Prostate Cancer Molecular Test Grid - Grand Rounds in Urology
78
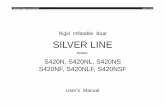
3 February 2016. NCCN is a registered trademark of the National Comprehensive Cancer Care Network. NCCN does not endorse any therapy or product. AUA is a registered trademark of American Urological Association. AUA does not endorse any therapy or product. 1 Adverse pathology is defines as high-grade and/or non-organ-confined disease. *NCCN Prostate Cancer Guidelines (NCCN Guidelines Version 1.2015): “Men with clinically localized disease could consider use of a tumor-based molecular assay to stratify better risk of adverse pathology at radical prostatectomy or chance of biochemical recurrence or disease-specific mortality after radical prostatectomy.” Prostate Cancer Molecular Test Grid Test Description Validated Endpoint(s) Biomarker Selection Specific for Prostate Cancer Specimen Patient Access Genomic Health Genomic Prostate Score (GPS) Predicts the likelihood of adverse pathology 1 using multiple genetic pathways Adverse Pathology at RP Likelihood of high-grade disease Likelihood of non-organ-confined disease 5-year BCR NCCN Guidelines®* YES Positive Biopsy NCCN Very Low, Low, Low-intermediate risk GS 3+3, 3+4 Medicare Covered for NCCN Very Low/Low Financial Assistance Available: Patient contacted if out-of-pocket >$100 Prolaris ® Myriad Genetics Cell Cycle Progression Score (CCP) Reports the risk of dying from untreated disease in 10 years, using a single pathway In a biopsy setting: 10-year Untreated Mortality in a post-RP setting: 10-year BCR Metastasis NCCN Guidelines®* NO Prostatectomy Positive Biopsy AUA® Low-High Risk Medicare Reimbursed for NCCN Very Low/Low Financial Assistance Available: Patient contacted if out-of-pocket >$375 ProMark ® Metamark Genetics ProMark Score Predicts likelihood of adverse pathology using protein staining Adverse Pathology at RP Likelihood of high-grade disease Likelihood of non-organ-confined disease YES Positive Biopsy GS 3+3, 3+4 Financial Assistance Available: Patient contacted if out-of-pocket >$350 ConfirmMDx ® MDx Health ConfirmMDx result Predicts likelihood of negative repeat biopsy Negative Repeat Biopsy YES Negative Biopsy HGPIN Biopsy Medicare Reimbursed Financial Assistance Available: Patient contacted if out-of-pocket >$500 Decipher ® GenomeDx Bioscience Genomic Classifier Predicts the probability of metastasis after surgery 5 -year Metastasis YES Prostatectomy pT3 or pT2 w/positive margin Medicare Reimbursed Financial Assistance Available: Patient contacted if out-of-pocket >$395 4KScore ® Opko 4KScore Provides probability of aggressive cancer Likelihood of GS 3+4 and higher at biopsy YES Blood Biopsy-eligible patients Financial Assistance is not reported on website
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Prostate Cancer Molecular Test Grid - Grand Rounds in Urology

