Wednesday, 6 September 2006 - Oxford Academic
159
Wednesday, 6 September 2006 Downloaded from https://academic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Wednesday, 6 September 2006 - Oxford Academic
Wednesday, 6 September 2006
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Long-term results of drug-eluting stents 829
LONG-TERM RESULTS OF DRUG-ELUTINGSTENTS
4862(W) Long-term suppression of restenosis bysirolimus-eluting coronary stents - Five year resultsof the Ravel trial
M.-C. Morice1, P.W. Serruys2, C. Bode3, P. Barragan4,J. Fajadet5 , E. Sousa6, M.A. Perin7, E. Ban Hayashi8 on
behalf of The Ravel investigators. 1Institut Cardiovasculaire Paris Sud,Cardiology, Massy, France; 2Thoraxcenter, Cardiology, Rotterdam, Netherlands;3Albert-Ludwigs-Universitatkliniken, Cardiology, Freiburg, Germany; 4CliniqueBeauregard, Cardiology, Marseille, France; 5Clinique Pasteur, Cardiology,Toulouse, France; 6Instituto Dante Pazzanese, Cardiology, Sao Paulo, Brazil;7Instituto Albert Einstein, Cardiology, Sao Paulo, Brazil; 8Instituto Nacional deCardiologia, Cardiology, Mexico, Mexico
Background and study objectives: The RAVEL trial was the first randomized,double blind drug-eluting-stent trial comparing sirolimus eluting stent (SES) withan identically appearing bare metal stent (BMS, BX Velocity). Angiographic follow-up at 6 months showed complete suppression of late loss resulting in 0% resteno-sis in the SES group. The protocol defined clinical follow-up over 5 years to assessthe long term safety and efficacy of the SES. The purpose of this abstract is topresent the final long-term data.Patient population and methods: The study enrolled 238 patients with a singlede novo native coronary artery lesion. Survival free from target lesion revascular-ization (TLR), target vessel failure (TVF), and MACE up to 5 years of follow-upwas compared between the groups.Results: Rates of survival free from clinically driven target lesion revasculariza-tion (TLR), and target vessel failure (TVF) at 1-, 2-, 3- and 4-year follow-up were99.2%, 96.5%, 94.6%, 92.7 (TLR), and 96.6%, 94.0%, 89.4% and 85.5% (TVF),respectively, in the SES group, versus 85.9%, 85.9%, 84.9%, and 84.0% (TLR),and 80.0%, 78.2%, 75.5% and 74.6% (TVF) in the BMS group. The differenceswere significant at 4 years (P = 0.010 for TLR, and P <0.001 for TVF). Free-dom from MACE at 4 years was 78.4% in patients randomized to the SES group,versus 75.5% in patients assigned to BMS (P=0.23) due to a higher rate of non-cardiac death in the SES group (8.5% versus 1.7% in BMS).Conclusions: Treatment of de novo coronary artery stenoses with SES is asso-ciated with a sustained significant reduction of TLR and TVR in the SES group at4 years. Five year follow-up results will be available at the time of presentation.
4863 the european multicenter, randomized, double-blindstudy of the sirolimus-eluting stent in the treatment ofpatients with de novo coronary artery lesions(E-SIRIUS): 4-year clinical outcomes
J. Schofer1, G. Breithardt2, E. Garcia3, A. Gershlick4, M. Schlueter1,T. Wichter4, W. Wijns5 on behalf of E-SIRIUS investigators. 1Center onCardiology & Vascular Intervention, Interventional cardiology, Hamburg,Germany; 2University Hospital, Interventional cardiology, Muenster, Germany;3University Hospital, Interventional cardiology, Madrid, Spain; 4GlenfieldHospital, Interventional cardiology, Leicester, United Kingdom; 5CardiovascularCenter, Interventional cardiology, Aalst, Belgium
The randomized double-blind E-SIRIUS trial enrolled 352 patients at 35 centersin Europe and Israel to compare the safety and efficacy of the Sirolimus-elutingstent (SES, n = 175) vs the identically appearing bare-metal stent (BMS, n = 177)in the treatment of native de novo coronary artery lesions. The primary endpointwas in-stent minimum lumen diameter (MLD) at 8-month follow-up. Among thesecondary endpoints were major adverse cardiac events (MACE) at 1, 6, 9 and12 months - and annually up to 5 years -, as well as target lesion revascularization(TLR), target vessel revascularization (TVR) and target vessel failure (TVF) at9 months. The superiority of the SES over the BMS was clearly demonstratedangiographically, with a binary in-lesion restenosis rate at 8 months of 5.8% (vsBMS 43.9%, p<0.001). At 3 years, the clinical benefit of the SES over the BMSwas maintained, with a statistically significant lower incidence of major adversecardiac events (death, TV-MI, CABG and TLR) (11.4% vs 32.2%, p<0.001). Thisdifference in incidence was primarily driven by a statistically significant differencein TLR rates (5.7% vs 28.8%, p<0.001). With event-free survival curves for SESand BMS patients still diverging at 3 years, there was no indication of a "late catch-up" phenomenon. Four-year clinical follow-up of patients enrolled in E-SIRIUS willbe analyzed by July 2006. Results for the overall patient cohort will be availableat the time of presentation.
4864 Long-term durability of the polymer-based,paclitaxel-eluting stent for coronary artery lesions:4-year clinical follow-up of TAXUS II
A. Colombo1, A. Banning2, S. Silber3, K.E. Hauptmann4,J. Drzewiecki5, J. Koglin6, M.E. Russell1, E. Grube7. 1EMO - Centro
Cuore Columbus, Milan, Italy; 2John Radcliffe Hospital, Oxford, United Kingdom;3Internistische Klinik Dr. Muller, Munchen, Germany; 4Krankenhaus derBarmherzigen Bruder, Trier, Germany; 5Samodzielny Publiczny Szpital KlinicznyNr 7, Katowice, Poland; 6Boston Scientific Corporation, Natick, United States ofAmerica; 7Heart Center Siegburg, Siegburg, Germany
Purpose: TAXUS II demonstrated that both slow-release (SR) and moderate-release (MR) polymer-based, paclitaxel-eluting TAXUS stents reduce restenosisversus bare metal stents (BMS) while not posing any significant safety concernsin patients with de novo, focal lesions. This report will focus on the outcomes ofTAXUS versus BMS out to 4 years.Methods: TAXUS II is a randomized, double-blind clinical trial conducted at 38sites comparing the safety and efficacy of TAXUS SR (n=131) and TAXUS MR(n=135) versus BMS (n=270) in patients with focal, de novo lesions in the fourthyear of a 5-year follow-up.Results: The primary endpoint of % net volume obstruction as measured byIVUS was met with significant reductions in the TAXUS groups versus BMS. Ad-ditionally, significant reductions in target lesion revascularization (TLR) and majoradverse cardiac event (MACE) rates have been consistently demonstrated forTAXUS versus BMS through the 3-year follow-up. From 1 to 3 years, there wasonly 1 TLR in the TAXUS groups versus 9 in BMS, demonstrating that TAXUSstents continue to reduce restenosis up to 3 years. As a result, the TLR rateswere significantly lower for TAXUS versus BMS at 3 years (TLR: 5.5% SR and4.1% MR vs. 16.4% BMS, p=0.0001). Concordantly, overall 3-year MACE ratesremained low for TAXUS versus BMS (15.7% SR and 16.4% MR vs. 27.3% BMS,p=0.0096). From 2 to 3 years, there were no new stent thromboses in TAXUScompared to 1 in BMS. There were no statistically significant differences in stentthrombosis rates across groups at 3 years (2.4% SR and 1.7% MR vs. 0.4%BMS, p=0.14). The 4-year clinical follow-up of TAXUS II is currently being con-ducted to expand the long-term clinical profile of both SR and MR TAXUS stents.As of February 14 2006, 93.7% of patients had completed the 4-year follow-upevaluation. The results will be finalized in July, 2006.Conclusions: The TAXUS SR and MR stents are associated with markedly fewerTLR than BMS and are safe over a prolonged period of time up to 3 years. Thepresent analysis will extend the long-term data for the TAXUS stent by providing4-year clinical follow-up for the largest patient population with TAXUS to date.
4865 Long-term cost-effectiveness of drug-eluting stentsversus bare-metal stents in a real world setting: 18months results of the BAsel Stent Kosten EffektivitaetsTrial (BASKET)
C. Kaiser, H.P. Brunner-La Rocca, P. Buser, P. Rickenbacher,P. Hunziker, R. Jeger, C. Mueller, M. Pfisterer on behalf of BASKET Investigators.University Hospital, Cardiology, Basel, Switzerland
Background: The 6 months results of the BAsel Stent Kosten-Effektivitäts Trial(BASKET) showed that, despite a lower incidence of adverse events, using ofdrug-eluting stents (DES), their routine use is less cost-effective compared tobare metal stents (BMS) since higher DES costs are not fully balanced by thesomewhat higher follow-up costs with a BMS strategy (Lancet 2005;366:921-29).However, due to the limited follow-up of 6 months, late events and costs were notcaptured so far.Methods: All 811 patients (82%) patients of BASKET who survived the first 6months were prospectively followed with respect to additional events (cardiacdeath, non-fatal myocardial infarction and clinically driven target-vessel revascu-larization (TVR)) up to 18 months. Costs were ascertained on the basis of pro-cedures, stents used and day spent in hospital and ICU. Patients were advisedto stop clopidogrel after 6 months. The protocol did not allow control angiographywithout clinical indication.Results: Of a total of 826 consecutive patients enrolled in BASKET, 753 (91%)had no major events up to 6 months. Patients had been randomised to DES(Cypher, n=264; Taxus, n=281) or to bare metal stents (BMS (Vision), n=281)in a 2:1 allocation. The total population consisted of 79% men with an averageage of 64+11 years presenting with stable angina in 42%, acute MI in 21% andunstable coronary syndromes in 36%. Patients had received 1.9+1.1 stents for atotal stent length of 34+20mm per patient. There were no significant differencesbetween the 3 patient groups in any of these parameters. Clinical follow-up up to18 months is presently complete in 813 (98%) of patients and, hopefully, 100%complete cost-effectiveness data can be presented at the meeting.Conclusions: 18 months clinical effectiveness findings from BASKET will demon-strate 1) whether there were differences in late events between DES and BMS af-ter stopping clopidogrel and 2).whether eventual higher long-term follow-up costsin BMS patients will compensate the higher DES costs at baseline. Thus, thesefindings will add important new long-term data which may impact current stentingpractice.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

830 Long-term results of drug-eluting stents / Drug-eluting stents in acute myocardial infarction
4866 Do sirolimus-eluting stents remain superior to baremetal stents in patients with acute myocardialinfarction after 3 years of follow-up? Insights into theRESEARCH registry
J. Daemen, G. Sianos, H.M. Garcia-Garcia, M. Patterson, S. Tanimoto,P.T. De Jaegere, R.T. Van Domburg, P.W. Serruys. Erasmus MC, Thoraxcenter,Rotterdam, Netherlands
Background Sirolimus-eluting stents (SES) were proven superior to bare-metalstents for both clinical and angiographic restenosis in patients with ST-segmentelevation myocardial infarction (STEMI) at 1 year of follow-up. Currently, no dataare available on the long-term (3 years) clinical outcome of these high-risk pa-tients.Methods We compared the outcome of 186 consecutive patients presenting withSTEMI treated with percutaneous coronary intervention with SES implantationwith a control group of 183 patients treated with bare metal stents (BMS) inthe immediate preceding period. The incidence of death, reinfarction, and repeatrevascularization was assessed at 3 years of follow-up.Results Follow-up was available for 98% of the patients in both groups. Post-procedural vessel patency and enzymatic release were similar between bothgroups. The cumulative incidence of the composite endpoint of death or rein-farction was comparable in both groups: SES 14.5% versus BMS 17.1%, p=0.43.At three years, treatment with SES significantly reduced the crude cumulativeincidence of major adverse cardiac events (26.8% versus 17.8%; hazard ratio[HR] 0.61; 95% confidence interval [CI] 0.39 - 0.96; p=0.03); when adjusting forindependent predictors (cardiogenic shock, treatment of left main and left ante-rior descending coronary artery, postprocedural TIMI flow and current smoking),the superiority of SES became non-significant (adjusted HR 0.70; 95% CI 0.44 -1.14). There was a trend in a reduction of target vessel revascularization in theSES-group (7.1% versus 12.4; HR 0.51; 95% CI 0.24 - 1.06; p=0.07).Conclusions: At three years of follow-up, in an unselected cohort of patients pre-senting with ST-segment elevation acute MI, the use of SES was no longer asso-ciated with superior clinical outcome compared to BMS, mainly due to a greaterincrease in late TVR in the SES-group.
DRUG-ELUTING STENTS IN ACUTE MYOCARDIALINFARCTION
4868 A randomized trial of sirolimus eluting and bare metalstents in patients with acute myocardial infarction:in-hospital and 30 days outcome of the MISSIONIntervention Study
B. Van Der Hoeven, S.S. Liem, J.W. Jukema, D.E. Atsma, M. Bootsma,K. Zeppenfeld, E.E. Van Der Wall, M.J. Schalij. Leiden University Medical Center,Cardiology, Leiden, Netherlands
Introduction: The MISSION! Intervention Study is a randomized, single centerstudy in 316 patients comparing drug eluting stents and bare metal stents in pa-tients with acute myocardial infarction (AMI).Methods Patients with ST-segment elevation AMI (<9 hours) due to a de novocoronary artery lesion with a reference diameter of 2.25 to 3.75 mm were in-cluded. Key exclusion criteria were: age >80 years, need for mechanical ventila-tion, previous PCI or CABG of the infarct related artery, triple vessel disease, leftmain stenosis of 50% or more and contraindication for abciximab. Either a CypherSelect sirolimus eluting stent or a cobalt chromium Vision stent was implanted.The primary angiographic endpoint of the study is in-lesion late loss at 9 months.Secondary endpoints include MACE (major adverse cardiac events: death, re-current myocardial infarction, any revascularization), target lesion revasculariza-tion rate at 12 months and minimum lumen area (intracoronary ultrasound) at 9months. All patients received abciximab during the procedure, aspirin indefinitelyand clopidogrel for 12 months after the procedure.Results All patients are included and have completed 30-days follow-up. Patientcharacteristics: age 59±12 years, male 78%, diabetes mellitus 10%, family his-tory of CAD 44%, hyperlipidemia 20%, hypertension 29%, smoking 54%, pre-vious myocardial infarction 4%, previous PCI 2%, previous CABG 1%. Targetvessel: LAD 54%, RCA 30%, LCX 16%. Stent length 26±12 mm, stent diam-eter 3.3±0.3 mm, average number of stents implanted within the culprit lesion1.3±0.6. Procedural results: device success 99%, non-culprit vessel interven-tion 6.0%. In-hospital cumulative MACE: death 1.3%, recurrent myocardial in-farction 0.9%, target vessel revascularization 0.1%, Non-target vessel revascu-larization 2.8%. Cumulative MACE at 1 month: death 0.9%, recurrent myocardialinfarction 1.6%, sub-acute stent thrombosis 1.3%, target vessel revascularization0.9%, non-target lesion revascularization 3.2%. MACE free survival at 30 dayswas 93.1%.Conclusion The randomized MISSION! Intervention Study comparing a drugeluting stent and a cobalt chromium stent in patients with AMI demonstrates ex-cellent acute and 30 days preliminary results and low rates of target lesion revas-cularization and subacute stent thrombosis.
4869 Long-term follow-up patients with ST-segmentelevation acute myocardial infarction treated withsirolimus-eluting stent and paclitaxel-eluting stent
S. Nakamura1, J.H. Bae2, Y.H. Cahyadi3 , W. Udayachalerm4 ,D. Tresukosol5 , S. Tansuphaswadikul6 . 1New Tokyo Hospital,
Department Of Cardiology, Matsudo, Japan; 2Konyang University Hospital,Daejeon, Korea, Republic of; 3Husada Hospital, Jakarta, Indonesia; 4KingChulalongkorn Memorial Hospital, Bangkok, Thailand; 5Siriraj Hospital, Bangkok,Thailand; 6Chest Disease Institute, Bangkok, Thailand
Background: Previous clinical study utilizing Sirolimus-eluting stent (SES) andPaclitaxel-eluting stent (PES) in simple coronary lesions demonstrated an impres-sive reduction in intimal hyperplasia and restenosis. However, clinical efficacy ofSES and PES in treating patients with ST-segment elevation myocardial infarction(STEMI) has not been validated.Methods: We assessed baseline clinical and angiographic characteristics, in-hospital and 12, 24-month major adverse cardiac events (MACE) in 1838 con-secutive STEMI patients who received on SES, PES or bare metal stents (BMS)without cardiogenic shock undergoing emergent PCI.Results: The baseline clinical characteristics between 3 groups were similar. Seetable for the clinical results.
BMS (n=388) SES (n=843) PES (n=607) p
In-hospital Clinical success (%) 98.5 98.8 99.0 NSDeath (%) 1.0 0.8 1.0 NSStent thrombosis (%) 0.5 0 0 NS
12-month Death (%) 1.3 0.9 1.2 NSAngiographic restenosis (%) 16.0 3.8* 3.3* 0.01Repeat PCI (%) 10.8 3.0* 2.5* 0.01
24-month Death (%) 1.3 0.9 1.2 NSAngiographic restenosis (%) 17.5 3.8* 3.3* 0.01Repeat PCI (%) 11.9 3.0* 2.5* 0.01
Conclusion: Implantation of Sirolimus-eluting stent and Paclitaxel-eluting stent inSTEMI patients is not associated with any risk of adverse in-hospital events, andreduced the need for repeat PCI at follow-up.
4870 Short- and long-term clinical benefit ofsirolimus-eluting stents compared to conventional barestents for patients with acute myocardial infarction
A. Assali, I. Teplitsky, I. Ben-Dor, S. Fuchs, D. Hasdai, D. Brosh,A. Battler, R. Kornowski. Rabin Medical Center, cardiology,
Petah-Tikva, Israel
Background: Sirolimus-eluting stents (SES) have been proven to reducerestenosis and reintervention compared with bare stents (BMS). Both safety and6 months outcomes of primary PCI with SES in ST-segment elevation acute my-ocardial infarction [AMI] are scarce.Objectives: This study investigated the clinical outcomes of patients with AMItreated with SESs or with conventional bare stents.Methods: Primary PCI was performed with SESs in 53 patients with AMI whowere compared with 628 patients treated with BMS. Patients with cardiogenicshock were excluded. The incidence of death, reinfarction, and repeat revascu-larization was assessed at 30 and 6 months.Results: see table 1.
Table 1
BMS(N=628) SES (N=53) P
Age (yrs) 61±13 59±13 0.4Male 79% 77% 0.8Anterior AMI 48% 70% 0.02DM 27% 32% 0.52/3 Vessel disease 55% 68% 0.1Post PCI TIMI 3 94% 98% 0.51 month
Death 3.7% 0% 0.3Stent thrombosis 2.45% 0% 0.5
Six monthsDeath 6.05% 0% 0.2Re-AMI 7% 0% 0.1TVR 9.2% 5.7% 0.3TLR 8.6% 1.9% 0.09MACE 17% 5.6% 0.05
Conclusions: Compared to conventional bare stents, the SESs were not associ-ated with an increased risk of stent thrombosis and were effective in reducing theincidence of adverse events at six months patients with AMI referred for primaryangioplasty.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Drug-eluting stents in acute myocardial infarction / Medical and surgical treatments for pulmonary hypertension 831
4871 In-hospital and long-term clinical outcomes of patientstreated with sirolimus-eluting stents versus bare-metalstents during primary angioplasty
M. Vasconcelos1, R. Almeida1, A. Azevedo2, J. Silva1, D. Magalhaes1,J. Mota Garcia1, F. Rocha-Goncalves1. 1Sao Joao Hospital Medical
School, Department of Cardiology, Porto, Portugal; 2University of Porto MedicalSchool, Department of Hygene and Epidemiology, Porto, Portugal
Purpose: We aimed to compare in-hospital and long-term clinical outcomes ofpts treated with sirolimus-eluting stents (SESs) versus bare-metal stents (BMSs)for ST elevation myocardial infarction (STEMI).Methods: We analyzed 343 pts (mean age 58±13 years; 63% male; n=164 inSESs group, n=179 in BMSs group) consecutively admitted in our cardiology de-partment with acute (<12h) STEMI, between January 2003 and December 2005.Our end-point was a composite of adverse events (death, non-fatal myocardial in-farction and target vessel revascularization) during hospitalization and two-yearsfollow-up (data obtained from medical records and telephone contact).Results: Clinical and angiographic baseline characteristics were similar betweenthe two groups, except for dyslipidemia (62.2.% SESs group vs 51.4% BMSsgroup, p=0.05), anterior STEMI (64.0% SESs group vs 38.0% BMSs group,p<0.001) and left ventricular systolic dysfunction (61.0% SESs group vs 49.2%BMSs group, p=0.03). The procedural characteristics including the number ofstents per lesion, rates of stenting success and complications were similar. All pa-tients received clopidogrel and most received glicoprotein IIb/IIIa inhibitors (83.5%SESs group vs 86.0% BMSs group, p=0.22). The mean length of hospitalizationwas 8 days in both groups. Mean follow-up time was 355 days in SESs group and495 days in BMSs group. The rate of in-hospital and long-term adverse eventswas, respectively, 2.4% in SES group vs 8.9% in BMSs and 9.1% in SESs groupvs 16.7% in BMSs group. In-hospital adverse events were significantly less fre-quent in pts treated with SESs (OR 0.27; 95%CI 0.09-0.84) even after adjust-ment for other variables (age, diabetes, dyslipidemia, smoking, heart failure dur-ing hospitalization, left ventricular systolic dysfunction, multivessel disease, meantime to angioplasty, glicoprotein IIb/IIIa inhibitors, maximum troponin I, creatinine,haemoglobin and glucose levels on admission) using a binary logistic regressionmodel (adjusted OR 0.18; 95% CI 0.33-0.98). Long-term event-free survival up totwo years was not significantly different between the groups after adjustment forthe above mentioned variables using a forward stepwise Cox regression model(adjusted HR 0.92; 95% CI 0.45-1.90).Conclusions: In our sample of STEMI pts those receiving SESs during primaryangioplasty had less in-hospital adverse events, although long-term event freesurvival was not significantly different from pts receiving BMSs. Whether theseresults apply to most pts in this setting needs to be confirmed by larger scalerandomized trials.
4872 Impact of paclitaxel-eluting stent implantation inpatients with STEMI on anti-inflammatoryIL-10-producing T regulatory 1 (Tr1) cells
G. Sardella1, M. Paroli2, M. Mancone1 , R. Colantonio1, B.L. N’guyen1,L. De Luca1, G. Conti1, F. Fedele1 . 1Pol. Umberto I-Dept of Cardiology,
Cardiovascular Sciences, Roma, Italy; 2Pol. Umberto I-Dept of Internal Medicine,Internal Medicine, Roma, Italy
Background: Few data are available on the effect of different types of stentson peripheral redistribution of T cell subsets with either anti-inflammatory orpro-inflammatory properties in ischemic and therapeutically reperfused my-ocardium.We investigated the effect of primary percutaneous coronary interven-tion (PCI) with implantation of bare (BS) or paclitaxel-eluting stents (PES) on thebalance between T helper 1 cells (Th1) producing pro-inflammatory interferon- gand T regulatory 1 cells (Tr1) producing anti-inflammatory inteleukin-10.Methods: We randomized 40 patients with ST-elevation myocardial infarction(STEMI) threated with Primary PCI respectively to BS (n=20),Group 1(G1) orPES (n=20),Group 2(G2) implantation. Peripheral Blood Monocyte Cells (PBMC)were isolated before, 48 h and 6 days after primary PCI and basicly in 20 normalhealty subjects (Control Group,CG). Tr1 and Th1 cells were identified by IFN- g orIL-10 flow cytometer intracellular staining. RESULTS: Basal peripheral Th1 andTr1 frequencies were both reduced in STEMI patients of G1 and G2 as comparedwith control subjects (G1=2.8%Th1, 0.9%Tr1 and G2=3.0%Th1, 0.9%Tr1 vs CG=4.3%Th1, 2.0%Tr1; p< 0.02), and further decreased 48 h after PCI (G1=1.6%Th1, 0.7% Tr1 and G2=1.4% Th1, 1.3% Tr1). Moreover, mean Th1:Tr1 ratio wassignificantly lower in patients receiving PES (G2) as compared with those receiv-ing BS (G1) (1.2:1 vs 2.1:1, p< 0.05) 48 h after PCI.Conclusions: Our data suggest that reduced frequency of circulating both pro-and anti-inflammatory T cells in STEMI respect to control subjects might reflecttheir local recruitment into the ischemic myocardium and this might result in a ben-eficial effect on healing and remodeling of injured myocardium, that is known tobe associated with the presence of pro-inflammatory cytokines during the reperfu-sion phase.A greater percentage of Tr1 producing anti-inflammatory inteleukin-1048h after PES implantation in primary PCI comparing with BS might confirm ananti-inflammatory DES action with a consequent impact on stent restenosis.
4873 Incidence and predictors of stent thrombosis inpatients treated with percutaneous coronaryintervention and drug-eluting stent implantation foracute ST elevation myocardial infarction
G. Sianos, M.I. Papafaklis, J. Daemen, S. Vaina, C.A. Van Mieghem,R.T. Van Domburg, L.K. Michalis, P.W. Serruys. Thoraxcenter, Erasmus MC,Thoraxcenter - Bd 408, Interv. Cardiology, Rotterdam, Netherlands
Purpose: To investigate the incidence and predictors of angiographic stent throm-bosis (ST) in an unselected patient population undergoing percutaneous coronaryintervention (PCI) with drug-eluting stent (DES) implantation for ST elevation my-ocardial infarction (STEMI).Methods: From April 2002, when DES became commercially available, untilDecember 2004, 812 consecutive patients with STEMI were treated with PCIand DES implantation [204 patients with sirolimus-eluting (SES) and 608 withpaclitaxel-eluting (PES) stents]. Thrombus burden (TB) was scored as small(TBS) when greatest thrombus dimension was ≤2 vessel diameters and large(TBL) when >2 vessel diameters by visual assessment. In SES patients dualantiplatelet medication was prescribed for 3 months and in PES patients for 6months. Rheolytic thrombectomy (RT) (the only thrombectomy device used in ourinstitution) was at the discretion of the operator. The incidence of ST was com-puted by the Kaplan-Meier method and multivariate Cox regression analysis wasused for identifying the independent predictors for ST.Results: Complete follow-up was available in 798 patients (98.3%) with a meanduration of 18.2 ± 7.8 months. Thrombus burden was classified in 792 (TBS71.6%, TBL 28.4%) and RT was used in 63 (8%) patients [59 (93.6%) in TBL pa-tients]. During the whole follow-up period (33 months) there were 23 ST events;9 (39.1%) in ≤30 days (early ST) and 14 (60.9%) after 30 days (late ST, latestevent at 884 days). Seventeen (21.5%) occurred in the group of TBL without RT.The 24-month cumulative ST rate (± SEM) was 3.2 ± 0.007%. The cumulativeST rate was significantly higher in the TBL compared to the TBS group (8.2 ±0.02% vs. 1.3 ± 0.01% at 24 months respectively, p<0.0001). In the TBL groupa significantly lower 24-month cumulative ST rate was observed when thrombec-tomy was performed (0% vs. 11.3 ± 0.03%, p<0.0001). Independent predictorsfor ST were TBL (HR: 5.65, 95% CI: 2.2-14.6, p<0.001), stent thrombosis aspresentation at the index procedure (HR: 5.5, 95% CI: 1.8-16.7, p=0.003), bifur-cation stenting (HR: 4.6, 95% CI: 1.8-11.8, p=0.001), and RT (HR: 0.12, 95% CI:0.02-0.86, p=0.036). Stent type was not a predictor for ST.Conclusions: High incidence of ST was observed in patients undergoing DESimplantation for STEMI. This is mainly due to the very high incidence in patientswith large thrombus burden. Thrombus aspiration, in this group of patients, usingRheolytic Thrombectomy prevents this complication.
MEDICAL AND SURGICAL TREATMENTS FORPULMONARY HYPERTENSION
4874 Therapy with subcutaneous treprostinil improvessurvival in patients with pulmonary arterialhypertension: four-year follow-up
R.J. Barst1, N. Galie2, R. Naeije3, G. Simonneau4, C. Arneson5,L.J. Rubin6. 1Columbia Univ Coll of Physicians & Surgeons, New York,
Ny, United States of America; 2Istituto di Malattie Dell’Apparato Cardiovasc,Bologna, Italy; 3Erasmus University Hospital, Brussels, Belgium; 4Hopital AntioneBeclere, Service de Pneumologie, Clamart, France; 5United Therapeutics, SilverSpring, Md, United States of America; 6University of California at San Diego, LaJolla, Ca, United States of America
Background: Pulmonary arterial hypertension (PAH) is a progressive diseasewith a high mortality. Administration of intravenous epoprostenol improves ex-ercise capacity and hemodynamics in PAH, and increases survival in idiopathicPAH (IPAH). The longer acting prostacyclin analogue treprostinil (TRE) offers anadditional mode of therapy for PAH.Methods: To determine the effect of subcutaneous (SC) TRE on long term out-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
832 Medical and surgical treatments for pulmonary hypertension
come in PAH, we collected survival data from 6-25-98 to 12-1-03 on 860 PAHpts (412 with IPAH) treated with SC TRE for up to 4 years. Observed survival isreported as Kaplan-Meier (K-M) estimates; for 332 IPAH pts with baseline hemo-dynamics, observed survival was also compared with predicted survival, usingthe NIH Registry formula. Use of additional PAH treatments was at the discretionof the treating physician.Results: Of the total 860 pts, 199 discontinued due to AEs (predominantly sitepain), 136 died, 117 discontinued due to deterioration, 29 withdrew consent and11 underwent transplantation. 97 were switched from SC TRE to an alternativeprostacyclin analogue; in addition, bosentan was started in 105 and sildenafil in25. K-M survival estimates were 87%, 78%, 71% and 68% at 1, 2, 3 and 4 years,respectively, for all 860 patients. For the IPAH subset with baseline hemodynam-ics (n=332), observed survival rates were 91%, 82%, 76% and 72% at 1, 2, 3and 4 years, respectively; in contrast, predicted survival was 69%, 56%, 46%and 38% at 1, 2, 3 and 4 years, respectively (Fig). The overall safety profile forlong-term SC TRE was consistent with previous short-term clinical trials, with nounexpected pattern of serious or non-serious AEs seen with long-term treatment.Conclusions: Therapy with SC TRE improves survival in IPAH pts who tolerateSC TRE, and may improve survival in PAH.
4875 Ambrisentan improves 6-minute walk distance anddecreases brain natriuretic peptide in patients withpulmonary arterial hypertension
N. Galie1, H. Olschewsky2, H.A. Ghofrani3, M.R. Kramer4,B.L. Wiens5, C. Dufton4, L.J. Rubin6 on behalf of ARIES-2 Study
Group. 1Institute of Cardiology-University of Bologna, Bologna, Italy; 2Med. UnivGraz, Graz, Austria; 3Med. Univ. Giessen, Giessen, Germany; 4Rabin Med.Ctr., Tel Aviv, Israel; 5Myogen, INC, Westminster-Co, United States of America;6UCSD, San Diego-Ca, United States of America
Purpose: Plasma brain natriuretic peptide (BNP), a hormone secreted primar-ily from the cardiac ventricles, has been proposed as a prognostic indicator ofmortality in patients with pulmonary arterial hypertension (PAH). Furthermore,reductions in BNP have been shown to parallel improvements in hemodynam-ics and 6-minute walk distance (6MWD) in patients with PAH. Ambrisentan isa propanoic acid-class, ETA-selective endothelin receptor antagonist that wasshown to significantly improve 6MWD and delay clinical worsening in a Phase3 placebo-controlled PAH study (ARIES-2).Methods: In the ARIES-2 study, 192 patients with idiopathic PAH or PAH associ-ated with connective tissue disease, anorexigen use or HIV were randomized toreceived placebo, 2.5 mg or 5 mg ambrisentan for 12 weeks. Post-hoc analysesare presented for all subjects with BNP data prior to first dose and after 12 weeksof ambrisentan therapy.Results: As previously reported, the placebo-corrected change from baseline in6WMD at week 12 improved by 59.4 m (95% CI: 29.6-89.3; p<0.001) in patientsreceiving 5 mg ambrisentan and 32.3 m (95% CI: 1.5-63.1; p = 0.022) in patientsreceiving 2.5 mg ambrisentan. 153 of these patients had BNP data pre-dose andat week 12: placebo (n = 46); 2.5 mg group (n = 55); or 5 mg group (n = 52).At baseline, mean plasma BNP was similar for the placebo group (252.4 ± 33.5pg/mL), 2.5 mg group (267.7 ± 37.1 pg/mL) and the 5 mg group (267.7 ± 65.2pg/mL). At week 12, mean plasma BNP decreased from baseline in the 2.5 mg (-98.6 ± 26.4 pg/mL; p<0.001) and 5 mg groups (-121.4 ± 58.0 pg/mL; p = 0.041),but increased in the placebo group (47.6 ± 30.9 pg/mL; p = 0.130). The changein BNP from baseline to week 12 was greater for both the 2.5 mg (p<0.001) and 5mg groups (p = 0.015), compared to placebo, but was similar in both ambrisentandose groups (p = 0.717). Regression analysis of all groups combined (n = 153)suggested that decreased BNP was associated with increased 6MWD at week12 (p = 0.050).Conclusions: During the 12-week study, ambrisentan significantly improved6MWD and decreased plasma BNP concentrations, compared to placebo. De-creased plasma BNP appeared to be associated with improvement in 6MWD andmay reflect underlying improvements in cardiopulmonary hemodynamics.
4876 A novel echocardiographic predictor of in-hospitalmortality and mid-term outcome of pulmonaryendarterectomy (PEA) for chronic thromboembolicpulmonary hypertension (CTEPH)
M. Hardziyenka, H.J. Reesink, B.J. Bouma, H.A.C.M. Rianne DeBruin-Bon, M.E. Campian, J.J. Kloek, P. Bresser, H.L. Tan. Academic MedicalCenter, Experimental and Clinical cardiology, Amsterdam, Netherlands
Background: PEA is the most effective treatment of CTEPH. Persistent pul-monary hypertension after PEA is associated with increased in-hospital mortalityand impaired functional recovery. It is believed to result mostly from distal vascu-lar obstruction and/or secondary small-vessel arteriopathy. Pulmonary artery sys-tolic flow deceleration (notch), an echocardiographic feature found in pulmonaryhypertension patients, occurs later in systole in more distal obstruction. We in-vestigated the association between preoperative notch timing and PEA outcome.Methods: Fifty-eight of 61 CTEPH patients (aged 53 ± 14 years; 36 women) whounderwent PEA between June 2002 and June 2005 were studied. Clinical, hemo-dynamic and echocardiographic variables were assessed preoperatively and at 3months post-PEA. Notch timing was quantified by notch ratio calculation (t1/t2),
where t1 is the time interval from the onset of pulmonary artery systolic flow to themaximal systolic flow deceleration, and t2 is the time interval from the maximalsystolic flow deceleration to the end of pulmonary artery systolic flow. Patientswith t1/t2 >1.0 were arbitrarily defined as having a late notch (LN). Data are pre-sented as means±SD.Results: Preoperatively, 7 patients had no notch (NN), 33 an early notch (EN),and 18 LN. EN and LN patients had similar hemodynamic and echocardiographicvariables, except t1/t2. Six of 61 patients died perioperatively (overall in-hospitalmortality was 9.8%). Non-survivors all had LN with t1/t2 significantly higher than insurvivors (1.47±0.38 vs. 0.77±0.28, p<0.001). At follow-up, survivors with pre-operative LN had worse functional outcome, as reflected by higher pulmonaryartery systolic pressure (PAPs)(55.1±25.8 mmHg vs. EN, 35.8±17.7 mmHg vs.NN, 32.4±5.1 mmHg, p<0.05), larger right ventricular end-diastolic diameter(RVEDD) (3.8±0.7 cm vs. EN, 3.4±0.6 cm vs. NN, 3.2±0.4 cm, p<0.05), andhigher plasma brain natriuretic peptide (BNP) levels (24.3±19.4 pmol/l vs. EN,10.0±7.8 pmol/l vs. NN, 7.6±4.6 pmol/l, p<0.05). Multivariate analysis identifiedt1/t2 as the only independent determinant of in-hospital mortality (p<0.01), andPAPs (p<0.01), RVEDD (p<0.01), and BNP (p<0.01) at 3 months follow-up afterPEA. In contrast, more traditional variables (e.g., pulmonary vascular resistance,mean pulmonary artery pressure) were no independent determinants.Conclusions: The timing of systolic notch is an independent determinant of in-hospital mortality and mid-term functional PEA outcome. LN is associated withunfavorable outcome and may be considered as a parameter of eligibility for PEA.
4877 Functional impairment of Endothelial Progenitor Cellsin hypoxic pulmonary hypertension
G. Marsboom, P. Pokreisz, P. Vermeersch, H. Gillijns, M. Pellens,M. Swinnen, S. Janssens. University of Leuven (CTG/VIB3), CTG(VIB-3), Leuven, Belgium
Introduction: Functional impairment of Endothelial Progenitor Cells (EPCs) is ahallmark of coronary artery disease and diabetes, but remains largely unstudiedin pulmonary hypertension.Methods: Spleen-derived mononuclear cells from normoxic (NX) or chronicallyhypoxic (CHX, 3 weeks FiO2 10%) C57BL/6 mice were cultured in EBM-2medium and after 7 days characterized as EPCs by the uptake of acetylatedLDL and BS-1 lectin binding. Adhesive properties were assessed on fibronectin-coated wells, migration was investigated using a modified Boyden chamber in thepresence or absence of mevastatin (1_M) and incorporation into a vascular net-work was studied by coplating EPCs and HUVECs on matrigel. Integrin expres-sion was determined using qPCR and apoptosis was induced by staurosporineand quantified by determination of DNA content on a FACSCalibur.Results: The number of circulating EPCs in CHX mice was significantly increasedcompared to NX mice (152±57 vs. 73±28 AcLDL+/BS1+ EPCs/HPF, respec-tively, n=7, P=0.03). Adhesion to fibronectin of EPCs derived from CHX micewas significantly lower compared to EPCs derived from normoxic mice (52±6 vs.73±10, n=7, P=0.03). Migration towards SDF-1_ was also impaired in CHX mice(99±28 vs. 169±27 migrating EPCs/HPF, n=7, P=0.02). Finally, incorporation ofEPCs from CHX mice into a vascular network was decreased by 22±6% (n=3,P=0.07). Integrin _v and _1 were downregulated in EPCs derived from CHX miceby 45±11 and 21±7% respectively (P<0.05 vs. NX for both, n=6). In contrast,EPCs derived from CHX mice were less sensitive to apoptosis following stau-rosporine (20±2% of EPCs derived from NX vs. 14±1% of EPCs derived fromCHX n=7, P=0.03) but failed to improve their migratory capacity to levels seen inNX mice following statin treatment.Conclusion: Chronic hypoxia increases the number of circulating EPCs and theirresistance to apoptosis, but is associated with a functionally impaired EPC pheno-type. The latter may hinder cell-mediated repair in pulmonary vascular disease,which in contrast to cell repair for atherosclerotic heart disease is refractory tostatin treatment.
4878 the effect of atorvastatin on monocrotaline-inducedpulmonary hypertension
H. Xie, L.D. Xie, C.S. Xu. 1st Affiliated Hospital Of FMU, FujianResearch Institute Of Hypertension, Fuzhou, China, People’s Republicof
Purpose To explore the effect of atorvastatin on monocrotaline-induced pulmonary hypertension.Methods Thirty two Sprague-Dawley rats were randomly divided into four groups:normal control (Ctr), untreated pulmonary hypertension (PHT), pulmonary hyper-tension treated with losartan (Los, 50mg/kg/d losartan by gavage after monocro-taline injection), and the group of pulmonary hypertension treated with atorvas-tatin (Ato, 5mg/kg/d of atorvastatin intragastrically after monocrotaline injection).The pulmonary hypertension was induced byinjection of 60 mg/kg monocro-taline intraperitoneally. After 4 weeks treatment, right ventricular systolic pres-sure (RVSP) and ratio of right ventricle to left ventricle plus septum (RV/LV+S)were measured. MT% (MT%=2*WT/ED,WT:wall thickness,ED:external diameter)of pulmonary arterioles were evaluated by image analysis software. Differencesbetween the groups were tested by analysis of variance (ANOVA) using the SPSSv.10.Results 1.RVSPs in losartan and atorvastatin treated group were significantly
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Medical and surgical treatments for pulmonary hypertension / Novel aspects in surgical treatment of valvular disease 833
decreased than that in untreated PHT group (RVSPs in mmHg:Ato 30.1±3.4; Los30.5±4.6 vs PHT 44.7±2.4, P<0.001 respectively), but not to the normal controllevel(21.1±2.2 mmHg). There was no marked difference between losartan andatorvastatin treated groups; 2.In comparison with PHT group, RV/LV+S in groupLos and group Ato were also obviously reduced (Ato 35.9±4.8; Los 36.4±4.3vs PHT 42.8±5.0, P<0.05 respectively). No significant difference was found be-tween group Los and Ato;3.A significant reduction in MT% of pulmonary arteri-oles was showed after administration of Losartan or Atorvastatin as comparedwith that in PHT group(Ato 22.5±2.4; Los 24.4±2.3 vs PHT 35.3±3.3, P<0.001respectively). there was no significant difference between group Los and Ato.
Data of RVSP and morphology
Group n RVSP(mmHg) RV/(LV+S)% MT%
Ctr 8 21.1±2.2 19.5±2.8 14.3±2.0PHT 8 44.7±2.4 42.8±5.0 35.3±3.3Los 8 30.5±4.6 ** 36.4±4.3 * 24.4±2.3**Ato 8 30.1±3.4 ** 35.9±4.8 * 22.5±2.4**
*P<0.05 versus group PHT, **P<0.001 versus group PHT.
Conclusions: Atorvastatin could attenuate pulmonary arterial structural remod-eling and right ventricular hypertrophy in pulmonary hypertension in rats inducedby monocrotaline, as effective as Losartan.
4879 Acute vasoreactivity and BMPR2 mutations inIPAH/FPAH children and adults
E. Berman Rosenzweig1, J.H. Morse2, J.A. Knowles3, A.M. Khan3,S. Rich4, B.E. Diamond3, R.J. Barst3. 1Columbia University,Pediatrics, New York, United States of America; 2Columbia University,
New York, United States of America; 3Columbia University, New York Ny, UnitedStates of America; 4University of Chicago, Section of Cardiology, Chicago,United States of America
Background: Mutations of Bone Morphogenic Protein Receptor II gene (BMPR2)have been identified in patients with idiopathic pulmonary arterial hypertension(IPAH) and patients with familial pulmonary arterial hypertension (FPAH), howeverthe impact of these mutations on disease severity and clinical course has yetto be determined. We analyzed whether BMPR2 mutations are associated withresponse to acute vasodilator testing (AVT) since AVT, has been used to predict:1) acute pulmonary vascular bed "reactivity" as well as 2) response to long-termtreatment with calcium channel blockade, i.e. patients who are responsive to AVTcan be treated successfully with calcium channel blockade.Methods: BMPR2 mutations were determined by nucleic acid sequencing of all13 exons and exon counting using MLPA kits. All comparisons were made us-ing the Fisher’s exact test. Acute pulmonary vasoreactivity was defined and ana-lyzed by two different criteria: #1) decrease in mean pulmonary arterial pressure(PAPm) > 20% without a decrease in cardiac output and the more recently de-scribed criteria #2) decrease of PAPm >10mmHg to PAPm < 40mmHg with anormal cardiac output.Results: In total, 163 patients, 114 patients (49 adult; 65 children) with IPAH and49 patients (34 adult; 15 children) with FPAH were included in this analysis. 55patients were acute responders, and 107 were non-responders, according to def-inition #1. According to definition #2, 46 patients were responders, and 116 werenon-responders. 76% (n=124) of patients were BMPR2 negative and 24% (n=39)of patients were BMPR2 positive. We found that patients with BMPR2 mutationswere less likely to have a positive response to AVT than BMPR2 negative pa-tients (p<.0001). In addition, regardless of BMPR2 status, FPAH patients wereless likely to respond to AVT than IPAH patients (p<0.0001). IPAH/FPAH childrenwere also more likely to respond to AVT than IPAH/FPAH adults.Conclusions: Patients who are positive for BMPR2 mutations are less likely torespond to AVT than BMPR2 negative patients. In addition, previously not re-ported 1) regardless of BMPR2 status, FPAH patients are less likely than IPAHpatients to respond to AVT, and 2) FPAH children were more likely to respond toAVT than adult FPAH patients. Furthermore, overall, children were more likely torespond to AVT than adults. While these data support the utility of determiningBMPR2 mutation in identifying patients who are unlikely to respond to CCB ther-apy, identifying additional genetic polymorphisms that may predict efficacy withother targeted PAH therapeutic modalities are warranted.
NOVEL ASPECTS IN SURGICAL TREATMENT OFVALVULAR DISEASE
4880 Impact of Prosthesis-Patient Mismatch on SurvivalAfter Mitral Valve Replacement
J. Magne1, P. Mathieu1, J.G. Dumesnil1, D. Tanne2, F. Dagenais2 ,D. Doyle2, P. Pibarot2. 1Laval Hospital Research Center, Sainte Foy,Canada; 2Cardiovascular Biomechanics Team, Marseille, France
Background: We recently reported that valve prosthesis-patient mismatch (PPM)is associated with persisting pulmonary hypertension after mitral valve replace-ment (MVR). The objective of this study was thus to evaluate the impact of PPMon mortality in patients undergoing MVR.
Methods and results: The indexed valve effective orifice area (EOA) was esti-mated for each type and size of prosthesis being implanted in 929 consecutivepatients and used to define PPM as not clinically significant if >1.2 cm2/m2, asmoderate if >0.9 cm2/m2 and < 1.2 cm2/m2 and as severe if < 0.9 cm2/m2.Moderate PPM was present in 69% of patients and severe PPM in 9%. For pa-tients with severe PPM, 6-year survival (74±5%) and 12-year survival (63±7%)were significantly less than for patients with moderate PPM (84±1% and 76±2%;p=0.027) or non-significant PPM (90±2% and 82±4%; p=0.002). On multivari-ate analysis, severe PPM was associated with higher mortality (hazard ratio: 3.2[95% confidence interval: 1.5-6.8], p=0.003).Conclusion: Severe PPM is an independent predictor of mortality after MVR. Asopposed to other independent risk factors, PPM may be avoided or its severitymay be reduced with the use of prospective strategy at the time of operation. Forthe patients who are identified to be at risk of severe PPM, every effort shouldthus be made to implant a prosthesis with a larger EOA.
4881 Low molecular weight heparin versus unfractionatedheparin for the perioperative anticoagulant therapy inpatients undergoing mechanical prosthetic valvereplacement
L. Iliuta, D. Filipescu, H. Moldovan, B. Radulescu, D.P. Gherghiceanu,C. Macarie. Institute of Cardiovasc Diseases"C.C.Iliescu", Cardiac Surgery I,Bucharest, Romania
Background: Immediate postoperative anticoagulation regimens in mechanicalprosthetic valve replacement are only regulated for unfractionated heparinAim: comparing the efficacy and safety of Enoxaparin (E) versus unfractionatedheparin (UH) during the immediate postoperative period in patients undergoingmechanical prosthetic valve replacementMaterial and method. Open-label, randomized clinical trial enrolling 680 mechani-cal prosthetic valve patients in the immediate postoperative period that were givenE or UH in combination with oral anticoagulation until achieving INR optimal level.The primary endpoints were the composites of 30-day mortality, in-hospital pros-thesis thrombosis (safety endpoints), duration of hospital stay and immobilization,quality of life, and the above endpoint plus in-hospital intracranial hemorrhage orin-hospital major bleeding complications (efficacy plus safety endpoint). Statisti-cal analysis used Systat and SPSS programs for multivariate regression analysisand relative risk and correlation coefficient calculation.Results: 1. Anticoagulation with Enoxaparin was proven more effective than UHin the immediate postoperative management of mechanical prosthetic valve pa-tients, with an better cost-benefit report. 2. Subjective measures in Enoxaparingroup patients included clinical improvement with decreased immobilization andhospitalization periods, less gluteal ulcerations and less postoperative depressionepisodes. 3. Objective measures of Enoxaparin efficacy included maintenance ofnormal echographic prosthetic parameters, absence of early prosthesis thrombo-sis and rapid achievement of optimal INR with decreased parenteral anticoagula-tion period 4. The probability of death was smaller in the E group compared withthe UH group. 5. Minor hemorrhage and thrombocytopenia were more commonin the UH group. 6. Patient compliance was good, and quality of life improved dueto shortened hospital stay, less coagulation tests, increased dosing convenience,shortened immobilization in the immediate postoperative period with subsequentimprovement in the psychological status, as well as due to lack of significant sideeffects.Conclusions: Taking into account efficacy and safety, the anticoagulation of me-chanical valve prosthesis with Enoxaparin emerged as the best treatment in thistrial. Because of the better cost-benefit report and additional advantages suchas the ease of administration, the lack of need for monitoring of anticoagulation,reduction of the hospitalization duration, Enoxaparin should be regarded as anattractive alternative pharmacological anticoagulation strategy.
4882 Influence of socioeconomic status on survival afterprimary aortic or mitral valve replacement. Doesgender play a role?
J.P. Bagger, M.B. Edwards, K.M. Taylor. Hammersmith Hospital,Division Of Cardiology, London, United Kingdom
Background: Socioeconomic deprivation has been associated with morbidityand mortality in a variety of diseases. We sought to evaluate whether socioe-conomic status influences survival after first-time single aortic or mitral valve re-placement.Methods: Between 1st January 1986 and 31st December 2001, 51,844 consec-utive patients (mean age 64.6 ± 11.8 years; 29,089 males and 22,755 females)who underwent primary aortic or mitral valve replacement were registered on theUnited Kingdom Heart Valve Registry. Data included age, gender, valve position,type of valve implant, follow-up time, date and cause of death, and the Carstairsdeprivation score (1991 Census).Results: The study was 98.3% complete with 861 patients lost to follow-up giv-ing a total number of 268,830 patient follow-up years. Aortic valve replacementaccounted for 72% (n=37,079) of implants compared to 28% (n=14,765) mitralvalves. More men (n=23,565, 81%) than women (n=13,514, 59%) had aortic valvereplacement and conversely more women (n=9,241, 41%) than men (n=5,524,19%) had mitral valve replacement. 31,663 (61%) had a mechanical valves versus
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

834 Novel aspects in surgical treatment of valvular disease / Syncope – From genes to the elderly
20,181 (39%) with a bioprosthesis with no difference between men and women.Overall survival at 15 years did not differ between males (40%) and females(39%). Both 30-day and 1-year survival rates were similar across all (five) so-cioeconomic levels. However, long-term survival rate (15 years) was significantlyhigher in the least deprived socioeconomic level as compared to the two most de-prived levels (P<0.000). Neither age nor type of valve (mechanical/bioprosthesis)or site of valve (aortic/mitral) could explain this. There was a 18% long-term lowersurvival rate amongst women in the most deprived group (35.9%, 95% CI: 32.4-39.4) versus the least deprived group (43.7%, 95% CI: 38.1-49.2, P<0.004). Inmales, survival in the most deprived group (39.5%, 95% CI: 36.4-42.5) was 7%lower than in the least deprived group (42.7%, 95% CI: 37.7-47.7, P< 0.005). In amultivariate analysis, older age, female gender, bioprosthesis, mitral position andsocioeconomic deprivation were all associated with death. The ratio of cardiac tonon-cardiac related deaths did not differ between socioeconomic groups.Conclusions: A disadvantaged social background influences negatively long-term survival after aortic or mitral valve replacement especially among women.
4883 Autograft or allograft AVR in young adult patients withcongenital aortic valve disease?
J.J.M. Takkenberg, L.M.A. Klieverik, J.A. Bekkers, J. Roos,A.J.J. Bogers. Erasmus University Medical Center, Dept. ofCardio-Thoracic Surgery, Rotterdam, Netherlands
Purpose: Optimal prosthetic valve selection for young adult patients who requireaortic valve replacement (AVR) for congenital valve disease remains a topic ofdebate. We studied outcome of all young adult patients with congenital aorticvalve disease who underwent primary autograft or allograft AVR and are part ofour ongoing annual prospective follow-up study.Methods: Between 1987 and 2004 146 patients with congenital aortic valve dis-ease age 16-50 underwent autograft or allograft AVR (84 allografts (33 subcoro-nary, 51 roots) and 62 autograft roots). Patient and perioperative characteristics,cumulative survival and freedom from reoperation and valve-related events wereanalyzed.Results: Mean age was 36 versus 29 years for allograft and autograft recipi-ents respectively (SD 9, range 16-49;p<0.01), 67% males. Etiology was bicuspidvalve 85% and other congenital 15% (indication endocarditis:13%). 24% under-went prior cardiac or coarctation surgery; 10% had an ascending aorta aneurysm.Thirty-day mortality was 1.4% (2 autograft recipients). During follow-up (mean8.6 yrs, max 18.8 yrs, total 1254 patient-years, 99.3% complete) 5 patients died(4 valve-related), there were 32 valve-related reoperations (5 for non-structural(all subcoronary allografts), 26 for structural valve deterioration (16 allografts, 9autografts), 1 for endocarditis (allograft)), 1 TIA, 1 endocarditis. Thirteen-year cu-mulative survival was 90.5% (SE 4.7) versus 96.8% (SE 2.2) for allografts andautografts respectively (p=0.05), freedom from valve-related reoperation 55.5%(SE 8.5) versus 65.3% (SE 11.0) (p=0.04), and freedom from any valve-relatedcomplications 51.7% (SE 8.2) versus 61.7% (SE 10.6) (p=0.12).Conclusions: In patients with congenital aortic valve disease autograft AVR isassociated with better late survival compared to allograft AVR. Although freedomfrom reoperation is better for autograft recipients, both valve substitutes showalarmingly high reoperation rates in the second decade after operation.
4884 Sutureless Implantation Of Stented 3 F TherapeuticsATS Enable Aortic Pericardial Bioprosthesis
K. Bartus1, J. Sadowski1, B. Kapelak1, J. Myc1, R.C. Quijano2.1Jagiellonian University, Dept. of Cardiovascular Surgery andTransplan, Krakow, Poland; 23 F Therapeutics Inc, Lake Forest, USA
Objectives: This abstract presents clinical and hemodynamic experience with theSutureless Stented 3F Therapeutics/ATS Enable Aortic Bioprosthesis™. Valve ismade of equine pericardium and located in a specially designed self-expandingNitinol stent. This feasibility human clinical trial intends to validate and verify thedesign for AVR in humans. Primary focus is to evaluate ease of use, safety andefficacy.Methods: Seven patients have received the 3F Therapeutics Enable heart valveat the time of this abstract writing. Patients met the inclusion and exclusion cri-teria, and were between 70 and 80 years of age. The primary objective is toevaluate the safety of the device, with primary end-points of safety analyzing mi-gration, hemolysis and adverse device effects and outcomes in the small popula-tion at risk. Its Efficacy would be assessed by cardiac status evaluated by NYHAClassification and hemodynamic performance.Results: After typical transection of aorta and debridement, the device deploy-ment required <60 seconds to complete in all cases. Three patients received 27mm valve, three patients 25 mm valve, only one patient received 23 mm valve. Nomigration, no obstruction of coronary flow, no perivalvular leak or central regurgi-tation has been observed in one year follow up. Immediate post- operative echoshowed a peak gradient of 9 mmHg for 25 mm device. Peak systolic gradient forall patients was 11.5 mm Hg at discharge, 11.4 mm Hg at 3-6 months, 10.8 mmHg at one year follow-up. Mean gradient was 6.5 at discharge, 5.9 at 3-6 monthsand 5.8 mm Hg at one year follow up.Conclusions: Sutureless implantation of the 3F Enable Aortic Valve is feasibleand requires short cadiopulmonary bypass and aortic cross-clamp times, needingless than a minute to position and engage the self-expanding stent into patient’s
aortic annulus without any evidence of migration. No complications were found inone year follow up. To date, in this small cohort of patients, no adverse effects oroutcomes are evident.
4885 Clinical outcome following second pump run to reviseinitial mitral valve repair
A.R. Raney1, P.M. Shah2, A.A. Raney2. 1Newport Beach, UnitedStates of America; 2Hoag Heart and Vascular Institute, Cardiology,Newport Beach, United States of America
Purpose: Mitral Valve repair is the preferred treatment for degenerative valvedisease associated with mitral valve prolapse. In the arrested heart, the repairsuccess is tested and if the valve competence is deemed satisfactory, the patientis weaned off extracorporeal circulation. Subsequently, the valve competence inthe beating heart is tested by intraoperative transesophageal echocardiography(IOTEE). If moderate or greater residual regurgitation is observed, it is a commonprocedure to replace the valve. We hypothesized that IOTEE guided revision offailed repair may result in improved rate of successful repair and obviate needlessvalve replacement.Methods: A total of 207 consecutive patients with degenerative mitral valve dis-ease were subjected to valve repair between January 1, 2000 and December31, 2005. A total of 24 patients (12%) underwent second pump run after IOTEEdemonstrated moderate or greater residual valve regurgitation. Precise patho-logic anatomy responsible for persistent regurgitation was demonstrated. Addi-tional surgical procedures were performed in 15 of 24 patients consisting of coro-nary bypass graft in 6, MAZE procedure in 4, tricuspid valve surgery in 3, 1 closureof fistula and one closure of PFO.Results: IOTEE demonstrated post-repair SAM in eight cases, and residual re-gurgitation through distinct sites within the valve apparatus. Nineteen patients(79%) underwent successful revision of the valve repair. The surgical proceduresconsisted of a change in annuloplasty band size (10/19), addition or adjustment ofartificial chords (7/19) closure of "cleft" between leaflet scallops (6/19) and leafletreduction (4/19). Five patients underwent valve replacement (21%). The secondpump run resulted in an increase in perfusion time from 194 + 72 minutes to 284+ 69 minutes. Postoperative echocardiograms obtained between 5 days and 4months demonstrated mean left ventricular ejection fraction was 59 + 2.9%. Theseverity of regurgitation was none in 3, trace in 10, mild in 5, and moderate in 1.Conclusion: IOTEE may provide anatomic and pathophysiologic basis for failedinitial mitral valve repair. We conclude that in vast majority of cases a revisionof valve repair can be successfully carried out, thus avoiding needless valve re-placement. No adverse effects of prolonged perfusion time were observed.
SYNCOPE – FROM GENES TO THE ELDERLY
4886 Polymorphism of the human b1-adrenergic receptorand susceptibility to faint during head-up tilt test
G. Hernandez Pacheco, M.F. Marquez, M. Cardenas, G. VargasAlarcon, A.G. Hermosillo. Instituto Nacional de Cardiologia I Chavez,Physiology, Mexico D.F., Mexico
Background: Vasovagal syncope (VVS) is a common clinical problem. The β1-adrenergic receptor (β1AR) is the predominant subtype in the heart and its poly-morphisms are associated with both inotropic and chronotropic alterations. Thispaper describes the allelic and genotype frequencies of two polymorphisms ofβ1AR in subjects submitted to head up tilt test (HUT) because of VVS.Methods and Results: Fifty patients [mean age 27±13, 29 females (58%)] wereincluded in the study. All patients were submitted to a conventional HUT proto-col of two phases ("drug-free" and "isosorbide-challenge"). Thirty-three patients(66%) had a positive HUT, 11 at the spontaneous phase and 22 at the pharma-cological phase. A peripheral blood venous sample was obtained before HUT toisolate genomic DNA by a rapid nonenzymatic method assay. Polymorphisms atpositions 389 (Arg389Gly) and 49 (Ser49Gly) were determined by a polymerasechain reaction-restriction fragment length polymorphism method.Patients with apositive HUT had a significantly higher genotype frequency of Arg389Gly com-pared with those with a negative test (54% vs 6%; OR 13; p=0.005). The allelicfrequency of Gly389 in positive HUT patients was higher than in the negativegroup (30% vs 3%; OR 13; p = 0.006). No differences were found in genotypeand allelic frequencies of polymorphisms at position 49 among positive or nega-tive patients.
β-1 adrenergic-receptor in syncope
Positive (n=33) n/% Negative (n=17) n/% P OR
GF Arg-Arg 14/42.4 16/94 0.003 0.07Arg-Gly 18/54.5 1/6 0.005 13Gly-Gly 1 /3 0/0 0.397 –AF Arg 46/69.7 33/97 0.006 0.07Gly 20/30.3 1/3 0.006 13
P value corrected by Bonferroni. OR = odds ratio. GF = genotype frequencies. AF = Allelic fre-quencies
Conclusion: Polymorphic variation of the human β1AR at amino acid 389 mayconfers an increased risk of developing vasovagal syncope
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Syncope – From genes to the elderly 835
4887 Minor psychiatric disorders and vasovagal syncope
D. Leftheriotis1, I. Michopoulos2 , P. Flevari1, C. Koborozos1,A. Douzenis1 , G. Theodorakis3 , L. Lykouras1 , D. Kremastinos1.1ATTIKON University Hospital, Department of Cardiology, Atrhens,Greece; 2ATTIKON University Hospital, Department of General
Hospital Psychiatry, Athens, Greece; 3Onassis Cardiac Surgery Center, 2ndDepartment of Cardiology, Athens, Greece
Background: A high prevalence of minor psychiatric disorders (MPDs), whichare often underdiagnosed, has been observed among patients (pts) with vasova-gal syncope (VVS). However, the hypothesis that MPDs may predispose VVSepisodes has not been systematically tested.Additionally, the prevalence andmechanism of syncope observed in patients with MPDs has not been fully in-vestigated.Aim: To assess a) the sensitivity of the VVS reflex expressed as a positive re-sponse to head-up tilt test (HUTT) in pts with MPDs, and b) the efficacy of psy-chiatric treatment in reducing syncopal episodes in pts with MPDs and history ofsyncopes.Methods: We assessed the rate of a positive clomipramine-HUTT in 40 consec-utive pts (age 43±12 years) with recently diagnosed MPDs (22 with anxiety and18 with affective mood disorders), according to the DSM-IV-TRTM criteria. Theresults were compared with those in 40 age- and sex-matched pts with docu-mented VVS, and 40 matched normal controls. Pts with MPDs were treated withantidepressants and/or benzodiazepines for the next 12 months, and we com-pared the recurrence of their syncope during this period with that during the 12months before therapy.Results: The prevalence of unexplained syncope in the MPD group was 55%,which is higher than in the general population (Table). The rate of positive HUTTwas also higher than in controls (50% vs 5%). Among the 22 pts with MPD andsyncopal episodes this rate was similar to that in VVS pts (19/22, 86% and 34/40,85%, respectively). After psychiatric treatment, only 6 of these 22 pts reportedsyncopal episodes (p<0.01). The mean number of syncopal events per year wasalso decreased from 2.7±0.32 to 0.36±0.14 (p<0.01).
Table 1
Groups MPDs VVS Controls
Pts with syncopal events 22 (55%)*† 40 (100%)* 0 (0%)Pts with positive HUTT 20 (50%)*† 34 (85%)* 2 (5%)
Yates corrected X2 (*p<0.05 compared to Controls, p<0.05 compared to VVS).
Conclusions: MPDs are associated with an increased vulnerability to VVS, whichis reduced after psychiatric therapy. This implies that MPDs might be involved inthe pathophysiology of VVS, and their diagnosis and therapy may be important intreating effectivelly pts with recurrent vasovagal episodes.
4888 Association between beta2 adrenoceptor genepolymorphisms and neurocardiogenic syncope
D. Hachul1, A.C. Pereira2, M. Macatrao-Costa2, F.C. Darrieux2,C. Pisani2, M.I. Scanavacca2, J.E. Krieger2, E. Sosa2. 1Heart Institute(InCor) Sao Paulo University, Arrhythmia, Sao Paulo, Brazil; 2Heart
Institute (InCor) Sao Paulo University, Genetics, Sao Paulo, Brazil
Background: Neurocardiogenic syncope is a common disorder that affects atleast 20% of people at some time in their lives. Nevertheless, probably half ofthese patients faint recurrently. Despite the known familial aggregation of recur-rent syncope, few studies have aimed at identifying genetic markers for this con-dition. Here we have studied the distribution of beta2 adrenoceptor gene poly-morphisms in a population of patients with recurrent neurocardiogenic syncopewithout structural heart disease.Material and Methods: We have studied 112 consecutive patients with recur-rent syncope (74% female, mean age 21.6±13.6) and a positive tilt-table testing.Control group was composed of 1576 individuals selected from the general pop-ulation with no history of syncope and no structural heart disease. Beta2 adreno-ceptor gene polymorphisms (namely, the Arg16Gly, Gln27Glu and Thr164Ile poly-morphisms) were genotyped by PCR-RFLP in each participant. Baseline demo-graphic data and tilt-table testing result were available for cases and demographicdata were available from controls. Hardy-Weinberg Equilibrium was determinedby the Chi-square test. Chi-square test was used for univariate comparison ofgene frequencies and logistic regression analysis was used for multivariate com-parison.Results: The most common pattern of tilt-table testing response was mixed(50.0%), followed by vasodepressor (37.2%), cardio-inhibitory (10.6%) and POTS(1.1%). Allele and genotype frequencies were in Hardy-Weinberg Equilibriumin cases and controls. No association regarding the Arg16Gly (p=0.87), theThr164Ile (p=0.95) was observed in univariate analysis comparing genotype fre-quencies in cases against controls. Interestingly, presence of the GlnGln geno-type for the Gln27Glu polymorphism conferred a significantly increased the riskof recurrent syncope, (p=0.03, OR 1.54).Conclusions: A positive association between beta2 adrenoceptor Gln27Glupolymorphism and recurrent syncope was verified in our study. These data shouldbe replicated and extended. The investigation of genetic markers associated withsyncope may not only shed light in its pathophysiological determinants, but alsoconstitute clinical markers for disease prediction and stratification.
4889 Clinical features related to orthostatic hypotension inan elderly community-dwelling population
C. Mussi, M. Foroni, A. Travaglione, M.D. Campanozzi, F. Salsi,G. Salvioli. Chair of Geriatrics, Ospedale di Baggiovara, Geriatrics,Modena, Italy
Background: The evaluation of orthostatic hypotension (OH) is easy, cheap andquick, but it is not already routinarily assessed in clinical practice, even though itis a well known cause of syncope and falls, and frequently it may represent anadverse drug reaction. The aim of the study is to identify clinical factors related toOH in an elderly community-dwelling population.Methods: 750 subjects consequently recruited during ambulatory cardiogeriatricvisits from september 1st, 2000 to March, 30th, 2005, were submitted to phys-iologic, clinical and pharmachologic history, antropometric evaluation, standard12-leads ECG and measurement of heart rate variability (HRV, index of auto-nomic nervous system activity). Blood pressure (BP) was measured at the end ofthe visit, in sitting position, and after 1 and 3 minutes of active standing. OH wasdefined as a reduction of systolic BP (SBP) greater than 20 mmHg from sittingto standing. 19 patients were excluded because of the incapacity of maintainingstanding position; 731 subjects (mean age 75.8 ± 6.8 years, 41% males) weredivided in 2 groups, according to the presence of OH: no OH, N=559, OH, N=172.Results: There were no differences between the two groups in terms of age, sex,and antropometric variables. Sitting SBP (161.9 ± 19.3 vs. 150.9 ± 22.3 mmHg,p<0.001) and diastolic BP (95.3 ± 14,6 vs. 88.0 ± 14,6 mmHg, p<0.001) werehigher in OH group. OH patients had a reduced HRV (6.6 ± 3.4 vs. 11.5 ± 5.9bpm, p=0.004), and took a greater number of calcium-channel blockers (29.2%vs. 22.6%, p=0.042), benzodiazepines (32.1% vs. 22.1%, p=0.006) and neurolep-tics (5.4% vs. 1.8%, p=0.018). Patients with OH were more likely to complaindizziness and light-headedness (55.6% vs. 33.9%, p=0,008), and the number offalls was higher in this group (median value: 2 vs. 0, p=0.034). Multivariate analy-sis confirmed the association between OH and high blood pressure at rest (SBP:p=0.003, DBP: p=0.005); also the use of benzodiazepines (p=0.014) and neu-roleptics (p=0.010) is associated to a higher risk of OH, independently from age,sex, and comorbidity.Conclusions: While antihypertensive drugs are commonly described as the ma-jor cause of OH, our data show a strong correlation between OH and a poorcontrol of BP, suggesting that uncontrolled hypertension blunts baroreflex sensi-tivity; medications active on the central nervous system, like benzodiazepines orneuroleptics, show the same association. Clinicians should pay attention to thesefindings to reduce the risk of falling in the old patient.
4890 A new therapeutic approach to neurocardiogenicsyncope
A. Kostopoulou, G. Theodorakis, E. Livanis, D. Leftheriotis, P. Flevari,D.T. Kremastinos. Onassis Cardiac Surgery Center, Athens, Greece
Purpose: Multiple mechanisms, central and peripheral, have been im-plicated in the pathophysiology of neurocardiogenic syncope (NCS). We testedthe efficacy of a therapeutic strategy that could block both central and peripheralfactors in patients (pts) with NCS.Methods: Eighty-seven pts with a clinical history suggestive of NCS underwenta head-up tilt-test with clomipramine challenge since October 2004. The test waspositive in 64 patients. Twenty-five pts (mean age 38.2±14.5 years, 9 men and15 females) with a positive head-up tilt test and > 5 total syncopal spells or 2episodes in the previous 6- months were included in the study after written in-formed consent. They randomly (1:1) received the combination of a serotonin re-uptake antagonist (SSIR- fluoxetine 20 mg per day) and a beta- blocker (atenonol12.5-25 mg per day) or placebo. Pts were followed-up at 3-month periods. Sta-tistical analysis: Results are expressed as mean±SD. Kaplan Meier analysis wasperformed with the Log-Rank test.Results: Thirteen pts received the combination of fluoxetine and atenolol and 12received placebo. There was one withdrawal from the placebo group. We followedup our pts for a period of 9±3.6 months (range: 2.5 to 14.5 months). Syncopalepisodes 6 months prior to inclusion in the study were 3.3±2.5 in the fluoxetine-atenolol group and 2.7±1.5 in the placebo group (p: non significant). Total synco-pal episodes during follow up decreased significantly in both groups when com-pared to baseline 6-month episodes (0.3±0.6 in the fluoxetine- atenolol groupand 1.2±1.0, in the placebo group, p<0.05). Ten (76.9%) pts remained free ofsyncope in the fluoxetine- atenolol group and 4 (36.3) in the placebo group. Ka-plan Meier analysis with respect to the first recurrence of syncope revealed thatfluoxetine - atenolol was significantly more effective than placebo (Log-Rank testp=0.035). One pt from each group had syncope with severe trauma and had apacemaker implanted.Conclusions: Primary results show that a combined therapeutic strategy thatblocks both central and peripheral mechanisms, implicated in the pathophysiologyof NCS, might be very promising.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

836 Syncope – From genes to the elderly / Management of stroke risk in the atrial fibrillation – new insights
4891 Medium term prognosis of cardiogenic syncope
A. Bartoletti1, P. Fabiani2 , L. Bagnoli3, C. Cappelletti3, M. Cappellini2,R. Gianni2, A. Lavacchi2, G.M. Santoro1. 1Cardiology Un.-N.S.Giovanni di Dio Hospital, Cardiology, Florence, Italy; 2InternalMed.-N.S.Giovanni di Dio Hospital, Internal Medicine, Florence,
Italy; 3Emergency Dpt-N.S.Giovanni di Dio Hospital, Emergency Department,Florence, Italy
Aim: Clinical reports published in the 80ies demonstrated a greater medium termmortality for patients (pts) with cardiogenic syncope (card-s) compared with thosewith other origin syncope (noncard-s) and mainly due to sudden death. In thepresent study pts with card-s were compared with those with noncard-s and non-syncopal (n-s) transient loss of consciousness (TLC) regarding the medium termoutcome.Methods: Starting from August 2002, all the patients referred to our EmergencyDepartment (ED) for a TLC were evaluated according to the specific EuropeanSociety of Cardiology Guidelines. Clinical data were collected in a dedicated database. Twelve months after the first observation, total mortality (TM), sudden mor-tality (SM), and recurrencies (REC) were investigated by phone call.Results: Between 09/01/2002 and 03/31/2004, 848 patients with TLC (493 M,age 60±23 years) were observed. The main clinical data are reported in the tablebelow. The main causes of death were stroke for n-s pts while non-cardiovascularco-morbidities for both card-s and noncard-s subjects.
Table 1. Clinical data according to TLC type
TLC type N. Pts SM p* TM p* REC p*
n-s 90 2 ns 14 ns 23 0.01card-s 79 2 / 10 / 8 /noncard-s 679 8 ns 36 0.02 30 ns
*vs card-s; ns: not-significant.
Conclusions: Our data, quite different from previous clinical observations, sug-gest a favourable impact of therapeutic tools now available for card-s. As a con-sequence guidelines-based, in-hospital models of care and management of syn-cope are warranted.
MANAGEMENT OF STROKE RISK IN THE ATRIALFIBRILLATION – NEW INSIGHTS
4892 Use of warfarin and performance of stroke riskstratification models in atrial fibrillation
A. Palacio, D. Parris, J. Chirinos, B. Lopez-Sanabria, G. Chen,H. Florez, L. Tamariz. Miami, United States of America
Purpose: Stroke is the main complication of atrial fibrillation (AF). Riskstratification models are used to predict stroke rates and guide therapy. We aimedto determine the use of warfarin in patients with AF by their risk of stroke andcompare the different stroke risk stratification models.Methods: The study consisted of a retrospective cohort of 18,197 subjects from alarge health benefits company with AF who used rate-controlling medications andwere continuously enrolled for a period of 12 months. We compared the follow-ing stroke risk stratification models: CHADS2 (an acronym for congestive heartfailure, hypertension, age > 65, diabetes, prior stroke), AFI (atrial fibrillation in-vestigators), SPAF (stroke prevention atrial fibrillation) and Framingham scores.We determined the incidence of stroke over 12 months of follow-up by categoriesof risk on each risk stratification model using person-time analysis and the areaunder the receiver operating characteristic curve (ROC) of each risk stratificationmodel.Results: Only fifty percent of the cohort used warfarin despite increasing risk ofstroke (table). The areas under the ROC curves were: CHADS2 score 0.66 (95%CI 0.65-0.67), SPAF 0.58 (95% CI 0.57-0.59), for AFI 0.55 (95% CI 0.55-0.56)and for the Framingham score 0.66 (0.65-0.68).
Table 1. Risk of stroke and warfarin use by risk stratification model
Stroke risk Categories Annual risk of stroke % Use of Area under the ROCstratification model of risk per 1000 peson-years warfarin (95% CI)
CHADS2 Low 0.12 51 0.66 (0.65-0.68)Moderate 0.29 49
High 0.98 50Framingham Low 0.087 52 0.66(0.65-0.67)
High 0.40 49AFI Low 0.10 50 0.58 (0.57-0.59)
High 0.41 50SPAF Low 0.16 51 0.55 (0.55-0.56)
High 0.45 49
Conclusions: There is a need to improve anticoagulation use in patients withAF. The CHADS2 and Framingham risk scores are better predictors of stroke riskthan other risk stratification models.
4893 Usefulness of antithrombotic therapy among elderlyhigh risk patients with atrial fibrillation
A. Macchia, S. Monte, M. Romero, A. D’ettorre, V. Lepore, G. Tognoni.Consorzio Mario Negri Sud, Clinical Pharmacology and Epidemiology,Santa Maria Imbaro, Italy
Despite evidence suggesting mandatory the use of antithrombotic treatment(ATT) in patients with atrial fibrillation (AF), observational studies demonstratedthat physicians and patients are reluctant to prescribe/receive anticoagulation(ACO). The impact of these decisions are unknown.Aim: to investigate the determinants of ATT with ACO and antiplatelet agents(APL) after an hospitalization with AF and the attributable effectiveness of ATTduring follow-up.Methods: Population study, linking administrative datasets from hospital dis-charge, prescription databases and vital statistics, including all consecutive pa-tients aged 65 years or older with AF in 3 regions in Italy from 1/00 to 12/03.Comorbidities were identified using previous prescription patterns and hospital-izations. Follow-up was extended up to 1 year. Cox proportional hazard modeladjusted for major confounders was fitted.Results: AF was present in 1,920 out of 25,012 patients (7.7%). Mean age was79 ± 7 years. Patients had high rate of cardiovascular and non cardiovascularcomorbidities: only 190 patients (9.9%) had age alone as risk factor for stroke.Among the 1,812 patients discharge from hospital, 521 (28.7%) received ACO,392 (21.6%) APL, and 89 (4.9%) both agents. Factors significantly associatedwith ATT were age (0.93 [0.92-0.95], p<0.001), malignancy (0.57 [0.39-0.82],p=0.003), COPD (0.77 [0.59-1.00], p=0.05) and previous use of ATT (4.56 [3.67-5.67], p<0.001). Patients exposed to ATT had a significantly lower mortality, -77%(-65% to -85%) with ACO and -34% (-14% to -50%) with APL. ACO was associ-ated with 0.52 (0.25 - 1.07) (p=0.07) reduction on thrombo-embolic events. Theseresults were homogeneous among different subgroups of patients.Conclusion: High risk community patients were undertreated with ACO and APLafter an hospitalization with AF. Age and comorbid conditions are related to under-treatment. ATT was associated with a significant reduction in total mortality andACO was associated with reduction of thrombo-embolic events.
4894 Antithrombotic drug prescription and its rationaleamong general practitioners, internal medicinespecialists and cardiologists in The Netherlands. TheEXAMINE-AF study
N.H.T. Dinh1, R. Nieuwlaat1, H.R. Buller2, N.A. Mensing VanCharante3, H.J.G.M. Crijns3. 1University Hospital Maastricht, CardiologyDepartment, Maastricht, Netherlands; 2Academic Medical Centre, VascularMedicin, Amsterdam, Netherlands; 3Amsterdam, Netherlands
Background: Guidelines on atrial fibrillation (AF) mainly focus on prevention ofthromboembolism. The EXAMINE-AF study recorded antithrombotic treatment(ATT) and adherence to the present guidelines in patients with AF in the dailypractice of Dutch general physicians (GPs), internists and cardiologists.Methods: Between October 2004 and March 2005, 300 Dutch GPs, internistsand cardiologists filled in questionnaires of consecutive AF patients for stroke riskfactors (SRF) and significant bleeding risk factors (BRF). Guideline were adheredif patients had (a) no SRF or BRF and received aspirin or no ATT, (b) ≥1 SRF andno BRF and received oral anticoagulation (OAC), or (c) ≥1 SRF and ≥1 BRF andreceived aspirin. Patients were overtreated if they had (a) no SRF but received noOAC, and (b) ≥1 BRF and received OAC. Patients were overtreated if they had≥1 SRF and no BRF but received to OAC.Results: 86 GPs, 93 internists and 99 cardiologist enrolled 1596 patients. Cardi-ologists patients were younger, had less hypertension and heart failure. Internistspatients were older and had more BRF factors. Numbers of patients who wereovertreated, undertreated or treated correctly according to the guidelines are de-picted in table 1. A cardiologist was indicated to be the main treating physicianfor AF in 82% of all patients and they prescribed current ATT in 80%. When se-lecting the physician who prescribed current ATT, cardiologists treated more oftenaccording to the guidelines (58, 55 and 70%: p<0.001).
Table 1. Overview of antithrombotic treatment
GP Internist Cardiologist p-valuen=365 n=351 n=880
Guideline followed 68% 63% 71% <0.001Undertreatment 20% 14% 11%Overtreatment 12% 23% 18%Physician prescribing current ATT n=161 n=99 n=1292Guideline followed 58% 55% 70% <0.001Undertreatment 33% 28% 11%Overtreatment 9% 17% 19%
Conclusion: Antithrombotic treatment is mainly handled by cardiologists andcompared to GPs and internist, cardiologists adhere best to the guidelines. There-fore, patients with AF should at least be seen by cardiologist once, as cardiolo-gists seem to be more aware of the guidelines.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Management of stroke risk in the atrial fibrillation – new insights / CVD risk prediction in Europe: where do we stand? 837
4895 Additive role of plasma von Willebrand Factor levels toclinical risk stratification in patients with atrialfibrillation
G.Y.H. Lip1, D.A. Lane1, C. Van Walraven2, R.G. Hart3. 1City Hospital,University Department of Medicine, Birmingham, United Kingdom;
2Ottawa Health Research Institute, Ottawa, Canada; 3University of Texas HealthScience Center, Texas, United States of America
Background: Several risk stratification schemes predicting stroke risk based onclinical and echocardiographic features have been published to aid decisionsfor thromboprophylaxis in atrial fibrillation (AF). von Willebrand factor (vWf) isa plasma marker of endothelial damage/dysfunction and is associated with in-creased risk of stroke and vascular events in AF patients. This study determinedthe additive role of plasma vWF levels to clinical factors for risk stratification in AFpatients.Methods: We classified 994 AF patients [mean (SD) age 69.3 (9.4) years; 75%male] enrolled in the SPAF III trial as being at low, moderate, or high risk ofstroke or thromboembolism, using the Birmingham and CHADS2 risk stratifica-tion schemes. vWf levels were classified as elevated if 158iU/dL or more. Ratesof ischemic stroke and vascular events within each clinical risk strata ± plasmavWf levels were compared.Results: Both clinical risk stratification schemes were similar in their accuracy forpredicting event rates with and without the addition of categorized vWf levels. An-nualised event rates were greatest on both risk stratification schemes for patientscategorised as ‘high risk clinical criteria plus high risk vWf levels’ (Table 1). Clearseparation of the annualised event rates (95% CI) for ‘moderate risk on clinicalcriteria plus low vWf levels’ compared to ‘high risk on clinical criteria plus low vWflevels’ was evident for both ischaemic stroke and vascular events. When addedto the Birmingham and CHADS2 clinical risk stratification, high vWf levels wereindependently associated with an increased risk of vascular events [HR (95% CI),2.05 (1.30-3.22) and 2.01 (1.27-3.18), respectively] but not ischaemic stroke [HR(95% CI), 1.72 (0.94-3.14) and 1.61 (0.87-2.96), respectively].
Annualised event rates by clinical risk & vWf
Hazard ratio (95% CI) Low risk Moderate risk High riskLow vWf High vWf Low vWf High vWf Low vWf High vWf
Ischaemic stroke (n=43)Birmingham 0 0 1.44 3.18 4.88 6.98
(0.69-2.48) (1.44-5.59) (2.51-8.04) (3.59-11.5)CHADS2 0.54 1.09 2.24 3.73 5.68 8.37
(0.05-1.56) (0.00-4.27) (1.22-3.56) (1.85-6.26) (2.04-11.1) (3.79-14.7)Vascular events (n=77)
Birmingham 1.2 0 1.88 5.02 8.66 16.3(0.12-3.58) (1.00-3.04) (2.74-8.00) (5.35-12.8) (10.8-23.1)
CHADS2 1.09 2.21 4.02 7.23 6.62 17.6(0.28-2.42) (0.21-6.33) (2.60-5.74) (4.47-10.6) (2.63-12.4) (10.4-26.7)
CI, confidence intervals; vWf, von Willebrandfactor
Conclusions: Plasma vWf levels, when added to clinical risk scores, refined clini-cal risk stratification for stroke and vascular events among AF patients. vWf levelsmay aid decisions about thromboprophylaxis, particularly among AF patients atmoderate risk.
4896 Atrial fibrillation: bridging of chronically anticoagulatedpatients with low molecular weight heparin prior tointerventional procedures - experience in 455 patientsfrom the BRAVE-registry
C. Hammerstingl, H. Schmidt, A. Schmitz, C. Platen, G. Von DerRecke, H. Omran. St. Marien Hospital, Internal Medicine, Bonn, Germany
Background: It is recommended to discontinue oral anticoagulation (OAC) inchronically anticoagulated patients (pts) with atrial fibrillation (AF) and concomit-tant thromboembolic (TE) risk factors prior to interventions with high risk of bleed-ing. To prevent TE complications, pts should receive weight adapted bridgingtherapy with unfractioned heparin intravenously. Low molecular weight heparins(LMWH) have a higher bioavailability and more predictive anticoagulatory effect,therefore, effective anticoagulant therapy can be achieved by subcutaneous ap-plication of LMWH. We recommend TE-risk adjusted dosage of LMWH in pts withAF. The aim of this registry was to assess the safety and practicability of bridgingtherapy with LMWH in TE-risk adapted dosage.Methods: Chronically anticoagulated pts with AF and indication for interruption ofOAC were included in the registry. Pts at high TE-risk (AF and several concomi-tant risk factors; LAA thrombus and/or dense spontaneous echocontrast; historyof thromboembolism; chronic heart failure) received weight adapted enoxaparins.c. twice a day (0,1mg/kgBW/12h). The remaining patients (n = 131) recievedenoxaparin in half therapeutic dosage. Procedures were performed at INR<1.5.After procedure OAC was reintroduced under LMWH therapy until effective INRwas reachieved. All pts were followed up regarding bleeding complications, oc-currence of clinical signs of thromboembolism and other adverse events underLMWH-therapy.Results: 455 pts were treated with enoxaparin, 324 with AF at high thromboem-bolic risk, 131 pts at intermediate thromboembolic risk. Age 73.3±10.5 y; meantreatment time 7.2±5.1 d; 44 pts underwent major surgery, 411 minor surgeryor other interventions with high risk of bleeding. In 19 pts occurred minor bleed-
ing, 0 major bleeding. No thromboembolic complication evolved due to bridingtherapy.Conclusions: Bridging therapy with low molecular weight heparin (enoxaparin)is safe and feasible in a large cohort of patients with atrial fibrillation. We recom-mand dose adjusted treatment according to the individual thromboembolic risk.
4897 Ischemic cerebrovascular events in the long-termfollow-up after intraoperative catheter ablation of atrialfibrillation
H. Tanner, G. Hindricks, C. Piorkowski, R. Kobza, J.H. Gerds-Li,H. Kottkamp. Leipzig, Germany
Background: The occurrence of ischemic strokes after catheter ablation of atrialfibrillation (AF) has not been reported so far. It is unclear, whether and whencessation of oral anticoagulation after successful ablation therapy can be donesafely.Methods: In this study, patients (pts) were treated with the specific left atrial lin-ear lesion line concept targeting at the perpetuation of AF using intraoperative ab-lation with minimal invasive surgical techniques (IRAAF). The aim of the presentstudy was to prospectively analyse the occurrence of ischemic strokes in the long-term follow-up.Results: In 118 pts (age 53 ± 9, 78% males) a mean follow-up of 3.8 ± 0.7 yearswas available. Freedom from AF using 7-days-ECGs measured 78%. Oral antico-agulation was stopped in 79% after a median duration of 6 months (range 0-56).A low risk for ischemic cerebrovascular events (CHADS2-score 0-1) was presentin the majority of pts (n=112, 95%). Six pts (5%) had a high CHADS2-score of 2or 3, all of them with a history of ischemic stroke before the intervention. Duringfollow-up, a total of 6 (5%) ischemic events (TIA n=2, Stroke n=4) were identi-fied. Three of them were directly related to the left atrial AF ablation procedurewith symptoms occurring during or immediately after the intervention. One is-chemic event happened during cessation of oral anticoagulation for implantationof a pacemaker and AV-node ablation because of recurrent AF. Two pts withoutAF recurrence during follow-up (one during ongoing oral anticoagulation) had anischemic stroke, both of them with a history of ischemic stroke before the proce-dure having a CHADS2-score of 2 or more. Therefore, 2 of 6 pts (33%) having ahistory of ischemic stroke before AF ablation had such an event during follow-up.Conclusions: In pts with low-risk for ischemic cerebrovascular events and suc-cessful intraoperative ablation of AF cessation of oral anticoagulation 6 monthsafter the procedure seems to be safe. However, in high-risk pts with a history ofischemic stroke, the risk of future ischemic cerebrovascular events seems to besubstantial, even if ablation is successful.
CARDIOVASCULAR DISEASE RISK PREDICTION INEUROPE: WHERE DO WE STAND?
4923 Different results of the Procam-Score,Framingham-Score and for Germany regionalisedESC-Score for detection of coronary high risk patients:results of 48623 persons
S. Silber1, B. Bischoff2, P. Lochow2, B.M. Richartz2, L. Pieper3,J. Klotsche3, H.U. Wittchen3. 1Cardiology Practice And Hospital, Cardiology,Munchen, Germany; 2Cardiology Practice and Hospital, Munich, Germany;3Technical University of Dresden, Dresden, Germany
Background: It is reasonable to evaluate the individual risk for a coronaryevent in persons without typical angina pectoris or if no sign of ischemia ispresent (primary prevention). For this purpose the Framingham-Score in theUnited States was created (5251 individuals, age 20-79). In Europe the Procam-Score is more widely used (5389 individuals, age 35-65). Both scores prognosethe coronary morbidity and mortality. In 2003 the European Society of Cardiol-ogy (ESC) developed a score to prognose the cardiovascular mortality includingstroke (205178 individuals). This ESC-score was recently regionalised for Ger-many (Heart Score). "High risk" is a Framingham- and Procam-Score risk of over20%/10 years (morbidity and mortality), an ESC-Score of over 5%/10 years (mor-tality). The goal of this analysis was to determine the percentage of high riskpatients in general practices in Germany using these different scores.Methods: On September 16th or September 18th, 2003, between 7 a.m. and1 p.m. or between 1 p.m. and 6 p.m. all patients in 3795 general practices inGermany were counted. 6895 patients had known coronary artery disease (CAD).The following analysis includes 48623 patients with no known CAD. The everageage of this patients was 51.8 ± 17.1 years, 38.5% were male, 27.5% smoker,18.5% former smoker, 25% had hypelipidemia, 11.9% were diabetic, 31.4% hadhypertension and 13.8% had a positive family history of CAD.Results: The high risk patients generated from the different scores are shown inTable 1. The rate of coronary/cardiovascular high risk patients in general practices
Table 1
Procam Framingham ESC-Germany
Male (%) 13.1 43.6 33.6Female (%) 9.2 21.7 10.1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

838 CVD risk prediction in Europe: where do we stand?
is different according to the scores used. According to the regionalised ESC-Score for Germany every third male and every tenth female would be consideredas "high risk".
4924 Social deprivation confounds equity when applying theFramingham coronary risk score to the Scottishpopulation
H. Tunstall-Pedoe1 , M. Woodward2 on behalf of the SIGN groupon risk estimation. 1Ninewells Hospital And Medical School,
Cardiovascular Epidemiology Unit, Dundee, United Kingdom; 2George Institute,Sydney, Australia
Purpose The objective of cardiovascular risk scores is to target preventive treat-ment equitably to those in greatest need, while many national policies seek todiminish social gradients in disease. The effect of social deprivation on cardio-vascular risk is known to be inadequately explained by conventional risk factors.How much does this matter when the Framingham and similar scores are used inpractice?Methods 6419 men and 6618 women free of coronary heart disease in theSHHEC study were recruited randomly from the Scottish population from 1984onwards and followed for coronary morbidity and mortality to March 1997. Base-line risk factor data were used to calculate a Framingham score for all coronaryheart disease. Home address was used to allocate each participant to a fifth ofthe Scottish Index of Multiple Deprivation (SIMD) (1=least and 5 = most deprived)which is based on census and other administrative data on many different socialvariables.Results Women showed a greater social gradient in observed coronary diseasethan men. With sexes combined, age standardized results showed a gradient inobserved relative risk by SIMD fifth of 1.00, 1.81, 1.98, 2.22 and 2.57. The Fram-ingham score overestimated coronary risk overall but seriously underestimatedthe social gradient, predicting a social gradient (relative risk) of only 1.00, 1.17,1,19, 1.28, and 1.36. The ratio of observed, to this expected (predicted) risk whichdetermines preventive treatment, therefore showed a strong residual social gra-dient of 1.00, 1.56, 1.66, 1.74 and 1.88.Conclusions: Using the Framingham score unadjusted, the most socially de-prived would receive only half as much preventive treatment in relation to theiractual risk as would the least deprived. To the extent that prevention works, uni-form application of the Framingham score in Scotland would exacerbate socialgradients in coronary disease, frustrating national policies to reduce these gradi-ents. We are exploring with the Scottish Intercollegiate Guideline Network (SIGN)alternative strategies: either of adjusting the Framingham score to take accountof social deprivation; or of developing and implementing a cardiovascular riskscore which includes an index of social deprivation along with conventional riskfactors. Similar problems arise in populations with different ethnic groups. For var-ious reasons, however, existing risk scores remain preferable to unguided clinicaljudgement.
4925 SCORE estimated and true observed CVD deaths inEast Finland: the kuopio ischaemic heart disease riskfactor (KIHD) study
T.-P. Tuomainen, J.A. Laukkanen, S. Kurl, V.-P. Valkonen,K. Ronkainen, J.T. Salonen. University of Kuopio, Atherosclerosis
Research Unit, Kuopio, Finland
Total risk assessment is recommendable and has gained popularity among physi-cians in the evaluation of cardiovascular risk of a single patient. There are severalCVD risk assessment tools available, like the U.S. Framingham Risk Index andthe European SCORE. We wanted to test the predictive performance of suchtool, using true observed cardiovascular deaths (in SCORE evaluations) in a highrisk population. For this purpose, we compared the SCORE estimated and ob-served cardiovascular deaths in 2 682 42 to 60 years old men who participated inthe KIHD cohort study in East Finland. We also used a logistic regression modelwith more variables than included in the SCORE model, for further comparison.During a 10-year period from study baseline in 1984-89, 147 CVD deaths wereobserved. Using SCORE model with baseline risk factors, 63 fatal CVD eventswere expected, producing a 57.1% underestimate. A multivariate logistic regres-sion model, allowing for age, smoking, socio-economical status, obesity, physicalactivity, blood pressure, blood lipids, glucose homeostasis and family history ofCHD, predicted 103 CVD deaths (vs. 128 observed), in 2408 subjects with non-missing data, producing a 19.6% underestimate. Overall accuracy of the modelwas 94.7%. If prior CHD was used as a stratifier, total performance of SCOREwas somewhat better among CHD-free than those with prior CHD. Logistic re-gression performed equally well in both groups. Risk functions in form of tablesare easy to use and they can be very helpful in fast total risk assessment. Also theimpact of a change in any risk factor used is instantly demonstrable to a patient,and can be used to motivate the patient in adopting a healthier life style, for ex-ample. However, our findings warrants population-area -tailored risk assessmenttools to take full advantage of the already large knowledge base of CVD risk func-tions. The general risk functions should be tested and, when needed, adjusted toaccommodate local variance.
4926 Acute coronary syndrome risk models: validation usingthe Myocardial Infarction National Audit Projectdatabase
C.P. Gale1, S.O.M. Manda2, P.D. Batin3, J. Birkhead4, A.S. Hall1.1Leeds General Infirmary, Department Of Cardiology, Leeds, United
Kingdom; 2University of Leeds, Biostatistics Unit, Leeds, United Kingdom;3Pinderfields General Infirmary, Department Of Cardiology, Wakefield,United Kingdom; 4Northampton General Hospital, Department Of Cardiology,Northampton, United Kingdom
Risk models help medical decision-making for patients with acute coronary syn-dromes (ACSs) but many are developed from randomised controlled trials and areonly validated in the derivation cohort. We used the MINAP database, a UK reg-istry of ACSs, to externally validate popular ACS risk models and to see if modelsdeveloped on different populations may be applied to our UK population. We haddata for 187,069 patients and validated the following risk scores and models: TIMIscore for unstable angina/NSTEMI, TIMI score for STEMI, and Simple Risk Index;and the PURSUIT, GUSTO-1, EMMACE, and GRACE risk models. We found thatthe TIMI and SRI showed a significant increased risk of death with increasing riskscore at 30-days (TIMI OR = 1.288 and 1.604, respectively, per unit increase inscore; upper quintile versus lower quintile SRI = 34% to 1.6%). We found that theGRACE, GUSTO-1 and PURSUIT risk models had better performance in discrim-inating death (table).
ACS risk model performance
Model C index 95% CI P value
TIMI (NSTEMI/UA) 0.584 0.574 to 0.594 <0.001GRACE in-hospital 0.804 0.798 to 0.810 <0.001GRACE 30-day 0.789 0.783 to 0.796 <0.001GRACE 180-day 0.799 0.794 to 0.804 <0.001PURSUIT 0.788 0.779 to 0.797 <0.001GUSTO-1 0.800 0.793 to 0.807 <0.001EMMACE 0.774 0.769 to 0.778 <0.001EMMACE (Our P30) 0.776 0.771 to 0.781 <0.001
However, the EMMACE models require less baseline data to obtain a comparableprediction of 30-day death. The commonly used TIMI unstable angina/NSTEMIrisk score was not a good predictor of 14-day death in a UK community-basedpopulation. Risk scores should be validated in the population to which they are tobe applied, so that accurate predictions of clinical end points may be made.
4927 European and American prevalence of subclinicalatherosclerosis and risk factors: similarities anddifferences of the Heinz Nixdorf Recall Study (HNRS)and Multi-Ethnic Study of Atherosclerosis (MESA)
R. Erbel1, S. Mohlenkamp1, S. Moebus2, A. Schmermund3 ,A. Stang4, N. Dragano5, E.-M. Beck3, K.-H. Joeckel3 on behalf of Heinz NixdorfRecall Study Group. 1West-German Heart Center Essen, Dept. of Cardiology,Essen, Germany; 2University Clinic Essen, Essen, Germany; 3CardiologischesCentrum Bethanien, Frankfurt, Germany; 4University Clinic Halle, Halle,Germany; 5University Clinic Dusseldorf, Dusseldorf, Germany
The Heinz Nixdorf Recall Study (HNRS) and the Multi-Ethnic Study of Atheroscle-rosis (MESA) are ongoing population-based cohort studies on the prognosticvalue of measuring subclinical atherosclerosis - especially coronary artery cal-cium (CAC) - versus established and new markers of cardiovascular (CV) risk.Here, we compare the trials in design, methodology and results of the screeningperiod.Methods: MESA (performed in 6 US-centers) assesses differences among eth-nic populations (aged 45-84); HNRS (performed in 1 center) is performed in cau-casians only (aged 45-74). HNRS were randomly recruited from city registries,which was not possible in MESA. MESA uses EBT- and MSCT-scanners; HNRSuses EBT only. A stress-ECG is part of HNRS only. Aortic compliance and en-dothelial dysfunction is assessed only in MESA. Both trials also include carotidIMT, ankle-arm-index, resting ECG, and genetic markers of CV risk.Results: Blood pressure and lipid values are higher in HNRS (Tab). The rate ofwomen (52%), smokers (57%), known hypertension (36%) and diabetes (7.7%)is similar as is the BMI (28±5). The prevalence of a positive CAC is 82% vs. 70%(MESA vs. HNRS) in men and 55% vs 45% in women. Yet, percentile ranks arelower in HNRS in both sexes (Table).
HNRS MESA
RR syst [mmHg] 133±20 124±20LDL [mg/dL] 147±38 117±30HDL [mg/dL] 59±29 52±16Caucasian men [n] 1918 1259
50th Percentile 55 4875th Percentile 240 29890th Percentile 722 1595
Caucasian women [n] 2147 136050th Percentile 1.5 075th Percentile 38 5490th Percentile 188 291
Conclusion: Both studies provide important data on the prevalence and prog-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

CVD risk prediction in Europe: where do we stand? / Novel indicators of diabetes 839
nostic value of risk factors and subclinical atherosclerosis measures in Europeand the US. Differences in cohort selection, methodology and design render bothstudies unique for this purpose.
NOVEL INDICATORS OF DIABETES
4929 E-selectin levels are elevated and associated withincreased risk of ischemic cardiovascular events indiabetic but not in non-diabetic patients with chronicheart failure
C. Kistorp1, A.Y. Chong2, F. Gustafsson3, S. Galatius4, J. Faber5 ,I. Raymond2 , G.Y.H. Lip6, P. Hildebrandt3. 1Frederiksberg University Hospital,Department of Cardiology and Endocrinology, Copenhagen, Denmark;2City Hospital, Birmingham, United Kingdom; 3Rigshospitalet, Departmentof Cardiology, Copenhagen, Denmark; 4Gentofte University Hospital,Department of Cardiology, Gentofte, Denmark; 5Herlev University Hospital,Department of Endocrinology, Herlev, Denmark; 6City Hospital, Birmingham,United Kingdom
Purpose: Soluble E-selectin and von Willebrand factor levels (vWf) are markersof abnormal endothelial function. Both biomarkers are elevated in plasma in pa-tients with chronic heart failure (CHF), but the impact of diabetes mellitus (DM)on these indices, and the relation to prognosis in patients with CHF remains un-known.Methods: In cross-sectional analyses, we measured plasma levels of E-selectin,vWf and C-reactive protein (CRP, an index of inflammation) in 195 CHF patientswith (n=48, 24.5%), and without DM, who were compared to 116 age-matchedhealthy controls. Prognostic information was determined in patients with CHF,after a median of 2.6 (0.5-3.9) years (range) follow up.Results: Compared with controls, median plasma E-selectin levels were higherin diabetic CHF patients (49 ng/ml vs 36 ng/ml in controls, P=0.012), but wasnot in non-diabetic CHF patients (34 ng/ml, P=0.45); vWf levels were also higherin diabetic CHF patients (120 IU/dl vs 81 IU/dl in controls, P<0.001), but notsignificantly higher in non-diabetic CHF patients (89 IU/dl, P=0.108). Plasma lev-els of CRP were markedly higher in the CHF patients compared with controls(P<0.001), irrespective of DM.During follow up, 46 (23.5%) of the patients with CHF died and 45 (23.1%) hada major ischemic cardiovascular event. Increasing levels of plasma E-selectinwere associated with future cardiovascular events [adjusted hazard ratio (HR)2.60 (95% CI, 1.26-5.34; P=0.009) per 1 SD increment in log transformed vari-able] among the diabetic CHF patients, but not among the non-diabetic patients.High CRP levels were associated with increased risk of mortality [adjusted HR1.36 (95% CI, 1.02-1.83; P=0.038)], independently of severity of CHF, and no in-teraction with DM was found. In contrast, vWf levels were not related with any ofthe outcome measurements.Conclusions: Plasma levels of E-selectin and vWf are elevated in CHF patientswith DM, but not without DM. Soluble E-selectin, but not vWf, was independentlyassociated with future ischemic cardiovascular events in CHF patients with di-abetes, and such no association was observed in the non-diabetic patients. Incontrast, CRP levels were not influenced by DM status in CHF patients, and re-lated to prognosis. Endothelial activation and inflammation may both play a rolein the prognosis in CHF, especially in diabetic patients.
4930 In hospital daily insulin load (DIL) is an independentpredictor of adverse outcome after successful primaryPCI (PPCI) in diabetic patients (DM) with ST-elevationmyocardial infarction (STEMI)
T. Jezewski, T. Bendinger, M. Kidawa, M. Plewka, J.Z. Peruga,J. Drozdz, J.D. Kasprzak, M. Krzeminska-Pakula. Medical University of Lodz, IIChair and Dept. of Cardiology, Lodz, Poland
Objectives: Evaluation of factors describing on admission metabolic status ofconcomitant type 2 diabetes mellitus in patients undergoing PPCI in acute STEMI.Background: Diabetic patients suffering STEMI are at particular risk of short andlong term cardiac events. PPCI is an efficient way of restoring patency of IRA. Thedata about prognostic role of factors depicting metabolic status at the moment ofprocedure are sparse.Methods: Analysis of clinical (mean daily short acting insulin load during first 3days of hospitalization) and laboratory (level of blood glucose, HbA1c, presenceof microalbuminuria) factors in group of 112 diabetic patients (58% female) withSTEMI treated within first 6 hours with PPCI. Insulin was given in all patients toobtain mean, daily glucose level < 7,8mmol/L. Mortality and MACE rate (death,re-AMI, repeated coronary revascularization) were collected during 12 month fol-low up.Results: Non-survivors were younger (55,9 vs 64,2 p=0,005). T.2 diabetes mel-litus (DM) was de novo diagnosed in 15 (13,6%) patients, in 28 (24,7%) patientshad history of MI, Abciximab was used in 75% of procedures. Microalbuminuirawas present in 68 (60,5%) patients, mean HbA1c level was 7,9%. During followup 12 deaths (11,1%) and 33 (29,6%) MACE were reported. In multivariate logis-tic regression model only DIL>44 IU remained an independent risk factor for bothmortality (p=0,02 OR=18,3) and MACE (p=0,02 OR=5,2).
Conclusions: High DIL during acute phase of STEMI is a strong and independentpredictor of long term mortality and serious MACE in diabetic patients treated withPPCI. Not age but degree of metabolic disturbances best described in our analy-sis with DIL allows estimation of long term prognosis in this subset of patients.
4931 Insulin-like growth factor binding protein-1 predictscardiovascular morbidity and mortality in patients withacute myocardial infarction and type 2 diabetes.A report from the DIGAMI 2 trial
M. Wallander, K. Brismar, K. Malmberg, A. Norhammar, J. Ohrvik,L. Ryden on behalf of On behalf of the DIGAMI 2 Study Group. KarolinskaInstitutet, Dep of Medicine, Cardiology Unit, Stockholm, Sweden
Background: Although not a consistent finding there are indications that highlevels of insulin-like growth factor binding protein-1 (IGFBP-1) may be relatedto cardiovascular (CV) mortality and morbidity. The aim of this study was totest the hypothesis that high levels of IGFBP-1 predict future CV mortality andmorbidity in patients with acute myocardial infarction (AMI) and type 2 diabetes(T2DM).Methods: The DIGAMI 2 trial recruited 1253 patients with T2DM and suspectedAMI of which 575 patients (men 67%), the present material, were enrolled ina biochemical program with repeated blood sampling. Primary and secondaryendpoints were CV mortality and a composite of CV events (CV death, reinfarctionor stroke). Biochemical and clinical factors at admission where analyzed by amultiple Cox proportional hazard regression analysis. The results are presentedas HR and 95% CI.Results: During a median follow-up of 2.2 years, 102 out of the 575 patients(18%) died from CV reasons while 175 (30%) suffered from a CV event. Age(+5 years; 1.6, 1.4-1.8; p<0.001), Ln S-IGFBP-1 (1.5, 1.2-1.9; p<0.001) and LnS-Creatinine (2.0, 1.2-3.5; p=0.013) remained independent predictors of CV mor-tality. The model predicting major CV events contained the same variables and inaddition previous congestive heart failure (1.5, 1.1-2.1; p=0.025). Variables thatwere eliminated in best subset analyses were B-glucose, HbA1c, S-Potassium, S-cholesterol, S-triglycerides, BMI, gender, duration of diabetes, smoking, previousAMI and U-albumin. Figure 1 is presenting Kaplan-Meier curves of CV mortalitystatified for IGFBP-1 tertiles (p<0.001).
Fig. 1
Conclusion: High levels of IGFBP-1 in the acute phase of an AMI indicate in-creased risk for CV mortality and morbidity in patients with T2DM.
4932 Increased thromboxane A2 and COX-2 plateletexpression in diabetic patients
S. Giubilato1, L.M. Biasucci1, A. Leo1, D. Pitocco2, G. Liuzzo1,G. Ghirlanda3, F. Pulcinelli4, F. Crea1. 1Cardiology Institute, Rome,Italy; 2Internal Medicine Institute, Rome, Italy; 3Medicine Institute
Institute, Rome, Italy; 4Clinical Pathology Institute, Rome, Italy
Background: Recent studies suggest that aspirin is less efficient in reducing car-diovascular events in diabetic subjects. Little is known regarding the mechanismsaccounting for this phenomenon. We supposed that a role might be played by anexcess in TxA2 biosynthesis in diabetic subjects that could derive either from aresidual activity of COX-1, despite aspirin treatment, and/or from a platelet ex-pression of COX-2 in diabetic patients.Methods: To this aim, we studied in vitro collagen-induced platelet TxA2 produc-tion in 50 type 2 diabetic subjects and 50 non diabetics; all subjects were re-ceiving aspirin (100/160 mg/die for >7 days), but no other antiplatelet agent. Wealso measured the expression of both isoforms of cyclooxygenase, COX-1 and
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

840 Novel indicators of diabetes / The electrocardiogram – still evolving after more than 100 years
COX-2, assessed with western blot analysis using anti-human COX-1 or COX-2monoclonal antibodies in 20 diabetics and 20 control subject. The activity of COX-1 and -2 in the diabetic subjects was investigated considering collagen-inducedplatelet TxA2 levels after in vitro pre-treatment with aspirin, with a COX-2 inhibitor(NS-398) and with a combination of both.Results: Collagen-induced TxA2 levels were significantly higher in diabetic sub-jects than in controls (896.4 ± 232.3 pmol/108 cells vs 130.5 ± 31.5 pmol/108cells, p<0.005). Western blot analysis demonstrated that COX-2 was expressedin all diabetic patients analysed (n=20) but only in 8/20 of control patients. COX-1was highly expressed in both groups. The presence of both platelet COX-2 activ-ity and residual COX-1 activity in diabetic patients was also confirmed by the sig-nificant decrease of collagen-induced TxA2 production after in vitro pre-treatmentwith aspirin (51.4 ±11.5 pmol/108 cells, p<0.001) and with NS398 (461.9 ±167.5pmol/108 cells, p<0.005). A further reduction of TxA2 production was obtainedafter the combined use of aspirin and NS-398 (46.3±9.6 pmol/108 cells), whichwas significantly higher than that obtained with aspirin (p<0.05) or NS-398 alone(p<0.01).Conclusions: our study demonstrates that diabetic patients have enhancedplatelet production of TxA2 despite aspirin treatment that depends both on aresidual COX-1 activity and from platelet COX-2.
4933 A prospective cohort study of predictive value ofhomocysteine in patients with type 2 diabetes andcoronary artery disease
G. Ndrepepa, A. Kastrati, S. Braun, W. Koch, K. Koelling, J. Mehilli,A. Schoemig. Deutsches Herzzentrum, Munich, Germany
Background: Little evidence exists on the role of homocysteine as a predictor ofmortality in patients with type 2 diabetes. The aim of this study was to investigatewhether elevated plasma homocysteine levels are independently associated withall-cause or cardiovascular mortality in patients with type 2 diabetes and coronaryartery disease.Methods: This is a prospective cohort study that included 507 patients with type2 diabetes and angiographically proven coronary artery disease. Patients weredivided into 2 groups according to homocysteine level above or below medianvalue (12.4 mcmol/L): the high homocysteine group (255 patients) and the lowhomocysteine group (252 patients). The primary end-point of the study was all-cause mortality.Results: There were 103 deaths during a 4-year follow-up: 62 deaths in the highhomocysteine group and 41 deaths in the low homocysteine group (Kaplan-Meierestimates of mortality 25.6% and 17.4%, respectively (odds ratio [OR] 1.53, 95%confidence interval [CI] 1.03 to 2.27, P=0.031). Sixty two of 103 deaths (60.2%)were of cardiovascular origin: 37 deaths (14.5%) occurred in the high homo-cysteine group and 25 deaths (9.9%) occurred in the low homocysteine group(P=0.115). Cox proportional hazards model showed that plasma homocysteinewas not an independent correlate of all-cause (adjusted hazard ratio [HR] 1.10,95% CI 0.89 to 1.33; P=0.397 for 5 mcmol/L increase in concentration) or cardio-vascular (adjusted HR 1.04, 95% CI 0.80 to 1.36, P=0.753, for 5 mcmol/L increasein concentration) mortality.Conclusion: In patients with type 2 diabetes and coronary artery disease, ele-vated levels of homocysteine are an associate of increased cardiovascular riskbut not an independent predictor of cardiovascular mortality.
4934 Serum concentrations of adiponectin and risk of type 2diabetes mellitus in apparently healthy middle-agedmen. Results from the 18 year follow-up of a largecohort from Southern Germany
W. Koenig1, J. Baumert2, N. Khuseyinova2, H. Loewel1, C. Meisinger1.1University of Ulm Medical Center, Internal Medicine II - Cardiology, Ulm; 2GSFNational Research Center, Inst. of Epidemiology, Neuherberg, Germany
Purpose: Adiponectin, an obesity related hormone produced by adipocytes is in-volved in several crucial steps in atherogenesis. Adponectin induces nitric oxideexpression from endothelial cells, inhibits proliferation and migration of vascularsmooth muscle cells, and interferes with the transformation from macrophages tofoam cells. It is also linked to insulin resistance and has anti-inflammatory prop-erties. Thus, it has been postulated that high serum concentrations may be pro-tective against type 2 diabetes (T2DM).Methods: Serum concentrations of adiponectin were determined by ELISA (R&D,Wiesbaden, Germany) in 887 apparently healthy men aged 45-64 years, sampledfrom the general population in 1984 and followed until 2002.Results: During this period 115 of 887 men had a newly diagnosed T2DM. Me-dian baseline levels of adiponectin were lower in subjects with incident T2DMcompared to event-free subjects (5.0 μg/ml versus 6.4 μg/ml, p< 0.001). In aCox model, adjusted for age, subjects in the top tertile compared to the bot-tom tertile had a significantly decreased risk for a new-onset T2DM (HR 0.44;95% CI, 0.28-0.70, p for trend 0.0007). After controlling for BMI, smoking, phys-ical activity, alcohol consumption, actual hypertension, history of MI and totalcholesterol the RR slightly increased but still remained statistically significant (HR0.55; 95% CI, 0.34-0.88, p for trend 0.015). Only after further inclusion of to-tal cholesterol/HDL-cholesterol ratio in the model, the estimate for the predictivevalue of low adiponectin formally lost its statistical significance (HR 0.67, 95% CI
0.41-1.08; p for trend 0.105). Additional adjustment for CRP, Lp-PLA2 and plasmaviscosity did not further alter the relationship.Conclusions: Lower serum concentrations of adiponectin are associated withincreased risk of future T2DM in apparently healthy middle-aged men. The pro-tective effect of high serum concentrations might, at least in part, be explainedthrough its strong positive correlation with HDL-cholesterol.
THE ELECTROCARDIOGRAM – STILL EVOLVING AFTERMORE THAN 100 YEARS
4951 Mismatch between localization of Q waves in 12-leadelectrocardiogram and localization of myocardialinfarction at magnetic resonance imaging
D. Rovai1, G. Di Bella1, G. Rossi1, E. Strata1, M. Lombardi1 ,A. L’abbate2, A. Pingitore1. 1CNR, Clinical Physiology Institute,
Cardiology, Pisa, Italy; 2Scuola Superiore Sant’Anna, Medicine, Pisa, Italy
The electrocardiogram (ECG) is currently utilized to define the localization ofmyocardial infarction (MI), which can be precisely studied in vivo by contrast-enhanced magnetic resonance imaging (MRI). The aim of this study was to in-vestigate whether the localization of pathologic Q waves (duration > 0.04 sec orQS pattern in at least two contiguous leads) reflects the anatomical localizationof MI at contrast-enhanced MRI.In a group of patients with one old MI (age 62 ± 11 years), undergoing contrast-enhanced MRI, a 12-lead ECG was recorded and analyzed by two experiencedcardiologists. Patients with Left Bundle Branch Block were excluded. The infarc-tion was classified as anterior (Q waves in V1-V4), inferior (Q waves in II, III, aVF),lateral (Q waves in V5, V6, I, aVL or great and broad R wave in V2) or non-Q-wave.Contrast-enhanced MRI images were analyzed by a semi-automatic program thatdivided left ventricular myocardium according to a 17 segment model and calcu-lated the percent of MI in each segment. The segments were attributed to theclassical perfusion territories of left anterior descending (LAD), right (RCA) or leftcircumflex (LCx) coronary arteries. Of the entire group of 90 patients, 13 had apurely anterior MI at ECG, 13 a purely inferior, 11 a purely lateral and 11 a non-Qwave MI. In the patients with purely anterior MI, 80% of the infarction was local-ized in the LAD perfusion territory; however, 14% of the infarction was localizedin the RCA and 6% in the LCx perfusion territories. In the patients with purelyinferior MI, 57% of the infarction was localized in the RCA, 13% in the LAD and30% in the LCx perfusion territory. In the patients with purely lateral MI, 27% ofthe infarction was localized in the LCx, 39% in the LAD and 34% in the RCAperfusion territory. In non-Q-wave MI patients 50% of the infarction was localizedin the LAD, 30% in the RCA and 20% in the LCx perfusion territory. At MRI theinfarction was localized solely in the LAD perfusion territory in 11 patients, solelyin the RCA perfusion territory in 10 patients and solely in the LCx perfusion terri-tory in 6 patients; the ECG showed a purely anterior, a purely inferior or a purelylateral MI in only 4 (36%), 4 (40%) and 2 (33%) of these patients, respectively.In conclusion, the localization of pathologic Q waves weakly predicts the anatom-ical location of MI.
4952 Tako-tsubo syndrome and acute coronary syndrome:different entity?
B. Ibanez1, A. Pinero2, B. Choi2, F. Navarro1, M. Orejas1,J. Benezet-Mazuecos1 , P. Marcos-Alberca1, J. Farre1. 1Mount SinaiHospital, Cardiovascular Institute, New York, United States of America;
2Fundacion Jimenez Diaz, Cardiology, Madrid, Spain
The ECG of Tako-tsubo síndrome has been said to be similar to that of ante-rior wall AMI, however coronary arteries in tako-tsubo show no narrowing. Theetiology is still unknown. Recently, based on the presence of ruptured atheroscle-rotic plaques on left anterior descending (LAD) on IVUS examination, it has beenpostulated that tako-tsubo could be an anterior AMI with early spontaneous reper-fusion (Heart 2005).To test this hypothesis, we have compared the ECG of 20 consecutive tako-tsubopatients (Pts) with that of 40 consecutive anterior wall AMI Pts (20 with sponta-neous reperfusion: TIMI 3 on initial angiography, and 20 with instrumental reper-fusion: LAD occluded on angiography).Results Admission ECG showed pathological Q waves in 45% of tako-tsubo, 22%in spontaneous AMI reperfusion, and 65% in the intrumental group, disappearingin a 90%, 50%, and 8% respectively. The ST segment was elevated in 85%, 50%,and 100% respectively.The ECG evolved to deep negative T waves in 90% of the Pts in all 3 groups.However on days 2, and 3 the T waves were deeper in Pts with tako-tsubo andspontaneous reperfusion AMI (the sum of the T waves voltage is shown on Fig.1, left picture). QT interval was longer in tako-tsubo and spontaneous reperfusionAMI Pts (Fig. 1, right picture).Differences were statistically significant only between tako-tsubo and instrumentalreperfused AMI Pts (both for T waves voltage [p=.02], and for QT interval [p<.05]).Conclusions: ECG of tako-tsubo syndrome is very similar to that of anterior AMIPts with spontaneous reperfusion (high rate of Q wave disappearance, deepernegative T waves, and longer QT interval). This support the hypothesis that tako-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

The electrocardiogram – still evolving after more than 100 years 841
Fig. 1
tsubo syndrome could be a form of anterior wall AMI with early spontaneousreperfusion of LAD.
4953 Evaluation of QRS complex morphology discriminatorin patients undergoing cardiac resynchronizationtherapy
G. Boriani1, L. Padeletti2, M.G. Bongiorni3, M. Biffi3, C. Martignani3,A. Colella1, P. Silvestri4, A. Branzi3. 1S.Orsola-Malpighi, Cardiology,
Bologna, Italy; 2Ospedale Careggi, Cardiology, Firenze, Italy; 3OspedaleCisanello, Cardiology, Pisa, Italy; 4St.Jude Medical, Milano, Italy
Purpose: No data are currently available on rhythm discrimination by QRS com-plex analysis in patients with biventricular cardioverter defibrillators (ICDs). Mor-phology Discriminator (MD) is a diagnostic feature implemented in the algo-rithms for rhythm discrimination; it is based on automatic comparison, for de-tected events, between each single sensed QRS complex and a previously storedpatient-specific QRS template. Aim of this study was to evaluate QRS MD inbiventricular ICDs after 6 and 12 months of resynchronization therapy (CRT).Methods: All data were collected at the time of device implantation and after 6and 12 months. 38 patients were paced in both ventricles (BIV), 7 in left ven-tricle only (LV) mode. All patients were costantly paced using negative A-V/P-Vhystheresis with search.Results: 45 patients with wide QRS (>140ms) and drug refractory heart failureimplanted with a biventricular ICD (St Jude Medical) were considered. A templateof spontaneous right ventricular electrogram (EGM) was acquired at implant andreassessed after 6 and 12 months of follow-up to evaluate if any change in sponta-neous QRS complex, potentially related to CRT, was detectable by MD. The QRSwidth of the EGM during spontaneous rhythm resulted shorter after 6 months and12 months in comparison with baseline, as shown in the table. In 5 patients thechanges in QRS complex occurred at 6 months had the potential to influencethe discrimination performed by MD since the mean QRS percent matching com-pared to the template (evaluated in a window of 8 complexes) was below thethreshold (at least 65% similarity) for classifying the rhythm as supraventricular.In a follow up of 12 months, performed in 27 pts, MD template was reacquireddue to a lack of 100% matching percentage 14 times over 27 manual follow-up(52%).
Basal EGM width 6-month EGM width 12-month EGM width(ms) (ms) (ms)
Mean and St Dev 137±21 120±24 108±21p value p=0,001 vs basal p<0,001 vs basal p=0,03 vs 6 month
Conclusions: CRT for more than 6 months appears to be associated withchanges in spontaneous QRS complex, as detected by right ventricular EGM,that may reflect an electrocardiographic remodeling. Reacquisition of the tem-plate for MD is recommended in the months that follow the implant of a device forbiventricular pacing with this discrimination algorithm.
4954 Predischarge QRS score after acute ST-elevationmyocardial infarction independently predicts mid-termincidence of new-onset heart failure
A. Kalogeropoulos, J. Chiladakis, I. Sichlimiris, N. Koutsogiannis,D. Alexopoulos. University Hospital Of Patras, Division Of Cardiology,
Patras, Greece
Background: Early studies have validated the modified 32-point QRS scoringsystem (Selvester score) as a reliable tool for estimating myocardial infarct sizeand as a useful prognosticator of mortality after acute ST-elevation myocardialinfarction (STEMI). However, the value of the QRS score in identifying patients atrisk for heart failure following a STEMI has not been investigated.Methods: We calculated the QRS score prior to hospital discharge in 100 con-secutive survivors of a first acute STEMI (64±13 yrs, 77% male, BMI: 26.9±3.1kg/m2, Killip class: 1.7±0.6, anterior location: 44%, primary PCI: 12%, fibrinol-ysis: 79%, peak CPK: 1973±1616 u/l). Patients with LBBB or paced rhythmwere excluded from the study. Predischarge left ventricular systolic function (EF:0.47±0.09) and BNP levels (median: 240, 25%-75%: 119-494 pg/ml) were de-termined in all patients. The composite end-point of death and new-onset heartfailure was recorded during a 12-week follow-up period.Results: Predischarge QRS score was 2.4±1.7 points. During follow-up, 6 pa-tients died and 16 patients developed heart failure. In univariate analysis, apredischarge QRS score >2 was found to be highly predictive of subsequentevents (Figure). In multivariate Cox regression models, a QRS score >2 emerged
as an independent predictor of the composite endpoint (OR=3.9, 95% CI 1.4-10.9, p=0.009), in addition to supramedian BNP levels (OR=14.6, 95%1.9-114.2,p=0.011), and age >60yrs (OR=5.0, 95% CI 1.5-16.9, p=0.010).
Fig. 1. Kaplan-Meier curves by QRS score.
Conclusions: Electrocardiographic extent of myocardial damage, as reflected bya simple QRS score measurement prior to hospital discharge, is a powerful andindependent predictor of subsequent death or new-onset heart failure in the mid-term post-infarction period.
4955(W) Abnormal heart rate turbulence predicts totalmortality but not sudden death in patients withcongestive heart failure
I. Cygankiewicz1, W. Zareba2, R. Vazquez3, M. Valdes4,J. Gonzalez-Juanatey5 , M. Fiol6, P. Caminal7, A. Bayes De Luna2
on behalf of MUSIC Investigators. 1Hospital Sant Pau-ICCC, Barcelona, Spain;2University of Rochester, Rochester, Ny, United States of America; 3Hospital deValme, Cardiology, Sevilla, Spain; 4Hospital Virgen Arrixaca, Cardiology, Murcia,Spain; 5Hospital Universitario, Cardiology, Santiago De Compostela, Spain;6Hospital Son Dureta, Cardiology, Palma De Mallorca, Spain; 7PolitechnicalUniversity of Catalonia, Barcelona, Spain
Background: Heart rate turbulence (HRT) predicts total mortality (TM) and sud-den death (SD) in postinfarction patients. Data regarding its prognostic value inpatients with congestive heart failure (CHF) is limited. We aimed to evaluate theprognostic significance of HRT for predicting TM and SD in a large cohort of pa-tients with CHF in NYHA class II-III.Methods: In 576 sinus rhythm patients with CHF in NYHA class II-III, enrolled inthe MUSIC (Muerta Subita e Insuficiencia Cardiaca) study, 24-hour Holter moni-toring was performed at enrollment to assess HRT parameters - turbulence onset(TO) and slope (TS). TO≥0% and TS=<2.5 ms/RR were considered abnormal.Then patients were categorized as those with normal HRT (HRT0) or abnormalHRT (HRT 1 or 2). Patients were followed for median of 26 months with primaryendpoint defined as TM and secondary endpoint as SD.Results: HRT analysis was posible to perform in 487 pts (353M), mean age 63yrs. The majority of patients were in class II NYHA II (82%). Etiology of heart fail-ure was ischemic in 49%, idiopathic in 23% and hypertensive in 12%. Mean LVEFwas 37% including 25% of patients with preserved LVEF (>45%). There were35% of patients with diabetes, 56% with hypertension and 46% with previousmyocardial infarction. Median value of TO was -0.48% and median value of TSwas 2.62 ms/RR. Abnormal HRT parameters (TS=<2.5 ms/RR and/or TO≥0%)were found in 59% of patients. During follow up of median 26 months 48 patientsdied, in this 24 from SD. Nonsurvivors were characterized by higher values ofTO and lower values of TS. Abnormal TS and HRT category 2 were associatedwith increased total mortality in univariate and in multivariate analysis after adjust-ment for significant clinical covariates (ischemic etiology, hypertension, diabetes).HRT 2 was the strongest multivariate risk predictor for TM (HR 2.81, p=0.007)followed by NYHA class III, diabetes and abnormal TS (HR 2.05, p=0.028). A de-creased TS and HRT 2 were associated with increased risk for SD in univariateanalysis (HR 4.23, p=0.007 for HRT2) but they lost their predictive value afteradjustment for clinical covariates. Abnormal TO alone showed no prognostic sig-nificance.Abnormal HRT failed to predict TM and SD in patients with LVEF<35%,whereas in patients with LVEF>35% HRT was predictive for TM but not for SDConclusions: CHF patients present high percentage of HRT abnormalities. Ab-normal HRT predicts total mortality but fails to predict sudden cardiac death inCHF patients. From two HRT descriptors TS, but not TO, presents prognosticvalue.
4956 A further simplified new algorithm in the differentialdiagnosis of wide complex QRS tachycardias
A. Vereckei1, D.P. Zipes2, J.M. Miller1. 1Semmelweis University,School Med., 3rd Department of Medicine, Budapest, Hungary;2Krannert Institute of Cardiology, Indianapolis, USA
Background: Our previously devised ECG algorithm for the differential diagnosisof regular wide complex QRS tachycardias (WCT), that proved to be superiorto the Brugada algorithm, was further simplified by converting it to a stepwise,decision-tree algorithm, total omission of complicated morphological criteria andlimiting the leads to be studied to lead aVR.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

842 The electrocardiogram – still evolving after more than 100 years / Non-invasive studies in arrhythmias
Methods: 349 WCT [271 ventricular tachycardias (VT), 78 supraventricular tachy-cardias (SVT)] episodes from 226 patients with proven electrophysiological (EP)diagnosis were prospectively analyzed by the first author blinded to the EP diag-nosis. The following criteria were analyzed in lead aVR: 1) presence of an initial Rwave?, 2) if the QRS starts with an r or q wave its width is >30 ms?, 3) if there is aQS wave or a predominantly negative QRS with a negative onset, is there a notchon the downsloping limb of the QRS?, 4) estimation of initial (vi) and terminal (vt)ventricular activation velocity ratio (vi/vt) by measuring the distance in mV on theECG the impulse traveled vertically during the initial (vi) and terminal 40 ms (vt)of the QRS complex. When the answer to any of the first three questions wasyes, the final diagnosis was VT, when the answer was no, one had to proceed tothe next criterion. A vi/vt>1 suggested SVT and a vi/vt<1 suggested VT in the4th step. The simplified new algorithm was compared with our previous and theBrugada algorithms.Results: Using the new algorithm 90.0%, our previous algorithm 90.3% and theBrugada algorithm 84.5% of the WCT episodes were correctly classified. For VTdiagnosis the ability to make the correct diagnosis (p<0.001), the (-) predictivevalue (p<0.001) and the test accuracy (p=0.0563) of the new aVR algorithm weresuperior or borderline superior, for SVT diagnosis the specificity (p<0.05) and (+)predictive value (p<0.001) of the new algorithm were superior to those of theBrugada algorithm. There was no significant difference in any of the statisticalparameters between the new aVR and our previous algorithms.Conclusions: The much simplified new aVR algorithm was able to classify theWCT episodes with the same accuracy as reported for the application of all stan-dard criteria and our previous algorithm and proved to be superior to the Brugadaalgorithm.
NON-INVASIVE STUDIES IN ARRHYTHMIAS
4957 24 hour Holter monitoring to investigate palpitation orsyncope: an analysis of diagnostic efficacy in 8,052patients
S. Sulfi1, D. Balami1, N. Sekhri1, K. Ranjadayalan1 , A. Suliman1,R.A. Archbold2, A. Kapur1, A.D. Timmis1. 1Newham University
Hospital, Cardiology, London, United Kingdom; 2London Chest Hospital,Cardiology, London, United Kingdom
24 hour Holter monitoring is widely used to investigate palpitation and alteredconsciousness (dizziness, presyncope, syncope). The diagnostic usefulness ofHolter monitoring, however, has not been systematically evaluated. We haveprospectively recorded data in 8,052 consecutive patients who underwent 9,72924 hour Holter recordings over a 13 year period.Data included demographics, indications for Holter monitoring and electrocardio-graphic analysis of the recording.Palpitation was the indication in 3,066 patients who underwent 3,537 Holterrecordings. Diagnostic tachy-arrhythmias were recorded in 20.4% of patients onthe first recording, rising to 30.8% and 38.4% on second and third recordings(p<0.0001). Age was a major determinant of a diagnostic recording, rates ris-ing from 8.2% in patients aged <30 years to 39.5% in patients aged >70 years(p<0.0001). Altered consciousness was the indication in 3,299 patients who un-derwent 3,987 Holter recordings. Diagnostic tachy- or brady-arrhythmias wererecorded in 13.7% of patients on the first recording, rising to 17.9% and 15.2%on second and third recordings (p=0.03). Age was a major determinant of a di-agnostic recording, rates rising from 7.3% in patients aged <30 years to 16.9%in patients aged >70 years (p<0.0001). In conclusion, the diagnostic usefulnessof Holter monitoring in patients with palpitation or altered consciousness is agedependent, with pick-up rates for arrhythmias of <10% in younger patients butconsiderably higher in patients aged >70 years. Diagnostic yield increases withrepeat recordings but these data suggest that the threshold for Holter monitoringshould be higher in younger patients.
4958 Cardiac memory versus likelihood of ischemic heartdisease in hypertensive patients with ventricularrepolarization abnormalities after repetitive uniformventricular extrasystoles
A.M. Hegazy, B.A. Abdulkader. Farwania Hospital, Non-InvasiveCardiac Unit, Kuwait, Kuwait
Objectives: To investigate the value of changes in ventricular repolarization af-ter PVC’S for prediction of the hypertensive patients with likelihood of ischemicheart disease (IHD) and to identify receiver operating characteristic curve (ROC)derived cut-off values of ventricular repolarization changes after PVC’S to predictIHD in hypertensive patients.Methods: Two hundred and ten hypertensive patients were included and stratifiedinto: Group I: included 80 patients with T wave inversion after PVC’S and group II:included 130 patients with normal T wave after PVC’S. Ambulatory 24-hour ECG,ambulatory 24-hour blood pressure recording, transthoracic echocardiography,treadmill exercise ECG test and stress thallium scintigraphy were performed.Results: With regards to the ventricular repolarization, there was 62 patients hadsymmetrical T wave inversion and 18 patients had isoelectric or biphasic T wave.There was a significant increased time needed for resolution of T wave inversion
in the patients who had positive stress thallium scintigraphy compared with thosewho had negative stress thallium scintigraphy (32.5±8.9 versus 12±4.3 minutes,P<0.05). Predictive indices revealed that persistent symmetrical T wave inver-sion after repetitive uniform PVC’S = 30 minutes can be considered as indicatorsfor prediction of IHD in hypertensive patients as sensitivity was 80%, specificity=73%, accuracy =78%, positive predictive value =83% and negative predictivevalue=69%, respectively. Kappa coefficient value (K) indicated that there was agood agreement between changes in ventricular repolarization after PVC’S andthe results of stress thallium scintigraphy (K=0.827). ROC curve data revealedthat the best cut-off value of T wave inversion voltage to predict IHD in hyperten-sive patients was 2.2 mV with sensitivity=66% and false positive =35%, and areaunder curve was 0.716, but the best cut off value of time for resolution of T waveinversion was 34 minutes with sensitivity =83% and false positive =18% and areaunder curve was 0.873.Conclusion: Inspite of limitations and confounders, we propose that changes inrepolarizing current after repetitive uniform PVC’S could be due to cardiac mem-ory or IHD but persistent symmetrical T wave changes following resumption ofsinus rhythm is an independent variable which may provide statistically significantprediction to identify hypertensive patients with likelihood of IHD.
4959 Atrial fibrillatory rate and sinus rhythm maintenance inpatients undergoing cardioversion of persistent atrialfibrillation
F. Holmqvist1, M. Stridh1, J.E.P. Waktare2, L. Sornmo2, S.B. Olsson2,C.J. Meurling2. 1Lund, Sweden; 2The Cardiothoracic Centre,
Liverpool, United Kingdom
Aims: The study set out to explore whether an index of atrial electrical electro-physiology can be used to predict atrial fibrillation (AF) relapse, and if the predic-tive properties differ as a result of arrhythmia duration.Methods and results: The study comprised 175 consecutive patients with per-sistent AF (median duration 94, range 2 to 1044 days) referred for cardioversion.Twenty-nine patients had arrhythmia duration under 30 days (median 5, range 2 to26). Atrial fibrillatory rate (AFR) was estimated using frequency power spectrumanalysis of QRST-cancelled ECG.At one-month follow-up 56% of the patients had relapsed to AF. The pre-cardioversion mean AFR of those was 399±52 fpm compared to 363±63 fpmamong patients maintaining SR (p<0.0001). In patients with short AF duration thedifference was even more pronounced (424±52 fpm vs. 345±65 fpm, p<0.01).In this group a finding of an AFR above the mean value of the study populationpredicted AF relapse with high accuracy (figure).
Conclusion: In patients undergoing cardioversion of persistent atrial fibrillation,AF relapse is predicted by a higher AFR. A stronger association is seen i n pa-tients with short arrhythmia duration, reflecting either rapid remodeling or pre-existing changes in those who relapse to AF.
4960 Increased diurnal QT/RR slope predicts total mortalityand sudden death in heart failure patients with ejectionfraction >35%
I. Cygankiewicz1, W. Zareba2, R. Vazquez3, J. Almendral4,J. Villacastin5, A. Bardaji6, V. Nieto7, A. Bayes De Luna6 on behalf
of MUSIC Investigators. 1Hospital St Pau-ICCC, Barcelona, Spain; 2Universityof Rochester, Rochester, NY, USA; 3Hospital de Valme, Cardiology, Sevilla,Spain; 4Hospital Gregorio Maranon, Cardiology, Madrid, Spain; 5Hospital Clinico,Cardiology, Madrid, Spain; 6Hospital Joan XXIII, Cardiology, Tarragona, Spain;7Hospital Insular, Cardiology, Las Palmas De Gran Canaria, Spain
Background: Repolarization dynamics is considered as a marker of myocar-dial vulnerability contributing to increased risk of arrhythmic events and sudden
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Non-invasive studies in arrhythmias / Epidemiology and diagnosis of LV "diastolic dysfunction" 843
death (SD). Increased slope of QT/RR was reported as an independent risk pre-dictor in postinfarction patients. We aimed to evaluate the prognostic value ofQT/RR in prediction of total mortality (TM) and SD in patients with chronic heartfailure (CHF). Additional analysis was performed in subgroup of patients withLVEF>35%.Methods: In 576 sinus rhythm patients with CHF in NYHA class II-III 24-hourHolter monitoring was performed at enrollment to assess slope of the QTa/RR(QTapex) and QTe/RR (QTend) during entire 24-hour recording and separatelyduring day and night periods. Since values of QT/RR slopes indicating high riskindividuals in CHF population are unknown, we relied on quartile division consid-ering a priori values in 4th quartile as abnormal. Patients were followed for medianof 26 months after inclusion with primary endpoint defined as TM and secondaryas SD.Results: Analysis of repolarization dynamics was posible to perform in 466 pts(353M), mean age 63 yrs. The majority of patients was in class II NYHA (82%).Regarding CHF etiology ischemic (49%) followed by idiopathic (23%) were themost frequent. Mean LVEF was 37% including 198 patients with LVEF> 35%.Mean value of QTa/RR slope was 0.171 and QTe/RR was 0.195. During followup, there were 45 deaths including 23 SD. Nonsurvivors were characterized bysteeper QT/RR slopes. An increased diurnal QTe/RR slope (>0.22) was associ-ated with increased TM in multivariate analysis after adjustment for clinical co-variates with HR 2.36, p=0.006. None of repolarization parameters was associ-ated with increased risk of SD in the entire population. However, when analyz-ing subgroup of patients with LVEF>35% increased diurnal QT/RR slopes werethe only significant risk predictors of SD with HR 4.12 for QTa/RR slope>0.20(p=0.011) and HR 6.36 (p=0.001) for QTe/RR slope>0.22. On the other hand inthe subgroup of patients with LVEF<35% repolarization parameters showed noprognostic value.Conclusions: Abnormal repolarization dynamics is an independent risk strati-fier of mortality in patients with CHF. Furthermore, in patients with LVEF>35%increased daytime QT/RR slopes are strong predictors of sudden death. SinceCHF patients with EF< 35% could be qualified for prophylactic ICD therapy re-gardless of risk stratifiers, our findings showed that abnormal QT dynamics maybe helpful in identifying CHFpatients with relatively preserved LV function whomight benefit from an ICD.
4961 A comparison of T-wave alternans and programmedventricular stimulation for arrhythmia risk stratificationin athletes
G. Inama, M. Nanetti, C. Pedrinazzi, O. Durin, G. Donato, P. Agricola.Ospedale Maggiore, Department of Cardiology, Crema, Italy
Introduction: The usefulness of TWA in predicting the risk of ventricular tach-yarrhythmias (VT) has been widely demonstrated in several clinical conditions.Aim of our study was to evaluate the role of TWA to stratify the risk of suddencardiac death in athletes (ath) with complex VT, and to document a possible cor-relation between TWA and electrophysiological testing (EPT) results.Methods: We studied 43 ath (31 M, mean age 34 + 12 years). All subjects wereath engaged in 10 different sports, affected by VT (> 50 premature ventricularcomplexes/hour or non-sustained VT). In all cases a basic cardiological evalua-tion was performed, including ECG, 24-hour ambulatory ECG, echo, exercise test,TWA and EPT. Coronary angiogram, magnetic resonance imaging, right and leftventriculogram and endomyocordial biopsy were performed depending on basiccardiological evaluation. The patients were evaluated during a mean follow-up of25 + 22 months.The end-point was the occurrence of sudden death or malignantVTs.Results: TWA was negative in 28 ath (65%), positive in 8 (19%) and undeter-mined in 7 (16%). All subjects with negative TWA did not show induction of malig-nant VTs (sustained VT or FV) at EPT, with significant correlation between nega-tive TWA and negative EPT (p<0.01). All ath with positive TWA also had malig-nant VT induced by a EPT, with significant correlation between positive TWA andpositive EPT (p<0.01). In 5 ath with undetermined TWA (71%) malignant VT wereinduced at EPT. Our data did not show significant correlation between indetermi-nate TWA and positive or negative EPT (p>0.05). During follow-up, the patientstreated with ICD showed appropriate device interventions to terminate sponta-neous VT. In all other subjects we observed no episodes of malignant VT. Duringfollow-up we observed a significant difference in end-point occurrence betweenath with negative or positive TWA (0% vs 37.5%, p<0.05)Conclusion: TWA confirm its role as a simple and non-invasive test, and it seemsuseful for prognostic stratification of ath with VT. Similarly to the literature, TWApredictivity values are promising also in such a specific population, even if largercohorts are required to refine such calculations.
4962 Autonomic markers and non-fatal acute coronaryevents in postinfarction patients
J.S. Perkiomaki, V. Jokinen, J. Tapanainen, H.V. Huikuri. University ofOulu, Oulu, Finland
Background: Autonomic markers, such as heart rate variability (HRV),heart rate turbulence (HRT) and baroreflex sensitivity (BRS) provide informationon the risk of all-cause mortality after an acute myocardial infarction (AMI), buttheir value in predicting non-fatal cardiac events is not well known.
Methods: A consecutive series of 601 patients with an AMI underwent a 24-hour Holter recording, and assessment of BRS using phenylephrine test. Severalparameters of HRV and HRT were determined.Results: After up to 30 months of follow-up, 84 patients (14%) had a non-fatalacute coronary event. Among the studied variables, the short-term scaling expo-nent alpha1 (p=0.002), power-law slope beta (p=0.008), low-frequency compo-nent of HRV power spectrum (p<0.001), turbulence slope (p<0.001), and BRS(p<0.001) had the strongest association with the occurrence of non-fatal acutecoronary events in univariate comparisons. After adjustment with relevant clini-cal variables (such as age, gender, ejection fraction, functional class, medication,diabetes) in the Cox proportional hazards model, alpha1 and beta remained asstatistically significant predictors of non-fatal acute coronary events (HR=1.9 [1.2-3.1, 95% CIs, p=0.009] for alpha1 </= 1.025), (HR=1.9 [1.2-3.1, p=0.009] for beta</= -1.507).Conclusion: Several autonomic markers provide information on the risk of recur-rent acute coronary events after an AMI. Altered fractal heart rate behavior seemsto be the strongest independent predictor of such events.
EPIDEMIOLOGY AND DIAGNOSIS OFLEFT VENTRICULAR "DIASTOLIC DYSFUNCTION"
4963 Systolic and diastolic heart failure: a prospectivecommunity study
F. Bursi1, S.A. Weston2, M.M. Redfiled1, S.J. Jacobsen1 ,S. Pakhomov1, V.T. Nkomo1, R.A. Meverden1, V.L. Roger1. 1MayoClinic, Division Of Cardiovascular Diseases, Rochester, United States
of America; 2Mayo Clinic and Foundation, Health Sciences Research, Rochester,Mn, United States of America
Purpose: To prospectively measure ejection fraction (EF), diastolic function, andbrain natriuretic peptide (BNP) in all community subjects with heart failure (HF).HF is a heterogeneous syndrome that can be characterized by EF and diastolicfunction. Data on the characteristics of HF in the community are scarce as studiesare mostly retrospective relying on clinically indicated tests of hospitalized casesof prevalent HF. Furthermore, diastolic function is infrequently assessed and doesnot rely on standardized, current techniques.Methods: All Olmsted County, MN residents presenting with HF as in or and out-patients (n=886) between 09-10-2003 and 10-27-2005 were prospectively iden-tified through the electronic medical record. Of these, 607 (69%) consented toparticipate and 556 underwent echocardiogram. 22% were diagnosed as out-patients. EF and diastolic function were measured by echocardiography and BNPby the Shionoria® assay.Results: Echocardiography was performed at a median (25th-75th percentile) of1 (1-4) day after diagnosis. EF was preserved (≥50%) in 55% of subjects Pre-served EF was associated with older age, female sex, and no history of myocar-dial infarction (all p<0.05). Isolated diastolic dysfunction (DD) (DD with preservedEF) was present in 44% of subjects. DD was more common and severe whenEF was reduced (4% mild, 56% moderate, and 23% severe) versus preserved(7% mild, 63% moderate, and 8% severe) (p<0.001). The distributions of EF andDD were similar for non-incident and incident cases, and for in- and out-patientcases. Both low EF and DD were independently related to higher levels of BNP.At 6 months, mortality for reduced and preserved EF was 16% and 15% (age andsex-adjusted hazard ratio 0.83, 95% CI 0.58, 1.20; p=0.32 for preserved versusreduced EF).Conclusion: In the community, more than half of the subjects with HF have pre-served EF and isolated DD is present in more than 40% of cases. EF and DD areindependently related to higher levels of BNP. HF with preserved EF is associatedwith a severe prognosis, comparable to that of patients with reduced EF.
4964 Heart failure with preserved left ventricular function:prevalence and clinical correlates in over 3500 patientsfrom the ALPHA registry
G.M. De Ferrari1, R. Massa2, M. Tritto3, L. Manca4, P. Devecchi5,S. Rogiani6, S. Sarzi Braga7, J.A. Salerno-Uriarte8. 1IRCCS
Policlinico San Matteo, Cardiology Dept., Pavia, Italy; 2Univ of Torino, San GBattista Hospital, Torino, Italy; 3Univ of Insubria, Clinical Inst. Mater Domini,Castellanza (Va), Italy; 4F. Ferrari Hospital, Casarano (Le), Italy; 5Univ ofPiemonte Orientale, Maggiore Hospital, Novara, Italy; 6Spedali Civili Hospital,Brescia, Italy; 7IRCCS S. Maugeri Found., Scientific Institute, Tradate (Va), Italy;8Univ of Insubria, Circolo Hosp. Macchi Found., Varese, Italy
Conflicting data are present regarding the prevalence of preserved left ventricularfunction (PLVF) among patients with heart failure (HF). Most estimates derivefrom either population-based echocardiographic studies of from cohort studies ofpatients hospitalized for HF, not from unselected series of stable HF patients.Goal of the present study was to assess the prevalence and the clinical corre-lates of HF with PLVF in the large population of the ALPHA (T-wave Alternans inPatients with Heart fAilure) study registry. The registry included 3513 consecutiveoutpatients were evaluated in the HF clinic of 9 centers in Italy: 71% males, age67 ± 13 years, LVEF 34 ± 10%, 37% had QRS complex duration ≥120ms; 9%,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

844 Epidemiology and diagnosis of LV "diastolic dysfunction"
56%, 29% and 6% of patients were in NYHA class I-II-III-IV, respectively. Etiol-ogy was ischemic in 47%, idiopathic in 27%, hypertensive in 13%, valvular in 9%,combined in 4%.PLVF, defined as LV ejection fraction >45%, was present in 20% of the patients,who were slightly older than the remaining patients (69 ± 13 vs 66±13 yrs,p<0.0001). PLVF was present in 13%, 13%, 38% and 43% of patients with is-chemic, idiopathic, hypertensive and valvular etiology, respectively (p<0.0001),more frequently in females (32 vs 15% p<0.0001). On the other hand, PLVF wasless frequently present in advanced (III&IV) NYHA class (15 vs 23% p<0.0001)and in patients with QRSd>120 ms (12 vs 25% p<0.0001). Multivariate analysisfound that increasing age, female gender, hypertensive or valvular etiology (vsischemic) and less advanced NYHA class were all significantly (p<0.001) asso-ciated with PLVF.In conclusion, preserved LV function is present in one out of five unselected pa-tients with stable heart failure. It is more common in older patients, in women thanin men, in patients with hypertensive or valvular heart failure, and in patients withless advanced NYHA class and with narrow QRS.
4965 Predictors of diastolic dysfunction in the community
W.P. Abhayaratna1 , W.T. Smith2, N.G. Becker1 on behalf of TheCanberra Heart Study. 1Canberra, Australia; 2Newcastle, Australia
Background: Despite emerging evidence for the adverse prognosticsignificance of left ventricular (LV) diastolic dysfunction (DD), there are
limited data to document the risk factors of DD in the community. We evaluatedthe clinical predictors of DD in a population-based sample of older adults.Methods: Randomly selected adults of age 60-86 years (n=1275; 50% men) un-derwent assessment of clinical risk factors by history and physical examination,and LV diastolic function by comprehensive Doppler-echocardiography. Predic-tors of DD (grades 1-4) were determined using ordinal logistic regression analy-sis.Results: The prevalence of any DD was 34.7% (95%CI 32.1%- 37.4%) andmoderate-severe DD was 7.3% (95%CI 5.9%-8.9%). Predictors of DD includedincreasing age, LV ejection fraction (EF) ≤ 50%, overweight/obesity and history ofhypertension (all p<0.001); diabetes (p=0.02) or myocardial infarction (p=0.003).Age/gender-adjusted associations between these parameters and DD are dis-played in the Table. In multivariable analysis, independent predictors of DD in-cluded age, EF ≤ 50%, myocardial infarction and overweight/obesity.
Adjusted Odds Ratio P-value
Men 0.97 (0.76-1.23) 0.78Age group (referent: 60-69 years)
70-79 years 2.5 (1.9-3.2) <0.000180-86 years 5.7 (3.9-8.4) <0.0001
Hypertension 1.5 (1.2-2.0) 0.002Diabetes 1.4 (1.03-2.0) 0.029Myocardial infarction 2.8 (1.8-4.4) <0.0001Coronary disease 1.8 (1.3-2.4) <0.0001Body mass index (referent: <25 kg/m2)
25-29.9 kg/m2 1.5 (1.1-2.0) 0.01≥30 kg/m2 1.9 (1.3-2.6) <0.0001
EF =≤ 50% 5.4 (3.3-8.8) <0.0001
Conclusion: Classical risk factors for heart failure are associated with echocar-diographic evidence of DD in the community. Whether targeted screening of high-risk subgroups will facilitate early identification of subjects with DD who may ben-efit from more intensive medical therapy remains to be determined.
4966 Elevated plasma markers of matrix metalloproteinasestype 2 and 9 are independent predictors of diastolicheart failure
R. Martos1, J. Baugh2, M. Ledwidge1, C. O Loughlin1 , C. Conlon1,S. Donnelly2, K. Mc Donald1 . 1St Vincent’s University Hospital, Heart
Failure Services, Dublin, Ireland; 2University College Dublin, Conway Institute,Dublin, Ireland
Background: We have previously demonstrated that procollagen type III amino-terminal peptide levels are elevated in a well-defined diastolic heart failure (DHF)population. However, the role of Metalloproteinases (MMP’s) in the pathophysi-ology of DHF, in particular type 2 (MMP-2) and 9 (MMP-9), remain unclear. Inexperimental data, upregulation of MMP-2 and MMP-9 have been implicated inan abnormal collagen metabolism in DHF.Aim: The aim of our study was to determine whether increased activity of MMP-2and MMP-9 levels were present in a well-defined DHF population.Methods: Eighty-six patients were enrolled: 32 patients with DHF and 54 hy-pertensive patients without DHF (No-DHF). DHF was defined by dyspnoea, hos-pitalization for heart failure (HF), normal left ventricular systolic function (LVEF>45%) and echo Doppler indices of diastolic dysfunction. Plasma levels of MMP-2 and MMP-9 were assayed by ELISA. Plasma b-type natriuretic peptide (BNP)levels were also measured by (Biosite Triage, USA) in all patients. Comparisonsbetween DHF and No-DHF groups were conducted using independent samplet-tests and Mann-Whitney test and ANCOVA (two-sided, α = 0.05) where appro-priate. Multivariable analysis was conducted using logistic regression.
Results: Patients with DHF were significantly older (72±11 vs. 67±9 years,p=0.03). MMP-2 (1826.7±231.0 vs. 1485.8±152.6 ng/ml, p<0.01), MMP-9(202.8±131.1 vs.90.6±49.3 ng/ml, p<0.01) and BNP levels (264 ±182 vs. 101±129pg/ml, p= <0.001) were greater in the DHF group in comparison to patientswith No-DHF. M ultivariable analysis (controlling for age, gender and urea lev-els), identified MMP-2 (OR=1.013, p<0.01, 95% CI: 1.005, 1.021) and MMP-9(OR=1.037, p<0.01, 95% CI: 1.011, 1.065) as independent predictors of DHF.Conclusions: These data demonstrate serological evidence of an active fibroticprocess in a well-defined DHF population. Furthermore, we have found that MMP-2 and MMP-9 levels are independent predictors of DHF. This may help explain thepathophysiology of DHF and suggest new avenues for screening and therapeuticintervention.
4967 Impact of NTproBNP and NTproANP for the diagnosisof diastolic or systolic dysfunction
C. Luers1 , S. Kleta2, R. Wachter2, J. Koschack2, C. Herrmann-Lingen3, B. Pieske2, L. Binder2, M.M. Kochen2. 1Goettingen,Germany; 2University of Goettingen, Cardiology and Pneumology,
Goettingen, Germany; 3University of Marburg, Psychosomatics andPsychotherapy, Marburg, Germany
Background: Increase in wall stress causes secretion of NTproANP (NANP) fromatrial, and NTproBNP (NBNP) predominantly from ventricular myocardium. Dias-tolic dysfunction (DD) is often characterised by increased atrial pressure and nor-mal ventricular wall stress, at least in earlier stages of the disease and severediastolic heart failure and systolic heart failure are characterised by increasedatrial and ventricular wall stress. We tested the hypothesis that the combined as-sessment of NANP and NBNP may help to identify patients with isolated DD atearlier stages.Methods: 542 patients without known heart failure but cardiovascular risk fac-tors (hypertension, diabetes mellitus, stable CAD) were classified by standardisedechocardiographic evaluation including pulse doppler and tissue doppler analysisaccording to the absence or presence of diastolic (American Society of Echocar-diography (ASE) stage I (mild) vs. ASE stage II without evidence of elevated leftventricular enddiastolic pressure (moderate) and vs. ASE stage II and III with ev-idence of elevated left ventricular enddiastolic pressure (severe)) or systolic dys-function (SD). Echocardiographic parameters were related to LgNANP, LgNBNPplasma levels and the ratio of LgNBNP/LgNANP (NP-Ratio).Results: In mild DD, NBNP and NP-Ratio are elevated above baseline. Asymp-tomatic SD was associated with the largest increase in NBNP and NANP plasmalevels and an increase in the NP-Ratio. All 3 parameters can distinguish betweenmoderate and severe DD, but none of the parameters allows to separate severeDD from SD.
Natriuretic peptides in DD and SD
LgNANP LgNBNP NP N(Median [25-75 percentile]; (Median [25-75 percentile]; Ratio
fmol/ml) pg/ml)
No DD/SD 3.46 [3.36-3.60] 1.91 [1.59-2.19] 0.55 [0.47-0.62] 153Mild DD 3.47 [3.34-3.60] 2.05 [1.73-2.32]* 0.60 [0.51-0.66]* 300Moderate DD 3.62 [3.41-3.68]*$ 2.21 [2.00-2.39]*$ 0.61 [0.56-0.67]* 47Severe DD 3.72 [3.61-3.88]*$+ 2.75 [2.13-2.95]*$ 0.71 [0.56-0.78]*$+ 19SD (EF<50%) 3.74 [3.59-3.91]*$ 2.83 [2.32-3.03]*$+ 0.75 [0.63-0.79]*$+ 23
*p<0.05 vs. "No DD/SD"; $p≤0.001 vs. "Mild DD"; +p≤0.05 vs. "Moderate DD"
Conclusion: DD and SD may be detected by both natriuretic peptides, whereasNANP best identifies moderate and severe DD. The NP-Ratio may be an addi-tional indicator for the early detection of mild DD and SD.
4968 Heart failure with a preserved systolic function anddiastolic heart failure are not synonymous
J.-C. Eicher1, O. Barthez1, F. Saint-Pierre1, P. Dobsak2, J.-E. Wolf1.1CHU du Bocage, Service De Cardiologie, Dijon, France; 2St AnnUniversity Hospital, KFDR, Brno, Czech Republic
Background: Congestive heart failure (CHF) associated with a normal left ven-tricular ejection fraction (LVEF) is highly prevalent. Usually, this type of CHF isconsidered to be due to diastolic dysfunction, but the definition of this syndromeis still an unsolved problem. European guidelines recommend the association ofsymptoms of heart failure, a normal LVEF, and evidence of an impaired diastolicfunction. However, the proposed diagnostic criteria for diastolic dysfunction arerather complicated and difficult to apply in clinical practice. American guidelinesrequire typical symptoms of CHF and a normal systolic function, but they alsoprecise that "every effort should be made to exclude other disorders that maypresent in a same manner".Methods: We enrolled 145 consecutive patients hospitalized for acute pulmonaryedema. A dosage of NT pro-BNP was performed on admission. Patients under-went an initial echocardiogram with evaluation of LVEF using biplane Simpsonmethod. Each patient with a LVEF > 45% underwent a second complete echocar-diographic study including valvular functions, regional wall motion, and Doppleranalysis of diastolic function.Results: Study patients were 57% females; mean age was 78,6. 57% of them hada preserved systolic function (P group, LVEF > 45%) and 43% had an altered sys-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Epidemiology and diagnosis of LV "diastolic dysfunction" / Novel pathophysiological mechanisms involved in myocardial dysfunction 845
tolic function (A group, LVEF < 45%). 25% of patients of P group had significantcoronary artery disease; 24% had severe valve disease; 22% had atrial fibrilla-tion; 5% had severe bradycardia; 2% had hypertrophic obstructive cardiomyopa-thy; in 3 patients the initial diagnosis of pulmonary edema was considered wrong(2 pulmonary embolism, 1 bilateral pneumonia). Finally, only 18% of the P groupwere found to have isolated diastolic dysfunction. NT pro-BNP levels were signif-icantly higher in the A group than in the P group; in the P group, patients withpure diastolic dysfunction had lower levels of NT pro-BNP than others, withoutstatistical significance.Conclusion: This study confirms that a preserved LVEF is a common findingamong patients with acute CHF, but also shows that in most cases an alternativeexplanation can be found, rather than pure diastolic dysfunction. These alterna-tive mechanisms predominantly include valve diseases, coronary artery disease,or arrhythmias. The correct identification of these factors is of high importancesince therapeutic options will be fundamentally different. Finally, lower NT pro-BNP levels in pure diastolic dysfunction suggest either misdiagnosis, or conges-tion occurring at lower levels of filling pressure.
NOVEL PATHOPHYSIOLOGICAL MECHANISMSINVOLVED IN MYOCARDIAL DYSFUNCTION
4969 C-kit positive cardiac progenitor cells and cyclingcardiomyocytes in human myocardium
M.B. Arnold1, A. Schuetz1, V. Kufer1, T. Fischlein2, W.G. Daniel2,C.D. Garlichs2. 1Dept. of Cardiology, University of Erlangen,Cardiology/Angiology, Erlangen, Germany; 2Dept. of Cardiac Surg.
University of Erlangen, Cardiac Surgery, Erlangen, Germany
Background: Over the last years increasing data support the hypothesis that theheart is not a terminally differentiated organ. C-kit+/CD34-/CD45- adult cardiacprogenitor cells were found to be part of the physiological regeneration processof the myocardium in animal studies. Therefore we evaluated in human hearttissue the presence of a) adult cardiac progenitor cells (C-kit+/CD34-/CD45-) andb) of cardiomyocytes (Ki67+ cells) undergoing the cell cycle.Methods: 64 different specimens of human myocardium were studied. Formalinfixed sections were stained with antibodies against C-kit, CD34, and CD45. Cy-cling cardiomyocytes were labelled by antibodies against Ki67, a nuclear proteinexpressed during G1 to metaphase. C-kit+/CD34-/CD45- cells and Ki67+ cellswere counted by lightmicroscopy and their distribution noted with regard to theanatomic localization.Results: C-kit+/CD34-/CD45- cells as well as Ki67+ cardiomyocytes wereidentified in human myocardium. There was no difference in the distribu-tion of C-kit+/CD34-/CD45- cells with regard to anatomic localization (RA1.42±1.2*10-6 cells/μm2, RV 3.81±2.9*10-6 cells/μm2, LA 1.27±1.5*10-6cells/μm2, LV1.91±4.1*10-6 cells/μm2). In all tissue sections, Ki67 + cells werefound in significantly higher numbers as compared to the C-kit+/CD34-/CD45-cells (p=0.0001). There were significantly higher numbers of Ki67+ cells in theright atrium (p=0.007), left atrium (p=0.003), and right ventricle (p=0.04) as com-pared to the left ventricle, with absolute numbers decreasing from the right atrium,left atrium to the right ventricle (RA 4.97±5.4*10-6 cells/μm2, LA 4.83±3.9*10-6cells/μm2, RV 4.30±2.6*10-6 cells/μm2, LV 1.73 ±2.2*10-6 cells/μm2). No sta-tistical difference of cell numbers in Ki67+ cells was measured between the atriaand the right ventricle.Conclusion: C-kit+/CD34-/45- putative adult progenitor cells can also be iden-tified in human myocardium. Furthermore, Ki67+cardiomyocytes were detectedin all four heart chambers, a finding necessitating further studies. These specificcardiomyocytes are predominantly present in the "low"-pressure compartmentsof the heart.
4970 Age dependent development of contractile dysfunctionin MLP null myocardium
B. Unsoeld, H. Schotola, C. Jacobshagen, H. Koegler, G. Hasenfuss.Universitaetsklinikum Goettingen, Abteilung Kardiologie UndPneumologie, Goettingen, Germany
Muscle LIM protein (MLP) null mice display the phenotype of a dilated cardiomy-opathy, which starts to develop at approximately 4 weeks of age. Previous stud-ies have shown decreased contractility in MLP null myocardium whereas dataon the myofilament Ca2+-sensitivity is not available. We systematically analyzedcontractile phenotype, myofilament Ca2+-sensitivity and passive myocardial elas-ticity in MLP null mice at ages 4 and 12 weeks. Whereas in 4 week old animalsthere was no significant difference in the force-frequency relationship (FFR) be-tween WT and MLP null myocardium, at 12 weeks WT myocardium exhibiteda significantly positive FFR, while that of litter mate MLP null mice was signif-icantly negative. mRNA expression analysis by real-time-PCR showed a signif-icant downregulation of Sarcoplasmic/Endoplasmic Reticulum Calcium ATPase(Serca2a) mRNA in 12 week old MLP null myocardium to 56% of the level inWT myocardium. In contrast expression levels of Phospholamban (PLN) and theSodium/Calcium Exchanger (NCX) were not significantly influenced by genotype.The reduced expression of Serca2a with unaltered levels of PLN and NCX most
likely explains the contractile deficit observed in these mice. Myofilament Ca2+-sensitivity measured in Triton X-100 permeabilized muscle strips was not affectedby genotype, irrespective of age (EC50 values for 12 week old animals WT 3.61e-6 ± 5,36e-7 mol/L (n=13) vs. KO 2,8e-6 ± 1,48e-7 mol/L (n=14)). In 12 week oldbut not in 4 week old mice maximum Ca2+-activated force was significantly lowerin KO myocardium compared to WT myocardium (22,13 ± 1,49 mN/mm2 (n=14)vs. 38,2 ± 4,91 mN/mm2 (n=13)). Passive elastic properties were examined inskinned fibers obtained from LV papillary muscles by stretching to 150% of rest-ing length in 10-% increments. While in 4 week old animals MLP null myocardiumshowed a trend to an increased compliance compared to WT (not significant),myocardium of 12 week old MLP null mice was significantly less compliant thanWT myocardium. Preliminary histologic examination revealed increased fibrosisin MLP null hearts at 12 weeks which is consistent with previously publishedobservations. Our data show that the altered contractile function of MLP null my-ocardium is not due to changes in the contractile apparatus itself but is caused bydefects in calcium cycling and increased tissue fibrosis with secondary effects onmyocardial function.
4971 Comparative analysis of the matrix turn over bypatients with and without inflammatory cardiomyopathy
A. Kallwellis-Opara1, M. Bock2, K. Puhl1, S. Rutschow1, H.-P. Schultheiss1, M. Pauschinger1 . 1Charite, Med. Klinik II, Berlin,Germany; 2Charite, Med. Klinik II, Berlin, Germany
Different studies showed that the development of heart failure correlates withaltered collagen content and compositions. In addition, patients with clinicallysuspected dilated cardiomyipathy (DCM) have myocardial inflammation and vi-ral persistence in a high percentage, which are both effectors on matrix re-modeling. This study quantified the myocardial collagen content and collagendegradation in DCM patients with or without myocardial inflammation. Endomy-ocardial biopsies were obtained from 29 DCM patients without inflammation(2,64±0,47 CD3) and 24 DCM patients with inflammation (DCMi) (10,71±1,97;analyzed by immunohistochemistry). Both groups did not differ in age (53±2,47vs. 53±2,54years), LVEDD mean (69,48±1,72 vs. 66,75±1,44mm) and EF(28,65±1,87 vs. 28,5±1,96%). Collagen content were quantified by picosiriusred staining and the serum ICTP content (Collagen type I C-terminal peptide;serum marker of collagen remodeling) were measured and compared to 30comparable healthy blood donors. The MMP9 and TIMP expression in biopsiesand serum were quantified by immunhistochemistry and Elisa. ICTP serum levelof DCM and DCMi patients are significantly elevated in comparison to healthyblood donors (2.62±0,15μg/l vs. 7,12±1,06 μg/l by DCM vs 6,22±1,04 μg/l byDCMi) and correlates significantly with LVEDD (r2=0,2021; p=0,0025), LVEDP(r2=0,1582, p=0,0032) and EF (r2=-0,2092; p=0,0006). Following, whereas theICTP serum level did not differ significantly between DCM patients with orwithout inflammation, the collagen content was significantly increased by in-flammation (1,09±0,12% by DCMi vs. 0,54±0,10% DCM, p<0,0001; picosir-ius red staining) indicating a essential role of inflammation during fibrotic inclu-sion. The remodeling process seems to be a local process, because DCMi pa-tients showed a slightly increased MMP9 expression in biopsies (194,14±45,73cells/mm2 by DCMi vs 107,79±28,69 cells/mm2 by DCM) compared to DCM pa-tients, whereas neither the MMP9 expression in serum (31,22±2,90 μg/l by DCMivs 37,41±4,47μg/l by DCM) nor the expression of its inhibitor TIMP1 in biop-sies (4,72±1,12 cells/mm2 by DCMi vs 4,28±0,90 cells/mm2 by DCM) or serum(319,98±13,63 μg/l by DCMi vs 336,60±24,55 μg/l by DCM) differed betweenthee groups resulting in an increased MMP9/TIMP1 ratio in biopsies of DCMi pa-tients.Cardiac dysfunction of DCM patients is strongly correlated to the local degree ofthe collagen content, which is further increased by inflammation in DCMi patientsfollowed by a local rising MMP9 expression.
4972 Reduced stretch-induced delayed force response andmaintained Frank-Starling mechanism in failing humanmyocardium
D. Von Lewinski, J. Kockskamper, D. Zhu, A. Lauterbach, A. Elgner,B. Pieske. Universitat Gottingen, Abt. Kardiologie Und Pneumologie,
Gottingen, Germany
Stretch induces immediate and delayed inotropic effects in mammalian my-ocardium via distinct mechanosensitive pathways. The immediate phase is knownas Fank-Starling mechanism (FSM) and attributed to an increase in myofilamentsensitivity. The latter depends on the activation of membrane-bound proteinsand is Ca2+-dependent. Regulation of FSM is controversial in failing human my-ocardium and there is no data on the delayed phase in non-failing human my-ocardium. Therefore, we tested the effects of stretch on immediate and delayedforce responses in failing and non-failing human myocardium.Methods: Experiments were performed in muscle strips from 21 failing (F) and 9non-failing (NF) human hearts (physiological conditions: 37°C, 1 Hz, bicarbonatebuffer). Muscles were stretched from 88% to 98% of optimal length. The result-ing immediate (i.e. Frank-Starling mechanism; FSM) and delayed (i.e. slow forceresponse, SFR) increases in twitch force were assessed without and after block-ade of NO synthases (NOS; 500mmol/L L-NAME), PI-3-kinase (PI3K; 0.1μmol/LWortmannin) or reverse-mode Na+/Ca2+ exchange (rNCX; 5mmol/L KB-R7493).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

846 Novel pathophysiological mechanisms involved in myocardial dysfunction / Myocardial contrast echo in ischaemic substrates
We also measured [Na+]i using SBFI and tested the phosphorylation state ofp44/42MAPK -a potentially relevant signal transduction kinase- using WesternBlots for the protein and its phosphorylated form.Results: Stretch induced an immediate (<10 beats) followed by a slow (5-10min) force response (SFR). Immediate force response was comparable in bothgroups (NF vs. F: 226±16% vs. 232±14% of pre-stretch value, respectively),whereas the SFR was greater in non-failing myocardium (to 126±3%(NF) vs.120±2%(F) of force of FSM, respectively, p<0.05). Inhibition of NOS (F n=8; NFn=6) or PI-3-kinase (F n=6; NF n=6) did neither alter FSM nor SFR. The SFR wasaccompanied by an increase in [Na+]i in both F and NF myocardium. It was almostcompletely abolished by inhibition of rNCX (F 121±4% vs. 107±3%, n=7 andNF 129±8% vs. 108±2%, n=6; both p<0.05). The basal ratio of phosphorylatedp42/44MAPK and total protein was higher in F than NF (1.2±0.2 vs. 0.8±0.1desitometric units; p<0.05).Conclusion: The data demonstrate an unaltered FSM in failing human my-ocardium. In contrast, SFR is reduced in failing compared to non-failing humanmyocardium although signal transduction is qualitatively identical. The reducedSFR in F may be due to quantitative differences in the phosphorylation state ofstretch-regulated kinases.
4973 The novel role of urotensin II on the diastolic propertiesof myocardium
A.P. Fontes-Sousa, C. Bras-Silva, D. Monteiro-Sousa, A.F. Leite-Moreira. Faculty of Medicine, Dept. of Physiology, Porto, Portugal
Background: Urotensin II (U-II) is a peptide expressed, together withits receptor, in the central nervous system and in many peripheral tissues, includ-ing the cardiovascular system. In the latter, U-II has been shown to modulate thevascular tonus, myocardial contraction, heart rate and cardiac fibrosis and hyper-trophy. In the current study, we investigated the, yet unknown, acute effects of U-IIon the diastolic properties of the myocardium.Methods: Effects of increasing concentrations of U-II (10-8 to 10-6M) were evalu-ated in isolated right papillary muscles (n=13) from male New Zealand White rab-bits (Krebs-Ringer: 1,8mM CaCl2, 35°C). Reported parameters include: activetension (AT; mN/mm2), maximum velocities of tension rise and tension decline(dT/dtmax e dT/dtmin, respectively; mN/mm2/s), resting tension (RT; mN/mm2)and muscle length (L; L/Lmax). Only significant results (means±SEM, p<0.05)are given, expressed as % change from baseline.Results: U-II had no significant effects on AT, dT/dtmax and dT/dtmin in the con-centration range of this study. It, however, promoted a concentration-dependentincrease in resting muscle length up to 1.007±0.0016 L/Lmax at the highest con-centration. Correcting muscle length to its initial value resulted in a 20.6±3.59%decrease of RT, indicating decreased muscle stiffness.Conclusion: The present study demonstrated a novel effect of U-II on the dias-tolic properties of the myocardium, which consisted on a concentration dependentacute decrease of myocardial stiffness. This effect is a potentially powerful phys-iologic mechanism, as it may allow the heart to reach the same diastolic volumewith up to 20% lower filling pressures. Furthermore, as the plasmatic levels of U-IIare increased in heart failure, these results might help to better understand thephysiopathology of this syndrome.
4974 The acute increase in myocardial distensibility inducedby beta-adrenergic stimulation is mediated by PKA,PKC AND NA+/H+ exchanger
I. Falcao-Pires, P. Fontes-Sousa, C. Bras-Silva, A. Leite-Moreira.Faculty of Medicine, Physiology Department, Porto, Portugal
Purpose: Recent studies suggested that titin phosphorylation by PKA inducesan increase of myocardial distensibility. As β-adrenergic stimulation is one of themost important stimuli for PKA activation, the present study investigated its effectson myocardial distensibility, as well as some of the underlying mechanisms.Methods: Effects of increasing concentrations of isoproterenol (ISO; 10-10 to 10-5M) were evaluated in isolated right papillary muscles from male New ZealandWhite rabbits (Krebs-Ringer: 1,8mM CaCl2, 35°C) in the absence (n=9) orpresence of: (i) PKA inhibitor, KT5720 (10-6M; n=9); (ii) PKC inhibitor, chel-erythrine (CHE; 10-5M; n=9); or (iii) Na+/H+ exchanger inhibitor, 5-(N-metil-N-isobutil)-amiloride (MIA; 10-6M; n=8). Reported parameters include: active ten-sion (AT; mN/mm2), maximum velocities of tension rise and decline (dT/dtmaxand dT/dtmin, respectively; mN/mm2/s), passive tension (PT; mN/mm2) and mus-cle length (L; L/Lmax). Only significant results (means±SEM, p<0.05) are given,expressed as % change from baseline.Results: At baseline, ISO induced concentration-dependent positive inotropicand lusitropic effects maximal at 10-5M, which increased 106.6±17.9% AT,296.9±35.8% dT/dtmax and 198.9±21.1% dT/dtmin. These effects were not sig-nificantly affected by any of the inhibitors used in this study. Concerning myocar-dial distensibility, increasing concentrations of ISO progressively increased rest-ing muscle length up to 1.03 L/Lmax. Correcting muscle length to its initial valueresulted in a 27.1±5.22% decrease of RT, indicating decreased stiffness or anincrease of myocardial distensibility. This effect was almost abolished by the inhi-bition of PKA, PKC or Na+/H+ exchanger.Conclusion: The present study demonstrated that β-adrenergic stimulation pro-motes an increase of myocardial distensibility, modulated by the activation of sev-
eral intracellular pathways, including PKA, PKC and Na+/H+ exchanger. This ef-fect represents a novel mechanism of modulation of the diastolic properties of themyocardium by the sympathetic nervous system. This might have pathophysio-logic implications in heart failure, as this syndrome is characterized by sympa-thetic hyperactivation and β-adrenoceptor desensitization.
MYOCARDIAL CONTRAST ECHO IN ISCHAEMICSUBSTRATES
4975 Detection of myocardial viability by intravenouscontrast echocardiography in predicting the recoveryof left ventricular systolic function in patients withacute myocardial infarction
M. Olszowska, W. Tracz, M. Kostkiewicz, M. Hlawaty, P. Podolec.Institute of Cardiology, Department Cardiac and Vascular Disease, Krakow,Poland
Background: Despite angiographically successful opening of an infracted-related artery, some patients do not recover left ventricular regional wall functionin the infarct zone after an acute myocardial infarction (AMI). Myocardial contrastechocardiography (MCE) offers a promising modality for non-invasive evaluationof myocardial perfusion.Objective: The present study aimed to assess the role of MCE in predicting therecovery of left ventricular systolic function in patients with acute myocardial in-farction (AMI).Methods: Eighty-sixt subjects (68 M, 18 F; mean age 58.4±11.2) underwent pri-mary percutaneous coronary angioplasty (PCI) for acute anterior myocardial in-farction. MCE and two-dimensional echocardiography were performed in all sub-jects. Wall motion and segmental perfusion were estimated in real time beforeand immediately after PCI and on the third day after PCI, using low MI (0.3) after0.3 ml bolus injection of intravenous Optison. MCE was scored semiquantitativelyas: 1-homogenous contrast enhancement, 0.5- patchy contrast enhancement, 0-no contrast. Regional wall motion score index (RWMSI) and regional perfusionscore index (RPSI) within the risk area were calculated. Segments with homoge-nous perfusion were assessed as viable. Regional left ventricular function was re-assessed after 3 months. Segments with improvement contractility were deemedviable.Results: On the third day after PCI among 358 dyssynergics segments in 233segments (89 akinetic, 144 hipokinetic) perfusion defect was observed. Threemonths after PCI 238 dyssynergic segments (68 akinetic, 170 hipokinetic) weredetected. 90% of segments without perfusion on the third day had hypokinesis, orakinesis after 3 months. 90% of segments with normal perfusion on the third dayhad normal wall motion at follow-up. Strong relationship between RPSI in the riskarea assessed by myocardial contrast on the third day after PCI and RWMSI in therisk area after 3 months (R2 =0.7696) was observed. Sensitivity, specificity, andaccuracy in predicting wall motion recovery was 88%, 80%, 86%, respectively.Conclusion: Serial MCE facilitated identification of myocardial perfusion abnor-malities in patients with AMI. The presence of perfusion within the infarct zoneon the third day After PCI predicts the maintenance of perfusion and recovery ofresting systolic function.
4976 The extent of residual contrast perfusion and not leftventricular function predicts late recovery of globalcontractile function after acute myocardial infarctionand reperfusion therapy
G. Dwivedi, R. Janardhanan, K. Greaves, T.K. Lim, S. Hayat, R. Senior.Northwick Park Hospital, Cardiology, Harrow, United Kingdom
Background: Myocardial contrast echocardiography (MCE) by virtue of its abil-ity to assess both myocardial blood volume and velocity can be used to assessstatus of microvascular perfusion. Although the impact of residual microvascularperfusion assessed by MCE after acute myocardial infarction (AMI) and reperfu-sion therapy on late regional functional recovery has been demonstrated exten-sively, studies assessing its value on global left ventricular (LV) contractile func-tion, which is an important determinant of prognosis are sparse.Methods: Accordingly, 95 patients with ST elevation AMI underwent low-powerMCE and two-dimensional echocardiography after reperfusion therapy. Both sys-tolic wall thickening and contrast opacification were scored on a 16 segment LVmodel. Systolic wall thickening was scored as: 1=normal, 2=reduced, 3=absent,4=systolic wall thinning. Global LV function was calculated by adding the sys-tolic wall thickening scores in all 16 segments divided by 16. Myocardial perfu-sion was assessed over 15 cardiac cycles following the destruction of microbub-bles with high-energy pulses. A 3-point scoring system was used with 2=nor-mal;1=reduced;0=minimal/absent contrast opacification. Contrast perfusion index(CPI), a measure of extent of myocardial perfusion, was defined as sum of thecontrast opacification score in all 16 LV segments divided by 16. Echocardiogra-phy was repeated 12 weeks after the reperfusion therapy to assess recovery ofLV contractile function.Results: All patients but 2 had abnormal resting LV systolic function, of which 64(69%) demonstrated improvement in LV function at 3 months. The area under thereceiver operator characteristic curve for predicting recovery of global contractile
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Myocardial contrast echo in ischaemic substrates 847
function for MCE and LV function at baseline were 0.79 and 0.59 respectively.Furthermore, CPI was significantly higher (P<0.001) in the 64 patients, whichshowed late recovery of LV function (1.68±0.27) compared to CPI in patients whodid not show recovery of function (1.27±0.04). No significant difference was notedin the indices of baseline LV function inpatients with (1.67±0.32) and without(1.78±0.35) recovery of LV function. Of the 62 patients with minimal perfusiondefect (CPI>1.5), 54 (87%) showed recovery of LV function, conversely, 21 (66%)out of 31 patients with significant perfusion defect failed to recover function.Conclusion: The extent of residual contrast perfusion and not LV function pre-dicts late recovery of global LV function after acute myocardial infarction andreperfusion therapy.
4977(W) Myocardial contrast echocardiography providesadditional information about viability in 2-D akineticsegments in patients treated by a myocardialrevascularization procedure
A.V. Moraes, L. Araujo, W. Pereira, M. Carrinho, R. Morcerf,A.C. Nogueira, F. Morcerf. ECOR, Ecocardiografia, Rio De Janeiro, Brazil
Background: Infarcted zone (IZ) after myocardial infarction (MI) is often akineticon rest 2-D echo. Zones of viable myocardium are frequently found within the IZ,and this may have both therapeutic and prognostic implications. We sought tocorrelate the perfusion patterns of a 2-D akinetic segment with the follow-up aftermyocardial revascularization procedure (MRP) in pts with coronary artery disease(CAD).Methods: In 164 pts (104 male, 63±14 years), with at least one 2-D akinetic seg-ment, adenosine contrast echocardiography (ACE) was obtained to investigatethe extension of CAD after MI. Triggered 2nd harmonic imaging with infusion ofPESDA, at rest and after a bolus injection of adenosine (ADN) was the used pro-tocol. For each patient 3 LV territories were considered (total of 492 territories). Amarked contrast enhancement after ADN was normal perfusion (NP); a decreasecontrast enhancement after ADN was a reversible defect (RD), and a decreasecontrast enhancement at rest without changes after ADN was a fixed perfusiondefect (FD). MRP success was defined by the rest wall motion recovery in the 2-Decho performed 3 to 6 months later.Results: Akinesis was observed in 278 segments. NP, RD and FD were found in18, 54 and 206 territories respectively. Successful MRP (PCI in 87 pts and CABGin 77 pts) were observed in all 18 territories with NP (100%) and in 37/54 (68.5%)territories with RD (Figure). By the other hand 178/206 (86.5%) territories with FDwere related to unsuccessful MRP (p<0.001).
Fig. 1
Conclusion: ACE provides additional information about the different types of per-fusion defects in pts with 2-D akinetic segments that could be useful in the man-agement of myocardial viability.
4978 End-diastolic myocardial thickness, myocardialperfusion and reserve in predicting myocardialrecovery after revascularization in patients withoccluded coronary artery disease
C. Aggeli, S. Tapanlis, G. Giannopoulos, E. Christoforatou,G. Roussakis, S. Brili, J. Barbetseas, C. Stefanadis. 1st card. dep. Un.of Athens,Hippocration hos, Athens, Greece
Purpose: The aim of this study was to evaluate the impact of end-diastolic my-ocardial thickness (EDDT), myocardial perfusion using contrast echocardiogra-phy (MCE) and myocardial reserve using dobutamine stress echocardiography(DSE), in predicting recovery of dysfunctional myocardium after revascularizationin patients with an occluded coronary artery disease.Methods: 45 patients (mean age 60±3 y) with LAD disease, 25 with severestenosis >70% (group A) and 20 with occluded LAD (group B) and regional dys-function underwent MCE and DSE 2-5 days before revascularization. MCE wasperformed using real-time low mechanical index power modulation imaging dur-ing continuous infusion of SonoVue® (Bracco). All patients underwent coronarybypass grafting and follow-up low dose dobutamine stress test was repeated 2-3months after revascularization.Results: There were no differences in age, rest ejection fraction, and rest wallmotion score index between the two groups. Of 264 dysfunctional LAD territorysegments having undergone revascularization, 185 (112 in group A and 73 ingroup B) recovered as revealed at follow-up. The EDDT was significantly higher
in group A compared with group B (0.68±0.04 vs. 0.56±0.03, p<0.05). In groupA, MCE and DSE exhibited similar values of sensitivity, specificity and accuracy(86% vs. 85%, 68% vs. 72%, 77% vs. 76%, respectively) whereas in group B,MCE showed higher sensitivity and negative predictive value than DSE (82% vs.56%, p<0.001 and 80% vs. 65%, p<0.05, respectively) in predicting segmentalmyocardial recovery. These differences in sensitivity and negative predictive valuebetween MCE and DSE were more pronounced in akinetic segments of group B(78% vs. 42%, p<0.001 and 72% vs. 60%, p<0.05). The combination of EDDT>0.5 cm and presence of myocardial perfusion had the higher sensitivity 88%and a specificity of 56% to predict myocardial recovery of akinetic segments.Conclusions: The combination of EDDT>0.5cm and presence of myocardialperfusion (evaluated using MCE), has the higher sensitivity in predicting post-revascularisation recovery of dysfunctional myocardium supplied by totally oc-cluded LAD.
4979 Prediction of hibernating myocardium by myocardialcontrast echocardiography. Comparison with lategadolinium-enhanced cardiovascular magneticresonance
P. Tousek1 , M. Penicka1, J. Tintera2, H. Linkova1, Z. Straka1,P. Gregor1. 1Prague, Czech Republic; 2IKEM,ZRIR-MR, Prague,
Czech Republic
Background: Very little is known about the accuracy of intravenous myocardialcontrast echocadiography (MCE) in detection of myocardial hibernation. Thereare also currently no data on the comparison of MCE to late gadolinium-enhancedcardiovascular magnetic resonance (LGE-CMR) in this clinical setting.Methods: Twenty four patients (92% males, age 64 ± 7,3 years) with chroniccoronary artery disease and left ventricular dysfunction (EF 31,8 ± 4,3%) under-went MCE + LGE-CMR (n=15) within one month before bypass surgery. MCE wasperformed using continuous Optison infusion with intermittent imaging (PowerHarmonic Doppler). Control echocardiography was repeated at 6 months afterbypass surgery. 16 segment model of the left ventricle was used for the analysis.Myocardial perfusion was graded semi-quantitatively as 1=normal, 2=patchy and3= absent. By LGE-CMR, segments were scored according the severity of my-ocardial scar as 1=without scar, 2=less than 50% of myocardial thickness, 3=morethan 50% of myocardial thickness, which reflects nonviable myocardiumResults: Of the 321 revascularized dysfunctional segments, MCE was ade-quately visualized in 289 (90%) segments. Contractile function recovered in 106(37%) dysfunctional segments, out of which 66 (23%) segments where akinetic.The sensitivity of preserved myocardial perfusion (score 1+2) for segmental con-tractile function recovery (hibernating myocardium) of akinetic segments was 80%and was similar to LGE-CMR (88%, p-NS). Specificity of MCE was higher thanfor LGE-CMR (70%, and 52%, respectively; p<0,05)Conclusion: MCE identifies hibernating myocardium in patients with chroniccoronary artery disease undergoing bypass surgery. Accuracy of MCE to predictsegmental functional recovery is superior to LGE-CMR.
4980 Adenosine myocardial contrast echocardiographyversus positron emission tomography in assessmentof microvascular dysfunction in hypertrophiccardiomyopathy patients
O. Soliman1, P. Knaapen2, M.L. Geleijnse1, A.M. Anwar1,A. Nemes1, F.J. Ten Cate1. 1Thoraxcenter, Erasmus MC, Cardiology, Rotterdam,Netherlands; 2Vu Medical Center, Amsterdam, Netherlands
Background: Microvascular dysfunction in Hypertrophic cardiomyopathy (HCM)may be presented by serious manifestations ranging from dyspnoea to suddendeath, therefore its quantification is important in clinical assessment of HCM.Aim: To investigate dynamic changes in myocardial blood flow (MBF) and my-ocardial blood flow reserve (MBFR) by two non-invasive techniques for quan-tification, Myocardial Contrast Echocardiography (MCE) and Positron EmissionTomography (PET).Methods: Ten consecutive HCM patients with NYHA class III and angina pectoris(8males, age 54± 12.98 years) with normal coronary angiogram. All underwentMCE using continuous intravenous infusion of SonuVue® and PET using oxygenlabelled water [H215O]. All examinations done at rest and 5 minutes after infusionof 140-μg.kg.min adenosine. MCE was done using Philips Sonos 7500, mechani-cal index 0.1. Data stored for off-line analysis. Two experienced investigators anal-
Fig. 1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

