KLP7 jurnal ilmiah kedokteran

of 12
-
Upload
arya-kusuma -
Category
Documents
-
view
235 -
download
0
Transcript of KLP7 jurnal ilmiah kedokteran
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
1/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;25 www.nejm.org december 20, 2007 2589
Outcomes of Care by Hospitalists,
General Internists, and Family PhysiciansPeter K. Lindenauer, M.D., Michael B. Rothberg, M.D., M.P.H.,
Penelope S. Pekow, Ph.D., Christopher Kenwood, B.S., Evan M. Benjamin, M.D.,and Andrew D. Auerbach, M.D., M.P.H.
From the Center for Quality and SafetyResearch, Baystate Medical Center,
Springfield, MA (P.K.L., M.B.R., P.S.P.,E.M.B.); the Department of Medicine,Tufts University School of Medicine, Bos-ton (P.K.L., M.B.R., E.M.B.); the Schoolof Public Health and Health Sciences,University of Massachusetts, Amherst(P.S.P., C.K.); and the Department ofMedicine, University of California at SanFrancisco, San Francisco (A.D.A.). Ad-dress reprint requests to Dr. Lindenauerat the Center for Quality and Safety Re-search, Baystate Medical Center, 759Chestnut St., P-5928, Springfield, MA01199, or at [email protected].
N Engl J Med 2007;357:2589-600.
Copyright 2007 Massachusetts Medical Society.
A B S T RA C T
BACKGROUND
The hospitalist model is rapidly altering the landscape for inpatient care in the UnitedStates, yet evidence about the clinical and economic outcomes of care by hospital-
ists is derived from a small number of single-hospital studies examining the prac-tices of a few physicians.
METHODS
We conducted a retrospective cohort study of 76,926 patients 18 years of age orolder who were hospitalized between September 2002 and June 2005 for pneumonia,heart failure, chest pain, ischemic stroke, urinary tract infection, acute exacerba-tion of chronic obstructive pulmonary disease, or acute myocardial infarction at 45hospitals throughout the United States. We used multivariable models to comparethe outcomes of care by 284 hospitalists, 993 general internists, and 971 familyphysicians.
RESULTS
As compared with patients cared for by general internists, patients cared for byhospitalists had a modestly shorter hospital stay (adjusted difference, 0.4 day;P
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
2/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;25 www.nejm.org december 20, 20072590
Since they were first describedlit-tle more than a decade ago, hospitalistshave emerged as one of the fastest growing
physician groups in the United States.1-3Recentdata suggest that 29% of hospitals, including 55%of hospitals with 200 or more beds, have hospital-ists on their medical staffs, and more than 12,000
hospitalists practice in the United States.4If thehospitalist model of inpatient care becomes pre-dominant, it has been estimated that hospitalistswill eventually number as many as 30,000 ap-proximately the same as the number of cardiolo-gists in the United States.5
As compared with traditional inpatient care,the hospitalist model offers many potential ad-vantages.6 First, their availability all day (andsometimes around the clock) allows hospitaliststo respond quickly to acute symptoms or new testresults, reducing delays and potentially improv-
ing outcomes. Second, physicians who are basedwithin a hospital may learn to navigate its com-plex environment more efficiently. Third, hospi-talists may develop greater clinical expertise asa result of added experience.7Fourth, the finan-cial support provided by many hospitals to meetthe operating expenses of hospitalist programsis often associated with explicit or implicit incen-tives to reduce the length of hospital stay andcosts.8Finally, the presence of hospitalists allowsprimary care physicians to increase their avail-ability and productivity in the office setting be-cause they no longer need to travel to the hospi-tal to see one or two patients. Being allowed tofocus on one clinical setting may also improvethe quality of work life for physicians who referpatients to hospitalists.
