






Bahasa
Halaman
Hukum


1
Cognitive and affective disturbances following focal cerebellar damage in
adults: A neuropsychological and SPECT study
Hanne Baillieux1, Hyo Jung De Smet1, André Dobbeleir2, Philippe F. Paquier1, 3, Peter P. De
Deyn 4, & Peter Mariën1, 4
1 Department of Linguistics, Vrije Universiteit Brussel, Brussels, Belgium 2 Department of Nuclear Medicine, ZNA-AZ Middelheim, Antwerp, Belgium and Universitair
Ziekenhuis Gent, Ghent, Belgium 3 Department of Neurology, Hôpital Universitaire Erasme ULB, Brussels, Belgium and Unit of
Neurosciences, Universiteit Antwerpen, Antwerp, Belgium 4Department of Neurology, ZNA-AZ Middelheim, Antwerp, Belgium and Laboratory of
Neurochemistry and Behaviour, Institute Born-Bunge, Universiteit Antwerpen, Antwerp,
Belgium
Correspondence address: Prof. Dr. Peter Mariën
ZNA - Middelheim
Department of Neurology
Lindendreef 1
B-2020 Antwerp
Belgium
Tel: 0032/3/280.31.36
Fax: 0032/3/281.37.48
E-mail: [email protected]
Acknowledgements: This study was supported by grant G.0209.05 of the Fund for Scientific
Research – Flanders (F.W.O. – Vlaanderen), by Onderzoeksraad (OZR-VUB), by Nationale
Vereniging tot Steun aan Gehandicapte Personen (NVSG-ANAH), by Stichting Integratie
Gehandicapten (SIG), and by Deloitte Belgium.

2
Abstract
The traditional view on cerebellar functioning has recently been challenged by results from
neuroanatomical, neuroimaging and clinical studies. In this contribution, eighteen patients with
primary cerebellar lesions (vascular: n=13; neoplastic: n=5) were systematically investigated by
means of an extensive neuropsychological test battery. Fifteen patients (83%) presented with a
broad variety of cognitive and linguistic deficits following cerebellar damage. Disturbances of
attention (72%), executive functioning (50%) and memory (50%) were most commonly found.
Analyses of our results tend to support the hypothesis of a lateralization of cognitive modulation
within the cerebellum, the right cerebellar hemisphere being associated with logical reasoning
and language processing and the left cerebellum mediating right-hemispheric functions including
attentional and visuo-spatial skills. In addition, nine patients (50%) presented with frontal-like
behavioural and affective alterations. In an attempt to determine the working-mechanism
underlying cerebellar induced cognitive and affective disturbances, all patients were investigated
by means of quantified ECD-SPECT studies. From a semiological point of view, damage to the
cerebellum can cause a broad spectrum of clinically significant cognitive and affective
disturbances. From a pathophysiological point of view, quantified SPECT data, reflecting the
phenomenon of cerebello-cerebral diaschisis, support the functional impact of the cerebellar
lesion on cortical functioning through disruption of cerebello-cerebral connections.
Keywords: cerebellum, adults, cognition, cognitive-affective syndrome, SPECT

3
Introduction
At the beginning of the 20th century, neurophysiologists such as Luigi Rolando and
Marie-Jean-Pierre Flourens observed coordination difficulties, clumsiness and staggering gait
following isolated cerebellar ablation in animals (Fine et al., 2002). Additionally, Gordon Holmes
studied a family with hereditary cerebellar degeneration and described the family members as
small in stature with poor coordination and an unsteady walk. A decade later, Holmes (1922)
published his famous “Croonian Lectures” in which he reported hypotonia, dysmetria and
abnormal speech, characterized by an indistinct articulation in patients with acute cerebellar
lesions. As a result, coordination, balance and motor speech regulation were defined as the core
functions of the cerebellum. This view persisted during the 20th century.
Recently, however, results from neuroanatomical, neuroimaging and clinical studies have
challenged this traditional view on the cerebellum’s functions. Neuroanatomical studies have
shown bidirectional pathways between the cerebellum and cortical structures involved in
cognitive regulation. More specifically, the prefrontal cortex sends information to the cerebellum
via pontine nuclei, while the cerebellum sends information back to the prefrontal areas through
dentatothalamic pathways (Leiner et al., 1986; Middleton & Strick, 1994; Murdoch, this issue).
However, the functional implications of the cerebello-cerebral connectivity still evoke many
questions. There is no consistency with regard to the precise clinical consequences of acquired
cerebellar lesions and the pathophysiological substrate remains unclear. Numerous reports of a
broad variety of linguistic, cognitive and affective disturbances following isolated cerebellar
damage have been published (for a review see Baillieux et al., 2008). Clinical investigations of
patients with acquired cerebellar lesions have demonstrated cerebellar involvement in attentional
disturbances (Baillieux et al., 2006; Gottwald et al., 2004), executive dysfunctioning
4
(Schmahmann & Sherman, 1998), visuo-spatial disturbances (Molinari et al., 2004) and a variety
of language disorders such as agrammatism (Silveri et al., 1994), anomia (Schmahmann &
Sherman, 1998), adynamia (Mariën et al., 1996) and reading/writing disorders (Vlachos et al.,
2007) (see De Smet et al., 2007 for a review).
In this contribution, we describe the neurocognitive symptoms and behavioural
characteristics of eighteen patients with isolated cerebellar damage. In addition, functional
neuroimaging by means of quantified ECD-SPECT studies was conducted to evaluate the
pathophysiological hypothesis that cerebellar-induced cognitive and affective disturbances
constitute a diaschisis phenomenon (Mariën et al., 1996, 2001; Baillieux et. al., 2006).
Method
Population
All patients with focal cerebellar lesions admitted to the neurology department of ZNA
AZ-Middelheim hospital between January 2006 and November 2007 were included in this study.
Exclusion criteria consisted of: 1) lesions involving cortical or subcortical non-cerebellar
damage, 2) a neurological status that did not allow reliable neurocognitive testing, 3) age younger
than 18 years, 4) a history of psychiatric disease and 5) a history of substance abuse. Approval by
the local Ethics Committee was obtained. All patients were given a standard neurological
evaluation within 24 hours of onset of the symptoms.
Neuroimaging
Each patient underwent structural neuroimaging by means of Computed Tomography
(CT) and/or Magnetic Resonance Imaging (MRI) scan on admission to determine the precise
localization and nature of the cerebellar lesion. Based upon the templates provided by Savoiardo

