• Multiple Lessons • Interactive Exercises • References ...
107
Developmental Care by Speech-Language Pathologists in the Neonatal Intensive Care Unit ASHA Self-Study 4400 1 © 2011 American Speech-Language-Hearing Association • Multiple Lessons • Interactive Exercises • References • Related Resources • CEU Test
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of • Multiple Lessons • Interactive Exercises • References ...

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 1
© 2011 American Speech-Language-Hearing Association
• Multiple Lessons• Interactive Exercises• References• Related Resources• CEU Test

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 2
NAVIGATION PANELAccess content by clicking ontopics, or by title search.
PRESENTER PANELProvides information aboutthe presenter.
TOOLBARAccess relevant resources,references, and links; or exit theprogram.
PLAYBACK CONTROLSAdjust volume, play or pause theprogram, jump to the previous ornext slide.
CONTENT PANELDisplays slides, movies, simulations, and videos.
• Print a PDF copy of the testquestions in AdditionalResources.
• Refer to program contentduring the test.
• Complete test in its entirety.
• You have 3 attempts to passthe test (80%).
• Notice of completion will bemailed after successfulcompletion.
• CEUs are recordedautomatically for members ofthe ASHA CE Registry.

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 3
This course is offered for 0.3 ASHA CEUs (Intermediate level, Professional area).
Claire Miller, PhD, CCC-SLP, BRS-SAnn Clonan, MEd, CCC-SLP
Brenda Thompson, MA, CCC-SLP

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 4
• Implementation of developmentally-supportive care leads to improvedoutcomes for preterm infants
• Explore terminology and diagnoses specific to the NICU• History of developmental care and knowledge• Etiologies of oral motor and feeding problems in premature infants• Clinical indicators highlighting the need for objective swallowing
assessment• Develop supportive non-nutritive and nutritive oral motor stimulation
plans in the context of the overall developmental care plan.
• Recognize infant states, cues of stress, and levels of comfort• Utilize appropriate assessment/management methods• Discuss the role of speech-language pathology in interdisciplinary
assessment and treatment• Identify clinical indicators of swallowing dysfunction that signal the
need for objective assessment• Design treatment goals that can be implemented in the infant's
overall developmental care plan

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 5
Ann Clonan, MEdInpatient Speech
Pathology ProgramCincinnati Children's
Hospital Medical Center
Brenda Thompson, MARegional Center for
Newborn Intensive CareCincinnati Children's
Hospital Medical Center
Claire Miller, PhDAerodigestive CenterCincinnati Children's
Hospital Medical Center
II. Diagnoses: Impact on Feeding
III. Developmental Care
IV. Assessment and Intervention
V. Instrumental Assessment of Swallowing
VI. Using Current Evidence to Guide Intervention
I. Introduction to the NICU Click ona sectionto begin
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 6
Section I: Objectives
• Overview of the NeonatalIntensive Care Unit (NICU)
• ASHA Policy Documents
(see Additional Resources)
– Position Statement
– Technical Report
– Guidelines
– Required knowledge andskills
TOOLBARAccess Additional
Resources

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 7
Levels of Care
• Level I: Newborn Nursery
– Cares for healthy, term infants or infants who arephysiologically stable and born at 35-37 weeksgestation
• Level II: Special Care Nursery
– Provides level I care plus care for infants >32 weeksgestation and >1500 grams with physiologicalimmaturity (poor feeding, temperature instability,apnea)
– Infants in need of respiratory assistance such asmechanical ventilation for < 24 hours
Levels of Care (cont.)
• Level III: Neonatal Intensive Care Unit
– Levels I and II in addition, depending onintensity of needs, gestational age (<28weeks) and weight (<1000 grams)
• Advanced respiratory support, major surgicalrepairs, cardiopulmonary bypass, ECMO, accessto subspecialty consultants, access to advancedimaging (CT, MRI, echocardiography)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 8

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 9
Multidisciplinary Environment
• Neonatologists
• Neonatal nursepractitioners
• Resident physicians
• Nurses
• Registered Dietitians
• Pharmacists
• Respiratory therapists
• Pediatric Specialists (ENT,cardiology, neurology, GI,etc.)
• Speech-languagepathologists
• Occupational therapists
• Physical Therapists
• Audiologists
• Social Workers
• Chaplin
• Psychologists
• Holistic Health
• Child Life
• Developmental Specialists

