ACPNews NovDec2012_ACPNews - Alberta College of ...
16
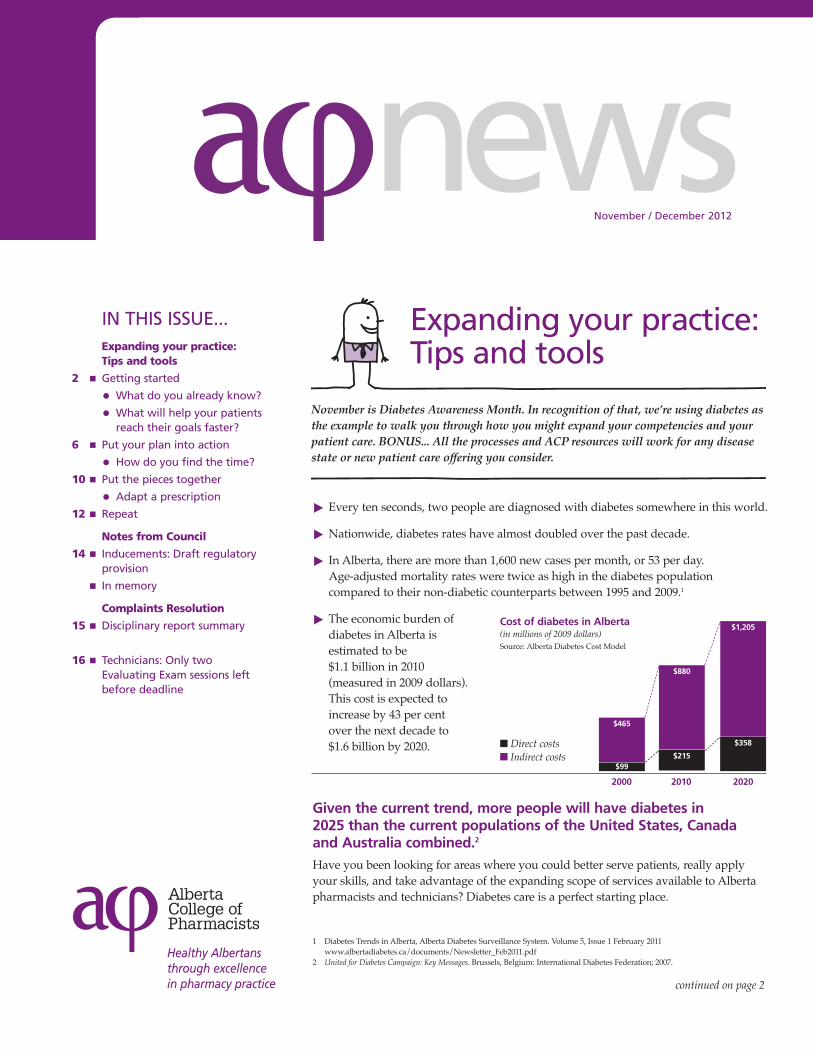
news November / December 2012 IN THIS ISSUE... Expanding your practice: Tips and tools 2 n Getting started l What do you already know? l What will help your patients reach their goals faster? 6 n Put your plan into action l How do you find the time? 10 n Put the pieces together l Adapt a prescription 12 n Repeat Notes from Council 14 n Inducements: Draft regulatory provision n In memory Complaints Resolution 15 n Disciplinary report summary 16 n Technicians: Only two Evaluating Exam sessions left before deadline Healthy Albertans through excellence in pharmacy practice November is Diabetes Awareness Month. In recognition of that, we’re using diabetes as the example to walk you through how you might expand your competencies and your patient care. BONUS... All the processes and ACP resources will work for any disease state or new patient care offering you consider. ® Every ten seconds, two people are diagnosed with diabetes somewhere in this world. ® Nationwide, diabetes rates have almost doubled over the past decade. ® In Alberta, there are more than 1,600 new cases per month, or 53 per day. Age-adjusted mortality rates were twice as high in the diabetes population compared to their non-diabetic counterparts between 1995 and 2009. 1 ® The economic burden of diabetes in Alberta is estimated to be $1.1 billion in 2010 (measured in 2009 dollars). This cost is expected to increase by 43 per cent over the next decade to $1.6 billion by 2020. Given the current trend, more people will have diabetes in 2025 than the current populations of the United States, Canada and Australia combined. 2 Have you been looking for areas where you could better serve patients, really apply your skills, and take advantage of the expanding scope of services available to Alberta pharmacists and technicians? Diabetes care is a perfect starting place. 1 Diabetes Trends in Alberta, Alberta Diabetes Surveillance System. Volume 5, Issue 1 February 2011 www.albertadiabetes.ca/documents/Newsletter_Feb2011.pdf 2 United for Diabetes Campaign: Key Messages. Brussels, Belgium: International Diabetes Federation; 2007. $99 $465 $880 $215 $358 $1,205 2020 2010 2000 Cost of diabetes in Alberta (in millions of 2009 dollars) Source: Alberta Diabetes Cost Model n Direct costs n Indirect costs continued on page 2 Expanding your practice: Tips and tools
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ACPNews NovDec2012_ACPNews - Alberta College of ...
newsNovember / December 2012
IN THIS ISSUE...Expanding your practice: Tips and tools
2 n Getting startedl What do you already know?l What will help your patients
reach their goals faster?
6 n Put your plan into actionl How do you find the time?
10 n Put the pieces togetherl Adapt a prescription
12 n Repeat
Notes from Council
14 n Inducements: Draft regulatoryprovision
n In memory
Complaints Resolution
15 n Disciplinary report summary
16 n Technicians: Only twoEvaluating Exam sessions leftbefore deadline
Healthy Albertansthrough excellencein pharmacy practice
November is Diabetes Awareness Month. In recognition of that, we’re using diabetes asthe example to walk you through how you might expand your competencies and yourpatient care. BONUS... All the processes and ACP resources will work for any diseasestate or new patient care offering you consider.
® Every ten seconds, two people are diagnosed with diabetes somewhere in this world.
® Nationwide, diabetes rates have almost doubled over the past decade.
® In Alberta, there are more than 1,600 new cases per month, or 53 per day. Age-adjusted mortality rates were twice as high in the diabetes populationcompared to their non-diabetic counterparts between 1995 and 2009.1
® The economic burden ofdiabetes in Alberta isestimated to be $1.1 billion in 2010(measured in 2009 dollars).This cost is expected toincrease by 43 per centover the next decade to$1.6 billion by 2020.
Given the current trend, more people will have diabetes in 2025 than the current populations of the United States, Canada and Australia combined.2
Have you been looking for areas where you could better serve patients, really applyyour skills, and take advantage of the expanding scope of services available to Albertapharmacists and technicians? Diabetes care is a perfect starting place.