848 Myocardial contrast echo in ischaemic substrates / Echo assessment of left ventricular function: new insights
ysed images using Qlab Region Of Interest (ROI) quantification software. ThreeROIs (were drawn at base, mid and apical septum. Time intensity curves werecalculated and fitted by mono-exponential function. MBF calculated from formula[MBF=A*β], where A is the peak plateau intensity representing myocardial bloodvolume (MBV), β is the rate of signal intensity (SI) rise reflecting the mean bubblevelocity (MBF velocity).Results: see figure.Absent vasodilator reserves (stress-rest ratio) after adenosine infusion detectedin 28/30 ROIs. MCE and PET derived MBF correlated well at rest and stress.(Rest MCE vs. PET r = 0.91, p<0.01), (Stress MCE vs. PET r =0.81, p <0.01).
ECHO ASSESSMENT OF LEFT VENTRICULARFUNCTION: NEW INSIGHTS
4981 The analysis of Doppler-derived end-systolicintraventricular pressure gradients provides a reliableestimation of the rate of ventricular relaxation
R. Yotti Alvarez1, C. Cortina1, J.C. Antoranz2, M. Desco1,J.L. Rojo-Alvarez3, C. Allue1, M.A. Garcia-Fernandez1 , J. Bermejo1.
1Hospital General Gregorio Maranon, Cardiology Dept., Madrid, Spain;2Universidad Nacional de Educacion a Distancia, Department of MathematicalPhysics and Fluids, Madrid, Spain; 3Universidad Carlos III, Signal Theory andCommunication, Madrid, Spain
Background: Current non-invasive indices of diastolic function have importantlimitations, and an accurate evaluation of ventricular relaxation is a pending is-sue in the clinical practice. We hypothesized that the end-systolic features of theDoppler-derived ejection intraventricular pressure difference (EIVPD) curve couldprovide a reliable estimation of the invasive time constant of ventricular relaxation(tau).Methods and Materials: Color-Doppler M-mode images of LV outflow, and highfidelity pressure and volume (conductance) signals were simultaneously acquiredin mini-pigs undergoing load (caval and aortic occlusions) and inotropic inter-ventions (acute ischemia and beta-adrenergic modulation). Tau was measuredusing the Weiss method. Using the data obtained in 9 open-chest animals, weperformed a wave intensity analysis (WIA) and developed a predictive model toestimate tau from EIVPD parameters. Then, another sample of 5 closed-chestanimals were used to validate the model.Results: By WIA, we demonstrated that the energy of the LV relaxation wave (Iw-)closely correlated in time and magnitude with tau, as well as with the peak reverseEIVPD and with the time to EIVPD abolishment (See Figure A). Accordingly, alinear correlation was observed between tau and peak reverse EIVPD and timeto EIVPD abolishment. Using both parameters, we derived a model that, in theseparate validation sample, showed a high predictive power for estimating tau(Rintraclass=0.77, n=607 beats) (see Figure B).
Conclusions: Doppler-derived end-systolic intraventricular pressure gradientsprovide a noninvasive and accurate estimation of tau, that can potentially improvethe characterization of diastolic function in clinical practice.
4982 Velocity vector imaging demonstrates paradoxicalabnormalities in longitudinal and circumferentialmyocardial function in patients with hypertrophiccardiomyopathy and normal ejection fraction
S. Moir, S.R. Ommen, F. Miller, J.K. Oh, S.L. Mulvagh. Mayo Clinic,Rochester Mn, United States of America
Background: Patients with hypertrophic cardiomyopathy (HCM) commonly havepreserved systolic ejection fraction despite significant longitudinal myocardialfiber dysfunction. This is believed to be due to compensatory normal or supra-normal radial and circumferential function. Velocity vector imaging (VVI) is a newmodality for quantification of myocardial function, and enables assessment of lon-gitudinal and circumferential strain and strain rates.Methods: We compared 20 patients with known HCM and preserved ejectionfraction (with no history of pacing or septal reduction therapy) and 20 controls(patients with no coronary risk factors and no evidence of myocardial ischemia bystress echocardiography). All patients were studied using a commercially avail-able machine (Acuson Sequoia - Siemens) and underwent off line VVI analysis,
utilizing the apical four chamber view for calculation of longitudinal strain andstrain rates, and the mid ventricular para-sternal short axis view for calculation ofcircumferential stain and strain rates.Results: There was no difference in age, gender or resting ejection fraction be-tween the two groups - see table. Compared with controls, patients with HCMhad significantly reduced mean longitudinal strain and stain rate - see table. Con-versely, patients with HCM had significantly increased circumferential strain, withno difference in circumferential strain rate compared with controls.
HCMn=12 Controln=12 p
Age (years) 48 ± 14 45 ± 14 0.58Males 11 13 .66Resting EF (%) 60.8 ± 8.9 61.6 ± 3.4 .65Longitudinal Strain (%) -15.2 ± 3.7 -20.2 ± 3.2 <0.001Longitudinal Strain Rate (/sec) -0.87 ± 0.28 -1.09 ± 0.26 0.01Circumferential Strain (%) -31.8 ± 8.7 -26.4 ± 4.3 0.02Circumferential Strain Rate (/sec) -1.73 ± 0.64 -1.63 ± 0.24 0.56
Conclusion: In patients with HCM, velocity vector imaging analysis demonstratessignificant abnormalities in longitudinal myocardial function, with paradoxicallysupra-normal circumferential myocardial function, which contributes significantlyto their normal ejection fraction.
4983 Is cardiac torsion and untwisting by speckle trackingechocardiography more sensitive than TDI in detectionof subclinical LV dysfunction in apparently healthyobese subjects?
C. Wong, R. Leano, T.H. Marwick. University of Queensland, School ofmedicine, Brisbane, Australia
Background: Speckle tracking echocardiography (STE) has been proposed as asensitive measure of LV function. We evaluate the LV rotation and untwisting inobese subjects comparing to TDI.Methods: After exclusion of overt LV dysfunction or ischemia, 44 asymptomaticobese pts underwent conventional and novel echocardiographic studies. Apicaland basal rotation and rotational velocities by STE measured from short axis im-ages by automatic frame-to-frame tracking of grey-scale speckle patterns. LV tor-sion was calculated as difference between clockwise rotation at base and counter-clockwise rotation at apex. Comparisons were made with 43 non-obese controls.Associations were sought between myocardial measures with STE and longitu-dinal tissue velocity (TDI), clinical characteristics. Subclinical LV dysfunction de-fined by presence of tissue velocities >1 SD below age adjusted mean values ofnormal-weight controls.Results: Obese subjects demonstrated reduced systolic LV torsion and basalrotation (Table), but preserved systolic apical velocities. The untwisting rotationalvelocities in diastole were similarly reduced. Systolic longitudinal tissue velocitysm correlated significantly with LV basal rotation (r=0.27, p<0.05) and overalltorsion (r=0.36, p<0.01). LV torsion also correlated with waist (r=-0.24, p<0.05).Basal rotation and LV torsion were significantly reduced even in pts without LVdysfunction by TDI.
Table 1. Clinical and STE characteristics
Obese Controls p(n=44, 33f, 11m) (n=43, 24f,19m)
Age (yrs) 44±10 51±8 <0.05BMI (kg/m2) 39±8 27±4 nsBP (mmHg) 125/77±13/8 126/79±17/10 ns
LVD by TDI Non LVDBasal rotation (°) 3.3±3.2 4.7 ±2.8 6.7±2.8 0.001Apical rotation (°) 7.2±2.0 6.0±3.4 7.7±6.0 nsLV torsion (°) 10.0±4.0 10.2±4.2 14.4±6.8 0.01Apical diastolic rotational velocity (°s-1) 46±23 54±22 65±26 <0.05Apical systolic rotational velocity (°s-1) 54±10 60±2 65±28 ns
LVD = LV dysfunction, TDI = Tissue Doppler Imaging.
Conclusion: Obese pts had reduced LV torsion, regional rotation at the base anddiastolic rotational velocities. Compared to TDI, STE may be a more sensitivemeasure of subclinical myocardial disease in metabolic disease.
4984 Determinants of left ventricular untwist rate: Is it allabout end-systolic volume?
A. Opdahl, T. Helle-Valle, T. Vartdal, E. Pedersen, T. Edvardsen,O.A. Smiseth. Rikshospitalet University Hospital, Institute for SurgicalResearch, Oslo, Norway
Background: Left ventricular diastolic untwist rate (UTR) has been proposed asa marker of recoil forces that account for diastolic suction. The mechanisms ofchanges in UTR, however, are not well defined. This study investigates the re-lationship between UTR and LV contractility, loading conditions and myocardialischaemia, respectively.Methods: In 7 anaesthetized dogs with micromanometers we measured LV twistby sonomicrometry as the difference between apical and basal rotations, andtwist rate as the time derivate of twist. In addition we measured apical rotation
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Echo assessment of left ventricular function: new insights / How important is high-sensity lipoprotein cholesterol? 849
and rotation rate by speckle tracking echocardiography (STE). LV volume wasmeasured by sonomicrometry. Measurements were done during different loadingconditions, increased contractility by dobutamine, and after 15-20 minutes of LADocclusion.Results: Volume loading caused no change in UTR or end-systolic volume (ESV).Dobutamine increased UTR from 64.9 ±8.8 (SEM) to 125.6 ±10.3°/s (p<0.01),and decreased ESV from 35.2 ±2.5 to 32.7 ±2.5 ml (p<0.01), whereas LAD oc-clusion decreased UTR from 64.9 ±8.8 to 57.1 ±6.0°/s (ns) and increased ESVfrom 35.2 ±2.5 to 44.0 ±3.8 ml (p<0.01). Importantly, at comparable ESV lev-els measurements during dobutamine showed essentially similar UTR as duringbaseline and volume loading. Furthermore, there was no reduction of UTR dur-ing ischaemia at comparable ESV levels before ischaemia. Similar results wereobserved for apical rotation by STE.
Conclusions: Changes in peak UTR during changes in contractility and is-chaemia were attributed to accompanying changes in ESV. Therefore, changesin contractility and ischaemia do not appear to have specific effects on peak UTR.These results support that diastolic untwist is caused by restoring forces that aredetermined by end-systolic dimension.
4985 Variations in systolic strain rate and strain parameters:a multiple regression analysis amongst normalindividuals
L. Herbots1, E. Eroglu2, J. Ganame2, D. Thys2, P. Boettler2,P. Claus2, F. Rademakers2 , J. D’hooge2. 1Uz Gasthuisberg (University
Hospital), Dept. Of Cardiology, Leuven, Belgium; 2UZ Gasthuisberg, KULeuven,Cardiology, Leuven, Belgium
Introduction: Strain rate and strain parameters have been introduced to quantifyregional myocardial function. Normal values have been reported before, howeverthe patient characteristics that influence these values have never been investi-gated extensively.Aim: To determine the dependency of systolic deformation parameters on patientcharacteristics.Methods: Myocardial Velocity Imaging data were acquired (GE Vivid7) from 149normal subjects (age 17-79y; 95 male) at high frame rate (> 140 fps) from theapical 2-, 3- and 4-chamber views. All subjects were free of any known cardio-vascular disease based on a thorough history, physical examination and a normalelectrocardiogram. Regional longitudinal function was analysed in a 18-segmentmodel of the left ventricle by extracting segmental strain and strain rate usingdedicated software. Peak systolic strain rate (SRsys) and maximal systolic strain(Ssys) were averaged over all segments per patient. As independent predictorsgender, age, heart rate, systolic and diastolic blood pressure, diastolic posteriorwall thickness, left ventricular end-diastolic short-axis diameter and body mass in-dex (BMI) were evaluated. Statistical analysis was performed using forward step-wise multiple regression.Results: Averaged SRsys was -1.58±0.28s-1 and Ssys was -21.4±2.6%. Aver-aged SRsys was negatively correlated with BMI (partial correlation coefficient [r2]0.45, p < 0.001) and age (r2=0.28, p=0.02) while Ssys was only correlated withBMI (r2=0.33, p<0.01). When BMI was not entered into the stepwise regressionmodel, SRsys correlated with age (r2=0.26, p<0.02) and diastolic posterior wallthickness (r2=0.23, p<0.04) and Ssys correlated with gender (r2=0.23, p<0.04).
Conclusions: Variations in systolic strain and strain rate parameters amongstnormal individuals can mostly be attributed to BMI. Also age and gender showedto be secondary predictors for changes in SR and strain respectively. This shouldbe taken into account when setting out normal values.
4986 A novel method of assessing regional strain and strainrate values using speckle tracking
N. Artis1, D.L. Oxborough1 , L.B. Tan1, G. Williams2, C.B. Pepper1.1University of Leeds, Leeds, United Kingdom; 2Leeds GeneralInfirmary, Leeds, United Kingdom
Introduction: 2-D Strain imaging using speckle-tracking is a new method en-abling simultaneous analysis of myocardial strain in both radial and circumfer-ential dimensions. 2-D derived values of radial (Rad) and circumferential (Circ)strain, systolic and diastolic strain rate (SRs’ and SRe’) of segmental left ven-tricular (LV) function have not been reported in patients with severely impaired LVfunction. We compared the values and patterns obtained from a cohort of patientswith LV dysfunction (LVD) vs healthy controls.Methods: Thirty-two subjects with no known history of cardiac disease and 22subjects with LV dysfunction (LVEF<35%) were assessed. Ultrasound imageswere acquired using a Vivid 7 (GE Vingmed) system and analyzed offline usingdedicated 2-D strain software. A parasternal short-axis view just below the levelof the mitral valve was used to assess circumferential and radial values. Strain,SRs’ & SRe’ were measured from Septal, Lateral, Inferior, Anterior, Anteroseptumand Posterior segments of the LV.Results: Table 1 shows the mean±SD of the two groups for peak Strain, SRs’& SRe’. There was a highly statistically significant difference between the twogroups (p<0.001) for Strain, SRs’ and SRe’. Higher strain values were seen in theradial dimension than in the circumferential dimension. There were no significantdifferences between segments of the left ventricle. The inter- and intra-observervariability for strain measurements was between 6 and 11% showing good repro-ducibility.
Peak Strain and Strain Rate values
Value Normal Impaired
Circ Strain (%) 19.4±4.5 6.67±4.21Circ Sys Strain Rate (s’) 1.27±0.36 0.59±0.33Circ Dia Strain Rate (e’) 1.84±0.78 0.72±0.48Rad Strain (%) 42.99±13.15 9.61±7.70Rad Sys Strain Rate (s’) 1.38±0.31 0.80±0.48Rad Dia Strain Rate (e’) 1.87±0.88 0.76±0.60
Conclusions: The difference in strain and strain rate between the two groupsis clear and this new method of quantifying strain shows great promise and us-ability. Its independance of the angle of insonation and reproducibility makes itpotentially superior to tissue doppler derived data and may allow strain imagingto be incorporated into daily clinical use.
HOW IMPORTANT IS HIGH-SENSITY LIPOPROTEINCHOLESTEROL?
4987 Drivers of low HDL-C in a dyslipidaemic population: ananalysis from the pan-European survey of HDL-C
E. Bruckert1, M. Baccara-Dinet2, H. Drexel3. 1Groupe HospitalierPitie-Salpetriere, Service d’Endocrinologie Metabolique, Paris, France;2Merck KGaA, Darmstadt, Germany; 3Academic Teaching Hospital,
Feldkirch, Austria
The Pan-European Survey of HDL-C evaluated the prevalence of low HDL-C(NCEP; <1.03 mmol/L in men and <1.29 mmol/L in women) and other cardio-vascular risk factors in 8545 patients receiving treatment for dyslipidaemia in 11European countries. Of the total population (n=8545), 40% of women and 33%of men receiving lipid-modifying treatment had low HDL-C. The overall populationand patients with low HDL-C had similar mean age (62 y), body mass index (BMI;30 vs. 29 kg/m2), and waist (103 cm), but subjects with low HDL-C were morelikely to be overweight or obese (BMI >25 kg/m2; 86% vs. 79%) or hypertensive(78% vs. 72%) or type 2 diabetic (55% vs. 45%) or to have prior myocardial in-farction (MI; 30% vs. 24%) or coronary heart disease (52% vs. 45%). Among thelow HDL-C group, 41% (19% of women and 57% of men) had very low HDL-C(<0.9 mmol/L). The table shows principal drivers for low HDL-C. Women were
Odds ratios (95% CI) for low HDL-C
All Women Men
BMI > or = 25 kg/m2 2.04 (1.80-2.32) 2.18 (1.80-2.63) 2.04 (1.72-2.42)BMI > or = 30 kg/m2 1.98 (1.79-2.19) 1.97 (1.68-2.30) 1.94 (1.70-2.21)Waist >NCEP 1.81 (1.64-1.99) 2.01 (1.69-2.38) 1.60 (1.41-1.81)Sport >once/week 0.75 (0.68-0.84) 0.75 (0.63-0.89) 0.79 (0.69-0.89)Alcohol > or = once/day 0.67 (0.61-0.74) 0.79 (0.68-0.93) 0.67 (0.59-0.77)Smoking 1.45 (1.28-1.65) 1.30 (1.03-1.63) 1.65 (1.41-1.92)Prior MI 1.31 (1.18-1.46) 1.52 (1.24-1.85) 1.38 (1.21-1.57)Type 2 diabetes 1.79 (1.63-1.97) 2.22 (1.90-2.58) 1.51 (1.33-1.71)
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

850 How important is high-sensity lipoprotein cholesterol?
more sensitive than men to the effects of prior MI and diabetes on the risk of lowHDL-C. Physical activity and moderate alcohol consumption were associated witha favourable effect on HDL-C in both women and men. Low HDL-C is commonin Europe, and is significantly associated with abdominal obesity, smoking andcardiometabolic comorbidity.Supported by an educational grant from Merck KGaA, Germany.
4988 Impact of low high density lipoproteins on in-hospitalevents and twelve-month clinical outcomes in patientswith non-STEMI acute coronary syndrome treated withdrug eluting stent implantation
R. Wolfram, Z. Xue, A. Pichard, L. Satler, K. Kent, B. Brewer,R. Waksman. Washington Hospital Center, Cardiology, Washington, Dc, UnitedStates of America
Objectives: We aimed to investigate the impact of baseline high density lipopro-tein cholesterol (HDL-C) on the outcomes of patients undergoing drug-elutingstent implantation for acute coronary syndrome.Background: HDL-C is known to have protective cardiovascular effects.Methods: Since March 2003, 1032 consecutive patients were, according to theirbaseline HDL-C, included into a low HDL-C group (n=550; male: 40mg/dl; female:>45mg/dl; mean: 55±19 mg/dl). End points were death, Q-wave myocardial in-farction, target lesion revascularization, and a composite of major adverse cardiacevents at 30 days and 1 year. We assessed the relationship between HDL-C andend points.Results: Low HDL-C patients had more diabetes, a higher body mass index,higher triglyceride-, and lower total cholesterol levels. Low-density lipoproteincholesterol (LDL-C) and statin treatment (98% in both groups) were comparable.Incidence of mortality and major adverse cardiac events at 30 days were higher inthe low- versus the high HDL-C group (chi square: p <.001, p = 0.002). At 1 year,more deaths occurred in the low HDL-C group (chi square: p <.001) as did majoradverse cardiac events (chi square: p <.001). Multivariate analysis revealed lowHDL-C at baseline (hazard ratio = 2.61; 95% confidence interval: 1.33 - 5.12) tobe a key predictor of major adverse cardiac events and death (hazard ratio = 0.30;95% confidence interval: 0.10 - 0.87) at 1 year.Conclusion: Regardless of baseline LDL-C levels and statin therapy, additionalstrategies to increase HDL-C should be evaluated in acute coronary syndromepatients.
4989 Hypoadiponectinemia contributes more strongly todecreased high-density lipoprotein cholesterol thaninsulin resistance or obesity
K. Matsushita, H. Yatsuya, K. Tamakoshi, T. Kondo, T. Murohara,H. Toyoshima. Nagoya University Graduate School Of Medicine,
Department Of Cardiology, Nagoya, Japan
Purpose: There is an inverse association between high-density lipoproteincholesterol (HDL-C) and cardiovascular disease (CVD), so that interventionsto prevent lowering or raise HDL-C seem to be promising to prevent CVD.It has been broadly known that decreased HDL-C is deeply involved with in-sulin resistance and obesity. Recently, a novel adipocytokine, adiponectin, hasemerged as an important molecule which may affect circulating HDL-C concen-tration in human. However, respective magnitude of insulin resistance, adiposity,or adiponectin in relationship to low HDL-C has not been entirely evaluated.Methods: We studied 3030 middle-aged Japanese (2347 men and 683 women),who had no medical history of CVD, cancer, diabetes, hypertension, or hyperlipi-demia. Following analyses were conducted for male and female separately. As theindex of insulin resistance and obesity, homeostasis model assessment of insulinresistance (HOMA-IR) and body mass index (BMI) were calculated respectively.To conduct direct comparison among these indexes and adiponectin, odds ratios(ORs) for low HDL-C (<40 mg/dL in men or <50 in women) of a 1-SD increasein BMI and log-transformed HOMA-IR and a 1-SD decrease in log-transformedadiponectin were calculated with multivariate logistic regression analyses.Results: Serum adiponectin was significantly correlated with HDL-C, while bothHOMA-IR and BMI were inversely correlated. In multivariate logistic regressionanalyses, decreased adiponectin was more strongly associated with low HDL-Cthan HOMA-IR and BMI in both genders (men: adiponectin, OR 1.98 [95% con-fidence interval 1.64-2.34], P<0.001, HOMA-IR, 1.30 [1.10-1.54], P=0.003 andBMI, 1.28 [1.07-1.55], P=0.008; women: adiponectin, 1.75 [1.31-2.36], P<0.001,HOMA-IR, 1.15 [0.84-1.15], P=0.392 and BMI, 1.40 [1.05-1.88], P=0.022). Moreimportantly, when potential confounding factors, i.e. age, smoking status, alcoholconsumption, or parental history of dyslipidemia were adjusted for, adiponectin,but not HOMA-IR and BMI, was significantly associated with low HDL-C in female.Conclusion: Hypoadiponectinemia was more strongly associated with low HDL-C rather than insulin resistance or obesity themselves. The present study mayhave important implications both for inferring the etiological mechanisms by whichHDL-C decreases in insulin resistant or obese condition and for clinical strategyto raise HDL-C.
4990 Prognostic value of classical and modern markers oflipoprotein-metabolism among elderly with CAD, onlyapoA-I is an independent predictor for eventfreesurvival
A. Schlitt1, S. Blankenberg2, H.J. Rupprecht1 , M. Russ2, M. Buerke2,K. Werdan2, X.C. Jiang3, C. Bickel2. 1Martin Luther-University,
Department of Medicine III, Halle, Germany; 2Johannes Gutenberg-University,Department of Medicine II, Mainz, Germany; 3Downstate Medical CenterBrooklyn, Department of Anatomy and Cell Biology, New York, United States ofAmerica
Introduction: Lipoproteins and their subfractions are associated with the inci-dence of atherosclerotic diseases. In patients with coronary artery disease (CAD)high serum concentrations of high density lipoprotein (HDL) and low serum con-centrations of low-density lipoproteins (LDL) are related to eventfree survival.We have previously shown that apolipoprotein A-I (apoA-I) is the only(apo)lipoprotein independently related to clinical outcome in patients with CAD.However, age dependency on lipoproteins and their relation to clinical outcome inelderly patients with CAD has been hardly investigated.Methods In 2,114 patients with angiographically documented CAD serumconcentrations/-activity of total-cholesterol (TC), LDL-cholesterol (LDL-C), HDL-cholesterol (HDL-C), triglycerides, Lp(a), apoA-I, apolipoprotein B (apoB),cholesteryl-ester transfer protein (CETP), phospholipid transfer protein (PLTP),and sphingomyelin (SM) were investigated in dependence on age stratified byquartiles (Q1: <50 years, n=304; Q2: 50-65 years, n=1075; Q3: 65-75 years,n=652; Q4 >75 years, n=83). Furthermore, baseline variables including CRPwere compared. We investigated in a median follow up of 4.4 years (min 0.1,max 7.6 years) the association of lipoprotein markers in dependence on age withthe incidence of a combined endpoint (myocardial infarction and cardiovasculardeath).Results Elderly were more often diabetics or hypertensive. They were lighter andsmoked less in comparison to younger patients. Three vessel disease and femalesex were more frequent in elderly, as expected. CRP was significantly elevatedin elderly (15.3 mg/l in patients >75 years vs. 8.3 mg/l in patients <50 years,p<0.001). TC, Non-HDL-C, apoB, Lp(a), and PLTP showed no age dependency.Triglycerides, LDL/HDL-quotient, CETP, and SM were significantly decreased inelderly patients, whereas HDL-C and apoA-I were significantly increased. ApoA-Iwas the only lipoprotein marker significantly related to outcome in patients >65years in both higher quartiles (Q3: HR 1.5, 95%CI 1.1-2.2, p=0.027, Q4: HR 3.2,95%CI 1.2-8.5, p<0.018) as shown by multvariate Cox-Regression analyses.Conclusion: Markers of postprandial lipoprotein metabolism such as triglyc-erides and SM, and markers related to HDL-metabolism such as HDL-C, apoA-I,CETP, and LDL-C/HDL-C quotient showed age dependency. However, only apoA-I was an independent predictor for outcome of elderly patients with CAD.
4991 Effects of long-term pioglitazone therapy on serumlipid profiles in high-risk type 2 diiabetes patient s:results from PROactive
R. Spanheimer1 , M. Tan2, J. Yates2 on behalf of The PROactiveinvestigators. 1Lincolnshire, United States of America; 2Indianapolis,
United States of America
Diabetic dyslipidemia is characterized by high triglyceride (TGs) and low HDL-Clevels. These lipid abnormalities contribute to the increased risk of atherosclerosisin patients with type 2 diabetes (T2D). We evaluated the effects of pioglitazone(PIO) therapy on lipid profiles over 2.5 years in patients with T2D in the PROactivestudy.The PROactive study was a double-blind, placebo-controlled study in which 5,238patients with T2D and macrovascular disease were randomized to PIO or match-ing placebo (PBO) in addition to their existing glucose-lowering and CV medica-tions, including anti-hypertensive, antiplatelet, and lipid-modifying drugs. Patientsstarted with 15 mg of PIO (or matching PBO), and, as tolerated, were titrated toa maximum dose of 45 mg, which was continued for the study duration. Meanfollow up was 34.5 months, and mean exposure to study drug was 30 months.Laboratory assessments for fasting lipid levels were performed every 6 months.At baseline, 1311 (50.3%) PIO patients and 1382 (52.5%) PBO patients were oneither fibrate or statin therapy. During the study, investigators were instructed toaim for the IDF treatment targets for lipids.At study entry, mean TGs (197.5 and 199.3 mg/dL), HDL-C (44.9 and 44.9mg/dL), and LDL-C (114.5 and 114.8 mg/dL) levels were similar in the PIO andPBO groups.
Mean percent change from baseline in lipid profile
PIO, % (n=2605) PBO, % (n=2633) Between-group P-Value
TGs -1.7 +12.5 <0.0001HDL-C +21.2 +11.3 <0.0001LDL-C +12.1 +8.4 0.0034LDL-C/HDL-C -4.39 -0.04 <0.0001
Treatment with PIO significantly improved abnormalities in TG and HDL-C asso-ciated with diabetic dyslipidemia. The LDL-C/HDL-C ratio was also significantlyimproved compared to PBO, despite a greater increase in LDL-C. These between-group differences were seen as early as 6 months after initiating treatment and
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

How important is high-sensity lipoprotein cholesterol? / The metabolic syndrome: risk and management 851
remained significant throughout the study. At study end, 1485 (61.5%) PIO pa-tients and 1515 (62.5%) PBO patients were on statin or fibrate therapy. Thus, im-provements in lipid values with PIO compared to PBO were seen despite knownbenefits of the lipid-altering medications being taken in a similar proportion ofpatients in the two treatment groups.
4992 Triglyceride-to-HDL cholesterol ratio as an emergentmarker of predictor of worse outcome in patients withchronic coronary artery disease at 3 year follow-up: theMASS II study
A.F.T. Gois, N.H.M. Lopes, D. Favarato, A.C. Pereira, P.L. Luz,S.A. Oliveira, W. Hueb, J.A.F. Ramires. Heart Institute, Sao Paulo, Brazil
Background: It is known that insulin resistance leads to increased assembly andsecretion of triglyceride-rich VLDL and decrease HDL cholesterol. Hence, thetriglyceride-to-HDL cholesterol ratio (TG/HDL-C) is strong correlate of insulin re-sistance. Therefore, we hypothesized that TG/HDL-C concentration ratio mightbe a marker of worse outcome in patient with chronic CAD. In the present study,we examine the association between higher TG/HDL-C ratio with the incidenceof cardiovascular end-points in a group of individuals prospectively followed-up inthe MASS II Study (Medical, Angioplasty or Surgery Study II, a randomized studyto compare treatments for multivessel CAD and preserved left ventricle function.Methods: We have evaluated 574 individuals enrolled in MASS II study, prospec-tively followed during 3 years regard the presence of higher triglyceride-to-HDLcholesterol ratio (TG/HDL-C > 5, based on units of mg/dL). The incidence ofthe composite end-point of cardiac death, myocardial infarction and refractoryangina was compared based on TG/HDL-C ratio levels. Survival curves were cal-culated with the Kaplan-Meier method and evaluated with log-rank statistic. Therelationship between baseline variables and the composite end-point of death,myocardial infarction and refractory angina was assessed using a Cox propor-tional hazards survival model.Results: 44.25% patients presented higher TG/HDL-C ratio. Most of the base-lines characteristics were similar in both groups, except for more smokers, highercholesterol total and predominant of men in the group of higher TG/HDL-C ra-tio. At three years of follow-up, there was no difference significant in compositeend-points in patients regarding TG/HDL-C ratio. However, patients with higherTG/HDL-C levels were associated with an increased cardiac mortality (p=0.034),even when we excluded the diabetes patients (p=0.032). Moreover, the presenceof the higher TG/HDL-C implied at 1.97 fold increased the risk of mortality amongpatients in a multivariate model. (p=0.047, 95% CI 1,008-3,854). Also, we dis-close an association with higher TG/HDL-C ratio and worse survival in patientstreated by PCI (p=0.015), but not by CABG or medical treatment.Conclusion: These results indicate a strong correlation between elevatedTG/HDL-C with mortality in patients with stable coronary artery disease, regard-less of LDL or HDL cholesterol level as well as the presence of diabetes. So, thismarker is an independent predictor of events in patients who are at risk of worsecardiovascular outcome in 3 years of follow-up.
THE METABOLIC SYNDROME: RISK AND MANAGEMENT
4993 Contribution of the metabolic syndrome to suddencoronary death risk in asymptomatic men. The ParisProspective Study I
J. Empana1, P. Ducimetiere2, B. Balkau2, A. Kane2, X. Jouven3.1Inserm U258, Villejuif, France; 2INSERM U258, Villejuif, France;
3INSERM U258/G Pompidou European Hospital, Villejuif/Paris, France
Objective: The metabolic syndrome (MetS) has been suggested to increasecoronary heart disease (CHD) mortality in healthy subjects. Our aim was to as-sess and compare the risk of sudden coronary death (SCD) and non-suddencoronary death (NSCD) associated with the MetS in the general population.Methods: The study population comprises 6678 men, 43 to 52 years, from theParis Prospective Study I, who were free of diabetes and CHD at the baselineexamination in 1967-1972, and whose vital status has been followed up over 21years. The MetS was identified by three of four abnormalities defined accordingto the NCEP criteria, but the sagittal abdominal diameter (SAD) was used insteadof waist circumference, and HDL-cholesterol was not measured.Results: The MetS was present in 14.4% of the men. Of the 1915 deaths thatwere registered, 315 were due to CHD, including 180 and 105 from NSCD andSCD respectively. The MetS at baseline was associated with a two-fold increasein the risk of SCD (HR: 1.95; 95% CI: 1.17-3.25), after adjustment for CHD riskfactors not included in the MetS. The association between the MetS and NSCDwas of lower strength (HR: 160; 95% CI: 1.07-2.39), but was not statistically dif-ferent (p=0.58). Elevated abdominal adiposity (upper quintile of SAD) had asso-ciations with mortality risk including SCD risk that paralleled that found with theMetS.Conclusion: In healthy middle-aged men, the MetS increases by two-fold the riskof SCD. However, the MetS may not discriminate asymptomatic subjects from thegeneral population who are at increased risk of SCD versus NSCD.
4994 An index of fasting glucose and HDL-cholesterol is astrong predictor for death and cardiovascular events inpatients with coronary artery disease
J. Ohrvik, K. Malmberg, L. Ryden on behalf of the Euro HeartSurvey Investigators. Karolinska Institute, Department of Medicine,
Stockholm, Sweden
Objectives: Abnormal glucose regulation (AbnGR) is known to have seriousprognostic implications in patients with coronary artery disease (CAD). More con-troversial is the prognostic impact of the metabolic syndrome (MS) in such pa-tients. This study tried to develop prognostic criteria based on variables in the MSaccording to NCEP criterion and compare these with an oral glucose tolerancetest (OGTT).Methods: CAD patients were enrolled at 110 centers in 25 countries and fol-lowed for one year. Fasting plasma glucose (FPG) and 2-h post load glucosewere obtained in patients without known AbnGR. The gluco-metabolic status wasclassified according to WHO as normal, impaired fasting glucose (IFG), impairedglucose tolerance (IGT) or diabetes (T2DM). Classification methods - ordinal lo-gistic regression and a neural network (NNET) - were assessed to find rules tocharacterize the gluco-metabolic status.Results: OGTT and the MS variables were available for 1 283 patients. Accord-ing to WHO criterion they were classified as normal (555), IFG or IGT (494) andT2DM (234). The percentages of patients who died or experienced a major car-diovascular event (myocardial infarction or stroke) (MCVE) during the follow upperiod were 4.5%, 5.9% and 8.6% (p = 0.087) respectively. The best classifica-tion algorithm for the gluco-metabolic status, a NNET with using FPG, age andHDL-cholesterol as input variables characterized 807 as normal, 246 as border-line and 208 as having disturbed gluco-metabolic status, when classifying intothree categories. The percentages of patients who died or experienced a MCVEduring follow up were 5.4%, 3.7% and 9.6% (p = 0.020) for the three categories.Conclusions: The prognostic criterion based on the NNET algorithm can identifypatients at high risk of dying or experience a MCVE better then an OGTT (9.6%vs 8.6%). Further the NNET criterion is much faster and cheaper to determineand patients in an acute stage do not have to run the risk of a glucose load.
4995 Metabolic syndrome diagnosis predictive value forhypertension development during seven years of followup
J. Bellwon, K. Chlebus, D. Zielinska, W. Sobiczewski, M. Gruchala,D. Ciecwierz, A. Rynkiewicz. Medical University Of Gdansk, Ist DeptOf Cardiology, Gdansk, Poland
Objective: The metabolic syndrome (MS) definition contains risk factors not in-cluded in commonly used cardiovascular risk algorithms and probably improvesrisk estimation. The aim of our study was to compare the predictive value of MSdiagnosis for development of cardiovascular diseases based on two, ATP III andIDF, MS definitions.Methods: We have examined 511 subjects, mean age 44,7 ± 8,2 years, who didnot have any symptoms of cardiovascular diseases. History, physical examina-tion, ECG, blood pressure twice in the sitting position, lipids and fasting glucosemeasurements were performed at baseline and repeated after seven years of fol-low up. MS was diagnosed according to ATP III and IDF criteria. Hypertensionand diabetes were diagnosed by GPs according to current guidelines. Myocardialinfarctions were confirmed by information from discharge letters.Results: At baseline 111 (21,7%) subjects fulfilled ATP criteria of MS and 152(29,7%) subjects fulfilled IDF criteria of MS (p<0,005). After 7 years 141 (27,6%)subjects fulfilled ATP criteria and 213 (41,7%) IDF criteria, p<0,001.Systolic blood pressure (SBP) increased significantly from 132±20 to 136±19mmHg (p<0,05) and diastolic (DBP) from 84±12 to 86±11 mmHg (p<0,05)mainly due to aging. Age adjusted blood pressure change was not significant,mean SBP 133 mmHg (ns) and mean DBP 85 mmHg (ns). During follow up arte-rial hypertension was diagnosed in 135 subjects, diabetes in 37 and 28 survivedmyocardial infarction. Overall there were 65 cardiovascular events.Positive predictive value (PPV) n of MS diagnosis based on ATP and IDF criteriafor arterial hypertension diagnosis during seven years of follow up were respec-tively 50% and 46%, negative predictive value (NPV) 79% and 80%, sensitivity39% and 49% and specificity 85% and 79%, all ns. PPV of MS diagnosis basedon ATP and IDF criteria for diabetes mellitus diagnosis were respectively 22%and 18%, NPV 96% and 97%, sens. 62% and 70% and spec. 82% and 75%,all ns. PPV of MS diagnosis based on ATP and IDF criteria for myocardial in-farction diagnosis during seven years of follow up were respectively 8% and 7%,NPV95% and 95%, sens. 29% and 36% and spec. 79% and 72%, all ns. PPV ofMS diagnosis based on ATP and IDF criteria for any cardiovascular event wererespectively 24% and 25%, NPV 87% and 89%, sens. 34% and 48% and spec.81% and 74%, all ns.Conclusion: The predictive value of metabolic syndrome diagnosis for arterialhypertension diabetes and myocardial infarction development during seven yearsfollow up are similar for both ATP III and IDF definitions of metabolic syndrome.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

852 The metabolic syndrome: risk and management / Preserved vs depressed left ventricular function
4996 The metabolic syndrome: aetiology, identifying criteria,pathologic anatomy, utility for CVD risk prediction –data from the Progetto CUORE
S. Giampaoli1, L. Palmieri1, C. Donfrancesco1 , S. Panico2,D. Vanuzzo3 , G. Cesana4, M. Ferrario5, J. Stamler6 on behalf of
Research Group of the Progetto CUORE. 1Istituto Superiore di Sanita’, CentroNazionale di Epidemiologia, Rome, Italy; 2Universita’ degli Studi FedericoII, Dipartimento di Medicina Clinica Sperimentale, Naples, Italy; 3AgenziaRegionale della Sanita’, Centro per la Prevenzione Cardiovascolare, Udine,Italy; 4Universita’ degli Studi Milano-Bicocca, Centro Ricerche PatologiaCronico-degenerativ, Monza, Italy; 5Universita’ degli Studi dell’Insubria,Dipartimento di Scienze Cliniche e Biologiche, Varese, Italy; 6NorthwesternUniversity, Department of Preventive Medicine, Chicago, United States ofAmerica
Introduction: The metabolic sindrome (MS) is being widely used for clinical CVDrisk assessment despite unresolved questions: 1. its causes; 2. its pathologicanatomy, involving consequences of any 3 or more of 5 variables dichotomized; 3.consequences of non-inclusion of major risk factors (total cholesterol/non-HDL-Cholesterol/LDL-Cholesterol, smoking); 4. is the whole better for CVD risk pre-diction than the sum of its parts? Better than other tools for risk evaluation? Thisstudy gives data on those questions.Methods: The Progetto CUORE data from 12 Italian population samples, 11,354women and 5,898 men, baseline ages 35-69 CVD free, followed for average 10years, with validated major CVD events.Results: There was a strong, graded relation of overweight/obesity to each ofthe 4 other MS defining variables (blood pressure [BP], HDL-C, triglycerides,glycemia/diabetes), and to combinations, e.g., women normal weight (BMI 18.5-22.9 and 23.0-24.9 kg/m2) – prevalence of any 3 or all 4 traits: 1.8% and 3.9%;overweight (BMI 25.0-29.9) – 6.3%; obese (BMI 30.0-34.9 and ≥35.0) – 10.9%and 13.1%. BMI≥25.0 was here used for MS definition (other 4 traits from ATPIII-definition). Prevalence of MS overall was 21.2% (women) and 34.6% (men); any 3of the 5 defining traits, 14.6% and 21.5%; any 4 only 5.8% and 11.0%. Of 16 pos-sible combinations of MS traits, the most common in both genders was BMI≥25.0,TG>150 mg/dl, elevated BP (5.3% and 9.2%); these 3 plus low HDL-C was alsocommon (4.5% and 6.4%); several combinations were rare. In multivariate Coxanalyses on relation of MS to 10-year CVD events, MS was significantly relatedto risk; however, in both genders the model of MS traits considered singly yieldedsignificantly enhanced prediction, as did total cholesterol, non-HDL-C, LDL-C andsmoking. Hazard ratios were less for MS than for its 5 traits considered togetheras continuous variables.Conclusion: Caloric imbalance producing overweight/obesity is a key populationwide exposure causing epidemic MS prevalence. MS as a CVD risk predictorneed re-appraisal, given limitations shown here and in other studies.
4997 Long-term effects of various physical activity levels inpreventing obesity and metabolic syndrome inmiddle-aged men
W. Drygas1, M. Kwasniewska1, T. Kostka1, A. Jegier2, M. Pasowicz3.1Department of Preventive Medicine, University, Lodz, Poland;
2Department of Sports Medicine, University, Lodz, Poland; 3Center forPrevention, Diagnosis and Rehabili, Cracow, Poland
Background and aim: Regular physical activity is considered as an effectivemethod in preventing obesity and influencing positively several metabolic risk fac-tors. There are only few studies analyzing longitudinal effects of various trainingprograms in middle-aged subjects.The aim of the study was to assess the influ-ence of leisure-time physical activity level (LTPA) on the prevalence of obesity andmetabolic syndrome (MS) in long-term observation.Methods: Between 1977 and 2004 (mean observation time 17,4 yrs) a group of305 men aged 30-59 years (baseline mean age 41,8 yrs) participated in regularhealth status examinations (detailed interview, physical examination, blood pres-sure, glucose and lipids profile, anthropometric measurements, exercise tests).According to self-reported LTPA all participants were divided into three groups:sedentary (S) (LTPA <1000 kcal/wk), moderate (M) LTPA (LTPA between 1000-2000 kcal/week) and highly (H) active group (LTPA > 2000 kcal/week). In thesubgroup of men with the highest aerobic capacity indices calcium scoring wasperformed using 64-slice computed tomography (MSCT) and Agatston’s algoritm.Results: Mean values of body weight, BMI and body fat increased in all groupshowever the mean values in H group are more favourable as compared withsedentary and moderate LTPA group. Only H group was able to maintain BMIvalue about 25,0 and to increase significantly HDL (51,7 vs. 56,6 mg/dl) in thefollow-up. At final examination we diagnosed obesity (BMI = or > 30,0 kg/m2)in 23,3% of sedentary men, 20,0% of moderate activity and 12,% of highly ac-tive group. Frequency of obesity increased above twofold in sedentary individuals(10,8 vs 23,3). Metabolic syndrome (MS) as defined by ATP III has been diag-nosed by 26,6% of sedentary, 23,1% of moderate and only 8,4% of highly activemiddle-aged men at final examination. In the group of men with the highest aero-bic capacity at final examination (VO2max >35 ml/min/kg) prevalence of obesityincreased form 2,4% to only 3,5%, and there were no cases of MS. Mean calciumscore was in the 8,4 with score=0 in 63% of highly active men.Conclusion: Prevalence of obesity and metabolic syndrome depends on leisuretime physical activity volume in middle-aged men. High aerobic capacity is strong
protective factor in development of obesity and metabolic syndrome, even moreimportant than leisure time energy expenditure related to the training. High LTPAcorrelates with low coronary calcium score.
4998 Reversing metabolic syndrome with high intensitytraining
A.E. Tjonna1, Ø Rognmo1, P.M. Haram1, T. Stolen1, J.P. Loennechen2 ,S. Slordahl1, U. Wisloff1. 1Institute Of Circulation And MedicalImaging, Department Of Medicine, NTNU, Trondheim, Norway; 2St.
Olavs Hospital, Trondheim, Norway
Background: The worldwide epidemic of the metabolic syndrome requires cost-effective tools such as endurance training for prevention and rehabilitation. Thepresent study determines the effects of moderate- and high-intensity (interval-training) exercise upon the metabolic syndrome.Methods 28 persons with the metabolic syndrome were randomized to either 16weeks, 3-times per week of high-intensity interval training (HIT) (92.5% of maxi-mal heart rate), moderate intensity (MIT) (70% of maximal heart rate; covered thesame distance as individuals in the HIT-group so that only exercise-intensity dif-fered) or a control group that received advice from their regular doctor. Endothelialfunction in the brachial artery was measured by ultrasound.Results: 46% in the HIT and 37% in the MTG, trained themselves out of the syn-drome. Body weight decreased significantly (p ≤ 0.05) in both training-groups.HIT significantly decreased systolic (p = 0.004) and diastolic (p = 0.033) bloodpressure, MIT significantly (p = 0.03) decreased systolic blood pressure, nochanges occurred in the control group. HIT had a 22% increase in HDL choles-terol (p = 0.036), and a decrease in fasting glucose (p ≤ 0.05). ox-LDL was signif-icantly (p = 0.003) reduced in the HIT group. Maximal oxygen uptake increased35% in HIT (p ≤ 0.001) and 16% in MIT (p ≤ 0.001). Endothelial dysfunctionwas reversed in both training group, but the effect on flow mediated dilatation wasmost pronounced in the HIT group.Conclusion: High-intensity training is superior to moderately-intensity and advicefrom the regular doctors to reduce the markers of the metabolic syndrome.
PRESERVED VS DEPRESSED LEFT VENTRICULARFUNCTION: IS LEFT VENTRICULAR EJECTION
FRACTION A PROGNOSTIC PARAMETER?
4999 Prognostic value of brain natriuretic peptide levels andleft ventricular functional parameters in chronic heartfailure patients with preserved or deteriorated systolicfunction
K.G. Adamyan, L.R. Tumasyan, A.B. Nargizyan, L.G. Budagyan.Institute of cardiology, Yerevan, Armenia
The aim of study was to assess the predictive power of BNP levels and left ventric-ular (LV) functional parameters in pts with chronic heart failure (CHF) in relationto preserved or deteriorated systolic function.Methods: 64 pts (age 65.8±1.2) with preserved and 86 pts (age 57.7±0.9) withdeteriorated systolic function and NYHA III functional class CHF in sinus rhythmwere prospectively studied. LV ejection fraction (LVEF, %), transmitral peak early(E) and late (A) filling velocities, E/A ratio, the deceleration time (DT, msec) ofE-wave, LV myocardial performance index (LVMPI) were obtained using echocar-diography. BNP (pg/ml) levels were assessed simultaneously.Results: During mean follow-up of 37±1.2 months from cardiac causes died total58 (38.7%) pts, 24 (37.5%) pts with preserved and 34 (39.5%) pts with deterio-rated systolic function. Mean plasma level of BNP in group of systolic CHF wassignificantly higher than in group of pts with preserved systolic function (874±112vs. 372±55, p<0.001). All pts with adverse outcomes had higher levels of BNP(935±152 vs. 257±80, p<0.001). In addition, the probability of death was pre-dicted by plasma level of BNP in both groups with reduced (986±116 vs. 471±75)or preserved (528±120 vs. 281±75) systolic function (p<0.001). The survivedpts of both groups had lower LVMPI (0.19±0.04 vs. 0.32±0.03 and 0.22±0.03 vs.0.33±0.03), E/A (0.78 ± 0.14 vs. 2.3 ± 0.5 and 0.8 ± 0.2 vs. 2.2 ± 0.4), higherLVEF (39.1±2.7 vs. 30.2±1.6 and 65.1±3.3 vs. 54.2±1.2) and longer DT (230 ±31 vs. 118 ± 25 and 240 ± 32 vs. 120 ± 23), (p<0.01 for all) compared with diedpts.Multivariate Cox analysis revealed that only BNP, E/A and DT were the indepen-dent predictors of cardiac death.Kaplan-Meier survival curves demonstrated a survival rate of 63% and 63.5% forpts with DT<150 and E/A>2.2, and 85% and 83% for those with DT>150 (85%)and E/A<2.2 (p<0.01). Distribution of pts with reduced and preserved systolicfunction according to cut-off values of BNP<600 and BNP≥600 and BNP<450and BNP≥450, respectively allowed to identify patients with low (18.6% and19.2%) and high risk (42.1% and 44.1%) of death from cardiac causes (p<0.001).In conclusions, despite higher LV EF, lower plasma levels of BNP, lower LVPMI,pts with CHF and preserved systolic function had a similar mortality to pts withreduced systolic function. BNP and parameters of the LV diastolic, but not sys-tolic function are the strong prognosticators in pts with severe CHF, regardless ofpresence and absence of systolic dysfunction.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Preserved vs depressed left ventricular function 853
5000 Prognostic significance of left ventricular fillingparameters in subjects with preserved systolicfunction from the general population
F. Pedersen1, I. Raymond1, D. Atar2, J. Mehlsen2, P. Hildebrandt2.1Frederiksberg University Hospital, Depart. of Cardiology/
Endocrinology, Copenhagen, Denmark; 2Aker University Hospital, University ofOslo, Depart. of Clinical Physiology, Oslo, Norway
Background: Knowledge about the prognostic value of left ventricular (LV) fillingparameters in the general population is limited.Purpose: To assess the prognostic value of: (i) low mitral ratio of peak early tolate diastolic filling velocity (E/A-ratio), (ii) prolonged E-wave deceleration time(E-DT), and (iii) a combination of (i) + (ii) indicating LV impaired relaxation.Methods: A total of 764 subjects, aged 50 years or more (median age 66 years,range 50-89), recruited from the background population answered a heart fail-ure questionnaire and underwent echocardiography. Excluding subjects with a LVejection fraction <50% or atrial fibrillation, diastolic function was evaluated in 647subjects. Of these, 179 subjects complained of exertional dyspnea. Cut-off valuesof low E/A-ratio (<0.67) and prolonged E-DT (>218 ms) were arbitrarily definedas the values that best separated poor from good prognosis after observing themortality in relation to quintiles of E/A-ratio (1. vs. 2.-5. quintiles) and E-DT (1.-4.vs. 5. quintiles).Results: After a median observation time of about 3 years (1135 days), 42 of 647subjects died (6.5%, all cause mortality). In univariate analysis, E/A-ratio <0.67(p =.0003), E-DT >218 ms (p <.0001), and the combination of E/A-ratio <0.67and E-DT >218 ms (p <0.0001, log rank test) were associated with increasedall-cause mortality, respectively.In three different Cox analysis, after adjusting for age, gender, systolic blood pres-sure, and exertional dyspnea, E/A-ratio <0.67 (hazard ratio [HR] 1.95, confidenceinterval [CI] 1.00 to 3.80, p <.05), E-DT >218 ms (HR 2.56, CI 1.35 to 4.87, p=.004), and the combination of E/A-ratio <0.67 and E-DT >218 ms (HR 2.62,CI 1.25 to 5.49, p =.01) were associated with increased all-cause mortality, re-spectively. In the subgroup with exertional dyspnea and preserved LV systolicfunction, 22 of 179 died. In Cox analysis, after adjusting for age and gender, E/A-ratio <0.67 (HR 2.46, CI 1.01 to 6.00, p <.05), E-DT >218 ms (HR 6.39, CI 2.70to 15.1, p <.0001), and the combination of E/A-ratio <0.67 and E-DT >218 ms(HR 5.70, CI 2.31 to 14.1, p <.0001) were associated with increased all-causemortality, respectivelyConclusion: In this sample of middle-aged and elderly subjects with preservedLV systolic function from the general population, LV filling parameters indicatingimpaired relaxation were associated with 2 - 2 1
2 -fold increased all-cause mortality.In a subgroup of subjects with dyspnea and preserved LV systolic function thisassociation were even stronger.
5001 Prevalence, clinical characteristics, outcomes andprognosis of diastolic heart failure in 519 elderlypatients. A clinical study with 5 years follow-up
F. Al Shaer1, W. Hassan2, N. Elkum1, M. Fawzy1, M. Nawaz1,S. Kharabsheh1 , N. Akhras1, C. Canver1. 1Riyadh, Saudi Arabia;
2King Faisal Specialist Hospital And Research, Cvd, Riyadh, Saudi Arabia
Background: To assess the prevalence, patient characteristics, repeated hospi-talization and prognosis in elderly patients with diastolic heart failure (DHF) withpreserved systolic function (PSF) in comparison to systolic heart failure (SHF).Methods: A clinical analysis of 519 adult patients above age 65 years admittedwith congestive heart failure and was followed up for 5 years. We assessed ejec-tion fraction, prevalence of hypertension, hypertrophy, diabetes, atrial fibrillation,pulmonary hypertension, coronary disease, management, repeated hospitaliza-tion, length of hospital stay, morbidity, and mortality and 5 years survival.Results: Diastolic dysfunction (DHF) with PSF was present in 61% of our studypatients. Compared to SHF, DHF was more predominant in; elderly female (53vs. 29%, P <. 0001), hypertensive (85 vs.60%, P <. 0001), with LV hypertrophy(67 vs. 24%, P <. 0001). Pulmonary systolic pressures, left atrial size were lowerin DHF (Table) as well as treatment with B-blockers, diuretics, ACEI, and digoxin.Repeated hospitalization, length of stay and mortality were significantly less inDHF (P <. 05, <. 0001, <. 0001).
Variable DHF (321 Pts) SHF (198 Pts) P Value
Age 73.3 ± 7.4 71 ±5.9 NSFemale Gender % 53 29 <. 0001 *Hypertension % 85 60 <. 0001 *Ejection Fraction % 66 ± 9 35 ± 14 <. 0001 *Left Ventricular Hypertrophy % 67 24 <. 0001 *PASP mmHg 34 ± 11 42 ± 17 <. 0001 *Seum Cr 115 ± 80 156 ± 171 0.0024 *Digoxin % 3 36 <. 0001ACE_Inhibitors % 43 78 <. 0001Loop Diuretics % 37 69 <. 0001Three admission or more % 2.5 6 <. 005 *Length of stay (Days) 23 ± 19 39 ± 30 <. 0001 *Mortality % 4 9 <. 0001 *
Conclusion: Diastolic cardiac failure is common, more prevalent in elderly femalehypertensive patients, less repeat hospitalization, length of stay and carry betterprognosis compared to SHF.
5002 Death causes in heart failure patients with depressedand preserved left ventricular ejection fraction. Isejection fraction relevant?
L. Grigorian, A. Varela Roman, F. Otero Ravina, E. Abu Assi, R. VidalPerez, J.R. Gonzalez-Juanatey. Santiago De Compostela, Spain
Background: Nothing is really known for sure about the relative incidences ofdifferent causes of death among congestive heart failure (CHF) patients with pre-served left ventricular systolic function (LVSF), even though this form of CHF isincreasingly prevalent.Aim: To examine the causes of death in patients admitted to hospital for CHF, andevaluate the differences in this respect between patients with and without LVSFdysfunction.Method and Results: All patients hospitalized in a tertiary hospital between 1998and 2002 for CHF were assessed. LVSF was defined as normal when left ven-tricular ejection fraction measured during hospitalization was at least 50%. Aftera mean follow-up of 2.8 years (range 1.6-4.1 years), 351 cases terminated indeath. The most common causes in the whole group were refractory heart fail-ure (38%) and sudden death (23%). There was no significant difference in sur-vival time between the two groups [mean 4.4 years (range 4.1-4.7 years) amongthose with normal LVSF, mean 4.3 years (range 4.0-4.5 years) among those withdepressed LVSF; p=0.67. Similarly, there was no significant difference betweenthe normal LVSF and depressed LVSF subgroups as regards the distribution ofdeaths among the five types of cause distinguished in this study, although thelatter group had a rather greater incidence of sudden death (27% as against 21%in the normal LVSF group) and a rather smaller incidence of non-cardiac vascularcauses (10% as against 16%). In both subgroups, the most common cause ofdeath was the same as in the whole group, refractory heart failure.Conclusions: Not only is the long-term death rate among patients hospitalizedwith CHF and normal LVSF similar to that found among patients with depressedLVSF, but the causes of death are also similar in the long term in these two groups.The high prevalence of deaths due to refractory heart failure among patients withnormal LVSF, suggests that beside pharmacological treatment optimization, othertherapeutic approaches, should be investigated in this prevalent group of patients.
5003 Does systolic function determine the prognosis ofhospitalized patients due to worsening heart failure?
A. Goncalves, A.N.A. Azevedo, R.U.I. Almeida, J.O.A.N.A. Mascaren-has, M.A.R.T.A. Patacho, F. Rocha Goncalves, P.A.U.L.O. Bettencourt.Hospital S. Joao, Porto, Portugal
Introduction: Preserved left ventricular systolic function (LVSF) is observed in upto 50% of patients with Heart Failure (HF). We aimed to determine the prognosticsignificance of LVSF in patients hospitalized due HF.Methods: We included 304 patients (72.7±11.6 years, 54.3% females) admit-ted due to decompensated HF. All patients had clinical, routine laboratorial eval-uation, ECG, Echocardiogram and plasma NT-proBNP. LVSF was preserved in31.6% and depressed in 68.4%. Preserved LVSF was defined by Ejection Frac-tion >45%. The primary end point was death or readmission in up to 6 months.Results: Patients with preserved LVSF were older (73.3± 11.2 vs. 70.7±12.7p=0.13), more frequently women (72.9% vs. 45% p<0.001), had a higher preva-lence of arterial hypertension (55.9% vs. 50.7% p=0.48) and were more fre-quently on atrial fibrilation (56.3% vs. 35.6% p<0.001). Patients with depressedLVSF were more frequently diabetic (43.7% vs. 38.0% p=0.43) and had morecommonly HF of ischemic etiology (59.6% vs. 27.1% p<0.001). NT-proBNP val-ues at discharge were higher in patients with depressed LVSF (median 5291 vs.2146 pg/ml; p<0.001). The primary end point occurred in 135 (44.4%) patients, in40 patients with preserved LVSF and 95 with depressed LVSF. The figure showsthe Kaplan-Meier curves for cumulative survival according to systolic function(HR=1.20 (CI: 0.83-1.73) for depressed versus preserved LVSF).
Fig. 1. Cumulative hospitalisation-free survival.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

854 Preserved vs depressed left ventricular function / Acute heart failure: how to diagnose and treat
Conclusions: Our results suggest an ominous prognosis of acute HF, regard-less of LVSF. This sample of HF patients with preserved LVSF (more frequentlywomen, and with higher prevalence of atrial fibrillation) is probably a representa-tive sample, reinforcing the need of closer follow-up and more aggressive strate-gies.
5004 Predictors of long term outcome in patients withdiastolic heart failure and atrial fibrillation
V. Lennie1 , J. Zamorano1 , L. Perez De Isla2, C. Almeria2,J.L. Rodrigo2, D. Herrera2, A. Garcia2, C. Macaya2. 1HospitalClinico San Carlos, Unidad de Imagen Cardiovascular, Madrid,
Spain; 2Hosp.Clinico San Carlos,Instituto Cardiovasc., Unidad De ImagenCardiovascular, Madrid, Spain
Mortality predictors in patients with heart failure (HF) and depressed left ventric-ular ejection fraction (LVEF) are well known. Heart failure with preserved LVEFhas been less studied. Our aim was to describe the incidence and predictors oflong term events in patients admitted to hospital for HF with preserved LVEF withatrial fibrillation.Method: 458 consecutive patients with a first admission due to diastolic HF withatrial fibrillation were enrolled. Uni and multivariate analysis were performed toobtain those factors related to long term outcome. The end-point was the com-bined one of long term mortality and new admissions due to heart failure.Results: Mean age was 82.15 (71% women). Twenty eight patients (6.2%) diedduring admission and 118 (25.8%) died or suffered readmissions due to HF dur-ing long-term follow up. Age, chronic obstructive air disease and ischemic heartdisease were identified as risk factors in a univariate analysis, but in multivariateone, only age and ischemic heart disease were identified as independent riskfactors for long-term events.
Multivariate analysis results
RR 95% CI p
PAH 1.01 0.99-1.02 0.26Renal failure 1.11 0.66-1.9 0.69COAD 1.6 0.98-2.61 0.06IHD 1.66 1.05-2.63 0.03Age 1.04 1.02-1.08 0.03ICD 1.01 0.99-1.03 0.33
95% CI: 95% confidnce interval, COAD: chronic obstructive airway disease, ICD: implantablecardio defibrillator, IHD: ischemic heart disease, RR: relative risk.
Conclusions: HF in patients with preserved LVEF and atrial fibrillation is frequentand long-term prognosis is poor. Age and ischemic heart disease are indepen-dent risk factors of bad long-term outcome.
ACUTE HEART FAILURE: HOW TO DIAGNOSE ANDTREAT
5005 Should N-terminal probrain natriuretic peptide beroutinely measured at admission in patients withacutely decompensated heart failure for long term riskstratification?
E.R. Perna1, S.M. Macin2, J.P. Cimbaro Canella2, J.O. Kriskovich2,A.P. Bayol2, W. Vargas Morales2, V. Franciosi2 , B. Gonzalez Arjol2. 1Corrientes,Argentina; 2Instituto de Cardiologia "J. F. Cabral", Heart Failure Clinic, Corrientes,Argentina
N-terminal probrain natriuretic peptide (NT-proBNP) is commonly used in patientswith acutely decompensated heart failure (ADHF) as a diagnostic or prognostictool, and its variation are potentially useful in the evaluation of treatment efficacy.We sought to identify the clinical markers of high levels of NT-proBNP in patientswith ADHF, and to evaluate the long-term prognostic role of a single measure atadmission.Methods: Clinical data, electrocardiogram, echocardiogram and laboratory testwere prospectively obtained in 76 consecutive patients admitted for ADHF, withoutacute coronary syndrome. NT-proBNP was measured in a single sample obtainedwithin 6-hr period after admission by an electro-chemiluminescent immunoassaywith an Elecsys 2010 automatic analyzer. Mean follow-up was 200±130 days.Results: The mean age was 62.3±15 years, 71% were male and 45% hadan ischemic aetiology. The mean level of NT-proBNP was 6235±7420 pg/mL,range 115-35000, median 4009 (25-75% interquartile interval [IQI]: 1873-7087).There was a moderated correlation between NT-proBNP level with creatinine level(r=0.44, p<0.001) and BUN (r=0.43, p<0.001), but there was not correlation withage (r=0.03, p=ns). The area under curve ROC of NT-proBNP for predicting thecombined end point of death or hospital readmission for ADHF was 0.74±0.06,and a cut-off of 4000 pg/mL showed a sensitivity and specificity of 73% and65%, respectively. NT-proBNP levels higher than 4000 pg/mL were associatedwith male gender, non-sudden decompensation, BUN, creatinine, glycemia, LVsystolic diameter (LVSD) and LV ejection fraction. However, in multiple regressionanalysis only BUN (RR=1.9, 95%CI=2.2-66.4) and LVSD (RR=1.08, 95%CI=1.02-1.14) were independently associated with high NT-BNP levels. Free ADHF-rehospitalization survival was 36% en patients with NT-BNP >4000 compared
with 74% in those with lower levels (p=0.0005). In Cox proportional hazard model,the prognostic markers of events were NT-BNP >4000 (HR=4.1, 95%CI=1.7-9.9, p=0.002), systolic blood pressure (HR=0.98, 95%IC=0.96-0.99, p=0.019) andheart rate (HR=0.97, 95%CI=0.94-0.99, p=0.018)Conclusions: NT-BNP measurement is a useful tool for early identification ofhigh-risk patients with ADHF. Renal impairment and LV dimension were predictorsof high level of the biomarker. NT-BNP >4000 pg/mL within 6-hr after admissionwas associated with poor long-term outcome.
5006 BNP and cardiac troponin T combination predictscardiac events in patients hospitalized for acute heartfailure
N. Aspromonte1, A.B. Scardovi1, M. Feola2 , A. D’eri3, P. Giovinazzo1,F. Noventa1, L. Milani1, R. Valle1. 1S.Spirito Hospital, CardiologyDepartment, Rome, Italy; 2S.Croce Hospital, Cardiology Department,
Carle, Cuneo, Italy; 3Heart Failure Unit, Cardiology Department, San Dona’ DiPiave, Italy
Aims: We prospectively evaluated whether the combination of pre-dischargeplasma B-type natriuretic peptide (BNP) and peak serum cardiac troponin T(cTnT) would effectively stratify patients with acute heart failure (HF).Patients and methods: We studied 200 consecutive patients (49% males) hos-pitalized for acutely decompensated HF: age (mean.±SD) 77.±10, 35 - 96 years;NYHA functional class on admission/discharge 3.7±0.5, 3-4 and 2.3.±0.8, 1-4respectively), ischaemic etiology 40%, atrial fibrillation 39%, left ventricular ejec-tion fraction (LVEF) 48.±16%, 15 - 70), preserved LVEF (> 50%) 46%, renalfailure (serum creatinine > 2.0 mg/dl) 18%, BNP on discharge 433+616 pg/ml,18 - 5000, 0,2.±0.7, 0 - 4,8 ng/ml.Results: During a six months follow-up, 31 deaths and 44 readmissions for wors-ening heart failure occurred. In a stepwise Cox regression analysis, includingthe all the above quoted variables, only age (HR=1.0, p=0.0018), NYHA classon discharge (HR=2.4, p=0.0000), LVEF (HR=1.0, p=0.0173), cTnT (HR=14.7,p=0.0001), renal failure (HR=3.0, p=0.0000) and pre-discharge BNP (HR=1.0,p=0.0000) were found to be significantly independent predictors of both cardiacdeath (p <0.05) and cardiac events (p <0.01). Cox Multivariate regression anal-ysis confirms that a combination of BNP (250 pg/ml) and cTnT (0.04 ng/ml) cut-off values identified on ROC analysis are the most accurate predictor of events,hazard ratios increasing from the lowest for BNP < 250 pg/ml and cTnT < 0.04ng/ml (event rate: 13%), through for either BNP > 250 pg/ml or cTnT >0.04 ng/ml(event rate: 42%; HR = 3.1; p=0.0021), to the highest for BNP > 250 pg/ml andcTnT >0.04 ng/ml (event rate: 78%; HR = 6.2; p=0.0000). Kaplan-Meier anal-ysis revealed that this combination could reliably stratify the patients into low-,intermediate-, and high-risk groups for cardiac events.Conclusion: A combination of concentration of peak cTnT and pre-dischargeBNP may be a highly effective in risk stratification of patients hospitalized foracute heart failure.
5007 Biological effects of the novel peptide apelin areuniquely suited to the treatment of acute heart failure
E. Ashley1, D. Charo2, K. Ernst1, M. Chen1, G. Fajardo1, M. Kawana1,D. Bernstein1, T. Quertermous1. 1Stanford University, CardiovascularMedicine, Stanford, United States of America; 2University of
Rochester, Rochester, United States of America
Targets of acute heart failure therapy include vascular resistance, cardiac con-tractility, the renin-angiotensin system, and arginine vasopressin. We previouslyreported a role for the G protein coupled apelin-APJ receptor signaling system inhuman heart failure and went on to show exogenous apelin-mediated changesin vascular resistance and ventricular elastance in mice. To investigate the effectof endogenous apelin production in normal and pathological conditions, we gen-erated by homologous recombination, a mouse with deletion of the apelin genelocus. These viable, fertile animals have lower exercise capacity, lower restingand maximal oxygen consumption, lower ejection fraction, and lower left ventric-ular elastance than wild type controls. To determine a mechanism for these ef-fects, we compared isolated left ventricular myocytes from apelin-/- and apelin+/+mice. Myocytes from apelin null mice exhibited decreased sarcomere shorten-ing suggestive of a previously unrecognised autocrine effect of apelin signalingon contractile processes. Despite overall decreased contractility, intracellular cal-cium concentration as indicated by Fura2 fluorescence was similar in the twogroups, consistent with an effect of apelin in the regulation of tonic myofilamentcalcium sensitivity. To investigate this further, we assessed phosphorylation of themyofilament protein troponin I using immunoblotting. In accordance with a previ-ously hypothesised downstream effect of PKC on myofilament sensitivity, troponinI phosphorylation was significantly decreased in myocardial tissue from apelinnull mice. In summary, apelin has effects which make it uniquely attractive asa therapeutic agent in acute heart failure. It counter-regulates renin-angiotensin,inhibits vasopressin release in the brainstem, reduces vascular resistance andincreases ventricular elastance. Here we report a novel autocrine effect of en-dogenous apelin on sarcomeric function likely mediated in part by changes incalcium sensitization at the level of troponin I.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Acute heart failure: how to diagnose and treat / What can we learn from Meta-analyses of statin and antihypertensives trials? 855
5008 Effects of levosimendan versus dobutamine onimmune activation, central hemodynamics, and cardiaccontractile performance in patients with acutelydecompensated chronic heart failure
S. Adamopoulos1 , J. Parissis2, E. Iliodromitis1, D. Farmakis1 ,D. Tsiapras2, I. Paraskevaidis2 , G. Karavolias2, D. Kremastinos1. 1OnassisCardiac Sugery Center, Athens, Greece; 2Attikon University Hospital, Athens,Greece
Introduction: Congestive heart failure (CHF) is characterized by increased in-flammatory and apoptotic processes, while the improvement of the underlyinghemodynamics has beneficial effects on both inflammation and apoptosis. Wecompared the effects of levosimendan and dobutamine on plasma levels of proin-flammatory cytokines and pro-apoptotic markers as well as on echocardiographicand hemodynamic parameters of left ventricular contractile performance in pa-tients with decompensated CHF.Methods: Sixty-nine patients with decompensated CHF (aged 70 ± 2.1 years,NYHA III-IV, LVEF <30%) were randomly allocated into three groups and received24-hour intravenous infusions of either levosimendan (n=23, 0.1 μg/kg/min),dobutamine (n=23, 5μg/kg/min), or placebo (n=23). End-systolic wall stress(ESWS), central hemodynamics, plasma N-terminal pro-B-type natriuretic pep-tide (NT-pro-BNP), interleukin (IL)-6, tumor necrosis factor (TNF)-α, soluble (s)Fas, and sFas Ligand (L) were measured at baseline and 48 hours after the initi-ation of treatment. All patients were monitored for a follow-up period of 4 monthsfor disease progression (death or re-hospitalization).Results: ESWS was significantly decreased only in the levosimendan group(from 782 ± 41 to 674 ± 42 gr/cm2, p<0.05). A more significant reductionin pulmonary capillary wedge pressure (p<0.01) and an increase in cardiacindex (p<0.001) were observed with levosimendan as compared with dobu-tamine treatment. Plasma levels of NT-pro-BNP, TNF-α, and sFasL were sig-nificantly decreased in the levosimendan group (from 1900±223 to 1378±170pg/ml, 13.4±1.0 to 12.3±1.2 pg/ml, and 68.2±3.7 to 59.8±3.6 pg/ml, respec-tively, p<0.05 for all), but remained unchanged in the other groups. Plasma sFaswas decreased in the levosimendan group (7.5±0.7 to 6.1±0.6 ng/ml, p<0.001),remained unchanged in the placebo group, and was significantly increased in thedobutamine group (7.5±0.6 to 8.2±0.8 ng/mL, p<0.05). Levosimendan-inducedreductions in ESWS were significantly correlated with respective decreases ofplasma NT-pro-BNP (r=0.671, p<0.01), TNF-α (r=0.586, p<0.01), sFas (r=0.441,p<0.05) and sFasL (r=0.614, p<0.01). Event-free survival was significantly longerin the levosimendan group (log-rank test p<0.05) compared with the dobutamineand placebo groups.Conclusions: Levosimendan (at low dosing) seems superior to dobutamine inpatients with decompensated CHF in improving central hemodynamics and car-diac contractile performance, and reducing the expression of proinflammatory cy-tokines and pro-apoptotic mediators.
5009 Right bundle branch block and long-term mortality inpatients with acute congestive heart failure
C. Mueller, K. Laule-Kilian, L. Purek, A.P. Perruchoud, M. Christ.University Hospital, Department Of Internal Medicine, Basel,Switzerland
Aim: The aim of the present study was to assess the impact of rightbundle brunch block (RBBB) on long-term mortality in patients presenting withacute congestive heart failure (ACHF).RBBB is a predictor of adverse outcome inacute myocardial infarction. The clinical relevance of RBBB in patients with ACHFis unknown.Methods: In a secondary analysis of the BASEL study, the initial 12-lead electro-cardiogram was analyzed for RBBB in 192 consecutive patients presenting withACHF to the emergency department. The primary endpoint was all-cause mortal-ity during 720-day follow-up.Results: This study included an elderly cohort (mean age 74 years) of ACHF pa-tients. Nearly half of patients were women, and comorbidity including pulmonarydisease was extensive. RBBB was present in 27 patients (14%). Although morepatients with RBBB had pulmonary comorbidity, other baseline characteristicsincluding age, sex, B-type natriuretic peptide level and initial management weresimilar in patients with RBBB as compared to patients without RBBB. A total of 84patients died during follow-up. Kaplan-Meier analysis revealed that 720-day sur-vival rate was significantly lower in patients with RBBB as compared to patientswithout RBBB (37% versus 61%, p=0.004). In Cox proportional hazard analysis,RBBB was associated with a two-fold increase in mortality (hazard ratio 2.15, 95%CI 1.26-3.66; p=0.005). This association persisted after multivariate adjustment(hazard ratio 1.95, 95% CI 1.06-3.61; p=0.033).Conclusions: RBBB is a powerful and independent predictor of mortality in pa-tients with ACHF. Early identification of this high-risk group may help to offer tai-lored treatment in order to improve outcome.
5010 Clinically assessed hemodynamic profiles predictsoutcome in patients admitted with severe heart failure
A. Chinaglia, G. Gaschino, B. Demichelis, M. Giuggia, S. Forno,A. Ghisio, F. Beqaraj, R. Trinchero. Cardiology Department, ASL 3,Cardiology Department, Turin, Italy
Background: Stevenson and coll. have recently proposed a simple clinical as-sessment to define hemodynamic profiles in patients admitted with heart failure(HF). The profiles could predict outcomes and could be used to guide therapy, butthe value of this assessment requires further confirmation.Aim: to verify the feasibility of the proposed clinical assessment in patients admit-ted with severe HF, to analyze the hemodynamic profile, the subsequent outcomeand the pharmacological therapy required.Methods: patients admitted with severe HF to the intensive care unit betweenOctober 2002 and June 2004 were prospectively analyzed. Patients were classi-fied by clinical assessment into 4 profiles: profile A: patients with no evidence ofcongestion or hypoperfusion (dry-warm), profile B: congestion with adequate per-fusion (wet-warm), profile C: congestion and hypoperfusion (wet-cold), and profileL: hypoperfusion without congestion (dry-cold). Baseline clinical characteristics,therapy administered during the hospital stay, death and urgent transplantationwere evaluated. Patients were followed up for 12 ± 4 months.Results: the analysis included 75 consecutive admissions related to 70 patientsadmitted for severe HF (age 67 ± 12 years, 52 men, mean ejection fraction 30± 11%). Of the 75 patients 33 were classified as profile B, 40 as profile C, 2 asprofile L; no patient was classified as profile A, considering the analysis criteria.Patients with profile B and C differed in systolic and diastolic blood pressure (143vs 107 mmHg, p=0.0004; 79 vs 66 mmHg, p=0,001), ejection fraction (35 vs 26%,p=0.008), serum creatinine (1,2 vs 1.9, p<0,0001) and serum sodium (139 vs134, p=0,001). They did not differ in age (68 vs 67 years), hospitalization length(11 vs 15 days) and heart rate (95 vs 97 bpm). Profiles B and C did not differ forintravenous diuretic therapy (100% in each profile) and vasodilator therapy (72%vs 70%). Patients in profile C were treated more frequently with inotropic therapythan B (60% vs 3%, p<0.01) and less frequently with betablockers during hospitalstay (17 vs 56%). At follow up 22 patients died, 2 were transplanted urgently; 20of these patients were classified as profile C (50%), 1 as profile B (4%) (p<0.01,OR 0,63, 95% IC 0,36-0,89) and 1 as profile L.Conclusions: a clinical assessment can be used to define profiles in patients ad-mitted with severe HF. These profiles predict outcomes and may be used to guidetherapy, identifying a low risk group, in which inotropic therapy can be frequentlyavoided and betablocker therapy early implemented.
WHAT CAN WE LEARN FROM META-ANALYSES OFSTATIN AND ANTIHYPERTENSIVES TRIALS?
5011 Intensive statin therapy and all-cause mortality:a meta-analysis of randomized controlled trials
J. Afilalo, A.A. Majdan, M.J. Eisenberg. Jewish General Hospital,McGill University, Internal Medicine, Montreal, Canada
Purpose: Compared with moderate statin therapy, intensive statin ther-apy has been shown to reduce major adverse cardiac events but not all-causemortality. We sought to determine the effect of intensive statin therapy on all-cause mortality in patients with recent acute coronary syndromes and stablecoronary artery disease. Secondarily, we sought to determine the frequency ofserious adverse drug events.Methods: We searched MEDLINE, EMBASE, and the Cochrane Library from1995 to 2006 to identify randomized controlled trials examining intensive statintherapy (80 mg/day of atorvastatin or simvastatin) versus moderate statin therapy.In addition, we searched abstracts from cardiology conferences and the Internetto identify unpublished trials. Results were analyzed by a random-effects modeland were reported as relative risks (RR) with 95% confidence intervals (CI).Results: We included 10 trials encompassing 30,555 patients. The mean follow-up period was 3.9 years. The mean achieved LDL cholesterol was 2.0 mmol/literin intensive regimens and 2.6 mmol/liter in moderate regimens. All-cause mortal-ity was reduced by 24% in patients with recent acute coronary syndromes (RR0.76; 95% CI 0.62 to 0.94) but not in patients with stable coronary artery dis-ease (RR 0.99; 95% CI 0.90 to 1.10) (Figure 1). Major adverse cardiac events
Fig. 1. All-cause mortality.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
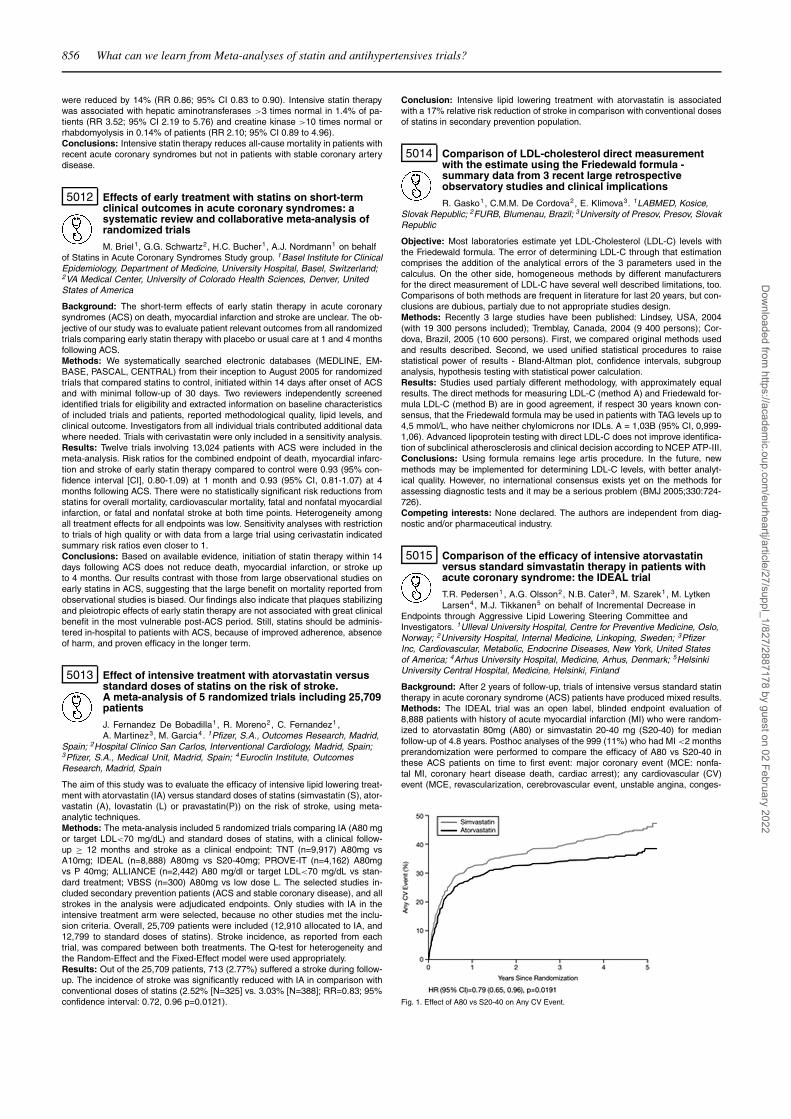
856 What can we learn from Meta-analyses of statin and antihypertensives trials?
were reduced by 14% (RR 0.86; 95% CI 0.83 to 0.90). Intensive statin therapywas associated with hepatic aminotransferases >3 times normal in 1.4% of pa-tients (RR 3.52; 95% CI 2.19 to 5.76) and creatine kinase >10 times normal orrhabdomyolysis in 0.14% of patients (RR 2.10; 95% CI 0.89 to 4.96).Conclusions: Intensive statin therapy reduces all-cause mortality in patients withrecent acute coronary syndromes but not in patients with stable coronary arterydisease.
5012 Effects of early treatment with statins on short-termclinical outcomes in acute coronary syndromes: asystematic review and collaborative meta-analysis ofrandomized trials
M. Briel1, G.G. Schwartz2, H.C. Bucher1, A.J. Nordmann1 on behalfof Statins in Acute Coronary Syndromes Study group. 1Basel Institute for ClinicalEpidemiology, Department of Medicine, University Hospital, Basel, Switzerland;2VA Medical Center, University of Colorado Health Sciences, Denver, UnitedStates of America
Background: The short-term effects of early statin therapy in acute coronarysyndromes (ACS) on death, myocardial infarction and stroke are unclear. The ob-jective of our study was to evaluate patient relevant outcomes from all randomizedtrials comparing early statin therapy with placebo or usual care at 1 and 4 monthsfollowing ACS.Methods: We systematically searched electronic databases (MEDLINE, EM-BASE, PASCAL, CENTRAL) from their inception to August 2005 for randomizedtrials that compared statins to control, initiated within 14 days after onset of ACSand with minimal follow-up of 30 days. Two reviewers independently screenedidentified trials for eligibility and extracted information on baseline characteristicsof included trials and patients, reported methodological quality, lipid levels, andclinical outcome. Investigators from all individual trials contributed additional datawhere needed. Trials with cerivastatin were only included in a sensitivity analysis.Results: Twelve trials involving 13,024 patients with ACS were included in themeta-analysis. Risk ratios for the combined endpoint of death, myocardial infarc-tion and stroke of early statin therapy compared to control were 0.93 (95% con-fidence interval [CI], 0.80-1.09) at 1 month and 0.93 (95% CI, 0.81-1.07) at 4months following ACS. There were no statistically significant risk reductions fromstatins for overall mortality, cardiovascular mortality, fatal and nonfatal myocardialinfarction, or fatal and nonfatal stroke at both time points. Heterogeneity amongall treatment effects for all endpoints was low. Sensitivity analyses with restrictionto trials of high quality or with data from a large trial using cerivastatin indicatedsummary risk ratios even closer to 1.Conclusions: Based on available evidence, initiation of statin therapy within 14days following ACS does not reduce death, myocardial infarction, or stroke upto 4 months. Our results contrast with those from large observational studies onearly statins in ACS, suggesting that the large benefit on mortality reported fromobservational studies is biased. Our findings also indicate that plaques stabilizingand pleiotropic effects of early statin therapy are not associated with great clinicalbenefit in the most vulnerable post-ACS period. Still, statins should be adminis-tered in-hospital to patients with ACS, because of improved adherence, absenceof harm, and proven efficacy in the longer term.
5013 Effect of intensive treatment with atorvastatin versusstandard doses of statins on the risk of stroke.A meta-analysis of 5 randomized trials including 25,709patients
J. Fernandez De Bobadilla1, R. Moreno2, C. Fernandez1 ,A. Martinez3, M. Garcia4. 1Pfizer, S.A., Outcomes Research, Madrid,
Spain; 2Hospital Clinico San Carlos, Interventional Cardiology, Madrid, Spain;3Pfizer, S.A., Medical Unit, Madrid, Spain; 4Euroclin Institute, OutcomesResearch, Madrid, Spain
The aim of this study was to evaluate the efficacy of intensive lipid lowering treat-ment with atorvastatin (IA) versus standard doses of statins (simvastatin (S), ator-vastatin (A), lovastatin (L) or pravastatin(P)) on the risk of stroke, using meta-analytic techniques.Methods: The meta-analysis included 5 randomized trials comparing IA (A80 mgor target LDL<70 mg/dL) and standard doses of statins, with a clinical follow-up ≥ 12 months and stroke as a clinical endpoint: TNT (n=9,917) A80mg vsA10mg; IDEAL (n=8,888) A80mg vs S20-40mg; PROVE-IT (n=4,162) A80mgvs P 40mg; ALLIANCE (n=2,442) A80 mg/dl or target LDL<70 mg/dL vs stan-dard treatment; VBSS (n=300) A80mg vs low dose L. The selected studies in-cluded secondary prevention patients (ACS and stable coronary disease), and allstrokes in the analysis were adjudicated endpoints. Only studies with IA in theintensive treatment arm were selected, because no other studies met the inclu-sion criteria. Overall, 25,709 patients were included (12,910 allocated to IA, and12,799 to standard doses of statins). Stroke incidence, as reported from eachtrial, was compared between both treatments. The Q-test for heterogeneity andthe Random-Effect and the Fixed-Effect model were used appropriately.Results: Out of the 25,709 patients, 713 (2.77%) suffered a stroke during follow-up. The incidence of stroke was significantly reduced with IA in comparison withconventional doses of statins (2.52% [N=325] vs. 3.03% [N=388]; RR=0.83; 95%confidence interval: 0.72, 0.96 p=0.0121).
Conclusion: Intensive lipid lowering treatment with atorvastatin is associatedwith a 17% relative risk reduction of stroke in comparison with conventional dosesof statins in secondary prevention population.
5014 Comparison of LDL-cholesterol direct measurementwith the estimate using the Friedewald formula -summary data from 3 recent large retrospectiveobservatory studies and clinical implications
R. Gasko1, C.M.M. De Cordova2, E. Klimova3. 1LABMED, Kosice,Slovak Republic; 2FURB, Blumenau, Brazil; 3University of Presov, Presov, SlovakRepublic
Objective: Most laboratories estimate yet LDL-Cholesterol (LDL-C) levels withthe Friedewald formula. The error of determining LDL-C through that estimationcomprises the addition of the analytical errors of the 3 parameters used in thecalculus. On the other side, homogeneous methods by different manufacturersfor the direct measurement of LDL-C have several well described limitations, too.Comparisons of both methods are frequent in literature for last 20 years, but con-clusions are dubious, partialy due to not appropriate studies design.Methods: Recently 3 large studies have been published: Lindsey, USA, 2004(with 19 300 persons included); Tremblay, Canada, 2004 (9 400 persons); Cor-dova, Brazil, 2005 (10 600 persons). First, we compared original methods usedand results described. Second, we used unified statistical procedures to raisestatistical power of results - Bland-Altman plot, confidence intervals, subgroupanalysis, hypothesis testing with statistical power calculation.Results: Studies used partialy different methodology, with approximately equalresults. The direct methods for measuring LDL-C (method A) and Friedewald for-mula LDL-C (method B) are in good agreement, if respect 30 years known con-sensus, that the Friedewald formula may be used in patients with TAG levels up to4,5 mmol/L, who have neither chylomicrons nor IDLs. A = 1,03B (95% CI, 0,999-1,06). Advanced lipoprotein testing with direct LDL-C does not improve identifica-tion of subclinical atherosclerosis and clinical decision according to NCEP ATP-III.Conclusions: Using formula remains lege artis procedure. In the future, newmethods may be implemented for determining LDL-C levels, with better analyt-ical quality. However, no international consensus exists yet on the methods forassessing diagnostic tests and it may be a serious problem (BMJ 2005;330:724-726).Competing interests: None declared. The authors are independent from diag-nostic and/or pharmaceutical industry.
5015 Comparison of the efficacy of intensive atorvastatinversus standard simvastatin therapy in patients withacute coronary syndrome: the IDEAL trial
T.R. Pedersen1, A.G. Olsson2, N.B. Cater3, M. Szarek1, M. LytkenLarsen4, M.J. Tikkanen5 on behalf of Incremental Decrease in
Endpoints through Aggressive Lipid Lowering Steering Committee andInvestigators. 1Ulleval University Hospital, Centre for Preventive Medicine, Oslo,Norway; 2University Hospital, Internal Medicine, Linkoping, Sweden; 3PfizerInc, Cardiovascular, Metabolic, Endocrine Diseases, New York, United Statesof America; 4Arhus University Hospital, Medicine, Arhus, Denmark; 5HelsinkiUniversity Central Hospital, Medicine, Helsinki, Finland
Background: After 2 years of follow-up, trials of intensive versus standard statintherapy in acute coronary syndrome (ACS) patients have produced mixed results.Methods: The IDEAL trial was an open label, blinded endpoint evaluation of8,888 patients with history of acute myocardial infarction (MI) who were random-ized to atorvastatin 80mg (A80) or simvastatin 20-40 mg (S20-40) for medianfollow-up of 4.8 years. Posthoc analyses of the 999 (11%) who had MI <2 monthsprerandomization were performed to compare the efficacy of A80 vs S20-40 inthese ACS patients on time to first event: major coronary event (MCE: nonfa-tal MI, coronary heart disease death, cardiac arrest); any cardiovascular (CV)event (MCE, revascularization, cerebrovascular event, unstable angina, conges-
Fig. 1. Effect of A80 vs S20-40 on Any CV Event.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
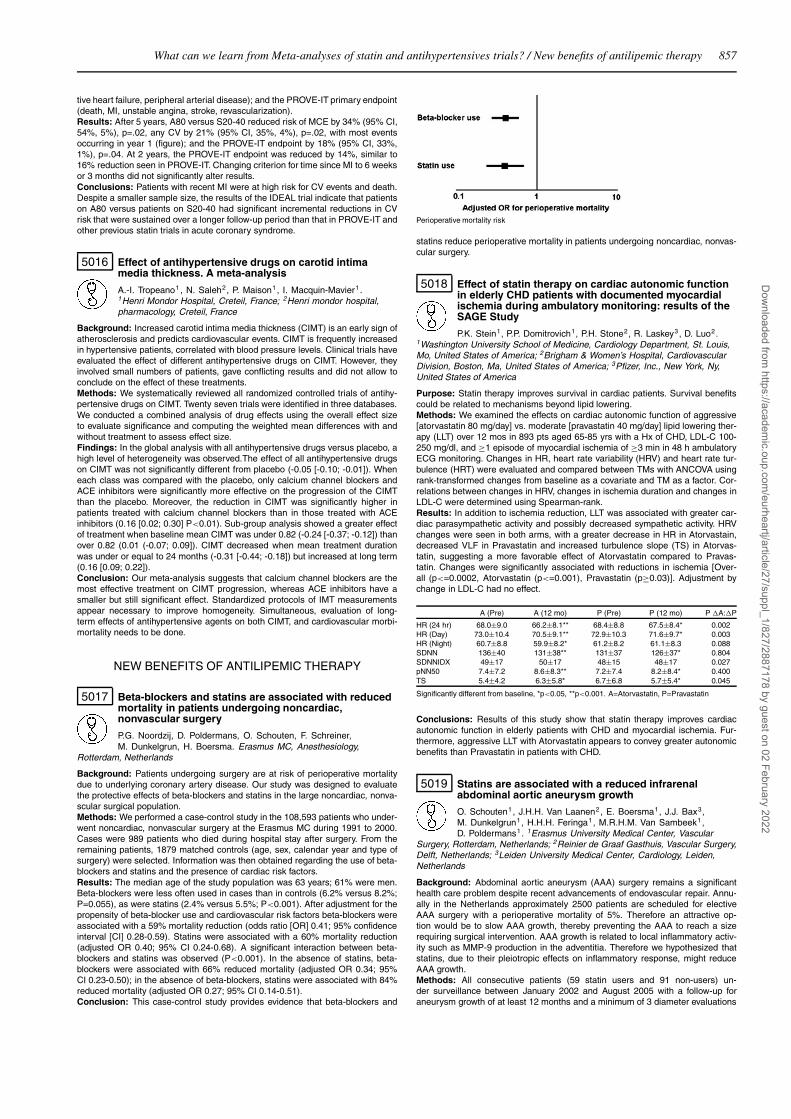
What can we learn from Meta-analyses of statin and antihypertensives trials? / New benefits of antilipemic therapy 857
tive heart failure, peripheral arterial disease); and the PROVE-IT primary endpoint(death, MI, unstable angina, stroke, revascularization).Results: After 5 years, A80 versus S20-40 reduced risk of MCE by 34% (95% CI,54%, 5%), p=.02, any CV by 21% (95% CI, 35%, 4%), p=.02, with most eventsoccurring in year 1 (figure); and the PROVE-IT endpoint by 18% (95% CI, 33%,1%), p=.04. At 2 years, the PROVE-IT endpoint was reduced by 14%, similar to16% reduction seen in PROVE-IT. Changing criterion for time since MI to 6 weeksor 3 months did not significantly alter results.Conclusions: Patients with recent MI were at high risk for CV events and death.Despite a smaller sample size, the results of the IDEAL trial indicate that patientson A80 versus patients on S20-40 had significant incremental reductions in CVrisk that were sustained over a longer follow-up period than that in PROVE-IT andother previous statin trials in acute coronary syndrome.
5016 Effect of antihypertensive drugs on carotid intimamedia thickness. A meta-analysis
A.-I. Tropeano1 , N. Saleh2, P. Maison1, I. Macquin-Mavier1 .1Henri Mondor Hospital, Creteil, France; 2Henri mondor hospital,pharmacology, Creteil, France
Background: Increased carotid intima media thickness (CIMT) is an early sign ofatherosclerosis and predicts cardiovascular events. CIMT is frequently increasedin hypertensive patients, correlated with blood pressure levels. Clinical trials haveevaluated the effect of different antihypertensive drugs on CIMT. However, theyinvolved small numbers of patients, gave conflicting results and did not allow toconclude on the effect of these treatments.Methods: We systematically reviewed all randomized controlled trials of antihy-pertensive drugs on CIMT. Twenty seven trials were identified in three databases.We conducted a combined analysis of drug effects using the overall effect sizeto evaluate significance and computing the weighted mean differences with andwithout treatment to assess effect size.Findings: In the global analysis with all antihypertensive drugs versus placebo, ahigh level of heterogeneity was observed.The effect of all antihypertensive drugson CIMT was not significantly different from placebo (-0.05 [-0.10; -0.01]). Wheneach class was compared with the placebo, only calcium channel blockers andACE inhibitors were significantly more effective on the progression of the CIMTthan the placebo. Moreover, the reduction in CIMT was significantly higher inpatients treated with calcium channel blockers than in those treated with ACEinhibitors (0.16 [0.02; 0.30] P<0.01). Sub-group analysis showed a greater effectof treatment when baseline mean CIMT was under 0.82 (-0.24 [-0.37; -0.12]) thanover 0.82 (0.01 (-0.07; 0.09]). CIMT decreased when mean treatment durationwas under or equal to 24 months (-0.31 [-0.44; -0.18]) but increased at long term(0.16 [0.09; 0.22]).Conclusion: Our meta-analysis suggests that calcium channel blockers are themost effective treatment on CIMT progression, whereas ACE inhibitors have asmaller but still significant effect. Standardized protocols of IMT measurementsappear necessary to improve homogeneity. Simultaneous, evaluation of long-term effects of antihypertensive agents on both CIMT, and cardiovascular morbi-mortality needs to be done.
NEW BENEFITS OF ANTILIPEMIC THERAPY
5017 Beta-blockers and statins are associated with reducedmortality in patients undergoing noncardiac,nonvascular surgery
P.G. Noordzij, D. Poldermans, O. Schouten, F. Schreiner,M. Dunkelgrun, H. Boersma. Erasmus MC, Anesthesiology,
Rotterdam, Netherlands
Background: Patients undergoing surgery are at risk of perioperative mortalitydue to underlying coronary artery disease. Our study was designed to evaluatethe protective effects of beta-blockers and statins in the large noncardiac, nonva-scular surgical population.Methods: We performed a case-control study in the 108,593 patients who under-went noncardiac, nonvascular surgery at the Erasmus MC during 1991 to 2000.Cases were 989 patients who died during hospital stay after surgery. From theremaining patients, 1879 matched controls (age, sex, calendar year and type ofsurgery) were selected. Information was then obtained regarding the use of beta-blockers and statins and the presence of cardiac risk factors.Results: The median age of the study population was 63 years; 61% were men.Beta-blockers were less often used in cases than in controls (6.2% versus 8.2%;P=0.055), as were statins (2.4% versus 5.5%; P<0.001). After adjustment for thepropensity of beta-blocker use and cardiovascular risk factors beta-blockers wereassociated with a 59% mortality reduction (odds ratio [OR] 0.41; 95% confidenceinterval [CI] 0.28-0.59). Statins were associated with a 60% mortality reduction(adjusted OR 0.40; 95% CI 0.24-0.68). A significant interaction between beta-blockers and statins was observed (P<0.001). In the absence of statins, beta-blockers were associated with 66% reduced mortality (adjusted OR 0.34; 95%CI 0.23-0.50); in the absence of beta-blockers, statins were associated with 84%reduced mortality (adjusted OR 0.27; 95% CI 0.14-0.51).Conclusion: This case-control study provides evidence that beta-blockers and
Perioperative mortality risk
statins reduce perioperative mortality in patients undergoing noncardiac, nonvas-cular surgery.
5018 Effect of statin therapy on cardiac autonomic functionin elderly CHD patients with documented myocardialischemia during ambulatory monitoring: results of theSAGE Study
P.K. Stein1, P.P. Domitrovich1, P.H. Stone2, R. Laskey3, D. Luo2.1Washington University School of Medicine, Cardiology Department, St. Louis,Mo, United States of America; 2Brigham & Women’s Hospital, CardiovascularDivision, Boston, Ma, United States of America; 3Pfizer, Inc., New York, Ny,United States of America
Purpose: Statin therapy improves survival in cardiac patients. Survival benefitscould be related to mechanisms beyond lipid lowering.Methods: We examined the effects on cardiac autonomic function of aggressive[atorvastatin 80 mg/day] vs. moderate [pravastatin 40 mg/day] lipid lowering ther-apy (LLT) over 12 mos in 893 pts aged 65-85 yrs with a Hx of CHD, LDL-C 100-250 mg/dl, and ≥1 episode of myocardial ischemia of ≥3 min in 48 h ambulatoryECG monitoring. Changes in HR, heart rate variability (HRV) and heart rate tur-bulence (HRT) were evaluated and compared between TMs with ANCOVA usingrank-transformed changes from baseline as a covariate and TM as a factor. Cor-relations between changes in HRV, changes in ischemia duration and changes inLDL-C were determined using Spearman-rank.Results: In addition to ischemia reduction, LLT was associated with greater car-diac parasympathetic activity and possibly decreased sympathetic activity. HRVchanges were seen in both arms, with a greater decrease in HR in Atorvastain,decreased VLF in Pravastatin and increased turbulence slope (TS) in Atorvas-tatin, suggesting a more favorable effect of Atorvastatin compared to Pravas-tatin. Changes were significantly associated with reductions in ischemia [Over-all (p<=0.0002, Atorvastatin (p<=0.001), Pravastatin (p≥0.03)]. Adjustment bychange in LDL-C had no effect.
A (Pre) A (12 mo) P (Pre) P (12 mo) P �A:�P
HR (24 hr) 68.0±9.0 66.2±8.1** 68.4±8.8 67.5±8.4* 0.002HR (Day) 73.0±10.4 70.5±9.1** 72.9±10.3 71.6±9.7* 0.003HR (Night) 60.7±8.8 59.9±8.2* 61.2±8.2 61.1±8.3 0.088SDNN 136±40 131±38** 131±37 126±37* 0.804SDNNIDX 49±17 50±17 48±15 48±17 0.027pNN50 7.4±7.2 8.6±8.3** 7.2±7.4 8.2±8.4* 0.400TS 5.4±4.2 6.3±5.8* 6.7±6.8 5.7±5.4* 0.045
Significantly different from baseline, *p<0.05, **p<0.001. A=Atorvastatin, P=Pravastatin
Conclusions: Results of this study show that statin therapy improves cardiacautonomic function in elderly patients with CHD and myocardial ischemia. Fur-thermore, aggressive LLT with Atorvastatin appears to convey greater autonomicbenefits than Pravastatin in patients with CHD.
5019 Statins are associated with a reduced infrarenalabdominal aortic aneurysm growth
O. Schouten1, J.H.H. Van Laanen2, E. Boersma1, J.J. Bax3,M. Dunkelgrun1, H.H.H. Feringa1, M.R.H.M. Van Sambeek1,D. Poldermans1. 1Erasmus University Medical Center, Vascular
Surgery, Rotterdam, Netherlands; 2Reinier de Graaf Gasthuis, Vascular Surgery,Delft, Netherlands; 3Leiden University Medical Center, Cardiology, Leiden,Netherlands
Background: Abdominal aortic aneurysm (AAA) surgery remains a significanthealth care problem despite recent advancements of endovascular repair. Annu-ally in the Netherlands approximately 2500 patients are scheduled for electiveAAA surgery with a perioperative mortality of 5%. Therefore an attractive op-tion would be to slow AAA growth, thereby preventing the AAA to reach a sizerequiring surgical intervention. AAA growth is related to local inflammatory activ-ity such as MMP-9 production in the adventitia. Therefore we hypothesized thatstatins, due to their pleiotropic effects on inflammatory response, might reduceAAA growth.Methods: All consecutive patients (59 statin users and 91 non-users) un-der surveillance between January 2002 and August 2005 with a follow-up foraneurysm growth of at least 12 months and a minimum of 3 diameter evaluations
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
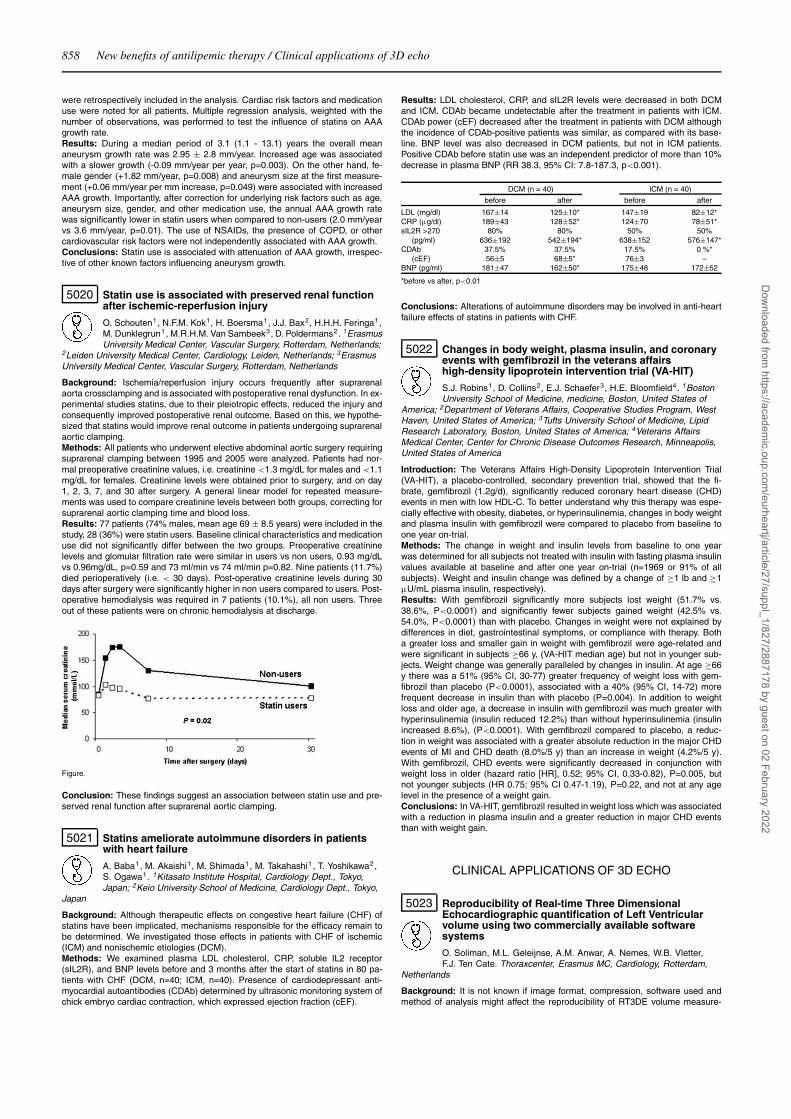
858 New benefits of antilipemic therapy / Clinical applications of 3D echo
were retrospectively included in the analysis. Cardiac risk factors and medicationuse were noted for all patients. Multiple regression analysis, weighted with thenumber of observations, was performed to test the influence of statins on AAAgrowth rate.Results: During a median period of 3.1 (1.1 - 13.1) years the overall meananeurysm growth rate was 2.95 ± 2.8 mm/year. Increased age was associatedwith a slower growth (-0.09 mm/year per year, p=0.003). On the other hand, fe-male gender (+1.82 mm/year, p=0.008) and aneurysm size at the first measure-ment (+0.06 mm/year per mm increase, p=0.049) were associated with increasedAAA growth. Importantly, after correction for underlying risk factors such as age,aneurysm size, gender, and other medication use, the annual AAA growth ratewas significantly lower in statin users when compared to non-users (2.0 mm/yearvs 3.6 mm/year, p=0.01). The use of NSAIDs, the presence of COPD, or othercardiovascular risk factors were not independently associated with AAA growth.Conclusions: Statin use is associated with attenuation of AAA growth, irrespec-tive of other known factors influencing aneurysm growth.
5020 Statin use is associated with preserved renal functionafter ischemic-reperfusion injury
O. Schouten1, N.F.M. Kok1, H. Boersma1, J.J. Bax2, H.H.H. Feringa1,M. Dunklegrun1, M.R.H.M. Van Sambeek3, D. Poldermans2. 1ErasmusUniversity Medical Center, Vascular Surgery, Rotterdam, Netherlands;
2Leiden University Medical Center, Cardiology, Leiden, Netherlands; 3ErasmusUniversity Medical Center, Vascular Surgery, Rotterdam, Netherlands
Background: Ischemia/reperfusion injury occurs frequently after suprarenalaorta crossclamping and is associated with postoperative renal dysfunction. In ex-perimental studies statins, due to their pleiotropic effects, reduced the injury andconsequently improved postoperative renal outcome. Based on this, we hypothe-sized that statins would improve renal outcome in patients undergoing suprarenalaortic clamping.Methods: All patients who underwent elective abdominal aortic surgery requiringsuprarenal clamping between 1995 and 2005 were analyzed. Patients had nor-mal preoperative creatinine values, i.e. creatinine <1.3 mg/dL for males and <1.1mg/dL for females. Creatinine levels were obtained prior to surgery, and on day1, 2, 3, 7, and 30 after surgery. A general linear model for repeated measure-ments was used to compare creatinine levels between both groups, correcting forsuprarenal aortic clamping time and blood loss.Results: 77 patients (74% males, mean age 69 ± 8.5 years) were included in thestudy, 28 (36%) were statin users. Baseline clinical characteristics and medicationuse did not significantly differ between the two groups. Preoperative creatininelevels and glomular filtration rate were similar in users vs non users, 0.93 mg/dLvs 0.96mg/dL, p=0.59 and 73 ml/min vs 74 ml/min p=0.82. Nine patients (11.7%)died perioperatively (i.e. < 30 days). Post-operative creatinine levels during 30days after surgery were significantly higher in non users compared to users. Post-operative hemodialysis was required in 7 patients (10.1%), all non users. Threeout of these patients were on chronic hemodialysis at discharge.
Figure.
Conclusion: These findings suggest an association between statin use and pre-served renal function after suprarenal aortic clamping.
5021 Statins ameliorate autoimmune disorders in patientswith heart failure
A. Baba1, M. Akaishi1, M. Shimada1, M. Takahashi1 , T. Yoshikawa2,S. Ogawa1. 1Kitasato Institute Hospital, Cardiology Dept., Tokyo,Japan; 2Keio University School of Medicine, Cardiology Dept., Tokyo,
Japan
Background: Although therapeutic effects on congestive heart failure (CHF) ofstatins have been implicated, mechanisms responsible for the efficacy remain tobe determined. We investigated those effects in patients with CHF of ischemic(ICM) and nonischemic etiologies (DCM).Methods: We examined plasma LDL cholesterol, CRP, soluble IL2 receptor(sIL2R), and BNP levels before and 3 months after the start of statins in 80 pa-tients with CHF (DCM, n=40; ICM, n=40). Presence of cardiodepressant anti-myocardial autoantibodies (CDAb) determined by ultrasonic monitoring system ofchick embryo cardiac contraction, which expressed ejection fraction (cEF).
Results: LDL cholesterol, CRP, and sIL2R levels were decreased in both DCMand ICM. CDAb became undetectable after the treatment in patients with ICM.CDAb power (cEF) decreased after the treatment in patients with DCM althoughthe incidence of CDAb-positive patients was similar, as compared with its base-line. BNP level was also decreased in DCM patients, but not in ICM patients.Positive CDAb before statin use was an independent predictor of more than 10%decrease in plasma BNP (RR 38.3, 95% CI: 7.8-187.3, p<0.001).
DCM (n = 40) ICM (n = 40)
before after before after
LDL (mg/dl) 167±14 125±10* 147±19 82±12*CRP (μg/dl) 189±43 128±52* 124±70 78±51*sIL2R >270 80% 80% 50% 50%
(pg/ml) 636±192 542±194* 638±152 576±147*CDAb 37.5% 37.5% 17.5% 0 %*
(cEF) 56±5 68±5* 76±3 –BNP (pg/ml) 181±47 162±50* 175±48 172±52
*before vs after, p<0.01
Conclusions: Alterations of autoimmune disorders may be involved in anti-heartfailure effects of statins in patients with CHF.
5022 Changes in body weight, plasma insulin, and coronaryevents with gemfibrozil in the veterans affairshigh-density lipoprotein intervention trial (VA-HIT)
S.J. Robins1, D. Collins2, E.J. Schaefer3, H.E. Bloomfield4. 1BostonUniversity School of Medicine, medicine, Boston, United States of
America; 2Department of Veterans Affairs, Cooperative Studies Program, WestHaven, United States of America; 3Tufts University School of Medicine, LipidResearch Laboratory, Boston, United States of America; 4Veterans AffairsMedical Center, Center for Chronic Disease Outcomes Research, Minneapolis,United States of America
Introduction: The Veterans Affairs High-Density Lipoprotein Intervention Trial(VA-HIT), a placebo-controlled, secondary prevention trial, showed that the fi-brate, gemfibrozil (1.2g/d), significantly reduced coronary heart disease (CHD)events in men with low HDL-C. To better understand why this therapy was espe-cially effective with obesity, diabetes, or hyperinsulinemia, changes in body weightand plasma insulin with gemfibrozil were compared to placebo from baseline toone year on-trial.Methods: The change in weight and insulin levels from baseline to one yearwas determined for all subjects not treated with insulin with fasting plasma insulinvalues available at baseline and after one year on-trial (n=1969 or 91% of allsubjects). Weight and insulin change was defined by a change of ≥1 lb and ≥1μU/mL plasma insulin, respectively).Results: With gemfibrozil significantly more subjects lost weight (51.7% vs.38.6%, P<0.0001) and significantly fewer subjects gained weight (42.5% vs.54.0%, P<0.0001) than with placebo. Changes in weight were not explained bydifferences in diet, gastrointestinal symptoms, or compliance with therapy. Botha greater loss and smaller gain in weight with gemfibrozil were age-related andwere significant in subjects ≥66 y, (VA-HIT median age) but not in younger sub-jects. Weight change was generally paralleled by changes in insulin. At age ≥66y there was a 51% (95% CI, 30-77) greater frequency of weight loss with gem-fibrozil than placebo (P<0.0001), associated with a 40% (95% CI, 14-72) morefrequent decrease in insulin than with placebo (P=0.004). In addition to weightloss and older age, a decrease in insulin with gemfibrozil was much greater withhyperinsulinemia (insulin reduced 12.2%) than without hyperinsulinemia (insulinincreased 8.6%), (P<0.0001). With gemfibrozil compared to placebo, a reduc-tion in weight was associated with a greater absolute reduction in the major CHDevents of MI and CHD death (8.0%/5 y) than an increase in weight (4.2%/5 y).With gemfibrozil, CHD events were significantly decreased in conjunction withweight loss in older (hazard ratio [HR], 0.52; 95% CI, 0.33-0.82), P=0.005, butnot younger subjects (HR 0.75; 95% CI 0.47-1.19), P=0.22, and not at any agelevel in the presence of a weight gain.Conclusions: In VA-HIT, gemfibrozil resulted in weight loss which was associatedwith a reduction in plasma insulin and a greater reduction in major CHD eventsthan with weight gain.
CLINICAL APPLICATIONS OF 3D ECHO
5023 Reproducibility of Real-time Three DimensionalEchocardiographic quantification of Left Ventricularvolume using two commercially available softwaresystems
O. Soliman, M.L. Geleijnse, A.M. Anwar, A. Nemes, W.B. Vletter,F.J. Ten Cate. Thoraxcenter, Erasmus MC, Cardiology, Rotterdam,
Netherlands
Background: It is not known if image format, compression, software used andmethod of analysis might affect the reproducibility of RT3DE volume measure-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Clinical applications of 3D echo 859
ments. We compared two commercially available software systems in our lab forquantification and reproducibility of LV volume measurements.Methods: Sixty cardiomyopathy patients duo to dilated (D)(n=20), non-compaction (NC) (n=20) and hypertrophic (H) (n=20) and control group (n=20)were investigated by RT3DE. Acquisition was done by Philips Sonos7500® . Datawere electronically stored and transferred by CD-ROM to two workstations. Vox-els in Sonos format (non-compressed) were sent to AD- QLab® (Q) software foranalysis by semi-automated border detection (SABD) in 20 2D cut-planes. DI-COM format (30% compressed) were sent to another workstation, and analysiswas done by TomTec® 4D (T) using SABD and ellipse formation in 8 2D cut-planes. Analysis was done by two investigators in LV long axis after definition ofmitral plane by four points in 4 and 2 chambers views and apical plane by onepoint. Then measurement of end-diastolic (EDV) and end systolic (ESV) volumesfor both systems were done.Results: Agreement and correlation coefficient among the total population (TP)for LV EDV, ESV and ejection fraction (EF) was excellent (r= 0.98, 0.99, 0.96 p <
0.0001) for Q and (r= 0.91, 0.93, 0.83 p <0.001) for T. Inter-methods correlationwas (r= 0.91, 0.93, 0.83 p < 0.001). Inter-method mean difference was significantfor H and D. Inter-observer variability was Greater in T for H.
n Paired difference (QLab-TomTec) Correlation
mean 95% CI p Value r p Value
Total population (TP) 80 5.4 ± 10 1.1 to 3.2 0.001 0.83 0.001(H) 20 9.8 ± 8.8 5.7 to 13.9 0.001 0.46 .05(D) 20 6.5 ± 1.5 -0.9 t0 6.9 0.01 0.85 0.0001(NC) 20 2.6 ± 6.8 - 0.6 to 5.8 0.1 0.85 0.0001Control 20 5.3 ± 14.9 -1.6 to 12.3 0.1 0.15 0.6
Conclusion: Reproducibility of RT3DE might be affected by technical factors likeimage format, software used, method of analysis and type of patients studied.This may influence application for clinical practice.
5024 Quantitative assessment of right ventricular volumeand function with real-time three-dimensionalechocardiography: comparison with cardiovascularmagnetic resonance
C. Pamboucas, E. Liodakis, D. Dawson, P. Nihoyannopoulos.Hammersmith Hospital, Echocardiography, London, United Kingdom
Background: Cardiovascular magnetic resonance (CMR) has been successfullyused as an accurate and reproducible tool to quantify right ventricular (RV) vol-umes in both normal and pulmonary arterial hypertension (PAH) subjects. Real-time three-dimensional echocardiography (RT-3DE) has emerged as an attractivemodality for measurement of left ventricular function but its accuracy for RV as-sessment has not yet been validated. The aim of this study is to compare RT-3DEand CMR, in the RV assessment, in patients with PAH and healthy subjects.Methods: We studied 14 PAH patients paired with 6 normal controls. CMR imag-ing was performed on a high field 3.0-Tesla. Calculation of the end-diastolic(EDV), end-systolic (ESV) volumes and ejection fraction (EF) from the echocar-diographic data were performed using dedicated offline software.Results: The RT-3DE data correlated highly with CMR in all variables tested(EDV: r=0.96 p<0.001, ESV: r=0.93 p<0.001 and EF: r=0.86 p<0.001). How-ever, RV volumes were underestimated by RT-3DE compared with CMR (EDV-27.5± 14.4 ml, p =0.002; ESV -17.3± 14.3 ml, p =0.004). The difference for EFwas not significant between the two methods (EF -1.1± 13%, p =0.79). Intra- andinterobserver agreement was good for both techniques.Conclusions: The RT-3DE is a fast and reproducible technique which allowsaccurate determination of RV cardiac volumes and function compared with CMR.Larger studies are needed in order to further validate this novel modality.
5025 Equal accuracy of semi-automated 3Dechocardiography estimates of left ventricular mass inpatients with and without wall motion abnormalities:comparison with cardiac magnetic resonance
J.-B. Le Polain De Waroux1, A.C. Pouleur1, D. Vancraeynest1 ,A. Pasquet1, B. Gerber1, O. Gerard2, P. Alain2, J.L. Vanoverschelde1. 1CliniquesUniversitaires Saint-Luc, Department Of Cardiology, Brussels, Belgium; 2PhilipsMedical System Research, Paris, France
Purpose: Assessment of left ventricular mass (LV mass) by 2D-echo is an im-portant prognostic factor in patients (pts) with hypertension. However, becausethis method relies on geometric assumptions, it is less accurate in pts with wallmotion abnormalities (WMA). 3D-echo (RT-3DE) is a promising new method forLV mass assessment that could be less sensitive to geometric distorsions of theLV. Therefore, the aim of the present study was to evaluate if RT-3DE is similarlyaccurate in estimating LV mass in pts with and without WMA by using cardiacmagnetic resonance (cMR) as the reference standard.Methods: 63 pts (28 with WMA) underwent RT-3DE and cMR. RT-3DE datasetswere analysed using a prototype version of the QLab software that allows for theautomatic detection of endocardial and epicardial contours by using a deformableshell model and for the calculation of LV mass from voxel counts. With cMR, LVmass was calculated by manually tracing endocardial and epicardial contours on
short-axis slices. The accuracy of RT-3DE in pts with and without WMA was thenevaluated by comparing LV mass by RT-3DE and cMR in the 2 groups (linearregression, Bland-Altman).Results: RT-3DE and cMR yielded similar values for LV mass in pts with (174±37g vs 168±40 g) and without (152±38 g vs 161±47 g) WMA. In both groups, RT-3DE and cMR LV masses were highly correlated (r = 0.92 and r = 0.91), with onlysmall biases (6±31 g and -9±32 g, respectively). In addition, no differences in Yintercept or regression slope were noted between the 2 groups.
Conclusion: RT-3DE accurately measures LV mass, irrespective of the presenceor absence of regional WMA. It can therefore be used to assess remodeling aftermyocardial infarction in a manner similar to cMR.
5026 Accuracy of 3D echocardiography in assessing leftintra-ventricular synchronicity using tissuesynchronization imaging
L. Badano1, M. Baldassi2, E. Tosoratti3 , E. Zakja1 , D. Pavoni1,E. Dall’armellina1, P. Gianfagna1, P.M. Fioretti1. 1Ospedale S M Della
Misericordia, Chief Echo.Lab., Dept.Cardiovascular Sciences, Udine, Italy; 2A.OS maria della Misericordia, Dpt of Cardiopulmonary Sciences, Udine, Italy;3University of Udine, Post-graduate School of Sport Medicine, Udine, Italy
Response to cardiac resynchronization therapy (CRT) mainly depends on the de-gree of left ventricular (LV) dyssynchrony which appears to be best quantitatedby LV dispersion as determined by tissue synchronization imaging (TSI). The aimof our study was to investigate normal values for measurement currently used asTSI criteria for LV dyssynchrony, and to compare synchronicity values obtainedusing real-time single-beat 3D multiplane echo (3D TSI) to values obtained usingcurrent 2D TSI acquisition modality. Accordingly, we studied 44 healthy adult vol-unteers (34±12 year, range 15-61 years, 55% M). Apical 4- and 2-chamber, andlong axis views were acquired from all patients with 2D (Frame rate= 140-160 fps)and 3D echo at 95-100 fps (Vivid 7-Dimension, GE Healthcare, Horten,Norway).Heart rate was similar among the 3 LV views (68±12 bpm in 4-CH, 67±11 bpm in2-CH, and 67±11 in apical LAX; F= 0.60, p=0.94). Intra-ventricular dyssynchronywas measured by TSI using the time to regional peak systolic velocity measuredin ejection phase, and a 6-basal-6-mid-segment model of LV. Comparison be-tween dyssynchrony parameters measured by 2D and 3D echo (median, 95%CI)are summarized in the Table.
Table 1. Comparison between synchronicity parameters measured by 2D and 3D Tissue Syn-chronization Imaging (TSI) echocardiography in normal subjects
2D TSI 3D TSI P value r P value
Heart Rate(bpm) 67±12 66±11 0.20 0.86 <0.000112 segment Ts-SD (ms) 22(20-27) 23(20-27) 0.90 0.87 <0.000112 segments Ts-diff (ms) 68(64-85) 67(62-84) 0.62 0.81 <0.0001Basal segment Ts-SD (ms) 20(19-27) 20(17-25) 0.14 0.77 <0.0001Basal segment Ts-diff (ms) 55(50-69) 51(46-64) 0.20 0.71 <0.0001
Seven controls (16%) showed LV dyssynchrony (12 segment SD>34 ms) at 2DTSI, and 6/7 were confirmed by 3D echo. Acquisition and measurement timeswere 185±29 s using 2D and 123±60 s using 3D (-34%, p= 0.001). Thus, despitea significantly lower frame rate, 3D TSI is accurate in comparison to standard2D TSI in measuring LV synchronicity. Furthermore, 3D TSI allows single-beatassessment of LV synchronicity (useful in patients with unstable heart rhythm oratrial fibrillation), and reduces time of synchronicity assessment.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

860 Clinical applications of 3D echo / New advances in stress echo
5027 Benefit of cardiac resynchronization therapy isdepending on the optimal lead position as defined by3D-Echocardiography
M. Becker1, A. Sasse2, C. Knackstedt1, P. Schauerte1 , R. Hoffmann1,H. Kuehl1, M. Kelm1, A. Franke1 . 1University Hospital Aachen,
Cardiology Dept., Aachen, Germany; 2Aachen, Germany
Background: 3D-Echocardiography (3DE) allows an exact quantitative analysison temporal course of contraction in each single left ventricular (LV) segment.We sought to define in a serial study using 3DE the impact of echocardiographi-cally defined LV lead position on the efficacy of cardiac resynchronization therapy(CRT).Methods: 22 consecutive patients (52±9 years,9 men) with heart failure (HF)were included in the study. 16 patients had an ischemic, 6 patients a non-ischemicheart disease. Echocardiograms were performed before CRT and at 3 monthsfollow-up using a 3D digital ultrasound scanner (iE33, Philips, Andover, MA). Anal-ysis of temporal course of contraction in 16 LV segments (ASE definition) wasperformed offline with using a semiautomatic contour tracing software (LV Analy-sis, TomTec, Unterschleissheim). Based on the resulting volume-time-curves thesegment with the latest minimum of systolic volume in each patient was iden-tified preoperatively (=segment A). Additionally the temporal difference betweenpre- and postoperative minimum of systolic volume was determined (Dts) for eachsegment. The segment with the longest Dts was defined to show the greatest ef-fect of CRT. The location of LV lead position was assumed within this segment(=segment B). LV lead position was defined as optimal when segments A and Bwere equal as non-optimal when they were different.Results: Using this definition 13 patients showed a non-optimal, 9 patients anoptimal LV lead position. Before CRT ejection fraction (EF) and peak oxygen con-sumption (VO2max) were equal in both groups (EF 32+4 vs. 31+6%, VO2max14.3+1.4 vs.14.6+1.5 ml/min/kg). At 3 months follow-up patients with an assumednon-optimal LV lead position showed an increase of 6+3% (EF) and 1.5+0.4ml/min/kg (VO2max), patients with an assumed optimal LV lead position 10+1%(p<0.001) and 2.4+0.3 ml/min/kg(p<0.01).Conclusion: A correspondence of the assumed LV lead position (segment B) andthe segment with the latest preoperative LV contraction (segment A) results in asignificant greater benefit of EF and cardiopulmonary exercise in CRT patients.
5028 Assessment of left ventricular volumes withtransthoracic real-time three-dimensionalechocardiography in patients with a first ST-elevationacute myocardial infarction
V. Delgado, M. Sitges, B. Vidal, M.T. De Caralt, R.J. Perea, M. Heras,M. Azqueta, C. Pare. Hospital clinic, cardiology, Barcelona, Spain
Combination of novel semiautomatic contour detection algorithm and high-resolution transthoracic real-time three-dimensional echocardiography (RT-3DE)has improved the accuracy of the assessment of left ventricular volumes (LVV)avoiding the need of time-consuming off-line postprocessing for volume quantita-tion.Objectives: To compare the accuracy of RT-3DE with a semiautomatic borderdetection algorithm and cardiac magnetic resonance (CMR) for quantitation ofLVV in patients with a first ST-elevation acute myocardial infarction (STEMI).Methods: Nineteen patients with a first STEMI (12 anterior, 5 inferoposterior, 2inferior) were prospectively investigated undergoing a RT-3DE and a CMR withinthe first week from hospital admission. LVV at end-diastole and end-systole wereobtained by both modalities, and the concordance and agreement between themwere compared. Volumes were determined from RT3DE scans using a dedicatedsoftware based on a semiautomatic contour detection algorithm that requires todelineate 5 points in the LV shape. Volumes from CMR were obtained by manuallytracing the endocardial border from LV short axis slices.Results: Mean LVV assessed with RT-3D and CRM were84.4 ± 35.3 ml and 96.2± 47.3 ml, respectively (Range 25-190 ml). Despite RT-3D tended to underesti-mate LVV as compared to CMR (mean difference -12 ± 24 ml), there was a goodcorrelation and agreement between both methods (Figure).
Conclusion: RT-3D in combination with a semiautomatic border detection allowsa rapid and accurate quantitation of LVV among patients with a first STEMI, com-pared to CMR as the reference standard. This technique may be useful as abedside imaging tool to evaluate LVV in the acute setting of STEMI, even in thepresence of LV wall motion and geometrical abnormalities.
NEW ADVANCES IN STRESS ECHO
5029 The diagnostic and prognostic value of tissue Dopplerimaging during dobutamine stress echocardiography inend stage renal disease
R. Sharma1, R.L. Mehta1, S.J.D. Brecker2, D.C. Gaze2,P.O. Collinson2, H. Gregson2, C.H. Streather2, D. Pellerin3.
1Southampton University Hospital, Cardiology, Southampton, United Kingdom;2St Georges Hospital, Cardiology, London, United Kingdom; 3The Heart Hospital,Cardiology, London, United Kingdom
Background: This study aimed to determine whether a quantitative tissueDoppler measurement of peak systolic velocity (PSV) during dobutamine stressecho cardiography (DSE) predicts significant coronary artery disease (CAD) andmortality in patients with end stage renal disease (ESRD).Methods: 140 renal transplant candidates were prospectively studied. An is-chaemic response defined by the development of a new wall motion abnormality(WMA) in one or more resting normal segments or deterioration of wall motionscore in one or more resting hypokinetic segments. Colour tissue Doppler im-ages (TDI) were acquired in digital cine-loop format. The mean PSV in the basaland mid segments of apical 2, 3, 4 chamber views were measured off-line. MeanPSV was compared with visual wall motion and the presence of significant CADat coronary angiography (defined as luminal stenosis > 70% by visual estima-tion).Results: 41 (30%) patients developed an ischaemic response during DSE and40 (29%) had significant CAD. Out of 1542 segments analysed, 134 demon-strated an ischaemic response during DSE as determined by visual analysis.Segments identified as having normal and abnormal wall motion showed signifi-cant differences in mean PSV (8.1±3.6 cm/s and 5.6±3.1 cm/s respectively; p =< 0.001). Mean PSV increased ≥100% in those segments without an ischaemicresponse compared to a 40-70% rise in ischaemic segments. From Receiver Op-erator Characteristic curve analysis, failure of the baseline PSV to rise by 50%predicted an ischaemic response with sensitivity 86% and specificity 90% (AreaUnder Curve 0.79, p = 0.01). Using this TDI cut off value, 42 (31%) patients de-veloped ischaemia during DSE. The sensitivity, specificity and accuracy valuesfor visual analysis of DSE to detect severe CAD were 84%, 91% and 88%. Thesame values for TDI assessment were 86%, 92% and 89% respectively. Forty -six (34%) patients developed ischaemia according to visual or TDI criteria. Forthese patients, the sensitivity, specificity and accuracy to detect significant CADwere 88%, 94% and 91%. There were 21 deaths over a mean follow-up period of2.2 ± 0.7 years. A positive DSE result, as defined by TDI analysis, was associatedwith significantly increased mortality (p = 0.001, log rank test).Conclusion: A fully quantitative interpretation of DSE, using tissue Doppler ve-locities, accurately predicts significant CAD and mortality in patients with ESRD.
5030 Comparison of 2- and 3-dimensional exerciseechocardiography for the detection of coronary arterydisease
P. Pinon, J. Peteiro, R. Perez, D. Perez, R. Estevez, E. Barga,R. Campo, A. Castro-Beiras on behalf of Study supported by theSpanish Network of Cardiovascular Studies (RECAVA). . Juan
Canalejo Hospital, Cardiology, A Coruna, Spain
Although 3-dimensional echocardiography (3-DE) has been applied during dobu-tamine stress echocardiography it has not been used during exercise echocardio-graphy (EE). We sought to evaluate the feasibility and accuracy of 3-DE as com-pared with 2-DE during EE for the prediction of coronary artery disease (CAD)Methods: 80 patients referred for treadmill EE were submitted to both peak (Pk)and post-exercise (PEx) 2-DE, and Pk- and PEx-3DE in separate days. SignificantCAD (≥50% stenosis) was detected in 50 patients (multivessel CAD in 34). Thequality of the studies was assessed by a score that assigned 0 to 3 points to eachwall (apicoseptal, posterolateral, anterior, inferior) according to the visualization ofmyocardial thickness and motion, as followed: 0, bad visualization or not acquired;1, visualization of <70%; 2, visualization of 70-95%; and 3, visualization of 95-100% of the extension of the wall.Results: Feasibility of Pk-2DE, Pk-3DE, PEx-2DE, and PEx-3DE was 99%, 94%,100%, and 97%, respectively. Inter- and intra-observer agreement (positive ornegative EE) was 92% and 88% for Pk-2DE (k=0.83 and k=0.75), 93% and88% for Pk-3DE (k=0.93 and k=0.63), 92% and 88% for PEx-2DE (k=0.85 andk=0.74), and 96% and 87% for PEx-3DE (k=0.96 and k=0.65). Agreement be-tween 2DE and 3DE was 84% at Pk (k=0.68), similar to agreement between2DE and 3DE at PEx (79%, k=0.57). Global imaging quality score was betterwith 2DE (Pk 2.9±0.4, PEx 3.0±0.1), than with 3DE (Pk 2.4±0.8, PEx 2.5±0.8,p<0.0001). Inadequate quality of images (score 0 to 1) were seen in 1% of thewalls by Pk-2DE, in none by PEx-2DE, in 18% by Pk-3DE and in 15% by PEx-3DE (p<0.0001 between 3DE and 2-DE). These scores by wall <2 were morefrequently seen in the inferior and anterior walls in contrast to the septoapicaland posterolateral walls (79% vs. 21%, p<0.0001). Acquisition time was shorterwith 3-DE (Pk 22±8 secs, PEx 15±5 secs) than with 2-DE (Pk 43±14 secs, PEx31±14 secs, p<0.0001 between Pk-3DE and Pk-2DE, p<0.0001 between PEx-3DE and PEx-2DE). Sensitivity was 80% with Pk-2DE, 74% with Pk-3DE, 64%with PEx-2DE, and 55% with PEx-3DE (p=0.01 vs. Pk-2DE). Specificity was sim-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

New advances in stress echo 861
ilar (Pk-2DE 87%, Pk-3DE 83%, PEx-2DE 97%, PEx-3DE 87%). Accuracy was82% with Pk-2DE (AUC 0.86, 95% CI=0.77-0.96), 77% with Pk-3DE (AUC 0.79,95% CI=0.68-0.90), 76% with PEx-2DE (AUC 0.84, 95% CI=0.75-0.94), and 68%with PEx-3DE (AUC 0.73, 95% CI=0.62-0.85; p=0.03 vs. Pk-2DE).Conclusions: 3-DE is feasible during EE but, at present, is not superior to 2-DEexercise echocardiography.
5031 Three-dimensional evaluation of dobutamine-inducedchanges in regional myocardial deformation inischemic myocardium using ultrasonic strainmeasurements: the role of circumferential myocardialshorte
H. Tanaka, Y. Mizuguchi, Y. Oishi, S. Emi, T. Ishimoto, N. Nagase,T. Oki. Higashi Tokushima National Hospital, Cardiovascular Section, Itano,Japan
Early identification of myocardial ischemia during high-dose dobutamine stress(DOB) has important clinical implications. Myocardial strain imaging can evalu-ate regional myocardial contractility in the radial, meridional, and circumferentialdirections. The aim of the present study was to assess precisely the differencesin deterioration of myocardial deformation between the 3 directions in patientswith newly developed myocardial ischemia during high-dose (20 μg/kg/min) DOBinfusion. Color tissue Doppler 2-dimensional images were recorded during DOBinfusion in 20 patients without myocardial ischemia and 25 patients with scinti-graphically diagnosed myocardial ischemia due to left anterior descending coro-nary artery stenosis. In the off-line analysis, systolic radial strain (Sr), longitudinalstrain (Sl), and circumferential strain (Sc) were determined in the anteroseptal andanterolateral left ventricular walls. In 20 patients without myocardial ischemia, thepeak systolic strains significantly increased in all 3 directions during DOB infusionat rates between 5 and 10 μg/kg/min (Sr; 50% to 69%, Sl; 27% to 36%, Sc; 29%to 38%, all p < 0.01) with a greater rate of change in the Sr (1.8 and 1.9 times,respectively, p < 0.001) than in the Sl and Sc. However, the peak systolic strainsdecreased significantly during DOB infusion at rates between 5 and 10 μg/kg/minin all 3 directions (Sr; 56% to 35%, Sl; 27% to 13%, both p < 0.01, Sc; 29% to7%, p < 0.001) with the greatest rate of change in the Sc in 25 patients with newlydeveloped myocardial ischemia.
In conclusion, circumferential myocardial shortening deteriorated to a greater ex-tent during DOB infusion in patients with coronary artery stenosis, and its mea-surement is a promising tool for detecting newly developed ischemia.
5032 Strain rate imaging improves septal analysis in patientswith left bundle branch block undergoing stress echo -an angiographic comparison
L. Hanekom1, M. Burgess2, C. Jenkins1, T.H. Marwick1. 1University OfQueensland, Department Of Medicine, Brisbane, Australia; 2University
of Queensland, Medicine, Brisbane, Australia
Background: Difficulty in distinguishing dyssynchrony due to left bundle branchblock (LBBB) from septal wall motion (WM) abnormalities can compromise theaccuracy of dobutamine echocardiography (DbE) for diagnosis of coronary arterydisease (CAD). Strain rate imaging (SRI) allows measurement of thickening andtiming of contraction. We compared the accuracy of SRI quantitation and colormap assessment with WM scoring (WMS) in pts with LBBB undergoing coronaryangiography.Methods: In 54 pts (21 women, age 64±9yrs) with LBBB and known or sus-pected CAD, undergoing DbE, 40 underwent coronary angiography within 74±43days of DbE (significant CAD = stenosis quantified as >50% by an independentobserver) and 14 with normal WMS were used to define normalcy. Previously de-fined SRI cut-offs were used to assess accuracy of SRI on a segt and pt basis.SRI color maps (SRCM) (at rest, low dose and peak stress) were assessed byan independent observer for color changes indicative of ischemia, and accuracycompared with WMS.Results: Feasibility of SRI was 88% at peak stress. Of 40 pts undergoing angiog-raphy, 31 had CAD (17 with LAD disease). Abnormal segments had significantlylower SR (-0.7±0.5/s vs. -1.4±0.8/s, p<0.0001, AUC 0.83), end systolic strain(ESS) (-8.9±7% vs. -14.3±8%, p<0.0001, AUC 0.73) and higher time to end ofsystole (tes) (0.25±0.06s vs. 0.20±0.05s, p<0.0001, AUC 0.74) and post-systolicindex (PSI) (0.52±0.3 vs. 0.4±0.3, p=0.07, ROC 0.65) at peak stress comparedwith normal segts. Table 1 summarizes the accuracy of SRI parameters and colormaps versus WMS in the diagnosis of CAD.
Table 1
WMS Peak Peak Peak PSI>0.2 SRCMSR<-0.9/s ESS<-9% tes>0.22s
CAD Sensitivity (%) 97 94 90 85 80 82Specificity (%) 56 78 78 25 56 50
p=0.5 p=0.6 p=1 p=1 p=1Normalcy (%) 83 91 78 35 65 62
LAD disease Sensitivity (%) 94 94 72 83 71 80Specificity (%) 56 78 78 25 56 50
p=0.5 p=0.6 p=1 p=1 p=1Normalcy (%) 62 81 84 35 76 84
Conclusion: SRI may improve the accuracy of DbE for the diagnosis of CAD inpts with LBBB, especially in the LAD territory.
5033 Differences in long axis systolic/diastolic couplingresponse to beta-adrenergic stimulation betweenpatients with dilated cardiomyopathy and normals.A stress tissue doppler imaging study
C. Robin, K. Isaaz, Y. Jamon, J. Thevenin, C. Romeyer, A. Da Costa,A. Cerisier, M. Lamaud. University of Saint Etienne, Cardiology, Saint Etienne,France
Background: Mitral anulus early diastolic velocity (Ea) measured by tissueDoppler imaging (TDI) is related to the rate of relaxation. A few invasive studieshave shown that relaxation rate response to beta-adrenergic stimulation is sur-prisingly preserved in dilated cardiomyopathy (DCM) despite attenuated inotropicresponse. However, the interrelationships between inotropic and lusitropic re-sponse to beta-adrenergic stimulation have not been investigated non-invasivelyusing TDI measurements.Methods: Using TDI, we measured Ea and mitral anulus systolic wave velocity(Sa) in 11 normal control subjects (Nls) and 11 patients with dilated cardiomy-opathy (DCM) at baseline conditions and during intravenous dobutamine infusion(max dose 10 microg/kg/min).Results: Baseline Sa and Ea (in cm/sec) were lower in DCM than in Nls (8.9±1.6vs 3.8±1.3 p < 0.0001 and 12.7± 2.5 vs 4.9 ±1.2 p< 0.0001). Stress Sa and Eawere also lower in DCM than in Nls (13.4±1.9 vs 5.3 ±1.9 p< 0.0001 and 16.9 ±2.7 vs 6.7±1.8 p< 0.0001). All stress values were higher than those at baseline ineach group (p < 0.005). The mean percent variation (%) from baseline to stressfor Sa was 53±20 in Nls vs 37±13 in DCM (p =0.04) and was 35±16 in Nls vs35±15 in DCM (ns). From baseline to peak stress, Ea values were linearly relatedto Sa values in each individual of Nls and DCM groups (r = 0.84 to 0.97 in Nls; r =0.85 to 0.96 in DCM, p < 0.0001) but the slope of the linear relation was higher inDCM than in Nls (1.37 vs 0.86, p = 0.019). At peak stress, the correlation betweenEa and Sa values was much higher in the DCM group (r = 0.92, p < 0.0001) thanin the Nls group (r = 0.71, p = 0.01).Conclusion: In DCM patients, the relative magnitude of lusitropic response tobeta-adrenergic stimulation is similar to that of Nls despite a blunted inotropicresponse due to a magnified lusitropy/inotropy interaction in DCM that may com-pensate the loss of intrinsic active relaxation process. These findings should betaken into account when evaluating diastolic function by TDI in heart failure.
5034 Velocity Vector Imaging can be an useful tool in theanalysis of stress echocardiography
J. Gomez De Diego, I. Caso, V. Montero Gato, A. Estevez Paniagua,R. Del Castillo Medina, E. Perez David, M. Moreno Yanguela,M.A. Garcia Fernandez. Hospital Gregorio Maranon, Cardiologia,
Madrid, Spain
Background: Velocity Vector Imaging (VVI) is a new tool that allows the analy-sis of regional myocardial function without the limitation of doppler-angle depen-dence.Methods: We studied the contraction pattern in the transversal short axis atthe mitral valve and the papillary muscle levels in 12 clinical dobutamine echostress studies (7 from normal patients and 5 with ischemic heart disease) with theVVI algorithm (Siemens, CA). VVI draws velocity vectors from the endocardiumspeckle-tracking that can be used to calculate radial velocity, strain, strain rateand radial displacement of the myocardium. The VVI results were compared withthe clinical interpretation of our echo stress experts in a blinded way.
Fig. 1. Segmental analysis (strain) by VVI.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
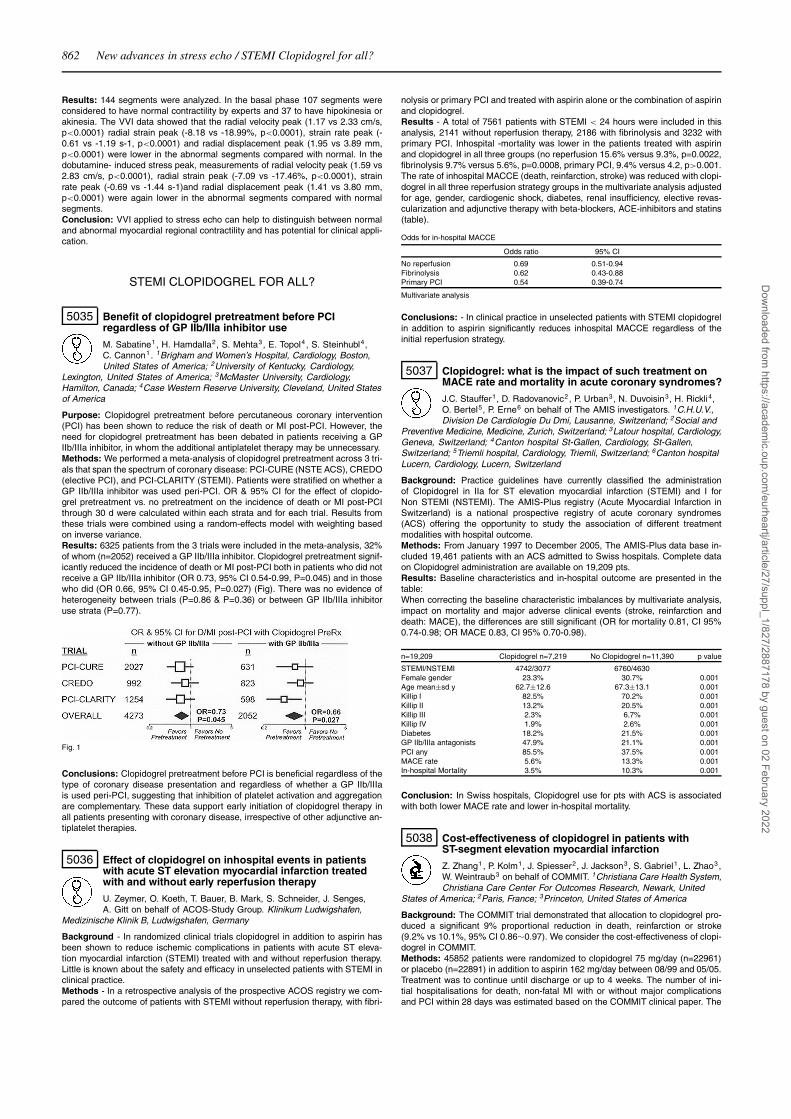
862 New advances in stress echo / STEMI Clopidogrel for all?
Results: 144 segments were analyzed. In the basal phase 107 segments wereconsidered to have normal contractility by experts and 37 to have hipokinesia orakinesia. The VVI data showed that the radial velocity peak (1.17 vs 2.33 cm/s,p<0.0001) radial strain peak (-8.18 vs -18.99%, p<0.0001), strain rate peak (-0.61 vs -1.19 s-1, p<0.0001) and radial displacement peak (1.95 vs 3.89 mm,p<0.0001) were lower in the abnormal segments compared with normal. In thedobutamine- induced stress peak, measurements of radial velocity peak (1.59 vs2.83 cm/s, p<0.0001), radial strain peak (-7.09 vs -17.46%, p<0.0001), strainrate peak (-0.69 vs -1.44 s-1)and radial displacement peak (1.41 vs 3.80 mm,p<0.0001) were again lower in the abnormal segments compared with normalsegments.Conclusion: VVI applied to stress echo can help to distinguish between normaland abnormal myocardial regional contractility and has potential for clinical appli-cation.
STEMI CLOPIDOGREL FOR ALL?
5035 Benefit of clopidogrel pretreatment before PCIregardless of GP IIb/IIIa inhibitor use
M. Sabatine1, H. Hamdalla2, S. Mehta3, E. Topol4 , S. Steinhubl4,C. Cannon1. 1Brigham and Women’s Hospital, Cardiology, Boston,United States of America; 2University of Kentucky, Cardiology,
Lexington, United States of America; 3McMaster University, Cardiology,Hamilton, Canada; 4Case Western Reserve University, Cleveland, United Statesof America
Purpose: Clopidogrel pretreatment before percutaneous coronary intervention(PCI) has been shown to reduce the risk of death or MI post-PCI. However, theneed for clopidogrel pretreatment has been debated in patients receiving a GPIIb/IIIa inhibitor, in whom the additional antiplatelet therapy may be unnecessary.Methods: We performed a meta-analysis of clopidogrel pretreatment across 3 tri-als that span the spectrum of coronary disease: PCI-CURE (NSTE ACS), CREDO(elective PCI), and PCI-CLARITY (STEMI). Patients were stratified on whether aGP IIb/IIIa inhibitor was used peri-PCI. OR & 95% CI for the effect of clopido-grel pretreatment vs. no pretreatment on the incidence of death or MI post-PCIthrough 30 d were calculated within each strata and for each trial. Results fromthese trials were combined using a random-effects model with weighting basedon inverse variance.Results: 6325 patients from the 3 trials were included in the meta-analysis, 32%of whom (n=2052) received a GP IIb/IIIa inhibitor. Clopidogrel pretreatment signif-icantly reduced the incidence of death or MI post-PCI both in patients who did notreceive a GP IIb/IIIa inhibitor (OR 0.73, 95% CI 0.54-0.99, P=0.045) and in thosewho did (OR 0.66, 95% CI 0.45-0.95, P=0.027) (Fig). There was no evidence ofheterogeneity between trials (P=0.86 & P=0.36) or between GP IIb/IIIa inhibitoruse strata (P=0.77).
Fig. 1
Conclusions: Clopidogrel pretreatment before PCI is beneficial regardless of thetype of coronary disease presentation and regardless of whether a GP IIb/IIIais used peri-PCI, suggesting that inhibition of platelet activation and aggregationare complementary. These data support early initiation of clopidogrel therapy inall patients presenting with coronary disease, irrespective of other adjunctive an-tiplatelet therapies.
5036 Effect of clopidogrel on inhospital events in patientswith acute ST elevation myocardial infarction treatedwith and without early reperfusion therapy
U. Zeymer, O. Koeth, T. Bauer, B. Mark, S. Schneider, J. Senges,A. Gitt on behalf of ACOS-Study Group. Klinikum Ludwigshafen,
Medizinische Klinik B, Ludwigshafen, Germany
Background - In randomized clinical trials clopidogrel in addition to aspirin hasbeen shown to reduce ischemic complications in patients with acute ST eleva-tion myocardial infarction (STEMI) treated with and without reperfusion therapy.Little is known about the safety and efficacy in unselected patients with STEMI inclinical practice.Methods - In a retrospective analysis of the prospective ACOS registry we com-pared the outcome of patients with STEMI without reperfusion therapy, with fibri-
nolysis or primary PCI and treated with aspirin alone or the combination of aspirinand clopidogrel.Results - A total of 7561 patients with STEMI < 24 hours were included in thisanalysis, 2141 without reperfusion therapy, 2186 with fibrinolysis and 3232 withprimary PCI. Inhospital -mortality was lower in the patients treated with aspirinand clopidogrel in all three groups (no reperfusion 15.6% versus 9.3%, p=0.0022,fibrinolysis 9.7% versus 5.6%, p=0.0008, primary PCI, 9.4% versus 4.2, p>0.001.The rate of inhospital MACCE (death, reinfarction, stroke) was reduced with clopi-dogrel in all three reperfusion strategy groups in the multivariate analysis adjustedfor age, gender, cardiogenic shock, diabetes, renal insufficiency, elective revas-cularization and adjunctive therapy with beta-blockers, ACE-inhibitors and statins(table).
Odds for in-hospital MACCE
Odds ratio 95% CI
No reperfusion 0.69 0.51-0.94Fibrinolysis 0.62 0.43-0.88Primary PCI 0.54 0.39-0.74
Multivariate analysis
Conclusions: - In clinical practice in unselected patients with STEMI clopidogrelin addition to aspirin significantly reduces inhospital MACCE regardless of theinitial reperfusion strategy.
5037 Clopidogrel: what is the impact of such treatment onMACE rate and mortality in acute coronary syndromes?
J.C. Stauffer1, D. Radovanovic2 , P. Urban3, N. Duvoisin3, H. Rickli4,O. Bertel5, P. Erne6 on behalf of The AMIS investigators. 1C.H.U.V.,Division De Cardiologie Du Dmi, Lausanne, Switzerland; 2Social and
Preventive Medicine, Medicine, Zurich, Switzerland; 3Latour hospital, Cardiology,Geneva, Switzerland; 4Canton hospital St-Gallen, Cardiology, St-Gallen,Switzerland; 5Triemli hospital, Cardiology, Triemli, Switzerland; 6Canton hospitalLucern, Cardiology, Lucern, Switzerland
Background: Practice guidelines have currently classified the administrationof Clopidogrel in IIa for ST elevation myocardial infarction (STEMI) and I forNon STEMI (NSTEMI). The AMIS-Plus registry (Acute Myocardial Infarction inSwitzerland) is a national prospective registry of acute coronary syndromes(ACS) offering the opportunity to study the association of different treatmentmodalities with hospital outcome.Methods: From January 1997 to December 2005, The AMIS-Plus data base in-cluded 19,461 patients with an ACS admitted to Swiss hospitals. Complete dataon Clopidogrel administration are available on 19,209 pts.Results: Baseline characteristics and in-hospital outcome are presented in thetable:When correcting the baseline characteristic imbalances by multivariate analysis,impact on mortality and major adverse clinical events (stroke, reinfarction anddeath: MACE), the differences are still significant (OR for mortality 0.81, CI 95%0.74-0.98; OR MACE 0.83, CI 95% 0.70-0.98).
n=19,209 Clopidogrel n=7,219 No Clopidogrel n=11,390 p value
STEMI/NSTEMI 4742/3077 6760/4630Female gender 23.3% 30.7% 0.001Age mean±sd y 62.7±12.6 67.3±13.1 0.001Killip I 82.5% 70.2% 0.001Killip II 13.2% 20.5% 0.001Killip III 2.3% 6.7% 0.001Killip IV 1.9% 2.6% 0.001Diabetes 18.2% 21.5% 0.001GP IIb/IIIa antagonists 47.9% 21.1% 0.001PCI any 85.5% 37.5% 0.001MACE rate 5.6% 13.3% 0.001In-hospital Mortality 3.5% 10.3% 0.001
Conclusion: In Swiss hospitals, Clopidogrel use for pts with ACS is associatedwith both lower MACE rate and lower in-hospital mortality.
5038 Cost-effectiveness of clopidogrel in patients withST-segment elevation myocardial infarction
Z. Zhang1, P. Kolm1, J. Spiesser2, J. Jackson3, S. Gabriel1, L. Zhao3,W. Weintraub3 on behalf of COMMIT. 1Christiana Care Health System,Christiana Care Center For Outcomes Research, Newark, United
States of America; 2Paris, France; 3Princeton, United States of America
Background: The COMMIT trial demonstrated that allocation to clopidogrel pro-duced a significant 9% proportional reduction in death, reinfarction or stroke(9.2% vs 10.1%, 95% CI 0.86∼0.97). We consider the cost-effectiveness of clopi-dogrel in COMMIT.Methods: 45852 patients were randomized to clopidogrel 75 mg/day (n=22961)or placebo (n=22891) in addition to aspirin 162 mg/day between 08/99 and 05/05.Treatment was to continue until discharge or up to 4 weeks. The number of ini-tial hospitalisations for death, non-fatal MI with or without major complicationsand PCI within 28 days was estimated based on the COMMIT clinical paper. The
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

STEMI Clopidogrel for all? / The strong platelet – fighting platelet resistance 863
CURE papers were used to estimate the number of subsequent hospitalisationsfor death, non-fatal MI, stroke, bleeding, angina and revascularisation between29 days and 1 year. Hospitalisations were assigned a diagnosis-related group(DRG). Costs for each DRG (year 2003) were estimated from Medicare reim-bursement rates. Physician costs were estimated as a % of hospital costs byDRG. Clopidogrel was assumed to be given as 1 year and priced at $3.80/day.Life expectancy gains due to the prevention of death, MI, and stroke were es-timated using Framingham data. Cost-effectiveness analysis was performed asincremental costs per life year gained (LYG).Results: Within 28 days, adding clopidogrel to aspirin is a dominant strategy,lowering event rate without an increase in costs. For the life time period, the in-cremental cost-effectiveness ratio of clopidogrel is $7806/LYG.
Clopidogrel (n=22961) Placebo (n=22891) Difference
Cost ($)28 days 7,745 7,748 -329 days to 1 year 5,968 4,831 1,137Within 1 year 13,712 12,579 1,134
Event rate of death, MI or stroke (%)28 days 9.25 10.12 -0.8729 days to 1 year 5.20 6.30 -1.10Within 1 year 14.45 16.42 -1.97
Life years lost (yrs) 0.7110 0.8562 0.1452
Conclusions: Addition of clopidogrel to aspirin, given up to 1 year, in the settingof ST-segment elevation MI is highly a cost-effective strategy.
5039 A double-blind randomized comparison between twodifferent clopidogrel maintenance doses afterpercutaneous coronary intervention (ISAR-CHOICE 2Trial)
N.V.B. Von Beckerath, A.K. Kastrati, A.W. Wieczorek, G.P.M. Pogatsa-Murray, D.S. Sibbing, A.S. Schoemig. Deutsches Herzzentrum
Muenchen, Cardiology, Muenchen, Germany
Background: Currently a daily dose of 75 mg is the standard dose for chronicclopidogrel therapy. This dose is chosen because it provides a degree of plateletinhibition similar to that achieved by 500 mg of ticlopidine per day. Recently, weshowed that administration of a 600 mg loading dose of clopidogrel in patientsalready on chronic clopidogrel therapy (75 mg/day) results in an additional sig-nificant increase in inhibition of ADP-induced platelet aggregation. We designedthis double-blind randomized trial to test whether an increase of the maintenancedose of clopidogrel from 75 mg to 150 mg per day results in additional suppres-sion of ADP-induced platelet aggregation.Methods: Consecutive patients (n=60) who were treated with elective PCI at leasttwo hours after administration of a 600 mg loading dose of clopidogrel partici-pated in this trial. Exclusion criteria included use of glycoprotein IIb/IIIa antag-onists during the intervention or during the preceding 14 days and therapy withclopidogrel within the last 28 days. After PCI, patients received aspirin and onecapsule containing either 75 or 150 mg of clopidogrel according to the random-ization sequence. Platelet function was evaluated with optical aggregometry atthe 30-day follow-up visit. The primary endpoint of the study was maximal ADP(5μmol/L)-induced platelet aggregation at this follow-up visit.Results: The Figure demonstrates the results of optical aggregometry at the 30-day follow-up visit.
Conclusions: An increase of the daily dose of chronic clopidogrel therapy from75 mg to 150 mg results in additional suppression of ADP-induced platelet ag-gregation. The safety and clinical benefit of using a chronic clopidogrel regimenbased on a daily dose of 150 mg should be evaluated in a large and specificallydesigned clinical trial.
5040 Short term vs. long term therapy with clopidogrel, inPTCA with bare stent, 2 years follow up
V. Bernardi1, J. Szarfer2, J. Ponce1, J. Gabay3, C. Sztejfman4,G. Sumay5, O. Mendiz6, R. Sarmiento7. 1Clinica del Sol, CapitalFederal, Argentina; 2Hospital Argerich, Capital Federal, Argentina;
3Hospital Italiano, Capital Federal, Argentina; 4IMAC Hospital, Capital Federal,Argentina; 5Hospital Churruca, Capital Federal, Argentina; 6Fundacion Favaloro,Capital Federal, Argentina; 7Hospital Frances, Capital Federal, Argentina
Background: The optimal duration of treatment with clopidogrel after PCI withstent placement remains controversial.Methods and Results: RACS is a prospective randomized, non-blinded study of1004 patients (pts) undergoing PCI who were randomized after successful barestent placement to 30 vs. 180 days of clopidogrel. Pts were eligible if they hadpresented with an ST elevation MI, acute coronary syndrome, or stable angina(CSA). The 1° end point was a composite of death, MI and stroke, at 180 days,1 year. The study has 80% power to detect a 21% reduction in events between30 days and 6 months, assuming a 12 month event rate of 23,4% in the groupreceiving therapy for 30 days, with significance at the 0.05 level. Baseline clini-cal characteristics revealed no differences between the groups in terms of age,gender, previous history, risk factors, or incidence of diabetes; 69,5% presentedwith an ACS, 15,7% an MI at study entry. At hospital discharge and 30 days therewere no differences between groups in the frequency of death, MI, or stroke. Theoutcome between 30 days and 1 year among the 921 pts who have completed 1year follow-up is presented at the table.
Table 1. Events from 30 day to 1 year follow up
Events 30 Days Clopidogrel 180 days Cloidogrel p
n 461% (n) 460%(n)Death 4.77 (22) 2.39 (11) 0.051Cardiovascular Death 3.47 (16) 2.17 (10) nsAMI 3.69 (17) 3.04 (10) nsTVR 9.32 (43) 9.57 (44) nsStroke 0.43 (2) 0 nsDeath + AMI+ Stroke 7.59 (35) 4.35 (20) 0.05
Conclusions: This analysis reveals that the reduction in events among ptstreated with long-term clopidogrel has reached statistical significance at 6months, a similar trend was observed at 1 year. 2 year follow-up data will bepresented.
THE STRONG PLATELET – FIGHTING PLATELETRESISTANCE
5041 Association between the effectiveness of differentantiplatelet therapies, fibrinogen levels and ageing in5136 vascular patients
K. Koltai1, G. Feher1 , P. Kenyeres1, T. Alexy2, B. Horvath1,Z.S. Marton1, G. Kesmarky1, K. Toth1. 1Medical School, University of
Pecs, 1st Department of Medicine, Pecs, Hungary; 2USC, School of Medicine,Dept. of Physiology and Biophysics, Los Angeles, United States of America
Purpose: In our present study we investigated the association between the ef-fectiveness of the most widely used antiplatelet therapies (100 and 300-325 mgacetylsalicylic acid (ASA), 75 mg clopidogrel, 500 mg ticlopidine and the combi-nation of 100 mg aspirin and 75 mg clopidogrel), fibrinogen levels and ageing.Methods: Between 2001 and 2005 we measured the effectiveness of antiplatelettherapy in 5136 vascular patients (mean age: 63 ±11 years, 2282 females, 2854males) according to the method of Born in Carat TX-4 aggregometer. Platelet ag-gregation was tested with 5 and 10 μM adenosine-diphosphate, 2 μg/ml collagenand 10 μM epinephrine inducers. Fibrinogen level was measured in 3038 patientsaccording to Clauss’ method. Correlation was detected between maximal aggre-gation, fibrinogen levels and patients’ age. Association was determined betweenthe duration and the effectiveness of antiplatelet therapy in 352 patients.Results: According to our results, the effectiveness of both 100 and 300-325 mgASA decreases significantly with the advancing age (p<0.001). In ASA treatedpatients fibrinogen levels increase with aging (p=0.01 with 300-325 mg ASA,p<0.001 in the case of 100 mg ASA). At the same time there was no associ-ation between antiplatelet effectiveness or fibrinogen levels and aging neither inpatients treated with 75 mg clopidogrel nor with 500 mg ticlopidine. However,in the case of combination therapy with 100 mg aspirin and 75 mg clopidogrelthe association between platelet aggregation and age was similar to that seenin patients treated only with ASA. Fibrinogen levels significantly correlated withplatelet aggregation obtained with all inducers in patients treated with 100 mgASA (p<0.001). No association was found between fibrinogen levels and plateletaggregation in thienopyridine treated individuals. The proportion of aspirin resis-tance is significantly higher when the duration of ASA therapy is longer than 2years than in patients receiving ASA therapy for less than 6 months (p<0.05). Inthe case of thienopyridines the duration of antiplatelet therapy does not affect itseffectiveness.Conclusions: Our results suggest that long-term aspirin therapy is associatedwith a reduction in antiplatelet effect. The elevation of fibrinogen level with agingmay contribute to the decrease of ASA effectiveness associated with older age.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
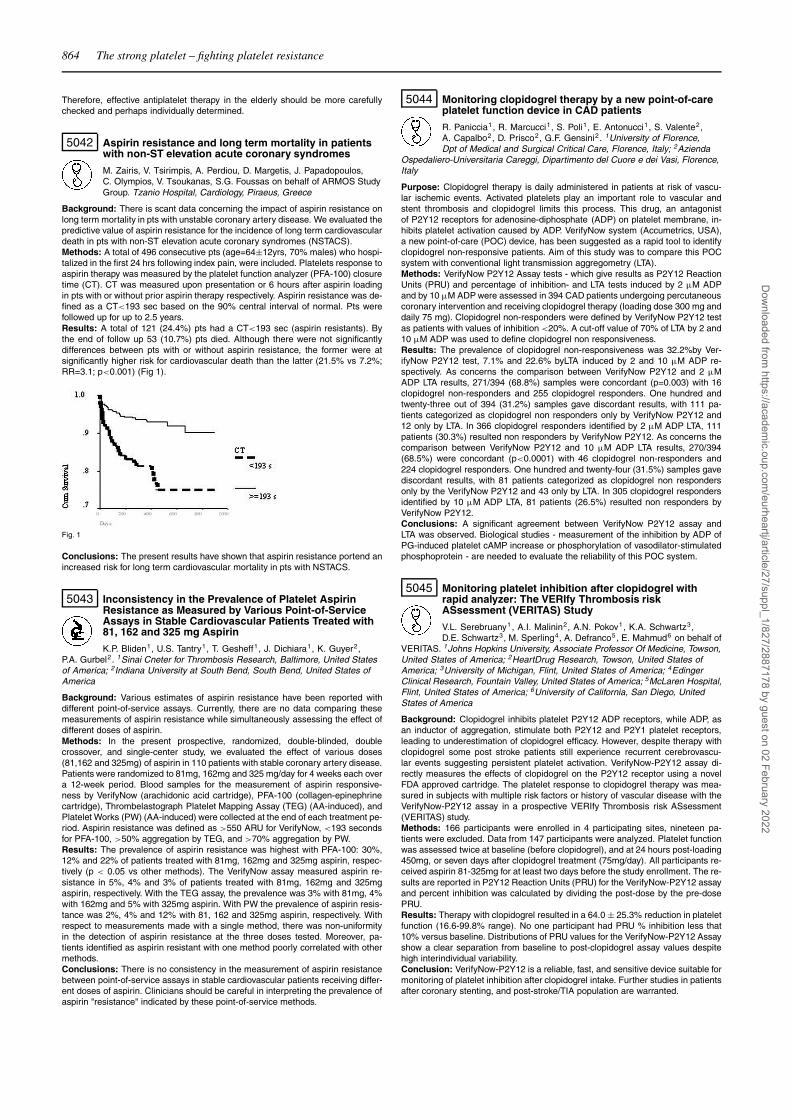
864 The strong platelet – fighting platelet resistance
Therefore, effective antiplatelet therapy in the elderly should be more carefullychecked and perhaps individually determined.
5042 Aspirin resistance and long term mortality in patientswith non-ST elevation acute coronary syndromes
M. Zairis, V. Tsirimpis, A. Perdiou, D. Margetis, J. Papadopoulos,C. Olympios, V. Tsoukanas, S.G. Foussas on behalf of ARMOS StudyGroup. Tzanio Hospital, Cardiology, Piraeus, Greece
Background: There is scant data concerning the impact of aspirin resistance onlong term mortality in pts with unstable coronary artery disease. We evaluated thepredictive value of aspirin resistance for the incidence of long term cardiovasculardeath in pts with non-ST elevation acute coronary syndromes (NSTACS).Methods: A total of 496 consecutive pts (age=64±12yrs, 70% males) who hospi-talized in the first 24 hrs following index pain, were included. Platelets response toaspirin therapy was measured by the platelet function analyzer (PFA-100) closuretime (CT). CT was measured upon presentation or 6 hours after aspirin loadingin pts with or without prior aspirin therapy respectively. Aspirin resistance was de-fined as a CT<193 sec based on the 90% central interval of normal. Pts werefollowed up for up to 2.5 years.Results: A total of 121 (24.4%) pts had a CT<193 sec (aspirin resistants). Bythe end of follow up 53 (10.7%) pts died. Although there were not significantlydifferences between pts with or without aspirin resistance, the former were atsignificantly higher risk for cardiovascular death than the latter (21.5% vs 7.2%;RR=3.1; p<0.001) (Fig 1).
Fig. 1
Conclusions: The present results have shown that aspirin resistance portend anincreased risk for long term cardiovascular mortality in pts with NSTACS.
5043 Inconsistency in the Prevalence of Platelet AspirinResistance as Measured by Various Point-of-ServiceAssays in Stable Cardiovascular Patients Treated with81, 162 and 325 mg Aspirin
K.P. Bliden1, U.S. Tantry1, T. Gesheff1, J. Dichiara1, K. Guyer2,P.A. Gurbel2. 1Sinai Cneter for Thrombosis Research, Baltimore, United Statesof America; 2Indiana University at South Bend, South Bend, United States ofAmerica
Background: Various estimates of aspirin resistance have been reported withdifferent point-of-service assays. Currently, there are no data comparing thesemeasurements of aspirin resistance while simultaneously assessing the effect ofdifferent doses of aspirin.Methods: In the present prospective, randomized, double-blinded, doublecrossover, and single-center study, we evaluated the effect of various doses(81,162 and 325mg) of aspirin in 110 patients with stable coronary artery disease.Patients were randomized to 81mg, 162mg and 325 mg/day for 4 weeks each overa 12-week period. Blood samples for the measurement of aspirin responsive-ness by VerifyNow (arachidonic acid cartridge), PFA-100 (collagen-epinephrinecartridge), Thrombelastograph Platelet Mapping Assay (TEG) (AA-induced), andPlatelet Works (PW) (AA-induced) were collected at the end of each treatment pe-riod. Aspirin resistance was defined as >550 ARU for VerifyNow, <193 secondsfor PFA-100, >50% aggregation by TEG, and >70% aggregation by PW.Results: The prevalence of aspirin resistance was highest with PFA-100: 30%,12% and 22% of patients treated with 81mg, 162mg and 325mg aspirin, respec-tively (p < 0.05 vs other methods). The VerifyNow assay measured aspirin re-sistance in 5%, 4% and 3% of patients treated with 81mg, 162mg and 325mgaspirin, respectively. With the TEG assay, the prevalence was 3% with 81mg, 4%with 162mg and 5% with 325mg aspirin. With PW the prevalence of aspirin resis-tance was 2%, 4% and 12% with 81, 162 and 325mg aspirin, respectively. Withrespect to measurements made with a single method, there was non-uniformityin the detection of aspirin resistance at the three doses tested. Moreover, pa-tients identified as aspirin resistant with one method poorly correlated with othermethods.Conclusions: There is no consistency in the measurement of aspirin resistancebetween point-of-service assays in stable cardiovascular patients receiving differ-ent doses of aspirin. Clinicians should be careful in interpreting the prevalence ofaspirin "resistance" indicated by these point-of-service methods.
5044 Monitoring clopidogrel therapy by a new point-of-careplatelet function device in CAD patients
R. Paniccia1, R. Marcucci1, S. Poli1, E. Antonucci1, S. Valente2,A. Capalbo2, D. Prisco2, G.F. Gensini2. 1University of Florence,Dpt of Medical and Surgical Critical Care, Florence, Italy; 2Azienda
Ospedaliero-Universitaria Careggi, Dipartimento del Cuore e dei Vasi, Florence,Italy
Purpose: Clopidogrel therapy is daily administered in patients at risk of vascu-lar ischemic events. Activated platelets play an important role to vascular andstent thrombosis and clopidogrel limits this process. This drug, an antagonistof P2Y12 receptors for adenosine-diphosphate (ADP) on platelet membrane, in-hibits platelet activation caused by ADP. VerifyNow system (Accumetrics, USA),a new point-of-care (POC) device, has been suggested as a rapid tool to identifyclopidogrel non-responsive patients. Aim of this study was to compare this POCsystem with conventional light transmission aggregometry (LTA).Methods: VerifyNow P2Y12 Assay tests - which give results as P2Y12 ReactionUnits (PRU) and percentage of inhibition- and LTA tests induced by 2 μM ADPand by 10 μM ADP were assessed in 394 CAD patients undergoing percutaneouscoronary intervention and receiving clopidogrel therapy (loading dose 300 mg anddaily 75 mg). Clopidogrel non-responders were defined by VerifyNow P2Y12 testas patients with values of inhibition <20%. A cut-off value of 70% of LTA by 2 and10 μM ADP was used to define clopidogrel non responsiveness.Results: The prevalence of clopidogrel non-responsiveness was 32.2%by Ver-ifyNow P2Y12 test, 7.1% and 22.6% byLTA induced by 2 and 10 μM ADP re-spectively. As concerns the comparison between VerifyNow P2Y12 and 2 μMADP LTA results, 271/394 (68.8%) samples were concordant (p=0.003) with 16clopidogrel non-responders and 255 clopidogrel responders. One hundred andtwenty-three out of 394 (31.2%) samples gave discordant results, with 111 pa-tients categorized as clopidogrel non responders only by VerifyNow P2Y12 and12 only by LTA. In 366 clopidogrel responders identified by 2 μM ADP LTA, 111patients (30.3%) resulted non responders by VerifyNow P2Y12. As concerns thecomparison between VerifyNow P2Y12 and 10 μM ADP LTA results, 270/394(68.5%) were concordant (p<0.0001) with 46 clopidogrel non-responders and224 clopidogrel responders. One hundred and twenty-four (31.5%) samples gavediscordant results, with 81 patients categorized as clopidogrel non respondersonly by the VerifyNow P2Y12 and 43 only by LTA. In 305 clopidogrel respondersidentified by 10 μM ADP LTA, 81 patients (26.5%) resulted non responders byVerifyNow P2Y12.Conclusions: A significant agreement between VerifyNow P2Y12 assay andLTA was observed. Biological studies - measurement of the inhibition by ADP ofPG-induced platelet cAMP increase or phosphorylation of vasodilator-stimulatedphosphoprotein - are needed to evaluate the reliability of this POC system.
5045 Monitoring platelet inhibition after clopidogrel withrapid analyzer: The VERIfy Thrombosis riskASsessment (VERITAS) Study
V.L. Serebruany1, A.I. Malinin2, A.N. Pokov1, K.A. Schwartz3,D.E. Schwartz3, M. Sperling4, A. Defranco5, E. Mahmud6 on behalf of
VERITAS. 1Johns Hopkins University, Associate Professor Of Medicine, Towson,United States of America; 2HeartDrug Research, Towson, United States ofAmerica; 3University of Michigan, Flint, United States of America; 4EdingerClinical Research, Fountain Valley, United States of America; 5McLaren Hospital,Flint, United States of America; 6University of California, San Diego, UnitedStates of America
Background: Clopidogrel inhibits platelet P2Y12 ADP receptors, while ADP, asan inductor of aggregation, stimulate both P2Y12 and P2Y1 platelet receptors,leading to underestimation of clopidogrel efficacy. However, despite therapy withclopidogrel some post stroke patients still experience recurrent cerebrovascu-lar events suggesting persistent platelet activation. VerifyNow-P2Y12 assay di-rectly measures the effects of clopidogrel on the P2Y12 receptor using a novelFDA approved cartridge. The platelet response to clopidogrel therapy was mea-sured in subjects with multiple risk factors or history of vascular disease with theVerifyNow-P2Y12 assay in a prospective VERIfy Thrombosis risk ASsessment(VERITAS) study.Methods: 166 participants were enrolled in 4 participating sites, nineteen pa-tients were excluded. Data from 147 participants were analyzed. Platelet functionwas assessed twice at baseline (before clopidogrel), and at 24 hours post-loading450mg, or seven days after clopidogrel treatment (75mg/day). All participants re-ceived aspirin 81-325mg for at least two days before the study enrollment. The re-sults are reported in P2Y12 Reaction Units (PRU) for the VerifyNow-P2Y12 assayand percent inhibition was calculated by dividing the post-dose by the pre-dosePRU.Results: Therapy with clopidogrel resulted in a 64.0 ± 25.3% reduction in plateletfunction (16.6-99.8% range). No one participant had PRU % inhibition less that10% versus baseline. Distributions of PRU values for the VerifyNow-P2Y12 Assayshow a clear separation from baseline to post-clopidogrel assay values despitehigh interindividual variability.Conclusion: VerifyNow-P2Y12 is a reliable, fast, and sensitive device suitable formonitoring of platelet inhibition after clopidogrel intake. Further studies in patientsafter coronary stenting, and post-stroke/TIA population are warranted.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

The strong platelet – fighting platelet resistance / Molecular biology of atrial fibrillation 865
5046 Platelet inhibition with prasugrel (CS-747) versusclopidogrel: the JUMBO platelet substudy
V.L. Serebruany1, M.G. Midei2, H. Meilmann2, A.I. Malinin3,D.L. Lowry3. 1Johns Hopkins University, Associate ProfessorOf Medicine, Towson, United States of America; 2Midatlantic
Cardiovascular, Towson, United States of America; 3HeartDrug Research,Towson, United States of America
Background - Based on the preclinical and Phase 1 studies, prasugrel, a novelplatelet ADP P2Y12 receptor blocker, may be a more potent platelet inhibitor thanclopidogrel. We compared the antiplatelet properties of prasugrel and clopidogrelin a Phase 2 randomized trial (JUMBO).Methods - One hundred seventy eight patients undergoing coronary stentingwere screened, and nine were randomized to the study. Aspirin and GP IIb/IIIainhibitors were allowed. Platelet activity was assessed at baseline, at 4, and 24hours, and at 30 days after stent implantation in substudy participants, and com-pared to 124 historic controls who received clopidogrel.Results: Independent of the loading, or maintenance dose, patients treated withprasugrel exhibited significantly more potent platelet inhibition as determined byADP- (p=0.002), and collagen-induced aggregation (p=0.0001), Ultegra Analyzer(p=0.003), and surface expression of PECAM-1 (p=0.006), GPIIb/IIIa antigen(p=0.04), and activity with PAC-1 antibody (p=0.002), GPIb (p=0.008), P-selectin(0.002), CD40-ligand (p=0.01), GP37 (p=0.007), and thrombospondin receptorexpression (p=0.003) when compared with those treated with clopidogrel. Therewere no differences between antiplatelet agents with regard to vitronectin, LAMP-1, PAR-1 (intact and cleaved epitopes) thrombin receptor expression, or formationof platelet-monocyte microparticles. Expression of GPIIb antigen, vitronectin, andLAMP-3 receptor were not affected by both agents. Two patients treated with pra-sugrel 10 mg/daily exhibited complete inhibition of collagen-induced aggregationat 30 days.Conclusion: At the dosing regimens chosen in the JUMBO trial, it appears thatprasugrel is a more potent antiplatelet agent than clopidogrel. Two episodesof profound platelet inhibition, which are not observed with clopidogrel, raisethe possibility of higher bleeding risks especially during chronic prasugrel use.Whether stronger platelet inhibition will yield better clinical outcomes and/or in-creased bleeding remains to be determined in an ongoing comparative Phase 3superiority trial (TRITON).
MOLECULAR BIOLOGY OF ATRIAL FIBRILLATION
5047 Chronic atrial fibrillation and pacemaker current, IF: anelectrophysiological, molecular and pharmacologicalstudy in human atrium
F. Stillitano1, G. Lonardo1, G. Giunti2, P.L. Stefano1, E. Cerbai2,A. Mugelli3. 1Center of Molecular Medicine C.I.M.M.B.A., University
of Firenze, Firenze, Italy; 2Azienda Ospedaliero-Universitaria Careggi, Unitof Cardiosurgery, Firenze, Italy; 3Center of Molecular Medicine C.I.M.M.B.A.,University of Florence, Firenze, Italy
Background: Chronic atrial fibrillation (AF) involves functional remodeling of hu-man atrial myocytes (HuAM) associated with changes in ion channel expres-sion. The Hyperpolarization-activated, Cyclic Nucleotide-gated current IF, codedby HCN genes, is constitutively present in HuAM and over-expressed in manycardiac diseases at ventricular level, where it might exert a proarrhythmic role.However, little is known about changes in IF expression in fibrillating atria. Thus,we assessed the biophysical properties of IF, mRNA and protein expression ofcorresponding HCN isoforms, in right atrial appendages obtained from patientsin sinus rhythm (SR) and suffering from chronic (>1 year) AF, undergoing cardiacsurgery.Methods and results: HuAM were isolated from samples and utilized for patch-clamp recording. mRNA level of HCN2 and HCN4 isoforms was measured byReal-Time PCR. Protein amount was evaluated by Western Blot. Membrane ca-pacitance (Cm) and IF amplitude measured at -120 mV (p<0.01 and p<0.02, re-spectively) were both significantly increased in HuAM from AF group. Maximal IFdensity (amplitude normalized vs. Cm) was unchanged (SR: 2.9±0.1 pA/pF; AF:3.3±0.6 pA/pF). Activation curve of IF was slightly shifted toward less negativepotentials in AF vs. SR group (midpoint: -86.5±2.2 and -90.0±1.3 mV, respec-tively; n.s.). No changes in mRNA expression and protein amount of HCN2 weredetected in AF samples, while HCN4 expression was decreased at mRNA (86%of SR, p<0.0001) and protein level (40% of SR, p<0.02). Pharmacological stim-ulation of Gs-coupled receptors (β1- and β2-adrenergic and 5-HT4 receptors),which increases intracellular cAMP levels, significantly and equally shifted IF acti-vation curve in both groups. Atrial natriuretic peptide (ANP), which positively mod-ulates IF through the stimulation of guanylate cyclase-coupled receptors, eliciteda smaller effect in HuAM from AF patients (p<0.02).Conclusions: Detailed analysis of biophysical, pharmacological and molecularproperties of IF in atrial specimens demonstrates that chronic AF causes com-posite modifications, such as a selective down-regulation of HCN4 isoform (atmRNA and protein level) and ANP receptor system. The proarrhythmic role of IFin AF remains controversial, and might be clinically evaluated by using F-channelblockers.
5048 Induction of heat-shock response protects fromtachycardia induced T-Type Ca2+ channel remodeling
B.J.J.M. Brundel1, X.Y. Qi2, D. Chartier1, R.H. Henning2,H.H. Kampinga2, S. Nattel1. 1University Medical Center Groningen,Radiation And Stress Cell Biology, Groningen, Netherlands; 2Montreal
Heart Institute, Montreal, Canada
Background: There is evidence that heat shock proteins (Hsps) protect againstcardiac injury and remodeling in a variety of clinically-relevant paradigms. Wefound a prominent T-type Ca2+ current in HL-1 atrial myocytes and evaluated theeffect of Hsp induction on tachycardia-induced T-type Ca2+ channel remodeling.Methods: We studied the effects of tachycardia in HL-1 myocytes (3 Hz, 0-4 hrs)on T-type Ca2+ current (ICaT) and corresponding calcium transients (CaT), withand without Hsp-inducing pre-treatment including heat-shock pretreatment (20min 43°C + 16 h 37°C), the heat shock stress response co-inducer geranylger-anylacetone (GGA, 10 μM, 2 hrs before and during pacing) or transient transfec-tion with constructs encoding human Hsp70 wildtype (wt), human Hsp27wt or theHsp27 phosphorylation-altered mutants pHsp27AAA (phosphorylation deficient),or Hsp27DDD (phosphorylation mimicking).Results: Pacing significantly and progressively reduced ICaT in HL-1 myocytes by56% after 4 hours of pacing, with associated decreases in CaT by 61%. Both HSpre-treatment and GGA treatment before and during pacing almost completelyprevented tachycardia-induced reductions in ICaT and CaT. Myocytes transfectedwith Hsp27wt or Hsp27DDD were also protected against ICaT and CaT reductions,in contrast to Hsp70 and Hsp27AAA transfected myocytes, for which no preven-tion was observed, indicating that Hsp27 is sufficient for protection and protectionis phosphorylation dependent.Conclusions: Augmentation of Hsp expression, especially Hsp27, protectsagainst tachycardia-induced reductions in T-type Ca2+ channel and Ca2+ tran-sients in a tachy-paced atrial cell model. These findings support the hypothesisthat Hsp may be an important endogenous suppressor of clinically-relevant car-diac remodeling and provide a potential rationale for Hsp system manipulation fortherapeutic prevention of remodeling-promoted conditions like AF.
5049 Increased expression of atrial adenosine A2A receptorscontributes to abnormal sarcoplasmic reticulumcalcium handling in patients with atrial fibrillation
L. Hove-Madsen1 , C. Prat1, A. Llach1, C.E. Molina1, C. Lluis2,F. Ciruela2, R. Franco2 , J. Cinca1. 1Hospital de la Santa Creu i Sant
Pau, Cardiology, Barcelona, Spain; 2Universidad de Barcelona, Biochemistryand Molecular Biology, Barcelona, Spain
Atrial fibrillation induces remodeling of membrane receptors and alterations incAMP-dependent regulation of sarcoplasmic reticulum calcium handling.Purpose: To investigate whether expression and function of adenosine A2A re-ceptors (A2AR), known to regulate cAMP production, were altered in atrial my-ocytes from patients with atrial fibrillation.Methods: Atrial tissue was obtained from 46 patients undergoing cardiac surgery.Twenty-three patients had atrial fibrillation whereas 33 did not have this arrhyth-mia. Immunolabelling, real time PCR, and western blotting were used to study theexpression of the A2AR. Effects of A2AR stimulation on spontaneous calcium re-lease from the sarcoplasmic reticulum (Ca-sparks and Ca-waves) were assessedin fluo-4 loaded atrial myocytes using confocal microscopy. The inward Na-Caexchange current induced by spontaneous calcium release was recorded usingperforated patch-clamp technique.Results: Expression of the functional dimeric form of the A2AR was increasedfour-fold in patients with atrial fibrillation. In these patients, agonist stimulation ofthe A2AR with 200 nM CGS21680 increased the frequency of both spontaneouscalcium waves (from 2.2±0.8 to 14.3±3.3 waves/min, p=0.01) and spontaneousNa-Ca exchange currents (from 3.2±1.1 to 8.3±2.1 currents/min, p<0.04). Incontrast, atrial myocyes from patients without atrial fibrillation did not exhibit sig-nificant changes in calcium wave (0.6±0.3 vs. 3.0±1.3 waves/min) or Na-Ca ex-change current frequency (1.0±0.3 vs. 1.7±0.8 currents/min) under CGS21680stimulation. The stimulatory effect of CGS21680 on spontaneous calcium releasein myocytes from patients with atrial fibrillation was not associated with alterationsin calcium spark amplitude (1.49±0.13 vs. 1.54±0.11), decay of calcium sparks(42±5 vs. 52±6 ms), or caffeine releasable sarcoplasmic reticulum calcium con-tent at rest (6.9±0.6 vs. 7.0±0.4 amol/pF).Conclusions: Atrial myocytes from patients with atrial fibrillation show an in-creased expression of atrial adenosine A2A receptors. These receptors have thepotential to increase spontaneous calcium release from the sarcoplasmic reticu-lum and therefore, may contribute to the reported abnormal calcium handling inmyocytes from the fibrillating human atrium.
5050 Losartan prevents stretch induced electricalremodelling in cultured atrial myocytes
C. Zobel1 , E. Saygili1, O.R. Rana1, H. Reuter1, J. Muller-Ehmsen1,R.H. Schwinger2. 1University of Cologne, Clinic III for InternalMedicine, Cologne, Germany; 2Clinic Weiden, Clinic II for Internal
Medicine, Weiden, Germany
Background: Atrial fibrillation (AF) is the most frequent arrhythmia found in clin-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

