
Usefulness of ultrasonography in children with right iliac fossa ...
Upload
independentCategory
view
0download
0
Ultrasound in Med. & Biol., Vol. 34, No. 10, pp. 1554–1563, 2008© 2008 Published by Elsevier Inc. on behalf of World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/08/$–see front matter
doi:10.1016/j.ultrasmedbio.2008.03.010
● Original Contribution
ULTRASONOGRAPHY FOR THE MONITORING OF SUBCUTANEOUSDAMAGE IN MYCOBACTERIUM ULCERANS INFECTION (BURULI ULCER)
GIORGIO LEIGHEB,* TERESA CAMMAROTA,† ELISA ZAVATTARO,* ANTONINO SARNO,†
ALESSANDRO CARRIERO,‡ ANNA CLELIA LUCIA GAMBARO,‡ ANGE DOSSOU,§
FRANCESCO POGGIO,� CLAUDIO CLEMENTE,¶ ROCH CHRISTIAN JOHNSON,# GHISLAIN SOPOH,§
and FABRIZIO LEIGHEB***Dermatologic Clinic, University of Piemonte Orientale “A. Avogadro,” Novara, Italy; †Radiology 5, San Giovanni
Battista Hospital, Torino, Italy; ‡Department of Radiology, University of Piemonte Orientale “A. Avogadro,”Novara, Italy; §Centre de Dépistage et de Traitement de l’Ulcère de Buruli (CDTUB), Allada, Benin; �Scientific
Committee on Buruli Ulcer Program, Rotary Club Milano Aquileia, Rotary International, Milano, Italy; ¶Pathologyand Cytopathology Division, S. Pio X Hospital, Milano, Italy; #Programme National de Lutte contre l’Ulcère de
Buruli et la Lèpre, Ministère de la Santé Publique, Cotonou, Benin; and **Hygiene and Public Health Unit,University of Piemonte Orientale “A. Avogadro,” Novara, Italy.
(Received 20 July 2007; revised 18 February 2008; in final form 10 March 2008)
Abstract—We used ultrasonography to evaluate the nature and the extent of subcutaneous damage provoked byMycobacterium ulcerans (M. ulcerans) and to investigate the possible involvement of the tributary lymph nodes duringthe various stages of progression of Buruli ulcer. Nineteen patients affected by M. ulcerans infection in Benin, WestAfrica, were studied. Ultrasonography was performed on all subjects, except one, at the site of nonulcerated lesionsand/or at perilesional site. The tributary lymph nodes were also studied in six patients. Ultrasound (US) evaluation wascarried out using a 10 MHz linear probe and all lesions were compared with the homologous unaffected controlateralsite. The ultrasonography showed relevant alterations at the dermo-hypodermic level, in agreement with histologicalspecimens. In the active forms of the disease, these alterations are characterized by significant oedematous imbibitionof the adipose tissue and necrosis (adiponecrosis) that leads to varying irregularities in the echogenicity of thehypodermis, which is generally thicker. In agreement with the clinical examination, the lymph nodes in six patientsevaluated, despite their possible histological involvement with necrotic phenomena described in literature in M.ulcerans infection, did not display significant alterations visible by ultrasonography. The US scanning we haveperformed is the first use of this technique for M. ulcerans infection. We have shown that it can reveal thesubcutaneous depth and the peripheral extent of the pathological process and it is particularly useful for monitoringthe efficacy of or resistance to antibiotic treatment, especially in extensive ulcero-oedomatose forms. Such monitoringoffers also a useful guide to the surgeon allowing the reduction or postponement of the removal of the large cutaneousareas that were carried out until recently. (E-mail: [email protected]) © 2008 Published by ElsevierInc. on behalf of World Federation for Ultrasound in Medicine & Biology.
Key Words: Buruli ulcer, Mycobacterium ulcerans infection, Skin sonography, Soft tissue, Ultrasonography,
Ultrasound, Lymphoedema, Adiponecrosis.INTRODUCTION AND LITERATURE
Buruli ulcer (BU) is an obscure and severe disease causedby Mycobacterium ulcerans that affects mainly childrenand young adults living in subtropical areas. Most of thecases are present in western, sub-Saharan Africa.
Address correspondence to: Prof Giorgio Leigheb, Dermatologic
Clinic, University of Piemonte Orientale “A. Avogadro,” Novara, Italy.E-mail: [email protected]1554
The transmission of the disease is thought to be me-diated by aquatic insects or through human abraded skinand the development of cutaneous symptoms has beensuggested to be related to the production of a toxin namedmycolactone (Marsollier et al. 2005; Van der Werf et al.2003).
The clinical picture is not always pathognomonic,but polymorphous and indolent cutaneous lesions areobserved ranging from small nodules to wide ulcers (Fig.1) and multiple, disseminated lesions, sometimes accom-
panied by severe musculoskeletal involvement (Pszolla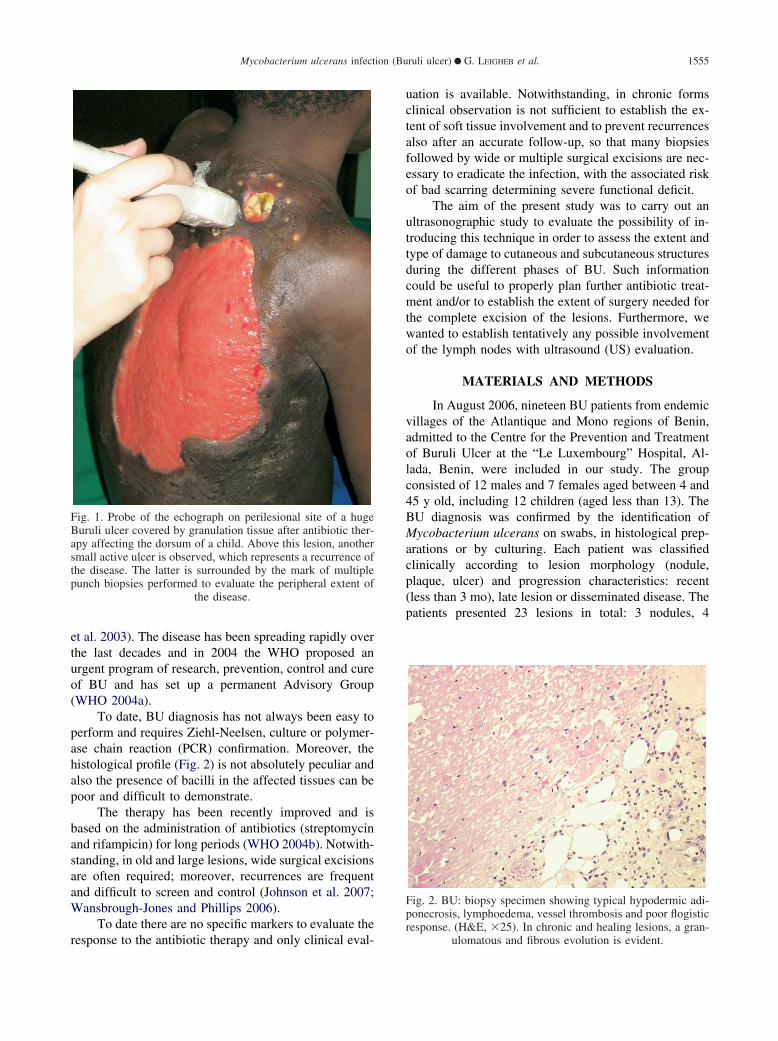
Mycobacterium ulcerans infection (Buruli ulcer) ● G. LEIGHEB et al. 1555
et al. 2003). The disease has been spreading rapidly overthe last decades and in 2004 the WHO proposed anurgent program of research, prevention, control and cureof BU and has set up a permanent Advisory Group(WHO 2004a).
