![[Intradiverticular bladder tumours: review of the Cancer Committee of the French Association of Urology]](https://static.fdokumen.com/doc/165x107/633918e8ab09c360bf02de97/intradiverticular-bladder-tumours-review-of-the-cancer-committee-of-the-french.jpg)
What's New in Surgery for BPH? - Grand Rounds in Urology
64
What’s New in Surgery for BPH? Steven A. Kaplan, M.D. Professor of Urology Director, Benign Urologic Diseases and The Men’s Health Program Icahn School of Medicine at Mount Sinai
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of What's New in Surgery for BPH? - Grand Rounds in Urology

What’s New in Surgery for BPH?
Steven A. Kaplan, M.D. Professor of Urology
Director, Benign Urologic Diseases and The Men’s Health Program Icahn School of Medicine at Mount Sinai

Surgical Options
§ Minimally invasive options • Office based • Ambulatory based • Minimal anesthestic • High risk patients • Low morbidity
§ Advanced Invasive Options • Improved versions of prostatectomy

Technology Based Treatment of LUTS related to BPH
§ ALL surgical approaches based on removing bladder outlet obstruction1 (? Tissue)
§ Minimally Invasive Therapies1 § Thermotherapies1 § Novel hybrid therapies2
§ Surgical Debulking Procedures1 • Vaporizers and Enucleators1
• Robots Vs. Lasers Vs Electrosurgical Technologies3
1. Kacker R, Williams SB. J Urol 2011: 8; 171-176. 2. Hoffman RM et al. Cochrane Database Syst Rev 2009;(1):CD001987
3. Lee N et al. AUA 2011. Abstract 2098.
LUTS: lower urinary tract symptoms BPH: benign prostatic hypertrophy

Minimally Invasive Therapies: Update
FDA APPROVED § Prostatic Lifts1
• Transurethral Suture Tacking
§ Robotic/Laparoscopic Technology • Single Port2 and Transvesical Approaches3
§ Vapor Ablation (Steam)
Investigational § Photodynamic Therapy4 § Histotripsy (focused ultrasound) § Prostatic Arterial Ablation § WaterJet/Laser Technology § Intraprostatic Injections5
• Botox, NX 1207, ethanol and other compounds 1. Woo, H. et al. BJU Int 2011;108: 82-8
2. Fareed K, et al. BJU Int 2012: DOI: 10.1111/j.1464-410X.2012.10954.x 3. Granberg CF, et al. J Endourol. 2009 May;23(5):747-52
4. Tiwari A, et al. Exp Opin Invest Drugs 2005; 5. Denmeade S, et al. Eur Urol 2011; 59:747-54. Epub 2010 Nov 24.

The Prostatic Urethral Lift
§ Compress encroaching lateral lobe § Deliver UroLift® implant to hold in
place § An average of 4.9 implants for
prostates ≤ 80cc

AnterolateralLoca,on
§ Mechanicallyopensprosta0curethra
§ Resultisvisibleundercystoscopy
§ Implantsareanterolateral,awayfromNVbundlesordorsalvenouscomplex
PRE POST

Prosta0cUrethralLiEProgress
PUBLISHED
RandomizedCrossoverStudy
Posi0veGuidance
N.I.C.E.PUBLISHED
2YearDurability
DeNovoApproval
HCPCSCoding
CoverageAETNA
PUBLISHEDRandomizedBlindedStudy
PUBLISHEDSexualFunc0on
Over2,000treated
PUBLISHED
2YearRandomizedDurability
PUBLISHED
BPH6Study:RandomizedtoTURP
Coverage
Medicare23statesSeveralprivates
PUBLISHED
‘Real-World’EuropeanRegistry
PUBLISHED
Safety&Feasibility
Category1CPTCodes[Effec0veJan’15]
PUBLISHED
LOCALStudy
Where does UroLift® fit?
§ Men with moderate to severe LUTS due to BPH who… • Want to preserve sexual function • Concerned about possible TURP/laser complications • Want rapid return to daily life • Unhappy with BPH drugs due to insufficient relief or
bothersome side effects
Widely Studied
Publications to Date § J Urology USA randomized
(n=206, 1yr) § J Sexual Medicine USA sexual function
(n=140, 1 yr) § EU J Urology EU registration (n=102,
1yr) § Urology J. 2 yr Multi-Center Study
(n=64,2 yr) § J. Sexual Medicine Sexual Function (n=64,
1yr) § British J. Urology First-in-Man (n=19,1 yr) § Canadian J. Urology Technique § Multiple small studies from France, Spain, Germany

