
Variability of presentation in medial temporal lobe epilepsy: a study of 30 operated cases
11
Acta Neurol Scand 1996: 94: 1-11 Printed in UK - all rights reserved Copyright 0 Munksgaard 1996 ACTA NEUROLOGICA SCANDINAVICA ISSN 0001-6314 Variability of presentation in medial temporal lobe epilepsy: a study of 30 operated cases Adam C. Clemenceau S. Semah E Hasboun D. Samson S. Aboujaoude N. Samson Y. Baulac M. Variability of presentation in medial temporal lobe epilepsy: a study of 30 operated cases Acta Neurol Scand 1996: 9 4 1-11. 0 Munksgaard 1996. Introduction - To evaluate the homogeneity of patients operated on for MTLE. Material and methods - 30 consecutive patients prospectively investigated with clinical, EEG, neuropsychology, MRI, FDG-PET criteria and eventually intracranial EEG, who underwent antero-medial temporal resection (follow-up: 24 months). Results - Clear and well-lateralisedMTLE was non-invasively ascertained in 22 patients (73%). Eight patients (27%) had a less pure presentation due to divergent scalp EEG features (bitemporal, widespread or extratemporal), unusual auras or absence of MRI-based hippocampalsclerosis or FDG-PET hypometabolism. They were explored by invasive monitoring which confirmed medial temporal origin of seizures. Outcome was excellent in 95% of the pure cases (Engel's class I) and less favorable in the more difficult ones (65% of class I). Conclusions - MTLE criteria, including the strong contribution of brain imaging, permit to select accurately a large percentage of patients. However a consistant number of patients present a less pure presentation suggestingmore complex I epileptogenic networks. Several recent reports have contributed to define the characteristics of the epilepsies of the medial temporal lobe (MTLE). A retrospective study ana- lysed the preoperative data from 67 patients explored with intracranial electrodes, who became seizure-free after resection including the medial temporal lobe structures (1, 2). The non-invasive diagnostic criteria of this population comprised early events, natural history of the disease, seizure characteristics, neuropsychological profiles, surface EEG-video data and brain imaging abnormalities. One of the major characteristics was the presence of medial temporal sclerosis (MTS). This latter point is supported by a large body of publications about the localising and lateralising value of MRI- based MTS (2-10). The presence of these criteria has enabled to simplify the procedure of presurgi- cal evaluation while obtaining non-invasively very good post-operative results (11). From a prospective point of view, however, these criteria which correspond to a pure culture analysis are not found in all the patients for whom MTLE is suspected. There is some degree of heterogeneity C. Adam It, S. Clemenceau w, F. Semah 25, D. Hasboun u, S. Samson ', N. Aboujaoude ', Y. Samson ', M. Baulac 'Service de Neurophysiologie,'Unit6 d'Epileptologie, Clinique Neurologique Paul Castaigne, 'Service de Neurochirurgie,4Service de Neuroradiologie, HGpital de la Piti6-SalpBtribre.Paris, %serm U 334. Service hospitalier F. Joliot. DRIPP. CEA, Orsay, France Key words: temporal lobe epilepsy; neurosurgery; medial temporal sclerosis; positron emission tomography; magnetic resonance imaging; electroencephalography; implanted electrodes M. Baulac, Clinique Neurologique Paul Castaigne, HBpital de la Salpetribre, 47, boulevard de I'HOpital, 75651 Paris c6dex 13, France Accepted for publication April 1, 1996 in the clinical and EEG pictures and for a given patient some critical information can be either not present or not congruent with the other parame- ters. In spite of the strong contribution of brain imaging, confirmation of MTLE diagnosis and its lateralisation may still require depth recordings in these cases. But the demarcation between patients who can be processed non-invasively and those for whom intracranial recordings should be recom- mended is arbitrary, depending on the weight attributed to the various evaluation parameters and finally on individual center's experience. This series has evaluated 30 patients taken consecutively and not selected on post-operative outcome. The non-invasive evaluation process included also a FDG PET scan looking for the characteristic pattern of MTLE (12, 13). Twenty patients (73%) were directly referred for surgery, whilst in eight of them (27%) additional pre- operative information was sought by intracranial recordings. We report and discuss the clinical, paraclinical characteristics and the post-operative outcomes in these two groups of patients 1
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Variability of presentation in medial temporal lobe epilepsy: a study of 30 operated cases
Acta Neurol Scand 1996: 94: 1-11 Printed in UK - all rights reserved
Copyright 0 Munksgaard 1996 ACTA NEUROLOGICA
SCANDINAVICA ISSN 0001-6314
Variability of presentation in medial temporal lobe epilepsy: a study of 30 operated cases
Adam C. Clemenceau S. Semah E Hasboun D. Samson S. Aboujaoude N. Samson Y. Baulac M. Variability of presentation in medial temporal lobe epilepsy: a study of 30 operated cases Acta Neurol Scand 1996: 9 4 1-11. 0 Munksgaard 1996.
Introduction - To evaluate the homogeneity of patients operated on for MTLE. Material and methods - 30 consecutive patients prospectively investigated with clinical, EEG, neuropsychology, MRI, FDG-PET criteria and eventually intracranial EEG, who underwent antero-medial temporal resection (follow-up: 24 months). Results - Clear and well-lateralised MTLE was non-invasively ascertained in 22 patients (73%). Eight patients (27%) had a less pure presentation due to divergent scalp EEG features (bitemporal, widespread or extratemporal), unusual auras or absence of MRI-based hippocampal sclerosis or FDG-PET hypometabolism. They were explored by invasive monitoring which confirmed medial temporal origin of seizures. Outcome was excellent in 95% of the pure cases (Engel's class I) and less favorable in the more difficult ones (65% of class I). Conclusions - MTLE criteria, including the strong contribution of brain imaging, permit to select accurately a large percentage of patients. However a consistant number of patients present a less pure presentation suggesting more complex
I epileptogenic networks.
