What Engineering Technology Could Do for Quality of Life in Parkinson’s Disease: a Review of...
11
2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. See http://www.ieee.org/publications_standards/publications/rights/index.html for more information. This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI 10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics JBHI-00260-2015-R2 1 Abstract—Parkinson’s Disease (PD) involves well known motor symptoms such as tremor, rigidity, bradykinesia, and altered gait but there are also non-locomotory motor symptoms (e.g., changes in handwriting and speech) and even non-motor symptoms (e.g., disrupted sleep, depression) that can be measured, monitored, and possibly better managed through activity based monitoring technologies. This will enhance quality of life (QoL) in PD through improved self-monitoring, and also provide information which could be shared with a health care provider to help better manage treatment. Until recently, non- motor symptoms (“soft signs”) had been generally overlooked in clinical management yet these are of primary importance to patients and their QoL. Day-to-day variability of the condition, the high variability in symptoms between patients, and the isolated snapshots of a patient in periodic clinic visits makes better monitoring essential to the proper management of PD. Continuously monitored patterns of activity, social interactions, and daily activities could provide a rich source of information on status changes, guiding self correction and clinical management. The same tools can be useful in earlier detection of PD and will improve clinical studies. Remote medical communications in the form of telemedicine, sophisticated tracking of medication use, and assistive technologies that directly compensate for disease related challenges are examples of other near term technology solutions to PD problems. Ultimately, a sensor technology is no good if it is not used. The Parkinson’s community is a sophisticated early adopter of useful technologies and a group for which engineers can provide near term gratifying benefits. Index Terms—review article, activity, nonmotor symptoms, cognition, depression, sleep quality, exercise, patient perspective I. INTRODUCTION N the first World War, Winston Churchill described the gap between inventors and potential beneficiaries: A hiatus exists between the inventor who knows what they could invent, if they only knew what was wanted, and the soldiers who knew, or ought to know, what they want and would ask for it if they only knew how much science could do for them [1]. J.A. Stamford is a neuroscientist with Parkinson’s and a co-founder of Parkinson’s Movement. (e-mail: [email protected]). P.N. Schmidt is a bioengineer and the CIO and Vice President for Research at the National Parkinson’s Foundation (e-mail: [email protected]). K.E. Friedl is an endocrine physiologist, currently supported by the ORISE Knowledge Preservation Program for the US Army Research Institute of Environmental Medicine and a Professor (adjunct) of Neurology at the University of California, San Francisco (e-mail: [email protected]). Parkinson’s Disease (PD) has attracted numerous engineering innovations, especially around classical signals associated with movement disorders but patients are concerned about other symptoms that affect their quality of life. This paper describes problems of people with PD and technological solutions that might help improve quality of life. Parkinson’s Disease (PD) is a neurological condition that has been traditionally characterized by motor symptoms such as tremor, rigidity, slowed movement (bradykinesia), and altered gait. Research starting in the 1950’s identified the association between specific brain regions and motor function resulting in the characterization of PD as a disease of dopamine [2]. Dopamine replacement therapies have revolutionized outcomes of motor function and pre-clinical research is currently largely focused on characterizing and targeting effects that go beyond the dopamine system, including a panoply of motor and non-motor symptoms with no specific symptom or domain obviously dominating the patient experience. Better management of many non-motor symptoms awaits success of these pre-clinical efforts [3-5]. With this as context for the status of Parkinson’s management, monitoring technologies for PD patients offer the potential to increase quality of life through objective, continuous, and on demand self-monitoring. These technologies also provide important information which could be shared with a health care provider to help better manage treatment [6]. Parkinson’s care is typically informed by history taking based on patient recall, observation of the patient for the duration of the encounter, and follow-up intervals timed to sample clinically relevant change. However, many aspects of the disease fluctuate broadly across the frequency space, from gait asymmetry (seconds) to medication pharmacokinetic cycles (hours) to days-to-months cycles of fatigue, constipation, psychosis, and depression [7]. The high variability in symptoms between patients, and the isolated snapshots of a patient in periodic clinic visits makes better monitoring essential to the proper management of PD. Technologies such as remote medical communications in the form of telemedicine [8,9] and assistive technologies such as sophisticated tracking of medication use can also provide near term solutions to PD problems. This review outlines some of the current advances in non- locomotory motion-based technologies and explores additional needs and opportunities in PD. What Engineering Technology Could Do for Quality of Life in Parkinson’s Disease: a Review of Current Needs and Opportunities Jonathan A. Stamford, PhD, DSc, Peter N. Schmidt, PhD, and Karl E. Friedl, PhD, Fellow, AIMBE I
Transcript of What Engineering Technology Could Do for Quality of Life in Parkinson’s Disease: a Review of...

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
1
Abstract—Parkinson’s Disease (PD) involves well known
motor symptoms such as tremor, rigidity, bradykinesia, and
altered gait but there are also non-locomotory motor symptoms
(e.g., changes in handwriting and speech) and even non-motor
symptoms (e.g., disrupted sleep, depression) that can be
measured, monitored, and possibly better managed through
activity based monitoring technologies. This will enhance quality
of life (QoL) in PD through improved self-monitoring, and also
provide information which could be shared with a health care
provider to help better manage treatment. Until recently, non-
motor symptoms (“soft signs”) had been generally overlooked in
clinical management yet these are of primary importance to
patients and their QoL. Day-to-day variability of the condition,
the high variability in symptoms between patients, and the
isolated snapshots of a patient in periodic clinic visits makes
better monitoring essential to the proper management of PD.
Continuously monitored patterns of activity, social interactions,
and daily activities could provide a rich source of information on
status changes, guiding self correction and clinical management.
The same tools can be useful in earlier detection of PD and will
improve clinical studies. Remote medical communications in the
form of telemedicine, sophisticated tracking of medication use,
and assistive technologies that directly compensate for disease
related challenges are examples of other near term technology
solutions to PD problems. Ultimately, a sensor technology is no
good if it is not used. The Parkinson’s community is a
sophisticated early adopter of useful technologies and a group for
which engineers can provide near term gratifying benefits.
Index Terms—review article, activity, nonmotor symptoms,
cognition, depression, sleep quality, exercise, patient perspective
I. INTRODUCTION
N the first World War, Winston Churchill described the gap
between inventors and potential beneficiaries: A hiatus
exists between the inventor who knows what they could invent,
if they only knew what was wanted, and the soldiers who
knew, or ought to know, what they want and would ask for it if
they only knew how much science could do for them [1].
J.A. Stamford is a neuroscientist with Parkinson’s and a co-founder of
Parkinson’s Movement. (e-mail: [email protected]). P.N. Schmidt is a bioengineer and the CIO and Vice President for Research
at the National Parkinson’s Foundation (e-mail: [email protected]).
K.E. Friedl is an endocrine physiologist, currently supported by the ORISE Knowledge Preservation Program for the US Army Research Institute of
Environmental Medicine and a Professor (adjunct) of Neurology at the
University of California, San Francisco (e-mail: [email protected]).
Parkinson’s Disease (PD) has attracted numerous
engineering innovations, especially around classical signals
associated with movement disorders but patients are
concerned about other symptoms that affect their quality of
life. This paper describes problems of people with PD and
technological solutions that might help improve quality of life.
Parkinson’s Disease (PD) is a neurological condition that
has been traditionally characterized by motor symptoms such
as tremor, rigidity, slowed movement (bradykinesia), and
altered gait. Research starting in the 1950’s identified the
association between specific brain regions and motor function
resulting in the characterization of PD as a disease of
dopamine [2]. Dopamine replacement therapies have
revolutionized outcomes of motor function and pre-clinical
research is currently largely focused on characterizing and
targeting effects that go beyond the dopamine system,
including a panoply of motor and non-motor symptoms with
no specific symptom or domain obviously dominating the
patient experience. Better management of many non-motor
symptoms awaits success of these pre-clinical efforts [3-5].
With this as context for the status of Parkinson’s
management, monitoring technologies for PD patients offer
the potential to increase quality of life through objective,
continuous, and on demand self-monitoring. These
technologies also provide important information which could
be shared with a health care provider to help better manage
treatment [6]. Parkinson’s care is typically informed by
history taking based on patient recall, observation of the
patient for the duration of the encounter, and follow-up
intervals timed to sample clinically relevant change.
However, many aspects of the disease fluctuate broadly across
the frequency space, from gait asymmetry (seconds) to
medication pharmacokinetic cycles (hours) to days-to-months
cycles of fatigue, constipation, psychosis, and depression [7].
The high variability in symptoms between patients, and the
isolated snapshots of a patient in periodic clinic visits makes
better monitoring essential to the proper management of PD.
Technologies such as remote medical communications in the
form of telemedicine [8,9] and assistive technologies such as
sophisticated tracking of medication use can also provide near
term solutions to PD problems.
This review outlines some of the current advances in non-
locomotory motion-based technologies and explores additional
needs and opportunities in PD.
