
Experimental study on the fatigue behaviour of welded tubular ...
Upload
independentCategory
view
1download
0
Received
publishe
R.S. has
nothing
disclose
M.S. ha
Supported
the fram
23616/2
M�ario S
Biomed
Reprint req
Laborat
Abel Sa
Salazar,
0015-028doi:10.10
Ultrastructure of tubular smooth endoplasmicreticulum aggregates in human metaphase II oocytesand clinical implications
Ros�alia S�a, M.Sc.,a Mariana Cunha, B.Sc.,c Joaquina Silva, M.D.,c Ana Lu�ıs, M.D.,a Cristiano Oliveira, M.D.,c
Jos�e Teixeira da Silva, M.D.,c Alberto Barros, M.D., Ph.D.,b,c and M�ario Sousa, M.D., Ph.D.a
a Department of Microscopy, Laboratory of Cell Biology, Unit for Multidisciplinary Investigations in Biomedicine, Abel Salazar
Institute of Biomedical Sciences, b Department of Genetics, Faculty of Medicine, University of Porto, and c Center for
Reproductive Genetics Alberto Barros, Porto, Portugal
Objective: To compare demographic, embryologic, pregnancy, and newborn outcomes after intracytoplasmicsperm injection (ICSI) cycles with or without mature oocytes (metaphase II [MII]) showing visible aggregatesof tubular smooth endoplasmic reticulum (aSERT) and to describe the ultrastructure of this dysmorphism.Design: Retrospective study.Setting: Private fertility center and university cell biology and genetics departments.Patient(s): There were 721 ICSI cycles, 520 carrying morphologically normal MII (control group) and 60 contain-ing aSERT-MII (study group).Intervention(s): None.Main Outcome Measure(s): Embryologic and clinical and live birth outcomes, including malformations andultrastructural characterization of aSERT-MII.Result(s): Compared with the control group there was a significant decrease in the fertilization, embryo cleavage,and blastocyst rates in the study group. The only child born after transfer of embryos derived from aSERT-MIIpresented a major cardiovascular malformation. Ultrastructurally, large aSERT were surrounded by abnormal-shaped mitochondria and clusters of small dense bodies formed by very small vesicles, and they had curvilineardense tubules in the interior. The same pathology was observed in small peripheral aSERT.Conclusion(s): The presence of large aSERT, showing attainment of the periphery, demonstrated that thecytoplasm is pathologic. The compromised embryo development and implantation was associated with decreasedclinical outcomes and newborn malformations. Therefore, oocytes with large aSERT should not be used for embryotransfer. (Fertil Steril� 2011;96:143–9. �2011 by American Society for Reproductive Medicine.)
Key Words: Large tubular smooth endoplasmic reticulum aggregates, human oocyte, ultrastructure, oocytedysmorphism, ICSI, pregnancy rates, newborn outcomes
A large proportion of human oocytes recovered from exogenousgonadotropin-stimulated cycles display dysmorphic phenotypesthat can be extracytoplasmatic and/or intracytoplasmatic (1, 2).
In most of the cases reported in the literature, authors studieddifferent dysmorphisms simultaneously, pooling data for pregnancyand implantation rates. In general, the results indicate that onlysevere dysmorphisms of both types of dysmorphic phenotypes (i.e.,extracytoplasmatic and intracytoplasmatic) affect clinical outcomes.
Studies on single dysmorphisms included extracytoplasmicabnormalities such as the first polar body (PB1) (3, 4), and the zona
October 22, 2010; revised and accepted April 25, 2011;
d online May 31, 2011.
nothing to disclose. M.C. has nothing to disclose. J.S. has
to disclose. A.L. has nothing to disclose. C.O. has nothing to
. J.T.d.S. has nothing to disclose. A.B. has nothing to disclose.
s nothing to disclose.
in part by the Foundation for Science and Technology (FCT), in
ework of a Ph.D. scholarship granted to Ros�alia S�a (SFRH/BD/
005) and research scholarships granted to Ros�alia S�a and
ousa through the Unit for Multidisciplinary Investigation in
icine (UMIB).
uests: M�ario Sousa, M.D., Ph.D., Department of Microscopy,
ory of Cell Biology (Director), Institute of Biomedical Sciences
lazar (ICBAS), UMIB, University of Porto, Largo Prof. Abel
2, 4099-003 Porto, Portugal (E-mail: [email protected]).
2/$36.0016/j.fertnstert.2011.04.088 Copyright ª2011 American S
pelucida (5), as well as several cytoplasmic dysmorphisms, such ascentral granulation (6), smooth vacuoles (7, 8), vacuoles (9), refractilebodies (10, 11), increased cytoplasmic viscosity (12), and oval oocytes(5, 13). The abnormal expression of genes was associated withfragmented PB1, central granular area, and abnormal-shaped oocytes(14). Thus, dysmorphisms are important predictors of pregnancy andtake-home baby rates in intracytoplasmic sperm injection (ICSI)treatment programs.
The present work aimed to compare demographic, embryologic,pregnancy, and newborn outcomes after ICSI cycles, with or withoutmature oocytes showing visible aggregates of tubular smooth endo-plasmic reticulum (aSERT). In addition, the study aimed to describethe ultrastructure of this dysmorphism (i.e., smooth vacuoles) com-pared with normal oocytes from the same cohort. The results showedthat dysmorphism is associated with an abnormal cytoplasm anda significant decrease in fertilization and embryo development.
MATERIALS AND METHODSEach patient’s material was used with her informed consent. Women under-
went controlled ovarian hyperstimulation with a GnRH antagonist protocol
(Cetrorelix, Merck-Serono; Ganirelix; Organon) and recombinant FSH
(Puregon, Organon; Gonal-F, Merck-Serono). The agonist protocol (Busere-
line, Sanofi-Aventis) and hMG (Menopur, Ferring) were used in the remain-
ing cases. For ovulation induction, hCG (Pregnyl, Organon) was
Fertility and Sterility� Vol. 96, No. 1, July 2011 143ociety for Reproductive Medicine, Published by Elsevier Inc.

administered 35 hours before oocyte retrieval (15). Estradiol serum levels
were assayed at the day of hCG or 1 day before (Elecsys-2010, Roche;
Supplemental Materials and Methods, available online at www.fertstert.org).
Two different media (Medicult-Origio, Jyllinge; Vitrolife, Kungsbacka)
were interchanged every 2 months for gamete and embryo handling. Semen
preparation, gamete handling, ICSI, embryo culture, embryo grading, em-
bryo transfer, luteal supplementation, implantation, and clinical pregnancy
were performed as previously described (15–18).
Electron MicroscopyTwo oocytes showing a visible (large) aSERTwere collected after failed ICSI
(14–18 hours). Four excedentary MII oocytes were additionally processed:
one with a large aSERT, another morphologically normal oocyte, and a third
with a large aSERT from the same patient (cohort); the fourth was a normal
oocyte from a cycle without dysmorphic oocytes. Oocytes were measured
with the use of Cronus-3 (Research-Instruments) on an inverted microscope.
Oocytes were processed according to previously published protocols
(10, 19). Ultrathin sections were observed in a Jeol 100CXII transmission
electron microscope operated at 60 kV.
Statistical AnalysesData were analyzed with the use of SPSS-18 (PASW Statistics 18) software.
Means were compared by independent-sample t test for equality of means.
Other variables were analyzed by descriptive statistics and Pearson chi-
square test with continuity correction. All tests were performed with the
use of two-tailed significance (P<.05).
RESULTSDuring 2008, there were 761 ICSI treatment cycles, with 40 can-celed, resulting in 721 cycles with retrieval of 5,527 (7.7/cycle)cumulus-oocyte complexes (COCs). Out of these, 4,352 were MII.We studied 60 ICSI cycles with at least one oocyte with a large ag-gregate of tubular smooth endoplasmic reticulum (aSERT-MII) anda control group formed by 520 cycles with at least one MII oocytewithout morphologic abnormalities and no aSERT-MII. Fifty-fiveout of the 60 cycles had embryo transfer, 40 originated only from
TABLE 1Embryologic outcomes.
Parameter Control cycles Cycles with aSERT
Cycles 520 60
COC 4,458 577
Total MII (mixed) 3,606
MII (pure) 1,868 499COC (per cycle) (8.6) 577 (9.6)
COC immaturity, % 19.1 13.5a
Total MII/COC 8.1 8.6
2PN (2PN/MII) 1,419 (76) 349 (69.9)a
Day 2 (d/2PN) 1,398 (98.5) 337 (96.6)a
Day 3 (d/2PN) 1,310 (92.3) 298 (85.4)a
Day 4 (d/2PN) 866 (61) 181 (51.9)a
Day 5 (d/2PN) 828 (58.4) 131 (37.5)a
Note: Embryo transfer cycles with aSERT-MII: normal: from only normal MII; mix
MII. Rates were significantly lower compared with embryo A/B grade, espec
regarding day 5 blastocysts. 2PN ¼ two pronuclei; 2PN/MII ¼ fertilization ra
cumulus-oocyte complexes; d/2PN ¼ cleavage rate; MII ¼ metaphase II.a Significant difference between study and control groups.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
144 S�a et al. aSERT clinical and ultrastructural features
normal MII, 11 from a mixed transfer (originated from one normalMII and one aSERT-MII), and 4 only from aSERT-MII.