5
et al. (1987) and Cormier et al. (1992), vascular lesions were attributed to the following vascular
territories independently of the neuropsychological data: superior cerebellar artery (SCA),
posterior inferior cerebellar artery (PICA) or anterior inferior cerebellar artery (AICA). In
addition, a quantified Tc-99m-ECD SPECT study was administered in the acute phase and during
follow-up after onset of the cerebellar damage. Using a previously fixed butterfly needle 740
MBq (20 mCi) Tc-99m-ECD was administered to the patient sitting in a quiet and dimmed room,
eyes open and ears unplugged. Acquisition was started 40 min after injection using a three-
headed rotating gamma camera system (Triad 88; Trionix Research Laboratory, Twinsburg,
Ohio, USA) equipped with lead super-fine fanbeam collimators with a system resolution of 7.3
mm FWHM (rotating radius 13 cm). Projection data were accumulated in a 128 x 64 matrix,
pixel size 3.56 mm, 15 seconds per angle, 120 angles for each detector (3° steps, 360° rotation).
Projection images were rebinned to parallel data, smoothed and reconstructed in a 64 x 64 matrix,
using a Butterworth filter with a high cut frequency of 0.7 cycles/cm and a roll-off of 5. No
attenuation or scatter correction was performed. Trans-axial images with a pixel size of 3.56 mm
were anatomically standardized using SPM and compared to a standard normal and SD image
obtained from 15 normal ECD perfusion studies in healthy adults. Using a 31 ROI template, the
z-scores (SD) were then calculated for each region. A regional z-score of >2.0 was considered
significant.
Neuropsychological assessment
All patients were extensively investigated by means of a neuropsychological protocol.
Patients with vascular lesions were evaluated following the time frame model of Mazzochi &
Vignolo (1979) for the study of vascular aphasia and were examined during the lesion phase with
an average of 30 days following onset of the cerebellar lesion. Follow-up examinations were

6
conducted during the late phase with an average of 6 months and 24 days post-onset. Patients
with cerebellar tumours were investigated before the surgical resection of the tumour and with an
average of 3 weeks after removal of the tumour.
The Wechsler Memory Scale-Revised (Wechsler, 1987) was administered to assess
general memory skills in patients below 74 years of age. Patients above the age of 74 were tested
with the Hierarchic Dementia Scale (HDS, Cole & Dastoor, 1983) or the Repeatable Battery for
the Assessment of Neuropsychological Status (R-BANS, Randolph, 1998). In addition, executive
functioning and problem solving were investigated by means of the Wisconsin Card Sorting Test
(WCST) (Heaton et al., 1993), the Stroop Color-Word Test (Hammes, 1971), and the
Trailmaking Test (Reitan, 1958). The D2 test of attention (Brickenkamp & Zilmer, 1998) was
used to evaluate visual-motor attention and a copy of the Rey-Osterrieth Figure (Osterrieth, 1944)
was used to examine visuo-constructive praxis. Working memory was assessed by verbal and
visual memory spans (WMS-R), while the Raven Matrices tests (Raven Progressive and Raven
Coloured) were used to evaluate non-verbal problem solving (Raven, 1938, 1958).
Neurolinguistic assessments consisted of a semantic verbal fluency test (1 minute generation of
four semantic categories: animals, transportation, vegetables and clothing; unpublished norms)
and the Boston Naming Test (BNT) (Kaplan et al., 1983; Mariën et al., 1998). In addition, to
evaluate possible behavioural-affective abnormalities and personality changes, the patient’s
behaviour and emotional coping were observed and family members of all patients were
interviewed.
Results
Group characteristics
Demographic data
7
Eighteen patients matching our criteria were included in the study. Demographic
characteristics and neurological symptoms are summarized in Table 1.
Insert Table 1 near here
Twelve patients were men with an average age of 64 years (X=63.6; SD=11; range 50-88)
and six patients were women with an average age of 67 years (X=67.1; SD=12; range 50-86). All
patients were right-handed as formally assessed by the Edinburgh Handedness Inventory
(Oldfield, 1971).
Lesion localization
Eight patients (patients 1 to 8) presented with right-sided cerebellar lesions, of whom six
patients had a vascular lesion: three were located in the PICA territory (patient 2, 3, 6; Figure
1A), while three patients presented with lesions in the SCA territory (patient 1, 4, 5; Figure 1B).
Two patients presented with a right-sided cerebellar tumour (patient 7 and 8).
Insert Figure 1A-B-C near here
Six patients (patients 9 to 14) had lesions confined to the left cerebellar hemisphere, of
whom five patients presented with vascular lesions: four located in the PICA territory (patient 10,
11, 13, 14; Figure 2A), while one patient had an infarction in the SCA territory (patient 9). MRI
in one patient showed a left cerebellar tumour (patient 12; Figure 2B).
Insert Figure 2A-B
One patient (patient 14) presented with bilateral cerebellar infarctions in the SCA
territory.
In addition, three patients presented with lesions confined to the vermis (AVM rupture in
patient 17 and tumours in patient 16 and 18; Figure 3).
Insert Figure 3 near here

8
Neuropsychological results
Three patients (patients 3, 5 and 8) obtained normal neuropsychological and
neurolinguistic results and had no affective disturbances. Analysis of neuropsychological data
revealed cognitive symptoms and/or behavioural-affective abnormalities in fifteen patients
(83%). Statistical analysis by means of the chi-square test revealed no significant relation
between gender and neuropsychological outcome (Pearson χ2=1.80; p=0.18). Cognitive and
affective symptoms are summarized in Table 2.
Insert Table 2 near here
Speech was characterized by dysarthria and an indistinct articulation in nine patients
(50%; patient 1, 2, 4, 5, 7, 13-15, 17). Comprehension however was normal in all patients.
Language symptoms mostly consisted of naming deficits (22%; patient 1, 4, 13, 15) and disturbed
semantic verbal fluency (39%; patient 1, 2, 4, 7, 13, 15, 18). Two patients (patients 4 and 15)
presented with apractic agraphia. No ideomotor or ideational apraxia was found in any of the
patients.
Executive dysfunction (disturbed divided attention, mental flexibility, problem solving
and organization skills) was found in nine patients (50%; patient 1, 2, 4, 7, 10, 13, 16, 17, 18). In
addition, attentional deficits were present in thirteen patients (72%; patient 1, 2, 4, 7, 9-17). Five
patients presented with visuo-spatial disturbances including disrupted non-verbal problem-
solving (28%; patient 1, 9, 10, 13, 14). Verbal memory as assessed by WMS-R was disturbed in
five patients (28%, patient 2, 4, 7, 14, 18) and deficient recent memory (WMS-R) was found in
four patients (22%; patient 2, 6, 14, 18). In addition, a disruption of verbal working memory as
assessed by verbal memory span (WMS-R) was found in four patients (22%; patient 1, 2, 4, 7).
Two patients presented with abnormal visual memory spans (11%; patient 9, 11) (Table 2).

