BPH
57
Presentasi Kasus
-
Upload
mak-chin-jian -
Category
Documents
-
view
48 -
download
0
description
BPH
Transcript of BPH

Presentasi Kasus

Identitas Pasien
Nama : Tn. T Jenis kelamin : Laki-laki Usia : 67 tahun Alamat : Tegal anak RT 03/05 Kedungrejo
Cilacap Status pernikahan : menikah Nomor RM : 921.953 Tanggal periksa : 14 Maret 2012

Keluhan Utama
Gangguan buang air kecil

Riwayat Penyakit Sekarang
3 HSMRS: os mengeluhkan tidak bisa BAK, ketika ingin BAK, BAK yang keluar hanya berupa tetesan. Urine yang keluar berwarna jernih kekuning2an. Tidak ada keluhan BAK. Pada malam hari sering terbangun malam hari karena ingin buang air kecil hingga lebih dari 2 kali.
1 HSMRS : keluhan os sejak 3 hari tetap disertai dengan nyeri perut bagian bawah.

Riwayat Penyakit Dahulu Belum pernah mengalami keluhan seperti
ini. Riwayat sakit batu pada saluran kemih
disangkal. Riwayat buang air kecil berdarah (-)

Riwayat Penyakit Keluarga Hipertensi (-). DM (-) Riwayat pada keluarga (+) pada saudara
kandung dengan keluhan yang sama dan sudah dioperasi.

IPSS Score
Incomplete emptying 5 Frequency (BAK setiap 2 jam) 5 Intermittency 5 Urgency 5 Weak stream 5 Straining 5 Nocturia 5
Quality of live 6 (terrible)

Resume Anamnesis
Gangguan buang air kecil, urin yang keluar berupa tetesan. Nyeri perut terutama kanan bawah. Semakin lama tidak bisa buang air kecil.
Riwayat keluhan serupa pada saudara kandung.
IPSS score 35

Pemeriksaan Fisik KU : baik Kesadaran : CM VS: TD= 130/90mmHg, HR =72 x/m,
RR=20x/m, t: afebris

• Kepala : conjunctiva anemis -/-
• Leher : lnn ttb, JVP tidak meningkat
• Thorax : simetris, sonor pada perkusi +/+, vesicular +/+
• Jantung: S1 S2 tunggal, bising -/-.
• Abdomen : datar, BU+ N, 10x/menit, timpani +/+
• Ekstremitas : pucat (-), edema (-)

Status Lokalis Urologis
Flank region : masa -/-, nyeri tekan -/-, nyeri ketok -/-,
Supra pubik : distended (+), nyeri tekan (+) OUE : discharge -, lesi kulit -, warna kulit dbn.

Rectal Toucher
TMSA : positif Mukosa licin Ampula recti tidak kolaps Teraba masa 2 ruas jari sekitar jam 12, ujung
pool/kutub tidak dapat teraba Darah - , feses -, lendir -

Assessment
Susp. BPH

Plan Cek Darah Rutin, Ureum Kreatinin, Asam
urat, Gula darah sewaktu Cystography USG Abdomen Pro Prostatectomy Pasang DC

Px penunjang
Darah rutin : Hb 14.3, AL 6.630, AT 338.000 Waktu perdarahan : 5, waktu pembekuan : 10 Faal ginjal : ureum 20, kreatinin 0,9 GDS : 114

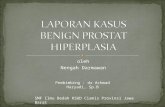
Diagnosis
Benign Prostate Hyperplasia

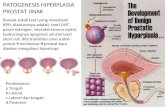
Pembahasan

Prostate
Walnut-shaped gland that forms part of the male reproductive systemSurrounds the urethra - the tube that carries urine from the bladder out of the body
n
n

Secretes semen which carries sperm
During orgasm, prostate muscles contract and propel ejaculate out of the penis
Prostate
n
n

The size of prostate enlarged microscopically since the age of 40.Half of all men over the age of 60 will develop an enlarged prostate
By the time men reach their 70’s and 80’s, 80% will experience urinary symptoms
But only 25% of men aged 80 will be receiving BPH treatment
BPH
n
n

Benign Prostatic Hyperplasia

Normal Prostate Anatomy• Prostate weights ~20g
• Measures 3 x 4 x 2 cm (walnut sized)
• Apex = inferior portion of prostate, continuous with striated sphincter.
• Base = superior portion and continuous with bladder neck.

