and ileorectal anastomosis
Ho [34] 1997 7 NR** 9.2 NR 14 43.0 29 0 0 0
Xu [20] 2008 44 197 7.6 NR 4.5 18.2 11.4 4.5 2.3 0
Pinedo [51] 2009 20 248 7.0 10.0 NR NR 15.0 5.0 5.0 0
Xu [20] 2012 32 122 8.5 NR NR NR 0 3.1 3.1 0
Wang [55] 2013 56 223 8.7 0 5.3 7.1 1.8 0 0 0
Author Year Operation N Time LOS Bleed Inf Total cx POI* Re-op Leak Mort
(d) Subtotal colectomy and ileosigmoid anastomosis (ISA); isoperistaltic caecorectal anastomosis (IPCCA); antiperistaltic caecorectal
anastomosis (APCCA); lap: laparoscopic
de Graaf [28] 1996 ISA 24 NR NR NR NR NR NR NR NR 4.2
Feng [22] 2008 ISA 45 135 13.1 NR NR 20 NR 0 0 0
Sun [58] 2015 ISA 22 NR NR NR NR NR NR NR NR 0
Feng [22] 2008 IPCRA 34 120 12.5 NR NR NR NR 0 0 0
Li F [57] 2014 IPCRA 32 NR NR 0 3.1 28.1 12.5 3.1 3.1 0
Sun [58] 2015 IPCRA 26 NR NR NR NR NR NR NR NR 0
Marchesi [47] 2007 APCRA (5 lap) 17 NR 11.9 NR NR 9.3 5.9 11.8 5.9 0
Jiang [50] 2008 APCRA 17 130 14.5 NR 5.9 NR NR NR 0 0
Marchesi [54] 2012 APCRA 15 184 10.9 NR NR 13.3 0 0 0 0
Marchesi [54] 2012 APCRA lap 15 232 9.3 NR NR 13.3 0 0 6.7 0
Cx, complications; NR, not reported.
*Includes prolonged ileus and early mechanical obstruction.†In patients with STC only.‡70 min shorter than laparoscopic procedures in same series (actual duration not reported).§5 patients had colectomy and end ileostomy.¶Includes ‘intestinal obstruction, POI, nausea and vomiting, and haemorrhage’. POI, postoperative ileus.
**+/� rectopexy.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 21
C. H. Knowles et al. Surgery for constipation

problems) were similarly heterogeneous 13.3%, (95%CI:
8.6–18.7%) I2 = 87.7%, including study rates from 0%
to 45% (Fig. 4b). Particular to colectomy for constipa-
tion is the concept that laparoscopy might reduce the
well-established high incidence of post-operative SBO.
The review provided only limited data from small stud-
ies comparing open with laparoscopic procedures,
although SBO rates appeared much lower. Ho et al.
[34] found that early adhesion formation leading to
bowel obstruction was more frequent in patients under-
going laparoscopically assisted colectomy (29%) com-
pared to open (13%). A larger series of 124 patients
also showed no differences in post-operative morbidity
between approaches [55]. Conversely, a low quality
case-control study of 15 laparoscopic vs 15 open subto-
tal colectomy with antiperistaltic CRA showed that
bowel obstruction rates were halved (from 13.3 to
6.7%) in the laparoscopic groups [54]. The follow up in
these studies (12–20 months) was generally shorter
than the average (47 months) although very high rates
of SBO were reported by a study of exclusively open
CIRA with 12 months follow up [52]. Finally, while
the results for laparoscopic approach offer some opti-
mism based on the small numbers of patients in these
studies, no differences were observed in complication
rates between open and laparoscopic procedures in the
US nationwide survey of 2377 colectomies [19].
However, the most revealing conclusions can be
drawn from further analysis of US national database
study in which longitudinal data were recorded on 166
patients recorded on State Inpatient Databases of Flor-
ida and California (2005–2011). These data agreed with
the whole national dataset (n = 2377) in confirming
high perioperative (30-day) complication and re-admis-
sion rates, but also showed that resource utilisation in
the form of emergency department visits, hospitalisation
and surgical intervention remained high in the following
1 year. Excluding the colectomy itself, these 166
patients had a total of 2355 encounters, which included
1494 emergency department visits and 861 hospitalisa-
tions by 149 and 144 patients, respectively. Among the
1494 emergency department visits, the 674 that
occurred postoperatively were shared across 119 (72%)
patients; among the 861 hospitalisations, 488 occurred
after colectomy and affected 110 (66%) patients. A
breakdown of the motivation for these attendances
reveals the well-described issue of ongoing abdominal
pain, which as well as other gastrointestinal symptoms
and postoperative complications, increased after colec-
tomy.
Figure 2 Forest plot showing totalcomplications (percentage of patients)
after colectomy by procedure type.
CIRA, colectomy and ileorectal
anastomosis; lap, laparoscopic; ISA,ileosigmoid anastomosis; IPCRA,
isoperistaltic caecorectal anastomosis;
APCRA, antiperistaltic caecorectal
anastomosis.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3622
Surgery for constipation C. H. Knowles et al.
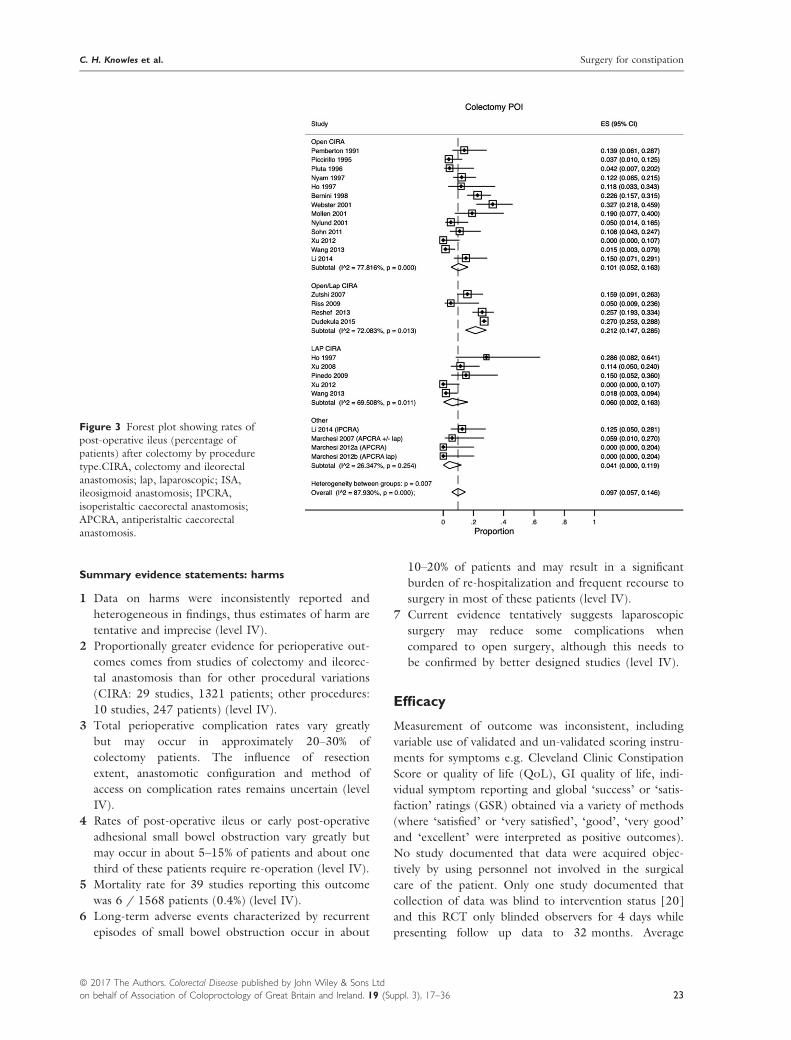
Summary evidence statements: harms
1 Data on harms were inconsistently reported and
heterogeneous in findings, thus estimates of harm are
tentative and imprecise (level IV).
2 Proportionally greater evidence for perioperative out-
comes comes from studies of colectomy and ileorec-
tal anastomosis than for other procedural variations
(CIRA: 29 studies, 1321 patients; other procedures:
10 studies, 247 patients) (level IV).
3 Total perioperative complication rates vary greatly
but may occur in approximately 20–30% of
colectomy patients. The influence of resection
extent, anastomotic configuration and method of
access on complication rates remains uncertain (level
IV).
4 Rates of post-operative ileus or early post-operative
adhesional small bowel obstruction vary greatly but
may occur in about 5–15% of patients and about one
third of these patients require re-operation (level IV).
5 Mortality rate for 39 studies reporting this outcome
was 6 / 1568 patients (0.4%) (level IV).
6 Long-term adverse events characterized by recurrent
episodes of small bowel obstruction occur in about
10–20% of patients and may result in a significant
burden of re-hospitalization and frequent recourse to
surgery in most of these patients (level IV).
7 Current evidence tentatively suggests laparoscopic
surgery may reduce some complications when
compared to open surgery, although this needs to
be confirmed by better designed studies (level IV).
Efficacy
Measurement of outcome was inconsistent, including
variable use of validated and un-validated scoring instru-
ments for symptoms e.g. Cleveland Clinic Constipation
Score or quality of life (QoL), GI quality of life, indi-
vidual symptom reporting and global ‘success’ or ‘satis-
faction’ ratings (GSR) obtained via a variety of methods
(where ‘satisfied’ or ‘very satisfied’, ‘good’, ‘very good’
and ‘excellent’ were interpreted as positive outcomes).
No study documented that data were acquired objec-
tively by using personnel not involved in the surgical
care of the patient. Only one study documented that
collection of data was blind to intervention status [20]
and this RCT only blinded observers for 4 days while
presenting follow up data to 32 months. Average
Figure 3 Forest plot showing rates of
post-operative ileus (percentage ofpatients) after colectomy by procedure
type.CIRA, colectomy and ileorectal
anastomosis; lap, laparoscopic; ISA,ileosigmoid anastomosis; IPCRA,
isoperistaltic caecorectal anastomosis;
APCRA, antiperistaltic caecorectal
anastomosis.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 23
C. H. Knowles et al. Surgery for constipation

reported follow-up of studies was 4.3 years (range 1–11 years).
Accepting these methodological limitations, there are
many reports supporting the assertion that most patients
undergoing colectomy are satisfied; meta-analysis of
studies found an overall global satisfaction rating of
85.6% (95%CI: 81.4–89.3%), I2 = 76.9% based on data
from 1616 patients (Table 4; Fig. 5). Again study find-
ings are heterogeneous, with no clear advantage for any
particular procedure or surgical approach. However, such
Table 3 Long-term small bowel obstruction and re-operation rates.
Author Year Operation N SBO Re-operation*
(a) Open colectomy and ileorectal anastomosis
Pemberton [26] 1991 CIRA 36 11.1 8.3
Piccirillo [27] 1995 CIRA 54 9.3 3.7
Redmond [21] 1995 CIRA 37 18.0 NR
Lubowski [29] 1996 CIRA 52 17.0 14.0
Pluta [31] 1996 CIRA 24 21.0 8.4
Ghosh [32] 1996 CIRA 21 71.0 42.0
Nyam [33] 1997 CIRA 74 9.5 6.7
Bernini [36] 1998 CIRA 106 29.0 18.0
Pikarsky [39] 2001 CIRA 62 7.3 (21.4)† 2.4 (14.3)†
Pikarsky [40] 2001 CIRA 30 20.0 10.0
Mollen [42] 2001 CIRA 21 19.0 9.5
Nylund [43] 2001 CIRA 40 42.5 42.5
Fitzharris [45] 2003 CIRA 75 38.0 17.0
Hassan [46] 2006 CIRA 65 0 0
Jiang [50] 2008 CIRA 21 15.0 NR
Sohn [53] 2011 CIRA 37 10.8 2.7
Wang [55] 2013 CIRA 68 2.9 0
Kamm [23] 1988 Mix 44 NR 38.0
Vasilevsky [24] 1988 Mix 52 36.0 24.0
Yoshioka & Keighley [25] 1989 Mix 40 NR 30.0
Platell [30] 1996 Mix 96 10.4 36.0
Hasegawa [37] 1998 Mix 61 NR 45.0
Fan [38] 2000 Mix 24 21.0 4.2
de Graaf [28] 1996 Segmental on transit 42 2.0 2.0
You [35] 1998 Segmental on transit 40 NR 7.5
Lundin [44] 2002 Segmental on transit 28 19.2 25.0
Feng [22] 2008 IPCRA 34 8.9 NR
Feng [22] 2008 ISA 45 6.7 NR
Jiang [50] 2008 APCRA 17 11.8 NR
Marchesi [54] 2012 APCRA 15 13.3 13.3
(b) Series including open and laparoscopic procedures
Marchesi [47] 2007 APCRA 23 5.9 11.8
Zutshi [48] 2007 CIRA 69 20.0 11.6
Riss [52] 2009 CIRA 20 65.0 45.0
Reshef [56] 2013 CIRA 144 NR 20.0
Dudekula [19] 2015 CIRA 56 NR 30 additional surgeries
in 12 months F up
(c) Laparoscopic procedures only
Pinedo [51] 2009 APCRA 20 5.0 5.0
Marchesi [54] 2012 APCRA 15 6.7 0
Wang [55] 2013 CIRA 56 0 0
SBO, small bowel obstruction; NR, not reported.
*Includes all reported for bowel complications although majority are for adhesional SBO.†(Values) for age 65–85 years.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3624
Surgery for constipation C. H. Knowles et al.

levels of satisfaction can be related to marked changes in
bowel frequency (generally from a mean of once per week
to three times per day in the 14 studies reporting both
variables) (Table 5), and where recorded (three studies
only), marked changes in summative symptom scores e.g.
the Cleveland Clinic Constipation score reduced from a
mean of > 20 points pre-operatively (indicative of severe
constipation) to approx. 2–3 points (low normal range)
post-operatively. Individual symptom outcomes high-
lighted the well documented problems of diarrhoea: 9.8%
(95%CI: 4.7–16.4%), I2 = 76.9% (Fig. 6); and inconti-
nence: 7.4%, (95%CI: 2.2–14.7%), I2 = 90.8% following
colectomy, ongoing or recurrent constipation: 18.2%,
(95%CI: 9.3–29.2%), I2 = 91.4%; persistent (or wors-
ened) abdominal pain: 39.3%, (95%CI: 28.8–50.1%),I2 = 89.0%; and bloating 23.9%, (95%CI: 11.9–38.1%),I2 = 92.7%. Poor functional outcomes contributed to
further resection or permanent stoma: median 5% (range
0–28%) patients when reported (by only seven studies;
data not shown).
Meta-analyses of efficacy outcomes featured consider-
able heterogeneity, not explained by procedure or age
of publication. Given the different duration of studies
and variable follow up within studies there is also the
potential for time-confounding. Studies limited only to
laparoscopic procedures are characterized by small num-
bers limiting scope for comparison with open proce-
dures and no adjustment has been attempted for
potential differences in the populations recruited into
individual studies. Consequently efficacy estimates are
tentative.
Accepting the caveat that only a minority of studies
reported functional variables, several observations can
be made regarding functional outcomes in studies of
less radical colonic resections (Tables 5b and c) com-
pared to those for CIRA (Table 5a). The general pre-
mise of such procedures is to reduce the risk of long-
term diarrhoea and incontinence and this concept is in
part supported by data that, accepting small study num-
bers and heterogeneity, suggest potential to reduce
rates of diarrhoea for segmental and subtotal resections
(Fig. 6). However, this was at the cost of increased
ongoing or recurrent constipation (median 8.7% for
CIRA compared to 26.8% for more conservative
Figure 4 Forest plot showing (a) long-term rates of small bowel obstruction
(percentage of patients) after colectomy
by procedure type with focus on openand laparoscopic approach; (b) rates of
re-operation for small bowel obstruction
(percentage of patients) after colectomy
by procedure type. CIRA, colectomy andileorectal anastomosis; lap, laparoscopic.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 25
C. H. Knowles et al. Surgery for constipation

resections). The latter has proved a particular problem
for segmental resections (right or left hemicolectomy)
with generally poor results compared to colectomy
mainly due to unresolved constipation requiring further
intervention (Table 5c). De Graaf et al. [28] used seg-
mental transit (radio-opaque marker) methodology to
select patients for partial left sided colectomy or subto-
tal colectomy. Whilst results as a whole were disappoint-
ing, the study concluded that in terms of complications
and functional outcome, there was little difference
between procedures, and that a more limited resection
was therefore a reasonable option in this selected group.
You et al. [35] reported the use of left, right or subto-
tal colectomy based on segmental transit time measure-
ments with excellent results. Further, in the three cases
where constipation recurred following segmental resec-
tion, a subtotal colectomy was undertaken successfully
at a later date. This experience was not however
repeated by Lundin et al., [44] when recurrent consti-
pation was experienced by 46% patients despite transit-
guided resection. Thus, while in the laparoscopic era
where there is a greater theoretical advantage of not
meeting the technical challenges of mobilizing both
colonic flexures laparoscopically, the tailoring of seg-
mental resections using these specialist investigations of
transit is inconsistently supported by published data.
Further, the tests required to accurately determine
resection level e.g. isotope scintigraphy have limited
availability.
Subtotal resection with ileosigmoid anastomosis is
generally considered less effective than ileorectal anasto-
mosis based on several relatively small case series mixing
both procedures (Table 4d). Contemporary data on
subtotal resections with CRA come mainly from a few
institutions in Italy and China. Conclusions from these
studies vary. For example, Li et al. [57] demonstrated
good results for both isoperistaltic CRA and CIRA. Feng
et al. [22] compared isoperistaltic CRA with SCISA. Sur-
gical safety outcomes and length of stay were similar but
patients were more satisfied after ileosigmoid anastomo-
sis mainly due to ongoing constipation in caecorectal
group. However patients experienced slightly less
Figure 4 Continued
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3626
Surgery for constipation C. H. Knowles et al.

Table 4 Percentage success based on global satisfaction ratings (GSR).
Author Year FU (mean) Operation N % success
(a) Colectomy and ileorectal anastomosis
Pemberton [26] 1991 36 Open 36 100
Piccirillo [27] 1995 27 Open +/� rectopexy 54 94
Redmond [21] 1995 90 Open 34 90*
Lubowski [29] 1996 42 Open 52 90
Pluta [31] 1996 65 Open 24 92
Nyam [33] 1997 56 Open 74 97
Ho [34] 1997 24 Open 17 96
Ho [34] 1997 24 Laparoscopic 7 100
Bernini [36] 1998 78 Open 106 78†
Fan [38] 2000 23 Open‡ 24 88
Pikarsky [40] 2001 60 Open 30 100
Webster & Dayton [41] 2001 12 Open (5 ileostomy) 55 89
Mollen [42] 2001 62 Open 21 76
Nylund [43] 2001 132 Open 40 73
Fitzharris [45] 2003 47 Open 75 69
Hassan [46] 2006 68 Open 65 85
Zutshi [48] 2007 130 Open & laparoscopic (n = 7) 69 79
Jiang [50] 2008 48 Open 21 65
Hsiao [49] 2008 12 Laparoscopic 44 89
Sohn [53] 2011 41 Open 37 84
Reshef [56] 2013 43 Open & laparoscopic (n = 7) 144 89§
Li [57] 2014 64 Open 40 93
(b) Subtotal colectomy and ileosigmoid anastomosis (ISA); isoperistaltic caecorectal anastomosis (IPCRA);
antiperistaltic caecorectal anastomosis (APCRA); lap: laparoscopic
de Graaf [28] 1996 46 ISA 24 67
Feng [22] 2008 47 ISA 45 93
Marchesi [47] 2007 72 APCRA (lap n = 5) 17 88
Jiang [50] 2008 48 APCRA 17 88
Feng [22] 2008 47 IPCRA 34 74
Li [57] 2014 33 IPCRA 32 97
(c) Segmental colectomy (all based on regional transit measurement)
de Graaf [28] 1996 46 Lt hemicolectomy 18 62.5
You [35] 1998 24 Segmental based on transit 40 92
Lundin [44] 2002 50 Segmental based on transit¶ 28 86
(d) Mixed procedures
Kamm [23] 1988 > 12 CIRA / IPCRA (11) 44 50
Vasilevsky [24] 1988 46 CIRA (5) / ISA 51 79
Yoshioka & Keighley [25] 1989 36 CIRA / ISA (1) / IPCRA (5) 40 58
Platell [30] 1996 60 CIRA / IPCRA (10) 96 81.3
Hasegawa [37] 1999 84 CIRA, ISA, IPCRA, segmental 61 39–95**
FU, mean follow up in months; NR, not reported.
*12.5% with generalized intestinal disorder (see text).†56% with associated rectal evacuatory disorder.‡2 patients had caecorectal anastomosis.§85% with associated rectal evacuatory disorder.¶26 of 28 had left hemicolectomy (6 with rectopexy) and 2 right.
**Outcome dependent on psychiatric disease and concomitant rectal evacuation disorder.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 27
C. H. Knowles et al. Surgery for constipation
diarrhoea and incontinence after caecorectal anastomosis.
Jiang et al. [50] compared antiperistaltic CRA with ileo-
rectal anastomosis. Again there were no differences in
post-operative course, however patients undergoing
caecorectal anastomosis had less diarrhoea, higher post-
operative quality of life (not recorded pre-operatively)
and overall reported GSR (88 vs 65%).
Laparoscopic surgery has the theoretical advantages
of better cosmesis (especially in young women) and per-
haps lower long-term complication rates (see above).
Such factors have not however yet translated into
improved functional outcomes mainly because these
have not yet been the focus of comparative studies. Ho
et al. [34] found no difference in GSR between open
and laparoscopic CIRA (96 vs 100%). In the case-con-
trol study of Marchesi et al. [54], despite the halving of
SBO rates (from 13.3 to 6.7%) in the laparoscopic
groups, long-term functional outcomes and GI quality
of life were very similar.
Summary evidence statements: efficacy
1 Proportionally greater evidence for efficacy comes
from studies of colectomy and ileorectal anastomosis
than for other procedural variations (CIRA: 25 stud-
ies, 1209 patients; mixed: 5 studies, 280 patients;
other procedures: 9 studies, 247 patients; and seg-
mental procedures 4 studies, 99 patients (level IV).
Figure 5 Forest plot showing global
success rates as defined by percentage of
patients who were ‘satisfied’ or ‘verysatisfied’ with outcome, or where
outcome was defined as ‘good’ or
‘excellent’ after colectomy by procedure
type. CIRA, colectomy and ileorectalanastomosis; lap, laparoscopic; ISA,
ileosigmoid anastomosis; IPCRA,
isoperistaltic caecorectal anastomosis;
APCRA, antiperistaltic caecorectalanastomosis; mixed, mix of resection
types reported in each case series.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3628
Surgery for constipation C. H. Knowles et al.

Table
5Functional
outcomes
byprocedure.
Author
Year
Procedure
NBFpre
BFpost
CCSpre
CCSpost
DI
AP
LB
RC
(a)Colectomyandileo
rectal
anastomosis
Pem
berton[26]
1991
Open
36
NR
14.0
NR
NR
00
NR
00
0
Red
mond[21]
1995
Open
37
NR
26/5*
NR
NR
NR
NR
0/69*
0/44*
0/44*
NR
Piccirillo[27]
1995
Open
†54
NR
26
NR
NR
24
24
NR
1.9
NR
NR
Lubowski[29]
1996
Open
52
NR
28.0
NR
NR
14
12
52
NR
NR
26.9
Pluta
[31]
1996
Open
24
1.4
18.0
NR
NR
33
NR
58
NR
29
NR
Ghosh
[32]
1996
Open
‡21
NR
NR
NR
NR
NR
NR
90
NR
NR
NR
Nyam
[33]
1997
Open
74
NR
28
§14
NR
NR
<10
1NR
2§9
NR
0
Ho[34]
1997
Open
17
0.3
11.2
17115.4
NR
NR
00
NR
00
0
Bernini[36]
1998
Open
90
NR
19.6
§14.6
DD
NR
NR
14
§15
21
§20
44
§37
NR
45
§43
4§38
Fan
[38]
2000
Open
24
1.4
22.8
NR
NR
8.3
0NR
8.3**
NR
8.3**
Pikarsky[39]
2001
Open
62
1.4
††1.0
20.3
††26.6
NR
NA
9††27
17
††36
NR
0††9
NR
NR
Pikarsky[40]
2001
Open
30
NR
17.5
NR
NR
NR
17
NR
623
NR
Web
ster
&Dayton[41]
2001
Open
‡‡
55
NR
21.0
NR
NR
54
19
NR
10
9
Mollen
[42]
2001
Open
21
0.8
19.6
NR
NR
NR
10
86
62
90
76
Nylund[43]
2001
Open
40
1.1
3.8
NR
NR
NR
7.5
38
NR
NR
NR
Fitzh
arris[45]
2003
Open
75
NR
2.5
NR
NR
25
45
41
20
NR
NR
Zutshi[30]
2007
Open
&lap
69
1.0
21.0
NR
NR
NR
NR
37
NR
66
51
Jiang[50]
2008
Open
21
1.4
23.8
NR
NR
15
NR
20
NR
25
NR
Pined
o[51]
2009
Lap
20
NR
NR
22.3
1.8
NR
NR
5NR
NR
5
Riss[52]
2009
Open
orlap
20
NR
NR
NR
11.5
§§
NR
NR
NR
NR
NR
50§§
Sohn[53]
2011
Open
37
NR
NR
19.3
2.1
NR
NR
NR
NR
NR
NR
Xu[20]
2012
Open
32
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Wang[55]
2013
Open
orlap
114
NR
35.0
NR
NR
NR
NR
NR
6NR
6
Reshef
[56]
2013
Open
orlap
144
NR
31.0
(33.0)
NR
NR
NR
11(15)
31(33)
13(26)
NR
NR
Li[57]
2014
Open
40
NR
NR
27.3
NR
2.5
2.5
13
NR
7.5
NR
(b)Subtotalcolectomyandileo
sigmoid
anastomosis(ISA);isoperistaltic
caecorectal
anastomosis(IPCRA);andantiperistaltic
caecorectal
anastomosis(A
PCRA);lap:laparoscopic
deGraaf
[28]
1996
ISA
24
NR
NR
NR
NR
12.5
8.3
62.5
20.8
50
29.2
Fen
g[22]
2008
ISA
45
1.6
15.5
NR
NR
4.5
2.2
17.8
6.7
15.6
6.7
Sun[58]
2015
ISA
22
1.1
34.3
NR
5NR
NR
NR
NR
NR
NR
Marchesi[47]
2007
APCRA
17
NR
19.6
20.3
2.6
NR
NR
NR
NR
NR
NR
Fen
g[22]
2008
IPCRA
34
1.5
10.2
NR
NR
NR
024
26.8
24
26.8
Jiang[50]
2008
APCRA
17
1.5
16.8
NR
NR
0NR
NR
NR
23.5
NR
Marchesi[54]
2012
APCRA
30
NR
18.2
20
3NR
NR
NR
NR
NR
NR
Li[57]
2014
IPCCRA
32
NR
NR
27
NR
3.1
03.1
NR
3.1
NR
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 29
C. H. Knowles et al. Surgery for constipation

Table
5(C
ontinued
).
Author
Year
Procedure
NBFpre
BFpost
CCSpre
CCSpost
DI
AP
LB
RC
Sun[58]
2015
IPCCRA
26
1.1
16.1
NR
3.2
NR
NR
NR
NR
NR
NR
(c)Segmen
talcolectomy
deGraaf
[28]
1996
Lthem
icolectomyontransit
18
NR
NR
NR
NR
5.6
5.6
33.3
16.7
22.2
16.7
You[35]
1998
Segmen
talontransit
40
114
NR
NR
0NR
NR
NR
08
Hasegaw
a[37]
1999
Segmen
talmix
13
NR
NR
NR
NR
NR
NR
NR
NR
NR
62
Lundin
[44]
2002
Predom.lefthem
iontransit
28
17
NR
NR
NR
NR
50
067
46
(d)Mixed
procedures
Kam
m[23]
1988
IRA
/APCRA
44
NR
NR
NR
NR
39
14
71
45
45
11
Vasilevsky[24]
1988
IRA
/ISA
(predom)
52
NR
19.6
NR
NR
NR
2NR
20
NR
NR
Yoshioka&
Keighley[25]
1989
IRA
/ISA
/IPCRA
40
0.3
21.0
NR
NR
33
NR
39
NR
NR
NR
Platell[30]
1996
IRA
/IPCRA
96
NR
NR
NR
NR
NR
52
55
NR
NR
NR
Hasegaw
a[37]
1999
IRA,ISA,IPCRA
48
NR
NR
NR
NR
NR
NR
NR
NR
NR
33
NR,notreported
;BF,Bowel
freq
uen
cy/week;
CCS,ClevelandClinic
Constipationscore;D,diarrhoea;I,
incontinen
ce;AP,abdominal
pain;L,laxatives;
B,bloating;RC,recurren
t
constipation.
*If
associated
gen
eralized
intestinal
disorder
(GID
).†5withrectopexy.
‡Includes
onesegmen
talresection.
§Values
ifSTC
associated
withconcomitantRED;values
forlaparoscopic
wherethesediffered.
**In
2/24patients
undergoingcaecorectal
anastomosis.
††Age65–8
0(compared
to21–6
1years).
‡‡Includes
oneen
dileo
stomy.
§§Based
on12patients
infollow
up.
Studiesnotreportingacohort
average,
i.e.
only
subgroupswereexcluded
from
themeta-analysis.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3630
Surgery for constipation C. H. Knowles et al.

2 Data on efficacy were inconsistently reported and
heterogeneous in findings, thus estimates were tenta-
tive and imprecise. Studies varied in their follow-up
of patients, the mean follow-up in studies was
4.3 years (range 1–11 years) (level IV).
3 Colectomy (based on the global rating of success)
benefits the majority of patients with slow transit
constipation: overall mean 85.6% (95% CI: 81.4–89.3%) at > 12 months follow up (level IV).
4 Negative long term functional outcomes persist in a
minority of patients: diarrhoea and incontinence in
about 5–15% of patients; abdominal pain in 30–50%of patients; recurrent constipation in 10–30% of
patients and bloating in 10–40% (level IV).
5 Tailoring of segmental resections using specialist
regional transit measurements provides uncertain
benefit (level IV).
6 There are insufficient data to conclude: (a) that alter-
native procedures (subtotal or segmental) perform
better than CIRA; (b) that one type of subtotal
resection (caecorectal vs ileosigmoid) or anastomosis
(iso- or anti-peristaltic) is superior to another; (c)
that laparoscopic approach has benefit over open sur-
gery (level IV).
7 Subtotal colectomy may reduce long-term rates of
diarrhoea compared to CIRA although this finding is
tentative and should be verified with better designed
studies (level IV).
Patient selection
While clinical experience suggests careful patient selec-
tion for procedures is important, few studies systemati-
cally addressed this issue [12]. Main findings from
studies that stratified outcomes based on baseline phe-
notype are included in Table 6. These studies provide
some information on clinical characteristics but more so
on results of specialist physiological testing.
Pikarsky et al. [39] studied whether colectomy can
be performed in elderly patients (defined 65–80 years in
their series). Although overall success was diminished
on the older age group (64% vs 95%, P = 0.01), the
authors concluded that the results were acceptable and
that the procedure was safe based on no increase in
observed morbidity. The question of whether the pres-
ence of severe psychological problems adversely influ-
ences outcome has been discussed by studies that noted
both poor outcomes and a number of post-operative
psychological problems including suicide [23]. Others
have made post-hoc correlations between prior psychi-
atric disease and poor outcome [31]. This factor was only
addressed as a stated aim by Hasegawa et al. [37], who
Figure 6 Forest plot showing rates of
long-term diarrhoea (percentage of
patients) after colectomy by procedure
type. CIRA, colectomy and ileorectalanastomosis; lap, laparoscopic; ISA,
ileosigmoid anastomosis; IPCRA,
isoperistaltic caecorectal anastomosis;APCRA, antiperistaltic caecorectal
anastomosis; mixed, mix of resection
types reported in each case series.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 31
C. H. Knowles et al. Surgery for constipation

Table
6Summaryofprognostic
findings.
Author
Year
Factorstudied
Op
NFU
Mainfindings:
perioperative
Mainfindings:functional
Mainfindings:long-
term
morbidity
Red
mond[21]
1995
GID
CIR
A34
90
Increasedperioperative
morbidity(44%vs
24%)withGID
and
increasedLOS:13.1
vs
12.1
days
GRA
12.5%vs
90%satisfied
withoutcomein
GID
group;
at2years:BH
5vs
28p.w,rec.
constipation&
pain56%
inGID
vs5%in
noGID
group.Sim
ilar
findingsfor
bloating,abdominal
painandlaxative
requirem
ents
at
2yearsandworseat
5years
1death
inboth
groups:
GID
secondaryto
TPN
catheter
Nyam
[33]
1997
RED
CIR
A74
56
NR
Resultssimilar
(nos.d)betweenRED
andnoRED
forall
studied
NR
Hasegaw
a[37]
1999
RED
&psych
Mix
61
84
NR
Failure
in11%withoutvs
39%withRED;failure
in70%
withpsychological
problems(incs-fold
increase
in
admissions,further
surgery,
and5fold
increase
in
even
tual
stoma
Bernini[36]
1998
RED
CIR
A106
78
NR
GRA
decreased
ifRED:56vs
78%;weeklyBF14.7
vs
19.6;nodiffin
other
symptoms
SBO
only
inCIgroup-
23vs
0%
Pikarsky[39]
2001
Age<or>65years
CIR
A59
105
SBO
21%in
ageover
65vs
7%in
younger
patientgroup
WeeklyBFhigher
(n.s)in
older
group(26.6
vs20.3);
excellen
toutcomein
64%older
vs95%;increasedFIin
older
(36%vs
17%)
1/14older
group
required
stoma
Hassan[46]
2006
RED
CIR
A104
68
NR
Nodiffin
KESSandSF-12withorwithoutRED
Reshef
[56]
2013
RED
CIR
A144
43
LOSlonger
withRED
9.7
vs7.8
days;overall
morbidityotherwise
similar
61vs
54%POI;
re-operation41vs
26%
Inc.
laxuse
inRED
group(26vs
13%)other
variables
similar
inc.
overallsatisfaction:GRA
89vs
85
Nodiffin
ileo
stomy
rates(5%both
groups)
orre-admissions(30%
both
groups)
RED,rectal
evacuation
disorder;GID
,gen
eralized
intestinal
disorder;BF,biofeed
back;
CIR
A,colectomyand
ileo
rectal
anastomosis;
KESS,Knowles-Eccesley-Scott
score;LOS,
length
ofstay.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3632
Surgery for constipation C. H. Knowles et al.

reported a statistically significant prejudicial influence of
‘severe psychological disorder’.
Outcomes of colectomy are improved by selection of
patients with proof of slow colonic transit. Although it
could be argued that other factors may have also influ-
enced outcomes (e.g. mix of surgical approaches, surgi-
cal technique and equipment), this statement is
corroborated by comparing outcome data from an era
when specialist investigations of transit were variably
applied [23–25,37] with subsequent studies that always
performed transit studies and used these as a selection
criteria. Most contemporary studies also evaluated
anorectal physiology especially in relation to the diagno-
sis of a combined slow-transit and defaecatory disorder
phenotype. The management of this patient group
remains contentious. Bernini et al. [36] in a study of
106 patients demonstrated that despite preoperative
biofeedback training, patients with non-relaxing pelvic
floor (n = 16) had significantly higher rates of recurrent
defaecatory difficulty (38 vs 4%), and lower rates of sat-
isfaction after colectomy (56 vs 78%). However, three
other studies (Table 6) found little effect on functional
outcome or complication rates when functional or
structural defects were addressed prior to colectomy.
These studies included the contemporary Cleveland
Clinic experience of 144 patients where obstructed
defaecation (n = 41) had no influence on outcome from
laparoscopic or open colectomy [56].
It is generally accepted that some patients with slow
colonic transit also manifest upper GI symptoms (espe-
cially nausea and vomiting). Abnormalities of oesopha-
geal, gastric and small bowel function can be
demonstrated in a proportion of patients by a variety of
methods [18]. Ghosh et al. [32] showed that the high
proportion of patients undergoing colectomy who sub-
sequently developed SBO episodes (71% with 42%
requiring surgery in their series) were more likely to
have non-colonic visceral and autonomic nervous system
abnormalities on post-operative testing. This observa-
tion has been considerably strengthened by the prospec-
tive cohort study of Redmond et al. [21]. A significant
fall in long-term success rate (to 10 years) as a result of
persistent constipation, abdominal pain and distension)
was observed in patients defined as having a generalized
intestinal disorder (GID) on the basis of having both
upper and lower GI dysmotility using a battery of intra-
luminal tests. Successful outcome was observed in only
12.5% patients with GID vs 90%: without.
Summary evidence statements: patient selection
1 Outcomes of colectomy may be poorer in patients
with significant psychological disorder (level IV).
2 Outcomes of colectomy may be improved by selec-
tion of patients with definitive proof of slow colonic
transit (level IV).
3 Outcomes of colectomy are inconsistently influenced
by concomitant rectal evacuation disorder although
data suggest that structural and functional defecation
disorders, if evident, should be treated prior to colec-
tomy (level IV).
4 Outcomes of colectomy may be prejudiced by pre-
operative evidence of upper gastrointestinal dysmotil-
ity (level IV).
Conclusions
A systematic review of evidence for the perioperative
and long-term benefits and harms of colectomy identi-
fied no high quality studies. The evidence base is char-
acterised by observational studies of variable and often
uncertain methodological quality. Current data suggest
a balance of harms against efficacy with evidence that
outcomes are at best variable. Future studies should
provide high quality evidence for clinicians to support
patient decision making, both in terms of the incremen-
tal benefits and harms of colectomy and in understand-
ing the effects of prognostic factors upon treatment
success.
Acknowledgments
We would like to acknowledge the following people in
relation to the NIHR CapaCiTY working group: Mr
Steven Brown, Sheffield Teaching Hospitals NHS
Foundation Trust; Mr Kenneth Campbell, The Univer-
sity of Dundee, NHS Education for Scotland; Mr Mark
Chapman, Heart of England NHS Trust; Mr Andrew
Clarke, Poole Hospital NHS Foundation Trust; Mr Neil
Cruickshank, Sandwell and West Birmingham Hospitals
NHS Trust; Mr Anthony Dixon, University of Bristol,
Bristol, UK; Dr Christopher Emmett, County Durham
and Darlington NHS Foundation Trust; Mr Ugo
Grossi, Queen Mary University of London; Dr Richard
Hooper, PCTU, Queen Mary University of London;
Miss Emma Horrocks, University Hospital Southamp-
ton NHS Foundation Trust; Professor Charles Knowles,
Queen Mary University of London; Mr Jon Lacy-Col-
son, Shrewsbury and Telford Hospital NHS Trust; Mr
Ian Lindsey, Oxford University Hospitals NHS Trust;
Professor James Mason, University of Warwick, Coven-
try; Mr Mark Mercer-Jones, Gateshead Health NHS
Foundation Trust; Mr Andrew Miller, University
Hospitals of Leicester NHS Trust; Mr David Pares,
Hospital Germans Trias i Pujol, Barcelona, Spain; Miss
Sophie Pilkington, University Hospital Southampton
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 33
C. H. Knowles et al. Surgery for constipation

NHS Foundation Trust; Mr Neil Smart, Royal Devon
& Exeter NHS Foundation Trust; Ms Natasha Stevens,
PCTU, Queen Mary University of London; Professor
Douglas Tincello, University Hospitals of Leicester
NHS Trust; Miss Karen Telford, South Manchester
NHS Foundation Trust; Mr Paul Vollebregt, Queen
Mary University of London; Mr Andrew Williams,
Guy’s and Thomas’ NHS Foundation Trust; Professor
Yan Yiannakou, County Durham and Darlington NHS
Foundation Trust.
Conflict of interest
All authors have no conflict of interest in relation to the
content of the manuscript. In the last 2 years, C.H.
Knowles has received speaker fees and consultancy pay-
ments from Medtronic Inc. Mark Chapman has received
funding to attend courses from Medtronic Inc.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opinions
expressed in this report are those of the authors and are not
those of the PGfAR Programme, NIHR, the UK National
Health Service, or the UKDepartment of Health.
References
1 Smith JL, Lane A. Sir Arbuthnot Lane, chronic intestinal
stasis, and autointoxication. Ann Intern Med 1982; 96:
365–9.
2 Sarli L, Costi R, Sarli D, Roncoroni L. Pilot study of
subtotal colectomy with antiperistaltic cecoproctostomy for
the treatment of chronic slow-transit constipation. Dis
Colon Rectum 2001; 44: 1514–20.
3 Nicholls RJ, Kamm MA. Proctocolectomy with restorative
ileoanal reservoir for severe idiopathic constipation. Report
of two cases. Dis Colon Rectum 1988; 31: 968–9.
4 Hosie KB, Kmiot WA, Keighley MR. Constipation:
Another indication for restorative proctocolectomy. The
British journal of surgery 1990; 77: 801–2.
5 Kalbassi MR, Winter DC, Deasy JM. Quality-of-life assess-
ment of patients after ileal pouch-anal anastomosis for
slow-transit constipation with rectal inertia. Dis Colon Rec-
tum 2003; 46: 1508–12.
6 Li N, Jiang J, Feng X, Ding W, Liu J, Li J. Long-term fol-
low-up of the Jinling procedure for combined slow-transit
constipation and obstructive defecation. Dis Colon Rectum
2013; 56: 103–12.
7 Ding W, Jiang J, Feng X et al. Novel surgery for refractory
mixed constipation: Jinling procedure - technical notes and
early outcome. Archives of medical science: AMS 2014; 10:
1129–34.
8 Zhu X, Li J, Fu T, Sun P, Jing Y, Tian W. Laparoscopic-
assisted subtotal colectomy combined with modified Duha-
mel procedure for mixed constipation. JSLS 2015; 19:
e2014.00131
9 Peng H-Y, Xu A-Z. Colonic exclusion and combined ther-
apy for refractory constipation. World J Gastroenterol 2006;
12: 7864–8.
10 Pfeifer J, Agachan F, Wexner SD. Surgery for constipation:
a review. Dis Colon Rectum 1996; 39: 444–60.
11 Pfeifer J. Surgery for constipation. Acta Chir Iugosl 2006;
53: 71–9.
12 Knowles CH, Scott M, Lunniss PJ. Outcome of colectomy
for slow transit constipation. Ann Surg 1999; 230:
627–38.
13 Sheng QS, Lin JJ, Chen WB et al. Comparison of hand-
assisted laparoscopy with open total colectomy for slow
transit constipation: a retrospective study. J Dig Dis 2014;
15: 419–24.
14 Raahave D, Loud FB, Christensen E, Knudsen LL. Colec-
tomy for refractory constipation. Scand J Gastroenterol
2010; 45: 592–602.
15 Sarli L, Costi R, Iusco D, Roncoroni L. Long-term results
of subtotal colectomy with antiperistaltic cecoproctostomy.
Surg Today 2003; 33: 823–7.
16 Howick J, Chalmers I, Glasziou P et al. Explanation of the
2011 Oxford Centre for Evidence-Based Medicine
(OCEBM) Levels of Evidence. Oxford Centre for Evi-
dence-Based Medicine. (http://www.cebm.net/index.aspx?
o=5653)
17 Reshef A, Gurland B, Zutshi M, Kiran RP, Hull T. Colec-
tomy with ileorectal anastomosis has a worse 30-day out-
come when performed for colonic inertia than for a
neoplastic indication. Colorectal Dis 2013; 15: 481–6.
18 Scott SM, Picon L, Knowles CH et al. Automated quanti-
tative analysis of nocturnal jejunal motor activity identifies
abnormalities in individuals and subgroups of patients with
slow transit constipation. Am J Gastroenterol 2003; 98:
1123–34.
19 Dudekula A, Huftless S, Bielefeldt K. Colectomy for con-
stipation: time trends and impact based on the US Nation-
wide Inpatient Sample, 1998-2011. Aliment Pharmacol
Ther 2015; 42: 1281–93.
20 Xu LS, Liu WS. A prospective, randomized, single-blind
comparison of laparoscopic versus open colectomy for
slow-transit constipation. Am Surg 2012; 78: 495–6.
21 Redmond JM, Smith GW, Barofsky I, Ratych RE, Golds-
borough DC, Schuster MM. Physiological tests to predict
long-term outcome of total abdominal colectomy for
intractable constipation. Am J Gastroenterol 1995; 90:
748–53.
22 Feng Y, Jianjiang L. Functional outcomes of two types of
subtotal colectomy for slow-transit constipation: ileosig-
moidal anastomosis and cecorectal anastomosis. Am J Surg
2008; 195: 73–7.
23 Kamm MA, Hawley PR, Lennard-Jones JE. Outcome of
colectomy for severe idiopathic constipation. Gut 1988;
29: 969–73.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3634
Surgery for constipation C. H. Knowles et al.