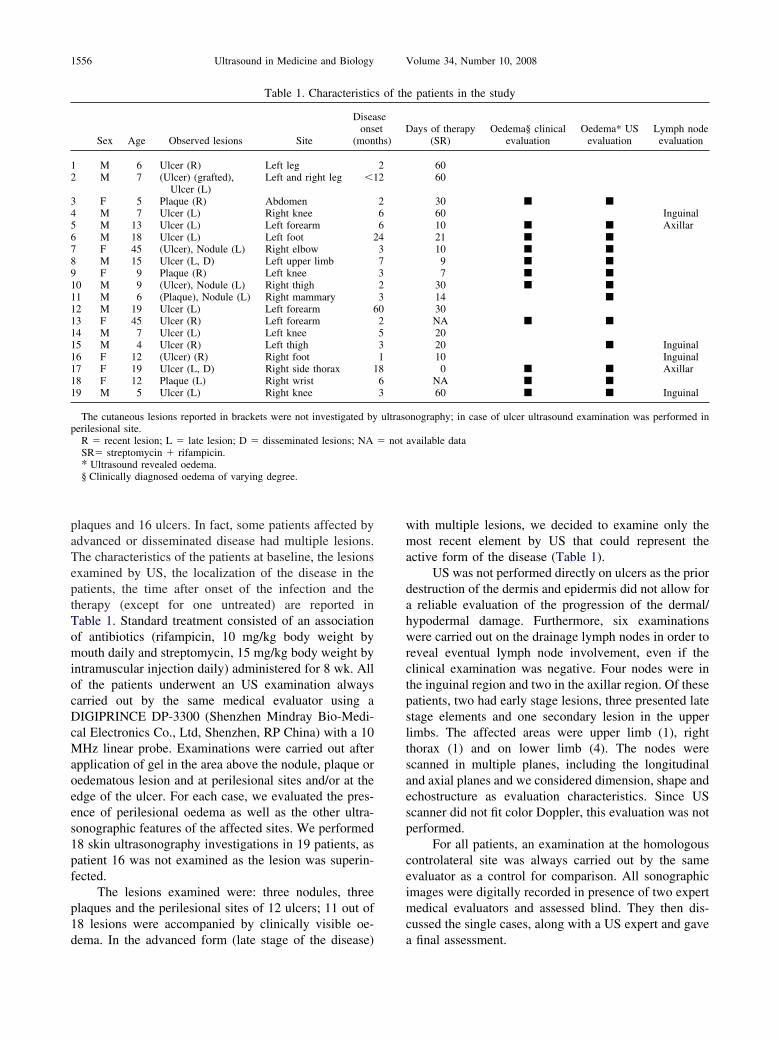
To date, BU diagnosis has not always been easy toperform and requires Ziehl-Neelsen, culture or polymer-ase chain reaction (PCR) confirmation. Moreover, thehistological profile (Fig. 2) is not absolutely peculiar andalso the presence of bacilli in the affected tissues can bepoor and difficult to demonstrate.
The therapy has been recently improved and isbased on the administration of antibiotics (streptomycinand rifampicin) for long periods (WHO 2004b). Notwith-standing, in old and large lesions, wide surgical excisionsare often required; moreover, recurrences are frequentand difficult to screen and control (Johnson et al. 2007;Wansbrough-Jones and Phillips 2006).
To date there are no specific markers to evaluate the
Fig. 1. Probe of the echograph on perilesional site of a hugeBuruli ulcer covered by granulation tissue after antibiotic ther-apy affecting the dorsum of a child. Above this lesion, anothersmall active ulcer is observed, which represents a recurrence ofthe disease. The latter is surrounded by the mark of multiplepunch biopsies performed to evaluate the peripheral extent of
the disease.
response to the antibiotic therapy and only clinical eval-
uation is available. Notwithstanding, in chronic formsclinical observation is not sufficient to establish the ex-tent of soft tissue involvement and to prevent recurrencesalso after an accurate follow-up, so that many biopsiesfollowed by wide or multiple surgical excisions are nec-essary to eradicate the infection, with the associated riskof bad scarring determining severe functional deficit.
The aim of the present study was to carry out anultrasonographic study to evaluate the possibility of in-troducing this technique in order to assess the extent andtype of damage to cutaneous and subcutaneous structuresduring the different phases of BU. Such informationcould be useful to properly plan further antibiotic treat-ment and/or to establish the extent of surgery needed forthe complete excision of the lesions. Furthermore, wewanted to establish tentatively any possible involvementof the lymph nodes with ultrasound (US) evaluation.
MATERIALS AND METHODS
In August 2006, nineteen BU patients from endemicvillages of the Atlantique and Mono regions of Benin,admitted to the Centre for the Prevention and Treatmentof Buruli Ulcer at the “Le Luxembourg” Hospital, Al-lada, Benin, were included in our study. The groupconsisted of 12 males and 7 females aged between 4 and45 y old, including 12 children (aged less than 13). TheBU diagnosis was confirmed by the identification ofMycobacterium ulcerans on swabs, in histological prep-arations or by culturing. Each patient was classifiedclinically according to lesion morphology (nodule,plaque, ulcer) and progression characteristics: recent(less than 3 mo), late lesion or disseminated disease. Thepatients presented 23 lesions in total: 3 nodules, 4
Fig. 2. BU: biopsy specimen showing typical hypodermic adi-ponecrosis, lymphoedema, vessel thrombosis and poor flogisticresponse. (H&E, �25). In chronic and healing lesions, a gran-
ulomatous and fibrous evolution is evident.