1 Diabetes Trends in Alberta, Alberta Diabetes Surveillance System. Volume 5, Issue 1 February 2011www.albertadiabetes.ca/documents/Newsletter_Feb2011.pdf
2 United for Diabetes Campaign: Key Messages. Brussels, Belgium: International Diabetes Federation; 2007.
$99
$465
$880
$215
$358
$1,205
202020102000
Cost of diabetes in Alberta(in millions of 2009 dollars)Source: Alberta Diabetes Cost Model
n Direct costsn Indirect costs
continued on page 2
Expanding your practice:Tips and tools
aφnews is published six times per yearby the Alberta College of Pharmacists.Send submissions for publication [email protected]
The deadline for submissions for theJan/Feb 2013 issue is Dec. 7.
Alberta College of Pharmacists1100, 8215 - 112 Street NWEdmonton AB T6G 2C8780-990-0321 / 1-877-227-3838Fax: 780-990-0328
President: Kaye Moran President Elect: Kelly OlstadVice President: Krystal WynnykPast President: Anjli Acharya
Councillors:Brad Willsey, District 1Clayton Braun, District 2Rick Hackman, District 3Ahmed Metwally, District 3Krystal Wynnyk, District 3Kelly Olstad, District 4Kamal Dullat, District 5Kaye Moran, District 5Kelly Boparai, Pharmacy Technician
Public members:Vi BeckerBob KruchtenPat Matusko
Pharmacy technician observer:Robin Burns
You can contact council members by emailvia our website under About ACP/ Council,or by using the search feature to locatethem by name.
Staff DirectoryAll staff are available at 780-990-0321 or 1-877-227-3838 or by fax at 780-990-0328.
Their email addresses are available onour website at pharmacists.ab.ca underContact Us.
Registrar: Greg EberhartDeputy Registrar: Dale CooneyComplaints Director: James KrempienPractice Development Director:
Debbie LeeProfessional Practice Director: Shao LeePharmacy Practice Consultants:
Tom Curr, Monty Stanowich, Jennifer Voice
Operations and Finance Director: Lynn Paulitsch
Registration and Competence Director:Heather Baker
Registration Manager: Linda HagenCommunications Director: Karen Mills
pharmacists.ab.ca
news
2
Expanding your practice continued from page 5
Pharmacists are generally the most accessible health care providers. On average,patients with diabetes see their pharmacist seven times more often than they see otherprimary care providers.3 This increased patient contact – combined with pharmacists'medication knowledge, therapeutic experience, and ability to effectively deliverpatient education – has positioned pharmacists to assume a major role in providingoptimal diabetes management.
So, what are we waiting for? Let’s get started!
Gettingstarted
((( Expanding your practice )))
You’ve decided you want to expand yourcare for diabetics. You start thinkingabout the diabetic patients you alreadyhave and your patients who are at riskfor diabetes, and the questions start tocome fast and furious.
n How can I assess patients thoroughly,but quickly, so that I can identifythose at risk and help them?
n Are my skills up to snuff?
n What are some good CE courses I cantake to get the most up-to-dateinformation?
n Would having any authorizations orcertifications help my patients andme?
n How can I shift my workload so Ihave enough time for thoroughcounseling and follow up?
What now?
You need a plan: your continuing professionaldevelopment plan. Log into your registrant profile on theACP homepage and dive in. Theonline CPD system is much more thansimply a place to log your continuing
education credits. It takes you throughthe whole continuing professionaldevelopment cycle:
1. performing a self-assessment,
2. creating a learning plan,
3. learning, and
4. evaluating the entire process.
So, to figure out your starting point withdiabetic patients, you’ll need to start byassessing what skills and knowledge youalready have, and what you might needto brush up on.
If we look at the questions that poppedinto your mind, it looks like you mightwant to assess your skills in assessment,sterile product preparation,communication, documentation, andfollow up.
All of these topics are covered in theCompetency Profile for Alberta Pharmacists.This profile details 66 competency topicsacross six practice areas: pharmacypractice, communication skills, safety,operational and business management,professionalism, and foundationalknowledge and skills.
Let’s look at assessment in more detail.
3 Wubben DP, Vivian EM. Effects of pharmacist outpatient interventions of adults with diabetes mellitus: a systematic review.Pharmacotherapy. 2008;28(4):421-436.
The initial evaluation of a patient athigh risk for diabetes is used to classifythe patient's blood glucose status,detect complications, and direct thefocus of the treatment plan.
Components of the evaluation includemedical history, physical exam,laboratory evaluation, and lifestyleassessment.4 Providers must assess thehistory and progression of symptoms,the progression of complications,previous and current treatmentstrategies, and the risks for furtherdisease progression. Pertinent baselinelab tests include A1C, fasting lipidprofile, liver function tests, serumcreatinine, thyroid-stimulatinghormone, and urinalysis. Referrals toclinical specialists may be required forfurther evaluation.4
You’ve got a lot of information-gathering goals and limited time. Howcan you be sure you get the mostinformation during your assessment inthe least amount of time?
While you’ve learned a few tricks of thetrade (e.g., ask open ended questions,start questions with “Is there a reason…”rather than “Why do you…” to avoidmaking people defensive), you knowimproving your assessment skills willbe important to your success indiabetes care.
To determine what learning will benefityou and your patients most, start bytaking an inventory of the knowledgeand skills you already have and thenidentify the gaps. An easy way to dothat is to compare your competencieswith those listed in the CompetencyProfile for Alberta Pharmacists.
aφnews – November / December 2012 3
What do you already know?The Competency Profile associates the following competencies with patient assessment:
COMPETENCY A-1 Patient Care Practice
A-1-2 Patient Assessment
A pharmacist will... A-1-2-1 Demonstrate the ability to conduct an appropriate patient assessment,
including but not limited to • Identifying patient’s needs • Systematically finding, analyzing, evaluating and applying
information from multiple sources, such as the patient, the patient’scaregiver(s), other health care providers, medication profile (inpharmacy and/or on Netcare), and electronic health record
• Gathering relevant information to enable an appropriate assessment,e.g., physical assessment, relevant laboratory values, medical history,etc.
A-1-2-2 Demonstrate the ability to systematically find, analyze, evaluate andapply information in order to identify factors that impact drug therapy. • Drug information, for example in the form of texts, journal articles,
research papers, advertising materials, etc. • Clinical practice guidelines • Financial constraints of the patient • Lifestyle of the patient • Nutrition of the patient • Concurrent drug use
A-1-2-3 Demonstrate an understanding of, and the ability to identify, thevarious types of drug therapy problems.
A-1-2-4 Demonstrate the ability to assess the patient data collected, synthesizethe information, and critically evaluate the patient’s drug therapy-related needs.
A-1-2-5 Demonstrate the ability to prioritize the patient’s drug therapyproblems.
4 National Diabetes Fact Sheet: General Information and National Estimates on Diabetes in the United States, 2007. Atlanta, GA: US Department of Health and Human Services, Centers for DiseaseControl and Prevention; 2008.
