
Whooping Cough and Parkinson's Disease
11
International Journal of Epidemiology © International Epidemiological Association 1996 Vol. 25, No. 6 Printed in Great Britain Whooping Cough and Parkinson's Disease JESUS DE PEDRO-CUESTA,*** GRETAR GUDMUNDSSON,* VICTOR ABRAIRA,* GUNNAR GUDMUNDSSON.t ARTHUR LOVE, 5 HRAFN TULINIUS," JORGE VEIGA,* JAVIER ALMAZAN* AND INGOLF J PETERSEN 11 FOR THE EUROPARKINSON PREPARATORY ACTIVITY RESEARCH GROUP de Pedro-Cuesta J (Instituto de Salud Carlos III, Centro Nacional de Epidemiologia, Departamento de Epidemiologia Aplicada, d Sinesio Delgado, 6, 28029 Madrid, Spain), Gudmundsson G, Abraira V, Gudmundsson G, Love A, Tulinius H, Veiga J, Almazan J and Petersen I J for the EUROPARKINSON Preparatory Activity Research Group. Whooping Cough and Parkinson's Disease. International Journal of Epidemiology 1996; 25: 1301-1311. Background. We reported high levodopa use and prevalences of Parkinson's Disease (PD) in periodically, time-clustered, Icelandic cohorts born after major whooping cough epidemics (MWCE). Methods. In order to quantify a possible relationship between age at first post-birth MWCE and risk of PD we: 1) calcu- lated cumulative incidences of PD during the period 1954-1963 in one-year Icelandic cohorts born between 1869 and 1927, using raw material from a reported survey; 2) identified MWCE from 1869 onwards in Iceland; 3) estimated cohort ages at onset of incidence period and at first MWCE; and 4) combined the above-mentioned information using log-linear models. In addition, we studied the prevalence of levodopa users in Icelandic birth cohorts during a recent period. Results. The curves of the above-mentioned incidences and prevalences in one-year birth-cohorts showed: 1) a similar, age-related, inverted V profile; and 2) a systematic notchy pattern, with peak values for one or both measurements for cohorts born during or after each of nine MWCE identified during the period 1869-1927. When 13 cohorts born in years with MWCE were excluded from the analysis, the risk of PD rose with age at first defined MWCE, with the linear increase being 8.4% per year (95% Cl : -0.1-18.3%). Conclusions. These results are consistent with reported effects of age at exposure in animal models of toxic parkin- sonism, age-related changes in the dopamine receptor-GPT-binding protein-adenylatecyclase system observed in rats treated with pertussis toxin, and some PD epidemiological features. They suggest that pertussis neurotoxicity could be causally related to PD worldwide. Keywords: dopamine, drug use, epidemiology, aetiology, Parkinson's disease, pertussis Parkinson's disease (PD) is a disorder characterized by progressive Lewy-body neuronal degeneration, located mainly in substantia nigra (SN) and other brainstem nuclei. 1 This lesion might precede the onset of clinical symptoms by several decades.' 2 The disease appears * Department of Applied Epidemiology, National Centre for Epidemiology, Carlos III Institute of Health, Madrid, Spain. *• Division of Neurology, Department of Clinical Neuroseience and Family Medicine, Huddinge University Hospital, Karolinska Institute, Huddinge, Sweden. 'Department of Neurology, National University Hospital, Reykjavik, Iceland. ' Biostatistics Unit, Ram6n y Cajal Hospital, and the REUNI Centre, Carlos III Institute of Health, Madrid, Spain. 8 Department of Microbiology, National University, Reykjavik, Iceland. "Department of Social Medicine, National University, Reykjavik, Iceland. ' Pharmaceutical Division, Ministry of Health, Reykjavik, Iceland. Reprint requests: Jesus de Pedro Cuesta. Instituto de Salud Carlos III, Centro Nacional de Epidemiologfa, Departamento de Epidemiologia Aplicada, c/ Sinesio Delgado, 6, 28029 Madrid, Spain. to be ubiquitous, is not present in animals, and may have undergone similar historical changes worldwide linked to modernization. 3 - 4 The highest reported PD incidence and prevalence for ages under 70 years and Parkinsonism-related mortality are to be found in Iceland. 4 " 7 The causes of PD are unknown. Nowadays, the most plausible aetiological hypothesis is a combination of hereditary—most probably polygenic—and toxic envir- onmental factors. 8 " 10 However, while a two- to threefold risk of PD associated with a genetic defect linked to cytochrome P450 mono-oxygenase activity, a protect- ive factor against toxic environmental compounds, has been reported,"" 13 environmental toxins potentially linked to PD remain unidentified. In the West, recent studies report that 76-83% of all prevalent diagnosed patients are being treated with levodopa (LD). 14 Furthermore, LD use (LDU) is highly specific for PD treatment. 15 Geographical evaluation of sales of LD in 92 regions from Denmark, Iceland, Greece, Spain, and Sweden, 16 " 18 pointed to highest LDU 1301 by guest on August 10, 2016 http://ije.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Whooping Cough and Parkinson's Disease
International Journal of Epidemiology© International Epidemiological Association 1996
Vol. 25, No. 6Printed in Great Britain
Whooping Cough and Parkinson'sDiseaseJESUS DE PEDRO-CUESTA,*** GRETAR GUDMUNDSSON,* VICTOR ABRAIRA,*GUNNAR GUDMUNDSSON.t ARTHUR LOVE,5 HRAFN TULINIUS," JORGE VEIGA,*JAVIER ALMAZAN* AND INGOLF J PETERSEN11 FOR THE EUROPARKINSON PREPARATORYACTIVITY RESEARCH GROUP
de Pedro-Cuesta J (Instituto de Salud Carlos III, Centro Nacional de Epidemiologia, Departamento de EpidemiologiaAplicada, d Sinesio Delgado, 6, 28029 Madrid, Spain), Gudmundsson G, Abraira V, Gudmundsson G, Love A, Tulinius H,Veiga J, Almazan J and Petersen I J for the EUROPARKINSON Preparatory Activity Research Group. Whooping Coughand Parkinson's Disease. International Journal of Epidemiology 1996; 25: 1301-1311.Background. We reported high levodopa use and prevalences of Parkinson's Disease (PD) in periodically, time-clustered,Icelandic cohorts born after major whooping cough epidemics (MWCE).Methods. In order to quantify a possible relationship between age at first post-birth MWCE and risk of PD we: 1) calcu-lated cumulative incidences of PD during the period 1954-1963 in one-year Icelandic cohorts born between 1869 and1927, using raw material from a reported survey; 2) identified MWCE from 1869 onwards in Iceland; 3) estimated cohortages at onset of incidence period and at first MWCE; and 4) combined the above-mentioned information using log-linearmodels. In addition, we studied the prevalence of levodopa users in Icelandic birth cohorts during a recent period.Results. The curves of the above-mentioned incidences and prevalences in one-year birth-cohorts showed: 1) a similar,age-related, inverted V profile; and 2) a systematic notchy pattern, with peak values for one or both measurements forcohorts born during or after each of nine MWCE identified during the period 1869-1927. When 13 cohorts born in yearswith MWCE were excluded from the analysis, the risk of PD rose with age at first defined MWCE, with the linear increasebeing 8.4% per year (95% Cl : -0.1-18.3%).Conclusions. These results are consistent with reported effects of age at exposure in animal models of toxic parkin-sonism, age-related changes in the dopamine receptor-GPT-binding protein-adenylatecyclase system observed in ratstreated with pertussis toxin, and some PD epidemiological features. They suggest that pertussis neurotoxicity could becausally related to PD worldwide.Keywords: dopamine, drug use, epidemiology, aetiology, Parkinson's disease, pertussis