866 Molecular biology of atrial fibrillation / Electrophysiological imaging studies. New insights with new tools
ical practice. In recent studies, a decrease in the development or recurrence ofAF was found in patients with hypertension treated with angiotensin-convertingenzyme (ACE) inhibitors or angiotensin receptor-blocking agents (ARBs). Hyper-tension is related to an increased wall tension in the atria resulting in increasedstretch on the level of the individual myocytes which is one of the major stimuli forthe remodelling process.Aims: In the present study we used a model of cultured stretched atrial neonatalrat cardiomyocytes to provide insight in the mechanisms resulting in the preven-tive effect of the ARB losartan against AF on a molecular level.Methods: Static stretch was applied for 48h. Hypertrophy was assessed by mea-surement of protein/DNA ratio and ANP mRNA expression. Ion channels (IK1 andIto) were characterised on mRNA and current density level.Results: Stretch induced a significant increase in protein/DNA ratio (control(n=12) 1 vs. stretch (n=12) 1.16±0.026, p<0.05) and ANF mRNA expression(control (n=5) 1 vs. stretch (n=5) 1.49±0.02, p<0.05) indicating hypertrophy. Ex-pression of genes encoding for IK1 were significantly increased (Kir2.1: control(n=5) 1 vs. stretch (n=5) 1.14±0.03, p<0.05); Kir2.2: not detected; Kir2.3: control(n=5) 1 vs. stretch (n=5) 2.77±0.10, p<0.05). In contrast, mRNA expression ofKv4.2 was significantly reduced in stretched myocytes (control (n=5) 1 vs. stretch(n=5) 0.5±0.03, p<0.05). The alterations on the level of gene expression cor-related with the corresponding current densities. IK1 density at -130 mV was in-creased in stretched myocytes (control (n=6) -10.82±0.79 pA/pF vs. stretch (n=6)-28.2±1.77 pA/pF, p<0.05) while Ito density at +60 mV was reduced (control(n=6) 4.09±0.11 pA/pF vs. stretch (n=5) 3.21±0.18 pA/pF, p<0.05). Treatmentof stretched myocytes with the ARB losartan (1μM) prevented stretch inducedincreases in protein/DNA ratio (1.03±0.01, p<0.05) and ANP mRNA expression(1.02±0.02, p<0.05). The stretch induced increase in IK1 density ((n=5) -15.81pA/pF, p<0.05) and gene expression (Kir 2.3 (n=5) 1.64±0.06, p<0.05) was at-tenuated in the presence of losartan. Alterations in Ito function ((n=5) 5.06±0.06pA/pF, p<0.05) and gene expression (Kv4.2 (n=5) 1.39±0.01, p<0.05) were pre-vented as well.Conclusion: Prevention of stretch induced electrical remodelling might contributeto the clinical effects of losartan against atrial fibrillation.
5051 Tissue plasminogen activator in human atrialfibrillation: effects of angiotensin-converting enzymeinhibitors
E.H. Hatzinikolaou, D. Tziakas, D. Floros, D. Stakos, A. Hotidis,G. Chalikias, A. Mavridis, D.I. Hatseras. Demokritus University ofThrace, Academic Cardiology Department, Alexandroupolis, Greece
Aim: The aim of this study was to evaluate 1) whether the tissue-plasminogenactivator (tPA) is reduced in human atrial fibrillation (AF) indicative of reducedfibrinolytic activity which is probably an additional risk of thrombogenicity and2) whether angiotensin-converting enzyme (ACE) inhibition favorably alters thefibrinolytic balance probably regulated by bradykinin (BK).Methods: Sixty-five patients (pts) with paroxysmal lone AF were randomly as-signed to two groups. Thirty-three pts were treated with the ACE inhibitor (ACE-G) {perindopril for a duration of one month} and 32 pts were not treated with theACE inhibitor (non-ACE-G). All of the pts underwent an electrophysiology studyfor ablation procedure and they were catheterized for taking blood samples fromthe aorta (Ao) and coronary sinus (CS) simultaneously. We measured the tPA ac-tivator levels and the plasminogen activator inhibitor-1 (PAI-1) levels at baselineand after graded doses of sodium nitroprusside (SN) (7.5 to 60 μg/min), and BK(0.2 to 0.5 and 2.0 μg/min for 3 min) administered into the Ao. We performed TEEin all patients and we followed them for a period of 38 ±5 months.Results: The tPA antigen levels at the Ao were similar to those in CS inboth groups but in the non-ACE-G were significantly lower than that in ACE-G(p<0.0001). The level of PAI- 1 in either the Ao or the CS did not differ betweenthe two groups but there was a trend towards to be higher in the non-ACE-G(p<0.075). BK induced an increase in the release of the net tPA in both groups.The extent of that increase was significantly greater in the ACE-G than in the non-ACE-G (p<0.0002). With an increase in BK dosage, the level of PAI-1 in the CStended to decrease compared to that in the Ao in both groups; however there wasa trend towards to a greater decrease in the non-ACE-G (p=0.087). These effectscould not be attributed to changes in blood flow because doses of equivalent po-tency of the vasodilator SN did not increase tPA. The TEE detected thrombusformation in 5 pts (16%) in non-ACE-G and in none patient in ACE-G.Conclusions: The human AF is associated with reduced levels of tPA without anysignificant change in PAI-1 levels in human vasculature. Intraarterial infusion ofBK stimulates tPA release without causing any change in PAI-1 levels. In addition,this effect of BK is augmented in pts treated with an ACE inhibitor. The ACEinhibitor stimulates the tPA release without causing any change in PAI-1 levelsprobably through the BK pathyway.
5052 Effects of renin angiotensin system blockade on atrialremodeling and the second factor in a goat model ofatrial fibrillation
M.C.S. Hall1, S. Kirubakaran1, N.S. Peters2, C.J. Garratt1.1Manchester Royal Infirmary, Manchester Heart Centre, Manchester,
United Kingdom; 2St. Mary’s Hospital, London, United Kingdom
Several groups have suggested that atrial remodeling and AF self-perpetuationmay be suppressed by renin angiotensin system (RAS) blockade. Published workis limited by short-term protocols, high doses of RAS blockers and confoundingeffects of LV impairment. We evaluated candesartan in a long-term goat model oflone AF in which electrical remodeling and second factors are well characterisedand in which candesartan is orally active.Methods: We adapted Wijffels’s goat model to deliver atrial burst pacing via apacemaker-based system. The effect of RAS blockade on acute electrical remod-eling was assessed in 24 goats (12 candesartan 0.5mg/kg/day, 12 placebo) dur-ing a 4 week protocol. Atrial refractory period (AERP) and AF stability (durationof induced AF episodes) were measured. To assess the effects of RAS blockadeon second factors, 16 of these goats underwent further 4 week periods of burstpacing (total 2 months in 16 goats, 3 months in 8 goats) each separated by 7days of sinus rhythm.Results: There was no effect of candesartan on acute electrical remodeling; thehalf time (for AERP to fall to half of the difference between baseline and nadir)was 20.0±4.7 hours (placebo) and 18.3±2.5 hours (candesartan) (p=ns). Therewas a progressive increase in AF stability from month 1 to month 3 in both groups(ANOVA p<0.05) but there was no difference between candesartan and controlgroups (Figure).
Conclusion: This study found no effect of RAS blockade on acute electrical re-modeling or AF self-perpetuation due to second factors in a chronic goat modelof lone AF. These findings suggest that the benefit of RAS blockade seen in se-lected patients with AF is likely to be due to improvements in haemodynamics orleft ventricular function rather than any direct effects on the remodeling processitself.
ELECTROPHYSIOLOGICAL IMAGING STUDIES. NEWINSIGHTS WITH NEW TOOLS
5053 3D myocardial scar reconstruction based on delayedenhancement MRI; comparison with electroanatomicmapping in patients with ventricular tachycardia andchronic myocardial infarction
A. Codreanu1, F. Odille2, M. Andronache2 , I. Magnin-Poull2, C. DeChillou2, P.-Y. Marie2, J. Felblinger1, E. Aliot2. 1University Hospital, CardiologyDept., Nancy, France; 2INSERM ERI 13, Nancy, France
Purpose: Electroanatomic mapping (CARTO™) of myocardial scar substantiallyhelps the identification of target sites for radiofrequency (RF) ablation of ventric-ular tachycardia (VT) of ischemic origin. The aim of the study was to analyze therelation between left ventricular (LV) pathologic areas in CARTO and the 3D scarmap based on MRI with delayed enhancement (DE).Methods: Seven patients with VT and chronic myocardial infarction were studiedby: (i) 3D CARTO in sinus rhythm (87 to 268 points/patient), with analysis of thetopography and extent of areas defined by the <0.5 mV, 0.5 - 1.5 mV and 1.5 - 2.0mV bipolar amplitude thresholds; (ii) MRI with 3D DE analysis. A 3D MRI recon-struction of the LV was created using the MATLAB software, providing informationon the topography of myocardial scars, on their position within the ventricular wall(endocardial, intramural, epicardial) and allowing for quantification of their areaand transmural extent. The transmural extent of the scar for the areas defined inCARTO was so calculated.Results: Good agreement was found between the endocardial scar in MRI andthe <1.5 and <2.0 mV areas (r2>0.85), but not with the <0.5 mV area. All pa-tients had distinct amounts of intramural (20±11%) and subepicardial (6±5%)scar, unsuspected in CARTO. The transmural extent of the scar was highly het-erogeneous within any of the pathologic areas defined in CARTO (Figure: endo-cardial = yellow; transmural = red; strictly intramural = dark green). Endocardialscar car still represented 35±15% of the 1.5 - 2.0 mV areas.Conclusions: 3D MRI endocardial scar correlates well with the pathologic areas
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Electrophysiological imaging studies. New insights with new tools 867
3D MRI scar map compared to CARTO
in CARTO. MRI provides supplemental information on the transmural extent ofthe scar and its’ location within the ventricular wall.
5054 Three-dimentional electroanatomic voltage mappingand histologic evaluation of patients undergoingcatheter ablation of right ventricular outflow tracttachycardia
D. Corrado1, C. Basso2, L. Leoni2 , P. Turrini2, A. Ramondo2, G. Buja2,S. Iliceto2, G. Thiene1. 1University Hospital of Padova, University of
Padova, Padova, Italy; 2Institute of Pathological Anatomy, University of Padova,Padova, Italy
Background: Distinction between patients with idiopathic right ventricular out-flow tract (RVOT) tachycardia and arrhythmogenic right ventricular cardiomyopa-thy/dysplasia (ARVC/D) is critically important because it implies different clini-cal outcome and management strategy. The aim of the present study was touse 3-D electroanatomic voltage mapping in combination with endomyocardialbiopsy (EMB) in patients presenting with RVOT tachycardia to test whether atleast some cases of this tachycardia that have been classified as "idiopathic" af-ter non-invasive evaluation, in fact represent an early stage or a form frusta ofARVC/D.Methods: The study population comprised 27 consecutive patients (15 males and12 females, age 33.9±8 years) with recurrent RVOT tachycardia and no echocar-diographic evidence of RV dilatation/dysfunction, who were referred for charac-terization of the ventricular tachycardia (VT) substrate and catheter ablation. Allpatients underwent detailed invasive-study including activation and voltage map-ping and EMB for histological study.Results: Activation mapping showed that all VTs arose from the RVOT in all pa-tients: anteroseptally in 14, anterolaterally in 9, posterolaterally in 3, and close tothe His bundle in one. Voltage mapping was normal in 20 of 27 patients (74%,Group A), with electrogram voltage > 1.5 mV throughout the RV. The other 7patients (26%, Group B), showed 2±1.4 electroanatomic scar areas (bipolar volt-age <0.5 mV) that correlated with histopathologic evidence of fibrofatty myocar-dial replacement at endomyocardial biopsy (p<0.0001). Two patients had a seg-mental RVOT involvement, while the remaining 5 patients showed multiregionalelectroanatomic scars. Independent predictors of scar were right precordial QRSprolongation (p<0.001) and VT inducibility at programmed ventricular stimula-tion (p <0.01). Catheter ablation successfully eliminated VT in 18 of 20 patients(90%). During a follow-up of 36±4 months, 3 out of 7 patients (57%) from GroupB received an ICD after having experienced syncope or cardiac arrest, whereasall patients from Group A had an uneventful outcome (p=0.016).Conclusions: Early/minor form of ARVC/D may present clinically as RVOT tachy-cardia in absence of RV dilatation/dysfunction, thus mimicking idiopathic RVOTtachycardia. Three-D electroanatomic voltage mapping is able to identify suchsubclinical ARVC/D variants by detecting RV electroanatomic scars that correlatewith diagnostic histopathologic features of the disease and may predispose tolife-threatening arrhythmias.
5055 Evaluation of a new 3D mapping system to guidecommon flutter ablation and validate cavotricuspidisthmus block
A. Bortone, N. Combes, J.C. Macia, F. Leclercq, J.L. Pasquie. CHU Ade Villeneuve, Montpellier, France
Introduction: Radiofrequency catheter ablation (RF) of common atrial flutter is aneveryday practice procedure whose definite endpoint is creation of cavotricuspidisthmus (CTI) block. However, in various circumstances CTI ablation may still bechallenging and validation of CTI block requires extreme accuracy. The aim ofour study is to assess the efficiency and accuracy of the 3D Realtime PositionManagement System (RPM) for anatomic guidance of common flutter ablationand validation of post-ablation CTI block.Methods: 15 patients (64 ± 12 yo, 11M, 4 F) underwent common right atrial (RA)flutter ablation guided by the 3D electroanatomic mapping system RPM (versionRPMi:0, Boston Scientific) based on an ultrasound technique. Catheter ablationwas performed during flutter in 12 patients and in sinus rhythm in 3 patients. Two7F reference catheters were positioned at the RV apex and in the coronary sinus(CS) respectively. Mapping and ablation were performed with a 7F temperature-
controlled 5 mm-tip quadripolar catheter (BLAZER RPMÔ, Boston Scientific). Atthe beginning of the procedure, reconstruction of the RA and CS shell was per-formed during flutter (n=12) or in sinus rhythm (n=3) in order to guide ablation linecreation within the CTI. At the end of the procedure, validation of CTI block wasassessed during pacing from the proximal CS by a conventional electrophysio-logical approach and compared to the activation and propagation maps obtainedwith the RPM system.Results: The RPM system allowed precise anatomic reconstruction of the RA inless than 30 minutes in all patients and accurate catheter positioning along theablation line. RF ablation was successfully achieved in all patients with creationof CTI block. However, in 5 patients conversion to an irrigated-tip catheter wasnecessary to obtain complete CTI block. Assessment of CTI block with the RPMsystem provided a rapid and clear visualization of the activation fronts and wastotally identical to the results obtained by conventional electrophysiological mea-surements. Mean total procedure time was 100.4 ± 37.5 min with a mean totalfluoroscopy exposure of 18.9 ± 11.7min (including catheter positioning).Conclusion: The RPM system appeared an accurate 3D reconstruction and navi-gation system. Data obtained from the activation map were highly concordant withstandard EP techniques in validating CTI block. Moreover, use of this system wasassociated to rapid map reconstruction and a short fluoroscopy exposure aftercatheter positioning.
5056 Abnormal low voltage areas in patients with rightventricle outflow tract arrhythmia- are they associatedwith arrhythmia’s characteristics?
S. Nowak, A. Hoffmann, C. Czerwinski, A.M. Wnuk-Wojnar, A. Rybicka-Musialik, I. Wozniak-Skowerska, K. Szydlo, M. Trusz-Gluza. Silesian
Medical University, I Dept. Of Cardiology, Katowice, Poland
Background: Electroanatomical voltage mapping in patients (pts) with right ven-tricle outflow tract arrhythmia (RVOT), provides insight into the size and locationof electrical abnormalities of endocardium, which are sometimes present despitenormal ECG, echocardiography and even magnetic resonance imaging (MRI).Therefore, the purpose of our study was to analyze voltage maps of RV recordedin pts with RVOT and correlate presence and size of endocardial voltage abnor-malities with arrhythmia’s characteristics.Methods and results: Between 2001and 2006 72 consecutive pts (43 woman,mean age 36±18) with severely symptomatic RVOT (sustained/non-sustainedVT, polymorfic VT-pVT, frequent premature ventricular beats-PVB) underwentcathether ablation with the use of CARTO system. All pts had arrhythmia withLBBB morphology and an inferior axis. One pt had sustained polymorfic VT trig-gered by PVB, cardiac arrest and ICD implanted. No structural heart disseasewas detected by physical examination, ECG and echocardiography. MRI per-formed in 16 cases showed no signs pointing ARVD/C. A 3-D voltage map ofRV was obtained. Low voltage areas, defined as regions of bipolar electrograms< 1,8mV were found in 17 pts (24%) and ranged from 6 to 52 cm2. Areas of bipo-lar electrograms<0,5mV (assumed as a scar) were present in 11 pts (15%). Allmentioned above areas were measured with "area measurement"- application ofCARTO-Merge system.In vast majority "scar" area didn’t exceed 3,5 cm2 but in 1 pt it was 23,8cm2 (pthad sustained pVT triggered by PVB, cardiac arrest and ICD implanted) In all ptsearliest activation sites were located in the scar area or in tranzition zone betweenlow voltage and scar area, on anterior RVOT wall.
Low-voltage areas-distribution in pts
Area < 10cm2 Area > 10cm2
Number of pts 7 10Arrhythmia’s characteristics PVB’s Couplets, triplets, nsVT - 6 pts
pPVBs (2 morphologies) - 1 ptMonomorphic VT - 2 ptsPolymorphic VT - 1 pt
Conclusions: In pts with RVOT arrhythmia abnormal low voltage areas in RV oc-cur but are not frequent. They usually correspond with arrhythmia’s site of origin.Large areas and/or presence of multiple low voltage regions are observed in ptswith malignant outcome. Further follow-up will show if such findings can predictfuture development of ARVD/C.
5057 A comparison of two different diagnostic strategies forcatheter ablation using the magnetic navigation system
S. Ernst, K.J.R. Chun, F. Ouyang, A. Ujeyl, B. Koektuerk, A. Metzner,M. Antz, K.H. Kuck. St. Georg Hospital, Ii. Med. Abteilung/CardiologyDept., Hamburg, Germany
The magnetic navigation system (MNS) Niobe allows remote-controlled naviga-tion by changing the orientation of a small magnet embedded in the tip of anablation catheter using two outer permanent magnets (0.08 Tesla). In addition,using a motor unit, advancement and retraction of the magnetic catheter can beperformed from the control room.Methods and Results: A total of 155 pts (93 f, mean age 46 ± 16 yrs) underwentan invasive electrophysiologic (EP) study of narrow QRS complex tachycardiaidentified as either AV nodal or AV reentry using the MNS from May 2003 to July2005. In the intial series (n = 104 pts) a conventional EP study using 4 diagnostic
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
868 Electrophysiological imaging studies. New insights with new tools / Endothelial progenitor cell mobilisation by diet, drugs and stents
non-magnetic catheters was performed to investigate the underlying tachycardiasubstrate (multi DX). In the later patients (n = 51 pts) only one diagnostic non-magnetic catheter was used in addition to the magnetic ablation catheter (singleDX) to perform a sequential EP study. Using the single DX approach, all proce-dural data were reduced for both AVNRT and AP ablation as compared to themulti DX group. Most importantly, the total fluoroscopy duration was reduced by55% to a median of 3.2 min for AVNRT and by 58% to a median of 6.5 min for APablation, which is significantly lower compared to the multi DX group.
Table 1
AVNRT (multi DX) AVNRT (single DX) AVRT (multi DX) AVRT (single DX)n = 67 pts n = 37 pts n = 27 pts n = 14 pts
duration (min) 140 (60-390) 95 (55 - 200)* 190 (105 - 360) 150 (90 - 300)*Fluoro(min) 7.1 (2.5 - 48.3) 3.2 (1.3 - 8.1)* 15.2 (3.2 - 72.3) 6.5 (3.4 - 34.4)*# HFS 7 (1 - 28) 4 (1 - 16)* 3 (1 - 20) 4.5 (1 - 14)
Data is given with median and interquartile range
Conclusions: Remote catheter ablation of supraventricular tachycardia using thenew magnetic navigation system Niobe is highly effective. Using a sequential di-agnostic approach, a further significant reduction of procedural parameters couldbe demonstrated with special emphasis on total radiation exposure.
5058(W) Brugada Syndrome: the registry of the Piemonteregion of Italy
C. Giustetto1, S. Drago1, P. Carvalho2, R. Riccardi3,E. Occhetta4, P.G. Golzio5, P. Pinna Pintor6, F. Gaita4. 1CardinalMassaia Hospital, Cardiology, Asti, Italy; 2 Edoardo Agnelli
Hospital, Cardiology, Pinerolo, Italy; 3Mauriziano Hospital, Cardiology, Torino,Italy; 4 Hospital, Cardiology, Novara, Italy; 5Molinette Hospital, Cardiology, Torino,Italy; 6 Pinna Pintor Clinic, Torino, Italy
Background: The issue of risk stratification in Brugada syndrome is still unan-swered. In this study the data of patients from the Registry of the Piemonte Re-gion are reported. In this Registry patients were prospectively evaluated usinga standardized approach, especially regarding the electrophisiologic study (EP)protocol.Methods: Patients were enrolled if they had type 1 ECG spontaneously or afterflecainide or ajmaline test. Clinical and familial history were collected and the pa-tients were evaluated for the presence of a structural heart disease. Programmedstimulation was performed from two right ventricular sites, at two pacing cyclelengths with up to two extrastimuli to the ventricular refractory period. ICD wasimplanted in patients with previous cardiac arrest and in those with sustainedventricular arrhythmias induced at EP study.Results: Eighty-nine patients were included: 76 males (85%) and 13 female(15%). Forty-five patients were asymptomatic (51%) and 44 symptomatic (49%):3 patients with aborted sudden death and 41 patients with syncope (45% syncopewithout prodromes and 55% vaso-vagal syncope). The first symptom occurred atthe mean age of 45±12 years. EP study was performed in 74 patients (83%). Sus-tained ventricular arrhythmias were induced in 36 patients (49%): 54% of symp-tomatic patients and 38% of asymptomatic were induced (p=0.15). Sustainedventricular arrhythmias were induced in 50% of the patients with vaso-vagal syn-cope as compared to 60% of patients with syncope without prodromes (p=0.66).Thirty-nine patients (44%) underwent ICD implantation. At a mean follow-up of23±17 months 6 events occurred. Five patients received an appropriate ICDshock and an asymptomatic patient who had refused EP study died suddenlyduring sleep. Two ICD shocks occurred in asymptomatic patients (4%) and 4 insymptomatic (9%) (p=0.64): 3 occurred in the group with vaso-vagal syncope andone in the group with previous cardiac arrest. No event was observed in the pa-tients not induced at EP study (Log-Rank 2.2; p=0.02).Conclusions: In this study the high risk patients were correctly identified by EPstudy. Vaso-vagal syncope does not imply a good prognosis.
ENDOTHELIAL PROGENITOR CELL MOBILISATION BYDIET, DRUGS AND STENTS
5063 The effect of green tea on endothelial function andcirculating endothelial progenitor cell in chronicsmoker
W. Kim, M.H. Jeong, J.H. Kim, Y.K. Ahn, J.G. Cho, J.C. Park,Y.J. Hong, J.C. Kang. Gwangju, Korea, Republic of
Background and Objectives: Circulating endothelial progenitor cells (EPC) withan endothelial phenotype contribute to the regeneration and repair of the artery.The number of circulating EPC has an inverse correlation with chronic smokingand endothelial dysfunction. Green tea cathechin mary improve endothelial dys-function. The effect of green tea cathechin on the number of circulating EPCs andendothelial dysfunction in chronic smoker is not known. Materials and Methods:In 20 young healthy smokers (27.6±3.6 years, male), endothelial functions de-fined by flow-mediated endothelium dependent vasodilation (FMD) of the brachialartery, as well as the number of EPC isolated from peripheral blood, were deter-mined by baseline and at 2 weeks after taking green tea (8 g/day). Circulating
EPCs were quantified by flow cytometry as CD45lowCD34+KDR2+ cells and byacyl-LDL and FITC-lectin double positive cells after culture for 7 days.Results: Changes of clinical characteristics and laboratory findings were not dif-ferent between the baseline and at 2 weeks after green tea intake. EPC levelswere inversely correlated with the number of smoked cigarettes. Circulating EPCsby flow cytometry and cultured EPCs increased rapidly at 2 weeks after greentea consumption (78.6±72.6/ml vs. 156.1±135.8/ml, p<0.001; 118.2±35.7/10field vs. 169.31±58.3/10 field, p<0.001). FMD was significantly improved after2 weeks (7.2±2.8 vs. 9.3±2.4, p<0.001). FMD was correlated with EPC countbefore treatment (r=0.67, p=0.003) and after 2 weeks (r=0.60, p=0.013).Conclusion: The number of circulating EPCs and FMD are reduced in chronicsmokers. Green tea induces rapid improvements of EPC levels and FMD. A short-term of green tea consumption may be effective in the reduction of cardiovascularrisk in chronic smoker.
5064 Angiogenesis and endothelial progenitor cells. Anexperimental and clinical study in patients with criticallimb ischemia
M.C. Barsotti1, T. Santoni1, R. Di Stefano1, C. Armani2, E. Melillo1,M.C. Iorio1, A. Leone1, A. Balbarini1. 1University Of Pisa, Cardiac
and Thoracic Department, Pisa, Italy; 2University of Pisa, Cardiac and ThoracicDepartment, Pisa, Italy
Purpose: Angiogenesis induced by endothelial progenitor cells (EPCs) has beenwidely assessed by recent studies, although in vivo results are fast to be clearlydemonstrated. Moreover, doubts exist yet on those different factors able to in-crease EPCs number. A stable prostacyclin analog (Iloprost) would seem an ef-fective stimulus to both in vitro and, probably, in vivo angiogenesis in other exper-imental settings. The aim of this study was to assess the angiogenic effects dueto Iloprost in vitro and in patients (pts) suffering critical limb ischemia (CLI).Methods: For in vitro angiogenesis assay, 7 x 10*4 HUVECs in M199 with 5%FCS were seeded on Matrigel-coated plates, with or without 10 m M Iloprost.Networks were observed with a microscope equipped with a digital camera. 23patients (age: 79.6 ± 6.8) with CLI (n = 10: III stage and n = 13: IV stage) weretreated with Iloprost i.v. for 14 days. The effect of iloprost treatment was assessedby clinical parameters and transcutaneous oxygen and CO2 tension. Response totreatment was considered positive (R= responder pts) if at least one of the aboveparameters improved its value, negative (NR= nonresponder pts) if there was noparameter improving. Mononuclear cells (MNCs) were isolated from peripheralblood, before and after the end of Iloprost treatment and 10 x 10*6 MNCsplatedon fibronectin in EGM-2-MV. After 6 days, the uptake of DiI-AcLDL and the bindingof UEA-I was analyzed by FACS and the number of double-positive cells (EPCs)per ml of peripheral blood was assessed. Pre- and post-iloprost levels of EPCswere compared. Ptts were followed up 1 yearResults: In the Matrigel tubule assay, Iloprost significatively enhanced networkformation by HUVECs.CLI pts showed an increase in the EPCs number after iloprost treatment (averageper cent increase: +199.2%, p=0.005), although with a striking individual variabil-ity. There were two types of pts: R (n=14) and NR (n=9). The differences in thepre/post-iloprost EPCs numbers were normally distributed. No significant differ-ence was found between R and NR patients. No significant association emergedbetween the increase in the EPCs number after the treatment or the basal EPCslevels and age, sex and AOCP stage.After 1 year follow up, no pt underwent major limb amputation.Conclusions: Stable prostacyclin analog seemed to have a proangiogenic ef-fect, enhancing both in vitro network formation by mature endothelial cells andcirculating EPCs in CLI pts. Also clinical improvement was seen.
5065 The effects of granulocyte-colony stimulating factor inbare stent and drug-eluting stent in pigs followingmyocardial infarction
Y. Ahn, S.Y. Lim, Y.S. Kim, M.H. Jeong, J.G. Cho, J.C. Park. ChonnamNational University Hospital, Cardiology Dept, Gwangju, Korea,
Republic of
Objectives: The purpose of this study was to compare the effects of G-CSFon ISR in bare and drugeluting stents (DES) in a porcine myocardial infarctionmodel. Background: Using granulocyte-colony stimulating factor (G-CSF) to mo-bilize stem cells has shown promise in infarcted heart. However, G-CSF mayaggravate in-stent restenosis (ISR) and an aggressive strategy to prevent ISR isneeded.Methods: Bare stents and DES were implanted in coronary arteries (bare stents,Group I; bare stents with G-CSF, Group II; DES, Group III; DES with G-CSF,Group IV, n=10 in each group). G-CSF (10 μg/kg/day) was injected for 7 daysfrom 24 hours after stent implantation.Results: Area stenosis was 27.9±9.6% in Group I and 76.7±12.0% in GroupII at 28 days (P<0.001). The ratio of inflammatory cells in the neointima washigher in Group II (P<0.001). No significant differences were observed betweenGroup III and IV. In Group II, phosphorylated signal transducers and activatorsof transcription (STAT)-3, STAT-3, and vascular endothelial growth factor (VEGF)showed increased neointimal expression. In porcine aortic smooth muscle cells(PASMC), G-CSF increased the growth rate, migration, STAT-3 phosphoryla-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Endothelial progenitor cell mobilisation by diet, drugs and stents / Pulmonary vein isolation to cure atrial fibrillation 869
tion, and VEGF, which were suppressed by rapamycin and AG490, a STAT-3inhibitor.Conclusions: STAT-3 and VEGF are important in the development of enhancedISR by G-CSF in bare stents. DES could be a good strategy to prevent the G-CSF-stimulated proliferation and migration of smooth muscle cells, which couldbe responsible for neointimal hyperplasia.
5066 Increased EPC-recruitment by a novel cRGD-coatedpolymer stent reduces neointimal hyperplasia
R. Blindt1, F. Vogt2, I. Astafieva3, C. Fach1, M. Hristov1,J. Bernhagen1 , R. Hoffmann1, C. Weber1 . 1University Hospital RwthAachen, Medical Clinic I, Aachen, Germany; 2Aachen, Germany;
3Guidant Corporation, Santa Clara, United States of America
Background: Re-endothelialization is important for healing after arterial injury.Novel stents loaded with a cyclic integrin-binding RGD-peptide (cRGD) were an-alyzed for their potential to limit coronary neointima formation and to accelerateendothelialization by attracting endothelial progenitor cells (EPCs).Methods: Effects of cRGD on EPC number, recruitment in flow and invasion wereanalyzed in vitro. A durable polymer coating containing 67μg cRGD/stent was de-veloped for Guidant Tetra TM stents. Twelve cRGD-loaded polymer, 12 unloadedpolymer, and 12 bare metal stents were deployed in porcine coronary arteries.Quantification of cRGD in peri-stent tissue was established by HPLC and massspectrometry (MS). Histomorphometry and immunostaining were performed after4 and 12 weeks. Recruitment of labeled porcine EPCs was assessed 7 days afterintracoronary infusion.Results: cRGD clearly supported the outgrowth, recruitment, and migration ofEPCs in vitro. At 4 weeks, there was no difference for mean neointimal area(NA) and percent area stenosis in the cRGD-loaded, polymer, or bare metal stentgroup. At 12 weeks, NA (2.2±0.3 mm 2) and percent area stenosis (33±5%) weresignificantly reduced compared to polymer (3.8±0.4 mm 2, 54±6%; P=0.010) orbare metal stents (3.8±0.3 mm 2, 53±3%; P<0.001). HPLC/MS confirmed cRGDtissue levels of 1-3 μg/stent at 4 weeks, whereas cRGD was not detectable at 12weeks. Staining for CD34 and scanning electron microscopy indicated enhancedendothelial coverage on cRGD-loaded stents at 4 weeks associated with a signif-icant increase in the early recruitment of infused EPCs.Conclusions: Stent coating with cRGD may be useful to reduce in-stent resteno-sis by accelerating endothelialization.
5067(W) Endothelial progenitor cell capture by stentscoated with antibody against integrin alphaVbeta3
K.C. Hwang1, Y.S. Yoo2, J.M. Ahn1, M.H. Jeong1, Y.S. Jang1.1Yonsei University College Of Medicine, Cardiology, Seoul,Korea, Republic of; 2Seoul, Korea, Republic of
Objectives: The aim of this study was to develop the coating method of an-tibody to Co-Cr surface and to evaluate the effect of antibody against integrinalphavbeta3 which was coated on stent surface for capturing endothelial progeni-tor cells (EPC) and induction of endothelialization processes.Backgrounds: Even though drug-eluting stents has dramatically reduced the in-cidence of in-stent restenosis, the drugs interfere with the formation of functionalendothelial lining over the stent as well as neointimal formation. It is believed thatstent surface which was coated with antibody against integrin alphavbeta3 mayenhance the capturing of EPC from blood flow and the formation of endotheliallining.Methods: Deposition of amine groups on Co-Cr surface was conductedby plasma polymerization of ethylendiamine. Then amino groups were con-verted to carboxyl groups treated with succinic anhydride and subsequentlytreated with EDAC (1-ethyl-3-(3-dimethylaminopropyl)carbodiimide) and NHS (N-hydroxysuccinimide) with various molar ratio. After thoroughly washing, 200 mg/ml of antibody against alphavbeta3 as well as CD34+ antibody solution wasadded to bind for 2h. Human EPC used in this study was cultured from umbilicalcord blood.Results: The most effective molar ratio for antibody against alphavbeta3 aswell as CD34+ antibody immobilization was 0.6:20:50 of antibody against a vb 3:EDAC:NHS. Immobilized amounts of antibody against alphavbeta3 as wellas CD34+ antibody after treatment under optimum conditions were 122.4 mg/cm2. No more release of Antibody against alphavbeta3 was absorbed after 1day until 14 days. Adhesion of EPC enhanced about 2-fold on antibody againstalphavbeta3-coated surface than on CD34+-coated surface and cell spreadingwas significantly affected by antibody against alphavbeta3 coating comparedto CD34+-coating. The phosphorylation of adhesion-related proliferation signal,FAK, Akt and downstream regulator ERKs in EPC increased by 3-, 1.5-, and 1.5-fold, respectively, on antibody against alphavbeta3-coated plate compared thanCD34+-coated plate.Conclusion: These results suggest that stent coated with antibody againstalphavbeta3 shows higher capturing ability for EPC and more potent activitiesfor adhesion-related proliferation signals, which may enhance the formation ofendothelial lining over the stent surface and significantly reduce the restenosis.
PULMONARY VEIN ISOLATION TO CURE ATRIALFIBRILLATION – BENEFITS AND RISKS
5073 Isolation of pulmonary veins with a new 28/23 mmcryoballoon in atrial fibrillation - first experience
J. Vogt, A. Dorszewski, L. Luong Thanh, J. Heintze, H. Buschler,D. Horstkotte. Heart Center North Rhine-Westphalia, BadOeynhausen, Germany
Purpose: In the treatment of paroxysmal atrial fibrillation (af) a reliable anatomi-cally oriented approach to isolate the pulmonary veins (pv) seems optimal. How-ever, segmental isolation with radiofrequency energy showed a reconduction in90% and pv stenoses in about 5% of patients (p). Substrate modification unfortu-nately associated with the risk of esophago-left atrial fistulas may be an overtreat-ment in trigger induced af. This study reports on the first experience in isolatingpv with a new balloon technique with cryoenergy.Methods: After pv angiography and Lasso mapping of sleeve potentials isolationwas performed with a new 28/23mm balloon (Arctic Front, Cryocath, Canada).After inflation the over a wire balloon occludes the venous ostium and freezesdown to -50 to - 70°C 8 minutes two times per vein with nitrous oxide. Lassomapped rest potentials were eliminated with additional balloon freezes or with the9 french Freezor Max catheter.Results: We treated 33 patients (p) (7 women, mean age 59±12 years, 28 withparoxysmal, 5 persistent af, left atrium 42±5 mm, 16 with lone af, 10 hyperten-sion, 7 mild structural heart disease, mean drug refractory af duration 75±50months) with the new Arctic Front balloon, 24 p with 28, 6 p with 23 mm, 3 p withboth. Mean vein diameter was 18.9±4 mm angiographically. With a mean numberof 2.4±0.6 impulses and a mean temperature of - 47±18°C we could isolate 73%of the left pv,70% of the right upper and 58% of the right lower pv. After touchup of rest potentials in 32% of 132 pv we isolated 100% of all pv. The proceduretime was 231±41 min, the X-ray burden 42 ±12 min. We observed phrenic nervepalsy in two p with the 23 mm balloon. During the 3 months follow up 5 of 15 phad a redo, 8 of remaining 10 p were free of af during 2 seven day holters, 2 pmarkedly improved.Conclusion: The new cryoballoon technique is safe and acutely highly effec-tive. The advantage in comparison with other innovative tools is the high coolingpower, isolation of parts of venous antrum and a high percentage of stand alonepv isolation. Avoidance of prenic nerve palsy and efficacy of different balloon sizeshas to be focused.
5074 Preprocedural predictors of recurrences afterelectroanatomical encircling of pulmonary veins
A. Berruezo, D. Tamborero, B. Vidal, M. Sitges, M. Matiello, I. Molina,J. Brugada, L.L. Mont. Hospital Clinic de Barcelona, Barcelona, Spain
Succes rate of electroanatomical encircling of pulmonary veins (EE)to treat atrial fibrillation (AF) ranges from 60 to 90% depending on the series.The aim of the study was to identify the predictors of recurrences of AF after astandardized procedure of EE.Methods and results: A series of 145 consecutive patients submitted to EE forparoxysmal (66%) persistent (23%) or permanent (11%) AF were included in thestudy and completed more than 6 months follow-up. Inclusion criteria were: drugrefractory AF, age >18 AND <75 years and antero-posterior left atrial diameter(LAD) <56 mm. No patient was excluded on the basis of their AF duration. EE withcreation of supplementary block lines along posterior wall and mitral istmus wasperformed in all patients. Structural heart disease was present in 20% and hyper-tension in 38%. After a mean follow-up of 14.3±8.5 months, 70% of patients werearrhythmia free. At univariate analysis, hypertension (44,2% vs 22.8%, p=0.014)and larger LAD (44.2±6.2 vs 40.2±5.6 mm, p<0.001) were associated with re-currence. Cox regression analysis showed that hypertension (OR = 2.4; 95% CI:1.2 - 4.5; p=0.01) and LAD (OR = 1.13; 95% CI: 1.06 - 1.2; p<0.001) were inde-pendent predictors of recurrence. P redicted probability of the multivariate modelshowed a linear relation between increase of LAD and the increase of the proba-bility of late recurrence, influenced in each LAD by the presence of hypertension(see graphic).
Predicted probability model
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

870 Pulmonary vein isolation to cure atrial fibrillation
Conclusion: Antero-posterior LAD and hypertension are independent predictorsof recurrence after EE to treat AF. The probability of late recurrence increaseslinearly with the increase of LAD. The data may help in patient selection for AFablation.
5075 Relationship between early recurrence within threedays from successful Extensive Encircling PulmonaryVein isolation for atrial fibrillation and chronicrecurrence
H. Suzuki1, Y. Yoshida1, N. Tsuboi2, T. Itou3, T. Yamada4,Y. Murakami1, Y. Indenn5, T. Murohara5. 1Nagoya Daini Red Cross
Hospital, Cardiology, Nagoya, Japan; 2Chukyo Hospital, Cardiology, Nagoya,Japan; 3Nagoya National Central Clinic, Cardiology, Nagoya, Japan; 4AichiCardiovascular and Respiratory Center, Cardiology, Nagoya, Japan; 5NagoyaUniversity, Cardiology, Nagoya, Japan
Background: We often experiment early recurrence after Extensive EncirclingPulmonary Vein isolation(EEPVI) for atiral fibrillation(AF). But it is unclear whetherthere is any relationship between early recurrence and chronic recurrence.Methods: We retrospectively evaluated 224 consecutive patients who were re-ceived EEPVI for their AF. We included 158 patients who were considered asacute success case and whose data were available in acute and late phase. Inthe session of EEPVI, Pulmonary veins (PVs) could be completely isolated withcontinuous circular lesions (CCLs) around the right-sided and left-sided ipsilateralPVs guided by 3D anatomical mapping and double Lasso (DL) placed at ipsilat-eral superior and inferior PVs. In case there were remaining PV potentials (PVP),additional irrigated ablation was segmentally underwent to ostia of PVs whichgenerated PVP. The outcome of the procedure was determined as acute suc-cess when the disappearance of PVP at DL was confirmed. After EEPVI session,we observed monitoring electrocardiogram for three consecutive days. We haddetermined as acute recurrence when the patient had atrial fibrillation for morethan one minutes. We had determined as chronic success as disappearance ordecrease of self-awareness of paroxysmal palpitation for paroxysmal AF patientsand maintaining sinus rhythm for persitent/chronic AF patients.Results: In 158 patients, there were 125 males(79.1%). Average age was59.0±10.6. There were 95 paroxysmal AF patients(60.1%), 27 persistent AF pa-tients(17.1%) and 36 chronic AF patients(22.8%). The average of followed upperiod was 9.3±7.9 months. Cases of chronic success were 145patients(91.8%)and cases of chronic fail were 13 patients(8.2%). Within three consecutive daysfrom EEPVI, the patients who had paroxysmal or sustained AF were 44 cases(asgroup F), another patients who maintained sinus rhythm were 114 cases(as groupS). In group F, the cases who had recurrence of AF at day1 were 2cases(4.5%),at day2 were 29 cases(65.9%) and at day 3 were 13 cases(29.5%). There wereno statistical significant difference between group F and group S about type ofAF, duration time of AF and rate of dependence from medication after EEPVI.Chronic success cases were 40 cases in group F(90.1%) and 105 cases in groupS(92.1%). P value was 0.75, there were also no statistical significant differencebetween chronic success rate of group F and group S.Conclusion: Acute recurrence of AF within three consecutive days from EEPVInever predicts chronic recurrence.
5076 Visualization of the oesophagus during catheterablation of atrial fibrillation: comparison betweenelectro-anatomic tagging and MSCT reconstruction
R. Littmann1, G. Moennig1 , J. Wessling2, R. Fischbach2 ,K. Wasmer1, P. Milberg1, G. Breithardt1, L. Eckardt1. 1Department
of Cardiology and Angiology, Hospital of the Westfaelische Wilhelms-Univer,Muenster, Germany; 2Department of Radiology, Hospital of the WestfaelischeWilhelms-Univer, Muenster, Germany
Background: During left atrial catheter ablation, atrio-oesophageal fistulas maydevelop as a result of thermal injury of the oesophagus. Various studies thatinvestigated the topographic variability of relation between oesophageal andleft atrium, stressed the importance of visualization of the oesophagus duringcatheter ablation. We therefore aimed at comparing computed tomographic (CT)imaging of the oesophagus with real-time tagging of the oesophagus during theablation procedure.Methods: In 25 consecutive patients, 16-slice CT was performed within 2 daysbefore circumferential radiofrequency catheter ablation of the pulmonary veins.CT data were imported to the Carto electroanatomic mapping system. Usingthe new CartoMerge Image Integration Module, CT images and electroanatomicmaps were aligned. In addition, tagging of the oesophagus was performed afterLA reconstruction prior to ablation using a Carto catheter advanced through aconventional gastric tube into the oesophagus. Tagging was started while slowlywithdrawing the catheter.Results: Using the CartoMerge Module the oesophagus could be segmented inall patients. CT visualization in a posterior-anterior view revealed a highly vari-able proximity of the oesophagus to different areas of the posterior LA, which in21 patients lay within the AF ablation zone. However, there was a good correlationbetween the CT segmentation and the real-time Carto tagging. The mean mini-mal distance between the segmented CT oesophagus and the tagged Carto oe-sophagus was 7.1± 7.6mm, the maximal deviation measured 13.1± 8.3mm. The
mean differences at the roof, the centre, and the base of the LA were 11.1±8.4mm, 10.3±7.4 mm, and 9.6±8.9 mm, respectively.Conclusion: There is good correlation between CT visualization and real-timeelectroanatomic tagging of the oesophagus. Thus, CT cannot only be used forfusion with electroanatomic maps but also for localization of important adjacentanatomic structures such as the oesophagus. Although this technique does notaccount for oesophageal movement, identification of the oesophagus may dimin-ish the potential risk of atrio-oesophageal fistulas.
5077 Left atrium ablation for atrial fibrillation: a multicenterperspective registry on procedural safety
E. Bertaglia1, F. Zoppo1, A. Colella2, N. Bottoni3, G. Stabile4,F. Zerbo3, D. D’este3, P. Pascotto3. 1Ospedale Civile, Cardiologia,Mirano, Italy; 2Azienda Ospedaliera/Universitaria, Cardiologia,
Firenze, Italy; 3Ospedale Civile, Cardiology, Reggio Emilia, Italy; 4Casa Di CuraSan Michele, Cardiology, Maddaloni, Italy
Background and objective: not univocal data are available about proceduralsafety of left atrium (LA) ablation for curing atrial fibrillation (AF). Our aim wasto assess the safety of left atrium radiofrequency ablation (RFCA) procedures tocure AF by means of pulmonary veins (PV) circumferential isolation, PV segmen-tal disconnection and linear LA lesions, in patients (pts) with drug refractory atrialfibrillation.Methods and results: data were perspectively collected in a multicenter registry.From January 2005 and September 2005, 355 consecutive pts underwent RFCAfor AF. There were 273 (77%) male, mean age 57.9+9.9 years. Paroxysmal AFwas present in 55%, persistent in 37%, and permanent in 8% of pts. History ofcerebrovascular accident was present in 4% of pts. Pre-ablation transesofagealechocardiographic assessment was performed in 346 pts (97%). Activation clot-ting time during the procedure was set between 250 and 350 sec.Mean vascular cannulations were 2.97±0.8. In 277 pts (78%) a single transseptalpuncture was necessary; in 50 pts (14%) a double puncture; in 2 pts (0.6%) atriple, while a patent foramen ovalis was found in 27 pts (8%). In 323 (90%) pts atridimensional non-fluoroscopic mapping technique was used (CARTO system).In 81 (23%) pts a LASSO catheter and in 45 (13%) pts a BASKET catheter wereused. Cooled tip catheter was used in 252 pts (71%) with a mean power set up to40 Watts; 8-mm tip catheter and 4 mm tip were used respectively in 83 (23%) andin 21 (6%) pts, with a mean power set up to 80 Watts. A mean of 4.5±1.2 PVswere isolated. Linear lesions were added in 202 pts (57%) at cavotricuspidalicisthmus, in 186 pts (52%) at mitral isthmus, and in 89 pts (25%) along the LA roof.Mean procedure time was 128.3+85.6 min; mean fluoroscopy time 31.1+25.4 min;mean RF delivery time 45.7+17.3 min.We collected all complications occurred during the first month after the ablation,classified in major (not spontaneously solved), and minor (when spontaneouslysolved). No patient died for the procedure. Cumulative rate of major complicationswas 3%: there were 2 (0.5%) cases of cardiac tamponade, 1 (0.2%) pleuric ematiceffusion, 5 (1.4%) pseudoaneurisms, 2 (0.5%) artero-venous fistula and 1 (0.2%)major ischemic stroke. All minor complications were accounted for a 2.5%, with4 (1%) inguinal hematoma, 1 (0.2%) left arm phlebitis, 1 TIA, 1 pt with 50% PVstenosis and 2 (0.6%) pericardial effusions conservately treated.Conclusion: In comparison with other literature data, in this series of pts a slightlower rate of complication was recorded.
5078 Unexpected absence of atrial fibrillation after hearttransplantation
P. Hlivak, M. Luknar, J. Fabian, R. Hatala. National CardiovascularInstitute, Department Of Arrhythmias and Cardiac Pacing, Bratislava,Slovak Republic
Aim: Heart transplant (HTx) patients often have co-morbities which are indepen-dent risk factors for atrial fibrillation (AF). We would expect a higher incidence ofAF in this population. The operative technique for orthotopic heart transplantationshares some common features with catheter ablation of AF, (i.e. the electrical iso-lation of the pulmonary veins). The aim of our study was to determine the long -term incidence of AF after HTx in relation to risk factors for AF.Patients and methods: Patients who survived a minimum of 6 months after HTxwere studied retrospectively. The m ean time post-orthotopic cardiac transplan-tation was 77±45 months. We analyzed clinical and echocardiographic variablesand therapy status with possible relation to AF occurrence [age, gender, hyperten-sion (HT), diabetes mellitus (DM), left atrium size (LA), and impaired left ventricle(LV) diastolic function]. ECG tracings from 1743 visits were reviewed.Results: One-hundred and five patients met the inclusion criterion (survival ≥6 months after HTx). Mean age of these patients was 51±12 years, with malepreponderance (89%). Hypertension and diabetes were found in 91% and 26%of pts, respectively. LA dilatation was reported in 71 pts (68%), mean LA diameterin all subjects was 45±7 mm. LV diastolic dysfunction was present in 83% ofpts, a mean LV ejection fraction was 58±9%. Calcium channels blockers, beta-blockers, ACE inhibitors, and angiotensin II receptor blockers were used in 50%,51%, 50%, and 22% of patients respectively. We did not observe any case ofAF. In four patients, atrial reentrant tachycardias were recorded (2 pts underwenttransplant with the bicaval and 2 with biatrial technique).Conclusion: The incidence of risk factors for AF is high in patients after car-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Pulmonary vein isolation to cure atrial fibrillation / Computers in cardiology, from artificial intelligence to mobile echo in Africa 871
diac transplantation. The absence of AF in 105 patients followed for a mean of77 months suggests a preventive and therapeutic effect of the transplant surgerywhich included pulmonary vein isolation. However, we recorded reentrant atrialtachyarrhytmias, which can also occur after AF ablation and which require subse-quent specific treatment.
COMPUTERS IN CARDIOLOGY, FROM ARTIFICIALINTELLIGENCE TO MOBILE ECHO IN AFRICA
5079 Artificial neural networks are a potential tool forestimating prognosis in coronary artery disease -preliminary experience
J.D. Kasprzak1, A. Michalak2, A. Nowakowski2. 1Medical University OfLodz, Ii Chair Of Cardiology, Lodz, Poland; 2University of Lodz, Lodz,
Poland
Aim: Artificial neural networks (ANN) may be used for creation of expert systemsin cardiology. We aimed to create and test the ability of ANN for the prediction ofindividual risk in patients with coronary disease.Methods: We based our study on the database of 250 patients with coronarydisease with known follow-up of 18±6 months duration. Every patient was rep-resented with one input vector, containing data on age, sex, BMI, CSS, historyof infarction, diabetes, dyslipidemia, smoking and hypertension and output vectorwas expressed as 4 grades of clinical course: death/infarction or revasculariza-tions/other acute coronary syndromes/uneventful course. Tested ANNs were pre-pared using different methods: 1. Backpropagation algorithm - networks with oneor two hidden layers included 3-40 neurons, with tanh activation function; 2.RadialBasis Function Network (RBFN) with 20-30 neurons in hidden layers; 3. CascadeCorrelation of Fahlman (CCF) with 50,60 and 100 maximal neuron in hidden layer,tanh or Gauss activation function; 4. Kohonen Algoritm (40 neurons)Results: Tested ANNs differed in their ability to predict the clinical course: 50-75%correct answers for Backpropagation algorithm, 40-75% for RBFN, 50% for CCFand 75% for Kohonen ANN. The most promising approach was using linked Ko-honen learning algorithm with Backpropagation algoritm (different networks had1 or 2 hidden layers with 20-70 neurons), providing 85% correct answers when 1hidden layer with 40 neurons, 0.6 learning rate and 500 learning cycles in Koho-nen algoritm, 0.1 learning rate and 500 cycles in Backpropagation algorithm wasused. We expected that neurons would specialize in recognizing certain samplesin the same disease categories, but this was not observed. Increasing learningcycles numbers gave the effect of overfiting.Conclusions: ANNs are potential means for creation of advanced prognostictools in cardiovascular disease. With a proper combination of network structureand learning algorithms, it was possible to obtain >80% correct prediction of clin-ical course. The results of our initial work warrants optimization using modifieddatasets and larger test cohorts.
5080 Databases in the coronary care unit: towards thetwenty-first century
P.F. Monteiro, F. Goncalves, L.M. Goncalves, M. Freitas,L.A. Providencia. Coimbra University Hospital & Medical School,Cardiology, Coimbra, Portugal
Introduction: In current days, efficient databases are crucial to improve medicalrecords and achieve an optimal medical care, particularly in acute care settings,were most of the therapies are based in widely accepted protocols.Aim: To analyse the impact of the introduction of a fully computerized database ina single coronary care unit. Population and methods: Using the latest technologyin wireless broadband communications, we set up in May 2004 a fully computer-ized system to process medical information in the coronary care unit (CCU). Sincethen, data from 956 patients was collected, from admission to discharge. This in-formation included demographics, risk factors, previous history and medications,admission diagnosis, clinical evaluation (through the entire hospital stay), resultsfrom laboratory and other exams, complications and their outcome and dischargediagnosis and medications. Patient rounds were made using a portable digitalassistant (PDA) and information was immediately sent to the server via a wire-less broadband communication system. The system was also used to make allmedical prescriptions, to order exams and automatically collected the results fromthe laboratory exams, inserting them in the patient chart. The database is pass-word protected and available from every computer in our hospital (for authorizedusers), allowing instant access to the patient records regarding current admissionand previous ones.Results: Since the introduction of this system, the quality of the data gathered foreach patient increased sharply. Prescription omissions were virtually banned (be-cause the program has a built-in prescribing assistance system) and medicationerrors due to misinterpretation of handwriting were also eliminated (the systemautomatically prints prescription orders to the pharmacy and nursing staff). Pa-tient and primary care physician information also improved, because they nowget a copy of the discharge note, including a summary of the clinical condition,treatments performed, medication prescribed, future appointments and list of riskfactors to be controlled. Besides all this clinical advantages, this database has
been proven as an excellent scientific tool, allowing to produce more and betterscientific works. This system is now going to be implemented nationwide as thestandard CCU medical records program.Conclusion: In the CCU, computerized databases can be used to improve pa-tient care, facilitate prescriptions and exam ordering, as well as to build a com-prehensive clinical records tool to be used to produce new scientific knowledge.
5081 Successful real time ECG recording and transmissionin cardiac patients with a wearable system based onsmart textiles: first clinical experience of the WEALTHYproject
S. Coli1, F. Grassi1, N. Taccini2, G. Loriga1, G. Calori2, A. Gemignani3,B. Ghelarducci2, D. Cianflone3. 1University Vita-Salute, San Raffaele IRCCS,Cardiothoracic and Vascular diseases, Milan, Italy; 2Smartex s.r.l., Prato, Italy;3University of Pisa, Physiology and Biochemistry G. Moruzzi, Pisa, Italy
Background: Smart textiles (textiles with electrophysical properties) allow thedevelopment of wearable devices for telemedicine. The EU supported WEALTHYproject has developed a wearable shirt made with smart textiles, integrated witha transmission module (bluetooth/GPRS), for the remote monitoring of cardiacpatients (pts). The shirt contains various sensors and tissue electrodes for ECG(standard peripheral leads, V2, V5). We present the first data regarding ECGquality and patient comfort with the WEALTHY shirt (WS) in cardiac pts.Materials and Methods: 15 male pts (median age 57 years) admitted for CAD(10), rehabilitation after CABG (4) or myo-pericarditis (1) wore the WS for 45minutes, at rest and during physical activity. WS ECG was recorded and trans-mitted in real time with a bluetooth connection to a computer, where the datawere stored. Simultaneously, the ECG was recorded and digitally stored with astandard telemetry system (Mortara-Rangoni, MR) for in hospital monitoring ofambulatory pts. For each patient 10 seconds ECG strips of 4 leads (DI, DII, V2,V5), during 3 levels of activity (rest, light exercise, moderate exercise), simultane-ously recorded with the two systems (a total of 24 strips for each patient) wererandomly selected among the stored data and evaluated off-line by two blindedcardiologists. ECG quality was scored on a 1 to 5 scale (1 worst, 5 best). At theend of the protocol pts scored shirt comfort on a 1 to 5 scale (1 worst, 5 best).ECG quality scores were compared by ANOVA for repeated measures with Bon-ferroni corrections for post-hoc contrasts.Results: ECG quality score was not different between the two systems (p=0.59)and not dependent on the reader (p=0.36), while there was a significant as-sociation with the level of physical activity (p=0.0002) and the lead examined(p<0.0001). ECG quality modestly decreased during exercise compared to restwith both systems (ECG score, mean ± sd: rest, WS 3.78 ± 0.94, MR 3.73 ±0.93; light exercise, WS 3.10 ± 1.12, MR 3.18 ± 1.32; moderate exercise, WS2.84 ± 1.12, MR 3.08 ± 1.18). V5 performed significantly better than V2 and DI,while V2 was better than DI (ECG score, mean ± sd: DI, WS 2.47 ± 1.00, MR3.08 ± 1.01; DII, WS 3.73 ± 1.03, MR 3.54 ± 1.14; V2, WS 3.17 ± 1.02, MR 2.99± 1.31; V5, WS 3.60 ± 1.04, MR 3.69 ± 1.13). Patient comfort was good (meanscore ± sd: 3.93 ± 0.80).Conclusion: the WS is capable of recording and transmitting in real time ECGof comparable quality to a commonly used telemetry system and appears to becomfortable. The WS may be a useful device for the remote care of cardiac pts.
5082 New ECG criteria of inferolateral myocardial infarctionassessed by contrast enhanced-cardiovascularmagnetic resonance based on the morphology of QRSin V1
A.J. Bayes De Luna1, J. Cino1, A. Kotzeva1, F. Carreras2,S. Pujadas1, M. Fiol3, J. Cinca1, G. Pons-Llado1. 1Institut Catala
Ciencies Cardiovasculars, Hospital Sant Pau, Barcelona, Spain; 2HospitalSant Pau, Cardiology, Barcelona, Spain; 3Hospital Universitario Son Dureta,Cardiology, Palma, Spain
Purpose: It has been considered by an AHA statement (Cerqueira 2002) thatthe term posterior wall has to be abandoned and the classical posterior wall thatcorresponds to segment 4 has to be named inferobasal segment. According tothis statement, the left ventricle may be divided in 4 walls, anterior, septal, inferiorand lateral, and 17 segments. Therefore, we may divide the myocardial infarctionof the inferolateral zone according the location detected (CE-CMR), in three types:inferior (segments 4, 10, and part of 15,3 and 9), lateral (segments 5,6,11,12,16)and inferolateral that encompass both types. Our purpose is to check the QRSmorphology in V1 to know in which type of MI of the inferolateral zone the classiccriteria of true posterior MI (RS morphology in V1) is present.Methods: We studied a series of 45 consecutive patients with inferolateral MI (9lateral MI, 14 inferior MI and 22 inferolateral MI). We defined the 3 groups accord-ing the location of infarction by CE-CMR. We checked the presence of pathologi-cal R wave in V1 (R≥S and width of R≥ 40 mm) according to the classical criteriaof MI of segment 4-(old posterior MI as was described by Perloff in 1964), and wechecked if new ECG criteria may be defined.Results: Classical criteria: 1) RS >I in V1 was present in 2 of 9 (22%) of lateralMI, 0 of 14 (0%) of inferior MI, and 6 of 22 (27%) of inferolateral MI. 2) R≥ 40 mswas present in 5 of 9 (56%) of lateral MI, 0 of 14 (0%) MI of inferior and 12 of 22(55%) of inferolateral MI. The correlation with CE-CMR allowed us to define the
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

872 Computers in cardiology, from artificial intelligence to mobile echo in Africa / The latest on non coronary cardiac interventions
following new criteria: 1) R/S ratio in V1 is never >0.5 in inferior infarction, thatin 80% of cases includes infarction of segment 4 (classical posterior MI). 2) Thewidth of R in V1 is never > 30 msec in inferior infarction. 3) A new ECG criteria isthe amplitude of R in V1 > 3 mm that is only seen in patients with lateral MI.Conclusions: 1) The classical criteria of posterior MI based on the presenceof tall R in V1 are due to lateral infarction and not to inferobasal (segment 4 orposterior) infarction. 2) New ECG criteria of lateral infarction (and not of posteriorinfarction) are the presence in V1 of a) R/S > 0,5. b) R width > 30 msec and c)R amplitude > 3 mm. 3) We have to abandon the term posterior wall and trueposterior MI and consider that the MI that presents abnormal RS pattern in V1 isdue to lateral MI.
5083 Clinical significance of a new ultrasound method forthe simultaneous assessment of radial and longitudinalmyocardial deformation in myocardial infarction:validation with contrast-enhancement MRI
F. Tona1, R. Montisci2, A. Cati2, M. Ruscazio1 , F. Corbetti3,L. Cacciavillani2, M. Perazzolo2 , S. Iliceto2. 1Cardiology, University of Padova,Padova, Italy; 2Cardiology, University of Cagliari, Cagliari, Italy; 3Radiology,University of Padova, Padova, Italy
Strain (S) has been proposed as a tool to quantify regional myocardial function.One of the major pitfalls of the current methodology is its angle dependency. Toovercome this problem, a new method for estimation of S -2D Velocity VectorImaging (2DVVI) (Siemens, California)-, independent of angle, has been devel-oped. We aimed to clarify the clinical significance of 2DVVI in assessing the trans-mural extent of acute myocardial infarction (AMI) by comparing 2DVVI to delayedcontrast-enhancement (DCE) of magnetic resonance imaging (MRI).Methods: We examined 2DVVI and contrast-enhanced MRI in 30 patients withAMI. The new methodology was used to perform simultaneous measurements ofradial and longitudinal S. According to the 16 segments as recommended by theAmerican Society of Echocardiography, a total of 129 infarcted segments wereenrolled and divided into 2 groups based on the extent of DCE by MRI: group1= hyperenhancement >/= 75% of whole myocardial layer (n=91) and group 2=hyperenhancement <75% (n=38). Group 1 and 2 were also independently com-pared with normal segments of age-matched healthy volunteers.Results: In all segments, it was possible to obtain adequate 2DVVI analysis.Both longitudinal and radial S were lower in transmural (group 1) (10 ± 6% vs 17± 3%, p<0.0001 and 10 ± 7% vs 16 ± 4%, p<0.0001, respectively) and non-transmural (group 2) (10 ± 5% vs 17 ± 3%, p<0.0001 and 10 ± 5% vs 16 ± 4%,p<0.0001, respectively) compared with corresponding normal segments. Therewas a significant relationship between longitudinal and radial S obtained by 2DVVIand increasing extent of DCE by MRI (longitudinal S group 1: 6 ± 4%, group 2 10± 5%, p=0.001; radial S group 1: 6 ± 4%, group 2 10 ± 5%, p<0.0001).Conclusions: Strain measurement obtained by 2DVVI appeared to illustratetransmural extent of AMI. 2DVVI may have clinical significance in assessing my-ocardial viability in patients with AMI.
5084 First experience using a truly mobile digital echolaboratory in Africa for planning congenital heartsurgery in children
R. Motz1, K. Kronberg1, M.S. Claus2, S. Urban2, G.H. Reil1. 1KlinikumOldenburg, Oldenburg, Germany; 2OFFIS Research Institute,
Oldenburg, Germany
Purpose: Within the scope of humanitarian aid in Eritrea a team of cardiac sur-geons and one cardiologist work 7 days every year to examine and operate chil-dren with congenital heart defects. On the plane the cardiologist carried along ahandheld echo machine (Acuson Cypress) and a notebook. The aim was to doc-ument all echoes with measurements, a structured report, final diagnosis, imagesand film-loops.Methods: The notebook was equipped with a software (GO-Kinderecho) collect-ing all data in a database. The images and films were acquired via a local areanetwork in the DICOM format. They could additionally be converted to a MotionPicture Expert Group format version 4 (MPEG-4). The reports used diagnosisrelated texts according to the DICOM structured report supplement 72. All docu-ments were imported afterwards in the home based database.
Fig. 1. Mobile digital echo laboratory.
Results: A mean of 126 children were examined each visit. 40 were scheduledfor operation on the basis of the echocardiography. Cardiac defects included coro-nary fistulas, unroofed coronary sinus, sinus venosus defect, atrioventricular sep-tal defects and other. The digital documents were reviewed and confirmed pre-,intra- and postoperatively from the surgeons. There was no relevant discrepancy.Four patients were transfered to a German heart centre, one child was scheduledfor re-operation in Rome after sending images and films via email. A mean of 5still images and 8 films were documented per patient (8.1 megabytes).Conclusions: The truly mobile digital echo laboratory lead to excellent image andreport documentation. Due to the small system size it could be taken along withthe hand luggage on the airplane and deployed all over the world. The possibilityof MPEG-4 conversion allows telemedicine consultation with experts anywhere inthe world per email.
THE LATEST ON NON-CORONARY CARDIACINTERVENTIONS
5085 PFO closure without implantable devices
M. Skowasch, M. Leetz, E. Fischer, N. Majunke, A. Baranowski,C. Heinisch, N. Wunderlich, H. Sievert. CardioVascular CenterFrankfurt, Frankfurt Am Main, Germany
Introduction: Currently available techniques for catheter PFO closureto prevent paradoxical embolism rely on placement of a permanent implant and,therefore, carry the disadvantages associated with a foreign structure remainingin the body. The PFXTM Closure System, (Cierra, Inc., Redwood City, CA) em-ploys monopolar radiofrequency (RF) energy as the closure mechanism withoutthe necessity of an implantable device. Procedural and mid-term outcomes usingthis device were evaluated at a single center.Patients and Methods: The device is composed of a disposable catheter withan electrode housing, an radiofrequency (RF) generator and a vacuum pump.The catheter is advanced over a guidewire until the distal housing is positionedover the PFO on the right atrial surface. Once in place, vacuum is applied topull the tissues of both septa together. Between April and November 2005, in thefirst clinical use of the device, 40 patients with history of stroke or TIA due toparadoxical emboli underwent PFO closure under local anesthesia. Mean patientage was 49 ± 12 years (18-65 yrs). The mean balloon measured PFO diameterwas 8.1 ± 2.6 mm (3 - 15). Septal aneurysm was present in 35% of patients.Procedure time averaged 35.5 ± 12.8 minutes. Average energy application was26.6 ± 3.6 Watts for a duration of 6.6 ± 2.0 min. All patients received aspirin (100mg minimum) and clopidogrel (75 mg) for at least 6 weeks. TransesophagealEchocardiography (TEE) and ECG were performed at 1, 3 and 6 months post-procedure.Results: In 37 out of 40 patients (93%), the device was successfully introduced,positioned at the PFO and energy applied. Size and shape of the PFOs preventedadequate closure in two and vacuum position was lost twice during energy ap-plication in one case, necessitating conversion to a conventional PFO implantclosure device. One patient whose PFO was not closed with RF successfully re-ceived an implantable device at 3 month follow- up (FU). FU interval ranged from1 to 7.5 months (3.8 ±2) with a c losure rate of 44% at last FU. During the courseof patient enrollment, modifications to the device and treatment were made. Atotal of 16 patients of the whole collective have been treated sicne then with thenew device. Their FU period ranged from 1 to 3 months with a closure rate of 69%(11/16). Complications due to the device or energy induced pains or arrhythmiaswere not observed.Conclusions: Thus, PFO closure with radiofrequency is technically feasible andsafe. Important changes in the treatment device and technique resulted in promis-ing clinical outcomes. Longer term FU data will be presented.
5086 Percutaneous closure of Atrial septal defect in adults:longterm results and complications
C. Heinisch, H. Sievert, A. Baranowski, N. Wunderlich, N. Majunke,M. Leetz, E. Fischer. CardioVascular Center, Frankfurt, Germany
Background: Transcatheter closure of ASDs is well established. How-ever, information about long-term results is limited.Methods: Since Mai 1992 730 patients underwent percutaneous ASD-closurein our center. Mean age was 47.2 ± 17.1 years. Mean stretched diameter 20 ±6.4mm. Mean Qp/Qs ratio 1.83 ± 0.68. 79 patients had multiple defects. The fol-lowing devices were used: 563 Amplatzer, 51 Helex, 42 StarFlex, 10 AngelWings,31 ASDOS, 4 CardioSeal, 25 Sideris, 1 Sideris-Patch, 1 Rashkind, 2 SolySafe.The patients underwent TEE, X-ray and EKG one and six months after procedure,thereafter follow up was performed clinically and by questionnaries (follow-up 1-127 months).Results: Implantation was successful in 715/730 (97.9%). Mean procedure time:47.7 ± 26.8 min, mean X-ray time: 9 ± 9.2 min. Mean hospital stay was 1.3 ±1.1 days. 4 patients developed a haemopericardium after intervention (surgeryuneventful), in 3 patients the occluder embolized, 1 patient developed retroperi-toneal haematoma without further sequelae. After 6 months a hemodynamicallyrelevant shunt was diagnosed in 0.5%. Mean Qp/Qs ratio after 6 months was1.0 ± 0.28. During follow-up 4 patients underwent surgery because of persisting
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

The latest on non coronary cardiac interventions / Improving viability in the ischaemic heart 873
shunt. 22 pts developed atrial fibrillation, 10 patients were diagnosed with smallpericardial effusion (no further clinical consequences), 6 patients developed athrombus on the occluder, 7 patients suffered from a TIA, 8 patients had a stroke.9 patients died during follow-up due to non-procedure related reasons.Conclusion: Percutaneous closure of atrial septal defects is feasible and safe.Complications are rare even during long-term follow-up.
5087 Procedural Characteristics and clinical results ofpercutaneous Atrial Septal Defect Closure using asimplified Intracardiac Echo guidance
M. Abeytua, G. Linares, A. Forns, F. Sarnago, T. Datino, E. Garcia.Hospital General Gregorio Maranon, Cardiology, Madrid, Spain
Background: Atrial Septal Defect (ASD) Closure is usually performed by trans-esophageal echo guidance and simultaneous balloon correlation. We have evalu-ated the results of ASD closure guided by intracardiac echo (ICE) without sizing-balloon correlation.Methods: We have analyze the efficacy and safety of intracardiac echo guidanceusing the ICE catheter by Boston Scientific hooked to the Ultraview or Galaxyconsole for percutaneous ASD closure with the Amplatzer device. The procedurewas performed with only local anaestesia and the mean procedural and fluorotime were 32±12 and 8±4 minutes respectively. All the patients referred for per-cutaneous ASD closure were accepted for independent of the size observed byechocardiography.Results: We attempted percutaneous ASD closure in 112 consecutive patientswith echocardiographic diagnosis of ASD. 82 (73,2%) were female and the aver-age age was 42,36 years (SD 15,38). Sizing-balloon correlation was needed onlyin 10 patients (8,9%) and Transesophageal Echo in 1 patient (0,9%). Proceduralsuccess was achieved in 102 patients (91,1%). In 10 patients the defect was tolarge for percutaneous closure and the procedure was abandoned without com-plications. Transthoracic echocardiography control at 24 hours showed residualshunt in 8 patients (7,1%) which was not longer present at 1 month in 7. Only1(0.9%) patient remained with small residual shunt at 6 months Conclusions: In-tracardiac echocardiography is a very useful tool to guidee ASD percutaneousclosure in adult patientsand makes the procedure easy to performed and confort-able for the patients.
5088 Immediate results of percutaneous mitralcommissurotomy. Analysis of a series of 3709 patients
M. Majdoub, S. Tawn, B. Iung, D. Messika-Zeitoun, E. Brochet,J.M. Juliard, D. Himbert, A. Vahanian. Bichat Hospital, Cardiology,Paris, France
Purpose A large single-centre series enables the results of percutaneous mitralcommissurotomy (PMC) to be accurately assessed and predictive factors to beidentified with an adequate statistical power.Methods Between 1986 and 2005, 3709 consecutive patients underwent PMC inour institution. Their mean age was 48±15 yrs [9-86], 2950 (80%) were female,639 (17%) had had previous commissurotomy, 1182 (32%) were in atrial fibrilla-tion, 1210 (32%) were in NYHA class I or II, 2367 (64%) in class III, and 132 (4%)in class IV. Echocardiographic examination showed that 337 pts (9%) had pliablevalves and mild chordal thickening (group I), 2256 (61%) had pliable valves andextensive subvalvular disease (group II), while 1116 (30%) had calcified valves(group III).Results There were 40 cases of technical failure (1%). The effective proceduresused a single- or double balloon in 616 cases and the Inoue balloon in 3053. AfterPMC, valve area (VA), as assessed by planimetry, increased from 1.03±0.23 to1.87±0.30 cm2 (p<0.0001). Adverse events were in-hospital death, 14 (0.4%);tamponade, 7 (0.2%); and mitral regurgitation (MR) ≥3/4, 162 (4.4%). Good im-mediate results were defined as a final VA ≥ 1.5 cm2 without MR >2/4 and wereobtained in 3284 pts (88.5%). This proportion did not change significantly overthe years (p=0.27). Multivariate logistic regression analysis identified the follow-ing predictors of poor immediate results: older age (p<0.0001), higher NYHAclass (p=0.0007), higher echocardiographic group (p<0.0001), female gender(p=0.004), smaller initial VA (p<0.0001), higher initial gradient (p<0.0001), thepresence of mild initial MR (p=0.0004), and the non-use of an Inoue balloon(p=0.0008).Conclusions: The results of this series 1) Confirm the safety and efficacy of PMCin a variety of patient subsets. 2) Show that prediction of the immediate resultsof PMC is multifactorial and that, besides anatomy, a number of other patientcharacteristics should be taken into account in patient selection.
5089 Percutaneous mitral valve annuloplasty for ischemicmitral regurgitation. First in man experience with atemporary implant
O. Dubreuil, A. Basmadjian, B. Thibault, L. Bilodeau. Montreal HeartInstitue, Hemodynamic, Montreal, Canada
Background: Functional moderate to severe mitral regurgitation (MR) occurs in19% of patients after myocardial infarction and 15% of dilated cardiomyopathy.Although surgical annuloplasty remains the standard treatment, its application
is limited by high morbidity and mortality and is rarely performed without surgi-cal revascularization. After animal study, we evaluated the human feasibility andacute efficacy of a novel percutaneous annuloplasty device (PTMA-Viacor) placedin the coronary sinus (CS): the implant remodels the mitral annulus, by reducingthe anterior-posterior (A-P) annular dimension, thus improving leaflet co-aptationand reducing MR.Methods: Patients referred to our institution with NYHA functional class II or III,ischemic mitral regurgitation graded 2+ to 4+ and severe coronary artery diseaserecurring surgical revascularization and mitral annuloplasty were screened. Con-traindications to PTMA included abnormal mitral leaflets or any morphological mi-tral apparatus abnormality. Preoperatively, under general anaesthesia and trans-esophageal echocardiography guidance, a temporary PTMA device was placedpercutaneously through the right internal jugular vein in the CS.Results: Three patients were included with ischemic MR graded 2+ or 3 withmitral annular dilatation. All had dilated ventricle (diastolic diameter: 62,7 ± 6,5mm), left ventricle dysfunction (39 ± 14% LVEF) and at least some segmental hy-pokinesia. After device placement, MR and regurgitant volume were substantiallyreduced (≥ 2 grade reduction) via mitral annular A-P diameter reduction (see ta-ble) in 2 patients. In one patient, despite proper advancement of the sheath in theCS, the PTMA device could not be deployed due to extreme angulated anatomy.After device removal, all patients were subsequently operated without adverseevents including visual inspection of the CS.
Patient no. 1 Patient no. 3
Baseline Treatment Baseline Treatment
MAD A-P diastolic, mm 37 32,3 38,4 35,5MAD A-P systolic, mm 36 34 39 34,6Regurgitant volume (ml) 37,6 21,7 26,1 8,4
MAD = Mitral annular diameter
Conclusion: Temporary percutaneous mitral annuloplasty in CS reduce ischemicMR by reducing mitral annular A-P diameter. Permanent implants are being de-veloped.
5090 Pulmonary valvuloplasty in adults using the Inoueballoon catheter
H.U.N.G. Pham, L.H. Nguyen, M.H. Nguyen, N.Q. Nguyen, D.L. Do,L.V. Nguyen, K.G. Pham. Vietnam Heart Insitute, Vietnam HeartInstitute, Hanoi, Viet Nam
Background: Although pulmonary valvular stenosis is not uncommon in adults.There are few reports of percutaneous pulmonary valvuloplasty in adults, espe-cially using Inoue balloon. OBJECTIVES: This report describes the experiencein adult patients undergoing Pulmonary valvuloplasty using Inoue balloon andevaluates its effectiveness and tolerance.Methods: Over an 4-year period (2000-2004), pulmonary valvuloplasty using In-oue balloon was considered in 35 adult patients [19 men, 16 women; mean age28.0 years ± standard deviation (SD) 10.3; range 16-53 years] with congenitalpulmonary valve stenosis. Sixteen patients were asymptomatic with pulmonarysystolic murmurs, although 19 patients presented with dyspnea. Before the pro-cedure, the peak-to-peak transpulmonary valve gradient was 91±40 mmHg SD,with a mean right ventricular systolic pressure of 107±41 mmHg SD.Results: The procedure was technically successful in all patients but one (98%).One falure because balloon could not pass throught pulmonary orifice valve dueto very tight valve stenosis. Among all patients with technical success all toleratedwell and free of major complications. The mean right ventricular systolic pres-sure and the pulmonary valvular peak-to-peak systolic gradient decreased from107±41 to 56±19 mm Hg (p = 0.001) and 91±40 to 21±7 mm Hg (p = 0.0002),respectively. An infundibular peak-to-peak systolic gradient either developed (n =13) or increased (n = 5). None of the patients were treated with beta-adrenergicblockers before or after the valvuloplasty. Eighteen patients underwent echo fol-low up study 12-24 months (mean 14) after treatment, and had no evidence ofvalvular restenosis. The mean right ventricular systolic pressure and the meaninfundibular peak-to-peak systolic gradient decreased, compared to the valuesimmediately after valvuloplasty (56 to 47 mm Hg, p = 0.03, and 28 to 10 mm Hg,p = 0.03, respectively).Conclusions: The study suggests that pulmonary valvuloplasty in adults usingthe Inoue balloon catheter technique is feasible, safe, and effective.
IMPROVING VIABILITY IN THE ISCHAEMIC HEART
5095 Inotropic effects of substances released afterischaemia on isolated rat cardiomyocytes
K. Birkenmeier1, A. Staudt1, W.-H. Schunck2, I. Janke2, C. Labitzke2.1Universitaetsklinikum Greifswald, Klinik Fuer Innere Medizin B,Greifswald, Germany; 2Max-Delbrueck-Institut Molekulare Medizin,
Berlin, Germany
Background: During reperfusion, cardiodepressive factors are released from iso-lated rat hearts after ischaemia. The present study analyzes the mechanisms by
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

874 Improving viability in the ischaemic heart
which these post-ischaemically released substances mediate their cardiodepres-sive effect.Methods: After 10 min of global ischaemia, isolated rat hearts were reperfusedand coronary effluent was collected over a period of 30 s. We tested the effect ofthis post-ischaemic effluent on cell shortening and calcium metabolism, by appli-cation of fluorescence microscopy of field-stimulated rat cardiomyocytes stainedwith Fura-2AM. Cells were pre-incubated with various inhibitors: e.g., the non-specific COX inhibitor indomethacin (5 μmolar), the specific COX-1 inhibitor SC-560 (0.25 μmolar), the specific COX-2 inhibitor NS-398 (0.25 μmolar), and thenon-selective potassium (ATP) channel blocker glibenclamide (1 μmolar). Lysatesof cardiomyocytes were tested for expression of COX-1 and COX-2 in Westernblot.Results: In contrast to non-ischaemic effluent (control), post-ischaemic effluentinduced a concentration-dependent reduction of calcium transient (dilution 1:4:-15 ± 2%) und cell shortening (dilution 1:4: -39 ± 4%, p < 0.001 vs. control) inthe rat cardiomyocytes. After pre-incubation of cells with indomethacin, the neg-ative inotropic effect was attenuated: i.e., with calcium-transient (dilution 1:4: -0.2± 0.1) and contractility (dilution 1:4: -11.1 ± 1). SC 560 had no influence on theeffect of post-ischaemic effluent on calcium transient and systolic cell shorten-ing. After pre-incubation with NS-398, effects on calcium transient (dilution 1:4:-0.3 ± 0.1) and contractility (dilution 1:4: -7.7 ± 1) were reduced (p < 0.001).The inducibly expressed COX-2 was detected in freshly isolated cardiomyocytesprepared for fluorescence microscopy. The effect of the ischaemic effluent waseliminated in applications of glibenclamide. The potential protective effect of post-ischaemic effluent was investigated while extracellular calcium was increased.Post-ischaemic effluent significantly reduced the intracellular diastolic and systoliccalcium increase (p < 0.01). When cells were incubated with the non-ischaemiceffluent (control) the intracellular diastolic and systolic calcium metabolism wasn‘tinfluenced.Conclusion: The cardiodepressive effect of post-ischaemic effluent is COX-2-dependent and is cardioprotective.
5096 Ischemic preconditioning prevents calpain-mediatedimpairment of Na+/K+-ATPase activity during earlyreperfusion
V. Hernando, D. Garcia-Dorado, J. Inserte, I. Barba, J. Soler-Soler.Hospital Universitari Vall d’Hebron, Cardiology, Barcelona, Spain
Objectives: Ischemic preconditioning (IPC) attenuates calpain activation dur-ing reperfusion. Herein, we tested the hypothesis that enhancement of Na+/K+-ATPase activity during early reperfusion as a result of calpain inhibition is involvedin the protection afforded by myocardial IPC.Methods: Intracellular Na+ concentration ([Na+i]) measured using 23Na-magnetic resonance spectroscopy, Na+/K+-ATPase activity, detachment ofNa+/K+-ATPase alpha subunits from the membrane cytoskeleton, degradationof fodrin and ankyrin, and calpain activation were analysed in isolated rat heartsreperfused after 60 min of ischemia with or without previous IPC and differenttreatments aimed to mimic or blunt the effects of IPC.Results: In non-treated hearts subjected to ischemia, reperfusion for 5 minseverely reduced Na+/K+-ATPase activity, and dissociated α1 and α2 subunitsof Na+/K+-ATPase from the membrane-cytoskeleton complex in parallel with pro-teolysis of α-fodrin and ankyrin-B and calpain activation. IPC accelerated recov-ery of [Na+i], increased Na+/K+-ATPase activity and prevented dissociation ofNa+/K+-ATPase from the membrane-cytoskeleton complex, loss of α-fodrin andankyrin-B and calpain activation, effects that were associated to attenuated LDHrelease and infarct size and improved contractile recovery. These effects of IPCwere reproduced by perfusing the hearts with the calpain inhibitor MDL-28170and by transient stimulation of cAMP-dependent protein kinase (PKA) with CPT-cAMP, while they were reverted by perfusing with the PKA inhibitor H89.Conclusion: The results of the present study are consistent with the hypothesisthat enhanced recovery of Na+/K+-ATPase activity during reperfusion as a resultof attenuated calpain-mediated detachment of the protein from the membrane-cytoskeleton complex contributes to the protection afforded by IPC.
5097(W) Cardioprotection by intracellular delivery of heatshock protein 27 in ischemia/reperfusion heartinjury model
J.H. Chung, J.B. Kim, J.H. Kwon, Y. Jang. Yonsei UniversityCollege Of Medicine, Cardiovascular Research Institute, Seoul,
Korea, Republic of
Heat shock proteins (Hsps) provide one kind of defense against stresses suchas high temperature, hypoxia/ischemia and oxidative stress in all mammalian celltypes. One such protein which is highly induced during the stress response isHsp27, and its expression is correlated with the cellular survival in responseto cytotoxic insults. Previous findings have suggested that augmentation of thelevel of Hsp27 represents a potential therapeutic strategy for the treatment ofcritically ill patients. In this study, using protein delivery approach, we studiedthe potential cardiac protective effect of Hsp27 in rat cardiac myoblast and is-chemia/reperfusion model. Human Hsp27 gene was fused with a Tat-proteintransduction domain vector at its N-terminus. The Tat-Hsp27 fusion protein wasexpressed in E. coli and purified. The Tat-Hsp27 fusion protein was efficiently
delivered to cardiomyocytes, and its transduction showed cytoprotective effectagainst the hypoxic stress in vitro. Moreover, transduction of Tat-Hsp27 also atten-uated hypoxia-induced apoptosis, which was accompanied by reduced caspase-3 activity. In addition, intraperitoneal injection of Tat-Hsp27 into rat resulted inefficient protein transduction in heart tissues within 2 h, decreased infarcted my-ocardium (control vs Tat-Hsp27, 39.1% vs 29.5%, p<0.05) and preserved heartfunction (fractional shortening and 2D strain of myocardium, 15.6% vs 33.4%,4.83 vs 9.59, p<0.05), as determined at 7 d after ischemia/reperfusion. These ex-perimental findings suggest that the intracellular delivery of therapeutic proteinsmay represent a novel strategy of protein therapy for ischemic heart diseases.
5098 Cardiomyocyte-specific overexpression of Nitric OxideSynthase 3 confers protection against apoptoticcardiomyocyte cell death
G. Marsboom1, M. Pellens1, H. Gillijns1, P. Jans1, M. Jiang2,S. Janssens1. 1University of Leuven, Leuven, Belgium; 2University of
Leuven, Leuven, United States of America
Introduction: After coronary artery occlusion, programmed cell death of car-diomyocytes in the peri-infarct zone contributes to infarct expansion and to thedevelopment of heart failure. Nitric oxide dose-dependently regulates apoptosisand may confer cytoprotective as well as cytotoxic effects. We investigated theeffect of cardiomyocyte-specific overexpression of NO synthase 3 on cardiomy-ocyte apoptosis in vitro and in vivo.Methods: Neonatal murine cardiomyocytes were isolated from transgenic micewith cardiomyocyte-restricted overexpression of NOS3 (NOS3-TG) or wild typeC57Bl/6 littermates (WT). Cardiomyocytes were plated on 12-well dishes at adensity of 50,000 cells and cultured in DMEM medium containing 14% serum.After 3 days, apoptosis was induced by incubation with staurosporin for 24 hoursand the number of beating cardiomyocytes was compared in both genotypesbefore and after stau. Apoptosis was quantitated by measuring the number ofTUNEL immunoreactive cardiomyocytes and by FACS analysis of cardiomyocyteploidy before and after 24 h incubation with 0.25 and 1.0 μM stau, resp. Apop-totic cardiomyocyte cell death in vivo was semi-quantitatively evaluated 72 h afterproximal LAD ligation in the infarct core and border zone of NOS3-TG (n=7) andWT (n=8) mice using TUNEL and activated caspase 3 immunohistochemistry.Results: After 24h stau, the residual percentage of beating NOS3-TG cardiomy-ocytes remained significantly higher than WT cardiomyocytes (56±13% versus36±7%, P=0.001) and the percentage of TUNEL immunoreactive cardiomyocytesfrom NOS3-TG was less than from WT (19±6% vs 38±12%, P=0.03). FACS anal-ysis of stau-exposed cardiomyocytes using propidium iodide staining indicated asignificantly greater proportion of WT cells with DNA fragmentation compared tocells from NOS3-TG. Proximal LAD ligation caused a similar infarct size compris-ing 21±4 and 23±1% of the LV resp, but TUNEL immunoreactivity was muchmore predominant in the infarct core, border zone and remote myocardium of WTmice compared to the more focal TUNEL immunoreactivity, confined to the bor-der zone of NOS3-TG with little detectable apoptosis in remote area’s. Similarly,activated caspase 3 immunoreactivity was markedly reduced in the infarct borderin NOS3-TG compared to WT mice.Conclusion: Cardiomyocyte-restricted overexpression of NOS3 confers protec-tion against staurosporin-induced in vitro apoptotic cell death and limits in vivoapoptotic cardiomyocyte death in the infarcted myocardium. The important anti-apoptotic role of NOS3 in cardiac myocytes may contribute to its beneficial role inpost-infarction LV remodeling.
5099 Neuregulin/Erb2 is involved in regulation of oxidativestress in adult rat ventricular cardiomyocytes
F. Timolati1, D. Ott2, L. Pentassuglia2 , T.M. Suter2, J.C. Perriard3,C. Zuppinger3 . 1Inselspital Bern, Dkf, Bern, Switzerland; 2Inselspital,Cardiology, Bern, Switzerland; 3Federal Institute of Technology, Cell
Biology, Zurich, Switzerland
Objective: A new cancer therapy (trastuzumab) in form of antibodies against theerbB2 signaling system is associated with worsening of anthracycline-inducedcardiotoxicity. Cardiotoxicity of doxorubicin (Doxo) cancer therapy has a complexaetiology involving the formation of reactive oxygen species (ROS) and alterationsof calcium homeostasis. We hypothesized that neuregulin-1 beta (NRG), a ligandof the cardiac erbB receptor tyrosine kinases, attenuates Doxo-induced cellulardamage and changes of excitation-contraction coupling by stimulating antioxidantmechanisms in cultured adult rat ventricular cardiomyocytes (ARVM).Methods: ARVM were isolated and treated for 18-48 hours. SERCA protein levelwas analyzed by Western Blot, SR calcium content by rapid application of caf-feine 20mM, EC-coupling parameters by Fura-2 and by phase contrast, geneexpression by RT-PCR and ROS by DCF fluorescence microscopy (defined 0%in untreated and 100% in H2O2).Results: Doxo caused an increase in systolic calcium at 1 m M (135±11%),followed by a decrease at higher doses (65±2% in 10μM, 18±2% in 20μM),but diastolic calcium was raised at all the doses (120-150%). NRG alone didnot change calcium amplitude, but it protected from Doxo-induced alterations(91±7% vs 134±7% in Doxo 1μM; 83±5% vs 68±5% in Doxo 10μM), similarlyas the antioxidant N-acetylcystein (112±4 vs 135±11% in Doxo 1μM; 88±5%vs 65±2% in 10μM). Doxo treatment decreased SERCA protein and SR calcium
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
Improving viability in the ischaemic heart / Ageing and senescence: cellular and molecular aspects 875
content only at 10μM and NRG attenuated this damage (62±6% in Doxo 10μMvs 77±6% adding NRG, 112±7% in NRG alone). Therefore, NRG was tested forstimulating antioxidant gene expression. NRG and Doxo regulated oppositely theglutathione reductase gene (215±40% in NRG, 19±4% in Doxo, 38±11% in thecombined treatment). We confirmed the anti-oxidant role of erb2 activation com-bining NRG with H2O2 and measuring total ROS by DCF fluorescence. NRG de-creased H2O2-induced oxidative stress (69±3% vs 100%). The peroxide-induceddecrease in SERCA protein (56±2%) was attenuated by pretreatment with NAC(72±5%) or NRG (110±19%). The antioxidant action of NRG vs H2O2 was abol-ished by preincubating with LY 294002, but not by U126 suggesting that this effectdepends on the Akt and not on the MAPK pathway.Conclusions: NRG attenuates Doxo-induced alterations of EC-coupling by re-ducing oxidative stress in ARVM. Inhibition of the erbB2/NRG signaling pathwayby trastuzumab in patients concomitantly treated with Doxo might prevent benefi-cial effects of NRG in the myocardium.
5100 Stimulation of glucose transport by insulin or byactivation of AMP-activated protein kinase (AMPK) isdefective in insulin resistant cardiac myocytes: the roleof nuclear receptors
L. Derouette, I. Papageorgiou, R. Lerch, C. Montessuit. GenevaUniversity Hospitals, Cardiology, Geneva, Switzerland
Background: The survival of cardiomyocytes in conditions of metabolic stress,such as ischemia or reperfusion, critically depends on an acceleration of the gly-colytic flux fueled by increased glucose transport. The stimulation of glucosetransport results from the recruitment of the glucose transporter GLUT4 fromintracellular pools towards the cell surface. In physiological situations, GLUT4translocation obeys to signals triggered by insulin binding to its receptor. Duringmetabolic stress, the AMP-dependent protein kinase (AMPK), deemed the "cel-lular fuel gauge", senses the low energy charge and stimulates the translocationof GLUT4.Purpose: To determine whether insulin-resistant cardiomyocytes are also resis-tant to activation of AMPK and whether restoration of insulin responsiveness alsorestores AMPK-induced glucose transport.Methods and Results: Experiments were performed in adult rat cardiomyocytes(ARC) exhibiting insulin resistance. Treatment of ARC for three days with theinsulin-sensitizing agent 9-cis retinoic acid (RA) increased insulin-stimulated glu-cose transport. Stimulation of glucose transport in response to insulin requiresthe phosphorylation of the signaling intermediate Akt/PKB on the residues Thr308and Ser473. Although phosphorylation of Akt/PKB on Ser473 was normal, phos-phorylation of Thr308 in response to insulin was rather low in insulin resistantARC. However, treatment with 9-cis RA markedly increased Thr308 phosphory-lation in response to insulin.Activation of AMPK by a combination of the pharmacological agonists AICARand metformin stimulated glucose uptake in insulin-sensitive ARC. In contrast,AICAR/metformin failed to increase glucose transport in insulin-resistant ARC.The restoration of insulin responsiveness by 9-cis RA in insulin resistant ARCwas associated with improved glucose transport in response to AICAR/metformin-mediated AMPK activation.Conclusion: Insulin resistance of cardiac myocytes is associated with a defec-tive stimulation of glucose transport in response to AMPK activation. Insulin re-sistance may therefore aggravate ischemic or post-ischemic injury. The defectivesignaling component common to the insulin- and AMPK-triggered pathways re-mains to be identified.
AGEING AND SENESCENCE: CELLULAR ANDMOLECULAR ASPECTS
5101 Molecular basis for the increased vulnerability of theaging heart to injury
A. Jahangir, E.L. Holmuhamedov, C.C. Cabrera Aguilera, A.S. Oberlin,N. Ashfaque, A.E. Alekseev, A. Terzic. Mayo Clinic, Cardiology,Rochester, Minnesota, United States of America
While aging is associated with increased vulnerability of the heart to injury, themolecular basis for this is not clear. Using young (6 month) and aged (24 monthold) Fischer 344 rats, we demonstrated that the tolerance of the aged wholeheart, isolated cardiomyocytes and mitochondria to ischemia-reperfusion, Ca2+-overload and hypoxia-reoxygenation stress was reduced. The protection con-ferred by ischemic preconditioning (IPC), robust in the young was lost in thesenescent heart, which demonstrated poor functional recovery compared to theyoung. The energetic reserve and Ca2+ handling capacity of the aged mito-chondria was reduced, which exhibited an increased susceptibility to injury, butmaintained responsiveness to the protective effect of modulators of mitochondrialmembrane potential. Metabolic regulation of the ATP-sensitive potassium (KATP)channel, the major regulator of the endogenous cardioprotective response wasreduced in the aging heart with decreased activation by changes in ATP/ADPratio; however, channel responsiveness to activation by potassium channel open-ers was preserved. Expression of several genes coding for proteins involved instress responses, cardiac energetics and mitochondrial oxidative phosphoryla-
tion was decreased in the aging heart. This included, decrease in the expressionof both the genes KCNJ11 and ABCC9 that codes for the two subunits (Kir6.2 andSUR2A, respectively) of the cardioprotective KATP channels. Thus, age-relateddown-regulation of the message and function of the sarcolemmal KATP channel,as well as genes coding for mitochondrial proteins may underlie reduction in tol-erance of the aging heart to stress. The aging heart can be protected againstmetabolic injury by modulation of the sarcolemmal KATP channels and mitochon-drial function.
5102 Characterisation of human endothelial cells lackingmitochondrial DNA (Rho0 cells): a model system tostudy the involvement of mitochondria in cellularsenescence
J.R. Wilkinson1, S.L. Colombo1, J. Erusalimsky2. 1University CollegeLondon, Cardiovascular Research Group, Wing 2.3, London, United
Kingdom; 2University of Wales Institute Cardiff, Cardiff School of HealthSciences, Cardiff, United Kingdom
Background and purpose: Mitochondria are the major cellular energy gener-ators. They also play an important role in other cellular activities including: pro-duction of reactive oxygen species, regulation of calcium homeostasis and or-chestration of apoptosis. The feasibility of culturing mammalian cells depleted ofmitochondrial DNA, and hence lacking functional mitochondria (Rho0 cells), is avaluable tool for studying the participation of mitochondria in the above processes.Mitochondria might also be involved in cellular senescence, a process that can-not be studied using immortalized cell lines, from which the majority of Rho0 cellsare normally derived. Endothelial cell senescence may be involved in vasculardisease (reviewed in Exp.Gerontol 2005.40:634). The aim of our study was toascertain the feasibility of producing Rho0 human umbilical vein endothelial cells(HUVEC) that could be used to investigate the involvement of mitochondria inoxidative stress-induced senescence.Methods: HUVEC were cultured in medium supplemented with high-glucose, uri-dine and 50ng/ml ethidium bromide (EB) to generate Rho0 cells. Rho0 status wasevaluated by measuring cell growth in uridine-free medium and real time PCR ofmitochondrial gene expression.Results: Culture of HUVEC with EB for 12 days caused a decline in the expres-sion of cytochrome-C oxidase subunit-1 and ATPase subunit-6, to <1% of theinitial levels. At this time no growth was detected in uridine-free medium. Thecontinuous presence of EB was required to maintain the Rho0 phenotype. Therewas no apparent decline in viability, although Rho0 grew at a reduced rate com-pared to wild type (WT) cells. ATP levels were 990 and 727 (pmole/mg protein)in WT and Rho0 cells respectively (p<0.01). Incubation with metabolic inhibitorsindicated that in both cell types ATP levels were maintained primarily by glycoly-sis; mitochondria contributing marginally to ATP levels in WT cells. Treatment ofWT HUVEC with tert-butyl-hydroperoxide (25-50μM) increased apoptosis (mea-sured by caspase activity) and the percentage of senescent cells (measured bysenescence-associated β-galactosidase staining). In contrast, in Rho0 HUVECthis treatment had no significant effect on apoptosis and caused significantly lesssenescence.Conclusions: HUVEC rely mainly on glycolysis for their energetic demands, thusenabling the derivation of Rho0 cells. Our initial results using this system suggestthat in endothelial cells mitochondria are involved in the induction of senescenceby oxidative stress.
5103 Mice overexpressing mitochondrial-targeted catalaseare protected against cardiac aging
D.F. Dai, N.J. Linford, L.F. Santana, P. Treuting, W. Ladiges,P.S. Rabinovitch. University of Washington, Pathology, Seattle, UnitedStates of America
We have previously shown that mice overexpressing mitochondrial-targeted cata-lase (MCAT) mice have 21% extension of median lifespan. These mice wereshown to be protected from oxidative damages to mitochondria. Since heart isan organ rich in mitochondria and high in oxygen utilization, we hypothesize thatmitochondrial overexpression of catalase might protect against cardiac aging.Methods and Results: Echocardiography was performed for 170 mice in thelongevity cohort study. These mice were fed regular chow diet and were notsubjected to any other experimentation. In non transgenic mice, we found age-dependent increases in left ventricular mass index and left atrial dimension, de-crease in Em/Am as measured by Tissue Doppler Imaging of mitral annulus, andworsening of myocardial performance (Tei) index as well as increased preva-lence of diastolic dysfunction. All of the above findings were significantly betterin age-matched MCAT mice (p<0.001 to 0.04 for different ages). Systolic func-tion (fractional shortening) was relatively preserved during aging and not differentbetween MCAT and non transgenic mice. Real-time gene expression analysis ofcalcium-handling proteins revealed that Sarcoplasmic reticulum Ca-ATPase 2a(SERCA2a), sodium calcium exchanger (NCX), ryanodine receptors (RyRs) andcalsequestrins (casq) were significantly down-regulated in aging non-transgenicmice. These genes were much better preserved in aging MCAT mice (SERCA2aand NCX, p<0.005; RyRs and casq, p∼0.08). By using Ca-transient analysis, wedemonstrated that MCAT mice had slightly faster rate of cytoplasmic calcium re-uptake and significantly lower increase of end-diastolic cytoplasmic calcium after
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

876 Ageing and senescence: cellular and molecular aspects / Prognostic factors in ACS: the new, the old and the useless
incremental pacing (0.5 to 4 Hz). These results are consistent with, but extendprevious histologic observations that MCAT mice were protected against arte-riosclerosis and cardiomyopathy during aging.Conclusion: Mitochondrial-targeted overexpression of catalase can protectagainst cardiac aging changes, which include left ventricular hypertrophy and di-astolic dysfunction. These protective effects are partly mediated through preser-vation of SERCA2a and NCX.
5104 Lysophosphatidic acid decreases survival andproliferation of senescent human cardiomyocytes inculture: potential implication for cardiomyocyte ageing
S.I. Svetlov1, V.L. Serebruany2. 1University of Florida, Neuroscience,Gainesville, United States of America; 2HeartDrug Research,
Baltimore, United States of America
Molecular signals linking platelet or endothelial activation and sur-vival/proliferation of cardiomyocytes are poorly recognized. The capacityof ageing human cardiac myocytes to survive and regenerate upon injuriousor inflammatory insult compared to younger cells has not been investigated.Lysophosphatidic acid (LPA) is a simple phospholipid growth factor released fromactivated platelets and endothelial cells in response to inflammatory stimulation.LPA is known to promote survival and proliferation of various cells via three typesof LPA receptor (LPA1, LPA2 and LPA3) encoded by Endothelial DifferentiationGene (EDG) family. In this study, we investigated cell survival and proliferation inhuman cardiomyocytes maintained in cultures for 3 days (‘young’) and 21 days(‘ageing’). Concomitant expression and cell distribution of LPA receptors wasassessed using semi-quantitative RT-PCR and immunocytochemistry. In ‘young’cardiomyocytes, LPA elicited an increase in cell viability and DNA synthesis at 1and 10 μM of LPA, and a slight decrease at high LPA concentration of 50 μM. Incontrast, human cardiomyocytes ageing in culture for 21 days responded to 1and 10 μM LPA by a profound decrease of cell viability and DNA synthesis. Both‘young’ and ‘ageing’ cardiomyocytes expressed similar levels of LPA1 (EDG2)receptor subtype. The cells cultured for 3 days presented LPA3 receptor isoform(EDG3), which disappeared upon cardiomyocyte senescence in culture for 21days. On the contrary, LPA2 (EDG4) receptor was not present in ‘young’ cells,and was up-regulated in ‘ageing’ cardiomyocytes. Thus, the observed differencesin LPA responses may be explained by switching the LPA receptor profileduring ageing of cardiomyocytes in culture. These data suggest that LPA/LPAreceptor system plays a role linking platelet activation and cardiomyocytesurvival/proliferation, and that these responses are altered significantly duringageing.
5105 Long-term exercise training prevents age-relateddiastolic dysfunction by altering myocardial collagencross-linking
S.Y. Choi1, H.J. Chang2, K.I. Kim1, Y.S. Cho1, T.J. Youn1, I.H. Chae1,D.J. Choi1, C.H. Kim1. 1Seoul National University Hospital, Internal
Medicine, Seoul, Korea, Republic of; 2Seoul National University BundangHospital, Internal Medicine, Seongnam, Korea, Republic of
Objective: Heart failure due to diastolic dysfunction remarkably increases withage. There are several reports that long-term exercise prevents diastolic dysfunc-tion in senescent men. The glycation reactions following maturation are true agingprocesses, and attempts at their inhibition presented the sucessful reduction ofvascular and myocardial stiffness.We tested the hypothesis that long-term exercise training will improve age-relateddiastolic stiffness of the myocardium by reducing advanced glycation end prod-ucts(AGEs) cross-linked collagen.Methods: Young (3 month) and old (21 month) male Fischer 344 rats were as-signed to controls (young control: YC, old control: OC), and an exercise group (oldtrained: OT). After 12-week treadmill exercise, the cardiac performance at differ-ent preloads was assessed using the Millar Pressure-Volume system. Histologicand biochemical analysis of extracellular matrix were performed.Results: In OC, compared with YC, cardiac contractility and diastolic functionwere impaired, but EDV was increased. The improvement of diastolic function,especially in diastolic stiffness, by exercise was proved in old rats (table). My-ocardial collagen pepsin solubility (as an index of AGE associated cross-linking)decreased in old rats, consistent with increased cross-linked collagen by AGEs(YC 43.6%, OC 38.1%; p=0006). However, this senescent increment was pre-vented by long-term exercise training (OT 43.9%, OC 38.1%; p=0.032).
Hemodynamic parameters
YC OC OT p-value p-value(YC vs. OC) (OC vs. OT)
LVEDP, mmHg 5.3±0.4 13.2±3.1 11.8±2.2 0.042 0.711CI, ml/min/100g 18.6±0.8 20.5±3.2 26.1±2.3 0.568 0.173EF, % 67.2±3.0 62.4±5.2 72.3±1.2 0.448 0.113+dP/dt, mmHg/s 13,609±1334 6,520±682 9,275±747 0.001 0.027-dP/dt, mmHg/s 9,922±436 4,899±709 6,892±654 0.000 0.070t (Weiss), ms 8.2±0.3 17.3±2.6 12.2±0.61 0.014 0.107LVEDV, μl 203.4±10.6 367.5±21.1 290.2±12.0 0.000 0.003EDPVR slope, mmHg/μl 0.035±0.007 0.073±0.015 0.033±0.010 0.044 0.041
Values are means ± SE.
Conclusions: Long-term exercise training in old rats prevents senescent deteri-oration in diastolic function and LV geometry. The AGEs cross-linking of collagenin myocardium might be a majour determint in senescent diastolic dysfunction.
5106 Arginase inhibition attenuates vascular stiffness inaged rats
A.M. Benjo, S. Ryoo, A.R. White, H. Lim, L. Pellakuru,M. Anderson, D. Nyhan, D.E. Berkowitz. Johns Hopkins Hospital,Anesthesiology/Medicine, Baltimore, United States of America
Purpose: We have recently demonstrated that Arginase (Arg) reciprocally reg-ulates nitric oxide (NO) production in the endothelium and is upregulated in oldrats. Arg inhibition restores NO signaling and endothelial function ex vivo in oldrat vessels. We hypothesized that Arg inhibition decreases age-related vascularstiffness in vivo.Methods: 24 months Wistar rats were implanted with osmotic infusion pumpscontaining the specific Arg inhibitor (S)-(2-boronoethyl)-L-cysteine (BEC) (O) orplacebo (C) for 1 month; a young (Y) cohort, 3-6 months, received placebo.Vascular stiffness was determined pre and post-treatment by pulse wave ve-locity (PWV) using an EKG triggered 10 MHz Doppler probe (Indus Instr.)at thoracic and abdominal aorta locations; PWV was calculated as quotientof separation distance and time difference between pulse arrivals, as mea-sured from EKG’s R-peaks. We used colorimetric determination of urea with α-isonitrosopropriophenone in aortic tissue to quantify Arg activity. Data was an-alyzed with paired t-tests and one-way and repeated measurements ANOVA(GraphPad Prism 4).Results: Vascular Arg activity was significantly higher in the O controls com-pared to the C (427 ± 11.87 vs. 532 ± 31.85, p<0.001); actually the chronic BECtreatment resulted in a vascular Arg activity similar to Y (429 ± 9.45). PWV wassignificantly higher (∼2 fold) in O vs. Y. BEC treatment significantly decreasedPWV in O rats compared with C invoking Arg as a modulator of vascular stiffnessin O rats (Figure 1).
Fig. 1
Conclusions: Arg inhibition in decreases vascular stiffness associated with theaging process, as measured by the PWV, most likely by an NO dependent mech-anisms. This has important implications for therapies to improve vascular compli-ance and ventricular-vascular coupling in aging.
PROGNOSTIC FACTORS IN ACS: THE NEW, THE OLDAND THE USELESS
5111 In troponin positive patients with non-ST-elevationACS, additional risk stratification can not identifycandidates for an early invasive strategy
A. Hirsch1, F. Windhausen1 , J.G.P. Tijssen1, G.T. Sanders1,J.H. Cornel2, H.R. Michels3, R.J. De Winter1 on behalf of the ICTUS
investigators. 1AMC, Cardiology, Amsterdam, Netherlands; 2MCA, Cardiology,Alkmaar, Netherlands; 3Catharina hospital, Cardiology, Eindhoven, Netherlands
Background: Subgroup analysis of previous strategy trial in patients with ACSrevealed that benefit from an early invasive strategy (CAG and revascularizationwithin 24-48 hours) was primarily confined to patients at intermediate or high riskfor adverse outcomes. In the ICTUS trial we could not confirm the general supe-riority of an early invasive strategy in troponin positive ACS patients. Therefore,we assessed whether high risk patients from the ICTUS trial would specificallybenefit from an early invasive strategy.Methods: We developed a multivariate logistic regression model for the predictionof the primary endpoint of death, MI or rehospitalization for anginal symptomswithin one year. The risk factors were selected from: age, sexe, medical history,cardiovascular risk factors, ST deviation and baseline levels of NT-proBNP, cTnTand creatinine. Patients were divided in four risk categories by the calculated riskscore.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Prognostic factors in ACS: the new, the old and the useless 877
Results: The predictive model was based on 1141 of 1200 patients with non-missing values of all risk factors. Diabetes mellitus, prior aspirin use, ST deviation≥1mm, and creatinine clearance <70 were identified as independent predictors,with odds ratios between 1.2 and 1.5. The observed event rates varied from 17%in lowest quartile to 33% in the highest quartile. The event rates for early andselective invasive strategy were virtually the same in all risk categories (figure 1).
Fig. 1
Conclusion: Regardless of the risk at admission no benefit of an early invasivestrategy could be demonstrated in nSTE-ACS patients with an elevated troponinT. These observations challenge the paradigm that patients with the highest riskparticularly benefit from early invasive management.
5112 Polymorphism of endothelial NOS gene promoter hasnegative prognostic impact after ACS
Y.A. Lutay1, A. Parkhomenko1, V. Dosenko2, N. Dovgan1,S. Kozhukhov1 , A. Moibenko2. 1Institute of Cardiology, Ccu, Kyiv,Ukraine; 2Institute of Physiology, Kyiv, Ukraine
An endothelial nitric oxide synthase (eNOS) gene polymorphism (-786T>C) inpromoter region has been associated with cardiovascular disease. We inves-tigated whether carriage of the polymorphism was associated with functionalchanges in the endothelium, and how it affected prognosis in patients with ACS.332 patients with ACS (142 patients without ST elevation and 190 patients withST elevation ACS) and 83 controls were investigated. The eNOS gene polymor-phism has been analyzed by PCR-RFLP (restriction fragment length polymor-phism) analysis. Endothelium-dependent, flow-mediated brachial artery dilatation(FMD) was measured using high-resolution ultrasound.A significant difference in genotype distribution was observed between patientsand controls. Pathological CC genotype was more often determined in ACSpatients (16,6% vs. 6,0%, p<0,01). The multivariate analysis showed that CCgenotype in the eNOS gene promoter was associated with increased risk ofrecurrent ischemic events (death/myocardial infarction) during one-year follow-up.Homozygosity for the CC variant of the eNOS gene promoter in ACS patientswas associated with lower flow-mediated brachial artery dilatation (6.4±1.4% vs9.0±0.7%, p<0.05)
Death/myocardial infarction
Our results suggest that CC genotype of eNOS gene promoter may predisposeto the development of ACS and among ACS patients this genotype is associ-ated with poor prognosis that can be explained by more pronounced endothelialdysfunction.
5113 Osteoprotegerin is an independent predictor oflong-term mortality in patients with acute coronarysyndromes
T. Omland1, T. Ueland2, A.M. Jansson3, A. Persson4, T. Karlsson4,P. Aukrust5, M. Hartford5, K. Caidahl2. 1Akershus Univ Hosp, Univ ofOslo, Dept of Medicine, Oslo, Norway; 2National Univ Hosp, Section
of Endocrinol, Oslo, Norway; 3Karolinska Univ Hosp, Dept of acute medicine,Stockholm, Sweden; 4Sahlgrenska Univ Hosp, Dept of Clin Physiol, Goteborg,Sweden; 5Rikshosp Univ Hosp, Res Inst Int Med, Dept of Medicine, Oslo,Norway
Background: Osteoprotegerin (OPG), a member of the tumor necrosis factor
receptor superfamily, is a potent inhibitor of osteoclastogenesis and regulator ofbone metabolism. The relationship between OPG on admission and long-termmortality in patients with acute coronary syndromes is unknown.Methods: Plasma OPG levels were measured on admission in 1311 patients(median age 66 y, 70% male) with acute coronary syndromes. The median follow-up time was 79 months. The association between OPG concentration and long-term mortality was assessed using Cox proportional hazards regression.Results: 311 patients died during follow-up. Compared with the 1st quartile, anOPG level in the 4th quartile was significantly associated with long-term mortality(Hazard ratio (HR) 4.90 (95% CI 3.33 - 7.22), p<0.0001). After adjustment forage, gender, index diagnosis (ST elevation myocardial infarction (STEMI), non-STEMI, unstable angina), smoking status, prior MI, diabetes, hypertension, Killipclass, serum creatinine and peak CK-MB the hazard ratio was 2.09 (1.31-3.32).The relationship remained significant in subgroups of patients in whom echocar-diographically determined left ventricular ejection fraction was available and ad-justed for (n=509; HR:1.82 (1.06-3.13), p=0.03) and in patients in Killip class I onadmission (n=611, HR: 2.04 (1.25-3.34), p=0.004).
Survival in OPG quartiles 1 to 4
Conclusions: Plasma OPG is strongly predictive of long-term mortality in pa-tients with acute coronary syndromes, independently of conventional risk mark-ers. These findings suggest that this novel biomarker may have clinical utilityfor risk stratification purposes in patients presenting with acute coronary syn-dromes.
5114 Prognostic significance of monoclonal cardiac troponinI assay compared to conventional polyclonal troponin Itest in patients assessed for myocardial ischemia
B. Hassunizadeh, D. Cunningham, A. Shah, Y. Kardouh, H. Ghanbari,M. Daccarett, A. Braunstein, C. Machado. Providence Hospital,
Cardiology, Southfield, Michigan, United States of America
Purpose: Cardiac troponin-I ADV is a new recombinant assay that utilizes mon-oclonal antibodies for detection of cardiac troponin I. The conventional cardiacTn-I assay (cTn-I) uses polyclonal antibodies. The objective was to evaluate riskof death after a six-month follow-up of hospitalized patients with suspected my-ocardial infarction assessed with biomarkers of myocardial damage including themonoclonal cTn-I ADV assay and a simultaneous polyclonal c-Tn-I test.Methods: Blood specimen from hospitalized patients being assessed for myocar-dial infarction were simultaneously analysed for cTn-I ADV and cTn-I. The highestlevels for each patient were used for further analysis. Manufacturer recommen-dations were utilized (cTn-I ADV: negative < 0.04 ng/ml, borderline 0.04 to <0.4ng/ml, positive > 0.4; conventional cTn-I: negative < 0.99 ng/ml, borderline 1.0-3.9 ng/ml, positive > 4.0 ng/ml). Patient survival at 6 months was assessed byreviewing the National Death Index Database and death certificates.Results: The study comprised of 804 prospectively enrolled patients. The meanage was 63 ± 4 years. cTn-I ADV and cTn-I were strongly correlated (r=0.82,p<0.005). Overall 60 deaths in the study cohort were noted. Patients with bor-derline (B) or positive (P) cTn-I ADV elevation (180/804 patients) had significantlyhigher risk of death at six months (32 deaths, RR=3.96 [2.45-6.39], p<0.0001)than patients with negative cTn-I ADV. Patients with a B or P cTn-I elevation(61/804) also had significantly increased risk of death (10 deaths, RR=2.44 [1.3-4.55]; p<0.0057) compared to patients with a negative cTn-I. Patients with B orP cTn-I ADV elevation and simultaneously negative cTn-I (70/804) had signifi-cantly higher risk of death (16 deaths, RR=4.49 [2.61-7.7]; p<0.0001) comparedto patients with both simultaneously negative cTn-I ADV and cTn-I levels.Conclusion: 1) In a large cohort of hospitalized patients assessed for myocardialinfarction, an increased risk of death at six months was seen in the group ofpatients with borderline or greater values of monoclonal cTn-I ADV and also in thegroup of patients with borderline or greater values of polycloncal cTn-I comparedto patients with negative values at baseline. 2) Patients with borderline or greatervalues of monoclonal cTnI ADV and simultaneously negative polyclonal cTn-I hada significantly higher risk of death than patients with simultaneously negative cTn-I ADV and cTn-I. Monoclonal cTn-I ADV may identify a specific group of patientswith a very high risk of death not identified by the polyclonal cTn-I test.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

878 Poster session 7 / Moderated Posters: Metabolism and oxidative stress in endothelial function
5115 Activated Factor XII type A strongly predicts all causemortality after hospitalisation with TnT negative chestpain
V. Poenitz1, T. Brugger-Andersen1, D. Pritchard2, H. Grundt2,D.W.T. Nilsen2. 1Stavanger University Hospital, Cardiology
Department, Stavanger, Norway; 2Axis-Shield AS, Dundee, United Kingdom
Background: The study aim was to assess the utility of activated Factor XII (XIIa)in predicting mortality in patients admitted with chest pain. Recent research hasdemonstrated that in-vivo XIIa exists in several different forms, and that XIIaRconcentrations are strongly predictive of subsequent MI at 30 days follow-up.Methods: All cause mortality within each quartile of XIIaA and XIIaR were com-pared at 30 day, 6 month, 12 month and 24 month follow-up in 871 patients ad-mitted with chest pain. Plasma XIIaA and XIIaR concentrations were determinedby ELISA at admission. A key difference between XIIaA and XIIaR is that assayof the latter requires treatment of the sample (for example, by addition of Triton) tomake the XIIaR available for measurement, whereas for XIIaA no such treatmentis required.Results: Of 871 patients, 396 had a TnT concentration [TnT]>0.05 ng/mL at ad-mission whilst 475 had a [TnT] ≤ 0.05ng/mL (of the latter group, 64% had knownpre-existing coronary heart disease). At 24 months follow-up, 130 (14.9%) pa-tients had died. At all follow-up timepoints, XIIaA concentrations were stronglyassociated with all cause mortality with the strongest association at one-yearfollow-up. Mortality was significantly higher in patients with XIIaA in Q4 as com-pared to Q1, both in all patients (30 Days: OR 4.24, p=0.0055; 6 months: OR 6.08,p<0.0001; 12 months: OR 3.86, p<0.0001, 24 months: OR 2.79, p<0.0001) andespecially in patients with [TnT] ≤ 0.05 ng/mL at admission [30 Days: OR 16.14,p=0.0057; 6 months: OR 15.7; (p<0.0001); 12 months: OR 23.88; p<0.0001, 24months: OR 6.69; p<0.0001].
2 years survival for TnT neg. patients
Conclusion: XIIaA strongly predicts mortality in patients admitted with acutechest pain, particularly in those without significant TnT release at admission.
5116 Cystatin C is a strong independent predictor ofmortality by one year in nSTE-ACS patients with anelevated troponin T
F. Windhausen1 , A. Hirsch1, J.H. Cornel2, J.P. Straalen Van1,G.T.B. Sanders1, R.J. De Winter1 on behalf of The ICTUS
investigators. 1AMC, Cardiology Dept., Amsterdam, Netherlands; 2MCA,cardiology, Alkmaar, Netherlands
Introduction: Even mild renal disease has been shown to be a major risk fac-tor for cardiovascular complications after an acute myocardial infarction. CystatinC is a serum marker of renal function which has a linear relationship beweenplasma levels and glomerular filtration rate, independent of age,gender race andbodysurface area. The prognostic value of Cystatin C in patients with a non ST el-evation acute coronary syndrome with an elevated cardiac troponin T is unknown(cTnT). Therefore we assessed whether Cystatin C is an independent predictorof mortality and myocardial infarction in nSTE-ACS patients with an elevated tro-ponin T.Methods and results: Baseline samples for central Cystatin C measurementswere available in 1128 nSTE-ACS patients with an elevated cTnT randomizedto an early or a selective invasive strategy. Patients were divided into quartilesof Cystatin C level at baseline. Mortality by one year was 7.3% in the highestquartile compared to 1.1% of patients in the lower three quartiles (p<0.0001).
Fig. 1
In a binary logistic regression analyses, Cystatin C was a strong independentpredictor of one-year mortality (OR 5.8 (95% CI 2.5 - 13.4; p<0.001). ReceiverOperating Characteristic curve for the prediction of one-year mortality for CystatinC and creatinine showed a larger area under the curve for Cystatin C comparedto creatinine (figure 1). The rate of myocardial infarction within one year was 8.4%in the highest quartile versus 8.9% in the lower three quartiles (p=0.80).Conclusion: We showed that Cystatin C is a strong independent predictor ofmortality by one year in nSTE-ACS patients with an elevated cTnT. However, wecould not demonstrate an association between Cystatin C levels at baseline andthe incidence of recurrent myocardial infarction by one year.
POSTER SESSION 7
MODERATED POSTERSMETABOLISM AND OXIDATIVE STRESS IN
ENDOTHELIAL FUNCTION
P5126 Inhibition of the ubiquitin-proteasome systemprotects endothelial cells from oxidative stress
S. Meiners, A. Weller, A. Ludwig, K. Stangl, V. Stangl.Universitaetsmedizin Berlin, Charite, Med. Klinik, Kardiologie,Campus Mitte, Berlin, Germany
Enhanced generation of reactive oxygen species (ROS) contributes to the for-mation of atherosclerotic lesions. Anti-oxidative enzymes convert these reactiveoxygen molecules into non-toxic products and thereby reduce oxidative stress.The ubiquitin-proteasome system plays a central role in the degradation of mostintracellular proteins. It has been implicated in the controlled proteolysis of severaltranscriptional factors involved in the induction of anti-oxidative enzymes. Here,we analyzed the effects of partial inhibition of the proteasome on the expressionof anti-oxidative enzymes and the generation of ROS in endothelial cells.Primary HUVECS were pretreated with low and non-toxic doses of the protea-some inhibitors MG132 (70 nM) or MG262 (4 nM) for 24 hours and then stressedwith 100 μM hydrogen peroxide for 30 minutes. Quantification of the intracellularROS levels using 2’, 7’dichloro-fluorescein diacetate revealed that partial protea-some inhibition by low and non-toxic doses of proteasome inhibitors efficientlysuppressed hydrogen peroxide-mediated increase in ROS in endothelial cells.These protective effects were accompanied by increased expression of severalanti-oxidative enzymes, such as glutathione peroxidase-3, superoxide dismutase1, and heme oxygenase 1, as quantitated by real-time RT-PCR analysis. Protea-some inhibitor-mediated induction was analyzed in detail by transient transfec-tions of HUVECs with reporter gene constructs containing the human promoterof glutathione peroxidase-3. Mutation analysis of the promoter revealed that tran-scriptional up regulation was completely abrogated by deletion or point mutationof an anti-oxidative response element, indicating an essential function for thiselement in the transcriptional activation of glutathione peroxidase-3 by protea-some inhibition. Western blot analysis of the antioxidant transcription factor Nrf2revealed stabilization of Nrf2 upon proteasome inhibition suggesting that Nrf2 isinvolved in the transactivation of glutathione peroxidase-3 via the anti-oxidant re-sponse element.Our data indicate a causal relationship between partial proteasome inhibition,regulation of anti-oxidative transcription factors, and up regulation of anti-oxidativeenzymes. Importantly, our results show for the first time that non-toxic doses ofproteasome inhibitors are able to protect endothelial cells from oxidative stress.
P5127 Proteasome inhibition improves TNFalpha-inducedendothelial dysfunction
V. Stangl, N. Wilck, M. Lorenz, A. Ludwig, S. Meiners, G. Baumann,K. Stangl. Universitaetsmedizin Berlin, Charite Mitte, Cardiology,Berlin, Germany
The ubiquitin-proteasome system is the major pathway for protein degrada-tion in eukaryotic cells. Recently we have shown that inhibition of the protea-some with MG132 increased endothelial nitric oxide synthase (eNOS) expres-sion and activity in endothelial cells. The aim of our study was to investigatewhether MG132 is capable of improving TNFα-induced endothelial dysfunc-tion. Endothelium-dependent (acetylcholine) and endothelium-independent (pa-paverine) vasorelaxation was performed in phenylephrine-precontracted rat aor-tic rings. Compared to control, in vitro incubation of the rings with TNFα for 48h resulted in a significant dose-dependent reduction of acetylcholine-induced va-sorelaxation by 34±9% (250 pg/ml) and 49±8% (500 pg/ml). Co-incubation withTNFα (250 pg/ml) and MG132 (50 and 100 nM) for 48 h resulted in a dose-dependent improvement of endothelium-dependent vasorelaxation (22,9±6% for50 nM MG132; 35±5,9% for 100 nM MG132) in comparison to TNFα-treatedrings. Endothelium-independent vasorelaxation remained unaffected in all rings.To explore the underlying mechanisms we analysed mRNA levels of importantdeterminants of vascular function by real-time RT-PCR. MG132 significantly in-creased SOD1 mRNA expression and reduced mRNA levels of several subunitsof the NAD(P)H oxidase complex: gp91phox, Nox4, p47phox, p40phox, p22phox.Consequently, superoxide production was reduced in rings incubated with 100nM MG132 in comparison to controls as shown by lucigenin chemiluminescence.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Moderated Posters: Metabolism and oxidative stress in endothelial function 879
Interestingly, mRNA expression of the potent vasoconstrictor endothelin-1 wasupregulated by TNFα and markedly decreased in rings incubated with MG132.eNOS mRNA levels in rat aortic rings did not correlate with their improved vas-cular function after treatment with MG132. In conclusion, low-dose proteasomeinhibition with MG132 improves vascular function in an aortic ring model of TNFα-induced endothelial dysfunction. By reducing the expression of the NAD(P)H ox-idase complex and by enhancing the expression of the antioxidant SOD, subse-quent amelioration of NO bioavailability is presumably one underlying mechanismfor MG132-induced improvement in endothelial function. Moreover, by suppres-sion of endothelin-1 mRNA levels in MG132 treated rings the balance betweenvasoconstriction and vasodilatation is shifted in favour of endothelium-dependentvasodilatation.
P5128 Diabetes mellitus alters the intrinsic constrictor anddilator mechanisms regulating the tone of humancoronary microvessels: Role of cyclooxygenase-2
T. Szerafin1, N. Erdei1, I. Edes1, A. Koller2, Z. Bagi1. 1Instituteof Cardiology, Debrecen, Hungary; 2Institute of Pathophysiology,
Budapest, Hungary
Based on findings of experimental models of diabetes mellitus (DM) showing al-terations in vascular prostaglandin synthesis, we hypothesized that the tone andresponses of human coronary microvessels from patients with or without DM toagonists are impaired. Arterioles were dissected from the right atrial appendagesobtained at the time of cardiac surgery. Isolated arterioles (89±15 μm in diam-eter) were cannulated and pressurized (at 80 mmHg) and changes in diameterwere measured with videomicroscopy. After spontaneous tone developed, acetyl-choline (ACh, 1 nM-1 μM) elicited dilations of coronary arterioles from non-DMpatients (at 1 μM: 82±5%), whereas it induced constrictions in arterioles from DMsubjects (at 1 μM: -29±7%). In contrast, dilations to bradykinin (1 nM-1 μM) weresignificantly (P<0.05) greater in arterioles of DM patients (at 10 nM: 77±10%)compared to that of non-DM (at 10 nM: 38±14%). In both groups, dilations weresimilar to the NO-donor sodium nitroprusside. ACh-induced responses were notaffected by indomethacin, a non-selective inhibitor of cyclooxygenases (COX-1and COX-2) in both groups of vessels. However, in arterioles of DM patientsbradykinin-induced dilations were reduced by indomethacin or by the selectiveCOX-2 inhibitor, NS-398 (at 10 nM: to 20±4% and 16±5%, respectively). In addi-tion, a marked COX-2 immunostaining was detected in coronary arterioles of DMpatient compared to those of non-DM. We conclude that in isolated coronary arte-rioles from DM patients ACh elicits prostaglandin-independent vasoconstrictions,whereas bradykinin induces enhanced COX-2-derived prostaglandin-mediateddilations. These findings are the first to suggest that in humans, diabetes mel-litus alters both the intrinsic constrictor and dilator mechanisms regulating thetone of coronary microvessels.
P5129 Essential role of NOXA1 in generation of reactiveoxygen species induced by oxidized low-densitylipoprotein in human vascular endothelial cells
T. Honjo, N. Inoue, K. Otsui, R. Shiraki, S. Kawashima,M. Yokoyama. Kobe University Graduate School Of Medicine,
Division Of Cardiovascular Medicine, Kobe, Japan
Purpose: Oxidative stress induced by superoxide in vasculature plays an in im-portant role in pathogenesis of various cardiovascular diseases, and NAD(P)Hoxidase is a principal enzymatic origin for superoxide in vascular cells. Re-cently, novel homologues of cytosolic regulatory components of NAD(P)H oxi-dase, p47phox and p67phox, are identified, that is, Nox organizer 1 (NOXO1)and Nox activator protein 1 (NOXA1), respectively; however, their functional rolesin the activation of vascular NAD(P)H oxidase remains to be elucidated. On theother hand, it is reported that oxidized low-density lipoprotein (ox-LDL) generatesreactive oxygen species (ROS) in endothelial cells via lectin-like oxidized low-density lipoprotein receptor-1 (LOX-1). In the present investigation, we examinedthe role of NOXA1 in ox-LDL-induced ROS generation in vascular endothelial cellsusing RNA interference.Methods: The expression of NOXA1 in EAhy926, a cell line of human umbilicalvein endothelial cells, was examined by RT-PCR. The generation of intracellularreactive oxygen species (ROS) was detected with Dihydroethidium method. Theexpression of NOXA1 was suppressed by transfection of siRNA.Results: RT-PCR confirmed the expression of NOXA1 in EAhy926 cells and itsexpression was increased by ox-LDL in time- and dose- dependent manner. Dihy-droethidium method demonstrated that ox-LDL (30 μg/ml) and angiotensin II (10-7M) increased in ROS generation in EAhy926 cells. Transfection of siRNA of thep22phox gene dramatically suppressed the ROS generation, which indicated theinvolvement of p22phox-based NAD(P)H oxidase. Furthermore, treatment withantibody against LOX-1 potently suppressed ox-LDL-induced ROS generation,and also transfection of siRNA of the NOXA1 gene significantly suppressed theexpression of NOXA1 mRNA expression as well as ROS generation induced byangiotensin II and ox-LDL. In contrast, transfection of si RNA of scramble controlhad no effects.Conclusion: LOX-1-mediated NOXA1 activation is essential for generation ofROS induced by ox-LDL in vascular endothelial cells.
P5130 Enhanced vascular arginase II activity is involved inendothelial dysfunction in insulin-resistant mice fedhigh-fat diet
X.-F. Ming1, C. Sartori2, P.-Y. Jayet1, G. Gajanajake2, U. Scherrer1,Z. Yang2. 1University of Fribourg, Department of Medicine, Fribourg,
Switzerland; 2CHUV, University of Lausanne, Lausanne, Switzerland
Background: Insulin resistance plays a central role in type 2 diabetes, increasescardiovascular risk, is associated with decreased endothelial nitric oxide (NO)bioavailability. Arginase II competes with endothelial NO synthase (eNOS) for thesubstrate L-arginine, is involved in endothelial dysfunction. This study investigatedthe role of arginase in endothelial dysfunction associated with insulin resistancein a mouse model.Methods and results: Female C57BL/6J mice were fed low fat (LFD, energycontent 12%) or high-fat diet (HFD, 55% fat) for 10 weeks. Endothelial func-tion was analyzed in isolated aortic rings suspended in organ chambers filledwith physiological salt solution (37oC) aerated with 95%O2/5% CO2 for isometrictension recording. Protein levels of eNOS and arginase II in aortas were ana-lyzed by immunoblotting and arginase activity by urea production. Compared tomice fed LFD, mice fed HFD revealed a decreased endothelium-dependent relax-ation (LFD: 79±2% and HFD: 49±8%, p<0.05) to acetylcholine (ACh, 10nmol/L -0.1mmol/L) despite of higher eNOS protein levels (166% increase, p<0.01). Incu-bation of aortic rings with the arginase inhibitor L-norvaline (20mmol/L) improvedthe endothelium-dependent relaxations to ACh (71±5%) in mice fed HFD, withouthaving effects on endothelium-independent relaxations to the NO-donor sodiumnitroprusside, and did not affect the endothelium-dependent relaxations to ACh inmice fed LFD. In line with this finding, increased arginase II protein level (230%increase) and enzymatic activity (156% increase) were observed in mice fed HFD(p<0.05).Conclusions: Increased vascular arginase II activity is involved in endothelialdysfunction in insulin resistant mice fed HFD. Vascular arginase II may be a noveltherapeutic target for cardiovascular disease associated with insulin resistance.
P5131 5-Methyl-tetrahydrofolate acid improves endothelialfunction and decreases superoxide production byimproving eNOS coupling and increasingtetrahydrobiopterin bioavailability in human vesselsin vivo
C. Antoniades, C. Shirodaria, J. Lee, P. Leeson, N. Warrick,C. Ratnatunga, R. Pillai, K.M. Channon. University Of Oxford, CardiovascularMedicine Dept, Lab 3, Oxford, United Kingdom
Uncoupled endothelial nitric oxide synthase (eNOS) appears to be a source ofsuperoxide radicals (SOO) in human atherosclerosis.Aim: We hypothesized that 5-methyl-tetrahydrofolate (5MTHF), the circulatingmetabolite of folic acid, may improve eNOS coupling by preventing the intracellu-lar oxidation of eNOS cofactor tetrahydrobiopterin (BH4), decreasing in this waySOO- production in human vessels.Methods: Fifty-six patients undergoing CABG were randomized to receive intra-venous bolus 5MTHF (0.13 mg/kg BW, n=24) or placebo (n=32) preoperatively,45 minutes before graft harvesting. Vascular SOO production was determined inpaired samples of saphenous veins (SV) and internal mammary arteries (IMA)using lucigenin chemiluminescence, in the presence or absence of NOS inhibitorLNAME. Vasomotor responses of SV to acetylcholine (Ach) and nitroprusside(SNP) were determined in an organ bath, while vascular 5-MTHF and biopterinswere measured by HPLC.Results: 5MTHF improved vasomotor response to Ach (Fig. 1a) and decreasedSOO- production in both SV and IMA (1.0±0.15 and 0.97±0.15 RLU/sec/mg in5MTHF vs 2.27±0.37 and 5.01±0.62 RLU/sec/mg in placebo, p<0.01 for both).LNAME reduced SOO- in both SV and IMA in placebo group, an effect reversedby 5MTHF (Fig. 1b). 5MTHF increased BH4 and BH4/total biopterin (tBio) ratio(Fig. 1c). Vascular 5MTHF was correlated with BH4/tBio ratio (r=0.406, p=0.001in SV and r=0.334 p=0.043 in IMA respectively) and the maximum relaxations ofSV to Ach (r=0.314, p=0.016).
Fig. 1
Conclusions: Intravenous administration of 5MTHF rapidly increases nitric oxidebioavailability, improves eNOS ‘coupling’ and decreases superoxide production inhuman vessels, partly by preventing intracellular BH4 oxidation in vivo.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

880 Moderated Posters: Metabolism and oxidative stress in endothelial function / AF – occurrence, clinical management and prevention
P5132 Effects of CETP inhibition on endothelial function intype II hyperlipidemia
F. Hermann, L.E. Spieker, I. Sudano, F. Ruschitzka, R. Corti, G. Noll,T.F. Luescher. University Hospital, Cardiology, CardiovascularCenter, Zurich, Switzerland
Background: Reduced high-density lipoprotein cholesterol (HDL-C) levels area powerful risk factor for coronary artery disease. Besides its role in reverse-cholesterol transport, HDL-C exhibits anti-inflammatory, antithrombotic and pro-fibrinolytic effects. Whereas conventional treatment with statins, fibrates or nico-tinic acid only modestly affectes HDL-C, the discovery of cholesteryl ester-transferprotein (CETP) inhibitors provided new means to substantially increase HDL-Clevels. In hypercholesterolemic men, reconstituted HDL-C normalizes endothelialfunction and increases NO bioavailability. Aims: We investigated whether CETP-Inhibition with JTT-705 600mg once daily improves endothelial function, and in-flammatory markers in patients with type II hyperlipidemia.Methods and Results: In 18 patients with hyperlipidemia (mean age 58±3years), flow-mediated dilation (FMD) was measured using high-sensitive ultra-sonography of the brachial artery. Statin treatment was suspended for at least6 weeks before study entry. After a 3 week screening phase, patients receivedJTT-705 600mg daily or matching placebo over a period of 4 weeks. FMD andblood samples were analyzed after 2 and 4 weeks of therapy. After 4 weeks oftreatment with JTT-705, FMD slightly improved. Baseline vasodilation was en-hanced from 3.1%±0.6 to 3.6%± 0.4 (ANOVA: P=0.11). In the control group FMDslightly decreased from 2.9%±0.6 at baseline to 2.7%±0.4 (ANOVA: P=0.18) af-ter 4 weeks. Glycerol trinitrate induced vasodilation was not affected by neitherJTT-705 nor placebo (JTT-705: 8.9%±1.4 vs. 9.3%±1.3, P=0.48 and placebo:9.1%±0.6 vs. 8.7%±1.0, P=0.91). Under therapy with the CETP Inhibitor JTT-705, HDL-C was significantly increased by 26% from 1.14 mmol/l to 1.44 mmol/l(P<0.05), whereas triglyceride concentration was significantly reduced from 2.52mmol/l to 1.97 mmol/l, P<0.05 respectively. Total cholesterol, low-density lipopro-tein cholesterol and inflammatory markers remained unchanged both in the treat-ment and in the control group. In a secondary analysis patients were analyzedaccordingly to baseline HDL-C levels. Using a median split analysis, FMD im-proved significantly in those patients treated with JTT-705 with a lower than me-dian HDL-C level compared to those patients with a higher than median HDL-Clevel (P=0.01).Conclusion: In hypercholesterolemics, the CETP inhibitor JTT 705 safely andeffectively increases HDL-C and lowers triglycerides but does not affect inflam-matory markers. JTT 705 improved function particularly in patients with a lowbaseline HDL-C level.
P5133 Improvement of vascular dysfunction in diabetes bychronic guanylyl cyclase activation
A. Schaefer, C. Vogt, D. Fraccarollo, M. Leutke, G. Ertl,J. Bauersachs. University of Wuerzburg, Department of InternalMedicine - Cardiology, Wuerzburg, Germany
Background: Vascular endothelial dysfunction and the so-called "non-contractile" phenotype of smooth muscle cells are well described in diabetesmellitus. Endothelial dysfunction results in decreased signalling through theNO/cGMP pathway leading to decreased levels of cGMP in diabetes. We inves-tigated whether chronic stimulation of guanylyl cyclase with the novel activatorHMR1766 would improve vascular reactivity in diabetic rats.Methods and Results: Male Wistar rats received a single intravenous injectionof streptozotocin (STZ) to induce diabetes. 2 weeks after STZ injection, ratswere randomized to treatment with either placebo or the guanylyl cyclase acti-vator HMR1766 (10 mg/kg twice daily) for another 2 weeks. Afterwards, vascu-lar function in the thoracic aorta of these animals was assessed in organ bathstudies. Aortae from diabetic rats displayed a highly significant reduction in con-tractile response compared to healthy control animals as described for the dia-betic, non-contractile phenotype (contraction in g by phenylephrine 1 μM: Con-trol 2.55±0.08; STZ-Placebo 1.59±0.09, p<0.01). Treatment with HMR1766 nor-malized vascular contraction (STZ-HMR 2.51±0.09, p<0.01 vs. STZ-Placebo).Endothelium-dependent, nitric oxide-mediated vasorelaxation was significantlyimpaired in diabetic placebo-treated animals, which was completely normalizedby treatment with HMR1766. This was at least partially dependent on a re-duced smooth muscle sensitivity to nitric oxide as demonstrated by endothelium-independent relaxation to DEA-NONOate, which was significantly impaired in di-abetic placebo-treated rats and normalized by guanylyl cyclase activation.Conclusion: Chronic guanylyl cyclase activation in diabetes improves vascularreactivity by improving release of and sensitivity for nitric oxide. HMR1766 sig-nificantly enhanced the reduced signaling through the NO/cGMP pathway in dia-betes and may be a new potential therapeutic approach for treatment of vasculardysfunction in diabetes.
ATRIAL FIBRILLATION – OCCURRENCE, CLINICALMANAGEMENT AND PREVENTION
P5134 A randomized trial of atorvastatin for reduction ofpost-operative atrial fibrillation in patientsundergoing cardiac surgery
G. Patti1, M. Chello1, D. Candura1 , V. Pasceri2, A. D’ambrosio1,A. Nusca1, E. Covino1, G. Di Sciascio1. 1Campus Bio-Medico
University, Cardiovascular Sciences, Rome, Italy; 2S. Filippo Neri Hospital,Interventional Cardiology, Rome, Italy
Purpose: Atrial fibrillation after cardiac surgery is associated with increased riskof cardiovascular complications. As inflammatory mechanisms may be involved inthe pathogenesis of post-operative atrial fibrillation, statin therapy might reducethe incidence of such complication through its anti-inflammatory effects. Thus, wetested this hypothesis in a randomized, prospective, double-blind study.Methods: Two-hundred patients undergoing elective cardiac surgery with car-diopulmonary bypass (CPB), no previous statin treatment and no history of atrialfibrillation were enrolled. Patients were randomized to atorvastatin (40 mg/day,N=101) or placebo (N=99) starting 7 days before operation. Primary endpointwas the incidence of post-operative atrial fibrillation. C-reactive protein (CRP) lev-els were routinely measured before surgery and every 24 hours post-operativelyuntil discharge.Results: The occurrence of atrial fibrillation was significantly lower in the statinvs. placebo arm (35% vs 57%; P=0.003); no difference was found in durationand time of onset of the arrhythmic episodes. Peak post-operative CRP levelswere significantly lower in patients without atrial fibrillation, vs. those with atrialfibrillation (P ≤ 0.025), irrespective of randomization assignment. Multivariableanalysis showed that pre-treatment with atorvastatin conferred 60% risk reductionof atrial fibrillation (OR 0.39, 95% CI 0.18-0.85; P=0.017), whereas high post-operative CRP levels were associated with increased risk (2.0, 1.2-7.0; P=0.01).Conclusions: Pre-treatment with atorvastatin 40 mg/day for 7 days significantlyreduces incidence of post-operative atrial fibrillation after elective cardiac surgerywith CPB; anti-inflammatory effects of statin therapy may contribute to this clin-ical benefit. These results may influence practice patterns concerning adjuvantpharmacological therapy prior to cardiac surgery.
P5135 Prevalence of atrial fibrillation in cardiology clinics inSpain; the FAMA study
J. Muniz1, J.L. Llisterri2, S.G. Chapman3, J. Aznar4 on behalfof The FAMA study group. 1Hospital Maritimo de Oza, InstitutoCiencias da Saude, A Coruna, Spain; 2Centro de Salud Ingeniero
Joaquin Benlloch, Valencia, Spain; 3AstraZeneca Farmaceutica Spain, MedicalDepartment, Madrid, Spain; 4Hospital Nuestra Senora de Gracia, CardiologiaExtrahospitalaria, Zaragoza, Spain
Purpose: The prevalence of atrial fibrillation (AF) in Spain is poorly quantifiedboth in the general population and in specialist centres. A primary objective of thiscross-sectional multicentre study was to quantify the prevalence of AF in PrimaryCare, as a proxy of population prevalence, as well as its burden in outpatientCardiology Clinics across Spain. Here we report the cardiology centre resultsonly.Methods: The first 50 patients over 18 years of age attending the out-patient clinicof 117 cardiologists from all regions of Spain were included in the study. Age, sexand risk factors for AF were recorded for each patient. Any prior diagnosis of AFwas also recorded, or new cases detected by taking the patient’s pulse and thenproceeding to confirmatory ECG in case of any rhythm irregularity or tachycardia.Each case of AF was classified as either permanent, persistent, paroxysmal orfirst episode.Results: 5770 patients were included (45% women), mean age 65 ± 15 years,of which 1173 were diagnosed as having AF, the prevalence in these specialistcentres therefore being 20%. AF cases were classified as 66% permanent, 16%persistent, 11% paroxysmal and 7% detected as a first episode. The prevalenceof AF in each of the risk factors was as follows: hypertension 24%, previous strokeor TIA 28%, type 2 diabetes 21%, IHD 14%, COPD 25%, smoking 15%.Conclusions: This study demonstrated that 20% of patients in cardiology clinicsin Spain have AF. These data, together with the individual risk factor data, mayhelp to orientate appropriate resource allocation to adequately diagnose and treatAF in at risk patients in Spain.
P5136 Incidence of atrial fibrillation in redo cases afterOPCABG aorta non touch operations
S.N. Prapas1, D.C. Karatza1, I. Panagiotopoulos2 , I. Raptis2,V.N. Kotsis2, A. Michalopoulos2. 1Henri Dunant Hospital, Dept. ofCardiac Surgery, Athens, Greece; 2Henri Dunant Hospital, Dept. of
Cardiac Surgery, Athens, Greece
Atrial fibrillation (AF) remains the most common complication after cardiacsurgery. This study aimed to determine the incidence of postoperative AF in redoCABG without the use of extracorporeal circulation.1281 pts undergoing first time beating heart aorta non touch coronary artery
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – occurrence, clinical management and prevention 881
revascularization(Group A) and 78 pts undergoing a redo off pump by pass graft-ing operation(Group B) were enrolled. A 24-hour ECG monitoring was performedin all pts perioperatively and postoperatively, until hospital discharge. Patientshaving a medical history of AF episodes, thyroid gland dysfunction, severe COPD(defined as FEV1<50%), as well as those needing prolonged mechanical venti-lation support (more than 48 hours), were excluded.The groups were compared using the Fischer’s exact test and ANOVA.Incidence of AF was found to be lower in the redo group(Group B) comparedto the primary cases(10.3 vs 20.7%, P<0.028). It is noteworthy that in the redogroup the number of distal and arterial anastomoses was smaller (2.78+0.91,2.65+0.97, P<0.005); there were also fewer grafts off the LIMA (1.81+0.76 vs1.30+0.60, P<0.005).Although the redo heart operations result in a higher morbidity compared to pri-mary ones, according to our findings the incidence of AF in redo cases seems tobe significantly lower. The smaller number of anastomoses used in redos couldresult in a limited extent of injury and consequently in a diminished inflammatoryprocess.Further study is needed to elucidate this very important point.
P5137 Atrial arrhythmias in symptomatic patients with longQT syndrome: under daily life conditions - an ICDfollow-up study
P. Kirchhof1, S. Zellerhoff1, R. Pistulli1, G. Moennig1, M. Hinterseer2,J. Koebe2, S. Kaab1, D. Boecker2. 1University Hospital Muenster,
Cardiology And Angiology, Muenster, Germany; 2University Hospital Muenchen,Muenchen, Germany
The long QT syndromes are inherited channelopathies with a propensity to poly-morphic ventricular tachycardias due to prolonged ventricular repolarization. Thesame ion channels that cause ventricular repolarization also contribute to atrialrepolarization, and we have previously found polymorphic atrial arrhythmias inpatients with long QT syndrome undergoing invasive electrophysiological test-ing. To investigate whether such atrial arrhythmias occur in patients with long QTsyndrome under daily-life conditions, we performed a nested case-control studyof long QT patients treated with an implantable defibrillator and matched controlsubjects without structural heart disease. The devices were used to systematicallysearch for atrial arrhythmias. A systematic database search of the long QT patientfiles at the University hospitals in Munich and Münster identified 21 long QT syn-drome patients with a defibrillator that were followed up locally (3male, mean age39 years, 18 on β blocker therapy, mean ICD therapy duration 6.1 years, 4 LQT1, 6LQT2, 2 LQT3). These were matched to 24 control patients (mean age 50 years,13 male, 3 on β blocker therapy, mean pacemaker therapy duration 8.5 years)with an indication for permanent DDD pacemaker therapy without pre-existingatrial fibrillation, (13 with 3rd degree AV block, 5 with 2nd degree AV block, 1 withLBBB and 1st degree AV block, 2 unexplained syncope). 7/21 LQTS patients de-veloped atrial arrhythmias during follow-up, while only 1 control patient developeda single episode of post-operative atrial fibrillation (p<0.05). Atrial cycle lengthwas < 250 ms in all patients with analyzable frequency histograms during thearrhythmias. Episodes were always self-terminating and clearly related to symp-toms (dizziness and fatigue) in 2 patients.Conclusions: The ion channel dysfunction in LQT appears to affect the atria insymptomatic LQT patients under daily-life conditions. Palpitations in patients witLQTS may at times be of atrial origin. The mechanisms of atrial arrhythmias inLQT warrant further investigations.
P5138 Increased physical activity in patients with idiopathicAtrial Fibrillation: a case-control study
I. Molina, D. Tamborero, B. Collvinent, R. Elosua, J. Brugada,M. Sitges, B. Vidal, L. Mont. Hospital Clinic de Barcelona, Barcelona,Spain
Etiology of atrial fibrillation (AF) remains unknown in about 30% of patients. Theaim of study was to analyze whether physical activity may play an etiologic factorin idiopathic AF.Methods: A group of 112 consecutive patients younger than 65 years seen at theemergency room because of idiopathic AF were included. Controls were recruitedfrom healthy individuals matched for age and sex. They all answered a detailedvalidated questionnaire of the physical activity they performed during their life toestimate cumulated lifetime hours in four intensity levels of effort.Results: There were 54% of patients with paroxysmal and 46% with persistentAF. There were 68% of men, mean age 48±11 years. Mean cumulated life-time hours in both, moderate-high intensity and high intensity physical activitypractice, was higher in patients than in controls (9748±11971 vs 2968±4619and 2000±3553 vs 1367±3782 hours respectively; p<0.001). Overall, more than1500 cumulated hours of high intensity physical activity practice was associatedwith higher AF risk (OR=2.8; 95% CI: 1.5 - 5.1; p=0.001).Conclusions: Cumulated lifetime high intensity physical activity seems to be apredisposing factor for development of idiopathic AF in healthy young individuals.
P5139 Prospective registration of serious adverse eventswithin the Network of Competence on AtrialFibrillation
M. Oeff1, U.E. Wolf1, K.G. Haeusler2, G. Steinbeck3, G. Breithardt4
on behalf of Network of Competence of Atrial Fibrillation .1Stadt-Klinikum Brandenburg, Cardiology, Brandenburg/Havel,
Germany; 2Charite Universitaetsmedizin Berlin, Neurology, Berlin, Germany;3Klinikum Grosshadern, Cardiology, Munich, Germany; 4UniversitaetsklinikumMuenster, Cardiology, Muenster, Germany
Background: Atrial fibrillation (AF), the most common sustained rhythm distur-bance, is associated with a significantly enhanced mortality and morbidity due tothromboembolic events, and other cardiac and noncardiac complications. There-fore the "Network of Competence on Atrial Fibrillation (AFNET)" supported by theGerman Ministry for Education and Research (BMBF) was established in orderto collect clinical data on patients (pts) with AF (paroxysmal, persistent, perma-nent) over a study period of 5 years with an expected sample size of 10,000 pts.Incidence, clinical relevance and outcome after serious advers events (SAE) isrecorded and assessed by a Critical Event Committee (CEC).Methods: The CEC-members (experts in cardiology and neurology) defined asSAE any death with or without relationship to AF, cardioembolic events (stroke,peripheral arterial embolism), bleeding complications due to antithrombotic ther-apy, acute heart failure, syncope, resuscitation; additionally, the complication ofinterventional strategies for AF-treatment and other AF-independent SAE. Over a5-year follow-up period, during 6-monthly and unscheduled visits, the SAEs aresystematically documented, blinded and their relationship to AF will be interpretedin detail by the CEC.Results: Within the first 24 months of registration, nearly 8,500 pts were enrolled.Out of these, 702 (male: 63%, age 70 ± 11yrs, female: age 73 ± 11yrs) SAEswere recorded: death not due to SAE 19%, stroke 10%, peripheral embolism3%, bleeding 10%, acute heart failure 19%, syncope 7%, resuscitation 2% andother SAE 30%. Reclassification of SAE was necessary in almost 18% of events.The CEC categorized no correlation between AF and SAE in more than 50%of the reported cases. Most of them were due to the underlying serious heartor pulmonary diseases. But nevertheless over one third of them were definite,probable or possible associated with AF especially bleeding complications andcerebrovascular events.Conclusion: Serious Adverse Events of AF in 8,500 of expected 10,000 ptsare presently monitored within the "Network of Competence on Atrial Fibrillation(AFNET)". These data do allow detailed and complete assessment of their corre-lation to AF by the CEC and, thus, will be suitable for the modification of presentdiagnostic and therapeutic guidelines for AF.
P5140 Cardiovascular complications in a cohort of atrialfibrillation over a 5 years period
A. Ruigomez1, S. Johansson2 , M.-A. Wallander3, L.-A. Garcia-Rodriguez3. 1Spanish Centre Pharmacoepidemiology, Ceife,Madrid, Spain; 2Prev.Cardiology:Goteborg Univ., R&D Az, Molndal,
Sweden; 3Public Health.Uppsala Univ., R&D Az, Molndal, Sweden
Background: Atrial fibrillation is a common disease frequently associated withcardiovascular morbidity and mortality. Heart failure (HF), ischemic heart disease(IHD) and cerebrovascular ischemic accident (CVA) are common complicationsamong atrial fibrillation (AF) patients.Objective: The aims of this study were to estimate the incidence rates of HF,IHD and CVA among newly diagnosed atrial fibrillation patients attending generalpractice in the UK.Research Design and Methods: From a previous prospective cohort study usingdata from the GPRD database, we identified a cohort of newly diagnosed AF pa-tients in 1996, aged 40 to 90 years (N=1,635). From the same source population,we identified a comparison group of patients free of atrial fibrillation (N=10,000).In both cohorts we excluded individuals with prior recorded diagnosis of HF, IHDor CVA. We followed-up the two study cohorts until December 2001 to ascer-tain patients with a first ever diagnosis of heart failure, ischemic heart diseaseor cerebrovascular ischemic accident (Stroke or TIA), whichever was diagnosedfirst. Among the AF cohort, we detected 366 patients with an incident diagnosisof HF, IHD or CVD, and 715 among the cohort free of AF. We estimated incidencerate (IR) for the different outcomes (HF, IHD, CVA) by age and sex groups in ourtwo cohorts and calculated the relative risk (RR) of developing HF,IHD or CVA as-sociated with AF diagnosis. We also ascertained the IR separetely for paroxysmalAF and permanent/chronic AF.Results and Conclusion: Patients with AF were more likely to develop HF, IHDor CVD than patients free of AF (incidence rate 15.5 vs. 2.4 cases per 100 person-years). The age and adjusted relative risk associated with AF was 4.5 (95%CI:3.9-5.1). Patients with permanent/chronic AF had a higher incidence rate of devel-oping any of the studied cardiovascular outcomes than paroxysmal AF patients,and the major difference was observed with heart failure. The risk of developingHF was greater than two fold among chronic/permanent AF than among paroxys-mal AF patients (age and sex adjusted RR: 2.4, 95% CI: 1.7-3.4).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

882 Atrial fibrillation – occurrence, clinical management and prevention
P5141 Feasibility and benefits from the implementation ofthe ACC/AHA/ESC guidelines on atrial fibrillation indaily practice. The GEFAUR-3 study
A. Martin, C. Del Arco, P. Laguna, A. Lozano, B. Coll-Vinent,C. Suero, P. Pinera, M. Cancio on behalf of GEFAUR-3 investigators.
Spanish Society of Emergency Medicine, Arrhythmia Division, Madrid, Spain
Background: Although recommendations for management of atrial fibrillation(AF) are detailed in widely available clinical guidelines, some reluctance to fol-low them and doubts about their applicability exist in routine practice.Objectives: To determine the feasibility and benefits of implementing the inter-national guidelines on atrial fibrillation (AF) in daily clinical practice.Methods: Interventional prospective multicenter case-control study carried out in12 emergency departments (ED) in April, 2002. Controls: GEFAUR-1 prospectiveobservational study (same hospitals, July 2000). Intervention: systematic appli-cation of the recommendations of the ACC/AHA/ESC guidelines on AF (copies,posters and 1 clinical session in every ED, no other educational efforts). Rate con-trol (RATE-C) if HR at rest > 100 bpm (effective if achieved 60-90 bpm): Calciumand βblockers (Ca-BB) rather than digoxin (systolic dysfunction, heart failure, dis-ability). Rhythm Control (RHY-C) in recent onset episodes (lasting <48 hours)(successful if achieved stable sinus rhythm >2h.): amiodarone in structural HD,flecainide if not, DC-cardioversion (DC-CV) in hemodynamic unstability or drugfailure. Thromboprofilaxis: anticoagulation (ACO) if risk factors for stroke.Results: controls 1178; cases 1069 patients (58% female), mean age 75y.(60%>75y.). Demographics and co-morbidity of both groups were comparable.Symptoms that caused ED visit were attributable to AF in 68% of patients.HR>100 in 40% of patients, RATE-C to 70% (NS) with higher effectivenessin GEFAUR-3 (76vs44%, OR=3.85) and more suitable use of drugs (78vs64%,OR=1.9). Recent onset AF in 20%, Rhy-C attempt to 58% of them in GEFAUR-3 (vs 41%, OR=1.6), global effectiveness 67% (NS), 2-fold increase of DC-CV(12%, all effective). RF for stroke in 90%, ACO prescribed in 68 (vs40%, OR=4.5).The implementation of guidelines was 74% (RATE-C in 76%, Rhy-C 83%, ACO79%) with higher proportion of symptom relieving (50vs10%, OR=9.7) and with-out increasing the ED length of stay or the number of admissions (34%, mainlyrelated with heart failure and stroke).Conclusions: The implementation of guidelines on AF in the acute setting routinepractice is feasible without major efforts by the own ED physicians. It is also advis-able due to the superior success in relieving of symptoms and the improvementin patients’ prognosis (increasing strategies to prevent stroke and LV dysfunc-tion, main causes of morbidity and admission). Therefore, we recommend theirsystematic implementation in the acute setting daily clinical practice.
P5142 Correlates and outcome of atrial fibrillation in stablesymptomatic coronary disease
J.E. Otterstad1, B.-A. Kirwan2, J. Lubsen2, S. De Brouwer2,K.A.A. Fox3, P. Hildebrandt4, P.A. Poole-Wilson5 on behalf ofThe ACTION Investigators. 1Hospital Of Vestfold, Cardiology,
Toensberg, Norway; 2SOCAR RESEARCH SA, Cardiovascular dpt., Nyon,Switzerland; 3University of Edinburgh, Division of Medical & RadiologicalSciences, Edinburgh, United Kingdom; 4University Hospital, Fredriksberg,Cardiology Clinic, Copenhagen, Denmark; 5National Heart and Lung Institute,Imperial C, Cardiac Medicine, London, United Kingdom
Background: Data on the prevalence, incidence and impact on prognosis of ex-isting and new onset atrial fibrillation (AF) in large cohorts of patients with stable,symptomatic coronary artery disease (CAD) without overt heart failure is scarce.Methods: We examined the prevalence, incidence and prognosis of AF in 7665participants with stable angina and left-ventricular ejection fraction ≥ 40% in theplacebo-controlled ACTION (A Coronary disease trial Investigating Outcome withNifedipine GITS) trial.Results: AF was present in 4.1% of patients. During a mean follow-up of 4.9years, the incidence of recurrent AF in patients with AF at baseline was 13.5/100patient-years while the incidence of new AF in patients without AF at baselinewas 1.64/100 patient-years. During follow-up, 35% of patients with new onsetAF had sustained either a myocardial infarction or an episode of heart failure orhad undergone coronary bypass surgery within 4 weeks before the AF on-set.AF at baseline was associated with increased mortality (adjusted hazard ratio(aHR) 1.42, 95% CI (confidence interval) 1.03-1.96) and new over heart failure(aHR 1.67, 95% CI 1.02-2.74). New onset AF was associated with increasedmorbidity and mortality throughout the study, and in particular soon after onset(adjusted 30-day relative risk (aRR30d) for mortality 23, 95% CI 14-36;aRR30dfor debilitating stroke 37, 95% CI 18-77; aRR30d for heart failure 54, 95% CI32-03). The incidence of AF was not affected by treatment with nifedipine GITS.Conclusion: The presence of AF in patients with stable symptomatic CAD isan independent risk factor for subsequent mortality and cardiovascular morbidity.New-onset AF in patients not previously known with AF is associated with a poorprognosis and requires careful medical care.
P5143 Amiodarone prophylaxis for atrial fibrillation ofhigh-risk patients
M. Budeus1, P. Feindt2 , E. Gams1, K. Reimert1, O. Felix1,H. Wieneke2, S. Sack2, R. Erbel2. 1West-German Heart Centre,Cardiology, Essen, Germany; 2Heinrich-Heine-University, Thorax-
and Cardiovascular Surgery, Duesseldorf, Germany
Aims: Atrial fibrillation (AF) occurs often in patients after coronary artery bypassgrafting (CABG) and can result in increased morbidity and mortality. Previousstudies using P-wave signal-averaged electrocardiogram have shown that pa-tients with a longer filtered P wave duration (FPD) have a high risk of AF afterCABG. We have shown that patients with a FPD ≥ 124 ms and a root-mean-square voltage of the last 20 ms of the P wave 20 ≤ 3.7 μV have an increased riskof AF after surgery. Accordingly, the aim of this study was to investigate whetheror not prophylactic perioperative administration of amiodarone could reduce inci-dence of AF in this high-risk group undergoing CABG.Methods and results: In this prospective, double-blinded, placebo-controlled,randomized study, 106 patients received either amiodarone (n = 53) or placebo(n = 53). Amiodarone was given as 600 mg oral single dose one day before andfrom days 2 through 7 after surgery. In addition, amiodarone was also admin-istered intravenously during surgery in a 300-mg bolus for one hour and as atotal maintenance dose of 20 mg/kg weight over 24 hours on the first day fol-lowing surgery. The primary endpoint was the occurrence of AF after CABG. Thesecondary endpoint was hospital length of stay after CABG. The baseline charac-teristics were similar in both treatment groups. The incidence of postoperative AFwas significantly higher in the placebo group compared to the amiodarone group(85% vs. 34% of patients, P < 0.0001). The prophylactic therapy with amiodaronesignificantly reduced the intensive care (1.8 ± 1.7 vs. 2.4 ± 1.5 days, P< 0.05)and hospitalization length of stay (11.3 ± 3.4 vs. 13.0 ± 4.3 days, P< 0.03). Inthe amiodarone group, concentrations of amiodarone and desethylamiodaronediffered significantly between patients with AF and sinus rhythm (amiodarone: 0.96± 0.5 vs. 0.62 ± 0.4 μg/mL, P< 0.02; desethylamiodarone: 0.65 ± 0.2 vs. 0.48± 0.1 μg/mL, P < 0.04).Conclusion: The incidence of postoperative AF among high-risk patients wassignificantly reduced by a prophylactic amiodarone treatment resulting in a shortertime of intensive care unit and hospital stay. Our data supports the prophylacticuse of amiodarone in perioperative period in patients at high-risk for AF afterCABG.
P5144 Atrial fibrillation and mortality in a population oflong-term haemodialysis patients
A. Vincenti1, M.G. Valsecchi2, E. Rossi2, D. Pogliani2,I. Acquistapace2, A. Stella2, S. Genovesi2 . 1St Gerardo Hospital,Cardiology, Monza, Italy; 2University of Milano Bicocca, DIMEP,
Monza, Italy
Introduction: AND AIMS: The prevalence of atrial fibrillation (AF) in a populationof long-term haemodialysis (HD) patients, as recently assessed in a epidemio-logic multicentric study, was 26.6%. In detail, the prevalence of the paroxysmalform was 3.2%, the persistent form was 9.4% and the permanent was 13.9%. AFwas significantly associated to age, duration of HD history and left atrial dilatation.In the present study we analyzed the death rate in this cohort of patients and wetried to evaluate the impact of AF and other clinical features on mortality risk.Methods: The follow-up study included 476 HD patients (men, 58%; age,66.2±13.4 years; duration of HD therapy, 74.1±84 months). An history of is-chemic heart disease (previous acute myocardial infarction, coronary artery by-pass graft or coronary angioplasty) was present in 23.5% subjects, hypertensionin 81.3% and diabetes in 19.1% patients. Left ventricular (LV) hypertrophy waspresent in 71.8% of patients and a low LV ejection fraction (<40%) in 9.5% sub-jects.Results: At 2 years from the enrollement, 112/476 patients were dead (23.5%).Cardiovascular death was 40%, sudden death (within 1 hour from the beginningof symptoms) was 18.8% of the overall mortality; 49.1% of all deaths were noncardiovascular; death cause was not assessed in 10.7% of cases. A significantassociation of total mortality was found with age (9.9% <60 years, 21.3% 61-70years, 34.7% > 70 years, p<0.0001), with duration of HD (19% if < 37 months,27.2% if >37 months, p<0.048), with the history of ischemic heart disease (40.2%vs 18.4%, p<0.0001) and with AF (38.6% vs 18.1, p< 0.0001). No associationof total mortality rate was found with LV hypertrophy and low LV ejection fraction.The multivariate statistical analysis showed that age (p<0.0001), ischemic heartdisease (p<0.0001) and AF (p<0.0009) were independent predictive factors ofall causes mortality.Conclusions: In a population of long-term haemodialysis patients the two-yearsmortality rate was 23.5%; death was cardiovascular in 40% of cases, and suddenin about 1/5 of cases. Besides age and the presence of ischemic heart disease,AF was identified as an independent predictor of mortality in the long-term period.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – occurrence, clinical management and prevention 883
P5145 Statin drugs suppress the incidence of the prolongedand fractionated right atrial electrograms in patientswith idiopathic paroxysmal atrial fibrillation
K. Nakao, R. Shibata, S. Fukae, K. Matsuo, K. Yano. NagasakiUniversity School of Medicine, Third Department of Internal
Medicine, Nagasaki, Japan
Purpose: Statin drugs reduce the risk of development or recurrence of parox-ysmal atrial fibrillation (PAF). Although the prolonged and fractionated right atrialelectrograms have been reported as predictors of the development of chronicatrial fibrillation (CAF) in patients with idiopathic PAF, the effects of statin drugson these electrophysiologic abnormalities remain unknown. The purpose of thisstudy was to evaluate whether statin drugs have attracted some attention to suchatrial electrophysiologic abnormalities in patients with PAF.Methods: While taking oral statin drugs for hyperlipidemia, 10 patients (statingroup) with idiopathic PAF underwent electrophysiologic study, including cathetermapping of 12 right atrial sites during sinus rhythm. An abnormal atrial electro-gram was defined as having a duration of 100 ms or longer, or eight or morefragmented deflections, or both. Right atrial extrastimulation was also performedfor atrial vulnerability. Twenty age-matched patients with idiopathic PAF but nottaking oral statin drugs were included as a control group.Results: The longest duration of the right atrial electrogram was significantlyshorter and the maximum number of fragmented deflections per patient was sig-nificantly lower in the statin group than in the control group (86 ± 22 ms ver-sus 101 ± 15 ms, P<0.05; 5.5 ± 2.0 versus 7.9 ± 2.6, P<0.05, respectively).The total number of abnormal atrial electrograms per patient was significantlylower in the statin group than in the control group (0.6 ± 1.6 versus 2.2 ± 1.8,P<0.05). The percentage of patients with at least one abnormal atrial electro-gram was significantly lower in the statin group than in the control group (20.0%versus 80.0%, P<0.001). No significant difference was found between the statinand control group in the terms of the effective refractory period of atrium, repet-itive atrial firing zone, fragmented atrial activity zone, interatrial conduction delayzone, and maximal interatrial conduction delay.Conclusions: Statin drugs use is associated with a decrease of prolonged andfractionated right atrial electrograms in patients with idiopathic PAF. In addition,we suggest that statin drugs may help prevent idiopathic PAF from becomingchronic.
P5146 Validation of new parameters based on therelationship between RR interval and performance forleft ventricular function in atrial fibrillation
C.J. Kim, H.S. Ko, W.S. Ryu. Chung Ang University Hospital,Department of Internal Medicine, Seoul, Korea, Republic of
Purpose: This study was designed to validate new parameters based on the rela-tionship between RR interval and left ventricular (LV) performance, representingLV function independent of irregular RR intervals in atrial fibrillation (AF).Methods: Echocardiography was performed in 107 consecutive patients with AF.The logarithmic equation between pre-preceding RR interval (RR-2) and LV out-flow peak ejection velocity (Vpe) was obtained in the coordinates with precedingRR interval (RR-1) ≥ 0.5 second. By removing the coordinates RR-1 < 0.5 sec-ond, the squared correlation coefficient (r2) between RR-2 and Vpe was improvedfrom 0.19 to 0.25 (p=0.000). Using this equation, Vpe was adjusted for the effectof RR-2 assuming that RR-2 is fixed to the mean RR interval. By this adjust-ment, r2 between RR-1 and Vpe was improved from 0.61 to 0.71 (p=0.000). Thelogarithmic equation between RR-1 and adjusted Vpe was calculated in the coor-dinates with RR-1 ranged from 0.6 to 1 second. From this relationship, r2, slope,Vpe at RR-1 = 1 second (Vpe-1), and the ratio of slope to Vpe-1 (Slope/Vpe-1)were calculated.Results: When patients were divided into two groups according to the historyof heart failure (HF, New York Heart Association, Functional Class ≥ 3, n=54),forward logistic regression analysis showed that old age, high Slope/Vpe-1, mi-tral regurgitation, and LA enlargement independently predict the occurrence ofHF. Ejection fraction and fractional shortening were not different between twogroups. Slope/Vpe-1 was associated with systolic LV dimension (LVIDs, r=0.45,p=0.000), diastolic LV dimension (r=0.41, p=0.000), ejection fraction (EF, r=-0.34,p=0.000), fractional shortening (r=-0.33, p=0.001), history of heart failure (HF,r=0.29, p=0.003), and LV mass (0.29, p=0.004). Among those, LVIDs and his-tory of HF were independent parameters in multiple stepwise regression analysis(r=0.49, p=0.000). To minimize the effect of systolic dysfunction, same analyseswere repeated in patients with normal LV size and without significant regurgitation(n=69). Old age and high Slope/Vpe-1 independently predicted the occurrence ofHF (n=27). Slope/Vpe-1 was independently associated with thickness of interven-tricular septum and the history of HF (r=0.45, p=0.001).Conclusions: A new parameter, Slope/Vpe-1, is superior to the classic param-eters for the evaluation of LV function. This parameter is determined not only bythe systolic dysfunction but also by the diastolic dysfunction resulting in the mostuseful predictor in predicting the occurrence of HF in AF.
P5147 Risk factors in patients with atrial fibrillation: resultsfrom the REduction of Atherothrombosis forContinued Health (REACH) Registry
S. Goto1, J. Rother2, Y. Ikeda3, P.W. Wilson4, A. Hirsch5,E.M. Ohman6, D.L. Bhatt7, P. Gabriel Steg8 on behalf of REACH
Registry Investigators. 1Tokai University School of Medicine, Department ofMedicine, Kanagawa, Japan; 2Klinikum Minden, Director of Neurology, Minden,Germany; 3Keio University School of Medicine, Department of Internal Medicine,Tokyo, Japan; 4Medical University of South Carolina, Department of Medicine,Charleston, United States of America; 5University of Minnesota School PublicHealth, Epidemiology and Community Health, Minnneapolis, United States ofAmerica; 6Duke University Medical Center, Program for Advanced CoronaryDisease, Durham, United States of America; 7Cleveland Clinic Foundation,Cardiac, Peripheral and Cartoid Intervention, Cleveland, United States ofAmerica; 8AP-HP Hopital Bichat-Claude Bernard, Cardiologue, Paris, France
Atrial fibrillation (AF) is a risk factor for cardiogenic stroke. To evaluate risk factorsrelated to AF, baseline characteristics of patients (pts) with AF were comparedwith those without AF.REACH Registry recruited >68,000 pts with established atherothrombosis (doc-umented coronary artery, cerebrovascular or peripheral arterial disease) or ≥3risk factors. The risk factor profile of the 7,143 pts with AF was similar to that ofpts without AF (Table). (Preliminary results: not yet age-adjusted.) The percent-age of younger pts with AF increased in proportion to the number of risk factors(diabetes mellitus, hypertension, hyperlipidemia, obesity) (Figure).
Risk factors in AF vs non-AF patients
Risk factor only CAD CVD PAD(n=12,420) (n=40,440) (n=18,991) (n=8,320)
AF+ AF- AF+ AF- AF+ AF- AF+ AF-
Sample size (n) 745 11,438 4,945 34,516 2,544 15,963 927 7,168Men (%) 53.2 49.2 68.2 70.1 60.0 59.4 72.0 70.4Age (mean±SD) 73.4 68.7 67.7 68.9 73.5 68.9 73.2 68.8
±8.5 ±9.9 ±10.1 ±10.1 ±9.18 ±10.1 ±9.2 ±9.8Diabetes (%) 70.4 75.3 39.3 38.0 38.0 37.2 46.5 43.7Hypertension (%) 92.8 90.1 84.1 79.7 84.7 82.9 86.4 80.4Hyperlipidemia (%) 78.1 80.6 71.4 77.7 56.3 58.2 60.1 66.9Obesity (BMI>30; %) 62.6 58.2 48.9 44.8 45.0 41.9 45.2 43.6
Risk factors for AF patients by age
In this large, global registry of stable outpatients with/at high risk of atherothrom-bosis, prevalence of atrial fibrillation in younger participants increased with thenumber of atherothrombotic risk factors.
P5148 Pacing to prevent atrial fibrillation - high right septumimplantation guided by intracardiacechocardiography
M. Rosiak, R. Pietruszynski, A. Bissinger, W. Grabowicz,L. Markuszewski. University Hospital No. 2, Invasive Cardiology,
Lodz, Poland
Atrial pacing is an accepted therapy for sick sinus syndrome (SSS) patients. Thepurpose: to prospectively evaluate whether in comparison to appendage pacing,atrial septal lead localization could lower the incidence of atrial fibrillation (AF).Additionally, the influence of atrial lead localization on P-wave duration (PWD).Methods: Study participants: 59 SSS patients (23 men, 36 women, age68.6±5.1). 29 patients were assigned to the right atrial appendage (RAA) pac-ing group and the other 30 to the suprafossal (SF) pacing group. The SF groupimplantation was performed both under X-ray fluoroscopy and intracardiac echo-cardiography (ICE). The area above the fossa ovalis was the target implantationsite. PWD in the 12-lead ECG was measured at a paper speed of 100 mm/s.Follow-up - a minimum of 6 months. An AF event was defined as an episode thatlasted 15 minutes or more and was verified by ECG.Results: The mean number of AF episodes: 7.5 in the RAA group and 5.5 in theSF group (p=0.033). A significantly longer mean PWD was recorded in the RAAgroup compared to the SF group (134±11.6 vs. 127±25.0 ms, p=0.027). Themean PWD change: +1.8 ms (increase) in the RAA group in comparison to -3.2
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

884 Atrial fibrillation – occurrence, clinical management and prevention
ms (reduction) in the SF group. AF-free 6-moth period rate was 17.4% for the SFgroup and 4.1% for the RAA group (p=0.0016) - the Kaplan-Meier estimates.
Table 1. Results
RAA (n=29) SF (n=30) P value
PWD (ms) 134±11.6 127±25.0 0.027PWD change (ms) 1.8±6.5 -3.2±6.5 0.020Mode switch counter 6-month 41 (28-58) 32 (19-42) 0.025No. of AF episodes 7 (5.0-9.25) 5 (3.0-7.0) 0.003
Data are given as medians (25%-75% quantiles) or mean ± SD; PWD - P wave duration
Conclusions: The SF pacing results in a shorter P-wave on a 12-lead ECG andin a reduced number of AF episodes.
P5149 The prognostic impact of a first episode of atrialfibrillation during a 5-year follow-up: a single centerexperience
T. Becker, T. Kleemann, K. Doenges, B. Gut, J. Senges, K. Seidl.Klinikum der Stadt Ludwigshafen, Herzzentrum, Ludwigshafen,
Germany
Objective: To evaluate for the prognostic impact of a first episode of atrial ar-rhythmia compared to pts with already recurrent episodes.Methods: 1053 pts with atrial fibrillation or flutter were included in this single cen-ter registry designed on an intention to cardiovert base and thereafter followed-upfor 5 years regarding their long-term outcome and antithrombotic treatment (ATT)during this period.Results: 618 pts (59%) presented with a first episode of atrial arrhythmia vs. 435pts (41%) with recurrent episodes. Baseline characteristics at index admissionwere as follows (first vs. recurrent): male 71% vs. 74%, median age 65 vs. 64years, structural heart disease 58% vs. 59%, EF<40% and NYHA II+ 13% vs.8%. In 27% of pts with a first episode compared to 13% of pts with recurrentepisodes (OR 2.4, 95% CI 1.7-3.3) a new diagnosis of structural heart diseasewas made. Long-term outcome and ATT during 5 year follow-up are shown inTbl.1, whereat a first episode was alos independently associated with mortality ina multivariate model (HR 1.4, 95% CI 1.02-1.98).
Death Embolic events Severe bleeding Oral anticoagulation(OAC)
First episode 27 % 5% 1.2% 58%Recurrent episodes 16% 4% 0.9% 70%OR (95% CI) 2.0 (1.4-2.7) 1.4 (0.6-3.4) 1.4 (0.3-0.7) 0.5 (0.4-0.7)
Conclusions: 1. The first episode of atrial fibrillation serves as a marker for un-derlying cardiac diseases and is associated with impaired prognosis. 2. The dis-tinction between first and recurrent episodes does not apply for thromboembolicrisk stratification, nevertheless the prescription rate of OAC at the end of follow-upwas significantly lower in pts with a first episode.
P5150 Permanent VVI pacing versus ventricular backuppacing in patients with chronic atrial fibrillation andnormal left ventricular systolic function
I. Chiladakis1, N. Koutsogiannis2, A. Kalogeropoulos2 ,N. Vlassopoulou2, P. Arvanitis2, D. Alexopoulos2. 1Patras, Greece;
2University Hospital, Cardiology, Rion-Patra, Greece
Background: Atrial fibrillation and rhythm irregularity itself may negatively im-pact the cardiac performance. However, it remains uncertain whether any benefitsachieved by rate regularization may be counterbalanced by the adverse effects ofthe pacing induced ventricular dyssynchrony. We investigated whether rate reg-ularization itself affects the ventricular performance in patients with chronic atrialfibrillation and normal left ventricular (LV) systolic function by evaluating conven-tional doppler, tissue doppler (TD) and color M-Mode (CMM) echocardiographicstudies and B-type natriuretic peptide (BNP) measurements.Methods: We examined 18 patients (mean age 76 ± 9 years) with chronic atrialfibrillation and normal LV systolic function (ejection fraction > 55%) who wereimplanted with a VVI pacemaker. Baseline echocardiographic data and BNP [logmean, 95% CI] levels were obtained during underlying atrial fibrillation (meanheart rate 58±5 beats/minute) with the pacemaker programmed to ventricularbackup pacing at 45 beats/min. The baseline data were compared with thosemeasurements after a two-week period of continuous VVI pacing ensuring per-manent ventricular capture at 70 beats/minute.Results: Permanent VVI pacing, compared to the irregular atrial fibrillationrhythm, resulted in significant decreases in stroke volume (63 ± 12 ml vs. 78± 17 ml, p < 0.001) and TD-Sa index (7.3 ± 1.1cm/s vs. 7.8 ± 1.0 cm/s, p <
0.05), and trends of increases in isovolumetric relaxation time (117 ± 22 ms vs.107 ± 25 ms, p = 0.06). Other measurements including TD and CMM derivedE/Ea and E/Vp indexes, and cardiac output did not significantly change. The BNPlevels following permanent VVI pacing increased by 20% [177 (128-244) pg/ml vs.147 (98-221) pg/ml, p = 0.07]. Both modes of heart rhythm were well tolerated,but 4 patients preferred the permanent VVI pacing rhythm.Conclusions: Rate control with permanent VVI pacing, compared to slower irreg-
ular heart rhythm, seems to worsen slightly the cardiac function during mid-termfollow-up in patients with atrial fibrillation and normal LV systolic function.
P5151 Prevention of onset of atrial fibrillation bybeta-blockers treatment in heart failure.A meta-analysis
I. Abi-Nasr, A. Bouzamondo, J.S. Hulot, P. Lechat. Pitie Salpetrierehospital, Clinical Pharmacology, Paris, France
Introduction: Atrial fibrillation (AF) is an important morbidity-mortality risk fac-tor, especially in patients with heart failure (HF). Angiotensin converting enzyme(ACE) inhibitors and Angiotensin II receptor antagonists have been shown to re-duce its occurrence. The preventive efficacy of beta-blockers on such AF occur-rence has not yet been evaluated.Methods A systematic review of the literature was performed to identify all clini-cal trials evaluating beta-blockers efficacy in heart failure. Eligible studies had tobe randomised, placebo-controlled and providing information on the number ofpatients with occurrence of AF during follow up among those with a sinus rhythmat baseline. We calculated a weighted relative risk of AF occurrence for each trial,a Chi2 test of association and a Chi2 test of heterogeneity.Results A total of 7 studies could be found which included 11952 patients receiv-ing a background treatment with ACE inhibitors. Overall, β blockers significativelyreduced incidence of onset of AF from 5.3% to 3.8% (Table 1): relative risk reduc-tion= 27% (95% confidence interval [CI] 14% to 38%, p<0.001).Heterogeneitytest: p=0,096. A same trend of efficacy was observed in all trials except in theSENIORS study where no effect of Nebivolol was observed. In this trial whichincluded aged patients (>70 years) and patients with systolic or diastolic HF, ahigher prevalence of AF at baseline (35%) was observed compared to the meanbaseline prevalence of 13% in the other similar trials (range 11%-15%).
Table 1. Incidence of onset of AF in each trial in HF
β-blockers (events/patients) Placebo (events/patients)
CIBIS I (bisoprolol) 9/280 13/276MERIT HF (metoprolol) 33/1677 54/1681WAAGSTEIN F (metoprolol) 1/86 8/79SENIORS (nebivolol) 78/706 74/684BEST (bucindolol) 78/1208 111/1197COPERNICUS (carvedilol) 12/1156 22/1133CAPRICORN (carvedilol) 16/895 31/894Total 227/6008 (3.8%) 313/5944 (5.3%)
Conclusion β blockers appear to effectively prevent occurrence of AF in patientswith heart failure in the prevention of systolic HF related AF.
P5152 Valsartan amlodipine combination and prevention ofatrial fibrillation recurrence in hypertensive diabeticpatients
R. Fogari, P. Preti, M. Destro, P. Lazzari, A. Rinaldi, A. Zoppi,A. Mugellini. University of Pavia, Department of Internal Medicine,
Pavia, Italy
Aim: to evaluate the effect of antihypertensive treatment with valsartan-amlodipine combination as compared to atenolol-amlodipine combination in pre-venting the recurrence of atrial fibrillation in hypertensive patients with a historyof recent atrial fibrillation.Methods: we studied 220 mild hypertensive (SBP > 130 mmHg 80 < 100 mmHg)out patients with well controlled type 2 diabetes (HbA1c < 7%). They were insinus rhythm but with at least two ECG documented episodes of atrial fibrillationin the previous 6 months. After one week placebo period, they were randomizedto valsartan 160 mg plus amlodipine 2.5 mg or to atenolol 100 mg plus amlodipine2.5 mg in 1:1 ratio with an amlodipine dose titration after 4 (5 mg.), 8 (7.5 mg),and 12 weeks (10 mg) weeks, and were followed for 1 year. Blood pressure wasevaluated and a 24 hours ECG was recorded every month; the patients wereasked to report any episode of symptomatic atrial fibrillation and to perform anECG as early as possible.Results: One hundred and ninety nine patients completed the study, 100 invalsartan-amlodipine group and 99 in atenolol-amlodipine group. After 12 monthsof treatment the blood pressure mean values were significantly reduced bothin valsartan-amlodipine group (from 154/96 to 126/76 mmHg, p< 0,001) and inatenolol-amlodipine group (from 155/95 to 128/78 mmHg, p<0,001) without anydifference between the two treatments. At least one symptomatic or non symp-tomatic ECG documented episode of atrial fibrillation was reported in 13% of thepatients treated with valsartan-amlodipine and in 33% of the patients treated withatenolol-amlodipine (p<0,01).Conclusions: the valsartan-amlodipine combination seems to be more effectivethan atenolol-amlodipine in preventing new episodes of atrial fibrillation in hyper-tensive diabetic patients with recurrent atrial fibrillation. These data suggest thatangiotensin II type 1 receptor blockade could be able to favourably impact theatrial electrical and structural remodelling in this type of patients.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – occurrence, clinical management and prevention 885
P5153 Progressive structural heart disease results in biatrialmechanisms of atrial fibrillation in humans
N.D. Skadsberg1, H.B. Rao2, S. Saksena2. 1Medtronic, Inc.,Minneapolis, United States of America; 2RWJ Medical School,Warren, United States of America
Background: The impact of different diseases on the right and left atrial substratefor atrial fibrillation (AF) is unknown. OBJECTIVES: We mapped spontaneous AFin pts with coronary artery disease (CAD), systemic hypertension (HTN) or bothdiseases (CAD+HTN) during simultaneous biatrial catheter and 3-dimensionalnon-contact mapping (NCM).Methods: Spontaneous atrial premature beats (APBs) and atrial tachyarrhyth-mias (ATs) were mapped. Regional origin of APBs, mechanisms of ATs and theircycle length were analyzed.Results: 38 pts (Gp.1: CAD n=11, Gp.2: HTN n=17, Gp.3: CAD+HTN n=10)were studied. Mean LA diameter (Gp.1 = 4.6 cm, Gp.2 = 4.1 cm, Gp.3 = 4.4cm; p>0.35) and mean LV ejection fraction (Gp.1 = 49%, Gp.2 = 55%, Gp.3 =47%) were comparable. Mean P-wave duration in the 3 groups was 145±34 ms,152±16 ms, and 136±45 ms, respectively (p=ns). The origin of APBs and theirmean coupling interval was similar in the 3 groups. % of pts having APBs orig-inating in both the right and left atrium was comparable (Gp.1 = 40%, Gp.2 =27%, Gp.3 = 30%; p=ns). Distribution of ATs was biatrial in Gps 1 and 2 but pre-dominated in the RA and septum in Gp 3 (Fig). AT cycle lengths did not differby disease state (Gp.1 = 237±92 ms, Gp.2 = 234±42, and Gp.3 = 268±47 ms;p=ns).
Conclusions: 1. In symptomatic AF pts with either CAD or HTN, NCM find-ings suggest biatrial disease already exists and results in similar mechanismsof AF onset. This biatrial substrate may explain failure of unilateral interventionsor monotherapies. 2. A shift to the RA/septum in AF onset mechanisms occurswith progressive coexistence of CAD and HTN disease states.
P5154 Effect of dronedarone on exercise in patients withpermanent atrial fibrillation
J.M. Davy1, M. Herold2, C. Hoglund3, D. Radzik4,A.J.M. Timmermans5. 1CHU Arnaud de Villeneuve, Mont-pellier, France; 2Fakultni Nemocnice-Kral, Praha, Czech Republic;
3Stockholm Heart Center, Seville, Spain; 4Sanofi-Aventis SMA, Paris, France;5Medisch Spectrum Twente, Enschede, Netherlands
Background: The ERATO study demonstrated that dronedarone (D) effectivelycontrols heart rate (HR) during atrial fibrillation (AF) in a broad range of patientsincluding those on concomitant standard HR-lowering therapies. The purpose ofthis substudy was to assess the ability of D compared to placebo (P) in improvingexercise performance defined as the control of ventricular rate during exercisewith maintained exercise duration in patients participating in the ERATO study.Methods: Patients with permanent AF were randomly assigned to receive D 400mg bid (n=85) or P (n=89) for six months. Exercise response was assessed atbaseline and day 14 using a symptom-limited exercise test with an incrementalexercise workload using cycle ergometry. Systolic blood pressure (SBP) and HRwere measured at rest, at sub-maximal (50% of max workload at baseline andmaximal exercise) and at maximal exercise. Exercise performance (defined as thedifference in HR at sub- and maximal exercise, and maximal exercise duration)was compared at day 14 versus baseline in the D and P groups using an analysisof covariance model.Results: Mean change from baseline in ventricular rate on day 14 was signifi-cantly greater in the D group compared to P both at sub- (-25.6, [95% CI -30.1to -21.1] D vs. -2.2 [95% CI -6.7 to 2.4] P, p<0.001) and maximal exercise (-27.4[95% CI -32.5 to -22.3] D vs.-2.9 [95% CI -8.0 to 2.3] P, p<0.001). At maximalexercise at day 14, mean ventricular rate change from baseline was 24.5 bpmlower in the D group compared to P. Despite a powerful control of ventricularrate exercise, duration was maintained as no significant effect on maximal ex-ercise duration at day 14 compared to baseline was observed (0.14 minutes Dvs 0.26 minutes P). There was no difference between the two treatment groupsin changes from baseline to day 14 for SBP, measured at maximal exercise.D was well tolerated with no incidences of torsades de pointes or organ toxic-ity.Conclusion: Treatment with dronedarone decreased HR from baseline duringboth sub-maximal and maximal exercise without decreasing exercise duration.
P5155 Prognostic significance of atrial fibrillation in patientswith systolic heart failure: does sex matter?
P. Corell1, F. Gustafsson2, M. Schou3, J. Markenvard4,T. Nielsen5, P. Hildebrandt6. 1Frederiksberg University Hospital,Cardiology, Frederiksberg, Denmark; 2Copenhagen University
Hospital,Rigshospitalet, Cardiology, Copenhagen, Denmark; 3FrederiksbergUniversity Hospital, Cardiology, Copenhagen, Denmark; 4Fredericia Hospital,Internal Medicin, Fredericia, Denmark; 5Ribe County Hospital, InternalMedicin, Esbjerg, Denmark; 6Frederiksberg University Hospital, Cardiology,Frederiksberg, Denmark
Purpose: Atrial fibrillation (AF) is the most frequent sustained arrhythmia amongpatients with systolic heart failure (HF). Despite the hemodynamic consequencesof AF, the prognostic influence of AF is controversial because of conflicting datafrom clinical studies. The aim of our study was to examine the prognosis of AF inan unselected outpatient population with HF due left ventricular systolic dysfunc-tion.Methods: We included 1019 consecutive HF patients (70% men, 71 years) withLVEF ≤ 45% referred to outpatient HF clinics.Results: At baseline 26.4% had AF, and 18.7% developed new onset AF (an-nual incidence 6%). Patients with AF were older (p<0.001), more often male(p=0.04), more likely to have a history of stroke (p=0.03), but less likely to haveIHD (p<0.001). Patients with AF and SR had similar mean LVEF, NYHA class andheart rate. After a mean follow-up of 742 ± 498 days, 267 patients died and 716reached the combined end-point (all cause mortality or all cause admission tohospital). AF at baseline was associated with increased all-cause mortality (HR1.38; CI 1.07-1.78, p=0.01) and all-cause mortality/hospitalisation (HR 1.43; CI1.22-1.68, p<0.001). By multivariable analysis baseline AF were significantly as-sociated with increased risk of experiencing the combined endpoint (HR 1.29; CI1.05-1.58; p=0.02). Baseline AF was not an independent predictor of mortality.By multivariable analysis new onset AF was associated with increased risk ofall-cause mortality/hospitalisation (HR 1.45; CI 1.05-2.00; p=0.02).We found significant interaction between AF and sex and between AF and LVEF.Females with AF had a significantly increased mortality (HR 1.65; CI 1.03-2.65;p=0.04) compared with females with SR. We found no significant difference inmortality between males with AF and SR (p=0.09).In patients with LVEF above the median (LVEF ≥ 30%) presence of AF at base-line significantly increased mortality (HR 1.46; CI 1.04-2.07; p=0.03) compared topatients with SR. In patients with LVEF below the median (LVEF<30%) we foundno significant difference between patients with AF and SR.Conclusion: In outpatients with systolic HF, AF is a common comorbidity withwhich importantly affects morbidity and mortality. The specific prognostic impactof AF in women with HF deserves further investigation.
P5156 Antitachycardia pacing and preventive pacingalgorhythms decrease the atrial fibrillation burden inpatients with brady-tachy syndrome. Results of thePrevention Or Termination (POT) trial
L. Mont1, R. Ruiz-Granell2, J.G. Martinez3, J. Carmona4,M. Fidalgo5, M. Riera6, X. Navarro6 on behalf of POT study investigators.1H.Clinic, Arrhythmia Unit, Barcelona, Spain; 2H.Clinico, Arrhythmia Unit,Valencia, Spain; 3H.General, Cardiologia, Alicante, Spain; 4H. de Navarra,Cardiology, Pamplona, Spain; 5H. de Leon, Cardiology, Leon, Spain; 6MedtronicIberica, Scientific & Clinical, Barcelona, Spain
The effect of preventive pacing algorithms (PPA) and Antitachycardia pacing(ATP) in reducing atrial fibrillation episodes remains controversial. The aim ofthe study was to prospectively assess whether ATP on top of preventive pacingalgorithms (PPA) decreases AF burden in patients (pts) with documented AF (>2AF episodes in <6 months) and Class I ACC/AHA indication for pacing.Methods: A total of 160pts were included in the study. They received an AT500™pacemaker. There was 1 month of stabilization. After 3months of conventionalDDDR pacing at 60bpm, AF burden was analyzed. If patients had >30 min/weekof AF, they were randomized to 3m period of PPA or to PPA+ATP (Period 1).Afterwards, they were crossed to the alternative therapy for additional 3m (Period2) with a 1m wash out period (total study duration 11m). A group of 75p fulfilledrandomization criteria and were included in the analysis.
Fig 1. AFB after 3m (1P) and 7 m (2P)
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

886 Atrial fibrillation – occurrence, clinical management and prevention / Atrial fibrillation – optimizing the cardioversion outcome
Results: Mean age 68±8 years, 50% men. Group A (n=43) received first PPA andat month 4 PPA+ATP. Whereas Group B (n=42) were randomized in the reverseorder. There were no differences in the initial AF burden between both groups.Both groups showed a significant decrease in AF burden at the end of period 1(60% and 70% respectively p<0.01). After period 2, there was a further decreasein AF burden, without differences between both groups (fig 1). There was also asignificant decrease in the number of episodes in group A and B at period 1 (40%and 31% respectively) that continue decrease at period 2, without differencesbetween the 2 groups.Conclusions: Both PPA and PPA+ATP diminish burden of AF. The addition ofATP does not seam to increase the reduction in AF burden nor the number ofepisodes in this cross-over design.
P5157 High prevalence of Sleep Apnoea (SA) syndrome inpatients with paroxysmal Atrial Fibrillation (pAF)
A. Mueller, T. Vogtmann, J. Vivell, I. Fietze, G. Baumann, H. Theres.Charite, Universitaetsmedizin Berlin, Department of Cardiology,Berlin, Germany
Background: A strong association of AF and obstructive SA has been docu-mented recently by Gami (Circ 2004) by means of Berlin questionnaire. Addi-tionally our group used a new automatic detection algorithm based on transtho-racic impedance measurement (TTI) integrated in a standard Holter ECG (Car-dioMem 3000, getemed, Germany) to detect SA. The method was validated withpolysomnography with a 0.80 sensitivity, specificity 0.93, positive predictive value0.78 and negative predictive value 0.93 before.Purpose of the study: Prospective evaluation of the association of SA in unse-lected pts. with a history of pAF admitted to a university cardiology departmentfor any reasons.Methods: PAF patients were not known to suffer from SA so far. An impedanceapnoe hypopnoe index ≥10 as detected with TTI was defined positive for SA. TheBerlin questionnaire (validated for the detection of obstructive SA) and Epworthsleepiness scale (with a cut-off value of ≥ 9 for SA positive) were used.Results: 30 consecutive pts. (13 f), mean age 63 ± 11 y,14 with structural heartdisease (8 valve disorders, 5 CAD, 1 ASD), mean EF 57±7% with a history of3.1± 5.6 y (range 0.1-25) of paroxysmal atrial fibrillation (17± 26 episodes/mon,range 1-90) were studied. A high prevalence of SA was shown in the study pop-ulation highlighting the clinical relevance of screening AF patients for SA.
Transthoracic Impedance Berlin EpworthHolter recording Questionnaire Sleepiness Scale
SA positive 13/30 13/30 14/3043% 43% 47%
Conclusion: 1) Our results prove a high prevalence of SA in patients with pAF.2) These results were confirmed by the questionnaires as with the TTI systemintegrated in a Holter ECG.3) Further studies are needed to elucidate the pathophysiological link betweenpAF and SA.4) TTI integrated in a standard Holter ECG might be a helpful screening tooldetecting sleeping disorders in patients with arrhythmias.
P5158 Persistent atrial fibrillation predicts appropriateshocks and heart failure in patients with leftventricular dysfunction treated with an implantablecardioverter defibrillator
M. Rienstra, M.D. Smit, W. Nieuwland, E.S. Tan, A.C.P. Wiesfeld,R.G. Anthonio, D.J. Van Veldhuisen, I.C. Van Gelder. University Medical CenterGroningen, Cardiology, Groningen, Netherlands
Introduction: The impact of AF on cardiovascular morbidity and mortality in thesetting of CHF is still uncertain.Aim: To investigate the impact of persistent AF on appropriate ICD shocks, car-diovascular mortality and CHF in ICD patients with left-ventricular dysfunction.Methods: We included 319 consecutive patients with a LVEF ≤0.35, who under-went a first ICD implantation. The impact of persistent AF on appropriate ICDshocks, cardiovascular mortality, and CHF was investigated.Results: History of persistent AF was present in 71 of 319 (22%) patients,and 44 (14%) patients had AF at implantation. They had more frequently valvedisease and previous cardiac surgery, and less often coronary artery disease,compared to patients without a history of persistent AF. Persistent AF patientshad higher NYHA functional class, but LVEF was comparable (0.28±0.07 ver-sus 0.29±0.08, p=ns). During a mean follow-up of 2.4±1.9 years, patients witha history of persistent AF more often received appropriate shocks (25 [35%] ver-sus 58 [23%], p=0.045), and developed (deterioration of) CHF (22 [31%] versus36 [15%], p=0.003). Multivariate regression analysis revealed history of persis-tent AF as independent risk indicator for appropriate ICD shocks (adjusted HR1.8 [1.1-3.0], p=0.01), and development or progression of CHF (adjusted HR 1.7[1.0-3.0], p=0.04) (Figure). Patients with new-onset AF (20 patients, 9%) devel-oped more often (deterioration of) CHF (9 [45%] versus 24 [12%], p=0.001), andcardiovascular mortality (8 [40%] versus 19 [10%], p=0.001) predominantly dueto CHF.
Conclusion: In ICD patients with left-ventricular dysfunction, a history of per-sistent AF is associated with appropriate ICD shocks and (deterioration of) ofCHF. New-onset AF is related to (deterioration of) CHF and cardiovascular mor-tality.
ATRIAL FIBRILLATION – OPTIMIZING THECARDIOVERSION OUTCOME
P5159 Pharmacological cardioversion compared to electricalcardioversion predicts maintenance of sinus rhythm
X. Vinolas1, J.M. Alegret1, J. Sagrista1, A. Hernandez-Madrid2 onbehalf of REVERSE Investigators. 1Cardiology, Barcelona, Spain;2Cardiology, Madrid, Spain
It is known that a proportion of patients (P) with persistent AF reverts to SR whentreated with antiarrhythmic drugs (AAD) before electrical cardioversion (ECV), butthe clinical implications regarding the maintenance of sinus rhyhtm (SR) are notwell known.Matherial & methods: The REVERSE (Registro Cardioversion Eléctrica Espaf-plusmn;a - Spanish Registry of Electrical Cardioversion) included prospectivelyall P without organic heart disease and persistent AF (>7days) submitted to ECVin 97 hospitals from march to june 2004 (n=800). An attempt of pharmacologicalcardioversion before ECV was performed in 412 P. We compared clinical charac-teristhics and maintenance of SR at 3 m follow-up in the patients in whom AADrestored SR (n=99) with patients needing an effective ECV(n=269) to restore SR.P with a failed ECV or inmediate recurrence of AF were excluded.Results: AAD used were amiodarone in 80% and IC drugs in 16% restoring SRin 24% (n=99). In the remaining 313 P an ECV was performed restoring SR at dis-charge in 86% (n=269). P with pharmacological cardioversion has a smaller bodysurface area (1,83 vs 1,94); smaller left atrium (41 vs 44) and less percentaje ofAF longer than 6 m (26% vs 12%).83% of P with pharmacological CV were in SR at 3 m compared to 64% of the Pneeding ECV. Table I shows the factors predicting maintenance of SR in univariateanalysis.
AF at 3m (n=109) SR at 3 m (n=259) p
Body surface area (BSA) 1,96±0,17 1,89±0,17 .02Left atrium 44±6mm 42±5mm .05Previous ECV 31% 18% .05Pharmacol. cardioversion 11% 33% .001
In the multivariate analysis pharmacological cardioversion (p=.002;OR 2,8); bodysurface area (p=0.02;0,19) and previous ECV (p=.01; OR 1,98) were independentpredictors of maintenance of SR.Conclusions: Pharmacological cardioversion with drugs previous to an ECV inP eith persistent AF defines a subgroup of P with higher maintenance of SR atmid-term follow-up.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – optimizing the cardioversion outcome 887
P5160 Clinical predictors of unsuccessful cardioversion foratrial fibrillation - a key to therapeutic management?Data from the atrial Fibrillation Italian REgistry (FIRE)
I.M. Suliman, D. Lucci, D. Casella, D. Fumagalli, L. Gonzini,C. Mazzone, G. Zanotto, A.P. Maggioni on behalf of The FIRE
Investigators. ANMCO Research Center, Florence, Italy
Background: The identification of clinical predictors of unsuccessful cardiover-sion for atrial fibrillation (AF) could be very useful in the decision making to taylorthe most proper strategy (rate control vs rhythm control). The aim of this analysiswas to define the clinical predictors of unsuccessful cardioversion for AF.Methods AND RESULTS. 2473 pts with AF enrolled in the FIRE study, a sur-vey conducted by 207 Italian Centers, underwent cardioversion during hospitalstay (electric 38.6%, pharmacologic 61.4%). Univariate and multivariable (logis-tic regression model) analyses were performed to identify the predictors of AFat hospital discharge. Mean age of pts was 67.6±11.9 years; 45% of them wereof female gender. Sinus rhythm at discharge was obtained in 2052 pts (83%)while 17% remained in AF. Pts who remained in AF after cardioversion attemptwere older, with more previous episodes of AF, with a duration of AF longer than48 h, in long-term anticoagulation (OAT) therapy, with neurological/heart failuresymptoms, admitted in a non-Cardiology Department and pharmacologically car-dioverted. The independent predictors for AF identified by multivariable analysisare shown in the Table (statistical significance was defined as p<0.01).
Variable Chi-Square OR 95%CI p
Heart failure 31.8 2.14 1.64-2.88 <0.0001OAT 21.6 2.15 1.56-2.96 <0.0001Pharmacological cardioversion 19.9 2.25 1.57-3.20 <0.0001Neurological symptoms 17.2 4.82 2.29-10.12 <0.0001AF onset >48h 13.7 1.73 1.29-2.31 0.0002Age (as a continuous variable) 13.1 1.02 1.01-1.03 0.0003Non cardiology department 12.3 1.65 1.25-2.17 0.0004Symptomatic AF 11.7 2.22 1.41-3.50 0.0006
Conclusions: The strongest predictors of persisting AF were the presence ofheart failure, duration of AF, severity of symptoms, choosing pharmacologicalcardioversion and the admission to a non cardiology department. Identificationof independent clinical markers of AF can allow a more appropriate selection be-tween the available strategies.
P5161 Effects of Polyunsaturated Fatty Acids n-3 (PUFA n-3)in the prophylaxis of atrial fibrillation relapses afterexternal electric cardioversion
S. Nodari, A. Manerba, A. Madureri, N. Berlinghieri, E. Pulcini,S. Frattini, M. Metra, L. Dei Cas. University of Brescia, Chair of
Cardiology, Brescia, Italy
Background: The most important problem in management of Atrial Fibrillation(AF) is the high incidence of relapses at short and mid term after pharmacologi-cal or electric cardioversion (ECV). Data from literature show Amiodarone as themost effective antiarrhythmic drug in synus rhythm mantainance, with about a 50-60% effectiveness at six months. Moreover recent studies have shown positiveeffects on atrial remodeling and reduction of AF relapses of non-antiarrhythmicdrugs like Renin Angiotensin System Blockers (RAS inhibitors). The antiarrhyth-mic properties of PUFA n-3 are known, too. There are many evidences about pos-itive effects on ventricular tachiarrhythmias and sudden death; on the contrary it’snot proved their efficacy on AF.Aim: To evaluate effects of PUFAs n-3, on top of traditional treatment, in theprevention of AF relapses in patients (pts) undergone ECV.Methods: We have evaluated 70 consecutive pts, 46 males and 24 females, withpersistent AF, different AF etiology and previous relapses neverthless antiarrhyth-mic therapy. All pts underwent laboratory routine analysis and echocardiogrambefore bifasic wave ECV. After the restore of synus rhythm pts were monitoredwith telemetry for at least six hours and, before discharge, were randomized toreceive placebo or PUFAs n-3 (1 gr/day), in addition to therapy with amiodarone,beta-blockers and RAS inhibitors. All pts were evaluated with Holter monitoringafter 1, 3 and 6 months.Results: Control group enrolled 40 pts (26 males and 14 females), mean age69.9 ± 7.2; PUFAs n-3 group enrolled 30 pts (20 males and 10 females), meanage 70.4 ± 6.2. There were not significat differences between the two groupsfor age, mean AF duration and echocardiographic parameters. The AF etiologywas ischemic cardiopathy (20% vs 18%), dilated cardiomiopathy (ischemic or id-iopathic) (20% vs 22%), hypertension (32% vs 40%), valvular heart disease 25%vs 15%), "lone AF" (3% vs 5%), in PUFAs n-3 versus placebo group respectively.The restore of synus rhythm was obtained in all pts. No complications were ob-served. In the PUFAs n-3 group AF relapses were significantly lower than placebogroup at a mounth (3.3% vs 10%; p=0.043), at 3 mounths (10% vs 25%; p=0.004)and at 6 mounths (13.3% vs 40%; p<0.0001).Conclusions: Our study shows a significantly reduction in AF relapses after PU-FAs n-3 treatment, in addition to optimized therapeutic protocol (amiodarone,beta-blockers and RAS inhibitors) in pts with persistent AF, confirming the roleof PUFAs n-3 in the prevention of AF relapses.
P5162 The efficacy and safety of new class III antiarrhythmicdrug nibentan for cardioversion in patients withpersistent atrial fibrillation
I.N. Bregvadze, E.B. Maykov, S.F. Sokolov, S.P. Golitsyn,L.V. Rozenshtraukh, E.I. Chazov. Institute Of Clinical Cardiology,
Clinical Electrophysiology, Moscow, Russian Federation
Purpose: To study the efficacy and safety of intravenous (i.v.) class III antiar-rhythmic drug-nibentan (Nb) for restoration of sinus rhythm (SR) (pharmacologi-cal cardioversion) in patients (pts) with persistent atrial fibrillation (AF) in dosageof 0,0625-0,125 mg/kg.Methods: Sixty-four pts (45 male, mean age 54 years) with persistent AF witha median duration of 6,7±6,8 months (8 days to 36 mon.) were included in thestudy. Hypertension was diagnosed in 43,7% of pts (n=28), ischaemic heart dis-ease - in 12,5% (n=8), compensated thyrotoxicosis - in 4,6% (n=3), 4,6% (n=3)were after mitral valve replacement and 33,4% (n=22) had idiopathic AF.Nb i.v. was used in 2 bolus injections (0,0625 mg/kg each), performed in theinterval of 15 minutes. The infusion was terminated in case of: 1) SR restoration;2) Increase of QT interval > 500 mc; 3) "Torsade de pointes" (tdp) development.Nb administration was controlled by 12 leads 24 hours Holter ECG monitoring.Results: Cardioversion was successful within 15 minutes after the first bolus in-jection in 29,6% of pts (n=19/64) and after the second bolus - in 42,1% (n=27/64).The overall conversion rate to SR was 71,8% (n=46/64). The average effectivedose of 1 bolus was 5,3 mg (4,5-7 mg), and of 2 boluses - 10,6 mg (8-17mg).The mean period to arrhythmia conversion was 7 and 115 minutes after 1 and 2boluses, respectively. No side effects were registered at doses < 0,0625 mg/kg.At the moment of SR restoration QT and QTc intervals were 458±54 mc and468±53 mc, respectively after 1 bolus and 474±52 mc and 487±50 mc, respec-tively after 2 boluses. Sinus bradycardia was noted in 4,6% (3/64 pts). "Tdp" de-veloped in 3% (2/64 pts) after administration of 2 boluses (0,125 mg/kg). In onecase DCC was required.Conclusion: Nb in studied doses is an effective drug for pharmacological car-dioversion of persistant AF with low rate of side effects.
P5163 Efficacy and safety of RSD1235 Injection in thetreatment of atrial fibrillation: combined analysis oftwo phase III trials
C. Torp-Pedersen1 , D. Roy2, C. Pratt3, J. Camm4, G.N. Beatch5,T. Kitt6, B. Yan2, B. Mangal6 . 1Copenhagen, Denmark; 2Montreal,
Canada; 3Houston, United States of America; 4London, United Kingdom;5Vancouver, Canada; 6Deerfield, United States of America
Background: RSD1235 is a novel atrial selective drug for the treatment of atrialfibrillation (AF). The efficacy and safety of intravenous RSD1235 for the conver-sion of AF to sinus rhythm (SR) in patients with AF of >3 hours to 3 hours to 3hrs to ≤7 days duration (short duration subgroup). Additional analyses includedefficacy in the overall population (>3 hours to <45 days). Safety was assessedby collection of adverse events (AEs), laboratory values, vital signs, and ECG andHolter recordings.Results: Patient demographics were similar in the RSD1235 and placebo groups:mean age was 62 years with 68% male. RSD1235’s efficacy was consistentacross the 2 studies. In the short duration subgroup, 51% and 52.3% RSD1235patients converted to SR compared to 4% and 3.6% of placebo patients, respec-tively (combined analysis: 51.1% vs. 3.8%, P<0.0001), and in the overall pop-ulation, 35.3% and 39.8% of RSD1235 patients converted to SR compared to2.6% and 3.3% of placebo patients, respectively (combined analysis: 36.9% vs.3.0%, P<0.0001). Of the RSD1235 patients who converted within 90 minutes,the median time to conversion was 10 minutes (from the start of the first infusion)in the short duration subgroup and 11 minutes in the overall population. Of theshort duration RSD1235 patients who converted within 90 minutes, 97.4% werein SR at 24 hrs and 92.9% were in SR at 7 days; similarly in the overall popula-tion, 97.2% and 92.3%, respectively. Symptom relief was significantly greater inthe RSD1235 group compared to Placebo in both the short duration and overallpopulations (P<0.001) 90 minutes post-infusion. Serious AEs occurred in 15.7%(37/236) of placebo and 12.1% (41/339) of RSD1235 patients in the 30-day follow-up period. There were no investigator assessed drug-related torsade de pointeswithin the first 24 hours. There were 4 deaths in the RSD1235 group, due to lungcancer; aortic dissection; ventricular fibrillation in a patient with severe chronicheart disease; and worsening dyspnoea and heart failure in the 30 day follow-up.The most common AEs reported in the RSD1235 group were transient dysgeusia(28.3%) and sneezing (17.1%).Conclusion: RSD1235 Injection safely achieved a rapid and high rate of conver-sion of AF to SR, with a low rate of relapse.
P5164 Acute management of Atrial Fibrillation with oralFlecainide or Propafenone in patients on top 1 Cantiarrhythmic drug therapy
G.Q. Villani, M.F. Piepoli, D. Aschieri, M.S. Pisati, G. Rusticali,A. Capucci. General Hospital Guglielmo da Saliceto, Cardiology
Division, Piacenza, Italy
The management of patient on chronic antiarrhythmic therapy, with recurrences
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