Increase yourknowledgeOnce you’ve completed your knowledgeand skills inventory, ask yourself, “Whatcan I do to help my patients reach theirgoals faster?” This is a simple (andmotivating!) way to uncover andprioritize your professional developmentneeds. You become a more competentprofessional and your patients get bettercare – it’s a win-win situation.
Let’s go back to our assessment example.Say that while reviewing thecompetencies, you realized you want toknow more about interviewing. Wherecould you go to learn about that?
Start with the ACP website. The Events, Practice Resources, andContinuing Competence pages arechockablock with courses, guidelines,and tips to help you improve yourpractice.
To upgrade your interviewing skills, youcould start with the Chat, Check andChart tool card and worksheet. Both areavailable under Practice Resources > Infosheets & posters.
NEW RESOURCE: Look to the newPrescription Adaptation Guide to leadyou step-by-step through the Chat,Check and Chart method of assessingand documenting. The Guide is postedunder Practice Resources > Forms > Tools.
For even more sources of education, lookto the Learning Links tab in theContinuing Competence section of theACP website. Here are just a fewexamples of the diabetes-related offeringswe found.
rx BriefCase
1. Enhancing Communication:Understanding Issues and ChallengesFaced by Many Patients [CCCEP FileNumber: 1066-2012-614-I-P (1 CEU)]
2. Diabetes Education: A ComprehensiveReview (12 CCCEP-accreditedmodules)
3. Insulin Dose Calculation Support: Anew feature in diabetes control[CCCEP File Number: 1066-2012-425-I-P (1 CEU)]
4. "The How to of ManagingDiabetes…A Prescription forPharmacists", the CanadianPharmacists Association's (CPhA)diabetes educational program (10CCCEP-accredited modules/ 12CEUs)
Mylan Learning Center
1. Smoking Cessation in the AdolescentPopulation (1.5 CEUs)
Canadian Pharmacist’s Letter
1. Many supplements are promoted forDiabetes Special Report: NaturalMedicines in the ClinicalManagement of Diabetes
2. Prevention and Treatment of DiabeticFoot Infections
3. Which Diabetic Patients should takeAspirin
What will help your patients reach their goals faster?
Adapting a prescription using Chat, Check, Chart
Step 1: Gather information (Chat) from the patient and other sources (e.g., Netcare) to determine if it is appropriate to adapt a prescription.
Ask your patient the 3 prime questions to efficiently gather information.
1. Purpose
2. Direction
3. Monitoring
What are you taking this medication for?
How are you using this medication?
How are you doing on this medication? What are your expectations?
Step 2: Assess (Check) the patient and therapy (including renewals).
Ask the following questions to evaluate the appropriateness of therapy in order to identify and prevent any potential drug therapy problems.
I
E
S
U
Is the therapy indicated?
Is the therapy effective?
Is the therapy safe?
Is the patient willing to use/adhere to the therapy?
Is there a clinical indication for the therapy? Can the medical condition identified benefit from the chosen therapy?
Is this one of the most effective options? Is the dosage of the medication sufficient to achieve the goals
of the therapy? For ongoing therapy, are the goals of the therapy being achieved?
(Patient’s signs and symptoms, vital signs, lab test results, blood glucose levels, etc.)
Is the dose safe? (No contraindications or interactions) For ongoing therapy, are there NO signs of toxicity or adverse reactions?
Is the patient willing and able to take/use this therapy as prescribed? (Cost, concerns, culture, etc.)
Step 3: Develop care plans for any drug therapy problems by determining goals of therapy and potential solutions to each drug therapy problem.
Step 4: If the drug therapy problem can be resolved by adapting the prescription, obtain informed consent from the patient.
Adaptation options:
Dosage change
Formulation change
Regimen change
Therapeutic substitution
Renewal for continuity of care
The patient is assessed personally There is evidence of current ongoing therapy There is an immediate need for drug therapy It is not reasonably possible to have the prescription
transferred to you or for the patient to attend the original pharmacy
The original pharmacy is notified regarding the renewal
Pharmacists may only renew a prescription without the original prescription if:
Please refer to Standards 11-15 in the Standards of Practice for Pharmacists and Pharmacy Technicians for more information on pharmacist adapting.
aφnews – November / December 2012 4
aφnews – November / December 2012 5
Rogers Healthcare Group
1. Type 2 Diabetes and Chronic KidneyDisease [CCCEP File Number: 1065-2011-308-I-P (2 CEUs)]
2. Type 2 Diabetes: A Fresh NewApproach with Incretin Agents[CCCEP File Number: 1065-2010-050-I-P (1 CEU)]
3. Integrating Incretin-based Therapiesinto the Management ofHyperglycaemia in Type 2 Diabetes[CCCEP File Number: 1065-2010-166-I-P (1.5 CEUs)]
Ontario Pharmacists’ Association
1. Diabetes Level 1 Certificate Programonline program (13 CEUs)
Upgrade your skillsWhat if it’s a hands-on skill you wantto brush up on? Again, look to theACP website.
First, look to the Competency Profile forAlberta Pharmacists again. It definescompetency clusters for various skillsand activities. One example is thepreparation of sterile products (asshown below).
Does reading this make you realize it hasbeen a while since you had to pre-fill aninsulin syringe? If so, you can check thePractice guidelines and references listings onthe Practice Resources page of the ACPwebsite and find the guideline for pre-filling insulin syringes.
Check the Events pageWhile you’re on the website, don’t forgetto look at the Events page for courses.Here are just two examples of what youwill find there that would help youexpand your practice.
COMPETENCY A-16 Preparation of Sterile Products
A pharmacist will... A-16-1 Demonstrate the ability to select and use the appropriate equipment
required for sterile compounding.
A-16-2 Demonstrate knowledge of, and ability to comply with, the requirementsfor preparation of sterile products as defined by the Alberta College ofPharmacists, including USP Chapter 797, and by workplace standards,policies and procedures.
A-16-3 Demonstrate knowledge of, or ability to locate information in thefollowing areas:
• Aseptic technique and contamination factors
• Facilities, equipment and supplies
• Parenteral routes of drug administration
• Methods and equipment for administration of drugs
• Procedures for the preparation, compounding, distribution andstorage of sterile products (including incompatibilities, pH andosmolality)
• Documentation, quality control and quality assurance procedures
• The chemical, pharmaceutical and clinical properties of all theingredients in a sterile product
• Sterilization techniques and process validation
• The principles of microbiology
• Issues related to home parenteral therapy
A-16-4 Demonstrate knowledge of, and ability to apply quality control processesin, the preparation of sterile products.
This course has been designed tohelp you enhance your practice bygiving a boost to your patientassessment and documentationskills. It runs from the beginning ofFebruary to mid-March, 2013 andincludes a one-and-a-half dayworkshop (February 8 & 9, 2013)and two assignments.
Registration Deadline: January 4, 2013
Please visit the PracticeDevelopment website for moreinformation.www.pharmacy.ualberta.ca/PD/courses/bootcamp/bootcamp.htm
continued on page 6
aφnews – November / December 2012 6
Put your plan into actionHow do you find the time?