9
Behavioural-affective disturbances consisted of a variety of frontal-like behavioural
abnormalities and were present in eight patients (45%; patient 1, 2, 4, 6, 10, 16-18). Three
patients (patient 2, 4, 10) presented with a behavioural profile characterized by inhibition, apathy,
flattening of affect and reduced initiative. Five patients (patient 1, 6, 16-18), however, presented
with a disinhibition syndrome characterized by overfamiliarity, irresponsible behaviour,
inappropriate comments and verbal disinhibition. One patient (patient 17) developed a
behavioural profile resembling obsessive-compulsive disorder and was referred to psychiatric
counselling.
Right versus left cerebellar damage
Comparison of right (n=8) versus left (n=6) cerebellar damage revealed a tendency to
lateralization of cerebellar involvement in cognitive processing. Five out of eight patients with
right cerebellar lesions (patients 1, 2, 4, 6, 7) and all six patients with left-sided cerebellar lesions
developed cognitive disturbances. Statistical analysis by means of the chi-squared test revealed
no significant difference between right or left cerebellar damage and the occurrence of
neuropsychological deficits (Pearson χ2= 2.86; p=0.09).
However, a difference was found in the type of neuropsychological impairment following
right versus left cerebellar damage. The majority of the patients with right-sided cerebellar
lesions showed typical left-hemispheric dysfunctions, including disorders in executive functions,
logical reasoning and language skills, such as disturbed verbal working memory, naming deficits
and reduced verbal fluency. By contrast, all six patients with left-sided cerebellar lesions (patients
9 to 14) demonstrated significant deficits in attention, visuo-spatial functioning, non-verbal
problem-solving and/or visual working memory, which are typically associated with right-
hemispheric dysfunctioning. Statistical analysis by means of a chi-squared test revealed a

10
significant difference in the type of neuropsychological symptoms following left versus right
cerebellar infarction (Pearson χ2= 11,00; p=0.001).
Analysis of behavioural-affective abnormalities revealed that four patients (patient 1, 2, 4,
6) with right-hemispheric cerebellar damage presented with behavioural-affective abnormalities.
By contrast, only one patient (patient 10) with left cerebellar damage experienced behavioural-
affective symptoms.
Vascular territory: SCA lesions versus PICA lesions
Cerebellar lesions of twelve patients with a vascular aetiology were attributed to a
vascular territory (SCA, PICA, AICA) within the cerebellum. One patient (patient 17) presented
with a vermian AVM. Seven patients had vascular lesions in the territory of the PICA (patients 2,
3, 6, 10, 11, 13, 14) and five patients presented with vascular lesions in the SCA territory
(patients 1, 4, 5, 9, 15).
Comparing the cognitive and affective deficits in relation to the vascular territory reveals
that six out of seven patients (patient 2, 6, 10, 11, 13, 14) with cerebellar lesions in the PICA
territory presented with clinically significant cognitive symptoms and/or behavioural
disturbances. One patient however with a PICA lesion did not develop neurocognitive symptoms
(patient 3). Similar results were obtained regarding the five patients with vascular lesions in the
SCA territory. Four patients out of five (patient 1, 4, 9, 15) developed post-stroke cognitive
and/or behavioural-affective symptoms. One patient remained free of any cognitive or
behavioural disturbances following the SCA infarction (patient 5). Statistical analyses by means
of a chi-square test revealed no significant difference between the vascular territory and the
occurrence of neuropsychological symptoms (Pearson χ2=0.69; p=0.79). In addition, no
difference was found in neuropsychological impairment following infarction in the SCA or PICA

11
territory. Attentional deficits were observed five times following PICA infarction and four times
following SCA infarction. Executive deficits were found in three patients following PICA
infarction and in two patients with SCA infarction. Disruption of linguistic skills (naming and
verbal fluency) was observed in two patients with PICA infarction and in three patients with SCA
infarction. Memory disturbances were found four times following PICA infarction and two times
following SCA infarction. Visuo-spatial deficits were observed in three patients with an
infarction in the vascular territory of the PICA and in two patients with an infarction in the SCA
territory.
Functional neuroimaging
Quantified ECD-SPECT studies were conducted in thirteen patients (patient 1, 2, 4, 5, 6,
8, 9, 10, 11, 13, 15, 16, 17). In all patients with vascular lesions a SPECT study was performed
with an average of four weeks after the stroke. In two patients (patient 8 and 16) with cerebellar
tumours a SPECT study was performed before the surgery and four weeks after surgical removal
of the tumour. Results of the quantified ECD-SPECT studies are summarized in table 3.
Insert Table 3 near here
Supratentorial perfusional deficits (more than 2SD below average) were observed in ten
of the thirteen patients (77%; patient 1, 2, 4, 5, 6, 8, 9, 13, 15, 17). Three patients presented
exclusively with infratentorial hypoperfusion (patients 10, 11 and 16). Eight patients presented
with frontal hypoperfusion (patients 1, 2, 4-6, 13, 15, 17) and two patients with parietal
hypoperfusion (patients 4 and 15). Analysis of cognitive data revealed an association between
supratentorial hypoperfusion and the observed neuropsychological deficits. Seven out of eight
patients with frontal hypoperfusion presented with associated neuropsychological deficits
(patients 1, 2, 4, 6, 9, 13, 15, 17), including executive dysfunction and/or behavioural

12
disturbances. No frontal lobe hypoperfusions were found in patients 10 and 16 despite executive
dysfunctions. Two patients with parietal hypoperfusion (patients 4 and 15) both presented with
apraxic apgraphia, a symptom commonly associated with parietal dysfunctioning (Heilman,
1974). Two patients, however, had normal neuropsychological results despite supratentorial
hypoperfusions (patient 5 and 8).
Figure 4A-B-C shows quantified ECD-SPECT studies following the onset of the
cerebellar lesion in three patients (patient 2, 13 and 17).
Insert Figure 4A-B-C near here
Discussion
In this prospective study, cognitive and functional neuroimaging findings of 18 adult
patients with isolated cerebellar damage are presented. Fifteen patients (83%) presented with
significant cognitive impairment and/or behavioural-affective disturbances. Analysis of the
neuropsychological data revealed a clear tendency to lateralization of cognitive functioning
within the cerebellum: left cerebellar damage relates to right-hemispheric dysfunctioning, such as
attention deficits and visuo-spatial disturbances, while right cerebellar damage relates to typical
left-hemispheric deficits, such as disrupted language skills. In addition, analysis of the
neuropsychological symptoms revealed no significant difference between SCA and PICA lesions.
Functional neuroimaging studies by means of quantified ECD-SPECT showed that supratentorial
hypoperfusional deficits could be related to neuropsychological symptoms, in which frontal
hypoperfusions were associated with executive dysfunctions while two patients with parietal
hypoperfusions presented with apractic agraphia.
In the late 1990s, Schmahmann and Sherman (1998) introduced the concept of cerebellar-
cognitive-affective-syndrome (CCAS) to identify a spectrum of cognitive and affective