24 Vasilevsky CA, Nemer FD, Balcos EG, Christenson CE,
Goldberg SM. Is subtotal colectomy a viable option in the
management of chronic constipation? Dis Colon Rectum
1988; 31: 679–81.
25 Yoshioka K, Keighley MR. Clinical results of colectomy for
severe constipation. Br J Surg 1989; 76: 600–4.
26 Pemberton JH, Rath DM, Ilstrup DM. Evaluation and sur-
gical treatment of severe chronic constipation. Ann Surg
1991; 214: 403–11; discussion 411-3.
27 Piccirillo MF, Reissman P, Wexner SD. Colectomy as treat-
ment for constipation in selected patients. Br J Surg 1995;
82: 898–901.
28 de Graaf EJ, Gilberts EC, Schouten WR. Role of segmental
colonic transit time studies to select patients with slow
transit constipation for partial left-sided or subtotal colec-
tomy. Br J Surg 1996; 83: 648–51.
29 Lubowski DZ, Chen FC, Kennedy ML, King DW. Results
of colectomy for severe slow transit constipation. Dis Colon
Rectum 1996; 39: 23–9.
30 Platell C, Scache D, Mumme G, Stitz R. A long-term fol-
low-up of patients undergoing colectomy for chronic idio-
pathic constipation. Aust N Z J Surg 1996; 66: 525–9.
31 Pluta H, Bowes KL, Jewell LD. Long-term results of total
abdominal colectomy for chronic idiopathic constipation.
Value of preoperative assessment. Dis Colon Rectum 1996;
39: 160–6.
32 Ghosh S, Papachrysostomou M, Batool M, Eastwood MA.
Long-term results of subtotal colectomy and evidence of
noncolonic involvement in patients with idiopathic slow-
transit constipation. Scand J Gastroenterol 1996; 31: 1083–
91.
33 Nyam DC, Pemberton JH, Ilstrup DM, Rath DM. Long-
term results of surgery for chronic constipation. Dis Colon
Rectum 1997; 40: 273–9.
34 Ho YH, Tan M, Eu KW, Leong A, Choen FS. Laparo-
scopic-assisted compared with open total colectomy in
treating slow transit constipation. Aust N Z J Surg 1997;
67: 562–5.
35 You YT, Wang JY, Changchien CR et al. Segmental colec-
tomy in the management of colonic inertia. Am Surg
1998; 64: 775–7.
36 Bernini A, Madoff RD, Lowry AC et al. Should patients
with combined colonic inertia and nonrelaxing pelvic floor
undergo subtotal colectomy? Dis Colon Rectum 1998; 41:
1363–6.
37 Hasegawa H, Radley S, Fatah C, Keighley MRB. Long-
term results of colorectal resection for slow transit consti-
pation. Colorectal Dis 1999; 1: 141–5.
38 Fan CW, Wang JY. Subtotal colectomy for colonic inertia.
Int Surg 2000; 85: 309–12.
39 Pikarsky AJ, Efron J, Hamel CT, Weiss EG, Nogueras JJ,
Wexner SD. Effect of age on the functional outcome of
total abdominal colectomy for colonic inertia. Colorectal
Dis 2001; 3: 318–22.
40 Pikarsky AJ, Singh JJ, Weiss EG, Nogueras JJ, Wexner SD.
Long-term follow-up of patients undergoing colectomy for
colonic inertia. Dis Colon Rectum 2001; 44: 179–83.
41 Webster C, Dayton M. Results after colectomy for colonic
inertia: a sixteen-year experience. Am J Surg 2001; 182:
639–44.
42 Mollen RM, Kuijpers HC, Claassen AT. Colectomy for
slow-transit constipation: preoperative functional evaluation
is important but not a guarantee for a successful outcome.
Dis Colon Rectum 2001; 44: 577–80.
43 Nylund G, Oresland T, Fasth S, Nordgren S. Long-term
outcome after colectomy in severe idiopathic constipation.
Colorectal Dis 2001; 3: 253–8.
44 Lundin E, Karlbom U, P�ahlman L, Graf W. Outcome of
segmental colonic resection for slow-transit constipation.
Br J Surg 2002; 89: 1270–4.
45 FitzHarris GP, Garcia-Aguilar J, Parker SC et al. Quality of
life after subtotal colectomy for slow-transit constipation:
both quality and quantity count. Dis Colon Rectum 2003;
46: 433–40.
46 Hassan I, Pemberton JH, Young-Fadok TM et al. Ileo-
rectal anastomosis for slow transit constipation: long-term
functional and quality of life results. J Gastrointest Surg
2006; 10: 1330–6; discussion 1336-7.
47 Marchesi F, Sarli L, Percalli L et al. Subtotal colectomy
with antiperistaltic cecorectal anastomosis in the treatment
of slow-transit constipation: long-term impact on quality of
life. World J Surg 2007; 31: 1658–64.
48 Zutshi M, Hull TL, Trzcinski R, Arvelakis A, Xu M. Sur-
gery for slow transit constipation: are we helping patients?
Int J Colorectal Dis 2007; 22: 265–9.
49 Hsiao KC, Jao SW, Wu CC, Lee TY, Lai HJ, Kang JC.
Hand-assisted laparoscopic total colectomy for slow transit
constipation. Int J Colorectal Dis 2008; 23: 419–24.
50 Jiang CQ, Qian Q, Liu ZS, Bangoura G, Zheng KY, Wu
YH. Subtotal colectomy with antiperistaltic cecoproc-
tostomy for selected patients with slow transit constipation-
from Chinese report. Int J Colorectal Dis 2008; 23: 1251–
6.
51 Pinedo G, Zarate AJ, Garcia E, Molina ME, Lopez F,
Z�u~niga A. Laparoscopic total colectomy for colonic inertia:
surgical and functional results. Surg Endosc 2009; 23: 62–
5.
52 Riss S, Herbst F, Birsan T, Stift A. Postoperative course
and long term follow up after colectomy for slow transit
constipation–is surgery an appropriate approach? Colorectal
Dis 2009; 11: 302–7.
53 Sohn G, Yu CS, Kim CW et al. Surgical outcomes after
total colectomy with ileorectal anastomosis in patients with
medically intractable slow transit constipation. J Korean Soc
Coloproctol 2011; 27: 180–7.
54 Marchesi F, Percalli L, Pinna F, Cecchini S, Ricco’ M,
Roncoroni L. Laparoscopic subtotal colectomy with
antiperistaltic cecorectal anastomosis: a new step in the
treatment of slow-transit constipation. Surg Endosc 2012;
26: 1528–33.
55 Wang DY, Lin JJ, Xu XM, Liu FL. The role of hand-
assisted laparoscopic surgery in total colectomy for colonic
inertia: a retrospective study. J Korean Surg Soc 2013; 85:
123–7.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–36 35
C. H. Knowles et al. Surgery for constipation

56 Reshef A, Alves-Ferreira P, Zutshi M, Hull T, Gurland B.
Colectomy for slow transit constipation: effective for
patients with coexistent obstructed defecation. Int J
Colorectal Dis 2013; 28: 841–7.
57 Li F, Fu T, Tong W et al. Effect of different surgical
options on curative effect, nutrition, and health status of
patients with slow transit constipation. Int J Colorectal Dis
2014; 29: 1551–6.
58 Sun JW, Gu JN, Du P, Chen W. Comparison of two types
of colectomy in treating slow transit constipation with or
without melanosis coli. World J Gastroenterol 2015; 21:
9736–40.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 17–3636
Surgery for constipation C. H. Knowles et al.

Surgery for constipation: systematic review and practicerecommendations
Results II: Hitching procedures for the rectum (rectal suspension)
U. Grossi*, C. H. Knowles*, J. Mason†, J. Lacy-Colson‡ and S. R. Brown§ on behalf of the NIHR
CapaCiTY working group¶ and Pelvic floor Society**
*National Bowel Research Centre, Blizard Institute, Queen Mary University London, London, UK, †University of Warwick, Coventry, UK, ‡RoyalShrewsbury Hospital, Shrewsbury, UK, §Sheffield Teaching Hospitals, Sheffield, UK, ¶National Institute for Health Research: Chronic Constipation
Treatment Pathway, London, UK, and **Affiliate section of the Association of Coloproctology of Great Britain and Ireland, London, UK
Abstract
Aim To assess the outcomes of rectal suspension proce-
dures (forms of rectopexy) in adults with chronic con-
stipation.
Method Standardised methods and reporting of bene-
fits and harms were used for all CapaCiTY reviews that
closely adhered to PRISMA 2016 guidance. Main con-
clusions were presented as summary evidence statements
with a summative Oxford Centre for Evidence-Based
Medicine (2009) level.
Results Eighteen articles were identified, providing data
on outcomes in 1238 patients. All studies reported only
on laparoscopic approaches. Length of procedures ran-
ged between 1.5 to 3.5 h, and length of stay between 4
to 5 days. Data on harms were inconsistently reported
and heterogeneous, making estimates of harm tentative
and imprecise. Morbidity rates ranged between 5–15%,with mesh complications accounting for 0.5% of
patients overall. No mortality was reported after any
procedures in a total of 1044 patients. Although
inconsistently reported, good or satisfactory outcome
occurred in 83% (74–91%) of patients; 86% (20–97%)of patients reported improvements in constipation after
laparoscopic ventral mesh rectopexy (LVMR). About 2–7% of patients developed anatomical recurrence. Patient
selection was inconsistently documented. As most com-
mon indication, high grade rectal intussusception was
corrected in 80–100% of cases after robotic or LVMR.
Healing of prolapse-associated solitary rectal ulcer syn-
drome occurred in around 80% of patients after LVMR.
Conclusion Evidence supporting rectal suspension pro-
cedures is currently derived from poor quality studies.
Methodologically robust trials are needed to inform
future clinical decision making.
Keywords Rectopexy, chronic constipation, laparo-
scopic ventral mesh rectopexy (LVMR), robotic ventral
mesh rectopexy (RVMR), laparoscopic resection recto-
pexy (LRR), open rectopexy (OR)
Introduction
Background and procedural variations
Constipation, in a proportion of patients and in the broad
sense of the term, is related to an inability to evacuate the
rectum. This obstructed defaecation or rectal evacuation
disorder is characterized by excessive straining, the feeling
of incomplete evacuation, post-defaecatory seepage and
often mucous discharge and pelvic pain [1]. In some of
these patients there is clinical and proctographic evidence
of a rectocoele and/or intussusception. These anatomical
variants are considered to cause obstructed defaecation by
a process of loss of force vector (ballooning of the rectum
into a rectocoele or invagination of the rectum into an
intussusception rather than evacuation of stool on strain-
ing) or mucosal obstruction (in the case of an intussus-
ception) [1]. It follows that clinical resolution of
symptoms could be achieved by restoration of normal
anatomy by surgery. Resuspension of the rectum aims to
hitch the prolapsing or redundant rectal wall thus
straightening the intussusception and/or effacing the rec-
tocoele. This concept while anatomically rational remains
clinically controversial for a number of reasons. First, such
anatomical variants are common and are often found in
healthy individuals with no symptoms of obstructed
defaecation [2]. Secondly, resuspension operations when
employed to patients with full thickness rectal prolapse,
Correspondence to: Mr Steven Brown, Consultant Colorectal and General
Surgeon, Department of Surgery, Northern General Hospital, Herries Road,
Sheffield S5 7AU, UK.
E-mail: [email protected]
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–48 37
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13773

may themselves cause increasing constipatory symptoms
[3]. Such procedures include posterior rectopexy [4].
The potential for worsening constipation is thought to
relate to fibrosis caused by insertion of foreign material or
mobilization of the lateral ligaments of the rectum. These
ligaments contain nerves to the rectal wall and the resul-
tant denervation may be the cause. In the process of
developing alternative resuspending procedures, surgeons
have attempted to limit the effect of the foreign material
by using sutures only [5], added a resection of the sig-
moid colon to the rectopexy [6–8] or more recently, lim-
iting the dissection of the rectum to the ventral surface by
supporting the rectum with mesh [9–23]. In addition,
laparoscopy has become the favoured approach procedu-
rally, not only allowing a more rapid recovery but also
easing access to, and visibility in the pelvis.
Scope
The purpose of the overall CapaCiTY review process is to
assess the efficacy and harms of surgical procedures for
chronic constipation in adults. Thus, the aim of this
review is to assess the outcomes of rectal suspension pro-
cedures in adults presenting with chronic constipation
symptoms. In effect, this is however limited to patients
with obstructed defaecation and internal prolapse (intus-
susception). Procedures considered beyond the scope of
systematic review included rectal excisional procedures,
e.g. STARR [9], rectal reinforcement procedures, e.g.
transanal/transperineal repair of rectocele [10], and
uncommon variant of suspension procedures, e.g. laparo-
scopic promonto-fixation [11]. Studies where outcomes
could not be segregated by eligible procedure were also
excluded due to a mixed patient population with internal
and external rectal prolapse [12–19], mixed indications
including numerous pelvic floor abnormalities [20] or
limited postoperative outcomes [21].
Previous reviews
Seven systematic [3, 22–27] and 4 narrative [28–31]reviews have focused on the outcome of rectal suspen-
sion. Of the systematic reviews, 3 [3,23,26] focused on
full thickness external rectal prolapse, 2 included both
full-thickness prolapse and constipation participants, and
2 [22,25] analysed outcomes of robotic surgery.
Summary of search results and study quality
The search yielded a total of 47 manuscripts for full text
review (Fig. 1). From these, 18 articles published
between 1995 and 2015 contributed to the systematic
review, providing data on outcomes in a total of 1238
patients (range 20–233 patients per study) based on 18
defined patient cohorts (Table 1). Specific exclusions
after full-text review (and after exclusion of non-English
language publications) included 4 studies where the pop-
ulation sample was confirmed to be less than 20 patients
[5,36–38], 4 studies of out-of-scope procedures [9–11,39], 2 studies where data were considered a duplicate
Figure 1 PRISMA diagram of search results.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–4838
Rectal suspension for constipation U. Grossi et al.

[34,40], and 10 studies where outcomes could not be
segregated by eligible procedure; [12–21] other exclusioncriteria were: constipation not representing an indication
(n = 2) [32,41], follow-up less than 12 months (n = 5)
[8,33,35,42,43], and lack of primary patient data (one
international survey on 391 surgeons) [44].
The general quality of studies was poor due to inade-
quate description of methods. The 18 included studies
were all observational with no randomised controlled
trials. These comprised two good quality prospective
cohort studies [45,46] (level IIB), and 16 (level IV)
studies comprising two poor quality case-control studies
[34,47], eight prospective case series [6,7,48–53], andsix retrospective case series [4,54–58]. Mean patient fol-
low-up ranged from 12 to 72 months (median
25 months). Fifteen studies derived from European
centres, with one each from Australia, Iran and Japan.
Perioperative data
Perioperative data were reported by all 18 studies
(Table 2). Reporting of procedure duration was incon-
sistent but median procedural duration for laparoscopic
ventral mesh rectopexy (LVMR) was 159 (range 75–198) min; for robotic ventral mesh rectopexy (RVMR),
205 (range 191–218) min; for laparoscopic resection
rectopexy (LRR), 123 min (one study) [45,46].
Although robotic procedures appeared to take longer,
substantial non-reporting of other procedures
precluded a clear finding. The two papers on RVMR
were from the same centre. It is interesting to note a
decrease in duration of operation, which may indicate a
learning curve. Conversion to laparotomy was rare (me-
dian 2%, range 0–8%) (Table 2), with the most com-
mon reason being adhesions. The median length of
stay (LOS) was similar for procedures: LVMR, median
3.3 (range 1.0–7.1) days; RVMR, median 4.3 (range
4.0–4.6) days (data from one centre via two reports)
[45,46]; LRR, 4 days (data from one study) [7]. LOS
possibly reflected local policy rather than clinical need,
since day case procedures have been shown to be feasi-
ble [59,60]. The reason to keep patients in hospital for
up to 1 week was not documented. Only one paper
commented on LOS after open rectopexy (OR)
(8.5 days) [54].
Summary evidence statements: perioperative data
1 Procedures are reported to take from 1.5 to 3.5 h,
with consequent typical LOS of 4–5 days (level IV).
2 There was no clear variation between procedures in
perioperative measures, although non-reporting by
studies may have concealed differences (level IV).
Harms
There was a considerable heterogeneity in surgical
morbidity reported as well as in overall procedural
Table 1 All studies included in systematic review.
Author Year Centre Country Total N FU* Design Level†
van Tets[4] 1995 Groot Netherlands 37 72 RCS IV
Tsiaoussis [6] 2005 Heraklion Greece 27 45 PCH IV
Vermeulen [54] 2005 Rotterdam Netherlands 20 18 RCS IV
Von Papen [7] 2006 Herston Australia 56 44 PCS IV
Collinson [48] 2009 Oxford UK 75 12 PCS IV
Kargar [55] 2011 Shaid Sadoughi Iran 39 32 RCS IV
Portier [49] 2011 Toulouse France 40 22 PCS IV
Wong [45] 2011 Nantes France 41 12 PCH IIB
Wong [50] 2011 Nantes France 84 29 PCH IV
Sileri [51] 2012 Rome Italy 34 12 PCS IV
Wahed [52] 2012 Gateshead UK 65 12 PCS IV
Evans [34] 2013 Oxford UK 30 36 PCS IV
Formijne Jonkers [56] 2013 Amersfoort Netherlands 233 30 RCS IV
Gosselink [57] 2013 Oxford UK 151 12 RCS IV
Mantoo [46] 2013 Nantes France 128 16 PCH IIB
Borie [58] 2014 Montpellier France 52 18 RCS IV
Franceschilli [53] 2015 Rome Italy 100 20 PCS IV
Tsunoda [47] 2015 Kamogawa City Japan 26 16 PCS IV
PCH, prospective cohort study; RCS, retrospective case series; PCS, prospective case series study.
*Mean follow up in months.
†Oxford CEBM [34]. A median time follow up time was not provided.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–48 39
U. Grossi et al. Rectal suspension for constipation

Table
2Perioperativedatabyprocedure.(a)Laparoscopic
ventral
meshrectopexy(L
VMR).(b)Roboticventral
meshrectopexy(R
VMR).(c)Laparoscopic
resectionrectopexy
(LRR).(d)Open
rectopexy(O
R).
(a)
Author
Year
N
Duration,
mins
LOS
Totalcx,%
Re-op,%
Mesh
comps,%
Conv,%
Stoma,
%Mort,%
Collinson[48]
2009
75
NR
24
00
1.3
00
Kargar
[55]
2011
39
NR
NR
NR
NR
NR
NR
NR
NR
Portier[49]
2011
17(40*)
NR
NR
7.5
00
NR
00
Wong[45]
2011
25
159
4.6
NR
00
80
0
Wong[50]
2011
84
NR
58.3
1.2
1.2
3.6
00
Sileri[51]
2012
34
110
223.5
2.9
00
00
Wahed
[52]
2012
65
NR
27.6
1.5
01.5
00
Form
ijneJonkers
[56]
2013
233
NR
54.7
0.4
0.9
2.5
0.4
0
Gosselink[57]
2013
151
NR
NR
NR
NR
NR
NR
NR
NR
Mantoo[46]
2013
74
163
511
00
40
0
Borie[58]
2014
25
NR
7.1
24
0NR
80
0
Evans[34]
2015
30
NR
NR
10
03.4
NR
00
Franceschilli[53]
2015
100
75
216
10
10
0
Tsunoda[47]
2015
26
198
17.6
00
00
0
(b)
Wong[45]
2011
16
218
4.6
10.5
00
6.3
00
Mantoo[46]
2013
44
191
40
00
50
0
(c)
Tsiaoussis[6]
2005
23(27)‡
NR
NR
22
NR
NA
NR
NR
0
VonPapen
[7]
2007
56
123
413
70
20
0
(d)
Author
Year
Operation
NDuration,mins
LOS
Totalcx,%
Re-op%
Meshcomps,%
Conv,
%Stoma,
%Mort,%
vanTets[4]
1995
Posteriormeshrectopexy
37
NR
NR
NR
NR
NR
NA
NR
NR
Vermeu
len[54]
2005
Anteriormeshrectopexy
20
NR
8.5
15
00
NR
00
Portier[49]
2011
Anteriormeshrectopexy
23(40)*
NR
NR
7.5
00
NR
00
LOS,length
ofstay;Cx,
complications;Re-op,reoperation;Conv,
conversion;Mort,mortality;
NR,notreported
.
*17werelaparoscopic,23open
.
‡4open
.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–4840
Rectal suspension for constipation U. Grossi et al.

complication rates (Fig. 2), with individual study rates
varying from 0.0% to 23.5% (Table 2). Such hetero-
geneity may reflect different inclusion, thresholds or
conventions for recording complications. Complica-
tions typically occurred in about 5–15% of patients.
Pooled findings suggest that LRR might be associated
with higher morbidity (total complications 15% for
LRR vs 10% LVMR) although the findings were not
statistically significant (Z-test, P = 0.30), and absolute
patient numbers were small for LRR. The majority of
complications were minor and included urinary tract
infections (the most common reported), wound infec-
tions, haematoma formation, persistent pain and uri-
nary retention. There were some more serious
complications including port-site hernia, small bowel
obstruction (usually after conversion but also related
to mesh or suture adhesions), osteomyelitis and blad-
der injury (often when associated to bladder prolapse
surgery). Specific mesh complication rates were rare,
with only five occurrences after 939 procedures
(0.53%). Overall, procedures were safe: conversion to
laparotomy was rare (median 2%, range 0–8%)(Table 2), with the most common reason being adhe-
sions; stoma was only reported in one study; no peri-
operative deaths were reported. Two open rectopexy
procedures (posterior mesh) were described, but data
concerning post-operative complications were limited.
There was no mortality recorded after any resuspension
procedures.
Summary evidence statements: harms
1 Data on harms were inconsistently reported and
heterogeneous, making estimates of harm tentative
and imprecise (level IV).
2 Complications typically occurred in about 5–15% of
procedures (level IV).
3 Mesh complications were reported in a minority of
studies and occurred in about 0.5% (range 0–3.9%)of patients overall (level IV).
4 No mortality was recorded after any resuspension
procedure, in a total of 1044 patients reporting this
outcome (level IV).
Efficacy
Measurement of clinical outcomes was inconsistent and
included the variable use of validated and un-validated
scoring instruments for symptoms, such as Patient
Assessment of Constipation Quality of Life (PAC-
Figure 2 Forest plot showing rates of
total procedural complications
(percentage of patients) after rectopexy
by procedure type. KEY: LVMR,laparoscopic ventral mesh rectopexy;
RVMR, robotic ventral mesh rectopexy;
LRR, laparoscopic resection rectopexy;OR, open rectopexy.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–48 41
U. Grossi et al. Rectal suspension for constipation

QOL) and Patient Assessment of Constipation-Symp-
toms (PAC-SYM) scores (one study only) [57], Cleve-
land Clinic Constipation score [34,47,48,50,51,53,56],
obstructed defecation syndrome (ODS) score
[46,50,56,58], Knowles-Eccersley-Scott score (KESS)
[48], Cleveland Clinic Incontinence score [46,49,56],
Faecal Incontinence Severity Index (FISI) [47,48,51–53,56–58] and St Marks Incontinence score [48]. Glo-
bal ‘success’ or ‘satisfaction’ ratings (GSR) were
obtained via a variety of methods in 7 studies (where
‘satisfied’ or ‘very satisfied’, ‘good’, ‘very good’, and
‘excellent’ were interpreted as a positive outcome or
overall improvement). Further studies also reported
individual symptoms. No study reported acquiring data
objectively using personnel not involved in the surgical
care of the patient or data collection blinded to inter-
vention status. Average reported studies follow-up was
31 months (range 12–72 months).
Accepting these methodological limitations, several
reports assert that most patients undergoing rectal sus-
pension procedures were satisfied. Meta-analysis of stud-
ies reporting a summary measure found considerable
heterogeneity, which may reflect variation in measure-
ments, patients or procedures. Overall improvement (a
good or satisfactory outcome) was reported in 83%
(95%CI: 74–91%, I2 = 77%) of cases, based on 328
patients (Table 3; Fig. 3). Similar levels of improvement
were recorded for LVMR and OR; only one small study
reported improvement after LRR, and data were not
available for RVMR.
The initial aim of ‘suspension’ procedures is to
treat symptoms. Functional assessment of constipation
is therefore the most important outcome. However,
many patients also suffer from incontinence, typically
post-defaecatory seepage. The various scoring instru-
ments and functional outcomes employed are reported
in Table 4. Generally, measures are too sparsely
reported to be informative. For LVMR, Cleveland
Clinic Constipation score improved from a median of
14 (range 7–18) to a median of 5 (range 4–7) in 6
studies providing pre- and post-operative data.
Improvement in constipation was highly heteroge-
neous and only reported in a minority of studies,
varying from 20% to 97%. By pooling data for LVMR,
the reported improvement in constipation was 86%
(95%CI: 20–97%).While the clinical outcome has primacy, the most
immediate visible consequence of surgery is to correct
anatomy. Therefore, an assessment of anatomical recur-
rence is also important (although necessarily represent-
ing only a surrogate outcome). Anatomical recurrence
rates varied between 0 to 21% (Fig. 4), but typically
occurred in 2–7% of patients in most studies. Functional
outcome data on robotic surgery and LRR were rarely
available, but again anatomical correction was very likely
achieved with both procedures. No conclusions about
functional or anatomical outcomes could be made for
the other rectopexy procedures.
Table 3 Overall improvement based on global satisfaction rat-
ings (GSR). (a) Laparoscopic ventral mesh rectopexy (LVMR).
(b) Robotic ventral mesh rectopexy (RVMR). (c) Laparoscopic
resection rectopexy (LRR). d) Open rectopexy (OR).
(a)
Author Year
Follow
up
(months) N
%
success
Collinson [48] 2009 12 75 NR
Kargar [55] 2011 22 39 74
Portier [49] 2011 32 40 (17*) 97
Wong [45] 2011 12 25 NR
Wong [50] 2011 29 84 NR
Sileri [51] 2012 12 34 NR
Wahed [52] 2012 12 65 71
Formijne
Jonkers [56]
2013 30 233 NR
Gosselink [57] 2013 12 151 NR
Mantoo [46] 2013 16 74 NR
Borie [58] 2014 NA 25 NR
Evans [34] 2015 36 30 NR
Franceschilli [53] 2015 20 100 89
Tsunoda [47] 2015 16 26 NR
(b)
Wong [45] 2011 12 16 NR
Mantoo [46] 2013 16 44 NR
(c)
Tsiaoussis [6] 2005 45 23 (27)‡ 93
Von Papen [7] 2007 44 56 NR
(d)
Author Year Operation
Follow
up
(months) N
%
success
van Tets [4] 1995 Posterior
mesh
rectopexy
72 37 70
Vermeulen
[54]
2005 Anterior
mesh
rectopexy
18 20 63
Portier [49] 2011 Anterior
mesh
rectopexy
22 40 (23*) 97
Cx, complications; NR, not reported.
*17 were laparoscopic, 23 open.
‡4 open.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–4842
Rectal suspension for constipation U. Grossi et al.

Summary evidence statements: efficacy
1 Data on efficacy were inconsistently reported and
findings heterogeneous, making estimates tentative
and imprecise (level IV).
2 Although inconsistent, patient GSR suggest that a
good or satisfactory outcome typically occurs in 83%
(74–91%) of patients (level IV).3 Similar levels of satisfaction were recorded for all pro-
cedures where data were available (LVMR, OR,
LRR) (Level IV).
4 Patient-reported improvements in constipation
occurred in 86% (95%CI: 20–97%) of patients after
LVMR (Level IV).
5 Limited evidence found consistently improved Cleve-
land Clinic Constipation scores for patients undergo-
ing LVMR (level IV).
6 Anatomical recurrence typically occurred in about 2–7% of patients (level IV).
Patient selection
Patient selection is perceived by many experts as extre-
mely important when choosing the surgical approach.
Whilst these procedures may be efficient at correcting
normal anatomy (median 95%, range 79–100%), many
underlying functional and organic pathologies may
jeopardize the success of surgery in the attempt of ‘cur-
ing’ the patient [61]. Fifteen of 18 papers highlight the
fact that all patients had undergone a period of conser-
vative management. Other than this common feature,
selection was inconsistent. Even the diagnosis of abnor-
mal anatomy varied throughout the literature. Studies
described interventions for patients with: ungraded
intussusception [7,54]; ‘rectoanal’ intussusception
[6,47]; ‘high grade’ intussusception [57]; ‘grade 3 or 40
intussusception [48,49,51,53,56]; ‘anterior or circum-
ferential’ intussusception [4]; rectocoele +/- intussus-
ception [52,54,58] or +/- cystocoele [13]; complex
rectocoele of above 2–3 cm [50]; multi-compartment
pelvic floor disorders [46]; solitary rectal ulcer syn-
drome (SRUS) [34,55]. Thus, it was difficult to draw
any conclusions as to which group could benefit from
intervention. When summarising the data, the most
common theme regarding patient selection is a high
grade intussusception (i.e. rectoanal or Oxford grade
≥ 3). Table 5 lists the papers where this inclusion crite-
rion has been adopted and one of the primary indica-
tions along with a summary of the outcome measures
reported (if given in more than one paper). The conclu-
sions from this sub-analysis resemble those described in
the whole review.
SRUS deserves specific mention as two papers
included patients specifically diagnosed with this condi-
tion [34,55]. Patients report passage of mucus and
bloody liquid on defaecation, with an ulcer seen within
the rectum. Treatment is conservative, initially using
biofeedback and behavioral intervention. A proportion
of patients present an element of internal intussuscep-
tion, which may reflect the ulcerated area as the apex of
the intussusception, repetitively traumatised with strain-
ing. The surgical correction of a prolapse (when
Figure 3 Forest plot showing rates of
overall improvement (percentage of
patients) after rectopexy by proceduretype. KEY: LVMR, laparoscopic ventral
mesh rectopexy; LRR, laparoscopic
resection rectopexy; OR, open rectopexy.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–48 43
U. Grossi et al. Rectal suspension for constipation

Table
4Functional
andclinical
outcomes
byprocedure.(a)Laparoscopic
ventral
meshrectopexy(L
VMR).(b)Roboticventral
meshrectopexy(R
VMR).(c)Laparoscopic
resection
rectopexy(L
RR).(d)Open
rectopexy(O
R).
(a)
Author
Year
NCCSpre
CCSpost
ODS
pre
ODS
post
FISIpre
FISIpost
Constipation
improved%
Anatomical
recurren
ce%
Collinson[48]
2009
75
12
5NR
NR
28
886
5
Kargar
[55]
2011
39
NR
NR
NR
NR
NR
NR
NR
NR
Portier[49]
2011
40
NR
NR
NR
NR
NR
NR
Worse
2.5
Wong[45]
2011
25
NR
NR
NR
NR
NR
NR
NR
0
Wong[50]
2011
84
75
NR*
NR*
NR
NR
Improved
6.3
Sileri[51]
2012
34
16
7NR
NR
93
NR
5.9
Wahed
[52]
2012
65
NR*
NR*
NR
NR
NR*
NR*
97
3.7
Form
ijne
Jonkers
[56]
2013
233
NR
8.1
NR*
NR*
NR*
NR*
81
2.6
Gosselink[57]
2013
151
NR
NR
NR
NR
NR*
NR*
NR
NR
Mantoo[46]
2013
74
NR
NR
NR†
NR†
NR
NR
NR
8
Borie[58]
2014
25
NR
NR
16
7.6
24
220
NR
Evans[34]
2015
30
17
6NR
NR
19
NR
NR
21
Franceschilli[53]
2015
100
18.4
5.5
NR
NR
NR*
NR*
89
14
Tsunoda[47]
2015
26
11
4NR
NR
30
6NR
3.8
(b)
Wong[45]
2011
16
NR
NR
NR
NR
NR
NR
NR
NR
Mantoo[46]
2013
44
NR
NR
NR
NR
NR
NR
NR†
8
(c)
Tsiaoussis[6]
2005
23(27)‡
NR
NR
NR
NR
NR
NR
NR
0
VonPapen
[7]
2007
56
NR
NR
NR
NR
NR
NR
53
3.6
(d)
Author
Year
Operation
NCCSpre
CCS
post
ODS
pre
ODSpost
FISI
pre
FISI
post
Constipation
improved%
Anatomical
recurren
ce%
vanTets[4]
1995
Posteriormeshrectopexy
37
NR
NR
NR
NR
NR
NR
NR
NR
Vermeu
len[54]
2005
Anteriormeshrectopexy
20
NR
NR
NR
NR
NR
NR
NR
NR
Portier[49]
2011
Anteriormeshrectopexy
40(23�)
NR
NR
NR
NR
NR
NR
Worse
2.5
NR,notreported
;CCS,ClevelandClinic
Constipationscore.
*significantim
provemen
t(nodatagiven
).
†decreased
orim
provedbutnotsignificantly(nodatagiven
).
‡4open
;�23open
procedures.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–4844
Rectal suspension for constipation U. Grossi et al.

detected) may be reasonable in the hope of resolving
the ulcer. Data on a total of 75 patients with SRUS
who have undergone LVMR are available from the two
papers. Healing of the ulcer occurred in 78% of patients
after surgery.
Summary evidence statements: patient selection
1 Although patient selection is perceived as vital in pre-
dicting outcome, it was inconsistently documented
(level IV).
Figure 4 Forest plot showing rates of
anatomical recurrence (percentage of
patients) after rectopexy by proceduretype. KEY: LVMR, laparoscopic ventral
mesh rectopexy; RVMR, robotic ventral
mesh rectopexy; LRR, laparoscopic
resection rectopexy; OR, open rectopexy.
Table 5 Summary of papers where participants had a high grade internal intussusception (rectoanal, Oxford grade ≥ 3).
Author Year Op N FU % success
CCS
pre
CCS
post
FISI
pre
FISI
post
Constipation
improved
Anatomical
recurrence
Tsiaoussis [6] 2005 † 27 45 93 NR NR NR NR NR 0
Collinson [48] 2009 LVMR 75 12 NR 12 5 28 8 86 5
Portier [49] 2011 * 40 22 97 NR NR NR NR Worse 2.5
Wong [45] 2011 ‡ 41 12 NR NR NR NR NR NR 6.3
Sileri [51] 2012 LVMR 34 12 NR 16 7 9 3 NR 5.9
Formijne
Jonkers [56]
2013 LVMR 233 30 NR 8.1 NR NR NR NR 2.6
Gosselink [57] 2013 LVMR 151 12 NR NR NR NR NR NR NR
Borie [58] 2014 LVMR 52 1–18 NR NR NR 24 2 20 NR
Evans [34] 2015 LVMR 30 36 NR 17 6 19 NR NR 21
Franceschilli [53] 2015 LVMR 100 20 89 18.4 5.5 NR NR 89 14
Tsunoda [47] 2015 LVMR 26 16 NR 11 4 30 6 NR 3.8
*Lap and Open Ant mesh rectopexy.
†Lap resection rectopexy.
‡LVMR and RVMR.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–48 45
U. Grossi et al. Rectal suspension for constipation

2 One common indication appears to be high grade
rectal intussusception (level IV).
3 For high grade intussusception, LVMR, RVMR and
resection rectopexy typically correct anatomy in
about 80–100% of cases (level IV).
4 If SRUS is associated with prolapse, a LVMR typi-
cally results in healing of the ulcer in around 80% of
patients (level IV).
Discussion
A systematic review of evidence for the perioperative
and long terms benefits and harms of rectal suspension
procedures identified no high quality studies. The evi-
dence base is characterised by observational studies of
variable and often uncertain methodological quality.
Definitions are poor, e.g. grading of complications was
inconsistent. Future studies should provide robust and
comparative evidence for clinicians to support patient
decision making, in terms both of the incremental bene-
fits and harms of suspension procedures. A Clavien-
Dindo (or equivalent) classification is essential. Greater
understanding is required of the mediating effects of
prognostic factors particularly preoperative definition of
both functional and radiological parameters that impact
upon treatment success. Relevant to future research
would be to define a minimum set of outcomes for
reporting future studies. Finally, and most obviously,
the evidence base requires urgent augmentation with
some high quality studies focused on having at least
one well powered randomized controlled trial to inform
future clinical decision making.
Acknowledgments
We would like to acknowledge the following people in
relation to the NIHR CapaCiTY working group: Mr
Steven Brown, Sheffield Teaching Hospitals NHS
Foundation Trust; Mr Kenneth Campbell, The Univer-
sity of Dundee, NHS Education for Scotland; Mr Mark
Chapman, Heart of England NHS Trust; Mr Andrew
Clarke, Poole Hospital NHS Foundation Trust; Mr Neil
Cruickshank, Sandwell and West Birmingham Hospitals
NHS Trust; Mr Anthony Dixon, University of Bristol,
Bristol, UK; Dr Christopher Emmett, County Durham
and Darlington NHS Foundation Trust; Mr Ugo
Grossi, Queen Mary University of London; Dr Richard
Hooper, PCTU, Queen Mary University of London;
Miss Emma Horrocks, University Hospital Southamp-
ton NHS Foundation Trust; Professor Charles Knowles,
Queen Mary University of London; Mr Jon Lacy-Col-
son, Shrewsbury and Telford Hospital NHS Trust; Mr
Ian Lindsey, Oxford University Hospitals NHS Trust;
Professor James Mason, University of Warwick, Coven-
try; Mr Mark Mercer-Jones, Gateshead Health NHS
Foundation Trust; Mr Andrew Miller, University
Hospitals of Leicester NHS Trust; Mr David Pares,
Hospital Germans Trias i Pujol, Barcelona, Spain; Miss
Sophie Pilkington, University Hospital Southampton
NHS Foundation Trust; Mr Neil Smart, Royal Devon
& Exeter NHS Foundation Trust; Ms Natasha Stevens,
PCTU, Queen Mary University of London; Professor
Douglas Tincello, University Hospitals of Leicester
NHS Trust; Miss Karen Telford, South Manchester
NHS Foundation Trust; Mr Paul Vollebregt, Queen
Mary University of London; Mr Andrew Williams,
Guy’s and Thomas’ NHS Foundation Trust; Professor
Yan Yiannakou, County Durham and Darlington NHS
Foundation Trust.
Conflict of interest
The authors declare no conflict of interest.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opin-
ions expressed in this report are those of the authors
and are not those of the PGfAR Programme, NIHR,
the UK National Health Service, or the UK Depart-
ment of Health.
References
1 D’Hoore A, Penninckx F. Obstructed defecation. Colorectal
Dis 2003; 5: 280–7.
2 Shorvon PJ, McHugh S, Diamant NE, Somers S, Steven-
son GW. Defecography in normal volunteers: results and
implications. Gut 1989; 30: 1737–49.
3 Tou S, Brown SR, Nelson RL. Surgery for complete (full-
thickness) rectal prolapse in adults. Cochrane Database Syst
Rev, 2015; 11: CD001758.
4 Vantets WF, Kuijpers JHC. Internal rectal intussusception -
fact or fancy. Dis Colon Rectum 1995; 38: 1080–3.
5 Graf W et al. Functional results after abdominal suture rec-
topexy for rectal prolapse or intussusception. Eur J Surg
1996; 162: 905–11.
6 Tsiaoussis J et al. Rectoanal intussusception: presentation
of the disorder and late results of resection rectopexy. Dis
Colon Rectum 2005; 48: 838–44.
7 von Papen M et al. Functional results of laparoscopic resec-
tion rectopexy for symptomatic rectal intussusception. Dis
Colon Rectum 2007; 50: 50–5.
8 Johnson E et al. Long-term outcome after resection rec-
topexy for internal rectal intussusception. ISRN Gastroen-
terol 2012; 2012: 824671.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–4846
Rectal suspension for constipation U. Grossi et al.

