
Turkish Nursing Students’ Perceptions and Experiences of Bullying Behaviors in Nursing Education
36
Turkish Nursing Students’ Perceptions and Experiences of Bullying Behaviors in Nursing Education Serap Palaz University of Balikesir Abstract Objective: This descriptive study aimed to determine the bullying and harassment experiences of nursing students’ in various Nursing Schools in Turkey. The types and frequency of bullying behaviors, the sources of bullying behaviors, and students’ emotions towards these experiences were investigated. Methods: Study participants were 370 undergraduate nursing students from four different Turkish Nursing Schools. To estimate bullying at nursing school I used a short version of the Negative Acts Questionnaire that adapted according to the earlier studies on bullying against nursing students particularly those conducted by Cooper et al. and Celik and Bayraktar. Results: A total of 222 respondents (60%) reported that they had experienced at least one of the thirteen bullying behaviors at daily and weekly frequencies during the last six months. Work related bullying was the most frequently encountered type of bullying behaviors which is followed by personal related bullying behaviors. Also, an interesting result from this study is that most students reported clinic nurses as their bully, indicating that the perpetrators were mostly females and older than them. Conclusions: This study supports previous reports of bullying against Turkish student nurses and adds to the scant body of literature showing that nursing students often experience bullying and harassment from clinical nurses (horizontal
Transcript of Turkish Nursing Students’ Perceptions and Experiences of Bullying Behaviors in Nursing Education
Turkish Nursing Students’ Perceptions and Experiences of
Bullying Behaviors in Nursing Education
Serap Palaz
University of Balikesir
Abstract
Objective: This descriptive study aimed to determine thebullying and harassment experiences of nursing students’ invarious Nursing Schools in Turkey. The types and frequency ofbullying behaviors, the sources of bullying behaviors, andstudents’ emotions towards these experiences were investigated.
Methods: Study participants were 370 undergraduate nursingstudents from four different Turkish Nursing Schools. Toestimate bullying at nursing school I used a short version ofthe Negative Acts Questionnaire that adapted according to theearlier studies on bullying against nursing studentsparticularly those conducted by Cooper et al. and Celik andBayraktar.
Results: A total of 222 respondents (60%) reported that theyhad experienced at least one of the thirteen bullying behaviorsat daily and weekly frequencies during the last six months.Work related bullying was the most frequently encountered typeof bullying behaviors which is followed by personal relatedbullying behaviors. Also, an interesting result from this studyis that most students reported clinic nurses as their bully,indicating that the perpetrators were mostly females and olderthan them.
Conclusions: This study supports previous reports of bullyingagainst Turkish student nurses and adds to the scant body ofliterature showing that nursing students often experiencebullying and harassment from clinical nurses (horizontal

bullying), and importantly, this may influence their futureemployment choices.
Introduction
Violence, verbal abuse and bullying at work have been widely
studied by researchers in the field of occupational health and
safety particularly among researchers in the nursing
professions from different parts of the world (Cox, 1987;
Einarsen, Matthiesen, & Skogstad, 1998; Quine, 2001; Stevens,
2002; Inoue, Tsukano, Muraoka, Kaneko, & Okamura, 2006, Lewis,
2006; Celik & Celik, 2007; Cooper, Walker, Askew, Robinson, &
McNair, 2011). Although the study of types, sources and
frequency of bullying/mobbing behaviors encountered by Turkish
nurses in the workplace attracted noticeable attention recently
(Uzun, 2003; Oztunc, 2006; Yildirim & Yildirim, 2007; Kisa,
2008; Ozturk, Sokmen, Yilmaz, & Cilingir 2008; Efe & Ayaz,
2010; Pinar & Ucmak, 2010) according to the best of our
knowledge there has been paid a little attention to the
investigation of bullying and harassment against nursing
students in Turkey (Celik & Bayraktar, 2004; Celebioglu,
Akpinar, Kucukoglu, & Engin, 2010).
National and international literature reveals that the
prevalence of bullying and harassment in the health sector
workplace is well known problem and the risk of being subjected
to psychological violence among nurses are three times higher
than in other professional groups in the service sector (Keely,
2002; Celebioglu, et al, 2010). Also Ferns and Meerabeau
(2007: 437) quote that nursing students have the highest risk
of experiencing aggression because of inexperience, frequent
ward changes and the challenge of meeting new environments.