• Prospec0ve,1:1randomizedstudycomparingPULtoTURP
Design
• 80subjectsenrolledat10Europeancenters• UK,Germany,Denmark
Enrollment
• 50yearsold• IPSS>12• Qmax≤15ml/s,PVR≤350ml• Prostatevolume≤60cc• ISI<5• Noac0veinfec0ons,urinaryreten0on,stones,obstruc0vemedianlobe
• Sexuallyac0ve• Ruledoutforprostatecancer• Washedoutfroman0coagulants
Criteria
BPH6RandomizedStudyOverview
Sonksenetal.EurUrol2015;DOI10.1016/j.eururo.2015.04.024

Pa0entcohortswerecomparable
Characteris,cs
PUL(N=44*) TURP(N=35)
Mean,SD[min-max],(n)Age(yrs) 63,6.8[50-84],(44) 65,6.4[51-78],(35)
Prostatevolume(cc) 38,11.6[16-59],(44) 41,13.4[17-68],(35)
Prostatelength(mm) 46,6.4[24-56],(43) 47,5.8[37-60],(34)
PSA 2.4,1.8[0.4–8.2],(43) 2.6,2.1[0.3–8.6],(33)
IPSS 22,5.7[12-33],(44) 23,5.9[13-34],(35)
Qmax(mL/s)† 9.2,3.5[3-15],(39) 9.5,3.2[3-15],(32)
PVR(mL) 86,71.6[0-344],(44) 102,86.9[0-328],(35)
ISI 1.8,1.0[1–4],(44) 2.0,1.0[1–4],(35)
SHIM 20,4.9[7–25],(44) 18,5.5[7–25],(35)
MSHQ-EjDfunc0on 11,2.7[4–15],(44) 9,2.3[4–13],(35)
MSHQ-EjDbother 1.7,1.8[0–5.0],(44) 2.0,1.5[0–4.0],(35)
*Onesubjectwasexcludedfromanalysisforviola0onofinclusioncriteria
Sonksenetal.EurUrol2015;DOI10.1016/j.eururo.2015.04.024

SymptomImprovementsasExpected• UroLiEshowsmorerapidimprovement,andTURPsurpassesat12months
(11.4vs15.4pointIPSSimprovements)
p=0.05
Sonksenetal.EurUrol2015;DOI10.1016/j.eururo.2015.04.024

Peakflowrate(Qmax)improvesmorewithTURP
• PULQmaxnormalizesto15mL/sec,whileTURPissuper-physiologicat22mL/sec.
Sonksenetal.EurUrol2015;DOI10.1016/j.eururo.2015.04.024

AUA2015Update:3YearL.I.F.T.Durability
Mean,95%CI
Roehrborn.AUA2015
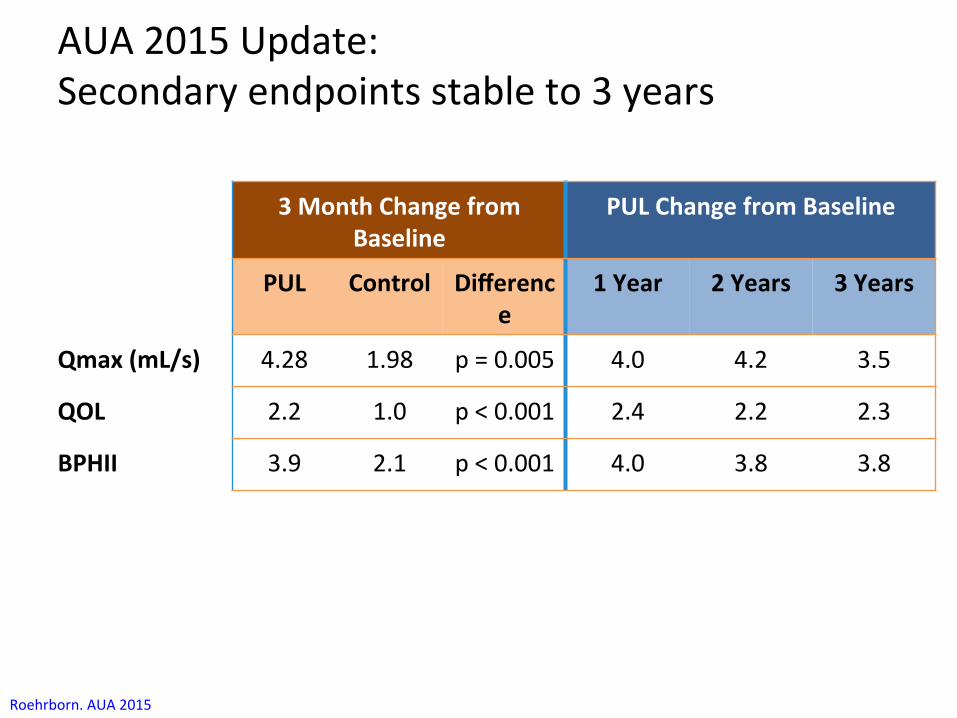
AUA2015Update:Secondaryendpointsstableto3years
3MonthChangefromBaseline
PULChangefromBaseline
PUL Control Difference
1Year 2Years 3Years
Qmax(mL/s) 4.28 1.98 p=0.005 4.0 4.2 3.5
QOL 2.2 1.0 p<0.001 2.4 2.2 2.3
BPHII 3.9 2.1 p<0.001 4.0 3.8 3.8
Roehrborn.AUA2015

