
Verification of the fetal valproate syndrome phenotype
15
American Journal of Medical Genetics 29171-185 (1988) Verification of the Fetal Valproate Syndrome Phenotype Holly H. Ardinger, Joan F. Atkin, R. Dwain Blackston, Louis J. Elsas, Sterling K. Clarren, Susan Livingstone, David B. Flannery, John M. Pellock, Mary Jo Harrod, Edward J. Lammer, Frank Majewski, Albert Schinzel, Helga V. Toriello, and James W. Hanson Division of Medical Genetics, Department of Pediatrics, University of Iowa, Iowa City (H.H.A., J. W. H.); Division of Medical Genetics, Department of Pediatrics, University of Virginia, Charlottesville (J. F. A.); Division of Medical Genetics, Department of Pediatrics, Emory University, Atlanta (R. D. B., L. J. E.); Department of Pediatrics, University of Washington, Seattle (S. K. C., S. L.); Department of Human Genetics (0. B. F.) and Division of Child Neurology, Department of Neurology (J.M.P.), Medical College of Virginia, Richmond; Department of Obstetrics and Gynecology, University of Texas, Dallas (M.J.H.); Embryology/ Teratology Unit, Massachusetts General Hospital, Boston (E. J. L .); Institute of Human Genetics, Dusseldorf, Federal Republic of Germany (F. M.); Department of Medical Genetics, University of Zurich (A. S.); Genetics/Birth Defects/Neurology Clinic, Blodgett Memorial Medical Center, Grand Rapids, Michigan (H. V. T.) We have evaluated 19 children who were exposed to valproic acid (VPA) in utero to look for manifestations of a fetal valproate syndrome (FVS), as proposed by Di Liberti et al. [1984]. We found no consistent alterations of pre- or postnatal growth with exposure to VPA monotherapy. Postnatal growth deficiency and microcephaly were present however, in two thirds of children exposed to VPA in combination with other anticonvulsants. Developmental delay or neurologic abnormality was found in 71% of those exposed to VPA monotherapy, and in 90% of those exposed to VPA and other anticonvulsants. Craniofacial anomalies, which can be seen with other anticonvulsant exposures, including midface hypoplasia, short nose with a broad and/or flat bridge, epicanthal folds, minor abnormalities of the ear, philtrum or lip, and micrognathia were also found in infants whose mothers used VPA. Prominent metopic ridge and Presented in part at the Society for Pediatric Research meetings, San Francisco, May, 1984. Received for publication April 20, 1987; revision received July 17, 1987. Address reprint requests to Dr. Holly H. Ardinger, Division of Medical Genetics, Department of Pediatrics, University of Iowa, Iowa City, IA,52242. 0 1988 Alan R. Liss, Inc.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Verification of the fetal valproate syndrome phenotype

American Journal of Medical Genetics 29171-185 (1988)
Verification of the Fetal Valproate Syndrome Phenotype
Holly H. Ardinger, Joan F. Atkin, R. Dwain Blackston, Louis J. Elsas, Sterling K. Clarren, Susan Livingstone, David B. Flannery, John M. Pellock, Mary Jo Harrod, Edward J. Lammer, Frank Majewski, Albert Schinzel, Helga V. Toriello, and James W. Hanson
Division of Medical Genetics, Department of Pediatrics, University of Iowa, Iowa City (H. H. A., J. W. H.); Division of Medical Genetics, Department of Pediatrics, University of Virginia, Charlottesville (J. F. A.); Division of Medical Genetics, Department of Pediatrics, Emory University, Atlanta (R. D. B., L. J. E.); Department of Pediatrics, University of Washington, Seattle (S. K. C., S. L.); Department of Human Genetics (0. B. F.) and Division of Child Neurology, Department of Neurology (J. M. P.), Medical College of Virginia, Richmond; Department of Obstetrics and Gynecology, University of Texas, Dallas (M. J.H.); Embryology/ Teratology Unit, Massachusetts General Hospital, Boston (E. J. L .); Institute of Human Genetics, Dusseldorf, Federal Republic of Germany (F. M.); Department of Medical Genetics, University of Zurich (A. S.); Genetics/Birth Defects/Neurology Clinic, Blodgett Memorial Medical Center, Grand Rapids, Michigan (H. V. T.)
We have evaluated 19 children who were exposed to valproic acid (VPA) in utero to look for manifestations of a fetal valproate syndrome (FVS), as proposed by Di Liberti et al. [1984]. We found no consistent alterations of pre- or postnatal growth with exposure to VPA monotherapy. Postnatal growth deficiency and microcephaly were present however, in two thirds of children exposed to VPA in combination with other anticonvulsants. Developmental delay or neurologic abnormality was found in 71% of those exposed to VPA monotherapy, and in 90% of those exposed to VPA and other anticonvulsants. Craniofacial anomalies, which can be seen with other anticonvulsant exposures, including midface hypoplasia, short nose with a broad and/or flat bridge, epicanthal folds, minor abnormalities of the ear, philtrum or lip, and micrognathia were also found in infants whose mothers used VPA. Prominent metopic ridge and
Presented in part at the Society for Pediatric Research meetings, San Francisco, May, 1984.
Received for publication April 20, 1987; revision received July 17, 1987.
Address reprint requests to Dr. Holly H. Ardinger, Division of Medical Genetics, Department of Pediatrics, University of Iowa, Iowa City, IA,52242.
0 1988 Alan R. Liss, Inc.

172 Ardinger et al.
outer orbital ridge deficiency or bifrontal narrowing and certain major anomalies such as tracheomalacia, talipes equinovarus (with intact spine) and lumbosacral meningomyelocele seem to be peculiar to infants with VPA exposure. Other defects such as urogenital anomalies, inguinal or umbilical hernias, and minor digital anomalies that are common to other prenatal anticonvulsant exposures are also occasionally found in those exposed to VPA. Heart defects have been found in infants exposed to nearly every class of anticonvulsant although the types of defects associated with maternal VPA use may be clarified when classified by pathogenetic mechanism. Our findings overall are in agreement with the report of Di Liberti et al. [1984].