In the control cycles, the mean (range) female and male ages were36.96 (22–49) and 38.96 (23–60) years, respectively. FSH was usedin 367 (70.6%) of the cases, hMG in 3 (0.6%), and FSH and hMG in150 (28.8%). Regarding the stimulation protocol, 463 (89%) usedthe antagonist and 57 (11%) the agonist protocol. In the 60 cycleswith aSERT-MII, the mean (range) female and male ages were34.5 (23–43) and 37.5 (27–54) years, respectively. FSH was usedin 33 (55%) of the cases, hMG in one (1.7%), and FSH and hMGin 26 (43.3%). Regarding the stimulation protocol, 52 (86.7%)used the antagonist and 8 (13.3%) the agonist protocol. In the studygroup, there were more cycles with rFSH þ hMG and more mixedfactors of infertility (77% vs. 47%). Cycles with transfer of embryosderived only from aSERT-MII showed significative differences re-garding higher doses of FSH needed, both initial and total, as wellas higher duration of stimulation (Supplemental Results;Supplemental Table 1; available online at www.fertstert.org).
Compared with embryologic outcomes for MII oocytes(Supplemental Table 2, available online at www.fertstert.org), outof the 60 cycles (499 MII) with a large aSERT, there were 405 nor-mal MII and 94 aSERT-MII. Comparisons among case subgroups(total, normal MII, and aSERT-MII) showed significantly lower fer-tilization (FR), embryo cleavage (ECR), and blastocyst formationrates with aSERT-MII.
Comparisons inside case subgroups showed similar FR, ECR, andblastocyst formation rates, with the exception of the FR withinaSERT-MII.
Compared with control oocytes (520 cycles, 1,868 MII), the FR(1,419/1,868: 76% control; 18.7% total study group, 16.4% normalMII, and 2.2% aSERT-MII), ECR (1,398/1,419: 98.5% control;23.7% total study group, 20.8% normal MII, and 3% aSERT-MII),and the blastocyst formation rates (828/1,419: 58.4% control; 9.2%total study group, 8% normalMII, and 1.3% aSERT-MII) were signif-icantly lower in the study group, especially within aSERT-MII.
Embryo transfer cycles with aSERT
Subgroup
TotalNormal-MII Mixed-MII aSERT-MII
40 11 4 55
434 101 24 559
371 91 24 486434 (10.9)a 101 (9.2) 24 (6) 559 (10.2)a
14.5a 9.9a 0a 13.1a
8.5 9.0 100 8.7
257 (69.3)a 70 (76.9) 17 (70.8) 344246 (95.7)a 69 (98.6) 17 (100) 332
219 (85.2)a 62 (88.6) 12 (70.6)a 293
132 (51.4)a 38 (54.3) 7 (41.2) 177
96 (37.4)a 26 (37.1)a 5 (29.4)a 127
ed: from one normal MII and one aSERT-MII; aSERT-MII: from only aSERT-
ially within cycles of mixed and aSERT-MII transfer, and only in these two
te; aSERT ¼ aggregates of tubular smooth endoplasmic reticulum; COC ¼
Vol. 96, No. 1, July 2011
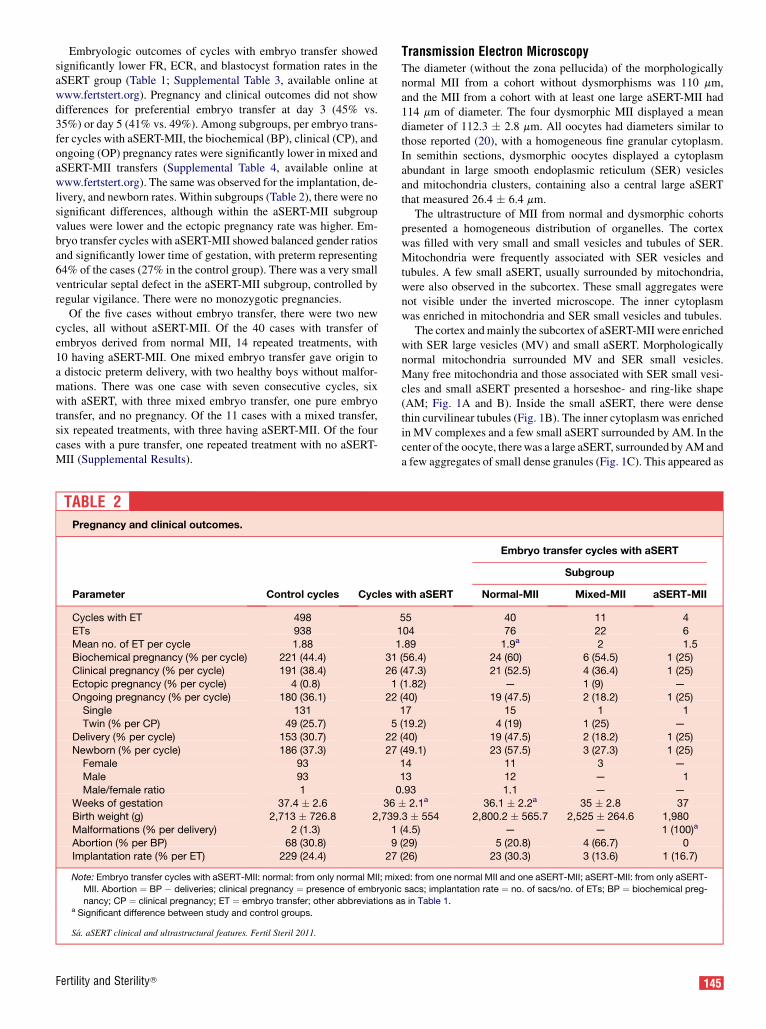
Embryologic outcomes of cycles with embryo transfer showedsignificantly lower FR, ECR, and blastocyst formation rates in theaSERT group (Table 1; Supplemental Table 3, available online atwww.fertstert.org). Pregnancy and clinical outcomes did not showdifferences for preferential embryo transfer at day 3 (45% vs.35%) or day 5 (41% vs. 49%). Among subgroups, per embryo trans-fer cycles with aSERT-MII, the biochemical (BP), clinical (CP), andongoing (OP) pregnancy rates were significantly lower in mixed andaSERT-MII transfers (Supplemental Table 4, available online atwww.fertstert.org). The samewas observed for the implantation, de-livery, and newborn rates. Within subgroups (Table 2), there were nosignificant differences, although within the aSERT-MII subgroupvalues were lower and the ectopic pregnancy rate was higher. Em-bryo transfer cycles with aSERT-MII showed balanced gender ratiosand significantly lower time of gestation, with preterm representing64% of the cases (27% in the control group). There was a very smallventricular septal defect in the aSERT-MII subgroup, controlled byregular vigilance. There were no monozygotic pregnancies.
Of the five cases without embryo transfer, there were two newcycles, all without aSERT-MII. Of the 40 cases with transfer ofembryos derived from normal MII, 14 repeated treatments, with10 having aSERT-MII. One mixed embryo transfer gave origin toa distocic preterm delivery, with two healthy boys without malfor-mations. There was one case with seven consecutive cycles, sixwith aSERT, with three mixed embryo transfer, one pure embryotransfer, and no pregnancy. Of the 11 cases with a mixed transfer,six repeated treatments, with three having aSERT-MII. Of the fourcases with a pure transfer, one repeated treatment with no aSERT-MII (Supplemental Results).
TABLE 2Pregnancy and clinical outcomes.
Parameter Control cycles Cycles w
Cycles with ET 498
ETs 938 1
Mean no. of ET per cycle 1.88 1Biochemical pregnancy (% per cycle) 221 (44.4) 31
Clinical pregnancy (% per cycle) 191 (38.4) 26
Ectopic pregnancy (% per cycle) 4 (0.8) 1
Ongoing pregnancy (% per cycle) 180 (36.1) 22Single 131
Twin (% per CP) 49 (25.7) 5
Delivery (% per cycle) 153 (30.7) 22
Newborn (% per cycle) 186 (37.3) 27Female 93
Male 93
Male/female ratio 1 0
Weeks of gestation 37.4 � 2.6 36Birth weight (g) 2,713 � 726.8 2,739
Malformations (% per delivery) 2 (1.3) 1
Abortion (% per BP) 68 (30.8) 9Implantation rate (% per ET) 229 (24.4) 27
Note: Embryo transfer cycles with aSERT-MII: normal: from only normal MII; mix
MII. Abortion ¼ BP � deliveries; clinical pregnancy ¼ presence of embryonic
nancy; CP ¼ clinical pregnancy; ET ¼ embryo transfer; other abbreviations aa Significant difference between study and control groups.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
Fertility and Sterility�
Transmission Electron MicroscopyThe diameter (without the zona pellucida) of the morphologicallynormal MII from a cohort without dysmorphisms was 110 mm,and the MII from a cohort with at least one large aSERT-MII had114 mm of diameter. The four dysmorphic MII displayed a meandiameter of 112.3 � 2.8 mm. All oocytes had diameters similar tothose reported (20), with a homogeneous fine granular cytoplasm.In semithin sections, dysmorphic oocytes displayed a cytoplasmabundant in large smooth endoplasmic reticulum (SER) vesiclesand mitochondria clusters, containing also a central large aSERTthat measured 26.4 � 6.4 mm.
The ultrastructure of MII from normal and dysmorphic cohortspresented a homogeneous distribution of organelles. The cortexwas filled with very small and small vesicles and tubules of SER.Mitochondria were frequently associated with SER vesicles andtubules. A few small aSERT, usually surrounded by mitochondria,were also observed in the subcortex. These small aggregates werenot visible under the inverted microscope. The inner cytoplasmwas enriched in mitochondria and SER small vesicles and tubules.