Upgrade your skills continued from page 5
Are you holding off on expandingyour patient services because youthink you don’t have time to fitanything more in your already packedday? Well, as the old saying goes,where there’s a will there’s a way.
Life will always be busy, so if youwant to break out of the status quoyou have two choices: be moreefficient yourself or delegate. Why nottry both? First, let’s look at how to bemore efficient.
Get lean in 30 seconds a dayIf you can reduce the time it takes tocarry out your daily tasks by just 30
seconds every business day for one year,at the end of the year, your productivitywill have increased by 26%.
How? Use lean management!
Lean is a philosophy that originatedwith the Toyota Production System inJapan over 50 years ago. It focuses onpeople working together to add valuewithout creating waste. Theunderlying principle of lean isproviding value to the end user – inthis case, your patients.
You can become lean by better usingexisting resources, improving work flow,standardizing work, eliminating wastes,and empowering employees by allowingthem to make changes to their workprocesses to enhance work flow.
Lean but not skimpy
Keep three things in mind as youembark on your lean process. Theywill help you get the greatest impactfor your efforts.
1. Make safety an underlyingphilosophy for your pharmacy andyour patients. This will help you keeppriorities straight and make decisionsabout what needs to stay and whatcan go.
2. When setting your goals forimprovement, make sure they’reSMART: Specific, Measurable,Achievable, Relevant and Timely. Thiswill allow you to measure progressand celebrate success.
((( Expanding your practice )))
ADAPT is a forward-thinking, 19-weekCE course designed specifically forpractising pharmacists. It wasdeveloped by the CanadianPharmacists Association (CPhA) andthe Canadian Society of HospitalPharmacists (CSHP).
ADAPT provides proven practiceexpertise using interactive onlinelearning, supportive moderators andplenty of peer interaction.
Through this course, you will masterskills and build confidence in:
n Medication assessment
n Collaboration
n Patient interviewing and assessment
n Making evidence-based clinicaldecisions
n Documentation
n Developing and implementingpatient care plans
ADAPT is accredited for 76.0 CEUs.Pharmacists who successfully completeADAPT may also challenge aCertificate Assessment process and beawarded a Certificate in Patient CareSkills. CPhA anticipates thatparticipation will require 4-6 hours aweek of your time.
See the Canadian PharmacistsAssociation website for registrationdetails (www.pharmacists.ca).
ADAPT
aφnews – November / December 2012 7
3. Remember that lean is an ongoingprocess, not a one-time sweep.Remember to:
n Make one improvement at a timeusing current resources.
n Take a walk around yourpharmacy and observe yourprocesses with “lean eyes.”
n Involve your entire team.
How do you get lean?
Use the Lean Management Toolworksheet found on the ACP websiteunder Registration & Licensure>Pharmacies> Pharmacy Assessment toguide you through the process.
ACP Pharmacy Practice Consultants canhelp you and your staff become a lean,mean, pharmacy team.
1. First, think about areas or processesyou would like to enhance toimprove patient care and safety,meet or exceed their expectations or
improve patient retention andrelationships. Now, follow thesesteps through the lean process.
2. Sort out your pharmacy.
a. Decide what is needed and notneeded.
b. Establish a place for everythingand put everything in its place.
c. Store frequently used items so thatthey are easily accessible.
d. Clean and keep the pharmacyorganized so you can see anddispose of waste quickly.
3. Once you’re finished sorting, developand follow operating procedures toimprove and sustain work flow andconduct an audit to identify any gapsin your processes.
4. Once you’ve identified and filled yourprocess gaps, standardize yourprocesses. Consistent processes meanconsistent results! Check equipment,sequence activities, post clearinstructions, monitor and measureperformance, and adjust to improve.
5. Remember that lean is aboutcontinuous improvement. If your firstimprovement doesn’t work out theway you expected, make anadjustment and keep trying. If youhave success, great! Find anotherimprovement and repeat the process.
6. Now, eliminate wastes. Do youdocument patient care notes manually and electronically?Streamline by only using one method.Are pharmacists performing non-professional tasks such as ringing upsales at the cash register? Arrange
workflow and staff to maximizepharmacist skills and time.
Let us know how you lean
Lean management should not use up alot of resources and you should be ableto make a big impact in a short amountof time. We’d love to hear about whatlean practices you put into place and theimpact they had on your practice andteam. Send your stories (successes,valiant attempts or utter disasters) [email protected].
Resources
For more information about leanmanagement, please contact yourpharmacy practice consultants orpharmacy practice administrator, JenShuman [email protected]
Find and fix common pharmacy deficienciesACP pharmacy practice consultantscontinue to help pharmacy teams correctdeficiencies, improve work flow andenhance practice. Over the last sixmonths, the consultants have identifiedthe most common deficiencies inpharmacies across Alberta. We arereviewing them in aφnews and TheLink over the coming months.
While we know that change isn’t alwayseasy or fast, we hope that with oursupport and educational tools, pharmacyteams will be able to make incrementalchanges to their practice and operationsthat are SMART (Specific, Measurable,Achievable, Relevant, and Timely).
Lean focuses on:1. 2. 3. 4. 5.
What is lean management?
1.
2.
3.
Ideas:
vorP. 1cofn eaL
t ahW
toteualvgnidiv:noes suc
namn aels i
tneitapeht
?tnegeman
pmE. 5imilE. 4
natS. 3pIm. 2
hpehtgnirewopsetsawgnitanimisksatgnizidrdanwoflkrowgnivor
g
maetycarmah
sw
p
pIm. 3
eeM2.
pIm. 1
hinu toyn aC
noitnetertneitapevor
xetneitapdeecxerotee
sndaeractneitapevor
t ahs tessecorf pok hin
?spihnsoitalernda
?snoitatcpex
?ytefas
:otd ecanhnee bn ac
:saedI
continued on page 8

aφnews – November / December 2012 8
The deficiency: Lack of formal,written policies and procedures
Do you have formal, written policies andprocedures in your pharmacy? Were youaware that this is required by theStandards for the Operation of LicensedPharmacies (1.2b)?
Compiling policies and procedures is apretty big task if you are starting fromscratch. To help you, ACP has recentlyupdated our Pharmacy Policies andProcedures manual template. Thetemplate is easy to use; and can bedownloaded, edited and saved so youcan fill in all the sections relevant to yourspecific pharmacy. You can find it underPractice Resources > Forms > Pharmacies onthe ACP website.
There are six main areas you need tofocus on when you start your manual:
1. Relief section – provides the basicinformation required by a reliefpharmacist (including someone whohas to come work in an emergencysituation when your regular staff are
not available). Include computersign-on information, location ofessential documents and keys, andimportant phone numbers.Essentially this is information that apharmacist, even if they have neverbeen in your pharmacy before,would require to be able to safelyprovide care to your patients.
