
ulrike schütz-fransson - DIVA
118
LICENTIATE THESIS IN ODONTOLOGY ULRIKE SCHÜTZ-FRANSSON FIXED MANDIBULAR RETAINERS A controlled 12-year follow-up LICENTIATE THESIS
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ulrike schütz-fransson - DIVA

LIC
EN
TIA
TE
TH
ES
IS IN
OD
ON
TO
LOG
Y
UL
RIK
E S
CH
ÜT
Z-F
RA
NS
SO
N
MA
LM
Ö U
NIV
ER
SIT
Y 2
01
8F
IXE
D M
AN
DIB
UL
AR
RE
TAIN
ER
S
ULRIKE SCHÜTZ-FRANSSON FIXED MANDIBULAR RETAINERS A controlled 12-year follow-up
L I C E N T I A T E T H E S I S


F I X E D M A N D I B U L A R R E T A I N E R S

© Copyright Ulrike Schütz-Fransson, 2018
Illustrations: Ulrike Schütz-Fransson
ISBN 978-91-7104-935-3 (print)
ISBN 978-91-7104-936-0 (pdf)
ISSN 1650-6065
Holmbergs, Malmö 2018

ULRIKE SCHÜTZ-FRANSSON FIXED MANDIBULAR RETAINERS A controlled 12-year follow-up
Department of OrthodonticsFaculty of Odontology
Malmö University, Sweden 2018

Publikationen finns även elektroniskt på:http://muep.mau.se/handle/2043/25665
Publikationen finns även elektroniskt,se www.mau.se/muep

To my family Christer, Anna and Erik


”There is nothing permanent, except change”Heraclitus of Ephesus
6th Century B.C.

CONTENTS
PREFACE ..................................................................... 11
THESIS AT A GLANCE ................................................... 12
ABSTRACT .................................................................. 13Paper I ................................................................................14Paper II ...............................................................................14PAR Index evaluation ............................................................15Key conclusions and clinical implications .................................15
POPULÄRVETENSKAPLIG SAMMANFATTNING .................. 16Konklusioner i delarbete I ......................................................17Konklusioner i delarbete II .....................................................17Konklusion i PAR Index utvärderingen .....................................17Klinisk betydelse ...................................................................18
INTRODUCTION .......................................................... 19Background .........................................................................19Retention methods ................................................................22Mandibular anterior segment stability .....................................25Mandibular anterior segment in untreated patients ...................26Biology during tooth movement and histological changes during orthodontic relapse .....................................................26Peer Assessment Rating .........................................................30
SIGNIFICANCE ............................................................ 32
AIMS ......................................................................... 34Paper I ................................................................................34Paper II ...............................................................................34PAR Index evaluation ............................................................34

HYPOTHESIS ............................................................... 35Paper I ................................................................................35Paper II ...............................................................................35PAR Index evaluation ............................................................35
SUBJECTS AND METHODS ............................................ 36Subjects ..............................................................................36PAR Index evaluation ............................................................39
Ethical considerations and consent ....................................40Methods ..............................................................................40
Papers I and II .................................................................40Paper II ...........................................................................42PAR Index evaluation ........................................................43Statistical analysis ............................................................43
RESULTS ..................................................................... 45Paper I ................................................................................45Paper II ...............................................................................48PAR Index evaluation ............................................................51
DISCUSSION ............................................................... 56Irregularity of mandibular anterior segment ..............................56Causative factors of relapse ..................................................59Irregularity of mandibular anterior segment in untreated cases ...59Overjet and overbite ............................................................60Cephalometric outcomes .......................................................60Gender ...............................................................................62Extractions versus non-extractions ...........................................62Retention for how long time? ..................................................63Failures and retainer breakages .............................................64Unexpected effects of fixed retainers .......................................65PAR Index evaluation ............................................................69Maintenance of fixed retainers ..............................................70Methodological aspects.........................................................71Future research.....................................................................72
CONCLUSIONS ........................................................... 73Key conclusions and clinical implications .................................74
ACKNOWLEDGEMENTS ............................................... 75
REFERENCES ............................................................... 78
PAPER I ..................................................................... 87PAPER II ...................................................................... 99

11
PREFACE
The following papers, on which this thesis is based, are referred to in the text as Paper I and Paper II.
I. Schütz-Fransson U, Lindsten R, Bjerklin K, Bondemark L. Twelve-year follow-up of mandibular incisor stability: Comparison between two different bonded lingual orthodontic retainers. Angle Orthod. 2017; 87:200-208.
II. Schütz-Fransson U, Lindsten R, Bjerklin K, Bondemark L. Mandibular incisor alignment in untreated subjects compared with long-term changes after orthodontic treatment with or without retainers. Accepted for publication by Am J Orthod Dentofacial Orthop. March 2018.
These papers are reprinted with kind permission from the copyright holders, The Angle Orthodontist and the American Journal of Orthodontics and Dentofacial Orthopedics.

12
THES
IS A
T A
GLA
NC
E T
HES
IS A
T A
GLA
NC
E
Study
Purpose
Study design
Sample
Main
outcom
e parameter
Main findings
I
To com
pare the long-te
rm
outcom
e 9 years after rem
oval of
two different types of fixed
retainers used for stabilisation of
the mandibular a
nterior segment;;
canine-to
-canine retainer and
Twistflex re
tainer
Retrospective
Contro
lled
Longitudinal
64 children
Little’s
Irregularity
Index (LII)
Both a canine-to-canine retainer and a Twistflex
retainer 3-3 can be recommended, as both are
equally effective when they are in place.
None of the retention types prevent long-term
changes of mandibular incisor irregularity after
removal of the re
tainers.
II
To analyse the dental and
skeletal changes 12 years after
treatment in patients tre
ated with
fixed orth
odontic appliances, w
ith
or without retention appliances
and to com
pare the changes with
untre
ated subjects
Retrospective
Contro
lled
Longitudinal
130 children
Little’s
Irregularity
Index (LII)
No differences were found in Little’s Irregularity
Index 12 years after treatment for the
mandibular incisors between the group that had
a retainer and the group that had no retainer
after treatment.
In the untre
ated group
, LII increased over time,
but not to the same extent as in the tre
ated
groups.
Correction of overjet and overbite was stable
long
-term
.
To evaluate the orthodontic
treatment outcome after
treatment and long
-term
, 12
years after treatment for tw
o different re
tainer groups and one
non-retention group
Retrospective
Contro
lled
Longitudinal
94 children
PAR Index
Twelve years after treatment, the mean
reduction in PAR
score was over 7
0 per cent for
the groups who had a mandibular retainer a
fter
treatment.
The non-retention group had a reduction of 66
per cent.
The cases that were ‘greatly im
proved’ and/or
‘improved’ 12 years after treatment w
ere 56 per
cent in the non-retention group, 64 per cent in
the canine-to
-ca n
ine retention group and 60
per
cent in the Tw
istflex re
tainer group.

13
ABSTRACT
A fixed retainer is a retention appliance that is often used after orthodontic treatment. For the mandibular incisors, two types of fixed retainer are commonly used – a canine-to-canine retainer bonded only to the canines or a Twistflex retainer bonded to each of the mandibular incisors and canines.
The increase in mandibular incisor irregularity seems to be a continuous process throughout life even in untreated patients. The natural physiological changes of aging causes the types of changes that occur after orthodontic treatment and the removal of a retainer. There are few long-term studies that compare patients who have had a mandibular fixed retainer with those patients who have not had any retention appliance after treatment, and then compare the treated patients with untreated subjects.
The overall aims of this thesis were to compare and evaluate two different mandibular fixed retainers and to compare orthodontically treated cases with those untreated long-term. The mandibular anterior region was evaluated.
This thesis is based on two studies, and a PAR Index evaluation is presented in the frame story.
The retrospective longitudinal study of Paper I focuses on the dental casts and lateral head radiographs of patients who had received either a canine-to-canine retainer or a Twistflex retainer after treatment. The study measured different variables, where Little’s Irregularity Index was the main outcome measure. The measurements were taken

14
at four different occasions, with the last registration occurring 12 years after treatment (i.e. nine years after the removal of the retainer).
Paper II is also a retrospective longitudinal study, but with three different groups. One group received a fixed mandibular retainer, one group did not receive any retention appliance after treatment, and the third group was composed of untreated subjects. Measurements were taken on dental casts and lateral head radiographs at four different occasions to analyse dental and skeletal changes 12 years after treatment. Here, Little’s Irregularity Index was also the main outcome measure.
The PAR Index evaluation was conducted to get an overall assessment of the orthodontic treatment outcome and not only to evaluate the mandibular anterior region, both directly after treatment and in the long-term for two different retainer groups and one non-retention group.
The following conclusions were drawn:
Paper I
• Both the canine-to-canine retainer and the Twistflex retainer can be recommended, as both are equally effective during the retention period.
• None of the retention types prevent long-term changes of mandibular incisor irregularity or available space for the mandibular incisors after removal of the retainers.
Paper II
• There were no differences found 12 years after treatment in Little’s Irregularity Index for the mandibular incisors between the group that had a retainer and the group that had no retainer after treatment.
• In the untreated group, Little’s Irregularity Index increased over time but not to the same extent as in the treated groups.
• The crowding before treatment did not explain the crowding at the last registration.

15
• The use of fixed mandibular retainers for two to three years does not appear to prevent long-term changes.
• The overjet and overbite were stable long term.
PAR Index evaluation
• Twelve years after treatment, the mean reduction in PAR score was over 70 per cent for the groups who had a mandibular retainer after treatment while the non-retention group had a PAR score reduction of 66 per cent.
• The cases that were ‘greatly improved’ and/or ‘improved’ 12 years after treatment were 56 per cent in the non-retention group, 64 per cent in the canine-to-canine retention group and 60 per cent in the Twistflex retainer group.
Key conclusions and clinical implicationsFor retention of the mandibular incisors after orthodontic treatment, the canine-to-canine retainer and the Twistflex retainer can both be recommended, as they are equally effective during the retention period.
The use of fixed mandibular retainers for two to three years does not appear to prevent long-term changes.
In untreated cases the mandibular incisor irregularity will increase over time but not to the same extent as in treated cases where the retainer has been removed.
Patients must be informed about the development of natural physiological changes that appear of the mandibular incisors through aging. If the patient wants to constrain natural development and changes, lifelong retainers are needed.

16
POPULÄRVETENSKAPLIG SAMMANFATTNING
Efter att ha genomgått tandregleringsbehandling (ortodontibehand-ling) måste tänderna ofta fixeras i sina nya lägen, eftersom de har en tendens att vilja flytta sig tillbaka till sina ursprungliga lägen (recidiv). Därför behöver tänderna hållas kvar efter behandling med t.ex. en metalltråd (retainer) som limmas på baksidan av framtänderna. För underkäkens framtänder finns det vanligen två olika typer av reta-inrar, antingen cuspid-retainern, som är styvare och limmas enbart på hörntänderna eller Twistflex-retainern, som är mer flexibel och limmas till samtliga framtänder och hörntänder.
Ökad trångställning av underkäkens framtänder är en kontinuerlig fysiologisk process som sker under hela livet både bland obehandlade och behandlade patienter. Det finns få långtidsuppföljningar som har jämfört patienter som har haft en retainer i underkäksfronten med individer utan retainer efter behandling, och dessutom jämfört behandlade med obehandlade individer.
Licentiatexamen är baserad på följande studier:
I en retrospektiv kontrollerad studie av studiemodeller samt profil-röntgenbilder var syftet i Studie I att i ett långtidsperspektiv jämföra cuspid-retainern med Twistflex-retainern ur stabilitetssynpunkt.
I studie II var syftet att jämföra ortodontiskt behandlade patienter med och utan retainer efter behandling med obehandlade, vad gäller underkäkens framtänder.

17
I ramberättelsen utfördes dessutom en PAR Index utvärdering (Peer Assessment Rating) för att analysera det totala behandlingsre-sultatet och inte bara utvärdera förändringarna av underkäksfram-tänderna. Utvärderingen gjordes direkt efter behandling samt 12 år efter behandling, för grupperna med olika retainrar samt gruppen utan retention.
Konklusioner i delarbete ISex och 12 år efter tandregleringsbehandling, och i genomsnitt 9,2 år efter att retainrarna hade avlägsnats kunde följande resultat och slutsatser dras:
• Både cuspid-retainern och Twistflex-retainern kan rekommenderas eftersom båda är lika effektiva under retentionsperioden.
• Ingen av retainrarna kunde förhindra trångställning av underkäkens framtänder på lång sikt efter att retainrarna har tagits bort.
Konklusioner i delarbete IIEn jämförelse mellan patienter som fått en bondad retainer med patienter utan någon retention efter behandling och en obehandlad grupp, gav följande slutsatser:
• Det förelåg inga skillnader mellan gruppen som hade haft en retainer och gruppen utan retainer, 12 år efter behandling med avseende på trångställningsgraden av underkäkens framtänder.
• I den obehandlade gruppen ökade också trångställningen av underkäkens framtänder över tid men inte lika mycket som i de behandlade grupperna.
Konklusion i PAR Index utvärderingen
• Tolv år efter behandling är förbättringsprocenten fortfarande bra men lägre än direkt efter behandling. Detta visar att förändringar har skett för många variabler i bettet. Detta gäller för samtliga 3 grupper.

18
Klinisk betydelseFör att retinera underkäksframtänderna efter tandreglerings-behandling är cuspid-retainern och Twistflex-retainern likvärdiga.
Hos obehandlade individer ökar också trångställningen av underkäksframtänderna, dock inte lika mycket som hos behandlade patienter, där retainern har tagits bort.
Om patienten vill ha jämna tänder livet ut och därmed förhindra de förändringar som sker genom naturlig fysiologisk utveckling, behöver retentionstrådarna sitta kvar hela livet.

19
INTRODUCTION
BackgroundIn Sweden, all children and adolescents receive free dental care until they are 22 years old, with the exception of some counties where the cut-off age is 24 years. There are several studies (Linder-Aronson et al. 2002; Holm 2005; Bjerklin et al. 2012) that have shown various prevalence of objective treatment need in Sweden. In most of the studies, 30–35 per cent of the children, adolescents, and young adults in this age range are offered free orthodontic treatment to correct their malocclusions.
The goal for orthodontic treatment is to achieve good function, good aesthetics and stable occlusion. Later, it is important to retain the treatment result to avoid relapse, and this is a great challenge in orthodontic treatment.
Relapse can be defined as the tendency of treated teeth to return to their former positions. Back in 1936, Mershon explained, “You can move teeth to where you THINK they belong; NATURE will place them where they best adapt themselves to the rest of the organism” (Mershon 1936).
The tendency of treated teeth to move back to their former position was already known by Coleman back in 1865 in England. A year later, Marvin described the physiological reasons for retention, and in 1881, James W. Smith designed the first retainer in the USA (Weinberger 1926). This retainer consisted of a vulcanite plate with a bar to keep the maxillary incisors in place. Since then, much has changed in the concept of how teeth should be retained. In 1887, Edward H. Angle suggested that a retaining appliance should hold

20
the teeth so firmly that there will be no movement to disturb or in any way interfere with the new bone formation (Angle 1887).
Riedel shared his ideas on stability and proposed nine retention rules (Riedel 1960). In the nine rules, he claims that
1) teeth tend to return to their former positions,2) mandibular arch form should be maintained during orthodontic
treatment,3) a proper diagnosis based on determining the cause of
malocclusion is invaluable, 4) overcorrection of malocclusion is a safety factor in retention, 5) occlusion is an important factor in retention,6) bone and adjacent tissues must be allowed to reorganise
around the newly positioned teeth for some length of time, 7) placing the mandibular incisors upright over basal bone will
result in a more stable correction of a malocclusion,8) corrections carried out during periods when the patients are
growing are less likely to relapse, and9) the farther teeth have been moved the less the likelihood of
relapse.
Retention is central for establishing long-term stability. Thus, after orthodontic treatment, the retention period has to be taken into consideration in the treatment plan, which involves considering how to retain and for how long. Therefore, it is important to understand the relapse process. Orthodontic relapse is a term to describe the post-treatment adaptation of the dentoalveolar system to changes in the mechanical conditions caused by the withdrawal of orthodontic forces. Usually, this change is distinguished between fast relapse, which occurs during the remodelling of the periodontal ligament, and slow relapse, which refers to changes later in life, i.e. natural physiological changes, (Thilander 2000). These later changes cannot be separated from normal age-related changes that appear independently whether orthodontic treatment has been carried out or not.
The amount and nature of relapse is unpredictable and variable. In most studies, we do not find any clinical, biometric or cephalometric variables that can predict the post-retention crowding. This is because relapse is considered as a multifactorial process. Among the factors that may cause relapse following orthodontic tooth movement are

21
tooth size, arch form, abnormal muscle function, occlusal stress, patient age, length of retention, mandibular rotation, apical base, craniofacial growth and mainly, the contraction of displaced fibrous tissue rearrangement that may be observed even after several years. In a study by Glenn et al. (1987), eight years post-retention, out of retention for a minimum of three years in non-extraction cases, the mandibular incisor mesiodistal and faciolingual dimensions were not associated with either pre-treatment or post-treatment incisor crowding. Another study with extraction cases, 5.1 years post-treatment and a fixed mandibular retainer for mean 1.6 years, showed that the mandibular-incisor-crown morphology was not significantly correlated with the amount of mandibular-anterior-crowding relapse (Freitas et al. 2006a).
If a malocclusion is caused by muscular or other soft tissue dysfunctions (i.e. cheek/lip/tongue pressure), and if the correction of this malocclusion is performed without any alteration in muscular or dysfunctional behaviour, then there will be an obvious risk of relapse (Proffit 1986).
Other important factors for long-term stability are a good occlusion, unchanged intermolar and intercanine distance (Proffit 2013). Changing the original dental arch form during treatment and the expansion of the transverse distance between the canines and molars increase the risk of relapse (de la Cruz et al. 1995). In cases with small apical bases, expansion treatment should be avoided to reduce the risk of relapse. The position of the incisors is recommended to be within normal range, i.e. the incisors have to be positioned over the apical base.
Also, the growth pattern of an individual patient is an important factor. Orthodontic corrections are likely to relapse during periods of growth, which include the eruption of teeth. It seems that the pattern of late mandibular growth is one contributor to the crowding tendency (Nanda & Nanda 1992). Moreover, there are researchers who claim that early treatment of malocclusions provides greater final stability (Kerosuo et al. 2013).
A mesially acting force emanating from the back of the dental arch is another possible factor (Samspon 1995), but the theory that pressure from the developing third molars causes late incisor crowding has not been confirmed. The presence of third molars does not appear

22
to produce a greater degree of mandibular anterior crowding after the cessation of retention than that which occurs in patients with third molar agenesis (Kaplan 1974). A study examined 51 subjects with intact lower arches and bilateral third molars present at the ages of 13 and 18 years. It was considered that the third molars are one of the causes of late mandibular arch crowding (Richardson 1989). The principal conclusion from another study was that the removal of third molars to reduce or prevent late mandibular incisor crowding could not be justified (Harradine et al. 1998). In addition, a review study concluded that long-term studies in untreated individuals do not suggest evidence of a cause and effect relationship between third molars and late mandibular incisor crowding. Thus, asymptomatic and pathology-free third molars should not be extracted to prevent post-retention crowding or to prevent late mandibular crowding in untreated individuals (Sumitra & Arundhati 2005).
Periodontal force is a potential cause of relapse (Reitan 1967; Johnston & Littlewood 2015). The periodontium exerts a continous force on the mandibular dentition and this force acts to maintain the contacts of approximating teeth in a state of compression. This force is increased after occlusal loading and may help to explain long-term crowding of the mandibular anterior teeth, physiologic drifting of teeth, and maintenance of posterior dental contacts after interproximal wear (Southard et al. 1992).
Genetic factors must also be considered, as it also constitutes a factor during retention following treatment. For instance, the influence caused by hereditary factors may be observed in certain cases in which overlapping by one or both lateral incisors are observed in the patient as well as in his/her mother or father (Reitan 1969).
One reliable predictor of relapse has been found by (Renkema et al. 2008 and 2011). They reported that the number of retainer failures, i.e. the number of detachments and/or breakages of the retainer, contributed to the relapse.
Retention methods‘Retention’ is derived from the Latin verb, retinere, which means ‘to hold back or maintain in place’.

23
Retention is necessary in cases where
• the supporting tissues of the teeth need to be reorganised around the teeth in their new position
• there is a (neuro)muscular imbalance, as the teeth may be in an inherently unstable position after treatment
• there is continued bone growth and remodelling after orthodontic treatment
• persistent unwanted habits could be present
To prevent relapse after orthodontic treatment, a fixed retainer was advocated 45 years ago (Knierim 1973), when enamel etching and modern adhesive systems became more common. Prior to that, a lingual wire soldered to canine bands for the fixed mandibular retainer had been used. Various combinations of stainless steel or beta titanium alloys were used on rectangular or round wires that were either braided or twisted and in various sizes ranging from 0.016 to 0.032-inch. Later, a multi-strand 0.0175-inch wire bonded on six anterior teeth was used (Zachrisson 1977). The next generation of fixed retainers was introduced in 1982. These were composed of heavier, flexible, round multi-strand 0.032-inch wires bonded only to the canines. Unfortunately, this heavy multi-strand wire caused an increase of plaque accumulation and reduced wearing comfort (Årtun & Zachrisson 1982). Further clinical experience resulted in a new generation of fixed retainers constructed on a plaster model from a smooth stainless-steel wire (0.030 to 0.032-inch) sandblasted at both ends to increase composite retention (Zachrisson 1995).
Another retention method is the vacuum-formed retainer such as the Essix retainer (Sheridan et al. 1993). This retainer can be used alone or in combination with bonded retainers.
Interproximal enamel reduction, or interproximal stripping of the mandibular anterior teeth has been shown to be an alternative strategy for preventing relapse. Often, it is done in combination with over-correction of rotated teeth. In a study by Aasen and Espeland (2005), 56 patients were treated with over-correction of rotated teeth and systematic enamel reduction of the approximal surfaces in the mandibular anterior region. In 45 per cent of the patients, the change in Little’s Irregularity Index was less than 0.5 mm three years

24
post-treatment, indicating that this treatment approach may be an alternative strategy to mandibular fixed retainers.
In another study by Edman Tynelius et al. (2015) five years out of retention, three different retention strategies were compared: bonded canine-to-canine retainer, positioner, and stripping of the mandibular anterior teeth. The results showed that all three retention methods gave equally favourable clinical results.
Surgical peri-incision of the supra-alveolar tissue (i.e. fiberotomy) has been proposed as a method to prevent relapse of rotated incisors. This method has been combined with serial reproximation early in treatment, six months after debond, and further on post-retention (Boese 1980). In a prospective study, the surgical procedure appeared to be more effective in alleviating pure rotational relapse than in labiolingual relapse (Edwards 1988). In addition, patients treated with circumferential supracrestal fiberotomy one week before debond were compared with a control group with no fiberotomy. In the group treated with fiberotomy, no significant increase of the irregularity index was noted, but in the control group, a significant increase of irregularity index was noted for both maxillary and mandibular anterior segment (Taner et al. 2000).
The two most common retention methods for the mandibular anterior segment are bonded retainers, either a Twistflex retainer bonded to all incisors and the canines or a rigid retainer bonded to the canines only (Zachrisson 1997; Proffit 2013). They are independent of patient cooperation, except for tooth brushing, nearly invisible, and easy to fabricate, but they need regular check-ups. Many studies have shown that bonded retainers are an efficient and reliable retention appliance in the long-term (Al Yami et al. 1999; Segner & Heinrici 2000; Zachrisson 2007; Booth et al. 2008; Renkema et al. 2011). Thus, these retainers are widely used, but few studies have evaluated the long-term effectiveness. Moreover, a Cochrane review (Littlewood et al. 2016) revealed that only two randomized controlled trials assessed the mandibular anterior segment long-term five and six years after treatment (Bolla et al. 2012; Edman Tynelius et al. 2015). It can also be pointed out that few studies have analysed the long-term outcome after removal of the retainers (Edman Tynelius et al. 2015), and in many studies, the retainers are still in place at the follow-up, five years post-treatment (Renkema et al. 2008 and 2011).

25
Mandibular anterior segment stabilityMost of the studies on retention and relapse that have been published refer to the mandibular anterior arch. The first published studies considered the intercanine distance a key factor for the stability of the mandibular anterior segment. It was published in 1944 by McCauley who stated that the two mandibular dimensions – molar width and canine width – are of such an uncompromising nature that one should establish them as fixed quantities (McCauley 1944). Many studies have later also shown that increasing the intercanine distance during treatment will later end up with a reduction in intercanine distance and increased mandibular incisor crowding after the follow-up period (Fastlicht 1970; Sondhi et al. 1980; Uhde et al. 1983; Zachrisson 1997).
When comparing extraction and non-extraction cases, some studies have shown a greater reduction in intercanine distance in cases treated with extractions (Shapiro 1974; Gardner & Chaconas 1976), while another study showed a larger mandibular intercanine dimension in extraction cases after treatment (Gianelly 2003).
The studies by Little and co-workers at the University of Washington in Seattle, where they studied more than 600 treated cases for more than 35 years, have given us much knowledge about mandibular incisor crowding, both in treated cases and in normal occlusions without treatment (Sinclair & Little 1983; Little 1990 and 1999). The conclusions from their studies are that the mandibular arch length progressively decreases and the intercanine distance also decreases in both treated and untreated cases. There is a tendency towards mandibular incisor crowding over time that continues at least up to the age of 40. There were no statistics to predict which cases would relapse and which would remain stable (Little 1999). Park and co-workers studied arch length changes over time in adolescents and adults. They found that arch length and intercanine width showed statistically significant decreases over time in both groups. Over the 16-year-long post-treatment period, adolescents showed a significantly greater increase in mandibular incisor irregularity than adults (Park et al. 2010).

26
Mandibular anterior segment in untreated patientsIncreased mandibular incisor irregularity has also been reported to be a continuous process throughout life in untreated patients (Eslambolchi et al. 2008; Tsiopas et al. 2013; Bondevik 2015). Continuous changes of the dental arches occur from the primary until the adult period, with individual variations. This change could be explained as a biological migration of the dentition, which will result in anterior crowding, especially in the mandible. Crowding depends on the relationship between the size of the teeth and the dimensions of the dental arches (Thilander 2009). The length, width, and depth of the jaws, as well as the size of the teeth, are all integrated parts of this equation.
The natural physiological changes that appear in the dental arches throughout aging are similar to those after orthodontic treatment once the retainers have been removed, but are they of the same amount? Are the post-treatment changes a result of relapse or are they part of the normal aging process? Studies have compared mandibular irregularity in treated and untreated patients long-term and found that normal, untreated patients showed similar physiological changes as treated cases (Little 1999).
Thilander (2000) found that late changes occurring during the post-retention period could not be distinguished from normal aging processes that occur regardless of whether a person has been treated orthodontically or not. Freitas et al. (2013) studied three groups: one treated with four premolar extractions, one treated non-extraction, and one untreated group. They concluded that the post-treatment change of the mandibular anterior crowding of the treated extraction cases was greater than the mandibular crowding caused by physiologic changes in the untreated group. On the contrary, another study that compared extraction and non-extraction cases with untreated subjects concluded that the long-term development of mandibular anterior crowding was unfavourable in subjects treated without extractions (Jonsson & Magnusson 2010).
Biology during tooth movement and histological changes during orthodontic relapseThe stability of tooth position is determined by the principal fibres of the periodontal ligament (PDL) and the supra-alveolar gingival fibre

27
network. These fibres contribute to a state of equilibrium between the tooth and the soft-tissue envelope. Orthodontic tooth movement will cause disruption of the PDL and the gingival fibre network, and a period of time is required for reorganisation of these fibres after orthodontic treatment.
Newly formed bone tissue, the adjacent bone tissue, and the fibre bundles of the periodontal membrane must be allowed to reorganise around the newly positioned teeth. Histologic evidence shows that bone and the tissue around the teeth that have been moved are altered, and it takes a considerable amount of time before complete reorganisation occurs.
Orthodontic relapse starts very fast and slows down until a stable situation is attained. The time at which half of the relapse takes place, i.e. the time it takes for half of the total amount of collagen to be replaced, varies among species, areas, and applied forces from less than one day to approximately 11 days. The total amount of immediate relapse ranges from 30 to 90 per cent of active tooth movement (Maltha & Von den Hoff 2017).
Histological studies have shown that the process of orthodontic relapse is similar to active tooth movement. The pressure side during active tooth movement can be considered the new tension side during orthodontic relapse. The initial reaction is physical due to the strain of the extracellular matrix of the PDL and the alveolar bone. This strain leads to a fluid flow in the PDL and the canaliculi of the alveolar bone, and later to cell strain of the periodontal fibroblasts, osteoblasts and osteocytes. This will then lead to cascades of molecular events and finally to the synthesis of many neurotransmitters, cytokines, growth factors, and colony-stimulating factors. The tooth movement is then facilitated by local stimulation of extracellular matrix synthesis or degradation and bone deposition or resorption (Maltha & Von den Hoff 2017).
The PDL, which is about 0.25 mm wide, joins the root cementum with the lamina dura or the alveolar bone. In the coronal direction, the PDL is continuous with the lamina propria of the gingiva and is separated from the gingiva by the collagen fibre bundles, which connect the alveolar bone crest with the root.