Parkinson's disease (PD) is a disorder characterized byprogressive Lewy-body neuronal degeneration, locatedmainly in substantia nigra (SN) and other brainstemnuclei.1 This lesion might precede the onset of clinicalsymptoms by several decades.'2 The disease appears
* Department of Applied Epidemiology, National Centre forEpidemiology, Carlos III Institute of Health, Madrid, Spain.*• Division of Neurology, Department of Clinical Neuroseience andFamily Medicine, Huddinge University Hospital, Karolinska Institute,Huddinge, Sweden.'Department of Neurology, National University Hospital, Reykjavik,Iceland.' Biostatistics Unit, Ram6n y Cajal Hospital, and the REUNI Centre,Carlos III Institute of Health, Madrid, Spain.8 Department of Microbiology, National University, Reykjavik,Iceland."Department of Social Medicine, National University, Reykjavik,Iceland.' Pharmaceutical Division, Ministry of Health, Reykjavik, Iceland.Reprint requests: Jesus de Pedro Cuesta. Instituto de Salud Carlos III,Centro Nacional de Epidemiologfa, Departamento de EpidemiologiaAplicada, c/ Sinesio Delgado, 6, 28029 Madrid, Spain.
to be ubiquitous, is not present in animals, and mayhave undergone similar historical changes worldwidelinked to modernization.3-4 The highest reported PDincidence and prevalence for ages under 70 years andParkinsonism-related mortality are to be found inIceland.4"7
The causes of PD are unknown. Nowadays, the mostplausible aetiological hypothesis is a combination ofhereditary—most probably polygenic—and toxic envir-onmental factors.8"10 However, while a two- to threefoldrisk of PD associated with a genetic defect linked tocytochrome P450 mono-oxygenase activity, a protect-ive factor against toxic environmental compounds, hasbeen reported,""13 environmental toxins potentiallylinked to PD remain unidentified.
In the West, recent studies report that 76-83% of allprevalent diagnosed patients are being treated withlevodopa (LD).14 Furthermore, LD use (LDU) is highlyspecific for PD treatment.15 Geographical evaluationof sales of LD in 92 regions from Denmark, Iceland,Greece, Spain, and Sweden,16"18 pointed to highest LDU
1301
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

1302 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
in Greenland, the Faroe Islands and Iceland, whichhistorically constituted small-sized, geographicallyisolated populations. Results of a survey of LD pre-scriptions in 1990-1991, reanalysis of raw data on PDprevalence in 1963 plus historical reports on severalchildhood infections in Iceland suggested that cohortsborn after whooping cough epidemics (WCE) mightaccount, at least in part, for the high prevalence of PDand high LDU level.18 The purpose of this paper wasto quantify a possible relationship between age atwhooping cough infection and risk for PD in Iceland.
METHODSParkinson's Disease FrequencyThe raw material produced by the late K R A Gud-mundsson, generated from the PD survey he conductedas a PhD Thesis in Iceland in the mid-1960s (reportedin 1967),6 was retrieved. The numbered, 29-pagedocument, entitled 'Parkinsonism 1954-1963. Allcases', was undated. It consisted of a manuscript listingdates of birth and death, diagnostic category—idio-pathic (IP), postencephalitic, post-traumatic or arterio-sclerotic (AP) parkinsonism—and age at clinical onsetfor 470 patients. All the information, was legible. Inter-pretation of the data did not prove problematic, exceptfor one patient classified as having both IP and AP, andone patient for which death was quoted but not dated.Data for three patients, one of them deceased in 1966,had been appended on the last page. The calendar yearof clinical onset for patients with IP or AP, an item ofinformation crucial for inclusion in incidence counts forthe above-mentioned period, had not been recorded.Hence, this was calculated from the date of birth andage at onset of clinical manifestations. Sixteen caseswith post-encephalitic parkinsonism and one classifiedas post-traumatic were excluded from this analysis.Information on the Icelandic population at 31 Decem-ber 1950, 1960, 1965 and 1990, was obtained from theIcelandic National Office for Statistics. The Icelandicpopulations by one-year groups as at I January 1954and 31 December 1963 were estimated by taking theaverage of the above-mentioned population figures for1950 and I960, and 1960 and 1965. Cumulative incid-ences during the period 1954-1963 for IP+AP werecalculated for one-year birth cohorts born during theperiod 1860-1940.
Identification of WCEThe earliest summary reports on WCE in Iceland referto outbreaks in 1792, 1826, 1839 and 1841 but docu-ments are only available for certain years.19 Systematic,annually compiled reports on relevant epidemics in this
population were published in Danish official statisticsfor the period 1854-1914.20 The quality of the informa-tion on WCE from the annual 1854—1914 health reportsvaried considerably. The text printed in Gothic letteringwas sometimes difficult to read. The information fromreports for the period between 1854 and 1870 was briefand incomplete. From 1881 onwards notification dataon WC were collected annually. Reports for the period1881-1950 were compiled in 1961.2I The examiners—AL, GG and HT—found the reported data for the period1869 onwards to be reliable for purposes of identifica-tion of major WCE (MWCE). After verifying that thenotification data were in accordance with the reportedgraphs,22 we identified major WC outbreaks, whichwere denoted as defined major WCE (DMWCE) whenthey were reported: 1) as massive, in the time prior tonotification, or at least when one annual count of noti-fied cases numbered 400 or higher; and 2) as success-ively affecting populations resident in distant regions ofthe island, including always the most populated regionin the South. The nationwide spread of each DMWCEwas ascertained by identifying the residence of reportedWC cases in a minimum of four areas, namely,Reykjavik and three selected counties, Thingeyri,Hofs6s and Faskrudsfordur (whose names changed withtime), located in the northwestern, central-northern andeastern regions of the country, respectively. Calendaryears with DMWCE were defined as those when peaksof a DMWCE were judged to have occurred prior to1890, or those with 400 or more notified WC cases.