What Engineering Technology Could Do for
Quality of Life in Parkinson’s Disease: a
Review of Current Needs and Opportunities
Jonathan A. Stamford, PhD, DSc, Peter N. Schmidt, PhD, and Karl E. Friedl, PhD, Fellow, AIMBE
I

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
2
II. QUALITY OF LIFE PROBLEMS IN PARKINSON’S DISEASE
Parkinson's, in common with many other long-term
disabling conditions, presents a number of general and specific
challenges to the quality of life of patients. These challenges
inevitably have spawned many survey instruments which
purport to quantify and numericise health-related quality of
life in Parkinson's. While many are validated research
instruments, all are inevitably reductionist in nature. Some are
overtly generic and broadly applicable. Others such as the 39
item Parkinson’s Disease Questionnaire (PDQ-39) and the
Parkinson’s Disease Quality of Life Questionnaire (PDQLQ)
are designed specifically for Parkinson's [10].
Standardized instruments all have flaws. Firstly, the
scoring and assessment is often conducted by healthcare
professionals rather than the patients themselves. This induces
an inevitable, if rather comical, disconnect between the patient
and their "quality of life". One might reasonably assume that
the patient was better placed than the physician to pass
judgment on the patient's quality of life.
Secondly, and integral to their need to standardize, the
instruments work best at a population rather than individual
level. The capacity to generalize almost inevitably nullifies the
scope to personalize. At a population level, quality of life
instruments speak reasonably well of the population.
However, weightings given to specific domains may help
validate instruments at the population level but serve poorly as
a "one size fits all" approach to individual quality of life [11].
Thirdly, the distinction between quality of life and health-
related quality of life is a largely clinical construct. Many, if
not most patients fail to recognize the distinction. This is
particularly true for Parkinson's where the treatment drugs can
produce strange alterations in impulse control such as punding
behaviors. For instance, financial difficulties have enormous
bearing on quality of life but, at first sight, are not health-
related. Consider however that these financial difficulties
might arise from Internet gambling due to inappropriately high
doses of prescribed dopamine agonist [12]. Immediately the
perspective is different and this is now a health-related quality
of life issue. Some health quality of life instruments attempt
to identify these related factors.
A. Importance of “soft signs” to PD patients
Non-motor symptoms of PD were largely ignored by
clinicians as recently as during the development of the original
Unified Parkinson’s Disease Rating Scale (UPDRS) rating
scale [13]. Approximately contemporaneously with the
development of the UPDRS, a systematic review of key
disabling symptoms identified by patients resulted in a
questionnaire including indicators of clinical issues beyond
motor symptoms such as speech, depression, anxiety,
psychosis, sleep quality and daytime sleepiness, cognitive
impairment and pain on the PDQ-39 [14]. The patients
surveyed also cited the impact of the disease on social
functioning, citing the importance of the impact of PD on their
ability to function in public, the impact on relationships,
ability to perform eating tasks and dressing, hygiene tasks,
handwriting, and leisure activities. The final PDQ-39
questionnaire was psychometrically optimized to ensure that
each of these domains was statistically independent.
The social functioning domains are clearly important to
patient health-related quality of life however they are difficult
to assess during a clinical interview, where clinicians may
question the patients about difficulty eating rather than
concerns about eating in public and patients may consider
such issues not relevant as clinical concerns. Pain in PD is not
uncommon but rarely identified. In a study of patients
transitioning from a movement disorders clinic to a palliative
care program, investigators found an improvement in Health
Related Quality of Life (HRQL) largely driven by a reduction
in pain [15].
With the diagnoses for many patients in their early 50s [16],
a majority of patients are diagnosed while still at an age where
they expect to be active in the workforce. While motor
impairment is cited in disability claims, for many patients non-
motor symptoms such as daytime sleepiness are cited as the
primary cause of disability [17].
There is good evidence that patient priorities in
symptomatology do not consistently match those of the
treating physician's. Patients often put greater emphasis on
"soft signs" rather than the more readily quantifiable and overt
symptomatology [7]. For instance, in a survey conducted by
Parkinson's Movement (http://parkinsonsmovement.com),
there was little correlation between patient-reported quality of
life and motor symptoms, suggesting that motor symptoms,
the most visible to a physician, are an inadequate measure
upon which to base treatment decisions (figure 1).
FIGURE 1. Motor Symptoms and Patient Quality of Life.
Quality of life in chronic conditions correlates well with the
prevalence of mood disorders [18]. Anxiety and depression are
strong negative predictors of quality of life. Data from
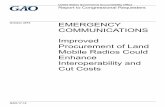
Parkinson's Movement shows that there is an increase in
multiply comorbid mood disorders (figure 2). These survey
data report higher prevalence of mood disorders than
previously recognized. In part this may be due to patients
being more comfortable reporting symptoms to other patients
(in the form of the Parkinson's Movement organization) than
to their treating physicians.

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
3
FIGURE 2. Mood Disorders Reported in Association with Parkinson’s.
This is only an approximate pictorial representation (see text for details).
Patients often underreport symptoms, especially those of an
embarrassing or stigmatizing nature, such as problems with
bladder control. Patients are also squeamish about reporting
mood disorders for fear that this may have stigmatizing
psychiatric implications. This is particularly true for
hallucinations, which are considerably underreported. In the
UK, patients who experience hallucinations may have their
driving license withdrawn, an action which itself has strong
negative implications for quality of life.
Although patients, as a group, tend to prioritize non-motor
symptoms over motor symptoms, the relative importance of
each symptom differs. Patients are as different in their
expression of non-symptoms as they are in their relative
predominance of tremor, rigidity and bradykinesia. Patients
with dystonia for instance will report pain as a major
determinant of quality of life, while those experiencing
chronic fatigue may talk more about sleep and sleep patterns.
These differences are difficult to capture in any single measure
or assessment and this emphasizes the importance of
personalization.
B. Access to care and the value of “virtual house calls”
The major problem with most current forms of clinician-
based assessment is the need for the patient to be physically in
the presence of the physician. For many mobility-impaired
patients this presents significant logistic challenges. Stressful
journeys to the clinic can make patients seem symptomatically
worse than they really are. This is particularly so for confused
and demented patients. Conversely, many patients alter the
timing of their medication or take additional tablets in order to
ensure that they arrive in good shape [19]. But whether the
patients seem worse or better, the issue is accuracy. In a brief
consultation under what are highly artificial circumstances, the
physician is likely to be misled and may consequently make
inappropriate prescribing decisions. To get an accurate
assessment of patients' health, it is best to make these
assessments in the patient's home. Clearly this is incompatible
with most modern medical resource allocation but it can be
elegantly addressed using simple telemedicine [20-22]. Skype
or other forms of audiovisual telecommunication can be
readily used to allow patients in their home to communicate
with physicians in their offices or clinics [22]. The vast
majority of the standard UPDRS assessments can be
conducted under such circumstances [23]. There are
substantial benefits in terms of time, but the real benefit lies in
the quality of information obtained from the patient in their
natural surroundings rather than the artificial environment of
the clinic.
The impact on patients and caregivers of the time and
expense of accessing care is also an important consideration.
In developing a telemonitoring system for depressed patients,
investigators realized that a 15-minute clinical assessment
required patients to dedicate a half day to getting from home
or work to the clinic, parking, walking to the clinic, signing in,
waiting to be seen, and then reversing the steps after the
encounter [24]. Programs offering telemedicine to the home
for PD care have shown the dramatic reduction in travel and
waiting times that can be achieved through telemedicine,
reflecting the longer average distances separating patients
from the scarce clusters of subspecialist neurologists [9].
Such “virtual house calls” are being evaluated in a randomized
controlled trial with one of us (PS) a co-investigator [8].
There are known risks as well as benefits to this approach that
must also be addressed, especially patient privacy and control,
data security, and remote provider training and credentials.
C. Patient Engagement
Patient use of technology and patient engagement in their
health status are implicitly interlinked. As a rule, the more
engaged a patient is with their condition, the more likely they
are to seek technological assistance. The converse however is
also true. Technological solutions are unlikely to appeal to the
disengaged and there is also a technological threshold in the
usage. Confused and demented patients, as well as those
struggling to come to terms with the reality of their illness, are
poor adopters of technology no matter how well meant. This
is reflected to some extent in the poor involvement of the
Parkinson's community in clinical trials [25].
Nonetheless, the diversity of Parkinson's symptoms and the
chronicity of the illness are, at once, a challenge to app
developers and technologists and a rich field of opportunity.
Necessity is the mother of invention and there seems little
doubt that the best solutions will be found when patients’
necessity is the driver for that burst of inventive flair.
Patients want technology that simplifies their lives rather
than complicates. An example of this might be the Lift Labs
spoon [26], designed with a simple servo mechanism that
counteracts the patient's tremor and allows the patient to enjoy
less messy meal times. This is an example of the technology
making life simpler but also addressing a real patient driven
need rather than a technologically driven solution.
Patients also want technology that is passive in the sense of
recording data without having to take active tests or decisions.
Clearly some measures are more amenable to this than others.
For instance, tremor can be monitored passively and
continuously without user intervention. Cognitive function on
ALL 3 SYMPTOMS
10% OF RESPONDENTS
ALL 3 SYMPTOMS
30% OF RESPONDENTS
ANXIETY
DEPRESSION
ANXIETY
DEPRESSION
OBSESSIONALTHOUGHTSOBSESSIONAL
THOUGHTS
ANXIETY &DEPRESSION26%
ANXIETY &DEPRESSION27%
BEFORE PARKINSON’S SINCE PARKINSON’S
NONE OF THESE 3 PROBLEMS: 36%NONE OF THESE 3 PROBLEMS: 13%

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
4
the other hand requires explicit testing and is therefore much
more temporally invasive and intrusive. Of necessity, such
measurements are also discrete rather than continuous.