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 10
Birth Weight Definitions
• Low birth weight (LBW): less than 2,500grams or 5 pounds, 8 ounces
• Very Low birth weight (VLBW): less than1,500 grams or 3 pounds, 4 ounces
• Extremely Low birth weight (ELBW): lessthan 1,000 grams
Premature Birth Rate
• More than 525,000 babies (12.7%)
• Current data shows continued increase
• 20% increase since 1990
• 60,000+ born with a birth weight of < 1500grams
• 90% survive
• 10% significant disability
• 25-50% experience later cognitive & behavioraldeficits
National Center for Health Statistics (www.cdc.gov/nchs)(Foster-Cohen et al., 2010; McCormick et al., 2011; Laughon et al., 2009)
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 11
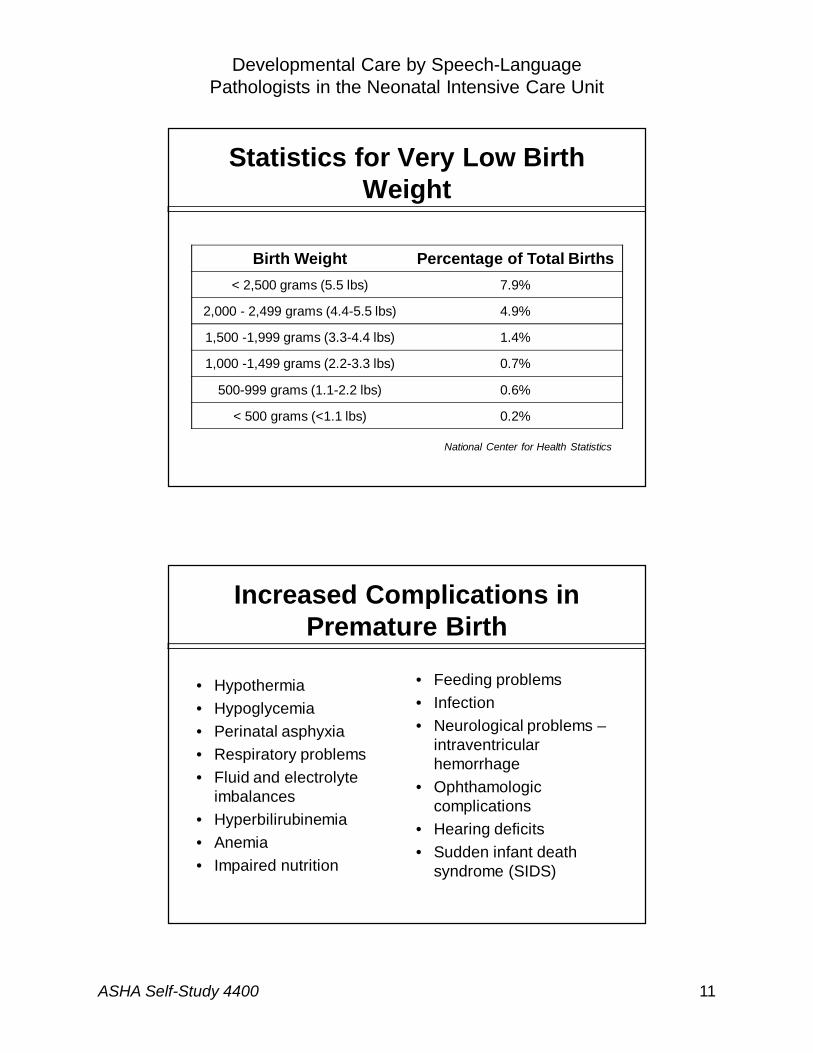
Statistics for Very Low BirthWeight
Birth Weight Percentage of Total Births
< 2,500 grams (5.5 lbs) 7.9%
2,000 - 2,499 grams (4.4-5.5 lbs) 4.9%
1,500 -1,999 grams (3.3-4.4 lbs) 1.4%
1,000 -1,499 grams (2.2-3.3 lbs) 0.7%
500-999 grams (1.1-2.2 lbs) 0.6%
< 500 grams (<1.1 lbs) 0.2%
National Center for Health Statistics
Increased Complications inPremature Birth
• Hypothermia
• Hypoglycemia
• Perinatal asphyxia
• Respiratory problems
• Fluid and electrolyteimbalances
• Hyperbilirubinemia
• Anemia
• Impaired nutrition
• Feeding problems
• Infection
• Neurological problems –intraventricularhemorrhage
• Ophthamologiccomplications
• Hearing deficits
• Sudden infant deathsyndrome (SIDS)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 12
Risks for Long TermComplications
• Generally the smallerthe baby, the higher therisk
• Increased likelihood of
– Cerebral palsy
– Blindness
– Deafness
– Developmental Delay
The Role of the SLP
• Communication evaluation and intervention
• Feeding and swallowing evaluation andintervention
• Parent/caregiver education and counseling, staff(team) education, and collaboration
• Active participant in the NICU in developingrelated protocols for infant care anddevelopment

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 13
Section I: Summary
• Preterm birth rate is on an upward trend
• Prematurity is associated with increasedrisk for neurodevelopmental problems
• The pediatric speech pathologist has aspecific role in the assessment andintervention of high risk preterm infants
Impact on Feeding

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 14
Section II: Objectives
• Prevalent medicaldiagnoses
• Implications forfeeding
• Equipment in theNICU
Prematurity Concerns
Issues of Prematurity• Periodic breathing, apnea of
prematurity (AoP),bradycardia, cyanosis
• Difficulty digesting andabsorbing food
• Temperature control
• Hyperbilirubinemia
• Metabolic: hypo andhyperglycemia, hypocalcemia,and problems with electrolytes
• Anemia
• Increased likelihood ofinfection
Possible Effects onFeeding
• Poor state modulation
• Reduced endurance
• Difficulty sucking: wide jawexcursions, anterior loss,tongue elevated
• Reduced coordination of suck-swallow-breathe

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 15
Video: Recognizing InfantStates
Video: Recognizing InfantStates

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 16
The infant shifted from a drowsy state to?
Question: Recognizing Infant States
Light sleep
Active alert state
Quiet alert state
Deep sleep
The infant shifted from a drowsy state to?
Question: Recognizing Infant States
Light sleep
Active alert state
Quiet alert state
Deep sleep

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 17
• State transition
– Quiet alert state
• Critical for supportinginfant development
– Discriminate infantstates
– Spot state transitions
– Cues for stimulation
Analysis: Recognizing InfantStates
Gastrointestinal (GI)Concerns
GI Conditions• Gastroesophageal Reflux
(GER)
• Necrotizing Entercolitis (NEC)
• Omphalocele
• Gastroschisis
• Hirschprung’s disease
• Pyloric Stenosis
• Midgut Volvulus
• Malabsorption
• Esophageal Atresia
Possible Effects onFeeding
• Delayed introduction of oralfeeding
• Motility
• Emesis
• Altered sensation in pharynx
• Oral aversion
• Reduced intake
• Possibly slow transition to oralintake

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 18
Video: GI Concerns
Video: GI Concerns

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 19
Question: GI Concerns
Coughing and choking
Gagging and grimacing
Vomiting
Rooting
The stress cues this infant displayedinclude?
Question: GI Concerns
Coughing and choking
Gagging and grimacing
Vomiting
Rooting
The stress cues this infant displayedinclude?

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 20
• Discern cues ofstress or acceptanceof feeding
– Break
– Pause
– Continue
Analysis: GI Concerns
Cardiac Concerns
Cardiac Anomalies• Patent Ductus Arteriosis (PDA)
• Coarctation of Aorta
• Tetrology of Fallot (TOF)
• Transposition of the GreatVessels
• Congenital Aortic Stenosis
• Congenital Pulmonic Stenosis
• Atrial Septal Defect (ASD)
• Ventricular Septal Defect(VSD)
Possible Effects onFeeding
• Fatigue
• Reduced endurance
• Reduced oral intake
• Reduced weight gain
• Tachypnea
• Apnea and Bradycardia
• Reduced coordination of suck-swallow-breathe

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 21
Neurological Concerns
Neurologic Conditions
• Hemorrhage: Intracranial,Intraventricular,Subarachnoid
• PeriventricularLeukomalacia (PVL)
• Myelomeningocele
• Chiari Malformation
• Hypoxic IschemicEncephalopathy (HIE)
• Central apnea
Possible Effects onFeeding
• State Modulation
• Endurance
• Tone Issues
• Reflexes
• Reduced coordination ofsuck-swallow-breathe
• Possibility of aspiration
Video: Neurological Concerns

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 22
Video: Neurological Concerns
Question: Neurological Concerns
Drifting into a sleep state
Grimacing
Calmed relaxed face and body
Arrhythmic suck
Best description of readiness cues forfeeding include?