Several recent reports have contributed to define the characteristics of the epilepsies of the medial temporal lobe (MTLE). A retrospective study ana- lysed the preoperative data from 67 patients explored with intracranial electrodes, who became seizure-free after resection including the medial temporal lobe structures (1, 2). The non-invasive diagnostic criteria of this population comprised early events, natural history of the disease, seizure characteristics, neuropsychological profiles, surface EEG-video data and brain imaging abnormalities. One of the major characteristics was the presence of medial temporal sclerosis (MTS). This latter point is supported by a large body of publications about the localising and lateralising value of MRI- based MTS (2-10). The presence of these criteria has enabled to simplify the procedure of presurgi- cal evaluation while obtaining non-invasively very good post-operative results (11).
From a prospective point of view, however, these criteria which correspond to a pure culture analysis are not found in all the patients for whom MTLE is suspected. There is some degree of heterogeneity
C. Adam I t , S. Clemenceau w, F. Semah 25, D. Hasboun u, S. Samson ', N. Aboujaoude ', Y. Samson ', M. Baulac 'Service de Neurophysiologie, 'Unit6 d'Epileptologie, Clinique Neurologique Paul Castaigne, 'Service de Neurochirurgie, 4Service de Neuroradiologie, HGpital de la Piti6-SalpBtribre. Paris, %serm U 334. Service hospitalier F. Joliot. DRIPP. CEA, Orsay, France
Key words: temporal lobe epilepsy; neurosurgery; medial temporal sclerosis; positron emission tomography; magnetic resonance imaging; electroencephalography; implanted electrodes
M. Baulac, Clinique Neurologique Paul Castaigne, HBpital de la Salpetribre, 47, boulevard de I'HOpital, 75651 Paris c6dex 13, France
Accepted for publication April 1, 1996
in the clinical and EEG pictures and for a given patient some critical information can be either not present or not congruent with the other parame- ters. In spite of the strong contribution of brain imaging, confirmation of MTLE diagnosis and its lateralisation may still require depth recordings in these cases. But the demarcation between patients who can be processed non-invasively and those for whom intracranial recordings should be recom- mended is arbitrary, depending on the weight attributed to the various evaluation parameters and finally on individual center's experience.
This series has evaluated 30 patients taken consecutively and not selected on post-operative outcome. The non-invasive evaluation process included also a FDG PET scan looking for the characteristic pattern of MTLE (12, 13). Twenty patients (73%) were directly referred for surgery, whilst in eight of them (27%) additional pre- operative information was sought by intracranial recordings. We report and discuss the clinical, paraclinical characteristics and the post-operative outcomes in these two groups of patients
1
Adam et al.
Patients and methods
Thirty consecutive adult patients were included on following criteria: 1) severe medically intractable epilepsy, 2) final diagnosis of MTLE, 3) no macro- scopic brain abnormality except medial temporal sclerosis, 4) patient operated on (between June 1991 and March 1994).
The first phase of evaluation was non-invasive and comprised clinical data (past and epilepsy history, physical examination), EEG-video moni- toring, MRI with a special protocol for hippocam- pal study, 18-fluorodeoxyglucose (FDG) PET scan, neuropsychological and psychiatric assessement and intracarotid sodium amobarbital testing.
The EEG-video recordings were performed on a 32 channel BMSI system (Nicolet-BMSI, Madison, Wisconsin, USA) connected to a computerized sei- zure automatic detection system (Monitor software, Stellate systems, Montreal, Canada). Surface EEG was acquired according to the 10-20 system (14) with the restriction that F7FS were placed more posteriorly and inferiorly at a position Tl/T2 (15). The same recordings were written out in various montages. Seizures were activated by hyperventila- tion, progressive drug withdrawal and sleep depri- vation. Mean duration of continuous EEG-video monitoring was 10 days. A mean of 5 seizures (range: 2-9) per patient was recorded on the scalp.
The MRI acquisition was performed on a Siemens unit at 1 tesla until September 1992 and then at 1.5 tesla. Following scout sequence to insure symmetric positioning of the subject's head, three series of scans were taken at each examination: 1) sagittal, T1-weighted; 2) oblique coronal, T1- weighted, spin-echo (TR 400, TE 15, 4 excitations, 5 mm slice thickness, no gap) at 1 tesla, or Turbo- FLASH 3DFT (TR 10, TE 4, flip angle lo", 1.6 mm slice thickness) at 1.5 tesla; 3) coronal, T2-weighted (spin-echo TR 2200-2500 at 1 tesla or fast spin echo TR 6000 at 1.5 tesla, TE 30-90, 7 mm slice thick- ness). The oblique coronal plane imaging sequence was acquired perpendicular to the long axis of the hippocampus, which was defined on the sagittal images. One section was chosen so as to contain the anterior commissure. The presence of an hippo- campal atrophy was determined by visual inspec- tion (obvious hippocampal asymmetry and/or high T2 signal) and, in all the cases, hippocampal vol- ume measurements. The limits tolerated for normal hippocampal asymmetry index in this study were L2.2 SDs from the mean volume of 21 and 22 controls for each MRI acquisition technique respectively. A T2 weighted axial sequence was made for examination of all brain areas.
PET scan was performed interictally in 29 patients on the ECAT 953/31B (Siemens), a 31-
slice head-dedicated tomograph, which had in- plane resolution of 5mm. PET methods were recently published (13). The PET plane was paral- lel to the long axis of the hippocampus as deter- mined on MRI. A mean dose of 6 mCi of FDG was injected intravenously. Reconstructed images were corrected for attenuation using 68Ga-68Ge transmision scans. Local cerebral metabolic rate for glucose (CMRglu expressed in milligrams per minute per 100 g of tissue) was calculated accord- ing to Sokoloff's model, as modified by Phelps (16). Quantitative analysis was performed in 21 of 29 patients. Metabolic rates of glucose were deter- mined in three MRI-defined temporal regions (hip- pocampo-polar, anterior part of the lateral cortex, and posterior part of the lateral cortex). Individual analysis used indices of asymmetry, considered abnormal beyond 3 SDs from normal values obtained in 10 healthy volunteers. Visual analysis was performed in 8 of 29 patients by one of us blind to the other data. Extratemporal metabolism was controled by visual analysis.