At the same time, the hospitalist model intro-duces handoffs at the time of admission and atdischarge, transitions during which the risk oferrors and adverse events is high.9-14These discon-tinuities, coupled with a lack of previous knowl-edge of a patients care, may lead hospitalists to
order excessive diagnostic tests, resulting in highercosts with no benefit to hospitalized patients.Concerns regarding the potentially negative ef-fect of hospitalist programs on the satisfactionof primary care physicians and patients have notbeen borne out.15-18
Although hospitalists have captured the atten-tion of both medical and lay audiences,19knowl-edge regarding their effect on outcomes is derived
from a small number of studies of academic cen-ters and is based on the practices of few hospi-talists.15,18,20-27Given the effect the hospitalistmodel has had on inpatient care, we sought toaddress the limitations of previous studies by com-paring the outcomes for patients treated by a largenumber of hospitalists, general internists, and fam-
ily physicians throughout a wide range of practicesettings.
Methods
Setting and Participants
We conducted a retrospective cohort study usingdata from hospitals that participate in Perspec-tive (Premier Healthcare Informatics), a databasedeveloped for the measurement of health careuse and quality. In addition to the elements thatare available in standard hospital discharge data,
three quarters of the hospitals that part icipate inthe Perspective database report actual costs, andthe remainder provide cost estimates calculatedwith the use of Medicare cost-to-charge ratios.Participants in the Perspective database representall regions of the United States, are predominantlysmall-to-midsize nonteaching facilities, and servea largely urban patient population.
Among participants in the Perspective data-base, we identified 45 hospitals that used anexpanded set of physician-specialty codes thatincluded an option to categorize attending phy-sicians as hospitalists. Information provided tothese hospitals had defined hospitalists as phy-sicians, usually internists, who specialize in treat-ing hospitalized patients. Hospitals that reportedhaving hospitalists on their staffs were similar tothe entire group of participants in the Perspec-tive database in terms of size, teaching status,urban or rural location, and geographic region.
Patients were included in our analysis if theywere admitted to the hospital between Septem-ber 1, 2002, and June 30, 2005; if they were 18
years of age or older; and if they were cared forby an attending physician classified as being ageneral internist, family physician, or hospitalist.Given the administrative nature of our data set,we were unable to determine whether patientstreated by an attending physician who was not ahospitalist were actually cared for by their ownprimary care physician or by a covering physician.In order to focus on a set of conditions commonly
The New England Journal of Medicine
Downloaded from nejm.org on May 1, 2013. For personal use only. No other uses without permission.
Copyright 2007 Massachusetts Medical Society. All rights reserved.
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
3/12
Outcomes of Care by Hospitalists, General Internists, and Family Physicians
n engl j med 357;25 www.nejm.org december 20, 2007 2591
encountered by all three physician groups and ona group of diagnoses associated with a range ofexpected lengths of stay and in-hospital mortal-ity, we further limited our patient population tothose admitted with a principal diagnosis of pneu-monia, acute exacerbation of chronic obstructivepulmonary disease, ischemic stroke, chest pain,
acute myocardial infarction, heart failure, or uri-nary tract infection, as defined by the InternationalClassification of Diseases, Ninth Revision, Clinical Modi-
ficationcriteria. The institutional review board atBaystate Medical Center in Springfield, Massachu-setts, approved the study.
Data Elements
In addition to the patients age, sex, race or ethnicgroup, insurance information, and principal di-agnosis, we recorded the presence of coexistingconditions using Healthcare Cost and Utilization
Project Comorbidity Software, version 3.1 (Agen-cy for Healthcare Research and Quality); thissoftware is based on work by Elixhauser et al.28Data on the length of stay, cost, in-hospital deaths,and all-cause readmission rates at the index hos-pital at 14 days were obtained from the Perspec-tive discharge file. In addition, we identif ied thespecialty of each attending physician and thehospitals bed size, teaching status, geographicregion, and whether the institution served an ur-ban or rural population.
Statistical Analysis
Summary statistics were constructed at the pa-tient level with the use of means, standard devia-tions, medians, and interquartile ranges for con-tinuous data and frequencies and percentages forcategorical data. Chi-square tests of associationwere used to evaluate differences in proportionaccording to physician specialty for each categor-ical factor; KruskalWallis analysis of variancewas used to compare specialties for each contin-uous-scale factor. To estimate the effect of physi-
cian specialty independent of patient volume, wecalculated an annualized case volume for eachphysician by dividing his or her reported patientcount by the total number of months that thephysician contributed patients to the data set.This figure was multiplied by 12 to estimate thephysicians annualized case volume for the sevenconditions under study.