28
The principal fibres of the PDL associate into the following groups:
• Alveolar crest fibres• Horizontal fibres• Oblique fibres• Apical fibres• Interradicular fibres
The connective tissue of the gingiva consists of 60 per cent collagen fibres (including elastic-like oxytalan fibres), five per cent are fibroblasts and 35 per cent are vessels, nerves and matrix. The collagen fibres can usually be divided into four groups:
• Dentogingival fibres • Circular fibres• Transseptal fibres• Dentoperiosteal fibres
The tissue reactions in the gingiva differ from those in the PDL, which is important for the stability of an acquired tooth position (Thilander 2000). The remodelling of gingival connective tissue (collagenous and elastic fibres) is not as rapid as that of the PDL, as the supra-alveolar fibres are not anchored in a bone wall that is readily remodelled. The reason for the slow remodelling of the supra-alveolar tissues is probably related to the quality of particular fibre groups whose main function is to protect the alveolar process and conserve tooth position and interproximal contact (Rygh 1995). The difference in turnover rate between gingival and periodontal fibres might be related to the fact that the gingival fibres are generally only embedded in the root cementum and not in the alveolar bone (Thilander 2000).
Within four to six months, the collagenous fibre networks within the gingiva have normally completed their reorganisation, but the elastic supracrestal fibres remodel extremely slowly and can still exert forces capable of displacing a tooth at one year after removal of the orthodontic appliance (Proffit 2013).
The reorganisation or remodelling of the periodontal ligament occurs over a three to four month period. Several factors are essential for the re-establishment of an adequate supporting apparatus during and after tooth movement, and conversely, for a possible lack of stability after treatment:

29
• the main remodelling of the periodontal ligament takes place near the alveolar bone and is different on the tension side, and
• remodelling of the fibrous system on the tension side is related to the direction of pull on the tooth resulting in the production of new fibres only in that direction (Rygh 1995).
The experimental studies assessed by Reitan 1959 and 1967 found that there is no rearrangement of the fibrous structures in the marginal region of the tooth after a retention period of 28 days. Even after 232 days, the free fibre bundles of the labial and lingual surfaces of the root will remain stretched and displaced. Complete rearrangement in the middle and apical region of the tooth can be seen after 232 days. The most persistent relapse tendency is caused by the structures related to the marginal third of the root, whereas little relapse tendency exists in the area adjacent to the middle and apical thirds.
Much of the cellular activity in a bone consists of removal and replacement at the same site – a process called remodelling. Bone remodelling is a process where osteoclasts and osteoblasts work sequentially in the same bone remodelling unit. The osteoclasts resorb the bone by a strictly coordinated process, whereas the osteoblasts produce new bone of the same amount as the osteoclasts have resorbed.
The adult skeleton is renewed by remodelling every ten years (Mangolas 2000). In the time span of one year, 10 per cent of the skeleton is replaced by new bone, and every ten years, we get a new skeleton. In children and adolescents, the bone tissue is converted faster but no exact time periods can be found in the literature. During childhood and adolescence, bones are sculpted by a process called modelling, which allows for the formation of new bone at one site and the removal of old bone from another site within the same bone. Bones are shaped or reshaped by independent action of osteoblasts and osteoclasts (Langdahl et al. 2016). This process allows individual bones to grow in size and to shift in the space.
During derotation of teeth, the compressed gingiva that rotates with the tooth during the rotation movement will form an increased amount of elastic fibres. These fibres exert pressure on the tooth leading to relapse after the release of retention (Redlich et al. 1999).

30
It is possible to prevent relapse of rotated teeth by the surgical procedure of fiberotomy, which disconnects the compressed gingiva from the tooth thus preventing relapse (Taner et al. 2000).
Other fibres in the PDL may also play a role for the relapse tendency, namely, the presence of oxytalan fibres. Oxytalan fibres can be classified as belonging to the elastic fibre family. It has been claimed that stress induced by orthodontic force application leads to the increased amount, size and length of oxytalan fibres. This suggests a mechanical function for the oxytalan fibre network in the PDL. The oxytalan fibres may take up to six years to remodel (Kharbanda & Darendeliler 2016). Oxytalan fibres develop simultaneously with the root and the vascular system within the PDL. A close association between oxytalan fibres and the vascular system also remains later in life, suggesting a role in vascular support. Further research is required to clarify the exact mechanical function and possible role of oxytalan fibres in orthodontic tooth movement (Strydom et al. 2012).
Peer Assessment RatingIn orthodontics, it is important to objectively assess whether or not an improvement of the orthodontic treatment has been achieved in terms of overall alignment and occlusion. Therefore, to evaluate orthodontic treatment outcome, the Peer Assessment Rating (PAR) Index is often used (Richmond et al. 1992a). The PAR Index was developed to provide a single summary score for all the occlusal anomalies, which can be found in a malocclusion. The PAR Index is claimed to offer uniformity and standardisation in assessing the outcome of orthodontic treatment and is thereby used as an evaluation instrument for the orthodontist to measure his/her own quality as well as measuring the overall quality in larger samples. The PAR Index comprises 11 components: upper-right segment, upper-anterior segment, upper-left segment, lower-right segment, lower-anterior segment, lower-left segment, right buccal occlusion, left buccal occlusion, overjet, overbite and centreline. The score provides an estimate of how far a case deviates from normal alignment and occlusion.
The difference between the before and after treatment scores reflects the degree of improvement, which can be judged as ‘greatly improved’, ‘improved’ or ‘worse/not improved’. The mean reduction

31
in PAR Index should be as high as possible, e.g. greater than 70 per cent. At least a 30 per cent reduction in PAR score is the minimal requirement for a case to be judged as ‘improved’ (Richmond et al. 1992b). If the score is less than 30 per cent after treatment the case is found to be ‘worse or not improved’.
A change of 22 points or greater in a weighted PAR score is required for a case to be considered ‘greatly improved’. Weightings have been derived for individual components from validation studies in which panel assessments serve as the “gold standard”. The weighted score for each of the components are combined to form a single summary score.

32
SIGNIFICANCE
It can be noted that there are few long-term studies that have been performed more than five years after removal of the mandibular retainer, and furthermore, long-term follow-up studies conducted more than 10 years after treatment are lacking, and therefore, desirable. For this purpose, a unique material of both treated and untreated subjects with records dating back more than 10 years after orthodontic treatment at the Department of Orthodontics in Jönköping, Sweden, was used in the studies of this thesis. As these patients were treated with two different fixed mandibular retainers in addition to a group of patients who never got a retention appliance in the mandibular anterior region, this was an opportunity to analyse the cases. It became possible to compare the two most commonly used types of fixed retainers focusing, in particular, on the retainers’ ability to stabilise the mandibular anterior segment. The results of the studies are considered to help orthodontists when deciding which fixed retainer type to choose in order to avoid or minimise relapse.
Another challenge was to compare treated patients with aged-matched untreated subjects long-term regarding the mandibular incisor alignment, to find out what has been caused by relapse and what has been caused by natural physiological changes. To gain more insight into this problem could result in being able to make more clear what is a normal development of the occlusion and tooth positions and what is a relapse when explaining these to both patients and other professionals. Perhaps this could even lead to the patients’ greater understanding about how natural physiological changes may occur thus avoiding misplaced blame on the orthodontist for a relapse.

33
In the frame story of this thesis, a PAR evaluation was also carried out to get an overall assessment of the orthodontic treatment outcome and not only to evaluate the mandibular anterior region.

34
AIMS
Paper I
• To compare the long-term outcome 9 years after the removal of two different types of fixed retainers used for stabilisation of the mandibular anterior segment.
Paper II
• To analyse the dental and skeletal changes in patients treated with fixed orthodontic appliances, with or without retention appliances, and to compare the changes with a group of untreated subjects. In particular, mandibular incisor irregularity was studied.
PAR Index evaluationA further aim was to conduct a Peer Assessment Rating evaluation, which is presented in the frame story of this thesis.
The main purpose with the evaluation was to get an overall assessment of the orthodontic treatment outcome and not only to evaluate the mandibular anterior region. Firstly, the degree of improvement in malocclusion was determined after orthodontic treatment and also long-term, in terms of ‘greatly improved’, ‘improved’ or ‘worse/not improved’. Secondly, the pre-treatment weighted PAR score was compared with the weighted PAR score after treatment. In addition, the pre-treatment, weighted PAR score was compared with the weighted PAR score 12 years after treatment between the group without retention, the group with canine-to-canine retainer, and the group with Twistflex retainer.

35
HYPOTHESIS
Paper IThere would be no difference in mandibular incisor stability between the two different mandibular retainers in a long-term perspective.
Paper IIThe long-term mandibular incisor irregularity for the treated group without retainer is greater than for the group with retainer. Both groups who have undergone orthodontic treatment had a higher amount of irregularity than the untreated group.
PAR Index evaluationThe mean percentage reduction in weighted PAR score should be greater than 70 per cent in each of the three groups, after orthodontic treatment. Furthermore, 12 years after treatment, at least 70 per cent of the cases in each group should be ‘greatly improved’ and/or ‘improved’.

36
SUBJECTS AND METHODS
SubjectsIn Paper I, the study comprised 64 children who had their orthodontic treatment performed 1980–1995 at the Department of Orthodontics at the Institute for Postgraduate Dental Education in Jönköping, Sweden. The patients received orthodontic treatment for Class II malocclusions, large overjet, crowding and/or deep bites.
The sample was divided into two groups based on which type of fixed mandibular retainer was used after treatment. Twenty-eight of the patients received a canine-to-canine retainer (0.028-inch spring hard wire) bonded to the canines (Group 1), and 36 patients had a bonded Twistflex retainer (0.0195-inch) which was bonded to all mandibular incisors and canines (Group 2). Both types of retainers were custom-made in the laboratory and bonded with composite (Figure 1).
Figure 1
Canine-‐to-‐canine retainer Twistflex retainer
Figure 1
Canine-‐to-‐canine retainer Twistflex retainer
Figure 1. Canine-to-canine retainer Twistflex retainer

37
To participate in the study, long-term records were required. No interproximal enamel reduction or circumferential supracrestal fiberotomy was performed in either group. In both groups, extractions were carried out prior to treatment for the same number of patients (i.e. 64 per cent extraction cases and 36 per cent non-extraction cases in each group).
The orthodontic treatment consisted of fixed edgewise appliances (0.018-inch) in both jaws.
Figure 2 presents a flow chart of the patients in Paper I.
N=28 13 boys 15 girls
N=36 10 boys 26 girls
N=36 10 boys 26 girls
N=28 13 boys 15 girls
N=36 10 boys 26 girls
N=28 6 boys 22 girls
N=26 12 boys 14 girls
N=24 11 boys 13 girls
T0 1 reg/ before tx
T1 2 reg/ after tx
T2 3 reg/ 6 yrs after tx
T3 4 reg/ 12 yrs after tx
Canine-‐to-‐canine retainer Twistflex retainer Group 1 Group 2
Figure 2. Flow chart of the patients in Paper I.

38
In Paper II, three different groups were included with a total of 130 children: two groups who received orthodontic treatment (105 patients) and one untreated group (25 subjects). Long-term records were required for participation in the study. Sample exclusions were single arch treatment, cleft lip and/or palate, agenesis and extraction of anterior teeth. This was a retrospective material, and no cases have been added or excluded after applying the inclusion criteria.
One of the groups who had undergone orthodontic treatment with fixed appliances in both jaws received a fixed mandibular retainer after treatment. In total, there were 64 patients, and they were all patients from Paper I. This group received either a canine-to-canine retainer or a Twistflex retainer (Group 1, retention group). The mean retention time was 2.7 years (SD 1.50).
The other group consisted of 41 patients with similar orthodontic treatment as the retention group, but they did not receive any retainer in the mandibular arch at all (Group 2, non-retention group).
The decision to leave the treated patients without retention in the mandible was made by the orthodontists who treated the patients.
All of the treated cases had a removable appliance in the maxilla for retention. No interproximal enamel reduction or circumferential supracrestal fiberotomy had been performed in the groups who had orthodontic treatment.
The third group – the untreated subjects – was comprised of 25 cases that were age-matched with the subjects in the two other groups (Group 0, untreated group).
The indications for orthodontic treatment for the 105 patients in Paper II were the same as in Paper I. All participants in Paper II were also recruited from the Department of Orthodontics in Jönköping, Sweden, between 1980 and 1995.
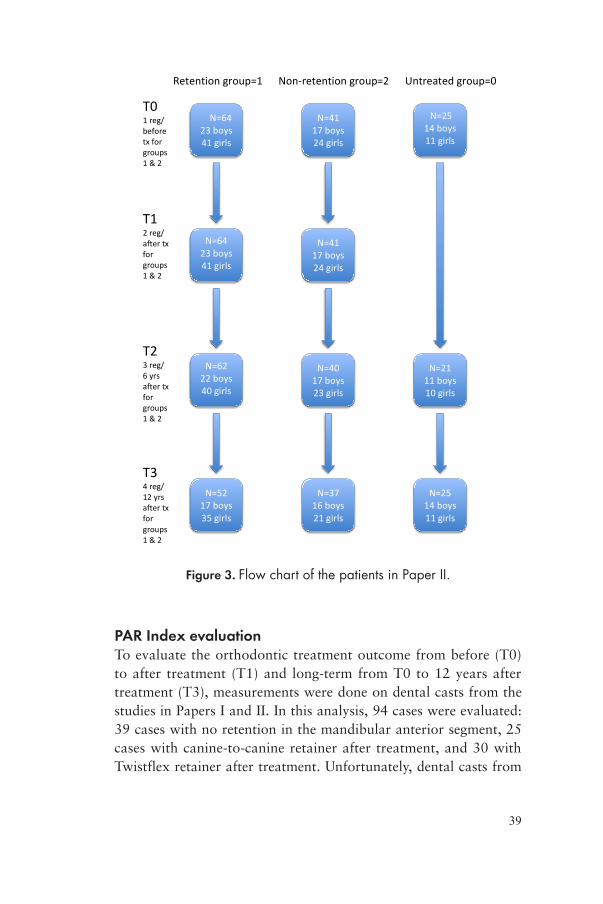
Twelve patients were excluded from the study, as the records did not meet the requirements and they were all from Group 2. In particular, there were missing registrations, especially at the last registration. Figure 3 shows a flow chart of the subjects in Paper II.
39
N=64 23 boys 41 girls
N=41 17 boys 24 girls
N=25 14 boys 11 girls
N=41 17 boys 24 girls
N=64 23 boys 41 girls
N=40 17 boys 23 girls
N=21 11 boys 10 girls
N=37 16 boys 21 girls
N=25 14 boys 11 girls
N=62 22 boys 40 girls
N=52 17 boys 35 girls
T0 1 reg/ before tx for groups 1 & 2
T1 2 reg/ after tx for groups 1 & 2
T2 3 reg/ 6 yrs after tx for groups 1 & 2
T3 4 reg/ 12 yrs after tx for groups 1 & 2
Retention group=1 Non-‐retention group=2 Untreated group=0
Figure 3. Flow chart of the patients in Paper II.
PAR Index evaluationTo evaluate the orthodontic treatment outcome from before (T0) to after treatment (T1) and long-term from T0 to 12 years after treatment (T3), measurements were done on dental casts from the studies in Papers I and II. In this analysis, 94 cases were evaluated: 39 cases with no retention in the mandibular anterior segment, 25 cases with canine-to-canine retainer after treatment, and 30 with Twistflex retainer after treatment. Unfortunately, dental casts from

40
11 cases were not available of which, 2 were distributed to the non-retention group, 3 to the canine-to-canine group, and 6 to the Twistflex retainer group.
Ethical considerations and consent The Ethics Committee of Linköping, Sweden, approved the protocol (2014/381-31).
Each patient and parent received verbal information at start of the treatment about the possibility of using their study models in future studies. There was no need for any written information according to the Ethics Committee.
MethodsPapers I and IIMeasurements were performed on dental casts using a sliding digital caliper (Mitutoyo 500-171 Kanagawa, Japan) with an accuracy of 0.01 mm.
The measurements were made at four occasions: T0 before treatment, T1 immediately after orthodontic treatment (i.e. at the start of retention), T2 six years after treatment (i.e. mean 3.6 years after the retainer was removed), and T3 12 years after treatment (i.e. mean 9.2 years after removal of the retainer).
The main outcome measure was Little’s Irregularity Index, LII (Little 1975) – the summed displacement of the anatomic contact points of the mandibular anterior teeth (Figure 4). Other measurements performed on dental casts were intercanine width (cusp tip to cusp tip of the mandibular canines), intercanine perimeter distance (arch perimeter length between the mesial contact points of the canines), available mandibular incisor space (intercanine perimeter distance minus summed tooth width for the four mandibular incisors), two different lateral arch lengths (from the mesial contact point of the mandibular first molar to the mesial contact point of the canines and to the mesial contact point of the central incisors), overjet, and overbite (Figure 5). In Paper II, one of the lateral arch lengths (to the central incisors) was not measured.

41
Figure 4. Little’s Irregularity Index = A+B+C+D+E
Measured variables
1.Intercaninewidth
2.Intercaninearchperimeterdistance
3.Lateralarchlengthle76-2
4.Lateralarchlengthright6-2
5.Lateralarchlengthle76-central
6.Lateralarchlengthright6-central
1
2
3
546
Figure 5. Measured variables
On lateral head radiographs the sagittal and vertical relationships between the jaws and the incisor inclination were evaluated. The cephalometric reference lines and points were assessed according to Björk (1947) and Solow (1966) (Figure 6). The measurements on the lateral head radiographs were made to the nearest half-degree or 0.5 mm with correction for enlargement.

42
SNA SNB ANB SN/ML ML/NL SN/NL U1/NL L1/Apg mm L1/ML Interincisal angle
Figure 6. Cephalometric reference lines and points
All registrations were made by one examiner (USF). At T2 and T3, no retention appliance was in place. As a result, a blinded evaluation was possible, i.e. the examiner was unaware to which group the patients belonged or if the casts were taken at T2 or T3.
Also in Paper I, the bonding failures for the different retainers were obtained from the patients’ records.
Paper IIFor the untreated group, dental casts and lateral head radiographs were available for the corresponding ages at T0, T2 and T3, but not at T1. In the retention group, no retention appliance was in place at T2 and T3.
The untreated control material consisted of subjects from two PhD dissertations: Infraocclusion of primary molars (Kurol 1984) and Ectopic eruption of maxillary first permanent molars (Bjerklin 1994). From these dissertations, it is clear that in cases with infraocclusion of primary molars with permanent successors, the growth and development of the dentition is normal. Also, cases with the reversible type of ectopic eruption of the maxillary first permanent molars show a normal growth and development of the dentition regarding eruption of the first, second and third permanent molars.

43
The subjects had Class I occlusion without any other malocclusions and registrations were performed for the above reasons.
PAR Index evaluationThe same examiner (USF) did the evaluation using a PAR ruler to take the measurements. The individual scores were summed to obtain an overall total score representing the degree a case deviates from normal alignment and occlusion. A score of zero indicates good alignment and occlusion whereas higher scores indicate increased levels of irregularity and deviation in occlusion.
The overall score was recorded on pre-treatment (T0), post-treatment (T1), and 12 years post-treatment dental casts (T3) for the three groups (non-retention, canine-to-canine retainer, and Twistflex retainer). The weighted PAR scores were calculated according to the British system of weights and measures (Richmond et al. 1992a). Points reduction and percentage reduction in the weighted PAR scores were calculated for each of the three groups.
Statistical analysisSample size calculation In Paper I, with its two groups, the sample size estimation was performed and based on an alpha significance level of 0.05 and a beta of 0.1 to achieve 90 per cent power to detect a clinically meaningful difference of 1.5 mm (SD 1.5) of Little’s Irregularity Index. The calculation revealed that 21 patients in each group were sufficient.
In Paper II, with its three groups, the sample size estimation was based on a significance level of 0.05 and 80 per cent power to detect a clinically meaningful difference of 1.5 mm (SD 1.5) in Little’s Irregularity Index. The estimation revealed that 22 patients in each group were sufficient.
The sample was normally distributed according to the Kolmogorov-Smirnov test.
Descriptive statisticsIn Papers I and II, the arithmetic means and standard deviations (SD) were calculated for each variable at group level at times corresponding

44
to pre-treatment (T0), end of active treatment (T1), six years after treatment (T2) and 12 years after treatment (T3).
For the PAR Index evaluation, the arithmetic means and standard deviations (SD) were calculated for each group at pre-treatment (T0), end of active treatment (T1) and 12 years after treatment (T3).
Differences between and within groupsSignificant differences in means in groups and between groups were assessed by one-way analysis of variance (ANOVA) using the IBM Statistical Package for Social Sciences (version 22.0; SPSS Inc., Chicago, Illinois, USA). P-values less than 5 per cent (P<0.05) were considered statistically significant. When significant differences were found between groups, the Bonferroni correction was used.
In Paper II, a regression analysis was also assessed to evaluate whether Little’s Irregularity Index (LII) at T3 was dependent on LII at T0 and to relate mandibular incisor inclination (L1/ML) to changes in LII.
Error of the methodIn Papers I and II, the same examiner (USF) measured on two separate occasions with at least a four-week interval 24 randomly selected cases, which included both the dental casts and the lateral head radiographs. The mean error of the measurements according to Dahlberg’s formula (Dahlberg 1940) for the linear variables was mean 0.1 mm. The largest measurement error was 0.5 mm for intercanine width, 0.5 mm for intercanine perimeter distance, and 0.5 mm for left lateral arch length. Error measurements for the cephalometric angular variables were, on average, 0.8°. The greatest measurement error was noted for the maxillary incisor inclination, 3.3°.
A paired t-test showed no significant differences between the two series of records in most of the measurements, except for left lateral arch length (range min -0.1 to max 0.5), available space (range min -0.3 to max 0.2), tooth width 32 (range min -0.1 to max 0.1), tooth width 41 (range min -0.1 to max 0.1) and L1/Apg (range min -0.1 to max 1.3). The systematic error was within the aforementioned boundaries.

45
RESULTS
Paper IDistribution according to age at the four registration occasions can be seen in Figure 7. There were no significant differences in age at the four registration occasions between the two groups (Paper I, Table 1, p. 201).
The orthodontic treatment started (T0) at a mean age of 12.5 years (SD 1.47) in Group 1 (canine-to canine retainer) and 13.2 years (SD 4.18) in Group 2 (Twistflex retainer).
The treatment lasted, on average, 2.6 years (SD 0.94) for Group 1 and 2.9 years (SD 1.76) for Group 2. Twelve years after treatment (T3), the post-retention time was 9.3 years (SD 2.79) for Group 1 and 9.1 years (SD 1.86) for Group 2. At T3, most of the patients were aged between 25 and 30 years (Paper I, Table 2, p. 202).
Figure 7. Mean ages at the four different registration occasions for the two retainer groups
Registration occasions
Age
Figure 7. Mean ages at the four different registration occasions for the two retainer groups

46
Little’s Irregularity Index (LII)LII was the main outcome measure. It showed that there were no significant intergroup differences. However, within each group, several significant differences were found between the four registrations. LII was 4.5 mm at T0 for Group 1 and 4.7 mm for Group 2. Nine years after retention (T3), LII was 4.2 mm for Group 1 versus 4.4 mm for Group 2 (Figure 8).
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
T0 T1 T2 T3
Canine-‐to-‐canine
Twist5lex
LII m
eans
(m
m)
Figure 8. LII (mean) at the four different registration occasions
Little’s irregularity Index
Registration occasions
Figure 8. LII (mean) at the four different registration occasions
The available spaceThe available space for the mandibular anterior segment showed similar results as LII. For both groups, the available space in the mandibular anterior segment increased after treatment. Six and 12 years after treatment, the available space had decreased in both groups, and for Group 1, it was almost equivalent to that before treatment, with no significant intergroup differences (Paper I, Table 3, p. 204).
Overjet and overbiteIn both groups, the overjet and overbite were reduced after treatment and stayed almost the same throughout the observation period. Thus, the overjet was reduced from mean 6.3 mm in the group with a
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
T0 T1 T2 T3
Retention
Non-‐retention
Untreated
0
2
4
6
8
10
12
14
16
0−10 11−20 21−30 31−40
Non-‐retention
Canine-‐to canine retainer
Twist5lex retainer
Time
LII m
eans
(m
m)
Little’s Irregularity Index
Figure 11. Pre-‐treatment PAR score categories for the three groups
Figure 12. Post-‐treatment PAR score categories for the three groups
Num
ber o
f cases
PAR score

47
canine-to-canine retainer to 3.2 mm after treatment. Twelve years after treatment, the mean overjet was 3.7 mm. The corresponding measures for the group with Twistflex retainer were 7.5 mm at T0, 3.3 mm at T1 and 4.0 mm at T3.
Overbite went from mean 3.7 mm in the canine-to-canine retainer group to 2.5 mm after treatment and from 3.5 mm in the Twistflex retainer group to 2.4 mm. At T3, the mean overbite was 2.9 mm in both groups.
There were no significant differences between the two groups for overjet and overbite (Paper I, Table 3, p. 204).
Intercanine widthThe intercanine width was almost the same in both groups before and after treatment. It decreased from T0 to T3, with about 1 mm in both groups.
Arch lengthThe arch length measures, both to the canine and to the central incisor, decreased after treatment for Group 1, 1.3-1.5 mm, and for Group 2, 0.5-0.9 mm. This includes some extraction-cases. It continued to decrease six and 12 years after treatment in both groups (Paper I, Table 3, p. 204).
Tooth widthThere was a small but significant difference in tooth width of the mandibular right lateral incisor between Groups 1 and 2.
Cephalometric variables There were no significant intergroup differences for any of the cephalometric variables at the four different occasions (Paper I, Table 4, p. 205).
Extraction versus non-extractionAccording to LII, there was no difference in mandibular incisor stability between the patients who had extractions prior to treatment and those who had no teeth taken out.

48
Bonding failuresBonding failures were found in 32 per cent of the patients who had a canine-to-canine retainer versus 44 per cent in the group with Twistflex retainer, but this difference was not statistically significant. In some patients, the Twistflex retainer came loose more than once.
Paper IIThe mean ages at the four registration occasions for Paper II can be seen in Figure 9.
No significant age differences were found at the four registration occasions between the three groups, but there was a larger number of girls in the two treated groups compared to the untreated group (Paper II, Table 1).
Figure 9. Mean ages at the four different registration occasions for the three groups
Age
Registration occasions
Figure 10. LII (mean) at the four diffrerent registration occasions
Figure 9. Mean ages at the four different registration occasions for the three groups
Little’s Irregularity IndexBefore treatment (T0), there were no significant differences according to Little’s Irregularity Index between the groups with and without retention wires (Paper II, Table 2).
Twelve years after treatment, no significant differences were found in Little’s Irregularity Index between the retention and non-

49
retention group. However, significant differences were found between the untreated and two treated groups at T3 (Figure 10) (Paper II, Table 2). The untreated group showed less LII at T0 and at the last registration. No registrations were available at T1 for the untreated group.
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
T0 T1 T2 T3
Retention
Non-‐retention
Untreated
0
2
4
6
8
10
12
14
16
0−10 11−20 21−30 31−40
Non-‐retention
Canine-‐to canine retainer
Twist5lex retainer
Time
LII m
eans
(m
m)
Little’s Irregularity Index
Figure 11. Pre-‐treatment PAR score categories for the three groups
Figure 12. Post-‐treatment PAR score categories for the three groups
Num
ber o
f cases
PAR score
Figure 10. LII (mean) at the four different registration occasions
The multiple regression analysis showed that LII at T2, six years after treatment, was the only variable that could explain LII at T3 (P=0.000). The incisor irregularity 12 years after treatment could not be related or predicted to LII before treatment.
Available spaceThe retention group had mean -2.0 mm available space at T0 compared with the non-retention group, which had -0.8 mm, and this was statistically significant. Compared with the untreated group, the available space was significantly less for treatment groups, but after 12 years, no significant differences were found between the three groups.

50
Intercanine widthExpansion of the intercanine width during orthodontic treatment was avoided in the groups that had orthodontic treatment and thus, no increase in intercanine width was seen.
No differences in intercanine width were found between the three groups at baseline or throughout the observation period.
Arch lengthIn the untreated group, the lateral arch length was significantly larger compared with the two treatment groups at all registrations. Some extraction cases were included in the treated groups. On average, the lateral arch length for the untreated group was 1.6–3.9 mm larger at all registrations, and in all groups, the arch length was decreased from T0 to T3 (Paper II, Table 2).
Tooth widthThe four mandibular incisors showed no statistically significant differences in tooth width between the three groups and over time.
Overjet and overbiteAt T0, there were statistically significant differences in overjet between the untreated group and the two treatment groups, P<.01 for the retention group and P<.001 for the non-retention group.
Overjet was reduced during orthodontic treatment in the two treatment groups, and at T1, it was almost the same as the untreated group had at T0, 3.6 mm, (SD 1.52) (Table 1).
Overbite was also reduced during treatment in the two treatment groups. Six and 12 years after treatment, both overjet and overbite stayed nearly the same in all three groups, and there were no statistically significant differences between the groups (Table 1).

