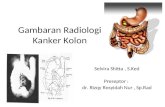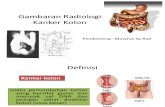
KANKER KOLON
29
00:00 Kanker usus besar
-
Upload
endahpramulat -
Category
Documents
-
view
30 -
download
10
description
TUGAS
Transcript of KANKER KOLON
-
00:00Kanker usus besar
-
Overview Ca ColonPengertianEpidemiologiEtiologiPathologiGejala klinisTerapiAskep
-
ABDC
-
Intestinal tumorsTumor epitel merupakan penyabab terbesar angka kesakitan dan kemarian di duniaUsus meliputi rektum merupakan organ pertama terkena neoplasma
Non-neoplastic PolypsHyperplastic polypsHamartomatous polypsJuvenile polypsPeutz-Jeghers polypsInflammatory polypsLymphoid polypsNeoplastic Epithelial LesionsBenign polypsAdenomasMalignant lesionsAdenocarcinomaSquamous cell carcinoma of the anusOther TumorsGastrointestinal stromal tumorsCarcinoid tumorLymphoma
-
Adenocarcinoma98% kanker berada di usus besar Kebanyakan kanker colorectal berkembang dari polip, oleh karena itu polypectomy colon mampu menurunkan kejadian kanker colorectal.
-
Epidemiologypeak incidence: 60 to 70 years of age< 20% cases before age of 50adenomas presumed precursor lesions for most tumorsmales affected 20% more often than females
-
Epidemiologyworldwide distribution World Cancer Report WHO, diperkirakan 944.717 kasus ditemukan di seluruh dunia pada tahun 2000. highest incidence rates in United States, Canada, Australia, New Zealand, Denmark, Sweden, and other developed countries
-
Etiologygenetic influences:kecenderungan genetik tertentu, seperti Hereditary Nonpolyposis Colorectal Cancer (HNPCC; 4-7% dari semua kasus) dan Familial Adenomatosa Polyposis (FAP, 1%) serta Inflammatory Bowel Disease (IBD; 1% dari semua kasus).
-
Etiologyenvironmental influences:dietary practiceslow content of unabsorbable vegetable fibercorresponding high content of refined carbohydrateshigh fat contentdecreased intake of protective micronutrients (vitamins A, C, and E)use of Aspirin and other NSAIDs: protective effect against colon cancer?cyclooxygenase-2 & prostaglandin E2
-
Carcinogenesischromosome instability pathway
-
Carcinogenesismismatch repair (microsatellite instability) pathway
-
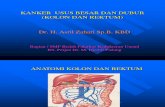
Karsinoma Colon Sebelah Kanan
Karsinoma pada caecum atau pada ascending colon biasanya memperlihatkan gejala nonspesifik seperti kekurangan zat besi (anemia). Kejadian anemia ini biasanya meningkatkan kemungkinan terjadinya karsinoma colon yang belum terdeteksi, yang lebih cenderung berada di proksimal daripada di colon distal. Beberapa tanda gejala yang terlihat yaitu berat badan yang menurun dan sakit perut pada bagian bawah yang relatif sering, tetapi jarang terjadi pendarahan di anus. Pada 50-60% pasien terdapat massa yang teraba di sisi kanan perut
-
Karsinoma Colon Sebelah KiriKarsinoma terletak pada bagian distal---gangguan buang air besarAdanya darah di feses. Beberapa karsinoma pada transversa colon dan colon sigmoid dapat teraba melalui dinding perut.Karsinoma sebelah kiri lebih cepat menimbulkan obstruksi, sehingga terjadi obstipasi. Tidak jarang timbul diare paradoksikal, karena tinja yang masih encer dipaksa melewati daerah obstruksi partial
-
Karsinoma RektumGangguan defekasi, misalnya konstipasi atau diare. Sering terjadi perdarahan yang segar dan sering bercampur lendir, berat badan menurun. Perlu diketahui bahwa rasa nyeri tidak biasa timbul pada kanker rectum. Kadang-kadang menimbulkan tenesmus dan sering merupakan gejala utama
-
Morphology25% of colorectal carcinomas berada di cecum atau ascending colonProporsi yang sama berada di rectum dan distal sigmoid25% di descending colon dan proximal sigmoidremainder scattered elsewheremultiple carcinomas present often at widely disparate sites in the colon
-
MorphologySemua kanker kolon dimulai dari in situ lesionstumors in the proximal colon: polypoid, exophytic masses dapat melebar sepanjang cecum dan ascending colon
-
MorphologyTumbuh berbentuk cincin menimbulkan napkin-ring. Pada permulaan, tumor tampak seperti massa berbentuk sesil, kemudian tumbuh berbentuk plak melingkar yang menimbulkan obstipasi. Kemudian bagian tengah mengalami ulserasi yang menimbulkan simtom diare, tinja campur lendir dan darah, konstipasi dan tenesmus mirip dengan sindrom disentri
-
Morphologyall colon carcinomas - microscopically similaralmost all - adenocarcinomasrange from well-differentiated to undifferentiated, frankly anaplastic massesmany tumors produce mucinsecretions dissect through the gut wall, facilitate extension of the cancer and worsen the prognosiscancers of the anal zone are predominantly squamous cell in origin
-
Clinical Features may remain asymptomatic for yearssymptoms develop insidiouslycecal and right colonic cancers:fatigueweaknessiron deficiency anemialeft-sided lesions:occult bleedingchanges in bowel habitcrampy left lower quadrant discomfortanemia in females may arise from gynecologic causes, but it is a clinical maxim that iron deficiency anemia in an older man means gastrointestinal cancer until proved otherwise
-
STADIUM KANKER
-
Lanjutan.......