PROSTATE histology
Prostatic tissue is formed of two components :•fibromuscular tissue (30%)
•glandular epithelial cells (70%)

Normal histology of the prostate formed of glands and stroma glands: lined by two layers of cells which are inner cuboidal cells and outer basal cells stroma :fibro muscular stroma

Prostate zonesCentral zone (CZ) •Cone shaped region that surround the ejaculatory ducts (extends from bladder base to the verumontanum) •Only 1-5% of prostate cancer from this region . Peripheral zone (PZ) •Posteriolateral prostate •Majority of prostatic glandular tissue •Origin of up to 70% of prostate adenocarcinoma
Transitional zone (TZ) •Surrounds the prostatic urethra •Commonest site for benign prostatic hyperplasia.


What causes BPH?
BPH is part of the natural aging process, like getting gray hair or wearing glasses
BPH cannot be prevented
BPH can be treated
n
n
n

Half of all men over the age of 60 will develop an enlarged prostate.
By the time men reach their 70’s and 80’s, 80% will experience urinary symptomsBut only 25% of men aged 80 will be receiving BPH treatment

BPHProposed Etiologies
• 1-alterations in the testosterone/estrogen balance:enlarged prostate may be caused by lower levels of testosterone (male hormone) production in middle to old age. As men age, the levels of testosterone in their blood decreases, leaving a higher proportion of estrogen (female hormone), so a higher amount of estrogen within the prostate gland can increase activity that promotes cell growth.
•2-Induction of prostatic growth factors.
•3- Increased stem cells/decreased stromal cell death

BENIGN PROSTATIC HYPERTROPHY (BPH)—PATHOPHYSIOLOGY
• Common in older men; varies from mild to severe• Change is actually hyperplasia of prostate
– Nodules form around urethra• Not change to cancer prostate.• Rectal exams reveals enlarged gland• Incomplete emptying of bladder leads to infections• Continued obstruction leads to distended bladder,
dilated ureters, renal damage– If significant, surgery required


WHAT’S LOWER URINARY TRACT SYMPTOMS SECONDARY TO PROSTATIC URETHRA OBSTRUCTION?Abnormal Voiding
(obstructive)symptoms• Hesitancy• Weak stream• Straining to pass urine• Prolonged micturition• Feeling of incomplete
bladder emptying• Urinary retention
Storage (irritative orfilling) symptoms•Urgency:an increasingly strong desire to void)
•Frequency•Nocturia•Urge incontinence
LUTS is not specific to BPH – not everyone withLUTS is not specific to BPH – not everyone withLUTS has BPH and not everyone with BPH has LUTSLUTS has BPH and not everyone with BPH has LUTS

BPH—SIGNS AND SYMPTOMS
• Initial signs– Obstruction of urine flow
• Hesitancy : delay between trying to urinate and the flow actually beginning.
• dribbling • decreased force of urine stream• Incomplete bladder emptying
– Frequency,– nocturia : need to urinate at night – recurrent Urinary Tract Infections

BPH complications
• hypertrophy of the prostateàdetrussor muscle of the bladder undergo hypertrophy to overcome the obstruction in the prostatic urethra. Later on decompensation occur .
•Increase pressure inside bladder diverticula formation
increasing urine retention hydronephrosis renal failure.

Diverticula in bladder


Diagnosis of BPH• Symptom assessmentSymptom assessment
• Digital rectal examination(DRE)Digital rectal examination(DRE)–inaccurate for size but can detect shape and consistency
• Prostate Volume (PV) determination by ultrasonographyProstate Volume (PV) determination by ultrasonography
• Urodynamic analysisUrodynamic analysis
• Measurement of prostate-specific antigen (PSA) Measurement of prostate-specific antigen (PSA) –high correlation between PSA and PV,–men with larger prostates have higher PSA levels–PSA is a predictor of disease progression and screening tool for Cancer Prostate.–as PSA values tend to increase with increasing Prostatic Volume and increasing age, PSA may be used as a prognostic marker for BPH.

When should BPH be treated?
BPH needs to be treated ONLy IF:
Symptoms are severe enough to bother the patient and affect his quality of life
Complications related to BPH n
n

Medication :α blockers - relax the smooth muscle of prostate
and provide a larger urethral opening
Surgical approaches
1- Transurethral resection of the prostate (TURP)
2- Open simple prostatectomy
Treatment options

“WATCHFUL WAITING”
For mild symptoms. follow up1 to 2 times yearly
Offer suggestions that help reduce symptoms
Avoid caffeine and alcoholAvoid decongestants and antihistamines
n
n
n
n