9 Biviano I et al. Comparative outcome of stapled trans-anal
rectal resection and macrogol in the treatment of defeca-
tion disorders. World J Gastroenterol 2011; 17: 4199–205.
10 Hirst GR et al. The role of rectocele repair in targeted
patients with obstructed defaecation. Colorectal Dis 2005;
7: 159–63.
11 Sabbagh R et al. Long-term anatomical and functional
results of laparoscopic promontofixation for pelvic organ
prolapse. BJU Int 2010; 106: 861–6.
12 Sitzler PJ et al. Long-term clinical outcome of surgery for
solitary rectal ulcer syndrome. Br J Surg 1998; 85: 1246–
50.
13 Bruch HP et al. Laparoscopic surgery for rectal prolapse
and outlet obstruction. Dis Colon Rectum 1999; 42:
1189–94.
14 Schultz I et al. Whole gut transit is prolonged after Rip-
stein rectopexy. Eur J Surg 1999; 165: 242–7.
15 Badrek-Amoudi AH et al. Laparoscopic ventral mesh rec-
topexy in the management of solitary rectal ulcer syndrome:
a cause for optimism? Colorectal Dis 2013; 15: 575–81.
16 Laubert T et al. Obstructive defecation syndrome: 19 years
of experience with laparoscopic resection rectopexy. Tech
Coloproctol 2013; 17: 307–14.
17 Mackenzie H, Dixon AR. Proficiency gain curve and pre-
dictors of outcome for laparoscopic ventral mesh rectopexy.
Surgery 2014; 156: 158–67.
18 Owais AE et al. Laparoscopic ventral mesh rectopexy in
male patients with internal or external rectal prolapse.
Colorectal Dis 2014; 16: 995–1000.
19 Gravie JF, Maigne C. “Wrap technique”: a new operative
procedure using a self-adhesive prosthesis for laparoscopic
ventral rectopexy. Tech Coloproctol 2015; 19: 361–3.
20 Gultekin FA et al. Safety of laparoscopic ventral rectopexy
in the elderly: results from a nationwide database. Dis
Colon Rectum 2015; 58: 339–43.
21 Abet E et al. Sexual function and laparoscopic ventral rec-
topexy for complex rectocoele. Colorectal Dis 2012; 14:
e721–6.
22 Ramage L et al. Is robotic ventral mesh rectopexy better
than laparoscopy in the treatment of rectal prolapse and
obstructed defecation? A meta-analysis Tech Coloproctol
2015; 19: 381–9.
23 Faucheron JL et al. Anterior rectopexy for full-thickness
rectal prolapse: technical and functional results. World J
Gastroenterol 2015; 21: 5049–55.
24 Gouvas N et al. Ventral colporectopexy for overt rectal
prolapse and obstructed defaecation syndrome: a systematic
review. Colorectal Dis 2015; 17: O34–46.
25 Rondelli F et al. Robot-assisted or conventional laparoscoic
rectopexy for rectal prolapse? Systematic review and meta-
analysis. Int J Surg 2014; 12(Suppl 2): S153–9.
26 Cadeddu F et al. Focus on abdominal rectopexy for full-
thickness rectal prolapse: meta-analysis of literature. Tech
Coloproctol 2012; 16: 37–53.
27 Samaranayake CB et al. Systematic review on ventral rec-
topexy for rectal prolapse and intussusception. Colorectal
Dis 2010; 12: 504–12.
28 Shastri-Hurst N, McArthur DR. Laparoscopic rectopexy
for rectal prolapse: will it be the gold standard? Indian J
Surg 2014; 76: 461–6.
29 Cullen J, Rosselli JM, Gurland BH. Ventral rectopexy for
rectal prolapse and obstructed defecation. Clin Colon Rec-
tal Surg 2012; 25: 34–6.
30 Harmston C, Jones O. The evolution of laparoscopic sur-
gery for rectal prolapse. Int J Surg 2011; 9: 370–3.
31 Senagore AJ. Management of rectal prolapse: the role of
laparoscopic approaches. Semin Laparosc Surg 2003; 10:
197–202.
32 Lahr SJ et al., Operative management of severe constipa-
tion. Am Surg 1999; 65: 1117–21: discussion 1122-3.
33 Silvis R et al. Abdominal rectovaginopexy - Modified tech-
nique to treat constipation. Dis Colon Rectum 1999; 42:
82–8.
34 Evans C et al. Laparoscopic ventral rectopexy is effective
for solitary rectal ulcer syndrome when associated with rec-
tal prolapse. Colorectal Dis 2014; 16: O112–6.
35 Schultz I et al. Continence is improved after the Ripstein
rectopexy - Different mechanisms in rectal prolapse and
rectal intussusception? Dis Colon Rectum 1996; 39: 300–
6.
36 Orrom WJ et al. Rectopexy is an ineffective treatment
for obstructed defecation. Dis Colon Rectum 1991; 34:
41–6.
37 Tweedie DJ, Varma JS. Long-term outcome of laparo-
scopic mesh rectopexy for solitary rectal ulcer syndrome.
Colorectal Dis 2005; 7: 151–5.
38 van den Esschert JW et al. Laparoscopic ventral rectopexy
for obstructed defecation syndrome. Surg Endosc 2008; 22:
2728–32.
39 Portier G et al. Malone antegrade colonic irrigation: ileal
neoappendicostomy is the preferred procedure in adults.
Int J Colorectal Dis 2006; 21: 458–60.
40 Johnson E et al. Resection rectopexy for internal rectal
intussusception reduces constipation and incomplete evacu-
ation of stool. Eur J Surg Suppl 2003; 588: 51–6.
41 Maggiori L et al. Laparoscopic ventral rectopexy: a
prospective long-term evaluation of functional results and
quality of life. Tech Coloproctol 2013; 17: 431–6.
42 Schultz I et al. Long-term results and functional outcome
after Ripstein rectopexy. Dis Colon Rectum 2000; 43: 35–
43.
43 Wong MTC et al. Robotic versus laparoscopic rectopexy
for complex rectocele: a prospective comparison of short-
term outcomes. Dis Colon Rectum 2011; 54: 342–6.
44 Formijne Jonkers HA et al. Evaluation and surgical treat-
ment of rectal prolapse: an international survey. Colorectal
Dis 2013; 15: 115–9.
45 Wong MT et al. Minimally invasive ventral mesh rectopexy
for complex rectocoele: impact on anorectal and sexual
function. Colorectal Dis 2011; 13: e320–6.
46 Mantoo S et al. Is robotic-assisted ventral mesh rectopexy
superior to laparoscopic ventral mesh rectopexy in the man-
agement of obstructed defaecation? Colorectal Dis 2013;
15: e469–75.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–48 47
U. Grossi et al. Rectal suspension for constipation

47 Tsunoda A et al. Laparoscopic ventral rectopexy for rec-
toanal intussusception: postoperative evaluation with proc-
tography. Dis Colon Rectum 2015; 58: 449–56.
48 Collinson R et al. Laparoscopic ventral rectopexy for inter-
nal rectal prolapse: short-term functional results. Colorectal
Dis 2010; 12: 97–104.
49 Portier G et al. The effect of abdominal ventral rectopexy
on faecal incontinence and constipation in patients with
internal intra-anal rectal intussusception. Colorectal Dis
2011; 13: 914–7.
50 Wong M et al. Safety and efficacy of laparoscopic ventral
mesh rectopexy for complex rectocele. Colorectal Dis 2011;
13: 1019–23.
51 Sileri P et al. Laparoscopic ventral rectopexy for internal
rectal prolapse using biological mesh: postoperative and
short-term functional results. J Gastrointest Surg 2012; 16:
622–8.
52 Wahed S et al. Short-term results for laparoscopic ventral
rectopexy using biological mesh for pelvic organ prolapse.
Colorectal Dis 2012; 14: 1242–7.
53 Franceschilli L et al. Laparoscopic ventral rectopexy using
biologic mesh for the treatment of obstructed defaecation
syndrome and/or faecal incontinence in patients with inter-
nal rectal prolapse: a critical appraisal of the first 100 cases.
Tech Coloproctol 2015; 19: 209–19.
54 Vermeulen J et al. Anterolateral rectopexy for correction of
rectoceles leads to good anatomical but poor functional
results. Tech Coloproctol 2005; 9: 35–41; discussion 41.
55 Kargar S et al. Laparoscopic rectopexy in solitary rectal
ulcer. Acta Med Iran 2011; 49: 810–3.
56 Formijne Jonkers HA et al. Laparoscopic ventral rectopexy
for rectal prolapse and symptomatic rectocele: an analysis of
245 consecutive patients. Colorectal Dis 2013; 15: 695–9.
57 Gosselink MP et al. Impact of slow transit constipation on
the outcome of laparoscopic ventral rectopexy for
obstructed defaecation associated with high grade internal
rectal prolapse. Colorectal Dis 2013; 15: e749–56.
58 Borie F et al. Laparoscopic ventral rectopexy for the treat-
ment of outlet obstruction associated with recto-anal intus-
susception and rectocele: a valid alternative to STARR
procedure in patients with anal sphincter weakness. Clin
Res Hepatol Gastroenterol 2014; 38: 528–34.
59 Powar MP, Ogilvie JW Jr, Stevenson AR. Day-case laparo-
scopic ventral rectopexy: an achievable reality. Colorectal
Dis 2013; 15: 700–6.
60 George R et al. Re: day-case laparoscopic ventral rectopexy.
Colorectal Dis 2013; 15: 1450–1.
61 Pescatori M, Spyrou M and Pulvirenti d’Urso A. A prospec-
tive evaluation of occult disorders in obstructed defecation
using the ‘iceberg diagram’. Colorectal Dis 2007; 9: 452–6.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 37–4848
Rectal suspension for constipation U. Grossi et al.

Surgery for constipation: systematic review and practicerecommendations
Results III: Rectal wall excisional procedures (Rectal Excision)
M. Mercer-Jones*, U. Grossi†, D. Pares‡, P. F. Vollebregt†, J. Mason§, C. H. Knowles†, on behalf
of the NIHR CapaCiTY working group¶ and the Pelvic floor Society**
*Queen Elizabeth Hospital, Gateshead NHS Trust, Gateshead, UK, †National Bowel Research Centre, Blizard Institute, Queen Mary, University London,
London, UK, ‡Hospital Germans Tr�ıas i Pujol, Barcelona, Spain, §University of Warwick, Coventry, UK, ¶National Institute for Health Research: Chronic
Constipation Treatment Pathway, London, UK and **Affiliate section of the Association of Coloproctology of Great Britain and Ireland
Abstract
Aim To assess the outcomes of rectal excisional proce-
dures in adults with chronic constipation.
Method Standardised methods and reporting of bene-
fits and harms were used for all CapaCiTY reviews that
closely adhered to PRISMA 2016 guidance. Main con-
clusions were presented as summary evidence statements
with a summative Oxford Centre for Evidence-Based
Medicine (2009) level.
Results Forty-seven studies were identified, providing
data on outcomes in 8340 patients. Average length of
procedures was 44 min and length of stay (LOS) was
3 days. There was inadequate evidence to determine vari-
ations in procedural duration or LOS by type of proce-
dure. Overall morbidity rate was 16.9% (0–61%), with
lower rates observed after Contour Transtar procedure
(8.9%). No mortality was reported after any procedures in
a total of 5896 patients. Although inconsistently
reported, good or satisfactory outcome occurred in 73–80% of patients; a reduction of 53–91% in Longo scoring
system for obstructive defecation syndrome (ODS)
occurred in about 68–76% of patients. The most common
long-term adverse outcome is faecal urgency, typically
occurring in up to 10% of patients. Recurrent prolapse
occurred in 4.3% of patients. Patients with at least 3 ODS
symptoms together with a rectocoele with or without an
intussusception, who have failed conservative manage-
ment, may benefit from a rectal excisional procedure.
Conclusion Rectal excisional procedures are safe with
little major morbidity. It is not possible to advise which
excisional technique is superior from the point of view
of efficacy, peri-operative variables, or harms. Future
study is required.
Keywords surgery, constipation, rectal excision,
STARR, TRANSTAR
Introduction
Background and procedural variations
Chronic constipation is related to an inability to evacu-
ate the rectum in over half of all adults presenting for
specialist advice. This phenomenon, which may be vari-
ably described as obstructed defaecation or rectal evacu-
ation disorder (and many other terms) is characterized
by excessive straining, the feeling of incomplete evacua-
tion, post-defaecatory seepage and often mucous dis-
charge and pelvic pain [1]. In some of these patients,
there is clinical and radiological (usually proctographic)
evidence of a dynamic structural abnormality, leading
to physical impediment to emptying during defaecation.
The most common abnormalities are rectocoele and/or
intussusception. Theoretically, these anatomical variants
could lead to the features of obstructed defaecation by
a process of loss of force vector (ballooning of the rec-
tum into a rectocoele or invagination of the rectum
into an intussusception, rather than evacuation of stool
on straining) or mucosal obstruction (in the case of an
intussusception) [1]. Correction of these variants can
be carried out by surgically excising the redundant rec-
tal wall, i.e. that ballooning out or prolapsing in, thus
restoring ‘normal’ anatomy.
Techniques
The stapled transanal rectal resection (STARR) proce-
dure uses two circular procedure for prolapsing
Correspondence to: Mr Mark Mercer-Jones, Queen Elizabeth Hospital, NE9
6SX Gateshead NHS Trust, Gateshead, UK.
E-mail: [email protected].
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 49
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13772

haemorrhoids (PPH)01 stapling devices (Ethicon Endo-
surgery, INC., Cincinnati, Ohio, USA), or at times,
two circular PPH03 devices. They are used sequentially
to remove the anterior rectal wall prolapse and then the
posterior rectal wall prolapse. These full thickness rectal
wall excisions result in defects that are anastomosed
with staples contained within the device. The STARR
procedure was derived from the technique of stapled
haemorrhoidopexy and was introduced into clinical
practice by Antonio Longo using the PPH01 device
[2]. Initially, most STARR procedures were performed
with PPH01; however, subsequently the PPH03 device
was developed, essentially for haemorrhoidopexies, to
reduce intra-operative staple line bleeding. The two
devices, PPH01 and PPH03, differ only with respect to
the closed staple height, which varies between 1–2.5 mm and 0.75–1.5 mm, respectively. The PPH03
device is no longer licensed for use for STARR because
of concerns that the staple line height was insufficient
for the thickness of tissue that was resected and anasto-
mosed. As with all new techniques, in order to ensure
that safety and efficacy concerns were addressed, a num-
ber of initiatives were put in place by the manufacturer.
The procedure could only be performed by trained sur-
geons who then mentored other surgeons. In the UK,
the PPH01 device is no longer used for haemor-
rhoidopexies, and consequently Ethicon will only per-
mit the sale of this device to institutions with surgeons
trained in the STARR technique. The European
STARR registry was established through collaboration
between Ethicon Endosurgery and the colorectal soci-
eties in the UK, France, Germany and Italy. Outcomes
from this registry have been published and, in response,
the National Institute for Health and Care Excellence
(NICE) issued interventional procedure guidance in
2010. The NICE guidance concluded that ‘the current
evidence on safety and efficacy of stapled transanal rec-
tal resection (STARR) for obstructed defaecation syn-
drome (ODS) is adequate . . . . . . the procedure may
therefore be used with normal arrangements for clinical
governance, consent and audit.’ [www.nice.org.uk/
ipg351].
Despite its proven safety and efficacy, the STARR
procedure still had limitations. These were primarily
related to the stapling device itself. The two biggest
concerns were that the rectal resection was performed
‘blind’ within the low rectum and that the volume of
the resected tissue was entirely dependent upon the
capacity of the stapling device housing, rather than the
extent of the prolapse. As such, the surgeon was
unable to modify the extent of resection in relation to
the size of the prolapse. Consequently, a new stapling
device, the Contour Transtar curved cutter stapler
(Ethicon Endosurgery, INC.), was introduced [3] in
order to allow a tailored correction of the prolapse by
removing more tissue. It would also allow this resec-
tion to be performed under direct vision. The Contour
Transtar stapler utilises replaceable staple cartridges
allowing multiple firings with a single device.
Although STARR has been heavily popularized, it is
not the first procedure to use of rectal excision as a
means of treating prolapse. Edward Delorme originally
described his procedure for full-thickness external rectal
prolapse in 1900 [4]. There have been several modifica-
tions, one being an intra-anal Delorme’s procedure for
the treatment of recto-anal intussusception [5]. Unlike
STARR and Contour Transtar, there is no full-thickness
rectal wall excision and only the redundant mucosa is
excised. The mucosa is stripped cephalad, and the
underlying muscle is plicated together with sutures to
concertina the prolapse.
Scope
The purpose of this review was to assess the efficacy
and harms of rectal excisional procedures for internal
prolapse and/or rectocoele in adults. Procedures con-
sidered beyond the scope of systematic review included:
(i) those where ‘tightening’ is effected without excision
(covered in rectovaginal reinforcement systematic
review); (ii) those where only mucosa is excised (muco-
sectomy) and there is no plication of the muscular wall;
(iii) those where a mucosectomy and plication are lim-
ited to the anterior wall (covered in rectovaginal rein-
forcement systematic review); (iv) those where the
whole rectum is resected rather than a component of
the wall, i.e. as occasionally performed for megarectum
[6]. Studies where outcomes could not be segregated
by eligible procedure were also excluded, due to a
mixed patient population with internal and external rec-
tal prolapse, mixed indications, including numerous pel-
vic floor abnormalities or limited postoperative
outcomes, transanal endocopic microsurgery proce-
dures, technical reports, or cost analyses only.
Previous reviews
One previous meta-analysis including 26 studies [7]
addressed the outcome of rectal excisional procedures
for constipation.
Summary of search results and studyquality
The search yielded a total of 84 articles for full text
review (Fig. 1). From these, 47 published between
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7250
Rectal excision for constipation M. Mercer-Jones et al.

2000 and 2014 contributed to the systematic review,
providing data on outcomes in a total of 8340 patients
(range 20–2224 patients per study) (Table 1). Specific
exclusions after full-text review (and after exclusion of
non-English language publications) included nine stud-
ies where the population sample was confirmed to be
< 20 patients, eight where follow-up was < 12 months;
five studies with out of scope procedures [8–11], threestudies where data were considered duplicate [12,13],
and three where outcomes could not be segregated by
eligible procedure. Other exclusion criteria were: indica-
tion not constipation (n = 1) and lack of extractable
outcome data (n = 5).
The quality of studies varied. The 47 included stud-
ies (Table 1) included 42 observational studies and five
randomised controlled trials (RCTs). The latter
included three good quality RCTs (level IB) with low
levels of predicted bias, and two with less well described
methodology (level IIB). The remaining 42 observa-
tional studies encompassed several good quality
prospective cohort studies with low levels of bias includ-
ing four prospectively maintained funded registries
(level IIB). Other studies were a mix of prospective and
retrospective case series. Mean study follow-up was
1.9 years (range 1.0–5.5 years); 36 studies originated
from European centres, three from the USA and eight
from other countries.
Perioperative data
Perioperative data were reported by 47 studies reporting
55 procedures (Tables 2 and 3). Measures of variation
of continuous measures included ranges or standard
deviations but were inconsistently reported. Average
procedural duration and length of stay (LOS) varied
between procedures but design heterogeneity, small
numbers of studies and large range of values precluded
any clear conclusions (Table 3). The overall average
duration of procedures reported by cohorts was 44
(range 23–95) min, and the overall average LOS was
3.0 (range 1.0–8.0) days (Figs 2 and 3). In one RCT
of 100 patients (STARR vs Contour Transtar) [37],
Contour Transtar took significantly longer to perform
(52.2 vs 42.4 minutes P = 0.008). However this reduc-
tion was not apparent more broadly within the pooled
findings (Fig. 2). While LOS for intra-anal Delorme’s
procedure was shorter (2 days) this was based on only
one study reporting this outcome in 34 patients.
Figure 1 PRISMA diagram of search results.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 51
M. Mercer-Jones et al. Rectal excision for constipation

Table 1 All studies included in systematic review.
Author Year Centre Country Total N FU* Design Level†
Liberman [14] 2000 Omaha USA 34 43 RCS IV
Boccasanta [15] 2004 Milan Italy 50 23 RCT IB
Boccasanta [16] 2004 Milan Italy 90 16 PCH IIB
Pescatori [17] 2006 Rome Italy 26 36 RCS IV
Arroyo [18] 2007 Elche Spain 37 24 PCH IIB
Gagliardi [19] 2008 Multicentre Italy 85‡ 17 RCS IV
Dindo [20] 2008 Zurich Switzerland 24 18 PCH IIB
Lehur [21] 2008 Multicentre France, Italy, UK 119 12 RCT IIB
Arroyo [22] 2008 Multicentre Spain 104 26 PCH IIB
Lenisa [3] 2009 Multicentre Europe 75 12 PCH IIB
Harris [23] 2009 Orlando USA 75 12 RCH IV
Jayne [24] 2009 Multicentre UK, Germany, Italy 2224§ 12 PCH IIB
Reboa [25] 2009 Genoa Italy 33 18 PCH IIB
Boccasanta [26] 2010 Milan Italy 142 24 PCH IIB
Isbert [27] 2010 Nuremberg Germany 150 12 RCH IIB
Zhang [28] 2010 Beijing China 50 12 PCH IIB
Madbouly [29] 2010 Alexandria Egypt 46 42 PCH IIB
Schwandner [30] 2010 Regensburg Germany 379 12 PCH IIB
Ram [31] 2010 Ramat Aviv Israel 30 26 PCS IV
Zehler [32] 2010 Hamburg Germany 20 66 PCS IV
Goede [33] 2011 Bristol UK 344 12 PCS IV
Meurette [34] 2011 Nantes France 30 48 PCS IV
Martellucci [35] 2011 Siena Italy 133 19 PCS IV
Patel [36] 2011 Houston Texas 37 20 PCH IIB
Boccasanta [37] 2011 Milan Italy 100 36 RCT IB
Stuto [38] 2011 Pordenone Italy 2171 12 PCH IIB
Song [39] 2011 Seoul South Korea 58 34 RCH IV
Ding [40] 2011 Beijing China 86 12 PCH IIB
Renzi [41] 2011 Naples Italy 61 24 RCT IB
Reibetanz [42] 2011 Wuerzburg Germany 170 18 RCH IIB
Naldini [43] 2011 Pisa Italy 30 24 PCH IIB
Biviano [8] 2011 Rome Italy 60 38 PCH IIB
Savastano [44] 2012 Vicenza Italy 64 27 PCH IIB
Jiang [45] 2012 Wuhan China 43 12 RCS IV
Boenicke [46] 2012 Wuerzburg Germany 181 19 PCH IIB
Kohler [47] 2012 Dresden Germany 80 39 PCS IV
Hasan [48] 2012 Cairo Egypt 40 12 PCH IIB
Ganio [49] 2013 Vercelli Italy 167 36 RCS IV
Adams [50] 2013 London UK 37 13 RCS IV
Masoni [51] 2013 Rome Italy 187 12 RCS IV
Bock [52] 2013 St Gallen Switzerland 70 48 RCS IV
Zhang [53] 2013 Beijing China 75 30 PCH IIB
Panicucci [54] 2014 Pisa Italy 54 12 PCH IIB
Borie [55] 2014 Nimes France 52 18 RCH IV
Ribaric [56] 2014 Multicenter Europe 100 12 PCH IIB
Gentile [57] 2014 Naples Italy 66 12 RCT IIB
Leardi [58] 2014 L’Aquila Italy 51 36 PCS IV
RCS, retrospective cohort study; PCS, prospective case series; RCT, randomised controlled trial; PCH, prospective cohort study.
*Mean follow up in months.
†Oxford CEBM [13].
‡Report on 123 patients, but only 85 operated on.
§Report on 2838 patients for complications, 2224 reached 12 months follow-up.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7252
Rectal excision for constipation M. Mercer-Jones et al.

Table 2 Perioperative data by procedure.
Author Year N
Time
(minutes) LOS (days)
Post-op
bleed
Req.
Treatment %
Sepsis
%
Post-op
anastomotic
dehiscence
%
Total
complications
%
Mortality
%
(a) PPH-01
Boccasanta [15] 2004 25 41.8 � 6 2.1 � 0.8 4 0 0 40 0
Boccasanta [16] 2004 90 43.3 � 9 2.1 � 0.8 4.4 0 0 16.5 0
Arroyo [18] 2007 17 45.9 (9.8) NR 6 0 0 NR 0
Gagliardi [19] 2008 85 † NR NR 2.3 3 0 18 0
Dindo [20] 2008 24 60 (40–110) 3 (1–10) 4.1 0 0 25 0
Lehur [21] 2008 119 40 (15–56) 2.1 (1–6) 1.8 1.8 0 15 0
Arroyo [22] 2008 37‡‡ 46.7 (9.3) 2.2 (0.7) 2.8 0 0 NR 0
Boccasanta [26] 2010 74 35.8 � 6.1 2.6 � 0.5 4 0 0 28.3 0
Harris [23] 2009 36 52.7 2.6 19.4§§ 2.8 0 61.1¶¶ 0
Isbert [27] 2010 68 57 � 15.4 3.4 � 1.6 3 0 2 7.3 0
Jayne [24] 2009 2224‡ 44 (15–210) 3.7 (1–36) 5 4.4 3.5* 36 0
Reboa [25] 2009 33 37 � 7 1.5 � 0.6 0 0 0 15.1 0
Zhang [28] 2010 50 28 NR 0 0 0 NR 0
Madbouly [29] 2010 46 48.4 � 9.6 1 0 0 0 15.2 0
Schwandner [30] 2010 379 40 5.5 2.9 1.6 7.1* 21.2 0
Ram [31] 2010 30 40 (35–80) 2 (1–4) 0 0 NR 36.7 0
Zehler [32] 2010 20 53.5 (45–65) 8 (3–22) 15 0 0 20 0
Goede [33] 2011 344 NR NR 2.7 NR NR 16.3 0
Meurette [34] 2011 30 40 � 8 3 � 1 NR NR NR 27 0
Patel [36] 2011 37 NR 1 0 NR NR 35.1 0
Boccasanta [37] 2011 50 42.4 (6.9) 3.2 (0.6) 2 0 0 4 0
Stuto [38] 2011 2171¶ 95 (15–230) 3.6 (1–21) NR NR NR NR NR
Song [39] 2011 58 35.1 � 11.3 3.91 � 0.84 4 0 NR NR 0
Ding [40] 2011 86 30 � 7 5 � 1.8 0 0 0 NR 0
Renzi [41] 2011 30 28.1 (11.5) 1.2 (0.5) 6.6 0 NR NR 0
Reibetanz [42] 2011 170§ NR NR 0 0 0.6 7 0
Naldini [43] 2011 15 NR 3.4 (3–6) 0 NR NR 0 0
Biviano [8] 2011 30 NR NR 0 0 0 6 0
Savastano [44] 2012 32 28 (20–45) 2 (1–3) 13 0 0 NR 0
Boenicke [46] 2012 181** NR NR 1 0 0.5 8.2 0
Kohler [47] 2012 80 67 (34–182) NR 6 1 1 22.5 0
Hasan [48] 2012 40 35 � 10 1.7 � 2.3 0 0 0 NR 0
Adams [50] 2013 37 NR 1 (0–8) 5.4 2.7 0 32 0
Zhang [53] 2013 75 NR NR 0 0 0 NR 0
Panicucci [54] 2014 54 †† NR NR NR NR NR NR NR
Borie [55] 2014 25 NR 5.6 � 2.1 0 0 0 24 0
Leardi [58] 2014 51 NR 3 2 0 0 2 0
(b) PPH03
Arroyo [18] 2007 20 40.1 (10.4) NR 0 0 0 NR 0
Arroyo [22] 2008 67*** 46.7 (9.3) 2.2 (0.7) 2.8 0 0 NR 0
Jiang [45] 2012 43 23 � 4 5 (4–6) 0 0 0 NR 0
Gentile [57] 2014 30 40 NR NR NR NR 20 NR
(c) Contour Transtar
Lenisa [3] 2009 75 45 (24–90) 4 (1–16) 2.6 0 0 7 0
Isbert [27] 2010 82 51 � 18.2 3.6 � 2.3 3 0 0 7.5 0
Martellucci [35] 2011 133 42 (26–71) NR 1.5 NR 1.5 15.7 0
Boccasanta [37] 2011 50 52.2 (8.7) 3.5 (1.0) 2 0 0 2 0
Renzi [41] 2011 31 33.1 (15.7) 1.25 (0.5) 3.2 0 NR NR 0
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 53
M. Mercer-Jones et al. Rectal excision for constipation

Summary evidence statements: perioperative data
1 The average duration of procedures was 44 min,
although this ranged widely between studies from 23
to 95 min (level II).
2 The average length of stay was 3 days although this
ranged widely between studies from 1 to 8 days
(level II).
3 There was inadequate evidence to determine varia-
tions in procedural duration or length of stay by type
of procedure (level IV).
Harms
Perioperative complications
Five measures of perioperative harm were reported by a
majority of studies within the review. In general, there was
considerable heterogeneity between cohort findings. This
heterogeneity may have reflected (for example) differing
inclusion, procedural content, context of care, or thresh-
olds or conventions for recording complications.
Overall procedural complication rates varied between
cohorts from 0% to 61% Fig. 4. Random effects meta-
analysis found the overall complication rate to be 16.9%
(95% CI: 12.7–21.5%), I2 = 93%. The Contour Transtar
procedure reported a lower overall complication rate of
8.9% (95% CI: 5.1–13.5%), I2 = 70%, although cohort
findings within this category were heterogeneous and
non-comparative. The two RCTs (IB) comparing STARR
to Contour Transtar reported no difference in periopera-
tive complication rates [37,41], although these included
only 161 patients in total and six events. A more general-
isable estimate of the overall complication rate may come
from the European STARR registry which reported an
overall morbidity rate of 36% from 2838 patients [24].
The inclusion criteria for morbidity in this registry incor-
porated urgency (20%), but this was not universally
applied in most other studies, explaining its discrepancy
from the pooled findings.
Rates of post-operative bleeding requiring treatment
varied between cohorts from 0% to 19% (Fig. 5). Ran-
dom effects meta-analysis found the pooled bleed rate
to be 1.6% (95% CI: 0.9–2.5%), I2 = 63%. Regarding
Table 2 (Continued).
Author Year N
Time
(minutes) LOS (days)
Post-op
bleed
Req.
Treatment %
Sepsis
%
Post-op
anastomotic
dehiscence
%
Total
complications
%
Mortality
%
Naldini [43] 2011 15 NR 3.1 (2–5) 3.3 NR NR 3.3 0
Savastano [44] 2012 32 43 (32–65) 4 (3–7) 6 0 9.3 NR 0
Masoni [51] 2013 187 48 (32–78) < 3 0 0 0 7.4 0
Bock [52] 2013 70 NR NR 0 0 0 23 0
Ribaric [56] 2014 100 43.8 � 13.9 4.36 � 2.75 1 0 0 11 0
(d) Intra-anal Delorme’s procedure
Liberman [14] 2000 34 NR 1.8 (2.4) 3 8.8 0 35.3 0
Pescatori [17] 2006 26 NR NR 15.4 16††† 12.5††† 45††† 0
Ganio [49] 2013 167‡‡‡ NR NR 0 1.2 1.8 10.2 0
Gentile [57] 2014 36 65 NR NR NR NR 19.4 0
NR, not recorded.
All PPH03, except Jiang [45] translinear stapler.
*Reported as staple line complications, including dehiscence.
†Report on 123 patients, but only 85 operated on.
‡Report on 2838 patients for complications, 2224 reached 12 months follow-up.
§101 patients had Countour Transtar.
¶208 patients had Contour Transtar.
**Some patients had Contour Transtar.
††18 patients had Contour Transtar.
‡‡Complications are reported for 104 patients (67 had PPH03).
§§It is uncertain if this required intervention as recorded as ‘rectal bleeding’.
¶¶Total complications included tenesmus, diarrhoea, faecal incontinence, and pruritis ani.
***Complications are reported for 104 patients (37 had PPH01); NR: not recorded.
†††These percentages are based upon analysis of 40 patients (14 patients having had PPH01 or PPH01 with manual mucosectomy).
‡‡‡91 patients also had levatoroplasty.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7254
Rectal excision for constipation M. Mercer-Jones et al.

intra-operative bleeding from staple lines, results from
one prospective cohort study (IIB) showed that less
intraoperative staple line sutures were required with
PPH03 compared with PPH01 [18]. Details of treat-
ments provided (e.g. transfusion or re-operation) were
unclear in many instances.
Sepsis rates varied from 0% to 16%, but were consis-
tently low, occurring in no patients in 78% of cohorts
reported. Random effects meta-analysis found the sepsis
rate to be 0.2% (95% CI: 0.0–0.7%), I2 = 63%. Septic
complications were mostly related to urinary tract
infections, C. difficile infection, or more rarely, pneu-
monia. Sepsis rates for Delorme’s procedure appeared
high at 6.2% (95% CI: 0.0–19.4%), I2 = 82%, but find-
ings from the three studies were highly heterogeneous
and the only moderately large study [49] reported a
1.2% sepsis rate. The rate of post-operative anastomotic
dehiscence (wound rupture) varied between cohorts
from 0% to 13% but was consistently low, occurring in
no patients in 76% of cohorts reported. Random effects
meta-analysis found the pooled rate of anastomotic
dehiscence to be 0.3% (95% CI: 0.0–0.8%), I2 = 62%.
Table 3 Procedural data.
Procedure
Procedure duration (mins) Length of stay (days) Follow-up (months)
N Mean Range N Mean Range N Mean Range
PPH-01 25 44.6 (28.0–95.0) 25 2.9 (1.0–8.0) 37 23.0 (12.0–66.0)
PPH-03 4 37.5 (23.0–46.7) 2 3.6 (2.2–5.0) 4 18.5 (12.0–26.0)
Contour Transtar 8 44.8 (33.1–52.2) 7 3.4 (1.3–4.4) 10 22.6 (12.0–48.0)
Delorme’s 1 65.0 – 1 1.8 – 3 38.3 (36.0–43.0)
Total 37 43.8 (23.0–95.0) 35 3.0 (1.0–8.0) 54 23.5 (12.0–66.0)
Figure 2 Forest plot showing procedureduration by operation type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 55
M. Mercer-Jones et al. Rectal excision for constipation

There was inadequate evidence to select between proce-
dures on the basis of individual complications.
No deaths were reported in any cohort of patients
reporting mortality, which included a total of 5896
patients (Table 3). Incidences of serious complications
were reported but these were rare. These included: one
case of sepsis with retropneumoperitoneum [19], two
cases of intra-operatively recognized rectal perforation
requiring diverting colostomy [32,35], one case of rec-
tovaginal abscess requiring diversion [50], one case of
suture line disruption requiring diversion [30], and one
case of rectal necrosis requiring a colostomy [24]. There
were no cases of inadvertent small bowel injury as a
result of peritoneal inclusion with anterior rectal wall
excision and enterocoele excision. This is despite the
fact that in one study [42], 84 of 101 patients who had
Contour Transtar, and 14 of 69 patients who had
PPH01, had peritoneum present in the resected tissue.
Long-term adverse outcomes
Although obstructed defecation is a benign condition,
it may have a significant impact on a patient’s quality
of life. Studies have consistently reported a number of
long-term conditions and symptoms occurring after
stapled rectal excision procedures that may have a fur-
ther negative impact upon quality of life. Measures
reported by more than half of cohorts include: rectal
stenosis (83% of cohorts), recto-vaginal fistula (76%),
pain/proctalgia (70%), and urgency after defaecation
(72%); those less consistently reported include recur-
rent prolapse (46%) and dyspareunia (33%) (Table 4).
Random effects meta-analysis found that reported
rectal stenosis rates were 0.2% (95% CI: 0.0–0.6%),I2 = 30%, although individual cohorts varied from 0.0%
to 7.4%, with no stenosis reported in 67% of cohorts.
Recto-vaginal fistula was a very rare outcome, occurring
in just 3 of 4851 patients (0.062%) studied. Rectal pain
or proctalgia lasting > 6 months post-procedure was
reported by 0.7% of patients (95% CI: 0.1–1.6%),I2 = 79%, although individual cohorts varied from 0%
to 17%, with no proctalgia reported in 53% of cohorts.
Similarly to pooled findings, there was no difference in
pain comparing STARR and Contour Transtar in the
two level 1B RCTs [37,41]; at 36 months, the inci-
dence of pain was significantly less compared with pre-
Figure 3 Forest plot showing length of
stay by operation type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7256
Rectal excision for constipation M. Mercer-Jones et al.

operative values in both groups [37]. The two studies
with the highest reported incidence of proctalgia were
both PCHs (IIB). At 38 � 18 months post-STARR
(n = 30), 17% complained of intermittent anal pain,
however despite the fact that pre-operative Cleveland
Clinic Constipation scores were recorded, there was no
analysis about de novo pain [8]. At 12 months post-
STARR (n = 2838), 7.1% complained of persistent pain
[24]. Again there was no analysis regarding the de novo
nature of this pain.
Urgency of defecation, at least one year post-proce-
dure, was reported by 5.2% of patients (95% CI: 2.7–8.2%), I2 = 92%, although findings were heterogeneous
and individual cohorts varied from 0% to 34% (Fig. 6).
The European STARR registry reported higher urgency
rates of 20% at 12 months [24] and the German
STARR registry reported rates of 25% at 12 months
[30]. Both groups of authors pointed to poor record-
ing of pre-operative urgency symptoms, relying on the
subset scores from patients’ Symptom Severity Score
(SSS). Schwander et al.[30] suggest that this high
incidence reflected numbers with new onset urgency
with a score of > 1 in SSS, 5.5% had score > 3, and
8% of patients observed a reduction in urgency com-
pared with pre-op. Jayne et al. [24] acknowledged in a
subsequent reply to an invited expert’s analysis of their
paper, that de novo urgency was not recorded in their
registry but 20% of patients reported this as a compli-
cation. Analysis of the subset question in their SSS
suggested that 39.9% of patients experienced urgency
pre-operatively and this fell to 26.8% at 12 months
post-STARR. The highest reported incidence of
urgency came from an RCT (IB) comparing STARR/
PPH01 (34% at 3 years) with Contour Transtar (14%
at 3 years) (P = 0.035) [37]. Urgency was reported as
being de novo in both groups. However, the text in
the results reports that the symptoms resolved in all
but one patient (it is probable that this refers to tenes-
mus which is reported for one patient post-op). The
other RCT (level IB) comparing STARR/PPH01 with
Contour Transtar showed no difference in urgency
rates after 24 months [41].
Figure 4 Forest plot showing rates of
complications by operation type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 57
M. Mercer-Jones et al. Rectal excision for constipation

Summary evidence statements: harms
1 Evidence is largely drawn from observational stud-
ies and comparisons. Findings were heteroge-
neous, making estimates tentative and imprecise
(level IV).
2 Overall procedural complication rates ranged from 0%
to 61%. However, these complications may typically
occur in about 13–22% of procedures (level II).
3 The Contour Transtar procedure may feature a
lower overall complication rate although this needs
to be confirmed with better research (level IV).
4 Post-operative bleeding requiring treatment may
typically occur in 1–3% of patients (level II).
5 Post-operative sepsis and anastomotic dehiscence
are rare complications rare typically occurring in less
than 1% of patients (level II).
6 Serious acute post-operative complications are very
rare occurring in about one in a thousand patients
(level II).
7 In the longer term (12 months or more), rectal
stenosis is a rare complication typically occurring in
less than 1% of patients (level II).
8 The most common longer term adverse outcome is
urgency of defaecation, typically occurring in up to
10% of patients (level II).
9 Longer term pain is experienced typically by less
than 2% of patients (level II).
Figure 5 Forest plot showing rates ofbleeding by operation type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7258
Rectal excision for constipation M. Mercer-Jones et al.