Key words: birth defect, epilepsy, spina bifida, teratogen, anticonvulsant
Valproic acid (VPA) is a relatively new anticonvulsant, having been approved for use in the United States in 1978. The main indication for its use is in treatment of absence seizures although it has been used in a variety of seizure disorders, often in combination with other anticonvulsants. Although VPA, as a carboxylic acid, is structurally unrelated to other kinds of anticonvulsant drugs, prenatal exposure to it, like other prenatal anticonvulsant exposures, has been associated with congenital malformations in laboratory animals [Brown et al., 1980; Kao et al., 1981: Diaz and Shields, 1981; Bruckner et al., 1983; Paulson et al., 19851. VPA is known to cross the human placenta and is present in higher concentration in the infant than in the mother [Dickinson et al., 1979; Nau et al., 19811.
Single case reports of birth defects occurring in offspring of women taking VPA during pregnancy have been published since 1980 suggesting that VPA might have teratogenic properties in humans as well [Dalens et al., 1980; Gomez, 1981; Thomas and Buchanan, 1981; Clay et al., 1981; Stanley and Chambers, 1982: Bailey et al., 1983; Blaw and Woody, 1983; Bantz, 1984: Garden et al., 1985; Tein and MacGregor, 19851. In September, 1982, utilizing data from the Birth Defects Surveillance Program in Lyon, France, for the years 1976 and 1978-1982, Robert and Guibaud [ 19821 reported that an unusually high proportion of infants with spina bifida were born to women with epilepsy treated with VPA. Further analysis of these data [Robert et al., 19841 and data from other birth defect registries [Bjerkedal et al., 1982; CDC, 19821 has confirmed this association and has led to an estimated risk of spina bifida of 1-2% in children of women using VPA during pregnancy. The risk is similar to the recurrence risk for a family with one child with an open spinal defect so that prenatal testing for open spinal defects is recommended for women using VPA during the first trimester [CDC, 1983; AAP, 19831.
Other major malformations reported in association with prenatal VPA exposure from the Lyon birth defects registry include cardiac defects (relative risk 4.3) and oral clefts (relative risk 5.4) [Robert and Rosa, 19831. Minor anomalies have been enumerated in single case reports, although a comprehensive definition of a fetal valproate syndrome (FVS) was not available with photographs until recently. Di Liberti et al. [ 19841 described seven children with prenatal VPA exposure who had a consistent facial phenotype including epicanthal folds, flat nasal bridge, small upturned nose, long upper lip, shallow philtrum, thin upper lip and downturned mouth. They also suggested an association with other anomalies including low birth weight, psychomotor delay, congenital heart defects, neural tube defects, hypospadias, strabismus and nystagmus. A prospective study of 14 infants with prenatal VPA exposure showed a similar pattern of craniofacial anomalies and suggested that fetal growth was not affected. The risk for perinatal distress increased with increased dose of VPA and the number of minor anomalies appeared to be dose

Fetal Valproate Syndrome 173
related [Jager-Roman et al., 19861. We present data from 19 infants born to 18 mothers with seizure disorders who took VPA during pregnancy which verifies and extends the phenotype of FVS.
METHODS
Case reports were collected after a general request was made for information on outcome of pregnancies associated with maternal valproate use. The cases come from diverse populations and it is not possible to calculate risk estimates for the various associated anomalies. We have not made an attempt to obtain a comparison group because our goal was to identify a group of abnormalities common to individuals with prenatal VPA exposure which may be subjected to future epidemiologic testing.
Our findings are presented in Table I. Four of the patients are described in short case reports to illustrate the variety of ways these children come to medical attention.
TABLE Ia. Manifestations of Eight Patients with Prenatal VPA Exposure Only
Clinical data (patient no.) 1 2 3 4 5 6 7 8 Total (7%)
Prenatal exposure Dose VPA/day (mg) Other anticonvulsants
Family history of birth defects and/or mental retardation
Growth Prenatal growth deficiency Prenatal growth excess Postnatal growth deficiency
Microcephaly Brain abnormality on CT scan,
ultrasound or autopsy Developmental delay and/or
neurologic abnormality
Prominent metopic ridge and/or trigonocephaly
Bifrontal narrowing Epicanthal folds Midface hypoplasia Short nose with anteverted
Broad or flat nasal bridge External ear abnormalities Flat philtrum Long philtrum Thin vermilion border Micrognat hia Oral cleft
Development
Craniofacial anomalies
nostrils
Respiratory tract abnormality Cardiovascular defect Abdominal wall defect Genital abnormality Limb abnormality Spinal defect
750 2,250 750 2,000 1,500 1,500 1,500 1,000 - - - - - - - -
- - + - ? ? ? -
- - ? ? + ? ? ?
- + ? + - + + +
+ + + + - + ? - + ? + + ? ? + + + + + + ? ? + ? - + - + ? ? + ?
+ + - + ? ? + + + + - + ? ? + + - + + + ? + + - - + - + ? + + -
? - i - + + - - - + - + ? + + ? + + + + ? + - ?
- - - + + - f - + + - - - - f - + + + + + + + -

TABL
E Ib
. M
anif
esta
tions
of 1
1 Pa
tient
s with
Pre
nata
l VPA
Plu
s Oth
er A
ntic
onvu
lsan
t(s) E
xpos
ure
Clin
ical
dat
a (p
atie
nt n
o.)