888 Atrial fibrillation – optimizing the cardioversion outcome
of symptomatic AF episode is a main clinical problem and at present the terapeu-tical approach in the Emergency Department is empirical and no accepted guide-lines are available. Ninety-six of 100 consecutive pts admitted for a recurrenceof symptomatic, short-lasting (< 72 hours), paroxysmal AF, with clinical history ofAF and in chronic therapy with Propafenone (PNF) or Flecainide (Fl), were con-sidered for a further oral loading antiarrhythmic treatment. Each enrolled patientwere randomised to a further oral loading dose of the same drug taken chron-ically (Fl-Treatment ie. Fl-T 100 mg, PNF-Treatment ie. PNF-T 300 mg) or to aclinical observation without therapy (Fl-Control ie. Fl-C, PNF-Control ie. PNF-C).After drug administration the pts kept a supine position, while cardiac rhythm wasmonitored by 24 hour ECG. After the antiarrhythmic treatment we observed sinusrhythm restoration in 15/26 patient of Group PNF-T (58%), in 17/24 pts of GroupFl (72%) (p 0.05), in 7/21 pts in the Fl-C group and in 5/25 patients in PNF-Cgroup (21%), (p 0.001); furthermore the terapeutical goal was reached faster in Flpts (Group PNF 6 ± 2.9 hours vs group Fl 3 ± 0,5 hours, p 2:1 were observed in5/26 (21%) pts of Group PNF-T and in 7/24 (28%) pts of group Fl. Sinus pauses(< 2 sec) were observed in 6/26 pts of Group PNF-T (22%) and in 4/24 pts ofgroup Fl (15%) at the time of sinus rhythm restoration. None of the pts presentedan AFl with 1:1 atrio-ventricular conduction. The results of this study indicatesthat in pts with recurrences of Atrial Fibrillation (AF), on top of class IC agents forrhythm control, a further oral loading dose of PNF or Fl can be safe and success-ful in restoring sinus rhythm. This terapeutical approach may cut hospitalisationcosting.
P5165 Pharmacological conversion of recent AtrialFibrillation: A randomized study of threeantiarrhythmic
I. Balla, G. Bardhaj, E. Shota, E. Petrela, A. Gace, A. Kondili onbehalf of Idriz Balla, Gazmend Bardhaj, Eduart Shota, Ela Petrela,Artur Gaçe, Anesti Kondili,. Department of Cardiology, University
Hospit, Department of Cardiology, University Hospit, Tirana, Albania
Conversion of atrial fibrillation (AF) to sinus rhythm is commonly attempted toreduce the risk of embolism and of hemodynamic deterioration. Drug selectionis usually empirical or based on limited comparative studies. Comparison of oralamiodarone (A), flecainide (Fl), propafenone (Pf) versus placebo (Pl.) for the con-version of recent AF was made in a randomized single-blind, placebo-controlledstudy. 165 consecutive patients (pts), that were of mean age 58.08 ± 10.3 withrecent AF (not older than 48 hour), and heart rate > 100 beats/min were enrolledin the study, they were randomly assigned to one of 4 groups: to receive 30 mg/kgof amiodarone (n=40), or flecainide 3 mg/kg (n=40), or propafenone 8.5 mg/kg ofbody weight (n=40) or placebo (n=40). The initial clinical and echocardiographycharacteristics were similar. Conversion to SR was verified by 24-hour monitoringin CCU. Longer duration of AF and therapy with Pl were associated with lowerconversion rate in stepwise logistic regression analysis.The results of therapy were assessed at 3, 6, 12 and 24 hours from the startingtime.
Fln=40 A(n=40) Pfn=45 PlN=40
CR at 3h 18 ** (45%) 0 23** (51.1%) 4 (10%)CR at 6h 11 (27.5%) 5 (12.5%) 6(13.3%) 3(7.5%)CR at 12h 5 (12.5%) 18 (45%) 3(6.6%) 0CR at 24h 1 (2.5%) 11 (27.5%) 2(4.5%) 0unconverted 5 (12.5%) 6(15%) 6(15%) 33(82.5%)
CR conversion rate (%): *p<0.05 in comparison to the other drugs.
Conclusion It was found that there is a statistically significant difference aboutconversion time between flecainide and amiodarone (p=0.001) and betweenpropafenone and amiodarone (p=0.001) (within 3 hours from initiation of treat-ment), whereas it was not found statistically significant difference between fle-cainide and propafenone (p=0.92).It was observed that it exists a positive linearrelationship, statistically significant between the time of presentation and conver-sion, what means that the faster the patients present to the hospital, the earlier isthe time of conversion.
P5166 Efficacy and safety of nibentan for cardioversion inpatients with persistent atrial fibrillation with andwithout amiodarone therapy
A. Berkowitsch1, A. Rivin2, M. Medvedev2 , S. Zaltsberg1, I. Shubik2.1Kerckhoff-Klinik, Cardiology, Bad Nauheim, Germany; 2North-West
Center for Diagnostic and Treatmen, St. Petersburg, Russian Federation
Potassium channel blocker nibentan was shown to be highly effective for phar-macological cardioversion of persistent AF but not for long term maintenanceof sinus rhythm (SR). The aim of this prospective study was to investigate ef-ficacy of cardioversion with nibentan in patients receiving amiodarone therapyand those without amiodarone. Fifty nine patients with persistent AF (42 male,age: 55; IQR:51-61 yrs, 11 lone AF, 5- Hypertension, 43 structural heart disease)were enrolled into the study. The median duration of AF was 12 (IQR: 4-75) days.The median left atrial size (LAS) was 4.55 (IQR: 4.20-5.00) cm. Twenty eightpatients were on amiodarone (200-400 mg daily) prior to cardioversion. Nibentanwas infused intravenously. Median dose of nibentan was 0.119 (IQR: 0.113-0.143)
mg/kg. The primary effect was achieved in 52 patients (median time to restore SRwas 12 (IQR:5-18) min). The failed cardioversion was significantly associated withenlarged left atrium (5.10 (IQR: 4.40-5.30) vs. 4.40 (IQR: 4.20-4.90) cm; p<.05).Seven patients, in whom cardioversion failed were excluded from further analysis.After the successful cardioversion patients without amiodarone were in median 3(IQR: 2-7) days on SR whereas those being on amiodarone had in median 30(IQR: 4-364) days stable SR (p<.01). The multivariate analysis revealed absenceof amiodarone and increased LAS to be independent predictors for new onset ofAF after adjustment for clinical variable. After restoring of SR the median QTs was475 (IQR: 450-500) ms. There was no difference in QTs between patients withand without amiodarone. Proarrhythmic effects (non sustained VT and substan-tial suppression of sinus rhythm automatism) were registered in 4 and 15 patients,respectively. However, no association between proarrhythmic effects and use ofamiodarone was found in our patients. Proarrhythmic effects were significantlyassociated with enlarged LA (4.25 (IQR: 4.13-4.82) vs. 4.70 (IQR: 4.40-5.56) cm,female gender (10 (71.3%) women vs. 9 (24.3%) men) and long duration of AF(9(IQR: 3-28) vs. 67(IQR: 6.25-160) days; p<.01 for all. The multivariate anal-ysis revealed enlarged LA and female gender to be independent predictors forproarrhythmic effects of nibentan. (p<.01 for both parameters). Administration ofamiodarone prior to and after the pharmacological cardioversion with nibentan iseffective for long term maintenance of sinus rhythm in patients with persistent AF.However, patients with enlarged left atrium and women are on increased risk toexperience proarrhythmic effects of nibentan.
P5167 Relationship between C-reactive protein andrecurrence of atrial fibrillation after successfulcardioversion: a meta-analysis
T. Liu1, G.P. Li1, L.J. Li2. 1Second Hospital Of Tianjin MedicalUniversity, Department of Cardiology, Tianjin, China, People’s
Republic of; 2Tianjin Medical University, Department of Epidemiology Research,Tianjin, China, People’s Republic of
Background: Recently, the role of inflammation on genesis and perpetuation ofatrial fibrillation(AF) has been evaluated, and inflammatory biomarker C-reactionprotein(CRP) was elevated in patients with AF. The objective of this systematic re-view is to evaluate the relationship between CRP concentration before cardiover-sion and recurrence of AF after successful cardioversion.Methods: We searched MEDLINE (January 1966 to October 2005), theCochrane controlled Trials Register (Cochrane Library Issue 4, 2005), EMBASE(January 1980 to October 2005). Using the keywords "C-reaction protein", "in-flammation" and "atrial fibrillation" to identify relevant studies which evaluated thepotential relationship between CRP and recurrence of AF after successful car-dioversion. Additionally, a manual search was conducted using all review articleson this topic, bibliographies of original papers, and abstracts from conference pro-ceedings. Two reviewers evaluated trial quality and extracted data independently,and discrepancies were resolved by consensus of a third reviewer.Results: Five studies with 317 patients were identified (181 with and 136 withoutrecurrence of AF). Overall, CRP concentration was higher in patients with recur-rence of AF, the standardised mean difference in the CRP levels between thepatients with and without AF was 0.32mg/dL (95%CI: 0.08 to 0.56)(Fig 1). Het-erogeneity test showed there were no significant differences between individualstudies(P=0.52); the Z score for overall effect was 2.58(P=0.010).
Fig. 1
Conclusions: Our meta-analysis suggests increased CRP concentration is as-sociated with higher risk of recurrence of AF after successful cardioversion.
P5168 High plasma B-type natriuretic peptide levels predictatrial fibrillation after cardiac surgery
S. Sarzi Braga, R. Vaninetti, D. Aieta, F. Santoro, R.F.E. Pedretti.IRCCS Fondazione Salvatore Maugeri, Cardiology, Tradate, Italy
Background: Atrial fibrillation (AF) is a frequent event after cardiacsurgery. Risk factors for arrhythmia development include older age, low ejectionfraction and electrolyte imbalance. Few information are available on the relation-ship between elevated B-type natriuretic peptide (BNP) plasma levels and AFafter cardiac surgery.Aim: Evaluation of potential association between plasma BNP levels and AF aftercardiac surgery.Methods: We enrolled 153 pts undergoing rehabilitation after cardiac surgery:coronary artery by pass 97 (63%); valve replacement 43 (28%); coronary arteryby pass & valve replacement 13 (8%). At admission all pts had sinus rhythm
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
Atrial fibrillation – optimizing the cardioversion outcome 889
and the following characteristics: mean age 66±10 yrs, male 76%, left ventricularejection fraction 56±9%. Plasma BNP levels were determined 10±5 days aftersurgery using the Biosite Diagnostic Assay.Results: At admission BNP levels were 431±453 pg/ml (normal value < 100pg/ml). In the early post-operative period at least one AF episode was observedin 55 (36%) pts. During the rehabilitation period a total of 27 (18%) pts expe-rienced AF. Of these arrhythmias, 18 (66%) represented recurrences, versus 9(33%) occurring in pts with no prior episodes (p=0.001). Pts with AF episodes(either early and late after cardiac surgery; n=64) had significantly higher plasmaBNP levels when compared with event-free pts (573±633 vs 329±207, p=0.001).Female gender (p=0.03), older age (p=0.002), lower kaliemia values (p=0.004),left atrial size (p=0.02) and valvular surgery (p=0.03) were significantly associatedwith post-surgical AF at univariate analysis. At multivariate analysis only BNP lev-els (p=0.02) and kaliemia (p=0.03) showed an independent association with AF.Conclusions: AF recurrence during rehabilitation is a frequent event. Elevatedplasma BNP levels are still present at the beginning of the rehabilitation programafter cardiac surgery, and are independently related with the occurrence of post-operative AF. These results suggest a more aggressive therapeutical approachduring the rehabilitation phase in patients with lower kaliemia, history of AF soonafter surgery and elevated plasma BNP levels.
P5169 Predictive value of NT-proBNP for recurrence of atrialfibrillation after successful electrical cardioversion
H. Moellmann, H. Nef, M. Weber, M. Stanisch, C. Hamm,A. Elsaesser. Kerckhoff Heart Centre, Dept Of Cardiology, BadNauheim, Germany
Purpose: Atrial fibrillation causes an increase in NT-proBNP. The purpose of ourstudy was to determine the predictive value of BNP-levels after elective electricalcardioversion concerning the rhythm stability. Furthermore, the predictability ofBNP levels regarding the short-term success of cardioversion was investigated.Methods: 51 Patients with atrial fibrillation (duration 178±14 d, age 65.2±8.1 a)were provided with an event-recorder for a follow-up period of three weeks afterelective cardioversion. NT-proBNP serum levels were measured before and threeweeks after cardioversion using an electrochemiluminescence immunoassay. Pa-tients with reduced left ventricular function (EFII°), and increased retention val-ues were excluded. Values for NT-proBNP are given as median and interquartilerange.Results: All patients with atrial fibrillation presented with increased NT-proBNPserum levels (median 836 pg/ml, IQR 613-102). 29 patients were in stable si-nus rhythm during the follow-up. These patients showed a significant decreaseof the NT-proBNP (from 792 pg/ml, 549-912 to 283 pg/ml, 88-345, p<0.001) andreached normal values after three weeks or showed a decrease of NT-proBNP>60%. In 19 patients a relapse of atrial fibrillation after primarily successful car-dioversion during follow-up was documented. NT-proBNP was significantly higherprior to cardioversion in comparision to patients without relapse and remainedunchanged during follow-up (1033 pg/ml, 778-1317 vs. 1061 pg/ml, 811-1426,p=n.s.). In 3 patients short periods of asymptomatic atrial fibrillation were doc-umented in the event-recorder. The duration of these periods was consistentlyunder 48 h. These patients showed a less pronounced decrease in NT-proBNPthan the collective with stable sinus rhythm upon cardioversion (816 pg/ml, 661-907 vs. 513 pg/ml 407-599).Conclusions: NT-proBNP values are higher in patients with atrial fibrillation anddecrease after cardioversion if a stable sinus rhythm can be achieved. The prob-ability of a successful cardioversion correlates inversely with the NT-proBNP val-ues. Additionally, the short term success of a cardioversion might be predicted bydetermination of the NT-proBNP level prior to cardioversion.
P5170 Ablate and pace therapy in patients withdrug-refractory atrial fibrillation. Is the treatedpopulation changed in the last fifteen years?
D. Pavoni1, A. Proclemer1, D. Facchin1 , C. Bonanno2 , R. Ometto2,R. Mantovan3, M. Crosato1, V. Calzolari1. 1Cardiology, Udine, Italy;
2Cardiology, Vicenza, Italy; 3Cardiology, Treviso, Italy
Radiofrequency ablation of the atrioventricular junction followed by pacemakerimplantation, defined as "Ablate and Pace" (AP), is a well accepted therapy inpatients with disabling and medically refractory atrial fibrillation (AF). In the lastyears new AF ablation strategy, such as pulmonary vein isolation (PVI), seemedmodify the indications to AP.Aim: To compare the clinical characteristics and the main outcome in patientstreated by AP in the era before and after wide application in the clinical practiceof PVI.Methods: We analysed two patient’s groups with medically refractory AF treatedwith AP in two different periods: the first group underwent AP between 1992 to2001 (n=212), the second group between 2002 to 2005 (n=100).Results: The first group was characterized by younger patients treated for nonsignificative less prevalence of permanent AF. The second group was more oftenin NYHA class III-IV. No significative differences were evident between the twogroups if we considered gender, heart disease, ejection fraction, previous ineffec-tive drugs and use of dual chamber pacemaker (PM). Total mortality after 1 yearand 3 years appeared similar in the two groups (Table 1).
Table 1
1992-2001 2002-2005 P
Mean age (years) 69 ± 9 74 ± 8 <0.01Male 90 (42%) 42 (42%) nsHeart disease 140 (66%) 73 (73%) nsEjection fraction 52 ± 13 50 ± 13 nsParoxysmal AF 121 (58%) 47 (47%) nsPrevious ineffective drugs 2,5 ± 1,7 2,3 ± 0,7 nsNYHA class III-IV 43 (28%) 56 (56%) <0.01Dual chamber PM 106 (50%) 48 (48%) ns1 year total mortality 12 (6%) 7 (7%) ns3 year total mortality 24 (15%) 17 (17%) ns
Conclusions: In the era of PVI therapy for drug refractory AF the populationtreated with AP was changed, particularly by older age and higher prevalenceof advanced functional class. Despite these different clinical characteristics, totalmortality appears similar in the two groups of patients treated with AP in the twoperiods considered (before and after PVI).
P5171 Complications of electrical cardioversion forpersisting atrial fibrillation in a UK district generalhospital
A. Mirchandani, C. Gibson, S. Hood, P. Macintrye, I. Findlay. RoyalAlexandra Hospital, Cardiology, Paisley, United Kingdom
We audited 689 consecutive patients undergoing elective cardioversion for AF Weassessed cancellation and success rates, immediate complications, in-hospitalmortality, post-procedure complications and re-admission rates 6 weeks post pro-cedure. 689 cardioversions were planned over 87 months in 378 patients (age64.9 years) (233 males, 61.6%). 189 (27.1%) procedures were cancelled: 83(43.9%) due to reversal to SR, 68 (36.0%) due to INR <2. 500 procedures wereperformed in 380 patients. 407 (81.4%) were successful. There were no deathsand complication rate was 2.6% (13 cases). 11 had bradyarrhythmias, 4 had res-piratory complications. 9 (1.8%) required immediate admission, 14 (3.68%) within6 weeks of procedure (table). 54 patients (14.2%) who received electrical car-dioversion were re-admitted > 6 weeks during the study period (table).
Outcome following DC Cardioversion
Reason for Admission < 6weeks Total No. Prior Successful Cardioversion
AF and Dyspnoea 8 6Chest Pain (troponin -ve) 3 3Heart Failure 2 2Multi-organ Failure 1 1Reason for Admission > 6 weeks
AF/Palpitations 17 14Heart Failure 13 12Acute Coronary Syndrome 6 5Pacemaker insertion 5 4VT/VF 5 3Syncope/Collapse 3 3Transient ischaemic attack 1 1Pericarditis 1 0Other 3 2
Conclusions: Cardioversion is a relatively safe with only 1.8% requiring overnightobservation. The main reason for readmission was AF in both the early and lateperiods. Thrombo-embolic events were extremely low. The significant cancella-tion rate (27.1%) is largely unavoidable due to spontaneous reversal to sinusrhythm but a significant proportion could be prevented with improved anticoagu-lation monitoring.
P5172 Simple 24 hour holter data identify patients prone toatrial fibrillation recurrence within month afterelectrical cardioversion
C. Varounis, T. Maounis, N. Dagres, D. Panagiotakos,G. Athanassopoulos, G. Karatasakis, D.V. Cokkinos. Onassis
Cardiac Surgery Center, 1st Cardiology, Athens, Greece
Background: The recurrence of atrial fibrillation (AF)after electrical cardiover-sion(CV) remains high. We investigated the significance of heart rate(HR) andatrial arrhytmias measured during Holter recording for 24 hours(24H)after car-dioversion.Methods: We prospectively studied 46 consecutive patients (mean age±SD:65±10 and 47% men) subjected to CV. All underwent echocardiography(ECHO)and 24H after CV. At one month the recurrence of AF was studied by standardelectrocardiography or by interim report of AF.Results: Twenty-four pts remained in sinus rhythm (SR) (group I). The rest hadAF recurrence (Group II). Age, gender, underlying disease left atrial size andleft ventricular fractional shortening as well as drug therapy were similar. (AllPs>0.05). Specifically 50% Group I and 45% Group II pts were receiving amio-darone but only 16% and 13.6% sotalol respectively. Group I pts had lower maxi-mal HR compared to group II(82.04±14.3 vs 99.38±19.39 bpm) (P=0.004). Cut-off analysis showed that HR=90.5 bpm discriminate pts between the two groups(sensitivity=69%, specificity=73%). Those with HR >90.5 bpm had 6.6 times
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

890 Atrial fibrillation – optimizing the cardioversion outcome / Atrial fibrillation – miscelaneous
higher risk of AF recurrence (OR=6.68 with 95% C.I= 1.3-34.9) (sensitivity=69%,specificity=75%). Group I also had fewer atrial premature contractions per hour(APCs/h) (P=0.002).Those with >32 APCs/h had 10 times higher risk of AF recur-rence(OR=10.4 with 95% C.I= 2.3-47.4)(sensitivity=75%, specificity=77%). Ptswith combination of HR>90.5 bpm and >32 APCs/h had 25.2 times higher risk ofAF recurrence (OR=25.28 with 95% C.I= 1.8-352.5). The occurrence of supraven-tricular tachycardia of any duration was non-predictive.Conclusion: Two simple 24 H indices may help identify pts at higher risk of AFrecurrence after CV. These findings may prompt drug therapy changes to preventthis occurrence.
P5173 Outcome of pharmacological rhythm control fornew-onset persistent atrial fibrillation in patients withsystolic heart failure: is it really bad?
M.E.W. Hemels, A.C.P. Wiesfeld, M.P. Van Den Berg, D.J. VanVeldhuisen, I.C. Van Gelder. University Medical Center Groningen,
Thoraxcenter, Department Of Cardiology, Groningen, Netherlands
Background: Rhythm control is preferred in patients with symptomatic persistentatrial fibrillation (AF), also in patients with heart failure.Objective: To investigate outcome of a serial cardioversion strategy in patientswith and without systolic heart failure.Methods: Patients with a first episode of persistent AF and symptomatic systolicheart failure (NYHA class II-III and left ventricular ejection fraction (LVEF) lessthan 0.40) were included and outcome of a serial electrical cardioversion (ECV)strategy, including antiarrhythmic drug use, was compared with a control groupof patients with symptomatic persistent AF without heart failure and a normalsystolic LV function. Follow-up was 18 months in both groups.Results: A total of 64 consecutive patients with heart failure (mean age 64±12years, 72% male, 50% coronary artery disease, LVEF 0.30±0.07) were enrolledand compared with 48 consecutive patients without heart failure (mean age 66±8years, 60% male, all LVEF > 0.50, 40% lone AF). Duration of AF was longer inpatients with heart failure (median of 4 months versus 3 months, respectively,p=0.03). Recurrence pattern after ECV was comparable (Table). At follow-up AFwas accepted in 45% versus 29% of the patients with versus patients withoutheart failure, respectively (p=0.03).
Table 1
Heart Failure No Heart Failure P-value
Shock Failure 9% 6% NSImmediate reinitiation of AF after ECV 5% 6% NSSubacute recurrence of AF (within 30 days) 44% 46% NSLate recurrence of AF (> 30 days after ECV) 28% 21% NSNo AF recurrence 14% 21% NSRate control after first relapse 23% 4% < 0.01Serial re-ECVs, no antiarrhythmic drugs 20% 4% < 0.01Number of re-ECVs - median (range) 0 (0-3) 1 (0-4) < 0.01Sotalol and/or Amiodarone institution 42% 75% < 0.01
Conclusions: Interestingly, the recurrence pattern of AF after ECV is compa-rable between patients with and without systolic heart failure. However, a serialcardioversion and antiarrhythmic drug approach is often not followed in patientswith systolic heart failure. Change of approach of rhythm control may improvesuccessful maintenance of sinus rhythm.
ATRIAL FIBRILLATION – MISCELANEOUS
P5174 Expression of NO-synthases in the left atrial appendixin a sheep model of permanent atrial fibrillation
I. Lenaerts, R. Willems, W. Anne, S. Janssens, H. Heidbuchel.Cardiology, University of Leuven, Leuven, Belgium
Background: Endocardial NO-synthase is downregulated in pigs af-ter 1 week of rapid atrial pacing (Cai et al. Circulation 2002). We wanted to evalu-ate the expression of different NO-synthases in the left atrial appendix in a sheepmodel of permanent atrial fibrillation (AF).Method and results: Fourteen ewes (55.8 ± 14.9 kg; 27.7 ± 13.7 months old)were rapidly atrially paced at 600 bpm for a median of 57 weeks (range 12 - 166weeks). At the time of sacrifice all animals were in permanent AF for 24 weeks(median, 1 -144 weeks). Left atrial tissue was collected and snap frozen at -80°C.Ten non-stimulated sheep (55.5 ± 11.2 kg; 28.2 ± 11.7 months, p = ns) servedas controls. Total RNA was isolated and cDNA was constructed. eNOS, nNOSand iNOS expression was measured by quantitative PCR (Taqman). The resultswere normalized for expression levels of GAPDH. Fold differences between thetwo groups were calculated based on the cycle threshold values. All 3 isoforms ofNOS were expressed in the atrium. Expression of atrial eNOS mRNA was 26.3%lower in AF group vs control (p<0.05). No significant differences were seen innNOS and iNOS mRNA expression between both groups.Conclusion: In our sheep model the development of AF is associated with adecreased expression of endothelial NO-synthase, suggesting a possible role fornitric oxide synthase in the remodeling processes occurring during permanent AF.
P5175 Cytotoxin-associated gene-A bearing strains ofHelicobacter pylori and atrial fibrillation due toischemic origin. Is there a link?
H. Badran1, M. Mahfouz2. 1Tanta, Egypt; 2Tanta University,Biological science, Tanta, Egypt
Objectives: Previous studies suggested an association between infection by cy-totoxic CagA bearing Helicobacter pylori (Hp) strains and atherosclerosis. Wehypothesized that CagA strains could increase the risk for atrial fibrillation(AF)in patients with chronic coronary heart disease (CHD) by induction of systemicinflammatory reactions. Our aims were: (1) to confirm the association betweenCagA strains and CHD. (2) to evaluate the presence of Cag A strains in AF dueto ischemic etiology.Methods and subjects: Serological status for Hp cagA by a semiquantitativecommercial (ELISA) kit against the p120 antigen of CagA, C-reactive protein,total leucocytic count and atrial size using echocardiography were determined in185 patients with proved CHD. Patients were assigned to (Group A, n= 82) CHDand AF & (Group B, n= 103) CHD with sinus rhythm. 80 subjects from the samegeographical area free of clinical cardiovascular disease matched for age and sexassigned to control group.Results: 52 (63%) patients were seropositive for Hp Cag A in Group A versus40(39%) in Group B (odds ratio 3.95 with 95% confidence interval 1.94-6.0).Only 25(31%) of the control were seropositive. There was a significant associ-ation between seropositivity for (Hp Cag A) and having previous myocardial in-farction (68 versus 53%, odds ratio 2.04 with 95% CI:1.02-2.82, P=0.034). Thesefindings remained valid in a multivariate analysis including possible confoundingfactors (age, sex, smoking and hypertension; odds ratio 2.35 with 95% CI 2.01-4.83). Left atrial dimension & CRP were significantly increased in seropositivesubgroups (4.31±0.66 vs 3.1±0.58 cm & 3.32±0.86 vs 1.79±0.72 mg/l in groupA and 3.7±0.62 vs 2.85±0.66cm & 2.5±0.54 vs 1.62±0.5 mg/l in group B re-spectively (P<0.01)Conclusions: The positive association between Hp(Cag A) with elevated CRPand increased atrial size and having AF in CHD may reflect the inflammatorychanges in the atrial structure that promotes the development or persistence ofAF. This study provides further support for the hypothesis that there is a causalrelationship between chronic infection with Hp and CHD especially if AF super-vene.
P5176 Combined effects of upstream and downstreamtherapies for the prevention of atrial electricalremodeling. Studies in the canine rapid atrialstimulation model
H. Fukaya, S. Niwano, D. Satoh, H. Niwano, Y. Masaki, T. Izumi.Kitasato University School of Medicine, Cardiology, Sagamihara,
Japan
Background: We previously reported the effects of bepridil (Bep), a multi-channelblocker including that of IKs currents, on atrial electrical remodeling (ER), i.e.,promotion of reverse ER even with a downstream therapy. In the present study,the effects of Bep and olmesartan (Olm), a angiotensin II receptor blocker, on ERwere evaluated in a canine rapid atrial stimulation model.Methods and Results: In 15 beagle dogs, the right atrial appendage was pacedat 400 bpm for 6 weeks. The atrial effective refractory period (AERP) and conduc-tion velocity (CV) were evaluated along the time course of the rapid pacing. For10 dogs, Bep (10 mg/kg/day) was orally administered as a downstream therapystarting at 2 weeks after the rapid pacing. In 5 of those 10 dogs, Olm (2mg/kg/day)was orally administered as an upstream therapy starting 2 weeks before the rapidpacing. In the control group (n=5), the AERP exhibited a gradual and continuousshortening. In the Bep group, the AERP exhibited a relatively quick prolongationafter the Bep administration in the first week then the AERP kept gradually recov-ering to the day 0 level which was understood to be a reverse ER effect. However,the change in the CV and atrial fibrosis was not affected by Bep. In contrast in theBep+Olm group, in addition to the recovery of the AERP, the decrease in the CVand atrial fibrosis was suppressed in comparison to the control.
Changes in AERP
Conclusions: In a canine rapid atrial stimulation model, Bep caused a recov-ery of the AERP, i.e., reverse ER effect, as a downstream therapy, but could notsuppress the change in the CV and fibrosis. The combination of Bep and Olmshowed an ideal suppression of the ER which can be considered a benefit of thecombination of the downstream and upstream therapies for ER in atrial fibrilla-tion.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – miscelaneous 891
P5177 QT/RR relation and its day-to-night differences inpatients with paroxysmal idiopathic atrial fibrillationtreated with circumferential pulmonary veins catheterablation: prospective follow-up
K. Szydlo, A.M. Wnuk-Wojnar, M. Trusz-Gluza, C. Czerwinski,I. Wozniak-Skowerska, S. Nowak, A. Hoffmann, K. Wita. Silesian MedicalUniversity, I Dept. Of Cardiology, Katowice, Poland
QT/RR relation representing the heart rate dependency of the QT interval is underintensive investigation. Autonomic imbalance with adrenergic predominance, aswell vagal withdrawal, may enhance the QT/RR relation.The purpose of the study was to analyze the QT/RR relation obtained in patientswith paroxysmal idiopathic atrial fibrillation (PAF) treated with circumferential pul-monary veins (PVs) catheter ablation (RFCA) in regard to the recurrences of ar-rhythmia.Methods: Twenty five highly symptomatic pts with drug refractory PAF who un-derwent RFCA of PVs, according to Pappone technique (17 males, age: 51±9years; with left ventricular EF >50%) were examined. 24-hour Holter recordings(Reynolds) were performed before (H0) and 6-12 months (median 9 months, H1)after the procedure. The QT/RR linear regression slope was calculated from thewhole recording (whole) and from daytime (D) (6 a.m.- 9 a.m and 2 p.m.- 10 p.m.)and nighttime (N) (10 p.m.- 6 a.m.) periods.Results: 6-12 months after RFCA 10 pts had relapses of PAF (AF+) and 15 ptswere free of PAF (AF-). They did not differ in age, gender and medical treatment.There were no significant differences in QT/RR between AF- and AF+ pts- inH0. QT/RR slope was steeper in H1 than in H0. The comparison of parametersobtained in H1 revealed remarkable differences between both groups (table). In-terestingly, after RFCA, there were no differences between daytime and nighttimeperiods.
QT/RR slope in study population
H0 (AF-) H0 (AF+) H1 (AF-) H1 (AF+) AF- vs AF+ (H1)
Whole 0.164±0.011 0.145±0.03 0.154±0.01 0.178±0.016 <0.01D 0.144±0.02 0.14±0.035 0.151±0.01 0.174±0.022 <0.001N 0.12±0.02 0.115±0.02 0.148±0.01 0.174±0.016 <0.001D vs N ns <0.05 ns ns
Conclusion: Despite on the period of analysis QT/RR slope was significantlysteeper after the RFCA, the most significantly in patients with recurrences of atrialfibrillation. This fact and the lack of daytime and nighttime differences in QT/RRslopes, may suggest the presence of sympatho-vagal imbalance with vagal with-drawal in all patients who underwent RFCA. The usefulness of QT/RR slope as astratifier of AF recurrences should be further investigated.
P5178 Dominant frequency gradient between right atrial andcoronary sinus electrograms to identify potentialdrivers of atrial fibrillation outside left atrium
H. Miyazaki1, W.G. Stevenson1, T. Hruczkowski1, M.E. Field1,K. Stephenson1, K. Inada2, T. Yamane2, K. Sugimoto2. 1Brigham
and Women’s Hospital, Cardiology, Div of Clinical Electrophysiology, Boston,United States of America; 2Jikei University School of Midicine, Div of Cardiology,Dept of Medicine, Tokyo, Japan
Purpose: To determine whether a gradient of dominant frequency (DF) be-tween the right atrium (RA) and coronary sinus (CS) during atrial fibrillation (AF)suggests the location of potential driving sites where ablation terminates AF.BACKGROUND: Ablation at some sites with complex fractionated electrograms(CFEGM) that can be in either the left atrium (LA), RA or CS terminates AF, sug-gesting that they are drivers helping to maintain AF.Methods: In 66 patients with sustained AF either present or induced, continu-ous RA and CS electrograms were recorded from a 20-pole catheter positionedalong the tricuspid annulus with its tip advanced into the CS. Ablation targetedareas of CFEGM in the LA followed by RA and/or CS until AF terminated or allidentified CFEGM sites had been ablated. DFs in the RA and CS were calculatedfrom a spectral analysis using fast Fourier transform of simultaneous 15-secondrecordings.Results: During AF, the gradient of DFs between CS and RA was > 0.15 Hz (CSfaster than RA) in 32 patients (Group I), -0.15 to 0.15 Hz in 10 patients (Group II),< -0.15 Hz (CS slower than RA) in 24 patients (Group III). AF terminated duringablation in 56 of 66 patients (table). In group I, LA ablation terminated AF in 20patients and LA+RA+CS ablation terminated AF in 10 patients. Termination of AFduring RA ablation was observed only in patients in group III.
Calculated gradient of dominant frequency between coronary sinus (CS) and right atrium (RA)
Group I (CS > RA) Group II (CS = RA) Group III (CS < RA) Total
Terminated in LA 20 9 8 37Terminated in RA 0 0 9 9Terminated in CS 10 0 0 10No termination 2 1 7 10Total 32 10 24 66
CS > RA, CS = RA and CS < RA means CS faster than, equal to and slower than RA, respec-tively.
Conclusion: Simultaneous recordings show a DF gradient between CS electro-
grams, which reflect both LA and CS activation, and the RA in the majority ofAF patients undergoing ablation. RA drivers can be suspected from analysis ofDF gradient between CS and RA. However, even when the gradient favors RAdrivers, LA ablation may terminate AF.
P5179 Combination of ablation and pacing therapies to treatatrial fibrillation: study in a biophysical model
N. Virag1, L. Dang2, L. Kappenberger3 . 1Medtronic Europe, R.& D. Dept., Tolochenaz, Switzerland; 2Swiss Federal Institute ofTechnology, Lausanne, Switzerland; 3Service of Cardiology, CHUV,
Lausanne, Switzerland
Introduction: Complex ablation procedures have proven to be effective in treat-ing chronic atrial fibrillation (AF), but they may have undesirable side effects. Atrialpacing so far has not shown to be effective. We studied here if ablation lines se-lected from the commonly used patterns could improve the success of therapeu-tical pacing.Methods: A biophysical model of AF using an anatomical geometry of the atriabased on human MR images and a membrane kinetics model were used. Dur-ing sustained chronic AF several combinations of ablation and pacing therapieswere tested. The following ablation patterns were applied: P1=isthmus line be-tween inferior vena cava and mitral valve, P2=line between superior and inferiorvena cava, P3=isolation of pulmonary veins, P4=P1+P3, P5=P2+P3, P6=P1+P2,P7=P1+P2+P3. Rapid pacing was applied from different sites in the left and rightatrium: LAA (left atrial appendage), LAFW (left atrial free wall), BB (Bachmann’sbundle), RAA (righ atrial appendage), RAFW (right atrial free wall), and RAI (rightatrial isthmus). For each combination ablation/pacing, 11 simulations were per-formed and the percentage of return to sinus rhythm was documented.Results: Results are summarized in Table 1. The most successful ablation pat-terns are P5 and P7, involving both an isolation of pulmonary veins and a linebetween superior and inferior vena cava. The best areas for pacing were the rightatria free wall and the Bachmann’s bundle.
Table 1
LAA LAFW BB RAA RAFW RAI Average
P1 9.1% 0.0% 0.0% 0.0% 9.1% 0.0% 3.0%P2 0.0% 0.0% 0.0% 9.1% 0.0% 0.0% 1.5%P3 9.1% 0.0% 18.2% 0.0% 9.1% 9.1% 7.6%P4 0.0% 9.1% 18.2% 27.3 % 18.2% 9.1% 13.7%P5 18.2% 18.2% 27.3% 9.1% 36.4% 36.4% 24.3%P6 0.0% 0.0% 9.1% 0.0% 18.2% 0.0% 4.6%P7 27.3% 0.0% 45.5% 36.4% 54.5% 9.1% 27.1%Average 9.0% 3.9% 16.9% 11.7% 20.8% 9.1%
% AF termination (horizontal: pacing sites, vertical: ablation patterns)
Conclusion: Our biophysical computer model of human atria suggests that thesuccess of pacing of AF can be increased by introducing minimal ablation pat-terns, but cannot lead to termination in all cases. The model is currently used forsearching the optimal combination of therapies.
P5180 High C-reactive protein (CRP) serum levels are notassociated with CRP 1059 G/C and interleukin-6 (IL-6)-174 G/C polymorphisms in atrial fibrillation patients
A.M. Gori, B. Giusti, R. Marcucci, E. Romano, I. Lapini, A. Michelucci,R. Abbate, G.F. Gensini. University of Florence, Medical and
Surgical Critical Care, Florence, Italy, Italy
Purpose: Nonvalvular atrial fibrillation (NVAF) is the most common arrhythmiain clinical practice and is a potential cause of thromboembolic events. Recently,the involvement of inflammatory processes in NVAF has been demonstrated. Weinvestigated the prevalence of C-Reactive Protein (CRP) 1059G/C and Interleukin6 (IL-6) -174G/C polymorphisms, and the influence of these polymorphisms onCRP circulating levels in 456 patients with NVAF and in 912 apparently healthysubjects.Methods: CRP 1059G/C and IL-6 -174G/C polymorphisms were analyzed byusing microarray technology; hsCRP circulating levels were assessed with a high-sensitivity nephelometric assay.Results: CRP GG or GC as well as IL-6 GG or GC genotypes did not conferreda significant protection against NVAF in a multivariate analysis adjusted for age,sex, traditional cardiovascular risk factors and hsCRP levels.After adjustment for age, sex, smoking habit and BMI, hsCRP levels were sig-nificantly higher in NVAF patients [3.42 (2.84-4.11) mg/L] than in controls [2.44(2.26-2.62) mg/L; p<0.01]. hsCRP levels were lower in controls carrying CRP1059 GC and 1059 CC genotypes [2.04 (1.67-2.48) mg/L] than in controls with1059 GG genotype [2.51 (2.32-2.72) mg/L; p=0.056]. This genotype-phenotypeassociation was not found in NVAF patients.This genotype-phenotype associationwas not found in NVAF patients.No significant genotype-phenotype association between IL-6 -174 G/C polymor-phism and hsCRP levels was observed in both NVAF patients and controls.Raised hsCRP levels were significantly associated with NVAF at both the univari-ate (OR=1.84 95% CI, 1.12-2.39, p=0.001) and multivariate analysis after adjust-ment for potential confounding variables and inflammatory gene polymorphisms(OR=2.5 95%CI 1.1-5.9, p=0.033).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

892 Atrial fibrillation – miscelaneous
Conclusions: our results demonstrate, in NVAF patients, the lack of associationbetween the CRP 1059 G/C, IL-6 -174 G/C polymorphisms and AF, confirm therole of elevated hsCRP levels in NVAF and extend the relationship between 1059CC CRP genotype and hsCRP levels in elderly controls.
P5181 N-3 polyunsaturated fatty acids treatment reducevulnerability to inducible atrial fibrillation and lowerexpression levels of connexins in dogs
F. Molin, J.F. Sarrazin, G. Comeau, P. Daleau, J. Kingma, I. Plante.Heart Institute, Hopital Laval, Electrophysiology Department,
Quebec, Canada
Objectives: The aims of this open-label, uncontrolled study were to assesswhether omega-3 or n-3 polyunsaturated fatty acids (n-3 PUFAs) prevent atrialfibrillation (AF) induced by vagal stimulation in a canine model and to evaluatetheir impact on atrial tissue expression levels of connexins (Cx) 40 and Cx43.Background: AF is a common arrhythmia with limited successful treatment. N-3PUFAs have demonstrated cardio-protective properties by protecting against ven-tricular arrhythmias and reducing postoperative AF, but their exact mechanismsof action remain unclear.Methods: A total of twenty-five dogs were studied using the vagally-induced AFmodel. Eight dogs were studied after treatment with 1.2 g PO of n-3 PUFAs dailyfor 14 days. Seventeen additional control dogs were studied to find 8 dogs witheasily inducible AF which were immediately restudied after intravenous treatmentwith n-3 PUFAs. Episodes of AF induced by extra stimuli or burst induction werecompared. Atrial tissue biopsies were obtained for western blot analysis of Cx40and Cx43 protein levels.Results: No changes were observed for hemodynamic or electrocardiographicparameters. Atrial refractory periods were not affected by oral treatment. Thenumber of episodes of sustained AF in the orally treated group was reduced by79% with the extra stimulus technique (10.5 vs. 48.9%, p = 0.001) and by 42%with burst induction (22.5 vs. 38.8%, p = 0.034). Cx40 and Cx43 protein levelswere lower in orally treated dogs (average decrease of 60% (p = 0.019) and 42%(p = 0.038), respectively). In the IV acutely treated group, n-3 PUFAs did not showeffect.Conclusions: Induction of AF was significantly diminished with n-3 PUFA oraltreatment in this canine model. Protection against AF by n-3 PUFAs could berelated to modulation of expression levels of Cx.
P5182 Impact of decreased capillary density in atrialmyocardium on result of electrical cardioversion inpatients after mitral surgery
T. Mularek-Kubzdela, W. Seniuk, S. Grajek, A. Marszalek,M. Jemielity, M. Lesiak, M. Prech, A. Cieslinski. University School of
Medical Sciences, 1-st Cardiology Department, Poznan, Poland
The purpose of this study was to investigate which histopathologic abnormalitiesof left atrium are predictive for unsuccessful electrical cardioversion in patientswith mitral valvular disease after mitral surgery. 101 consecutive patients (male25, female 76) aged 23 to 71 (mean 52) with mitral valvular disease admittedfor mitral surgery were enrolled in the study.36 patients were in sinus rhythm, 65had chronic atrial fibrillation. Biopsies of the posterior wall of the left atrium wereobtained during open heart surgery. Tissue was analyzed for cell size, percentof fibrosis and capillaries density using Leica Q500MC image analyzer. We alsosemiquantitatively measured the amount of intramyocardial adipose tissue (grade0 to IV), inflammatory infiltrates (grade 0 to IV), area (percentage of myolyticcells) and degree (A,B,C) of myolysis. After operation 45 patients were in sinusrhythm, 55 had atrial fibrillation (one patient died during surgery).Before discharge33 patients (without contraindications, who gave consent) underwent electricalcardioversion. According to the result of cardioversion patients were divided into:success group - N = 21 and failure group - N = 12.Results: Univariate analysis revealed a significant difference between successand failure group in capillary density only (table). We did not find any other signif-icant differences.
Successful cardioversion Unsuccessful cardioversion p valueN=21 N=12
Percent of fibrosis 35,5% ± 12,2% 38,7% ± 8,3% p=0,291Cell size 18,1 μm ± 3,2 μm 15,7 μm ± 2,5 μm p=0,099Capillaries density 1892/mm2 ± 494/mm2 1578/mm2 ± 194/mm2 p=0,007
Conclusion: The decreased capillaries density in left atrial myocardium corre-lates with failure of electrical cardioversion in patients after mitral surgery.
P5183 Mild cognitive impairment (MCI) in patients with AtrialFibrillation
G. Novo1, D. Puccio1, V. Baiamonte2, G. Fazio1, E. Corrado1,A. Nuccio1, I. Muratori1, S. Novo1. 1Cardiology Unit, UniversityHospital, Internal Medicine and Cardiovascular Disease, Palermo,
Italy; 2Neurology Unit, University Hospital, Neuroscience, Palermo, Italy
Purpose: Atrial Fibrillation (AF) is the most common cardiac arrhythmia and itsprevalence increases with age. AF increases the risk of stroke or TIA due tomacroembolism. Moreover it may produce multiple ischemic areas due to mi-croembolic phenomena and so lead to a progressive cognitive impairment andeven to acclaimed vascular dementia after some years.Purpose of our study wasto evaluate the prevalence of a mild cognitive impairment (MCI) in patients withAF.Method: we studied 42 patients with a history of non valvular AF and 40 controlsin sinus rhythm matched for sex and age. All subjects underwent careful anamne-sis, physical examination, biochemistry and instrumental tests (EKG, echocardio-gram and echo-Doppler duplex scanning of the epiaortic trunks). Inclusion criteriawere: age between 60 and 80 years, ejction fraction above 45%, negative his-tory of previous cerebrovascular diseases and the absence of haemodinamicallysignificant carotid plaque. Moreover to investigate cognitive status all subjectsunderwent the following neuropsychological tests: Mini Mental State Examina-tion (MMSE), Clinical Dementia Rating Scale (CDR), Global Deterioration Scale(GDS) and Hachinski Ischemic Score (HIS). Patients with a diagnosis of demen-tia defined by a score < 18 at MMSE, > 1 at CDR and > 2 at GDS were alsoexcluded.Results: patients with AF had a lower score at GDS (4,21 ± 3,65 vs 2,85 ± 3,26;p =0,07), CDR (0,13 ± 0,25 vs 0,05 ± 0,15; p = 0,07), HIS (1,4 ±1,77 vs 0,30 ±1,18, p=0,001) vs controls; no significant differences were found for MMSE evenafter correction for education, (27,13 ± 2,77 vs 27,38 ± 2,63, p > 0.05; 28,48 ±1,88 vs 28,43 ± 1,88, p > 0.05) between case and controls. Among patients withAF those treated with warfarin, compared with aspirin, had a lower rate of MCIat MMSE (28,2 ± 1,7 vs 26,1 ± 3,2, p = 0.07), CRD (0,03 ± 0,1, vs 0,3 ± 0,3,p 0,04) and GDS (2,4 ± 2,6 vs 6 ± 4,3 p=0,03); no difference was found for HIS(0,9 ± 1,4 vs 1,9 ± 2,1, p >0.05).Conclusion: AF may be responsible of a mild cognitive impairment probablydue to microembolism, detectable with the more accurate neuropsycological testssuch as GDS, CDR, HIS. Anticoagulation therapy may play a protective role; how-ever more evidence are needed.
P5184 Interleukin-1 Beta -511 C/T poymorphisms isassociated with atrial fibrillation
A.M. Gori, B. Giusti, R. Marcucci, C. Fatini, E. Sticchi, A. Capalbo,R. Abbate, G.F. Gensini. University of Florence, Medical andSurgical Critical Care, Florence, Italy
Purpose: Nonvalvular atrial fibrillation (NVAF) is the most common arrhythmiaand is associated with a high risk in cardiovascular mortality and morbidity. Thereis a growing body of evidences that inflammation may be involved in the patho-genesis of NVAF. Aim of this study is to evaluate in a case-control study, theassociation between the interleukin-1Beta polymorphism -511C/T (IL-1beta -511C/T) and the presence of atrial fibrillation.Methods: 456 NVAF patients and 912 matched controls were genotyped by anelectronic microchip technology for IL-1beta -511 C/T polymorphism.Results: The genotype distribution of IL-1Beta -511 C/T polymorphism signifi-cantly differed between NVAF patients and controls. The prevalence of CT andTT genotype was significantly lower in NVAF patients (56.1%) than in control sub-jects (64.6%) (p<0.05).In normotensive subjects no significant difference in genotype distributions of in-flammatory gene polymorphisms between patients and controls was observed.In subjects in whom hypertension was documented, a significant difference ingenotype distributions between NVAF patients (n=265) and controls (n=379) wasfound. In a dominant model of inheritance, the presence of IL-1Beta CT or TTgenotypes, conferred a significant protection against NVAF at both univariate (IL-1Beta CT+TT vs CC genotype: OR: 0.70, 95% 0.56-0.88; p<0.01) and multivari-ate (OR: 0.73, 95% CI 0.56-0.94, p=0.016) analyses. In normotensive subjectsthe presence of IL-1Beta CT or TT genotypes was not independently associatedwith NVAF at both univariate (OR=0.89, 95% CI 0.63-1.25, p=0.49) and multivari-ate analysis (IL-1Beta polymorphism: OR=0.95, 95% CI 0.63-1.45, p=0.82).In the subgroup of hypertensive subjects, a significant association betweenIL-1Beta polymorphisms and NVAF was observed at the univariate analysis(OR=0.61, 95% CI 0.44-0.83, p=0.002). In the multivariate analysis adjusted forsex, age, traditional cardiovascular risk factors, IL-1 Beta polymorphism remaineda significant and independent protective factor for NVAF (OR: 0.69, 95% CI 0.48-0.99, p=0.048).Conclusions: Our results, obtained in a large number of NVAF and controls, andafter adjustment for all potential confounders, show that the presence of the IL-1Beta -511 C/T polymorphisms has an independent protective effect on NVAF.Furthermore, this association was found among hypertensive subjects, but not innormotensive subjects, so suggesting that the protective effect of the inflamma-tory alleles may be evident particularly in a condition, in which tissue injury orendothelial impaired function are present.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – miscelaneous 893
P5185 Effects of sympathetic activation on fibrillatoryfrequency recorded at right and left atrial sites
F. Lombardi1, M. Mantica2, C. Tondo2, V. Corino3, L. Lombardi1,L. Mainardi2. 1Cardiologia, Osp. San Paolo, Univ. of Milan, Medicina,Chirurgia, Odont., Univ. Di Milano, Milan, Italy; 2Lab. Elettrofisiologia,
Ist. S. Ambrogio, Milan, Italy; 3Ingegneria Biomedica, Politecnico di Milano,Milan, Italy
Background: Sympathetic activation, by increasing conduction velocity and re-ducing atrial refractory period, may contribute to atrial fibrillation (AF) onset andmaintenance. Aim of the present study was to evaluate the effects of Isoproterenol(I) infusion on dominant frequency (DF) of atrial electrical activity recorded at dif-ferent right and left atrial sites during AF.Methods: We studied 13 patients (58±6 years) with an indication for pulmonaryvein radiofrequency catheter ablation for persistent AF. Adrenergic activation wasinduced by I infusion (0.2 μg/kg/min).Atrial electrograms were at right atrial (RA)site (n= 5), coronary sinus (CS) ostium and left atrium (LA, n=4) through a 20polar catheter inserted into the CS. Recordings from left upper pulmonary vein(n=5) were obtained with a Lasso catheter. All signals were digitized to a 1000 Hzsampling rate. The averaged ventricular interference signal was computed andsubtracted from each atrial signal. The local atrial period series were derived as asequence of temporal distances between two consecutive atrial activations. FFTanalysis over sequential 5 sec periods was used to obtain the power spectrum ofelectrograms. Data are presented as mean±SD; *= p<0.05.
RA 9-10 RA 5-6 RA 1-2 CS 9-10 CS 5-6 CS 1-2 Lasso 3-4 Lasso 9-10
AF (Hz) 5.45 5.04 4.61 4.99 4.82 4.75 5.13 5.40±1.11 ±1.48 ±1.64 ±2.03 ±1.23 ±1.41 ±2.06 ±1.88
AF+I (Hz) 5.58 5.21 5.23 5.35 5.10 5.14 5.98 5.74±1.23 ±1.58* ±1.33* ±1.74* ±1.16* ±1.43* ±1.95* ±2.20
Results and Conclusions: During AF, DF was not homogeneous varying from4.33±1.71 at proximal coronary sinus area to 5.56±1.78 at upper left pulmonaryvein ostium. I infusion was associated with a significant increase in DF with great-est values measured on electrograms recorded with Lasso catheter. These dataindicate that sympathetic activation, by increasing high frequency activity duringAF, may favour arrhythmia maintenance. Identification of sites with greater re-sponse to I infusion could represent a novel approach for identifying the substratemaintaining AF.
P5186 Influence of different atrial lead positions on atrialfibrillation in patients with sick-sinus-syndrome -results of the pastra-trial after 24 months
S.G. Spitzer1, P. Wacker2, K. Malinowski3, S. Gazarek4,V. Schibgilla5 on behalf of PASTA Investigators. 1Praxisklinik Herz
Und Gefaesse, Kardiologie-Angiologie-Radiologie-Nuklearmed., Dresden,Germany; 2Klinikum Barnim GmbH, Eberswalde, Germany; 3Helios Klinikum,Aue, Germany; 4Vitatron GmbH, Koeln, Germany; 5Klinikum Coburg gGmbH,Coburg, Germany
The atrial lead position is suspected to affect the incidence of atrial fibrillation(AF). PASTA (Pacing of the Atria in Sick Sinus Syndrome Trial) is a prospectiveand randomized trial, assessing the effect of different atrial lead positions on theAF incidence in patients with with sick sinus syndrome (SSS). The atrial leadposition is randomized to: a) free right atrial wall, b) right atrial appendage (RAA),c) coronary sinus ostium (CS-Os), or d) dual site right atrial pacing (CS-Os +RAA). Pacemakers (Vitatron Selection 9000 or Prevent AF, Vitatron B.V. Arnhem,The Netherlands) are programmed in DDDR 70 mode. Total follow-up duration is24 months.Method: To describe the atrial rhythm state pacemaker derived data (arrhythmiacounter) were assessed for AF episodes. AF was considered as evident, if AFburden (time in AF related to follow up interval) was >1% (i.e. 15min/d). Followup data after 24 months were evaluated.The analysis evaluates 114 of 138 enrolled patients (76 male, 74,2 yrs. ± 7,8).Also there was no statistic significant difference with respect to the mean AFburden between the 4 groups after 24 months (A: 11%; B:18%, C: 21%, D 19%).The percentage of atrial/ventricular pacing was A: 74/85% B: 77/86% C: 81/66%D: 80/70%. Differences are not significant.Results: Results of analysis:
Total Number of pts. (%) with AF burden > 1% p-valueEnrolled within 24 months (Z test)
A: Free wall 33 11/28 (39%) VS. B: 0,51 n.s.VS. C: 0,57 n.s.VS. D: 0,61 n.s.
B: RAA 36 9/29 (31%) VS. A: 0,51 n.s.VS. C: 0,91 n.s.VS. D: 0,24 n.s.
C: CS-Os 37 10/31 (32%) VS. A: 0,57 n.s.VS. B: 0,24 n.s.VS. D: 0,28 n.s.
D: CS-Os+ RAA 32 12/26 (46%) VS. A: 0,61 n.s.VS. B: 0,24 n.s.VS. C: 0,28 n.s.
Conclusion: The evaluation of AF burden >1% and total AF burden after 24months did not show differences in the incidence of atrial fibrillation in patientswith sick sinus syndrome. The incidence for AF seems not to be affected by dif-ferent atrial lead positions.
P5187 The Extent of myocardial fibrosis determined bydelayed enhancement correlates with plasma BNPconcentration in hypertrophic cardiomyopathy
A. Alsaileek, S. Ommen, U. Valeti, J. Tajik, R. Nishimura, J. Glockner,J. Seward. Mayo Clinic, Cardiovascular, Rochester, United States of
America
Introduction: Plasma level of brain natriuretic peptide (BNP) is related to thepresence and magnitude of heart failure and is reported to be elevated in pa-tients with hypertrophic cardiomyopathy (HCM). Myocardial delayed enhance-ment (MDE), assessed by magnetic resonance (CMR), can quantify myocardialfibrosis. We hypothesize that in HCM patients, the extent of myocardial fibrosis(MDE) is associated with diastolic heart failure and higher BNP.Methods: Cine and gadolinium-enhanced CMR was performed in 63 HCM pa-tients (54.1+15.8 year old and 33 [52.4%] were men). The extent of MDE wasquantified from short-axis delayed contrast-enhanced images. BNP was per-formed within 3 months and the echo within one month of CMR.Results: BNP ranged from 5 to 1540 pg/mL (207.9+258.4 pg/mL). BNP was ele-vated (> the upper limit for age) in 44 (80%) patients. BNP (log BNP) was foundsignificantly associated with increasing MDE (r=0.46, p=<0.0001, LV mass index(r=0.55, p<0.0001), E/e’ ratio (r=0.41, p=0.002), severity of diastolic dysfunctiongrades (p<0.0001), but not LV outflow tract gradient (r=0.19, p=0.1313). On ageand sex-adjusted linear regression analysis, increased BNP was found to be in-dependently associated with extent of MDE (p=0.022) after adjusting for othervariables found significant on univariate analysis (table).
Table 1. Univariate and multivariate linear regression analysis of the plasma BNP (log BNP)
Univariate Analysis Multivariate Analysis
Estimate p value Estimate p value
Age, years 0.007 0.468 -0.005 0.594Male Sex -0.445 0.152 0-.442 0.138MDE, g 0.092 <0.0001 0.062 0.022Paroxysmal AF 1.24 0.007 -0.098 0.846E/e’ ratio 0.063 <0.0001 0.045 0.007LVmass index, g/m2 0.02 <0.0001 0.005 0.389Mitral Regurgitation > mild 0.660 0.044 0.073 0.806LA Volume Index, mL/m2 0.02 <0.0001 0.012 0.165
Conclusion: BNP is elevated in the majority of HCM patients which is stronglyrelated to the extent of myocardial fibrosis and the magnitude of diastolic dysfunc-tion. The findings support the role of myocardial fibrosis in HCM associated heartfailure.
P5188(W) Atrial fibrillatory rate and sinus rhythmmaintenance in patients undergoingcardioversion of persistent atrial fibrillation
F. Holmqvist1, M. Stridh1, J.E.P. Waktare2, L. Sornmo2,S.B. Olsson2, C.J. Meurling2. 1Lund, Sweden; 2The
Cardiothoracic Centre, Liverpool, United Kingdom
Aims: The study set out to explore whether an index of atrial electrical electro-physiology can be used to predict atrial fibrillation (AF) relapse, and if the predic-tive properties differ as a result of arrhythmia duration.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

894 Atrial fibrillation – miscelaneous
Methods and results: The study comprised 175 consecutive patients with per-sistent AF (median duration 94, range 2 to 1044 days) referred for cardioversion.Twenty-nine patients had arrhythmia duration under 30 days (median 5, range 2 to26). Atrial fibrillatory rate (AFR) was estimated using frequency power spectrumanalysis of QRST-cancelled ECG.At one-month follow-up 56% of the patients had relapsed to AF. The pre-cardioversion mean AFR of those was 399±52 fpm compared to 363±63 fpmamong patients maintaining SR (p<0.0001). In patients with short AF duration thedifference was even more pronounced (424±52 fpm vs. 345±65 fpm, p<0.01).In this group a finding of an AFR above the mean value (384 fpm) of the studypopulation predicted AF relapse with high accuracy, illustrated in the Figure.Conclusion: In patients undergoing cardioversion of persistent atrial fibrillation,AF relapse is predicted by a higher AFR. A stronger association is seen i n pa-tients with short arrhythmia duration, reflecting either rapid remodeling or pre-existing changes in those who relapse to AF.In this subset of patients AFR, may well prove to add clinical value.
P5189 Experience with the use of a coronary ballooncatheter for the implant of the left ventricular lead forcardiac resynchronization therapy
E. Arbelo Lainez, A. Garcia Quintana, C. Amador, J. Suarez DeLezo, R. Ramirez, J.R. Ortega, L. Ramirez Burgos, A. Medina.
Hospital de Gran Canaria Dr. Negrin, Cardiology, Las Palmas De Gran Canaria,Spain
Introduction: The implant of an epicardial electrode in a coronary vein can bevery challenging due to various unfavourable anatomical factors. Manoeuvreswith a ballon catheter used in interventional cardiology may facilitate the implantin complex coronary venous anatomies.Objective: We have studied our experience with the use of a balloon during theimplant of the left ventricular electrode for cardiac resynchronization.Materials and Methods: In 16 (11%) out of 143 patients (p) (age 70 ± 7 years,79% males, NYHA class 3 ± 0.4, ejection fraction 27 ± 5, QRS 159 ± 27 ms)an angioplasty balloon-catheter was used during the implantation of a coronaryvenous left ventricular lead.Results: The reasons for using the balloon during the implantation of the LV leadwere: 1) Restrictive and perforated Tebesian valve (2p/1.4%) (figure), 2) Focalstenosis of the target vein (7p/4.9%), 3) Hypoplasia of the target vein (4 p/2.8%)and 4) To possibilitate the advance of the guiding catheter over the shaft of ananchored balloon in the target vein (8p/5.6%) (figure). In 5p, there was more thanone reason for the use of the balloon. The diameter of the balloon was 3.66 ± 0.6mm and the mean inflation pressure was 9.6 ± 3.8 atmospheres. The electrodewas successfully positioned in the target vein in all p. The stimulation thresholdwas 2.2 ± 1.5 V (at 0.5 ms) and the local electrogram amplitude was 13 ± 7.1mV. No complications were observed.
Conclusion: The use of a coronary balloon catheter in the coronary venous sys-tem is safe and it may increase the success rate of the implant of the left ventric-ular lead in patients with complex anatomy.
P5190 NYHA functional class influences the relationship ofdiabetes and cardiac autonomic function
P. Deedwania1 , P.K. Stein2, L. Tereshchenko2 , P.P. Domitrovich2,A. Perez3. 1VACCHCS/UCSF School Of Medicine, CardiologyDepartment, Fresno, United States of America; 2Washington
University School of Medicine, Cardiovascular Division, St. Louis, Mo, UnitedStates of America; 3Takeda Pharmaceuticals of North America, Chicago, Il,United States of America
Purpose: Both diabetes and heart failure are associated with decreased heartrate variability (HRV), reflecting pathological alterations in cardiac autonomicfunction in both conditions. It is unclear whether the cardiac autonomic deficitsof diabetes and heart failure are cumulative.Methods: 24-hr HRV in 79 diabetic vs. 75 non-diabetic heart failure patients wascompared by functional class (NYHA II or III) among patients entered into a heartfailure drug treatment evaluation study. Entry criteria included: stable class II/IIICHF, treated with ACE-I or ARB, LVEF<40% and BNP>200. Traditional and non-linear HRV and heart rate turbulence (HRT) were determined before randomiza-tion.Results: Class II non-diabetic patients were older than each of the other groupsbut no other clinical or demographic differences were seen. As seen in the table,after adjustment for age, time and frequency domain and non-linear HRV were
significantly better in class II non-diabetic patients compared with all other groups.Also, HRV was similar in class II diabetic and both groups of class III patients.Prevalence of abnormal HRT was lowest in class II diabetic patients and similarin the other groups. Only SD12, measuring randomness of HR patterns was moreabnormal in class III diabetic compared to class II diabetic patients.
Representative HRV by Group
Class II Class III p-value
No Diabetes Diabetes No Diabetes Diabetes
Heart rate (bpm) 68± 21 72± 2 75 ± 2 76±2 0.002SDNN (ms) 117 ± 62 92± 6 91 ± 7 92 ± 7 0.012Ln VLF 7.1 ± 0.22 6.3 ± 0.2 6.4±0.2 5.9 ± 0.2 <0.001Ln LF 5.6 ± 0.22 4.7± 0.2 4.7 ± 0.2 4.6 ± 0.2 0.003DFA1 1.02 ± 0.032 0.88±0.03 0.92 ± 0.03 0.89 ± 0.04 0.013Power law slope -1.29±0.032 -1.40± 0.03 -1.39 ± 0.03 -1.44 ± 0.03 0.006SD12 25.1 ± 1.51 30.5 ± 1.6a 27.8 ±1.7 32.9 ± 1.8a 0.0081Significantly different class II non-diabetic: all class III, 2Significantly different class II non-diabetic: all groups.
Conclusions: The effects of diabetes and heart failure on autonomic function ap-pear to be cumulative in class II patients, but diabetes may have little additionaleffect on HRV in class III patients. Only SD12, which is not a measure cardiac au-tonomic function but of heart rate patterns, appears to be associated with NYHAclass in diabetic patients with CHF.
P5191 Relationship of Carotid Intima-Media thickness,unstable carotid plaques and severe carotid stenosiswith the severity of coronary artery disease
N. Cicorella, L. Franceschini, L. Zanolla, A. Rossi, B. De Cristan,G. Cacici, M. Arieti, C. Vassanelli. University of Verona, Institute of
Cardiology, Verona, Italy
Purpose: Carotid intima-media thickness (IMT) is widely used as a surrogatemarker of systemic atherosclerosis. The purpose of this study was to assess therelationship between IMT, the presence of plaques instability or severe stenosisof the carotid arteries, and the extent of coronary artery disease (CAD).Methods: We examined retrospectively 1337 patients (mean age: 67 years ±9) who performed both coronary angiography (for suspected or symptomatic is-chemic heart disease (IHD) or as a standard pre-surgery evaluation in valvulardisease) and carotid ultrasound evaluation from 1995 to 2005. Carotid plaqueswas defined as unstable when characterized by a low echogenity or disomoge-neous aspect and as a severe plaque when >70%. We considered as affected bysignificant CAD patients with at least one lesion > 50% within the main branchesof the coronary arteries.Results: In our population 1023 patients (75%) had a IHD (both symptomatic oroccasionally diagnosed), 256 (19.1%) had a severe valvular disease, 67 (5.0%)had a dilatated cardiomyopathy. We observed that patients with known IHD had asignificantly higher IMT (0.94 mm ± 0.19 vs 0.99 ± 0.16 p<0.0001). A significantprogressive increase in IMT was observed in patients with one, two or three ves-sel CAD (0.95 ± 0.18, 0.99 ± 0.16, 1.01 ± 0.15) (p =0.0002). This association isalso present in patients without known IHD: 0.90 ± 0.18 in patients without signif-icant CAD and 0.96 ± 0.18, 0.99 ± 0.16, 1.00 ± 0.19 respectively. (p <0.0001).In our population the extent of coronary disease and the presence of unstablecarotid plaques were significantly associated: 7% of patients without CAD had anunstable carotid plaques and 21.3%, 18.5%, 23.5% respectively in one, two, threevessel disease (p<0.001). Significant CAD and severe carotid disease were sig-nificantly associated: severe carotid stenosis was found in 68.8% of patients withCAD vs 31.8% of patients without CAD (p=0.03) Moreover, in patients withoutknown IHD the presence of severe carotid plaques was associated with a highincidence of three vessel coronary disease (14.4%, 8.5%, 20.0%, 57.1% respec-tively in zero, one, two, three vessel disease).Conclusions: In our study we confirmed that there is a high correlation betweencarotid artery disease and the presence and severity of CAD. This is demon-strated not only by the because IMT increases with advancing CAD, but also bythe higher frequency of unstable plaques and severe plaque in patients with CAD.In patients with severe carotid plaque there is high probability of three vessel dis-ease.
P5192 T-wave alternans for cardiac events prediction afteracute infarction and early PCI
A. Filipecki, K. Wita, Z. Tabor, M. Turski, D. Urbanczyk,W. Kwasniewski, W. Orszulak, M. Trusz-Gluza. Silesian MedicalUniversity, I Dep. of Cardiology, Katowice, Poland
The era of early primary coronary intervention (PCI) for acute MI has changed thepatients’ outcome, thus we undertook study to assess prognostic value of T-wavealternans (TWA) and other established risk indices in these settings. Prospec-tively, we enrolled 96 consecutive pts with acute anterior MI undergoing PCI<12hours from symptoms onset, with successful LAD opening, treated according tocurrent guidelines. Demographics, established RFs and index event data wereassessed. Major adverse cardiac events (MACE) - death, recurrent MI, rehospi-talization due to heart failure - were recorded at 6 month follow-up. At day 30 dayTWA test was performed.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Atrial fibrillation – miscelaneous / Mitral valve disease 895
Results: 14 pts experienced MACE at 6 months (3 died, 1 reinfarcted and 10were rehospitalized for HF). There were no differences in demographics, comor-bidities, treatment, arrhythmias (bedside and 5th day Holter), time from symptomsonset to PCI, TIMI and MBG before/after PCI, as well as ECG and SAECG inboth groups. MACE(+) pts had significantly lower EF at day 1 (36±4 vs. 42±8%,p<0.01), higher maximum Troponin I and CK MB levels (42±14 vs 30±20ng/mland 396±243 vs 261±251 IU, respectively, both p<0.05), more frequent TWA+(8/14 vs 17/82, p<0.01), lower HRV (SDRR 77±22 vs 109±31 ms, p<0.05) andhigher Holter 3-lead QTd (36.0±8.4 vs 27.6±9.8, p<0.05). MACE free survivalwas 93% in all pts and was significantly lower for TWA+ (96% vs 71%, p<0.001)- figure 1. In univariate Cox proportional hazard model TWA+, low EF and SDRRwere significant for MACE and in multivariate model the best for MACE predictionwas combination of EF and TWA.
Fig. 1
Conclusions: TWA alone or in combination with ejection fraction is a powerfulpredictor of mid-term cardiac events occurrence in patients after acute MI whowere successfully treated with early PCI.
MITRAL VALVE DISEASE
P5193 Differences in the presentation of candidates forpercutaneous mitral commissurotomy across theworld: do they influence the results of the procedure?
E. Marijon1, A.O. Hausse-Mocumbi2 , H. Gamra3, N. Vo Thanh4,J. Kamblock5, C. Esteves6, I. Palacios7, A. Vahanian1. 1Bichat
Hospital, Cardiology Department, Paris, France; 2ICOR, Cardiology Department,Maputo, Mozambique; 3Fattouma Bourguiba Hospital, Cardiology Department,Monastir, Tunisia; 4Choray Hospital, Cardiology Department, Ho Chi MinhCity, Viet Nam; 5Taaone Hospital, Cardiology Department, Papeete, FrenchPolynesia; 6Dante Pazzanese Institute, Cardiology Department, Sao Paulo,Brazil; 7Massachusetts General Hospital, Cardiology Division, Boston, UnitedStates of America
Purpose Despite marked differences in the epidemiology of rheumatic fever, littleis known on the geographic differences in the characteristics of patients (pts)with mitral stenosis and on the results of percutaneous mitral commissurotomy(PMC). To address this issue, we analysed 350 pts in 7 centres located acrossthe 5 continents.Methods The study included 50 consecutive pts scheduled for PMC in each cen-tre from 5 non-Western countries (Mozambique, Tunisia, French Polynesia, Viêt-Nam, and Brasil) and 2 Western countries (USA and France).Results Baseline characteristics of the 350 pts are detailed in the Table. Therewere no significant differences in complication rates between non-Western andWestern countries, respectively 0.8% and 1.0% for in-hospital death (p=0.85),1.6% and 0% for tamponade (p=0.47), 2.8% and 5.0% for mitral regurgitationgrade ≥3/4 (p=0.31), 3.2% and 4.0% for the need of surgery within the first month(p=0.71). Good immediate results, defined as valve area ≥1.5 cm2 without mitralregurgitation grade >2/4, were observed in 90% of pts from non-Western centresand 88% of pts from Western centres (p=0.58).
Table 1
Non-Western Western p(n=250) (n=100)
Age (years) 35 ± 15 57 ± 15 <0.0001Female (%) 80 82 0.73Previous embolism (%) 8 20 0.009Previous commissurotomy (%) 15.6 16.0 0.40NYHA class III or IV (%) 48 63 0.01Atrial fibrillation (%) 16 45 <0.0001Wilkins score 8.8 ± 1.4 8.6 ± 2.0 0.35Systolic pulmonary artery pressure (mmHg) 57 ± 21 42 ± 14 <0.0001Mean gradient (mmHg) 15 ± 6 8 ± 4 <0.0001Indexed valve area (cm2/m2 BSA) 0.57 ± 0.14 0.62 ± 0.14 0.006
Baseline characteristics of the 350 patients(BSA: body surface area)
Conclusions: As compared with pts from Western countries, candidates for PMCfrom non-Western countries 1) Are younger, have more severe valve stenosis andpulmonary hypertension, but a lower frequency of atrial fibrillation and previousembolism. 2) However, PMC achieves good immediate results in a similarly highproportion of pts, showing further the wide applicability of this technique.
P5194 Balloon mitral valvotomy versus closed surgicalcommissurotomy, up to ’15 years’ follow up of arandomized study
O.E.A. Rifaie1, M.K. Abdul Dayem2, A.L.I. Ramzi1, H.E.Z.Z. Attia1,A.D.E.L. El Atribi1, T.A.R.E.K. Zaki1, H. El Sayed1, P.S. Redy3. 1Iain
Shams University, Cardiology Department, Abbasseya, Egypt; 2Cairo, Egypt;3Pittsberg, Pensylvania, United States of America
Background: The immediate and intermediate term results of balloon mitralvalvotomy(BMV) are comparable to closed surgical commissurotomy(CSC). How-ever,longterm data of randomized trials are scanty. Objective: To present thelongterm results of a randomized study of BMV versus CSC up to 15 years.Methods: Fourty patients had been randomized to balloon mitral valvotomy(BMV) or closed surgical commissurotomy (CSC) in 1988. Each group consistedof 20 cases with symptomatic rheumatic mitral stenosis with minimal calcification.No difference was noticed at baseline data including age, sex, rhythm and echoscore. Double balloon technique was used for (BMV) (18, 20mm).Hemodynamicstudy & left ventriculography were done for all patients of both groups before &after BMV & CSC.Results: Doppler mitral valve area increased from 0.9±2 to 1.9±2 cm2 in BMVgroup versus 0.9±2 to 2.1 cm2 CSC group (P>0.05). Mean pulmonary arterypressure dropped from 38±10 to 21±7 mmHg, in PBMV group versus 46±12 to25±6 mmHg in CSC group P0.05. New mitral regurgitation (MR) was noted in 2patients in both groups (10%) but none had severe MR. No mortality or seriouscomplications were noted in either groups. One patient developed stroke afterBMV. Patients were followed up to 15 years by clinical examination & colouredDoppler echocardiography for a mean of 99±24 months. Only 2 patients droppedfrom follow up in CSC group versus one patient in BMV group. The Doppler valvearea was 1.8±0.3 cm2 in CSC group versus 1.8±0.4 cm2 in BMV group (P>0.05).The Doppler gradient was 7±4 mmHg in PBMV group versus 6.6±4 mmHg inCSC group (P>0.05). Restenosis was noted in 3 patients in CSC group (16.6%)versus 4(20%) in the BMV group (P>0.05). MR grade decreased from grade 2/4to 1/4 in one patient in one patient to PBMV group and remained the same inthe other patient. In CSC group, MR disappeared in one of the two patients &dropped from 2/4 to 1/4 in the other. New atrial fibrillation (AF) was noted in 4patients (20%) of CSC group versus 3 (15%) of PBMV group (P>0.05).Conclusion: BMV yields comparable results to CSC on immediate & long termoutcome. The good results of BMV are sustained up to 15 years following up,being still similar to CSC.
P5195 Sustained reduction of functional mitral regurgitationwith cardiac resynchronization therapy is related toclinical response and independent of underlyingcardiomyopathy etiology
V. Delgado, M. Sitges, B. Vidal, L. Mont, D. Tamborero, E. Roig,M. Azqueta, C. Pare. Hospital clinic, cardiology, Barcelona, Spain
Few studies have assessed the quantitative impact of cardiac resynchronizationtherapy (CRT) on mitral regurgitation (MR) over time and its clinical implications;also, the particular effect on ischemic MR has not been analyzed.Objectives: We analyzed the evolution of MR in patients (pts) treated with CRTat 1 year follow-up (FU) according to their clinical evolution and the etiology of theunderlying cardiomyopathy.Methods: 89 pts with heart failure, LV ejection fraction (EF) < 35% and LBBBwere studied with color-Doppler echo before (OFF), immediately after (ON), at6 and 12 month FU after CRT. MR was quantified determining regurgitant ori-fice area (ROA) and regurgitant volume (RV). We considered clinical respondersthose pts who were alive without cardiac transplantation and who improved by10% in the 6 minutes walking test at one year FU.Results: There were 34 pts (38%) with non-trivial MR (RV > 10 ml/beat). Etiol-ogy of LV dysfunction was ischemic heart disease in 13 (38%) pts and idiopathicdilated cardiomyopathy in 21 (62%) pts. At 12 month FU, 14 pts were clinical nonresponders. CRT induced an acute and sustained reduction of MR in clinical re-sponders along 12 month FU; in non responders, however, the acute effect onMR reduction was not sustained over time (Table1). Additionally, sustained MRreduction was observed both in pts with ischemic cardiomyopathy (n = 13, ROAat 12 months FU 15 ± 9 mm2 vs ROA baseline 27 ± 12 mm2, p < 0.05) and non-ischemic cardiomyopathy (n=21, ROA at 12 months FU 24 ± 21mm2 vs ROAbaseline 38 ± 21mm2, p < 0.05).
Table 1. Mitral ROA (mm2) in pts with CRT
OFF ON 6m 12m
Responders 27 ±16 18 ±12* 23 ±10* 17 ±15*Non-responders 42 ±19 20 ±16* 33 ±19 32 ±19
CRT induced and acute and sustained reduction of MR in clinical responders along 12 monthsof follow-up. In non-responders this acute reduction was not significantly sustained. *p<0.005 vsOFF.
Conclusions: CRT induced a sustained reduction of MR in pts who were clinicalresponders, but not in non responders. Sustained MR reduction was observedregardless of the etiology of the underlying cardiomyopathy. CRT may be an al-ternative to treat functional ischemic or non-ischemic MR
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
896 Mitral valve disease
P5196 Survival after coronary revascularization, with andwithout mitral valve repair, in patients with ischemicmitral regurgitation. Importance of pre-operativemyocardial viability
J.-B. Le Polain De Waroux1, A.C. Pouleur1, A. Pasquet1 ,B.L. Gerber1, G. El Khoury1, P. Noirhomme1, A. Robert2, J.L. Vanoverschelde1 .1Cliniques Universitaires Saint-Luc, Department Of Cardiology, Brussels,Belgium; 2Ecole de Sante Publique, Brussels, Belgium
Background: The impact of adding mitral valve repair (MVR) to coronary bypassgrafting (CABG) in patients (pts) with ischemic mitral regurgitation (iMR) is un-clear. This study aimed at comparing the 30-day and 4-year survival of pts withiMR undergoing CABG or CABG+MVR and to investigate the role of myocardialviability (VM) in the prognostic response to MVR.Methods: We studied 76 coronary pts (61 men, 62±9 yrs) with poor LVEF(37±10%) and ≥ 2 iMR who underwent low-dose dobutamine echo to identifyVM before CABG. Survival of 34 pts undergoing CABG+MVR (restrictive annulo-plasty) was compared to that of the 42 pts who underwent CABG alone. Groupswere further substratified according to preoperative VM.Results: At baseline, the 4 groups were similar. During follow-up, 30 pts (39%)died. 30-day survival tended to be lower in CABG+MVR (83%) than in CABGalone (96%, p=0.06), irrespective of VM. 4-yr survival was better in pts withVM, irrespective of MVR, (76±10%) than in those without VM, whether under-going CABG (56±9%) or CABG+MVR (35±11%, p<0.01 vs VM). At 1 yr, resid-ual iMR was lower in CABG+MVR+VM pts (1.2±0.9) than in the other groups(CABG+MVR nonviable: 1.6±0.5; CABG viable: 1.8±0.5; CABG nonviable:2.0±0.9, p<0.05). Cox’s porportional hazard analysis identified VM (OR=0.14,95%CI [0.05; 0.38] p<0.001), MVR (OR=3.54, 95%CI [1.48; 8.50], p=0.004), ad-ditive Euroscore (OR=1.29, 95%IC [1.08; 1.55], p=0.005) and LVEF (OR=0.93,IC95% [0.59; 1.02], p=0.002) as independent predictors of long term outcome inthis population.
Conclusions: In pts with iMR, survival after CABG is mainly influenced by thepresence of VM. By contrast, adding MVR to CABG does not affect survival ex-cept in pts without VM in whom it increases early mortality.
P5197 Implantation of a coronary sinus stent improves acuteischemic mitral valve regurgitation; an experimentalstudy
S. Karagiannis1 , A. Manginas1, G. Karatasakis1, A. Papalois2,A. Papalambrou2, P. Daphnomili2, L. Khaldi2, D.V. Cokkinos2.
1Onassis Cardiac Surgery Center, 1st Cardiology, Athens, Greece; 2ELPENResearch Unit, Athens, Greece
Introduction: Mitral valve regurgitation worsens the hemodynamic strain of thefailing LV by causing volume overload and leads to further deterioration of the clin-ical status in heart failure patients. Several coronary sinus annuloplasty methodsare under development, in an attempt to find a safe and efficient device with long-term durable effects. We sought to determine the effect of a stent placement aspercutaneous mitral anulloplasty device in the coronary sinus of pigs in a modelof experimental ischemic mitral regurgitation (IMR).Methods: Five consecutive male pigs (weight 20±5kg), were anesthetized, in-tubated and catheterized through the right femoral artery approach, after dailypretreatment with aspirin (325 mg) and clopidogrel (75 mg) for one week. An an-gioplasty balloon was repeatedly inflated in the proximal left circumflex artery forfive minutes each time to induce mitral regurgitation. Mitral regurgitation was esti-mated by transthoracic echo measuring the color jet area, the regurgitant flow andthe proximal isovelocity surface area (PISA) radius. The balloon inflation and theMR assessment were repeated 3 times at baseline. Consequently a large (8.0-9.0 mm) diameter stent was implanted in the coronary sinus through the rightfemoral vein and the degree of IMR was again evaluated in the same manner.The measurements after stent placement were again repeated 3 times, and thevalues were averaged. Stent placement was possible in all animals and the totalprocedure time was 225±17.8 min (mean±SE)Results: Immediately following stent implantation IMR improved in all experi-
ments as it is shown in the Table (mean values± SD).Three animals were allowed to recover. They were sacrificed at 30 days and his-tology was performed, documenting endothelialization of the coronary sinus stentwithout thrombosis.
Table
MR area (cm2) PISA MR flow(ml/sec) PISA radius(cm)
Pre-stent 2.36±0.37 63.9±37.3 0.46±0.08Post-stent 1.12±0.60 44±35.0 0.30±0.05P value 0.016 0.029 0.09
Conclusion: Percutaneous mitral annuloplasty by coronary sinus stent implan-tation is feasible and improves experimental acute IMR. This method is easy toperform within acceptable operator times.
P5198 Left atrial size independently predicts outcome inasymptomatic severe mitral regurgitation
R. Rosenhek1, F. Rader2, M. Krejc1, D. Kalbeck1, H. Gabriel1,U. Klaar1, G. Maurer1, H. Baumgartner1 . 1Medical University OfVienna, Department Of Cardiology, Wien, Austria; 2Vienna, Austria
Background: Left atrial (LA) size is affected by left ventricular (LV) diastolic pres-sure, the degree of ventricular remodeling, the occurrence of atrial fibrillation andthe presence of mitral regurgitation (MR) itself. LA size has been proposed tobe a predictor of outcome after mitral valve replacement with preserved LV func-tion. However, the predictive value of LA size for development of symptoms or LVdysfunction among pts with severe MR has not been studied.Methods: 132 consecutive asymptomatic pts (age 55±15 yrs, 49 female) withsevere degenerative MR and normal LV function were prospectively followed for amedian of 69 months. Pts underwent serial clinical and echocardiographic exams.The following potential predictors of outcome were studied: LA size, endsystolicand enddiastolic LV diameter, pulmonary artery pressure and clinical risk factors.Results: Kaplan-Meier event-free survival for the entire pt. group, with endpointsdefined as development of symptoms or LV dysfunction (n=38) and death relatedto MR (n=0) was 92±2% at 2 yrs, 78±4% at 4yrs, 65±5 at 6 yrs and 55±6% at 8yrs. LA size was the strongest independent predictor of outcome: No events wereobserved in the group with a LA < 50 mm. Event-free survival for patients with aLA 50 to 69 mm was 94±3% at 2 yrs, 82±5% at 4 and 51±8% at 8 yrs versus85±8% at 2 yrs, 47±12% at 4yrs and 40±12% at 8 yrs for patients with a LA ≥70 mm (p=0.0001). None of the other studied parameters reached significanceas predictors of outcome in multivariate analysis.
Fig.1. Event-free survival according to LA-size.
Conclusion: LA size is a strong and independent predictor of outcome in patientswith asymptomatic severe MR. Patients can be stratified by LA size in groups atlow, intermediate and high risk for subsequent symptom or LV dysfunction devel-opment requiring surgery.
P5199 Percutaneous transvenous mitral commissurotomy isa safe and effective procedure in restenosis aftersurgical commissurotomy
M.A. Rahman1, M. Ahmed1, T. Haque1, A. Khan1, M. Amin1,H.S. Chaudhury2 , M. Rashid1, M. Rahman1. 1National Institute
of Cardiovascular Diseases, Department Of Cardiology, Dhaka, Bangladesh;2Shahabuddin Medical College, Department of Biochemistry, Dhaka, Bangladesh
Purpose: The percuteneous transvenous mitral commissurotomy (PTMC) hasbeen reported to be less good in patients with prior surgical commissurotomy(CMC). The purpose of this study was to evaluate the immediate results of PTMCin patients with restenosis after CMC.Methods: Using a cross-sectional analytical design, a total of 210 consecutivepatients who underwent PTMC for mitral restenosis after CMC (Group I) andmitral stenosis without prior CMC (Group II), in the Department of Cardiology,National Institute of Cardiovascular Diseases, from January 2003 to December2005, were included. PTMC was done by Inoue method. Step wise dilatationtechnique was used. Finally atrial septal puncture was carried out by lateral view.Outcomes measures were: mitral valve area (MVA) by echocardiography; trans-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Mitral valve disease 897
mitral gradient both by echocardiography and cardiac catheterization. Acute com-plications were also compared.Results: In Group I (n=43), 34 (79%) were female and 9 (21%) were male. Themean duration of CMC was 7.0 ± 3.2 years. In Group II (n=167), 143 (86%)were female and 24 (14%) were male. Compared to Group I, younger subjectswere present in Group II (Group I vs. II: 30.27 ±9.78 vs. 24 ± 8 years, P<0.05).Wilkins’s Echo score were comparable between the two groups (Group I vs. II:6.39 ± 1.19 vs. 6.12 ± 1.10, P=ns). Before PTMC, MVA and transmitral gradientwere similar in both groups (mean ± SD, Group I vs. II: MVA 0.78 ± 0.14 vs. 0.79± 0.12 cm2 (P=ns); and transmitral gradient 21.79 ± 5.27 vs. 23.05 ± 6.42 mmHg (P=ns)). After PTMC, MVA and transmitral gradient were again comparable(Group I vs. II: MVA 1.79 ± 0.31 vs. 1.86± 0.28 cm2, (P=ns); transmitral gradient6.26 ± 1.95 vs. 6.50± 2.06 mm Hg, (P=ns)). MVA was increased and transmitralgradient was reduced significantly after PTMC in both groups (P <0.001). Acutecomplications in both the groups were very less frequent, and were compara-ble.Conclusions: PTMC is a safe and effective procedure in patients with Post-CMCrestenosis. Post CMC status is not itself is the predictor of outcome of PTMC.IAS puncture in the lateral view is easy and safe technique. Stepwise inflation ofInoue balloon during PTMC avoids acute complication.
P5200 Percutaneous Mitral Valve Repair. A Single Center’sExperience
L.L. Rodriguez, P. Whitlow, W. Stewart, S. Kapadia, M. Tuzcu,R. Savage. Cleveland Clinic Foundation, Dept. Of Cardiology,Cleveland, United States of America
Background: The Evalve ® MitraClip™ device in the EVEREST I Trial (Endovas-cular Valve Edge-to-Edge REpair Study) evaluates a percutaneous transseptalapproach for treatment of mitral regurgitation (MR).Methods: Under transesophageal echo guidance and standard transseptal ac-cess, the central portion of mitral leaflets is grasped with a clip, to reduce MR.The primary safety endpoint is significant adverse events (SAE), the efficacy end-point is core lab MR severity <2+. Surgical candidates with moderately severeor severe central MR and symptoms (or asymptomatic with EF,60% or LVESD>
45 mm) were included. Patients with EF<30%, LVESD> 55 mm, endocarditis orrheumatic disease were excluded.Results: We report our institutional experience, in 12 patients enrolled at our cen-ter; Six patients had functional MR and 6 had myxomatous mitral valve disease.Five had prior cardiac surgery. Six patients received one clip, 5 patients received2 clips. We excluded from analysis one patient because problems with transsep-tal puncture led to the clip not being delivered. A systematic echocardiographicTEE evaluation was used to guide the procedure.Results: Device time (DT), from guide insertion to clip delivery system removal,decreased with experience. DT in single clip patients decreased from 161 min-utes in the first 3 pts to 145 minutes the last 3. In patients requiring two clipsfor the repair, DT decreased from 301 minutes in the first 3 pts to 166 minutesthe last 2 pts. There were no procedural deaths. One patient had a small strokewithout residual neurological deficit. Six (6) pts have completed 30-day core labMR severity assessment, 5 of the 6 (83%) had MR severity ≤1+ (mild) and onept had 2+ MR. One patient had increased diastolic gradients after the procedurebut improved at 1 month follow up. None have required subsequent operation.Conclusion: Percutaneous Edge-to-Edge valve repair for mitral regurgitation canbe accomplished safely and successfully, with significant reduction of mitral re-gurgitation. The steep learning curve is improved by combined use of fluoroscopyand selected TEE views. The device time of the procedure was nearly cut in halfin patients requiring 2 clips.
P5201 Mitral valve surgery for dilated cardiomyopathy:impact of right ventricle function on early outcome
S. Gallina, M. Di Mauro, M. Pano, F. Palma, A. Tatasciore, R. DiPillo, M. Giancane, G. Di Giammarco. G. D’Annunzio University,Cardiology and Cardiac Surgery Department, Chieti, Italy
Aim of study: Mitral valve (MV) repair is a worldwide accepted surgical optionfor treatment of dilated cardiomyopathy (DCM). This study was aimed to evaluatewhich preoperative variables can impact 30-day outcome.Methods: From January 1997 to January 2006, 150 patients with DCM under-went to MV repair, 111 ischemic and 39 non-ischemic. Mean age was 66±10years. Average NYHA class and mitral regurgitation (MR) degree were 3.2±0.7and 3.4±0.8, respectively; right ventricle function was evaluated by echocardio-graphic parameters (excursions of the tricuspid annular plane:TAPSE, Dopplertissue imaging peak systolic velocity: TDIs, systolic pulmonary artery pressure:PAPs) Stepwise logistic regression was used to find which independent variablescan impair early outcome. ROC analysis was used to identify the cut-off values.Results: Thirty-day mortality was 8.6% (13 patients). Predictors were reported inthe table. Either preoperative clinical status or excessive MV apparatus remod-elling can result in worse prognosis. Moreover, the right ventricular (RV) functioncan play an important role in the first postoperative month. Any attempt to corre-late left ventricular dysfunction and dilatation to early outcome failed.Conclusions: MV repair can be considered a safe procedure for treatment ofDCM but we should carefully evaluate preoperative hemodynamics, MV appara-
Logistic regression ROC analysis
OR p-value AUC, p-value Sensitivity - Specificity
Heart Failure 2.8 0.018 – –MR degree 1.1 0.033 – –MVA<39mm 7.5 0.003 0.80, 0.001 70% - 77%MVCD>10mm 6.1 0.012 0.78, 0.001 77% - 65%TAPSE <13mm 7.1 0.036 0.84, 0.007 72% - 72%TDIs <11cm/s 13.1 0.022 0.78, 0.027 87% - 68%PAPs>50mmHg 11.5 0.015 0.90, 0.001 88% - 93%
MVCD: mitral valve coaptation distanceMVA: Mitral valve annulus
tus changes and RV function to improve early outcome. This study clear demon-strates that RV function has a very strong impact on early outcome of this partic-ular subset of patients.
P5202 Association Between Nanobacteria and MitralAnnular Calcification
C. Ozdol1, F.S. Ertas1, T. Hasan1, C. Conkbayir1 , I. Dincer1,K. Aho2, N. Ciftcioglu2, E.O. Kajander2. 1Ankara University Schoolof Medicine, Cardiology Deparment, Ankara, Turkey; 2Nanobac Life
Sciences, Tampa, Finland
Background and Aim: Mechanisms leading to vascular and tissue calcificationremains incompletely understood. Previous studies demonstrated an associationbetween Nanobacteria (NB), a controversial, slow-growing and calcifying agent,and vascular calcification and kidney stone formation. The aim of the presentstudy was to evaluate a possible pathogenetic link between the development ofmitral annular calcification (MAC) and NB infection.Methods: We evaluated 93 consecutive patients with MAC detected by 2D echo-cardiography. Asymptomatic 94 subjects with no evidence of calcifications wereselected as control group. Patients with rheumatic valve disease and renal dis-ease were excluded. Severity of MAC was prospectively classified as mild (thick-ness of the calcium deposit <6mm), moderate (6-10mm) and severe (>10mm).Results: Mean titers of NB-antibodies were higher in individuals with MAC(p<.0001). Multivariate logistic regression analysis revealed that age (OR:1.09;95%CI:1.05-1.14), hypertension (OR: 4.4; 95%CI: 1.7-11.4), diabetes (OR: 5.3;95%CI: 1.4-19.8), low HDL-C (OR: 11.4; 95%CI: 3.5-36.8) and high NB titers(OR: 5.4; 95%CI: 2.1-14) as independent correlates of MAC. Increasing titers ofNB antibodies were significantly associated with increased severity of MAC (Fig-ure 1).
Fig. 1
Conclusion: These results suggest that NB may play an important role in thepathogenesis of mitral annular calcification.
P5203 Myocardial 123I-metaiodobenzylguanidinescintigraphic uptake and heart rate variability inpatients with mitral valve prolapse
E.A. Zacharis, G.E. Kochiadakis, I.K. Karalis, S.I. Koukouraki,M.E. Marketou, A.P. Patrianakos, N.S. Karkavitsas, P.E. Vardas.
Heraklion University Hospital, Cardiology, Heraklion, Greece
Purpose: Mitral valve prolapse (MVP) is associated with autonomic nervoussystem abnormalities. We undertook this study to evaluate myocardial sympa-thetic innervation and cardiac vagal activity by simultaneous assessment of 123-I-metaiodobenzylguanidine (MIBG) scintigraphy and heart rate variability (HRV)in patients with MVP.Methods: MIBG myocardial scintigraphy and time-domain heart rate variability(HRV) were analysed in 33 patients with MVP (21 female, 36 ± 12 years) and25 healthy controls. None of the participants had any other disease that mayhave affected myocardial adrenergic innervation or autonomic nervous system.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

898 Mitral valve disease
A 24-hour ECG ambulatory Holter monitoring was performed in all the subjectswho also underwent a planar and a SPECT myocardial imaging of the heart afterintravenous infusion of 5mCi MIBG. Heart to mediastinum ratio (H/M) was usedfor quantitative assessment of adrenergic innervation, 10 minutes and 4 hoursafter drug infusion, while SPECT scintigraphy evaluated the regional distributionof adrenergic activity. The percent washout rate (WR) was determined for the4-hour period.Results: Forty percent of the MVP was located in the posterior leaflet, 40% inthe anterior leaflet and 20% in both leaflets. Patients with MVP showed enhancedWR (7.7 ± 3.4 in MVP versus 2.2 ± 2.3 in controls) and regional adrenergic inner-vation defects mostly in the inferoposterior and septal walls in anterior MVP andin inferior and lateral walls in posterior MVP. HRV analysis revealed a significantreduction of cardiac vagal tone in MVP patients (pNN50 (%): 4.7 ± 2.2, rMSSD(ms): 16.8 ± 6.5, SDNN (ms): 210 ± 65) compared to controls (pNN50 (%): 8.6 ±5.1, rMSSD (ms): 32.9 ± 7, SDNN (ms): 160 ± 79, p<0.05 for all). WR correlatedadversely with pNN50 (r= - 0.65, p= 0.02) and tended to correlate with rMSSD (r=- 0.059, p= 0.055).Conclusions: Patients with MVP revealed an increased clearance of MIBG up-take and regional myocardial adrenergic innervation defects, which are relatedto a depressed cardiac vagal tone. These findings add important information toexisting knowledge concerning the disturbed autonomic drive in MVP syndromebut further studies are necessary to assess if these findings are the cause or theresult.
P5204 Clinical outcome of significant MR following PMV
S.H. Kim, E.S. Jeon, S.H. Lee, S.W. Park, J.Y. Park, S.C. Lee.Samsung Medical Center, Sungkyunkwan University School OfMedicine, Seoul, Korea, Republic of
Background: Mitral regurgitation(MR) is a frequent complication af-ter percutaneous mitral valvuloplasty(PMV). We sought to investigate the naturalhistory of moderate or severe MR after PMV.Methods: From August, 1995 to September, 2003, PMV was performed in 183consecutive patients with severe mitral stenosis. Baseline and follow-up echocar-diographic and clinical data of 29 patients who developed moderate or severe MRafter PMV were reviewed retrospectively.Results: Among the 29 patients, 19 patients developed moderate MR and 10 se-vere MR. Their mean age was 42 ±9 years. Mean follow-up period was 4.0±2.4years. Excluding 2 patients who underwent emergency surgery immediately afterPMV and 1 patient who refused follow up, baseline post-procedural echocardio-graphy was performed in 26 patients 1 day after PMV. Within three years, thegrade of MR seemed to improve in 35% after 1 year and in 13% after 3 years.Thereafter, however, the grade of MR progressed in 27% and 36% of patientsafter 3 and 5 years, respectively. The overall progression rate for initial moderateMR (n=18) was 15% and 53% in 3 and 5 years after PMV. Left atrial size alsoshowed a significant increase with time (p=0.02). A total of 8 cases of major clini-cal events occurred during follow-up, with a 5-year event rate of 32%. The eventswere; 2 cases of elective operation, 2 cases of new atrial fibrillation, 1 case ofheart failure and 1 case of stroke.Conclusion: PMV-associated moderate MR shows relatively rapid progressionand frequent clinical events on follow-up. Special attention is required in thesepatients including detailed history taking and annual echocardiographic examina-tion.
P5205 Can exercise haemodynamics help in the decision forsurgery in asymptomatic patients with severe mitralinsufficiency by echo criteria?
H. Gohlke, C. Gohlke-Baerwolf, N. Jander, M. Allgeier, K. Peters,W. Zeh, T. Comberg, F.-J. Neumann. Herz-Zentrum, Cardiology, Bad
Krozingen, Germany
Echocardiographic determination of severity of mitral insufficiency (MI) is of prog-nostic importance. Patients (Pts) with an effective regurgitant orifice (ERO) of >
40 mm2 have a guarded prognosis, which lead to a recommendation for surgeryeven in asymptomatic Pts. According to ESC/AHA Guidelines a systolic pul-monary artery pressure (PAPs) at rest of > 50mmHg or of > 60mmHg duringexercise is considered an indication for surgery in asymptomatic Pts with severeMI.The goal of this study was to examine the role of a haemodynamic evaluationwith a Swan-Ganz balloon tipped catheter at rest and during submaximal supinebicycle ergometry in Pts with severe MI to identify Pts who fulfill ESC/AHA criteriafor mitral valve surgery.In 219 consecutive Pts with severe MI (mean age 59, 4 + 0,8 yrs, 72% male)haemodynamics at rest and during exercise were evaluated.Results: According to the PAPs at rest Pts were divided into three groups. ThePAPs during exercise was analysed in these three groups and results are shownin table 1.The PAPs at rest was below 50 mmHg in 180/219 Pts (82%), 108 (60%) of whichdeveloped a PAPs of > 60mm Hg during exercise. 42% of Pts with a PAPs of 30mmHg or less manifested an indication for surgery with a PAPs of > 60 mmHgConclusion: Exercise haemodynamics identify Pts fulfilling ESC/AHA criteria formitral valve surgery, who are not identified by resting haemodynamics. Exercise
Table 1
PAPs at Rest (mmHg) <31 mmHg 31-49 mmHg > 49 mmHg(n=111) (n=69) (n=39)
PAPs Exercise >60 mmHg N=47 (42%) N=61 (88%) N=39 (100%)*
*p�0,0001.
haemodynamics can be helpful in the decision for surgery particularly in asymp-tomatic Pts with PAPs < 31 mmHg at rest. This applies also to Pts in whom PAPscan not be determined by echo at rest.
P5206 Long-term follow-up of ischemic mitral valve repair:survival analysis
J. Biernat, K.S. Golba, M.A. Deja, K. Widenka, W. Domaradzki,M. Jasinski, R. Bachowski, S. Wos. Medical University of Silesia,Cardiology, Katowice, Poland
Mitral valve repair is considered to be the standard in treating mitral regurgitation.To determine the outcome of mitral valve repair for ischemic mitral regurgitation(IMR) patients were prospectively followed.Methods: 198 consecutive pts, mean age 59.0±14.37, median=61.1 (52.58-67.70), females 23.6%, with mitral regurgitation of ischemic origin, who under-went mitral valve repair between 1999 and 2005 entered the study. CABG wasperformed in all cases (2.8±0.95 distal anastomoses per patient). The operationswere performed with undersized ring annuloplasty. IMR severity was determinedwith ratio of regurgitant jet to left atrial area (up to 20%-mild, 20-40%-moderate,more then 40%-severe). Mean observation time was 3.47±1.65, median=3.27(0.10-7.34) years. Ejection fraction (EF), end systolic volume index (ESVI) andIMR grade impact on outcome were assessed. Cut-off value for EF and ESVIwere determined with receiver operating characteristic (ROC) curve analysis.Event rates after surgery were estimated by Kaplan-Meier method. End-pointswere overall survival and composition of cardiovascular (CVS) death or hospital-ization.Results: The ROC curve analysis showed cut-off values for EF for overallsurvival and composite end-point 32% (AUC=0.644±0.051, p=0.005) and 36%(AUC=0.646±0.05, p=0.003) respectively. For ESVI cut-off value was equal 64ml/m2 (AUC=0.732±0.043, p=0.056) for both end-points. Impact of preoperativeEF, ESVI and IMR grade on analyzed end-points is presented in table.
Cumulative survival
Overall Composite
EF<32% 66.1% EF<36% 42.4%EF>32% 86.5% p<0.001 EF>36% 62.1% p=0.012ESVI >64 ml/m2 83.5% ESVI >64 ml/m2 60.1%ESVI <64 ml/m2 68.2% p=0.213 ESVI <64 ml/m2 37.5% p=0.025IMR severe 83.2% IMR severe 40.1%IMR moderate 79.6% p=0.525 IMR moderate 68.3% p=0.014
Overall: free from death, Composite: free from CVS death or hospitalization.
Conclusion: In pts with IMR preoperative low EF is associated with excess long-term overall mortality and more frequent incidence of composite end-point (CVSdeath or hospitalization). Preoperative large ESVI and severe IMR are connectedwith higher incidence of CVS death or hospitalization.
P5207 Repeat percutaneous mitral valvuloplasty (PMV) inpatients with restenosis after prior PMV
M. Ghasemi, E. Nematipour on behalf of Research Center ofEndovascular Intervention. Tehran University of Medical Sciences,Catheterization Laboratory/Interventional CAR, Tehran, Iran (Islamic
Republic of)
Background: Symptomatic mitral restenosis developed in 4% - 39% of patientsafter PMV. It is unknown whether these patients may benefit from repeat percuta-neous mitral valvuloplasty (PMV). This study assesses the immediate and earlyoutcome of repeat PMV in patients experienced restenosis after their initial PMV.Materials and Methods: Our study reports the immediate and early outcome of54 patients (average age 38±8.2 years, 40 females and 14 males) with symp-tomatic mitral restenosis after their initial PMV. These patients underwent a sub-sequent PMV around 3.8±2.4 years after the initial procedure.Results: After the procedure, there was a substantial increase in mitral valve area(MVA): from1.0 ± 0.2 to 2.2 ± 0.4 cm2 (p<0.001), a decrease in left atrial pres-sure: from 27 ± 8 to 15 ± 6 mm Hg (p<0.001) and in mitral valve gradient from17±4 to 2±1 mm Hg (P <0.001). The mean pulmonary artery pressure did notchange significantly after repeat PMV. Except for one, none of the other patientsdeveloped severe mitral regurgitation (3+) after the second PMV. Successful pro-cedural outcome (post-PMV mitral valve area ≥1.5 cm2, pulmonary/systemic flow
Echocardiographic results of the repeat
Variables Before PMV Post PMV p
Mitral Valve Area (cm2) 1.0±0.2 2.2+/- <0.001Left Atrial pressure (mmHg) 27±8 15±6 <0.001Mean Valve gradient (mmHg) 17±1 2+/- <0.001
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Mitral valve disease 899
ratio =<1.5:1 and <2+increase in mitral regurgitation with a post- PMV mitralregurgitation<+3) was achieved in 50 or 92.5% of the patients.Conclusion: A repeat percutaneous mitral valvuloplasty in patients who experi-enced restenosis after the first percutaneous valvuloplasty can be accomplishedwith acceptable results. The patients were selected on the basis of favorable char-acteristics and the echocardiographic analysis of the restenotic mitral valve.and unequivocal predictor of restenosis by multivariate analysis
P5208 Three dimensional versus two dimensinaltransesophageal echocardiography in mitral valverepair
R. Garcia Orta1, E. Moreno Escobar2, M. Vidal Alarcon2, M.F. RuizLopez2, J.M. Oyonarte Ramirez2, J. Lara Torrano2 , T. MorenoHerrero2, J. Azpitarte Almagro2. 1Hospital Virgen de las Nieves,
Cardiology Dept., Granada, Spain; 2Hospital Clinico San Cecilio, Cardiology,Granada, Spain
Objectives Our aim was to compare the diagnostic performance of three-dimensional echocardiogram versus two-dimensional in patients with regurgitantmitral valve.Background An accurate assessment of morphology and function of the mi-tral valve is essential for surgical repair. Two-dimensional (2D) transesophagealechocardiography has certain spatial limitations that could be overcome by three-dimensional (3D) imaging.Methods Patients undergoing surgical repair due to severe mitral regurgitation.Preoperative 2D and 3D transesophageal echocardiographic studies were com-pared to surgical findings (standard of reference). 3D images of the MV wereobtained unaware of 2D or surgical findings.Results Eighty-one consecutive patients underwent surgical repair (2002-2004).Concordance regarding segments affected between the 2- and 3D studies andsurgery was high, (2D: 88%-98%, 3D: 89%-100%). An increment of accuracyfor 3D imaging was observed in A1 segment defects (p=0.05) and commissuraldysfunction (p=0.02). 2D study incorrectly classified 22 segments mainly corre-sponding to complex disease. The three-dimensional study incorrectly classified14 segments, unrelated to complex disease. Five (6%) patients with complex dis-ease, who suffered complex repair surgery, were incorrectly diagnosed with 2Dbut adequately with 3D echocardiography. A non-expert observer analysis of the3D images vas in accordance (94%, κ 0.845) with data of the experienced author.Conclusions: Three-dimensional echocardiography offers high precision in theevaluation of the mitral valve, and it may complement two-dimensional study inpatients with complex valve anatomy where surgical decisions are even more dif-ficult. It provides easily interpretable images and thus a high degree of experienceis not required.
P5209 Assessment of the mitral valve area in patients withmitral stenosis by computed tomography
D. Messika-Zeitoun, J.M. Serfati, J.P. Laissy, M. Berhili, E. Brochet,B. Iung, A. Vahanian. Hopital Bichat, Cardiology, Paris, France
Background: Management of patients with mitral stenosis (MS) re-lies on accurate evaluation of the mitral valve area (MVA). Planimetry is con-sidered as the reference method but is operator dependent and requires precisemeasurement at the tips of the mitral leaflet with a correct plane orientation. Multi-slices computed tomography (MSCT), providing a three-dimensional acquisitionof the entire heart, which can be sliced as desired along any plane, seems ideallysuited for MVA measurements but has never been evaluated. We sought to as-sess the feasibility and accuracy of MSCT for MVA measurement in patients withMS.Methods: MSCT measurements of the MVA (MVACT) were performed by two ex-perienced operators and one non-experienced operator (Radiology Technologistwith no previous experience in valvular disease) in 29 patients with MS in sinusrhythm and compared to the planimetry measured by echocardiography (MVAE-CHO).Results: CT measurements could be performed in all patients in 3±1 minutes.MVACT (1.51±0.47 cm2, range 0.85-2.4 cm2) did not differ and correlated wellwith MVAECHO (1.44±0.53 cm2; range 0.7-2.3 cm2; p=0.15; r=0.88, p<0.0001;mean difference 0.20±0.17 cm2). Intra and inter-observer variability were re-spectively 0.14±0.12 and 0.17±0.13 cm2. CT measurements performed by thetechnician (1.45±0.55 cm2) also did not differ from and correlated well withMVACT (p=0.70; r=0.89, p<0.0001) and MVAECHO (p=0.25; r=0.82, p<0.0001)assessed by experienced operators.Conclusion: MSCT provides an accurate and reproducible MVA evaluation andis not operator dependent. Therefore, MSCT can be considered as an alternativefor MVA measurements in patients with poor echocardiographic windows or forteams not accustomed to evaluating patients with MS.
P5210 Left Atrial Appendage systolic Tissue Dopplervelocity is an important echocardiographic parameterin predicting thromboembolism in patients with mitralstenosis
M. Cayli, E. Acarturk, M. Demir, M. Kanadasi. Cukurova University,Cardiology Department, Adana, Turkey
Background: The incidence of systemic embolism remains high in patients withmitral stenosis (MS). Thromboembolic risk can be determined on the basis ofclinical and echocardiographic parameters. Although left atrial appendage (LAA)dysfunction has been found to be an important indicator of thromboembolism,new parameters will help in more accurate risk prediction.Aim: To investigate the value of the LAA velocities obtained by tissue Dopplerimaging (TDI) in predicting the risk of thromboembolism in patients with MS.Methods: Sixty patients with isolated MS were included. Patients were dividedinto two groups as Group I (n=20) with thromboembolism and Group II (n=40)without thromboembolism. Left ventricular ejection fraction (EF) and mitral valvearea (MVA) were calculated. Transmitral mean (MG) and peak gradients (PG)were measured. The presences of spontaneous echo contrast (SEC) and throm-bus were investigated by using transesophageal echocardiography. The LAA lateemptying flow velocity (LAAEV) was measured. LAA late systolic (LAASV) anddiastolic (LAADV) tissue velocities were recorded by putting the sample volumeof the TDI on the LAA lateral wall.Results: Group I had significantly higher incidence of dense SEC (85.0% vs.25.0%) and thrombus (50.0% vs. 17.5%) than Group II. Mean MVA, EF, LAAEV,LAASV and LAADV were significantly lower in Group I. Left atrial dimension,MG and PG were similar in both groups. Multivariate logistic regression analy-sis showed that LAASV, LAAEV and dense SEC were independent predictors ofthromboembolic events (Table).
Independent predictors of the risk of th
p Wald r OR 95% CI
Mitral valve area 0.3 1.7 0.00 0.04 0.01-5.04Ejection fraction 0.8 0.06 0.00 1.03 0.83-1.29Dense spontaneous echo contrast 0.03 4.7 0.20 3.19 1,71-13.68Thrombus 0.2 1.8 0.00 1.9 0.61-11.14LAA late emptying flow velocity 0.04 4.4 -0.19 0.62 0.40-0.97LAA late systolic tissue velocity 0.01 5.5 -0.22 0.25 0.08-0.88LAAlate diastolic tissue velocity 0.5 0.4 0.00 0.87 0.57-1.34
Conclusion: Besides LAAEV and SEC, LAASV seems more reliable and usefulparameter in predicting the risk of thromboembolism in MS.
P5211 Single shot for rheumatic mitral stenosis: a simpleand effectual usage of the Inoue technique
T. Bozat, H. Ozkan, S. Tiryakioglu, O. Tiryakioglu, V. Koca. BursaYuksek Ihtisas Egitim ve Arastirma Hast, Department of Cardiology,Bursa, Turkey
Background: Percutaneous balloon mitral valvuloplasty (PBMV) is an effectivetherapy in patients with mitral stenosis. PURPOSE: To obtain optimal result fromPBMV, more than half of patients need larger size than ideal Inoue balloon size.We thought that, using larger balloon size with single inflation would be moreeffective than using larger balloon following ideal balloon size because of inade-quate results.Method: 336 patients with rheumatic mitral stenosis were studied between 1994-2005. PBMV was performed with Inoue balloon. Ideal balloon size was measuredaccording to patients’ height. Stepwise method was used in 222 of 336 patients.115 of these 222 patients (51%)(Group 1) needed a larger inflation because ofinadequate results. Because the percentage of overinflation was high,we usedsingle inflation of +2 mm larger balloon size in 116 of 336 patients(Group 2).We compared these two groups with each other. All patients underwent standarttransesophageal (TEE) and transthoracic (TTE) echocardiographic examinationbefore and after PBMV. Follow-up was scheduled every 6 months in the first yearand yearly thereafter.Results: Baseline characteristics of group1 (n=115, 37,2±9,6 age) and group 2(n=116, 38±11,4 age) were similar. TTE and invasive measurements were simi-lar too. However, procedure time was significantly lower in group 2 (31,55±11,5min v.s. 25,2±11 min.,p<0.001). Follow-up duration was 49,5±19,2 months (24-84 months). At the last follow-up, measurements demonstrated that MVA wassignificantly higher (1,65±0,3 v.s. 1,42±0,34 cm2 p=0.02) and mean transmitralgradient was lower (9±3,6 v.s 6,7±3 mmHg p=0,017) in group 2. The change ofMVA is shown in Table 1.
Table 1. Change of MVA during follow-up period
MVA PRE-PBMV POST-PBMV 6 MONTH 2 YEAR LAST FOLLOW-UP
GROUP1 1,2±0,3 1,93±0,34 1,85±0,29 1,64±0,33 1,42±0,34GROUP2 1,13±0,21 2,02±0,28 1,89±0,26 1,82±0,3 1,65±0,3
Conclusion: The need for larger balloon size with stepwise method resulted bet-ter than expected. Excellent immediate results were obtained with both stepwiseoverdilatation and single overinflation. However, long-term results were signifi-cantly better with single overinflation. The ideal balloon size to achieve optimal
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

900 Mitral valve disease
results still remains unclear. As a result, using +2 mm larger balloon size withsingle inflation is an alternative and effective therapy with low procedure time.
P5212 Percutaneous mitral valvuloplasty during pregnancy
H. Pham, L.H. Nguyen, N.Q. Nguyen, D.L. Do, L.V. Nguyen,G.K. Pham. Vietnam Heart Institute, Vietnam Heart Institute, Hanoi,Viet Nam
Background: Circulatory changes in gestation, a hyperdynamicadaptive state in general, cause an additional burden on the cardiovascular sys-tem of women with rheumatic mitral stenosis (MS). Percutaneous Mitral Valvulo-plasty (PMV) has emerged as an effective nonsurgical technique for the treatmentof patients with symptomatic MS during pregnancy.Methods: From November 1999 to Dec. 2004, 35 pregnant women (among 3000PMV patients) were performed PMV using Inoue balloon at Vietnam Heart Insti-tute. The transthoracic echocardiography was used in combination with intermit-tent fluoroscopy to limit the radiation exposure time. A detailed clinical, echocar-diographic, hemodynamic assessment was analyzed pre, post procedure, at ev-ery 3 months for the first year and at 6-month interval thereafter. The pregnancyand newborn babies outcomes were also followed.Results: MS pregnant women were 27,6 years old on average (ranged 22-42)and the mean length of pregnancy was 24,2 ± 5,6 weeks. Echo score of mitralvalve was 7,1 ± 2,3. The procedure was technically successful in all cases withoutany complications. The total mean duration of the procedure was 35,25 ± 14,28min and that of fluoroscopy 2,55 ± 1,28 min (from 1 min 59 sec to 3 min 15sec). The fluoroscopy time was significantly shorter than that of usual patients notusing echo guided (2 min 23 sec vs. 7 min 23 sec, p< 0,01). The mitral valve areaincreased from 0,7 ± 0,3 to 1,9 ± 0,4 cm2 (on 2D echocardiography) and from 0,8± 0,4 to 2,0 ± 0,4 cm2 (on PHT) (p< 0.01). A reduction in mean transmitral valvegradient (MVG) was from 22 ± 6 to 8 ± 2 mmHg. There were no maternal or fetaldeaths. All patients delivered at full term but 2 (without major complications), 14vaginally and 21 by caesarean section. After average 18 months follow-up (range,3 to 36) all children had normal growth.Conclusions: During pregnancy, Percutaneous Mitral Valvuloplasty could beconsidered as the treatment of choice of severe pliable mitral stenosis which arerefractory to medical treatment. Using echocardiography guided can reduce thefluoroscopy time.
P5213 Balloon mitral valvotomy in pregnancy With mitralstenosis
P. Manoria1, S.K. Trivedi2, R.K. Singh2. 1Bhopal, India; 2BhopalMemorial Hospital And Research Centre, Cardiology, Bhopal, India
Purpose: To evaluate the efficacy and safety of balloon mitral valvo-tomy for the treatment of mitral stenosis during pregnancy.Method: Balloon mitral valvotomy (BMV) was performed in 16 (5%) pregnantwomen with tight mitral stenosis (MS) among 307 patients of MS, who underwentthis procedure in our institution between 2001-2005. Mean age of the pregnantpatients who underwent BMV was 24 years (range: 18-36 years). The averagegestational period was 22 ±5 weeks (range: 12-28 weeks). Out of 15 patients,ten (62%) patients were primigravidas. Two out of fifteen patients (12%) were inNYHA class IV, 5 (32%) were in class III and 9 (56%) were in class II. Atrial fibril-lation was present in 2 patients. Wilkins score was <8 in 62%, 8-10 in 26% and>10 in 12% patients. BMV was performed using flow guided Inoue balloon tech-nique. To protect the foetus from radiation, pelvic-abdominal area was shieldedwith a lead apron (2mm thick). Film badge dosimeters were used to measure ra-diations. The various haemodynamic parameters were assessed by transthoracicand transesophageal echocardiography. Results were expressed as mean ± SD.Quantitative data before and after BMV were compared using Wilcoxon’s test.The results were analyzed by statistical software Programme (SPSS).Result: BMV was successful in all cases. Pre-BMV mitral valve area was0.9±0.01 cm2 and post BMV was 1.9 ± 0.3 cm2 (p value 0.005). Pre-BMV meangradient was 22 ±3 mm Hg and post BMV it was 7± 2 mm Hg (p value 0.005) . LAmean pressure was 28 ±5 mmHg pre-BMV and 12 ±5 mmHg post BMV (p value0.005) . PA pressure decreased from 55±17mmHg pre BMV to 43±15mmHg postBMV. Mean fluoroscopy time was 4.7 ±1.5 minutes. Mitral regurgitation increasedby grade I in 32% patients and grade II or more in 12% patients. Abdominal radi-ation was always < 0.2 mSv, which is the threshold of dosimeter. In all patientsthe pregnancy went to term without any complications and all had a normal vagi-nal delivery except for one, who had a caesarian section at 35 weeks becauseof breech presentation. On an average follow up of 3 months after delivery, allpatients remain symptom free and babies were growing normally.Conclusion: BMV during pregnancy is a safe and effective procedure for treat-ment of mitral stenosis, provided due care is taken to protect foetus from radiationand care of the expectant mother is ensured.
P5214 Three-dimensional evaluation of the mitral valve areaand commissural opening before and afterpercutaneous mitral commissurotomy in patients withmitral stenosis
D. Messika-Zeitoun, E. Brochet, D. Rosenbaum, B. Cormier,J.M. Serfati, B. Iung, A. Vahanian. AP-HP, Hopital Bichat, 75018, Paris, France
Background: Management of patients with mitral stenosis (MS) relies on accu-rate evaluation of the mitral valve area (MVA). Planimetry (MVA2D) is consideredas the reference method but must be performed at the tips of the leaflets withthe correct plane orientation and therefore requires experienced operators. Real-time three-dimensional echocardiography (RT3DE) may overcome this limitationbut its usefulness for experienced compared to less experienced operators hasnot been evaluated. In addition, superiority of RT3DE for the evaluation of com-missural splitting after percutaneous mitral commissurotomy (PMC) is unknown.Methods: Sixty patients were prospectively evaluated by 2D and RT3DE beforeand after PMC by 2 experienced operators and one less experienced operator.Results Before PMC, MVA3D was slightly higher than MVA2D (1.15±0.25vs. 1.06±0.22 cm2, p=0.0001) but correlation between methods was excellent(r=0.73, p<0.0001), mean difference small (0.15±0.13 cm2) and clinically mean-ingless (3 patients misclassified, 2 of whom had borderline MS severity). AfterPMC, MVA3D did not differ from and correlated well with MVA2D (1.87±0.37vs. 1.85±0.32 cm2, p=0.36; r=0.76, p<0.0001; mean difference 0.18±0.17 cm2).MVA3D assessed by the less experienced operator (1.54±0.48 cm2) did notdiffer from MVA3D (1.52±0.44 cm2) and only slightly from MVA2D (1.44±0.47cm2) measured by experienced operators (p=0.66 and 0.05 respectively). Inter-observer variability was low and similar for experienced and less experiencedoperators. Compared to RT3DE, 2DE underestimated the degree of commissuralopening in 33% of patients (p<0.0001) and agreement between methods wasweak (kappa=0.41).Conclusion: RT3DE provides accurate MVA measurements similar to 2Dplanimetry performed by experienced operators. Thus, it does not provide a realadvantage for experienced operators whereas it seems particularly helpful for lessexperienced operators. In addition, RT3DE improves the description of valvularanatomy.
P5215 Mixomatous degeneration of mitral valves in humansis associated with herpes simples viral infection
L.B. Mitrofanova1, V.E. Karev1, P.G. Platonov2. 1Research Instituteof Cardiology, St.Petersburg, Russian Federation; 2Lund UniversityHospital, Department of Cardiology, Lund, Sweden
Background: the rolemixomatous degeration (MD) as a cause of valvular defectsin humans is increasingly appreciated. Abnormal function of myofibroblasts isbeleived to contribute to development of MD. Whether this is due to a primaryinherited defect in myofibroblast function or it is secondary to other conditionsthat affect their function is not clear. Aim of the present study was to evaluatepossible role of herpes simplex viral infection in the pathogenesis of MD.Material and Methods: seventeen mitral valve specimens with documented MDwere obtained from patients undergoing operation of mitral valve replacement andcompared with mitral valve samples obtained during autopsies of 10 age-matchedindividuals without structural heart disease. PCR for DNA of herpes simplex virus(HSV) and immunohistochemical analyses with DakoCytomation antibodies toHSV type 1 and type 2, proliferation marker Ki-67 and apoptosis marker Bcl-2were performed on all mitral valve samples.Results: 1) HSV-1 was identified in fibroblasts of all 17 MD vs. 2 of10 controlspecimens (p<0.01) and in endothelial cells of 15 of 17 MD vs 3 of 10 controls(p<0.01); 2) HSV-2 was identified in fibroblasts of 15 of 17 MD vs 3 of 10 controls(p<0.01) and in endothelial cells of 14 of 17 MD vs 4 of 10 control specimens(p<0.01); 3) PCR technique revealed HSV DNA only in one MD patient and in noone control subject; 4) Proliferation and apoptosis markers Ki-67 and Bcl-2 didnot show any difference between MD and control group neither in fibroblasts or inendothelial cells.Conclusion: presence ofHSV-1 and HSV-2 in fibroblasts and endothelium ap-peared to be a common finding in mixomatous degeneration of mitral valves inhumans. The HSV infection could therefore be considered as an important con-tributor to the dysfunction of myofibroblasts.
P5216 Left ventricular long axis contraction in patients withasymptomatic non-ischemic mitral valve regurgitationand normal systolic function
I. Paraskevaidis1, S. Kyrzopoulos1, D. Tsiapras2 , D. Farmakis1 ,E. Iliodromitis1, J. Parissis1, D. Kremastinos1. 1Attikon University
Hospital, Athens, Greece; 2Onassis Cardiac Sugery Center, Athens, Greece
Aim: To investigate the role of ventricular long axis contraction in patients withasymptomatic non-ischemic mitral regurgitation (ANIMR).Methods: Eighty-nine patients aged 59.9±13.5 yrs with ANIMR and normal rest-ing left ventricular (LV) ejection fraction (EF) were studied by resting echocardio-graphy, including tissue Doppler imaging at LV lateral wall, inter-ventricular sep-tum and right ventricular lateral wall. Exercise radionuclide cineangiography andcoronary angiography were also performed.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
Mitral valve disease 901
Results: 50/89 patients (56.2%) had a normal LVEF response to exercise (>5%increase). Differences in echocardiographic markers at LV lateral wall accordingto the LVEF response are shown in the Table. Indexes measured at right ventric-ular lateral wall did not differ in two groups. Maximal systolic wave velocity at LVlateral wall was the index that best predicted LVEF response to exercise; a cutoffvalue of 9.5 cm/sec predicted an impaired LVEF response with a specificity andsensitivity of 100%. A concordance of MR severity, as defined by vena contractawidth and by maximal systolic wave velocity, was observed in 69.2% of patients.
EF>5% (n=50) EF<5% (n=39) p value
L Ea (cm/sec) 10.4±3.5 10.7±4.1 NSL Aa (cm/sec) 9.1±2.7 8.3±2.6 NSL tissue systolic wave VTI (cm) 1.7±0.4 1.9±0.5 NSL tissue systolic wave slope (cm/sec2) 50.6±17.5 39.0±11.0 <0.001L tissue systolic wave velocity (cm/sec) 11.2±1.1 7.7±1.4 <0.001IVS Ea (cm/sec) 8.1±3.4 8.4±3.0 NSIVS Aa (cm/sec) 7.8±3.3 7.6±2.0 NSIVS tissue systolic wave VTI (cm) 1.8±0.8 1.7±0.6 NSIVS tissue systolic wave slope (cm/sec2) 46.2±9.0 30.5±13.9 <0.001IVS tissue systolic wave velocity (cm/sec) 8.7±1.3 6.6±1.6 <0.001E/L Ea 6.8±2.4 7.5±3.0 NS
EF= LVEF response to exercise, L= lateral mitral annulus, Ea= tissue Doppler early diastolicwave velocity, Aa= tissue Doppler late diastolic wave velocity, VTI= velocity time integral, IVS=interventricular septum, E= transmitral early diastolic wave velocity
Conclusion: LV long axis contraction at rest can unmask a subnormal LV func-tional status in patients with ANIMR and normal systolic function.
P5217 Beta adrenergic blockade and its effect on ET-1, BNP,inflammatory markers and ventricular remodeling inheart failure
J. Nessler1, B. Nessler1, M. Kitlinski2, M. Stepniewski3,M. Pasowicz4, R. Willenheimer4, W. Piwowarska1. 1Institute of
Cardiology, Department of Coronary Disease, Cracow, Poland; 2UniversityHospital, Department of Cardiology, Malmoe, Sweden; 3Institute of Pharmacy,Radioligand Laboratory, Cracow, Poland; 4John Paul II Memorial Hospital,Centre for Heart and Lung Diagnosis., Cracow, Poland
Aim: to evaluate the effect of beta adrenergic blockade on endothelin-1 (ET-1), brain natriuretic peptide (BNP), proinflammatory cytokines (TNF-alpha, IL-6),CRP in heart failure patients and to define their relationship with left ventricularfunction.Material: We studied 86 patients (81 men) aged 35 to 70 years (56.8±9.19) withheart failure (NYHA class II and III), LVEF below 40%, not receiving beta blockersbut ACEI, diuretics and/or digoxin for at least 3 months.Methods: Before and at 3 and 12 months after carvedilol we measured ET-1,BNP, TNF-alpha, IL-6 and CRP. Remodeling was assessed by echocardiographyin 86 patients and by MRI additionally in 19 patients.Results: Mean carvedilol dose during follow-up was 25.0±13.5 mg/24h. Therewas a positive correlation between HR at rest (HRs) and ET-1 (r=0.28; p=0.04),BNP(r=0.25; p=0.02) and CRP (r=0.30; p=0.03) and between BNP and LVEDd(r=0.23; p=0.04), and a negative correlation between BNP and LVEF (r=-0.23;p=0.03). Table nr 1 summarizes changes during treatment.
Table nr 1
Variable Baseline 0-12 months 0-3 months 3-12 monthsvalue change p % change of p % change of p
(%) total change total change
BNP (pg/ml) 464±214 -98,0(21) 0,001 14,0 NS 8,3 NSET-1 (pg/ml) 49,3±94 -18,6(47) 0,002 37,7 0,024 15,3 NSIL-6 (pg/ml) 9,4±8,5 -4,1 (43) 0,004 20,2 NS 29,3 NSTNF-α (pg/ml) 12,2±8,7 -6,9 (56) 0,001 12,3 NS 50,5 0,001CRP (mg/l) 14,5±14 -9,1 (63) 0,001 51,0 0,001 23,9 NSHRs (1/min) 87±18 -8,0(7,2) 0,0001 17,2 0,0001 0,0 NSLVEDd (mm) 68,8±7,4 -2,9(4,2) 0,002 3,5 0,014 1,0 NSLVEF % 28,7±6,2 +8,1 (20) 0,0001 15,8 0,0001 7,6 NSLVESVI 67,9±27 -4,8(18,6) 0,001 7,1 NS 12,4 0,002
Changes of the selected parameters during treatment.
Conclusions: 1. Decreased sympathetic tone significantly reduces the concen-trations of ET-1, TNF-alpha, IL-6, CRP and BNP. 2. 12-month treatment withcarvedilol leads to favorable left ventricular remodeling (reverse remodeling) andis significantly related with reduced levels of inflammatory cytokines.
P5218 Gender differences in the management and outcomeof patients hospitalized with heart failure
S. Gottlieb1, A. Shotan2, M. Moriel3, B.S. Lewis4, S. Behar5,J. Leor5, A. Caspi5, M. Garty6 on behalf of the Steering Committeeand Investigators of HFSIS 2003. 1Bikur Cholim Hospital, Heart
Institute, Jerusalem, Israel; 2Hillel Yaffe Hospital, Cardiology, Haderah, Israel;3Shaare Zedek Medical Center, Cardiology, Jerusalem, Israel; 4Lady DavisCarmel Medical Center, Cardiology, Haifa, Israel; 5Sheba Medical Center,Neufeld Cardiac Research Institute, Tel-Hashomer, Israel; 6Rabin MedicalCenter, Recanati Insitute, Petach Tikva, Israel
Background: Results of previous studies on the influence of gender on prognosisin heart failure (HF) have been conflicting and have been conducted in selectedpopulations. The aim of this study was to determine whether mortality risk inwomen and men hospitalized with HF is different.Methods: A prospective 2-month nationwide survey of consecutive HF pts ad-mitted to all 25 public hospitals in Israel in 2003, included 4102 pts; 1764 women(W) 43%, and 2338 men (M).Results: W were older than M (median age 77 vs 73 yrs), and more often haddiabetes (53 vs 48%), hypertension (81 vs 71%), anemia [Hb<12gr%] (61 vs39%), pre-hospital NYHA class III-IV (43 vs 36%) and Killip class III-IV on ad-mission (48% vs 38%), but less often had IHD (75 vs 88%), ACS (32 vs 40%)and renal failure [creatinine >1.5 gr%] (34 vs 46%). In-hospital use of IV diuretics(67 vs 56%) and blood transfusions (9 vs 6%) was more frequent in W than in M,whereas, the use of IV inotropics or IV vasodilators was comparable. At discharge,use of ACE-I/ARB (67 vs 68%), aldospirone (19 vs 21%), digoxin (14 vs 15%)was comparable in W and M, whereas, W received less often beta-blockers (55vs 59%), aspirin (62 vs 71%) and statins (34 vs 43%), but more often furosemide(79 vs 69%), thiazides (6 vs 4%) and calcium-channel blockers (31 vs 21%). In-hospital mortality was significantly higher in W than in M (6.2 vs 3.6%, p=0.0001,age-adj. OR=1.54[95% CI 1.14-2.07], covariate adj. OR=2.04[1.46-2.86]), while1-yr mortality rate among hospital survivors was comparable (25.4 vs 23.9%, age-adj. OR=0.92[0.79-1.07], covariate adj OR=1.00[0.85-1.18]). In both genders vari-ables associated with worse 1-yr outcome were: age, NYHA class III-IV, systolicBP<115 mmHg, anemia, renal failure and prior stroke. In M but not in W, COPDand ACS were also associated with increase 1-yr mortality, whereas, history ofhypertension was associated with a better outcome.Conclusion: In HFSIS 2003 national survey of hospitalized HF pts, in-hospitalmortality was 2-fold higher in W than in M, a difference that disappeared laterat 1-yr. Gender disparities in outcome most probably relate to W’s older age,differences in HF etiology and presentation.
P5219 Beneficial effects of thymulin in MCT-inducedpulmonary hypertension and its modulation of IL-6gene expression
T. Henriques-Coelho1, F.L.F. Carvalho1, S.M. Oliveira1, A. Brandao-Nogueira1 , M. Santos1, R. Roncon-Albuquerque1 , J. Correia-Pinto2,
A.F. Leite-Moreira1. 1Faculty of Medicine, University of Porto, PhysiologyDepartment, Porto, Portugal; 2Life and Health Sciences Research Institute,ICVS, Braga, Portugal
Inflammation has an important pathophysiologic role in Pulmonary Hypertension(PH). Indeed, inflammatory cells recruitment and activation, with the release ofcytokines (such as IL-6 and IL-1) and growth factors, may underlie the pulmonaryvasoconstrition and vascular remodeling that characterize PH. Thymulin, pro-duced by thymic epithelial cells, is a nonapeptide neuroendocrine hormone withimmunoregulatory actions, depressing C-C and CXC cytokines in the lung. In thisstudy, we evaluated thymulin effects in a model of monocrotaline (MCT)-inducedPH.Adult Wistar rats randomly received a subcutaneous injection of MCT (60 mg/kg)or an equal volume of vehicle. At D1, animals were randomly assigned to receivea subcutaneous injection of thymulin (10 ng/100g, qd for 3 wk) or saline. Threegroups were analyzed: normal rats injected with saline (Sham, n = 7), MCT rats in-jected with saline (MCT, n = 9) and MCT rats treated with thymulin (MCT+Thym, n= 9). At the end of the third week, right ventricular (RV) hemodynamic parameterswere measured: peak systolic RV pressure (RVPmax), peak rates of RV pressurerise (RV dP/dtmax) and RV end-diastolic filling pressures (RVEDP). Heart andlungs were weighted and samples were collected for real-time PCR analysis ofIL-6 mRNA levels.Results are summarized in the table below and expressed as means±SE.P<0.05: a vs Sham; b vs MCT.
Results
Sham MCT MCT+Thym
RV/LV, g/g 0.38±0.01 0.50±0.07 a 0.34±0.03 bLung/BW, g/kg 4.17±0.2 12.4±1.0 a 6.62±0.4 bIL6 lung, AU 1.0±0.32 17.4±3.8 a 3.8±1.3 bIL6 RV, AU 1.0±0.34 8.0±2.1 a 0.6±0.3 bRVPmax, mmHg 25±2 56±8 a 24±3 bdP/dtmax, mmHg/s 1231±108 1669±181 a 1191±90 bRVEDP, mmHg 1.6±0.3 2.6±1.2 a 0.7±0.4 b
Chronic thymulin administration, started simultaneously with the first inflammatorychanges induced by MCT, completely reversed PH, RV hypertrophy and attenu-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

902 Mitral valve disease
ated IL6 activation. Thymulin immunomodulatory potential may thus be exploredas a new therapeutic tool in PH management.
P5220 Altered cardiac glucose uptake incardiomyocyte-specific PPARgamma knockout mice
E. Caglayan1, M.C. Kreissl2, D.B. Stout2, F. Blaschke1,S. Rosenkranz3, R.K. Tangirala1 , H.R. Schelbert1, W.A. Hsueh1.1University of California, Endocrinology, Diabetes and Hypertension,
Los Angeles, United States of America; 2University of California Los Angeles,Pharmacology, Los Angeles, United States of America; 3University of Cologne,Internal Medicine III, Cologne, Germany
Diabetic cardiomyopathy is characterized as ventricular dysfunction of the dia-betic heart in the absence of coronary artery disease. The underlying morpho-logical and structural changes include cardiomyocyte hypertrophy and fibrosis.In the diabetic heart, cardiac energy metabolism is altered towards increasedfree fatty acid utilization and a decrease in insulin-mediated glucose uptake. Theligand-activated insulin sensitizer nuclear receptor PPARgamma is expressed incardiac myocytes and has been demonstrated to play a role in cardiomyocytehypertrophy. We have previously shown that cardimyocyte-specific PPARgammaknockout mice develop increased interstitial cardiac fibrosis and cardiac hyper-trophy upon infusion with pressor doses of angiotensin II. However, the functionalrole of cardiomyocyte PPARgamma regarding cardiac energy metabolism has notyet been determined. Using the Cre-lox P system we generated mice with a con-ditional cardiomyocyte specific deletion of PPARgamma (cardioPPARg-/-). Litter-mate control mice not expessing the cre-recombinase under the cardiomyocytespecific promoter MLC2v were used as controls throughout the study (WT). Non-fasted cardioPPARg-/- and WT mice (n=5/group) were imaged on 2 different daysusing small animal positron emisson tomography (microPET) technology with andwithout prior subcutaneous insulin (2 IU/kg*BW) injection. The cardiac uptakewas determined after a 45-min wait period in a Siemens microPET Focus220 anda single set of images reconstructed. Standardized uptake values (SUV) weredetermined using the average of 4 small regions in the myocardial wall, normal-ized for body weight and injected dose. Under conscious uptake, a significantdifference was measured between WT and cardioPPARg-/- mice (0.61%±0.08%vs 1.76%±0.29%; p<0.05). Insulin significantly increased cardiac FDG uptake inWT (p<0.01),but not in cardioPPARg-/- (1.82%±0.07% vs. 1.81%±0.13%).Therewas no alteration in insulin-mediated glucose uptake in skeletal muscle or liverand no difference in systemic glucose tolerance measured by oral glucose toler-ance testing (OGTT). In addition, cardioPPARg-/- showed an attenuated insulinresponse of the glucose transporter-4 (GLUT4) translocation to the plasma mem-brane, although total GLUT4 expression was not altered. These results suggestthat PPARgamma in the cardiac myocyte is an important mediator in mecha-nisms involving angiotensin II-induced cardiac hypertrophy and fibrosis as well asinsulin-mediated cardiac glucose uptake. Modulation of PPARgamma in diabeticcardiomyopathy may therefore provide new therapeutic benefit.
P5221 A prognostic risk index for long-term mortality inpatients with peripheral arterial disease
H.H.H. Feringa1, V.H. Van Waning1, J.J. Bax2, A. Elhendy3,E. Boersma1, O. Schouten1, M. Dunkelgrun1, D. Poldermans1.1Erasmus MC, Cardiology, Rotterdam, Netherlands; 2Leiden
Unversity Medical Center, Cardiology, Leiden, Netherlands; 3University ofNebraska, Internal Medicine, Section of Cardiology, Omaha, United States ofAmerica
Background: Prognostic information in patients with peripheral arterial disease(PAD) may provide the basis for optimal treatment strategies. In this study, a prog-nostic risk index for 10-year mortality was developed in a derivation cohort andvalidated in a comparable cohort.Methods and results: A total of 2642 patients with PAD were randomly dividedinto derivation (n=1332) and validation (n=1310) cohorts. During 10 years follow-up, all-cause mortality was recorded in 42.2% patients in the derivation cohortand 40.4% patients in the validation cohort. Multivariate hazard regression anal-ysis identified independent predictors of 10-year mortality and weighted pointswere assigned to each variable based on the beta-coefficient: renal failure (+12),heart failure (+7), ST-segment changes (+5), age >65 years (+5), hyperlipidemia(+5), ankle-brachial index <0.60 (+4), Q-waves (+3), diabetes (+3), stroke (+3).
Survival curves in different risk groups
Statins (-6), aspirin (-4), and β-blockers (-4) were independently associated with10-year mortality risk. These variables constituted the prognostic risk index witha discrimination of 0.70. Patients were stratified into four different risk categories:low (<0), low intermediate (0-5), high intermediate (6-9), high (>9). In the low, lowintermediate, high intermediate and high risk category in the derivation cohort, 10-year mortality rate was 22.1%, 32.2%, 45.8% and 70.4%, respectively (p<0.001).Using the prognostic risk index from the derivation cohort, similar mortality rateswere observed in the validation cohort.Conclusion: A prognostic risk index for 10-year mortality stratifies patients withperipheral arterial disease into different risk categories, which may be useful forpatient counselling and medical decision making.
P5222 Leptin levels in Chagas heart disease
F.F. Fernandes1 , F.J.A. Ramires2, B.M. Ianni2, S.A. Dantas2,P.C. Buck1, H.F. Lopes2, V.M.C. Salemi2, C. Mady2. 1Heart Institute,Sao Paulo, Brazil; 2Heart institute, Sao Paulo, Brazil
Purpose: In addition to its direct effects on energy metabolism andcaloric intake, leptin exerts several circulatory effects that appear to be mediatedby an interaction with the sympathetic nervous system and the major reflexogenicarea involved in cardiovascular homeostatic control. Chagas’disease results inautonomic nervous system damage and in a cardiac neuronal depopulation whichmay contribute to cardiac impairment.Objective: The aim of this study was to investigate the leptin plasma levels andtheir relation to different stages of Chagas heart disease.Methods: We studied 52 chagasic patients and 15 controls matched for age andbody mass index (BMI). All subjects underwent anthropometric, leptin and NT-proBNP levels measurements and were evaluated by echocardiography, 12-leadelectrocardiogram (ECG) and chest x-ray. Chagasic patients were divided in threegroups: group I (indetermined form, IF group) consisted of 24 subjects with nocardiac involvement as evaluated by chest x-rays, ECG and 2-dimensional echo-cardiography; group II (showing ECG abnormalities and normal left ventricularsystolic function, ECG group) consisted of 14 patients; group III consisted of 14patients with heart failure (HF group) and left ventricular dysfunction.Results from chagasic and control groups are showed in the Table bellow:
Results in chagasic patients and control
Group IF ECG HF Controls p value
Age(years) 48.4±10.8 42.9±8.1 47.8±9.1 43.9±5.9 0.39BMI (kg/m2) 24.7±2.7 23.2±3.1 24.0±2.0 24.6±2.2 0.34Leptin (ng/ml) 5.3±5.3 9.7±10.7 1.4±0.8* 8.1±7.8 <0.01NT-ProBNP(pg/ml) 53.2±33.3 83.3±57.4 831.8±800.1* 32.0±22.7 <0.01LVSD(cm) 31.7±5.9 31.4±3.5 52.4±10.9* 31.3±4.2 0.02LVEDV(ml) 116.1±40.8 114.1±25.6 273.4±137.2* 115.1±33.2 0.05LVESV(ml) 35.2±21.2 32.2±11.3 161.6±109.8* 33.1±12.2 0.006EF 0.71±0.07 0.71±0.05 0.44±0.12* 0.71±0.05 < 0.01
*Comparing to controls. LVSD, left ventricular systolic dimension; LVEDV, left ventricular end-diastolic volume; LVESV, left ventricular end-systolic volume; EF, ejection fraction
Conclusion: We conclude that leptin metabolism is involved on advanced stageof heart failure and can be used as a marker to determinate severity of the cardiacdysfunction in patients with Chagas’disease.
P5223 Non-linear indexes applied to detect cardiovascularautonomic neuropathy and follow-up of diabeticpatients
O.P. Pacheco1, C. Egoavil1, A.F. Pacheco2, D.A. Hofelmann2,R.H. Heinisch2. 1Universidade Federal de Santa Catarina,
Florianopolis, Brazil; 2UNISUL Universidade do Sul de Santa Catarina, Curso deMedicina, Tubarao, Brazil
Objectives: Determining two non-linear indexes of time series generated by HRV,to identify the presence of cardiovascular autonomous neuropathy (CAN) and toassess the prognostic influence of CAN on mortality in diabetes.Methods: Electrocardiographic records were processed applying digital signalprocessing techniques. Once calculated the RR intervals of the electrocardio-grams, the largest exponent of Lyapunov (LE) and Pearson’s coefficient (PC) oftime series provided by HRV were calculated. Subjects were gathered in twogroups clinically defined: i) patients with diabetes mellitus with CAN (DCAN)(n=37); ii) patients with diabetes mellitus without CAN (DWOCAN) (n =15) All sub-jects selected passed by tests proposed by Ewing et al. (1985) that let classify DMsubjects by CAN stage. There were 22% in the definitive stage. Kaplan-Meier es-timates were used to describe the follow-up experience. To compare differencesbetween groups log-rank test was applied.Results: Patients’ characteristics: mean age 60.9 ± 10.1 years and 70.6% males.Application of the nonlinear indicators of the CAN. The largest exponent of Lya-punov resulted in a correct rate of 76.8%, sensibility 80.5% and specificity of70%, that could be applied as CAN detector and Pearson’s coefficient, that couldbe applied to classify CAN severity, resulted in a correct rate of 96.4%, sensibility97.2% and specificity of 95%. The mortality rate was 11.5% in 3 years (Figure1). The relative risk of death related to definitive CAN was 1.79 (95% CI: 1.04 to3.07; p<0.01).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Mitral valve disease / Echocardiography: miscellaneous 903
Survival probability and CAN
Conclusion: Nonlinear analysis application in HRV signals can generate indexesthat could detect and discriminate CAN in patients with DM. Diabetic patientswith definitive CAN had higher risk of death than those without cardiovascularautonomic neuropathy.
ECHOCARDIOGRAPHY: MISCELLANEOUS
P5224 The ultrasound stethoscope: experience of dailycardiologist’s practice
V. Vysniauskas, R. Alminiene. Marijampole Central Hospital,Marijampole, Lithuania
Limited or/and focussed echocardiography(L/F Echo) performed to-gether with echocardiography of other organs have been applied since1987 in ourcardiologist’s consultations. The aim of the study is to evaluate the advantages ofthe above mentioned consultations.Methods About 50000 patients (pts) have been consulted from 1987 to 2005year. L or/and F Echo have been performed after interviews with pts and thenphysical examination(inspection, palpation, auscultation). Morphological data instandard cardiac views, basic linear measurements of structures and cavities andDoppler blood flow imaging have been obtained. In case of cardiac derangementsstandard full Echo with quantitative Doppler function has been performed. In caseof clinical indication limited Echo of liver, kidney, pancreas, spleen, thyroid, carotidarteries, law extremities veins, abdominal aorta has been performed as well.Results: This methodology allowed rapid diagnosis of followed cardiacdisorders: shunts(195 pts,0.39%), cavity dilation(15000 pts,30%),valvularheart diseases(4700pts,9.4%),LV hypertrophy(33500pts,67%),pericardial effu-sion(107pts,0,24%), emergency cardiac tamponade(11pts,0,02%),wall motionabnormalities(9000pts,18%). Cardiac abnormalities have been excluded with ahigh degree of certainty in 25% of the cases. The agreement between stan-dard Echo and goal-oriented Echo was 96%(kappa value 0,941). The ultrasoundstethoscope screening allowed to rapidly identify unexpected non cardiac disor-ders: 460(0,92%) cases of liver diseases, 29(0,06%) cases of aortic abdominalaneurism, 185(0,37%) cases of kidney diseases, 43(0,09%)cases of pancreasdiseases, 35(0,07%)cases of spleen enlargement, 290(0,58%) cases of thyroiddiseases,164(0.32%) cases of deep veins thrombosis. All pts with visualized ab-normalities of these internal organs have been sent to the appropriate specialist(agreement 93%, kappa value 0.870).Conclusions: 1. A limited goal-oriented echocardiographic examination is un-doubtedly valuable to identify or exclude the cardiac diagnoses-60% of consul-tant pts need standard Echo protocol. 2.Echo/Doppler examination revealed thelimitations of the physical examinations in many clinical situations, particularly inthe early stages of the disease. 3.The ultrasound stethoscope helped to identifythe incidental non cardiac disorders in 2.5% cases. 4.It is highly prestigious touse echostethoscope in daily cardiologist’s consultations. 5.The disadvantagesof the mentioned consultations are as follows: prolonged time, limited imagingperformance and reimbursement issues.
P5225 Can portable echocardiography in the cath labreplace left ventricular angiography?
O.A. Breithardt, G. Teerling, D. Haghi, T. Sueselbeck, J.J. Kaden,M. Borggrefe. University Hospital, I. Medizinische Klinik, Mannheim,Germany
Left ventricular (LV) angiography (ANGIO) is standard practice during diagnosticcardiac catheterization (CATH) for the assessment of global LV function, regionalwall motion abnormalities, mitral regurgitation, aortic stenosis and diastolic func-tion by end-diastolic pressure (LVEDP). This information can also be obtainednon-invasively by echocardiography with 2D imaging, Doppler echocardiographyand tissue Doppler imaging (for estimation of LVEDP).Methods: We examined 80 consecutive patients (mean age65±12 years) imme-diately before CATH (incl. PTCA) with the patients lying in a full supine positionon the catheterization table. A brief echo exam was performed with a portableecho scanner (VIVIDi, GE Vingmed, Horten, Norway) to obtain the following views
(each 3 beats, digital storage): apical 4- and 2-chamber views, colour Doppler ofmitral and aortic valve, mitral inflow by pulsed-wave Doppler, aortic outflow bycontinuous-wave Doppler, pulsed-wave tissue Doppler of septal and lateral mitralannulus. ANGIO was performed immediately after the echo exam. Time require-ments (Echo: start to end of echo exam; ANGIO: insertion of pigtail catheter toinsertion of coronary catheter) and the feasibility for each exam were compared.Results: Complete diagnostic information was available in 100% of patients byANGIO within 3:54±1:35 minutes (range 1:45 to 11:50) with the use of 60.3±17ml(36 to72ml) contrast media and a x-ray Dose-area product of 2.88±1.9 (2 to 63.2)Gy cm2 on average. Complete echocardiographic recordings of diagnostic valuefor all parameters were available in 65 of 80 patients (81%) within 2:43±0:43minutes (1:32 to 4:51) on average.Conclusions: Portable echocardiography within the cathetzerization laboratoryis feasible in the majority of patients. Image acquisition is less time consuming forecho than for conventional LV angiography. The use of disposable material (pigtailcath, angio contrast syringe) and the amount of contrast media and x-ray expo-sure for the patient can be reduced significantly, thereby increasing the safety andcost-effectiveness of the invasive procedure. New portable digital echo scannerscan be easily integrated in existing laboratories in order to improve patient safetyand reduce costs in the long-term
P5226 Visualization of coronary arteries and stents usingfragment reconstructed transesophagealechocardiography
P. Wild1, A. Abushi2, R.J. Zotz2. 1Johannes-Gutenberg-University,Int. Medicine II, Mainz, Germany; 2Klinikum Herford, Cardiology,
Herford, Germany
Background: A method has been developed for non-invasive visualization ofcoronary arteries using reconstruction and compilation of coronary fragments bya rationally performed steering of a transesophageal echocardiographic trans-ducer (FRC-TEE).Methods and Results: We studied 50 patients (33 men, 17 women) with FRC-TEE being admitted for coronary angiography. For fragment reconstruction thenewly developed software USIP was used. FRC-TEE and angiography findingswere compared visually and by quantitative measurements. All transesophagealstudies were performed without any complications and provided valuable results.In total 171 vessels (right coronary artery 42, left main coronary artery 49, left cir-cumflex artery 49, left anterior descending artery 28, ramus intermedius 3) wereexamined by FRC-TEE. The total lengths visualized were [95% confidence inter-val]: 9,6±1,8 cm [9,1;10,2] for right coronary artery, 7,1±1,2 cm [6,7;7,4] for leftcircumflex artery, 3,9±1,2 cm [3,4;4,4] for left anterior descending artery, 4,9±1,3cm [3,5;6,3] for ramus intermedius and 1,5±0,8 cm [1,3;1,7] for left main coronaryartery. There was a high concordance between coronary angiography and FRC-TEE. 63 stenoses were detected by FRC-TEE. The mean stenosis degree was51,6±18,7% using FRC-TEE and 51,3±19,5% using angiography. The mean dif-ference in stenosis degree was 0,2±5,1%. In 19 segments stents could be visu-alized. A limitation of the method is the detection of distal stenosis of the coronaryarteries. Thus 14 stenoses, predominantly in the left anterior descending artery(n=11) and 2 stents (left anterior descending artery) could not be examined byFRC-TEE.We furthermore analyzed 37 patients (27 men, 10 women, aged 64,3 ± 12,0years, with coronary stents. A FRC-TEE was performed 6,4 ± 5,5 days afterstent implantation as a reference and repeated 156,6 ± 40,4 days after stentimplantation as a follow-up. In 6 patients a restenosis was detected using FRC-TEE at follow-up and they were treated with a drug-eluting stent.Conclusions: In this study the findings of FRC-TEE show good agreement tothose of angiography concerning stenosis localization, stenosis degree and stentstatus. The method allows an additional demonstration of the vessel wall and ves-sel occlusions. With improvement in visualization of the LAD and distal parts ofcoronary vessels, with further automation, the method might gain further impor-tance.
P5227 Cardiac output estimation by transesophagealDoppler monitoring versus thermodilution in theintensive coronary care unit
A. Mehta, R. Passey, J.P.S. Sawhney, R.R. Mantri, B. Kandpal,R. Jain, S. Dhawan, A. Mohanty. Sir Ganga Ram Hospital,
Department of Cardiology, New Delhi, India
The measurement of cardiac output using the thermodilution technique is as-sociated with considerable morbidity in critically ill patients. The present studywas conducted to assess the validity of cardiac output measurement usingtransesophageal Doppler. A total of 23 patients with severe left ventricular (LV)dysfunction, who underwent off-pump coronary artery bypass grafting (CABG),were enrolled from the cardiac ICU over a period of 6 months. The study in-cluded patients who were already mechanically ventilated, sedated and moni-tored with a pulmonary artery catheter. Simultaneous measurements of cardiacoutput were obtained by thermodilution using a pulmonary artery catheter andtransesophageal Doppler. A good correlation was found between the cardiac out-put thermodilution technique (COTD) and cardiac output transesophageal Doppler(COTED) (r=0.95), with a small systematic underestimation (bias: 0.24 L/min) us-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

904 Echocardiography: miscellaneous
ing transesophageal Doppler. The limits of agreement between COTD and COTED
were +2 L/min and -1.5 L/min. Variations in cardiac output between the two con-servative measures using either transesophageal Doppler or the thermodilutiontechnique were similar in direction and magnitude (bias:0 L/min; limits of agreee-ment: ±1.7 L/min). These results confirm that transesophageal Doppler can pro-vide a non-invasive, clinically useful estimate of cardiac output and detect hemo-dynamic changes in critically ill patients.
P5228 Transcranial Doppler ultrasonography versustransesophageal echocardiography in PFO diagnosis
G.P. Ussia, S. Mangiafico, A. Privitera, R. Calaciura, M. Mule’,E. Caruso, C. Tamburino. Ferrarotto Hospital, Cardiology Institute,Catania, Italy
Background: Patent foramen ovale is frequently associated with embolic cere-brovascular accidents, mainly in young adults patients. A Patent Foramen Ovale(PFO) is present in 25% of population, but its occurrence is higher in patientswith prior cryptogenic stroke. The reference standard for identifying a PFO andfor follow-up those patients submitted to percutaneous transcatheter closure iscontrast-enhanced transesophageal echocardiography, a semi-invasive methodnot readly available in all units.The contrast-enhanced transcranial doppler ultrasonography (TCD), a non inva-sive method, has been recently proposed as an alternative technique to detectthe passage of a contrast material injected into a peripheral vein to the cerebralcirculation during the valsalva manouver.We sought to evaluate the feasibility of the transcranial Doppler and its diagnosticsensitivity compared to transesophageal echocardiography.Materials and Methods: A total of 78 patients (42 females, 35 males, mean age38), referred to our Institute with diagnosis of migraine with aura, prior crypto-genic embolic cerebrovascular accidents, scotoma and syncope. All patients un-derwent, in the same day, to TCD and TEE evaluation, both performed by twoindependent operators.The TCD and TEE tests were performed according to a standardized procedure:In brief,10 mL of air-mixed saline was injected into the right antecubitalvein inthree different times, while the Doppler signal was recorded during Valsalva ma-neuverDuring TCD the contrast passage into the right-middle cerebral artery wasrecorded 25 seconds after valsalva manouver.Results: We detected a right-to-left shunt in 40 patients (51%) and no-shunts in32 patients (41%) with both TCD and TEE. In three patients TEE evaluation didn’tshow a contrast passage that we after detected with TCD. In three patients onlythe TEE revealed a PFO. The feasibility of both method was 100%.Conclusions: TCD is a feasible method and has an equal sensitivity comparedto TEE in PFO diagnosis. TCD, in our experience, had a sensitivity of 93% andthe specifity of 91%.These methods are complementary for PFO diagnosis anddefinition, but for us TCD is an ideal tool for screening and follow-up purposesbecause of its low cost, and high feasibility.
P5229 Percutaneous closure of patent foramen ovale indivers: incidence of decompression illness at 1- and3-year follow-up
R. Zbinden1, M. Billinger2, L. Remonda1, M. Schwerzmann1,R. Vogel1, S. Windecker1, B. Meier1, C. Seiler1. 1Ealing, United
Kingdom; 2Bern, Switzerland
Background: Patent foramen ovale (PFO) is related to an increased risk of de-compression illness (DCI) in SCUBA divers. It is unknown whether closure of PFOreduces the incidence of major and/or minor DCI.Methods: 104 divers were included in the study (mean age 39±7 years; 84men), 65 with a PFO on transesophageal contrast echocardiography, 39 controls.PFO was occluded percutanously using an Amplatzer-PFO-Occluder in 26 divers(PFO-occlusion group). All divers completed a questionnaire to assess a minorDCI-score (e.g. headache, paresthesia, joint-pain etc), and major DCI (treatmentin decompression chamber) at inclusion, at 1-year and at 3-year follow-up.Results: Mean total follow-up time was 2.7±0.3 years and there were 13831dives in total. There were no significant differences in baseline characteristics(age, gender, mean number of dives, mean diving depth, number of dives be-yond 40 meters) between the three groups. There were no procedure relatedcomplications. Minor DCI-score at 1-year follow-up differed significantly betweenthe PFO-occlusion group and the PFO group (PFO-occlusion group: 1.1±1.2 mi-nor DCI-score, PFO group: 2.4±2.0 minor DCI-score; p=0.006). The differencebetween the control-group and the PFO group, and between the control-groupand the PFO-occlusion group was not significant. The difference in minor DCI-score was no longer significant after 3-years of follow-up (PFO-occlusion group:1.3±1.6 minor DCI-score, PFO group: 2.0±1.8 minor DCI-score, control-group:1.7±1.7 minor DCI-score; p=NS). 3 major DCI were reported during the 3-yearfollow-up period: 2 in the PFO group, 1 in the control group and none in the PFO-occlusion group (p=0.43 ANOVA overall).Conclusion: PFO occlusion reduces minor DCI in SCUBA divers after 1-year offollow-up. However, after 3 years of follow-up, the difference in minor DCI is nolonger significant. Major DCI requiring treatment in a decompression chambertend to be reduced with PFO occlusion.
P5230 Detection of baffle leaks by echocardiography inadults after Mustard repair for transposition of thegreat arteries
M. Schwerzmann1, O. Salehian2, C.K. Silversides2, J.M. Colman2,G. Webb3, S.C. Siu3. 1Swiss Cardiovascular Center Bern,
Cardiology Dept., Bern, Switzerland; 2TCCCA, Toronto, Canada; 3AdultCongenital Heart Disease Program, Philadelphia, United States of America
Introduction: Baffle-related complications following atrial switch procedures forcomplete transposition of great arteries (d-TGA) are common. Atrial baffle leakscan be found in as many as 10% of patients and may warrant re-intervention.Due to the complexity of atrial anatomy following Mustard repair, baffle leaks caneasily be missed on transthoracic echocardiography. The purpose of this studywas to determine if the dimensions of the subpulmonary left ventricle (LV) couldhelp to identify patients with baffle leaks.Methods: We studied the echocardiographic data of 45 adult patients late afterMustard repair for d-TGA. Seven patients had a significant left-to-right shunt (con-firmed by cardiac catheterization [n=4], by magnetic resonance imaging [n=2], orduring surgery [n=1]), 8 patients had predominant LV outflow tract obstruction(LVOTO), and 30 randomly selected patients were reported to have none of thesecomplications ("controls"). Assuming that a significant left-to-right shunt causesa volume overload of the subpulmonic LV, we assessed LV dimensions in Mus-tard patients with and without known baffle leaks. LV and right ventricular (RV)dimensions were measured in standard echo imaging planes (parasternal longaxis view [PLAX], parasternal short axis view [PSAX], four chamber view [4CV])and compared among the three groups.Results: The mean LV to PA gradient in the 8 patients with LVOTO was 65 ±27 mmHg. Biventricular echocardiographic dimensions are shown in table 1. Fiveof 7 patients with a baffle leak had a 4CV LV:RV>1. Two controls had PLAXLV:RV>1, 4 controls had SAX LV:RV>1, but none of the controls had a 4CVLV:RV>1.
Table 1
BSA PLAX LV:RV PSAX LV:RV 4CV LV:RV
Controls 1.85 m2 0.84 ±0.21 0.81 ±0.27 0.67 ±0.15Baffle leak 1.90 m2 1.13 ±0.18 1.10 ±0.25 0.96 ±0.24*LVOTO 1.91 m2 1.20 ±0.45* 1.14 ±0.45* 0.91 ±0.34*P-value 0.722 0.003 0.008 0.001
BSA: body surface area; LV:RV: ratio of end-diastolic LV to RV diameter. * denotes p<0.05 whencompared to controls.
Conclusions: In adult patients after Mustard repair, a LV:RV ratio >1 in the apical4CV indicates significant pressure or volume overload of the subpulmonic LV. Inpatients with this finding without significant LVOTO, a thorough assessment for anatrial baffle leak should be performed.
P5231 Real-time three-dimensional echocardiographyprovides novel and useful anatomic insights ofperimembranous ventricular septal aneurysm
J.R. Wu1, J.H. Hsu2, M.H. Lee1, Z.K. Dai1. 1Kaohsiung MedicalUniversity Hospital, Pediatrics, Kaohsiung, Taiwan; 2Kaohsiung
Medical University Hospital, Pediatrics, Kaohsiung, Taiwan
Background: R eal-time three-dimensional echocardiography (RT3DE) is a newimage modality, and it can display a unique image reconstruction in a varietyof heart diseases. However, clinical assess ment of ventricular septal aneurysm(VSA) by RT3DE has not been reported. This pilot prospective study is to surveywhat kinds of new insights of VSA can be provided by RT3DE as compared withconventional 2-dimensional echocardiography (2DE).Methods: We investigated the diagnostic value of RT3DE and 2DE in 60 con-secutive patients with VSA. From different transthoracic windows, structures ofinterest can be displayed from any orientation through adjusting cropping andslicing the RT3DE datasets. The results were compared with those in 2DE.Results: RT3DE reconstruction of VSA was feasible in 56 of 60 patients (93%).When compared with 2DE, additional information provided by RT3DE includedblood flow through left ventricle to right ventricle, visualization of VSD en-faceborder in 56 patients (93%), morphology of the VSA from apical short axis viewin 48 patients (86%), hypertrophied margin of the interventricular septum in 26patients (43%), dynamic changes of VSA and tricuspid valve in 18 patients (30%),adhesion of chordae tendineae in VSA in 16 patients (26%).Conclusions: Structures of interest can be evaluated from unique RT3DE in anyorientation during scanning. RT3DE offers additional novel views and has theadvantages of not only displaying better visualization of VSA, but also adequatelyshowing the spatial relationship with its adjacent structures. It can provide noveland useful anatomic insights than 2DE while assessing patients with VSA.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Echocardiography: miscellaneous 905
P5232 Mitral and tissue Doppler diastolic parameters areincremental for risk stratification of patients with leftventricular dysfunction with or without significantNT-proBNP elevation
F.L. Dini, U. Conti, D. Andreini, S. Banti, P. Fontanive, R. Arena,S.M. De Tommasi. Cardiovascular Diseases Unit 2, Santa Chiara Hospital, Pisa,Italy
Background: It is well known that symptomatic and asymptomatic left ventric-ular (LV) dysfunction is associated with increased circulating concentrations ofnatriuretic peptide hormones. The amino-terminal fragment of the proBNP (NT-proBNP) has proved to be a good marker of prognosis in both patients with overtheart failure (HF) or asymptomatic LV dysfunction.Aim: To investigate whether LV diastolic parameters are useful to improve riskassessment of patients with symptomatic or asymptomatic LV dysfunction cate-gorized according to NT-proBNP levels.Methods: Echocardiograms were obtained in 325 patients with LV systolic dys-function (ejection fraction <45%). They were judged symptomatic if the had anHF score >/=2 (n=98). Pulsed-Doppler mitral wave velocities, E wave decelera-tion time (EDT) and tissue Doppler (TD) diastolic annular velocities were mea-sured. The primary end-point was cardiac death, the secondary end-point wascardiac death or hospitalization for worsening HF. Survival and event-free sur-vival analyses were performed by univariate and multivariate Cox models and theKaplan-Meier method. Median follow-up duration was 21 months.Results: The median NT-proBNP was 3553 pg/ml in symptomatic and 921 pg/mlin asymptomatic patients. At 24 months, survival was 80% in patients with HF,86% in asymptomatic patients with NT-proBNP >921 pg/ml and 98% in thosewith a lower NT-proBNP (Log-rank statistics =0,002). Survival free from cardiacdeath or HF hospitalization was 60% in symptomatic, 70% and 93% in asymp-tomatic patients with and without elevated NT-proBNP levels, respectively (Log-rank statistics <0.0001). In a stepwise model of event-free survival, the additionof EDT <140 msec and early septal annular velocity (Ea) <8 cm/sec significantlyimproved the chi-square either in symptomatic (from 23.5 to 27.5) or in asymp-tomatic with lower NT-proBNP levels (from 23.3 to 25.9). An Ea <8 cm/sec wasthe only diastolic variable that significantly improved the chi-square over demo-graphic, clinical and conventional echocardiographic parameters in asymptomaticpatients with NT-proBNP >921 pg/ml (from 24.1 to 25.3).Conclusion: Patients with persistent HF and those asymptomatic but with ele-vated NT-proBNP plasma levels were at higher risk for adverse events as com-pared with those with lower NT-proBNP levels. An EDT <140 msec and a TD Eavelocity <8 cm/sec had incremental predictive power over clinical and conven-tional echocardiographic parameters.
P5233 Determinants of brain natriuretic peptide levels at restand at exercise in patients with systolic heart failure
P. Lancellotti1, M. Lempereur2 , C. Brogneaux2 , B. Cosyns3,D. Karsera4, G. Tumminello3, P. Melon3, L. Pierard3. 1CHU SartTilman, Service de Cardiologie, Batiment B 35, Liege, Belgium;
2University Hospital, Cardiology, Liege, Belgium; 3CHIREC, Cardiology, BraineAlleud, Belgium; 4University Hospital, Cardiology, Liege, Belgium
Background - Plasma brain natriuretic peptide (BNP) is an emerging diagnosticand prognostic biomarker in heart failure (HF). In these patients, dynamic mitralregurgitation (MR) contributes to exercise intolerance and conveys a poor prog-nosis. Whether exercise-induced increases in MR severity might be a trigger ofBNP release has never been investigated. This study sought to examine the effectof exercise on levels of BNP and to assess the determinants of exercise-inducedchanges in plasma BNP in patients with systolic HF.Methods - Forty-six consecutive patients with systolic left ventricular (LV) dys-function and functional MR underwent quantitative analysis of BNP, MR, systolicand diastolic (early diastolic transmitral (E) and annular (Ea) velocities) LV func-tion and LV dyssynchrony at rest and during exercise. None of them had inducibleischemia on perfusion imaging.Results: With stepwise multiple regression analysis, the LV end-systolic volume(p=0.0001), the E/Ea ratio (p=0.007) and the severity of MR (p=0.019) emergedas independent determinants of BNP. During test, BNP increased in 39 patients.The maximal increment occurred at peak exercise in 30 patients. In multivariateanalysis, a larger increase in systolic dyssynchrony index (p=0.013) and in effec-tive regurgitant orifice (p=0.037) during exercise and higher end-diastolic volumeat peak test (p=0.048) emerged as independent determinants of exercise-inducedchanges in BNP.Conclusions: MR severity, volume overload and LV filling pressure are surrogateof BNP under resting conditions. During exercise, changes in BNP reflect thepresence of dynamic changes in both MR severity and LV dyssynchrony in theabsence of inducible ischemia.
P5234 Increased inflammatory and coagulant activity inpatients with spontaneous echocardiographiccontrast in the thoracic aorta
C. Aggeli, G. Giannopoulos, E. Economou, G. Roussakis,E. Christoforatou, C. Kokkinakis, J. Barbetseas, C. Stefanadis. 1st
Cardiology Dept., Athens Medical School, Hippokration Hospital, Athens, Greece
Background: Spontaneous echocardiographic contrast (SEC) is a phenomenonof discrete smoke-like reflections appearing in the blood inside the cardiac cham-bers or vessels, without previous injection of echocontrast medium.Aim: The purpose of this study was to evaluate the level of inflammatory andcoagulation activation in patients with incidentally observed SEC in the thoracicaorta (AoSEC) on transesophageal echocardiography (TEE).Methods: We studied 299 consecutive patients (age 61 ± 13) without aorticaneurysm or dissection and without rheumatic or inflammatory disease, who un-derwent TEE in our laboratory. AoSEC was observed in 35 patients (11.7%).We measured C-reactive protein, serum amyloid A, factor VII, fibrinogen and fi-bronectin levels in these patients, as well as in a control group of subjects withoutAoSEC, matched for age, gender, smoking habit, presence of atrial fibrillation andcoronary heart disease, selected among the rest of the patients who underwentTEE.Results: Patients with AoSEC exhibited significantly higher levels of C-reactiveprotein (30.25 mg/l vs. 4.48 mg/l, p=0.029) and serum amyloid A (36.96 μg/mlvs. 8.66μg/ml, p<0.001) [see Figure], as well as increased fibrinogen levels (438mg/dl vs. 320 mg/dl, p=0.039). Factor VII and fibronectin levels also tended to behigher in patients with AoSEC without achieving statistical significance.
Conclusion: These findings strongly associate AoSEC with enhanced inflamma-tory activity, a finding reported for the first time, as well as increased fibrinogenlevels. Both are established predictors of adverse cardiovascular events. We con-clude that AoSEC, when observed on TEE, is a finding which should prompt acomprehensive cardiovascular risk evaluation of the patient, leading to appropri-ate risk factor modifications.
P5235 Onset of myocardial and blood flow motion duringisovolumic relaxation
P. Lindqvist1, S. Morner2 , K. Karp1, A. Waldenstrom1. 1PublicHealth And Medicine, Clinical Medicine, Umea, Sweden; 2NorrlandUniversity Hospital, Cardiology, Umea, Sweden
Background: Isovolumic relaxation (IVR) is a phase in the cardiac cycle con-sidered to be constant in volume. Colour m-mode propagation (cP) and tissueDoppler imaging (TDI) are two methods useful in the evaluation of blood flow andmyocardial motion. cP depicts blood flow and TDI depicts cardiac wall motion.This study was performed to assess if the left ventricle (LV) alters shape duringthe IVR period.Methods: Forty-seven healthy subjects (42-78 years, mean age 61±11 years, 25males) were studied. cP was measured at the mitral valve inflow tract and used todetermine the onset of blood flow during IVR. We measured the time from R-wavein ECG to the onset of cP (R-cP) of the first colour signal after the second heartsound but before mitral valve opening. Myocardial IVR was measured by TDI atthe basal septal segment in the apical four chamber view. The time interval fromelectrical activation (R-wave in EGC) to onset of myocardial motion from TDI [IVRnegative (R-IVRn and IVR positive (R-IVRp)] was measured, see figure.Results: The R-cP time interval (405±47ms) was significantly longer comparedwith R-IVRn (341±23 ms) and also compared to R-IVRp (374±27 ms, p< 0.001for both).Conclusion: Wall motion during myocardial isovolumic relaxation precedes theblood motion within the chamber during the isovolumic relaxation period. We pro-pose that during IVR (aortic and mitral valves closed) the LV alters shape resultingin internal ventricular blood motion towards the apex. This phenomenon indicatesthat the cavity takes a more spherical form just before LV filling. This conforma-tional change of the left ventricular chamber may be a prerequisite for a better"suction effect".
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

906 Echocardiography: miscellaneous / Acute myocardial infarction: metabolism and anaemia
P5236 Tissue Doppler Imaging and ContrastEchocardiography: new methods in diagnosingintracardiac masses
M.B. Hlawaty, W.T. Tracz, M. Olszowska, M. Kostkiewicz,M. Pasowicz, P. Podolec. Institute of Cardiology, John Paul IIHospita, Dept. of Cardiac and Vascular Diseases, Krakow, Poland
Background: Standard echocardiography is currently used to assess patients(pts) with intracardiac masses. However, there are pts for whom 2D gray-scaleecho features are not clear. The precise morphologic characteristic of intracar-diac tumors has important implications for further treatment. The aim of the studywas to assess the role of Tissue Doppler Imaging (TDI) and Contrast Echocar-diography (CE) in identifying intracardiac masses.Methods and results: Echocardiographic study (TTE, TEE) with TDI was per-formed in 85 pts: 20 pts with aortic and 14 with mitral valve diseases, 18 withatrial myxoma, 5 after pulmonic emboli, 3 with angiosarcoma and 25 pts after my-ocardial infarction. In difficult echocardiograms CE (Optison) was used to improvedetection on endocardial border, clots or tumors and reduce artifacts. Comparingthe motion of intracardiac masses with the surrounding tissue three types of mo-tion were differentiated related to direction, velocity and phase: A-concordant mo-tion with no difference in direction, velocity and phase; B-coherent motion with aphase difference depending on motion of the surrounding tissue but out of phase;C- incoherent motion due to free oscillation. Concordant motion was found inrigidly fixed left ventricular clot (n-15), small left atrial myxoma (n-3) and angiosar-coma (n-3). Coherent motion was present in pts with mural left atrial clot (n-10)and large myxoma (n-15). Incoherent motion was noted in valvular vegetation (n-24) and in right heart clot (n-5). Out of 85 pts 18 (21%) had one or more embolicevents. The incidents of embolism were compared with the echocardiographiccharacteristics (localization, size and mobility) of the vegetations, clots and tu-mors. In 10 pts with dense spontaneous echo contrast and artifacts CE excludedclots in the left ventricular aneurysm.Conclusions: TDI improves the detection of intracardiac masses and allows cor-rect definition of their morphology and motion. The morphologic characteristicsof vegetations and tumors or clots is helpful in predicting embolic events andsuggests urgent operation. CE is a useful additional diagnostic tool in evaluatingcardiac tumors and clots as it markedly improves their visualization and reducesartifacts.
P5237 Furosemide comet-stress test for differentialdiagnosis of cardiogenic versus pneumogenicdyspnoea
L. Gargani1, F. Frassi1 , M. Agrusta2, G. Soldati3, E. Poggianti3,S. Gligorova1, G. Mottola1, E. Picano3. 1CNR, Institute ofClinical Physiology, Pisa, Italy; 2Cardiology Clinic "Montevergine",
Mercogliano, Italy; 3Castelnuovo Garf.na Hospital, Lucca, Italy
Background: Ultrasound Lung Comets (ULCs) are a simple echographic signof extra-vascular lung water originating from water-thickened interlobular septa.ULCs can also have a pneumogenic origin due to fibrotic septa in presence ofchronic lung pathology. Aim: To assess whether an acute furosemide challengecan differentiate cardiogenic from pneumogenic ULCs.Methods: We considered 77 consecutive patients (15 females, age= 69±9 yrs)admitted to our Cardio-Pulmonary Department with acute dyspnoea and ULCs.ULC score has been obtained with an echocardiographic scanner by summingthe number of comets in each of the scanning spaces in the anterior right and lefthemithorax from second to fifth intercostal space. ULCs have been assessed atentry and 7 hours (range 4-13) after clinically-driven therapy with i.v. furosemide(40-120 mg). Final etiologic diagnosis of dyspnoea (pneumogenic or cardiogenic)was established by the "standard of truth" of a multidisciplinary expert panelblinded to ULCs findings and with access to clinical, cardiac imaging and labora-tory data. Results: Dyspnoea was cardiogenic in 66 (Group 1) and pneumogenicin 11 (Group 2) patients. ULCs number was similar at baseline (Group 1=29±18vs Group 2=34±23, p=ns). NT-proBNP was more frequently abnormal (>500pg/mL) in patients of Group 1 (Group 1=94% vs Group 2=27%, p<.01). Followingfurosemide, ULC score decreased in Group 1 (18±13, p<.0001 vs baseline) butnot in Group 2 patients (30±22, p=ns vs baseline).
Conclusion: ULCs are a dynamic sign of extra-vascular lung water usually de-tectable in cardiogenic dyspnoea. Fibrotic ULCs due to underlying lung and/orpleural pathology can be separated from cardiogenic comets by a furosemide"stress" test, since watery cardiogenic comets are usually reversible.
P5238 Weight loss after bariatric surgery normalizes aorticdistensibility and left ventricular function in subjectswith morbid obesity: a 3-year follow-up study
I. Ikonomidis1, A. Mazarakis2 , C. Papadopoulos1 , N. Patsouras2,F. Kalfarentzos2, D.T. Kremastinos1, D. Alexopoulos2. 1University
of Athens,Attikon Hospital, Athens, Greece; 2University of Patras,Rio Hospital,Cardiology, Patras, Greece
Mordid obesity is associated with high incidence of heart failure. Aortic distensi-bility (AoD) is an important determinant of left ventricular (LV) function. We inves-tigated whether a) increased body mass index (BMI, kg/m2) is associated withimpaired AoD and LV function b) weight loss after bariartic surgery (gastric by-pass) is associated with changes of AoD and LV function in subjects with morbidobesity after 3 and 36 months of follow-up.Methods: We studied 60 subjects (mean age 35±11 years) with morbid obesity(BMI>40 kg/m2) by 2D, and Doppler Echocardiography. AoD was calculated us-ing the formula 2 x (pulsatile change in aortic diameter)/[diastolic aortic diameter x(aortic pulse pressure)](normal range:2.4-4.4 cm2 dyn-1 × 10-6). Aortic diameterswere measured 3cm above the aortic valve by 2D guided M-mode echocardio-graphy and aortic pulse pressure was obtained simultaneously by cuff sphygmo-manometry 3 and 36 months after surgery.Results: All patients had normal systolic function and impaired AoD beforesurgery (table). Increasing BMI was related to decreasing AoD (r=0.43,p<0.01)and increased interventicular septum (IVS) and posterior (PW) wall thickness(IVS: r=0.57, PW: r=0.58, p<0.01) before surgery. Decreasing AoD was relatedto prolonged IVRT (r=0.43, p<0.01) and DT (r=0.40, p<0.05). Three months af-ter surgery, BMI, LV diastolic diameter (LVDmm), IVS(mm), PW(mm), isovolumicrelaxation time (IVRT sec) and decelaration time (DTsec) were reduced whereasAoD was increased. (table, p<0.01). After 36 months, there was a further im-provement in AoD and BMI The decrease of BMI was related to improvement ofAoD at 36 months of f/u (r=0.40 p=0.008).
Table
Surgery BMI AoD LVD IVS PW IVRT DT
Before (1 week) 49±7 1.6±1 50±4.8 11.2±1 11.2±1 91±13 214±60After(3 months) 38±9 3.4±1.1 46.7±3 9.3±1.3 9.2±1.3 72±11 189±49F/U (36 months) 32±6 4.2±1.6 48±3.6 9.5±1.1 9.1±0.96 82±9 195±36p <0.01 <0.01 NS <0.01 <0.01 0.048 0.024
Conclusion: Morbid obesity is associated with impaired aortic distensibility andLV hypertrophy leading to significant LV diastolic dysfunction. Weight reductionafter bariatric surgery normalises aortic distensibility, reduces LV hypertrophy andthus, improves LV diastolic function early and 36 months after surgery
ACUTE MYOCARDIAL INFARCTION: METABOLISMAND ANAEMIA
P5239 Importance of acute and chronic glucosedysregulation in non-diabetic patients withST-segment elevation myocardial infarction
S. Rasoul1, J.P. Ottervanger1, H.J.G. Bilo1, A.W.J. Van ’T Hof1,L.D. Dikkeschei1, F. Zijlstra2 on behalf of the GIPS II investigators.
1Isala Klinieken, cardiology, Zwolle, Netherlands; 2University Medical Center,cardiology, Groningen, Netherlands
Purpose: Admission hyperglycaemia is associated with an increased risk of mor-tality after acute myocardial infarction. Whether long-term glucose dysregulationis more important than acute hyperglycaemia is unknown. We evaluated the prog-nostic value of admission glucose and long term glucose dysregulation, assessedby HbA1c levels, in non diabetic patients with ST-segment elevation acute my-ocardial infarction (STEMI).Methods: In 504 unselected, consecutive patients with STEMI, glucose andHbA1c levels were measured on admission. Patients with previously diagnoseddiabetes were excluded from the study. Glucose was categorised as <11.1mmol/L (n= 422) and ≥11.1 mmol/L (n=82). HbA1c levels were categorised as< 6.0% (n=416) and ≥ 6.0% (n=88). Mean follow up was 1.6 ± 0.6 years.Results: Patients with hyperglycaemia on admission were comparable to thosewith normoglycaemia. There were, however, important differences between pa-tients with or without increased HbA1c. Patients with HbA1c>6.0% were older,more often used beta blockers and more frequently had multivessel disease. Mor-tality in the subsequent glucose categories (<11.1 mmol/L and ≥11.1 mmol) was8% and 22% (p <0.001). In patients with HbA1c of < 6.0% mortality was 9%compared to 18% in patients with a HbA1c ≥6.0% (p=0.015). After multivariableanalyses admission glucose (OR 2.66; 95%CI: 1.31 - 5.42) but not HbA1c (OR1.44; 95%CI: 0.567 - 3.10) was significantly associated with higher mortality.Conclusion: Elevated admission glucose is an important predictor of outcomeafter STEMI, while prior long-term glucose dysregulation is a covariate of otherhigh risk clinical characteristics.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Acute myocardial infarction: metabolism and anaemia / Acute myocardial infarction strategies 907
P5240 Impact of anemia and thrombocytosis on mortalityfollowing acute myocardial infarction
E. Tay1, K.T. Ho2, W.D. Tan3, L.L. Sim2, J.A.M.E.S. Yip4, B.L. Chia2,M.A.R.K. Chan2, T.C. Yeo2. 1Singapore, Singapore; 2TTSH,Cardiac, Singapore, Singapore; 3SCDB, Singapore, Singapore;
4NUH, Cardiac, Singapore, Singapore
Background Anemia can exacerbate ischemia and worsen outcomes in patientswith acute myocardial infarction (AMI). Similarly, elevated platelet levels may pre-cipitate thrombotic events in these patients. Data relating hemoglobin and plateletlevels to mortality in patients presenting with an AMI is limited.Methods: We identified 5378 consecutive patients with confirmed MI admittedto 2 major public hospitals in Singapore between January 2000 and December2003. Data on baseline demographics, co-morbidities and in- hospital manage-ment were collected. The patients were divided into quintiles based on their pre-senting hemoglobin and platelet levels. One year mortality was adjusted for differ-ences in baseline characteristics and index hospitalization treatments. Adjusted1 year mortality was then compared between the groups.Results: Mean age was 62±13 with 71%% males. Adjusted 1 year mortality waslowest in patients with hemoglobin levels in the highest quintile (>16g/dl). Table1 showed that compared with this group, patients with hemoglobin levels in thelowest 2 quintiles had significantly higher adjusted 1 year mortality. With regardsto platelet levels, no difference in mortality was in seen in the different groupscompared with the lowest quintile (Table 1).
Table 1
Hemoglobin Odds 95% CI P value Platelet levels Odds 95% CI P valueg/dL ratio x109/L ratio
<11 1.45 1.03-2.06 0.036 <197 1.0011- 13.9 1.39 1.01-1.92 0.045 198 - 235 0.81 0.61-1.07 0.1314-14.9 1.17 0.83-1.65 0.372 236 - 269 1.02 0.77-1.35 0.8815-15.9 1.29 0.88-1.87 0.189 270 - 316 1.13 0.85-1.49 0.40≥16 1.00 ≥317 1.11 0.89-1.52 0.26
Conclusions: Anemia is a powerful and independent predictor of 1 year mortalityin patients presenting with an AMI. Thrombocytosis is not associated with highermortality in these patients.
P5241 Anaemia at admission is a strong predictor forin-hospital and long term mortality in patients withhigh risk acute myocardial infarction treated withprimary angioplasty
J.A. Gomez Hospital, G. Roura, M. Rodriguez, J. Gonzalez-Costello,J. Maristany, E. Iraculis, A. Cequier, E. Esplugas. Hospital Universitari Bellvitge,Interventional Cardiology, Barcelona, Spain
Aims: Anaemia is a predictor of long term mortality in stable patients (pts) withischemic cardiomyopathy treated with percutaneous coronary intervention (PCI).The aim of our study was to evaluate the impact of anaemia on short and longterm outcomes after primary angioplasty in the context of a high risk acute my-ocardial infarction (AMI).Methods: Patients treated with primary PCI in the context of a high risk acuteST elevation myocardial infarction (anterior AMI, rescue PCI or haemodynamicinstability).were prospectively included in the study. Anaemia was defined as avalue of haemoglobin of less than 11.5 g/dL prior to PCI. In hospital mortality andlong term major adverse cardiac events (death, AMI or repeat revascularization)were collected for analysis.Results: We included 292 consecutive pts with high risk AMI, with a mean ageof 61±13 years old, 81.5% males, 25% diabetics. Anterior AMI was present in52.7% of pts. Stent implantation was performed in 86.6% and final angiographicsuccess was achieved in 92.3%. Anaemia was detected in 21 pts (7.2%). In hos-
Cumulative Survival
pital global mortality was 16.8%, and was higher in patients with anaemia com-pared with those without anaemia (38.1% vs 15.3%, p= 0.014). After a meanfollow-up of 1260 days, anaemia was also associated with an reduced survival(57.1% vs 81.7%%, Log Rank 8.17, p=0.0043). Cox multivariate analysis alsodetected anaemia an independent predictor factor for long term mortality (OR 19;p= 0.044) with Insulin dependent diabetes (OR 45, p=0.021), cardiogenic shock(OR 127; p=0.01), and the need of antiarhytmic therapy for ventricular arrhythmia(OR 46; p= 0.032).Conclusion: In pts with a high risk AMI treated with primary PCI, anaemia onadmission is a strong predictor of in-hospital and long term mortality.
P5242 Prognostic impact of anemia in patients with acutecoronary syndromes
J. Feliciano, A.J. Fiarresga, A. Mamede, R.M. Fernandes,A.T. Timoteo, D.N. Cacela, R. Ferreira, J. Quininha. Hospital SantaMarta, Cardiology Department, Lisboa, Portugal
Anemia is considered an independent risk factor for cardiovascular outcome inheart failure and coronary artery disease. However, in the acute setting, its influ-ence on short term prognosis remains unclear.Aim: To evaluate the impact of anemia on short term outcomes in patients withacute coronary syndromes (ACS).Population and methods: We studied 285 consecutive patients (66% male,mean age 64±13 years, 55% hypertensive, 40% dyslipidemic, 34% smokers,21% diabetic), admited for ACS (57% with ST-elevation ACS, 13% in Killip Class≥II, 79% underwent coronary angiography and 50% underwent angioplasty). Acomplete hemogram was carried out at baseline. Patients were categorized ac-cording to the the presence of anemia, as defined by the World Health Organi-zation criteria (hemoglobin levels < 13g/dl in male and <12 g/dl in women). Theevents considered were: congestive heart failure and in-hospital mortality.Results: Seventy-eight patients (28%) were anemic. In this group, patients wereolder (mean age 72±12 vs 62±12 years; p<0.0001), mostly male (77% vs 62%;p<0.05), with a higher prevalence of diabetes (31% vs 18%; p<0.05), less preva-lence of smoking habits (17% vs 40%; p<0.0001). Anemic patients presentedwith a higher incidence of congestive heart failure (23% vs 8%; p<0.001) andin-hospital mortality (14% vs 4%; p<0.005). In multivariate analysis, and afterajustment for age, gender and comorbidities, anemia kept its association with ahigher in-hospital mortality (odds ratio 0.71; 95% CI 0.55-0.93; p<0.05).Conclusion: In the setting of ACS, anemia is a frequent entity, and is stronglyassociated with a higher risk of in-hospital complications and mortality.
ACUTE MYOCARDIAL INFARCTION STRATEGIES
P5243 Guideline based treatment of STEMI patients in twoEuropean regions: Berlin and Florence
B. Maier1, D. Balzi2, R. Matteucci Gothe3, A. Barchielli2, H. Theres1
on behalf of Berlin Myocardial Infarction Registry, Acute MyocardialInfarction Registry Florence . 1(Berlin Myocardial Infarction
Registry), Berlin, Germany; 2Florence, Italy; 3Innsbruck, Austria
Background: Surveys suggest that differences among countries exist in treat-ment of patients with ST-elevation myocardial infarction (STEMI). The extent ofthese differences on outcome of hospital care delivered to patients in everydayroutine is largely unknown. It was the aim of this study to evaluate differences incharacteristics, hospital care, and outcome for patients from 2 regional registriesin Berlin and in Florence.Methods: The two registries are population-based and data were collectedprospectively from unselected populations from 1.3.2000 - 28.2.2001 in the Flo-rence area (N=876) and from 1.1.2000 - 31.12.2001 in Berlin (N=1714). Datadisclose a comprehensive picture for treatment, patients’ characteristics and out-come in the areas covered by the registries. Berlin and Florence data-sets weremerged, and determinants of hospital mortality were evaluated by logistic regres-sion analysis.Results: Essential differences exist among characteristics and hospital care ofSTEMI patients in the two regions. Florentine patients were on average 7 yearsolder than Berlin patients, smoked less, and suffered less from hypercholes-terolemia and hypertension. The percentage of patients receiving reperfusiontherapy ranged from 56% (Florence) to 81% (Berlin): Primary PCI was performedfor 35% in Berlin and 51% in Florence; thrombolysis for 46% in Berlin and 5%in Florence. Hospital mortality as outcome was very similar in the two regions(10.6% for Florence and 10.2% for Berlin, unadjusted). After adjustment for agein years (OR=1.06; 95% CI: 1.04-1.08), severity of disease on admission (Kil-lip class IV compared to Killip class I with OR=16.0; 95% CI: 10.24-25.06; Killipclass II/III compared to Killip class I with OR=2.98; 95% CI: 2.1-4.22), ex-smokingcompared to never smoking (OR=0.57; 95% CI: 0.34-0.95), and reperfusion ther-apy (OR=0.69; 95% CI: 0.49-0.96), differences in hospital mortality among thetwo populations were significant ("enclosed in Florence region" showed OR=0.64;95% CI: 0.46-0.89).Conclusion: After adjustment for differences in patients’ characteristics,population-based differences remain in short-term outcome between patients in
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