All patients underwent a neuropsychological (evaluating intellectual, memory and language abil- ities) and a psychiatric examination. The intraca- rotid sodium Amobarbital procedure (17) was performed in 28 patients to provide evidence for cerebral language laterality and to evaluate risks for developing significant post-surgical memory deficits. A description of the current procedure can be found elsewhere (18,19). With one exception, both hemispheres were tested on two consecutive days. The memory test was composed of 7 items presented during the effect of the drug.
When informations of the first phase were not sufficiently congruent or clear, a second phase could be undertaken consisting of invasive record- ings with intracerebral and subdural electrodes (Ad-Tech Medical Instruments, Racine, Wisconsin, USA). The intracerebral electrodes were com- posed of 8 contacts 0.8 cm apart mounted on a 1 mm wide flexible plastic probe. The subdural elec- trodes were strips of 4, 6 or 8 contacts 1 cm apart. The electrode location was determined according to the hypotheses resulting from the previous phase. Eight patients have been invasively investi- gated. Three were explored bilaterally by medio- temporal intracerebral electrodes introduced through postero-anterior trajectory. These elec- trodes recorded the medial structures of the tem- poral lobe (amygdala and hippocampus) and the temporo-occipital cortical junction. The five other patients had also frontal intracerebral electrodes (introduced parasagittally) exploring medial struc- tures: orbitofrontal cortex, anterior cingulate gyrus and prefrontal portion of the first frontal gyrus. Subdural strips inserted through burr holes were
2

Variability of MTLE presentation
added in one patient to sample lateral or inferior cortices of frontal and temporal lobes. The post- implantation location of the electrodes was con- troled by MRI. The duration of EEG-video moni- toring with intracranial electrodes was a mean of 2 weeks. Eight spontaneous seizures per patient were recorded during the session.
Surgical treatment was identical whatever the side of operation (15 right, 15 left). It consisted of removal of the temporal pole, the uncus, the amy- gdala and the largest part of hippocampal forma- tions with the parahippocampal gyrus. In 2 patients who failed at the sodium amytal tests temporal resection removed only the amygdala and the uncus. Pathological examination of resected tissue was performed in all patients. Mean duration of postoperative follow-up was 24 months (range: 12 to 44). Patients were left with their preoperative medical treatment during the first year. When the treatment combined a tritherapy, it was reduced to a bitherapy, After the first year treament was simplified but not systematically. None has been
Statistical analyses between non-implanted and implanted groups were performed with chi-square tests with Yates’ correction or Student’s t-test.
lost to follow-up.
Results
Twenty two patients (73%) were directly operated on after the non-invasive phase. Eight patients (27%) were explored with intracranial electrodes because they did not present a clear set of charac- teristics of well-lateralised MTLE for one or sev- eral of the following reasons (Table 5): absence of brain imaging abnormality (n=l), unusual first subjective symptoms (n=3), somatosensitive com- ponent of aura suggesting an extratemporal partic- ipation (n=l), conflicting lateralisation between EEG and brain imaging such as temporal spiking activity contralateral to MRI-based MTS (n=3 including one predominant on the normal side of MRI) or seizure build-up contralateral to MTS (n=3 including one expressing exclusively on the normal side of MRI), and occasionally or exclu- sively extratemporal or widespread seizure onsets suggesting a potential extratemporal origin (n=4). All these difficulties justified, in our experience, the use of intracranial explorations.
The intracranial recordings confirmed the medial temporal lobe (MTL, amygdala and/or hippocam- pus) origin of seizures in all cases and showed that no seizure originated from another suspected area. Yet, in 4 patients, seizures emanated independantly from either temporal lobe, but usually with a high predominance (more than 80% of seizures) on the operated side. In one case (no 3 in Table 5 , Fig. l),
Table 1. Demographic data
non-implanted implanted ~ ~~~~
19female. 11 male 25 right-handed, 4 left-handed, 1 ambidextrous Age at epilepsy onset. 9 years (2-25) Age at surgery: 29 years (1&44) 29 (18-44) 28 (22-37)
9 (2-25) 8 (3-17)
Post-operative follow-up: 24 months ( 1 2 4 ) 25 (12-41) 21 (1344)
however, seizures appeared equally distributed on both sides (6 right, 6 left).
Demographic data/early events/risk factors
Demographic data of these two subgroups were not significantly different (Table 1).
Early events were retrieved in 26 patients (87% of patients). Nineteen patients (63% of all, 68% of non-implanted, 50% of implanted patients) expe- rienced early convulsions at the mean age of 15 months (range: 3 4 8 months). Habitual seizures began after a mean latency of 8 years after early convulsions. Other early events have been noted less frequently: head trauma (17% of all, 14% of non-implanted, 25% of implanted patients) some- times with convulsions (7%), coma (7%), pre- sumed meningitis (7%), operated craniostenosis (3%) and, in one patient, an association of familial febrile convulsions and generalized epilepsy. Head trauma without convulsions was mild in 2 cases and its significance might be discussed.
Seizure characteristics
Seizure types - All patients had complex partial seizures according to the international classifica- tion of seizures (20), 19 also had simple partial seizures (14 non-implanted (64%), 5 implanted patients (71%)) and 17 rare secondarily general- ized seizures (10 non-implanted (45%), 7 implanted patients (87%), no statistical difference). No status epilepticus was reported.
Auras - All patients except one had auras (97% of all, 100% of non-implanted, 87% of implanted patients (Table 2)). The most frequent one was an abdominal (usually epigastric) visceral sensation (73% of all, 77% of non-implanted, 62% of implanted patients) often ascending. The second most frequent was a feeling of fear or anxiety (43% of all, 44% of non-implanted, 37% of implanted patients) accompanying visceral sensation in 27% of patients. The other components of auras are listed in Table 2. During the conscious phase of seizures, they appeared always later than vis- cerovegetative or affective sensation, except some-
3
Adam et al.
