university of calgary - Alberta College of Social Workers
142
UNIVERSITY OF CALGARY Decolonizing Home Assessment Practice at the Kitchen Table: A Thematic Analysis Identifying the Crucial Elements in the Assessment of Kinship Caregivers by Julie Mann-Johnson A THESIS SUMBITTED TO THE GRADUATE PROGRAM IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SOCIAL WORK GRADUATE PROGRAM IN SOCIAL WORK EDMONTON, ALBERTA APRIL 2016
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of university of calgary - Alberta College of Social Workers

UNIVERSITY OF CALGARY
Decolonizing Home Assessment Practice at the Kitchen Table:
A Thematic Analysis Identifying the Crucial Elements in the Assessment of Kinship
Caregivers
by
Julie Mann-Johnson
A THESIS
SUMBITTED TO THE GRADUATE PROGRAM
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE
DEGREE OF MASTER OF SOCIAL WORK
GRADUATE PROGRAM IN SOCIAL WORK
EDMONTON, ALBERTA
APRIL 2016
Crucial Elements of Kinship Care Home Assessment
ii
Abstract
Literature suggests that children placed in kinship care achieve positive
outcomes. Literature also suggests the experience for kinship caregivers is very different
from adoption and foster care; however assessment practice and policy do not reflect
these unique elements. Using thematic analysis of secondary qualitative data, this study
discusses crucial elements required for kinship care home assessments in Alberta. These
elements which influence the practitioner, process, policy, legislation and systemic issues
can then be used to inform kinship home assessment practice, policy and legislation. By
using secondary data analysis, this study endeavored to honour the voices of people who
have already shared their perspectives at public consultations and information gathering
events sponsored by the Government of Alberta. An anti-colonizing lens and critical
ecological framework ground this research in an approach that is sensitive to the impacts
of structural colonization on Indigenous children and families through child welfare
practice, policy and legislation.
Crucial Elements of Kinship Care Home Assessment
iii
Acknowledgements
I would like to start by acknowledging the children, youth and families that I
have been honoured to work with throughout my career. I have been blessed to be
a part of their journey and they have transformed mine. Caring for children is a
sacred gift, and kinship caregivers are unique and special gifts for the children they
care for and love. Like all of us, these families want the best for the children whom
they care about deeply.
My family are also my gift. My daughters transform me daily and were
cheerleaders throughout my process. Their kind-hearted nature gives me an
energetic and hopeful lens in this work. My loving and encouraging husband helped
me get through this marathon in an endless manner of emotional ways but also
often as IT support and editor! My mom first instilled the importance of lifelong
learning for me helped me right along the journey through transcription. My wise
dad has always grounded me to how family and community worked together to
care for kids back in the day along the shores of the Red River.
My thesis sisters and faculty members at the Faculty of Social Work listened
endlessly to my ideas that sometimes led to dead ends and others that stuck. The
support and sense of community within the faculty is a powerful force.
I thank my committee for sharing their wisdom and expertise to strengthen
my work. Anne-Marie, my thesis supervisor listened and helped filter a TON of
ideas in this journey. Thank you for keeping me focused.
I acknowledge these members of my kin network and the many others.
Crucial Elements of Kinship Care Home Assessment
iv
Table of Contents: Abstract ii Acknowledgements iii Table of Contents iv Introduction 1 Locating Myself 1 What is Kinship Care 3 Research Question 3 Literature Review 5 Colonization and Child Welfare 6 The Meaning and Historical Development of Kinship Care 9 Kinship Care Internationally 11 Kinship Care in Indigenous Communities 12 Benefits of Placement in Kinship Care 13 Challenges in Kinship Care Practice 16 Assessing Kinship Homes 22 Alternatives in Kinship Care Home Assessment 28 Conclusion 32 Home Assessment Policy and Practice – Various Jurisdictions 33 Home Assessment in Alberta 33 Kinship Home Assessment in Other Jurisdictions 35 Methodology 39 Theoretical Framework 39 Secondary Data Analysis 41 Thematic Analysis 47 Rigour 50 Data Analysis 52 Findings 59 Assessor Characteristics 62 Important Areas to Address 65 Home Assessment Process 70 Safety 75 Policy and Legislated Requirements 77 Systemic 81 Discussion 87 Implications for Practice 93 Limitations of the Study 96 My Journey 99 References 101 Appendix A 113 Appendix B 117 Appendix C 119 Appendix D 121 Appendix E 122

Crucial Elements of Kinship Care Home Assessment
1
Introduction
Locating myself
I have been a social worker in Alberta for 18 years. Most of my practice has been
in the field of child intervention and now in the area of policy and program development
for child intervention. For a number of years I worked primarily as a Home Assessment
writer completing home assessments on families who were applying as adoptive, foster
or kinship parents. Kinship care is a formal placement for children in care with family or
someone who they have a significant relationship with. I was always keenly interested in
kinship care assessments and these assessments would make me always consider my
own kinship networks. I am a mother, step-mother, wife, auntie, cousin, daughter, sister,
niece, and friend. With these roles I have an extensive kin network of caregivers for my
children, but also of children that I could potentially be a caregiver for, and have. I have
first-hand knowledge of the unique joys and challenges of kinship care. In keeping with
anti-oppressive practice, I would like to note my social location. I am a white woman,
raised in rural, northern Alberta but living in urban setting for most of my adult life.
In my career I have worked with many Indigenous families and communities and
observed the unique experiences had by this population within our system. Canada’s
Child Welfare system has a long history of colonizing Indigenous people (Strega &
Carrier, 2015; Ing, 2006; Hart, 2002). This tragic legacy started with the Residential
Schools, through to the sixties scoop and to the current state which includes a significant
over representation of Indigenous children in care. Today in Alberta, 69% of children in
care are Aboriginal (Human Services, 2015), yet Aboriginal people represent only 6% of
the provincial population (Government of Canada, 2011). Since a strong majority of
Crucial Elements of Kinship Care Home Assessment
2
children in care are Indigenous, child welfare practices and policies impact the
Indigenous community more than any other ethnic group. As a result, this analysis will
focus particularly on Indigenous children and families.
First Nation people place great significance on familial relationships and
relatedness (Hart, 2002; Bodor, Makokis & Friesen, 2014). Children are considered
sacred beings and highly respected as gifts from the spirit world (Bodor et al, 2014).
Caregiving relationships are fluid and it is both the parents’ and community’s
responsibility to provide each child the best opportunities to develop. Traditionally,
Indigenous families and communities have cared for each other this way (Greenwood &
De Leeuw, 2006). Colonization, however, disrupted these relationships when children
were removed and re-educated through the institutions of colonizers (Hart, 2002).
Punitive-based and rigid systems of child rearing were forced on First Nation people and
misaligned with their traditional beliefs (Bodor et al, 2014). Because of these traditional
beliefs, it was common practice in the First Nation community for kin to care for
children when biological parents were unable to do so.
What is kinship care?
When children come into the care of child welfare, they are placed formally in
various caregiving arrangements. They could be placed in foster care, which is
temporary, family based care (Alberta Human Services, 2016). These families are
typically unknown to the child or family. Children or youth could also be placed in
group or residential care (Alberta Human Services, 2016). These settings range from
being community-based to more institutional.
Crucial Elements of Kinship Care Home Assessment
3
Kinship care is another option for placement. Kinship care in Alberta conforms to
the policy definition of the Government of Alberta, Ministry of Human Services and is
considered to be the “placing of a child with a caregiver who is an extended family
member of a child, or a person who has a significant relationship with the child, or is a
member of the child’s cultural community (Ministry of Human Services, 2014, 2.0).
Many other jurisdictions, such as England (Selwyn & Nandy, 2014) and Ontario
(Brisebois, Kernsmith, Carcone, 2013) adopt a similar operational definition. Currently
in Alberta, Kinship care is the preferred placement option recognizing that placement
with family or community members ensures the strongest possible connection for that
child to their culture and community (Alberta Human Services, 2016).
Research Question
Most western, government sponsored child welfare systems, including Alberta’s,
have only recently recognized kinship care as a legitimate placement option
(Government of Alberta, 2009). Once kinship care was recognized as a formal
placement option by most child welfare jurisdictions, the government’s response was to
apply the same policies and processes as other placement resources. Currently, in
Alberta, home study methods used in the kinship care program utilize the same
approaches and tools used for foster care and adoption, otherwise known as stranger
care. This is problematic for a number of reasons: current practices do not recognize
traditional kin network practices amongst Indigenous people; they do not highlight the
inherent strengths in children being cared for by family and community; and they fail to
recognize structural challenges such as poverty, inadequate housing, and the racism
faced by many of these families.

Crucial Elements of Kinship Care Home Assessment
4
The Alberta Government has a legislated responsibility to ensure the survival,
security, and development of all children (Child, Youth and Family Enhancement Act,
2004). For children under the care and guardianship of the province, the Government
becomes the parent and as such must ensure the survival, security, and development of
those children. The Alberta Government therefore is compelled to ensure caregiving
arrangements are safe and nurturing. However, by applying the same practices and
policies of other non-kin placement resources to kinship care, it could be said that
governments have continued a practice of colonialism through the child welfare system.
There has been inadequate recognition that kinship providers want what is best for their
children.
With the stated assumptions that the current situation for kinship care providers is
inadequate and that current practice inadvertently excludes or punishes potential kinship
caregivers, this project asks “what are the crucial elements required for Kinship
caregiver assessments in Alberta?” In pursuit of this question, I have employed a
secondary analysis of previously collected data from community consultations and other
dialogues that the government of Alberta has conducted in good faith, in order to answer
this question.
Crucial Elements of Kinship Care Home Assessment
5
Literature Review
Assessing potential kinship caregivers is a complex process. In order to provide a
thorough understanding of kinship care, this literature review covers issues related to the
definition and historical development of kinship care, international experiences of
kinship care, barriers and challenges of kinship care, benefits of kinship care, and
assessment practices in kinship care.
There has been an explosion in research into kinship care in recent years. This
literature review includes international research into these issues with a general focus on
research from the past decade. Older studies were included if they were considered to
have made lasting contributions to the field and/or have formed the basis of other
investigations, or if they relate specifically to assessment of caregivers. There is limited
research specifically into the assessment of kinship caregivers, but a significant amount
that speaks to the experience of kinship care.
In addition to government sponsored and supported kinship care placements,
there are situations where families may be caring for kin informally and without
significant supports. These informal kinship care situations are still occurring in
situations where a child is not considered to be in government care and the parents still
remain the only guardians. These are situations where, for example, a parent may
directly ask a grandparent, other relative, or friend to care for their child and no
government authority is involved. The literature refers to these arrangements as informal
kinship. While this practice is a significant area, this writing will not explore informal
kinship. The focus of this overall study is to address the assessment of formal kinship
care.

Crucial Elements of Kinship Care Home Assessment
6
Also not included in this literature review are studies and theoretical texts that
speak to the experience of specific types of kin. For example, there is literature that
speaks to the experience of grandparents or siblings as kinship caregivers. While these
experiences are significant within the general field of kinship care, my investigation in
interested in more of a general experience of kinship care.
Colonization and Child Welfare
In considering any aspect of child welfare practice, it is important to understand
the colonizing impacts of legislation and policy. Since the time of first contact with
Europeans, Indigenous people in Canada have experienced significant losses
including land, culture, children and language (Strega & Carriere, 2015).
Starting in the sixteenth century (Ing, 2006) and formalized in 1876
through the Indian Act (Greenwood & DeLeeuw, 2006), Indian residential
schools were established and typically operated by various religious organizations. With
a goal of cultural assimilation, these institutions contributed to severed ties between
children and their families, children were forbidden to speak their First Nations
languages, and they suffered a number of other atrocities and indignities (Ing, 2006).
The impact of the residential schools has been generational. Future generations felt the
impacts as the children placed in residential schools did not encounter “healthy parental
role models and, as adults, frequently had diminished capacity to care for their own
children.” (Trocmé, Knoke, Blackstock, 2004, 578).
The current generation continues to feel these affects. This is not surprising
when you consider that the last of these schools closed in the mid-1990’s, even though
the Federal Government started to close these institutions in the 1950’s (Truth and
Crucial Elements of Kinship Care Home Assessment
7
Reconciliation Commission of Canada(TRC), 2012). Residential schools have been
identified as the cause of multi-generational dysfunction in First Nations communities as
individuals struggle to cope with the trauma from the loss of community, culture, and
family (Blackstock, 2004; TRC, 2012). The attempt to eradicate Indigenous culture, left
children who attended these schools ashamed of themselves and their families (Ing,
2006) and challenged to pass on cultural connection and pride. Long term detrimental
effects have been passed on to the children of those survivors of residential school.
These children and subsequent generations have been “deprived of learning and knowing
the positive and beautiful things about their culture” (Ing, 2006).
In 1951, an amendment to the Indian Act made all provincial and territorial laws
applicable on reserve. This meant that child protections services delivered to individuals
and families living on reserves became a provincial or territorial responsibility. With this
change in legislation, non-indigenous social workers began to enter reserves to
investigate cases of perceived child maltreatment, and in many cases apprehended the
child (Strega & Carriere, 2012). These services were often delivered by social workers
“who had little or no knowledge about colonization and residential schools who often
mistook symptoms of systemic discrimination as parental failure” (Blackstock, 2011, p.
188). In 1951, the percentage of Indigenous children in care was 1 percent, while at the
end of the 1960’s this percentage was between 30-40%. This rapid increase in the
apprehension rate of Indigenous children became known as the “sixties-scoop” (Strega
& Carriere, 2012).
Indigenous children continue to enter government care at rates vastly
disproportionate to the rest of the population. As indicated previously, 69% of the
Crucial Elements of Kinship Care Home Assessment
8
children in government care in Alberta are Indigenous (Human Services, 2015). In some
parts of the country, rates of Indigenous children in care are higher than at the height of
the “sixties scoop”. The term “millennium scoop” (Beaucage, 2011) was coined to
describe the continuing disproportionate rates of substantiated investigations with
Indigenous children and families compared non-indigenous children and families (Sinha
et al., 2011).
First Nation communities and other Aboriginal advocates lobbied government for
control over the welfare of their children and families (Blackstock, 2011). In response to
these efforts and in a attempt to acknowledge the effects of colonialism, provincial and
territorial statutes began to mandate consultation with First Nations for case planning and
prior to permanency planning for a First Nation child (Child, Youth and Family
Enhancement Act, 2004; Trocmé et al. 2004). More importantly was the development
by the Federal Government through recognition of First Nation child and family services
agencies beginning in the early 1990’s through what has been termed Directive 20-1.
Directive 20-1 established a funding formula which allowed First Nation communities to
delivery child welfare services within their communities (Singha et al, 2011). However,
complicated and often inadequate funding formulas and jurisdictional challenges resulted
in limited capacity and other structural challenges. “The [First Nation child and family
services] agencies must wear the straightjackets of provincial legislation and federal
government funding regimes that are often not culturally appropriate and are rarely
grounded in research evidence relevant to First Nations” (Blackstock, 2011, p. 188). In
practice, First Nations have little autonomy in their child and family services due to strict
administrative guidelines.
Crucial Elements of Kinship Care Home Assessment
9
The Meaning and Historical Development of Kinship Care
Historically, it was common for relatives to care for children when biological
parents were unable to do so. However, western child welfare systems have only recently
recognized kinship care as a legitimate placement option (Farmer, 2009; Leos-Urbel,
Bess, Geen, 2002). As a result the practice of kinship care has begun to expand
significantly in recent years.
The formal use of kinship homes in Alberta began with the proclamation of the
Child, Youth and Family Enhancement Act in 2004, which mandated the inclusion of
family, and significant others as potential placement options considered for a child who
is coming into the care of the government. (Government of Alberta, 2009). Alberta was
in line with many other jurisdictions that began to consider family and those with other
significant relationships to provide day-to-day care in situations where parents were
unable to, and the government had become responsible to ensure the needs of these
children were being met.
Ontario, for example, recognized and adopted a policy mandating child welfare
agencies to explore potential placements with a relative, extended family member, or a
member of the child’s community upon removal from the child’s home (Brisebois,
Kernsmith & Carcone, 2013). This shift came in 2006 with the passing of Bill 210
which highlighted the importance of seeking relatives for placement for children in care,
but at the same time emphasized the need to ensure the safety of children placed with
relatives. Similar to foster care, safety standards were adopted for kinship caregivers
including criminal record checks and a review of child welfare history (Brisebois et al.,
Crucial Elements of Kinship Care Home Assessment
10
2013). These standards resulted in complications for a system that often requires
placement decisions to be made quickly. For example a lack of clarity existed
concerning how to make decisions when potential kinship caregivers had a criminal or
child welfare history. This challenge was unique to kinship caregivers as foster parents
were pre-screened and awaited children to be placed in their care when required.
Kinship caregivers, however, generally respond to crisis and urgent need for placement.
Research trends in kinship care have followed a timeline similar to its growing
use in practice. O’Brien identifies three periods or phases in kinship care research. Early
studies incorporated kinship care into research of general foster care practices. In the
1990’s research shifted into practice and policy development as many jurisdictions were
implementing specific policies and legislation regarding kinship care. Since the late
1990’s the emphasis, in both qualitative and quantitative research, has been on
comparing the experiences of kinship and non-kin placements (2012).
In the early 2000’s governing authorities struggled to adapt policies and approval
processes developed for traditional foster care to fit the needs of this evolving and
increasingly popular kinship care alternative (Leos-Urbel et al, 2002). This approach
failed to bring clarity to the field. According to Selwyn and Nandy (2014) the use of
kinship care involves considerable legal complexities. The rapid expansion in use of this
practice has been confusing for both the general public and for social workers. This
confusion extends to unclear definitions and boundaries between different types of
kinship care, variances in levels of support, access to information, and rules regarding
assessment, licensing, and financial compensation. In many jurisdictions, this policy
Crucial Elements of Kinship Care Home Assessment
11
confusion has created structural barriers to kinship care. These structural barriers will be
discussed more specifically.
Kinship Care Internationally
Internationally, developments in kinship care practices have occurred in countries
such as Australia, New Zealand, Spain, Holland, Sweden, India, Poland, the United
Kingdom, and the United States. In the United States, the use of kinship care drastically
increased in the late 1980’s and 1990’s due to an increase of children requiring out of
home placements and a shortage of non-kin foster care (Leos-Urbel, Bess & Geen,
2002). Along with this operational need to access kinship homes was an attitude shift
resulting from federal and state court rulings that recognized the rights of relatives to act
as foster parents and to be financially compensated (Leos-Urbel et al., 2002). Also
critical to the American expanded use of kinship care in the United States was the Indian
Child Welfare Act of 1978, which stated that Native American children should be placed
“near their home and with their extended family if possible” (Leos-Urbel et al., 2002, p.
40). In 1997, the Adoption and Safe Families Act provided a tentative endorsement of
the use of kinship care by stating that “a fit and willing relative” could provide a
“planned permanent living arrangement.” However financial compensation could only be
provided if the kinship care provider met foster care licensing standards (Leos-Urbel et
al., 2002, p. 40). The implications of these policies discussed below, were signficant.
Spain adopted a formal kinship care system in 1987 under Law 21. As was the
case in other western child welfare systems, caseworkers in Spain were reluctant to place
children with grandparents due to attitudes and assumptions regarding intergenerational
transmittance of child maltreatment. A shortage of placements and increased research
Crucial Elements of Kinship Care Home Assessment
12
into the positive outcomes and stability of kinship care contributed to a shift towards
increased acceptance of grandparents as alternative care givers (Fuentes-Pelaez, Amoros,
Pastor, Molina & Mateo, 2015). Kinship care rates in England have been increasing
since 1989 with the passing of the Children Act, which legislated the importance of
maintaining children with their family and social networks as much as possible (Farmer,
2009).
Kinship Care in Indigenous Communities
Kinship care is a significant issue for Indigenous populations in Canada.
Indigenous children in Canada were forcibly removed from their families and
communities in large numbers during the residential school era and again during the
sixties scoop (Blackstock, 2011; Truth and Reconciliation Commission, 2012).
Furthermore, through colonization, punitive-based and rigid systems of child rearing
were forced on First Nation people (Bodor, Makokis & Friesen, 2014) that did not align
with their traditional beliefs.
First Nation people place great significance on children and familial
relationships. Loppie and Pauly indicate “family is a key feature of Indigenous wellness”
(2015, p. 218). A belief of particular significance within the Cree culture is the
“sacredness of children” (Hart, 2002, p. 48). Cree elders teach that understanding the
meaning of life comes from relationship with children. “Children help people to see their
purpose and then recognize their responsibilities to the many generations to come” (Hart,
2002, p. 48). Because of these traditional beliefs, it was common practice in First Nation
communities for kin to care for children when biological parents were unable to do so.

Crucial Elements of Kinship Care Home Assessment
13
Yet most western child welfare systems, including Alberta, have only recently
recognized kinship care as a legitimate placement option (Government of Alberta, 2009).
In Australia, a similar tragic history of assimilationist policies and a “stolen
generation” has led to a community of Indigenous people who struggle with the loss of
their identity. They also experience the over-representation of Indigenous children in
government care and in the criminal justice systems, significant health issues and welfare
dependency (Ban, 2005). Australia commissioned the Bringing them Home Report in
1997 that suggested that, since extended family are often significantly involved in the
raising of children in Indigenous communities, the extended kinship network and
community as a whole should be considered as resources (Ban 2005). This highlighted
an Aboriginal child placement principle that had driven practice in Australia since the
1980’s. According to this principle, an Aboriginal child should be placed with: (i) with
the child’s extended family; (ii) with the child’s Aboriginal community; or (iii) with
other Aboriginal people (Victorian Government Department of Human Services, 2002, p.
7).
Benefits of Placement in Kinship Care
Government systems have begun to implement enabling policies for kinship care
in recognition that these placements are beneficial for children. Alberta’s Enhancement
Policy of 2014 recognizes that placing a child with a caregiver with whom a connection
has already been established “reduces the trauma of coming into care, provides
familiarity during a difficult time, and helps reduce the need for multiple moves for the
child and the likelihood of the child coming back into care over time” (Ministry of
Human Services, 2014, 2.0).
Crucial Elements of Kinship Care Home Assessment
14
While kinship placements may not be permanent, they can in fact be stable (Koh,
2010; Farmer, 2010). Messing differentiated these experiences (2006) and described
from the child’s perspective that stability did not need to be permanent because children
were confident that their families would always provide care in some way. Farmer found
that grandparents were least likely to experience placement disruption of any group of
kinship caregivers (2010). Even in cases of children with very troubled backgrounds or
behaviours, these kinship placements persevere. Placements for these children are more
likely to disrupt in non-kin foster care (Farmer, 2010). Denby suggests that placement
with a caregiver who has an existing, significant connection with the child represents a
protective factor (2011).
It is the quality of the relationship and the ongoing contact between children and
their biological family that contributes to kinship placements being more stable (Berrick,
1997; Koh, 2010; O’Brien, 2012). In kinship care separation of siblings is less likely and
contact with the biological parent is common (Terling-Watt, 2001). While there are
situations where contact with biological parent may present risk or concern, contact is
“desirable for most maltreated children” (Terling-Watt, 2001). Of further benefit, the
contact that occurs is more “natural” and without agency intervention or resource
intensive supported visits (O’ Brien, 2012). Even if a kinship placement breaks down at
some point, the time spent in kinship placement will have created opportunities for
extended family connection that continues on after the placement. This builds capacity
for that child to maintain a lifelong connection. A child who has spent time with an aunt
and uncle is more likely to stay connected with, or initiate contact with them when they
are independent adults (O’Brien, 2012).

Crucial Elements of Kinship Care Home Assessment
15
Additionally, kinship care can contribute to healthy identity formation in children
since family and community membership helps answers questions of “who am I?” and
“where do I come from?” (O’Brien, 2012). This also has a significant impact on the
creation of one’s cultural identity (Ban, 2005). Shlonsky and Berrick highlight this as an
important issue. In considering the overrepresentation of certain minority groups and the
high number of non-minority foster parents within the child welfare system, many
minority children are being placed with non-minority foster parents. This then creates
many placements with “ethnic dissimilarities” (2001, p. 64) and complications in the
identity formation for the children placed there.
Messing suggested that much of the research regarding the reduced trauma and
stigma for children placed in kinship care did not represent children’s’ voices. However,
when she studied the issue while incorporating children’s voices, she found that the
children’s voices actually supported existing research that kinship placements resulted in
reduced trauma (Messing, 2006). Children described the transition to kinship care as
being natural and that their family relationships remained fluid. In a cohort studied by
Berrick it was found that kinship caregivers believed the children placed in their care
were less emotionally traumatized by past experiences than those children who were
placed in non-kin homes (Berrick, 1997).
Children placed in kinship care have been found to have fewer
emotional/behavioural problems than children placed in non-kin care (Keller et al.,
2001). Keller et al. (2001) found the clinical scores in emotional/behavioural domains for
children placed in kinship very closely match the general child population. While this
finding is interesting, a limitation to this study is differences in scores on
Crucial Elements of Kinship Care Home Assessment
16
emotional/behavioural functioning for children placed in kinship care compared to those
placed with non-kin may occur because fewer services are offered to kinship families
(Keller et al., 2001). And with fewer services, the children placed in kinship care cannot
be tracked using similar indicators. It is also suggested that kinship caregivers may
inaccurately describe or minimize the emotional and behavioral issues of the children
placed in their care (Berrick, 1997).
Children placed in kinship care may be in care longer, but have lower rates of
recidivism. That is, once returned to parental care they are less likely to be removed
again from parental care (Berrick, 1997; Koh & Testa, 2011; Perry et al., 2012). While
this phenomenon could be impacted by different demographics of kinship versus non-
kinship type placements, there is evidence that these two groups of children are
becoming more and more demographically similar (Koh et al., 2011).
Farmer found that kinship homes that had gone through formal approval methods
and were receiving financial and practical support were more successful in providing
longer term, stable placements than those placements that had not (2010). Along with
this finding, Farmer’s UK study involving 270 file reviews found the practice and
attitudes of social workers involved in supporting kinship care work varied greatly in
different regions (2010) indicating a need for consistency in kinship care practice.
Challenges in Kinship Care Practice
A number of challenges exist within kinship care practice. Government and child
welfare authorities grapple with the notion of ensuring safety and managing risk for
children in care while also maintaining their connection to family. Authorities have a
duty to ensure that children, particularly those in their care, are not maltreated and
Crucial Elements of Kinship Care Home Assessment
17
receive quality care. Shlonsky and Berrick (2001) describe a minimum standard for
parents providing care for their biological children. When these standards are not met,
the state intervenes and is expected to be responsible to provide care that is higher than
the usually accepted minimum. Furthermore, children who have been maltreated may
require a higher level of care. By definition (having required apprehension from original
families) these children present unique and challenging needs to their caregivers
(Shlonsky & Berrick, 2001). These considerations speak to the need for and importance
of robust systems of care.
A number of structural barriers exist for the general kinship caregiver population.
Poverty is a significant issue affecting kinship families. According to Falconnier,
Tomasello, Doueck, Wells, Luckey and Agathen (2010), the American Bar Association
reported that over half of the children in kinship care live in extreme poverty. Other
authors have described poverty as being a unique challenge faced and experienced by
kinship caregivers (Farmer, 2009). According to Shlonsky and Berrick (2001), “kinship
caregivers are more likely than nonrelated foster parents to be poor”.
In the United States, a number of jurisdictions require that licensing standards be
met before financial support can be provided to kinship caregivers. However, these
licensing standards, such as limited number of children per bedroom, window sizes, and
physical repair of the home, are often difficult for these caregivers to meet due to poverty
(Shlonsky & Berrick, 2001). The crisis nature of practice is such that a child may still be
placed with a kinship caregiver even if they do not meet licensing standards. In these
cases, they may be placed informally. If they are not licensed, they will not receive
supports. This further marginalizes poor families as they are forced to care for their kin
Crucial Elements of Kinship Care Home Assessment
18
without financial compensation because they are too poor to qualify. The financial needs
of kinship caregivers are generally significant when considering their typical
demographics.
In addition to poverty, kinship caregivers are more likely than non-kin care
providers to be older women, less educated, ethnic minorities, live in “compromised
neighbourhoods” and experience health challenges (Berrick, 1997; Christenson &
McMurty, 2009; Keller, Wetherbee, LeProhn, Payne, Sim & Lamont, 2001). Yet even
with these disadvantages, kinship caregivers receive less services for the children placed
with them and have less regular contact with their caseworkers than non-kin foster
parents (Fuentes-Palaez, 2015; Keller et. al, 2001). It is unclear if this discrepancy is
because kinship parents prefer it this way or whether agency and professional variables
contribute to the lower services received by kinship caregivers (Falconnier et al., 2010).
Research also highlights that kinship caregivers are less prepared than non-kin
care providers, with little or no preparation before placement, limited formal training and
inadequate understanding of the child welfare system (Christenson & McMurty, 2009).
Kinship caregivers often receive little or no notice before a child is placed with them
and/or they begin fostering during a crisis. On the other hand, foster parents generally
become caregivers very intentionally and have made the decision to become caregivers
over a period of time (Coakley, et al., 2007). They also attend training, receive formal
supports from both they system and other formal caregiver colleagues.
There is a significant degree of strain on kinship caregivers. Compared to their
non-kin counterparts, kinship caregivers are 45% more likely to have trouble coping with
the children in their care. Because they are committed to the children in their care, they
Crucial Elements of Kinship Care Home Assessment
19
often put the children’s needs ahead of their own (Farmer, 2010). However, the strain of
this kind of caregiving can eventually jeopardize the quality of the placement (Farmer,
2010), which highlights the needs for formal and informal support.
Kinship caregivers are more likely to care for children where there have been
concerns of parental substance abuse compared to other children in care (Coakley, et al.,
2007; Falconnier et al., 2010). Prenatal exposure to substances is often associated with
negative developmental consequences, which leaves children placed in kinship care more
likely to experience such challenges. Unfortunately, there is little research comparing
kinship versus non-kin placed children on developmental trajectories.
Some studies suggest that children placed in kinship care tend to stay longer in
placement than their peers placed in non-kin placements (Berrick, 1997; Leos-Urbel et.
al, 2002, O’Brien, 2012; Perry, Daly & Kotler, 2012), yet eventual reunification rates are
similar (Berrick, 1997, O’Brien, 2012). Furthermore, as indicated above, children placed
in kinship care have lower rates of recidivism (the likelihood a child returning to
government care after being returned to parental care) compared to children in non-kin
placements (Berrick, 1997; Koh & Testa, 2011; Perry et al., 2012). Overall though,
research into permanency outcomes that compare children in kinship and non-kin
placements is inconsistent and not generalizable (Koh, 2010). Blakey (2012) indicates
that mothers in her study identified feeling that having their children in kinship care
represented the “best of both worlds” where they could continue being a part of their
child’s lives without addressing lifestyle or addiction issues. Kinship placements in these
instances were viewed as enabling addictive and maladaptive behavior (2012). Blakey
speculates that higher levels of access in kinship care contributed to a reduced incentive
Crucial Elements of Kinship Care Home Assessment
20
for birth parents to work towards the return of their children thereby delaying
reunification.
A significant challenge in kinship care practice may also derive from caseworkers
attitudes (Farmer, 2009). Caseworkers may hold beliefs that the relative of an abusive or
neglectful biological parent is more likely to be abusive or neglectful; such beliefs can
create a barrier to kinship placement and practice. Research has found that caseworkers
sampled felt that if grandparents, for example, were “responsible for creating or
participating in the problematic behavior by having raised adult children who abused or
neglected their children, why should they be supported in raising a new generation of
children?” (Lorkovich, Piccola, Groza, Brinda & Mark, 2004). Yet Lorkovich et al.’s
research actually found in most cases, the birth parent’s abusive or neglectful behavior
was the exception within their family of origin (2004). Furthermore, other research
suggests that some maternal grandmothers describe pride in being able to care for their
grandchildren even though they were unable to care adequately for their children. This
ability to “right a wrong” becomes a motivating factor for some kinship caregivers
(Blakey, 2012).
Caseworker’s attitudes toward kinship care in Ontario were explored by
Brisebois, Kernsmith and Carcone in 2013. Even though previous research found an
overall support of shifting practice towards family-based care, Brisebois et al. found
“moderate, generally negative attitudes about kinship foster care” (p. 412) among their
sample of caseworkers. They further found that this attitude and skepticism influenced
decisions to remove children from kinship care placements due to what was deemed to
be safety concerns by caseworkers. They also found that another compounding factor in
Crucial Elements of Kinship Care Home Assessment
21
case decisions were worker’s attitudes regarding financial responsibility. Workers in this
study indicated kinship homes should not be financially supported by the agency were
more likely to have removed a child from the kinship home (Brisebois et al, 2013).
While this research is quite recent, provides Canadian context, and examines the role that
caseworker attitudes may play in the removal of a child placed in kinship care, it was
quantitative in nature and relied on self-reporting on survey instruments. A qualitative
approach would provide deeper insight into the rationale of case decisions and the
influence that experience and attitudes have had on these decisions.
Lorkovich, Piccola, Groza, Brindo and Marks also explored caseworker attitudes
towards kinship care as a potential barrier specifically to kinship adoption (2004).
Caseworkers who were identified as having rigid definitions of who could be included as
kin and also caseworkers or who believed a potential kinship caregiver should not have
close ties to the abusive or neglectful parent, were found to have allowed these attitudes
to negatively influence their placement decisions. The research noted “practitioners
often had difficulty separating some of their concerns and attitudes about the biological
family from kinship caregivers” (Lorkovitch et al, 2004). These attitudes have had an
impact on policies and practice in kinship care in general even though a growing body of
research results indicate that placement in kinship care is preferred (Lorkovitch et al,
2004; Christenson & McMurty, 2007; Scannapieco & Hegar, 1996; Falconnier et. Al,
2010).
While considerable knowledge has been gained regarding the experience of
kinship caregivers and the children placed in their care, understanding in the areas of
how best to support caregivers through training, formal supports, and information