13
disturbances in patients with isolated cerebellar lesions. Based upon bedside screening and formal
neuropsychological testing of 20 patients, the authors grouped a constellation of cognitive,
linguistic and affective symptoms following cerebellar damage. The core features of this
syndrome consist of executive dysfunctions, disrupted spatial cognition, impaired visual-spatial
memory, language disturbances and personality and behavioural disorders (Schmahmann &
Sherman, 1998). Since the first description of the syndrome, CCAS has been reported in a
number of aetiologically different patients, both children and adults, with acquired (Levisohn et
al., 2000; Baillieux et al., 2006) and congenital cerebellar damage (Duggal, 2005; Mariën et al.,
2008). Analyses of the spectrum of cognitive symptoms and behavioural abnormalities in our
patients revealed full-blown CCAS in only four cases (patient 1, 2, 4 and 10). The majority of our
patients, however, presented with a broad spectrum of cognitive and/or linguistic deficits,
including disturbances in executive functioning (50%), attention (72%), verbal and recent
memory (50%), visuo-spatial skills (28%) and linguistic functions such as naming deficits (22%)
and disrupted verbal fluency (39%). Additionally, various degrees of severity were found in our
patient group, indicating that neuropsychological deficits following cerebellar lesions may vary
among the population.
A possible explanation for the clinical diversity in our patient group might be found in the
functional lateralization (left versus right) and/or topographical organization (SCA versus PICA)
of the cerebellum. Comparing the neurocognitive deficits of our patients with right-sided versus
left-sided cerebellar lesions provides support for a lateralized involvement of cerebellar structures
in cognition. Eight patients presented with right-sided cerebellar damage, of whom five patients
showed typical left hemisphere dysfunction, including disrupted linguistic skills (disrupted
naming and verbal fluency), disturbed verbal working memory, impaired planning and deficits in
logical reasoning (executive dysfunctions). By contrast, only one patient with left-sided

14
cerebellar damage presented with linguistic deficits (disturbed verbal fluency), while none of the
patients with left-sided cerebellar damage showed disturbances in verbal working memory. By
contrast, all six patients with left cerebellar damage had typical symptoms of right hemisphere
dysfunctioning, such as visual attention disturbances, visual working memory deficits and
disrupted visuo-spatial skills. In summary, our data show that patients with right-sided cerebellar
lesions were generally more impaired in linguistic processing and logical reasoning than patients
with left-sided cerebellar damage who had significant deficits in attention, visuo-spatial
functioning and non-verbal problem solving, mimicking typical right hemisphere dysfunctioning.
The lateralized functional involvement of the cerebellum in typical dominant and non-dominant
hemisphere dysfunctions is subserved by strong crossed cerebello-cerebral connections. The
cross-wise functional impact of focal cerebellar damage on supratentorial regions subserving
cognitive functioning has been amply documented. Early evidence in support of this finding was
presented by Botez-Marquard et al. (1994) and Mariën et al. (1996). In the early 1990s Botez-
Marquard et al. (1994) described typical right-hemisphere dysfunction, such as attention deficits
and disrupted visuo-spatial skills following a left cerebellar lesion. A few years later, Mariën et
al. (1996) introduced the concept of a lateralized linguistic cerebellum based upon a longitudinal
follow-up study of a patient with cerebellar-induced aphasia following a right cerebellar infarct.
The authors attributed the modulating role of the right cerebellar hemisphere to crossed cerebello-
cerebral connections. Their hypothesis was supported by SPECT results revealing cerebello-
cerebral diaschisis, a phenomenon that represents the functional impact of the cerebellar lesion on
cortical functioning. More recently, neurocognitive studies of Allin et al. (2001), Gottwald et al.
(2004) and Hokkanen et al. (2006) have provided evidence that patients with right-sided
cerebellar lesions are generally more impaired in verbal functions, while patients with left-sided
cerebellar lesions show more difficulty in visuo-spatial tasks. It may be hypothesized that the

15
cerebellar involvement in cognitive functioning reflects a lateralized functional organization of
the cerebellum: left cerebellar lesions lead to right-hemisphere dysfunction, whereas in right
cerebellar lesions left-hemispherical symptoms are more prominent. In addition, functional
neuroimaging studies by means of SPECT (Baillieux et al., 2006; Mariën et al., 2007) and fMRI
(Fink et al., 2000; Jansen et al., 2005) have convincingly shown the importance of the
contralateral cerebello-cerebral network in cognitive modulation.
A second factor that can possibly account for the various clinical expressions in our
patient group is the topographical organization of the cerebellum (Exner et al., 2004; Mariën et
al., 2008). Based upon neuroanatomical and neuroimaging studies, the anatomic specificity of the
cerebellar-cerebral connections implies a functional topography of cognitive modulation within
the cerebellum in which different cerebellar areas interact with specific and different cortical
areas. According to Schmahmann (2004), these anatomical subcircuits consist of the feed-
forward loop of the cortico-ponto-cerebellar system and the feed-back loop of the cerebello-
thalamo-cortical pathway. These anatomical subcircuits constitute the structural basis for
functional subunits reflecting a topographic organization of motor and cognitive functions within
the cerebellum: the posterior parts of the cerebellum seem to be predominantly involved in
cognitive modulation, while the anterior cerebellar lobe is mainly involved in motor functions.
Recently, Exner et al. (2004) investigated the hypothesis that vascular lesions in different
vascularization areas of the cerebellum result in differential cognitive and affective impairments.
According to their results, patients with SCA lesions generally did not present with cognitive
symptoms or affective abnormalities, while patients with PICA lesions presented with a variety
of cognitive, linguistic and affective disturbances, including memory deficits, executive
disturbances and emotional withdrawal. These conclusions are supported by other studies (Paulus
et al., 2004; Willert et al., 2005). Additionally, Schmahmann and Sherman (1998) showed that

16
the majority of their patients (10/13) presented with CCAS following PICA-lesions. However,
neuropsychological findings in our patients challenge these results. No statistically significant
difference was found between cognitive and/or affective symptoms following cerebellar lesions
in the PICA or SCA territory. Two patients out of 13 with vascular lesions (cases 3 and 5) had
normal neuropsychological results. One of these patients had an infarction in the vascular
territory of the PICA and the other patient had an SCA infarction. In addition, full-blown CCAS
was found four times in our patient group, twice after a SCA infarction and twice after lesions
within the PICA territory. Additionally, the majority of the patients with cerebellar lesions
confined either to the SCA territory (80%) or the PICA territory (87%) presented with clinically
significant neuropsychological disturbances. No indications of a difference in the type of
neuropsychological impairment following ischaemic damage in the SCA or PICA territory were
found. Infarction in the territory of the SCA and PICA were both associated with deficits in
executive functioning, attention, linguistic skills, memory and visuo-spatial abilities.
Accordingly, Mariën et al. (2008) recently reported cognitive, linguistic and affective
disturbances in a patient with a SCA lesion and Neau et al. (2000) found no significant
differences between the neuropsychological consequences of vascular lesions in the PICA or
SCA territory. From an anatomical point of view, there is still no consistency in findings with
regard to the parts of the cerebellum that subserve cognitive modulation. Several studies and case
reports, including our own, demonstrate that variability may exist with regard to the functional
anatomy of the cerebellum (Neau et al., 2000; Mariën et al., 2008).
In addition to cerebellar involvement in language and cognition, 19th century reports
anecdotally mentioned behavioural alterations and affective abnormalities in patients with
isolated cerebellar damage (Combettes, 1831; Otto, 1873). Due to lack of standardized
investigations and pathological verification these observations did not receive much attention