It is also worth asking the question, Who does the
technology serve? Holter electrocardiographic monitoring
provides data to the physician. A personal fitness monitor
provides data primarily to the user. Patients have an entirely
different relationship with data they ‘own.’
D. Three important QoL problems that could be addressed by
technology
In practice, there are broadly speaking three areas where
technology either could or already does provide assistance.
These are medication monitoring, symptom logging and
cognitive assessment.
Medication monitoring is an area where technology already
provides simple solutions. Parkinson's, more than almost any
other condition, calls for precise timing of medication. There
are several apps available where medication reminders are
provided at user-set times and intervals. Many are generic,
equally usable for any chronic medication condition. Some are
more specific for Parkinson's [27]. However all such apps
make the tacit assumption that accurate reminders mean
accurate compliance although, in reality, there is little reason
to believe that such a close relationship holds. Many apparent
medication failures are in fact compliance failures. A better
system would be one that monitors actual ingestion of tablets.
This is the real problem in search of a solution.
Symptom logging is an area of widespread development
with many apps taking advantage of smart phone gyroscopes
and accelerometers to analyze complex movement patterns
and, with the assistance of complex software solutions, to
tease out tremor, bradykinesia, dyskinesia and gait instability
therefrom [28]. These are often technically elegant and, it has
to be conceded, may be of assistance to physicians in their
decision-making. However, this is also an example of
technology offering solutions ahead of problems. Patients, as
discussed earlier, place far greater emphasis on non-motor
symptoms which have been, so far, less amenable to
gyroscopic or accelerometer analysis. There is the sense that
motor dimensions of symptomatology are given greater weight
by technologists simply because the solutions are already
available.
Mood and cognition monitoring is a tough nut to crack.
Although simple technological solutions for smart phones
exist, all require user intervention either to answer questions
or to perform reasoning based tasks. Such complex biological
constructs as mood and cognition are not amenable to simple
technological solutions. Indeed most such offerings are
fundamentally little more than paper exercises transferred to
the smart phone rather than solutions conceptualized for the
phone. Most such current solutions involve discrete testing at
certain times of day with the logging of the data, either
manually or automatically in some form of diary. It is worth
noting some success in on-line monitoring of depression,
where it was found that the patients most in need of care were
the ones most adherent to the system [24].
III. POTENTIAL TECHNOLOGY SOLUTIONS TO SOME OF THE
SOFT-SIGN (NON-LOCOMOTORY) PROBLEMS
Human behavior is signaled by body movements and other
physical and physiological patterns - so called “honest
signals.” Much of this is detectable body language but more
subtle behavior may be reliably deciphered from continuous
measurements using relatively simple monitors with the aid of
signal analysis and pattern recognition tools. The more
extreme deviations in patterns associated with disease
conditions may also help to identify common features that
reflect performance fluctuations in healthy individuals with
more subtle presentation. In this role, PD is a prototypical
disease for activity studies that include activity-based patterns
of non motor problems. These non motor issues include mood
and depression, cognitive decline and dementia, fatigue, and
various types of disordered sleep. These have not been
typically included as part of the rest of the data analysis in
research studies involving activity measurements in
Parkinson’s, even though these are interrelated and important
to daily functioning for an individual with Parkinson’s
[29,30]. From a technologist’s perspective, it is likely that
many motor and non-motor features of PD can be
stochastically modeled using data as simple as that collected
with a single wearable sensor system involving triaxial
accelerometry [31-34]. Sensitivity and specificity may benefit
from additional data such as heart rate, skin conductance, or
speech components (Table 1).
TABLE 1. NON MOTOR SYMPTOM TRACKING USING ACTIVITY
MONITORING AND OTHER MEASURES.
Note: REM – rapid eye movement sleep stage; SWS – slow wave sleep
Approaches to modeling, mining, and crowd sourcing
behavior from complex monitoring data have been proposed
[58-60]. Similar techniques could be applied to PD data.
A. The importance of purposeful exercise in PD
Exercise can provide remarkable benefits to Parkinson’s
patients, improving clinical evaluation and sustaining or even
improving HRQL, and specifically improving motor function,
mood, and cognition. This non-pharmacological benefit
appears to involve more than one mechanism including
increases in dopamine D2 receptors and BDNF secretion [61-
64]. Walking, Tai Chi, dance, and cycling are popular forms
of exercise in Parkinson’s but all forms of activity appear to
provide benefits, especially if they include high physical
intensity, high-amplitude motion, and cognitive challenges
[65-71]. Monitoring technologies that quantify physical
Problem Feature/Marker Other measures Reference
Exercise activity intensity, duration 35-39
Sleep and alertness REM, SWS
heart rate, skin
conductance 40-43
sleep movements bed monitor 44-47
Fatigue eye tracking 48
Depression voice 49-54
Psychosis 55,56
Cognition memory, confusion,
executive function
instrumented
home, GPS 57

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
5
activity frequency and intensity provide feedback to patients
and care providers to establish the individually useful exercise
prescription. Data from such monitoring will help to further
define optimal exercise dosing. Monitoring also helps to
promote exercise compliance, and this is especially important
in PD because of the recognized therapeutic benefits and
because of barriers to exercise not present in the non-PD
population [36,37,72]. Activity level is also a marker for
declining health and progression of disease, even in the
absence of gait changes, decreasing activity levels are a
marker for the emergence of several clinically relevant
symptoms such as depression [18,38].
Many commercially available devices rely on some form of
actigraphy to provide estimates of activity in steps taken,
distance traveled, or calories expended. Currently available
systems and their applications to PD patients have been well
reviewed elsewhere [33]. Longitudinal monitoring of activity
in PD has revealed differences in intensity and volume of
exercise without changes in frequency or duration, requiring
more than “steps counted” as a useful monitoring approach
[38]. Traditional methods used by researchers to estimate
energy expenditure in free living individuals (ie., outside of a
metabolism chamber) relied on continuous heart rate
monitoring [73] but the combination of continuous heart rate
and actigraphy has been demonstrated to provide greater
accuracy for energy expenditure in healthy active individuals
[74]. Other novel measures such as foot contact time can
accurately assess locomotory activity and categories of
activity [75]. A sensor on a necklace was applied to
quantification of daily activity and energy expenditure
estimates in PD patients [35]. Interpretation of sensor data
requires specific validation with a Parkinson’s population
where altered gait, asymmetrical loss of arm swing, etc. could
conceivably change usual assumptions [76].
The useful interpretation of large continuous data streams
from activity and motion from smart shoes, other wearable
monitors, and home area monitoring, is an important current
focus [31,33]. As activity monitoring increases in the general
population, the observed association between physical activity
and PD risk can also be parsed into whether exercise is
protective or diminished exercise is a result of PD onset [77].
Further development of systems involving social
interaction with peers or coaches and with real or virtual
humans to motivate regular activity could be an important tool
in enhancing quality of life for PD patients [78-80].
B. Sleep quantification and implications for PD
Sleep disturbance is a disabling symptom for many PD
patients and the characterization of sleep disturbance is
important in treatment [7,81-83]. There are effective therapies
for many causes of PD sleep disturbance and rapid
identification of the specific nature of disturbance could speed
beneficial therapy and prevent disability.
Methods to assess sleep quality have been offered in
numerous forms including commercial activity, biometric, and
sleep actigraphy monitors. The simplest form of sleep
monitoring is a well established wearable wrist monitor using
triaxial accelerometry, with movements interpreted using
simple algorithms [40]. In PD patients this also works
reasonably well when compared to the gold standard of
polysomnography in a sleep laboratory, but some of the
measures such as time for sleep onset are complicated by the
disease and scoring algorithms need further work [41].
Inclusion of additional sensor data such as heart rate, skin
conductance, and skin temperature could be expected to
improve sleep assessments, including perhaps isolation of
important phases of sleep (e.g., slow wave sleep; REM sleep).
For example, a simple wearable device that distinguishes
REM sleep with some accuracy would be an important
advance in assessment of REM Sleep Behavior Disorder
(RBD) which occurs in one third of PD patients and is an early
predictive symptom for PD [83].
Another aspect of sleep quality involves large body
movements, measured with instrumented beds or with
accelerometers mounted on the legs or the back [44-46]. In
PD patients compared to healthy controls, smaller and shorter
axial movements are observed but these have not been tied to
any laboratory measures of sleep quality in these studies
[45,46].
Some patients have reported another phenomenon referred
to as “sleep benefit”, where a sleep that is perceived as restful
improves physical symptoms the next day. This effect has
been difficult to establish with questionnaire data and requires
a better practical method of objective quantification of sleep
quality [84].
Sleepiness and sudden sleep onset (“sleep attacks”) have
been reported for some PD patients and this is especially
problematic during driving [85]. Vigiliance monitoring
systems to detect onset of a sleep attack might be beneficial to
PD patients but would require high specificity and rapid
response time; current systems to assess drowsiness may be
inadequate for this purpose.