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 23
Question: Neurological Concerns
Drifting into a sleep state
Grimacing
Calmed relaxed face and body
Arrhythmic suck
Best description of readiness cues forfeeding include?
• Discern cuesindicating readinessfor feeding
– Quiet alert state isideal
Analysis: NeurologicalConcerns

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 24
Respiratory Concerns
Respiratory Conditions• Pulmonary Hypertension
• Tracheoesophageal Fistula(TEF)
• Laryngomalacia
• Tracheomalacia
• Bronchopulmonary Dysplasia(BPD)
• Obstructive Apnea
• Congenital DiaphragmaticHernia (CDH)
Possible Effects onFeeding
• State and Endurance
• Reduced coordination of suck-swallow-breathe
• Tachypnea, increased work ofbreathing
• Increased potential foraspiration due to reducedcoordination and highrespiratory rate
• Possibly reduced weight gain
Craniofacial Concerns
Craniofacial Anomaliesand Syndromes
• Cleft lip
• Cleft palate
• Combined cleft lip and palate
• Pierre Robin Sequence(micrognathia, glossoptosis,+/- cleft palate) (PRS)
• Goldenhar syndrome
• CHARGE
Possible Effects on Feeding
• Reduced lip seal resulting inanterior loss
• Functional compression of nippletypically
• Reduced negative pressure
• Nasal regurgitation
• Need for specialized feeder thatprovides assistive squeeze tocompensate for reduced negativepressure
• Arousal, endurance, tachypnea,hypoxia particularly withobstruction with PRS
• Possibility of aspiration due tofeeder assistance variability
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 25
Video: Craniofacial Concerns
Video: Craniofacial Concerns
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 26
Question: Craniofacial Concerns
Provide an assistive squeeze with eachsuck
Watch the infant’s cues to determinewhen to squeeze
Provide squeezing when infant stopssucking
Provide squeezing towards the end ofthe feed
When feeding using a specialized feeder, itis important to?
Question: Craniofacial Concerns
Provide an assistive squeeze with eachsuck
Watch the infant’s cues to determinewhen to squeeze
Provide squeezing when infant stopssucking
Provide squeezing towards the end ofthe feed
When feeding using a specialized feeder, itis important to?

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 27
Equipment in the NICU
The Infant’s Environment
• Beds:
– Incubators: closedenvironment
– Cribs: openenvironment
• Monitors
– Heart rate
– Respiratory rate
– Oxygen saturation
It is important to developthe ability to read the
infant’s cues and signs ofstress without total reliance
on monitors for feedback
Oxygen Delivery Systems
• Oscillator
• Ventilator
• Continuous positive air pressure (CPAP)
– uses mild air pressure to maintain anopen airway during sleep
• High Flow
– refers to oxygen delivery, inspired gasesat a preset oxygen concentration"
• Nasal Cannula
– oxygen delivered via a nasal cannula(tubing with nasal prongs from whichoxygen flows)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 28
Section II: Summary
• There are a number of medical and feedingconcerns that are associated with prematurity
• Infants can have associated or isolatedproblems that affect the gastrointestinal, cardiac,respiratory, neurological, or craniofacial system
• There are several common pieces of equipmentwithin the NICU environment that allow closemonitoring and support of infants.
Recognizing Infant States
Maximizing Oral Potential

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 29
Section III: Objectives
• Developmental Care
• Infant states and cues
– Respond appropriately
• Maximize oralpotential
Developmental Care
• Infant’s neurobehavioralorganization and how NICUenvironment care can fosterdevelopment
• Defines “competence” ofnewborn’s functioning as
– interplay between infant’sautonomic, motor, state/regulatory,attentional/interactional, and self-regulatory systems and theenvironment
(Lawhon, 2003)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 30
NIDCAP
• Newborn Individualized Developmental Careand Assessment Program (NIDCAP)
– Process-oriented approach
– Focuses on a relationship based, individualized,developmentally focused framework of care
(Als, 1996)
Caregivers
• Parents should understand
– Infant’s strengths and challenges
– How the infant communicates
– How to best interact with the environment
• Can become a guide for all caregivers

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 31
Infant Behavior
• Infant communicatesthrough behaviors
– State
– Movement
– Autonomic system
• React appropriately toensure optimalsupportive interventions
Environment
• Alter sensorial input to supportneurobehavioral organizationand development
– tactile, auditory, olfactory,vestibular, visual, taste
• For example:
– lighting, sound, positioning,containment, touch

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 32
Infant States of Consciousness
• Relate to sleeping and waking cycles
• Each state has a unique set of behavioral,neurological and physiologicalcharacteristics
• Indicates when infants may be ready foran activity
State Transitions
• Indicator of infant’s maturation
• Maintenance of state supports infant’sability to take advantage of theirorganization to learn, sleep for recovery,grow
• Smooth transition between state supportsinfant’s organization

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 33
Quiet Sleep
• Face relaxed
• Eyelids closed, still
• Relaxed body
• No body movements; rarestartles
• Breathing regular
• Decreased heart rate andblood pressure
• Decreased brain activity
Active Sleep
• Eyes closed butinconsistently flutter
• Motor activity varies
• Rapid eye movement
• Breathing irregularand faster than quietsleep
• May suck or “chew”with mouth

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 34
Drowsy
• Typically, as infant wakesup or falls asleep
• Slow movements withsome smiling, frowning,lip pursing
• May stretch
• Eyes may be opened(glazed, rolling up) witheyelids droopy or shut
Quiet Alert
• Eyes open and bright
• Looking at caregiversface/eyes
• Motor activitysuppressed
• Energy seemsfocused onhearing/seeing

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 35
Active Alert
• Frequent movements
• Eyes looking about
• Making small sounds
• Attention less focused
• Often occurs prior tofeeding or when fussy
Crying
• Eyes open or closed
• Breathing irregular
• Obvious sign ofcommunication
• Occurs with infanthunger, discomfort, orlonely

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 36
StabilityCopingStress
InfantCues
Identifying Cues
• Attention
• State
• Motor
• Physiologic

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 37
Stability
• Attention:
– smiling, mouthing, cooing/ooh face, looking at you
• State:
– awake and relaxed
• Motor:
– hands to face, limbs moving smoothly, minimal motoractivity
• Physiologic:
– pink color, easy breathing, good heart rate
Coping
• Attention:
– looking away
• State:
– shifting to a lower state
• Motor:
– grasping, leg bracing, fisting, hands to mouth,clasping hands or feet
• Physiologic:
– sucking, yawning