3
February 2016
NCCN is a registered trademark of the National Comprehensive Cancer Care Network NCCN does not endorse any therapy or product AUA
is a registered trademark of American Urological Association AUA does not endorse any therapy or product1Adverse pathology is defines as high-grade andor non-organ-confined disease
NCCN Prostate Cancer Guidelines (NCCN Guidelines Version 12015)ldquoMen with clinically localized disease could consider use of a tumor-based molecular assay to stratify better risk of adverse pathology
at radical prostatectomy or chance of biochemical recurrence or disease-specific mortality after radical prostatectomyrdquo
Prostate Cancer Molecular Test Grid
Test Description Validated Endpoint(s)
Biomarker
Selection Specific
for Prostate
Cancer
Specimen Patient Access
Genomic Health
Genomic Prostate
Score (GPS)Predicts the likelihood of
adverse pathology1 using
multiple genetic pathways
Adverse Pathology at RPLikelihood of high-grade disease
Likelihood of non-organ-confined
disease
5-year BCR
NCCN Guidelinesreg
YES
Positive BiopsyNCCN Very Low Low
Low-intermediate risk
GS 3+3 3+4
Medicare Covered for
NCCN Very LowLowFinancial Assistance Available
Patient contacted if out-of-pocket
gt$100
Prolarisreg
Myriad Genetics
Cell Cycle
Progression Score
(CCP)Reports the risk of dying from
untreated disease in 10 years
using a single pathway
In a biopsy setting
10-year Untreated Mortality in a post-RP setting
10-year BCR
Metastasis
NCCN Guidelinesreg
NOProstatectomy
Positive BiopsyAUAreg Low-High Risk
Medicare Reimbursed for
NCCN Very LowLowFinancial Assistance Available
Patient contacted if out-of-pocket
gt$375
ProMarkreg
Metamark
Genetics
ProMark ScorePredicts likelihood of adverse
pathology using protein
staining
Adverse Pathology at RPLikelihood of high-grade disease
Likelihood of non-organ-confined
disease
YES Positive BiopsyGS 3+3 3+4
Financial Assistance Available
Patient contacted if out-of-pocket
gt$350
ConfirmMDxregMDx Health
ConfirmMDx resultPredicts likelihood of
negative repeat biopsy
Negative Repeat Biopsy YESNegative Biopsy
HGPIN Biopsy
Medicare Reimbursed Financial Assistance Available
Patient contacted if out-of-pocket
gt$500
Decipherreg
GenomeDx
Bioscience
Genomic ClassifierPredicts the probability of
metastasis after surgery
5 -year Metastasis YESProstatectomy
pT3 or pT2 wpositive
margin
Medicare Reimbursed Financial Assistance Available
Patient contacted if out-of-pocket
gt$395
4KScorereg
Opko
4KScoreProvides probability of
aggressive cancer
Likelihood of GS 3+4 and
higher at biopsyYES
BloodBiopsy-eligible patients
Financial Assistance is not reported
on website
Focal (non-radical) Therapy Debate- Pro
Innovations Conference
Prostate Cancer Session
Santa Fe NM 9152018
Jeffrey A Jones MD MS FACS FACPM FAsMA
Professor Baylor College of Medicine
Chief of Urology ME DeBakey VAMC
Topics
bull Debate defined
ndash What are we debating today
ndash Why does this topic need debating
bull Localized Disease Therapy Options
ndash Similar issues as that for Salvage (post XRT) Therapy
bull Current Outcome Data for RALP or RRP Cryotherapy HIFU (Descriptions for info)
ndash Trifecta
bull Oncologic control
bull Continence
bull Erectile Function
ndash Operative and Post-operative Complications
bull Discussion Reduce side effects Improve quality of life not just quantity
ndash A little unfair to Dr Davis since I put together and moderating the session and didnrsquot tell Dr Davis about my planhellip
bull But I knew I could not win a traditional argument in that I myself do not believe it
ndash Will not argue that radical prostatectomy is a better oncologic control operation
bull Same is true for radical nephrectomy radical mastectomy etc
ndash The debate from my perspective is can we achieve the desired oncologic outcome while reducing
bull Operative and Post-operative Complications
bull Incontinence
bull Erectile dysfunction
ndash We have learned from other cancer operations that more (radical) is not always better
ndash What is the best surgical strategy to achieve all of our outcome objectives for Prostate Cancer
Debate defined
ndash Active Surveillance Watchful Waiting
ndash Intervention
raquo Invasive
bull RRPRPP
raquo Less Invasive- Minimally Invasive
bull RALP- Robotic Assisted Laparoscopic +- PLND dominates current mgmt
bull EBRTBrachytherapy (HDRLDR) Proton Combination
bull EBRT- Conformal is being supplanted by IMRT
bull Brachy- isotope LDR still dominates
bull Proton- show me the cost effectiveness efficacy side effect data
bull Combination for higher risk and higher stage
bull Cryotherapy
bull Whole Gland Focal
raquo Minimally Invasive - Non-Invasive
bull HIFU - Physics Technique Current amp Future Role in PCA Management
Localized Disease Therapy Options
bull gt 15 published meta-analysis of radical prostatectomy surgical outcomes
bull gt 50 published comparison studies mostly retrospective reviews of single institutional series
bull Only a few prospective studies
bull Bottom line
ndash Improvements in blood loss hospital stay return to work post-op pain with RA
ndash But despite radical excision and robotic assistance
bull gt25 biochemical recurrence
bull 30+ with PP SUI and 10+ severe incontinence
ndash 5 of prostatectomy patients undergo continence surgery
bull 40+ with PP erectile dysfunction
RALP RARP and RP Outcomes
bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Focal (non-radical) Therapy Debate- Pro
Innovations Conference
Prostate Cancer Session
Santa Fe NM 9152018
Jeffrey A Jones MD MS FACS FACPM FAsMA
Professor Baylor College of Medicine
Chief of Urology ME DeBakey VAMC
Topics
bull Debate defined
ndash What are we debating today
ndash Why does this topic need debating
bull Localized Disease Therapy Options
ndash Similar issues as that for Salvage (post XRT) Therapy
bull Current Outcome Data for RALP or RRP Cryotherapy HIFU (Descriptions for info)
ndash Trifecta
bull Oncologic control
bull Continence
bull Erectile Function
ndash Operative and Post-operative Complications
bull Discussion Reduce side effects Improve quality of life not just quantity
ndash A little unfair to Dr Davis since I put together and moderating the session and didnrsquot tell Dr Davis about my planhellip
bull But I knew I could not win a traditional argument in that I myself do not believe it
ndash Will not argue that radical prostatectomy is a better oncologic control operation
bull Same is true for radical nephrectomy radical mastectomy etc
ndash The debate from my perspective is can we achieve the desired oncologic outcome while reducing
bull Operative and Post-operative Complications
bull Incontinence
bull Erectile dysfunction
ndash We have learned from other cancer operations that more (radical) is not always better
ndash What is the best surgical strategy to achieve all of our outcome objectives for Prostate Cancer
Debate defined
ndash Active Surveillance Watchful Waiting
ndash Intervention
raquo Invasive
bull RRPRPP
raquo Less Invasive- Minimally Invasive
bull RALP- Robotic Assisted Laparoscopic +- PLND dominates current mgmt
bull EBRTBrachytherapy (HDRLDR) Proton Combination
bull EBRT- Conformal is being supplanted by IMRT
bull Brachy- isotope LDR still dominates
bull Proton- show me the cost effectiveness efficacy side effect data
bull Combination for higher risk and higher stage
bull Cryotherapy
bull Whole Gland Focal
raquo Minimally Invasive - Non-Invasive
bull HIFU - Physics Technique Current amp Future Role in PCA Management
Localized Disease Therapy Options
bull gt 15 published meta-analysis of radical prostatectomy surgical outcomes
bull gt 50 published comparison studies mostly retrospective reviews of single institutional series
bull Only a few prospective studies
bull Bottom line
ndash Improvements in blood loss hospital stay return to work post-op pain with RA
ndash But despite radical excision and robotic assistance
bull gt25 biochemical recurrence
bull 30+ with PP SUI and 10+ severe incontinence
ndash 5 of prostatectomy patients undergo continence surgery
bull 40+ with PP erectile dysfunction
RALP RARP and RP Outcomes
bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Topics
bull Debate defined
ndash What are we debating today
ndash Why does this topic need debating
bull Localized Disease Therapy Options
ndash Similar issues as that for Salvage (post XRT) Therapy
bull Current Outcome Data for RALP or RRP Cryotherapy HIFU (Descriptions for info)
ndash Trifecta
bull Oncologic control
bull Continence
bull Erectile Function
ndash Operative and Post-operative Complications
bull Discussion Reduce side effects Improve quality of life not just quantity
ndash A little unfair to Dr Davis since I put together and moderating the session and didnrsquot tell Dr Davis about my planhellip
bull But I knew I could not win a traditional argument in that I myself do not believe it
ndash Will not argue that radical prostatectomy is a better oncologic control operation
bull Same is true for radical nephrectomy radical mastectomy etc
ndash The debate from my perspective is can we achieve the desired oncologic outcome while reducing
bull Operative and Post-operative Complications
bull Incontinence
bull Erectile dysfunction
ndash We have learned from other cancer operations that more (radical) is not always better
ndash What is the best surgical strategy to achieve all of our outcome objectives for Prostate Cancer
Debate defined
ndash Active Surveillance Watchful Waiting
ndash Intervention
raquo Invasive
bull RRPRPP
raquo Less Invasive- Minimally Invasive
bull RALP- Robotic Assisted Laparoscopic +- PLND dominates current mgmt
bull EBRTBrachytherapy (HDRLDR) Proton Combination
bull EBRT- Conformal is being supplanted by IMRT
bull Brachy- isotope LDR still dominates
bull Proton- show me the cost effectiveness efficacy side effect data
bull Combination for higher risk and higher stage
bull Cryotherapy
bull Whole Gland Focal
raquo Minimally Invasive - Non-Invasive
bull HIFU - Physics Technique Current amp Future Role in PCA Management
Localized Disease Therapy Options
bull gt 15 published meta-analysis of radical prostatectomy surgical outcomes
bull gt 50 published comparison studies mostly retrospective reviews of single institutional series
bull Only a few prospective studies
bull Bottom line
ndash Improvements in blood loss hospital stay return to work post-op pain with RA
ndash But despite radical excision and robotic assistance
bull gt25 biochemical recurrence
bull 30+ with PP SUI and 10+ severe incontinence
ndash 5 of prostatectomy patients undergo continence surgery
bull 40+ with PP erectile dysfunction
RALP RARP and RP Outcomes
bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