Identifying poor sleep quality and characterizing other
aspects of the sleep is an important goal for wearable devices
that has not yet been fully achieved but is vitally important for
effective self monitoring. Currently, clinical labs evaluate
characteristics of sleep disorders through electromyographic,
kinemetric, and electroencephalographic measurements
generally involving complex systems. Wearable systems have
been proposed to obtain continuous EEG and manage data
artifacts and these show some promise for the future [86,87].
C. Fatigue - a significant but poorly quantified problem
Fatigue is a separate disabling symptom reported in a
majority of Parkinson’s patients, not necessarily associated
with sleep quality, cognitive impairment, or depression
[10,88,89]. Patients report fatigue as a key limiter in physical
and social functioning [88]. Distinguishing this symptom
from other problems such as daytime sleepiness and
depression through biomonitoring is a key technological
challenge [90]. Novel approaches to unobtrusive detection of
changes in mental state, perhaps including mental fatigue, are
suggested by a recent study that used key-hold times from
normal interactions with a computer keyboard to detect

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
6
psychomotor impairments. These were changes were induced
with testing during night time waking (“sleep inertia”) [91].
D. Mood disorders and psychosis
Depressive mood is associated with lowered activity levels
[50] and disordered sleep [42,29], and there is some evidence
that aspects of mood (depression, anxiety, mania) and
psychotic features (confusion, hallucination, delusion) affect
motor presentation in PD. There is sparse-to-none data on
changes in daily patterns of activity as indicators of depressed
status, yet this seems to be an obvious target for productive
activity-based monitoring research. Combined with other
biological signals such as changes in vocal acoustics, this
could be extraordinarily useful. Changes in speech
characteristics are themselves a symptom of PD motor
changes but specific components have been used to track
depression severity in other patients [54].
Other techniques could evaluate mood and psychosis. Signs
from EEG, ECG, or EMG monitoring have the potential to
assist with identification and may do so in conjunction with
sleep monitoring. One system (iCalm) has explored a
combination of activity, skin conductance, temperature, and
photoplethysmography on wrist and foot to detect changes in
autonomic activity [56]. Another similar system (PSYCHE)
has been tested in bipolar patients to detect mood transitions
including hypomanic and depressive episodes over a course of
treatment [91].
Affect can also be assessed with everyday technologies.
For example, facial expressions in Parkinson’s patients are
often misunderstood because of motor changes affecting facial
muscles (the “Parkinson’s mask”) but an advanced facial
recognition system could conceivably learn its patient in a
webcam application and detect alterations reflecting emotional
changes [80,93,94].
Increasing isolation is another measureable component of
depression. Socialization was monitored in one study by
providing all participants within a network of peers with smart
phone software that detected and recorded proximity to other
software equipped phones, charting frequency of in person
social interactions [43]. In another test of phone-based motion
sensors, developers inadvertently recorded audio data using
the phone’s microphone and analysts evaluated social
interaction using the audio data [95]. The integration of
tracking of broadcast identifiers from 802.11 wifi, Bluetooth,
NFC, or other wireless signature could automate identification
of social interaction through tracking interaction with other
individuals’ devices, tracking frequency and duration of
contact, and a count of unique devices encountered. Many
MAC addresses (wifi or NFC) or numbers (Bluetooth) can be
identified as belonging to a fixed or mobile transmitter (e.g.,
access point or portable client) and in many cases can be
linked to a specific manufacturer, providing more detailed
resolution of social versus infrastructure encounters.
Treatments for depression and anxiety may include
gaming therapies which are being explored for their
effectiveness and lower incidence of side effects compared to
pharmacotherapy [51,52].
E. Mild cognitive impairment and dementia
Many aspects of cognition may be monitored effectively
through gamification of cognitive tests, with set shifting,
memory, and fluency easily tested in engaging ways [96].
Such systems are being developed for a range of
neurocognitive testing applications but could be tailored to
cognitive domains most affected in Parkinson’s, as that
information becomes clearer [97]. Further, activity monitors
may identify erratic behavior patterns characteristic of
executive dysfunction in early cognitive decline and may
compliment cognitive testing or provide insight if the
frequency of dedicated cognitive self-monitoring declines.
Specific types of activities that might be built into an
engaging test system could include simple measures such as
finger tapping. Finger tapping has recently been defined with
29 subtest parameters which can now be characterized in
studies with Parkinson’s patients to define aspects of cognition
and motor function [98]. Impaired driving ability in
Parkinson’s is explained in part by cognitive decline [99].
This can be tested with driving simulations although PD
patients with current licenses are not likely to volunteer to
have their driving assessed in research studies [100]. Driver
assistance systems with warning information about speeds and
following distances improved traffic performance of PD
patients and demonstrate the importance of simple assistive
technologies for safer driving [101].
Monitoring of ambient audio could track verbal fluency
(speech rate) and speaking levels (e.g., polysyllabic words,
sentence structures) to establish baseline and track change in
these markers for cognitive status. Speech content changes
over long duration distinguish declining mental status for
President Reagan compared to President Bush during their
terms in office [102]. Similar evaluations could be conducted
through monitoring the frequency and characteristics of
electronic communications, including e-mail, phone calls, and
online social networking.
Remembering to follow the usually complicated
medication regimes can be a problem in PD. Simple timed
reminders are helpful. Actual detection of pill intake with
individual edible bar codes or other microtags is a feasible
technology that could provide additional help to patients.
IV. BIG DATA STUDIES TECHNOLOGY
A. Previous and current initiatives
Data collected through the approaches identified in section
III will rapidly achieve a scale putting it into the domain of
“big data,” which in this context would suggest very large N
studies with high enough sampling rates as to be considered
effectively continuous. Note that this does not preclude the
huge importance of small sample studies that can identify
large individual effects.
The standard for large dataset studies in neuroscience
was set by the Alzheimer’s Disease Neuroimaging Initiative
(ADNI) [103,104]. This study of 800 subjects collected
longitudinal clinical, genetic, and diverse imaging data from
individuals with Alzheimer’s disease and controls. The ADNI

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
7
has been successful in identifying an imaging biomarker for
Alzheimer’s. The FDA’s tentative but positive-leaning
response has inspired researchers in other diseases to consider
replicating the ADNI approach for the identification of
biomarkers. The ADNI model of public data sharing inspired
the Michael J. Fox Foundation to launch the Parkinson’s
Progression Marker Initiative (PPMI)(http://www.ppmi-
info.org/) [105]. This was also based, in part, on proof of
feasibility in the establishment of an enriched cohort to
identify premotor (prodromal) biomarkers of PD in the Army-
funded Parkinson Associated Risk Syndrome Study
(PARS)[106]. The PPMI, with a cohort expanded beyond the
original 600 PPMI cases and controls, is being supplemented
with body-fixed sensor data.
A different approach builds on a quality improvement
model pioneered by the Northern New England
Cardiovascular Study Group [107] and improved upon in
cystic fibrosis [108]. Using this experimental design, the
National Parkinson Foundation (NPF) launched the
Parkinson’s Outcomes Project (POP). This study is focused
on patient reported outcomes and their clinical care, with the
express purpose of optimizing care [109]. The POP study also
includes mobility as an outcome and has collected data on
subjects using body-fixed sensors [110]. POP, with
approximately 8,000 subjects and 20,000 clinical evaluations,
is the largest clinical study of Parkinson’s disease ever
conducted. With comprehensive clinical characterization,
these studies offer a different set of benefits from the addition
of monitoring technology. Split sample approaches with a
validation dataset held back enable analyses with reduced risk
of spurious findings [111].
A third initiative in Parkinson’s tests the value of wearable
self monitoring devices in improving quality of life for
patients (https://www.michaeljfox.org/). This involves a
collaboration between Intel and Michael J. Fox Foundation.
With patient consent, the data are being aggregated to
compare the device data to patient diaries, medication use, and
clinical observations. The device tested provides 24 hour
measurements of activity but also estimates of sleep quality.
The large volume of data (300 observations/s from each
patient) is managed through a big data analytics cloud
infrastructure at Intel with real time detection of patient status.
Such large scale assessment of free living patients using
wearable monitoring could revolutionize clinical trials. More
importantly, self monitoring technologies could empower
patients to more effectively manage their own healthcare.
Finally, this concept has been extended into the open source
concept in research through Apple’s Research Kit, announced
in March 2015. Research Kit is described as a “software
framework made specifically for medical research” by
providing access to sensors in the iPhone and other Apple
devices [112]. It is too early to determine the success of this
effort which will reflect skew due to (unquantified)
availability bias. Apple’s Research Kit is being utilized in the
mPower tool [113].
B. Importance of frequency-space information
While machine learning will enable new insight to be drawn
from the large studies such as PPMI and POP, their low
frequency of data collection will limit insight into higher
frequency events, signs, and symptoms. Patient data reflects
several frequency-space domains, ranging from falls, which
include delta function-like spikes as ground contact results in
rapid deceleration, through tremor, dyskinesia, and medication
effects to disease progression which is measured on scale of
years (Table 2). TABLE 2
CHARACTERISTIC PERIODS OF SEVERAL FEATURES OF PD
Feature Characteristic Period
Falls
Tremor
Dykinesia
Medication effects
Sleep/fatigue
Hospitalization
Depression
Psychosis
Disease progression
Instantaneous to 1 second
0.25-0.5 seconds
1 second
2-4 hours
1 day
Several days
Months
1-2 years to develop
Years
Continuous data collection from sensors could record these
key events and track motor and other information to
extrapolate the rate of change in features with different
characteristic periods. Such approaches could dramatically
increase the insight available from studies such as PPMI and
POP, identifying some features and tracking change in other
features that are identified through clinical evaluation or
testing. Although currently no kinemetric biomarkers are
available to track many features, a Fourier-transform
approach, analyzing continuous data or a frequency-level
analysis of discontinuous data could be valuable in identifying
to-date unknown associations between monitoring data and
clinically-identified symptoms.