17
(Dow & Moruzzi, 1958). However, the introduction of the CCAS (Schmahmann & Sherman,
1998), renewed interest in the role of the cerebellum in behavioural and affective regulation. In
our study group, frontal-like behavioural abnormalities were present in nine patients. Three
patients presented with an inhibitory behavioural profile, characterized by apathy, flattening of
affect and reduced initiative (patient 2, 4, 10) and five patients presented with the opposite
behavioural condition consisting of a disinhibition syndrome characterized by overfamiliarity,
irresponsible behaviour, inappropriate comments and verbal disinhibition (patient 1, 6, 16-18).
Schmahmann and Sherman (1998) observed that behavioural and affective symptoms in their
patient group were most notable when the lesion involved the vermis or paravermian region. This
finding is supported by the affective disturbances in patients with vermian malformations
(Steinlin, 1997) and in children following posterior fossa tumour resection who have undergone
surgical splitting of the vermis. In our patient group only two patients presented with isolated
lesions of the vermis. Patient 16 presented with severe behavioural-affective disturbances
following vermian tumour resection, while patient 17 presented with obsessive-compulsive
behavioural symptoms that needed psychiatric counselling.
Finally, the cerebello-cerebral diaschisis phenomenon is advanced as a possible
explanation for cerebellar-induced cognitive symptoms, linguistic deficits and behavioural
abnormalities (Mariën et al., 2001). It reflects a disturbance of the excitatory impulses from deep
cerebellar nuclei through dentatothalamic connections to the cortical areas subserving cognitive
processes. Data in support of this hypothesis comes from SPECT studies, evidencing perfusional
deficits in cortical areas which are crucially involved in cognitive functioning (Hassid, 1995;
Mariën et al., 1996, 2001; Zettin et al., 1997; Baillieux et al., 2007). To test this hypothesis, we
conducted ECD-SPECT studies in the immediate and follow-up phase in the vascular and
tumoural patient group. An association between the hypoperfusional deficits and the

18
neuropsychological profile was found in the majority of patients. Patients with frontal
hypoperfusions presented with executive dysfunctions and /or behavioural abnormalities, while
parietal hypoperfusions in two patients were associated with apractic agraphia, a rare writing
disorder often linked to parietal dysfunctioning (Valenstein & Heilman, 1979). However, some
inconsistency could be observed: patient 5 for example had normal neuropsychological results
while a SPECT study conducted two weeks post-stroke revealed discrete bilateral medial frontal
hypoperfusions. In addition, patient 10 presented with executive dysfunctions and behavioural
abnormalities in the absence of frontal hypoperfusions. Similar inconsistencies were observed by
Gasparini et al. (1999), Pollack et al. (1995) and Ersahin et al. (2002). In addition, it is likely that
post-infarction phenomena such as oedema or tissue swelling influence supratentorial perfusional
blood-flow and can account as a possible explanation for the observed inconsistency in SPECT
data following acquired cerebellar lesions. It seems plausible that the relation between
supratentorial hypoperfusion following an acquired cerebellar lesion and the neuropsychological
outcome is not a strict causal relationship, but an important part of a complex network underlying
cerebellar-induced cognitive and behavioural symptoms.
In summary, converging evidence from numerous clinical reports and neuroimaging
studies shows that the cerebellum is crucially involved in cognitive functioning, behavioural
processing and affective regulation. However, many questions concerning the functional
cerebello-cerebral connectivity remain unanswered. In order to determine the extent and the
precise nature of the cerebellar contribution more systematic studies are necessary to unravel this
complex network.

