
Vendor-to-Vendor Education to Improve Malaria Treatment by ...
20
QUALITY ASSURANCE PROJECT Center for Human Services • 7200 Wisconsin Avenue, Suite 600 • Bethesda, MD 20814-4811 • USA • www.qaproject.org OPERATIONS RESEARCH RESULTS Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya February 2002
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Vendor-to-Vendor Education to Improve Malaria Treatment by ...

Q U A L I T Y
A S S U R A N C E
P R O J E C T
Center for Human Services • 7200 Wisconsin Avenue, Suite 600 • Bethesda, MD 20814-4811 • USA • www.qaproject.org
O P E R A T I O N S R E S E A R C H R E S U L T S
Vendor-to-Vendor Education toImprove Malaria Treatment by
Drug Outlets in Kenya
February 2002

The Quality Assurance (QA) Project is funded by the U.S. Agency for International Development(USAID), under Contract Number HRN-C-00-96-90013. The QA Project serves countries eligible forUSAID assistance, USAID Missions and Bureaus, and other agencies and nongovernmental organiza-tions that cooperate with USAID. The QA Project team consists of prime contractor Center for HumanServices (CHS), Joint Commission Resources, Inc. (JCI), and the Johns Hopkins University School ofHygiene and Public Health (JHSPH), Center for Communication Programs (JHU/CCP), and Program forInternational Education in Reproductive Health (JHPIEGO). The QA Project provides comprehensive,leading-edge technical expertise in the design, management, and implementation of quality assuranceprograms in developing countries. CHS, the nonprofit affiliate of University Research Co., LLC (URC),provides technical assistance and research for the design, management, improvement, and monitoringof healthcare systems and service delivery in over 30 countries.

O P E R A T I O N S R E S E A R C H R E S U L T S
Continued on page ii
Table of Contents
1.0 INTRODUCTION.............................................................................................. 1
2.0 BACKGROUND ............................................................................................... 2
3.0 OBJECTIVES OF THE STUDY......................................................................... 3
4.0 DESCRIPTION OF INTERVENTION ................................................................ 3
5.0 EVALUATION METHODOLOGY ...................................................................... 5
5.1 Use of Mystery Shoppers ......................................................................... 5
5.2 Sample Design and Data Analysis ........................................................... 5
6.0 FINDINGS ........................................................................................................ 6
6.1 Characteristics of Respondents Interviewed and Outlets Visited ........... 6
6.2 Estimated Coverage and Acceptability of the Intervention ..................... 8
6.3 Impact of the Interventiion ........................................................................ 9
6.4 Summary of Key Indicators ..................................................................... 10
6.5 The Effect of Explicit Consumer Demand .............................................. 11
6.6 Cost-Effectiveness of the Intervention ................................................... 11
7.0 DISCUSSION ................................................................................................. 12
8.0 CONCLUSIONS AND RECOMMENDATIONS ............................................. 13
APPENDIX 1: CALCULATION OF THECOST-EFFECTIVENESS OF THE INTERVENTION .............................................. 15
REFERENCES ....................................................................................................... 16
Vendor-to-Vendor Education toImprove Malaria Treatment byDrug Outlets in Kenya
Abstract
Private drug outlets have grownincreasingly important as the mainsource of malaria treatment for resi-dents of malaria endemic areas.Unfortunately, the quality of infor-mation and the quantity and qual-ity of drugs provided is oftendeficient. The World Health Orga-nization has included the privatesector in its Roll Back Malaria strat-egy, but has noted that it is notori-ously difficult to change privatesector practices without burdeningthe governments of developingcountries. In the Bungoma districtof Kenya, the Quality AssuranceProject (USA) teamed up with theBungoma District Health Manage-ment Team and African Medicaland Research Foundation to testan innovative, low-cost approachfor improving the prescribingpractices of private drug outlets.The intervention, called Vendor-to-Vendor Education, involved train-ing and equipping wholesalecounter attendants and mobilevendors with customized job aidsfor distribution to small rural andperi-urban retailers. The job aidsconsisted of: (a) a shopkeeperposter that described the newmalaria guidelines, provided atreatment schedule, and gaveadvice on the appropriate actionsto take in various scenarios; and(b) a client poster that depicted thefive approved malaria drugs andadvised clients to ask for them. Thetraining of wholesalers began inApril 2000.

Abstract Continued
Six months after the training started,the authors evaluated the programusing mystery shoppers, who posedas caretakers of sick children need-ing medication. The evaluation re-vealed that outlets receiving job aidshad significantly better malaria knowl-edge and prescribing practices thanthose that did not. It was estimatedthat about 500 drug outlets (of 1500in Bungoma district and 2400 in neigh-boring districts) were reached by theintervention and that about 82,000additional malaria clients receivedproper treatment as a result of theintervention. Since the interventioncost about $8300 to conduct (exclud-ing the cost of the mystery shopperevaluation), the cost is $0.10 per ben-eficiary. For greater impact, it wouldbe necessary to strengthen consumerdemand for the correct drugs, to de-velop ways to continue to motivate thewholesale counter attendants, and toachieve proper packaging and qual-ity enforcement at the national level.
Acknowledgements
The authors wish to acknowledge the valuable contribution of otherBungoma district team members who implemented the intervention:Terry Wefwafwa, Richard Wanyonyi, Joachim Mwanza, and TomKangere. Dr. Muthoni Kariuki and Hezron Ngugi (African Medical andResearch Foundation or AMREF) and Dr. Bart Burkhalter (QualityAssurance Project) provided important technical input and guidanceduring the study. Victor Masbayi, Project Manager at USAID/Kenya; Dr.Alan Gohole, Bungoma District Medical Officer of Health; and Dr.Dennis Carroll, Senior Malaria Advisor at USAID/Washington gavesupport and encouragement throughout the study.
Funding for this study was provided by the U.S. Agency for Interna-tional Development through the African Integrated Malaria Initiative aspart of the Bungoma District Malaria Initiative.
While we acknowledge the valuable contributions of the partiesmentioned above, all errors of omission and/or interpretation remainthe sole responsibility of the authors.
Recommended citation
Tavrow, P., J. Shabahang, and S. Makama. 2002. Vendor-to-VendorEducation to improve malaria treatment by drug outlets in Kenya.Operations Research Results. 2(3). Bethesda, MD: Published for theU.S. Agency for International Development (USAID) by the QualityAssurance (QA) Project.
About this series
The Operations Research Results series presents the results of QAProject country or area research to encourage discussion and com-ment within the international development community. To obtain the fullresearch report with the relevant data collection instruments, pleasecontact [email protected].
Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 1
Abbreviations
AMREF African Medical andResearch Foundation
AQ Amodiaquine
BDMI Bungoma District MalariaInitiative
CQ Chloroquine
DHMT District Health ManagementTeam
Ksh Kenyan shilling
MOH Ministry of Health
NMCC National Malaria ControlCommittee
NS Not significant
QA Quality Assurance
RBM Roll Back Malaria
SP Sulfadoxine-pyrimethamine
USAID United States Agency forInternational Development
WHO World Health Organization
Paula Tavrow, Jennifer Shabahang, and Sammy Makama
Vendor-to-Vendor Education to ImproveMalaria Treatment by Drug Outlets in Kenya
1.0 Introduction
Malaria is one of the most seriouspublic health issues worldwide. Itkills at least one million people eachyear: about 3,000 per day. Almost300 million people suffer from acutemalaria each year, causing not onlydeath and morbidity but severeeconomic losses (Roll Back Malariawebsite 2001). Current strategies tocombat malaria, led by the WorldHealth Organization’s “Roll BackMalaria” initiative, focus on early andeffective treatment, along withmultiple prevention strategies.Effective treatment is hampered bythe lack of universally efficaciousand inexpensive drugs. It is alsohindered by frequently incorrectdosing—either under- or over-dosing—and the widespread use inendemic areas of anti-malarial drugswithout a laboratory diagnosis.These factors lead to the rapid riseof drug resistance, which necessi-tates constant change in malariatreatment guidelines.
Contributing to the difficulty ofmalaria control is the decreasing use
of public health services. Animportant consequence of healthsector reform in developing coun-tries has been the increased use ofprivate practitioners and drugoutlets. Previously, free public healthfacilities had been most people’sprime source of medical care,especially in sub-Saharan Africa.However, public facilities often havea number of drawbacks—such asdistance from people’s homes,inconvenient operating times, longwaits, inconsiderate providers, anddrug shortages. In contrast, privateservices are usually closer topeople’s homes, have short queues,are open in the evening, and stocksufficient drugs. When publicfacilities charge for medical consul-tations and drugs, people opt forprivate services. It is estimated thatfor certain common ailments, suchas malaria, as many as 60 to 80percent of people in developingcountries now first visit private drugoutlets or practitioners for treatment(McCombie 1996). Because caretak-ers of sick children generallyacquire their knowledge on anti-malarial drugs from the site wherethey obtain them (WHO TechnicalReport 2000), the quality of privatesector services has grown moreimportant.
Unfortunately, the technical qualityof private medical and pharmaceuti-cal services is often questionable,

2 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
mainly because they are outsidemost governments’ capacity toinform, update, monitor, and regu-late. Governments in endemic areasgenerally do little more than requireprivate establishments to beregistered by a licensed doctor orpharmacist. Yet it is widely acknowl-edged that untrained personnel,whom a licensed practitioner mayonly nominally supervise, frequentlystaff these establishments. Thesepersonnel may not be able to giveconsumers correct information aboutthe drugs they purchase. Also,interest in making money may takeprecedence over healing people.