51
Table 1. Mean and standard deviation (SD) values for overjet and overbite at the four registration points, and the differences in mean values between the three groups (P). The four registration points are T0 before treatment, T1 after treatment, T2 six years after treatment, T3 12 years after treatment. For the untreated group measured at T0, T2 and T3 for the corresponding ages.
Retention group=1
Non-retention group=2
Untreated group=0
Mean SD Mean SD Mean SD P
Overjet T0 7.00 3.20 6.36 4.41 3.64 1.52
0≠1**, 0≠2***
T1 3.26 1.03 3.37 1.20 - - NS
T2 3.77 1.63 3.28 2.07 3.06 1.33 NS
T3 3.81 1.67 3.30 2.45 3.43 1.95 NS
Overbite T0 3.59 2.18 2.72 2.55 3.33 1.57 NS
T1 2.41 1.09 2.34 1.15 - - NS
T2 2.76 1.56 2.38 1.69 2.20 1.32 NS
T3 2.91 1.51 2.38 1.61 2.57 1.55 NS
NS= not significant, ** P<.01; ***P<.001
Cephalometric variablesAfter treatment (T1), the mandibular incisors were significantly more proclined in the retention group compared with the non-retention group (Paper II, Table 3).
From the multiple regression analysis, it was found that the change in incisor irregularity (LII) from T0-T3 was explained by the change of incisor inclination (L1/ML) from T0-T3 in only 10.4 per cent (P=0.004). Accordingly, the mandibular incisor inclination was not an important cofactor for increased mandibular incisor crowding.
PAR Index evaluationThe improvement after treatment in percentage was 75 for the non-retention group, 88 for the canine-to-canine group and 86 per cent for the Twistflex retainer group.
The pre-treatment, post-treatment and 12 years post-treatment PAR scores were divided into four categories, as shown in Figures 11, 12 and 13.

52
Most of the pre-treatment PAR scores were in the 21–30 group for all three groups and after treatment the post-treatment PAR scores were mostly in the 1–10 group for all three groups.
Twelve years after treatment, most of the cases were still in group 1–10, but the 11–20 group has increased for all three groups.
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
T0 T1 T2 T3
Retention
Non-‐retention
Untreated
0
2
4
6
8
10
12
14
16
0−10 11−20 21−30 31−40
Non-‐retention
Canine-‐to canine retainer
Twist5lex retainer
Time
LII m
eans
(m
m)
Little’s Irregularity Index
Figure 11. Pre-‐treatment PAR score categories for the three groups
Figure 12. Post-‐treatment PAR score categories for the three groups
Num
ber o
f cases
PAR score
Figure 11. Pre-treatment PAR score categories for the three groups
0
5
10
15
20
25
30
35
0−10 11−20 21−30 31−40
Non-‐retention
Canine-‐to-‐canine retainer
Twist5lex retainer
N
umbe
r of c
ases
PAR score
Figure 12. Post-treatment PAR score categories for the three groups

53
0
5
10
15
20
25
30
0−10 11−20 21−30 31−40
Non-‐retention
Canine-‐to-‐canine retainer
Twist5lex retainer
0 2 4 6 8 10 12 14 16 18 20
Greatly improved
Improved Worse/no different
Post-‐treatment
12 years post-‐treatment
Figure 13. 12 years post-‐treatment PAR score categories for the three groups
Num
ber o
f cases
PAR score
Figure 14. Non-‐retention group
Num
ber o
f cases
Figure 13. Twelve years post-treatment PAR score categories for the three groups
The mean pre-treatment, post-treatment, and 12 years post-treatment PAR scores are shown in Table 2.
Table 2. Mean PAR score (weighted)
GroupsNon-
retentionCanine-to-canine
retainerTwistflex retainer
PAR score Mean SD Mean SD Mean SD
Pre-treatment T0 24.7 10.73 25.4 7.51 24.2 6.81
Post- treatment T1 6.2 6.84 3.0 3.73 3.4 3.41
12 years post-treatment T3
8.4 8.67 7.1 6.77 7.1 5.64
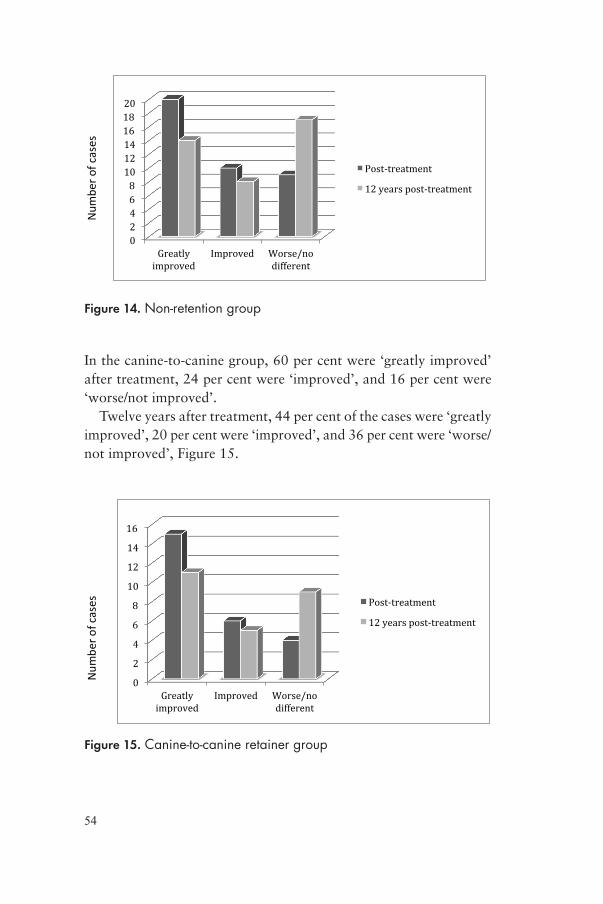
The distribution of cases according to improvement categories for the three different groups can be seen in Figures 14, 15 and 16.
After treatment, 51 per cent of the cases in the non-retention group fell into the ‘greatly improved’ category, 26 per cent were ‘improved’, and 23 per cent were ‘worse/not improved’.
Twelve years after treatment, 36 per cent of the cases were ‘greatly improved’, 20 per cent were ‘improved’, and 44 per cent were ‘worse/not improved’, Figure 14.
54
0
5
10
15
20
25
30
0−10 11−20 21−30 31−40
Non-‐retention
Canine-‐to-‐canine retainer
Twist5lex retainer
0 2 4 6 8 10 12 14 16 18 20
Greatly improved
Improved Worse/no different
Post-‐treatment
12 years post-‐treatment
Figure 13. 12 years post-‐treatment PAR score categories for the three groups
Num
ber o
f cases
PAR score
Figure 14. Non-‐retention group
Num
ber o
f cases
Figure 14. Non-retention group
In the canine-to-canine group, 60 per cent were ‘greatly improved’ after treatment, 24 per cent were ‘improved’, and 16 per cent were ‘worse/not improved’.
Twelve years after treatment, 44 per cent of the cases were ‘greatly improved’, 20 per cent were ‘improved’, and 36 per cent were ‘worse/not improved’, Figure 15.
Figure 16. Twistflex retainer group
0
2
4
6
8
10
12
14
16
Greatly improved
Improved Worse/no different
Post-‐treatment
12 years post-‐treatment
0
2
4
6
8
10
12
Greatly improved
Improved Worse/no different
Post-‐treatment
12 years post-‐treatment
Num
ber o
f cases
Nub
er of c
ases
Figure 15. Canine-‐to-‐canine retainer group
Figure 15. Canine-to-canine retainer group

55
In the Twistflex retainer group, 37 per cent were ‘greatly improved’ after treatment, 40 per cent were ‘improved’, and 23 per cent were ‘worse/not improved’.
Twelve years after treatment, 27 per cent of the cases were ‘greatly improved’, 33 per cent were ‘improved’, and 40 per cent were ‘worse/not improved’, Figure 16.
Figure 16. Twistflex retainer group
0
2
4
6
8
10
12
14
16
Greatly improved
Improved Worse/no different
Post-‐treatment
12 years post-‐treatment
0
2
4
6
8
10
12
Greatly improved
Improved Worse/no different
Post-‐treatment
12 years post-‐treatment
Num
ber o
f cases
Nub
er of c
ases
Figure 15. Canine-‐to-‐canine retainer group
Figure 16. Twistflex retainer group

56
DISCUSSION
Irregularity of mandibular anterior segmentThe main findings of Paper I were that there were no differences in Little’s Irregularity Index and available space at the long-term follow-up between the two different retainers. Thus, the null hypothesis was confirmed. Both a canine-to-canine retainer and a Twistflex retainer can be recommended, as they are equal from a stability point of view, as long as the retainers are in place. When the retainers were removed, the long-term follow-up at T3 showed that 42 per cent of the patients (64 patients) had an irregularity of 3.5 mm or less, and similar results have been found 14 years post-retention by Årtun et al. (1996), where 47.4 per cent showed LII of 3.5 mm or less.
The most important and main result of Paper II was that, 12 years after treatment, the mandibular incisor irregularity showed no significant differences between the non-retention and retention groups. The hypothesis that Little’s Irregularity Index would be greater for the group long-term without retainers than for the retainer group could not be confirmed. The irregularity of the incisors was almost at the same level before and 12 years after treatment. This is also shown in the studies by Little in which more than 70 per cent of the cases had moderate to severe crowding before treatment, and later, at least 10 years after removal of all retainer devices, the same number of cases showed moderate to severe crowding but in different proportions (Little et al. 1981 and 1988).
To illustrate, Figure 17 shows how three cases with the highest irregularity of the mandibular incisors, 12 years after treatment for Groups 0, 1 and 2 are compared with LII before treatment. Nearly the same teeth with contact point displacements at T0 were displaced at

57
T3 and also in the same angulation as before treatment. In Figure 18, three cases with the lowest irregularity of the mandibular incisors, 12 years after treatment are presented. They show a fairly well-aligned mandibular anterior segment at T3.
The highest irregularity of the mandibular incisors 12 years after treatment in the three different groups and the corresponding start registration
Non-retention group at T0 Non-retention group at T3
Retention group at T0 Retention group at T3
Untreated group at T0 Untreated group at T3
Figure 17. The highest irregularity of the mandibular incisors 12 years after treatment in the three different groups and the corresponding start registration.

58
Figure 18. The lowest irregularity of the mandibular incisors 12 years after treatment in the three different groups and the corresponding start registration.
The lowest irregularity of the mandibular incisors 12 years after treatment in the three different groups and the corresponding start registration
Non-retention group at T0 Non-retention group at T3
Retention group at T0 Retention group at T3
Untreated group at T0 Untreated group at T3

59
Causative factors of relapse Pre-treatment variables such as initial mandibular incisor crowding, increased mesiodistal incisor dimension, arch length deficiency, and arch constriction have been found to be associated factors in the post-retention process resulting in increased crowding and incisor irregularity (Kahl-Nieke et al. 1995; Årtun et al. 1996; Ormiston et al. 2005; Bjering et al. 2017).
In Paper II, the multiple regression analysis showed that the initial crowding at T0 could not be related to the crowding at T3, but the crowding at T2 could explain the crowding at T3. It is clear that, in some studies (Reitan 1969; Kahl-Nieke et al. 1995; Årtun et al. 1996) we can see a connection between initial crowding and post-retention crowding, and this is important to take into consideration when planning for the retention appliance.
Irregularity of mandibular anterior segment in untreated casesIn the untreated group, Little’s Irregularity Index also increased over time but not to the same extent as in the two treated groups. The hypothesis, which claims that the two groups who have had orthodontic treatment would have more irregularity in the mandibular anterior segment than the untreated group long-term was confirmed. This has also been confirmed by Freitas et al. (2013), although the observation period was just over five years, the mandibular crowding caused by physiologic changes in the untreated group was less than the post-treatment changes of the treated extraction group. Sinclair and Little (1983) also showed that incisor irregularity changes in untreated subjects were similar in nature but to a lesser extent than post-treatment changes in treated cases.
Most of the changes in irregularity occurred between the ages of 14.9–21.8 years. Bushang and Shulman (2003) showed that crowding increased most during the late teens and early twenties. A retrospective longitudinal study by Driscoll-Gilliland et al. (2001) where they compared treated subjects with untreated cases concluded that from late adolescence through early-to-middle adulthood, the mandibular incisor irregularity increased at a similar rate in both groups.

60
Overjet and overbite Overjet and overbite decreased during treatment and was stable 12 years after treatment. This result was almost the same in both the treated groups and the untreated group. This is an encouraging finding as the mandibular incisor stability was not optimal. The same was found by Little and co-workers (1988) in patients treated with four premolar extractions followed 10- and 20 years post-retention. Both the overjet and overbite were corrected and did not relapse. The overbite apparently does not play a role in the anterior malalignment, but there are different opinions about this. Francisconi et al. (2014) found significant and positive correlations of overjet and overbite relapses with mandibular anterior crowding relapse, and consequently, between overjet and overbite relapses. In their study, fixed mandibular retainers were used for less than two years, and the patients were followed five years after treatment. Once mandibular crowding relapse occurs, the mandibular incisors are lingually tipped and there are consequent increases in overjet and overbite.
In Figure 19, the overjet in the three different treated groups from Paper II can be seen before treatment and 12 years after treatment.

61
Overjet before and 12 years after treatment in three different groups Before treatment Canine-to canine retainer 12 years after treatment
Before treatment Twistflex retainer 12 years after treatment
Before treatment Non-retention 12 years after treatment
Figure 19. Overjet before and 12 years after treatment in three different groups
Cephalometric outcomesIn Paper I, it was found that the two groups were equal when comparing cephalometric outcomes. In Paper II, the cephalometric analysis disclosed only a small number of significant intergroup differences. For instance, the group with a retainer had more proclined mandibular incisors after treatment, but at T3, no differences between the groups were found. In just 10.4 per cent of the group, Little’s Irregularity Index could be explained by the change in incisor inclination (L1/ML) from T0 to T3. Given that the mandibular incisor inclination to ML did not change much over time in any of the groups in Paper II, this was probably not a cofactor for increased mandibular incisor crowding. In a long-term study by Schütz-Fransson et al. (2006), deep bites treated non-extraction were compared with untreated subjects. The mandibular incisors proclined significantly in relation to ML during treatment and was normalised

62
8.2 years after retention. Despite this, the available mandibular incisor space was less, -1.8 mm, in the control group compared with the treatment group, -0.9 mm.
Thilander (2000) found no relation between various cephalometric variables and post-retention changes in mandibular incisor crowding, but an anterior rotation of the mandible could be a factor. Oh et al. (2016) also did not find any associations between different cephalometric measurements and changes in mandibular incisor irregularity. Both studies are in accordance with Paper II.
The untreated subjects showed normal cephalometric values at all registrations, which were expected. Thordarson et al. (2006) have shown that the inclination of the mandibular incisors increased over time from 6–16 years of age, but this could not be found in Paper II, as the inclination was almost the same during the whole observation period.
GenderIn both Papers I and II, more girls were in the treatment groups than in the untreated group. The reason for this is probably that girls are more likely to request and/or accept orthodontic treatment compared with boys. Studies have shown that there are no statistical differences between genders for Little’s Irregularity Index measured in untreated subjects (Eslambolchi et al. 2008; Tsiopas et al. 2013). However, a study by Zinad (2016) reported some gender-specific differences: the pattern of physiological changes in dentition for participants aged 12–39 years was different between the sexes. Females showed more relapse than males between 10–15 years post-treatment. Thus, the importance of gender for relapse seems to be unclear.
Extractions versus non-extractionsIn Paper I, both groups were treated with the same amount of extractions and non-extractions - 64 per cent respectively 36 per cent. In Paper II, extractions were carried out in 71 patients (68 per cent) and 34 patients (32 per cent) were treated non-extraction. Here, there was also exactly the same proportion of extraction and non-extraction cases in the group with and without retainers. There was no difference in mandibular incisor stability, regardless of extractions, and this has also been confirmed by Rossouw et al. (1999), Erdinc et al. (2006) and Zafarmand et al. (2014).

63
Retention for how long time?How long a retainer should be in place is a question that is constantly discussed. Sadowsky et al. (1994) showed that an average period of 8.4 years with a fixed mandibular retainer resulted in a relatively good alignment at the long-term stage, five years without retainer. Al Yami et al. (1999) claimed that about half of the total relapse takes place during the first two years after retention. Also, another study (Kuijpers-Jagtman 2002) found that nearly 50 per cent of the relapse occurred during the first two years after retention. After that period, certain stability was reached except for the mandibular front teeth. Edman Tynelius et al. (2013) showed that major relapse took place during the first year of retention, and only small changes and differences occurred during the second year of retention. Thus, the first year of retention seems to be the most important to retain the treatment result, and that is also the time it takes for the surrounding tissues to adapt.
The rearrangement of bone tissue is very small after a retention period of 15 days, and partial rearrangement can be seen after 28 days. During retention, new bone or bone spicules are formed along stretched fibre bundles. This rearrangement and calcification of the new bone spicules result in a fairly dense bone tissue, which, for a certain period, prevents relapse of the tooth moved. Therefore, to avoid relapse, a tooth should be retained until total rearrangement of the structures involved occurs. After retention for 28 days, new bone is added between the first bone spicules. After a retention period of 232 days, a more complete reorganisation of bone tissue has taken place (Reitan 1959), although the oxytalan fibres may take up to six years to remodel (Kharbanda & Darendeliler 2016).
Relapse that occurs during this period of remodelling of periodontal structures must be distinguished from late changes during post-retention period. The changes that occur later are more related to craniofacial growth, dental development and muscle function. However, according to the studies by Reitan (1959 and 1967) and Malta & Von den Hoff (2017), a two to three years retention period as in Papers I and II, ought to be enough to prevent relapse of the orthodontic treatment results.
The normal development of the dental arch is characterised by a gradual reduced dimension and increased crowding in both arches

64
starting in late adolescence and continuing during adulthood. This is not easily separable from the real treatment relapse. Occlusal and dentoalveolar changes in untreated subjects from either the primary or early permanent dentition up to early and late adulthood are well documented (Thilander 2009; Jonsson & Magnusson 2010; Tsiopas et al. 2013). In the study by Thilander (2009), 436 subjects of Swedish origin aged between 5–31 years were studied. They had normal occlusion and no orthodontic treatment. The results verified that continuous changes of the dental arches occur from the primary dentition to the adult period, with individual variations. These changes could be interpreted as a biological migration of the dentition resulting in anterior crowding especially in the mandible, even in subjects with congenitally missing third molars.
The dental arch dimension and incisor irregularity changes from the ages between 20–60 years have also been longitudinally investigated (Tsiopas et al. 2013). A correlation was found between an increase in mandibular incisor irregularity and decreases in mandibular arch length and intercanine width. In general, the decrease in intercanine width is more pronounced in the mandibular than in the maxillary arch.
Failures and retainer breakagesOne disadvantage of bonded retainers is that the placement procedure is time-consuming and technique sensitive. The technique-related problem with fixed retainers entails frequent bond failures. It could be either at the wire/composite interface if too little composite is added or at the adhesive/enamel interface when moisture contamination or movement of the retainer during the bonding procedure has taken place (Zachrisson 1977). Placement of insufficient resin or use of a resin with inadequate abrasion resistance seems to be the main reasons for failure of bonded fixed retainers (Bearn 1995). Other reasons for failure are a result of wear and direct trauma to the retainer.
The bonding failures in Paper I were frequently reported in both retainer groups: 32 per cent of the patients who had a canine-to-canine retainer and 44 per cent in the group with Twistflex retainer but the difference was not statistically significant. The bonding failure rate was most common during the first year after treatment, and this could be one reason for a small amount of incisor irregularity.

65
A 3-year follow-up study of three different retainers (Årtun et al. 1997) – two of the retainers were bonded to the canines only and one to all incisors and canines - showed failure of the retainers in 22.9 per cent, but there was no difference between the failure rates of the three types of bonded retainers. Scheibe and Ruf (2010) evaluated the survival and failure rates in a retrospective study of 1062 patients with mandibular fixed retainers, 30±19.5 months after treatment. In their study, 34.9 per cent of all patients experienced retainer failure, with the canine-to-canine retainer failing significantly less often than the retainer with six bonding sites. The failure rate in a prospective study by Taner and Aksu (2012) where they used an eight-braided stainless-steel retainer was 37.9 per cent over a 6-month period after debond.
A survival analysis of different orthodontic retainers (Jin et al. 2018) concluded that the survival time was the longest for lingual fixed retainers and Hawley retainers, median 1604 days versus 1529 days compared to 258 days for a combination of two different retainers in the same arch and 105 days for vacuum-formed retainers. The reasons for failures were mainly mechanical (debond and fracture) and patient-related (loss).
The wide divergence in findings is explained by differences in the types of retainers and/or bonding materials used as well as differences in the registration method. However, it seems that a failure rate of around 30–40 per cent is the average in most studies, including Paper I.
A review by Iliadi et al. (2015) evaluated the risk of failure of fixed orthodontic retention protocols and concluded that there was a lack of evidence to guide orthodontists in the selection of the best protocol and materials for fixed orthodontic retention.
Unexpected effects of fixed retainersLong-time wear of fixed retainers is associated with unexpected negative side effects. Even if they are rare, they can be serious enough to produce biological damage.
The Twistflex retainer affords physiologic stimulation to the periodontium. For instance, a twisted retainer can, after a certain number of years, start to derotate or detwist, although the progress is likely to be extremely slow. Consequently, the tooth may gradually perform a torqueing movement with lingual or buccal root torque, see Figure 20.

66
Figure 20. Twistflex retainer with torque discrepancy of the left lateral incisor. Courtesy of Dr Krister Bjerklin
Twistflex retainers bonded to all the teeth appear most likely to produce inadvertent tooth movement. One reason is that the patient might not notice partial debonding. Early detection of bonding failures, wire breakage, and tooth movement created by the retainer is critical in preventing major problems (Shaughnessy et al. 2016). These unexpected changes are not found in cases of thick stainless-steel canine-to-canine retainer bonded to the canines only, even at five years post-treatment (Renkema et al. 2008).
A study by Pazera et al. (2012) presents a serious complication of a mandibular fixed retainer. Four years after orthodontic treatment, a patient sought treatment for a broken retainer. One tooth had 35° buccal root torque and the root, and the apex of the tooth were almost completely out of the bone on the buccal side. These unexpected movements might be to such an extent that retreatment is necessary.
The exact aetiological factors for these unexpected changes described above are unknown, but they show certain clinical patterns. A round, Twistflex retainer is produced by twisting multiple strands to form one spiral wire. Forces within the wire might be generated through an untwisting of these single strands. Another reason could be that the mechanical properties of some retainer wires cannot

67
prevent or may lead to certain types of tooth movement. Clinicians must carefully and thoughtfully select the wires for fixed retainers, as the difference in resistance to torque is great. High torque control must be achieved, for instance, with plain 0.016x.0016-inch or braided 0.016x0.022-inch stainless steel wires (Arnold et al. 2016). Other possible factors could be the torquing moments that can be present within the retainer wire due to the manufacturing process, i.e. multi-stranded spiral wires with a left-handed or right-handed twist or mechanical deformation from masticatory forces (Katsaros et al. 2007; Renkema et al. 2011).
It is important that the wire is bonded passively across the surfaces of the teeth, and any elastic deflection during bonding should be avoided (Sifakakis et al. 2015). A tooth attached by a retainer wire to only one neighbouring tooth is less torque resistant than a tooth connected to two neighbouring teeth (Arnold et al. 2016). This could lead to the clinical consideration to retain a tooth, which is exposed to the heavy forces of mastication or has been severely torqued during orthodontic treatment, with a retainer connected to both neighbouring teeth to improve stability. Annealing the wire with a flame reduces the stiffness of retainer wires markedly and can lead to a non-uniform and non-reproducible effect (Arnold el al. 2016).
Other adverse effects are on oral health, including demineralisation, caries, gingivitis or marginal bone loss. When comparing patients who had a retainer bonded to all mandibular anterior teeth with patients who had a retainer bonded to the mandibular canines only, it seems that the patients with the retainer bonded to all anterior teeth showed more plaque accumulation and gingivitis. The plaque accumulation and gingivitis differed significantly between the two groups (Rody et al. 2016). They pointed out that the results of their study agree with other research that did not find a relationship between bonded retainers and severe clinical damage of periodontal tissues. A review article by Westerlund et al. (2014) which included two systematic reviews, two randomized controlled trials, four non-randomized controlled studies and five case series concluded that there was very low quality of evidence whether periodontal outcomes, dental caries prevalence, or presence of calculus differ between various types of retainer regimes, such as a fixed or removable retainer for more than two years after treatment, no retainer or fiberotomy.

68
The effects of fixed retainers on marginal bone level have been studied with cone-beam computed tomographic evaluation by Westerlund et al. (2017). Ten years after orthodontic treatment they found that long-term retention, in general, did not seem to cause any adverse effects on the marginal bone level. They also showed that a low marginal bone level was associated with a basal open vertical relationship, posterior rotation of the mandible, pre-treatment of the incisor protrusion, and extraction therapy.
Another adverse effect is the development of gingival recession. Renkema et al. (2013) assessed the prevalence of gingival recessions in patients before, immediately after, and two and five years after orthodontic treatment. They found that the prevalence of gingival recessions steadily increases after orthodontic treatment. The type of retainer did not influence the development of recessions in the mandibular front region. The recessions were more prevalent in older than in younger patients. No variable except for age at the end of treatment seemed to be associated with the development of gingival recessions. In addition, in a study by Juloski et al. (2017), orthodontically treated patients were followed for five years after treatment and compared with untreated age-matched subjects. The results showed that the long-term presence of fixed mandibular retainers did not increase the development of mandibular gingival recessions but did increase the accumulation of calculus. The prevalence of gingival recessions in patients five years after orthodontic treatment, with and without retainers, was similar to the prevalence in untreated individuals of the same age. An example of a gingival recession can be seen in Figure 21.

69
Figure 21. Gingival recession and attachment loss of the right central incisor. Courtesy of Dr Krister Bjerklin
PAR Index evaluationAs the mean percentage reduction in weighted PAR score should be greater than 70 per cent in each of the three groups after orthodontic treatment, the hypothesis was confirmed. The improvement after treatment in percentage was 75 for the non-retention group, 88 for the canine-to-canine group and 86 per cent for the Twistflex retainer group.
Twelve years after treatment the mean reduction in PAR score was 66 for the non-retention group, 72 for the canine-to-canine retainer group and 71 per cent for the Twistflex retainer group. These relatively good results depend on overjet and overbite remaining fairly the same at the long-term follow-up, as overjet and overbite are weighted high. On the other hand, the mandibular anterior segment showed a return to crowding.
The other hypothesis – that at least 70 per cent of the cases in each of the three groups should be ‘greatly improved’ and/or ‘improved’ 12 years after treatment – was not confirmed. The cases that were ‘greatly improved’ and/or ‘improved’ 12 years after treatment were
70
56 per cent in the non-retention group, 64 per cent in the canine-to-canine retention group and 60 per cent in the Twistflex retainer group. After treatment, between 16 and 23 per cent of all the cases were ‘worse or not improved’. However, between 36 and 44 per cent of the total cases were ‘worse or not improved’ 12 years after treatment, (less than 30 per cent PAR score reduction).
However, it must be pointed out that there were both severe and easy cases in the groups and in cases with low initial PAR scores (below 20) it is more difficult to attain a relative PAR score reduction.
Otuyemi et al. (1995) studied 50 cases 10 years after retention utilising the PAR Index, and the results showed that a high standard of treatment result was demonstrated with a mean reduction in PAR score of 82.5 per cent, which was almost in accordance with the present study. However, 10 years post-retention, the mean PAR score change was reduced to 48.6 per cent. The cases that were ‘greatly improved’ and ‘improved’ 10 years after retention were 76 per cent. Birkeland et al. (1997) reported a 76.7 per cent reduction in PAR score after treatment, and five years out of retention, the reduction was 63.8 per cent.
Freitas et al. (2006b) also had a reduction in PAR score after treatment of 78.5 per cent but they concluded that the quality of orthodontic treatment outcomes was not related to the long-term occlusal stability. In another study (Bjering et al. 2017), with a similar long-term evaluation as in this frame story the PAR Index percentage improvement decreased from 73.1 per cent post-treatment to 53.5 per cent 10 years out of retention.
Maintenance of fixed retainers This clinical routine with increasingly more fixed retainers generates an increasing number of patients in need of retainer maintenance, which will lead to an increased workload for orthodontists and general dentists. Increased costs for the patients will also be a result.
There is a need to inform patients about long-term expectations of the treatment. One must remember that the patients’ satisfaction in the follow-up stage is associated only with their occlusal status at that moment and not with the initial malocclusion or with their occlusion when the treatment ended.
Before starting orthodontic treatment, it is the orthodontist’s responsibility to provide the patient with truthful information

71
about the importance of retainers, the frequency of relapse, natural physiological changes and the long-term costs. It is important to ask the patient to report a failure immediately so that a repair can be made as soon as possible. Patients should also be clearly informed about maintaining good oral hygiene and how to detect problems at an early stage. However, considering the potential risks of bonded retainers for oral health, it is reassuring that fixed retainers appear to be compatible with oral health. The condition of the gingiva in the anterior region of the mandible, with and without retainers, was comparable after 20 years of use of fixed retainers (Booth et al. 2008).
Routine and periodic control of retention is indispensable. Orthodontists and dentists should be aware of the possible complications of bonded retainers. The responsibilities of the patient’s general dentist in their role of taking over the long-term maintenance of the retainers means that it may be necessary to increase training for dentists in regard to the placement and repair of fixed retainers.
Is it realistic to expect a long-term and stable incisor position after orthodontic treatment? From the literature, the only thing we know is that retention decreases the amount of orthodontic relapse. No conclusion can be drawn regarding how long retention is necessary to reach stability, particularly for the mandibular incisors, as relapse is inevitable.
Methodological aspectsIn these retrospective studies, one of the selection criteria was that sufficient registrations had been performed of the patients as well as dental casts and radiographs had been taken. In a retrospective study the risk of selection bias is high because often the successfully treated patients have been registered while the unsuccessful patients have been omitted at registration. Thus, the level of evidence provided by a retrospective study is considered to be low, and especially, compared to a prospective study or a randomized controlled trial, i.e. the “gold standard”. Nevertheless, a RCT follow-up study of 12 years can be difficult to perform. The long post-retention time makes it useful from a clinical point of view. However, it is essential to have a retrospective evaluation as a starting point because it inspires future studies with a prospective design.