TO2
TO3
LOTA
H1
H2
H3
TO1
TO3
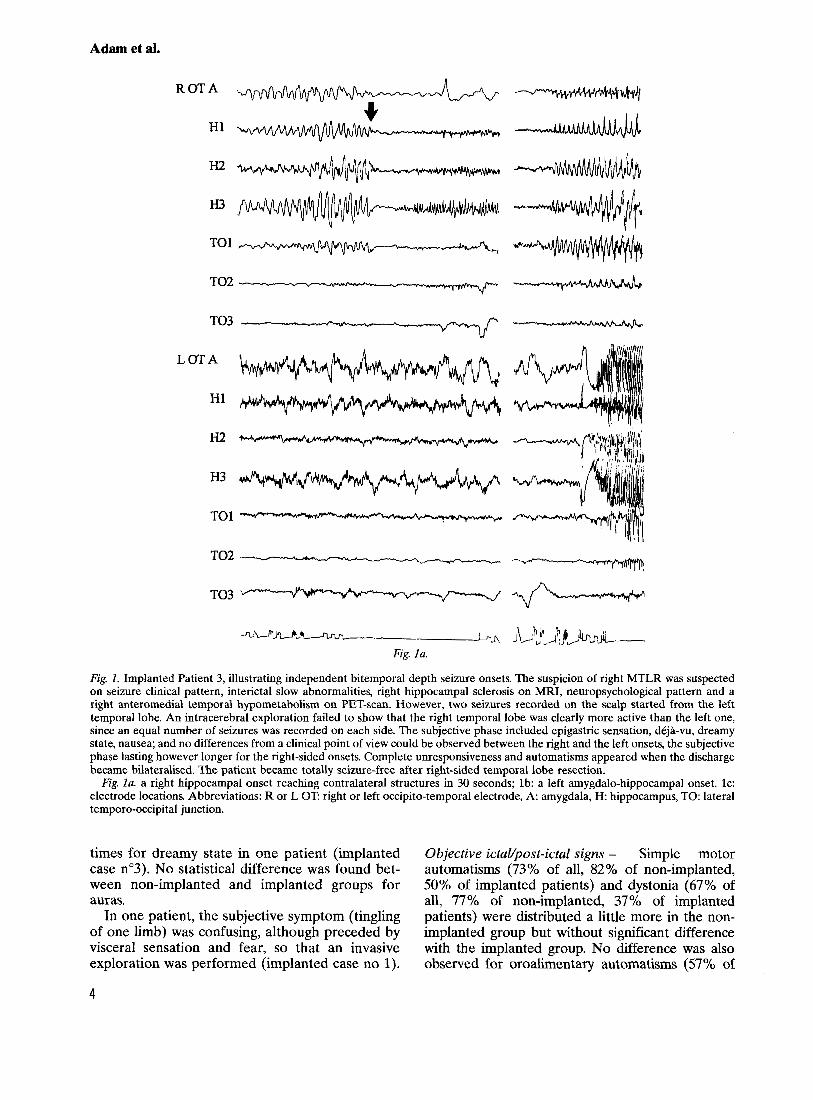
Fig. 1. Implanted Patient 3, illustrating independent bitemporal depth seizure onsets. The suspicion of right MTLR was suspected on seizure clinical pattern, interictal slow abnormalities, right hippocampal sclerosis on MRI, neuropsychological pattern and a right anteromedial temporal hypometabolism on PET-scan. However, two seizures recorded on the scalp started from the left temporal lobe. An intracerebral exploration failed to show that the right temporal lobe was clearly more active than the left one, since an equal number of seizures was recorded on each side. The subjective phase included epigastric sensation, dkja-vu, dreamy state, nausea; and no differences from a clinical point of view could be observed between the right and the left onsets, the subjective phase lasting however longer for the right-sided onsets. Complete unresponsiveness and automatisms appeared when the discharge became bilateralised. The patient became totally seizure-free after right-sided temporal lobe resection. Fig. la. a right hippocampal onset reaching contralateral structures in 30 seconds; lb: a left amygdalo-hippocampal onset. lc:
electrode locations. Abbreviations: R or L OT right or left occipito-temporal electrode, A amygdala, H hippocampus, TO: lateral temporo-occipital junction.
times for dreamy state in one patient (implanted case n"3). No statistical difference was found bet- ween non-implanted and implanted groups for auras.
In one patient, the subjective symptom (tingling of one limb) was confusing, although preceded by visceral sensation and fear, so that an invasive exploration was performed (implanted case no 1).
Objective ictaUpost-ictat signs - Simple motor automatisms (73% of all, 82% of non-implanted, 50% of implanted patients) and dystonia (67% of all, 77% of non-implanted, 37% of implanted patients) were distributed a little more in the non- implanted group but without significant difference with the implanted group. No difference was also observed for oroalimentary automatisms (57% of
4

Variability of MTLE presentation
ROTA
H1
H2
H3
TO1
-w TO2 4 4
TO3
all, 59% of non-implanted, 50% of implanted patients), verbal automatisms (30% of all, 36% of non-implanted, 12% of implanted patients) and post-ictal aphasia (47% of all, 45% of non- implanted, 50% of implanted patients). For the whole population, dystonia was most of time (57% of patients) opposite to the side of the subsequent operation and post-ictal aphasia occurred in seizures beginning in the dominant hemisphere in all patients (43% of patients) but one.
Scalp EEG findings
In one patient, no seizure was recorded on surface EEG but the presence of 2 very active independent spiking foci led to perform an intracranial EEG monitoring. Fig. 1 c.
5

Adam et al.