9 10
11
12
13
14
15
16
17
18
19
To
tal (
%)
Pren
atal
expo
sure
D
ose
VPA
/day
(m
g)
Oth
er a
ntic
onvu
lsan
ts*
Fam
ily h
isto
ry o
f birt
h de
fect
s an
d/or
men
tal r
etar
datio
n G
row
th
Pren
atal
gro
wth
def
icie
ncy
Pren
atal
gro
wth
exc
ess
Post
nata
l gro
wth
def
icie
ncy
Mic
roce
phal
y B
rain
abn
orm
ality
on C
T sc
an,
ultra
soun
d or
aut
opsy
D
evel
opm
enta
l del
ay an
d/or
ne
urol
ogic
abno
rmal
ity
Dev
elop
men
t
Cra
niof
acia
l ano
mal
ies
Prom
inen
t met
opic
ridg
e an
d/or
trig
onoc
epha
ly
Bifr
onta
l nar
row
ing
Epic
anth
al f
olds
M
id fa
ce h
ypop
lasi
a
Broa
d or
flat
nas
al b
ridge
Ex
tern
al e
ar a
bnor
mal
ities
Fl
at p
hiltr
um
Long
phi
ltrum
Th
in v
erm
illio
n bo
rder
M
icro
gnat
hia
Ora
l cle
ft
Shor
t nos
e w
ith a
ntev
erte
d no
stril
s
Res
pira
tory
trac
t abn
orm
ality
C
ardi
ovas
cula
r def
ect
Abd
omin
al w
all d
efec
t G
enita
l abn
orm
ality
Li
mb
abno
rmal
ity
SDin
al de
fect
? C
BZ,
PD
750
DPH
75
0 ?
DPH
,PD
,MS
PB
? PB
? 50
0 60
0 PB
D
PH,P
B
DPH
,CB
Z 30
0 PB
1,
500
DPH
.MPB
1,
250
CB
Z,A
Z
I
+a
-
? ?
? +
+ + -
died
-
-
-
+ di
ed
+ ?
-
6/10
(60
)
114
(25)
+ +
+ -
+ +
? ?
-
? ?
? ?
+
-
1011
1 (9
0)
+ +
+ +
+ +
+
+?
-
? -
?-
-
-?
+
? -
?+
?
+?
-
? -
?+
+
+?
-
+ -
?-
?
+?
-
? I
?-
?
-?
-
?
719
(78)
51
9 (5
5)
517
(71)
51
8 (6
2)
718
(87)
81
9 (8
9)
4/10
(40
) 31
8 (3
7)
317
(43)
51
8 (6
2)
118
(12)
1/
11 (
9)
2/11
(18
) 6
1 11
(54)
2/
11 (
18)
311
1 (2
7)
9/11
(81
) 3/
11 (
27)
+ + + + + + -
- + +
+ + 1
+ + + ? ?
+
++
-
+ -
-
-
-+
-
- I
-+
+
- +
+
*AZ
= ac
etaz
olam
ide,
CB
Z =
carb
amaz
epin
e, D
PH =
diph
enyl
hyda
ntoi
n. M
PB =
mep
hoba
rbita
l, M
S =
mes
anto
in, P
B =
phe
noba
rbita
l. P
D =
prim
idon
e, V
PA =
valp
roic
acid
. a
= si
blin
gs.
Fetal Valproate Syndrome 175
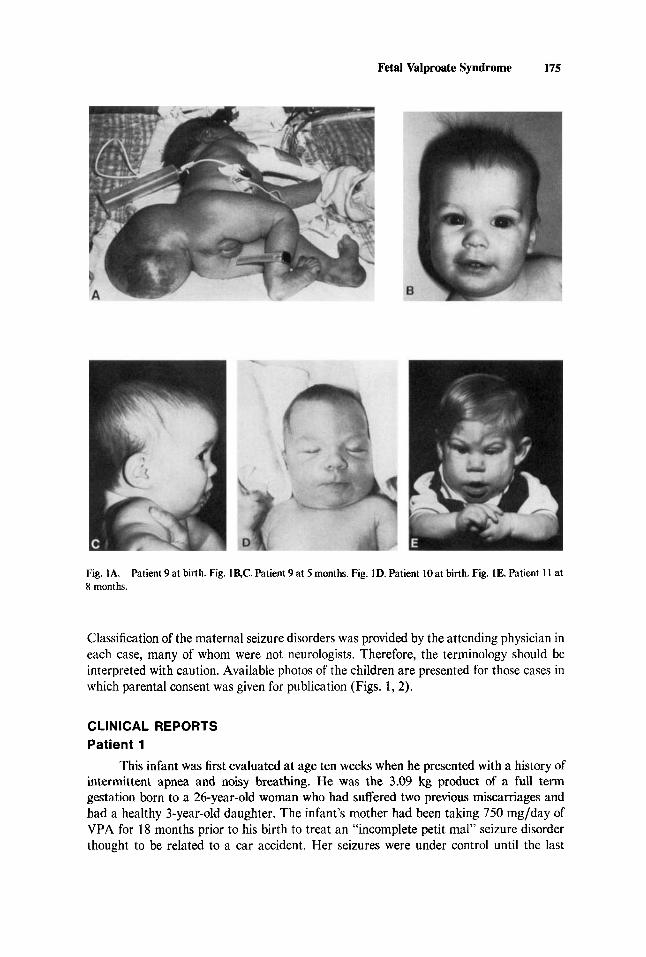
Fig. IA. 8 months.
Patient 9 at birth. Fig. lac. Patient 9 at 5 months. Fig. ID. Patient 10 at birth. Fig. 1E. Patient 11 at
Classification of the maternal seizure disorders was provided by the attending physician in each case, many of whom were not neurologists. Therefore, the terminology should be interpreted with caution. Available photos of the children are presented for those cases in which parental consent was given for publication (Figs. 1,2).