2. Assistant and technician roles –formal policies and proceduresoutlining the roles of your pharmacytechnicians and assistants in thedispensing process and how they aresupervised by the pharmacists.
3. Compounding activities – includethe steps involved in preparing,dispensing, monitoring, andevaluating your products. More detailson what to include in this section will becovered in a future article.
4. Medication error management –this should describe how you wantyour staff to respond to amedication incident that isdiscovered in your pharmacy orbrought to your attention. Includewhat steps are to be taken to ensure
the health and safety of anyoneinvolved, as well as the stepsrequired to document, investigate,and review the incident with theintent to determine the root causeand make any necessary changesand prevent that error fromoccurring in the future.
5. Compliance packaging – you canmodel this section after yourcompounding policy and procedureas it would include the preparation,dispensing, monitoring, andevaluating of the process to dispensecompliance packages. You want tomake certain that you have a safesystem that is easily audited toensure quality assurance. Note aswell the labelling requirements forcompliance packs (see Standard 7)that are often found deficient inpharmacy assessments.
6. Methadone (if your pharmacydispenses methadone) – this can bemodelled after the compoundingpolicy and procedure as well. Inaddition, you need to ensure you arecompliant with the MethadoneTreatment in Alberta Guidelines(copy available on the ACP website),and the labelling requirements foryour methadone stock bottles (seethe Summer 2010 edition of theTransition Times: Best of FAQ). Besure to detail your system foridentifying patients and signing offon drink doses, as well as directionsfor how you keep a log record ofyour bulk compounding of yourstock solution.
Once you have your policies andprocedures in place for these six areas,you can continue to work through theremainder of the ACP template andcomplete your comprehensive manual.
Finally, turn your manual into action,not just dusty papers on a shelf.Regularly review your policies andprocedures with your team. Put stepsin place to ensure the policies are beingfollowed. Make revisions and additionswhen necessary so your manual iscurrent and relevant.
Common pharmacy deficienciescontinued from page 7
aφnews – November / December 2012 9
Streamline yourdocumentationA patient record must containdemographic information about thepatient, a profile of drugs provided and arecord of care provided. The details ofwhat must be included in each of thesecomponents are provided in Appendix Ato the Standards of Practice for Pharmacistsand Pharmacy Technicians.
However, think quality not quantitywhen documenting. Use the eDAP(efficient Data, Assessment, Plan) formatfrom Chat, Check and Chart to help youfocus your information gathering. UseStep 6 of the Prescription Adaption Guide(above) to walk you through the process.Using a standardized style alsoencourages complete data and consistentprocesses, and improves the organizationof your thoughts.
DelegateIf you are as efficient as you can beand you still don’t have time, thenwhat? It’s time to see if you are reallyspending your time as effectively aspossible. What should you delegate?
As you are making your pharmacylean (see page 6), don’t forget to makesure you are using your humanresources as effectively as possible.Technicians who are knowledgeableabout diabetes can contributesignificantly to the pharmacy team.
Helping patients select and use bloodglucose meters is certainly not a newrole for pharmacy technicians incommunity practice settings. With anewly diagnosed diabetic, atechnician can:
n help the patient choose a glucosemeter,
n explain what it does and how to useit,
n outline the best times to check theirblood sugar,
n guide the patient through a practicerun so they feel confident using thedevice,
n provide the patient with a log bookand show them how to keep track oftheir glucose levels, and
n discuss the importance of a gooddiet, exercise, and keeping someform of sugar with them if theirglucose falls too low.
Pharmacy technicians who supportdiabetes education by assisting withblood glucose device training can alsohelp by keeping application forms forfunding programs on hand in thepharmacy or know how to access themonline when needed.
Before you delegate…
Is your pharmacy prepared to adapt itsworkflow to accommodate regulatedpharmacy technicians and make moretime available for pharmacists to focuson patient assessment, follow-up, and other non-dispensing services? Do you have a formal Policy andProcedure for the roles of yourAssistants/Technicians in thedispensing/compounding/compliancepackaging process in your pharmacy?