ndash A little unfair to Dr Davis since I put together and moderating the session and didnrsquot tell Dr Davis about my planhellip
bull But I knew I could not win a traditional argument in that I myself do not believe it
ndash Will not argue that radical prostatectomy is a better oncologic control operation
bull Same is true for radical nephrectomy radical mastectomy etc
ndash The debate from my perspective is can we achieve the desired oncologic outcome while reducing
bull Operative and Post-operative Complications
bull Incontinence
bull Erectile dysfunction
ndash We have learned from other cancer operations that more (radical) is not always better
ndash What is the best surgical strategy to achieve all of our outcome objectives for Prostate Cancer
Debate defined
ndash Active Surveillance Watchful Waiting
ndash Intervention
raquo Invasive
bull RRPRPP
raquo Less Invasive- Minimally Invasive
bull RALP- Robotic Assisted Laparoscopic +- PLND dominates current mgmt
bull EBRTBrachytherapy (HDRLDR) Proton Combination
bull EBRT- Conformal is being supplanted by IMRT
bull Brachy- isotope LDR still dominates
bull Proton- show me the cost effectiveness efficacy side effect data
bull Combination for higher risk and higher stage
bull Cryotherapy
bull Whole Gland Focal
raquo Minimally Invasive - Non-Invasive
bull HIFU - Physics Technique Current amp Future Role in PCA Management
Localized Disease Therapy Options
bull gt 15 published meta-analysis of radical prostatectomy surgical outcomes
bull gt 50 published comparison studies mostly retrospective reviews of single institutional series
bull Only a few prospective studies
bull Bottom line
ndash Improvements in blood loss hospital stay return to work post-op pain with RA
ndash But despite radical excision and robotic assistance
bull gt25 biochemical recurrence
bull 30+ with PP SUI and 10+ severe incontinence
ndash 5 of prostatectomy patients undergo continence surgery
bull 40+ with PP erectile dysfunction
RALP RARP and RP Outcomes
bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