72
Future researchAs patient-centred care becomes increasingly important, the patient should be actively involved in the decision-making process about therapy options, even those involving the retention phase. Patient satisfaction with the treatment should be one of the ultimate measures of therapeutic success. Today, little is known about the satisfaction of patients wearing various types of retainers and what is important to them about retainers. To conduct a prospective study to evaluate the level of satisfaction, from the start of the retention and in the long run would be of interest. It is important to identify what the patients regard as most important about retainers.
More research is also needed to gain further knowledge about the causative factors and individual variations of long-term changes in incisor irregularity.
A PAR Index evaluation of untreated subjects would also be of interest to perform.

73
CONCLUSIONS
When comparing a canine-to-canine retainer and a Twistflex retainer long-term, six and 12 years after orthodontic treatment and mean 9.2 years after removal of the retainers, the conclusions were:
• Both a canine-to-canine retainer and a Twistflex retainer can be recommended, given that both are equally effective when they are in place.
• None of the retention types prevent long-term changes of mandibular incisor irregularity or available space for the mandibular incisors after removal of the retainers.
After analysing the dental and skeletal changes in patients treated with fixed orthodontic appliances, with or without fixed mandibular retainer, and comparing the changes with untreated subjects, the following conclusions can be drawn:
• There were no differences found in Little’s Irregularity Index 12 years after treatment for the mandibular incisors between the group that had a retainer and the group that had no retainer after treatment.
• In the untreated group, Little’s Irregularity Index increased over time, but not to the same extent as in the treated groups.
• The crowding before treatment did not explain the crowding at the last registration.
• The use of fixed mandibular retainers for two to three years does not appear to prevent long-term changes.
• The overjet and overbite were stable long term.

74
From the weighted Peer Assessment Rating, the conclusions were:
• Twelve years after treatment, the mean reduction in PAR score was over 70 per cent for the groups who had a mandibular retainer after treatment while the non-retention group had a reduction of 66 per cent.
• The cases that were ‘greatly improved’ and/or ‘improved’ 12 years after treatment were 56 per cent in the non-retention group, 64 per cent in the canine-to-canine retention group and 60 per cent in the Twistflex retainer group.
Key conclusions and clinical implicationsFor retention of the mandibular incisors after orthodontic treatment, the canine-to-canine retainer and the Twistflex retainer can both be recommended, as they are equally effective during the retention period.
The use of fixed mandibular retainers for two to three years does not appear to prevent long-term changes.
In untreated cases the mandibular incisor irregularity will increase over time but not to the same extent as in treated cases were the retainer has been removed.
Patients must be informed about the development of natural physiological changes that appear of the mandibular incisors through aging. If the patient wants to constrain natural development and changes, lifelong retainers are needed.

75
ACKNOWLEDGEMENTS
I wish to express my deepest and sincerest thanks to everyone who has helped and supported me during these years with my project. Especially, I would like to thank:
Professor Lars Bondemark, my main supervisor and co-author, for excellent research guidance, for never-failing enthusiasm, critical thoughts and stimulating discussions. Thank you for leading the way, giving support, making me believe in myself and for always being there for me throughout this work. It has been a true privilege to work with you.
Associate Professor Rune Lindsten, my co-supervisor, co-author and friend, for stimulating discussions, valuable advice and your positive attitude to the project. You have shared your great wisdom and your warmth and always positive support. I am very proud to have worked with you.
Associate Professor Krister Bjerklin, my co-supervisor and co-author, for your steadfast belief in this project, for sharing your scientific knowledge, generous support and for your never-failing energy when it came to finding all those study models. I am grateful that we could use the dental casts and radiographs from the Department of Orthodontics in Jönköping.
Per-Erik Isberg for excellent help with all the statistical analysis.
Janet Feenstra for excellent revision of the English text.

76
Dr Maria Tyreman Bandhede, Head of the Orthodontic Department in Uddevalla, Region Västra Götaland and my dear friend. Thank you for always supporting, encouraging me during these years and allowing me time for research.
Dr Dan Turesson, my colleague at the Orthodontic Department in Uddevalla, for helping me with the photo for the front page.
Eva Lindqvist Buhr, my dental technician, for producing the retainers for the front page.
The staff and colleagues at the Orthodontic Department in Uddevalla, the County Orthodontic Clinic, for always understanding me when my mind was in the world of science.
Andrea, my sister for interesting discussions every week about the real world.
Ulf, my brother in law for being my IT-guru.
My mom Petra for hosting me during my frequent visits to Malmö.
My husband Christer, our loving children Anna and Erik for their help and never-failing support and patience while I had to study. Thank you for always being there for me. After October the 12th my time is yours.
Lovisa, my grandchild for keeping me updated with Pippi Longstocking and her adventures.
All my friends who have stimulated me with their different interests and through nice gatherings with e.g. dinners, winetasting, gardening, travelling and nice discussions.

77
The following financial support is gratefully acknowledged:
Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden
Department of Orthodontics, The Institute for Postgraduate Dental Education, Jönköping, Sweden
Region Västra Götaland, Sweden
Gothenburg Dental Society

78
REFERENCES
Aasen, T.O. & Espeland, L. (2005). An approach to maintain orthodontic alignment of lower incisors without the use of retainers. Eur J Orthod. 27:209-214.
Al Yami, E.A., Kuijpers-Jagtman, A.M. & van’t Hof, M.A. (1999). Stability of orthodontic treatment outcome: Follow-up until 10 years postretention. Am J Orthod Dentofacial Orthop. 115:300-304.
Angle, E.H. (1887). Notes on Orthodontia with a new system of regulation and retention. The Ohio Journal of Dental Science. 7:457-464.
Arnold, D.T., Dalstra, M. & Verna, C. (2016). Torque resistance of different stainless steel wires commonly used for fixed retainers in orthodontics. J Orthod. 43:121-129.
Bearn, D.R. (1995). Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Orthop. 108:207-213.
Birkeland, K., Furuvik, J., Bøe, O.E. & Wisth, P.J. (1997). Evaluation of treatment and post-treatment changes by the PAR Index. Eur J Orthod. 19:279-288.
Bjering, R., Sandvik, L., Midtbø, M. & Vandevska-Radunovic, V. (2017). Stability of anterior tooth alignment 10 years out of retention. J Orofac Orthop. 78:275-283.
Bjerklin, K. (1994). Ectopic eruption of the maxillary first permanent molar. An epidemiological, familial, aetiological and longitudinal clinical study. Diss. Göteborg: Göteborgs Universitet. Swed Dent J Suppl. 100:1-66.
Bjerklin, K., Lindsten, R., Sagevik Tunge, J. & Sjövall, C. (2012). Orthodontic treatment need, outcome and residual treatment need in 15- and 20-year-olds. Swed Dent J. 36:157-165.
Björk, A. (1947). The face in profile. Svensk Tandl Tidskr. 40:suppl 1.
Boese, L.R. (1980). Fiberotomy and reproximation without lower retention 9 years in retrospect: Part II. Angle Orthod. 50:169-178.

79
Bolla, E., Cozzani, M., Doldo, T. & Fontana, M. (2012). Failure evaluation after a 6-year retention period: a comparison between glass fiber-reinforced (GFR) and multistranded bonded retainers. Int Orthod. 10:16-28.
Bondevik, O. (2015). A longitudinal study of dental arches and occlusal chan-ges in adults from 22 to 33, and 33 to 43 years of age. J Orofac Orthop. 76:79-89.
Booth, F.A., Edelman, J.M. & Proffit, W.R. (2008). Twenty-year follow-up of patients with permanently bonded mandibular canine-to-canine retainers. Am J Orthod Dentofacial Orthop. 133:70-76.
Buschang, P.H. & Shulman, J.D. (2003). Incisor crowding in untreated per-sons 15-50 years of age: United States, 1988-1994. Angle Orthod. 73:502-508.
Dahlberg, G. (1940). Statistical methods for medical and biological students. London, United Kingdom: Allen and Unwin, Ltd.
de la Cruz, A., Sampson, P., Little, R.M., Årtun, J. & Shapiro, P.A. (1995). Long-term changes in arch form after orthodontic treatment and retention. Am J Orthod Dentofacial Orthop. 107:518-530.
Driscoll-Gilliland, J., Buschang, P.H. & Behrents, R.G. (2001). An evaluation of growth and stability in untreated and treated subjects. Am J Orthod Dentofacial Orthop. 120:588-597.
Edman Tynelius, G., Bondemark, L. & Lilja-Karlander, E. (2013). A ran-domized controlled trial of three orthodontic retention methods in Class I four premolar extraction cases-stability after 2 years in retention. Orthod Craniofac Res. 16:105-115.
Edman Tynelius, G., Petrén, S., Bondemark, L. & Lilja-Karlander, E. (2015). Five-year postretention outcomes of three retention methods - a randomi-zed controlled trial. Eur J Orthod. 37:345-353.
Edwards, J.G. (1988). A long-term prospective evaluation of the circumferen-tial supracrestal fiberotomy in alleviating orthodontic relapse. Am J Orthod Dentofacial Orthop. 93:380-387.
Erdinc, A.E., Nanda, R.S. & Işiksal, E. (2006). Relapse of anterior crowding in patients treated with extraction and nonextraction of premolars. Am J Orthod Dentofacial Orthop. 129:775-784.
Eslambolchi, S., Woodside, D.G. & Rossouw, P.E. (2008). A descriptive study of mandibular incisor alignment in untreated subjects. Am J Orthod Dento-facial Orthop. 133:343-353.
Fastlicht, J. (1970). Crowding of mandibular incisors. Am J Orthod. 58:156-163.
Francisconi, M.F., Janson, G., Freitas, K.M., Gobbi de Oliveira, R.C., Gobbi de Oliviera, R.C., Freitas, M.R. & Henriques, J.F. (2014). Overjet, overbite, and anterior crowding relapses in extraction and nonextraction patients, and their correlations. Am J Orthod Dentofacial Orthop. 146:67-72.

80
Freitas, M.R., Ribeiro de Castro, R.C., Janson, G., Freitas, K.M. & Henri-ques, J.F. (2006a). Correlation between mandibular incisor crown morpho-logic index and postretention stability. Am J Orthod Dentofacial Orthop. 129:559-561.
Freitas, K.M., Freitas, M.R., Janson, G., Pinzan, A. & Henriques, J.F. (2006b). Retrospective analysis of orthodontic treatment outcomes and its relation to postretention stability. J Appl Oral Sci. 14:324-329.
Freitas, K.M., Janson, G., Tompson, B., Freitas, M.R., Simão, T.M., Valarelli, F.P. & Cançado, R.H. (2013). Posttreatment and physiologic occlusal chan-ges comparison. Angle Orthod. 83:239-245.
Gardner, S.D. & Chaconas, S.J. (1976). Posttreatment and postretention chan-ges following orthodontic therapy. Angle Orthod. 46:151-161.
Gianelly, A.A. (2003). Arch width after extraction and nonextraction trea-ment. Am J Orthod Dentofacial Orthop. 123:25-28.
Glenn, G., Sinclair, P.M. & Alexander, R.G. (1987). Nonextraction ortho-dontic therapy: Posttreatment dental and skeletal stability. Am J Orthod Dentofacial Orthop. 92:321-328.
Harradine, N.W., Pearson, M.H. & Toth, B. (1998). The effect of extraction of third molars on late lower incisor crowding: a randomized controlled trial. Br J Orthod. 25:117-122.
Holm, A. (2005). Bettavvikelser och tandreglering i ett hälsoperspektiv. En systematisk litteraturöversikt. Stockholm: Statens beredning för medicinsk utvärdering (SBU). p.121.
Iliadi, A., Kloukos, D., Gkantidis, N., Katsaros, C. & Pandis N. (2015). Failu-re of fixed orthodontic retainers: A systematic review. J Dent. 43:876-896.
Jin, C., Bennani, F., Gray. A., Farella, M. & Mei, L. (2018). Survival analysis of orthodontic retainers. Eur J Orthod. Epub ahead of print.
Johnston, C.D. & Littlewood, S.J. (2015). Retention in Orthodontics. Br Dent J. 218:119-122.
Jonsson, T. & Magnusson, T.E. (2010). Crowding and spacing in the dental arches: long-term development in treated and untreated subjects. Am J Orthod Dentofacial Orthop. 138:384.e1-384.e7.
Juloski, J., Glisic, B. & Vandevska-Radunovic, V. (2017). Long-term influence of fixed lingual retainers on the development of gingival recession: A retro-spective, longitudinal cohort study. Angle Orthod. 87:658-664.
Kahl-Nieke, B., Fischbach, H. & Schwarze, C.W. (1995). Post-retention crow-ding and incisor irregularity: A long-term follow-up evaluation of stability and relapse. Br J Orthod. 22:249-257.
Kaplan, R.G. (1974). Mandibular third molars and postretention crowding. Am J Orthod. 66:411-430.

81
Katsaros, C., Livas, C. & Renkema. A.M. (2007). Unexpected complications of bonded mandibular lingual retainers. Am J Orthod Dentofacial Orthop. 132:838-841.
Kerosuo, H., Heikinheimo, K., Nyström, M. & Väkiparta, M. (2013). Out-come and long-term stability of an early orthodontic treatment strategy in public health care. Eur J Orthod. 35:183-189.
Kharbanda, O.P. & Darendeliler, M.A. (2016). Occlusion and Orthodontics. In: Klineberg, I., Eckert, S.E., (eds.) Functional Occlusion in Restorative Dentistry and Prosthodontics 1st ed. St Louis: Elsevier Mosby. p.201-214.
Knierim, R.W. (1973). Invisible lower cuspid to cuspid retainer. Angle Orthod. 43:218-220.
Kuijpers-Jagtman, A.M. (2002). Repair and revision 8. Relapse of lower inci-sors: retreatment? Ned Tijdschr Tandheelkd. 109:42-46.
Kurol, J. (1984). Infraocclusion of primary molars. An epidemiological, fami-lial, longitudinal clinical and histological study. Diss. Göteborg: Göteborgs Universitet. Swed Dent J Suppl. 21:1-67.
Langdahl, B., Ferrari, S. & Dempster, D.W. (2016). Bone modeling and remo-deling: potential as therapeutic targets for the treatment of osteoporosis. Ther Adv Musculoskel Dis. 8:225-235.
Linder-Aronson, S., Bjerrehorn, K. & Forsberg, C.-M. (2002). Objective and subjective need for orthodontic treatment in Stockholm County. Swed Dent J. 26:31-40.
Little, R.M. (1975). The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod. 68:554-563.
Little, R.M., Wallen, T.R. & Riedel, R.A. (1981). Stability and relapse of mandibular anterior alignment-first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 80:349-365.
Little, R.M., Riedel, R.A. & Årtun, J. (1988). An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop. 93:423-428.
Little, R.M. (1990). Stability and relapse of dental arch alignment. Br J Ort-hod. 17:235-241.
Little, R.M. (1999). Stability and relapse of mandibular anterior alignment: University of Washington studies. Semin Orthod. 5:191-204.
Littlewood, S.J., Millett, D.T., Doubleday, B., Bearn, D.R. & Worthing-ton, H.V. (2016). Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. (1):CD002283.
Maltha, J.C. & Von den Hoff, J.W. (2017). Biological basis for orthodontic relapse. In: Katsaros, C. & Eliades, T, (eds.) Stability, Retention & Relapse in Orthodontics. 1st ed. United Kingdom: Quintessence Publishing. p.15-27.

82
Mangolas, S.C. (2000). Birth and death of bone cells: Basic regulatory mecha-nisms and implications for the pathogenesis and treatment of osteoporosis. Endocrine Reviews. 21:115-137.
McCauley, D.R. (1944). The cuspid and its function in retention. Am. J. Ort-hod. 30:196–205.
Mershon, J.V. (1936). Failures. Int J Orthod Oral Surg. 22:338-342.
Nanda, R.S. & Nanda, S.R. (1992). Considerations of dentofacial growth in long-term retention and stability: Is active retention needed? Am J Orthod Dentofacial Orthop. 101:297-302.
Oh, H., Ma, N., Feng, P.P., Kieu, K., Boero, R., Dugoni, S., Aubert, M. & Chambers, D. (2016). Evaluation of posttreatment stability after ortho-dontic treatment in the mixed and permanent dentitions. Angle Orthod. 86:1010-1018.
Ormiston, J.P., Huang, G.J., Little, R.M., Decker J.D. & Seuk, G.D. (2005). Retrospective analysis of long-term stable and unstable orthodontic treat-ment outcomes. Am J Orthod Dentofacial Orthop. 128:568-574.
Otuyemi, O.D. & Jones, S.P. (1995). Long-term evaluation of treated class II division 1 malocclusions utilizing the PAR Index. Br J Orthod. 22:171-178.
Park, H., Boley, J.C., Alexander, R.A. & Bushang, P.H. (2010). Age-related long-term posttreatment occlusal and arch changes. Angle Orthod. 80:247-253.
Pazera, P., Fudalej, P. & Katsaros, C. (2012). Severe complication of a bonded mandibular lingual retainer. Am J Orthod Dentofacial Orthop. 142:406-409.
Proffit. W.R. (1986). On the aetiology of malocclusion. The Northcroft lec-ture, 1985 presented to the British Society for the Study of Orthodontics, Oxford, April 18, 1985. Br J Orthod. 13:1-11.
Proffit, W.R. (2013). Retention. In: Proffit, W.R., Fields, H.W & Sarver, D.M, (eds.) Contemporary Orthodontics. 5th ed. St Louis: Elsevier Mosby-Year Book. p.606-620.
Redlich, M., Shoshan, S. & Palmon, A. (1999). Gingival response to ortho-dontic force. Am J Orthod Dentofacial Orthop. 116:152-158.
Reitan, K. (1959). Tissue rearrangement during retention of orthodontically rotated teeth. Angle Orthod. 29:105-113.
Reitan, K. (1967). Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthod. 53:721-745.
Reitan, K. (1969). Principles of retention and avoidance of posttreatment relapse. Am J Orthod. 55:776-790.
Renkema, A.-M., Al-Assad, S., Bronkhorst, E., Weindel, S., Katsaros, C. & Lisson, J.A. (2008). Effectiveness of lingual retainers bonded to the canines in preventing mandibular incisor relapse. Am J Orthod Dentofacial Ort-hop. 134:179.e1-179.e8.

83
Renkema, A.-M., Renkema, A., Bronkhorst, E. & Katsaros, C. (2011). Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop. 139:614-621.
Renkema, A.-M., Fudalej, P.S., Renkema, A., Kiekens, R. & Katsaros, C. (2013). Development of labial gingival recessions in orthodontically treated patients. Am J Orthod Dentofacial Orthop. 143:206-212.
Richardson, M.E. (1989). The role of the third molar in the cause of late lo-wer arch crowding: A review. Am J Orthod Dentofacial Orthop. 95:79-83.
Richmond, S., Shaw, W.C., O’Brien, K.D., Buchanan, I.B., Jones, R., Stephens, C.D., Roberts, C.T. & Andrews, M. (1992a). The development of the PAR Index (Peer Assessment Rating): reliability and validity. Eur J Orthod. 14:125-139.
Richmond, S., Shaw, W.C., Roberts, C.T. & Andrews, M. (1992b). The PAR Index (Peer Assessment Rating): methods to determine outcome of ortho-dontic treatment in terms of improvement and standards. Eur J Orthod. 14:180-187.
Riedel, R.A. (1960). A review of the retention problem. Angle Orthod. 30:179-199.
Rody, W.J., Elmaraghy, S., McNeight, A.M., Chamberlain, C.A., Antal, D., Dolce, C., Wheeler, T.T., McGorray, S.P. & Shaddox, L.M. (2016). Effects of different orthodontic retention protocols on the periodontal health of mandibular incisors. Orthod Craniofac Res. 19:198-208.
Rossouw, P.E., Preston, C.B. & Lombard, C. (1999). A longitudinal evaluation of extraction versus nonextraction treatment with special reference to the posttreatment irregularity of the lower incisors. Semin Orthod. 5:160-170.
Rygh, P. (1995). Orthodontic forces and tissue reactions. In: Thilander, B., Rönning, O, (eds). Introduction to Orthodontics. 2nd ed. Förlagshuset Gothia AB. p.191-194.
Sadowsky, C., Schneider, B.J., BeGole, E.A. & Tahir, E. (1994). Long-term sta-bility after orthodontic treatment: Nonextraction with prolonged retention. Am J Orthod Dentofacial Orthop. 106:243-249.
Samspon, W.J. (1995). Current controversies in late incisor crowding. Ann Acad Med Singapore. 24:129-137.
Scheibe, K. & Ruf. S. (2010). Lower bonded retainers: survival and failure ra-tes particularly considering operator experience. J Orofac Orthop. 71:300-307.
Schütz-Fransson, U., Bjerklin, K. & Lindsten, R. (2006). Long-term follow-up of orthodontically treated deep bite patients. Eur J Orthod. 28:503-512.
Segner, D. & Heinrici, B. (2000). Bonded retainers - clinical reliability. J Oro-fac Orthop. 61:352-358.
84
Shapiro, P.A. (1974). Mandibular dental arch form and dimension. Treatment and postretention changes. Am J Orthod. 66:58-70.
Shaughnessy, T.G., Proffit, W.R. & Samara, S.A. (2016). Inadvertent tooth movement with fixed lingual retainers. Am J Orthod Dentofacial Orthop. 149:277-286.
Sheridan, J.J., LeDoux, W. & McMinn, R. (1993). Essix retainers: fabrication and supervision for permanent retention. J Clin Orthod. 27:37-45.
Sifakakis, I., Eliades, T. & Bourauel, C. (2015). Residual stress analysis of fixed retainer wires after in vitro loading: can mastication-induced stresses produce an unfavorable effect? Biomed Tech (Berl). 60:617-622.
Sinclair, P.M. & Little, R.M. (1983). Maturation of untreated normal occlu-sions. Am J Orthod. 83:114-123.
Solow, B. (1966). The pattern of craniofacial associations. Acta Odontol Scand. 24:suppl 46.
Sondhi, A., Cleall, J.F. & BeGole, E.A. (1980). Dimensional changes in the dental arches of orthodontically treated cases. Am J Orthod. 77:60-74.
Southard, T.E., Southard, K.A. & Tolley, E.A. (1992). Periodontal force: a potential cause of relapse. Am J Orthod Dentofacial Orthop. 101:221-227.
Strydom, H., Maltha, J.C., Kuijpers-Jagtman, A.M. & Von den Hoff, J.W. (2012). The oxytalan fibre network in the periodontium and its possible mechanical function. Arch Oral Biol. 57:1003-1011.
Störmann, I. & Ehmer, U. (2002). A prospective randomized study of different retainer types. J Orofac Orthop. 63:42-50.
Sumitra & Tandur, A.P. (2005). Third molars and late mandibular incisor crowding - A review. J Ind Orthod Soc. 38:100-111.
Taner, T., Haydar, B., Kavuklu, I. & Korkmaz, A. (2000). Short-term effects of fiberotomy on relapse of anterior crowding. Am J Orthod Dentofacial Orthop. 118:617-623.
Taner, T. & Aksu, M. (2012). A prospective clinical evaluation of mandibular lingual retainer survival. Eur J Orthod. 34:470-474.
Thilander, B. (2000). Biological basis for orthodontic relapse. Semin Orthod. 6:195-205.
Thilander, B. (2009). Dentoalveolar development in subjects with normal occlusion. A longitudinal study between the ages of 5 and 31 years. Eur J Orthod. 31:109-120.
Thordarson, A., Johannsdottir, B. & Magnusson, T.E. (2006). Craniofacial changes in Icelandic children between 6 and 16 years of age - a longitudinal study. Eur J Orthod. 28:152-165.
Tsiopas, N., Nilner, M., Bondemark, L. & Bjerklin, K. (2013). A 40 years follow-up of dental arch dimensions and incisor irregularity in adults. Eur J Orthod. 35:230-235.

85
Uhde, M.D., Sadowsky, C. & BeGole, E.A. (1983). Long-term stability of den-tal relationships after orthodontic treament. Angle Orthod. 53:240-252
Zachrisson, B.U. (1977). Clinical experience with direct-bonded orthodontic retainers. Am J Orthod. 71:440-448.
Zachrisson, B.U. (1995). Third-generation mandibular bonded lingual 3-3 retainer. J Clin Orthod. 29:39-48.
Zachrisson, B.U. (1997). Important aspects of long-term stability. J Clin Ort-hod. 31:562-583.
Zachrisson, B.U. (2007). Long-term experience with direct-bonded retainers: update and clinical advice. J Clin Orthod. 41:728-737.
Zafarmand, A.H., Qamari, A. & Zafarmand, M.M. (2014). Mandibular inci-sor re-crowding: is it different in extraction and non-extraction cases? Oral Health Dent Manag. 13:669-674.
Zinad, K., Schols, A.M. & Schols, J.G. (2016). Another way of looking at treatment stability. Angle Orthod. 86:721-726.
Weinberger, B.W. (1926). Orthodontics: An historical review of its origin and evolution. Vol I. ST. Louis: The CV Mosby Company.
Westerlund, A., Daxberg, E.-L., Liljegren, A., Oikonomou, C., Ransjö, M., Samuelsson, O. & Sjögren, P. (2014). Stability and side effects of ortho-dontic retainers - A systematic review. Dentistry. 4:258. doi:10.4172/2161-1122.1000258.
Westerlund, A., Oikonomou, C., Ransjö, M., Ekestubbe, A., Bresin, A. & Lund, H. (2017). Cone-beam computed tomographic evaluation of the long-term effects of orthodontic retainers on marginal bone levels. Am J Orthod Dentofacial Orthop. 151:74-81.
Årtun, J. & Zachrisson, B. (1982). Improving the handling properties of a composite resin for direct bonding. Am J Orthod. 81:269-276.
Årtun, J., Garol, J.D. & Little, R.M. (1996). Long-term stability of mandibu-lar incisors following successful treatment of Class II, Division 1, malocclu-sions. Angle Orthod. 66:229-238.
Årtun, J., Spadafora, A.T. & Shapiro, P.A. (1997). A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod. 19:501-509.