Table 4 Long-term adverse outcomes after rectal excisional procedures.
Author Year N Stenosis
Recto
vaginal
fistula
Recurrent
Prolapse
Pain/
proctalgia > 6
months Dyspareunia
Urgency
after 12
months
(a) PPH01
Boccasanta [15] 2004 25 4 0 0 0 0 0
Boccasanta [16] 2004 90 3.3 0 0 0 0 1.1
Arroyo [18] 2007 17 6 0 6 0 NR 0
Gagliardi [19] 2008 85* 0 0 9.4 1.1 1.1 8.2
Dindo [20] 2008 24 0 0 NR 4.1 0 NR
Lehur [21] 2008 119 0 0 NR 1.8 0 NR
Arroyo [22] 2008 37†† 0 0 5.7 0.9 NR 5.8
Harris [23] 2009 36 0 0 2.7 2.7 10.5 16.7E
Jayne [24] 2009 2224† 0.6 0.04 NR 7.1 0.1 20
Reboa [25] 2009 33 0 0 NR 0 NR 6
Boccasanta [26] 2010 74 1.3 0 0 0 0 2.7
Isbert [27] 2010 68 0 0 2.9 3 NR 4.4
Zhang [28] 2010 50 0 0 2 2 0 2
Madbouly [29] 2010 46 6.5 0 NR 0 NR 0
Schwandner [30] 2010 379 2.1 NR NR 0.5 NR 25.3§§
Ram [31] 2010 30 NR NR NR 0 NR NR
Zehler [32] 2010 20 0 0 NR NR NR NR
Goede [33] 2011 344 2.9 NR NR NR NR 11.5***
Meurette [34] 2011 30 NS NR NR 0 NR 6.8
Patel [36] 2011 37 2.7 NR NR NR 5.4 NR
Boccasanta [37] 2011 50 0 0 12 0 NR 34¶¶
Stuto [38] 2011 2171§ NR NR NR NR NR NR
Song [39] 2011 58 1.7 NR NR 0 NR 0
Ding [40] 2011 86 0 0 NR 0 NR 0
Renzi [41] 2011 30 NR 0 NR NR 3.3 10
Reibetanz [42] 2011 170‡ 0 0 NR 0 NR NR
Naldini [43] 2011 15 NR NR NR NR NR 20
Biviano [8] 2011 30 0 0 3 17 0 6
Savastano [44] 2012 32 6.25 0 NR 0 0 0
Boenicke [46] 2012 181¶ 0 0 NR 0 NR NR
Kohler [47] 2012 80 0 0 5 0 NR 12.5
Hasan [48] 2012 40 0 0 0 2.5 NR 2.5
Adams [50] 2013 37 2.7 0 5.4 NR NR NR
Zhang [53] 2013 75 0 0 4 NR NR 1.3†††
Panicucci [54] 2014 54** NR NR NR NR NR 7.4
Borie [55] 2014 25 0 0 NR NR 12‡‡ NR
Leardi [58] 2014 51 0 0 2 NR NR 0
(b) PPH03
Arroyo [18] 2007 20 0 0 5 0 NR 0
Arroyo [22] 2008 67‡‡‡ 0 0 5.7 0.9 NR 5.8
Jiang [45] 2012 43 0 0 NR 2 NR NR
Gentile [57] 2014 30 NR NR NR NR 16.6 NR
(c) Contour Transtar
Lenisa [3] 2009 75 0 0 NR 0 NR 13
Isbert [27] 2010 82 0 0 0 3 NR 4.8
Martellucci [35] 2011 133 0 0.8 NR 1.5 NR 6.8
Boccasanta [37] 2011 50 0 0 0 0 0 14
Renzi [41] 2011 31 NR NR NR NR 0 9.6
Naldini [43] 2011 15 NR NR NR NR NR 13
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 59
M. Mercer-Jones et al. Rectal excision for constipation

10 Rectovaginal fistula is a very rare longer term
complication, occurring in about one in about one
in every one thousand six hundred patients (level
II).
11 There was insufficient evidence to establish whether
specific post-operative or longer term complications
varied between procedures (level IV).
12 In all studies where mortality was recorded, there
were no deaths in a total of 5896 patients studied
(level II).
Efficacy
Measurement of clinical outcome was consistently
recorded in many studies using a variety of the available
subjective summative scoring instruments for constipa-
tion symptoms (Table 6). These included the Cleveland
Clinic Constipation Score (21 studies), obstructed defe-
cation syndrome (ODS) score (30 studies), Symptom
Severity Score (SSS) (eight studies).
The Longo scoring system for ODS was reported for
56% of cohorts. Reduction in ODS occurred in 72.2%
of patients (95% CI: 68.5–75.8%), I2 = 83% (Fig. 7).
There was considerable heterogeneity between findings,
which varied from 53–91% and may reflect multiple
causes. Although findings are imprecise, there was no
robust evidence that one procedure produced greater
score reductions than another. Improvement in consti-
pation was reported in all studies where it was recorded.
In many publications regarding surgical treatment of
constipation, success has been defined as > 50%
improvement in objective scores. A total of 18/21 stud-
ies reported > 50% improvement in CCS; all studies
(30/30) reported > 50% improvement in ODS; 5/8
studies reported > 50% improvement in SSS. Significant
improvement in ODS was seen in both arms of the two
RCTs (IB) comparing STARR (PPH01) and Contour
Transtar [37,41] and in the other level IB RCT com-
paring STARR with PPH01 and mucosectomy (with
PPH01) together with levatoroplasty [15]. Whilst this
Table 4 (Continued).
Author Year N Stenosis
Recto
vaginal
fistula
Recurrent
Prolapse
Pain/
proctalgia > 6
months Dyspareunia
Urgency
after 12
months
Savastano [44] 2012 32 0 0 NR 0 0 3.2
Masoni [51] 2013 187 0 0.5 NR NR NR 0
Bock [52] 2013 70 0 NR 8.6 NR NR 0
Ribaric [56] 2014 100 0 0 NR 1 NR 3
(d) Intra-anal Delorme’s procedure
Liberman [14] 2000 34 3 0 3 0 NR NR
Pescatori §§§ [17] 2006 26 7.5 0 35 2.5 NR NR
Ganio [49] 2013 167 ¶¶¶ 1.8 0 5.4 2.4 NR NR
Gentile [57] 2014 36 NR NR NR NR 11.1 NR
NR, not recorded.
All PPH03, except Jiang [45] translinear stapler.
*Report on 123 patients, but only 85 operated on.
†Report on 2838 patients for complications, 2224 reached 12 months follow-up.
‡101 patients had Countour Transtar.
§208 patients had Contour Transtar
¶Some patients had Contour Transtar
**18 patients had Contour Transtar.
††Complications are reported for 104 patients (67 had PPH03).
‡‡Not stated if de novo.
§§This reflects numbers with score of > 1 in Symptom Severity score, 5.5% had score > 3, and 8% of patients observed a reduction
in urgency compared with pre-op.¶¶Table refers to this incidence at 3 years, however text reports that all urgency resolved in all but one patient.
***Authors report that 74% of patients had pre-op urgency.
†††Uncertain if this is de novo.
‡‡‡Complications are reported for 104 patients (37 had PPH01).
§§§These percentages are based upon analysis of 40 patients (14 patients having had PPH01 or PPH01 with manual mucosec-
tomy).
¶¶¶91 patients also had levatoroplasty.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7260
Rectal excision for constipation M. Mercer-Jones et al.

improvement was maintained at three years, without
difference between procedures in one trial [37], in the
other at 24 months the improvement was maintained in
the Contour Transtar group but not in the STARR
group and there was a significant difference in scores
between the two groups [41]. In the other two RCTs
of lesser quality (IIB), STARR (PPH01) was shown to
be significantly better for functional outcome compared
with biofeedback (although there was > 50% attrition
rate in the biofeedback group) [21], and STARR
(PPH01) was shown to give similar functional results
compared with Intra-anal Delorme’s with levatoroplasty
[57]. In other non-randomised (level IIB) comparisons
of STARR (PPH01) vs Contour Transtar [8,27,43]
there was no difference in functional outcome. One
prospective cohort study (level IIB) compared PPH01
with PPH03 [18] and showed no difference in func-
tional outcome, and a further compared STARR with
macrogol therapy [8]. There was no difference in out-
come when looking at response rates, however it was
unclear if groups were matched and no report on differ-
ent laxative use was included in inclusion criteria. One
would normally assume that macrogol or other medical
management would have been tried before selecting a
patient for a rectal excisional procedure.
The effect of time post-procedure and efficacy was
examined in the four level I/IIB studies with a follow-
up of > 30 months [8,37,53,57]. Three studies showed
greater than 75% reduction in subjective scores
[8,37,57] and the other greater than 50% reduction,
regardless of the procedure provided.
Global ‘success’ or ‘satisfaction’ ratings (GSR) were
obtained via a variety of methods in 28 of 55 cohorts
(Table 5), where ‘satisfied’ or ‘very satisfied’, ‘good’,
‘very good’ and ‘excellent’ were interpreted as positive
outcomes. Further studies also reported individual
symptoms. No study reported acquiring data objectively
using personnel not involved in the surgical care of the
patient or data collection blind to intervention status.
Most reports assert that the majority of patients
Figure 6 Forest plot showing rates ofrectal urgency after 12 months by
operation type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 61
M. Mercer-Jones et al. Rectal excision for constipation
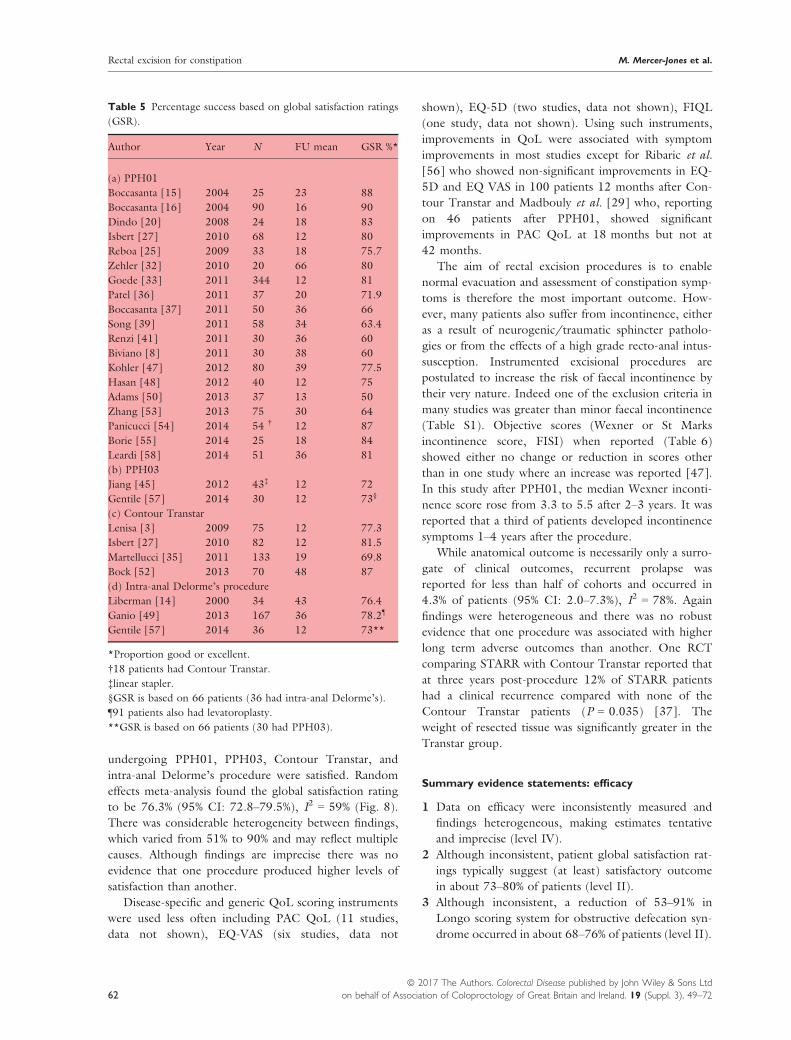
undergoing PPH01, PPH03, Contour Transtar, and
intra-anal Delorme’s procedure were satisfied. Random
effects meta-analysis found the global satisfaction rating
to be 76.3% (95% CI: 72.8–79.5%), I2 = 59% (Fig. 8).
There was considerable heterogeneity between findings,
which varied from 51% to 90% and may reflect multiple
causes. Although findings are imprecise there was no
evidence that one procedure produced higher levels of
satisfaction than another.
Disease-specific and generic QoL scoring instruments
were used less often including PAC QoL (11 studies,
data not shown), EQ-VAS (six studies, data not
shown), EQ-5D (two studies, data not shown), FIQL
(one study, data not shown). Using such instruments,
improvements in QoL were associated with symptom
improvements in most studies except for Ribaric et al.
[56] who showed non-significant improvements in EQ-
5D and EQ VAS in 100 patients 12 months after Con-
tour Transtar and Madbouly et al. [29] who, reporting
on 46 patients after PPH01, showed significant
improvements in PAC QoL at 18 months but not at
42 months.
The aim of rectal excision procedures is to enable
normal evacuation and assessment of constipation symp-
toms is therefore the most important outcome. How-
ever, many patients also suffer from incontinence, either
as a result of neurogenic/traumatic sphincter patholo-
gies or from the effects of a high grade recto-anal intus-
susception. Instrumented excisional procedures are
postulated to increase the risk of faecal incontinence by
their very nature. Indeed one of the exclusion criteria in
many studies was greater than minor faecal incontinence
(Table S1). Objective scores (Wexner or St Marks
incontinence score, FISI) when reported (Table 6)
showed either no change or reduction in scores other
than in one study where an increase was reported [47].
In this study after PPH01, the median Wexner inconti-
nence score rose from 3.3 to 5.5 after 2–3 years. It was
reported that a third of patients developed incontinence
symptoms 1–4 years after the procedure.
While anatomical outcome is necessarily only a surro-
gate of clinical outcomes, recurrent prolapse was
reported for less than half of cohorts and occurred in
4.3% of patients (95% CI: 2.0–7.3%), I2 = 78%. Again
findings were heterogeneous and there was no robust
evidence that one procedure was associated with higher
long term adverse outcomes than another. One RCT
comparing STARR with Contour Transtar reported that
at three years post-procedure 12% of STARR patients
had a clinical recurrence compared with none of the
Contour Transtar patients (P = 0.035) [37]. The
weight of resected tissue was significantly greater in the
Transtar group.
Summary evidence statements: efficacy
1 Data on efficacy were inconsistently measured and
findings heterogeneous, making estimates tentative
and imprecise (level IV).
2 Although inconsistent, patient global satisfaction rat-
ings typically suggest (at least) satisfactory outcome
in about 73–80% of patients (level II).
3 Although inconsistent, a reduction of 53–91% in
Longo scoring system for obstructive defecation syn-
drome occurred in about 68–76% of patients (level II).
Table 5 Percentage success based on global satisfaction ratings
(GSR).
Author Year N FU mean GSR %*
(a) PPH01
Boccasanta [15] 2004 25 23 88
Boccasanta [16] 2004 90 16 90
Dindo [20] 2008 24 18 83
Isbert [27] 2010 68 12 80
Reboa [25] 2009 33 18 75.7
Zehler [32] 2010 20 66 80
Goede [33] 2011 344 12 81
Patel [36] 2011 37 20 71.9
Boccasanta [37] 2011 50 36 66
Song [39] 2011 58 34 63.4
Renzi [41] 2011 30 36 60
Biviano [8] 2011 30 38 60
Kohler [47] 2012 80 39 77.5
Hasan [48] 2012 40 12 75
Adams [50] 2013 37 13 50
Zhang [53] 2013 75 30 64
Panicucci [54] 2014 54 † 12 87
Borie [55] 2014 25 18 84
Leardi [58] 2014 51 36 81
(b) PPH03
Jiang [45] 2012 43‡ 12 72
Gentile [57] 2014 30 12 73§
(c) Contour Transtar
Lenisa [3] 2009 75 12 77.3
Isbert [27] 2010 82 12 81.5
Martellucci [35] 2011 133 19 69.8
Bock [52] 2013 70 48 87
(d) Intra-anal Delorme’s procedure
Liberman [14] 2000 34 43 76.4
Ganio [49] 2013 167 36 78.2¶
Gentile [57] 2014 36 12 73**
*Proportion good or excellent.
†18 patients had Contour Transtar.
‡linear stapler.
§GSR is based on 66 patients (36 had intra-anal Delorme’s).
¶91 patients also had levatoroplasty.
**GSR is based on 66 patients (30 had PPH03).
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7262
Rectal excision for constipation M. Mercer-Jones et al.

Table 6 Functional outcomes by procedure.
Author Year N FU‡‡
% reduction
in CCS
% reduction
in Longo/
ODS score
% reduction
in SSS score
Any significant
increase or
decrease in
FI scores
(a) PPH01
Boccasanta [15] 2004 25 23 68.6 \ \ N
Boccasanta [16] 2004 90 16 65.3 \ \ N
Arroyo [18] 2007 17 24 \ \ 68 \
Gagliardi [19] 2008 85 * 17 \ \ \ \
Dindo [20] 2008 24 18 54.5 \ \ \
Lehur [21] 2008 119 12 \ 71 \ \
Arroyo [22] 2008 37†† 26 62.3 \ \ \
Boccasanta [26] 2010 74 24 \ 88.4 \ \
Harris [23] 2009 36 12 \ 88 \ \
Isbert [27] 2010 68 12 46.8 65.5 \ N
Jayne [24] 2009 2224† 12 \ 67.3 76.1 Decrease
Reboa [25] 2009 33 18 72.4 \ \ \
Zhang [28] 2010 50 12 63.5 66.3 70.3 \
Madbouly [29] 2010 46 42 \ 75.3 \ \
Schwandner [30] 2010 379 12 \ \ 49.4 N
Ram [31] 2010 30 26 \ \ \ \
Zehler [32] 2010 20 66 \ 65 40 Decrease
Goede [33] 2011 344 12 \ 89 \ Decrease
Meurette [34] 2011 30 48 \ 58.6 \ N
Patel [36] 2011 37 20 \ 58.6 \ \
Boccasanta [37] 2011 50 20 \ 83 \ N
Stuto [38] 2011 2171§ 12 \ 70 \ Decrease
Song [39] 2011 58 34 58.5 \ \ \
Ding [40] 2011 86 12 \ 60.5 \ N
Renzi [41] 2011 30 36 \ 59.6 \ \
Reibetanz [42] 2011 170‡ 18 47 \ \ \
Naldini [43] 2011 15 24 \ 73.4 \ \
Biviano [8] 2011 30 38 76.1 \ \ \
Savastano [44] 2012 32 27 \ 87 \ \
Boenicke [46] 2012 181¶ 19 58.9 \ \ N
Kohler [47] 2012 80 39 54.8 \ \ Increase
Hasan [48] 2012 40 12 83.8 \ \ \
Adams [50] 2013 37 13 \ \ \ \
Zhang [53] 2013 75 30 54.6 53.5 \ N
Panicucci [54] 2014 54 ** 12 68.5 74.4 \ \
Borie [55] 2014 25 18 \ 59 \ \
Leardi [58] 2014 51 36 \ 76 \ Decrease
(b) PPH03
Arroyo [18] 2007 20 24 \ \ 68 \
Arroyo [22] 2008 67R 26 62.3 \ \ \
Jiang [45] 2012 43 12 62.9 \ \ \
Gentile [57] 2014 30 12 \ \ \ \
(c) Contour Transtar
Lenisa [3] 2009 75 12 \ 83 50.2 N
Isbert [27] 2010 82 12 50 68 \ N
Martellucci [35] 2011 133 19 48 \ \ \
Boccasanta [37] 2011 50 36 \ 85 \ N
Renzi [41] 2011 31 24 \ 64.5 \ \
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 63
M. Mercer-Jones et al. Rectal excision for constipation
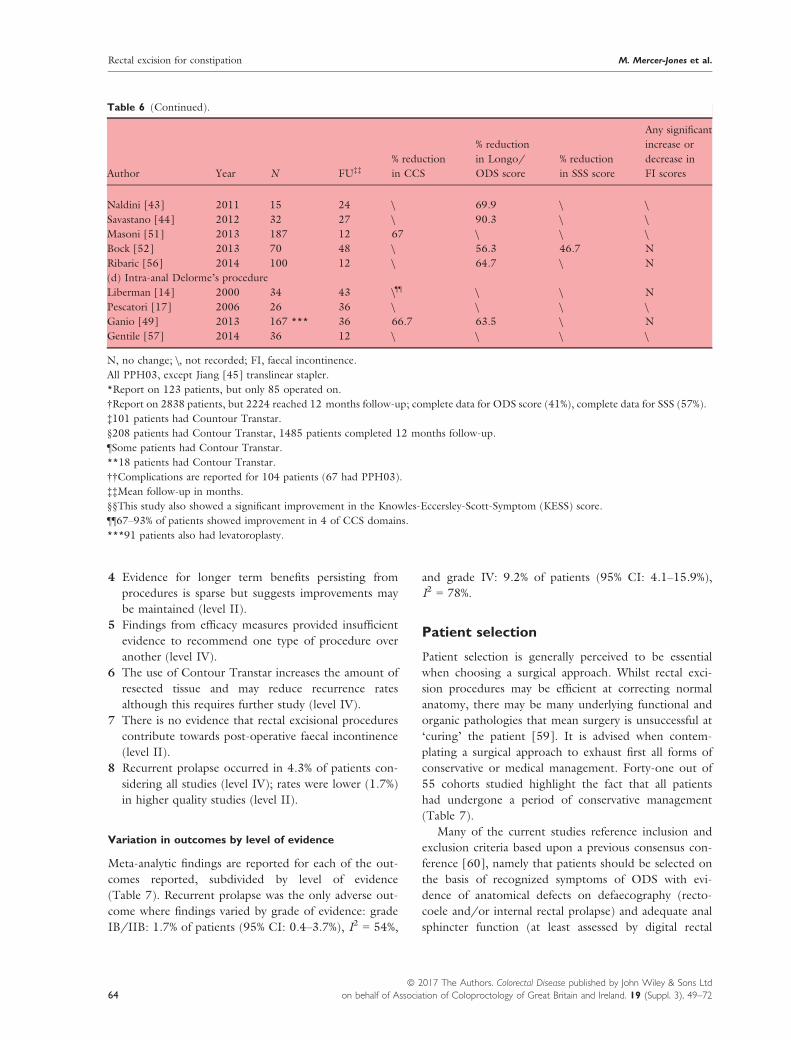
4 Evidence for longer term benefits persisting from
procedures is sparse but suggests improvements may
be maintained (level II).
5 Findings from efficacy measures provided insufficient
evidence to recommend one type of procedure over
another (level IV).
6 The use of Contour Transtar increases the amount of
resected tissue and may reduce recurrence rates
although this requires further study (level IV).
7 There is no evidence that rectal excisional procedures
contribute towards post-operative faecal incontinence
(level II).
8 Recurrent prolapse occurred in 4.3% of patients con-
sidering all studies (level IV); rates were lower (1.7%)
in higher quality studies (level II).
Variation in outcomes by level of evidence
Meta-analytic findings are reported for each of the out-
comes reported, subdivided by level of evidence
(Table 7). Recurrent prolapse was the only adverse out-
come where findings varied by grade of evidence: grade
IB/IIB: 1.7% of patients (95% CI: 0.4–3.7%), I2 = 54%,
and grade IV: 9.2% of patients (95% CI: 4.1–15.9%),I2 = 78%.
Patient selection
Patient selection is generally perceived to be essential
when choosing a surgical approach. Whilst rectal exci-
sion procedures may be efficient at correcting normal
anatomy, there may be many underlying functional and
organic pathologies that mean surgery is unsuccessful at
‘curing’ the patient [59]. It is advised when contem-
plating a surgical approach to exhaust first all forms of
conservative or medical management. Forty-one out of
55 cohorts studied highlight the fact that all patients
had undergone a period of conservative management
(Table 7).
Many of the current studies reference inclusion and
exclusion criteria based upon a previous consensus con-
ference [60], namely that patients should be selected on
the basis of recognized symptoms of ODS with evi-
dence of anatomical defects on defaecography (recto-
coele and/or internal rectal prolapse) and adequate anal
sphincter function (at least assessed by digital rectal
Table 6 (Continued).
Author Year N FU‡‡
% reduction
in CCS
% reduction
in Longo/
ODS score
% reduction
in SSS score
Any significant
increase or
decrease in
FI scores
Naldini [43] 2011 15 24 \ 69.9 \ \
Savastano [44] 2012 32 27 \ 90.3 \ \
Masoni [51] 2013 187 12 67 \ \ \
Bock [52] 2013 70 48 \ 56.3 46.7 N
Ribaric [56] 2014 100 12 \ 64.7 \ N
(d) Intra-anal Delorme’s procedure
Liberman [14] 2000 34 43 \¶¶ \ \ N
Pescatori [17] 2006 26 36 \ \ \ \
Ganio [49] 2013 167 *** 36 66.7 63.5 \ N
Gentile [57] 2014 36 12 \ \ \ \
N, no change; \, not recorded; FI, faecal incontinence.
All PPH03, except Jiang [45] translinear stapler.
*Report on 123 patients, but only 85 operated on.
†Report on 2838 patients, but 2224 reached 12 months follow-up; complete data for ODS score (41%), complete data for SSS (57%).
‡101 patients had Countour Transtar.
§208 patients had Contour Transtar, 1485 patients completed 12 months follow-up.
¶Some patients had Contour Transtar.
**18 patients had Contour Transtar.
††Complications are reported for 104 patients (67 had PPH03).
‡‡Mean follow-up in months.
§§This study also showed a significant improvement in the Knowles-Eccersley-Scott-Symptom (KESS) score.
¶¶67–93% of patients showed improvement in 4 of CCS domains.
***91 patients also had levatoroplasty.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7264
Rectal excision for constipation M. Mercer-Jones et al.

examination). In 42 out of the 55 cohorts studied,
patients had at least 3 ODS symptoms (Table 8). In
general when selecting patients for functional surgery it
has also been advised to select patients with a high
symptom load [61]. A criticism made to the authors of
the European STARR Registry (n = 2224) was that the
median ODS score was low (15.7 out of a possible 40)
and that the range was high (1–31) [24]. The two level
I RCTs reported inclusion criteria of an ODS score
> 12 in one [41] and 15 in the other [37]. The major-
ity of studies reported an inclusion criterion of rectal
intussusception and/or rectocoele, (38 out of 55 study
groups). Thirty-two out of the 55 study groups
reported a rectocoele > 2 cm, and in 26 of these, more
than 75% of patients had a rectocele > 2 cm. Thirty-
seven out of the 55 study groups reported on recto-rec-
tal or recto-anal intussusception, and in 28 of these
more than 60% of patients had an intussusception. Mul-
tiple classifications were used for diagnosing an intussus-
ception including Pescatori [62], Shorvon [63], and
Oxford [64]. Other studies stated that inclusion
required a rectal intussusception greater than 10 mm
[41] or recto-anal intussusception > 10 mm [31]. One
study reported on outcome at five years following
PPH01 for patients with a symptomatic rectocoele
when the authors specifically excluded intussusception
[32]. This study found an 80% satisfaction rate at one
year, which remained at five years. It was not possible
to draw conclusions regarding efficacy according to
either the presence of an intussusception (whichever
grade/stage) or rectocoele size.
It is pertinent to discuss exclusion criteria as this may
influence the surgeon in their choice of procedure (rein-
forcement/suspension/excision). Reference was again
made in many studies to the consensus statement [60]
and a decision making algorithm for STARR [65] when
defining exclusion criteria. Specifically, external rectal
prolapse, solitary rectal ulcer syndrome (SRUS),
anatomical enterocele, and ‘significant gynaecological
pelvic floor abnormality requiring treatment’ were
Figure 7 Forest plot showing reduction
in Longo’s obstructed defacation
syndrome (ODS) score by operation
type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 65
M. Mercer-Jones et al. Rectal excision for constipation

stated as exclusions. Less than 50% of the reviewed
studies excluded external rectal prolapse or other pelvic
organ prolapse, and no study excluded SRUS
(Table S1). Only one study graded pelvic organ pro-
lapse (rectocoele, cystocoele, vault, uterine) with a stan-
dardized grading system e.g. POP-Q (data not shown)
[26]. Whilst it is sensible to exclude patients with exter-
nal rectal prolapse, no conclusion can be made regard-
ing excluding patients with SRUS, or concomitant
pelvic organ prolapse.
Anatomical enterocoele is generally regarded as a
contraindication to an anterior rectal wall excision
[60,65], however many studies did not exclude this
(Table S1). Irrespective of this, there were no cases of
iatrogenic small bowel injury reported. One study
examined the outcome with respect to harms in
patients with a functional enterocoele, and those with-
out [42]. All patients had either PPH01 or Contour
Transtar and outcomes with respect to harms were
similar.
Summary evidence statements: patient selection
1 Patient selection, although perceived as vital in pre-
dicting outcome, is inconsistently documented and
poorly informed by current evidence (level IV).
2 Patients with at least three ODS symptoms together
with a rectocoele with or without an intussusception,
who have failed conservative management may bene-
fit from a rectal excisional procedure (level II).
3 It is not possible to advise on excluding patients with
concomitant pelvic organ prolapse or SRUS when
considering a rectal excisional procedure (level IV).
Conclusions
A systematic review of evidence for the perioperative
and long term benefits and harms of rectal excisional
procedures identified a modest number of high quality
studies together with a larger number of observational
lesser quality studies. Whilst the evidence is superior to
the level of evidence for other procedures for
Figure 8 Forest plot showing global
satisfaction rating (%) by operation type.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7266
Rectal excision for constipation M. Mercer-Jones et al.

constipation it is still rather poor in the field of medi-
cine systematic reviews. Notwithstanding this, certain
conclusions can be drawn:
1 In the presence of a rectocoele with or without an
intussusception, together with at least three symp-
toms of ODS, a rectal excisional procedure may ben-
efit the patient after all conservative measures have
been exhausted.
2 Reliance on proving efficacy using GSR and unvali-
dated scoring systems (Longo) is not satisfactory and
greater emphasis should be placed in future studies
on the use of disease-specific and generic QoL scor-
ing instruments.
3 It is not possible to advise which excisional technique
is superior from the point of view of efficacy, peri-
operative variables, or harms (peri-operative or long
term adverse outcomes). Future study is required.
4 Both short- and long-term harms may have been
exaggerated in previous reports. Rectal excisional
procedures appear to be safe with little major mor-
bidity. Rectal urgency appears to be a problem, but
findings are inconsistent because of poor reporting.
5 Despite evidence of mixed grade (IB, IIB and IV)
being available for rectal excision procedures, there
was little evidence that outcomes varied by grade of
evidence. Recurrent prolapse was the only adverse
outcome where findings varied by grade of evidence
and thus may be a chance finding in the absence of
any systematic pattern across outcomes.
Acknowledgements
We would like to acknowledge the following people in
relation to the NIHR CapaCiTY working group: Mr
Steven Brown, Sheffield Teaching Hospitals NHS
Foundation Trust; Mr Kenneth Campbell, The Univer-
sity of Dundee, NHS Education for Scotland; Mr Mark
Chapman, Heart of England NHS Trust; Mr Andrew
Clarke, Poole Hospital NHS Foundation Trust; Mr Neil
Cruickshank, Sandwell and West Birmingham Hospitals
NHS Trust; Mr Anthony Dixon, University of Bristol,
Bristol, UK; Dr Christopher Emmett, County Durham
and Darlington NHS Foundation Trust; Mr Ugo
Grossi, Queen Mary University of London; Dr Richard
Hooper, PCTU, Queen Mary University of London;
Miss Emma Horrocks, University Hospital Southamp-
ton NHS Foundation Trust; Professor Charles Knowles,
Queen Mary University of London; Mr Jon Lacy-Col-
son, Shrewsbury and Telford Hospital NHS Trust; Mr
Ian Lindsey, Oxford University Hospitals NHS Trust;
Professor James Mason, University of Warwick, Coven-
try; Mr Mark Mercer-Jones, Gateshead Health NHS
Foundation Trust; Mr Andrew Miller, University
Hospitals of Leicester NHS Trust; Mr David Pares,
Hospital Germans Trias i Pujol, Barcelona, Spain; Miss
Sophie Pilkington, University Hospital Southampton
NHS Foundation Trust; Mr Neil Smart, Royal Devon
& Exeter NHS Foundation Trust; Ms Natasha Stevens,
PCTU, Queen Mary University of London; Professor
Table 7 Outcomes by level of evidence.
IB/IIB IV Combined
IB/IIB
vs IV
Effect size (95%CI), I2 Effect size (95%CI), I2 Effect size (95%CI), I2 p
Perioperative data
Procedure duration (mins) 44.3 (39.9–48.7), 99.2% 44.4 (35.4–53.5), 99.5% 44.3 (40.5–48.1), 99.5% 0.98
Length of stay (days) 2.8 (2.5–3.2), 98.1% 3.6 (2.5–4.7), 98.7% 3.0 (2.6–3.4), 98.8% 0.18
Total complication rate (%) 13.5% (8.3–19.6%), 94.0% 22.0% (15.9–28.7%), 85.5% 16.9% (12.7–21.5%), 92.6% 0.052
Perioperative harm
Bleeding rate (%) 1.5% (0.7–2.4%), 52.7% 2.2% (0.6–4.3%), 72.4% 1.6% (0.9–2.5%), 63.0% 0.56
Sepsis rate (%) 0.0% (0.0–0.5%), 67.1% 0.8% (0.0–2.2%), 48.8% 0.2% (0.0–0.7%), 62.6% 0.090
Anastomotic
dehiscence rate (%)
0.2% (0.0–0.9%), 67.3% 0.2% (0.0–0.9%), 11.2% 0.3% (0.0–0.8%), 61.6% 0.98
Long term adverse outcomes
Rectal stenosis (%) 0.1% (0.0–0.5%), 24.4% 0.4% (0.0–1.2%), 36.4% 0.2% (0.0–0.6%), 30.3% 0.52
Rectal pain (%) 0.6% (0.0–1.9%), 83.6% 0.8% (0.1–1.8%), 0.0% 0.7% (0.1–1.6%), 78.7% 0.76
Rectal urgency (%) 5.6% (2.7–9.3%), 90.7% 4.2% (0.9–9.2%), 89.1% 5.2% (2.7–8.2%), 91.8% 0.51
Rectal prolapse (%) 1.7% (0.4–3.7%), 53.9% 9.2% (4.1–15.9%), 82.0% 4.3% (2.0–7.3%), 78.7% 0.006
Efficacy
Global satisfaction
rating (%)
76.4% (71.3–81.1%), 59.0% 76.0% (71.1–80.7%), 62.4% 76.3% (72.8–79.5%), 59.0% 0.94
Longo ODS (%) 71.9% (68.5–75.1%), 70.7% 71.3% (58.0–83.0%), 90.9% 72.2% (68.5–75.8%), 83.2% 0.93
M. Mercer-Jones et al. Rectal excision for constipation
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 67

Table 8 Inclusion criteria for procedures.
Author Year N
Rectocele
> 2 cm %
Recto-rectal /
Recto-anal
Intussusception %
Rectocele +
Intussusception %
Failure of
conservative RX
At least 3
ODS symptoms
(a) PPH01
Boccasanta [15] 2004 25 100 100 100 Yes Yes
Boccasanta [16] 2004 90 97 100 97 Yes Yes
Arroyo [18] 2007 17 92 27 NR Yes Yes
Gagliardi [19] 2008 85* 80 93 73 Yes Yes
Dindo [20] 2008 24 79 83 NR Yes Yes
Lehur [21] 2008 119 92 61 NR No Yes
Arroyo [22] 2008 37†† NR NR NR Yes Yes
Boccasanta [26] 2010 74 100 100 100 Yes Yes
Harris [23] 2009 36 81 39 39 No Yes
Isbert [27] 2010 68 100 80 80 Yes Yes
Jayne [24] 2009 2224† 99 80 NR Yes Yes
Reboa [25] 2009 33 67 97 NR Yes Yes
Zhang [28] 2010 50 NR NR NR No No
Madbouly [29] 2010 46 59 41 NR Yes Yes
Schwandner [30] 2010 379 NR NR NR No Yes
Ram [31] 2010 30 67 13 67 No Yes
Zehler [32] 2010 20 100 0 0 Yes Yes
Goede [33] 2011 344 NR 100 NR No Yes
Meurette [34] 2011 30 100 100 100 Yes No
Patel [36] 2011 37 100 81 81 Yes Yes
Boccasanta [37] 2011 50 100 100 100 No Yes
Stuto [38] 2011 2171§ 82 95 NR No Yes
Song [39] 2011 58 62 80 NR Yes Yes
Ding [40] 2011 86 90 94 77 Yes Yes
Renzi [41] 2011 30 NR NR NR Yes Yes
Reibetanz [42] 2011 170‡ NR NR NR No No
Naldini [43] 2011 15 NR NR NR Yes Yes
Biviano [8] 2011 30 77 50 NR Yes Yes
Savastano [44] 2012 32 NR NR NR No No
Boenicke [46] 2012 181¶ NR NR 100 Yes Yes
Kohler [47] 2012 80 100 100 NR No Yes
Hasan [48] 2012 40 90 55 NR Yes Yes
Adams [50] 2013 37 NR NR NR Yes Yes
Zhang [53] 2013 75 NR 87 NR Yes No
Panicucci [54] 2014 54 ** NR NR NR Yes Yes
Borie [55] 2014 25 100 65 65 Yes Yes
Leardi [58] 2014 51 43 57 0 Yes No
(b) PPH03
Arroyo [18] 2007 20 92 27 NR Yes Yes
Arroyo [22] 2008 67§§ NR NR NR Yes Yes
Jiang [45] 2012 43 100 56 56 Yes Yes
Gentile [57] 2014 30 NR NR NR Yes No
(c) Contour Transtar
Lenisa [3] 2009 75 NR NR NR Yes Yes
Isbert [27] 2010 82 100 65 65 Yes Yes
Martellucci [35] 2011 133 NR NR NR Yes Yes
Boccasanta [37] 2011 50 100 100 100 No Yes
Renzi [41] 2011 31 NR NR NR Yes Yes
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7268
Rectal excision for constipation M. Mercer-Jones et al.