The cortex andmainly the subcortex of aSERT-MII were enrichedwith SER large vesicles (MV) and small aSERT. Morphologicallynormal mitochondria surrounded MV and SER small vesicles.Many free mitochondria and those associated with SER small vesi-cles and small aSERT presented a horseshoe- and ring-like shape(AM; Fig. 1A and B). Inside the small aSERT, there were densethin curvilinear tubules (Fig. 1B). The inner cytoplasmwas enrichedin MV complexes and a few small aSERT surrounded by AM. In thecenter of the oocyte, therewas a large aSERT, surrounded byAManda few aggregates of small dense granules (Fig. 1C). This appeared as
ith aSERT
Embryo transfer cycles with aSERT
Subgroup
Normal-MII Mixed-MII aSERT-MII
55 40 11 4
04 76 22 6
.89 1.9a 2 1.5(56.4) 24 (60) 6 (54.5) 1 (25)
(47.3) 21 (52.5) 4 (36.4) 1 (25)
(1.82) — 1 (9) —
(40) 19 (47.5) 2 (18.2) 1 (25)17 15 1 1
(19.2) 4 (19) 1 (25) —
(40) 19 (47.5) 2 (18.2) 1 (25)
(49.1) 23 (57.5) 3 (27.3) 1 (25)14 11 3 —
13 12 — 1
.93 1.1 — —
� 2.1a 36.1 � 2.2a 35 � 2.8 37.3 � 554 2,800.2 � 565.7 2,525 � 264.6 1,980
(4.5) — — 1 (100)a
(29) 5 (20.8) 4 (66.7) 0(26) 23 (30.3) 3 (13.6) 1 (16.7)
ed: from one normal MII and one aSERT-MII; aSERT-MII: from only aSERT-
sacs; implantation rate ¼ no. of sacs/no. of ETs; BP ¼ biochemical preg-
s in Table 1.
145
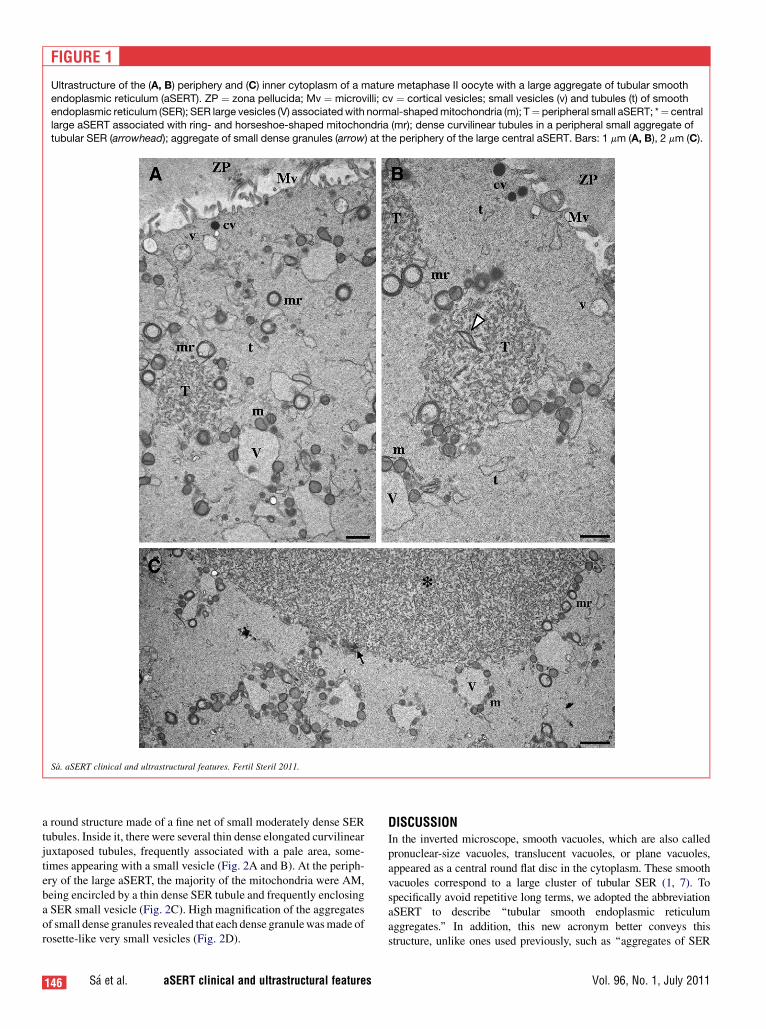
FIGURE 1
Ultrastructure of the (A, B) periphery and (C) inner cytoplasm of a mature metaphase II oocyte with a large aggregate of tubular smooth
endoplasmic reticulum (aSERT). ZP ¼ zona pellucida; Mv ¼ microvilli; cv ¼ cortical vesicles; small vesicles (v) and tubules (t) of smoothendoplasmic reticulum (SER); SER large vesicles (V) associatedwith normal-shapedmitochondria (m); T¼ peripheral small aSERT; *¼ central
large aSERT associated with ring- and horseshoe-shaped mitochondria (mr); dense curvilinear tubules in a peripheral small aggregate of
tubular SER (arrowhead); aggregate of small dense granules (arrow) at the periphery of the large central aSERT. Bars: 1 mm (A, B), 2 mm (C).
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
a round structure made of a fine net of small moderately dense SERtubules. Inside it, there were several thin dense elongated curvilinearjuxtaposed tubules, frequently associated with a pale area, some-times appearing with a small vesicle (Fig. 2A and B). At the periph-ery of the large aSERT, the majority of the mitochondria were AM,being encircled by a thin dense SER tubule and frequently enclosinga SER small vesicle (Fig. 2C). High magnification of the aggregatesof small dense granules revealed that each dense granulewasmade ofrosette-like very small vesicles (Fig. 2D).
146 S�a et al. aSERT clinical and ultrastructural features
DISCUSSIONIn the inverted microscope, smooth vacuoles, which are also calledpronuclear-size vacuoles, translucent vacuoles, or plane vacuoles,appeared as a central round flat disc in the cytoplasm. These smoothvacuoles correspond to a large cluster of tubular SER (1, 7). Tospecifically avoid repetitive long terms, we adopted the abbreviationaSERT to describe ‘‘tubular smooth endoplasmic reticulumaggregates.’’ In addition, this new acronym better conveys thisstructure, unlike ones used previously, such as ‘‘aggregates of SER
Vol. 96, No. 1, July 2011

FIGURE 2
Ultrastructure of the mature metaphase II oocyte with a centrally located large aSERT. (A) View of the whole aSERT (*). Aggregate of small
dense granules (arrow). (A, B) Dense curvilinear tubules (arrowheads) inside the large aSERT. (C, D) Periphery of the central large aSERT. (C)Ring- and horseshoe-shapedmitochondria encircling SER small vesicles and closely encircled by thin SER tubules. (D) The aggregate of small
dense granules are apparently formed by rosettes of very small vesicles (arrowhead). Bars: 3 mm (A), 0.5 mm (B, C), 0.15 mm (D). Abbreviationsas in Figure 2.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
tubuli’’ (1), ‘‘tubular-type smooth endoplasmic reticulum clusters,sERCs’’ (7), and SER cluster, SER aggregation (8).
In our observations, the large aSERTwas surrounded by a densepopulation of horseshoe- and ring-like mitochondria, and by smallaggregates of dense granules containing tiny vesicles. The interiorpresented dense fine curvilinear tubules. This pattern was alsoobserved in the peripheral small aSERT, the number of which wasincreased. In addition, there appeared to be an increase in numberof large and medium-sized SER vesicles, which were surroundedby normal mitochondria.
Fertility and Sterility�
It has been suggested that aSERTarise as a consequence of ovaryhyperstimulation, because these forms have never been observed ingerminal vesicle oocytes aspirated from antral follicles in nonstimu-lated ovaries (1). These dysmorphic oocytes presented a high aneu-ploidy rate (18%–37%) (2), but the organization of the meioticspindle is not affected by the large aSERT (21).
In gonadotropin-stimulated cycles, the incidence of large aSERTin oocytes that had not been inseminated was <1%, and in IVF un-fertilized MII oocytes it was 2.5% (1). In studies where the oocyteswere stimulated with the agonist protocol, the rates were 1.9% (22),
147

10% (7, 23), and 0.5% (24), and 2%–4% (25) when stimulated withantagonists. In the present study, the incidence was 1.7% per COCand 2.2% per uninseminated MII from cycles stimulated with theantagonist protocol.
Besides the present study of 60 cycles with at least one aSERT-MII, two other studies have been exclusively dedicated to aSERT.These studies were by Otsuki et al. (7) with 18 cycles, and Ebneret al. (8) with 30 cycles. Similarly to these authors, we found no sig-nificant difference regarding patient and stimulation characteristics.However, similarly to Ebner et al. (8), we showed higher initial andtotal FSH doses as well as duration of stimulation. Large aSERTmay be recurrent and appeared to be related with higher E2 (7)and antimullerian hormone (25) levels. Earlier authors found nodifference regarding FR, ECR, high quality embryo grade (7, 8),and the number of embryos transfered (7), although the blastocystformation rate was lower in large aSERT-positive cycles, with nodifference regarding blastocyst quality (8). Our data showed a signif-icant decrease in FR, ECR, and blastocyst formation rates. We alsofound no difference in embryo grade (inside subgroup) and in themean number of transfered embryos. Otsuki et al. (7) found a signif-icant decrease in the CP and implantation rates from cycles withlarge aSERT. In contrast, Ebner et al. (8) found no significant differ-ence regarding the BP, CP, implantation, and twin rates and newborngender ratios, but found a higher abortion rate. Our results demon-strated lower BP, CP, OP, delivery, newborn, and implantation rateswith the transfer of mixed or pure aSERT-MII, with no differencesregarding gender ratios. However, this difference was not observedwhen comparisons were madewithin subgroups. The transfer of em-bryos derived from oocytes presenting aSERT-MII resulted inBeckwith-Wiedmann syndrome (7), one diaphragmatic-hernia (8),two polymalformations (26), and a small ventricular septal defect(present results).