ndash Active Surveillance Watchful Waiting
ndash Intervention
raquo Invasive
bull RRPRPP
raquo Less Invasive- Minimally Invasive
bull RALP- Robotic Assisted Laparoscopic +- PLND dominates current mgmt
bull EBRTBrachytherapy (HDRLDR) Proton Combination
bull EBRT- Conformal is being supplanted by IMRT
bull Brachy- isotope LDR still dominates
bull Proton- show me the cost effectiveness efficacy side effect data
bull Combination for higher risk and higher stage
bull Cryotherapy
bull Whole Gland Focal
raquo Minimally Invasive - Non-Invasive
bull HIFU - Physics Technique Current amp Future Role in PCA Management
Localized Disease Therapy Options
bull gt 15 published meta-analysis of radical prostatectomy surgical outcomes
bull gt 50 published comparison studies mostly retrospective reviews of single institutional series
bull Only a few prospective studies
bull Bottom line
ndash Improvements in blood loss hospital stay return to work post-op pain with RA
ndash But despite radical excision and robotic assistance
bull gt25 biochemical recurrence
bull 30+ with PP SUI and 10+ severe incontinence
ndash 5 of prostatectomy patients undergo continence surgery
bull 40+ with PP erectile dysfunction
RALP RARP and RP Outcomes
bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull gt 15 published meta-analysis of radical prostatectomy surgical outcomes
bull gt 50 published comparison studies mostly retrospective reviews of single institutional series
bull Only a few prospective studies
bull Bottom line
ndash Improvements in blood loss hospital stay return to work post-op pain with RA
ndash But despite radical excision and robotic assistance
bull gt25 biochemical recurrence
bull 30+ with PP SUI and 10+ severe incontinence
ndash 5 of prostatectomy patients undergo continence surgery
bull 40+ with PP erectile dysfunction
RALP RARP and RP Outcomes
bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull Published Series Examples
RALP RARP and RP Outcomes
Author Pts Follow-Up (Months) Potency Rates ()
BNS UNS NNS Total McCammon et al[51] 203 42 452 305 167
Geary et al[52] 459 12 319 133 11 mdash
Penson et al[12] 1288 18 44 414 344 mdash
Catalona and Basler[32] 295 12 63 41 mdash
Leandri et al[53] 106 12 mdash mdash mdash 71
Drago et al[54] 151 mdash mdash mdash mdash 66
Walsh et al[7] 64 18 mdash mdash mdash 86
Kao et al[9] 1069 gt6 mdash mdash mdash 116
Guillonneau et al[14] 40 6 mdash mdash __ 45
Salomon et al[15] 143 12 875 50 30 56 __
Su et al[55] 177 12 76 mdash mdash 48
Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Outcome of interest No of studies Noof patientsRARPRRP ORWMD(95CI) dagger p-value Study heterogeneity
Chi2 df I2 p-value
Operation time min 10 15231435 4443[8018084] dagger 002 116656 9 99 lt00001
Estimated blood loss ml 8 10801102 -49341[-67209- 31474] dagger lt0001 21736 7 97 lt00001
Transfusion rate 18 162497209 016[009028] lt0001 11644 17 85 lt00001
Remove the catheter day 3 1173735 -178[-250-106] dagger lt0001 1952 2 90 lt00001
Hospital stay day 6 15681117 -075[-126-024] dagger 0004 7572 5 93 lt00001
Overall complications 14 27822767 050 [027 092] 003 15813 13 92 lt00001
Urinary continence-3mo 7 945818 121[074198] 045 1333 6 55 004
Urinary continence- 12mo 4 9421409 097[078120] 079 1089 6 45 009
Potent recovery-3mo 4 722685 450[1911062] lt0001 1764 3 83 lt0001
Potent recovery-12mo 4 9421409 158[105236] 003 1033 3 71 002
RALPRARP Outcomes
Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Readmission rate 4 28503025 053[023121] 013 2410 3 88 lt0001
Pathologic T stage
lepT2a 10 17251871 102[083126] 083 702 9 0 063
pT2b 9 16751821 099[080121] 090 807 8 1 043
gepT2c 12 19792212 098[079121] 084 948 11 0 058
Pathological Gleason score
le6 27 58476576 099[087113] 088 4537 26 43 001
7 27 58476576 114[102128] 002 4680 26 44 0007
ge8 27 58476576 079[067092] 0003 3831 26 32 006
PSM 39 1399217806 087[076099] 004 12338 37 70 lt0001
PSM for T2 16 66497986 071[053095] 002 5153 15 71 lt0001
PSM for T3 12 14231713 139[119163] lt0001 938 11 0 059
Mean LN yield 2 375275 377[-5871341] dagger 044 10654 1 99 lt0001
Positive lymph node 10 26683684 069[052090] 0006 931 9 3 041
BCR for free survival 5 11921797 116[071189] 055 2376 4 83 lt0001
RALP RARP Outcomes
bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull Up to ~ 60 of patients with PCA are potentially candidates for alternative local treatment
ndash PCA who do not wish to remain on active surveillance due to up-grading up-staging or PSA rise ldquostressrdquo
ndash Localized disease who are not RALP candidates
ndash Localized disease who refuse RALPRRP due to concern for side effects
ndash Localized disease who are concerned about XRT effects
ndash Failed XRT for localized disease- next discussion
Candidates for Cryotherapy or HIFU
Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Cryotherapy Technique
Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Ice ball control varies by probe Endocare vs Galil
Cryotherapy Technique continued
Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Focal Cryotherapy Results
bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull Not all HIFU is created equally
bull 2 major manufacturers
ndash EDAP-
bull Ablatherm
bull Focus One
ndash Sonacare-
bull Sonoblate
bull Sonotherm
HIFU- High Intensity Focused UltrasoundTechnique device comparison- technical features
Device (Focal One-FO Sonablate-SB) FO SB
Size of Rx Focal Zone (mm) 5 11
Tissue Change Monitoring - +
Power Control Adjustment - +
Duty Cycle Options - +
RIM box monitoring (Reflectivity Ind) - +
Automatic Margin around Target - +
Reference US for assessment - +
Auto-Overlapping Treatment Zones - +
Multi-modality with other probes - +
BU Probe provided - +
HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

HIFU- High Intensity Focused UltrasoundTechnique device comparison- outcomes
References
Ahmed SCM 2016
Mortezim Swiss Urol 2017
Perez-Reggeti Acta Urol Esp 2017
Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Physics of Ultrasound HIFU- Effect
Diagnostic 1 ndash 20MHz
Therapeutic ndash HIFU 1-5MHz
Ablative Lesion-
3 x 3 x 12mm
Ultrasound energy is absorbed and converted to
heat in the focal zone- Temperature elevation
melts lipid membranes denatures proteins
produces vascular endothelial cell damage and
ultimately leads to coagulative necrosis
A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

A New Management Paradigm
TargetFocal Ablation offers a clinical option between Surveillance and Surgery
SurgerySurveillance TargetFocal
Ablation
Earlier cancer diagnosis calls for surgeons to
expand their treatment paradigm
Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate HIFU System
bull 65 MHz imaging
bull 40 MHz transducer for treatment
bull Can be used with standard operating table
bull Single treatment protocol
bull Real-time power modulation control by the physician
bull Tissue change monitoring measures RF backscatter
bull Rectal wall cooling and rectal wall auto measurement
bull Reflex Index Monitoring for HIFU reverberation
bull Automatic rectal wall distance measurement
bull 3x2x12mm HIFU lesion
bull 40mm anterior to posterior (AP) reach
bull MRI fusion with several vendors ndash Phillips Eigen MiMrsquos UroNav
Imaging Crystal Therapy Crystal
40 mm geometric focus
30 mm geometric focus
bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull 2-4 hour outpatient ldquoSurgery Center Basedrdquo procedure
bull Non-invasive transrectal probe using sound to create heat
bull 1-2 hour recovery
bull Most patients resume normal
lifestyle within a few days
bull Lower side effectives
bull Options for targeted ablation
bull Repeatable procedure
Sonablate Prostate HIFU Procedure
Robert Pugach MD
TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