1556 Ultrasound in Medicine and Biology Volume 34, Number 10, 2008
plaques and 16 ulcers. In fact, some patients affected byadvanced or disseminated disease had multiple lesions.The characteristics of the patients at baseline, the lesionsexamined by US, the localization of the disease in thepatients, the time after onset of the infection and thetherapy (except for one untreated) are reported inTable 1. Standard treatment consisted of an associationof antibiotics (rifampicin, 10 mg/kg body weight bymouth daily and streptomycin, 15 mg/kg body weight byintramuscular injection daily) administered for 8 wk. Allof the patients underwent an US examination alwayscarried out by the same medical evaluator using aDIGIPRINCE DP-3300 (Shenzhen Mindray Bio-Medi-cal Electronics Co., Ltd, Shenzhen, RP China) with a 10MHz linear probe. Examinations were carried out afterapplication of gel in the area above the nodule, plaque oroedematous lesion and at perilesional sites and/or at theedge of the ulcer. For each case, we evaluated the pres-ence of perilesional oedema as well as the other ultra-sonographic features of the affected sites. We performed18 skin ultrasonography investigations in 19 patients, aspatient 16 was not examined as the lesion was superin-fected.
The lesions examined were: three nodules, threeplaques and the perilesional sites of 12 ulcers; 11 out of18 lesions were accompanied by clinically visible oe-
Table 1. Characteristic
Sex Age Observed lesions Site
Diseaons
(mon
1 M 6 Ulcer (R) Left leg2 M 7 (Ulcer) (grafted),
Ulcer (L)Left and right leg �1
3 F 5 Plaque (R) Abdomen4 M 7 Ulcer (L) Right knee5 M 13 Ulcer (L) Left forearm6 M 18 Ulcer (L) Left foot 27 F 45 (Ulcer), Nodule (L) Right elbow8 M 15 Ulcer (L, D) Left upper limb9 F 9 Plaque (R) Left knee10 M 9 (Ulcer), Nodule (L) Right thigh11 M 6 (Plaque), Nodule (L) Right mammary12 M 19 Ulcer (L) Left forearm 613 F 45 Ulcer (R) Left forearm14 M 7 Ulcer (L) Left knee15 M 4 Ulcer (R) Left thigh16 F 12 (Ulcer) (R) Right foot17 F 19 Ulcer (L, D) Right side thorax 118 F 12 Plaque (L) Right wrist19 M 5 Ulcer (L) Right knee
The cutaneous lesions reported in brackets were not investigated byperilesional site.
R � recent lesion; L � late lesion; D � disseminated lesions; NASR� streptomycin � rifampicin.* Ultrasound revealed oedema.§ Clinically diagnosed oedema of varying degree.
dema. In the advanced form (late stage of the disease)
with multiple lesions, we decided to examine only themost recent element by US that could represent theactive form of the disease (Table 1).
US was not performed directly on ulcers as the priordestruction of the dermis and epidermis did not allow fora reliable evaluation of the progression of the dermal/hypodermal damage. Furthermore, six examinationswere carried out on the drainage lymph nodes in order toreveal eventual lymph node involvement, even if theclinical examination was negative. Four nodes were inthe inguinal region and two in the axillar region. Of thesepatients, two had early stage lesions, three presented latestage elements and one secondary lesion in the upperlimbs. The affected areas were upper limb (1), rightthorax (1) and on lower limb (4). The nodes werescanned in multiple planes, including the longitudinaland axial planes and we considered dimension, shape andechostructure as evaluation characteristics. Since USscanner did not fit color Doppler, this evaluation was notperformed.