Table 2. Auras in non-implanted and implanted patients groups (YO of patients in each group in parentheses)
non-implanted implanted total
Patients with aura
Types of aura:
-Visceral sensation (abdominal or thoracic) only aura Fear or anxiety
Warmth DBjd-vu. deja-vecu Sound modification (increase. echo) Dreamy state/complex visual hallucinations Removal Gustatory Tachycardia Faintness Tachypnea Thrill h g l i n g of one limb Olfactory Auditory (elementary) Micro-macropsia-heautoscopy Forced idea Levitation sensation Depersonalisation
-Aura without visceral sensation or fear Thrill Indescribable
-Symptoms accompanying visceral and/or fear sensation
-No aura
The spiking activity (Table 3) was frequently tempo- ral (87% of all, 95% of non-implanted, 62% of implanted patients) and likewise for the seizure onsets (Table 4) but to a lesser degree (70% of all, 82% of non-implanted, 37% of implanted patients). These temporal interictal and ictal changes were unilateral respectively in 63% and 60% of all patients and significantly more often (p<0.05) in non-implanted patients (77% and 77% respectively) than in implanted ones (25% and 12% respectively). Comparison between the two groups showed a tendency to more frequent bitemporal spiking in implanted cases (37% of implanted versus 18% of non-implanted patients), to extratemporal spiking (12% versus 0% respectively) and to absence of spikes (25% versus 5% respectively). Regarding ictal onsets, they tended to be more frequently independent bitemporal in implanted cases (25% of implanted versus 0% of non-implanted patients), widespread (lateralised (25% versus 5%) or bilat- eral (25% versus 14%)) or extratemporal (12% versus 0%).
MRI findings (Table 5)
Medial temporal sclerosis was detected in 29 patients (97% of all, 100% of non-implanted, 87%
of implanted patients), as hippocampal atrophy (27 patients) associated with hyperintensity (15 patients) or as an hippocampal hyperintensity alone in 2 patients. The temporal resection was always performed on the side of MRI-based MTS. In the patient without MRI-based abnormality, interictal and ictal EEG informations suggested an epileptic process involving the 2 temporal lobes and consequently intracranial EEG monitoring was undertaken.
PET findings (Table 5)
Unilateral temporal hypometabolism was found in 28 of 29 examined patients (97% of all, 100% of non-implanted, 87% of implanted patients). The PET scan was normal in one patient, precisely in the patient with no MRI-based MTS. The hypome- tabolism involved the amygdalo-hippocampal area and the temporal pole in all cases and to a various extent the lateral part of the temporal lobe (13). No significant extratemporal .hypometabolism was noted. Interictal PET hypometabolism was lateral- ised on the side of operation and so, there was no discordance between PET and MRI data in terms of lateralisation.
6

Variability of MTLE presentation
Table 3. lnterictal EEG: epileptic abnormalities in non-implanted and implanted patient groups (% of patients in each group in parentheses)
non-implanted implanted total
no. of patients Temporal
unilateral
bilateral independent concordant*
with concordant predominance with discordant" predominance without predominance
Frontal (bilateral) No abnormalities
*with operated side
Table 4. lctal scalp EEG onset in non-implanted and implanted patient groups (% of patients in each group in parentheses)
non-implanted implanted total
no. of patients* Temporal
unilateral concordant** discordant
with concordant predominance without predominance
bilateral independent (from both sides)
bilateral synchronous""
concordant
with concordant maximal amplitude with no lateralised maximum
Widespread (lateralised)x***
Widespread (bilateral)+***
Frontal Uninterpretable No seizure obtained
*different kinds of onsets could coexist in an individual patient (3 cases) **with operated side ***with concordant maximal amplitude ****maximum usually temporo-frontal
Neuropsychological findings and arnobarbital tests
The mean full-scale IQ (WAIS-R) of the patients was 88 (range: 51-113). Sixteen patients (57% of all tested patients, 65% of non-implanted, 37% of implanted tested patients) displayed a memory def- icit on Amobarbital tests during injection contralat- era1 to the proposed surgery (Table 5). Three patients presented a s i m c a n t memory impairement fol- lowing injection ipsilateral to the future surgery. 7his led to a restricted surgical removal for 2 cases
Surgical results (Table 5)
Surgical outcome was evaluated after a mean fol- low-up of 24 months (12 to 44 months) and most of patients were still under antiepileptic drugs, although often reduced compared to preoperative treatment.
Twenty six patients (87%) can be considered as belonging to Engel's class I (21). Three patients (10%) responded to class I1 criteria and one patient (3%) to class JIIA of Engel. In detail, 17 patients (57%) became completely seizure-free, sometimes after rare auras disappeared within a few weeks after surgery for more than one year (2 cases). Six patients (20%) experienced persistent auras only. Six patients have had very rare seizures (less than 3/year): 4 experienced very rare generalized tonic clonic seizures (GTCS), e.g. one GTCS during a febrile gastroenteritis with drug discontinuation (1 patient), one unprovoked GTCS (1 patient), two GTCS in the year following surgery in the context of familial generalized epilepsy but seizure-free for more than two years (1 patient) and very few GTCS, less than 3/year (implanted Case no 2); 2 had very few complex partial seizures (CPS), less than 3/year: during sudden drug discontinuation in
7

Adam et al.
Table 5. Most of data in implanted cases (the eight first) and the other patients (the next)
Unusual first- EEG Memory Outcome Onset ( y ) l subjective Depth ictal deficit (Engel's Follow-up
Patient Early event symptom spikes" seizures* MRI PET onsets* (Wada) Surgev classification) (months)
8/rr 1 OIFC 17/FC 6/rr
1 OIFC 3IFC 31-
1 llcoma 9 8/FC
10 1 l/FC 11 24/FC 12 121FC 13 4/FC 14 1 O/rr,EC 15 Z/mn 16 13/cranio,EC 17 12/FC 18 14lmn 19 31- 20 5/FC
22 1 O/Tr,EC 23 12/FC 24 3f l r 25 1 O/FC 26 9/FC 21 1 l /FC
29 7/FC 30 16/coma
21 251-
28 151-
- R T
dreamlike - - L T (R)
no aura R FIL) L T (R)
- L T -
- - indescribable R T (L)
L T R T U-1
L T - R T - R T
R T R T L T
- R T
L T L T L T
thrill L T - R=L T - L T - R=L T - R T - R T
R T - L T - L=R T
-
-
-
-
-
-
-
-
-
- -
-
1 R TF, Bi
L T F
L T (8) L Hemis R=L T, Bi
L T R T I T R T R T R T R T L T
R TF L l L T L T b i l L T biTF L T biTF R T R T
? L T
biTF. L T
-
R R R R R R L L L L L L L L
L L R R L L R R R R R R R R L L R R L L L L L L L L L nd R R L L R R R R R R R R L L L L
- -
R R R L L
L"" L R L R L R R R R L R L L L L L R
L" R R R R L L
la Ilb la la Ic
llla la Ilb la Ib la Ib Id la la Ic Ib Ilb la la la Ib la lb Ib la la la la la
22 19 13 16 44 23 15 20 40 38 17 36 25 24 16 36 30 12 28 25 18 30 14 41 12 31 14 31 21 25
cranio: craniostenosis, EC: early non febrile convulsions, FC: early febrile convusions, mn: menigitis. nd: not done, Tr: head trauma, Bi: bilateral widespead, F: frantal, Hemis: hemispheric, L left. R: right, T. temporal, -: negative or absent, *: in parentheses the less frequent events, **: respecting most of hippocampus. 7: uninterpretable
early postsurgical period but now seizure-free for more than two years (implanted Case no 5, com- plicated by severe psychiatric disturbances) and a few CPS since operation (implanted Case no 8, the only one without brain imaging abnormality). The last case (implanted No 6), in whom most of hippocampus was left at operation, experienced 4 CPS/year, that represented however a 95% improvement in seizure frequency. Seizure control was better in the non-implanted subgroup (95% of Engel's class I) compared to implanted patients (63% of Engel's class I (statis- tical significance being not reached however)).