86


Original Article
Twelve-year follow-up of mandibular incisor stability:
Comparison between two bonded lingual orthodontic retainers
Ulrike Schutz-Franssona; Rune Lindstenb; Krister Bjerklinc; Lars Bondemarkd
ABSTRACTObjective: To compare the long-term outcome 9 years after removal of two different types of fixedretainers used for stabilization of the mandibular anterior segment.Materials and Methods: Sixty-four children who had undergone orthodontic treatment with fixedappliances in both arches were divided into two groups depending on which kind of retainer beingused. Twenty-eight of the patients had a canine-to-canine retainer bonded to the canines and 36had a bonded twistflex retainer 3-3, bonded to each tooth. Measurements were made on studymodels and lateral head radiographs, before and after treatment, 6 years after treatment, and 12years after treatment, with a mean of 9.2 years after removal of the retainers.Results: No significant differences were found between the two groups at the long-term follow-upaccording to Little’s Irregularity Index or available space for the mandibular incisors. The overjetand overbite were reduced after treatment in both groups and stayed stable throughout theobservation period. Also, no differences in bonding failures between the two retainers were found.Conclusions: Both a canine-to-canine retainer bonded only to the canines and a twistflex retainer3-3 bonded to each tooth can be recommended. However, neither of the retention types preventedlong-term changes of mandibular incisor irregularity or available space for the mandibular incisorsafter removal of the retainers. (Angle Orthod. 2017;87:200–208)
KEY WORDS: Long-term stability; Irregularity Index; Orthodontic retainers; Relapse
INTRODUCTION
Bonded lingual retainers are an important and often-
used retention appliance in orthodontic treatment
because they are independent of patient cooperation,
nearly invisible, and easy to fabricate, but they need
regular check-ups. Studies have shown that bonded
retainers represent an efficient and reliable retention
appliance for long-term use.1–6
For retention of the mandibular incisors with a fixed
retention appliance, two different fixed retainers can be
used, either a canine-to-canine retainer bonded only to
the canines or a retainer bonded to each of the
mandibular incisors and canines.7,8 Although these
retainers are widely used, only a limited number of
studies can be found concerning their long-term
effectiveness. In a Cochrane review,9 there was only
one randomized clinical trial10 that assessed the
mandibular incisor alignment after 3 years of retention.
Furthermore, few studies have analyzed the long-
term outcome after removal of the retainers.11 In most
studies, the retainers were still in place at follow-up,
and the long-term follow-up was only 5 years post-
treatment.5,6
When tooth positions during 24 months of retention
were compared, it was found that the canine-to-canine
retainer induced frequent relapse of incisors not
bonded to the retainer compared with the retainer
attached to six teeth.12 In addition, another study13
concluded a high failure rate, 34.9% for each of these
two retainers, but the canine-to-canine retainer failed
significantly less often than did the retainer with six
a Research student, Faculty of Odontology, Malmo University,Sweden, Specialist in Orthodontics, The County OrthodonticClinic in Uddevalla, Vastra Gotaland, Sweden.
b Associate Professor and Head, Department of Orthodontics,Institute for Postgraduate Dental Education, Jonkoping, Sweden.
c Associate Professor, Department of Orthodontics, Faculty ofOdontology, Malmo University, Sweden.
d Professor and Head, Department of Orthodontics, Faculty ofOdontology, Malmo University, Sweden.
Corresponding author: Dr Ulrike Schutz-Fransson, Special-istcentrum, Uddevalla Sjukhus, SE 451 80 Uddevalla, Sweden(e-mail: [email protected])
Accepted: July 2016. Submitted: March 2016.Published Online: August 23, 2016.
2017 by The EH Angle Education and Research Foundation,Inc.
Angle Orthodontist, Vol 87, No 2, 2017 DOI: 10.2319/031716-227.1200

Original Article
Twelve-year follow-up of mandibular incisor stability:
Comparison between two bonded lingual orthodontic retainers
Ulrike Schutz-Franssona; Rune Lindstenb; Krister Bjerklinc; Lars Bondemarkd
ABSTRACTObjective: To compare the long-term outcome 9 years after removal of two different types of fixedretainers used for stabilization of the mandibular anterior segment.Materials and Methods: Sixty-four children who had undergone orthodontic treatment with fixedappliances in both arches were divided into two groups depending on which kind of retainer beingused. Twenty-eight of the patients had a canine-to-canine retainer bonded to the canines and 36had a bonded twistflex retainer 3-3, bonded to each tooth. Measurements were made on studymodels and lateral head radiographs, before and after treatment, 6 years after treatment, and 12years after treatment, with a mean of 9.2 years after removal of the retainers.Results: No significant differences were found between the two groups at the long-term follow-upaccording to Little’s Irregularity Index or available space for the mandibular incisors. The overjetand overbite were reduced after treatment in both groups and stayed stable throughout theobservation period. Also, no differences in bonding failures between the two retainers were found.Conclusions: Both a canine-to-canine retainer bonded only to the canines and a twistflex retainer3-3 bonded to each tooth can be recommended. However, neither of the retention types preventedlong-term changes of mandibular incisor irregularity or available space for the mandibular incisorsafter removal of the retainers. (Angle Orthod. 2017;87:200–208)
KEY WORDS: Long-term stability; Irregularity Index; Orthodontic retainers; Relapse
INTRODUCTION
Bonded lingual retainers are an important and often-
used retention appliance in orthodontic treatment
because they are independent of patient cooperation,
nearly invisible, and easy to fabricate, but they need
regular check-ups. Studies have shown that bonded
retainers represent an efficient and reliable retention
appliance for long-term use.1–6
For retention of the mandibular incisors with a fixed
retention appliance, two different fixed retainers can be
used, either a canine-to-canine retainer bonded only to
the canines or a retainer bonded to each of the
mandibular incisors and canines.7,8 Although these
retainers are widely used, only a limited number of
studies can be found concerning their long-term
effectiveness. In a Cochrane review,9 there was only
one randomized clinical trial10 that assessed the
mandibular incisor alignment after 3 years of retention.
Furthermore, few studies have analyzed the long-
term outcome after removal of the retainers.11 In most
studies, the retainers were still in place at follow-up,
and the long-term follow-up was only 5 years post-
treatment.5,6
When tooth positions during 24 months of retention
were compared, it was found that the canine-to-canine
retainer induced frequent relapse of incisors not
bonded to the retainer compared with the retainer
attached to six teeth.12 In addition, another study13
concluded a high failure rate, 34.9% for each of these
two retainers, but the canine-to-canine retainer failed
significantly less often than did the retainer with six
a Research student, Faculty of Odontology, Malmo University,Sweden, Specialist in Orthodontics, The County OrthodonticClinic in Uddevalla, Vastra Gotaland, Sweden.
b Associate Professor and Head, Department of Orthodontics,Institute for Postgraduate Dental Education, Jonkoping, Sweden.
c Associate Professor, Department of Orthodontics, Faculty ofOdontology, Malmo University, Sweden.
d Professor and Head, Department of Orthodontics, Faculty ofOdontology, Malmo University, Sweden.
Corresponding author: Dr Ulrike Schutz-Fransson, Special-istcentrum, Uddevalla Sjukhus, SE 451 80 Uddevalla, Sweden(e-mail: [email protected])
Accepted: July 2016. Submitted: March 2016.Published Online: August 23, 2016.
2017 by The EH Angle Education and Research Foundation,Inc.
Angle Orthodontist, Vol 87, No 2, 2017 DOI: 10.2319/031716-227.1200

bonding sites. As to comfort, the canine-to-canine
retainer was given a significantly poorer rating.12
There are different advantages and disadvantages
ascribed to the two types of retainers. However, few
studies have been published that compare different
types of bonded mandibular retainers and their
capacity for maintaining long-term stability, that is,
more than 5 years after retention removal. Therefore,
the aim of the present study was to compare the long-
term outcome 9 years after removal of two different
types of fixed retainers used for stabilization of the
mandibular anterior segment.
The null hypothesis was that there would be no
difference in mandibular incisor stability between the
two different mandibular retainers in a long-term
perspective.
MATERIALS AND METHODS
The study comprised 64 children (23 boys and 41
girls) who had undergone orthodontic treatment be-
tween 1980 and 1995 for Class II malocclusion, deep
and/or bite, and/or crowding of the maxillary and
mandibular incisors at the Department of Orthodontics,
Institute for Postgraduate Dental Education in
Jonkoping, Sweden. Long-term records were required
for participation in the study. Treatment consisted of
fixed edgewise appliances (0.018-inch) in both jaws.
No interproximal enamel reduction or circumferential
supracrestal fiberotomy was performed.
The sample was divided into two groups, depending
on which kind of mandibular retainer was used.
Twenty-eight of the patients had a canine-to-canine
retainer (0.028-inch spring hard wire) bonded to the
canines (group 1, Figure 1a), and 36 had a bonded
twistflex retainer (0.0195-inch) bonded lingually to all
mandibular incisors and canines (group 2, Figure 1b,
Table 1). Each group consisted of both extraction
(64%) and nonextraction (36%) cases. All retainers
were custom-made in the laboratory and were bonded
with composite.
Methods
The Ethics Committee of Linkoping, Sweden, ap-
proved the protocol (2014/38131).The measurements were performed on dental casts
using a sliding digital calliper (Mitutoyo 500171Kanagawa, Japan) with an accuracy of 0.01 mm.
Measurements were made at four time points: T0,
before orthodontic treatment; T1, immediately after
treatment, that is, at the start of retention; T2, 6 years
after treatment, that is, a mean of 3.6 years after the
retainer was removed; and T3, 12 years after
treatment, that is, a mean of 9.2 years after retainer
removal (Table 2). There were no registrations at
retainer removal; thus, the study measured changes
after retainer removal.
Figure 1. Twistflex retainer and canine-to-canine retainer.
Table 1. Mean Age and Number of Subjects (Boys/Girls) in Groups 1 And 2, at the Four Registration Points
T0a T1 T2 T3
n Boys Girls Mean SD n Boys Girls Mean SD n Boys Girls Mean SD n Boys Girls Mean SD
Group 1b 28 13 15 12.5 1.47 28 13 15 15.1 1.57 26 12 14 21.2 2.45 24 11 13 27.0 2.51
Group 2 36 10 26 13.2 4.18 36 10 26 16.1 4.36 36 10 26 22.4 4.13 28 6 22 27.8 4.14
a T0 indicates before treatment; T1, after treatment; T2, 6 years after treatment; T3, 12 years after treatment.b Group 1 indicates canine-to-canine retainer; group 2, twistflex retainer.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 201
The measured variables were Irregularity Indexaccording to Little14 (LII; the summed displacement ofthe anatomic contact points of the mandibular anteriorteeth), intercanine width (cusp tip to cusp tip of themandibular canines), intercanine perimeter distance(arch perimeter length between the mesial contactpoints of the canines), available mandibular incisorspace (intercanine perimeter distance minus summedtooth width of the four mandibular incisors), twodifferent lateral arch lengths (mesial contact point ofthe mandibular first molar to the mesial contact point ofthe canines or to the mesial contact point of the centralincisors), overjet, and overbite (Figures 2 and 3). Also,the tooth width of the mandibular incisors wasmeasured at T0 and T3.
Sagittal and vertical relationships between the jawsas well as incisor inclination and mandibular lengthwere evaluated on lateral head radiographs. Referencelines and points are shown in Figure 4. All measure-ments on the lateral head radiographs were made tothe nearest half-degree or 0.5 mm with correction forenlargement. Cephalometric reference points andmeasurements were assessed according to Bjork15
and Solow16 with the following addition: Ar-B, which isthe distance from articulare to point B.
All registrations and measurements were made byone author. At T2 and T3, there were no retentionappliances in place and thereby a blinded evaluationwas possible, that is, the examiner was unaware as towhich group the patients belonged to or whether casts
were taken at T2 or T3. In addition, notes of any retainerbonding failures were obtained from the patient files.
Statistical Analysis
Sample size estimation was based on a significancelevel of 0.05 and 90% power to detect a clinicallymeaningful difference of 1.5 mm of LII.14 The estimaterevealed that 21 patients in each group was sufficient.Arithmetic means and standard deviations (SDs) ongroup level were calculated for each variable at T0, T1,T2, and T3.
The sample was normally distributed according tothe Kolmogorov-Smirnov test.
Significant differences in means in and betweengroups were tested by one-way analysis of varianceusing the Statistical Package for Social Sciences(version 22.0, SPSS Inc, Chicago, Ill). P values lessthan 5% (P , .05) were considered statisticallysignificant. When significant differences were foundbetween groups, the Bonferroni correction wasused.
Error of the Measurements
The same examiner measured 24 randomly selectedcases at two separate time points with a 4-weekinterval. The mean error of the measurements accord-ing to Dahlberg’s formula17 for the linear variables was0.1 mm. The largest measurement error was 0.5 mmfor intercanine width, 0.5 mm for intercanine perimeterdistance, and 0.5 mm for left lateral arch length. Errormeasurements for the cephalometric angular variableswere a mean 0.88. The greatest measurement errorwas noted for the maxillary incisor inclination, 3.38.
No significant differences between the two series ofrecords were found using paired t-tests in most of themeasurements (in mm) except for the left lateral archlength (range, 0.1 to 0.5), available space (range,0.3 to0.2), tooth width 32 (range,0.1 to 0.1), tooth width 41(range,0.1 to 0.1), and L1/Apg (range,0.1 to 1.3). Thesystematic error was within the boundaries given above.
RESULTS
Distribution according to age and gender can beseen in Table 1. Teatment started in group 1 at a mean
Table 2. Number of Years with Retention and Time After Retention for Groups 1 and 2
Reta Time Ret Out–T2b Ret Out–T3 Time, T0–T1 Time, T1–T2 Time, T1–T3
n Y SD n Y SD n Y SD n Y SD n Y SD n Y SD
Group 1c 28 2.6 2.48 26 3.7 2.52 24 9.3 2.79 28 2.6 0.94 26 6.2 1.99 24 11.7 2.05
Group 2 36 3.0 1.66 35 3.5 1.93 28 9.1 1.86 36 2.9 1.76 36 6.3 2.26 28 12.2 1.82
a Ret indicates retainer or retention.b T0 indicates before treatment; T1, after treatment; T2, 6 years after treatment; T3, 12 years after treatment.c Group 1 indicates canine-to-canine retainer; group 2, twistflex retainer.
Figure 2. Little’s Irregularity Index.
Angle Orthodontist, Vol 87, No 2, 2017
202 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

bonding sites. As to comfort, the canine-to-canine
retainer was given a significantly poorer rating.12
There are different advantages and disadvantages
ascribed to the two types of retainers. However, few
studies have been published that compare different
types of bonded mandibular retainers and their
capacity for maintaining long-term stability, that is,
more than 5 years after retention removal. Therefore,
the aim of the present study was to compare the long-
term outcome 9 years after removal of two different
types of fixed retainers used for stabilization of the
mandibular anterior segment.
The null hypothesis was that there would be no
difference in mandibular incisor stability between the
two different mandibular retainers in a long-term
perspective.
MATERIALS AND METHODS
The study comprised 64 children (23 boys and 41
girls) who had undergone orthodontic treatment be-
tween 1980 and 1995 for Class II malocclusion, deep
and/or bite, and/or crowding of the maxillary and
mandibular incisors at the Department of Orthodontics,
Institute for Postgraduate Dental Education in
Jonkoping, Sweden. Long-term records were required
for participation in the study. Treatment consisted of
fixed edgewise appliances (0.018-inch) in both jaws.
No interproximal enamel reduction or circumferential
supracrestal fiberotomy was performed.
The sample was divided into two groups, depending
on which kind of mandibular retainer was used.
Twenty-eight of the patients had a canine-to-canine
retainer (0.028-inch spring hard wire) bonded to the
canines (group 1, Figure 1a), and 36 had a bonded
twistflex retainer (0.0195-inch) bonded lingually to all
mandibular incisors and canines (group 2, Figure 1b,
Table 1). Each group consisted of both extraction
(64%) and nonextraction (36%) cases. All retainers
were custom-made in the laboratory and were bonded
with composite.
Methods
The Ethics Committee of Linkoping, Sweden, ap-
proved the protocol (2014/38131).The measurements were performed on dental casts
using a sliding digital calliper (Mitutoyo 500171Kanagawa, Japan) with an accuracy of 0.01 mm.
Measurements were made at four time points: T0,
before orthodontic treatment; T1, immediately after
treatment, that is, at the start of retention; T2, 6 years
after treatment, that is, a mean of 3.6 years after the
retainer was removed; and T3, 12 years after
treatment, that is, a mean of 9.2 years after retainer
removal (Table 2). There were no registrations at
retainer removal; thus, the study measured changes
after retainer removal.
Figure 1. Twistflex retainer and canine-to-canine retainer.
Table 1. Mean Age and Number of Subjects (Boys/Girls) in Groups 1 And 2, at the Four Registration Points
T0a T1 T2 T3
n Boys Girls Mean SD n Boys Girls Mean SD n Boys Girls Mean SD n Boys Girls Mean SD
Group 1b 28 13 15 12.5 1.47 28 13 15 15.1 1.57 26 12 14 21.2 2.45 24 11 13 27.0 2.51
Group 2 36 10 26 13.2 4.18 36 10 26 16.1 4.36 36 10 26 22.4 4.13 28 6 22 27.8 4.14
a T0 indicates before treatment; T1, after treatment; T2, 6 years after treatment; T3, 12 years after treatment.b Group 1 indicates canine-to-canine retainer; group 2, twistflex retainer.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 201
The measured variables were Irregularity Indexaccording to Little14 (LII; the summed displacement ofthe anatomic contact points of the mandibular anteriorteeth), intercanine width (cusp tip to cusp tip of themandibular canines), intercanine perimeter distance(arch perimeter length between the mesial contactpoints of the canines), available mandibular incisorspace (intercanine perimeter distance minus summedtooth width of the four mandibular incisors), twodifferent lateral arch lengths (mesial contact point ofthe mandibular first molar to the mesial contact point ofthe canines or to the mesial contact point of the centralincisors), overjet, and overbite (Figures 2 and 3). Also,the tooth width of the mandibular incisors wasmeasured at T0 and T3.
Sagittal and vertical relationships between the jawsas well as incisor inclination and mandibular lengthwere evaluated on lateral head radiographs. Referencelines and points are shown in Figure 4. All measure-ments on the lateral head radiographs were made tothe nearest half-degree or 0.5 mm with correction forenlargement. Cephalometric reference points andmeasurements were assessed according to Bjork15
and Solow16 with the following addition: Ar-B, which isthe distance from articulare to point B.
All registrations and measurements were made byone author. At T2 and T3, there were no retentionappliances in place and thereby a blinded evaluationwas possible, that is, the examiner was unaware as towhich group the patients belonged to or whether casts
were taken at T2 or T3. In addition, notes of any retainerbonding failures were obtained from the patient files.
Statistical Analysis
Sample size estimation was based on a significancelevel of 0.05 and 90% power to detect a clinicallymeaningful difference of 1.5 mm of LII.14 The estimaterevealed that 21 patients in each group was sufficient.Arithmetic means and standard deviations (SDs) ongroup level were calculated for each variable at T0, T1,T2, and T3.
The sample was normally distributed according tothe Kolmogorov-Smirnov test.
Significant differences in means in and betweengroups were tested by one-way analysis of varianceusing the Statistical Package for Social Sciences(version 22.0, SPSS Inc, Chicago, Ill). P values lessthan 5% (P , .05) were considered statisticallysignificant. When significant differences were foundbetween groups, the Bonferroni correction wasused.
Error of the Measurements
The same examiner measured 24 randomly selectedcases at two separate time points with a 4-weekinterval. The mean error of the measurements accord-ing to Dahlberg’s formula17 for the linear variables was0.1 mm. The largest measurement error was 0.5 mmfor intercanine width, 0.5 mm for intercanine perimeterdistance, and 0.5 mm for left lateral arch length. Errormeasurements for the cephalometric angular variableswere a mean 0.88. The greatest measurement errorwas noted for the maxillary incisor inclination, 3.38.
No significant differences between the two series ofrecords were found using paired t-tests in most of themeasurements (in mm) except for the left lateral archlength (range, 0.1 to 0.5), available space (range,0.3 to0.2), tooth width 32 (range,0.1 to 0.1), tooth width 41(range,0.1 to 0.1), and L1/Apg (range,0.1 to 1.3). Thesystematic error was within the boundaries given above.
RESULTS
Distribution according to age and gender can beseen in Table 1. Teatment started in group 1 at a mean
Table 2. Number of Years with Retention and Time After Retention for Groups 1 and 2
Reta Time Ret Out–T2b Ret Out–T3 Time, T0–T1 Time, T1–T2 Time, T1–T3
n Y SD n Y SD n Y SD n Y SD n Y SD n Y SD
Group 1c 28 2.6 2.48 26 3.7 2.52 24 9.3 2.79 28 2.6 0.94 26 6.2 1.99 24 11.7 2.05
Group 2 36 3.0 1.66 35 3.5 1.93 28 9.1 1.86 36 2.9 1.76 36 6.3 2.26 28 12.2 1.82
a Ret indicates retainer or retention.b T0 indicates before treatment; T1, after treatment; T2, 6 years after treatment; T3, 12 years after treatment.c Group 1 indicates canine-to-canine retainer; group 2, twistflex retainer.
Figure 2. Little’s Irregularity Index.
Angle Orthodontist, Vol 87, No 2, 2017
202 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

age of 12.5 years (SD 1.47) and 13.2 years (SD 4.18)in group 2 (Table 1). T0–T1 was 2.6 years (SD 0.94) forgroup 1 and 2.9 years (SD 1.76) for group 2 (Table 2).Mean postretention time was 9.3 years (SD 2.79) forgroup 1 and 9.1 years (SD 1.86) for group 2 (Table 2).Most of the patients were between 25 and 30 years ofage at the last registration (T3).
Little’s Irregularity Index
LII14 was 4.5 mm for group 1 and 4.7 mm for group2 before treatment and after treatment LII was 1.9 mmand 1.6 mm, respectively. Nine years after retention,LII was 4.2 mm in group 1 vs 4.4 mm in group 2.
There were no significant intergroup differences, butwithin each group, several significant differences werefound between the four registrations (T0–T3).
Available Space
Available space in the mandibular anterior segmentshowed similar results as LII (Table 3). For bothgroups, the available space in the mandibular anteriorsegment increased after treatment. Six and 12 yearsafter treatment, the available space had decreased inboth groups, and for group 1, it was equivalent to thatbefore treatment with no significant intergroup differ-ences (Table 3).
Figure 3. Variables measured on dental casts.
Figure 4. Cephalometric reference points and lines.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 203
Overjet, Overbite
Both overjet and overbite were reduced aftertreatment in both groups and then fairly stablethroughout the observation period. There were nosignificant differences between the two groups (Table3).
Intercanine Width
The intercanine width was almost the same beforeand after treatment in both groups, and over time, theintercanine width decreased approximately 1 mm inboth groups (Table 3).
Intercanine Perimeter Distance
Intercanine perimeter distance increased duringtreatment by 0.6 mm in both groups. At T2, it haddecreased, and it further decreased at T3, 0.9 mm forgroup 1 and 0.8 mm for group 2 (Table 3).
Arch Length
Both variables for arch length (from the first molar tothe canine or to the central incisor) decreased aftertreatment and continued to decrease 6 and 12 yearsafter treatment in both groups (Table 3).
Tooth Width
There was a small but significant difference inmandibular right lateral incisor width between groups1 and 2 (Table 3).
Cephalometric Variables
No significant intergroup differences were found forany of the variables measured on the lateral headradiographs at the four time points (Table 4).
Extraction Vs Nonextraction
There was no difference in mandibular incisorstability between the patients who had extractions
Table 3. Mean Values MM and Number of Subjects for 14
Variables at the 4 Registration Points Measured on Study Models
and the Differences in Mean Values Between Groups 1 and 2.
Variables
Group 1
(Canine-to-Canine
Retainer)
Group 2
(Twistflex
Retainer)
n Mean SD n Mean SD P
Little’s Irregularity Index
T0a 28 4.5 3.46 35 4.7 2.96 NSb
T1 28 1.9 1.36 36 1.6 1.07 NS
T2 26 3.2 2.01 36 3.4 2.16 NS
T3 24 4.2 2.52 28 4.4 2.31 NS
Available space, mand 3-3
T0 28 1.9 2.59 35 2.1 2.51 NS
T1 28 0.1 0.45 36 0.1 0.30 NS
T2 26 1.3 1.16 36 0.8 0.84 NS
T3 24 2.0 1.45 28 1.3 1.01 NS
Intercanine width
T0 27 26.3 1.92 34 25.6 1.72 NS
T1 28 26.2 1.63 36 25.8 1.66 NS
T2 26 25.7 1.49 36 25.2 1.63 NS
T3 24 25.2 1.62 28 24.7 1.66 NS
Intercanine perimeter distance
T0 27 24.3 1.24 34 23.5 1.42 NS
T1 28 24.9 1.12 36 24.1 1.59 NS
T2 26 24.1 0.89 36 23.3 1.66 NS
T3 23 23.4 1.13 28 22.7 1.88 NS
Lateral arch length, left 2-6
T0 28 20.2 2.60 36 20.3 2.49 NS
T1 28 18.9 3.65 36 19.4 3.32 NS
T2 26 18.6 3.64 36 18.9 3.52 NS
T3 24 18.4 3.57 28 18.8 3.46 NS
Lateral arch length, right 2-6
T0 28 19.9 2.47 36 20.0 2.45 NS
T1 28 18.4 3.57 36 19.5 3.35 NS
T2 26 17.7 3.80 36 19.1 3.28 NS
T3 24 17.4 3.69 28 19.0 3.29 NS
Lateral arch length, left central-6
T0 28 29.8 2.26 36 29.6 2.38 NS
T1 28 28.5 3.28 36 28.9 3.10 NS
T2 26 27.6 3.34 36 27.9 3.04 NS
T3 24 27.2 3.05 28 27.7 3.07 NS
Lateral arch length, right central-6
T0 28 29.5 2.19 36 29.6 2.57 NS
T1 28 28.0 3.22 36 29.0 3.20 NS
T2 26 27.2 3.26 36 28.1 3.13 NS
T3 24 26.8 3.11 28 27.9 3.12 NS
Tooth width, 32
T0 28 6.3 0.32 36 6.1 0.36 NS
T3 24 6.3 0.30 28 6.0 0.39 NS
Tooth width, 31
T0 28 5.7 0.33 36 5.5 0.31 NS
T3 24 5.7 0.32 28 5.5 0.33 NS
Tooth width, 41
T0 28 5.6 0.32 36 5.5 0.36 NS
T3 24 5.6 0.31 27 5.4 0.37 NS
Tooth width 42
T0 28 6.3 0.40 36 6.0 0.39 *
T3 24 6.3 0.41 28 5.9 0.36 **
Overjet
T0 28 6.3 3.32 36 7.5 3.04 NS
T1 28 3.2 0.91 36 3.3 1.13 NS
T2 26 3.6 1.58 36 3.9 1.68 NS
T3 24 3.7 1.91 28 4.0 1.46 NS
Table 3. Continued
Variables
Group 1
(Canine-to-Canine
Retainer)
Group 2
(Twistflex
Retainer)
n Mean SD n Mean SD P
Overbite
T0 28 3.7 2.62 36 3.5 1.79 NS
T1 28 2.5 1.12 36 2.4 1.07 NS
T2 26 2.8 1.80 36 2.7 1.39 NS
T3 24 2.9 1.85 28 2.9 1.20 NS
a T0 indicates before treatment; T1, after treatment; T2, 6 yearsafter treatment; T3, 12 years after treatment.
b NS indicates not significant; * P¼ .05; **P¼ .01.
Angle Orthodontist, Vol 87, No 2, 2017
204 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

age of 12.5 years (SD 1.47) and 13.2 years (SD 4.18)in group 2 (Table 1). T0–T1 was 2.6 years (SD 0.94) forgroup 1 and 2.9 years (SD 1.76) for group 2 (Table 2).Mean postretention time was 9.3 years (SD 2.79) forgroup 1 and 9.1 years (SD 1.86) for group 2 (Table 2).Most of the patients were between 25 and 30 years ofage at the last registration (T3).
Little’s Irregularity Index
LII14 was 4.5 mm for group 1 and 4.7 mm for group2 before treatment and after treatment LII was 1.9 mmand 1.6 mm, respectively. Nine years after retention,LII was 4.2 mm in group 1 vs 4.4 mm in group 2.
There were no significant intergroup differences, butwithin each group, several significant differences werefound between the four registrations (T0–T3).
Available Space
Available space in the mandibular anterior segmentshowed similar results as LII (Table 3). For bothgroups, the available space in the mandibular anteriorsegment increased after treatment. Six and 12 yearsafter treatment, the available space had decreased inboth groups, and for group 1, it was equivalent to thatbefore treatment with no significant intergroup differ-ences (Table 3).
Figure 3. Variables measured on dental casts.
Figure 4. Cephalometric reference points and lines.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 203
Overjet, Overbite
Both overjet and overbite were reduced aftertreatment in both groups and then fairly stablethroughout the observation period. There were nosignificant differences between the two groups (Table3).
Intercanine Width
The intercanine width was almost the same beforeand after treatment in both groups, and over time, theintercanine width decreased approximately 1 mm inboth groups (Table 3).
Intercanine Perimeter Distance
Intercanine perimeter distance increased duringtreatment by 0.6 mm in both groups. At T2, it haddecreased, and it further decreased at T3, 0.9 mm forgroup 1 and 0.8 mm for group 2 (Table 3).
Arch Length
Both variables for arch length (from the first molar tothe canine or to the central incisor) decreased aftertreatment and continued to decrease 6 and 12 yearsafter treatment in both groups (Table 3).
Tooth Width
There was a small but significant difference inmandibular right lateral incisor width between groups1 and 2 (Table 3).
Cephalometric Variables
No significant intergroup differences were found forany of the variables measured on the lateral headradiographs at the four time points (Table 4).
Extraction Vs Nonextraction
There was no difference in mandibular incisorstability between the patients who had extractions
Table 3. Mean Values MM and Number of Subjects for 14
Variables at the 4 Registration Points Measured on Study Models
and the Differences in Mean Values Between Groups 1 and 2.
Variables
Group 1
(Canine-to-Canine
Retainer)
Group 2
(Twistflex
Retainer)
n Mean SD n Mean SD P
Little’s Irregularity Index
T0a 28 4.5 3.46 35 4.7 2.96 NSb
T1 28 1.9 1.36 36 1.6 1.07 NS
T2 26 3.2 2.01 36 3.4 2.16 NS
T3 24 4.2 2.52 28 4.4 2.31 NS
Available space, mand 3-3
T0 28 1.9 2.59 35 2.1 2.51 NS
T1 28 0.1 0.45 36 0.1 0.30 NS
T2 26 1.3 1.16 36 0.8 0.84 NS
T3 24 2.0 1.45 28 1.3 1.01 NS
Intercanine width
T0 27 26.3 1.92 34 25.6 1.72 NS
T1 28 26.2 1.63 36 25.8 1.66 NS
T2 26 25.7 1.49 36 25.2 1.63 NS
T3 24 25.2 1.62 28 24.7 1.66 NS
Intercanine perimeter distance
T0 27 24.3 1.24 34 23.5 1.42 NS
T1 28 24.9 1.12 36 24.1 1.59 NS
T2 26 24.1 0.89 36 23.3 1.66 NS
T3 23 23.4 1.13 28 22.7 1.88 NS
Lateral arch length, left 2-6
T0 28 20.2 2.60 36 20.3 2.49 NS
T1 28 18.9 3.65 36 19.4 3.32 NS
T2 26 18.6 3.64 36 18.9 3.52 NS
T3 24 18.4 3.57 28 18.8 3.46 NS
Lateral arch length, right 2-6
T0 28 19.9 2.47 36 20.0 2.45 NS
T1 28 18.4 3.57 36 19.5 3.35 NS
T2 26 17.7 3.80 36 19.1 3.28 NS
T3 24 17.4 3.69 28 19.0 3.29 NS
Lateral arch length, left central-6
T0 28 29.8 2.26 36 29.6 2.38 NS
T1 28 28.5 3.28 36 28.9 3.10 NS
T2 26 27.6 3.34 36 27.9 3.04 NS
T3 24 27.2 3.05 28 27.7 3.07 NS
Lateral arch length, right central-6
T0 28 29.5 2.19 36 29.6 2.57 NS
T1 28 28.0 3.22 36 29.0 3.20 NS
T2 26 27.2 3.26 36 28.1 3.13 NS
T3 24 26.8 3.11 28 27.9 3.12 NS
Tooth width, 32
T0 28 6.3 0.32 36 6.1 0.36 NS
T3 24 6.3 0.30 28 6.0 0.39 NS
Tooth width, 31
T0 28 5.7 0.33 36 5.5 0.31 NS
T3 24 5.7 0.32 28 5.5 0.33 NS
Tooth width, 41
T0 28 5.6 0.32 36 5.5 0.36 NS
T3 24 5.6 0.31 27 5.4 0.37 NS
Tooth width 42
T0 28 6.3 0.40 36 6.0 0.39 *
T3 24 6.3 0.41 28 5.9 0.36 **
Overjet
T0 28 6.3 3.32 36 7.5 3.04 NS
T1 28 3.2 0.91 36 3.3 1.13 NS
T2 26 3.6 1.58 36 3.9 1.68 NS
T3 24 3.7 1.91 28 4.0 1.46 NS
Table 3. Continued
Variables
Group 1
(Canine-to-Canine
Retainer)
Group 2
(Twistflex
Retainer)
n Mean SD n Mean SD P
Overbite
T0 28 3.7 2.62 36 3.5 1.79 NS
T1 28 2.5 1.12 36 2.4 1.07 NS
T2 26 2.8 1.80 36 2.7 1.39 NS
T3 24 2.9 1.85 28 2.9 1.20 NS
a T0 indicates before treatment; T1, after treatment; T2, 6 yearsafter treatment; T3, 12 years after treatment.
b NS indicates not significant; * P¼ .05; **P¼ .01.
Angle Orthodontist, Vol 87, No 2, 2017
204 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