Although The World Health Organizations, the International
Council of Nurses, and Public Services International recognize
the incidence of violent episodes as a major health priority,
the number of nurses affected by this problem still continues
to rise (Hinchberger, 2009; Kuehn, 2010).
Bullying and harassment are emotional issues for nurses who are
exposed to abusive behaviors and have negative influences on
both their own physical and psychological health and the
quality of service they provide. Especially Celik and
Bayraktar (2004) and Longo (2007) contend that when nursing
students a practice setting encounter bullying behaviors, their
approach to practice, as well as their intent to become a nurse
can be affected. The nursing shortage is considered to be a
world-wide problem and it is suggested that unhealthy work
environments cause the recruitment and retention problem (Gok &
Kocaman, 2011). Yet there is limited research on the
phenomenon of bullying and harassment in the nursing education
and possible impact of this on future employment choices. This
present study attempts to make a contribution to redressing
this gap by determining perceived bullying and harassment
behaviors which experienced by nursing students in four Turkish
Nursing Schools. More specifically, this study intended to
achieve the followings:
1. To describe the types and frequency of bullying and
harassment behaviors that is faced by nursing students in
Nursing Schools, and the association between bullying behaviors
and demographic variables such as gender, year at school,
marital status and participant’s place of living;
2. To describe the sources of bullying and harassment
experienced by nursing students in both their educational and
clinical settings;
3. To determine the effect of bullying behaviors on nursing
students’ academicals and professional achievement and also
physical and psychological health; and
4. To determine the type of behaviors used by students to cope
with bullying and harassment, and to find out whether any
Nursing School has special programs to overcome this problem.
Background
The concept of workplace bullying sometimes referred to as
mobbing (Leymann, 1990), workplace abuse (Keashly, 1998),
victimization (Aquino & Stefan, 2009), workplace harassment
(Brodsky, 1976), and verbal abuse (Ferns & Meerabeau, 2007)
refers to situations where a person repeatedly and over a
period of time feels subjected to negative treatment on the
part of one or more persons, and where the person(s) exposed to
the treatment have difficulty in defending them selves against
this actions (Einarsen, 2000). Also all various constructs
applied in the literature to describe the phenomenon of
systematic and prolonged mistreatment at work share that the
experienced aggression has harmful effects on targets’ health
and well-being.
Although there are numerous words to describe the same
phenomenon including aggression, harassment, mobbing,
intimidation in the literature we use workplace bullying and
harassment in this paper, as suggested by Einarsen, Hoel, Zapf
and Cooper (2011), and the following definition will be applied
to refer to the concept of workplace bullying and harassment;
Bullying at work means harassing, offending, or
socially excluding someone or negatively affecting
someone’s work. In order for the label bullying (or
mobbing) to be applied to a particular activity,
interaction, or process, the bullying behavior has to occur
repeatedly and regularly (e.g., weekly) and over a period
time (e.g., about six months). Bullying in an escalating
process in the course of which the person confronted ends
up in an inferior position and becomes the target of
systematic negative social acts. A conflict cannot be
called bullying if the incident is an isolated event or if
two parties of approximately equal strength are in conflict
(Einarsen, Hoel, Zapf & Cooper, 2003:15).
Considering the present study, the power imbalance between
parties needs to be taken into account particularly.
Typically, targets of bullying find it difficult to defend
themselves against the negative behavior, as their opportunity
for retaliation is more or less ruled out. The imbalance of
power may mirrors the formal power structure of the
organizational context in which the bullying scenario unfolds
(Notelaers, 2011). This would be the case when supervisors to
be more often in the role of the perpetrator as compared to
subordinates. But the source of power may also be informal,
based on knowledge and experiences. The imbalance of power can
be originated in the target’s dependence on the perpetrators,
which may be of a social, physical, economic, or as in our
case, academic dependency. As is indicated by Einarsen (1999)
knowledge about someone’s weak points and deficiencies may also
be exploited and become s a strong source of power in the
development of bullying cases.
Bullying and harassment in the workplace are not new phenomena
however there are growing epidemic of bullying in the health
sector is raising great interest among employers, health care
workers, and governmental agencies across the world
(Hinchberger, 2009). For the reason that explained by Zapf,
Escartin, Einarsen, Hoel & Vartia (2011) health sector jobs
such as nursing profession require a high level of personal
involvement which means that sensing and expressing emotions
and building up personal relationships. The higher the level
of personal involvement, the more personal information is
available and the more possibilities for being attacked exist.