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 38
Stress
• Attention:– avoid social interaction
• State:– gaze aversion, glassy eyes,
irritability, decreased alertness
• Motor:– limb stiffening, finger/toe splaying,
arching, frowning, tonguethrusting, generalized hypotonia
• Physiologic:– color change, heart rate change,
drop in O2, apnea, hiccoughs,yawning, coughing, sneezing
Aversion Development
• Long term NPO
• Reflux
• Neurological issues
• Significant medicalinterventions aroundface/mouth/throat
• Negative intraoralexperiences
• Limited experiencewith oral sensoryexperiences: taste,smell, touch
• General sensoryissues of prematurity
• Aspiration
• “Forced” experiences(i.e., infant not incontrol)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 39
Care to Maximize OralPotential
• Proactive intervention
• Developmental Care/nursing
• Oral Care
• Taping
• Tube Feeding
• Gavage Feeding Support-held/pacifier during feed
• Kangaroo care
• Respiratory Care
– Choice of suctioning
• Whole body sensory input
– Massage
• Maximizing pleasant oral/facialexperiences
– Non-nutritive suckingopportunities
• Pacifier
• Empty breast
• Inclusion of Parents
• Oral Intake of any volume:tastes/ sham
– Interplay of sensory-motorreceptivity
– Capability in handlingactivity of PO feeding
Section III: Summary
• Developmental care:
– Interventions designed to minimize the stressof the environment
• Newborn Individualized DevelopmentalCare and Assessment Program(NIDCAP):
– Individual strategies combined into a program
• Behavioral cues guide the timing ofinteraction

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 40
Section IV: Objectives
• Key components of theevaluation of non-nutritiveand nutritive skills
• Typical and atypicalmaturation characteristicsof nutritive sucking
• Assessment andintervention strategies

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 41
CreateOpportunity for
Success
Continuum of Care
• Assessment directs intervention
• Integration of multiple systems
• Focus on quality
IdentifyStrength’s andChallenges
Perspectives in Feeding
Readiness considerations go beyond oralmotor and swallowing considerations
• Consider whole infantand how to maximizetheir abilities
• Team approachrequired

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 42
Considerations forAssessment and Intervention
• Neurobehavioral organization– State– Cues
• Caregiver–Infant psychodynamics• Nutrition Issues• Physiological/Autonomic• Anatomy/Structure• Non-nutritive skills• Nutritive skills• Swallow function and assessments
Formal Assessments
• Few in number and limited in range ofassessment
• Only a few have been tested for validity:
– SAIB (Systematic Assessment of the Infant at theBreast)
– PIBBS (Preterm Infant Breast-Feeding BehaviorScale)
– The Early Feeding Skills Assessment for PretermInfants (Thoyre, et al., 2005)
– NOMAS (Neonatal Oral-Motor Assessment Scale)• Useful for full-term infants, less reliable for preterm (Mizuno,
2005)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 43
• Full range of states– Oral feed only with infant in drowsy or quiet alert
state
• Coordinate suck/swallow (McCain, et al, 2001)– Pattern is more 3/4:1 which can result in deglutition
apnea
• Non-nutritive suck for calming (Lemons, 2001)
• Coordinate SSB with 1/1/1 pattern forappropriate burst (Lemons, 2001)
• Nutritive suck with longer bursts (10 to 30)(Lemons, 2001)
32
34
38
40
36
Weeks
Nutritional Readiness
• Demonstrating adequate growth
• Sequence
– Total Parenteral Nutrition and lipids
– Supplemental Enteral
• Nasojejunal, nasoduodenal, nasogastric
– Flow rate
• Continuous
• Bolus

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 44
Nutritional Readiness (cont.)
• Formula or Breast Milk
• Schedule:
– Hourly timed
– Ad lib
– On-demand
• Remain aware of how supplemental feedingtransitions are affecting oral intake
– Change in caloric density, volume or time
– Motility
Maturation
• Ability to:
– Tolerate handlingand transitions
– Achieve andmaintainappropriate state
– Remain organizedfor length offeeding

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 45
Physiological Considerations
• Respiratory Status
– Between 20-50 breaths per minute, no greaterthan 70 bpm (Shaker & Woida, 2007)
• Cardiac Status:
– Between 120 and 160 beats per minute
• Color:
– Remains pink, not mottled, pale, or blue
• Effects of positioning on physiologicalsystem (non-nutritive and nutritive skills)
Anatomy
• Physiological flexion
– Cheeks/fat pads lateralsupports
– Tongue fills oral cavity
– Jaw supported withapproximation of neck/chest
– Hard palate close withapproximation and sealsanteriorly
– Soft palate is posterior seal

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 46
Anatomical Considerations
• Less support
• Less efficient/effective
• More fatiguing
How do anomalies impact feeding?
Initial Observation
• Management ofsecretions
• Both non-nutritive andnutritive activities
• Sensory and motorresponsiveness
• Lip placement andtongue cupping
• Strength of suck

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 47
Initial Evaluation (cont.)
• Rhythmicity of suck
– Non-nutritive: 2sucks/second
– Nutritive: 1 suck/second
– Premature infants:arrhythmic with morecompression affect withvariable suction
• Length of sucking burst
Nutritive Evaluation
• Suck/swallow/breath coordination
– Sucking Bursts
– Ability to handle flow of intake
• Liquid viscosity
• Taste
• Nipple
• Endurance

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 48
Nipples
No one size fits all
• Pliability
• Shape
• Size and length
• Hole type and size
• Individualize to:
– Support infant’s structure and function
– Matching nipple’s structure and function

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 49
Pacifiers (cont.)
• Helps with statemodulation (calming,arousing)
• Positive effect onoxygenation, GI function
• Match shape with one tobe used for feeding
Ability to suck on a pacifier does notassure success at oral feeding
Video: Pacifier

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 50
Video: Pacifier
Video: Pacifier
• Lack of fat pads incheeks
• Still behavior
• Short bursts withgood pauses

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 51
Considerations of Bottleand/or Breast Feeding
• Typically dictated by medical status
– Volume limits
– Inability to control flow
– Oral coordination
• Coordinate with lactationconsultant
• Activities that support eventualBreastfeeding
– Kangaroo care
– “Dry breast”
Interventions
• Oral Feeding is one component
– QUALITY not QUANTITY
– Assure for experience with stable:• Coordination of SSB
• Maintenance of autonomic system, state
– Competent caregiver• Understanding global process
• Successful provider
Remember Infant’s Goals

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 52
Intervention: SpecificConsiderations
• Stimulation Control
– Environment
– Tactile Input
– Timing of care
• Position
– No one size fits all
– Adjust per infantissues/stability
Interventions (cont.)
• Supports for autonomic system
– Increase O2
– More frequency respiratorybreaks
• Coordination with enteral feeds
– Max. calories/min. volume
– Therapeutic feedings
– Minimal volumes
– Sham feedings
• Caregiver Training