-
Clinical Featuresspread by direct extension into adjacent structures and by metastasis through lymphatics and blood vesselsfavored sites for metastasis:regional lymph nodesliverlungsbonesother sites including serosal membrane of the peritoneal cavitycarcinomas of the anal region locally invasive, metastasize to regional lymph nodes and distant sites
TNM Staging of Colon Cancer
Tumor (T)T0 = none evidentTis = in situ (limited to mucosa)T1 = invasion of lamina propria or submucosaT2 = invasion of muscularis propriaT3 = invasion through muscularis propria into subserosa or nonperitonealized perimuscular tissueT4 = invasion of other organs or structures
Lymph Nodes (N)0 = none evident1 = 1 to 3 positive pericolic nodes2 = 4 or more positive pericolic nodes3 = any positive node along a named blood vessel
Distant Metastases (M)0 = none evident1 = any distant metastasis
5-Year Survival RatesT1 = 97%T2 = 90%T3 = 78%T4 = 63%Any T; N1; M0 = 66%Any T; N2; M0 = 37%Any T; N3; M0 = data not availableAny M1 = 4%
-
Clinical Featuresdetection and diagnosis:digital rectal examinationfecal testing for occult blood lossbarium enema, sigmoidoscopy and colonoscopyconfirmatory biopsycomputed tomography and other radiographic studiesserum markers (elevated blood levels of carcinoembryonic antigen)molecular detection of APC mutations in epithelial cells, isolated from stoolstests under development: detection of abnormal patterns of methylation in DNA isolated from stool cells
-
Therapychemotherapyradiotherapyphotodynamic therapyradical surgerygene therapy
-
ASUHAN KEPERAWATAN
-
True or false?98% of all cancers in the large intestine are adenocarcinomas.
Use of Aspirin and other NSAIDs may cause development of colon cancer.
Chromosome instability and the mismatch repair are two carcinogenesis pathways.
Tumors in the proximal colon tend to be annular, encircling lesions that produce napkin-ring constrictions of the bowel and narrowing of the lumen, while those in the distal colon tend to grow as polypoid, exophytic masses.
Colorectal carcinoma may remain asymptomatic for years.
-
References:http://www.liebertonline.com/doi/abs/10.1089/pho.2008.2238http://clincancerres.aacrjournals.org/cgi/content/abstract/5/9/2359Elsevier. Kumar et al: Robbins Basic Pathology 8eZahari Ari. Deteksi Dini diagnosis dan penatalaksanaan kanker kolon dan rektum. Suplemen majalalah kesehatan AndalasTimothy J Yeatman, Cancer colon. University of South Florida, Tampa, Florida, USA
Two of the earliest genes affected in the development ofcolon cancer are the adenomatous polyposis coli (APC)gene and the RAS gene (Fearon and Vogelstein, 1990)*Makanan mempunyai peranan penting pada kejadian kanker colorectal. Mengkonsumsi serat sebanyak 30 gr/hari terbukti dapat menurunkan risiko timbulnya kanker colorectal sebesar 40% dibandingkan orang yang hanya mengkonsumsi serat 12 gr/hari. Orang yang banyak mengkonsumsi daging merah (misal daging sapi, kambing) atau daging olahan lebih dari 160 gr/hari (2 porsi atau lebih) akan mengalami peningkatan risiko kanker colorectal sebesar 35% dibandingkan orang yang mengkonsumsi kurang dari 1 porsi per minggu*