Crucial Elements of Kinship Care Home Assessment
22
sharing is lagging (Denby, 2011). Hong, Algood, Chiu and Lee suggest that because of
these complexities, an ecological approach is required in the development of these
kinship specific processes and policies (2011). These authors suggest there are multiple
layers of influence on the developmental outcomes for children in care. Further, the
interrelations of the child, and kinship caregivers’, environment must be understood
(Hong et al., 2011).
Furthermore, some authors have criticized the research done to date for its
reliance on Western approaches. For example, Love warned that the danger of applying
these western, dominant perspectives to Indigenous communities, for example, is the
“continuation of colonial processes, with the practice of oppression and cultural
dismemberment overlaid with the rhetoric of caring and altruism” (2000, p. 29).
Assessing Kinship Homes
One apparent detrimental impact of kinship policy on practice is in the area of
assessments and home studies. Alberta, like many other jurisdictions, requires a formal
kinship home study as part of the approval process. Prospective kinship caregivers
typically undergo a home assessment based on tools developed for middle class adoptive
families and based on modernist, empirical approaches (Calder& Talbot, 2006). These
structured tools do not consider cultural traditions or context, and only peripherally
consider the opinions of other family members. Modernist home study practices exclude
many potential kinship caregivers based on “class bias and are ignorant of the outcomes
for children who live in kinship placements” (Calder & Talbot, 2006, p. 31).
Furthermore, while family’s may appreciate the requirement for a formal evaluation of
their homes, an extended assessment process can be an “unwelcome, incomprehensible,

Crucial Elements of Kinship Care Home Assessment
23
intrusive and worrying intervention” while they are adjusting to the unexpected provision
of child care (O’Brien, 2014, p. 356.)
The Structure Analysis Family Evaluation (SAFE) home study tool has been used
in Alberta and a number of home study practitioners have been trained in its use. SAFE
was developed in 1989 based on adoption home study practices and loosely based on the
Family Assessment Form (FAF) (Crea et al., 2007). Its intent was to create a uniform
home study methodology that would more thoroughly assess adoptive families through
uniformity, efficiency, and psychosocial evaluation (Crea, Barth, & Chintapalli, 2007;
Crea, Barth, Chintapalli, & Buchanan, 2009b). SAFE was a response to inconsistencies
in adoption practices and decision making, and an effort to meet the three purposes of an
adoption home study: i) to educate and prepare adoptive families for adoption, ii) to
gather information for the purpose of matching and, iii) to evaluate the fitness of the
family (Crea et al., 2007).
A differential use of home studies has developed throughout North America.
Over time, SAFE has not only been used for adoption but, but has been applied as an
assessment tool for different placement types such as foster care, and then kinship care
(Crea et al., 2007). This differential use of home studies has been based on the
assumption that “every person caring for a child with special needs should meet the same
standards” (Crea et al., 2007, p. 151). But, this differential use for foster care and
adoption does not recognize the difference in motivations or caregivers’ ability to make
short or long term commitments to children (Crea et al., 2007). Kinship care then adds
another level of complexity in the differential use of a home study. The motivation,
demographic, experience, challenges and outcomes are not necessarily the same for kin
Crucial Elements of Kinship Care Home Assessment
24
and non-kin caregivers. Ironically, Crea et al. point out that state administrators
expressed the view that facilitating permanency and concurrent planning would be
facilitated with one single home study instrument methodology for all types of caregivers
(Crea et al, 2009b). This perspective is not supported in other research.
Research on the use of SAFE has focused on the perceptions by child welfare
professionals in its use and impact rather than on outcomes where it has been used (Crea
et al., 2007; Crea, Barth, Chintapalli & Buchanan, 2009a). An interesting finding has
been the differentiation between less experienced and more experienced staff in the use
of SAFE as a home study approach. Less experienced staff are more positive about the
use and impact of SAFE than more experienced staff (Crea et al., 2009a). This may
suggest that inexperienced workers require a structured decision making tool or
highlights an issue of change-management among senior staff. This underscores the
need for additional training in the home study process such as interviewing skills,
engaging with clients, and assessment (Crea et al., 2009a). SAFE is now identified as a
tool that is used for adoption, foster care and kinship. However research into its
differential effectiveness is extremely limited and the practice implications of differential
use have not been addressed.
Concerns have also been raised in the use of SAFE with Indigenous families and
caregivers. The Aboriginal Advisor’s report on the status of Aboriginal child welfare in
Ontario raised the issue that home study programs like SAFE should be removed until
they could be modified to reflect Indigenous values and cultures. The report further
suggested that home study programs and standards be developed that are specifics to
Indigenous communities (Beaucage, 2011).
Crucial Elements of Kinship Care Home Assessment
25
Some jurisdictions have focused on group training programs as part of a home
assessment process (Crea et al., 2007). The Parents Resources for Information
Development and Education (PRIDE) is one such development program. The PRIDE
program, developed by the Illinois Department of Children and Family Services, consists
of nine 3-hour training sessions delivered over a two-and-a-half months (Christenson &
McMurty, 2009). In addition to these training sessions families meet with a social
worker for assessment and information meetings in the family’s home (Christenson &
McMurty, 2009). PRIDE curriculum is based on five competencies: protecting and
nurturing children; meeting children’s developmental needs and addressing
developmental delays; supporting relationships between children and their families;
connecting children to safe, nurturing relationships intended to last a lifetime; and
working as members of a professional team (Christenson & McMurty, 2007). Research
showed participants of the PRIDE training program gained competencies in the area of
protection and nurturing of children, connecting children to safe, nurturing relationships
intended to last a lifetime, and working as a member of the professional child welfare
team (Christenson & McMurty, 2009). The rationale for the development of PRIDE is
embedded in the recognition that foster parent training is associated with outcomes such
as placement stability, parenting skills and parent satisfaction (Christenson & McMurty,
2007). Furthermore, social supports have been found to be crucial in the retention of
caregivers (Christenson & McMurty, 2007). However, as with other tools in the
assessment and initiation of caregivers, the effectiveness and impact of PRIDE with
kinship caregivers specifically is unknown and under researched.
Crucial Elements of Kinship Care Home Assessment
26
Shlonsky and Berrick (2001) argue that a substitute caregiver’s home should
undergo the same scrutiny as does a biological family’s home in the course of an
“investigation” (p.61). This is often done through the licensing process. However this
process typically addresses safety and supervision only, and not other domains related to
child well-being (2001). Shlonsky and Berrick further suggest that placement in
unlicensed (unapproved) kinship care leaves these children are at risk of receiving
substandard care. Shlonsky and Berrick measured quality of care in terms of child safety
including maltreatment, physical safety of the home, physical environment,
neighbourhood, medical and dental care, educational support, mental health and
behavioural support, as well as developmental factors (2001). They did not consider
domains such as child attachment and connection, social supports, emotional supports,
community connection, cultural identity, stability, and ongoing connection to informal
and natural supports, all of which are areas in that children placed in kinship care
experience positive outcomes. Furthermore, licensing for kinship caregivers becomes
complex as requirements are typically based on middle class standards (number of
bedrooms, home insurance, fences) making it difficult for extended family who live in
poverty to qualify (Falconnier, Tomaselloa, Doueck, Wells, Luckey & Agathen, 2010).
Some research suggests leniency and flexibility with standards is acceptable in
kinship placements (O’Brien, 2012). The extent to which children are safe in a given
placement, factors into the consideration of leniency and flexibility of standards (Font,
2015). Research has suggested that kinship care may be safer when compared to
traditional foster care (Font, 2015; Winokur, Crawford, Longoardi & Valentine, 2008).
In a study that compared outcomes for children placed in kinship are to those placed in

Crucial Elements of Kinship Care Home Assessment
27
foster care, Winokur et al. found that children in foster were 10.1 times more likely to
have an allegation of abuse or neglect while in care (2008). Font found allegations of
maltreatment to be higher for out of home placements within the first three months of
placement, suggesting the needs to support and screening to be imperative at initial
placement (2008). It should be noted, however, for this particular finding Font looked at
the allegations of maltreatment and not cases of substantiated maltreatment.
Lorkovitch et al. suggest home assessment processes for kinship families should
be comprehensive and examine not only the viability of the kinship caregivers as a
permanency option, but also the family’s needs in order to provide them with necessary
informational, financial, and social service supports (Lorkovitch et al, 2004). The focus
of this research was on the barriers to kinship adoption, and did not consider what
barriers families face when caring for kin temporarily.
Recently, a Spanish participatory action research project created an evaluation
instrument and questionnaire specific to kinship home assessment. Few researchers
identify and describe specific methodology to assessing kinship caregivers. This
particular project comprised of six open-ended questions to gather information on six
domains. These included: personal and social demographic data; coverage of basic
needs; collaboration with foster program professional teams, family structure and
dynamics; relationship between the foster family, the child and the biological family;
motivation and attitude toward fostering; and a final synthesis (Fuentes-Pelaez et al.,
2015). A number of limitations existed within this suggested framework including
methodology, a failure to recognize the clinical differences between kinship and foster
care, and a theoretical framework that failed to recognize marginalized populations and

Crucial Elements of Kinship Care Home Assessment
28
instead furthered the dominant perspective. Furthermore, this participatory action
research included only child protection professionals and no kinship caregivers.
Until now, Spain has not had any home assessment process for kinship care. It is
interesting that Spain is applying foster care assessment strategies to kinship care in
Spain in a similar evolution with kinship care practice as North America. The Spanish
researchers make the connections that “reviewing the research helps us identify the
elements that are associated with disruptions in foster care and therefore could be
explored in an assessment of kinship foster caregivers” (Fuentes-Pelaez et al., 2015, p.
4). They further suggest that factors associated with a good foster care process for some
types of foster care appear to be the same for other foster care modalities. As an
example, issues and experiences for specialized foster care is similar in nature to general
foster care (Fuentes-Pelaez, 2015).
Alternatives in Kinship Care Home Assessment
Understanding the characteristics of successful kinship arrangements can help
inform appropriate assessment methodology. Coakley, Cuddeback, Buehler and Cox
identified characteristics of successful kinship arrangements through interviews with
kinship caregivers as “support of family, commitment of children, faith, good parenting
abilities, church involvement, flexibility and adequate resources” (2007, p. 92).
Characteristics that inhibited successful placements included “strained relationship with
the birth family, poor discipline strategies, inability to deal with the ‘system’, lack of
resources and inability to deal with children’s emotional, behavioural, physical problems
(Coakley et al., 2007, p. 93). This understanding can help guide the development of
assessment approaches in the context of the population identified by Coakley. However
Crucial Elements of Kinship Care Home Assessment
29
this may not be representative of caregiving experiences for Indigenous populations or
other unique and diverse groups.
An important component of practice in kinship care and home assessment is
reflexivity (Mills & Usher, 1996; O’Brien, 2014; Fairbairn & Strega, 2015). A
practitioner’s reflection on their own particular set of values and their understanding of
the personal impact of their family history can provide insight into their attitudes about
kinship care. As discussed earlier, caseworker attitudes have a large bearing on this area
of practice and prevailing attitudes are not necessarily grounded in evidence. O’Brien
(2012) suggests practitioners in this area of practice must ask themselves a number of
questions regarding their own extended family networks, history, and experiences to
develop a reflexive position. This reflexive position ensures critical thinking applied to
this area of practice and the ability to apply principles of social justice.
Assessments may be considered as an ongoing process progressing through a
number of steps. Mills and Usher suggested a three-stage process that is family-centred
and strengths-based (1996). Because of the many cross-cultural situations and the
heterogeneity of kinship networks, Mills and Usher’s approach highlights a culturally
competent approach. This model suggests the assessment leads into case management
where a similar focus and principles are applied for “intensive wraparound service
delivery” (p. 602). The model also applied the following principles of attention to
cultural diversity; family participation and decision-making; systematic assessment; and
comprehensive services under a highly coordinated service delivery plan (Mills & Usher,
1996). Systemic assessment involves a three stage protocol using an ecological
theoretical approach to first encourage the families to self-identify their resources,
Crucial Elements of Kinship Care Home Assessment
30
second to identify what supports would be required (including financial, child care,
stressors, and housing), and finally identify child-specific needs.
To self-identify resources, tools such as an ecomap and genogram are used to
further understand the resources, supports and relationships available within a family
system. A “pathways exercise” helps the case manager and family identify strengths
within the family and existing supports including a “family communicator” (Mills &
Usher, 1996, p. 606). The family communicator and case manager then organize the
FGC to explore further placement options and alternatives. Mills and Usher’s model uses
a Family Group Conference (FGC) to ensure family participation and empowerment.
Family decision-making is a key element of FGC (Mills & Usher, 1996) where family
members come together to make decisions about case planning and the use of family and
community resources.
The second step of the protocol is in understanding the formal services and
supports, which would be necessary to maintain the child in the kinship caregiver’s
home. The third step is focused on what the child’s needs would be. Both steps describe
the use self-assessment as foundational elements to the assessment. Children who are old
enough to describe their wishes are engaged in this self-assessment.
The family uses the information from the self-assessment, ecomap and genogram
to negotiate a service plan that incorporates attention to cultural diversity, family
participation, systemic assessment and comprehensive services.
Children placed in the demonstration project’s kinship homes, experienced
greater placement stability and caregivers reported a positive care experience and an
increased receipt of support services (Mills & Usher, 1996). This research dates back to
Crucial Elements of Kinship Care Home Assessment
31
1996, and while ecological approaches to assessment and FGC are fully entrenched in
child welfare practice, the Mills and Usher model of kinship care case management has
not received widespread implementation. No updated research is available on this
framework.
O’Brien offers a conceptual model for kinship care assessment that addresses the
practice of assessing kinship homes, but also considers the political and legislative
impacts on kinship care assessment (2014). O’Brien identified the key parental capacities
required of kinship caregivers as: “insight into self; understanding the child’s needs and
be committed to meeting them; understanding and ability to deal with family dynamics,
especially one’s own position in it; and allowing the agency provide support to the child
and family” (O’Brien, 2014, p. 357). These parental capacities, however, must occur
within a context that is supported by the government or supporting agency. Enabling and
clear legislation and policy that recognize and encourage the preference for keeping
children within their family and community are required, but this model also recognizes
the role of the child’s family network and their participation as essential. Similar to
Mills and Usher, O’Brien suggests the use of family group decision making to mobilize
natural supports within the family or community (2014).
O’Brien’s work which is based in a social constructivist theoretical framework
ensures that context is recognized and ensures a critical stance towards practice and
theory. However, this work was completed in Ireland where the impacts of colonization
on Indigenous populations have not impacted the overrepresentation of Indigenous
populations the same way as it has in Alberta. This conceptual model suggested by

Crucial Elements of Kinship Care Home Assessment
32
O’Brien omits the cultural factors, which may be more relevant in Indigenous
populations.
Conclusion
The literature indicates that to be successful, kinship home assessments should be
approached in a manner that is unique and different than traditional foster care (Hegar &
Scannapieco, 2014). Kinship families in many instances are the preferred option to care
for children, however they face unique challenges that differ from traditional foster care
(Hegar & Scannapieco, 2014). Terling-Watt indicates that a good kinship home
assessment addresses “an important distinction between what relatives plan to do and
what they are able to do in terms of providing permanent homes for these children”
(2001, p. 114). Kinship home assessments that are completed with kinship caregivers
should help identify this distinction. However a well-done assessment can also identify
where a child welfare agency can fill the gaps in terms of providing required support to
ensure success for children and their kinship caregivers.