For all patients, an examination at the homologouscontrolateral site was always carried out by the sameevaluator as a control for comparison. All sonographicimages were digitally recorded in presence of two expertmedical evaluators and assessed blind. They then dis-cussed the single cases, along with a US expert and gave
e patients in the study
ays of therapy(SR)
Oedema§ clinicalevaluation
Oedema* USevaluation
Lymph nodeevaluation
6060
30 � �
60 Inguinal10 � � Axillar21 � �
10 � �
9 � �
7 � �
30 � �
14 �
30NA � �
2020 � Inguinal10 Inguinal
0 � � AxillarNA � �
60 � � Inguinal
nography; in case of ulcer ultrasound examination was performed in
available data
s of th
seetths)
D
22
26643732302531863
ultraso
� not
a final assessment.
thicke
Mycobacterium ulcerans infection (Buruli ulcer) ● G. LEIGHEB et al. 1557
Informed verbal consent was obtained from eachpatient or from the parents of the patient for minors. Thisstudy was carried out according to the principles of theDeclaration of Helsinki.
RESULTS
The sonographic images showed diverse clinicalpictures corresponding to the various clinical and evolu-tionary phases of the characteristic lesions of M. ulceransinfection (nodule, plaque, massive and diffuse lymphoe-dema, ulcer, fibrosis).
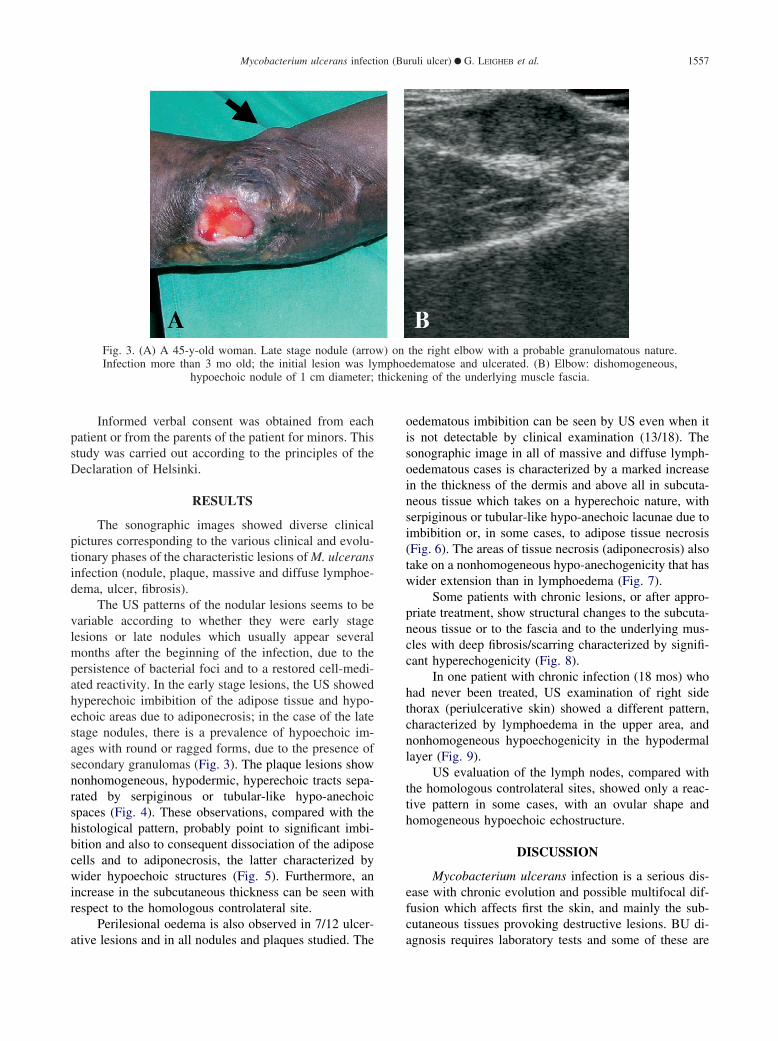
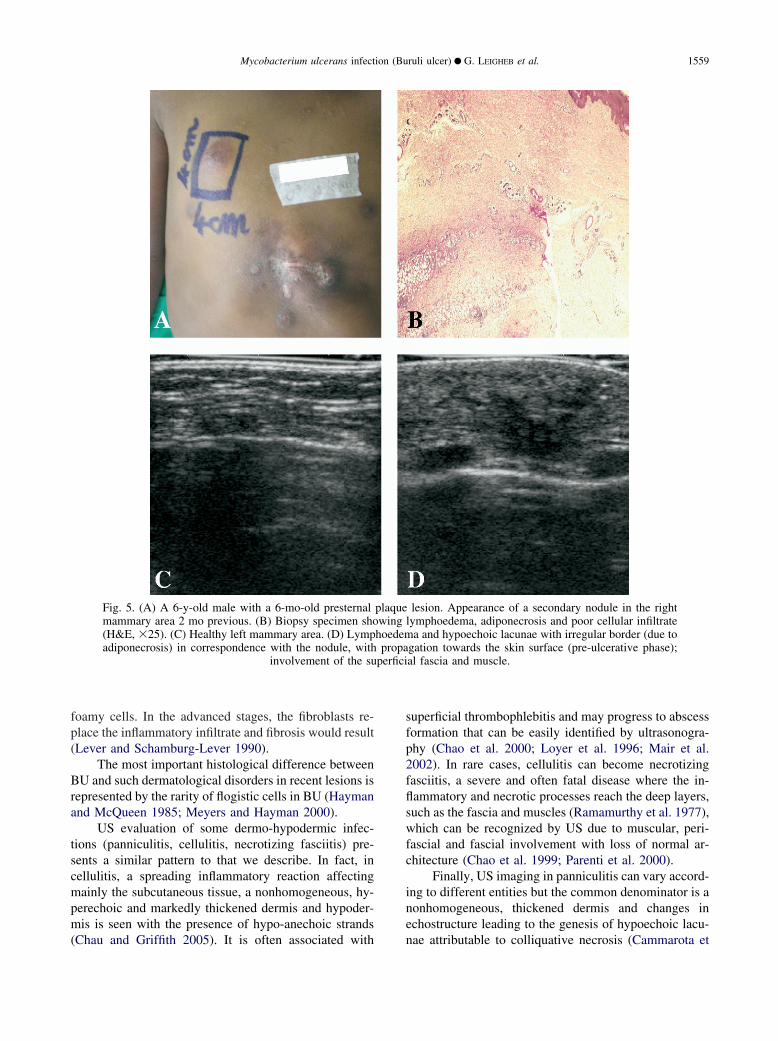
The US patterns of the nodular lesions seems to bevariable according to whether they were early stagelesions or late nodules which usually appear severalmonths after the beginning of the infection, due to thepersistence of bacterial foci and to a restored cell-medi-ated reactivity. In the early stage lesions, the US showedhyperechoic imbibition of the adipose tissue and hypo-echoic areas due to adiponecrosis; in the case of the latestage nodules, there is a prevalence of hypoechoic im-ages with round or ragged forms, due to the presence ofsecondary granulomas (Fig. 3). The plaque lesions shownonhomogeneous, hypodermic, hyperechoic tracts sepa-rated by serpiginous or tubular-like hypo-anechoicspaces (Fig. 4). These observations, compared with thehistological pattern, probably point to significant imbi-bition and also to consequent dissociation of the adiposecells and to adiponecrosis, the latter characterized bywider hypoechoic structures (Fig. 5). Furthermore, anincrease in the subcutaneous thickness can be seen withrespect to the homologous controlateral site.
Perilesional oedema is also observed in 7/12 ulcer-
Fig. 3. (A) A 45-y-old woman. Late stage nodule (arroInfection more than 3 mo old; the initial lesion was ly
hypoechoic nodule of 1 cm diameter;
ative lesions and in all nodules and plaques studied. The
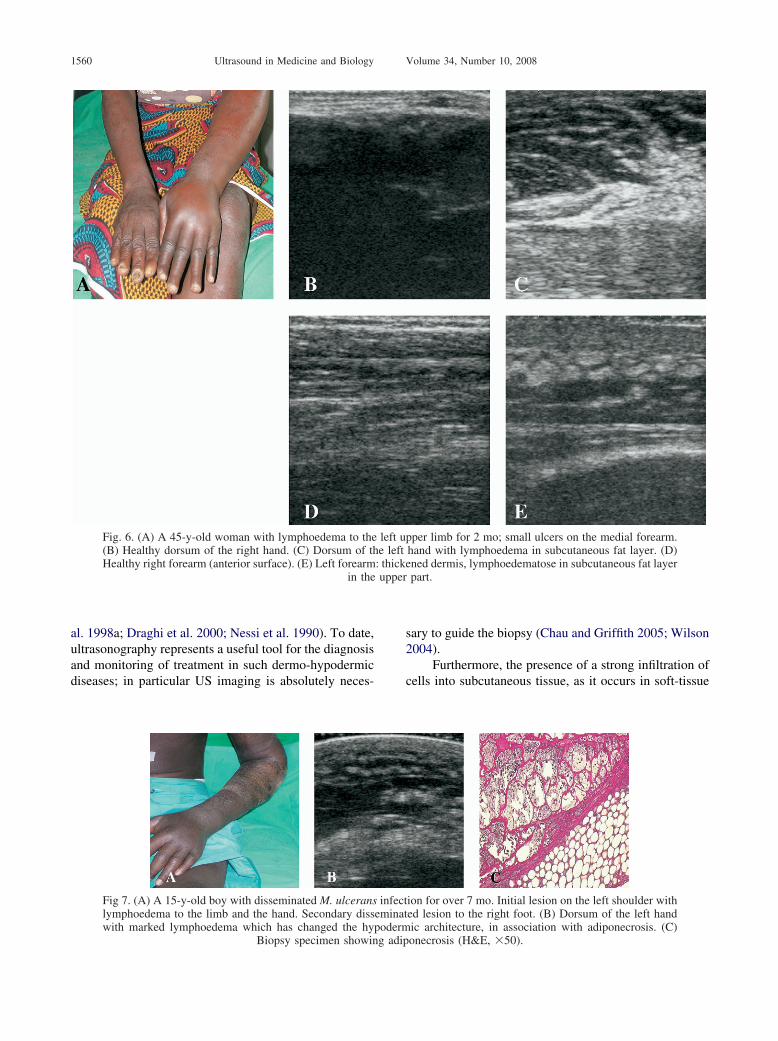
oedematous imbibition can be seen by US even when itis not detectable by clinical examination (13/18). Thesonographic image in all of massive and diffuse lymph-oedematous cases is characterized by a marked increasein the thickness of the dermis and above all in subcuta-neous tissue which takes on a hyperechoic nature, withserpiginous or tubular-like hypo-anechoic lacunae due toimbibition or, in some cases, to adipose tissue necrosis(Fig. 6). The areas of tissue necrosis (adiponecrosis) alsotake on a nonhomogeneous hypo-anechogenicity that haswider extension than in lymphoedema (Fig. 7).