C. Challenges and technology needs
In large-scale characterization studies such as these “big
data” studies, clinical motion data should be collected with
minimal filtering, as the frequency-space associations with PD
features are insufficiently established. A critical need is the
better characterization of these relationships. Key technology
questions are:
How can we address issues of data compression and
power requirements to create more usable sensors that still
provide a sufficient level of resolution to address patient
monitoring needs?
How effectively can unilateral measurement characterize
bilateral symptoms? Are asymmetric features different in the
frequency space depending on position of sensor?
Increasing evidence suggests that motor control
compensation in the forebrain may result in different motor
characteristics. Could frequency-space motor measurement
identify specific pathology?
A recent analysis has shown that not just medication

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
8
effects but differences in effect between medications may be
identifiable through sensitive motor measurement. Can this be
delivered at scale?
How do we organize data flow so that patients have their
desired level of privacy and security controls?
What is the business model that will encourage device
manufacturers to provide raw data, perhaps through an open
API, to access an evolving set of algorithms?
How do we effectively manage genome data for
personalized data interpretation?
V. CONCLUSIONS AND BROAD IMPLICATIONS
Parkinson’s patients want to be involved in decisions about
them. Monitoring technologies can help arm PD patients to
take greater responsibility in their own health care and quality
of life. They may also choose to share these data with health
care providers, especially remotely through emerging
telemedicine capabilities, and this will enable clinicians to
provide better care targeting the specific needs of their
individual patients. The science that can drive development of
important monitoring and other assistive technologies in PD
already largely exists today and is simply waiting for clever
engineering technologists to harness and apply to the right
problems. This paper has outlined the patient perspective
which includes a focus on the often overlooked nonmotor
symptoms and problems. Many of these problems can be
tracked using noninvasive technologies that have been
developed to address each specific symptom (e.g., depressed
mood, inadequate restorative sleep, impaired cognition, etc)
but a combined differential assessment of these various
problems in a single relevant disease (Parkinson’s) has not
been undertaken. The patient community will readily provide
feedback on the desirable features of such a monitoring device
if it is developed and, for the first time, the research
community will be able to access data on free living
populations to address earlier detection and effectiveness and
complications of treatment interventions.
DISCLAIMERS
The opinions and assertions in this paper are those of the
authors and do not necessarily represent the official views or
policies of their institutions. Mention of any specific
commercial products, process, or service by trade name,
trademark, manufacturer, or otherwise does not necessarily
constitute or imply its endorsement, recommendation, or
favoring by the authors or the organizations they represent.
REFERENCES
[1] W. Churchill, The World Crisis, v. 4, p. 192, 1923.
[2] H. Ehringer and O. “Hornykiewicz. Verteilung von Noradrenalin und Dopamin (3-Hydroxytyramin) im Gehirn des Menschen und ihr
Verhalten bei Erkrankungen des extrapyramidalen Systems.” Klinische
Wochenschrift, vol. 38, pp. 1236-1239, 1960. [3] G.C. Cotzias, P.S. Papavasiliou, and R. Gellene. “Modification of
Parkinsonism—chronic treatment with L-dopa.” N Engl J Med, vol.
280, pp. 337-345, 1969.
[4] A.Y. Hung and M.A. Schwarzschild. “Treatment of Parkinson’s
Disease: What’s in the Non-dopaminergic Pipeline?” Neurotherapeutics,
vol. 11, pp. 34-46, 2014.
[5] M.R. Lemke, H.M. Brecht, J. Koester, P.H. Kraus, and H. Reichmann.
“Anhedonia, depression, and motor functioning in Parkinson’s disease during treatment with pramipexole.” J Neuropsychiat, vol. 17, pp. 214-
220, 2005.
[6] P. Wicks, J. Stamford, M.A. Grootenhuis, L. Haverman, and S. Ahmed. “Innovations in e-health.” Qual Life Res, vol. 23, pp. 195-203, 2014.
[7] K.R. Chaudhuri, D.G. Healy, and A.H..V. Schapira. “Non-motor
symptoms of Parkinson's disease: diagnosis and management.” The Lancet Neurology, vol. 5, pp. 235-245, 2006.
[8] M.A. Achey, C.A. Beck, D.B. Beran, et al. “Virtual house calls for
Parkinson disease (Connect.Parkinson): study protocol for a randomized, controlled trial.” Trials, vol. 15, 465 (13 pp), 2014.
[9] M.A. Achey, J.L. Aldred, N. Aljehani, et al. “The past, present, and
future of telemedicine for Parkinson's disease.” Mov Disord, vol. 29, pp. 871-883, 2014.
[10] P. Martinez-Martin, C. Rodriguez‐Blazquez, M.M. Kurtis, and K.
Chaudhuri. “The impact of non‐motor symptoms on health‐related quality of life of patients with Parkinson's disease.” Mov Disord, vol. 26,
pp. 399-406, 2011.
[11] K.R. Chaudhuri, P. Odin, A. Antonini, P. Martinez-Martin. “Parkinson’s disease: the non-motor issues.” Parkinsonism Relat Disord, vol. 17, pp.
717-723, 2011.
[12] M. Samuel, M. Rodriguez‐Oroz, A. Antonini, et al. “Management of
impulse control disorders in Parkinson's disease: Controversies and future approaches.” Mov Disord, vol. 30, pp. 150-159, 2015.
[13] Movement Disorder Society Task Force on Rating Scales for
Parkinson's Disease. “The Unified Parkinson's Disease Rating Scale (UPDRS): status and recommendations.” Mov Disord, vol. 18, p. 738,
2003.
[14] V. Peto, C. Jenkinson, and R. Fitzpatrick. “PDQ-39: a review of the development, validation and application of a Parkinson’s disease quality
of life questionnaire and its associated measures.” J Neurol, vol. 245,
pp. S10-S14, 1998. [15] J.M. Miyasaki, J. Long, D. Mancini, et al. “Palliative care for advanced
Parkinson disease: an interdisciplinary clinic and new scale, the ESAS-
PD.” Parkinsonism Relat Disord, vol. 18, pp. S6-S9, 2012. [16] A. Hassan, S.S. Wu, P. Schmidt, I.A. Malaty, Y.F. Dai, J.M. Miyasaki,
and M.S. Okun. “What are the issues facing Parkinson's disease patients
at ten years of disease and beyond?: Data from the NPF-QII study.” Parkinsonism Relat Disord, vol. 18, pp. S10-S14, 2012.
[17] U. Wüllner, T. Schmitz‐Hübsch, G. Antony, et al. “Autonomic dysfunction in 3414 Parkinson's disease patients enrolled in the German
Network on Parkinson's disease (KNP eV): the effect of ageing.” Eur J Neurol, vol. 14, pp. 1405-1408, 2007.
[18] D. Bega, S.S. Wu, Q. Pei, P.N. Schmidt, and T. Simuni. “Recognition
and Treatment of Depressive Symptoms in Parkinson's Disease: The NPF Dataset.” J Parkinson's Dis, vol. 4, pp. 639-643, 2014.
[19] J.A. Cramer, R.D. Scheyer, R.H. Mattson. “Compliance declines
between clinic visits.” Arch Intern Med, vol. 150, pp. 1509-1510, 1990. [20] V. Venkataraman, S.J. Donohue, K.M. Biglan, P. Wicks, and E. R.
Dorsey. “Virtual visits for Parkinson disease A case series.” Neurology:
Clin Prac, vol. 4, pp. 146-152, 2014. [21] J.P. Hubble, R. Pahwa, D.K. Michalek, C. Thomas, and W.C. Koller.
“Interactive video conferencing: a means of providing interim care to
Parkinson's disease patients.” Mov Disord, vol. 8, pp. 380-382, 1993. [22] E.R. Dorsey, V. Venkataraman, M.J. Grana, et al. “Randomized
controlled clinical trial of “virtual house calls” for Parkinson disease.”
JAMA Neurol, vol. 70, pp. 565-570, 2013. [23] A. Abdolahi, N. Scoglio, A. Killoran, E.R. Dorsey, and K.M. Biglan.
“Potential reliability and validity of a modified version of the unified
Parkinson's disease rating scale that could be administered remotely.” Parkinsonism Relat Disord, vol. 19, pp. 218-221, 2013.
[24] E.M. Hunkeler, W.A. Hargreaves, B. Fireman, et al. “A web-delivered
care management and patient self-management program for recurrent depression: a randomized trial.” Psychiatr Services, vol. 63, pp. 1063-
1071, 2012.