Physicians from each group with annualized
case volumes that met or exceeded the 25th per-centile for hospitalists (i.e., a volume attained by75% of all hospitalists) were categorized as be-ing high-volume providers. This threshold provideda comparison group of general internists and fam-ily physicians whose inpatient volumes approachedthose of a mainstream group of hospitalists. In
exploratory analyses, we examined the effect ofchanging the threshold to the 50th percentile forhospitalists. These analyses yielded similar effectestimates with greatly reduced power as a resultof the small numbers of internists and familyphysicians who met this volume threshold.
We developed a series of multivariable modelsto assess the independent effect of physician spe-cialty on the length of stay, cost, inpatient mor-tality, and rate of readmission; these models wereadjusted for principal diagnosis, all other patientcharacteristics, all hospital characteristics, and
the annualized physician case volume. General-ized estimating equations (the GENMOD proce-dure in SAS software, version 9.1; SAS Institute)were used to account for the clustering of patientswith physicians and physicians with hospitals. Aninteraction term between physician specialty andprincipal diagnosis was included in all models.Logit-link generalized estimating equations wereused to assess in-hospital mortality and 14-dayreadmission. Analyses of length of stay and costswere restricted to cases with values within 3 SD ofthe mean because of the extremely skewed natureof these data, and identity-link normal-distribu-tion generalized estimating equations were usedto assess log-transformed length of stay and cost.
In a secondary analysis, we generated a pro-pensity score derived from a nonparsimoniousmultinomial logit model performed with theGLIMMIX procedure in SAS software, version9.1 (SAS Institute). This model used attending-physician specialty as the outcome variable, there-by producing three predicted probabilities, eachrepresenting the likelihood of being assigned to
one of our physician groups (and summing to100%). Because these probabilities are a linearcombination of each other, two scores were thenused as additional covariates in subsequent pro-pensity-adjusted multivariable models.
To explore the relationship among physicianspecialty, case volume, and outcome, we developedmodels that excluded case volume, as well as mod-els that included an interaction term between the
The New England Journal of Medicine
Downloaded from nejm.org on May 1, 2013. For personal use only. No other uses without permission.
Copyright 2007 Massachusetts Medical Society. All rights reserved.
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
4/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;25 www.nejm.org december 20, 20072592
Table 1.Characteristics of Hospitals and of Patients Cared for by Hospitalists, General Internists, and Family Physicians at 45 Hospitals.*
Characteristic
Care Providedby Hospitalists
(N = 24,772)
Care Provided byGeneral Internists
(N = 33,341)
Care Provided byFamily Physicians
(N = 18,813) P Value
Patients
Age
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
5/12
Outcomes of Care by Hospitalists, General Internists, and Family Physicians
n engl j med 357;25 www.nejm.org december 20, 2007 2593
Table 1.(Continued.)
Characteristic
Care Providedby Hospitalists
(N = 24,772)
Care Provided byGeneral Internists
(N = 33,341)
Care Provided byFamily Physicians
(N = 18,813) P Value
Payer category no. (%)
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
6/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;25 www.nejm.org december 20, 20072594
annualized volume and specialty. In addition, allregression models were repeated with an interac-tion term to examine whether the effect of physi-cian specialty varied according to hospital teach-ing status.
Using the estimates from our models, we pre-sent differences in adjusted length of stay and
costs between hospitalists and general internistsand between hospitalists and family physiciansat the individual-hospital level. All analyses werecarried out with the use of SAS software, version9.1 (SAS Institute).
Results
Characteristics of Patients and Hospitals
Between September 2002 and June 2005, a totalof 76,926 patients 18 years of age or older weredischarged with a principal diagnosis of pneu-
monia, heart failure, chest pain, ischemic stroke,urinary tract infection, acute exacerbation ofchronic obstructive pulmonary disease, or acutemyocardial infarction from 1 of 45 hospitals thatcontributed data on hospitalists. Of these pa-tients, 32% were cared for by 284 hospitalists,43% were cared for by 993 general internists, and25% were cared for by 971 family physicians. Themean age of the patients was 69 years, 57% werewomen, and 66% were white (Table 1). Pneumo-nia accounted for 28% of cases. Overall, the meanlength of stay was 4.9 days, costs averaged $7,796,and approximately three of four patients were dis-charged home. A total of 3351 patients (4.4%) diedduring hospitalization, and 6.7% were readmittedwithin 14 days after discharge.