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 53
Interventions (cont.)
• Pre-feeding oralstimulation (touch,pacifier)
• Bottle / Nipple systems
• Flow rate:
• Bolus size and rate
• Single and/or slowchain
• Dipped tastes on pacifier ornipple
• Syringepresented/controlled
• Pacifier/nipple
• Thickening:developmentally ormedically appropriate?
Interventions (cont.)
• Pacing
– Self
– External
– Burping
• Extending trunk/abdomen
• Gentle: patting
• Respiratory break
• Oral supports
– Jaw/cheek support
– Caution
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 54
Video: NNS to NS
Video: NNS to NS

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 55
Video: NNS to NS
• Positioning
• Stimulated
• From NNS withpauses to NS
• Pacing
Video: Pacing Cues

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 56
Video: Pacing Cues
Video: Pacing Cues
• Gulping
• Pulling back
• Eyes widening
• Labored breathing

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 57
Section IV: Summary
• Gestational age, medical status andstability in physiologic, motor, and statesystems determines readiness for feedingin preterm infants
• Interventions should be individualized tomatch an infant’s skills
Options in the NICU

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 58
Section V: Objectives
• Clinical indicators
• Available tests
– Strengths
– Limitations
• Video examples
Instrumental Assessments
Only appropriate on physiologically stable infants
• Indirect Assessment– Cervical auscultation: used in conjunction with clinical
observation in some settings, but not standardized
– Dye testing: used to assess evidence of aspiration, but poorspecificity
– Scintigraphy/Radionuclide scanning
• Direct Assessment– Videofluoroscopy
– Endoscopy
– Ultrasonography

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 59
Infant Swallowing Patterns
• Relation between swallowing and respiration changes withmaturation
• Mature infants:
– Swallowing occurs at end of inspiration, .672 sec (apnea), rhythmicalternation of compression, suction, expression, swallow-breath (SW-BR) (Gewolb & Vice, 2006)
– Observations: Intermittent nasopharyngeal reflux, hesitation in cervicalesophagus (Newman, et al., 1991)
– Swallowing occurs during pauses in respiration at 32-33 weeks(Bu’Lock et al., 1990; Lau et al., 2000)
– Sucking behavior matures ~ 34 weeks in regard to number of sucks perswallow, intensity of sucking pressure (Gewolb et al., 2001)
• Preterm infants:
– Immature pattern, can be successful, but not as efficient (Lau et al.,2003)
Other Considerations
• Preterm infants
– physiologically stable
– medical complications
– co-morbid conditions
• Term infants
– medical diagnoses that may impactupon coordination of respiration,sucking, swallowing

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 60
Suck, Swallow, andRespiration
• Sucking rate and strength
• Ability to integrate breathing with sucking, swallowing
• Bolus volume, consistency, and delivery
• Impact of swallowing on respiration– During swallowing, respiration is inhibited
– Feeding supersedes normal ventilatory chemoreceptor controlmechanisms
– Swallowing rhythm maintained (Goldfield, et al., 2006) (Vice &Gewolb, 2008)
• Implications of respiratory compromise (i.e., BPD)
• Implications of poor oxygen saturation on strength ofsucking, ability to maintain airway protection
Cervical Auscultation
• Screening Tool
• Auditory assessment ofrespiration/swallow, changes duringfeeding
• Make inferences about the pharyngealphase
• Reliability/Validity questionable
• Therapist dependent– Reynolds, et al., 2002

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 61
Ultrasonography
• Use to assess suckingbehavior and oral transittimes in both breast-fedand bottle-fed infants
• Non-invasive
• Not used extensively byclinicians in clinicalpractice
– Miller & Kang, 2007
Scintigraphy
• Radionuclide isotope inbuccal cavity
• Indicates aspiration inlungs
• Scanning done at intervalsover a 2 hour period
• Questionable: materialaspirated duringswallowing of saliva orduring a reflux event
• Not a “true” evaluation ofswallowing function

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 62
Dye Testing
• Dye added to feeds
• Trached patients– can monitor presence of
dye via tracheal suctioning
• Issues with reliability andvalidity– Use of dye contraindicated
in medically fragile patients
– Evidence questionable asto from above or below insome cases
– More research is needed
Signs of Swallowing Dysfunction
• Coughing, choking while feeding
• Noisy, wet respiration associatedwith feeding
• Color changes
• Physiologic signs:– apneic spells, bradycardia, increased
respiratory rate
• Evidence in tracheotomy tube
• Unexplained respiratory illnesses– Consider patient’s diagnosis (Newman,
et al., 2001)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 63
When to Use Swallow Study
Consider:
• Medical history
• Overall development
– Motor skills (whole bodyand oral-NNS, NS)
– State
– Results of feedingevaluation
• Made in consultationwith team
Video Swallow Study (VSS)Goals
• Obtain dynamic images during swallowing:
– oral phase and transit
– pharyngeal response
– upper esophageal function
• Focus on airway protection capability duringswallowing
• Identify problems:
– Why do they occur and at what point
• Obtain holistic view of suck-swallow-respirationcoordination

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 64
Ensuring Success
Preparation is key!
• Positioning
– Fluoroscope table is tilted vertically
– Use optimal positioning for infant, based oninformation from clinical assessment
• Time the VSS for the “right” time
– State and hunger
• Be ready with feeder and equipment
• Establish a collaborative plan with the radiologistto execute the study

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 65
Observations During VSS
• Barium via selected nipple or syringe
Analyze sucking response, in terms of:
• Rate, strength, and rhythm
• Even, uneven, slow, in bursts
• Loss of formula
• Other difficulties
Monitoring During VSS
• Monitor physiologic state during feeding
Know the normal baseline!
• Work with team to monitor:– Heart rate, respiratory rate, and effort
• Note any changes
– Oxygen saturation• Note initial saturation and document any changes

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 66
Typical Interventions During VSS
• Altering Position– Neutral head position, watch for extension and flexion
• Pacing– Certain number suck-swallows, impose pause
• Changing viscosity– Altering fluid thickness to slow rate of flow, facilitate organization
of airway protection prior to swallowing
• Nipple change– Alter flow rate
• Clearing “dry” swallows– To assist with hypopharyngeal clearance in between nutritive
swallows
Fatigue Effect
• Assess suck-swallow-breathe synchrony
– initially, during, and at end of feeding
• Obtain images of initial sucking bursts andpauses
• Ask radiologist for interval fluoroscopy imagesas the infant continues to feed
– Allows assessment of fatigue effect (e.g., if infant tiresas feeding progresses and has difficulty withmaintenance of airway protection)
– Helpful information for intervention planning