Crucial Elements of Kinship Care Home Assessment
33
Home Assessments Policy and Practice - Various Jurisdictions
To further understand current policy and its impact on practice, I sought to
understand policy and practice on kinship home assessment in various jurisdictions
throughout Canada and some international jurisdictions as well. This information was
compiled either by emailing specific contacts responsible for this area of policy and
practice in other provinces or by directly contacting them through phone or electronic
means such as Skype. Contacts were asked directly what the process was for kinship
home assessment; if there was a specific standardized tool or assessment form being used
for kinship assessment; and if any other practices, such as Family Group Conferencing,
were foundational to the assessment process. In the course of this sharing, contacts in
other jurisdictions were also made aware of Alberta processes for kinship care home
assessment. A summary of these findings are presented in detail in Appendix C.
Home Assessment in Alberta
Currently, kinship home assessments in Alberta are completed using either the
Structured Assessment Family Evaluation (SAFE) tool or completed using a regulated
form known as the Home Assessment Record (HAR). Attempts were made to
implement the SAFE tool provincially for all caregivers (adoption, foster care, and
kinship) by providing training and supports to this structured home assessment approach.
However, a significant barrier to this implementation was resistance amongst the
Delegated First Nation Agencies (DFNA’s) who saw the SAFE tool as not culturally
relevant and offensive to cultural practices of kinship. As a result, policy states that
home assessments can be made using either approach.
Crucial Elements of Kinship Care Home Assessment
34
An unintended consequence to this flexibility in policy, has been that home
assessment training has been only offered to and accessed by those home assessment
practitioners who are using SAFE. While the SAFE training is specifically training in
the use of the structured tool, it does include elements of general home assessment
training. Those practitioners or agencies who have continued using the HAR have not
had opportunities to attend home assessment specific training outside of SAFE. It should
also be considered that aside from SAFE training no other home assessment specific
training is available for practitioners.
Child Intervention service delivery in Alberta is provided through eight Child and
Family Service regions and seventeen Delegated First Nation Agencies who are
responsible for delivering child intervention services in several First Nation
communities. Home assessment practice in each region and DFNA looks different. In
addition to the home assessment approach used, practitioners may be experienced staff
with experience in supporting caregivers. Or, in some areas, they maybe externally
contracted service providers with no child intervention experience. These service
providers, if practicing with the SAFE model, would have attended SAFE training.
However they would not have attended any other home assessment training and may or
may not have previous experience in child intervention. The majority of home
assessments in Alberta are completed with use of external service providers.
The external providers make recommendation for approval or non-approval based
on their assessment. However the authority to approve or not approve is delegated to the
child intervention supervisor. The information in the assessment report informs this
decision.
Crucial Elements of Kinship Care Home Assessment
35
Some regions, primarily rural, complete home assessments internally. In these
situations, these internal staff completing the home assessments, are experienced
caseworkers or caregiver support workers with twenty or more years of experience. In
these sites, home assessment practice is recognizes as a highly specialized area of
practice requiring higher level of skill. Decision to approve or not approve homes
assessed in this manner sits with the supervisor who makes the decision in consultation
with the assessor.
Kinship Home Assessment in Other Jurisdictions
In preparation for this work, I completed an informal scan of home assessment
practice in other provinces. In April 2015, contacts from the provincial and territorial
placement services table were contacted via email and asked the following questions:
what, if any, home study tool is used? Who completes them? How are they trained or
supported in their role? And are there any other integral components to the kinship care
assessment process over and above the home study? The Provincial/Territorial
placement services table is comprised of government representatives from each province
and territory who have some responsibility for the creation and implementation of policy
and program development for child welfare placement resources.
Six of twelve jurisdictions replied to these questions and I charted their responses
of informal and comparative analysis. The chart of their responses was shared with the
jurisdictions for their own information and is attached as appendix C.
This scan showed the practice of contracting home assessments appears to be
unique to Alberta. All responses showed that internal staff complete the kinship care
home assessments. In some areas a placement specialists (ie: foster care social worker,
Crucial Elements of Kinship Care Home Assessment
36
placement resources team, or residential services unit staff) complete the kinship home
assessment and while in others it may be the caseworker or social worker assigned to the
child’s file with decision making authority. It should be noted that in jurisdictions where
a placement specialist complete kinship home assessments, they are also completing
foster care and adoption home assessments. This is significant to note as previously
discussed in the literature review a differential approach to these different types of
assessment is required to meet the unique experience of kinship care.
Many of the jurisdictions identified using the SAFE structured assessment tool
and some other jurisdictions described developing their own tools for what they
described as the unique nature of kinship care as compared to adoption or foster care. It
is important to note that one of the jurisdictions that did develop developed a kinship
specific approach also developed additional assessment elements for kinship care to
augment the assessment used for other placement resources (adoption and foster care).
These additional elements include the ability to “maintain and manage healthy
boundaries with the birth family” and the family’s “ability to work with the Director in
an open and cooperative manner when the birth parents may not be in agreement with the
case plan.” The addition of these elements could suggest an attitude within the
jurisdiction that kinship caregivers may be problematic because of their alignment with
birth parents. A more in depth discourse analysis of jurisdictional policy would be
required to further understand underlying attitudes about kinship care in policy, practice
and program development in various jurisdictions.
Through this jurisdiction scan it was discovered that the requirements of kinship
care practice such as annual reviews, support plans or training greatly varied throughout
Crucial Elements of Kinship Care Home Assessment
37
the Canadian jurisdictions. Only one jurisdiction identified the involvement of family in
all case and safety planning and the importance of family involvement in this work.
Because this scan approached particular individuals who are involved in
placement resources work, the information shared was their policy interpretation. Policy
interpretation and information shared could have been reflective of personal biases,
professional attitudes towards kinship care practice or perception. This review gives a
partial picture of kinship care practices throughout Canada.
Contact was also made with child intervention practitioners in Western Australia
and New Zealand. These jurisdictions are a significant source of comparison to
Alberta’s practice because of similar histories of colonization and resulting over-
representation of Indigenous children in care. These jurisdictions have adopted the Signs
of Safety approach to child intervention and Alberta is in the midst of implementing this
approach provincially (Alberta Human Services, 2014). This is a strengths-based,
solution-focused and safety-organized approach to child intervention work (Turnell,
2012) developed by child intervention practitioners, Andrew Turnell and Steve Edwards,
in the 1980’s. The approach serves as a model and a set of tools where professionals and
families engage together in partnership to address situations of child abuse and
maltreatment (Turnell, 2012). Family participation in case and safety planning and
decision-making is an outcome of this approach. In attempts to engage kin in case
planning and the placement provision, this approach has been used (Turnell & Essex,
2014).
Western Australia developed a new home assessment form that
incorporates elements of Signs of Safety practice in relative or significant other
Crucial Elements of Kinship Care Home Assessment
38
assessment. Elements of Appreciative Inquiry for a strengths-based approach are
present in addressing questions on certain required elements in the form of “what is
working well.” The assessment is formatted to address five carer competencies that are
legislated and regulated in Western Australia. The competencies include: provides care
for a child in a way that promotes the wellbeing of the child, promotes the child’s family
and interpersonal relationships, and protects the child from harm; is able to provide a
safe living environment for the child; is able to work co-operatively with officers, a
child’s family and other people when providing care for a child; is able to take
responsibility for the development of his or her competency and skills as a carer; and is a
person of good character and repute. Inherent in these legislated competencies are value
laden statements which complicate professional assessment. However the application of
Signs of Safety model and focus on solution-focused approaches is embedded in the
assessment. Following completion of the assessment, the report and recommendations go
through a series of panels for final approval, which further removes the family from final
decision-making.
Similar to Western Australia, New Zealand has embedded Signs of Safety
strengths-based and solution focused approaches into their caregiver assessment. In a
New Zealand home assessment, a number of identified domains of assessment are
described in the language and context of the Indigenous Maori people. This inclusive
approach to language, together with solution-focused and strengths-based approaches
ensures family engagement in the home assessment process. Furthermore, typically a
kinship care home assessment begins following a Family Group Conference, which have
been mandatory in New Zealand since 1989 (Connolly, 2006).
Crucial Elements of Kinship Care Home Assessment
39
Methodology Theoretical Framework
Because of the history of structural colonialism in the child welfare system, this
research is grounded in an anti-colonialist perspective. This perspective is the most
appropriate approach in addressing the over-representation of Indigenous children in care
(Pon, Gosine, & Phillips, 2011; Hart, 2009). Many authors have pointed out that child
welfare systems have “become the contemporary manifestation of colonization” (Strega
& Carriere, 2015, p. 2, TRC, 2012). Colonization occurs when hierarchical and dominant
discourses are adopted and clients who are typically marginalized are seen as the ‘other’
or less than (Strega & Carriere, 2015). Colonization is driven by a worldview that
embraces “dominion, self-righteousness and greed” and can impact both the colonized
and colonizer at many levels – nation, community, family and individual (Hart, 2002, p.
24). When societal and institutional structures produce and reproduce inequalities based
on race, class, sexual and gender location, colonization is deemed to be structural (Sefa
Dei, 2000).
This perspective differs from anti-oppressive approaches, which have failed to
address over-representation because they have failed to recognize the continuing issue of
white supremacy in the dominant culture (Pon et al, 2011). An anti-colonialist approach
considers colonialism to be persistent. Hart (2009) argues that, while relationships
between the state and Indigenous people have been redefined and re-negotiated,
dominant structures and marginalization continue through these re-negotiated structures
(p. 28). Since colonialism continues, anti-colonialism should not be confused with post-
colonialism, which considers colonization as an event in the past (Hart, 2009). Rather
Crucial Elements of Kinship Care Home Assessment
40
anti-colonialism is the embracing of an alternative or oppositional paradigm as well as
“cultural revitalization” (Hart, 2009, p. 32). In practice, anti-colonialism focuses on the
recovery of traditional Indigenous knowledge (Hart, 2009, p. 32). An anti-colonialist
would suggest a reorganization that embraces the Indigenous traditional ways of
knowing, helping, doing and being, which suggests an anti-colonialist perspective by
recognizing traditional Indigenous knowledge and proficiency. The community
conversations hosted by the Government of Alberta heard a number of comments
suggesting traditional Indigenous knowledge should inform the child welfare system
(Alberta Government, 2014).
Alberta has recently adopted an Aboriginal Experience principle as part of the
Child Intervention Practice Framework that describes an anti-colonialist approach. The
principle states:
Aboriginal people have always had their own ways of ensuring that vulnerable members, including children, are safe, protected and nurtured. We honour this by recognizing their expertise in matters concerning their children, youth and families. (Alberta Human Services, 2014)
This principle suggests that an exploration of how traditional kin networks are
approached and understood by the child welfare system is vital. Processes and policy
must start supporting the perspective represented in the principles. Intrusive home
assessment practices have been criticized for failing to honour the expertise of
community or family.
This investigation is also grounded in critical ecological systems theory. This
theoretical approach integrates principles of social justice through questioning and self-
reflective application of theory (Rothery, 2008). Ecological theory gives “equal weight
Crucial Elements of Kinship Care Home Assessment
41
to the individuality of our clients as people and to the social environments that determine
their well-being” (Rothery, 2008, p. 90). By taking a relational perspective, this theory
recognizes that the person and environment are intricately connected and “reciprocally
sustaining and shaping one another” (Rothery, 2008, p. 91). Integrating concepts of
social justice into ecological theory has evolved this theoretical perspective into critical
ecological theory. This theoretical approach has significant influence, not only on child
intervention practice, but also on the practice of approving caregivers for children in
care. Assessment practices for caregivers often use an ecological framework
(Scannapieceo & Hegar, 1996). However, adding a critical lens to the consideration of
kinship caregivers is of significant importance to ensure a socially just approach to this
typically marginalized population.
The recognition of people’s social context and the influence of societal constructs
suggest that postmodernist philosophy influences critical ecological systems theory. As a
result, approaches to research influenced by this theory lend themselves to being
investigated through qualitative means. Qualitative research aims to explore a
phenomenon by understanding the meaning individuals attribute to the social problem
(Creswell, 2014). Qualitative research is suited to studies that incorporate transformative
worldviews, seek to examine the oppression of individuals or to examine the impacts of
social constructs on marginalized populations (Creswell, 2014).
Secondary Data Analysis
This study identified existing qualitative data from previous government
consultations and conducted a secondary analysis on this data to isolate the crucial
elements of kinship home assessment. Using existing data to inform and reform child
Crucial Elements of Kinship Care Home Assessment
42
intervention practices honours the voices and expertise of community members who
have previously shared this information for the purposes of making changes to child
intervention practice.
Secondary data analysis is “the use of an existing data set to find answers to a
research question that differs from the question asked in the original or primary study”
(Hinds, Vogel, Clarke-Steffen, 1997, P. 408). The secondary use of data in quantitative
studies has been common (Gillies et al., 2005; Irwin et al., 2011). However the
secondary analysis of qualitative studies is far less common and has only begun to be
discussed in the literature (Gillies et al., 2005). Analyzing secondary data sets is a
complex approach, yet archived sources of qualitative data have been described as a
potential repository of valuable knowledge. They are “a rich and unique yet often
unexploited source of research material that can be reanalyzed, reworked, and compared
with contemporary data” (Corti, et al., 2005, p. 1).
Irwin and Winterton (2011) identify areas of investigation that can benefit from a
secondary analysis of qualitative data. Examples include assessing the credibility of new
research, supplementing one’s own data, providing rich descriptive information,
revealing new methodological insights by reflecting on previously conducted research,
generating new findings by analyzing old data from a new lens, or gaining further insight
on hard to reach populations or sensitive topics without further intrusion into vulnerable
populations. Justification for this thesis research focuses on the latter area. It is well
documented that Indigenous communities have been victimized and oppressed in the
name of science (Smith, 1999; Hart, 2002). De-colonizing and anti-oppressive
approaches that acknowledge power differences within the history of research with
Crucial Elements of Kinship Care Home Assessment
43
Indigenous populations, seek to understand the ‘truth’ for Indigenous populations rather
then the ‘fact’ identified by Western knowledge (Smith, 1999).
Some members of the Indigenous community in Alberta have identified that
further consultations could be viewed as intrusive. Using secondary data analysis will
honour the information they have already shared with government agencies. The
government of Alberta hosted a number of Community Conversations from 2011 to
2013. At these conversations, participants expressed frustration and exploitation from
constant consultation. The following comment from the community conversation echoes
this frustration:
Been to SO MANY of these – this is ANOTHER conversation – where are all the other volumes of reports, all the ideas, all the good things – so frustrating – it’s just talk, it’s always just talk – nothing has changed.
Many benefits exist for the increased use of qualitative secondary data analysis in
general. Bishop (2009) highlights some of these as, “making ‘unmined data’ available,
avoiding duplication, reduced burden on research participants, greater transparency of
research procedures, alignment with open access principles, recognizing that publicly
funded research is a public asset” (p. 256). The practice of secondary data analysis
aligns with those governmental organizations’ that are moving towards open data sharing
policies (Bishop, 2009). This data sharing movement comes from recognition that
transparency and openness makes the fullest use of publicly funded research (Bishop,
2009). Whiteside et al (2012) identifies the benefits as “efficiencies in time, money, and
other resources and the maximization of the use of potentially important data that might
otherwise lie dormant” (p. 504). Secondary data analysis research can prevent existing
Crucial Elements of Kinship Care Home Assessment
44
data sets from being underused and can generate new knowledge and hypotheses or
support for existing theories (Hinds et al., 1997).
However, challenges exist in secondary data analysis. While the description of
these challenges differ amongst authors, they generally align with Whiteside et al.’s three
categories of methodological challenges: quality of data, data “fit” and the nature of the
relationship between the research and the data (2012).
In a secondary analysis of primary data, there must be consideration paid to the
quality of the primary data. The quality of secondary data may be problematic if the
data is outdated, if some data or information is missing, if there were weaknesses in the
original research design, or there was a poorly documented methodology (Whiteside et
al, 2012). Assessing the quality of the primary research design can be challenging,
unless the researcher has access to or was involved in the primary research. One must
have access to the principal investigator and the study team in order to assess quality
(Hinds et al, 1997). With access one can measure the completeness including a measure
of the condition of the data set, accuracy of transcription, comprehensibility of the data,
and how interpretable the data set is (Hinds et al., 1997). This closeness can help the
research, however too much closeness can skew the secondary data investigator to
existing knowledge of the phenomena (Hinds et al., 1997).
The research question within the secondary data analysis must “fit” with the
purpose, context and time period of the primary research. Furthermore it’s important
that secondary study has a similar theoretical framework to the primary study (Van den
Berg cited in Corti, 2005) and a similar time frame (Vall Gillies and Edwards cited in
Corti, 2005). This idea of currency of the data set is important as qualitative research
Crucial Elements of Kinship Care Home Assessment
45
may study a phenomena’s change over time. Therefore, the timing of a secondary
analysis should be carefully considered (Hinds et al., 1997).
Hammersley (2010) points out the weaknesses attributed to secondary data
analysis are the same as the weaknesses identified for qualitative research in general.
For example, consider the critique that secondary data analysis uses data received in
response to the primary research question to answer a different secondary research
question. This can also be the case in qualitative, primary research. Often this type of
investigation will start off looking at one phenomenon but the iterative nature of
qualitative research, brings it into another direction. In addition the context of a
phenomenon is more fully revealed during the course of research, therefore the context
understood at the beginning of an investigation is different than it is at the end (Irwin &
Winterton, 2011).
Finally, the nature of the relationship between the research and data must be
considered. Qualitative research is strongly connected to the interaction between
participant and researcher (Gillies et al, 2005). Secondary data analysts need to be
sensitive to the emotions and cognitions experienced by the participants in the primary
study. Primary study investigators can help sensitize the secondary analysts into a sense
of “having been there” (Hinds et al., 1997). It’s a challenge to secondary analysts who
do not experience facial expressions, gestures or comments made that were not recorded.
These help set the context of the original data (Hinds et al, 1997). However, research
assistants or research teams themselves are often removed from qualitative data and the
interviews themselves as they review transcripts or recording carried out by others

Crucial Elements of Kinship Care Home Assessment
46
similar to a secondary analysis (Hammersley, 2010). Generally speaking we know more
about the research process and flaws in that methodology when we create the data.
Ethics are a significant issue in the use of secondary data analysis as well, and
issues regarding consent are particularly important. Ideally consent would have been
received in the primary study to use data in secondary analysis. (Hinds et al, 1997) and it
is suggested that contemporary primary researchers should consider incorporating this
into their consent forms. When historical data is used, going back to get consent is time-
consuming and can be impossible (Gillies et al., 2005). Researchers completing
secondary analysis must consider if reusing the data breaches the contract between the
primary researchers and the participants (Whiteside et al., 2012). Bishop (2009)
proposes that full consent is non-existent anyway. We cannot ever inform participants of
all consequences, as they may not be known. If they were well known there would be no
reason to research. Ethical codes also highlight a duty to benefit society by increasing
knowledge and understanding. This duty must be weighed against harm towards
participants (Bishop, 2009). Prior to undertaking secondary analysis researchers must
consider if harm will come to the participants.
Ethics can also support the use of secondary data analysis. Internationally, most
ethical codes for research prescribe that participants should be exempt from unnecessary
intrusion (Bishop, 2009). Suggesting secondary data analysis is one way to minimize
this unnecessary intrusion. There is also a duty for openness and transparency within the
research community.
Irwin and Winterton (2011) advise, “the difficulties for secondary analysis will
be more or less severe depending on whether there is a risk of systematic interpretation
Crucial Elements of Kinship Care Home Assessment
47
of data and whether there are checks that can be made on our interpretations with
reference to other forms of data” (p. 10). Similarly Whiteside et al suggests the use of
literature can strengthen the secondary analysis as an additional source of comparative
data (2012). My approach to secondary data analysis included comparison to the
literature. In addition, this study ensured rigour by presenting key themes from the
secondary analysis to a group of practitioners.
I have confidence that secondary data analysis was an appropriate approach in my
thesis investigation. I was confident because I had access to the data and the
methodology in which the data was collected, the data “fits” this research endeavour and
furthermore, it honours the voices that were shared in past data collection. The primary
data collection was grounded in a similar anti-colonialist theoretical framework which
matches this investigation.
Thematic Analysis
Thematic analysis is a common approach to data analysis within the qualitative
research. Simply, it focuses on “identifiable themes and patterns of living and/or
behaviour” (Aronson, 1994). It is a “method for identifying, analyzing and reporting
patterns (themes) within data. It minimally organizes and describes your data set in
(rich) detail. However, frequently it goes further than this, and interprets various aspects
of the research topic” (Braun & Clarke, 2006, p. 79). Furthermore they describe
thematic analysis as the search across a data set to find repeated patterns of meaning
(2006).
Thematic analysis has been described as foundational to qualitative research
(Braun & Clark, 2006). They further identify the benefits of thematic analysis as
Crucial Elements of Kinship Care Home Assessment
48
flexibility and theoretical freedom. However, critics argue that thematic analysis has
historically struggled in ensuring rigour due to an absence of guidelines, tools, and
techniques (Attride-Stirling, 2001; Braun & Clarke, 2006). While the field of qualitative
research has gained popularity (Attride-Stirling, 2001) and developed strategies for
ensuring rigour in data collection and analysis, thematic analysis as an approach within
the qualitative approach has been poorly described and acknowledged (Braun & Clarke,
2006).
However, there are several authors who have suggested guidelines and applied
strict methodology to thematic analysis (Braun & Clarke, 2006; Aronson, 1995; Tuckett,
2005; Attride-Stirling, 2001). Braun and Clarke (2006) describe the process that begins
with the collection of data and familiarizing oneself with the data. This may be through
transcribing recordings or repeated readings of the entire data set. The second step is to
generate initial codes based on your familiarity with the entire data set. Codes identify a
feature of the data. These codes are then organized into meaningful groups or categories
of codes. Themes then start to develop from the analysis of these categories or groups.
Analysis includes thinking about the relationship between categories and potential
themes and main themes or sub-themes may emerge.
Significant effort must be put into reviewing and refining codes and possible
themes and ensuring there are clear and identifiable distinctions between themes (Braun
& Clarke, 2006). As themes are refined and defined, they require a detailed analysis and
what Braun and Clarke refer to as a story that connects to the broader “story” (2006).
Attride-Stirling (2001) describes the use of thematic networks as an
organizational aide to thematic analysis by facilitating the depiction of themes and their
Crucial Elements of Kinship Care Home Assessment
49
interrelationship. Themes are mapped out in a web-like manner based on groupings of
various similarity and filter down in increasing specificity. Similar to the constructs and
processes of grounded theory, (Corbin and Strauss, 1990; Attride-Stirling, 2001), basic,
organizing and global themes are identified through the thematic network. Basic themes
are the simplest representation of the data and are grouped together to form an organizing
theme. Organizing themes bring basic themes into clusters of similar issues and become
more abstract ideas of what is represented in the textual data. These organizing themes
come together to form global themes which can present an assertion about a given issue
or reality (Attride-Stirling, 2001). These networks can be visually represented and create
a descriptive aid in documented research.
Although the literature review is a critical piece of thematic anlalysis, there is
some disagreement with when to engage in a literature review relative to data analysis.
An early literature review may narrow the analytic field of vision and create focus
(Braun & Clarke, 2006). On the other hand, a literature review may interfere with an
inductive approach to data analysis. These critics argue the data should be informing the
identification of themes and not the current body of research (Braun & Clarke, 2006).
In reviewing thematic analysis for quality, it is important to ensure that an
analysis of the data has occurred and not just a collection of data. Other potential
weaknesses include the use of data collection questions as an overall theme, and themes
that overlap and fail to be differentiated, or where there is inconsistency. Other potential
weaknesses to watch for, similar to other qualitative research data pitfalls, include when
there is no support for analytic claims and a mismatch between analysis and theoretical
Crucial Elements of Kinship Care Home Assessment
50
framework (Braun & Clarke, 2006). In this project, an anti colonizing framework aligns
with the framework of the community conversations for example.
Thematic analysis, when done carefully and correctly, provides a robust
methodology for data analysis. Its flexibility brings benefit to research endeavours
through various theoretical frameworks. The flexibility inherent in thematic analysis
makes it appropriate for use in secondary qualitative data analysis. As an example,
grounded theory would not be an appropriate approach in secondary qualitative data
analysis because I do not have access to the sample to go back an ensure saturation in
each theme or category, nor can I use theoretical sampling. Approaches that require
direct observation or interaction such as ethnography are also not possible in secondary
qualitative data analysis.
For this project, the use of thematic analysis through thematic network mapping
(Attride-Stirling, 2001)was used to identify the crucial elements of kinship care as
identified through the existing data sets.
Rigour
This project design used rigor criteria as described by Lincoln (1995) for
qualitative research. I chose Lincoln’s framework specifically because it promotes
qualitative inquiry that displays commitments to its participants; an ability to foster
professional, personal and political action; and research that promotes social justice and
diversity (Lincoln, 1995). Elements described by Lincoln of positionality, voice, critical
subjectivity, and sacredness are embedded throughout this project.

Crucial Elements of Kinship Care Home Assessment
51
Identifying and articulating my positionality early on ensured ongoing reflection
on my position and biases. Lincoln (1995) describes the criteria of voice as ensuring
someone is speaking for the silenced, the disengaged, or the marginalized.
This project was designed to ensure the voices shared in previous inquiry were
not silenced and were further honoured and validated by exploring answers to this
particular research question. I employed journaling while designing the project,
identifying the methodology and during data analysis which generated opportunities to
support critical subjectivity and reflexivity.
The aim of this project is to more deeply understand the experience of assessment
for kinship caregivers in order to gain a more fulsome approach to this area of practice. It
is intended that this deeper understanding in turn, will support the caregivers. Sacredness
is gained in research that is based on the “granting of dignity, and deep appreciation of
the human condition” (Lincoln, 1995, p. 284). This is relevant as the construct of
kinship care aligns with Indigenous world views.
As described earlier, Irwin and Winterton (2011) suggest specific checks be used
to check on interpretations of data in secondary qualitative data analysis. In the case of
this project, a comparison to the body of literature on kinship care and home assessment,
and the use of a focus group to discuss findings is used to check on interpretations made
in the data analysis.
Crucial Elements of Kinship Care Home Assessment
52
Data Analysis
My process for data analysis comprised of two elements. First, the secondary
data sets were themed using thematic analysis. Then, preliminary themes were presented
to a focus group for discussion. Themes were then further developed with feedback from
the focus group. Within this secondary data analysis, data from two sources were used:
the DM Summit Meetings and Community Conversations.
Data set 1: DM Summit Meeting. On October 27 and 28, 2011 and on February
22, 2012, the Government of Alberta held Deputy Minister’s summit meetings with
directors of Delegated First Nation Agencies (DFNAs), Chief Executive Officers (CEOs)
of Child and Family Services Authorities (CFSAs) and representatives from First
Nations receiving services from CFSA. Forty to fifty participants attended these
meetings to discuss home study practice and policy, guiding principles, and outcomes.
The goal was to develop a shared understanding and a province-wide approach to
completing a home study that was culturally appropriate, based on good outcomes and
solid foundational principles. All participants held leadership positions such as Director
or Senior Manager.
Participants were divided into three groups according to Treaty Area. DFNA
Directors and representatives from First Nations met and CEO’s from the regions
corresponding with that particular Treaty Area met together. As a result, Treaty Areas 6,
7 and 8 met as separate groups and each had unique conversations. Each group was
asked to carefully draft and identify the principles and outcomes and to also fine tune
their responses after some reflection at the second meeting. The groups were further
asked to identify specific qualifications and training needed by people doing the home

Crucial Elements of Kinship Care Home Assessment
53
study, and essential specifications of an instrument that could be used by the person
doing the home study.
Each group included a facilitator who was employed within the Ministry of
Human Services and a note taker. Facilitator guides and an orientation were provided to
both facilitators and note takers to ensure a consistent approach within all three separate
groups. Notes were made onto large flipchart paper whereby participants could, and did,
provided clarification or correction as needed while notes were being taken. The notes
from all three conversations were amalgamated together and shared with all participants.
Data Set 2: Community Conversations. From December 2011 to May 2013, the
Aboriginal Engagement and Strategy Division conducted 16 Community Conversations
as a means to understand the complexity of the issue of the overrepresentation of
Indigenous children and youth in government care. The Community Conversation
model was adopted from the Tamarack Institute processes (Tamarack Institute, 2016).
The intent of a community conversation is to “bring together people with diverse
perspectives to share their insights on a topic of common importance” (Alberta
Government, 2014). Community conversations are open ended and are based on the
premise that solutions to complex problems lie within the diversity of skills, perspectives
and strengths that exist within the community; incorporate the views of people who play
a variety of roles within the community; do not start out with a solution in mind; start
with a sense of curiosity about the variety of perspectives on the topic; and are structured
to build a common understanding of the issue and the roles of people connected to the
issue (Alberta Government, 2014).

Crucial Elements of Kinship Care Home Assessment
54
This community conversation approach aligns with an anti-colonialist perspective
where the community is seen to be an expert on themselves, and that expertise is
embraced. For this reason, it was important to include data gained through this process
within my study. Furthermore a very large amount of data was collected through this
process and it is important to honour those who in good faith provided this information.
In fact comments were recorded from participants at the community conversations that
spoke to the need to honour the information. Participants stated:
How many more stories do our people need to tell? We need to leave today with action.
It is disrespectful to ask people to share their stories and not make change happen.
Been to SO MANY of these – this is ANOTHER conversation – where are all the other volumes of reports, all the ideas, all the good things – so frustrating – it’s just talk, it’s always just talk – nothing has changed. same things over and over and over.
We meet and we meet… we need to be heard this time and the change has to happen!
There were 1628 individuals from 126 communities were invited to attend the
conversations and 782 participated. These included youth, elders, First Nation and Metis
community members, individuals with lived experience, Aboriginal and non-Aboriginal
service providers (ie: health, education, law enforcement), and staff from Delegated First
nation Agencies (DFNAs) and Child and Family Services Authorities (CFSAs).
Participants were from both government and non-government agencies and represented
rural and urban populations. Each event was planned by a steering committee that
identified local invitees and the logistics of the day. Local Indigenous elders played a
crucial role at each community conversation. Participants were advised the information
Crucial Elements of Kinship Care Home Assessment
55
would be used in the future to inform practices and policies within the child welfare
system, thus setting the stage for using this data in the current project.
The conversations started with open-ended questions about what was happening
in the field of child intervention for Indigenous children, youth, families and
communities. Following this, participants were asked about what changes they would
like to see and what steps could be taken to make these happen. The discussion at each
conversation was captured by note takers who sat at each table and wrote down the
comments made by participants. Each of the 13,000 comments was then entered into an
excel database and sorted into primary and secondary themes. However, the un-themed
comments were still accessible allowing for secondary analysis of the pure comments.
In the fall of 2013, each community where a community conversation was held
was visited by the Aboriginal Engagement and Strategy Division of the Alberta
Government and presented with the information as it was heard.
Analysis of Secondary Data. The raw data for each of the two data sets was
obtained through formal channels and permission for the Ministry of Human Services.
Then, in the case of the Community Conversations, this data was stored in a large excel
database of 13,000 comments. These comments were from table conversations that had
been transcribed by facilitators at the Community Conversations. They were then
entered into large database for later analysis. The comments themselves were used for
the secondary data analysis.
Data from the DM Summit Meetings were in the form of flip chart notes from the
2 events which were then transcribed to Word documents. These meetings each had
facilitators and note takers taking notes on large flip charts during the conversation.

Crucial Elements of Kinship Care Home Assessment
56
While there were no audio recordings from these meetings, it can be assumed that note
taking through flip charts ensures accuracy in the note taking. Because the participants
are able to correct the note taker on the accuracy of the notes being taken, we can be
assured that any misinterpretation is caught by the participants themselves at the time of
the note taking.
After I read all of the comments from both data sets in their entirety, I returned
and started to code comments line by line. A list of these codes is presented in Appendix
D. I used NVivo 10 as a qualitative software analysis tool to code and organize my
research. During the coding, various memos and journals were made to ensure
appropriate reflection and consistency in the theming process. For example, while all
13,000 comments from the Community Conversations were analyzed. Several of those
comments were not relevant to this particular research question on kinship care. As a
result I generated a memo describing that comments were being included that related to
kinship, extended family, caregivers, recruitment of caregivers or caregiving. Data that
did not include these constructs were excluded.
Starting with a process of open coding, comments from both data sets were
individually coded to describe the topic or issue being described in the comment. Over
time, these comments were then grouped and categorized using NVivo 10, and organized
into global themes. The coding from NVivo 10 then pictorially became a thematic
network map to be described in the findings. I returned to the themes and codes a
number of times and continued refining the themes.
Focus Group. After an initial thematic network map was developed, early
findings were presented to a group of practitioners involved in kinship care home
Crucial Elements of Kinship Care Home Assessment
57
assessment in Alberta for feedback and discussion. The feedback from this group of
practitioners augmented the data from the secondary data analysis and together with the
secondary data analysis informed the findings. The focus group provided rigour and a
check on the quality of the secondary data analysis.
A purposive sampling approach was used for the focus group. This group of
practitioners were recruited from an existing working group of the Child and Family
Services Division of the Ministry of Human Services. I presented information on the
research question, methodology and consent process at one of this group’s regular
meetings. This was followed up with an email invitation to the group for participation in
a two-hour focus group and included the same information on the purpose of the focus
group. Informed consents were attached to the email invitation that included contact
information in the event there were any questions. This consent form is included as
Appendix A.
Of the fourteen practitioners invited to participate, there were nine who
participated and one who was sent as a proxy. It should be noted that the proxy was also
a practitioner with significant experience in the area of kinship care. One participant was
represented an agency providing services exclusively to an Indigenous community.
Three of the participants connected to the focus group through video conferencing. All
participants signed consent forms.
A focus group protocol was developed and is attached here as Appendix B. The
focus group was audio recorded and then later transcribed. The focus group was advised
of this at the outset of the meeting. As per the focus group protocol, they were also
advised that the information shared within the focus group was confidential and
Crucial Elements of Kinship Care Home Assessment
58
participants were asked to also respect the confidentiality of fellow participants. They
were further advised they were free to withdraw their consent at any time and leave the
group, however because of the format of the group the information they had shared until
the point of leaving would be included in the findings. After the explanation, all
participants confirmed they were prepared to continue with their participation and the
audio recording began.
A power point presentation was presented to the group, as per the focus group
protocol, and included a brief overview of the project, research question, and
methodology. This included a brief overview of secondary data analysis, an overview of
the secondary data sources, and an overview of thematic analysis and thematic network
mapping.
Feedback and discussion emerged after the presentation of some themes. This
discussion helped refine and reinforced or confirmed certain key areas that had arisen
from the secondary data analysis or the participants presented elements that they
identified as crucial or requiring further consideration. The discussion also focused on
elements of disagreement or areas they felt the secondary data sources had not
considered, but in the perspective of the practitioners was worth consideration.
Crucial Elements of Kinship Care Home Assessment
59
Findings
The research set out to discover the perceived crucial elements of kinship care
home assessment. A descriptive approach to analysis was chosen rather than interpretive
due to the secondary analysis nature. An interpretive approach to data analysis would
risk erroneous assumptions there was no relationship to the participants or the data itself.
A descriptive approach maintains a closer portrayal of the data (Irwin & Winterton,
2011). Analysis of the data revealed seven global themes or crucial elements as
identified by the secondary data and focus group. The final global themes were:
Assessor Characteristics; Important Areas to Address; Home Assessment Process;
Safety; Policy and Legislated Requirements; and Systemic Issues.
Notably these global themes identify issues from the micro to the macro systems
level. There is value in considering the crucial elements from this ecological systems
approach to firmly understand from a critical perspective the experience between the
practitioner and the family or caregivers at the micro level of practice. But, this
approach also considers the macro influences that occur at a larger systemic or societal
level that potentially impact the experience of families within child welfare and
specifically those pursuing kinship care. This considers “all people or groups of people
in a system share a reciprocal influence on each other” (Rothery, 2008, p. 96). These
systems at the micro and macro level mutually impact each other in a circular rather than
linear manner (Rothery, 2008). Diagramming becomes a useful approach to
conceptualize the person within the larger environment or ecology (Rothery, 2008). The
crucial elements of kinship care home assessment can be visually represented in the
following figure.
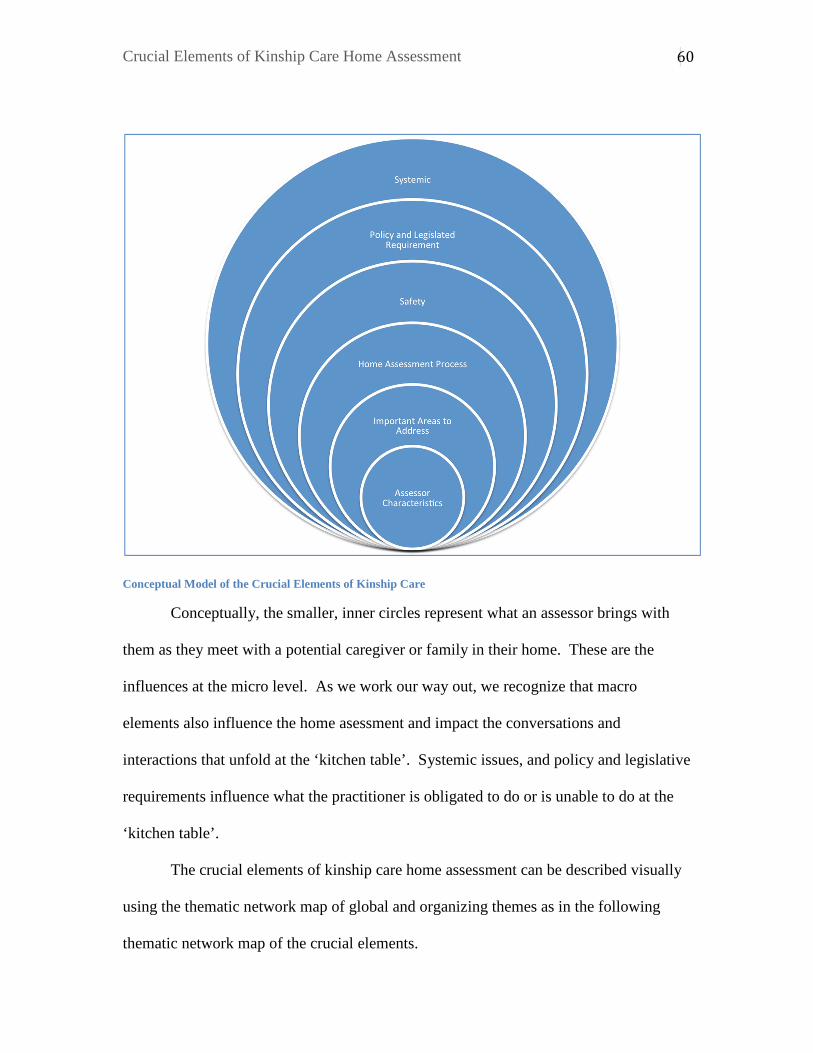
Crucial Elements of Kinship Care Home Assessment
60
Conceptual Model of the Crucial Elements of Kinship Care
Conceptually, the smaller, inner circles represent what an assessor brings with
them as they meet with a potential caregiver or family in their home. These are the
influences at the micro level. As we work our way out, we recognize that macro
elements also influence the home asessment and impact the conversations and
interactions that unfold at the ‘kitchen table’. Systemic issues, and policy and legislative
requirements influence what the practitioner is obligated to do or is unable to do at the
‘kitchen table’.
The crucial elements of kinship care home assessment can be described visually
using the thematic network map of global and organizing themes as in the following
thematic network map of the crucial elements.