Surgical complications comprised persistent upper limb deficit due to per-operative infarction in the deep territory of middle cerebral artery (1 patient), persistent hemianopsia and regressive speech disorder in relation to necrosis of temporal lobe white matter (1 patient) and psychiatric dis- turbances (severe psychosis in 1 patient, lasting depression in 2 patients, reappearance of a former bipolar illness in 1 patient).
Pathology
Resected tissues comprised specimen taken from the temporal pole and the medial structures, uncus and hippocampus. These medial structures were removed as small consecutive blocks on slices 0.5 to 10 mm thick. In some cases, dissection was difficult and the resected material could not pro- vide proper hippocampal samples. Finally, 18 spec- imens have been available and all showed clear medial temporal sclerosis. The case where struc- tural abnormalities could not be detected on brain imaging presented nevertheless obvious lesions of medial temporal sclerosis.
Discussion
The concept of MTLE relies on the hypothesis of a network of epileptogenic tissues involving prima- rily the hippocampal formations, the amygdala and presumably the adjacent limbic cortex such as parahippocampal and perirhinal cortices. The pre-
8
Variability of MTLE presentation
cise distribution of this epileptogenic network remains a matter of speculation. The two golden criteria used for its delimitation, intracranial ictal onset recordings and seizure relief after surgery, have the disadvantage to be invasive or a posteri- ori. Futhermore, their total accurracy is question- nable. Depth recordings provide limited spatial resolution and can show different kinds of seizure onsets (focal, regional or diffuse) sometimes vari- able in the same patient (22,23). Surgical resection, even the selective amygdalohippocampectomy, may partly act through disconnecting mechanisms whereas all the extensions of epileptogenic tissue are not fully excised.
The identification of MTLE can also be approached differently, through a syndromic anal- ysis. A set of non-invasive criteria was proposed from the study of a pure culture of MTLE patients all explored with intracranial electrodes and sei- zure-free after surgery (1, 2). The same team has reported very good postsurgical results in 22 patients using these non-invasive criteria (11). In our study these criteria were used prospectively as guidelines for presurgical evaluation, but not all of them were considered as mandatory. Priority was given to the nature of the initial subjective symp- toms, the EEG pattern and brain imaging, whereas the lack of febrile convulsion or of the typical pattern of automatisms, for example, was not con- sidered as critical.
Our evaluation process mainly based on non- invasive criteria led to refer 73% of patients directly for surgery and tended to be validated a posteriori since 95% of these patients belonged to Engel’s class I. By opposition, the subgroup of patients investigated with intracranial electrodes (27 Yo) had less favorable postsurgical outcome (63% of class I) than the non-implanted patients. They presented some heterogeneous features in their clinical, EEG and imaging presentation.
Clinical data
The clinical informations tended to differ little between the two subgroups, as demographic data were almost similar in each group and early con- vulsions, auras, clinical signs of seizures (automa- tisms and dystonia) were just a little more frequent and secondarily generalized seizures just a little less frequent in the non-implanted subgroup in com- parison with the implanted patients (but with no statistical significance).
For the whole population, the presence of an aura was the rule (97% of all, 100% of non- implanted, 87% of implanted patients), and its nature was viscerovegetative or affective in 90% of the cases. These subjective phenomena are consid-
ered as characteristic of MTLE (24), despite the fact that they are probably elicited by a propaga- tion to extrahippocampal, even extratemporal, areas, presumably the insula for epigastric sensa- tion (25). In our experience, the signal symptom was of great importance, as its absence or the absence of its viscerovegetative or affective com- ponent contributed in some patients to the decision of invasive explorations. It was also the case with the patient presenting quite misleading somatosen- sitive phenomena.
Most of the other subjective manifestations reported by the patients (dreamy state, dkji-vu or vCcu, auditory, gustatory, olfactory hallucinations or illusions) were quite less frequent than vis- cerovegetative and affective symptoms. Some of them led to suspect an engagement, early in the course of the seizure, of neocortical areas of the temporal lobe. However, in the present series, these symptoms occurred in most of the cases after neurovegetative or affective sensations. Dreamy state illustrates this point. It seems to result from the simultaneous engagement of medial and lateral temporal structures, especially the superior tempo- ral gyrus (26). In the 3 cases with dreamy state of this series, this symptom occurred most of the time as a second symptom, this sequential organization suggesting a propagation phenomenon. Two of these patients became totally seizure-free after surgery and one remained with a few auras consist- ing of the viscerovegetative component only. As most of the lateral neocortex was left in place at operation (and especially the superior temporal gyrus), this suggests that the resection of the medial structures can be sufficient to inactivate the neuro- nal network underlying dreamy state.