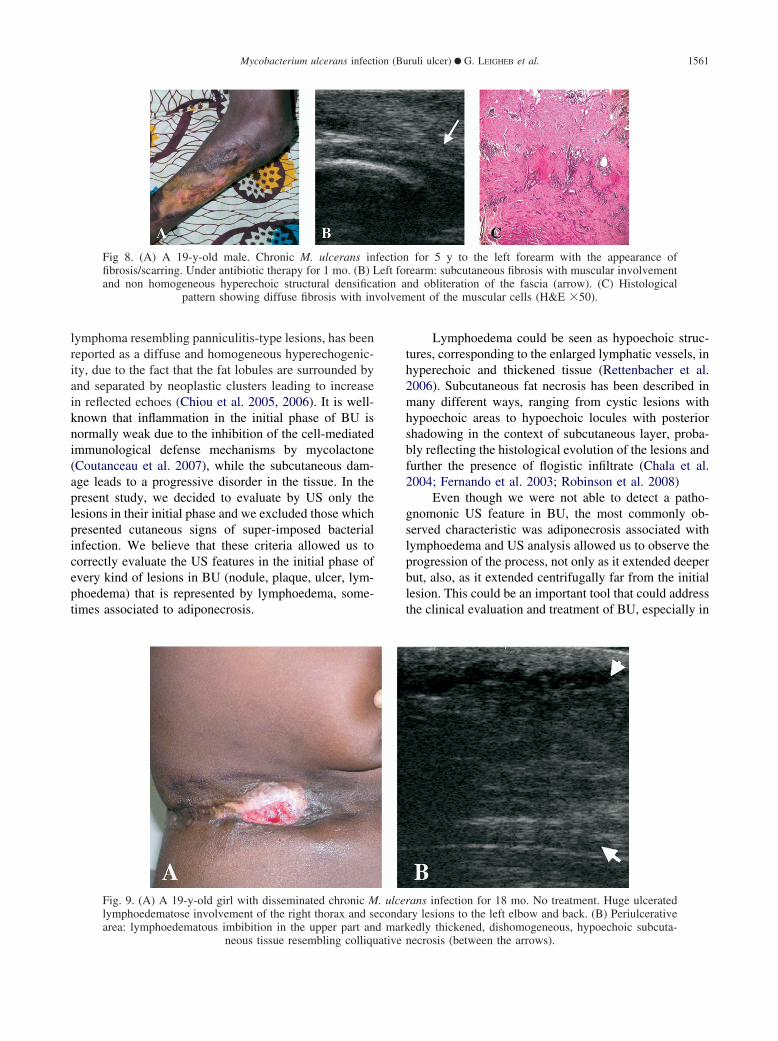
Some patients with chronic lesions, or after appro-priate treatment, show structural changes to the subcuta-neous tissue or to the fascia and to the underlying mus-cles with deep fibrosis/scarring characterized by signifi-cant hyperechogenicity (Fig. 8).
In one patient with chronic infection (18 mos) whohad never been treated, US examination of right sidethorax (periulcerative skin) showed a different pattern,characterized by lymphoedema in the upper area, andnonhomogeneous hypoechogenicity in the hypodermallayer (Fig. 9).
US evaluation of the lymph nodes, compared withthe homologous controlateral sites, showed only a reac-tive pattern in some cases, with an ovular shape andhomogeneous hypoechoic echostructure.
DISCUSSION
Mycobacterium ulcerans infection is a serious dis-ease with chronic evolution and possible multifocal dif-fusion which affects first the skin, and mainly the sub-cutaneous tissues provoking destructive lesions. BU di-
the right elbow with a probable granulomatous nature.dematose and ulcerated. (B) Elbow: dishomogeneous,
ning of the underlying muscle fascia.
w) onmphoe
agnosis requires laboratory tests and some of these are

ciated
1558 Ultrasound in Medicine and Biology Volume 34, Number 10, 2008
very expensive or not available in most subtropical areas,where the disease is mainly distributed. Moreover, treat-ment of BU consists of very long administration ofantibiotics, and in some cases, even this is not sufficientto eradicate the infection and surgery is needed. Further-more, advanced and chronic cases often require numer-ous huge surgical excisions, due to the unpredictableextension of the affected areas, with serious complica-tions in term of scarring and functional deficits, also afterskin grafting (Wansbrough-Jones and Phillips 2006).
Due to such difficulties, we used US scanning toevaluate different clinical stages of the disease and todiscover whether distinctive images could be observed.Even if it was not the aim of the present study to correlatethe US image with histological specimens, we were ableto detect by US all of the reported histological charac-teristics of the cutaneous disease, except for vesselthrombosis. This may be due to the fact that thrombosisoccurs in small vascular structures which cannot be seenby ultrasonography.
The main characteristic that we were able to detectin every stage, was a marked lymphoedematose imbibi-tion of the subcutaneous tissue, shown by the majority ofpatients, even when oedema was not clinically evident,sometimes associated with adiponecrosis; consequently,a marked increase of the thickness of dermis and subcu-taneous tissue was observed. Upon US examination,adiponecrosis appears as large, nonhomogeneous, hypo-anechoic subcutaneous tissue with hyperechoic foci in-side, while in lymphoedema the hypoechoic lacunae aresmaller with a serpiginous form.
The only patient never treated with antibiotics or
Fig. 4. (A) A 5-y-old female with a 2-mo-old lesion (a h- arrow - ) on the upper abdomen, under antibiotic thhypodermis with echostructural changes typical of lymph
cellular infiltrate asso
surgery was affected by a chronic form of the infection
on the right thorax and disseminated lesions on left upperlimb and back. US evaluation of the right thorax showeda different pattern corresponding to lymphoedematousimbibition in the upper part and dishomogeneous, hypo-echoic subcutaneous tissue resembling colliquative ne-crosis.