Douglas Tincello, University Hospitals of Leicester
NHS Trust; Miss Karen Telford, South Manchester
NHS Foundation Trust; Mr Paul Vollebregt, Queen
Mary University of London; Mr Andrew Williams,
Guy’s and Thomas’ NHS Foundation Trust; Professor
Yan Yiannakou, County Durham and Darlington NHS
Foundation Trust.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opin-
ions expressed in this report are those of the authors
and are not those of the PGfAR Programme, NIHR,
the UK National Health Service, or the UK Depart-
ment of Health.
Conflicts of interest
M Mercer-Jones has no conflict of interest in relation
to the content of the manuscript. In the last 2 years
he has received fees as a preceptor for Medtronic Inc.
C.H.Knowles has no conflict of interest in relation to
the content of the manuscript. In the last 2 years he
has recieved speaker fees and consultancy payments
from Medtronic Inc. remaining authors no conflict.
References
1 D’Hoore A, Penninckx F. Obstructed defecation. Colorectal
Dis 2003; 5: 280–7.
2 Longo A. Treatment of hemorrhoids disease by reduction
of mucosa and hemorrhoidal prolapse with a circular sutur-
ing device: a new procedure. 6th World Congress of Endo-
scopic Surgery, Pts 1 and 2. 1998. Pp. 777–84.
3 Lenisa L, Schwandner O, Stuto A et al. STARR with Con-
tour Transtar: prospective multicentre European study.
Colorectal Dis 2009; 11: 821–7.
4 Delorme R. Sur le traitment des prolapses du rectum
totaux pour l’excision de la muscueuse rectale ou rectocol-
ique. Bull Mem Soc Chir Paris 1900; 26: 499–518.
5 Dippolito A, Esser S, Reed J 3rd. Anterior modification of
Delorme procedure provides equivalent results to Delorme
procedure in treatment of rectal outlet obstruction. Curr
Surg 2005; 62: 609–12.
6 Gladman MA, Scott SM, Lunniss PJ, Williams NS. System-
atic review of surgical options for idiopathic megarectum
and megacolon. Ann Surg 2005; 241: 562–74.
7 Van Geluwe B, Stuto A, Da Pozzo F et al. Relief of
obstructed defecation syndrome after Stapled Transanal
Rectal Resection (STARR): a meta-analysis. Acta Chir Belg
2014; 114: 189–97.
Table 8 (Continued).
Author Year N
Rectocele
> 2 cm %
Recto-rectal /
Recto-anal
Intussusception %
Rectocele +
Intussusception %
Failure of
conservative RX
At least 3
ODS symptoms
Naldini [43] 2011 15 NR NR NR Yes Yes
Savastano [44] 2012 32 NR NR NR No No
Masoni [51] 2013 187 84 97 NR Yes Yes
Bock [52] 2013 70 NR NR NR Yes No
Ribaric [56] 2014 100 80 73 NR Yes No
(d) Intra-anal Delorme’s procedure
Liberman [14] 2000 34 NR 100 70.6 Yes Yes
Pescatori [17] 2006 26 NR 100 37.5*** No No
Ganio [49] 2013 167 NR 77.2 66.5 Yes No
Gentile [57] 2014 36 NR NR NR Yes No
NR, not recorded.
All PPH03, except Jiang [45] translinear stapler.
*Report on 123 patients, but only 85 operated on.
†Report on 2838 patients for complications, 2224 reached 12 months follow-up.
‡101 patients had Countour Transtar.
§208 patients had Contour Transtar.
¶Some patients had Contour Transtar.
**18 patients had Contour Transtar.
††Inclusions are reported for 104 patients (67 had PPH03).
§§Reported for 104 patients (37 had PPH01).
***Based on total number of 40 cases.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 69
M. Mercer-Jones et al. Rectal excision for constipation

8 Biviano I, Badiali D, Candeloro L et al. Comparative out-
come of stapled trans-anal rectal resection and macrogol in
the treatment of defecation disorders. World J Gastroenterol
2011; 17: 4199–205.
9 Hirst GR, Hughes RJ, Morgan AR, Carr ND, Patel B,
Beynon J. The role of rectocele repair in targeted patients
with obstructed defaecation. Colorectal Dis 2005; 7: 159–
63.
10 Portier G, Ghouti L, Kirzin S, Chauffour M, Lazorthes F.
Malone antegrade colonic irrigation: ileal neoappendicos-
tomy is the preferred procedure in adults. Int J Colorectal
Dis 2006; 21: 458–60.
11 Sabbagh R, Mandron E, Piussan J, Brychaert PE, le Tu M.
Long-term anatomical and functional results of laparo-
scopic promontofixation for pelvic organ prolapse. BJU Int
2010; 106: 861–6.
12 Johnson E, Carlsen E, Mjaland O, Drolsum A. Resection
rectopexy for internal rectal intussusception reduces consti-
pation and incomplete evacuation of stool. Eur J Surg
2003; 588: 51–6.
13 Evans C, Ong E, Jones OM, Cunningham C, Lindsey I.
Laparoscopic ventral rectopexy is effective for solitary rectal
ulcer syndrome when associated with rectal prolapse.
Colorectal Dis 2014; 16: O112–6.
14 Liberman H, Hughes C, Dippolito A. Evaluation and out-
come of the delorme procedure in the treatment of rectal
outlet obstruction. Dis Colon Rectum 2000; 43: 188–92.
15 Boccasanta P, Venturi M, Salamina G, Cesana BM, Ber-
nasconi F, Roviaro G. New trends in the surgical treatment
of outlet obstruction: clinical and functional results of two
novel transanal stapled techniques from a randomised con-
trolled trial. Int J Colorectal Dis 2004; 19: 359–69.
16 Boccasanta P, Venturi M, Stuto A et al. Stapled transanal
rectal resection for outlet obstruction: a prospective, multi-
center trial - The authors reply. Dis Colon Rectum 2004;
47: 1296–7.
17 Pescatori M, Boffi F, Russo A, Zbar AP. Complications
and recurrence after excision of rectal internal mucosal pro-
lapse for obstructed defaecation. Int J Colorectal Dis 2006;
21: 160–5.
18 Arroyo A, Perez-Vicente F, Serrano P et al. Evaluation of
the stapled transanal rectal resection technique with two
staplers in the treatment of obstructive defecation syn-
drome. J Am Coll Surg 2007; 204: 56–63.
19 Gagliardi G, Pescatori M, Altomare DF et al. Results, out-
come predictors, and complications after stapled transanal
rectal resection for obstructed defecation. Dis Colon Rec-
tum 2008; 51: 186–95.
20 Dindo D, Weishaupt D, Lehmann K, Hetzer FH, Clavien
PA, Hahnloser D. Clinical and morphologic correlation
after stapled transanal rectal resection for obstructed defe-
cation syndrome. Dis Colon Rectum 2008; 51: 1768–74.
21 Lehur PA, Stuto A, Fantoli M et al. Outcomes of stapled
transanal rectal resection vs. biofeedback for the treatment
of outlet obstruction associated with rectal intussusception
and rectocele: a multicenter, randomized, controlled trial.
Dis Colon Rectum 2008; 51: 1611–8.
22 Arroyo A, Gonzalez-Argente FX, Garcia-Domingo M et al.
Prospective multicentre clinical trial of stapled transanal
rectal resection for obstructive defaecation syndrome. Br J
Surg 2008; 95: 1521–7.
23 Harris MA, Ferrara A, Gallagher J, DeJesus S, Williamson
P, Larach S. Stapled transanal rectal resection vs. transvagi-
nal rectocele repair for treatment of obstructive defecation
syndrome. Dis Colon Rectum 2009; 52: 592–7.
24 Jayne DG, Schwandner O, Stuto A. Stapled transanal rectal
resection for obstructed defecation syndrome: one-year
results of the European STARR Registry REPLY. Dis Colon
Rectum 2009; 52: 1213–4.
25 Reboa G, Gipponi M, Logorio M, Marino P, Lantieri F.
The impact of stapled transanal rectal resection on anorec-
tal function in patients with obstructed defecation syn-
drome. Dis Colon Rectum 2009; 52: 1598–604.
26 Boccasanta P, Venturi M, Spennacchio M, Buonaguidi A,
Airoldi A, Roviaro G. Prospective clinical and functional
results of combined rectal and urogynecologic surgery in
complex pelvic floor disorders. Am J Surg 2010; 199:
144–53.
27 Isbert C, Reibetanz J, Jayne DG, Kim M, Germer CT,
Boenicke L. Comparative study of contour transtar and
STARR procedure for the treatment of obstructed defeca-
tion syndrome (ODS) – feasibility, morbidity and early
functional results. Colorectal Dis 2010; 12: 901–8.
28 Zhang B, Ding JH, Yin SH, Zhang M, Zhao K. Stapled
transanal rectal resection for obstructed defecation syn-
drome associated with rectocele and rectal intussusception.
World J Gastroenterol 2010; 16: 2542–8.
29 Madbouly KM, Abbas KS, Hussein AM. Disappointing
long-term outcomes after stapled transanal rectal resection
for obstructed defecation. World J Surg 2010; 34: 2191–
6.
30 Schwandner O, Furst A, Grp GSRS. Assessing the safety,
effectiveness, and quality of life after the STARR procedure
for obstructed defecation: results of the German STARR
registry. Langenbecks Arch Surg 2010; 395: 505–13.
31 Ram E, Alper D, Atar E, Tsitman I, Dreznik Z. Stapled
transanal rectal resection: a new surgical treatment for
obstructed defecation syndrome. Isr Med Assoc J 2010; 12:
74–7.
32 Zehler O, Vashist YK, Bogoevski D et al. Quo vadis
STARR? A prospective long-term follow-up of stapled
transanal rectal resection for obstructed defecation syn-
drome. J Gastrointest Surg 2010; 14: 1349–54.
33 Goede AC, Glancy D, Carter H, Mills A, Mabey K, Dixon
AR. Medium-term results of stapled transanal rectal resec-
tion (STARR) for obstructed defecation and symptomatic
rectal-anal intussusception. Colorectal Dis 2011; 13: 1052–
7.
34 Meurette G, Wong M, Frampas E, Regenet N, Lehur PA.
Anatomical and functional results after stapled transanal
rectal resection (STARR) for obstructed defaecation syn-
drome. Colorectal Dis 2011; 13: e6–11.
35 Martellucci J, Talento P, Carriero A. Early complications
after stapled transanal rectal resection performed using the
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7270
Rectal excision for constipation M. Mercer-Jones et al.
Contour(R) Transtar device. Colorectal Dis 2011; 13:
1428–31.
36 Patel CB, Ragupathi M, Bhoot NH, Pickron TB, Haas
EM. Patient satisfaction and symptomatic outcomes follow-
ing stapled transanal rectal resection for obstructed defeca-
tion syndrome. J Surg Res 2011; 165: e15–21.
37 Boccasanta P, Venturi M, Roviaro G. What Is the Benefit
of a New Stapler Device in the Surgical Treatment of
Obstructed Defecation? Three-Year Outcomes from a Ran-
domized Controlled Trial. Dis Colon Rectum 2011; 54:
77–84.
38 Stuto A, Renzi A, Carriero A et al. Stapled trans-anal rectal
resection (STARR) in the surgical treatment of the
obstructed defecation syndrome: results of STARR Italian
Registry. Surg Innov 2011; 18: 248–53.
39 Song KH, Lee DS, Shin JK et al. Clinical outcomes of sta-
pled transanal rectal resection (STARR) for obstructed
defecation syndrome (ODS): a single institution experience
in South Korea. Int J Colorectal Dis 2011; 26: 693–8.
40 Ding JH, Zhang B, Bi LX, Yin SH, Zhao K. Functional
and morphologic outcome after stapled transanal rectal
resection for obstructed defecation syndrome. Dis Colon
Rectum 2011; 54: 418–24.
41 Renzi A, Brillantino A, Di Sarno G, Izzo D, D’Aniello F,
Falato A. Improved clinical outcomes with a new contour-
curved stapler in the surgical treatment of obstructed defe-
cation syndrome: a mid-term randomized controlled trial.
Dis Colon Rectum 2011; 54: 736–42.
42 Reibetanz J, Boenicke L, Kim M, Germer CT, Isbert C.
Enterocele is not a contraindication to stapled transanal
surgery for outlet obstruction: an analysis of 170 patients.
Colorectal Dis 2011; 13: E131–6.
43 Naldini G, Cerullo G, Menconi C et al. Resected specimen
evaluation, anorectal manometry, endoanal ultrasonography
and clinical follow-up after STARR procedures. World J
Gastroenterol 2011; 17: 2411–6.
44 Savastano S, Valenti G, Cavallin F, Missaglia C. STARR
with PPH-01 and CCS30 contour Transtar for obstructed
defecation syndrome. Surg Innov 2012; 19: 171–4.
45 Jiang C, Ding Z, Wang M et al. A transanal procedure
using an endoscopic linear stapler for obstructed defecation
syndrome: the first Chinese experience. Tech Coloproctol
2012; 16: 21–7.
46 Boenicke L, Reibetanz J, Kim M, Schlegel N, Germer CT,
Isbert C. Predictive factors for postoperative constipation
and continence after stapled transanal rectal resection. Br J
Surg 2012; 99: 416–22.
47 Kohler K, Stelzner S, Hellmich G et al. Results in the
long-term course after stapled transanal rectal resection
(STARR). Langenbecks Arch Surg 2012; 397: 771–8.
48 Hasan HM, Hasan HM. Stapled transanal rectal resection
for the surgical treatment of obstructed defecation syn-
drome associated with rectocele and rectal intussusception.
ISRN Surg 2012; 2012: 652345.
49 Ganio E, Martina S, Novelli E et al. Internal Delorme’s
procedure for rectal outlet obstruction. Colorectal Dis
2013; 15: e144–50.
50 Adams K, Papagrigoriadis S. Stapled transanal rectal resec-
tion (STARR) for obstructive defaecation syndrome:
patients with previous pelvic floor surgery have poorer
long-term outcome. Colorectal Dis 2013; 15: 477–80.
51 Masoni L, Mari FS, Favi F et al. Stapled transanal rectal
resection with contour transtar for obstructed defecation
syndrome: lessons learned after more than 3 years of sin-
gle-center activity. Dis Colon Rectum 2013; 56: 113–9.
52 Bock S, Wolff K, Marti L, Schmied BM, Hetzer FH.
Long-term outcome after transanal rectal resection in
patients with obstructed defecation syndrome. Dis Colon
Rectum 2013; 56: 246–52.
53 Zhang B, Ding JH, Zhao YJ et al. Midterm outcome of
stapled transanal rectal resection for obstructed defecation
syndrome: a single-institution experience in China. World J
Gastroenterol 2013; 19: 6472–8.
54 Panicucci S, Martellucci J, Menconi C, Toniolo G, Naldini
G. Correlation between outcome and instrumental findings
after stapled transanal rectal resection for obstructed defe-
cation syndrome. Surg Innov 2014; 21: 469–75.
55 Borie F, Bigourdan JM, Pissas MH, Guillon F. Laparo-
scopic ventral rectopexy for the treatment of outlet
obstruction associated with recto-anal intussusception and
rectocele: a valid alternative to STARR procedure in
patients with anal sphincter weakness. Clin Res Hepatol
Gastroenterol 2014; 38: 528–34.
56 Ribaric G, D’Hoore A, Schiffhorst G, Hempel E, Grp
TRS. STARR with CONTOURA (R) TRANSTAR (TM)
device for obstructed defecation syndrome: one-year real-
world outcomes of the European TRANSTAR registry. Int
J Colorectal Dis 2014; 29: 611–22.
57 Gentile M, De Rosa M, Cestaro G, Vitiello C, Sivero L.
Internal Delorme vs. STARR procedure for correction of
obstructed defecation from rectocele and rectal intussuscep-
tion. Ann Ital Chir 2014; 85: 177–83.
58 Leardi S, De Santis G, Lancione L, Sista F, Schietroma M,
Pietroletti R. Quality of life after treatment of rectal intus-
susception or rectocele by means of STARR. Ann Ital Chir
2014; 85: 347–51.
59 Pescatori M, Spyrou M, Pulvirenti d’Urso A. A prospec-
tive evaluation of occult disorders in obstructed defecation
using the ‘iceberg diagram’. Colorectal Dis 2006; 8: 785–
9.
60 Corman ML, Carriero A, Hager T et al. Consensus confer-
ence on the stapled transanal rectal resection (STARR) for
disordered defaecation. Colorectal Dis 2006; 8: 98–101.
61 Mercer-Jones MA, D’Hoore A, Dixon AR et al. Consensus
on ventral rectopexy: report of a panel of experts. Colorec-
tal Dis 2014; 16: 82–8.
62 Pescatori M, Quondamcarlo C. A new grading of rectal
internal mucosal prolapse and its correlation with diagnosis
and treatment. Int J Colorectal Dis 1999; 14: 245–9.
63 Shorvon PJ, McHugh S, Diamant NE, Somers S, Steven-
son GW. Defecography in normal volunteers: results and
implications. Gut 1989; 30: 1737–49.
64 Collinson R, Cunningham C, D’Costa H, Lindsey I. Rectal
intussusception and unexplained faecal incontinence:
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–72 71
M. Mercer-Jones et al. Rectal excision for constipation

findings of a proctographic study. Colorectal Dis 2009; 11:
77–83.
65 Schwandner O, Stuto A, Jayne D et al. Decision-making
algorithm for the STARR procedure in obstructed defeca-
tion syndrome: position statement of the group of STARR
Pioneers. Surg Innov 2008; 15: 105–9.
Supporting Information
Additional Supporting Information may be found in the
online version of this article:
Figure S1. Forest plot showing rates of sepsis by opera-
tion type.
Figure S2. Forest plot showing rates of anastomotic
dehiscence by operation type.
Table S1. Exclusion tables. (a) PPH-01; (b) PPH03;
(c) Contour Transtar; (d) Intra-anal.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 49–7272
Rectal excision for constipation M. Mercer-Jones et al.

Surgery for constipation: systematic review and practicerecommendations
Results IV: Recto-vaginal reinforcement procedures
U. Grossi*, E. J. Horrocks*, J. Mason†, C. H. Knowles*, A. B. Williams‡, on behalf of the NIHR
CapaCiTY working group§ and The Pelvic floor Society¶*National Bowel Research Centre, Blizard Institute, Queen Mary University of London, London, UK, †Health Economics, University of Warwick,
Coventry, UK, ‡Guy’s and St Thomas’ NHS Foundation Trust, London, UK, §National Institute for Health Research: Chronic Constipation Treatment
Pathway, London, UK, and ¶Affiliate section of the Association of Coloproctology of Great Britain and Ireland, London, UK
Abstract
Aim To assess the outcomes of recto-vaginal reinforce-
ment procedures in adults with chronic constipation.
Method Standardised methods and reporting of bene-
fits and harms were used for all CapaCiTY reviews that
closely adhered to PRISMA 2016 guidance. Main con-
clusions were presented as summary evidence statements
with a summative Oxford Centre for Evidence-Based
Medicine (2009) level.
Results Forty-three articles were identified, providing
data on outcomes in 3346 patients. Average length of
procedures ranged between 20 and 169 min, and
length of stay between 1 and 15 days. Complications
typically occurred after 7–17% of procedures (range 0–61%). Post-operative bleeding was uncommon (0–4%)as well as haematoma or sepsis (0–2%). Fistulation did
not occur in most studies. Two procedure-related
deaths were observed for 3209 patients. Although
inconsistent, 78% of patients reported a satisfactory or
good outcome, with 30–50% experiencing reduced
symptoms of straining, incomplete emptying or reduced
vaginal digitation. About 17% of patients developed
anatomical recurrence. Considering measures of harm
and global satisfaction rating scales, there was insuffi-
cient evidence to prefer one type of procedure over
another. There was no evidence to support better out-
comes based on selection of patients with a particular
size or grade of rectocoele.
Conclusion Evidence supporting recto-vaginal rein-
forcement procedures is currently derived from observa-
tional studies and comparisons, with only one high
quality study. Large trials are needed to inform future
clinical decision making.
Keywords Recto-vaginal reinforcement, constipation,
rectocele, STARR, transvaginal repair, transanal repair
Introduction
Background and procedural variations
Chronic constipation is related to an inability to evacu-
ate the rectum in over half of all adults presenting for
specialist advice. This phenomenon, which may be vari-
ably described as obstructed defaecation or rectal evacu-
ation disorder (and many other terms), is characterised
by excessive straining, the feeling of incomplete evacua-
tion, post-defaecatory seepage and often mucous dis-
charge, and pelvic pain [1]. In some of these patients
there is clinical and radiological (usually proctographic)
evidence of a dynamic structural abnormality leading to
physical impediment to emptying during defaecation.
By far away, the way most common abnormalities are
rectocoele and/or intussusception.
Traditionally a rectocoele may be considered either a
bulge into the vagina, giving vaginal prolapse symp-
toms, or the sensation of a lump or mass. Also, a herni-
ation of the rectum into the vagina preventing complete
evacuation may lead to ‘trapping’ of faeces in the
‘pocket’ and subsequent incomplete evacuation (bal-
looning may also lead to loss of vector forces along the
anorectal axis). This process can lead to dissatisfaction
with emptying and repeated visits to the toilet, post-
defaecatory soiling and the need to apply pressure to
the posterior vaginal wall or perineum to splint the rec-
tocoele and maximise emptying. Many women will also
‘digitate’ or manually assist emptying using a finger
Correspondence to: Andrew B. Williams, Consultant Colorectal and General
Surgeon, Guy’s and St Thomas’ NHS Foundation Trust, St Thomas’ Hospital,
Westminster Bridge Road London, SE1 7EH UK.
E-mail: [email protected]
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 73
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13781

either in the rectocoele via the anus to aid with com-
plete emptying or in the vagina to splint against the
posterior vagina to prevent trapping and direct evacua-
tory forces down along the axis of the anus.
It follows that strategies have been employed to
anatomically correct a rectocele by reinforcing the barrier
between the rectum and vagina (rectovaginal septum).
Access for rectovaginal reinforcement varies with three
main approaches described: the posterior vagina (poste-
rior repair [2]), the perineum (transperineal repair [3]),
or via the anus (transanal repair [4,5]). Vaginal repairs all
involve an incision in the posterior wall either longitudi-
nally to open the entire length of the rectocoele or trans-
versely to produce a broad based flap and expose the
entirety of the rectocoele, or a combination of the two
incisions in the shape of an inverted ‘T’. In most repairs
the redundant rectal wall is plicated outside the bowel
wall. The vaginal wall is then reconstructed with resec-
tion of any excess vaginal mucosa. Many repairs include
some degree of approximation of the levator ani and pel-
vic side wall muscles to formally reinforce the reconstruc-
tion of the rectovaginal septum, although with the
reputed higher risk of dyspareunia. More recently
attempts have been made to localise specific defects in
the rectovaginal septum. This has led to ‘site specific’
repairs [6,7], where the individual defects are repaired
before the vaginal wall is closed. All of these types of
repairs may be augmented by mesh reinforcement, usu-
ally using one of a variety of collagen meshes.
The rectovaginal septum may be entered through a
transperineal route. A transverse or curved incision is
made in the perineal body towards the vagina and the dis-
section extended anterior to the sphincter complex to gain
access to the rectovaginal septum. Having gained expo-
sure, a repair is made in the same way as in a transvaginal
approach. The potential advantage to this route is that it
may be combined with a sphincteroplasty in those women
with a deficient sphincter and a concurrent rectocoele.
Finally, a rectocoele can be considered as a redundant
pocket of rectum, rather than a weakness in the rectovagi-
nal septum leading to herniation of the rectum. A transa-
nal repair addresses the rectal redundancy with either an
anterior Delorme’s style repair (Sarle’s repair [5]) or with
a sutured pexy of the anterior rectal wall (Block repair
[4]). In the former repair, the mucosa is dissected free
from the rectal muscle and excised. Following this, the
rectal muscle coat is plicated longitudinally to obliterate
the rectocoele pocket and the mucosa is re-approximated
to close the defect. In the Block repair, full thickness lon-
gitudinal sutures are placed anteriorly to draw together
the redundant anterior rectal pocket and close the recto-
coele. It is evident that these procedures necessitate a
degree of rectal wall excision or suspension respectively.
Scope
The overall purpose of the CapaCiTY review series is to
assess the efficacy and harms of procedures for chronic
constipation in adults. The focus is therefore directed to
a population presenting with symptoms of obstructed
defecation, rather than women with only prolapse, uri-
nary symptoms or both (see overview and methods
paper). One group of procedures considered beyond
the scope of this systematic review included those where
excision is effected without reinforcement, e.g. rectal
excision only, such as stapled transanal resection of the
rectum (STARR). As is noted above, anterior Delorme’s
or Sarle’s procedures are included, which include a
degree of resection, but also have an significant element
of reinforcement with muscle wall plication (targeted at
the rectovaginal plane), which is not present in pure
resection. This noted, a small number of studies have
specifically focused stapled resection to the obliteration
of a rectocele by anterior deployment of a stapler to
exact mucosal excision (much like stapled haemor-
rhoidopexy). In a sense, these reinforce the RV septum
by tightening tissue and have been included for comple-
tion in this review. Further, most compare this
approach with one of the other approaches also covered
in this review. The separate review covering rectal exci-
sion includes numerous studies of STARR in which the
device is used to excise circumferential full-thickness
excision and the reviews overlap in only one study [8].
Circumferential Delorme’s procedures are excluded
from this review as their focus is not on reinforcement
of the rectovaginal septum but rather on general resec-
tion for prolapse (covered in rectal suspension review).
Studies where outcomes could not be segregated by eli-
gible procedure were also excluded, due to a mixed
patient population with internal and external rectal pro-
lapse, mixed indications including numerous pelvic floor
abnormalities or limited postoperative outcomes.
Previous reviews
There have been no systematic reviews of the results of
rectocoele repair for the treatment of obstructed defae-
cation or constipation. There has been a systematic
Cochrane review (with updates) on the surgical man-
agement of pelvic organ prolapse in women [9–13],which includes review of posterior vaginal repair for rec-
tocoele. This review included seven randomised trials
on women with posterior vaginal wall prolapse [3,14–19], three trials comparing vaginal and transanal
approaches [3,14,18]. In addition, another trial pro-
vided data for women with rectocele undergoing poste-
rior repair with and without absorbable mesh [16].
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9174
Recto-vaginal reinforcement for constipation U. Grossi et al.

There has been one systematic review of the use of bio-
logics in urogynaecological repairs [20]. In addition,
the International Continence Society, 5th International
Consultation on Incontinence, Paris, February 2012,
pages 1411–1414 [21], covers posterior repair. Neither
this, nor the Cochrane process focussed on the specific
management of patients with constipation.
Summary of search results and study quality
The search yielded a total of 72 citations for full text
review (Fig. 1). From these, 44 articles published
between 1990 and 2016 contributed 43 studies to the
systematic review (one cohort was spread across two
publications with a focus on perioperative morbidity
[22] and clinical outcomes [23], respectively). Data on
outcomes were provided for a total of 3346 patients
(study mean: 78, range 13–307) (Table 1). Specific
exclusions after full-text review (and after exclusion of
five non-English language publications) included: four
studies where the population sample was confirmed to
be <20 patients; eight studies where follow up was less
than 12 months; two studies of out of scope proce-
dures; four studies where data were considered as dupli-
cate; three studies where outcomes could not be
segregated by eligible procedure; and two studies with
no relevant outcome data.
The quality of studies varied. The 43 included stud-
ies included three randomised controlled trials (RCTs)
and 40 observational studies. The former included one
good quality RCT (level IB) with a low level of suscep-
tibility to bias and two with less well described method-
ology (level IIB). The 40 observational studies included
eight good quality cohort studies with low susceptibility
to bias (level IIB). Other studies were a mix of prospec-
tive and retrospective case series. Mean study follow-up
was 2.1 years (range 0.7–6.2 years); 19 studies origi-
nated from European centres, 12 from the USA and 12
from other countries. The studies covered the full spec-
trum of types of repair and are shown in Fig. 2.
Results
Perioperative data
The 43 studies included 62 patient cohorts receiving one
of eight procedures (Table 2). Perioperative data were
reported inconsistently by studies, with 24 (39%) cohorts
reporting average procedural duration and 29 (47%)
reporting average length of stay (Tables 2 and 3). There
was considerable variation in these measures when com-
paring procedures: design heterogeneity, small numbers
of studies and large range of values precludes any clear
pattern. The overall average duration of procedures was
67 (range 20–169) minutes, and the overall average
length of stay was 3.9 (range 1–15) days.
Summary evidence statements: perioperative data
• The average duration of procedures was about one
hour, although this is inconsistently reported and ran-
ged widely between studies from 20 to 169 min
(level IV).
• The average length of stay was about 4 days although
this is inconsistently reported and ranged widely
between studies from 1 to 15 days (level IV).
• There was inadequate evidence to determine varia-
tions in procedural duration or length of stay by type
of procedure (level IV).
Figure 1 PRISMA diagram of searchresults.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 75
U. Grossi et al. Recto-vaginal reinforcement for constipation
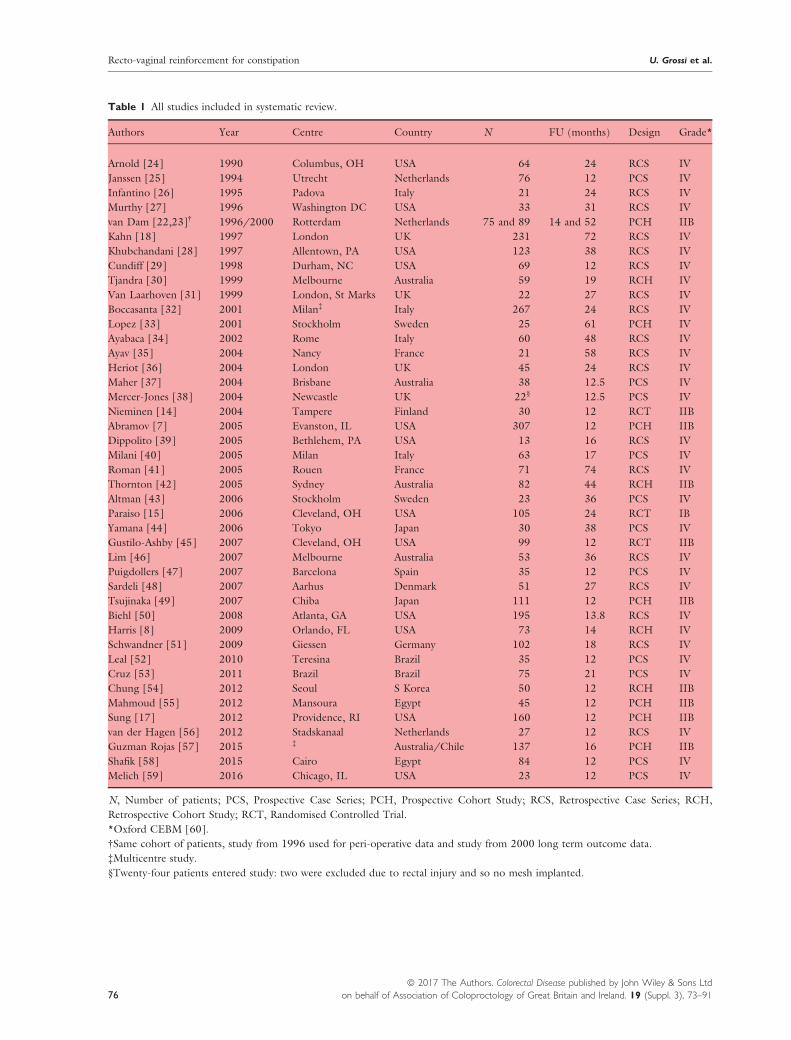
Table 1 All studies included in systematic review.
Authors Year Centre Country N FU (months) Design Grade*
Arnold [24] 1990 Columbus, OH USA 64 24 RCS IV
Janssen [25] 1994 Utrecht Netherlands 76 12 PCS IV
Infantino [26] 1995 Padova Italy 21 24 RCS IV
Murthy [27] 1996 Washington DC USA 33 31 RCS IV
van Dam [22,23]† 1996/2000 Rotterdam Netherlands 75 and 89 14 and 52 PCH IIB
Kahn [18] 1997 London UK 231 72 RCS IV
Khubchandani [28] 1997 Allentown, PA USA 123 38 RCS IV
Cundiff [29] 1998 Durham, NC USA 69 12 RCS IV
Tjandra [30] 1999 Melbourne Australia 59 19 RCH IV
Van Laarhoven [31] 1999 London, St Marks UK 22 27 RCS IV
Boccasanta [32] 2001 Milan‡ Italy 267 24 RCS IV
Lopez [33] 2001 Stockholm Sweden 25 61 PCH IV
Ayabaca [34] 2002 Rome Italy 60 48 RCS IV
Ayav [35] 2004 Nancy France 21 58 RCS IV
Heriot [36] 2004 London UK 45 24 RCS IV
Maher [37] 2004 Brisbane Australia 38 12.5 PCS IV
Mercer-Jones [38] 2004 Newcastle UK 22§ 12.5 PCS IV
Nieminen [14] 2004 Tampere Finland 30 12 RCT IIB
Abramov [7] 2005 Evanston, IL USA 307 12 PCH IIB
Dippolito [39] 2005 Bethlehem, PA USA 13 16 RCS IV
Milani [40] 2005 Milan Italy 63 17 PCS IV
Roman [41] 2005 Rouen France 71 74 RCS IV
Thornton [42] 2005 Sydney Australia 82 44 RCH IIB
Altman [43] 2006 Stockholm Sweden 23 36 PCS IV
Paraiso [15] 2006 Cleveland, OH USA 105 24 RCT IB
Yamana [44] 2006 Tokyo Japan 30 38 PCS IV
Gustilo-Ashby [45] 2007 Cleveland, OH USA 99 12 RCT IIB
Lim [46] 2007 Melbourne Australia 53 36 RCS IV
Puigdollers [47] 2007 Barcelona Spain 35 12 PCS IV
Sardeli [48] 2007 Aarhus Denmark 51 27 RCS IV
Tsujinaka [49] 2007 Chiba Japan 111 12 PCH IIB
Biehl [50] 2008 Atlanta, GA USA 195 13.8 RCS IV
Harris [8] 2009 Orlando, FL USA 73 14 RCH IV
Schwandner [51] 2009 Giessen Germany 102 18 RCS IV
Leal [52] 2010 Teresina Brazil 35 12 PCS IV
Cruz [53] 2011 Brazil Brazil 75 21 PCS IV
Chung [54] 2012 Seoul S Korea 50 12 RCH IIB
Mahmoud [55] 2012 Mansoura Egypt 45 12 PCH IIB
Sung [17] 2012 Providence, RI USA 160 12 PCH IIB
van der Hagen [56] 2012 Stadskanaal Netherlands 27 12 RCS IV
Guzman Rojas [57] 2015 ‡ Australia/Chile 137 16 PCH IIB
Shafik [58] 2015 Cairo Egypt 84 12 PCS IV
Melich [59] 2016 Chicago, IL USA 23 12 PCS IV
N, Number of patients; PCS, Prospective Case Series; PCH, Prospective Cohort Study; RCS, Retrospective Case Series; RCH,
Retrospective Cohort Study; RCT, Randomised Controlled Trial.
*Oxford CEBM [60].
†Same cohort of patients, study from 1996 used for peri-operative data and study from 2000 long term outcome data.
‡Multicentre study.
§Twenty-four patients entered study: two were excluded due to rectal injury and so no mesh implanted.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9176
Recto-vaginal reinforcement for constipation U. Grossi et al.

Harms
Perioperative complicationsFour measures of harm were reported by a majority of
studies within the review: overall complications, bleed-
ing, fistulation and haematoma/sepsis. There was con-
siderable heterogeneity in surgical morbidity, reported
as overall procedural complication rates; with individual
study rates varying from 0% to 61% (see Table 2). This
heterogeneity may have reflected (for example) differ-
ing inclusion, procedural content, context of care, or
thresholds or conventions for recording complications.
Random effects meta-analysis found the overall compli-
cation rate to be 11.5% (95% CI: 7.2–16.6%),I2 = 87% (Fig. 3). Overall complication rates varied
within and between procedures without evidence to
favour one or more procedures. Although variable, the
bleeding complication rate was generally low being
reported as zero in 50% of cohorts of procedures. Ran-
dom effects meta-analysis found the pooled bleed rate
to be 2.0% (95% CI: 0.7–3.6%), I2 = 68%. The
reported fistulation rate was consistently low (0% in
80% of cohorts). Random effects meta-analysis found
the fistulation rate to be 0.0% (95% CI: 0.0–0.1%),I2 = 0%. The rate of haematoma or sepsis varied
between studies but was generally low (0% in 56% of
cohorts). Random effects meta-analysis found the
pooled rate of haematoma or sepsis to be 0.9% (95%
CI: 0.2–2.0%), I2 = 54% (Fig. 4). Although there was
some evidence of variation by procedure, sub-group
findings are based on selective reporting of relatively
few and small studies and should be viewed with cau-
tion.
Other measures of short term harm were less consis-
tently reported: perioperative pain (37% of cohorts),
urine retention (6%) and UTIs (10%).
Long term adverse outcomesMeasures of long term harm were poorly reported:
urgency (19%) and anal stenosis (13%). Although 37
cohorts (60%) made some assessment of dyspareunia,
these assessments were not made in an adequately com-
parable fashion. Wide variations between studies may
reflect inconsistency in the studies when reporting
improvement, deterioration or de novo dyspareunia. Rates
of mesh erosion were as high as 30% but were only
reported in two studies [40,46]. This adverse outcome is
devastating for the female sufferer and is rightly receiving
extensive media coverage, focus by some regulatory bod-
ies (e.g. Scottish Government) and much interest by sur-
geons themselves. It is thus unfortunate that in the
narrowly defined context of this systematic review, evi-
dence regarding this outcome was of poor quality.
Summary evidence statements: harms
• Evidence is drawn from observational studies and
comparisons. Most comparisons featured considerable
heterogeneity, which may have multiple causes (level
IV).
• Overall procedural complication rates ranged from 0%
to 61%. However, these complications typically
occurred in about 7–17% of procedures (level IV).
• Post-operative bleeding rates were low, typically rang-
ing from 0% to 4% (level IV).
• Fistulation was a very rare complication, not occur-
ring at all in most studies (level IV).
• Mesh erosion was a common complication, but only
reported in two studies (level IV).
• The occurrence of haematoma or sepsis was typically
low at around 0–2% (level IV).
• Considering measures of harm, there was insufficient
evidence to prefer one type of procedure over another
(level IV).
• Long term adverse outcomes were poorly reported
(level IV).
• Dyspareunia was reported too inconsistently to make
meaningful comparisons between procedures,
although it may be central to patient decision making
(level IV).
• Only two procedure-related deaths were reported for
3209 patients included in studies (level IV).
Efficacy
Most studies used ad hoc questionnaire assessment of
symptoms (n = 27) to assess efficacy; other tools used
included Cleveland Clinic Constipation score (n = 2),
Wexner constipation score (n = 3), obstructed defaeca-
tion score (n = 4) with single studies using the follow-
ing: PAC QOL; Short Form-36 (SF-36); St Mark’s
Figure 2 Venn diagram showing the distribution of studies
between different types of repair. KEY: Box denotes number of
studies in each category. *includes only one Level IB RCT
[15].
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 77
U. Grossi et al. Recto-vaginal reinforcement for constipation

Table
2Perioperativedatabyprocedure.
Author
Year
N
Len
gth
of
procedure*
Len
gth
ofstay
†TotalCx
rate
Bleed
ing
Fistulation
Pain
Haematoma/
Sepsis
Urgen
cy
Anal
sten
osis
Urine
retention
UTI
Dyspareu
nia
(new
)Other
(a)Transvaginalrepa
ir:standard
Arnold
[24]
1990
29
NR
5.6
(3–1
4)
34
00
17
3NR
NR
NR
NR
23
NR
Infantino[26]
1995
8NR
NR
12.5
00
012.5
NR
NR
NR
NR
NR
NR
Kahn[18]
1997
231
NR
NR
NR
NR
NR
22
NR
13
NR
NR
NR
9NR
Cundiff[29]
1998
69
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
�10
NR
Lopez
[33]
2001
25
NR
6.3
(3–1
6)
28
00
020
0NR
4%
4%
13§
NR
Maher
[37]
2004
38
52(10–1
25)
4.3
(3–1
0)
7.9
00
02.6
0NR
NR
2.6%
�32
2.6%inadverten
t
proctotomy
Nieminen
[14]
2004
15
35(20–5
0)
NR
00
00
00
NR
NR
NR
0NR
Abramov[7]
2005
183
NR
NR
5.4
30
NR
0NR
NR
NR
NR
33
NR
Paraiso
[15]
2006
37
150(SD68)
2(1–1
9)
43.2
50
NR
14
NR
NR
NR
11%
01ileu
s
Yam
ana[44]
2006
30
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
7NR
Gustilo-A
shby
[45]
2007
33
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Tsujinaka[49]
2007
40
63.5
(19–1
23)
15(10–2
2)
NR
50
17.5
0NR
NR
NR
NR
NR
NR
Harris[8]
2009
37
85.5
318.9
2.7
00
5.4
NR
NR
NR
NR
12
NR
Schwandner
[51]
2009
102
36.5
(29–6
7)
4.1
(2–7
)11
20
NR
2NR
NR
NR
2%
NR
NR
Chung[54]
2012
24
74
212.5
00
00
0NR
NR
NR
8NR
Sung[17]
2012
81
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Shafik[58]
2015
84
45(35–5
5)
4.2
(3.1–5
.6)
NR
01.2
00
8.3
NR
NR
NR
2.4
6%constipation
(b)Transvaginalrepa
ir:site-specific
Abramov[7]
2005
124
NR
NR
6.4
30
NR
0NR
NR
NR
NR
33
0%
Paraiso
[15]
2006
37
151(69)
2(1–7
)30
00
NR
0NR
NR
NR
NR
0
Gustilo-A
shby
[45]
2007
37
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Sardeli[48]
2007
51
32.5
(15–9
0)
2.1
(1–1
4)
24
12
2NR
4NR
NR
NR
NR
4Urinary
incontinen
ce2%
Guzm
anRojas[57]
2015
137
NR
NR
00
0NR
0NR
NR
NR
NR
15
NR
(c)Transanalrepa
ir:blocksuturedrepa
ir
Arnold
[24]
1990
35
NR
5.6
(3–1
4)
34
00
17
3NR
NR
NR
NR
21
NR
Infantino[26]
1995
13
NR
NR
00
00
0NR
NR
NR
NR
NR
0
Van
Laarhoven
[31]
1999
7NR
NR
14
4.5
NR
NR
NR
NR
NR
NR
NR
NR
NR
Boccasanta
[32]
2001
44
79.6
4.5
1.5
25
5NR
0NR
NR
NR
NR
00
Tsujinaka[49]
2007
71
30.5
(16–9
7)
9(6–1
7)
NR
5.6
011
0NR
NR
NR
NR
0NR
(d)Transanalrepa
ir:stapled
transanalresection
Boccasanta
[32]
2001
15
79.6
4.5
1.5
00
00
NR
7NR
NR
0NR
Ayav[35]
2004
21
NA
3.3
(2–5
)0
00
00
00
NR
NR
�4.7
NR
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9178
Recto-vaginal reinforcement for constipation U. Grossi et al.