Crucial Elements of Kinship Care Home Assessment
61
Thematic Network Map – Global and Organizing Themes of the Crucial Elements of Kinship Care Home Assessment
Throughout this section, basic and organizing themes will be broken down
further in thematic network maps for for each global theme followed by further
description and discussion. Detailed examples of comments demonstrating each theme
are represented in tables in Appendix E. Sections on these tables left blank, represent
Crucial Elements of Kinship Care Home Assessment
62
areas in which there were no comments provided. Findings from the focus group will be
integrated throughout the discussion of the themes.
Assessor Characteristics
Those elements that are in the centre of the visual model represent the Assessor
Characteristics. Assessors are the social workers, typically, who completed the home
assessment by meeting with the family members individually, and with the whole family
and assess the ability of potential caregivers to care for the identified children. The
themes presented here are the elements and competencies that an assessor1 brings with
them to the home they are assessing. Within this global theme, comments were further
analyzed into organizing and basic themes and visually portrayed in the following figure.
Three organizing themes included Assessor Skill, Assessor Perspective and Professional
Supports highlighted comments pertaining to those topics.
1 The terms assessor, home assessor or practitioner are used interchangeably throughout this section and all describe the social worker who completes the home assessment.
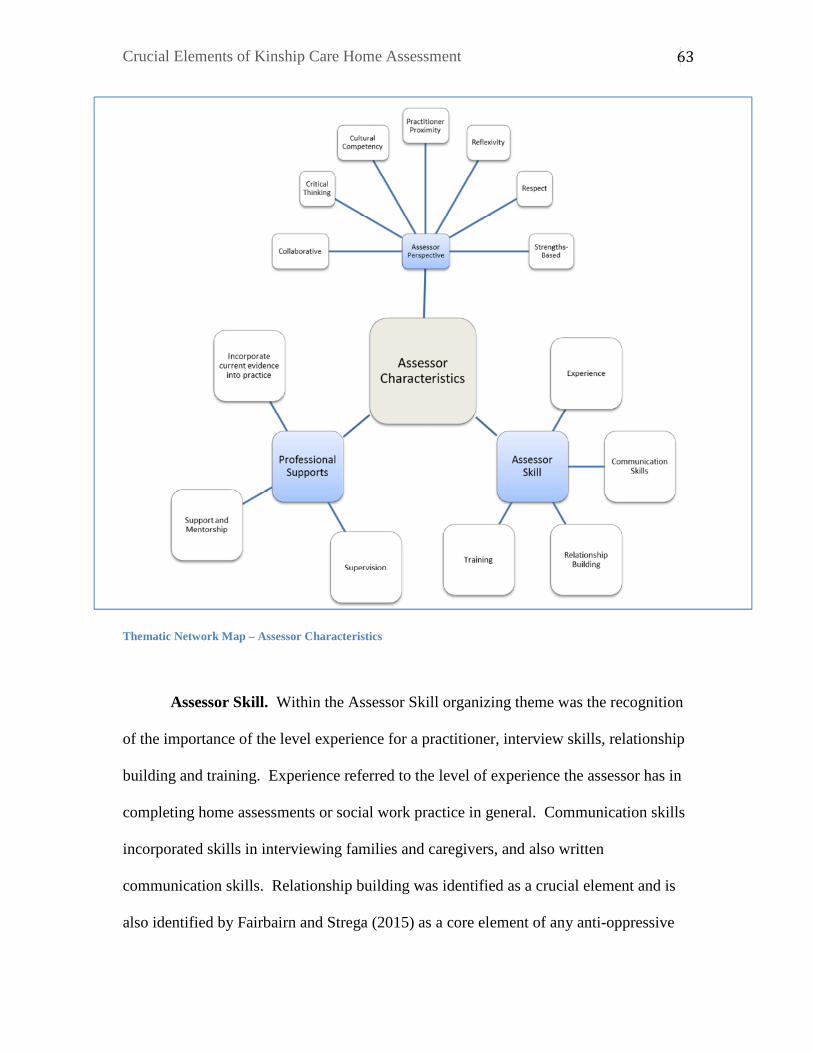
Crucial Elements of Kinship Care Home Assessment
63
Thematic Network Map – Assessor Characteristics
Assessor Skill. Within the Assessor Skill organizing theme was the recognition
of the importance of the level experience for a practitioner, interview skills, relationship
building and training. Experience referred to the level of experience the assessor has in
completing home assessments or social work practice in general. Communication skills
incorporated skills in interviewing families and caregivers, and also written
communication skills. Relationship building was identified as a crucial element and is
also identified by Fairbairn and Strega (2015) as a core element of any anti-oppressive

Crucial Elements of Kinship Care Home Assessment
64
child welfare assessment. Training refers to the formal training that an assessor has in
completing home assessments. It also can refer to training in other crucial elements
outlined within the findings.
Assessor Perspective. Also under Assessor Characteristics was the organizing
theme of Assessor Perspective. This includes elements that form an assessor’s
perspective or innate qualities that were identified as being important for a home assessor
to possess. These qualities included being collaborative, possessing critical thinking,
cultural competency, reflexivity, respect, strengths-based, and practitioner proximity.
An assessor who incorporates collaboration and critical thinking into the
assessment was described as being important. Cultural competency within this theme
refers to the assessor’s understanding of the family’s culture, their ability to approach
families in a cultural relevant manner and their ability to appreciate the role of culture in
families. Reflexivity is identified often in the literature as a key element to assessment
work, assessors must be keenly aware of their social location, that of the agency and
critically affect on how these positions may impact the assessment itself as well as the
outcomes (Fairbairn & Strega, 2015). From the focus group, this reflexivity was
highlighted as important because so much is depending on the neutrality and objectivity
of the practitioner.
An assessor who is respectful with the families they work with and incorporates
this element into their work with the family was described within the theme of respect.
“A respectful relationship is always in the child’s best interests” (Fairbairn & Strega,
2015). An assessor who can see strengths in families and caregivers was also identified

Crucial Elements of Kinship Care Home Assessment
65
as crucial. Comments organized within this theme specifically relate to the strengths-
based perspective of the assessor themselves.
Practitioner proximity described a group of comments that suggested that an
assessor or practitioner who lives within a community may best be able to assess a
prospective kinship family. The comments suggest that an assessor who possesses direct
community knowledge may best be able to complete a home assessment for kinship
families.
Professional Support. The final organizing theme within Assessor
Characteristics is Professional Supports. Comments in this area described supervision,
support and mentorship and ensuring that current evidence is incorporated into home
assessment practice.
The assessor’s ability to access supervision and opportunities for support and
mentorship were described as being crucial to this area of practice. Providing
opportunities or ensuring that current evidence is incorporated into assessment practice
was also identified. It should be noted that Fairbairn and Strega (2015) suggest caution
and reflection in the consideration of evidence-based practice to consider the heavy
influence of socio-political ideologies as well as personal and professional biases on
what we consider to be evidence.
Important Areas to Address
The next global theme represents data that identified important areas to address
within the home assessment and required elements required within the home assessment
report. This impacts practice at the mirco level or direct practice with the family, but
may be influenced by the organization. Thus they are further away from the center
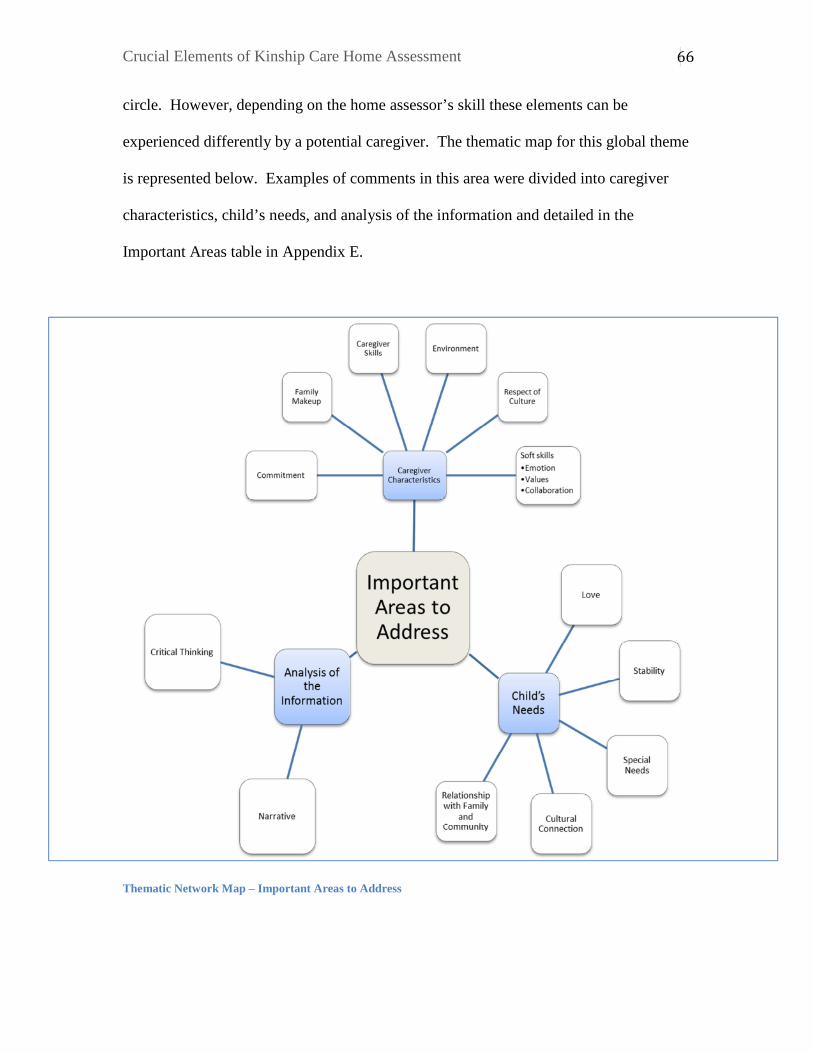
Crucial Elements of Kinship Care Home Assessment
66
circle. However, depending on the home assessor’s skill these elements can be
experienced differently by a potential caregiver. The thematic map for this global theme
is represented below. Examples of comments in this area were divided into caregiver
characteristics, child’s needs, and analysis of the information and detailed in the
Important Areas table in Appendix E.
Thematic Network Map – Important Areas to Address

Crucial Elements of Kinship Care Home Assessment
67
Caregiver Characteristics. A number of elements under caregiver
characteristics were identified and comments were categorized under this organizing
theme. They included: commitment, family makeup, caregiver skills, environment,
respect of culture and soft skills, which included emotion, values and collaboration.
Commitment describes comments that described a potential caregiver’s
commitment to a child and their case plan which could be reunification with their parents
or remaining in the kinship home long term. The focus group suggested going beyond
the notion of commitment and suggested also considering motivation. The focus group
felt that motivation is different than commitment and should be evaluated specifically.
Motivation is currently an area requiring evaluation in Alberta home assessments. The
focus group also suggested considering the evaluation of economic motivation.
Family makeup describes comments that described the importance of analysis of
the whole family structure being included in the assessment. These comments also
highlighted specifically that Indigenous families make look different than families of the
dominant culture. An assessor should be cognizant of this while assessing this area.
The focus group provided many comments in this area and discussed the
importance of evaluating possible impacts that age could play on family dynamics. The
focus group also identified the importance of understanding potential changes in roles
post placement. From a family structural perspective, roles can change if, for example,
the grandmother is caring for a grandchild, but has children in the home of similar age.
In this case the child placed (the grandchild) is in relationship with the other children in
the home as siblings rather than cousins, aunt/niece, etc. This may not be the case if the
family unit is not nuclear in composition as is common in Western families, and more
Crucial Elements of Kinship Care Home Assessment
68
communal as is common in traditional Indigenous communities (Fairbairn & Strega,
2015). Comments in the secondary data did suggest that Indigenous families can look
different than those of the dominant culture.
Caregiver skill included two different subthemes. These were parenting skills
and knowledge that caregivers may already possess or need to be trained to. An
assessment would include analysis on what the family’s parenting skills are or what their
approach to parenting has been in the past. It would also include commentary on the
specific knowledge the parents possess, which could be specific to the unique or, in some
cases, special needs of the child. The focus group commented that kinship families may
not have the same degree of skill as foster parents may have. Data also suggested a need
to assess the caregiver’s environment to ensure it is stable for a child. Respect of culture
is noted in the data and while one of the benefits of kinship care is connection to culture,
there are situations where children are placed with significant others who are not family
members or there is not a shared culture between the paternal or maternal extended
family. Respect of the child’s culture(s) becomes relevant in these situations.
The data described a number of elements such as the caregiver’s values, emotions
and collaboration. These were grouped together and themed as soft skills or skills that
consider emotion and affection. Comments in the data described the importance of a
child experiencing love and affection in a potential kinship home and the importance that
these be incorporated in the home assessment. The focus group had a number of thoughts
to consider in the evaluation of love and its subjectivity. Discussion suggested a need to
ensure reflexivity of the practitioner in their evaluation and assessment of these areas.
Because of the subjectivity of this issue, the focus group commented it is important the
Crucial Elements of Kinship Care Home Assessment
69
practitioner have personal insight into how they are evaluating it. There was much
discussion and cautioning on the assessment of these soft skills within the focus group
discussion.
Connection to family is more often facilitated in kinship placements than other
out of care placements and the data highlighted the importance of ensuring caregivers are
willing to facilitate through the assessment. This area was another area of discussion
with the focus group. There appeared to be two components to this: willingness to
collaborate with the caseworkers and willing to collaborate with the family.
The focus group also suggested the need to look at history, grief and loss and
trauma within the assessment. This would suggest an assumption from the focus group
that caregiver’s have a history of trauma and grief and loss. Interestingly, the secondary
data identified the focus on history as being a barrier in the home assessment process.
This will be discussed further under Home Assessment Process and is noted here in the
findings, but is not identified as a theme.
Child’s Needs. Another identified theme important to include in the home
assessment is the identification and understanding of the child’s needs and how
caregivers will be able to meet these needs. Comments were themed according to love,
stability and permanency, special needs, cultural connection, and relationship with
family and community.
Comments categorized in the theme of love, referred specifically to a child’s need
for love. Similar to comments themed as soft skills under caregiver characteristics, these
comments were specific to articulating a child’s needs rather than assessing a caregiver’s
abilities to meet emotional needs. Comments regarding a child’s need for stability and
Crucial Elements of Kinship Care Home Assessment
70
permanency were themed together and describe comments that indicated a child needs
consistent and stable caregiving and minimal moves between placements.
A caregiver’s ability to meet a child’s special needs was identified as being
crucial. This would include trauma informed approaches, disability, and the ability to
provide specialized supports when necessary. In considering research that suggests
many children placed in kinship care have come into care due to issues of addictions
(Falconnier et al., 2010), special needs due to possible prenatal substance exposure are a
consideration.
Comments also described a child’s need for cultural connection and relationship
with family and community. These elements are often met through placement in kinship
care because the child is placed with family or community. However, as described with
caregiver characteristics, there are circumstances in kinship care placements where these
need to be considered. For example, if paternal and maternal sides of the family do not
share the same culture or a kinship placement is outside of the community.
Analysis of the Information. Another area identified was the analysis of the
assessment itself. It was described that the report should contain both narrative and
analytical elements. This was a source of considerable conversation within the focus
group. It was suggested that the assessment must be more than just a narrative story
about the family, but that it must contain considerable analysis into the family’s ability
and potential to care for the identified child.
Home Assessment Process
As mapped below, the next global theme is the Home Assessment Process itself.
Conceptually, these comments are still micro in nature and impact the experience for the
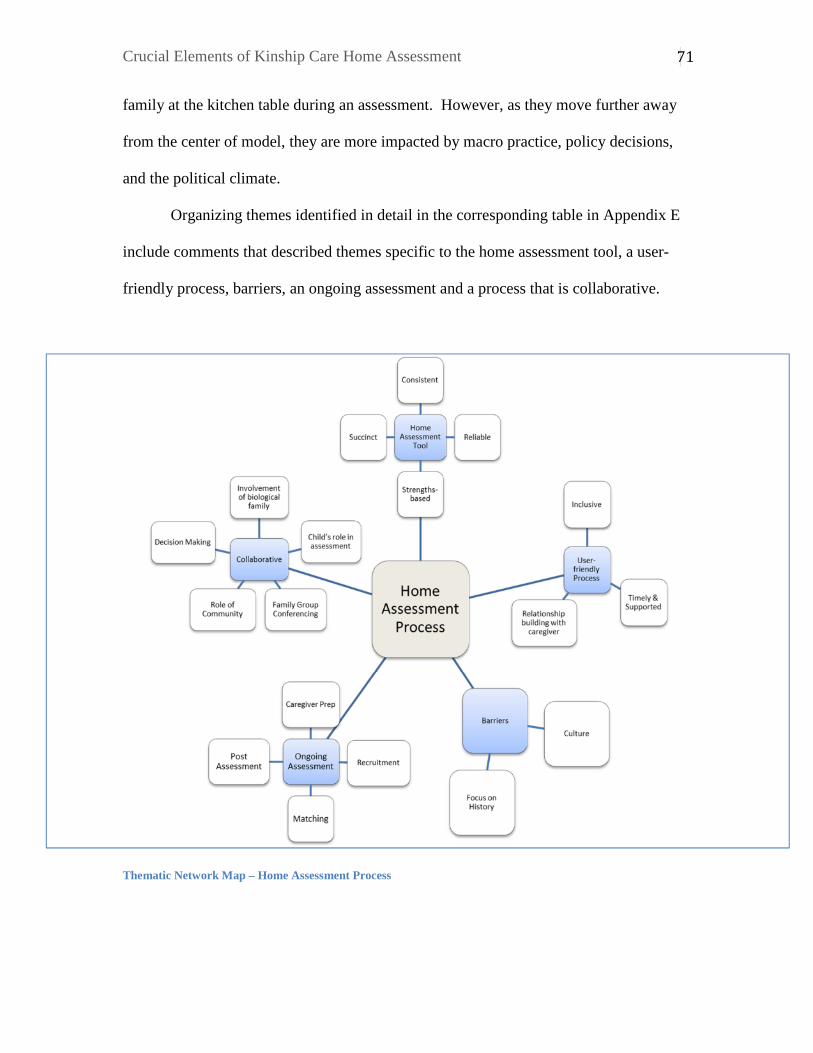
Crucial Elements of Kinship Care Home Assessment
71
family at the kitchen table during an assessment. However, as they move further away
from the center of model, they are more impacted by macro practice, policy decisions,
and the political climate.
Organizing themes identified in detail in the corresponding table in Appendix E
include comments that described themes specific to the home assessment tool, a user-
friendly process, barriers, an ongoing assessment and a process that is collaborative.
Thematic Network Map – Home Assessment Process

Crucial Elements of Kinship Care Home Assessment
72
Home Assessment Tool. Comments suggested that if a standardized home
assessment tool is to be used, it was important that it be consistent, reliable, succinct, and
strengths-based.
The comments categorized under strengths-based tool differed from the
comments describing a strengths-based practitioner. Here, they were specifically
focused on a strengths-based form, tool, or process rather than a practitioner who is
grounded in a strengths-based approach.
User-friendly Process. Other comments within the Home Assessment Process
identified the need for a user-friendly process. Within this organizing theme an
inclusive, timely and supported home assessment process was described. Participants
also described a home assessment process that focuses on relationship building.
Comments described a process that is inclusive. An inclusive assessment process
would recognize barriers that some participants may face such as language or geography
and ensure flexibility to meet the needs of the participants or potential caregivers.
A timely and supported home assessment was described as necessary in the
secondary data and highlighted the urgency of these assessments in considering that
children are potentially waiting placement while they are being done. In discussing this
theme, focus group participants highlighted the barriers that families or caregivers face in
completing required documentation or tasks related to completing the home assessment
in a timely manner. Suggestions highlighted the need for supports to be provided during
this process. As a result this theme was renamed to “timely and supported”. Some of the
elements of the conversation could have been themed under “barriers,” however the
Crucial Elements of Kinship Care Home Assessment
73
comments were made in the context of a user-friendly home assessment process, and
they were coded and categorized under this section.
A process that recognizes and allows opportunity for the assessor to build a
relationship with the caregiver was described in the comments. The comments
categorized in this section were specific to a process that allows for relationship building
as opposed to the comments that were themed as Assessor Characteristics.
Barriers. Comments within the data also highlighted a number of barriers within
the current home assessment process. While there were comments related to barriers in
general, there were also comments that were focused more specifically on a lack of
understanding of Indigenous culture within the assessment and being judged negatively
as a result. Also, there were frustrations expressed at the current home assessment’s
focus on history without opportunity to discuss the context or areas of change.
Ongoing Assessment. The data described the need for the assessment to be
ongoing and not just a snapshot in time describing a caregiver and their home.
Comments described the importance of caregiver preparation, recruitment, matching and
support post assessment. Comments included within these organizing themes are related
to practice specific elements. Systematic issues on recruitment and caregiver supports
are included in systemic themes to be discussed later on.
The focus group provided commentary specifically on recruitment efforts within
the home assessment process. The focus group identified the risks of not deeply
exploring all potential caregivers and potentially excluding some. They also describe
that matching can speak to other themes as well. Matching overlaps in considering
Crucial Elements of Kinship Care Home Assessment
74
parenting skills and caregiver characteristics under the global them of Important Areas to
Address.
Collaborative. A collaborative process was also described by the data. This
collaborative process was described as including involvement from the biological family,
identifying the child’s role in the assessment, Family Group Conferencing, the role of
community and the manner in which decision making occurs.
Comments regarding Family Group Conferencing (FGC) were intentionally
included within the secondary data analysis for a number of reasons. FGC was not
specifically identified in the comments as a crucial element to kinship home assessment.
However it was identified as a key practice important to the reform of child intervention
practice. FGC is suggested in the literature as a potential element in kinship care home
assessment and thus was included within this analysis. Furthermore, FGC has been
identified as an important process in the reunification of children and youth with their
extended family and community. This is also one of the intents of kinship care.
The focus group agreed that FGC was a crucial element to the home assessment.
The benefit to FGC was also identified as the ability to locate more possible caregivers
or even supports to the identified caregiver. There was also an identification that this
practice needs to happen more.
The role of community, involvement of biological family and child’s role in the
assessment all described notions that the community, biological family and child
respectively potentially have knowledge about potential caregivers and should be able to
have input into the approval of a kinship home. Decision-making speaks to the process
of deciding whether or not to approve or not approve a kinship home. Comments from

Crucial Elements of Kinship Care Home Assessment
75
the secondary data sources highlighted a consideration that these occur as a group
decision-making process.
Conversation with the focus group of practitioners on decision making was more
focused on how to support the family in situations of non-approval. This reflects an
approach, similar to status quo, in which the decision is made by the professionals
assigned to the case and not the family or community through a group decision making
process.
Safety
Child safety and standards were significantly present throughout the data. As
such they were grouped into a global theme of Safety and visually represented in the
thematic network map below. This theme contains comments that were child focused in
nature and focused on micro practice issues. This global theme also contained more
macro level concepts and issues including safety standards and systemic or political
notions of standards as applied to community and are described in the Safety table found
in Appendix E.
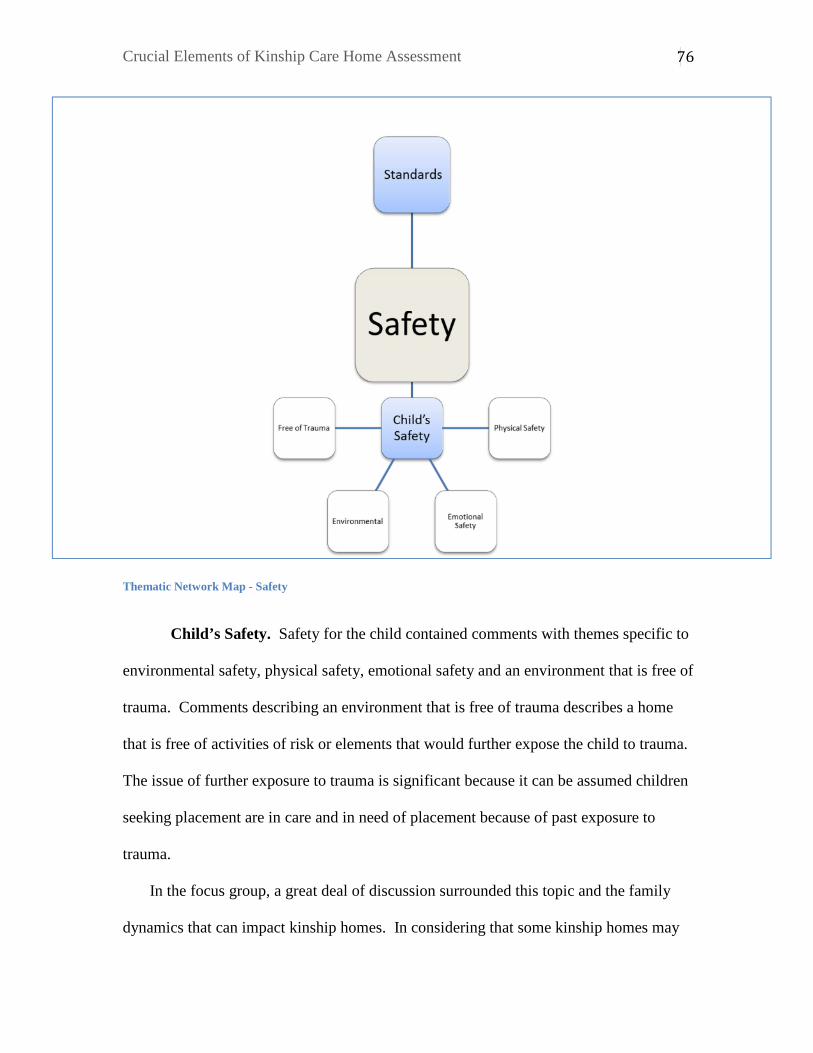
Crucial Elements of Kinship Care Home Assessment
76
Thematic Network Map - Safety
Child’s Safety. Safety for the child contained comments with themes specific to
environmental safety, physical safety, emotional safety and an environment that is free of
trauma. Comments describing an environment that is free of trauma describes a home
that is free of activities of risk or elements that would further expose the child to trauma.
The issue of further exposure to trauma is significant because it can be assumed children
seeking placement are in care and in need of placement because of past exposure to
trauma.
In the focus group, a great deal of discussion surrounded this topic and the family
dynamics that can impact kinship homes. In considering that some kinship homes may