19
Table 1: Demographic and neurological data of the patient group
Pt. Nr.
Gender/ Age/
Hand.
Aetiology R vs. L
Terri-tory
Neurological symptoms at onset
1 de laet
M/58/R infarction R SCA right-sided ataxia, dysmetria, dysarthria gait disturbances
2 matthé
M/52/R infarction R PICA right-sided hypotonia, disequilibrium, dysarthria
3 DERWA
EL??
M/50/R infarction R PICA gait disturbances, disequilibrium,
4 schelkens
M/75/R infarction R SCA right-sided ataxia, hypotonia, gait disturbances, disequilibrium, dysarthria
5 schellens
M/61/R infarction R SCA disequilibrium, gait disturbances, vertigo, dysarthria
6 vleugels
M/67/R infarction R PICA left-sided paresthesia and dysmetria, vertigo, gait disturbances
7 VAN
AGGELPEOL??
F/53/R tumour R - disequilibrium, visual disturbances, dysarthria, nausea
8 florus
M/55/R tumour R - disequilibrium
9
M/88/R infarction L SCA left-sided ataxia, hypotonia, discrete facial palsy, gait disturbances, vertigo
10 verschuer
en???
F/68/R infarction L PICA gait disturbances, left-sided paresthesia, dysmetria, ataxia
11
smet
M/52/R infarction L PICA disequilibrium, gait disturbances
12 langenhu
yzen
F/68/R tumour L - disequilibrium, nausea
13 janssens
M/80/R infarction L PICA dizziness, disequilibrium, dysarthria
14 palinckx
F/78/R infarction L PICA disequilibrium, hypotonia, dysarthria
15 geerts
F/86/R infarction BL SCA right-sided hemiparesis, disequilibrium, dysarthria
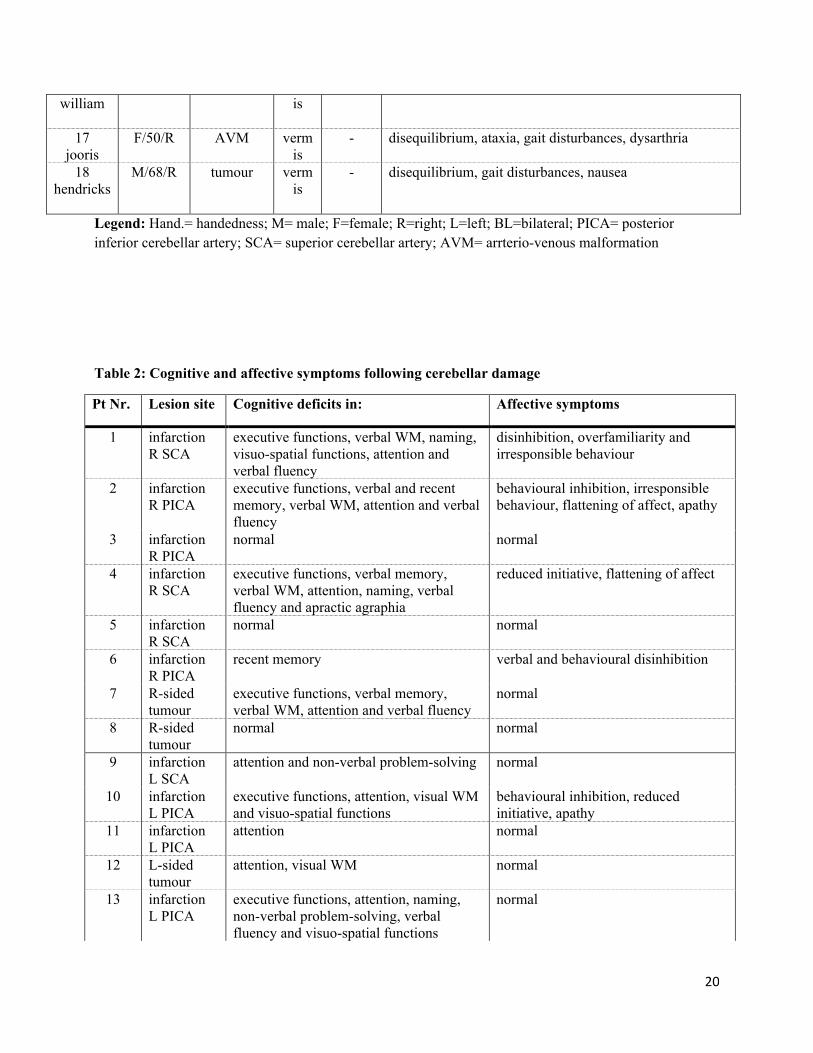
16 M/57/R tumour verm - disequilibrium, gait disturbances, ataxia
20
william
is
17 jooris
F/50/R AVM vermis
- disequilibrium, ataxia, gait disturbances, dysarthria
18 hendricks
M/68/R tumour vermis
- disequilibrium, gait disturbances, nausea
Legend: Hand.= handedness; M= male; F=female; R=right; L=left; BL=bilateral; PICA= posterior inferior cerebellar artery; SCA= superior cerebellar artery; AVM= arrterio-venous malformation
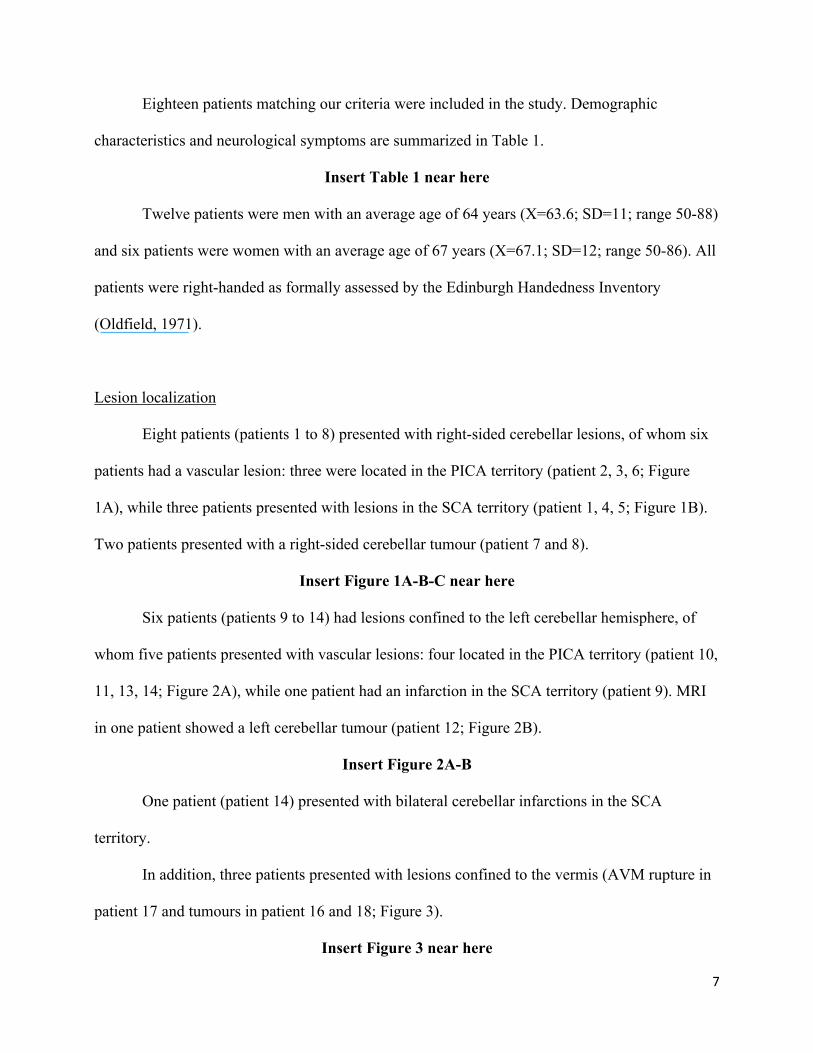
Table 2: Cognitive and affective symptoms following cerebellar damage
Pt Nr. Lesion site Cognitive deficits in: Affective symptoms
1 infarction R SCA
executive functions, verbal WM, naming, visuo-spatial functions, attention and verbal fluency
disinhibition, overfamiliarity and irresponsible behaviour
2 infarction R PICA
executive functions, verbal and recent memory, verbal WM, attention and verbal fluency
behavioural inhibition, irresponsible behaviour, flattening of affect, apathy
3 infarction R PICA
normal normal
4 infarction R SCA
executive functions, verbal memory, verbal WM, attention, naming, verbal fluency and apractic agraphia
reduced initiative, flattening of affect
5 infarction R SCA
normal normal
6 infarction R PICA
recent memory verbal and behavioural disinhibition
7 R-sided tumour
executive functions, verbal memory, verbal WM, attention and verbal fluency
normal
8 R-sided tumour
normal normal
9 infarction L SCA
attention and non-verbal problem-solving normal
10 infarction L PICA
executive functions, attention, visual WM and visuo-spatial functions
behavioural inhibition, reduced initiative, apathy
11 infarction L PICA
attention normal
12 L-sided tumour
attention, visual WM normal
13 infarction L PICA
executive functions, attention, naming, non-verbal problem-solving, verbal fluency and visuo-spatial functions
normal