The World Health Organization(WHO) recognizes that governmenthealth services are often not thepredominant source of malariatreatment and recommends thatprivate health services be includedin strategies to control and treatmalaria. It recommends that re-searchers investigate approachesfor collaborating with the privatesector, especially drug sellers.WHO acknowledges, however, thatachieving rational prescribing in theprivate sector is “notoriouslydifficult” due to influences frompatient demand, drug advertising,and profit margins (WHO TechnicalReport 2000).
Monitoring and influencing thequality of private services has beena major challenge for resource-constrained governments. Evencommunicating new standards ofdiagnosis and treatment to privatepractitioners poses immensechallenges to governments withlimited resources. To date, mostapproaches for improving theperformance of the private sectorinvolve direct shopkeeper training toimprove malaria treatment practices,such as is being tested in Kilifi
district, Kenya (Marsh et al. 1999).Given the multitudes of shopkeepersin these countries, as well as theconstantly changing counterattendants, approaches that requirethree to eight days of classroomtraining per drug outlet are notfeasible for most governments.Innovative approaches are neededto achieve greater quality of privateservices without significantlyincreasing the burden or cost to thegovernment.
In late 1999, the Quality Assurance(QA) Project, together with membersof the Bungoma District HealthManagement Team in Kenya and theAfrican Medical and ResearchFoundation (AMREF), developedand introduced a new intervention toimprove private sector dispensingpractices. This intervention, called“Vendor-to-Vendor Education,” relieson wholesale vendors to communi-cate malaria guidelines to retailersvia a customized job aid. Thisintervention was evaluated inOctober 2000 using mysteryshoppers. This paper describes theintervention and presents the mainresults.
2.0 Background
In Kenya, approximately 26,000children die each year from malaria.About a third of out-patient atten-dance in health facilities throughoutthe country is attributable to malaria.Adult disability due to malariatranslates to an economic loss ofabout 160 million working days peryear. Bungoma district, located inWestern Province, is a malariaendemic area with a population ofabout one million. Malaria inBungoma district accounts for 39percent of out-patient visits, 36percent of in-patient mortality, and
42 percent of hospital in-patientadmissions (Bungoma DHMT 1998).Malaria transmission occurs yearround, peaking in the rainy seasonmonths of April and May.
In 1998 the government of Kenyachanged its first-line anti-malarialtreatment from chloroquine tosulfadoxine-pyrimethamine (SP).Currently, SP is the first-line drug,available over the counter for homeuse, and amodiaquine is to be usedas the second-line drug. Chloro-quine can be sold only by prescrip-tion. However, the current drugpolicy is not enforced: chloroquineand amodiaquine are widelyavailable in shops. In 1999, thegovernment of Kenya conductedefficacy-testing of 33 SP brands.Five were approved for malariatreatment: Fansidar, Laridox,Falcidin, Orodar, and Metakelfin.However, because of lack ofenforcement, the 28 SP drugs thatwere not approved still remained onthe market.
Several earlier studies in Bungomadistrict contributed to the initiation ofthis research. In 1998 the BungomaDistrict Health Management Team(DHMT) conducted a survey toidentify groups and individualsinvolved in the actual distribution ofanti-malarials and anti-pyretics in thedistrict. The research team inter-viewed private clinicians, pharma-cists, drug vendors, and communitypharmacies. Shops or kiosks werefound to be the main source ofdrugs for people in rural areas. Thesurvey revealed that 87 percent ofthe shopkeepers surveyed hadnever received training on drug use,but 60 percent of them gave someinstruction on dosages to theircustomers. Additionally, 27 percentof the shopkeepers surveyed did notknow the difference between anti-
Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 3
malarials and anti-pyretics(Bungoma DHMT 1998).
A formative study for the BungomaDistrict Malaria Initiative (BDMI),conducted in 1996, interviewedcaretakers of 315 recently febrilechildren under the age of five.According to caretakers, 47 percentof children received home treatmentwith an anti-malarial, and one-thirdof children received their only anti-malarial treatment at home. Thestudy also found that 29 percent ofanti-malarials for home treatmentwere purchased in a small shop orkiosk (Hamel et al. 2001).
3.0 Objectives of theStudy
The purpose of this study was totest whether a low-cost outreacheducation strategy would increaseprivate drug outlets’1 knowledge ofand compliance with nationalmalaria treatment guidelines inBungoma district, Kenya. Unlike“academic detailing,” where out-reach educators are health provid-ers or experts, in this study theoutreach educators were mobilevendors and counter attendantsfrom wholesale pharmacies andgeneral shops. The strategy pro-moted a unique partnership betweenthe public health system (namely theBungoma DHMT) and the privatesector.
The study sought to answer thefollowing questions:
■ Will wholesale counter attendantsand mobile vendors widely andeffectively communicate newmalaria treatment standards toprivate drug outlets?
■ Do private drug outlets thatreceive the job aids understandand comply with malariaguidelines better than thosethat do not?
■ What is the cost-effectivenessof the vendor-to-vendorintervention?
4.0 Description ofIntervention
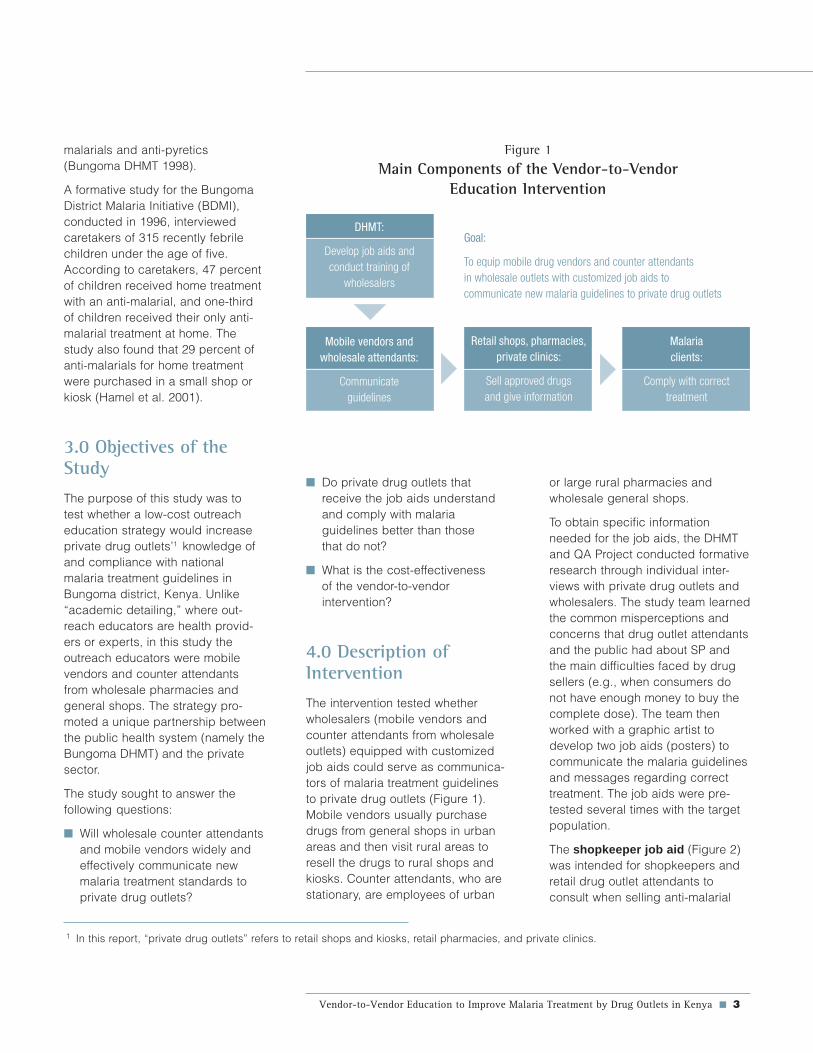
The intervention tested whetherwholesalers (mobile vendors andcounter attendants from wholesaleoutlets) equipped with customizedjob aids could serve as communica-tors of malaria treatment guidelinesto private drug outlets (Figure 1).Mobile vendors usually purchasedrugs from general shops in urbanareas and then visit rural areas toresell the drugs to rural shops andkiosks. Counter attendants, who arestationary, are employees of urban
1 In this report, “private drug outlets” refers to retail shops and kiosks, retail pharmacies, and private clinics.
Goal:
To equip mobile drug vendors and counter attendantsin wholesale outlets with customized job aids tocommunicate new malaria guidelines to private drug outlets
or large rural pharmacies andwholesale general shops.
To obtain specific informationneeded for the job aids, the DHMTand QA Project conducted formativeresearch through individual inter-views with private drug outlets andwholesalers. The study team learnedthe common misperceptions andconcerns that drug outlet attendantsand the public had about SP andthe main difficulties faced by drugsellers (e.g., when consumers donot have enough money to buy thecomplete dose). The team thenworked with a graphic artist todevelop two job aids (posters) tocommunicate the malaria guidelinesand messages regarding correcttreatment. The job aids were pre-tested several times with the targetpopulation.