Crucial Elements of Kinship Care Home Assessment
77
have close relationships with the biological parents who may have been the source of
trauma leading a child to come into care, it is quite possible that there could be some
exposure. The issue then becomes how these can be mitigated, as it was felt by the focus
group that you cannot prevent some of this potential exposure through non-contact.
Contact is likely in situations where, for example, a child is being placed with a
grandmother who still cares for her son or daughter while also caregiving for her
grandchild.
Standards. An organizing theme in the area of safety was also standards.
Standards speak to social or formal expectations and requirements within a home.
Homes that meet these pre-determined standards are deemed to be safe. However
comments in the secondary data questioned who determines what these standards are and
how are they applied in different communities with different realities.
The focus group identified this as an ongoing challenge in practice. Particularly
they identified confusion and misunderstanding in what the standards are and how they
are applied. This leads to confusion in practice and in the ability to articulate the standard
itself.
There was also a keen awareness by the focus group of the role of poverty in this
area of standards and community standards. There was recognition that some home
assessment writers will confuse poverty with what is “safe enough”. This also highlights
that conceptually the issue of safety and standards is both a micro and macro issue.
Policy and Legislated Requirements As we continue moving outwards of the conceptual model, the data shows us
how policy and legislative requirements impact the home assessment. These themes are
Crucial Elements of Kinship Care Home Assessment
78
highlighted in the figure below. While these elements do not “sit at the kitchen table”
with the potential caregivers and the assessor, they impact the experience and the
outcomes. These elements create the context around the home assessment and are within
the control of policy makers and program developers. Within this global theme and
identified in Appendix E, we have organizing themes of proceduralism or being rule-
based which includes themes of reporting and documenting requirements, risk
management, and principle-based practice. We also have organizing themes of Making
Kinship a Priority, which includes basic themes of flexible kinship criteria and
recognizing the rights of kinship caregivers. Caregiver Policies is also an organizing
theme.
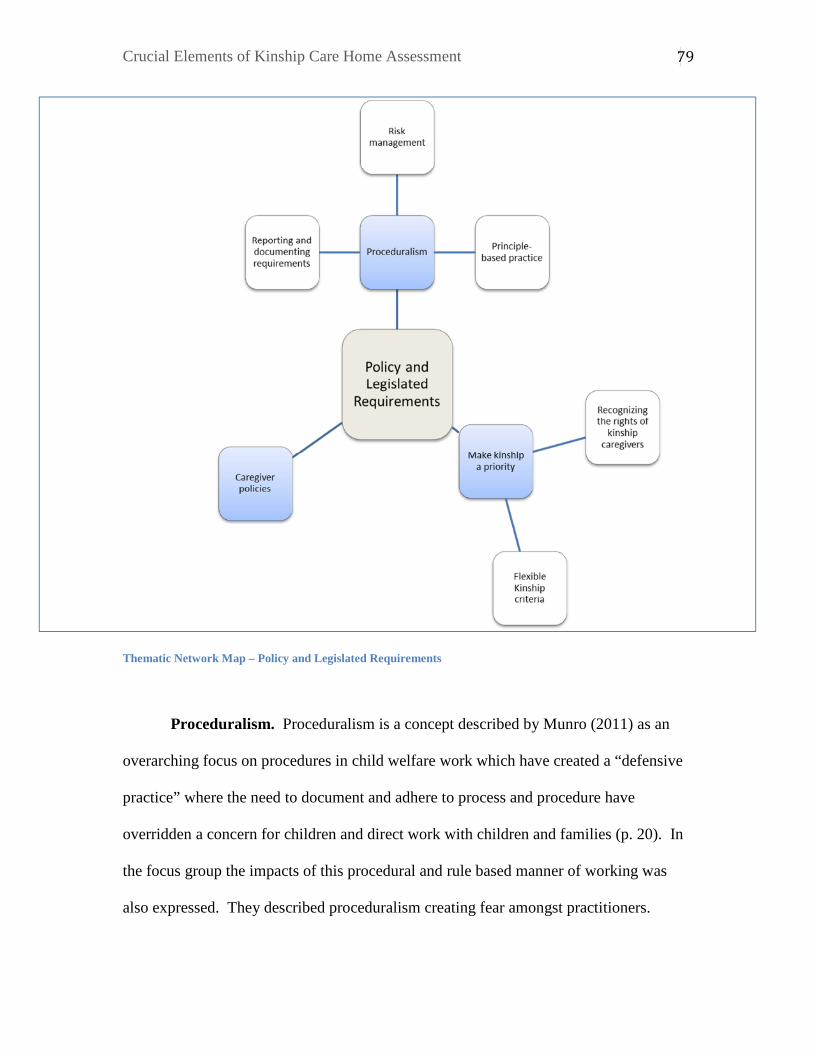
Crucial Elements of Kinship Care Home Assessment
79
Thematic Network Map – Policy and Legislated Requirements
Proceduralism. Proceduralism is a concept described by Munro (2011) as an
overarching focus on procedures in child welfare work which have created a “defensive
practice” where the need to document and adhere to process and procedure have
overridden a concern for children and direct work with children and families (p. 20). In
the focus group the impacts of this procedural and rule based manner of working was
also expressed. They described proceduralism creating fear amongst practitioners.
Crucial Elements of Kinship Care Home Assessment
80
Proceduralism includes themes of risk management, reporting and documenting
requirements and proposed notions of principle-based practice to oppose proceduralism.
Munro (2011) states it would be ideal if risk management could ensure eradication of
risk, but it is simply not possible. The search for certainty in an uncertain field of
practice, creates complexity and difficulty. “Uncertainty and risk are features of child
protection work: risk management can only reduce risks, not eliminate them” (Munro,
2011, p. 23). Caseworkers and practitioners in this field of practice have come to believe
that it is their inherent responsibility to prevent all harm to children and even though
human behaviour is unpredictable, child protection professionals feels they will be held
accountable for any sort of unpredictable harm (Fairbairn & Strega, 2015). As a result
strict and rigid procedures are implemented and expected which do not allow for
flexibility for families.
Make Kinship a Priority. Make kinship a priority is an organizing theme,
which also included a number of comments related to kinship care in comparison to
foster care or other out of home placement. This included comments that suggested
flexibility in kinship criteria and a recognition of the rights of kinship caregivers. The
focus group further recognized concerns that in practice, kinship caregivers do not seem
to have the same amount of rights as foster parents. The focus group identified a number
of policy and legislated requirements that have created challenges in making kinship care
a priority. Legislation can sometimes be contradictory in that it supports placement with
kin as a priority, but also allows for foster parents to review or appeal these decisions to
place with kin. In those cases foster parents receive more rights than a kinship caregiver
and the caseworker or home assessment practitioner’s hands may be tied.
Crucial Elements of Kinship Care Home Assessment
81
Caregiver Policies. The secondary data highlighted challenges from caregiver
policies that are unclear. The focus group also highlighted that some policies are just not
feasible. For example, a discussion was held on the reasonableness that a caregiver can
protect a child from future trauma if they are going to be having ongoing contact with
their biological parent. As well, some policies are barriers to normal family functioning.
One example provided was a policy that states the biological parent cannot reside in the
kinship caregiver’s home while the child is placed there. However, the focus group
identified circumstances where a biological parent having made significant gains and
changes wanted to live in the kinship caregiver’s home. The case plan at that time was
for a return to the parent’s care. However while the child remained in kinship care, that
biological parent could not reside in the home. This can become a barrier for placement
and also a barrier towards reunification and family healing overall.
Systemic Finally, the outer ring of the conceptual model, are systemic issues that impact
kinship caregiving or the ability for kin to care for in general. These are concepts that
require multiple level of government to address and may also require significant societal
shifts in attitude and approach. They also remind us that kinship care is a complex issue
beyond its assessment. Organizing themes under systemic issues as described in the
figure below are Resources, Colonization, Family Preservation, Collaborative Casework,
Supports for Caregivers, and Worries with kinship. The table in Appendix E identifies
the themes and examples of comments.
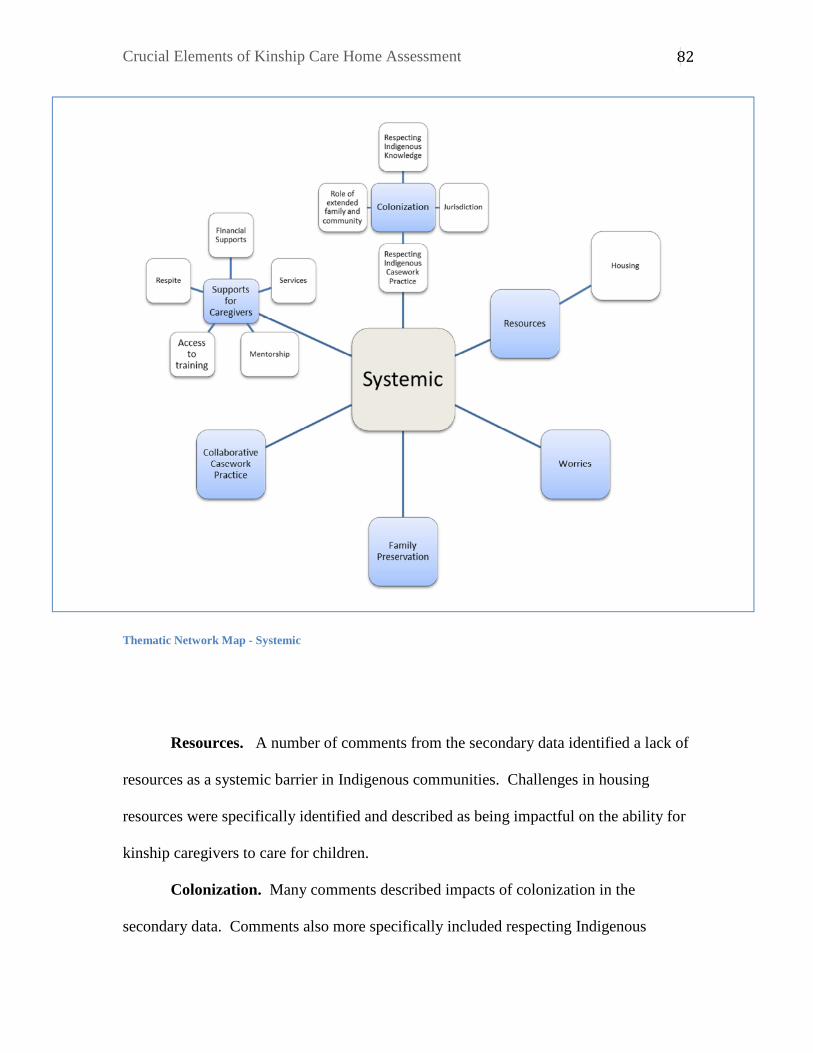
Crucial Elements of Kinship Care Home Assessment
82
Thematic Network Map - Systemic
Resources. A number of comments from the secondary data identified a lack of
resources as a systemic barrier in Indigenous communities. Challenges in housing
resources were specifically identified and described as being impactful on the ability for
kinship caregivers to care for children.
Colonization. Many comments described impacts of colonization in the
secondary data. Comments also more specifically included respecting Indigenous
Crucial Elements of Kinship Care Home Assessment
83
knowledge, issues of jurisdiction, respecting Indigenous casework practice, and
respecting traditional connections to family and community.
Jurisdiction refers to challenges in negotiating between federal, provincial, and
on reserve jurisdiction. Respecting Indigenous knowledge is a key element in the
consideration of an anti-colonizing approach. Indigenous knowledge includes the “good-
sense ideas and cultural knowledges of local peoples concerning the everyday realities of
living” (Sefa Dei, 2000. P. 114). The use and recognition of Indigenous knowledge,
becomes an “entry point” into an anti-colonizing approach (Sefa Dei, 2000, p. 117).
Respecting traditional connections to family and community builds upon the
recognitions of Indigenous knowledge, but these comments are more specific to the
traditions of connections to extended family and community within Indigenous cultures.
The theme of Indigenous casework practice recognizes social work practice developed,
practiced, and recognized as leading practice in Indigenous communities.
Family Preservation. Comments were made and themed as Family Preservation
that referred to the notion that if children were supported to remain with their biological
families in the first place, out of home placements would not be required.
Collaborative Casework Practice. Collaborative Casework Practice describes
comments that sought overall approaches to casework that are collaborative and reflect
shared decision-making. These are comments that were not specific to collaboration in
kinship assessment, but casework in general. The focus group also identified this
importance of collaborative casework. They highlighted the importance that kinship
caregivers be part of the service team meeting and understand the case plan. In their
Crucial Elements of Kinship Care Home Assessment
84
experience, that does not happen and makes it difficult for a kinship caregiver to
successfully work collaboratively.
Supports for Caregivers. Supports for caregivers were described in a number of
comments. Because these supports are beyond the practice scope of an assessor and may
also speak to supports within the community that involve a number of systems, they have
been themed under the systemic issues global theme. They could have been under the
policy and legislative requirements, however they are larger in nature as they involve
community and other system responses. Support for caregivers were comments general
in nature, but also more specific and spoke to financial supports, services, mentorship,
access to training, and respite.
The focus group identified a number of challenges in the area of financial
supports. While these challenges may not be specific to home assessment, these supports
impact caregivers’ experiences and thus their ability to provide quality care to the child
placed in their home. The focus group identified a frustration and barriers with
caseworker attitudes in funding kinship care.
It was also identified by the focus group that the financial supports create a
challenge or create dependency. This may happen if a kinship caregiver makes decisions
based on financial supports, which are being provided during the course of caregiving.
However, later these supports may be taken away if the child returns home. For
example, a caregiver may choose to move into a larger home to facilitate the placement.
The system supported them to make that move, but once the children have returned the
caregiver must move again in order to be able to afford their housing. It was also noted
by the focus group that kinship caregivers may not receive the same degree of supports,
Crucial Elements of Kinship Care Home Assessment
85
once they pursue a permanency status (ie: private guardianship or adoption) under the
Supports for Permanency program.
The focus group further commented on the need to offer continued services in
navigating the various systems and resources that may potentially be supporting the child
who is placed in the kinship caregiver’s home. This is similar to the focus group’s
identification of a need for a support person to help the home assessment process, but
this speaks to the importance of support in navigating systems overall and for an ongoing
period.
It was also identified by the focus group that the policies of other systems need to
understand the unique nature of kinship care and be aware when their policies create a
barrier to those supports. An example provided was that kinship caregivers are no longer
eligible for day care subsidy or that the federal government has been considering taxing
the maintenance payments that kinship caregivers receive.
Worries. The theme of worries grouped together comments that expressed
concern with kinship care in general or the potential for negative dynamics or
experiences.
Areas that the focus group found missing from the themes of crucial elements
included a lack of mention around initial assessment, which is assessment upon
immediate placement. They also suggested a need for more focus on getting concrete
support in the home assessment process such as a support person to help getting the
documents gathered, accessing supporting documentation or help with language and
literacy in the documents. The focus group also suggested various wording changes in

Crucial Elements of Kinship Care Home Assessment
86
some elements. The discrepancy between the community comments and the focus group
will be discussed further in the next section.

Crucial Elements of Kinship Care Home Assessment
87
Discussion
The findings and themes highlight the complexity of kinship care home
assessment. The intent of a kinship care home assessment, as indicated in the literature
and confirmed in the focus group conversation, is to compare the care that a caregiver
intends to provide a child with an analysis of what the caregiver reasonably can provide
a child based on a number of aspects. The complexity comes from a number of
systemic, political and legislative influences. Adding to the complexity are the
influences of values, worldviews, and standards. These all become the lenses through
which an assessment is viewed and analyzed making assessor characteristics crucial to
the experience and the process in general. However, the interplay of all six global
themes; Assessor Characteristics, Important Areas to Address, Home Assessment
Process, Safety, Policy and Legislated Requirements and Systemic, are crucial elements
in understanding this area of home assessment practice. They all influence the practice
at the kitchen table.
The continuing legacy of colonization exists and is apparent in the analysis of this
issue. The assumptions surrounding who gets to decide what is safe enough or good
enough for a child strikes at the core of colonization and the institutions, legislation and
other structures that surround each decision suggest structural colonization. For example
the reported difficulties with meeting imposed standards, coupled with a lack of
resources, further marginalizes these families.
Data from the community suggested a desire to return to traditional ways of
communal caring for children through the involvement of community, elders, and
extended family. Yet, a western child intervention system demands a level of

Crucial Elements of Kinship Care Home Assessment
88
proceduralism, which does not align with the traditional, Indigenous ways. Still, it
continues to be the priority and drives current practice.
Proceduralism drives the priorities in practice, but it has also become status quo,
and makes it difficult to entertain the possibility that another approach could be within
the realm of possibility. As the participants identify what was required in kinship home
assessment practice, it is possible that their description was also influenced by status quo
and a discomfort that any deviation from status quo is not only wrong, but potentially
dangerous. No one ever wants a child to be placed at risk in any placement, but does this
mean that status quo is the only way to reach a level that is “safe enough”? Critical
theorists suggest that there cannot be one universal truth or approach as there are
complex existing realities (Swift & Callahan, 2009).
Part of the current status quo is the use of a standardized assessment tool. The
rise of risk assessment tools was welcomed in the mid-1990’s (Swift & Callahan, 2009).
However there has since been recognition that these risk assessment tools apply
universal truths and assumptions, that fail to recognize social context and individuality
(Swift & Callahan, 2009). The use of a standardized assessment tool for caregivers has
been controversial and largely rejected by the Indigenous community (Beaucage, 2011).
This rejection drove the DM Summit meetings which are one of the secondary data
sources. Noted in the DM Summit discussions, this tool was rejected by the Indigenous
community, but it was welcomed within the government agencies as an approach that
would create strengthened assessments. This position supports a belief that a
standardized assessment can prevent future harm (Fairbairn & Strega, 2015).
Standardized assessment tools have generally been found to be problematic for use with
Crucial Elements of Kinship Care Home Assessment
89
marginalized populations. These tools neglect the social and political context in which
individual problems appear to arise. Standardized assessments can reproduce the
gendered, classed and raced constructions and parenting expectations of the dominant
culture and impose them on marginalized populations (Fairbairn & Strega, 2015; Choate
& McKenzie, 2015). They become colonizing actions.
Another aspect to the status quo is a focus on history and historical concerns.
These findings suggest the focus on history becomes an unnecessary barrier; however the
focus group identified the need to address history and potential “legacies” in order to
fully assess a potential caregiver’s suitability. While many acknowledge the challenges
related to the unique demographics for many kinship caregivers such as poverty, health
challenges, other structural issues, the literature review did not indicate past trauma or
legacies for kinship caregivers. In fact Lorkovitch et al. (2004) found this attitude
amongst caseworkers created barriers and were unfounded.
The findings also suggest that a “one-size” fits all approach to kinship care home
assessment is not appropriate in a diverse society. The measurement of what is “good-
enough” or “safe enough” may not be the same for every population or community.
Critics of standardized assessment tools suggest this is the case for standardized
assessments. If dominant culture definitions of parenting are being used, then
Indigenous families and parents are at an immediate disadvantage (Choate & McKenzie,
2015).
Valerie O’Brien identified a conceptual model similar to that which I have
presented here. It incorporates a systems approach to considering what impacts the
assessment of kinship homes and the context in which they exist (O’Brien, 2014).

Crucial Elements of Kinship Care Home Assessment
90
However, elements like cultural diversity or impacts from colonization are not
mentioned within her model. This is likely because her model is developed for a
European (Irish) population where marginalized populations exist, but not within a
context of colonization.
It is also interesting to note that caregiver training is a significant part of the
current kinship care program in Alberta (Alberta Human Services, 2016) and current
status quo. Training for kinship caregivers was identified only briefly in the data. It
would be worth considering how community members value this in comparison to
practitioners. Training could be considered an element that meets systemic needs for
accountability, but perhaps it is not a meaningful support for caregivers or seen as crucial
by practitioners.
The concept of love demonstrates how groups differ on the crucial elements. It
was uncomfortable for the focus group of practitioners as they saw it as too complex and
difficult to measure or analyze in an assessment, as it is strongly dependent on the
practitioner’s lens or worldview. It was, however, identified by the community as being
very important and relevant. While practitioners agreed that a child being loved and
experiencing love was important, they reported in the focus group that love may not get
the caregiver through difficult times or through the challenges of caregiving. To the
contrary, the community reported that “love can make up for a lack of skills, but skills
cannot make up for a lack of love.” Experts may not agree that this emotional interaction
exceeds the importance of westernized skill and insight in parenting, however from an
anti-colonizing perspective, the community’s position must be respected and honoured as
the authority.

Crucial Elements of Kinship Care Home Assessment
91
Similarly, the concept of standards is significant within this theoretical
framework. The community data described standards as colonizing. As the standards
being applied are western standards, we must accept that they are colonizing.
Practitioners using reflexivity recognize the influence of western standards and their
application with marginalized and Indigenous communities as problematic. However,
western standards are entrenched in the practice through environmental checklists and
policy requirements. The question of “whose standards” must be addressed. However,
in order to address the issue from an anti-colonizing perspective, the community must
define these standards. The question remains whether or not the system will be able to
accommodate and accept an external definition and identification of community
standards.
In comparing the focus group information to that of the secondary data from the
community, differing world-views becomes apparent. It appears that Indigenous
families are being viewed through a western lens. For example, comments relating to
role shift and the impacts of these shifts on caregivers and children assume a nuclear
family approach to family structure. Indigenous communities traditionally provide care
to their children and elders communally. The assumption is that a role shift from
grandmother to parent may be difficult. However, this may not be the case in an
Indigenous family or in other cultures where communal and multi-generational family
caregiving is common. This challenge may be an assumption based on the dominant
culture’s worldview.
Alberta recently adopted an approach to principle-based practice. One of these
principles is reflective of anti-colonizing practice (Alberta Human Services, 2014).

Crucial Elements of Kinship Care Home Assessment
92
Principle-based practice requires reflexivity on the part of the practitioner, but also from
within the organization. Rather than focusing on what we do, principle-based practice
focuses on how we do the work (Lonne, Parton, Thomson & Harries, 2009). It means, in
this case, that in following this anti-colonizing principle workers must focus on how to
practice from an anti-colonizing manner and less on procedures and process that is what
we do.
As part of this implementation, the province has provided tools and strategies for
staff to be reflective on their worldview and the effects that particular worldview has on
the decisions being made for children and youth. This approach would support reflective
decisions being made in the assessing and approval of kinship caregivers. However,
these decisions continue to be made within the context of a structured home assessment
process, an approach to safety and standards, and legislation that has not been created to
reflect the principles. Principle-based practice must be integrated throughout practice to
truly practice from these principles (Lonne et al., 2009). This suggests that an anti-
colonizing approach must be integrated throughout the home assessment process,
assessment tools, policies, and standards.
In addition to the assessment of kinship caregivers, the data also highlights the
importance of recognizing supports for kinship care as significant. Literature suggests
kinship caregivers receive less contact from caseworkers compared to non-kin caregivers
(Fuentes-Palaez, 2015; Keller et al., 2001). Participants in both the secondary data sets
and the focus groups described ongoing supports and services to be a crucial element in
kinship care practice. This is a worthy consideration in the analysis of kinship care
practice in general.
Crucial Elements of Kinship Care Home Assessment
93
Implications for Practice and Further Inquiry
Social workers practicing in the field of home assessments must contemplate the
crucial elements and also employ a critical ecological approach to this work. Aligning
with the themes identified as crucial elements of home assessment, a critical ecological
approach considers a potential caregiver’s social context. Assessment from a critical
ecological perspective reflects on the “goodness of fit” between the person and the
circumstances of their environment (Rothery, 2008). This assessment will inform what
the caregiver intends to do in the care of the child and what they are capable of doing
based on a number of influences. This approach would also inform the supports and
services required to mitigate any potential challenges in the care of a potential child. The
analysis of this study has identified elements to include in an assessment reflective of
critical ecological approach. It also identifies the systemic influences important to
consider in the assessment. Without this theoretical approach, assessments can be
oppressive and continue colonizing legacies.
This study can inform how social workers completing home assessments should
be supported by child welfare organizations through training, supervision and
mentorship. It also suggests the characteristics that social workers practicing in this area
should possess and considerations in the hiring and performance management of these
staff.
Leaders within child welfare organizations should consider the micro and macro
elements of this practice and their opportunities to support both areas. Leaders may
make operational and human resource decisions that support staff to integrate the crucial
elements into their practice and meet community needs. However, they also have
Crucial Elements of Kinship Care Home Assessment
94
opportunities to advocate for systemic, or policy and legislative changes that are
suggested here to impact kinship caregivers and assessment. The data suggests potential
areas to consider in ensuring kinship caregivers are appropriately and adequately
assessed in considering their roles and experiences. With this data, a practitioner could
inform their practice by considering what elements they bring with them to a home
assessment and its interviews. Policy makers and program developers can also consider
these elements in their decision making on kinship care program design, supports,
training, etc. However these crucial elements should not be used to inform the
development of a standardized assessment tool.
In this area of practice, standardized assessment should be approached with
caution. The dominant culture’s notions of parenting, safety, standards and the ‘good
enough parent’ could be irrelevant to marginalized group including Indigenous
populations. Therefore it could be further suggested that the crucial elements for
assessment in one community or population, are different than others based on values,
history, tradition and social norms. In the data references to the differences between
Indigenous cultures or other multicultural communities and “our culture” were
mentioned. This again suggests the development of an approach that suits the dominant
culture, may not fit all cultures. I would caution that the crucial elements identified in
this research, should not be used to create standardized assessment tools. Rather, it could
inform practice, process, legislation, policy and other systemic issues.
This study focused specifically on the impacts of kinship home assessment
practices on Indigenous children, caregivers and families. Because a great majority of
children in the care of child welfare are Indigenous, an Indigenous focus is justified.

Crucial Elements of Kinship Care Home Assessment
95
Moreover, Ban (2005) suggests that non-indigenous populations can benefit from
Indigenous approaches in child welfare programs and policies. Similar to the
implementation of Family Group Conferencing in New Zealand, Indigenous approaches
can be advantageous to the dominant culture as well.
The complexity of the issue is evident in the sheer amount of themes presented in
the findings. While it could have been possible to continuously refine and widen themes
in order to have a more interpretive description of the themes, I opted for a descriptive
approach. The descriptive approach keeps the data closer to that which was presented by
the community and participants and honours their voice by keeping the findings more
closely represented by their words. An interpretive approach would have made a number
of assumptions, which could very likely by erroneous or colonizing. Particularly so
because of the secondary data methodology, staying close to the comments was
important to ensure authenticity as it is difficult to be inductive without relationship to
the participants or data (Irwin & Winterton, 2011). Were there the opportunity to
reconnect with the community for member checking or confirmation of the data, a more
interpretive approach would have been possible.
Participatory action research is done collaboratively with participants or insiders
of an organization (Rudestam & Newton, 2015) and would be an effective way to further
understand the crucial elements of kinship care. This type of approach requires
participants and researchers become co-researchers and partners in the process. While the
elements will need to be refined by and accepted by participants in such a research
design, this approach would ensure an anti-colonizing approach to a shift in practice.
Crucial Elements of Kinship Care Home Assessment
96
Limitations of the Study A limitation in secondary data analysis is that the data is only as good as the
primary data methodology. Some limitations in the methodology of both data sets were
noted. For example in the community conversations, comments were not audio recorded
and the data that was used in this secondary data analysis was that from facilitator notes
taken from table conversations. Because notes were taken with pen and paper by note
takers, there were no opportunities for participants to comment on the accuracy of the
recording. Some of the comments recorded did not provide context or detail and for the
purposes of secondary data analysis were unusable. As a result, some comments were
unusable due to the quality of the note taking. Examples include:
Young girl at our table shared her story of foster care. Then spoke.
Non Aboriginal person had her perspective and our perspective-embraced/affirmed our perspective-we share I think some …….. and making these kinds of things a priority. 1 bedroom, 1bathroom, 1 bedroom
It should be noted, however, that considering the quantity of comments from the
community conversations (13,000), there were very few that were unusable (10).
The data from the DM Summit meetings was recorded using flip charts. I would
suggest these notes are more accurately reflective of the participants’ comments than by
using a note taker. By using flip charts, there are natural opportunities for participants to
provide feedback based on the notes they are able to see.
A further limitation in the design is recognition that the comments from the data
sets were not specifically related to kinship care. While many comments reference
kinship care, extended family caregiving, family relationships, etc it can only be assumed
Crucial Elements of Kinship Care Home Assessment
97
that the participants were specifically commenting on kinship care. Some data from the
DM summit meetings was unusable because they commented specifically on other forms
of caregiving assessment. Comments that described kinship care specifically or that
were not specific were included in the secondary data analysis. However, without
specific reference to kinship care or an ability to confirm the data, it cannot be certain
they referred to kinship care. Considering that the elements for stranger care – foster
care and adoption– may not be relevant to kinship care, this is a limitation.
In the analysis, a single coder was used. This can be a limitation because the
analysis relies on one person’s interpretation of the data. This limitation was mitigated
through regular journaling and memoing throughout the analysis.
The data in the secondary analysis is from 2011-2013. It should be noted, a
number of policy changes may have impacted the relevance of some of the comments
made in the primary data collection. By 2016, a number of kinship policy changes had
been made which may or may not have impacted some of the comments made under the
policy and legislative requirement theme. For example kinship policy in Alberta was
amended in 2014 to be more enabling by removing requirement for managerial approval
and financial stability requirements. This quite possibly could have addressed comments
such as
Kinship care has a lot more potential. Need to look more into this and reduce barriers/policies that hinder kinship care. The focus group provided an opportunity for practitioners in the field of kinship
care home assessment to provide comment on the crucial elements identified in the
secondary data analysis. While this created an opportunity for feedback from experts in
the field and also ensure rigour within the research design, it should be noted that this
Crucial Elements of Kinship Care Home Assessment
98
process functions somewhat contradictory to an anti-colonizing approach. An anti-
colonizing approach would accept the comments from the Indigenous community as
being experts. A true anti-colonizing approach would have brought the comments to the
community to provide the feedback and not to a group of experts who are member of
dominant and colonizing society. Lincoln also advocates for the use of community as
“arbiter of quality” (Lincoln, 1995, p. 280).
Because of the nature of this secondary data analysis, not all elements described
by Lincoln to ensure qualitative rigor could be followed. For example, Lincoln also
identified reciprocity and the sharing of perquisites (1995). Without an established
relationship with the participants, this sharing and reciprocity are difficult or not
possible. Lincoln does acknowledge that some criteria may be applicable in certain
settings or stages of inquiry (1995). This applies for this project.
Indigenous research methodologies would also advocate for the inclusion of
community as this arbiter and also as a participant (Smith, 1999). Historically, research
with Indigenous people was a colonizing activity. Indigenous people were studied,
observed, and documented as the ‘other’ by members of dominant, western society
(Smith, 1999). The community agreed to the use of this information to further inform
child welfare practice and policy, however they should have been consulted in its use and
to be engaged as an arbiter.
Crucial Elements of Kinship Care Home Assessment
99
My Journey
I chose an anti-colonizing and critical ecological approach as my theoretical
framework because they resonated with me. Upon reflection when I was a home
assessment practitioner, I always struggled with the idea of “how am I to judge” if this
family is good enough for this child or not. We always want to children to be safe and
nurtured, and the authority to decide who would be safe and nurturing is difficult.
Since delving into the data and comparing the various perspectives on home
assessment, I feel even more strongly that an anti-colonizing approach is the appropriate
one and one that is necessary in this field of practice. Without reflecting upon status quo
and the policy or legislation that permeates and protects our practice from changing, we
are perpetuating colonization in contemporary times. We cannot practice in a manner
that presumes extended family or community are a potential risk to children and youth
and required the same extended family or community to prove their worth. This
presumption is not different than action taken in the height of residential school trauma
or the sixties scoop.
Community was able to identify what is crucial in the caring for children in the
context of kinship care: they used words like love, connection, voice, and care.
Practitioners and leadership use words like analysis, standards, requirements, and
documentation. We are left to consider what is more important to the life of a child: love
or documents?
My intention was to identify what the crucial elements of kinship care home
assessment are based on the feedback from the Indigenous community, practitioners, and

Crucial Elements of Kinship Care Home Assessment
100
child intervention leadership. A model reflective of critical ecological system theory was
created based on the secondary data analysis and a focus group source of data to inform
this descriptive model. The merging of the perspectives of all involved, could be viewed
as collaborative and an integration of perspectives, however I reflect on the elements of
colonization that crept their way into my research design. Seeking approval and
feedback from a group of practitioners rather than the community is such an example.
By looking at the individual comments from the community conversations, I was
transformed into hearing the voices of the community that are too often silenced and
have been silenced for centuries. There is value in honouring these voices and looking to
these voices for direction and opportunity for future social policy decisions. The
expertise is within the community and the community shared their expertise with us. We
must honour it and act on it, just as they asked us to do. When the Indigenous
community’s expert voice truly guides our work, we will move towards an anti-
colonizing context.