Age at Clinical Onset, Age at Infection andModelling StrategiesData from 59 one-year birth cohorts, those for theperiod 1869-1927 which generated the majority of theIP+AP cases, were taken as a preliminary selection foranalytical purposes. For each cohort, age at 1 January1954 was calculated, taken as a surrogate for age atclinical onset for said cohort and denoted for our pur-poses as cohort age. The cohorts were further classifiedinto categories, taken as surrogates of age at infectionaccording to the number of years elapsed between yearof birth and 1 January of the first year with a DMWCE.This measurement would correspond to a minimumaverage age at first possible, i.e. post-birth, pertussisinfection (PI). A considerable shortcoming of the ageat first DMWCE measurement in this ecologicalapproach—particularly if the WCE started in the earlymonths of the birth year—is its low validity as a proxyof age at PI for cohorts born in years with DMWCE.This is because many individual members of suchcohorts could have been born after the epidemic hadaffected the population in the residential area of their
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

WHOOPING COUGH AND PARKINSONS DISEASE 1303
mothers, and so conceivably remained uninfectedduring such an epidemic. In fact, the minimum possibleage at PI for this proportion—non-existent in cohortsborn in periods free of WCE—would be much higherthan a few months since, at the very least, they oughtto have become infected after the immediate inter-epidemic interval. The analysis was therefore run ona subset of the above birth cohort data, namely, thatresulting after exclusion of all cohorts born in yearswith DMWCE.
The relationship between age at first DMWCE andrisk of PD was assessed using a log-linear Poissonmodel where the predictor variables were cohort ageand cohort age at first DMWCE, and the dependentvariable the cumulative incidence of IP+AP for eachcohort. In the model, the following steps were carriedout: 1) cohort age was categorized into nine age inter-vals (0-44, seven 5-year intervals, and 80 years andover), and cohort age at first DMWCE into five cat-egories, from one to five and more years; 2) both factorswere then coded as dummy; and lastly, 3) introducedinto the final model, since the relationship of PD incid-ence with age is well established.4'5 With regard to effectof age at first DMWCE, the reference for comparison ofrisks were the cohorts born in the year immediatelypreceding that for the first post-birth DMWCE. Aninteraction term was then introduced but the modeldid not converge; hence, interaction was not tested.Output values from this model for effect of age at firstDMWCE would be interpretable as RR, with effect ofage at onset of clinical manifestations being controlledfor. Goodness-of-fit was evaluated by comparing thedeviance of the two-factor 'cohort age + age at firstDMWCE' model against that of: 1) the base model withthe intercept term; and 2) the model with cohort age asthe only independent variable.
Prevalence of LD UsersIn order to verify whether the birth-cohort pattern foundfor reported prevalences of LD users in Icelandic birthcohorts for the period 1 October 1990 to 31 March1991 (based on data obtained from a drug prescriptionsurvey)18 fitted the findings for PD incidence during theperiod 1954-1963 and for MWCE, the three data setswere plotted on the same graph.
RESULTSThe differences between reported and reanalysed datafrom the Icelandic PD survey, grouped in diagnosticand epidemiological categories, are shown in Table 1.There were 272 reported versus 270 retrieved IP+APpatients incident during the study period, the youngest
TABLE 1 Reported and reanalysed information from a data set ofparkinsonian syndromes, used as a basis for a descriptive sur\>eyon Parkinsonism in Iceland
Category
Diagnostic group:IdiopathicArterioscleroticPosl-encephaliticPost-traumaticAll groups
Epidemiological counts (IP+AP):All casesIncident during the period 1954-1963Prevalent at 31 December 1963Incident before 1954Incident before 1954 and deceased
before 1964(excluded from counts)
Number of cases
Reported
3876616
1470
453272304181
-
Reanalysed
3936016
1
470
453270316183
86
being born in 1925. The variations with possible impactin the analysis were small.
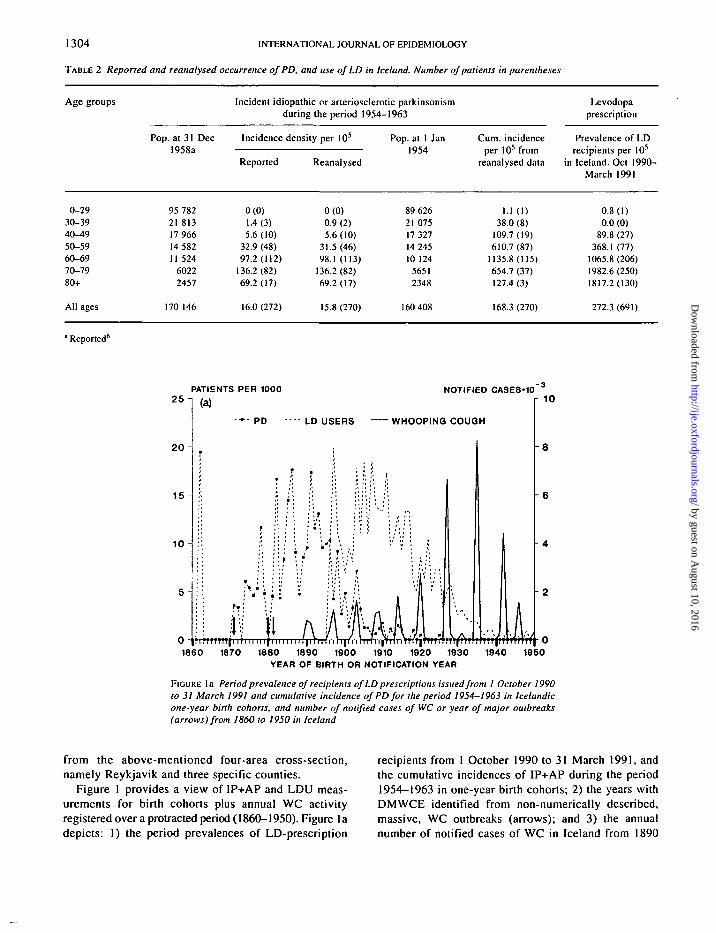
The age-specific, reported and reanalysed incidencesand cumulative incidences of IP or AP in Iceland duringthe period 1954-1963, as well as the age-specific pre-valences of LD recipients during the 6-month period,October 1990-March 1991, are listed in Table 2. Ratesand proportions increase with age, particularly so in thecase of prevalences of LD users. With regard to differ-ences between reported and recalculated counts, a slightvariation in the distribution of incidences of IP+AP byage at clinical onset is observed.