21
14 infarction L PICA
verbal and recent memory, visuo-spatial functions and attention
normal
15 BL infarction SCA
attention, naming, verbal fluency and apraxic agraphia
normal
16 vermian tumour
executive functions, attention disinhibition and overfamiliarity
17 vermian AVM
executive functions, attention and severe logorrhea
verbal disinhibition, behavioural profile resembling obsessive-compulsive disorder
18 vermian tumour
executive functions, verbal and recent memory and verbal fluency
verbal disinhibition
Legend: L= left; R= right; BL= bilateral; PICA= posterior inferior cerebellar artery; SCA= superior cerebellar artery; AVM= arterio-venous malformation; WM= working memory

22
Table 3: Results from quantified SPECT studies in patients with vascular or neoplastic lesions
Pt Nr. Lesion site X weeks
po Hypoperfusional deficits (x standard-scores below average)
supratentorial infratentorial 1 infarction
R SCA 5w po frontal medial L (-2.21) cerebellum R (-3.15)
2 infarction R PICA
10w po bilateral frontal medial (-5.38 R, -4.15 L); motor cortex R (-2.62)
/
4 infarction R SCA
3w po premotor cortex L (-2.82) parietal lobe L (-4.41)
cerebellum R (-2.41)
5 infarction R SCA
2w po bilateral frontal medial (-2.34 R, -3.28 L)
/
6 infarction R PICA
1w po bilateral frontal medial (-3.17 R, -4.02 L), caudate nucl L (-2.20); thalamus L (-2.09)
8
R-sided tumour
4w post-op
bilateral temporal (-2.81 R, -2.85 L)
/
9 infarction L SCA
3w po occipital lobe R (-3.42), caudate nucl L (-2.74); thalamus L (-2.44)
10 infarction L PICA
12w po caudate nucl L (-2.88); thalamus L (-2.73)
cerebellum left (-3.83); vermis (-2.63)
11 infarction L PICA
2w po caudate nucl L (-4.27); thalamus L (-2.32)
13 infarction L PICA
2w po bilateral frontal medial (-2.09 R, -2.82 L); motor cortex L (-2.52), bilateral caudate nucl (-2.13 R; -4.8 L); thalamus L (-4.38)
vermis (-2.20) cerebellum L (-4.75)
15 BL infarction SCA
1w po frontal medial R (-3.24); motor cortex R (-4.81); parietal R (-4.91)
cerebellum R (-3.09)
16 vermian tumour
4w post-op
bilateral caudate nucl (-2.39 R, -2.88 left); thalamus R (-2.37)
vermis (-5.04)
17 vermian AVM
10w po bilateral frontal medial (-3.86 R, -3.74 left)
/
Legend: w=weeks; po=post-onset; post-op.= post-operative; R=right; L=left; BL=bilateral; PICA= posterior inferior cerebellar artery; SCA= superior cerebellar artery; AVM= arterio-venous malformation; nucl.=nucleus

23
References
Allin M, Matsumoto H, Santhouse AM, Nosarti C, Alasady MH, Stexard AL, Rifkin L and
Murray RM. Cognitive and motor functions and the size of the cerebellum in adolescents
born very pre-term. Brain, 124: 60-66, 2001
Baillieux H, De Smet HJ, Lesage G, Paquier PF, De Deyn PP and Mariën P. Neurobehavioral
alterations in an adolescent following posterior fossa tumor resection. The Cerebellum, 5:
289-295, 2006.
Baillieux H, Weyns F, Paquier PF, De Deyn PP and Mariën P. Posterior fossa syndrome after a
vermian stroke: a new case and review of the literature. Pediatric Neurosurgery, 43: 386-
395, 2007
Baillieux H, De Smet HJ, Paquier PF, De Deyn PP, and Mariën P. Cerebellar neurocognition:
insights into the bottom of the brain. Clinical Neurology and Neurosurgery, 110 : 763-773,
2008
Botez-Marquard T, Léveillé J and Botez MI. Neuropsychological functioning in unilateral
cerebellar damage. Canadian Journal of Neurological Sciences, 21: 353-357, 1994.
Brickenkamp R and Zillmer E. D2 Test of Attention. Göttingen: Hogrefe, 1998.
Cole M, and Dastoor D. The hierarchic dementia scale. Journal of Clinical and Experimental
Gerontology, 5: 219-234, 1983.
Combettes M. Absence complete du cervelet, des pédoncules postérieures et de la protubérance
cérébrale chez une jeune fille morte dans sa onzième année. Bulletin de la Société Anatomique
Paris, 5: 148-157, 1831.
Cormier PJ, Long ER. and Russell EJ. MR imaging of posterior fossa infarctions: vascular
territories and clinical correlates. Radiographics, 12 : 1079-1096 , 1992
De Smet HJ, Baillieux H, Mariën P, De Deyn PP, and Paquier PF. The cerebellum and language:
the story so far. Folia Phoniatrica et Logopaedica, 59: 165-170, 2007
Dow RS and Moruzzi G. The Physiology and Pathology of the Cerebellum. Minneapolis:
University of Minnesota Press, 1958.
Duggal HS. Cognitive affective psychosis syndrome in a patient with sporadic
olivopontocerebellar atrophy. Journal of Neuropsychiatry and Clinical Neurosciences, 17:
260-261, 2005.

24
Ersahin Y, Yararbas U, Duman Y, and Mutluer S. Single photon emission tomography following
posterior fossa surgery in patients with and without mutism. Child’s Nervous System, 18:
318-325, 2002
Exner C, Weniger G and Irle E. Cerebellar lesions in the PICA but not SCA territory impair
cognition. Neurology, 63: 2132-2135, 2004.
Fine EJ, Ionita CC, and Lohr L. The history of the development of the cerebellar
examination. Seminars in Neurology, 22: 375-384, 2002
Fink GR, Marshall JC, Shah NJ, Weiss PH, Haligan PW, Gros-Ruyken M, Ziemons K, Zilles K
and Freund HJ. Line bisection judgments implicate right parietal cortex and cerebellum as
assessed by fMRI. Neurology, 54: 1342-1331, 2000
Folstein M, Folstein S, and McHugh P. Mini-Mental State Examination. USA : Psychological
Assessment Resources, Inc, 2000
Gasparini M, Di Piero V, Ciccarelli O, Cacioppo MM, Pantano P. and Lenzi GL. Linguistic
impairment after right cerebellar stroke: a case report. European Journal of Neurology, 6:
353-356, 1996
Gottwald B, Mihajlovic Z, Wilde B and Mehdorn HM. Does the cerebellum contribute to specific
aspects of attention? Neuropsychologia, 41: 1452-1460, 2003.
Gottwald B, Wilde B, Mihajlovic, Z and Mehdorn HM. Evidence for distinct cognitive deficits
after focal cerebellar lesions. Journal of Neurology, Neurosurgery and Psychiatry, 74:
1524-1531, 2004
Hammes JGW. Stroop Kleur Woord Test. Swets & Zeitlinger B.V.: Lisse, 1971.
Hassid EI. A case of language dysfunction associated with cerebellar infarction. Journal of
Neurological Rehabilitation, 9: 157-160, 1995
Heaton RK, Chelune GJ, Talley JL, Kay GG and Curtiss, G. Wisconsin Card Sorting Test:
Revised and expanded. Psychological Assessment Resources Inc.: Lutz, 1993.
Hokkanen, L.S.K., Kauranen V, Roine RO, Salonen O and Kotila M. Subtle cognitive deficits after
cerebellar infarcts. European Journal of Neurology, 13: 161-170, 2006
Holmes G. A form of familial degeneration of the cerebellum. Brain, 30: 466-480, 1907
Holmes G. The cerebellum. The Croonian lectures on the clinical symptoms of cerebellar diseases
and their interpretation. Brain, 44: 522-591, 1922
Jansen A, Flöel A, Van Randenborgh J, Konrad C, Rotte M, Förster A, Deppe M and Knecht S.