[25] S. Chowdhury, C.C. Meunier, L. Cappelletti and T.B Sherer. “Improving patient participation in Parkinson’s clinical trials: the
experience of the Michael J Fox Foundation.” Clin Invest, vol 4, pp.
185-192, 2014.

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
9
[26] A. Pathak, J.A. Redmond, M. Allen, and K.L. Chou. “A noninvasive
handheld assistive device to accommodate essential tremor: A pilot
study.” Mov Disord, vol. 29, pp. 838-842, 2014.
[27] T. Keränen and S. Liikkanen. “Medication reminder service for mobile
phones: An open feasibility study in patients with Parkinson's disease.” Telemed e-Health vol. 19, pp. 888-890, 2013.
[28] S. Das, B. Amoedo, F. De la Torre, J. Hodgins. “Detecting Parkinsons’
symptoms in uncontrolled home environments: a multiple instance learning approach.” 34th Annual Int Conf IEEE EMBS, San Diego, CA.
Pp. 3688-3691, 2012.
[29] N.J. Weerkamp, G. Tissingh, P.J.E. Poels, S.U. Zuidema, M.Munneke, R.T.C.M. Koopmans, and B.R. Bloem. “Nonmotor symptoms in nursing
home residents with Parkinson's disease: prevalence and effect on
quality of life.” J Am Geriatr Soc, vol. 61, pp. 1714-1721, 2013. [30] D.A. Gallagher, A.J. Lees, and A. Schrag. “What are the most important
nonmotor symptoms in patients with Parkinson's disease and are we
missing them?” Mov Disord, vol. 25, pp. 2493-2500, 2010. [31] E. Fuster-Garcia, A. Bresó, J. Martínez-Miranda, J. Rosell-Ferrer, C.
Matheson, and J.M. García-Gómez. “Fusing actigraphy signals for
outpatient monitoring.” Information Fusion, vol. 23, pp. 69-80, 2015. [32] J. Cancela, M. Pastorino, A.T. Tzallas, M.G. Tsipouras, G. Rigas, M.T.
Arredondo, and D.I. Fotiadis. “Wearability assessment of a wearable
system for Parkinson’s Disease remote monitoring based on a body area network of sensors.” Sensors, v. 14, pp. 17235-17255, 2014.
[33] W. Maetzler, J. Domingos, K. Srulijes, J.J. Ferreira, and B.R. Bloem.
“Quantitative wearable sensors for objective assessment of Parkinson's disease.” Mov Disord, vol. 28, pp. 1628-1637. 2013.
[34] S. Patel, H. Park, P. Bonato, L. Chan, and M. Rodgers. “A review of wearable sensors and systems with application in rehabilitation.” J
Neuroengineer Rehabil, vol. 9, pp. 21, 2012.
[35] M.L. Dontje, M.H.G. de Greef, A.D. Speelman, et al. “Quantifying daily physical activity and determinants in sedentary patients with Parkinson's
disease.” Parkinsonism Related Disord, vol. 19, pp. 878-882, 2013.
[36] M. van Nimwegen, A.D. Speelman, K. Smulders, et al. “Design and
baseline characteristics of the ParkFit study, a randomized controlled
trial evaluating the effectiveness of a multifaceted behavioral program to
increase physical activity in Parkinson patients.” BMC neurology, vol. 10, pp. 70, 2010.
[37] A.D. Speelman, M. van Nimwegen, B.R. Bloem, M. Munneke.
“Evaluation of implementation of the ParkFit program: A multifaceted intervention aimed to promote physical activity in patients with
Parkinson's disease.” Physiotherapy, vol. 100, pp. 134-141, 2014.
[38] J.T. Cavanaugh, T.D. Ellis, G.M. Earhart, M.P. Ford, K.B. Foreman, and L.E. Dibble. “Capturing Ambulatory Activity Decline in Parkinson
Disease.” J Neurologic Physical Ther, vol. 36, pp. 51, 2012.
[39] K.R. Evenson, F. Wen, J.S. Metzger, and A.H. Herring. “Physical activity and sedentary behavior patterns using accelerometry from a
national sample of United States adults.” Int J Behav Nutr Phys Act, vol.
12, pp. 20, 2015. [40] S. Ancoli-Israel, R. Cole, C. Alessi, M. Chambers, W. Moorcroft, C.
Pollak. “The role of actigraphy in the study of sleep and circadian
rhythms. American Academy of Sleep Medicine Review Paper.” Sleep, vol. 26, pp. 342-392, 2003.
[41] J. Maglione, L. Liu, A.B. Neikrug, T. Poon, et al. "Actigraphy for the
Assessment of Sleep Measures in Parkinson's Disease." Sleep, vol. 36, pp. 1209-1217, 2013.
[42] G. Jean–Louis, M.V. Mendlowicz, J.C. Gillin, et al. “Sleep estimation
from wrist activity in patients with major depression.” Physiol Behav, vol. 70, pp. 49-53, 2010.
[43] M. Butt, T.B.M.J. Ouarda, S.F. Quan, A.S. Pentland, and I. Khayal.
“Technologically sensed social exposure related to slow-wave sleep in healthy adults.” Sleep Breath, vol. 19, pp. 255-261, 2015.
[44] A.M. Adami, M. Pavel, T.L. Hayes, A.G. Adami, C. Singer. “A method
for classification of movements in bed.” In Engineering in Medicine and Biology Society, EMBC, 2011 Annual International Conference of
the IEEE, pp. 7881-7884. IEEE, 2011.
[45] M Louter, R.J.G. van Sloun, D.A.A. Pevernagie, J.B.A.M. Arends, P.J. Cluitmans, B.R. Bloem, and S. Overeem. “Subjectively impaired bed
mobility in Parkinson disease affects sleep efficiency.” Sleep Med, vol.
14, pp. 668-674, 2013. [46] M. Louter, W. Maetzler, J. Prinzen, et al. “Accelerometer-based
quantitative analysis of axial nocturnal movements differentiates patients
with Parkinson's disease, but not high-risk individuals, from controls.” J Neurol Neurosurg Psychiatr, vol. 86, pp. 32-37, 2015.
[47] D.T. Plante. “Leg actigraphy to quantify periodic limb movements of
sleep: A systematic review and meta-analysis.” Sleep Med Rev, vol. 18,
pp. 425-434, 2014.
[48] J.I. Hoff, J.J. Van Hilten, H.A.M. Middelkoop, and R.A.C. Roos.
“Fatigue in Parkinson's disease is not associated with reduced physical activity.” Parkinsonism Relat Disord, vol. 3, pp. 51-54, 1997.
[49] A. Korszun, E.A. Young, N.C. Engleberg, C.B. Brucksch, J.F. Greden,
and L.A. Crofford. “Use of actigraphy for monitoring sleep and activity levels in patients with fibromyalgia and depression.” J Psychosom Res,
vol. 52, pp. 439-443, 2002.
[50] J. Kim, T. Nakamura, H. Kikuchi, T. Sasaki, and Y. Yamamoto. “Co-variation of depressive mood and locomotor dynamics evaluated by
ecological momentary assessment in healthy humans.” PloS One, vol. 8,
pp. e74979, 2013. [51] C.V. Russoniello, K. O’Brien, and J.M. Parks. “EEG, HRV and
psychological correlates while playing Bejeweled II: A randomized
controlled study.” Stud Health Technol Inform, vol. 144, pp. 189-92, 2009.
[52] C.V. Russoniello, M. Fish, K. O'Brien. “The efficacy of casual
videogame play in reducing clinical depression: A randomized controlled study.” Games for Health, vol. 2, pp. 341-346, 2013.
[53] A.A. Rizzo, B. Lange, J. G. Buckwalter, et al. “An intelligent virtual
human system for providing healthcare information and support.” Studies Health Technol Informatics, vol. 163, pp. 503, 2011.
[54] J.C. Mundt, A.P. Vogel, D.E. Feltner, and W.R. Lenderking. “Vocal
acoustic biomarkers of depression severity and treatment response.” Biol Psychiatr, vol. 72, pp. 580-587, 2012.
[55] G. Valenza, M. Nardelli, A. Lanata, C. Gentili, G. Bertschy, R. Paradiso, and E.P. Scilingo. “Wearable monitoring for mood recognition in
bipolar disorder based on history-dependent long-term heart rate
variability analysis.” IEEE J Biomed Health Inform, vol. 18, pp. 1625-1635, 2014.
[56] R.R. Fletcher, K. Dobson, M.S. Goodwin, et al. “iCalm: Wearable
sensor and network architecture for wirelessly communicating and
logging autonomic activity.” IEEE Trans Inform Technol Biomed, vol.
14, pp. 215-223, 2010.
[57] D.F. Mahoney, R.B. Purtilo, F.M. Webbe, et al. “In-home monitoring of persons with dementia: Ethical guidelines for technology research and
development.” Alz Dementia, vol. 3, pp. 217-226, 2007.
[58] K. Bousmalis, S. Zafeiriou, L. Morency, and M. Pantic. “Infinite hidden conditional random fields for human behavior analysis.” IEEE Trans
Neural Networks Learning Sys, vol. 24, pp. 170-177, 2013.
[59] M. Chatterjee, G. Stratou, S. Scherer, and L.P. Morency. “Context-based signal descriptors of heart-rate variability for anxiety assessment.” IEEE
Int Conf Acoust, Speech Signal Processing, pp. 3631-3635, 2014.