Crucial Elements of Kinship Care Home Assessment
101
References
Alberta Government (2014). What we heard: A summary of the community
conversations. Retrieved from:
http://humanservices.alberta.ca/documents/community-conversations-what-we-
heard.pdf.
Alberta Human Services (2014). Child Intervention Practice Framework. Retrieved from:
http://humanservices.alberta.ca/abuse-bullying/17242.html.
Alberta Human Services (2015). Becoming a kinship caregiver. Retrieved from:
http://humanservices.alberta.ca/foster-kinship-care/15440.html.
Alberta Human Services (2016). Children in care. Retrieved from:
http://humanservices.alberta.ca/abuse-bullying/17183.html.
Aronson, J. (1995). A pragmatic view of thematic analysis. The Qualitative Report, 2(1),
1-3.
Attride-Stirling, J. (2001). Thematic networks: An analytical tool for qualitative
research. Qualitative Research, 1(3), 385-405.
Ban, P. (2005). Aboriginal child placement principle and family group conferences.
Australian Social Work, 58(4), 384-394.
Beaucage, J. (2011). Children first: The Aboriginal advisor’s report on the status of
Aboriginal child welfare in Ontario. Retrieved from:
http://www.children.gov.on.ca/htdocs/english/documents/topics/aboriginal/child_
welfare_EN.pdf.

Crucial Elements of Kinship Care Home Assessment
102
Berrick, J. (1997). Assessing quality of care in kinship and foster family care. Family
Relations, 46(3), 273-280.
Bishop, L. (2009). Ethical sharing and reuse of qualitative data. Australian Journal of
Social Issues. 44(3), 255-272.
Blackstock, C. (2004). Keeping the promise: The Convention of the Rights of the Child
and the lived experiences of First Nations Children and Youth. Retrieved from
http://site.ebrary.com/id/10079794?.
Blackstock, C. (2011) The Canadian Human Rights Tribunal on First Nations Child
Welfare: Why if Canada wins, equality and justice lose. Children and Youth
Services Review, 33(1), 187-194.
Blakey, J.M. (2012). The best of both worlds: How kinship care impacts reunification.
Families in Society: The Journal of Contemporary Social Services, 93(2), 103-
110.
Bodor, R., Makokis, L. & Friesen, S. (2014). Indigenous concepts and frameworks vital
for human service workers: The practice of omanitew. Journal for Services for
Children and Families, 7, 54-71.
Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative
Research in Psychology, 3(2), 77-101.
Brisebois, K., Kernsmith, P.D., & Carcone, A.I. (2013). The relationship between
caseworker attitudes about kinship care and removal decisions. Journal of
Family Social Work, 16(5), 403-417.
Calder, M.C. & Talbot, C. (2006). Chapter 3- Contemporary Assessment: A Critique,
Assessment in kinship care. Russell House Publishing, Dorset, UK.
Crucial Elements of Kinship Care Home Assessment
103
Child, Youth and Family Enhancement Act, Province of Alberta. S 107 (2004).
Choate, P. & Mckenzie, A. (2015). Psychometrics in parenting capacity assessments: A
problem for Aboriginal parents. First People Child and Family Review, 10 (2),
31-43.
Christenson, B., & McMurty, J. (2007). A comparative evaluation of preservice training
of kinship and nonkinship foster/adoptive families. Child Welfare, 86(2), 125-
140.
Christenson, B., & McMurty, J. (2009). A longitudinal evaluation of the preservice
training and retention of kinship and nonkinship foster/adoptive families one and
a half years after training. Child Welfare, 88(4), 5-22.
Coakley, T.M., Cuddeback, Buehler, C., & Cox, M.E. (2007). Kinship foster parents
perceptions of factors that promote or inhibit successful fostering. Children and
Youth Services Review, 29, 92-109.
Connolly, M. (2006). Fifteen Years of Family Group Conferencing: Coordinators talk
about their experiences in Aotearoa New Zealand. British Journal of Social
Work, 36, 523-540. doi: 10.1093/bjsw/bch273.
Corbin, J. & Strauss, A. (1990). Grounded theory research: Procedures, canons and
evaluative criteria. Qualitative Sociology, 13(1), 3-21.
Corti, l., Witzel, A., & Bishop, L. (2005). On the potentials and problems of secondary
analysis: An introduction to the FQS special issue on secondary analysis of
qualitative data. Research Forum: Qualitative Social, 6(1), Art. 49.

Crucial Elements of Kinship Care Home Assessment
104
Crea, T.M., Barth, R.P. & Chintapalli, L.K. (2007). Home study methods for evaluating
prospective resource families: history, current challenges, and promising
approaches. Child Welfare, 86(2), 141-159.
Crea, T.M., Barth, R.P., Chintapalli, L. & Buchanan, R.L. (2009a). Structured home
study evaluations: Perceived benefits of SAFE versus conventional home studies.
Adoption Quarterly, 12, 78-99.
Crea, T.M., Barth, R.P., Chintapalli, L.K., & Buchanan, R.L. (2009b). The
implementation and expansion of SAFE: Frontline responses and the transfer of
technology to practice. Children and Youth Services Review, 31, 903-910.
Creswell, J. (2014). Research design: Qualitative, quantitative and mixed methods
approaches (4th Ed.). Los Angeles, California: Sage.
Denby, R.W. (2011). Kinship liaisons: A peer-to-peer approach to supporting kinship
caregivers. Children and Youth Services Review, 33, 217-225.
Fairbairn, M. & Strega, S. (2015). Anti-oppressive approaches to child protection:
Assessment and file recording. In J. Carriere & S. Strega (Eds.), Walking this
path together: Anti-racist and anti-oppressive child welfare practice (2nd ed.) (pp.
157-175). Winnipeg, Manitoba: Fernwood Publishing.
Falconnier, L.A., Tomasella, N.M., Doueck, H.J., Wells, S.J., Luckey, H. & Agathen,
J.M. (2010). Indicators of quality in kinship foster care. Families in Society: The
Journal of Contemporary Social Services, 91(4), 415-420.
Farmer, E. (2009). Making kinship care work. Adoption and Fostering, 33(3), 15-27.
Farmer, E. (2010). What outcomes relate to good placement outcomes in kinship care?
British Journal of Social Work, 40, 426-444.

Crucial Elements of Kinship Care Home Assessment
105
Font, S. (2015). Are children safer with kin? A comparison of maltreatment risk in out-
of-home care. Children and Youth Services Review, 54, 20-29.
Fuentes-Pelaez, N., Amoros, P., Pastor, C., Molina, M.C., & Mateo, M. (2015).
Assessment in kinship foster care: A new tool to evaluate strengths and
weaknesses. Social Sciences, 4, 1-17. Doi: 10.3390/socsci4010001.
Gill, H., Higginson, L., & Napier, H. (2003). Family group conferences in permanency
planning. Adoption & Fostering, 27(2), 53-63. doi:
10.1177/030857590302700208
Gillies, V., & Edwards, R. (2005). Secondary analysis in exploring family and social
change: addressing the issue of context. Forum: Qualitative Social Research, 6(1),
Art. 44.
Government of Alberta, Children and Youth Services. (2009). Kinship Care Review
Report. Retrieved from http://site.ebrary.com/id/10397956?ppg=1.
Government of Canada. Statistics Canada. (2011). National Household Survey (NHS)-
Analytical products, 2011. Aboriginal People in Canada: First Nations, Métis and
Inuit. Retrieved from http://www12.statcan.gc.ca/nhs-enm/2011/as-sa.
Greenwood, M. & DeLeeuw, S. (2006) Fostering indigeneity: The role of Aboriginal
mothers and Aboriginal early child care in response to colonial foster-care
interventions. In D.M. Lavell-Harvard & J. Corbiere Lavell (Eds.), Until our
hearts are on the ground: Aboriginal mothering, oppression, resistance and
rebirth. (pp. 173-183). Toronto, Ontario: Demeter Press.
Crucial Elements of Kinship Care Home Assessment
106
Hammersley, M. (2010). Can we re-use qualitative data via secondary analysis? Notes
on some terminological and substantive issue. Sociological Research Online,
15(1), 1-13.
Hart, M.A. (2002). Seeking Mino-Pimatisiwin: An Aboriginal approach to healing.
Halifax, Nova Scotia: Fernwood Publishing.
Hart, M.A. (2009). Anti-colonial Indigenous Social Work: reflections on an Aboriginal
approach. In R. Sinclair, M.A. Hart & G. Bruyere (Eds.), Wicihitowin Aboriginal
social work in Canada (pp. 25-41). Halifax, Nova Scotia: Fernwood Publishing.
Hegar, R.L. & Scannapieco, M. (2014). Kinship Care. In G.P. Mallon & P. Hess (Eds.),
Child welfare for the twenty-first century: A handbook of practices, policies and
programs. New York, NY: Columbia University Press.
Hinds, P.S., Vogel, R.J. & Clarke-Steffen, L. (1997). The possibilities and pitfalls of
doing a secondary analysis of a qualitative data set. Qualitative Health Research,
7(3), 408-424.
Hong, J.S., Algood, C.L., Chiu, Y-L, Lee, S. (2011). An ecological understanding of
kinship foster care in the United States. Journal of Child and Family Studies, 20,
863-872.
Human Services. (2015). Child intervention information and statistics summary
2015/2016 third quarter (December) update. Retrieved from:
http://humanservices.alberta.ca/documents/child-intervention-info-stats-
summary-2015-16-q3.pdf.
Ing, R. (2006). Canada’s Indian residential schools and their impacts on mothering. In
D.M. Lavell-Harvard & J. Corbiere Lavell (Eds.), Until our hearts are on the

Crucial Elements of Kinship Care Home Assessment
107
ground: Aboriginal mothering, oppression, resistance and rebirth. (pp. 157-172).
Toronto, Ontario: Demeter Press.
Irwin, S. & Winterton, M. (2011). Debates in qualitative analysis: critical reflections
(Timescapes Working Paper Series No. 4). Retrieved from:
http://www.timescapes.leeds.ac.uk/assets/files/WP4-March-2011.pdf
Keller, T.E., Wetherbee, K., LeProhn, N.S., Payne, V., Sim, K. & Lamont, E.R. (2001).
Competencies and problem behaviours of children in family foster care:
Variations by kinship placement status and race. Children and Youth Services
Review, 23(12), 915-940.
Koh, E. (2010). Permanency outcomes of children in kinship and non-kinship foster care:
Testing the external validity of kinship effects. Children and Youth Services
Review, 32, 389-398.
Koh, E & Testa, M.F. (2011). Children discharged from kin and non-kin foster homes:
Do the risks of foster care re-entry differ? Children and Youth Services Review,
33, 1497-1505.
Lambert, V.A. & Lambert, C.E. (2010). Conducting a scholarly literature review. Pacific
Rim International Journal of Nursing Research, 14(2), 101-111.
Leos-Urbel, L., Bess, R., & Geen, R. (2002). The evolution of federal and state policies
for assessing and supporting kinship caregivers. Children and Youth Services
Review, 24(1/2), 37-52.
Levi, Y. & Ellis, T.J. (2006). A systems approach to conduct an effective literature
review in support of information systems research. Informing Science Journal, 9,
181-212.

Crucial Elements of Kinship Care Home Assessment
108
Lincoln, Y. (1995). Emerging criteria for quality in qualitative and interpretive research.
Qualitative Inquiry, 1(3), 275-289.
Lonne, B., Parton, N., Thomson, J. & Harries, M. (2009). Reforming child protection.
New York, NY: Routledge.
Loppie, C. & Pauly, B. (2015). Indigenous families: Substance use and child welfare. In
J. Carriere & S. Strega (Eds.), Walking this path together: Anti-racist and anti-
oppressive child welfare practice (2nd ed.) (pp. 217-239). Winnipeg, Manitoba:
Fernwood Publishing.
Lorkovich, T.W., Piccola, T., Groza, V., & Marks, J. (2004). Kinship care and
permanence: guiding principles for policy and practice. Families in Society: The
Journal of Contemporary Social Services, 85 (2), 159-164.
Love, C. (2000). Family group conferencing: Cultural origins, sharing and appropriation-
a Maori reflection. In G. Burford & J. Hudson (Eds.), Family group
conferencing: New directions in community-centred child and family practice (pp
15-30). New York: Aldine de Gruyter.
Messing, J.T. (2006). From the child’s perspective: a qualitative analysis of kinship care
placements. Children and Youth Services Review, 28, 1415-1434.
Mills, C.S., & Usher, D. (1996). A kinship care case management approach. Child
Welfare, 75(5), 600-618.
Ministry of Human Services (2014). Enhancement Act Policy Manual. Retrieved from:
humanservices.alberta.ca/documents.Enhancement-Act-Policy_Manual.pdf.
Munro, E. (2011). The Munro review of child protection: Final report. United Kingdom:
The Stationery Office Limited.

Crucial Elements of Kinship Care Home Assessment
109
O’Brien, V. (2012). The benefits and challenges of kinship care. Child Care in Practice,
18(2), 127-146.
O’Brien, V. (2014). Responding to the call; A conceptual model for kinship care
assessment. Child and Family Social Work, (19), 355-366.
Perry, G., Daly, D. & Kotler, J. (2012). Placement stability in kinship and non-kin foster
care: A Canadian study. Children and Youth Services Review, 34, 460-465.
Pon, G., Gosine, K. & Phillips, D. (2011). Immediate response: Addressing anti-native
and anti-black racism in child welfare. International Journal of Child, Youth and
Family Studies, 3&4, 385-409.
Rothery, M. (2008). Critical ecological systems theory. In N. Coady & P. Leahmann
(Eds.), Theoretical perspectives for direct social work practice (pp. 89-118).
New York, NY: Springer Publishing Company.
Rudestam, K.E. & Newton, R.R. (2015). Surviving your dissertation: A comprehensive
guide to content and process (4th Ed.). Los Angeles, California: Sage.
Scannapico, M., & Hegar, R.L. (1996). A nontraditional assessment framework for
formal kinship homes. Child Welfare, 75(5), 567-582.
Sefa Dei, G.J. (2000). Rethinking the role of Indigenous knowledges in the academy.
International Journal of Inclusive Education, 4(2), 111-132.
Selwyn, J. & Nandy, S. (2014). Kinship care in the UK: using census data to estimate the
extent of formal and informal care by relatives. Child and Family Social Work,
19, 44-54.
Shlonsky, A.R, & Berrick, J.D. (2001). Assessing and promoting quality in kin and
nonkin foster care. Social Service Review, 75(1), 60-83.

Crucial Elements of Kinship Care Home Assessment
110
Sinha, V., Trocme, N., Fallon, B., MacLaurin, B., Fast, E., Thomas Prokop, S., et al
(2011). Kiskisik Awasisak: Remember the children. Understanding the
overrepresentation of First Nations children in the child welfare system. Ontario:
Assembly of First Nations. Retrieved from:
http://cwrp.ca/sites/default/files/publications/en/FNCIS-
2008_March2012_RevisedFinal.pdf.
Smith, L.T. (1999). Decolonizing methodologies: Research and Indigenous peoples.
New York, NY: Zed Books Ltd.
Strega, S. & Carriere, J. (2015). Anti-racist and anti-oppressive child welfare. In J.
Carriere & S. Strega (Eds.), Walking this path together: Anti-racist and anti-
oppressive child welfare practice (2nd ed.) (pp. 1-24). Winnipeg, Manitoba:
Fernwood Publishing.
Swift, K. & Callahan, M. (2009). At risk: Social justice in child welfare and other
human services. Toronto, Ontario: University of Toronto Press.
Tamarack Institute (2016). Introduction: A new era in community building. Retrieved
from:http://tamarackcci.ca/files/cc2ed_introduction.pdf?__hstc=163327267.abcb
b030211d06f8428b2a3595305421.1460837777991.1460837777991.1460837777
991.1&__hssc=163327267.1.1460837777991&__hsfp=1667286275.
Terling-Watt, T. (2001). Permanency in kinship care: An exploration of disruption rates
and factors associated with placement disruption. Children and Youth Services
Review, 23 (2), 111-126.

Crucial Elements of Kinship Care Home Assessment
111
Trocmé, N., Knoke, D., Blackstock, C., (2004) Pathways to the Overrepresentation of
Aboriginal Children in Canada’s Child Welfare System. Social Service Review,
78 (4), 577-600.
Truth and Reconciliation Commission of Canada (2012). Canada, Aboriginal peoples,
and residential schools: They came for the children. Retrieved from:
http://publications.gc.ca/collections/collection_2012/cvrc-trcc/IR4-4-2012-
eng.pdf.
Tuckett, A.G. (2005). Applying thematic analysis theory to practice: A researcher’s
experience. Contemporary Nurse, 19(1-2), 75-87.
Turnell, A. (2012). The Signs of Safety: Comprehensive Briefing Paper. Retrieved from:
www.signsofsafety.net/briefing-paper.
Turnell, A. & Essex, S. (2014). It takes a village: Placing grandparents and extended
family at the center of safeguarding vulnerable children. In D. Pitch (Ed.) Inside
kinship care: Understanding family dynamics and providing effective support (pp
96-121). London: Jessica Kingsley Publishers.
Whiteside, M., Mills, J. & McCalman, J. (2012). Using secondary data for grounded
theory analysis. Australian Social Work, 65(4), 504-516.
Winokur, M., Crawford, G., Longobardi, C. & Valentine, D. (2008). Matched
comparison of children in kinship care and foster care on child welfare outcomes.
Families in Society: The Journal of Contemporary Social Services, 89(3), 338-
347.
Victorian Government Department of Human Services (2002). Aboriginal Child
Placement Principle. Retrieved from:
Crucial Elements of Kinship Care Home Assessment
112
http://www.cyf.vic.gov.au/__data/assets/pdf_file/0019/17083/placement_aborigin
al_cppguide_2002.pdf
Crucial Elements of Kinship Care Home Assessment
113
Appendix A
Consent Form: Focus Group
Name of Researcher, Faculty, Department, Telephone & Email :
Graduate Student:
Julie Mann-Johnson, RSW, Faculty of Social Work, University of Calgary 780-460-8494 [email protected]
Principle Investigator:
Anne-Marie McLaughlin, PhD, Faculty of Social Work, University of Calgary Title of Project:
Identifying the Crucial Elements of Kinship Care Home Assessment
This consent form, a copy of which has been given to you, is only part of the process of informed consent. If you want more details about something mentioned here, or information not included here, you should feel free to ask. Please take the time to read this carefully and to understand any accompanying information. The University of Calgary Conjoint Faculties Research Ethics Board has approved this research study.
Purpose of the Study:
This project will explore social work practice in the area of kinship care. This study will identify the crucial elements required for kinship care home assessments in Alberta. These elements can then be used to inform kinship home assessment practice. The literature suggests that children placed in kinship care achieve more positive. Even so, practice and policy regarding kinship care has been slow to develop and in most jurisdictions foster care and adoption policies were applied to kinship care. Literature suggests the experience for kinship caregivers is very different from stranger care – adoption and foster care. As a result the home assessment process may require a unique approach with unique elements. Many public consultations and information gathering events have occurred in recent years within government in Alberta. This study endeavors to looks at these sources of data to answer the question what are the crucial elements of kinship care assessment in Alberta? This secondary data analysis endeavors to honour the voices of people who have already shared their perspectives. Secondary qualitative data analysis endeavors to gain further insight on existing data without further intrusion on populations who have shared the information previously, thus reducing a burden on research participants and avoiding duplication.
Crucial Elements of Kinship Care Home Assessment
114
Irwin and Winterton advise, “the difficulties for secondary analysis will be more or less severe depending on whether there is a risk of systematic interpretation of data and whether there are checks that can made on our interpretations with reference to other forms of data” (2011, p. 10). A focus group of subject matter experts will provide one of these checks as well as a comparison to the current body of literature. What Will I Be Asked To Do?
You will be asked to participate in an in-depth audio-recorded focus group of approximately 2 hours. The focus group will be facilitated by the graduate student researcher. During the focus group the facilitator will share with you some themes that have arisen from the secondary data analysis of kinship care home assessment. The facilitator will ask for your comments, experiences and feelings regarding the themes presented and you will be asked to engage in a discussion concerning these with other members of the focus group. All focus groups will be digitally recorded. Participation is Voluntary Your participation is completely voluntary. It is your choice to take part in this study. You do not have to answer any questions that you don’t want to answer. You are free to discontinue at any time during the study by informing to the researcher, but your contributions to the point of withdrawal will remain a part of the data. If at any time you wish to withdraw from the focus group simply raise your hand and the discussion will end until you have left the room. What Type of Personal Information Will Be Collected?
Should you agree to participate, you will be asked to provide your area of employment and years of experience. Direct quotes may be used in reporting the findings and data-themes will be presented in aggregate form. All reasonable attempts will be made to protect confidentiality; audio recordings will be transcribed verbatim and all personal identifying information will be removed from the transcripts. Transcribed documents will be assigned a pseudonym. There are several options for you to consider if you decide to take part in this research. You can choose all, some or none of them. Please put a check mark on the corresponding line(s) that grants me your permission to I wish to choose my own pseudonym: ______________________________________ Yes: ___ No: ___
I wish to receive the final report (address provided on next page) Yes: ___No: ___ Are there Risks or Benefits if I Participate?
Possible Risks: We do not anticipate any harm accruing to you as a function of your participation in this research project. However, although we are committed to the principles of confidentiality and we will ask this from all participants we cannot guarantee that others in the focus group will not share information outside of the group.
Crucial Elements of Kinship Care Home Assessment
115
Benefit: The findings of this study will benefit children in government care in increasing their access to placements with extended family or significant others. Research indicates better outcomes for children who are placed in kinship homes. Furthermore, kinship caregivers who are more appropriately assessed, trained, and supported will create more successful or stable placements for these children. You may personally benefit by developing a clearer understanding of what has been identified by other stakeholders as crucial elements to kinship care home assessment through discussion within the focus group. What Happens to the Information I Provide?
The information you provide will be used to inform best practice in the area of child intervention and caregiver assessment. The research may also be used for educational purposes, including public presentations and research publications. The research team will have access to the audio tapes before they are transcribed. All digital files will be stored in locked filing cabinets inside locked offices. All signed consent forms will be stored there as well. Any information stored in electronic format on computers or other electronic storage devices will be kept in password-protected files on computers that are also password-protected. No information that can be used to identify you will be included in electronic files. Audio- and video-tapes will be erased after 5 years or sooner. Computer files may be stored indefinitely but will remain password-protected and contain no information that can be used to identify you.
Signatures (written consent)
Your signature on this form indicates that you 1) understand to your satisfaction the information provided to you about your participation in this research project, and 2) agree to participate as a research subject. In no way does this waive your legal rights nor release the investigators, sponsors, or involved institutions from their legal and professional responsibilities. You are free to withdraw from this research project at any time. You should feel free to ask for clarification or new information throughout your participation.
Participant’s Name: (please print) _____________________________________________
Participant’s Signature __________________________________________Date: _______________
Participant’s email address (to receive the final report)
_____________________________________________________________________
Researcher’s Name: (please print) ________________________________________________
Researcher’s Signature: ________________________________________Date: _______________
Crucial Elements of Kinship Care Home Assessment
116
Questions/Concerns
If you have any further questions or want clarification regarding this research and/or your participation, please contact:
Julie Mann-Johnson Graduate Student
Faculty of Social Work University of Calgary
780-460-8494 [email protected]
If you have any concerns about the way you have been treated as a participant, please contact the Research Ethics Analyst, Research Services, University of Calgary.
A copy of this consent form has been given to you to keep for your records and reference. The investigator has kept a copy of the consent for
117 Crucial Elements to Kinship Care Home Assessment
Appendix B
Focus group Protocol This project will explore social work practice in the area of kinship care. The literature suggests that children placed in kinship care achieve more positive outcomes. Even so, practice and policy regarding kinship care has been slow to develop and in most jurisdictions foster care and adoption policies were applied to kinship care. However the literature suggests the experience for kinship caregivers is very different from stranger care – adoption and foster care. In this study, data was reviewed from previous public consultations and information gathering events have occurred in recent years within government in Alberta where information was gathered regarding kinship caregiver assessment. This data was analyzed and used to inform this project to honour the voices of people who have already shared their perspectives. Secondary qualitative data analysis endeavors to gain further insight on existing data without further intrusion on populations who have shared the information previously, thus reducing a burden on research participants and avoiding duplication. I would like to present what this data identified as being crucial to kinship caregiver assessment and I would invite you to share your thoughts regarding these findings. This process will serve to ensure checks on the secondary data analysis. Our conversation will be digitally recorded. However aside from my research supervisor, no one will have access to this recording or the transcripts of the recording. Our conversation today is completely confidential and I ask that the participants in the room respect these principles of confidentiality and refrain from sharing information from other participants. If for any reason you wish to end your participation in the focus group, you are always free to withdraw your consent and leave the room. However the information that you have shared until that point may be used.