Your pharmacy must have policies andprocedures outlining the roles of yourpharmacy technicians and assistants inthe dispensing process and how theyare supervised by your pharmacists(Standard 3, Standards for the Operationof Licensed Pharmacies). This will allowyou to regularly monitor compliancewith these procedures to ensure thesafety and integrity of your dispensingprocesses. You can also refer toStandard 20 of the Standards of Practicefor Pharmacists and Pharmacy Technicianswhich outlines the roles andresponsibilities of each regulatedmember including the supervisionrequirements of employees in thepharmacy.
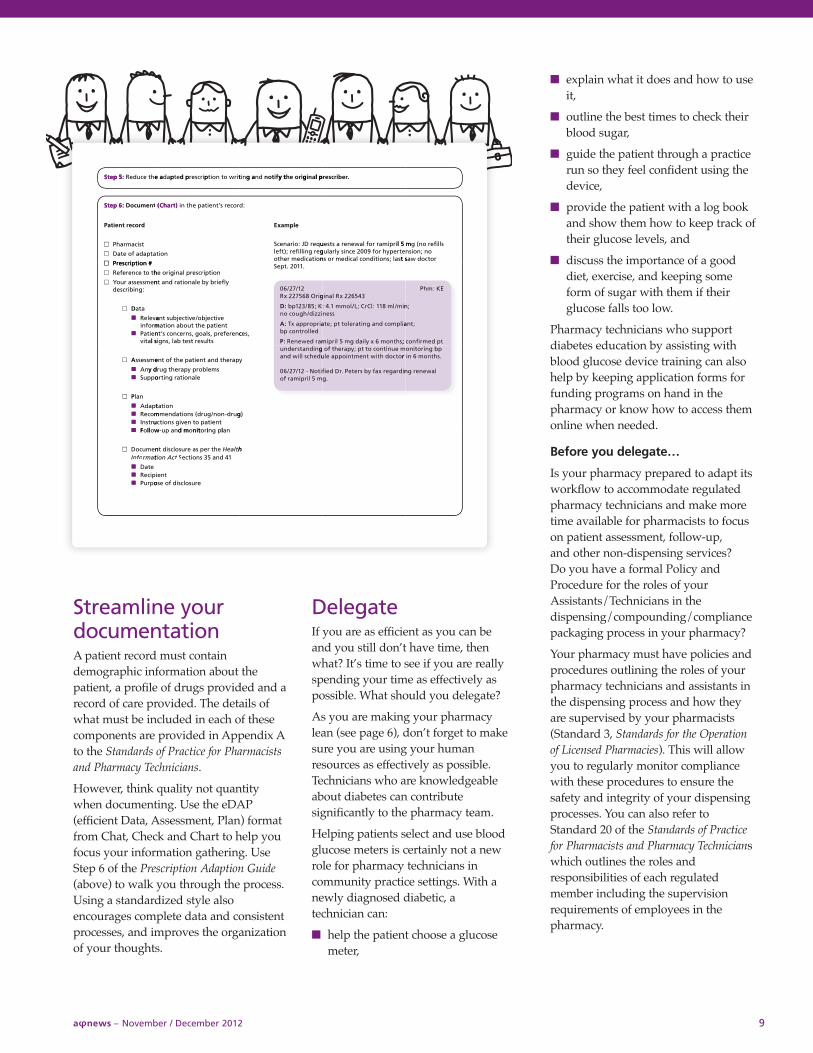
Step 5:
Step 6: (Chart)
: p 5etS e ahe tcudeR
tiro wn toitpircserd petpade a
d ng anit l panigire ohy tfiton
.rebircser
p 5
: p 6etS nemucoD t
tsicamrahP
atpadf ae otDa
n #oitpircserP
drocet rneitaP
pd pp
) t)rahC ( roces r’tneitae phn ti
noit
g a l pgy t
:d
elpmaxE
uqeD r: JoiranecSgeg rnilfile; r)tfelnoitacider mehto
l 5 mirpimar rol fawenes a rtseuetrepyr ho9 f00e 2cniy slralugt ssa; lsnoitidnol cacider ms on
s lfileo rng (l 5 mo ; nnoisn
r otcow dat s
n #oitpircserP
ho te tcnerefeR
nemssessr auoY:gnibircsed
D a ta
aveleRmrofnineitaP
l sativ
noitpircserl panigire oh
y fleiry be blanoitad rnt an
e vitcejbo/evitcejbut snatneitae pht tuobn aoitam
cnerefer, pslao, gsnrecnos c’tnstluset rseb ta, lsngil s
2
, sec
.110. 2tpeS
1/72/60gir8 O6572x 2R
:D ; K58/321p bizzid/hguoo cn
:A airproppx a Tp b dellrotnoc
: P mad reweneR
34562x 2l Ranig
nim/l8 m1: 1lCr; CL/lom1 m.: 4ssen
ailpmod cng anitarelot t; peta
; cshtnoy x 6 mlaig dl 5 mirpim
E: KmhP
; n
; tna
t d pemrfino; c
A emssess
y dnAoppuS
P nal
tpadAmoceRurtsnI
llF
parehd tnt aneitae phf tt one
smelbroy pparehg tury delanoitag rnitro
noitatgurd-non/gurds (noitadnemm
tneitao pn tevis gnoitculitnid m
g o
y
)g
nidnatsrednuudehcl slid wna
fiito2 - N1/72/60l 5 mirpimaf ro
e munitnoo ct t; pyparehf tg or iotcoh dtit wnemtnioppe alu
nidragex ray fs brete. Prd Defi.g
p g bnirotnio.shtnon 6 mr i
l aweneg rn
wolloF
nemucoDtamronffoI
etDapiceRopruP
nalg pnirotniod mnp au-w
e hr tes pe arusolcsit dn h tlaeHt cn Aoit 1d 4n5 as 3noitce St
tneierusolcsif de oso
h

aφnews – November / December 2012 10
How to ensure continuity ofcare for your diabetic patients
You feel confident in your assessmentskills. You’ve fine tuned yourdocumentation system. Now it’s timeto apply these skills. How might thatlook in practice?
Example:
One of your Type 2 diabetic patientspresents to you at your communitypharmacy. He is out of Metforminrefills and can’t get in to see thedoctor for his annual check up at theend of the month.
Sound familiar?
The Standards of Practice for Pharmacistsand Pharmacy Technicians (Std. 11.3) state:
A pharmacist may prescribe a Schedule 1drug by adapting a prescription fromanother prescriber by:
a) altering the dosage, formulation orregimen;
b) substituting another drug that isexpected to have a similar therapeuticeffect; or
c) renewing a prescription to ensurecontinuity of care.
What are the fundamentals ofprescribing? (Std. 11.8)
A pharmacist must only engage inprescribing a drug or blood productwhere the pharmacist:
a) has or develops a professionalrelationship with the patient,
b) has adequate knowledge andunderstanding of the condition beingtreated and the drug being prescribed,
c) has adequate information about thepatient’s health status and the diseaseor condition being treated,
d) takes reasonable steps to besatisfied that the patient hasenough information to participatein the decision-making process andobtains the patient’s informedconsent to prescribe,
e) is satisfied that the patient is notinappropriately seeking drug therapyfrom the pharmacist in circumstanceswhere that therapy has been refusedby another prescriber, and
f) takes responsibility for the prescribing decision.
You know this patient and his healthhistory, have checked Netcare and his labvalues, have completed your assessmentand are knowledgeable about diabetes.Based on this, you decide to adapt hisMetformin prescription.
What must be documented?Std. 11.10 - A pharmacist who prescribesa drug or blood product must reduce theprescription to writing in a clear, conciseand easy to read format that includes allinformation required in a completeprescription as outlined in Standard 6.7.
Std. 11.11 - A pharmacist who prescribesa drug or blood product must documentin the patient’s record:
a) the prescribing decision, the rationalefor it and the information required inStandard 11.9;
b) a follow-up plan; and
c) a record of the notification of anyother health professional.
Put the pieces together
Adapt a prescription
((( Expanding your practice )))
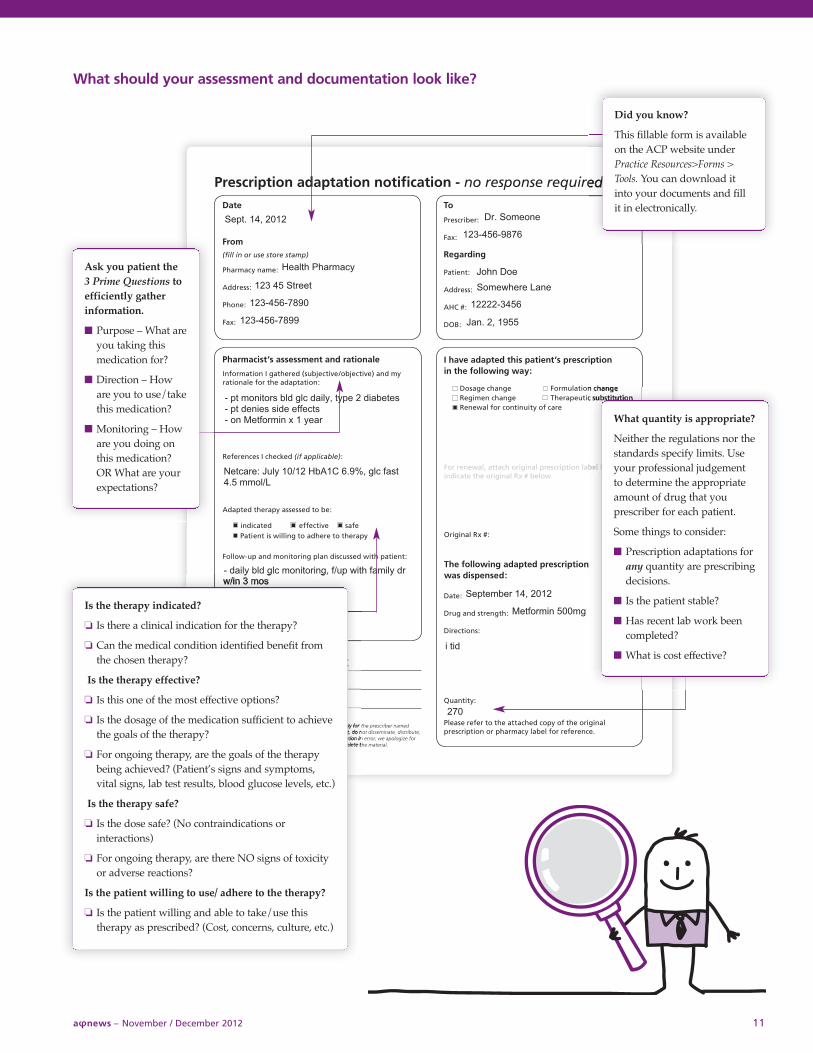
What should your assessment and documentation look like?