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 67
Scoring the Infant VSS
• Evaluation of overall suck-swallow-breathecomponent
• Document:
– Premature spillage
– Episodes of laryngeal penetration
– Episodes of laryngeal aspiration
– Infant responses:
• Clearing response, no protective response
Strengths and Limitations of theInfant Video Swallow Study
Strengths:
• Overall look at all phases
– Detailed analysis oforopharyngeal andpharyngoesophageal phase
• Anatomical and physiologicabnormalities
• Assess protective reactions
• Determine effectiveness ofcompensatory strategies
– Flexibility to try strategies toimprove feeding/swallowingfunction: i.e. differentpositions, alter flow rate,different viscosities
Limitations:
• Brief sample of feeding in alimited time
• Addition of barium (taste)
• Effects of radiation
• Requires ability to ingestsufficient amounts

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 68
Possible Findings on VSS
• Oral transfer problems resulting in poor timing ofairway protection and swallowing
• Reduced strength of oropharyngeal andpharyngeal musculature
• Incomplete airway closure during swallowingresulting in penetration into airway
• Aspiration: material in airway with reaction
• Silent aspiration: material into airway with noprotective response
Assessing Poor AirwayProtection
• Before the swallow:
– Poor oral phase collection/delivery
– Delayed initiation/sensory
• During the swallow:
– Incomplete closure or airway protection
• Poor coordination of SSB
– Anatomic issues
– Function/strength

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 69
Aspiration
• After the swallow
– Aspiration of persistentresidue secondary to poorpharyngealsqueeze/peristalsis
– Failure of the UES to relax(e.g., cricopharyngealachalasia)
– Poor sensory awarenessof residual material
Objective SwallowingAssessment: VSS

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 70
Video: Infant Swallow
Video: Infant Swallow

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 71
Question: Infant Swallow
Five to six sucks per swallow
Variable pattern, but a tendency toward1-2 sucks per swallow
No appreciable pattern, the infantseems disorganized
None of the above
1. The pattern of sucks can best bedescribed as:
Five to six sucks per swallow
Variable pattern, but a tendency toward1-2 sucks per swallow
No appreciable pattern, the infantseems disorganized
None of the above
1. The pattern of sucks can best bedescribed as:
Question: Infant Swallow

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 72
Question: Infant Swallow
Two episodes that cleared
One large episode of aspiration
Three small episodes of aspiration
Deep penetration but noaspiration
2. How many episodes of aspirationoccurred?
Question: Infant Swallow
Two episodes that cleared
One large episode of aspiration
Three small episodes of aspiration
Deep penetration but noaspiration
2. How many episodes of aspirationoccurred?
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 73
Video: Infant Swallow #2
Video: Infant Swallow #2

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 74
Question: Infant Swallow #2
Disorganized with no real rhythm established
Unorganized initially, with only slightly betterorganization as the swallow sequences continued
Smooth and efficient anterior posterior tongue motion,overall a coordinated 1:1 suck-swallow pattern
Coordinated pattern with basically two-three suckcompressions per swallow
How would you describe the suck-swallowpattern in clip #2?
Question: Infant Swallow #2
Disorganized with no real rhythm established
Unorganized initially, with only slightly betterorganization as the swallow sequences continued
Smooth and efficient anterior posterior tongue motion,overall a coordinated 1:1 suck-swallow pattern
Coordinated pattern with basically two-three suckcompressions per swallow
How would you describe the suck-swallowpattern in clip #2?

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 75
Analysis: Infant Swallow #2
• More compressionsprior to swallow
• Changes to typicalsuck, swallow,breath pattern
Video: Infant Swallow #3

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 76
Video: Infant Swallow #3
Question: Infant Swallow #3
Consistent
Unable to be fully visualized
Incomplete
None of the above
In video clip # 3, palatal contact with theposterior pharyngeal wall is:

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 77
Question: Infant Swallow #3
Consistent
Unable to be fully visualized
Incomplete
None of the above
In video clip # 3, palatal contact with theposterior pharyngeal wall is:
Role in the NICU

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 78
Pediatric FEES
• Transnasal passageof endoscope to viewpharyngeal andlaryngeal structures
• Assessment of abilityto protect airway
• Collaborative exam
• Conduct feedingportion as with VSS
Equipment
• Nasopharyngoscope
• Light source
• Recording equipment
– Camera
– Recording device• Video
• Digital

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 79
Scope and Anesthetic
• Scopes sizes:– 2.2, 3.5, 3.7, 4.0 mm
– 2.2 most common forNICU
• Topical anesthesia:– 1:1 mixture of
oxymetazoline and 2%pontocaine spray
– Not used in the NICU
– Can use viscous lidocaineon the scope
(Willging & Miller, 2007. PediatricFEES Conference, Cincinnati
Children’s)
Strengths and Limitations ofFEES
Advantages
• Allows assessment of secretionmanagement ability
• Clear view of structures andfunction
• May assist with seeing tissueirritation secondary to reflux
• Assessment of sensation
• No radiation
• Can be done at the bedside
• Possible to do duringbreastfeeding
• Overall assessment of ability toprotect airway from secretions andfeeds
Disadvantages
• Invasive procedure, athough mostinfants adapt quickly anddemonstrate functional skills
• May be difficult for infants with asensitive gag reflex
• Contraindication – choanalatresia, tongue base prolapse
• Presence of scope may limitwillingness to eat during exam
• Difficult to assess chainswallowing – loss of view
(FEES in the NICU, Pediatric FEESConference - Willging, Miller & Clonan,
2007)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 80
Structural Changes with Age
Hypopharynx
Pharyngeal wall
PyriformSinus
Pharyngoepiglotticfold
Vocal cord
Arytenoid
Epiglottis

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 81
Detecting Secretions and IdentifyingEvents During the Exam
• Food color contraindicated
– Increased gut permeability
• Betacarotene
– 50 mg capsules mixed with water, heated
• Aquadex
– Opague color advantage

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 82
FEES Findings
• Directly view secretions
– Rate: secretion management, oral phase andfunction, pharyngeal response, swallowdynamics, protective reaction
• No time limit to compensatory strategies
Secretion Management
• Presence of spontaneous clearingswallows
• Pooling within the laryngeal vestibule
• Evidence of leakage into the subglottis
• Response to secretions:
– Normal spontaneous swallows to clear
– Ineffective attempts to clear
– No attempt to clear

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 83
Video: Prone PositioningDuring FEES
Video: Prone PositioningDuring FEES

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 84
Video: Prone PositioningDuring FEES
• Could you detect acoordinated suckpattern?
• Did you recognizethe internalstructures?
Video: FEES

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 85
Video: FEES
Video: FEES
• Do you think theunilateral vocal foldparalysis had animpact on theinfant’s ability tofeed?