before fixed appliances and those who had no teethtaken out.
Bonding Failures
Bonding failures were found in 32% of the patientswith the canine-to-canine retainer and 44% in thetwistflex group. The group differences were notstatistically significant, however, in some patients; thetwistflex retainer came loose more than once.
DISCUSSION
The main result of this study was that there were no
differences at the long-term follow-up between the two
groups. Thus, the null hypothesis was confirmed. In
addition, LII and available space in the mandible were
equivalent for both groups before treatment and 12
years after treatment. Furthermore, the important
treatment outcomes, overjet and overbite, decreased
during treatment and were stable 12 years after
treatment. Consequently, either retention method can,
from a stability point of view, be recommended as long
as the retention is in place.Studies published on long-term stability of the
mandibular incisors after orthodontic treatment showthat long-term alignment of the mandibular anteriorsegment is variable and unpredictable.18 More than70% of the cases had moderate or severe crowdingprior to treatment whereas after retention (at least 10years after removal of all retainer devices), more than70% were classified as showing moderate or severecrowding but in different proportions.18 In anotherstudy, only 10% of the cases had an acceptablemandibular alignment (LII , 3.5 mm) 20 yearspostretention.19
In our study, we found patterns similar to those ofearlier studies,18,19 that is, relapse of the correctedmandibular incisor irregularity and available incisorspace. Consequently, in our study of 64 patients, 42%had an LII of 3.5 mm or less 12 years after treatment.Similar results have also been presented 14 yearspostretention20; thus, in 78 patients, 47.7% had an LIIof 3.5 mm or less.
A long-term follow-up study found that postretentioncrowding and incisor irregularity increased morefrequently in the mandible than in the maxilla.21
Different pretreatment variables such as increasedmesiodistal incisor dimension, severe crowding andincisor irregularity, arch length deficiency, and archconstriction, were found to be associated factors in theprocess of postretention and the resultant increase ofcrowding and incisor irregularity.
Another study pointed out that more factors than justthe type of retention appliance can influence the long-
Table 4. Mean Values MM and Number of Subjects for the
Cephalometric Variables at the Four Registration Points, Measured
on Lateral Head Radiographs and the Differences in Mean Values
Between Groups 1 and 2
Variables
Group 1
(Canine-to-Canine
Retainer)
Group 2
(Twistflex
Retainer)
n Mean SD n Mean SD P
SNA, 8T0a 28 81.0 3.55 35 81.3 3.03 NSb
T1 17 80.4 3.33 31 80.0 3.35 NS
T2 14 79.5 3.84 24 79.8 3.23 NS
T3 18 80.5 4.31 22 79.5 2.99 NS
SNB, 8T0 28 76.7 4.02 35 76.0 2.64 NS
T1 17 77.3 4.43 31 76.2 3.16 NS
T2 14 76.8 5.16 24 75.9 3.20 NS
T3 18 78.0 5.54 22 75.7 3.07 NS
ANB, 8T0 28 4.3 2.88 35 5.3 3.76 NS
T1 17 3.2 2.35 31 3.7 1.35 NS
T2 14 2.7 2.54 24 3.9 1.79 NS
T3 18 2.4 2.50 22 3.9 1.89 NS
SN/ML, 8T0 28 32.8 6.10 35 35.4 4.90 NS
T1 17 32.4 7.25 31 34.7 6.02 NS
T2 14 31.8 8.71 24 33.4 6.56 NS
T3 18 30.7 8.35 22 35.4 4.60 NS
ML/NL, 8T0 28 26.0 5.28 35 28.9 5.04 NS
T1 17 26.2 7.58 31 28.2 6.15 NS
T2 14 23.8 8.18 24 26.5 5.89 NS
T3 18 23.7 7.39 22 28.3 4.93 NS
SN/NL, 8T0 28 6.8 3.31 35 6.5 3.11 NS
T1 17 6.1 2.67 31 6.4 3.32 NS
T2 14 8.0 3.14 24 6.9 3.30 NS
T3 18 7.1 3.81 22 7.0 3.07 NS
U1/NL, 8T0 28 110.7 10.47 34 108.2 8.84 NS
T1 17 105.3 10.72 31 103.4 6.48 NS
T2 14 109.2 9.93 24 106.0 6.45 NS
T3 18 108.8 11.79 22 103.9 7.59 NS
L1/Apg, mm
T0 28 1.1 3.81 34 0.4 2.67 NS
T1 17 0.9 3.01 31 1.8 2.03 NS
T2 14 1.4 3.10 24 1.9 1.85 NS
T3 18 1.2 3.59 22 1.4 2.05 NS
L1/ML, 8T0 28 93.8 5.57 34 92.3 7.81 NS
T1 17 92.9 6.29 31 95.8 8.59 NS
T2 14 95.1 7.28 24 96.9 7.71 NS
T3 18 93.2 7.14 22 94.1 5.96 NS
Interincisal angle, 8T0 28 128.8 11.42 34 127.6 12.42 NS
T1 17 134.6 8.36 31 130.7 9.51 NS
T2 14 131.8 11.01 24 129.7 6.67 NS
T3 18 133.2 11.85 22 132.9 8.31 NS
Ar-B, mm
T0 28 94.7 5.64 30 97.1 10.10 NS
T1 17 99.4 7.42 26 102.4 9.63 NS
T2 14 103.3 7.61 20 103.3 5.42 NS
T3 18 108.1 6.17 20 105.6 5.72 NS
a T0 indicates before treatment; T1, after treatment; T2, 6 yearsafter treatment; T3, 12 years after treatment.
b NS indicates not significant.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 205
term stability of the mandibular incisors, for example,
soft tissue pressure, growth, function, the contact
relationship between the maxillary and mandibular
incisors, and length of retention.22
In our study, the length of retention was a mean 2.6
years (SD 2.48) for the canine-to-canine retainer and a
mean 3.0 years (SD 1.66) for the twistflex retainer. In
the study by Edman Tynelius et al.,11 the retention time
Table 5. Mean Values MM Between the Four Registrations (T0, T1, T2, T3) for Subjects Measured on Study Models at the Four Registration
Points for Groups 1 and 2
Group 1 Canine-to-Canine-Retainer Group 2 Twistflex Retainer
Mean SD P Mean SD P
Little’s Irregularity Index
T0a 4.5 3.14 T0 „ T1** 4.9 3.23 T0 „ T1***
T1 1.8 1.44 T1 „ T2*, T1 „ T3* 1.5 1.10 T1 „ T2, T3***
T2 3.4 2.07 T2 „ T3* 3.5 2.28 T2 „ T3***
T3 4.1 2.56 4.3 2.32
Available space, mand 3-3
T0 1.8 2.48 T0 „ T1* 1.9 2.26 T0 „ T1**
T1 0.1 0.50 T1 „ T2**, T1 „ T3*** 0.1 0.33 T1 „ T2, T3***
T2 1.4 1.20 T2 „ T3* 0.9 0.91 T2 „ T3***
T3 1.9 1.51 1.3 1.02
Intercanine width
T0 26.4 1.75 T0 „ T3*, 25.6 1.61 T0 „ T3**
T1 26.2 1.57 T1 „ T2*, T1 „ T3** 25.8 1.75 T1 „ T2, T3**
T2 25.6 1.58 25.0 1.57 T2 „ T3*
T3 25.3 1.68 24.6 1.68
Intercanine perimeter distance
T0 24.4 1.20 T0 „ T3* 23.4 1.52
T1 24.9 1.12 T1 „ T2, T3*** 23.9 1.72 T1 „ T2, T3***
T2 23.9 0.86 T2 „ T3* 23.1 1.74 T2 „ T3*
T3 23.5 1.06 22.6 1.90
Lateral arch length, left 2-6
T0 20.5 2.51 T0 „ T2, T3* 20.4 2.22 T0 „ T3*
T1 19.1 3.66 T1 „ T2**, T1 „ T3*** 19.5 3.20 T1 „ T2*, T1 „ T3**
T2 18.5 3.66 T2 „ T3* 19.0 3.46 T2 „ T3***
T3 18.4 3.57 18.8 3.46
Lateral arch length, right 2-6
T0 20.1 2.42 T0 „ T2, T3** 20.2 2.01 NSb
T1 18.3 3.61 T1 „ T2, T3** 19.7 3.28
T2 17.6 3.76 19.2 3.22
T3 17.4 3.80 19.0 3.29
Lateral arch length, left central-6
T0 29.9 2.32 T0 „ T2**, T0 „ T3*** 29.6 2.10 T0 „ T2*, T0 „ T3**
T1 28.6 3.30 T1 „ T2, T3*** 28.9 3.00 T1 „ T2, T3***
T2 27.5 3.29 T2 „ T3* 27.9 3.00 T2 „ T3**
T3 27.2 3.17 27.7 3.10
Lateral arch length, right central-6
T0 29.6 2.20 T0 „ T2**, T0 „ T3*** 29.7 2.11 T0 „ T2*, T0 „ T3**
T1 28.0 3.31 T1 „ T2**, T1 „ T3*** 29.1 3.16 T1 „ T2, T3***
T2 27.1 3.22 T2 „ T3* 28.2 3.06 T2 „ T3**
T3 26.8 3.21 27.9 3.12
Overjet
T0 6.1 3.33 T0 „ T1, T2, T3** 7.4 3.10 T0 „ T1, T2, T3***
T1 3.1 0.92 3.3 0.94
T2 3.5 1.67 3.8 1.57
T3 3.7 1.98 4.0 1.46
Overbite
T0 3.5 2.64 NS 3.6 1.65 T0 „ T1*
T1 2.2 0.93 2.4 0.84
T2 2.8 1.82 2.8 1.17
T3 2.8 1.87 2.9 1.20
a T0 indicates before treatment; T1, after treatment; T2, 6 years after treatment; T3, 12 years after treatment.b NS indicates not significant.* P¼ .05; ** P¼ .01; *** P¼ .001.
Angle Orthodontist, Vol 87, No 2, 2017
206 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

before fixed appliances and those who had no teethtaken out.
Bonding Failures
Bonding failures were found in 32% of the patientswith the canine-to-canine retainer and 44% in thetwistflex group. The group differences were notstatistically significant, however, in some patients; thetwistflex retainer came loose more than once.
DISCUSSION
The main result of this study was that there were no
differences at the long-term follow-up between the two
groups. Thus, the null hypothesis was confirmed. In
addition, LII and available space in the mandible were
equivalent for both groups before treatment and 12
years after treatment. Furthermore, the important
treatment outcomes, overjet and overbite, decreased
during treatment and were stable 12 years after
treatment. Consequently, either retention method can,
from a stability point of view, be recommended as long
as the retention is in place.Studies published on long-term stability of the
mandibular incisors after orthodontic treatment showthat long-term alignment of the mandibular anteriorsegment is variable and unpredictable.18 More than70% of the cases had moderate or severe crowdingprior to treatment whereas after retention (at least 10years after removal of all retainer devices), more than70% were classified as showing moderate or severecrowding but in different proportions.18 In anotherstudy, only 10% of the cases had an acceptablemandibular alignment (LII , 3.5 mm) 20 yearspostretention.19
In our study, we found patterns similar to those ofearlier studies,18,19 that is, relapse of the correctedmandibular incisor irregularity and available incisorspace. Consequently, in our study of 64 patients, 42%had an LII of 3.5 mm or less 12 years after treatment.Similar results have also been presented 14 yearspostretention20; thus, in 78 patients, 47.7% had an LIIof 3.5 mm or less.
A long-term follow-up study found that postretentioncrowding and incisor irregularity increased morefrequently in the mandible than in the maxilla.21
Different pretreatment variables such as increasedmesiodistal incisor dimension, severe crowding andincisor irregularity, arch length deficiency, and archconstriction, were found to be associated factors in theprocess of postretention and the resultant increase ofcrowding and incisor irregularity.
Another study pointed out that more factors than justthe type of retention appliance can influence the long-
Table 4. Mean Values MM and Number of Subjects for the
Cephalometric Variables at the Four Registration Points, Measured
on Lateral Head Radiographs and the Differences in Mean Values
Between Groups 1 and 2
Variables
Group 1
(Canine-to-Canine
Retainer)
Group 2
(Twistflex
Retainer)
n Mean SD n Mean SD P
SNA, 8T0a 28 81.0 3.55 35 81.3 3.03 NSb
T1 17 80.4 3.33 31 80.0 3.35 NS
T2 14 79.5 3.84 24 79.8 3.23 NS
T3 18 80.5 4.31 22 79.5 2.99 NS
SNB, 8T0 28 76.7 4.02 35 76.0 2.64 NS
T1 17 77.3 4.43 31 76.2 3.16 NS
T2 14 76.8 5.16 24 75.9 3.20 NS
T3 18 78.0 5.54 22 75.7 3.07 NS
ANB, 8T0 28 4.3 2.88 35 5.3 3.76 NS
T1 17 3.2 2.35 31 3.7 1.35 NS
T2 14 2.7 2.54 24 3.9 1.79 NS
T3 18 2.4 2.50 22 3.9 1.89 NS
SN/ML, 8T0 28 32.8 6.10 35 35.4 4.90 NS
T1 17 32.4 7.25 31 34.7 6.02 NS
T2 14 31.8 8.71 24 33.4 6.56 NS
T3 18 30.7 8.35 22 35.4 4.60 NS
ML/NL, 8T0 28 26.0 5.28 35 28.9 5.04 NS
T1 17 26.2 7.58 31 28.2 6.15 NS
T2 14 23.8 8.18 24 26.5 5.89 NS
T3 18 23.7 7.39 22 28.3 4.93 NS
SN/NL, 8T0 28 6.8 3.31 35 6.5 3.11 NS
T1 17 6.1 2.67 31 6.4 3.32 NS
T2 14 8.0 3.14 24 6.9 3.30 NS
T3 18 7.1 3.81 22 7.0 3.07 NS
U1/NL, 8T0 28 110.7 10.47 34 108.2 8.84 NS
T1 17 105.3 10.72 31 103.4 6.48 NS
T2 14 109.2 9.93 24 106.0 6.45 NS
T3 18 108.8 11.79 22 103.9 7.59 NS
L1/Apg, mm
T0 28 1.1 3.81 34 0.4 2.67 NS
T1 17 0.9 3.01 31 1.8 2.03 NS
T2 14 1.4 3.10 24 1.9 1.85 NS
T3 18 1.2 3.59 22 1.4 2.05 NS
L1/ML, 8T0 28 93.8 5.57 34 92.3 7.81 NS
T1 17 92.9 6.29 31 95.8 8.59 NS
T2 14 95.1 7.28 24 96.9 7.71 NS
T3 18 93.2 7.14 22 94.1 5.96 NS
Interincisal angle, 8T0 28 128.8 11.42 34 127.6 12.42 NS
T1 17 134.6 8.36 31 130.7 9.51 NS
T2 14 131.8 11.01 24 129.7 6.67 NS
T3 18 133.2 11.85 22 132.9 8.31 NS
Ar-B, mm
T0 28 94.7 5.64 30 97.1 10.10 NS
T1 17 99.4 7.42 26 102.4 9.63 NS
T2 14 103.3 7.61 20 103.3 5.42 NS
T3 18 108.1 6.17 20 105.6 5.72 NS
a T0 indicates before treatment; T1, after treatment; T2, 6 yearsafter treatment; T3, 12 years after treatment.
b NS indicates not significant.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 205
term stability of the mandibular incisors, for example,
soft tissue pressure, growth, function, the contact
relationship between the maxillary and mandibular
incisors, and length of retention.22
In our study, the length of retention was a mean 2.6
years (SD 2.48) for the canine-to-canine retainer and a
mean 3.0 years (SD 1.66) for the twistflex retainer. In
the study by Edman Tynelius et al.,11 the retention time
Table 5. Mean Values MM Between the Four Registrations (T0, T1, T2, T3) for Subjects Measured on Study Models at the Four Registration
Points for Groups 1 and 2
Group 1 Canine-to-Canine-Retainer Group 2 Twistflex Retainer
Mean SD P Mean SD P
Little’s Irregularity Index
T0a 4.5 3.14 T0 „ T1** 4.9 3.23 T0 „ T1***
T1 1.8 1.44 T1 „ T2*, T1 „ T3* 1.5 1.10 T1 „ T2, T3***
T2 3.4 2.07 T2 „ T3* 3.5 2.28 T2 „ T3***
T3 4.1 2.56 4.3 2.32
Available space, mand 3-3
T0 1.8 2.48 T0 „ T1* 1.9 2.26 T0 „ T1**
T1 0.1 0.50 T1 „ T2**, T1 „ T3*** 0.1 0.33 T1 „ T2, T3***
T2 1.4 1.20 T2 „ T3* 0.9 0.91 T2 „ T3***
T3 1.9 1.51 1.3 1.02
Intercanine width
T0 26.4 1.75 T0 „ T3*, 25.6 1.61 T0 „ T3**
T1 26.2 1.57 T1 „ T2*, T1 „ T3** 25.8 1.75 T1 „ T2, T3**
T2 25.6 1.58 25.0 1.57 T2 „ T3*
T3 25.3 1.68 24.6 1.68
Intercanine perimeter distance
T0 24.4 1.20 T0 „ T3* 23.4 1.52
T1 24.9 1.12 T1 „ T2, T3*** 23.9 1.72 T1 „ T2, T3***
T2 23.9 0.86 T2 „ T3* 23.1 1.74 T2 „ T3*
T3 23.5 1.06 22.6 1.90
Lateral arch length, left 2-6
T0 20.5 2.51 T0 „ T2, T3* 20.4 2.22 T0 „ T3*
T1 19.1 3.66 T1 „ T2**, T1 „ T3*** 19.5 3.20 T1 „ T2*, T1 „ T3**
T2 18.5 3.66 T2 „ T3* 19.0 3.46 T2 „ T3***
T3 18.4 3.57 18.8 3.46
Lateral arch length, right 2-6
T0 20.1 2.42 T0 „ T2, T3** 20.2 2.01 NSb
T1 18.3 3.61 T1 „ T2, T3** 19.7 3.28
T2 17.6 3.76 19.2 3.22
T3 17.4 3.80 19.0 3.29
Lateral arch length, left central-6
T0 29.9 2.32 T0 „ T2**, T0 „ T3*** 29.6 2.10 T0 „ T2*, T0 „ T3**
T1 28.6 3.30 T1 „ T2, T3*** 28.9 3.00 T1 „ T2, T3***
T2 27.5 3.29 T2 „ T3* 27.9 3.00 T2 „ T3**
T3 27.2 3.17 27.7 3.10
Lateral arch length, right central-6
T0 29.6 2.20 T0 „ T2**, T0 „ T3*** 29.7 2.11 T0 „ T2*, T0 „ T3**
T1 28.0 3.31 T1 „ T2**, T1 „ T3*** 29.1 3.16 T1 „ T2, T3***
T2 27.1 3.22 T2 „ T3* 28.2 3.06 T2 „ T3**
T3 26.8 3.21 27.9 3.12
Overjet
T0 6.1 3.33 T0 „ T1, T2, T3** 7.4 3.10 T0 „ T1, T2, T3***
T1 3.1 0.92 3.3 0.94
T2 3.5 1.67 3.8 1.57
T3 3.7 1.98 4.0 1.46
Overbite
T0 3.5 2.64 NS 3.6 1.65 T0 „ T1*
T1 2.2 0.93 2.4 0.84
T2 2.8 1.82 2.8 1.17
T3 2.8 1.87 2.9 1.20
a T0 indicates before treatment; T1, after treatment; T2, 6 years after treatment; T3, 12 years after treatment.b NS indicates not significant.* P¼ .05; ** P¼ .01; *** P¼ .001.
Angle Orthodontist, Vol 87, No 2, 2017
206 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

was 2 years, and LII increased during the 5-year period
without retention.
The question is, For how long can the retainer wirebe expected to retain the treatment corrections andwhen is the wire only obstructing normal development?
It is likely that 2.5 to 3 years is enough. When retainersare used long-term, it is important to have continuous
check-ups to minimize negative side effects such asgingival retraction, buccally standing premolars, andchanges in mandibular arch form.
It was found that the groups were equal whencomparing cephalometric outcomes, but greater man-dibular growth was found in group 1, the group with
more boys than girls. However, at the last registration,all patients had reached adulthood, but in both groups,a certain amount of growth can be seen, in agreement
with Pancherz et al.23
In this study, some cases had extractions carried outand some were nonextraction cases, with the same
distribution of extractions in each group. No differencein mandibular incisor stability was found, regardless ofextractions. Similar results have been shown in two
other studies.24,25
In both groups, retainer breakage was frequent; forinstance, 32% in group 1 and 44% in group 2
experienced retainer failure, meaning retainers hadbecome unattached from one or more teeth. The
bonding failure rate was highest during the first yearafter treatment. This could be one reason for a verysmall amount of incisor irregularity. The failure rate in
another study26 was 46.9% over a 6-month period afterdebond. Moreover, a review by Iliadi et al.27 evaluatedthe risk of failure of fixed orthodontic retention
protocols and concluded that there was a lack ofevidence in selecting the optimal protocol and mate-
rials for fixed orthodontic retention.
CONCLUSIONS
Both retention methods, a mandibular canine-to-
canine retainer bonded to the canines or a mandib-ular twistflex retainer 3-3 bonded to each tooth, canbe recommended since both are equally effective
during the retention period. However, after removal of the retainers, neither of theretention types prevent long-term changes in man-
dibular incisor irregularity or available space therefor.
REFERENCES
1. Zachrisson BU. Long-term experience with direct-bonded
retainers: update and clinical advice. J Clin Orthod.
2007;41:728–737.
2. Al Yami EA, Kuijpers-Jagtman AM, van’t Hof MA. Stability of
orthodontic treatment outcome: follow-up until 10 years
postretention. Am J Orthod Dentofacial Orthop .
1999;115:300–304.
3. Segner D, Heinrici B. Bonded retainers-clinical reliability. J
Orofac Orthop. 2000;61:352–358.
4. Booth FA, Edelman JM, Proffit WR. Twenty-year follow-up of
patients with permanently bonded mandibular canine-to-
canine retainers. Am J Orthod Dentofacial Orthop.
2008;133:70–76.
5. Renkema AM, Al-Assad S, Bronkhorst E, Weindel S,
Katsaros C, Lisson JA. Effectiveness of lingual retainers
bonded to the canines in preventing mandibular incisor
relapse. Am J Orthod Dentofacial Orthop. 2008;134:179e1–
e8.
6. Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Long-
term effectiveness of canine-to-canine bonded flexible spiral
wire lingual retainers. Am J Orthod Dentofacial Orthop.
2011;139:614–621.
7. Zachrisson BU. Important aspects of long term stability. J
Clin Orthod. 1997;31:562–583.
8. Profitt WR. Retention. In: Contemporary orthodontics. Proffit
W, Fields, H, Sarver, D, eds. 5th ed. St Louis, MO: Elsevier
Mosby-Year Book; 2013:615–616.
9. Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Wor-
thington HV. Retention procedures for stabilizing tooth
position after treatment with orthodontic braces. Cochrane
Database Syst Rev. 2006(1): CD002283.
10. Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study
of various types of orthodontic canine-to-canine retainers.
Eur J Orthod. 1997;19:501–509.
11. Edman Tynelius G, Petren S, Bondemark L, Lilja-Karlander
E. Five-year postretention outcomes of three retention
methods—a randomized controlled trial. Eur J Orthod.
2015;37:345–353.
12. Stormann I, Ehmer U. A prospective randomized study of
different retainer types. J Orofac Orthop. 2002;63:42–50.
13. Scheibe K, Ruf S. Lower bonded retainers: survival and
failure rates particularly considering operator experience. J
Orofac Orthop. 2010;71:300–307.
14. Little RM. The irregularity index. A quantitative score of
mandibular anterior alignment. Am J Orthod. 1975;68:554–
563.
15. Bjork A. The face in Profile. Uppsala, Sweden: Svensk Tandl
Tidsk; 1947;40(suppl 1).
16. Solow B. The pattern of craniofacial associations. Acta
Odontol Scand. 1966;24(suppl 46).
17. Dahlberg G. Statistical Methods for Medical and Biological
Students. New York: Interscience Publications; 1940.
18. Little RM, Wallen TR, Riedel RA. Stability and relapse of
mandibular anterior alignment—first premolar extraction
cases treated by traditional edgewise orthodontics. Am J
Orthod. 1981;80:350–365.
19. Little RM, Riedel RA, Artun J. An evaluation of changes in
mandibular anterior alignment from 10 to 20 years post-
retention. Am J Orthod. 1988;93:423–428.
20. Artun J, Garol JD, Little RM. Long-term stability of
mandibular incisors following successful treatment of Class
II, Division 1, malocclusions. Angle Orthod. 1996;66:229–
238.
21. Kahl-Nieke B, Fischbach H, Schwarze CW. Post-retention
crowding and incisor irregularity: A long term follow-up.
Evaluation of stability and relapse. Br J Orthod.
1995;22:249–257.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 207
22. Johnston CD, Littlewood S. Retention in orthodontics. Br
Dent J. 2015;218:119–122.23. Pancherz H, Bjerklin K, Hashemi K. Late adult skeletofacial
growth after adolescent Herbst Therapy: a 32-year longitu-dinal follow-up study. Am J Orthod Dentofacial Orthop.
2015;147:19–28.24. Rossouw PE, Preston CB, Lombard C. A longitudinal
evaluation of extraction versus nonextraction treatment withspecial reference to the posttreatment irregularity of the
lower incisors. Semin Orthod. 1999;5:160–170.
25. Zafarmand AH, Qamari A, Zafarmand MM. Mandibular
incisor re-crowding: is it different in extraction and non-extraction cases? Oral Health Dent Manag. 2014;13:669–
674.26. Taner T, Aksu M. A prospective clinical evaluation of
mandibular lingual retainer survival. Eur J Orthod.2012;34:470–474.
27. Iliadi A, Kloukos D, Gkantidis N, Katsaros C. Failure of fixedorthodontic retainers: a systematic review. J Dent.
2015;43:876–896.
Angle Orthodontist, Vol 87, No 2, 2017
208 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK

was 2 years, and LII increased during the 5-year period
without retention.
The question is, For how long can the retainer wirebe expected to retain the treatment corrections andwhen is the wire only obstructing normal development?
It is likely that 2.5 to 3 years is enough. When retainersare used long-term, it is important to have continuous
check-ups to minimize negative side effects such asgingival retraction, buccally standing premolars, andchanges in mandibular arch form.
It was found that the groups were equal whencomparing cephalometric outcomes, but greater man-dibular growth was found in group 1, the group with
more boys than girls. However, at the last registration,all patients had reached adulthood, but in both groups,a certain amount of growth can be seen, in agreement
with Pancherz et al.23
In this study, some cases had extractions carried outand some were nonextraction cases, with the same
distribution of extractions in each group. No differencein mandibular incisor stability was found, regardless ofextractions. Similar results have been shown in two
other studies.24,25
In both groups, retainer breakage was frequent; forinstance, 32% in group 1 and 44% in group 2
experienced retainer failure, meaning retainers hadbecome unattached from one or more teeth. The
bonding failure rate was highest during the first yearafter treatment. This could be one reason for a verysmall amount of incisor irregularity. The failure rate in
another study26 was 46.9% over a 6-month period afterdebond. Moreover, a review by Iliadi et al.27 evaluatedthe risk of failure of fixed orthodontic retention
protocols and concluded that there was a lack ofevidence in selecting the optimal protocol and mate-
rials for fixed orthodontic retention.
CONCLUSIONS
Both retention methods, a mandibular canine-to-
canine retainer bonded to the canines or a mandib-ular twistflex retainer 3-3 bonded to each tooth, canbe recommended since both are equally effective
during the retention period. However, after removal of the retainers, neither of theretention types prevent long-term changes in man-
dibular incisor irregularity or available space therefor.
REFERENCES
1. Zachrisson BU. Long-term experience with direct-bonded
retainers: update and clinical advice. J Clin Orthod.
2007;41:728–737.
2. Al Yami EA, Kuijpers-Jagtman AM, van’t Hof MA. Stability of
orthodontic treatment outcome: follow-up until 10 years
postretention. Am J Orthod Dentofacial Orthop .
1999;115:300–304.
3. Segner D, Heinrici B. Bonded retainers-clinical reliability. J
Orofac Orthop. 2000;61:352–358.
4. Booth FA, Edelman JM, Proffit WR. Twenty-year follow-up of
patients with permanently bonded mandibular canine-to-
canine retainers. Am J Orthod Dentofacial Orthop.
2008;133:70–76.
5. Renkema AM, Al-Assad S, Bronkhorst E, Weindel S,
Katsaros C, Lisson JA. Effectiveness of lingual retainers
bonded to the canines in preventing mandibular incisor
relapse. Am J Orthod Dentofacial Orthop. 2008;134:179e1–
e8.
6. Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Long-
term effectiveness of canine-to-canine bonded flexible spiral
wire lingual retainers. Am J Orthod Dentofacial Orthop.
2011;139:614–621.
7. Zachrisson BU. Important aspects of long term stability. J
Clin Orthod. 1997;31:562–583.
8. Profitt WR. Retention. In: Contemporary orthodontics. Proffit
W, Fields, H, Sarver, D, eds. 5th ed. St Louis, MO: Elsevier
Mosby-Year Book; 2013:615–616.
9. Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Wor-
thington HV. Retention procedures for stabilizing tooth
position after treatment with orthodontic braces. Cochrane
Database Syst Rev. 2006(1): CD002283.
10. Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study
of various types of orthodontic canine-to-canine retainers.
Eur J Orthod. 1997;19:501–509.
11. Edman Tynelius G, Petren S, Bondemark L, Lilja-Karlander
E. Five-year postretention outcomes of three retention
methods—a randomized controlled trial. Eur J Orthod.
2015;37:345–353.
12. Stormann I, Ehmer U. A prospective randomized study of
different retainer types. J Orofac Orthop. 2002;63:42–50.
13. Scheibe K, Ruf S. Lower bonded retainers: survival and
failure rates particularly considering operator experience. J
Orofac Orthop. 2010;71:300–307.
14. Little RM. The irregularity index. A quantitative score of
mandibular anterior alignment. Am J Orthod. 1975;68:554–
563.
15. Bjork A. The face in Profile. Uppsala, Sweden: Svensk Tandl
Tidsk; 1947;40(suppl 1).
16. Solow B. The pattern of craniofacial associations. Acta
Odontol Scand. 1966;24(suppl 46).
17. Dahlberg G. Statistical Methods for Medical and Biological
Students. New York: Interscience Publications; 1940.
18. Little RM, Wallen TR, Riedel RA. Stability and relapse of
mandibular anterior alignment—first premolar extraction
cases treated by traditional edgewise orthodontics. Am J
Orthod. 1981;80:350–365.
19. Little RM, Riedel RA, Artun J. An evaluation of changes in
mandibular anterior alignment from 10 to 20 years post-
retention. Am J Orthod. 1988;93:423–428.
20. Artun J, Garol JD, Little RM. Long-term stability of
mandibular incisors following successful treatment of Class
II, Division 1, malocclusions. Angle Orthod. 1996;66:229–
238.
21. Kahl-Nieke B, Fischbach H, Schwarze CW. Post-retention
crowding and incisor irregularity: A long term follow-up.
Evaluation of stability and relapse. Br J Orthod.
1995;22:249–257.
Angle Orthodontist, Vol 87, No 2, 2017
MANDIBULAR INCISOR STABILITY WITH BONDED LINGUAL RETAINERS 207
22. Johnston CD, Littlewood S. Retention in orthodontics. Br
Dent J. 2015;218:119–122.23. Pancherz H, Bjerklin K, Hashemi K. Late adult skeletofacial
growth after adolescent Herbst Therapy: a 32-year longitu-dinal follow-up study. Am J Orthod Dentofacial Orthop.
2015;147:19–28.24. Rossouw PE, Preston CB, Lombard C. A longitudinal
evaluation of extraction versus nonextraction treatment withspecial reference to the posttreatment irregularity of the
lower incisors. Semin Orthod. 1999;5:160–170.
25. Zafarmand AH, Qamari A, Zafarmand MM. Mandibular
incisor re-crowding: is it different in extraction and non-extraction cases? Oral Health Dent Manag. 2014;13:669–
674.26. Taner T, Aksu M. A prospective clinical evaluation of
mandibular lingual retainer survival. Eur J Orthod.2012;34:470–474.
27. Iliadi A, Kloukos D, Gkantidis N, Katsaros C. Failure of fixedorthodontic retainers: a systematic review. J Dent.
2015;43:876–896.
Angle Orthodontist, Vol 87, No 2, 2017
208 SCHUTZ-FRANSSON, LINDSTEN, BJERKLIN, BONDEMARK



Mandibular incisor alignment in untreated subjects compared with
long-term changes after orthodontic treatment with or without retainers
Ulrike Schütz-Franssona; Rune Lindstenb; Krister Bjerklinc; Lars Bondemarkd
Accepted for publication
This is a pre-copyedited, author-produced version of an article accepted for publication in the
American Journal of Orthodontics and Dentofacial Orthopedics. The version of record of this article
can be found at the journals website:
https://www.ajodo.org/
____________________________________________________________ a Research student, Faculty of Odontology, Malmö University, Sweden
Specialist in Orthodontics, The County Orthodontic Clinic Uddevalla, Västra Götalands Regionen,
Sweden b Associate Professor and Head, Department of Orthodontics, Institute for Postgraduate Dental
Education, Jönköping, Sweden c Associate Professor, Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden d Professor and Head, Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden
Corresponding author: Dr Ulrike Schütz-Fransson, Specialistcentrum, Uddevalla Sjukhus, SE 451 80
Uddevalla, Sweden (email:[email protected])

Mandibular incisor alignment in untreated subjects compared with
long-term changes after orthodontic treatment with or without retainers
Ulrike Schütz-Franssona; Rune Lindstenb; Krister Bjerklinc; Lars Bondemarkd
Accepted for publication
This is a pre-copyedited, author-produced version of an article accepted for publication in the
American Journal of Orthodontics and Dentofacial Orthopedics. The version of record of this article
can be found at the journals website:
https://www.ajodo.org/
____________________________________________________________ a Research student, Faculty of Odontology, Malmö University, Sweden
Specialist in Orthodontics, The County Orthodontic Clinic Uddevalla, Västra Götalands Regionen,
Sweden b Associate Professor and Head, Department of Orthodontics, Institute for Postgraduate Dental
Education, Jönköping, Sweden c Associate Professor, Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden d Professor and Head, Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden
Corresponding author: Dr Ulrike Schütz-Fransson, Specialistcentrum, Uddevalla Sjukhus, SE 451 80
Uddevalla, Sweden (email:[email protected])

Schütz-Fransson et al. – Mandibular incisor alignment
2
ABSTRACT
Objective: To analyze the dental and skeletal changes in patients, treated with fixed orthodontic
appliances, with or without retention appliances and to compare the changes with untreated subjects.
Specifically, mandibular incisor irregularity was analyzed.
Materials and Methods: Totally 105 children who had undergone orthodontic treatment with fixed
appliances in both jaws were examined in two groups: 64 had a lingual mandibular retainer and 41
had no retainer. Retention time was 2.7 years (SD 1.50). The untreated group consisted of 25
subjects. Measurements were done on study casts and lateral head radiographs before and after
treatment, six and twelve years after treatment. Little’s Irregularity Index (LII) was the most important
variable.
Results: No differences were found 12 years after treatment in LII between a group that had a
retainer and a group without a retainer after treatment. In the untreated group, LII was increased over
time, but not to the same extent as in the treated groups.
Correction of overjet and overbite was stable long-term. At the last registration, the amount of overjet
was almost the same in all three groups.
Conclusion: The routine use of mandibular retainers for two to three years does not appear to
prevent long-term relapse. If the patient wants to constrain natural development and changes, lifelong
retainers are needed.
KEY WORDS: Long-term stability, Irregularity Index, Dental arch, Growth/Development, Relapse
Schütz-Fransson et al. – Mandibular incisor alignment
3
INTRODUCTION
After orthodontic treatment, one challenge is to
keep the teeth in their new positions and to avoid
relapse. More specifically, the alignment of the
mandibular incisors after treatment has become
an issue in orthodontics. The mandibular incisors
tend to move back to nearly the same position
they were in before treatment and after the
retainer has been removed.1-4 However, some of
the posttreatment changes can be explained by
relapse and other posttreatment changes by the
continued growth and compensatory eruption
and migration of the teeth.5 Changes occurring
up to one year postretention are likely to be a
combination of true orthodontic relapse and late-
growth changes.
The etiology of the undesirable incisor
irregularity changes is complex. Mandibular
incisor irregularity is both unpredictable and
variable. Many possible interacting factors are
likely such as: tooth size, arch form, forces from
the periodontal fibers, deflecting occlusal
contacts, facial growth patterns, continuing late
growth, and a mesially acting force emanating
from the back of the dental arch.6-8
Increased mandibular incisor irregularity seems
to be a continuous process throughout life even
in untreated patients.9-11 The natural physiological
changes during aging cause changes like those
that occur after orthodontic treatment and the
removal of retainers. Nevertheless, the question
remains if the posttreatment changes are a result
of relapse or the normal aging and maturational
process.
Some studies have compared mandibular
irregularity in treated and untreated patients long-
term.12-14 However, very few long-term studies, if
any, have compared patients who have had a
bonded lingual retainer with a group without a
retention appliance after treatment and then
compared those patients with an untreated
group.
The aim of this retrospective longitudinal study
was to analyze the dental and skeletal changes
in patients, treated with fixed orthodontic
appliances, with or without retention appliances
and to compare the changes with a group of
untreated subjects. Specifically, mandibular
incisor irregularity was studied. The hypothesis was that the long-term
mandibular incisor irregularity for the treated
group without retainers would be higher than for
the group with retainers and that both groups
who have had orthodontic treatment would have
a higher amount of irregularity than the untreated
group.
SUBJECTS AND METHODS
Material
Three different groups were included (Table 1),
and long-term records were required for
participation in the study. Sample exclusions
were single arch treatment, orthognatic surgery
treatment, cleft lip and/or palate, agenesis and
extraction of anterior teeth. This was a
retrospective material and no cases have been
added or excluded after applying the inclusion
criteria.
The group with retainers consisted of 64 children,
(23 boys and 41 girls) who have had orthodontic
treatment with fixed appliance in both jaws. After
treatment, the retention appliance for the
mandibular anterior segment was either a
canine-to-canine retainer (0.028 inch, spring hard
wire bonded to the canines only) or a twistflex
retainer (0.0195 inch, bonded to all mandibular
incisors and canines). Both retainers were
custom-made in the laboratory and were bonded
with composite. The two different retainer types

Schütz-Fransson et al. – Mandibular incisor alignment
2
ABSTRACT
Objective: To analyze the dental and skeletal changes in patients, treated with fixed orthodontic
appliances, with or without retention appliances and to compare the changes with untreated subjects.
Specifically, mandibular incisor irregularity was analyzed.
Materials and Methods: Totally 105 children who had undergone orthodontic treatment with fixed
appliances in both jaws were examined in two groups: 64 had a lingual mandibular retainer and 41
had no retainer. Retention time was 2.7 years (SD 1.50). The untreated group consisted of 25
subjects. Measurements were done on study casts and lateral head radiographs before and after
treatment, six and twelve years after treatment. Little’s Irregularity Index (LII) was the most important
variable.
Results: No differences were found 12 years after treatment in LII between a group that had a
retainer and a group without a retainer after treatment. In the untreated group, LII was increased over
time, but not to the same extent as in the treated groups.
Correction of overjet and overbite was stable long-term. At the last registration, the amount of overjet
was almost the same in all three groups.
Conclusion: The routine use of mandibular retainers for two to three years does not appear to
prevent long-term relapse. If the patient wants to constrain natural development and changes, lifelong
retainers are needed.
KEY WORDS: Long-term stability, Irregularity Index, Dental arch, Growth/Development, Relapse
Schütz-Fransson et al. – Mandibular incisor alignment
3
INTRODUCTION
After orthodontic treatment, one challenge is to
keep the teeth in their new positions and to avoid
relapse. More specifically, the alignment of the
mandibular incisors after treatment has become
an issue in orthodontics. The mandibular incisors
tend to move back to nearly the same position
they were in before treatment and after the
retainer has been removed.1-4 However, some of
the posttreatment changes can be explained by
relapse and other posttreatment changes by the
continued growth and compensatory eruption
and migration of the teeth.5 Changes occurring
up to one year postretention are likely to be a
combination of true orthodontic relapse and late-
growth changes.
The etiology of the undesirable incisor
irregularity changes is complex. Mandibular
incisor irregularity is both unpredictable and
variable. Many possible interacting factors are
likely such as: tooth size, arch form, forces from
the periodontal fibers, deflecting occlusal
contacts, facial growth patterns, continuing late
growth, and a mesially acting force emanating
from the back of the dental arch.6-8
Increased mandibular incisor irregularity seems
to be a continuous process throughout life even
in untreated patients.9-11 The natural physiological
changes during aging cause changes like those
that occur after orthodontic treatment and the
removal of retainers. Nevertheless, the question
remains if the posttreatment changes are a result
of relapse or the normal aging and maturational
process.
Some studies have compared mandibular
irregularity in treated and untreated patients long-
term.12-14 However, very few long-term studies, if
any, have compared patients who have had a
bonded lingual retainer with a group without a
retention appliance after treatment and then
compared those patients with an untreated
group.
The aim of this retrospective longitudinal study
was to analyze the dental and skeletal changes
in patients, treated with fixed orthodontic
appliances, with or without retention appliances
and to compare the changes with a group of
untreated subjects. Specifically, mandibular
incisor irregularity was studied. The hypothesis was that the long-term
mandibular incisor irregularity for the treated
group without retainers would be higher than for
the group with retainers and that both groups
who have had orthodontic treatment would have
a higher amount of irregularity than the untreated
group.
SUBJECTS AND METHODS
Material
Three different groups were included (Table 1),
and long-term records were required for
participation in the study. Sample exclusions
were single arch treatment, orthognatic surgery
treatment, cleft lip and/or palate, agenesis and
extraction of anterior teeth. This was a
retrospective material and no cases have been
added or excluded after applying the inclusion
criteria.
The group with retainers consisted of 64 children,
(23 boys and 41 girls) who have had orthodontic
treatment with fixed appliance in both jaws. After
treatment, the retention appliance for the
mandibular anterior segment was either a
canine-to-canine retainer (0.028 inch, spring hard
wire bonded to the canines only) or a twistflex
retainer (0.0195 inch, bonded to all mandibular
incisors and canines). Both retainers were
custom-made in the laboratory and were bonded
with composite. The two different retainer types

Schütz-Fransson et al. – Mandibular incisor alignment
4
have been evaluated in a previous study2, and it
was reported that no differences were found
between the two retention types considering their
capacity in keeping the mandibular incisors
aligned in a long-term perspective. Therefore, in
this study the two types of bonded retainers were
merged to one group. The mean retention time
for the mandibular incisors was 2.7 years (SD
1.50). The maxillary arch had a removable
appliance for retention.
The non-retention group consisted of 41
patients, (17 boys and 24 girls) with similar
orthodontic treatment as the retention group,
although no retention appliance was used for the
mandibular anterior segment after treatment. The
decision to leave the treated patients without
retention in the mandible was made by the
orthodontists who treated the patients. This
group also had a removable appliance in the
maxilla for retention.
The orthodontic treatments were performed at
the Department of Orthodontics, the Institute for
Postgraduate Dental Education in Jönköping,
Sweden, between 1980 and 1995. The patients
received orthodontic treatment for Class II
malocclusions, large overjet, crowding and/or
deep bites. The treatment consisted of fixed
edgewise appliances (0.018 inch) in both jaws,
and both extraction and non-extraction cases
were included. Extractions were carried out in 71
patients (68%) and 34 patients (32%) were
treated non-extraction. There was exactly the
same proportion of extraction and non-extraction
cases in the groups with and without retainers. Expansion of the intercanine width during
orthodontic treatment was avoided, and no
interproximal enamel reduction or circumferential
supracrestal fiberotomy was performed in the
groups who had undergone orthodontic
treatment.
The untreated group comprised 25 patients, (14
boys and 11 girls) who were age-matched with
the subjects in the two other groups. In this
group, the subjects had Class I occlusion with
normal overjet and overbite and with minor or no
crowding. This group was also recruited from the
Department of Orthodontics in Jönköping,
Sweden between 1980 and 1995.
Methods
The Ethics Committee of Linköping, Sweden,
approved the protocol (2014/381-31).
Measurements were performed on dental casts
using a sliding digital caliper (Mitutoyo 500-171
Kanagawa, Japan) with an accuracy of 0.01 mm.
Schütz-Fransson et al. – Mandibular incisor alignment
5
The measurements for the treatment groups
were taken on four occasions: before treatment
(T0); immediately after orthodontic treatment and
start of retention (T1); six years after treatment
(T2); and 12 years after treatment (T3).
For the untreated group, study casts were
available for the corresponding ages at T0, T2,
and T3. In the retention group, no retention
appliance was in place at T2 and T3. The mean
retention time for the mandibular incisors was 2.7
years (SD 1.50).
The main outcome measures (Figures 1 and 2)
were irregularity index according to Little (LII), the
summed displacement of the anatomic contact
points of the mandibular anterior teeth15,
intercanine width, intercanine arch perimeter
distance, available mandibular incisor space
(intercanine arch perimeter distance minus
summed tooth width for the four mandibular
incisors), lateral arch length, overjet, and
overbite. Also, the tooth width of the mandibular
incisors was measured, at T0 and T3.
Sagittal and vertical relationships between the
jaws and incisor inclination were evaluated on
lateral head radiographs, and the cephalometric
reference points and measurements were
assessed according to Björk16 and Solow17
(Figure 3). All measurements on lateral head
radiographs were made to the nearest half-
degree or 0.5 mm with correction for
enlargement. No lateral head radiographs were
available at T1 for the untreated subjects.
Figure 1. Figure 2.
Figure 3.
All registrations and measurements were made
by one author (USF) and because there was no
retention appliance in place at T2 and T3, a
blinded evaluation was possible, meaning that
the examiner was unaware of which of the three
groups the patients belonged to or if the casts
were taken at T2 or T3.

Schütz-Fransson et al. – Mandibular incisor alignment
4
have been evaluated in a previous study2, and it
was reported that no differences were found
between the two retention types considering their
capacity in keeping the mandibular incisors
aligned in a long-term perspective. Therefore, in
this study the two types of bonded retainers were
merged to one group. The mean retention time
for the mandibular incisors was 2.7 years (SD
1.50). The maxillary arch had a removable
appliance for retention.
The non-retention group consisted of 41
patients, (17 boys and 24 girls) with similar
orthodontic treatment as the retention group,
although no retention appliance was used for the
mandibular anterior segment after treatment. The
decision to leave the treated patients without
retention in the mandible was made by the
orthodontists who treated the patients. This
group also had a removable appliance in the
maxilla for retention.
The orthodontic treatments were performed at
the Department of Orthodontics, the Institute for
Postgraduate Dental Education in Jönköping,
Sweden, between 1980 and 1995. The patients
received orthodontic treatment for Class II
malocclusions, large overjet, crowding and/or
deep bites. The treatment consisted of fixed
edgewise appliances (0.018 inch) in both jaws,
and both extraction and non-extraction cases
were included. Extractions were carried out in 71
patients (68%) and 34 patients (32%) were
treated non-extraction. There was exactly the
same proportion of extraction and non-extraction
cases in the groups with and without retainers. Expansion of the intercanine width during
orthodontic treatment was avoided, and no
interproximal enamel reduction or circumferential
supracrestal fiberotomy was performed in the
groups who had undergone orthodontic
treatment.
The untreated group comprised 25 patients, (14
boys and 11 girls) who were age-matched with
the subjects in the two other groups. In this
group, the subjects had Class I occlusion with
normal overjet and overbite and with minor or no
crowding. This group was also recruited from the
Department of Orthodontics in Jönköping,
Sweden between 1980 and 1995.
Methods
The Ethics Committee of Linköping, Sweden,
approved the protocol (2014/381-31).
Measurements were performed on dental casts
using a sliding digital caliper (Mitutoyo 500-171
Kanagawa, Japan) with an accuracy of 0.01 mm.
Schütz-Fransson et al. – Mandibular incisor alignment
5
The measurements for the treatment groups
were taken on four occasions: before treatment
(T0); immediately after orthodontic treatment and
start of retention (T1); six years after treatment
(T2); and 12 years after treatment (T3).
For the untreated group, study casts were
available for the corresponding ages at T0, T2,
and T3. In the retention group, no retention
appliance was in place at T2 and T3. The mean
retention time for the mandibular incisors was 2.7
years (SD 1.50).
The main outcome measures (Figures 1 and 2)
were irregularity index according to Little (LII), the
summed displacement of the anatomic contact
points of the mandibular anterior teeth15,
intercanine width, intercanine arch perimeter
distance, available mandibular incisor space
(intercanine arch perimeter distance minus
summed tooth width for the four mandibular
incisors), lateral arch length, overjet, and
overbite. Also, the tooth width of the mandibular
incisors was measured, at T0 and T3.
Sagittal and vertical relationships between the
jaws and incisor inclination were evaluated on
lateral head radiographs, and the cephalometric
reference points and measurements were
assessed according to Björk16 and Solow17
(Figure 3). All measurements on lateral head
radiographs were made to the nearest half-
degree or 0.5 mm with correction for
enlargement. No lateral head radiographs were
available at T1 for the untreated subjects.
Figure 1. Figure 2.
Figure 3.
All registrations and measurements were made
by one author (USF) and because there was no
retention appliance in place at T2 and T3, a
blinded evaluation was possible, meaning that
the examiner was unaware of which of the three
groups the patients belonged to or if the casts
were taken at T2 or T3.

Schütz-Fransson et al. – Mandibular incisor alignment
6
Statistical analysis
The sample size estimation was based on a
significance level of 0.05 and 80% power to
detect a clinically meaningful difference of 1.5
mm (SD 1.5) of Little’s Irregularity Index. The
estimation revealed that 22 patients in each
group were sufficient.
Arithmetic means and standard deviations (SD)
on group level were calculated for each variable
at pre-treatment (T0), the end of active treatment,
and at the start of retention (T1), six years after
treatment (T2), and 12 years after treatment (T3).
The sample was normally distributed according
to the Kolmogorov-Smirnov test.
Significant differences in means within groups
and between groups were tested by one-way
analysis of variance (ANOVA), using the
Statistical Package for Social Sciences (version
22.0; SPSS Inc., Chicago, Illinois, USA). P-
values less than 5% (P<.05) were considered
statistically significant. When significant
differences were found between groups, the
Bonferroni correction was used.
A regression analysis was performed for Little’s
Irregularity Index to assess if LII at T3 was
dependent of LII at T0 and to relate mandibular
incisor inclination (L1/ML) to changes in Little’s
Irregularity Index.
Error of the measurements
The same examiner measured 24 randomly
selected cases at two separate occasions with at
least a four-week interval.
The mean error of the measurements according
to Dahlberg’s formula18 for the linear variables
was 0.1 mm. The largest measurement error was
0.5 mm for intercanine width, 0.5 mm for
intercanine perimeter distance, and 0.5 mm for
left lateral arch length. Error measurements for
the cephalometric angular variables were mean
0.8 degrees. The greatest measurement error
was noted for the maxillary incisor inclination, 3.3
degrees.
No significant differences between the two
series of records were found using paired t-test in
most the measurements, except for left lateral
arch length (range min -0.1 to max 0.5), available
space (range min -0.3 to max 0.2), tooth width 32
(range min -0.1 to max 0.1), tooth width 41
(range min -0.1 to max 0.1) and L1/Apg (range
min -0.1 to max 1.3). The systematic error was
within the boundaries given above.
RESULTS The distribution of age and gender can be seen
in Table 1. No significant difference in age at T0
between the three groups could be found;
however, a higher number of girls were observed
in the two treated groups compared to the
untreated group.
Little’s Irregularity Index, LII
No significant differences in mandibular incisor
irregularity between the retention and non-
retention group at T3 (12 years after treatment)
were found. However, significant differences
were found between the untreated and the two
treated groups at T3 (Table 2). The untreated
group had less LII at baseline (T0) and at the last
registration (T3).
At T0, Little’s Irregularity Index was less for the
untreated group compared with the retention
group.
The multiple regression analysis revealed that LII
at T2 was the only variable that could explain LII
at T3 (p=0.000). However, the incisor irregularity
at T3 could not be predicted by LII at T0.
Schütz-Fransson et al. – Mandibular incisor alignment
7
Available space
There was a significant difference at T0 in
available space between the non-retention and
retention group, i.e. mean -0.8 mm versus -2.0
mm. Also at T0, the available space was
significant less in the two treatment groups
compared with the untreated group. However,
after 12 years (T3), no significant differences
between the three groups were found.
Intercanine width
The intercanine width had not increased during
the orthodontic treatment. There were no
differences found between the three groups at
baseline or throughout the observation period.
Intercanine arch perimeter distance
The distance was slightly increased in the
treatment groups from T0 to T1. After T1, the
distance decreased in all three groups.
Arch length
Lateral arch length was significantly larger in the
untreated group compared with the two treatment
groups, except at T1 (Table 2).
Tooth width
There were no statistical significant differences in
tooth width for the four mandibular incisors
between the three groups and over time.
Overjet, Overbite
Overjet was reduced during treatment for the two
treatment groups and the reduction in overjet
corresponded to the amount of overjet for the
untreated group at T0.
At T2 and T3, the overjet stayed fairly the same
in all three groups. The same development could
also be seen for the overbite.
Cephalometric variables
Results for the cephalometric variables are
presented in Table 3, and a small number of
significant intergroup differences were found.
After treatment (T1), the mandibular incisors
were significantly more proclined in the retention
group compared with the non-retention group.
The multiple regression analysis showed that the
change in incisor irregularity (LII) T0-T3 was
explained by the change of incisor inclination
(L1/ML) from T0-T3 in 10.4%, (p=0.004).