AUA2015Update:Ejaculatoryanderec0lefunc0onpreserved• Erec0lefunc0onunchanged,whileEjaculatoryfunc0onimprovedmodestly
**
*
*
***
**
*
*
*
*
Mean,95%CI*p<0.05
Roehrborn.AUA2015

AUA2015Update:Addi0onalfollowontreatment
• 10.7%requiredreinterven0onby3years:• 6(4.3%)receivedaddi0onalPULimplants• 9(6.4%)underwentTURPorPVP
• 14of642implants(2.1%)weredeployedsuchthatexposedtobladderandshowedencrusta0on:
• Over3years,9implantswereremoved(endoscopicgraspers)
• Importanttechniquepoint:Ifdeployedtooproximally,removeimplantduringindexprocedurewithendoscopicgraspersorscissors.
Roehrborn.AUA2015

Summary
§ Novel approach to BPH • Symtom reduction • Sexual function preserved
§ Concerns • Retreatment rates high • Encrustation • Reproducibility
TIME WILL TELL !!!

Introduction: Convective WAVE™ Technology
A NEW Technology Platform for Tissue Ablation
Convective Water Vapor Energy (WAVE™)
A NEW Technology
CONVECTIVE Thermal Heat Transfer WATER VAPOR (STEAM) to Ablate Tissue
19

Differences in Thermal Energy Transfer CONVECTION Conduction
Prostate Capsule
• Vapor rapidly disperses through interstices • Condensation releases stored thermal energy • Cell membranes are gently denatured, thereby
causing cell death
Vapor Injection
Heat Source
• Heat is conductively transferred from cell to cell • Conductive heating of prostate capsule occurs • Temp gradient results in cells near source being
heated substantially more than those far away
20

Vapor Ablation (Steam) Rezum System: NxThera, Inc
510 K FDA Clearance in Sept 2015

Methods: Rezūm FIM and Pilot Treatment Summary
FIM Pilot
Mean ± SD Range Mean ± SD Range
Treatment Time per Injection (seconds) 8.9 ± 0.9 (7,10) 9 -
Calories/Treatment 218 ± 26 (190,289) 208 -
Total Treatments in Both Lateral Lobes 5.1 ± 1.6 (2,8) 3.8 ± 1.1 (2,6)
Treatments/Median Lobe 2.5 ± 0.6 (2,3) 1.8 ± 0.8 (1,3)
Total Treatments/Prostate 4.9 ± 1.9 (4,9) 4.4 ± 1.9 (2,9)
22

Results: MRI and 3D Renderings Analysis Volume Reduction From 1 Wk
Post Rx Time N Mean
(cm3) Mean ∆ (cm3)
Mean % ∆
Lesion Volume
1 Week 30 9.5
1 Month 29 3.3 -6.2 -65.3%
3 Months 28 0.7 -8.8 -92.6%
6 Months 28 0.3 -9.2 -96.8%
Transition Zone Volume
1 Week 30 44.3
1 Month 29 36.1 -8.2 -18.5%
3 Months 28 30.4 -13.9 -31.4%
6 Months 28 27.2 -17.1 -38.6%
Prostate Volume
1 Week 30 75.2
1 Month 29 64.1 -11.1 -14.8%
3 Months 28 55.8 -19.4 -25.8%
6 Months 28 50.7 -24.5 -32.6%
23