In some of the patients examined, when chronicinfection is established and despite therapy, we couldalso detect fascial and even muscular involvement, con-sisting of hyperechoic structures of various degrees dueto fibrotic processes. This last element represents a se-vere feature because fibrosis can easily compromise thefunction of the limbs.
US evaluation of the lymph nodes in the six patientswe have studied did not show significant alterations inexamined parameters. The drainage lymph nodes studieddid not show characteristics significantly different tocontrolateral lymph nodes. Notwithstanding the smallnumber of patients, the data seem to confirm the appar-ently poor lymph node involvement, which characterizeBU clinically. We did not see the necrotic phenomena,which should be recognizable by ultrasonography, thathave described histologically in some cases in the liter-ature (Meyers and Hayman 2000).
Adiponecrosis or fat necrosis is the most importanthistological feature of BU lesions but it can be seen innumerous dermatological disorders, such as panniculitis,Weber-Christian syndrome, Rothmann-Makai panniculi-tis and different diseases affecting newborn children orassociated with pancreatic disorders. Such diseases alsoshow the distinctive and remarkable presence of flogisticcells on histological examination, mainly corresponding
aque with extensive lymphoedema and initial ulcerationfor 1 mo. (B) Notable thickening of the dermis anda; the dermal hypoechogenicity was due to the massivewith lymphoedema.
uge plerapyoedem
to macrophages or histiocytes, sometimes collected in
perfici
Mycobacterium ulcerans infection (Buruli ulcer) ● G. LEIGHEB et al. 1559
foamy cells. In the advanced stages, the fibroblasts re-place the inflammatory infiltrate and fibrosis would result(Lever and Schamburg-Lever 1990).
The most important histological difference betweenBU and such dermatological disorders in recent lesions isrepresented by the rarity of flogistic cells in BU (Haymanand McQueen 1985; Meyers and Hayman 2000).
US evaluation of some dermo-hypodermic infec-tions (panniculitis, cellulitis, necrotizing fasciitis) pre-sents a similar pattern to that we describe. In fact, incellulitis, a spreading inflammatory reaction affectingmainly the subcutaneous tissue, a nonhomogeneous, hy-perechoic and markedly thickened dermis and hypoder-mis is seen with the presence of hypo-anechoic strands
Fig. 5. (A) A 6-y-old male with a 6-mo-old presternalmammary area 2 mo previous. (B) Biopsy specimen sho(H&E, �25). (C) Healthy left mammary area. (D) Lympadiponecrosis) in correspondence with the nodule, with
involvement of the su
(Chau and Griffith 2005). It is often associated with
superficial thrombophlebitis and may progress to abscessformation that can be easily identified by ultrasonogra-phy (Chao et al. 2000; Loyer et al. 1996; Mair et al.2002). In rare cases, cellulitis can become necrotizingfasciitis, a severe and often fatal disease where the in-flammatory and necrotic processes reach the deep layers,such as the fascia and muscles (Ramamurthy et al. 1977),which can be recognized by US due to muscular, peri-fascial and fascial involvement with loss of normal ar-chitecture (Chao et al. 1999; Parenti et al. 2000).
Finally, US imaging in panniculitis can vary accord-ing to different entities but the common denominator is anonhomogeneous, thickened dermis and changes inechostructure leading to the genesis of hypoechoic lacu-
lesion. Appearance of a secondary nodule in the rightlymphoedema, adiponecrosis and poor cellular infiltrate
a and hypoechoic lacunae with irregular border (due togation towards the skin surface (pre-ulcerative phase);al fascia and muscle.
plaquewinghoedempropa
nae attributable to colliquative necrosis (Cammarota et
upper
1560 Ultrasound in Medicine and Biology Volume 34, Number 10, 2008
al. 1998a; Draghi et al. 2000; Nessi et al. 1990). To date,ultrasonography represents a useful tool for the diagnosisand monitoring of treatment in such dermo-hypodermicdiseases; in particular US imaging is absolutely neces-
Fig. 6. (A) A 45-y-old woman with lymphoedema to the(B) Healthy dorsum of the right hand. (C) Dorsum of thHealthy right forearm (anterior surface). (E) Left forearm
in the
Fig 7. (A) A 15-y-old boy with disseminated M. ulceranslymphoedema to the limb and the hand. Secondary disswith marked lymphoedema which has changed the hy
Biopsy specimen showing adip
sary to guide the biopsy (Chau and Griffith 2005; Wilson2004).
Furthermore, the presence of a strong infiltration ofcells into subcutaneous tissue, as it occurs in soft-tissue
pper limb for 2 mo; small ulcers on the medial forearm.hand with lymphoedema in subcutaneous fat layer. (D)ned dermis, lymphoedematose in subcutaneous fat layerpart.
ion for over 7 mo. Initial lesion on the left shoulder withed lesion to the right foot. (B) Dorsum of the left handic architecture, in association with adiponecrosis. (C)
left ue left: thicke
infecteminatpoderm
onecrosis (H&E, �50).
volvem
Mycobacterium ulcerans infection (Buruli ulcer) ● G. LEIGHEB et al. 1561
lymphoma resembling panniculitis-type lesions, has beenreported as a diffuse and homogeneous hyperechogenic-ity, due to the fact that the fat lobules are surrounded byand separated by neoplastic clusters leading to increasein reflected echoes (Chiou et al. 2005, 2006). It is well-known that inflammation in the initial phase of BU isnormally weak due to the inhibition of the cell-mediatedimmunological defense mechanisms by mycolactone(Coutanceau et al. 2007), while the subcutaneous dam-age leads to a progressive disorder in the tissue. In thepresent study, we decided to evaluate by US only thelesions in their initial phase and we excluded those whichpresented cutaneous signs of super-imposed bacterialinfection. We believe that these criteria allowed us tocorrectly evaluate the US features in the initial phase ofevery kind of lesions in BU (nodule, plaque, ulcer, lym-phoedema) that is represented by lymphoedema, some-times associated to adiponecrosis.