More than half of the hospitals were locatedin the South, 74% served an urban population,35% had 200 to 399 beds, and one quarter wereinvolved in the training of house staff. As com-pared with the hospitals included in the 2003 an-nual survey of the American Hospital Association,the hospitals included in our analysis were larger,
more often urban, and more likely to be engagedin the training of house staff.
Practices of Hospitalists, General Internists,
and Family Physicians
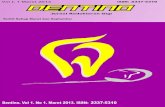
On average, physicians categorized as family phy-sicians cared for approximately 20 patients withone of the seven selected diagnoses each year,general internists cared for 30, and hospitalistscared for 75 (Fig. 1). As compared with patients
cared for by general internists or family physi-cians, patients cared for by hospitalists tended tobe younger, were more likely to be male, black orHispanic, and enrolled in a managed-care plan(Table 1). Patients treated by hospitalists weremore likely to receive care at larger hospitals, inurban settings, and in the South and not in theMidwest. There were few clinically signif icant dif-ferences in the case mix and coexisting condi-tions of patients cared for by the three physician
groups, and unadjusted in-hospital death rateswere similar. Fourteen-day readmission ratesranged from 6.3% among patients cared for byhospitalists to 6.9% for those cared for by gen-eral internists. The mean length of stay rangedfrom 4.7 days for patients cared for by hospital-ists to 5.2 days for those cared for by general in-ternists. Mean costs ranged from $7,077 per casefor patients cared for by family physicians to$8,078 for those cared for by hospitalists.
400
Patients(n
o./yr)
300
200
100
0Hospitalists(N=284)
Internists(N=993)
FamilyPhysicians(N=971)
40/yr
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
7/12
Outcomes of Care by Hospitalists, General Internists, and Family Physicians
n engl j med 357;25 www.nejm.org december 20, 2007 2595
Results of Multivariable Analyses
In multivariable models adjusted for the principaldiagnosis, patient characteristics, hospital charac-teristics, case volume, and clustering of patientswith physicians and of physicians with hospitals,patients cared for by hospitalists, as compared
with those cared for by general internists, had a0.4-day shorter length of stay (P
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
8/12
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
9/12
Outcomes of Care by Hospitalists, General Internists, and Family Physicians
n engl j med 357;25 www.nejm.org december 20, 2007 2597
in length of stay were observed for all seven diag-noses and costs differed significantly for threediagnoses. We noted relatively little variation inthese patterns among the 45 hospitals we studied(Fig. 2). As compared with the length of stay amongpatients cared for by family physicians, the lengthof stay among patients cared for by hospitalistswas 0.4 day shorter (P
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
10/12
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;25 www.nejm.org december 20, 20072598
more, cost and length of stay for high-volumehospitalists as compared with high-volume gen-eral internists (cost, $251 [P = 0.06]; length of stay,0.4 day [P
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
11/12
Outcomes of Care by Hospitalists, General Internists, and Family Physicians
n engl j med 357;25 www.nejm.org december 20, 2007 2599
own patients, the patients of their partners, orpatients without primary care physicians who hadbeen assigned to them through a roster. The rela-tively similar outcomes we observed among thethree physician groups may therefore reflect alarge percentage of patients cared for by physi-cians who did not benefit from a longitudinal
relationship with them.In addition, although our cost data were de-
rived from the cost-accounting systems of par-ticipating hospitals, these data were not calcu-lated and reported uniformly among sites, andthis inconsistency may have introduced bias. Wefocused our analysis on several important out-comes; however, we were limited to informationconcerning in-hospital deaths, and we would nothave been able to detect differences in deathsthat occurred after discharge. Moreover, althoughhospitalists were no more likely than other phy-
sicians to discharge patients to nonacute carefacilities, we were unable to fully assess down-stream costs. Although the seven conditions westudied are extremely common, they make up arelatively small percentage of the annual caseload
for physicians who care for hospitalized patients.Consequently, there is a risk that our findingsmay not be generalizable to the full spectrum ofinpatient medicine. Finally, we relied on admin-istrative data to identify hospitalists, so we mayhave misclassified physicians. However, the def-inition used to identify hospitalists was consis-
tent with that of the Society of Hospital Medi-cine and produced results that were not affectedby adjustment for case volume.