Results: IPSS
24
Baseline
N=30
Week 1 N=30
Month 1 N=30
Month 3 N=28
Month 6 N=28
Year 1 N=27
IPSS 23.0 ± 6.3 19.0 ± 8.7 13.2 ± 7.9 8.7 ± 6.9 8.3 ± 7.1 10.8 ± 6.7
IPSS ∆ (0) -4.0 ± 11.3
-10.8% -9.8 ± 10.8
-37.2% -14.7 ± 8.3
-61.9% -15.0 ± 8.7
-63.0% -12.8 ± 6.9
-54.3%

Rezūm II Study Design
TotalEnrolledN=197
Treatmentn=136
2WeekFollow-Up
Controln=61
1MonthFollow-Up
3MonthFollow-Up
2WeekFollow-Up
1MonthFollow-Up
3MonthFollow-Up
BLINDED
6MonthFollow-Up
12MonthFollow-Up
2,3,4,and5YearFollow-Up
OPEN
PRIMARY ENDPOINT 3 Month ITT Randomized Comparison Rezūm IPSS Reduction > 125% Control
1 Year Rezūm Durability
LongTermFollowUpto5Years
6MonthFollow-Up
SubjectCrossovern=53
25

Procedural Results Treatment (N=136)
Control (N=61)
Mean ± SD (n)
Mean ± SD (n)
Treatment Time (min) 5.3 ± 3.5 (135) 3.3 ± 1.3 (61)
% subjects with middle lobe treated or
identified
31.1%
(42/135) 18.0% (11/61)
Number of treatments total 4.5 ± 1.8
(135) N/A
TypeofMedica,on
#ofSubjects(N=196)
PercentageofSubjects
OralSeda0on 135 68.88%ProstateBlock 41 20.92%IVSeda0on 20 10.20%Procedural Pain
Management
26

Primary Efficacy Endpoint – As Treated
Metpre-specifiedprimaryefficacyendpoint!
TreatmentArm ControlArm
Baseline 3Months Change Baseline 3
Months Change P-value
IPSSScore 22.0±4.8
10.7±6.5
-11.3±7.6
21.9±4.7
17.5±7.6 -4.3±6.9<0.0001
Improvement in LUTS as measured by IPSS change for subjects in the Treatment Arm as compared to those in the Control Arm at 3 months post-treatment.
27

IPSS - As Treated
N=61 N=135 N=59 N=130 N=61 N=132 N=61 N=134 N=129 N=77 28

Qmax - As Treated
N=61 N=135 N=61 N=133 N=61 N=133 N=125 N=75 29
1 Mo 3 Mo 6 Mo

Primary Safety Endpoint
Met primary safety endpoint!
Patients% (n/N)
Primary Safety Composite Endpoint: 1 0.7% (1/136) 3.40% <0.000
1Upper CI ≤ 12% Yes
1) Device perforation of rectum or GI tract 0 0.0% (0/136)
2) Device related formation of fistula between the rectum and urethra 0 0.0%
(0/136)3) De novo severe urinary retention lasting more than 21 consecutive days post treatment
1 0.7% (1/136)
1 One-sided 95% Exact Binomial CI
Treatment ArmEvents Upper
CI¹ P-value Endpoint Criteria
Endpoint Met?
Demonstrate that the composite observed rate of post-procedure device-related serious complications in the Treatment Arm is <12% at 3 months.
30

Safety Profile • 3 device or procedure-related SAEs (2 treatment subjects)
– Subj. 1 – extended retention (significant intravesical lobe protrusion) – Subj. 2 – allergic reaction to Xanax (nausea and vomiting)
• 12 unrelated SAEs (9 treatment subjects) – 3 bowel obstructions; 1 hemorrhoid; 1 UTI, 1 syncope; 1 injury, Other; 1 pneumonia; 1
spinal stenosis; 1 pulmonary embolism; 1 pyelonephritis, 1 cancer • Most common AEs
– Mild-to-moderate, typically resolved by 2 weeks (% subjects per arm)
TreatmentSubjects(N=136)
ControlSubjects(N=61)
Dysuria 23(16.9%) 1(1.6%)
Hematuria,Gross
17(12.5%) 0(0%)
Hematospermia
10(7.4%) 0(0%)
UrinaryFrequency
9(6.6%) 2(3.3%)
UrinaryUrgency
8(5.9%) 1(1.6%)
31