Also in health sector, it is difficult to evaluate or apprise
jobs objectively then this lack of objectivity offers a lot of
opportunity for attacking each other. The studies show that
bullying is rife in the health sector, especially in the
nursing profession and has a negative impact on both nurses own
physical and psychological welfare (Celebioglu et al, 2010;
Lewis, 2006; Pranjic, Males-Bilic, Beganlic, & Mustajbegovic,
2006; Quine, 2001). The previous studies on bullying against
Turkish nurses report wide prevalence rates ranging from 33 %
to 86.5 % (Yildirim & yildirim, 2007; Efe & Ayaz, 2010)
similarly as is found in international studies (Hinchberger,
2009). Workplace bullying and harassment can be both internal
to the workplace, i.e. bullied by nurse, doctor, and manager
and external, i.e. perpetrated by a patient, patient relatives
and visitors. Although nurses often come a cross bullying and
harassment in the healthcare environment, they are reluctant to
complain because they tend to accept it as just “part of the
job”. Therefore workplace abuse in the healthcare sector is
severely underreported (Ferns, 2006; Magnavita & Heponiemi,
2011).
Nursing students are also exposed to horizontal (negative
behavior directed from colleagues on the same level) and
vertical (negative behavior directed from superiors towards
subordinates) bullying and harassment in nursing school and
workplace. Randle (2003: 395) claims that bullying was found
to be commonplace in the transition to becoming a nurse;
students were bullied and also witnessed patients being bullied
by qualified nurses. The internalization of nursing norms meant
that students then bullied others. This means that if the
student is socialized into a nursing culture that accepts
bullying as a routine practice, then the results can be
destructive (Cooper et al, 2011). In addition, Hodgkinson,
Mclvor, & Phillips (1985) propose that nursing students have
the highest risk of experiencing negative behaviors because of
being younger nurses, less experience, less education, frequent
ward changes and the challenge of meeting new environments and
being vulnerable to patient aggression. Cooper et al (2011:4)
cite that Magnussen and Amundson (2003) in their U.S study
identify some nursing instructors actually impede their
educational experiences, undervalue nursing students, or treat
students in uncaring ways. In Turkey, Celik and Bayraktar
(2004) investigated all types of abuse in the nursing school
and found that students experienced high rates of verbal abuse
as well as academic, physical, and sexual abuse. Nearly all
participants identified their classmates as a source of verbal
abuse and they reported some instances of sexual and physical
violence while in nursing school and clinical placement.
Moreover, Celebioglu et al (2010) investigated the violence
experiences of nursing students’ in clinical settings and they
indicated that similar to nurses, nursing students also
experienced violence in areas of practice. According to their
findings 50.3% of the students were subjected to violence, and
91.6% of these students were subjected to verbal abuse and
anger, fury, and enmity are their most frequent responses after
confronting violence. Consequently, a systematic review of
studies on bullying and harassment in nursing school
demonstrate that in spite of different culture, countries, and
research designs, and settings, high level of workplace
bullying and harassment is a problem for nurses and their
responses to abuse are similar and include anger, anxiety,
guilt, self-blame, and shame (Magnussen & Amundson 2003; Celik
and Bayraktar, 2004; Frens & Meerabeau, 2007; Celebioglu et al,
2010; Cooper et al, 2009; Magnavita & Heponiemi, 2011).
Materials and Methods
Participants and Settings
This descriptive study on bullying and harassment against
nursing students was conducted in four different Nursing
Schools in the wide area of the southern Marmara and Aegean
region of Turkey, namely Balikesir, Bandirma, Canakkale, and
Aydin. In Turkey, the new Nursing Law which passed in 2007
changed the minimum nursing education requirement to a four
year undergraduate baccalaureate degree program and lifted the
barrier to men becoming nurses. Before the new Law introduced,
the Turkish nurses had been educated in a variety of
educational settings. These include diploma from vocational
high school; associate degree from two year college;
baccalaureate degree from four year undergraduate program.
Currently, nursing education is given by 89 undergraduate
nursing programs at the university level.