[60] S. Park, P. Shoemark, and L.P. Morency. “Toward crowdsourcing micro-level behavior annotations: the challenges of interface, training,
and generalization.” Proc 19th Int Conf Intelligent User Interfaces, pp.
37-46, 2014. [61] B.E. Fisher, Q. Li, A. Nacca, et al. “Treadmill exercise elevates striatal
dopamine D2 receptor binding potential in patients with early
Parkinson’s disease.” Neuroreport, vol. 24, pp. 509-514, 2013. [62] G. Frazzitta, P. Balbi, R. Maestri, G. Bertotti, N. Boveri, G. Pezzoli.
“The beneficial role of intensive exercise on Parkinson disease
progression.” Am J Phys Med Rehabil, vol. 92,pp. 523-532, 2013. [63] G. Frazzitta, R. Maestri, M.F. Ghilardi, et al. “Intensive Rehabilitation
Increases BDNF Serum Levels in Parkinsonian Patients.” Neurorehab
Neural Repair, vol. 28,pp. 163-168, 2014. [64] G.M. Petzinger, B.E. Fisher, S. McEwen, J.A. Beeler, J.P. Walsh, M.W.
Jakowec. “Exercise-enhanced neuroplasticity targeting motor and
cognitive circuitry in Parkinson's disease.” The Lancet Neurology, vol. 12, pp. 716-726. 2013.
[65] J.E. Ahlskog. “Does vigorous exercise have a neuroprotective effect in
Parkinson disease?” Neurology, vol. 77, pp. 288-294, 2011. [66] A.D. Speelman, B.P. van de Warrenburg, M. van Nimwegen, G.M.
Petzinger, M. Munneke, B.R. Bloem. “How might physical activity
benefit patients with Parkinson disease?” Nature Reviews Neurology, vol. 7, pp. 528-534, 2011.
[67] Y. Yang, X.Y. Li, L. Gong, Y.L. Zhu, and Y.L. Hao. “Tai chi for
improvement of motor function, balance and gait in Parkinson's disease: a systematic review and meta-analysis.” PloS One, vol. 9, e102942,
2014.
[68] C. Fox, G. Ebersbach, L. Ramig, and S. Sapir. “LSVT LOUD and LSVT BIG: behavioral treatment programs for speech and body movement in

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
10
Parkinson disease.” Parkinson’s Dis, vol. 2012, 12 pp,
http://dx.doi.org.ezproxy.nihlibrary.nih.gov /10.1155/2012/391946.
[69] G. Ebersbach, A. Ebersbach, F. Gandor, B. Wegner, J. Wissel, and A.
Kupsch. “Impact of Physical Exercise on Reaction Time in Patients
With Parkinson's Disease—Data From the Berlin BIG Study.” Arch Phys Med Rehabil, vol. 95, pp. 996-999, 2014.
[70] D. Conradsson, N. Löfgren, H. Nero, M. Hagströmer, A. Ståhle, J. Lökk,
and E. Franzén. “The Effects of Highly Challenging Balance Training in Elderly With Parkinson’s Disease A Randomized Controlled Trial.”
Neurorehabil Neural Repair, 1545968314567150, 2015.
[71] C.J.M. Ayan, A. Cancela, A. Gutiérrez-Santiago, and I. Prieto. “Effects of two different exercise programs on gait parameters in individuals with
Parkinson's disease: a pilot study.” Gait Posture, vol. 39, pp. 648-651,
2014. [72] T. Ellis, J.K. Boudreau, T.R. DeAngelis, et al. “Barriers to exercise in
people with Parkinson disease.” Phys Therapy, vol. 93, pp. 628-636,
2013. [73] G.B. Spurr, A.M. Prentice, P.R. Murgatroyd, G.R. Goldberg, J.C. Reina,
N.T. Christman. “Energy expenditure from minute-by-minute heart-rate
recording: comparison with indirect calorimetry.” Am J Clin Nutr, vol. 48, pp. 552-559. 1988.
[74] S. Brage, N. Brage, P.W. Franks, et al. “Branched equation modeling of
simultaneous accelerometry and heart rate monitoring improves estimate of directly measured physical activity energy expenditure.” J Appl
Physiol, vol. 96, pp. 343-351, 2004.
[75] R.W. Hoyt, M.J. Buller, W.R. Santee, M. Yokota, P.G. Weyand, and J.P. Delany. “Total energy expenditure estimated using foot-ground contact
pedometry.” Diab Technol Therapeutics, vol. 6, pp. 71-81, 2004. [76] M.D. Lewek, R. Poole, J. Johnson, O. Halawa, and X. Huang. “Arm
swing magnitude and asymmetry during gait in the early stages of
Parkinson's disease.” Gait Posture, vol. 31, pp. 256-260, 2010. [77] H. Chen, S.M. Zhang, M.A. Schwarzschild, M.A. Hernan, A. Ascherio.
“Physical activity and the risk of Parkinson disease.” Neurology, vol. 64,
pp. 664-669, 2005.
[78] F. Ofli, G. Kurillo, S. Obdrzalek, R. Bajcsy, H. Jimison, M. Pavel,
“Design and evaluation of an interactive exercise coaching system for
older adults: lessons learned.” IEEE J Biomed Health Informatics, in press, 2015, DOI 10.1109/JBHI.2015.2391671.
[79] A.A. Rizzo, B. Lange, J. G. Buckwalter, et al. “An intelligent virtual
human system for providing healthcare information and support.” Stud Health Technol Informatics vol. 163, pp. 503-509, 2010.
[80] J. Gratch, N. Wang, A. Okhmatovskaia, F. Lamothe, M. Morales, R.J.
van der Werf, and L.P. Morency. “Can virtual humans be more engaging than real ones?” In, Human-Computer Interaction. HCI Intelligent
Multimodal Interaction Environments, pp. 286-297. Springer Berlin
Heidelberg, 2007. [81] S. Paus, H.M. Brecht, J. Köster, G. Seeger, T. Klockgether, and U.
Wüllner. “Sleep attacks, daytime sleepiness, and dopamine agonists in
Parkinson's disease.” Mov Disord, vol. 18, pp. 659-667, 2003.
[82] U. Wüllner, T. Schmitz‐Hübsch, G. Antony, et al. “Autonomic
dysfunction in 3414 Parkinson's disease patients enrolled in the German Network on Parkinson's disease (KNP eV): the effect of ageing.” Eur J
Neurol, vol. 14, pp. 1405-1408, 2007. [83] C.H. Schenck, J. Y. Montplaisir, B. Frauscher, et al. “Rapid eye
movement sleep behavior disorder: devising controlled active treatment
studies for symptomatic and neuroprotective therapy—a consensus statement from the International Rapid Eye Movement Sleep Behavior
Disorder Study Group.” Sleep Med, vol. 14, pp. 795-806, 2013.
[84] M.M. van Gilst, M. Louter, C.R. Baumann, B.R. Bloem, and S. Overeem. “Sleep benefit in Parkinson's disease: time to revive an
enigma?” J Parkinson's Dis, vol. 2, pp. 167-170, 2012.
[85] C. Meindorfner, Y. Körner, J.C. Möller, K. Stiasny‐Kolster, W.H. Oertel, H.P. Krüger. “Driving in Parkinson's disease: mobility,
accidents, and sudden onset of sleep at the wheel.” Mov Disord, vol. 20, pp. 832-842, 2005.
[86] A.J. Casson, D. Yates, S. Smith, J.S. Duncan, and E. Rodriguez-
Villegas. “Wearable electroencephalography.” IEEE Engineer Med Biol Mag, vol. 29, pp. 44-56, 2010.
[87] V. Mihajlovic, B. Grundlehner, R. Vullers, and J. Penders. “Wearable,
Wireless EEG Solutions in Daily Life Applications: What are we Missing?” IEEE J Biomed Health Informatics, vol. 19, pp. 6, 2015.
[88] K. Herlofson and J.P. Larsen. “The influence of fatigue on health-
related quality of life in patients with Parkinson’s disease.” Acta Neurol Scand, v. 107, pp. 1-6, 2003.
[89] M. Amboni, G. Santangelo, P. Barone. “Depression, Apathy,
Anhedonia, and Fatigue in Parkinson’s Disease.” In, Neuropsychiatric Symptoms of Mov Disord, pp. 1-28. Springer Publ, 2015.
[90] W.J. Kop, A. Lyden, A.A. Berlin, et al. “Ambulatory monitoring of
physical activity and symptoms in fibromyalgia and chronic fatigue syndrome.” Arthritis Rheum, vol. 52, pp. 296-303, 2005.
[91] L. Giancardo, A. Sanchez-Ferro, I. Butterworth, C.S. Mendoza, J.M.
Hooker. Psychomotor impairment detection via finger interactions with a computer keyboard during natural typing. Sci Reports, vol. 5, article
no. 9678, 2015.
[92] A. Lanata, G. Valenza, M. Nardelli, C. Gentili, and E.P. Scilingo, “Complexity index from a personalized wearable monitoring system for
assessing remission in mental health.” IEEE J Biomed Health
Informatics, v. 19, pp. 132-139, 2015. [93] T. Baltrusaitis, D. McDuff, N. Banda, M. Mahmoud, R. El Kaliouby, P.
