Kelainan jantung bawaan
29
Panel 3 rd Module : Congenital Heart Disease 1 st Scenario Presented By 1A Group Thanks to our Tutor : dr. Sulhana Mochtar Medical Faculty Moeslim University Of Indonesian 2010
-
Upload
zarah-dzulhijjah -
Category
Health & Medicine
-
view
595 -
download
1
description
Tutorial cardivascular
Transcript of Kelainan jantung bawaan

Panel 3rd Module : Congenital Heart Disease
Panel 3rd Module : Congenital Heart Disease
1st ScenarioPresented By1A Group
1st ScenarioPresented By1A Group
Thanks to our Tutor : dr. Sulhana Mochtar
Medical Faculty Moeslim University Of Indonesian
2010

1A Group
• Maria Ulfah (1102090049)• Irfan Thamrin (1102090056)• Rizki Rahmadhan (1102090063)• Akhmad Edwin Indra Pratama (1102090064)• Fakhrurrazi (1102090065)• Muh. Fadly Aditya (1102090070)• Muhammad Assadul Malik (1102090072)• Inna Mthmainnah Musa (1102090084)• Andi Firman Mubarak (1102090088)• Ainun Martoni (1102090093)• Andi Fajar Apriani (1102090106)• Dzul Ikram (1102090108)• Zarah Alifani Dzulhijjah (1102090115)• Sigit Dwi Pramono (1102090133)• Andi Anugrah Suci (1102090142)• Nur Sabriany Lihawa (1102100156)

1st Scenario
A ten year old girl comes with her lips and fingers blue. This has happened since she was a baby.This worsens when she cries or plays. She often have to sit on her knees when she is tired playing. Physical examination shows small and skinny appearance. Cyanosis appears on her lips,end of her tongue, her fingers and toes. Pulse and blood pressure are normal. Thorax examination reveals right ventricle activity increases, followed by thrill at LSB 3. Heart sound 1 and 2 are pure, intensity increases. Systolic ejection murmur (degree 3/6 p.m LSB 4), is found. Femoral artery palpation is normal. She’s got drum stick fingers.

Difficult Words
• Thrill : Palpable fibration that can be found in palpation
• LSB 3 : Left Side Branch 3• Cyanosis : a bluish color of the skin and
mucous membranes resulting from an increased quantity of reduced hemoglobin, or of hemoglobin derivatives, in the small blood vessels of those areas. It is usually most marked in the lips, nail beds, ears, and malar eminences.

• Systolic ejection murmur degree 3/6 P. In LSB 4 : also called Midsystolic Murmurs which are often crescendo-decrescendo in shape, and occur when blood is ejected across the aortic or pulmonic outflow tracts
• Clubbing Fingers : The selective bullous enlargement of the distal segments of the fingers and toes due to proliferation of connective tissue, particularly on the dorsal surface,

Keywords
• A girls 10-year-old• Lips and nail cyanosis• Sit on her knee when she is tired• Cyanoisis getting wordt when she is
craying• Right ventricle contraction is rising• Thrill LSB 3 • systolic ejection murmurs, 3/6 degree p.
m LSB 4• Clubbing fingers• Pulse of femoral artery are normal

Questions and
Answers
Questions and
Answers

1. How is the mechanism of cyanosis?
In the central type, the O2 is reduced or an abnormal hemoglobin de- 2 derivative is present, and the mucous membranes and skin are both affected.

Peripheral cyanosis is due to a slowing of blood flow and abnormally great extraction of O2 from normally saturated arterial blood. It results from vasoconstriction and diminished peripheral blood flow, such as occurs in cold exposure, shock, congestive failure, and peripheral vascular disease. Often in these conditions the mucous membranes of the oral cavity or those beneath the tongue may be spared
Reference: Harrison’s Principles of Internal Medicine vol. Vol 1 ed.16

2. Why is she feel more comfort when she’s squatting?
It results in obstruction of venous return of desaturated blood and an increase in the peripheral systemic vascular resistance. This leads to a reduced right-to-left shunt and improved cerebral oxygenation.
Reference: Kumar & Clark: Clinical Medicine ed.6

3. Why is the cyanosis getting worst when she is craying? • Exercise increases resistance to
pulmonary blood flow but reduces systemic vascular resistance.
• Hypoxia in exercised muscles

4.Is there any relation between all the symptoms and growth reterdation? • Yes..• Saturated oxigen really urgent for
metabolism system, aand when it decreases, the metabolism sytem also disturbed


5. Why is the intensity of 1st and 2nd Heart sounds increasing?• S1 is louder if diastole is shortened
because of tachycardia, if AV flow is increased because of high cardiac output or prolonged because of mitral stenosis, or if atrial contraction precedes ventricular contraction by an unusually short interval, reflected in a short PR interval.

• S2 is louder cause the stenosis of pulmonal semilunar valve

6. Why is the predilection of cyanotis always found in the peripher?
• Have the most resistance capillaries and get less saturated oxygen

7. Explain the etiology of cyanosis!CENTRAL CYANOSIS
Decreased arterial oxygen saturation, Decreased atmospheric pressure—high altitude, Impaired pulmonary function Alveolar hypoventilation, Uneven relationships between pulmonary ventilation and perfusion (perfusion of hypoventilated alveoli), Impaired oxygen diffusion, Anatomic shunts, Certain types of congenital heart disease, Pulmonary arteriovenous fistulas, Multiple small intrapulmonary shunts, Hemoglobin with low affinity for oxygen, Hemoglobin abnormalities, Methemoglobinemia—hereditary, acquired, Sulfhemoglobinema—acquired, Carboxyhemoglobinemia (not true cyanosis)

PERIPHERAL CYANOSIS• Reduced cardiac output• Cold exposure• Redistribution of blood flow from
extremities• Arterial obstruction• Venous obstruction

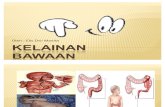
8. Why is the right ventricle contraction increase?
Obstruction in pulmonary trunk (pulmonary stenosis) RVH.
VSDPS
OvA
RVH
AO
AP
LV
LA
RA

9. What is the compensation of tha body, so she has still alive?
• Squatting position• Mixed unsaturated n saturated
blood

10.Establish betwen central and peripheral cyanosis!• Central : decreased saturation,
general and severe• Peripheral : normally saturation, local
and low

11. How is the mechanism of clubbing fingers?
• Hypoxia at the tissue• proliferation of connective
tissue, particularly on the dorsal surface,

12 . Why is the systole ejection murmur can be heard?• blood is ejected across the aortic or
pulmonic outflow tracts)• starts shortly after S1, when the
ventricular pressure becomes high enough to open the semilunar valve
• As the velocity of ejection increases

13. Explain the Differential Diagnosis!

TGAClinical Manifestation of scenario
Clinical manifestation in TGA
Cyanosis apparent with stress or crying.
Single second HS and loudPansystolic Murmur or continuous murmur
RVH


Thank youso much !