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 86
Parameter VSS FEES
Velopharyngeal closure good excellent
Vocal cord mobility and closure Good/fair excellent
Laryngeal elevation excellent good
Oral phase excellent Fair
Pharyngeal squeeze good excellent
Pooling of secretions poor excellent
Premature spillage excellent excellent
Penetration good excellent
Aspiration excellent good (loss of view)
Residue excellent excellent
Comparing VSS and FEES(Willging & Miller, Pediatric FEES Course 2007)
Section V: Summary
• Videofluoroscopy and endoscopy areinstrumental assessments available whichboth provide important informationregarding anatomy and function key tosafe swallowing
• Defining safety of swallowing is key todevelopment of an appropriateintervention plan by the SLP

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 87
Speech PathologyIntervention in the NICU
Section VI: Objectives
• Evidence based practice
• Recognize goodevidence
• Efficacy of specificclinical interventions
– What Exists
– Ongoing Research

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 88
ASHA PositionStatement
Evidence-Based Practice inCommunication Disorders, ASHA,2005
• “SLPs should incorporate theprinciples of evidence-based practicein clinical decision making to providehigh quality clinical care”
See Additional Resources
TOOLBARAccess Additional
Resources
Evidence Based Practice (EBP)
“Evidence-based clinician”uses clinical expertiseand the best availableexternal evidence
Coyle and Leslie,Perspectives, December
2006 (15:4)

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 89
Searching for Evidence
• EBSCO Host: searches numerous databases
• Ovid: searches certain bibliographical databases
• PubMed: http://www.ncbi.nlm.gov/entrez/query
• Medline Plus: designed for consumers, indexes web pages, portal to info
• Medline: professionals
• Eric: educational journals
• Cochrane Database of Systematic Reviews: experts, constant process,systematic reviews
• Scopus: in-depth reviews
Types of Research
• Qualitative
– Collecting data
– Survey research, case reports, caseseries
• Quantitative
– Test hypothesis
– Clinical trials
– Correlation: relationship among 2 ormore variables
– Casual-comparative: identify possiblecauses for variations between groups

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 90
Meta-Analysis
• Analysis of findings frommultiple studies on a topic
– Effect and outcomes can becompared
– Provides a more powerfulestimate of true treatmenteffect
– Example: The CochraneCollaboration
Treatment Plan
• Establishing short and long term goalstoward realistic outcomes using bestevidence available and clinical judgment
• What’s available and pertinent to the SLP?
– Effects of some selected feeding interventions

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 91
Non-Nutritive Sucking (NNS)
What effect does non-nutritivestimulation have?
• Measel & Anderson, 1979
– Earlier readiness for bottle feeds
• Schwartz et al., 1987 (meta analysis results)
– Decreased time to nipple feeding (NNS duringgavage feeds)
– Decreased length of hospital stay
Effect of NNS
• Pickler et al., 1996
– Decreased heart rate, improved oxygen saturationand behavioral state, and improved duration of firstnutritive sucking burst
• Fucile et al., 2002
– Faster transition from tube to oral feeds, increasedvolume of oral intake, but no reduce length of stay
• Pickler and Reyna, 2004
– NNS prior to oral feed did not affect suckingcharacteristics, behavioral state, or feeding efficiency

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 92
Effect of NNS
• Lau and Kusnierczyk, 2001
– No conclusive evidence that NNS facilitatesdevelopment of NS
• McCain, 1995
– Decreased behavioral state changes duringfeeding
– Increased quiet awake state during feeds
– No change in heart rate between NNS/control
Systematic Review of NNS
• Pinelli & Symington, 2005
– No significant associations with weight gain,improved increased energy or digestion ofenteral feeds
– Consistent trend of decreased hospital lengthof stay
– No negative outcomes of intervention wereidentified

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 93
Introduction of Oral Feeds
What is the best way to present oralfeeds? Standard care or cue-based?
• McCain, et al., 2001
– Semi-demand feeding protocol
– Faster transition to oral feeds
– Did not compromise weight gain
Cue-Based Oral Feeding
• Oral feeding based on clinical cues ofinfant readiness
– Achieve and maintain appropriate state,physiologic readiness, etc.
• Kirk and Alder, 2007
– Earlier achievement of full oral feeding

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 94
Cue-Based Oral Feeding
• Evidence-based guideline (McCain, 2003)
– Based on:
• Behavioral organization, rhythmic suck-swallow-breathe pattern, cardiorespiratory regulation inhealthy preterm infants
• Used “semi-demand” feeding method
• Non-nutritive sucking to promote “awake” behavior,use of behavioral assessment to identify readinessfor oral feeds, systematic observation of infantbehavior cues to regulate frequency, length, andvolume of oral feeds
• Earlier discharge
Nipples and Flow Rates
Does the choice of nipple affect feedingperformance?
• Lau and Schanler, 1990
– Comparison of unrestricted milk flow via standard nipple and use ofspecialized nipple with self-paced flow
– Measured feeding efficiency (ml/minute)
– Concluded bottle feeding can be enhanced with self-paced system
• Scheel, Schanler, and Lau, 2005
– Comparison of 3 different nipples in healthy VLBW infants
– Infants modified sucking to maintain rate of milk transfer appropriate toSSB pattern
– Conclusion: focus on suck-swallow-breathe coordination, not typeof nipple

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 95
Oral Support and Facilitation
What is the evidence to support the useof oral facilitation techniques?
• Widely used
• Very little supporting evidence
• Einarsson-Backes et al., 1994
– Increase return to pre-feeding oxygen saturation
• Hill, 2000
– No interference with cardiopulmonary function
Oral Stimulation
Does oral stimulation accelerate transitionfrom tube feeding to oral feeding?
• Fucile, Gisel, and Lau, 2002
– N = 32, pre-term infants (26-29 weeksgestational age)
– Oral stimulation x 15 minutes, experimentalgroup, sham in control group
– Accelerated transition to oral feeds inexperimental group

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 96
Pacing
Is there evidence that using pacing as afeeding strategy is beneficial?
• Laws-Morstatt et al., 2003
– Significant decrease in bradycardia episodesduring oral feeds
– More efficient sucking patterns at discharge
Need for Pacing Intervals in BPD
• Gewolb & Vice, 2006
– Apneic swallows frequency increased
– Decreased rhythmic coordination ofswallowing and respiration during feeding

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 97
Thickening Fluids
Is there evidence to support use ofthickened fluid as a feeding strategy?
• No efficacy studies as yet
• Clinical judgment
Thickening Liquids
Formula selection, concentration, and deliveryare all dependent on many medical and
nutritional issues
• Consult the NICU team
• Carefully evaluate the nutritional implications of eachthickening method, the infant’s needs, and the feasibilityof the family’s ability to obtain and prepare the product
CAUTION