148 S�a et al. aSERT clinical and ultrastructural features
In normal oocytes, cortical and subcortical SER vesicles, smallaSERT, and associated normal-shaped mitochondria act as calciumstores. After fertilization, these organelles were displaced towardthe oocyte center, around pronuclei, with a decrease in large SERvesicles and the disappearance of small aSERT. This change waslinked to the intensity and localization of calciumwaves. At fertiliza-tion, strong calciumwaves started from the periphery, whereas at thezygote stage calcium waves started from the center and were weaker(27, 28). Therefore, it is possible that the anomalies found in the SERand mitochondria of oocytes with large aSERT may disturb calciumstores and calcium oscillations during fertilization, embryodevelopment, and implantation (29). It was also suggested that thisdysmorphism is related to cell deterioration (apoptosis) (7, 8).
In summary, from our study and other published data, large aSERT-MIIwere associatedwith lower embryologic, clinical, and newborn out-comes, as well as with imprinting disorders, major malformations, andfetal polymalformations. These alarming outcomes suggest that the ef-fect of this type of dysmorphism is lethal, and therefore the advice is tostrictly avoid the transfer of embryos derived from large aSERT-MII.
Acknowledgments: The authors acknowledge all those who contributed to this
work: Jorge Beires, M.D., Ph.D., gynecologist (Director, Department of Ob-
stetrics); Jos�e Manuel Teixeira da Silva, M.D., gynecologist (oocyte retrieval);
Jos�e Correia,M.D., anesthetist (Department of Anesthesiology), from the Hos-
pital de S. Jo~ao, Porto, Portugal); Luis Ferraz, M.D., urologist (andrology
patient evaluation), Director, Department of Urology, Centro Hospitalar de
Vila Nova de Gaia, Portugal; Paulo Viana, B.Sc., clinical embryologist–
ESHRE (execution, IVF Lab, data collection); Ana Goncalves, B.Sc.; Cl�audia
Os�orio, M.Sc.; Nuno Barros, B.Sc. (andrology lab); Elsa Oliveira, higher
technician (transmission electron microscopy assistance); Margarida Cardoso,
Ph.D., Assistant Professor; Cor�alia Vicente, Ph.D., Cathedratic Professor
(statistics), Instituto de Ciencias Biom�edicas Abel Salazar; and Milaydis
Sosa Napolskij, higher technician (English revision).
REFERENCES
1. van Blerkom J. Occurrence and developmental con-
sequences of aberrant cellular organization in meiot-
ically mature human oocytes after exogenous ovarian
hyperstimulation. J Elect Microsc Tech 1990;16:
324–46.
2. van Blerkom J, Henry G. Oocyte dysmorphism and
aneuplody in meiotically mature human oocytes after
ovarian stimulation. Hum Reprod 1992;7:379–90.
3. Sousa M, Tesarik J. Ultrastructural analysis of fertil-
ization failure after intracytoplasmic sperm injection.
Hum Reprod 1994;9:2374–80.
4. Ebner T, Moser M, Yaman C, Feichtinger O, Hartl J,
Tews G. Efective transfer of embryos selected on the
basis of first polar body morphology is associated
with increased rates of implantation and pregnancy.
Fertil Steril 1999;72:599–603.
5. Ebner T, Yaman C, Moser M, Sommergruber M,
Feichtinger O, Tews G. Prognostic value of first polar
body morphology on fertilization rate and embryo
quality in intracytoplasmic sperm injection. Hum Re-
prod 2000;15:427–30.
6. Esfandiari N, Ryan EAJ, Gotlieb L, Casper RF.
Successful pregnancy following transfer of em-
bryos from oocytes with abnormal zona pellucida
and cytoplasm morphology. Reprod BioMed On-
line 2005;11:620–3.
7. Kahraman S, Yakin K, Donmez E, Samh H, Bahce M,
Cengiz G, et al. Relationship between granular cyto-
plasm of oocytes and pregnancy outcome following
intracytoplasmic sperm injection. Hum Reprod
2000;15:2390–3.
8. Otsuki J, Okada A, Morimoto K, Nagai Y, Kubo H.
The relationship between pregnancy outcome and
smooth endoplasmic reticulum clusters in MII oo-
cytes. Hum Reprod 2004;19:1591–7.
9. Ebner T, Moser M, Shebl O, Sommerguber M,
Tews G. Prognosis of oocytes showing aggregation
of smooth endoplasmic reticulum. Reprod BioMed
Online 2008;16:113–8.
10. Ebner T, Moser M, Sommerguber M, Gaiswinkler U,
Shebl O, Jesacher K, et al. Occurrence and develop-
mental consequences of vacuoles throughout
preimplantation development. Fertil Steril 2005;83:
1635–40.
11. el ShafieM, SousaM,WindtM-L, Kruger TF, editors.
An atlas of the ultrastructure of human oocytes. A
guide for assisted reproduction. New York: Parthe-
non; 2000.
12. Otsuki J, Nagai Y, Chiba K. Lipofuscin bodies in hu-
man oocytes as an indicator of oocyte quality. JAssist
Reprod Genet 2007;24:263–70.
13. Ebner T, Moser M, Sommergruber M, Puchner M,
Wiesinger R, Tews G. Developmental competence
of oocytes showing increased cytoplasmic viscosity.
Hum Reprod 2003;18:1294–8.
14. Ebner T, Shebl O, Moser M, Sommergruber M,
Tews G. Developmental fate of ovoid oocytes. Hum
Reprod 2008;23:62–6.
15. Wells D, Berm�udez MG, Steuerwald N, Malter HE,
Thornhill AR, Cohen J. Association of abnormal mor-
phology and altered gene expression in human preim-
plantation embryos. Fertil Steril 2005;84:343–55.
16. Pinto F, Oliveira C, Cardoso MF, Teixeira da
Silva JM, Silva J, Sousa M, et al. Impact of
GnRH stimulation protocols on intracytoplasmic
sperm injection outcomes. Reprod Biol Endocrinol
2009;7:5.
17. SousaM, Cremades N, Silva J, Oliveira C, Teixeira da
Silva J, Viana P, et al. Predictive value of testicular
histology in secretory azoospermic subgroups and
clinical outcome after microinjection of fresh and
frozen-thawed sperm and spermatids. Hum Reprod
2002;17:1800–10.
18. Vandervorst M, Liebaers I, Sermon K, Staessen C, de
Vos A, van de Velde H, et al. Successful preimplanta-
tion genetic diagnosis is related to the number of
available cumulus-oocyte complexes. Hum Reprod
1998;13:3169–76.
19. Gardner DK, Phil D, Lane M, Stevens J, Schlenker T,
Schoolcraft WB. Blastocyst score affects implanta-
tion and pregnancy outcome: toward a single blasto-
cyst transfer. Fertil Steril 2000;73:1155–8.
20. Veeck LL, editor. An atlas of human gametes and
conceptuses. An illustrated reference for assisted re-
productive technology. New York: Parthenon; 1999.
21. Chamayou S, Ragolia C, Alecci C, Storaci G,
Maglia E, Russo E, et al. Meiotic spindle presence
and oocyte morphology do not predict clinical ICSI
outcomes: a study of 967 transferred embryos.
Reprod BioMed Online 2006;13:661–7.
22. Alikani M, Palermo G, Adler A, Bertoli M, Blake M,
Cohen J. Intracytoplasmic sperm injection in dysmor-
phic human oocytes. Zygote 1995;3:283–8.
Vol. 96, No. 1, July 2011

23. Meriano JS, Alexis J, Visram-Zaver S, Cruz M,
Casper RF. Tracking of oocyte dysmorphisms for
ICSI patients may prove relevant to the outcome in
subsequent patient cycles. Hum Reprod 2001;16:
2118–23.
24. Rienzi L, Ubaldi FM, Iacobelli M, Minasi MG,
Romano S, Ferrero S, et al. Significance of metaphase
II human oocyte morphology on ICSI outcome. Fertil
Steril 2008;90:1682–700.
25. Ebner T, Sommerguber M, Moser M, Shebl O,
Schreier-Lechner E, Tews G. Basal level of
Fertility and Sterility�
anti-mullerian hormone is associated with oocyte
quality in stimulated cycles. Hum Reprod 2006;
21:2022–6.
26. Akarsu C, Caglar G, Vicdan K, Sozen E,
Biberoglu K. Smooth endoplasmic reticulum
aggregations in all retrieved oocytes causing recur-
rent multiple anomalies: case report. Fertil Steril
2009;92:1496e1–3.
27. Sousa M, Barros A, Tesarik J. Developmental
changes in calcium dynamics, protein kinase C distri-
bution and endoplasmic reticulum organization in
human preimplantation embryos. Mol Hum Reprod
1996;2:967–77.
28. Sousa M, Barros A, Silva J, Tesarik J. Developmental
changes in calcium content of ultrastructurally
distinct sucellular compartments of preimplantation
human embryos. Mol Hum Reprod 1997;3:83–90.
29. Sousa M, Barros A, Mendoza C, Tesarik J. Effects of
protein kinase activation and inhibition on sperm-, thi-
merosal-, and ryanodine-induced calcium response of
human oocytes. Mol Hum Reprod 1996;2:699–708.
149

SUPPLEMENTAL MATERIALS AND METHODS
PatientsUnder informed consent, during 2008 a total of 761 intracytoplasmic sperm
injection (ICSI) cycles for infertility treatment were analyzed. There were 60
cycles with at least one oocyte with a smooth endoplasmic reticulum large
tubular aggregate (aSERT). A control group formed by 520 cycles (68.3%)
with at least one oocyte without morphologic abnormalities was included.