25
Crossed cerebro-cerebellar language dominance. Human Brain Mapping, 24: 165-172,
2005.
Kaplan E, Goodglass H and Weintraub S. Boston Naming Test. USA: Lei and Febiger, 1983.
Leiner HC, Leiner AL and Dow RS. Reappraising the cerebellum: what does the hindbrain
contribute to the forebrain? Behavioral Neuroscience, 103: 998-1008, 1989.
Levisohn L, Cronin-Golomb A and Schmahmann JD. Neuropsychological consequences of
cerebellar tumor resection in children: cerebellar cognitive affective syndrome in a
pediatric population. Brain, 123: 1041-1050, 2000.
Mariën P, Baillieux H, De Smet HJ, Engelborghs S, Wilssens I, Paquier P, and De Deyn PP.
Cognitive, linguistic and affective disturbances following a right superior cerebellar artery
infarction: a case study. Cortex, Epub, 2008
Mariën P, Engelborghs S, Fabbro F and De Deyn PP. The lateralized linguistic cerebellum: a
review and a new hypothesis. Brain and Language, 7: 580-600, 2001.
Mariën P, Mampaey E, Vervaet A, Saerens J and De Deyn PP. Normative data for the Boston
Naming Test in native Dutch-speaking Belgian elderly. Brain and Language, 65: 447-
467, 1998.
Mariën P, Saerens J, Nanhoe R, Moens E, Nagels G, Pickut BA, Dierckx RA and De Deyn PP.
Cerebellar induced aphasia: case report of cerebellar induced prefrontal aphasic language
phenomena supported by SPECT findings. Journal of the Neurological Sciences, 144: 34-
43, 1996.
Mazzocchi F. and Vignolo LA. Localisation of lesions in aphasia: clinical-CT scan correlations in
stroke patients. Cortex, 15: 627-654, 1979
Middleton FA. and Strick PL. Anatomical evidence for cerebellar and basal ganglia involvement
in higher cognitive function. Science, 266: 458-461, 1994
Molinari M, Petrosini L, and Misciagna S. Visuospatial abilities in cerebellar disorders. Journal of
Neurology, Neurosurgery and Psychiatry, 75: 235-240, 2004
Neau JP, Arroyo-Anllo E, Bonnaud V, Ingrand P and Gil, R. Neuropsychological disturbances in
cerebellar infarctions. Acta Neurologica Scandinavia, 102: 363-390, 2000.
Oldfield RC. The assessment and analysis of handedness; the Edinburgh inventory.
Neuropsychologia, 9: 97-113, 1971
Osterrieth PA. Rey's Complexe Figuur Test. Swets & Zeitlinger Publishers: Amsterdam, 1944.

26
Otto A. Ein Fall von Verkummerung des Kleinhirns. Archives fur Psychiatry und Nervenkranken,
4: 730-746, 1873.
Paquier PF and Mariën P. A synthesis of the role of the cerebellum. Aphasiology, 19: 3-19, 2005.
Paulus KS, Magnano I, Conti M, Galistu P, D'Onofrio M, Satta W and Aiello I. Pure post-stroke
cerebellar cognitive affective syndrome: a case report. Neurological Sciences, 25: 220-224, 2004.
Pollack IF, Polinko P, Albright AL, Towbin R. and Fitz C. Mutism and pseudobulbar symptoms after
resection of posterior fossa tumours in children: incidence and pathophysiology. Neurosurgery,
37, 885-893, 1995
Randolph C. Repeatable battery for the assessment of neuropsychological status. San Antonio:
Psychological Corporation, 1998
Raven JC. Raven Standard Progressive Matrices. San Antonio: The Psychological Corporation, 1996
Reitan RM. Validity of the Trail Making Test as an indicator of organic brain damage.
Perceptual and Motor Skills, 8: 271-276, 1958.
Savoiardo M, Bracchi M, Passerini A, and Visciani A. The vascular territories in the cerebellum
and brainstem : CT and MR study. American Journal of Neuroradiology, 8: 199-209, 1987
Schmahmann JD. The cerebrocerebellar system: anatomic substrates of the cerebellar
contribution to cognition and emotion. International Review of Psychiatry, 13: 247-260,
2001
Schmahmann JD. Disorders of the cerebellum: ataxia, dysmetria of thought and the cerebellar
cognitive affective syndrome. Journal of Neuropsychiatry and Clinical Neuroscience, 16: 367-
378, 2004.
Schmahmann JD and Sherman JC. The cerebellar cognitive affective syndrome. Brain, 121: 561-
579, 1998.
Silveri MC, Misciagna S, Leggio M and Molinari M. Spatial dysgraphia and cerebellar lesion: a case
report. Neurology, 48: 1529-1532, 1997
Steinlin M. Non-progressive congenital ataxias. Brain and Development, 20: 199-208, 1997
Vlachos F, Papathanasiou I, and Andreou G. Cerebellum and Redding. Folia Phoniatrica et
Logopeadica, 59: 177–183, 2007
Wechsler D. Wechsler Memory Scale - Revised (WMS-R). San Antonio: The Psychological
Corporation, 1987.
Willert C, Schaumann-Kuchling C, Adamaszek M and Spitzer C. Neuropsychological

27
dysfunction after cerebellar stroke. Nervenartz, 76: 988-991, 2005.
Zettin M, Cappa SF, D'Amico A, Rago R, Perino C, Perani D, and Fazio F. Agrammatic speech
production after a right cerebellar haemorrhage. Neurocase, 3: 375-380, 1997
Top Related
Copyright © 2022 FDOKUMEN