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 98
Commercial Thickeners
• Corn starch based
– add calories but noother nutrients
– Advantage• Easy to use
– Limitations• Continuous thickening
• Diarrhea
• Skews nutrient ratios
• Xanthan gum based
– adds no nutrients
– Advantages:• Easy to use
• Always a consistentthickness
• Flavorless
– Limitation:• *Availability
Electrical Stimulation
Does electrical stimulation assist withimproving swallowing function in
infants?
• No empirical evidence currently
• Research studies currently underway

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 99
Oral Feeding Experience
Does early introduction of oral feedingaccelerate transition time to full oral feeding?
• Simpson, Schanlder, and Lau, 2002
– Decreased time to oral feeds
– Progress in maturation of sucking characteristics
• Pickler, Best, Reyna, Gutcher, Wetzel, 2006
– Sucking activity (# sucks, sucks/burst, sucks/minute)predicted by morbidity, maturity, feeding experience,and pre-feeding state
Developmental Care
What is the efficacy of developmental care?
• Symington and Pinelli, 2006– Short term growth, decreased respiratory support, decreased
length of stay, improved neurodevelopmental outcomes up to 24months of age
• More research is needed!– Which aspects of developmental care are most effective?
– What are the long term neurodevelopmental outcomes of infantsreceiving developmental care?

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 100
Multi-Center Trial Studying Effects ofIndividualized Developmental Care
• Als, et al., 2003
– Sample of very low birth weight infants (<1250grams, <28 weeks), N = 92
– Outcome measures: medical,neurodevelopmental, and family function
– Effects noted:
• Shorter duration of parenteral feeds , decreasedtime to transition to oral feeds, decreased time inNICU, enhanced autonomic, motor, state,attention, and self-regulatory functioning, loweredfamily stress
Additional Developmental CareStudies
• Symington & Pinelli, 2006
– 36 studies
– Reviewed four categories of developmentalcare
• Positioning
• Clustering of nursery care activities– no randomized trial were found
• Modification of external stimuli
• Individualized developmental care

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 101
Conclusions of DevelopmentalCare Studies
• Difficulties identifying intervention effects
• Overall,
– Evidence for limited benefit
– no major harmful effects
Need additional studies on short andlong term outcomes
Comprehensive Follow-Up Care
What do follow-upstudies of high risk
(VLBW) infants show?
• Increased risk ofrespiratory, nutritional,neurologic, anddevelopmental problems
• Longer term outcomestudies underway

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 102
Developing anEvidence Base
• Summary of evidence related tooutcomes of treatment
– Roles of Speech-LanguagePathologists in the NeonatalIntensive Care Unit: TechnicalReport
See Additional Resources
– Sheppard & Fletcher, 2007
TOOLBARAccess Additional
Resources
Predicting Success
What does the research show the predictorsare for success in oral feeding?
• Vice and Gewolb, 2008– Developmentally regulated
• Howe et al., 2007– OM skills, feeding techniques, feeding practice
• Pickler et al, 2006– Relationship between number of sucks in first nutritive suck burst
& feeding outcomes
• Mizuno and Ueda, 2005– Successful transition to oral feeding does appear to be a
predictor of developmental outcome

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 103
Example Treatment Goals
• Long Term:
– To demonstrate appropriate state to support nutritiveinput
• Short Term:
– Transition to state to support nutritive input followingcare, use of gentle arousal techniques, positionchanges, gentle stimulation
– Demonstrate ability to maintain state supportive toparticipate in nutritive activity
– Maintain organization for duration of nutritivestimulation
Example Treatment Goals
• Long Term Goals:
– To encourage infant seeking stimulation, rooting, and sucking
• Short Term Goals:
– Accept tactile sensory input to peri-oral area
– Accept tactile sensory input to the peri-oral and intraoral area
– Accept non-nutritive peri and oral input via pacifier, pt.’s hands/fingers, therapist’sgloved finger
– Demonstrate rooting in response to tactile input
– Display open mouth to tactile input
– Demonstrate ability to cup and move tongue anteriorly during non-nutritive sucking
– Display ability to approximate lips on nipple during non-nutritive sucking
– Increase ability to depress jaw to generate negative pressure during non-nutritivesucking
– Display prompt sucking initiation in response to nipple placement on tongue
– Demonstrate appropriate sucking burst length
– Maintain sucking strength
– Demonstrate sucking on pacifier with tastes of formula/breast milk without difficulty
Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 104
Example Treatment Goals
• Long Term:
– To demonstrate emerging oral feeding skills
• Short Term:
– Demonstrate a prompt rooting response to tactile input peri-orally
– Respond with lip closure to intraoral nipple placement
– Demonstrate adequate lip rounding on the nipple
– Demonstrate lingual groove around nipple
– Display prompt sucking initiation in response to nipple placement on tongue
– Demonstrate ability to transition from non-nutritive suck to nutritive suck withintroduction of liquid (using graded jaw depression and elevation).
– Display acceptance of small measured bolus/volumes presented in coordinationwith suck of liquid with syringe and free nipple
– Show ability to extract and accept bolus from nipple without clinical signs of beingoverwhelmed for X ml. (1.5ml/min, 30ml – 20min, 9ml/5min.)
– Display ability to coordinate respiration with suck and swallow with oral intake withuse of external pacing every X sucks for X ml.
– Demonstrate increased coordination of respiration with suck and swallow with oralintake for X sucks with self pacing
Section VI: Summary
• There is evidence to support feedinginterventions
• Nutritive sucking and feeding behaviors areemerging as predictors of developmentaloutcomes
• Write measurable treatment goals that supportprogression of nonnutritive and nutritive skills;stay current in knowledge and utilization ofevidence based interventions

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 105
Thank You
• When you are ready to take the CEU test, pleaseclick the link above.
• You will need your ASHA Web site login andpassword to access the test.
• If you encounter any problems, please [email protected]
Click here to take the test

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 106
Service Delivery andPractice Management
Swallowing Disorders Other ASHA Programs
www.asha.org/shop
It’s Easy!
Find RelatedPrograms
Your First Choice for ASHA CEUs
On the Web at www.asha.org/profdev
• Earn CEUs online at ASHAeLearning
• Browse Web/Telephone Seminars,Replays & Self-Studies
• Browse the Products Catalog• View information about upcoming
Conferences
Have a question about Professional Development products?Contact our Professional Development at [email protected].

Developmental Care by Speech-LanguagePathologists in the Neonatal Intensive Care Unit
ASHA Self-Study 4400 107
Jack Coursen
Educational Program Manager, Professional Development
Sharon Willig, MA, CCC-SLP
Associate Director, Clinical Issues in Speech-Language Pathology
Parrish Swann
Instructional Technology Manager, Professional Development
Matthew Cutter
Managing Editor, Professional Development
Rohan Mahadevan
Program Coordinator, Professional Development
© 2011 American Speech-Language-Hearing Association