TCM is a unique quantitative software module that displays real-time
changes in prostate tissue destruction resulting from the HIFU ablation
Sonablate Real-Time Tracking
Tissue Change Monitoring (TCM)
Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Validation of TCM with Real-Time Thermometry
During HIFU in PCa Patients
83 ORANGE ( gt 75degC)
17 YELLOW (60-75degC)
Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Prostate Ablation
Whole Gland Ablation
bull Sonablate ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissue
Hemi Gland Ablation Focal Gland Ablation
Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Prostate Multiparametric MRI
Diffusion Weighted (DWI)
Dynamic Contrast Enhancement
TMRI 2-Weighted
MR Spec
Post MRI Processing
Prostatic Margin Section
ROI Annotation
Anatomical Annotation
PIRAD Rating
Target Biopsy Systems
UroNav Invivo
Artemis Eigen
Symphony MiMS
Koelis (Q4 2016)
MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

MRI Ultrasound Fusion
TRUS Surface
MRI Contours
TRUS Contours
MRI Surface
Sonablate Ultrasound
Dataset Contours
MRI Dataset
Section Annotation
MRIUSRegistration
Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Prostate Technology Workflow
Sonablatebull DynaCAD-MRUS Fusion
bull HIFU Planning
bull HIFU Prostate Ablation
(TCM)
mpMRIbull T2W
bull DWI
bull DCE
bull Spec
UroNavbull DynaCAD-MRUS Fusion
bull Bx Navigation
bull Bx Reporting
DynaCADbull Segmentation
bull ROI
Annotation
bull PIRADrsquos
Seamless platform for precise
diagnostics ablation and systematic
follow-up
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Focal HIFU AblationWith DynaCADUS Fusion
DynaCAD is a proprietary MRI post processing software from Invivo Inc A DynaCAD-MRI data set can be fused with
ultrasound within the UroNav Target Biopsy System and the Sonablate Prostate HIFU Ablation System
Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Prostate Tissue Ablation
bull Ultrasound image guided HIFU ablation allows for a customizable ablation plan tailored to each patientrsquos prostate
bull This tailored ablation plan allows the user to ablate a whole or partial prostatic tissueWhole Gland Ablation
Hemi Gland Ablation Focal Gland Ablation
Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Study
Improved Outcomes with
Advancements in High
Intensity Focused Ultrasound
Devices for the Treatment of
Localized Prostate Cancer
Toyoaki Uchida Tetsuro Tomonaga Hakushi Kim
Mayura Nakano
Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
From the Department of Urology Tokai University
Hachioji Hospital (TU TT HK MN SS YN)
Hachiojiand Department of Urology Tokai University
Isehara (TT) Japan
0022-5347151931-01030THE JOURNAL OF UROLOGYregcopy 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH INC
bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull A total of 918 patients
bull Three different Sonablate models
bull Median follow up by Sonablate model
SB Model n FU
1 SB200500 408 108 months
1 SB500(v4) 239 83 months
2 SB500(TCM) 271 47 months
Sonablate Study Overview
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

SB500(TCM)
Sonablate Study Highlights
Improved Outcomes with Advancements in High Intensity Focused Ultrasound Devices for the Treatment of Localized Prostate Cancer Toyoaki Uchida Tetsuro
Tomonaga Hakushi Kim Mayura Nakano Sunao Shoji Yoshihiro Nagata and Toshiro Terachi
SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

SB500(TCM)
Sonablate Study Highlights
Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Sonablate Study Highlights
Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Medium-term Outcomes after Whole-gland High-intensity
Focused Ultrasound for the Treatment of Nonmetastatic
Prostate Cancer from a Multicenter Registry Cohort
L Dickinson M Arya N Afzal P Cathcart SC Charman A Cornaby R Hindley H Lewi N
McCartan CM Moore S Nathan C Ogden R Persad J van der Meulen S Weir M
Emberton Hashim U Ahmed Division of Surgery and Interventional Sciences University College London London UK Department of Urology UCLH
NHS Foundation Trust London UK Department of Urology Princess Alexandra Hospital NHS Trust Harlow UK Department of Urology Dorset County Hospital Dorchester UK
Department of Health Services Research and Policy London School of Hygiene and Tropical Medicine London UK Clinical Effectiveness Unit The Royal College of Surgeons of
England London UK Department of Urology Basingstoke Hospital Hampshire Hospitals NHS Foundation Trust Hampshire UK Department of Urology Broomfield Hospital Mid
Essex NHS Trust Chelmsford UK Department of Academic Urology The Royal Marsden Hospital NHS Foundation Trust London UK Department of Urology North Bristol NHS
Trust Bristol UK wwwsciencedirectcom journal homepage wwweuropea nurologycom Article history Accepted February 18 2016
Abstract- Background High-intensity focused ultrasound (HIFU) is a minimally-invasive treatment for
nonmetastatic prostate cancer Objective To report medium-term outcomes in men receiving primary
whole-gland HIFU from a national multi-center registry cohort Design setting and participants 569
patients at eight hospitals were entered into an academic registry Intervention Whole-gland HIFU
(Sonablate 500) for primary nonmetastatic prostate cancer Redo-HIFU was permitted as part of the
intervention Outcome measurements and statistical analysis Our primary failure-free survival outcome
incorporated no transition to any of the following (1) local salvage therapy (surgery or radiotherapy) (2)
systemic therapy (3) metastases or (4) prostate cancer-specific mortality Secondary outcomes included
adverse events and genitourinary function Results and limitations Mean age was 65 yr (47ndash87 yr)
Median prostate-specific antigen was 70 ngml (interquartile range 44ndash102) National Comprehensive
Cancer Network low- intermediate- and high-risk disease was 161 (28) 321 (56) and 81 (14)
respectively 163 569 (29) required a total of 185 redo-HIFU procedures Median follow-up was 46
(interquartile range 23ndash61) mo Failure-free survival at 5 yr after first HIFU was 70 (95 confidence
interval [CI] 64ndash74) This was 87 (95 CI 78ndash93) 63 (95 CI 56ndash70) and 58 (95 CI 32ndash77) for
National Comprehensive Cancer Network low- intermediate- and high-risk groups respectively 58 754
(77) had one urinary tract infection 22574 (29) a recurrent urinary tract infection 22754 (3)
epididymo-orchitis 227754 (30)
Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Medium Term Outcomes Following Focal HIFU for the
Treatment of Non-Metastatic Prostate Cancer a UK Registry
Analysis of 625 Cases
Guillaumier S1 Hamid S1 Charman S
C1 van der Meulen J1 McCartan N1
Shah K1 Hindley R3 Nigam R4
Dudderidge T4 Afzal N6 Cornaby A6
Lewi H7 Persad R8 Moore CM12
Arya M1 Emberton M12 Ahmed
HU12
UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