Stimulation ProtocolAll women underwent controlled ovarian hyperstimulation with a GnRH
short antagonist multiple-dose flexible protocol in the large majority of the
cases and the long agonist protocol (buserelin; Suprefact; Sanofi Aventis)
in the other cases (1). For stimulation, subcutaneous recombinant FSH was
used, with or without previous oral contraceptive pretreatment (Puregon, Or-
ganon; Gonal-F, Merck Serono). In some cases hMG (Menopur; Ferring) was
added to rFSH, and in a very few cases only hMGwas used. The initial rFSH
dose was chosen according to the subject’s characteristics. The GnRH antag-
onist cetrolelix (Cetrotide; Merck Serono) or ganirelix (Orgalutran; Orga-
non), 0.25 mg/d subcutaneously, was added daily, starting when the leading
follicle reached a diameter of 12 mm and until either the leading follicle
reached amean diameter of 18mmor two ormore follicles reached a diameter
of 17 mm. Urinary hCG (5,000–10,000 IU intramuscular/subcutaneous; Pre-
gnyl;Organon)was administered 35 hours before recovery. In a small number
of cases, rhCG (Ovitrelle; Merck Serono) was used, and an agonist was used
instead of hCG in cases of ovarian hyperstimulation risk. Estradiol serum
levels were assayed at the day of hCG or 1 day before (pg/mL; 1 � 10�12
g/mL; Elecsys 2010, Roche; Vidas Estradiol II, Biomerieux).
Oocyte RetrievalFor oocyte collection, handling, microinjection, embryo culture, and transfer,
two different media (Medicult and Vitrolife) were used, and they were inter-
changed every 2 months.
Cells, plates, and media manipulations were performed in a grade II hor-
izontal laminar flow cabinet (Labcaire Systems HLF 18, Labcaire Systems;
MDH, Braun), without light and over a thermostatic plate (Minitub; Tiefen-
bach) at 37�C with the use of sterile micropipette tips. Except for sperm
handling (33�C, 5% CO2, in filtered humidified air atmosphere, using
commercial purified water), all incubations were performed at 37�C, 6%CO2, 5% O2, and 89% N2 in a 0.2-mm filtered atmosphere humidified with
purified water). There were three large Sanyo incubators for ICSI and day
0 culture, another for days 2–3, and another for prolonged culture. There
was a small Galaxy-A incubator for transitory storage, one large Sanyowhich
was disrupted of CO2 for medium (3-(N-morpholino)propanesulfonic) that
did not require it, and another large CO2 Sanyo incubator at 33�C for testic-
ular specimens. Air in the IVF room was purified by a Coda-Tower system,
using HEPA, activated carbon, and 0.2-mm filters. Also in the IVF Lab, there
were two nonrefrigerated centrifuges (Sigma).
The patient was sedated with intravenous administration of 1% propofol
(Fresenius). Oocyte retrieval of large ovarian follicles was performed by
ultrasonically guided transvaginal follicular aspiration, using a syringe of
10 mL (BD Plastipack) containing 1–2 mL prewarmed Synvitro Flush
Medium (with heparin; Medicult Origio) or G-MOPS-Plus (Vitrolife). Aspi-
ration was performed in an Aloka apparatus (JP-1233) and probe (Vaginal
probe for follicle aspirations) with the use of a Swemed needle (Follicle as-
piration set, gauge, single lumen, Luer with tubing, 1.6 � 350 mm, tubing
600 mm, usually 16 gauge and occasionally 17 gauge).
The syringe fluid containing the cumulus-oocyte complexes were ex-
pelled into large Petri plates (10 cm cell culture plastic dishes, embryo tested;
Falcon 100� 20) and isolated under a binocular stereomicroscope (SMZ-2B;
Nikon) with the use of sterile glass pipettes (Gilson; Blaubrand Intramark);
they were then washed in G-MOPS-Plus or Sperm Preparation Medium
(SPM; Medicult), and allocated in the central well of a tissue culture plate
(Falcon; Becton Dickinson) in G-IVF-Plus (Vitrolife) or IVF (Medicult) me-
dium for maturation culture (1–4 hours) inside a Sanyo incubator.
149.e1 S�a et al. aSERT clinical and ultrastructural features
Semen PreparationAfter complete liquefaction inside an incubator (37�C, 30 minutes), the
ejaculates were submitted to a two-gradient (90%, 45%) separation using
PureSperm 100 (Nidacon; 1 mL semen, 2 mL 55%, 2 mL 80%) and centri-
fuged at 500 g (1,500 rpm) for 20–30 minutes at room temperature with
the use of 15 mL sterile plastic conic graduated tubes (Nunc), to collect at
the bottom of the tubes the sperm fraction showing a higher concentration
of motile spermatozoa with normal morphology. The pellet was then washed
twice in 1–3 mL SPM (HEPES buffer prewarmed in an incubator with 5%
CO2) or G-MOPS (Vitrolife; prewarmed in an incubator without CO2) by
centrifugation at 500 g (1,500 rpm) for 5–10 minutes. Over the pellet, 500
mL (0.1–1 mL) swim-up medium (Universal IVF Medium, Medicult;
G-IVF-Plus) was cautiously added to collect the swim-up fraction. The
tube (10–15 mL, sterile) was incubated for 1–2 hours to allow spermatozoa
migration. This was to collect motile normal sperm that actively migrated
from the pellet to the upper aqueous phase. The gradient step was not per-
formed in cases with very low sperm concentration (<1 � 106/mL), which
were only washed and submitted to the swim-up technique. In the andrology
laboratoty, for normal sperm, the centrifuge used was a Hehich Universal II
(MCS), the incubator was a Minigalaxy-A (Biotech), and the horizontal lam-
inar flow cabinet Labcaire Systems HLE Clean Air). For seropositive men,
the incubator was a Sanyo (5% CO2) and the vertical laminar flow cabinet
Nuaire Class II.
Oocyte DenudationOn sterile Petri dishes (60 mm; Falcon), cumulus-oocyte complexes were in-
cubated with recombinant hyaluronidase as denudation enzyme (80 UI; ICSI
Cumulase, Medicult; Hyase-10�, Vitrolife) for 30 seconds, to disaggregate
cumulus cells, washed in 5 drops of SPM, and then mechanically dissociated
in SPM or G-MOPS-Plus with an oocyte denudation micropipette
(0.130–0.190 mm, 0.134–0.145 mm; Swemed) to remove all granulosa cells
at the stereomicroscope with a thermostatic plate (37�C). Denudation was
performed under paraffin oil (light mineral oil; Liquid Paraffin, Medicult;
Ovoil-100, Vitrolife). Denuded oocytes were then incubated in 4-well plastic
tissue culture dishes (embryo tested; Nunc) in IVF medium (Universal IVF
Medium, G-IVF-Plus) for 1–2 hours until microinjection for recovery
(4 cumulus-oocyte complexes/500 mL/well).
ICSIMicroinjection was performed as previously described (2) with the use of
a sterile cell culture plastic Petri dish (60 mm; Falcon), under paraffin oil,
in SPM or G-MOPS-Plus. One spread drop of 10% polyvinylpyrrolidone
(PVP)–SPM, where 1–10 mL of the swim-up fraction was added (generally
at the top of the drop, to allow sperm migration), one spread drop of PVP
to immobilize the sperm, and 10 mL drops of SPMwithout albumin (Synvitro
ICSI Holding Medium; Medicult), corresponding to the total number of oo-
cytes to inject (four). From the drop of PVP-SPM, each spermatozoon (gen-
erally at the border) was selected based on sperm normal morphology and
rapid progressive motility with rotating head. This was transfered to the
PVP drop and washed in another site to avoid medium contamination, and
the tail was squeezed at the distal tip to immobilize the cell, avoiding themid-
piece where mitochondria are present. The spermatozoon was then aspirated,
tail first, and microinjected using the strong dislocation of the cytoplasm
(3, 4). To immobilize the spermatozoon, we used PVP (Clinical Grade,
Medicult; ICSI Immobilization Medium, Vitrolife). To hold the oocyte,
a holding micropipette (0.009–0.017 mm; Swemed) was used, and to
select and microinject the spermatozoon a microinjection micropipette
(ICSI Micropipette, 0.005 mm; Swemed) was used. Only mature oocytes
(metaphase II [MII], first polar body) were microinjected. Microinjection
was performed in an inverted microscope (Nikon Diaphot 200) with
Hoffman optics (Nikon) on a thermal stage (37�C), and with Narishige
micromanipulators (MO-188).
Embryo CultureAfter microinjection, oocytes were washed with SPM or G-MOPS-Plus, and
cultured in 4-well plates (Nunc) with 500 mL culture medium or in multi–
Vol. 96, No. 1, July 2011

small well EGPS plates (Nunc) with 50 mL medium under oil. Embryos were
cultured in sequential media. For Medicult, after microinjection (day 0) em-
bryos were cultured in ISM1/BlastAssist System Medium 1 up to the third
day, and then in ISM2/BlastAssist System Medium 2 up to day 5. For trans-
fer, they were placed in 0.5–1 mL UTM (containing human serum albumin
[HSA] and hyaluronan) for 30 minutes to 1 hour. For Vitrolife (Series G3/
G5), after microinjection embryos were cultured in G-1 Plus medium during
day 1 (pronucleus visualization), day 2 (E2–5 cells), and up to the end of day-
3 (E6–14). From the end of day 3 and up to day 5 (blastocyst), embryos were
transferred to G-2 Plusmedium. For embryo transfer, embryos were placed in
a central well of a tissue culture plate (Falcon) with EmbryoGlue (containing
HSA and hyaluronan). In these three media, hyaluronan concentrations were
progressively increased.
Normal fertilization was assessed 14–18 hours after injection (two pronu-
clei, second polar body), and embryo quality was evaluated according to the
number, size, and regularity of the blastomeres and the percentage of frag-
ments; high-quality embryos were those with the correct number of cells,
of similar size and regularity, and with <25% fragments (A/B) (5, 6).
Blastocysts were scored according to Gardner et al. (7–9). High-quality blas-
tocysts were BL1 and BL2 with good morphology and BL3–BL5 if the inner
cell mass and trophectoderm were A/B.