During the period 1869-1927, nine major WC out-breaks were identified, with the duration of DMWCE-free intervals ranging from 4 to 8 years. The first WCEreported for this period was that in 1871-1872. Detailsregarding spread were sparse in some cases, particu-larly for the early epidemics with onset in 1871 and1880, for which a lack of reported cases from somecounties was observed. At that time, physicians werescarce, their reporting habits varied and they mighthave been absent from some places just when the resid-ent population was affected. The 1871-1872 epidemicaffected the capital and, subsequently, the southernregions—where most infants aged below one year died—reaching western and northern Iceland the followingyear. The 1880-1882 outbreak traced a similar pattern,with deaths reported solely in 1881. For each of theseven remaining DMWCE recorded over the period1869-1927, WC case notification came, at the minimum,
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from
1304 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
TABLE 2 Reported and reanalysed occurrence of PD, and use of LD in Iceland. Number of patients in parentheses
Age groups
0-2930-3940-4950-5960-6970-7980+
All ages
Pop. at 31 Dec1958a
95 78221 81317 96614 58211 524
60222457
170 146
Incident idiopathic or arteriosclerotic parkinsonismduring the period 1954-1963
Incidence density per 105
Reported
0(0)1.4 (3)5.6(10)
32.9 (48)97.2 (112)
136.2(82)69.2(17)
16.0 (272)
Reanalysed
0(0)0.9 (2)5.6(10)
31.5(46)98.1 (113)
136.2(82)69.2(17)
15.8(270)
Pop. at 1 Jan1954
89 62621 07517 32714 24510 124
565!2348
160 408
Cum. incidenceper 105 from
reanalysed data
1.1 (1)38.0 (8)
109.7(19)610.7 (87)
1135.8(115)654.7 (37)127.4(3)
168.3 (270)
Levodopaprescription
Prevalence of LDrecipients per 105
in Iceland. Oct 1990-March 1991
0.8(1)0.0 (0)
89.8 (27)368.1 (77)
1065.8(206)1982.6(250)1817.2(130)
272.3 (691)
" Reported6
25-1
2 0 -
PATIENTS PER 1000
LD USERS WHOOPING COUGH
1860 1870 1880 1890 1900 1910 1920 1930YEAR OF BIRTH OR NOTIFICATION YEAR
1940 1950
FIGURE la Period prevalence of recipients of LD prescriptions issued from I October 1990to 31 March 1991 and cumulative incidence of PD for the period 1954-1963 in Icelandicone-year birth cohorts, and number of notified cases of WC or year of major outbreaks(arrows) from I860 to 1950 in Iceland
from the above-mentioned four-area cross-section,namely Reykjavik and three specific counties.
Figure 1 provides a view of IP+AP and LDU meas-urements for birth cohorts plus annual WC activityregistered over a protracted period (1860-1950). Figure ladepicts: I) the period prevalences of LD-prescription
recipients from 1 October 1990 to 31 March 1991, andthe cumulative incidences of IP+AP during the period1954-1963 in one-year birth cohorts; 2) the years withDMWCE identified from non-numerically described,massive, WC outbreaks (arrows); and 3) the annualnumber of notified cases of WC in Iceland from 1890
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

WHOOPING COUGH AND PARKINSON'S DISEASE 1305
PATIENTS PER 100018-1
1 6 -
NOTIFIED CASES-10r 1 0
1860 1870 1880 1890 1900 1910 1920 1930YEAR OF BIRTH OR NOTIFICATION YEAR
1940 1950
FIGURE lb Same data: VIC notification, unchanged; incidence and prevalence measure-ments, smoothed (triennial, centred, one-step-ahead moving averages)
onwards. The incidences and prevalences in birthcohorts are unstable and show similar variations: a) aninverted V-skewed shape linked to cohort age; andb) notchy profiles, where peak birth-cohort values aresuggested for calendar time-clustered cohorts bornconsecutively and immediately after 1870, 1880, 1889,1901, 1908 and 1912 for incidences, and 1896, 1902,1910, 1912, 1919 and 1926 for prevalences. The in-dentations overlapping the age-related pattern are moreclearly perceived when plotting smoothed incidencesand prevalences in the form of 3-year, centred, one-step-ahead moving averages (Figure lb). In the Figure,most peak values for PD occurrence or prevalence ofLD users corresponded to cohorts born consecutively,during or immediately after WCE. For some cohorts,such as those born after 1896 and 1903, peak values forboth measurements are seen. To sum up: 1) the notchypattern described in periodically time-clustered Ice-landic cohorts for LD use in 1990-1991, and preval-ences of PD in 1963 shown elsewhere,18 with peaks incohorts born immediately after MWCE years, isobserved from IP+AP cumulative incidences during anearlier period; and 2) followed-up cohorts, surveyed attime points approximately 30 years apart, presentparallel, overlapping peak frequencies for IP+AP andLD users.
The information on 59 cohorts born and WCE re-gistered during the period 1869-1927, taken as a prelim-inary selection for analytical purposes, is presented
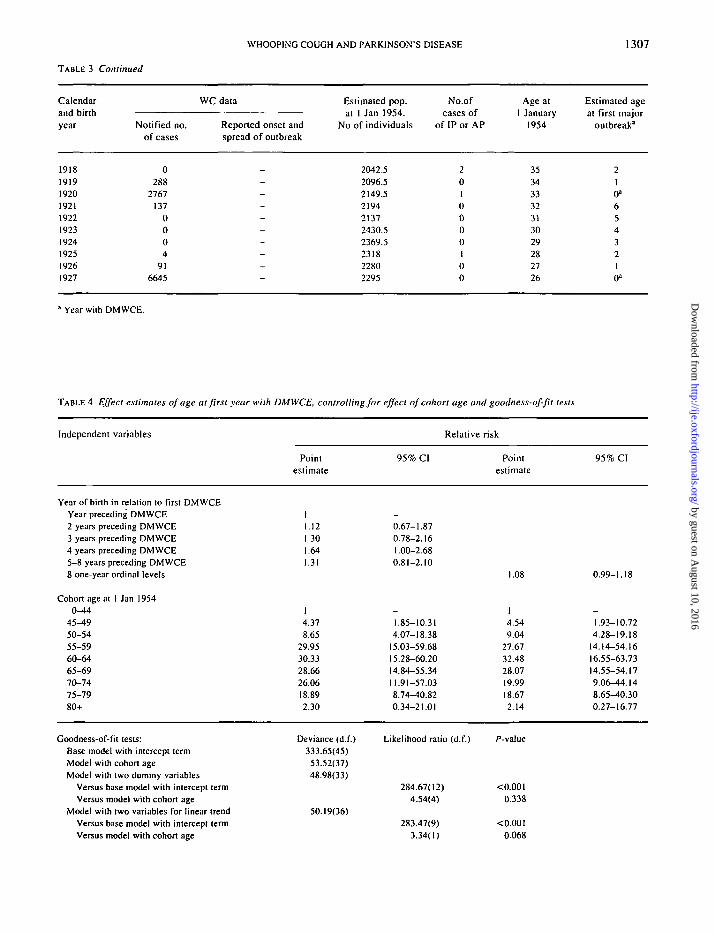
in Table 3. More specifically, the Table lists detailedannual information for the period 1869-1927 on:1) numerators and denominators of cumulative incid-ences of IP+AP in birth cohorts; 2) identified DMWCEyears; 3) cohort age at 1 January 1954 and; 4) theestimated age at first DMWCE for each birth cohort.Some epidemics, such as those with onset in 1896 and1902—years of birth for cohorts with a considerablecontribution to incidence counts—started in the spring.Since 13 out of the above-mentioned 59 cohorts wereborn in years with DMWCE, the remaining 46 cohortswere selected for analysis. Because WC epidemicsquite often spread during years immediately precedingor following those with DMWCE, pertussis infectiveactivity in Iceland was observed to a remarkable extentduring years free of DMWCE, such as 1870, 1882,1902 and 1910. This phenomenon particularly affectedthose cohorts born one and five-or-more years beforeDMWCE.