118 Crucial Elements to Kinship Care Home Assessment
Potential questions: Do these comments seem to reflect your practice experience? Would you like to add anything? Do you see things differently? Do you disagree with anything presented? Can you elaborate? Was anything else overlooked? Left out? Do you see certain elements as being most/least crucial? Can you elaborate?
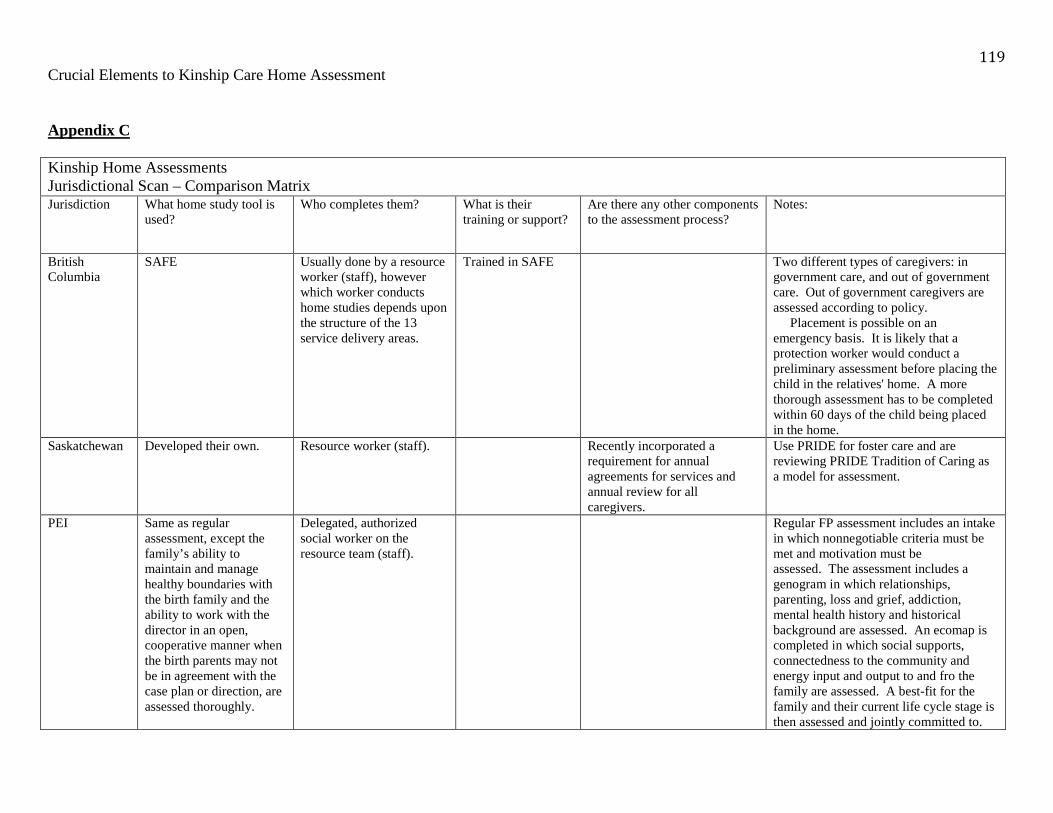
119 Crucial Elements to Kinship Care Home Assessment
Appendix C Kinship Home Assessments Jurisdictional Scan – Comparison Matrix Jurisdiction What home study tool is
used? Who completes them? What is their
training or support? Are there any other components to the assessment process?
Notes:
British Columbia
SAFE Usually done by a resource worker (staff), however which worker conducts home studies depends upon the structure of the 13 service delivery areas.
Trained in SAFE Two different types of caregivers: in government care, and out of government care. Out of government caregivers are assessed according to policy. Placement is possible on an emergency basis. It is likely that a protection worker would conduct a preliminary assessment before placing the child in the relatives' home. A more thorough assessment has to be completed within 60 days of the child being placed in the home.
Saskatchewan Developed their own. Resource worker (staff). Recently incorporated a requirement for annual agreements for services and annual review for all caregivers.
Use PRIDE for foster care and are reviewing PRIDE Tradition of Caring as a model for assessment.
PEI Same as regular assessment, except the family’s ability to maintain and manage healthy boundaries with the birth family and the ability to work with the director in an open, cooperative manner when the birth parents may not be in agreement with the case plan or direction, are assessed thoroughly.
Delegated, authorized social worker on the resource team (staff).
Regular FP assessment includes an intake in which nonnegotiable criteria must be met and motivation must be assessed. The assessment includes a genogram in which relationships, parenting, loss and grief, addiction, mental health history and historical background are assessed. An ecomap is completed in which social supports, connectedness to the community and energy input and output to and fro the family are assessed. A best-fit for the family and their current life cycle stage is then assessed and jointly committed to.

120 Crucial Elements to Kinship Care Home Assessment
Nova Scotia An initial assessment
followed with full SAFE. Foster care social workers (staff) complete both. In some parts of the province, SAFE assessments are completed by social workers who are designated to complete SAFE assessments for both foster care and adoption.
SAFE training and supported and trained in the agencies by their social work supervisors in the application of the initial assessment.
PRIDE - A tradition of caring (training) is mandatory. Usual gamut of checks is required - home safety, child abuse register, criminal records/vulnerable sector search, medical, references, and financials.
New Brunswick
SAFE Children’s Residential Services Unit social workers (staff). All are certified to complete SAFE assessments.
Attending PRIDE is encouraged but not required. All individuals over the age of 19 living in the home must also have a Child Welfare Check completed and a Criminal record check. An Environment of Care Assessment is completed as well. Immediate response Conference, Family Group Conference and Permanency Planning Conferences - all with the focus on working with the family to develop a safety plan for their child.
These are interim Kinship services and policy as legislative changes are being worked on. If a child is in the Minister's care and living with a family member or kin (someone known to the child) they are viewed as a provisional home and we proceed with assessing the family following the SAFE Assessment model.
Newfoundland Kinship home assessment. Social worker (staff). Kinship care is not an in-care status. Children are placed through agreement or order to the Kinship caregiver’s care. If they do not approve after assessment, child may remain but no supports are provided and parents are advised that an investigation may occur.
Western Australia
Developed own tool based on regulated competencies.
Social worker (staff). Not specific to home assessment.
Certain parts of assessment are completed at initial placement and others are completed within five days. Approved by a panel.
New Zealand Form incorporates Signs of Safety.
May be done by outside contractor who becomes involved through facilitation of FGC.
Signs of Safety training.
FGC is component of all cases as per legislation.
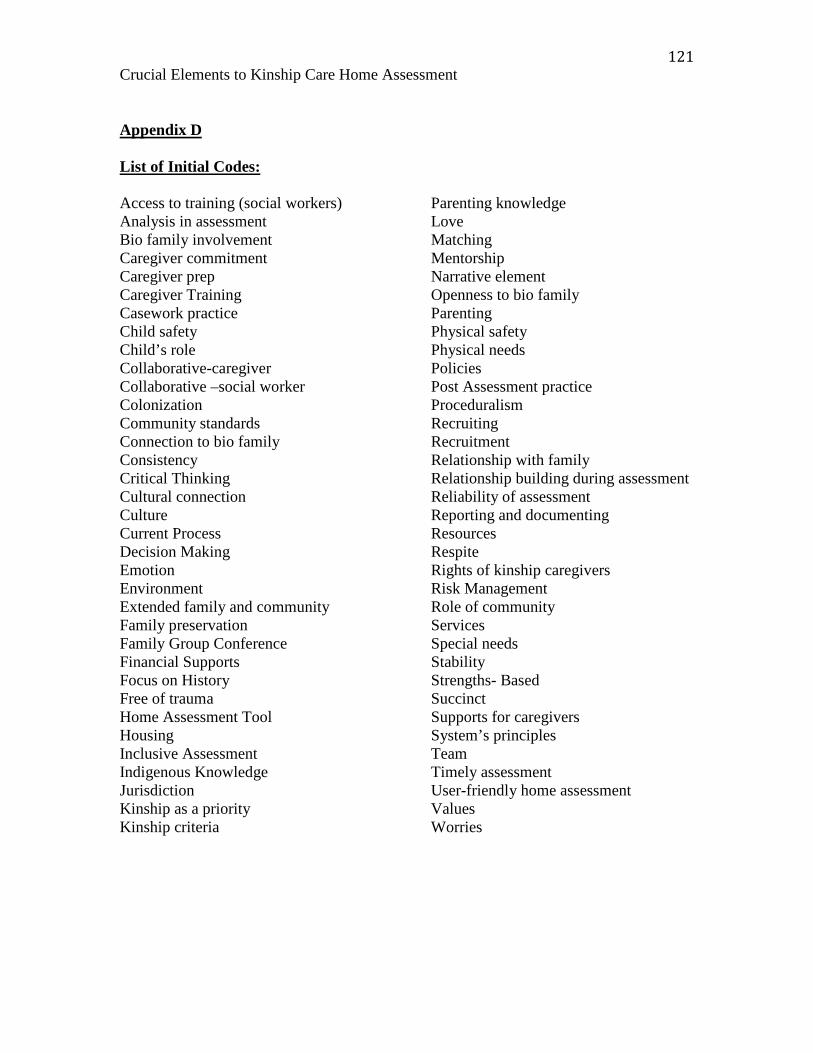
121 Crucial Elements to Kinship Care Home Assessment
Appendix D List of Initial Codes: Access to training (social workers) Analysis in assessment Bio family involvement Caregiver commitment Caregiver prep Caregiver Training Casework practice Child safety Child’s role Collaborative-caregiver Collaborative –social worker Colonization Community standards Connection to bio family Consistency Critical Thinking Cultural connection Culture Current Process Decision Making Emotion Environment Extended family and community Family preservation Family Group Conference Financial Supports Focus on History Free of trauma Home Assessment Tool Housing Inclusive Assessment Indigenous Knowledge Jurisdiction Kinship as a priority Kinship criteria
Parenting knowledge Love Matching Mentorship Narrative element Openness to bio family Parenting Physical safety Physical needs Policies Post Assessment practice Proceduralism Recruiting Recruitment Relationship with family Relationship building during assessment Reliability of assessment Reporting and documenting Resources Respite Rights of kinship caregivers Risk Management Role of community Services Special needs Stability Strengths- Based Succinct Supports for caregivers System’s principles Team Timely assessment User-friendly home assessment Values Worries
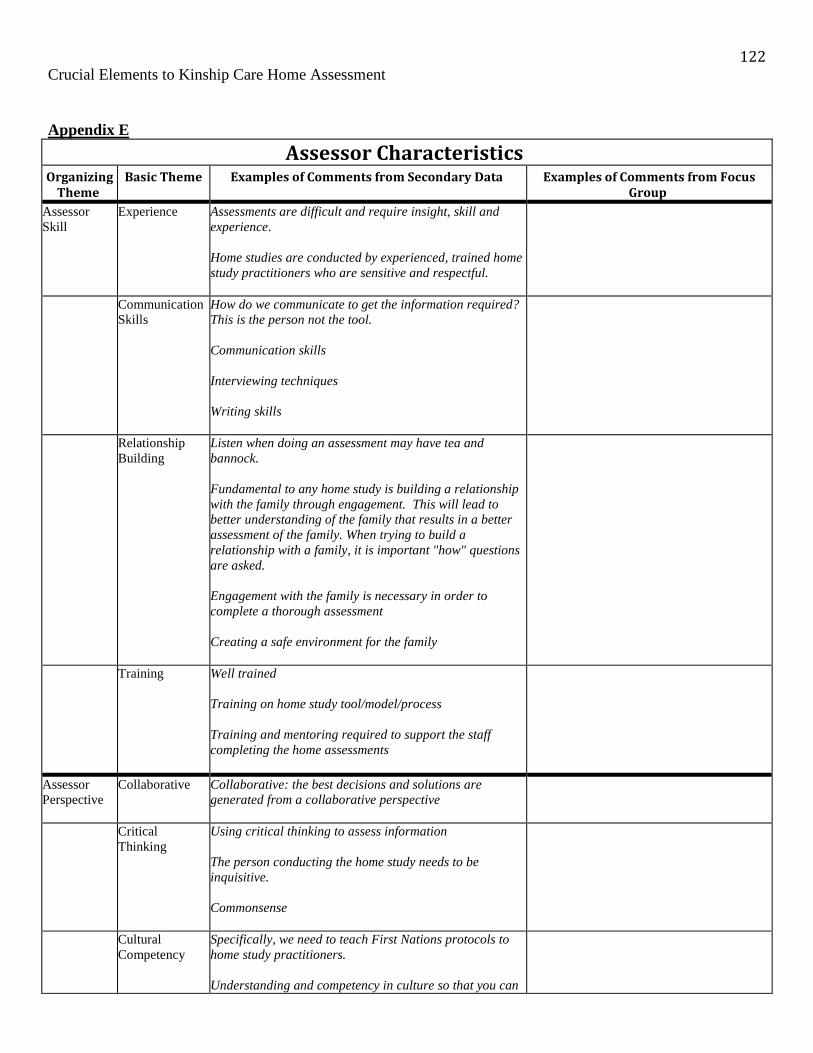
122 Crucial Elements to Kinship Care Home Assessment
Appendix E
Assessor Characteristics Organizing
Theme
Basic Theme Examples of Comments from Secondary Data Examples of Comments from Focus
Group
Assessor Skill
Experience Assessments are difficult and require insight, skill and experience. Home studies are conducted by experienced, trained home study practitioners who are sensitive and respectful.
Communication Skills
How do we communicate to get the information required? This is the person not the tool. Communication skills Interviewing techniques
Writing skills
Relationship Building
Listen when doing an assessment may have tea and bannock.
Fundamental to any home study is building a relationship with the family through engagement. This will lead to better understanding of the family that results in a better assessment of the family. When trying to build a relationship with a family, it is important "how" questions are asked.
Engagement with the family is necessary in order to complete a thorough assessment
Creating a safe environment for the family
Training Well trained Training on home study tool/model/process Training and mentoring required to support the staff completing the home assessments
Assessor Perspective
Collaborative Collaborative: the best decisions and solutions are generated from a collaborative perspective
Critical Thinking
Using critical thinking to assess information The person conducting the home study needs to be inquisitive. Commonsense
Cultural Competency
Specifically, we need to teach First Nations protocols to home study practitioners.
Understanding and competency in culture so that you can
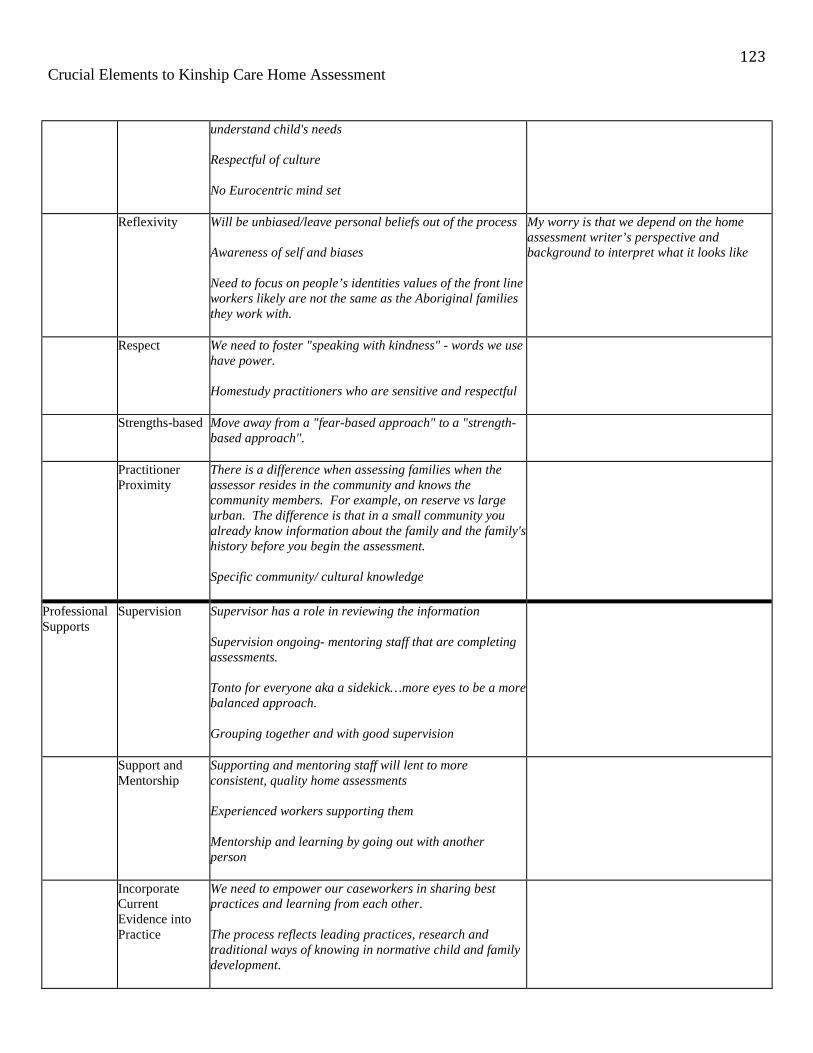
123 Crucial Elements to Kinship Care Home Assessment
understand child's needs
Respectful of culture
No Eurocentric mind set
Reflexivity Will be unbiased/leave personal beliefs out of the process Awareness of self and biases Need to focus on people’s identities values of the front line workers likely are not the same as the Aboriginal families they work with.
My worry is that we depend on the home assessment writer’s perspective and background to interpret what it looks like
Respect We need to foster "speaking with kindness" - words we use have power. Homestudy practitioners who are sensitive and respectful
Strengths-based Move away from a "fear-based approach" to a "strength-based approach".
Practitioner Proximity
There is a difference when assessing families when the assessor resides in the community and knows the community members. For example, on reserve vs large urban. The difference is that in a small community you already know information about the family and the family's history before you begin the assessment.
Specific community/ cultural knowledge
Professional Supports
Supervision Supervisor has a role in reviewing the information Supervision ongoing- mentoring staff that are completing assessments. Tonto for everyone aka a sidekick…more eyes to be a more balanced approach. Grouping together and with good supervision
Support and Mentorship
Supporting and mentoring staff will lent to more consistent, quality home assessments
Experienced workers supporting them
Mentorship and learning by going out with another person
Incorporate Current Evidence into Practice
We need to empower our caseworkers in sharing best practices and learning from each other.
The process reflects leading practices, research and traditional ways of knowing in normative child and family development.

124 Crucial Elements to Kinship Care Home Assessment
Important Areas to Address Organizing
Theme Basic Theme Examples of Comments from Secondary
Data Examples of Comments from Focus
Group
Caregiver Characteristics
Commitment and Motivation
Caregivers need to commit to the child.
Caregivers capacity/ability and commitment to care for children in the long term
Will confirm the caregivers' commitment to help the children remain connected (or return) to their families, communities and culture.
Will also confirm the family's commitment to re-unite the child and help the child remain connected with his/her family of origin, community and culture
The acceptance of the child and their needs and behaviors by caregivers
To me, motivation is very different than commitment….You may have a grandparent who is very committed…but they may be motivated more by a sense of obligation. They don’t want to do this. This is not how life was supposed to be….but you don’t want to risk not seeing this child again.
I don’t want to do this, but I have to do this.
A red flag for me is if it’s based in economics. Creates family conflict.
Once we tied in the kinship rates, all the people who identified kokum were saying I’m the one.
Adding ability to provide permanency. Circumstance changes all the time. Maybe that is motivation and commitment as well.
Family Makeup The whole family has to be assessed Government’s definition of a family is not suitable for Aboriginal families. Indigenous tradition of families living with families is frowned upon but Eastern religions and cultures do the same thing but it is considered ok
You need a plan B. We have 75 year olds caring for 5 year olds. What if something happens to them? They need to be aware that plan B caregivers may not be eligible for supports.
Under caregiver characteristics. Is the caregiver aware around the change in their role. They are no longer auntie. Their kokum but now they’re the parent. And the cousins who live there are now their siblings. Renegotiating roles. Maybe you can get your head around that, but what about everyone else in the home.
Grief and loss-especially for grandparents. So many losses, loss of relationship, loss of role as grandparents. Your role as a parent is so different than that as a grandparent.
Caregiver Skill: Parenting skills
Knowledge (including proof) of the parenting styles of the primary caregivers
The willingness of the caregivers to provide and/or get the supports to care for children who may have unique and special needs.
The parental skills to deal with the child’s needs
We know that kinship caregivers do not have as much skill at the table as foster parents, but do they have enough?
The interplay together – can they do that and how do we support that
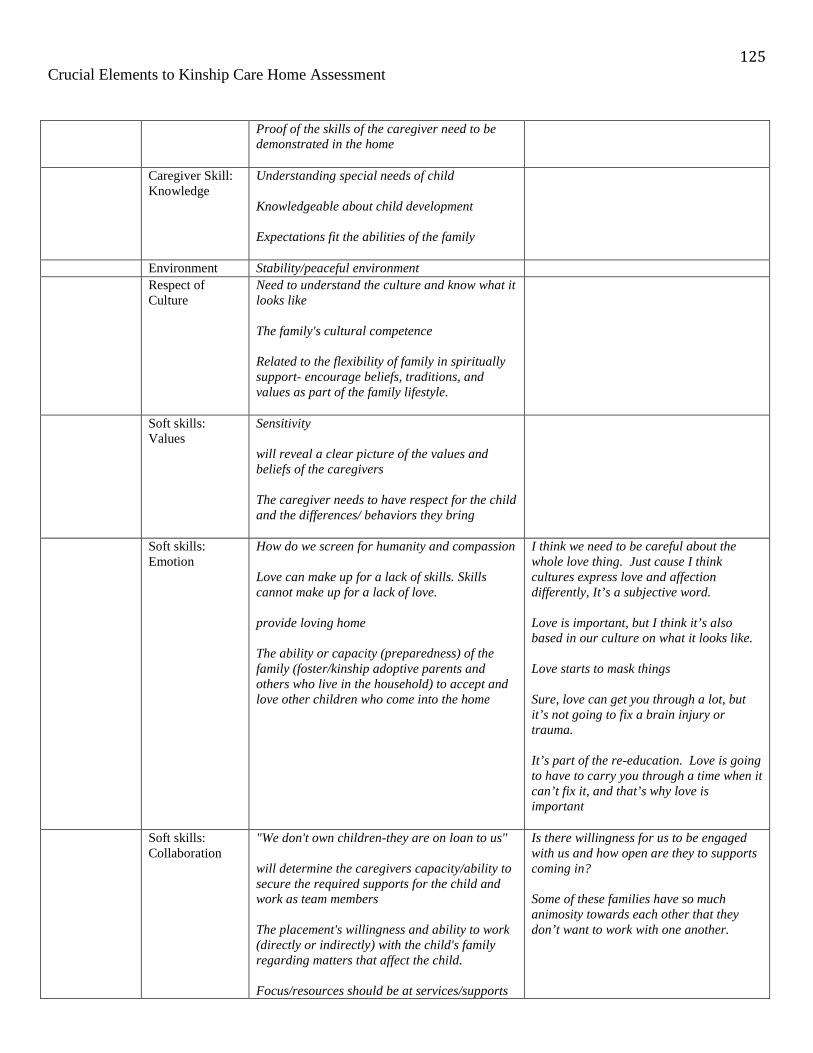
125 Crucial Elements to Kinship Care Home Assessment
Proof of the skills of the caregiver need to be demonstrated in the home
Caregiver Skill: Knowledge
Understanding special needs of child Knowledgeable about child development Expectations fit the abilities of the family
Environment Stability/peaceful environment
Respect of Culture
Need to understand the culture and know what it looks like The family's cultural competence Related to the flexibility of family in spiritually support- encourage beliefs, traditions, and values as part of the family lifestyle.
Soft skills: Values
Sensitivity
will reveal a clear picture of the values and beliefs of the caregivers The caregiver needs to have respect for the child and the differences/ behaviors they bring
Soft skills: Emotion
How do we screen for humanity and compassion Love can make up for a lack of skills. Skills cannot make up for a lack of love. provide loving home The ability or capacity (preparedness) of the family (foster/kinship adoptive parents and others who live in the household) to accept and love other children who come into the home
I think we need to be careful about the whole love thing. Just cause I think cultures express love and affection differently, It’s a subjective word.
Love is important, but I think it’s also based in our culture on what it looks like.
Love starts to mask things
Sure, love can get you through a lot, but it’s not going to fix a brain injury or trauma.
It’s part of the re-education. Love is going to have to carry you through a time when it can’t fix it, and that’s why love is important
Soft skills: Collaboration
"We don't own children-they are on loan to us" will determine the caregivers capacity/ability to secure the required supports for the child and work as team members
The placement's willingness and ability to work (directly or indirectly) with the child's family regarding matters that affect the child.
Focus/resources should be at services/supports
Is there willingness for us to be engaged with us and how open are they to supports coming in?
Some of these families have so much animosity towards each other that they don’t want to work with one another.

126 Crucial Elements to Kinship Care Home Assessment
that prevent children from coming into care - However, if a child comes into care the focus needs to be at returning the child to their parents/family/community. Home study needs to assess a family's ability to support this principle.
One of the struggles we have with family caregivers who have experienced trauma, but time may have passed or they’re in a different place, but often it is similar to what the child has experienced.
What kind of legacy are they carrying and not projecting that onto the child in their home. Are they able to know what their history is, their legacy and how to interrupt it? Do they have any insight?
Child’s Needs Love We need to change how we support these kids – they need connection to some member of their family that loves them They need family love
Child requires "love" not just a placement
Love them for who they are
Children have the caregivers’ time and attention and feel loved, accepted, and emotionally safe
Stability and permanency
Experiences "normalcy" It needs to be a guide to gather information toward a specific goal such as adoption, private guardianship, foster care or return home.
We need to decrease the number of moves in care - let's make the match of the child to the caregiver a good one from the beginning.
Special Needs It must be recognized that the child has undergone trauma We need to ensure the child receives the support he/she needs including things like counseling. Children experience loss, sorrow and grief when removed from their families and placed in a new environment.
Cultural Connection
The gov’t has a responsibility to support extended family to care for their kin. Exten, teach them how to believe in the Creator.
identifying, supporting and implementing what is needed to support the child's connection to culture

127 Crucial Elements to Kinship Care Home Assessment
Cultural planning and connectedness
Children need a healthy well rounded sense of self based in traditions, beliefs, values, spirituality and family lifestyle.
Relationship with Family and Community
We cannot look at a child in isolation but rather we need to look at a child in terms of attachment to their families and communities. We need to recognize and respect the child's relationships to parents and siblings
emotional/relationship needs met - placed near/in the community the child has knowledge of and connection to family and community
Analysis of the Information
Narrative A comprehensive story will be told about the family Tell a story about the family that includes information about the individual's history, extended family, community, willingness/ability to work to return the child home (facilitating visits with the family, etc.)
Critical Thinking Good documentation of the assessment piece - not just collecting information Analysis of the information Critical thinking is key
I wonder about different language other than narrative. The old format was very much narrative. The idea of SAFE was more of an assessment. We need to move away from storytelling and it’s great what families tell us in 30 pages, but we need assessment pieces. Crux of any home assessment is analyzing all your information. Taking everything we talked about today, bringing it together to somehow make a case for approving or not approving this family. Would be neat to have some more guidelines for how you do this. Honouring their story, presenting solution for the issues we are worried about, your plan of how you would support them. Analysis is the key to the whole home study.
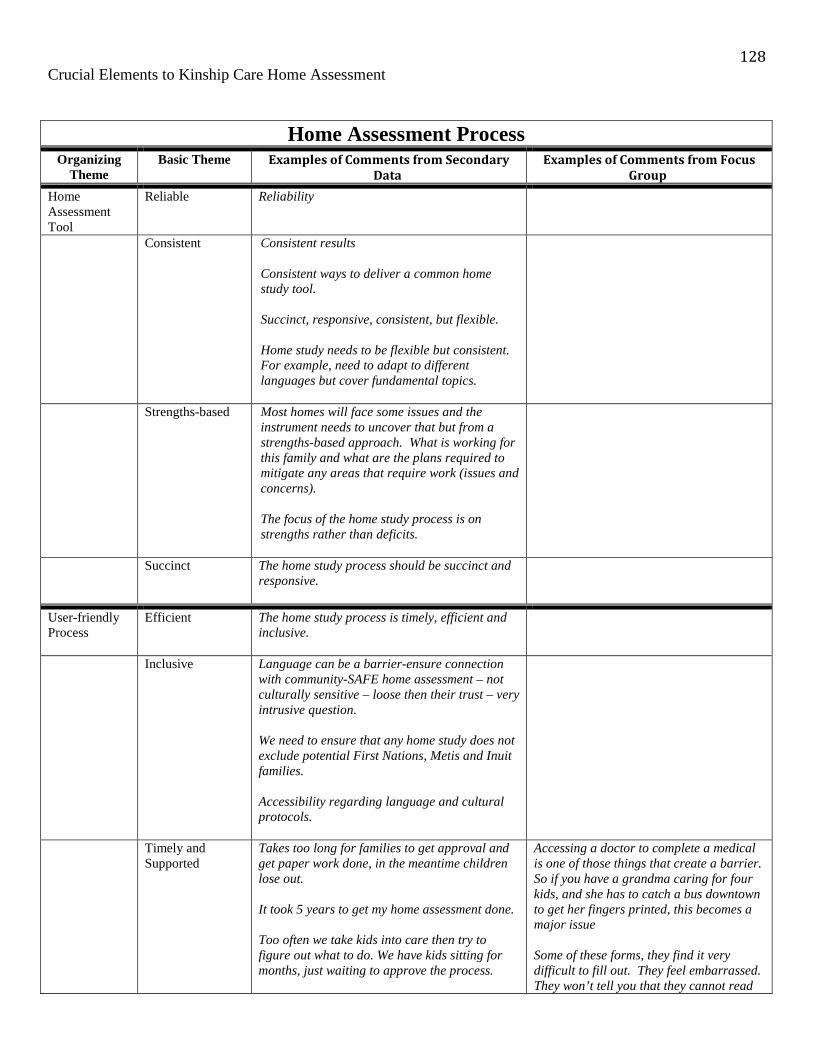
128 Crucial Elements to Kinship Care Home Assessment
Home Assessment Process Organizing
Theme Basic Theme Examples of Comments from Secondary
Data Examples of Comments from Focus
Group
Home Assessment Tool
Reliable Reliability
Consistent Consistent results Consistent ways to deliver a common home study tool. Succinct, responsive, consistent, but flexible. Home study needs to be flexible but consistent. For example, need to adapt to different languages but cover fundamental topics.
Strengths-based Most homes will face some issues and the instrument needs to uncover that but from a strengths-based approach. What is working for this family and what are the plans required to mitigate any areas that require work (issues and concerns). The focus of the home study process is on strengths rather than deficits.
Succinct The home study process should be succinct and responsive.
User-friendly Process
Efficient The home study process is timely, efficient and inclusive.
Inclusive Language can be a barrier-ensure connection with community-SAFE home assessment – not culturally sensitive – loose then their trust – very intrusive question. We need to ensure that any home study does not exclude potential First Nations, Metis and Inuit families. Accessibility regarding language and cultural protocols.
Timely and Supported
Takes too long for families to get approval and get paper work done, in the meantime children lose out. It took 5 years to get my home assessment done. Too often we take kids into care then try to figure out what to do. We have kids sitting for months, just waiting to approve the process.
Accessing a doctor to complete a medical is one of those things that create a barrier. So if you have a grandma caring for four kids, and she has to catch a bus downtown to get her fingers printed, this becomes a major issue
Some of these forms, they find it very difficult to fill out. They feel embarrassed. They won’t tell you that they cannot read