In conclusion, the hospitalist model is associ-ated with relatively modest improvements in ef-ficiency as compared with traditional approachesto caring for hospitalized patients. Given the largeand growing presence of hospitalists, there re-mains a need to understand how hospitalist sys-tems should be structured in order to improve thequality and outcomes of care.
Supported by a Patient Safety Research and Training Grant
from the Agency for Healthcare Research and Quality (K08HS11416-02, to Dr. Auerbach) and a Doris Duke Clinical Scien-tist Development Award (to Dr. Rothberg).
No potential conflict of interest relevant to this article wasreported.
We thank Bill Saunders, Ph.D., of Premier Healthcare Infor-matics, for technical assistance.
References
Wachter RM, Goldman L. The emerg-ing role of hospitalists in the Americanhealth care system. N Engl J Med 1996;335:514-7.
Auerbach AD, Chlouber R, Singler J,Lurie JD, Bostrom A, Wachter RM. Trendsin market demand for internal medicine1999 to 2004: an analysis of physician jobadvertisements. J Gen Intern Med 2006;21:1079-85.
Lindenauer PK, Pantilat SZ, Katz PP,Wachter RM. Hospitalists and the prac-tice of inpatient medicine: results of asurvey of the National Association of In-patient Physicians. Ann Intern Med 1999;130:343-9.
Kralovec PD, Miller JA, Wellikson L,Huddleston JM. The status of hospitalmedicine groups in the United States.J Hosp Med 2006;1:75-80.
Lurie JD, Miller DP, Lindenauer PK,
Wachter RM, Sox HC. The potential sizeof the hospitalist workforce in the UnitedStates. Am J Med 1999;106:441-5.
Wachter RM. An introduction to thehospitalist model. Ann Intern Med 1999;130:338-42.
Halm EA, Lee C, Chassin MR. Is vol-ume related to outcome in health care? Asystematic review and methodologic cri-tique of the literature. Ann Intern Med2002;137:511-20.
Pham HH, Devers KJ, Kuo S, Beren-son R. Health care market trends and the
1.
2.
3.
4.
5.
6.
7.
8.
evolution of hospitalist use and roles.J Gen Intern Med 2005;20:101-7.
Cornish PL, Knowles SR, MarchesanoR, et al. Unintended medication discrep-ancies at the time of hospital admission.Arch Intern Med 2005;165:424-9.
Forster AJ, Murff HJ, Peterson JF,Gandhi TK, Bates DW. Adverse drugevents occurring following hospital dis-charge. J Gen Intern Med 2005;20:317-23.
Roy CL, Poon EG, Karson AS, et al.Patient safety concerns arising from testresults that return after hospital dis-charge. Ann Intern Med 2005;143:121-8.
Dudas V, Bookwalter T, Kerr KM,Pantilat SZ. The impact of follow-up tele-phone calls to patients after hospitaliza-tion. Am J Med 2001;111:Suppl 9B:26S-30S.
van Walraven C, Mamdani M, Fang J,Austin PC. Continuity of care and patient
outcomes after hospital discharge. J GenIntern Med 2004;19:624-31.Goldman L, Pantilat SZ, Whitcomb
WF. Passing the clinical baton: 6 princi-ples to guide the hospitalist. Am J Med2001;111:Suppl 9B:36S-39S.
Davis KM, Koch KE, Harvey JK, Wil-son R, Englert J Gerard PD. Effects of hos-pitalists on cost, outcomes, and patientsatisfact ion in a rural health system. Am JMed 2000;108:621-6.
Fernandez A, Grumbach K, Goitein L,Vranizan K, Osmond DH, Bindman AB.
9.
10.