aφnews – November / December 2012 11
Did you know?
This fillable form is availableon the ACP website underPractice Resources>Forms >Tools. You can download itinto your documents and fillit in electronically.
Is the therapy indicated?
o Is there a clinical indication for the therapy?
o Can the medical condition identified benefit fromthe chosen therapy?
Is the therapy effective?
o Is this one of the most effective options?
o Is the dosage of the medication sufficient to achievethe goals of the therapy?
o For ongoing therapy, are the goals of the therapybeing achieved? (Patient’s signs and symptoms,vital signs, lab test results, blood glucose levels, etc.)
Is the therapy safe?
o Is the dose safe? (No contraindications orinteractions)
o For ongoing therapy, are there NO signs of toxicityor adverse reactions?
Is the patient willing to use/ adhere to the therapy?
o Is the patient willing and able to take/use thistherapy as prescribed? (Cost, concerns, culture, etc.)
Ask you patient the 3 Prime Questions toefficiently gatherinformation.
n Purpose – What areyou taking thismedication for?
n Direction – Howare you to use/takethis medication?
n Monitoring – Howare you doing onthis medication?OR What are yourexpectations?
What quantity is appropriate?
Neither the regulations nor thestandards specify limits. Useyour professional judgementto determine the appropriateamount of drug that youprescriber for each patient.
Some things to consider:
n Prescription adaptations forany quantity are prescribingdecisions.
n Is the patient stable?
n Has recent lab work beencompleted?
n What is cost effective?
aφnews – November / December 2012 12
Adapting pointers 1. All standards regarding prescribing
apply to both adapting and initialprescribing.
2. You must make all decisions in thebest interests of the patient.
3. Appropriately assess each patientwho may require you to prescribe adrug for them.
n Good decisions require goodinformation – use Netcare,therapeutic indicators (e.g., labinformation, blood pressure),
medication histories and any otherinformation available to supportyour decisions. Also consider thegoals of therapy and why anotherprescriber may have made thechoice they did.
4. You must take responsibility for thedecision. Sign your name on anyprescriptions you write.
5. Use ACP’s Code of Ethics andStandards as a foundation toensure that you and yourpharmacy team are best positionedto meet your patients’ needs.
6. Work with the patient’s team. Thestandards require that other healthprofessionals who are caring for apatient must be notified of pharmacistprescribing decisions as soon asreasonably possible.
Use Chat, Check and Chart to help youincorporate assessment anddocumentation within your practice. ThePrescription Adaptation Guide, postedunder Practice Resources > Forms > Tools,will walk you through the process.
((( Expanding your practice )))
Repeat
One of the hallmarks of a professional isa demonstrated commitment to lifelonglearning. The status quo is never goodenough. Pharmacists and pharmacytechnicians in Alberta have demonstratedtime and again that your success stemsdirectly from your ability to learn andadapt, and your drive to provide the bestcare for your patients. The expandedscope of practice now just broadens theareas in which your can apply yourknowledge and drive.
We hope these tips and tools help yousave time, enjoy results faster and serveyour patients better as you apply it inwhatever practice areas you decide topursue.
We’d love to hear your feedback,suggestions, and results. Please sendthem to [email protected].
aφnews – November / December 2012 13
Are pharmacypractitionersgetting the creditthey deserve?
Do you work with some unsung heroes? Here’s a chance to shine a light on them and their good work.
Recognizing pharmacy professionals through the APEX Awards helps identify role models, celebrate great patient care, and raise the profile of pharmacy in Alberta – and it feels good!
Consider nominating a colleague for one of the following awards.
With seven categories to choose from, the awards capture all facets of pharmacy practice.
1. M.J. Huston Pharmacist of Distinction honours apharmacist who has consistently demonstrated outstandingprofessional excellence in the practice of pharmacy over time.
2. Award of Excellence pays tribute to an Alberta pharmacistfor individual outstanding achievement in the field ofpharmacy. This award is granted for a single uniqueaccomplishment thus differing in this way from the Pharmacistof Distinction Award.
3. W.L. Boddy Pharmacy Team of the Year is presented to apharmacy staff team in Alberta who, by virtue of theirpractice, positively impact the health of their community.The Awards Committee will consider how the teamincorporates factors such as staffing, workflow, staff trainingand development, policies and procedures, technology andinnovative programs to offer excellent.
4. Future of Pharmacy is presented to up to three pharmacists per year who exude enthusiasm and passion for pharmacy, are visionary, and offer extraordinary promise to the profession.
5. Partners in Practice recognizes a collaborative effort betweena pharmacist and one or more other non-pharmacy healthprofessionals to optimize patient care and/or safety.
6. Friend of Pharmacy is presented to a non-pharmacist whohas contributed to the success of the profession of pharmacy.
7. Pfizer Consumer Healthcare Bowl of Hygeia celebrates apharmacist who has compiled an outstanding record ofcommunity service that, apart from his/her specificidentification as a pharmacist, reflects well on the profession.
View the awards’ terms of reference and nominate online ordownload the forms from the ACP website under About ACP >APEX Awards.
The APEX (Alberta Pharmacy Excellence) Awards are jointly sponsored by the Alberta Pharmacists’ Association (RxA)and the Alberta College of Pharmacists.
Nominations must be received at the ACP office by Dec. 14, 2012.
Those are the messages we received loudand clear as we conducted research intoinducements. We also recognize theexpectation inherent in the fact that 75%of registrants believe it is appropriate forthe Alberta College of Pharmacists topursue a prohibition. Therefore, we arecirculating a draft regulatory provisionand are inviting your feedback.
All feedback is due at the ACP office by4:30 p.m. on Mon., Dec. 3.
To comment on the draft standard, pleaseemail, mail, or fax your comments to:
Leslie AinslieExecutive Assistant to the RegistrarAlberta College of Pharmacists1100-8215 112 Street NWEdmonton, AB T6G [email protected] – 780-990-0328
Council will consider your feedbackwhen determining its next steps at itsmeeting on December 6, 2012.