Table
2(C
ontinued
).
Author
Year
N
Len
gth
of
procedure*
Len
gth
ofstay
†TotalCx
rate
Bleed
ing
Fistulation
Pain
Haematoma/
Sepsis
Urgen
cy
Anal
sten
osis
Urine
retention
UTI
Dyspareu
nia
(new
)Other
Harris[8]
2009
36
52.7
2.6
61
19
02.7
0NR
NR
NR
NR
10.5
NR
Leal[52]
2010
35
45(33–7
0)
114
23
00
08.5
8.5
NR
NR
NR
NR
Cruz[53]
2011
75
42
113
17
04
0NR
9.3
NR
NR
NR
NR
Mahmoud[55]
2012
22
20(sd5)
2.0
(0.8)
NR
NR
NR
NR
NR
NR
NR
NR
NR
�58
4.4%overall
denovoFI
(e)Transanalrepa
ir:Delorme’sor
Sarle’sStyle
Janssen
[25]
1994
76
NR
NR
2.6
1.3
01.3
0NR
0NR
NR
NR
Murthy[27]
1996
33
NR
3.7
(1–8
)21
NR
3NR
NR
NR
NR
18
NR
NR
NR
Khubchandani[28]
1997
123
NR
NR
NR
NR
1NR
NR
NR
NR
NR
NR
NR
2.8%flap
retraction
Tjandra
[30]
1999
59
NA
NR
3.4
1.7
0NR
0NR
NR
2NR
NR
NR
Boccasanta
[32]
2001
82
79.6
4.5
1.5
81
NR
NR
NR
2.1
3.5
NR
0NR
Ayabaca[34]
2002
13
NR
NR
30
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Nieminen
[14]
2004
15
35(6)
NR
13
00
00
0NR
NR
NR
70
Dippolito
[39]
2005
13
NR
1.9
30
NR
NR
NR
NR
0NR
NR
NR
NR
Minor
complication
Roman
[41]
2005
71
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Thornton[42]
2005
40
NA
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Puigdollers[47]
2007
11
NA
NR
NR
00
NR
NR
NR
NR
NR
NR
NR
NR
Chung[54]
2012
26
61.5
20
00
00
0NR
NR
NR
00
Mahmoud[55]
2012
23
45(6)
4.0
(1.6)
NR
NR
NR
NR
NR
NR
NR
NR
NR
�58
4.4%de
novoFI
(f)Com
bined
transvaginalandtransanalDelormes/Sarlesstyle
vanDam
[22]
1996
75
NR
NR
NR
NR
4NR
5.30
NR
NR
NR
20
NR
NR
(g)Transperinealrepa
ir
Boccasanta
[32]
2001
126
73.4
5.2
00
0NR
NR
NR
NR
NR
NR
17
1Death
Ayabaca[34]
2002
11
NR
NR
30
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
Puigdollers[47]
2007
24
NR
NR
8.3
00
NR
8.3
NR
NR
NR
NR
NR
NR
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 79
U. Grossi et al. Recto-vaginal reinforcement for constipation

Author
Year
N
Len
gth
of
procedure*
Len
gth
of
stay
†Total
Cxrate
Bleed
ing
Fistulation
Pain
Haematoma/
Sepsis
Urgen
cy
Anal
sten
osis
Urine
retention
UTI
Dyspareu
nia
(new
)Other
Repair
type
Mesh
type
(h)Meshrepa
irs
Van Laarhoven
[31]
1999
15
NR
NR
14
4.5
NR
NR
9.1
NR
NR
NR
NR
NR
NR
TP
Syn
thetic
marlex
Mercer-Jones
[38]
2004
24
NR
2(1–6
)14
00
014
0NR
NR
NR
4.5
TP
Syn
thetic
prolene/
Vipro
II
Milani[40]
2005
63
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
18%
19.5%mesh
erosion
TV
Syn
thetic
prolene
Altman
[43]
2006
23
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
VAS‡2
pre
1,6
post
NR
TV
PX
Paraiso
[15]
2006
31
169(62)
2(1–6
)42
30
NR
6NR
NR
NR
19
0NR
TV
PX
Gustilo-
Ashby[45]
2007
29
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
TV
PX
Lim
[46]
2007
53
39
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
26%
19%vaginal
discharge;
30%
mesherosion;
63%atrophic
vaginitis
TV
Syn
thetic
vipro
II
Biehl[50]
2008
95
NR
NR
NR
11
NR
1NR
3–
NR
NR
25
11%incision
deh
iscence
TV
PDX
Biehl[50]
2008
100
NR
NR
NR
10
NR
NR
NR
7.4
–NR
NR
36
5.3
incision
deh
iscence
TV
HDA
Sung[17]
201
79
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NR
NA
NA
TV
PSS
vander
Hagen
[56]
2012
27
56(50–6
8)
3(2–6
)7.4
NR
NR
NR
NR
NR
NR
NR
NR
3.70%
7.4%port
site
infection
TV
Syn
thetic
prolene
Melich[59]
2016
23
NR
NR
40
00
4NR
NR
NR
NR
11%
NR
TV
PDX
strattice
Allratesarepercentages
wherenegativevalues
indicatereductionfrom
preoperativestate;
Cx,
complication;NR,Notrecorded
;TV,transvaginal
repair;
TP,transperinealrepair;
PX,
porcinexenograft;PDX,porcinedermal
xenograft;HAD,human
dermal
allograft;PSS,porcinesub-intestinal
submucosa.
*Meanminutes(range).
†Mean(range)
days.
‡Visual
analoguescore
2pre,1.6
post.
§Twen
ty-seven
percentageat
5yearsfollow
up.
¶Vaginal
sten
osis.
Table
2(C
ontinued
).
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9180
Recto-vaginal reinforcement for constipation U. Grossi et al.

Table 3 Summary of selected data from Table 2.
Procedure
Procedure duration (min) Length of stay (days) Follow-up (months)
N Mean Range N Mean Range N Mean Range
Standard TVR 8 67.6 (35.0–150.0) 9 5.2 (2.0–15.0) 17 22.9 (8.0–72.0)
Site-specific TVR 2 91.8 (32.5–151.0) 2 2.1 (2.0–2.1) 5 18.2 (12.0–27.0)
Block sutured TAR 2 55.1 (30.5–79.6) 3 6.4 (4.5–9.0) 5 22.2 (12.0–27.0)
Delormes/Sarles TAR 3 62.0 (45.0–79.6) 5 3.2 (1.9–4.5) 13 27.2 (12.0–74.0)
Delormes/Sarles TAR + TVR 0 – – – – (0.0–0.0) 1 52.0 –
Stapled transanal resection 5 47.9 (20.0–79.6) 6 2.4 (1.0–4.5) 6 20.4 (8.0–58.0)
Transperineal repair 1 73.4 – 1 5.2 – 3 28.0 (12.0–48.0)
Mesh repair 3 88.0 (39.0–169.0) 3 2.3 (2.0–3.0) 12 19.0 (12.0–36.0)
All procedures 24 66.6 (20.0–169.0) 29 3.9 (1.0–15.0) 62 23.1 (8.0–74.0)
Figure 3 Forest plot showing rates oftotal procedural complications
(percentage of patients) by procedure
type. KEY: TVR, transvaginal repair;TAR, transanal repair; TV, transvaginal;TP, transperineal.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 81
U. Grossi et al. Recto-vaginal reinforcement for constipation

incontinence score; Pelvic Floor Distress Inventory-20
(PFDI-20) questionnaire; Pelvic Floor Impact-7 (PFI-
7) questionnaire; Pelvic Organ Prolapse/Urinary Incon-
tinence Sexual Questionnaire (PISQ-12). Global ‘suc-
cess’ or ‘satisfaction’ ratings (GSR) were obtained via a
variety of methods for 47 of the 62 cohorts (where ‘sat-
isfied’ or ‘very satisfied’, ‘good’, ‘very good’ and ‘excel-
lent’ were interpreted as positive outcomes) (Table 4).
Further, some studies also reported individual symp-
toms. No study reported acquiring data objectively
using personnel not involved in the surgical care of the
patient or data collection blind to intervention status
(RCTs were not observer-blinded).
Data were too inconsistently reported to usefully
analyse efficacy outcomes either in their natural units or
after standardisation. Instead a binary response of global
improvement (yes/no) was derived for each cohort of
patients. Reported in 76% of procedures, random effects
meta-analysis found global improvement to be 72.8%
(95% CI: 66.8–78.3%), I2 = 86% (Fig. 5); again there
was considerable heterogeneity between findings. Given
the crudeness and imprecision of estimates, as well as
small numbers of studies/patients for some procedures,
there is insufficient evidence that particular procedures
provide higher levels of improvement.
For individual symptoms, changes in percentage of
patients experiencing each symptom were not reported
for a majority of studies. Straining was reported for
45% of total procedures; incomplete emptying for 47%;
vaginal digitation for 50%. Other symptoms were less
frequently reported. All symptom measures featured
considerable heterogeneity and selective reporting by
(generally) small studies limiting any comparison
between procedures. These caveats accepted, the overall
Figure 4 Forest plot showing rates ofhaematoma or sepsis (percentage of
patients) by procedure type. KEY: TVR,
transvaginal repair; TAR, transanal repair;
TV, transvaginal; TP, transperineal.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9182
Recto-vaginal reinforcement for constipation U. Grossi et al.

Table 4 Percentage success based on global satisfaction ratings and individual recorded symptoms.
Authors Year N FU
Global %
improved
% Reduction in symptom
Straining
Incomplete
empty
Vaginal
digitation
Anal
digitation
Perineal
digitation
(a) Transvaginal repairs (including site specific repair)
Transvaginal
Arnold [24] 1990 29 24 77 NR NR NR NR NR
Infantino [26] 1995 8 36 75 88 75 75 NR NR
Kahn [18] 1997 231 72 NR �11 �11 67 77 77
Cundiff [29] 1998 69 12 * 30 NR NR NR NR
Lopez [33] 2001 25 61 NR NR 91 48 NR NR
Maher [37] 2004 38 12.5 97 60 NR 84 NR 84
Nieminen [14] 2004 15 12 93 NR NR 66 66 66
Abramov [7] 2005 183 12 NR 18 NR NR NR NR
Paraiso [15] 2006 37 24 74 32 17 24 NR 24
Yamana [44] 2006 30 38 90 90 60 42 NR NR
Gustilo-Ashby [45] 2007 33 12 48 31 28 34 NR 34
Tsujinaka [49] 2007 40 12 80 NR NR 35 NR 35
Harris [8] 2009 37 8 78 † NR NR NR NR
Schwandner [51] 2009 102 18 70 NR 83 67 NR 67
Chung [54] 2012 24 12 75 NR NR NR NR NR
Sung [17] 2012 81 12 NR 9 30 18 NR 18
Shafik [58] 2015 84 12 94 NR NR NR NR NR
Site specific
Abramov [7] 2005 124 12 NR 20 NR NR NR NR
Paraiso [15] 2006 37 24 88 35 18 37 NR 37
Gustilo-Ashby [45] 2007 37 12 50 31 28 34 NR 34
Sardeli [48] 2007 51 27 NR NR 14 NR NR NR
Guzman Rojas [57] 2015 137 16 85 36 NR NR NR NR
(b) Transanal repairs
Block sutured
Arnold [24] 1990 35 NR 83 80 NR NR NR NR
Infantino [26] 1995 13 24 85 92 77 86 NR NR
Van Laarhoven [31] 1999 7 27 43 NR 0 17 NR NR
Boccasanta [32] 2001 44 24 42 NR NR NR NR NR
Tsujinaka [49] 2007 71 12 83 NR NR 34 NR 34
Stapled
Boccasanta [32] 2001 15 11.3 42 NR NR NR NR NR
Ayav [35] 2004 21 58 76 NR 76 67 NR NR
Harris [8] 2009 36 8 83 † NR NR
Leal [52] 2010 35 12 88 ‡ NR NR NR NR
Cruz [53] 2011 75 21 NR NR NR NR NR NR
Mahmoud [55] 2012 22 12 78 51 45 45 NR NR
Delorme’s style
Janssen [25] 1994 76 12 84 56 41 21 NA NA
Murthy [27] 1996 33 31 62 19 19 NR NR NR
Khubchandani [28] 1997 123 38 82 NR NR NR NR NR
Tjandra [30] 1999 59 19 NR NR 78 39 39 NR
Boccasanta [32] 2001 82 24 42 NR NR NR NR NR
Ayabaca [34] 2002 13 48 69 68 NR NR NR NR
Nieminen [14] 2004 15 12 73 NR NR 39 39 39
Dippolito [39] 2005 13 16 92 NR 86 NR NR NR
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 83
U. Grossi et al. Recto-vaginal reinforcement for constipation

pooled finding for reduction in strain was 38.0% (95%
CI: 27.1–49.6%), I2 = 94%; reduction in incomplete
emptying was 44.4% (95% CI: 30.2–58.9%), I2 = 96%;
and reduction in vaginal digitation was 42.7% (95% CI:
34.9–50.6%), I2 = 86%.
The aim of reinforcing the rectovaginal septum is
to restore normal anatomy which theoretically will
enable normal evacuation. Given the underlying aim of
surgery is to correct anatomy, an assessment of
anatomical recurrence is also important (although this
is necessarily only a surrogate of clinical outcome).
Studies variously and inconsistently reported clinical,
radiological and symptom recurrence (Table 5). Clini-
cal recurrence was reported for 44% of cohorts
(Fig. 6). The overall clinical recurrence rate was 17.1%
(95% CI: 11.7–23.3%), I2 = 89%, with individual
findings for procedures varying from 0% to 55%. There
is a suggestion that site specific TVR features a higher
clinical recurrence rate that other procedures, based on
four studies and 349 patients, although this may be a
chance finding given the selective reporting by studies
(Fig. 6). One study showed that the results of a site
specific repair are further compromised by the concur-
rent use of collagen mesh [15].
Summary evidence statements: efficacy
• Data on efficacy were inconsistently measured and
findings heterogeneous, making estimates tentative
and imprecise (level IV).
• Although inconsistent, assessments of patient global
improvement typically suggest a good outcome in
about 67–78% of patients (level IV).
Table 4 (Continued).
Authors Year N FU
Global %
improved
% Reduction in symptom
Straining
Incomplete
empty
Vaginal
digitation
Anal
digitation
Perineal
digitation
Roman [41] 2005 71 74 29.6 NA 50.7 42.30 42.3 NA
Thornton [42] 2005 40 44 28 NR NR NR NR NR
Puigdollers [47] 2007 11 12 66 52 74 52 NR 52
Chung [54] 2012 26 12 77 NR NR NR NR NR
Mahmoud [55] 2012 23 12 78 51 45 45 NR NR
Combined TV and TA
van Dam [22] 2000 89 52 69 NR NR NR NR NR
(c) Transperineal repairs
Boccasanta [32] 2001 50 24 41 NR NR NR NR NR
Ayabaca [34] 2002 11 48 73 NR NR NR NR NR
Puigdollers [47] 2007 24 12 66 52 74 52 NR 52
(d) Mesh repairs
Mesh
Van Laarhoven [31] 1999 15 27 87 NA 67 47 NA NA
Mercer-Jones [38] 2004 22 12.5 55 30 50 23 NA NA
Milani [40] 2005 63 17 NA NA NA NA NA NA
Altman [43] 2006 23 36 NA 16 6 15 �6 NA
Paraiso [15] 2006 31 24 90 27 65 44 NA 44
Gustilo-Ashby [45] 2007 29 12 76 31 28 34 NA 34
Lim [46] 2007 53 36 47 31 NA NA NA NA
Biehl [50] 2008 95 13.8 NA NA NA NA NA NA
Biehl [50] 2008 100 13.8 NA NA NA NA NA NA
Sung [17] 2012 79 12 NA 9.2 30 18 NA 18
van der Hagen [56] 2012 27 12 NA NA NA NA NA NA
Melich [59] 2016 23 12 NA NA NA NA NA NA
Negative values indicate increase in symptoms.
*Global improvement over all studied = 8.6 (scale from 0 to 10).
†ODS score Post 1.86 (no data pre).
‡Cleveland Clinic Constipation score Pre 15.2 vs Post 4.4 (P = 0.001).
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9184
Recto-vaginal reinforcement for constipation U. Grossi et al.

• Findings for global improvement, derived from global
satisfaction rating scales, provide insufficient evidence
to prefer one type of procedure over another (level
IV).
• Other patient symptom scores were inconsistently
reported (level IV).
• Approximately 30–50% of patients may experience
reduced symptoms of straining, incomplete empty-
ing or reduced vaginal digitation (level IV).
• Anatomical recurrence (as judged by a variety of mea-
sures) occurred in approximately 17% patients at
mean follow up of 23.4 months (range 12–74) (level
IV).
Patient selection
Patient selection is generally perceived by experts as impor-
tant when choosing a surgical approach. There was a vast
variation in the preoperative investigation of patients in the
studies. Most studies included evacuation imaging (33 out
of the total 43) where defaecation proctography was used
in all but one (which used isotope imaging) [36]. There
was selective use of anal ultrasound, anorectal physiological
assessment, with colonic transit studies being recorded in
12 studies. There was however little correlation between
the results of surgery and preoperative investigation results.
Key features include the presence of a symptomatic
Figure 5 Forest plot showing rates ofglobal rating of satisfaction (percentage
of patients) by procedure type. KEY:
TVR, transvaginal repair; TAR, transanalrepair; TV, transvaginal; TP,
transperineal.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 85
U. Grossi et al. Recto-vaginal reinforcement for constipation
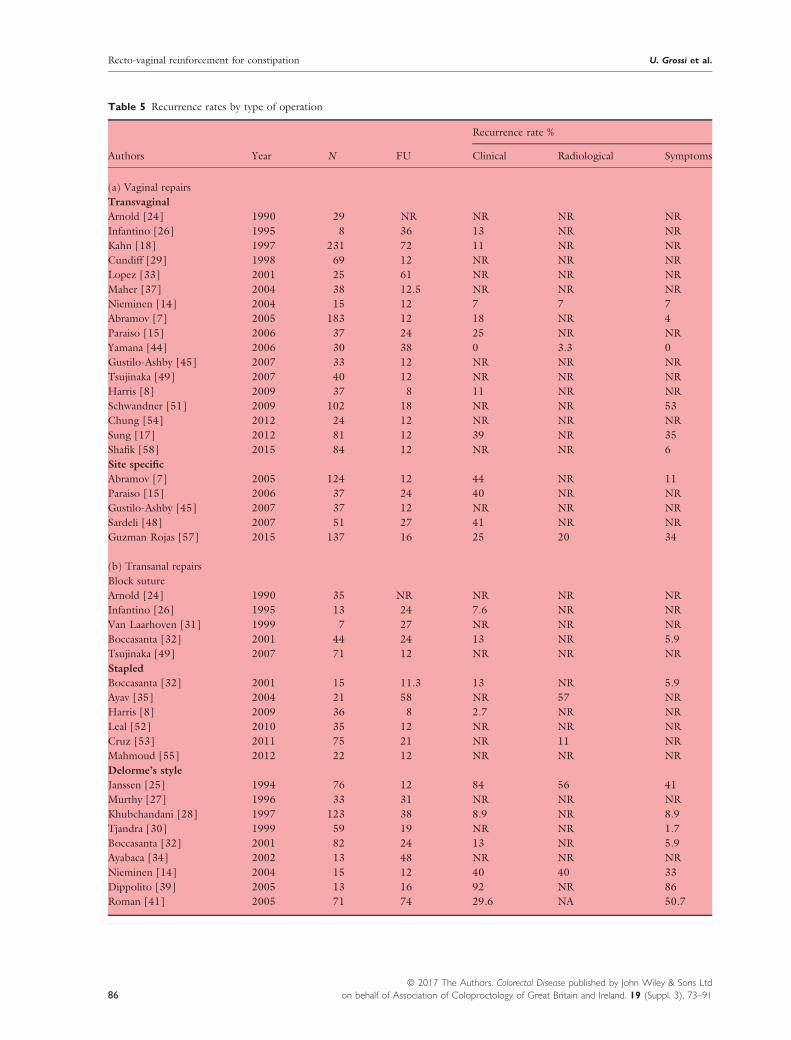
Table 5 Recurrence rates by type of operation
Authors Year N FU
Recurrence rate %
Clinical Radiological Symptoms
(a) Vaginal repairs
Transvaginal
Arnold [24] 1990 29 NR NR NR NR
Infantino [26] 1995 8 36 13 NR NR
Kahn [18] 1997 231 72 11 NR NR
Cundiff [29] 1998 69 12 NR NR NR
Lopez [33] 2001 25 61 NR NR NR
Maher [37] 2004 38 12.5 NR NR NR
Nieminen [14] 2004 15 12 7 7 7
Abramov [7] 2005 183 12 18 NR 4
Paraiso [15] 2006 37 24 25 NR NR
Yamana [44] 2006 30 38 0 3.3 0
Gustilo-Ashby [45] 2007 33 12 NR NR NR
Tsujinaka [49] 2007 40 12 NR NR NR
Harris [8] 2009 37 8 11 NR NR
Schwandner [51] 2009 102 18 NR NR 53
Chung [54] 2012 24 12 NR NR NR
Sung [17] 2012 81 12 39 NR 35
Shafik [58] 2015 84 12 NR NR 6
Site specific
Abramov [7] 2005 124 12 44 NR 11
Paraiso [15] 2006 37 24 40 NR NR
Gustilo-Ashby [45] 2007 37 12 NR NR NR
Sardeli [48] 2007 51 27 41 NR NR
Guzman Rojas [57] 2015 137 16 25 20 34
(b) Transanal repairs
Block suture
Arnold [24] 1990 35 NR NR NR NR
Infantino [26] 1995 13 24 7.6 NR NR
Van Laarhoven [31] 1999 7 27 NR NR NR
Boccasanta [32] 2001 44 24 13 NR 5.9
Tsujinaka [49] 2007 71 12 NR NR NR
Stapled
Boccasanta [32] 2001 15 11.3 13 NR 5.9
Ayav [35] 2004 21 58 NR 57 NR
Harris [8] 2009 36 8 2.7 NR NR
Leal [52] 2010 35 12 NR NR NR
Cruz [53] 2011 75 21 NR 11 NR
Mahmoud [55] 2012 22 12 NR NR NR
Delorme’s style
Janssen [25] 1994 76 12 84 56 41
Murthy [27] 1996 33 31 NR NR NR
Khubchandani [28] 1997 123 38 8.9 NR 8.9
Tjandra [30] 1999 59 19 NR NR 1.7
Boccasanta [32] 2001 82 24 13 NR 5.9
Ayabaca [34] 2002 13 48 NR NR NR
Nieminen [14] 2004 15 12 40 40 33
Dippolito [39] 2005 13 16 92 NR 86
Roman [41] 2005 71 74 29.6 NA 50.7
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9186
Recto-vaginal reinforcement for constipation U. Grossi et al.

rectocoele greater than 2 cm on proctography with evi-
dence of contrast trapping at the end of maximal evacua-
tion. Where graded, generally rectocoeles operated upon
were grade 2 or 3. Only one study measured the rectocoele
clinically with POPQ assessment [37]. Other than medical
co-morbidity precluding surgery there were very few con-
sistent exclusion criteria in any of the studies, although sev-
eral excluded those women with slow transit constipation.
Furthermore, in the few studies that related preoperative
assessment to outcome, none could show an association
between baseline symptoms or size of rectocoele and func-
tional outcome. The need to digitate to assist evacuation
did not appear to predict outcome following surgery, but
may predict the need to digitate postoperatively.
Summary evidence statements: patient selection
• Although patient selection is perceived as vital in pre-
dicting outcome it was inconsistently documented
(level IV).
• There was no evidence to support better outcomes
based on selection of patients with a particular size or
grade of rectocoele (level IV).
Conclusions
A systematic review of evidence for the perioperative
and long terms benefits and harms of recto-vaginal rein-
forcement procedures to treat symptoms of constipation
identified only one high quality study. Two further ran-
domized controlled trials were identified although these
were small and had methodological limitations. The evi-
dence base was therefore characterised almost exclu-
sively by observational studies of variable and often
uncertain methodological quality. Future studies should
provide robust and comparative evidence for clinicians
to support patient decision making, both in terms of
the incremental benefits and harms of procedures.
Table 5 (Continued).
Authors Year N FU
Recurrence rate %
Clinical Radiological Symptoms
Thornton [42] 2005 40 44 NR NR 56
Puigdollers [47] 2007 11 12 NR NR NR
Chung [54] 2012 26 12 NR NR NR
Mahmoud [55] 2012 23 12 NR NR NR
Combined TV and TA
van Dam [22] 2000 89 52 NR NR 29
(c) Transperineal repairs
Boccasanta [32] 2001 50 24 13 11 6.40
Ayabaca [34] 2002 11 48 NR NR NR
Puigdollers [47] 2007 24 12 NR NR NR
Authors Year N FU
Recurrence rate %
Repair type Mesh typeClinical Radiological Symptoms
(d) Mesh repair
Van Laarhoven [31] 1999 15 27 NA NA NA TP/TA Synthetic marlex
Mercer-Jones [38] 2004 24 12.5 4.50 NA NA TP Synthetic prolene/Vipro II
Milani [40] 2005 63 17 NA NA NA TV Synthetic prolene
Altman [43] 2006 23 36 NA NA NA TV Porcine xenograft
Paraiso [15] 2006 31 24 55 NA NA Site specific Porcine xenograft
Gustilo-Ashby [45] 2007 29 12 NA NA NA TV Porcine xenograft
Lim [46] 2007 53 36 22 NA NA TV Synthetic vipro II
Biehl [50] 2008 95 13.8 1 NA NA Site specific Porcine dermal xenograft
Biehl [50] 2008 100 13.8 7 NA 3 Site specific Human dermal allograft
Sung [17] 2012 79 12 38.9 NA 34.8 TV Porcine subintestinal submucosa
van der Hagen [56] 2012 27 12 NA NA NA TV Synthetic prolene
Melich [59] 2016 23 12 4 4 4 TV Porcine dermal xenograft strattice
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 87
U. Grossi et al. Recto-vaginal reinforcement for constipation

Greater understanding is required of the mediating
effects of prognostic factors particularly preoperative
definition of both functional and radiological parame-
ters that impact upon treatment success.
Acknowledgements
We would like to acknowledge the following people in
relation to the NIHR CapaCiTY working group: Mr
Steven Brown, Sheffield Teaching Hospitals NHS
Foundation Trust; Mr Kenneth Campbell, The Univer-
sity of Dundee, NHS Education for Scotland; Mr Mark
Chapman, Heart of England NHS Trust; Mr Andrew
Clarke, Poole Hospital NHS Foundation Trust; Mr Neil
Cruickshank, Sandwell and West Birmingham Hospitals
NHS Trust; Mr Anthony Dixon, University of Bristol,
Bristol, UK; Dr Christopher Emmett, County Durham
and Darlington NHS Foundation Trust; Mr Ugo
Grossi, Queen Mary University of London; Dr Richard
Hooper, PCTU, Queen Mary University of London;
Miss Emma Horrocks, University Hospital Southamp-
ton NHS Foundation Trust; Professor Charles Knowles,
Queen Mary University of London; Mr Jon Lacy-Col-
son, Shrewsbury and Telford Hospital NHS Trust; Mr
Ian Lindsey, Oxford University Hospitals NHS Trust;
Professor James Mason, University of Warwick, Coven-
try; Mr Mark Mercer-Jones, Gateshead Health NHS
Foundation Trust; Mr Andrew Miller, University
Figure 6 Forest plot showing rates of clinical recurrence (percentage of patients) by procedure type. KEY: TVR, transvaginal repair;TAR, transanal repair; TV, transvaginal; TP, transperineal.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9188
Recto-vaginal reinforcement for constipation U. Grossi et al.

Hospitals of Leicester NHS Trust; Mr David Pares,
Hospital Germans Trias i Pujol, Barcelona, Spain; Miss
Sophie Pilkington, University Hospital Southampton
NHS Foundation Trust; Mr Neil Smart, Royal Devon &
Exeter NHS Foundation Trust; Ms Natasha Stevens,
PCTU, Queen Mary University of London; Professor
Douglas Tincello, University Hospitals of Leicester NHS
Trust; Miss Karen Telford, South Manchester NHS
Foundation Trust; Mr Paul Vollebregt, Queen Mary
University of London; Mr Andrew Williams, Guy’s and
Thomas’ NHS Foundation Trust; Professor Yan Yian-
nakou, County Durham and Darlington NHS Founda-
tion Trust.
Conflicts of interest
The authors declare no conflict of interest.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opin-
ions expressed in this report are those of the authors
and are not those of the PGfAR Programme, NIHR,
the UK National Health Service, or the UK Depart-
ment of Health.
References
1 D’Hoore A, Penninckx F. Obstructed defecation. Colorectal
Dis 2003; 5: 280–7.
2 Mellgren A, Anzen B, Nilsson BY et al. Results of rectocele
repair. A prospective study. Dis Colon Rectum 1995; 38:
7–13.
3 Farid M, Madbouly KM, Hussein A, Mahdy T, Moneim
HA, Omar W. Randomized controlled trial between per-
ineal and anal repairs of rectocele in obstructed defecation.
World J Surg 2010; 34: 822–9.
4 Block IR. Transrectal repair of rectocele using obliterative
suture. Dis Colon Rectum 1986; 29: 707–11.
5 Sarles JC, Arnaud A, Selezneff I, Olivier S. Endo-rectal
repair of rectocele. Int J Colorectal Dis 1989; 4: 167–71.
6 Miklos JR, Kohli N, Lucente V, Saye WB. Site-specific fas-
cial defects in the diagnosis and surgical management of
enterocele. Am J Obstet Gynecol 1998; 179: 1418–22. dis-
cussion 822-3.
7 Abramov Y, Gandhi S, Goldberg RP, Botros SM, Kwon C,
Sand PK. Site-specific rectocele repair compared with stan-
dard posterior colporrhaphy. Obstet Gynecol 2005; 105:
314–8.
8 Harris MA, Ferrara A, Gallagher J, DeJesus S, Williamson
P, Larach S. Stapled Transanal Rectal Resection vs.
Transvaginal Rectocele Repair for Treatment of
Obstructive Defecation Syndrome. Dis Colon Rectum
2009; 52: 592–7.
9 Maher C, Feiner B, Baessler K, Adams EJ, Hagen S, Glaz-
ener CM. Surgical management of pelvic organ prolapse in
women. Cochrane Database Syst Rev 2010; 14:
CD004014.
10 Maher C, Baessler K, Glazener CM, Adams EJ, Hagen S.
Surgical management of pelvic organ prolapse in women: a
short version Cochrane review. Neurourol Urodyn 2008;
27: 3–12.
11 Maher C, Baessler K, Glazener CM, Adams EJ, Hagen S.
Surgical management of pelvic organ prolapse in women.
Cochrane Database Syst Rev 2007; 18: CD004014.
12 Maher C, Baessler K. Surgical management of posterior
vaginal wall prolapse: an evidence-based literature review.
Int Urogynecol J Pelvic Floor Dysfunct 2006; 17: 84–8.
13 Maher C, Baessler K, Glazener CM, Adams EJ, Hagen S.
Surgical management of pelvic organ prolapse in women.
Cochrane Database Syst Rev 2004; 18: CD004014.
14 Nieminen K, Hiltunen KM, Laitinen J, Oksala J, Heinonen
PK. Transanal or vaginal approach to rectocele repair: a
prospective, randomized pilot study. Dis Colon Rectum
2004; 47: 1636–42.
15 Paraiso MF, Barber MD, Muir TW, Walters MD. Rectocele
repair: a randomized trial of three surgical techniques
including graft augmentation. Am J Obstet Gynecol 2006;
195: 1762–71.
16 Sand PK, Koduri S, Lobel RW et al. Prospective random-
ized trial of polyglactin 910 mesh to prevent recurrence of
cystoceles and rectoceles. Am J Obstet Gynecol 2001; 184:
1357–62. discussion 62-4.
17 Sung VW, Rardin CR, Raker CA, LaSala CA, Myers DL.
Changes in bowel symptoms 1 year after rectocele repair.
Am J Obstet Gynecol 2012; 207: 423. e1–5.
18 Kahn MA, Stanton SL. Posterior colporrhaphy: its effects
on bowel and sexual function. Br J Obstet Gynaecol 1997;
104: 82–6.
19 Vijaya G, Dell’Utri C, Derpapas A et al., editors. A
prospective randomised trial comparing two surgical tech-
niques for posterior vaginal wall prolapse using subjective
and objective measures. Neurourology and Urodynamics;
2011: Wiley-Blackwell Commerce Place, 350 Main St, Mal-
den 02148, MA USA.
20 Yurteri-Kaplan LA, Gutman RE. The use of biological
materials in urogynecologic reconstruction: a systematic
review. Plast Reconstr Surg 2012; 130(5 Suppl 2): 242S–
53S.
21 Karram M, Maher C. Surgery for posterior vaginal wall
prolapse. Int Urogynecol J 2013; 24: 1835–41.
22 van Dam JH, Schouten WR, Ginai AZ, Huisman WM,
Hop WC. The impact of anismus on the clinical outcome
of rectocele repair. Int J Colorectal Dis 1996; 11: 238–42.
23 van Dam JH, Hop WC, Schouten WR. Analysis of patients
with poor outcome of rectocele repair. Dis Colon Rectum
2000; 43: 1556–60.
24 Arnold MW, Stewart WR, Aguilar PS. Rectocele repair. Four
years’ experience.Dis Colon Rectum 1990; 33: 684–7.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 89
U. Grossi et al. Recto-vaginal reinforcement for constipation

25 Janssen LW, van Dijke CF. Selection criteria for anterior
rectal wall repair in symptomatic rectocele and anterior rec-
tal wall prolapse. Dis Colon Rectum 1994; 37: 1100–7.
26 Infantino A, Masin A, Melega E, Dodi G, Lise M. Does
surgery resolve outlet obstruction from rectocele? Int J
Colorectal Dis 1995; 10: 97–100.
27 Murthy VK, Orkin BA, Smith LE, Glassman LM. Excellent
outcome using selective criteria for rectocele repair. Dis
Colon Rectum 1996; 39: 374–8.
28 Khubchandani IT, Clancy JP 3rd, Rosen L, Riether RD,
Stasik JJ Jr. Endorectal repair of rectocele revisited. Br J
Surg 1997; 84: 89–91.
29 Cundiff GW, Weidner AC, Visco AG, Addison WA, Bump
RC. An anatomic and functional assessment of the discrete
defect rectocele repair. Am J Obstet Gynecol 1998; 179:
1451–6. discussion 6-7.
30 Tjandra JJ, Ooi BS, Tang CL, Dwyer P, Carey M. Transa-
nal repair of rectocele corrects obstructed defecation if it is
not associated with anismus. Dis Colon Rectum 1999; 42:
1544–50.31 Van Laarhoven CJ, Kamm MA, Bartram CI, Halligan S,
Hawley PR, Phillips RK. Relationship between anatomic
and symptomatic long-term results after rectocele repair for
impaired defecation. Dis Colon Rectum 1999; 42: 204–10.
discussion 10-1.
32 Boccasanta P, Venturi M, Calabro G et al. Which surgical
approach for rectocele? A multicentric report from Italian
coloproctologists. Tech Coloproctol 2001; 5: 149–56.
33 Lopez A, Anzen B, Bremmer S et al. Durability of success
after rectocele repair. Int Urogynecol J Pelvic Floor Dysfunct
2001; 12: 97–103.
34 Ayabaca SM, Zbar AP, Pescatori M. Anal continence after
rectocele repair. Dis Colon Rectum 2002; 45: 63–9.
35 Ayav A, Bresler L, Brunaud L, Boissel P. Long-term results
of transanal repair of rectocele using linear stapler. Dis
Colon Rectum 2004; 47: 889–94.
36 Heriot AG, Skull A, Kumar D. Functional and physiologi-
cal outcome following transanal repair of rectocele. Br J
Surg 2004; 91: 1340–4.
37 Maher CF, Qatawneh AM, Baessler K, Schluter PJ. Midline
rectovaginal fascial plication for repair of rectocele and
obstructed defecation. Obstet Gynecol 2004; 104: 685–9.
38 Mercer-Jones MA, Sprowson A, Varma JS. Outcome after
transperineal mesh repair of rectocele: a case series. Dis
Colon Rectum 2004; 47: 864–8.
39 Dippolito A, Esser S, Reed J 3rd. Anterior modification of
Delorme procedure provides equivalent results to Delorme
procedure in treatment of rectal outlet obstruction. Curr
Surg 2005; 62: 609–12.40 Milani R, Salvatore S, Soligo M, Pifarotti P, Meschia M,
Cortese M. Functional and anatomical outcome of anterior
and posterior vaginal prolapse repair with prolene mesh.
BJOG 2005; 112: 107–11.41 Roman H, Michot F. Long-term outcomes of transanal
rectocele repair. Dis Colon Rectum 2005; 48: 510–7.
42 Thornton MJ, Lam A, King DW. Laparoscopic or transanal
repair of rectocele? A retrospective matched cohort study.
Dis Colon Rectum 2005; 48: 792–8.
43 Altman D, Zetterstrom J, Lopez A et al. Functional and
anatomic outcome after transvaginal rectocele repair
using collagen mesh: a prospective study. Dis Colon Rec-
tum 2005; 48: 1233–41. discussion 41-2; author reply
42.
44 Yamana T, Takahashi T, Iwadare J. Clinical and physiologic
outcomes after transvaginal rectocele repair. Dis Colon Rec-
tum 2006; 49: 661–7.
45 Gustilo-Ashby AM, Paraiso MF, Jelovsek JE, Walters MD,
Barber MD. Bowel symptoms 1 year after surgery for pro-
lapse: further analysis of a randomized trial of rectocele
repair. Am J Obstet Gynecol 2007; 197: 76. e1-5.
46 Lim YN, Muller R, Corstiaans A, Hitchins S, Barry C,
Rane A. A long-term review of posterior colporrhaphy with
Vypro 2 mesh. Int Urogynecol J Pelvic Floor Dysfunct 2007;
18: 1053–7.
47 Puigdollers A, Fernandez-Fraga X, Azpiroz F. Persistent
symptoms of functional outlet obstruction after rectocele
repair. Colorectal Dis 2007; 9: 262–5.
48 Sardeli C, Axelsen SM, Kjaer D, Bek KM. Outcome of
site-specific fascia repair for rectocele. Acta Obstet Gynecol
Scand 2007; 86: 973–7.
49 Tsujinaka S, Tsujinaka Y, Matsuo K, Akagi K, Hamahata Y.
Changes in bowel function following transanal and
transvaginal rectocele repair. Dig Surg 2007; 24: 46–53.
50 Biehl RC, Moore RD, Miklos JR, Kohli N, Anand IS, Mat-
tox TF. Site-specific rectocele repair with dermal graft aug-
mentation: comparison of porcine dermal xenograft
(Pelvicol) and human dermal allograft. Surg Technol Int
2008; 17: 174–80.
51 Schwandner T, Roblick MH, Hecker A et al. Transvaginal
rectal repair: a new treatment option for symptomatic rec-
tocele? Int J Colorectal Dis 2009; 24: 1429–34.
52 Leal VM, Regadas FSP, Regadas SMM, Veras LR. Clinical
and functional evaluation of patients with rectocele and
mucosal prolapse treated with transanal repair of rectocele
and rectal mucosectomy with a single circular stapler
(TRREMS). Tech Coloproctol 2010; 14: 329–35.
53 Cruz JV, Regadas FS, Murad-Regadas SM et al. TRREMS
procedure (transanal repair of rectocele and rectal mucosec-
tomy with one circular stapler): a prospective multicenter
trial. Arq Gastroenterol 2011; 48: 3–7.
54 Chung CS, Yu SH, Lee JE, Lee DK. Comparison of long-
term clinical outcomes according to the change in the rec-
tocele depth between transanal and transvaginal repairs for
a symptomatic rectocele. J Korean Soc Coloproctol 2012;
28: 140–4.
55 Mahmoud SA, Omar W, Farid M. Transanal repair for
treatment of rectocele in obstructed defaecation: manual or
stapled. Colorectal Dis 2012; 14: 104–10.
56 van der Hagen SJ, van Gemert WG, Soeters PB, de Wet
H, Baeten CG. Transvaginal posterior colporrhaphy com-
bined with laparoscopic ventral mesh rectopexy for isolated
Grade III rectocele: a prospective study of 27 patients.
Colorectal Dis 2012; 14: 1398–402.
57 Guzman Rojas R, Kamisan Atan I, Shek KL, Dietz HP.
Defect-specific rectocele repair: medium-term anatomical,
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–9190
Recto-vaginal reinforcement for constipation U. Grossi et al.