CLINICAL REPORTS Patient 1
This infant was first evaluated at age ten weeks when he presented with a history of intermittent apnea and noisy breathing. He was the 3.09 kg product of a full term gestation born to a 26-year-old woman who had suffered two previous miscarriages and had a healthy 3-year-old daughter. The infant’s mother had been taking 750 mg/day of VPA for 18 months prior to his birth to treat an “incomplete petit mal” seizure disorder thought to be related to a car accident. Her seizures were under control until the last
176 Ardinger et al.
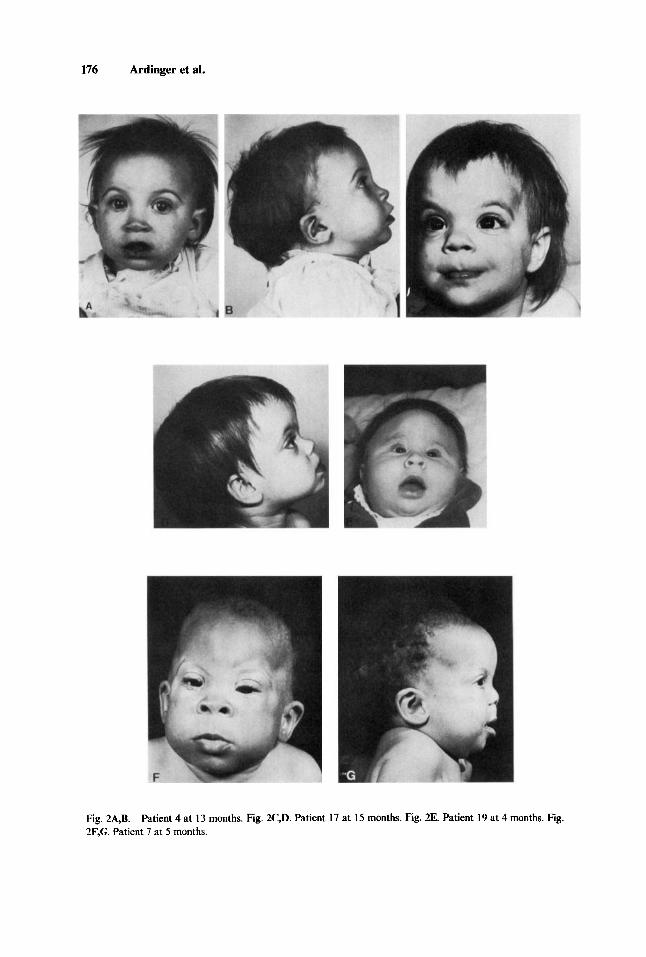
Fig. 2A.B. 2F,G. Patient 7 at 5 months.
Patient 4 at 13 months. Fig. 2C,D. Patient 17 at 15 months. Fig. 2E. Patient 19 at 4 months. Fig.

Fetal Valproate Syndrome 177
trimester of pregnancy when she had three to four convulsive episodes described as “mini-blackouts.” In addition, she inadvertently used oral contraceptive pills for the first 12 weeks of pregnancy and smoked one-half pack of cigarettes per day.
The infant’s first apneic episode occurred at age 13 days and he was subsequently placed on an apnea monitor. He had intermittent episodes of 20-30 sec of apnea which always resolved spontaneously. After three hospitalizations for respiratory ailments, he underwent a bronchoscopy which demonstrated tracheomalacia. Results of a head CT scan was normal. His growth and development was normal. Physical examination showed minor craniofacial anomalies (Table I).
Patient 9
(Figs. lA,B,C) This female infant was born to a 26-year-old primigravida who had a 12 year history of “petit mal” and grand ma1 seizures. She took primidone, carbamazepine and VPA during the first 14 weeks of her pregnancy. She had daily “petit mal” seizures throughout her pregnancy. She allegedly stopped the VPA after reading a newspaper article describing an increased risk of open spine defects associated with prenatal VPA exposure. An obstetrical ultrasound study subsequently showed that her fetus had a large sacral mass for which an elective cesarean section was performed at term.
The infant had Apgar scores of 7 and 8 at one and five minutes, respectively. Her birth weight was 3,240 g (55th centile) and her head circumference (OFC) was 31.8 cm (2nd centile). She had a large skin-covered low lumbosacral mass which measured 29 cm in circumference. She had a partial sensory deficit of S, and S2 and a complete sensory deficit of S3 through S5 segments. She had a motor deficit below L5. Spinal radiographs showed the vertebral bodies to be intact, but slightly widened. At surgery, two fluid-filled sacs were found within the mass, the smaller of which contained nerve roots that left the neural canal and attached to the sac. The defect was repaired and a brain ultrasound was found to be normal. Other remarkable physical features are listed in Table I.
On follow-up at five months, her OFC was 41 cm (30th centile) while her length and weight were at the 30th and 25th centiles, respectively. She tested low average to average on the Bayley Scales of Infant Development and the Wisconsin Behavior Rating Scale with expressive language skills being the greatest area of weakness. Motor skills were judged to be approximately one month below chronologic age. She was lost to further follow-up after the family moved away.
Patient 10 (Fig. 1D) This male infant was born to a 36-year-old gravida three woman. The
pregnancy was complicated by maternal epilepsy (underlying cause unknown) with monthly generalized convulsions. She took 750 mg/day of VPA and 500 mg/day of diphenylhydantoin (DPH) with blood levels recorded in the third trimester as VPA 19.1 mcgjml (normal range = 50-100) and DPH 18.1 mcg/ml (normal range = 1C-20). During two previous pregnancies, this mother’s epilepsy had been treated with DPH and phenobarbital and had resulted in the birth of a healthy son (who, at ten years, required special education), and the fetal demise of twin girls.
This infant was meconium stained at birth and required intubation for resuscitation. Apgar scores were 4 and 8 at one and five minutes, respectively. He had an uneventful course in the newborn nursery and was evaluated only because of his prenatal exposure to VPA. OFC was 36.2 cm (90th centile). Spine films were normal.
178 Ardinger et al.
At eight months, his OFC was 45.5 cm (50th centile) and his length and weight were in the 90th centile. He was mildly hypotonic and was at the six month developmental level by the Denver Developmental Screening Test. He began walking at 13 months and at 16 months his developmental skills were appropriate for age. His OFC was 47.5 cm (40th centile) and his height and weight were at the 50th centile.