Embryo Transfer and Pregnancy ConfirmationEmbryo transfer was performed under ultrasonography (JP-1233 Abdominal
Probe for Embryo Transfer; Aloka) with the use of a Sure View Wallace
Embryo Replacement Catheter (23 cm; CE123); for more difficult cases
a new stylet (more rigid sheath) was introduced (Wallace Malleable Stylet,
for use with the 23 cm catheter; Smiths Medical). The endometrial appear-
ance was evaluated (thickness 8–13 mm, ecogeneicity triple layer). All
patients had luteal supplementation with intravaginal administration of two
endovaginal tablets of 100 mg natural-micronized progesterone every 8
hours (600 mg/d; Utrogestan 100 mg; Jaba, Besins) beginning 3 days before
embryo transfer was scheduled. Implantation was confirmed by a rise in
serum b-hCG on days 11–14 after embryo transfer (2 consecutive days 2
weeks after embryo transfer). A clinical pregnancy was established by
ultrasonography at 5–7 weeks of gestation. Progesterone was maintained
until b-hCG serum assay. If positive, it was continued.
Transmission Electron MicroscopyTwo oocytes showing aSERTs were collected after failed ICSI, without
showing no signs of fertilization as assessed 14–18 hours after injection
(no pronucleus, first polar body). Four excedentary MII oocytes were addi-
tionally used, one showing an aSERT, one normal from a cycle without ab-
normal oocytes, and one morphologically normal and one with an aSERT
from the same patient. In all cases, oocytes were collected after controlled
ovarian hyperstimulation during ICSI treatment cycles with the patient’s in-
formed consent. Oocytes were selected after denudation and classified in an
inverted microscope with Hoffman optics on a thermal stage (37�C). Oocytemeasures were obtained with the use of a Cronus-3 (Research Instruments).
Oocytes with smooth endoplasmic reticulum tubular aggregates were
fixed with Karnovsky (2.5% glutaraldehyde in 4% paraformaldehyde in
0.15 mol/L cacodylate buffer, pH 7.3) for 4 hours at room temperature,
washed in buffer (overnight, 4�C), postfixed in 2%OsO4 in buffer, containing
0.032 g FeCnK (19 mmol/L potassium ferrum cyanide) for 2 hours at 4�C,washed in buffer (10 minutes), serially dehydrated in ethanol, equilibrated
with propylene oxide, and embedded in Epon. Semithin sections were ob-
tained in an ultramicrotome (Reichert-Jung Ultracut S; Leica Microsystems)
with a diamond knife (Diatome) at 1 mm and stained (1% methylene blue in
1% borax aqueous solutionþ 1%Azur II in aqueous solution, 1:1) to localize
the aSERT (Fig. 2). Semithin sections were photographed in an optical mi-
croscope (Leitz DM-RBE) with a digital camera (Leica DFC-480-R2), and
then ultrathin sections were obtained at 500–700 �A. Sections were collected
Fertility and Sterility�
in 200-mesh copper grids (TAAB). They were then contrasted with 3% aque-
ous uranyl acetate (20 minutes) and Reynolds lead citrate (10 minutes).
Ultrathin sections were observed and photographed in a Jeol 100CXII trans-
mission electron microscope operated at 60 kV (10).
Unless otherwise noted, all chemicals were obtained from Sigma-Aldrich
and Merck.
Statistical AnalysesData were analyzed with the use of SPSS-18 (PASW Statistics 18) software.
Means were compared by the independent-sample t test for equality of
means. Two variables had to be tested using one-sample t test to compare
with reference value. The other variables were analyzed by descriptive statis-
tics and Pearson chi-square test with continuity correction. One variable had
to be tested by the Fisher exact test. All tests were performed using two-tailed
significance (P<.05).
SUPPLEMENTAL RESULTS
Control group (n ¼ 520) ages (y) were as follows: %30 (28, 5.4%), 31–34
(114, 21.9%), 35–39 (239, 46%), R40 (139, 26.7%), <35 (142, 27.3%),
and R35 (378, 72.7%).
Case group (n¼ 60) ages (y) were as follows:%30 (8, 13.3%), 31–34 (25,
41.7%), 35–39 (20, 33.3%),R40 (7, 11.7%), <35 (33, 55%), andR35 (27,
45%).
Regarding updated data from the 60 cycles with at least one MII oocyte
containing a large aSERT (aSERT-MII), we observed that out of the five
cases without embryo transfer (ET), one had a previous cycle canceled due
to poor ovarian response and for a new cycle without an aSERT-MII there
was no pregnancy; one had a healthy baby after oocyte donation; one had
a new cycle without an aSERT-MII canceled due to poor endometrium and
then a thaw cycle with no pregnancy; one had a previous cycle canceled
due to poor ovarian response; and one had a thaw cycle from the initial cycle
(present study) with transfer of normal MII and a healthy baby was born.
Out of the 40 cases with transfer of embryos derived from MII (normal
MII) without a large aSERT, 14 repeated treatments, 4 had no aSERT-MII,
and 10 had aSERT-MII again. Out of the latter, 15 cycles were performed,
11 with transfer of embryos derived from normal MII, 3 were mixed ET (1
normal MII þ 1 aSERT-MII), and 1 was a pure ET (only aSERT-MII). In
ten cases there was no pregnancy: 7 from normal MII ET (3 thaw), 2 mixed
ET (1 thaw), and 1 pure ET. From these 15 cycles, there was also one bio-
chemical pregnancy (normal MII ET), two healthy ongoing pregnancies
(normal MII ET), and two deliveries (normal MII thaw ET and mixed ET).
This cycle from a mixed ET gave origin to a distocic preterm (35 weeks) de-
livery, with two healthy boys (2,180 g, 46 cm; 2,160 g, 47 cm) without mal-
formations. In three cases there was recurrence for the presence of aSERT-
MII. Twelve patients had 19 previous treatment cycles, 18 without aSERT-
MII and 1 with aSERT-MII. In all cases there was no pregnancy. There
was one case with seven consecutive cycles, six with aSERT, two normal
ET, three mixed ET (one thaw), and one pure ET. No pregnancy ensued.
Out of the 11 cases with a mixed transfer (embryo originating from one
normal MII and one aSERT-MII), six repeated treatments, three with and
three without aSERT-MII. Out of the cases with aSERT-MII, there were
four ET cycles, all from normal MII oocytes, three with no pregnancy (one
thaw) and one biochemical pregnancy. Seven patients had previous treatment
cycles, with eight ET cycles, and out of these, three had aSERT-MII and none
resulted in a pregnancy. Recurrencewas observed only in the case of a couple
that did not repeat any cycle but had two previous unsuccessful cycles (nor-
mal MII ET, mixed ET) and one biochemical pregnancy (mixed ET).
Out of the four cases with a pure transfer (embryo originated only from
aSERT-MII), only one repeated treatment and had no aSERT-MII. Three
cases had previous treatments, undergoing five ET cycles from normal MII
oocytes. Neither pregnancy nor recurrence was observed.
149.e2

REFERENCES1. Pinto F, Oliveira C, Cardoso MF, Teixeira da
Silva JM, Silva J, Sousa M, et al. Impact of
GnRH stimulation protocols on intracytoplasmic
sperm injection outcomes. Reprod Biol Endocrinol
2009;7:5.
2. Sousa M, Cremades N, Silva J, Oliveira C, Teixeira
da Silva J, Viana P, et al. Predictive value of testicular
histology in secretory azoospermic subgroups and
clinical outcome after microinjection of fresh and fro-
zen-thawed sperm and spermatids. Hum Reprod
2002;17:1800–10.
3. Tesarik J, Sousa M, Testart J. Human oocyte activa-
tion after intracytoplasmic sperm injection. Hum Re-
prod 1994;9:511–8.
4. Tesarik J, Sousa M. Key elements of a highly efficient
intracytoplasmic sperm injection technique: Ca2+
fluxes and oocyte cytoplasmic dislocation. Fertil
Steril 1995;64:770–6.
5. Staessen C, Camus M, Bollen N, Devroey P, Van
Steirteghem AC. The relatioship between embryo
quality and the occurrence of multiple pregnancies.
Fertil Steril 1992;57:626–30.
6. Vandervorst M, Liebaers I, Sermon K, Staessen C, De
Vos A, Van de Velde H, et al. Successful preimplan-
tation genetic diagnosis is related to the number of
available cumulus-oocyte complexes. Hum Reprod
1998;13:3169–76.
7. Gardner DK, Schoolcraft WB. In-vitro culture of
human blastocysts. In: Jansen R, Mortimer D,
eds. Towards reproductive certainty: infertility
and genetics beyond. Canforth: Parthenon Press,
1999:378–88.
8. Gardner DK, Lane M. Embryo culture systems. In:
Trouson AL, Gardner DK, eds. Handbook of in vitro
fertilization, 2nd ed. Boca Raton, Florida: CRC Press,
2000:205–64.
9. Gardner DK, Phil D, Lane M, Stevens J, Schlenker T,
Schoolcraft WB. Blastocyst score affects implanta-
tion and pregnancy outcome: towards a single blasto-
cyst transfer. Fertil Steril 2000;73:1155–8.
10. Sousa M, Tesarik J. Ultrastructural analysis of fertil-
ization failure after intracytoplasmic sperm injection.
Hum Reprod 1994;9:2374–80.