ContextAt its September meeting, ACP councilreviewed the input received fromregistrants, stakeholders, and patientsand then considered a range of optionsfor dealing with inducements. Councildecided to take a two-pronged approach:circulate a draft regulatory provision toregistrants for discussion and work withthe government to ascertain their interestin this issue.
The draft regulatory provision isinformed by policies, standards andlegislation in other jurisdictions. Councilexamined documents from otherpharmacy regulatory bodies, as well asthose of other health professions. Thedraft you see today represents the bestand most relevant of those policies. Itwould be mandatory and would apply toall registrants and pharmacies.
aφnews – November / December 2012 14
Inducements: Draft regulatoryprovision for discussion
Notes fromCouncil
�
�In memory...� Inge Kinna passed away onOct. 16, 2012 at the age of 64 years.Inge received her BScPharm fromthe U of A in 1970. She went on tobe a very dedicated communitypharmacist, spending the last 14years of her career with Zellersin Edmonton.
� Mary Logue passed away on Oct. 4, 2012 in Calgary at theage of 57. Mary was born in St. Paul, AB and graduatedpharmacy at the U of A in 1977.Mary’s career was dividedbetween both hospital andcommunity pharmacy in Calgary.
� Arthur Pedlar passed awayon Sept. 13, 2012 at the age of 86 years. Art was raised inLougheed, AB, and studiedpharmacy at the University ofAlberta, graduating in 1950. Art worked for Crook’s Drugs inCalgary before opening Pedlar'sPharmacy. After closing hisbusiness upon his “retirement”, he worked for Pinder’s Drugs.
n Pharmacists want to provide good care to their patients.
n Pharmacists are health professionals and their relationships with patientsshould be based on the quality of advice and service.
n Providing inducements in return for professional pharmacy services does notpromote professional relationships or good patient care.
DisciplinaryreportsummaryAn investigation and hearing into theprofessional conduct of a pharmacist hasrecently concluded. Following is asummary of the hearing tribunal report.You can view the full report on ACP’swebsite under Complaints Resolution/Investigating & hearing tribunal reports.
A hearing tribunal made a finding ofunprofessional conduct against SaeedSattari when the following allegationswere proven to be true. Mr. Sattari:
1. Breached his professional declarationof May 28, 2010 that he wouldmaintain valid professional liabilityinsurance while on the clinicalregister when in fact he did notobtain the required professionalliability insurance;
2. Was on the clinical register fromJuly 1, 2010 to on or about May 9,2011 without valid professionalliability insurance;
3. Practised as a pharmacist withoutvalid professional liability insuranceduring the period of July 1, 2010 toOctober 12, 2010;
4. Breached his regulatory obligation tothe Alberta College of Pharmacists byfailing to maintain the requiredprofessional liability insurance; and
5. Breached his ethical obligation to hispatients and the public by failing tomaintain the required professionalliability insurance.
The hearing tribunal made thefollowing orders.
1. A reprimand. [The decision servedas the written reprimand.]
2. A fine of $1,000.
3. The payment of all costs of theinvestigation and hearing[$11,908.01].
aφnews – November / December 2012 15
Prohibition on the provision of inducements1. In this regulatory provision
a. “licensee” means a clinical pharmacist who holds a license issued under thePharmacy and Drug Act;
b. “regulated member” means
i) a clinical pharmacist,
ii) a courtesy pharmacist,
iii) a provisional pharmacist,
iv) student pharmacist,
v) a pharmacy technician,
vi) a courtesy pharmacy technician, and
vii) a provisional pharmacy technician;
c. “professional products” means
i) Schedule 1 and Schedule 2 drugs as defined in the Pharmacy and DrugAct, and
ii) blood products,
d. “professional services” means
i) the practice of pharmacists as described in section 3(1) of Schedule 19to the Health Professions Act, and
ii) the practice of pharmacy technicians as described in section 3(2) ofSchedule 19 to the Health Professions Act; and
e. “proprietor” has the same meaning as in the Pharmacy and Drug Act.
2. No regulated member, licensee or proprietor shall provide or distribute or be aparty to the provision or distribution of any inducement to a patient orpatient’s agent for obtaining a professional product from a licensed pharmacyor a professional service from a regulated member, including cash, gifts,points, loyalty points, coupons, discounts, goods, rewards and similar schemeswhich can be redeemed for a gift or other benefit.
3. Section 2 does not prohibit regulated members, licensees or proprietors from:
a. providing free or discounted parking to patients who are receivingprofessional products or professional services from a licensed pharmacy;
b. providing free professional services or professional products oncompassionate grounds;
c. providing free or discounted delivery services in respect of professionalproducts or professional services;
d. establishing the price for a professional product or professional service;
e. permitting patients or patients’ agents to pay for professional products orprofessional services by using major credit cards that are linked toinducements like points, loyalty points or rewards, except where, directlyor indirectly, the inducements are awarded specifically for the purchase ofprofessional products or professional services.
4. Guideline 13 of Article 15 of the Code of Ethics is repealed.
ComplaintsResolution
5. Guideline 13 to Article 1 of the Code of Ethics reads: 13. Do not provide rewards or incentives that have the potential to cause harm to a patient. It will be replaced by the proposed regulatory provision.
Canadian Publication Agreement Number: 40008642
Return undeliverable Canadian addresses to:Alberta College of Pharmacists1100, 8215 - 112 Street NW, Edmonton, AB T6G 2C8news
aφnews – November / December 2012 16
Technicians: Only twoEvaluatingExam sessionsleft beforedeadline
ACP emails and newsletters are official methods of notification to pharmacists andpharmacy technicians licensed by the college. In addition to providing you with timelyinformation that could affect your practice, college emails serve inadministrative hearings as proof of notification. Make sure you get theinformation you need to practice legally and safely by reading collegenewsletters and ensuring ACP emails are not blocked by your system.!
Effective Jan. 1, 2014, only individualswho have graduated from a CCAPP-accredited training program or whohave completed the PEBC EvaluatingExam (or the PTCB-AB or OCP exam)will qualify to be on the provisionalpharmacy technician register.
The PEBC only offers the EvaluatingExam two times per year; this meansthere are only two more opportunitiesto challenge the exam. The October2013 sitting of the exam will be thefinal opportunity to complete thisrequirement.
The PEBC Evaluating Exam is designedto determine if candidates have theknowledge and skills comparable to thatof a graduate of a CCAPP-accreditedprogram. Completion of bridgingprogram courses is not required to sitthis exam.
PEBC Evaluating Exam Schedule
Application deadline Exam date
January 2013 April 2013
July 2013 October 2013
Please see www.pebc.ca for additionalinformation about the exam and exactapplication deadlines.
HappyHolidaysBest wishes from ACP staff to you for a happy, healthy holiday season and New Year.Note: The ACP office will be closed between 1 p.m., Mon., Dec. 24 and 8 a.m., Wed., Jan. 2.