Patient 11
(Fig. 1 E) This male infant was the 3 100 g product of a 37 week gestation born to a 22-year-old primigravida. Prenatal care was not sought until 23-24 weeks gestation. The mother was mentally retarded (cause unknown) and had a complex convulsive disorder consisting of both grand ma1 seizures and short staring spells. She was treated with VPA 750 mg/day, DPH 300 mg/day, primidone 1,500 mg/day and mesantoin 300 mg/day.
The infant was born via low forceps vaginal delivery with Apgar scores of 7 and 10 at one and five minutes, respectively. By age 24 hours, he had developed projectile vomiting and was transferred for evaluation. The vomiting resolved and he was found to have moderate gastroesophageal reflux on barium swallow. He was observed to have a poor suck and uncoordinated swallow and required gavage feeding.
He had a markedly abnormal facial appearance and distal phalangeal hypoplasia. Vertebral radiographs were normal. He was microcephalic with an OFC of 31 cm. A systolic heart murmur was thought to be functional.
He was placed in foster care and despite a caloric intake of up to 170 Kcal/kg/day (without vomiting or diarrhea), his length and weight fell to well below the 5th centile. At one month, he was noted to have large inguinal herniae and an incompletely descended left testis which were surgically corrected.
By four months he had obvious microrRphaly (OFC was 35 cm) with pronounced metopic ridging and asymmetry of his face. Skull radiographs did not conclusively show signs of premature synostosis.
At nine months, his gross motor skills were at the six and one-half month level with overall cognitive skills (using the Bayley Scales of Infant Development) of five to five and one-half months.
At 16 months, his heart murmur was re-evaluated and thought to be due to a small ventricular septa1 defect. His speech/language skills were judged to be at the seven month level while gross motor skills were at the ten month level. His OFC was 40.5 cm (50th centile for a 2 month old) and his length and weight persisted below the 5th centile. CT scan of his head showed evidence of premature fusion of the metopic sutures and asymmetry of the cranial structures but no gross brain abnormalities.
RESULTS
Table I summarizes the clinical findings among the 19 patients. In all cases, VPA was used in the first trimester and the total daily doses (where known) ranged from 300 to 2,250 mg, all probably under the maximum recommended dose of 60 mg/kg/day. In 8 pregnancies, VPA was used alone; in the other 1 1 pregnancies, it was used in combination with one or more different anticonvulsants. We looked for common abnormalities within the group of children as a whole and have also considered those children exposed to VPA monotherapy as a separate group (Group 1) from those exposed to VPA in combination with other anticonvulsants (Group 2).
Fetal Valproate Syndrome 179
Fetal VPA exposure does not seem to be strongly associated with prenatal growth deficiency since only one of 19 infants was small for gestational age. In fact, two infants from Group 1 and one infant from Group 2 were large at birth. Postnatal growth deficiency (6/8) and microcephaly (6/10) were found in children in Group 2, but none of the infants in Group 1. However, 15 of 18 children had mild to moderate developmental delay or neurologic abnormalities (five of seven (71%) of those in Group 1 and 10 of 11 (91%) of those in Group 2 ) . Abnormalities noted on brain CT scan included asymmetric lateral ventricles in Patient 4 and mild ventriculomegaly in Patient 18.
Common craniofacial anomalies in the group as a whole included prominent metopic ridging and/or trigonocephaly, bifrontal narrowing with an indentation (or deficiency) in the outer orbital ridge, midface hypoplasia, short and upturned nose, a broad and/or flat nasal bridge, thin vermilion border and flat and/or long philtrum. Minor abnormalities in ear position or shape were common as was relative micrognathia. Cleft lip and palate was present in only one patient (Patient 15).
Abnormalities of other systems, while not consistently present, were distinctive enough to warrant mention. Three unrelated infants exposed to VPA alone had significant stridor found to be due to tracheomalacia on bronchoscopy. A fourth infant from Group 2 had a lower respiratory tract anomaly (abnormal lung lobation) found on autopsy. Nearly one-half of all our cases had a documented or suspected cardiovascular abnormality. Although no one specific type of heart defect was present in each affected individual (Table 11), the 3 individuals with a precise anatomic diagnosis (Patients 4, 13, 17) all had lesions related by a similar mechanism of cardiac dysmorphogenesis (altered blood flow) as proposed by Clark [ 19861.
Inguinal hernias were observed in three patients in Group 1 and two patients in Group 2. A variety of genital anomalies were present in males. These consisted of second degree hypospadias (Patients 2, 4, 16), small penis (Patient 3), bifid scrotum (Patient 10) and cryptorchidism (Patient 16). One female infant (Patient 13) was found to have complete duplication of vagina, cervix and uterus at autopsy.
There were a number of minor limb anomalies of low frequency including clinodactyly (Patients 1, 14, 15 and 16), arachnodactyly (Patients 2, 4 and IS), camptodactyly (Patients 5 and 18), distal phalangeal hypoplasia (Patients 9, 11, 13, 16, and 17, all of whom were exposed to additional anticonvulsants), hyperextended terminal phalanges (Patient 6), small hands and feet (Patient 17) and “dysplastic” nails (Patient 18). Limb anomalies of more consequence included two cases of bilateral talipes
Table II. Types of Cardiovascular Lesions Associated With Prenatal Exposure to VPA
VPA alone Case 3 VSD Case 4
Case 11 VSD Case 12 Case 13 Hypoplastic left heart Case 15 Heart murmur Case 17 Case 18 Dysrhythmia
Membranous.VSD, mild CoA, PDA VPA in combination
Heart murmur and left axis deviation on ECG
Perhembranous VSD, PDA, mild PPS and persistent LSVC
CoA = coarctation of the aorta, LSVC = left superior vena cava. PDA = patent ductus arteriosus, PPS =
peripheral pulmonic stenosis. VSD = ventricular septa1 defect.