Robinson, and R. Picard. “Real-time inference of mental states from
facial expressions and upper body gestures.” IEEE Int Conf Automatic Face & Gesture Recognition and Workshops, pp. 909-914, 2011.
[94] T. Baltrusaitis, P. Robinson, L. Morency. “3D constrained local model
for rigid and non-rigid facial tracking.” In, IEEE Conf Computer Vision and Pattern Recognition, pp. 2610-2617, 2012.
[95] J. Liddle, D. Ireland, S.J. McBride, et al. “Measuring the lifespace of
people with Parkinson’s disease using smartphones: proof of principle.” JMIR mHealth uHealth, vol. 2, 2014.
[96] S. Hagler. “Computational modeling of cognitive processes for
continuous in-home assessment of cognitive performance.” PhD Dissertation, Oregon Health and Science University. Scholar Archive.
Paper 3559, 2014. http://digitalcommons.ohsu.edu/etd/3559 [97] M. Balzer-Geldsetzer, A. S. Costa, M. Kronenbürger, et al. “Parkinson's
disease and dementia: a longitudinal study (DEMPARK).”
Neuroepidemiology, vol. 37, pp. 168, 2011. [98] D. Austin, J. McNames, K. Klein, H. Jimison, and M. Pavel. “A
Statistical Characterization of the Finger Tapping Test: Modeling,
Estimation, and Applications.” IEEE J Biomed Health Inform, in press, 2015.
[99] A.M. Crizzle, A.M. Myers, E.A. Roy, and Q.J. Almeida. “Drivers with
Parkinson’s disease: are the symptoms of PD associated with restricted driving practices?” J Neurol, vol. 260, pp. 2562-2568, 2013.
[100] A.M. Crizzle, A.M. Myers, and Q.J. Almeida. “Drivers with parkinson's
disease: Who participates in research studies?” Parkinsonism Relat Disord, vol. 18, pp. 833-836, 2012.
[101] M. Dotzauer, S.R. Caljouw, D. De Waard, and W.H. Brouwer. “Longer-
term effects of ADAS use on speed and headway control in drivers diagnosed with Parkinson's disease.” Traffic Injury Prev, vol. 16, pp. 10-
16, 2015.
[102] V. Berisha, S. Wang, A. LaCross, and J. Liss. “Tracking Discourse Complexity Preceding Alzheimer's Disease Diagnosis: A Case Study
Comparing the Press Conferences of Presidents Ronald Reagan and
George Herbert Walker Bush.” J Alz Dis, vol. 45, pp. 959-963, 2015. [103] S.G. Mueller, M.W. Weiner, L.J. Thal, et al. “Ways towards an early
diagnosis in Alzheimer’s disease: The Alzheimer’s Disease
Neuroimaging Initiative.” Alzheimers Dement, vol. 1, pp. 55-66, 2005. [104] G. Miller. “Alzheimer's biomarker initiative hits its stride.” Science, vol.
326, pp. 386-389, 2009.
[105] K. Marek, D. Jennings, S. Lasch, et al. “The Parkinson Progression Marker Initiative (PPMI).” Prog Neurobiol, vol. 95, pp. 629-635, 2011.
[106] D. Jennings, A. Siderowf, M. Stern, J. Seibyl, S. Eberly, D. Oakes, K.
Marek, and the PARS Investigators. “Imaging prodromal Parkinson disease: the Parkinson Associated Risk Syndrome Study.” Neurology,
vol. 4, pp. 1739-46, 2014.
[107] G.T. O'Connor, S.K. Plume, E.M. Olmstead, et al. “A regional prospective study of in-hospital mortality associated with coronary
artery bypass grafting. The Northern New England Cardiovascular
Disease Study Group.” JAMA vol. 266, pp. 803-809, 1991. [108] A. Gawande. “The Bell Curve.” The New Yorker, 6 December 2004.
[109] M.S. Okun, et al. “Piloting the NPF data-driven quality improvement
initiative.” Parkinson’s Related Disorders, vol. 16, pp. 517-521, 2011. [110] P. Schmidt, E.C. Nelson, M. Guttman et al. “The analysis of the use of
kinemetric devices to predict outcomes: Results from NPF-QII”
Movement Disorders Society Annual Congress, 2015 (In press.) [111] S. Young, S. Stanley, and A. Karr. “Deming, data and observational
studies.” Significance, vol. 8, pp. 116-120, 2011.
[112] Apple. https://developer.apple.com/researchkit/ Accessed: 1 July 2015. [113] S.H. Friend, et al. http://parkinsonmpower.org/ Accessed: 1 July 2015.

2168-2194 (c) 2015 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission. Seehttp://www.ieee.org/publications_standards/publications/rights/index.html for more information.
This article has been accepted for publication in a future issue of this journal, but has not been fully edited. Content may change prior to final publication. Citation information: DOI10.1109/JBHI.2015.2464354, IEEE Journal of Biomedical and Health Informatics
JBHI-00260-2015-R2
11
Jonathan A. Stamford DSc is a
neuroscientist with a double interest in
Parkinson's.
He took a BSc in pharmacology from
the University of Bath (1980). Following
a doctoral thesis on the neurophysiology
of the dopaminergic forebrain (London
Hospital Medical College), and
postdoctoral experience in the UK (LHMC) and USA (Indiana
University and University of California, Riverside), he headed
a research lab (Royal London Hospital) for more than a
decade looking at the effects of drugs on brain dopamine
systems with particular reference to Parkinson's. He was the
author of three academic books and over 200 research
publications and communications.
He was also diagnosed with Parkinson's in 2006 and, since
2011 has been strongly involved in patient advocacy. He
currently works for The Cure Parkinson's Trust and is a
director and co-founder of Parkinson's Movement, a global
patient advocacy collective. He was an ambassador for the
2013 World Parkinson Congress in Montréal.
Since diagnosis, he has also written and published four
books on living with Parkinson's and co-authored a series of
articles on technology tools for Parkinson’s patients including:
P. Wicks, J.A. Stamford, et al. Innovations in e-health. Qual
Life Res, vol. 23, pp. 195-203, 2014; R. Lakshminarayana, et
al. Smartphone-and internet-assisted self-management and
adherence tools to manage Parkinson’s disease (SMART-PD):
study protocol for a randomised controlled trial. Trials, vol.
15, pp. 374, 2014; and R. Narayana, et al. Self-management
in long term conditions using smartphones: A pilot study in
Parkinson’s disease. Int J Integrated Care, vol. 14, 2014.
Dr. Stamford is a frequent invited speaker and also writes a
humorous and influential weekly blog “Slice of Life” about
life with young onset Parkinson's.
Peter N. Schmidt, PhD, earned his
bachelor’s degree at Harvard University
and was awarded an M.S. and Ph.D. from
Cornell University, Sibley School of
Mechanical Engineering where he studied
gait and balance and total joint replacement.
He completed a fellowship at the Hospital
for Special Surgery in New York.
He joined NPF as Chief Information
Officer and Vice President, Research and Professional
Programs in June 2009 where he is responsible for the
Parkinson’s Outcomes Project (POP), a longitudinal study of
Parkinson’s disease with the three aims to (1) identify and
disseminate best practices in care, (2) to identify, track, and
study clinical outcome outliers, and (3) to optimize care in
order to improve the statistical power of clinical trials. With
over 17,500 clinical evaluations of over 7,500 patients, POP is
the largest clinical study of Parkinson’s disease ever
conducted and includes the largest set of patient-reported
outcome measures ever collected in a prospective study.
His career has focused on the intersection of math and
medicine, addressing such problems as engineering
simulations of insults to biological systems, stochastic systems
for chronic disease management, and interoperable electronic
medical records. Along the way, Schmidt contributed to early
versions of Linux, built an encryption system for a Wall Street
brokerage, and published articles on veterinary surgery,
hedging currency risk, and sector-specific characteristics of
stock market valuations. Schmidt holds patents on a total knee
replacement and a mobile device-based video game.
Karl E. Friedl, PhD is an endocrine
physiologist. He received B.A. and M.A.
degrees in zoology from the University of
California at Santa Barbara (UCSB) and
the Ph.D. degree in biology (integrative
physiology) at the Institute of
Environmental Stress, UCSB, in 1984.
From 1983 to 2013, he was a military
officer conducting physiology research and leading medical
research programs for the US Army. His last Army
assignment was as the Director, Telemedicine and Advanced
Technology Research Center (TATRC, 2006-2012). He is
now a physiology consultant in Frederick, Maryland;
Professor (adjunct), Department of Neurology, University of
California, San Francisco; a member of the Board of Directors
for the Parkinson’s Action Network; and a Fellow of the
American Institute of Medical and Biological Engineering.
His research interests include the metabolically optimized
brain, wearable biosensing/physiological models, and limits of
human performance.
Dr. Friedl’s awards and honors include the French Ordre
national du Mérit, US Army Legion of Merit (2nd
OLC), Order
of Military Merit, Morris K. Udall Award for Parkinson’s
Research Advocacy, Ronald and Nancy Reagan Alzheimer’s
Research Award, Diabetes Technology Society Research
Leadership Award, and Outstanding Research and
Development Scientist Award (SAFMLS).