908 Acute myocardial infarction strategies
Berlin and in Florence. This difference may result from a different risk factor pro-file (e.g. different genetic background or dietary habits) that was not covered bythe study - and by differences in therapeutic effectiveness of reperfusion therapy.Further studies are required to better understand these phenomena.
P5244 Importance of time of day and day of week in thetreatment of ST-elevation myocardial infarction withprimary PCI
D. Becker, G. Fulop, G.Y. Szabo, G.Y. Barczi, L. Geller, L. Molnar,E. Zima, B. Merkely. Semmelweis University Cardiovascular Surgery,
Cardiovascular Center, Budapest, Hungary
Introduction: Recent data shows that the prognosis of STEMI patients who weretreated with primary PCI during off-hours is worse than during regular hours.Since 2003 in Budapest acute myocardial infarction is treated by organized pri-mary PCI. During regular hours five centres, during off-hours one centre is re-sponsible to fulfil this task. Our clinic covers a part of the surrounding region, andevery Wednesday night and every Sunday Budapest and its surrounding region.Purpose: In-hospital and 30 day mortality of patients treated by primary PCI be-tween 2003 and 2005 at our clinic on two tables were evaluated who were dividedinto two groups: patients treated during regular and during off-hours.Methods: Evaluation of the data of patients who were seen at the clinic after thePCI using the computer-based patient registry, and using a telephone-interviewwith the patient or relative if had no contact since then.Results: Between 2003 and 2005, 1890 STEMI patients were admitted. 1888STEMI patients underwent primary PCI; due to longer pre-PCI waiting period 2patients received thrombolysis. 671 patients (35.5%) were admitted during reg-ular and 1219 patients (65.5%) during off-hours. There was no significant differ-ence between mean age (63.1/63.3 years), nor between mean length of symp-toms (5.8/6.1 hours). During off-hours mean door-to-balloon time was signifi-cantly shorter (off-hours: 41±5 min, regular hours: 45±6 min - p<0.01), sincein the former case there were no elective intrventions. There was no signifi-cant difference between the number of patients who were admitted in a se-vere hemodynamic state [68/671 (10.1%) - 136/1219 (11.16%)], nor betweenthe use of intraaortic balloon pump [63/671 (9.4%) - 120/1219 (9.8%)] or res-pirator [84/671 (12.5%) - 160/1219 (13.13%)]. Follow-up rate was 98.7% (1865patients). In-hospital mortality was 3.2% during regular hours (n=21/664), 3.7%during off-hours (n=44/1201); 30 day mortality was 7.68% (n=51/664) and 7.83%(n=94/1201), respectively (p=NS).Conclusion: Treatment of acute STEMI with primary PCI with a well organizedon-call system, with the availability of adequate number of skilled staff can achievesimilar good results during off-hours compared to regular hours.
P5245 Coordinated aggressive medical and interventionaltherapy for acute myocardial infarction: pre-hospitaladministration of thrombolysis with urgent culpritartery revascularization (PATCAR)
G.M. Giesler1, S. Sdringola2, M. Vooletich1, V. Julapalli1,H.V. Anderson1, A. Denktas1, D. Persse3, R.W. Smalling2. 1U. Texas HealthScience Center, Cardiology, Houston, United States of America; 2U. TexasHealth Science Center, Cardiology, Houston, United States of America; 3HoustonFire Department, Houston, United States of America
Background: Percutaneous coronary intervention (PCI) has improved outcomesin patients presenting with ST-elevation myocardial infarction (STEMI). PrimaryPCI has been limited by facility availability and prolonged time to reperfusion. Pre-vious trials (DANAMI, PRAGUE-2, CAPTIM) of transport to a primary PCI centerdemonstrated pain onset to balloon times of 188 to 277 minutes, initial infarctrelated artery (IRA) patency (TIMI III flow) of 17-20% and a 30-day mortality of5-7%. The PATCAR Pilot aims to evaluate the hypothesis that pre-hospital 1
2 dosethrombolysis followed by immediate PCI will significantly reduce time from onsetof pain to IRA patency and improved reperfusion scores compared to standardprimary PCI.Methods: Patients in a large metropolitan area who activate emergency medicalservices (EMS) are evaluated by EMS personnel for STEMI. Patients meetinginclusion criteria are given in-field thrombolytic therapy (10 units Retevase®) andtransported directly to the Level I Cardiovascular Center, with the interventionalteam activated during transport. Those who are ineligible for thrombolysis aretaken emergently to the cath lab for primary PCI.Results: To date, 140 patients have been enrolled in the Pilot trial. No patientrandomized has had an adverse event prior to hospital arrival. 83% of patientswith facilitated PCI, compared to 43% with direct PCI, had TIMI II/III flow on arrivalto the cath lab suggesting IRA patency occurred earlier than indicated by doorto balloon time. In field activation of cath personnel led to earlier door to balloontime in the facilitated PCI arm (78 vs. 115 minutes; p=0.02). Complete reperfusionbased on an angiographic perfusion score >/= 10 was also higher with facilitatedPCI (% APS >10: 71% vs. 31%; p=0.05). PCI was successful in all patients withno neurological complications.Conclusion: Pre-hospital thrombolysis with facilitated PCI has shifted the timefrom onset of pain to IRA patency earlier than current primary PCI strategies. Thisearly IRA patency may further reduce the 30-day mortality to less than 5-7%. Thebenefits of 1
2 dose pre-hospital lysis with urgent culprit artery revascularization
(pre-hospital facilitated PCI) compared to primary PCI will be evaluated in thePATCAR pivotal trial.
P5246 Good survival rates in patients with acute myocardialinfarction treated with an intra aortic balloon pump
S.D.A. Valk, W.K. Lagrand, A.J.M. Van De Sande, R.T. VanDomburg, M.L. Simoons. Erasmus Medical Centre, Cardiology,Rotterdam, Netherlands
Introduction: The intra aortic balloon pump (IABP) is used as a mechanical sup-port in addition to pharmacological treatment in patients with low cardiac outputor sustained myocardial ischemia. In patients with acute myocardial infarction(AMI) it may reduce myocardial ischemia by augmenting coronary perfusion andreduce afterload. Its use has been proven valuable in patients treated with reper-fusion therapy (percutaneous coronary intervention (PCI), coronary artery bypassgrafting (CABG) or trombolysis) by improving coronary patency. However, little isknown about long-term survival or predictors of survival in these patients.Methods AND PATIENT CHARACTERISTICS: All consecutive patients (N=238)with AMI treated with IABP between January 1990 and July 2004 were reviewedusing data from a local database. Survival rates were obtained by contactingthe civil registry, follow up was complete in 99.6%. Multivariate Cox regressionanalysis was performed to identify predictors of in-hospital and long-term survival.Mean age was 61 years, 78% were male. The observed median follow up periodwas 6.1 [0.5-15] years. Previous AMI was present in 37%, 11% had a previousPCI and 9% had undergone CABG. The AMI was located in the anterior wallin 53%. Severely depressed left ventricular function (LVF) was found in 31% ofthe patients. Three vessel and left main disease was present in 36% and 14%,respectively.Results: In-hospital survival was 66%. The cumulative 5, 10 and 15 years sur-vival rates were 45%, 30% and 12%, respectively. So, if discharged from thehospital alive, almost 50% of the patients were still alive after 10 years. Moderateto severely depressed LVF and IABP running time were independently associ-ated with lower in-hospital survival (Hazard ratio= (HR) 2.8 [1.1-8.2] and 2.1 [1.1-4.1], respectively). PCI or CABG was associated with higher in-hospital survival(HR=0.4 [0.2-0.8] and 0.3 [0.1-0.4], respectively). Predictors of lower long-termsurvival were age (HR=1.0 [1.01-1.05]), diabetes mellitus (HR=2.1 [1.3-3.6]), de-pressed LVF (HR=1.9 [1.1-3.4]) and longer IABP running time (HR=1.7 [1.1-2.8]).Only CABG was associated with higher long-term survival (HR=0.3 [0.1-0.8]).Conclusion: From the patients, treated with IABP, who were discharged fromhospital alive almost 50% were still alive after 10 years follow-up. Lower in-hospital and long-term survival were related to depressed LVF and IABP runningtime. PCI and CABG were associated with higher in-hospital survival while CABGwas also associated with better long-term outcome.
P5247 Decreasing rate of reperfusion therapy withincreasing clinical risk in patients with acute STelevation myocardial infarction
U. Zeymer, A. Gitt, C. Juenger, T. Heer, H. Wienbergen, J. Senges.Klinikum Ludwigshafen, Medizinische Klinik B, Ludwigshafen,
Germany
Background: Guideline recommended therapy has been shown to reduce mor-tality in patients with acute ST elevation myocardial infarction. However, high riskpatients often are not treated with reperfusion therapy and guideline adherentadjunctive therapies. Aim of the study was to investigate the impact of TIMI riskscore on the rate of reperfusion and adjunctive therapies in patients with acuteST elevation myocardial infarction.Methods: Patients with STEMI < 12 h enrolled in two prospective registries(ACOS and GOAL) with patients with acute coronary syndromes were dividedinto 4 groups according to their TIMI risik score.Results: The rates of guideline adherent therapies and hospital mortality accord-ing to the TIMI risk score are shown in the table.
TIMI risk score 0-1 (n=1968) 2-3 (n=2478) 4-5 (n=2517) > 5 (n=1810)
Reperfusion therapy 89.9% 79.5% 65.0% 47.3%Aspirin 91.6% 92.6% 90.9% 87.3%Beta-blocker 86.0% 84.5% 78.3% 62.3%ACE-Inhibitor 64.6% 63.3% 67.1% 56.2%Mortality 0.8% 3.2% 9.0% 26.7%
Conclusions: In clinical practice higher risk patients are undertreated with re-spect to early reperfusion and adjunctive therapies, which is associated with asteep increase in hospital mortality. Therefore all efforts should be made to in-crease guideline adherent therapies in higher risk groups, to reduce overall mor-tality in patients with STEMI.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Acute myocardial infarction strategies 909
P5248 After successful primary PTCA is still needed routineadmission of all patients to CCU?
M.L. De Benedictis1, N. De Cesare2, R.A. El-Kheir2, V. Trani2,D. Falchetti2, S. Zanotti2, A. Polese2. 1Policlinico San Marco,Cardiology, Zingonia-Osio Sotto Bg, Italy; 2Policlinico San Marco,
Cardiology, Zingonia-Osio Sotto Bg, Italy
Background: In pre-reperfusion era, the diffusion of CCU decreased significantlyin-hospital AMI mortality, as result of better complication management. PrimaryPTCA, because of high success reperfusion rate and very low reocclusion risk,when associated to stent use, allowed to achieve a remarkable reduction of AMIcomplications. The aim of this study was to assess if after successful primaryPTCA routine CCU stay is still needed in all pts with AMI, including those at lowrisk.Methods and results: In our institution from July 1.2002 to December 31.2005we performed primary PTCA and stent implantation in 369 pts with AMI. Afterprocedure, 60 high risk pts (pre-hospital cardiac arrest, cardiogenic shock, pul-monary oedema non drug responding, unsuccessful PTCA) were admitted toCCU. The remaining low risk pts (310) were admitted to Cardiology Ward with12-lead EKG monitoring for at least 72 h. In the high risk group in-hospital deathwas reported in 10 cases (16.6%) (hemorrhagic stroke 1, post-anossic come 2,refractory cardiogenic shock 7), while in low risk group, 4 exitus occurred (0.7%)(hemorrhagic stroke 2, cardiogenic shock 2).Observations: Low risk pts successfully treated with primary PTCA have a verylow in-hospital complication incidence, allowing their management in CardiologyWard, at least when 12-lead EKG is monitored. As a consequence, in CardiologyUnits that use primary PTCA as first choice treatment of AMI, the number ofpts admitted to CCU could significantly decrease, saving economic resourcesand allowing a reduction of the total cost of the hospital stay of pts with AMItreated with primary PTCA. The remarkable mortality rate in high risk pts of ourpopulation may be explained by the very strict selection criteria, that identify ptsat extremly high risk.
P5249 Immediate vs delayed angioplasty in STEMI patientswith TIMI III flow infarct-related artery,thrombus-containing lesion and ST segmentresolution
N. Meneveau, F. Schiele, P. Legalery, M.F. Seronde, V. Descotes-Genon, K. Didier-Petit, Y. Bernard, J.P. Bassand. University Hospital
Besancon, Dept of Cardiology, Besancon, France
Background: Early management of patients (pts) with ST segment elevation my-ocardial infarction (STEMI) and TIMI III flow infarct-related artery (IRA) has neverbeen assessed. Immediate PCI is associated with distal embolisation, delayedPCI with increased risk of recurrent MI; both these adverse events unfavourablyimpact long-term outcome.Methods: Matched comparison of immediate vs delayed PCI in STEMI pts re-ferred for primary or rescue PCI (50%) at diagnostic angiography. Primary end-point was procedural success defined as final DS <30%, with TIMI III flow andwithout slow flow, no reflow, or distal embolisation. Pts were matched for age, riskfactors & lesion site. GPIIb/IIIa inhibitors were administered before or during PCIin all pts except rescue PCI. All pts received a 300mg loading dose of clopidogrelwith 500mg iv aspirin and 30mg iv bolus of enoxaparin at diagnostic angiography.Enoxaparin and antiplatelets were maintained until PCI in the delayed group.Results: (Table) There were significantly more procedure-related complicationsand enzyme release in the immediate PCI group. In the delayed group, no is-chemic event occurred before PCI, and there was a significant reduction in throm-bus burden score at PCI procedure as compared with baseline (83% vs 38% forscores 3 and 4; p=0.039). There was no difference in in-hospital major adversecardiac events between groups.
Immediate (n=39) Delayed (n=39) P
Onset to angiogram (hrs) 5.3±2.2 5.5±2.1 0.82Onset to PCI (days) 0.22±0.1 2.2±0.93 <10-5Thrombus score at baseline 3.0±0.7 3.5±0.75 0.12Abciximab 19 (49%) 39 (100%) <10-5TIMI 3 flow 35 (90%) 39 (100%) 0.04Distal embolisation 7 (18%) 2 (5%) 0.076No reflow/slow flow 6 (15%) 1 (3%) 0.047Procedural success 30 (77%) 37 (95%) 0.022Peak CK 1634±810 1215±745 0.02
Conclusion: In STEMI pts with TIMI III flow IRA and ST resolution, delayed PCIresults in significantly greater procedural success, and lower enzyme release, ascompared with immediate PCI
P5250 Does rescue angioplasty improve survival?A quantitative review of randomized trials
M. Masotti, A. Betriu. Hospital Clinic - Thorax Institute, Cardiology,Barcelona, Spain
Background: Contrary to primary coronary angioplasty (PCI), thepotential benefit of rescue PCI in the early hours of acute myocardial infarction
(MI) remains unclear, as individual studies have yielded controversial results. Inparticular, the impact of rescue PCI on mortality was not been established.Objective: To assess whether a policy of routine rescue PCI following failedthrombolysis results in better outcomes than conservative treatment.Methods: We combined data from all control randomized trials (Belenkie, RES-CUE I, LIMI, PRAGUE I, MERLIN, REACT and WEST) comparing rescue PCIwith conservative management. We focused on hard end-points, death and reMI,assessed at 30 days.Results: Our analysis included a total of 1323 patients; of them, 665 underwentrescue PCI while the remaining 658 were managed conservatively. Rescue PCIwas performed after a mean of 288 minutes after symptom onset. The 30-dayoutcomes (rescue PCI vs conservative treatment, respectively) were as follows:mortality 7% vs 10% (OR 0.66, 95% CI 0.46-0.98; p=0.04), reMI 5.1% vs 8.8%(OR 0.55, 95% CI 0.35-0.88; p=0.013), and the combined death/reMI 12.2% vs19.0% (OR 0.59, CI 0.43-0.82; p=0.002). This translates into 37 lives saved per1000 patients treated.Conclusions: Early rescue PCI following unsuccessful thrombolysis significantlyreduces both death and non-fatal reMI rates. Whether this benefit extends to pa-tients treated beyond the time window of the randomized trials remains to beelucidated.
P5251 Mild hypothermia as adyuvant treatment tofibrinolytic therapy in acute myocardial infarction withST segment elevation
N. Avilla, E. Chuquiure-Valenzuela, G. Vieyra, C. Martinez-Sanchez,E. Lupi, J. Casanova, U. Juarez, H. Gonzalez. Instituto Nacional de
Cardiologia, Coronary Care Unit, Mexico City, Mexico
Objective: To reduction in metabolic demands in patients with acute myocardialinfarction treated with fibrinolysis and moderate hypothermia.Material and Methods: From March 2002 to March 2003, 42 consecutive malepatients with acute myocardial infarction with ST segment elevation were in-cluded. Patients had less than 6 hours from the start of symptoms, and weretrombolyzed with rt-PA. Hypothermia was assigned on a balanced basis duringthe first 24 hours of hospitalization in a special preconditioned area. The groupswere compared with controls who received rt-PA at room temperature, and pairedby age and infarction localization. Metabolic, hemodynamic, gasometrical andlaboratory data were obtained every two hours.Results: Body temperature of 32-34°C was accomplished in most patients at5 hours (± 1 hour). Once hypothermia was established significant difference inheart rate was observed between the hypothermia group (60 + 11 bpm) and thecontrol group (86 + 16 bpm) (p<0.01). Systolic blood pressure was 102 ± 11mmHg in the hypothermia group and 119.48 ± 25.39 mmHg in the control group(p<0.008). Inflammation, as measured by serum leukocyte increase was lower inthe hypothermia group (10.24 ± 2.69) than in the control group (13.81 ± 2.95)(p<0.04). Patients treated with hypothermia had lower troponin release than con-trols (64.34 ± 55.40 vs. 98.22 ± 47.61) (p<0.05).Conclusions: Mayor determinants of cardiac output like heart rate and systolicblood pressure in a state of hypothermia are significantly lowered, which de-notes the preservation of high-energy phosphates from ischemic tissue. Reduc-tion in troponin release correlates with less myocardial necrosis. Inflammatorymechanisms activated during acute ischemia were minimized in the experimen-tal group. Hypothermia, besides being a safe method to treat patients with acuteST-segment elevation myocardial infarction, promises to reduce infarct size, andpreserve contractile function.
P5252 Is transfer for primary PCI for STEMI feasible in theUnited States? 3 year results of the Minneapolis HeartInstitute Level 1 Myocardial Infarction Program
T.D. Henry, B.T. Unger, S.W. Sharkey, I.J. Chavez, W.R. Pedersen,D.L. Lips, J.D. Madison, D.M. Larson. Minneapolis Heart Institute
Foundation at ANW, Research Unit, Minneapolis, United States of America
Purpose: Primary PCI for STEMI is superior when performed in a timely man-ner in high volume centers, however, 75% of STEMI patients present to non PCIhospitals. Current total door to balloon times for patients in the United States areunacceptably long (median 178 min, only 12% <120 min).Methods: A standardized protocol for transfer of STEMI patients to Abbott North-western Hospital (ANW), a tertiary cardiac center in Minneapolis, from 28 ruraland community hospitals was implemented. This includes immediate activationof transport services, mobilization of the cath lab team by the Emergency Physi-cian and administration of adjunctive medications. Hospitals < 60 miles away useprimary PCI (Zone 1). Hospitals 60-210 miles away (Zone 2) use facilitated PCIwith 1
2 dose TNK prior to transfer.Results: From 3/03 to 1/06, of a total of 924 consecutive patients with STEMI,720 were transferred for primary PCI by ambulance (n= 220, 31%) or helicopter(n=500, 69%). During the same period, 204 STEMI pts presented directly to ANW.There were no deaths during transfer. No patients were excluded from transferincluding patients with cardiac shock and out of hospital cardiac arrest. Mediandoor to balloon times (mins) and 30 day outcome (no significant differences) areshown in the table.Conclusions: Rapid transfer of STEMI patients from community hospitals up to
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

910 Acute myocardial infarction strategies
In door 1 - Transport In door 2 - Total door - Mortality Stroke Reinfarctionout door 1 time balloon balloon 30 days 30 days 30 days
ANW (n=204) NA NA 65 65 5.4% 2.0% 2.9%Zone 1 (n=441) 49 22 20 95 4.1% 1.1% 1.6%Zone 2 (n=279) 60 32 18 120 5.4% 1.1% 0%p-value 0.0018 0.005 <0.001 <0.001 0.65 0.95 0.05
210 miles from PCI Centers in the US is safe and effective with an integrated re-gional system of acute cardiac care. Outcomes for transferred patients are similarto those who present to PCI Centers directly.
P5253 Myocardial salvage in patients with acute myocardialinfarction presenting beyond 12 hours after onset ofsymptoms
G. Parodi1, G. Ndrepepa2, A. Kastrati1, A. Conti2, J. Mehilli1,M. Schwaiger1, D. Antoniucci2, A. Shomig1. 1Division of Cardiology,
Careggi Hospital, Florence, Italy; 2Deutsches Herzzentrum, TechnischeUniversitat, Munich, Germany
Context: No data exist about potential myocardial salvage in asymptomatic pa-tients with ST-segment elevation myocardial infarction (STEMI) presenting >12hours after symptom onset.Objective: Comparison of the effects on myocardial salvage of mechanical reper-fusion and conservative tratment strategy (CTS).Design, setting and patients: International, multicenter, unblinded, randomizedcontrolled trial based on two-hundred and sixty-one consecutive patients withSTEMI admitted between 12 and 48 hours after symptom onset and undergo-ing paired technetium (Tc) 99m-sestamibi scintigraphies prior to randomizationand 5 to 10 days later. Intervention: There were 131 patients randomly assignedto the invasive treatment (mainly percutaneous coronary intervention) and 130patients assigned to the conservative treatment.Main outcome measure: Myocardial salvage index (proportion of initial perfusiondefect salvaged by reperfusion) was the primary end-point.Results: The amount of myocardium at risk (median [25th, 75th percentiles]) didnot differ between groups (17.0% [9.0-28.5] versus 16.0% [9.0-37.5]; P=0.99).The final infarct size was significantly smaller in patients assigned to the inva-sive treatment than in those assigned to the conservative treatment (8.0% [2.0-16.0] versus 12.0% [3.2-25.0]; P=0.004). Myocardial salvage was revealed in bothgroups. However, myocardial salvage index was higher in the invasive group (0.44[0.13-0.80]) as compared to the conservative group (0.23 [0.0-0.50]; P<0.001).Anterior infarct location emerged as the only independent predictor of myocardialsalvage after PCI.Conclusion: The currently recommended CTS leads to salvage myocardium inpatients with STEMI presenting more than 12 hours after onset of symptoms.However, primary PCI allows an almost two times greater myocardial salvage inthis subgroup of patients when compared to the CTS. The late reperfusion benefitis higher in patients with anterior infarction.
P5254 Emergency revascularization in cardiogenic shockcomplicating acute myocardial infarction: ameta-analysis of randomized controlled trials
R. Jeger1, P. Urban2, J. Stauffer3, S. Harkness4, L. Sleeper3,M. Pfisterer4, J. Hochman5. 1University Hospital Basel, Department
Of Cardiology, Basel, Switzerland; 2Hopital de La Tour, Meyrin-Geneva,Switzerland; 3Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland;4New England Research Institutes, Watertown, United States of America; 5NewYork University, New York, United States of America
Background: Enrollment in randomized controlled trials (RCT) testing emer-gency revascularization (ERV) vs. initial medical stabilization (IMS) in cardiogenicshock complicating acute myocardial infarction was difficult with some trials beingterminated before completion.Methods: A comprehensive survey using PubMed, the Cochrane Controlled Clin-ical Trials Register, and published literature reviews revealed 244 abstracts ofwhich 242 (99%) were excluded based on detailed evaluation. Only 2 abstractsreported data on an RCT in cardiogenic shock testing ERV vs. IMS, i.e., the SwissMulticenter evaluation of early Angioplasty for SHock following myocardial infarc-tion (SMASH) and the SHould we revascularize Occluded Coronaries for car-diogenic shocK? (SHOCK) Trial. These databases were combined for a randomeffects meta-analysis using individual patient data.Results: Both trials combined enrolled 357 patients, of which 9 (3%) were ex-cluded to analysis because shock was due to a mechanical complication or aor-tic dissection leaving 348 patients for analysis. Due to different inclusion cri-teria, SMASH patients (n=54) had more often congestive heart failure (26 vs.6%, p<0.001) and a lower systolic (77±12 vs. 100±22mmHg, p<0.001) anddiastolic blood pressure on support (46±11 vs. 56±16mmHg, p<0.001) thanSHOCK patients (n=294). SMASH patients were treated less often with vasopres-sors/inotropic agents (96 vs. 100%, p=0.024), fibrinolysis (35 vs. 56%, p=0.007),intra-aortic balloon counterpulsation (7 vs. 87%, p<0.001), and cardiac catheter-ization (63 vs. 82%, p=0.03) than SHOCK patients. Due to the more severerisk profile, 1-year mortality was higher in SMASH than SHOCK (77 vs. 59%,
p=0.014). After adjustment for baseline differences and performance of coronaryangiography, mortality was similar (odds ratio 0.87, 95% confidence interval 0.61-1.25, p=0.45). In both trials, ERV compared with IMS resulted in lower 1-yearmortality (73 vs. 83% for SMASH and 52 vs. 66% for SHOCK, respectively). Therelative risk of ERV vs. IMS for 1-year mortality in both trials combined was 0.82(95% confidence interval 0.70-0.96; test of heterogeneity p=0.49).Conclusions: This is the first meta-analysis of ERV in cardiogenic shock. Only 2RCT have been published so far, emphasizing the difficulty of enrolling criticallyill patients in randomized trials. Despite large differences in shock severity andpatient mortality between the trials, treatment effect of ERV on 1-year outcome issimilar across the whole spectrum of cardiogenic shock.
P5255 The MITRA score: a new score for the quality of carein hospitals treating patients with acute ST elevationmyocardial infarction
U. Zeymer1, A. Gitt2, C. Juenger1 , H. Wienbergen1, J. Senges1
on behalf of MITRA-Study group. 1Klinikum Ludwigshafen,Medizinische Klinik B, Ludwigshafen, Germany; 2Ludwigshafen, Germany
Background: A variety of scores have been proposed to estimate the risk ofpatients admitted with acute coronary syndromes. However, so far there are noscores to evaluate the quality of care provided by hospitals in these patient popu-lation and its influence on outcome. Therefore our aim was to propose a hospitalscore which might allow to estimate the quality of the individual hospital treatingpatients with acute coronary syndromes.Methods: We used the database of the MITRA-Plus registry to search for hospitalparameters which were related to outcome in patients with acute ST elevationmyocardial infarction. These were related to structure (availibility of a cath-lab withinterventional capacities), organisation (short time to reperfusion intervals, highrate of reperfusion therapies, high rate of reperfusion therapies during off-hours)and implementation of guideline adherent therapies (acutely and at discharge).Each parameter was than counted as one point for a total of 7 possible points.Hospitals were divided into three groups: low (0-2 points), medium (3-4 points)and high (5-6 points) MITRA score.Results: Inhospital mortality and major adverse cardiovascular and cerebralevents (MACCE) were significantly associated with the MITRA score, being 6%,5% and 4% (p =0.0013) and 13%, 9% and 6% in the three groups, respectively.The hospital MACCE rate in relation to the TIMI risk score of the patients is shownin the table.
MITRA score 0-2 MITRA score 3-4 MITRA score 5-6
TIMI risk score 0-3 3.0% 5.0% 7.7%TIMI risk score 4-6 6.8% 11.7% 14.3%TIMI risk score > 6 11.5% 14.4% 26.3%
In hospital MACCE related to TIMI risk score of the patients and MITRA score of the hospital
Conclusion: The MITRA score provides an easy tool for estimating the qualityof the hospital treating patients with STEMI. Even after adjusting for the baselinerisk of the patients these score is closely linked to clinical outcome. It thereforecan be used to improve structure, organization and adherence to guidelines ofhospitals treating patients with STEMI.
P5256 Effects of intravenous nicorandil before reperfusionfor ST-elevation acute myocardial infarction inpatients with a higher white blood cell count
H. Ishii1, S. Sakai1, Y. Ogawa1, S. Ichimiya2, M. Kanashiro2,T. Matsubara3, T. Murohara2. 1Nagoya University School Of
Medicine, The Department Of Cardiology, Nagoya, Japan; 2Yokkaichi MunicipalHospital, Yokkaichi, Japan; 3Aichi-Gakuin University, Nagoya, Japan
Background: In patients with acute myocardial infarction (AMI), a high whiteblood cell (WBC) count at admission is associated with impaired epicardial andmyocardial perfusion, and an important prognosis factor for adverse outcomes.We aimed to assess effects of intravenous nicorandil administered before reper-fusion on ST-elevation AMI (STEMI) patients with a higher WBC count at admis-sion.Methods: A total of 368 first STEMI patients undergoing percutaneous coronaryintervention (PCI) were randomly assigned to receive 12mg of nicorandil or aplacebo intravenously just before reperfusion. Patients were classified accordingto the WBC count at admission and the use of nicorandil or a placebo: 96 patientsgiven placebo with WBC count < 10000 cells/mm3 (Group L-p), 87 patients givenplacebo with WBC count ≥ 10000 cells/mm3 (Group H-p), 101 patients givennicorandil with WBC count < 10000 cells/mm3 (Group L-n) and 84 patients givennicorandil with WBC count ≥ 10000 cells/mm3 (Group H-n). We examined cor-rected TIMI (cTIMI) frame count and ST-segment resolution as immediate dataand 5 years freedom from MACE (coronary heart disease death or unplannedreadmission due to congestive heart failure) as late phase data.Results: Baseline data about cTIMI frame count and electrocardiograms werecomparable. Postprocedural cTIMI frame count was 24.2 ± 11.2, 26.1 ± 16.9,20.3 ± 10.0 and 21.8 ± 7.9 in Groups L-p, H-p, L-n and H-n, respectively (p =0.02). ST-segment resolution >50% was observed in 63.5%, 56.3%, 85.1% and73.8% of Groups L-p, H-p, L-n and H-n, respectively (p = 0.02). On Kaplan Meier
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Acute myocardial infarction strategies / Acute myocardial infarction registries and surveys 911
analysis, 5 years freedom from MACE was 80.3% in Group L-p, 75.4% in GroupH-p, 94.4% in Group L-n and 88.3% in Group H-n (p = 0.009).Conclusions: For STEMI patients with a higher WBC count at admission, ad-junctive therapy with administration of intravenous nicorandil before reperfusionsignificantly improves epicardial flow and prevents the occurrence of severe mi-crovascular reperfusion injury, resulting in better outcome in these patients.
P5257 Impact of patient characteristics on response toenoxaparin vs UFH in STEMI: an ExTRACT-TIMI 25analysis
E.M. Antman, D.A. Morrow, C.H. Mccabe, E. Braunwald on behalfof ExTRACT-TIMI 25 Investigators. TIMI Study Group, Brigham andWomen’s Hospital, Boston, United States of America
Since pharmacologic reperfusion is the most common treatment for patients(pts) with ST-elevation myocardial infaction (STEMI) worldwide and enoxaparin(ENOX) has several advantages (reliable anticoagulation,greater antiXa:IIa ac-tivity, more convenient sc administration), a definitive evaluation of its potentialsuperiority over unfractionated heparin (UFH) is needed.ExTRACT-TIMI 25 was a large (N=20,506) phase 3 double-blind, double-dummy,international (674 sites, 48 countries) trial comparing a strategy of ENOX (duringindex hospitalization) to the current guideline recommended weight-based dos-ing of UFH (for at least 48 hrs) for prevention of death (D) or nonfatal recurrentMI (D/MI) through 30 days in subjects receiving fibrinolysis for STEMI. Subjectscould be treated with any of the following fibrinolytics: tenecteplase, alteplase,reteplase, streptokinase.While pts less than 75 yrs received ENOX as a 30 mg IV bolus and 1.0 mg/kg sctwice daily, a novel regimen of no IV bolus and reduced sc dosing of 0.75 mg/kgtwice daily was used in pts 75 yrs or older. For all pts with estimated creatinineclearance less than 30 ml/min, ENOX was given as 1.0 mg/kg once daily. Blindedstudy drug was used when PCI was performed. Blinded aPTT or ACT measure-ments for UFH dosing were coordinated centrally.The results for the primary endpoint (D/MI), key secondary endpoints(D/MI/Urgent Revascularization), net clinical benefit (D/MI/Nonfatal DisablingStroke) and bleeding will be reported, stratified by key baseline characteristicsof the subjects such as the following (% in trial shown):1. Age (continuous variable)2. Age > 75 (12.4%)3. Gender (Male 77%)4. History of Diabetes (15.0%)5. History of Prior MI (13%)6. Prior ASA use (13.5%)7. Infarct Location (Anterior 43.2%)8. Fibrinolytic Administered (Fibrin-specific 79.8%, SK 20.2%)9. Time from symptoms to treatment (median=3.3 h)10. TIMI Risk score (0-<3=64%; 3 or greater = 36%)
P5258 The impact of using age as a clinical determinant ofappropriateness for early revascularisation (ERV) incardiogenic shock (CS) complicating AcuteMyocardial Infarction (AMI)
P.J. Sheridan, A. Al-Mohammad. Northern General Hospital,Cardiology, Sheffield, United Kingdom
Clinical trials have shown prognostic benefit from early revascularisation (ERV) incardiogenic shock (CS) complicating AMI. The adherence to international guide-lines recommending ERV and intra-aortic balloon counterpulsation (IABC) in thiscontext remains low. The factors which influence the management of CS in thereal world and the effectiveness of an individualised approach in CS is unclear.Fifty consecutive patients with CS complicating AMI presenting to two univer-sity teaching hospitals in a 12 month period were identified from a prospectiveregistry. Clinical details including baseline characteristics, management and out-comes were examined.The causes of CS were pump failure (86%), ventricular septal rupture (10%), car-diac rupture (2%) and papillary muscle rupture (2%). An individualised approachto the management of pump failure was demonstrated with low rates of coronaryangiography (46%) and IABC (44%). The overall survival rate in the ERV groupwas 43% compared to 23% in the non-ERV group. A decision to proceed to leftheart catheterisation (LHC) was made in 48%, LHC was deemed inappropriate in22% and no documented decision was found in 30%. Age >75yrs was associatedwith a delayed decision for LHC (median shock-decision time 12h vs 2h), a lowerERV rate (28% vs 68%; p=<0.05) and lower survival (20% vs 50%). Following thepresentation of a 6 month interim report the use of both ERV and IABC increasedin those >75yrs, but not in those <75yrs, and overall survival rates increasedfrom 20% to 40%.Although other baseline characteristics will contribute to the decision to proceedto ERV, age was the single most important predictor governing the use of ERV inCS complicating AMI by cardiologists in our study. In the clinical setting, recon-sidering the appropriateness of ERV in CS may improve overall outcomes.
P5259 Relative adrenal insufficiency in patients withCardiogenic Shock
N. Lellouche, A. Mekontso-Dessap, L. Brochard, C. Brun-Buisson,J.L. Dubois-Rande. Hopital Henri Mondor, Cardiology, Creteil,France
Introduction: Relative adrenal insufficiency has been demonstratedto be associated with increased mortality in septic shock patients. Cardiogenicshock (CS) induces a stress response involving the adrenal cortex, but func-tional hypoadrenalism has never been investigated in this setting. The aim of thepresent study was to prospectively evaluate adrenal function in patients admittedto intensive and coronary care unit for cardiogenic shock.Methods: 40 consecutive patients (35 men) admitted for CS, with a mean age of66 ± 16 years were included. Patients submitted to any steroid therapy or eto-midate were excluded. 4 patients needed mechanical ventilation and 4 patientswere equipped with an intraaortic balloon pump. Causes of CS included acutemyocardial infarction (n=14), cardiomyopathy (n=13), arrrythmia (n=3), and oth-ers (n=10). Patients underwent a high dose short corticotrophin test (SCT) andrelative adrenocortical insufficiency (nonresponders) was defined by a rise in cor-tisol less than 90 microg/L after stimulation.Results: 13 (32.5%) patients were classified as nonresponders and 27 (67.5%)as responders. No significant difference was evidenced between responders andnonresponders concerning clinical characteristics and outcome (Table 1).
Table 1. Patients with CS classified according to the response to the SCT
Parameter Nonresponders (n=13) Responders (n=27) p
MAP, mmHg 70 [62-77] 73 [58-81] 0.98LVEF, % 20 [15-22] 23 [18-30] 0.14Inotrope duration,d 5 [3-10] 5 [3-8] 0.87ICU stay, d 7.0 [3.5-15] 6.5 [4.0-11.5] 0.88ICU death 6 (46%) 10 (37%) 0.73
Conclusion: About one third of patients with cardiogenic shock exhibit relativeadrenocortical insufficiency. Further studies are needed to clarify its prognosticsignificance in this setting.
ACUTE MYOCARDIAL INFARCTION REGISTRIESAND SURVEYS
P5260 Impact of heart failure complicating ST-elevationmyocardial infarction on hospital outcome in clinicalpractice: results of MITRAplus
A.K. Gitt, H. Wienbergen, T. Heer, C. Juenger, F. Towae,M.G. Gottwik, J. Senges on behalf of MITRAplus Study Group.
Herzzentrum Ludwigshafen, Senior Physicican, Dept. Of Cardiology,Ludwigshafen, Germany
Background: After the advances of the treatment of STEMI in the last decade,little data exist about the impact of heart failure complicating myocardial infarctionin clinical practice.Methods: Between 1994 and 2002 a total of 64207 consecutive patients withacute coronary syndromes were enrolled into the MITRAplus registry in Germany.We examined the impact of heart failure complicating STEMI on hospital course in32707 consecutive patients with STEMI. Heart failure was defined as LV-EF<40%and symptoms NYHA II-IV.Results: Out of 32707 STEMI patients, 3005 (9%) developed complicating heartfailure during the hospital course. Patients with heart failure were older, moreoften female and significantly more often had prior myocardial infarctions, priorcoronary interventions and concomitant diseases, but did receive acute reper-fusion therapy significantly less often than patients without heart failure. Afteradjustment for these differences by multivariate regression analysis, heart failurecomplicating STEMI was associated with significant higher hospital mortality (OR2.03, p<0.01).
Heart failure complicating STEMI
Heart Failure No Heart Failure p-value(n=3005) (n=29702)
Age (years) 74 66 < 0.01Female Gender 43.2% 31.3% < 0.01Prior MI 26.9% 15.2% < 0.01Prior PCI/CABG 11.8% 9.1% < 0.01Hypertension 49.7% 46.4% < 0.01Diabetes 31.3% 25.0% < 0.01Renal Failure 7.2% 2.5% < 0.01Hyperlipidemia 40.5% 44.2% < 0.01Prior Stroke 4.2% 2.3% < 0.01Acute Reperfusion 42.6% 61.2% < 0.01Hospital Mortality 22.5% 6.7% < 0.01Hospital MACCE (Death/MI/Stroke) 29.4% 10.6% < 0.01
Conclusion: Patients with heart failure complicating acute STEMI significantlyless often received acute reperfusion therapy. Even after adjustment for thesedifferences in treatment and for the differences in baseline characteristics, heartfailure complicating STEMI was associated with 2-fold higher hospital mortality.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

912 Acute myocardial infarction registries and surveys
P5261 Impact of renal failure on hospital outcome ofconsecutive patients with STEMI in clinical practice:Results of the ACOS-Registry
A.K. Gitt1, H. Wienbergen1, F. Towae1, U. Zeymer1 , C. Hausdorf2,H. Darius2, M.G. Gottwik1, J. Senges1 on behalf of ACOS-Study-
Group. 1Herzzentrum Ludwigshafen, Senior Physicican, Dept. Of Cardiology,Ludwigshafen, Germany; 2Vivantes Klinik Neukoelln, Cardiology, Berlin,Germany
Background: Patients with renal failure have a higher cardiovascular morbidityand mortality. Little is known about the influence of renal failure on the acuteoutcome of ST-elevation myocardial infarction (STEMI) in clinical practice.Methods: Between 2000 and 2002 a total of 8303 consecutive patients withSTEMI were enrolled into the multicenter ACOS-registry in Germany. We exam-ined the impact of renal failure on hospital outcome in clinical practice. Renalfailure was defined as serum creatinine > 2.0 mg/dl.Results: Patients with renal failure were older and more often female than pa-tients without renal failure. Patients with renal failure significantly more often hadprior myocardial infarctions and coronary interventions as well as a higher preva-lence of concomitant diseases. They less often did receive acute reperfusion ther-apy. After adjustment for these differences by multivariate regression analysis, re-nal failure was associated with significant higher hospital mortality (OR 3.49, CI2.54-4.79).
Renal failure in STEMI
Renal Failure No Renal Failure p- valuen=272 n=8031
Age (years) 74.3 65.6 < 0.001Female Gender 35.3% 30.1% < 0.001Prior MI 37.5% 15.8% < 0.001Prior PCI/CABG 20.2% 9.7% < 0.001Hypertension 78.7% 58.2% < 0.001Diabetes 51.8% 25.7% < 0.001Hyperlipidemia 60.3% 61.9% < 0.001pAVD 22.8% 5.9% < 0.001Smoking 17.6% 36.2% < 0.001Reperfusion Therapy 47.1% 71.3% < 0.001Hospital Mortality 37.5% 8.5% < 0.001Hospital MACCE (Death/MI/Stroke) 41.2% 13.3% < 0.001
Conclusion: In consecutive STEMI-patients renal failure was associated with amore than 3-fold increased hospital mortality in clinical practice.
P5262 Influence of low BMI on early and one-year mortalityin patients treated with primary PCI for acutemyocardial infarction or the "obesity paradox".Results from the nationwide French USIC 2000 study
L. Sabbah1 , J.M. Lablanche2 , D. Blanchard2, N. Genes2, P. Gueret2,G. Hanania3 , J.P. Cambou4, N. Danchin5 on behalf of USIC 2000 investigators.1Paris, France; 2Lille, France; 3Aulnay, France; 4Toulouse, France; 5HopitalEuropeen Georges Pompidou (Hegp), Service De Cardiologie, Paris, France
Background: Obesity is a recognised risk factor for cardiovascular disease. Lit-tle is known, however, on the influence of BMI on outcomes in patients havingsustained an acute myocardial infarction (AMI).The aim of this study was to assess the prognostic role of BMI in patients treatedwith primary PCI (PPCI) for ST elevation AMI.Methods: The USIC 2000 registry included all patients hospitalised within 48hours of symptom onset in 83% of ICUs in France in November 2000. Of the 2,320patients included, 2,067 had information on their BMI available, and 411 of themwere treated with PPCI. Quintiles of BMI were determined and their relationshipwith early and late survival was assessed.Results: Compared with patients in the 4 upper quintiles, BMI-Q1 patients had aless frequent history of hypertension ((27% vs 43%, p<0.01), but all other base-line characteristics were not significantly different. 5-day mortality was highestin the lowest quintile of BMI (<23.7 for men and <21.5 for women) (BMI-Q1)(9.4% v 1.1%, 1.2%, 3.8%, 2.5%, respectively for each quintile of increasing BMI,p=0.02). Using multiple regression analysis, odds ratio for 5-day mortality was 7.0(95% CI: 2.0-24.1, p=0.002) for BMI-Q1 vs all 4 upper quintiles (other indepen-dent predictors of early mortality were diabetes mellitus, female sex, chronic renalfailure). One-year mortality (Kaplan-Meier) was significantly higher in patients inBMI-Q1 (16%) compared with all 4 other quintiles (10%) (p<0.001). When only5-day survivors were included in the long-term analysis, however, BMI-Q1 was nolonger associated with increased subsequent mortality (8% vs 6%, 5%, 4%, and9%, respectively for each BMI quintile, p=NS).Conclusion: in this real world setting of patients with acute myocardial infarc-tion treated with PPCI, lean patients had a higher early mortality than patients inthe 4 upper quintiles of BMI. The correlation of low BMI with early mortality wasindependent of other predictors of mortality. In contrast, there was no excess ofmortality in patients in the highest quintile of BMI.
P5263 Effect of clopidogrel on 1-year mortality in survivorsof ST-elevation myocardial infarction (STEMI)undergoing fibrinolytic therapy
O. Koeth, T. Bauer, F. Towae, J. Senges, U. Zeymer. KlinikumLudwigshafen, Kardiologie Department, Ludwigshafen, Germany
Background: Randomized trials demonstrate that clopidogrel reduces the inci-dence of cardiovascular complications in patients undergoing fibrinolytic therapy.Rare data are available about the longterm benefit of clopidogrel in unselectedpatients with STEMI undergoing fibrinolytic therapy.Objectives: To investigate the impact of clopidogrel treatment in patients dis-charged after fibrinolytic therapy for STEMI.Methods: Retrospective analysis of the prospective ACOS-registry in survivors ofSTEMI undergoing fibrinolytic therapy on aspirin with or without additional clopi-dogrel.Results: Overall 1872 patients with STEMI treated with fibrinolytic therapie anddischarged alive were studied; 969 (51,8%) received clopidogrel at discharge,908 (48,2%) did not. The incidence of death, non fatal recurrent MI or non fatalstroke is demonstrated in the table below.In the multivariate analysis clopidogrel treatment reduces highly significant 1- yearmortality (odds ratio 0.45, 95% CI 0.28-0-72, p<0.001).
Complications at 1 year Clopidogrel at discharge No clopidogrel at discharge p-valuefollow up n=969 n= 903
Death 3,3% (32/969) 8,9% (80/903) <0,00001Non fatal recurrent MI 3,0% (24/804) 4,5% (31/696) 0,13Non fatal stroke 1,5% (12/804) 1,2% (8/689) 0,58
Conclusion: In the daily clinical practice clopidogrel treatment resulted in a highlysignificant reduction in 1-year mortality in unselected survivors of STEMI treatedfibrinolytic therapy
P5264 Patients with acute ST-elevation myocardial infarctionand prehospital delay to presentation >12 hours: highrisk of worse outcomes and selective use ofreperfusion therapies. The GRACE registry
G. Oliveira1, C.B. Granger2 , F. Van De Werf3, G. Montalescot4 ,K.A.A. Fox5, D. Gulba6, J. Allegrone7, A. Avezum6 on behalf of GRACEInvestigators. 1Sao Paulo, Brazil; 2Durham, United States of America; 3Leuven,Belgium; 4Paris, France; 5Edinburgh, United Kingdom; 6Duren, Germany;7Worcester, United States of America
Background: STEMI patients (pts) presenting <12h since onset of symptomsshould receive reperfusion therapy, which results in important mortality reduction.Currently, it is controversial whether late-presenters (>12h) should receive fibri-nolytics (lytics) or primary angioplasty (PCI).Methods: We analyzed the GRACE registry to determine factors associated withprehospital delay of 12-24h, use of lytics, PCI, or either, and hospital outcomes(death; heart failure [HF]). Pts with contraindications to lytics were excluded. Mul-tivariable models were applyed to assess the independent relationship of reper-fusion and outcomes.Results: We report data from 9670 pts: 709 (7.3%) pts presented between 12-24h (age 66yrs; 33% female). Compared with early-presenters (<12h), thosewith long prehospital delay were significantly older, more likely to be female,more often had new or presumed new left bundle branch block (LBBB), and hadmore history of angina, hypertension and diabetes. PCI was performed in 15%(>12h) vs 23% (<12h), lytics in 12% vs 42%, any reperfusion therapy in 27%vs 65%, respectively (P<.001), and time from admission to initiation of reper-fusion was longer for either lytics (41 vs 33min, P=.01) or PCI (110 vs 80min,P<.001). No significant differences were observed in proportions of teaching hos-pitals, catheterization facilities, geographic regions, and number of cardiac cathor CABG procedures. Although late-presenters had significantly higher incidenceof death (9% vs 7%, P=.04) and HF (23% vs 19%, P=.02), prehospital delayof 12-24h was not independently associated with outcomes after adjustment forbaseline risk and hospital therapies (death, OR 1.11 [0.7-1.6]; HF, OR 1.12 [0.89-1.42]). Overall, PCI was independently associated with lower risk of death (OR0.63 [0.47-0.86], P=.003] relative to no reperfusion, but there was no significantinteraction between early- and late-presenters and reperfusion therapy.Conclusions: In STEMI, elderly, women, pts with history of angina, hyperten-sion, and diabetes, and those with LBBB are more likely to present with longprehospital delay. These late-presenters are selectively treated with reperfusion,often with longer time from admission, and are at high risk of worse outcomes.The independent relationship of PCI and better survival in the overall cohort didnot significantly differ in early- and late-presenters, suggesting that PCI may bebeneficial in selected late-presenters. Randomized trials are needed to determinewhich pts will benefit from reperfusion strategies when presenting with prehospitaldelay >12h.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Acute myocardial infarction registries and surveys 913
P5265 Gender differences in the treatment of patientsadmitted with a primary diagnosis of acutemyocardial infarction in US community hospitals
A.D. Kugelmass1, P.P. Brown2, L.G. Tarkington1, S.D. Culler3,A.W. Simon4 on behalf of HCA CCMN Committee. 1Henry Ford
Health System, Cardiology, Detroit, United States of America; 2HCA, Inc, Quality,Nashville, United States of America; 3Emory University, Rollins School ofPublic Health, Atlanta, United States of America; 4Cardiac Data Solutions, Inc.,Research, Atlanta, United States of America
Purpose: To examine if women admitted to a hospital with a primary diagnosisof Acute Myocardial Infarction (AMI) receive fewer procedures and have worseoutcomes than men.Methods: A retrospective analysis was conducted using the HCA (Hospital Cor-poration of America) Casemix Database, an administrative database of consecu-tive patients admitted to any HCA hospital. The study population includes 26,400patients admitted with a primary diagnosis of AMI in one of 82 full service UScommunity heart hospitals (hospitals performing both PCI and CABG) that treatedmore than 52 AMI patients between 10/1/2004 and 9/31/2005. A logistic regres-sion equation (controlling for age, gender, race and 19 co-morbidities) was es-timated to predict the risk-adjusted probability of in hospital mortality for eachpatient. Treatments received were coded based on ICD-9-CM contained in theHCA Casemix Database. Student t-tests were used to test for gender differencesin treatment and outcomes between men and women.Results: The average hospital in our study treated 448 patients (patient volumeranged from 59 to 1,191) and approximately 37.3% of the patients admitted tostudy hospitals were women. A greater percent of men were transferred into fullservice hospitals than women (20.5 versus 17.2, p<0.001). In addition, the per-cent of men receiving each treatment studied was significantly higher than forwomen, with the exception of thrombolytics (p=0.106). Women also had a signifi-cantly higher risk-adjusted mortality rate than men (relative risk of dying that was1.37 times higher than for a comparable man).
Treatment and Mortality Rates
All Patients Women Men p-Value
% Transferred In 19.3 17.2 20.5 <0.001Treatment Received:
% Any Thrombolytics 0.87 0.75 0.94 0.106% Any GIIb/IIIa 28.0 22.4 31.4 <0.001% Any PCI 52.2 44.3 56.9 <0.001% Any CABG 13.8 10.5 15.9 <0.001
Risk-Adjusted Mortality Rate 7.1 8.5 6.2 0.002
Conclusion: This analysis indicates that women experience a gender disadvan-tage in treatments received and risk-adjusted mortality rates among AMI patientstreated in US community hospitals.
P5266 J-curve relation between body mass index andmortality after acute myocardial infarction.Preliminary results of the HELIOS study
G.K. Andrikopoulos1, S. Tzeis1 , A. Gotsis2, A. Kartalis3,A. Synetos1, K. Kalantzi4, P. Kalogeropoulos1, J. Lekakis1 on
behalf of HELIOS investigators. 1Hellenic Cardiological Society, Athens, Greece;2Hellenic Cardiological Society, Komotini, Greece; 3Hellenic CardiologicalSociety, Chios, Greece; 4Hellenic Cardiological Society, Ioannina, Greece
Background: We investigated in-hospital and 30-day mortality after acute my-ocardial infarction (AMI) in relation to body mass index (BMI).Methods: Data from 1266 patients (age 67±14 years, 77% males) hospitalizedfor AMI who have been enrolled in the HELlenic Infarction Observational Study,were analyzed. The HELIOS study was organized by the Hellenic CardiologicalSociety to investigate the incidence and clinical course of AMI using stratified ran-dom sampling in a countrywide basis. Availability of a catheterization laboratory,geographical location and proportion of urban population were taken into consid-eration in the selection of the thirty centers that participated in this study.Results: Unadjusted in-hospital and 30-day mortality rates differed significantlybetween the five quintiles of BMI (8.5, 7.2, 3.1, 2.8 and 8.3%, P=0.009 and 15.3,11.2, 5.5, 3.9 and 10.9%, P<0.001, respectively) (Figure). In univariate analysismortality rates were higher among patients belonging in the upper (BMI>30.2
Fig. 1. Mortality in relation to BMI
kg/m2) and in the lower (BMI<24.2 kg/m2) quintiles. In multivariate analysis ad-justed for age, gender, diabetes mellitus, smoking, thrombolysis and/or primaryPCI, and advanced Killip class (III-IV) the upper quintile was significantly and in-dependently associated with in-hospital mortality (RR=1.938, 95%CI=1.086-3.46,P=0.025), while the lower quintile (BMI<24.2 kg/m2) was significantly and in-dependently associated with 30-day mortality (RR=1.697, 95%CI=1.042-2.764,P=0.034).Conclusions: Obese and underweight patients are at increased risk after acuteMI. The responsible mechanisms accounting for their worse prognosis are inde-pendent from the major established prognostic risk factors and should be furtherinvestigated.
P5267 Clinical factors associated with thrombolysis failurein patients transferred to an interventional cardiacunit for myocardial infarction: data from RICO survey
E. Vigreux1, G. Dentan2, J.-C. Beer1, Y. Laurent3 , I. L’huillier2,L. Janin-Manificat4, M. Zeller3, Y. Cottin3 on behalf of the RICO
survey working group.. 1CHU Bocage, RICO, Service de Cardiologie, Dijon;2Clinique de Fontaine, RICO, Service de Cardiologie, Fontaine Les Dijon;3Centre Hospitalier, RICO, Service de Cardiologie, Semur En Auxois; 4CentreHospitalier, RICO, Service de Cardiologie, Beaune, France
Purpose: Randomised studies have shown the benefits of hospital transfer forpatients with acute myocardial infarction (AMI) to an interventional center partic-ularly in the event of thrombolysis failure. However, the characteristics of thesepatients and management outcomes have never been clearly established.Methods: Based on the non-selected AMI population from RICO (obseRvatoiredes Infarctus de Côte d’Or), we set out to compare patients who, after receivingthrombolysis therapy following MI, were transferred to interventional centers be-tween 1st January 2001 and 25th November 2003. The criteria for thrombolysisfailure were those used in routine clinical practice (persistent >50% ST segmentelevation on ECG).Results: 301 patients were analysed:group 1: failed thrombolysis; group 2: suc-cessful thrombolysis. Thrombolysis failed in 47% of cases. Angiographic dataconfirmed the absence of coronary reperfusion (TIMI flow 0 or 1 on IRA) in only49% of cases in group 1. In contrast, 11% of patients in group 2 had TIMI 0or 1, even though they had been considered as reperfused. Rescue PCI wasperformed in 77% of patients with failed thrombolysis, within 534(419-810) min)after symptom onset, which resulted in a return to normal flow (TIMI 3) on IRA in99% of cases. Thrombolysis failure is associated with more extensive necrosis,increased onset of cardiac events (recurrent MI, AF, cardiogenic shock), and ofhospital death (12% vs 4%, p=0.007). The independent predictors of thrombolysisfailure in multivariate analysis are diabetes, anterior wall location, and the pres-ence of cardiogenic shock on admission. In contrast, patients who present withchest pain within the days or weeks preceding MI are at a lower risk of thrombol-ysis failure.Conclusions: Our work revealed a substantial incidence of failed thrombolysis inpatients transferred to an interventional center after thrombolytic therapy, which isassociated with a poor in-hospital prognosis. Our data also highlight the existenceof subgroups of patients, including those with diabetes or with anterior location MI,at an increased risk of thrombolysis failure, and thus identify patients who requiremore aggressive therapy in the context of acute MI.
P5268 Current European practice in post MI patients: interimanalysis of the first 804 patients enrolled in amulticentre registry
G. Boriani1, M. Santini2, M. Lunati3, G. Botto4, A. Proclemer5,A. Erdogan6, B. Shmidt7, M. Russo8 on behalf of the Search-
MI/Bakken Research Center Study teams. 1Inst. of Cardiology, S.Orsola Hosp.,Bologna, Italy; 2San Filippo Neri Hospital, Cardiology, Roma, Italy; 3Niguarda CaGranda Hospital, Cardiology, Milano, Italy; 4S. Anna Hospital, Cardiology, Milano,Italy; 5S. Maria della Misericordia Hospital, Cardiology, Udine, Italy; 6Klinikum derJustus-Liebig-Universitat, Cardiology, Giessen, Germany; 7Universitatsklinikum,Cardiology, Freiburg, Germany; 8San Filippo Neri Hosp., Cardiology, Russo, Italy
Objective: Search-MI is a prospective observational multi-centre registry on Eu-ropean ICD implants in patients with previous myocardial infarction (MI)Population and Method: Between 2002 and 2005, 804 patients were enrolled<1 month after ICD implant. Each device-based electrogram was randomized to2 of 5 blinded reviewers (a third when necessary).Results: There were 787 patients with an interim 10 month mean follow-up.Thebaseline data are shown in the table. There were 154 patients adjudicated with
Study Madit II Search-MI
Enrollment countries 71 USA, 5 UE 84 UEurope,5 Middle-EastN patients (ICD arm) 742 (84% Men) 804 (89% men)LVEF (%) 23% 27%ICD mode VR/DR/CRT 56% : 44% : 0% 57% : 29% : 14%NYHA class I/II/III/IV% 35/35/25/5 9/49/40/2CABG % 58 36LBBB % 19 25Amiod./Statins/Diuretics/Beta Blockers% 13/67/72/70 25/55/85/80
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

914 Acute myocardial infarction registries and surveys
a documented VT/VF by blinded reviewers (11 could not be adjudicated and 16required an additional review). This signifies that 24% of the patients display anappropriate ICD intervention for VT/VF at 1 year, a value higher than the 17%reported in previous primary prevention trials.Conclusion: In the post- Madit-II European population one ICD in 4 will show anappropriate VT/VF therapy at 1-year follow-up
P5269 Registry of acute coronary syndromes in Latvia: STelevation myocardial infarction subgroup analysis
A. Erglis, I. Zakke, A. Maca, S. Jegere, I. Narbute. Pauls StradinsClinical Univ. Hospital, Latvian Centre of Cardiology, Riga, Latvia
Purpose The registry of acute coronary syndromes (ACS) in Latviais a retrospective-prospective, national study of patients hospitalised with diag-nosis of ACS. The purpose of this registry was to create an electronic databaseon patient management practice patterns and clinical outcomes in Latvia. Ourgoal was to analyse the quality of care for patients with ST elevation myocardialinfarction (STEMI).Methods Registry started in June 2005 and has collected data on patients hos-pitalised with ACS from January 1, 2005 to December 31, 2005 in 35 hospitalsacross all Latvia. A standardized web-based data collection form captured infor-mation on demographic characteristics, risk factors, medical history, time betweensymptom onset and presentation, diagnostic and treatment approaches, diagno-sis and clinical outcomes. The comparison was made to the results from previousregistry that took place in 2001. Also separately the results from Latvian Centreof Cardiology (LCC) at Pauls Stradins Clinical University Hospital as the leadinginterventional hospital in Riga were analysed.Results Of the 9881 patients enrolled in ACS registry, 1815 presented withSTEMI, including 317 patients at LCC. Of these, 60% in Latvia and 35% at LCCdid not receive any reperfusion. Hospital mortality in 2005 compared to 2001 hasdecreased by 5% in Latvia and 10% at LCC. The main results are shown in Table.
Reperfusion and outcomes in STEMI
Latvia LCC
Year 2001 Year 2005 Year 2001 Year 2005
Patient number, n 1895 1815 326 317Reperfusion:
Primary PCI, n (%) 20 (1%) 109 (6%) 20 (6%) 100 (32%)Thrombolysis, n (%) 575 (30%) 624 (34%) 122 (37%) 106 (33%)
Clinical outcomes:Hospital mortality, n (%) 415 (22%) 312 (17%) 72 (22%) 37 (12%)
Conclusions: Registry describes the quality of care for patients with ACS inLatvia and the current state to the awareness of and adherence to the nationaland European guidelines. Since 2001 clinical outcomes of STEMI patients haveimproved via more expansive use of mechanical reperfusion. Although a sub-stantial proportion of patients who are eligible for reperfusion therapy still do notreceive this treatment. Registry may facilitate the development and improvementof the national health care strategy.
P5270 Clinical covariates of NSTEMI and STEMI: report fromSerbian CCU registry
D. Matic1, Z. Vasiljevic1, N. Mickovska2, N. Milic3, D. Cvetkovic-Matic1, M. Krotin4, B. Putnikovic5, G. Panic6. 1Institute forCardiovascular Diseases, Belgrade, Serbia and Montenegro;
2Institute for Health Care of Serbia, Belgrade, Serbia and Montenegro; 3Institutefor Medical Statistics, Belgrade, Serbia and Montenegro; 4Clinical CenterBezanijska Kosa, Belgrade, Serbia and Montenegro; 5Clinical Center Zemun,Belgrade, Serbia and Montenegro; 6Institute for Cardiovascular Diseases,Sremska Kamenica, Serbia and Montenegro
Background: Taking the historical events on the area of ex-Yugoslavia during
last 15 years into consideration, that influenced the social, economic and healthstate of the population, we analyzed the most important demographic and clinicalcharacteristics in patients with acute myocardial infarction (AMI).Methods: In 50 coronary care units (CCU), of the 12351 patients presentingwith acute coronary syndrome in 2004, data from 8284 patients with AMI wereanalyzed. The others had non stable angina pectoris. Of these with AMI, 6393(77,17%) patients had an AMI with ST-segment elevation (STEMI), and 1891(22,83%) patients had an AMI without ST-segment elevation (NSTEMI). Base-line demographic characteristics and other co morbidities in patients with STEMIand NSTEMI were analyzed.Results: Patients with NSTEMI had, except smoking, significantly higher rates ofall cited risk factors and co morbid conditions then patients with STEMI (Table).Multivariate logistic regression analysis identified four independent predictors forNSTEMI: hypertension (OR=1,4; 95% CI for OR 1,2-1,5; p<0,001), previous my-ocardial infarction-MI (OR=1,4; 95% CI for OR 1,2-1,6; p<0,001), previous anginapectoris-AP (OR=1,3; 95% CI for OR 1,1-1,5; p<0,001), previous coronary arterybypass grafting-CABG (OR=1,7; 95% CI for OR 1,3-2,3; p<0,001). Only one in-dependent predictor for STEMI was identified-smoking (OR=0,8; 95% CI for OR0,7-0,9; p<0,001).
Characteristics of STEMI and NSTEMI
Patients % p value
STEMI NSTEMI
Mean age in years ±SD 63.3±11.47 64.0±11.15 0.016Male 65.4 62.7 0.035Previous MI 11.6 17.8 <0.001Previous angina 20.6 27.6 <0.001Previous CABG 2.1 4.7 <0.001Diabetes mellitus 24.9 25.9 0.374Smoking 38.7 32.6 <0.001Hypertension 59.6 68.0 <0.001Hyperlipidemia 37.9 40.5 0.046In hospital mortality 12.4 8.0 <0.001
Conclusion: Findings from the CCU registry in Republic of Serbia indicated thatmore patients had STEMI than NSTEMI which were different than other nationalregistries and surveys (Euro Heart Survey, ENACT, GRACE). Hypertension andprevious coronary artery disease (MI, AP and CABG) were independent predic-tors for NSTEMI.
P5271 Does gender influence the recommendation oftherapy after coronarography in patients with acutecoronary syndrome without ST elevation? Resultsfrom the ALKK registry
J. Friedrich1, M. Hochadel1 , U. Tebbe2, M. Weber3, T. Bonzel4,U. Sechtem5, J. Senges4, U. Zeymer4 on behalf of ALKK (ArbeitsgemeinschaftLeitende Kardiologische Krankenhausärzte). 1Klinikum Ludwigshafen,Medizinische Klinik B, Ludwigshafen, Germany; 2Klinikum Lippe-Detmold,Cardiology, Detmold, Germany; 3Amper-Klinikum, Cardiology, Dachau, Germany;4Klinikum Fulda, Cardiology, Fulda, Germany; 5Robert-Bosch-Krankenhaus,Cardiology, Stuttgart, Germany
Objective: To evaluate if there is a gender difference in the recommendation toconservative treatment or revascularisation procedures after coronarography inpatients with acute coronary syndrome (ACS) without ST elevation.Methods: In 2003, 78683 invasive procedures at 86 non university hospitals wereconsecutively included in the ALKK quality control registry. 11259 angiographieswere performed in patients with ACS without ST elevation. 31% of them werefemale, the mean age was 68, in men 66 and in women 72 years (p<0.001).Coronary artery disease (CAD) was defined as presence of at least one epicardialcoronary stenosis > 50%. Patients with additional valvular disease were excludedfrom the analysis.In the multivariate analysis, influence of gender on recommended therapy, i.e.revascularisation vs. medical treatment, was calculated.Results: Table 1
Table 1
Men Women p-value
Diagnosis n=7731 n=3528No CAD (%) 3.2 7.3 <0.001Significant CAD (%) 89.2 78.7 <0.001Others (%) 7.6 14.0 <0.001
Treatment recommendation in patients with significant CAD n=6861 n=2762PCI (%) 57.9 49.9 <0.001CABG (%) 15.8 13.0 <0.001Conservative (%) 24.3 34.8 <0.001
Variable OR 95%CLMale 1.16 1.03-1.30 0.01
Conclusions: 1) In clinical practice female ACS patients without ST elevationless often have relevant CAD. 2) The probability for revascularisaion in this studyis significantly higher in men than in women, even after adjustment for age.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Acute myocardial infarction registries and surveys / Angiography in acute myocardial infarction 915
P5272 Temporal trends in risk factors, practice patterns andin-hospital outcome among patients with acutemyocardial infarction. Five years (1998 to 2003)experience from a South Asian center
S.N. Nadeem1, A. Pathan2, A.R. Quraishi3, S.H. Dhakam1. 1AgaKhan University, Cardiology Section, Department Of Medicine, Karachi, Pakistan;2National Institute of Cardiovascular Diseases, Cardiology, Karachi, Pakistan;3Dalhousie University, Cardiology Division, Halifax, Canada
Background: With the epidemiologic transition in South Asia, prevalence of riskfactors for cardiovascular diseases (CVD) is increasing rapidly. Similarly, despiteadvances in the management of CVD based on randomized clinical trial data andpublished guidelines, the extent to which such treatments are applied in clinicalpractice remains uncertain.Objective: To analyze the shifts in the prevalence of CVD risk factors over fiveyears period in our patients with acute myocardial infarction (AMI) over 5 yearsperiod (1998-2003). We also aim to study changes in hospital management andreport temporal trends for in-hospital outcome over these two time periods.Method: All consecutive patients with AMI at our institution from 1/2003 to12/2003 database (n=587) were compared with those from 1/1998 to 12/1998database (n=261).Results: Patients with AMI in 2003 were older (mean age 62+12 vs. 60+12;p=0.03), had higher prevalence of diabetics (50.1% vs. 39.1%; p=0.003); hy-pertensive (62.9% vs. 48.3%; p<0.001), elevated cholesterol (46.5% vs. 21.1%;p<0.001), prior MI (27.4% vs. 17.2%; p=0.001), previous percutaneous coro-nary angioplasty [PCI] (5.3% vs. 0.4%; p<0.001) and lower LVEF (49% vs. 42%;p<0.001). No change was observed for duration of symptoms at presentationover 5 years (median 4 hrs). Overall reperfusion therapy in ST-segment eleva-tion MI (STEMI) was similar (53.1% in 1998 vs. 51.0% in 2003), however pri-mary PCI was performed more frequently in 2003 (12.0% vs. 0.6%; p<0.001).Use of non-invasive tests for risk assessment declined in 2003, whereas coro-nary angiography was done more frequently in 2003 (45.8% vs. 29.9%; p<0.001)along with an increase in PCI (19.3% vs. 5.7%; p<0.001). Surgical revasculariza-tion rates were similar over two time periods. Use of medications with prognosticbenefit was higher in 2003; Aspirin (96.1% vs. 89.7%; p<0.001), beta-blockers(84.7% vs. 58.6%; p<0.001), lipid lowering (79.4% vs. 30.7%; p<0.001) and ACE-Inhibitors (65.6% vs. 59.4%; p=0.08). Hospital stay was shorter in 2003 (median4 vs. 7 days). Overall in-hospital mortality was significantly lower in 2003 (7.2%vs. 12.6%, RR 0.62; p=0.01) with similar for trends for STEMI (16.1% vs. 10.0%;p<0.001) and non-STEMI (8.5% vs. 5.5%; p=0.04).Conclusion: Prevalence of CVD risk factors was significantly increased amongpatients with AMI over 5 year’s period. Increasing use of evidence based man-agement strategies with established prognostic benefit was clearly evident. Im-provement in clinical practices was associated with decline in hospital stay andoverall in-hospital mortality.
P5273 Impact of symptom-onset-to-balloon time on leftventricular remodeling, 30-day and long-termmortality in patients with acute myocardial infarctiontreated by primary angioplasty. Poznan Registry
M. Lesiak1, S. Grajek2, A. Araszkiewicz1, M. Pyda2, W. Skorupski2,P. Mitkowski2, M. Grygier2, A. Cieslinski2. 1University Of Medical Sciences,Department Of Cardiology, Pozman, Poland; 2University Of Medical Sciences,Department of Cardiology, Poznan, Poland
Multiple studies have shown the importance of treatment delay in patients withacute ST-segment elevation myocardial infarction (STEMI) treated by primary an-gioplasty (pPCI). We prospectively analyzed the influence of symptom-onset-to-balloon time on late ventricular remodelling, as well as on short- and long-termmortality of unselected patients treated by primary angioplasty.Methods: In 2002, in Department of Cardiology in University Hospital in Poz-nan, a total number of 488 consecutive STEMI patients were treated with pPCI.According to treatment delay patients were divided into three groups: I - thosetreated in less than three hours (n=164), II - patients treated between 3 and 6hour (n=187), and III - patients treated after 6 hours from the symptom onset(n=137). TIMI flow and myocardial blush grade (MBG) were analysed in all ofthem. In a subset of patients with anterior STEMI, a 2-dimensional echo exam-ination of the left ventricular (LV) function was performed within 72 hours from,and 6 moths after pPCI. Thirty-day, 12-month and long term (31.4 ± 4.2 months)mortality data were analysed.Results: The median values of time delays were significantly greater in elderlypatients (300 min for patients > 70 years old vs. 222,5 min for younger patients;p=0.00008), women (320 min vs. 230 min in men; p=0.0001), diabetics (320 minvs. 240 min in nondiabetics; p=0.00003) and patients with three-vessel disease(280 min vs. 240 min in patients with < 3 vessel disease; p=0,0002). Time totreatment was significantly associated with the MBG, in groups I, II and III, MBG3 was obtained in 47.6%, 32.6% and 29.9% of patients respectively (p=0.002). Ina multivariate analysis MBG < 2 was an independent risk factor of late cardiacdeath (12 months: HR 10.1, 95% CI 8.55-11.5, p = 0.002, and end of follow-up: HR 5.05, 95% CI 3.99-6.11, p=0.003). The LV remodeling (increase after 6months in EDV ≥20%) was diagnosed in 28% of patients with MBG 0&1, andonly in 10% of patients with MBG 2&3, p=0,02. After adjustment for baselineparameters, time-to-treatment significantly correlated with mortality only in a long-
term observation. The adjusted odds ratios OR (95% CI) for 30-day, 12-month andtotal observation time were as follow: OR 1.067 (0.979-1.155), p=0.14; OR 1.061(0.996-1.126), p=0.07; OR 1.060 (1.007-1.113), p=0,032.Conclusion: In STEMI patients treated with pPCI prolonged ischemic time is anindependent risk factor of the impairment of myocardial perfusion, this in turntranslates into LV remodeling and late mortality of these patients.
P5274 Intervention in acute coronary syndrome in Scotland:Impact on readmission and mortality
I.N. Findlay1, J. Bishop2, J. Craig3, K. Oldroyd4. 1Royal AlexandraHospital, Cardiology Dept, Paisley, United Kingdom; 2ScottishExecutive, ISD, Edinburgh, United Kingdom; 3Scottish Executive,
NHSQIS, Glasgow, United Kingdom; 4Western Infirmary, Glasgow, UnitedKingdom
Scotland has a well developed and validated ability to track admissions to hos-pital and subsequent outcomes. We used data provided by the Information andStatistics Division of the Scottish Health Service to look at outcomes for 22441patients with a first ever recorded admission diagnosis of angina/acute myocar-dial infarction for the period 2002-4. The analysis was restricted to those hospitalswith more than 500 such discharges. 13.2% underwent angiography on the indexadmission, 9.5% underwent PCI, 2.0% CABG. Thirty day was mortality was 9.1%and 1 year mortality 16.3% There were 5614 admissions to hospitals equippedto do angiography and CABG/PCI; 1498 to hospitals equipped to do angiography+ PCI, 4342 to angiography equipped only and 10987 to the remainder "trans-fer hospitals". Data were age/sex/deprivation standardized. The % undergoingangiography during the index admission was CABG/PCI =23.6, angiography +PCI =19.5, angiography only = 8.9 and transfer hospitals =8.4%. The figures forthose undergoing PCI on that admission was 15.8, 20.9, 4.8, 6.4% respectively.Subsequently 4.8, 8.3, 5.7, 7.4% were readmitted for PCI The median time tointervention PCI-was 3, 3, 8 and 13 days respectively. The % undergoing CABGon the index admission was 3.9, 1.3, 1.7, 1.2 respectively with a subsequent 5.4,5.0, 6.0, 5.2 readmitted for CABG The % patients readmitted with a diagnosis ofangina/AMI within 30 days was 2.5, 2.7, 4.9, 4.1. and by 1 year was 8.7, 10.5,15.1, 13.5% respectively. The % of patients readmitted and specifically codedas an emergency readmission to their index hospital at 1 year was 4.1, 3.0, 5.9,5.5% respectively The 30 day mortality was 8.5, 8.9, 9.5, 9.4% respectively and1 year mortality was 15.6, 15.8, 16.6, 16.6% respectively. There are clear differ-ences in rates of investigation and outcome with the main outcome benefit beinga reduced incidence of readmission with angina/AMI with higher rates of interven-tion. One year mortality suggests that higher intervention rates in this unselectedpopulation results in only modest benefit
ANGIOGRAPHY IN ACUTE MYOCARDIAL INFARCTION
P5275 Impact of baseline thrombus on the clinical outcomein patients with ST segment elevation myocardialinfarction. Validation of a pre-existing and propositionof a new simplified classification
G. Sianos, M.I. Papafaklis, S. Vaina, J. Daemen, C.A. Van Mieghem,R.T. Van Domburg, L.K. Michalis, P.W. Serruys. Thoraxcenter, Erasmus MC,Thoraxcenter - Bd 408, Interv. Cardiology, Rotterdam, Netherlands
Purpose: To determine the impact of thrombotic burden on clinical outcome inpatients with ST segment elevation myocardial infarction (STEMI).Methods: From April 2002 to December 2004, 900 consecutive patients withSTEMI were retrospectively analysed. The majority were treated with drug-elutingstents (90.1%). Thrombus burden was scored as following: grade 0 (G0)= nothrombus, grade 1 (G1)= possible thrombus (reduced contrast density, haziness,irregular lesion contour) grade 2 (G2)=small [greatest dimension <1/2 vesseldiameter (VD)], grade 3 (G3)=moderate (≥1/2 but <2VD), grade 4 (G4)=large(≥2VD), grade 5 (G5)=unable to assess thrombus burden due to total vessel oc-clusion. Patients with G5 were reclassified to one of the other categories afterflow achievement with wire crossing or a small (1.5 mm) balloon passage or di-latation. The incidence of Major Adverse Cardiac Events (MACEs) defined asdeath, non-fatal myocardial infarction, and infarct related artery revascularisationwas computed using the Kaplan-Meier method.Results: Complete follow-up was available in 886 patients (98.4%); median dura-tion was 18.5 months. G5 group constituted 57.7% of all patients. Reclassificationof thrombus was achieved in 97.9% of the G5 group. Thrombotic burden after re-classification was G0:8.1%, G1:19%, G2:24.5%, G3:16.6%, G4:30%, G5:1.9%.Distal embolization was comparable between the G5 and G0-4 groups (9.1% vs.8% respectively, p=ns). The cumulative MACE rate at 24 months was compa-rable in the reclassified groups G1, G2, G3 (15.5%, 14.1%, 12.6% respectively,p=ns), while groups G0 and G4 did significantly worse (24.2% and 25% respec-tively) compared to the former ones (p<0.0001). After stratification in two largegroups (G4 and G0-1-2-3) G4 was found to be an independent predictor for death(HR: 1.66, 95% CI: 1.04-2.68, p=0.035), death/MI (HR: 2.07, 95% CI: 1.39-3.08,p<0.001) and MACE (HR: 2.04, 95% CI: 1.44-2.88, p<0.001).Conclusions: In patients with STEMI: A) Thrombotic burden can be reliably es-timated in angiographically occluded vessels after flow achievement. B) Large
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

916 Angiography in acute myocardial infarction
thrombus (≥ 2 VD) is a significant independent predictor for MACEs. C) Throm-bus burden <2 VD represents a category with lower risk and should be gradedas one unified category of small thrombus. D) Patients without visible thrombusconstitute a specific category with increased risk for MACEs necessitating furtherinvestigation. These findings might have significant impact on the interpretationof the results of trials using thrombectomy devices during STEMI.
P5276 Left anterior descending coronary artery flow aftersuccessful primary angioplasty in acute anteriormyocardial infarction is suboptimal early andincreases later
D. Sharif1, A. Sharif-Rasslan2, A. Khalil1, C. Shahla1,U. Rosenschein1 . 1Bnai Zion Medical Center, Dept. Of Cardiology,
Haifa, Israel; 2Technion, Technology and Science, Haifa, Israel
Primary angioplasty (PCI) is the treatment of choice an acute myocardial infarc-tion (MI). Achievement of TIMI grade 3, and myocardial blush grade 3 is the ul-timate target of primary angioplasty, however these are invasive and not easilyrepeatable. Trans-thoracic Doppler sampling of velocities in the left anterior de-scending coronary artery (LAD) is feasible.Aim: Assessment of LAD flow after primary angioplasty and during hospitalizationin patients with acute anterior MI.Methods: Velocities in the LAD were recorded within 6 hours after PCI, 48 hourslater and pre-discharge in 36 patients presenting with acute anterior MI. Calcu-lation of estimates of flow in the LAD were performed using heart rates, Dopplertime velocity integrals and LAD color Doppler diameters.Results: Diastolic LAD flow immediately after PCI was 35±11ml/min increasedto 44±23 ml/min and pre-discharge 51±23 ml/min, p<0.05. Systolic LAD flow im-mediately after PCI was characterized by early systolic flow reversal in 6 subjectswhich contributed to reduced average systolic flow, while pre-discharge systolicforward flow was 14±17ml/min.Conclusions: Early after successful primary-PCI, flow in the LAD is suboptimal.Diastolic flow increases steadily during follow-up. Early systolic flow reversal con-tributes to reduced flow early after PCI, while on late follow-up forward systolicflow increases.
P5277 Clinical descriptors and impaired microvascularperfusion after mechanical intervention for STEMI:The EMERALD experience
R. Baeza1, A. Lansky2, P. Johanson3 , Y. Na2, R. Mehran2, D. Cox4,G. Stone3, M. Krucoff5. 1Duke Clinical Research Institute, Durham,
United States of America; 2New York, United States of America; 3Goteborg,Sweden; 4Charlotte, United States of America; 5Durham, United States ofAmerica
Background: Clinical descriptors are predictive of outcome in patients withSTEMI however the mechanism responsible for this effect is unknown. Biomark-ers of microvascular perfusion after mechanical infarct artery recanalization werecorrelated with key clinical descriptors in the EMERALD study.Methods: All 433 patients in the EMERALD trial with TIMI 3 flow after PCI wereanalyzed for 1) final myocardial perfusion grade (MPG) and 2) % ST segment re-covery 30 minutes after PCI (%STR) as determined by blinded core laboratories.Key descriptors were age, gender (F/M), infarct related artery (LAD v/s Non LAD),diabetes (DB), time to reperfusion (TTR) and Killip Class (KC) were correlated.Results: Patients older that 55 y/o had a median %STR of 81 v/s 86 in patientsunder that age (p=0.02). No age cutoff point could be detected for MPG. Patientswith TTR up to 5 hrs from the onset of symptoms had a MPG=3 of 65% v/s 51%in those treated later (p=0.040). Results for categorical variables are shown in theTable 1.
Results for categorical variables
F M LAD Non LAD DM Non DM KC≥2 KC<2
%STR 88 81* 60 93* 67 84* 74 84*75,100 56,100 38,79 78,100 49,100 60,100 52,99 62,100
MPG=3 % pts 61 61 47 69 * 56 62 38% 64%*
Values expressed as percentages or median and 25th, 75th percentiles. *p<0.05
Conclusion: Impairment of both ST segment recovery and myocardial blushgrade was observed in patients with LAD infarct location and Killip class >2,suggesting that microcirculatory dysfunction might be the mechanism of poor out-come even after mechanical restoration of epicardial TIMI 3 flow.
P5278 High-grade infarct related stenosis after successfulthrombolysis: strong predictor of reocclusion but notassociated with adverse clinical outcome
P.C. Kievit1, M.A. Brouwer1, P.J.P.C. Van Den Bergh1, H.J. Dieker1,G. Veen2, W.R.M. Aengevaeren1 , F.W.A. Verheugt1 . 1Radboud
University Medical Center, 670 Cardiology, Nijmegen, Netherlands; 2VU MedicalCenter, Amsterdam, Netherlands
Background: Previously we reported that in the APRICOT-1 trial (1987-1991),
a high-grade stenosis at 24-hour angiography after successful thrombolysis wasstrongly predictive of reocclusion but not of death or reinfarction. To investigatewhether this finding holds true in the current era, we extended our analysis topatients from the more recent APRICOT-2 trial (1995-2000).Methods: In both Antithrombotics in the Prevention of Reocclusion In COro-nary Thrombolysis (APRICOT) trials 499 patients with ST-elevation MI who hada patent infarct related artery 24 hours after thrombolysis had 3-month repeatangiography to assess reocclusion. QCA-analysis was possible in 478 patients(96%). An ischemia-guided revascularization strategy was followed. Five-yearclinical follow-up was collected.Results: On the basis of the optimal discriminative stenosis severity (63.2%) atROC-analysis, reocclusion rates were 39% (80/203) in patients with a high-graderesidual stenosis versus 13% (37/275) in patients with a low-medium-grade steno-sis (OR 4.18; 95% CI 2.68-6.54, p < 0.01). Median clinical follow-up was 1804days. Survival free from death or reinfarction was 76% in both groups (p=ns). Mul-tivariate analysis identified a high-grade stenosis as an independent predictor ofreocclusion (OR 4.15; 95% CI 2.50-6.89, p< 0.01) but not of death or reinfarction(HR 1.12; 95%CI 0.75-1.67, p=ns).Conclusions: Following an ischemia-guided revascularization strategy after suc-cessful thrombolysis, a high-grade infarct related stenosis is strongly associatedwith reocclusion but not with adverse clinical outcome. These findings appear notto be affected by the improvements in medical treatment over the years. Our ob-servations challenge the suggested benefit of routine revascularization to improveclinical outcome in this setting. The effect of routine angioplasty in the preventionof reocclusion is currently investigated in the APRICOT-3 trial.
P5279 Right ventricular infarction in the Cath-Lab:independent risk factor for increased mortality whichmay be improved by complete revascularization of theright coronary artery
A. Assali, I. Teplitsky, I. Ben-Dor, A. Solodky, D. Brosh, S. Fuchs,A. Battler, R. Kornowski. Rabin Medical Center, cardiology, Petah-Tikva, Israel
Background: Right ventricular (RV) involvement during acute inferior myocardialinfarction (MI) is associated with increased early morbidity and mortality. Withrecent improvement in percutaneous coronary intervention (PCI) techniques it isunclear which factors may improve the outcomes of these patientsObjectives: We sought to assess the prognostic significance of the presenceof RV-MI in patients undergoing primary PCI and explore factors associated withimproved outcomes using a large data base representing the "real-life" of patientswith acute MI treated by primary PCI.Methods: we analyzed our data base of acute MI patients undergoing primaryPCI within 12 hours of chest pain between 1/2000 and 6/2005 excluding patientswith cardiogenic shock.Results: Of the 666 consecutive patients with MI fulfilling our inclusion criteria329 had anterior wall MI, 264 inferior [230 inferior + 34 lateral] wall MI and 73were found to have RV-MI. Mortality at hospital discharge, 30 days and 6 monthswas highest in patients with RV-MI involvement (5.5%, 9.6% and 12.3%, respec-tively) intermediate in patients anterior MI (2.4%, 4.6% and 7.3%, respectively),and lowest in patients without RV myocardial involvement (0.8%, 1.1% and 3%,respectively) [P<0.05 for hospital discharge and 30 days, p=0.1 for six months].After adjustment for the CADILLAC score, odds ratio for 30 days morbidity was5.2 [95% CI, 1.6-17; P=0.005) for patients with RV-MI vs. those without RV-MI.Within the group of patients with RV-MI, complete revascularization of the rightcoronary artery including the major RV branch was associated with improved 30days mortality (OR =0.4; 95% CI: 0.1-1.05; P=0.06).Conclusions: Right ventricular infarction is an independent risk factor for in-creased mortality even in these days of primary PCI. Complete revascularizationincluding the restoration of blood flow into the right coronary artery including themajor RV branch may improve clinical outcomes.
P5280 Relationship between pre-PCI TIMI-3 flow and 30-daymortality in acute MI pts treated by emergency PCIpreceded (or not) by pre-hospital thrombolysis
P. Garot1, T. Lefevre2 , Y. Louvard1, C. Pouges3, J.Y. Le Tarnec4 ,T. Unterseeh2, J.C. Robart4, K. Tazarourte5 . 1ICPS, Quincy, France;
2ICPS, Massy, France; 3SAMU 91, Corbeil-Essonnes, France; 4SAMU 77,Melun, France; 5SAMU 77, Massy, France
Background: When performed within the first hour of acute MI (golden hour),pre-hospital thrombolysis has shown very favourable outcome including improvedsurvival rate.Objectives: We sought to serially assess the pre and post-PCI TIMI-flow in acohort of 2,033 pts treated from 1995 to 2005 for acute MI in our institution.Methods and results: A total of 2,300 patients were treated for acute MI be-tween 1995 and 2005. Shock was present on admission in 267 patients whowere excluded from the present analysis. A total of 2,033 pts were included in thepresent analysis. Seventy-nine percent (79%) were males and their mean agewas 61±14 years-old. The mean time elapsed between chest pain onset and ad-mission to the cath-lab was 294±249 minutes and 23% of pts were treated by pre-hospital thrombolysis. Pts treated by pre-hospital thrombolysis were treated by di-rect stenting in 56% (vs. 40% in pts treated by primary PCI, P<0.0001) and their
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Angiography in acute myocardial infarction 917
30-days survival rate was 2.2 (vs. 4.4% in pts treated by primary PCI, P<0.05).Pre- and post- PCI TIMI flow as well as 30-days mortality are presented in thetable below.
Time between pain onset to lytics of PCI 0-1 2-3 4-6 7-9 10-12
Pre-PCI TIMI 3 Flow Lytics + PCI 67% 58%1 44%2 36%3 40%3
PCI alone 17% 19% 14% 15% 13%Post-PCI TIMI 3 Flow Lytics + PCI 100% 90%1 89%1 93% 90%1
PCI alone 93% 94% 94% 93% 84%1
30-day mortality Lytics + PCI <1% 2%1 4%1 <1% 2%1
PCI alone 2% 4%1 4%1 4%1 7%2
1p<0.05, 2p<0.01, 3p<0.001, #p<0.0001 (vs.0-1)
Conclusion: The improved survival rate observed in pts treated by pre-hospitalthrombolysis and emergency PCI is associated with higher rates of pre-PCI TIMI-3 flow, especially during the golden hour.
P5281 Clinical and angiographic characteristics of acutemyocardial infarction due to vasospastic anginawithout organic coronary heart disease
D.B. Kim1, K.B. Seung2, P.J. Kim1, D.I. Shin1, C.S. Park1,H.J. Park1, S.H. Baek1, K.B. Choi1. 1St. Paul hospital, Internal
Medicine, Seoul, Korea, Republic of; 2Kangnam St. Mary’s Hospital, Cardiology,Seoul, Korea, Republic of
Background and Objectives: In some patients with the diagnosis of variantangina, dangerous complications, such as acute myocardial infarction (AMI) thatcan lead to sudden death, are observed during an ischemic attack. We evalu-ated the characteristics of AMI associated with vasospastic angina (VA) withoutorganic coronary heart disease.Methods: VA was defined as a transient luminal narrowing, greater than 99%, ofthe coronary artery, and chest pain during a coronary spasm provocation test afterinjection of intra-coronary acetylcholine. AMI associated with VA was defined bycardiac marker (troponin-I and CK-MB) elevation and no organic coronary heartdisease by angiography.Result: We evaluated 672 coronary spasm provocation tests performed betweenJanuary 2003 and June 2005. We diagnosed coronary spastic angina in 292 pa-tients. Among the 292 patients, 21 patients (7.2% of all VA patients) experiencedan AMI. There were 20 patients who initially visited the emergency room for AMIwithout suffering prior VA. Among the 20 patients, 16 patients had a ST eleva-tion in the initial ECG (anterior wall 8 patients, Inferior wall 6 patients). One pa-tient with a history of VA experienced an AMI during medication discontinuation.There were no observed differences between baseline characteristics of VA groupwith AMI and the VA group without AMI except for the hs-CRP. For the results ofthe echocardiography, except for the ejection fraction (42±19% vs. 67± 13%,p<0.001), there were no differences observed between the two groups. Ten pa-tients, among 21, experienced severe emotional stress, which was evaluated bythe Beck Depression Inventory. The spasm provocation test showed that the AMIpatients had more multivessel and diffuse spasm compared to the VA patientswithout AMI (respectively, 76% vs. 57%, p=0.008; 86% vs. 59%, p=0.013). Whiletaking medication for VA, none of the VA patients experienced AMI.Conclusion: Clinically, AMI patients with VA usually had their first attack of severechest pain while discontinuing medication; this could be a cause of AMI amongknown VA patients. Half of the AMI patients with VA had emotional stress beforethe AMI attack. Angiographically, the spasm provocation test, in AMI patients,showed more multivessel and diffuse spasm compared to VA patients withoutAMI.
P5282 Predictors of infarct related artery patency aftercombined fibrinolytic therapy in patients withST-elevation myocardial infarction treated withfacilitated percutaneous coronary intervention
D. Dudek, T. Rakowski, A. Dziewierz, L. Rzeszutko, W. Mielecki,M. Wizimirski, K. Zmudka, J.S. Dubiel. Jagiellonian University, Krakow, Poland
Background: Patency of infarct related artery (IRA) before percutaneous coro-nary intervention (PCI) for ST-elevation myocardial infarction (STEMI) is associ-ated with better outcome. Little is known about clinical or angiographic predictorsof IRA recanalization after administration of combined fibrynolytic therapy beforePCI.Methods and Results: A total of 225 non shock pts with STEMI <12 h, admit-ted to remote hospitals with anticipated transfer time to cathlab >90 min wereenrolled. All pts received iv bolus of 40U/kg heparin, 15 mg alteplase and bo-lus of 0.25 mg/kg abciximab at the remote hospital and were immediately trans-ferred for angiography. Infusion of alteplase (35mg/60 min) and abciximab (0.125ug/kg/min) was continued during transfer.Occluded IRA (TIMI 0+1) was found in 14.2% of pts (group A, n= 32) and patentIRA (TIMI 2+3) in 85.8% of pts (group B, n=193) at baseline angiography. Therewere no significant differences in clinical and demographical characteristics andtime from chest pain onset to lysis or from lysis to angiography between studygroups except for smoking rate (A vs B: 50% vs 73.1%; p=0.009). In angiographicanalysis culprit lesion (CL) was defined as the minimal lumen diameter (MLD)
point in IRA (CLMLD) (in group with occluded IRA measurement was done af-ter first pass of guide wire). Angiography revealed similar IRA localization, similarproximal, distal and mean reference diameter, and lesion length in both groups.The distance from CLMLD point to the nearest proximal side branch was longer ingroup A (gr A vs B: 21.2±10.3 mm vs 13.8±11.2 mm; p=0.002). Longer distancefrom vessel ostium to CLMLD in group A was also observed (A vs B: 41.4±28mm vs 32.8±20 mm p=0.05). In multivariate analysis smoking and distance fromCLMLD to the nearest proximal side branch (analysis per each millimeter) werethe independent predictors of IRA patency at baseline angiography (OR 0.3;95%CI 0.11-0.83 p=0.022 and OR 1.066; 95%CI 1.02-1.1 p=0.002 respectively).Using receiver-operating characteristic curve analysis the optimal CLMLD to sidebranch distance cutoff was >11.05mm, with 92.6% sensitivity and 49.6% speci-ficity for predicting TIMI 0+1 at baseline angiography.Conclusions: Angiographic (anatomical) IRA parameters as the distance fromostium to CLMLD and from CLMLD point to nearest proximal side branch mayinfluence efficacy of combined fibrynolytic therapy before PCI despite the similarclinical characteristics and time delay to angiography. A paradoxical beneficialeffect of smoking was also observed.
P5283 What predicts early patency ofthe infarct relatedartery after pre hospital thrombolysis. A prospectivestudy
J. Puel1, Y. Cottin2, L. Belle3, D. Savary1, S. Charpentier3,L. Soulat4, D. Miljkovic5, P.G. Steg6 on behalf of OPTIMAL StudyGroup. 1Toulouse, France; 2Dijon, France; 3Annecy, France;
4Chateauroux, France; 5Boehringer Ingelheim, Reims, France; 6Paris, France
Background: Preshospital thrombolysis (PHT) allows early implementation ofreperfusion therapy in patients with ST elevation myocardial infarction (STEMI).However, PHT fails to result in early recanalization of occluded infarct arteries ina substantial fraction of treated patients.Aim: To identify predictors of successful recanalization of the infarct related artery(IRA) after PHT.Methods: The OPTIMAL registry is a nationwide prospective multicenter cohortof STEMI patients receiving PHT and who underwent coronary angiography 90min to 6h after PHT onset. Demographics, risk factors, and logistic factors will beanalyzed in relation to patency, which will be assessed by an independent blindedcore laboratory.Results: From November 2004 to November 2005, 1236 patients received PHTat a median time of 1.92 hours (Q1 25%: 1.25 h; Q3 75%: 2.83 h) after symptomonset and had an angiogram at a median time of 1.83 hours (Q1 25%: 1.33 h; Q375%: 2.5 h). TIMI flow grades in the IRA were TIMI 3 in 58.02%, 2 in 16.23% and0-1 in 25.75%. Detailed results in terms of univariate and multivariate predictorsof patency will be presented in September.Conclusion: This will be the largest ever cohort to analyze early angiographicpatency of the infarct artery after PHT. It may also identify "optimal" versus "poor"candidates to PHT.
P5284 Cyclic flow variations following primary angioplastyis poor short-term outcome
M. Albertal, F. Cura, M. Trivi, R. Henkin, L. Padilla, J. Thierer,J. Belardi. Instituto Cardiovascular de Buenos Aires, Cardiology,Buenos Aires, Argentina
Background: Recent studies have shown that coronary cyclic flow variation(CCFV) is a platelet-related phenomenon that occurred following reperfusion. Al-though CCFV predicts acute complications following thrombolytic therapy, its im-pact following primary angioplasty has not been evaluated yet.Methods: A total of 141 patients with St-segment myocardial infarction who un-derwent primary angioplasty were included in the analysis. All patients had 12-lead ST-segment monitoring for 24 hours, each analyzed by an independent,blinded core laboratory. The development of CCFV was defined as >3 transi-tions occurring prior to the onset of stable ST-segment recovery. The relationbetween CCFV and in-hospital mortality were analyzed using a multivariate logis-tic regression model using the following variables: age, sex, diabetes, smoking,anterior infarct, Killip class, final TIMI flow grade, the development of coronarydistal embolization during the procedure and 90-minute percentage ST-segmentresolution.Results: A total of 14 patients (9,9%) developed CCFV. Clinical and angiographiccharacteristics were similar between patients with and without CCFV. In-hospitalmortality occurred in 3 patients with CCFV (21,4%) and 3 patients without CCFV(2,4%, p=0,022). Multivariate logistic analysis showed that the presence of CCFV(OR 16.1; 95% CI 2,0-128; P=0,009), a high Killip Class (OR 12.7; 95% CI 1,5-107; P=0,019) and the presence of distal embolization (OR 8,1; 95% CI 1,0-65,9;P=0,049) independently predicted in-hospital mortality.Conclusion: The development of CCFV following primary angioplasty is predic-tive of short-term clinical outcome
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

918 Angiography in acute myocardial infarction / Electrocardiogram in acute myocardial infarction
P5285 Full reperfusion after myocardial infarction asassessed with angiographic perfusion score andtrifecta is associated with improved left ventricleremodeling in patients treated with facilitated PCI
R. Sanz1, P.L. Sanchez1, G. Pena1, J.B. Lopez-Messa2 ,R. Hernandez-Antolin3 , J. Alonso-Briales4, C.M. Gibson5, F. Fernandez-Aviles3
on behalf of GRACIA II investigators. 1Heart Sciences Institute (ICICOR),Valladolid, Spain; 2Rio Carrion Hospital, Palencia, Spain; 3Clinic San CarlosHospital, Madrid, Spain; 4University Clinic Hospital, Malaga, Spain; 5Brighamand Womens Hospital, Boston, United States of America
New angiographic full perfusion parameters like angiographic perfusion score(APS) and trifecta have never been correlated with left ventricle (LV) post-infarction remodeling. The aim of this study was to analyze the relationship be-tween the full perfusion after acute myocardial infarction (MI) and LV remodeling.Methods: 212 patients (pts) with ST-elevation MI (STEMI) within 12 hours ofsymptom onset were randomized to primary PCI within 3 hours ± abciximab(n=108) or TNK-facilitated PCI (TNK bolus and enoxaparin immediately and stentor CABG within 3-12 hours) (n=104). Angiograms (TIMI flow grade [TFG], TIMImyocardial perfusion grade [TMPG], LV ejection fraction [LVEF] and volumes) andelectrocardiograms (ST-elevation resolution [STRes]) were analyzed by a corelaboratory blinded to randomization and outcomes, at baseline and at 6-weekfollow-up. APS was defined as the sum of the TFG and TMPG before and afterPCI (range 0-12), and trifecta was defined as TFG=3, TMPG=3 and STRes>70%.Results: full perfusion (APS 10-12) was more frequent in the facilitated PCI arm(49%vs9%,p<0.001) and the trifecta was achieved more frequently in the facil-itated PCI arm as well (21%vs6%,p=0.002). Pts with an APS of 10-12 had areduction in systolic LV volume (SV) and an increase in ejection volume (EV) at6-week follow-up in relation to pts with APS of 0-3 (�SV - 4cc vs 6.2cc, p=0.015;�EV 12.2 cc vs 0 cc, p=0.009). In the facilitated PCI group the APS and thetrifecta were associated with LVEF evolution (figure) indicating a more favorableLV remodeling in pts with full reperfusion after STEMI. This relationship was notobserved in the primary PCI arm.
Delta-LVEF (6months FU in both arms)
Conclusion: pts with STEMI treated with TNK-facilitated PCI show more com-plete reperfusion parameters and this is associated with more favorable LV re-modeling.
P5286 Impact of angiographic slow/no flow duringpercutaneous coronary intervention on long-termprognosis in patients with acute myocardial infarction
K. Suenari, N. Shiode, K. Shirota, H. Ishii, K. Gotou, A. Sairaku,S. Mikami. Matsue Red Cross Hospital, Department Of Cardiology,
Matsue, Japan
Background: Angiographic slow/no flow during percutaneous coronary interven-tion (PCI) in patients with acute myocardial infarction (AMI) is associated withunfavorable results. The aim of this study was to investigate the predictive factorsand long-term prognosis of AMI patients with angiographic slow/no flow duringPCI.Methods: We evaluated 228 consecutive AMI patients without cardiogenic shockwho admitted within 24 hours after the onset of symptoms and underwent emer-gency PCI. The patients were classified as either slow/no flow (N=36) or normalflow (TIMI-3 flow) (N=192) based on cineangiograms during procedure. We eval-uated clinical and angiographic characteristics and mortality during 1-year follow-up period in both groups.Results: No significant differences were seen between two groups in baselineclinical characteristics. Multivariate logistic regression analysis revealed that hy-perglycemia on admission (>180 mg/dl) (odds ratio [OR] 2.25; 95% confidenceinterval [CI] 1.07-4.73; P=0.034) and long lesion in the infarct-related artery (>10mm) (OR 3.15; 95% CI 1.47-6.72; P=0.003) were significant and independentpredictors of angiographic slow/no flow during PCI. Total mortality estimated us-ing Kaplan-Meier method was significantly higher in slow/no flow group than innormal flow group during follow-up period (Figure).
Kaplan-Meier survival analysis
Conclusions: In AMI patients, acute hyperglycemia on admission and long lesionin the infarct-related artery were strong independent predictors of angiographicslow/no flow during PCI. In addition, angiographic slow/no flow was significantlyassociated with 1-year mortality.
ELECTROCARDIOGRAM IN ACUTE MYOCARDIALINFARCTION
P5287 ST-elevation 0.5 mm or more in lead aVL and/or anyST-elevation in aVR - a simple ECG marker forproximal LAD occlusion
M.J. Eskola1, K.C. Nikus1, L. Holmvang2, S. Sclarovsky3,H.H. Tilsted4, H. Huhtala5, K.O. Niemela2, P. Clemmensen3.
1Heart Center Tampere University Hospital, Department of Cardiology, Tampere,Finland; 2Heart Centre, Rigshospitalet, Copenhagen, Department of CardiologyB, Copenhagen, Denmark; 3University of Tel Aviv, Tel Aviv, Israel; 4AalborgUniversity Hospital, Aalborg, Denmark; 5University of Tampere, School of PublicHealth, Tampere, Finland
Objectives: The study assessed the value of the electrocardiogram (ECG) topredict the site of occlusion in relation to the diagonal branches in patients withacute anterior myocardial infarction (AMI).Background: In acute anterior AMI the site of occlusion of the LAD is importantbecause proximal occlusion is associated with less favorable outcome and prog-nosis. This subgroup of AMI patients should be recognized by simple non-invasivemethods for immediate primary PCI.Methods: In a prospective post-hoc DANAMI-2 substudy we compared two pre-specified ECG patterns to determine the level of LAD occlusion based on the12-lead ECG in 155 patients treated with primary PCI. Occlusion in the proximalpart of the LAD was defined by 1) concomitant ST-elevation ≥ 0.5 mm in lead aVL(aVL+ pattern) or 2) either ST-elevation ≥ 0.5 mm in lead aVL or any ST-elevationin lead aVR (aVR+ pattern). An additional analysis was performed after excludingpatients (n=9) with concomitant ST-elevation ≥ 1 mm in all inferior leads (proximalpattern). Both the ECG:s and the angiograms were analyzed by independent corelaboratories blinded to the clinical data.Results: Table 1 describes the sensitivity, specificity and predictive values in thedifferent groups. We found that a proximal occlusion of the LAD could be pre-dicted with a sensitivity of 94% and specificity of 49% when the ST-segment waselevated in lead aVL or aVR and patients with ST-elevation in all inferior leadswere excluded from the analysis.
Table 1. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value(NPV) for the different ECG patterns to predict proximal occlusion of the LAD
ECG pattern Sensitivity (%) Specificity (%) PPV (%) NPV (%)
aVL+ 82 50 84 45aVR+ 87 50 85 55Proximal 94 49 85 71
Conclusions: ST-elevation ≥ 0.5 mm either in lead aVL or any ST-elevation inaVR in association with precordial ST-segment elevation in at least two contigu-ous leads (including V2, V3 or V4) is an ECG marker with good sensitivity, positiveand negative predictive values for a culprit lesion proximal to a medium-sized orbig diagonal side branch.
P5288 Normal limits of STj in V3R-V6R and V7-V9
P.W. Macfarlane1, J. Petryka2, E. Kaczmarska2. 1University ofGlasgow, Cardiology, Royal Infirmary, Glasgow, United Kingdom;2University of Warsaw, Warsaw, Poland
Introduction: It is well established that age and sex significantly in-fluence the standard 12 lead ECG morphology. Normal limits of STj amplitudein the conventional 12 lead ECG amply demonstrate this. On the other hand, lit-tle is known about the effect of constitutional variables on normal limits of ST-Tmeasurements in right sided chest leads V3R-V6R and additional posterior leadsV7-V9 which are often recommended for use in cases of suspected acute my-ocardial infarction. The aim of the present study, therefore, was to measure the
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Electrocardiogram in acute myocardial infarction 919
upper limits of normal ST-T amplitudes in V3R-V6R and V7-V9, to determine ifthey are age and sex dependent and to set criteria for abnormal ST elevation inthese leads.Methods: Standard 12 lead ECGs as well as right sided leads V3R - V6R and ad-ditional posterior ECG leads V7 - V9 were obtained from 200 apparently healthyvolunteers. There were 88 men with a mean age of 42.2 ± 14.3 (20 - 85 years)and 112 women with a mean age of 42.3 ± 13.3 (19 - 89) years. For some analy-ses, they were divided into 4 age groups namely < 30 years; 30-39 years; 40-49years; >49 years of age. All ECGs were analysed by the Glasgow ECG analysisprogram and upper limits of normal were obtained by excluding 2% of measuresat the top end of a range.Results: No subject had any significant ECG abnormality. No consistent corre-lation between STj amplitude and age was found. In females, there was a cor-relation of STj with age only in V7 (r=-0.22, p=0.02) and in males STj correlatedwith age in V8 (r=0.21, p=0.05) and in V3R (r=-0.23, p=0.034). In V3R, males inthe three younger age groups had significantly higher maximal STj than femalesbut there was no other consistent difference in STj between sexes in V3R-V6R.Max STj amplitude clearly exceeded 0.05mV only in V3R in males. In V3R, V6R,V7 and V9, there were statistically significant differences in mean STj amplitudebetween males and females but the differences were of no clinical significancebeing of the order of a few microvolts. Indeed, max STj < 40 μV in V7 and < 30μV in V8, V9.Conclusion: As far as is known, these unique age and sex based results arederived from the largest set of normal ST-T measurements in V3R-V6R ever ac-quired and from the first ever large set of normal V7-V9 leads. They are of directrelevance in detecting acute STEMI and suggest that STj>0.05mV would be aspecific criterion for abnormal ST elevation in additional leads V7-V9 and V3R-V6R both for males and females with the exception of V3R where STj > 0.1mVfor males is the recommended threshold for abnormality.
P5289 Early ST segment resolution in STEMI: spontaneousreperfusion in acute myocardial infarction
K.R. Bainey1, Y. Fu1, G. Wagner2 , S.G. Goodman3, A. Ross4,C. Granger1 , F. Van De Werf5, P.W. Armstrong4 on behalf ofASSENT 4 PCI Investigators. 1University of Alberta, Department
of Medicine, Edmonton, Canada; 2Duke Clinical Research Institute, Durham,United States of America; 3University of Toronto, Toronto, Canada; 4GeorgeWashington University Medical Center, Washington, United States of America;5University Hospital Gasthuisberg, Leuven, Belgium
Spontaneous reperfusion (SR) in STEMI has traditionally been assessed by coro-nary angiography; however the frequency of SR appears variable and the clinicalimplications remain unclear. Accordingly, in a unique data set derived from theASSENT 4 PCI study we undertook a systematic comparison between ECG andangiographic assessment of SR. Six hundred and four patients randomized to theprimary PCI arm alone of ASSENT 4 PCI in whom both core lab ECG and investi-gator determined TIMI flow grade data were available approximately 60 min afterrandomization and prior to PCI were studied. Sixty minutes after randomizationand prior to PCI, ECG SR (≥70% STR) occurred in 15.6% (94/604) vs.14.9%(90/604) pts with angiographic SR (TIMI grade 3). The table shows clinical out-comes according to each SR method; notably only 37% of ECG SR pts also hadangiographic SR.Whereas the frequency of SR was comparable by ECG and angiographic criteria,clinical outcome differences best tracked the ECG measures. These data lendfurther support to the role of the ECG in assessing reperfusion and are presum-ably a reflection of not just infarct-related artery patency, but overall myocardialperfusion.
P5290 Comparison of ST resolution in primaryPercutaneous Coronary Intervention for anteriorversus Inferior STEMI
A. Yeung, A. Farshid, D. Coles, D. Mc Gill, S. O’ Connor, I. Jeffery,R.P. Tan on behalf of Department of Cardiology, The Canberra
Hospital.. The Canberra Hospital, Department of Cardiology, Canberra, Australia
Anterior ST elevation MI [STEMI] confers a higher mortality than inferior STEMI.Early complete ST resolution [STR] post reperfusion therapy is an independentpredictor for mortality.Aim: To compare the degree of STR in anterior vs inferior STEMI in patients
Abstract P5289 – Table 1
Electrocardiographic spontaneous reperfusion Angiographic spontaneous reperfusion
Spontaneous (≥70% STR) Non-spontaneous (<70% STR) P value Spontaneous (TIMI=3) Non-spontaneous (TIMI<3) P value
N= 94 510 90 514�ST at baseline (mm) 13 (9,20) 13 (9.18) 0.762 13 (8,16) 13 (9,19) 0.144Time from symptom onset to randomization (min) 133 (92,214) 140 (91, 220) 0.69 125 (80, 211) 140 (94, 224) 0.1Time from randomization to 60 min ECG (min) 67 (50,100) 64 (45, 90) 0.101 76 (56, 105) 62 (45, 89) 0.001Time from randomization to Angiography (min) 85 (70, 115) 85 (70.120) 0.92 97 (80, 130) 84 (69, 115) <0.00130 day clinical outcomes
Reinfarction % 0 3.3 0.089 1.1 3.1 0.490Death % 0 3.5 0.092 2.2 3.1 1.00Death/reinfarction % 0 5.7 0.015 2.2 5.3 0.290Death/shock/CHF% 8.5 12.5 0.303 10.2 12.2 0.722
undergoing primary percutaneous coronary intervention [PCI] and its effect on 30day mortality.Method: 120 consecutive patients undergoing primary PCI for STEMI from Jan-uary 2004 to June 2005 were recruited for the study. Percent [%] STR was cal-culated by measuring the difference in sum ST elevation in all leads in paired 12lead ECGs. Early STR was measured at 1 hour post-PCI and late STR at 18-24hrs post-PCI. STR was defined as complete [>70%], partial [30-70%] and none[<30%].Results: See Table 1.
Table 1
Anterior Inferior
Pt Nos [%] 50 [41.6%] 70 [58.3%]Mean age, years 62.6 61.5Female 32.9% 34.0%Early STR analysis*
Complete 46.9% 71.0%Partial 32.7% 13.0%None 20.4% 16.0%Mean time between ECGs hrs:mins 3:02 3:56
Late STR analysis*Complete 57.2% 91.2%Partial 26.5% 4.4%None 16.3% 4.4%Mean time between ECGs hrs:mins 18:45 23:08
Overall 30day mortality† 8.0% 4.4%>70% Early STR 30day mortality† 4.3% 4.1%<70% Early STR 30day mortality* 11.5% 5.3%
*p value significant, †p value non-significant.
Conclusion: Anterior STEMI have less early and late STR respectively post pri-mary PCI. The mortality for anterior STEMI may be higher only when early STRis not complete.
P5291 Symptom onset to balloon time in patients withST-segment elevation myocardial infarction (STEMI)treated by primary angioplasty. Influence onST-segmento resolution and on prognosis
F. Soto Loureiro1 , E. Abu Assi1, E. Paredes Galan2, A.N.A. Garcia1,R. Vidal Perez1, R. Trillo Nouche1, C. Iglesias Carreno1, A. Amaro Cendon1.1Hospital clinico universitario de santiago, Santiago De Compostela, Spain;2Hospital Meixoeiro de vigo, Pontevedra, Spain
Background and objectives: With controversy in the field, we wanted to assessthe influence of symptom onset to balloon time in the context of STEMI on the STsegment resolution and on the mortality.Methods: we conducted a retrospective study from January 1997 to August 2004.The study was based on a sample of 558 consecutive patients with STEMI treatedby primary percutaneous coronary intervetion. Symptom to balloon time was de-fined as the elapsed time between symptom onset and the first balloon inflation.The mean meassure was the resolution of ST segment immediatly and at 8 hoursafter PCI as a clinical marker of myocardial reperfusion. The mean (SD) clinicalfollow up was 51 (20) months.Results: Table 1 summarises clinical features according to symptom to balloontime.
Table 1
Symptoms to ballon time < 2 h 2-4 h 4-6 h > 6 h p value
Age (> 70 years) % 32 30 17 21 < 0,0001Male % 46 29 12 13 0,047Diabetes mellitus 28 32 17 23 0,052ST segment resolution (%) 36 29 19 15 <0,0001Procedural success(%) 47 29 13 12 < 0,0001Left ventricular ejection fraction >50% (%) 49 30 11 10 0,001Mortality (%) 11 21 30 38 <0,001
h: hours
After adjustment of other potentially confounding variables, sypmtom to balloontime was the variable associated with less ST segmento resolution (HR 1,772,95% CI 1,46 to 5,15).Conlusions: This study shows that, in patients with STEMI treated by primaryangioplasty, symptom onset-to-balloon time is related to ST segment resolution,less procedural and mortality.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

920 Electrocardiogram in acute myocardial infarction
P5292 Admission ECG of patients with inferior myocardialinfarction may predict high risk cases requiringcoronary angiography following in-hospitalmanagement
A.S. Majumder, M.S. Kabir, A.W. Chowdhury, A.E.M.M. Islam,A. Hossain, M.U. Ahmed, A. Muttalib, S.A.M. Husnayen. NICVD,
Cardiology, Dhaka, Bangladesh
Background: Isolated inferior myocardial infarction (MI) is supposed to involvea small area of myocardium. One would think of significant lesion involving onlysingle coronary artery like right coronary artery (RCA) or uncommonly left cir-cumflex artery (LCX) in such cases. We frequently come across cases of inferiorMI having multiple lesions in coronary angiogram. It will be useful if we can pre-dict the extent of the disease on coronary angiogram from the admission ECG.To find out whether an admission ECG can predict these high risk cases we un-dertook a study by performing CAG in every patient having inferior MI.In a thirdworld country, like Bangladesh, where patients fail to have regular follow up orfail to undergo non-invasive evaluation for ischaemic myocardium after an acuteMI we may perform coronary angiography after stabilization of the acute event inthose high risk cases determined by presenting ECG on admission.Patients and method: CAG was performed in a total of 202 consecutive patientshaving inferior MI, who gave consent for it, in a single unit of the departmentof Cardiology, at NICVD, Dhaka. Admission ECG was correlated with the angio-graphic finding.Results: Only 13 out of total 202 patients were female. Triple vessel diseasewas found in 106 (52.5%) patients; out of whom 94 patients had anterior is-chaemia (ST- depression) besides inferior MI. Double vessel disease was foundin 47 (23.26%) patients; out of whom 43 patients had ST depression in pre-cordialleads. Posterior extension of inferior MI was found in 16 patients, 15 of whom haddouble vessel disease. Right ventricular infarction was found in 14 patients, 6 ofwhom had double vessel disease and 4 patients had triple vessel disease. Amongthe remaining 19 patients, 17 had single vessel disease and 2 had double vesseldisease.Conclusion: Anterior ischaemia as evident by ST-depression in pre-cordial leadsin patients with inferior MI strongly suggests double or triple vessel involvementof coronary arteries. Patients having associated posterior or RV infarction alsohave more chance of suffering from multi vessel disease. It may be concludedthat inferior MI patients whose admission ECG suggests multivessel involvementshould undergo coronary angiography regardless of their clinical or non-invasiveevaluation for residual ischaemia.
P5293 Dynamic of the ST-segment elevation and the CK-MBpeak in risk stratification of thrombolysed patients foracute myocardial infarction
G. Tatu-Chitoiu, C. Teodorescu, M. Dan, M. Guran, P. Capraru,N. Caea, M. Dorobantu. Spitalul Clinic de Urgenta, Cardiologie,
Bucharest, Romania
Background: 1.Rapid reduction of the ST-elevation by more than 50% from theinitial value and a peak of the CK-MB within the first 12 hours are the bed-side cri-teria for coronary reperfusion (CR) in patients (pts) with thrombolytic therapy (TT)for ST-elevation myocardial infarction (STEMI). 2.There are poor data regardingthe behaviour and clinical significance of the CK-MB curves in pts without ECGsigns of CR.Objective: To compare the in-hospital mortality in pts with early (4-12 hours) andlate (12-24 hours) CK-MB peak and with and without ECG criteria of CR and inpts. without TT for STEMI (non-TT pts) as well.Methods: A group of 786 consecutive pts. have been treated either with (560pts) or without TT (226 pts) within the first 6 hours after the onset of STEMI.All pts received aspirin, unfractionated heparin or enoxaparin, beta-blockers andconverting enzyme inhibitors if no contraindicated. In all pts. a 12 lead ECG wasrecorded at admission and at every 24 hours thereafter. In TT pts. additional 12-lead ECGs were recorded before the onset of the TT and every 10 min. for thenext 180 min. In all pts the CK-MB levels were measured at admission and at4,9,12,16,20,24,36,48,72 and 96 hours thereafter.Results: ECG criteria of CR was seen in 392 pts. In 303 (77.29%) of these ptsthe ECG sign of CR was also sustained by an early CK-MB peak. A similar earlyCK-MB peak was also seen in 101 pts (60.11%) without ECG criteria of CR. Innon-TT pts. an early CK-MB peak was seen in only 29.64%. In pts who met theECG criteria of CR the in-hospital mortality was 3.96% in subgroup with an earlyCK-MB peak and 4.49% in the one showing a late CK-MB peak. In pts withoutECG criteria of CR the in-hospital mortality was 8.91% if an early CK-MB peakwas detected and 19.40% if the CK-MB peak appeared after 12 hours. In non-TTpts. the in-hospital mortality was 19.49%Conclusions: Our data suggest that the dynamics of the ST-segment elevationand of the CK-MB allow a risk stratification of STEMI thrombolysed pts. In ptsshowing the ECG criteria of CR the in-hospital mortality is low, irrespective if anearly or a late CK-MB peak is recorded. Patients without ECG signs of CR can bedivided in two subgroups: 1. pts showing an early CK-MB peak (these pts. havean intermediate risk); 2. pts showing a late CK-MB peak (these pts. have a similarhigh mortality compared with the non-TT pts). This stratification could be used fora better rescue PTCA strategy.
P5294 Improved clinical outcome of diabetic patients withacute myocardial infarction treated with antioxidantvitamins C and E. Substudy of randomized,multicenter MIVIT trial
T. Jaxa-Chamiec, B. Bednarz, L. Ceremuzynski on behalf ofPolish MIVIT Trial Investigators. Postgraduate Medical School, Department ofCardiology, Grochowski Hospital, Warszawa, Poland
Background: There is a lot of evidence that reactive oxygen species play a cru-cial role in ischemia/reperfusion injury and in the pathogenesis of diabetes. Ex-perimental and biochemical data suggest that vitamins C and E have substantialantioxidant properties.Aim: to elucidate the clinical effects of vitamins C and E in diabetic patients withacute myocardial infarction (AMI).Methods: 800 patients (male 69%, mean age 63±12) with AMI were randomlyassigned to receive, on top of routine medication, one of two treatments: vitaminC (infusion of 1000 mg/12h) followed by vitamin C (orally 1200 mg/24h) togetherwith vitamin E (600 mg/24h) or placebo for one month.Results: There was a significant reduction in 30-day cardiac mortality in diabeticpatients treated with antioxidant vitamins C+E.
Diabetes Cardiac mortality n (%) OR [95% CI] p
Placebo (n=398) Vitamins (n=402)
Yes (n=122) 14 (22) 5 (8) 0.32 [0.11-0.93] 0.036No (n=678) 19 (6) 19 (6) 0.98 [0.51-1.86] NS
Conclusion: In this relatively small group of diabetic patients with AMI we ob-served significant improvement of clinical outcome of those treated with antioxi-dant vitamins C and E. This study encourages the initiation of a large-scale trialto confirm the usefulness of this inexpensive and safe therapy.
P5295 Are all glycoprotein IIb-IIIa inhibitors equal when usedupon angioplasty in patients with ST-elevationmyocardial infarction?
P.F. Monteiro on behalf of on behalf on the Portuguese AcuteCoronary Syndrome Registry Investigators. Coimbra University
Hospital & Medical School, Cardiology, Coimbra, Portugal
Introduction: Each glycoprotein IIB/IIIA inhibitor (GPI) claims for itself a superiorclinical efficacy, but which one is the best when used in the real world?Aim: To evaluate, in ST-elevation acute myocardial infarction (STEMI) patientstreated with GPI following percutaneous coronary intervention (PCI), if the GPIused influences in-hospital prognosis. Population and methods: Retrospectiveanalysis of a nationwide database containing 1315 patients admitted since 2002for STEMI and treated with GPI in the context of PCI. Population was subdividedin three groups: Abciximab (n=850), Eptifibatide (n=176) and Tirofiban (n=289).Results: Patients treated with tirofiban had more previous use of aspirin andstatins. The highest rate of smoking habits was in patients treated with abcix-imab, which had also less previous angina and infarction and were more sub-mitted to acute reperfusion and primary PCI, double antiplatelet therapy, hepain,angiotensyn-converting enzyme (ACE) inhibitors and statins, having had less re-current angina, lower maximal killip class and lower rate of in-hospital morbidity.Patients on eptifibatide were more often male and had more hypertension, an-terior wall STEMI, severe left ventricular dysfunction, reinfarction and in-hospitalmortality. Multivariate analysis showed that the GPI used was not an independentpredictor of in-hospital morbidity or mortality, unlike catecholamines (higher mor-bidity and mortality), ACE inhibitors (lower mortality), statins (lower morbidity) andsevere left ventricular dysfunction (higher mortality) - Figure 1.
Fig. 1. Results
Conclusion: In STEMI patients submitted to PCI and GPI therapy, the GPI useddoes not independently influences in-hospital prognosis, unlike other cardiovas-cular therapies anf left ventricular function.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
Electrocardiogram in acute myocardial infarction / Bifurcation 921
P5296 Impact of clopidogrel on 1-year mortality in hospitalsurvivors of STEMI without early reperfusion-therapy
B. Mark, A.K. Gitt, H. Wienbergen, U. Zeymer on behalf ofACOS-study group. Herzzentrum Ludwigshafen, Kardiologie,Ludwigshafen, Germany
Randomized trials showed a better short-term outcome in patients (pts.)treated with clopidogrel in acute ST-elevation infarction (STEMI) with or with-out reperfusion-therapy. Less is known about the long-term effect of clopidogrel-treatment in pts. without early reperfusion.Methods: From 2000 to 2002, 7732 consecutive pts with an acute STEMI were in-cluded in the prospective, multicentric ACOS-registry (Akutes COronar-Syndrom-Registry). We analysed all STEMI pts. without early reperfusion-therapy dis-charged alive after the index event. We compared the 1-year-outcome of pts.on aspirin with and without additional clopidogrel at discharge.Results: Out of 2049 pts. without reperfusion-therapy, 635 pts. (31%) receivedclopidogrel (+) at discharge and 1414 pts. (69%) did not (-). Differences in clinicalcharacteristics and outcome are shown in the table.After multivariate adjustment (for age, gender, diabetes, cardiogenic shock andejection fraction), treatment with clopidogrel at discharge was an independentpredictor of a lower 1-year-mortality (ORadj. 0.64 [95%-CI 0.45-0.92]).
Clinical characteristics and outcome
+ Clopidogrel - Clopidogrel p-valuen=635 n=1414 univariate
Age (years) 68 (60-77) 73 (64-80) <0.0001Male gender 63% 56% <0.0001Diabetes 32% 36% 0.05Prehospit delay (hours) 9.0 (3.0-21.0) 8.3 (2.8-19.2) 0.6Cardiogenic shock 4.1% 6.4% 0.04Ejec.fraction <40% 32% 38% 0.021-year-mortality 11% 21% <0.0001
Conclusion: Clopidogrel-treatment at discharge is associated with an improved1-year-survival in STEMI-pts. without early reperfusion-therapy.
P5297 Long acting calcium channel blocker azelnidipineprevents left ventricular remodeling after myocardialinfarction
D. Nishiya1, T. Omura2, M. Yoshiyama2, T. Kusuyama2,S. Enomoto2, R. Matsumoto2, Y. Izumi2, K. Takeuchi2 . 1Osaka,
Japan; 2Osaka City University Medical School, Osaka City, Japan
Long acting calcium channel blocker has been reported to be effective for treat-ment of ischemic heart disease. However, the effects of long acting calcium chan-nel blocker on cardiac remodeling after myocardial infarction (MI) are still unclear.The purpose of this study was to examine the effect of azelnidipine on the leftventricular remodeling, including systolic and diastolic dysfunction in the myocar-dial infarcted rats. MI was made by ligation of the left anterior descending artery.Then, the rats were separated by 3 groups of sham-operated group, untreated MIgroup and azelnidipine treated MI group. The rats of azelnidipine treated MI groupwere orally administered azelnidipine (5 mg/kg), in a volume of 3 ml/kg, by gastricgavage once per day for four weeks (n=10). Four weeks after MI, hemodynamicmeasurement and Doppler echocardiographic assessment were performed. Asthe results, the left ventricular weight was increased in the untreated MI group(2.21±0.04 g/kg, n=10), compared with the sham-operated group (1.87±0.02g/kg, n=9). Azelnidipine significantly prevented the increase in weight of the leftventricle (2.07±0.02 g/kg, P<0.05). The left ventricular end-diastolic dimension(LVDd) in the untreated MI group (10.0±0.4 mm) was higher than that of thesham-operated group (7.6±0.3 mm). Azelnidipine significantly prevented the in-crease in LVDd (8.9±0.3 mm, P<0.05). Azelnidipine also improved the ejectionfraction (42±3%, P<0.05), compared with the untreated MI group (31±3%). A pa-rameter of diastolic dysfunction, the ratio of E wave to A wave in the untreated MIgroup (5.3±0.8) was significantly increased, compared with that of azelnidipine-treated group (3.2±0.5, P<0.05). In conclusion, azelnidipine can prevent left ven-tricular remodeling, and improve systolic and diastolic function after MI in rats.Administrations of long acting calcium channel blocker for long time can be effec-tive strategies for treating MI.
P5298 The Post Infarction Nurse Practitioner project: theoutcomes of a nurse practitioner led clinical pathwayfor infarction patients
C.J.M. Broers, J.H. Ruiter, J.O.J. Peels, V.A.W.M. Umans. MedicalCenter Alkmaar, Cardiology, Alkmaar, Netherlands
Purpose: In follow-up of our randomized study "Post Infarction Nurse Practitionerproject; a randomized task shifting trail between cardiologist and nurse practi-tioner", we started a prospective study evaluating the implementation of a nursepractitioner led clinical pathway for infarction patients.Aims: This prospective study evaluates the clinical outcomes of a nurse-led clinicfor stable patients recovering from a recent myocardial infarction using a newdesigned clinical pathway.Methods: During a 3 year period, 370 consecutive infarction patients received
medical treatment by a registered nurse practitioner on the cardiology ward un-til discharge. The NP replaced the residents. The NP designed, evaluated andredesigned a clinical pathway using the plan-do-check act cycle.Results: The patients were predominantly males (72%) with a mean age of 63years. 8% of the patients suffered an earlier infarction, 12% had diabetes, 48%were smokers and 48% had high cholesterol. 35% of the patients had a anteriorinfarction and 32% an inferior infarction. 65% of all patients were eligible for revas-cularisation therapy and received a primary PCI, the mean CK level was 1471 u/land there was a mean of 10mm ST deviation on the admission EKG. During thestudy period the admission time dropped from 10.7 days in 2003 until 5.1 day in2005 (p=0.000). The post infarction complications were low (table 1).
Table 1. Admission time and 30 days follow up
2003 2004 2005 total p
N 110 133 127 370Admission time in days 10.7 7.0 5.1 0.000Death no. 0 0 1 1 nsRe-infarction no. 1 0 2 3 nsPCI TV no. 1 1 0 2 ns
PCI TV = Percutan Coronary Intervention Target Vessel
Conclusions: This prospective study shows the effectiveness of a nurse-practitioner led post infarction clinic using a clinical pathway for infarction patients.The admission time reduced significantly in 3 years while the post infarction com-plication rate stayed low.
P5299 Inhibition of histone deacetylase on ventricularremodeling in infarcted rats
T.-M. Lee1, M.S. Lin2, C.H. Tsai1, N.C. Chang3. 1Chi-Mei MedicalCenter, Dept. of Int. Med., Cardiology Section, Tainan, Taiwan;2National Taiwan University Hospital, Department of Pharmacy,
Taipei, Taiwan; 3Taipei Medical University and Hospital, Department of Medicine,Taipei, Taiwan
Objective: Histone deacetylase (HDAC) determines the acetylation status of hi-stones, and thereby control the regulation of gene expression. HDAC inhibitorshave been found to inhibit the cardiomyocyte growth in vitro and in vivo. HDACinhibitors have emerged recently as promising antihypertrophic agents. We as-sessed whether HDAC inhibitors exert beneficial effect on the remodeling heartin infarcted rats.Methods and Results: Twenty-four hours after ligation of the anterior descend-ing artery, male Wistar rats were randomized to either vehicle, HDAC inhibitorsvalproic acid and tributyrin, an agonist of HDAC theophylline, or a combinationof valproic acid and theophylline or tributyrin and theophylline for 4 weeks. Sig-nificant ventricular hypertrophy was detected by increased myocyte size at theborder zone isolated by enzymatic dissociation after infarction. Rats in the val-proic acid- and tributyrin-treated groups significantly attenuated cardiomyocytehypertrophy with similar potency, as compared with the vehicle-treated group (54± 14x103 μm3, 52 ± 10 x103 μm3 vs. 80 ± 18 x103 μm3 in the vehicle group,both P<0.0001, respectively). Left ventricular shortening fraction was significantlyhigher in the valproic acid- or tributyrin-treated groups compared with the vehicle-treated group. Increased synthesis of atrial natriuretic peptide mRNA after infarc-tion was confirmed by reverse transcription-polymerase chain reaction, consistentwith the results of immunohistochemistry and Western blot for acetyl histone H4.The beneficial effects of valproic acid and tributyrin were abolished by adminis-tering theophylline, implicating HDAC as the relevant target.Conclusions: Inhibition of HDAC by either valproic acid or tributyrin administra-tion can attenuate ventricular remodeling after infarction.
BIFURCATION
P5300 Bifurcational lesions treated with paclitaxel elutingstents: a substudy of the TRUE trial (TAXUS in reallife usage evaluation)
N. Morici1, C. Godino1, O. Goktekin2, R. Barbagallo3,C. Tamburrino4, A. Colombo4, M.G. Sangiorgi5, C. Di Mario4. 1San
Raffaele Research Institute, Cardio-Thoracic and Vascular Department, Milan,Italy; 2Royal Brompton Hospital, Cardio-Thoracic and Vascular Department,London, United Kingdom; 3Careggi Hospital, Cardio-Thoracic and VascularDepartment, Florence, Italy; 4Ferrarotto Hospital, Cardio-Thoracic and VascularDepartment, Catania, Italy; 5Columbus Hospital, Milan, Italy
Previous studies of drug-eluting stents (DES) on bifurcations were focused onspecific techniques and plagued by the lack of control and independent dataanalysis typical of single centre studies. We reviewed the results obtained in 149patients with 158 bifurcational lesions involving a side branch (SB) of sufficientdiameter (average reference diameter 2.3+0.45 mm) to be treated with a polymerbased paclitaxel eluting stent (PES, TAXUS) and at high risk of occlusion (pre-PTCA DS 51%), as part of a prospective multicenter trial enrolled between June2003 and December 2004. Only patients with AMI and left main disease wereexcluded. Diabetes was present in 23% of patients, in-stent restenotic lesion in
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

922 Bifurcation
10%. Two stents (DS) were used in 118 lesions (75%) with the majority treatedwith crush stenting (73 patients, 62%). T-stenting was used in 23 patients, 20%,culotte in 5 patients, 4%, V-stenting in17 patients, 14%. In 40 lesions a cross-oversingle stent technique (C-OSS) was used (25%). Final kissing balloon inflationwas used in 113 lesions (83%): 100/118 lesions (85%) treated with DS and 13/40(32%) with C-OSS. Mean stent length was 22.3+7.2 mm for the main vessel (MV)and 20.5+6.5 mm for the SB. Despite a final dilatation at 20 atm for the mainvessel and 15 atm for the SB in the DS group, residual stenosis was 24% both inthe MV and SB. With 73% angiographic follow-up at 6 months (recommended inall patients) and 100% 1 year clinical follow-up the following clinical outcome wasobserved.Only 1 stent thrombosis occurred after 1 month. Unlike previous reports, revas-cularization involved the main vessel in the majority of patients (21/149, 14%).In conclusion, in a real life setting of consecutive bifurcational lesions treatmentwith PES yields high immediate clinical success. Possibly because of the greaterdifficulty to obtain full stent expansion despite high pressure postdilatation anduniversal final kissing balloon dilatation, the thrombosis rate, concentrated in theDS group, and the need for target lesion revascularization remain higher thanin less complex lesion subgroups treated with PES. No differences in immediatesuccess and TLR were observed between DS and C-OSS groups.
P5301 Procedural and long term results of Taxus stent incomplex bifurcation lesions. A single center registry
G. Gasparini, D. Zavalloni Parenti, M.L. Rossi, G. Belli, P. Pagnotta,M. Scatturin, P. Presbitero. Istituto Clinico HUmanitas, Cardiology,Rozzano - Milano, Italy
Background: Treatment of bifurcation lesions with Paclitaxel-eluting stents (PES)is associated with a high restenosis rates. In-stent restenotic bifurcation lesionsrepresent a difficult subset to treat, with long term efficacy of PES still unknown.A single-center registry was established to evaluate the efficacy of PES in thetreatment of de novo and in-stent (bare metal) bifurcation restenotic lesions.Methods: A total of 125 patients with 128 bifurcation lesions were included inour registry. Bifurcation lesions were treated with two strategies: only main vesselstenting or both vessels stenting. Immediate and long-term clinical and angio-graphic outcome was analyzed in the whole population.Results: See Table 1 for results.
De novo Restenotic Bifurcation
Patients (lesions) 90 (93) 35 (35)Mean age (%men) 63.4 (86%) 65.1 (85%)Current smokers/hypertension/hypercolesterolemia 59/60/76% 55/73/68%Diabetes mellitus 33% 40%Technique used: only main branch stenting/2 stents 82/18% 58/42%RD (mm) (MV = main vessel; SB = side branch) (MV) 2.95 (MV) 2.86
(SB) 2.58 (SB) 2.28MLD pre (mm) 0.61 0.69 0.78 0.84MLD post (mm) 3.19 2.77 3.09 2.51MLD 6-mo follow up (mm) 3.08 2.57 2.95 2.26Late loss (mm) 0.11 0.20 0.14 0.25
Diameter stenosis at 6-mo FU 16% 23% 14% 19.9%Procedural success 95.6% 91.5%In hospital MACE 4.4% 5.6%Clinical (and Angiographic) Follow up 100% (62.2%) 100% (71%)6-mo cumulative MACE (TLR) 10.8% (8.6%) 22.8% (11.4%)Stent thrombosis 1.1% 2.8%RR % (MV = main vessel; SB = side branch) (MV) 5.3% (MV) 8%
(SB) 12.5% (SB) 16%
MACE: major adverse cardiac events; TLR: target lesion revascularization.
Conclusion: Treatment of de novo and in-stent restenotic bifurcation lesions withPES is feasible and associated with high procedural success rate and low episodeof stent thrombosis. The TLR rate of 8.6% and of 11.4% is a good result in thissubset of high-risk patients. Restenosis at the side branch remains a problem tobe solved.
P5302 Is the presence of diffuse coronary diseaseassociated with the outcome of bifurcation stentingwith drug eluting stents?
T.C. Aranzulla, J. Cosgrave, R. Babic, M. Ferraro, F. Airoldi, G. Melzi,A. Colombo. Milano, Italy
Background: The impact of atherosclerotic burden on the outcome following per-cutaneous treatment of coronary lesions has never been well demonstrated.Objective: Aim of our study was to assess the relationship between the extent ofcoronary artery disease and the outcome after drug eluting stent (DES) implan-tation in bifurcation lesions.Method: The SYNTAX score, which is based on the number of vessels and le-sions affected and the characteristics of the lesions was calculated in consecu-tive patients treated in bifurcation lesions. Patients were divided into two groups:Group 1 included all patients treated with a DES in both branches, and Group 2all patients who underwent provisional stenting as intention to treat.Results: A total of 200 patients with 263 bifurcation lesions (group 1: 127 pa-tients; group 2: 73 pts) treated between April 2002 and March 2005 were anal-
ysed. Baseline characteristic were similar in both groups. In the provisional grouponly 6 patients required an additional stent on the side branch. In the overallcohort SYNTAX score was associated with the occurrence of MACE: patientswithout MACE had SYNTAX score of 31.6 ± 20; patients with MACE 40.5 ± 26(p=0.01). In group 1 the SYNTAX score was not associated with the occurrenceof MACE: patients without MACE had SYNTAX score of 36.49 ± 21.3; patientswith MACE 41.8 ± 27 (p= 0.233). In contrast, in group 2 the SYNTAX score wasassociated with the occurrence of MACE: patients without MACE had the scoreof 24.5 ± 15, patients with MACE 36.4 ± 24 (p<0.02).Conclusion: Our data suggest that in patients with higher SYNTAX score, cor-relating with the presence of diffuse disease, the treatment of bifurcation lesionsmay require the implantation of stents both in main and side branches.
P5303 Impact of paclitaxel-eluting stents on the one-yearoutcome of patients with bifurcation lesions:multicenter registry in Asia
S. Nakamura1 , J.H. Bae2, Y.H. Cahyadi3, W. Udayachalerm4 ,D. Tresukosol5 , S. Tansuphaswadikul6 . 1New Tokyo Hospital,
Department Of Cardiology, Matsudo, Japan; 2Konyang University Hospital,Daejeon, Korea, Republic of; 3Husada Hospital, Jakarta, Indonesia; 4KingChulalongkorn Memorial Hospital, Bangkok, Thailand; 5Siriraj Hospital, Bangkok,Thailand; 6Chest Disease Institute, Bangkok, Thailand
Background: Previous clinical study utilizing Paclitaxel-eluting stents (TAXUS) insimple coronary lesions demonstrated an impressive reduction in intimal hyper-plasia and restenosis. However, long-term efficacy of TAXUS in treating patientswith true bifurcation lesions is still unknown. A prospective Asian multicenter reg-istry was set up in five high volumes Asian centers to evaluate the efficacy ofTAXUS in the treatment of bifurcation lesions.Methods: A total of 708 patients, 821 lesions (male 70.6%, mean age 68.2) withbifurcation lesions (defined as more than 50% stenosis in both parent vesseland side branch, LMT/bifurcation 11.3%, LAD/diagonal 50.2%, LCX/OM 20.5%,and RCA/PD 18.0%) were treated with 4 strategies: stenting both vessels utiliz-ing TAXUS with Y-stenting (n=204), modified T-stenting (semi-crushing stenting)(n=184), stenting the parent vessel utilizing TAXUS and balloon angioplasty ofthe side branch (n=278) and stenting both vessels utilizing TAXUS with crushingstenting (n=155). We evaluated immediate and long-term clinical results by 6 and12 months coronary angiography.Results: See table for clinical results.
Y-stenting Modified Single CrushingT-stenting stenting stenting
Number of patients 204 184 278 155MACE at 30 days (%) 0 0 0 0Angiographic restenosis rate (12 mo)
Both vessels (%) 6.4 3.3 5.8 5.8Parent vessel (%) 6.9 3.3 5.8 5.8Side branch (%) 10.8 6.5 18.0 14.2
TLR: any vessels (%) 11.8 4.9* 12.2 11.6
Conclusion: Our results suggest that stenting both vessels utilizing TAXUS withmodified T-stenting can dramatically reduce the restenosis rate at follow-up.
P5304 Does stenting modify the angle between daughterbranches of bifurcational lesions and do thesechanges affect clinical outcome?
C. Godino1, N. Morici1, F. Airoldi1, R. Barbagallo2, C. Tamburrino3,A. Colombo3, G.M. Sangiorgi4, C. Di Mario5. 1San Raffaele Institute,
Cardio-Thorac and Vascular Department, Milan, Italy; 2Careggi Hospital,Cardio-Thorac and Vascular Department, Florence, Italy; 3Ferrarotto Hospital,Cardio-Thorac and Vascular Department, Catania, Italy; 4Columbus Hospital,Milan, Italy; 5Royal Bromton Hospital, Cardio-Thorac and Vascular Department,London, United Kingdom
The angle (Â) between distal main vessel (MV) and side-branch (SB) of bifurca-tional lesions influences the technique used for stent implantation and has beensuggested to be a predictor of long term results. This observation, however, camefrom a small retrospective analysis and no studies have measured this  afterstent implantation, which straightens the stented segments and possibly narrowsÂ. We hypotetised that large variations of  and the consequent vessel stretch-ing may induce chronic wall damage and affect restenosis and clinical outcome.We reviewed the results obtained in 188 patients with 200 bifurcational lesionstreated with the polymer based paclitaxel eluting TAXUS Express stent (PES)in a prospective multicenter trial. The bifurcations treated were on the distal leftmain (42, 22%). The  was measured before and after stenting in the angio-graphic projection showing the greatest opening of the 2 branches. A dedicatedQCA program (CMS 5.2 Medis, Leiden, NL) was used to draw the two centerlinesof the daughter vessels joining in the middle of the bifurcation and defining Â. Thedifference of  before and after stenting was also calculated.Culotte stenting was used to treat bifurcations with wider pre treatment  (NS).Double stenting induced a significant reduction of  (-7+18°, p<.0001) while aslight non significant increase (+2°, p=.5) was observed when SS was used. TheDS techniques inducing the greatest decrease in  were crush and culotte. Angio-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Bifurcation / Chronic total occlusion 923
graphic follow-up was performed in 130 patients (69%) at an average of 196+73days. No correlation was observed in the entire population or in the double stent-ing (DS) and single stenting (SS) groups between  pre or the procedure induced change and MV or SB restenosis (Figures 1 & 2).Similarly, the three tertiles of Âchange showed similar rates of target lesion revascularization (TLR)(17%, 13%,14%, p=.4). In conclusion, in a large group of bifurcational lesions the implantationof two PES induced a significant distortion of the lesion geometry, with the largestreduction of the bifurcation angle induced by the crush and culotte techniques.However, this change did not translate in differences of restenosis and TLR.
P5305 Treatment of true coronary bifurcation lesion with themodified crush technique. Thirty-day clinical andeight-month angiographic results
A.R. Galassi, C. Grasso, S.D. Tomasello, R. Barbagallo, F. Marza’,L. Costanzo, G.P. Ussia, C. Tamburino. Ferrarotto Hospital - Catania
University, Cardiology, Catania, Italy
Background: Recent evidence suggest that in true coronary bifurcation lesionsrestenosis at side branch remains a problem despite the use of drug eluting stents(DES) either stenting of both branches or when stenting only the main branch.Methods and results: We report a new stenting technique which was employedin 45 consecutive patients (52 lesions) to treat true bifurcation lesions using DESin both branches. Predilation of the bifurcation lesion with kissing balloons is firstaccomplished. Then a stent in the side branch and a balloon in the main branchare advanced at the site of the bifurcation lesion. The proximal marker of the sidebranch stent must be situated right at the level of the main branch guide wire ata distance of 1- 2 mm proximal to the carina of the bifurcation. The side-branchstent is firstly deployed; after that, the balloon positioned in the main branch isdeployed crushing the protruding segment of the side branch stent. The mainbranch stent is then advanced to cover the ostium of the side branch and it isdeployed. Final kissing balloon is then accomplished. Using this technique pro-cedural success was 100% for both branches, without complications and withexcellent angiographic result in 98% of cases. Pre-procedure reference vessel di-ameter and minimal lumen diameter (MLD) were 2.79+ 0.25 mm and 0.44+ 0.30mm for the main branch, respectively and 2.47+ 0.30 mm and 0.40+ 0.31 mmfor the side branch, respectively. Post-procedure MLD was 2.98+ 0.22 mm for themain branch and 2.57+ 0.15 mm for the side branch. Jailed wire technique wasemployed in 70% of cases. Recrossing of the side branch was possible in 95% ofcases. No MACE were observed at 30-day. Angiographic follow up at 8 monthsshowed a reference vessel diameter of 2,82± 0,15 mm and 2,53± 0,23 mm anda MLD of 2,37± 0,11 mm and 2,21± 0,20 mm for the main branch and the sidebranch respectively; restenosis in the main branch was 8,7% while in the sidebranch was 4,3%. Clinical follow up at 8 months, showed only one case of sidebranch stent thrombosis (2,2%), occurring at 72 days after procedure, resultingin non Q-wave MI. TLR was 13%. No death and Q-wave MI were observed, totalMACE at 8-month were 17%.Conclusions: Immediate and 30-day outcome indicates that "the modified crushtechnique" for true bifurcation lesions with DES is a safe technique, easy to apply.It provides excellent in-hospital and 8-month outcome with very low side branchrestenosis and total MACE rate. These results confirmed the advantage of thisspecific technique to give complete coverage of the ostium of the side branchwith a drug eluting stent.
CHRONIC TOTAL OCCLUSION
P5306 Total Occlusion, Basic Equipments for LesionInterrogation, Evaluation, Visualization andEndoluminal Reopening Study (TO BELIEVERS)
W. Kadro, M. Turkmani, D.A.N.A. Kadro, A. Dbs, I. Eid, A. Hamwi.Golden Cardiovascular Center, Interventional Cardiolgy, Damascus,
Syria Arab Republic
Background: Chronic total occlusion (CTO) is a challenging dilemma for the in-terventional cardiologist. The success rate ranges between 30% and 80% de-pending on the tools used and the patience of the interventional cardiologist whoshould always be ready for the unexpected. We report our results for CTO inter-vention using simple and economic tools.Method: our group did 172 consecutive cases of CTO intervention over the pasttwo years using the simple approach. The tools consist of one guiding catheter,one stiff hydrophilic glide wire, one balloon and one stent in most cases unless thelesion is too long requiring more than one stent. Contra lateral injection to assessthe collaterals was not allowed in this basic equipments protocol for CTO interven-tion. 57% of the cases were turned down for PCI by other cardiologists (group1).CTsurgeons turned down 37% of the patients for CABG (group2). 20.42% of thecases failed attempted PCI by another cardiologists (group3).Results: Overall Angiographic success with TIMI III flow and no significant resid-ual stenosis was achieved in 93% of the cases. There were no death or emer-gency CABG during hospital stay or one month after PCI. Protocol violation (us-age of more than one wire or more than one balloon) was done in 3 cases. Per-foration occurred in 3 (1.74%) cases, one of them required pericardial window.In hospital MI occurred in 2 cases (1.14%). There was no need for GP IIb/IIIa
inhibitors in any case. Success rate were 87%, 92%, 100% in groups 1,2,3 re-spectively. One month follow up results were: 0% mortality, 0% CABG, 0% rein-tervention, 2% rehospitalization for CHF, 1.4% rehospitalization for ACS.Conclusion: CTO is a challenging dilemma for the interventionalist. CTO requiresendless patience from the cardiologist. There is no need to abuse the resourcesof the cath lab if we follow the protocol of TO BELIEVERS. Excellent results canbe obtained if CTO intervention done by using these basic equipments
P5307 Stenting in chronic total occlusions reducesrestenosis compared with balloon angioplasty but isassociated with a higher risk of non-fatal MI
B. Kunadian, J. Dunning, K. Vijayalakshmi, A. Sutton, D. Muir,R. Wright, J. Hall, M.A. De Belder. The James Cook University
Hospital, Middlesbrough, United Kingdom
Background: Stenting reduces the need for repeat revascularisation comparedwith percutaneous transluminal coronary angioplasty (PTCA) alone in chronic to-tal occlusions (CTOs); the impact on short and long-term mortality and frequencyof non-fatal myocardial infarction is unclear.Methods: We performed a meta-analysis of all published randomised trials com-paring stenting with PTCA in CTOs. A full systematic review was performed. Thestudies were combined using the DerSimonian and Laird Random Effects Modelfor dichotomous clinical outcomes. Heterogeneity was also assessed.Results: The 10 trials enrolled 1547 patients, with 771 patients randomised toelective stenting and 776 patients randomised to balloon angioplasty with a meanangiographic follow-up time of 6 months. Random effect odds ratios (OR) fordeath, non-fatal myocardial infarction (MI), repeat revascularization (RptR), ma-jor adverse cardiac events (MACE), reocclusion, and restenosis at 6 months andclinical follow-up to 6 years were computed. No significant difference was ob-served between the stent and PTCA groups in the rates of death (OR 0.74; 95%CI0.28, 1.96; P=0.55) but more non-fatal MI occurred in the stent group (OR 1.94;95%CI 1.01, 3.72; P=0.045). Stented patients had lower rates of MACE (OR 0.45;95%CI 0.31, 0.66; P<0.01),primarily due to less RptR (OR 0.41; 95%CI 0.32,0.53; P<0.01). The restenosis (OR 0.38; 95%CI 0.24, 0.59; P<0.01) and reoc-clusion (OR 0.36; 95%CI 0.22, 0.59; P<0.01) rates at 6 months were lower in thestent group.
Non-fatal MI at 6 months
Conclusions: Restenosis and RptR is reduced by stenting in patients with CTOs.Compared to balloon angoplasty there is a higher rate of non-fatal MI followingstenting, but has no impact on mortality rates.
P5308 Results of a second attempt to open chronicallyoccluded coronary arteries after failed first procedure
M. Scholz, R. Degenhardt, B. Abt, H. Koehler, M. Unverdorben,E. Wagner, C. Vallbracht. Center for Cardiovascular Diseases,Cardiology, Rotenburg A.D. Fulda, Germany
Purpose: Recanalisation of chronic coronary artery occlusions (>1 month) failsprimarily in 20 to 40%. It is unknown whether a second attempt may be performedsuccessfully.Methods: 115 consecutive patients with exercise induced angina pectoris or is-chemia due to a chronic coronary occlusion in whom a former attempt to open theartery had failed were proceeded to a second attempt. All films were examinedagain by two cardiologists. Length of occlusion, side branches, collaterals fromanother major coronary artery and a clear cut stump were noted.Results: The occlusions had a mean age of 25,9 months (1,5-180). The meantime from the first attempt of recanalisation was 6 weeks (6 days to 10 years).73 patients had had an infarction before. In 25 cases the left anterior descendingartery was occluded, in 14 cases the circumflex artery and in 57 cases the rightcoronary artery. In 19 cases large side branches were occluded. A Biotronik stiffwire was taken as standard coronary wire. In 18 cases a graphics PT interme-diate wire was taken additionally. 65 of 115 occlusion (57%) could be reopend(TIMI III: 51, TIMI I-II: 14)). Successrate was higher in younger occlusions (≥6months: 68%, >6 months: 45%; p<0,05) and in occlusions with a clear cut stump(stump: 63%, no stump: 41%; p<0,05). Success rate did not depend on the pres-ence of sidebranches next to the occlusion (yes: 57%, no: 56%) or collateralsfrom another coronary artery (yes: 50%, no: 54%). 3 minor complications wereseen (pseudoaneurysm of the femoral artery, perforation of the coronary wire withminor pericardial hemorrhage and hematoma at puncture site). Reangiography
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

924 Chronic total occlusion
after 4 to 6 months was performed in 52 of 65 patients with successful secondattempt. 70% of the vessels were still open if the primary result had been TIMI III-flow. 43% of arteries with formerly TIMI I-II-flow were still open. Restenoses werefound in 45% of the open arteries and were redilated. In the reoccluded arteriesa re-recanalisation was successful in 42%.Conclusion: A second attempt to recanalise chronically occluded coronary ar-teries after a formerly failed first attempt is successful in more than 50% of thecases. Occlusion age under 6 months and a clear cut stump are indicators for asuccessful recanalisation.
P5309 Successful prevention of lesion recurrence in chronictotal coronary occlusions treated with apaclitaxel-eluting polymer-based stent: long-termresults from the Paclitaxel in chronic total occlusion
G.S. Werner1 , P. Glaser2, M. Fritzenwanger1 , M. Ferrari1,H.R. Figulla1. 1Klinikum Darmstadt, Medizinische Klinik I, Darmstadt, Germany;2Friedrich-Schiller-University, Cardiology, Jena, Germany
Background: The reduction of restenosis by drug-eluting stents provides a newtherapeutic approach to improve the high recurrence rate after percutaneouscoronary intervention (PCI) in chronic total coronary occlusions (CTO). In viewof the unknown risk of late recurrence, the long-term benefit of this novel therapyremains to be established.Methods: In 92 consecutive patients a CTO (duration >2 weeks) was success-fully recanalized with implantation of paclitaxel-eluting stents (Taxus, Boston Sci-entific Corp.). Each of these patients was matched to a patient treated with baremetal stents (BMS) in the preceding time period based on lesion characteristicsand clinical parameters. Angiographic results after 6 months and major clinical ad-verse events (MACE: death, MI, CKMB increase above the upper limit of normal,repeat revascularization) after 24 months were compared. Patients with lesion re-currence underwent repeat PCI, and secondary patency was assessed by repeatangiography.Results: Clinical and demographic data were similar in both groups with a highrate of diabetes in 29% (Taxus) and 23% (BMS). Duration of CTOs was >3months in 70% of patients. The number of stents was 1.7±0.9 in both groups,with a mean diameter of the implanted stent of 3.0±0.3 mm. The mean stentedsegment length was similar in the BMS group with 36±17 mm and the Taxusgroup with 40±20 mm. Periprocedural MACE consisted only of asymptomatic in-crease of CKMB in 2.2% with BMS and 5.4% with Taxus (p=0.44). At 6 monthsrepeat angiography the target vessel failure was significantly lower with Taxusthan with BMS (9.8% vs. 57.2%; p<0.001). Notably, the rate of late reocclusionwas lower with Taxus in 1.1% vs. 23.1% (p<0.001). The clinical MACE rate at 24months was 15% with Taxus and 61% with BMS (p<0.001). In the BMS group6 cardiovascular deaths and none in the Taxus group occurred during follow-up(p=0.015). All 8 restenotic lesions in the Taxus group were focal and were suc-cessfully treated by a repeat PCI with an additional Taxus stent. All underwent arepeat angiography and showed a restenosis in only one patient. The secondarypatency rate was 98.5%. One late stent thrombosis was observed 18 months afterPCI.Conclusions: The implantation of Taxus stents in CTOs lead to a more than80% reduction of MACE and TVF with a secondary patency of 98.5%. Theremay be even a prognostic advantage of the Taxus stent in CTOs. The one latestent thrombosis raises the question about further close observation of this lesiongroup during long-term follow-up.
P5310 Recanalisation of chronically occluded coronaryarteries: experience in 1250 cases, includinglong-term angiographic follow-up
M. Lins, A. Tiroke, N.E. El Mokhtari, D. Krueger, G. Herrmann,R. Simon. Kiel, Germany
PCI of chronically occluded coronary arteries continues to be a challenge of in-terventional cardiology. To elucidate inital success and long-term angiographicfollow-up a consecutive series of 1250 patients, who underwent recanalisation(R) procedure between 1988 and 2002 in our department were investigated.Mean time of occlusion (TIMI 0) was documented for 21 weeks. There were Rof RCA in 43.1%, RCX in 17.3%, LAD in 36.4%, SVG in 3.2%. For R a standardguidewire (14/1000 inch) was used in about 80% of the procedures, less oftenother techniques such as rotational wire or laser wire were performed. Overallsuccess rate was 69% (866/1250) with residual stenosis <50% (QCA, PhilipsDCI): RCA 65.3%, LCX 71.6%, LAD 73.7% and SVG 76.9%. Mean fluroscopytime was 26 min in successful cases and 34 min in unsuccessful cases, totaltime of procedure was 61 and 65 min respectively. Complication rate was 2.7%(35/1250, in- and out- of- hospital): 11 pts developed AMI, 7 pts underwent emer-gency CABG due to perforation or imminent vessel occlusion (in pre stent era).In 13 stented pts SAT was documented, 3 pts suffered from intracranial hem-orrhage and 3 pts died. In 676/866 pts (78%) angiographic follow-up was avail-able: 402/676 pts (60%) showed satisfying results with restenosis <50%, wherasrestenosis was found in 187/676 pts (28%). Reocclusion was less frequent in87/676 pts (12%). Those pts with restenosis underwent reintervention in 90%(168/187) and those with reocclusion in 30% (26/87). All other pts could be med-ically treated in most cases, however, bypass operation was rare. This series of
1250 pts who underwent recanalisation of an occluded coronary vessel shows ahigh primary success rate with standard wire technique. The high angiographicfollow-up rate of 78% shows a very acceptable long-term outcome.
P5311 Three-year clinical and angiographic outcomes aftercoronary stenting of chronic total occlusion usingsirolimus-eluting stents: insights from theRESEARCH registry
H.M. Garcia-Garcia, J. Daemen, K. Tsuchida, C. Van Mieghem,S. Tanimoto, M. Van Der Ent, P. De Feyter, P.W. Serruys. Thoraxcenter, ErasmusMC, Interventional Cardiology, Rotterdam, Netherlands
Background We previously reported that at one year the survival-free of targetlesion revascularization was 97.4% in patients with chronic total occlusion (CTO)treated with sirolimus-eluting stents (SES). Long-term results following percuta-neous coronary intervention (PCI) with SES are currently unknown. We assessedthe three-year clinical and angiographic outcomes of 76 patients with CTO treatedwith SES.Methods From April 2002, all patients in our institution were treated with SESas the device of choice during PCI. SES implantation was carried out in CTOs,defined as target lesion with >3 months of occlusion. The 3-year angiographicalfollow-up is still ongoing and will be presented at the meeting.Results A total of 76 consecutive patients were prospectively enrolled. Sixty-sixpercent was male and mean age was 61±11 years. At three years 13 majoradverse cardiac events occurred. Five patients died, 3 deaths were of cardiaccause, 1 patient died of cancer and the cause of 1 patient was unknown. ThreeMI’s occurred and target vessel revascularization was performed in 8 patients.The cumulative survival-free of MACE is shown in the figure. At 3-year follow-up, so far 30 patients underwent angiography, 4 patientes had binary restenosis(>50% diameter stenosis) and 2 CTOs were found to be reoccluded.Conclusions: Although this is a very high risk subset of lesions and usually thepatients have also high risk characteristics, the results are encouraging. Interest-ingly, 7 (54%) of the MACE events ocurred after one year of the index procedure.
P5312 Comparison of efficacy and safety betweenSirolimus-eluting stent (Cypher) and Paclitaxel-elutingstent (TAXUS) on the outcome of patients withchronic total occlusions: multicenter registry in Asia
S. Nakamura1 , J.H. Bae2, Y.H. Cahyadi3, W. Udayachalerm4 ,D. Tresukosol5 , S. Tansuphaswadikul6 . 1New Tokyo Hospital, Department OfCardiology, Matsudo, Japan; 2Konyang University Hospital, Daejeon, Korea,Republic of; 3Husada Hospital, Jakarta, Indonesia; 4King ChulalongkornMemorial Hospital, Bangkok, Thailand; 5Siriraj Hospital, Bangkok, Thailand;6Chest Disease Institute, Bangkok, Thailand
Background and Purpose: Both Sirolimus-eluting BX velocity stent (Cypher™,Cordis) and Paclitaxel-eluting Express stent (TAXUS™, Boston Scientific) havebeen reported to be effective in preventing neointimal formation and in-stentrestenosis. The aim of this study is to compare the safety and efficacy of these 2stents on the outcome of patients with chronic total occlusions (CTO).Methods: A prospective analysis of 808 patients with 922 CTOs (396 Cypher™and 526 TAXUS™) in five high volume Asian centers after successful recanal-ization of CTO (defined as TIMI flow trade 0 and the age of occlusion was morethan 3 months. Cypher™: LAD 53.5%, LCX 26.8%, RCA 19.7%. TAXUS™: LAD52.3%, LCX 22.1%, RCA 25.6%) was performed. The study endpoints were majoradverse cardiac events (MACE) at 30 days and restenosis rate at 12 months.Results: The baseline clinical characteristics between 2 groups were similar. Seetable for clinical results.
Cypher™ TAXUS™ p
Number of patients 396 526 –Procedural success (%) 100 100 NSMACE at 30 days (%) 0 0.4 NSReference diameter (mm) 2.86 ± 0.80 2.84 ± 0.90 NSMLD post (mm) 2.75 ± 0.80 2.70 ± 0.80 NSMLD at 12 months (mm) 2.70 ± 0.70 2.55 ± 0.75 NSRestenosis rate (%) 4.0 6.7 NSTVR (%) 3.6 6.7 NSMACE at 12 months (%) 3.6 6.7 NS
Conclusion: The use of both stents in patients with CTO was equally safe withlow acute complication and very low incidence of restenosis.
P5313 Late percutaneous coronary intervention for thetotally occluded infarct-related artery improvessurvival: a meta-analysis of 1193 patients
A. Abbate1, D. Appleton1, V. Ramachandran1 , M. Amin1,P. Agostoni2, G.W. Vetrovec2, G.G.L. Biondi-Zoccai3. 1Richmond,
United States of America; 2Antwerp, Belgium; 3Milan, Italy
Background: There is ongoing uncertainty about the risk-benefit ratio of late per-cutaneous coronary intervention (PCI) in stable patients with persistent infarct-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Chronic total occlusion / Saphenous vein grafts 925
related artery occlusion. We performed a meta-analysis of randomized controlledtrials comparing PCI with best medical therapy (medical Rx) in such patientsaimed at assessing impact on mortality.Methods: PubMed, CENTRAL, and mRCT were searched for eligible studies.Random-effect odds ratios (OR) were pooled for the dichotomous clinical out-comes of all-cause mortality. Power and heterogeneity analyses were also per-formed.Results: We combined data from 8 studies enrolling 1193 patients, with me-dian time from acute myocardial infarction to randomization of 8 days (range 1-26days), and median follow-up time of 9 months (range 3-56). Six-hundred-one pa-tients was randomized to PCI and 592 to medical treatment only. There were 17and 31 deaths in the 2 groups, respectively. Overall, PCI was associated withsignificantly greater survival (Peto OR 0.52 [0.29-0.93], P for effect=0.03, P forheterogeneity=0.53). The figure shows individual studies and cumulative analy-sis.
Conclusion: While waiting for larger randomized studies, pooled data from thelargest cohort ever of patients randomized to late PCI versus best Rx for postin-farction total coronary occlusion suggest that PCI is associated with greater sur-vival.
P5314 Chronic total occlusion and incidence of target lesionrevascularization rates after percutaneous coronaryintervention. Western Denmark Heart Registry
L.O. Jensen1, M. Maeng2, P. Thayssen3 , K.N. Hansen4,K. Rasmussen5, L. Krusell5, L. Thuesen5 . 1Odense University
Hospital, Dpt.of Cardiology, Catheterisation Laboratory, Odense C, Denmark;2Skejby Sygehus, University of Aarhus, Aarhus, Denmark; 3Odense UniversityHospital, Odense, Denmark; 4Odense University Hospital, Odense, Denmark;5Aalborg Sygehus, Aalborg, Denmark
Background: The technique of percutaneous coronary intervention (PCI) involv-ing chronic total occlusion (CTO) has improved over time. However, limited dataare available on acute and follow-up results in patients treated with PCI on CTOin recent years. Data from the Western Denmark Heart Registry was analysed toidentify the primary success rate and target lesion revascularization (TLR) within9 months.Methods: from January 2000 to September 2004 data from all PCI proceduresin patients with stable angina pectoris in Western Denmark were prospectivelyrecorded. TLR was defined as repeat PCI of the index lesion or CABG within 9months after the index PCI due to restenosis.Results: A total of 16.358 lesions were treated, and 2.313 lesions were CTO le-sions. Technical success was obtained in 83.8% of CTO lesions and failed attemptusing PCI was observed in 375 CTO lesions. TLR was significantly higher in CTO8.4% vs. 6.2%, p<0.001. In CTO lesions the TLR declined from 10.0% in 2000to 4.8% in 2004, p<0.001 and in non CTO lesions the TLR declined from 7.7%in 2000 to 3.9% in 2004, p<0.001. Compared to non CTO lesions, PCI treatedCTO lesions were longer (20.4 ± 12.3 mm vs. 12.9 ± 7.8 mm) p<0.001, weretreated with longer stents (22.3 ± 10.0 mm vs. 16.2 ± 7.2 mm) p<0.001, hadsmaller vessel size (3.1 ± 0.6 mm vs. 3.2 ± 0.6 mm) p<0.001 and the patientswere younger (61.4 ± 10.9 years vs. 63.7 ± 10.8 years) p<0.001. CTO lesionswere more often stented (bare metal stent) in 2000, 86.0% vs. 77.9%, p<0.001and DES were more often used in 2004, 61.3% vs. 42.9%, p<0.001. Indepen-dent predictors of TLR by multiple logistic regression analysis were: CTO (OR1.40; 95% CI 1.15-1.70, p<0.001) DES (OR 0.32; 95% CI 0.24-0.43, p<0.001),cobalt chromium alloy stent (OR 0.44; 95% CI 0.29-0.68, p<0.001), bare metalstent (OR 0.71; 95% CI 0.59-0.85, p<0.001).Conclusion: Successful PCI was achieved in a high percentage of CTOs andTLR was almost comparable to non CTO lesions. The use of stents with favour ofDES was an independent predictor of TLR.
SAPHENOUS VEIN GRAFTS
P5315 Long term evolution of patients with percutaneouscoronary revascularization and prior coronary arterybypass graft
J.A. Gomez Hospital, A. Sadek, J. Gonzalez-Costello, A. Cequier,E. Iraculis, J. Gomez-Lara, J.L. Ferreiro, E. Esplugas. Hospital
Universitari Bellvitge, Interventional Cardiology, Barcelona, Spain
Aim: Percutaneous coronary intervention (PCI) is increasingly been performed inpatients (pts) with chronic ischemic cardiomyopathy. To determine the long termevolution of pts with prior coronary artery bypass graft (CABG) in whom PCI wasperformed.Methods: We studied all consecutive pts with prior CABG who underwent PCIfrom 1997 to 2003. A Parsonet risk score was calculated for each pts in orderto assess the theoretical risk of a surgical procedure. Pts were prospectively fol-lowed and death, acute myocardial infarction (AMI) and repeat revascularization(RR) were collected.Results: We included 128 consecutive pts, with a mean age of 64±9 years old.CABG had been performed a mean of 7±5 years prior to PCI. Fifty two were di-abetics (40.6%), 72 had hypertension (56.3), and 105 had hyperlipidemia (82%).The mean Parsonet risk score was 12.5±6.5. PCI was performed in 183 lesions(1.4 lesions/pt). A native vessel was treated in 98 pts (76.6%) and a stent wasimplanted in 112 procedures (87.5%). Final angiographic success was achievedin 114 pts (89.1%). In hospital mortality was 3.8% (4 pts), significantly less thanpredicted by the Parsonet score (3.8% vs 12.5%, p< 0.001). Predictors of in-hospital death were pulmonary disease (OR 13, 1.8-93) and a high Parsonetscore (OR1.1, 1.04-1.2). During long term follow-up (41±20 months) 12 pts died(9.4%), 21 pts had an AMI (16.4%), and RR was performed in 29 pts (22.7%). Theindependent predictive factors for long term mortality were an impaired left ven-tricular function (OR 0.9; 0.8-0.9), an urgent PCI procedure (OR 23, 3.7-143) andthe use of beta blockers was found to be a protective factor (OR 0.2; 0.005-0.6).Conclusion: In pts with previous CABG, PCI offers a lower risk compared withpredicted surgical risk assessed by the Parsonet score. Pulmonary disease wasa predictor of in hospital mortality, while the predictors of long term mortality wereimpaired left ventricular function, and an urgent PCI procedure. Treatment withbeta blockers was found to be a protective factor.
P5316 Factors influencing long-term success in saphenousvein grafts angioplasty:Drug-eluting stents eficcacy
A. Pereira1, R. Teles1, P. Goncalves2, M. Almeida2, L. Raposo2,A. Ferreira2, F. Seixo2, A. Silva1. 1Hospital de Santa Cruz,UNICARV, Servico de Cardiologia, Carnaxide, Portugal; 2Hospital
de Santa Cruz, servico de Cardiologia Unidade Hemodinamica, Lisboa, Portugal
Background: Percutaneous coronary intervention (PCI) in degenerated saphe-nous vein grafts (SVG) has evolved scantly and, albeit widely used, drug-elutingstents (DES) benefit remains unclear.Purpose: To determine the prognostic factors that affect long-term success an-gioplasty in de novo SVG lesions.Methods: Retrospective study including 82 consecutive patients (pts) submittedto PCI of de novo SVG lesions between 2000 and 2005. Mean age was 69±9years, 83% were males and bypass surgery was done 11 ± 5 years before percu-taneous intervention. An acute coronary syndrome was the presentation in 44%of pts and 28% of the pts had diabetes, 68% hypertension, 61% dyslipidemiaand 22% were smokers; 47% had previous myocardial infarction (MI) and 38%had an ejection fraction <50%. Left main disease was present in 12% of pts and82% had 3 vessel disease. The primary endpoint was defined as the compositeoccurrence of major cardiac events (MACE): death, non-fatal MI or target vesselrevascularization (TVR).Results: One hundred and twenty lesions were treated. Distal protection deviceswere in place in 19,3% of the cases and IIbIIIa inhibitors were administrated in54,3%. A total of 120 stents (41 DES, 79 bare metal stents- BMS), 1,3±0,7 perpatient. The mean diameter was 3,41 ± 0,6 mm and mean total length 27±16mm. Event-free survival was 62,7% at follow-up (878 ± 160 days). There were 6deaths,11 myocardial infarctions (MI) and 27 TVR. The following MACE predictorswere identified: dyslipidemia (p=0.08) and DES use (p=0.05). By Cox regressiveanalysis the only independent predictor of clinical events was dyslipidemia.Conclusion: The long-term success of saphenous vein grafts angioplasty wasadversely influenced by dyslipidemia. Despite their increased use, drug-elutingstents did not improve results in this population.
P5317 Effectiveness of drug-eluting stents in the treatmentof bypass graft lesions
V. Voudris1, C. Kalianos1, S. Patsilinakos1, A. Manginas1,G. Pavlides1, C. Spargias1, N. Kafkas1, D.V. Cokkinos2. 1OnassisCardiac Surgery Center, 1st Cardiology, Athens, Greece; 2Onassis
Cardiac Surgery Center, 1st Cardiology, Athens, Greece
Background: Percutaneous coronary intervention (PCI) in patients (pts) with by-pass graft lesions (BGL) is associated with an increased rate of subsequent ad-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

926 Saphenous vein grafts / Left main disease
verse events. Encouraging results with drug-eluting stent (DES) have been re-ported in pts with native coronary artery disease (CAD). In this prospective singlecenter non-randomized study we assess the short- and long-term results of DESin pts with BGL as compared to base metal stent (BS).Methods: Forty-three consecutive pts treated with DES were compared with 40consecutive pts treated with BS. The in-hospital results and clinical outcome dur-ing follow-up (22.48 ± 9.4 months, range 4-38) were obtained. Major adversecoronary events (MACE) during follow-up were considered death, myocardial in-farction (MI), bypass surgery (CABG), target and non-target vessel PCI.Results: Clinical presentation of CAD, risk factor profile, previous MI, ejectionfraction < 40%, and stenosis location and characteristics were not different be-tween DES and BS pts; however the incidence of diabetes mellitus was higher inDES pts (51% vs. 25%, p=0.02). PCI was performed to dilate 45 saphenous veingrafts (SVG), or arterial conduits using sirolimus (90%) or paclitaxel (10%) DES,and 43 SVG or arterial conduits using BS. In addition 15 native vessels were di-lated in the DES and 8 in the BS group. The number of stent/pt was 1.67 ± 0.75in the DES and 1.58 ± 0.75 in the BS group (p=ns). Use of IIb/IIIa inhibitors anddistal embolization protection device were 21% and 14% in the DES and 25% and20% in the BS pts (p=ns). The clinical success rate (angiographic success with-out death, Q- wave MI, CABG) was 98% in the DES and 100% in the BS (p=ns).In-hospital complications included sub-acute thrombosis and non-Q-wave MI (de-fined as increases of CK-MB > 3 times normal) (0% vs. 2,5% and 2.3% vs. 2.5%in the DES and BS pts respectively); there was also one (2.3%) Q-wave MI in theDES group. Follow-up angiography performed in 26% and 23% of pts in the DESand BS group showed similar in-stent restenosis rate (33%). Clinical follow-upwas obtained in all pts. There were no differences in death (2.3% vs. 0%, p=ns),MI (2.3% vs. 5%, p=ns) or any revascularization (18% vs, 13%, p=ns) in the DESand BS group of pts and the MACE free survival was 79% and 85% respectively(p=ns). In the DES group these was a non-significant preponderance of MACE indiabetics.Conclusion: The implantation of DES in pts with BGL is associated with similarin-hospital and long-term results, compared to those treated with BS, despite ahigher incidence of diabetes mellitus in DES pts.
P5318 Sirolimus-eluting stents effectively inhibit neointimalproliferation as compared to bare metal stents indiseased saphenous vein grafts: 6-monthintravascular ultrasound results of a randomized trial
P. Agostoni1, P. Vermeersch1 , S. Verheye1, P. Van Den Heuvel1,C. Convens1, N. Bruining2, F. Van Den Branden1, G. Van Langenhove1 . 1AZMiddelheim, Antwerp, Belgium; 2Thoraxcenter, Rotterdam, Netherlands
Purpose: The RRISC trial is a randomized double blind comparison of sirolimus-eluting stent (SES) versus bare metal stent (BMS) in diseased vein grafts. The6-month angiographic and clinical benefits of SES, with significant reductions inrestenosis and repeated revascularizations, have been already reported. We de-scribe here the intravascular ultrasound (IVUS) analysis of our trial.Methods: 75 patients with 96 lesions localized in 80 diseased vein grafts wererandomly allocated to SES or BMS. Six-month angiographic follow up was man-dated for all patients and IVUS was recommended in all. Volumetric quantitativeIVUS analysis was obtained for stent and lumen with a validated software. Neoin-timal volume (NIV, defined as the difference between stent volume and lumenvolume) was the primary end point. Late incomplete apposition volume was alsoevaluated.Results: 38 patients received 60 SES for 47 lesions, while 37 patients received54 BMS for 49 lesions. IVUS analysis was performed in 59 patients (79% of allthe patients). Overall, 34 lesions (40 stents) were analyzed in the SES group,while 39 lesions (42 stents) were analyzed in the BMS group (p=0.40). Resultsare presented in the Table. Lack of NIV was evident in 47% SES vs. 2.5% BMSlesions (p<0.001). NIV <30 mm3, NIV between 30 and 60 mm3, NIV >60 mm3
were respectively 47%, 3% and 3% after SES, versus 56.5%, 28% and 13% afterBMS (p for trend <0.001). No late incomplete apposition was present in 47% SESvs. 5.5% BMS lesions (p <0.001). Minimal late incomplete apposition (<1 mm3)was detected in 44% SES versus 92% BMS lesions (p<0.001). More pronouncedlate malapposition (>1mm3) was seen in 9% SES versus 2.5% of BMS lesions(p=0.33).
IVUS volumetric analysis at follow up
BMS SES p-value
Stent length (mm), median [IQR] 21.2 [17.1-30.9] 23.4 [18.8-31.6] 0.14Stent volume (mm3), median [IQR] 211 [143-282] 214 [174-325] 0.23Lumen volume (mm3), median [IQR] 175 [125-243] 205 [174-310] 0.023Neointimal volume (mm3), median [IQR] 24 [8-34] 1 [0-13] <0.001Late malapposition volume (mm3), median [IQR] 0.21 [0.09-0.37] 0.03 [0-0.34] 0.033
IQR: interquartile range
Conclusions: In saphenous vein grafts, SES significantly reduce neointimal hy-perplasia formation as opposed to BMS. Late incomplete apposition is a commonfinding after vein graft stenting, and its incidence is not increased after SES.
P5319 Implantation of paclitaxel-eluting stents in saphenousvein grafts in comparison to bare metal stents.Clinical and angiographic follow-up results from amulticenter study
R. Hoffmann1, T. Pohl2, R. Koester3, R. Blindt1, K.P. Boeckstegers3 ,T. Heitzer2. 1University Aachen, Medical Clinic I, Aachen, Germany; 2UniversityMunich, Munich, Germany; 3University Hamburg, Hamburg, Germany
There is little data on the clinical and angiographic success of drug-eluting stentsin saphenous vein grafts. This multicenter study sought to define the follow-upclinical and angiographic results after implantation of paclitaxel-eluting stents(PES) in stenotic saphenous vein grafts in comparison to treatment using baremetal stents (BMS).Methods: 60 patients (67±11 years, 54 male) with 65 lesions located in 65saphenous vein grafts (mean age of vein grafts 11.3±5.7 years) treated with PES(V-Flex Plus Ò, 2.7μg/mm2 paclitaxel, Cook Inc) and 60 patients (66±12 years,52 male) with 60 saphenous vein graft lesions treated with BMS were included inthe study. Lesions had to be less than 20 mm in length and in saphenous veingrafts of 2.75 to 3.5 mm diameter. Angiographic follow-up was obtained on 51lesions (79%) of the PES group and 51 lesions (85%) of the BMS group.Results: Baseline clinical and angiographic characteristics were comparable be-tween both groups with lesion lengths of 11.8±4.1 and 10.8±3.8 mm (P=ns) andreference vessel diameters of 3.05±0.52 and 3.06±0.60 mm(P=ns) in the PESand the BMS groups, respectively. At angiographic follow-up 3 vein grafts in thePES group and 5 vein grafts in the BMS group were occluded. Angiographic andclinical 6 months follow-up results are given in the table.
Follow-up after PES vs BMS
PES BMS P
MLD at follow-up (mm) 2.28±0.72 1.71±0.62 0.001Late loss (mm) 0.61±0.81 1.06±0.72 0.021Restenosis (%) 12 33 0.012Target vessel failure (%) 14 34 0.022
Conclusion: Implantation of non-polymer based PES in saphenous vein grafts isassociated with a lower late loss and restenosis rate compared to those of BMS.However, there remains a substantial target vessel failure rate even at 6 monthsdue to graft occlusion, restenosis or new lesions within the graft.
LEFT MAIN DISEASE
P5320 Percutaneous treatment with drug eluting stentimplantation versus bypass surgery for unprotectedleft main stenosis: a single center experience
A. Chieffo, N. Morici, F. Maisano, J. Cosgrave, M. Montorfano,I. Michev, O. Alfieri, A. Colombo. San Raffaele Scientific Institute,
Interventional Cardiology Unit, Milan, Italy
Background: Improvements in results with percutaneous coronary intervention(PCI) with drug-eluting stent (DES) may extend their usage in patients with leftmain coronary artery (LMCA) stenosis.Methods: All consecutive patients, with unprotected LMCA stenosis, treated elec-tively with PCI and DES or with CABG in our center between March 2002 andJuly 2004. A propensity analysis was performed to adjust for baseline differencesbetween the two cohorts. Hierarchical study end-points were: the cumulative oc-currence, during hospitalization and at one year, of: death; death or myocardial in-farction (MI); death, MI or stroke; repeat revascularization; death, MI, stroke, or re-peat revascularization, major adverse cardiac cerebrovascular events (MACCE).Results: Two hundred forty nine patients were treated: 107 with PCI and DESimplantation and 142 with CABG. At one year, there was no statistical differencein the occurrence of death in PCI vs. CABG both for the unadjusted (OR= 0.291;95% CI= 0.054-1.085; p= 0.0710) and adjusted analysis (OR= 0.331; 95% CI=0.055-1.404; p= 0.1673). A potential advantage of PCI was suggested when thecomposite end-points of death and myocardial infarction (unadjusted OR= 0.235;95% CI= 0.048-0.580; p= 0.0002; adjusted OR= 0.260; 95% CI= 0.078-0.597; p=0.0005) and death, MI and cerebrovascular events (unadjusted OR= 0.300; CI95%= 0.102-0.617; p= 0.0004: adjusted OR= 0.385; 95% CI= 0.180-0.819; p=0.01) were analyzed. No difference was detected in the occurrence of MACCEat the unadjusted (OR= 0.675; 95% CI= 0.371-1.189; p= 0.1891) and adjustedanalysis (OR= 0.568; 95% CI= 0.229-1.344; p= 0.2266).Conclusions: At one year, in this single center retrospective experience, therewas no difference in the degree of protection against death, stroke, myocardialinfarction and revascularization between PCI with DES and CABG for LMCA dis-ease.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Left main disease 927
P5321 Short-term and intermediate-term results after leftmain stenting using Paclitaxel-eluting stents (Taxus)
S.M. Huehns, J. Waigand, C.M. Gross, M. Moeckel, M. Steeg,M. Stockburger, R. Dietz, W. Bocksch. Berlin, Germany
Background: Current gold standard in the treatment of left maincoronary artery (LM) stenosis consists of coronary artery bypass grafting(CABG). This is mainly due to a comparatively high re-intervention rate after per-cutaneous coronary intervention (PCI). The introduction of drug-eluting stents intoPCI in recent years represents the first alternative treatment regimen for this typeof stenosis. We sought to determine safety and short- intermediate-term resultsafter implantation of Paclitaxel-eluting stents (PES, Taxus?).Methods and Results: 89 patients (65±17 years, 30 [33.7%] diabetics, 20[22.5%] acute myocardial infarction, left ventricular ejection fraction 50±16%) un-derwent PES implantation for LM-stenoses (unprotected LM: n=66 [74.2%]); 24ostial LM [27%]; 9 mid LM [10%) 56 distal LM [63%]. All patients were followed-upfor 6 months. Stenting techniques were as follows: 28 of 56 (50%) distal stenoseswere treated with 1 stent only, the remaining 28 with reconstructive techniques(26 crush, 2 V-stenting). Angiographic success rate was 99%. 2 patients hadperi-interventional complications (2 non ST-segment elevation myocardial infarc-tion: 2.3%). 3 patients suffered subacute stent thrombosis (SAT, 3.4%; lethal in 2cases after aspirin discontinuation [1 patient after crush-stenting, 1 patient afterV-stenting]). 6 patients died in hospital (6.7%, cardiac death in 4 [4.5%] cases;3/4 had pre-existing shock before angioplasty). 3 (3.6%) of the remaining 83 pa-tients died during follow-up (2 patients of cardiac causes; 1 case of SAT, 1 case ofsudden cardiac death). Focal re-stenosis was found in 3 (3.6%) patients (1 geo-graphic miss after LM ostial PCI, 2 focal restenoses of left circumflex after Crushstenting). Re-do PCI was necessary in 2 patients; 1 patient underwent CABG forsevere disease progression.Conclusion: Short-term and intermediate-term results after LM-PCI using PESsuggest that this treatment is an effective and safe alternative to CABG. Theoccurrence of SAT represents the most serious limitation.
P5322 Provisional T stenting in patients with unprotected leftmain stem stenosis with low risk of cardiac surgery
D. Dudek, J. Legutko, D. Giszterowicz, R. Singh, G. Heba, S. Bartus,L. Rzeszutko, J. Dubiel. Institute of Cardiology, II Department ofCardiology, Krakow, Poland
Background: New data suggests that stenting of unprotected left main coronaryartery (LMCA) is safe and feasible,with reported late mortality. Restenosis caninfluence outcome after percutaneous coronary interventions (PCI) of LMCA butbaseline characteristics of patients could be more important. Low risk group asdefined by a EuroSCORE ≤ 5 are considered to have better long term outcomeafter LMCA stenting.Methods: 86 patients with a low risk of cardiac surgery underwent the procedureof elective stenting of unprotected LMCA. Provisional T stenting was performedin 82 patients. In 4 pts, V stenting was performed. All patients were scheduledfor control angiography between 2 - 6 months after PCI. Immediate and mid termmajor adverse cardiac events [death, non fatal myocardial infarction and TargetLesion Revascularization (TLR) and non-TLR] were assessed.Results: Stents were implanted in all patients (Drug Eluting Stents: 61.6%, BareMetal Stents: 38.4%). Clinical and angiographic success was 100%. Mean clin-ical observation period was 32.5 ± 20.5 weeks. No death or myocardial infarc-tions were recorded. TLR was higher in the BMS group [BMS: 5.8% vs DES: 0%,p=0.4]. Non TLR was 9.3% in all patients (DES: 9.3%, BMS: 9.2%, in 3 patientsdue to disease progression and in 5 patients due to restenosis).Conclusion: LMCA stenting in low risk patients provides good immediate andmid term results. Our data although, not statistically significant, suggests thatDES possibly offers a better outcome for patients undergoing UPLMS PCI. Largerstudies exploring the current theme would help highlight this issue.
P5323 Comparison of efficacy and safety betweenSirolimus-eluting stent (Cypher) andPaclitaxel-eluting stent (TAXUS) in unprotected leftmain coronary arteries: multicenter registry in Asia
S. Nakamura1, J.H. Bae2, Y.H. Cahyadi3 , W. Udayachalerm4,D. Tresukosol5 , S. Tansuphaswadikul6 . 1New Tokyo Hospital, Department OfCardiology, Matsudo, Japan; 2Konyang University Hospital, Daejeon, Korea,Republic of; 3Husada Hospital, Jakarta, Indonesia; 4King ChulalongkornMemorial Hospital, Bangkok, Thailand; 5Siriraj Hospital, Bangkok, Thailand;6Chest Disease Institute, Bangkok, Thailand
Background and Purpose: Both Sirolimus-eluting BX velocity stent (Cypher™,Cordis) and Paclitaxel-eluting Express stent (TAXUS™, Boston Scientific) havebeen reported to be effective in preventing neointimal formation and in-stentrestenosis. The aim of this study is to compare the safety and efficacy of these2 stents on the outcome of patients with unprotected left main coronary arteries(LMT).Methods: A prospective analysis of 420 patients with LMT stenosis (248Cypher™ and 172 TAXUS™, average ejection fraction were 42.8% in Cypher™,43.6% in TAXUS™) in five high volume Asian centers after successful stenting
in LMT was performed. Lesion location of LMT was ostial 76 cases (18.1%),mid shaft 78 cases (18.6%) and distal 266 cases (63.3%). The study endpointswere major adverse cardiac events (MACE) at 30 days and restenosis rate at 12months.Results: The baseline clinical characteristics between 2 groups were similar. Seetable for clinical results.
Cypher™ (n=248) TAXUS™ (n=172) p
Age (mean/yrs) 69.6 71.3 NSProcedural success (%) 100 100 NSMACE at 30 days (%) 0 0 NSReference diameter (mm) 3.63 ± 0.88 3.50 ± 0.77 NSY/single/crushing stenting (n) 75/87/86 52/40/80 NSMLD post (mm) 3.59 ± 0.86 3.30 ± 0.78 NSMLD at 12 months (mm) 3.50 ± 0.88 3.18 ± 0.78 NSRestenosis rate (%) 3.2 4.7 NSTLR (%) 3.2 3.5 NS
Conclusion: The use of both stents in patients with LMT was equally safe withlow acute complication and low incidence of restenosis.
P5324 Midterm results of Unprotected Left Main CoronaryArtery Stenosis treatment in the Drug Eluting StentEra
E. Garcia, F. Sarnago, M. Abeytua, G. Linares, T. Datino, A. Forns,A. Barrio. Hospital General Gregorio Maranon, Department of
Cardiology, Madrid, Spain
Background: Coronary Artery By-Pass Graft (CABG) has been the treatment ofchoice for Left Main Coronary Artery (LMCA), due to poor long-term results usingbare metal stents. Since the introduction of Drug Eluting Stent (DES), percuta-neous treatment is proposed as an alternative treatment in some centers.Objectives: To analyze midterm results of LMCA disease treated with DES.Methods: Since March 2003, we have performed elective LMCA percutaneousprocedure using DES in 108 patients.Results: Mean age was 68.5 years ±11.4 years, 80 (74.1%) were male, 68%had unstable angina 31% with Stable Coronary Disease. Multivessel disease wasobserved in 86 (79.6%) and the right coronary artery was occluded or stenotic in58 (53.7%). Ejection Fraction was 49.5±11.4%. Plaque modification was usedin 71 (65%), cutting balloon in 51 (47.2%), Rotational Aterectomy in 7 (6.5%),Abciximab in 53 (49,1%). Mechanical support with Intraaortic balloon pump wasused in 23 (21.3%) and left ventricular assist (Impella) in 2. Paclitaxel polymerbased DES were used in 91 (94,4%). Final IVUS evaluation was obtained in 65(60.2%). Two patients (1.8%) died in the hospital after the index procedure and 2more (1.8%) had non Q myocardial infarction. At 1 month follow up 100 (92.5%)were free of any cardiac event. At 6 months follow up 6 (5%) patients had died, 6more (5%) required target lesion revascularization and 93 (86%) were free of anycardiac event.Conclusions: Unprotected Left Main Coronary Artery treatment with Drug Elut-ing Stent appears like a valid alternative to surgical treatment waiting for the re-sults of randomized trials.
P5325 Clinical and angiographic outcomes one year afterelective implantation of Sirolimus-Eluting Stents inunprotected left main coronary arteries: final resultsof an European retrospective study
J. Fajadet1 , P. Barragan2, R. Seabra-Gomes3, J.-J. Goy4,C. Tamburino5, P. Rubino6, T. Lefevre7 on behalf of the Left Main investigators.1Clinique Pasteur, Unite de Cardiologie interventionelle, Toulouse, France;2Polyclinique Les Fleurs, Unite de Cardiologie interventionelle, Ollioules, France;3Hospital Santa Cruz - Instituto Do Coracao, Lisboa, Portugal; 4Clinique Cecil,Lausanne, Switzerland; 5University of Catania - Ferrarotto Hospital, Catania,Italy; 6Montevergine Clinic, Mercogliano, Avellino, Italy; 7Institut HospitalierJacques Cartier, Massy, Paris, France
Background: Sirolimus-Eluting Stents (SES) were proven to significantly reducerates of restenosis and reintervention compared to bare metal stents (BMS) invarious types of coronary artery lesions. However, only limited data are availablecharacterizing the safety and efficacy of SES after implantation in unprotected leftmain coronary (UPLM) arteries.Methods: A multicenter, retrospective study collecting data from approximately300 patients from 13 European centers was initiated to assess the safety andeffectiveness of SES for de-novo lesions in unprotected left main coronary arter-ies (UPLM). Consecutive patients were included if they were treated with SES forUPLM lesions between April 2002 and December 2004. Non-elective and bail-outstent implantations were excluded. The primary endpoint for analysis is cumula-tive MACE (Major Adverse Cardiac Events) defined as a composite of death,myocardial infarct and target vessel revascularization up to 1 year. Secondaryendpoints include target lesion and target vessel revascularization (TLR, TVR)as well as angiographic parameters measured by quantitative coronary analysis(QCA) between 6-12 months.Results and conclusion: Electronic data capture through a dedicated secure
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