The shopkeeper job aid (Figure 2)was intended for shopkeepers andretail drug outlet attendants toconsult when selling anti-malarial
Figure 1
Main Components of the Vendor-to-VendorEducation Intervention
DHMT:
Develop job aids andconduct training of
wholesalers
Mobile vendors andwholesale attendants:
Communicateguidelines
Retail shops, pharmacies,private clinics:
Sell approved drugsand give information
Malariaclients:
Comply with correcttreatment

4 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
Figure 2
Shopkeeper Job Aid
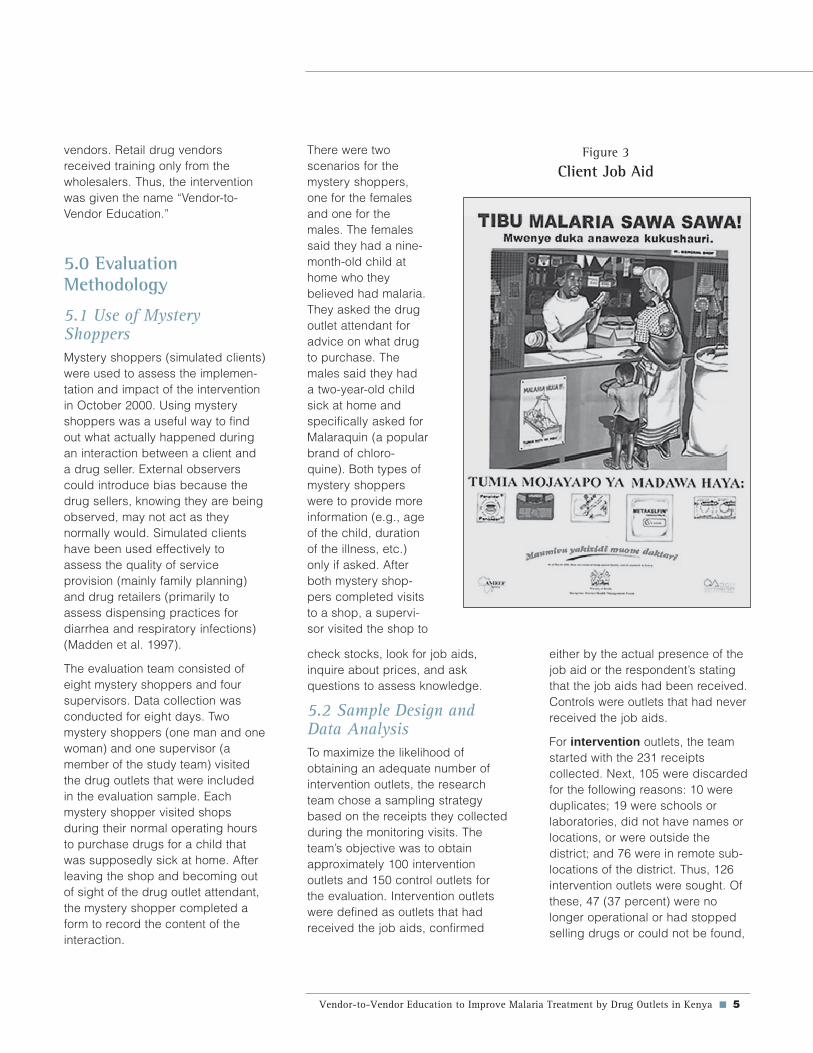
drugs. It was to be hung prominentlyin the shop so that the shopkeepercould easily use it when servingclients. The job aid contained thesigns of malaria, a dosage chart ofthe approved SPs and anti-pyretics,treatment advice, and commonsituations faced by shopkeepersand suggestions on how to deal withthem. The client job aid (Figure 3)was to be placed at the drug outletto communicate to clients that SPwas now available there. This wasparticularly important for shopsbecause previously they were notallowed to sell SP. The job aidreminded people to treat malariaproperly and depicted the fiveapproved SP drugs in their actual
packaging. Both jobaids were producedin Kiswahili, alanguage under-stood by all retailersin the district.
The DHMT and QAProject thendeveloped a three-hour orientation forwholesale ownersand a one-daycourse to traincounter attendantsand mobile ven-dors. In order toinvolve the counterattendants, orienta-tion sessions werefirst held with theowners of thewholesale pharma-cies and generalshops. During thisthree-hour sessionthe new malariaguidelines and theproposed interven-tion were explainedand discussed. Theowners then agreed
distribution. Out of approximately105 wholesale vendors identified,about three-quarters participated inthe training: 22 wholesale pharmacyattendants, 11 wholesale shopattendants, and 40 mobile drugvendors. All who were trainedreceived yellow caps and T-shirtswith the “Tibu malaria sawa sawa”(“Treat malaria correctly”) slogan.
The communication of the guidelineswas to occur during the normalbusiness interaction. For wholesalecounter attendants, they were tocommunicate the guidelines andgive the job aids to retailers whenthey came to the wholesale phar-macy or general shop to buy anti-malarials. For mobile vendors theinteraction would occur at the retailshop, pharmacy, or clinic, since themobile vendors travel to theseoutlets. The counter attendants andmobile vendors were asked to obtaina receipt from each shopkeeper whoreceived a job aid. By signing thereceipt, the recipient of the job aidagreed to follow the malaria guide-lines when serving clients.
Two to three months after training,the study team monitored wholesaleattendants and mobile vendors.During the monitoring visits, theteam checked their malaria knowl-edge with a quiz and collectedreceipts. The quiz consisted of keyissues covered during the training,and the attendants and mobilevendors were given feedback onquestions they answered incorrectly.Out of ten points the average scoreswere as follows: pharmacy atten-dants, 9.8; general wholesaleattendants, 9.5; and mobile vendors,9.1. This same quiz was used duringthe evaluation to assess the malariaknowledge of retailers. It is importantto note that we directly trained onlythe wholesale attendants and mobile
to send their attendants to thetraining and let them distribute thejob aids during the course of theirwork.
In April and May 2000, the DHMTconducted five separate one-daytraining sessions for mobile vendorsand counter attendants in the majorurban areas of Bungoma district.Topics were an overview of districtmalaria activities, general informa-tion on malaria, the government ofKenya’s policy on malaria treatment,inter-personal communication skills,and practical sessions on the use ofjob aids. At the end of the trainingthe wholesalers received about 20copies of each job aid to begin
Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 5
vendors. Retail drug vendorsreceived training only from thewholesalers. Thus, the interventionwas given the name “Vendor-to-Vendor Education.”
5.0 EvaluationMethodology
5.1 Use of MysteryShoppersMystery shoppers (simulated clients)were used to assess the implemen-tation and impact of the interventionin October 2000. Using mysteryshoppers was a useful way to findout what actually happened duringan interaction between a client anda drug seller. External observerscould introduce bias because thedrug sellers, knowing they are beingobserved, may not act as theynormally would. Simulated clientshave been used effectively toassess the quality of serviceprovision (mainly family planning)and drug retailers (primarily toassess dispensing practices fordiarrhea and respiratory infections)(Madden et al. 1997).
The evaluation team consisted ofeight mystery shoppers and foursupervisors. Data collection wasconducted for eight days. Twomystery shoppers (one man and onewoman) and one supervisor (amember of the study team) visitedthe drug outlets that were includedin the evaluation sample. Eachmystery shopper visited shopsduring their normal operating hoursto purchase drugs for a child thatwas supposedly sick at home. Afterleaving the shop and becoming outof sight of the drug outlet attendant,the mystery shopper completed aform to record the content of theinteraction.
Figure 3
Client Job AidThere were twoscenarios for themystery shoppers,one for the femalesand one for themales. The femalessaid they had a nine-month-old child athome who theybelieved had malaria.They asked the drugoutlet attendant foradvice on what drugto purchase. Themales said they hada two-year-old childsick at home andspecifically asked forMalaraquin (a popularbrand of chloro-quine). Both types ofmystery shopperswere to provide moreinformation (e.g., ageof the child, durationof the illness, etc.)only if asked. Afterboth mystery shop-pers completed visitsto a shop, a supervi-sor visited the shop to
check stocks, look for job aids,inquire about prices, and askquestions to assess knowledge.
5.2 Sample Design andData AnalysisTo maximize the likelihood ofobtaining an adequate number ofintervention outlets, the researchteam chose a sampling strategybased on the receipts they collectedduring the monitoring visits. Theteam’s objective was to obtainapproximately 100 interventionoutlets and 150 control outlets forthe evaluation. Intervention outletswere defined as outlets that hadreceived the job aids, confirmed
either by the actual presence of thejob aid or the respondent’s statingthat the job aids had been received.Controls were outlets that had neverreceived the job aids.
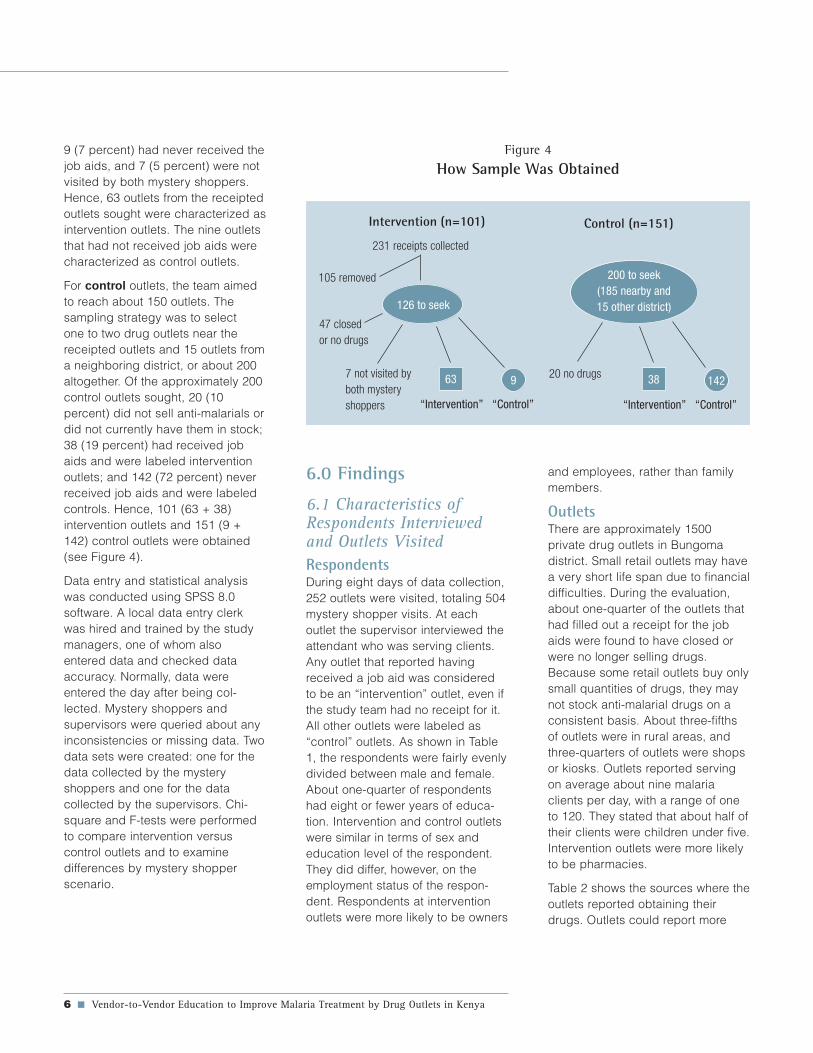
For intervention outlets, the teamstarted with the 231 receiptscollected. Next, 105 were discardedfor the following reasons: 10 wereduplicates; 19 were schools orlaboratories, did not have names orlocations, or were outside thedistrict; and 76 were in remote sub-locations of the district. Thus, 126intervention outlets were sought. Ofthese, 47 (37 percent) were nolonger operational or had stoppedselling drugs or could not be found,
6 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
9 (7 percent) had never received thejob aids, and 7 (5 percent) were notvisited by both mystery shoppers.Hence, 63 outlets from the receiptedoutlets sought were characterized asintervention outlets. The nine outletsthat had not received job aids werecharacterized as control outlets.