MedicationFirst line of defense against bothersome urinary symptoms
Two major types:α blockers - relax the smooth muscle of prostate and provide a larger urethral opening (Hytrin,Doxaben, Harnalidge)
5 α reductase inhibitor - Shrink the prostate gland (Proscar, Avodart)
n
n
n
n

Benefits
Convenient
No loss of work time
Minimal risk
Disadvantages
Drug Interactions
Must be taken every day
Manages the problem instead of fixing it
Medication
n
n
n
n
n
n

POSSIBLE SIDE EFFECTS OF
• Impotence
• Dizziness
• Headaches
• Fatigue
• Loss of sexual drive
medication
n
n
n
n
n

Α-ADRENERGIC BLOCKERS: RATIONALE
• Prostate smooth muscle tone is mediated via α1-adrenergic receptor
• Blockage of the receptor leads to improvement of flow rate and LUTS1
• Central α-receptors and the effect of agents on these receptors likely play an additional role
• Density of adrenergic receptors changes with prostate size and age
•Three α1-adrenergic receptor subtypes have been identified (A, B, D)
Schwinn DA. BJU Int. 2000;86(suppl 2):11-22.

Α-BLOCKERS• Nonselective
– Phenoxybenzamine• Short-acting selective α1-blocker
– Prazosin, Alfuzosin• Long-acting selective α1-blockers
– Terazosin– Doxazosin
• Long-acting selective α1A-subtype– Tamsulosin– Alfuzosin-SR

Indication of surgical intervention • Acute urinary retention • Gross hematuria• Frequent urinary tract infection (UTI)• Vesical stone • BPH related hydronephrosis or renal
function deterioration• Obstruction

Differential Diagnosisof BPH(i.e from other causes of urinary obstruction)
• Urethral stricture• Bladder neck contracture• Carcinoma of the prostate• Carcinoma of the bladder• Bladder calculi• Urinary tract infection and prostatitis• Neurogenic bladder

TURP
“Gold Standard” of care for BPH
Uses an electrical “knife” to surgically cut and remove excess prostate tissue
Effective in relieving symptoms and restoring urine flow
(transurethral resection of the prostate)
n
n
n

TURP• “Gold standard” of surgical treatment for
BPH• 80~90% obstructive symptom improved• 30% irritative symptom improved• Low mortality rate 0.2%

THE “GOLD STANDARD”- TURP
Benefits
Widely available
Effective
Long lasting
Disadvantages
Greater risk of side effects and complications
1-4 days hospital stay
1-3 days catheter
4-6 week recovery
n
n
n
n
n
n
n

Complication of TURP•Immediate complication bleeding
capsular perforation with fluid extravasation
TUR syndrome•Late complication urethral stricture
bladder neck contracture (BNC)
retrograde ejaculation
impotence (5-10%)
incontinence (0.1%)

Open Simple Prostatectomy
• “too large prostate” -- >100 gm • Combined with bladder diverticulum or
vesical stone surgery • Suprapubic or retropubic method

Minimally invasive therapy• During the last decade, numerous amounts of
minimally invasive therapy modalities have been developed to challenge the traditional surgery of TURP
• The aim of these therapies is to achieve results similar to TURP but with minimal anesthesia, complication, risk and hospital stay.

Minimally invasive therapy for BPH• transurethral balloon dilatation of the prostate (TUBDP) • transurethral incision of the prostate (TUI)• intraprostatic stent• transurethral microwave thermotherapy (TUMT)• transurethral needle ablation of the prostate (TUNA)• transurethral electrovaporization of the prostate (TUVP)• photoselective vaporization of the prostate (PVP), • Cryotherapy• Transurethral ethanol ablation of the prostate (TEAP),

Minimally invasive therapy for BPH• transurethral laser-induced prostatectomy (TULIP)• visual laser ablation of the prostate (VLAP)• contact laser prostatectomy (CLP)• interstitial laser coagulation of the prostate (ILC)• holmium:YAG laser resection of the prostate (HoLRP)• holmium:YAG laser enucleation of the prostate
(HoLEP)• high-intensity focused ultrasound (HIFU) coagulation• botulinum toxin-A injection of the prostate

Summary• Minimally invasive therapies for the treatment of BPH
has the advantages such as less blood loss, less occurrence of hyponatremia, quicker recovery, and reduced risk of urethral stricture.
• However, it also has the disadvantages such as long-lasting bladder irritation owing to higher temperature during therapy and possible longer catheterization period due to swelling of the prostate.
• It is still too early to make a definitive conclusion concerning the future role of these minimally invasive therapies for the treatment of BPH.

Thanks for Your Attention!