EEG data
In this series, the EEG data were the evaluation parameter which led the most frequently to further invasive investigations. A certain number of patients did not have a clear, and sufficiently well- lateralised, temporal lobe focus but presented some divergent EEG patterns suggesting a more complex epileptogenic network. These features were mainly independent bilateral foci of spikes or seizures, and ictal onsets projecting beyond or outside the temporal area.
These types of surface EEG patterns can be the result of specific modalities of electrophysiological propagation. The spread of epileptic activity from the medial temporal lobe to frontal lobes (27) could be particularly facilitated in the patients with widespread scalp abnormalities and could induce a large excitable zone beyond the limits of the tem- poral lobe (27-29).
9

Adam et al.
These divergent scalp EEG features rise also the question of another independent seizure generator. Extratemporal lobe onsets can sometimes be observed in patients with hippocampal sclerosis (23, 30). The most frequent situation with respect to the question of multiple generators is repre- sented by the bitemporal cases. Following So et al., independent bitemporal onsets recorded by depth electrodes is a major factor of less favourable prognosis. A predominance of lateralisation of seizures superior to 80% was suggested as a rea- sonable cutoff to benefit from surgery (31). How- ever, the other patients could be improved (to a lesser degree) after surgery and have, in other studies, good to excellent results (32, 33). Futher- more, all these reports did not benefit from the predictive value of MRI analyses. In the present series, the one patient with as many depth seizure onsets on either side presented presurgically a well- lateralised MTS which influenced strongly the indi- cation of resection. Her outcome was excellent after surgery. In that case, the decision making process would have been very difficult before the era of MRI/PET examinations (33).
Brain imaging
Almost all the patients of this study had a detect- able MTS at presurgical stage as they were spe- cially selected on this criterion. The presence of MTS has been shown in many studies to be predic- tive of a favorable outcome (3, 7, 10, 34) and the results of this series at two years of follow-up are in agreement with these litterature data. The dem- onstration of MTS has also a great neuropsycho- logical interest and this information can influence the decision-making process, in the way that surgi- cal resection of the MTL structures can be consid- ered only on the atrophic side. For all these reasons, the key role played by MRI-based MTS in the evaluation of partial epilepsy patients justifies all the strategies that are undertaken to optimize its identification (35).
FDG-PET scan, with its characteristic pattern of temporal lobe hypometabolism (13), has been shown to be more sensitive than MRI examination (12). In two cases of the present series, PET examination confirmed the TL changes which were suspected on signal alterations whilst hippocampal volumes were symmetrical. Moreover, PET can be positive even in absence of hippocampal signal change (12).
Yet, MRI and PET scan can be both negative and such situations represent a very difficult sub- group of MTLE. Non-contributive brain imaging may be due either to subtle structural changes or almost symmetrical bilateral abnormalities which
are not detected when scans are analysed by side- to-side comparison. This second eventuality was the most likely in our only one patient with nega- tive MRI and PET scans since the resected speci- men presented obvious signs of MTS.
Despite its very high value, however, the presence of a demonstrable MTS or of a PET scan pattern compatible with MTLE is not always synonymous of pure MTLE. Indeed, mild hippocampal asymme- try can be found by volumetric study in some cases of frontal lobe epilepsy (9). Depth electrode inves- tigations have proven that MTS does not exclude the possibility of complex, widespread, multifocal epileptogenic network (23, 30). The present study demonstrates that a marked hippocampal sclerosis does not rule out the eventuality of a contralateral temporal seizure focus (4 cases in our implanted patients). The lateralisation of that sclerosis has always been on the side of the most active epilep- togenic zone in these latter patients, except in one. Even in this case, the excellent surgery response tended to prove that the MRI abnormality indicated correctly the primary seizure focus.
In conclusion, the clinical and EEG criteria for MTLE and the very strong contribution of brain imaging enable an accurate non-invasive identifi- cation of MTLE patients with the best postsurgical prognosis. However, there are cases for which the clinical and EEG features suggest that the epilep- togenic network differs from the usual pattern, even in presence of MRI-based MTS and PET temporal hypometabolism. These patients have in particular more frequently bitemporal and/or extratemporal EEG abnormalities. According to the experience of each center, intracranial proce- dures may be used in order to confirm the existence of a predominant medial TL focus. These patients have a less favorable postsurgical outcome, but despite this they benefit greatly from a surgical procedure.
Acknowledgement
We are very grateful to Paul Boon who kindly accepted to comment on this manuscript.
References
1. FRENCH JA, WILLIAMSON PD, THADMI VM et al. Charac- teristics of medial temporal lobe epilepsy: I. Results of history and physical examination. Ann Neurol 1993: 34
2. WILLIAMSON PD, FRENCH JA, THADANI VM et al. Charac- teristics of medial temporal lobe epilepsy: 11. Interictal and ictal scalp electroencephalography, neuropsychological testing, neuroimaging, surgical results, and pathology. Ann Neurol 1993: 34: 781-787.
3. JACK CR, SHARBROUGH FW, WOMEY CK et al. Temporal lobe seizures: lateralization with MR volume measure-
774-780.
10
Variability of MTLE presentation
ments of the hippocampal formation. Radiology 1990: 175: 423-429.
4. JACKSON GD, BERKOVIC SF, ’IREss BM, KALNINS RM, FABINYI GCA, BLADIN PF. Hippocampal sclerosis can be reliably detected by magnetic resonance imaging. Neurol-
5. ASHTARI M, BARR WB, SCHAUL N, BOGERTS B. Three- dimensional fast low-angle shot imaging and computerized volume measurement of the hippocampus in patients with chronic epilepsy of temporal lobe. Am J Neuroradioll991:
6. COOK MJ, FISH DR, SHORVON SD, STRAUGHAN K, STEVENS JM. Hippocampal volumetric and morphometric studies in frontal and temporal lobe epilepsy. Brain 1992:
7. KUZNIECKY R, BURGARD S, FAUGHT E, MORAWETZ R, BARTOLUCCI A. Predictive value of magnetic resonance imaging in temporal lobe epilepsy surgery. Arch Neurol 1993: 50 65-69.