For control outlets, the team aimedto reach about 150 outlets. Thesampling strategy was to selectone to two drug outlets near thereceipted outlets and 15 outlets froma neighboring district, or about 200altogether. Of the approximately 200control outlets sought, 20 (10percent) did not sell anti-malarials ordid not currently have them in stock;38 (19 percent) had received jobaids and were labeled interventionoutlets; and 142 (72 percent) neverreceived job aids and were labeledcontrols. Hence, 101 (63 + 38)intervention outlets and 151 (9 +142) control outlets were obtained(see Figure 4).
Data entry and statistical analysiswas conducted using SPSS 8.0software. A local data entry clerkwas hired and trained by the studymanagers, one of whom alsoentered data and checked dataaccuracy. Normally, data wereentered the day after being col-lected. Mystery shoppers andsupervisors were queried about anyinconsistencies or missing data. Twodata sets were created: one for thedata collected by the mysteryshoppers and one for the datacollected by the supervisors. Chi-square and F-tests were performedto compare intervention versuscontrol outlets and to examinedifferences by mystery shopperscenario.
6.0 Findings
6.1 Characteristics ofRespondents Interviewedand Outlets VisitedRespondentsDuring eight days of data collection,252 outlets were visited, totaling 504mystery shopper visits. At eachoutlet the supervisor interviewed theattendant who was serving clients.Any outlet that reported havingreceived a job aid was consideredto be an “intervention” outlet, even ifthe study team had no receipt for it.All other outlets were labeled as“control” outlets. As shown in Table1, the respondents were fairly evenlydivided between male and female.About one-quarter of respondentshad eight or fewer years of educa-tion. Intervention and control outletswere similar in terms of sex andeducation level of the respondent.They did differ, however, on theemployment status of the respon-dent. Respondents at interventionoutlets were more likely to be owners
Figure 4
How Sample Was Obtained
7 not visited byboth mysteryshoppers
Intervention (n=101) Control (n=151)
231 receipts collected
105 removed
47 closedor no drugs
“Intervention” “Control”
126 to seek
963
200 to seek(185 nearby and15 other district)
“Intervention” “Control”
1423820 no drugs
and employees, rather than familymembers.
OutletsThere are approximately 1500private drug outlets in Bungomadistrict. Small retail outlets may havea very short life span due to financialdifficulties. During the evaluation,about one-quarter of the outlets thathad filled out a receipt for the jobaids were found to have closed orwere no longer selling drugs.Because some retail outlets buy onlysmall quantities of drugs, they maynot stock anti-malarial drugs on aconsistent basis. About three-fifthsof outlets were in rural areas, andthree-quarters of outlets were shopsor kiosks. Outlets reported servingon average about nine malariaclients per day, with a range of oneto 120. They stated that about half oftheir clients were children under five.Intervention outlets were more likelyto be pharmacies.
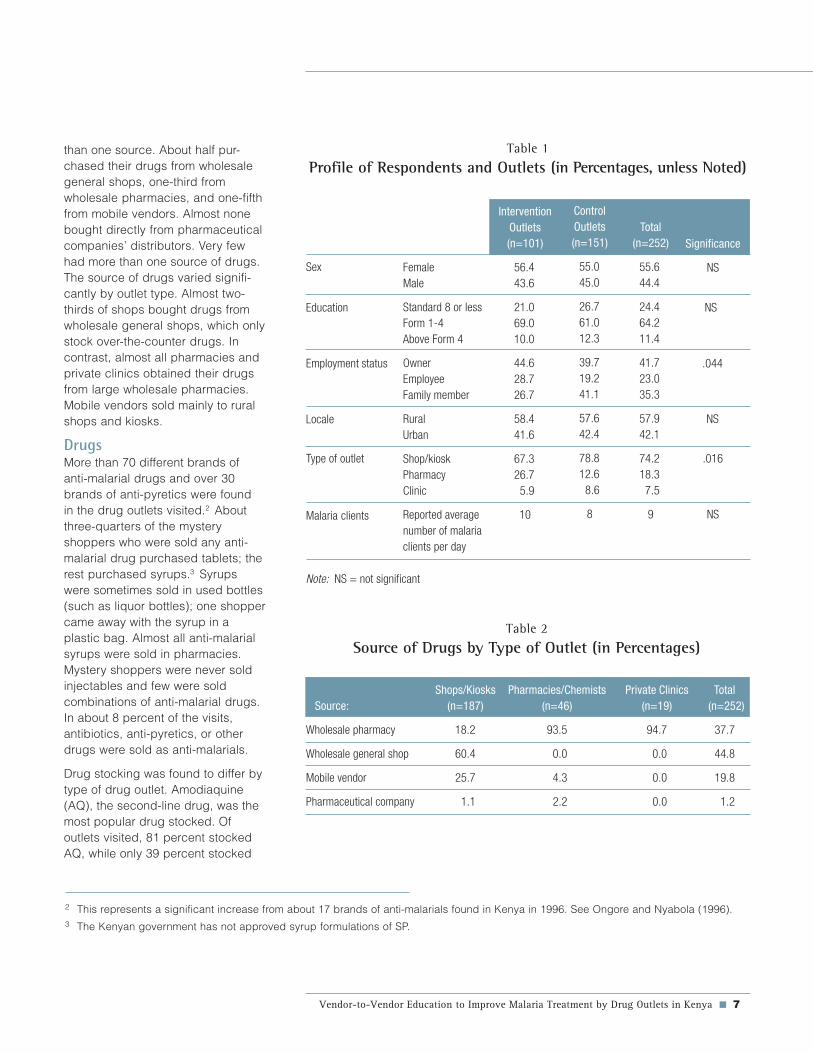
Table 2 shows the sources where theoutlets reported obtaining theirdrugs. Outlets could report more
Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 7
Table 1
Profile of Respondents and Outlets (in Percentages, unless Noted)
Sex FemaleMale
Standard 8 or lessForm 1-4Above Form 4
OwnerEmployeeFamily member
RuralUrban
Shop/kioskPharmacyClinic
Reported averagenumber of malariaclients per day
InterventionOutlets(n=101)
56.443.6
21.069.010.0
44.628.726.7
58.441.6
67.326.7
5.9
10
ControlOutlets(n=151)
55.045.0
26.761.012.3
39.719.241.1
57.642.4
78.812.6
8.6
8
Total(n=252)
55.644.4
24.464.211.4
41.723.035.3
57.942.1
74.218.3
7.5
9
Significance
NS
Note: NS = not significant
Education NS
Employment status .044
Locale
Type of outlet
NS
.016
NSMalaria clients
than one source. About half pur-chased their drugs from wholesalegeneral shops, one-third fromwholesale pharmacies, and one-fifthfrom mobile vendors. Almost nonebought directly from pharmaceuticalcompanies’ distributors. Very fewhad more than one source of drugs.The source of drugs varied signifi-cantly by outlet type. Almost two-thirds of shops bought drugs fromwholesale general shops, which onlystock over-the-counter drugs. Incontrast, almost all pharmacies andprivate clinics obtained their drugsfrom large wholesale pharmacies.Mobile vendors sold mainly to ruralshops and kiosks.
DrugsMore than 70 different brands ofanti-malarial drugs and over 30brands of anti-pyretics were foundin the drug outlets visited.2 Aboutthree-quarters of the mysteryshoppers who were sold any anti-malarial drug purchased tablets; therest purchased syrups.3 Syrupswere sometimes sold in used bottles(such as liquor bottles); one shoppercame away with the syrup in aplastic bag. Almost all anti-malarialsyrups were sold in pharmacies.Mystery shoppers were never soldinjectables and few were soldcombinations of anti-malarial drugs.In about 8 percent of the visits,antibiotics, anti-pyretics, or otherdrugs were sold as anti-malarials.