TABL
E III.
Com
paris
on o
f Man
ifest
atio
ns of
Pre
viou
slv R
ewrt
ed P
atie
nts T
o th
e Pr
esen
t Pat
ient
s
Tot
al
Gro
up 1
-VPA
on
ly
Gro
up 2-
VPA
pl
us o
ther
ant
imnd
sant
Clin
ical
dat
a L
itera
ture
* O
ur c
ases
To
tal
Lite
ratu
re*
Our
cases
Tota
l O
vera
ll
Pren
atal
expo
sure
D
ose
VPA
/day
(mg)
Oth
er an
ticon
vulsa
nts
Gro
wth
Pr
enat
al g
row
th d
efic
ienc
y Pr
enat
al g
row
th e
xces
s Po
stna
tal g
row
th d
efic
ienc
y
Mic
roce
phal
y B
rain
abn
orm
ality
on
CT
scan
or
aut
opsy
D
evel
opm
enta
l del
ay a
nd/o
r ne
urol
ogic
abn
orm
ality
Dev
elop
men
t
(n - 2
6)
300-
2,50
0 no
ne To
tal (
%)
5/25
(20
)
619
(66)
7/23
(30
)
1/24
(4)
111
(1W
518
(62)
(n =
9)
50&1
,500
D
PH;D
PH,P
B,C
BZ;
PD
( 3);
PD,C
BZ
PB,
CL;
MPB
;CB
Z
Tota
l (%
) To
tal (
%)
5/33
(15
) 21
9 (2
2)
3/32
(9)
119
(11)
6/
16 (
37)
216
(33)
7/30
(23
) 21
7 (2
9)
1011
5 (6
7)
112
(50)
(n =
11)
30
0-1,5
00
DPH
;DPH
,PB
DPH
, M
PB;D
PH,P
D,M
S;
DPH
,CB
ZPB
(4);
PD
,CB
Z;C
BZ,
AZ
Tota
l (%
) 1/
11 (9
) 3/
20 (
1 5)
618
(75)
8/
14 (5
7)
6/10
(60
) 8/
17 (
47)
1/11
(9)
2/20
(10
)
113
(33)
11
3 (3
3)
1011
1 (9
1)
11/1
3 (8
5)
8/53
(1 5
) 5/
52 (1
0)
14/3
0 (4
7)
15/4
7 (3
2)
317
(43)
21/2
8 (7
5)

Cra
niof
acia
l fea
ture
s Pr
omin
ent m
etop
ic ri
dge
2
trigo
noce
phal
y B
ifron
tal n
arro
win
g Ep
ican
thal
fold
s M
idfa
ce hy
popl
asia
Broa
d or
flat
nas
al b
ridge
Ex
tern
al ea
r abn
orm
aliti
es
Flat
phi
ltrum
Lo
ng p
hiltr
um
Thin
ver
mili
on b
orde
r M
icro
gnat
hia
Ora
l cle
ft
Shor
t nos
e with
ant
ever
ted n
ostri
ls
Res
pira
tory
trac
t abn
orm
ality
C
ardi
ovas
cula
r def
ect
Abd
omin
al wall
defe
ct
Gen
ital a
bnor
mal
ity
Lim
b ab
norm
ality
SD
inal
defe
ct
15/3
8 (3
9)
13/1
7 (7
6)
22/3
9 (7
6)
8/13
(61
) 24
/38
(63)
32
/45
(71)
22
/45
(49)
10
/23
(43)
17
/34
(50)
1013
1 (3
2)
21/3
7 (5
7)
1/54
(2)
5/54
(9)
14
/54
(26)
15
/54
(28)
15
/54
(28)
32
/54
(59)
2/19
(10
)
7/20
(80
)
9/21
(43
) 14
/22
(64)
10
121
(48)
21
5 (4
0)
8/18
(44
) 10
120
(50)
4/
17 (
23)
313
(100
)
-
0/26
(0)
01
26 (0)
5/26
(19
) 7/
26 (
27)
8/26
(31
)
7/26
(27
)
12/2
5 (4
8)
14/2
7 (4
6)
19/2
8 (6
8)
14/2
8 (5
0)
5/12
(42
) 1 1
/24
(46)
14
/26
(54)
9/
23 (
39)
0134
(0)
3/34
(9)
7/
34 (
21)
818
(100
)
315
(60)
1013
4 (2
9)
11/3
4 (3
2)
719
(78)
51
9 (5
5)
517
(71)
51
8 (6
2)
718
(87)
81
9 (8
9)
4/10
(40
) 31
8 (3
7)
317
(43)
51
8 (6
2)
118
(12)
1/
11 (9
) 2/
11 (
18)
2/11
(18
) 61
1 1 (5
4)
3/11
(27
)
8/12
(67
) 5/
9 (5
5)
1011
4 (7
1)
518
(62)
10
/1 I
(91)
13
/17
(76)
8/
17
(47)
5/
11 (
45)
6/10
(60)
7/
11
(64)
11
8 (1
2)
1/20
(5)
2/
20 (
10)
7/20
(35)
5/
20 (
25)
4/20
(20
) 14
/26
(54)
71
8 (8
7)
21/3
4 (6
2)
219
(22)
9/
11 (
81)
11/2
0 (5
5)
3/26
(1
1)
018
(0)
3/34
(9)
119
(11)
3/
11 (
27)
4/20
(20
) 7/
54 (
1 3)
*Ref
eren
ces G
roup
1: B
aile
y et
al.,
1983
; Ban
tz, 1
984;
Bla
w an
d W
oody
, 198
3; C
hess
a and
Iann
etti,
198
6; D
alen
s et a
l., 1
980;
Di L
iber
ti et
al.,
1984
; Gom
ez, 1
981;
Jage
r-R
oman
, et
al.,
1986
; Tei
n an
d M
acG
rego
r, 19
85. G
roup
2: C
lay
et a
l., 19
81; D
i Lib
erti
et al
., 19
84; N
au e
t al.,
1981
; Tho
mas
and
Buc
hana
n, 1
981.