8. TIEN RD, FELSBERG GJ, CAMPI DE CASTRO C et al. Complex partial seizures and mesial temporal sclerosis: evaluation with fast spin-echo MR imaging. Radiology 1993: 189: 835- 842.
9. ADAM C, BAULAC M, SAINT-HILAIRE J-M, LANDAU J, GRANAT 0, LAPLANE D. Value of magnetic resonance imaging-based measurements of hippocampal formations in patients with partial epilepsy. Arch Neuroll994: 51: 130- 138.
10. GARCIA PA, LAXER KD, BARBARO NM, DILLON Wl? Prognostic value of quantitative magnetic resonance imag- ing hippocampal abnormalities in patients undergoing tem- poral lobectomy for medically refractory seizures. Epilepsia 1994: 35: 520-524.
11. THADANI VM, WILLIAMSON PD, BERGER R et al. Successful epilepsy surgery without intracranial EEG recording: criteria for patient selection. Epilepsia 1995: 36: 7-15.
12. GAILLARD WD, BHATIA S, BOOKHEIMER SY, FAZILAT S, SATO S, THEODORE WH. FDG-PET and volumetric MRI in the evaluation of patients with partial epilepsy. Neurology
13. SEMAH F, BAULAC M, HASBOUN D et al. Is interictal temporal hypometabolism related to mesial temporal sclerosis? a PETMRI confrontation. Epilepsia 1995: 36 447456.
14. JASPER HH. The ten twenty electrode system of the Inter- national Federation. Electroenceph Clin Neurophysiol
15. SILVERMAN D. The anterior temporal electrode and the ten twenty system. Electroenceph Clin Neurophysiol 1960: 12: 735-737.
16. PHELPS ME, HUANG SC, HOFFMAN EJ, SELIN C, SOKOLOFF L, KUHL DE. Tomographic measurement of local cerebral glucose metabolic rate in humans with (F-18)2-fluoro-2- deoxy-D-glucose: validation of method. Ann Neurol 1979:
17. WADA J, RASMUSSEN T. Intracarotid injection of sodium Amytal for the lateralization of cerebral speech domi- nance: experimental and clinical observations. J Neurosurg 1960 17: 226-282.
18. MILNER B. Psychological aspects of focal epilepsy and its neurosurgical management. In: Purpura D, Penry J,
ogy 1990: 40: 1869-1875.
12: 941-947.
115: 1001-1015.
1995: 45: 123-126.
1958: 1 0 371-375.
6 371-388.
Walter R, eds. Advances in neurology. New York: Raven Press, 1975: 299-321.
19. JONES-GOTMAN M, P~ITO A, ZATORRE R. Deficits cognitifs associes aux ICsions cCrCbrales focaliskes. Rev Que Psycho1
20. Commission on classification and terminology of the Inter- national League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epi- leptic seizures. Epilepsia 1981: 22: 489-501.
21. ENGEL JJ, VAN NESS PC, RASMUSSEN TB, OJEMANN LM. Outcome with respect to epileptic seizures. In: Engel JJ, ed. Surgical treatment of the epilepsies. New York: Raven Press, 1993: 609-621.
22. So N, GLOOR P, QUESNEY LF, JONES-GOTMAN M, OLIVIER A, ANDERMANN F. Depth electrode investigations in patients with bitemporal epileptiform abnormalities. Ann Neurol 1989: 25: 423-431.
23. BAULAC M, SAINT HILAIRE J-M, ADAM C, MARTINEZ M, FONTAINE S, LAPLANE D. Correlations between magnetic resonance imaging-based hippocampal sclerosis and depth electrode investigation in epilepsy of the mesiotemporal lobe. Epilepsia 1994 35: 1045-1053.
24. PALMINI A, GLOOR l? The localizing value of auras in partial seizures: a prospective and retrospective study. Neurology 1992: 42: 801408.
25. PENFIELD W, JASPER H. Epilepsy and the functional anat- omy of the human brain. Boston: Little, Brown, 1954.
26. BANCAUD J, BRUNET-BOURGIN F, CHAUVEL P, HALGREN E. Anatomical origin of dijd vu and vivid ‘memories’ in human temporal lobe epilepsy. Brain 1994: 117: 71-90.
27. ADAM C, SAINT-HILAIRE J-M, RICHER F. Temporal and spatial characteristics of intracerebral seizure propagation: predictive value in surgery for temporal lobe epilepsy. Epilepsia 1994: 35: 1065-1072.
28. MORRELL F. Varieties of human secondary epileptogenesis. J Clin Neurophysiol 1989: 6 227-275.
29. BARRY E, SUSSMAN NM, O’CONNOR MJ, HARNER RN. Presurgical electroencephalographic patterns and out- come from anterior temporal lobectomy. Arch Neurol
30. SPENCER SS, MCCARTHY G, SPENCER DD. Diagnosis of medial temporal lobe seizure onset: relative specificity and sensitivity of quantitative MRI. Neurology 1993: 43: 2117- 2124.
31. So N, OLIVIER A, ANDERMANN F, GLOOR P, QUESNEY LF. Results of surgical treatment in patients with bitemporal abnormalities. Ann Neurol 1989: 25: 432-439.
32. ENGEL JJ, CRANDALL PH. Falsely localizing ictal onsets with depth EEG telemetry during anticonvulsant withdrawal. Epilepsia 1983: 24 344-355.
33. HIRSCH LJ, SPENCER SS, SPENCER DD, WILLIAMSON PD, MATTSON RH. Temporal lobectomy in patients with bitem- poral epilepsy defined by depth electroencephalography. Ann Neurol 1991: 30 347-356.
34. ~ O U - K H A L I L B, ANDERMANN E, ANDERMANN F, OLIVIER A, QUESNEY LF. Temporal lobe epilepsy after prolonged convulsions: excellent outcome after surgical treatment. Epilepsia 1993: 34 87-83.
35. JACKSON GD. New techniques in magnetic resonance and epilepsy. Epilepsia 1994 35(suppl. 6): S2-Sl3.
1984: 5: 83-104.
1992: 49: 21-27.
11




