149.e3 S�a et al. aSERT clinical and ultrastructural features Vol. 96, No. 1, July 2011
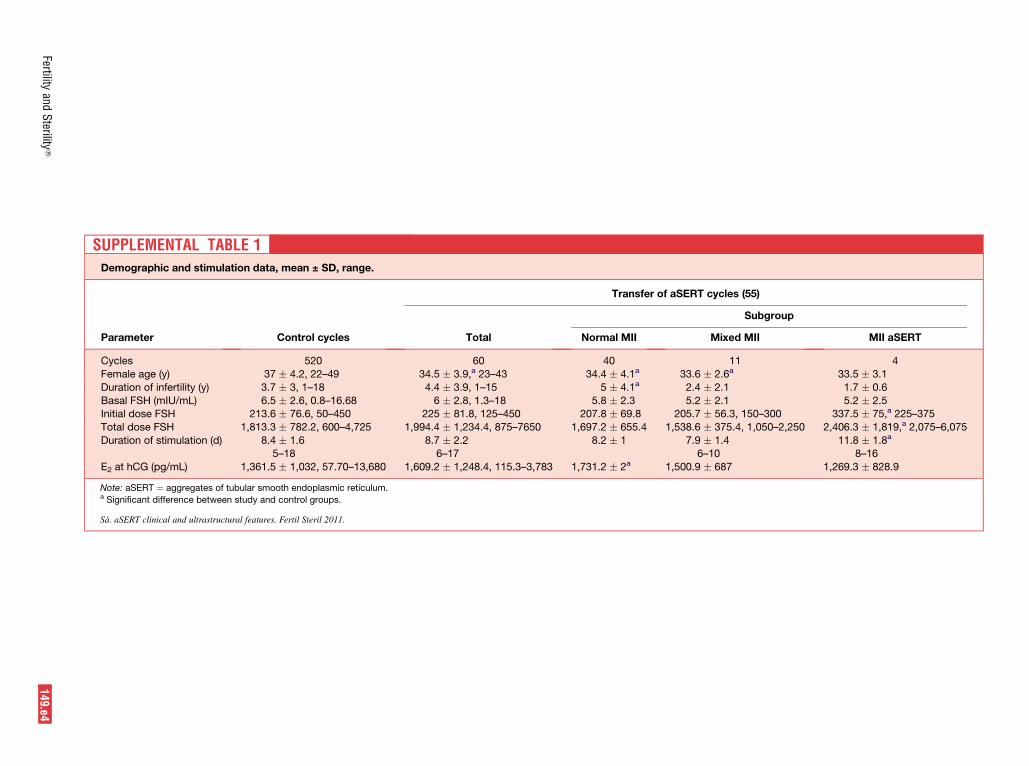
SUPPLEMENTAL TABLE 1Demographic and stimulation data, mean ± SD, range.
Parameter Control cycles
Transfer of aSERT cycles (55)
Total
Subgroup
Normal MII Mixed MII MII aSERT
Cycles 520 60 40 11 4
Female age (y) 37 � 4.2, 22–49 34.5 � 3.9,a 23–43 34.4 � 4.1a 33.6 � 2.6a 33.5 � 3.1
Duration of infertility (y) 3.7 � 3, 1–18 4.4 � 3.9, 1–15 5 � 4.1a 2.4 � 2.1 1.7 � 0.6
Basal FSH (mIU/mL) 6.5 � 2.6, 0.8–16.68 6 � 2.8, 1.3–18 5.8 � 2.3 5.2 � 2.1 5.2 � 2.5Initial dose FSH 213.6 � 76.6, 50–450 225 � 81.8, 125–450 207.8 � 69.8 205.7 � 56.3, 150–300 337.5 � 75,a 225–375
Total dose FSH 1,813.3 � 782.2, 600–4,725 1,994.4 � 1,234.4, 875–7650 1,697.2 � 655.4 1,538.6 � 375.4, 1,050–2,250 2,406.3 � 1,819,a 2,075–6,075
Duration of stimulation (d) 8.4 � 1.65–18
8.7 � 2.26–17
8.2 � 1 7.9 � 1.46–10
11.8 � 1.8a
8–16
E2 at hCG (pg/mL) 1,361.5 � 1,032, 57.70–13,680 1,609.2 � 1,248.4, 115.3–3,783 1,731.2 � 2a 1,500.9 � 687 1,269.3 � 828.9
Note: aSERT ¼ aggregates of tubular smooth endoplasmic reticulum.a Significant difference between study and control groups.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
Fertilityand
Sterility
�149.e4
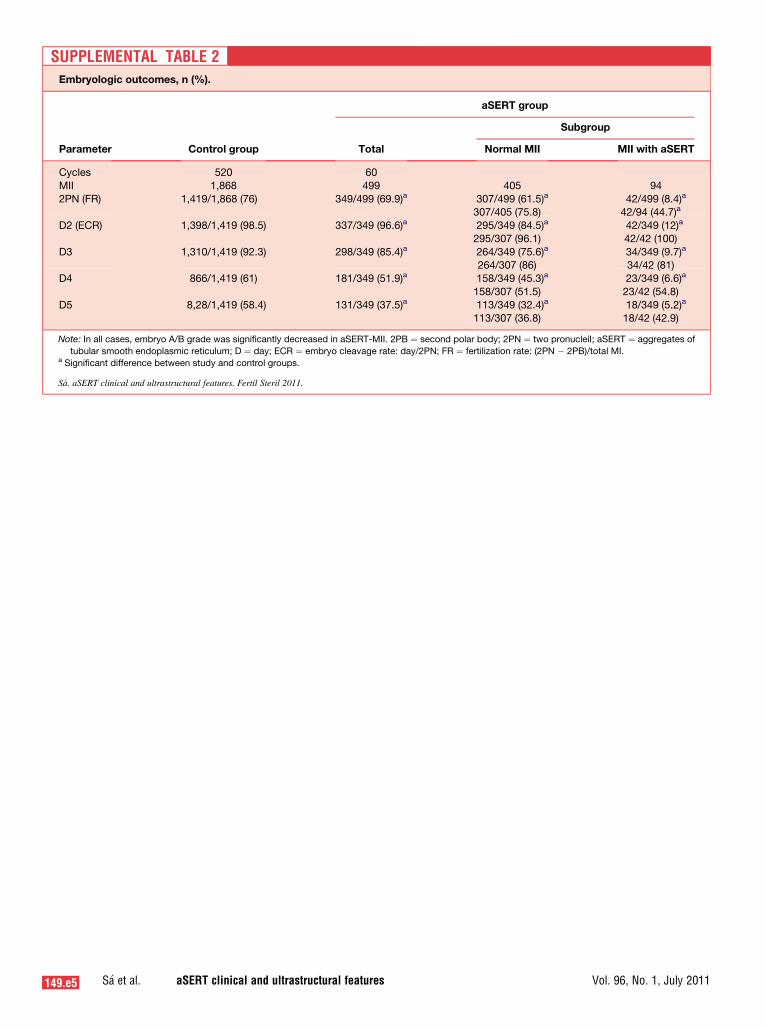
SUPPLEMENTAL TABLE 2Embryologic outcomes, n (%).
Parameter Control group
aSERT group
Total
Subgroup
Normal MII MII with aSERT
Cycles 520 60
MII 1,868 499 405 94
2PN (FR) 1,419/1,868 (76) 349/499 (69.9)a 307/499 (61.5)a
307/405 (75.8)42/499 (8.4)a
42/94 (44.7)a
D2 (ECR) 1,398/1,419 (98.5) 337/349 (96.6)a 295/349 (84.5)a
295/307 (96.1)
42/349 (12)a
42/42 (100)
D3 1,310/1,419 (92.3) 298/349 (85.4)a 264/349 (75.6)a
264/307 (86)34/349 (9.7)a
34/42 (81)
D4 866/1,419 (61) 181/349 (51.9)a 158/349 (45.3)a
158/307 (51.5)
23/349 (6.6)a
23/42 (54.8)
D5 8,28/1,419 (58.4) 131/349 (37.5)a 113/349 (32.4)a
113/307 (36.8)18/349 (5.2)a
18/42 (42.9)
Note: In all cases, embryo A/B grade was significantly decreased in aSERT-MII. 2PB ¼ second polar body; 2PN ¼ two pronucleiI; aSERT ¼ aggregates of
tubular smooth endoplasmic reticulum; D ¼ day; ECR ¼ embryo cleavage rate: day/2PN; FR ¼ fertilization rate: (2PN � 2PB)/total MI.a Significant difference between study and control groups.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
149.e5 S�a et al. aSERT clinical and ultrastructural features Vol. 96, No. 1, July 2011
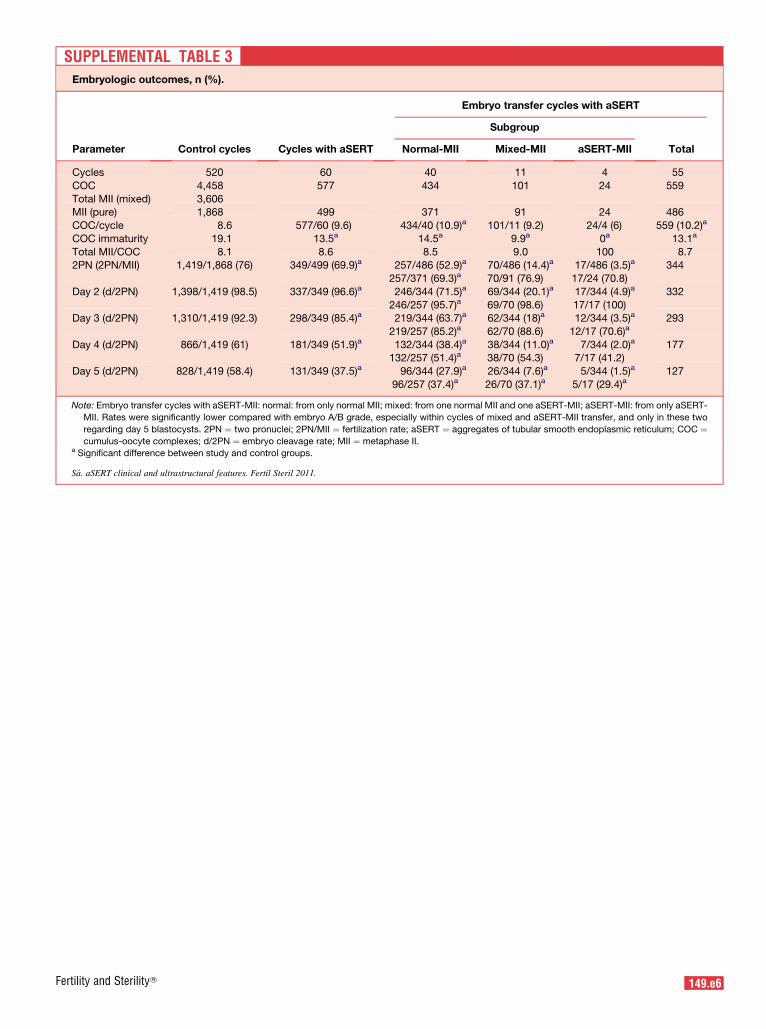
SUPPLEMENTAL TABLE 3Embryologic outcomes, n (%).