182 Ardinger et al.
equinovarus (Patients 2 and 3) one case of bilateral pes cavus (Patient 5) without a concurrent spinal cord defect, and a duplicated thumb (Patient 7).
Spinal anomalies included two cases of low lumbosacral meningomyelocele (LS MMC) (Patients 9 and 16). In both cases, other anticonvulsants had been used in conjunction with VPA during pregnancy and in neither case was ventricular shunting for hydrocephalus required. One additional child, (Patient 12) had a single thoracic “butterfly” vertebra discovered radiographically after being observed to have a pilonidal sinus and hair tuft over the sacrum.
Table I11 summarizes the abnormalities reported in the literature of children born to mothers taking VPA during pregnancy and compares those children to our patients.
DISCUSSION
Our results support the concept of a fetal valproate syndrome (FVS) in agreement with the conclusions of Di Liberti et al. [ 19841.
The existence of a FVS has been questioned because VPA is often given in combination with other anticonvulsants and it is difficult to separate the effects of each anticonvulsant in a multiply-exposed child. In addition, some abnormalities may occur only as the result of an interaction between two or more anticonvulsants. We have compared these anomalies of our cases with the abnormalities reported to be associated with prenatal exposure to DPH, trimethadione, and phenobarbital or primidone [Schar- dein, 19851 and have found some notable differences (Table IV).
There are no consistent pre- or postnatal growth alterations with fetal exposure to VPA alone. Prominent metopic ridge and outer orbital ridge deficiency or bifrontal narrowing seem to be especially characteristic of VPA exposure. Minor abnormalities in position (“low set” or posteriorly angulated) or configuration of the ears (“squared-off” helices, prominent antihelices, upfolded lobes or lobular hypoplasia), long or flat philtrum, thin upper lip and micrognathid common in VPA exposure can also be seen in infants exposed to other anticonvulsants. Craniofacial anomalies common to each of the other anticonvulsant exposures including midface hypoplasia, short nose with a broad and/or flat nasal bridge and epicanthal folds are also seen in association with fetal VPA exposure.
Certain major anomalies in the infant seem to be more likely to be associated with maternal VPA use. These include respiratory tract anomalies such as tracheomalacia limb anomalies such as talipes equinovarus, genital anomalies, and cardiac defects. Although many of the cardiac defects in our group of patients were not fully characterized, there is a suggestion that defects related to altered embryonic blood flow might occur more frequently than expected among the group with heart defects associated with prenatal VPA exposure.
The spinal defects associated with fetal VPA exposure deserve special mention. We are not aware of any reports of a significant association of anencephaly with maternal VPA use. A recent review of data collected by 13 birth defect study groups supported the view that maternal VPA use is associated specifically with spina bifida rather than NTD’s in general [Lindhout and Schmidt, 19861. In most of the case reports in which locations were given, meningomyeloceles (MMCs) were either sacral or lumbosacral. In our two patients with MMCs, the defects were both low lumbosacral MMCs and both were skin covered. This raises the possibility that the influence of VPA is caudal to the posterior neuropore. In susceptible embryos, VPA may preferentially affect the process of

Fetal Valproate Syndrome 183
TABLE IV. A Comparison of Manifestations Seen In Prenatal Exwsure to Variom Antkonvulsants
VPA DPH TMD PBIPD
Growth deficiency Developmental delay Craniofacial abnormalities”
Prominent metopic ridge Outer orbital ridge deficiency Ptosis Upslanting eyebrows Ears abnormal position
abnormal configuration Long philtrum with thin lip Micrognathia Prognathism Oral clefts
Respiratory tract anomalies Congenital heart defects Inguinal or umbilical hernias Urogenital abnormalities Limb anomalies (miscellaneous)
Distal phalangeal hypoplasia Talipes equinovarus
Spinal defects
+ + - - + f
+ + - f
+ + + + + + +
-
+ +
+ +
+ + +
+ +
+ +
“Midface anomalies such as midface hypoplasia, short nose with a broad or flat nasal bridge and epicathal folds are associated with exposures to any of the four agents. VPA = valproic acid, DPH = diphenylhydantoin, TMD = trimethadione, PB/PD = phenobarbital/primidone.
canalization which forms the caudal end of the neural tube and occurs later in embryonic life than neurulation [Lemire et al., 19751. If this hypothesis can be substantiated, comparative studies of pathogenetic mechanisms responsible for spinal, cardiac, respira- tory and genital tract anomalies should be carried out to identify a possible common basis for dysmorphogenesis.
Several counseling issues are raised. First, the lower spinal defects may be associated with fewer handicaps later in life than the higher spinal defects. Neither of our patients with a MMC developed hydrocephalus and at least one was ambulatory in childhood. Secondly, defects resulting from canalization are often skin-covered. Prenatal testing for NTDs generally consists of screening for elevations of alpha fetoprotein amniotic Auid (AF). These values usually are normal in skin-covered lesions. Therefore, prenatal evaluation of a fetus exposed to VPA must include careful ultrasonography of the caudal fetal spine, even in the presence of normal AFP levels.
Unfortunately, at the present time, besides the 1% risk for lower spinal defects, we do not have risk figures for the various abnormalities to use in counseling women using VPA who are contemplating pregnancy. Some of the associated major malformations are detectable using sophisticated obstetrical ultrasonography (eg., neural tube defects, some forms of congenital heart defect). Other abnormalities such as developmental delay which occurs in 71-90% of exposed children, while of major importance to the child and its parents, cannot be predicted prenatally. In addition, there are no data regarding recurrence risk of any of the abnormalities should the mother decide not to use VPA in subsequent pregnancies. For example, if a woman using VPA during her first pregnancy gives birth to a child with a MMC, it is not known whether she is at increased risk for

184 Ardinger et al.
MMC in future children if she does not use VPA during those pregnancies. We attempted to summarize data from the case reports in the literature even though
few had complete clinical details and only 3 presented photographs [Di Liberti et al., 1984; Tein and MacGregor, 1985; Chessa and Iannetti, 19861. Many reports focused on the major anomalies and described either “facial dysmorphia” or made no comment at all on the facial appearance. Nevertheless, a similar pattern of associated malformations emerged (Table 111).