Goals of Less Invasive BPH
§ Rapid Results • Feeling better within days • Symptoms improve > Rx
§ Minimal Adverse Effects • No serious adverse events • No ED, EjD • No Post Op Foley
§ Tolerable In-Office Treatment
Goals of Less Invasive BPH
§ Predictable § Reproducible § Reliable § Durable § Positive Economic Drivers
• Patient, Urologist, Insurers
Offer a Procedural Treatment that
Reduces Obstruction AND Competes with
Palliative MEDICAL Therapy
Medi Tate TIND Temporary Implantable Nitinol Device (TINDTM)

Medi Tate TIND Temporary Implantable Nitinol Device (TINDTM)
Medi Tate TIND Temporary Implantable Nitinol Device (TINDTM)
§ 5 minutes to deploy – The device can be deployed in any clinical setting that has standard rigid cystoscopy equipment. The deployment procedure is intuitive and does not require a post-procedure catheter. Once the device is deployed, the patient is free to return to normal activities immediately.
§ 5 days in position – TIND remains in position for 5 days. When deployed in the prostatic urethra, the device clears obstructive tissue by exerting pressure on prostate tissue from the inside, clearing the urethral path and enabling improved urination immediately following the procedure. The long-term effect is achieved by the reshaping of the prostate: channels are formed that permanently expand the cross-sectional area along the entire prostatic urethra.
§ 5 minutes to remove – 5 days later, the device is removed in just a few minutes.
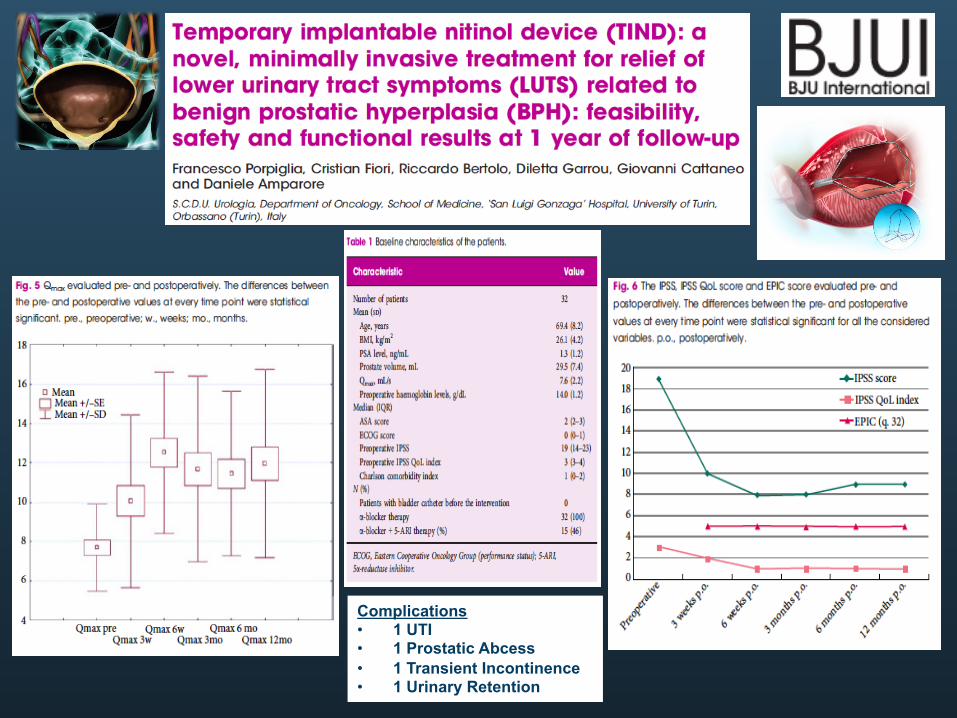
Complications • 1 UTI • 1 Prostatic Abcess • 1 Transient Incontinence • 1 Urinary Retention