Drug stocking was found to differ bytype of drug outlet. Amodiaquine(AQ), the second-line drug, was themost popular drug stocked. Ofoutlets visited, 81 percent stockedAQ, while only 39 percent stocked
Table 2
Source of Drugs by Type of Outlet (in Percentages)
Shops/Kiosks Pharmacies/Chemists Private Clinics Total Source: (n=187) (n=46) (n=19) (n=252)
Wholesale pharmacy 18.2 93.5 94.7 37.7
Wholesale general shop 60.4 0.0 0.0 44.8
Mobile vendor 25.7 4.3 0.0 19.8
Pharmaceutical company 1.1 2.2 0.0 1.2
2 This represents a significant increase from about 17 brands of anti-malarials found in Kenya in 1996. See Ongore and Nyabola (1996).3 The Kenyan government has not approved syrup formulations of SP.
8 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
SP, and 41 percent stocked chloro-quine (CQ). Among shops, morethan three-quarters stocked AQ andabout two-fifths stocked CQ, whileless than one-fourth stocked SP.Almost all pharmacies and aboutthree-quarters of private clinicsstocked both AQ and SP. (CQ canbe sold legally by pharmacies andprivate clinics, but not by shops.)
Outlet types varied significantly inthe number of brands and types ofanti-malarial drugs they had instock. Pharmacies had an averageof 10.4 different brands of anti-malarials in stock, while shops had1.7, and private clinics 4.5. Not onlydid the shops stock very few brandsat once, but it was common fornearby shops to be selling differenttypes or brands. The most com-monly stocked anti-malarial drugbrand was Malaratab, an AQproduced in Kenya.
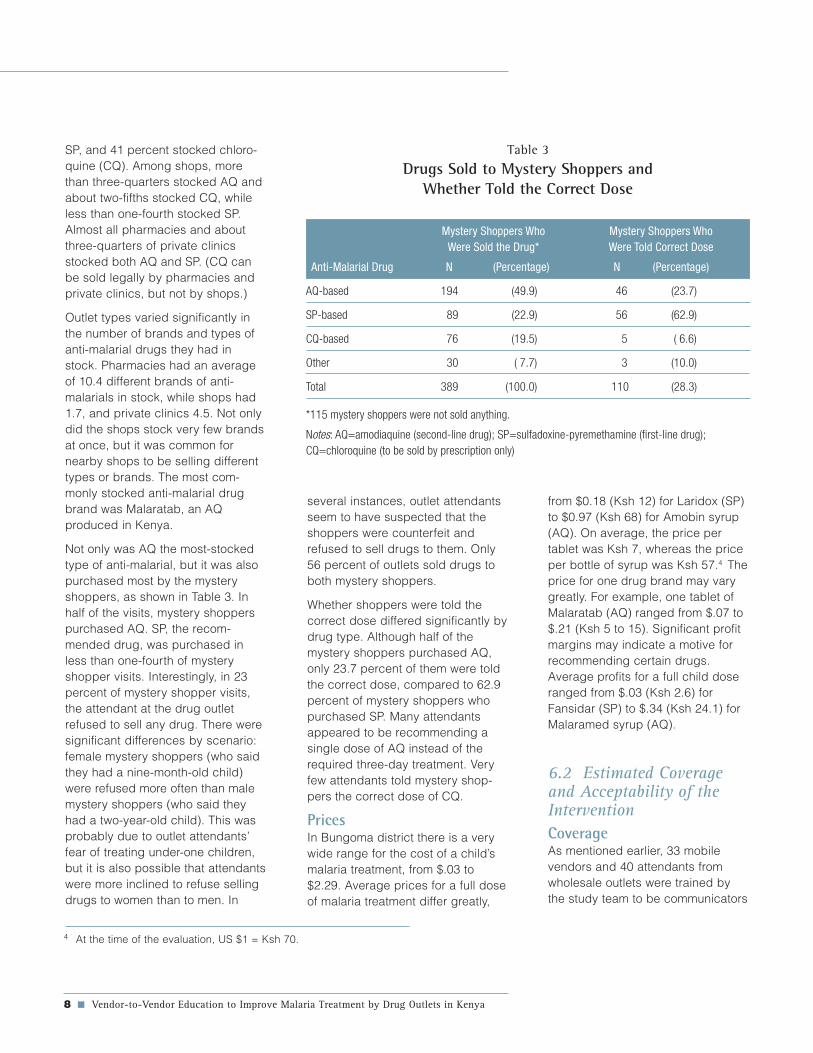
Not only was AQ the most-stockedtype of anti-malarial, but it was alsopurchased most by the mysteryshoppers, as shown in Table 3. Inhalf of the visits, mystery shopperspurchased AQ. SP, the recom-mended drug, was purchased inless than one-fourth of mysteryshopper visits. Interestingly, in 23percent of mystery shopper visits,the attendant at the drug outletrefused to sell any drug. There weresignificant differences by scenario:female mystery shoppers (who saidthey had a nine-month-old child)were refused more often than malemystery shoppers (who said theyhad a two-year-old child). This wasprobably due to outlet attendants’fear of treating under-one children,but it is also possible that attendantswere more inclined to refuse sellingdrugs to women than to men. In
several instances, outlet attendantsseem to have suspected that theshoppers were counterfeit andrefused to sell drugs to them. Only56 percent of outlets sold drugs toboth mystery shoppers.
Whether shoppers were told thecorrect dose differed significantly bydrug type. Although half of themystery shoppers purchased AQ,only 23.7 percent of them were toldthe correct dose, compared to 62.9percent of mystery shoppers whopurchased SP. Many attendantsappeared to be recommending asingle dose of AQ instead of therequired three-day treatment. Veryfew attendants told mystery shop-pers the correct dose of CQ.
PricesIn Bungoma district there is a verywide range for the cost of a child’smalaria treatment, from $.03 to$2.29. Average prices for a full doseof malaria treatment differ greatly,
Table 3
Drugs Sold to Mystery Shoppers andWhether Told the Correct Dose
Mystery Shoppers Who Mystery Shoppers WhoWere Sold the Drug* Were Told Correct Dose
Anti-Malarial Drug N (Percentage) N (Percentage)
AQ-based 194 (49.9) 46 (23.7)
SP-based 89 (22.9) 56 (62.9)
CQ-based 76 (19.5) 5 ( 6.6)
Other 30 ( 7.7) 3 (10.0)
Total 389 (100.0) 110 (28.3)
*115 mystery shoppers were not sold anything.
Notes: AQ=amodiaquine (second-line drug); SP=sulfadoxine-pyremethamine (first-line drug);CQ=chloroquine (to be sold by prescription only)
from $0.18 (Ksh 12) for Laridox (SP)to $0.97 (Ksh 68) for Amobin syrup(AQ). On average, the price pertablet was Ksh 7, whereas the priceper bottle of syrup was Ksh 57.4 Theprice for one drug brand may varygreatly. For example, one tablet ofMalaratab (AQ) ranged from $.07 to$.21 (Ksh 5 to 15). Significant profitmargins may indicate a motive forrecommending certain drugs.Average profits for a full child doseranged from $.03 (Ksh 2.6) forFansidar (SP) to $.34 (Ksh 24.1) forMalaramed syrup (AQ).
6.2 Estimated Coverageand Acceptability of theInterventionCoverageAs mentioned earlier, 33 mobilevendors and 40 attendants fromwholesale outlets were trained bythe study team to be communicators
4 At the time of the evaluation, US $1 = Ksh 70.

Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 9
of the malaria guidelines. During thetraining, about 1300 copies of eachjob aid were distributed to theattendants and mobile vendors fordissemination. It is estimated that insix months they reached approxi-mately 500 drug outlets, of whichabout one-fifth were outsideBungoma district.5
Job aids acceptability,visibility, and useAt all outlets, supervisors looked fordisplayed job aids and assessedtheir visibility. Supervisors found thatalmost two-thirds of the interventionoutlets were displaying the job aids.Of those, the majority were dis-played in a visible location, such ason the shelves behind the counter,on a wall, or on a door. Some jobaids were not displayed but werefound folded and placed in a drawer.Most were found in good condition,though some were torn or hadgotten wet and were not very legible.
Respondents who had job aids werealso asked about the usefulness ofthe job aids. For the shopkeeper jobaid, over half reported that theyused it a lot, and almost one quartersaid they used it sometimes. For theclient job aid, respondents wereasked how often they thought clientsused it. About a third thought that itwas used a lot, and a fourth thoughtit was used sometimes. An indica-tion of the usefulness of the shop-keeper job aid is that 31 percent ofrespondents who had received ashopkeeper job aid used it whenasked about the dosages of SPdrugs. (The supervisor observed useof the job aid before asking anyquestions about it.)
6.3 Impact of theInterventionKnowledge of correct malariatreatmentDuring the evaluation the supervi-sors administered a ten-questionmalaria knowledge quiz to therespondents. Intervention outletsscored significantly better thancontrol outlets on seven of tenquestions, and slightly better orequivalent on the remaining threequestions. As shown in Table 4, theintervention outlets had betterknowledge of important concepts,such as that SP is not too strong forchildren and that SP can be sold inshops.