Schütz-Fransson et al. – Mandibular incisor alignment
6
Statistical analysis
The sample size estimation was based on a
significance level of 0.05 and 80% power to
detect a clinically meaningful difference of 1.5
mm (SD 1.5) of Little’s Irregularity Index. The
estimation revealed that 22 patients in each
group were sufficient.
Arithmetic means and standard deviations (SD)
on group level were calculated for each variable
at pre-treatment (T0), the end of active treatment,
and at the start of retention (T1), six years after
treatment (T2), and 12 years after treatment (T3).
The sample was normally distributed according
to the Kolmogorov-Smirnov test.
Significant differences in means within groups
and between groups were tested by one-way
analysis of variance (ANOVA), using the
Statistical Package for Social Sciences (version
22.0; SPSS Inc., Chicago, Illinois, USA). P-
values less than 5% (P<.05) were considered
statistically significant. When significant
differences were found between groups, the
Bonferroni correction was used.
A regression analysis was performed for Little’s
Irregularity Index to assess if LII at T3 was
dependent of LII at T0 and to relate mandibular
incisor inclination (L1/ML) to changes in Little’s
Irregularity Index.
Error of the measurements
The same examiner measured 24 randomly
selected cases at two separate occasions with at
least a four-week interval.
The mean error of the measurements according
to Dahlberg’s formula18 for the linear variables
was 0.1 mm. The largest measurement error was
0.5 mm for intercanine width, 0.5 mm for
intercanine perimeter distance, and 0.5 mm for
left lateral arch length. Error measurements for
the cephalometric angular variables were mean
0.8 degrees. The greatest measurement error
was noted for the maxillary incisor inclination, 3.3
degrees.
No significant differences between the two
series of records were found using paired t-test in
most the measurements, except for left lateral
arch length (range min -0.1 to max 0.5), available
space (range min -0.3 to max 0.2), tooth width 32
(range min -0.1 to max 0.1), tooth width 41
(range min -0.1 to max 0.1) and L1/Apg (range
min -0.1 to max 1.3). The systematic error was
within the boundaries given above.
RESULTS The distribution of age and gender can be seen
in Table 1. No significant difference in age at T0
between the three groups could be found;
however, a higher number of girls were observed
in the two treated groups compared to the
untreated group.
Little’s Irregularity Index, LII
No significant differences in mandibular incisor
irregularity between the retention and non-
retention group at T3 (12 years after treatment)
were found. However, significant differences
were found between the untreated and the two
treated groups at T3 (Table 2). The untreated
group had less LII at baseline (T0) and at the last
registration (T3).
At T0, Little’s Irregularity Index was less for the
untreated group compared with the retention
group.
The multiple regression analysis revealed that LII
at T2 was the only variable that could explain LII
at T3 (p=0.000). However, the incisor irregularity
at T3 could not be predicted by LII at T0.
Schütz-Fransson et al. – Mandibular incisor alignment
7
Available space
There was a significant difference at T0 in
available space between the non-retention and
retention group, i.e. mean -0.8 mm versus -2.0
mm. Also at T0, the available space was
significant less in the two treatment groups
compared with the untreated group. However,
after 12 years (T3), no significant differences
between the three groups were found.
Intercanine width
The intercanine width had not increased during
the orthodontic treatment. There were no
differences found between the three groups at
baseline or throughout the observation period.
Intercanine arch perimeter distance
The distance was slightly increased in the
treatment groups from T0 to T1. After T1, the
distance decreased in all three groups.
Arch length
Lateral arch length was significantly larger in the
untreated group compared with the two treatment
groups, except at T1 (Table 2).
Tooth width
There were no statistical significant differences in
tooth width for the four mandibular incisors
between the three groups and over time.
Overjet, Overbite
Overjet was reduced during treatment for the two
treatment groups and the reduction in overjet
corresponded to the amount of overjet for the
untreated group at T0.
At T2 and T3, the overjet stayed fairly the same
in all three groups. The same development could
also be seen for the overbite.
Cephalometric variables
Results for the cephalometric variables are
presented in Table 3, and a small number of
significant intergroup differences were found.
After treatment (T1), the mandibular incisors
were significantly more proclined in the retention
group compared with the non-retention group.
The multiple regression analysis showed that the
change in incisor irregularity (LII) T0-T3 was
explained by the change of incisor inclination
(L1/ML) from T0-T3 in 10.4%, (p=0.004).

Schütz-Fransson et al. – Mandibular incisor alignment
8
Schütz-Fransson et al. – Mandibular incisor alignment
9
DISCUSSION
The most important and main result 12 years
after treatment was that mandibular incisor
irregularity revealed no significant differences
between the non-retention and retention groups.
Furthermore, in the two treatment groups, the
irregularity of the incisors was almost at the same
level before and 12 years after treatment.
Consequently, the hypothesis that long-term
mandibular incisor irregularity for the treated
group without retainers would be higher than for
the group with retainers could not be confirmed.
However, the hypothesis was partly confirmed in
that both treatment groups had a higher amount
of irregularity than the untreated group at the 12-
year follow-up.
Freitas et al.14 also confirmed our findings that
posttreatment change of the mandibular anterior
crowding was greater in a treated group
compared to mandibular crowding caused by
physiologic changes in an untreated group,
although the observation period was only five
years. Moreover, another sample of untreated
subjects was found to fall in line with our result
that incisor irregularity changes were similar in

Schütz-Fransson et al. – Mandibular incisor alignment
8
Schütz-Fransson et al. – Mandibular incisor alignment
9
DISCUSSION
The most important and main result 12 years
after treatment was that mandibular incisor
irregularity revealed no significant differences
between the non-retention and retention groups.
Furthermore, in the two treatment groups, the
irregularity of the incisors was almost at the same
level before and 12 years after treatment.
Consequently, the hypothesis that long-term
mandibular incisor irregularity for the treated
group without retainers would be higher than for
the group with retainers could not be confirmed.
However, the hypothesis was partly confirmed in
that both treatment groups had a higher amount
of irregularity than the untreated group at the 12-
year follow-up.
Freitas et al.14 also confirmed our findings that
posttreatment change of the mandibular anterior
crowding was greater in a treated group
compared to mandibular crowding caused by
physiologic changes in an untreated group,
although the observation period was only five
years. Moreover, another sample of untreated
subjects was found to fall in line with our result
that incisor irregularity changes were similar in

Schütz-Fransson et al. – Mandibular incisor alignment
10
nature but to a lesser extent than postretention
changes found in a sample of treated cases.19
In our study, most of the changes in the
irregularity of the mandibular incisors in the
treated groups occurred between 14.9 and 21.8
years of age. Similar findings were shown in a
study20 of untreated subjects, with most of the
mandibular incisor crowding occurring during late
teens and early twenties. In addition, other
studies have shown equal physiologic changes in
the mandibular incisor alignment in
orthodontically treated patients compared with
untreated patients. From late adolescence
through to early-to-middle adulthood, mandibular
incisor irregularity increased similarly in both
untreated and treated subjects.5
The crowding before treatment did not explain
the crowding at the last registration as Little’s
Irregularity Index six years after treatment was
the only variable that explained LII 12 years after
treatment. Studies have shown21,22 that relapse
of dental crowding depends on initial crowding. In
our study the explanation value for this was low.
Correction of overjet and overbite was stable
long-term. At the last registration, the amount of
overjet was almost the same in all three groups.
Eslambolchi et al.9 also pointed out that in an
untreated group of children who were followed for
29.8 years, overjet and overbite remained stable. The arch length variable, intercanine width, and
intercanine perimeter distance, decreased in all
three groups over time, and in the treatment
groups also because of extractions in some
cases. For patients treated in this study,
intercanine width did not increase during
treatment, which is an important predictor of
relapse.23,24
The cephalometric analysis revealed only a
small number of significant intergroup
differences. The group with a retainer had more
proclined mandibular incisors after treatment, but
at follow-up, no differences between the groups
were found.
Since the mandibular incisor inclination to ML did
not change much over time in any of the groups,
this was probably not a cofactor for increased
mandibular incisor crowding. Thilander25 has
claimed that no relationship has been found
between various cephalometric variables and
postretention changes in mandibular incisor
crowding. Mandibular incisor crowding is also
believed to be related to anterior rotation of the
mandible. In another study from 201626 no
associations were found between different
cephalometric measurements, for instance
mandibular incisor inclination (L1/ML) and
changes in incisor irregularity, and this lack of
association was also found in our study.
As expected, untreated subjects showed normal
cephalometric values at all registrations.
Thordarson et al.27 have shown in an untreated
group that the inclination of the mandibular
incisors increased over time from the ages of 6-
16 years. However, in our study, the inclination
was almost the same during the entire
observation period.
In our study, there were more girls in the
treatment groups compared with the untreated
group. The reason could be that girls are more
likely to request and/or accept orthodontic
treatment compared with boys. Nevertheless, no
statistically significant differences between
genders for Little’s Irregularity Index, measured
in untreated subjects was found.9,10 However, a
study has reported certain dental gender-specific
differences such as females showing more
relapse than males between 10-15 years
posttreatment.28 Consequently, the importance of
gender for relapse seems to be unclear.
Schütz-Fransson et al. – Mandibular incisor alignment
11
When studying stability after orthodontic
treatment, an important question must be asked:
“How much of the unwanted tooth movement is
relapse, and how much is due to natural
physiological changes?” Relapse is not only
caused by the muscle function but also, and to
an even greater extent, by a tendency to
rearrange the alveolar fibrous system. While the
principal fibers are rearranged after a certain
retention period, histological studies have shown
that the supra-alveolar structures may remain
displaced and stretched for more than seven
months after the cessation of orthodontic tooth
movement.29 So relapse occurring during this
period of remodeling of periodontal structures
must be distinguished from late changes during
the postretention period. Instead, the changes
that occur later are more related to craniofacial
growth, dental development and muscle function.
Edman Tynelius et al.30 showed that a major part
of relapse took place during the 1st year of
retention (different methods of retention used)
and only small changes and differences occurred
during the 2nd year of retention. This implies that
the 1st year of retention is the most important to
retain the treatment result. Furthermore, another
study has shown31 that nearly 50% of the relapse
occurred the first two years after retention. After
that period, certain stability is reached except for
the mandibular incisors. Consequently, a
retention time of about two years is probably
sufficient, and tooth movements after those years
are considered as natural physiological changes.
Sadowsky et al.32 showed an average period of
8.4 years with a fixed mandibular retainer was
more favorable than other studies using shorter
retention times. It seems that a life-long retention
for the mandibular anterior segment is needed.
Thus, for patients who want straight teeth
throughout their life, permanent retention is
recommended. It is important to stress that
improperly designed or inserted retainers may
cause inadvertent tooth movements; therefore,
retainers for long-term use require regular check-
ups.33 The permanent retention we used in our study
were two different bonded retainers which were
merged to one group, as we have shown in
another study2 that there were no differences in
their capacity in keeping the mandibular incisors
aligned in a long-term perspective.
It might be surprising that one group did not get
a retainer after treatment, although the crowding
situation was similar before treatment in both
groups. On the other hand this group made this
study possible. It is difficult to find an
orthodontically treated group without retainer
afterwards.
The untreated control material consisted of
subjects followed because of infraocclusion of
primary molars with permanent successors or the
reversible type of ectopic eruption of the
maxillary first permanent molars 34,35. The growth
and development of the dentition was normal in
these cases. These subjects had Class I normal
occlusion without any other malocclusions.
A limitation with this study was that the subjects
in the untreated control group only had minor
malocclusions. Ideally, the study should have
included an untreated group of subjects with
similar malocclusions to those of the treated
groups. However, the postponement of a needed
orthodontic intervention for about 12 years is
ethically unacceptable.

Schütz-Fransson et al. – Mandibular incisor alignment
10
nature but to a lesser extent than postretention
changes found in a sample of treated cases.19
In our study, most of the changes in the
irregularity of the mandibular incisors in the
treated groups occurred between 14.9 and 21.8
years of age. Similar findings were shown in a
study20 of untreated subjects, with most of the
mandibular incisor crowding occurring during late
teens and early twenties. In addition, other
studies have shown equal physiologic changes in
the mandibular incisor alignment in
orthodontically treated patients compared with
untreated patients. From late adolescence
through to early-to-middle adulthood, mandibular
incisor irregularity increased similarly in both
untreated and treated subjects.5
The crowding before treatment did not explain
the crowding at the last registration as Little’s
Irregularity Index six years after treatment was
the only variable that explained LII 12 years after
treatment. Studies have shown21,22 that relapse
of dental crowding depends on initial crowding. In
our study the explanation value for this was low.
Correction of overjet and overbite was stable
long-term. At the last registration, the amount of
overjet was almost the same in all three groups.
Eslambolchi et al.9 also pointed out that in an
untreated group of children who were followed for
29.8 years, overjet and overbite remained stable. The arch length variable, intercanine width, and
intercanine perimeter distance, decreased in all
three groups over time, and in the treatment
groups also because of extractions in some
cases. For patients treated in this study,
intercanine width did not increase during
treatment, which is an important predictor of
relapse.23,24
The cephalometric analysis revealed only a
small number of significant intergroup
differences. The group with a retainer had more
proclined mandibular incisors after treatment, but
at follow-up, no differences between the groups
were found.
Since the mandibular incisor inclination to ML did
not change much over time in any of the groups,
this was probably not a cofactor for increased
mandibular incisor crowding. Thilander25 has
claimed that no relationship has been found
between various cephalometric variables and
postretention changes in mandibular incisor
crowding. Mandibular incisor crowding is also
believed to be related to anterior rotation of the
mandible. In another study from 201626 no
associations were found between different
cephalometric measurements, for instance
mandibular incisor inclination (L1/ML) and
changes in incisor irregularity, and this lack of
association was also found in our study.
As expected, untreated subjects showed normal
cephalometric values at all registrations.
Thordarson et al.27 have shown in an untreated
group that the inclination of the mandibular
incisors increased over time from the ages of 6-
16 years. However, in our study, the inclination
was almost the same during the entire
observation period.
In our study, there were more girls in the
treatment groups compared with the untreated
group. The reason could be that girls are more
likely to request and/or accept orthodontic
treatment compared with boys. Nevertheless, no
statistically significant differences between
genders for Little’s Irregularity Index, measured
in untreated subjects was found.9,10 However, a
study has reported certain dental gender-specific
differences such as females showing more
relapse than males between 10-15 years
posttreatment.28 Consequently, the importance of
gender for relapse seems to be unclear.
Schütz-Fransson et al. – Mandibular incisor alignment
11
When studying stability after orthodontic
treatment, an important question must be asked:
“How much of the unwanted tooth movement is
relapse, and how much is due to natural
physiological changes?” Relapse is not only
caused by the muscle function but also, and to
an even greater extent, by a tendency to
rearrange the alveolar fibrous system. While the
principal fibers are rearranged after a certain
retention period, histological studies have shown
that the supra-alveolar structures may remain
displaced and stretched for more than seven
months after the cessation of orthodontic tooth
movement.29 So relapse occurring during this
period of remodeling of periodontal structures
must be distinguished from late changes during
the postretention period. Instead, the changes
that occur later are more related to craniofacial
growth, dental development and muscle function.
Edman Tynelius et al.30 showed that a major part
of relapse took place during the 1st year of
retention (different methods of retention used)
and only small changes and differences occurred
during the 2nd year of retention. This implies that
the 1st year of retention is the most important to
retain the treatment result. Furthermore, another
study has shown31 that nearly 50% of the relapse
occurred the first two years after retention. After
that period, certain stability is reached except for
the mandibular incisors. Consequently, a
retention time of about two years is probably
sufficient, and tooth movements after those years
are considered as natural physiological changes.
Sadowsky et al.32 showed an average period of
8.4 years with a fixed mandibular retainer was
more favorable than other studies using shorter
retention times. It seems that a life-long retention
for the mandibular anterior segment is needed.
Thus, for patients who want straight teeth
throughout their life, permanent retention is
recommended. It is important to stress that
improperly designed or inserted retainers may
cause inadvertent tooth movements; therefore,
retainers for long-term use require regular check-
ups.33 The permanent retention we used in our study
were two different bonded retainers which were
merged to one group, as we have shown in
another study2 that there were no differences in
their capacity in keeping the mandibular incisors
aligned in a long-term perspective.
It might be surprising that one group did not get
a retainer after treatment, although the crowding
situation was similar before treatment in both
groups. On the other hand this group made this
study possible. It is difficult to find an
orthodontically treated group without retainer
afterwards.
The untreated control material consisted of
subjects followed because of infraocclusion of
primary molars with permanent successors or the
reversible type of ectopic eruption of the
maxillary first permanent molars 34,35. The growth
and development of the dentition was normal in
these cases. These subjects had Class I normal
occlusion without any other malocclusions.
A limitation with this study was that the subjects
in the untreated control group only had minor
malocclusions. Ideally, the study should have
included an untreated group of subjects with
similar malocclusions to those of the treated
groups. However, the postponement of a needed
orthodontic intervention for about 12 years is
ethically unacceptable.

Schütz-Fransson et al. – Mandibular incisor alignment
12
CONCLUSION
There were no differences found 12 years after
treatment in Little’s Irregularity Index for the
mandibular incisors between the group that had a
retainer and the group that had no retainer after
treatment. In the untreated group, Little’s
Irregularity Index was increased over time, but
not to the same extent as in the treated groups.
The crowding before treatment did not explain
the crowding at the last registration.
The routine use of mandibular retainers for two to
three years does not appear to prevent long-term
relapse. If the patient wants to constrain the
changes that come with natural development,
then lifelong retention is needed.
It may be perceived discouraging that the
mandibular incisor stability was suboptimal, but
encouraging that the overjet and overbite were
stable long-term.
Acknowledgement
This study was supported by grants from the
Gothenburg Dental Society.
REFERENCES
1. Al Yami EA, Kuijpers-Jagtman AM, van’t Hof
MA. Stability of orthodontic treatment
outcome: Follow-up until 10 years
postretention. Am J Orthod Dentofacial
Orthop. 1999;115:300-4.
2. Schütz-Fransson U, Lindsten R, Bjerklin K,
Bondemark L. Twelve year follow-up of
mandibular incisor stability: A comparison
between two different bonded lingual
orthodontic retainers. Angle Orthod.
2017;87:200-8.
3. Bjering R, Birkeland K, Vandevska-
Radunovic V. Anterior tooth alignment: A
comparison of orthodontic retention
regimens 5 years posttreatment. Angle
Orthod. 2015;85:353-9.
4. Otuyemi OD, Jones SP. Long-term
evaluation of treated class II division 1
malocclusions utilizing the PAR index. Br J
Orthod. 1995;22:171-8.
5. Driscoll-Gilliland J, Buschang PH, Behrents
RG. An evaluation of growth and stability in
untreated and treated subjects. Am J Orthod
Dentofacial Orthop. 2001;120:588-97.
6. Samspon WJ. Current controversies in late
incisor crowding. Ann Acad Med Singapore.
1995;24:129-37.
7. Profitt WR. Retention. In: Contemporary
orthodontics. Profitt, W, Fields, H, Sarver, D,
eds. 5th ed. St Louis, MO: Elsevier Mosby –
Year Book; 2013:615-6.
8. Johnston CD, Littlewood S. Retention in
orthodontics. Br Dent J. 2015;218:119-22.
9. Eslambolchi S, Woodside DG, Rossouw PE.
A descriptive study of mandibular incisor
alignment in untreated subjects. Am J
Orthod Dentofacial Orthop. 2008;133:343-
53.
10. Bondevik O. A longitudinal study of dental
arches and oclusal changes in adults from
22 to 33, and 33 to 43 years of age. J
Orofac Orthop. 2015;76:79-89.
Schütz-Fransson et al. – Mandibular incisor alignment
13
11. Tsiopas N, Nilner M, Bondemark L, Bjerklin
K. A 40 years follow-up of dental arch
dimensions and incisor irregularity in adults.
Eur J Orthod. 2013;35:230-5.
12. Little RM. Stability and relapse of mandibular
anterior alignment: University of Washington
studies. Semin Orthod. 1999;5:191-204.
13. Jonsson T, Magnusson TE. Crowding and
spacing in the dental arches: l long-term
development in treated and untreated
subjects. Am J Orthod Dentofacial Orthop.
2010;138:384.e1-7.
14. Freitas KM, Janson G, Tompson B, de
Freitas MR, Simão TM, Valarelli FP,
Cançado RH. Posttreatment and physiologic
occlusal changes comparison. Angle
Orthod. 2013;83:239-45.
15. Little RM. The irregularity index. A
quantitative score of mandibular anterior
alignment. Am J Orthod. 1975;68:554-63.
16. Björk A. The face in profile. Svensk Tandl
Tidskr. 1947;40: suppl no 1.
17. Solow B. The pattern of craniofacial
associations. Acta Odontol Scand. 1966;24:
suppl 46.
18. Dahlberg G. Statistical methods for medical
and biological students. New York
Interscience Publications;1940.
19. Sinclair PM, Little RM. Maturation of
untreated normal occlusions. Am J Orthod.
1983;83:114-23.
20. Bushang PH, Shulman JD. Incisor crowding
in untreated persons 15-50 years of age:
United States, 1988-1994. Angle Orthod.
2003;73:502-8.
21. Kahl-Nieke B, Fischbach H, Schwarze CW.
Post-retention crowding and incisor
irregularity: a long-term follow-up evaluation
of stability and relapse. Br J Orthod.
1995;22:249-57.
22. Bjering R, Sandvik L, Midtbø M, Vandevska-
Radunovic V. Stability of anterior tooth
alignment 10 years out of retention. J Orofac
Orthop. 2017;78:275-83.
23. Zachrisson BU. Important aspects of long-
term stability. J Clin Orthod.
1997;31:562-83.
24. Artun J, Garol JD, Little RM. Long-term
stability of mandibular incisors following
successful treatment of Class II, Division 1,
malocclusions. Angle Orthod. 1996;66:229-
38.
25. Thilander B. Biological basis for orthodontic
relapse. Semin Orthod. 2000;6:195-205.
26. Oh H, Ma N, Feng PP, Kieu K, Boero R,
Dugoni S, Aubert M, Chambers D.
Evaluation of posttreatment stability after
orthodontic treatment in the mixed and
permanent dentitions. Angle Orthod.
2016;86:1010-8.
27. Thordarson A, Johannsdottir B, Magnusson
TE. Craniofacial changes in Icelandic
children between 6 and 16 years of age - a

Schütz-Fransson et al. – Mandibular incisor alignment
12
CONCLUSION
There were no differences found 12 years after
treatment in Little’s Irregularity Index for the
mandibular incisors between the group that had a
retainer and the group that had no retainer after
treatment. In the untreated group, Little’s
Irregularity Index was increased over time, but
not to the same extent as in the treated groups.
The crowding before treatment did not explain
the crowding at the last registration.
The routine use of mandibular retainers for two to
three years does not appear to prevent long-term
relapse. If the patient wants to constrain the
changes that come with natural development,
then lifelong retention is needed.
It may be perceived discouraging that the
mandibular incisor stability was suboptimal, but
encouraging that the overjet and overbite were
stable long-term.
Acknowledgement
This study was supported by grants from the
Gothenburg Dental Society.
REFERENCES
1. Al Yami EA, Kuijpers-Jagtman AM, van’t Hof
MA. Stability of orthodontic treatment
outcome: Follow-up until 10 years
postretention. Am J Orthod Dentofacial
Orthop. 1999;115:300-4.
2. Schütz-Fransson U, Lindsten R, Bjerklin K,
Bondemark L. Twelve year follow-up of
mandibular incisor stability: A comparison
between two different bonded lingual
orthodontic retainers. Angle Orthod.
2017;87:200-8.
3. Bjering R, Birkeland K, Vandevska-
Radunovic V. Anterior tooth alignment: A
comparison of orthodontic retention
regimens 5 years posttreatment. Angle
Orthod. 2015;85:353-9.
4. Otuyemi OD, Jones SP. Long-term
evaluation of treated class II division 1
malocclusions utilizing the PAR index. Br J
Orthod. 1995;22:171-8.
5. Driscoll-Gilliland J, Buschang PH, Behrents
RG. An evaluation of growth and stability in
untreated and treated subjects. Am J Orthod
Dentofacial Orthop. 2001;120:588-97.
6. Samspon WJ. Current controversies in late
incisor crowding. Ann Acad Med Singapore.
1995;24:129-37.
7. Profitt WR. Retention. In: Contemporary
orthodontics. Profitt, W, Fields, H, Sarver, D,
eds. 5th ed. St Louis, MO: Elsevier Mosby –
Year Book; 2013:615-6.
8. Johnston CD, Littlewood S. Retention in
orthodontics. Br Dent J. 2015;218:119-22.
9. Eslambolchi S, Woodside DG, Rossouw PE.
A descriptive study of mandibular incisor
alignment in untreated subjects. Am J
Orthod Dentofacial Orthop. 2008;133:343-
53.
10. Bondevik O. A longitudinal study of dental
arches and oclusal changes in adults from
22 to 33, and 33 to 43 years of age. J
Orofac Orthop. 2015;76:79-89.
Schütz-Fransson et al. – Mandibular incisor alignment
13
11. Tsiopas N, Nilner M, Bondemark L, Bjerklin
K. A 40 years follow-up of dental arch
dimensions and incisor irregularity in adults.
Eur J Orthod. 2013;35:230-5.
12. Little RM. Stability and relapse of mandibular
anterior alignment: University of Washington
studies. Semin Orthod. 1999;5:191-204.
13. Jonsson T, Magnusson TE. Crowding and
spacing in the dental arches: l long-term
development in treated and untreated
subjects. Am J Orthod Dentofacial Orthop.
2010;138:384.e1-7.
14. Freitas KM, Janson G, Tompson B, de
Freitas MR, Simão TM, Valarelli FP,
Cançado RH. Posttreatment and physiologic
occlusal changes comparison. Angle
Orthod. 2013;83:239-45.
15. Little RM. The irregularity index. A
quantitative score of mandibular anterior
alignment. Am J Orthod. 1975;68:554-63.
16. Björk A. The face in profile. Svensk Tandl
Tidskr. 1947;40: suppl no 1.
17. Solow B. The pattern of craniofacial
associations. Acta Odontol Scand. 1966;24:
suppl 46.
18. Dahlberg G. Statistical methods for medical
and biological students. New York
Interscience Publications;1940.
19. Sinclair PM, Little RM. Maturation of
untreated normal occlusions. Am J Orthod.
1983;83:114-23.
20. Bushang PH, Shulman JD. Incisor crowding
in untreated persons 15-50 years of age:
United States, 1988-1994. Angle Orthod.
2003;73:502-8.
21. Kahl-Nieke B, Fischbach H, Schwarze CW.
Post-retention crowding and incisor
irregularity: a long-term follow-up evaluation
of stability and relapse. Br J Orthod.
1995;22:249-57.
22. Bjering R, Sandvik L, Midtbø M, Vandevska-
Radunovic V. Stability of anterior tooth
alignment 10 years out of retention. J Orofac
Orthop. 2017;78:275-83.
23. Zachrisson BU. Important aspects of long-
term stability. J Clin Orthod.
1997;31:562-83.
24. Artun J, Garol JD, Little RM. Long-term
stability of mandibular incisors following
successful treatment of Class II, Division 1,
malocclusions. Angle Orthod. 1996;66:229-
38.
25. Thilander B. Biological basis for orthodontic
relapse. Semin Orthod. 2000;6:195-205.
26. Oh H, Ma N, Feng PP, Kieu K, Boero R,
Dugoni S, Aubert M, Chambers D.
Evaluation of posttreatment stability after
orthodontic treatment in the mixed and
permanent dentitions. Angle Orthod.
2016;86:1010-8.
27. Thordarson A, Johannsdottir B, Magnusson
TE. Craniofacial changes in Icelandic
children between 6 and 16 years of age - a

Schütz-Fransson et al. – Mandibular incisor alignment
14
longitudinal study. Eur J Orthod
2006;28:152-65.
28. Zinad K, Schols AM, Schols JG. Another
way of looking at treatment stability. Angle
Orthod. 2016;86:721-6.
29. Reitan K. Clinical and histologic
observations on tooth movement during and
after orthodontic treatment. Am J Orthod.
1967;53:721-45.
30. Edman Tynelius G, Bondemark L, Lilja-
Karlander E. A randomized controlled
trial of three orthodontic retention methods
in Class I four premolar extraction cases -
stability after 2 years in retention. Orthod
Craniofac Res. 2013;16:105-15.
31. Kuijpers-Jagtman AM. Repair and revision
8. Relapse of lower incisors: retreatment?
Ned Tijdschr Tandheelkd. 2002;109:42-6.
32. Sadowsky C, Schneider BJ, BeGole EA,
Tahir E. Long-term stability after orthodontic
treatment: Nonextraction with prolonged
retention. Am J Orthod Dentofacial Orthop.
1994;106:243-9.
33. Shaughnessy TG, Proffit WR, Samara SA.
Inadvertent tooth movement with fixed
lingual retainers. Am J Orthod Dentofacial
Orthop. 2016;149:277-86.
34. Kurol J. Infraocclusion of primary molars.
An epidemiological, familial,
longitudinal clinical and histological study.
Swed Dent J Suppl. 1984;21:1-67. (Thesis)
35. Bjerklin K. Ectopic eruption of the maxillary
first permanent molar. An epidemiological,
familial, aetiological and longitudinal
clinical study. Swed Dent J Suppl.
1994;100:1-66. (Thesis)


MALMÖ UNIVERSITY
205 06 MALMÖ, SWEDEN
WWW.MAU.SE
UL
RIK
E S
CH
ÜT
Z-F
RA
NS
SO
N
MA
LM
Ö U
NIV
ER
SIT
Y 2
01
8F
IXE
D M
AN
DIB
UL
AR
RE
TAIN
ER
S
isbn 978-91-7104-935-3 (print)
isbn 978-91-7104-936-0 (pdf)
issn 1650-6065
L I C












![Spurensuche in multimedialen Bildschichtungen/Retracing Multimedial Image Layers [Ulrike Rosenbach], in: Andrea Seamann/Katrin Grögel (eds.): Performance Saga. Interview 05: Ulrike](https://static.fdokumen.com/doc/165x107/63137401fc260b71020f1a0a/spurensuche-in-multimedialen-bildschichtungenretracing-multimedial-image-layers.jpg)