The results of the model and goodness-of-fit tests areshown in Table 4. When compared with cohorts born inyears immediately preceding those with DMWCE, andeffect of cohort age was controlled for, the risk ofIP+AP increased moderately with age at first DMWCE.In general, the 95% CI of RR for categories of age atDMWCE were wide. The increase was highest for co-horts born 4 years before a DMWCE (RR 1.64; 95%CI : 1.00-2.68). When a linear trend of RR, as deter-mined by age in years at first DMWCE, was calculated,
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

1306 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
TABLE 3 Annual registered whooping cough (WC) outbreaks during the period 1869-1927; estimated population at onset of incidenceperiod; number of incident cases of IP or AP during the period 1954-1963 in one-year birth-cohorts; and estimated cohort age and ageat first post-birth DMWCE
CalendarinA Uii-thana Dirtnyear
1869187018711872
18731874187518761877
1878187918801881188218831884
1885188618871888188918901891189218931894
18951896189718981899190019011902
19031904
1905190619071908190919101911191219131914191519161917
Notified no.
of cases
_
---
---_-------------
797672
59000
4071256
330
120
2381660
53
00
10861180239
100
1829329
03
WC data
Reported onset andspread of outbreak
_
-Started in Oct
In northern zone,Jan-July
--
---
--
StartedContinuedContinued
-
---
---
Latter monthsFirst half
---_
May-DecAll monthsJan-June
-
Oct-Nov-
May-DecAll months
Jan-Feb---_
----
--
-
-
Estimated pop.
at 1 Jan I 9 J 4 .No of individuals
215268.5282
299337332373439567.5602.5629.5611.5672722702842.5832.5909.5996.5
106010591051.51098112711481258130813651420142015011451.51467
15111544.515621618.516511744.51699.51787.51762
1793.518121897.52006198120062032
No.ofcases of
of IP or AP
001
1
022237303
1237
1216959
101913151213146
134725
11
5221
123021
3200
Age at
1 January1954
848382
81807978777675747372717069686766656463626160595857565554
5352
5150494847464544
4342414039383736
Estimated ageat first major
outbreak"
210"
87
654
3210a
0a
87654
321
0"0"4321
0a
0a
54
321
0*432
10"0"43210»543
Continued
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from
WHOOPING COUGH AND PARKINSON'S DISEASE 1307
TABLE 3 Continued
Calendarand birthyear
1918191919201921192219231924192519261927
Notified no.of cases
0288
2767137
0004
916645
WC data
Reported onset andspread of outbreak
_
-_--_--_
-
Estimated pop.at 1 Jan 1954.
No of individuals
2042.52096.52149.5219421372430.52369.5231822802295
No.ofcases of
of IP or AP
2010000100
Age at1 January
1954
35343332313029282726
Estimated ageat first major
outbreak"
210"6543210a
1 Year with DMWCE.
TABLE 4 Effect estimates of age at first year with DMWCE, controlling for effect of cohort age and goodness-of-fit tests
Independent variables Relative risk
Pointestimate
1.121.301.641.31
95% CI
0.67-1.870.78-2.161.00-2.680.81-2.10
Pointestimate
95% CI
Year of birth in relation to first DMWCEYear preceding DMWCE2 years preceding DMWCE3 years preceding DMWCE4 years preceding DMWCE5-8 years preceding DMWCE8 one-year ordinal levels
Cohort age at 1 Jan 19540^*4
45-4950-5455-5960-6465-6970-7475-7980+
1.08 0.99-1.18
4.378.65
29.9530.3328.6626.0618.892.30
Deviance (d.f.)333.65(45)
53.52(37)48.98(33)
50.19(36)
1.85-10.314.07-18.38
15.03-59.6815.28-60.2014.84-55.3411.91-57.038.74-40.820.34-21.01
Likelihood ratio (d.f.)
284.67(12)4.54(4)
283.47(9)3.34(1)
4.549.04
27.6732.4828.0719.9918.672.14
/•-value
<0.00l0.338
<0.0010.068
1.93-10.724.28-19.18
14.14-54.1616.55-63.7314.55-54.179.06-44.148.65-40.300.27-16.77
Goodness-of-fit tests:Base model with intercept termModel with cohort ageModel with two dummy variables
Versus base model with intercept termVersus model with cohort age
Model with two variables for linear trendVersus base model with intercept termVersus model with cohort age
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

1308 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
with such variable being coded as an ordinal value from1 to 8 years, and the effect of cohort age was controlledfor, the risk of PD increased by 8.4% per year of age atDMWCE (95% CI : -0.1-18.3). The goodness-of-fit ofthe two models improved when age at first DMWCEwas added.
DISCUSSIONThe results of this study suggest a relationship inIceland between age at events closely linked to WCinfection and incidence of parkinsonism, and that thisfactor underlies recently reported differences in pre-valences of LD users among birth cohorts. The patternrevealed by PD incidence and prevalence of LD userscould hardly be determined by events underlying theabove-mentioned disparity between reported and reana-lysed data, or by random or systematic error present inthe different studies and specific for certain birth cohorts,such as might result from 1) under- and misdiagnosisof PD, most likely present in the raw material fromthe 1954-1963 survey,4"6 2) use of diagnostic criteria,3) choice of drug for PD treatment or 4) mistakes in ourcalculations. However, the 'age-at-exposure' categoriesconsist of calendar time-aggregated measurements andthe underlying facts at the individual level are unknown.Therefore, although we have failed to identify anyhealth-related phenomena matching the pattern of WCEin Iceland, confounding by simultaneous phenomenacausally related to parkinsonism cannot be ruled out.