11.
12.
13.
14.
15.
16.
Friend or foe? How primary care physi-cians perceive hospitalists. Arch InternMed 2000;160:2902-8.
Auerbach AD, Aronson MD, Davis RB,Phillips RS. How physicians perceive hos-pitalist services after implementation:anticipation vs reality. Arch Intern Med2003;163:2330-6.
Wachter RM, Goldman L. The hospi-talist movement 5 years later. JAMA 2002;287:487-94.
Landro L. The informed patient: med-icines fastest growing specialty. WallStreet Journal. October 6, 2004:D1.
Auerbach AD, Wachter RM, Katz P,Showstack J, Baron RB, Goldman L. Im-plementation of a voluntary hospitalistservice at a community teaching hospital:improved clinical efficiency and patientoutcomes. Ann Intern Med 2002;137:859-65.
Lindenauer PK, Chehabeddine R, Pe-kow P, Fitzgerald J, Benjamin EM. Qualit yof care for patients hospitalized withheart fai lure: assessing the impact of hos-pitalists. Arch Intern Med 2002;162:1251-6.
Meltzer D, Manning WG, Morrison J,et al. Effects of physician experience oncosts and outcomes on an academic gen-eral medicine service: results of a trial ofhospitalists. Ann Intern Med 2002;137:866-74.
Myers JS, Bellini LM, Rohrbach J,
17.
18.
19.
20.
21.
22.
23.
The New England Journal of Medicine
Downloaded from nejm.org on May 1, 2013. For personal use only. No other uses without permission.
Copyright 2007 Massachusetts Medical Society. All rights reserved.
-
8/13/2019 KLP7 jurnal ilmiah kedokteran
12/12
n engl j med 357;25 www.nejm.org december 20, 20072600
Outcomes of Care by Hospitalists, General Internists, and Family Physicians
Shofer FS, Hollander JE. Improving re-source utilization in a teaching hospital:development of a nonteaching service forchest pain admissions. Acad Med 2006;81:432-5.
Phy MP, Vanness DJ, Melton LJ III, etal. Effects of a hospitalist model on el-derly patients with hip fracture. Arch In-tern Med 2005;165:796-801.
Kaboli PJ, Barnett MJ, Rosenthal GE.Associations with reduced length of stayand costs on an academic hospitalist ser-vice. Am J Manag Care 2004;10:561-8.
Rifkin WD, Holmboe E, Scherer H,Sierra H. Comparison of hospitalists and
24.
25.
26.
nonhospitalists in inpatient length of stayadjusting for patient and physician char-acteristics. J Gen Intern Med 2004;19:1127-32.
Wachter RM, Katz P, Showstack J,Bindman AB, Goldman L. Reorganizingan academic medical service: impact oncost, quality, patient satisfaction, and ed-ucation. JAMA 1998;279:1560-5.
Elixhauser A, Steiner C, Harris DR,Coffey RM. Comorbidity measures for usewith administrat ive data. Med Care 1998;36:8-27.
Halasyamani LK, Valenstein PN,Friedlander MP, Cowen ME. A compari-
27.
28.
29.
son of two hospitalist models with tradi-tional care in a community teaching hos-pital. Am J Med 2005;118:536-43.
Coffman J, Rundall TG. The impact ofhospitalists on the cost and quality of in-patient care in the United States: a re-search synthesis. Med Care Res Rev 2005;62:379-406.
Greenfield S, Nelson EC, Zubkoff M,
et al. Variations in resource utilizationamong medical specialties and systems ofcare: results from the Medical OutcomesStudy. JAMA 1992;267:1624-30.Copyright 2007 Massachusetts Medical Society.
30.
31.
APPLYFORJOBSELECTRONICALLYATTHENEJMCAREERCENTER
Physicians registered at the NEJM CareerCenter can apply for jobs electronicallyusing their own cover letters and CVs. You can keep track of your job-application
history with a personal account that is created when you registerwith the CareerCenter and apply for jobs seen online at our Web site.
Visit www.nejmjobs.orgfor more information.
The New England Journal of Medicine
Downloaded from nejm org on May 1 2013 For personal use only No other uses without permission