UK Registry Study Overview of 625 Cases
Study Protocol-
bull UK prospective academic HIFU registry 2004 to 2015 (11 years)
bull 625 with T1aN0M0 to T3aN0M0 prostate cancer were treated with focal-HIFU (Sonablate)
bull 8 UK centres
bull Disease located via mpMRI followed by transperineal mapping biopsies andor MR-targeted
biopsies
bull Intermediate and high-risk cases underwent radioisotope bone-scan andor cross-sectional
CT
bull Focal-HIFU according to disease location involving hemi-ablation quadrant or focal lesion
ablation
bull Follow-up consisted of serial PSA readings repeat MRI and biopsies if clinically indicated
bull Positive biopsies of the contralateraluntreated area are defined as lsquoout-of-fieldrsquo recurrence
and are not considered to as treatment failure but as metachronous disease development
A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

A B
UK Registry Data Results of 625 Cases
20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

20
60
40
80
10
0
0
Meta
sta
sis
-fre
e S
urv
iva
l (
) (9
5
CI)
0 1 2 3 4 5 6Time since Focal HIFU (years)
625 586 497 433 374 252 126 Number at risk
Kaplan-Meier curve showing Metastases-free survival 95 Kaplan-Meier curve showing salvage-free survivial
at 3 years 95 and at 5 years 91
UK Registry Study Results of 625 Cases
Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Scenarios
Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Prostate Cancer Treatment Landscape
Primary Prostate Cancer Radiation Therapy
Conformal EBRT IMRT Proton Beam
PCa Failure Following Radiation up to 30
Rising PSA+ biopsy
Local recurrence amenable to control
Salvage (post XRT) Treatment Options [NCCN]ndash Salvage Radical Prostatectomy- RALPRRPRPP
ndash Salvage Brachytherapy (Focal vs Whole Gland)
ndash Cryotherapy (Focal vs WG)
ndash HIFU- High Intensity Focused Ultrasound (Focal vs WG)
ndash +- Lymph Node Dissection- PLNDePLNDRPLND
Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Multi-Institutional Salvage RP Data
Chade DC et al Salvage RP for radiation-recurrent prostate cancer Eur Urol (2011) 60205-10
Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage RP Outcomes
Chade DC et al Cancer control and functional outcomes of salvage RP Eur Urol (2012) 61961-71
Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Perioperative
Conversion to open 0
Rectal injury 1
Ureteral injury 0 (0)
Vascular injury 0 (0)
OpT (min) 166
EBL (ml) 118
Blood transfusion 0
LOS (days) 23
MP45 - 1218Abstract 13-
1796
Results N = 88
Clavien grade
I - II 8
III - IV 4
Total 12
30-day Complications
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer
Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Results
MP45 - 1218Abstract 13-
1796
Results
Salvage robot-assisted radical prostatectomy for
recurrent prostate cancer safety and feasibility
Functional outcomes
SHIM gt 21 11
Continence (no pad) 48
Oncologic outcomes
Biochemical failure (PSAgt02)
28
BF free-survival 1 y2 y3 y
716359
Multivariable analysis for BF OR 95 CI p
PSA ngml 1044 1004 ndash 1085 0029
Pathology Gleason (8 - 10 vs 6 - 7) 2890 1020 ndash 8191 0045
Median 13 months follow up
Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Rationality for Salvage Focal Therapy
bull In the lsquosalvagersquo setting after radiation failure
bull Recurrent Pca is more likely to occur at the same site as the primary dominant tumour
ndash thus lsquosuggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to managementrsquo
bull Step-section specimens of 46 salvage RPsndash 72 had a single unilateral focus
ndash Total cancer volume of 068 cm3
ndash Total cancer volume of 343 cm3 (278 cm3 for the index tumour and 018 cm3 for secondary tumours) naiumlve tumors
bull Recurrent cancer ndash Less volume
ndash More likely to be a single unilateral focus
ndash More amenable to targeted focal therapy than is lsquoprimary treatment-nai versquo PCa
bull Arrayeh E et al Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor Results of a longitudinal MRI and MRSI study Int J Radiat Oncol Biol Phys 2012 82 e787ndash93
bull Pucar D et al Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor magnetic resonance imaging and step-section pathology evidence Int J Radiat Oncol Biol Phys 2007 69 62ndash9
bull Huang WC et al The anatomical and pathological characteristics of irradiated prostate cancers may influence the oncological efficacy of salvage ablative therapies J Urol 2007 177 1324ndash9 quiz 1591
Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Cryotherapy
Finley D and A Belldegrun Curr Urol Rep (2011) 12209-215
Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Cryo Functional Outcomes
Study Patients Follow-up Age y Incontinence Baseline Potency Rectal Ureth UTI Hematuria LUTS Per pain AUR 2oPr
(mo) ED 6mo fistula Sx
Ng et al 18 NR 709 Mi-mod37 NR NR 2 0 10 11 Transient 39 14 21 8
Severe 3 Persistent 10
Pisters etal 279 216 700 Any pads 44 692 NR 12 NR NR NR NR NR 68 32
any leakage102
Perrotte 150 167 680 64ge1 pad 59 152 NR NR NR NR NR 44 NR NR
72 any leak
Donnelly 46 NR 689 65 persistent 804 556 22 0 8 7 2 2 4 3 217 65 217
Ismail et al 100 335 668 ge 1 pad 13 78 429 1 0 NR NR 16 4 2 NR
Yin et al 100 24 NR 30 NR 56 6 NR NR 6 NR 23 22 25
Bahn et al 59 823 675 43 NR NR 34 NR NR NR NR NR NR NR
Eisenberg 15 18 71 67 pads NR 40 0 6 7 NR NR NR NR NR NR
a Among prepotent men
b Hemiablation
AUR acute urinary retention ED erectile dysfunction LUTS lower urinary tract symptoms NR not reported UTI urinary tract infection
Curr Urol Rep (2011) 12209ndash215
Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Brachytherapy
Allen GW et al Cancer (2007) 1101405-16
Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Radiother Oncol 2012 Nov105(2)198-202 Epub 2012 Oct 12
Locally recurrent prostate cancer after initial radiation therapy early salvage
high-intensity focused (HIFU) ultrasound improves oncologic outcomesCrouzet S Murat FJ Pommier P Poissonnier L Pasticier G Rouviere O Chapelon JY Rabilloud M Belot A
Megravege-Lechevallier F Tonoli-Catez H Martin X Gelet A Edouard Herriot Hospital Lyon France
METHODS AND MATERIALS A total of 290 men with biopsy-confirmed locally radio-recurrent
PCa underwent S-HIFU DAmico risk group before external beam radiotherapy (EBRT)
Prostate Specific Antigen (PSA) estimated Gleason score prior HIFU and post HIFU biopsies
were analyzed for predictive utility of local cancer control cancer-specific metastasis free and
progression free survival rates (PFSR)
RESULTS Local cancer control with negative biopsy results was obtained in 81 of the 208
patients who underwent post-S-HIFU biopsies Median PSA nadir was 014 ngml and 127
patients did not require androgen deprivation therapy (ADT) The mean follow up was 48
months for cancer-specific survival rates The cancer-specific and metastasis-free survival rates
at 7 years were 80 and 796 respectively The PFSR was significantly influenced by the
pre-HIFU PSA level (hazard ratio (HR) 109 95 CI 104-113) a Gleason score ge8 versus le6
(HR 117 95 CI 103-13) and a previous ADT (HR 128 95 CI 109-146) The rates of
recto-urethral fistula (04) and grade IIIII incontinence (195) indicate significant
reduction in serious side effects with use of dedicated post-radiation acoustic parameters
compared with standard parameters
CONCLUSION S-HIFU is an effective curative option for radio-recurrent PCa with acceptable
morbidity for localized radio-recurrent PCa but should be initiated early following EBRT failure
Use of prognostic risk factors can optimize patient selection
Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Focal HIFU
bull Focal salvage high-intensity focused ultrasound in radiorecurrentprostate cancer
ndash N = 150
ndash 35 months follow up
bull Kanthabalan A et al BJU Int 2017 Aug120(2)246-256
bull Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy Multi -institutional analysis of 418 patients
ndash Whole gland
ndash 35y follow up
ndash Crouzet S et al BJU Int 2017 Jun119(6)896-904
Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Outcomes Meta-analysisEur Urol Focus 2016 Jun2(2)158-171 doi 101016jeuf201509004 Epub 2015 Oct 4
Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus
Nonsurgical Therapies for Radiorecurrent Prostate Cancer A Meta-Regression AnalysisPhilippou Y Parker RA Volanis D Gnanapragasam VJ Dept Surgery Basildon and Thurrock University Hospital Essex UK
Health Services Research University Edinburgh Edinburgh UK Dept Urology Addenbrookes University Hospital Cambridge U
ABSTRACT
Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement We included 63
articles in the analysis (25 on salvage radical prostatectomy (SRP) 8 on salvage high-intensity focused
ultrasound (SHIFU) 16 on salvage cryotherapy (SCT) 14 on salvage brachytherapy (SBT))
EVIDENCE SYNTHESIS Median values of the following variables were extracted from each study patient age
length of follow-up prostate-specific antigen (PSA) before radiotherapy (RT) PSA before salvage therapy
Gleason score before RT and time interval between RT and salvage therapy Functional toxicity and
oncologic outcomes were measured according to rates of impotence incontinence fistula formation urethral
strictures and biochemical recurrence Meta-regression adjusting for confounders found no significant
difference in oncologic outcomes between SRP and nonsurgical salvage modalities SBT SCT and
SHIFU appeared to have better continence outcomes than SRP No significant difference in toxicity
outcomes between modalities was found although limitations such as reporting selection and
publication bias and between-study heterogeneity must also be considered with these conclusions
CONCLUSIONS Oncologic outcomes are comparable for SRP and all three nonsurgical salvage modalities
We found no significant differences in toxicity outcomes among modalities however SRP appears to be
associated with worse rates of urinary incontinence than SBT SCT and SHIFU
PATIENT SUMMARY We performed a meta-regression analysis to compare oncologic functional and toxicity
outcomes between salvage radical prostatectomy and nonsurgical salvage modalities Oncologic and toxicity
outcomes appear to be similar however all nonsurgical salvage modalities may be associated with
better continence outcomes
HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