Medi Tate TIND Temporary Implantable Nitinol Device (TINDTM)
§ Devices were implanted between May 2010 and July 2012, within a mean operative time of 5.8±2.9 min, and retrieved five days thereafter, within a mean operative time of 2.8±1.1 min.
§ No intra-procedural complications were recorded during implantation or retrieval procedures. • One case of urinary tract infection and one case of
temporary acute urinary retention were recorded and resolved.
§ All patients reported significant symptomatic improvement and terminated BPH medicinal regimens within 3 months of implantation, with an improvement of 51.96±19.16% and 51.79±68.66% in IPSS and Qmax, respectively, by that time point

Prostate Arterial Embolization
§ Reliance on image based reduction in prostate volume
§ Naïve prostato – centric concepts of LUTS • Lack of controls
§ Definitions of clinical improvement • ? Placebo effect
§ Tends to ignore LUTS / bother metrics
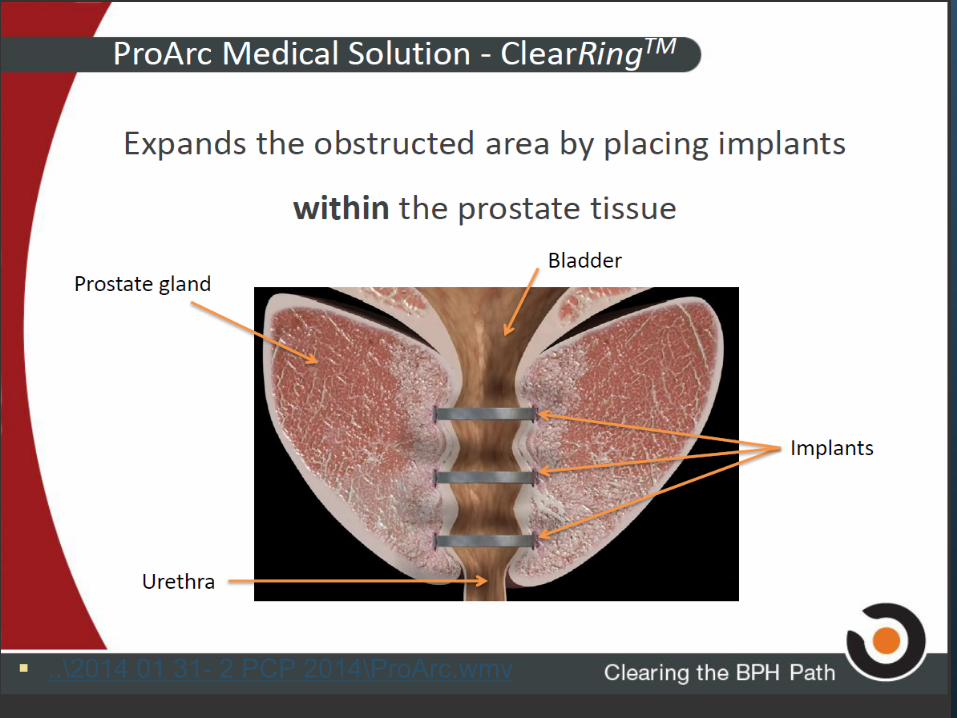
§ ..\2014 01 31- 2 PCP 2014\ProArc.wmv

HowItWorks?
Step3:Inaverysimpleandquickprocedure,theurologist
performsacircularincisionintheprostate0ssue,andsimultaneouslyplacestheimplantinsideofit

HowItWorks?
Step4:Thedeliverysystemisretracted,leavingtheimplantsto
expandthepreviouslyobstructedarea

SuccessfulPre-ClinicalTrials
• Theprocedurehasbeenfoundtobesafe:o Goodclinicalcondi0onsofanimalsduringtheen0refollow-upperiod
o Nosignificantadverse0ssueresponse
o Normalblood/urineparameters
o Normalbehavior
ExpandedareaBladder
Prostate
Significantenlargementoftheurethra90dayspostprocedure

• Preliminaryproofthattheprocedureissafeandfeasible
• Post12monthsreports(3pa0ents):
o Pa0entsarefeelinggoodwithnocomplaints
o Majorsymptomsimprovements
o Sexualfunc0onwaspreserved
• Strongefficacyindica0ons
• Nounexpectedsafetyissues
• Procedure0meislessthanfiveminutes
SuccessfulFirstinManTrial

VORTX RX Histotripsy Technology § Histotripsy applies high
intensity acoustic energy to fragment and homogenize cellular tissues through a process known as cavitation.
§ Cavitation appears as a “bubble cloud” on ultrasound imaging and is easily tracked and monitored by the surgeon throughout the procedure.