Definition of the FVS has been hampered by the lack of a comprehensive, prospective study of the outcomes of a large number of pregnancies during which the mother was on VPA. Even the European registries which were instrumental in detecting the increased risk of spina bifida in fetal VPA exposure have primarily monitored for major birth defects. In such a system, relatively subtle craniofacial alterations and abnormalities such as postnatal growth deficiency, developmental delay, and certain cardiac or respiratory tract defects which may only become apparent over time may be missed. Follow-up reports from Jager-Roman, et al., [ 19861 regarding the postnatal growth and mental development and the occurrence of any other health problems in their study of 14 VPA-exposed children will be quite valuable in this regard. In reviewing our cases, it is apparent that not all children with fetal VPA exposure have problems that would necessarily draw them to the attention of a pediatrician in the neonatal period, making ascertainment of associated problems even more difficult.
REFERENCES
American Academy of Pediatrics (AAP), Committee on Drugs (1983): Valproate teratogenicity. Pediatrics
Bailey CJ, Pool RW, Poskitt EME, Harris F (1983): Valproic acid and fetal abnormality. Br Med J 286:190. Bantz EW (1984): Valproic acid and congenital malformations. CIin Pediatr 23:352-353. Bjerkedal T, Czeizel A, Goujard J, Kallen B, Mastroiacovo P, Nevin N, Oakley G, Robert E (1 982): Valproic
Blaw ME, Woody RC (1983): Valproic acid embryopathy? [letter]. Neurology 33:255. Brown NA, Kao J, Fabro S (1980): Teratogenic potential of valproic acid. Lancet 1:660-661. Bruckner A, Lee YJ, OShea KS, Henneberry RC (1983): Teratogenic effects of valproic acid and
Centers for Disease Control (CDC) (1983): Valproate: A new cause of birth defects-Report from Italy and
Centers for Disease Control (CDC) (1982): Valproic acid and spina bifida: A preliminary report-France.
Chessa L, Iannetti P (1986): Fetal valproate syndrome [letter]. Am J Med Genet 24381-382. Clark EB (1986): Cardiac embryology. Its relevance to congenital heart disease. Am J Dis Child 140:4144. Clay SA, McVie R, Chen H (1981): Possible teratogenic effect of valproic acid [letter]. J Pediatr 99:828. Dalens B, Raynaud E-J, Gaulme J (1980): Teratogenicity of valproic acid [letter]. J Pediatr 97:332-333. Diaz J, Shields WD (1981): Effects of dipropylacetate on brain development. Ann Neurol 10465468. Dickinson RG, Harland RC, Lynn RK, Smith WB, Gerber N (1979): Transmission of valproic acid (Depakene)
Di Liberti JH, Farndon PA, Dennis NR, Curry CJR (1984): The fetal valproate syndrome. Am J Med Genet
Garden AS, Benzie RJ, Hutton EM, Gare DJ (1985): Valproic acid therapy and neural tube defects. Can Med
Gomez MR (1981): Possible teratogenicity of valproic acid [letter]. J Pediatr 98508-509. Jager-Roman E, Deichl A, Jakob S, Hartmann A-M, Koch S, Rating D, Steldinger R, Nau H, Helge H (1986):
Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 108:997-1004.
71:980.
acid and spina bifida [letter]. Lancet 21096.
diphenylhydantoin on mouse embryos in culture. Teratology 27:29-42.
follow-up from France. MMWR 32:438439.
MMWR 31:565-566.
across the placenta: Half life of the drug in mother and baby. J Pediatr 942332435,
19:473481.
Assoc J 132:933-936.

Fetal Valproate Syndrome 185
Kao J, Brown NA, Schmid B, Goulding EH, Fabro S (198 1): Teratogenicity of valproic acid: In vivo and in vitro investigations. Teratogenesis Carcinog Mutagen 1:367-382.
Lemire RJ, Loeser JD, Leech RW, Alvord EC (1975): “Normal and Abnormal Development of the Human Nervous System.” Hagerstown, M D Harper and Row, pp. 7143.
Lindhout D, Schmidt D (1986): In utero exposure to valproate and neural tube defects [letter]. Lancet 1:1392-1393.
Nau H, Rating S, Koch S, Hauser I, Helge H (1981): Valproic acid and its metabolites: Placental transfer, neonatal pharmacokinetics, transfer via mother’s milk and clinical status in neonates of epileptic mothers. J Pharmacol Exp Ther 219:768-777.
Paulson RB, Sucheston ME, Hayes TG, Paulson GW (1985): Teratogenic effects of valproate in the CD-1 mouse fetus. Arch Neurol4298G983.
Robert E, Guihaud P (1982): Maternal valproic acid and congenital neural tube defects [letter]. Lancet 2:937. Robert E, Lokvist E, Mauguiere F (1984): Valproate and spina bifida [letter]. Lancet 2:1392. Robert E, Rosa F (1983): Valproate and birth defects [letter]. Lancet 2:1142. Schardein JL (1985): “Chemically Induced Birth Defects.” New York: Marcel Dekker, pp 142-189. Stanley OH, Chambers TL (1982): Sodium valproate and neural tube defects [letter]. Lancet 21282. Tein I, MacGregor DL (1985): Possible valproate teratogenicity. Arch Neurol42291-293. Thomas D, Buchanan N (1981): Teratogenic effects of anticonvulsants [letter]. J Pediatr 99:163.
Edited by John M. Opitz and James F. Reynolds




