The independent variables for cohorts representimpure operative categories of age at WC infection andage at onset of clinical manifestations. The effect ofsuch a misclassification appears to be particularlyrelevant for age at first DMWCE in cohorts born five ormore years prior to DMWCE. This would give rise tounderestimation of the magnitude of an underlyingassociation for this exposure category and of the lineartrend. The expected magnitude of the association instudies based on individual age at infection would behigher too because, whereas the ecological measure-ments here computed correspond to 8 1 -year categoriesof age at WCE, actual age at exposure for individualsranged from 0 to at least 14 years in Iceland,23 despiteneonates and very young infants being highly suscept-ible to the disease.24
The distribution of 138 incident cases of parkinson-ism in Rochester, Minnesota for the period 1967-1979was: 85.5% IP, 1.4% AP, 7.2% drug-induced and 5.8%parkinsonism-plus syndromes (PPS).25 Some PPS casesmight have been classified as IP by K R A Gudmund-sson or, despite poor response to LD recorded for somePPS variants,26 have been on LD by 1990-1991, hence
accounting for the notchy pattern in both data sets.However, since the variability in age at PI is determinedby endemicity, closely related to demography23-27 (popu-lation size and concentration), geographical isolation,and duration of the interepidemic intervals (particularlylong in Iceland,22-23'29 )and population density wasproposed 8 years ago as a major common determinantof LD use and PD,14 this pattern could be attributable toa phenomenon in which PD is implicated. An inverserelationship between population concentration/densityand PD was suggested from a recent reanalysis of PDincidence in Europe (where most such surveys havebeen conducted), because incidence at ages below70 years was lowest, in the Netherlands, and signifi-cantly higher in southwest Finland and, above all, in Ice-land.16 With regard to risk factors for PD, while multipleinterpretations have been given to the well-established,modest, negative association with smoking,14'28~30 thisand other,9'31"41 (sometimes inconsistent)31'32 associa-tions such as those with residence in rural environ-ment9'31"36 (particularly in the first decades of life),9'33
well-water drinking,9'33'35"37 neoplasm incidence38 andmortality,39 plus a trend with age at measles infection,40
could all be interpreted as confounding by effects ofpopulation density, such as age at PI, since they maymerely constitute population-density-associated factorslinked to modernization.l4>16'41 In addition, results of asimilar pilot analysis conducted in December 1992 inthe Azores (San Miguel Island) suggest that, a hypo-thesis positing a causal link between PD aetiology andage at PI would also apply outside Iceland.16 This inter-pretation of our results would imply some reasonableassumptions, namely that: 1) there is an absence of aprotective effect or early-in-life PI, as suggested bythe historically high lethality of WC in infants;2442
2) the high PD incidences present in Iceland are not dueto high inbreeding rates, relevant for diseases (dis-similar to PD)10 which display a recessive pattern;43
and 3) PD behaves in populations and calendar timefollowing a Unitarian pattern.4
It has been argued that the geographically wide-spread PD distribution calls for a non-toxic aetiologyand alternative hypotheses.44 However, informationavailable at the present time allows for an eclectic viewand synthesis of different proposals. Age-at-infectiondeterminants of effect are a common characteristic oflaboratory infections by neurotropic agents.45'46 Infect-ive and toxic agents can be linked in the same causalprocess,47 and an L-dopa responsive disorder has beendescribed following Nocardia infection in mice.48
Infectious agents whose reservoir is the human hostmight underlie ubiquitous environmental neurotoxicity.We are not aware of any reports suggesting a possible
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

WHOOPING COUGH AND PARKINSON'S DISEASE 1309
relationship between exposure to WC agents and neuro-degenerative diseases. An odds ratio of 0.88 (95%CI : 0.60-1.3) for unreported PI at college entrance wasfound by Sasco and Paffenbarger,38 but this proportion—42% among cases—was disproportionately high,49 sug-gesting recall deficit; age at infection was not studied.
While there is extensive biological evidence of acuteneuronal pertussis toxicity,50 we are not aware of re-ported extrapyramidal symptoms during PI in humans.Pi-related diseases can be generated from an arrayof B.pertussis virulence factors, pertussis toxin (PT),heat-labile toxin, adenylate cyclase toxin and trachealcytotoxin. PT, perhaps the most studied of these, is anADP-ribosyltransferase capable of inactivating manyeukaryotic G proteins involved in cellular metabolism,and determines virulence and immunogenicity,51 Overthe last 7 years, evidence of the short-term effects of PTin striatal dopaminergic function has been accumulatedfrom approximately 100 laboratory reports (because PThas been routinely used to study said neuronal function)but the long-term effects are not known. PT interactsin vivo with the Ni regulatory protein coupled with thestriatal D2-dopamine receptor, involved in the receptor-adenyl cyclase system.52 Age-related changes in thedopamine receptor-GPT-binding protein-adenylatecyclase system have been identified using PT, anddifferences were shown between adult and infant rats inwhich the striatal function of said system is low.53
Latencies of considerable duration for exposure-relatedeffects are not uncommon in developmental neuro-toxicology.54 PT injected intracerebrally into miceinduced a durable motor neurological abnormality aftera log period of one week.55 However, this could be dueto a non-specific effect.
1 -methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)selective nigral neuronal toxicity in laboratory animalsis highest for the older rats and macaca,56'57 and, inthe mouse, can be inhibited pretreatment by specificenzymatic action or with a nerve growth factor,BDNF.58>59 Age-related changes in melanin content ormetabolic impairment of SN neurons,6061 BDNFgrowth factor availability, or individual variations incytochrome P450 expression""13 might constituteindividual conditions determining a neuronal substratesensitization for PT, potentially resulting, in the longrun, in a dying-back SN degenerative process. If, as seenin the animal models of MPTP toxic parkinsonism,56'57
there is a more extensive aspect (not age-at-exposure-related) of the SN toxic lesions, the foregoing mightindicate that the relevance of PI as a factor, potentiallyimplicated in a subtle, preventable lesion of thedopaminergic system, could be high in terms of PDaetiological fraction.
ACKNOWLEDGEMENTSTo the personnel of all the pharmacies in Iceland fortheir collaboration in the prescription survey; CarmenAmela, Isabel Pach6n and Gonzalo Lopez-Abente forscientific support; Martha Messman and MichaelBenedict for help with the English-language version.This study was supported by the Research Commissionof the European Union, the Swedish Council forMedical Research, (B-88-27-8330-01) the KarolinskaInstitute, Stockholm, the Spanish Health ResearchFund, and the Carlos III Institute of Health, Madrid.