§ Once treated, tissues change in ultrasound appearance from bright to dark, enabling the surgeon to easily track the treatment as it progresses.
§ The VORTX RX is an investigational device and is limited by law to investigational use by qualified investigators in the United States and Canada.

47
THE AQUABEAM® System Conformal Planning Unit
• Surgical planning & mapping • Controlled depth of resection • Integrated TRUS display
Aquablation • Submerged high velocity
saline jet • Tissue selectivity & depth
control • Non-thermal (room
temperature)
Handpiece • 24 Fr, precise sapphire nozzle • Cystoscopic visualization • Aspiration for tissue collection
NotavailableforsaleintheUnitedStates

48
0
2
4
6
8
10
12
14
16
18
20
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
Depth(m
m)
PowerLevel(0-100inincrementsof5)
DEPTHCONTROLAQUABEAMTECHNOLOGY

49
ANGLEPLANNING–TRANSVERSEVIEW

50
CONTOURPLANNING–SAGITTALVIEW

51
AQUABLATIONTREATMENT

52
Pa,entDemographics(n=21)
Age 70+5.1yrs(62–78yrs)
Prostatesize
57+19.4ml(30–102ml)
Medianlobe
57%(12/21pa0ents)
PrimaryEndpoints(Safety&Feasibility) TechnicalSuccess 100% Opera0veTime 38+9min(23–56min) Resec0onTime 5.0+2.9min(1–22min) Haemoglobin (post op)
5.7% reduction (143 to 135 g/l)
21SUBJECTSPHASEII–12MONTHFOLLOWUP
v Post-opera0vedysuriawasminimalv Nointra-op.complica0onsv Adverseeventsweretypicallymildandtransient

53
SecondaryEndpoints(Symptoms,UrinaryFlowRate,QOL)
Mediancatheterwithdrawal0me
One(1)day(1–7)
Pdet@Qmaxchange 40%reduc0on(65to39ml/cmH2O)
ProstateVolume 39%reduc0on(57to35ml)
v Nocasesofurinaryincon0nence,retrogradeejacula0onorerec0ledysfunc0onwerereported
21SUBJECTSPHASEII–12MONTHFOLLOWUP
*p<0.05;†p<0.01;‡p<0.001;§p<0.0001
23.0
10.7
7.0 7.1 6.8
0
5
10
15
20
25
30
0 13 26 39 52WEEKS
IPSSMEAN&95%CI
§ §§
§
8.6
14.816.6
18.9 18.3
0
5
10
15
20
25
0 13 26 39 52WEEKS
Qmax(ml/s)MEAN&95%CI
‡
§ §‡

54
*p<0.05;†p<0.01;‡p<0.001;§p<0.0001
5.0
2.31.8 1.7 1.7
0
1
2
3
4
5
6
0 13 26 39 52WEEKS
QoLMEAN&95%CI
§§ §§
143
84
5239
54
0
40
80
120
160
200
0 13 26 39 52
PVR(ml)MEAN&95%CI
*
†
†
†
21SUBJECTSPHASEII–12MONTHFOLLOWUP

55
WATERNCT02505919
• Prospec0vemul0centerrandomizedcontrolledtrial– Aquabla0onvs.TURP
• Targetpa0entpopula0on:moderate-to-severeBPH– Age45-80withLUTSduetoBPH– IPSS≥12– Prostatevolume30-80byTRUS– Qmax<15mL/s
• Randomiza0onPhase– 2:1randomiza0on,blockedbycenterandIPSS>20vs.<20
56
PrimaryEndpoints
• Safety• Clavien-Dindograde2orabovesurgicalcomplica0on
• Effec,veness• DecreaseinIPSS• Non-inferiorityapproach

Summary
§ All procedures do well in the hands of the specialized committed expert
§ Energy-based surgical techniques require comprehension of their unique tissue effects with specific technology

Summary
§ Small glands tend to do well with any technology • Large glands more difficult to do -- not for novice • No matter the surgical technology, surgeon attain
hemostasis

Technology Opportunities
§ We are drowning in data and starving for intelligence
§ Most of our metrics are static and not dynamic § Our ability to capture data is not fully realized § Science must direct analyses with objective
measures and NOT soft marketing measures