928 Left main disease
internet website was initiated in December 2005 and will be ongoing until April2006. Results of the analysis will be available by July 2006 and for the con-ference.
P5326 Clinical outcome after stenting or coronary arterybypass surgery for the treatment of left main disease
J.H. Yang, S.H. Choi, J.H. Choi, S.U.N.G. Kiick, H.C. Gwon, Y.T. Lee,S.H. Lee, P.W. Park. Samsung Medical Center, Dept of Medicine,Seoul, Korea, Republic of
Background: Left main disease stenting is increasingly performed as a valuablealternative to coronary artery bypass surgery (CABG), but clinical data regardingcomparison of stenting and surgery are limited.Methods: From 1997 to 2005, 298 consecutive patients were treated with elec-tive left main revascularization, using bare metal stent (BMS) (N=71); drug-elutingstent (DES) (N=63), or CABG (N=164). Six-month clinical follow-up was com-pleted in 234 patients (78.5%) and survival analysis was performed for this popu-lation.Results: There was no difference of clinical parameters except higher frequencyof diabetes (71%) in CABG than BMS (23%) and DES (32%) group. Freedomfrom all major adverse events (MACE)of DES at 6 month (96.6%) and 12 month(96.6%) was comparable to that of CABG (99.3%) (p=NS), and significantly higherthan that of BMS (83.6%) (p<0.001). Freedom from MACE of DES (94.7%) at 1year was also comparable to that of CABG (95.9%) and significantly higher thanthat of BMS (73.8%) (p<0.001). There was one periprocedural shock, who wasrecovered by percutaneous cardiopulmonary support, and two deaths includingone procedural failure and one subacute thrombosis in DES group.Conclusion: Although this is non-randomized retrospective study in a single cen-ter, our results shows that DES implantation for left main disease in selectedcases has favorable clinical midterm result.
P5327 Results of the left main TAXUS pilot study
T. Lefevre1, O. Darremont2, M.C. Morice2, M. Silvestri3, Y. Louvard2,P. Garot4, J.L. Leymarie5 , P. Dumas3. 1ICPS, Massy, France;2Clinique Saint-Henri, Bordeaux, France; 3UCV, Marseille, France;4ICPS, Quincy, France; 5Clinique Saint-Augustin, Bordeaux, France
Background: CABG is the gold standard treatment of unprotected left main (LM)stenosis. Percutaneous coronary intervention (PCI) using bare metal stents hasbeen proposed as an alternative treatment in some centers with excellent in-hospital results. However, these results were partially impaired by the occurrenceof restenosis.Methods: A pilot study using the TAXUS stent was set-up in 3 French centers witha wide experience in LM stenting. PCI was proposed as an alternative to CABG inpatients (Pts) with de novo unprotected LM stenosis. Technical recommendationwas to systematically cover the LM ostium with the stent and to use a provisionalT stenting approach in case of distal LM. Acute MI and cardiogenic shock werethe only criteria for exclusion. Prospective 6-8 months, 1, 2 and 3 years clinicalfollow-up was set up with a recommended angiogram at 6 months.Results: Between March 2003 and June 2005, 291 Pts were included. They were69±11 years old, 29% diabetic, 19% previous or recent MI, 37% unstable anginaand 26% with 3 vessel disease. Euroscore was 4.8±3.4. Reference LM diameterwas 3.71±0.49 mm and LM lesion was distal in 78% of cases. In Pts with distalLM, a second stent (T stenting) was used in 41% of cases and a final kissingballoon inflation was performed in 97% of cases. Other lesions were treated in78% and total stent length was 53±23 mm. Angiographic success was obtainedin 99.6% with an in-hospital MACCE rate of 3.8% (death 0.7%). Six-eight monthfollow-up was obtained in 98% of cases. Total MACCE rate was 11.6%, includ-ing death in 3.4% (cardiac 2.0%), TVR 5.2% and stroke 0.7%. Acute LM stentthrombosis (per procedural) occurred in 1 case and sudden death in 2 cases (8and 11 weeks). The total rate of documented or suspected LM stent thrombosiswas 1.0%. By univariate analysis, the only predictors of death were diabetes (78vs 27%, p=0.003) and dialysis (33 vs 1%, p<0.0001). Coronary angiogram wasperformed in 153 patients (53%). LM restenosis was observed in 9.5%: 5 in LMstent, 4 in the stented ostial Circ., 3 at the LM ostium (unstented), 1 distal to theLM stent and 1 an unstented ostial Circ. The only predictor of restenosis wasdiabetes (57 vs 27%, p=0.053).Conclusion: Left main PCI using the TAXUS stent with a strategy of provisionalT stenting in case of distal LM provide excellent acute angiographic results andacceptable mid-term outcome. Complete one year follow-up will be presented atthe meeting.
P5328 Long term (2 Years) outcome in patients withunprotected left main coronary artery stenosistreated with drug-eluting stent implantation
A. Chieffo1, N. Morici1, S. Corbett2, F. Airoldi2, G. Melzi2,M. Montorfano2, R. Babic1, A. Colombo2. 1San Raffaele Scientific
Institute, Interventional Cardiology Unit, Milan, Italy; 2EMO Centro CuoreColumbus, Interventional Cardiology Unit, Milan, Italy
Background: The long-term safety and efficacy of drug-eluting stent (DES) im-
plantation in the treatment of unprotected left main coronary artery (LMCA) steno-sis is still a matter of debate.Methods: Primary end-point of the study was 2 years major adverse cardiacevent (MACE) defined as the occurrence of any of the followings:cardiac death,myocardial infarction (MI), target lesion revascularization (TLR) and target vesselrevascularization (TVR). All consecutive patients (pts) who had sirolimus (SES,Cypher, Cordis, Johnson and Johnson Company, Warren, NJ) or paclitaxel-elutingstent (PES, Taxus, Boston Scientific, Natick, MA) electively implanted in de novolesions on ULM were analyzed.Results: A total of 107 pts were treated:52 with PES and 55 with SES.Twenty (18.7%) patients were diabetics, 34 (31.7%) unstable angina, mean age63.6±10.3 years, EF 52.0±10. High mortality risk scores (Euroscore >6 and/orParsonnet >15) were present in 43 (40%) of the patients. Eighty-seven (81.3%)patients had distal left main lesions: 77 bifurcation and 10 trifurcation. Bothbranches were stented in 64 (73.6%) pts: crush technique was performed in 38(59%) of them. Reference vessel diameter was 3.3±0.68mm. Procedural successwas achieved in all pts. During hospitalization 10 (9.3%) patients had non-Q waveMI. None of the patient had Q wave myocardial infarction (MI), died or had CABG.One patient had thrombosis in left anterior descending artery with MI at 3 months.At 2 years, 5(4.6%) patients died: 1 of lung cancer, 1 following elective CABG, 1of pulmonary edema (this patient had severe aortic and mitral regurgitation, andstent patency was demonstrated 20 days before death), 1 of possible cardiacdeath in a patient with multiorgan failure with pancreatitis and discontinuation ofantiplatelet therapy, 1 of sudden death following ICD discharge. TLR occurred in18 (16.8%) pts (13 re-PCI and 5 CABG), TVR in 23 (21.4%). Angiographic follow-up performed in 90 (84%) pts showed restenosis in 17 pts (18%); all restenosisoccurred in pts with treatment of distal left main and were focal.Conclusions: Treatment of LMCA stenosis with DES appears safe withfavourable and improved clinical results maintained at two years clinical follow-up.
P5329 Unprotected left main coronary artery treated withsirolimus-eluting stent: results from the e-cypherregistry
C. Lotan1, A.H. Gershlick2, G. Guagliumi3, P. Guyon4, J. Schofer5,J.E. Sousa6, P. Urban7, W. Wijns8 on behalf of The e-Cypher
Investigators. 1Hadassah-Hebrew University Medical Center, Heart Institute,Jerusalem, Israel; 2University Hospitals Leicester, Leicester, United Kingdom;3Ospedali Riunutu di Bergamo, Bergamo, Italy; 4Centre Cardiologique du Nord,Saint-Denis, France; 5Kardiologische Gemeinschaftpraxis, Hamburg, Germany;6Institute Dante Pazzanese of Cardiology, Saint-Denis, Brazil; 7La Tour Hospital,Geneva, Switzerland; 8Onze-Lieve-Vrouw-Ziekenhuis, Aalst, Belgium
Background and Aim: Sirolimus-eluting stents (SES) have been shown to behighly effective in lowering rates of restenosis and target lesion revascularization(TLR) in comparison with bare metal stents, in several subsets of patients. How-ever, there is insufficient data regarding the use of these stents in the high-riskgroup of patients with unprotected left main coronary artery (ULM) disease.The e-Cypher Registry was designed to assess "real life" treatment of coronarylesions with SES in a large population. In this report we present the e-Cypherregistry results of treatment of ULM lesions with SES.Method and Design: The present data were collected from a multi-center, in-ternational internet-based registry (the e-Cypher Registry) from April 2002 untilSeptember 2005. Clinical follow-up was done at 1, 6 and 12 months.Results: A total of 15,157 patients who underwent implantation of ≥1 SES in18,295 lesions, in 279 centers in 41 countries, were enrolled in the registry. 393(2.2%) of the lesions were in the LM. In the ULM subset, mean patient age was67.9 ± 12.4 years, 64.2% were males and 17.9% were diabetic. 17.9% had aprevious MI (84.2% Q wave) and 38.7% had previous PCI. Indication for PCIincluded acute MI (3.8%), stable angina (42.5%), unstable angina (41.5%) andsilent ischemia (5.7%). Mean lesion length was 9.98 ± 5.16 mm with a referencevessel diameter of 3.33 ± 0.42 mm. 43.4% were bifurcation lesions, comparedwith only 10.3% bifurcation lesions in the non-LM cohort.Major events at 360 days are shown in the table. TLR rates were similarly low inthe ULM subset and in the non-LM cohort. Total MACE and death rates, whichreflect the high-risk nature of these patients, are considerably lower than historicalof bare stent treatment in the ULM subset of patients.
MACE 360 days
ULM patients N=93 Non-LM patients N=11781 p
MI 0 136 (1.15%) nsTLR 3 (3.23%) 317 (2.69%) nsDeath 7 (7.53%) 235 (1.99%) 0.0029Total MACE 10 (10.8%) 611 (5.19%) 0.0298
Conclusions: The use of the CYPHER TM stent was shown to be safe and effec-tive in this high risk group, and these results may enable us to consider a changein present treatment strategies.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Left main disease 929
P5330 Are the results of drug-eluting stents for the electivetreatment of unprotected left main lesions different indiabetics
P. Garot1, T. Lefevre2, O. Darremont3, M. Silvestri4, Y. Louvard2,J.L. Leymarie1 , V. Decalf2, P. Dumas2. 1ICPS, Quincy, France;
2ICPS, Massy, France; 3Clinique Saint-Augustin, Bordeaux, France; 4UCV,Marseille, France
Background: Left main (LM) stenting using DES has emerged as an alternativeto cardiac surgery. However, whether the results of elective LM stenting usingDES are different in diabetics is unknown. Objectives: To determine the results ofelective LM stenting using DES in diabetics.Methods and results: Using the data of a French multicenter registry includ-ing 325 pts electively treated by DES for unprotected LM lesion, we sought tocompare the results of PCI and outcomes in diabetics (n=90) vs. non diabetics(n=235). Seventeen (n=17) pts presenting with acute MI and/or shock were ex-cluded from the present analysis. The procedural characteristics and outcomesare described.
Diabetics n=90 Non diabetics n=235 p
Euroscore 5.0±3.2 4.7±3.4 nsMales 76% 76% nsAge, yr 69±10 69±12 nsHypertension 73% 60% <0.05Unstable angina 34% 35% nsPost MI 4% 8% nsEjection fraction 60±12% 61±13% nsDistal left main stenting 76% 76% nsProvisional T stenting 64% 66% nsDistal LM ’T’ shape 33% 26% <0.05PCI success, n (%) 100% 98% nsnon Q-wave MI 3% 2% nsQ-wave MI 0% 0% nsIn-hospital MACE 7% 3% <0.05In-hospital death 2% <1% 0.076-mo MACCE/TVR 23% 5% <0.0016-mo TVR 5% 3% <0.056-mo death 11% 2% <0.00016-mo cardiac death 8% <1% <0.0001
Conclusion: Despite high PCI success rates in diabetics (similar to that of nondiabetics), diabetics had, compared to non-diabetics, higher rates of MACE duringhospital stay and higher rates of MACE, TVR and death at 6-Mo.
P5331 Left Main Stem Percutaneous Coronary Intervention -an unselected registry of all comers 2000 - 2005
A.C. Morton, A. Siotia, J. Gunn. Sheffield Teaching Hospitals NHSTrust, Cardiology, Sheffield, United Kingdom
Introduction: Left Main Stem (LMS) PCI remains a controversialarea. Stents have transformed the safety of the procedure and drug eluting stents(DES) promise a low restenosis rate. Bifurcation stenting techniques are also im-proving.Methods: We performed LMS stenting on an unselected, consecutive cohort ofpatients referred for revascularisation in the period 2000-2005. We followed upall patients clinically and with 4 and 8 month exercise tests. We did not performroutine follow-up angiography. Follow-up data were collected from patient notes,operator records and catheter laboratory records.Results: 114 procedures were carried out (55 up to 2005 and 62 in 2005). Meanfollow-up was 15 months. 32% of patients were female and the mean age was 58± 10 years. 47% were unsuitable for CABG of whom 11% were in a catastrophicstate. 12% of procedures were emergencies, 27% urgent and 61% elective and12% of procedures were performed as bailout. 26% of lesions involved the os-tium/body of the LMS and 74% the bifurcation. The mean number of vesselsdiseased (apart from the LMS) was 1.9 ± 1.07 and the mean number treated1.7 ± 1.0. 12% of LMS were protected and 96% of patients had stents inserted(100% deployment success). IVUS was performed in 4% of cases and a Pressurewire in 3%. Since becoming available, 73% of patients received a DES. 19% hadan IABP inserted and 56% were given a GPIIbIIIa inhibitor. 51% of patients un-derwent shotgun stenting, 43% single stenting and 6% another technique. TotalMACE was 21% consisting of 9% deaths, 4% MI, 3.5% CVA and 4% TVR/TLR(none of which occurred in DES). Of the deaths, 50% of patients were in a catas-trophic state.Conclusions: The results of unselected LMS stenting in the modern era aregood. Our results are comparable with other recent registries of LMS stenting.In the elective setting, the mortality rate is comparable to CABG. For patients inshock, this may represent a life saving strategy.
P5332 Acute coronary syndromes due to left main stemstenosis treatment options in a real world. Analysisfrom the PL-ACS Registry
L. Polonski1, D. Dudek2, M. Gasior2, M. Gierlotka2, A. Witkowski3,Z. Kalarus3, M. Zembala3, M. Tendera4 on behalf of on behalf of
the PL-ACS Investigators. 1Silesian Center for Heart Disease, 3rd Departmentof Cardiology, Zabrze, Poland; 2Medical Academy, Krakow, Poland; 3MedicalAcademy, Warsaw, Poland; 4Medical Academy, Katowice, Poland
The left main stenosis as a culprit lesion is a serious cause of acute coronary syn-dromes (ACS) leading to a high mortality despite revascularization procedures.The aim of the analysis was to present the treatment strategies in a population ofACS patients (pts) with a special respect to urgent and deferred revascularizationprocedures.Methods: All patients with ACS due to left main stem stenosis as a culprit le-sion who were registered in the prospective, population-based Polish Registry ofAcute Coronary Syndromes (PL-ACS) were included in the analysis. For theman urgent (coronary angioplasty or bypass surgery) or deferred (bypass surgeryor angioplasty after discharge) revascularization was chosen by the responsiblestaff.Results: In PL-ACS Registry 28 268 (38%) pts from 74 149 had coronary an-giography performed. There were 727 (2.6%) ACS caused by the left main stemstenosis. Urgent revascularization was performed in 40.5% pts with unstableangina (UA), in 58.9% pts with non-ST-segment elevation myocardial infarction(NSTEMI), and in 87.6% pts with ST-segment elevation myocardial infarction(STEMI) - table. These patients were of higher risk as compared to patients withdeferred revascularization planned. In 28 (3.9%) of pts revascularization was notplanned or possible and in-hospital mortality in those pts were 7.1%.
UA (N=321) NSTEMI (N=185) STEMI (N=193)Urgent Deferred Urgent Deferred Urgent Deferred
revascula- revascula- revascula- revascula- revascula- revascula-rization rization rization rization rization rizationN=130 N=191 N=109 N=76 N=169 N=24(40.5%) (59.5%) (58.9%) (61.1%) (87.6%) (12.4%)
PCI (%) 75.4 4.2 88.1 0.0 95.9 0.0CABG (%) 24.6 95.8 12.8 100.0 5.3 100.0Age (years) 63.9 64.7 66.1 66.9 62.5 63.0Male sex (%) 69.2 74.4 69.7 64.5 71.0 83.3Diabetes (%) 22.3 18.3 19.3 22.4 26.6 20.8Killip 3 or 4 (%) 0.8 0.0 16.5 6.6 36.1 12.5In-hospital mortality (%) 2.3 –* 11.9 –* 26.6 –*
*Mortality data for deferred revascularization patients will be available after completing the follow-up data.
Conclusions: Data from the PL-ACS Registry show that the rates of urgentrevascularization in ACS caused by left main stem stenosis increase togetherwith the severity of ACS. Deferred revascularization is chosen in lower risk pa-tients with non-ST-segment elevation acute coronary syndromes.
P5333 Percutaneous treatment of unprotected left main inelderly patients with non ST elevation acute coronarysyndrome
F. Barlocco1, T. Palmerini2, I. Sheiban3, G. Guagliumi4, F. Liistro5,A. Marzocchi5 , M. D’urbano1, S. De Servi1. 1Ospedale Civile
di Legnano, Cardiology, Legnano, Italy; 2Policlinico S. Orsola, Universita diBologna, Cardiology Institute, Bologna, Italy; 3Ospedale S. Giovanni Battista,Cardiology, Torino, Italy; 4Ospedali Riuniti di Bergamo, Cardiology, Bergamo,Italy; 5Ospedale di Arezzo, Cardiology, Arezzo, Italy
Background: P ercutaneous coronary interventions (PCI) for unprotected leftmain coronary artery disease (ULMCAD) are still controversial, however this op-tion can be reasonably provided to high risk patients (pts) unsuitable for surgery.Aims: To assess immediate and long term results in elderly pts (≥ 75 years old)with non ST elevation acute coronary syndrome (NSTE-ACS) undergoing PCI forULMCAD.Methods: Over the last 4 years, 167 elderly pts with NSTE-ACS and ULMCADwere treated with PCI in 5 Italian centers. PCI was performed in pts either deemedunsuitablefor surgery or for pts preference.Results: Mean age was 81.6 ± 4.2 years, 38% of pts were female. Diabetes,chronic renal failure and peripheral vascular disease were present in 27%, 21%and 34% of pts respectively. Multivessel coronary disease was found in 78% ofpts and left ventricular dysfunction in 56%. Angiographic success was obtainedin 99% of pts. Stenting was performed in all cases with drug-eluting stents usedin 42% of them. Rotational atherectomy and IAPB were used in 3% and 6% ofcases, respectively. GPIIb/IIIa inhibitors were used in 34% of cases and multives-sel coronary revascularization was accomplished in 77% of pts. Eight pts died(5%) during the hospitalization. At a mean follow-up of 13.9 ± 10.4 month, 29pts died (19.8%) and 6 pts (4%) had non-fatal myocardial infarction. Target vesselnew revascularization was necessary in 23 pts (16%) including CABG (1.5%) andrepeated PCI (14.5%). Four pts (2.7%) had ischemic stroke. Event free survivalwas 53%.Conclusion: In high risk elderly patients with NSTE-ACS, PCI of ULMCAD isfeasible with an acceptable mid-term outcome.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
930 Left main disease
P5334 Unprotected left main percutaneous coronaryinterventions. randomized study
A. Erglis1, I. Narbute1, I. Kumsars1, S. Jegere1, I. Mintale1,I. Zakke1, U. Strazdins1, A. Saltups2. 1Latvian centre of Cardiology,Invazive cardiology, Riga, Latvia; 2Cabrini Medical Centre, Invazive
cardiology, Melbourne, Australia
Background: In an effort to find the optimal intervention for LM disease we ran-domized bare metal stent (BMS) or drug eluting stent (DES) for unprotected LMIVUS guided PCI.Purpose: • To compare safety and efficacy of BMS and DES for unprotected LM.• To evaluate intra-hospital outcome. • To evaluate 6 months clinical, angiographicand IVUS outcome.Methods: Between January 2002 and January 2006 - 190 consecutive patientswith unprotected LM disease underwent PCI in our center. One hundred and eightpatients of them were randomized for BMS (n=53) or DES (n=55) implantation.In randomized cohort (n=108) all interventions were IVUS guided and underwentcutting balloon (CB) pretreatment before stenting. All patients were scheduled for6 months clinical, angiographic and IVUS follow-up.Results: In both cohorts (BMS and DES) baseline clinical characteristics werecomparable. Procedural success was obtained in 100%. Distal LM interventionwas done in 78%. No MACEs during intrahospital period occurred. Mean hospital-ization time were 3.3 days. During 6 months follow-up 2 deaths (one non-cardiacand one cardiac) obtained. Angiographic binary restenosis was obtained in 11 (9in BMS and 2 in DES group), TLR in 8 (7 in BMS and 1 in DES group) cases.
Table 1. IVUS results
DES group BMS group P values
MLD post PCI, mm 3.25±0.26 3.29±0.33 0.614MLD at f-up, mm 3.05±0.31 2.98±0.51 0.469MLD late loss, mm 0.20±0.14 0.41±0.28 0.002MSA post PCI, mm2 8.64±1.32 9.13±1.49 0.148MSA at f-up, mm2 7.62±1.48 7.58±2.39 0.936MSA late loss, mm2 0.88±0.56 1.84±1.17 0.001Intima volume, mm3 13.13±13.87 22.03±14.79 0.007
Conclusions: Left main PCI was safe and effective with excellent immediate andmid-term result in both groups. IVUS guidance and CB pretreatment may be ef-fective strategy to obtain better acute and mid-term result. However, IVUS resultsconfirm statistically significant benefit of DES implantations in the unprotected LMlesions in all stented segment measured dimensions over BMS.
P5335 Long term prognosis of patients submitted todrug-eluting stent implantation in unprotected leftmain coronary lesions
G. Musumeci, G. Guagliumi, R. Rossini, A. Vassileva, L. Mihalcsik,M. Tespili, A. Gavazzi, O. Valsecchi. Ospedali Riuniti di Bergamo,
Cardiovascular Dept, Bergamo, Italy
Although surgery remains the standard treatment for left main stenosis, prelimi-nary experience with drug-eluting stents appears promising.The aim of the study is to evaluate the long-term outcome following implantationof drug-eluting stents (DES) in unprotected left main (LM) lesions.Methods: since 2002, a total of 116 consecutive patients with unprotected leftmain stenoses treated with drug eluting stents (Cypher® 61.2% and Taxus®
38.8%) were included in the study. There were no exclusion criteria, except pa-tient refusal. Technical issues, such as IVUS guidance, use of glycoprotein IIbIIIainhibitors or predilatation method were left to operators’ discretion. Combined as-pirin and clopidogrel was maintained through a minimum of 6 months. A clinicalfollow-up was scheduled at 1 and 12 months after the indexed procedure. Majoradverse cardiac events (MACE) included death, myocardial infarction (MI) andtarget vessel revascularization (TVR). Acute, sub-acute and late stent thrombo-sis were also evaluated. Angiographic follow-up was recommended at 3 and 9months after the procedure.Results: baseline characteristics were as follows: mean age was 66.3 ± 10.4years (33-83), female patients were 31% and diabetics 28%. The revasculariza-tion procedure was performed in patients with acute coronary syndrome in 59.5%of the cases, with 18 patients presenting with ST elevation MI (15%). Mean leftventricular ejection fraction was 49.2 ± 7.8%. Transradial approach was used in64% of the cases. Fifty-three lesions (45.6%) were located at the bifurcation, in-cluding 18 cases (15.5%) with both LAD and CX ostia affected. The mean LMreference diameter was 3.6±0.6 mm. About 18% of the procedures were per-formed under IVUS guidance. Direct stenting was performed in 57%. A stent wasimplanted in LM in all patients (stent length 17.2±7.5mm). An additional stent,in LAD or CX, was used in 10 pts (8.6%). The procedure was successful in allpatients. One-month adverse events were recorded in 6,2% of patients: MI in1.8% and death in 4.4%. At 12 months, total mortality was 6.2% (cardiac death in5.3%). TVR was required in only 3.5% (two pts were submitted to re-PCI and twopts to CABG). A nine-month angiographic follow-up was obtained in 101 patients,with a restenosis rate of 6.9%.Conclusions: in our population, percutaneous treatment of left main coronaryartery disease with DES is safe and successful. It is associated with low rates oflong term mortality, MI, and TVR.
P5336 Favourable mid term outcome following drug elutingimplantation in non bifurcational lesions involvingunprotected left main: a multicenter registry
A. Chieffo1, S.J. Park2, M. Valgimigli3, Y.H. Kim1, I. Sheiban4,A. Truffa5, P.W. Serruys3, A. Colombo5. 1San Raffaele Scientific
Institute, Interventional Cardiology Unit, Milan, Italy; 2Asan Medical Center,University of Ulsan, Seoul, Korea, Republic of; 3Erasmus Medical Center,Thoraxcenter, Rotterdam, Netherlands; 4 San Giovanni Battista Hospital, Turin,Italy; 5San Giovanni Battista Hospital, Turin, Italy
Stenosis in the ostium and the body of unprotected left main not requiring bifur-cation treatment, are still considered a standard indication for surgical revascular-ization.Aim: Aim of the study To assess the safety and mid-term efficacy of drug-elutingstent (DES)implantation in ostial and the body of unprotected left main stenosis(LMCA).Methods: All consecutive patients (pts) in 5 Centres who had SES (Cypher,Cordis, Johnson and Johnson Company, Warren, NJ) or PES (Taxus, Boston Sci-entific, Natick, MA) electively implanted for the treatment of ostial and the body ofLMCA main stenosis not requiring the treatment of the bifurcation.Results: A total of 144 pts were treated: 39 with PES and 105 with SES. Seventy-five patients had ostial LMCA stenosis, 41 in the body and 28 had diffuse diseasein either ostium or the body of the left main. Twenty-eight (19.4%) patients werediabetics and 65 (45.1%) had unstable angina. Mean age was 62.6 ±12.3 yearsand LVEF 55.2± 11.3%. Euroscore was 5.4±5.8 and Parsonnet 7.7±7.7. Fifty-two (36.1%) patients had right coronary artery (RCA) disease; 22 had concomi-tant RCA treatment. Reference vessel diameter was 3.7 ± 0.9mm. Intra-aorticballoon pump was used in 5 (3.5%) patients (2 electively and 3 acutely). Glyco-protein IIb/IIIa inhibitors were used in 18 patients (12.5%). In 73 (50.7%) patientsIVUS guidance was performed. Predilation was performed in 57 (39.6%) pts: cut-ting balloon was used in 11 of them. Maximum balloon diameter was 3.7±0.9 mmand maximum pressure 17.0± 4.9 atm. In 2 patients rotational atherectomy wasperformed; none of the patients had directional atherectomy. Procedural successwas achieved in 143 (99%) of the pts; in one patients it was not possible to fully di-late the stenosis in the ostium of the left main and the residual stenosis was largerthan 30%. During hospitalization no patient had Q wave myocardial infarction (MI)or died; 1 patient had elective CABG following the unsuccessful procedure. Onepatient died after 19 days from the procedure because of pulmonary infection. At6 months no other patient died or had MI. Two patients had TVR (1 re-PCI and1 CABG). Angiographic follow-up performed in 100pts (69.4%) with a late loss of-0.09 mm. Restenosis in left main trunk occurred only in 1 (1%) patient (in-stentTaxus).Conclusions: In this early experience with DES in non bifurcational ULM lesionswe can state that this procedure appears safe with favourable clinical results atsix months with an encouraging 1% restenosis rate.
P5337 Influence of treatment in left main coronary arterydisease in a cohort of 548 patients: Percutaneouscoronary intervention (PCI) with stent deploymentversus coronary artery by- pass grafting (CABG)
J. Garcia-Lara, A. Bouzas Mosquera, J. Salgado Fernandez,R. Calvino Santos, G. Aldama Lopez, J.M. Vazquez Rodriguez, N. VazquezGonzalez, A. Castro-Beiras. Hospital Universitario Juan Canalejo, Servicio DeCardiologia, A Coruna, Spain
Background: Left main coronary artery (LMCA) disease has a poor short andmedium term prognosis if coronary revascularization is not accomplished. Today,treatment for this condition can be surgical CABG, PCI or pharmacological ther-apy. We sought to analyze the incidence of major adverse clinical events (MACE)in these patients according to treatment strategy received.Methods: Patients consecutively diagnosed as LMCA stenosis >50% from Jan-uary 2000 to December 2004 were studied.Results: 548 patients were included. 50 underwent PCI (Group A), 425 CABG(Group B) and 73 received only pharmacologic therapy. We found no significantdifferences between groups A and B regarding to age (68 ± 15.3 vs 67 ± 9.6years, p=NS) and gender (male 81 vs 80%, p=NS). There was significant differ-ence between groups A and B in ejection fraction (EF) (52 ± 15.2 vs 60 ± 15%,p=0.018), Euroscore (7.80 ± 3.76 vs 5.01 ± 3.13) and indication for catheteriza-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
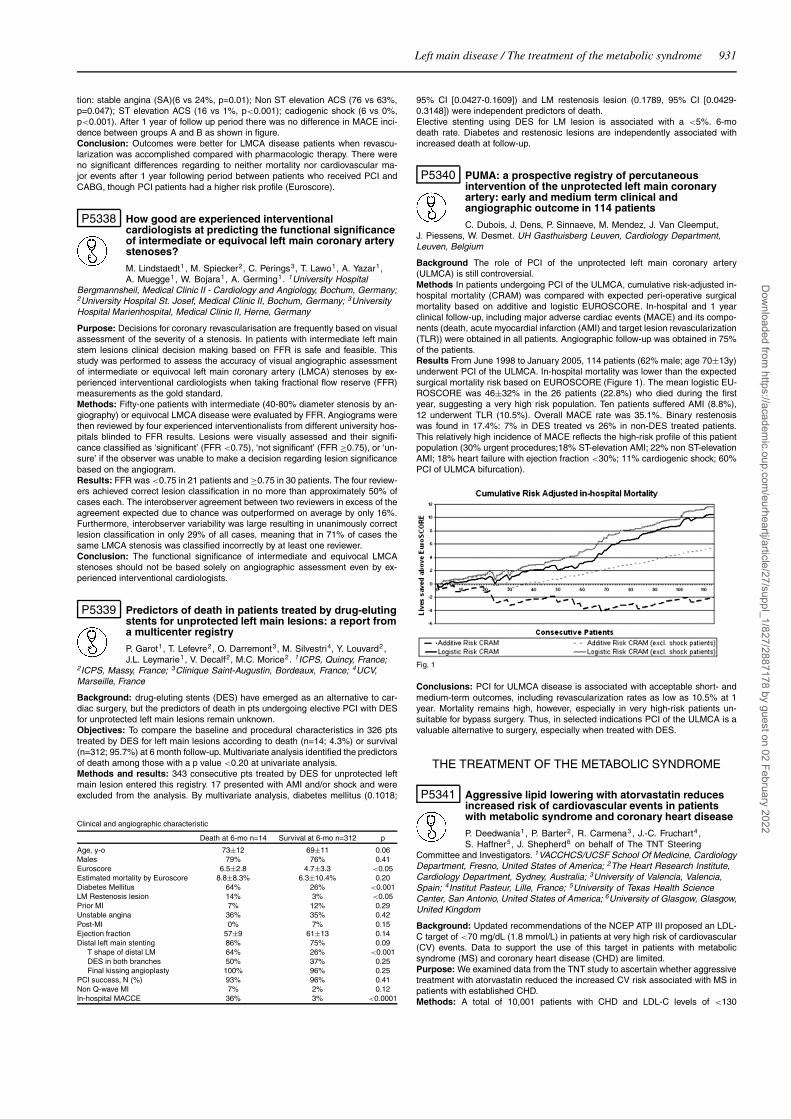
Left main disease / The treatment of the metabolic syndrome 931
tion: stable angina (SA)(6 vs 24%, p=0.01); Non ST elevation ACS (76 vs 63%,p=0.047); ST elevation ACS (16 vs 1%, p<0.001); cadiogenic shock (6 vs 0%,p<0.001). After 1 year of follow up period there was no difference in MACE inci-dence between groups A and B as shown in figure.Conclusion: Outcomes were better for LMCA disease patients when revascu-larization was accomplished compared with pharmacologic therapy. There wereno significant differences regarding to neither mortality nor cardiovascular ma-jor events after 1 year following period between patients who received PCI andCABG, though PCI patients had a higher risk profile (Euroscore).
P5338 How good are experienced interventionalcardiologists at predicting the functional significanceof intermediate or equivocal left main coronary arterystenoses?
M. Lindstaedt1 , M. Spiecker2, C. Perings3, T. Lawo1, A. Yazar1,A. Muegge1 , W. Bojara1, A. Germing1. 1University Hospital
Bergmannsheil, Medical Clinic II - Cardiology and Angiology, Bochum, Germany;2University Hospital St. Josef, Medical Clinic II, Bochum, Germany; 3UniversityHospital Marienhospital, Medical Clinic II, Herne, Germany
Purpose: Decisions for coronary revascularisation are frequently based on visualassessment of the severity of a stenosis. In patients with intermediate left mainstem lesions clinical decision making based on FFR is safe and feasible. Thisstudy was performed to assess the accuracy of visual angiographic assessmentof intermediate or equivocal left main coronary artery (LMCA) stenoses by ex-perienced interventional cardiologists when taking fractional flow reserve (FFR)measurements as the gold standard.Methods: Fifty-one patients with intermediate (40-80% diameter stenosis by an-giography) or equivocal LMCA disease were evaluated by FFR. Angiograms werethen reviewed by four experienced interventionalists from different university hos-pitals blinded to FFR results. Lesions were visually assessed and their signifi-cance classified as ‘significant’ (FFR <0.75), ‘not significant’ (FFR ≥0.75), or ‘un-sure’ if the observer was unable to make a decision regarding lesion significancebased on the angiogram.Results: FFR was <0.75 in 21 patients and ≥0.75 in 30 patients. The four review-ers achieved correct lesion classification in no more than approximately 50% ofcases each. The interobserver agreement between two reviewers in excess of theagreement expected due to chance was outperformed on average by only 16%.Furthermore, interobserver variability was large resulting in unanimously correctlesion classification in only 29% of all cases, meaning that in 71% of cases thesame LMCA stenosis was classified incorrectly by at least one reviewer.Conclusion: The functional significance of intermediate and equivocal LMCAstenoses should not be based solely on angiographic assessment even by ex-perienced interventional cardiologists.
P5339 Predictors of death in patients treated by drug-elutingstents for unprotected left main lesions: a report froma multicenter registry
P. Garot1, T. Lefevre2, O. Darremont3, M. Silvestri4, Y. Louvard2,J.L. Leymarie1, V. Decalf2, M.C. Morice2. 1ICPS, Quincy, France;
2ICPS, Massy, France; 3Clinique Saint-Augustin, Bordeaux, France; 4UCV,Marseille, France
Background: drug-eluting stents (DES) have emerged as an alternative to car-diac surgery, but the predictors of death in pts undergoing elective PCI with DESfor unprotected left main lesions remain unknown.Objectives: To compare the baseline and procedural characteristics in 326 ptstreated by DES for left main lesions according to death (n=14; 4.3%) or survival(n=312; 95.7%) at 6 month follow-up. Multivariate analysis identified the predictorsof death among those with a p value <0.20 at univariate analysis.Methods and results: 343 consecutive pts treated by DES for unprotected leftmain lesion entered this registry. 17 presented with AMI and/or shock and wereexcluded from the analysis. By multivariate analysis, diabetes mellitus (0.1018;
Clinical and angiographic characteristic
Death at 6-mo n=14 Survival at 6-mo n=312 p
Age, y-o 73±12 69±11 0.06Males 79% 76% 0.41Euroscore 6.5±2.8 4.7±3.3 <0.05Estimated mortality by Euroscore 8.8±8.3% 6.3±10.4% 0.20Diabetes Mellitus 64% 26% <0.001LM Restenosis lesion 14% 3% <0.05Prior MI 7% 12% 0.29Unstable angina 36% 35% 0.42Post-MI 0% 7% 0.15Ejection fraction 57±9 61±13 0.14Distal left main stenting 86% 75% 0.09
T shape of distal LM 64% 26% <0.001DES in both branches 50% 37% 0.25Final kissing angioplasty 100% 96% 0.25
PCI success, N (%) 93% 96% 0.41Non Q-wave MI 7% 2% 0.12In-hospital MACCE 36% 3% <0.0001
95% CI [0.0427-0.1609]) and LM restenosis lesion (0.1789, 95% CI [0.0429-0.3148]) were independent predictors of death.Elective stenting using DES for LM lesion is associated with a <5%. 6-modeath rate. Diabetes and restenosic lesions are independently associated withincreased death at follow-up.
P5340 PUMA: a prospective registry of percutaneousintervention of the unprotected left main coronaryartery: early and medium term clinical andangiographic outcome in 114 patients
C. Dubois, J. Dens, P. Sinnaeve, M. Mendez, J. Van Cleemput,J. Piessens, W. Desmet. UH Gasthuisberg Leuven, Cardiology Department,Leuven, Belgium
Background The role of PCI of the unprotected left main coronary artery(ULMCA) is still controversial.Methods In patients undergoing PCI of the ULMCA, cumulative risk-adjusted in-hospital mortality (CRAM) was compared with expected peri-operative surgicalmortality based on additive and logistic EUROSCORE. In-hospital and 1 yearclinical follow-up, including major adverse cardiac events (MACE) and its compo-nents (death, acute myocardial infarction (AMI) and target lesion revascularization(TLR)) were obtained in all patients. Angiographic follow-up was obtained in 75%of the patients.Results From June 1998 to January 2005, 114 patients (62% male; age 70±13y)underwent PCI of the ULMCA. In-hospital mortality was lower than the expectedsurgical mortality risk based on EUROSCORE (Figure 1). The mean logistic EU-ROSCORE was 46±32% in the 26 patients (22.8%) who died during the firstyear, suggesting a very high risk population. Ten patients suffered AMI (8.8%),12 underwent TLR (10.5%). Overall MACE rate was 35.1%. Binary restenosiswas found in 17.4%: 7% in DES treated vs 26% in non-DES treated patients.This relatively high incidence of MACE reflects the high-risk profile of this patientpopulation (30% urgent procedures;18% ST-elevation AMI; 22% non ST-elevationAMI; 18% heart failure with ejection fraction <30%; 11% cardiogenic shock; 60%PCI of ULMCA bifurcation).
Fig. 1
Conclusions: PCI for ULMCA disease is associated with acceptable short- andmedium-term outcomes, including revascularization rates as low as 10.5% at 1year. Mortality remains high, however, especially in very high-risk patients un-suitable for bypass surgery. Thus, in selected indications PCI of the ULMCA is avaluable alternative to surgery, especially when treated with DES.
THE TREATMENT OF THE METABOLIC SYNDROME
P5341 Aggressive lipid lowering with atorvastatin reducesincreased risk of cardiovascular events in patientswith metabolic syndrome and coronary heart disease
P. Deedwania1 , P. Barter2, R. Carmena3, J.-C. Fruchart4 ,S. Haffner5, J. Shepherd6 on behalf of The TNT Steering
Committee and Investigators. 1VACCHCS/UCSF School Of Medicine, CardiologyDepartment, Fresno, United States of America; 2The Heart Research Institute,Cardiology Department, Sydney, Australia; 3University of Valencia, Valencia,Spain; 4Institut Pasteur, Lille, France; 5University of Texas Health ScienceCenter, San Antonio, United States of America; 6University of Glasgow, Glasgow,United Kingdom
Background: Updated recommendations of the NCEP ATP III proposed an LDL-C target of <70 mg/dL (1.8 mmol/L) in patients at very high risk of cardiovascular(CV) events. Data to support the use of this target in patients with metabolicsyndrome (MS) and coronary heart disease (CHD) are limited.Purpose: We examined data from the TNT study to ascertain whether aggressivetreatment with atorvastatin reduced the increased CV risk associated with MS inpatients with established CHD.Methods: A total of 10,001 patients with CHD and LDL-C levels of <130
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

932 The treatment of the metabolic syndrome
mg/dL (3.4 mmol/L) were randomized to double-blind therapy with atorvastatin10 mg/day or 80 mg/day. Of these, 5584 had MS based on NCEP ATP III cri-teria (BMI >28 substituted for waist circumference). The primary end point wasoccurrence of a first major CV event (CHD death, nonfatal non-procedure-relatedmyocardial infarction, resuscitated cardiac arrest, or fatal or nonfatal stroke).Results: After a median follow-up of 4.9 years, 629 patients (11.3%) with MSexperienced a major CV event compared with 353 patients (8.0%) without MS(HR 1.44, 95% CI 1.26-1.64, P<0.0001). In all patients randomized to atorvas-tatin 10 mg, the risk of major CV events increased with the presence of eachadditional component of MS (Figure). This risk was reduced in patients receivingatorvastatin 80 mg, with increasing significance for each additional MS compo-nent. Atorvastatin 80 mg reduced CV events in patients with MS and diabetes(n=1231; 17.8% vs 14.0%; HR 0.76 [0.57-1.01]), as well as those without dia-betes (n=4353; 11.6% vs 8.2%; HR 0.70 [0.57-0.84]).
Conclusions: Patients with MS and CHD were at significantly higher CV risk thanthose with CHD only. This increased risk was significantly reduced by intensivetherapy with atorvastatin 80 mg.
P5342 Frequency and clinical correlates of aspirinresistance in metabolic syndrome
G. Kahraman, T. Sahin, N.Z. Baytugan, T. Kilic, U. Bildirici,G. Kozdag, D. Ural, B. Komsuoglu. Kocaeli University, MedicalFaculty, Cardiology, Kocaeli, Turkey
Purpose: Patients with metabolic syndrome (MetS) have elevations in fibrinogenand other coagulation factors that lead to a prothrombotic state. Low dose as-pirin therapy is usually suggested for primary prevention in MetS patients withhigh cardiovascular risk. This study sought to determine the frequency of aspirinresistance and its related factors in a group of patients with MetS.Methods: Aspirin resistance was assessed in 110 ambulatory patients with MetS(38 male, 72 female, aged 54±10 years). All patients received aspirin 100 mg/dayfor ≥7 days. Effect of antiplatelet therapy was evaluated with platelet functionanalyzer, PFA-100. A collagen-epinephrine closure time <186 s is accepted asaspirin resistance.Results: Aspirin resistance was found in 23 patiens (%20.9). Age, gender, glu-cose, lipids, fibrinogen and HbA1C levels were not statistically different betweenpatients with and without aspirin resistance, whereas uric acid, homocysteine andhs-CRP levels were significantly higher in those with aspirin resistance (p=0.035,p=0.037, p=0.026, respectively) (Table). Multivariate logistic regression analysisdemonstrated that level of hs-CRP is the most important factor for aspirin resis-tance in MetS (p=0.004, OR 5.3, 95% CI 1.7-16.8). In patients with a hs-CRP ≥1mg/dL, frequency of aspirin resistance was significantly higher than in patientswith lower levels (50% vs. 16%, p=0.005).
Table 1
Aspirin resistance (-) Aspirin resistance (+) p(n=87) (n=23)
Uric asid (mg/dL) 4.5±1.4 5.4±1.9 0.035hs-CRP (mg/dL) 0.49±0.49 1.12±1.43 0.026Homocysteine (mmol/L) 12±6 16±10 0.037
Conclusion: This study demonstrates that aspirin resistance may be a frequentfinding in MetS patients receiving low dose aspirin. Increased levels of uric acid,homocysteine and especially a hs-CRP ≥1mg/dL are significantly related to as-pirin resistance.
P5343 The combination of quinapril and dietary modificationresulting in weight loss improves insulin sensitivityand markers of obesity in patients with the metabolicsyndrome
B. Khan1, S. Sola1, A. Pandian1, Q. Khan1, S. Nagamia1,N. Merchant2 . 1Emory University, Division Of Cardiology, Atlanta, United Statesof America; 2InVasc Therapeutics, Atlanta, United States of America
Background: Patients with the metabolic syndrome (MBS) have activation ofpro-inflammatory mechanisms within the vasculature. We sought to determinewhether a combination of an angiotensin converting enzyme (ACE) inhibitor anddietary modification resulting in weight loss regulates markers of obesity and in-sulin resistance in MBS.
Methods: 44 patients with MBS were placed on a reduced calorie and fat regimento lose weight. Subjects were randomized in a double blinded manner to eitherthe ACE inhibitor quinapril (20 mg/day) or matching placebo for 24 weeks. Wemeasured serum markers of adiponectin and leptin. Additionally, estimations ofinsulin secretion and insulin sensitivity using homeostasis model assessment ofinsulin resistance (HOMA-IR) were obtained.Results: There was a similar reduction of body weight, systolic blood pressure,serum LDL cholesterol, triglyceride, and fasting glucose in both the placebo andquinapril groups. In the placebo group, there was a trend toward increased levelsof serum adiponectin in patients who underwent diet modification to lose weightat both 12 and 24 weeks of therapy. The difference was statistically significant at24 weeks in the placebo group (baseline: 1.40± 0.08 pg/ml, 24-weeks: 1.59 ±0.10 pg/ml; p=0.03 vs baseline). Moreover, in patients who were in the quinaprilgroup, the findings were statistically significant at both 12 weeks and 24 weeksof therapy (baseline: 1.50±0.12 pg/ml, 12-weeks: 1.97±0.14 pg/ml; p=0.009 vsbaseline, 24-weeks: 2.04±0.11 pg/ml; p=0.007 vs baseline). In comparison toplacebo, serum leptin levels were further reduced in the quinapril group (changein placebo: -5.28 ± 0.86; change in quinapril: -12.53 ± 2.16 ng/ml; p < 0.001quinapril vs placebo). The HOMA-IR was decreased by 13 percent in the placebogroup and by 31 percent in the quinapril group after 24 weeks of therapy. Therapywith quinapril was well tolerated.Conclusions: Dietary modification resulting in weight loss improves markers ofobesity and insulin resistance; moreover, this effect is potentiated with the additionof quinapril. These results may attenuate the progression of the pathophysiologyseen in individuals with MBS.
P5344 Changes in body composition in patients with leftventricular systolic dysfunction treated withbeta-blocker therapy
L. Ingle, A.S. Rigby, J.G.F. Cleland, A.L. Clark. University of Hull,Academic Cardiology, Hull, United Kingdom
Introduction: Patients with left ventricular systolic dysfunction (LVSD) have anincreased resting metabolic rate, which may be related to the development ofcachexia, an independent risk factor for mortality. There is some evidence in-creasing body mass index (BMI), cholesterol, and body fat are associated witha better prognosis in patients with LVSD. We aimed to investigate long-termchanges in body composition in patients with LVSD treated with beta-blocker ther-apy.Methods: We studied 575 patients at baseline (72% male) with LVSD (mean age72 ± 11 years; BMI 28.0 ± 5.3 kg m2; body mass 80.3 ± 15 kg; mean left ventricu-lar ejection fraction 32 ± 9%) who had body fat (30 ± 14%), fat mass (24 ± 12kg),and fat-free mass (56 ± 10kg), determined by bioelectrical impedance assess-ment (Tanita TBF 410-MA, Japan). 45% of patients were prescribed beta-blockers(carvedilol 16.0%; bisoprolol 13.6%; atenolol 11.2%; others 4.2%). 291 patientshad body composition re-assessed 1-year later. The relationship between changein body composition and beta blocker usage was investigated by least squares re-gression analysis taking beta blocker as a factor at two levels (any versus none),and beta-blocker type (none, atenolol, bisoprol, carvedilol and any other). Wealso looked for dose-response effects across all types of beta-blocker therapy. Allregression analyses were corrected for age, sex and BMI.Results: After 1 year, mean BMI was 28.4 ± 5.5 kg m2 (P>0.05); body masswas 81.2 ± 17 kg (P>0.05);% body fat was 32 ± 17%, P>0.05; fat mass was27 ± 14 kg, P>0.05; and fat-free mass was 56 ± 10 kg, P>0.05. 79% of pa-tients were prescribed beta-blockers (carvedilol 32.4%, bisoprolol 20.6%, atenolol17.4%, others 8.6%). There was an increase in usage over 1 year in these pa-tients (P<0.001). There was no statistical difference between beta-blocker us-age, beta-blocker type or beta-blocker dose, and changes in % body fat, basalmetabolic rate, impedance, fat-free mass, fat mass, and total body water. Therewere no significant differences between any of these measures and beta-blockerusage (any, type or dose). There was no evidence for dose-response effects withincreasing dosage of beta-blocker.Conclusion: After 1 year, changes in body composition are not influnced by beta-blocker therpay in patients with LVSD.
P5345 Effect of valsartan on adiponectine, leptin andresistine in hypertensive obese patients
R. Fogari, G. Derosa, A. Mugellini, P. Preti, P. Lazzari, A. Zoppi,M. Destro. University of Pavia, Department of Internal Medicine,Pavia, Italy
The aim of the study was to compare the effect of valsartan and amlodipine onblood pressure (BP), plasma adiponectine (pA), plasma leptin (pL), and plasmaresistine (pR) in hypertensive patients with obesity. Seventy-two obese patients(BMI > 30 kg/m2) with mild to moderate hypertension (DBP evaluated with ap-propriate size cuff > 90 mmHg < 110 mmHg) aged 31-65 years after a 4 weekwash out period were randomized to valsartan 160 mg (n= 36) or to amlodipine10 mg (n= 36) for 12 weeks. At the end of the wash-out period and of each treat-ment period BP was evaluated and a venous sample was drawn in the morningat the same hour to evaluate pA, pL and pR. Furthermore insulin resistance index(HOMA-R) was calculated using fasting glycemia and plasma insulin. No dietaryadvice was prescribed for the duration of the study. The main results are shown in
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

The treatment of the metabolic syndrome 933
the table. Both valsartan and amlodipine significantly decreased BP without anydifference between the two treatments; however valsartan improved insulin sen-sitivity and induced a significant reduction in pL and pR and an increase in pA;such an increase was significantly correlated with HOMA-R changes.
Main resuts
Baseline Valsartan Baseline Amlodipine
SBP (mmHg) 156.8±11 140.2±10 ** 157.5±12 139.8±10 **DBP (mmHg) 100.4±6 86.1±5 ** 100.1±5 85.8±4 **pA (ng/ml) 6.3±0.9 7.4±1.1 * 6.0±0.9 6.3±1.0pL (ng/ml) 34.8±15.6 31.1±13.3 * 35.2±16.7 34.9±16.5pR (ng/ml) 5.9±0.9 4.8±0.7 * 5.7±0.6 5.5±0.6HOMA-R 8.1±3.1 7.1±2.4 * 8.3±3.5 8.1±3.3
*p< 0.05 **p< 0.01 vs baseline
These data suggest that in obese hypertensive patients Angiotensin II antagonistsimprove insulin sensitivity as well the impaired adipocyte metabolism.
P5346 The effects of orlistat on intima media thickness andsome hemodynamic parameters of femoral arteries inpatients with metabolic syndrome
Z. Hajdukovic, A. Jovelic, S. Radjen. Military Medical Academy,Endocrinology, Belgrade, Serbia and Montenegro
Background: Insulin is a vascular hormone. Orlistat weight-losing treatment isassociated with increment insulin sensitivity and correction of dyslipidemia, butits influence on functional and morphologic parameters of peripheral arterial cir-culation in patients with metabolic syndrome (MS) is not fully elucidated.Aim: To evaluate the 6 months orlistat treatment compared with placebo on tradi-tional cardiovascular risk factors, insulin sensitivity, femoral arteries intima-mediathickness (IMT), pulse pressure (PP), mean blood flow velocity (MV) and resis-tance index (RI) in subjects with MS.Methods: Forty subjects (54.3% men; age 50.2±8.2 years, waist circumference(WC): 105.9±7.8 cm) were randomly assigned to receive either orlistat (120 mg3 times daily; n=20) or placebo (n=20), with a hypocaloric diet. MS was definedaccording to International Diabetes Federation. Insulin sensitivity index (ISI) wascomputed according to formula proposed by De Fronzo et Matsuda. The IMT,PP, MV and RI were determined with Doppler ultrasonography on femoral arter-ies.Results: Baseline both groups were comparable in regards to WC, blood glu-cose level, glycosylated hemoglobin (HbA(1c)), lipid status, PP, ISI, MV, RI andIMT (P>0.05). Orlistat therapy reduced weight (9.67±1.50 vs. 5.40±1.28 kg,p<0.001), WC (17.56 vs. 7.75 cm, p<0.001), systolic blood pressure (15.4 vs.6.9 mmHg, p=0.05), pulse pressure (10.2 vs. 1.9 mmHg, p=0.003), glucose (0.78vs. 0.35 mmol/l, p=0.007), HbA(1c) (0.57 vs. 0.07%, p=0.006) and triglycerides(1.40 vs. 0.29 mmol/l, p=0.04) to a greater extent than diet alone. ISI improvedsignificantly more in orlistat than in control group (15.9 vs. 5.63; p=0.001). Re-ductions of RI (0.024 vs. 0.006, p=0.04), MV (11.06 vs 2.75; p=0.05) and IMT(0.27 vs 0.11; p=0.018) were higher in the orlistat than in the placebo group. In amultiple regression analysis that included changes in HbA(1c) and ISI, incrementin ISI (β= -0.55, p=0.007) was the independent predictor of reduction of MV. Onlyunivariant predictors of RI and IMT reductions were increment of ISI (β= -0.439,p=0.008) and triglycerides (β= -0.482, p=0.003), respectively.Conclusion: In studied patients with metabolic syndrome we documented theimprovements of the early subclinical functional and morphologic parameters offemoral arteries, mean blood flow velocity, pulse pressure, resistance index andintima-media thickness witch could be associated with increment in insulin sensi-tivity following 6 months of orlistat weight-losing treatment.
P5347 Effects of orlistat on cardiovascular risk factors andliver fat in overweight Chinese patients withnon-alcoholic fatty liver
B. Tomlinson1, Y.-J. Fang1, T.T.W. Chu1, Y.-L. Chan1,N.W.Y. Leung2, W.-S. Chan3, I.F.F. Benzie4, K.K.C. Lee2. 1Chinese
University of Hong Kong, Medicine & Therapeutics, Shatin, Hong Kong, People’sRepublic of China; 2Alice Ho Miu Ling Nethersole Hospital, Medicine, Tai Po,Hong Kong, People’s Republic of China; 3North District Hospital, Radiology,Fanling, Hong Kong, People’s Republic of China; 4Hong Kong PolytechnicUniversity, Ageing & Health Section, School of Nursing, Kowloon, Hong Kong,People’s Republic of China
Background: Orlistat is known to promote weight reduction and help to preventthe onset of type 2 diabetes mellitus in patients with the metabolic syndromebut the effects on the frequently associated non-alcoholic fatty liver (NAFL) areuncertain.Methods: Chinese patients with BMI >23 kg/m2 were screened for NAFL byultrasound and 36 including 29 with hypertension and 13 with diabetes were ran-domised to treatment with orlistat 120 mg three times daily or placebo in additionto diet. Measurements of obesity, blood pressure (BP), plasma lipids, glucoseand insulin were made at baseline and after 6 months treatment. Liver volumewas assessed by MRI and liver fat estimated by the percentage signal loss in theopposed-phase as compared to the in-phase gradient echo T1-weighted imagesin a region of interest in the right lobe of the liver. The greater the percentage
signal loss, the higher the fat content of the liver. Measurements were repeatedafter 6 months treatment.Results: Orlistat treatment was well tolerated and resulted in reductions in bodyweight (orlistat -2.0 ± 1.9 vs. placebo +0.6 ± 1.3 kg, p<0.01), systolic BP (-8.5 ± 8.9 vs. +3.9 ± 14.9 mmHg, p<0.01), diastolic BP (-4.1 ± 6.0 vs. +0.7 ±10.1 mmHg, p<0.05), fasting plasma glucose (-0.4 ± 1.0 vs. +0.5 ± 1.1 mmol/L,p<0.01) and plasma insulin (-6.7 ± 8.9 vs. +4.8 ± 11.9 nmol/L, p=0.002). Therewas no significant change in the ratio of LDL-cholesterol to HDL-cholesterol ineither group. Liver volume was reduced from 2.3 ± 0.5 to 1.7 ± 0.2 L in theorlistat group and from 2.2 ± 0.8 to 1.8 ± 0.5 L in the placebo group (p<0.01between groups) and liver fat content was reduced more (p<0.01) with orlistat(33.0 ± 0.2 to 19.2 ± 0.1% signal loss) than with placebo (31.2 ± 0.2 to 29.0 ±0.2% signal loss).Conclusion: The weight reduction with orlistat treatment was associated withimprovements in BP, plasma glucose and insulin and marked reduction in liverfat content suggesting the beneficial effects exceed simple weight reduction andorlistat may be an effective treatment for NAFL.
P5348 Cardiorrespiratory fitness, metabolic syndrome andsubclinical inflammation in a primary preventioncardiology unit
M. Acevedo, G. Chamorro, R. Corbalan, J.A. Rodriguez, V. Kramer,C. Bambs, L. Orellana. Catholic University of Chile, Cardiovascular
Diseases, Santiago, Chile
The metabolic syndrome (MS) is present in 1 out of 4 adult subjects in Chile.It has been recognized that the presence of the MS is associated with a higherdegree of inflammation. Physical activity improves insulin resistance and mightinfluence the development of inflammation and metabolic risk factors. We soughtto determine whether a better cardiorespiratory fitness could attenuate the levelsof subclinical inflammation in subjects with metabolic risk factors including thosewith MS.Methods: We prospectively studied 1587 subjects (1016 men, mean age = 52± 12 yo) without history of CHD or CVD. We assessed CV risk factors anddetermined body mass index, waist circumference, systolic and diastolic bloodpressure, a fasting lipid profile and glycemia. Subclinical inflammation was deter-mined by ultrasensitive C-reactive protein (CRPus) and cardiorespiratory fitnesswith a maximal treadmill exercise test. Fitness was divided in quartiles of maximalmetabolic equivalents (METs).Results: In our cohort, 67% of the subjects were overweight/obese, and 25%had MS according to ATP III. Significant correlations were demonstrated betweenMETs and age (r=-0.6, p<0.001), logCRPus ((r=-0.2, p=0.001), glycemia (r=-0.2,p<0.001), systolic blood pressure (r=-0.3, p<0.001) and body mass index (r=-0.12, p<0.001). The table shows the distribution of MS components and CRPusby METs quartiles.CRPus levels were higher in the subjects with MS compared tothose without (2.9 versus 2.0 mg/L, p=0.03). In MS subjects, mean CRPus levelswere significantly higher in those in the lowest fitness quartile versus those in thehighest fitness quartile (4.8 versus 1.9 mg/L respectively, p=0.02).
MS components and CRP by METS quartiles
Risk Factor (mean) <8 METs 8-10 METs >10-12 METs >12 METs p for trend
SBP mmHg 133 129 125 122 <0.001Glycemia (mg/dL) 99 95 93 92 <0.001HDL mg/dL 51 57 56 60 0.007CRPus mg/L 3.7 2.3 2.1 1.9 0.003
SBP=systolic blood pressure; CRPus=ultrasensitive C-reactive protein.
Conclusions: Our findings show that metabolic risk factors and CRPus levelsimprove with a better fitness level. In people with MS an increased level of car-diorespiratory fitness might attenuate subclinical inflammation and decrease car-diovascular risk.
P5349 Management of lifestyle dependent on body massindex in post myocardial infarction patients in primarycare practice
R. Glowczynska1, M.E. Starczewska2, A. Pietrasik1, K.J. Filipiak1,G. Opolski1. 1Medical University Of Warsaw, 1St Department Of
Cardiology, Warsaw, Poland; 2Medical University of Warsaw, 1st Department ofCardiology, Warsaw, Poland
Background: High risk patients (pts) after myocardial infarction (MI) are at thesupreme priority for secondary preventive cardiology. The aim of this paper wasto determine in post MI pts, whether the ESC recommendations on cardiovascularevents (CVE) prevention were being followed in primary care practice.Methods: Data from representative sample of 1545 general practitioners, on8972 pts (mean age 63±10 years; 66,5% males) after MI were randomly se-lected from 31,116 out-patients charts database of POLKARD-SPOK survey.Both pts and practitioner questionnaires collected data on: cardiovascular riskfactors, lifestyle and medications applied. Value of normal BMI was defined as20-24.9 kg/m2. Compartment of BMI between 25-29.9 kg/m2 was described asoverweight. Value of BMI 30-34.9 kg/m2, 35-39.9 kg/m2 and over 40 kg/m2 deter-mined relatively obesity I°, II° and III°.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

934 The treatment of the metabolic syndrome / Diagnosing the metabolic syndrome
Management of lifestyle in post-MI pts
Indications BMI
Normal Overweight Obesity I° Obesity II° Obesity III°
Regular physical activityYes 71.59% 79.86% 85.80% 88.89% 91.89%No 7.08% 5.81% 4.54% 3.61% 2.70%Not concerned 21.34% 14.33% 9.66% 7.50% 5.41%
Diet modificationYes 59.05% 76.13% 89.14% 94.69% 95.95%No 13.84% 9.42% 5.07% 2.79% 1.35%Not concerned 27.12% 14.44% 5.79% 2.51% 2.70%
Normalization of weightYes 25.29% 66.02% 91.08% 96.95% 98.65%No 19.29% 11.66% 4.07% 1.39% 0.00%Not concerned 55.42% 22.32% 4.85% 1.66% 1.35%
Conclusions: In primary care practice doctors’ opinion almost every fourth pa-tient with value of BMI between 25-29.9 kg/m2 did not achieved criteria of over-weight diagnosis. That indicated this group of pts did not need weight normaliza-tion.
P5350 Effects of bariatric surgery on preclinical myocardialalterations in severes obesity
V. Di Bello1, F. Santini2, A. Di Cori1, E. Talini1, A. Pucci1, M.G. DelleDonne1, A. Barsotti1, M. Mariani1. 1University Of Pisa, DipartimentoCardio Toracico, Pisa, Italy; 2Pisa, Italy
Background: Obesity is a well established risk factor for Congestive Heart Failure(CHF) and is able to determine preclinical left ventricular functional alterations,well detected with ultrasonic Integrated Backscatter and Color Doppler MyocardialImaging.Objective: The aim is to clarify the effect of bariatric surgery with a consequentsubstantial weight loss, on structural and functional myocardial alterations ob-served in severe obese population.Material and methods. Twenty consecutive severely obese "healthy" patients (5males, 15 females, mean age 31.2±6 yr) were enrolled. Twenty age-matchednon-obese healthy subjects were also recruited as controls. All subjects under-went conventional 2D-Color Doppler echocardiography. The new ultrasonic tech-niques are: a) Integrated Backscatter (IBS) for the analysis of myocardial reflec-tivity, referred to pericardial interface as expression of myocardial structure (in-crease in collagen content) and of Cyclic Variation Index (CVI) as expression ofintrinsic myocardial contractility and b) Color Doppler Myocardial Imaging (CDMI)for the analysis of strain and strain rate (myocardial deformability). All subjectsunderwent bariatric surgery and were resubmitted to echocardiographic and bio-chemical examination within 6 months after surgery.Results: The main finding of the present study was a quite complete normal-ization of myocardial functional and structural alterations, evidentiated with IBSand CDMI, in severe obese patients after bariatric surgery. In particular, CVI atseptum level highly improves after surgery (before: 16.6 ± 5.0 vs. after surgery:25.7 ± 11.2 vs. controls: 36.2 ± 9.1; p<0.0001). Furthermore mean reflectivityat septum level significantly decreases after surgery (before: 52.8 ± 9.5 vs. aftersurgery: 46.5 ± 8.8 vs. controls: 43.0 ± 8.0; p<0.04). Also the strain at septumlevel significantly improves after surgery (before: -15.7 ± 3.2 vs. after surgery:-20.4 ± 5.3 vs. controls: -23.4 ± 9; p<0.001). Significant correlations were de-tected between BMI variation and left ventricular mass, CVI at septum level, meanseptum reflectivity and myocardial deformability (strain and strain rate) variations.Conclusion: Bariatric surgery appears to be efficient not only for the determi-nation of a substantial and durative weight loss but also for the improvement ofmyocardial metabolism and function. This study establishes the utility of new ul-trasonic techniques able to detect, in obese patients, very early structural andfunctional myocardial alterations and their substantial regression after bariatricsurgery.
DIAGNOSING THE METABOLIC SYNDROME
P5351 The diagnosis of the metabolic syndrome may besimplified using triglycerides and waistcircumference or BMI in healthy subjects
T.S.F. Leong1, Y. Rahman2, A.P. Fitzgerald3 , C. Mcgorrian1,G. Boran1, J. Nolan4, I.M. Graham1. 1Adelaide & Meath Hospital,
Cardiology, Dublin, Ireland; 2Charing Cross Hospital, London, United Kingdom;3University College, Epidemiology, Cork, Ireland; 4St James’s Hospital, Dublin,Ireland
Introduction: The metabolic syndrome (MS) is associated with increased risk ofcardiovascular disease (CVD). The NCEP definition uses 5 criteria to diagnosisthis. We propose to examine if the MS may be simplified in order to increase itsutility.Methods: Dataset 1: We used subjects from a staff screening initiative (n=471),and also controls from a diabetes study (n=206), all free from CVD and dia-betes, giving a total of 677 healthy subjects. Dataset 2: We used the control group
(n=800) free from CVD from ’The European Concerted Action Project: Homocys-teinaemia and Vascular Disease’ to test the findings from Dataset 1. The NCEPdefinition of the MS was used. The modified NCEP definition (MSBMI) used BMI≥30 as a proxy for waist.Results: The prevalence of the MS was 9.8% in Dataset 1 and 13% (MSBMI) inDataset 2. The agreement between the MS and MSBMI in Dataset 1 was 98%.We used the 5 components as continuous variables in a model and tested itsdiagnostic ability for the MS. Then, each component was removed step-wise andat each step, compared with the original model with 5 components. The areaunder the ROC curve (AUROC) for all 5 components was 0.97 (95% CI 0.96,0.98). The diagnostic ability did not significantly change until waist & triglyceridesremain, AUROC 0.96 (95% CI 0.94, 0.98). The results obtained using BMI insteadof waist were similar. We then used beta-coefficients from Dataset 1 derived froma model using only BMI and triglycerides as continuous variables and tested itas a risk score function in Dataset 2 - AUROC 0.94 (95% CI 0.92, 0.96). Table 1shows the discriminative ability of these models for the MS.
Table 1
Sensitivity Specificity Positive Negative(%) (%) predictive predictive
value (%) value (%)
Dataset 1: Increased waist (>102 cm men,>88 cm women) 95 86 43 99
Dataset 1: Triglycerides ≥1.7 mmol/L 76 90 46 97Dataset 1: Increased waist & triglycerides 71 98 83 96Dataset 2: BMI ≥30 37 97 68 92Dataset 2: Triglycerides ≥1.7 mmol/L 89 86 49 98Dataset 2: Increased BMI & triglycerides 27 100 100 90
Conclusions: The diagnosis of the MS can be simplified to only waist and triglyc-erides without great compromise in healthy subjects. Good predictive valuescould be achieved using the usual cut-points for both.
P5352 International Diabetes Federation Criteria do notimprove coronary disease risk stratification insubjects with the metabolic syndrome
J. Neubauer1 , R.D. Santos2, J.A.M. Carvalho2. 1Prev. Med CenterAlbert Einstein Hospital, Sao Paulo, Brazil; 2Heart Institute- InCor
Univ. of Sao Paul, Sao Paulo, Brazil
Purpose: Recently the International Diabetes Federation (IDF) determined thatabdominal obesity, becomes an obligatory criterion for the diagnosis of themetabolic syndrome (MS), furthermore it also reduced the waist girth measure-ment (> 94 cm in Europids) and blood glucose (>100 mg/dL) in comparison toATP III. There is no evidence that this new definition improves coronary heartdisease (CHD) risk stratification when compared with the classical ATP III defini-tion of the MS. Both Framingham risk scores and white blood cell count correlatewith atheroscelrosis risk. This study compares both the IDF and ATP III criteriaregarding clinical and inflammatory markers for CHD risk in white asymptomaticmen.Methods: 3,202 consecutive men (mean age 44 years) were evaluated in a struc-tured check-up. Subjects were divided in 4 groups: ATP: MS according to ATP cri-teria, however without waist girth > 102 cm, n=56 (1,7%); IDF: MS according toIDF criteria only, n= 327 (10.2%); ATP+IDF: MS according to both criteria n=617,(19.3%), and NoMS no MS according to both criteria, n=2,202 (68.8%).The CHDrisk markers evaluated were 10-year total predicted CHD risk calculated by Fram-ingham Risk Score (FRS) and white blood cell count (WBCC).Results: Subjects in NoMS group presented the lowest predicted risk and WBCC(respectively 5.6±3.7% and 6.1±1.6 1,000/mL, p<0.001 for both values vs. allMS groups). The individuals in IDF group, despite higher FRS and WBCC whencompared with NoMS individuals, expressed lower predicted risk and WBCCcompared with IDF+ATP group (8.5 ± 4.9% vs. 10.5 ± 6.4%, p<0.001 and 6.3 ±1.5 x1,000/mL vs 6.7 ± 1.5 x1,000/mL, p=0.002 respectively). On the other hand,ATP individuals presented no difference in these two parameters compared withIDF+ATP group (p>1.0).Conclusion: In our population the IDF criteria increased the number of individu-als diagnosed with the MS, however these subjects presented significantly lowerCHD risk when compared with those diagnosed by ATP III when FRS and inflam-matory parameters were used.
P5353 Abdominal obesity and physical activity: do they addsomething to the Framingham risk score?
M. Acevedo, G. Chamorro, C. Bambs, V. Kramer, L. Orellana,J.A. Rodriguez, R. Corbalan. Catholic University Of Chile,Cardiovascular Diseases, Santiago, Chile
Background: Abdominal obesity and sedentary behaviour are considered car-diovascular(CV) risk markers. However, there is little information to what extentthey add to cardiovascular risk prediction. Purpose: To determine the changes inFramingham risk score using abdominal obesity and time dedicated to physicalactivity as indicators of cardiovascular risk.Methods: We prospectively studied 1590 subjects (1016 men, mean age = 52 ±12 yo) without history of CHD or CVD presenting to a primary prevention unit. We
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Diagnosing the metabolic syndrome 935
assessed CV risk factors and determined waist (W) circunference, systolic anddiastolic blood pressure, a fasting lipid profile and glycemia. Abdominal obesitywas determined using the new cutoffs proposed by the International DiabetesFederation. Physical activity was measured as times per week of aerobic exercise≥ 30 minutes each time. We classified them in those doing < 1, 1-2 and ≥ 3times/week of aerobic exercise. Framingham risk score was calculated as thepercentage for 10-year CV risk in each individual.Results: Fifty-five percent of the subjects exercised < 1 time/week, 22% did it1-2 times/week and 23% ≥ 3 times/week. Mean W in males was 97 ± 9 cm and82 ±10 cm in females. Subjects with higher W exercised less than those with nor-mal W (p<0.001). A direct and significant correlation was found between CV riskmeasured by Framingham risk score and W (r=0.4,p<0.001). This relationshipwas independent of times/week of physical activity. The table shows the 10-yearCV risk according to W and physical activity in men and women.
Framingham Score by waist and exercise
Males Males Females Females
Physical Activity W<90cm W≥90cm W<80cm W≥80cm<1 time/week 5% (3-10) 10% (6-19)* 3% (2-6) 6% (4-11)*≥3 times/week 2% (2-7) 10% (6-16)* 3% (1-6) 6% (4-9)*Total 4% (2-8) 10% (6-16)* 3% (2-6) 6% (4-11)*
Results expressed as Median and interquartiles ranges;*p<0.001 for W≥90/80 versus <90/80cm in males/females respectively;W=waist
Conclusions: In this cohort, abdominal obesity confers more CV risk assessedby Framingham score in both men and women independently of time dedicated toaerobic exercise. Physical activity appears to have a beneficial role reducing 10-year CV risk only in men with normal W circunference. Abdominal obesity mightbe used as a rapid indicator of CV risk in some populations.
P5354 Clustering of borderline atherosclerotic risk factors iscomparable with an established factor regardingchange in inflammatory markers
K. Matsushita, H. Yatsuya, K. Tamakoshi, T. Kondo, T. Murohara,H. Toyoshima. Nagoya University Graduate School Of Medicine,
Department Of Cardiology, Nagoya, Japan
Purpose: Metabolic syndrome (MetS) is a cluster of atherosclerotic cardiovas-cular disease (CVD) risk factors. Recently, the clinical significance of MetS hasbeen opposed by some investigators who have insisted that persons with clus-tered MetS components obviously have a high risk for CVD, since each MetScomponent has been proved as a CVD risk factor (RF). Meanwhile, the impor-tant aspect of the conventional MetS definition is that the cutoff values of somecomponents are less stringent than required to identify an established RF. How-ever, the clinical significance of clustering of borderline RFs has not been wellinvestigated.Methods: We studied 2805 middle-aged Japanese men without a history of can-cer or CVD. MetS components except obesity were stratified as established (high-density lipoprotein cholesterol [HDL-C], <35 mg/dL; triglyceride, ≥200 mg/dL;glucose, ≥126 mg/dL; blood pressure, ≥140/90 mmHg) or borderline (HDL-C, 35-39 mg/dL; triglyceride, 150-199 mg/dL; glucose, 110-125 mg/dL; blood pressure,130-139/85-89 mmHg). All subjects were then further classified into 4 groups asfollows: (1) 2 to 4 established RFs, (2) 1 established RF, (3) 2 to 4 borderlineRFs, or (4) 0 or 1 borderline RF. Cardiac-event-predictive inflammatory markers(C-reactive protein [CRP], leptin, and adiponectin) were compared among these4 groups adjusting for covariates by ANCOVA with post-hoc analyses using theBonferroni method.Results: As expected, those with 2 to 4 established RFs showed the highestinflammatory condition among them. Although those with 2 to 4 borderline RFsshowed higher inflammatory state than those with 0 or 1 borderline RF, they werecomparable with those with 1 established RF (CRP [mg/L]: 0.47 vs. 0.36 [P<0.05]and 0.48 [P=n.s.], leptin [ng/mL]: 4.64 vs. 3.50 [P<0.001] and 4.57 [P=n.s.], andadiponectin [μg/mL]: 5.38 vs. 6.63 [P<0.001] and 5.68 [P=n.s.]).Conclusions: These results imply that persons with concomitant borderline RFsmight have a risk for cardiac events similar to patients with 1 established RF, whoare covered by conventional therapeutic guidelines. Therefore, a clinical strategyto treat patients with several borderline RFs would be warranted.
P5355 The relationship between metabolic syndrome,according to alternative definitions, and endothelialfunction among healthy, middle-aged men. Thefirefighters and their endothelium study
L. Title1, E. Lonn2, F. Charbonneau3 , M. Fung3, K.J. Mather4,S. Verma5, T.J. Anderson4 on behalf of FATE Study. 1Qe Ii Health SciencesCentre, Division Of Cardiology, Halifax, Canada; 2McMaster University,Hamilton, Canada; 3University of Calgary, Calgary, Canada; 4Indiana University,Indianapolis, United States of America; 5University of Toronto, Toronto, Canada
Background: The metabolic syndrome [MetSyn] is a risk factor for cardiovascu-lar disease [CVD]. It may predispose to CVD by causing endothelial dysfunctionand vascular inflammation. The aim of this study was to determine the relation-ship between the MetSyn, defined according to the World Health Organization
[WHO]; National Cholesterol Education Program [NCEP]; and International Di-abetes Federation [IDF], and endothelial function (brachial artery flow-mediateddilatation [FMD]), inflammation (high-sensitivity C-reactive protein [hsCRP]), andsubclinical atherosclerosis (carotid intimal-medial thickness [IMT]) among 1,555middle-aged men without CVD.Methods and Results: We prospectively evaluated 1,555 male, firefighters(mean age 49) in the Firefighter and Their Endothelium [FATE] study. Of these,358 (23%) met the WHO definition of MetSyn, 331 (21%) met NCEP criteria forMetSyn, and 492 (32%) met the newer IDF definition. Mean FMD was lower forthose with the NCEP and IDF criteria for MetSyn vs. no MetSyn (NCEP: 8.1±4.1vs. 8.7±4.0%, p=0.03; IDF: 8.2±3.9 vs. 8.7±4.1%, p=0.02). However, there wasno relationship between FMD and increasing number of MetSyn criteria using theNCEP and IDF definitions. Using the WHO criteria, FMD was similar for MetSynvs. no MetSyn (8.2±4.1 vs. 8.7±4.0; p=0.09). The median hsCRP was higherin those with MetSyn vs. no MetSyn according to all 3 definitions (WHO: 2.06vs. 1.11 mg/L, p<0.001; NCEP: 2.09 vs. 1.12 mg/L, p<0.001; IDF: 1.9 vs. 1.07mg/L, p<0.001) and median hsCRP increased with increasing number of Met-Syn criteria using all 3 definitions. Lastly, median carotid artery IMT was higherin those with MetSyn vs. no MetSyn according to all 3 definitions (WHO: 0.76vs. 0.70 mm, p<0.001; NCEP: 0.76 vs. 0.70 mm, p<0.001; IDF: 0.76 vs. 0.70mm, p<0.001) and median IMT increased with increasing number of MetSyn cri-teria using all 3 definitions. The results remained unchanged after excluding 66subjects with diabetes (fasting glucose>7mmol/L; history of diabetes; or usinganti-diabetic meds).Conclusions: The prevalence of MetSyn varied according to the definition usedfrom 21 to 32% among the middle-aged male firefighters in the FATE study. Usingall 3 definitions (WHO, NCEP, and IDF), MetSyn was associated with inflammationand subclinical atherosclerosis in the FATE study. The presence of the MetSynwas associated with worse endothelial function, according to the NCEP and IDFdefinitions. Thus, MetSyn may predispose to CVD and atherosclerosis by causingendothelial dysfunction and vascular inflammation.
P5356 Comparative analysis of current definitions anddiagnostic criteria of metabolic syndrome using theOlivetti heart study database
P. Strazzullo1, A. Barbato1, A. Siani2, F.P. Cappuccio3 , A. Venezia2,P.L. Schiattarella2, E. Farinaro2 on behalf of The Olivetti Heart
Study. 1University of Naples "Federico II", Dep. of Clinical and ExperimentalMedicine, Naples, Italy; 2 CNR, Institute of Food Sciences, Avellino, Italy;3Warwick Medical School, Clinical Sciences Research Institute, Coventry, UnitedKingdom
Purpose: To compare the ability of seven definitions of metabolic syndrome (MS)- WHO (1998), EGIR (1999), ATPIII (2001), AACE (2003), ATPIII (2004), IDF(2005) and AHA/NHLBI (2005) - to identify individuals with insulin resistance (Ins-R) and high cardiovascular (CV) risk.Methods: The definitions’ diagnostic criteria were applied to the population of 933men aged 59.5 yrs (33-81) attending the 2002-2004 examination of the OlivettiHeart Study, for whom standardized measurements were available of BMI, waistcircumference, BP, fasting serum T- and HDL-cholesterol, triglyceride, glucose, in-sulin, hs-CRP and 24-hr microalbuminuria (mALB). Ins-R was defined as a HOMAindex > 2.77 (80th pct of the HOMA distribution in an Italian adult non-obesemale population). The individual absolute risk of a heart attack in 10 years wasestimated by PROCAM algorithm. ROC curves were calculated to evaluate theability of the seven definitions to correctly identify individuals at high CV risk.Results AND CONCLUSIONS. a) MS prevalence ranged from 8.6% (AACE) to44.5% (IDF); b) Likewise, the prevalence of Ins-R spanned from 94.8% (EGIR) to49.2% (IDF); c) type 2 diabetes was highly prevalent by WHO (59.9%), much lessby ATPIII, IDF and AHA/NHLBI (22-24%) and was excluded by EGIR and AACEcriteria; d) MS+ subjects had greater estimated average CV risk than MS- sub-jects by all definitions except AACE or EGIR; e) In general, the ability to correctlyidentify individuals with PROCAM CV risk >20% was dampened by limited sen-sitivity (maximum 60% by IDF), the least sensitive definitions being those whichexclude diabetics (EGIR and AACE). The largest value of the area under ROCcurve was attained by the AHA/NHLBI definition (0.647, p<0.001). Lowering thecutoff for abdominal adiposity (waist circumference <94 cm) by IDF did not im-prove its performance in this regard albeit increasing the prevalence of MS; on theother hand, the IDF definition was able to pick up the largest number of individualswith mALB (56%) or elevated CRP (53%).
P5357 Prevalence and prognostic relevance of the metabolicsyndrome in patients with coronary artery disease:definition matters
P.W. Radke1, L.C. Harland2, F. Ullerich3, B. Nagel1, H. Schunkert3,R. Hoffmann1. 1University Hospital Schleswig Holstein, Cardiology
Department, Luebeck, Germany; 2University Hospital Schleswig-Holstein,Cardiology, Luebeck, Germany; 3RWTH University Hospital, Cardiology, Aachen,Germany
Purpose: The metabolic syndrome (MS) is an established risk factor for coronaryartery disease (CAD). The prevalence and prognostic relevance of the MS in pa-tients with known CAD, however, is unknown. Aim of this study was to compare
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

936 Diagnosing the metabolic syndrome / Characteristics of the metabolic syndrome
three established clinical definitions of the MS regarding prevalence and progno-sis in CAD patients.Methods: A total of 427 consecutive patients undergoing percutaneous coronaryintervention for CAD (95% stent implantation) form the study population. MS wasdefined using criteria of the 1.) ATP III (Adult Treatment Panel III) 2.) WHO (WorldHealth Organization) and 3.) AACE (American Association of Clinical Endocri-nologists). All major adverse cerebrovascular events (MACCE: death, myocardialinfarction, stroke, bypass operation, percutaneous coronary intervention) weredocumented over a five year period after index procedure (Table).Results: The prevalence of MS was a) ATP III 86 (20%), b) AACE 192 (45%) andc) WHO 42 (9%). MACCE-rates varied non-significantly between a) 40% (ATPIII), b) 35% (AACE) and c) 38% (WHO), respectively (Table).
Cumulative Event Rates
ATP III AACE WHO(n=86, 20%) (n=192, 45%) (n=42, 9%)
5 Year Follow Up MACCE° 40% 35% 38%Death 13% 11% 20%Myocardial infarction 5% 9% 3%Bypass-OP 9% 6% 3%Stroke 2% 4% 3%Re-PTCA† 21% 17% 15%
°Major Adverse Cardiac or Cerebral Event, †re-PTCA defined as re-intervention during 5-yearfollow-up.
Conclusions: The MS is commonly observed in patients with CAD. The preva-lence, however, varies significantly between established definitions. All definitionsidentify high-risk patients with comparable event rates. Prospective studies di-rectly assessing parameters of the glucometabolism (i.e. insulin-clamp, glucosetolerance test) are neccessary to correlate disease pathophysiology with clinicaldefinitions and outcome.
P5358 The diagnosis of metabolic syndrome: an addedvalue in the evaluation of cardiovascular risk?
M. Castellano, M.L. Muiesan, E. Agliozzo, R. Tosini, M. Giacche’,M. Salvetti, E. Belotti, E. Agabiti Rosei. University of Brescia,Scienze Mediche e Chirurgiche, Brescia, Italy
It has been suggested that cardiovascular risk in patients with metabolic syn-drome (MS) may be higher than indicated by traditional risk scoring systems. Ifthis could be confirmed, the clinical relevance of the concept of MS, still quite con-troversial, would be much strengthened. To verify this hypothesis, we have exam-ined, in a prospective study on a representative sample of general population, theprevalence of MS and its relationship with cardiovascular events and cardiovas-cular organ damage. In a sample of 557 subjects (250 males, 307 females), aged30 to 65 years, we have verified the presence of ATP-III criteria for the diagno-sis of MS and calculated individual cardiovascular risk in each subject, based onthe Framingham algorhytm (FRAM) and SCORE Project formula. In addition, wehave measured, by ultrasound techniques, left ventricular mass index (LVMI) andcarotid wall intima media thickness (IMT), and recorded cardiovascular eventsoccurred during a 5-year follow-up period. One fourth of the population (24.4%)was affected by MS (31.6% of males, 18.6% of females). Risk scoring was signif-icantly higher in subjects with MS (MS+) than in those without MS (MS-) (FRAM10-year percent risk:13.50.89 vs 5.80.33, p<0.001). The incidence of cardiovas-cular events was higher in MS+ subjects, though not significantly so, due to thelimited number of events in this general population at average low-risk (1.84 vs1.12 per 100 subjects/year, p=0.15). Cardiovascular damage indexes were alsosignificantly higher in MS+ subjects (LVMI: 95.72.46 vs 84.61.29, p<0.001; IMT:1.550.06 vs. 1.360.03, p=0.002). We have observed statistically significant corre-lations between indexes of cardiovascular risk scoring (either FRAM or SCORE)and organ damage (FRAM-risk and LVMI: r=0.454, p<0.001; FRAM-risk and IMT:r=0.265, p<0.001) in the whole population. However, the regression lines showedsignificantly reduced slope and higher intercept values in MS+ as compared toMS- subjects; in other words, in the range of low to medium risk (e.g.: up to 10 ofFRAM scoring, which includes the large majority of subjects) the diagnosis of MSis associated to higher indexes of cardiovascular damage than observed in MS-subjects. In conclusion, the occurrence of MS features in a subject with traditionalcardiovascular risk scoring not particularly elevated seems to represent an un-favourable prognostic element which should be taken into account in the clinicalevaluation.
P5359 Insulin resistance in patients with metabolicsyndrome with normal fasting glucose levels
A. Atar, I. Atar, O. Gulmez, C. Ertan, A. Yildirir, B. Ozin,H. Muderrisoglu. Baskent University, Ankara, Turkey
Purpose: The term metabolic syndrome (MS) refers to a group ofatherosclerotic risk factors, including dyslipidemia, high fasting blood glucose lev-els, obesity, and hypertension. The exact mechanism of accelerated atheroscle-rosis in MS is yet unknown. Fasting blood glucose levels are one of the diagnosticcriteria for MS. However, fasting insulin levels and postprandial insulin and glu-cose levels are important components of the glucose metabolism. In this study,our aim was to determine the state of glucose metabolism when the fasting blood
glucose levels are within normal limits in patients with metabolic syndrome com-pared to the normal population.Methods: The study included 114 patients. Patients with fasting glucose levels >
110 mg/dl were excluded. MS was diagnosed based on the criteria recommendedby ATP III. 47 patients were in MS group (Group1) and 67 patients were in controlgroup (Group2). All the participants received a breakfast of 904 kcal, consisting68% of lipids, 16% of protein and 16% of carbohydrates after fasting for 12 hours.Fasting and postprandial glucose and insulin levels were determined before theingestion of the breakfast and 2 hours after the ingestion. Insulin resistance wasdetermined using the homeostasis model assessment (HOMA).Results: The clinical and demographical characteristics and the laboratory find-ings of Group1 (n=38, mean age 59±10 years, 22 females) and Group2 (n=65,mean age 58±10 years, 22 females) were similar (p>0.05) except gender, HDLlevels and TG levels. Fasting glucose levels were similar in both groups (Group1:90±10 mg/dl vs Group2: 86±10mg/dl, p=0.09). Fasting insulin levels and post-prandial insulin and glucose levels were higher in Group1 (8.2±4.2 vs 6.2±4.4μU/mL, p=0.02; 61.2±40.7 vs 44.9±31.2 μU/mL, p=0.02; 111±30 mg/dl vs99±19 mg/dl, p=0.01 respectively). HOMA values were significantly higher inGroup1 than Group2 (1.83±0.98 vs 1.36±1.05, p=0.02).Conclusion: The results of this study indicate that even when the fasting bloodglucose levels are within normal limits postprandial glucose metabolism is dis-turbed and insulin resistance is present in patients with metabolic syndrome. Wethink that MS may be underdiagnosed when only the current ATP III criteria areused.
P5360 Prospective evaluation of International DiabetesFederation 2005 and Adult Treatment Panel III 2001criteria of the metabolic syndrome among womenundergoing coronary angiography
C.H. Saely1, L. Koch2, F. Schmid2, T. Marte1, S. Aczel1, P. Langer2 ,G. Hoefle1, H. Drexel1. 1Academic Teaching Hospital Feldkirch, InternalMedicine, Feldkirch, Austria; 2VIVIT Institute, Feldkirch, Austria
Purpose: The International Diabetes Federation (IDF) has recently established aworldwide consensus definition of the metabolic syndrome (MetS). The purposeof this study was to prospectively evaluate the cardiovascular risk associated withthe IDF and Adult Treatment Panel III (ATPIII) MetS definitions in women under-going coronary angiography.Methods: In a prospective study on 241 women undergoing coronary angiogra-phy for the evaluation of coronary artery disease we recorded vascular eventsover 4 years.Results: From the women enrolled in our study, 34.9% (n = 84) had the MetSaccording to the ATP III definition and 47.8% (n = 115) according to the IDF defi-nition. Concordance between the definitions was moderate (Cohen-Kappa coeffi-cient = 0.537; p <0.001). The MetS as defined by the ATP III criteria significantlypredicted vascular events (adjusted hazard ratio = 2.133 [1.111-4.094]; p = 0.023)but the MetS as defined by IDF criteria did not (adjusted hazard ratio = 1.214[0.635-2.319]; p = 0.558). Accordingly, event-free survival was significantly loweramong women who fulfilled the ATP III but not the IDF criteria than among thosewho met the IDF but not the ATP III criteria (p = 0.035).Conclusions: Among women undergoing coronary angiography for the evalua-tion of CAD, the ATP III and the IDF definitions of the MetS do not identify thesame patients. The ATP III definition of the MetS confers a significantly higherrisk of vascular events than the IDF definition.
CHARACTERISTICS OF THE METABOLICSYNDROME
P5361 Electrocardiographic characteristics amongindividuals with and without the metabolic syndrome:a population-based study
I. Ben-Dor1, M. Gillon2, A. Atamna3, G. Alpert1, D. Gofer2,A. Battler3, O. Kalter-Leibovici2. 1Rabin Medical Center, Petach
Tikva, Israel; 2Gertner Institute, Tel-Hashomer, Unit of CardiovascularEpidemiology, Ramat Gan, Israel; 3Clalit Health Services, Hadera, Israel
Background: The metabolic syndrome and electrocardiographic (ECG) changeshave been shown to predict cardiovascular disease.Aim: To describe the associations between ECG abnormalities and the metabolicsyndrome in the general population.Methods: Participants were derived from a random sample of the general pop-ulation of Hadera district, stratified by ethnicity (Arabs and Jews), gender andage (range: 25-64). Information on demographic and lifestyle characteristics wasobtained by personal interviews, and blood pressure and anthropometric mea-surements, fasting blood samples and resting ECG records were subsequentlyobtained. The metabolic syndrome was defined according to NCEP-III criteria.ECG records were coded using the Minnesota-coding-system.Results: ECG recodes were obtained in 549 participants (51.4% males, Table I).On multivariate analyses, controlling for the effects of age, gender, ethnicity andFramingham risk score, the metabolic syndrome was significantly associated withhigher heart rate (b =4.3, p<0.001) and longer QTc interval (b =0.005, p=0.04),
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Characteristics of the metabolic syndrome 937
Table I
Variable Metabolic syndrome P
Absent (N=375) Present (N=174)
Arab ethnicity 163 (43.2%) 99 (56.6%) 0.004Age (yrs.) 46.3+11.1 53.5+9.5 <0.001Heart-rate (bpm) 68.8+10.0 73.3+11.0 <0.001Q-Tc interval 0.410+0.031 0.418+0.022 0.002Any Q-wave 13 (3.4%) 22 (12.6%) <0.001Any S-T depression 8 (2.1%) 13 (7.4%) 0.002First degree A-V block 1 (0.3%) 4 (2.3%) 0.037Any major S-T elevation 18 (4.8%) 2 (1.1%) 0.047Any T-wave inversion 39 (10.3%) 34 (19.4%) 0.003
higher odds for any Q-waves (OR=2.9; 95% CI: 1.4, 6.2) and any S-T depression(OR=2.9; 95% CI: 1. 1, 7.9). In further analyses, apart from a low HDL-cholesterollevel, all the other components of the metabolic syndrome were significantly andindependently associated with ECG characteristics.Summery: Our findings show that the metabolic syndrome is associated withECG abnormalities, independent of gender, age, ethnicity and Framingham RiskScore.
P5362 A relationship between echocardiographicsubepicardial adipose tissue and metabolic syndrome
K. Okyay, A.S. Balcioglu, Y. Tavil, G. Tacoy, S. Turkoglu, A. Abaci.Gazi University Medical School, Cardiology, Ankara, Turkey
Visceral obesity leads to metabolic syndrome (MS) which is a com-posite of multiple cardiovascular risk factors. There are insufficient data about theimportance of subepicardial adipose tissue (SAT), a part of visceral adiposity. Inthis study, a relationship was sought between echocardiographic SAT thicknessand parameters of metabolic syndrome.Methods: One hundred twenty-three patients (76 women, 54±10 years) with MSwere enrolled in the study. One hundred twenty-three age- and gender-matchedpatients were constituted the control group. Echocardiographic measurements ofSAT thickness on the right ventricle were performed using 2D M-mode in bothparasternal long and short axis views by two different cardiologist. Maximum val-ues at any site were measured and the average value was used. Metabolic syn-drome was idendified by the criteria of International Diabetes Federation.Results: Patients with MS had significantly thicker SAT compared to the con-trol group (5.1±1.7 vs 3.4±1.6 mm, p<0.001). Theunivariate predictors ofSAT thickness were found to be body mass index (r=0.505, p<0.001), triglyc-eride level (r=0.364, p<0.001), hypertension (r=0.209, p=0.001), age (r=0.165,p=0.010), fasting glucose level (r=0.335, p<0.001), presence of diabetes mel-litus (r=0.327, p<0.001), presence of MS (r=0.484, p<0.001), female gender(r=0.222, p<0.001), smoking (r= -0.204, p=0.001), waist circumference (r=0.592,p<0.001), echocardiographic septum (r=0.199, p=0.02) and posterior wall thick-ness (r=0.275, p<0.001) and left atrial size (r=0.221, p=0.001). In multivariatestepwise linear regression analysis, the independent predictors of SAT thicknesswere the presence of MS (r=0.172, p=0.003), serum triglyceride level (r=0.178,p=0.001), female gender (r=0.256, p<0.001), age (r=0.111, p=0.017), and waistcircumference which had the most predictive value for SAT(r=0.499, p<0.001).Conclusion: Our study demonstrated a close relationship between MS and SATthickness. Assessment of the SAT thickness in routine echocardiographic exam-ination is a feasible and reliable method to predict the existence of MS and MSassociated cardiovascular risk factors.
P5363 Relation between Body Mass Index and cognitivefunction in healthy middle-aged men and women
M. Cournot1 , J.C. Marquie2 , D. Ansiau2, C. Martinaud3, H. Fonds4,J. Ferrieres2, J.B. Ruidavets5. 1INSERM U558, Department ofEpidemiology, Toulouse, France; 2Work and Cognition Laboratory,
CNRS UMR 5551, Toulouse, France; 3Service IU de Medecine Preventive,Toulouse, France; 4Direction Regionale du Travail et de l’Emploi, Toulouse,France; 5Department of Epidemiology, CHU Toulouse, Toulouse, France
Background: Whether Body Mass Index (BMI) is associated with cognitive func-tion and cognitive decline in healthy men and women, even young and non obese,is unknown.Methods: Prospective Cohort Study. Data from 2223 healthy workers aged 32to 62 years at baseline were analyzed. Medical, psychosocial and environmentaldata were collected in 1996 and 2001 and various clinical measurements wereperformed. Subjects’ cognitive functions were tested at baseline and at follow-upwith a word list learning (4 recalls), a digital symbol substitution test (DSST) anda selective attention test.Results: Cross-sectionally, a negative and linear association was found betweenBMI and cognitive scores, after adjustment for age, sex, educational level, bloodpressure, diabetes and other psychosocial covariables. BMI at baseline was alsonegatively associated with cognitive changes at follow-up, after adjustment for theabove-cited confounding factors. For the changes in scores at the word list learn-ing (delayed recall), regression coefficients were -0.008 ± 0.13; -0.09 ± 0.13;-0.17 ± 0.14 and -0.35 ± 0.14 (p for trend <0.001) for the 2nd, 3d, 4th and 5thquintile of BMI at baseline when compared with the first quintile. This association
was statistically significant for word list learning and DSST but not for the selec-tive attention test. No significant association was found between changes in BMIand cognitive function.
Conclusions: BMI was independently associated both with cognitive function(word list learning and DSST) and changes in word list learning in healthy non-dement middle-aged men and women, and this association could be observedwhatever the values of BMI, even in the lowest.
P5364 The profile of aortic pressure waveform is related tobody fat amount in healthy people
P. Guzik, A. Wykretowicz, T. Krauze, H. Wysocki. Poznan, Poland
Introduction: Overweight and obesity are acknowledged risk factorsfor the development of atherosclerosis, which affects the profile of
aortic pressure waveform and left ventricle afterload. This study aimed to ana-lyze the relationship between body fat amount and measures of aortic pressurewaveform in healthy people.Material and methods: Ninety six healthy volunteers aged 19 - 62 years old(31.8±11.6 yrs, 47 female) were recruited. Percentage of body fat was measuredwith total body impedance (BodyStat 1500, USA). Resting peripheral blood pres-sure signal was assessed noninvasively by tonometric measurement of radialpulse pressure wave (Colin BMP7000, Japan) and used for on-line reconstruc-tion of aortic pulse pressure waveform with the use of general transfer function(Sphygmocor Mx, Australia). Nonparametric Spearman correlation was applied toanalyze the relationship between percentage of body fat and measures of centralpressure waveform.Results: Relative body fat amount ranged from 6.8 to 41.2% (mean 20.2±7.4%).The mean values of the reconstructed aortic systolic blood pressure (SBP) was97.2±13.1 mmHg, the diastolic blood pressure (DBP) was 67.6±10.6 mmHgand the end-systolic blood pressure (ESBP) was 86.5±13.0 mmHg. The meantime to return (TR) of reflected wave was 154.8±18.9 ms, the central augmen-tation index (AI) was 110.7%±16.8% and cardiac time-tension index (TTI) was1958.7±366.7 mmHgs/min. The percentage of body fat was significantly and pos-itively correlated with DBP (r=0.26; p=0.0121), ESBP (r=0.32; p=0.0013), and AI(r=0.65; p<0.0001) and TTI (r=0.36; p=0.0002) and negatively with TR (r=-0.51;p<0.0001). The correlation between relative fat amount and SBP was not quitesignificant (r=0.19; p=0.0629).Conclusions: Characteristics of aortic pressure waveform are related to body fatamount. Greater relative body fat amount is associated with higher aortic bloodpressure, faster return of reflected wave and increased afterload in healthy peo-ple.
P5365 The obesity cardiomyopathy is it a reality?An ultrasonic tissue characterization study
V. Di Bello1, F. Santini2, A. Di Cori1, C. Palagi1, E. Talini1,M. Giannetti1, A. Barsotti1, M. Mariani1. 1University Of Pisa,Dipartimento Cardio Toracico, Pisa, Italy; 2Pisa, Italy
Obesity is a well established risk factor for Congestive Heart Failure (CHF). Evi-dence has been provided indicating that insulin resistance could be the mediatorbetween obesity and CHF, but the pathogenic mechanisms leading to myocar-dial alterations remain unclear. A im of this study was to investigate, by ultra-sonic integrated backscatter analysis (IBS), subclinical alterations of Left Ven-tricular (LV) structure and function in severe obesity. Sixty consecutive severelyobese, otherwise healthy subjects (O) (15 males, 45 females, mean age ± SD =31.8±7 yr) were enrolled. Forty-eight sex- and age-matched non-obese healthysubjects were recruited as controls (C). All subjects underwent conventional 2D-Color Doppler echocardiography, Pulsed Wave Tissue Doppler Imaging (PW-TDI)at mitralic annulus level and IBS. The homeostasis model assessment insulin re-sistance index (HOMA-IR) was used to assess insulin resistance. HOMA-IR val-ues in O were significantly higher (mean ± SD = 4.9 ±1.4) than in C (0.92 ±0.5, p<0.0001). O had a greater LVMh (58.5±14 g/m2.7) than C (37±8 g/m2.7,p<0.0001), because ofcompensation response to volume overload caused by agreater cardiac output (p<0.02). Preload reserve was increased in O, as demon-strated by the significant increase in left atrial dimension (p<0.0001). This volu-metric increase activated the Frank-Starling mechanism, and determined a sig-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

938 Characteristics of the metabolic syndrome
nificantly higher left ventricular ejection fraction (p< 0.03) in O as compared withC. A slightly reduced LV diastolic function was demonstrated in O (trans mitralE/A ratio = 1.1±0.7) as compared with C (1.5 ±0.5, p<0.02). PW-TDI showedan impairment of diastolic left ventricular longitudinal function and increased leftventricular diastolic filling pressure. The IBS values at septum level, indexed bypericardium interface, weresignificantly higher for septum in O (57.8 ± 8%) thanin C (42.3 ± 9%, p<0.0001). Additional IBS alterations were observed in O, witha significantly lower Cyclic Variation Index (CVI) both at septum (p<0.0001) andat posterior wall level (p<0.001). A significant association was found betweeninsulin resistance index and both the IBS index of myocardial reflectivity at sep-tum level (expression of increased myocardial collagen content) or left ventricularmass. In conclusion, this study demonstrates that obese patients exhibit myocar-dial structural and functional alterations related to insulin resistance and to leftventricular volume overload, which could be considered the very early stage onof an incipient "obesity cardiomyopathy".
P5366 The impact of obesity on the prognostic importanceof N-terminal pro brain natriuretic peptide, highsensitivity C-reactive protein and urinealbumin/creatinine ratio in apparently healthy people
M.H. Olsen1, T.W. Hansen2, M.K. Christensen3, F. Gustafsson3,H. Ibsen2, K. Borch-Johnsen4 , T. Joergensen2 , P.R. Hildebrandt5.1Rigshospitalet, Copenhagen University Hosp., Department Of Cardiology,Copenhagen, Denmark; 2Bispebjerg University Hospital, Department OfCardiology, Copenhagen, Denmark; 3Glostrup University Hospital, Dept. ofClinical Physiology and Nuclear Med., Copenhagen, Denmark; 4Steno DiabetesCenter, Gentofte, Copenhagen, Denmark; 5Frederiksberg University Hospital,Department Of Cardiology, Copenhagen, Denmark
Background: We have previously shown that obesity was associated with higherlevels of high sensitivity C-reactive protein (hsCRP) and lower levels of N-terminalpro brain natriuretic peptide (Nt-proBNP) in a general population aged 41, 51, 61or 71 years. Therefore, the aim of this study was to investigate the impact of obe-sity on the prognostic importance of Nt-proBNP, hsCRP and UACR in a subgroupof 2051 apparently healthy individuals without prior stroke or myocardial infarc-tion, who did not receive any cardiovascular (CV), anti-diabetic or lipid-loweringtreatment.Methods: In 1993 we measured CV risk factors, serum Nt-proBNP, UACR andserum hsCRP. The composite CV endpoint (CEP) of CV death and non-fatalstroke or myocardial infarction was assessed after 9.5 years. Obesity was definedas body mass index (BMI) ≥ 25 kg/m2 and found in 50% of the subjects. Abdomi-nal obesity was defined as abdominal circumference (AC) ≥ 80 cm for women and94 cm for men and found in 45% of the subjects. To make comparison of hazardratios (HR) from Cox regression analyses possible, log(Nt-proBNP), log(hsCRP)and logUACR were divided by their standard deviations (SD). HRs were adjustedfor age and gender.Results: In Cox regression analyses, CEP was predicted by log(Nt-proBNP),log(hsCRP) and logUACR in obese as well as in non-obese (Table 1). However,logUACR predicted CEP stronger in subjects without than in subjects with ab-dominal obesity (P<0.05 for interaction).
Table 1. Age and gender adjusted HRs for CEP
Log(Nt-proBNP)/SD Log(hsCRP)/SD LogUACR/SDStandard deviations 1.09 log(pg/ml) 1.09 log(mg/l) 0.6 log(mg/mmol)
BMI < 25 kg/m2 1.55, P<0.01 1.42, P<0.01 1.50, P<0.001BMI ≥ 25 kg/m2 1.35, P<0.05 1.46, P<0.01 1.58, P<0.001AC(w/m)<80/94 cm 1.54, P<0.01 1.55, P<0.01 1.74, P<0.001AC(w/m)<80/94 cm 1.35, P<0.05 1.32, P=0.06 1.42, P<0.001
Conclusion: Nt-proBNP, hsCRP and UACR predicted CEP independently of obe-sity although obesity was associated with lower levels of Nt-proBNP and higherlevels of hsCRP.
P5367 Structural and functional characteristics ofsubcutaneous small arteries in subjects affected byobesity and metabolic syndrome
G. Seravalle1, F. Scopelliti2, R. Dell’oro1, V. Ilardo1, L. Fattori1,E. Lattuada3, G. Grassi2, G. Mancia2. 1Ospedale St. Luca - Istituto
Auxologico Itali, Cardiology Dept, Milan, Italy; 2Clinica Medica, Osp. S. Gerardo,UNIMIB, Monza, Italy; 3Clinica Chirurgica, IRCCS Policlinico, Milano, Italy
Background: The obese state (O) is characterized by an impairment in largearteries structure and function. Whether this is the case also for small resistancearteries is unknown. It is also unknown whether and to what extent the effects of Oon arteries displaying a diameter <400μm are qualitatively and/or quantitativelydifferent from those observed in the metabolic syndrome (MS), i.e. a condition inwhich obesity is associated with other metabolic risk factors.Methods: In 7 normotensive control subjects (C, age:43.8±4.9yrs, body mass in-dex, BMI:22.7±4.8kg/m2, waist circumference, WC:89±1.2cm), in 6 patients withsevere visceral O (age:43.5±2.7yrs, BMI:40.3±1.8kg/m2, WC:130.7±5.4cm) andin 6 individuals with MS (ATP III criteria; age:38.7±3.8yrs, BMI 44.1±3.9kg/m2,WC:143.2±7.6cm) we assessed the structural and functional characteristics of
small arteries via the myographic technique. Bioptic samples were obtained fromsubcutaneous tissue of the abdominal area during laparoscopic surgery (gastricbanding in O and MS and cholecystectomy in C). Vessel segments were isolatedand mounted on a pressurized myograph to assess media thickness (M), lumendiameter (L) and to evaluate endothelial function (vasodilatatory responses toacetilcholine following maximal vasoconstriction induced by norepinephrine).Results: For similar sphygmomanometric mean arterial pressure (MAP,C:96.6±2.6, O:97.6±2.3mmHg) O showed M, L and M/L ratio values signifi-cantly greater than C (M:25.5±0.8 vs 15.9±1.2μm, p<0.05; L:248.2±30.9 vs237.5±17.1μm;M/L:0.10±0.01 vs 0.06±0.002, p<0.05). MS patients, althoughcharacterized by BMI and WC similar to O, showed a tendency to greater M/Lratio (0.12±0.01, p<0.05 vs C). A similar behaviour characterized endothelialfunction whose impairment was progressively more pronounced from O to MS(O:-38%, MS:-49% compared to C, p<0.05 for both), the degree of impairmentparallelling the observed alterations in HOMA index.Conclusions: Thus both O and MS are characterized by an arteriolar remodellingand an endothelial dysfunction. The magnitude of the structural and functionalvascular abnormalities appears, however, to be greater in conditions in which vis-ceral O is accompanied by other metabolic alterations, such as insulin resistance.
P5368 Echocardiographic assessment of pulmonary arterypressure in obese patients
Z. Sido1, B. Bachmann2, S. Makadi1, T. Honig1, I. Bernat1. 1CentralHospital Of Ministry Of Defense, Department Of Cardiology,Budapest, Hungary; 2Budapest, Hungary
Introduction: The authors pointed out in earlier works, that the obesity has sig-nificant effect as well to the heart’s geometry as to the systolic and diastolic func-tion of left ventricle. Patients and methods: Present study investigated how theleft ventricular diastolic function and pulmonary artery pressure changes in obe-sity. 73 male (46.3 ±6.0 y, BMI: 40.9 ± 7.4 kg/m2) and 85 female (41.3 ± 5.8 y,BMI: 37.8 ± 6.1 kg/m2) suffering from metabolic syndrome were examined from2003.01.01. to 2005.12.31. 41 male (46,1 ± 7.0 y, BMI: 21.9 ± 2.1 kg/m2) and57 female (41.5 ± 5.4 y, BMI: 21.1 ± 2.1 kg/m2) of normal weight served ashealthy control group. During echocardiographic examination the ratio (E/A) ofearly diastolic peak filling velocity (E) and late diastolic peak filling velocity (A),isovolumetric relaxation time (IVRT), as well as the ratio (E/Ea), with the help oftissue Doppler imaging (TDI) early diastolic velocity (Ea) and the transmitral earlyflow velocity (E) were determined. Pulmonary artery pressure (PASP) was calcu-lated from tricuspidal flow. All measurements were performed conforming to therecommendations of the American Society of Echocardiography.Results: IVRT in case of males suffering from obesity was 115.1 ± 13.4 msec,contrary to controll group where it resulted in 91.2 ± 24.6 msec. In case of femalesthe IVRT was 107.3 ± 15.5 msec, while in controll group 74.5 ± 15.7 msec. E/Ain males with obesity outcame 0.97 ± 0.2, meanwhile in control group this was1.72 ± 0.4. Females E/A yielded 1.1 ± 0.4, in contrast in controll group was 1.87± 0.4. Value of E/Ea in case of males was 9.5 ± 2.5, in contrast in control group5.5 ± 0.9. E/Ea in females resulted in 9.3 ± 1.7 the same time in control group5.6 ± 0.8. Calculated systolic pulmonary pressure in males yielded to 33.5 ±5.2 mm of mercury, contrary in control group 14.5 ± 3.2 mm of mercury. Thisparameter resulted in 36.6 ± 7.0 mm of mercury in females, in contrast to controlgroup 15.2 ± 3.4 mm of mercury. All of these differences in each parametersresulted in strong significance (p<0.0001). Summary: The obesity significantlyreduces the left ventricular diastolic function and the calculated pulmonary arterypressure remarkably increased in both gender. These parameters may explainthe deterioration of obese patient’s condition.
P5369 The relationship of metabolic risk factors with carotidartery intima-media thickness in military pilots
A. Jovelic, Z. Hajdukovic, S. Radjen. Military Medical Academy,Belgrade, Serbia and Montenegro
Background: The common carotid artery intima-media thickness(CCAIMT) is the independent predictor of cardiovascular events and diabetesmellitus in apparently healthy men. Relationship between features of metabolicsyndrome (MS) and CCAIMT is not fully elucidated.Aim: To assess the cross-sectional relationship between CCAIMT and cardiovas-cular risk factors (age, total cholesterol (TC), low density lipoprotein cholesterol(LDL-c), high density lipoprotein cholesterol (HDL-c), triglycerides (Tg), fastingglucose, glycosylated hemoglobin (HbA1c), blood pressure (BP), smoking habit,waist circumference (WC)) in military pilots on their regular annual medical con-trol.Methods: We studied 205 pilots (age 38±6 years) free of cardiovascular diseaseand diabetes mellitus. MS was defined according to International Diabetes Fed-eration. The CCAIMT was measured by high-resolution B-mode ultrasonographyin the posterior wall of the distal 1 cm of both common carotid arteries.Results: 66.5% patients had CCAIMT>1.0 mm. The means of CCAIMT in sub-jects grouped according to the absence and presence of 3, 4, and 5 features ofthe MS were 0.95mm, 0.99mm, 1.16mm, and 1.26 mm, respectively, (ANOVAp=0.001), with a statistically significant differences between those without andthose with 4 (p=0.008) and 5 (p=0.001) components, and between those withMS and those with 4 (p=0.047) and 5 (p=0.011) MS features. In a simple linear
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Characteristics of the metabolic syndrome 939
regression analyses only HDL-c was not associated with CCAIMT. In a multipleregression analysis, WC (β=0.316; p=0.001) and TC (β=0.372; p<0.001) were theindependent predictors of CCAIMT. Using ROC curve analysis with CCAIMT >1mm as outcome, WC (Area=0.733, p=0.000), age (Area=0.685, p=0.002) and TC(Area=0.642, p=0.017) were found to be significant predictive parameters, whileBP, LDL-c, HDL-c, Tg, glucose, HbA1c and smoking habit were not.Conclusions: With increasing number of metabolic syndrome features in stud-ied apparently healthy males, common carotid artery intima-media thickness in-creases. Besides total cholesterol, as a traditional cardiovascular risk factor, inour group waist circumference was the independent predictor of CCAIMT.
P5370 Insulin resistance and obesity as possiblemechanism of preclinical cardiac involvement innormal population
M. Kozakova1, E. Muscelli1, B. Astirraga1, S. Pinnola1, C. Morizzo1,A. Natali1, E. Ferrannini1 , C. Palombo2. 1University of Pisa,
Department of Internal Medicine, Pisa, Italy; 2Univ. Of Pisa & Cnr Inst. Of Clin.Physiology, Department Of Internal Medicine, Pisa, Italy
Background: development of left ventricular (LV) hypertrophy (H) depends onhemodynamic and nonhemodynamic factors. Within the second, hyperinsuline-mia, hyperglycemia and insulin resistance are considered pro-hypertrophic stim-uli. However, observations in humans yielded so far inconsistent results, possiblydue to the confounding effect of a relatively high prevalence of diabetic and/orhypertensive subjects in study populations. Insulin resistance evaluated by eug-lycemic hyperinsulinemic clamp is reported in a significant proportion of normalgeneral populations. Aim of the study was to assess the possible relationships ofLV mass, systolic performance and diastolic filling with insulin secretion, insulinsensitivity (IS) and associated lipid profile in healthy subjects.Methods: sixty-one normotensive, non-diabetic subjects (30 men, mean age43±8 years, mean BP 121±11/74±8 mmHg), with wide body mass index (BMI)range (18-39 kg/m2) and no evidence of cardiovascular diseases, underwent aDoppler-echocardiographic study and an euglycemic hyperinsulinemic clamp (in-fusion of 40mU insulin/m2 BSA for 2h) to measure insulin sensitivity, an O-GTTand IV-GTT to evaluate insulin secretion, and a complete plasma lipid profile de-termination.Results: Measure of insulin sensitivity (M value) ranged from 12 to 83μmol/kg*min, fasting insulin and stimulated insulin secretion also displayed alarge range distribution. LV mass (range 61-261 g) increased with BMI, waistgirth, systolic BP, Doppler-derived stroke work (SW), fasting plasma glucose,insulin and C peptide (r=+0.27-0.53, p<0.05-0.001), and decreased with HDL-cholesterol and M value (r=-0.52 and -0.32, p<0.001 and 0.02). In multivariateanalysis, SW, HDL and BMI were independent predictors of LV mass (adjustedr2=0.48). E/A ratio of LV filling flow was independently and inversely related toage, fasting plasma insulin and systolic blood pressure (adjusted r2=0.42), whileindices of LV systolic performance (ejection fraction and midwall shortening) werenot influenced by anthropometric or metabolic factors.Conclusions: even in normotensive non-diabetic subjects, relative insulin resis-tance and obesity seem to contribute to higher LV mass and lower LV filling func-tion.
P5371 The effect of obesity on outcome of acute coronarysyndromes: paradoxical or real risk factor?
C.M. Tavares Aguiar, J.M.S. Ferreira, A.M. Ferreira, S. Lima,P.A. Goncalves, J.M. Aniceto Silva. Hospital Santa Cruz, Cardiology,Carnaxide, Portugal
Background: Obesity is a major risk factor for cardiovascular disease and long-term mortality. Yet, in the setting of acute myocardial infarction (MI) or percuta-neous coronary intervention, obesity seems paradoxically associated with betteroutcome. The aims of the present study are to evaluate the prevalence of an ab-normal body mass index (BMI) in patients with acute coronary syndrome (ACS),and the relationship between BMI and intermediate-term outcome in this popula-tion.Methods: We studied 965 patients admitted to the Coronary ICU due to an ACS.Patients were divided into 3 BMI (kg/m2) categories: healthy weight (<25), over-weight (25.0 - 29.9), and obese (≥30.0). Patient clinical and laboratorial charac-teristics, treatments, and 6-month outcome by BMI category were assessed.Results: Of the 632 patients admitted due to non-ST-elevation ACS (NSTE-ACS),227 had a healthy weight, 296 (46.8%) were overweight, and 109 (17.3%) wereobese. Of the 333 patients admitted due to ST-elevation MI (STEMI), 114 hada healthy weight, 161 (48.4%) were overweight, and 58 (17.4%) were obese. Inthe NSTE-ACS group, obese patients were significantly younger, and more of-ten male, diabetic, hypertensive, and hypercholesterolemic. In the STEMI group,obese patients were significantly younger, and more often hypertensive. In bothACS types, in-hospital management was similar for all BMI categories. In theNSTE-ACS group, obesity did not significantly affect the rate of death or (re)MIat 6 months follow-up (17.4% vs. 18.9% in healthy weight patients), but it wasan independent predictor of 6-month mortality (11.0% vs. 4.0% in healthy weightpatients; adjusted HR 3.35; 95% CI, 1.38-8.10; p=0.007). In the STEMI group,obesity did not significantly influence the rate of death or (re) MI at 6 months(12.1% vs. 15.8% in healthy weight patients), or the 6-month mortality risk (8.6%
vs. 11.4%). Overweight (compared to healthy weight) was not a predictor of 6-month outcome, regardless of the ACS type.Conclusions: 1) Two of every 3 patients admitted due to ACS have an elevatedBMI. 2) Obese patients with ACS are younger, but have more comorbidities. 3)Obesity is present in 1 of every 3 NSTE-ACS patients who die in the intermediate-term, and is an independent predictor of 6-month mortality after NSTE-ACS. 4) InSTEMI patients, obesity neither adversely affects outcome, nor is it paradoxicallya predictor of more favourable prognosis.
P5372 The metabolic syndrome at hypertensive patientswith left ventricular hypertrophy
I. Tasic1 , B. Lovic2, D. Djordjevic1, D. Mijalkovic1, D. Petrovic1,N. Miladinovic Tasic3, D. Jankovic3 , M. Lovic3. 1Institute OfCardiology And Rheumatology, Cardiology, Niska Banja, Serbia and
Montenegro; 2Institute of Cardiology "Niska Banja", Cardiology, Nis, Serbia andMontenegro; 3School of Medicine, Nis, Serbia and Montenegro
Metabolic syndrome (MS) is one of the numerous risk factors for some patientswith cardiovascular diseases.Aim: 1. to prove the presence of MS at patients with hypertension and left ven-tricular hypertrophy (LVH) analyzing clinical parameters; 2. to estimate the impactof MS on patient prognosis.Method: There have been analyzed 73 hypertensive patients (43 male), averageage 56.3 ± 8.5 with echocardiographically proved LVH (average LVMI 163.5 ±31.8 g/m2).Results: 36 patients (55 ± 8 years) fulfilled the criterion of MS. They had signifi-cantly higher glucose level, lower HDL cholesterol, higher triglycerides and higherbody mass index (29.6 ± 3.8 vs. 27.8 ± 3, p<0.03). This group of patients hadmore frequent complex VA and significantly lower values of HRV. After 8 years ofobservation, 13 patients in this group had serious cardiovascular incidents (6 CVI- 3 deaths, 1 sudden death, 2 IM, 3 angina pectoris, 1 severely bilateral stenosisa. carotids), while in the second group 7 patients had serious cardiovascular in-cidents (2 deaths, 2 IM, 2 PTCA with inbuilt stent, 1 angina pectoris). At patientswith MS without serious cardiovascular incidents there was noticed an increasedglucose level (5.9 vs. 8.1; p<0.02), an increased LVMI (152.3 vs. 164.3 g/m2),an increased left atrium (36.9 vs. 41.8 mm), and mean carotid intima media thick-ness (IMT) was 1.03 mm. Patients with non-metabolic syndrome had a decreasedLVMI (172.1 vs. 168.1 g/m2), and mean IMT was 0.99 mm. By multivariable anal-ysis, metabolic syndrome (beta 0.320; p=0.009) and left ventricular mass (beta0.280; p=0.021), signifcantly associated with serious cardiovascular incidents (in-cluding baseline variables, age, diabetes, mean 24h systolic blood pressure, QTcdispersion, SDNN).Conclusion: Metabolic syndrome at hypertensive patients with LVH is connectedwith significantly higher activity of sympathetic nervous system (expressed inHRV), progression of left ventricular hypertrophy at hypertensive patients and in-creased risk of cardiovascular disease
P5373 Metabolic syndrome independently causessubclinical left ventricular dysfunction inasymptomatic Northern Europeans and Indian Asiansaged 35 to 75: a general population study
T.K. Lim1, E. Lim2, P. Jain1, J. Kooner1, R. Senior2. 1Northwick ParkHospital, Cardiology, Harrow, United Kingdom; 2Ealing Hospital, Cardiology,London, United Kingdom
Background Metabolic syndrome (MS) identifies individuals with elevated risk fordevelopment of atherosclerotic cardiovascular disease. However, its effects on leftventricular function are unknown. Tissue Doppler imaging(TD) during echocardio-graphy allows improved assessment of left ventricular (LV) function compared toconventional echocardiography. As Indian Asians are at high risk of MS, the aimof this study was to evaluate the relationship between MS and parameters of LVfunction in asymptomatic Northern Europeans and Indian Asians.Methods Asymptomatic Northern Europeans and Indian Asians aged 35 to 75from West London were randomly invited to participate. Each underwent 2D andTD echocardiography. The AHA 2005 definition of MS was used. Systolic param-eters assessed were left ventricular ejection fraction (LVEF) and S wave with TD(longitudinal function). Diastolic parameters assessed were Doppler mitral E/A,TD mitral annular e’, ratio of E/e’ mitral deceleration time (DT), isovolumatic re-laxation time (IVRT) and left atrial volume index (LAVI).Results Accordingly, 453 subjects (137 Northern European and 316 IndianAsian) were studied (80% male, mean age 51±10years) of which 101 (22%) hadMS. Of the 101 subjects with MS, 84 (83%) were Indian Asian and 17 (17%) wereNorthern European (p=0.001). Subjects with MS were found to have significantlyhigher LAVI(p=0.004), LV mass index (p<0.001), mitral E/e’ (p<0.001); but theyhad significantly lower S wave (p=0.003), mitral E/A (p<0.001) and TD annular e’(p<0.001) compared to those without MS. After adjusting for the effects of age,sex, ethnicity, diabetes, hypertension, systolic and diastolic blood pressure, lowersystolic longitudinal function (p=0.003) and higher LAVI (p=0.03) continued to besignificantly associated with MS as compared to those without MS.Conclusion Prevalence of MS was found to be significantly higher in IndianAsians compared to Northern Europeans and MS independently causes asymp-tomatic LV dysfunction.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

940 Characteristics of the metabolic syndrome / Lipids and antilipemics
P5374 Metabolic syndrome and gender differences inpostprandial lipaemia
K.D. Salpea1, K.K. Tsarpalis1, G.D. Kolovou1,K.K. Anagnostopoulou1 , A.N. Pavlidis1, D.P. Mikhailidis2,I.S. Hoursalas1, D.V. Cokkinos1. 1Onassis Cardiac Surgery Center,
1st Cardiology, Athens, Greece; 2Royal Free Hospital, London, United Kingdom
Introduction: The metabolic syndrome (MetS) increases the risk of coronaryartery disease (CAD). Postprandial lipaemia has also been associated with CAD.The aim of this study was to evaluate postprandial lipaemia after an oral fat toler-ance test (OFTT) in men and women with MetS.Methods: An OFTT was administered to 41 men and 21 women with MetS (de-fined by the National Cholesterol Education Program Adult Treatment Panel IIIcriteria), as well as to 14 healthy men and to 12 healthy women. Triglyceride(TG) levels were measured before and 2, 4, 6 and 8 h after the OFTT. A valueof greater than 219 mg/dl was taken as an abnormal response according to ourprevious studies. The postprandial response was quantified by the areas underthe curve (AUC) and the incremental-AUC of postprandial TG levels.Results: Although no gender difference was noticed in body mass index, menwere characterised by an increased waist circumference compared to women(108±10 vs 99±6 cm, p=0.002), as expected. Men also showed a greater plasmaTG response 8 h after OFTT (284±117 vs. 224±126 mg/dl, p=0.029). Thirty six(87.8%) men and 16 (76.2%) women were found to have an abnormal postpran-dial response. The response to the OFTT was significantly higher in MetS menand women when compared with male and female controls, respectively (AUCin mg/dl/h; 2395±973 vs. 1019±280 and 2014±933 vs. 732±197, respectively,p<0.001). In a linear regression analysis, only fasting TG levels were a signifi-cant predictor of the AUC (coefficient B=11.126, p<0.001) and incremental-AUC(coefficient B=3.348, p=0.002).Conclusions: A high percentage of both genders with MetS displayed an abnor-mal postprandial lipaemia, which was more pronounced in men. MetS men seemto have delayed TG clearance compared to MetS women. The fasting TG con-centration is the main determinant of postprandial lipaemia, another metabolicdisturbance likely associated with MetS.
LIPIDS AND ANTILIPEMICS
P5375 The change of low-dense lipoprotein particle size inLDL phenotype B can predict restenosis aftercoronary stent implantation
J.-S. Kim, H.M. Kwon, M.H. Kim, B.K. Hong, Y.W. Yoon, S.J. Rim,S.J. Yoon, H.S. Kim. Yong Dong Severance Hospital, Division of
Cardiology, Seoul, Korea, Republic of
Background: Although the use of drug-eluting stents have significantly reducedthe rate of in-stent restenosis (ISR), ISR is still a serious medical problem thatneeds to be addressed. The main mechanism of ISR has been known as neoin-timal hyperplasia, which is related to the endothelial dysfunction and vascularinflammation. Recently, small dense LDL is emerging as an important risk fac-tor for CAD and associated with endothelial function and vascular inflammation.Therefore, we investigated whether changes of LDL particle size after coronaryintervention is related to the development of ISR.Methods: A total of 331 stents (BMS: 237 lesions, DES: 94 lesions) in 217 pa-tients who underwent CAG with a stable angina or acute coronary syndrome wereenrolled in this study. Blood samples were collected at both initial and follow-upCAG and the particle size and fraction of LDL (Quantimetrix LipoprintTM LDLSystem), hs CRP and lipid profiles were measured. The development of ISR wasevaluated at 6 or 9 month after stetnt implantation.Results: ISR developed in 60 (18%) lesions at follow-up CAG. The change of LDLparticle size between initial and follow-up was associated with ISR in univariatateanalysis (p=0.002). Logistic multivariate analysis revealed the intial hsCRP (≥ 2.0mg/l) (p=0.019, OR=2.18) and stent length (≥ 24 mm) (p=0.008, OR=2.49) weresignificant predictors for ISR in all lesions. Non-increment of LDL particle size(< 0.5 nm) was not significant factor when considered for all lesions (p=0.286,OR=1.47). However, it was a significant predictor in subgroups demonstrated LDLphenotupe B (127 lesions) before coronary intervention (p=0.015, OR=5.98).Conclusions: In our study, change of LDL particle size (< 0.5 nm) at follow-upwas associated with in-stent restenosis in lesions with LDL phenotype B control-ling for the LDL level and hs-CRP. Therefore modification of LDL particle size maybe a new strategy to reduce ISR in patients with LDL phenotype B.
P5376 Effects of N-3 fatty acids of marine or plant origin onserum triglycerides and LDL-cholesterol: Influencesof initial BMI and LDL-cholesterol values
J. Sabate, J. Tazman, E. Haddad, S. Rajaram. Loma LindaUniversity, Department Of Nutrition, Loma Linda, United States of
America
Purpose: Regular consumption of n-3 fatty acids, whether from marine or plantsources results in cardiovascular health benefits, including improved serum lipids.However, fish oil supplementation resulted in a paradoxical increase in low density
lipoprotein (LDL)-cholesterol in some clinical trials. We investigated how the initialvalues of LDL-cholesterol and body mass index (BMI) of a subject may influencethe effects of two sources of n-3 fatty acids, salmon or walnuts, on serum LDL-cholesterol and triglyceride levels.Methods: In a randomized crossover metabolic trial, 25 normo- or hypercholes-terolemic subjects (14 males, 11 females) were fed three isocaloric diets for fourweeks each in random order. The diets conformed to the current dietary guide-lines for cardiovascular disease prevention and differed primarily in source andtype of polyunsaturated fat: walnut (42 g/2400 kcal diet, 6 days/week), fish (113 gof salmon/2400 kcal, 2 days/week), and control diet (no fish or walnuts).Results: The walnut diet significantly decreased serum total and LDL-cholesterolcompared to the fish and control diets. The fish diet increased serum HDL-cholesterol and decreased triglycerides compared to the control and walnut diets.Compared with the control diet, we observed an LDL-cholesterol-increasing ef-fect of fish that was magnified in subjects with higher baseline LDL-cholesterol(mean change ± SE: 3.2 ± 1.9 mg/dL for a baseline LDL-cholesterol of 110mg/dL versus 8.1 ± 2.0 mg/dL for a baseline LDL of 170 mg/dL; P value fordiet-baseline interaction 0.04). In contrast, we observed an LDL-C-lowering ef-fect of the walnut diet (-11.0 ± 2.0) that was not influenced by subjects’ base-line LDL-cholesterol level. We observed a triglyceride-lowering effect of fish thatattenuated with increasing BMI, reversed, and became a triglyceride-increasingeffect among obese (BMI >30kg/m2) subjects (-23.2 ± 5.5 mg/dL at BMI of 22,-0.6 ± 6.4mg/dL at BMI of 27.5, 25.4 ± 17.1 mg/dL at BMI of 33; P value fordiet-BMI interaction 0.02). No effect of the walnut diet was observed on triglyc-erides.Conclusions: Fish and walnut sources of n-3 fatty acids have distinct effectson serum lipids. High baseline values of LDL-cholesterol magnify the increasingeffect of fish on LDL-cholesterol, but does not influence the LDL lowering effectsof walnuts. A high BMI attenuates the triglyceride lowering effect of fish.
P5377 Uncontrolled dyslipidemia and previous statintherapy in patients presenting with acute myocardialinfarction
D. Mytas1, D. Billias2, S. Makrygiannis2 , O. Ampartzidou2,E. Adamopoulou2 , M. Zairis2, V. Pyrgakis1, S. Foussas2 .
1Cardiology Department, General Hospital, Corinthos, Greece; 2CardiologyDepartment, Tzanio Hospital, Piraeus, Greece
Purpose: Patients with uncontrolled dyslipidemia (UD) are at high risk for subse-quent major cardiovascular events. Our aim was to determine the prevalence ofuncontrolled dyslipidemia in patients presenting with acute myocardial infarction(AMI) and correlate former statin therapy with its clinical outcome.Methods: One hundred and sixty-three consecutive patients who were admittedto our cardiology department due to AMI were enrolled in the present study. Wereceived a detailed history registering baseline characteristics including all classicrisk factors. Furthermore, we determined lipid profile in the first 12h from admis-sion. Additional information was collected regarding the type of AMI, severity ofCAD, in-hospital complications and mortality.Results: Myocardial infarction with ST segment elevation (STEMI) was diag-nosed in 106 patients while 57 suffered from myocardial infarction without STsegment elevation (NSTEMI). 106 patients were male and 47 female. The meanage of the study sample was 65.3 (SD=12.3 yrs).The admission lipid profile re-vealed that 127 patients (77.9%) had UD. One hundred and three of them (81.1%)had known dyslipidemia, while 40 (31.5%) also had history of CAD. The over-all percentage of patients with CAD history that presented with well controlledlipidemic profile was less than 5%. Another 40.2% (51 patients) despite hav-ing known dyslipidemia and being advised to follow treatment ignored medicalinstructions; twelve of them were also diagnosed as CAD patients. Twenty-onepatients were on lipid-lowering diet (17 of them with UD on admission), while 28were on statins (23 with UD). Patients on previous statin therapy presented moreoften with NSTEMI (p<0.05). Additionally, there was a trend for these patients tohave less in-hospital events and in-hospital deaths, although this observation didnot reach statistical significance.Conclusions: The prevalence of uncontrolled dyslipidemia is substantial amongpatients presenting with AMI. Interestingly, this observation also applies to pa-tients aware of their high-risk condition, such as known dyslipidemic and CADpatients. On the other hand patients on statin therapy appear to suffer a morestable syndrome, may be due to plaque stabilization and inhibition of platelet ag-gregation. In the pursuit of a stricter lipidemic control, doctors that first diagnosedyslipidemia and CAD may and should play a key role.
P5378 Apolipoprotein B is a strong predictor of long-termoutcome in middle-aged women recovering from anacute coronary event
E. Nagy1, I. Janszky2, F. Al-Khalili3, K. Schenck-Gustafsson3 .1Karolinska University Hospital, Department of Cardiology,
Stockholm, Sweden; 2Karolinska Institutet, Department of of Public HealthSciences, Stockholm, Sweden; 3Danderyds Hospital, Department of Medicine,Stockholm, Sweden
Objectives: Previous studies suggested that apolipoprotein B (apo B) andapolipoprotein A (apo A-I) are better predictors of coronary heart disease risk
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Lipids and antilipemics 941
than total-cholesterol and LDL-cholesterol among healthy individuals and patientswith coronary artery disease.We assessed the 9-year predicitive value of apo B, apo A, total-cholesterol, LDL-and HDL-cholesterol in middle-aged women surviving an acute coronary event.Material and methods: The Stockholm Female Coronary Risk Study included fe-male patients aged <=66 years, resident in the greater Stockholm area, that wererecently hospitalized for an acute coronary event between February 1991 andFebruary 1994. A total of 292 patients were included. Extensive clinical screen-ing including blood test was performed 3-6 month after the coronary event andthan the patients were followed up for a median of 9 years. We measured con-centrations of total-cholesterol, HDL-cholesterol, LDL-cholesterol, apo B, apo Aand calculated apo B/apo A ratio.Results: Both in univariate models and when controlled for the potential con-founders such as age, BMI, index event, left ventricular function and history ofdiabetes mellitus the values for apo B were strongly and positively related to therisk of total mortality. The corresponding hazard ratio was 1,33 (1,03-1,72) in theunadjusted and 1,62 (1,07-2,45) in the adjusted analysis. Cardiovascular mortal-ity had a HR in the unadjusted:1,45 (1,1-1,99) respectively 1,98 (1,13-3,48) inthe adjusted analysis and combined clinical outcome of cardiovascular mortalityand recurrent events had a HR in the unadjusted: 1,31 (1,04-1,67) and HR in theadjusted model was 1,54 (1,05-2,27).The predictive value for the other lipid parameters was considerably weaker andoften non-significant.Conclusions: Among the lipid parameters investigated in this study apo B wasthe strongest predictor of total, cardiovascular mortality and of recurrent coronaryevents in middle-aged women recovering from an acute coronary syndrome.
P5379 Improvement of coronary vasodilation capacity byLDL apheresis: impact of the first application
K.-P. Mellwig, F. Van Buuren, D. Baller, O. Lindner, D. Horstkotte.Heart Center North Rhine-Westphalia, Department Of Cardiology,Bad Oeynhausen, Germany
Purpose: A major reduction of LDL cholesterol by LDL apheresis (APH) markedlyimproves coronary vasodilation capacity in patients undergoing chronic apheresistreatment. The aim of our study was to investigate whether this effect may alsobe achieved by one single APH.Methods: In 19 patients (3 women, age 48±9 y) with advanced coronary arterydisease and cholesterolemia in spite of maximal lipid-lowering medication anddiet therapy, myocardial blood flow at rest (MBF(bas)) and after pharmacologicalrecruitment of coronary reserve (CFR) by adenosine (MBF(A)) was determinedusing quantitative positron emission tomography (PET) immediately before and24 h after the first application of APH (H.E.L.P. procedure). CFR was calculatedas the MBA(A)/MBF(bas) ratio, minimal coronary resistance (MCR) as the ratiobetween mean arterial pressure and MBF(A). Laboratory data were obtained im-mediately before the first (pre) and second (post) PET scan.Results: Under continuous medication, the reduction of LDL cholesterol (> 50%)resulted in a significant improvement of viscosity and coronary vasodilation ca-pacity within 24 h as indicated by a decrease in MCR and an increase in CFR.
Pre Post
LDL chol (mg/dl) 176±42 80±25Fibrinogen (mg/dl) 335±54 168±38Viscosity (mPas) 1.25±0.07 1.16±0.08CFR 2.26±0.78 2.62±0.87*MCR (mmHg*min*100g/ml) 0.55±0.22 0.49±0.19*
*p<0.01
Conclusion: Even the first application of APH is successful in markedly reducingLDL cholesterol and fibrinogen with a positive impact on viscosity and vasodilata-tion capacity. Thus, one single LDL apheresis provides a curative effect.
P5380 Association of lipoprotein (a) levels with the severityof coronary artery stenosis in an Iranian population(according to Gensini score)
M.A. Boroumand, V. Rekabi, G.H. Davoodi, A. Amirzadegan,S. Saadat, S.H. Abbasi, G.H. Poorgholi. Tehran Heart Center,
Tehran University of Med, Resrach, Tehran, Iran (Islamic Republic of)
Background: Lipoprotein (a) [Lp(a)] is a known risk factor for developing coro-nary artery disease. However, the pattern of Lp (a) distribution in various racialand genetic groups has been found to be different. Furthermore, the associationof Lp (a) and the severity of coronary artery disease in different populations hasnot been clearly assessed. This study has been done to determine the relation-ship between Lp (a) and the severity of coronary artery stenosis in an Iranianpopulation.Methods: Between July 2004 and March 2005, 826 patients who had been candi-dates for angiography at TehranHeartCenter, were included. The severity of theircoronary artery stenosis was assessed through Gensini score. At the first part ofthe study, to check interobserver reliability, 60 angiographies were reported andtheir Gensini scores were determined by two cardiologists. During hospitaliza-tion, Lp(a), triglyceride, cholesterol, high density lipoprotein, low density lipopro-
tein and quantitative C reactive protein levels were measured and their correlationwith coronary artery stenosis were assessed.Results: Among 826 participants, 510 (62%) patients were male and 316 (38%)were female. Coronary angiography was normal in 283 (34%) while 543 (66%) pa-tients showed atherosclerosis. Mean Lp(a) levels in both normal and atheroscle-rotic participants showed significant difference (P<0.005). Fixing confoundingfactors such as age, sex and cigarette smoking, Lp(a) showed positive corre-lation with coronary atherosclerosis (p<0.01) and high levels of Lp(a) was morepronounced in participants with positive angiographic findings (OR=3).In participants with Lp(a) levels of <30, ≥31<60 and ≥61, mean Gensini scoreswere 40, 49 and 56 respectively (p=0.052).Conclusion: Lp(a) has a positive relationship with coronary artery stenosis in thisIranian population. Furthermore, Gensini score can be considered to assess therelationshipbetween Lp(a) levels and atherosclerosis.
P5381 Effects of exercise training on lipid transfer processto HDL in plasma
V.M. Silva, R.C. Maranhao, T. Solano, C.G. Vinagre. Heart of Intitute-Medical School, Laboratory of Lipid Metabolism, Sao Paulo, Brazil
Qualitative aspects of high density lipoprotein (HDL) may be involvedwith its protective function, as the capacity to accept lipids from other plasmalipoproteins. The objective of this study was to evaluate the effects of aerobicand anaerobic exercise on the lipid profile and on the lipid transfer to HDL. Forthis purpose, an articial emulsion (LDE) labeled with 14C-phospholipid (PL), 3H-tryglicerides(TG), 14C-cholesterol (C) and 3H-cholesteryl ester (CE) was incu-bated (1 h) with plasma from 9 cyclists, 6 weight lifters and 8 sedentary controls.After this, VLDL, LDL and LDE were precipitated and the radiactivity in the super-natant HDL was determined.Results: In regards to lipid profile, only HDL-cholesterol plasma levels werehigher (57 ± 3 mg/dL) and triglycerides were lower (68 ± 25 mg/dL) in cyclinggroup (n=15) compared to the hypertrophy (n=10) (42 ± 7, 129 ± 35 mg/dL,respectively) and control (n=15) (37 ± 6, 37 ± 6 mg/dL, respectively) groups,p<0.005. The transfer of all lipids from LDE to HDL was lower in cyclists com-pared to control group. However, in hypertrophy group, the transfer of cholesterolester (3H-CE) was similar to the controls. There was no difference in the lipidtransfer between the cycling and hypertrophy groups.
Lipid transfer (%) to HDL
Lipid transfer (%) Groups
Cycling (n=9) Hypertrophy (n=6) Control (n=8)3H-CE 0.85±0.47 * 1.23±0.26 1.79±0.6614C-PL 3.57±0.84 * 3.79±0.84 * 5.93±0.643H-TG 0.66±0.26 * 0.96±0.36 * 1.55±0.2514C-C 1.44±0.49 * 1.80±0.43* 2.24±0.27
CE,cholesteryl ester; PL, phospholipids; TG, triglycerides; C, cholesterol
Conclusion: Concluding, aerobic and anaerobic exercise raise the transfer oflipids from lipoproteins to HDL, in the bloodstream. This may be related to theantiatherogenic effects of the exercise.
P5382 Statin therapy post-infarction: what doctors perceive,recommend and communicate to their patients
S. Mann, N. Sapre, C.R. Elley. Wellington School of Medicine,Department of Medicine, Wellington, New Zealand
Aim: We wished to investigate how doctors perceive the degree ofbenefit from statin therapy following myocardial infarction (MI) and communicatethis to patients.Methods: We interviewed 22 cardiologists (Cs) and 20 General Practitioners(GPs) to determine treatment policies and ways of expressing its benefits to apost-MI patient with moderate dyslipidaemia (total cholesterol - TC - 6.24, HDLc1.03, LDLc 3.8, triglycerides - TG - 2.35, all units in mmol/l). We asked what drugand dosage they would recommend with or without current New Zealand fundingrestrictions.Main results: Nineteen Cs would commence (funded) simvastatin 40mg/day im-mediately whereas 12 GPs would start either diet alone or a lower dose (mostly20mg/day). Without funding restrictions on other drugs, 4 Cs and 6 GPs wouldprescribe atorvastatin for preference. Most (19) GPs used total cholesterol as atarget whereas Cs (18) focused on LDLc and pursuing more aggressive target lev-els vigorously. All but one C would justify therapy to the patient by citing a reducedchance of major adverse cardiovascular events (MACE), 12 quoting an estimateof relative risk reduction (RRR); 18 GPs also cited this but only 3 ventured a RRRestimate. All but 2 in each group felt the patient could expect a longer life withtherapy, 1 C and 9 GPs estimating >5 years extra life expectancy. Most (18) Cswere comfortable estimating a RRR for MACE (range 10-50%, median 40%), GPswere less likely to define this and only 50% of them estimated an absolute riskreduction (ARR) over 5 years. Estimates of ARR from each group varied widelyfrom 0-5% to >20%. When confronted with a hypothetical partial response (TC4.92, HDLc 0.98, LDLc 2.80, TG 2.15 mmol/l), Cs were again more aggressive, 11recommending a switch to high-dose atorvastatin and 5 adding ezetimibe. GPs
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

942 Lipids and antilipemics
suggested titrating simvastatin (10), low-dose atorvastatin (6), adding a fibrate (1)or ezetimibe (4). No interviewee was willing to quantify likely incremental benefitfrom higher doses or additional drugs. Both groups cited a range of sources fortheir policies, Cs relying more on original study publications and GPs on nationalguidelines.Conclusion: There were major disparities between the two groups of cliniciansin perception of benefits and dosing policy and a considerable overestimate ofeffect of treatment on life expectancy and ARR.
P5383 Obesity, but not waist circumference is a determinantof oxidized LDL in Slovak non-CHD subjects
B. Vohnout1 , A. Vachulova1, P. Blazicek2, G. Fodor3 , J. Lietava1.1Comenius University, 2nd Dept. of Internal Medicine, Bratislava,Slovak Republic; 2Military Hospital, Dept. of Biochemistry, Bratislava,
Slovak Republic; 3Ottawa Heart Institute, Ottawa, Canada
Introduction: Identification of persons with increased oxidized LDL (oxLDL) canimprove risk assessment of patients. Measurement of oxLDL levels is howevernot used as a standard method in clinical practice. We evaluated simple anthro-pometric variables that can be used in clinical practice as determinants of oxLDLlevels.Methods: We have examined 96 non-CHD subjects (18-75 years old) involved ina cross-sectional Homocystein Slovakia study. Plasma levels of lipids and oxLDLwere measured using standard methods. For statistical analysis categorical vari-ables were created from waist circumference (WC was evaluated as dummy vari-able based on WC>102 cm in men and WC>89 in women) and BMI (normal<25, overweight 25-29.9 and obese ≥30 kg/m2). General linear model (GLM)was used to evaluate determinants of oxLDL and lipids.Results: Main characteristic of subjects is shown in the table. In GLM using BMI,WC, smoking, age and sex as covariates only BMI has been significant determi-nant of oxLDL levels (p=0.011). There was significant difference in oxLDL accord-ing to BMI status with lowest levels in BMI < 25 kg/m2 group in univariate analysis(p<0.0001). Similar finding were seen for Tg levels. Both BMI and WC have notbeen significant determinants of cholesterol and LDL.
Characteristics of subjects
Age 43.3±12.7Chol (mmol/l) 5.9±1.2LDL 3.9±1.1Tg 1.3±0.6oxLDL 3.6±1.1BMI <25 kg/m2 (n) 36BMI 25-29.9 30BMI ≥30 30WC ≤ 102M/89F cm (n) 56WC >102M/89F 40Males/Females (%) 17.7/82.3
WC - waist circumference
Conclusions: Obesity evaluated by BMI but not WC was a significant determi-nant of oxLDL in Slovak non-CHD subjects. Simple measurements of weight andheight therefore might help in evaluation of oxLDL status in everyday clinical prac-tice.
P5384 The effect of ezetimibe administration in patients withdifferent apolipoprotein E genotypes
L. Mark, G. Dani, Ö Fazekas, O. Szule, H. Kovacs, A. Katona.Pandy Kalman Bekes County Hospital, 2nd Dept InternalMedicine-Cardiology, Gyula, Hungary
The genetic polymorphism of apolipoprotein E could influence the atheroscleroticprocess. Three common alleles are known: 2, 3 and 4. Allele 3 is the wild type.Subjects with allele 4 have a higher total cholesterol concentration and a higherintestinal cholesterol absorption. Ezetimibe is a selective cholesterol transportinhibitor which reduces the intestinal uptake of cholesterol. We investigated thecholesterol lowering effect of ezetimibe in subjects with different apolipoprotein Ephenotypes.Design: Fourteen patients with the E3/4 or E4/4, and 14 patients with E3/3 geno-type received 10 mg ezetimibe for 6 weeks. The mean age ± SD was 62.2±9.7in patients with allele 3 and 64.4±13.3 in those with allele 4. The patients wereon constant diet.Results: The baseline total cholesterol level was 5.03±0.84 mmol/l in patientswith wild type and 5.12±1.62 mmol/l in patients bearing allele 4. In subjects withwild type allele the total cholesterol level after the ezetimibe treatment decreasedby 13.7%, the LDL-cholesterol with 22.9%, the triglyceride with 9.2, and in thelevel of HDL-cholesterol a 8.0% increase was observed. In patients with allele 4the decrease of total cholesterol was 12.1%, LDL-cholesterol dropped by 19.6%,and triglyceride levels fell by 9.1%. The level of HDL-cholesterol increased by8.9%. There was no significant difference between the effect of ezetimibe on lipidlevels in patients with E4/4, E4/3 and E3/3 genotypes.Conclusion: the effect of ezetimibe was not influenced by the apolipoprotein Epolymorphism.
P5385 Effect of atorvastatin withdrawal on serumcoenzyme Q10 concentration in patients withhypercholesterolemia
C.S. Chu1, H.S. Kou2, C.J. Lee3, K.T. Lee1, S.W. Chen1,W.C. Voon2, S.H. Sheu2, W.T. Lai2. 1Kaohsiung Medical University
Hospital, Cardiology Dept, Kaohsiung, Taiwan; 2Kaohsiung Medical University,Graduate Institute of Pharmaceutical Science, Kaohsiung, Taiwan; 3KaohsiungMedical University, Department of Pharmacy, Kaohsiung, Taiwan
Background: Statin therapy inhibits HMG-CoA reductase and therefore de-creases the biosynthesis of cholesterol and other downstream end-products ofmevalonate, including coenzyme Q10. The issue of coenzyme Q10 supplement inpatients receiving statin therapy remains controversial. The e ffect of statin with-drawal on circulating coenzyme Q10 levels remained unknown.Methods and Results: Twenty-six patients with hypercholesterolemia receivedatorvastatin 10 mg/day for 3 months. Serum lipid profiles and coenzyme Q10 wereassessed before and immediately after 3 months’ atorvastatin therapy and werealso measured on the second and the third days after statin withdrawal. Afterstatin therapy for 3 months, serum levels of total cholesterol, low-density lipopro-tein (LDL) cholesterol and coenzyme Q10 (from 0.43 ± 0.23 to 0.16 ± 0.10 μg/mL)were all significantly reduced (all p values <0.001). After statin withdrawal, coen-zyme Q10 levels were significantly elevated (0.38 ± 0.18 μg/mL, p < 0.001 vs.after statin therapy) within 2 days and maintained the same levels on the third day(0.38 ± 0.18 μg/mL, p < 0.001 vs. after statin therapy), while total cholesteroland LDL cholesterol did not significantly change within the same 3 days of statinwithdrawal.
Conclusions: Atorvastatin therapy reduced serum coenzyme Q10 levels in pa-tients with hypercholesterolemia. Within 3 days of statin withdrawal, circulatingcoenzyme Q10 levels were restored toward baseline.
P5386 Lipoprotein(a) level is increased in healthy youngsubjects with parental history of prematuremyocardial infarction
G. Gaeta1, S. Cuomo2, M.C. Foglia1, G. Capozzi2, V. Stornaiuolo3,A. Caruso1, R. Calabro’3, M. Trevisan4. 1Antonio Cardarelli Hospital,
Cardiology, Naples, Italy; 2Second University of Naples, Cardiology - V. MonaldiHospital, Naples, Italy; 3S. Maria delle Grazie Hospital, Pediatrics, Pozzuoli, Italy;4University at Buffalo, School of Public Health & Health Professions, Buffalo,United States of America
Background: It has been previously reported that children, adolescents andyoung adults with family history of coronary artery disease have increased levelof lipoprotein(a) [Lp(a)]. However, some studies have not confirmed this finding.We reviewed our twelve-year database to assess if healthy children, adolescentsand young adults with parental history of premature myocardial infarction (PH-PMI) have increased [Lp(a)] level and are at risk for elevated (> 30 mg/dl) Lp(a)concentration.Methods: One hundred fifty healthy children, adolescents and young adultswith PHPMI (cases; 55% males; age 18±6.7 years) and 150 age- (±1 year)and gender-matched control subjects participated in the study. Concentration oftotal plasma cholesterol, low-density lipoprotein (LDL)-cholesterol, high-densitylipoprotein (HDL)-cholesterol, apolipoprotein (Apo) A-I and B, triglycerides andLp(a) was determined after fasting for 14 hours.Results: Cases had higher concentration of LDL-cholesterol (107.9±31.1 vs.99.2±28.7 mg/dl, p = 0.01), Apo B (89.6±26.4 vs. 82.8±20.2 mg/dl, p = 0.011)and Lp(a) (26.7±34.0 vs. 19.2±23.2 mg/dl, p = 0.012) and lower HDL-cholesterolconcentration (47.9±11.3 vs. 50.7±13.9 mg/dl, p = 0.038) in comparison to con-trols. Thirty percent of cases had elevated Lp(a) concentration vs. 16.7% of con-trols [p = 0.009; relative risk (RR): 2.14; 95% CI: 1.23 - 3.73). In a logistic regres-sion analysis, Lp(a) concentration was significantly and independently associatedto PHPMI.Conclusions: We found that healthy young subjects with PHPMI have increasedLp(a) level and a higher risk for elevated Lp(a) concentration. This is the single-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Lipids and antilipemics 943
centre hospital-based case-control study with the highest number of cases withdocumented PHPMI.
P5387 Gender differences in postprandial lipaemia inpatients with familial hypercholesterolaemia
G.D. Kolovou, K.K. Anagnostopoulou, K.D. Salpea, D.S. Damaskos,A.N. Pavlidis, T.E. Chimonas, V.N. Giannakopoulou, D.V. Cokkinos.Onassis Cardiac Surgery Center, 1st Cardiology Department ,
Athens, Greece
Introduction: Familial hypercholesterolaemia (FH) is a genetic disease that leadsto premature coronary heart disease (CHD). Postprandial hypertriglyceridaemiahas also been associated with cardiovascular disease but its study has been lim-ited in FH. The aim of the study was to evaluate gender differences in triglyceride(TG) response after a fatty meal in heterozygous (h) FH patients.Methods: Eighteen hFH men were age-matched (31±7 years) to 18 hFH pre-menopausal women (34±7 years). Plasma TG concentrations were measuredbefore and 2, 4, 6 and 8 h after a standardised fat load. A value of greater than219 mg/dl (2.5 mmol/L) was taken as an abnormal response to the fat load ac-cording to our previous studies. The postprandial lipaemia was quantified by theareas under the curve (AUC) of TG concentrations.Results: Men with hFH had a greater body mass index than hFH women (26±2vs. 21±2 kg/m2, p<0.001). Twelve out of 18 (67%) hFH men displayed an abnor-mal postprandial response, while only 3 out of 18 (17%) women had a TG valueover 219 mg/dl. The mean AUC value was also found to be higher in hFH mencompared with hFH women (1704±816 vs. 1045±537 mg/dl/h, p=0.004).Conclusions: By comparing men and women with a genetic trait as FH, it seemsthat premenopausal women are protected against postprandial hypertriglyceri-daemia. This may partially explain the observation that CHD onset occurs in hFHwomen 10-15 years later than in hFH men.
P5388 Simultaneous transfer to HDL of cholesterol,triglycerides and phospholipids in aging andcoronary artery disease
C.H.M.A. Heitmann Mares Azevedo, C.G. Puk, G.S. Feitosa-Filho,A.C. Lo Prete, T.M. Seydell, J. Diament, M. Wajngarten,
R.C. Maranhao. Heart Institute of University of Sao Paulo, Lipids MetabolismLaboratory, Sao Paulo, Brazil
Objective: We tested the hypothesis whether in younger patients the ability ofHDL to receive lipids is different from that of elderly patients with or without CAD.Methods: We studied 38 elderly patients (19 with CAD, 75±6 yo; 19 without CAD,72±6 yo), both evaluated by coronariography and/or perfusion scintilography and17 younger controls (44±16 yo). An artificial cholesterol-rich nanoemulsion la-beled with 3H- triglycerides (TG) and 14C-free cholesterol (FC) or 3H- cholesterylester (CE) and 14C- phospholipids (PL) was incubated with plasma. After pre-cipitation of other lipoproteins, the supernatant containing HDL was counted forradioactivity and lipids transfer was expressed as % of total radioactivity/10mgHDL/h. The HDL diameter (nm) was measured by laser-light-scattering.Results: Transfer of PL to HDL is greater in elderly patients with CAD than thosewithout CAD(5.4±0.3 and 4.4±0.3 p <0.05), but the transfer of other lipids andHDL size are equal. In elderly subjects without CAD, the transfer of all lipids (CE=0.5±0.08, PL= 4.4±0.3, TG= 1.0±0.06 and CL= 1.6±0.1)was smaller and HDLsize greater (10.2±1.5nm) when compared with young subjects (CE= 1.8±0.4,PL= 5.9±0.4, TG= 1.6±0.1, CL= 2.4±0.1 and HDL = 8.6±0.6 p=<0.0001).Conclusions: Lipid transfers and HDL size were not discriminative of the pres-ence of CAD in elderly subjects. However, decreased lipid transfers are associ-ated with aging. Due to HDL important antiatherogenic roles, this result can berelevant to establish new mechanisms and risk factors in CAD. Funding: CNPQand FAPESP
P5389 Effect of intensive cholesterol lowering withatorvastatin in patients with previous coronarybypass surgery: a Treating to New Targets (TNT)substudy
D. Waters1, P. Barter2, J.J.P. Kastelein3, S. Shah2, J. Shepherd4,N.K. Wenger5 , J.C. Larosa6 on behalf of the TNT Investigators. 1San
Francisco General Hospital, Division Of Cardiology, Room 5G1, San Francisco,United States of America; 2The Heart Research Institute, Sydney, Australia;3Academic Medical Center, University of Amster, Amsterdam, Netherlands;4University of Glasgow, Glasgow, United Kingdom; 5Emory University Schoolof Medicine, Atlanta, United States of America; 6State University of New YorkHealth Science C, Brooklyn, United States of America
Background and Aims: The Treating to New Targets (TNT) Study (N Engl JMed 2005;352:1425) showed that intensive LDL-cholesterol lowering to a levelof 2.0 mmol/L with atorvastatin 80 mg/day provided additional clinical benefitbeyond that afforded by LDL-cholesterol lowering to 2.6 mmol/L with atorvas-tatin 10 mg/day in patients with stable CHD. The development and progressionof atherosclerosis is accelerated in coronary venous bypass grafts. The aim ofthis post hoc analysis is to determine whether patients with previous coronary
bypass graft surgery (CABG) achieved clinical benefit in TNT from intensive LDL-cholesterol lowering.Methods: A total of 10,001 patients with clinically evident CAD, including 4,654with previous CABG, were randomized to atorvastatin 10 mg or 80 mg/day andwere followed for a median of 4.9 years. Entry criteria included an LDL-C between3.4-6.5 mmol/L off treatment and an LDL-C <3.4 mmol/L during a run-in periodon atorvastatin 10 mg/day. The primary endpoint was the occurrence of a firstmajor cardiac event (CHD death, nonfatal MI, resuscitated cardiac arrest, or fatalor nonfatal stroke).Results: Compared to patients without CABG, patients with prior CABG wereolder (63.8 versus 59.9 years), more likely to be diabetic (17.7% versus 12.7%)and to be male (83.4% versus 78.9%), to have peripheral vascular disease(15.6% versus 8.3%), hypertension (58% versus 50.8%) prior stroke (6.7% ver-sus 3.9%), a history of heart failure (10.4% versus 5.5%) and less likely to havehad a percutaneous coronary intervention (PCI, 31.3% versus 73.9%). A first ma-jor cardiac event occurred in 11.4% of the patients with prior CABG and 8.5% ofthose without prior CABG (hazard ratio 1.38, 95% CI 1.22-1.56, p<0.0001). Meanon-treatment LDL-cholesterol levels in patients with prior CABG were 2.0 mmol/Lin the 80 mg arm and 2.6 mmol/L in the 10 mg arm. In patients with prior CABG,the primary event rate was 9.7% in the 80 mg arm and 13.0% in the 10 mg arm(hazard ratio 0.73, 95% CI 0.62-0.87, p=0.0004). Repeat revascularization dur-ing follow-up, either CABG or PCI, was done in 11.3% of the CABG patients in80 mg arm and 15.9% in the 10 mg arm (hazard ratio 0.70, 95% CI 0.60-0.82,p<0.0001).Conclusion: Previous CABG identifies a group at high risk for cardiovascularevents. Intensive LDL-cholesterol lowering to a mean of 2.0 mmol/L with ator-vastatin 80 mg/day in patients with previous CABG reduces major cardiovascularevents by 27% and the need for repeat coronary revascularization by 30%, com-pared to less intensive cholesterol lowering with atorvastatin 10 mg/day.
P5390 Rosuvastatin plus ezetimibe for achievement oflow-density lipoprotein cholesterol and C-reactiveprotein goals: results from the EXPLORER study
C.M. Ballantyne1, F. Sosef2, E. Duffield1 on behalf of TheEXPLORER study investigators. 1Baylor College of Medicine,
Houston, Tx, United States of America; 2AstraZeneca, Macclesfield, UnitedKingdom
Background: Achievement of low-density lipoprotein cholesterol (LDL-C) goalsin high-risk patients presents a difficult challenge. If C-reactive protein (CRP) of<2 mg/L is also considered a target, clinical trials have shown poor success inachieving dual LDL-C and CRP goals. EXPLORER evaluated rosuvastatin (RSV)alone or in combination with ezetimibe (EZE) for achieving LDL-C and CRP goals.Methods: High-risk patients (n=469) with LDL-C 160-<250 mg/dL (4.1-6.5mmol/L) were randomised to 6 weeks’ treatment with RSV 40 mg alone or in com-bination with EZE 10 mg. The primary endpoint was achievement of the NCEPATP III LDL-C goal of <100 mg/dL (2.6 mmol/L) at week 6. Secondary endpointsincluded changes in lipids and lipoproteins. A post-hoc analysis assessed thepercentage of patients achieving LDL-C <100 mg/dL or <70 mg/dL (1.8 mmol/L)(depending on risk category) combined with CRP <2 mg/L.Results: Baseline characteristics were similar between groups. Significantlymore patients achieved the NCEP LDL-C and dual LDL-C/CRP goals at 6 weekswith RSV + EZE vs RSV alone (Table). Mean LDL-C in the RSV and RSV + EZEgroups respectively was 191 mg/dL (4.9 mmol/L) and 189 mg/dL (4.9 mmol/L)at baseline, and 82 mg/dL (2.1 mmol/L) and 57 mg/dL (1.5 mmol/L) at week 6.Furthermore, a LDL-C/HDL-C ratio of 1.1 was seen with RSV + EZE at week 6.Both treatments were well tolerated.
RSV 40 mg RSV 40 mg + EZE 10 mg(n=230) (n=235)
% change from baseline#LDL-C -57 -70*HDL-C +8.5 +10.8CRP -29 -46*
% patients reaching goalNCEP ATP III LDL-C1 79 94*Updated NCEP LDL-C2 42 82*Combined LDL-C and CRP3 24 58*
*p<0.001#LDL-C & HDL-C=mean, CRP=median. 1LDL-C <100 mg/dL (2.6 mmol/L), 2LDL-C<100 mg/dL or <70 mg/dL (1.8 mmol/L), depending on risk category, 3LDL-C <100 mg/dL or<70 mg/dL, depending on risk category, and CRP <2 mg/L
Conclusions: RSV enables the majority of patients to achieve LDL-C goals. Theaddition of EZE to RSV reduced LDL-C by 70% and allowed more patients toachieve LDL-C and dual LDL-C/CRP goals.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

944 Lipids and antilipemics
P5391 Statins are associated with reduced perioperativemyocardial ischemia during continuous 12-leadelectrocardiography, troponin T release and long-termmortality after major vascular surgery
H.H.H. Feringa1, O. Schouten1, J.J. Bax2, R.T. Van Domburg1,S.H. Meij1, M. Dunkelgrun1, P.G. Noordzij1, D. Poldermans1. 1ErasmusMC, Cardiology, Rotterdam, Netherlands; 2Leiden University Medical Center,Cardiology, Leiden, Netherlands
Background: HMG-CoA reductase inhibitors (statins) improve cardiac outcomein high-risk patients. In addition to the lipid-lowering effects of statins, pleiotropiceffects (inflammation reduction, stabilization of atheromatous plaques) may con-tribute to its beneficial properties. In this study, we examined whether statins areassociated with a reduced incidence of perioperative myocardial ischemia andimproved long-term outcome. In addition, we examined whether LDL-cholesterolreduction prior to surgery was associated with a reduction in myocardial ischemia.Methods: The study population consisted of 213 patients (mean age 68 ±10years, 79% male) scheduled for major non-cardiac vascular surgery. Serialcholesterol levels were measured 3 months prior to surgery and preoperatively.Myocardial ischemia was assessed during 72 hours by continuous 12-lead elec-trocardiographic monitoring (12-lead ECG), starting 1 day before surgery andcontinuing for 2 days after. Serial troponin T measurements were performed onday 1, 3 and 7 after surgery. During follow-up, all-cause mortality was noted. Inpatients receiving statins, the change (%) in LDL-cholesterol level prior to surgerywas correlated with the occurrence of perioperative myocardial ischemia and tro-ponin T release.Results: In this study cohort, 71 (33%) patients had myocardial ischemia on 12-lead ECG, 33 (15%) had troponin T release and 61 (29%) died during a me-dian follow-up of 3.3 years (IQ range: 0.7-6.8). Using multivariate regressionanalysis with adjustment for cardiac risk factors and beta-blockers, statin ther-apy was significantly associated with a reduced incidence of myocardial ischemia(OR: 0.36, 95% CI: 0.17-0.74, p=0.006), reduced troponin T release (OR: 0.43,95% CI: 0.19-0.95, p=0.038) and improved long-term survival (HR: 0.44, 95%CI: 0.25-0.76, p=0.003). In 118 patients who used statins, the reduction (%) inLDL-cholesterol level prior to surgery was not significantly associated with the oc-currence of myocardial ischemia (OR per % reduction: 0.99, 95% CI: 0.98-1.01,p=0.59) and troponin T release (OR per % reduction: 1.00, 95% CI: 0.98-1.02,p=0.97).Conclusion: Statin use in patients undergoing major non-cardiac vascularsurgery is associated with a reduced incidence of perioperative myocardial is-chemia, troponin T release and long-term mortality rate. In patients using statins,LDL-cholesterol reduction prior to surgery was not a predictor of myocardial is-chemia, suggesting that other than the lipid-lowering properties of statins may beresponsible for its beneficial effect.
P5392 Safety and tolerability of prolonged-release nicotinicacid in combination with a statin: results of theNAUTILUS study
A. Vogt1, U. Kassner1, U. Hostalek2, E. Steinhagen-Thiessen1 onbehalf of NAUTILUS Study Group. 1Charite-Universitaet Berlin,
Berlin, Germany; 2Merck KGaA, Darmstadt, Germany
The multiceNtre, open, uncontrolled sAfety and tolerability stUdy of a modified-release nicoTinic acId formuLation in sUbjects with dySlipidaemia and low HDL-cholesterol (NAUTILUS) was an open-label, uncontrolled, phase IIIb study.The study population included a total of 566 patients with dyslipidaemia inade-quately controlled after four weeks of diet and low HDL-cholesterol (<1.0 mmol/L[<40 mg/dL] in men and <1.2 mmol/L [<46 mg/dL] in women). Exclusion criteriaincluded uncontrolled diabetes, significant hepatic, and vascular or renal disease.The main objective was to evaluate the safety and tolerability of prolonged-releasenicotinic acid, particularly in combination with statins (incidence of adverse events(AE) and serious AE). Efficacy parameters (lipid parameters) were also mea-sured.Patients received once-daily treatment with prolonged-release nicotinic acid (tar-get dose 2000 mg/day) added to existing regimens for 15 weeks. At baseline,40.5% of patients were receiving an HMG-CoA reductase inhibitor (statin), mostlysimvastatin or atorvastatin.Patients with and without concomitant statin therapy reported a similar incidenceof all-cause adverse events (64.6% vs. 57.9%, respectively), treatment-relatedAE (54.6% vs. 47.2%), all-cause serious AE (3.9% vs. 3.6%), treatment-relatedserious AE (0.9% vs. 0.3%), and withdrawals for AE (17.5% in each case). Asexpected, the most frequent AE was flushing. The incidence of flushing was sim-ilar in patients with and without statin treatment (45.0% vs. 40.1%), as was theproportion of patients withdrawing for flushing (8.7% vs. 10.4%). Only about onequarter of patients flushed >5 times. The median duration of flushing was identi-cal in either group (60 minutes). For subjects, who flushed, the mean number offlushes/week was similar for statin users (1.8) and non-users (1.6).There was no sign of serious hepatic or muscle toxicity. In particular, there wereno elevations of AST (GPT) or ALT (GOT) to more than 3-fold higher than theupper limit of normal (ULN), and no elevations of CPK to more than 5-fold greaterthan the ULN.The addition of prolonged-release nicotinic acid markedly increased HDL-cholesterol irrespective of statin treatment (+20% and +24%, respectively).
Prolonged-release nicotinic acid was well tolerated and effective when combinedwith a statin in patients with dyslipidaemia.
P5393 Achievement of LDL-cholesterol goals by addition ofezetimibe to high dose statin therapy in HeterozygousFamilial Hypercholesterolemia patients: 12 monthsfollow up
L. Papadimitriou, J. Skoumas, C. Pitsavos, C. Masoura, N. Giotsas,M. Toutouza, T. Papaioannou, C. Stefanadis. Ippokration Hospital School ofMedicine, 1St Cardiology Dept Lipid Clinic, Athens, Greece
Background: Familial Heterozygous Hypercholesterolemia is a common autoso-mal inherited disorder characterized by very high levels of LDL-Cholesterol (LDL-C) and increased risk for premature cardiovascular disease. Despite the pivotalrole of statins in decreasing LDL-C levels, the addition of ezetimibe seems to bea safe and efficacious choice.We evaluated the effect of ezetimibe on hFH patients already receiving statin.Design: We administered ezetrol in 105 patients (mean age 54.84 years, 58 menand 47 women) with hFH, already treated with high dose statins at least for oneyear. The lipid changes between baseline -statin and statin-statin+ezetimibe at3 and 12 months were assessed. We investigated for differences between hFHsubjects regarding the achievement of the respective LDL-C levels, according tothe International Panel on the Management of Familial Hypercholesterolemia.Results: Among hFH subjects 5.7% reached the LDL-C goal with the adminis-tration of statin, 34.9% with the addition of ezetimibe at 3 month and 40.5% at12 month interval(5.7% vs. 34.9%, p<0.001 and 34.9% vs. 40.5%, p=0.54). To-tal cholesterol (TC), LDL-C and triglyceride (TGL) concentrations were reducedby 30.6% (p<0.001), 37.5% (277.92mg/dl vs. 159.13mg/dl, p<0.001) and 13.6%(p<0.001), respectively, after statin treatment compared to baseline levels. Atthe end of the 12 month follow up the levels of TC, LDL-C, and TGL were de-creased by 16.9% (p<0.001), 22.5% (159.13mg/dl vs. 120.61mg/dl, p<0.001),9.2% (91.26mg/dl vs. 79.26mg/dl, p<0.001) respectively compared to statin treat-ment. HDL cholesterol levels increased by 12.5% (47.16mg/dl vs. 54.88mg/dl,p<0.001), under statin treatment, while a minor reduction of 1.6% (54.88mg/dlvs. 52.73mg/dl, p=1.0) was observed with the co-administration of ezetimibe at12 months. The addition of ezetimibe to statin did not alter the inflammatory sta-tus at 12 months, as it is monitored with the measurement of C-reactive protein(0.935mg/dl vs. 0.937mg/dl, p=0.988) and did not worsen the levels of transam-inases and of creatinine phosphokinase (CPK) (SGPT, p=0.55 vs. SGOT, p=1.0vs. CPK, p=1.0)Conclusion: The co-administration of ezetimibe with high dose statins in patientswith hFH revealed significant reductions of total cholesterol, LDL-C and triglyc-erides compared with statin monotherapy, and reveals its pivotal role in accom-plishing the LDL-Cholesterol goal levels in this subgroup, whereas no side effectswere demonstrated. Ezetimibe exerted a constant beneficial effect during the 12months follow up in this high risk population.
P5394 Atorvastatin 80 mg has equal benefits in patients <and => 65 yrs with acute coronary syndrome:Myocardial Ischemia Reduction with AggressiveCholesterol Lowering (MIRACL) study
A. Olsson1, G. Schwartz2, M. Jamieson3, D. Luo1. 1Universityof Linkoeping, Department of Medicine and Care, Linkoeping, Sweden; 2VAMedical Center and University of Colarado, Health Sciences, Denver, UnitedStates of America; 3Pfizer Inc, New York, United States of America
Objective: Older patients are currently undertreated after ACS. This study in-vestigated the efficacy and safety of treatment with atorvastatin 80 mg in acutecoronary syndrome (ACS) patients aged < and =>65 years recruited in the MIR-ACL study.Methods: A total of 3086 patients (1414 patients aged =>65 yrs) began 16 weeksof randomized treatment with atorvastatin 80 mg/day or placebo within 24-96hours following hospital admission for ACS. The primary end point (PEP) wasa composite of death, nonfatal acute myocardial infarction (MI), cardiac arrest, orrecurrent unstable angina. Stroke was a secondary end point.Results: End points occurred more frequently in older patients. In patients as-signed to placebo, those aged =>65 yrs experienced a greater proportion of PEPsthan patients <65 yrs (N=179 [21.7%] vs N=90, [12.4%]), a fourfold increase inrate of death (N=55 [6.7%] vs 13 [1.8%]), and a three-times higher incidence ofstroke (2.1% vs 0.7%). Corresponding rates for nonfatal MI were 9.1% for thoseaged =>65 yrs and 5.2% for those <65 yrs. In atorvastatin-treated patients, a2.6% absolute and a significant 16% relative risk reduction (RRR) in the PEP wasobserved overall (P=0.048) versus placebo, with a 14% RRR in patients aged
Table 1. Summary of incidence of treatment-associated adverse events in patients aged <65years and ≥65 years
Patients aged <65 years, Patients aged ≥65 years,n (%) n (%)
Atorvastatin Placebo Atorvastatin Placebo(N=689) (N=725) (N=849) (N=823)
Discontinuations due to adverse events 24 (3.5%) 21 (2.9%) 45 (5.3%) 22 (2.7%)Serious adverse events 4 (0.6%) 5 (0.7%) 11 (1.3%) 2 (0.2%)
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Lipids and antilipemics 945
=>65 yrs (HR=0.86, 95% CI=0.70-1.07) and a 22% RRR in those aged <65years (HR=0.78, 95% CI=0.56-1.06). Absolute risk reductions in the PEP associ-ated with atorvastatin 80 mg were similar in patients < and=>65 years (2.5% and2.9%, respectively). The treatment-by-age test for heterogeneity was not signifi-cant (P>0.5), indicating no evidence of difference in treatment effect by age. Thesafety profile of atorvastatin 80 mg was similar in both age groups (Table 1).Conclusions: After ACS, cardiovascular event rates are high in those =>65years. Atorvastatin 80 mg is similarly beneficial in patients < or =>65 years ofage.
P5395 Effects of Ezetimibe/Simvastatin compared toSimvastatin monotherapy in reducing C-Reactiveprotein and low density Lipoprotein-Cholesterol
C.M. Ballantyne1, P. Ridker2, T. Pearson3, E. Veltri4, Y.B. Mitchel5,C.M. Mc Crary Sisk3, A. Shah3, D.L. Maccubbin3 . 1Baylor College
of Medicine, Houston, United States of America; 2Brigham and Women’sHospital, Boston, United States of America; 3Univ. Rochester School of Med.and Dentistry, Rochester, United States of America; 4Schering-Plough ResearchInstitute, Kenilworth, United States of America; 5Merck and Co., Inc., Rahway,United States of America
Background: In addition to lowering cholesterol, statins reduce C-reactive pro-tein (CRP) and may play a direct role in modifying atherosclerosis. Ezetim-ibe/simvastatin (EZE/SIM) reduces LDL-C to a greater extent than SIM alone.This study evaluated the CRP lowering effects of both agents.Methods: This post hoc analysis pooled data from 3 similar randomized, placebo(Pbo) controlled, double blind studies. After a 6 to 8 wk washout and 4 wk diet/Pborun in, 3083 hypercholesterolemic patients (LDL-C: 145 - 250 mg/dL; TG ≤ 350mg/dL) were randomized equally to Pbo, EZE 10 mg, EZE/SIM (10/10, 10/20,10/40, 10/80 mg), or SIM (10, 20, 40, 80 mg) for 12 wks. Changes in CRP andLDL-C and the percentage of patients achieving defined single and dual LDL-C(<70 and <100 mg/dL) and CRP (<1 and <2 g/L) levels were examined acrossindividual and pooled treatment groups.Results: EZE alone did not significantly reduce CRP vs Pbo. Pooled EZE/SIMproduced significantly greater CRP and LDL-C reductions vs pooled SIM alone(Table). Significantly more patients in the pooled groups achieved single LDL-Cand CRP, and dual LDL-C/CRP levels with EZE/SIM vs SIM alone (Table 1). Theenhanced CRP lowering effect was similar among subgroups based on age (<65vs ≥65 years), gender, body mass index (<30 vs ≥30 kg/m2), coronary heartdisease, diabetes and metabolic syndrome status.Conclusions: Although EZE alone did not significantly reduce CRP vs Pbo,EZE/SIM provided additional incremental CRP and LDL-C lowering beyond thatachieved with SIM alone.
P5396 Rosuvastatin promotes vasculogenesis and correctsendothelial dysfunction in patients with chronic heartfailure
E.B. Beck, S. Erbs, V. Adams, A. Linke, N. Kraenkel, S. Moebius-Winkler, G. Schuler, R. Hambrecht. University of Leipzig - Heart
Center, Cardiology, Leipzig, Germany
In patients with chronic heart failure (CHF), endothelial dysfunction has been par-tially attributed to an impaired regenerative capacity of circulating endothelial pro-genitor cells (CPCs). Given the beneficial effects of statins with regard to CPC re-lease and function, aim of the present trial was to elucidate, whether rosuvastatintreatment influences vasculogenesis through activation of CPCs and whether thisis associated with an improvement in endothelial function in patients with CHF.Methods: Forty patients with CHF (LVEF 30±1%, 12 with ischemic heart dis-ease, 28 with dilative cardiomyopathy) were randomized to 12 weeks of 40 mgrosuvastatin daily or placebo therapy in a double-blind manner. At begin and at12 weeks, AcLDL/lectin+ CPCs were recovered from blood-derived mononuclearcells by cell culture and counted using FACS analysis. Functional capacity ofCPCs was determined by migration and matrigel assay. Percutanous biopsies ofthe vastus lateralis muscle were obtained and capillary density was determined byimmunohistochemistry. Endothelium-dependent, flow-mediated dilatation of theradial artery was assessed by high resolution ultrasound.Results: Rosuvastatin decreased LDL cholesterol levels by -56±2% (from3.7±0.2 mmol/L at begin to 1.6±0.1 mmol/L at 12 weeks, p<0.05 vs. placebo).Rosuvastatin increased not only the number of CPCs by +409±138% (p<0.01
Abstract P5395 – Table 1
Mean % change from baseline Proportion of patients achieving individual and dual LDL-C and CRP levels §
CRP† LDL-C‡ LDL-C <100 LDL-C <70 CRP<2 CRP <1 LDL-C <100 + CRP <2 LDL-C <100 + CRP <1 LDL-C <70 + CRP <2 LDL-C <70 + CRP <1
Pooled SIM -14.3 -38.0 42.5 6.0 27.7 14.7 22.2 12.2 3.2 1.3Pooled EZE/SIM -31.0** -52.5** 78.8** 37.3** 34.2* 21.3** 47.7** 29.0** 21.6** 13.5**†Logarithm of (study end/baseline CRP) was modeled through ANOVA with terms for dose and baseline CRP, LDL-C, and HDL-C; (exponentiation of the model-based least square means - 1) x 100yielded geometric means.‡ Least square percent change in LDL-C was modeled through ANOVA with terms for dose and study.§Expressed as percentage of patients achieving level out of patients above level at baseline. For inclusion in the dual LDL-C/CRP analysis, patients had to be above the stated LDL-C and/or CRP levelat baseline.**One-sided p-value <0.001 versus pooled SIM.*One-sided p-value <0.050 versus pooled SIM.P-value for difference in CRP geometric means is based upon first order approximation of difference in geometric means.
vs. placebo), but also augmented migratory capacity of CPCs from 1.6±0.5 to2.8±0.6 cells per 100 plated cells (p<0.05 vs. placebo) and their ability to in-tegrate into endothelial networks from 1.5±0.5 to 2.9±0.6 cells per 100 coro-nary endothelial cells (p<0.05 vs. placebo for the change). This was associatedwith an increase in capillary density in the skeletal muscle by +14±3% (p<0.05vs. placebo) and an improvement in peripheral flow-mediated dilatation from6.7±1.0% to 17.7±2.5% (p<0.05 vs. placebo) in the rosuvastatin group. All ofthe above-mentioned parameters remained virtually unchanged during the studyperiod in the placebo group.Conclusion: Rosuvastatin therapy augments the regenerative capacity of circu-lating endothelial progenitor cells, which contribute to the correction of endothelialdysfunction and promote the formation of new vessels through vasculogenesis inpatients with chronic heart failure.
P5397 Effects of ezetimibe/simvastatin on lipoproteinsubclasses in patients with primaryhypercholesterolemia
L. Ose1, K.Q. Olegario2, R. Reyes2, A.O. Johnson-Levonas2 ,A. Sapre2, D. Tribble2. 1Lipid Clinic Rikshospitalet, Oslo, Norway;2Merck and Co., Inc., Rahway, United States of America
Background: Cholesterol-rich apo B-containing lipoproteins including LDL,IDL and VLDL, are known to promote atherosclerosis. Ezetimibe/simvastatin(EZE/SIM) is an efficacious lipid-lowering therapy that inhibits both the intestinalabsorption and biosynthesis of cholesterol. The current analysis compared theeffects of EZE, SIM, and EZE/SIM on apo B-containing lipoprotein subfractions.Methods: This was a multi-center, randomized, double-blind, placebo (Pbo)-controlled, parallel arm study. After a washout and diet/Pbo run-in, 1528 patientswith hypercholesterolemia (LDL-C 145-250 mg/dL; TG ≤350 mg/dL) were ran-domized to 1 of 10 daily treatments for 12 wks: EZE/SIM (10/10, 10/20, 10/40,10/80 mg); SIM alone (10, 20, 40, 80 mg); EZE 10 mg; or Pbo. Cholesterol as-sociated with lipoprotein subclasses was quantified by the vertical autoprofile IImethod. The primary analysis was median % change in subfraction cholesterolfor EZE/SIM (pooled across doses) vs SIM (pooled across doses) or EZE.Results: EZE/SIM produced significant reductions in VLDL-C1+2 and VLDL-C3,IDL-C, LDL-C 1-3 vs EZE, SIM, and Pbo (Table). EZE/SIM resulted in nearlyadditive reductions in VLDL-C1+2 and VLDL-C3, IDL-C, LDL-C 1-3 vs EZE andSIM alone. Compared to Pbo, numerically larger reductions in LDL-C 4 were seenwith SIM and EZE/SIM. Of the subfractions examined, with EZE/SIM, the greatestreductions were observed for IDL-C and LDL-C 1-3.
Median values Pbo EZE Pooled SIM Pooled EZE/SIM(mg/dL) (N = 140) (N = 139) (N = 569) (N = 549)
B Change (%)1 B Change (%)1 B Change (%)1 B Change (%)1
VLDL-C1+2 11.2 0a 11.6 -14.0a,b 12.1 -23.6a 12.0 -31.7VLDL-C3 14.0 -3.9a 15.0 -17.2a,b 15.0 -25.0a 15.0 -33.3IDL-C 19.5 -5.6a 20.0 -36.6a,b 20.0 -58.2a 20.0 -76.0LDL-C 1 27.2 -2.3a 28.0 -25.1a,b 27.4 -43.3a 27.0 -57.9LDL-C 2 35.2 -3.8a 31.9 -15.0a 31.3 -32.8a 31.2 -50.0LDL-C 3 78.0 0.3a 79.7 -13.2a,b 76.9 -35.6a 76.4 -50.3LDL-C 4 11.0 0 12.6 -10.1 13.0 -20.4 12.7 -21.2
VLDL-C = very-low density lipoprotein-cholesterol; IDL-C = intermediate density lipoprotein-cholesterol; LDL-C = low density lipoprotein-cholesterol; B= baseline value; Pooled SIM= simvas-tatin pooled across the dose range; Pooled EZE/SIM = EZE/SIM pooled across the dose range.1Expressed as median percent change from baselinea p<0.01 vs EZE/SIM; bp<0.010 EZE vsPbo.
Conclusion: EZE/SIM was particularly effective in reducing atherogenic lipopro-tein subfractions.
P5398 Follow-up of Patients on agressive lipid loweringtherapy: Correlation between outcomes, blood lipids,carotid arteries and gated SPECT datas
T. Vakhtangadze1 , F. Todua2 , M. Akhvlediani2, D. Gachechiladze2 ,R. Kharadze2 . 1Tbilisi, Republic of Georgia; 2Institute of Radiology,
Radiology, Tbilisi, Republic of Georgia
Objectives: Evaluation of the impact of aggressive statin therapy on the follow-upof patients with CAD.Methods: 27 consecutive male patients (mean age 57,7± 6.5yy) with stress-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

946 Lipids and antilipemics
inducible ischemia on Tc99m Sestamibi Gated SPECT were included in the study.We evaluated the effect of intensive lipid-lowering therapy on stress-inducible de-fect size, carotid arteries intima-media (CAIM) thickening and lipid profile. Patientswere receiving Atorvastatin or Simvastatin 40-80 mg daily maintaining goal ofLDLCh in range 65-70 mg/dl with a median follow-up of 18 (12-24) months. Bloodlipid profile, carotid arteries ultrasound and Tc99m sestamibi gated SPECT wereperformed at the beginning of the study and after every six months.Results: All of the patients revealed impairment in lipid profile, particularly in lev-els of LDL cholesterol and stress-inducible defects on the SPECT images at thebeginning of the study, 37,0% (10 patients) of the patients did not have any sig-nificant changes in CAIM. Statin therapy reduced serum LDLCh (-57%; P<0.001)in all patients; thickening of CAIM and/or plaque size also decreased in 94% ofpatients. All of the patients showed improvement of symptoms of CAD, which cor-related very well with levels of LDL and CAIM. However, gated SPECT showedimprovement in stress-inducible defect size in only 33% (9) of patients, whereasthere were no changes in 13 patients and other 5 revealed even worsening in re-versible defect sizes and perfusion scores. There were no major coronary eventsduring the study. Improvement of Gated SPECT data did not correlate with im-provement in CAIM thickening and/or reduction of plaque size.Conclusion: This study has shown that statin therapy has good effect on CADsymptoms, outcomes, lipid profile, CAIM, however there is less effect on the per-fusion score acquired by gated SPECT.
P5399 Intensive lipid-lowering therapy and ventriculararrhythmias in patients with coronary artery diseaseand internal cardioverter defibrillator implants
J.H.A.J. De Sutter1, G. De Bacquer1, L. Jordaens2, M. De Buyzere3,K. Matthys4, G. De Backer3, R. Tavernier4 on behalf of CLARIDI
investigators. 1University Gent, Public Health, Gent, Belgium; 2ErasmusUniversity Hospital, Cardiology, Rotterdam, Netherlands; 3University Hospital,Cardiology, Gent, Belgium; 4Pfizer, Medical Department, Brussels, Belgium
Background Lipid-lowering therapy reduces cardiovascular morbidity and mor-tality in pts with coronary artery disease (CAD). Since ventricular arrhythmiasare an important cause of death in these pts, we hypothesized that intensivelipid-lowering therapy would reduce the frequency of ventricular arrhythmias inhigh-risk CAD pts.Methods In this double-blind, placebo-controlled multicenter trial, 106 CAD ptswith implantable cardioverter/defibrillators (ICDs) and total cholesterol levelslower than 250 mg/dl were randomly assigned between 2000 and 2003 to re-ceive either 80 mg of atorvastatin daily or placebo for 12 months. The primaryend point was the first recurrence of an ICD intervention for ventricular tachy-cardia or fibrillation confirmed by stored electrograms. The combination of death,myocardial infarction, coronary revascularisation and stroke was investigated asa secondary endpoint.Results Fifty-three pts were assigned to atorvastatin and 53 to placebo. Baselineclinical characteristics, extent of CAD and concomitant medication were compa-rable between both groups. Serum total cholesterol remained at 210±41 mg/dl inthe placebo group and fell to 148± 36 mg/dl in the atorvastatin group (p<0.001).Serum low-density lipoprotein cholesterol remained at 139±29 mg/dl in theplacebo group and fell to 76±39 mg/dl in the atorvastatin group (p<0.001).Forthe primary endpoint, 11 of the 53 pts (21%) on atorvastatin had an appropriateICD intervention, while this was the case for 20 of the 53 patients (38%) who usedplacebo (hazard ratio 0.47, 95%CI 0.22-0.98, log-rank test: p=0.040). Also, treat-ment with atorvastatin resulted in a 59% reduction in the number of days with anappropriate ICD intervention (hazard ratio 0.41, 95%CI 0.28-60). The incidenceof the secondary endpoint was comparable: 9% for the atorvastatin group versus6% for the placebo group, p=0.72. Treatment related adverse events were alsocomparable: 11% for the atorvastatin group versus 4% for the placebo group,p=0.27, and were mainly related to gastro-intestinal symptoms.Conclusions: In this prospective randomized trial, intensive lipid lowering therapysignificantly reduced recurrences of ventricular arrhythmias in pts with CAD andICD implants
P5400 Fluvastatin improves arterial stiffness in patients withcoronary artery disease: a 5-year follow-up study
M. Hongo1, H. Tsutsui2, E. Mawatari2, M. Azegami1, A. Yamazaki1,Y. Yazaki2, O. Kinoshita2, U. Ikeda2. 1Shinshu University Schoolof Health Sciences, Dept Of Cardiovascular Medecine, Matsumoto
City, Japan; 2Shinshu University School of Medicine, Dept Of CardiovascularMedecine, Matsumoto City, Japan
Background: Recent studies suggest that statins act to exert direct benefi-cial cardiovascular effects and reduce adverse clinical events in patients at riskthrough not only the lipid-lowering action but also the lipid-independent anti-atherogenic properties. The present study was designed to test our hypothesisthat fluvastatin might improve aortic stiffness assessed by pulse wave velocity(PWV) in patients with coronary artery disease (CAD).Methods and Results: One hundred patients were randomly assigned to eitherfluvastatin (Group A, n = 50) or placebo (Group B, n = 50) and followed up for5 years. Patients had measurement of brachial-ankle PWV and serum lipid andC-reactive protein (CRP) before and 3, 6, 12, 24, 36, 48, and 60 months after
treatment. Age, blood pressure, heart rate, gender distribution, severity of CAD,prevalence and magnitude of diabetes mellitus and dyslipidemia, and medicationwere not different between the 2 groups. In Group A, the PWV (from 1719±313 to1616±308 cm/s, p < 0.001) and serum total cholesterol, low-density lipoproteincholesterol, and CRP levels were significantly decreased after 3 months of fluvas-tatin. This improvement was further enhanced for next 9 months and the variableskept constant thereafter. In Group B, despite identical lowering of serum lipid lev-els, the PWV was significantly increased (from 1681±337 to 1741±347 cm/s, p <
0.001) at 12 months after treatment and the increase lasted over the follow-up pe-riod. There was no change in the serum CRP levels. In a subgroup of patients (n= 22) who had clofibrate or probucol, the drug was switched to fluvastatin. Thesepatients showed significant improvement of the PWV and serum CRP levels 3months after the change of treatment.Conclusions: There is rapid improvement of the PWV as well as serum CRP lev-els after short-term treatment with fluvastatin in patients with CAD. Its beneficialeffects on arterial stiffness persist for long-term period.
P5401 Assessment of the dose-dependence of the influenceof statin on arterial elasticity in coronary artery heartdisease
M. Kurpesa, E. Trzos, T. Rechcinski, M. Krzeminska-Pakula. SecondChair&Department Of Cardiology, Medical University, Lodz, Poland
Purpose: Statins reduce the mortality of patients with coronary artery disease(CAD) even in those who have normal plasma cholesterol level. In this grouppleiotropic properties seem to be responsible for such benefficial effects of statins.One of the pleiotropic mechanisms of statins is the improvement of arterial elas-ticity. Pulse wave velocity (PWV) provides an indirect, non-invasive assessmentof the mechanical properties of arteries. The dose sufficient to achieve the non-lipid effects of statins in CAD with normal cholesterol level is still discussed. Theaim of this study was to assess whether the benefficial effect of statins on arterialdistensibility is a dose-dependent phenomenon.Methods: The study group consisted of 58 patients with CAD and normal choles-terol serum level (189±16 mg/dl). They were randomized into Group I (20 patientswho received simvastain 10 mg/d), Group II (20 patients who received simvastatin40 mg/d) and Group III (18 patients who received placebo). Groups were compa-rable according to demographic characteristics and treatment of CAD. Before andfollowing 6 months of treatment PWV was evaluated using a computer systemCOMPLIOR-Colson. For automatic measurement of PWV pressure waveformswere digitized at rate 500 Hz for carotid-femoral distance.Results: Initial PWV in all groups was similar (11,4 ± 0,7 m/s in Group I vs 12,1± 0,8 m/s in Group II vs 11,7 ± 04 m/s in Group III). After 6 months PWV inplacebo group did not change significantly. The significant lowering of PWV wasobserved in Group I (8,5 ± 0,8 m/s, p<0,05 vs initial) as well as in Group II (8,4 ±0,6 m/s, p<0,05 vs initial). PWV in Group I was reduced by 23% and in Group IIby 25% (NS). After 6-moth treatment the cholesterol level was significantly lowerin Group II (130±24 mg/dl) than in Group I (169±21 mg/dl), p<0,05.Conclusion: 1. The benefficial effect of statin on arterial elasticity seems to bea dose independent phenomenon. 2. In coronary artery disease without hyperc-holesterolemia 10 mg/d of simvastatin is sufficient to achieve the pleiotropic effecton arterial elasticity.
P5402 Simvastatin reduces monocyte adhesion expressionmediated by native LDL in hypercholesterolemicpatients
C.V. Serrano Jr1, M.F.V. Hunziker1, F.O. Toledo1, J.L. Fernandes1 ,A.E.P. Pesaro1, J.C. Nicolau1, V.M. Yoshida1, H.P. Monteiro2. 1Heart
Institute (InCor), Medical School, Univ. of Sao Paulo, Sao Paulo, Sp, Brazil;2Molecular Biochemistry/Biology Department, Med School Paulista, Fed. Univ.of Sao Paulo, Sao Paulo, Sp, Brazil
Introduction: Native LDL-cholesterol plays a pivotal role in the progression ofatherosclerotic lesions, however the mechanisms involved are not fully clear. Re-cent studies have suggested that native LDL may increase monocyte-endothelialcell adhesive interactions.Aim: Evaluate the local effect of elevated native LDL concentrations on monocyteadhesion molecule expression. We hypothesized that high levels of native LDLcould promote monocyte-endothelial cell interactions and that statins, through apleiotropic effect, could supress such process.Methods: Venous blood samples from twenty-three patients (56±12 years; 65%men) with hypercholesterolemia (plasmatic LDL= 152.4±6.4mg/dL) and stablecoronary artery disease were collected before and after a 12-week treatment with40 mg of simvastatin. Isolated native LDL, at a fixed concentration of 100 mg/dl,was added to monocyte suspensions, obtained before and after the simvastatintreatment. Cellular adhesion molecule expression (CD11b, L-selectin and CD14)was determined by flow cytometry. Normocholesterolemic individuals (plasmaticLDL=111±6.4 mg/dl) were used as controls (n=15; 54±11 years; 66% men).Results: After the lipid-lowering treatment, plasmatic LDL was reduced from152.4 ±15.7 to 101.5 ± 9.5 mg/dl (p<0.04). In addition, monocyte CD11b ad-hesion molecule expression was reduced from 174.2 ± 8.4 to 116.9 ± 12.5(p<0.03) and CD14 expression from 140.4 ± 5.0 to 107.5 ± 6.2 (p<0.04). Mono-cyte L-selectin adhesion molecule expression increased from 46.0 ± 3.5 to 58.7 ±
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Lipids and antilipemics / Childhood obesity 947
5.0 (p<0.04). Normocholesterolemic individuals presented CD11b, CD14 and L-selectin monocyte adhesion expression, respectively, of 98.4 ± 10.6, 90.5 ± 11.6and 67.7 ± 11.5. After statin treatment, hypercholesterolemic patients presentedsimilar monocyte adhesion expression compared to normocholesterolemic indi-viduals. Data expressed in mean ± SD.Conclusion: These data implicate that native LDL is capable of inducing an over-expression of monocyte adhesion molecule expression - facilitating monocyte ad-hesion to the vascular wall. Moreover, statins completely abolished the stimula-tory effect of native LDL on monocyte activation. This study contributes in under-standing the pleiotropic effects of statins particularly with regard to their use intreatment and prevention of cardiovascular disease.
CHILDHOOD OBESITY
P5403 Abnormal HDL subclasses distribution in childrenwith type 2 diabetes mellitus and insulin-resistantobesity
O. Perez-Mendez1, M. Torres-Tamayo2 , C. Posadas-Romero2 ,V. Vidaure2, J. Zamora-Gonzalez2 . 1National Institut of Cardiology,
Physiology, Mexico City, Mexico; 2IMSS, Mexico City, Mexico
Purpose: To investigate HDL size distribution in obese children with or withoutimpaired glucose tolerance (IGT), and in children affected by type 2 diabetesmellitus (T2DM).Methods: We transversally studied HDL size distribution assessed by polyacril-amide gradient gel electrophoresis, of HDL isolated from the plasma of 47 chil-dren with T2DM, 16 obese children with IGT, 43 with obesity and normal glucosetolerance, and 39 lean controls.Results: Diabetic children had significantly lower proportions of HDL2b andHDL2a, and higher proportions of HDL3b and HDL3c than the other threegroups. Obese subjects showed HDL size distributions similar to those of con-trols. However, when compared with obese insulin sensitive (homeostasis modelassessment <2.01), obese insulin resistant subjects had lower proportions ofHDL2b (7.99±4.80% vs. 15.60±7.02%, p=0.0002), and HDL2a (9.64±4.48% vs.13.98±3.07%, p=0.0037), and higher proportions of HDL3b (27.63±5.94% vs.19.81±4.17%, p=0.0002). Partial correlation analysis adjusted by age and gendershowed that homeostasis model assessment correlated with HDL2b (r=-0.284,p=0.001), HDL2a (r=-0.261, p=0.002), HDL3a (r=0.246, p=0.003), and HDL3b(r=0.174, p=0.038). No correlations were found between C-reactive protein andHDL size distribution.Conclusions: This study showed an abnormal HDL size distribution in pediatricpatients with type 2 diabetes mellitus and in children with or without impairedglucose tolerance. Insulin-resistance seems to be the principal factor responsiblefor the HDL size distribution shift to smaller particles; therefore, this parametermay be useful as a very early risk marker of incident diabetes and, probably, ofcoronary heart disease.
P5404 Abnormal myocardial deformation properties inobese, non-hypertensive, children: an ABPM,standard echocardiographic and strain rate imagingstudy
G. Di Salvo, G. Pacileo, G. Limongelli, A. Rea, B. Castaldi, P. Caso,L. Perrone, R. Calabro’. Second University of Naples, Chair of
Cardiology, Naples, Italy
The prevalence of obesity is increasing among children in the developed world.The association of obesity and abnormal cardiac function is still debated. The re-ported changes may reflect the role of comorbidities that contribute to ventriculardysfunction. Obese children, without arterial hypertension, may be a unique clin-ical opportunity to evaluate the effect of obesity, per se, on myocardial function,excluding the influence of possible comorbidities. We sought to define the pre-clinical effects of obesity on the cardiovascular system, of healthy children withexcess weight who have no other clinically appreciable cause of heart disease,by using the more sensitive ultrasonic derived strain rate (SR) imaging.Methods: We studied 278 subjects divided into 2 groups: 1- Obese children(Group O: n= 150; age: 12±3 years); 2- Healthy lean children, comparable forage, sex, and pubertal stage (Referents: n=128; mean age12±4 years).Results: Systolic (SBP) and diastolic blood pressure (DBP), as well as 24h-SBPand 24h-DBP were comparable between groups. Left ventricular (LV) mass/height2.7 was increased (p<0.0001) in Group O (46±12 g/m 2.7) compared to Ref-erents (31±14 g/m 2.7). Standard echocardiographic indices of global systolicfunction were similar in the 2 groups. Intima-media thickness measured at thecommon carotid artery was increased (p=0.4) in obese children (0.46±0.09mm)compared to Referents (0.45±0.07mm). Obese children showed regional longi-tudinal peak systolic SR (-1.4 ± 0.7 s-1) values lower (p<0.0001) than that ofReferents (-2.2± 0.5) in both left and right ventricle, even after correction for LVmass mass/height 2.7. In multivariable analysis, average peak systolic SR wassignificantly correlated with HOMA-IR (p<0.01; coefficient, -0.02; SE, 0.011), andinsulin serum concentration (p<0.01; coefficient, -0.05; SE, 0.023).Conclusions: Our study demonstrated that obesity, in absence of hypertension,is associated with impaired myocardial deformation properties already in child-
hood involving both right and left ventricle. Obesity not only is a risk factor forlater cardiovascular disease, but also is associated with contemporaneous andsignificant impairment of longitudinal myocardial deformation properties. Thus,our data support the prevention of obesity in pediatric age, because already inchildhood, obesity is responsible of abnormal systolic myocardial function.
P5405 Reducing cardiovascular risk factors in obeseadolescents
T. Stolen1, A.E. Tjonna1, R. Odegaard2 , U. Wisloff1. 1NTNU,Department of Circulation and Medical Imaging, Trondheim, Norway;2St. Olav Hospital, Trondheim, Norway
Objective: The aim of present study was compare the effects of a multidisci-plinary approach and intensity-controlled interval training on cardiovascular riskfactors in obese adolescents.Methods: Obese adolescents (body fat 39.5 ± 4.2%) were randomised to multi-disciplinary treatment or high intensity interval training after testing peak oxygenuptake and endothelial function (flow mediated dilatation). Multidisciplinary treat-ment: 3 hours of physical activity and/or practical cocking and 2 hours of grouptherapy each month for 13 weeks. Interval training: 4 times 4 minutes at 85-95%of maximal heart rate separated by 3 minutes active pauses twice a week for 13weeks. Preliminary Results: Interval training increased peak oxygen uptake by13.9%, maximal oxygen pulse by 17.6%, flow mediated dilatation by 140.9% anddecreased fasting blood-insulin levels by 44.2%, blood-insulin levels 2 hours af-ter a standard glucose test by 54.8% and fat percent by 4.8%. No change wasobserved in the multidisciplinary treatment group, except an improvement in max-imal oxygen pulse by 6.2%. The close correlation between body fat and flow medi-ated dilatation observed at pre test was absent after 13 weeks of interval training.Conclusions: Two weekly high intensity exercise training sessions for 13 weeksreduced several known cardiovascular risk factors, such as flow mediated dilation,low peak oxygen uptake, insulin resistance and fat mass, and resulted in that flowmediated was unrelated to fatness after the intervention period.
P5406 Non-invasive ultrasonic detection of endotheliumdysfunction in severely obese children
R. Bassil Eter1, B. Jouret2, A. Taktak1, J.P. Salles2, N. Lounis2,C. Arnaud2, M. Tauber2 , P. Acar1. 1Pediatric Cardiology, Toulouse,France; 2Pediatric Endocrinology, Toulouse, France
Aim: Obesity in childhood is associated with increased cardiovascular morbidityand mortality in adults. Impaired endothelium function is considered to be anindependent risk factor for cardiovascular events. The aim of our study was toevaluate arterial mechanics and endothelial function in obese children.Methods: Fifty-six severely obese children (median BMI; Z score = 4.68 [3.78- 5.96]) and 49 controls (BMI; Z score = 0.18 [-0.41 to 0.65]) aged between 7and 15 years old were enrolled in this prospective study. All children underwentnon-invasive ultrasonic measurements of common carotid artery luminal systolicand diastolic diameters, and intima-media thickness (QLab, Philips). The cross-sectional compliance and distensibility, and the incremental elastic modulus of thecommon carotid artery were calculated. The flow-mediated dilation of the brachialartery, defined as diameter changes in response to reactive hyperemia, was mea-sured.Results: The systolic and diastolic pressures were higher in obese children vscontrols (mean 111/60 vs 105/56; p < 0.05). The intima-media thickness wasincreased in obese children vs controls (median 0.48 [0.45 - 0.53] vs 0.45 [0.43- 0.49] mm; p < 0.05). The cross-sectional compliance (0.185 [0.16 - 0.225] vs0.24 [0.18 - 0.27] mm2 mmHg-1; p < 0.001) and distensibility (0.475 [0.36 - 0.58]vs 0.63 [0.52 - 0.76] mmHg-1.10-2; p < 0.001) were lower than in controls. Theincremental elastic modulus (3049 [2280 - 3781] vs 2093 [1700 - 2582]; p <
0.001) were significantly higher in obese than in controls. Endothelium-dependentfunction was blunted in obese children vs controls (5% [2.33 - 7.5] vs 6.66%[5.3 - 10]; p < 0.01). Intima-media thickness was positively correlated with waistcircumference (p < 0.01), BMI; Z score (p = 0.01), and total fat mass (p < 0.05).There was a tendancy of positive correlation between intima-media thickness andinsulin resistance (p = 0.096).Conclusions: Ultrasonic evaluation of arterial changes shows strong associationbetween severe childhood obesity, arterial wall stiffness and endothelial dysfunc-tion. This non-invasive method may be routinely performed in the assessmentof early cardiovascular risks in obese children, so that other cardiovascular riskfactors could be seriously addressed.
P5407 Physical activity and body mass index in schoolchildren: first results of the Leipzig School Project
C. Walther1, S. Fikenzer2 , E. Fiehn1, K. Drechsler1, M. Sonnabend1 ,B. Bublitzer1, M. Busse2, G. Schuler1. 1University of Leipzig,Heart Center, Cardiology, Leipzig, Germany; 2University of Leipzig,
Institute for Sports Medicine, Leipzig, Germany
The prevalence of obesity is continuously increasing among school children dur-ing the past years, caused by inadequate nutrition and decrease of physical activ-ity. The importance of physical activity on cardiovascular mortality and morbidity
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