functional and subjective outcomes. Aust N Z J Obstet
Gynaecol 2015; 55: 487–92.
58 Shafik AA, El Sibai O, Shafik IA. Rectocele repair with sta-
pled transvaginal rectal resection. Tech Coloproctol 2016;
20: 207–14.
59 Melich G, Pai A, Kwak M et al. Transverse incision
transvaginal rectocele repair combined with levatorplasty
and biological graft insertion: technical details and case ser-
ies outcomes. Tech Coloproctol 2016; 20: 51–7.
60 Evans C, Ong E, Jones OM, Cunningham C, Lindsey I.
Laparoscopic ventral rectopexy is effective for solitary rectal
ulcer syndrome when associated with rectal prolapse.
Colorectal Dis 2014; 16: O112–6.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 73–91 91
U. Grossi et al. Recto-vaginal reinforcement for constipation

Surgery for constipation: systematic review and practicerecommendations
Results V: Sacral Nerve Stimulation
S. A. Pilkington*, C. Emmett†, C. H. Knowles‡, J. Mason§, Y. Yiannakou†, On behalf of the
NIHR CapaCiTY working group¶ and Pelvic floor Society**
*University Hospital Southampton, Southampton, UK, †County Durham and Darlington NHS Foundation Trust, Durham, UK, ‡National Bowel
Research Centre, Blizard Institute, Queen Mary University London, London, UK, §Warwick Medical School, University of Warwick, Coventry, UK,
¶National Institute for Health Research: Chronic Constipation Treatment Pathway, London, UK, and **Affiliate section of the Association of
Coloproctology GB and Ireland, London, UK
Abstract
Aim To assess the outcomes of sacral nerve stimulation
in adults with chronic constipation.
Method Standardised methods and reporting of bene-
fits and harms were used for all CapaCiTY reviews that
closely adhered to PRISMA 2016 guidance. Main con-
clusions were presented as summary evidence statements
with a summative Oxford Centre for Evidence-Based
Medicine (2009) level.
Results Seven articles were identified, providing data on
outcomes in 375 patients. Length of procedures and
length of stay was not reported. Data on harms were
inconsistently reported and heterogeneous, making esti-
mates of harm tentative and imprecise. Morbidity rates
ranged between 13 and 34%, with overall device
removal rate between 8 and 23%. Although inconsis-
tently reported, pooled treatment success was typically
57–87% for patients receiving permanent implants,
although there was significant variation between studies.
Patient selection was inconsistently documented. No
conclusions could be drawn regarding particular pheno-
types that responded favourably or unfavourably to
sacral nerve stimulation.
Conclusion Evidence supporting sacral nerve stimula-
tion is derived from poor quality studies. Three
methodologically robust trials are have reported since
this review and all have all urged greater caution.
Keywords Constipation, sacral nerve stimulation, neu-
romodulation, slow transit constipation
Introduction
Background and procedural variations
Sacral nerve stimulation (SNS) is well established for pelvic
urinary indications and for the treatment of faecal inconti-
nence when conservative measures have failed [1,2]. Its
role in the management of chronic constipation (CC) has
been studied since 2001 [3], based on a century of experi-
mental (multiple species: physiological and anatomical)
and clinical data that the sacral innervation has a prokinetic
effect on the rectum and colon via ascending colonic
nerves [4]. Brindley stimulation has exploited this effect in
small numbers of patients since the 1980s [5,6] andmech-
anistic studies from Adelaide of SNS effects on transit and
colonic contractile activity have confirmed potential to
increase anterograde contractile activity, reduce retro-
grade activity and speed transit [7]. SNS in its current
form uses chronic low amplitude stimulation of a chosen
sacral nerve root (usually S3) via a percutaneously placed
quadripolar electrode and implanted pulse generator.
There are procedural variations in terms of testing phase
(temporary wire ‘basic’ vs tined lead ‘advanced’ evalua-
tion) however the final assembly of components is uniform
reflecting a single current manufacturer (Medtronic Inc
Medtronic Limited, Watford, Herts, UK) for this clinical
indication.
Scope
The purpose of this study was to assess the efficacy and
harms of implanted SNS for adult patients whose main
presenting complaint is chronic constipation. Proce-
dures beyond the scope of this review include other
forms of neurostimulation (e.g. transcutaneous, vaginal,
Correspondence to: Miss Sophie Pilkington, Mailpoint 134, University Hospital
Southampton, Tremona Road, Southampton, SO16 6YD, UK.
E-mail: [email protected]
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–10092
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13780

transanal, pudendal) and temporary SNS (i.e. where
data are only available during the testing phase).
Previous reviews
Two systematic Cochrane reviews have focused on
SNS for constipation, although faecal incontinence
was also included. The first (2007 [8]) concluded
that SNS can reduce symptoms in selected patients
with constipation, however this was based on a single
study which included two patients [9]. The second
included two RCTs and concluded that SNS did not
improve symptoms in patients with constipation,
although it recognised that the evidence was severely
limited [10].
Summary of search results and study quality
The search yielded a total of 20 citations for full text
review from a total of 121 abstracts found by initial
search criteria (Fig. 1: PRISMA diagram). From these,
only seven articles published between 2001 and 2015
contributed to the systematic review, providing data on
outcomes in a total of 375 patients (range 21–117patients per study) (Table 1. Specific exclusions after
full-text review (and after exclusion of non-English lan-
guage publications: n = 1) [11] included nine studies
where the population sample was confirmed to be less
than 20 patients [3,12–19], one study [20] which was a
dual publication reporting a patient cohort that over-
lapped with another study [21] and one study where
results were combined for mixed indication s [22].
Study follow up ranged from 20 to 51 months.
The general quality of studies was poor due to inade-
quate description of methods. The seven included stud-
ies were all observational and all provided uncontrolled
LEVEL IV evidence, including one low quality prospec-
tive cohort study, two prospective and four retrospec-
tive case series. Mean patient follow up ranged from 20
to 51 months (median 27 months). All studies derived
from European centres, with three from UK and one
each from Spain, The Netherlands, Italy and Sweden.
Perioperative data
There were few data concerning standard perioperative
variables. All studies failed to include data on duration
of procedure, number of cases performed as day surgery
or duration of inpatient stay. A summary of periopera-
tive data is provided in Table 2. Peculiar to SNS, data
were reported on paradigm of test stimulation i.e. there
is more than one way to perform test stimulation. The
use of a previously described ‘standard procedure’ is sta-
ted in the methods section in only three studies [23–25]. The duration of temporary SNS was reported as
2 weeks in two of the studies [25,26] and 3 weeks in
five of the studies [21,23,24,27,28]. The use of antibi-
otics during permanent SNS placement was reported by
one study only [23]. Type of anaesthesia for insertion
of temporary and permanent leads was reported in two
studies [20,27,28] and insertion of temporary wires in
the outpatient setting was described in one study [24].
Figure 1 PRISMA diagram of search results.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–100 93
S. A. Pilkington et al. Surgery for constipation

Most studies used a tined quadripolar lead for perma-
nent stimulation. Five studies used a single lead
[21,23,24,28] whilst one study used bilateral stimula-
tion [27] and another used either single or bilateral
[25]. Some additional data pertaining to the cohort of
patients in the Govaert [21] study were reported in an
earlier study by Maeda et al. [20].
Summary evidence statements: perioperative data1 Standard perioperative data (duration of procedure
and length of stay) were not reported by any study
(Level IV)
2 Where reported, general anaesthesia was used for
SNS procedures (Level IV)
3 The number of temporary unipolar SNS leads used
varied (1 or 2) between studies (Level IV)
4 Most studies used a single tined quadripolar lead for
permanent stimulation (Level IV)
Harms
Surgical morbidity, reported as overall procedural com-
plication rates, vary considerably with individual study
rates varying from zero to 39% [24] (Table 3). This
heterogeneity may have reflected (for example) differing
inclusion, procedural content, context of care, or
thresholds or conventions for recording complications.
Random effects meta-analysis found the overall compli-
cation rate to be 22.7% (95% CI: 12.9% to 34.1%),
I2 = 47% (Fig. 2). Device removal was similarly hetero-
geneous: the overall device removal rate was 14.4%
(95% CI: 7.8% to 22.5%), I2 = 47% (Fig. 3). There
were 51 re-operations: 30 for device removal although
five were replaced after resolution of pain or infection,
11 to move or replace the implant, 10 lead problems.
In addition six operations were carried out for treat-
ment of chronic constipation including three subtotal
colectomies [23,28], two stomas and one appendicos-
tomy [28]. Infection resulting in device removal was
reported in three patients. The commonest reason for
explantation was lack of effect and this was reported in
19 cases (Table 3). Two explantations were carried out
for pain associated with the implant and one for lead
migration. There appeared to be no relationship
between device explantation rate and length of follow
up (Table 1).
Patients with SNS for constipation had high levels of
reportable adverse events. Often this was resolved by
reprogramming but more than one-third required surgi-
cal intervention or discontinued therapy. Such data were
specifically reported in the sub-cohort of Govaert et al.
[21], reported separately by Maeda et al. [20] who car-
ried out a retrospective review of 38 patients who had
SNS for constipation and found that 22 patients (58%)
experienced at least one reportable event. The most
common event was lack or loss of efficacy. In 19 events
(33%), surgical intervention was required and the most
common intervention was electrode replacement (14
events). Three adverse events lead to discontinuation of
SNS. The remaining 35 patients were still using SNS
but with a variable degree of benefit.
Summary evidence statements: harms1 Data on harms were inconsistently reported and
heterogeneous (Level IV).
2 The overall procedural complication rate resulting in
reoperation was typically 13–34% (Level IV).
3 Common complications resulting in reoperation
included lack of efficacy, infection, lead problems,
pain at site of implant, unwanted effects relating to
stimulation such as pain (Level IV).
4 Infection rates varied from 0 to 7% (Level IV).
5 Overall device removal rate was typically 8–23% at
mean follow up of 31 months (Level IV)
Table 1 All studies included in systematic review.
Author Year Centre Country
Total
N
Implanted
N FU*
Number at final
follow up N (%)‡ Design Level†
Kamm [23] 2010 St Marks UK 62 45 28 38 (61) PCH IV
Sharma [26] 2011 Hull UK 21 11 34 10 (48) RCS IV
Ortiz [24] 2012 Navarra Spain 48 23 26 14 (29) RCS IV
Govaert [21] 2012 Maastricht Netherlands 117 68 37 61 (52) RCS IV
Khan [27] 2014 Durham UK 22 12 20 12 (55) PCS IV
Ratto [25] 2014 Rome Italy 61 42 51 32 (76) RCS IV
Graf [28] 2015 Uppsala Sweden 44 15 24 11 (25) PCS IV
*Mean follow up in months.
†Oxford 2009 CEBM.
‡Based on intent to treat RCT, Randomised controlled trial; PCH, prospective cohort study; RCS, retrospective case series; PCS,
prospective case series; NR, Not recorded.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–10094
Surgery for constipation S. A. Pilkington et al.

Efficacy
Reported clinical outcomes varied in assessment tools
used across the seven studies (Table 4). Most com-
monly, these consisted of validated summative symptom
scores or questionnaires. These included the Cleveland
Clinic Constipation score [23,25], the SF-36 question-
naire [23,25], the Wexner Score [21,24], and PAC-
SYM and PAC-QOL questionnaire [27]. Additionally,
patient bowel diaries were used by several studies, either
as the principal outcome measure [26] or alongside
other measures [21,24,28]. The definition of treatment
success varied between studies. Of the two studies using
the Wexner score, one [24] defined success as a 30%
improvement in this score. The other [21] defined this
as a statistically significant reduction in score from base-
line. Kamm et al. [23] defined success as either ≥ 3
bowel motions per week or ≥ 50% improvement in
straining or ≥ 50% improvement in incomplete evacua-
tion. Other definitions of sustained treatment success
included a statistically significant reduction in Cleveland
Clinic Score and SF-36 from baseline [25], patient
reported clinical improvement [27,28] and 50%
improvement in bowel function (recorded on bowel
diaries [26]). The percentage of initial study recruits
providing data at final follow up varied between studies,
from 25 to 76% (Table 1) denoting significant attrition
in prospective studies.
Accepting variation in definitions used, random effects
meta-analysis found the overall SNS response rate (i.e. to
those beginning treatment but not necessarily implanted)
to be 56.9% (95% CI: 46.8% to 66.7%), I2 = 71%. Long
term overall treatment success was 40.1% (95% CI:
26.3% to 54.7%), I2 = 87%, considering permanently
implanted patients only, treatment success was 73.2%
(95% CI: 57.5% to 86.6%), I2 = 80% (Fig. 4).
Overall, success seemed to be dichotomised with four
studies [21,23,25,26] demonstrating higher success
rates, both in the short and long term, than others. The
largest of these, by Govaert et al. [21], is a retrospective
study at two centres in The Netherlands and Denmark,
with follow up at 1, 3, 6 and 12 months (although this is
difficult to verify for a retrospective study). It appears that
data were collected during routine clinical follow up
rather than as part of a planned research study. There was
considerable drop-out with Wexner scores available for
only 32 (47% of implanted cases) at 6 months. A multi-
centre prospective cohort study [23] demonstrated the
highest positive response rate to temporary SNS, as well
as a high long term success rate (87% of patients with per-
manent implants); the primary outcome was an improve-
ment in one of three domains; bowel frequency, straining
and incomplete evacuation, assessed using questionnairesTable
2Perioperativedatabyprocedure.
Author
Total
N
Implanted
N
Duration
temporary
SNS
(weeks)
Tem
porary
SNS
under
GA
Permanen
t
SNSunder
GA
Typeof
temporary
SNSlead
Number
of
temporary
SNSleadsused
Number
of
Permanen
t
SNSleadsused
Permanen
t
SNSusing
tined
quadripolarlead
Antibioticcover
duringpermanen
tSNS
Kam
m[23]
62
45
3NR
NR
U1
1Y
Y
Sharma[26]
21
11
2NR
NR
NR
NR
NR
NR
NR
Ortiz
[24]
48
23
30
NR
14U:34Q
11
YNR
Govaert[21]
117
68
3NR
NR
U1
1Y
NR
Khan
[27]
22
12
3Y
YU
22
YNR
Ratto
[25]
61
42
2NR
NR
U1OR
21OR
2NR
NR
Graf[28]
44
15
3Y
YU
≥2
1Y
NR
NR,notreported
;U,unipolarlead;Q,quadripolarlead;UT,untined
lead;T,tined
lead;Y,yes.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–100 95
S. A. Pilkington et al. Surgery for constipation

and validated symptom scores. However, treatment suc-
cess was assessed on last follow up and there was a high
drop-out rate (38% drop-out at 24 months). A further
retrospective study [26] of 21 patients in a single centre
demonstrated a 47% success rate based on patient
reported outcomes and laxative use. Ratto et al. [25]
used a retrospective study design to evaluate outcome
based on validated questionnaires. Although 32/42
(76%) of patients still had implant at the end of follow up
(and therefore considered to be responders to some
degree), only 15 (35%) had a 50% reduction of Cleveland
Clinic Score. Three studies [24,27,28] demonstrated rel-
atively poor efficacy of treatment (Table 4). Two of these
are retrospective case series while the other [27] studied
neurological constipation only.
Summary evidence statements: efficacy1 Data on efficacy were inconsistently measured with
high drop-out rates and heterogeneous findings,
making estimates tentative and imprecise [level IV]
2 Pooled treatment success was typically 57–87% for
patients receiving permanent implants, although
there was significant variation between studies [level
IV]
Patient selection
Patient selection was inconsistent between the seven
studies. There was no unifying criteria for establishing
a diagnosis of chronic constipation (Table 5). Four
studies excluded patients with neurological disease and
one study only included patients with neurological
disease. The proportion of participants with slow tran-
sit constipation (STC) was recorded in six of the
studies. There was no significant difference in
response to SNS when studies were grouped by those
with less or more than 50% of patients with STC
(Fig. 5). Defaecating proctograms were performed in
six of the studies but only used to stratify patients in
two studies (Table 5).
Figure 2 Forest plot showing rates of total procedural compli-
cations (percentage of patients).
Figure 3 Forest plot showing rates of device explantation rate
(percentage of patients).
Table 3 Harms.
Author
Total
N
Implanted
N
Total complications
resulting in
reoperation
Total adverse
events
Infection
resulting in
device removal
Explantation
(permanent
device removal)
Additional
surgery
Kamm [23] 62 45 11/45 (24%) 101 2/45 (4%) 2/45 (4%)
(7/45 exit study)
Subtotal colectomy
1
Sharma [26] 21 11 3/11 (27%) NR 0 0 NR
Ortiz [24] 48 23 9/23 (39%) NR 1/23 (4%) 6/23 (27%) NR
Govaert [21] 117 68 9/68 (13%) NR 3/68 (4.4%) 9/68 (13%) NR
Khan [27] 22 12 0 1 0 0 NR
Ratto [25] 61 42 14/42 (33%) 9 0 8/42 (19%) NR
Graf [28] 44 15 5/15 (33%) 12 PNE
5 PERM
1/15 (7%) 4/15 (27%) Stoma 2
Colectomy 2
Appendicostomy 1
NR, not reported.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–10096
Surgery for constipation S. A. Pilkington et al.
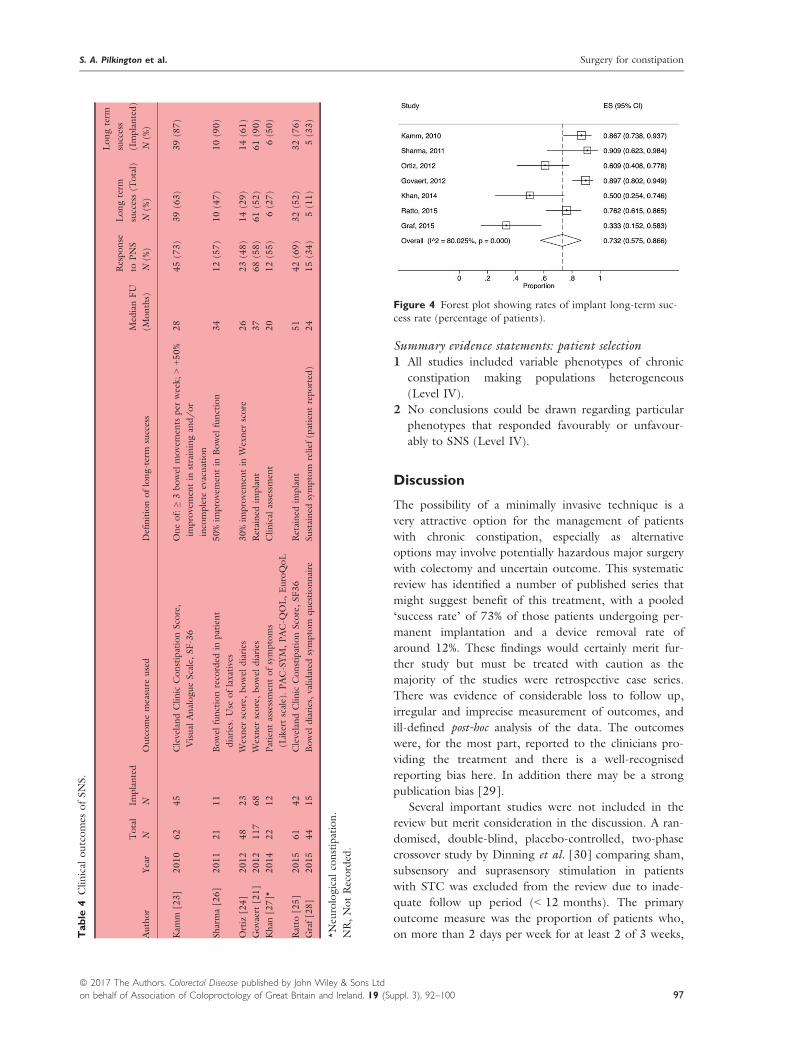
Summary evidence statements: patient selection1 All studies included variable phenotypes of chronic
constipation making populations heterogeneous
(Level IV).
2 No conclusions could be drawn regarding particular
phenotypes that responded favourably or unfavour-
ably to SNS (Level IV).
Discussion
The possibility of a minimally invasive technique is a
very attractive option for the management of patients
with chronic constipation, especially as alternative
options may involve potentially hazardous major surgery
with colectomy and uncertain outcome. This systematic
review has identified a number of published series that
might suggest benefit of this treatment, with a pooled
‘success rate’ of 73% of those patients undergoing per-
manent implantation and a device removal rate of
around 12%. These findings would certainly merit fur-
ther study but must be treated with caution as the
majority of the studies were retrospective case series.
There was evidence of considerable loss to follow up,
irregular and imprecise measurement of outcomes, and
ill-defined post-hoc analysis of the data. The outcomes
were, for the most part, reported to the clinicians pro-
viding the treatment and there is a well-recognised
reporting bias here. In addition there may be a strong
publication bias [29].
Several important studies were not included in the
review but merit consideration in the discussion. A ran-
domised, double-blind, placebo-controlled, two-phase
crossover study by Dinning et al. [30] comparing sham,
subsensory and suprasensory stimulation in patients
with STC was excluded from the review due to inade-
quate follow up period (< 12 months). The primary
outcome measure was the proportion of patients who,
on more than 2 days per week for at least 2 of 3 weeks,
Figure 4 Forest plot showing rates of implant long-term suc-
cess rate (percentage of patients).
Table
4Clinical
outcomes
ofSNS.
Author
Year
Total
N
Implanted
NOutcomemeasure
used
Definitionoflong-term
success
Med
ianFU
(Months)
Response
toPNS
N(%
)
Longterm
success(T
otal)
N(%
)
Longterm
success
(Implanted)
N(%
)
Kam
m[23]
2010
62
45
ClevelandClinic
ConstipationScore,
Visual
AnalogueScale,SF-36
Oneof:≥3bowel
movemen
tsper
week;
>+50%
improvemen
tin
strainingand/or
incomplete
evacuation
28
45(73)
39(63)
39(87)
Sharma[26]
2011
21
11
Bowel
functionrecorded
inpatient
diaries.Use
oflaxatives
50%im
provemen
tin
Bowel
function
34
12(57)
10(47)
10(90)
Ortiz
[24]
2012
48
23
Wexner
score,bowel
diaries
30%im
provemen
tin
Wexner
score
26
23(48)
14(29)
14(61)
Govaert[21]
2012
117
68
Wexner
score,bowel
diaries
Retained
implant
37
68(58)
61(52)
61(90)
Khan
[27]*
2014
22
12
Patientassessmen
tofsymptoms
(Likertscale).PAC-SYM,PAC-Q
OL,EuroQoL
Clinical
assessmen
t20
12(55)
6(27)
6(50)
Ratto
[25]
2015
61
42
ClevelandClinic
ConstipationScore,SF36
Retained
implant
51
42(69)
32(52)
32(76)
Graf[28]
2015
44
15
Bowel
diaries,validated
symptom
questionnaire
Sustained
symptom
relief
(patientreported
)24
15(34)
5(11)
5(33)
*Neu
rological
constipation.
NR,NotRecorded
.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–100 97
S. A. Pilkington et al. Surgery for constipation

reported a bowel movement associated with a feeling of
complete evacuation. This well-conducted trial showed
no clinical effect of sub- or suprasensory stimulation
over sham in 55 patients undergoing permanent SNS
implantation. The proportion of patients who met the
primary outcome measure did not differ between
suprasensory (30%) and sham (21%) stimulations nor
between subsensory (25%) and sham (25%) stimula-
tions. In addition there was no significant change in
quality of life scores. Long term data from this study
have been reported since the systematic review was
completed noting that 88% of patients in the original
study [30] had undergone device removal at median
follow up 5.7 years [31].
A French group have presented data on 20 patients
undergoing permanent SNS after a successful 3-week
temporary test. A randomised on/off sham controlled
sub-sensory stimulation was provided (8 weeks each
cycle) with no improvement during active stimulation.
At 1 year, only 11 (55%) patients were still responding
[32]. The results of a third study have been recently pre-
sented (nationally and internationally) from a multi-cen-
tre prospective randomised study [ISRCTN44563324].
The main aim of this study was to assess the efficacy of
sham controlled tined lead stimulation as a way of iden-
tifying true responders. Thirty-nine patients were
recruited to the test phase and 27 were implanted with
all but one followed up to 6 months. The findings
showed, once again, that temporary testing has no value
in determining long term response. The response at
6 months was assessed by a reduction of at least 0.5 on
Table 5 Patient baseline phenotypic data.
Authors N Inclusion criteria STC Neurological disease Proctogram
Kamm [23] 62 < 2 bowel movements per week and/or
straining or incomplete emptying > 25%
occasions
50 (81%) Excluded Performed not stratified
Sharma [26] 21 2 or fewer bowel movements per week, failed
conservative treatment over at least
12 months from GP referral
19 (86%) Excluded Performed used to rule out obstructive
defaecation but anismus not exclusion
criterion
Ortiz [24] 48 Rome III criteria, symptoms at least 1 year,
failed conservative treatment with laxatives,
suppositories, enemas and behavioural therapy
5 (10%) Excluded Performed not stratified
Govaert [21] 117 < 2 bowel movements per week and/or
straining or incomplete emptying > 25%
occasions. Persistent symptoms 1 year and
failed conservative treatment (NB includes 26
patients from Kamm study and 38 patients
from Maeda study)
75 (64%) Not excluded Performed not stratified
Khan [27] 22 Patients with neurological disease [including
multiple sclerosis (n = 14) and spinal cord
injury (n = 5)] and severe constipation
refractory to conservative treatment
NR Inclusion criterion None
Ratto [25] 61 Rome III criteria. Patients identified from
GINS: Italian group for sacral nerve
neuromodulation (NB may include some
patients from Ortiz study although not
specifically mentioned)
17 (28%) Not excluded Performed and patients with rectocoele,
intussusception, rectal prolapse and
enterocoele excluded
Graf [28] 44 History of ‘constipation’ for at least 6 months
and failure of conservative treatment
21 (48%) Excluded spinal
cord injury
Selective
Figure 5 Forest plot showing rates of SNS response rate by
level of STC patients (percentage of patients). KEY: STC, slow
transit constipation.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–10098
Surgery for constipation S. A. Pilkington et al.

PAC-SYM and this was achieved in 15(55%) of
patients.
These more recent prospective studies suggest that
the efficacy of SNS in constipation may be very limited,
but in particular, that prediction of responders using
various temporary testing regimens is poor. In view of
the cost and risk of the procedure, the inability to pre-
dict responders is likely to hamper the utility of the
treatment in the future.
There was a significant difference in the conclusions
between the largely retrospective early studies, which
supported the use of SNS, and the three recent well-
conducted prospective studies, which have all urged
greater caution. This is an example of the importance
and need for formally planned and robustly executed
studies to inform surgical practice and a warning against
over-reliance on retrospective cohort studies.
Acknowledgements
We would like to acknowledge the following people
in relation to the NIHR CapaCiTY working group:
Mr Steven Brown, Sheffield Teaching Hospitals NHS
Foundation Trust; Mr Kenneth Campbell, The
University of Dundee, NHS Education for Scotland;
Mr Mark Chapman, Heart of England NHS Trust;
Mr Andrew Clarke, Poole Hospital NHS Foundation
Trust; Mr Neil Cruickshank, Sandwell and West Birm-
ingham Hospitals NHS Trust; Mr Anthony Dixon,
University of Bristol, Bristol, UK; Dr Christopher
Emmett, County Durham and Darlington NHS
Foundation Trust; Mr Ugo Grossi, Queen Mary
University of London; Dr Richard Hooper, PCTU,
Queen Mary University of London; Miss Emma
Horrocks, University Hospital Southampton NHS
Foundation Trust; Professor Charles Knowles, Queen
Mary University of London; Mr Jon Lacy-Colson,
Shrewsbury and Telford Hospital NHS Trust; Mr Ian
Lindsey, Oxford University Hospitals NHS Trust;
Professor James Mason, University of Warwick,
Coventry; Mr Mark Mercer-Jones, Gateshead Health
NHS Foundation Trust; Mr Andrew Miller, University
Hospitals of Leicester NHS Trust; Mr David Pares,
Hospital Germans Trias i Pujol, Barcelona, Spain;
Miss Sophie Pilkington, University Hospital
Southampton NHS Foundation Trust; Mr Neil Smart,
Royal Devon & Exeter NHS Foundation Trust; Ms
Natasha Stevens, PCTU, Queen Mary University of
London; Professor Douglas Tincello, University
Hospitals of Leicester NHS Trust; Miss Karen Tel-
ford, South Manchester NHS Foundation Trust; Mr
Paul Vollebregt, Queen Mary University of London;
Mr Andrew Williams, Guy’s and Thomas’ NHS Foun-
dation Trust; Professor Yan Yiannakou, County
Durham and Darlington NHS Foundation Trust.
Conflict of interest
The authors declare no conflict of interest.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opin-
ions expressed in this report are those of the authors
and are not those of the PGfAR Programme, NIHR,
the UK National Health Service, or the UK Depart-
ment of Health.
References
1 Brazzelli M, Murray A, Fraser C. Efficacy and safety of
sacral nerve stimulation for urinary urge incontinence: a
systematic review. J Urol 2006; 175: 835–41.
2 Thin NN et al. Systematic review of the clinical effective-
ness of neuromodulation in the treatment of faecal inconti-
nence. Br J Surg 2013; 100: 1430–47.
3 Ganio E et al. Short-term sacral nerve stimulation for func-
tional anorectal and urinary disturbances: results in 40
patients: evaluation of a new option for anorectal functional
disorders. Dis Colon Rectum 2001; 44: 1261–7.
4 Knowles CH, Scott SM, Lunniss PJ. Slow transit constipa-
tion: a disorder of pelvic autonomic nerves? Dig Dis Sci
2001; 46: 389–401.
5 Brindley GS, Polkey CE, Rushton DN. Sacral anterior root
stimulators for bladder control in paraplegia. Paraplegia
1982; 20: 365–81.
6 Brindley GS. The first 500 patients with sacral anterior root
stimulator implants: general description. Paraplegia 1994;
32: 795–805.
7 Patton V et al. The effect of sacral nerve stimulation on
distal colonic motility in patients with faecal incontinence.
Br J Surg 2013; 100: 959–68.
8 Mowatt G, Glazener C, Jarrett M. Sacral nerve stimulation
for faecal incontinence and constipation in adults. Cochrane
Database Syst Rev 2007: CD004464.
9 Kenefick NJ et al. Double-blind placebo-controlled cross-
over study of sacral nerve stimulation for idiopathic consti-
pation. Br J Surg 2002; 89: 1570–1.
10 Thaha MA et al. Sacral nerve stimulation for faecal inconti-
nence and constipation in adults. Cochrane Database Syst
Rev, 2015: CD004464.
11 Zheng J et al. Sacral neuromodulation in the treatment of
intractable constipation. Zhonghua Wei Chang Wai Ke Za
Zhi 2014; 17: 1175–8.
12 Dinning PG et al. Sacral nerve stimulation induces pan-
colonic propagating pressure waves and increases defecation
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–100 99
S. A. Pilkington et al. Surgery for constipation

frequency in patients with slow-transit constipation.
Colorectal Dis 2007; 9: 123–32.
13 Kenefick NJ et al. Permanent sacral nerve stimulation for
treatment of idiopathic constipation. Br J Surg 2002; 89:
882–8.
14 Malouf AJ et al. Short-term effects of sacral nerve stimula-
tion for idiopathic slow transit constipation. World J Surg
2002; 26: 166–70.
15 Knowles CH et al. Prospective randomized double-blind
study of temporary sacral nerve stimulation in patients with
rectal evacuatory dysfunction and rectal hyposensitivity.
Ann Surg 2012; 255: 643–9.
16 Thomas GP et al. A double-blinded randomized multicen-
tre study to investigate the effect of changes in stimulation
parameters on sacral nerve stimulation for constipation.
Colorectal Dis 2015; 17: 990–5.
17 Carriero A et al. Sacral nerve stimulation for constipation:
do we still miss something? Role of psychological evalua-
tion. Int J Colorectal Dis 2010; 25: 1005–10.
18 Naldini G et al. Treatment of slow-transit constipation with
sacral nerve modulation. Colorectal Dis 2010; 12: 1149–52.
19 Holzer B et al. Sacral nerve stimulation in patients with
severe constipation. Dis Colon Rectum 2008; 51: 524–9;
discussion 529-30.
20 Maeda Y et al. Sacral nerve stimulation for constipation:
suboptimal outcome and adverse events. Dis Colon Rectum
2010; 53: 995–9.
21 Govaert B et al.Medium-termoutcome of sacral nervemodu-
lationforconstipation.DisColonRectum2012;55:26–31.
22 van Wunnik BP et al. Patient experience and satisfaction
with sacral neuromodulation: results of a single-center sam-
ple survey. Dis Colon Rectum 2011; 54: 95–100.
23 Kamm MA et al. Sacral nerve stimulation for intractable
constipation. Gut 2010; 59: 333–40.
24 Ortiz H et al. Functional outcome of sacral nerve stimula-
tion in patients with severe constipation. Dis Colon Rectum
2012; 55: 876–80.
25 Ratto C et al. Long-term results following sacral nerve
stimulation for chronic constipation. Colorectal Dis 2015;
17: 320–8.
26 Sharma A et al. Sacral neuromodulation for the manage-
ment of severe constipation: development of a constipation
treatment protocol. Int J Colorectal Dis 2011; 26: 1583–
7.
27 Khan U et al. A prospective trial of temporary sacral nerve
stimulation for constipation associated with neurological
disease. Colorectal Dis 2014; 16: 1001–9.
28 Graf W et al. Results after sacral nerve stimulation for
chronic constipation. Neurogastroenterol Motil 2015; 27:
734–9.
29 Timmer A et al. Publication bias in gastroenterological
research - a retrospective cohort study based on abstracts
submitted to a scientific meeting. BMC Med Res Methodol
2002; 2: 7.
30 Dinning PG et al. Treatment efficacy of sacral nerve stimu-
lation in slow transit constipation: a two-phase, double-
blind randomized controlled crossover study. Am J Gas-
troenterol 2015; 110: 733–40.
31 Patton V et al. Sacral nerve stimulation fails to offer long-
term benefit in patients with slow-transit constipation. Dis
Colon Rectum 2016; 59: 878–85.
32 Zerbib F et al. Randomized clinical trial of sacral nerve
stimulation for refractory constipation. Br J Surg 2017;
104: 205–13.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 92–100100
Surgery for constipation S. A. Pilkington et al.