Fig 8. (A) A 19-y-old male. Chronic M. ulcerans infibrosis/scarring. Under antibiotic therapy for 1 mo. (B) Land non homogeneous hyperechoic structural densifica
pattern showing diffuse fibrosis with in
Fig. 9. (A) A 19-y-old girl with disseminated chronic Mlymphoedematose involvement of the right thorax and sarea: lymphoedematous imbibition in the upper part an
neous tissue resembling colliquative
Lymphoedema could be seen as hypoechoic struc-tures, corresponding to the enlarged lymphatic vessels, inhyperechoic and thickened tissue (Rettenbacher et al.2006). Subcutaneous fat necrosis has been described inmany different ways, ranging from cystic lesions withhypoechoic areas to hypoechoic locules with posteriorshadowing in the context of subcutaneous layer, proba-bly reflecting the histological evolution of the lesions andfurther the presence of flogistic infiltrate (Chala et al.2004; Fernando et al. 2003; Robinson et al. 2008)
Even though we were not able to detect a patho-gnomonic US feature in BU, the most commonly ob-served characteristic was adiponecrosis associated withlymphoedema and US analysis allowed us to observe theprogression of the process, not only as it extended deeperbut, also, as it extended centrifugally far from the initiallesion. This could be an important tool that could addressthe clinical evaluation and treatment of BU, especially in
for 5 y to the left forearm with the appearance ofrearm: subcutaneous fibrosis with muscular involvementnd obliteration of the fascia (arrow). (C) Histologicalent of the muscular cells (H&E �50).
ans infection for 18 mo. No treatment. Huge ulceratedry lesions to the left elbow and back. (B) Periulcerativeedly thickened, dishomogeneous, hypoechoic subcuta-
fectioneft fotion a
. ulcerecondad mark
necrosis (between the arrows).

1562 Ultrasound in Medicine and Biology Volume 34, Number 10, 2008
countries where the health service is not well developed.In fact, in Africa the use of antibiotics in BU has per-mitted the reduction of the extension of the affectedareas, especially in the initial forms but it is not curativein every case. Moreover, despite the fact that BU repre-sents an evident and superficial disease, the damagedtissues cannot be identified easily only by clinical exam-inations: a small cutaneous lesion could be associatedwith histological changes that could extend far from theinitial lesion, probably due to the mycolactone action. Inthis way, a surgical excision of the lesion is not sufficientand BU would show very early recurrence. On the otherhand, the choice to carry out huge surgical excision maynot be acceptable either because of the localization of thelesions (face, neck, eye) or due to the risk of bad scarringleading to functional deficits (extremities) (WHO 2007).
Ultrasonography has been used in dermatology tostudy various dermatoses with a view to showing theextent of the lesions caused by both benign (cyst, lipoma)and malignant (melanoma, squamous cell carcinoma,sarcoma) tumours both for diagnosis and follow-up. Inthese malignant pathologies, US evaluation of the locallymph nodes represents a valid method for monitoringclinical progression and prognosis (Cammarota et al.1998a, 1998b; Dill-Müller and Maschke 2007; Gritz-mann et al. 2002; Rubaltelli et al. 2004; Schmid-Wendt-ner and Burgdorf 2005). Since it is a rapid, inexpensiveand easy-to-perform technique, it has also been used inclinical trials to monitor the efficacy of emollients andother local treatments, where it has allowed to highlightthe different stages of the healing process and, further-more, to better understand the pathogenesis of somediseases (Kreuter at al. 2005; Machet et al. 2006; Seide-nari 1995; Unholzer and Korting 2002).
We believe that US scanning could represent auseful tool to evaluate the efficacy of antibiotic therapyin BU lesions and the need to prolong treatment and/or toproperly plan surgery to permit the complete excision ofthe affected areas. Moreover, it could help to correctlyinvestigate the pathogenesis of this obscure disease.
To our knowledge, the present study represents thefirst use of ultrasonography in BU. Further studies areneeded to confirm these preliminary data and a largenumber of patients is required to establish the existenceof a correlation between histology and ultrasonography.Consequently, two important elements may be consid-ered in future investigations: the influence of therapy andcytokine pattern, as it is reported that a T helper 2cytokine pattern is predominant in early phases of thedisease (Gooding et al. 2002). In particular, a homoge-neous group of patients could be useful to correctlyevaluate the effect of different treatments; furthermore, itwould be interesting to correlate cytokine patterns of
patients with the clinical stage and US imaging.CONCLUSIONS
The data reported here represent the first use ofultrasonography in BU and, despite being limited to fewpatients and showing a relevant but not absolutely spe-cific pattern, demonstrate its usefulness to follow theevolution of cutaneous lesions. Given that US examina-tion is a rapid, simple, noninvasive technique that doesnot require a particular preparation of the patient, webelieve that it represents a valid and useful method toreveal the damage caused by the disease at the dermo-hypodermic level. Furthermore, US imaging could makethe job of the surgeon easier, limiting the vast excisionsthat were carried out in the past and making it easier tochoose the areas to remove. During the postinfectivehealing and sclerosing phase, the method is able to giveindications about the correct rehabilitative treatment.
Acknowledgments—The authors wish to thank Dr. Giorgio Crua, MrFrancesco Dadone and Mr Virgilio Petriello for lending us the USscanner in Benin, the Scientific Commission of the Rotary Club MilanoAquileia “Lotta all’Ulcera del Buruli”, the Rotary Clubs of New York(USA), Novara and Bergamo (Italy), and the medical and nursing staffof the Centre for the Prevention and Treatment of Buruli Ulcer(CDTUB) at the “Le Luxembourg” Hospital, Allada, Benin (supportedby the Fondation Luxembourgeoise Raoul Follereau). The authors alsothank Dr. Kingsley Asiedu, WHO, Global Buruli Ulcer Initiative, forhis help in encouraging the study of the disease and the research; andthe Franciscan Friars of Immacolata in Benin for their friendly hospi-tality during their stay in Allada. This non-profit work was made toscientific and humanitarian purposes. The Rotary Club Milano Aquileiasupported G. Leigheb, F. Poggio, C. Clemente, E. Zavattaro and F.Leigheb in their stay in Benin.
REFERENCES
Cammarota T, Bernengo MG, Bossi MC, Pippione M, Sarno A, Sol-biati L. Ecografia in dermatologia. Milano: Poletto, 1998a.
Cammarota T, Pinto F, Magliaro A, Sarno A. Current uses of diagnos-tic high-frequency US in dermatology. Eur J Radiol 1998b;27(Suppl 2):S215–S223.
Chala LF, de Barros N, de Carmago Moraes P, Endo E, Kin SJ,Pincerato KM, Carvalho FM, Cerri GG. Fat necrosis of the breast:Mammographic, sonographic, computer tomography, and magneticresonance imaging findings. Curr Probl Diagn Radiol 2004;33:106–126.
Chao HC, Kong MS, Lin TY. Diagnosis of necrotizing fasciitis inchildren. J Ultrasound Med 1999;18:277–281.
Chao HC, Lin SJ, Huang YC, Lin TY. Sonographic evaluation ofcellulitis in children. J Ultrasound Med 2000;19:743–749.
Chau CLF, Griffith JF. Musculoskeletal infections: Ultrasound appear-ances. Clin Radiol 2005;60:149–159.
Chiou HJ, Chou YH, Chiou SY, Chen WM, Chen W, Wang HK, ChangCY. High-resolution ultrasonography of primary peripheral softtissue lymphoma. J Ultrasound Med 2005;24:77–86.