948 Childhood obesity
was shown in large cohort studies. Aim of this trial is to teach a health-consciouslife-style, to improve physical activity and to reduce obesity in school children withadditional sport lessons. In the following the first results of the Leipzig SchoolProject are presented. A total of 60 boys and 55 girls (mean age 11.2 ± 0.4years) were evaluated. Two classes (51 children) of a city high school in Leipzig(LC) and two classes (45 children) of a country high school (CO) took part in thestudy. One class (19 children) of a high school with special focus on competi-tive sports (SP) served as control group. The regular exercise lessons were in-creased in one selected class of LC and CO respectively from two to five lessonsweekly for one year. Baseline investigations included physical examination, recordof anthropometric data, laboratory analysis, acquisition of fat free mass, spiroer-gometry and a standardised questionnaire on sport and leisure behaviour of thechildren. Motor abilities were determined by a body gross motor development testfor children (Koerperkoordinationstest fuer Kinder; KTK). Mean body mass index(BMI) did not differ significantly between the three schools (18.2 ± 2.5 kg/cm2 inLC, 18.9 ± 3.7 kg/cm2 in CO, 18.3 ± 2.1 kg/cm2 in SP). 14% of children in LCand 17.4% of children in CO had a BMI over the 97th percentile, compared to5% of children in SP. Maximal oxygen consumption (VO2max) was significantlybetter in children of SP (54.1 ± 7.4 ml/min/kg, p<0.001 vs. LC and CO) com-pared to children of the two other schools (42.8 ± 10.1 ml/min/kg in LC; 42.8 ±10.1 ml/min/kg in CO, p<0.01 versus LC). Children in SP reached a significantlyhigher average motor quotient (MQ) in the KTK (121.5 ± 7.5 in SP, p<0.01 vs.LC and CO) than children of the two other schools (110.4 ± 12.3 in LC; 106.5 ±16.8 in CO). VO2max and MQ were inversely correlated with BMI (MQ and BMIr=-0.553 (p<0.001); VO2max and BMI r=-0.441 (p<0.0001)). Higher BMI levelsare associated with poorer body gross motor development and endurance per-formance. Therefore, to prevent the negative consequences of physical inactivityand overweight/obesity early intervention to support exercise and movement isrecommended.
P5408 Obesity and metabolic syndrome in children andadolescents
I. Schusterova1, J. Saligova2, I. Riecansky3. 1Eastern Slovak HeartInstitute, Kosice, Slovak Republic; 2Children University Hospital,Metabolic disease, Kosice, Slovak Republic; 3Slovak Medical
University, Faculty of Cardiology, Bratislava, Slovak Republic
Background: Childhood obesity is a major risk factor, especially for the metabolicsyndrome and further cardiovascular diseases. By the definition, the metabolicsyndrome is a combination of obesity, arterial hypertension, hyperlipidemia ordyslipidemia, insulin resistance or type 2 diabetes mellitus. AIM: Aim of our studywas identify some of the insulin resistance associated cardiovascular risk factorsin children and adolescents.Methods: Study group consistent of 89 children aged 6-18 years (mean age12,5 ± 5,5) with hypercholesterolemia. Complete lipids analysis was performed(triglyceride -TAG, total -TCH, LDL and HDL cholesterol) and fasting insulin levelwas measured. Children were screened for obesity and overweight and BMI per-centiles were established. By echocardiography left ventricle mass - LVM (g) andLV geometry and intima-media thickness (IMT in mm) of the carotid arteries wasestablished. All children had an ambulatory blood pressure monitoring (ABPM).Results: Obesity was found in 20% children, same result was in overweight. Inchildren with combined DLP there was significantly higher BMI percentile - 73,59and the highest number of obese (18,51%) and overweight (33,3%). Left ven-tricle concentric remodeling was associated with significantly higher TCH leveland concentric hypertrophy with TAG level. Obesity and overweight were asso-ciated with significantly higher all values of blood pressure (BP) obtained fromABPM (i.e. mean average daily, nightly and 24 hour BP), higher IMT (0,52 and0,50 mm) compared with children with normal body weight (0,43 mm) and higherLVM (108,3 g; 135,2 g; 136,9 g in non obese, overweight and obese childrenrespectively) and with significantly higher (p < 0,01) fasting insulin level.Conclusion: Obesity and overweight in children and adolescents is associatedwith multiple insulin-resistant cardiovascular risk factors and that is why it is im-portant to screen for incipient metabolic syndrome in children.
P5409 Effects of different exercise programs on bloodpressure and body composition in obese Spanishchildren
E. Segura-Orti1, J.F. Lison-Parraga1, C. Sanchez-Juan2 ,M.D. Arguisuelas-Martinez1, J. Martinez-Gramage1, J.M. Real1.1CEU-Universidad Cardenal Herrera, Nursery & Physiotherapy
Dept., Moncada, Spain; 2Hospital General Valencia, Endocrinology, Valencia,Spain
Childhood obesity has reached epidemic proportions worldwide and is associ-ated with increased cardiovascular mortality and morbidity in adult life. It currentlyaffects 13,9% of children in Spain, and the prevalence appears to be increasingdramatically. Both dietary and physical activity patterns have been emphasizedas appropriate interventions for the prevention of childhood obesity.Purpose: To investigate the effects of two different exercise programs associatedwith diet on blood pressure and body composition in obese Spanish boys.Methods: Forty eight boys (mean age 12 + 1,2 years, BMI 31 + 3,2 kg/m2) wererandomly assigned to control group, aerobic exercise group (10 minutes warm-
up, 40 minutes above 70% HRmax, 10 minutes cool-down) or combined aerobicand resistance exercise group (10 minutes warm-up, 40 ‘circuit training’ and 10minutes cool-down). Both exercise programmes consisted of 3 supervised groupsessions per week, and were conducted for 4 months. All children followed anage-adjusted low-caloric diet during the study period. Baseline and outcome mea-sures consisted of calculation of body composition (tricipital and abdominal skinfolds, body circumferences and waist to hip ratio) and basal blood pressure.Results: We observed a significant reduction in BMI [from 31 + 3,2 kg/m2 to27 + 3,8 kg/m2 (aerobic group) and to 26 + 3,5 kg/m2 (combined aerobic andresistance exercise group), p<0.001], although no significant differences werefound between both exercise groups. There was a trend in basal blood pressureto decrease in both exercise groups compared to control, whilst results didn’tachieve statistical significance.Conclusion: Future studies implementing exercise programmes of longer dura-tion and higher intensity are needed to check their effects on body composition.
P5410 Cardiovascular, autonomic and antioxidant benefitsinduced by exercise training associated with estrogenreplacement in a menopause experimental model
K. De Angelis1, J. Paulini1, K. Flues1, S.M.R.R. Lima1,T.G. Fernandes2 , E.M. Krieger2, A. Bello-Klein1, M.C. Irigoyen2.
1Heart Insitute, University of Sao Paulo, Medical School, Sao Paulo, Brazil;2Federal University of Rio Grande do Sul, Porto Alegre, Brazil
The protection of young women from coronary events is sharply reduced withmenopause. Oxidative stress and impairment in baroreflex control of circulationhave been demonstrated to increase cardiovascular risk. On the other hand ex-ercise training has been indicated as non-pharmacological treatment for manycardiovascular and metabolic diseases. The aim of the present study was to eval-uate the effects of exercise training and estrogen replacement (ER) on arterialpressure (AP), baroreflex sensitivity, autonomic control of heart rate (HR) andantioxidant enzymes activities in ovariectomized rats. Female Wistar rats weredivided in sedentary ovariectomized (SO, n=9), sedentary ovariectomized+ER,(SOE, n=9) and trained ovariectomized+ER, (TOE, n=9). The ER was performedusing a 0.25 mg. 8-week sustained release pellet. Trained groups were submit-ted to an exercise training protocol on treadmill for 8 weeks. AP signals wererecorded using a data acquisition system (CODAS, 2 KHz). The baroreflex sen-sitivity was evaluated by the tachycardic (TR) and bradycardic (BR) responsesto AP changes induced by sodium nitroprusside and phenylephrine, respectively.Vagal (VT) and sympathetic (ST) tonus of HR were determined using methylat-ropine and atenolol. Catalase (CAT) and superoxide dismutase (SOD) activitieswere determined in myocardium. The TOE group showed mean AP reduction(115 ± 2 mmHg) as compared to SO group (122 ± 3 mmHg) and SOE group(121 ± 3 mmHg). The TOE rats presented an improvement in TR (3.2 ± 0.2bpm/mmHg) when compared to SO (2.7 ± 0.1 bpm/mmHg) and SOE rats (2.4 ±0.2 bpm/mmHg), however, BR was similar between groups. VT were reduced inSO group (31 ± 5 bpm) in relation to SOE (61 ± 7 bpm) and TOE (51 ± 6 bpm)groups. Exercise training decreased ST (TOE: 45 ± 10 vs. SO: 79 ± 7 bpm). ERinduced increase in SOD in SOE (48%) and TOE (54%) groups as compared toSO group. CAT activity was enhanced only in TOE animals (38%) in relation toSO animals. These results indicated that exercise training induced additional car-diovascular and antioxidant benefits in ovariectomized rats submitted to estrogenreplacement, suggesting a positive role of this association in the management ofcardiovascular risk factor in postmenopause women.
P5411 Carvedilol treatment does not limit the prognosticvalue of rest and exercise clinical variables in chronicheart failure patients
A.S. Ferraz1, M.M.F. Silva1, M.K. Arantes1, C.C.F. Carvalho1,A.C.B. Rodrigues1, T.S. Ferraz2, R.S. Meneghelo1 , L.S. Piegas1.
1Institute Dante Pazzanese of Cardiology, Cardiac Rehabilitation Department,Sao Paulo, Brazil; 2University of S Paulo R Preto Medical School, Cardiology,Sao Paulo, Brazil
Background: The ventilatory and gas exchange responses to exercise (CPX),particularly peak oxygen consumption (VO2), rest echocardiography (Echo) andsome clinical variables have been applied for the prognostic evaluation of patients(pts) with chronic heart failure (CHF). However, recent studies have suggestedthat carvedilol may decreases the prognostic value of these parameters. There-fore, we sought to investigate the prognostic value of those variables in pts treatedwith carvedilol.Methods: We analyzed 174 consecutive pts, 149 men, 49.8 ± 11.1 yrs (mean± sd), with CHF functional class II-IV (NYHA), 140 pts with non-ischemic dilatedcardiomyopathy, mean ejection fraction (LVEF) 32.0 ± 10.3%, left ventricle enddiastolic diameter (LVEDD) 72.5 ± 10.0 mm, VO2 16.0 ± 5.4 mL/kg/min. Patientswere followed during 32.9 ± 20.7 months and the composite end point was car-diac death or urgent heart transplantation (D/TX). Pts were divided in 2 groups:carvedilol treatment group (CT) - 68 pts and non-carvedilol (NC)- 106 pts. Atbaseline, all pts underwent maximal treadmill CPX - peak respiratory exchangerate (RER) = 1,18 ± 0,14 and Echo.Statistics: Analysis of covariance procedures were used to assess carvedilolinteraction to clinical, Echo data and exertional differences beween groups.The
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Childhood obesity 949
variables that showed significant association with outcome (p<0,02) at univari-ate Cox regression were included in the survival analysis on the basis of theCox proportional hazard model (multivariate analysis). Survival was estimated byKaplan-Meier method, significance: p < 0,05.Results: According to D/TX the univariate analysis showed significance to: hospi-talization (HO), functional class, peak VO2, slow periodic oscillation (SPO), peakoxygen pulse (VO2/HR), peak minute ventilation (VE), VE/VCO2 slope, VE/VCO2slope/VO2, Circulatory power (product of systolic arterial pressure and VO2),VE/VO2, % max. predicted VO2, LVEDD and LVESD. Carvedilol treatment andLVEF were not significant. After multivariate analysis only three variables still pre-sented statistical prognostic power: In CT - VO2 Hazard ratio (HR) = 0.909 (CI95% 0.829-0.996) p=0.040, SPO HR = 1.924 (CI 95% 1.083-3.419) p=0.026 andHO HR = 1.867 (CI 95% 1.151- 3.030) p=0.011. In NC - VO2 Hazard ratio (HR)= 0.901 (CI 95% 0.821-0.988) p=0.026, SPO HR = 2.074 (CI 95% 1.155-3.723)p=0.015 and HO HR = 1.811 (CI 95% 1.112- 2.947) p=0.017.Conclusions: In this CHF population peak VO2, SPO and HO were the mostpowerful predictors of D/TX and carvedilol did not limit its prognostic value.
P5412 First in man: effect of metoprolol CR/XL on exercisecapacity and subsequent variation in PulmonaryArtery Pressure in Heart Failure patients using aninnovative implant involving acoustic telemetry
K. Parikh1, H.A. Shah2, A.M. Naik2, H.A. Baxi2, M.C. Chag2,A.H. Chandarana2 , A. Hjalmarson3, Y. Rozenman4 on behalf of The Heart CareClinic. 1 The Heart Care Clinic, Dept. Of Cardiology, Ahmedabad, India; 2TheHeart Care Clinic, Ahmedabad, India; 3Goteborg University, Goteborg, Sweden;4The Edith Wolfson Medical Center, Tel Aviv, Israel
Purpose: Limitation of exercise capacity is seen in congestive Heart Failure(CHF) with increased Left Ventricular End Diastolic Pressure; Pulmonary ArteryPressure(PAP)and PA Diastolic Pressure(PADP). Metoprolol CR/XL(MXL) hashowever shown to improve morbidity and mortality in CHF. This study evaluatesthe effect of MXL on exercise capacity and PAP in patients with CHF, using Re-mon CHF implant (Impressure® ), a first of its kind device for the non-invasivemonitoring of PAP.Methods: It was a first-in-man, prospective, single arm study. 10 NYHA classIII/IV CHF patients (LVEF 26.5±4.3%) had Impressure placed via internal jugularvein permanently in the Right PA. Using ultrasonic signals it generates the PAPwaveforms on the desktop system. All the patients underwent Treadmill test (TMT)and PAP was measured before and after the exercise. MXL 25mg/day was thenloaded in all the patients and uptitrated two weekly using the MERIT-HF criteriato reach 200mg/d dose, with regular follow up TMT and PAP monitoring.Results: 8 out of 10 patients were taken into analysis.All the 8 patients had symp-tom limited TMT. The baseline mean±SD exercise time(EXtime) was 6.8±2.2mins and 8.4±2.2 METS (metabolic equivalents). The baseline rest PAP was30.6±9.1/16.1±8.0 mm Hg, which after TMT rose to 46.4±14.7/22.6±10.5mm Hg (p<0.05). After 2 weeks of loading 25mg/d MXL, the EXtime was6.96±2.2 mins and METS 8.6±2.3. The post TMT PAP was 51.6±15.9/23.7±9.9mmHg (p<0.05 for systolic PAP rise). After 50mg/d MXL dose EXtime was7.86±2.7 mins (p=0.09) and METS 9.4±2.6. PAP post TMT didnot show sig-nificant change as compared to previous follow up. On reaching 100mg/dMXL, there was no significant change in the Extime, METS or post TMT PAP(52.5±18.1/23.4±9.6 mmHg. On reaching the target dose of 200mg/d MXl, theEXtime and METS increased significantly to 8.0±2.6 mins and 9.7±2.6 respec-tively (p=0.03 for both), however no significant change was observed in post TMTPAP (52.1±17.7/23.6±8.6 mmHg). Post TMT Heart Rate decreased significantlyfrom 106±9 per min at baseline to 89±13 per min at 200mg/d MXL (p=0.01).Conclusions: MXL treatment in CHF patients produce a slight insignificant in-crease in systolic PAP at baseline and after exercise (with decrease in peak exer-cise systemic BP and HR) but improves the exercise capacity in selected patients.This supports the recommendation for slow and careful uptitration of MXL in CHFpatients.
P5413 First in Man: non invasive measurement of variationin Pulmonary artery pressure following exercise inheart failure patients using an innovative implantabledevice involving acoustic telemetry
K. Parikh1, H.A. Shah1, A.M. Naik1, H.A. Baxi1, M.C. Chag1,U.G. Shah1, A. Hjalmarson2, Y. Rozenman3 on behalf of The Heart Care Clinic.1The Heart Care Clinic, Dept. Of Cardiology, Ahmedabad, India; 2GoteborgUniversity, Goteborg, Sweden; 3The Edith Wolfson Medical Center, Tel Aviv,Israel
Purpose: Increase in Left Ventricular End Diastolic Pressure (LVEDP), Pul-monary artery (PA) pressure and limitation of exercise capacity are common find-ings in Congestive Heart Failure (CHF). An implantable device responding to ul-trasonic signals named the Remon CHF implant (Impressure®) is a first of its kindfor the noninvasive monitoring of PA pressure. The study investigates pulmonaryhemodynamic changes during exercise and its relationship with exercise capacityin CHF.Methods: It was a First-In-Man, prospective, single center, single arm study.10 NYHA class III/IV CHF patients with LVEF 26.5±4.3% were enrolled for
the Impressure® (3mm x 3mm x 16mm) implantation, a device placed percu-taneously via internal jugular vein, permanently in the Right Main PA. It respondsto ultrasonic signals to a desktop system and generates the PA pressure wave-form. Treadmill Exercise test (TMT) following standard Bruce Protocol was doneat the end of one month of the implantation. PA pressure was measured im-mediately before and after the exercise and on recovery using the noninvasiveImpressure® .Results: All the patients finished the symptom limited TMT with a peak heartrate of >90% of targeted heart rate. The mean±SD exercise time was 6.37±2.2minutes, corresponding to 8 ± 2 metabolic equivalents. Resting PA pressureswere 32.7±11.1/17.1±7.8 mm Hg. The PA pressure immediately after the TMTwas 49.0±17.9/24.1±11.2 mm Hg. The systemic blood pressure preTMT was111±18/71±7mmHg which post TMT rose to 144±28/82±10mmHg (p<0.01).The mean heart rate preTMT 81±3 beats/min after exercise increased to 105±19beats/min (p=0.001). The mean increase in the PA pressure due to exercisewas 16.3(±10.2) mm Hg systolic (p<0.001) and +6.9(±5.8) mm Hg diastolic(p=0.004).Conclusions: The study shows a significant rise in PA pressure and more impor-tantly, PA Diastolic pressure following exercise in CHF patients limiting their exer-cise capacity. This increase in PA pressure may be secondary to either ischemiaor Left ventricular dysfunction or both. Management of these CHF patients shouldbe tailored to avoid this exertional rise in PA Diastolic pressure either by avoidingischemia or by improving Left ventricular dysfunction. Noninvasive measurementby this novel device, Impressure® may assist in daily precise management ofthese patients.
P5414 NTproBNP: evaluation of a fast method for itsmeasurement
F. Marques, C. Fonseca, P. Morais Sarmento, R. Covas, A. Minez,J. Esperanca Pina, F. Ceia, A. Aleixo. S. Francisco Xavier Hospital,Medicine, Lisboa, Portugal
The N-terminal portion of the pro Brain Natriuretic Peptide (NT-proBNP) is an im-portant marker in establishing the diagnosis and the prognosis of cardiovascularpatients. Fast and precise assays for its evaluation are currently under investiga-tion.Aim: to compare two methods for NTproBNP evaluation, the ELECSYS 2010,Roche analyser, and the heterogeneous immunoassay utilising the DimensionRXL sandwich method (NTproBNP-DADE), in order to establish its feasibility andaccuracy in daily practice in a Heart Failure Unit, and in the Emergency room.Methods and Population: 192 tests were performed in 120 patients consecu-tively admitted to an Internal Medicine Department with a broad diagnosis specr-tum, 68 men, aged 69±12, and 52 women, aged 72±14. The two methods werecompared in the overall population, and according to gender and age (80), byWilcoxon t test and linear regression.Results: ELECSYS ranged between 9.9 and 65650, NTproBNP-DADE, 52 to47871. NTproBNP-DADE values (mean: 3467.99±5410.70, median 1554.5) werehigher than ELECSYS (mean: 3615.20±6813.35, median 1387.5). A strong cor-relation between the two methods was found: Global population: R2 = 0.96, forregression adjustment ELECSYS= 1.2362 x DADE - 672.1 (Fig). Men: R2 = 0.96,for regression adjustment ELECSYS = 1.211 x DADE - 685.3, women: R2 = 0.99for regression adjustment ELECSYS = 1.316 x DADE - 738.3. 80 (n = 47).
Fig. 1. NTproBNP ELECSYS and DADE correlation
Conclusions: We found good correlation between NTproBNP-DADE an ELEC-SYS measurement, independently of gender, and age; NTproBNP-DADE, amethod faster than the ELECSYS-NTproBNP, can be safely used in the dailypractice, namely in the Emergency room.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

950 Childhood obesity
P5415 Comparison of C-reactive protein level forcardiovascular disease and chronic disorders
L.L.H. Lund Haheim1, I.O. Olsen2, P.N. Nafstad2, P.S. Schwarze3,K.S.R. Skjold Ronningen1. 1Norwegian Knowledge Centre for theHealth Ser, Oslo, Norway; 2University of Oslo, Institute of Oral
Biology, Oslo, Norway; 3Norwegian Institute of Public Health, Oslo, Norway
Background: C-reactive protein (CRP) is a well known marker of unspecified in-fections. Its predictive role in myocardial infarction is being investigated. We com-pared the level of CRP in myocardial infarction, stroke, angina pectoris, diabetes,chronic bronchitis/emphysema, asthma, osteoporosis, fibromyalgia/chronic painsyndrome and oral infections.Methods: In all 5,323 men took part in the first and second health screeningof the Oslo Study in 1972/73 and 2000. Questionnaire information on medicalhistory recorded at the second screening is used to identify men with relevantdiseases. Serum samples collected in 2000 were stored for later analyses of C-reactive protein.Results: Men with myocardial infarction, asthma, chronic bronchitis, diabetes,osteoporosis or fibromyalgia and men without hey fewer, had significantly ele-vated levels of CRP versus non-cases. Other cardiovascular diseases as anginapectoris and stroke did not. Nor did current subjects with oral infections showelevated levels of CRP relative to non-cases. Men with a history of osteoporo-sis had the highest mean values, 6.53 versus 3.55μg/ml in subjects without dis-ease. Cases of asthma also had an increased mean CRP-level of 5.01 versus3.47μg/ml in subjects without disease. Diabetic men had 4.53 versus 3.53 μg/mlin non-diabetic men and, likewise, men with a history of myocardial infarction 4.27versus 3.59 μg/ml in non-cases. Quartile analyses of CRP-risk relative to lowestquartile value (Q1) showed differences that possibly reflect the acute or chronicstages of the diseases. Myocardial infarction, diabetes, asthma and chronic bron-chitis/emphysema showed highest relative risk for Q2 declining for higher quartilevalues. Osteoporosis had highest value for Q3 and fibromyalgia/chronic pain syn-drome for Q4.Conclusions: Significant elevated levels of CRP are confirmed in diseases ofnon-infectious origin. The CRP-level reflects both acute and chronic conditions.Chronic conditions have a different risk distribution per CRP-level than acute in-fections.
P5416 Impact of exercise training versus PCI uponinflammatory markers in stable coronary arterydisease: 2-year follow-up of a prospectivelyrandomized trial
C. Walther1, S. Moebius-Winkler1 , M. Bruegel2, G.M. Fiedler2,A. Linke1, J. Thiery2, G. Schuler1, R. Hambrecht1. 1University of
Leipzig, Heart Center, Cardiology, Leipzig, Germany; 2University of Leipzig,Institute of Laboratory Medicine, Leipzig, Germany
Chronic vascular inflammation may trigger ischemic heart disease whereas reg-ular physical exercise training has a protective potential. We investigated the im-pact of regular physical exercise training versus percutaneous intervention (PCI)on markers of chronic inflammation in patients with stable coronary artery disease(CAD). 101 male patients (pts) with stable CAD and an indication for revascular-ization were included into a prospectively randomized trial: 51 patients receivedregular exercise training (ET) and 50 percutaneous coronary intervention (PCI).Inflammatory markers (high sensitive C-reactive proteine (hsCRP), interleukin-6(IL-6), fibrinogen and leukocytes) were analyzed at baseline and after 2 years.Exercise capacity was determined by ergospirometry. Ischemic end-points (car-diovascular death, non-fatal myocardial infarction, cerebrovascular accident, needfor any revascularization procedure due to unstable angina pectoris and hospital-ization due to worsening of angina pectoris) were evaluated. At 2 years maximaloxygen consumption (VO2max) increased by 10% (ET, from 23.3 ± 0.6 to 25.7± 1.0 mL O2/kg/min; p=0.0171) versus 7% (PCI, from 22.3 ± 0.8 to 23.9 ± 1.2mL O2/kg/min; p=0.4248). ET led to a significant reduction in hsCRP levels by41% (from 3.08 ± 0.56 to 1.81 ± 0.25 mg/dL, p=0.025 versus baseline) and inIL-6 levels by 18% (from 43.7 ± 4.4 pg/L to 35.7 ± 3.1 pg/L, p=0.023). No rel-evant changes of inflammatory markers were seen in the PCI group. Event-freesurvival rates after 24 months were 78% (ET) versus 62% (PCI) (p=0.039). Pa-tients with ischemic events had significantly elevated hsCRP levels (4.8 ± 0.84versus 2.85 ± 0.58 mg/L in pts without ischemic events, p=0.0041). Regular phys-ical exercise leads to a reduction of hsCRP and ischemic events in patients withstable CAD. This finding is consistent with the hypothesis that exercise trainingreduces cardiovascular ischemic events in pts with stable CAD at least partiallyby an attenuated vascular inflammation.
Abstract P5418 – Table 1. 1-year incidence: Japan vs rest of world
Total (n=63,129) Multiple risk factor only (n=11,444) CAD (n=37,542) CVD (n=16,648) PAD (n=7,232)Japan Others Japan Others Japan Others Japan Other Japan Others
(n=4,844) (n=58,285) (n=814) (n=10,630) (n=2,151) (n=35,391) (n=1,893) (15,558) (n=599) (n=7,075)
Cardiovascular death (%) 0.76 1.59 0.28 0.63 0.91 1.86 0.74 1.94 0.42 2.54Non-fatal myocardial infarction(%) 0.79 1.18 0.59 0.77 1.04 1.47 0.45 1.06 1.00 1.43Non-fatal stroke (%) 1.83 1.62 1.39 0.78 1.14 1.35 3.01 3.85 2.27 1.75CV death/MI/stroke (%) 3.19 3.52 2.14 1.53 2.92 3.76 4.08 5.85 3.23 4.69CV death/MI/stroke/hospitalization for atherothrombosis(%) 6.31 13.40 2.39 5.47 8.04 15.77 6.19 15.57 11.76 23.07Hospitalization for bleeding events (%) 0.37 0.85 0.00 0.56 0.43 0.89 0.40 0.99 0.76 1.32Hospitalization for congestive heart failure (%) 0.78 3.54 0.22 1.91 1.48 4.64 0.53 3.69 1.22 4.71
P5417 Abdominal obesity is an additive marker of risk forcardiovascular disease in primary care patients inPortugal
M. Cardoso1, E. Mendes2, V. Gil3 on behalf of W-Risk investigators. 1Faculdade de Medicina, IHMS, Coimbra, Portugal; 2APMCG, -,
Lisboa, Portugal; 3Hospital Fernando Fonseca, Cardiology, Amadora, Portugal
Introduction: No reliable data exists about the role of abdominal obesity (AO) asa marker of cardiovascular risk (CVR) in Portugal.Purpose The importance of AO as a marker of CVR was analyzed through adescriptive analysis of a Primary Care Physician population aged 18 years orolder in Portugal.Methods W-Risk, a non-interventional cross-sectional study, allowed to deter-mine the prevalence of obesity (BMI: kg/m2), AO - measured by waist circumfer-ence (WC; cm), CVR factors and cardiovascular disease (CVD), using a standard-ized questionnaire, in 14,695 subjects (mean age 55.5 ±16.2 years; F: 65.8%)consulting their primary care physician (n=1,500) in Portugal. CVD was consid-ered to be present if patients had angina or previous myocardial infarction, strokeor transient ischemic attack.Results Prevalences of overweight, obesity and AO were respectively 46.9%,27.2% and 66.3% in men, and 35.9%, 34.6% and 82.9% in women. The stan-dardized prevalences of hypertension, diabetes and hypercholesterolemia wererespectively: 33.1%, 9.2% and 37.8%. The age adjusted odds ratio of the majorCVR factors and respective CIs (95%), for the presence of CVD, before and afteradding AO (IDF definition for WC: women >80 cm; men >94 cm) are shown intable 1.
Table 1. Addition of AO to major Risk Factors
RISK FACTOR OR for CVD OR for CVD
Hypertension 2.5 (2.1 - 3.0) Hypertension + AO 3.8 (2.8 - 5.1)Diabetes 1.6 (1.4 - 1.9) Diabetes + AO 2.4 (1.9 - 3.0)Hypercholesterolemia 1.6 (1.3 - 1.8) Hypercholesterolemia + AO 1.9 (1.5 - 2.5)
Conclusions: Abdominal obesity is an additive marker of CVR to traditional ma-jor risk factors, whenever present in a non-selected large cohort of patients inPrimary Care practice in Portugal.
P5418 Cardiovascular events of Japanese patients withatherothrombosis compared with other parts of theworld: results from the REduction ofAtherothrombosis for Continued Health (REACH)Registry
S. Goto1, T. Yamazaki2, Y. Ikeda3, P. Gabriel Steg4, D.L. Bhatt5,S. Uchiyama6, H. Origasa7 on behalf of REACH Registry Investigators. 1TokaiUniversity School of Medicine, Division of Cardiology, Kanagawa, Japan; 2TokyoUniversity, Tokyo, Japan; 3Keio University, Tokyo, Japan; 4AP-HP HopitalBichat-Claude Bernard, Department of Cardiology, Paris, France; 5ClevelandClinic Foundation, Department of Cardiovascular Medicine, Cleveland, UnitedStates of America; 6Tokyo Women’s Medical University, Tokyo, Japan; 7ToyamaMedical and Pharmaceutical University, Toyama, Japan
Background: The REACH Registry involves outpatients from around the worldwith documented or at high risk of atherothrombosis. One-year outcomes ofJapanese patients were compared with other parts of the world.Methods: A total of 68,223 patients at high risk of atherothrombosis (coronaryartery disease [CAD], cerebrovascular disease [CVD], or peripheral artery dis-ease [PAD]) were recruited from 44 countries including 27,739 patients fromNorth America, 23,728 from Europe, and 5,197 from Japan. One-year outcomesdata obtained so far for 4,844 Japanese patients with a follow-up rate of 91.4%(4,030 symptomatic atherothrombosis; 814 asymptomatic high-risk patients) werecompared with 58,285 patients recruited from the other 43 countries worldwide(47,655 symptomatic patients; 10,630 asymptomatic high-risk patients).Results: As shown in the table, the lower incidence of 1-year outcome of car-diovascular (CV) death, non-fatal myocardial infarction and equivalent onset ofnon-fatal stroke was demonstrated in Japanese patients compared with the othercountries, in spite of the fact that the use of aspirin (54.8% of total patients) andstatins (44.6%) was lowest in the world.Conclusions: Our results demonstrate a lower rate of CV death or non-fatal my-ocardial infarction in Japanese patients compared with the rest of world, despitethe lower use of aspirin and statins. This may be due to elements of the Japaneselifestyle and/or genetic characteristics.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 951
NOVEL ASPECT OF MYOCARDIAL AND PERICARDIALDISEASE
P5419 The significance of polymorphisms and intronicvariants in MYBPC3: Pitfalls in genetic diagnosis ofhypertrophic cardiomyopathy
R. Frank-Hansen1 , P.S. Andersen1, O. Havndrup2, H. Bundgaard1 ,W.J. Mckenna3, M. Christiansen2. 1Statens Serum Institut,
Department of Clinical Biochemistry, Copenhagen, Denmark; 2Rigshospitalet,The Heart Center, Copenhagen, Denmark; 3University College London, TheHeart Hospital, London, United Kingdom
Familial hypertrophic cardiomyopathy (FHC) is primarily caused by mutations ingenes encoding cardiac sarcomere proteins. Large mutation screening studiesfocusing on the coding sequence identify mutations in 35 - 65% of the examinedfamilies and 15-30% of those are found in MYBPC3 coding for the myosin bind-ing protein C. Apart from clearly disease-causing mutations, mutation screen-ing often leads to the identification of exonic polymorphisms and mutations inexon-near intronic sequence. The significance of these sequence variants is notclear, but theoretically they may interfere with pre-mRNA splicing by disruptingsplice enhancers or silencers, branch point sites or polypyrimidine tracts. In 81patients with FHC we identified 7 exonic polymorphisms (allelic frequency) inMYBPC3: V158M (9%), A179A (8%), S236G (9%), T262T (18%), V849V (3%),V896M (4%) and E1096E (38%). Using in silico prediction of interference withSR-protein exonic splice enhancers (ESEfinder), we found that 4 polymorphisms,T262T, V849V, V896M and E1096E, significantly reduced splice efficiency. In 250probands with FHC we screened the intronic sequences surrounding the micro-exons 10 and 14 in MYBPC3 for mutations and identified a total of 7 mutations(of which 5 were novel) and used in silico prediction (NetGene2) to assess theinterference with splicing. RT-PCR performed on mRNA isolated from periph-eral leukocytes was used to directly assess interference with splicing. Among theseven mutations identified c.1226+49C>T is a common polymorphism and wasnot found to affect splicing by RT-PCR. None of the other mutations were found innormal controls. The c.906-36G>A mutation introduces a new acceptor splicesitewith the final result that exon 10 increases to 37 bp, leading to a frameshift. Thec.906-1G>C mutation results in exclusion of the first 2 bases of exon 10, againcausing a frameshift. c.1224-19G>A generates de novo 3’-splicesites whereasc.906-1G>C and c.1224-2A>G disrupts the original 3’splicesite. The mutationsc.906-15G>C and c.908+39G>A do not affect splicing. Thus, both exonic poly-morphisms and intronic mutations in MYBPC3 may affect pre-mRNA splicing andthis should be taken into account when interpreting genotyping results in HCMfamilies. The effect of more subtle interference with splicing seen with exonicpolymorphisms could contribute to the phenotypic heterogeneity of HCM. Thespecific effect on the splicing of MYBPC3 pre-mRNA can be predicted using insilico methods and directly assessed by RT-PCR on mRNA from peripheral leuko-cytes.
P5420 Molecular analysis of Hypertrophic cardiomyopathy in380 index patients
P. Richard1, D. Brito2, A. Serio3, S. Morner4, A. Diaz5, A. Richter6,C. Hengstenberg7, R. Isnard8 on behalf of Eurogene Heart FailureGroup. 1Hopital Pitie-Salpetriere, UF Cardiogenetic et Myogenetic,
Paris, France; 2Lisboa, Portugal; 3Pavia, Italy; 4Umea, Sweden; 5Barcelona,Spain; 6Marburg, Germany; 7Rengensburg, Germany; 8Paris, France
Purpose: to evaluate the frequency and distribution of the main sarcomeric pro-tein genes mutations in an European cohort of patients with Hypertrophic car-diomyopathy (HCM) by direct sequencing.Patients and Methods: 380 unrelated index patients with familial (n=157) orsporadic HCM (n=223) were collected from 7 different European countries. Allthe coding sequences of the 2 major genes encoding beta myosin heavy chain(MYH7), and myosin binding protein C (MYBPC3) known to be responsible forHCM were sequenced. In patients without identified causative mutations, threeother genes encoding troponin T, troponin I, and myosin regulatory light chain(TNNT2, TNNI3 and MYL2) were then sequenced.Results: a mutation was identified in 205 patients (56%) ranging from 65% and35% according to centres. MYBPC3 and MYH7 were the most frequently involvedgenes (respectively, 64% and 30% of mutated patients). The same rate and distri-bution of mutations were found between familial and sporadic cases. Most of theobserved mutations (80% in MYBPC3 and 75% in MYH7) were described for thefirst time. Missense mutations were preferentially found in MYH7 and nonsensemutations (2/3) in MYBPC3. Finally, 10% of patients had two mutations: in someof them, both variations were pathogenic, but in others, one mutation seemed tohave only a modifier role on the phenotype.Conclusions: in this European cohort of unrelated index patients with HCM, themolecular defect is identified in 56% of patients. MYBPC3 and MYH7 are the mostfrequently involved genes in all the countries. More than 75% of the identifiedmutations are novel, indicating that the molecular diagnosis cannot be assessedby testing for known mutations, but needs the sequencing of the whole genes.
P5421 Uptake of predictieve genetic testing in hypertrophiccardiomyopathy
I. Christiaans, I.M. Van Langen, L.M. Dijksman, E. Birnie,G.J. Bonsel, A.A.M. Wilde. AMC, Klinische Genetica, Amsterdam,Netherlands
Introduction: Hypertrophic cardiomyopathy (HCM) is an autosomaldominant disease occasionally associated with sudden cardiac death (SCD) atyoung age if untreated. Genetic counselling and cascade-screening for HCMstarts with a proband. After the detection of a pathogenic mutation (in 60% ofcases, of which half is due to one founder mutation: the 2373insG MYBPC3 genemutation) the proband informs the relatives, by means of a family letter, about theaims and possibilities of predictive genetic testing. Carriers of a disease-causingmutation are referred for cardiological screening and regular follow-up aiming atreduction of SCD.Aim: This study focused on the family members’ uptake of genetic counsellingand predictive testing and the relationship between SCD in a first degree relativeand uptake.Results: In 46 families with the 2373insG Dutch founder MYBPC3 gene muta-tion, on average 2.41 first degree relatives attended for genetic counselling in thefirst year, corresponding with 43.9% of all eligible first degree relatives. This num-ber declines in more distant relatives (Table 1). All family members who attendedgenetic counselling proceeded with presymptomatic DNA-testing. The total num-ber of identified carriers was 1.74 per proband. There was a trend towards ahigher uptake in families in which SCD had occurred (odds ratio 3.00, 95%CI:[0.69-13.04]).
Table 1. Average number of family member
First degree Second degree Third degree Fourth degree Total(n= 111) (n= 38) (n= 22) (n= 3) (n= 174)
Mean (SD) 2.41 (2.65) 0.83 (1.32) 0.48 (1.33) 0.07 (0.33) 3.65 (3.95)
Conclusion: This is the first report on uptake of predictive genetic testing in ahereditary heart disease. Less than half of the eligible relatives opted for geneticcounselling. Research into the determinants of the uptake, including the processof invitation, is needed.
P5422 Cardiac manifestations and genotype-phenotypecorrelations in carriers with the STA gene mutations
K. Sakata1, H. Ino2, N. Fujino2, K. Uchiyama2, K. Hayashi2,T. Konno2, T. Fujita2, M. Yamagishi2. 1Ishikawa Prefectural CentralHospital, Cardiology Department, Kanazawa, Japan; 2Kanazawa
University, Cardilogy pepartment, Kanazawa, Japan
Purpose: Emery-Dreifuss muscular dystrophy (EDMD) is characterized by skele-tal myopathy and cardiac involvement. The STA gene encodes emerin and isone of genes that is affected in EDMD. We previously reported the cardiac man-ifestations in patients with X-linked recessive Emery-Dreifuss muscular dystro-phy (EDMD) caused by a nonsense mutation of the STA gene. However, thegenotype-phenotype correlations are not defined well. The aim of this study is toclarify the genotype-phenotype correlations in more patients with EDMD causedby the STA gene mutations.Methods: We surveyed additional family members of patients with Trp226Stopmutation in the STA gene, and analyzed STA gene mutations in a new patient withEDMD. Mutations were screened by the PCR-SSCP method and direct sequenc-ing analysis. Clinical phenotypes were determined using electrocardiography andechocardiography.Results: We identified totally 16 carriers (7 males and 9 females) in the two fam-ilies with a Trp226Stop mutation in the STA gene. In addition, we also identifieda de novo patient with a novel mutation (Gln222Stop) in the STA gene. Both car-riers with Trp226Stop or Gln222Stop mutation displayed atrial cardiomyopathy,atrial arrhythmia and dilatation. None of the patients demonstrated features sug-gestive of dilated cardiomyopathy at any age. And pacemaker implantation wasrequired for treatment of bradyarrhythmias (complete AV block, sinus node dys-function, and atrial fibrillation) in not only male carriers but also female carriers.The majority of carriers with Trp226Stop mutation had not been clinically diag-nosed as having EDMD prior to genetic testing because of extremely mild or non-existent skeletal myopathy. By contrast, skeletal myopathy was typical in thosewith Gln222Stop mutation.Conclusions: EDMD caused by STA gene mutations is characterized by infre-quent X-linked inheritance. Mutation screening for STA gene should be consid-ered in familial and sporadic cases of atrial cardiomyopathy such as atrial arryth-mias and dilatation even in females. The remarkable skeletal muscle phenotypevariability in the STA gene mutations suggests the existence of additional geneticand/or environmental factors.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

952 Novel aspect of Myocardial and Pericardial disease
P5423 Differences in diagnostic value of various criteria ofnegative T waves for hypertrophic cardiomyopathy ina genotyped population
T. Konno, H. Ino, N. Fujino, K. Hayashi, T. Hayashi, K. Uchiyama,Y. Sakamoto, M. Yamagishi. Kanazawa University, Molecular
Genetics of Cardiovascular Disorder, Kanazawa, Japan
Purpose: Negative T waves are one of the major ECG criteria for hypertrophiccardiomyopathy (HCM), and are frequently observed in patients with HCM. How-ever, differences in the diagnostic values of various definitions of negative Twaves for HCM have not yet been clarified in a genotyped population. We aimedto determine the most accurate diagnostic definition of negative T waves for de-tecting carriers of HCM, and to examine the association between phenotypes andthe diagnostic value of negative T waves.Methods and Results: Electrocardiographic and echocardiographic findingswere analyzed in 161 genotyped subjects (97 genetically affected, 64 unaffected)from 20 families with disease-causing mutations in 4 genes (MYH7, MYBPC3,TNNT2, TNNI3). We applied 3 different criteria for negative T waves that wereused in previous reports. The criteria for negative T waves were defined as fol-lows: Criterion 1, negative T wave >10mm in depth in any leads; Criterion 2,negative T wave >3mm in depth in at least two leads except aVR, V1 and V2;and Criterion 3, negative T wave >1mm in depth in at least two leads exceptaVR, V1 and V2. Of the 3 criteria, Criterion 3 showed the highest sensitivity (5%vs 26% vs 43%, p<0.0001) and retained a specificity of 100%, resulting in thehighest accuracy (43% vs 55% vs 66%). Using Criterion 3, carriers with negativeT waves showed greater maximal wall thickness than those without negative Twaves (19.0±5.2mm vs. 13.5±5.1mm, p<0.0001). Negative T waves were ob-served in only 12.9% of non-hypertrophic carriers, whereas abnormal Q waveswere seen in 22.6% of non-hypertrophic carriers.Conclusions: Criterion 3 for negative T waves may be the most accurate defini-tion for HCM based on genetic diagnoses. Furthermore, negative T waves maybe useful for detecting carriers with wall hypertrophy, whereas abnormal Q wavesmay be useful for non-hypertrophic carriers.
P5424 HLA DQB1 gene polymorphism in inflammatorydilated cardiomyopathy, dilated cardiomyopathy andmyocarditis in a german population
I. Portig1, A. Sandmoeller2, S. Kreilinger1, S. Pankuweit1,B. Maisch1. 1Philipps-University, Cardiology Department, Marburg,
Germany; 2Marburg, Germany
Dilated cardiomyopathy (DCM) is a genetically heterogenous disease with mul-tifactorial etiology. It may be idiopathic, familial/genetic, viral or autoimmune-mediated. Myocarditis is an inflammatory disease of the myocardium and mayheal or lead to DCM or inflammatory DCM (DCMi). In a patient subset, myocardi-tis, DCMi and DCM are thought to represent the acute and chronic stages of anorgan-specific disease of the myocardium. A pivotal role for autoimmunity in asubstantial proportion of these patients is supported by the presence of heart-specific autoantibodies and T cell infiltrates.Methods: To identify genetic factors in the immune system which might controlthe susceptibility to DCM, HLA class II gene polymorphisms were analyzed byusing the PCR/SSP techniques. HLA class II DQB1 allele typing was performedin 57 unrelated DCM and myocarditis patients (DCM in 22, DCMi in 19 with leftventricular enlargement plus reduced ejection fraction < 55% and myocarditis in16 with normal ejection fraction). Detailed clinical diagnoses were established byechocardiographic, hemodynamic and immuno-histochemical methods. The con-trol group consisted of 44 patients with non-inflammatory cardiac diseases otherthan DCM (arterial hypertension and arrythmias) and normal ejection fraction.Results: A significantly greater incidence of DQB1*0301 alleles in DCM, DCMiand myocarditis patients (36%, 57% and 44%) as compared to controls (14%)was found. Allelic frequencies of DQB1*0602, which is a dominant protective al-lele in Type I diabetes, were significantly lower in DCMi (11%) versus DCM (41%),myocarditis (38%) and control patients (27%).Conclusion: DQB1*02, especially DQB1*02-DQB1*03, is found in patients withmyocarditis less frequently than in those with DCMi and may thus be used asa prognostic marker in patients with myocarditis.On the other hand, DQB1*0602(and/or DQB1*02-DQB1*03) could be used as a diagnostic marker in patientswith dilated heart mucle disease and could aid in selection of patients who may begood candidates for specific anti-inflammatory therapeutic strategies and wouldtherefore profit from obtaining endomyocardial biopsies.
P5425 Prevalence and spectrum of mutations in thesarcomeric MYH7, TNNT2, MYBPC3 and TPM1 genesSpanish cardiac hypertrophy patients
M.G.C. Garcia Castro, J.R. Reguero, C. Alonso-Montes, D. Calvo,M. Martin, E. Coto, C.M. De La Tassa. Hospital Central de Asturias,
Molecular Genetics, Oviedo-Asturias, Spain
Background: Hypertrophy cardiomyopathy (HCM) is caused by mutations in atleast 11 cardiac sarcomeric genes. Three genes, MYH7, TNNT2, and MYBPC3,are responsible for most of the familial cases, and could be related with variableclinical outcomes.
Aim: The purpose of this study was to determine the spectrum and prevalence ofmutations in four sarcomere genes in a large cohort of HCM patients from Spain.Methods: DNA was obtained from 80 non-related patients diagnosed with anessential form of HCM. A total of 26 (32%) had a family history of HCM. Thecomplete coding exons of MYH7, TNNT2, MYBPC3 and TPM1 were screenedthrough SSCA and direct automated sequencing.Results: We found a total of 13 mutations in the 80 patients; 8 of the mutationswere not previously reported. The frequency of carriers of mutations in MYH7,MYBPC3, TNNT2 and TPM1 were 6%, 6%, 3% and 1%, respectively. Only two ofthese mutation carriers did not have a family history of HCM. We also determinedthe mutation-status in all the available relatives of the 13 patients, and informationabout genotype-phenotype correlations are discussed.
Main characteristics of the carriers
Gen Mutation Carriers SD Tx Septum IVS/PW EF Gradientand patients Index cases Index cases mm Hg
MYH7 F247L 2 N N 19 1.0 60% NoMYH7 R453C 2 Y Y 17 1.42 60% NoMYH7 R787C 2 Y N 19 1.46 60% 100MYH7 V822M 1 N Y 18 1.00 48% NoMYH7 R870H 2 N N 24 1.09 60% 180TNNT2 R92Q 2 Y N 19 1.4 55% NoTNNT2 R278C 4 N N 22 1.83 60% NoMYBPC3 V342D 3 N N 17 1.3 78% NoMYBPC3 Q820fs 1 N N 17 1.7 60% NoMYBPC3 A627V 4 N Y 28 1.6 58% NoMYBPC3 V771M 3 N N 18 1.6 59% NoMYBPC3 M844fs 5 Y N 17 1.0 73% 17TPM1 D175N 3 N N 32 2.46 60% 46
Y: yes; N: no. SD: sudden death.Tx: cardiac trasplantIVS/PW: interventricular septum/posteriorwall
Conclusions: Mutations in MYH7, MYBPC3, TNNT2 and TPM1 would explain16% of essential HCM in a large cohort (32% familial cases) of Spanish patients.
P5426 A newly recognized autosomal dominant isolatedquadriceps myopathy with cardiac involvement
J.C. Charniot1, M. Desnos2, K. Zerhouni3 , D. Bonnefont-Rousselot4 ,J.Z. Salama2, N. Vignat2, M. Komajda4, J.Y. Artigou2. 1Bobigny,France; 2European G. Pompidou Hospital, 75, Paris, France;
3Avicenne Hospital, 93, Bobigny, France; 4Pitie Salpetriere Hospital, 75, Paris,France
Thirty three members of a large family (75 members) with quadriceps myopa-thy and cardiac involvement underwent neurological, cardiological and ancillaryinvestigation.Cardiological abnormalities found in 12 patients (5 females) included dysrhyth-mias and atrioventricular conduction disturbances presenting as bradycardia,syncopal attacks necessitating pacemaker implantation or implantable cardiacdefibrillator (n=4), heart failure (n=2), sudden cardiac death (n=3) with 2 patientswere resuscitated following cardiac arrest.The mean age for cardiac involvement was 34 y (24-47). In 4 patients, cardiacinvolvement was associated with symmetrical weakness in the quadriceps muscleonly. Early contractures of the spine, contractures of elbows and Achilles tendonswere absent.Serum creatine kinase activity was normal in all patients. Electromyogramshowed polyphasic short duration, low amplitude motor unit action potentials withfast recruitment and muscle biopsies were consistent with muscular dystrophyand rimmed vacuoles without filamentous inclusion.In all patients, neuromuscular symptomatology preceded cardiological involve-ment.Early recognition of this myopathy with cardiac involvement offers an opportunityfor therapeutic intervention.
P5427 Mutations of the mitochondrial thioredoxin reductasegene (TXNRD2) in patients with dilatedcardiomyopathy
D. Sibbing1, S. Unwin1, H.E. Wichmann2, T. Meitinger2, A. Kastrati1,A. Schomig1, A. Pfeufer2, N. Von Beckerath1 . 1Deutsches
Herzzentrum Muenchen, Muenchen, Germany; 2GSF ForschungszentrumNeuherberg, Muenchen, Germany
Purpose: According to newer systematic studies about 20-30% of all patientsdiagnosed with dilated cardiomyopathy (DCM) have a positive family history. Fol-lowing general autosomal dominant inheritance patterns the currently known dis-ease genes and mutations account for not more than 10% of the familial andless than 5% of all DCM cases. The search for novel disease genes is ongoing.The mitochondrial thioredoxin reductase gene (TXNRD2) encodes a selenocys-tein containing enzyme important for mitochondrial radical scavenging. In Chinaan endemic cardiomyopathy (Keshan disease) exists caused by selenium defi-ciency possibly mediated via reduction of TXNRD2 enzyme activity. Heart-specificTXNRD2 knock-out mice display a phenotype with features of human DCM. Weintended to determine whether mutations of TXNRD2 would also explain a frac-tion of human DCM disease burden.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 953
Methods: We studied n=227 consecutively recruited DCM patients (n=177 male(78%), mean age=59.9±12.0yr, mean EF=26.9±9.5%) in whom secondary formsof DCM had been ruled out. Of these patients n=96 were sequenced for all 18 ex-ons of TXNRD2 - covering all three known splice variants - as well as for theselenocystein insertion sequence (SECIS) element encoded by the 3’ untrans-lated region of the mRNA. Detected amino acid exchanging variants were subse-quently genotyped in the remaining n=131 DCM patients and in n=702 personsfrom the general population (KORA survey S4).Results: Direct sequencing revealed Ala59Thr as a new, previously undescribedmutation of the TXNRD2 gene. It occurred once in a DCM patient from the se-quenced sample and was detected in a second, unrelated patient of the remain-ing sample. Ala59Thr was not observed in the exceedingly large general popu-lation sample. All other nonsynonymous variants were nsSNPs, three previouslyknown ones (Ala66Ser, Ser299Arg, Thr370Ile) and two novel ones (Arg286Ser,Gly384Ser). The nsSNPs occurred with similar genotype frequency in the generalpopulation and appeared not to be associated with DCM.Conclusions: For the first time we describe a mutation of the TXNRD2 gene inhumans. The observed mutation occurred twice in two unrelated patients diag-nosed with DCM. Follow up of mutations in relatives is ongoing as well as se-quencing of the remaining patient sample in search of additional mutations. Weconclude that mutations within TXNRD2 may explain a fraction of about 1% ofhuman DCM cases.
P5428 Serum vascular endothelial growth factor for riskstratification in patients with idiopathic dilatedcardiomyopathy
T. Ohtsuka, T. Uetani, M. Saito, T. Yoshii, A. Kurata, A. Ogimoto,H. Okayama, J. Higaki. Ehime University, 2Nd Dept Of Internal Med,
Ehime, Japan
Background: It has been proven that a disturbance in angiogenesis contributesto the progression of myocardial remodeling in idiopathic dilated cardiomyopathy(DCM). Vascular endothelial growth factor (VEGF) is a major angiogenic factorand also plays a key role in myocardial remodeling. Recent reports have demon-strated the aberrant expression of myocardial VEGF isoforms in human DCM.Moreover, vascular cell adhesion molecule (VCAM)-1 is known to have an angio-genic effect. We thus aimed to evaluate the utility of circulating angiogenic factorsfor predicting the prognosis of patients with DCM.Methods: We measured serum levels of VEGF and VCAM-1 using ELISA in 52patients (mean age, 60 ± 15 years; 44 males; mean LVEF, 28 ± 11%) with DCM(NYHA functional class II or III). Plasma levels of norepinephrine and B-type na-triuretic peptide (BNP) were also measured. The primary end point was the com-posite incidence of cardiac death and hospitalizations for worsening heart failure.Results: During the follow-up period (mean, 23 ± 17 months), 16 patients hadmajor cardiac events with cardiac death in 8 cases and hospitalizations for wors-ening heart failure in 8 cases. The multivariate Cox proportional analysis showedthat VEGF and BNP were significant independent predictors of cardiac events inpatients with DCM (both p< 0.05). According to the Kaplan-Meier analysis, car-diac event-free rates were significantly lower in the low VEGF group (VEGF< 34.0pg/ml) than in the high VEGF group (VEGF> 34.0 pg/ml) (p= 0.032).Conclusions: Our results indicate the capability of serum VEGF as a novel prog-nostic marker in DCM patients. We suggest that serum VEGF may provide impor-tant information for refining risk stratification in outpatients with DCM.
P5429 Antibodies against cardiac myosin light chain type 2in sera of patients with dilated cardiomyopathy
D. Haase1, H.H. Sigusch2, M. Czolbe2, H.R. Figulla2. 1University ofJena, Clinic Of Internal Medicine I, Jena, Germany; 2Heinrich BraunHospital, Clinic of Internal Medicine I, Zwickau, Germany
Purpose: In sera of patients with dilated cardiomyopathy (DCM), antibodiesagainst different antigens, including cell surface proteins and intracellularly lo-cated proteins, i. e. heat shock proteins 60 and 70, actin and myosin heavy chain,were found. Recently, we identified ventricular myosin light chain 2 (MLC2V) asselectively overexpressed in DCM. As a candidate gene for being involved in thepathogenesis of DCM, we examined sera of patients with DCM for the presenceof antibodies against MLC2V protein.Methods: Serum samples were obtained from 70 consecutive patients with DCMand from 70 patients with coronary artery disease (CAD). Control sera were ob-tained from 70 patients without any cardiac disorder. Recombinant human MLC2Vprotein was used as antigenic substrate in serial western blot analysis and directELISA. Diluted sera were used as first antibody and an alkaline phosphataseconjugated IgG as second antibody.Results: In four out of 70 (6%) DCM sera we found a reaction with the recom-binant MLC2V protein; none of the CAD patient sera and none of the controlsera contained antibodies against the MLC2V protein. Of these four patients withMLC2V antibody positive reactions, three were enterovirus negative in endomy-ocardial biopsy and one was enterovirus positive. A correlation between the pres-ence of antibodies against MLC2V and the course of disease, clinical status orhistological findings was not detected.Conclusions: These findings demonstrate for the first time the existence of anti-bodies against MLC2V in sera of DCM patients, but not in sera of CAD patients
or healthy persons. Thus, MLC2V could play a role as autoantigene and mightcontribute to the pathogenesis of DCM patients with a predisposing genetic back-ground.
P5430 Viral persistence and inflammatory cell infiltration inthe myocardium of the patients with DilatedCardiomyopathy
A. Ukimura, A. Iimori, H. Deguchi, F. Terasaki, Y. Kitaura. OsakaMedical College, The Third Division, Department Of Internal Me,
Takatsuki, Japan
Objective: Many papers showed an association of virus infection to myocardi-tis or cardiomyopathy. We evaluated viral persistence and cell infiltration in themyocardium of patients with end stage DCM (Dilated Cardiomyopathy) and IHD(Ischemic Heart Disease).Methods AND RESULTS: Myocardial specimens from 30 American patients withDCM (group AD), 30 Japanese patients with DCM (group JD), 20 American pa-tients with IHD (group AI), and 20 Japanese patients with IHD (group JI), were ob-tained at heart transplantation or volume reduction operation (PLV). Enterovirus(EV) and parvovirus B19 (PVB19) in heart specimens were examined by nestedPCR or RT-PCR. EV was detected in AD (7/30) and JD (9/30), not detected inAI (0/20) or JI (0/20). PVB19 was detected in AD (5/30), JD (9/30), AI (5/20) andJI (7/20). Sequencing showed detected viruses were Coxsackie B viruses, andPVB19 with mutations. However no viruses were isolated in cell culture by con-ventional methods in any of the hearts. Inflammatory cell infiltration was gradedfrom 0 to 3+. There were significant correlations between EV persistence and in-flammatory cell infiltration, however there was no significant correlation betweenPVB19 persistence and inflammatory cell infiltration. EV persistence influencedthe prognosis after PLV in JD group, however PVB19 persistence did not influencethe prognosis.Conclusions: The present study demonstrates that PVB19 genomes persist inthe myocardium in a significant proportion of patients with both end-stage DCMand IHD, and suggests the hypothesis that PVB19 infection is not specific to DCMand persists in hearts with chronic heart failure. EV was detected only in DCMpatients and showed significant correlations with inflammatory cell infiltration andthe prognosis after PLV. Specific anti-viral therapy for EV clearance should beconsidered in EV positive patients.
P5431 Novel mutation in the TCAP gene encodingtitin-cap/telethonin in a family with hypertrophiccardiomyopathy
A. Perrot, M.G. Posch, C. Geier, K.J. Osterziel. Charite-Universitaetsmedizin Berlin, Kardiologie Am Campus Buch &
Virchow-Klinikum, Berlin, Germany
Titin-cap/telethonin - a Z-disc protein interacting with muscle LIM protein, titin, andcalsarcin - plays an important role in the stretch sensor machinery of the heartmuscle. Therefore, we screened the TCAP gene encoding for titin-cap/telethoninin patients with hypertrophic cardiomyopathy (HCM).We clinically evaluated a cohort of 186 unrelated HCM patients on the basis ofmedical history, physical examination, 12-lead electrocardiogram, and echocar-diography after obtaining informed consent. The DNA of the patients was sys-tematically analyzed in the two coding exons of the TCAP gene using PCR, singlestrand conformation polymorphism (SSCP) analysis, and automated sequencing(ABI chemistry).We detected a novel heterozygous missense mutation in one patient. The muta-tion lead to an exchange of arginine to cysteine at codon 106 (R106C) and wasnot detectable in 400 control alleles. It affects a highly conserved residue closeto the titin interacting domain of the protein. The male patient was in NYHA func-tional class III and complained of dyspnoe on exertion and syncope. The echocar-diogram showed severe asymetrical hypertrophy with IVS=26 mm and PWT=15mm. His ECG had negative T-waves as well as a left anterior hemi-block. The 24-hours Holter ECG showed atrial fibrillation. The patient died at the age of 73 yearsbecause of sudden cardiac death. His son (45 years) and his nice (21 years), bothcarriers of the mutation, showed no HCM phenotype.In conclusion, we identified a novel mutation (R106C) in the recently describedHCM disease gene TCAP. This rare mutation showed a low disease penetrancein the family members. Sudden cardiac death of the index patient occurred at highage.
P5432 Effects of antibodies obtained from patients withdilated cardiomyopathy on the function of isolated rathearts
Y. Staudt, C. Trimpert, K. Birkenmeier, S.B. Felix, A. Staudt. Ernst-Moritz-Arndt-Universitaet, Innere klinik B, Greifswald, Germany
Background: Cardiac autoantibodies may play a pathophysiologicalrole in car-diac dysfunction of patients suffering from dilated cardiomyopathy (DCM). Im-munoadsorption (IA) which removes antibodies from patients’ plasma may con-sequently improve cardiac function in DCM. The functional effects of DCM anti-bodies are only partly understood.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

954 Novel aspect of Myocardial and Pericardial disease
Materials and methods: DCM patients (n = 10) were treated with IA by appli-cation of antibody columns directed against human immunoglobulin (Ig). IA wasalso performed with plasma taken from 10 healthy donors (controls). The an-tibodies eliminated and purified by IA were collected and dialyzed. Rat heartswere isolated and perfused retrogradely via the aorta in Langendorff mode. Dur-ing constant-pressure and constant-volume perfusion of the hearts the influenceof diluted antibodies on contractility, relaxation, and on coronary perfusion wasanalyzed.Results: Antibodies obtained from controls had no effect on contractility andrelaxation of isolated perfused hearts during constant-pressure and constant-volume perfusion. In contrast: during constant-pressure perfusion, collected DCMantibodies caused immediate and dose-related reduction of contractility (dLVPdt-max: dilution - 1:32 = -7.1 ± 1.1%; dilution - 1:2 = -20.1 ± 2.1%; p < 0.001) anddiastolic relaxation (dLVPdtmin: dilution - 1:32 = -11.1 ± 1.5%; dilution - 1:2 =-23.9 ± 2.2%; p < 0.001). The heart rate did not change significantly in eithergroup. The effects of DCM antibodies on contractility and relaxation remained de-tectable during constant-volume perfusion. The observed reduction of contractilityand diastolic relaxation was accompanied by impairment of coronary perfusion.Conclusion: In the rat heart, antibodies obtained from DCM patients may impaircontractility and relaxation; and thereby probably also coronary perfusion.
P5433 The effect of tranforming growth factor genepolymorphisms on exercise capacity of patients withdilated cardiomyopathy
F. Kolokathis1, S. Adamopoulos2, A. Chaidaroglou2, J. Parissis1,I. Paraskevaidis2 , A. Gouziouta3 , D. Degiannis2, D. Kremastinos2.
1Attikon University Hospital, Athens, Greece; 2Onassis Cardiac Sugery Center,Athens, Greece; 3Onassis Cardiac Surgery Center, Athens, Greece
Background: It is well known that inflammatory process plays a major role in thepathophysiology of exercise intolerance of heart failure patients,. Increased levelsof pro-inflammatory cytokines such as TNF- α and IL-6 as well as fibrotic factorTGF- β have been associated with cardiac fibrosis and worsening prognosis inpatients with dilated cardiomyopathy. However, the relathionship of cytokine genepolymorphisms (TNF-α 308A/G, IL-6 174G/C, TGF-β 10T/C, TGF-β 25C/G) withtheir exercise intolerance has not been investigated until now.Methods: This study enrolled 80 patients with dilated cardiomyopathy (aged 48± 5 years; 62 males and 18 females; mean LVEF: 30 ± 8%). Left ventricular (LV)funtion was evaluated by echocardiography, while VO2 max (as a marker of pa-tient exercise capacity) was estimated by cardiorespiratory stress test. Cytokinegenotyping was performed by using the sequence specific primers polymerasechain reaction (PCR-SSP) methodology, while cytokine serum levels were mea-sured by commercially available ELISA tests.Results: Mean VO2 max was 23.6 ± 8 ml/kg/min. The genotype frequencies ofTGF-β1 codon 10T/C and TGF-β1 codon 25G/C gene polymorphisms and theirrelationship with patient exercise capacity are shown in the Table. Genotypes T/C-G/C and C/C-G/G were significantly associated with worsening exercise capacity.Finally, no significant correlations of cytokine gene polymorphisms with respectiveserum cytokine concentrations were found in patient population.
TGF-β1 Population VO2 max p-value 95% C.I.10 25
T/T G/G 23(28.75%) 25.67 0.000 22.34 28.99T/C G/G 26 (32.50%) 27.64 0.426 -2.95 6.89T/C G/C 9 (11.25%) 18.5 0.018 -13.03 -1.30C/C G/G 12 (15%) 16.91 0.006 -14.86 -2.65C/C G/C 7 (8.75%) 21.10 0.183 -11.36 2.22C/C C/C 3 (3,75%) 23.67 0.658 -7.01 11.00
Regression analysis was performed
Conclusions: Genetic polymorphisms of TGF- β gene may be related with im-paired exercise capacity in dilated cardiomyopathy patients.
P5434 Gene expression analysis of myocardial tissue frompatients with pericarditis, myocarditis and dilatedcardiomyopathy by microarray analysis
B. Maisch1, V. Ruppert2, T. Jonsdottir1, S. Pankweit1. 1Philipps-University, Department Of Internal Medicine - Cardiology, Marburg,
Germany; 2Philipps-University, Internal Medicine & Cardiology, Marburg,Germany
Microarrays represent an exciting tool for gene expression analysis of manygenes in parallel in cardiac tissue to analyse pathogenetic pathways. Here wecompared mRNA expression profiles of patients with myocarditis, pericarditis, in-flammatory cardiomyopathy (DCMi) and with dilated cardiomyopathy (DCM).Methods: Total RNA was extracted from cardiac biopsies of patients with inflam-matory cardiac diseases and DCM. Each RNA pair (sample vs. reference) was hy-bridised against a Lab-Arraytor®60-combi microarray, comprising 578 probes for556 human genes involved in inflammatory processes and for 22 positive/negativecontrols. The RNA of patient samples was labelled with a red dye and referencesamples were green-labelled.Results: Differences in the gene expression between patients groups were ob-
served for approximately 45% of genes. A set of 42 genes, with a q-value ofless than 0.17 (corresponding to a p-value of less than 0.026) was consideredas being significantly changed. Differences in mRNA expression wer found ingenes involved in apoptotic processes and in the immune response. The meanexpression of CFLAR, C3, SERCA2, SERPING1, C1S and GALC was higher forpatients with myocarditis and pericarditis when compared to DCMi or DCM (Ta-ble). Opposite effects or minor differences were observed for a few genes, e.g.,TLR7, ICAM1, or SELL. Remarkably the expression of FOS, NPPB, MAP3K12,TNFRSF6 or PPBP was reduced in patients with pericarditis when compared tothe other groups.
Gene Gene function DCM DCMi Myocarditis Pericarditis
CFLAR Apoptosis 0.33 (±0.24) 0.16 (±0.28) 0.63 (±0.21) 0.7 (±0.42)SERPING1 Complement activation 0.03 (±0.18) 0.12 (±0.21) 0.35 (±0.22) 0.24 (±0.22)C3 Complement system 0.06 (±0.1) 0.05 (±0.2) 0.27 (±0.16) 0.24 (±0.17)C1S Complement system 0.18 (±0.17) 0.17 (±0.17) 0.43 (±0.22) 0.3 (±0.04)SERCA2 Ca2+-homeostasis 0.88 (±0.41) 0.69 (±0.42) 1.24 (±0.22) 1.37 (±0.36)GALC Fatty acid metabolism 0.18 (±0.21) 0.02 (±0.21) 0.3 (±0.17) 0.32 (±0.22)
mean expression [ln ratio]
Conclusions: By microarray analysis new pathways in the pathogenesis of my-ocardial and pericardial disease were identified. This enables a better characteri-zation of the underlying process, the clinical course and the prognosis.
P5435 Alpha 7 integrin is a major determinant of heart shapeand function
R. Nadif-Savey1, M. Emerson2, E.J. Cartwright3, U. Mayer4,L. Neyses3 on behalf of Cardiovascular Molecular Medicine Unit.1University Of Manchester, Molecular Medicine Unite, Manchester,
United Kingdom; 2Imperial College, Life Sciences, London, United Kingdom;3University of Manchester, Molecular Medicine Unit, Manchester, UnitedKingdom; 4Norwich University, Life Sciences, Norwich, United Kingdom
The unique structure of the heart is dependent on various cellular interactionsbetween the extracellular matrix (ECM), specific cell surface receptors (integrins)and the cytoskeleton. α7β1 integrin is the principal integrin-type receptor forlaminin in cardiac and skeletal muscle. We therefore investigated the structuraland functional role of integrin α7 in the heart of alpha7 null-mutant (α7-/-) mice.α7-/- mice have a shortened life span. Gross morphological analysis of theirhearts showed a reduction in the horizontal axis and an abnormally elon-gated structure compared with age matched controls. M-mode echocardiographydemonstrated a significantly shorter left ventricular end-diastolic diameter (α7-/-:3.01 ± 0.14mm, wt:3.88 ± 0.1mm; n=8; p<0.001), and a significantly thickeneddiastolic interventricular septum (α7-/-:0.92 ± 0.05mm; wt:0.80 ± 0.02mm; n=8;p<0.03) in six month old α7-/- mice. In addition, a significant decrease in leftventricular diameter/length ratio was noted by long-axis echocardiography (α7-/-:0.61 ± 0.03mm; wt:0.76 ± 0.06mm; n=6; p<0.001). The structural changesseen in the left ventricle were accompanied by significantly impaired stroke vol-ume (α7-/-:23.80 ± 2.11μl; wt: 41.97 ± 2.64μl; n=8; p<0.001). α7-/- mice exhib-ited cardiac hypertrophy by nine months of age indicated by a marked increase incardiomyocyte circumference (α7-/-:52.8 ± 5μm; wt:36.5 ± 3μm; n=3; p<0.01)and a significant increase in heart weight to body weight ratio (α7-/-:4.28 ± 0.10;wt:3.85 ± 0.13; n=8; p<0.03). From birth, both body and heart weights weresignificantly smaller in α7-/- mice compared to wild type controls leading to signif-icantly smaller heart weight to tibia length ratio in these mutant mice. α7-/- miceexhibited a significant decrease in heart weight after nine months of age suggest-ing cellular loss. TUNEL assay and electron micrographs from α7-/- and wild typehearts showed no morphological evidence of apoptosis. However, infiltration ofinflammatory cells, as an indicator of necrosis, was markedly increased in α7-/-hearts.In conclusion, ablation of the α7 gene in mice leads to small and abnormallyshaped hearts with low stroke volume; contrary to expectations, the individualcardiac myocytes are hypertrophied thus implying cell loss, likely due to necrosis.α7 integrin is therefore required for the maintenance of correct heart shape plac-ing it in the category of genes which determine the structure of the adult heart.
P5436 Structural changes of the conduction system underlieLenegre disease due to SCN5A gene mutations
C. Basso1, B. Bauce2, A. Rampazzo3, K. Pilichou1, D. Corrado2,E. Carturan3, G. Thiene3, A. Nava2. 1Pathology, Institute OfPathological Anatomy, Padova, Italy; 2Cardiology, Cardiology,
Padova, Italy; 3Biology, Biology, Padova, Italy
Background: Progressive cardiac conduction (Lenègre) disease is one of themost common cardiac conduction disturbances due to degenerative changes ofthe specialized conducting tissue. It constitutes the substrate for bundle branchblock and QRS complex widening leading to complete atrioventricular (AV) blockat risk of syncope and sudden death. Recently, SCN5A gene mutations have beendemonstrated to account for some familial form of Lenègre disease.Material and Methods. A detailed specialized conduction system investigation byserial section technique was carried out in two unrelated probands (M, 35; M,40) who died suddenly with previous history of syncope and an in vivo diagnosis
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 955
of AV conduction disturbances. SCN5A genetic screening as well as cardiologicevaluation was undertaken in family members.Results: Severe fibrosis of the bifurcating His and branch bundles with scleroticinterruption of the right bundle branch was detected in the two probands. Geneticscreening of family members revealed a mutation in exon 11 E473X (12 carriers)and exon 21 E1225K (3 carriers), respectively. The 12-lead ECG of 15 subjectscarrying a SCN5A mutation (of whom 2 probands were obligated carriers), 9 Mand 6 F, age 38,4±17 yrs (range18-72) was analysed. None of the non carriershad PQ interval prolongation. Twelve mutation carriers (80%) presented a rightventricular conduction delay and one (6,6%) a first degree left bundle branchblock. Mean PQ interval was 211±36 msec. A PQ interval > 200 msec waspresent in 10 (67%) (mean 232±20 msec, mean age 46,5±15 yrs vs 22,2±4,9yrs of those with normal PQ interval, p=0.0004); a QRS complex >110 msec waspresent in 11 subjects (mean 132±16 msec, mean age 43±17 yrs vs 26±6 yrsof those with normal QRS duration, p=0.01); and a coved ST-segment elevation>2 mm in V1-V2 was present in six cases (40%). In two SCN5A mutation carriersthe ECG was normal. Signal-averaged ECG in the time domain analysis showedlate potentials in 11 out of 13 SCN5A gene mutation carriers (84%).Conclusions: An organic substrate underlies Lenègre disease due to SCN5Amutations and consists of severe fibrosis of the bifurcating His bundle with scle-rotic interruption of the right bundle branch as to account for AV block and suddendeath in young people. Family members investigation revealed a PQ interval pro-longation and a QRS complex widening in two-thirds of SCN5A mutation carriersthus confirming the presence of a heritable conduction system disease.
P5437 In overweight patients cardiac structural adaptation ismodulated by the +1675 A/G angiotensin II receptortype 2 gene (AT2-R)
R. Schmieder1, C. Ott2, T. Schwarz2, S. Titze2, K.H. Hilgers2,M.P. Schlaich2. 1University Erlangen Nuernberg, Medizinische Klinik
4, Erlangen, Germany; 2University Erlangen-Nuremberg, Dept. of Nephrologyand Hypertension, Erlangen, Germany
Background: Overweight subjects without overt heart disease have subclinicalchanges of left ventricular (LV) structure and function. The genetic variation inAT2-R (+1675A/G polymorphism) is associated with LV structure in male youngpatients with hypertension. We questioned whether in overweight subjects LVstructure and function is influenced by AT2-R.Methods: In a homogenous cohort of 214 young (26.5±4.1years) male subjectswith normal or mildly elevated blood pressure, we assessed ambulatory bloodpressure, body mass index (BMI) and LV-structure and function by 2-D-guided M-mode-echocardiography. The intronic +1675A/G polymorphism was investigatedby single-strand conformational polymorphism analysis and DNA-sequencing.Results: Compared to lean subjects, 71 overweight subjects (bmi ≥ 25kg/m2)displayed an increased posterior and septal wall thickness as well as LV mass(255±51 vs. 226±42g, p< 0.001). Midwall fractional fiber shortening (16.9±2.4vs. 17.7±2.1U, p=0.011) and ejection fraction were decreased in these over-weight subjects. In the whole study cohort the A-allele (n=123) of the AT2-R genewas associated with an increased septal wall thickness and LV mass. Subsequentdivision of the study cohort according to BMI and AT2-R gene allele revealed thatin overweight subjects with the A-allele, LV mass (266±57 vs. 242±39g, p=0.045)and septal wall thickness (10.9±1.5 vs. 9.94±1.2mm, p=0.006) were greater thanin overweight subjects with the G-allele of the AT2-R gene, despite no differencesin potential confounding factors of LV structure and function, such as age, bloodpressure, BMI and sodium intake. Consistently, posterior (p=0.068) and relativewall thickness (p=0.072) tended to be increased in subjects with the A-allele. Inlean subjects no such clear relations were evident.Conclusion: The A-allele of the AT2-R emerged as a modulator of cardiac struc-tural adaptation, particularly in male overweight subjects.
P5438 Cardiac involvement in adults with m.3243A>GMELAS gene mutation
T. Vydt1, M.L. Geleijnse2, R. De Coo1, F.J. Ten Cate1. 1UniversityHospital Gasthuisberg, Cardiology, Leuven, Belgium; 2Erasmus MC,Cardiology, Rotterdam, Netherlands
Purpose: To study for the first time cardiac involvement in a consecutive series ofadults subjects with a MELAS (mitochondrial encephalomyopathy, lactic acidosis,and stroke-like episodes) - mitochondrial DNA point mutation m.3243A>G.Methods: Twelve subjects with a mean age of 35 ± 13 years with the mitochon-drial DNA point mutation m.3243A>G were enrolled in the study. Eight subjectshad the clinical syndrome of MELAS ("patients") and four subjects were asymp-tomatic gene carriers ("carriers"). Each subject underwent electrocardiography,exercise testing, Holter monitoring and echocardiography, which included systolicand diastolic tissue Doppler velocities at the mitral annular level. Histologic andgenetic analysis were performed together with biochemical analysis for respira-tory chain enzyme activity (complex I rest activity), all in skeletal muscle.Results: At electrocardiography and Holter monitoring none of the subjects hadevidence of pre-excitation, cardiac arrhythmias or conduction abnormalities. Pa-tients had significantly lower (42 ± 17% from normal vs. 103 ± 14%, P <0.02)exercise tolerance. All but one of the patients, but none of the gene carriers hadragged red fibers in the muscle biopsy. Mean percentage of gene mutation in
skeletal muscle tended to be higher in patients (53 ± 19%, range 19 to 73%)compared to gene carriers (33 ± 20%, range 15 to 62%). Mean complex I restactivity in patients (36 ± 18%, range 10 to 58%) was significantly (P <0.01) lowercompared to gene carriers (120 ± 60%, range 72 to 205%). Left ventricular (LV)abnormalities were confined to six MELAS patients. Three patients had LV hy-pertrophy, five patients had LV systolic abnormalities and five patients had LVdiastolic dysfunction. Apart from one patient with isolated diastolic abnormalityall patients with LV abnormalities had ragged red fibers. Patients with abnormalsystolic LV function had a trend towards a higher percentage of mutated skele-tal muscle (59.7 ± 10.7% vs. 35.8 ± 21.3%, P <0.10) and a significantly lowercomplex I rest-activity (26.7 ± 14.0% vs. 97.8% ± 57.9, P <0.01).Conclusions: None of the MELAS gene carriers had cardiac abnormalities. Con-versely, most phenotype MELAS patients, and in particular those with ragged redfibers, had LV involvement. These latter patients had the lowest complex I rest-activity in skeletal muscle. Whether the presence of ragged red fibers or complexI rest-activity in skeletal muscle may further select patients in whom a routinecardiac examination is really warranted should be subject to further studies.
P5439 Human insulin and leptin receptor number in healthyoffspring of hypertensives. The impact of ACE genepolymorphism
T.H. Makris1, D. Papadopoulos1 , U. Papazachou2, M. Daskakaki1 ,E. Sanidas1, S. Vichos1, A. Hatzizacharias1, V. Votteas1. 1Laiko
Hospital, Cardiology, Athens, Greece; 2Laiko Hospital, Cardiology, Athens,Greece
Essential hypertension is associated with increased insulin and leptin plasma lev-els and decreased human insulin (hINR) and leptin (hLR) receptor number. Thedeletion (D) allele of the insertion/deletion (ID) polymorphism of the angiotensinconverting enzyme (ACE) gene has been implicated in the pathogenesis of a va-riety of cardiovascular disorders. Aim of the study was to examine the possibleimpact of ACE gene polymorphism on leptin and insulin plasma levels, hINR andhLR number in healthy offspring of hypertensives.Methods: The I/D polymorphism of ACE gene was determined (PCR method)in 90 (56M and 34F) healthy offspring of hypertensives mean age 16 ± 2.5 yrs.and body mass index (BMI) 21.5 ± 2.8 kg/m2. Forty had DD genotype (Group A)and 50 ID and II genotype (Group B). The two groups were matched for age, sex,BMI and blood pressure levels. Leptin and insulin plasma levels (RIA method) andhINR and hLR number (ELISA method) were determined in the whole population.Results: The results and the comparison between the two groups are shownbelow:
Group A Group B p
Leptin (ng/L) 10.3±6 7.07±4 <.01Insulin (IU/ml) 17.3±6.2 14±5.6 <.05hINR (receptorX103/red cell) 8.5±3.1 10±4 <.001hLR (IU/ml) 18±6 25±9 <.01
Conclusion: Our findings suggest that the ACE/DD genotype is associated withsignificantly higher leptin and insulin plasma levels and lower hINR and hLR num-ber in healthy offspring of hypertensives. This finding needs further investigation.
P5440 Chronic occlusion of the infarct-related artery isassociated with decreased density of capillarynetwork and ongoing apoptosis
M. Prech1, S. Grajek1, A. Marszalek2, V. Filas3, M. Lesiak4,M. Jemielity5, A. Cieslinski2. 1Department of Cardiology, Cardiology,
Poznan, Poland; 2Department of Pathomorphology, Clinical Pathomorphology,Poznan, Poland; 3Department of Pathology, Oncology, Poznan, Poland;4Department of Cardiology, Cardiology, Poznan, Poland; 5Department ofCardiosurgery, Cardiosurgery, Poznan, Poland
Apoptosis has been shown as one of a key mechanism of cell loss in the settingof acute myocardial infarction (MI) and up to several weeks post MI. It hasn’tbeen investigated yet, whether it contributes to myocardiocyte death that occursmonths or even years post MI.Aim: To identify features of ongoing apoptosis in myocardiocytes that survivedacute phase of MI and to assess its relationship to alterations in capillary network.Materials and methods: Morphometric evaluation was performed in 51 humanhearts: group I (n=10) - non-cardiac death (control), group II (n=21) - post-Q-waveMI death (over 3 years post MI) and group III (n=20) - patients who survived QMIand who later (over 1 year) underwent aneurysmectomy. Apoptotic rate (AR) wascalculated at the site of infarction, within the aneurysms and in the unaffected LVregions (control) using immunohistochemistry (IHC) for caspase-3 and BCL2. Theextent of myocytolysis was assessed semiquantitatively from 0 (none) to severe(over 60% of myocytes shows loss of striation) while CD-34 IHC was applied toquantify density of capillary network.Results: A significant reduction in capillary density within infarcted area wasnoted in group II when compared to control group (1525.6 ± 378.5/mm2 vs.2968.7 ± 457.3/mm2; p<0.001). The most significant reduction (1204.6 ±156.9/mm2) was observed in patients with total infarct-related artery (IRA) occlu-sion (group IIB). Over 60% reduction in capillary density (1030.7 ± 241.8/mm2)
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

956 Novel aspect of Myocardial and Pericardial disease
was also observed in group III (IRA occlusion confirmed angiographically). Sucha reduction in capillary density was associated with a moderate (>30%) to se-vere (>60%) degree of myocytolysis (group IIB and III). In contrast less advancedalterations were observed in patients with patent IRA (group IIA). AR (based oncaspase-3 expression) was 8.2 ± 3.8 and 3.7 ± 2.4, respectively, while no differ-ence in BCL2 expression was observed when compared to control.Conclusions: 1. Loss of balance between number of capillaries and myocytes inpatients with chronic IRA occlusion is associated with extensive myocytolysis.2. Positive caspase-3 expression suggests apoptosis as a common metabolicpathway in hypoperfused cardiomyocytes that might contribute to cell deaths latepost MI.
P5441 NKX2.5 mutation frequency in patients withcongenital heart disease
L. Gioli-Pereira1, A. Pereira2, S. Mesquita2, J. Xavier-Neto2,A.A. Lopes2, J.E. Krieger2. 1Heart Institute, Sao Paulo, Brazil;2Heart Institute Sao Paulo, Laboratorio De Genetica, Sao Paulo,
Brazil
Background: Cardiac development is a complex and multifatorial biological pro-cess. Heterozygous mutations in the transcription factor NKX2.5 are among thefirst identified genetic causes for congenitalheart defects in humans.Aim: To evaluate the presence and frequency of mutations in the NKX2.5 genein 164 patients with non-familial, non-syndromic congenital heart disease.Methods: The coding region of the NKX2.5 locus was amplified by polymerasechain reaction and mutational analysis was performed using denaturing high per-formance liquid chromatography (dHPLC) and DNA sequencing.Results: We have studied 164 patients with different anatomical diagnosis:conotruncal defects 73; septation defects 57, Ebstein’s anomaly 21, and oth-ers. We were able to identify mutations in the NKX2.5 gene in 3 patients (1.8%):Arg25Cys in a patient with pulmonary atresia and VSD, Ala42Pro in a patient withEbstein’s anomaly and WPW, and Val315Leu in a patient with Tetralogy of Fallot.Mutation Arg25Cys has been previously described in patients with TOF, hypoplas-tic left heart, tricuspid atresia, interrupted aortic arch and trasposition of the greatarteries; mutations Ala42Pro and Val315Leu have never been described before.Conclusions: NKX2.5 mutations may cause a heterogeneous spectrum of con-genital malformations in humans. NKX2.5 gene mutations identification may helpthe clinical and counseling management of patients with congenital heart disease.
P5442 Impairment of cardiomyocyte cytoskeleton inarrhythmogenic right ventricular cardiomyopathy
E. Czarnowska1, M. Brudek2, E.K. Wlodarska3, A. Turska-Kmiec3,L. Ziolkowska3, W. Kawalec3, M. Pronicki3 on behalf of ARVC.1The Children Memorial Health Institute, Dept. Pathology, Warsaw,
Poland; 2The Children’s Memorial Health Center, Pathology, Warsaw, Poland;3Institute of Cardiology, Congenital Heart Diseases, Warsaw, Poland
Some aspects of myocyte structural abnormalities observed in arrhythmogenicright ventricular cardiomyopathy (ARVC) are not clear in the light of known genesmutations related to junctional and rianodine receptor RyR2 proteins, but sug-gest rather cytoskeleton injury. The aim of this study was to identify the stages ofmyocyte cytoskeleton injury and their specificity for ARVC.Materials and methods: EMBs from young (2M, 6F, mean age 10.8±3.7 yrs)and adult patients (4M, 3F mean age 48±8.8 yrs) patients with ARVC were anal-ysed. EMBs from ICM (4pts), DCM (4pts) and HF (4pts) served as controls.Routinely contrasted and then stained with bismuth chloride ultrathin sectionswere analysed under an electron microscope. Cytoskeletal proteins: desmin andbeta-tubulin (true cytoskeletal proteins), titin (sarcomeric skeleton), and vinculin(membrane-associated protein) were analysed immunohistochemically on serialparaffin sections.Results: Ultrastructural analysis of ARVC revealed an irregular or pale visiblecell cytoskeleton in the region of Z band and cell membrane invaginations whichformed T-tubules, and in the perinuclear area in many cardiomyocytes. The sitesof cell-matrix adhesion, i.e. lateral costamere junctions and focal contacts, inthese cells were numerous. Immunohistochemistry showed decreased expres-sion of titin in all sections, with small exceptions. The cytoskeletal proteins, desminand beta-tublin, and vinculin were highly up-regulated in some cardiomyocytesgathered in groups localized in normal myocardial tissue. This pattern of local-ization of cardiomyocytes with abnormally organized cytoskeletons was similar inboth young and adult patients. In EMBs from HF, cardiomyocytes exhibiting cy-toskeleton injury were not specificly dispersed, while in those from ICM and DCMthe injured cells were single, mainly in the area bordering fibrous tissue.Conclusions: It can not be excluded that in ARVC, loss of titin, a protein relatedto contractile machinery, may be an early event initiating an adaptive increase ofcytoskeleton proteins. The factors initiating this response remain, however, un-known. A specific pattern of localization of cardiomyocytes with an abnormal cy-toskeleton may be a feature contributing to the pathogenesis of ARVC and usefulin diagnosis of the disease when samples are not diagnostic in terms of replace-ment of cardiomyocytes by fibro-fatty tissue.
P5443 Peculiarities and alterations of myocardial gapjunctions in various models of cardiac injury
N. Tribulova, M. Fialova, K. Dlugosova, L. Okruhlicova, A. Brichtova,J. Slezak. Institute for Heart Research SAS, Bratislava, SlovakRepublic
Background: Rapid spreading of the electrical impulse throughout the heart isessential for synchronised contraction and is ensured by electrical coupling ofcardiomyocytes at the gap junctions (GJs). The latter contain high number of con-nexin channels, which in addition to electrical conduction allow molecular signaland Ca2+ waves propagation. GJs changes have been shown involved in arrhyth-mogenesis and/or contractile dysfunction. We examined topology and alterationsof GJs as well as impairment of intercellular coupling various models of cardiacinjury using electron microscopy.Methods: Chronic models of rat heart injury characterised by structural remod-elling were used, such as genetically- and L-NAME-induced hypertension andSTZ-induced diabetes. Acute models of rat heart injury characterised by Ca2+overload, such as ischemia, reperfusion, hypoxia and hypokalemia were per-formed on isolated heart preparation. These acute events were accompanied bydisorders in cardiac contraction and they often triggered arrhythmias, includingVF. All rats used were 3-4 month-old and ventricular tissues were examined.Results: Hypertensive and diabetic rat hearts exhibited structural remodelling(hypertrophy and/or fibrosis), which was accompanied by GJs remodelling. It wascharacterised by "lateralisation" and "internalisation" of GJs, i.e. neo-formation ofside-to-side and deterioration of end-to-end type of GJs associated with occur-rence of cytoplasmic annular profiles of GJs. There was a big variation in the size(0.3-3 m m) of new lateral GJs, whereby longer were more frequent in the heartsof hypertensive than diabetic rats. The longest (>3 m m) GJs located at the pe-riphery of intercalated discs and obviously seen in intact myocardium were morefrequent in diabetic rat hearts. Noteworthy, these GJs were close to mitochondriaor even enveloped them. Since temporal decline of cytosolic ATP or increase infree Ca2+ induce intercellular uncoupling, mitochondria can play a role in pro-tection and/or modulation of GJs function. Regardless the model of acute heartinjury, impairment of intercellular coupling and/or uncoupling were observed. Itwas indicated by disconnection of severely injured cardiomyocytes from adjacentslightly altered or normal ones and by presence of viable contracted cardiomy-ocytes in the neighbourhood of relaxed cardiomyocytes. Such changes were het-erogeneously distributed within myocardium.Conclusions: Gap junction remodelling and dispersion of intercellular couplingimpairment may contribute to re-entry arrhythmias and contractile dysfunction.
P5444 Favourable long-term outcome of percutaneousseptal ablation for symptomatic hypertrophicobstructive cardiomyopathy
D. Welge1, L. Faber1, D. Fassbender1 , H.K. Schmidt1,U. Gleichmann1, H. Seggewiss2, D. Horstkotte1. 1Heart Center
North Rhine-Westphalia, Bad Oeynhausen, Germany; 2Leopoldina Hospital,Schweinfurt, Germany
Purposeand methods: To define the role of septal ablation (PTSMA) as com-pared to surgical myectomy, we repeatedly analyzed the long-term outcome ofthe first 178 consecutive patients (pts.) treated with PTSMA for symptomatic hy-pertrophic obstructive cardiomyopathy (HOCM) between 1/1996 and 12/1998.We now report on the latest follow-up after a mean of 66±23 (maximum: 118)months, covering about 1000 pt.-years following the index intervention.Results: During the in-hospital phase, 3 pts. (1.7%) died (VF, pulmonary em-bolism, and pericardial tamponade in 1 pt. each). Mean CK rise was 599±300U/l. A DDD-pacemaker (DDD-PM) had to be implanted in 13 pts. (7%) for PTSMA-induced AV conduction problems. During follow-up, 20 pts. (11%) needed a re-intervention directed against residual or recurrent outflow obstruction (re-PTSMA:11; myectomy: 9). These cases included, at the most recent follow-up study satis-factory symptom control was reported by 141 pts. (81%), and gradient elimination(<30 mm Hg under any condition) was achieved in 94%. There were 6 (3%) ad-ditional DDD-PM implantations and 4 (2%) ICD implantations (2 for secondary, 2for primary prevention) in our pt. cohort. Overall, 14 pts. (8%) died 52±21 (8-86)months after their index PTSMA due to stroke (n=3), extracardiac disease (n=5),or cardiac causes (n=6).Conclusions: During long-term follow up following PTSMA, a persistent LVOTOreduction and exercise improvement can be observed. A second interventionwas needed in about 10% of our pts. A total mortality rate of 17/178 (9%) or1.5%/pt.-year, including all procedure-related deaths, compares favourably withthe reported natural course of this pt. group with severe disease.
P5445 Circulating T lymphocyte subpopulations may predictrecurrence of acute idiopathic pericarditis
A.C. Zacharoulis, D. Korres, A. Karavidas, C. Papadopoulos,A. Iniotaki, V. Vigklis, C. Stavropoulos-Giokas, A.P. Zacharoulis.General Hospital of Athens "G. Gennimatas", Cardiology, Athens,
Greece
Introduction: Acute Idiopathic Pericarditis (AIP) is a common, self-limited inflam-mation of the pericardium. Its major complication is recurrence that can reach up
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 957
to 30%. T lymphocytes have a central role in the inflammatory process, and stim-ulation of different subpopulations may predict the severity of the disease. AIM:To investigate the role of different T lymphocytes subpopulations in predicting re-currence of AIP.Methods: During the acute phase of AIP, we studied the circulating lym-phocyte subpopulations in 42 patients, using monoclonal antibodies (Becton-Dickinson) and flow cytometry technique.All patients initially received thesame medical treatment (NSAID) for 4 weeks.The investigated subpopula-tions were:CD3+,CD4+,CD4+/CD45RA+ naïve cells, CD4+/CD45R0+ memorycells,CD4+/CD25+ activated cells,CD8+, CD8+/HLA-DR+ and CD8+/CD38+ acti-vated cells, CD19+ B cells, and CD3-/CD16-56+ NK cells. Patients were followedclinically and by echocardiography every six months, for a mean follow-up pe-riod of 21.8 ± 31.6 months and recurrence was reported.Patients were allocatedinto two groups;Group I (patients with recurrence) and Group II (patients withoutrecurrence).Five healthy subjects were used as controls.Results: The percentage of CD4+/CD45RA+ naïve T cells in both groups (I andII) were significantly lower compared to the healthy controls (p=0.04). GroupI (n=14, patients with recurrence) had significantly lower percentage of naïveCD4+/CD45RA+ T cells and higher percentage of activated CD8+ T cells com-pared to group II (n=28, patients without reccurence).The results are shown onthe table (such differences were not noticed among other lymphocyte subpopula-tions).
T cells subpopulation Patients (% of lymphocytes) (mean±SD)
Group I Group II p Controls(n=14) (n=28) (between groups I and II) (n=5)
CD4+/CD45RA+ 10.14 ± 6.97 15.33 ± 6.99 0.028 28.02 ± 11.22CD4+/HLA-DR+ 7.21 ± 6.47 3.07 ± 2.84 0.034 1.60 ± 1.02CD8+/CD38+ 14.92 ± 6.74 10.86 ± 4.59 0.059 3.44 ± 2.21
Conclusion: Patients with recurrence of AIP have significantly high activationof their immune system during the acute phase. The regulatory mechanisms inthese patients may be impaired.Thus,during the acute phase of idiopathic peri-carditis, the percentage of CD45/RA+ and CD8+/HLA-DR+lymphocyte subpopu-lation may predict recurrence of the disease.
P5446(W) Prevalence and clinical features ofAnderson-Fabry disease in patients withsymptomatic hypertrophic cardiomyopathy: anendomyocardial biopsy study
Y. Yoshikazu1, H. Kasai1, H. Imamura1, O. Kinoshita1,M. Hongo1, U. Ikeda1, T. Takenaka2 , T. Tei1. 1Shinshu University, DivisionOf Cardiovascular Medicine, Matsumoto, Japan; 2Kagoshima University,Kagoshima, Japan
Background: Anderson-Fabry disease (AFD) is an X-linked recessive lysoso-mal storage disorder, resulting from a deficiency in alpha-galactosidaseA (alpha-GalA). AFD has been recognized as the cause of left ventricular hypertrophy in6% of men with hypertrophic cardiomyopathy (HCM). Although AFD is considereda recessive X-linked disorder, affected women are increasingly reported. The aimof our study was to determine the prevalence of AFD in patients with symptomaticHCM.Patients and Results: Endomyocardial biopsies were performed in 192 pa-tients with symptomatic HCM at our hospital and referral centers during thepast 14 years. There were 147 men and 45 women with an average age of58 years. Histological examination identified five cardiac AFD including 1 man(0.7%) and 4 women (8.9%), showing concentric hypertrophy in 2 patients, asym-metric hypertrophy in 2, and apical hypertrophy in 1. Mismatching between per-fusion (Thallium-201) and metabolism (Iodine-123 beta-methyliodophenyl pen-tadecanoic acid) in the hypertrophied myocardium was observed in 2 patients.Alpha-Gal A activity was reduced in 4 patients, and genetic analysis revealed thepresence of alpha-Gal A gene mutation in 2 cases.Conclusions: Heterozygous AFD is not rare in symptomatic patients with femaleHCM. Endomyocardial biopsy is a useful diagnostic tool for Heterozygous AFD.Distribution of hypertrophic portion varies from patients to patients in this disease.
P5447 Cardiac structural and functional changes inasymptomatic primary hyperparathyroidism afterparathyroidectomy
M. Birgander, E. Rydberg, R. Willenheimer. Malmo UniversityHospital, Department of Cardiology, Malmo, Sweden
Aim: Primary hyperparathyroidism (pHPT) is usually caused by hyperactivity ofone or more parathyroid glands, resulting in elevated serum (s) levels of parathy-roid hormone (PTH). The only curative therapy is parathyroidectomy. pHPT isassociated with hypertension, left ventricular hypertrophy and abnormal renin-angiotensin-aldosterone system activity, as well as increased risk of all-cause andcardiovascular mortality. We investigated changes in cardiac structural and func-tional parameters at echocardiography one year after successful parathyroidec-tomy in asymptomatic pHPT patients.Methods: We consecutively included 50 pHPT patients (age 62.9±11 years, 5men) and 50 healthy control subjects, evenly matched for age and sex. pHPT pa-
tients were examined preoperatively and 6 and 12 months postoperatively. Struc-tural and functional cardiac parameters were assessed by standard trans-thoracicechocardiography (TTE). The 3-group classification of left ventricular (LV) dias-tolic function was based on transmitral and pulmonary vein flow pattern, and leftatrial (LA) size. pHPT patients were divided into four subgroups based on medianpreoperative s-levels of PTH and calcium (Ca): high PTH/high Ca, high PTH/lowCa, high Ca/low PTH, and low PTH/low Ca.Results: After parathyroidectomy, s-Ca and s-PTH were normalized. At baseline,pHPT patients had greater LV mass (p=0.0023) and LA size (p=0.0002) versuscontrols. One year after PTX, LV mass, LA size, LV enddiastolic diameter, LVendsystolic diameter, LV posterior wall diameter and right ventricular enddiastolicdiameter increased, although non-significantly. Interventricular septum diameterincreased among pHPT patients, with significant progression in high PTH/lowCa patients (from 9.5±1.6 to 9.8±2.0 mm, p=0.0170). The Doppler-derived de-celeration time of the transmitral E-wave increased among pHPT patients, withsignificant progression in high PTH/low Ca patients (from 249±60 to 284±37ms, p=0.0011). There was deterioration of LV ejection fraction (from 62.7±7 to59.9±7.8%, p>0.05), and mean atrioventricular plane displacement (from 13.2±2to 12.6±2 mm, p=0.0286).Conclusion: One year after successful PTX, despite normalisation of serumcalcium and PTH, patients with asymptomatic pHPT, especially those with PTHabove median, showed progressive LV structural and functional impairment, in-dependent of blood pressure.
P5448 Multisystem primary defect of LAMP-2 in Danon’sdisease
P. Melacini, M. Fanin, A. Nascimbeni, L. Fulizio, M. Spinazzi,V. Pescatore, S. Iliceto, C. Angelini. University of Padua,Cardiac,Thoracic and Vascular Sciences, Padua, Italy
Background: Danon disease, an X-linked dominant disorder, results from mu-tations in the lysosome-associated membrane protein-2 (LAMP2) gene andpresents with hypertrophic cardiomyopathy, skeletal myopathy and mental retar-dation. We investigated the effects of LAMP2 gene mutations on protein expres-sion in different tissues.Methods and Results: We screened LAMP2 gene mutations and LAMP-2 pro-tein defect in the skeletal muscle of nine unrelated patients with hypertrophiccardiomyopathy and vacuolar myopathy. We identified 3 novel families (includingone affected mother) with unreported LAMP2 gene null mutations, and LAMP-2protein deficiency in skeletal and myocardial muscle, leukocytes and fibroblasts.LAMP-2 protein deficiency was detectable in various tissues,including leukocytes,explaining the multisystem clinical involvement. Skeletal muscle immunopathol-ogy showed that mutant protein was not localized in the Golgi complex, vacuolarmembrane expressed sarcolemmal-specific proteins, and the degree of musclefiber vacuolization correlated with clinical muscle involvement. In our female pa-tient, muscle histopathology and biochemical LAMP-2 protein analysis was incon-clusive. The random X-chromosome inactivation in muscle and leukocytes of ourfemale patient excluded the possibility that selective involvement of some tissuesin females is due to skewed X-chromosome inactivation.The identified patients had WPW syndrome. Severe and progressive heart failureassociated with end-stage systolic dysfunction led to death in two males at theage of 22 and 29 years and to transplantation in the female at 52 years.Conclusions: Biochemical diagnosis of leukocytes might be used for screening inmale patients with hypertrophic cardiomyopathy, but genetic screening is requiredin females.
P5449 Patients with cardiac events during long-termfollow-up after septal ablation for hypertrophicobstructive cardiomyopathy are characterized by the"classical" risk markers
L. Faber1 , D. Welge1, D. Fassbender1 , H.K. Schmidt1,U. Gleichmann1, H. Seggewiss2, D. Horstkotte1. 1Heart Center NorthRhine-Westphalia, Cardiology Dept., Bad Oeynhausen, Germany; 2LeopoldinaHospital, Schweinfurt, Germany
Purposeand methods: Various risk markers (RM) have been identified in non-selected cohorts of patients (pts.) with hypertrophic cardiomyopathy (HCM).Whether these RM also apply to pts. during long-term follow-up after septal ab-lation (PTSMA) for obstructive HCM is unknown. We compared pts. with an un-eventful course [group A; n=118], those who had a cardiovascular event (MACE:atrial fibrillation, any device implantation, heart failure hospitalization, stroke, ordeath [group B; n=57]), and those who died or survived a cardiac arrest (mortalityrate: 1.5%/pt.-year; [group C; n=16]).Results: At baseline, group C pts. were older (64±20 vs. 50±15 years; p=0.03),more severely impaired in terms of NYHA functional class (3.3±0.5 vs. 2.8±0.5;p=0.001), and had a thicker septum (5±10 vs. 21±4 mm; p=0.0008). At follow-up,the residual resting gradients were higher (24±5 vs. 25±33 mm Hg, p<0.0001).Severity of outflow obstruction (LVOTO) and impairment of diastolic LV function atbaseline, peri-interventional parameters, or other follow-up variables were not dif-ferent among the groups. Group B pts. also were older (60±15 years; p<0.0001)and had a larger left atrium (50±8 vs. 47±8 mm; p=0.03) at baseline. Other base-line or peri-interventional variables did not differ. At follow-up, LA dilatation was
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

958 Novel aspect of Myocardial and Pericardial disease
more pronounced (49±8 vs. 44±8 mm; p=0.001) and stressed residual gradientswere higher (26±27 vs. 14±20 mm Hg; p=0.006). Multiple logistic regressionanalysis testing these variables confirmed age and LA size as most potent pre-dictors of MACE, while septum thickness was the only predictor of subsequentcardiac death.Conclusions: During long-term follow up after PTSMA, persistent or progressiveLA dilatation characterizes pts. at risk for any type of cardiovascular events, whilepts. with severe hypertrophy appear to be at increased risk for cardiac death.These findings are in accordance with previous data on the natural history ofHCM, and may be helpful for the management of affected pts. apart from gradientreduction.
P5450 Poor prognostic predictors in acute pericarditis
M. Imazio, E. Cecchi, B. Demichelis, S. Ferro, D. Forno, S. Ierna,M. Novara, R. Trinchero. Cardiology Dept. Maria Vittoria Hospital,Cardiology, Torino, Italy
Background: Clinical search for poor prognostic predictors in acutepericarditis may be useful for the clinical triage of patients(pts) at high risk ofspecific etiologies or complications.Methods: After literature review, the following clinical features were consideredas possible poor prognostic predictors: fever>38°C, subacute course, immun-odepression, trauma, oral anticoagulants, myopericarditis, elevation of troponinI(TnI+), severe pericardial effusion, cardiac tamponade, aspirin or non-steroidalanti-inflammatory drugs(FANS) failure after 1 week, and use of corticosteroids.All consecutive cases of acute pericarditis were prospectively evaluated from Jan1996 to Aug 2004, excluding post-myocardial infarction pericarditis.Results: 453 pts were included(mean age 52 ± 18 years, 245 men). A spe-cific etiology(non-viral/idiopathic) was found in 76/453 pts(16.8%): autoimmunein 33 pts(7.3%), neoplastic in 23 pts(5.1%), tuberculous in 17 pts(3.8%), andpurulent in 3 pts(0.7%). In univariate analysis, a higher rate of the followingfeatures was found in pts with a specific etiology: fever>38°C(41.9% vs 9.5%),subacute onset(14.9% vs 1.1%), severe effusion and/or tamponade(17.6% vs1.0%), and aspirin failure(58.1% vs 11.1%; for all p<0.001). TnI+ was mainlyfound in pts with idiopathic/viral pericarditis(26.6% vs 5.4%; p<0.001). After mul-tivariate analysis, the following independent predictors for a specific etiology werefound: fever>38°C(OR 14.4 95% CI 5.2-39.9; p<0.001), subacute course(OR13.0 95% CI 3.1-54.8; p<0.001), severe effusion or tamponade(OR 5.5 IC 95%1.2-26.6; p=0.03), and aspirin failure(OR 4.6 95% CI 2.1-10.4; p<0.001). Aftera mean follow-up of 31 months, complications were detected in 95 pts(21.0%):recurrences in 83 pts(18.3%), tamponade in 14 pts(3.1%), and constriction in7 pts(1.5%). In univariate analysis, the following features were commoner inpts with complications: fever>38°C(29.5% vs 10.9%), subacute onset(10.5% vs1.4%), severe effusion or tamponade(14.7% vs 1.0%), oral anticoagulants(14.7%vs 3.9%), corticosteroid use(36.8% vs 7.3%), and aspirin failure(55.8% vs 8.9%;for all p<0.001). After multivariate analysis the following independent predictorsfor complications were found: severe effusion or tamponade(OR 12.8 95% CI2.2-74.6; p=0.005), aspirin failure(OR 7.2 95% CI 3.6-14.6; p<0.001), and corti-costeroids use(OR 3.0 95% CI 1.2-7.1; p=0.02).Conclusions: Fever >38°C, subacute course, severe pericardial effu-sion/tamponade, aspirin or FANS failure, and corticosteroids use are the mainpoor prognostic predictors in acute pericarditis.
P5451 Treatment of left-sided heart tumours based on a20-year experience
G. Knychov1, R. Vitovsky1, V. Popov1, V. Beshlyaga1,S. Andryevskya2. 1Amosov Institute of Cardiovascular surgery, Kiev,Ukraine; 2Cardiological center, Odessa, Ukraine
Objective: To present analysis of surgical treatment of left sided heart tumors(LSHT) and recommend optimum technique of LSHT removal based on theseresults.Methods: 362 consequtive patients (pts) with primary tumor of the LSHT were op-erated from 01.01.1984 till 01.01.2004 yy. Tumors based at the left atrium (LA)(n= 351 pts), left ventricle (LV) (n = 11 pts). Malignant forms were in 10 (2,8%) pts:LA (n= 9), LV (n=1). In other cases myxomas were marked in 98,9% (348/352):LA (100,0% - 342/342), LV (60,0% - 6/10). Mean age of pts was 52,6 ± 8,4 year(range 8-70 yy). Females - 282 (77,9%), males - 80 (23,2%). In the most of pts(95,7%) the bottom of the myxoma was based on any part of interatrial septum(frequently at fossae ovale). In 247 (68,2%) pts myxoma was in capsule and in106 (31,8%) pts without one. Episodes of emboli were occurred in 15 (4,2%)pts.Maternal basement was removed by wide resection of the interatrial septum(n = 195 pts) (group A) and without broad resection of the septum (n = 158 pts)(group B. Malignant tumor of the LA was removed with LA‘s wall and replaced thispart of the LA with the autopericardial patch. All operations were performed withCPB and moderate hypothermia. At the last 3 years modified biatrial approach toLA‘s myxoma was used.Results: Hospital mortality for malignant tumors was 20,0% (10/2): LA (n = 9/2),LV (n = 1/0) and for other forms - 9,4% (n = 352/33): LA (n = 342/31), LV (n =10/2) The main reasons of hospital mortality were heart failure and brain damagebecause pts had entered to clinic with heart failure (as a rule, giant myxoma) andwith previous episodes of emboli (absence of myxoma‘s capsule). At the late pe-
riod 293 (93,8%) pts were observed during 1 till 17 years after correction. Therewere 7 (1,9%) recurrences of myxoma (all left atrium). Four were successful re-operated. All pts belonged to group B. During last 5 years hospital mortality in thegroup with LA‘ tumors was 2,8% (141/4).Conclusion: Myxomas were occurred frequently in female age more than 45years old. The late result of myxoma‘s correction should be successful in caseswith broad resection of maternal bottom (interatrial septum) and replacement onewith autopericardial patch.
P5452 Excess mortality in presumed tuberculouspericarditis
C.S. Wiysonge1, M. Ntsekhe1, F. Gumedze1, G. Maartens1,J.A. Volmink1, P.J. Commerford1, B.M. Mayosi2 on behalf of IMPIAfrica Investigators. 1University of Cape Town, Medicine, Cape
Town, South Africa; 2University Of Cape Town, Department of Medicine, CapeTown, South Africa
Background: The mortality associated with tuberculous pericarditis in the humanimmunodeficiency virus (HIV) era is unknown.Objectives: The purpose of this study was to investigate the mortality rate, pre-dictors of death in presumed tuberculous pericarditis during six months of antitu-bercular therapy.Methods: Between March 1, 2004 and October 31, 2004, consecutive patientswith presumed tuberculous pericarditis were recruited from 15 referral hospitalsin Cameroon, Nigeria, and South Africa, and followed for 6 months. The diagno-sis of tuberculous pericarditis and HIV status was made on clinical and/or labo-ratory criteria. The mortality rate was determined by Kaplan-Meier analysis, andCox proportional regression was used to identify independent predictors of death.Mortality was stratified by clinical HIV status.Results: 185 patients (median age 33, range14 to 87 years) were studied. Theoverall mortality rate was 26% at 6 months. The presence of clinical features ofHIV infection conferred a mortality rate of 40%, compared to 17% in those with-out. The independent predictors of death were a proven non-tuberculosis diagno-sis (hazard ratio [HR] 7.33; 95% confidence interval [CI] 2.39, 22.50; P=0.001),residence outside South Africa (Ibadan, Nigeria: HR 3.22; 95% CI 1.38, 7.49;P=0.007; Yaoundé, Cameroon: HR 4.89; 95% CI 2.28, 10.49; P<0.001), pres-ence of clinical features of HIV infection (HR 3.1; 95% CI 1.52, 6.33; P=0.002),and age (HR 1.02; 95% CI 1.01, 1.05; P=0.028).Conclusion s: Patients with presumed tuberculous pericarditis have an exces-sively high mortality rate despite treatment with antituberculous drugs, especiallyin those with clinical signs of HIV infection.
P5453 Subxiphoid pericardiocentesis followed byintrapericardial infusion of antineoplastic drugsversus pericardial window via thoracotomy:management of malignant cardiac tamponade
C. Lafaras1, D. Platogiannis2, E. Mandala3 , N. Barbetakis3,A. Banti3, E. Verrou3, D. Mihou3, T. Bischiniotis3. 1Theagenion Cancer Hospital,Department of Cardiology, Thessaloniki, Greece; 2Theagenion Cancer Hospital,Department of Cardiology, Thessaloniki, Greece; 3Aristotle University ofThessaloniki, D’ Department of Internal Medicine, Thessaloniki, Greece
Introduction: Malignant involvement of the heart and/or pericardium is not un-common in patients with advanced cancer (10%) and is involved in the mecha-nism of mortality in 1/3 of the cases. Metastases may occur either from direct in-vasion by an adjacent primary tumour or by lymphatic or haematogenous spread.Acute treatment of malignant cardiac tamponade involves prompt complete re-moval of pericardial fluid, by pericardiocentesis or surgical intervention.Purpose: This study was performed in order to compare effectiveness and safetyof the two methods, which are used to manage large pericardial effusions.Methods: Since 2000, 95 patients with cancer, 58 men (median age of 63years) and 37 women (median age of 59 years), were studied. Fifty patients hadlung cancer (52.6%), 25 breast cancer (26.3%), 5 patients had bladder cancer(5.26%), 6 lymphoma (6.3%), 5 ovarian cancer (5.25%), one thymoma (1.1%)and 2 colon cancer (2.1%). Critically ill patients (group A, consisted of 70 pa-tients, 73.6%) underwent subxiphoid pericardiocentesis under ECG, echocardio-graphic and haemodynamic guidance. After the malignant aetiology of pericardialfluid had been confirmed by cytological examination intrapericardial chemother-apy was performed according to chemosensitivity of the primary tumour (10 mgcisplatin per day, instilled in three consecutive days, in lung cancer patients, 45mg theotepa in breast cancer and 30 mg bleomycin to the rest patients). Group B,consisted of 25 patients (26.4%), underwent left side thoracotomy and pericardialwindow fenestration. Clinical and echocardiographic evaluation was performedevery month thereafter.Results: There were no serious complications (except for transient electrical in-stability) and prompt clinical improvement was observed. Three of 70 patientsin group A relapsed (4.2%) and two developed constrictive pericarditis (2.8%).The patients who relapsed underwent surgical intervention, while pericardiectomywas performed in the two patients who developed constrictive pericarditis. On thecontrary, none of the patients of group B relapsed. Mean survival period was 6months.Conclusions: Both methods are effective and safe in confronting cardiac tam-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 959
ponade. After pericardiocentesis, intrapericardial chemotherapy according tochemosensitivity of the primary tumor, might be the method of choice in prevent-ing reaccumulation of pericardial fluid without significant side effects, in criticallyill patients. On the other hand, results of pericardial window formation are morepermanent, although the procedure is more invasive.
P5454 Apoptosis and cell cycles in cardiac myxoma
P.-H. Chu1, S.-M. Jung2. 1Chang Gung Memorial Hospital &University, The First Cardiovascular Dept., Taipei, Taiwan; 2ChangGung Memorial Hospital and University, Taipei, Taiwan
Background: Cardiac myxoma the most primary tumor of theheart, has multiple differentiating potentials, and recently various amounts ofcardiomyocyte-specific transcription factor genes are identified. This indicatesthat cardiac myxoma might arise from mesenchymal cardiomyocyte progenitorcells. This investigation will elucidate the possible pathways of apoptosis and cellcycle in the cardiac myxomas.Methods: This study included a cultured cardiac myxoma cell line, and 20 pa-tients with cardiac myxoma, who were treated with surgical excision of the lesion.Apoptosis signal transduction, Fas, Fas-ligand (FasL), tumor necrosis factor-α(TNF-α), Bcl-2, survivin, caspase-3, and terminal deoxynucleotidyl transferasenick-end labeling (TUNEL) assay; and cell cycles proteins, Ki-67 (MIB-1), p16,p53, and p63, were studied by both immunohistochemical and Western blot anal-ysis.Results: The patient population was comprised of 12 (60%) women and 8 (40%)men. All study patient cases were sporadic myxomas rather than familial myx-oma. The presentations included: asymptomatic (26%), dyspnea (44%), stroke(9%), chest pain (9%), and fever (11%). All lesions were located in the left atrium.The myxoma did not differ with location or clinical event in terms of patho-logical scores. Apoptosis documented by TUNEL (70.9+17.6%) and caspase-3 (66.5+32.5%) common final pathway in cardiac myxoma is characterized byextrinsic Fas/Fas-L (positive stained 70.9+19.2%; 26.0+17.2% each) dependentpathway, but not intrinsic TNF-α or Bcl-2 dependent pathway. On the other hand,survivin, suppressing apoptosis and regulating cell division, is strongly expressedin the cytoplasm (65.5+19.4%) to effect cell proliferation (Ki-67; 10.1+8.9%) andcell death (p63; 49.5+29.1%). The Western Blot analysis (Fas/Fas-L, TNF-α, p16,p53 p63 and caspase-3) of the cultured cardiac myxoma cells proved the im-munochemical results.Discussion: Cardiac myxomas exists both extrinsic dependent, Fas/FasL, andanti-apoptosis, survivin, pathways to control cell cycles with the changes of Ki-67,p16, p53 and p6, in cardiac myxoma.
P5455 Tissue Doppler imaging predicts the development ofFabry cardiomyopathy in preclinical stage
R. Toro1, J. Zamorano1 , G. Doxastakis1, L. Perez De Isla2,G. Pintos3, R. Torra4 , J. Ballarin1, J. Torras5. 1HospitalClinico San Carlos, Unidad de Imagen Cardiovascular, Madrid,
Spain; 2Hosp.Clinico San Carlos,Instituto Cardiovasc., Unidad De ImagenCardiovascular, Madrid, Spain; 3Hospital Trias i Pujol, Badalona, Spain;4Fundacion Puigvert, Barcelona, Spain; 5Hospital Bellvitge, Barcelona, Spain
Fabry disease (FD)is a rare X-linked lysosomal disorder caused by α-galactosidase A deficiency. Cardiovascular involvement appears to be a mayorcause of FD patients morbility and mortality. Systolic and diastolic myocardial ve-locities measure by tissue doppler imaging (TDI) were shown to be decreased insubjects who have mutations causing Fabry cardiomyopathy. We sought to deter-mine whether TDI predicts preclinical cardiac involvement of Fabry patients.Methods: We studied three groups of subjects: 18 healthy subjects, 42 Fabry pa-tients without left ventricular hypertrophy (LVH) and 17 with LVH. Patients with FDwere confirmed by enzyme essay and DNA analysis. In all patients 2-dimensionalechocardiography with tissue doppler analysis in the pulsed doppler mode wasperformed.Results: E TDI velocities were decreased and TCI and TRI were significantlyincreased compared with control sbjects (all P<0.05). TCI showed the best sen-sitivity and specificity in identifying patients with preclinical FC. See table.
E TDI (cm/s) TRI (ms) TCI (ms)
AUC 0.6 0.83 0.97OCP 15.5 60 105S (%) 44.4 27.8 100E (%) 93.2 96.6 91PPV (%) 66.7 71.4 78.2NPV (%) 84.6 81.4 100
Area under curve (AUC); Optimal cuttoff point (OCP); Sensitivity (S); Specificity (E); Positivepredictive value (PPV); Negative predictive value(NPV); Early diastolic myocardial wave velocity(E tdi); Ventricular isovolumetric contraction time (TCI);Ventricular isovolumentric relaxation time(TRI).
Conclusions: This results stablishes TDI as a reliable method for early identifica-tion of Fabry cardiomyopathy. Patients with LVH always show TDI abnormalities.But, moreover, there are patients without LVH that show TDI abnormalities.
P5456 Ischemic versus dilated cardiomyopathy. Incrementaldiagnostic value of Tissue Doppler Imaging
K. Papadopoulou, C.E. Papadopoulos, T.D. Karamitsos,E.G. Dalamanga, G. Giannakoulas, T. Zaglavara, H. Karvounis,G. Parharidis. AHEPA University Hospital, Cardiology, Thessaloniki,
Greece
Recently, early diastolic mitral annulus velocity (Em) has evolved as a powerfulpredictor of cardiac mortality in patients with left ventricular (LV) systolic impair-ment. Additionally, E/Em ratio correlates well with LV filling pressures.The aim of the present study was to evaluate these specific indexes in patientswith severely depressed LV systolic function and accordingly to investigate theirdiagnostic power to differentiate patients with ischemic cardiomyopathy (ICM)from those with dilated cardiomyopathy (DCM).Methods: Eighteen patients with ICM (mean age 62 ± 9, 16 males, mean EF 31± 8%) and 17 with DCM (mean age 45 ± 12, 12 males, mean 28 ± 7%) com-prised the study population. All patients underwent complete echo study, underrelative stable clinical and haemodynamic conditions. Using 2D echocardiogra-phy LV volumes, mitral valve tenting area (MVTA) and ejection fraction (EF) wereobtained. Mitral regurgitation (MR) was assessed using the PISA technique andeffective regurgitant orifice area (ERO) and regurgitant volume (RV) were cal-culated. Using conventional Doppler of mitral inflow E wave, A wave, E/A ratioand decceleration time were assessed. Finally mitral annulus velocities were ob-tained using Tissue Doppler Imaging (systolic-Sm, early diastolic-Em) and furtherassessment of E/Em index was performed.Results: The two groups had similar LV volumes, EF and standard Doppler di-astolic function indexes. Patients with ICM had more severe MR compared topatients with DCM according to ERO (0.16 ± 0.08 vs 0.1 ± 0.04 cm2, p<0.05)and RV (27 ± 18 vs 15 ± 9 ml, p<0.05). Additionally MVTA, that stands as anindex of LV remodeling and papillary muscle displacement was increased in ICMpatients compared to DCM (2.3 ± 0.8 vs 1.7±0.7 cm2, p<0.05). Tissue Dopplermitral annulus velocities were significantly lower in ICM group (Sm 2.3 ± 0.8 vs3.4 ± 0.9 cm/s, p=0.001, Em 2.5 ± 1.1 vs 4 ± 1.3 cm/s, p=0.001) and E/Em in-dex was increased (43 ± 31 vs 22 ± 7 p=0.009) compared to DCM group. Fromall indexes assessed, Em was the most significant predictor of ERO (R square0.520, p=0.002).Conclusions: Patients with ICM have lower mitral annulus velocities and in-creased LV filling pressures compared to patients with DCM and consequentlymay share worse prognosis. Em may quite accurately predict the severity of func-tional MR which in patients with severe heart failure is associated with the degreeof LV remodeling and thus to papillary muscle displacement and possibly dyssyn-chrony.
P5457 Morbidity and mortality of arrhythmogenic rightventricular cardiomyopathy: sudden cardiac death orheart failure?
S. Peters1, M. Truemmel2 . 1Klinikum D. Erxleben Quedlinburg,Innere Medizin Ii - Kardiologie, Quedlinburg, Germany; 2Klinikum
Quedlinburg, Cardiology, Quedlinburg, Germany
Arrhythmogenic right ventricular cardiomyopathy seems to be in most cases adisease of younger males with the risk of sudden arrhythmic death. Long-termfollow-up shows that progressive heart failure represents another important com-plication. The correlation of sudden cardiac death (SCD) and heart failure (HF)with regard to mortality and morbidity should be analysed in 243 symptomaticpatients (153 males, mean age 45.3 years) from different primary and tertiarycenters with a mean follow-up of 8.5 years.Results: The total rate of malignant arrhythmias in the follow-up was 13% witha mean age of 38.7 years. Five SCD’s and 27 adequate terminations of ventric-ular arrhythmias by ICD occurred in a mean time interval of 2.2 years (annualrate 6.0%). These observations were exclusively found in 166 patients with doc-umented ventricular arrhythmias and syncopes so that the event rate in this highrisk group was even higher with 19% (annual rate 9%). Symptomatic HF occurredin 13 cases (5%) with a mean age of 64.5 years in a mean time interval of 3 years(annual rate 0.5%). HF occurred in patients with initial ventricular arrhythmias,atrial arrhythmias, syncopes and atypical chest pain.Conclusions: Leading complication of ARVD/C in the follow-up remain malig-nant ventricular arrhythmias in younger patients. Highly therapy resistant HF rep-resents another significant complication in predominantly elderly patients.
P5458 Arrhythmogenic right ventricular cardiomyopathy: theEuropean Clinical Registry
C. Basso1, T. Wichter2, K. Wlodarska3, A. Nava4, W.J. Mckenna5,N. Protonotarios6, L. Antoniades7, G. Thiene7. 1Pathology,University of Padua, Padova, Italy; 2Cardiology, Muenster, Germany;
3Cardiology, Warsaw, Poland; 4Cardiology, University of Padua, Padua, Italy;5Cardiology, Heart Hospital, London, United Kingdom; 6Cardiology, Naxos, HoraNaxos, Greece; 7Cardiology, Nicosia, Cyprus
Aims: A multidisciplinary collaborative study has been established by the Euro-pean Commission with the aim to investigate the clinical, pathological and geneticfeatures of arrhythmogenic right ventricular cardiomyopathy (ARVC). The clinical
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

960 Novel aspect of Myocardial and Pericardial disease
registry has the following specific targets: validation of diagnostic criteria, riskstratification, epidemiology and familial occurrence, and Naxos disease.Methods and Results: Index cases with a definite diagnosis of ARVC and fam-ily members have been enrolled in a WEB constructed data base and labelledas affected, uncertain or non-affected based upon the currently available diag-nostic criteria. Blood samples from each case entering the clinical registry has tobe collected and tissue sample from biopsy and/or autopsy when available. Onlysubset fitting minimal conformance, ie with at least completed forms of clinicalhistory, medical history, 12-lead ECG, cardiac imaging-echo and/or angio and/orMRI-, and diagnostic test review) were considered in the preliminary analysis ofdata. In a 5 years interval (2001-2005) a total 1010 cases have been enrolled,consisting of 552 probands (372 M and 180 F) and 458 family members (230 Fand 228 M). Probands were collected from Italy (162, 29%), Poland (156, 28%),Germany (131, 24%), UK (79, 14%) Naxos (15 recessive form, 3%) and Cyprus(9, 2%). Among family members, 104 (23%) were considered borderline and 129(28%) affected accordingly to the Task Force diagnotic criteria. Mean age at di-agnosis was 36 yrs in the probands and 35 in the family members. Among theprobands, ARVC was diagnosed due to the onset of sustained VT in 166 (30%),non-sustained VT in 53 (10%), family history of ARVC and/or sudden death in 71(13%) and previous cardiac arrest in 31 (6%). Moreover, 310 (57%) are currentlyunder antiarrhythmic therapies, 76 (14%) underwent catheter ablation and 162(29%) received an ICD implantation. Tissue sample for histopathology analysis isavailable in 185 probands (33%).Conclusions: Because of the rarity of the disease, the ongoing multicenter largescale ARVC clinical database offers the unique opportunity to collect a significantnumber of patient population affected by either familial or sporadic forms, in orderto prospectively evaluate the accuracy of clinical diagnostic criteria, the long termoutcome and the efficacy of therapies.
P5459 In vitro validation of endomyocardial biopsy for the invivo diagnosis of arrhythmogenic right ventricularcardiomyopathy
C. Basso, F. Ronco, A. Abudureheman, G. Thiene. Pathology,Institute Of Pathological Anatomy, Padova, Italy
Background: Tissue characterization by endomyocardial biopsy (EMB) is a ma-jor criterion for in vivo diagnosis of arrhythmogenic right ventricular cardiomy-opathy (ARVC). Aim of our study was to in vitro assess the histomorphometricparameters in both physiologic and pathologic conditions, in order to define theirdiagnostic cut-off, sensibility and specificity.Methods: Sixty hearts were selected: 20 ARVC, 10 dilated cardiomyopathy, 10healthy controls, 10 adipositas cordis and 10 aged >80 yrs. An in vitro EMBwith Cordis bioptome was performed in the subtricuspid, apex, infundibulum andseptum of the RV and in the left ventricular free wall, for a total of 5 samplesper heart. Histomorphometric analysis was carried out on Heidenhain thricromestained EMB slides by Image ProPlus 4.0, to evaluate the amount of myocardium,fibrous and fatty tissue (percentage of the total EMB area). Data were comparedby ANOVA, and cut-off, sensibility and specificity were calculated by ROC curves.Results: The mean residual RV myocardium in ARVC was 54,5%± 16,8(p<0.001 vs the other groups), varying from 33,1%±29,8 in subtricuspid, to33,6%±22,7 in the apex, to 67,4%±21,4 in the infundibulum, to 83,9%±8,9in the septum. The ARVC diagnostic cut-off was a residual RV myocardium<64% (sensibility 80% and specificity 90%). The mean RV fatty tissue inARVC was 16,1%±13,2, with significant differences only vs controls (2,7%±3,6,p<0,001) and dilated cardiomyopathy (1,7%±1,9, p<0,001), but not vs adiposi-tas cordis group (10,6%± 8,1) and the elderly (7,2%±3,9). The RV fibrous tis-sue was increased both in ARVC (29,3%±11,5) and in dilated cardiomyopa-thy (19%±9,4; p=NS).When considering the RV apex sampling site, fatty tis-sue amount was higher in ARVC (31,9%±26,4) than in dilated cardiomyopa-thy (4,1%±5,1 p<0,05), but no significant differences were found vs controls(10%±15,1), adipositas cordis (30,8%±25,2) and the elderly (26,2 ± 14,3). Adiagnostic cut off of RV apex fibrosis>19% (85% sensibillity and 85% specificity)and of RV apex residual myocardium <42% (60% sensibillity and 90% specificity)have been calculated. No significant differences were found among the groupswhen considering the septum and the left ventricle.Conclusions: EMB’s sensibility and specificity change accordingly to the sam-pling site and to the analysed tissue parameter. Fatty tissue is mostly aspecificparticularly at the apex, whereas the residual RV myocardium and fibrous tissueappear the most relevant diagnostic parameters. Septal and left ventricular EMBare not useful for diagnostic purposes in ARVC.
P5460 Radiofrequency catheter ablation of septalhypertrophy in children with hypertrophic obstructivecardiomyopathy: initial experience
N. Sreeram1, J.V. Degiovanni2, M. Emmel3, K. Brockmeier4.1University Hospital Of Cologne, Dept Of Pediatric Cardiology,
Cologne, Germany; 2Birmingham Children’s Hospital, Pediatric cardiology,Birmingham, United Kingdom; 3University of Cologne, Pediatric cardiology,Cologne, Germany; 4University Hospital of Cologne, Pediatric cardiology,Cologne, Germany
Background: Surgical septal myectomy is at present the gold standard for ther-
apy of hypertrophic cardiomyopathy (HOCM) in children. Percutaneous radiofre-quency catheter ablation for septal reduction is however technically feasible, lessinvasive, and avoids the risk of permanent AV block.Aims: To describe the initial result and early follow-up data after RFA for reductionof septal hypertrophy in children with symptomatic HOCM.Patients and Methods: 8 children (5 female) ranging in age between 5 and 17years and in weight between 17 and 52 kg with symptomatic HOCM underwentRFA. Left ventricular angiography was performed to delineate the anatomical ex-tent of septal obstruction. Sequential AV pacing at varying AV intervals was thenperformed to assess the influence of pacing on the catheter withdrawal gradient.If no beneficial effect was seen, RFA was performed. The entire His bundle wasmarked and plotted using the using the Localisa navigation system (MedtronicUSA). Using an 8F cooled tip catheter (Sprinklr, Medtronic USA) with an infusionrate of 300 ml/minute during RF lesion application, ablation was commenced atthe most apical location of septal hypertrophy. Contiguous lesions were placedextending proximally to the aortic valve, taking care to stay away from the Hisbundle. Care was also taken to ensure that there were no gaps between adja-cent lesions, guided by the Localisa system. Three such lines of lesions wereproduced in each patient. The number of RF lesions (dictated by the anatomicalextent of septal hypertrophy) ranged between 10 and 50.Results: The left ventricular Doppler gradient changed from a median of 80 mmHg (range 50-112) pre-RFA to 30 mm Hg (20-50) at 72 hours post-procedure. Car-diac troponin T (5.1-8.6 micrograms/L; normal range <0.1) and CK-MB (45-397units/L; normal <20) were considerably elevated post-RFA, confirming significantmyocardial necrosis. All patients were discharged within 48 hours of the proce-dure, and none had AV block. All had relief of symptoms at 6 weeks’ follow-up.Recurrence of obstruction, or incomplete relief was observed in 3 patients within6 months of initial RFA; 1 underwent a second RFA with success, 1 patient isawaiting surgery and a third has been lost to follow-up (followed up elsewherewith no further data available).Conclusions: RFA for HOCM produces acute relief of LVOT obstruction with res-olution of symptoms. It avoids the risk of AV block, shortens hospital stay, and canbe repeated. Further experience appears to be warranted.
P5461 Septal ablation for hypertrophic cardiomypathy, byusing the patient’s own thrombosed blood
W. Kadro1, M.A.Y.A. Turkmani1, D.A.N.A. Kadro1, F.A.Y.A.Z. Shawl2.1Golden Cardiovascular Center, Interventional Cardiolgy, Damascus,Syria Arab Republic; 2Washington Adventist Hospital, Interventional
Cardiolgy, Takoma Park, United States of America
Background: Alcohol septal ablation has been recommended as a new treatmentfor reducing or removing dynamic LVOT obstruction in hypertrophic cardiomypa-thy (HOCM). This procedure carries the risk of alcohol spill over which could resultin a massive anterior myocardial infarction. We report a new method for septal ab-lation by injecting the patient’s own thrombosed blood into the septal branch of theleft anterior descending artey (LAD).Method: 3 patients with HOCM were treated in our center by this new method.After wiring the septal branch through the guiding catheter, an over the wire Bal-loon was advanced into the branch. After balloon inflation, the wire was removed.The patient’s own blood was obtained into a syringe through the side arm of the Yconnector. The appropriate septal branch was chosen by hemodynamic monitor-ing of the gradient during balloon inflation. After selecting the branch the balloonwas kept inflated in it. The thrombosed blood was injected into the septal branchthrough the lumen of the balloon; the thrombus was advanced through the bal-loon by advancing a wire through the balloon’s lumen at one time and injectingsaline through that lumen at a second time. The thrombus reached the lumenof the septal branch distal to the inflated balloon and caused total obliteration ofthe branch lumen. After flushing the balloon’s lumen with saline, the balloon wasdeflated and removed from the branch over a wire.Results: All the 3 patients tolerated the procedure well. There was no develop-ment of high degree AV block. No malignant ventricular arrhythmias were noted.There were no needs for another septal branch ablation in all the three caseshowever this procedure can be repeated easily in another branch by following thesame protocol.Conclusion: Using the patient’s own thrombosed blood is a safe method for sep-tal ablation in HOCM. Larger series are required for confirming its safety. A ran-domized trial comparing it with alcohol septal ablation is a good idea. Industryshould work on improving the way of thrombus delivery by giving us a low profilecoronary balloon with 2 mm diameter and a large lumen (e.g. 0.025 or larger).
P5462 The role of myocardial contrast echocardiographyduring percutaneous transluminal septal myocardialablation in predicting the site and size of myocardialinfarction
C. Van Der Lee1, W.G. Van Dockum2, M.L. Geleijnse1, R.T. VanDomburg1, A.C. Van Rossum2, F.J. Ten Cate1. 1Erasmus MC Rotterdam,Cardiology, Rotterdam, Netherlands; 2VU University Medical Center, Cardiology,Amsterdam, Netherlands
Background: Percutaneous transluminal septal myocardial ablation (PTSMA) in-duces a localized septal myocardial infarction (SMI) to reduce left ventricular
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 961
outflow tract obstruction in symptomatic patients with hypertrophic obstructivecardiomyopathy (HOCM). Myocardial contrast echocardiography (MCE) guidedPTSMA has been introduced to accurately predict site and size of SMI, whichparameters are both of importance to achieve optimal hemodynamic results andto maximally preserve left ventricular function after PTSMA. The present study isthe first to evaluate the role of MCE in predicting location and extension of SMI,assessed by 1-month follow-up magnetic resonance imaging (MRI).Methods and Results: Seventeen consecutive HOCM patients underwentSonoVue® MCE-guided PTSMA. All patients had SonoVue® opacification of themid anteroseptal and posteroseptal segments. At follow-up, 91% of these seg-ments showed SMI at MRI. SonoVue® opacification was present in 41% of thebasal anteroseptal and posteroseptal segments. Negative and positive predictivevalues of SonoVue® opacification for basal SMI at MRI were 10% and 86%, re-spectively. The correlation between SonoVue® opacified septal surface area andMRI determined SMI volume was poor (R = 0.09, P = NS). Injected ethanol vol-ume correlated significantly with mean peak CK-MB fraction (R = 0.73, P <0.001).Conclusions: MCE has an excellent positive predictive value for the desired mid-septal site of induced SMI. However, SMI frequently extended into more basalseptal parts and the correlation between the SonoVue® opacified area and MRIdetermined SMI size at follow-up is poor. SMI size depends primarily on injectedethanol volume.
P5463 Differences in diagnostic value of abnormal Q wavesbetween hypertrophic cardiomyopathy with a cardiactroponin I gene mutation and cardiac myosin bindingprotein-C gene mutations
K. Nakashima, H. Ino, N. Fujino, K. Hayashi, K. Uchiyama,T. Konno, T. Hayashi, M. Yamagishi. Kanazawa University, Molecular Genetics ofCardiovascular Disorder, Kanazawa, Japan
Purpose: Abnormal Q waves are one of the major diagnostic criteria of elec-trocardiography in hypertrophic cardiomyopathy (HCM). However, abnormal Qwaves may have different diagnostic value for HCM among various mutations be-cause clinical phenotypes differ for each genotype. We assessed the hypothesisthat the frequency and appearance time of abnormal Q waves for HCM may differfor different genotypes.Methods: We analyzed 43 carriers with a cardiac troponin I (TNNI3) gene muta-tion and 38 carriers with cardiac myosin-binding protein C (MYBPC3) gene mu-tations. Q waves were regarded as abnormal if depth was >1/4 of the ensuing Rwave and/or duration >0.04 second at least two leads except aVR.Results: In subjects aged <20 years, abnormal Q waves were found in 5 of 10(50%) carriers with the TNNI3 gene mutation. In contrast, they were found in onlyone of 6 (17%) carriers with the MYBPC3 gene mutation. In subjects aged >20years, abnormal Q waves were found in 13 of 33 (39%) carriers with the TNNI3gene mutation, while in 7 of 32 (22%) carriers with the MYBPC3 gene mutation.Conclusions: In conclusion, abnormal Q waves were found more frequently incarriers with the TNNI3 gene mutation compared with those with the MYBPC3gene mutations, especially in the young. These results suggest that abnormal Qwaves may have different diagnostic values for HCM according to genotype andage.
P5464 Systolic and diastolic echocardiographic evaluationin patients with Thalassemia major:correlation withferritin concentration, BNP and overload measured byMRI
M. Vieira, N. Hamerschlak, J.R. Parga, E. Lira Filho, L. Rosenberg,A. Cury, C.H. Fischer, S.S. Morhy. Hospital Israelita Albert Einstein, Sao Paulo,Brazil
Background: Patients with Thalassemia major (TM) submitted to regular bloodtransfusions may present heart failure in the clinical follow-up. The purpose ofthis study was to correlate systolic and diastolic echocardiographic evaluationwith serum ferritin concentration, B-type natriuretic peptide (BNP) and heart ironoverload measured by magnetic resonance imaging (MRI T2) in patients with TM.Methods: We studied 71 TM consecutive patients (41 males, age 22 ± 8 yrs). Inthe echocardiographic evaluation we measured LV systolic and diastolic volumesand diameters, LV Mass index (ASE formula), LVEF, E and A wave, E/A ratio,IRVT, DT, pulmonary vein flow evaluation (S wave, D wave, S/D ratio, A wave).By Doppler Tissue Imaging we measured E’ wave, A‘ wave, S wave, E’/A’ratioin the basal segment of the mitral valve annulus of the septum, lateral, anteriorand inferior walls, as well as in the basal segment othe tricuspid annulus of theRV lateral wall. We measured serum ferritin concentration (N: 10-291 ng/mL) andBNP (N<10 pg/mL). By MRI we measured LV volumes, LV Mass index, LVEFand cardiac iron overload by MRI T2 (N:T2>20ms; important cardiac overloadT2<8ms). Echocardiographic data was compared to ferritin concentration, BNPand MRI data by coefficient of determination-Spearman (r) 95% IC, p<0.05.Results: Serum ferritin concentration ranged from 59 to 9108 (2663 ± 1970)ng/mL; BNP ranged from 5 to 241 (33.5 ± 23. 34) pg/mL, MRI T2 ranged from 4to 52 (24.95 ± 14.11) ms. Fourteen patients presented MRI T2 < 8ms;32 pts withT2 between 8 and 20 ms; 25 patients presented MRI T2 > 20 ms. All patientspresented normal LVEF and LV Mass index (echo and MRI). Relative to diastolicevaluation: S/D ratio <1 correlated to serum ferritin concentration (p=0.047, r=
-0.23661); and to MRIT2 (p=0.0354; r= 0.25018). Septal E’/A’ratio<1 correlatedto MRI T2 (p=0.0676; r=0.21813); and RV E’/A’ratio<1 correlated to serum ferritinconcentration (p=0.0909, r=0.20219).Conclusions: In this Thalassemia major series, we observed normal LV systolicfunction as well as LV Mass index, despite important cardiac iron overload andhigh serum ferritin concentration. Diastolic disorders were observed, in spite ofweak correlations with MRI T2 and serum ferritin concentration.
P5465 A prospective study of biopsy-proven myocarditis:prognostic relevance of clinical and etiopathogeneticfeatures at diagnosis
A.L.P. Caforio1, F. Calabrese2, F. Tona3, A. Angelini1, A. Ramondo2,S. Iliceto2, G. Thiene1, L. Daliento2. 1Dept Cardiological Thoracic
Vascular Sciences, Division of Cardiology, Padua, Italy; 2Cardiac Pathology,Padua, Italy; 3Cardiological Thoracic Vascular Sciences, Padua, Italy
Myocarditis may be idiopathic, viral and/or immune; frequency of these forms andprognosis are ill defined.Purpose: To assess frequency of myocarditis forms and prognostic role of diag-nostic findings at presentation, including viral genome and serum anti-heart autoantibodies (AHA).Methods: We studied 174 myocarditis patients, 110 males, aged 36 ± 18 years,follow-up 35 ± 37 months. Endomyocardial biopsy (EMB) showed in 85 patientsactive, in 89 borderline myocarditis (Dallas criteria). AHA were detected by in-direct immunofluorescence on human myocardium and skeletal muscle. Poly-merase chain reaction (PCR) was used to detect virus on EMB.Results: Actuarial survival (Kaplan Meier) was of 73% at 6 years. AHA werefound in 56% of patients, in 26% PCR was positive for virus. Based upon AHAand PCR, myocarditis was autoimmune in 48% of patients, viral in 9%, viraland immune in 12%, idiopathic and/or cell-mediated in 31%. Univariate predic-tors of death/transplantation were: longer symptom duration, giant cell myocardi-tis, NYHA II-IV, positive PCR, presentation with left ventricular (LV) dysfunction,clinical signs/symptoms of heart failure, multiple echocardiographic and hemody-namic indexes of LV and right ventricular (RV) dysfunction. The only independentnegative predictor by Cox regression was RV end-diastolic pressure >6 mmHg(RR 6, p=0.01).Conclusions: In myocarditis, RV dysfunction at diagnosis was the main indepen-dent negative predictor in the mid-term. AHA identified immune-mediated my-ocarditis in 56% of cases. Viral genome by PCR had a negative prognostic valueby univariate analysis. The potential role of etiology as independent predictorshould be clarified in the long-term.
P5466 Thrombospondin 2 protects against uncontrolledcardiac inflammation and injury during viral anddoxorubicin-induced myocarditis
M. Swinnen1, D. Vanhoutte2 , Y.M. Pinto2, S. Heymans2. 1Universityof Maastricht/CARIM, Department Of Cardiology, Maastricht,
Netherlands; 2University of Leuven, Center of Transgene Technology & GeneTherapy, Leuven, Belgium
Background: The matricellular protein thrombospondin 2 (TSP2), a secretedextracellular matrix (ECM) glycoprotein, plays a crucial role in controlling cell-matrix interaction, inflammation and angiogenesis in cancer biology. Recently, ourgroup demonstrated that increased cardiac expression of TSP-2 during hyperten-sion reflects a protective mechanism against heart failure. Whether TSP-2 maybe involved in preventing exaggerated cardiac inflammation and thereby protectagainst heart failure during inflammatory cardiomyopathies remains, however, un-known.Methods and Results: Mortality, cardiac inflammation and function were inves-tigated in TSP2-null (KO) and wild type (WT) mice during coxsackie virus B3(CVB3)-induced (10E6 CCID50 ip CBV3, 7 days) and doxorubicin-induced (dox-orubicin: 6mg/kg/week for 4 weeks) myocarditis. Absence of TSP2 resulted inan increased mortality in TSP2-null as compared with WT mice in both viral my-ocarditis (KO: 37,5% vs. WT: 0%; n=8 per group) and doxorubicin-induced (KO:30% vs. WT: 0%; n=10 per group) myocarditis. Histological analysis revealed in-creased cardiac inflammation (CD3-positive T-lymphocytes), necrosis and evendisruption with fatal pericardial bleedings in TSP2-null compared to WT mice at 7days of viral myocarditis. Concordantly, influx of CD-45 positive leukocytes, car-diac necrosis and injury were increased in TSP2-null compared to WT mice at 4weeks of doxorubicin-injection. Detailed structural analysis revealed severe ma-trix disruption and myocyte injury in absence of TSP2 in both inflammatory car-diomyopathies. Increased inflammation and injury in absence of TSP2 resulted indepressed systolic function (% EF; 75.1 ± 6.8 in WT vs.77.3 ± 5.1 in KO mice,P<0.05) and increased cardiac dilatation (end-diastolic dimensions, mm; 2.3±0.2 in WT vs. 3.1± 0.3 in KO mice, P<0.05), as revealed by echocardiographicanalysis at 4 weeks of doxorubicin- induced myocarditis.Conclusion: Together, these data point towards a novel protective role of TSP2against uncontrolled inflammation, myocardial injury and dysfunction in inflamma-tory cardiomyopathy.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

962 Novel aspect of Myocardial and Pericardial disease
P5467 Presentation, patterns of myocardial damage andclinical course of viral myocarditis
H. Mahrholdt1, A. Wagner2, C.C. Deluigi2, G. Meinhardt2,H. Volgelsberg2, K. Klingel3, R. Kandolf3, U. Sechtem2. 1RobertBosch Medical Center, Cardiology, Stuttgart, Germany; 2Duke
Cardiovascular MR Center, Durham, United States of America; 3University ofTuebingen, Pathology, Tuebingen, Germany
Myocarditis is a common cardiac disease. It appears to be a major cause of sud-den death, and may progress to develop chronic dilated cardiomyopathy (DCM).Entero- and adenoviruses have been considered as the most common causesof viral myocarditis, but parvovirus B19 (PVB19) as well as human herpesvirus6 (HHV6) is increasingly found in endomyocardial biopsy samples. However, theprevalence of those new viruses in myocarditis patients, their clinical presentationas well as the clinical course is widely unknown.Consequently, our aim was to evaluate the prevalence and clinical presentationof cardiac PVB19 and/or HHV6 infection in a cohort of myocarditis patients aswell as to follow its clinical course. In addition, we sought to demonstrate patternsof myocardial damage and to determine predictors for recovery as well as forprogression towards chronic heart failure. Our study design consisted of a cardio-vascular magnetic resonance (CMR) protocol as well as endomyocardial biopsies(EMB) in the myocardial region affected as indicated by CMR.One-hundred-twenty-eight patients were enrolled by clinical criteria. In the groupof patients diagnosed with active myocarditis by Dallas criteria (n=87), PVB19(n=49), HHV6 (n=16) as well as combined PVB19/HHV6 infections (n=15) weredetected most frequently. The remaining forty-one patients were diagnosed withhealing myocarditis (n=15) or did not have myocarditis (n=26). Patients withPVB19 myocarditis clinically presented similar to myocardial infarction, mostlyhad typical subepicardial contrast enhancement in the left lateral wall and re-covered within a few months. Conversely, patients with HHV6 and especially withcombined HHV6/PVB19 infection usually presented with new onset of heart fail-ure, had septal contrast enhancement that over time remodeled towards "midwall-striae" like patterns as seen in DCM patients, and frequently progressed towardschronic heart failure.Our data indicate that PVB19 as well as HHV6 are the most important causesfor biopsy proven viral myocarditis in Germany and that the clinical presentationis related to the type of virus present in the myocardium. Furthermore, clinicalpresentation, type of virus as well as the pattern of myocardial damage are relatedto the clinical course.
P5468 High frequency of anti-heart autoantibodies in acutemyocardial infarction with angiographically normalcoronary arteries: evidence for undiagnosedimmune-mediated myocarditis
A.L.P. Caforio1, L. Daliento2, A. Angelini3, F. Tona4, A. Ramondo5,C. Basso1, G. Thiene1, S. Iliceto4. 1Dept Cardiological Thoracic VascularSciences, Division of Cardiology, Padua, Italy; 2Cardiological Thoracic VascularSciences, Padua, Italy; 3Cardiac Pathology, Padua, Italy; 4Cardiological ThoracicVascular Sciences, Padua, Italy; 5Cardiological Thoracic Vascular Sciences,Padua, Italy
Acute myocardial infarction with angiographically normal coronary arteries(MINC) is a poorly understood and highly heterogeneous entity. Although acutebiopsy-proven myocarditis (My) may present as MINC, differential diagnosis is of-ten not undertaken. Anti-heart autoantibodies (AHA) are specific serum markersof immune-mediated My.Purpose: To assess whether MINC may represent undiagnosed immune-mediated My, we compared features at diagnosis (dgn), including AHA, in consec-utive patients (pts) with MINC vs pts with biopsy-proven My and pseudo-ischemicpresentation (chest pain and abnormal troponin I).Methods: We studied 58 MINC pts, 31 males, aged 41± 21 years, 56 in NYHAI-II, 2 III, follow-up (f-u) 17 ± 22 months and 48 My pts, 36 males, aged 35 ±15 years, 47 in NYHA I-II, 1 III, f-u 35 ± 30 months. Left ventricular ejectionfraction (LVEF) by echocardiography and angiography was: 55 ± 10% and 64 ±12% in MINC; 55 ± 10% and 60 ± 13% in My respectively. Coronary angiogramwas always normal. Biopsy-proven My (Dallas criteria) was lymphocytic in 47 pts,giant cell in 1. AHA were detected by indirect immunofluorescence on humanmyocardium and skeletal muscle. Controls for AHA included 141 pts with angio-graphically proven coronary heart disease (CAD) (131 male, aged 51 ± 12 years)and 270 normal blood donors (NBD) (123 male, 35 ± 11 years). Features at dgnwere compared in MINC vs My by univariate analysis.Results: The proportion of females was higher in MINC (47%) than in My (25%,p=0.02). MINC was associated with lower left ventricular (LV) and right ventric-ular (RV) enddiastolic pressure (p=0.009; p=0.02), higher LV systolic (p=0.001)and lower RV systolic pressure (p=0.02); lower mean right atrial pressure (mRAP)(p=0.01) and lower pulmonary artery systolic pressure (PAS) (p=0.02). Peak tro-ponin I tended to be lower in MINC than in My (p=0.05). AHA were found in 51%of MINC and in 54% of My pts (p=NS). AHA frequency was higher in MINC or Mythan in CAD (2%, p=0.0001) or in NBD (5.5%, p=0.0001). At f-u 50 MINC and 44My pts were alive, of whom 1 transplanted, 12 lost to f-u; all pts were in NYHA I/II,with LVEF of 63 ± 8% in MINC and 64± 9% in My.Conclusions: The association with female gender and the high frequency ofAHA compared to CAD and NBD support an immune-mediated pathogenesis in
about 50% of MINC pts. MINC may represent undiagnosed mild My with pseudo-ischemic presentation in females.
P5469 Propranolol attenuates sympathetic hyperfunction,delays motor dysfunction, and prolongs life in amouse model of amyotrophic lateral sclerosis
T.G. Hampton1, A. Kale2, S. Mccue2, J.P. Morgan1, I. Amende1.1Harvard Medical School, Beth Israel Deaconess Medical Center,
Boston, United States of America; 2Mouse Specifics, Inc., R&D, Boston, UnitedStates of America
Autonomic dysfunction, in particular sympathetic hyperactivity, has been demon-strated in patients with amyotrophic lateral sclerosis (ALS), the most commonand invariably fatal human neurodegenerative disease. Treatment to restoresympathetic-parasympathetic balance to the heart could attenuate early cardio-vascular mortality in some ALS patients, although this has not yet adequatelybeen tested. We measured heart rate, heart rate variability, and gait in SOD1G93A mice (n=10), a widely studied animal model of ALS. We recorded electro-cardiograms in conscious mice through their paws as the animals rested quietly.We applied ventral plane videography to determine gait indices in ALS and controlmice walking on a transparent treadmill belt at a speed of 34 cm/s from 12 weeksto 17 weeks of age. Propranolol (0.5 g/l) was added to the drinking water of someSOD1 G93A mice (n=5) beginning at 6 weeks of age. We found that stride lengthwas significantly longer in untreated SOD1 G93A mice than control mice (7.1 ±0.1 cm vs. 6.8 ± 0.1 cm, P<0.05) at ∼12 and∼13 weeks of age, just prior to theonset of severe impairment of motor function. Increased stride length is often as-sociated with increased muscle sympathetic nerve activity. This presymptomatic"superathleticsm" was abolished in propranolol-treated mice. Gait disorders dur-ing walking became apparent earlier, at ∼14 weeks of age, in untreated SOD1G93A mice, with a significant decrease in stance width and an increase in thepaw placement angle. Paw placement angle exceeded 15° of the forelimbs and25° of the hind limbs during stance in untreated mice, characteristic of nerveinjury. Heart rate was significantly lower in propranolol-treated compared to un-treated SOD1 G93A mice (659 ± 14 bpm vs. 752 ± 18 bpm, P<0.05) at ∼15weeks of age, but heart rate variability, an index of cardiac autonomic nervoussystem balance, was not different (21 ± 5 bpm vs. 19 ± 1 bpm, NS). Paralysisand death occurred in untreated SOD1 G93A mice at ∼17 weeks of age; pro-pranolol delayed the onset of gait disturbances, delayed paralysis, and prolongedlife by ∼8%. We conclude that gait in the SOD1 G93A mouse model of ALS isinitially normal, then supernormal, then disturbed, the latter a consequence ofmotor neuron degeneration. Prophylactic treatment with propranolol could atten-uate aberrant sympathetic nerve hyperactivity, thereby delaying gait disturbancesand extending life in subjects with ALS.
P5470 Low-grade inflammation, arterial stiffness andthrombosis/fibrinolysis system: interrelationshipswith masked, white-coat and sustained hypertension
K. Dimitriadis, C. Tsioufis, D. Chatzis, E. Taxiarchou, P. Pavlidis,S. Lalos, C. Stefanadis, I. Kallikazaros. Department of Cardiology,
Hippokration, Athens, Greece
Purpose: The relation of "masked" hypertension (MHT) and "white-coat" hyper-tension (WCHT) to vascular damage is under debate, while inflammatory pro-cesses, impaired thrombosis/fibrinolysis and arterial stiffening are associated toatherosclerosis progression. In the present study, we examined the interrelation-ships of MHT, WCHT and sustained hypertension (SHT) with high-sensitivity C-reactive protein (hs-CRP), plasminogen-activator inhibitor type 1 (PAI-1), and ar-terial stiffness.Methods: 335 consecutive untreated non-diabetic subjects who referred to ouroutpatient clinic for 24-h ambulatory blood pressure (BP) monitoring, were clas-sified as subjects with sustained normal BP (office BP<140/90 mmHg anddaytime BP<135/85, n=44), MHT (office BP <140/90 mmHg and daytime BP>or=135/85 mmHg, n=32), WCHT (office BP >or=140/90 mmHg and daytimeBP <135/85 mmHg, n=81) and SHT (office BP >or=140/90 mmHg and daytimeBP >or=135/85 mmHg, n=178). Moreover, in all hypertensives arterial stiffnesswas evaluated on the basis of carotid to femoral pulse wave velocity (PWV), bymeans of a computerized method (Complior SP) and venous blood samples weredrawn for estimation of hs-CRP and PAI-1 levels.Results: Patients with SHT compared to WCHT and MHT group had higher 24-hsystolic BP (138 ± 10 vs 119 ± 7 vs 129 ± 15 mmHg, respectively; p<0.0001),while did not differ regarding sex, body mass index and metabolic profile (p=NS).P atients with SHT as compared to those with WCHT and MHT had greater levelsof hs-CRP (2.8 ± 0.7 vs 2.2 ± 0.6 vs 1.9 ± 0.4 mg/l, respectively; p<0.05), PAI-1(35.41 ± 5.1 vs 23.4 ± 2.3 vs 18.1 ± 1.8 ng/ml, respectively; p<0.05) and PWV(8.2 ± 1.4 vs 7.8 ± 1.2 vs 7.3 ± 0.9 m/sec, respectively; p<0.05). However, therewas no difference between the MHT and WCHT group regarding hs-CRP, PAI-1and PWV levels (p=NS for all cases). In the total hypertensive population, hs-CRP was associated with body mass index (r=0.285, p<0.0001), 24-h systolicBP (r=0.145, p<0.05) and PWV (r=0.232, p<0.0001), while PAI-1 was related to24-h diastolic BP (r=0.326, p<0.0001).Conclusions: Patients with SHT compared to those with MHT and WCHTare characterized by pronounced inflammatory involvement, impaired thrombo-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Novel aspect of Myocardial and Pericardial disease 963
sis/fibrinolysis and arterial stiffening, as reflected by hs-CRP, PAI-1 and PWV.These findings suggest that masking and white-coat effect may identify a state oflower cardiovascular risk, in this setting.
P5471 Ambulatory blood pressure monitoring and 2D echoin predicting non arrhytmic cardiac events inischemic cardiomyopathy after ICD implantation
L. Antonini, V. Pasceri, S. Greco, R. Ricci, S. Malfatti, M. Santini.San Filippo Neri Hospital, Cardiology, Rome, Italy
Background: Patients with ischemic cardiomyopathy and low ejection fraction(EF) who receive a defibrillator (ICD) are still at high risk of heart failure.Methods for predicting risk of heart failure in these patients are still unclear.Methods: We performed Ambulatory Blood Pressure Monitoring (ABPM) in 104consecutive patients (pts) (80 men). All patients received an ICD for MADIT2 criteria (75 pts with dual chamber ICD, 20 with cardiac resincronization, 9with single-chamber ICD). ABPM was performed 2 weeks after ICD implanta-tion on outpatient basis with Spacelabs 90207 system. ABPM variables consid-ered for predicting death and heart failure requiring hospitalization were: mean 24hour systolic blood pressure (m24hSBP), mean 24 hour diastolic blood pressure(m24hDBP), mean 24 hour heart rate (m24hHR). EF was calculated by 2D echo(Simpson rule) before ICD implantation.Results: At 1 year follow-up there were 21 events (20%) with 3 cardiac deaths(cardiogenic shock) and 18 cases of hospitalization for pulmonary oedema (n=8)or congestive heart failure (n=10).Only m24hDBP and age were independently associated with events (p < 0,03and p < 0,007 respectively), while EF, m24hSBP and m24hHR were not pre-dictive. ROC curves showed the best cut-off was 62 mmHg for m24hDBP (areaunder the curve 0.72, P=0.002) and 64 years for age (area under the curve 0.75,P=0.001). A Prognostic index was built from the age and m24hDBP according tothe formula: 120-age + m24hDBP and tested for the ability to predict events.ROC curves showed the best cut-off value for the PI was 108, with 80% sensibilityand 80% specificity (area under the curve 0.82, P<0.0001). A PI < 108 was highlypredictive of cardiac events with an Odds Ratio of 9.7 (95% confidence interval2.6-36) in multivariate analysis including EF and m24hSBP.Conclusion: The PI is predictive for death and heart failure in ischemic cardiomy-opathy. The ABPM could be a new simple method to predict non arrhythmic car-diac events in patients with uniformly low EF (≤30% by MADIT 2 criteria), whereEF values may not be predictive of new events.
P5472 Ambulatory arterial stiffness index as predictor forprognosis in pre and pot-menopausal women withacute coronary snydrome
I. Samuil1, M. Hashi2, A. Yuju2. 1Kawasaki, Kanagawa, Japan;2Kawasaki, Japan
Ambulatory arterial stiffness index (AASI) is derived from ambulatory blood pres-sure monitoring (ABPM) and reflects the arterial stiffness that predicts the cardio-vascular outcome.Methods: We examined 230 females with acute coronary syndromes, patientswere divided into group (A) 92 pre-menopausal patients, mean age 36 ± 8 yearsand group (B) 132 post-menopausal patients, mean age 48 ± 12 years who un-derwent ABPM. Diastolic blood pressure was plotted against systolic blood pres-sure and the regression slope was calculated. AASI was defined as one minusthis regression slope. Aortic pulse wave velocity (PWV) as well as echocardio-graphy were done. Patients were followed for 3 years for composite end pointsof cardiovascular morbidity and mortality (congestive heart failure, arrhythmia re-quiring hospitalization and cardiac death).Results: Mean AASI for group A was 0.58 compared with 0.66 for group B,p =0.01was significant. AASI correlated significantly with PWV for group (A)(r=0.42,p=0.001) and for group (B) (r=0.52,p=0.001). The rate of cardiovascularevents at 3 years follow up was 34% for group A Compared with 58% for groupB, p=0.001. At Cox model the hazard rate of ASSI for group A was (3.06, 95%CI =1.04-8.9,p=0.0001) for cardiovascular morbidity and for group B (4.56, 95%CI= 2.04-9.35,p=0.0001). After adjustment for age, history of current smoking,diabetes, body mass index, mean arterial pressure and pulse pressure the ad-justed hazard rates for group A (2.66, 95% CI=0.8-8.4,p=0.001) and for group B(4.1, 95%CI=1.7-8.8, p=0.001). The AASI correlated positively with left ventricu-lar ejection fraction(EF) for both groups and p=0.001 was significant. In group B,the AASI correlated positively with left ventricular mass(r=0.24,p=0.03) and leftventricular doppler E/A ratio(r=0.31,p=0.007). Multivariate analysis revealed bothAASI and EF were independent factors for cardiovascular events at 3 years followup.Conclusion: AASI is independent predictor for prognosis in female with acutecoronary syndrome.This simple non-invasive index of arterial stiffness can beeasily determined from ambulatory blood pressure recording and can be used forrisk stratification of both pre and post-menopausal women.
P5473 N-terminal ProBrain natriuretic peptide predictsaltered circadian variation in essential hypertension
S.M. Dogan, M. Aydin, M. Gursurer, G. Mungan, A. Dursun,T. Onuk. zonguldak karaelmas university, medicine fac, cardiology,Zonguldak, Turkey
Diminished nocturnal blood pressure (BP) fall in nondipper hypertensive patientsare closely associated with poor prognosis. N-terminal probrain natriuretic peptide(proBNP) can also identify poor prognosis in miscellanous heart diseases. In thisstudy, we aimed to clearify association between proBNP levels and diminishednocturnal BP fall in patients with essential hypertension. Twenty-six nondipper(age: 53 ± 8 years, 14 men) (group 1), and 26 dipper hypertensive patients (age:53 ± 9 years, 16 men) (group 2), based on ambulatory BP (ABP) monitoring, and28 normotensive subjects (age: 50 ± 11 years, 16 men) (group 3) were comparedeach others. Although systolic and diastolic ambulatory BP (ABP) values weresimilar in hypertensives during the day, those at night were higher in group 1 (p <
0.0001). Echocardiographic findings revealed that the left ventricular mass index(LVMI) was higher in both group 1 and group 2 (249 ± 65, 221 ± 47, 125 ±22, respectively p < 0.0001) but ejection fraction (EF) and relative wall thickness(RWT) were similar in all groups. The transmitral E wave decreased in group1 and group 2 compared with group 3 (0.62 ± 0.15 and 0.7 ± 0.14 and 0.95± 0.22 m/s, respectively p < 0.01), the transmitral E/A ratio decreased (0.71 ±0.12, 0.81 ± 0.2 and 0.79 ± 0.57, respectively p < 0.05), and the transmitral E-wave deceleration time increased in group 1 (217 ± 46, 195 ± 38 and 170 ± 42ms, respectively, p < 0.05). The isovolumic relaxation time increased (112 ± 23,110 ± 18 and 86 ± 11 m/s, respectively, p < 0.05). Although group 1 and group2 have similar numbers of patients with diastolic dysfunction (23/26 and 22/26,respectively, p > 0.05), there were great differences between plasma proBNP (88± 20, 58 ± 22 and 47 ± 20 pg/ml, respectively p<0.0001) levels. Also serum uricacid (6,5 ± 1.4, 5,3 ± 1,5 and 5,0 ± 1,9, respectively p <0.001), and creatininlevels (0,88 ± 0,2 and 0,78 ± 0,2 vs 0,72 ± 0,3, respectively p <0.05) were higherin group 1. These observations suggest that nondipper state is closely related tothe increase in LVMI and proBNP levels and increase in both plasma uric acidand creatinin levels.
P5474 Methylenetetrahydrofolate reductase genespolymorphisms in postmenopausal women withessential hypertension
E.I. Baranova1, O. Bolshakova1, V.I. Larionova2, A.A. Katsap2,O.S. Kolesnik2, M.A. Bogdanova1 . 1Saint-Petersburg Medical
University, Saint-Petersburg, Russian Federation; 2Saint-Petersburg MedicalAcademy, Saint-Petersburg, Russian Federation
Objective: to evaluate methylenetetrahydrofolate reductase (MTHFR) genespolymorphisms and their association with blood pressure (BP) level and param-eters of platelet aggregation in postmenopausal women with essential hyperten-sion.Material and methods: C677T, G1793A and A1298C MTHFR genes polymor-phisms were studied in 130 postmenopausal women with essential hypertension(mean age 53,7±3,5 years, mean BP 161,5±1,3/99,1±0,8 mm Hg). 24-hours BPmonitoring was performed and ADP-induced platelet aggregation (ADP concen-tration 2,5 mcmol/ml) was evaluated.Results: Allele distribution for C677T MTHFR gene polymorphism was 0,71 forC677 allele and 0,29 for 677T allele. The absence of C677-allele (TT genotype)was associated with higher diastolic BP level during 24-hours monitoring whencompared to patients with CC and CT genotypes (89,6±2,9 mm Hg vs 83,0±0,8mm Hg, p=0,048). TT genotype also corresponded with increased platelet ag-gregation: the grade of platelet aggregation was 84,1±3,5% in patients with TTgenotype and 71,1±1,5% in patients with CC and CT genotype (p=0,03), thetime of platelet aggregation was 329,1±12,3 sec and 459,8±30,1 sec accord-ingly (p=0,01). Allele distribution for G1893A MTHFR gene polymorphism was0,90 for G1893 allele and 0,10 for 1893A allele. 1793A allele was associated withhigher diastolic BP when compared to patients with GG genotype - 105,8±3,0mm Hg vs 95,2 mm Hg (p=0,02). Allele distribution for A1298C MTHFR genepolymorphism was 0,61 for A1298 allele and 0,39 for 1298C allele. We did notfind any associations between A or C alleles with BP level or platelet function.Mean homocysteine level was 13,42±0,38 mcmol/L and it did not vary depend-ing on different genotypes.Conclusion: MTHFR genes polymorphisms are associated with blood pres-sure level and parameters of platelet aggregation in postmenopausal hyperten-sive women. The present study did not reveal the association between differentMTHFR genes polymorphisms and homocysteine level in these patients.
P5475 Screening for Fabry disease in patients withhypertrophic cardiomyopathy
H. Bundgaard1 , O. Havndrup1, P.S. Andersen2, J. Hofman-Bang2,M. Christiansen2. 1Rigshospitalet, The Heart Center, Copenhagen,Denmark; 2Statens Serum Institut, Department of Clinical
Biochemistry, Copenhagen, Denmark
Fabry disease is a recessive X-linked lysosomal storage disease caused by muta-tions in the GLA gene coding for alpha galactosidase A. The disease may present
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

964 Novel aspect of Myocardial and Pericardial disease / Vascular smooth muscle cell proliferation and apoptosis
itself with left ventricular hypertrophy - the "cardiac variant" - as the sole symptom,and then it mimicks hypertrophic cardiomyopathy. We assessed the prevalence ofFabry disease in 61 probands with familial hypertrophic cardiomyopathy recruitedfrom a Danish tertiary referral center. All probands had been screened for muta-tions in the sarcomere genes and no mutations had been found. The GLA genewas screened for mutations by single strand conformation polymorphism anal-ysis and DNA sequencing. One male proband was found to be hemizygous forthe previously known missense mutation A156T and two female probands wereheterozygous for the novel missense mutations N139T and G239S, respectively.All probands has septal hypertrophy with maximum thickness ranging from 16 -20 mm. The N139T proband had a LVOT gradient of 75 mmHg and had sufferedfrom haemoptysis. The probands were diagnosed in the sixth decade. The G239Sproband had a markedly reduced enzyme activity, whereas an 18 year old asymp-tomatic female heterozygous carrier of the A156T mutation had a normal enzymeactivity. In conclusion, 3/61 (5%) of FHC probands without sarcomere mutationssuffer from Fabry disease and the GLA gene should thus be analysed as partof the genetic work-up of families with FHC. Fabry is associated with late-onsetFHC.
P5476 Clinical significance of troponin I efflux and troponinautoantibodies
K. Miettinen1, S. Eriksson2, J. Magga1, J. Kuusisto1, E.J. Vanninen1,K.R. Punnonen1 , K. Pettersson2, K.J. Peuhkurinen1 . 1KuopioUniversity Hospital, Department Of Internal Medicine, Kuopio,
Finland; 2University of Turku, Department of Biotechnology, Turku, Finland
Aim: To study the prevalence and clinical significance of serum troponin I (cTnI)levels and presence of cardiac troponin autoantibodies (cTnAbs) in patients withdilated cardiomyopathy (DCM).Methods: Circulating concentrations of cTnI and cTnAbs were determined in 95patients with idiopathic DCM using a novel, commercial immunoassay for cTnIwithout interference of cTnIAbs. The patients underwent laboratory testing, echo-cardiography, cardiopulmonary exercise testing, gated single photon emissioncomputed tomography and both-sided cardiac catheterization. Cardiovasculardeath, heart transplantation, and need for an automatic implantable cardioverterdefibrillator were considered as significant clinical end-points during a medianfollow-up time of 2.2 years.Results: cTnI positive (cTnI ≥ 0.01 ng/mL; n = 19) patients showed more promi-nent left ventricular enlargement, lower ejection fraction, and higher concentra-tions of vasoactive peptides than cTnI negative patients. The levels of neurohor-mones and inflammatory markers were similar in both groups. The cTnI positivegroup also suffered from clinical end-points more often than the cTnI negativegroup (p < 0.01; see picture). The commercial cTnT assay identified only 32% ofthe cTnI positive patients. The measured parameters did not differ significantly inthe patients with (n = 9) or without circulating cTnAbs.
Fig. 1. Survival curves for cTnI +/- patients
Conclusions: Patients with elevated serum cTnI levels demonstrate more promi-nent changes in the indices of left ventricular remodelling and function than pa-tients without signs of cTnI efflux. Elevated serum cTnI is also associated withless favorable clinical outcome. On the other hand, the presence of circulatingcTnAbs seems to have less utility in the clinical assessment of these patients.
P5477 Prevalence of organ specific autoantibodies(anti-human-tissue-transglutaminase,anti-endomysial, anti-actin and anti-thyreoperoxidasisantibodies) in DCM patients and their relatives
A. Di Lenarda1 , D. Chicco1, A. Taddio2 , L. Rubert1, M. Moretti2,E. Fabbro1 , G. Sinagra2, T. Not1. 1Ospedali Riuniti and University, Cardiology,Trieste, Italy; 2I.R.C.C.S. Burlo Garofolo and University, Pediadrics, Trieste, Italy
Background: Idiopathic dilated cardiomyopathy (DCM) is a relevant cause ofheart failure and the most common indication for heart transplantation. It maybe idiopathic, familial/genetic, viral, autoimmune or immune-mediated. The pres-ence of several autoantibodies or other immune factors in some patients andin their first degree relatives (FDR) contributes evidence to the hypothesis thatmultiple autoimmune mechanisms are involved in DCM. Coeliac disease (CD)
is a permanent intolerance to gluten and it’s often associated with autoimmuneextra-intestinal disorders. It has recently been shown an increased incidence ofCD in patients with DCM as compared to the general population. The aim of thisstudy was to establish the prevalence of some organ specific autoantibodies (anti-human-tissue-transglutaminase antibodies, anti-endomysial antibodies, anti-actinantibodies and anti-thyreoperoxidasis antibodies) in DCM patients and their FDR.Methods: We screened for anti-human-tissue-transglutaminase antibodies (IgAand IgG anti-h-tTG), anti-endomysial antibodies (AEAs), anti-actin antibodies andanti-thyreoperoxidasis antibodies 55 consecutive adult patients with inherited orsporadic DCM, 78 FDR and 200 healthy blood donors enrolled as control popula-tion. CD related HLADQ2-DQ8 was searched in tTG-positive subjects. Intestinalbiopsy was proposed to tTG-positive patients.Results: Three subjects were tTG-positive: two DCM patients (3,6%) and oneFDR (1,3%) (a daugther of a DCM patient). All the three subjects were AEA, andHLA-positive. Both of the tTG-positive subjects affected by DCM underwent duo-denal biopsy, that showed characteristic coeliac mucosal atrophy. 32/55 (58,2%)patients with DCM and 24/78 (30%) of FDR were tested positive for anti-actinantibodies. 18/55 (33%) patients with DCM and 20/78 (25%) FDR were testedpositive for anti-thyreoperoxidasis antibodies.2/200 (1%) of control population were tested positive for anti-thyreoperoxidasisautoantibodies, whereas 28/200 (14%) were tested positive for anti-actin autoan-tibodies. No one patient resulted positive for anti-human-tissue-transglutaminaseand for anti-endomysial autoantibodies screening research.Conclusions: High prevalence of CD in patients with DCM is confirmed. More-over a high presence of anti-actin antibodies and anti-thyreoperoxidasis antibod-ies was established both in patients with DCM and in their relatives as comparedwith controls. These preliminary data support the hypotesis that DCM could bean autoimmune disorder in a contest of unknown genetic predisposition.
VASCULAR SMOOTH MUSCLE CELL PROLIFERATIONAND APOPTOSIS
P5478 The forkhead transcription factor FoxO1a regulatesapoptosis of smooth muscle cells by controlingcaveolin-1 expression
D. Sedding1, S. Vogel1, H. Koenig1, H. Tillmanns1, W. Sellers2,R.C. Braun-Dullaeus3. 1Giessen University Clinic, Cardiology,
Giessen, Germany; 2Brigham and Womens’s Hospital, Internal Medicine,Boston, United States of America; 3Dresden University, Cardiology, Dresden,Germany
Background: The forkhead transcription factor FoxO1a represents an impor-tant physiological target of phosphatidylinositol-3 kinase (PI3-K)/protein kinaseB (Akt) signaling and we previously demonstrated that FoxO1a is a key regulatorfor the cell cycle entry of vascular smooth muscle cells (VSMC). In the presentstudy we sought to determine the effect of adenovirus-mediated expression of atransgene encoding a constitutively-active form of FoxO1a (Ad-FoxO1a;AAA) onVSMC apoptosis.Methods and Results: Following transduction with Ad-FoxO1a;AAA, the numberof apoptotic VSMC was increased compared to controls (14.8 ± 2.3 vs. 3.6 ±0.8%, P< 0.01) as determined by TUNEL assay. Caveolin-1 expression was in-creased at both, the mRNA and protein level in a dose-dependent manner. Overexpression of caveolin-1 itself reduced serum-induced Akt phosphorylation andsignificantly increased the number of apoptotic VSMC. Accordingly, knock downof caveolin-1 using antisense oligonucleotides significantly reduced the numberof apoptotic cells induced by 72 h serum starvation. Knock down of caveolin-1also significantly reduced the FoxO1a;AAA-induced apoptosis of VSMC. Similarly,VSMC isolated from caveolin-1-/- mice were resistant to FoxO1a;AAA-inducedapoptosis. For in vivo studies, the femoral artery of C57BL/6J mice was dilatedand adenoviral vectors were delivered intraluminally to the denuded segment.Four days after dilation, caveolin-1 expression as well as the apoptotic rate ofmedial VSMC in FoxO1a-transduced arteries was significantly increased as de-termined by TUNEL assay (9.7 ± 2.5 vs. 2.3 ± 0.9; P<0.05). Morphological anal-ysis of femoral arteries 28 days after dilation revealed a significantly reducedneointima/media ratio (0.7 ± 0.2 vs. 1.8 ± 0.4;P<0.005).Conclusion: By transactivating and increasing cellular caveolin-1 expressionlevels, FoxO1a interferes with cellular PI3-K/Akt-dependent survival signaling,thereby restoring the sensitivity of (neointimal) VSMC to apoptotic stimuli. Thispro-apoptotic effect adds to the anti-proliferative properties of FoxO1a resultingin impaired neointima formation in vivo. Thus, modulating FoxO1a-function mayrepresent a novel approach to prevent vascular proliferative disease.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Vascular smooth muscle cell proliferation and apoptosis 965
P5479 Inhibition of ROS liberation by the novel nox inhibitorVAS2870 attenuates PDGF-dependent src activationand chemotaxis, but not proliferation in vascularsmooth muscle cells
H. Ten Freyhaus1 , M. Huntgeburth1 , K. Wingler2, A.T. Baeumer1 ,M. Wartenberg3, H. Sauer4, M.M. Bekhite5, S. Rosenkranz4 . 1Universitaetzu Koeln, Klinik 3 Fuer Innere Medizin, Koeln, Germany; 2Vasopharm GmbH,Wuerzburg, Germany; 3Universitaet Potsdam, Institut fuer Biochemie undBiologie, Potsdam, Germany; 4Universitaet Giessen, Institut fuer Physiologie,Giessen, Germany; 5Inst. fuer Physiologie, Universitaet zu Koeln, Koeln,Germany
Reactive oxygen species (ROS) play a significant role in the pathogenesis of car-diovascular disease. They contribute to various cellular functions as second mes-sengers and are involved in the regulation of vascular tone, migration, and apop-tosis. NAD(P)H oxidases are the predominant source of ROS in the vascular wall.Expression and activity of these enzymes are regulated by growth factors such asangiotensin II and platelet-derived growth factor (PDGF). Recently, novel homo-logues of the membranous NAD(P)H oxidase subunit gp91phox have been identi-fied (nox1-5). We characterize the novel nox inhibitor VAS2870 in vascular smoothmuscle cells (VSMC). PDGF-BB increased NAD(P)H oxidase-activity (lucigenin-enhanced chemiluminescence) and intracellular ROS levels (detected by confocallaserscanning microscopy using 2,7 DCF) to 229±9% and 362±54% at 1 and 2h,respectively (p<0,05). Preincubation with VAS2870 (10 and 20 μM) completelyabolished PDGF-mediated NAD(P)H oxidase activation and ROS production.Since ROS are involved in various growth factor-induced cellular functions, theinfluence of VAS2870 on PDGF-induced DNA synthesis and chemotaxis was de-termined. PDGF promoted a 4,2±0,2-fold increase of VSMC migration (modifiedBoyden chamber, p<0,01) and concentration-dependently enhanced DNA syn-thesis to maximally 3,2±0,4-fold (BrdU incorporation, p<0,01). VAS2870 preincu-bation (0,1-20 μM) had no effect on PDGF-induced cell cycle progression. How-ever, it abolished PDGF-dependent chemotaxis in a concentration-dependentmanner (100% inhibition at 10 μM, p<0,05). These findings were related toPDGF-dependent signaling events. Western blot analyses using phospho-specificantibodies revealed that the downstream signaling molecules Akt, Erk, and Srcwere activated by PDGF. However, VAS2870 concentration-dependently blockedPDGF-dependent activation of Src, but not of Akt and Erk. Our data indicate thatthe novel nox inhibitor VAS2870 effectively suppresses growth factor-mediatedROS liberation in VSMC. Furthermore, it abolishes PDGF-dependent VSMCmigration, whereas it does not affect DNA synthesis. These divergent effectsdemonstrate the critical role of Src activity, which - in contrast to Akt and Erk - ap-pears to be redox-sensitive and is absolutely required for PDGF-induced chemo-taxis, but not cell cycle progression.
P5480 Cyclic nucleotides inhibit vascular smooth musclecell proliferation in vitro and in vivo bydownregulating Skp2 via a Rac1-dependent pathway
Y.J. Wu, G.B. Sala-Newby, A.C. Newby, M. Bond. Bristol HeartInstitute, CSSB, Bristol, United Kingdom
Cyclic nucleotides inhibit vascular smooth muscle cell (VSMC) proliferation phys-iologically and pharmacologically but the molecular mechanisms are uncertain.We investigated whether cyclic nucleotides lower cellular levels of S-phasekinase-associated protein-2 (Skp2), which we showed previously to be a keyregulator of p21Cip1 and p27Kip1 proteolysis and hence cell cycle progres-sion. In agreement with our hypothesis, we found that forskolin (0.01-0.1 mM)and dibutyryl-cAMP (0.1-1 mM) inhibited Skp2 transcription (promoter activityand mRNA expression, to 50 ± 5% and 48 ± 8% of control, respectively; n=3-4, p<0.05). Dibutyryl-cAMP also decreased Skp2 protein stability (t1/2: 3.1 ±1.2 vs. 8.4 ± 1.3 hours; n=3, p<0.05) and inhibited VSMC proliferation (8.4 ±3.1% vs. 69 ± 8%; n=3, p<0.05). Adenovirus-mediated Skp2 expression re-versed forskolin-induced p27Kip1 upregulation and rescued S-phase entry upto 50% (n=5, p<0.05). 8-Br-cGMP also reduced Skp2 (to 54 ± 5% of control;n=6, p<0.05) and VSMC proliferation (17 ± 2% vs. 30 ± 3%; n=3, p<0.05) inthe presence of 2% but not 10% serum. We noted that cyclic nucleotides alsochanged VSMC shape, which is thought to depend on the small GTPase, Rac1.Indeed forskolin and 8-Br-cGMP inhibited Rac1 activation (to 44 ± 6% and 60 ±15% of control, respectively; n=3, p<0.05) and forskolin, moreover, inhibit Rac1membrane/cytosol distribution (to 44 ± 10% of control; n=3, p<0.05). To definewhether Rac1 activation affected Skp2 levels we transduced cells with a con-stitutively active Rac1 mutant. This completely rescued Skp2 expression afterforskolin treatment. To demonstrate their role in vivo we showed that Skp2 expres-sion (mRNA and protein) and Rac1 activity were both upregulated after ballooninjury to the rat carotid artery. Local treatment with forskolin significantly reducedSkp2 expression (1.0 ± 0.2% vs. 7.5 ± 2.5%; n=5-6, p<0.05) and VSMC prolif-eration (3.8 ± 1.2% vs. 12 ± 2%; n=5-6, p<0.05). Clostridium difficile toxin B, aRho GTPase inhibitor produced similar effects (n=4-5, p<0.05; data not shown).These data demonstrate for the first time that cyclic-nucleotides inhibit VSMCgrowth in part by regulating Skp2 via a Rac1-dependent pathway.
P5481 Modification of calcium signalling during proliferationof human coronary and mammary arteries vascularsmooth muscle cells: a new target for drug-elutingstents?
L. Lipskaia1 , P. Leprince2, N. Bonnet1, S. Yacoubi2, I. Cantaloube2,C. Le Feuvre3, A.M. Lompre3. 1INSERM U 621, UPMC-CHU Pitie-Salpetriere,Paris, France; 2Chirurgie cardiaque, UPMC-CHU Pitie-Salpetriere, Paris, France;3Cardiologie Medicale, UPMC-CHU Pitie-Salpetriere, Paris, France
Coronary in-stent restenosis is related to proliferation of vascular smooth mus-cle cells (VSMC). We have previously shown in the rat that proliferation ofVSMC is associated with loss of RyR (ryanodine receptor) calcium channel andsarco/endoplasmic reticulum calcium ATPase, SERCA2a, leading to increasedcytosolic calcium. These alterations in Ca2+ handling induced activation of theCa2+-regulated transcription factor, NFAT, required for VSMC proliferation. Theaim of this study was to determine whether this phenomenon exists also in hu-man. We analyzed coronary arteries (CA) from explanted heart and mammaryarteries (MA) obtained after aorto-coronary bypass. The VSMC obtained fromthese arteries were used for in vitro studies. Atherosclerotic plaques were de-tected by Hematoxylin-Eosin staining on coronary arteries from explanted heart,but not on mammary arteries. VSMC were identified by expression (immunofluo-rescence) of SMMHC (smooth muscle myosin heavy chain 1 and 2) and NMMHC(non-muscular myosin heavy chain) in the media of CA and MA as well as in theneointima of CA. SERCA2a and RyR were expressed only in the VSMC from themedia from CA and CA but not in the VSMC from neointima. In freshly isolatedquiescent VSMC from CA and MA immunofluorescence revealed the presenceof SMMHC, NMMHC, SERCA2a, SERCA2b and RyR. Proliferation in vitro wasassociated with down-regulation of SMMHC, SERCA2a and RyR. The specificInhibitor of L-type calcium channels, diltiazem, had no effect on VSMC prolifer-ation, whereas nifedipine, mibefradil and 2APB, as well as cyclosporine A, aninhibitor of NFAT-signalling pathway, inhibited serum-induced VSMC proliferationin dose-dependent manner. In summary, proliferation of human vascular smoothmuscle cells is accompanied by down-regulation of RyR and SERCA2. Our datasuggest involvement of NFAT-signalling pathways in induction of proliferation inhuman. These findings could have potential implications in drug-eluting stent.
P5482 Inhibiting Calmodulin-cyclin E interactions arrestscell cycle progression of vascular smooth musclecells
J. Choi, N. Taulier, M. Husain. Toronto, Canada
Background: Understanding the molecular mechanisms mediatingcell cycle progression in vascular smooth muscle cells (VSMC) may
improve the design of therapies aimed at proliferative vascular diseases. We pre-viously showed that a coordinated elevation in free intracellular Ca2+ concentra-tions is required for G1-to-S phase cell cycle transitions in rodent VSMC. Morerecently, our studies suggest that Calmodulin (CaM)-dependent cyclin E/CDK2activity mediates Ca2+-sensitivity of this transition, and requires direct binding ofCaM to cyclin E. However, the molecular basis and physiological importance ofthis interaction was not known.Methods & Results: A CaM-target database suggested a putative CaM-bindingmotif that is highly conserved in mammalian cyclin E genes. Fluorescence titrationanalysis with purified CaM and a synthesized peptide of the CaM-binding motif inhuman cyclin E1 (named ‘CBS’ for CaM-Binding Sequence) confirmed the bindingof CaM to the putative CaM-binding motif (Kd= 1.5 ± 0.1 μM). Treatment with theCBS peptide inhibited Histone H1-phosphorylation-defined cyclin E/CDK2 activityin mouse VSMC, due to decreased CaM-cyclin E interactions. It also abrogatedCa2+-sensitive enhancement of cyclin E/CDK2 activity in vitro. Moreover, deliveryof the CBS peptide into primary mouse aortic SMC inhibited their proliferation ina dose-dependent manner (IC50: 187 μM). Flow-assisted cell sorting analysis(FACS) further demonstrated that the CBS peptide caused a G1-arrest in serum-stimulated primary mouse aortic SMC in culture. Delivery of the CBS peptide tothe site of an arterial injury model in animals will be tested to evaluate its anti-proliferative effects in vivo.Summary: These findings support the physiological relevance of a highly con-served CaM-binding motif in mammalian cyclin E genes, and suggest that inter-actions between CaM and cyclin E may represent a novel therapeutic target forproliferative vascular diseases.
P5483 PI 3-kinase and phospholipase C-g mediate thePlatelet-derived growth factor (PDGF)-induced cellcycle progression by different mechanisms
M. Vantler1, E. Caglayan1, F. Gerhardt1, M. Huntgeburth1 , H. TenFreyhaus1 , W.H. Zimmermann2, S. Rosenkranz3 . 1Universitaet zu
Koeln, Klinik III fuer Innere Medizin, Cologne, Germany; 2UniversitaetsklinikumHamburg-Eppendorf, Institut fur Experimentelle und Klinische Pha, Hamburg,Germany; 3Universitaet zu Koeln, Klinik III fuer Innere Medizin, Hamburg,Germany
Background: The platelet-derived growth factor b -receptor (bPDGFR)-mediatedproliferation of vascular smooth muscle cells (VSMC) plays a crucial role inatherogenesis and restenosis. The bPDGFR binds and activates cytoplasmic sig-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