To better understand the results ofthe quiz, a total exam score was
5 See Appendix 1 for an explanation of how the estimate was calculated.
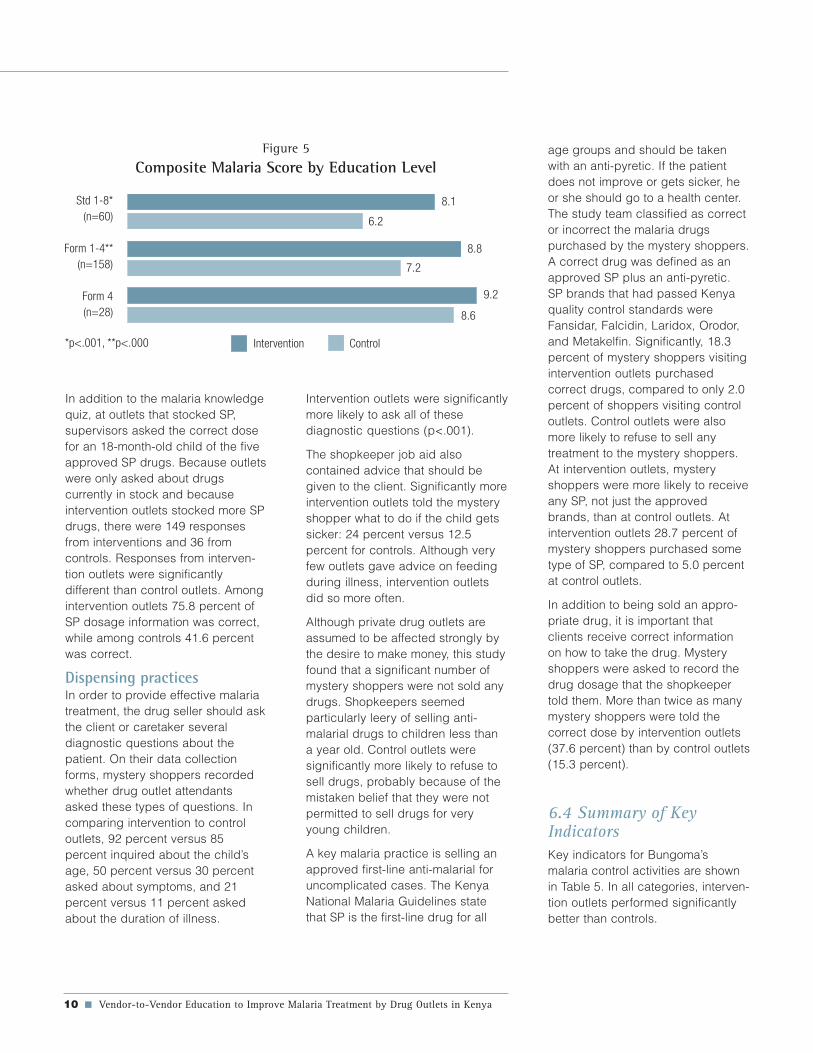
calculated by assigning one point toa correct answer and zero points foran incorrect answer or “don’t know.”Intervention outlets scored 8.7 onaverage while controls scored 7.1.Analysis by type of outlet showedthat for both shops and pharmacies,intervention outlets scored signifi-cantly better than controls. Interven-tion shops and pharmacies scoredon average 8.8 and 8.6, respec-tively, whereas control shops andpharmacies scored 7.0 and 7.5,respectively. There was no differ-ence among private clinics. Analysisof the malaria knowledge score byeducation level shows that, at eachlevel, intervention outlets scoredhigher than controls. These differ-ences were statistically significantfor respondents who had 12 years orless of education (see Figure 5).
Table 4
Specific Malaria Knowledge, by Intervention Status
Percentage of Correct Responses
Intervention Control Total Main Malaria Messages (n=101) (n=151) (n=252)
Fever is main symptom of malaria 94.1 94.7 94.4
Fansidar more effective than other drugs 92.1 85.4 88.1
Fansidar not too strong for children* 69.3 47.4 56.3
Fansidar and panadol is correct treatment* 88.1 64.2 73.8
Fansidar is a single dose treatment* 83.2 64.9 72.2
Fansidar can be sold in shops* 76.2 43.7 56.7
Continue feeding child with malaria 95.0 90.1 92.1
Don’t sell another drug if child gets worse* 91.1 71.5 79.4
Don’t always sell what is demanded* 87.1 65.6 74.2
Shouldn’t sell smaller doses of drug* 95.0 82.8 87.7
* Significant at p<.01
10 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
Figure 5
Composite Malaria Score by Education Level
In addition to the malaria knowledgequiz, at outlets that stocked SP,supervisors asked the correct dosefor an 18-month-old child of the fiveapproved SP drugs. Because outletswere only asked about drugscurrently in stock and becauseintervention outlets stocked more SPdrugs, there were 149 responsesfrom interventions and 36 fromcontrols. Responses from interven-tion outlets were significantlydifferent than control outlets. Amongintervention outlets 75.8 percent ofSP dosage information was correct,while among controls 41.6 percentwas correct.
Dispensing practicesIn order to provide effective malariatreatment, the drug seller should askthe client or caretaker severaldiagnostic questions about thepatient. On their data collectionforms, mystery shoppers recordedwhether drug outlet attendantsasked these types of questions. Incomparing intervention to controloutlets, 92 percent versus 85percent inquired about the child’sage, 50 percent versus 30 percentasked about symptoms, and 21percent versus 11 percent askedabout the duration of illness.
Intervention outlets were significantlymore likely to ask all of thesediagnostic questions (p<.001).
The shopkeeper job aid alsocontained advice that should begiven to the client. Significantly moreintervention outlets told the mysteryshopper what to do if the child getssicker: 24 percent versus 12.5percent for controls. Although veryfew outlets gave advice on feedingduring illness, intervention outletsdid so more often.
Although private drug outlets areassumed to be affected strongly bythe desire to make money, this studyfound that a significant number ofmystery shoppers were not sold anydrugs. Shopkeepers seemedparticularly leery of selling anti-malarial drugs to children less thana year old. Control outlets weresignificantly more likely to refuse tosell drugs, probably because of themistaken belief that they were notpermitted to sell drugs for veryyoung children.
A key malaria practice is selling anapproved first-line anti-malarial foruncomplicated cases. The KenyaNational Malaria Guidelines statethat SP is the first-line drug for all
age groups and should be takenwith an anti-pyretic. If the patientdoes not improve or gets sicker, heor she should go to a health center.The study team classified as corrector incorrect the malaria drugspurchased by the mystery shoppers.A correct drug was defined as anapproved SP plus an anti-pyretic.SP brands that had passed Kenyaquality control standards wereFansidar, Falcidin, Laridox, Orodor,and Metakelfin. Significantly, 18.3percent of mystery shoppers visitingintervention outlets purchasedcorrect drugs, compared to only 2.0percent of shoppers visiting controloutlets. Control outlets were alsomore likely to refuse to sell anytreatment to the mystery shoppers.At intervention outlets, mysteryshoppers were more likely to receiveany SP, not just the approvedbrands, than at control outlets. Atintervention outlets 28.7 percent ofmystery shoppers purchased sometype of SP, compared to 5.0 percentat control outlets.
In addition to being sold an appro-priate drug, it is important thatclients receive correct informationon how to take the drug. Mysteryshoppers were asked to record thedrug dosage that the shopkeepertold them. More than twice as manymystery shoppers were told thecorrect dose by intervention outlets(37.6 percent) than by control outlets(15.3 percent).
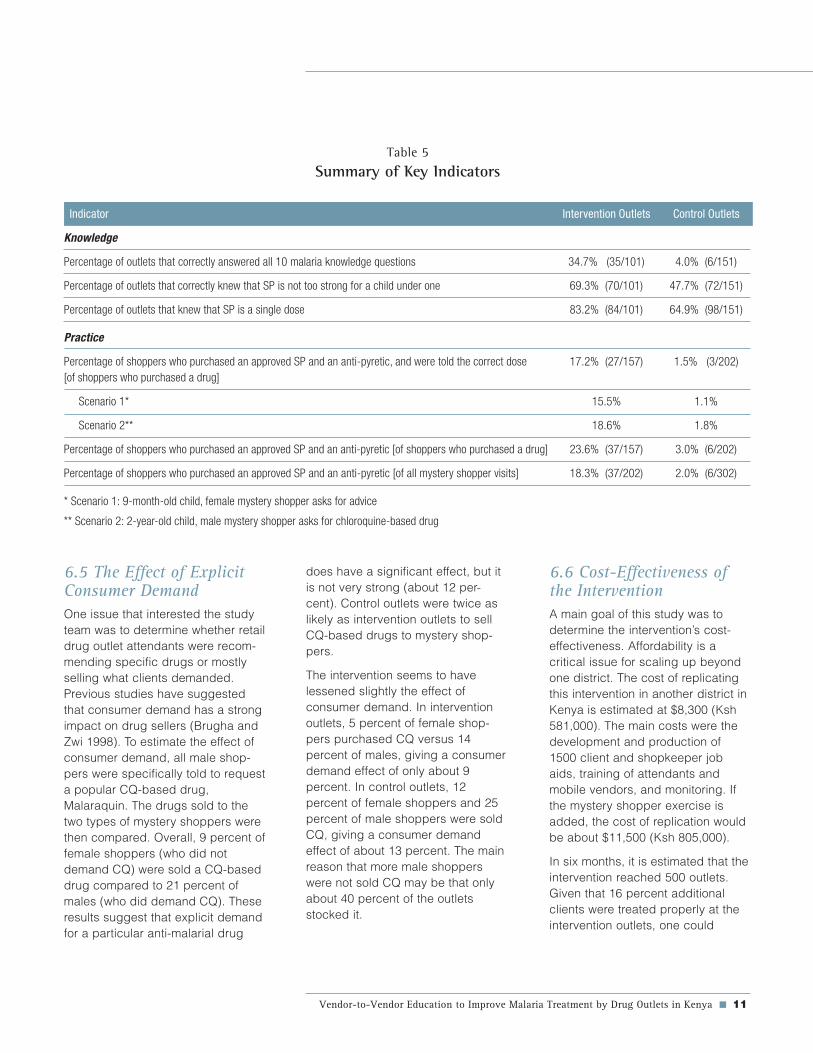
6.4 Summary of KeyIndicatorsKey indicators for Bungoma’smalaria control activities are shownin Table 5. In all categories, interven-tion outlets performed significantlybetter than controls.