Chiou HJ, Chou YH, Chiou SY, Chen WM, Chen W, Wan HK, ChaoTC, Chang CY. Superficial soft-tissue lymphoma: Sonographicappearance and early survival. Ultrasound Med Biol 2006;32:1287–1297.
Coutanceau E, Decalf J, Martino A, Babon A, Winter N, Cole ST,Albert ML, Demangel C. Selective suppression of dendritic cellfunctions by Mycobacterium ulcerans toxin mycolactone. J ExpMed 2007;204:1395–1403.
Dill-Müller D, Maschke J. Ultrasonography in dermatology. J DtschDermatol Ges 2007;5:689–707.

Mycobacterium ulcerans infection (Buruli ulcer) ● G. LEIGHEB et al. 1563
Draghi F, Fulle I, Madonia L, Coscia D. Panniculitis of the neck. Acase report. Radiol Med 2000;99:194–195.
Fernando RA, Somers S, Edmonson RD, Sidhu PS. Subcutaneous fatnecrosis. J Ultrasound Med 2003;22:1387–1390.
Gooding TM, Johnson PD, Smith M, Kemp AS, Robins-Browne RM.Cytokines profiles of patients infected with Mycobacterium ulcer-ans and unaffected household contacts. Infect Immun 2002;70:5562–5567.
Gritzmann N, Hollerweger A, Macheiner P, Rettenbacher T. Sonogra-phy of soft tissue masses of the neck. J Clin Ultrasound 2002;30:356–373.
Hayman J, McQueen A. The pathology of Mycobacterium ulceransinfection. Pathology 1985;17:594–600.
Johnson PD, Hayman JA, Quek TY, Fyfe JA, Jenkin GA, Buntine JA,Athan E, Birrell M, Graham J, Lavender CJ. Consensus recommen-dations for the diagnosis, treatment and control of Mycobacteriumulcerans infection (Bairnsdale or Buruli ulcer) in Victoria, Austra-lia. Med J Aust 2007;186:64–68.
Kreuter A, Gambichler T, Breukmann F, Rotterdam S, Freitag M,Stuecker M, Hoffmann K, Altmeyer P. Pulsed high-dose cortico-steroids combined with low-dose methotrexate in severe localizedscleroderma. Arch Dermatol 2005;141:847–852.
Lever WF, Schamburg-Lever G. Histopathology of the skin. Philadel-phia: Lippincott, 1990.
Loyer EM, DuBrow RA, David CL, Coan JD, Eftekhari F. Imaging ofsuperficial soft-tissue infections: Sonographic findings in cases ofcellulitis and abscess. Am J Roentgenol 1996;166:149–152.
Machet L, Ossant F, Bleuzen A, Grégoire J-M, Machet M-C, VaillantL. High-resolution ultrasonography: Utility in diagnosis, treatment,and monitoring dermatologic diseases. J Radiol 2006;87:1946–1961.
Mair MH, Geley T, Judmaier W, Gassner I. Using orbital sonographyto diagnose and monitor treatment of acute swelling of the eyelidsin pediatric patients. Am J Roentgenol 2002;179:1529–1534.
Marsollier L, Aubry J, Coutanceau E, André JP, Small PL, Milon G,Legras P, Guadagnini S, Carbonelle B, Cole ST. Colonization ofthe salivary glands of Naucoris cimicoides by Mycobacteriumulcerans requires host plasmatocytes and a macrolide toxin, myco-lactone. Cell Microbiol 2005;7:935–943.
Meyers W, Hayman J. Pathology. In: Asiedu K, Sherpbier R, Ravigli-one M, eds. Buruli Ulcer. Mycobacterium ulcerans infection. Ge-neva: WHO, 2000:35–36.
Nessi R, Betti R, Bencini PL, Crosti C, Blanc M, Uslenghi C. Ultra-sonography of nodular and infiltrative lesions of the skin and
subcutaneous tissues. J Clin Ultrasound 1990;18:103–109.Parenti GC, Marri C, Calandra G, Morisi C, Zabberoni W. Necrotizingfasciitis of soft tissues: Role of diagnostic imaging and review ofthe literature. Radiol Med 2000;99:334–339.
Pszolla N, Sarkar MR, Strecker W, Kern P, Kinzl L, Meyers WM,Portaels F. Buruli ulcer: A systemic disease. Clin Infect Dis 2003;37:e78–e82.
Ramamurthy RS, Scrinivasan G, Jacobs NM. Necrotizing fascitiis andnecrotizing cellulitis due to group B Streptococcus. Am J Dis Child1977;131:1169–1170.
Rettenbacher T, Tzankov A, Hollerweger A. Sonographic appearancesof subcutaneous and cutaneous oedema – correlation with histopa-thology. Ultrashall Med 2006;27:240–244.
Robinson P, Farrant JM, Bourke G, Merchant W, McKie S, Horgan KJ.Ultrasound and MRI findings in appendicular and truncal fat ne-crosis. Skeletal Radiol 2008;37:217–224.
Rubaltelli L, Tregnaghi A, Stramare R. Ultrasonography of superficiallymph nodes: Results acquired and new trials. Radiol Med 2004;107:388–406.
Schmid-Wendtner MH, Burgdorf W. Ultrasound scanning in derma-tology. Arch Dermatol 2005;141:217–224.
Seidenari S. High-frequency sonography combined with image analy-sis: A noninvasive objective method or skin evaluation and descrip-tion. Clin Dermatol 1995;13:349–359.
Unholzer A, Korting HC. High-frequency ultrasound in the evaluationof pharmacological effects on the skin. Skin Pharmacol Appl SkinPhysiol 2002;15:71–84.
Van der Werf TS, Stinear T, Stienstra Y, Van der Graaf WT, Small PL.Mycolactones and Mycobacterium ulcerans disease. Lancet 2003;362:1062–1064.
Wansbrough-Jones M, Phillips R. Buruli ulcer: Emerging from obscu-rity. Lancet 2006;367:1849–1858.
Wilson DJ. Soft tissue and joint infection. Eur Radiol 2004;14:E64–E71.
World Health Organization. 2004a. 57 World Health Assembly Advi-sory Group. Available: http://www.who.int/buruli/tag
World Health Organization. 2004b. Global Buruli Ulcer Initiative:Provisional guidance on the role of specific antibiotics in themanagement of Mycobacterium ulcerans disease (Buruli Ulcer).Available: http://www.who.int/buruli/information/antibiotics
World Health Organization. 2007. Summary Report of the WHOAnnual Meeting on Buruli Ulcer. Report of the Technical AdvisoryGroup Meeting. Available: http://www.who.int/buruli/events/Report_
2007_meeting_FINAL.pdfCopyright © 2022 FDOKUMEN




