HIFU as salvage first-line treatment for palpable TRUS-
evidenced biopsy-proven locally recurrent prostate
cancer after radical prostatectomy a pilot study
Asimakopoulos AD Miano R Virgili G Vespasiani G Finazzi Agrograve E Div Urology Univ Tor
Vergata Rome Italy
METHODS Nineteen patients with palpable TRUS-evidenced biopsy-proven local
recurrence of CaP after RP unwilling to undergo salvage radiotherapy (SRT) underwent
HIFU as a single-session procedure
RESULTS Median follow-up 48 months All cases overnight procedures No urethrorectal
fistula or anastomotic stricture was observed Two cases urinary retention were resolved
with urethral catheterization Four cases SUI 2 (mild incontinence) were resolved after
pelvic floor exercises within 6 mos 2 cases severe incontinence required surgical minimally
invasive treatment 1719 patients (89) were classified as success Two patients failed
to show a PSA nadir lt01 ngml During follow-up 817 patients (47) were classified as
failure with consequent total rate of failures 1019 (526) A statistically significant
difference was observed in pre-HIFU median PSA (2 vs 545 ngml respectively P = 0013)
and Gleason score of the RP specimen (P = 001) between the success and failure group
CONCLUSIONS Salvage first-line HIFU for palpable TRUS-evidenced biopsy-proven local
recurrence of CaP is a feasible minimally invasive day-case procedure with an acceptable
morbidity profile Fiar cancer control in the short- and mid-term Patients with lower pre-
HIFU PSA level and favorable pathologic Gleason score had better oncologic outcomes
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Concomitant
Salvage Left-Hemi HIFU + Robotic (Xi) ePLND
Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Concomitant
Salvage Right-Hemi HIFU + Robotic (Si) PLND
Side docking
Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Case Presentations
CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 1
bull JC ndash 57 YO plastic surgeon
bull PSA ndash 102
bull ~ 35 G prostate ndash felt benign
bull NBP ndash 512 cores ndash Gleason 4+4
bull ( - ) bone scan
bull ( - ) CT ndash abdomenpelvis
CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 1 ( 2 )
bull Elected radical prostatectomy ( open )
bull Pelvic exploration ndash suspicious LN ndash Lt side
bull Frozen section ndash positive for metastatic
adenocarcinoma
bull Proceed with prostatectomy
bull Abort the procedure
CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 1 ( 3 )
bull Had radical prostatectomy ndash 92006
bull Path Gl 4+4
18 cm ndash largest diameter
( + ) ECE
( + ) SVI
( + ) SM
( + ) LN ndash 10 cm in diameter
CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 1 ( 4 )
bull Was started on ADT post-op
bull Continued on ADT x total of 8 months
bull Had XRT to the prostate bed ndash 6 months post-op
bull Followed since
CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 1 ( 5 )
bull Last FU ndash 92017
bull Now 11 years since his operation
bull PSA - lt 0006 T ndash 487
bull Potent ( with viagra )
bull Continent ndash 0-1 padsday
CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 2
bull RM ndash 70 yo real estate agent
bull PSA 267 30 free
bull DRE - ~ 35 G prostate cw T3 Rt gt Lt
bull NBP ndash Rt side ndash all cores GL 5+4 4+5
Lt side ndash GL 4+4 amp 4+3
bull Bone scan ndash ( - )
bull CT ndash Enlarged LNrsquos ndash Internal Iliac
CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

CASE 2 ( 2 )
bull Elected multi ndash modal therapy
bull Had RALP + PLND 52017
bull Path 41 G prostate 65 replaced by tumor
bull GL 4+5 = 9
bull (+) SVI
bull (+) SM ndash Rt side amp apex
bull (+) LNrsquos ndash 28 ndash 21 mm largest diameter
bull Started ADT immediately post-op
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRITarget
PETCT Target
Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Case 3
bull 80 YO male
bull 2004 PSA 55ngmL Gleason 3+3 212 cores
bull 2010 EBRT
bull PSA 032 (2012) 38 (42014) 60 (42015) 48 (102015) 1098 (22016)
bull Bx 032016 Gleason 3+4 4+4 4+5 50 511 cores LB LM LA
bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

bull History of
ndash Urinary retention
ndash Radiation cystitis
ndash CICrsquos 2-3xday and void on own 3xday
bull SHIM 1025 ndash sexually active w PDEI
Case 3
Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Case 3
bull TRUS (62016) Prostate volume 18 cc
bull NaF BonePET DJD changes no definitive mets
bull CT AP No metastases
Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Case 3
MRI- Asymmetry in diffusion and perfusion on the left- No SV involvement- No metastases
Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage treatment options for
curative intentbull NCCN
ndashRadical prostatectomy + PLND
ndashCryoablation
ndashHIFU + PLND
ndashBrachytherapy
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43
Salvage Right-Hemi HIFU +
Robotic PLND
bull PLND
ndash Right 09
ndash Left 06
bull ORT 5hs
bull Complications No
bull LOS 1 day
Pre L sHIFU
Post L sHIFU
Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage Right-Hemi HIFU +
Robotic PLND
bull Same setting
ndash Not concomitant
bull sHIFU first
ndash R lateral decubitus
bull Change to lithotomy
ndash Prep + Ports + Docking hellip
bull Robotic PLND
Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Follow-up at 4 monthsbull PSA 1098 (22016) 06 (112016) 103 (12017)
Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Follow-up at 1 year
PSA 1098 (22016) 06 (112016) 103 (12017) 114 (52017) 123 (82017)
mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

mp-MRI + PSMA PETCT + TRUSFusion guided prostate biopsy
MRI targets orange and red All targeted and systematic BxPSMA PETCT target yellow
Adenocarcinoma of the prostate ASAP in the Right Base Only PSMA PET targeted Bx showed PCa
Prostatic adenocarcinoma with radiation associated changes
Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43

Salvage HIFU
Reference N FU (mos) Metric DFS ()
Gelet 71 148 BxPSA 44
Murat 167 181 BxPSA 42-53
Zacharakis 31 74 PSA(Bx) 71
Challacomb 12 21 PSA 25
Berge 46 9 PSA 61
Uchida 21 36 PSA 52
Ahmed 84 198 PSABx 43