966 Vascular smooth muscle cell proliferation and apoptosis
naling molecules such as Src, PI 3-kinase (PI3K), RasGAP, SHP-2 and phospho-lipase C-g (PLCg). The bPDGFR-induced signaling pathways leading to cell cycleprogression are largely unknown.Methods and Results: In order to characterize the signaling molecules, whichare important for PDGF-induced VSMC proliferation, we used mutated bPDGFRin which the tyrosine residues required for binding of each signaling moleculewere individually mutated to phenylalanine. To bypass endogenous PDGFR inVSMC we used chimeric receptors with altered ligand binding specificity, contain-ing the extracellular ligand binding domain of the M-CSF receptor, and the cyto-plasmic domain of the wild type or mutated b PDGFRs. BrdU incorporation assaysrevealed that stimulation of the chimeric wild type receptor (WT) with M-CSF (50ng/ml) led to a 2.8 ± 0.6-fold increase of DNA-synthesis (p<0.01). Deletion of thebinding sites for PI3K or PLCg diminished DNA-synthesis about 47 ± 6% or 54± 5%, respectively, whereas the deletion of the binding sites for Src, RasGAP, orSHP-2 had no influence. Accordingly, chimeric mutants which only bind PI3K orPLCg mediated 43 ± 4% or 52 ± 5% of the WT response.We investigated the influence of PI3K and PLCg on the expression of the key-players of cell cycle progression such as immediate early genes (IEGs), cyclins,and cyclin-dependent kinases (cdk). Real-time PCR analysis demonstrated thatIEGs are significantly upregulated after stimulation of VSMC with PDGF-BB (c-myc: 14.0 ± 2.1fold, c-fos: 101 ± 24fold and egr-1: 51 ± 14fold, p<0.01). Anal-ysis of the PDGFR mutants demostrated that up-regulation of IEG depends onboth PI3K and PLCg. Westernblot analysis of the protein expression levels of cy-clines and cdk-inhibitors in VSMC revealed that PI3K induced the upregulationof Cycline-D1, whereas PLC g mediated the down-regulation of the cdk-inhibitorp27kip1. Consistently, PDGF-dependent phosphorylation of the retinoblastomaprotein which is important for the G1/S transition was reduced when the bindingsites for PI3K or PLCg were deleted.Conclusions: Our results show, that the activated bPDGFR mediates prolifera-tion of VSMC via the activation of PI3K and PLCg. These signaling moleculesmediate the PDGF-induced DNA-synthesis by upregulation of IEGs and cyclinsand downregulation of cdk-inhibitors via redundant as well as different signalingpathways.
P5484 A novel mechanism underlying the regulation ofsmooth muscle cell proliferation by the small GTPaseRac-1
M. Bond, Y. Wu, G. Sala-Newby, A.C. Newby. University of Bristol,Dept. C.S.S.B., Bristol, United Kingdom
Late vein-graft failure, angioplasty restenosis and atherosclerosis all depend onvascular smooth muscle cell (VSMC) proliferation. Up-regulation of the cyclins,such as cyclin D and down- regulation of cyclin-dependent kinase inhibitors, suchas p27Kip1 are believed important but the regulatory mechanisms are not clear.We investigated the role of Rac-1, a member of the RhoGTPases that participatein both mitogenic and ECM-dependent signalling pathways. Adenovirus-mediatedexpression of a dominant-negative Rac-1 (Rac-N17) significantly inhibited VSMCproliferation measured by BrdU incorporation (from 79±4.3% to 18.6±4.0%,p<0.05, n=3), cell number (from 5.5±0.9x105 cells to 1.34±0.04x105, p<0.05,n=4) and hyperphosphorylation of retinoblastoma protein (to 1.1±0.063% of con-trol, p<0.05, n=3). Expression of Rac-N17 also down-regulated cyclinD1 and up-regulated p27Kip1 levels (to 142±8.1% of controls, p<0.05, n=3); up-regulationof p27Kip1 resulted from reduced expression of Skp2, the ubiquitin-ligase subunitimplicated in promoting p27Kip1 degradation. Exogenous expression of wild-typeSkp2 reversed the increase in p27Kip1 induced by Rac-N17 and rescued SMCproliferation (from 22.6±4.7% of control to 83.4±15.4%, p<0.05, n=3). In vivo,levels of active Rac1 were elevated 2 and 7 days after balloon injury to the ratcarotid artery. Treatment with the RhoGTPase inhibitor C. difficile Toxin B blockedupregulation of Skp2 and inhibited VSMC proliferation 2 days after injury. Thisdata shows that Rac-1-dependent regulation of Skp2 expression is a key stepin the initiation of SMC proliferation in vitro and in response to vessel injury. Todefine the mechanisms further we expressed a Rac-1Y40C mutant that is deficientin p21-activated kinase (PAK) binding. Rac-1Y40C expression inhibited cyclinD1expression but not expression of Skp2. However, expression of Rac-1F37A thatis defective in regulating the actin-cytoskeleton, did inhibit Skp2 expression. Fur-thermore, the cytoskeleton-disrupting agents cytochalasin D and Jasplakinolidealso inhibited expression of Skp2. Therefore, Rac-1 regulates SMC proliferationvia divergent pathways that include Rac/PAK-dependent regulation of cyclinD1and actin cytoskeleton-dependent regulation of Skp2.
P5485 The Platelet-derived growth factor (PDGF) b receptormediates pro- and anti-apoptotic effects via PI3-kinase-dependent signaling pathways
M. Vantler1, M. Huntgeburth1 , J. Sparwel1, E. Caglayan1,W.-H. Zimmermann2, S. Rosenkranz1 . 1Universitaet zu Koeln,
Klinik III fuer Innere Medizin, Cologne, Germany; 2UniversitaetsklinikumHamburg-Eppendorf, Institut fur Experimentelle und Klinische Pha, Hamburg,Germany
Background: The regulation of vascular smooth muscle cell (VSMC) apoptosisplays a critical role in atherosclerosis. The Platelet-derived growth factor b recep-tor (bPDGFR), which binds and activates cytoplasmic signaling molecules such
as Src, PI3K, RasGAP, SHP-2 and PLCg, mediates survival signals in many celltypes. We systematically investigated the relative role of each signaling moleculefor VSMC apoptosis.Methods and Results: Interestingly, stimulation of VSMC with PDGF-BB (50ng/ml) induced anti- as well as proapoptotic effects depending on the stimula-tion time. Incubation of VSMC with H2O2 (100 μM, 12 h) led to a 5.3 ± 1.1-foldincrease (p<0.05) of apoptosis as assessed by Cell Death Detection ELISA. Ad-dition of PDGF-BB (50 ng/ml) diminished H2O2-induced apoptosis (52 ± 7%,p<0.05). In contrast, chronic stimulation (96 h) with PDGF-BB led to a 3.1 ±0.4-fold increase of apoptosis (p<0.05). In order to characterize the anti- andproapoptotic pathways, we used mutated bPDGFR in which the binding sites forthe signaling molecules were individually deleted. To bypass endogenous PDGFRin VSMC we used chimeric receptors, containing the extracellular ligand bind-ing domain of the M-CSF receptor. Short term activation of the chimeric wildtype receptor (WT) with M-CSF (50 ng/ml) reduced H2O2-induced apoptosis tothe same extend as the endogenous PDGFR. Deletion of the PI3K binding sitecompletely abolished the antiapoptotic effect whereas deletion of other bindingsites had no influence. Exploration of downstream signaling events revealed thatPDGF-BB activates the antiapoptotic Akt signaling pathway in a PI3K dependentmanner, leading to the phosphorylation of BAD and Forkhead transcription fac-tors. Chronic stimulation of WT expressing VSMC with M-CSF (50 ng/ml, 96 h)led to a 2.8±0.6-fold increase of apoptosis (p<0.05). This effect correlates with andecreased expression of the antiapoptotic protein Bcl-2 as assessed by Real-timePCR and Westernblot analysis. Deletion of the binding site for PI3K completelyabolished the proapoptotic effect, whereas a mutant which only binds PI3K wasfully able to mediate the proapoptotic effect as the WT.Conclusions: Short-time activation of the bPDGFR induces cell survival by thetransient activation of the Akt signaling pathway, whereas the chronic stimulationwith PDGF leads to increased cell death by the regulation of genes such as theBcl-2 gene. Both effects are mediated by PI3K-dependent signaling pathways.
P5486 Urotensin II inhibition prevents smooth muscle cellproliferation and neointima formation followingballoon angioplasty through apoptosis modulationand G-betagamma signaling
G. Esposito1, E. Sanzari2, L. Di Serafino2, E. Cipolletta2, A. DeConcilio2, G. Iaccarino2, A. Rapacciuolo2 , M. Chiariello2. 1Federico II University,Naples, Division Of Cardiology, Naples, Italy; 2Federico II University, Geriatrics,Naples, Italy
Urotensin II (UT-II) is a somatostatin-like cyclic peptide mediating several cardio-vascular effects by interacting with a Gαq-coupled orphan receptor. Since UT-IIinduces vascular smooth muscle cells (VSMC) proliferation, we tested the hy-pothesis that inhibition of UT-II receptors might reduce restenosis following exper-imental angioplasty. In order to inhibit neointima formation, a newly synthesizedUT-II antagonist peptide (Urantide, UR) was locally delivered following ballooninjury of rat carotid arteries. 14 days after surgery, UT-II inhibition significantly re-duced neointima formation as expressed by neointima to media ratios (Vehicle:1.31 + 0.2; Urantide: 0.59 + 0.1, p<0.05). In cultured VSMC, UT-II administra-tion (100 nM) reduced apoptosis induced by serum deprivation, as measured byhypodiploidy of cells in flow cytometry. This effect was inhibited by Urantide ad-ministration in vitro. To address whether the anti-apoptotic effects of UT-II wereGβγ- related, we overexpressed the Gβγ-sequestering peptide βARKct in serum-starved VSMC. Interestingly, adenovirus-mediated βARKct overexpression com-pletely abolished UT-II effects on VSMC apoptosis. The proliferative effects of UTIIwere mediated by Erk-MAPK and p38-MAPK activation. Following UR pretreat-ment, Erk-MAPK and p38-MAPK activation was completely abolished. βARKctoverexpression inhibited MAPK activation UT-II induced. These data demonstratean important role of UT-II in modulating VSMC proliferation and apoptosis throughGβγ signalling and MAPK activation. These data may have important implicationsin preventing vasculoproliferative disorders including atherosclerosis and resteno-sis following percutaneous interventions.
P5487 PKA-activated p85alpha Prevents NeointimalHyperplasia After Vascular Injury Without AffectingRe-Endothelialization
D. Torella1, A. Curcio1, C. Gasparri1, A.L. Cavaliere1, A. Leone1 ,F.C. Surace1, E.V. Avvedimento2, C. Indolfi2. 1Magna Graecia
University, Cardiology, Catanzaro, Italy; 2Federico II University, Naples, Italy
Purpose: Impaired re-endothelialization of the stented arterial segment seemsto be a potential dangerous drawback of drug eluting stents (DES). One wayto circumvent this would be the identification of intracellular pathways/moleculesthat play differential roles on vascular smooth muscle cell (VSMC) and endothe-lial cell (EC) growth. cAMP/PKA-activated p85α, the regulatory subunit of phos-phatidylinositol 3’-Kinase (PI3K), inhibits ras protein function and consequentlythe proliferation of cancer cells. Importantly, the PI3K pathway has been shownto promote EC survival. Aim of the study were to evaluate: i) the differential role,if any, of p85α in the regulation of VSMC vs. EC growth in vitro and ii) the effectsof p85α on vascular healing after balloon injury in vivo.Methods: VSMCs and HUVECs were transfected in vitro with plasmids carry-ing a mutated cAMP/PKA-activated p85α (p85active) or dominant negative p85α
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
Vascular smooth muscle cell proliferation and apoptosis 967
(p85DN). VSMC and HUVEC proliferation and apoptosis were measured by BrdUand TdT staining, respectively. Balloon injury of the right carotid was produced inWistar rats. Straight after the vascular injury, the balloon-dilated arteries were ran-domly transfected with p85active (n=8), dominant negative p85 (p85DN) (n=8) orgreen fluorescent protein (GFP, n=6; controls).Results: Transfection of p85active decreased VSMC proliferation in the absenceof cAMP while cAMP inhibition of VSMC growth was prevented by p85DN.p85active formed a stable complex with ras proteins, resulting in a selectiveswitch-off of ras effectors in VSMCs. On the other hand, p85active did not af-fect HUVEC growth in vitro. Interestingly, p85active significantly reduced VSMCand HUVEC apoptosis in vitro. In both vascular cell lineages, p85active in-creased while p85DN decreased Akt phosphorylation. Importantly, the in vivotransfection of activated p85-active significantly reduced VSMC proliferation andthen neointimal formation after balloon injury. Finally, arterial healing with re-endothelialization of the injured segment occurred normally despite p85-activeefficient transfection.Conclusions: cAMP-PKA-activated p85α has protective vascular effects reduc-ing neointimal formation and being inhert on reendothelialization of injured arterialsegments. These data could be of relevance for the next generation of new DES.
P5488 Gut-enriched Kruppel-like factor (GKLF)-mediatedinduction of p53 is essential for inhibition ofproliferation of vascular smooth muscle cells
S. Wassmann, K. Wassmann, A. Jung, C. Mueller, G. Nickenig.Universitaetsklinikum Bonn, Medizinische Klinik II, Bonn, Germany
Enhanced proliferation of vascular smooth muscle cells (VSMC) plays an impor-tant role in the pathogenesis of atherosclerosis and restenosis. The transcrip-tion factor gut-enriched Kruppel-like factor (GKLF) is involved in redox-sensitivegrowth arrest of VSMC. We investigated the role of GKLF in VSMC proliferationand differentiation and the interaction with the tumor suppressor gene p53.Methods and Results: Cultured rat aortic VSMC were transfected with GKLFsense and antisense constructs by electroporation. To investigate the impact ofGKLF on VSMC phenotype, the expression of the differentiation markers SM22-α and α-smooth muscle actin was assessed (real-time RT-PCR, Western blot).Whereas GKLF had no effect on α-actin expression, SM22-α expression was sig-nificantly enhanced, indicating a shift to a more differentiated VSMC phenotype.Overexpression of GKLF significantly reduced VSMC proliferation (cell count).Because p53 is essential for proliferation processes, the effect of GKLF on p53gene expression was investigated. GKLF overexpression led to an enhanced p53promoter activity and increased p53 mRNA and protein expression (luciferasereporter assay, real-time PCR, Western blot). Co-transfection experiments re-vealed that the growth arrest induced by GKLF sense was completely abolishedby transfection of p53 antisense constructs, whereas the reduced proliferation ex-erted by p53 sense was not inhibited by GKLF antisense transfection, suggestingthat p53 induction is essential for the interference of GKLF with VSMC prolifera-tion.Conclusions: The transcription factor GKLF induces inhibition of proliferation ofVSMC which is mechanistically linked to a GKLF-induced enhancement of theexpression of the tumor suppressor gene p53.
P5489 New pullulan 3D matrices for in vitro and ex vivotransfection of rabbit vascular smooth muscle cells
A. San Juan1, H. Hlawaty1, F. Chaubet1 , D. Letourneur1 ,L.J. Feldman2. 1INSERM U698, Paris, France; 2AP-HP BichatHospital, INSERM U698, Cardiology, Paris, France
Clinical applications of arterial gene therapy are limited by the low efficiency ofgene vectors and the technical hurdles associated with local gene delivery at thetarget arterial site. The aim of this study was to formulate a plasmid DNA-elutingpolysaccharide 3D matrix for site-specific arterial gene transfer.Pullulan, a biodegradable polysaccharide, was chemically crosslinked andmolded as 3D hydrogel discs (figure), which were loaded with a plasmid vec-tor expressing a secreted form of alkaline phosphatase (pSEAP) complexed tothe cationic lipid FuGene. Transfection efficiency of FuGene/pSEAP-loaded pul-
Fig. 1. Pullulan hydrogel disc.
lulan discs was assessed in vascular smooth muscle cells (VSMCs) in vitroand ex vivo. Rabbit VSMCs (Rb-1 cell line) were incubated for 4 days with Fu-Gene/pSEAP (1μg)-loaded pullulan discs. Control VSMCs were incubated with aculture medium containing 1μg of naked pSEAP (no disc). Gene expression inthe conditioned cell culture medium and cell toxicity (MTT assay) were assessedat day 4. Preliminary ex vivo experiments were also performed on balloon-injuredrabbit aortas incubated with FuGene/pSEAP (4μg)-loaded pullulan discs for 6days. Control aortas were incubated with culture medium containing 4μg of nakedpSEAP (no disc).SEAP activity was 345-fold higher in VSMCs incubated with FuGene/pSEAP(1μg)-loaded pullulan discs than in VSMCs incubated with naked pSEAP, with-out significant cell toxicity. In addition, ex vivo incubation of balloon-injured aortaswith FuGene/pSEAP (4μg)-loaded pullulan discs resulted in significant SEAP ac-tivity at day 6.In conclusion, we have designed 3D pullulan-based hydrogel matrices which canbe used for in vitro and ex vivo gene transfer in VSMCs. Optimization of thismethod may lead to the design of new endovascular prosthetic tools for arterialgene transfer.
P5490 The subcellular localization of urokinase-typeplasminogen activator receptor is modulated byaggregated low density lipoproteins in migratinghuman coronary vascular smooth muscle cells
E. Pena, T. Padro, V. Llorente-Cortes, L. Badimon. CardiovascularResearch Center, CSIC-ICCC, Barcelona, Spain
Background and Objectives: Urokinase-type plasminogen (UPA) and its recep-tor UPAR facilitate a proteolytic cascade focused at the cell surface and elicitimportant cellular functional responses with a role in atherosclerosis, such as cellmigration and proliferation. Low density receptor related protein (LRP), the majorreceptor for aggregated LDL (agLDL) in vascular smooth muscle cells (VSMC) in-ternalizes lipids and among other functions binds UPA/UPAR facilitating internal-ization. In this study, we characterized the effects of agLDL internalization on ex-pression and subcellular localization of UPA and UPAR in human coronary VSMCand their interaction with the actin-cytoskeleton.Methods: Primary cultured human coronary VSMC were exposed during 24hours to agLDL (100ng/mL) under resting conditions and during migration in ascrape-wound model. UPA and UPAR levels in cell extracts were determined byWestern Blot analysis. Subcellular distribution was analyzed by fluorescence con-focal microscopy under permeabilization (detection of intracellular UPAR/UPA)and non-permeabilization (detection cell membrane GPI-UPAR) conditions.Results: agLDL did not significantly affect levels and distribution of UPAR in rest-ing cell. In control migrating cells, intracellular UPAR polarized to the leading edgeof the cells whereas agLDL-treated VSMC, with significantly lower migration rates,showed a wide distribution labelling for intracellular UPAR through the cell. A dif-ferent pattern was found for cell-membrane GPI-UPAR, that was detected in large(200-600μm2) aggregates concentrated at the migrating front of the cells. How-ever, cytofluorogram diagrams showed that GPI-UPAR in the migrating front colo-calized poorly with F-actin, which strongly differed from the high colocalizationlevel between UPAR and F-actin detected in control VSMC.In summary, our results showed that subcellular localization of UPAR in migratingcells and its colocalization with the actin-cytoskeleton is affected by the VSMCinternalization of agLDL. These processes may have clinical implications in theimpairing effect of LDL in atherosclerosis.
P5491 Small interfering RNA for in vitro and ex vivo MMP-2gene regulation in vascular smooth muscle cells
H. Hlawaty1, A. San Juan1, M.P. Jacob1, R. Vranckx1,D. Letourneur1 , L.J. Feldman2. 1INSERM U698, Paris, France;2L’AP-HP Hopital Bichat, INSERM U698, Paris, France
Objective: Matrix metalloproteinase 2 (MMP-2) is constitutively expressed in vas-cular smooth muscle cells (SMCs). Its active form induces extracellular matrixdegradation leading to SMC migration and proliferation, and plays an importantrole in atherosclerosis and restenosis. The aim of this study was to evaluate theability of small interfering RNA (siRNA) to knockdown MMP-2 gene expression inSMCs in vitro and ex vivo.Methods and Results: Rabbit aortic SMCs were transfected in vitro for 24hwith Tamra-tagged siRNA against MMP-2 mRNA (MMP-2 siRNA) in presenceof jetSI®-ENDO reagent. Control SMCs were transfected with scramble siRNA.Using flow cytometry and confocal microscopy, we showed that cellular uptakeof MMP-2 siRNA was ∼90%. MMP-2 activity, measured with gelatin zymogra-phy, was reduced by 68% at 48h after transfection with MMP-2 siRNA (P=0.005vs. scramble siRNA). Cell viability was not altered by MMP-2 siRNA transfec-tion (LDH and MTT test). MMP-2 gene expression, measured by real-time PCRwas reduced by 60%, 48h after MMP-2 siRNA transfection (P<0.005 vs. scram-ble siRNA). In a scrape wound assay, SMC migration was reduced by 57% at48h after transfection with MMP-2 siRNA (P<0.001 vs. scramble siRNA). More-over, preliminary experiments suggest that ex vivo transfection of stented rabbitcarotid arteries with MMP-2 siRNA/jetSI®-ENDO results in efficient siRNA arterialuptake (fluorescence microscopy, Figure) and up to 90% of inhibition of MMP-2gelatinolytic activity 48h after transfection.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

968 Vascular smooth muscle cell proliferation and apoptosis / Oxidative stress immunity and inflamation
Fig. 1. Ex vivo MMP-2 siRNA carotid transfection
Conclusions: Our results show that MMP-2 siRNA transfection significantly re-duces MMP-2 activity and cell migration in rabbit SMCs in vitro, as well as MMP-2activity in stented carotid arteries ex vivo, suggesting that siRNA is a promisingtechnique for gene silencing in the arterial wall.
OXIDATIVE STRESS IMMUNITY AND INFLAMATION
P5492 The regulatory role of redox-sensitive pathways oninflammatory process and vascular endothelium inyoung smokers: the anti-inflammatory effect ofhigh-dose combined antioxidant treatment
C. Antoniades, D. Tousoulis, C. Vasiliadou, K. Marinou, C. Tsioufis,E. Stefanadi, C. Vlachopoulos, C. Stefanadis. Athens, Greece
Smoking is associated with endothelial dysfunction and increased inflamma-tory process. Although smoking induces the release of reactive oxygen species(ROS), it is unclear whether ROS mediate the smoking-related inflammatory re-sponse through redox-sensitive pathways in humans.Aim: We examined the effect of high-dose combined administration of vitaminsC and E on endothelial function, lipid peroxidation and inflammatory process inyoung smokers.Methods: Forty-two healthy smokers (aged 36±2 yrs old) received vitamin C 2g/d(n=10, VITC), vitamin C 2g/d plus vitamin E 400IU/d (n=11, VITCE400), vitaminC 2g/d plus vitamin E 800IU/day (n=10, VITCE800) or no treatment (n=11, Con-trols), for 4 weeks. Venous occlusion strain gauge plethysmography was usedto estimate endothelium dependent dilation (EDD) and endothelium indepen-dent dilation (EID). Circulating levels of proinflammatory cytokines such as tumornecrosis factor alpha (TNF-α), interleukins 1b (IL-1b) and -6 (IL-6), and adhesionmolecules such as soluble vascular cell adhesion molecule (sVCAM-1) and sol-uble intercellular adhesion molecule (sICAM-1) were determined by ELISA andlipid hydroperoxide (LPO) were evaluated spectrocolorimentrically, at baselineand after treatment.Results: EDD was increased in VITCE400 (46.5±5.4 to 74.3±9.2%, p<0.01)and VITCE800 (43.6±3.9 to 74.9±4.2%, p<0.001), but not in VITC and con-trol groups. Similarly, LPO was reduced in VITCE400 and VITCE800 groups(14.5±1.2 and 15.4±2.9 to 8.8±1.6 and 8.3±1.7 μM respectively, p<0.05 forboth) only. However, in VITCE800, a significant decrease was observed in levelsof IL-1b (0.31±0.07 to 0.10±0.02 pg/ml, p<0.05), IL-6 (4.69±0.90 to 2.02±0.71pg/ml,p<0.05), sVCAM-1 (339±14 to 298±11 ng/ml, p<0.05) and sICAM-1(318±21 to 250±19 ng/ml, p<0.05), while TNF-α levels were slightly but not sig-nificantly decreased (1.76±0.343 to 1.27±0.074 pg/ml, p=NS). All the above pa-rameters remained unchanged in VITC, VITCE400 and control groups.Conclusions: High-dose combined administration of water-soluble vitamin C andlipid-soluble vitamin E, decreased lipid peroxidation and improved endothelialfunction in young smokers. Additionally it decreased the expression of IL-1b, IL-6, sVCAM-1 and sICAM-1, implying that targeting redox-sensitive pathways byhigh-dose combined antioxidant treatment, may have antiatherogenic effect.
P5493 Superoxide production in human aortic abdominalaneurysms: sources and relationship to aneurysmdiameter
B. Guzik1, A. Cencora2, M. Chwala2, R. Korbut1, T. Adamek-Guzik1 ,K. Zmudka1, K.M. Channon3 , T.J. Guzik4. 1Jagiellonian University,
Department of Hemodynamics, Krakow, Poland; 2St J. Grande Hospital,Department of Vascular Surgery, Krakow, Poland; 3University of Oxford,Department of Cardiovascular Medicine, Oxford, United Kingdom; 4EmoryUniversity, Division of Cardiology, Atlanta, United States of America
Increased superoxide (O2-) production by vascular cells may play important rolesin the pathogenesis of aortic abdominal aneurysms (AAA). However, the mech-anisms regulating oxidative stress in AAA are unclear. We have investigatedsources of O2- in human AAA, potential role of protein kinase C (PKC) in reg-ulating O2- production and the relationship between superoxide production andaneurysm diameter.Methods: Superoxide production was measured in AAA segments of from 40
patients undergoing AAA repair, using lucigenin enhanced chemiluminescence(5μM), and visualized by confocal microscopy (dihydroethidium fluorescence).Aneurysm diameter was determined in situ during the surgery. Malonylodialde-hyde (MDA) levels were measured as a marker of oxidative stress from 16 pa-tients with AAA and 16 without AAA.Results: MDA was higher in patient with AAA (4.87μM vs. 3.02μM; p<0,02);Basal superoxide production (O2-) was observed in all AAA segments and wassignificantly higher than in non-AAA segments (23.2±1.9 vs. 12.9 RLU/s/mg;p<0.001) Increased O2- production correlated with aneurysm diameter (R=0.425;p=0.038). O2- production was suppressed by preincubation with superoxide scav-enger Tiron or the superoxide dismutase (PEG-SOD; 450U/ml). O2- produc-tion was significantly inhibited by iNOS - 1400W (100μM) to 18% (4.2±2.4RLU/s/mg). O2- production was also significantly inhibited NAD(P)H oxidase in-hibitors: diphenyliodonium (DPI; 10μM) to 16% of control levels or by apocynin(500μM) to 51% of control levels (11.8±1.0 RLU/s/mg). Modest inhibition (to 60%of control levels) was also observed in response to the cyclooxygenase inhibitorindomethacin (10μM). Inhibitors of other oxidase systems (xanthine oxidase, mi-tochondrial) did not show significant effects. SOD inhibitable superoxide produc-tion in AAA was localised mainly in media and adventitia, as shown by dihy-droethidium staining. These data indicate that vascular NAD(P)H oxidase is thepredominant source of O2- in AAAs. Addition of NADPH (100μM) to intact AAAssegments increased of O2- production in AAA 19-fold (to 454±76 RLU/s/mg).Conclusions: iNOS and vascular NAD(P)H oxidase(s), are the predominantsource of superoxide production in AAA. Vascular O2- production is correlatedwith aneurysm diameter, as a measure of disease progression. Novel antioxidantapproaches directed on inhibiting iNOS and NAD(P)H oxidases may be useful intreatment of AAA.
P5494 Pro-atherogenic role of C-reactive protein viadendritic cells?
E.A. Van Vre1, V.Y. Hoymans2, H. Bult1, G. Nijs1, V.F. VanTendeloo1 , C.J. Vrints1, J.M. Bosmans1. 1University Of Antwerp,Cardiology, Wilrijk, Belgium; 2University of Antwerp, Cardiology,
Wilrijk, Belgium
Background: Dendritic cells (DC) are potent antigen-presenting cells that havebeen implicated in the development of atherosclerosis. Recent studies show var-ious pro-atherogenic effects of C-reactive protein (CRP), a powerful independentpredictor of cardiovascular disease, on different vascular cells. Since informationregarding effects of CRP on DC function is lacking, we analysed possible im-munomodulating effects on DC of human CRP in the absence and presence oflipopolysaccharide (LPS).Methods: Monocytes from healthy blood donors were differentiated into immatureDC and subsequently cultured with increasing CRP concentrations (0.06μg/ml to60μg/ml), with or without 0.1 μg/ml LPS. After 24h phenotypic changes wereexamined by flow cytometry. DC incubated with high CRP concentrations werecocultered with CFSE-labelled lymphocytes (ratio 1/9, DC/lymphocytes) to mea-sure T cell proliferation and IFNgamma secretion (ELISA) after 8 days.Results: Expression of the costimulatory molecules CD80 and CD40 increasedsignificantly after 24h incubation with respectively 6μg/ml and 20μg/ml CRP orhigher (p<0.01, one-way ANOVA, n=8), compared to control DCs. The maximumexpression of both CD80 and CD40 was equivalent to that seen with 0.1μg/mlLPS. We neither noticed a potentiation nor an inhibition of CRP on the effects ofLPS. In contrast to CD80 and CD40, LPS or CRP did not raise the expressionof CD83 or CD25. DCs incubated for 24 hours with 60μg/ml CRP showed mul-tiple enlarged cell clusters, and elongated cell morphology when compared withcontrol DCs. After 8 days of coculture, T lymphocytes incubated with these CRP-pulsed DC showed a strongly increased proliferation in comparison with controlDCs (p=0.03, n=3, average increase 53%). In addition IFNgamma concentrationof the supernatant was significantly increased compared to control supernatant(p=0.02, n=3, average increase 1925pg/ml).Conclusions: CRP induces a concentration-dependent maturation of DCs andof DC-mediated T cell proliferation and activation. In the current setting we didnot detect any anti-inflammatory, protective effects of CRP. These findings sug-gest that the increased CRP concentrations found in the blood and atheroscleroticarteries may promote inflammatory responses. This could contribute to an accel-eration of atherosclerosis and its complications.
P5495 Dendritic cells pulsed with oxidised low densitylipoprotein aggravate atherosclerosis
C. Hjerpe, D. Johansson, G. Hansson, X. Zhou. Karolinska Hospital,Stockholm, Sweden
Atherosclerosis is related not only to cholesterol deposition and cellproliferation in the lesions, but also to infiltration of immune cells involved in bothinnate and adaptive immunity. Dendritic cells (DCs), a professional antigen pre-senting cell that can prime T cells and stimulate B cell growth and antibody se-cretion in adaptive immunity, have been found in atherosclerotic lesions. Previ-ous findings suggest that DCs may be important in the initiation of immune re-sponses to plaque antigens. The effector mechanisms of DCs in atherosclerosishave not been studied. Meanwhile, oxidized low density lipoprotein (oxLDL) hasbeen identified as one of the most important candidate antigens for the immune
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Oxidative stress immunity and inflamation 969
response associated with atherosclerosis. To evaluate the function of DCs in thedevelopment of atherosclerosis, oxLDL-pulsed DCs derived from bone marrowwas transferred into apoE KO mice. The extent of the disease was estimatedby measuring lesion size in the root of aorta and was compared to control ani-mals transferred with either KLH-pulsed or untreated DCs. Mice receiving oxLDLpulsed DCs showed significantly increased atherosclerosis accompanied by el-evation of VCAM-1 expression in the lesions. Titers of antibodies to oxLDL orKLH were dramatically increased in the corresponding groups.Our results showthat transfer of bone marrow derived DCs pulsed with oxLDL can induce a strongantigen specific immune response and aggravate atherosclerosis.
P5496 Decreased arginase-1 and increased NO productionin foam-cell macrophages
A.C. Thomas1, G.B. Sala-Newby2, Y. Ismail1, A.C. Newby1.1University Of Bristol, Bristol Heart Institute, Bristol, United Kingdom;2University of Bristol, Bristol Heart Institute, Bristol, United Kingdom
Conversion of macrophages to foam-cell is a critical step in atherosclerosis.We used suppression subtraction hybridisation (SSH) to compare the transcrip-tome of non-foamy and foamy macrophages generated by placing subcutaneouspolyethylene sponges in rabbits fed a normal or cholesterol-enriched diet, re-spectively. Differential expression was confirmed at the mRNA level using semi-quantitative RT-PCR and at the protein level using enzymatic assays.SSH indicated decreased arginase-1 expression in foamy compared to non-foamy macrophages, which was confirmed using RT-PCR (n=6/group, P=0.0004).Arginase-1 converts arginine to urea plus ornithine, which is further metabolisedto other products including glutamate, proline and polyamines. Based on ureaproduction there was 60-fold less arginase activity in foamy compared tonon-foamy macrophages (n=6/group, P=0.0087). Using an HPLC assay, foamcell extracts catalysed less glutamine production than those from non-foamymacrophages (n=3/group, P=0.0481) and arginine consumption was 5-fold less(P=0.0260). Since arginine is also the substrate for nitric oxide synthase we hy-pothesised that NO production might be increased in foam cells. Indeed NOS ac-tivity measured using the Griess assay was 2.5 fold more in foamy macrophagescompared to the same number of non-foamy cells (n=6-12/group, P=0.0145), de-spite no differences in either neuronal NOS-3 or inducible NOS-2 mRNA levels(endothelial NOS-1 was undetectable).We conclude that decreased arginase-1 levels increased NO production in foamymacrophages. High levels of NO are believed to be proinflammatory, inhibitsmooth muscle cell proliferation and cause apoptosis of smooth muscle and en-dothelial cells. Low arginase-1 would tend therefore to favour atherosclerosisand plaque instability. Consistent with this, a polymorphism that leads to lowerarginase-1 activity in peritoneal macrophages promotes atherosclerosis in rab-bits.
P5497 Conversion of macrophages to foam cellsupregulates production of several matrixmetalloproteinases: role of ox-LDL
Y. Ismail1, G.B. Sala-Newby2, A.C. Thomas1, A.C. Newby1.1University Of Bristol, Bristol Heart Institute, Bristol, United Kingdom;
2University of Bristol, Bristol Heart Institute, Bristol, United Kingdom
Matrix metalloproteinases (MMPs) are thought to play a critical role in plaquerupture. We investigate whether conversion of macrophages (MF) to foam cells(FC) stimulates MMP expression and how this relates to uptake of oxidised-LDL(ox-LDL). Subcutaneous sponges were implanted into rabbits fed a normal dietto produce inflammatory MF or a cholesterol-rich diet to convert these to foamcells (FC). Human monocytes were differentiated into MF using hM-CSF beforeloading with 100mg/ml fully ox-LDL. MMP expression was investigated by RT-PCR, Western blotting and gelatin zymography. In the in vivo rabbit model, FChad 3.3-fold more MMP-1, 2-fold more MMP-12 and 1.3-fold more MT1-MMP but77% less MMP-9 than MF at the mRNA level. These results were confirmed atthe protein level with FC having 6-fold more MMP-1, 3.9-fold more MMP-12 and33-fold more MT1-MMP but 94% less MMP-9. FC had 1.6-fold more MMP-3 at themRNA level but this was not significant at the protein level (all differences p<0.05,n≥5/group). To investigate the role of ox-LDL loading, we used human MF in vitro.MMP-1 mRNA was significantly elevated 2.7-fold after lipid loading and MMP-9mRNA was reduced 33%, in keeping with the in vivo findings. In contrast, MMP-12 was down-regulated 70% by lipid loading while no differences were observedin MMP-3 or MT1-MMP at the mRNA level (all differences p<0.05, n=3/group).Our results show that conversion of MF to FC in vivo upregulates several MMPsthat have been implicated in plaque rupture. Ingestion ox-LDL appears to directlymodulate expression of MMP-1 and MMP-9. Since histological studies of bothhuman and rabbit atherosclerotic plaques demonstrate MMP-3, -12 and MT1-MMP expression in FC, mechanisms other than ox-LDL must also contribute.
P5498 A NCoR-dependent pathway mediates suppression ofcytokine-induced C-reactive protein gene expressionby LXR
F. Blaschke1, E. Caglayan2, Y. Takata1, F. Yin1, C. Lyon1,W. Hsueh1, R. Tangirala1 . 1University Of California, Endocrinology,
Diabetes, Hypertension, Los Angeles, United States of America; 2UCLA, LosAngeles, United States of America
Recent studies suggest that C-reactive protein (CRP), in addition to being anindependent risk predictor of future cardiovascular events, directly promotesatherosclerotic processes. We demonstrate here that the liver X receptors (LXR-alpha and -beta), members of the nuclear hormone receptor superfamily and im-portant regulators of cholesterol homeostasis and inflammatory gene expressionin macrophages, inhibit cytokine-induced expression of CRP. Treatment of pri-mary human hepatocytes and Hep3B cells with the LXR agonists T0901317 orGW3965 (0.1 - 5 μM) dose-dependently reduced cytokine (IL-6 10 ng/ml plus IL-1beta 20 ng/ml) induced CRP mRNA and protein expression as determined byNorthern blotting, real-time PCR and Western blotting. Transient transfection ofthe CRP promoter (- 964 bp to + 9 bp) in Hep3B cells revealed that LXR activa-tion dose-dependently inhibited CRP promoter activity. Analysis of truncated CRPpromoter constructs using series of 5’-deletions revealed that a region between-256 to -125 relative to the initiation site is required for the ability of LXR to in-hibit CRP promoter activity. This region contains binding sites for the hepatocytenuclear factor-1 alpha (HNF-1alpha) and Stat3. However, electrophoretic mobilityshift assays demonstrated that LXR ligands did not affect binding of these tran-scription factors, suggesting that LXR ligands might modulate binding of coac-tivator and corepressor complexes. Overexpression of the nuclear corepressorNCoR dose-dependently attenuated cytokine-induced CRP promoter activity, in-dicating that NCoR is involved in the regulation of CRP gene transcription. In-hibition of NCoR expression using an NCoR-specific short interfering (si) RNAresulted in an attenuation of LXR ligand mediated inhibition of CRP promoteractivity and mRNA expression, providing evidence that the mechanism of LXRligand-mediated inhibition of CRP gene transcription involves interaction of NCoRcomplexes with the CRP promoter. Chromatin immunoprecipitation experimentsdemonstrated that NCoR is present on the CRP promoter under basal conditions.In addition, cytokine-induced clearance of NCoR from the CRP promoter is in-hibited in cells treated with T0901317. In summary, our results demonstrate thatligand activation of LXR represses CRP gene transcription in hepatocytes and es-tablish an important role of NCoR in modulating CRP gene transcription. Theseresults define a novel function of LXRs in the control of liver CRP gene expressionand support the potential utility of LXR ligands in modulating inflammatory generesponses and inhibiting the development of atherosclerosis.
P5499 PTEN Reduces Cuff-induced Neointimal Formationand Vascular Inflammation
S. Koide, M. Okazaki, M. Tamura, K. Ozumi, H. Takatsu, A. Tanimoto,H. Tasaki, Y. Nakashima. Univ. of Occupa. and Environ. Health,Second Department of Internal Medicine, Kitakyusyu-Shi, Japan
Background: Vascular injury in percutaneous coronary intervention (PCI) causesan inflammatory response mediated in part by MCP-1, which results in thedevelopment of intimal hyperplasia and leads to post-PCI restenosis. Stimula-tion of angiotensin (Ang) II type 1 receptor increases vascular inflammation bystimulating MCP-1 expression in vascular smooth muscle cells (VSMCs). PTEN(phosphatase and tensin homolog deleted on chromosome 10) hydrolyzes the 3-phosphoinositide lipid products of phosphatidylinositol (PI) 3-kinase and inhibitsPI-3-kinase signaling, which regulates cell proliferation, migration, and survival. Inthis study, we examined whether adenovirus-mediated overexpression of PTENreduces cuff-induced inflammatory response and neointimal hyperplasia.Methods and Results: The femoral artery of male Wistar rat was isolated in situand sheathed with polyethylene tube. AxCALacZ or AxCAPTEN was injected be-tween the cuff and adventitia. Fourteen days later, rats were sacrificed and theartery examined histopathologically. Neointimal formation in AxCAPTEN-treatedvessel was significantly less than in AxCALacZ-treated artery (intima media ra-tio: 0.12±0.01 vs. 0.37±0.08, p<0.01, n=4, respectively). The ratio of the num-ber of PCNA (proliferating cell nuclear antigen)-stained cells to total cells waslower in AxCAPTEN- than in AxCALacZ-treated arteries (neointima: 0.12±0.05vs. 0.35±0.03, p<0.01, media: 0.16±0.04 vs 0.28±0.02, p<0.01, n=5, respec-tively). MCP-1 expression and macrophage invasion were both decreased inAxCAPTEN-treated vessels. MCP-1 expression was recognized in all vessel lay-ers, but macrophages were detected only in the intimal surface and adventitia. Incultured rat aortic VSMCs, PTEN inhibited Ang II-induced MCP-1 m-RNA expres-sion quantified by real-time PCR.Conclusions: These results suggest that overexpression of PTEN reducesneointimal formation, possibly in part through inhibition of inflammatory responseinvolving MCP-1 expression and macrophage invasion.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

970 Oxidative stress immunity and inflamation
P5500 AT1 receptor-independent effects of ACE inhibitionand angiotensin receptor blockade on vascularoxidative stress and atherogenesis?
S. Wassmann1 , T. Czech1, M. Van Eickels2, G. Nickenig2.1Universitaetsklinikum Bonn, Medizinische Klinik II, Bonn, Germany;
2Sanofi-Aventis TD CV, Frankfurt/Main, Germany
Activation of the angiotensin II type 1 (AT1) receptor is involved in the patho-genesis of atherosclerosis, which can be inhibited by ACE inhibition or AT1 re-ceptor blockade. The involvement of the bradykinin system in the effects of ACEinhibitors (ACE-I) and potential pleiotropic effects of angiotensin receptor blockers(ARB) and their contribution to the beneficial therapeutic effects of these agentsremain unclear. We investigated this issue in a mouse model of atherosclerosis.Methods and Results: Apolipoprotein E-deficent (ApoE-/-) mice and homozy-gous double-knockout animals deficient of ApoE and the AT1A receptor (ApoE-/-AT1-/- mice) were fed a high-cholesterol diet for 7 weeks. Vascular oxidative stress(L-012 chemiluminescence), atherosclerotic lesion formation in the aortic root andthe ascending aorta (oil red O staining), and endothelial dysfunction (organ cham-ber experiments with isolated aortic segments) were evident in ApoE-/- mice, butwere markedly reduced in double-knockout animals. Systolic blood pressure wassignificantly lower in ApoE-/-AT1-/- mice as compared with ApoE-/- animals (tail-cuff measurements). Oral treatment of cholesterol-fed ApoE-/-AT1-/- mice with ei-ther the ACE-I ramipril or the ARB telmisartan did not result in a significant furtherreduction of systolic blood pressure. Endothelium-dependent vasorelaxation andaortic reactive oxygen species release were identical in double-knockout animalstreated with placebo, ramipril, or telmisartan. Compared to placebo-treated ApoE-/-AT1-/- mice, atherosclerotic lesion formation was identical in double-knockoutanimals treated with the ARB, but was significantly increased in those treatedwith the ACE-I. AT2 receptor inhibition with PD123319 increased plaque forma-tion in ApoE-/-AT1-/- mice.Conclusions: Genetic disruption of the AT1A receptor reduces oxidative stressand atherogenesis in ApoE-/- mice. Our data provide no evidence for pleiotropiceffects of ARBs and the involvement of the bradykinin system in the effects of ACEinhibitors on vascular oxidative stress, endothelial dysfunction, and atherosclero-sis.
P5501 Prevention of experimental atherosclerosis withAgaricus sylvaticus: comparison with antioxidantvitamins C and E
S. Percario1, V.F. Odorizzi1, J.S. Penoni1, W.N. Ogawa1,D.R.S. Souza2 on behalf of Communitarian Health Research Group.
1Regional University of Gurupi, Communitarian Health Research Group, Gurupi,Brazil; 2Rio Preto Medical College, Molecular Biology, Sao Jose Do Rio Preto,Brazil
Only few studies highlight the real effects of antioxidant usage for the preventionor regression of atherosclerosis. The aim of the present study was to verify thepotential benefits of the consumption of a natural antioxidant-rich food in the pre-vention of the onset of atherosclerotic plaques in a rabbit model. This way, 27male New Zealand rabbits were fed a cholesterol-enriched diet (0.5g of choles-terol/kg/day) for a period of 10 weeks. Some also received a dietary supplementof the mushroom Agaricus sylvaticus (20mg of A. sylvaticus/kg/day/10 weeks)and constitute group MUSHROOM (N=10), whereas others received a vitaminsupplement (12mg of Vitamin E + 15mg of Vitamin C/kg/day/10 weeks) and con-stitute group VITAMINS (N=6). The remaining animals constitute group CHOLES-TEROL (N=11). As controls, 10 animals were kept under the same circumstances,but receiving normal rabbit chow only (group CONTROL). After the induction ofatherosclerosis (10 weeks), blood samples were drawn for biochemical evalua-tion of total cholesterol, oxidative stress (thiobarbituric acid reactive substances -TBARS; total antioxidant capacity - TAS) and uric acid. Additionally, aorta arter-ies were removed for evaluation of the surface taken by atherosclerotic plaquesby means of computerized planimetry. The results (Table) show an enormous in-crease in total cholesterol for the three cholesterol-fed groups, although differentmean areas of artherosclerotic plaques were observed, witch are correlated tothe alterations found in oxidative stress markers. Besides, group cholesterol pre-sented an increase in uric acid levels, suggesting the involvement of ischemia-reperfusion syndrome.
Mean ± SD values for all groups
Group N Cholesterol Uric acid TBARS TAS Plaques(mg/dL) (mg/dL) (ng/mol) (mmol/L) (%)
Mushroom 10 2113±243a 2.69±0.95a c 60.9±36.6c e 0.53±0.39a d 6±6a c e
Vitamins 6 1913±407a 2.05±0.33a 74.1±20.1b 0.56±0.14a 14±8a c
Cholesterol 11 2140±178a 24.50±17.90a 71.3±38.2b 0.41±0.34a 47±21a
Control 10 65±27 Not detected 52.4±39.7 0.98±0.17 Not detected
a = p≤0,01 against control; b = p≤0,05 against control; c = p≤0,01 against cholesterol; d =p≤0,05 against cholesterol; e = p≤0,01 against vitamins.
These findings strongly suggests that oxidative processes, rather tham choles-terol levels, are the main cause of atherosclerosis, and the use of antioxidantscan prevent it, even consumed in foods such as the A. sylvaticus mushroom.
P5502 Chronic treatment with nebivolol leads to stabilizationof atherosclerotic plaque in apoE-knockout mice
A. Kuroedov1, E. Osto1, M. Kurrer2, P. Francia3 , M. Eto2,M. Volpe1, T.F. Luscher2 , F. Cosentino2. 1Cardiology, University ofZurich, Cardiovascular Research, Zurich, Switzerland; 2Pathology,
University of Zurich, Zurich, Switzerland; 3Cardiology, University of Rome, Rome,Italy
Background: Attachment of activated monocytes to the endothelium and foamcell formation are crucial steps in atherogenesis. Recent studies suggestthat beta-blockers may affect monocytic-endothelial interaction. Although beta-adrenoceptors are present on circulating mononuclear cells, their role remain un-clear. The present study was designed to compare the effects of a new selectivebeta1-receptor antagonist nebivolol with atenolol on atherosclerotic plaque com-position in vivo and foam cell formation in vitro.Methods: Male apolipoprotein E knockout (ApoE-/-) mice (5-6 week old) werefed for 30 weeks with a Western type diet (42% milk fat, 0.15% cholesterol) inthe absence (control group) and in the presence of nebivolol (10 mg/kg/day) oratenolol (100 mg/kg/day). Animals were then sacrificed and the content of smoothmuscle cells and collagen fibers was calculated in atherosclerotic plaques ofaortic root. Furthermore, CD14 expression was used to determine the effect ofbeta1-receptor antagonists on IL-1 beta induced monocyte transformation of hu-man monocyte cell line, THP-1 cells (10-5g/L, incubation time=48 hours). Mousemacrophage cell line Raw 264.7 cells were exposed to DiI-labeled acetylatedLDLs (acLDLs, 5 μg/mL, 48 hours) in order to assess foam cell formation. Thefluorescence of Raw 264.7 cells was measured by flow cytometry after incuba-tion with acLDLs in control cells and cells treated with nebivolol or atenolol (10-6mol/L).Results: Chronic treatment with nebivolol reduced number of smooth musclecells in plaque shoulders and caps by 32 ±7% and increased their collagen con-tent by 24 ±7% (p<0.05 vs control, respectively). In contrast, atenolol did not ex-ert any significant change. Stimulation with IL-1beta of THP-1 cells increased ex-pression of CD14 (285±41%, n=3, p<0.01). Nebivolol totally blunted IL-1 beta in-duced CD14 upregulation (60±9%, n=3, p<0.01 vs control cells), whereas treat-ment with atenolol only reduced CD14 expression (173±14%, n=4, p<0.01 vscontrol cells). In Raw 264.7 cells, nebivolol reduced DiI-labeled acLDL-uptake(1228±150 and 616±173 relative units for control and nebivolol-treated cells, re-spectively, n=5, p<0.01). Atenolol did not affect acLDL uptake.Conclusions: Our findings suggest that only chronic treatment with third gener-ation beta1 selective antagonist nebivolol leads to stabilization of atheroscleroticplaque via inhibition of foam cell formation. Our future investigations will addressthe putative mechanisms involved.
P5503 Soluble CD31 gene transfer increases circulatingregulatory T cells and reduces atherogenesis inapolipoprotein E knockout mice
E. Groyer1, A. Nicoletti1, J. Khallou-Laschet1 , A.-T. Gaston1,O. Thaunat1 , S. Kaveri1, H. Stockinger2, G. Caligiuri1. 1INSERM,
UMRS 681, Paris, France; 2University of Vienna, Immunology, Vienna, Austria
Background: All the stages of atherosclerotic disease bear an imprint of theeffect of activated blood cells acting upon the arterial wall. CD31 is a transmem-brane glycoprotein expressed exclusively by the cells of the blood-vessel interface(endothelial cells, platelets, granulocytes, monocytes and lymphocytes) and canplay a regulatory role on these cells through its intracytoplasmic inhibitory motifs.We postulated that CD31 homophilic binding may regulate cell activation at theblood-vessel interface and thus contribute to prevent atherosclerosis.Objective: In the present study, we assessed the effect of circulating solubleCD31 gene transfer on circulating T cell activation/regulation and atherogenesis.Methods: Apolipoprotein E knockout (ApoE KO) mice (female, n=20) were sub-jected to plasmid transfer by muscle electroporation at 8, 13, 18 and 23 weeks ofage. Plasmid encoded a chimera of IgG1-Fc fused with a soluble form of the en-tire extracellular portion of CD31 (CD31Rg). Western blot and ELISA showed thatCD31Rg was still present in the serum at the time of sacrifice. Blood, aortic rootand spleen were collected from the anesthetized mice at 28 weeks of age. Lesionsize was analyzed on oil red-o stained aortic root cryosections. The percentageof regulatory T cells (Treg, CD4+/CD25hi/CD45RBLo) was evaluated by flow cy-tometry on blood leukocytes. Spleen cell proliferation in response to concanavalinA (ConA) was assessed by 3[H]Thymidine incorporation.Results: Atherosclerotic lesions were significantly reduced in CD31Rgtreated mice (16.8±0.9%; mean±SEM) as compared to controls (28.6±1.6%,p<0.0001). In parallel, the percentage of circulating Treg was increased (8.6±0.4vs 5.8±0.3%, p<0.05) while proliferative response of splenocytes to ConA wasreduced (108±3 vs 125±11 x1000 cpm, p<0.05).Conclusions: Circulating soluble CD31 overexpression reduces atherogenesisthrough a regulation of cell activation at the blood-vessel interface and, in partic-ular, of the T cell responses.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Oxidative stress immunity and inflamation 971
P5504 Potential role of secretory phospholipase A2 type IIAin the transition of innate to adaptive immunity duringatherosclerosis
E. Ibeas1, L. Fuentes1, M. Hernandez1 , R. Martin1, J. Carvalho1,F. Fernandez-Aviles2 , M.L. Nieto2. 1IBGM, I3U, Valladolid, Spain;
2Hospital Clinico Universitario, Cardiologia, Valladolid, Spain
Background: Acute coronary events commonly result from thrombosis triggeredby disruption of an atherosclerotic plaque. Migratory immune/inflammatory cellsare the key cellular elements at all stages of atherosclerosis and abound a sitesof plaque rupture. The recent finding of dendritic cells (DCs) accumulating inatherosclerotic lesions opens new vistas for the comprehension and treatmentof this disease. Dendritic cells (DCs) constitute a unique family of cells able toinduce primary immune responses. Frequency and maturation of DCs correlateswith the different stages of atherosclerotic plaques. Because of their unique abil-ity to stimulate naive T-cells, a relevance of DCs in atherosclerotic lesion initiationand progression can be assumed.Purpose of the study: Since recent reports have pointed to a member of the se-cretory phospholipase A2 family (sPLA2), the bee venom sPLA2-III, as a stimulusinvolved in DCs maturation, the aim of this study was to investigate the effectsonDCs of a secreted enzyme abundant in biological fluids/lesions of inflammatory-diseases such as atherosclerosis.Methods and Results: The secretory phospholipase A2 type IIA (sPLA2-IIA) isan enzyme strongly associated with the development of atherosclerotic lesion be-cause it has been detected in all stages of atherosclerotic arteries. To elucidateits role in the progression of the vascular lesion, we have studied the ability ofthis enzyme on the generation of functional human DCs derived from monocytes.The cellular response to sPLA2-IIA includes down-regulation of CD14 expressionand up-regulation of the phenotypic markers DC-SIGN, CD40, FasL, CD54 andCD106 (Flow cytometry and Western blot). This phenotype change endows thesecells with adhesive, migratory and endocitic functions similar to those observed inthe presence of PMA+IL-4, classical DCs-inducers. We have also observed mor-phological changes characteristic of monocyte-derived dendritic cells after 72hincubation with sPLA2-IIA (confocal microscopy). The presence of the mitogen-activated protein kinase kinase 1-extracellular signal-regulated kinase (ERK) in-hibitors PD98059 or U0126 significantly reduced the changes induced by thesPLA2-IIA, these results indicate that the ERK signaling pathways regulate thephenotypic markers acquiredduring monocyte-derived DCs differentiation.Conclusions: These data show that sPLA2 elicits important phenotypic changeson monocytes, linking the inflammatory and the immune responses.
P5505 Expansion of ζ-dim CD4+ T-cells and ζ-dimnatural-killer (NK)-cells correlates with C-reactiveprotein (CRP) in patients with acute coronarysyndromes (ACS)
E. Ammirati1, M. Banfi1, D. Cianflone1, A.P. Cope2, C. Godino2,M. Mussardo2 , A. Maseri2, C. Monaco1. 1Vita-Salute San Raffaele
University, Clinical Cardiovascular Biology, Milan, Italy; 2Kennedy Institute,Imperial College, Rheumatology, London, United Kingdom
Objective: Growing similarities are emerging between ACS and inflammatorydiseases. The down-regulation of the ζ-chain, a transmembrane protein associ-ated to the T-cell Receptor (TCR) and NK receptors has been reported in in-fectious and inflammatory diseases. Down-regulation of the ζ-chain has beenlinked to persistent antigenic and/or cytokine exposure in experimental models.We aimed to assess whether patients with ACS exhibit increased ζ-dim T-cellsand ζ-dim NK-cells frequencies, and whether such ζ-chain down-regulation corre-lates with the magnitude of systemic inflammation.Methods: We collected peripheral blood and serum of 35 patients with ACS onadmission, 10 with chronic Stable Angina (SA) and 20 controls. Peripheral bloodmono-nucleated cells were stained for CD3, CD4, TCRζ and for CD3, CD16,TCRζ. Frequencies of ζ-dim CD4+ T-cells and ζ-dim NK-cells were analysed byflow cytometry. We assessed hsCRP levels via nephelometric method.Results: ζ-dim CD4+ T-cell were expanded in ACS compared to SA (medianfrequencies: 4.4% vs 1.25% P=0.0006) and to controls (vs 1% P<0.0001). Alsoζ-dim NK-cells were increased in ACS compared to SA (5.05% vs 1.6% P=0.038).A significant correlation was found between hsCRP and ζ-dim CD4+ (r=0.44P=0.002) and ζ-dim NK-cells (r=0.4 P=0.016).Conclusions: Enrichment of ζ-dim CD4+T-cells and ζ-dim NK-cells is present inthe peripheral blood of patients with ACS compared to patients with SA and tohealthy controls. Expansion of ζ-dim cells could represent a new cellular markerof plaque instability as well as yet another similarity between ACS and inflam-matory diseases. The frequencies of ζ-dim populations appear to be correlatedwith the magnitude of ongoing systemic inflammation indicating that the expo-sure to infectious agents and/or inflammatory mediators might be the mechanismunderlying ζ downregulation.
P5506 Affinity of C-reactive protein towards FcgammaRI isstrongly enhanced by the gamma-chain
D.E. Manolov, C. Roecker, E. Kuzmenkina, H. Slatosch,G.U. Nienhaus, J. Torzewski. University of Ulm, Internal Medicine II,Ulm, Germany
Background: C-reactive protein (CRP), the prototype human acute phase pro-tein, is widely regarded to play a key role in atherogenesis. Its cellular receptor isstill under debate.Methods and Results: By using ultrasensitive confocal imaging analysis, wehave studied CRP binding to transfected COS-7 cells expressing the high affin-ity IgG receptor FcgammaRI. Here we show for the first time that CRP binds toFcgammaRI on intact cells, with a KD of (10 ± 3) μM. Transfection of COS-7cells with a plasmid coding for both FcgammaRI and its functional counterpart,the gamma-chain, markedly increases CRP affinity to FcgammaRI, resulting in aKD of (0.35 ± 0.10) μM. The affinity increase results from a ∼30-fold enhancedassociation rate coefficient. Dissociation of CRP is extremely slow, suggestingthat receptor clustering occurs upon binding.Conclusions: The pronounced enhancement of the affinity by the gamma-chainsuggests its crucial involvement in the CRP-receptor interaction. We suggest thatthe gamma-chain mediates interactions between the transmembrane parts of thereceptors. Considering the pentameric structure of CRP and the observed, ex-tremely slow dissociation of CRP from the receptors, our findings indicate thatmultivalent interaction and receptor clustering are crucially involved in the inter-action of CRP with nucleated cells.
P5507 Elevated thrombotic markers in diabetic mice arelowered by PPAR-alpha selective agonists
S. Youssef, D.E. Normandin, S. Seiler, R. Mukherjee, P.T. Cheng,M.L. Ogletree, B.J. Arey. Bristol-Myers Squibb Company, ThrombosisResearch, Pennington, United States of America
Purpose: Cardiovascular complications of diabetes and obesity are well docu-mented and represent a major cause of morbidity and mortality in patients withmetabolic disease. The cardiovascular disease profile associated with metabolicdysfunction includes elevation of markers associated with activation of throm-botic processes, including thrombin-antithrombin III complex (T-AT), soluble (s)P-selectin and plasminogen activator inhibitor (PAI-1). It has been noted clinicallythat thiazolidinediones such as troglitazone can lower levels of some thromboticmarkers. Our laboratory recently reported finding elevated levels of these andother thrombotic markers that correlate with shortened native clotting times indb/db mice. In the current experiments we studied the effects of selective PPAR-alpha and -gamma agonists on thrombotic markers in db/db mice.Methods: Diabetic mice at 12-14 weeks of age were administered PPAR agonistsp.o. once daily for 14 days prior to collection of blood for analysis of thromboticmarkers.Results: The PPAR-alpha agonists, fenofibrate and GW-9578, dose-dependentlylowered circulating levels of the thrombin generation marker, T-AT, but had no ef-fect on the platelet marker, sP-selectin. The PPAR-gamma agonists, rosiglitazoneand pioglitazone, did not affect the levels of either marker. However, both PPAR-alpha and -gamma agonists lowered circulating levels of the inflammation marker,IL-6, and elevated plasma PAI-1 activity. When co-administered at sub-thresholddoses of each agent alone, fenofibrate and rosiglitazone did not affect plasmaconcentrations of T-AT or sP-selectin.Conclusion: These data suggest that selective PPAR-alpha agonists, but notPPAR-gamma agonists, can beneficially lower some markers of both thrombo-sis and inflammation in diabetic mice. Moreover, these experiments describe apreclinical model for evaluating a potential therapeutic benefit of PPAR-alpha ag-onists on cardiovascular complications in metabolic disease.
P5508 T cell vaccination modulates experimentalatherogenesis
A. Varthaman, J. Khallou-Laschet, E. Groyer, A.-T. Gaston,S. Kaveri, G. Caligiuri, A. Nicoletti. INSERM, UMRS 681, Paris,France
Objective: T cell activation plays a critical role in atherogenesis.Clonal analysis of the T-cell infiltrate in lesions of apolipoprotein E knockout(ApoE°) mice showed an oligotypic prevalence of variable portion of the betachain (Vb)6 of the T cell receptor (TCR) of CD4+ T cells infiltrated in atheroscle-rotic lesions. By contrast, no Vb7+ T cells can be found in atherosclerotic plaquesof ApoE° mice. We have studied the role of the Vb6+ T cells in the formation of thelesions in ApoE° mice using the T cell vaccination procedure. T cell vaccinationrelies on the injection of an inactivated CD4+ T cell clone expressing the targetedVb chain that stimulates Vb-specific CD8+ regulatory T cells when portions ofthe Vb chain are presented within the Qa-1 type class II major histocompatibilitycomplex. The CD4+ T cells used for T cell vaccination and the targeted CD4+ Tcells can exhibit different antigen specificities provided that they express TCR Vbchains from the same family.Methods: Vb6+ or Vb7+ (Ctrl) CD4+ T cell hybridomas were stimulated with con-canavallina (con)A, irradiated and intravenously injected in 6-week old ApoE° fe-male mice (n=14). 2 months later, CD8+ T cells from lymphoid organs were tested
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

972 Oxidative stress immunity and inflamation / Lipids and metabolism
for their cytotoxicity against the 2 hybridomas. Lesions in the aortic root were an-alyzed on oil redO-stained slides.Results: CD8+ T cells from the immunized mice were found to lyse specificallythe hybridomas against which they were immunized. The blockade of the Vb6+clonal expansion in these mice by T cell vaccination resulted in a significant in-crease in lesion size (29% reduction, p<0.05).Conclusions: The T cell vaccination is a new strategy to control the activationof T-cell clones specific to atherosclerotic lesions. The blockade of the expansionof the CD4+Vb6+ population led to an increase in lesion density indicating anatheroprotective and possible immunomodulatory role of the prevalent CD4+ Tcell population in the early stages of lesion formation in ApoE° mice.
P5509 Inhibition of protein kinase C beta as a newtherapeutic strategy to prevent foam cell formation
E. Osto1, A. Kuroedov1, L. Rohrer2, A. Von Eckardstein2, M. Volpe3,T.F. Luscher2 , F. Cosentino2. 1Cardiology, University of Zurich,Cardiovascular Research, Zurich, Switzerland; 2Clinical Chemistry,
University of Zurich, Zurich, Switzerland; 3Cardiology, University of Rome, Rome,Italy
Background: Increasing evidence indicates that protein kinase C beta (PKCbeta) plays a role in several mechanisms promoting atherosclerosis. The presentstudy was designed to determine whether PKC beta signaling is involved inmonocyte-macrophage LDL uptake and foam cell formation.Methods: The transformation of human monocyte cell line THP-1 cells intomacrophages after 48 hours incubation with IL-1beta (10-5 g/mL) or phorbol es-ter 12-myristate 13-acetate (10-7 mol/L, PMA) was assessed by counting cell at-tachment and expression of CD14. Mouse macrophage cell line Raw 264.7 wasexposed for 48 hours to DiI-labeled acetylated LDLs (acLDLs, 5 μg/mL) in orderto study LDL uptake. The fluorescence of Raw 264.7 cells was measured by flowcytometry at baseline and after incubation with acLDLs.Results: Incubation of THP-1 cells with IL-1beta resulted in a significant in-crease of the number of attached cells (1628 cells/cm2 vs control 80 cells/cm2,n=5, p<0.001). The effect of PMA on cell adhesion elicited a similar increase(3496 cells/cm2, n=5, p<0.001 vs control). CD14 expression in THP-1 cellswas increased by IL-1beta or PMA (285±41% and 207±26% vs control, n=3,p<0.05 for IL-1beta and PMA respectively). LY 379196 (5x10-6 mol/L), a PKCinhibitor specific for beta isoforms, abolished attachment of THP-1 cells and re-duced CD14 upregulation (86±10%, p<0.01 and 83±29%, p<0.01 vs IL-1betaand PMA, respectively). Treatment of Raw 264.7 cells with LY379196 decreasedacLDL uptake (1228±150 vs 522±250 relative units in control, n=3). Further-more, LY379196 blunted PMA-induced formation of gigantic polynuclear cells.
Fig. 1. Stimulation of Raw 267.4 cells with PMA leads to the formation of gigantic polynuclearmacrophages (left panel), pretreatment with PKCβ inhibitor prevents such transformation (rightpanel). Bright particles in cytoplasm are the internalized acLDL.
Conclusions: Our results indicate that inhibition of PKCbeta reduce monocyte-derived macrophages as well as LDL uptake and foam cell formation.
P5510 The Multidrug Resistance Protein 1 (MRP1) mediatesexport of leukotrienes in vascular cells and affectsvascular function
C.F.H. Mueller1, J. Widder2, S. Wassmann2, T. Czech3,D.G. Harrison1, G. Nickenig2. 1Universitaetsklinik Bonn, Innere
Medizin - Kardiologie, Bonn, Germany; 2Emory University, Cardiology, Atlanta,United States of America; 3Universitaetskliniken des Saarlandes, Innere Medizin- Kardiologie, Homburg, Germany
Oxidative stress has been connected with endothelial dysfunction, apoptosis andplaque development in the vasculature. MRP1 is one of nine currently known MRPproteins. It has been shown that MRP1 is involved in oxidative stress manage-ment in Human Aortic Endothelial Cells (HAEC’s). Inhibition of MRP1 by MK571,a specific pharmacologic inhibitor, or downregulation by siRNA both efficientlyenhanced the intracellular redox-potential and decreased the rate of apoptosisunder ROS-exposure in HAEC’s. The aim of this study was to investigate the roleof MRP1 as transporter of leukotrienes and its role in the setting of atheroscle-rosis. Vascular smooth muscle cells (VSMC) were stimulated with Angiotensin II(10-6) and expression of MRP1 was analysed by western blot. MRP1 was notonly expressed in VSMC but also upregulated in a dose dependent manner in-
dicating an important role in the setting of cellular oxidative stress management.DCF fluorescence measurements revealed that pharmacologic inhibition of MRP1as well as downregulation by specific siRNA resulted in a reduced rate of ROSproduction under stimulation with Angiotensin II. These results were confirmedby using MRP-/- cells. Investigation of leukotriene export showed significantlyreduced rates of leukotriene release in cells lacking MRP1. To investigate therelevance of these findings in vivo three groups of ApoE-/-mice (n=6/group), ananimal model of rapid atherosclerotic lesion development, received Western dietfor 5 weeks. Additionally, one group was treated with MK 571, another group wastreated with Montelukast, a leukotriene-receptor antagonist. Blocking of MRP1as well as treatment with montelukast resulted in a reduction of atheroscleroticplaques area by 50%. Both goups showed a significantly improved endothelialfunction compared to the control group. These findings were supported by a re-duction in superoxide-production of more than 50%. Our results indicate a strongconnection between MRP1, vascular function and atherogenesis. MRP1 may pro-vide a potentially new therapeutic target for the treatment of endothelial dysfunc-tion and atherosclerosis
LIPIDS AND METABOLISM
P5511 HDL up-regulate cyclooxygenase-2 (Cox-2) in humanvascular smooth muscle cells through EndothelialDifferentiation Genes (EDGs)
M. Gonzalez-Diez, J. Martinez-Gonzalez, C. Rodriguez, L. Badimon.Cardiovascular Research Center, CSIC/ICCC, Barcelona, Spain
Background: HDL are lipoproteins inversely associated with cardiovasculardisease. One of the mechanisms by which HDL exert beneficial effects isthrough HDL the induction of prostacyclin (PGI2) release by up-regulatingcyclooxygenase-2 (Cox-2) expression in vascular cells. Sphingosine-1 phosphate(S1P) is a component of HDL that induces cell response acting through cell sur-face receptors called EDGs (endothelial differentiation genes).Objective: to assess the involvement of EDGs in the up-regulation of Cox-2 in-duced by HDL in human VSMC.Methods: The study was carried out inhuman coronary VSMC. Cox-2 protein lev-els were analyzed by Western blot and Cox-2 mRNA levels by real-time PCR us-ing TaqManTM probes. Prostacyclin (PGI2) was analyzed by EIA. Desensitizationof EDGs was performed pre-stimulating the cells with either S1P or dihydro-S1P(DhS1P), a S1P derivative that solely works through S1P cell surface receptors(EDGs). EDG-3 was inhibited using suramin. SR-BI was blocked using siRNA anda specific antibody (ab3811) that inhibits SR-BI biological function.Results: HDL (30 mg/dL) and S1P (0.1 microM) induced Cox-2 mRNA levels inhuman coronary SMC in a similar fashion. The effect of S1P was mimicked, atleast in a part, by DhS1P. Human VSMC exhibited significant expression levels ofEDG-3 and EDG-5. Desensitization of EDGs by either S1P or DhS1P abrogatedCox-2 up-regulation and PGI2 release induced by physiologically relevant HDLconcentrations (> 30 mg/dl). Suramin (inhibitor of EDG-3) significantly reducedHDL-, S1P- and DhS1P-induced Cox-2 up-regulation. By contrast, neither siRNAnor specific blocking antibodies against SR-BI prevented HDL-induced Cox-2 up-regulation.Conclusion: S1P receptors (EDGs), in particular EDG-3, could mediate the pro-tective effects of HDL on human VSMC.
P5512 Oleanolic acid potenciates the up-regulation ofcyclooxygenase-2 (Cox-2) induced by HDL in humanvascular smooth muscle cells
J. Martinez-Gonzalez1, R. Rodriguez-Rodriguez2, M. Gonzalez-Diez1, C. Rodriguez1, M.D. Herrera2, V. Ruiz-Gutierrez2.
1Cardiovascular Research Center, CSIC/ICCC, Barcelona, Spain; 2Instituto de laGrasa, CSIC, Sevilla, Spain
Background: Oleanolic acid (OLE) is a triterpenoid present in the un-saponifiedfraction of "orujo" olive oil that exerts vasorelaxant effects. Some lipid compoundsand lipoproteins such as HDL can induce prostacyclin (PGI2) release by up-regulating cyclooxygenase-2 (Cox-2) expression in vascular cells.Objective: to assess the effect of OLE on Cox-2 expression in human vascularsmooth muscle cells (VSMC) and to determine the signalling pathways involvedin such effect.Methods: The study was carried out inhuman coronary VSMC. HDL were iso-lated from human plasma. OLE was purified from "orujo" olive oil. VSMC weretreated with HDL or OLE in the presence of different signalling pathway in-hibitors. Cox-2 protein levels were analyzed by Western blot and Cox-2 mRNAlevels by real-time PCR using TaqManTM probes. Mitogen-activated protein ki-nase (MAPK) (p38MAPK and ERK1/ERK2) and c-Jun N-terminal kinase-1 (JNK-1) pathways were analyzed by Western blot.Results: OLE induced Cox-2 mRNA levels in human coronary VSMC in a time-and dose-dependent manner. Maximal inductions of Cox-2 mRNA levels (8.5-fold)and Cox-2 protein levels was observed 6 and 10 h after stimulus, respectively.The effect on Cox-2 mRNA levels was additive with that induced by physiolog-ical concentrations of HDL (30 mg/dL). OLE induced p38 MAPK phosphoryla-tion and JNK-1 in a lesser extent. SB203580 (p38MAPK inhibitor) and U0126
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Lipids and metabolism 973
(ERK1/ERK2 inhibitor) abrogated the up-regulation of both Cox-2 mRNA and pro-tein levels. A peptide inhibitor of JNK-1 did not produced any effect.Conclusion: OLE induces Cox-2 in human coronary VSMC via p38MAPK andERK1/ERK2. OLE exerts this effect through similar mechanisms to those acti-vated by HDL. OLE could be regarded as an active component of "orujo" olive oilthat contributes to the beneficial effects of the Mediterranean diet.
P5513 Palmitic acid reduces HDL catabolism in vivo:contribution of the negative charge density
O. Perez-Mendez, P. Alvarez-Salcedo. National Institut of Cardiology,Physiology, Mexico City, Mexico
Purpose: Non-esterified fatty acids (NEFA) are increased in type 2diabetes, pathology characterized by low HDL plasma levels and a high risk ofcoronary heart disease. However, little is known about the impact of NEFA onHDL metabolism. We report here the effect of one NEFA, palmitic acid, on HDLcatabolism and CETP lipid transfer.Methods: Phosphatidyl choline small unilamellar vesicles (SUV) prepared by ul-trasonication were used as vehicle for palmitic acid (PA). HDL enrichment with PA(HDL-PA) was performed by incubating SUV-PA with HDL isolated from 5 nor-molipidemic volunteers. HDL enriched only with phospholipids (HDL-Phl) andnative HDL were included as controls (HDL-N). Electric charge density (Cd)was estimated considering the HDL electrophoretic mobility values determinedin agarose gel, and their hydrodynamic diameter assessed by PAGE. ModifiedHDL were labelled with 3H-cholesteryl esters to determine the CETP-dependentcholesterol transfer to triglyceride-rich lipoproteins. In vivo turnover studies wereperformed by exogenous labelling of the HDL-protein with 125I, that were injectedintravenously to New Zealand white rabbits. Plasma radioactivity was counted atdifferent intervals during 72h. Data were adjusted to a bicompartimental model tocalculate de fractional catabolic rate (FCR).Results: At physiological pH, palmitic acid is mostly ionized in aqueous solution.As a consequence, HDL-PA Cd was 16.5 and 12.7% higher compared with HDL-Phl and HDL-N (2014.4±164.8 vs 1682.7±149.5 and 1758.2±124.3 esu/cm2,respectively, p<0.05). Both, HDL-PA and HDL-Phl are better substrate for CETPthan HDL-N (% of transfer, 13.02±3.8 and 12.7±4.5 vs. 7.8±2.7% in 16h, re-spectively, p<0.05). HDL-PA catabolism in vivo (FCR, 0.019±0.008 pools/h) wassignificantly lower than that of the HDL-Phl (FCR, 0.030±0.005 pool/h, p<0.001),and it was only about the 40% of that of the HDL-N (FCR, 0.047±0.003 pools/h,p<0.001).Conclusions: Enrichment with PA increases the negative surface charge of HDLat physiological pH, contributes to decrease their catabolism, and is associatedto an enhanced lipid transfer by CETP that has been related to the atherogenicprocess.
P5514 Elevated triglycerides/HDL ratio predicts extensivecoronary artery disease
P.L. Da Luz, D. Favarato, J.R. Faria Neto, A.C.P. Chagas, P. Lemos.Heart Institute (InCor), USP Medical School, Atherosclerosis, SaoPaulo, Brazil
Surrogate markers of coronary artery disease (CAD) are valuable for preventionof cardiovascular events. Smal LDL are atherogenic where large LDL are not.There is a strong correlation between the triglycerides/HDL ratio and small LDLconcentration. Objectives: To analyze the association among lipid variables andextension of coronary artery disease (CAD).Methods: Two hundred and seventy four patients who underwent diagnostic coro-nary angiography had total cholesterol, LDL, HDL, triglycerides and TG/HDL ra-tio calculated. CAD extension by the Friesinger index. Univariate analysis withchi-square for linear trend, and multivariate analysis by logistic regression wereperformed. The lipid variables were tested by quartile and Friesinger index di-chotomized at score 5.Results: There were 165 males (60.2%), 57.8±11.5 years-old; 34 with nocoronary lesion and the remaining had CAD ranging from irregularities to to-tal occlusions. The average Friesinger index was 6.9±4.4. Mean cholesterolwas 214.7±50.2; triglycerides 167.9±91.7 mg/dl, HDL 38.5±11.9 mg/dl; LDL142.9±45 mg/dl, and TG/HDL 5.11±4.03. There were 78.8% hypertensives,30.3% diabetics, 25.9% smokers, 60.6% hypercolesterolemics, 48.2% hyper-triglyceridemics, and 60.6% with low HDL-cholesterol <40 mg/dl. At univariateanalysis all lipids were associated with extensive CAD; however at multivariateanalysis only the TG/HDL maintained a significant association to extensive CAD(OR 1.33; p<0.0001) (table).
Variable OR P
Quartile Rel TG/HDL 1.34 <0.0001Quartile Total Cholesterol 1.41 0.235Quartile Triglycerides 0.32 0.574Quartile HDL 1.80 0.180Quartile LDL 1.20 0.238
Conclusion: The TG/HDL ratio was the only lipid variable independently associ-ated with extensive CAD regardless other lipid, and may be an useful surrogatemarker of CAD
P5515 The relation between oxidation products of lipidperoxidation (8-iso-prostaglandin F2a) or DNAdamage (8-hydroxydeoxyguanine) and coronaryatherosclerosis
J.Y. Kim, J. Yoon, M.S. Ahn, K.H. Lee, H.M. Choe, B.S. Yoo,S.H. Lee, K.H. Choe. Yonsei University, Wonju College Of Medicine,
Cardiology Department, Wonju, Korea, Republic of
Purpose: We evaluated urinary 8-iso-prostaglandin F2α (8-iso-PGF2α) and 8-hydroxydeoxyguanine (8-OHdG) as oxidative stress markers for the coronaryatherosclerosis.Methods: We assessed urinary 8-iso-PGF2α and 8-OHdG (OXIS InternationalInc, CA) levels by immunoassay in age-sex matched control (group1, n=43), min-imal disease or normal looking coronary artery (group 2, n=60) in coronary an-giography and presence of significant coronary artery disease (group 3, n=41) de-fined > 50% diameter stenosis of major coronary epicardial vessels. The patientswith acute coronary syndrome, heart failure, renal failure and infectious conditionwere excluded. The association between tertile of 8-iso-PGF2α or 8-OHdG andthree groups was compared by chi-square test.Results: Baseline demography showed more prevalent of hypertension and di-abetes in group 2 and 3. Urinary 8-iso-PGF2α were 7.2 ± 9.1, 11.9 ± 12.3, and18.4 ± 17.5ng/mg creatinine (p = 0.001) and 8-OHdG were 1.2 ± 1.0, 1.8 ± 1.8,and 2.0 ± 1.8ng/mg creatinine (p = 0.033) for group 1,2, and 3,respectively. Therewas significant association between the groups and tertile of urinary 8-iso-PGF2α
(group 1: 16.3%, group 2: 31.7%, and group 3: 51.2% in third tertile for 8-iso-PGF2α, p <0.001), not in 8-OHdG (p = 0.055). Urinary 8-iso-PGF2α levels werepositively correlated with hsCRP (r = 0.23; p=0.008) and LDL cholesterol(r = 0.18;p=0.043).
Group 1 (n=43) Group 2 (n=60) Group 3 (n=41) p
8-OHdG (%)1st tertile 20 (46.5) 17 (28.3) 12 (29.3) 0.0552nd tertile 19 (44.2) 17 (28.3) 13 (31.7)3rd tertile 4 (9.3) 26 (43.3) 16 (39.0)
8-iso-PGF2α (%)1st tertile 25 (58.1) 13 (21.7) 11 (26.8) <0.0012nd tertile 11 (25.6) 28 (46.7) 9 (22.0)3rd tertile 7 (16.3) 19 (31.7) 21 (51.2)
Conclusions: Urinary 8-iso-prostaglandin F2α might be more reliable and usefuloxidative stress marker than 8-hydroxydeoxyguanine in coronary atherosclerosis.
P5516 Lp(a) fibrin-binding and homocysteine are increasedin atherothrombotic disease
A. De La Pena1, M. Narduli2, H. Gonzalez1, E. Angles-Cano3.1Instituto Nacional de Cardiologia, Pharmacology, Mexico City,Mexico; 2University of Bari, Bari, Italy; 3INSERM, U698, Paris,
France
Lipoprotein Lp(a) and total homocysteine (tHcy) are currently considered as in-dependent cardiovascular risk factors. We emphasize the importance of Lp(a)in the inhibition of fibrinolysis and explore the role of tHcy on the antifibrinolyticeffect of Lp(a). A functional approach was designed, which allows evaluation ofphysiological molecular interactions that otherwise would remain masked if onlythe plasma concentration of Lp(a) and tHcy were determined. On the basis ofa previous study (Nardulli et al. Thromb Haemostas 2004) indicating that homo-cysteine dissociates apo(a) from the Lp(a) particle and that the free apo(a) hasa greater antifibrinolytic effect, we studied a group of fourteen survivors of acutecoronary syndrome (six with acute myocardial infarction and eight with unstableangina) and two with rheumatic cardiopathy. The antifibrinolytic effect of Lp(a) wasdetermined through a functional study, using a monoclonal antibody labeled withperoxide that detects the apo(a) binding to fibrin. The degree of apo(a) binding tofibrin is an indicator of its antifibrinolytic potential. The results were extrapolatedfrom a curve constructed with apo(a) recombinants of different lengths, from 10 to36 kringles. The tHcy was determined using a Biorad ELISA method. The resultsshowed that a statistically significant correlation exists, (0.647, p=0.007) betweenthe binding of apo(a) to fibrin and the concentration of tHCy.
P5517 Combination high-density lipoprotein infusion andatorvastatin significantly reduces experimentalatherosclerosis compared to either therapy alone:serial analysis with high-resolution MRI
K.S.L. Teo1, S.J. Nicholls2, P. Kee2, K. Rye1, P. Barter1,S.G. Worthley2 . 1University of Adelaide, Cardiovascular Research Centre,Adelaide, Australia; 2Heart Research Institute, Lipid Research Group, Sydney,Australia
Modest manipulations of serum HDL levels are associated with a significant im-pact on cardiovascular risk. High intensity lipid-lowering with statins however re-mains first line in the management of at risk individuals. We analysed the effectof combination HDL infusion and atorvastatin versus either therapy alone andplacebo in a rabbit model of atherosclerosis using MRI of the aortic atherosclero-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

974 Lipids and metabolism
sis as the end-point. Aortic atherosclerosis was established in New Zealand whiterabbits (n=12) over 17 weeks by balloon denudation and cholesterol feeding andbaseline MRI performed. Then rabbits received: (1) no treatment; (2) oral ator-vastatin 5 mg/kg/day; or (3) infusions of HDL (8 mg/kg apolipoprotein A-I) twiceper week; or (4) both, for a total of 12 weeks. A further MRI was performed. High-resolution vessel wall MR imaging of the aorta allowed analysis of the vessel wallarea (VWA) and abdominal aortic slices (n=8 per rabbit) were compared pre andpost treatment. Data is presented as mean±SEM (mm2) and paired t-testing per-formed. There was a small, nonsignificant increase in VWA over the 12 weeks inthe control group (6.10±0.16 vs 6.36±0.72, p=NS). There were non-significantdecreases in VWA in both the atorvastatin only (4.69±0.14 vs 4.45±0.14, p=NS)and HDL only (5.54±0.19 vs 5.22±0.28, p=NS) groups. However, there was asignificant decrease in VWA in the combination group (5.09±0.14 vs 4.60±0.15,p=0.03). Even infusing small amounts of HDL provides incremental regression ofatherosclerosis to atorvastatin using MRI in this rabbit model of atherosclerosis.
P5518 Paclitaxel Associated With a Lipid Nanoemulsion(LDE) Promotes Atherosclerosis Regression In TheRabbit
R.C. Maranhao, E.R. Tavares, A.F. Padoveze, C.J. Valduga,T.V. Oliveira, D.G. Rodrigues. INCOR-Heart Institute, University ofSao Paulo Medical School, Sao Paulo, Brazil
A cholesterol-rich nanoemulsion (LDE) binds to LDL receptors and after injectioninto the blood stream may concentrate in cells with LDL receptor overexpression,as occurs in neoplasias and other proliferative processes such as in atheroscle-rosis lesions. Thus, LDE may be used as vehicle to target drugs against thosecells. The association of a paclitaxel derivative, paclitaxel oleate, to LDE is stableand retains the cytostatic activity of drug.Purpose: To verify in rabbits whether LDE-paclitaxel oleate could reduce theatherosclerotic lesions produced by prolonged feeding of an atherogenic diet.Methods: 13 male New Zealand rabbits were fed a 1% cholesterol diet for twomonths. After one month, 7 animals were treated with LDE-paclitaxel oleate(4mg/kg/week, I.V. injection) and 6 with weekly I.V. saline solution injection. Phar-macokinetics of paclitaxel-oleate, was determined and after treatments the ani-mals were sacrificed for performance of morphometric analysis.Results: LDE-paclitaxel reduced lesion area by 75% compared with non-treatedrabbits and intima-media ratio was reduced fivefold. Hematologic parameters,weight and food intake evolution indicated that the treatment had no toxicity.Conclusions: Association with LDE endows paclitaxel to attain pharmacologicaleffect on the vessel lesion sites, so that dramatic lesion regression was achievedwith virtually no toxicity. Therefore, this preparation has remarkable potential incardiovascular therapeutics.
P5519 Aggregated Low Density Lipoprotein induces tissuefactor expression and activation by a Rho Adependent mechanism in human coronary vascularsmooth muscle cells
V. Llorente-Cortes, S. Camino-Lopez, L. Badimon. CardiovascularResearch Center, CSIC-ICCC, Hospital de la Santa Creu i Sant Pau, Barcelona,Spain
Background: LDL retention in the vascular wall is produced by binding to pro-teoglycans in the extracellular matrix. These resident LDL particles become ag-gregated in the arterial intima (agLDL). We have previously shown that the LowDensity Lipoprotein Receptor-Related Protein (LRP1) in human vascular smoothmuscle cells (VSMC) internalizes agLDL. This agLDL uptake induces tissue fac-tor (TF) expression and release in human VSMC. The objective of this study wasto analyze the mechanisms of TF induction by agLDL.Methods and Results: Human coronary VSMC were exposed to native LDL oragLDL (100 ug/mL) for 12-18 hours. TF expression was measured by real timePCR and Western blot analysis. TF activity was analyzed by the factor Xa Gener-ation Test. Rho A translocation was determined by detection of Rho A antigen incytoplasmic and membrane fractions. HMGCoA reductase was inhibited by sim-vastatin (2.5, 5,10 m mol/L) or pravastatin (0.25, 0.5 or 1 mmol/L) and Rho A byExoenzyme C3. AgLDL increased TF mRNA expression (by 1.3-fold), TF proteinexpression (agLDL: by 5.47-fold; nLDL: 1.5-fold) and activity (agLDL:3.44± 0.21vs nLDL:1.75± 0.19 or no LDL:0.84± 0.04 U/mg protein). AgLDL highly inducedRho A translocation to membrane (agLDL: by 2.56-fold vs nLDL: by 1.39-fold).Exoenzyme C3 and simvastatin completely abolished agLDL-TF protein overex-pression but only partially affected agLDL-TF activation. This effect of simvastatinwas reverted by geranylgeranyl pyrophosphate (GGPP) but not by farnesyl py-rophosphate (FPP).Conclusions: agLDL increases TF expression and activation through inductionof Rho A translocation, an effect that is blocked by a RhoA specific inhibitor and bystatins. Our results contribute to explain the mechanisms of prothrombotic trans-formation of the human vascular wall and the important role of Rho A activationon the pathogenesis of atherothombosis. Additionally, these results evidence thepotential of statins to induce cardiovascular protection.
P5520 Lipoprotein-associated phospholipase A2 (Lp-Pla2)gene is highly expressed in the aortic aneurysmsamples and carotid plaques and is associated withexpression of metalloproteinase
M. Madjid1, M. Haidari1, M. Ali1, D. Vela1, E.E. Porat2, A.L. Estrera2,H.J. Safi2, W. Casscells1. 1Univ. of Texas-Houston and Texas Heart Inst.,Houston, United States of America; 2Univ. of Texas-Houston, Houston, UnitedStates of America
Lipoprotein-associated phospholipase A2 (Lp-Pla2) is an enzyme produced byinflammatory cells specially macrophages in atherosclerotic lesions. High serumlp-pla2 levels are associated with increased risk of future cardiovascularevents.Lp-pla2 production in the coronary and carotid atherosclerotic lesions has beenreported before. We investigated the expression of lp-pla2 gene from aorticaneurysm lesions.Methods: We analyzed 40 aortic aneurysm and 33 carotid endarterectomy sam-ples. TaqMan real-time PCR technique was employed to assess the expression ofmRNA of lp-pla2, matrix metalloproteinase (MMP)-9, MMP-2, MMP-13, tissue in-hibitor of MMP (TIMP)-1, CD68 (marker of macrophages), and C-reactive protein(CRP). GAPDH, was used to standardize the quantity of total RNA. Spearman’scorrelation test was used to calculate rho coefficient of correlation (r).Results: Majority ofaortic aneurysm samples expressed lp-pla2 (73%), CD68(93%), MMP-2 (88%), MMP-9 (68%), MMP-13 (43%), and TIMP-1 (88%) genesbut none expressed CRP (0%) gene. Most ofthecarotid samples expressed lp-pla2 (97%), CD68 (94%), MMP-2 (93%), MMP-9 (91%), and TIMP-1 (96%)genes. In the aortic aneurysms, expression of lp-pla2 gene showed significantcorrelation with gene expression of CD68 (r=0.74, P<0.0001), MMP-9 (r=0.58,p=0.004), TIMP-2 (r=0.39, p=0.04), MMP-13 (r= 0.63, p=0.013), but not withMMP-2 (r=0.36, P=0.06).Expression of the CD68 gene in aortic aneurysms was significantly associatedwith gene expression of MMP-9 (r=0.76, p<0.0001), MMP-2 (r=0.39, p=0.019),and TIMP-1 (r=0.48, p=0.004) but not with MMP-13 (r= 0.45, p=0.068). In carotidsamples, lp-pla2 gene expression had significant correlation with gene expressionof CD68 (r=0.76, P<0.0001), MMP-9 (r=0.74, p<0.0001), and TIMP-1 (r=0.73,p<0.0001), but not with MMP-2 (r=-0.22, p=0.27). In carotid samples, expressionof CD68 gene was associated with the expression of MMP-9 (r=0.76, p<0.0001)and TIMP-1 (r=0.64, p<0.0001), but not with MMP-2 (r=-0.14, p=0.52) genes.Conclusion: We report, for the first time, that lp-pla2 gene is highly expressedin the aortic aneurysm samples removed at surgery. Lp-pla2 expression in aorticaneurysms is associated with expression of a macrophage marker and the relatedproteinases which may play role in aneurysm formation. Our data suggest inves-tigating the utility of measuring serum lp-pla2 as a biomarker to identify subjectsat high risk of aneurysm progression and testing the effect of lp-pla2 inhibitors incontrolling aneurysmal diseases.
P5521 HMGB-1 induces tissue factor expression in humanvascular smooth muscle cells
M. Ragni1, S. Musto D’amore1, G. Petrillo1, P. Cirillo1, F. GranatoCorigliano1, L. Sasso1, P. Calabro2, M. Chiariello2. 1UniversityFederico II, Cardiology, Naples, Italy; 2Second University of Naples,
Cardiology, Naples, Italy
High-mobility group box chromosomal protein (HMGB1, 30Kd) is an ubiquitari-ous nuclear protein present in many types of eukaryiotic cells. Recent studieshave unexpectedly shown that HMGB1 is also a cytokine that can be releasedby activated monocytes, macrophages, neutrophils and platelets and in turn me-diates inflammation and activation of endothelial cells. HMGB1 is also presentin atherosclerotic plaques, mainly expressed in macrophages and endothelialcells. Tissue factor (TF) is a transmembrane glycoprotein that activates the ex-trinsic pathway of coagulation and is the most represented thrombogenic proteinin atherosclerotic plaques. Aim of the study: to verify if HMGB1 may induce TFexpression and activity in human vascular smooth muscle cells.Methods: Quiescent cultured human smooth muscle cells were stimulated for 12
Fig. 1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

Lipids and metabolism 975
hours with human recombinant HMGB1 (100 ng/mL). After this period TF surfaceactivity was measured by chromogenic assay, whereas, in another set of experi-ments, TF surface antigen was measured by flow cytometry, using a monoclonalanti-TF fluorescein-conjugated antibody. Positive control included cells stimulatedwith endotoxin (LPS 100 ng/mL) or fetal calf serum (FCS 20%), negative controlincluded unstimulated cells. All experiments were made in quadruplicate.Results: HMGB1 at the dose of 100 ng/mL induced a significant TF surface ex-pression and activity with respect to unstimulated cells after 12 hours of stimula-tion (figure 1).Conclusion: HMGB1, a novel proinflammatory cytokine, may induce significantTF-dependent thrombogenic activity at the surface of cultured human smoothmuscle cells. Thus, HMGB1 may have in important pathophysiological role in dis-eases such as atherosclerosis in which there is a clear interplay between inflam-mation and thrombosis.
P5522 Erectile dysfunction precedes myocardial infarctionand stroke
M. Baumhaekel1, M. Boehm2. 1University Hospital Of The Saarland,Cardiology, Homburg, Germany; 2University Hospital of theSaarland, Cardiology, Homburg, Germany
Background: Erectile dysfunction (ED) is related to cardiovascular risk factors.Moreover, incidence and severity of endothelial dysfunction, as an initial stepin the development of atherosclerotic lesions and a predictor of cardiovascularoutcome, is known to be increased in patients with erectile dysfunction. Hence,symptoms of ED could precede cardiovascular events due to the same patho-physiologcial mechanisms and association of the same risk factors.Methods: The EROSS-Programme (Evaluation of Role of Sexual Dysfunction inthe Saarland-Programme) included 197 cardiovascular high risk patients since2003. Cardiovascular risk factors, previous events as well as concomitant drugtherapy were evaluated using medical records and personal interviews. Onsetand severity of ED was assessed with an ED-score generated from the five itemshort form of the International Index of Erectile Function (IIEF-5). Additionally,patients were asked regarding the year of onset of ED-symptoms as well as forsexual activity before diagnosis of their cardiovascular disease.Results: Average age was 62.3±10.8 years (32-86 years) with 92% of patientsliving in a stable partnership. Prevalence of ED was 81.1% with a mean ED-sum score of 12.0±5.7, indicating a moderate decrease of erectile function inthese patients. 158 patients reported about frequency of sexual contacts. In thesepatients, onset and diagnosis of cardiovascular disease was associated with asignificant decrease of sexual activity (p<0.001). Moreover, 48 patients with ahistory of myocardial infarction or ischemic stroke reported about first appearanceof symptoms of ED. In these patients, ED became clinically relevant 3.04±7.2years prior to the first major cardiovascular event (myocardial infarction or stroke,p=0.005).Conclusion: In cardiovascular high-risk patients, prevalence of ED is increasedcompared to the general population. Moreover, sexual activity is obviously influ-enced by cardiovascular diseases. In our patients, frequency of sexual contactsshowed a significant decline after onset and diagnosis of the cardiovascular dis-ease. In addition, symptoms of ED appeared about three years prior to a majorcardiovascular event. Probably, symptoms of impairment of the endothelial mono-layer of the corpus cavernosum and the penile arteries becomes clinically relevantprior to events in the coronary or cerebral arteries due to the distinct network ofendothelium in the penis. Thus, ED is suggested to be an early sign and symp-tome of generalized vascular disease with the opportunity of early detection andprevention of cardiovascular events.
P5523 Inverse association between C-reactive protein andmeasures of pulmonary function: implications for theincreased cardiovascular risk in pulmonary diseases
D. Aronson, I. Roterman, M. Yigla, A. Kerner, O. Avizohar, R. Sella,W. Markiewicz. Rambam Medical Center, Cardiology Dept., Haifa,
Israel
Background: Impaired lung function is a powerful predictor of cardiovascular dis-ease. Cytokine overexpression in lung tissue may occur secondary to inhaledmicroorganisms, smoking and other noxious particulate matter. Airspace inflam-matory responses promote tissue damage and a decline in lung function and, inparallel, may induce systemic inflammation.Methods: Pulmonary function tests, cardiorespiratory fitness (as determined bya maximal exercise test), components of the metabolic syndrome and high-sensitivity C-reactive protein (CRP) were measured in 1131 subjects.Results: There was a strong inverse association between CRP levels and quar-tiles of forced expiratory volume in 1 second (FEV1) in both smokers and non-smokers (Figure; P < 0.0001). The strong inverse association between CRPlevels and quartiles of FEV1 remaind significant (P < 0.0001) in a multivariablemodel adjusting for age, sex, smoking, statins use, components of the metabolicsyndrome (obesity, glucose intolerance, high triglycerides, low HDL and hyper-tension) and fitness level. Multivariate logistic regression models showed thatcompared to subjects at the highest FEV1 quartile, the adjusted odds ratio forhigh-risk CRP level (> 3 mg/L) were 2.5 in subjects in the lower FEV1 quartile(95% CI 1.50-4.0, P < 0.0001).
CRP According to FEV1 Quartile
Conclusions: Measures of pulmonary function are inversely related to CRP con-centrations. The association between respiratory impairment and cardiovascularrisk may be mediated, in part, through a proinflammatory mechanism.
P5524 Essential hypertensive subjects with extreme dippingof nocturnal blood pressure are not characterized byhypoadiponectinemia and arterial stiffening
K. Dimitriadis, C. Tsioufis, E. Vezali, F. Rozi, D. Tsiarchris,D. Tousoulis, C. Stefanadis, I. Kallikazaros. Department of
Cardiology, Hippokration, Athens, Greece
Purpose: There is evidence linking exaggerated nocturnal blood pressure (BP)dipping pattern with adverse stroke prognosis, while adiponectin and arterialstiffness are markers of atherosclerotic events. In this study we investigatedthe relationships of the extreme nocturnal BP dipping with arterial stiffness andadiponectin in essential hypertensive subjects.Methods: 287 newly diagnosed untreated patients with uncomplicated essen-tial hypertension [187 men, mean age=50 years, office BP=148/95 mmHg] wereclassified according to 24-h ambulatory BP monitoring as non-dippers (n=105)(<10% nocturnal systolic and diastolic BP fall), extreme-dippers (n=16) (>20%nocturnal systolic BP fall) and the remaining subjects as dippers (n=166). In theextreme-dipping and dipping group, arterial stiffness was evaluated on the basisof carotid to femoral pulse wave velocity (c-f PWV), by means of a computerizedmethod (Complior SP) and venous blood samples were drawn for estimation ofmetabolic profile and adiponectin levels.Results: Extreme-dippers compared to dippers had lower office diastolic BP (90± 7 vs 96 ± 7 mmHg, p=0.008), while did not differ regarding age, sex, body massindex, 24-h systolic/diastolic BP and left ventricular mass index (LVMI) (p=NS forall cases). Moreover, extreme dippers compared to dippers exhibited a trend to-wards greater c-f PWV levels (8 ± 1.3 vs 7.6 ± 1 m/sec, p=0.064) and a trendfor lower adiponectin levels (8.6 ± 3.4 vs 9.4 ± 2.6 μ g/ml, p=0.571) but with-out reaching statistical significance. In the total population, c-f PWV was relatedto age (r=0.377, p<0.0001), and diastolic BP fall (r=0.210, p<0.005), whereasadiponectin was negatively associated with diastolic BP fall (r=-0.380, p<0.0001).There was no correlation for both PWV and adiponectin with systolic BP fall(p=NS). Multiple regression analysis revealed that only age and LVMI were in-dependent predictors of systolic BP fall (p<0.05 for both).Conclusions: Extreme-dipping status is not accompanied by pronounced pro-atherosclerotic processes, as reflected by adiponectin and c-f PWV values. Thesefindings, although needing further validation, suggest that vascular damage isaccelerated through other pathways not associated with adiponectin and arterialstiffening, in this setting.
P5525 Prognosis and management of patients with lowerlimbs arterial disease in Brittany (France) with afollow-up of 5 years
L. Renault1, M. Mader2, B. Le Roux1, M. Varnoux1, L. Bressollette2,P. Gouny2, D. Mottier2, J. Mansourati2 . 1University Hospital of Brest,
Department of Cardiolgy, Brest, France; 2Dir. Regionale service medical deBretagne, Brest, France
Lower limbs arterial disease has a poor prognosis. The aim of our study was toevaluate the management and the prognosis of a cohort of patients with lowerlimbs arterial disease and moderate intermittent claudication in the French regionof Brittany with a follow-up (FU) of 5 years.Patients younger than 65, without any other known affection than lower limbsarterial disease and asking for 100% reimbursement for health costs to socialsecurity services between 01/03/99 and 30/06/00 were prospectively includedin this study. Patients were followed by a council physician from social securityservices at inclusion and after 3 years. At 5 years, all data concerning medical orsurgical treatment and mortality were collected from patients’ charts.Our cohort included 321 patients (53±7 years; M 89%). Main risk factors were:smoking 98%, dyslipidemia 57%, hypertension 31%, and diabetes 10%. Dopplerultrasound evaluation of lower limbs arteries was performed in 98% of the pa-tients. However, the ankle/brachial index measurement was not reported in 45%of these patients. Doppler ultrasound of cervical arteries was performed in 48% of
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

976 Lipids and metabolism / e-Poster session 10
the cases, an ECG in 78% of the cases and a stress-test in 35% of the cases. Anantiplatelet agent was prescribed in 86% of the cases, a vasoactive agent to im-prove functional status in 67%, a lipid lowering drug in 40%, an antihypertensivedrug in 34% and a hypoglycaemic drug in 10% of the cases.After 3 years of FU, the ankle/brachial index was only performed in 39% of thecases, Doppler ultrasound of cervical arteries was performed in 34% of the caseset no ECG was available in 10% of the cases. At 5 years, 37 patients died (totalmortality: 11.5%). 80% of the patients underwent surgery for lower limbs arterialdisease. An antiplatelet agent was used in 79% of the cases, a vasoactive agentin 58% of the cases, a lipid lowering drug in 58% of the cases, an antihypertensivedrug in 81% of the cases and a hypoglycaemic drug in 10% of the cases. Smokingwas ongoing in 50% of the cases.In conclusion, mortality in this cohort of young patients with moderately symp-tomatic lower limbs arterial disease is high. Management of these patients is notoptimal and their risk factors are not controlled adequately.
P5526 Disseminated atherosclerosis is associated withhigher mortality among patients with acute coronarysyndromes and should be treated more aggresively interms of invasive approach
D. Dudek, Z. Siudak, A. Dziewierz, T. Rakowski, S. Bartus,B. Witanek, W. Zasada, J.S. Dubiel. Institute of Cardiology, 2nd Department ofCardiology, Krakow, Poland
Background: Acute Coronary Syndromes (ACS) are associated with increasedmortality. Concomitant peripheral artery disease is often present in patients withACS. The aim was to assess the prevalence and outcome of patients with dis-seminated atherosclerotic diesease in a cohort of consecutive ACS patients.Methods: 29 non PCI centres with an established referral pattern with Percuta-neous Coronary Intervention (PCI) centre participated in the Registry of AcuteCoronary Syndromes in the Krakow Region in 2005. Patients were stratified ac-cording to the presence of coronary artery disease (CAD), CAD and periph-eral artery disease (CAD+PAD), CAD with PAD and cerebrovascular disease(CAD+PAD+CVD) in the presence of ACS. PAD and CVD were either confirmedby clinical symptoms (claudication, stroke) or imaging techniques (ultrasonogra-phy, angioCT).Results: Of 1313 patients with ACS, 1141 (85%) were in group CAD, 78 (6.8%)in group CAD+PAD, 79 (6.9%) were assigned to CAD+CVD, whereas 15 (1.3%)patients had CAD+PAD+CVD. There were no differences in the final diagnosisof ST-Elevation Mycoardial Infarction-STEMI (25% vs 22% vs 33% vs 20%; NS),Non ST-Elevation Myocardial Infarction (28% vs 40% vs 34% vs 33%; NS) andUnstable Angina (47% vs 38% vs 33% vs 47%; NS) among the groups. Thegroups differed substantially in demographic features like age (67±12 vs 71+/10vs 72+/10 vs 74±10; p=0.008) and past medical history of myocardial infarc-tion (31% vs 44% vs 35% vs 67%; p=0.003), heart failure (18% vs 33% vs 27%vs 53%; p<0.0001), diabetes mellitus (19% vs 28% vs 32% vs 27%; p=0.016)and renal insufficiency (4% vs 9% vs 13% vs 20%; p<0.0001). Antiplatelet, an-tithrombotic and statin treatment was similar in each group. Transfer to PCI centrefor invasive diagnostic and revascularisation was decreasing with diffuse disease(25% vs 13% vs 15% vs 13%; p=0.014). The in-hospital mortality for patients re-maining for conservative treatment were in non PCI centres was (8.2% vs 8.8%vs 11.9% vs 30.8%; p=0.044). Patients with STEMI and concomitant perpheraldisease were less likely transferred to PCI centres (45% vs 24% vs 25% vs 0%;p=0.022).Conclusions: Patients with ACS and concomitant atherosclerotic lesions in pe-ripheral arteries are less likely transferred to PCI centres for invasive treatment.The in-hospital mortality for patients remaining for conservative treatment in-creases with diffuse disease. It is this group that would benefit most from revascu-larization techniques. More aggresive complex invasive treatment strategy shouldbe applied to patients with peripheral and coronary artery disease.
P5527 Unilateral subclavian stenosis diagnosed by brachialsystolic pressure asymmetry is a prognostic markerfor mortality
V. Aboyans1, M.H. Criqui2, M. Mcgrae Mcdermott3 , M.A. Allison3,J.O. Denenberg3, A. Fronek3. 1Chru Dupuytren Limoges, Sce
De Chir.Cardiaque,Ctcv Et Angiologie, Limoges Cedex, France; 2University ofCalifornia, San Diego, Dept. of Family and Preventive Medicine, La Jolla, UnitedStates of America; 3Northwestern University, Feinberg School of Medicine,Chicago, United States of America
Background - Unilateral subclavian stenosis (USS) diagnosed by a brachial sys-tolic pressure difference (BSPD) >15 mmHg between both arms is associatedwith cardiovascular disease (CVD) risk factors and the presence of peripheral ar-terial disease (PAD). Yet, the predictive power of this condition has never beenassessed. We hypothesized that a BSPD >15 mmHg can be considered as aprognostic CVD marker.Methods - We analyzed baseline and longitudinal data from 3 cohorts. Two cor-responded to patients recruited from non-invasive vascular laboratories and thethird corresponded to a community-dwelling cohort. Cox survival models were runto explain correlates for total and CVD mortality.Results - Baseline and follow-up data (mean 9.8 years) were complete in 1778
participants. A USS was found in 157 (8.8%) subjects. Adjusted for age, gen-der, ethnicity and cohort of origin, the presence of USS was associated with total(OR: 1.42, p<0.005) and CVD mortality (OR: 1.50, p=0.05). This significant rela-tionship persisted after additional adjustment for CVD risk factors (pack-years ofsmoking, hypertension, diabetes, hypercholesterolemia) in the models (OR: 1.39,p<0.01 and 1.51, p<0.05 for total and CVD mortality). When a history of CVDor PAD or an ankle-brachial index <0.9 were added, USS remained an indepen-dent predictor for total mortality (OR: 1.35, p<0.02), with a similar trend for CVDmortality (OR: 1.43, p=0.09).Conclusion - Independently from CVD risk factors, the presence of USS, easilydiagnosed by comparing systolic pressures of both arms, can be considered asa clinical marker of total and CVD mortality.
P5528 Five-year angiographic follow-up in diabetic andnon-diabetics associated with progession of coronarydisease in MASS II study
A.F.T. Gois, J.C. Borges, N.H.M. Lopes, P.R. Soares, W. Hueb,L.A.M. Cesar, S.A. Oliveira, J.A.F. Ramires. Heart Institute, Sao
Paulo, Brazil
Introduction: Clinical and epidemiologic studies have shown and increase riskof coronary artery disease (CAD) among patients with diabetes mellitus (DM).Angiographic progression of coronary atherosclerosis is frequently observed inclinical practice and is used as end-point in clinical trials; however, its prognosticsignificance is unclear. In this study we analyze the significance of progression indiabetic and non diabetic group.Methods: It was performed an initial and 5 years follow-up angiograms in 392randomized patients. Progression was defined as an increase in diameter steno-sis by > 15% of at least one coronary lesion. We sought to evaluate the coronarydisease progression among medical, surgical and angioplasty on territory of LAD,LCX and RCA arteries in diabetic (136) and non-diabetics patients (256). Also,we analyzed the relationship with progression rate with morbidity and needing ofaddition intervention.Results: A total of 392 patients randomly assigned to either a CABG (n=136),PCI (n=146) or medical treatment (n=110) group were analyzed. There was nosignificant difference between the groups related to age, gender, hypertension,smoking or lipid disorders. We did not observed any difference in term of CADprogression when we compared diabetes with non-diabetic patients. When westratified by type of treatment, the surgery group presented less progression inboth diabetic (p= 0.014) and non-diabetic group (p= 0.007). In the PCI group, weobserved more progression in territory of RCA and LAD compared to non-diabeticpatients (p<0.05). There is no relation between progression and rate of events inboth groups.Conclusion: Diabetes was not associated with more progression of CAD in pa-tients with stable CAD and preserved ventricular function during 5 year of follow-up. However the diabetic patient submitted to CABG presented less progressionof CAD compared to PCI and MT.
e-POSTER SESSION 10
P5529 Gender-related differences in left ventricularhypertrophy and function in patients with aorticstenosis
C. David1, A.G. Almeida2, L. Pereira1, J. Marques1, M.G. Lopes1.1Hospital De Santa Maria, Cardiology, Lisbon, Portugal; 2Hospitalde Santa Maria, Cardiology, Lisbon, Portugal
Left ventricular (LV) hypertrophic response to aortic stenosis (AS) appears to begender-related with a trend to less compensatory increase in LV mass in women.The aim of this study was to detect gender-related differences in LV geometryand function in patients (pts) with AS.Methods: We studied 1035 consecutive patients (48% women; mean age69.9±12 years) with AS who underwent ecocardiographic examination in a uni-versitary hospital. In order to compare findings according to gender we analyzedthe following parameters: cardiac chambers dimensions, LV walls thickness andmass, fractional shortening (FS) and ejection fraction (EF); transmitral flow andpulmonary artery pressure.Results: Stenosis severity: 216 pts had severe AS (peak transaortic velocity ≥4.0m/s or aortic valve area ≤0.5 cm2/m2) and 819 pts had mild or moderate AS.Women had:– higher peak (53.1 vs 37.7 mmHg, p<0.001) and mean transaortic gradient (34.5vs 25.3 mmHg, p<0.001) but no significant differences in aortic valve area;– higher EF and FS (0.37 vs 0.33, p<0.001) and lower prevalence of LV systolicregional wall motion abnormalities. In the subgroup of patients without regionalabnormalities, women also had significantly higher EF;– smaller right atrium, right ventricle, LV and aortic root dimensions and lower LVmass (Devereux ASE convention adjusted equation) but, after indexing to bodysurface area, only smaller LV systolic diameter (18.9 vs 19.7 mm/m2, p=0.02)and LV mass (136.5 vs 146.0 g/m2, p=0.002). In spite of a lower LV mass, womenhad higher relative wall thickness (septal+posterior wall thickness/LV diastolic di-ameter; 0.50 vs 0.46, p<0,001) and higher prevalence of concentric remodelling
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

e-Poster session 10 977
(normal ventricular mass index and relative wall thickness >0.45) and concentrichypertrophy (increased ventricular mass index and relative wall thickness >0.45),while men had higher prevalence of eccentric hypertrophy (increased ventricularmass index and relative wall thickness <0.45);– higher left atrium diameter (28.0 vs. 24.4 mm/m2, p<0.001); higher transmitralE/A ratio (1.05 vs 1.19, p<0,001) and E wave desacceleration time (274 vs 238ms, p<0.001);– higher prevalence of pulmonary arterial hypertension (19.1 vs 14.6%, p<0.001).Conclusions: Women with AS have significantly lower LV mass, better LV sys-tolic function indices and lower prevalence of LV concentric hypertrophy buthigher prevalence of LA dilatation and pulmonary arterial hypertension suggest-ing higher LV filling pressures that may be explained by the higher prevalence ofLV concentric remodelling and hypertrophy.
P5530 Reproducibility and accuracy of left ventricular massmeasurement with real-time three-dimensionalechocardiography: comparison with magneticresonance imaging
A. Pouleur1, J.B. Le Polain De Waroux1, A. Pasquet1, B. Gerber1,D. Vancraeynest1 , P. Alain2, O. Gerard2, J.L. Vanoverschelde1 . 1CliniquesUniversitaires Saint-Luc, Departement De Cardiologie, Brussels, Belgium;2Philips Medical System Research, Paris, France
Purpose: Left ventricular (LV) mass is an important predictor of morbidity andmortality. Because the reproducibility of LV mass measurements is far better withcardiac magnetic resonance (cMR) than with 2D-echocardiography, cMR has be-come the reference method for LV mass assessment. Recently, real-time 3D-echocardiography (RT-3DE) has emerged as a promising method for assessingLV mass. The aim of the present study is to test the accuracy and the reproducibil-ity of this approach in comparison with cMR.Methods: 41 patients with normal or abnormal LV function were evaluated byRT-3DE and cMR. RT-3DE LV mass datasets were analyzed using a prototypeversion of the QLab software that allows for the automatic detection of endocardialand epicardial borders and the calculation of LV mass from voxel counts. WithcMR, LV mass was calculated by manually tracing endocardial and epicardialcontours on short-axis slices. All measurements were made twice by 2 differentobservers.Results: RT-3DE and cMR measurements of LV mass were highly correlated (r= 0.87) and not significantly different from each other (157 ± 33 g vs 159 ± 36g, p = 0.4). Intertechniques bias was -2.5 ± 37 g. Both RT-3DE and cMR showedexcellent interobserver agreement as shown by the small absolute (2 ± 29 g forRT-3DE and 3 ± 25 g for cMR) and relative (7 ± 7% for RT-3DE and 7 ± 5% forcMR) interobserver differences and high intraclass correlation coefficients (0.91for RT-3DE and 0.94 for cMR).
Conclusion: RT-3DE allows for the accurate determination of LV mass, whencompared to cMR. In addition, RT-3DE measurements of LV mass are as repro-ducible as those obtained with cMR. This suggests that RT-3DE can be used inthe follow-up of patients with LV hypertrophy and/or remodelling.
P5531 Left atrial volume does not accompany the leftventricular and aortic adaptations associated withwhite coat hypertension
E. Taxiarchou, C. Tsioufis, P. Stougiannos, I. Skiadas, K. Dimitriadis,I. Vlasseros, C. Stefanadis, I. Kallikazaros. Department of
Cardiology, Hippokration, Athens, Greece
Purpose: There are conflicting data regarding the effects of white coat hyperten-sion (WCHT) on target organ damage. The aim of our study was to investigatethe effect of WCHT on left atrial (LA) size, left ventricular (LV) hypertrophy andgeometry as well as aortic stiffness.Methods: Among291 untreated patients who referred to our clinic for 24-h ambu-latory blood pressure (BP) monitoring, we separated 89 subjects (aged 52 ± 10years, 46 males) with WCHT (defined as those with office BP>140/90 mmHg anddaytime BP<135/85 mmHg) and compared with 24 normotensives (defined asthose with office BP<140/90 mmHg and daytime BP<135/85 mmHg) that werematched for age and sex. All subjects underwent echocardiography study andLA volume and LV mass were indexed for body surface area to estimate LA vol-ume index (LAVI) and LV mass index (LVMI), respectively. Aortic stiffness wasevaluated on the basis of the carotid-femoral pulse wave velocity (c-f PWV) mea-surement by an automatic device (Complior SP).Results: The two groups did not differ regarding body mass index, metabolic pro-file and smoking status (p=NS for all cases). Subjects with WCHT compared tonormotensives had significantly increased 24-h systolic BP (120 ± 7 vs 113 ± 7,p<0.0001) and 24-h pulse pressure (48 ± 7 vs 43 ± 6 mmHg, p=0.005). Further-more, although WCHT compared to normotensives had increased LVMI (93.7 ±20.4 vs 79.4 ± 14.7 g/m2, p<0.0001), relative wall thickness (0.42 ± 0.05 vs 0.37± 0.04, p<0.0001) and c-f PWV (8.1 ± 1.4 vs 6.8 ± 0.85 m/sec, p<0.0001), therewas no difference in LA volume index (20.9 vs 19.5 ml/m2, p=NS).Conclusions: The haemodynamic load associated with WCHT apart from con-tributing to arterial stiffening seems to have differential effects on cardiac cavities.The clinical implications of these findings remain to be elucidated in properly de-signed trials.
P5532 Strain rate imaging detects diastolic abnormality ofthe heart without left ventricular hypertrophy
E. Miyajima, S. Harada, H. Yonezawa, A. Hoshi, A. Hanzawa,M. Watanabe, T. Ikeda. Yokohama City University, Dept. LaboratoryMed. And Clinical Invest., Yokohama, Japan
The purpose of this study was to clarify diastolic function in the hypertensive heartby a newly developed echocardiographic technique, strain rate imaging (SRI).Methods: A total of 300 consecutive patients (mean age 60 years, 152 male)with hypertension, excluding those with a history of coronary heart disease orrenal impairment (serum creatinine > 2.0 mg/dl) underwent clinical and laboratoryexaminations and echocardiographic evaluations using an Aplio (Toshiba, Tokyo).Left atrial (LA) and left ventricular (LV) dimension were measured, and the usualLV parameters such as LV mass index (LVMI) and relative wall thickness (RWT:ratio of wall thickness/LV cavity radius) were calculated. Peak and late diastolictransmitral velocity (E- and A-velocity, respectively) and deceleration time of E-velocity (DcT) were also measured. Peak systolic and diastolic SRI (SRI-S, SRI-D) were obtained by tissue Doppler imaging. Serum creatinine and plasma brainnatriuretic peptide (BNP) concentrations were also determined. These subjectswere divided into four groups; 125 normal LV (LVMI < 125 g/m2, RWT < 0.45),28 LV remodeling (LVMI < 125 g/m2, RWT > 0.45), 52 eccentric LVH (LVMI >
125 g/m2, RWT < 0.45), and 95 concentric LV hypertrophy (LVH) (LVMI > 125g/m2, RWT > 0.45).Results: Mean age, ejection fraction (EF), and SRI-S showed no significant dif-ference among the groups, whereas both plasma concentration of BNP and LAdimension were significantly different among the groups by analysis of variance,and were significantly increased in the eccentric and concentric LVH groups com-pared with the normal LV group. E-velocity, A-velocity, and DcT were significantlyincreased only in the concentric LVH group. In contrast, SRI-D was differentamong the groups (p < 0.001), and was significantly reduced in both the LVremodeling and concentric LVH groups compared with the normal LV group (p< 0.001; -9.23±0.32 in normal LV, -5.85±0.37 in LV remodeling, -8.07±0.51 ineccentric LVH, -6.87±0.31 in concentric LVH).Conclusion: Global diastolic function was significantly reduced in the eccentricand concentric LVH groups, accompanied by an increase in plasma BNP concen-tration, but was preserved in the LV remodeling group. However, strain rate imag-ing detected regional abnormality of the left ventricle during the diastolic phase inthe LV remodeling group.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

978 e-Poster session 10
P5533 Myocardial tissue Doppler imaging for early detectionof cardiomyopathy in patients with Fabry disease
R. Toro1, J. Zamorano1 , G. Doxastakis1 , L. Perez De Isla2,J. Gonzalez3, J. Paniagua4, A. Rivera5, J. Herrera6. 1HospitalClinico San Carlos, Unidad de Imagen Cardiovascular, Madrid,
Spain; 2Hosp.Clinico San Carlos,Instituto Cardiovasc., Unidad De ImagenCardiovascular, Madrid, Spain; 3Hospital Puerta del Mar, Cadiz, Spain; 4Hopitaldel Bierzo, Ponferrada, Spain; 5Hospital Xeral Cies, Vigo, Spain; 6HospitalCentral de Asturias, Oviedo, Spain
Fabry disease (FD) is an X-linked disorder caused by deficiency of lysosomal en-zyme α-galatosidase A. Cardiac involvement, consisting of progressive left ven-tricular hypertrophy (LVH) is very common and the most frequent cause of deathin FD. Conventional non invasive tools are unable to provide a preclinical diagno-sis allowing early institution of enzymatic therapy.Aim: To determinate the usefulnes of myocardial tissue doppler imaging (TDI) indetecting abnormalities before the development of LVH.Methods and results: We studied two groups of subjects: 18 healthy control sub-jects and 42 Fabry patients without LVH. In all patients 2-dimensional echocardio-graphy with tissue doppler analysis in the pulsed doppler mode was performed.
Results
Control FC without LVH p – S TDI (cm/s) TCI (ms) TRI (ms)
n (%) 18 (30%) 42 (70%) – AUC 0.5 0.9 0.8Age 26±6 29.3±13 NS – OCP 14 125 60S TDI (cm/s) 8.6±1.7 9.2±1.6 NS – S (%) 0 83 27E TDI (cm/s) 14±3 12±3.3 <0.03 – E (%) 98 97 97A TDI (cm/s) 8.5±2 8.5±2.4 NS – PPV (%) 66.7 88 81TCI (ms) 14.5±2.4 73±16 <0.01 – NPV (%) 76.3 95 81.4TRI (ms) 63±14 88±26 <0.01 –
Systolic myocardial wave velocity (S tdi); Early diastolic myocardial wave velocity (Etdi); Late dias-tolic myocardial wave velocity (A tdi); Ventricular isovolumetric contraction time(TCI); Ventricularisovolumentric relaxation time (TRI); Fabry cardiomyopathy (FC).AUC: Area under curve; OCP:Optimal cuttoff point;S: Sensitivity;E: Specificity; PPV Positive predictive value; NPV; Negativepredictive value.
Conclusions: Fabry cardiomyopathy is characterized by reduced contraction andrelaxation velocities at TDI and that such abnormalities are detectable before thedevelopment of LVH and alterations of traditional echocardiography. E tdi, TCI,TRI are the best parameters for detecting FC without LHV. TDI could provide apreclinical diagnosis of cardiac anomalies in FD.
P5534 The incremental prognostic significance of restrictivefilling pattern in hypertrophic cardiomyopathy:a Doppler echocardiographic study
B. Pinamonti1, A. Di Lenarda1 , D. Gregori2, G. Nucifora1 ,A. Perkan1, A. Aleksova1, M. Merlo1, G. Sinagra1. 1Ospedali Riuniti
and University, Cardiology, Trieste, Italy; 2University of Torino, Department ofPublic Health and Microbiology, Trieste, Italy
Aims: To study the frequency and incremental prognostic significance of restric-tive filling pattern (RFP) in hypertrophic cardiomyopathy (HCM) by Doppler echo-cardiography (DE). Background. At DE an abnormal relaxation pattern is the typ-ical diastolic abnormality reported in HCM. RFP has never been extensively eval-uated in HCM.Methods: From 1993 to 2001 we enrolled 87 pts with HCM (64%M, age 45±19y). At enrolment and during the follow-up, all pts underwent clinical examinationand DE examination.Results: 41 pts (48%) were symptomatic (NYHA ≥2), and 13 (15%) showedsigns of heart failure. Seven pts (8%) had LV systolic dysfunction (mean EF35±6%). At transmitral DE 18 pts (21%) had an impaired relaxation pattern(E/A<1), whereas RFP (E-deceleration time (EDT)<120 msec or E/A>2 andEDT<150 msec) was present in 14 pts (16%). Fifteen pts (17.2%) had a signif-icant intraventricular gradient (mean gradient 95±44 mmHg), and 14 (16%) hadsignificant mitral regurgitation (MR) (MR grade ≥ 2). During a mean follow-up of96±54 m, 23 pts (26%) died and 4 (5%) were transplanted. Duration of diseaseand NYHA were selected in a multivariate analysis as the only clinical predictorsof death or transplant. After entering DE variables, clinical data (NYHA class 2-3:HR 5.9, 95% CI: 1.3 - 26.4, p 0.02), indexed left atrial diameter (HR 1.7, 95%
Fig. 1
CI: 1.01-2.8, p 0.05) and RFP (HR 2.9; 95% CI: 1.2 - 6.9, p 0.01) were selected inthe clinical-DE model. Considering DE variables, the AUC of ROC curves signifi-cantly improved from 0.77 of the clinical model to 0.87 (p=0.048). Transplant-freesurvival was significantly lower in pts with RFP (p=0.0001) (Figure).Conclusions: In HCM left atrial dimension and RFP show an incremental prog-nostic value over clinical evaluation in predicting long-term outcome.
P5535 The impact of hypertension and hypertension relatedleft ventricle hypertrophy on right ventricle function
M. Tumuklu, O. Onalan, K. Ceyhan, A. Ocal. GaziosmanpasaUniversity, Faculty of Medicine, Cardiology, Tokat, Turkey
Aim: The aim of our study is to determine the effect of hyperten-sion and hypertension related LVH on RV morphology and function by using RVstandard Doppler echocardiographic indices, myocardial Doppler Imaging andStrain/strain rate Imaging indices.Methods: We studied 35 patients with arteriel hypertension and 30 age,sex -adjusted control subjects with had no other pathological conditions. Standarttransthorasic Doppler echocardiographical measurements, pulsed wave TissueDoppler from tricuspid anulus (Peak systolic - st, peak early diastolic - et, peak latediastolic velocity - at), reconstructed spectral pulsed wave tissue Doppler veloci-ties (Peak systolic-S, peak early-E, peak late diastolic velocity-A) and strain/strainrate imaging of RV free wall mid region (Peak systolic strain- Î, peak systolic strainrate-SR) were obtained.Results: Age, body surface area, blood pressure and heart rate were comprablebetween 2 groups. Hypertensive subjects had significantly increased LV end-diastolic septal and posterior wall thickness, left atrial diameter, LV mass, LV massindex, relative wall thickness during diastole (RWTd).At the level of right ventricular lateral tricuspid annulus without systolic changes,the majority of diastolic measurements were altered in hypertensives (early dias-tolic velocity et; 13±2 vs 18±4m/s, P<0.0001, late diastolic velocity at; 20±4vs 14±3 m/s, P<0.0001, early to late diastolic velocity ratio; 0,69±0,14 vs1,32±0,38, P<0.0001).The velocity data from 2-D colour myocardial imaging at the level of RV free wallmid region again showed altered diastolic measurements in hypertensives (earlydiastolic velocity Et; 8,01±2,6 vs 10,4±3,14m/s, P<0.00, late diastolic velocityA t; 11,5±2,6 vs 9,12±3,7 m/s, P<0.0001, early to late diastolic velocity ratio;0,75±0,41vs 1,87±0,48, P<0.00).The peak systolic strain of RV free wal mid region was significantly lower in hy-pertensive individuals than controls (25,66±5,64 vs30,03±6,78%, p<0,05).Conclusions: The present study demontrates that besides the manifest morpho-logic LV adaptations, significant RV functional alterations can be determined byTDI and strain/strain rate imaging in patients arteriel hypertension.Both tissue velocities by TDI and strain imaging may be new tools to define andquantitate subtle change in systolic and diastolic function of right ventricular func-tion in arteriel hypertension which can not be determined in standart echocardio-graphic parameters.
P5536 Sequential changes of myocardial hypertrophy andregional myocardial function in patients with severeaortic stenoses at baseline and during long termfollow-up after aortic valve replacement
F. Weidemann1 , S. Herrmann2, V. Lange1, M. Beer1, M. Niemann1,W. Voelker1, G. Ertl1, J.M. Strotmann1. 1University Hospital, Medical Clinic,Dept. Of Cardiology, Wurzburg, Germany; 2Wuerzburg, Germany
The purpose of this study was to investigate the change in left ventricular (LV)hypertrophy and regional myocardial function in patients with severe aortic valvestenoses at baseline and during follow-up after aortic valve replacement (AVR).Methods: 17 Patients with severe aortic stenoses were studied by conventionalechocardiography and strain rate imaging before (baseline), 2 weeks and 9months after AVR. Radial myocardial function was assessed in parasternal longaxis views from the posterior wall. By the use of apical four chamber views lon-gitudinal myocardial function was assessed in the septal and lateral wall. In eachwall peak systolic and early diastolic strain rates (SR) were measured. In addi-tion, end-diastolic wall-thickness, LV diameter (LVEDD) and ejection fraction (EF)were extracted.Results: For radial function a significant increase of systolic SR could be seenalready after 2 weeks (baseline=1.2±0.3 s-1; 2 weeks=1.7±0.5 s-1, 9 months=1.7±0.5 s-1). In contrast, systolic longitudinal SR increased only after 9 months
Change in function and hypertrophy.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

e-Poster session 10 979
significantly (Figure). For diastolic SR no change in the follow-up period couldbe documented. Parallel to the change of longitudinal systolic SR a significantreduction of LV wall-thickness could be seen only after 9 months (Figure). LVEDDand EF were normal at baseline and remained constant.Conclusions: These data implicate that in patients after AVR the initial increasein radial function can be due to the reduction of afterload. However, the long termremodelling after 9 months expressed as a reduction of wall thickness seems tobe associated with an increase of longitudinal contractile function.
P5537 Myocardial strain in Chagas disease. A new tool todiagnose subclinical disease
E.S. Silva1, L.D.C. Ferreira1 , C.G. Monaco1, J. Ortiz1, L.B. Peixoto2,W. Mathias Jr3, B.M. Ianni2, A.C.P. Barretto2. 1Omni-Ccni MedicinaDiagnostica, Echocardiography, Sao Paulo, Brazil; 2DASA, Echo,
Sao Paulo, Brazil; 3InCor, Echo, Sao Paulo, Brazil
Echocardiographic findings in Chagas’ disease are variable, both normal heartsand severe dysfunction can be found. Recently, tissue Doppler imaging lead to amore comprehensive evaluation of regional and global ventricular function.Objective: To measure myocardial strain in Chagas’ disease and evaluate ra-dial and longitudinal function in indeterminate and chronic forms of the diseasecomparing to normals.Methods: 39 individuals were studied (20 males, 51,3%) divided into four groups:Nl -17 normal (43,6%); Ind - 7 individuals with indeterminate form of Chagas’ dis-ease (17,9%); C1 - 7 individuals with chronic form and ejection fraction < 50%(17,9%) and C2 - 8 individuals with chronic form and ejection fraction > 50%(20,5%). After a complete echocardiogram four cine-loopings were stored dig-itally (paraesternal long and short axis; apical 2 and 4 chambers) to measuremyocardial strain in 16 different segments.Results: In Group C1 all segments of septal, posterior and inferior walls, and themedial segment of anterior wall have impaired contractility comparing to normal.Group C2 presented diminished strain in all segments of septal wall, basal andmedial segments of the posterior wall, medial and apical segments of the inferiorwall and medial segment of the anterior wall. Finally, in the Ind group, myocar-dial strain was diminished at the medial segment of posterior wall. Both radialand longitudinal functions were greater in group Nl than in C1 and C2, and inthe Ind group than in C1. All groups showed radial function greater than longitu-dinal. The mean radial strain values were 33,7% (30,4%; 38,2%) in the normalgroup; 32,3% (28,7%; 33,6%) in the Ind group; 21,7% (19,1%; 23,6%) in groupC1 e 24,7% (15,2%; 27,8%) in group C2. The mean longitudinal strain valueswere 25,9% (24,5%; 30,7%) in the normal group; 28% (24,7%; 29,7%) in the Indgroup; 16,8% (13,2%; 19,2%) in group C1 e 19,1% (15,8%; 22,3%) in group C2.Despite normal contractility on 2D echo, Indeterminate form showed abnormalstrain values in posterior wall. Kruskal-Wallis and Dunn and Mann-Whitney wereused for statistics.Conclusions: both radial and longitudinal functions were greater in normals thanin Chagas’ disease and in the indeterminate form than in chronics with low ejec-tion fraction. The radial function is always greater than longitudinal. Strain maydiagnose subclinical myocardial impairment in indeterminate form of Chagas’ dis-ease.
P5538 Doppler myocardial imaging in the diagnosis of earlysystolic LV dysfunction in diabetic rats
C. Weytjens1, S. Droogmans1, G. Van Camp1, B. Cosyns1,J. D’hooge2, P.R. Franken1 . 1AZ-VUB, Cardiology, Brussels,Belgium; 2UZ-Gasthuisberg, Cardiology, Leuven, Belgium
Background: Doppler myocardial imaging (DMI) can be used in small animals toquantitate regional myocardial function. We intent to use this technique to detectearly signs of LV dysfunction in a model of diabetic cardiomyopathy.Methods: A total of 20 male Wistar rats underwent baseline transthoracic echo-cardiography with TDI analysis of the anteroseptal and inferolateral wall in a short-axis view. A GE Vivid7 echo machine equipped with a 14 MHz linear probe wasused. In 12 rats Streptozotocin (STZ) 45 mg/kg was injected intravenously toinduce insulin dependent diabetes. Conventional M-mode and high frame ratecolour Doppler images were acquired at baseline and 12 weeks after STZ injec-tion.Results: A significant reduction in heart rate was seen in the diabetic rats after
Table
Normal Diabetes
Baseline 12 weeks Baseline 12 weeks
LV EDD (mm) 7.4 ±0.8 7.4 ±0.4 7.4 ±0.8 7.9 ±0.5a
LV FS (%) 43.4 ±4.5 45.4 ±6.3 41.6 ±6.7 44.0 ±4.7AS Peak Strain (%) 37 ±14 44 ±13 44 ±12 44 ±14IL Peak Strain (%) 51 ±18 55 ±12 55 ±14 56 ±13AS Peak Strain Rate (/s) 9.8 ±3.1 11.4 ±3.2 11.4 ±2.0 7.8 ±1.9a, b
IL Peak Strain Rate (/s) 15.3 ±5.6 15.4 ±2.8 16.4 ±3.6 13.8 ±3.4AS Mean Strain Rate (/s) 4.4 ±1.8 4.8 ±1.6 6.0 ±2.0 3.6 ±1.8a
IL Mean Strain Rate(/s) 6.6 ±3.0 5.8 ±2.0 7.6 ±1.5 5.4 ±1.3a
Mean values ± SD at baseline and after 12 weeks. a: p<0.05 compared to baseline (pairedStudent’s T-test);b: p<0.05 compared to normal (Student’s T-test). LV EDD: LV End diastolicdiameter. LV FS: LV Fractional shortening. AS: Anteroseptal; IL: Inferolateral
12 weeks (243 ± 21/min versus 315 ± 29/min). In the diabetic rats no changesin fractional shortening was present but a significant increase in LV EDD wasmeasured when compared to baseline (Table). Using DMI a significant decreasein peak and mean strain rate could be detected. The total amount of deformation(peak strain) remained unchanged but post systolic thickening derived from thestrain curves was present in 1 out of 16 segments in normal versus 10 out 24segments in diabetic rats (p < 0.05; Chi-square).Conclusion: Early systolic dysfunction can be detected in diabetic rats usingDoppler myocardial imaging.
P5539 Effect of obesity on left ventricular structure andmyocardial systolic function
M. Tumuklu, K. Ceyhan, A. Ocal, O. Onalan. GaziosmanpasaUniversity Faculty of Medicine, Cardiology, Tokat, Turkey
Background: Obesity is associated with heart failure, cardiovascularmorbidity and mortality.A direct effect of weight on Left Ventricle(LV) structure andmyocardial function is not well-established.Aim: The aim of our study is to determine the effect of obesity on LV morphologyand systolic function by using LV standard Doppler echocardiographic indices,myocardial Doppler Imaging and Strain/strain rate Imaging indices.Methods: We studied 33 obese and 34 age,sex -adjusted control subjects withhad no other pathological conditions. Standard transthorasic Doppler echocar-diographical measurements, reconstructed spectral pulsed wave tissue Dopplervelocities, strain and strain rate imaging of six different myocardial regions wereobtained. Peak systolic velocity (SR), peak systolic strain (Î), peak systolic strainrate(SR) for each region and as a global systolic longitidunal LV function mean ofpeak systolic strain of six myocardial regions (glsca) were compared.Results: Age, body surface area, blood pressure and heart rate were comprablebetween 2 groups. Obese subjects had significantly increased LV end-diastolicvolume„ septal wall thickness, left atrial diameter and decreased transmitral earlyto late diastolic velocity ratio.In obese subjects reconstructed spectral pulsed wave tissue Doppler analysisshowed significantly decreased basal lateral peak systoic (Sm) velocity (6.68 ±1.89vs 8.08 ± 2.50, p<0.05), mid lateral Sm (5.01 ± 2.17vs 6.78 ± 3.22, p<0.05).Differences in regional strain rate(mid septal SR-1.45 ± 0.23 vs 1.63 ± 0.18,p<0.05), regional strain (basal septum Î -19.13 ± 3.83vs 22.09 ± 4.60, p<0.05,mid septum Î -18.03 ± 2.91vs 20.25 ± 4.77, p<0.05, radial Î -27.50 ± 7.32vs35.53 ± 9.48, p<0.05) and global strain(glsca-19.38 ± 1.34vs 21.24 ± 2.82,p<0.05 were identified between obese and the referent subjects.Conclusions: Obesity is associated with morphologic alterations in left ventricleand left atrium and subclinical changes in left ventricle systolic function which canbe detected by Strain and strain rate imaging even without overt heart disease.
P5540 Effect of thyroid hormones on cardiac performanceestimated by tissue Doppler echocardiography
A. Minczykowski, K. Ziemnicka, J. Sowinski, H. Wysocki. PoznanUniversity of Medical Sciences, Department of Cardiology-IntensiveTherapy, Poznan, Poland
Objective: Thyroid hormones influence cardiac performance directly and in-directly via changes in peripheral circulation. Patients with a history of thyroidec-tomy for thyroid cancer present a unique model to investigate the cardiac effectsof acute hypothyroidism. The purpose of the study was to investigate the effectof hypothyroidism on heart systolic and diastolic function estimated by the tissueDoppler echocardiography (TDE).Patients and Methods: Eighteen patients with a history of thyroidectomy for thy-roid cancer (age 45.4±12.0 years, 2 males) in whom thyroid hormone replace-ment therapy (T4) was withheld for whole body radioiodine scanning, were in-vestigated before restoration of T4 therapy and after 5.5 months of replacementtherapy. A detailed two-dimensional and Doppler examination was made includingmeasurement of longitudinal mitral annular motion velocities by TDE.Results: During the first echocardiography study, both levels of free thyroidhormones were expectedly well below normal range, and TSH was increased,confirming the severe hypothyroid state. T4 medication resulted in a euthyroidstate at the time of the second study. Left ventricular diameter and wall thick-ness did not change after T4 treatment, although systolic increase in wall thick-ness increased significantly (IVS% 27.1±10.3% vs. 36.4±12.3% and PWT%33.5±14.6% vs. 42.9±18.6%, p<0.05, p<0.05, respectively). Ejection fraction in-creased from 0.57±0.11 to 0.65±0.05 (p<0.001) and cardiac output increasedfrom 3734±655 to 4400±866 ml/min. (p<0.001). During the second exami-nation the significant increase in mitral inflow and decrease of the E/A ratiowere noted. After restoration of T4 therapy there were significant increase insystolic (S’), and early diastolic (E’) mitral annular velocities (S’, 12.0±2.1 vs.13.4±1.9 cm/s, E’, 14.3±2.5 vs. 15.5±2.6 cm/s, p<0.05). Similarly during sec-ond examination tissue Doppler mitral annular late diastolic velocity (A’) increased(A’, 13.3±2.4 vs. 15.8±2.4 cm/s, p<0.001) and the ratio E’/A’ decreased from1.10±0.21 to 0.99±0.17 (p<0.01). The E/E’ ratio (E/E’, 4.82±1.18 vs. 5.08±1.20,p>0.05), isovolumic relaxation time and S’ duration remained unchanged. Themyocardial performance index (MPI) subnormal at the baseline (0.65±0.14, nor-mal range 0.37±0.05) decreased after 5,5 months of T4 treatment (0.55±0.08,p<0.05).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022
980 e-Poster session 10
Conclusion: Hypothyroidism is associated with the decrease in longitudinal mi-tral annular motion velocities. Cardiac performance improves after restoration ofthyroid hormone replacement therapy.
P5541 The relationship between conventional and tissueDoppler echocardiographic findings and plasmaN-Terminal pro Brain Natriuretic Peptide levels inhypertensive patients with left ventricular diastolic
C. Ceyhan1, S. Unal2, T. Tekten2, C. Yenisey3, I. Yilmaz3. 1AdnanMenderes Univ., Cardiology Dept., Aydin, Turkey; 2Adnan Menderes UniversityCardiology Dept, Aydin, Turkey; 3Adnan Menderes University Biochemistry Dept,Aydin, Turkey
Background: Brain Natriuretic Peptide (BNP) has been reported to be elevatedin patients with diastolic heart failure and in isolated left ventricular (LV) diastolicdysfunction. However, the utility of N-Terminal pro Brain Natriuretic Peptide (NT-proBNP) for detecting diastolic dysfunction in ambulatory hypertensive patientswithout heart failure symptoms is unclear. In this study, we investigated the rela-tion between NTproBNP plasma levels and LV diastolic dysfunction in hyperten-sive patients with normal ejection fraction and with no objective finding of heartfailure.Method: We studied 40 ambulatory patients (26 women, mean age 52±5) withcontrolled hypertension. Diastolic functions were evaluated with early diastolictransmitral E wave velocities, tissue Doppler mitral annulus early diastolic E’ wavevelocities and E/E’ ratios, respectively. Patients were divided in two groups ac-cording to E/E’ ratios >15 or not and NTproBNP levels were compared in twodifferent groups. The correlation between NTproBNP levels and E/E’ ratios werealso analyzed in all patients.Results: The NTproBNP levels are positively correlated significantly with E/E’ratio(R = 0.89, p<0.0001). Patients with elevated LV end diastolic pressure(LVEDP), defined as E/E’ >15 (n =10) had higher NTproBNP (203 ± 75 pg/ml)levels than the other group. (Table) A NTproBNP value of 119 pg/mL had a sen-sitivity of %87,5, a specificity of %100 for predicting E/E’ >15.
Table 1
Grup 1(n=10) Grup 2 (n =30) P
NT-pro-BNP(pg/mlt) 203 ± 75 55 ± 28 <0.0001
NTproBNp: N-Terminal pro Brain Natriuretic Peptide.
Conclusion: This study demonstrates for the first time the correlation of plasmaNTproBNP level with LV diastolic dysfunction and with E/E’ ratio and the com-bination of NTproBNP levels along with E/E’ ratios may be a better predictor ofelevated LV filling pressures in hypertensive patients with diastolic dysfunction.
P5542 Insulin Resistance is an independent predictor ofearly diastolic myocardial dysfunction inuncomplicated obesity
C. Palombo1, M. Kozakova2, E. Muscelli1, C. Morizzo1,S. Camastra1, M. Florescu3, E. Malshi2, E. Ferrannini2 . 1University
Of Pisa, Department Of Internal Medicine, Pisa, Italy; 2University of Pisa, InternalMedicine, Pisa, Italy; 3University Hospital, Cardiology, Bucharest, Romania
Obesity is an insulin resistant (IR) state associated with increased susceptibilityto heart failure. Whether or not IR may be a determinant of early subclinical LVdysfunction in "uncomplicated" obesity is still controversial.Aim of the study was to investigate the associations between fasting insulin, in-sulin secretion, IR and echocardiographic indices of LV performance in otherwisehealthy subjects with isolated obesity.Methods: We studied 44 subjects of either gender (age 18-68 yy, BMI 18-51kg/m2) free of organic heart disease, hypertension, diabetes, dyslipidemia. Ac-cording to a BMI < 25, ≥ 25 and < 30, or ≥ 30, subjects were classified as nor-mals (NL, 11), overweight (OW, 11) and obese (OB, 22). LV mass index, geometryand function were assessed by conventional echo. TDI-echo of the medium partof interventricular septum (Aloka SSD,5500, Tokyo) was used to assess myocar-dial performance. IR was estimated from plasma glucose and insulin responsesto O-GTT, by calculating OGIS index (Oral Glucose Insulin Sensitivity). C-peptidewas measured to estimate insulin secretion.Results: compared to NL, OW and OB showed higher (p<0.05) BP(118±11/69±8, 124±11/78±6, 131±9/83±6 mmHg) and HR (60±6, 67±11,74±12 bpm). Waist girth, fasting insulin, C-peptide and OGIS displayed a largerange of distribution and were significantly different between groups (p<0.05-0.01). Fasting glucose, LV mass index, and cardiac index were within normal limitsand comparable between groups.Peak systolic myocardial velocity measured by TDI did not differ between groups(6.9±1.1, 6.6±0.6, 7.3±1.4 cm/s), but it increased with fasting insulin in the en-tire population (r=0.41; p<0.01). Fasting insulin was also directly related to HR(r=0.49; p<0.01). Myocardial E/A ratio at TDI was lower in both OW and OB vsNL (1.2±0.4 and 1.2±0.4 vs 1.7±0.3; p<0.001). In the entire population, TDI E/Acorrelated inversely with age (r=-0.64; p<0.001), waist girth (r=-0.45; p<0.01),LV mass (r=-0.36; p<0.05), fasting glucose, insulin and C-peptide (r=-0.35, -0.35,-0.50; p<0.05-0.01), and directly with OGIS (r=0.43; p<0.001). In multivariateanalysis, age and OGIS (r2=0.55) were independent correlates of TDI E/A ratio.
Conclusions: In otherwise healthy subjects with a wide BMI range, IR is an inde-pendent predictor of LV diastolic performance, which shows a subclinical impair-ment in OW and OB groups in presence of preserved systolic function. A directrelation between fasting insulinemia and systolic myocardial velocities seems toreflect an insulin-related increased sympathetic drive to the heart.
P5543 Effect of preload reduction on ultrasound myocardialtissue characterization
A. Minczykowski, D. Zaremba-Drobnik, I. Pietrzak, S. Czekalski,H. Wysocki. Poznan University of Medical Sciences, Department ofCardiology-Intensive Therapy, Poznan, Poland
Objective: Several experimental and clinical studies have shown that the inte-grated backscatter signals (IBS) from the myocardium are affected by both struc-tural and functional properties of the myocardium. The aim of the present studywas to examine the effect of preload reduction by hemodialysis on the cyclic vari-ation of integrated backscatter (CV-IBS). PATIENTS AND METHODS: Fifty twopatients (age 51±17 years, 32 males) on maintenance hospital hemodialysis (4h three times a week) underwent echocardiography approx. 30 min prior to, andapprox. 30 min after, a routine hemodialysis session. The aim of fluid removal wasto achieve a clinically determined "dry weight". A detailed 2D and Doppler exam-ination was made to assess left ventricular (LV) structure and function includingCV-IBS.Results: Hemodialysis resulted in a mean reduction in weight of 2.1±1.0 kg. Fol-lowing HD, there were significant reduction in left ventricular end-diastolic andend-systolic dimensions and left atrial diameter (LVIDd, 4.8±0.6 vs. 4.4±0.7 cm,p<0.0001, LVIDs, 3.4±0.7 vs. 3.2±0.8 cm, p<0.0001, LA, 4.2±0.7 vs. 3.8±0.7cm, p<0.0001), consistent with a decrease in preload. Also consistent with a re-duction in preload there was a reduction in the peak early transmitral flow velocity(E, 97.5±29.0 vs. 74.6±26.1 cm/s, p<0.0001) and in the ratio of the peak E ve-locity to the peak late filling velocity (E/A, 1.29±0.59 vs. 0.95±0.34, p<0.0001).LV wall thickness and systolic increase in wall thickness did not change after HD.Stroke volume, cardiac output as well as LV ejection fraction decreased after HD(SV, 59.4±16.6 vs. 47.9±16.1 ml, p=0.0001, CO, 4295±1266 vs. 3581±1215ml/min, p<0.0001, LV EF, 58.1±9.3 vs. 55.5±10.0, p=0.0001). The cyclic vari-ation of integrated backscatter (CV-IBS) in the interventricular septum, the leftventricular lateral as well as in the inferior wall decreased significantly afterHD (7.87±2.19 vs. 6.86±1.78 dB for the interventricular septum, 7.04±2.11 vs.6.17±1.86 dB for the left ventricular lateral wall and 9.04±2.57 vs. 8.12±1.99 dBfor the left ventricular inferior wall, p=0.001, p=0.001, p=0.006, respectively). Thecalibrated integrated backscatter (cal-IBS) remained unchanged after dialysis incomparison with baseline. Correlation was found between change in CV-IBS andreduction in weight during HD.Conclusion: Preload reduction by hemodialysis has an influence on ultrasoundmyocardial tissue characterization - CV-IBS is strongly preload dependent. Thisfinding is in concordance with diminished LV performance during HD.
P5544 Systolic left ventricular function in patients withasymptomatic and mild aortic stenosis: the SEASstudy
K. Wachtell1, E. Gerdts2, D. Cramariuc1, M.H. Olsen3, K. Egstrup4,R. Willenheimer5, C. Gohlke-Barwolf6, S. Ray7. 1Rigshospitalet(Hospital), Dept. of Cardiology B2142, Copenhagen O, Denmark;
2Bergen, Norway; 3Copenhagen, Denmark; 4Svendborg, Denmark; 5Malmo,Sweden; 6Baden-Wurtemberg, Germany; 7Newcastle Upon Tyne, UnitedKingdom
Background: It is known that heart failure is a marker of poor prognosis in pa-tients with aortic stenosis (AS). However, it is unclear whether asymptomatic pa-tients with AS have impaired systolic left ventricular (LV) function. Furthermore, itis unclear whether systolic impairment is related to the concomitant LV hypertro-phy.Methods: Transthoracic Doppler echocardiography was performed at baselineon 1,762 patients with mild to moderate asymptomatic AS (transaortic Dopplervelocity ≥2.5 and <=4.0 m/s) randomised in to the Simvastatin and Ezetimibe inAortic Stenosis (SEAS) study.Results: Quartiles of aortic valve area indexed by body surface area (AVAI) and
Table 1
AVAI AVAI AVAI AVAI P
<0.34 ≥0.34 &<0.42 ≥0.42 &<0.51 ≥0.51No 421 423 430 419(%) 24.9 25.0 25.4 24.7Left ventricular mass index (g/m2) 74.9±22.9 71.0±22.0 71.1±21.8 70.8±22.8 <0.05Relative wall thickness 0.36±0.1 0.36±0.09 0.35±0.09 0.35±0.09 0.178Fractional shortening (%) 35.6±6.6 36.5±6.3 36.9±6.3 37.7±6.6 <0.001Low EFS < 27% (%) 6.2 5.0 4.2 4.1 0.457Midwall shortening (%) 16.64±3.5 17.14±3.3 17.41±3.4 17.73±3.3 <0.001Low midwall shortening <14% (%) 23.3 19.6 16.3 10.5 <0.001Circumpheren. end-systolic
stress (kdynes/cm) 162±52 162±49 162±50 163±57 0.984Stress-correct. midwall
shortening (%) 102±23 105±22 106±22 109±22 <0.001
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

e-Poster session 10 981
systolic LV function are shown in Table. AVAI was significantly related to endocar-dial fractional shortening (EFS) (r=0.111), midwall shortening (MWS) (r=0.122)and stress-corrected MWS (r=0.115, all p<0.001). Multivariate analyses showedthat low AVAI predicted low MWS (β=0.90) independent of higher LV mass index(β=-0.457, both p<0.001). Gender and systolic blood pressure did not enter themodel.Conclusion: In patients with mild to moderate AS smaller AVAI is related to lowersystolic LV function independent LV hypertrophy per se. Patients with the lowestAVAI quartile had highest prevalence of impaired systolic LV function. This indi-cates that AS impairs systolic LV function even in asymptomatic patients.
P5545 Global average of longitudinal strain imaging detectsearly impairment of left ventricular systolic functionin asymptomatic cardiac amyloidosis
D.B. Bellavia1, P. Pellikka1, J.K. Oh1, T.P. Abraham2, G. Al-Zharani2,C. Miyazaky2, F.A. Miller2. 1Mayo Clinic, Cardiovascular Diseases,
Rochester, United States of America; 2Jhons Hopkins University, CardiovascularDiseases, Baltimora, United States of America
Background: The purpose of the study was to clarify the potential role of tissuevelocity imaging (TVI), strain rate imaging (SRI) and strain imaging (SI) in theearly detection of cardiac amyloidosis (CA) and to define the minimum numberof segments necessary to assess longitudinal ventricular dysfunction in patientswith primary amyloidosis.Methods: 103 patients with primary amyloidosis and 27 healthy controls wereenrolled. Patients were divided into three groups according to left ventricular (LV)thickness, pulsed wave tissue Doppler imaging (PW-TDI), and clinical exams: 42non CA(normal LV wall thickness, and normal PW-TDI); 26 early CA(normal LVwall thickness and abnormal PW-TDI); and 35 overt CA(Increased LV wall thick-ness ± symptoms/signs of heart failure). TVI, SRI and SI longitudinal systolicpeak values were determined for the 16 LV segments considered individually, inclusters by level (average of the TDI values for the basal, middle and apical seg-ments) and by wall (average of the TDI basal, middle, and apical values for the 6LV walls). Diagnostic accuracy of all TDI modalities and variables were compared,and cut-off values were assessed by ROC curves for controls and for patients withovert, early, and non CA.Results: PW-TDI and TVI did not reach diagnostic accuracy in non CA patientsas compared to controls. In overt, early and non CA, SRI and SI of all LV basalsegments and all LV clusters were reduced as compared to controls. Global aver-age SI of all 16 LV segments AUC 0.946, cut-off -19.67%), or average SI of 6 basalsegments(AUC 0.943, cut-off -20.11) were the most accurate measurements todifferentiate overt, early and non CA from controls. SI of middle inferoseptum(AUC 0.90 cut-off -14.86) was the most accurate measurement to differentiateovert CA from non CA patients.Conclusions: SI was the most accurate technique, compared to TVI or SRI,to assess early longitudinal ventricular dysfunction in patients without traditionalechocardiographic signs of CA. The most accurate SI dataset to identify patientswith early CA were the average SI of the 16 LV or of the 6 basal segments. SI anal-ysis documented progressive regional cardiac impairment from non CA throughovert CA. Further studies are warranted to define the prognostic value of thesenew TDI modalities in predicting cardiac morbidity and mortality.
P5546 Strain rate imaging detects early myocardialabnormalities in patients with aortic regurgitation
A. Marciniak, G.R. Sutherland, M. Marciniak, T. Karu, A. Baltabaeva,E. Merli, B. Bijnens, M. Jahangiri. St. George’s Hospital, Departmentof Cardiology and Cardiac Surgery, London, United Kingdom
Early left ventricular (LV) dysfunction in patients (pts) with aortic regurgitation(AR) is often underestimated due to the lack of a sensitive diagnostic tool to mon-itor systolic function. Strain rate (SR) imaging could provide a new technique fordetecting early changes in regional LV systolic deformation.Aim: To asses the changes in regional LV function by SR imaging in predictingLV dysfunction in pts with AR.Methods: The study population consisted of 45 consecutive pts with isolatedAR (age 48±13) divided into 3 groups: mild, moderate, severe AR and 23 agematched healthy subjects. Pts were excluded if they had ischemic heart disease.All pts underwent a standard echo extended with a tissue Doppler study. ForLV radial deformation, the posterior wall (LVPW) was examined, for longitudinaldeformation, SR data were acquired from the LV lateral wall.
Fig. 1
Results: Radial peak systolic SR in the LVPW was significantly decreased inpts with severe AR compared to healthy subjects (1.6±0.6 s-1 vs 3.0±0.5 s-1,P<0.001), in addition SR was inversely correlated with LV end systolic diame-ter (ESD), (Figure 1 left) and end diastolic diameter (EDD), (P<0.001, R=-0.69).Longitudinal SR was significantly reduced for mid segment of LV lateral wall com-pared to controls (1.1±0.4 s-1 vs 1.6± 0.2 s-1, P<0.001). Longitudinal SR wasinversely correlated with ESD (Figure 1 right) and EDD (P<0.001, R=-0.51).There was no significant difference in radial or longitudinal peak systolic SR inthe groups with mild and moderate AR compared to controls.Conclusions: SR imaging is a sensitive tool in detecting subclinical changesin radial and longitudinal deformation in patients with severe AR. It could be anuseful tool in predicting LV dysfunction during patients follow-up.
P5547 Myocardial deformation by bidimensional strain inprofessional football players: comparison withcontrols and hypertrophic cardiomyopathy
V. Richand1, P. Reant2, K. Serri3, M. Lafitte2, A. Chalabi4,A. Kerouani2, R. Roudaut2 , S. Lafitte2. 1Bordeaux, France; 2Hopital
Cardiologique Haut-Leveque, Echocardiography, Bordeaux-Pessac, France;3Institut de cardiologie, Montreal, Canada; 4PSG Football club, Paris, France
In highly trained athletes, the extent of physiologic cardiac remodelling may oc-casionally be substantial and may raise a potential diagnosis of structural car-diac disease such as hypertrophic cardiomyopathy (HCM). Deformation analy-sis, which is now available by echocardiography using 2D strain, is a promisingtechnique to detect early systolic function abnormalities, especially in cases ofborderline left ventricular hypertrophy.Methods: 99 subjects (29 professional football players (PFP), 25 patients withhypertrophic cardiomyopathy (HCM) and 45 controls (CTL)) were investigatedat rest by conventional transthoracic echocardiography. 2D strain analysis wasperformed to measure deformation in 17 myocardial segments in the longitudinal,transverse, radial and circumferential axis.Results: Ejection fraction was 61.1±7%, 67±7%, 69±6% respectively for PFP,CTL and HCM. Compared to HCM (237±78g/m2), left ventricular mass was lowerfor PFP (119±22g/m2) and CTL (91±22 g/m2), p<0.05. Average radial and trans-verse myocardial deformation were significantly higher in PFP compared to CTLwhereas longitudinal strain was lower (table) (p<0.01). No significant differencewas observed in terms of circumferential strain between the 2 groups (p ns).Compared to HCM, athletes had higher values of transverse, radial and circum-ferential strain (p<0.01). Interestingly, no significant difference was observed be-tween PFP and HCM for longitudinal strain except when comparing pathologicalseptal hypertrophic segments to corresponding areas in PFP (-11.3±4.8% vs -15.8±2.4%, p<0.01). Finally, no strain apex-base gradient was observed in HCMwhereas it was found in PFP and CTL. Inter and intra-observer variabilities rangedbetween 9 and 13%.
2D strain (%) PFP CTL HCM
Longitudinal -16.9±4 -20.3±5.6 -14.9±7.7Transverse 34.7±4 27.3±14.9 23.5±17.6Circumferential -19.1±5.7 -19.8±8.2 -16.8±7Radial 39.3±16.2 36.6±18.2 25.1±13.9
Conclusion: 2D strain can identify specific patterns of myocardial deformationin PFP, CTL and HCM, particularly for transverse and radial components, andpathological segments. This technique is an easily clinically applicable method todistinguish between athlete’s heart and HCM.
P5548 Increased myocardial deformation in the left ventriclein chronic severe mitral regurgitation
A.N. Borg, M.R. Yusoff, S.M. Deepak, W. Khan, S.G. Williams,S.G. Ray. Wythenshawe Hospital, Cardiology, Manchester, UnitedKingdom
Background: It is difficult to assess left ventricular function in patients withchronic mitral regurgitation. Tissue Doppler-derived myocardial deformationimaging by may be a useful tool for monitoring these patients.Methods: 27 patients with moderate-to-severe mitral regurgitation due to mitralvalve prolapse (MVP) aged 65.1 ± 12.1 years, and 27 age-matched healthy con-trols (CONTR) were studied. Patients had no symptoms and an ejection frac-tion >60%. For radial deformation, peak systolic strain rate (SR) and end-systolicstrain (ESS) was obtained from the basal posterior wall. For longitudinal deforma-tion, SR and ESS were obtained from apex, mid and base of septal, lateral, infe-rior, anterior, posterior and anteroseptal walls. Post systolic strain that exceeded10% of ESS was measured. Radial ESS was divided by end systolic meridionalwall stress to derive a contractility index.Results: Radial SR was increased in MVP (3.88 ± 1.75 vs 1.8 ± 0.72/s,p<0.001). Longitudinal SR was also increased in most segments in MVP. Ra-dial ESS was increased in MVP (44.11 ± 18.32 vs 32.17 ± 12.91%, p=0.01),and longitudinal ESS tended to increase in most segments. Longitudinal SR inMVP peaked later than in CONTR (p<0.001), while systolic strain peaked signif-icantly earlier in MVP patients (p<0.001). In MVP, 38% of longitudinal segments
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

982 e-Poster session 10
demonstrated post-systolic shortening compared to 18% of segments in CONTR(p<0.001). Contractility Index was 8.50 MVP vs 6.05 KPa-1 CONTR, p=0.06.
Fig. 1. Mean strain rate.
Conclusion: Left ventricular longitudinal and radial deformation is increased inthe compensated stage of chronic MR, though the difference was less strikingwhen deformation was normalized for afterload. Serial monitoring of these indicesmight be useful as a marker of early left ventricular decompensation.
P5549 Left ventricular longitudinal function in hypertensivepatients with left ventricular hypertrophy regression
E. Pavlyukova. Institute Of Cardiology, Ischemic Heart Disease,Tomsk, Russian Federation
The aim of the study was to investigate longitudinal function of leftventricle (LV) in essential hypertension (EH) pts who had concentric LV hypertro-phy (LVH) and its regression by the end of the first year of ACE inhibitors moexipril(up to 15 mg/day) treatment.Material and methods. The analysis was performed in 50 pts (42 males, 8 femalesaged 51.2±5.4 yrs) with LV myocardial mass (LVMM) of 343.9± 30.9 g. Longitu-dinal LV function was assessed using pulse-wave Doppler Tissue Imaging fromapical view with scoring of systolic and diastolic velocities of all 18 segmentsand from fibrous rings of mitral valve (FRMV). Systolic wave (s) and two diastolicwaves (e, a) and their ratio and isovolumic relaxation time (ivrt) were assessed.24-h blood pressure monitoring (24 BPM) were performed in all pts before treatand the end of the first year of ACE inhibitors moexipril.Results: LVH regression was found in 44 (88%) of 50 LVH pts by the end of thefirst year of treatment. Longitudinal diastolic function was improved in 38 (86.4%)of 44 pts with LVH regression. Increase in systolic velocities from FRMV by theintraventricular septum was found in 21(47,7%) of 44 pts with LVH regression.They demonstrated e/a increase from FRMV of lateral, inferior, posterior and an-terior walls and ivrt decrease from posterior and lateral walls and intraventricularseptum. Systolic velocities from FRMV and basal, mid segments of anterior walland intraventricular septum were increased by the end of the first year of therapy.Changes in LVMM by the end of the first year of treatment correlated with changesin ivrt (r=-0.42-0.63), e/a (r=-0.50-0.76) and s (r=-0.74-0.88) of basal and mid LVsegments and from FRMV of posterior, anterior walls and intraventricular sep-tum (ivrt: r=-0.62-0.90; e/a:r=-0.45-0.63). Changes of s, e/a and ivrt from FRMVcorrelated with changes of parameters of 24 -h BPM.Conclusions: Improvement in LV longitudinal systolic and diastolic functions wasfound in pts with LVH regression by the end of the first year of ACE inhibitorstreatment.
P5550 Evaluation of right ventricular function using theDoppler Tei index in adenotonsiller hipertrophy
D. Duman, B. Naiboglu, H.S. Esen, R. Demirtunc. HaydarpasaNumune Training & Research Hosp, Cardiology Department,Istanbul, Turkey
Objective: Adenotonsillar hypertrophy (ATH) causing upper airway obstructionmay lead to the pulmonary hypertension and cor pulmonale. This study was de-signed to determine the clinical value of Doppler-derived index of combined sys-tolic and diastolic myocardial performance (Tei index) of right heart in ATH. Theeffects of adenoidectomy and tonsillectomy on Tei index was also asssessed.Methods: Seventeen children with ATH and sleep related breathing disordersand 20 age-and-sex matched healthy controls were enrolled.Tei index, defined asthe sum of isovolumetric contraction and relaxation time divided by ejection time(Figure 1), was measured by using Doppler echocardiography preoperatively andmean 6.7 ± 1.8 months postoperatively in all subjects.Results: When the right ventricular Tei index of study and control group com-pared preoperatively, Tei index was significantly higher in patients with ATH thanhealthy controls (0.37 ± 0.06 vs. 0.29 ± 0.08; P< 0.001). The right ventricularTei index decreased significantly after relief of upper airway obstruction by ade-noidectomy and/or tonsillectomy (from 0.37 ± 0.06 to 0.30 ± 0.07; P< 0.05). Theechocardiographic results in postoperative group were similar to control group.
Fig. 1. Doppler-derived index of Tei.
Conclusion: Our findings support that ATH is associated with impaired RV func-tion when compared with control subjects, which were recovered postoperatively.
P5551 Early changes in left ventricular deformation inpatients with asymptomatic mitral regurgitationdetected by strain rate imaging
A. Marciniak, G.R. Sutherland, M. Marciniak, B. Bijnens,A. Baltabaeva, T. Karu, E. Merli, M. Jahangiri. St. George’s Hospital,
Department of Cardiology and Cardiac Surgery, London, United Kingdom
Valvular heart disease with poor left ventricular (LV) function is recognized as animportant cause of morbidity and mortality. To date, there is no specific and widelyused diagnostic method to detect subclinical changes in systolic function beforeirreversible LV dysfunction occurs in mitral regurgitation (MR).Aims: To assess the changes in regional LV function by S imaging in patients(pts) with MR before development of clinical features.Methods: 77 individuals were studied: 54 asymptomatic pts with isolated MR(age 58±12) divided into 3 groups: mild, moderate, severe MR and 23 agematched controls. All pts underwent a standard echo examination with a tissueDoppler study. S data were acquired from the posterior wall (LVPW) - radial de-formation and from LV lateral wall (longitudinal deformation). Pts were excludedif they had ischemic heart disease. A mathematical modelling study was carriedout to predict how S should alter with increasing dimensions and potentially de-creasing contractility due to irreversible myocardial damage.Results: Radial peak systolic S in the LVPW was significantly decreased in ptswith severe MR compared to controls (39±14% vs 51±9%, P=0.002). Longitudi-nal S was significantly reduced in LV lateral wall compared to controls (15±5.6%vs 21±4.6%, P<0.05). The geometry compensated deformation index was cal-culated by dividing deformation by end diastolic diameter (S/EDD, Figure 1). Thisparameter was significantly reduced in patients with severe MR and this changewas most marked in the severe MR group with an ESD>4.5cm.
Fig. 1
Conclusions: S imaging index, corrected for geometry, could be a sensitive clin-ical tool in detecting subclinical deterioration in LV function in asymptomatic pa-tients with severe MR.
P5552 Prognostic value of non invasive studies in diabeticpatients assessed for simultaneous kidney-pancreastransplantation: 5 year experience of a single centre
A. Luz, F. Oliveira, L.S. Martins, M. Teixeira, H. Carvalho, S. Torres,A. Albuquerque, L. Gomes on behalf of Kidney-Pancreas Transplant
Team. Hospital Sto. Antonio, Porto, Portugal
Background and Purposes: Cardiac events are the leading cause ofdeath among patients undergoing simultaneous pancreas-kidney transplantation(SPKT), and different algorithms for coronary artery disease (CAD) detectionhave been described in the pre-transplant setting. We wanted to evaluate theprognostic value of myocardial perfusion scintigraphy (MPS) or dobutamine stressechocardiography (DSE) on cardiac risk stratification among candidates awaitingSPKT, on future myocardial infarction or cardiac death, at the single active centreof SPKT in our country.Materials and Methods: Records of 43 type 1 diabetic adult patients with endstage renal disease who underwent SPKT were reviewed, from the beginningof the program (May/2000) to July/2005. Mean age of candidates was 33,3±6.3years-old, 61% were female. Mean time of diabetes and dialysis evolution was
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

e-Poster session 10 983
23±14,2 years and 34.4±24.1 months, respectively. All had a non-invasive riskstratification within 6 months before surgery. 39 candidates were screened withMPS, 4 with DSE, along with a clinical evaluation plus ECG and standardechocardiogram. Coronary angiography was ultimately performed in 9 patients.Significant CAD was diagnosed if > 50% luminal stenosis was seen in a majorepicardial artery. We searched for major cardiac events (fatal or non-fatal infarc-tion, cardiac death) from date of surgery to December 2005 (mean follow-up time:2,53 years).Results: All candidates had normal left ventricular ejection fraction. Overall, 1DSE and 4 MPT were positive for ischemia, but significant CAD was diagnosedin only one MPS positive patient; intervention with stenting (PCIS) was then per-formed. Of the remaining 38 negative tests, 4 patients went on angiography: 1for angina-like chest pain (normal angio), two with new abnormal segmental wallmotion on standard echo while on awaiting list (PCIS in one patient, normal angioin the other) and 1 patient with previous MI (right coronary artery chronic total oc-clusion). Until now, we registered 3 deaths, two were non cardiac (septic shock)and one sudden death (a patient with failure of both grafts, again in dialysis, withpast PCIS due to new segmental wall abnormalities). No post-mortem evaluationwas carried on. No other major cardiac events were seen in this post-transplantcohort.Conclusions: In our experience, no major cardiac events were seen in the peri-operative and follow-up period of SPKT patients with pre-surgery normal left ven-tricular function and a negative MPT or DSE test. Coronary angiography shouldonly be dictated by clinical circumstances or a positive test for ischemia.
P5553 Left ventricular torsion in chronic mitral regurgitation:a potential marker for timing of mitral valve surgery
A.N. Borg, M.R. Yusoff, S.M. Deepak, D.J. Fox, S.G. Williams,S.G. Ray. Manchester, United Kingdom
Introduction: Left Ventricle (LV) torsion can be assessed by ultra-sonic 2D speckle tracking. Torsion is a sensitive index of LV function that couldbe useful in detecting early ventricular decompensation in chronic mitral regurgi-tation (MR).Methods: 14 patients with chronic moderate-severe MR secondary to mitral valveprolapse (aged 63 ± 12 years) and 14 age-matched controls (CONTR) were stud-ied. Short axis images of the LV at the level of the mitral valve and apex wereobtained. Torsion was plotted as the relative rotation of apex compared to baseat isochronal points. Peak systolic torsion (PST), peak systolic torsional velocity(PSTV), peak untwisting velocity (PUV) and time to PST (T-PST), corrected forheart-rate, were measured. Patients were further subdivided according to currentcriteria for mitral valve surgery, ie presence of symptoms, LV end-systolic diam-eter ≥ 4.5 cm, EF ≤ 60%: GROUP 1 (n=9) patients have not yet reached thesetime points, while GROUP 2 (n=5) require surgery.Results: There was no difference between patients and CONTR in all measuredtorsion parameters. PST in GROUP 1 (13.56 ± 6.82°) was increased comparedto CONTR (7.66 ± 3.04°, p=0.015) and to GROUP 2 (6.94 ± 5.65°, p=0.02).PSTV was also increased in GROUP 1 (75.04 ± 36.16°/s) compared to CONTR(47.53 ± 22.6°/s, p=0.03), and tended to increase compared to GROUP 2 (47.12± 28.39°/s, p=0.096). T-PST was decreased in GROUP 1 (334 ± 48) comparedto CONTR (368 ± 56, p=0.017). There were no differences in all measurementsbetween GROUP 1 and CONTR. PUV was the same in all subgroups.
Fig. 1. peak systolic torsion.
Conclusion: Systolic torsion is increased in compensated severe MR but de-clines to control levels as the LV decompensates. Alterations in systolic torsionmay be useful in timing mitral valve surgery.
P5554 Tissue Doppler imaging for risk stratification ofpatients with left ventricular systolic dysfunction withor without restrictive mitral flow
F.L. Dini, U. Conti, D. Andreini, S. Banti, P. Fontanive, R. Arena,S.M. De Tommasi. Cardiovascular Diseases Unit 2, Santa Chiara
Hospital, Pisa, Italy
Background: It is interesting to investigate whether the combined assessment of
mitral blood flow and tissue Doppler (TD) mitral annular velocities adds to prog-nostic stratification of patients with or without restrictive mitral flow.Aim: To evaluate the usefulness of early mitral annulus diastolic velocity (Ea) forpredicting the outcome of patients with left ventricular (LV) systolic dysfunction.Methods: Echocardiograms were obtained in 281 patients with LV systolic dys-function (ejection fraction <45%) in sinus rhythm. Restrictive mitral flow was de-fined by an E wave deceleration time (EDT) <140 msec. The nonrestrictive pat-tern was defined as E/A ratio </= 1 or E/A ratio >1 with EDT >/= 140 msec.TD velocities were acquired at the septal and lateral annular sites. Patients werefollowed-up for a median of 21 months. The primary end-point was cardiac death,the secondary end-point was cardiac death or hospitalization for worsening heartfailure (HF). Survival and event-free survival analyses were performed by univari-ate and multivariate Cox models and by the Kaplan-Meier method.Results: There were 24 (9%) cardiac deaths and 37(13%) hospitalizations forworsening HF. In multivariate analysis, older age, advanced NYHA class, LV ejec-tion fraction <25%, restrictive physiology and septal Ea <8 cm/sec were inde-pendent predictors of the combined end-point. When, demographics, clinical andechocardiographic measures were analyzed in hierarchic order, EDT <140 msecand Ea <8 cm/sec yielded the most valuable contributions in predicting the end-point (global chi-square from 35.7 to 51.21). In the nonrestrictive group (n=187;67%), Ea <8 cm/sec was the only independent echocardiographic predictor ofcardiac death or HF hospitalization. At 24 months, survival was 82% in those withrestrictive mitral flow, 92% in those with nonrestrictive mitral flow and a septalEa <8 cm/sec and 97% in those with nonrestrictive filling and a septal Ea >/=8cm/sec (Log-rank statistics =0,0082). Event free-survival was 59% in the restric-tive group, 76% and 92% in the nonrestrictive group with and without reduced Ea(Log-rank statistics <0,0001).Conclusion: The use of TD imaging of mitral annular diastolic velocities providesincremental information in patients with LV systolic dysfunction. In patients withnonrestrictive mitral flow, a reduced Ea velocity seems valuable for risk stratifica-tion.
P5555 A simple Doppler echocardiography method toevaluate pulmonary capillary wedge pressure inpatients with atrial fibrillation
M. Senechal, K. O’connor, J. Deblois, J. Magne, S. Bergeron,G. O’hara, J.G. Dumesnil, P. Pibarot. Laval Hospital, Cardiology
Department, Sainte-Foy, Canada
Purpose: Non-invasive estimation of pulmonary capillary wedge pressure (WP)in patients with atrial fibrillation (AF) is possible, but proposed formulas are com-plex and difficult to apply in routine clinical practice. The ratio of early mitral flowdiastolic velocity (E) to mitral annulus early diastolic velocity (E’) is a simple wellaccepted method to estimate WP in patients in sinus rhythm but few studies haveevaluated its feasibility and reliability in patients with AF.Methods: Twenty-four consecutive patients with AF with a Swan-Ganz catheterin place were studied. Of these, 22 were in the early postoperative phase of car-diac surgery and 19 had paroxysmal AF. Mitral inflow velocity was measured bypulsed wave Doppler and mitral annulus velocity was measured at the lateral andmedial aspects of the annulus by tissue Doppler imaging (TDI). The E/E’ ratiowas determined by 2 methods: 1) using the E and E’ velocities averaged over asample of 10 cardiac cycles; 2) using E and E’ obtained in the cycle of the samplewith the longest RR interval. WP was measured by catheter within 5 minutes ofechocardiographic evaluation.Results: Correlations of WP with E/E’ measured at the medial (r=0.47, p=0.021)or lateral (r=0.49, p=0.016) aspect of the mitral annulus were similar. ROC curvesfor prediction of WP > 15 mm Hg showed areas under the curve of 0.77 and 0.82respectively for the 10-cycle and 1-cycle methods when using E’ measured atthe lateral aspect, whereas the corresponding values were both 0.84 when usingE’ measured at the medial aspect. The best sensitivity and specificity were ob-tained with the E/E’ ratio measured at the medial aspect using the 1-cycle method(longest RR interval: mean RR interval 631±94 ms, heart rate 98±15/min): E/E’ratio > 16 predicted a wedge pressure > 15 mm Hg with a sensitivity of 91% andspecificity of 85%.Conclusions: The best performance for the prediction of elevated WP in patientswith atrial fibrillation is obtained with E/E’ measured in the cardiac cycle with thelongest RR interval using E’ measured at the medial aspect of the mitral annulus.This method is simple and accurately estimates WP in this population.
P5556 Strain rate imaging reveals right ventricular stunningassociated with troponin release after acutepulmonary embolism
T.C. Poerner1 , E. Koletzki2, I. Boehnisch2, B. Goebel1, D. Haghi2,H.R. Figulla1. 1University Hospital of Jena, Division of Cardiology,
Jena, Germany; 2University Hospital of Mannheim, Division of Cardiology,Mannheim, Germany
This study aimed to assess regional right ventricular (RV) myocardial functionand to investigate potential mechanisms associated with cardiac troponin releaseafter acute pulmonary embolism (APE).Methods: Conventional echocardiography with tissue Duppler and strain rateimaging (TDE/SRI) of basal, mid-wall and apical segments of free RV wall was
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

984 e-Poster session 10
performed in 72 consecutive patients with APE confirmed by computer tomogra-phy (CT). Strain and systolic strain rate were given as mean between peak valuesof the 3 RV segments. Post-systolic shortening (PSS), as typical pattern of acutetransmural ischemia, was defined as peak strain < 15% with a ratio post-systolicstrain/overall strain > 0.3. Serum troponin I (TnI) was determined in all patientson admission.Results: Pathologic TnI levels > 0.4 mcg/l were detected in 13 patients. TnI lev-els were significantly higher in patients presenting with PSS (0.46 ± 0.12 mcg/l)compared to the group without PSS (0.14 ± 0.04 mcg/l, p = 0.001, Fig. 1 - right).As shown in Fig. 1 - left, predictors for elevated TnI due to APE were: massiveextent of APE on CT scan (area under ROC curve [AUC] = 0.75, p = 0.004), thenumber of RV segments showing PSS (AUC = 0.71, p = 0.017) and the peak RVstrain (AUC = 0.72, p = 0.013), while the pressure gradient of tricuspid regurgi-tation, RV enddiastolic diameter and the visually assessed RV wall motion scorewere not predictive.
Figure 1
Conclusions: (1) The association between PSS and elevated TnI demonstratesthe role of severe persistent myocardial ischemia as the underlying mechanismof RV stunning. (2) Evaluation of RV mechanics by TDE/SRI is superior to visualassessment and gives insights into the pathophysiology of RV injury after APE.
P5557 Increased matrix metalloproteinase plasma levels areassociated with restrictive physiology in patients withdilated cardiomyopathy
S. Buralli1, F.L. Dini2, U. Conti1, S. Favilla2, P. Donati2, S. Taddei2 ,S.M. De Tommasi1 . 1Department of Internal Medicine, University of
Pisa, Pisa, Italy; 2Cardiovascular Diseases Unit 2, Santa Chiara Hospital, Pisa,Italy
Background: Left ventricular (LV) remodeling and the progression of LV dysfunc-tion are accompanied by alterations in myocardial extracellular matrix with eleva-tion in various matrix metalloproteinases (MMP) species. Plasma levels of MMP-3(stromelysin) have been found increased in patients with dilated cardiomyopa-thy, but information are lacking as regards their relationships with Doppler andechocardiographic parameters.Aim: To assess the relationships of MMP-3 and echo-Doppler parameters in pa-tients with either idiopathic or ischemic cardiomyopathy.Methods: MMP-3 and tissue inhibitors of metalloproteinases (TIMPS) plasmalevels were determined using high-sensitivity enzyme-linked immunosorbent as-say techniques in 36 consecutive patients diagnosed with heart failure (HF)due to dilated cardiomyopathy (58% ischemic). A complete M-mode and two-dimensional Doppler echocardiographic study was carried out in all patients.Results: Median plasma levels of MMP-3 and TIMPS were 22±18 ng/ml and4±3 ng/ml, respectively. Patients with symptomatic HF exhibited significant higherMMP-3 plasma levels; 37 ±24 ng/ml vs 21±9 ng/ml, p=0.016. As regards Dopplerand echocardiographic parameters, restrictive physiology and a low ratio of LVwall thickness to cavity radius (h/R <0.33) were associated with higher levels ofMMP-3; 38 ±24 ng/ml vs 21± 9 ng/ml, p=0.016 and 37 ±25 ng/ml vs 22±11ng/ml, p=0.033, respectively. No significant association was observed betweenTIMPS plasma levels and echo-Doppler variables in the study group. In patientsdivided according to MMP-3 median value, cardiac death or hospitalization forworsening HF occurred in 7 patients with higher MMP-3 levels and in 2 with lowerlevels.Conclusion: Among patients with dilated cardiomyopathy, those with signs andsymptoms of HF, restrictive mitral flow and reduced h/R ratio exhibited significantincreases in the plasma levels of MMP-3.
P5558 Left ventricular circumferential strain and rotation byultrasonic speckle tracking: An early marker ofdecompensation in chronic mitral regurgitation?
A.N. Borg1, M.R. Yusoff1, S.M. Deepak1, D.J. Fox2, S.G. Williams2,S.G. Ray2. 1Wythenshawe Hospital, Cardiology, Manchester, United
Kingdom; 2Manchester Heart Centre, Cardiology, Manchester, United Kingdom
Introduction: The early signs of left ventricular (LV) decompensation in chronicmitral regurgitation (MR) are difficult to detect with conventional echocardiogra-phy. Two-dimensional speckle tracking by ultrasound is a validated method for as-
sessment of circumferential deformation and rotation, which may be early mark-ers of functional deterioration.Methods: Echocardiographic parasternal short axis cuts of the left ventriclewere obtained for analysis by speckle-tracking. Global peak circumferential strain(PCS) and strain rate (PCSR), peak systolic rotation (PSR), rotation rate (PSRR)and untwisting rotation rate (PURR) were measured from base and apex.Results: 18 patients with chronic mitral regurgitation (aged 64 ± 12 years) sec-ondary to mitral valve prolapse and 18 age-matched controls (CONTR) were stud-ied. GROUP 2 (n=11) patients had reached one or more of the following criteriafor mitral valve surgery, while GROUP 1 (n=7) had none: presence of symptoms,LV end-systolic diameter ≥ 4.5 cm, EF ≤ 60%. At the base, PCS, PCSR, PSR andPSRR were all increased in GROUP 1 compared to CONTR (p<0.03), whereasvalues in GROUP 2 were similar to CONTR. At the apex, PCS and PCSR weresimilarly increased in GROUP 1 compared to CONTR (p<0.05), but reverted tocontrol values in GROUP 2. Apical rotation was similar for all 3 groups. PURRwas similar in all groups at both base and apex.
Fig. 1. Basal peak systolic rotation rate.
Conclusions: The onset of symptoms or depressed LV function with severe MRis associated with the normalisation of previously enhanced systolic circumfer-ential deformation and basal rotation. These measurements may be useful addi-tional markers of LV decompensation.
P5559 Tissue Doppler Imaging study assessment andN terminal pro-brain natriuretic peptide concentrationin the assessment of right ventricle function inpatients with dilated cardiomyopathy
J.U. Nowak, W. Streb, P. Rozentryt, A. Sliwinska, M. Kalinowski,L. Polonski, M. Zembala, T. Kukulski. Silesian Center for Heart Disease, 3rd Deptof Cardiology, Zabrze, Poland
Background: Right ventricle (RV) function in patients with dilated cardiomyopa-thy is not sufficiently explored. Tissue Doppler Imaging (TDI) may be useful in theevaluation of RV deformation in this cohort of patients.Thus the aim of the study was evaluate the RV function by TDI in patients withDCM and mild or moderate heart failure (HF).Methods: 29 consecutive patients were examined (27 men and 2 women, age46.6±12 yr, NYHA II - 24 pts, NYHA III - 5 pts, RV 30.2±4.2 mm, EDV 248.4±62ml, ESV 176.6±52 ml, EF 29.4±7.9%). The patients were divided into two groupsbased on NT-proBNP concentration (ECLIA technique) - Group I (n=19), withNT-proBNP ≥500 pg/ml (mean NT-proBNP 2372.7±724 pg/ml) and Group II(n=10) with NT-proBNP<500 pg/ml (mean NT-proBNP 240±177 pg/ml). The Tis-sue Doppler data were acquired from four chamber view for basal, medial andapical segments of free RV wall. The maximal and mean velocity (VEL), strain(S) and strain rate (SR) were calculated for ejection period. For the comparisonof both groups the analysis of variance was used.Results: The TDI parameters (strain, strain rate) of the medial and apical seg-ments of free RV wall were statistically significantly different between both groups.In patients with elevated NT-proBNP strain and strain rate had lower values -results are presented in the table below. No such differences were found for thesame parameters in basal segments.
Results of TDI for free RV wall
Apical segment Medial segment Basal segmentGroup I Group II Group I Group II Group I Group II
S max overall -0.19* -0.3* -0.146* -0.286* -0.149 -0.069SR max S -1.071 -1.56 -0.989* -1.551* -1.073 -0.996SR mean -0.494* -0.827* -0.449* -0.851* -0.564 -0.406S max S -0.17* -0.291* -0.13* -0.246* -0.14 -0.059S mean S -0.109* -0.193* -0.078* -0.150* -0.087 -0.033VEL max S 0.049 0.052 0.063 0.071 0.075 0.082VEL mean S 0.028 0.026 0.034 0.04 0.043 0.049
*= p<0.05
Conclusion: TDI parameters such as strain and strain rate during systole maybe useful in the assessment of segmental RV deformation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022

e-Poster session 10 985
P5560 Diastolic myocardial velocity of tissue Dopplerimaging predicts left ventricular revere remodelingafter one year repair or replacement in patients withsevere mitral insufficiency
M. Wang1, G. Yip2, I. Wan2, S. Wan2, C.M. Yu2, J.E. Sanderson3,A.A. Arifi3. 1The Chinese University of Hong Kong, Medical And TherapeticsDept., Hong Kong, People’s Republic of China; 2The Chinese University ofHong Kong, Medicine and Therapeutics, Hong Kong, China, People’s Republicof; 3Keele University Medical School, Cardiology, North Staffordshire, UnitedKingdom
Background: The importance of preservation of mitral valve subvalvular appara-tus for maintaining normal LV mechanics and contractile function has been em-phasized. Tissue Doppler imaging (TDI) provides rapid assessment of LV longaxis function, and the early diastolic mitral annulus velocity (Em) reflects myocar-dial relaxation and is relatively load-independent. We hypothesis that TDI is usefulto predict LV reverse remodeling after one year valve repair or replacement in pa-tients with mitral insufficiency.Methods: 103 patients undergoing isolated surgical correction of mitral insuffi-ciency by either mitral valve repair or complete chordal preserved replacementwere prospectively studied. Echocardiography with TDI systolic and diastolic ve-locities at basal myocardial segments was done preoperatively, 1 week, 3, 6, and12 months post operatively. LV ejection fraction by Simpson’ method (LVEF2d)was also determined.Results: 50 patients (30 male, mean age 59 ± 12 yrs) had MV repair. 53 pa-tients (20 male, mean age 52 ± 12 yrs) had completed subvalvular preservedreplacement. There was no significant difference between two groups in LVEF2d,LV end diastolic and systolic volume index (LVVd/LVVs index), left atrial diameterin systole (LADs), LVmass and ellipsoid index both in diastole and systole (EIdand EIs) preoperatively. After operation, LVEF2d, LVVd index and LADs signif-icantly decreased, EId/EIs significant increased over the time points comparedto baseline both groups. However, there were no differences in all variables ateach time point between the two groups. Em at baseline was significantly higher(7.4 ± 2.3 vs. 6.1 ± 1.8 p<0.05) in patients with LV reverse remodeling groupsafter one year (defined by LVVd reduction≥10%). Em ≥5.5cm/s provided inde-pendent and incremental value to predict LV revere remodeling [95%CI: 0.1(0.01to 0.5); p = 0.009] after adjusting for clinical risk factors (Age, mitral valve pro-lapse, rheumatic heart disease, ischaemic heart disease, Endocarditis and AF),LVEF2d<60%, LADs≥4.5cm and Sm≥5.5cm/sConclusion: Mitral valve replacement with total chordal preservation is compara-ble to mitral valve repair and both provide equivalent protection to the left ventricu-lar geometry and preservation of left ventricular systolic function. An Em≥5.5cm/scan predict LV revere remodeling at one year post surgery and is superior toLVEF2d and LADs.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/suppl_1/827/2887178 by guest on 02 February 2022