Std 1-8*(n=60)
Form 1-4**(n=158)
Form 4(n=28)
8.1
6.2
8.8
7.2
9.2
8.6
Intervention Control*p<.001, **p<.000
Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 11
Table 5
Summary of Key Indicators
Indicator Intervention Outlets Control Outlets
Knowledge
Percentage of outlets that correctly answered all 10 malaria knowledge questions 34.7% (35/101) 4.0% (6/151)
Percentage of outlets that correctly knew that SP is not too strong for a child under one 69.3% (70/101) 47.7% (72/151)
Percentage of outlets that knew that SP is a single dose 83.2% (84/101) 64.9% (98/151)
Practice
Percentage of shoppers who purchased an approved SP and an anti-pyretic, and were told the correct dose 17.2% (27/157) 1.5% (3/202)[of shoppers who purchased a drug]
Scenario 1* 15.5% 1.1%
Scenario 2** 18.6% 1.8%
Percentage of shoppers who purchased an approved SP and an anti-pyretic [of shoppers who purchased a drug] 23.6% (37/157) 3.0% (6/202)
Percentage of shoppers who purchased an approved SP and an anti-pyretic [of all mystery shopper visits] 18.3% (37/202) 2.0% (6/302)
* Scenario 1: 9-month-old child, female mystery shopper asks for advice
** Scenario 2: 2-year-old child, male mystery shopper asks for chloroquine-based drug
6.5 The Effect of ExplicitConsumer DemandOne issue that interested the studyteam was to determine whether retaildrug outlet attendants were recom-mending specific drugs or mostlyselling what clients demanded.Previous studies have suggestedthat consumer demand has a strongimpact on drug sellers (Brugha andZwi 1998). To estimate the effect ofconsumer demand, all male shop-pers were specifically told to requesta popular CQ-based drug,Malaraquin. The drugs sold to thetwo types of mystery shoppers werethen compared. Overall, 9 percent offemale shoppers (who did notdemand CQ) were sold a CQ-baseddrug compared to 21 percent ofmales (who did demand CQ). Theseresults suggest that explicit demandfor a particular anti-malarial drug
does have a significant effect, but itis not very strong (about 12 per-cent). Control outlets were twice aslikely as intervention outlets to sellCQ-based drugs to mystery shop-pers.
The intervention seems to havelessened slightly the effect ofconsumer demand. In interventionoutlets, 5 percent of female shop-pers purchased CQ versus 14percent of males, giving a consumerdemand effect of only about 9percent. In control outlets, 12percent of female shoppers and 25percent of male shoppers were soldCQ, giving a consumer demandeffect of about 13 percent. The mainreason that more male shopperswere not sold CQ may be that onlyabout 40 percent of the outletsstocked it.
6.6 Cost-Effectiveness ofthe InterventionA main goal of this study was todetermine the intervention’s cost-effectiveness. Affordability is acritical issue for scaling up beyondone district. The cost of replicatingthis intervention in another district inKenya is estimated at $8,300 (Ksh581,000). The main costs were thedevelopment and production of1500 client and shopkeeper jobaids, training of attendants andmobile vendors, and monitoring. Ifthe mystery shopper exercise isadded, the cost of replication wouldbe about $11,500 (Ksh 805,000).
In six months, it is estimated that theintervention reached 500 outlets.Given that 16 percent additionalclients were treated properly at theintervention outlets, one could

12 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
expect that about 82,000 additionalpeople were treated correctly. Thiswould mean that the interventioncost approximately $0.10 (Ksh 7)per case properly treated. If oneassumes that the effect of theintervention lasted at least anothersix months, the cost per beneficiarywould drop to about $0.06. Alterna-tively, one could say that theintervention cost about $17 (Ksh1200) per outlet reached. For a fullexplanation of how these estimateswere made, see Appendix 1.
7.0 Discussion
It seems likely that the private sectorwill continue as the dominant sourceof anti-malarial treatment for uncom-plicated cases of malaria in Kenya,as well as in other developingcountries. For this reason, strength-ening the capacity of private drugoutlets to provide quality anti-malarial drugs and information hasbecome one of Roll Back Malaria’sstrategic objectives. The challengeis to increase the capacity of privateoutlets at a cost low enough that theactivity can be scaled up nationally.At a cost of about $17 per outletreached, most countries couldprobably afford the Vendor-to-Vendor intervention.
Four strategies have been advancedfor improving the practices of retailpharmacies in developing countries:information, persuasion, incentives,and coercion (Goel et al. 1996). Themost successful strategy for chang-ing physician prescribing practicesin developing countries has beenthrough persuasion or “academicdetailing.” Persuasion is defined as“a successful, intentional effort toinfluence another’s mental statethrough communication in a setting
in which the target audience has ameasure of freedom” (Goel et al.1996). Indications are that persua-sion can have an impact on privatesector practices if doing so does notsignificantly reduce profits.
To date, very few interventions tochange retailer behaviors throughpersuasion (or by any other means)have been systematically introducedand evaluated. One intervention forpharmacy attendants in Kenya andIndonesia, called “face to faceeducational outreach,” resulted insignificant short-term improvementsin diarrheal product sales andcommunication with customers ondiarrhea treatment (Ross-Degnan etal. 1996). However, its long-termimpact and cost-effectiveness arenot known.
The Vendor-to-Vendor Educationintervention combined the strategiesof customized information andpersuasion to achieve improvedknowledge and dispensing prac-tices among private retailers.Formative research in setting up theintervention had revealed thatwholesalers were consideredcredible sources of information forprivate retail outlets on the test anti-malarial drugs. Hence, they weredesignated to serve as the“persuaders” for this activity.Informal interviews with wholesalersindicate that the mobile vendorswere more enthusiastic and ener-getic distributors of the job aids thanwere the counter attendants. Thereason seems to be that the inter-vention heightened the status ofmobile vendors more than counterattendants. Also, because themobile vendors do not face queuesof retailers, communicating theguidelines may have been morefeasible for them than the counterattendants.
Other studies have indicated thatjob aids tailored to the needs of thetarget audience can positively affectperformance (Knebel et al. 2000).The shopkeeper job aid seems to bethe other most important componentof the Vendor-to-Vendor intervention.Nearly two-thirds of shopkeepersreported that it was useful to them,and one-third used it spontaneouslywhen asked about SP dosages.Because no clients were interviewedduring the evaluation, we do notknow the impact of the client job aidon them. However, indications fromthe shopkeepers are that more thanhalf of the clients found them to beuseful.
The main alternate model forchanging shopkeeper anti-malarialdispensing behaviors has beenpiloted in Kilifi, Kenya. The corner-stone of the intervention was aseries of three workshops, eachlasting three days, followed by atwo-day refresher training for 46shopkeepers from 23 shops. Theactivity seems to have led todramatic improvements in anti-malarial prescribing practices andadvice given (Marsh et al.1999). Inour view, the main problems with theKilifi model are:
■ It is not clear that all of thetraining provided the shopkeep-ers is necessary for them to servethe public effectively
■ The training may be reachingmostly owners of shops, ratherthan many of those who actuallysell drugs to the public (e.g.,family members)
■ The turn-over among employeesin shops and short life spans ofmany small establishments wouldnecessitate constant retraining

Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 13
■ It seems to be quite costly(although cost information is notprovided) and time-consuming,which would make it difficult toachieve wide coverage
While the Vendor-to-Vendor interven-tion did seem to have significantlyimproved drug outlets’ knowledgeand behavior in a relatively shorttime (six months), the gap betweenactual and desired performance wasstill quite large. More than half thedrugs that intervention outlets soldto the mystery shoppers were notSP-based. This could be due toseveral factors. First, it is likely thatintervention outlets still had stocks ofold drugs that they needed to sell.Virtually all drug outlets operate onvery limited budgets and cannotafford to discard drugs that are nolonger recommended. Second,confusion and fear about SPs werestill common in the district. Manyoutlets still were not sure whetherthey were indeed entitled to sell SPsover the counter. Third, the interven-tion did not comment about the useof AQ, which had become extremelypopular in the district due to exten-sive advertising, high profit marginsfor sellers, and an apparentlycheaper price for consumers thanSP.6 Because SP is slow-actingwhereas AQ is fast-acting, AQseems to be more effective than SP.No one was aware of the long-termnegative side effects of long-termuse of AQ. Addressing these issueswould make the intervention moreeffective.
In general, the mystery shopperapproach, using “third person”scenarios, seems to have been very
effective in evaluating dispensingpractices of the outlets in Bungomadistrict. Including supervisory visitsto the outlets after the shopper visitsgave important additional informa-tion. The decision to vary thescenarios by gender of the mysteryshopper may not have been wise,however. It made it more difficult todiscern whether the differences inthe treatment given to shoppersrelated more to their scenario or totheir gender.
It is important to recognize thelimitations of the mystery shopperapproach. The main drawback tousing mystery shoppers is that theycannot evaluate certain institutionswhere they would be detected asoutsiders (such as school dispensa-ries) or where they are required tobring their child with them (such assome private clinics). If the mysteryshoppers had been actual clientswith children, private clinics prob-ably would have dispensed moreinjections. It is also possible that realclients, who are familiar with theshopkeepers, would be refusedtreatment less often than unknownclients (mystery shoppers). Inseveral situations, outlets may havebecome suspicious of the mysteryshoppers and given them differenttreatment than they would havenormally. A few shops locked theirdoors after the first shopper hadcompleted his or her visit, so thesecond shopper was never servedthere. These shops had to beexcluded from the analysis. Lastly, itseems likely that the mysteryshoppers received more informationabout the drugs than typical custom-
ers. Mystery shoppers noted that if areal customer asked for a drug bybrand name, the shopkeeper wasinclined to assume that they knewhow to take the drug and hencegave little information about it.