129 Crucial Elements to Kinship Care Home Assessment
those forms. So what they do is that they lose the forms. Huge language barrier. They signed it but they don’t know what the content of that document meant. The process is very confusing. Even when it’s explained to them. It’s that support piece.
Relationship building
Relationship with the family is essential There needs to be a team approach. Not “tool”/checklist focused. It needs to focus on relationship.
Barriers Focus on History Change policy around home study policy-requirements to difficult-e.g., if a problem (criminal) occurred 10 years ago and was minor they can’t get a home study When kinship is looked at, things are changing that past record where children weren’t harmed, it’s no reason to deny the application (eg. a drunk driving offence) Once a family comes into the system their file is active for 99 years. Grandparents are trying to get their grandkids but based on history and documentation we can’t hear each other Concern with things ‘in the record’.
Culture Government’s definition of a family is not suitable for Aboriginal families. tools/processes (e.g. assessments) don’t work well with Aboriginal families – staff do not feel supported to “push the envelope” and work outside of the rules. Now Elders are being assessed
Ongoing Assessment
Caregiver Prep Setting expectations of caregivers prior to assessment then ensuring assessment looks at the family’s commitment to these expectations. Family preparedness
Recruitment Look first in the child's family for placement options
Placing them with the immediate caregiver that was named or identified and no further searching is going on. They focused on bio mom and just shook her tree…I think a lot of times we neglect the dads.
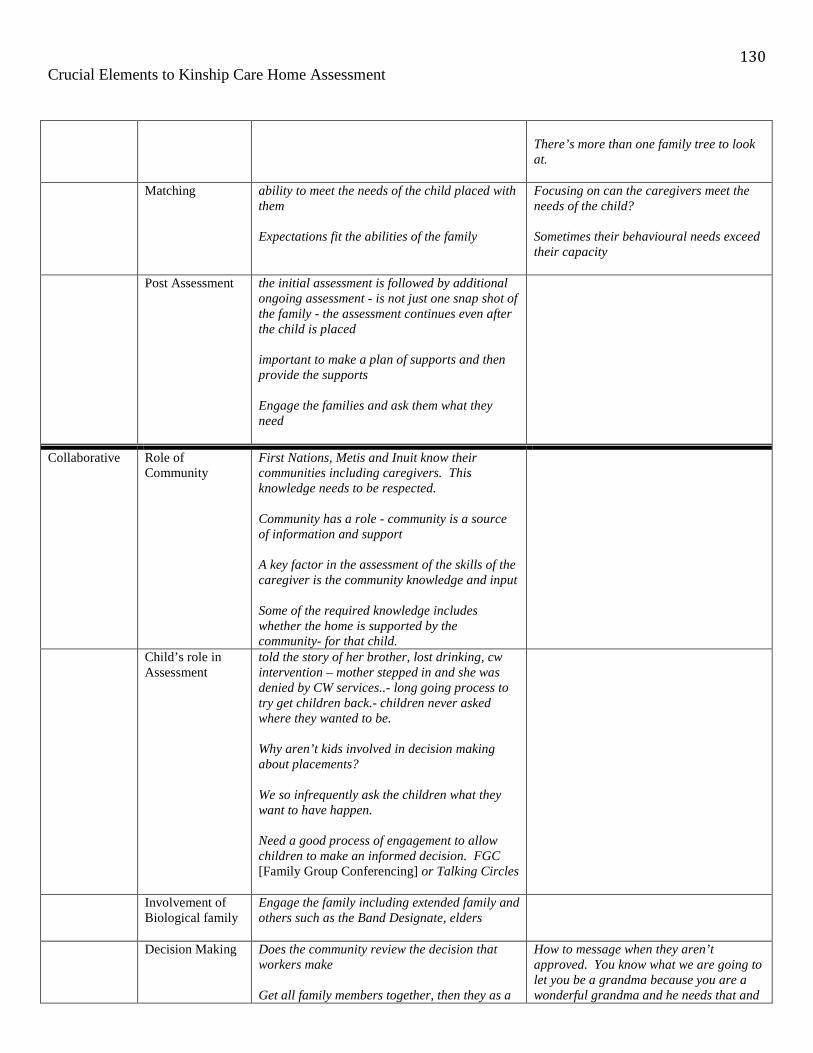
130 Crucial Elements to Kinship Care Home Assessment
There’s more than one family tree to look at.
Matching ability to meet the needs of the child placed with them Expectations fit the abilities of the family
Focusing on can the caregivers meet the needs of the child? Sometimes their behavioural needs exceed their capacity
Post Assessment the initial assessment is followed by additional ongoing assessment - is not just one snap shot of the family - the assessment continues even after the child is placed important to make a plan of supports and then provide the supports Engage the families and ask them what they need
Collaborative Role of Community
First Nations, Metis and Inuit know their communities including caregivers. This knowledge needs to be respected. Community has a role - community is a source of information and support A key factor in the assessment of the skills of the caregiver is the community knowledge and input Some of the required knowledge includes whether the home is supported by the community- for that child.
Child’s role in Assessment
told the story of her brother, lost drinking, cw intervention – mother stepped in and she was denied by CW services..- long going process to try get children back.- children never asked where they wanted to be. Why aren’t kids involved in decision making about placements? We so infrequently ask the children what they want to have happen. Need a good process of engagement to allow children to make an informed decision. FGC [Family Group Conferencing] or Talking Circles
Involvement of Biological family
Engage the family including extended family and others such as the Band Designate, elders
Decision Making Does the community review the decision that workers make Get all family members together, then they as a
How to message when they aren’t approved. You know what we are going to let you be a grandma because you are a wonderful grandma and he needs that and
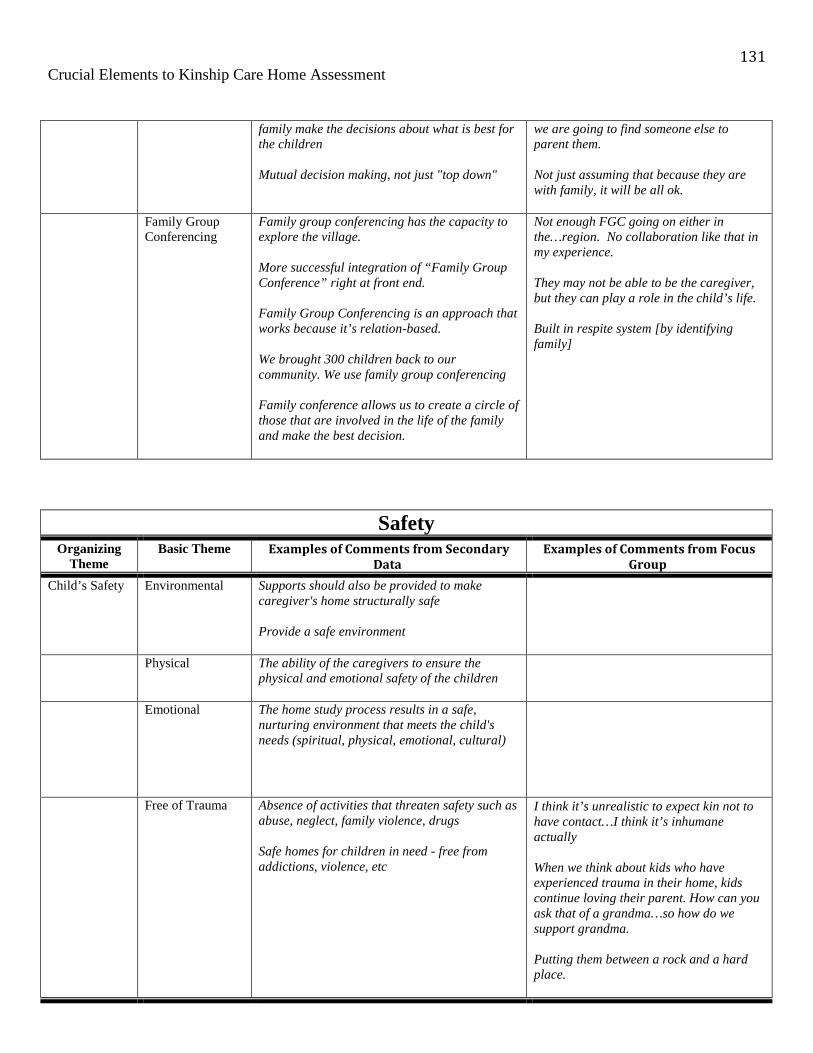
131 Crucial Elements to Kinship Care Home Assessment
family make the decisions about what is best for the children Mutual decision making, not just "top down"
we are going to find someone else to parent them. Not just assuming that because they are with family, it will be all ok.
Family Group Conferencing
Family group conferencing has the capacity to explore the village. More successful integration of “Family Group Conference” right at front end. Family Group Conferencing is an approach that works because it’s relation-based. We brought 300 children back to our community. We use family group conferencing Family conference allows us to create a circle of those that are involved in the life of the family and make the best decision.
Not enough FGC going on either in the…region. No collaboration like that in my experience. They may not be able to be the caregiver, but they can play a role in the child’s life. Built in respite system [by identifying family]
Safety Organizing
Theme Basic Theme Examples of Comments from Secondary
Data Examples of Comments from Focus
Group
Child’s Safety Environmental Supports should also be provided to make caregiver's home structurally safe Provide a safe environment
Physical The ability of the caregivers to ensure the physical and emotional safety of the children
Emotional The home study process results in a safe, nurturing environment that meets the child's needs (spiritual, physical, emotional, cultural)
Free of Trauma Absence of activities that threaten safety such as abuse, neglect, family violence, drugs
Safe homes for children in need - free from addictions, violence, etc
I think it’s unrealistic to expect kin not to have contact…I think it’s inhumane actually When we think about kids who have experienced trauma in their home, kids continue loving their parent. How can you ask that of a grandma…so how do we support grandma. Putting them between a rock and a hard place.
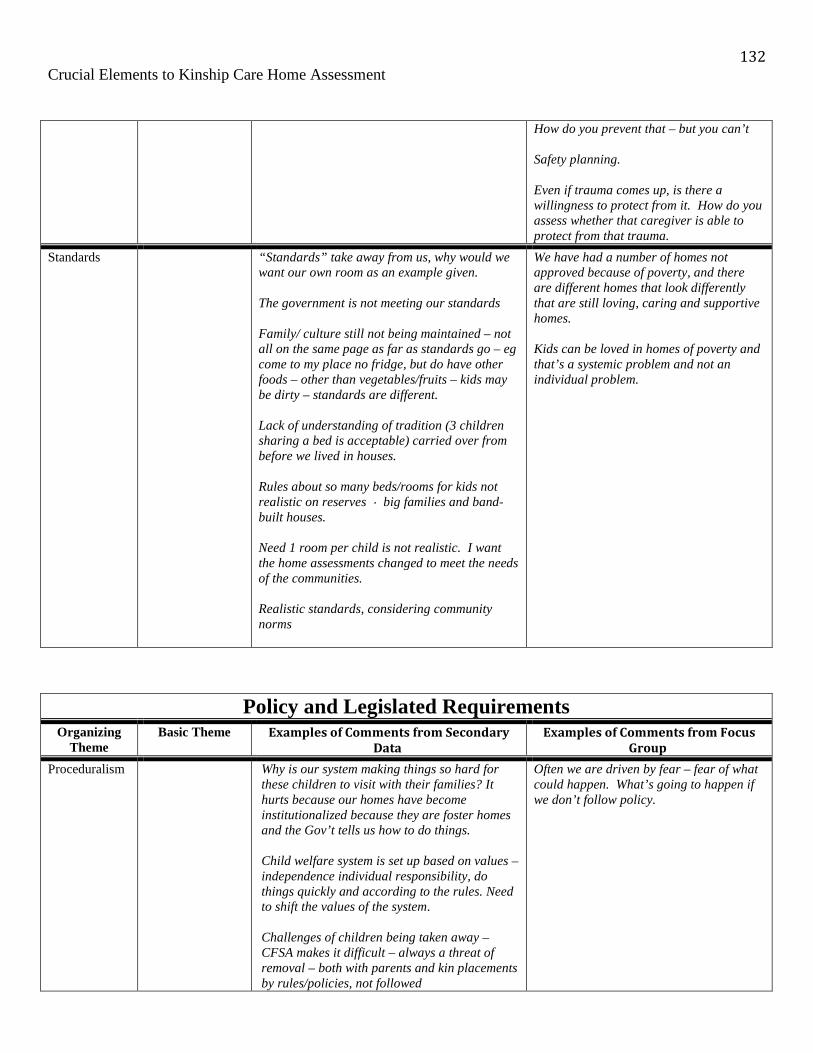
132 Crucial Elements to Kinship Care Home Assessment
How do you prevent that – but you can’t Safety planning. Even if trauma comes up, is there a willingness to protect from it. How do you assess whether that caregiver is able to protect from that trauma.
Standards “Standards” take away from us, why would we want our own room as an example given.
The government is not meeting our standards
Family/ culture still not being maintained – not all on the same page as far as standards go – eg come to my place no fridge, but do have other foods – other than vegetables/fruits – kids may be dirty – standards are different.
Lack of understanding of tradition (3 children sharing a bed is acceptable) carried over from before we lived in houses.
Rules about so many beds/rooms for kids not realistic on reserves big families and band-built houses.
Need 1 room per child is not realistic. I want the home assessments changed to meet the needs of the communities. Realistic standards, considering community norms
We have had a number of homes not approved because of poverty, and there are different homes that look differently that are still loving, caring and supportive homes.
Kids can be loved in homes of poverty and that’s a systemic problem and not an individual problem.
Policy and Legislated Requirements Organizing
Theme Basic Theme Examples of Comments from Secondary
Data Examples of Comments from Focus
Group
Proceduralism Why is our system making things so hard for these children to visit with their families? It hurts because our homes have become institutionalized because they are foster homes and the Gov’t tells us how to do things. Child welfare system is set up based on values – independence individual responsibility, do things quickly and according to the rules. Need to shift the values of the system. Challenges of children being taken away – CFSA makes it difficult – always a threat of removal – both with parents and kin placements by rules/policies, not followed
Often we are driven by fear – fear of what could happen. What’s going to happen if we don’t follow policy.
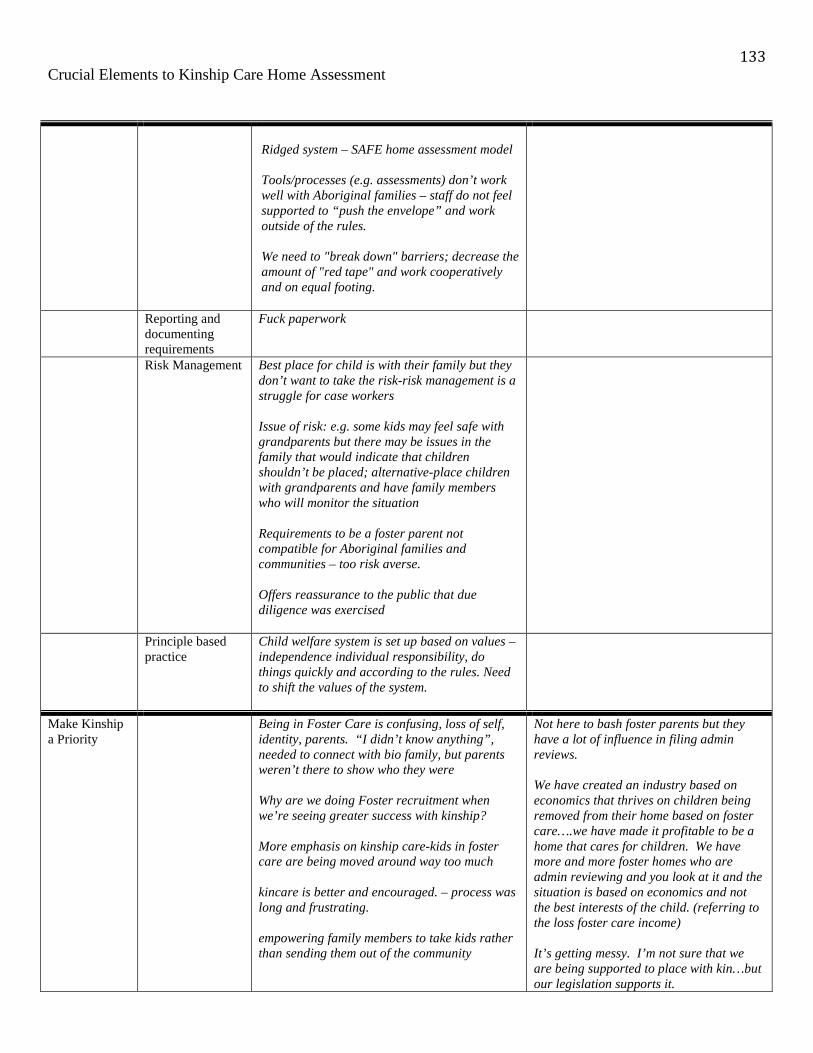
133 Crucial Elements to Kinship Care Home Assessment
Ridged system – SAFE home assessment model Tools/processes (e.g. assessments) don’t work well with Aboriginal families – staff do not feel supported to “push the envelope” and work outside of the rules. We need to "break down" barriers; decrease the amount of "red tape" and work cooperatively and on equal footing.
Reporting and documenting requirements
Fuck paperwork
Risk Management Best place for child is with their family but they don’t want to take the risk-risk management is a struggle for case workers
Issue of risk: e.g. some kids may feel safe with grandparents but there may be issues in the family that would indicate that children shouldn’t be placed; alternative-place children with grandparents and have family members who will monitor the situation
Requirements to be a foster parent not compatible for Aboriginal families and communities – too risk averse.
Offers reassurance to the public that due diligence was exercised
Principle based practice
Child welfare system is set up based on values – independence individual responsibility, do things quickly and according to the rules. Need to shift the values of the system.
Make Kinship a Priority
Being in Foster Care is confusing, loss of self, identity, parents. “I didn’t know anything”, needed to connect with bio family, but parents weren’t there to show who they were
Why are we doing Foster recruitment when we’re seeing greater success with kinship?
More emphasis on kinship care-kids in foster care are being moved around way too much
kincare is better and encouraged. – process was long and frustrating.
empowering family members to take kids rather than sending them out of the community
Not here to bash foster parents but they have a lot of influence in filing admin reviews.
We have created an industry based on economics that thrives on children being removed from their home based on foster care….we have made it profitable to be a home that cares for children. We have more and more foster homes who are admin reviewing and you look at it and the situation is based on economics and not the best interests of the child. (referring to the loss foster care income)
It’s getting messy. I’m not sure that we are being supported to place with kin…but our legislation supports it.

134 Crucial Elements to Kinship Care Home Assessment
I don’t know that the courts are willing to support us in that. We will get better at it as we go along, but we are in a catch up period.
Flexible kinship criteria
Kinship – more flexibility on who we approve as kinship families kinship has to go through same criteria as foster as foster home – too many barriers are being placed on family care
Have been told, grandma too old to care for grandchildren.
Want to see more kinship care, and that barriers are reduced for those wanted to take care of kin. Want courts to be more open to this.
Kinship care has a lot more potential. Need to look more into this and reduce barriers/policies that hinder kinship care.
Rights of kinship caregivers
As a kinship provider I should not need a lawyer. Has created a lot of mistrust right from the beginning of signing papers – lost my right as a human being – children became property of the government
Caregiver Policies
Clear guidelines regarding child management and discipline
Policy right now says that the bio parent cannot reside in the home. Dad got his act together….it’s working well. It’s one of the barriers. Family healing happens within the context of kinship care at a greater degree than we give it credit for. Love is a huge component in healing. Bring families together and see families heal. That’s my goal.

135 Crucial Elements to Kinship Care Home Assessment
Systemic Organizing
Theme Basic Theme Examples of Comments from Secondary
Data Examples of Comments from Focus
Group
Resources There are a number of barriers facing First Nation, Metis and Inuit families and communities. For example, the lack of housing on-reserve. How can we place a child in a home in their community when there is no housing? What about food security? How can we place a child in a home where there are food security issues? These issues are inter-connected and cannot be addressed in isolation.
Financial resources
Capacity and resources required to carry out tasks
Housing Work with what all communities need instead of building 3 bedroom houses build 5 rooms for Kokum.
Inadequate housing, 2 or 3 families living together in 1 house
Colonization Government rules, policies, procedures do not fit our culture. Entrenched in the dominant society of doing things. We have been programmed to have a nuclear family.
Prior to residential schools, aboriginal communities took care of their children
government is starting to realize that the Aboriginal people have the answers
How can we support or enhance a healing system? We need to get back our rights to make our own decisions; social workers make you feel like they own you.
Respecting Indigenous Knowledge
Aboriginal knowledge has been de-valued and continues to be de-valued. We need to learn to respect their knowledge.
feels shame when the community member is good and the policy states otherwise- the elders are good and they earned their place in the community- hard for workers to say no.
Some of the info out there is not very good. Starting with a literature review with poor info. What is the point? The wisdom is in the community

136 Crucial Elements to Kinship Care Home Assessment
Cultural sensitivity – for years gov’t has tried to figure out what’s important to us without once asking us. They don’t want to know the reality of what/who we are.
Jurisdiction Home study process should apply off reserve On reserve don’t have to do safe assessment (with feds) relationship with police criminal check immediate
Role of extended family and community
Our community always took care of us so we
didn’t go into care. Kids went into care when
they moved into the city, away from the
community.
We need to take care of our children as a
community.
Needs to be elder involvement – grandmas and
grandpas – they are useful people – no one is
looking for them
Grandparents are the glue
Aboriginal families don’t always have a mom
and dad that raise you. It’s aunties, uncles, and
grandparents that are integral to raising
children.
Kinship ties – traditional family connections
are critical for kids that can’t stay with their
parents.
We need to recognize that the best place for a
child is in the family and the community from
where they came from.
Consideration needs to be given to the child’s
larger family group/”clan”
Respecting Indigenous Casework Practice
First Nations practice standards inform the process and consider family and community norms
We elevate what is working and share First Nations best practices - this may include a provincial symposium of First Nations best practices
Family Preservation
If we pay group home 300 per day, why not pay this to keep kids in their own home.
Agreement around the table that children are

137 Crucial Elements to Kinship Care Home Assessment
better off in a bad situation in their biological family than in our system
Collaborative Casework Practice
A Voice, to be a true part of the team Involve all departments/ supports community resources.
Kinship are brought to the table at service team meeting so they understand the expectation of their child or the parents of the kid….they want to be part of it.
None of my kinship parents have been invited to service team meetings. They don’t have copies of the plans.
Support for Caregivers
A lot of grandparents have a lot of pressures and can’t take in children without support
Grandparents will not turn away their grandchildren, but they don’t have the ability to keep up and care for the grandkids. They need more supports.
Very hard for grandmother to take children in this system, young men used to hunt for grandma to feed children
At the moment kinship care is set up for failure
Financial The gov’t has a responsibility to support extended family to care for their kin. Extended family should not be expected to raise their family members without adequate financial supports.
Compensate family members who want to care for their children.
Dollars/$ should follow the children; going to the grandmothers who are raising them.
Sometimes they (caseworkers) seem to think it’s their money they’re spending
You’re family, you pay for it. (seems to be the attitude)
The caseworker told the kinship provider “you’re financially responsible for this kid. We’ll give you some help, but you need kick in some money.”
Sometimes our policy has too much discretion….sometimes one (office) will support buying winter clothing and another a worker will say I feel like I need to beg for things.
Sometimes we breed dependency…..they stop being self-reliant and hey I can get mileage for this and I’m not going to do this if I don’t get mileage. And then they have a really tough time. Or they move into a bigger house to accommodate the placement and then the kids go home and they are left with a larger home without the maintenance dollars. Don’t breed dependence. Sometime kinship families put the brakes on permanency when they hear that they
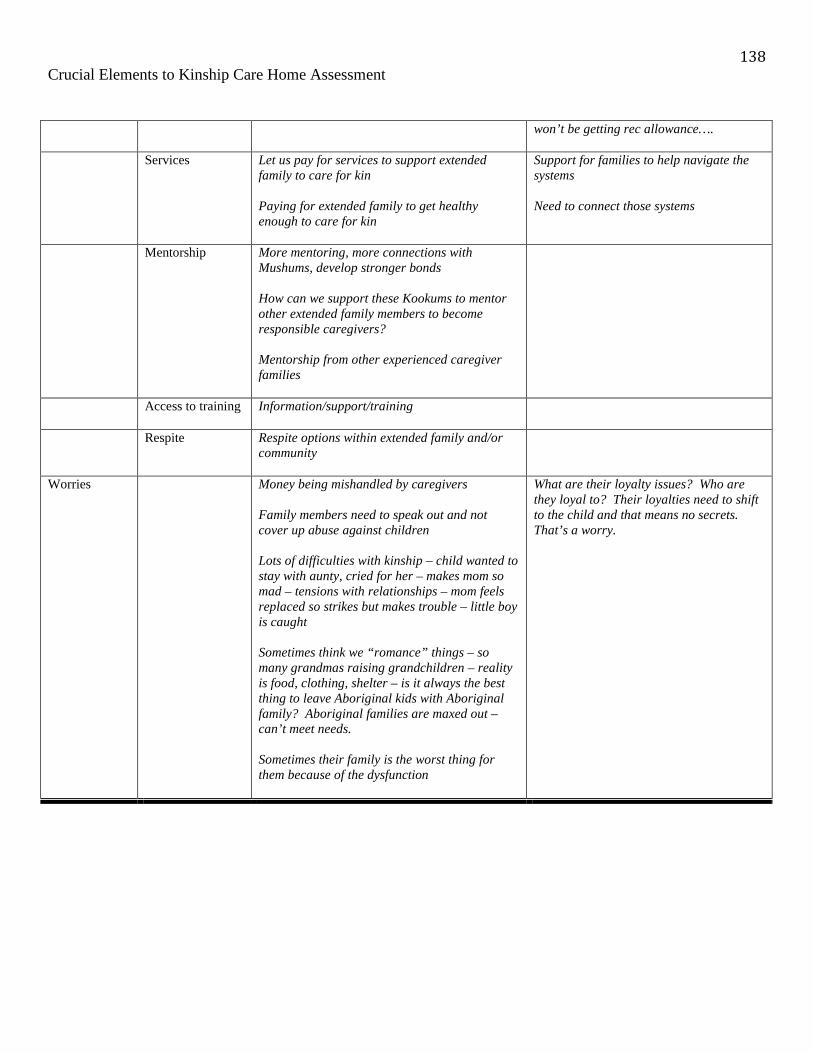
138 Crucial Elements to Kinship Care Home Assessment
won’t be getting rec allowance….
Services Let us pay for services to support extended family to care for kin Paying for extended family to get healthy enough to care for kin
Support for families to help navigate the systems
Need to connect those systems
Mentorship More mentoring, more connections with Mushums, develop stronger bonds How can we support these Kookums to mentor other extended family members to become responsible caregivers?
Mentorship from other experienced caregiver families
Access to training Information/support/training
Respite Respite options within extended family and/or community
Worries Money being mishandled by caregivers Family members need to speak out and not cover up abuse against children Lots of difficulties with kinship – child wanted to stay with aunty, cried for her – makes mom so mad – tensions with relationships – mom feels replaced so strikes but makes trouble – little boy is caught
Sometimes think we “romance” things – so many grandmas raising grandchildren – reality is food, clothing, shelter – is it always the best thing to leave Aboriginal kids with Aboriginal family? Aboriginal families are maxed out – can’t meet needs.
Sometimes their family is the worst thing for them because of the dysfunction
What are their loyalty issues? Who are they loyal to? Their loyalties need to shift to the child and that means no secrets. That’s a worry.