Surgery for constipation: systematic review and practicerecommendations
Graded practice and future research recommendations
C. H. Knowles*, U. Grossi*, E. J. Horrocks*, D. Pares†, P. F. Vollebregt*, M. Chapman‡,S. Brown§, M. Mercer-Jones¶, A. B. Williams**, Y. Yiannakou††, R. J. Hooper‡‡, N. Stevens‡‡and J. Mason§§, on behalf of the NIHR CapaCiTY working group¶¶, The Pelvic floor Society***
and European Society of Coloproctology†††*National Bowel Research Centre, Blizard Institute, Queen Mary University London, London, UK, †Hospital Germans Tr�ıas i Pujol, Barcelona, Spain,
‡Good Hope Hospital, Heart of England NHS Trust, Birmingham, UK, §Sheffield Teaching Hospitals, Sheffield, UK, ¶Queen Elizabeth Hospital,
Gateshead NHS Trust, Gateshead, UK, **Guy’s and St Thomas’ NHS Foundation Trust, London, UK, ††County Durham and Darlington NHS
Foundation Trust, Durham, UK, ‡‡NIHR Pragmatic Clinical Trials Unit, Blizard Institute, Queen Mary University of London, London, UK, §§University of
Warwick, Coventry, UK, ¶¶National Institute for Health Research: Chronic Constipation Treatment Pathway, ***Affiliate section of the Association of
Coloproctology of Great Britain and Ireland, and †††European Consensus groupa
Abstract
Aim This manuscript forms the final of seven that address
the surgical management of chronic constipation (CC) in
adults. The content coalesces results from the five system-
atic reviews that precede it and of the European Consensus
process to derive graded practice recommendations (GPR).
Methods Summary of review data, development of
GPR and future research recommendations as outlined
in detail in the ‘introduction and methods’ paper.
Results The overall quality of data in the five reviews was
poor with 113/156(72.4%) of included studies providing
only level IV evidence and only four included level I
RCTs. Coalescence of data from the five procedural
classes revealed that few firm conclusions could be drawn
regarding procedural choice or patient selection: no sin-
gle procedure dominated in addressing dynamic struc-
tural abnormalities of the anorectum and pelvic floor
with each having similar overall efficacy. Of one hundred
‘prototype’ GPRs developed by the clinical guideline
group, 85/100 were deemed ‘appropriate’ based on the
independent scoring of a panel of 18 European experts
and use of RAND-UCLA consensus methodology. The
remaining 15 were all deemed uncertain. Future research
recommendations included some potential RCTs but also
a strong emphasis on delivery of large multinational high-
quality prospective cohort studies.
Conclusion While the evidence base for surgery in CC
is poor, the widespread European consensus for GPRs
is encouraging. Professional bodies have the opportu-
nity to build on this work by supporting the efforts of
their membership to help convert the documented rec-
ommendations into clinical guidelines.
Keywords Constipation, surgery, obstructed defaecation
Introduction
This manuscript forms the final of seven that address
the surgical management of chronic constipation in
adults. The content coalesces results from the five sys-
tematic reviews that precede it and of the European
Consensus process to derive graded practice recommen-
dations.
Methods
These have been fully explained in the ‘Introduction
and Methods’ paper. Procedures have been grouped
as:
1 Colonic resection, including total colectomy, sub-
total and segmental colectomy (with some anasto-
motic variations for subtotal colectomy) by open and
laparoscopic approaches;
2 Rectal suspension procedures, including forms of
open and laparoscopic rectopexy;
3 Rectal excisional procedures, including stapled trans-
anal rectal resection (STARR) and intra-anal Delorme’s;
Correspondence to: Professor Charles H. Knowles, NBRC, 1st Floor Abernethy
Building, 2 Newark St, London E1 2AT, UK.
E-mail: [email protected]
aEuropean Society of Coloproctology members are listed in Appendix 1.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 101
This is an open access article under the terms of the Creative Commons Attribution License, which permits use,
distribution and reproduction in any medium, provided the original work is properly cited.
Systematic review doi:10.1111/codi.13775
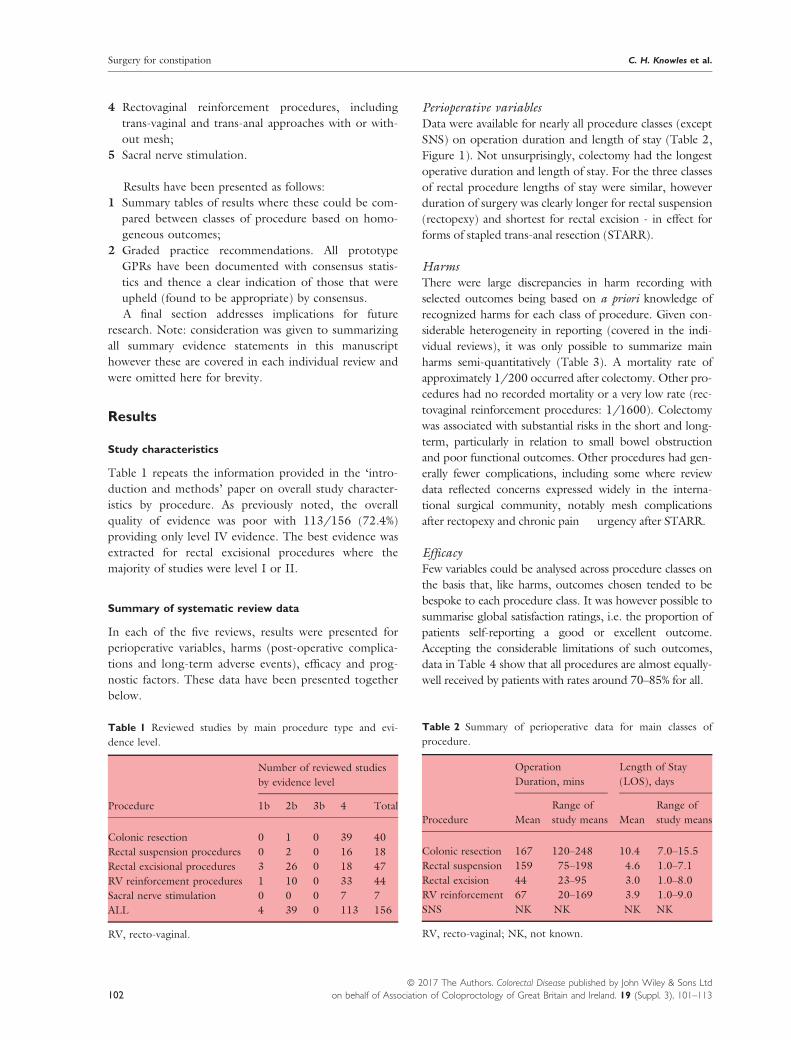
4 Rectovaginal reinforcement procedures, including
trans-vaginal and trans-anal approaches with or with-
out mesh;
5 Sacral nerve stimulation.
Results have been presented as follows:
1 Summary tables of results where these could be com-
pared between classes of procedure based on homo-
geneous outcomes;
2 Graded practice recommendations. All prototype
GPRs have been documented with consensus statis-
tics and thence a clear indication of those that were
upheld (found to be appropriate) by consensus.
A final section addresses implications for future
research. Note: consideration was given to summarizing
all summary evidence statements in this manuscript
however these are covered in each individual review and
were omitted here for brevity.
Results
Study characteristics
Table 1 repeats the information provided in the ‘intro-
duction and methods’ paper on overall study character-
istics by procedure. As previously noted, the overall
quality of evidence was poor with 113/156 (72.4%)
providing only level IV evidence. The best evidence was
extracted for rectal excisional procedures where the
majority of studies were level I or II.
Summary of systematic review data
In each of the five reviews, results were presented for
perioperative variables, harms (post-operative complica-
tions and long-term adverse events), efficacy and prog-
nostic factors. These data have been presented together
below.
Perioperative variablesData were available for nearly all procedure classes (except
SNS) on operation duration and length of stay (Table 2,
Figure 1). Not unsurprisingly, colectomy had the longest
operative duration and length of stay. For the three classes
of rectal procedure lengths of stay were similar, however
duration of surgery was clearly longer for rectal suspension
(rectopexy) and shortest for rectal excision - in effect for
forms of stapled trans-anal resection (STARR).
HarmsThere were large discrepancies in harm recording with
selected outcomes being based on a priori knowledge of
recognized harms for each class of procedure. Given con-
siderable heterogeneity in reporting (covered in the indi-
vidual reviews), it was only possible to summarize main
harms semi-quantitatively (Table 3). A mortality rate of
approximately 1/200 occurred after colectomy. Other pro-
cedures had no recorded mortality or a very low rate (rec-
tovaginal reinforcement procedures: 1/1600). Colectomy
was associated with substantial risks in the short and long-
term, particularly in relation to small bowel obstruction
and poor functional outcomes. Other procedures had gen-
erally fewer complications, including some where review
data reflected concerns expressed widely in the interna-
tional surgical community, notably mesh complications
after rectopexy and chronic pain � urgency after STARR.
EfficacyFew variables could be analysed across procedure classes on
the basis that, like harms, outcomes chosen tended to be
bespoke to each procedure class. It was however possible to
summarise global satisfaction ratings, i.e. the proportion of
patients self-reporting a good or excellent outcome.
Accepting the considerable limitations of such outcomes,
data in Table 4 show that all procedures are almost equally-
well received by patients with rates around 70–85% for all.
Table 1 Reviewed studies by main procedure type and evi-
dence level.
Procedure
Number of reviewed studies
by evidence level
1b 2b 3b 4 Total
Colonic resection 0 1 0 39 40
Rectal suspension procedures 0 2 0 16 18
Rectal excisional procedures 3 26 0 18 47
RV reinforcement procedures 1 10 0 33 44
Sacral nerve stimulation 0 0 0 7 7
ALL 4 39 0 113 156
RV, recto-vaginal.
Table 2 Summary of perioperative data for main classes of
procedure.
Procedure
Operation
Duration, mins
Length of Stay
(LOS), days
Mean
Range of
study means Mean
Range of
study means
Colonic resection 167 120–248 10.4 7.0–15.5
Rectal suspension 159 75–198 4.6 1.0–7.1
Rectal excision 44 23–95 3.0 1.0–8.0
RV reinforcement 67 20–169 3.9 1.0–9.0
SNS NK NK NK NK
RV, recto-vaginal; NK, not known.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113102
Surgery for constipation C. H. Knowles et al.

Patient selectionFor most classes of procedure, some information could
be obtained about prognostic baseline characteristics
that might guide patient selection. In all instances, the
level of evidence was poor with no formal stratified
medicine studies and very few (if any) adequately pow-
ered post-hoc analyses of good quality cohort studies.
Table 5 summarizes the broad phenotypes of patients
that may most benefit from each procedure and some
negative prognostic features.
Graded practice recommendations
A series of tables (Table 6 a-e) show all GPRs proposed by
the clinical guideline group by main procedure class. The
outcomes of the consensus process have been presented as
median score (1–9) and by classification based on RAND-
UCLA methodology: appropriate; uncertain and inappro-
priate. The reader is reminded that appropriateness is not
directly extrapolated from the median score but rather the
overall data distribution (see introduction andmethods).
Discussion
This manuscript summarises the body of data from five
systematic reviews and presents new graded practice
recommendations.
Figure 1 Summary of perioperative data for main classes of
procedure, showing range of study means.
Table 3 Summary of perioperative complications and long-term adverse events
Procedure
Total perioperative
complications* Mortality† Specific adverse events*
Colonic resection 24.4% (17.8–31.7%) 6/1568 (0.4%) Small bowel obstruction: 15.2%, (RE: 10.2% to 20.9%)
Re-op: 13.3%, (RE: 8.6% to 18.7%)
Poor function: abdominal pain, bloating (20–50%),
rec. constipation (10–30%), diarrhea & incontinence (5–15%)
Rectal suspension 9.5% (6.1–13.1%) 0/1044 Minor complications predominate e.g. UTI
Some major poorly documented e.g. SBO
Mesh complications 0.5% (range 0–3.9%)
Rectal excision 16.9% (12.7–21.5%) 0/5896 PO bleeding: 1.6% (0.9% to 2.5%)
Sepsis: 0.2% (0.0% to 0.7%)
Anastomotic dehiscence: 0.3% (0.0% to 0.8%)
Rectal stenosis: 0.2% (0.0% to 0.6%)
Chronic anorectal pain: 0.7% (0.1% to 1.6%)
Chronic urgency: 5.2% (2.7% to 8.2%)
RV reinforcement 11.5% (7.2–16.6%) 2/3209(0.06%) Post-op. bleeding: 2.0% (0.7% to 3.6%)
Haematoma or sepsis: 0.9% (0.2% to 2.0%)
Dyspareunia: inadequately reported to analyse
SNS 22.7% (12.9–34.1%) 0/375 At least one reportable event: 58%
Infection: 0–7%
Device removal: 14.4% (7.8% to 22.5%)
*Pooled estimates based on random effects (RE) models with (95% CI); RV: recto-vaginal.
†denominator represents only those studies where mortality was recorded and documented.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 103
C. H. Knowles et al. Surgery for constipation

Summary of systematic review data
The overall quality of data was poor with 113/156
(72.4%) of included studies providing only level IV evi-
dence, thus greatly limiting the number and grade of
summary evidence statements. This was a particular prob-
lem for colonic resection, rectal suspension procedures
and sacral nerve stimulation, where nearly all data were
derived from level IV studies. The limitations of such
observational data are well acknowledged and are a
source of concern when used as a basis for promoting
procedures. For instance, colectomy for slow-transit con-
stipation would, based on systematic review of 40 obser-
vational studies, appear to be an attractive prospect with
86% global satisfaction rate (the highest of any of the
studied classes of procedure). However, recently pub-
lished US retrospective cohort data on over 2000
patients [1] paint a very different picture of high compli-
cation rates and greater long-term post-procedural health
utilization (ambulatory care, hospital admissions, radiol-
ogy etc.) than before surgery. It is difficult to reconcile
such disparity [2], and the increasing rates of colectomy
for constipation in the US [1] also seem at odds with
international opinion (that promotes extreme caution).
Sacral nerve stimulation also had generally supportive
observational evidence based on seven included studies.
However, subsequent randomised studies [3,4] directly
contradict these data and most centres no longer offer
SNS for the constipation indication.
Perhaps the greatest area of academic contention in
the pelvic floor community concerns the choice of pro-
cedure to address dynamic structural abnormalities of
the pelvic floor that lead to prolapse and obstructed
defaecation symptoms. The results presented here do
little to help resolve this issue and certainly cannot help
underpin a much needed treatment algorithm for such
patients. In effect, all have similar global satisfaction rat-
ings, similar lengths of stay and complication profiles
that are to some extent procedure-specific. Based on
reviewed indications, rectal suspension and excision pro-
cedures can be applied to patients with rectal intussus-
ception and/or rectocoele and rectovaginal
reinforcement procedures to rectocoele only. Aside
from a generally longer operating time for rectopexy
(and shorter for STARR), decision making for a patient
with one or both of these abnormalities currently rests
with personal views about the acceptability of certain
complications and (possibly) surgeon enthusiasm for
Table 4 Summary of efficacy data based on global satisfaction ratings.
Procedure No studies Total No patients Follow up (mean and range of means, months) Global satisfaction*
Colonic resection 40 2045 47 (12–132) 86 (81–89)%
Rectal suspension 18 1238 25 (12–72) 83 (74–91)%
RV reinforcement 44 3499 25 (12–74) 72 (67–77)%
Rectal wall excision 47 8340 23 (12–66) 76 (73–80)%
SNS 7 375 27 (20–51) 73 (57–87)%
*Pooled estimates based on random effects models with (95% CI).
Table 5 Patient characteristics influencing selection for each class of procedure
Procedure Main positive characteristic Secondary positive characteristics Negative characteristics
Colonic resection Proven slow transit constipation Proven upper GI dysmotility
Proven psychiatric disorder
Inconsistent evidence for combined
defaecation disorder
Rectal suspension High grade intussusception
(Oxford grade III-V)
Solitary rectal ulcer syndrome
(SRUS)Rectocoele
None established
Rectal excision Minimum of 3 ODS symptoms;
Functioning rectocoele
High grade intussusception
(Oxford grade III-V)
None established
Rectovaginal
reinforcement
Functioning and significantly-
sized rectocoele
None established None established
SNS Chronic constipation None established None established
ODS, obstructed defaecation symptoms.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113104
Surgery for constipation C. H. Knowles et al.

Table 6 (a-e) Graded practice recommendations
Evidence level Grade Median score Decision
(a)
Colonic resection
Patient selection
1. Given uncertainty of outcome and potential for harm, colectomy
should only be offered to patients when all other relevant
treatments have failed
IV C 9 Appropriate
2. Given concerns regarding outcome, the following represent
absolute or relative contra-indications to colectomy
a Concomitant upper GI symptoms (relative) V N 6 Uncertain
b Proven upper GI dysmotility (absolute) IV C 8 Uncertain
c Unproven generalised delay in colon transit (absolute) IV C 8 Appropriate
d Concomitant defecation disorder (relative) IV D 6 Uncertain
e Significant symptoms of abdominal pain and bloating, including diag-
nosis of IBS (relative)
IV D 6 Uncertain
f Faecal incontinence and/or functionally impaired anal sphincter V N 9 Appropriate
3. As a consequence of the above, colectomy should not be
considered without precision phenotyping (clinical and radio-
physiological)
IV C 9 Appropriate
4. Given concerns regarding outcome, magnitude and irreversibility
of colectomy, patients with concomitant defecation disorder
should have this treated first including surgery for structural
causes where relevant
IV D 8 Appropriate
5. All patients considered for colectomy should have specialist
multidisciplinary discussion
V N 9 Appropriate
6. Formal psychological evaluation should be undertaken in all
patients considered for colectomy for constipation
V N 7 Appropriate
7. In view of need for specialist investigations and review, patients
should only undergo colectomy for constipation in centres with
access to appropriate specialist services
V N 9 Appropriate
Procedural considerations
1. Colectomy and ileorectal anastomosis (CIRA) should be
considered the default option considering weight of evidence
compared to other procedures
IV C 8 Appropriate
2. There are insufficient data to conclude that the following provide
certain benefit in terms of clinical outcome in comparison to CIRA
• Subtotal or segmental resection IV C 8 Appropriate
• Subtypes of subtotal resection (caecorectal vs ileosigmoid) IV D 7 Appropriate
• Variations in anastomotic configuration (iso- or anti-peristaltic) IV D 7 Appropriate
• Laparoscopic vs open approach IV D 5 Uncertain
• Tailoring of segmental resections using specialist regional tran-
sit measurements
IV D 6 Uncertain
3. Laparoscopic surgery should be considered in suitable patients
because of:
• Modest reductions in length of stay IV D 8 Appropriate
• Cosmesis and other generally-perceived benefits e.g. reduced
incisional hernia
V N 8 Appropriate
• Possible reduction in long-term small bowel obstruction and
re-operation rates
IV D 8 Appropriate
Patient counselling
1. Approximately 85% patients report some benefit at follow up
greater than 1 year after colectomy
IV C 8 Appropriate
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 105
C. H. Knowles et al. Surgery for constipation

Table 6 (Continued).
Evidence level Grade Median score Decision
2. Total perioperative complication rates vary greatly but may occur
in approximately 20–30% of colectomy patients regardless of
procedure choice, and include serious life-threatening
complications such as anastomotic leak (5% risk) and mortality
(0.4%)
IV C 8 Appropriate
3. Rates of post-operative ileus or early post-operative adhesional
small bowel obstruction vary greatly but occur in about 5–15% of
patients and about one-third of these patients require re-operation
regardless of procedure choice
IV C 8 Appropriate
4. Long-term adverse events characterized by recurrent episodes of
small bowel obstruction occur in about 10–20% of patients and
may result in a significant burden of re-hospitalization and
frequent recourse to surgery
IV C 8 Appropriate
5. Negative long term functional outcomes persist in a proportion of
patients: diarrhoea and incontinence in about 5–15% of patients;
abdominal pain in 30–50% of patients; recurrent constipation in
10–30% of patients and bloating in 10–40%
IV C 8 Appropriate
6. As a result of immediate and long-term complications,
approximately 5% patients will have a permanent ileostomy
IV C 6 Uncertain
(b)
Rectal suspension procedures
Patient selection
1. Rectal suspension procedures should be considered only for
patients failing appropriate non-surgical treatments
IV D 9 Appropriate
2. Rectal suspension procedures should be considered for patients
with the following anatomical abnormalities in conjunction with
symptoms suggestive of rectal evacuation disorder
• High grade intussusception (recto-anal e.g. Oxford grade: 3–5) IV C 8 Appropriate
• SRUS with associated intussusception IV C 8 Appropriate
3. Diagnosis of anatomical abnormalities should be conducted to a
standard where agreement exists that observed findings can be
deemed pathological based on appropriate normative data (derived
within the department or derived elsewhere but using identical
methodology e.g. for proctographic imaging)
V N 8 Appropriate
4. Given concerns regarding outcome, the following should be
regarded as relative contraindications to rectal suspension
procedures
• Significant psychiatric disorders V N 7 Appropriate
• Significant chronic pain syndromes including IBS V N 8 Appropriate
• Morbid obesity V N 8 Appropriate
• Known hostile abdomen/pelvis V N 8 Appropriate
• Joint hypermobility syndrome (EDS3)/connective tissue disor-
ders
V N 5 Uncertain
5. Patients considered for rectal suspension procedures should have
specialist multidisciplinary discussion
V N 8 Appropriate
6. In view of need for specialist investigations and review, patients
should only undergo rectal suspension procedures for constipation
in centres with access to appropriate specialist services
V N 8 Appropriate
7. Rectal suspension procedures (especially those employing mesh)
require special consideration in women who plan to become
pregnant
V N 8 Appropriate
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113106
Surgery for constipation C. H. Knowles et al.

Table 6 (Continued).
Evidence level Grade Median score Decision
Procedural considerations
1. There is insufficient current evidence to conclude that any one
rectal suspension procedure is clearly superior to another
IV C 7 Appropriate
2. Laparoscopic surgery should be considered in suitable patients
because of:
• Cosmesis and other generally perceived benefits such as
reduced incisional hernia
V N 8 Appropriate
• Possible reduction in adhesion formation V N 8 Appropriate
• Superior access to the deep pelvis V N 7 Appropriate
3. There is no current evidence to suggest superiority of robotic
surgery over a standard laparoscopic approach
IV D 8 Appropriate
4. Careful consideration should be given to the type of mesh and
fixation
V N 8 Appropriate
Patient counselling
1. Approximately 83% (73–91%) patients report some benefit at
follow up greater than 1 year after rectal suspension procedures
IV C 8 Appropriate
2. Total perioperative complication rates vary greatly but may occur
in approximately 5–15% of patients regardless of procedure choice
IV C 8 Appropriate
3. Serious complications such as mesh erosion occur in 0–4% of
patients however no mortality has not been reported
IV C 8 Appropriate
4. The effect on constipation symptoms is highly variable and data
are only available for lap VMR after which most patients (86%)
report an improvement in constipation symptoms
IV C 7 Appropriate
5. In patients with SRUS, ulcer healing is observed in 78% of
patients
IV C 8 Appropriate
(c)
Rectal excisional procedures
Patient selection
1. Rectal excisional procedures should be considered only for
patients failing appropriate non-surgical treatments
II B 9 Appropriate
2. Rectal excisional procedures should be considered for patients
with the following anatomical abnormalities in conjunction with
symptoms suggestive of rectal evacuation disorder
• Minimum of 3 ODS symptoms II B 7 Appropriate
• Rectorectal or rectoanal intussusception only IV D 5 Uncertain
• Rectocele only II B 5 Uncertain
• Rectocele and intussusception II B 7 Appropriate
3. Diagnosis of anatomical abnormalities should be conducted to a
standard where agreement exists that observed findings can be
deemed pathological based on appropriate normative data (derived
within the department or derived elsewhere but using identical
methodology e.g. for proctographic imaging for grade of
intussusception and size/functionality of rectocele)
V N 8 Appropriate
4. Given concerns regarding outcome, the following should be
regarded as relative contraindications to rectal excisional
procedures although none were supported by evidence in the
systematic review
• Significant psychiatric disorders V N 8 Appropriate
• Significant chronic pain syndromes (including IBS) or perceived
susceptibility to chronic post-surgical pain
V N 8 Appropriate
• Concomitant enterocele (because of perceived risk of bowel
injury
V N 9 Appropriate
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 107
C. H. Knowles et al. Surgery for constipation

Table 6 (Continued).
Evidence level Grade Median score Decision
• Reduced anal sphincter function (because of risk of urgency and
incontinence)
V N 7 Appropriate
• Solitary rectal ulcer syndrome V N 7 Appropriate
• Clear evidence of anal sphincter dyssynergia V N 7 Appropriate
• External rectal prolapse or other significant pelvic organ prolapse
syndrome
V N 9 Appropriate
5. Patients considered for rectal excisional procedures should have
specialist multidisciplinary discussion
V N 9 Appropriate
6. In view of need for specialist investigations and review, patients
should only undergo rectal excisional procedures for constipation
in centres with access to appropriate specialist services
V N 8 Appropriate
Procedural consideration
1. The evidence base of procedural choice is dominated by studies of
STARR procedures and all higher quality studies report STARR
outcomes; on this basis, it is reasonable to recommend STARR as
the default excisional procedure
II B 8 Appropriate
2. There is insufficient current evidence to conclude that any one
rectal excisional procedure is clearly superior to another in terms
of efficacy or complications
IV D 7 Appropriate
Patient counselling
1. Approximately 76% (73–80%) patients report some benefit at
follow up greater than 1 year after rectal excisional procedures
II B 7 Appropriate
2. Total perioperative complication rates vary greatly but may occur
in approximately 13–22% of patients regardless of procedure
choice
II B 7 Appropriate
3. Significant complications such as sepsis, anastomotic dehiscence
and bleeding occur in in approximately 2% (1–4%) of patients
II B 6 Uncertain
4. Life-threatening complications occur in in approximately 1: 1000
patients however no mortality was reported in recent review of
almost 6000 patients
II B 8 Appropriate
5. The effect on constipation symptoms is highly variable although
approximately 70% patients will obtain a significant reduction in
burden of obstructed defaecation symptoms
II B 7 Appropriate
6. Patients should be warned of long-term adverse functional
outcomes; rates of urgency (10%) and of chronic pain (2%) should
be cited
II B 8 Appropriate
7. Other long-term complications e.g. stenosis (< 1%)and fistula (1
in 1600) are rare
II B 7 Appropriate
(d)
Rectovaginal reinforcement
Patient selection
1. Rectovaginal reinforcement procedures should be considered for
patients with the following anatomical abnormalities in
conjunction with typical symptoms (vaginal bulging or prolapse
and problematic rectal evacuation)
• Significant dimensions (depth) based on clinical � imaging
assessment
IV C 7 Appropriate
• Evidence of functionality (trapping) on dynamic assessment IV C 8 Appropriate
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113108
Surgery for constipation C. H. Knowles et al.

Table 6 (Continued).
Evidence level Grade Median score Decision
2. Diagnosis of the above should be conducted to a standard where
agreement exists that observed findings can be deemed
pathological based on appropriate normative data (derived within
the department or derived elsewhere but using identical
methodology e.g. for imaging)
V N 8 Appropriate
3. Given concerns regarding outcome the following should be
regarded as relative contraindications to all forms of rectovaginal
reinforcement procedures
• Diagnosis of major psychiatric disorders V N 7 Appropriate
• Significant chronic pain syndromes including IBS V N 7 Appropriate
• Morbid obesity V N 7 Appropriate
• High grade recto-anal intussusception V N 8 Uncertain
4. Procedure-specific relative contraindications should include:
• Vaginal repairs: smoking V N 5 Uncertain
• Transanal repairs: sphincter incompetence, rectal inflammation
or anorectal stenosis
V N 8 Appropriate
5. Patients considered for rectovaginal reinforcement procedures
should have specialist multidisciplinary discussion
V N 9 Appropriate
6. In view of need for specialist investigations and review, patients
should only undergo rectovaginal reinforcement procedures for
constipation in centres with access to appropriate specialist services
V N 8 Appropriate
7. Rectovaginal reinforcement procedures require special
consideration in women who plan to become pregnant
V N 8 Appropriate
Procedural considerations
1. There is insufficient evidence to conclude that any one
rectovaginal reinforcement procedure is clearly superior to another
for the treatment of constipation
IV C 8 Appropriate
2. Evidence derived from other indications for rectovaginal
reinforcement procedures e.g. pelvic organ prolapse syndromes
suggests superiority of vaginal repair (although this has not been
demonstrated in the treatment of constipation)
V N 5 Uncertain
3. Limited evidence suggests that a site specific vaginal repair may
lead to a higher recurrence rate than other surgical approaches
IV C 5 Uncertain
4. There is no evidence that the use of mesh reinforcement in vaginal
or perineal surgery leads to net benefit
IV C 7 Appropriate
Patient counselling
1. Approximately 73% (67–78%) patients report some benefit at
follow up after 1 year after rectovaginal reinforcement procedures
IV C 7 Appropriate
2. Total perioperative complication rates vary greatly but may occur
in approximately 7–17% of patients regardless of procedural choice
IV C 8 Appropriate
3. Serious complications such as rectovaginal fistula occur rarely (< 1
in 1000 patients); mortality has been reported in 1 in 1600
patients
IV C 8 Appropriate
4. While dyspareunia may occur with any of the surgical procedures,
the particular risks of a vaginal approach should be discussed with
the patient
IV D 9 Appropriate
5. Evidence derived from other indications for rectovaginal
reinforcement procedures e.g. pelvic organ prolapse syndromes
suggests an increased risk of dyspareunia with a vaginal repair in
conjunction with levatorplasty
V N 7 Appropriate
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 109
C. H. Knowles et al. Surgery for constipation

type of approach and surgical instruments (flippantly
whether the surgeon prefers basic surgical instruments,
laparoscopy or staplers). With respect to complications,
limited reporting prevented much discussion beyond
the importance of counselling patients about established
complications (covered in GPRs). However, it is tempt-
ing to speculate that future stratification might provide
the opportunity to select patients for one or other pro-
cedure e.g. avoiding patients with certain prior pheno-
typic features or modifying risk. An example would be
chronic pain development, where perhaps STARR
should be relatively contra-indicated in patients with
preceding evidence of pain syndromes (e.g. migraine,
fibromyalgia or chronic back pain) or modified using
one of a number of available agents to prevent sensitiza-
tion during surgery e.g. pre-operative gabapentin or
intra-operative ketamine [5]. At the very least the data
provide the opportunity to appraise patients with the
options and their complication profiles where more than
one surgical option exists.
Another difficulty with interpretation was that inclu-
sion (in the review) necessarily reflected the availability
of studies, in turn reflecting the tendency to publish
studies of new techniques rather than well-established
ones. Higher quality data were available for rectal exci-
sional procedures due to several prospective cohort
studies and small RCTs of the STARR procedure (and
variations). It is well acknowledged that this body of
data, including over 8000 patients, reflects a period of
intense popularity for this procedure (nearly all pub-
lished in the decade 2004–14) with (interestingly) no
included papers arising from the final 18 months of the
review period. The large numbers are also known to
reflect industry investment in several data registries, two
of which included over 2000 patients. Anecdotal evi-
dence and expert opinion from international meetings is
that the popularity for this procedure has waned (even
in Italy – the origin of the procedure and its main pro-
ponents). Such a peak and decline in popularity was not
present for other procedures that were more evenly
spread across the review period.
Graded practice recommendations
The clinical guidelines group developed a total of 100
‘prototype’ graded practice recommendations by taking
forward summary evidence statements from the five
reviews and combining these with expert opinion and a
small number of RCTs (SNS only) published after the
extraction data (22/02/2016). These statements cov-
ered patient selection, procedural considerations and
patient counselling. The limitations in review evidence
meant that only 59/100 prototype GPRs were directly
derived from summary evidence (level II-IV; grades B-
D) with the remainder, 41/100 derived by expert opin-
ion only (level V; grade N). Of the 100 total, 85 were
deemed ‘appropriate’ based on the independent scoring
of 18 European experts and the remaining 15 were all
Table 6 (Continued).
Evidence level Grade Median score Decision
(e)
Sacral nerve stimulation
Patient selection
1. Recent trial data (from 2 independent RCTs) suggest no overall
benefit of SNS for chronic constipation regardless of type of
constipation; on this basis, the procedure cannot be recommended
for this indication
II B 7 Appropriate
Procedural considerations
1. Not applicable (follow manufacturer’s instructions and specific
training)
NA NA NA NA
Patient counselling
1. Patients should be counselled that the evidence base does not
support the use of SNS for chronic constipation
II B 9 Appropriate
2. If performed, patients should be warned of:
• Highly variable rates of device removal for adverse effects or
lack of efficacy
IV D 8 Appropriate
• Very high rates of reprogramming IV D 8 Appropriate
• Low eventual success rates II B 9 Appropriate
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113110
Surgery for constipation C. H. Knowles et al.

deemed uncertain, i.e. none was considered inappropri-
ate by the panel. This is a high level of consensus for a
single round of questioning and suggests that there is
reasonable European agreement as to selection of
patients for each class of procedure, which procedure to
perform and how to counsel the patient (often related
to outlining potential harms). However, this does not
signify unequivocal evidence of value for these recom-
mendations and they do not represent minimum stan-
dards, but can act as a basis for further research and
guideline development.
The 15 ‘uncertain’ GPRs were spread across proce-
dures with most in colectomy (n = 7) and least for
rectal suspension (1) and SNS (0). The majority con-
cerned patient selection (n = 8). Interestingly, only 5/
15 (33.3%) related to prototype GPRs based only on
expert opinion (level V, grade N). The remaining 10
included five where uncertainty by consensus accurately
reflected uncertainty by grade (D) (33.3%), three with
grade C summary evidence from the systematic reviews
(20.0%) and two with grade B evidence (13.3%).
There was thus no strong suggestion that grade
weighed panelist opinion. The two grade B statements
deemed uncertain both concerned rectal excision: first
that ‘rectocoele only’ was an indication in terms of
benefiting the patient; and secondly that significant
complications such as sepsis, anastomotic dehiscence
and bleeding can occur post-procedure in approxi-
mately 2% (1–4%) of patients. The panelist consensus
on these two GPRs is surprising since both would
seem to reflect widespread practice and knowledge,
respectively. Overall, while it would be possible to
have further rounds of consensus building among the
European panel, the GPRs as stands are a good start
to develop future clinical guidelines.
Future research recommendations
With the exception of rectal excision, there are clear
deficiencies in the current evidence base for all surgical
procedures directed at the management of chronic con-
stipation in adults. This was particularly true in terms of
availability of randomized controlled trials, where only
four reviewed studies met criteria for level I evidence.
The difficulties in conducting randomized trials for
complex interventions such as surgery are well rehearsed
[6], but their importance is exemplified by recent SNS
RCTs [3,4] that directly contradict observational data.
While it can be argued that sham surgery would be dif-
ficult to justify for patients with a chronic debilitating
condition, it is disappointing that no level I evidence
has been produced to compare classes of procedure
where more than one is appropriate. Such comparison
trials of different techniques may face problems of equi-
poise and interventional fidelity, and might need to
overcome a speciality divide e.g. posterior repair vs
transanal repair of rectocoele (the former performed lar-
gely by gynaecologists or urologists specializing in
female patients and the latter by colorectal surgeons).
An alternative is waiting-list designs where the wait time
for surgery can be randomized and analysis-based on
longitudinal outcomes before and after intervention [7].
An example of such a study is the CapaCiTY03
stepped-wedge randomised controlled study of laparo-
scopic ventral mesh rectopexy in adults with chronic
constipation [8].
Accepting the difficulty in performing RCTs, there is
still much opportunity to improve the evidence base by
encouraging high quality observational studies. Prospec-
tive cohort studies could benefit from incorporating
some of the scientific rigor of RCTs to limit obvious
sources of bias e.g. by multicentre recruitment and use
of blinded observers to collect outcomes. Awareness of
reporting standards by authors and journals may in turn
feed better protocol-driven research [9]. They should
incorporate the few validated patient-reported outcome
measures (PROMS) that are available e.g. PAC-QoL
and PAC-SYM, internationally-accepted HR-QoL mea-
sures e.g. EQ-5D-5L and monitor harms in a systematic
manner using established systems e.g. Clavien-Dindo
[6]. They should also consider collecting health utiliza-
tion data from patient information systems, the impor-
tance of which is illustrated by the Dudekula study [1]
of colectomy.
The CCG make the following recommendations as
research priorities:
1 Colonic resection: there is a need to determine
prospectively and robustly the risks and benefits of
this procedure. Considering its low incidence, a
prospective cohort study across Europe (or interna-
tionally) is recommended. Observer-blinded out-
comes (above) should be systematically recorded at
regular intervals to 5 years. Standardised baseline
phenotyping may permit determination of outcome
predictors if numbers are large enough. Considera-
tion could be given to a control group not undergo-
ing surgery (although selection bias is
acknowledged). All procedural variations could be
evaluated although the main comparison of interest
is now considered to be between more (total colec-
tomy) and less radical (subtotal) laparoscopic resec-
tions. A double-blind RCT of this latter comparison
might also be possible with international effort.
2 Rectal procedures for dynamic structural abnormali-
ties of the pelvic floor. A UK RCT is underway to
evaluate laparoscopic ventral mesh rectopexy [8]. A
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 111
C. H. Knowles et al. Surgery for constipation

further RCT is however recommended to determine
outcomes of repair of large rectocoele (in isolation),
comparing posterior repair of the vagina vs transanal
repair. It is acknowledged that this might require an
expertise-based design [6,10] but it is an unanswered
question for the indication of chronic constipation or
obstructed defaecation. Systematic review data would
also support a randomized comparison of STARR
with rectopexy for patients with high-grade intussus-
ception and rectocoele. However, expert opinion sug-
gests that STARR is no longer popular. An alternative
would be to perform a prospective cohort study (akin
to colectomy) capturing all current practice. This
could be performed internationally but might also be
possible in a single country where all three main
classes of procedure are still commonly utilized.
Conclusions
This manuscript concludes the series of seven, systemat-
ically detailing the outcomes of the main surgical proce-
dures directed toward patients with chronic
constipation. The current evidence base is poor and
heavily reliant on low-quality observational data. On
this basis, all procedures reviewed had generally positive
(supportive) data. Several authors expressed concern
that such data might not reflect the reality of clinical
practice. While bias in such observational study designs
is well recognized, it is possible that in surgical studies
(usually performed by the proponents of the surgery)
bias is both unidirectional (favouring the intervention)
and powerful. Not only should this lead to a greater
willingness to design and deliver high quality controlled
trials, but also to an essential understanding that retro-
spective observational studies should be interpreted with
caution. However the finding of widespread consensus
for graded practice recommendations is encouraging.
The stage is now set for recognised professional bodies
worldwide e.g. Societies of Coloproctology/Colorectal
surgery to build on this work by supporting the efforts
of their membership to address future research recom-
mendations and/or to help convert the recommenda-
tions documented in this series of papers into their
clinical guidelines.
Acknowledgments
We would like to acknowledge the following people in
relation to the NIHR CapaCiTY working group: Mr
Steven Brown, Sheffield Teaching Hospitals NHS
Foundation Trust; Mr Kenneth Campbell, The Univer-
sity of Dundee, NHS Education for Scotland; Mr Mark
Chapman, Heart of England NHS Trust; Mr Andrew
Clarke, Poole Hospital NHS Foundation Trust; Mr Neil
Cruickshank, Sandwell and West Birmingham Hospitals
NHS Trust; Mr Anthony Dixon, University of Bristol,
Bristol, UK; Dr Christopher Emmett, County Durham
and Darlington NHS Foundation Trust; Mr Ugo
Grossi, Queen Mary University of London; Dr Richard
Hooper, PCTU, Queen Mary University of London;
Miss Emma Horrocks, University Hospital Southamp-
ton NHS Foundation Trust; Professor Charles Knowles,
Queen Mary University of London; Mr Jon Lacy-Col-
son, Shrewsbury and Telford Hospital NHS Trust; Mr
Ian Lindsey, Oxford University Hospitals NHS Trust;
Professor James Mason, University of Warwick, Coven-
try; Mr Mark Mercer-Jones, Gateshead Health NHS
Foundation Trust; Mr Andrew Miller, University
Hospitals of Leicester NHS Trust; Mr David Pares,
Hospital Germans Trias i Pujol, Barcelona, Spain; Miss
Sophie Pilkington, University Hospital Southampton
NHS Foundation Trust; Mr Neil Smart, Royal Devon
& Exeter NHS Foundation Trust; Ms Natasha Stevens,
PCTU, Queen Mary University of London; Professor
Douglas Tincello, University Hospitals of Leicester
NHS Trust; Miss Karen Telford, South Manchester
NHS Foundation Trust; Mr Paul Vollebregt, Queen
Mary University of London; Mr Andrew Williams,
Guy’s and Thomas’ NHS Foundation Trust; Professor
Yan Yiannakou, County Durham and Darlington NHS
Foundation Trust.
Conflict of interest
All authors have no conflict of interest in relation to the
content of the manuscript. In the last 2 years, C.H.
Knowles has received speaker fees and consultancy pay-
ments from Medtronic Inc., S. Brown has received
speaker fees and consultancy payments from Allergan,
A.B. Williams has received speaker fees and consultancy
payments from Medtronic Inc. and acts as a nonpayed
consultant for Cook Medical, Y. Yiannakou has received
speaker fees and consultancy payments from Movetis
and Enteromed, and M. Mercer-Jones has received fees
as a preceptor for Medtronic Inc. Mark Chapman has
received funding to attend courses from Medtronic Inc.
Funding
This project was funded by the National Institute for
Health Research (NIHR) Programme Grant for Applied
Research (RP-PG-0612-20001). The views and opin-
ions expressed in this report are those of the authors
and are not those of the PGfAR Programme, NIHR,
the UK National Health Service, or the UK Depart-
ment of Health.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113112
Surgery for constipation C. H. Knowles et al.

References
1 Dudekula A, Huftless S, Bielefeldt K. Colectomy for consti-
pation: time trends and impact based on the US Nation-
wide Inpatient Sample, 1998–2011. Aliment Pharmacol
Ther 2015; 42: 1281–93.
2 Knowles CH. Defecation: Colectomy for constipation-a
time for renewed caution? Nat Rev Gastroenterol Hepatol
2015; 12: 675–6.
3 Dinning PG, Hunt L, Patton V et al. Treatment efficacy of
sacral nerve stimulation in slow transit constipation: a two-
phase, double-blind randomized controlled crossover study.
Am J Gastroenterol 2015; 110: 733–40.
4 Zerbib F, Siproudhis L, Lehur PA et al. Randomized clini-
cal trial of sacral nerve stimulation for refractory constipa-
tion. Br J Surg 2017; 104: 205–13.
5 Humble SR, Dalton AJ, Li L. A systematic review of thera-
peutic interventions to reduce acute and chronic post-surgi-
cal pain after amputation, thoracotomy or mastectomy. Eur
J Pain 2015; 19: 451–65.
6 Ergina PL, Cook JA, Blazeby JM et al. Challenges in
evaluating surgical innovation. Lancet 2009; 374: 1097–
104.
7 McCulloch P, Altman DG, Campbell WB et al. No surgical
innovation without evaluation: the IDEAL recommenda-
tions. Lancet 2009; 374: 1105–12.
8 ISRCTN.com; SRCTN#11747152. http://www.isrctn.com/
ISRCTN11747152.
9 von Elm E, Altman DG, Egger M et al. The Strengthening
the Reporting of Observational Studies in Epidemiology
(STROBE) statement: guidelines for reporting observa-
tional studies. Lancet 2007; 370: 1453–7.
10 Devereaux PJ, Bhandari M, Clarke M et al. Need for exper-
tise based randomised controlled trials. BMJ 2005; 330: 88.
Appendix 1
European Consensus group authorship: Donato Alto-
mare, Lars Boenicke, Steen Buntzen, Ken Campbell,
Peter Christensen, Andre D’Hoore, Eloy Espin, David
Jayne, Oliver Jones, Jens-Christian Knapp, Soren Lau-
rberg, Paul Lehur, Klaus Matzel, Ronan O’Connell,
Michel Prudhomme, Carlo Ratto, Mario Trompetto, and
Carolynne Vaizey.
ª 2017 The Authors. Colorectal Disease published by John Wiley & Sons Ltd
on behalf of Association of Coloproctology of Great Britain and Ireland. 19 (Suppl. 3), 101–113 113
C. H. Knowles et al. Surgery for constipation




