The sampling design also had somelimitations. Because outlets were notrandomly selected, one cannotextrapolate from the study toestimate the percentage of alloutlets in Bungoma district stockingSPs or giving correct advice tocustomers. Also, the decision toexclude receipted outlets in remotelocations due to logistical consider-ations may have led to someselection bias. It is also possible thatthere was a self-selection biasamong intervention outlets; somecontrol outlets may have beenoffered job aids but refused them.The occasional discrepancybetween “receipted” outlets andshopkeepers’ reports may also havebiased the sample to some extent.
8.0 Conclusions andRecommendations
The Vendor-to-Vendor Educationintervention, a low-cost outreacheducation strategy, seems to havehad a positive impact on privatedrug outlets’ compliance withmalaria treatment guidelines inBungoma district. Significantdifferences were discerned betweenintervention and control outlets ontypes of drugs sold, dosages sold,questions asked of clients, andadvice given. The intervention alsohad a significant positive impact on
6 Misleading packaging contributed to the misperception that AQ was cheaper than SP. For instance, the most popular AQ brand(Malaratab) was packaged in three-tablet blister packs, just like SP. But consumers actually need to purchase three blister packs ofMalaratab to get the correct dose. With SP (such as Falcidin), one blister pack is sufficient. Since one blister pack of SP was about 3-5shillings more costly than one blister pack of AQ, consumers were inclined to buy AQ.
14 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
knowledge of malaria treatmentguidelines. More intervention outletsknew key concepts about malariatreatment than control outlets. Theintervention appears to have had thegreatest impact on shops and kiosksand the least impact on privateclinics. Most outlets that receivedjob aids reported that they wereuseful and were displaying them in aprominent location.
To have greater impact, the interven-tion would have to address severalissues more intensively:
■ Build consumer demand for SP
■ Sustain the interest of wholesalecounter attendants as communi-cators of malaria guidelines
■ Encourage national-level enforce-ment of correct drug packagingand standard pricing
Based on the findings, the followingrecommendations were made toKenya’s policy-makers:
National level:
■ The National Malaria ControlCommittee (NMCC) shouldconsider replicating the Vendor-to-Vendor Education program inall endemic areas of the country
■ The MOH should revisit its policyabout amodiaquine as thesecond-line drug and make clearits concerns about wider use
■ The MOH should insist that majornational pharmaceutical compa-nies accurately indicate dosagesfor all age groups on drugpackages. Information should beclear enough for low-literateclients and shopkeepers tounderstand
■ The MOH should enforce thepolicy that unapproved anti-malarials do not reach the marketor are pulled from the market
District level:
■ The DHMT should designate anannual “malaria control month”just before the rains to engage invendor-to-vendor activities
■ To increase client demand forSPs, health facilities should beencouraged to include recom-mended anti-malarial drugs intheir micro-teachings
■ To address confusion regardingSP, an official letter needs to besent to wholesalers and vendors,which they can show to shops/kiosks
■ Ongoing misconceptions aboutmalaria treatment (e.g., that SP istoo strong for children) should beaddressed in subsequentactivities

Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya ■ 15
Appendix 1
Calculation of theCost-Effectiveness of theIntervention
To calculate the cost-effectivenessof the intervention, we began byestimating the coverage of theintervention in the 6 months betweenthe training of wholesalers and themystery shopper evaluation. Itshould be recalled that our sampleconsisted of several types of outlets:(a) receipted outlets that had indeedreceived the job aids, (b) receiptedoutlets that reported not receivingjob aids, (c) outlets without receiptsthat had in fact received the jobaids, and (d) outlets without receiptsthat had not received the job aids.7
Our first step was to calculate howmany of the 221 receipted outlets(after removing 10 duplicatereceipts) actually had received jobaids. Because of time constraints,we sought to visit only 126 receiptedoutlets. We found that 63 (50percent) of them had job aids. Weestimated therefore that 50 percentof the 95 receipted outlets that wedid not seek to visit also had jobaids, or 47. Next, we found that 19percent of the 200 unreceiptedoutlets in Bungoma district that wevisited actually had received jobaids, or 38. Consequently, weassumed that about 19 percent of allunreceipted outlets in the districthad in fact received job aids. TheDHMT estimated that the totalnumber of outlets selling anti-malarial drugs in Bungoma districtwas about 1500. Of that 1500, weexcluded in our calculations the 252
visited by the mystery shoppers andthe other 95 receipted outlets,leaving about 1150. If 19 percent ofthese 1150 outlets were reachedwith job aids, then 219 of the 1150were reached. Finally, 6 percent ofoutlets in a neighboring district werefound with job aids. If we estimatethat the spill-over effect to neighbor-ing districts was about 6 percent,and that there are about 2400 outletsin three neighboring districts toBungoma, then we need to add 6percent of 2400, or 144. Our totalcoverage is thus estimated at63+47+38+219+144 = 511, roundeddownward to 500 outlets reached.
Of the 500 outlets, it was estimatedthat about 75 percent (375) wereusing the job aids for about 5months or 120 working days. Onaverage, outlets reported that theysee about 9 malaria clients per day,or 405,000 clients in the period wewere evaluating (375 outlets x 9clients x 120 days = 405,000). Theremaining 125 outlets were esti-mated to have been using the jobaids for about 4 months or 90working days, which would yieldabout 101,250 clients (125 outlets x9 clients x 90 days = 101,250). Ourtotal estimated caseload at theintervention outlets is therefore405,000 + 101,250 = 506,250,rounded to 506,000 malaria clientsserved by the intervention outlets.
The percentage of malaria cases(mystery shoppers) treated properlydue to the intervention can beestimated at 18.3 percent (theamount treated properly in theintervention group) minus 2.0percent (the amount treated cor-rectly in the control group), or 16.3percent. We thus can assume that
16.3 percent of 506,000 malariacases, or 82,478 cases, receivedproper malaria treatment during thefirst 6 months because the outletsthey visited had received job aids.For ease of calculation, we roundedthis figure to 82,000 clients properlytreated due to the intervention inthe first 6 months. These peoplecould be considered the beneficia-ries of the program. If these outletscontinued to provide correcttreatment for at least another sixmonths, it is possible that there wereat least 150,000 beneficiaries.(Turnover among outlet attendantsand malaria seasonality coulddeflate this number somewhat.)
To determine the cost per benefi-ciary, we took the cost of theintervention, $8,300, and divided itby 82,000, the number of casesestimated to have been treatedproperly due to the intervention,resulting in $0.10 per beneficiaryin the first 6 months of the activity.If the number of beneficiariesreached 150,000 after one year, thecost of the intervention per benefi-ciary could fall to about $0.06.Alternatively, if we considered theoutlets as the beneficiaries, theintervention can be estimated ascosting about $17 per outlet ($8300/ 500 = $16.60).
7 Any outlet receiving the job aids was supposed to sign a receipt indicating that it would follow the new malaria guidelines.

16 ■ Vendor-to-Vendor Education to Improve Malaria Treatment by Drug Outlets in Kenya
References
Brugha, R., and A. Zwi. 1998. Improving the quality ofprivate sector delivery of public health services:Challenges and strategies. Health Policy and Planning13(2):107–20.
Bungoma DHMT. 1998. Report on community distributionoutlets for drug supply. Bungoma District Malaria InitiativeProject Report.
Goel, P., D. Ross-Degnan, P. Berman, and S. Soumerai.1996. Retail pharmacies in developing countries: Abehavior and intervention framework. Social Science andMedicine 42(8):1151–61.
Hamel, M.J., A. Odhacha, J.M. Roberts, and M.S. Deming.2001. Malaria control in Bungoma District, Kenya: A surveyof home treatment of children with fever, bednet use andattendance at antenatal clinics. Bulletin of the World HealthOrganization 79(11):1014–23.
Knebel, E., S. Lundahl, A. Edward Raj, and H. Abdallah.2000. “The use of manual job aids by health careproviders: What do we know?” Operations Research IssuePaper 1(1). Bethesda, MD: Published for the U.S. Agencyfor International Development (USAID) by the QualityAssurance (QA) Project.
Madden, J.M., J.D. Quick, D. Ross-Degnan, and K.K.Kafle. 1997. Undercover careseekers: Simulated clientsin the study of health provider behavior in developingcountries. Social Science and Medicine 45(10):1465–82.
Marsh, V.M., W.M. Mutemi, J. Muturi, A. Haaland, W.M.Watkins, G. Otieno, and K. Marsh. 1999. Changing hometreatment of childhood fevers by training shop keepers inrural Kenya. Tropical Medicine and International Health4(5):383–89.
McCombie, S.C. 1996. Treatment seeking for malaria: Areview of recent research. Social Science and Medicine43(6):933–45.
Ongore, D., and L. Nyabola. 1996. Role of shops andshopkeepers in malaria control. East African MedicalJournal 73(6):390–94.
Roll Back Malaria website: www.mosquito.who.int. May2001. “Malaria a global crisis.”
Ross-Degnan, D., S.B. Soumerai, P.K. Goel, J. Bates,J. Makhulo, N. Dondi, Sutoto, D. Adi, L. Ferraz-Tabor, andR. Hogan. 1996. The impact of face to face educationaloutreach on diarrhoea treatment in pharmacies. HealthPolicy and Planning 11(3):308–18.
Ruebush, T.K., M.K. Kern, C.C. Campbell, A.J. Oloo. 1995.Self-treatment of malaria in a rural area of Western Kenya.Bulletin of the World Health Organization 73(2):229–36.
WHO Technical Report 839. 2000. Implementation of theGlobal Malaria Control Strategy: Report of a WHO StudyGroup on the Implementation of the Global Plan of Actionfor Malaria Control (1993–2000).



