REFERENCES1 Gibb W R, Lees A J. The relevance of the Lewy body to the
pathogenesis of idiopathic Parkinson's disease. J NeuralNeurosurg Psychiatry 1988; 51: 745-52.
2 Riederer P, Wuketieh S. Time course of nigro-striatal degen-eration in Parkinson's Disease. J Neurol Transm 1976; 38:277-301.
3Schoenberg B S. Environmental risk factors for Parkinson'sdisease: The epidemiologic evidence. Can J Neurol Sci1987; 14: 407-13.
4 de Pedro-Cuesta J, Stawiarz L. Evaluation of how age modifiesthe risk for Parkinson's disease, based on stratified com-parisons of descriptive data. Acta Neurol Scand 1991; 84:295-302.
5de Pedro-Cuesta J, Stawiarz L. Parkinson's Disease incidence:magnitude, comparability, time trends. Acta Neurol Scand1991; 84: 382-88.
6Gudmundsson K R A. A clinical survey of Parkinsonism inIceland. Acta Neurol Scand 1967; 43: 9-61.
7de Pedro-Cuesta J. Parkinson's Disease occurrence in Europe.Acta Neurol Scand 1991; 84: 357-65.
8Tanner C M. Epidemiology of Parkinson's Disease. In:Cederbaum J M, Gaucher S T (eds), Parkinson's Disease,Neurologic Clinics. Philadelphia: W B Saunders, 1992,pp. 317-30.
9 Roller W, Vetere-Overfield B, Gray C et al. Environmental riskfactors in Parkinson's Disease. Neurology 1990; 40:1218-21.
l0Duvoisin R C, Johnson W G. Hereditary Lewy-body parkin-sonism and evidence for a genetic etiology of Parkinson'sDisease. Brain Pathol 1992; 2: 309-20.
11 Armstrong M, Daly A K, Cholerton S, Bateman D N, Idle 1 R.Mutant debrisoquine hydroxylation genes in Parkinson'sDisease. Lancet 1992; 339: 1017-18.
12 Smith C A D , Gough A C, Leigh P N et al. Debrisoquinehydroxylase gene polymorphism and susceptibility toParkinson's Disease. Lancet 1992; 339: 1375-77.
l3Plante-Bordeneuve INITIAL, Davis M B, Maraganore D M,Marsden C D, Harding A E. Debrisoquine hydroxylasegene polymorphism in familial Parkinson's disease.J Neurol Neurosurg Psychiatr 1994; 57: 911-13.
14 de Pedro-Cuesta J. Studies on the prevalence of ParalysisAgitans by tracer methodology. Acta Neurol Scand 1987;75 (Suppl.): 6-106.
15de Pedro-Cuesta J, Petersen I, Vassilopoulos F, Micheli F,Garcia-Inesta A. Epidemiological assessment of levodopa
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

1310 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
use by populations. Ada Neurol Scand 1991; 83:328-35.
16de Pedro-Cuesta J. Risk factors of Parkinson's Disease. In:Vuylsteek K and Hallen M (eds). Epidemiology. Amsterdam:IOS Press, 1994, pp. 182-211.
17de Pedro-Cuesta J, Wermuth L, Abraira V, Stawiarz L.Levodopa use in Denmark: high levels in Greenland andthe Faroe Islands. Ada Neurol Scand 1995; 91: 89-97.
18 de Pedro-Cuesta J, Petersen I J, Stawiarz L et al. High levodopause in periodically time-clustered, Icelandic birth cohorts.A vestige of parkinsonism etiology. Ada Neurol Scand1995; 91: 79-88.
19 Schleissner P A. Island undersdgt fra et laegevidenskabeligtsynspunkt. Copenhagen 1849, pp. 65-68.
20Del Kongelige Sundhedskollegium's Aarsberetning. AvsnitetIsland. Copenhagen: 1852-1910.
21 Reports on the Health of People in Iceland, from 1881 onwards.Reykjavik: Surgeon General's Office, 1961.
22 Cliff A D , Hagge t t P, O r d J K, Versey , G R. In: SpatialDiffusion. A historical geography of epidemics in an islandcommunity. Cambridge: Cambridge University Press,1981, pp. 192-93.
23Andersson R M, May R M. Age-related changes in the rate ofdisease transmission: implications for design of vaccina-tion programmes. J Hyg Camb 1985; 94: 365-436.
24 Christie A B. Whooping cough. In: Infectious diseases:Epidemiology and clinical practice. Fourth Edition. Vol 2.Edinburgh: Churchill Livingstone, 1987, pp. 927-58.
25 Rajput A H, Offord K P, Beard A M, Kur land L T. E p i d e m i o l o g yof Parkinsonism: Incidence, classification and mortality.Ann Neurol 1984; 16: 278-82.
26Parati E A, Fetoni V, Geminiani G C et al. Response to L-dopain multiple system atrophy. Clin Neuropharmacol 1993;16: 139-44.
27Andersson R M, May R M. Vaccination and herd immunity toinfectious diseases. Nature 1985; 318: 323-29.
28 Baron J A. Cigarette smoking and Parkinson's Disease.Neurology 1986; 36: 1490-96.
29Jansson A M. Protective actions of nicotine on lesionednigrostriatal dopamine systems. PhD Thesis. Stockholm1991.
30 Riggs J E. Cigaret te smoking and Parkinson disease: Theillusion of a neuroprotect ive effect. Clin Neuropharmacol1992; 15: 88-99.
31 Semchuk K M, Love E J, Lee R G. Parkinson's disease andexposure to rural environmental factors: a population-basedcase control study. Can J Neurol Sci 1991; 18: 279-86.
32 Tanner C M, Chen B, Wang W et al. Environmental factors andParkinson's Disease: a case control study in China.Neurology 1989; 39: 660-64.
33 Rajput A H, Uitti R J, S tern W, Laver t ry W. Ear ly-onse tParkinson's disease in Saskatchewan—Environmentalconsiderations for etiology. Can J Neurol Sci 1986; 13:312-16.
34 Ho S C, W o o J, Lee C M. Epidemiologic study of Park inson ' sd isease in Hong Kong. Neurology 1989; 390: 1314-18 .
" W o n g G F, Gray C S, Hassanein R S, Koller W C. Environ-mental risk factors in siblings with Park inson ' s disease.Arch Neurol 1991 ; 48 : 2 8 7 - 8 9 .
3 6 M o r a n o A, J imdnez-J imenez F J, Molina J A, Antolfn M A. Riskfactors for Parkinson's Disease: case-control study in theprovince of Caceres, Spain. Ada Neurol Scand 1994; 89:164-70.