Parameter Control cycles Cycles with aSERT
Embryo transfer cycles with aSERT
Subgroup
TotalNormal-MII Mixed-MII aSERT-MII
Cycles 520 60 40 11 4 55
COC 4,458 577 434 101 24 559
Total MII (mixed) 3,606MII (pure) 1,868 499 371 91 24 486
COC/cycle 8.6 577/60 (9.6) 434/40 (10.9)a 101/11 (9.2) 24/4 (6) 559 (10.2)a
COC immaturity 19.1 13.5a 14.5a 9.9a 0a 13.1a
Total MII/COC 8.1 8.6 8.5 9.0 100 8.72PN (2PN/MII) 1,419/1,868 (76) 349/499 (69.9)a 257/486 (52.9)a
257/371 (69.3)a70/486 (14.4)a
70/91 (76.9)
17/486 (3.5)a
17/24 (70.8)
344
Day 2 (d/2PN) 1,398/1,419 (98.5) 337/349 (96.6)a 246/344 (71.5)a
246/257 (95.7)a69/344 (20.1)a
69/70 (98.6)
17/344 (4.9)a
17/17 (100)
332
Day 3 (d/2PN) 1,310/1,419 (92.3) 298/349 (85.4)a 219/344 (63.7)a
219/257 (85.2)a62/344 (18)a
62/70 (88.6)
12/344 (3.5)a
12/17 (70.6)a293
Day 4 (d/2PN) 866/1,419 (61) 181/349 (51.9)a 132/344 (38.4)a
132/257 (51.4)a38/344 (11.0)a
38/70 (54.3)7/344 (2.0)a
7/17 (41.2)177
Day 5 (d/2PN) 828/1,419 (58.4) 131/349 (37.5)a 96/344 (27.9)a
96/257 (37.4)a26/344 (7.6)a
26/70 (37.1)a5/344 (1.5)a
5/17 (29.4)a127
Note: Embryo transfer cycles with aSERT-MII: normal: from only normal MII; mixed: from one normal MII and one aSERT-MII; aSERT-MII: from only aSERT-
MII. Rates were significantly lower compared with embryo A/B grade, especially within cycles of mixed and aSERT-MII transfer, and only in these two
regarding day 5 blastocysts. 2PN ¼ two pronuclei; 2PN/MII ¼ fertilization rate; aSERT ¼ aggregates of tubular smooth endoplasmic reticulum; COC ¼cumulus-oocyte complexes; d/2PN ¼ embryo cleavage rate; MII ¼ metaphase II.
a Significant difference between study and control groups.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
Fertility and Sterility� 149.e6
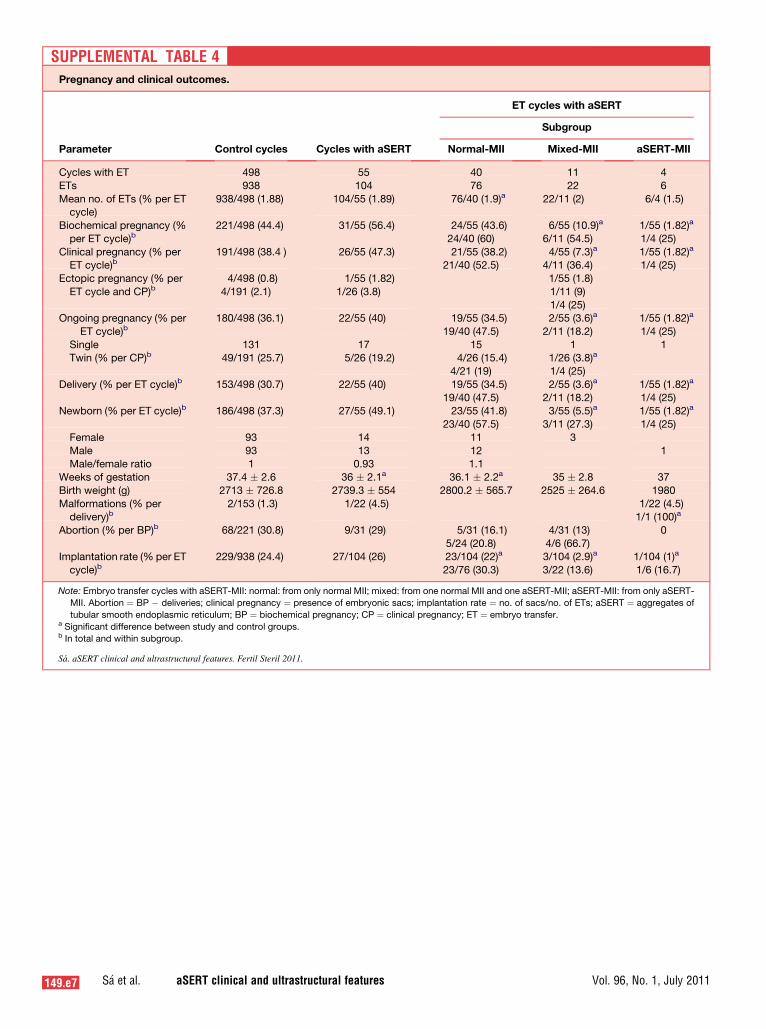
SUPPLEMENTAL TABLE 4Pregnancy and clinical outcomes.
Parameter Control cycles Cycles with aSERT
ET cycles with aSERT
Subgroup
Normal-MII Mixed-MII aSERT-MII
Cycles with ET 498 55 40 11 4
ETs 938 104 76 22 6
Mean no. of ETs (% per ETcycle)
938/498 (1.88) 104/55 (1.89) 76/40 (1.9)a 22/11 (2) 6/4 (1.5)
Biochemical pregnancy (%
per ET cycle)b221/498 (44.4) 31/55 (56.4) 24/55 (43.6)
24/40 (60)
6/55 (10.9)a
6/11 (54.5)
1/55 (1.82)a
1/4 (25)
Clinical pregnancy (% perET cycle)b
191/498 (38.4 ) 26/55 (47.3) 21/55 (38.2)21/40 (52.5)
4/55 (7.3)a
4/11 (36.4)1/55 (1.82)a
1/4 (25)
Ectopic pregnancy (% per
ET cycle and CP)b4/498 (0.8)
4/191 (2.1)
1/55 (1.82)
1/26 (3.8)
1/55 (1.8)
1/11 (9)
1/4 (25)Ongoing pregnancy (% per
ET cycle)b180/498 (36.1) 22/55 (40) 19/55 (34.5)
19/40 (47.5)
2/55 (3.6)a
2/11 (18.2)
1/55 (1.82)a
1/4 (25)
Single 131 17 15 1 1Twin (% per CP)b 49/191 (25.7) 5/26 (19.2) 4/26 (15.4)
4/21 (19)
1/26 (3.8)a
1/4 (25)
Delivery (% per ET cycle)b 153/498 (30.7) 22/55 (40) 19/55 (34.5)
19/40 (47.5)
2/55 (3.6)a
2/11 (18.2)
1/55 (1.82)a
1/4 (25)Newborn (% per ET cycle)b 186/498 (37.3) 27/55 (49.1) 23/55 (41.8)
23/40 (57.5)
3/55 (5.5)a
3/11 (27.3)
1/55 (1.82)a
1/4 (25)
Female 93 14 11 3
Male 93 13 12 1Male/female ratio 1 0.93 1.1
Weeks of gestation 37.4 � 2.6 36 � 2.1a 36.1 � 2.2a 35 � 2.8 37
Birth weight (g) 2713 � 726.8 2739.3 � 554 2800.2 � 565.7 2525 � 264.6 1980
Malformations (% perdelivery)b
2/153 (1.3) 1/22 (4.5) 1/22 (4.5)1/1 (100)a
Abortion (% per BP)b 68/221 (30.8) 9/31 (29) 5/31 (16.1)
5/24 (20.8)
4/31 (13)
4/6 (66.7)
0
Implantation rate (% per ET
cycle)b229/938 (24.4) 27/104 (26) 23/104 (22)a
23/76 (30.3)
3/104 (2.9)a
3/22 (13.6)
1/104 (1)a
1/6 (16.7)
Note: Embryo transfer cycles with aSERT-MII: normal: from only normal MII; mixed: from one normal MII and one aSERT-MII; aSERT-MII: from only aSERT-
MII. Abortion ¼ BP � deliveries; clinical pregnancy ¼ presence of embryonic sacs; implantation rate ¼ no. of sacs/no. of ETs; aSERT ¼ aggregates of
tubular smooth endoplasmic reticulum; BP ¼ biochemical pregnancy; CP ¼ clinical pregnancy; ET ¼ embryo transfer.a Significant difference between study and control groups.b In total and within subgroup.
S�a. aSERT clinical and ultrastructural features. Fertil Steril 2011.
149.e7 S�a et al. aSERT clinical and ultrastructural features Vol. 96, No. 1, July 2011
Copyright © 2022 FDOKUMEN



