Artificial Intelligence
winningAlgorithms | Portsmouth, NH | @winningAlgs
Webscraping à Event Matching àMobile Interface
• Scrape unstructured data from the Internet • Combine attributes with events • iOS mobile application for iPad and iPhone • Support real-time decisions with data

healthDeck healthDeck is a predictive engine used by
healthcare professionals to determine a patient’s risk and inform physician treatments
healthDeck
Cancer Alzheimer’s Diabetes Multiple Sclerosis HIV/AIDS Arthritis Heart
Disease
healthDeck Heart Disease is the tool that doctors will use for specific patients

healthDeck healthDeck is a predictive engine used by
healthcare professionals to determine a patient’s risk and inform physician treatments
healthDeck
Cancer Alzheimer’s Diabetes Multiple Sclerosis HIV/AIDS Arthritis Prostate
Disease
healthDeck Pprostate Disease is the tool that doctors will use for specific patients
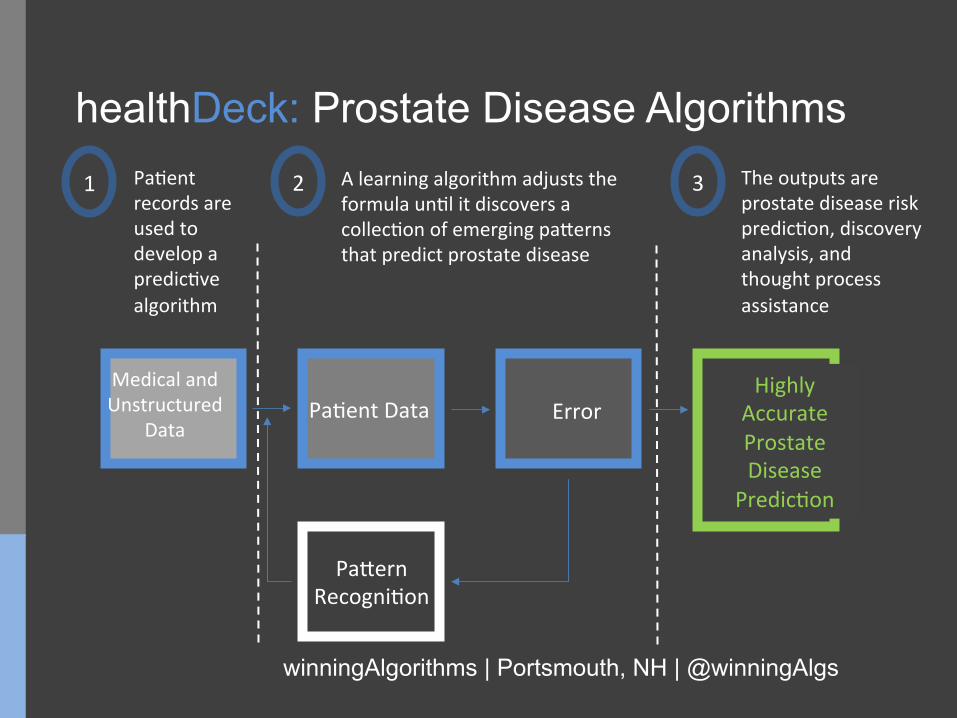
healthDeck: Prostate Disease Algorithms
winningAlgorithms | Portsmouth, NH | @winningAlgs
Pa0entDataMedicalandUnstructured
Data
Pa�ernRecogni0on
ErrorHighly
AccurateProstateDisease
Predic0on
1 2 3Pa0entrecordsareusedtodevelopapredic0vealgorithm
Alearningalgorithmadjuststheformulaun0litdiscoversacollec0onofemergingpa�ernsthatpredictprostatedisease
Theoutputsareprostatediseaseriskpredic0on,discoveryanalysis,andthoughtprocessassistance


![Preparation and Structural Characterization of Three Types of Homo and Heterotrinuclear Boron Complexes: Salen{[B−O−B][O 2 BOH]}, Salen{[B−O−B][O 2 BPh]}, and Salen{[B−O−B][O](https://static.fdokumen.com/doc/165x107/631bb28ea906b217b906972f/preparation-and-structural-characterization-of-three-types-of-homo-and-heterotrinuclear.jpg)

