37 Jimenez-Jimenez F J, Mateo D, Gimenez-Roldan S. Exposureto well-water and pesticides in Parkinson's disease: acase-control study in the Madrid Area. Mov Disorders1992; 7: 149-52.
38Jansson B, Jankovic J. Low cancer rates among patients withParkinson's disease. Ann Neurol 1985; 17: 505-09.
39Marmot M G. Mortality and Parkinson's disease. In: Rose F C,Capildeo R (eds). Research Progress in Parkinson'sdisease. Tunbridge Wells: Pitman Medical, 1981.
40Sasco A J, Paffenbarger R S. Measles infection and Parkinson'sdisease. Am J Epidemiol 1985; 122: 1017-31.
41 Nasca Ph C, Burnett W S, Greenwald P, Brennan K, Wolfgang P,Carlton K. Population density as an indicator of urban-rural differences in cancer incidence, upstate New York1968-1972. Am J Epidemiol 1980; 112: 362-75.
42 Gordon J E, Hood R I. W h o o p i n g cough and its ep idemio log ica lanomalies. Am J Med Sci 1951; 222: 333-61.
43 Khlat M, Khoury M . Inbreeding and diseases : d e m o g r a p h i c ,genetic, and epidemiologic perspectives. Epidemiol Rew1991; 13: 28-41.
44Rosswell E, Rocca W A, Ince S E. Parkinson's Disease:evidence against a toxic aetiology and for an alternativetheory. In: Markey P S (ed.) MPTP: A neurotoxin pro-ducing a parkinsonian syndrome. Academic Press, 1986,pp. 355-67.
45 Fishman P S, Gass J S, Swoveland P T, Lavi E, Highkin M K andWeiss S R. Infection of the basal ganglia by a murinecoronavirus. Science 1985; 229: 877-79 .
46 Mohammed A K, Magnusson O, Maehlen J et al. Behaviouraldeficits and serotonin depletion in adult rats after transientinfant nasal viral infection. Neuroscience 1990; 35: 355-63 .
47 Andersson T, Schultzberg M, Schwarcz R, Love A, Wickman C,Kristensson K. NMDA-recep tor antagonist preventsmeasles virus-induced neurodegeneration. Eur J Neurosci1991; 3: 61-77.
48 Kohbata S, Beaman B L. L-Dopa-responsive movement disordercaused by Nocardia asteroides localized in the brains ofmice. Infect lmmun 1991; 59 : 1 8 1 - 9 1 .
4 9 K r a n l z T , Taranger J ,Trollfors B. Estimating incidence of woopingcough over time - a cross-sectional recall study of fourSwedish birth cohorts. Int J Epidemiol 1989; 18: 9 0 1 - 0 5 .
5 0 Pi t tman M. Neurotoxici ty of Bordetella Pertussis: Neuroloxi-cology 1986; 7 : 5 3 .
51 Boyajian C L, Bickford-Wimer P, Kim M B, Freedman R,Cooper D M. Pertussis toxin lesioning of the nucleuscaudate-putamen attenuates adenylcyclase inhibition andalters neuronal electrophysiological activity. Brain Res1989; 495: 66-74.
52 Fujita N, Nakahiro M, Fukuchi I, Saito K, Yoshida H. Effects ofpertussis toxin on D2-dopamine receptor in rat str iatum.Brain Res 1985; 333: 2 3 1 - 3 6 .
53 Nomura Y, Arima T, Swgawa T. Influences of pertussis toxin,guanine nucleot ides and forskolin on adenylate cyclase instriatal membranes of infant, adult and senescent rats. Int JDev Neurosci 1987; 5 : 2 7 1 - 7 9 .
54 Rodier P M. Time of exposure and time of testing in develop-mental neurotoxicology. Neurotoxicology 1986; 7 : 69—76.
55 Sato I, Sato H. Animal models of pertussis. In: Wardlaw A C,Parton R (eds) . Palhogenesis and immunity in pertussis.Chichester: John Wiley, 1988, pp. 309-24.
56Langston J W, Irwing I, DeLanney L E. The biotransformationof MPTP and disposition of MPP+: the effects of aging.Life Sci 1987; 40: 749-54.
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from

WHOOPING COUGH AND PARKINSON'S DISEASE 1311
" R i c a u r t e G A, DeLanney L E, Irwin I, Langston J W. Olderdopaminergic neurons do not recover from the effects ofMPTP. Neuropharm 1987; 26 : 9 7 - 9 9 .
58 Pileblad E, Carlsson A. Catecholamine-uptake inhibitors preventthe neurotoxicity of l-methyl-4-phenyI-1,2,3.6-tetrahy-dropyridine (MPTP) in mouse brain. Neuropharmachol1985; 24: 689-92 .
59 Hyman C, Hofer M, Barde Y A el al. BDNF is a neurotrophicfactor for dopaminergic neurons of the substantia nigra.Nature 1991; 350: 230-32 .
' "Her re ro M T, Hirsch E C, Kastner A el al. Appearance ofneuromelanin with aging in catecholaminergic neurons ofthe brain-stem in macaca fascicularis. 10th InternationalSymposium on Parkinson's Disease, Abstracts book,Tokyo, 1991, pp. 228.
61 Bossi S R, Simpson J R, lsacson O. Age dependence of striatalneuronal death caused by mitochondrial disfunction.Neuroreport 1993; 4 : 73 -76 .
(Revised version received May 1996)
APPENDIXThe EUROPARKINSON PREPARATORY ACTIV-ITY RESEARCH GROUP was constituted as follows:Principal team investigators: DENMARK, E Dupont,L Wermuth; FINLAND, R J Marttila; FRANCE,A Alperovitch, F Boulesteix, J F Dartigues; GER-MANY, P Vieregge; GREECE, D Vassilopoulos;ICELAND, G Gudmundsson, I Petersen; ITALY,I Casetta, R D'Alessandro, V Govoni, E Granieri,W A Rocca, G Rosati; NORWAY, I Bekkelund;PORTUGAL, J A Aleixo-Dias, J Santos; SPAIN,
J Acosta-Varo; SPAIN-SWEDEN, J de Pedro-Cuesta(Project Leader); THE NETHERLANDS, M Breteler,A Hofman (COMAC liaison officer); UNITED KING-DOM, Y Ben-Shlomo, W J Mutch, R L G Sutcliffe.
Consultant experts: ARGENTINA, F Micheli;FRANCE, Y Agid, M Zuber; SPAIN, J Garcfa deYe"benes Prous; SWEDEN, K Kristensson; UNITEDKINGDOM, A Hughes, W Gibb, P Jenner, C D Ward,A C Williams; UNITED STATES, W G Johnson,W C Koller.
by guest on August 10, 2016
http://ije.oxfordjournals.org/D
ownloaded from




