The data of the study were obtained from four Nursing schools
(NS) of four year undergraduate program which are affiliated to
three different state universities namely, Balikesir University
(Bandirma NS and Balikesir NS), Adnan Menderes University
(Aydin NS), and 18 Mart University (Canakkale NS). The
sampling included only nursing students who were taking courses
in 2nd, 3rd, and 4th grades. First year students were not
included in the scope of the study because they have not
started to gain clinical experience yet. The survey was
anonymous and asked respondents to take part in the study
between March and May in 2011. In total, 400 questionnaires
were delivered and 374 returned. The initial examination of
the returned questionnaires showed that four were incomplete;
these were therefore excluded from the data analysis process.
The number of usable questionnaires was 370 (92 %).
Ethical Considerations
The study was approved by the university ethics committee of
researcher. Also before the research was initiated, legal
permission was obtained from the administrations of each
Nursing Schools. The questionnaires were administrated to the
dropout students by one of the instructor at the nursing
department. The purpose of the research was explained to them
and they were instructed about their right to refuse if they
wished to do so. In addition, respondents were informed that
any information that they shared would be used only for
scientific purposes. No information about the identity of the
volunteers was required.
Instruments
As is well explained by Nielsen, Notelaers, and Einarsen
(2011:150) measuring bullying is not an easy task because it is
a complex phenomenon with many facets. The difficulties in
measuring the phenomenon are reflected through the many
different measurement methods and inventories that have been
applied in research so far. Nonetheless, in most studies
bullying is measured by one of two methods; the operational or
behavioral experience method, and the self-labeling or
subjective method. In the first method, respondents are
usually presented with an inventory that includes various types
of unwanted and negative behaviors that may be called bullying
if occurring repeatedly over time. Then, the respondents are
asked to report how frequently they have been exposed to the
different behaviors listed in the inventory within a given time
period without any reference to the phrase “bullying” (i.e.,
the Negative Acts Questionnaire (NAQ), Einarsen & Raknes,
1997). In the latter method, respondents are provided with a
definition of bullying, and those who judge their experiences
within a particular timescale to fit the definition are
considered bullied. This method connotes the respondents’
overall feeling of being victimized by bullying.
Although the self-labeling method is the most frequently used
approach in research on workplace bullying, the method has some
disadvantages such as; it does not offer any insight in the
nature of the behaviors involved. Moreover, because people may
have different personal thresholds for labeling themselves as
bullied, this method is very subjective approach in which
personality, emotional factors, cognitive factors, and
misperception may figure as potential biases (Nielsen et al,
2011). On the other hand, the operational method seems to be
more objective than the self-labeling approach because it does
not require the respondents to label their experiences as
bullying and so the decision about whether or not someone is
bullied rests with the researcher through the use of a
statistical analysis (Notelaers, Einarsen, DE Witte, & Vermunt,
2006). In literature, there are 27 different inventories to
assess bullying or phenomena similar to workplace bullying.
Some of these have been used in only one study, whereas others,
such as the Leymann Inventory of Psychological Terror (Leymann,
1990), and the Negative Acts Questionnaire (NAQ) have been
employed in a range of study (Nielsen et al, 2011). Yet,
except the NAQ, they have not been thoroughly tested and
validated in separate validation studies. It was shown in a
study on the psychometric properties of the NAQ (Einarsen et
al, 2009) that the inventory has high internal stability and
excellent criterion and constructs validity. Therefore, to
estimate bullying at nursing school we used a short version of
the Negative Acts Questionnaire that adapted according to the
earlier studies on bullying against nursing students
particularly those conducted by Cooper et al (2011), Ferns and
Meerabeau (2007), and Celik and Bayraktar (2004). The scale
consists of thirteen items referring to personal related
bullying (e.g., being shouted, spreading gossip, socially
isolated), work related bullying (e.g., unmanageable workloads,
hostility after or failure to acknowledge significant clinical
or academic accomplishment), and physical intimidating forms of
bullying (e.g., threats of violence or physical abuse,
intimidating behavior such as finger pointing). The scale
showed a satisfactory internal consistency, measured by
Cronbach’s alpha (0.80). The questionnaire was discussed and
reviewed with three colleagues of Nursing Schools and their
opinions were sought with regard to face validity. In
addition, the questionnaire was tested for structure and
clarity in a pilot study, and no revisions to the questionnaire
were indicated. Data from the pilot study were not included in
this study. All items are given in behavioral terms with no
reference to the phrase “bullying”, thus measuring perceived
exposure to bullying behaviors without foreign the respondents
to label this situations as bullying. For each item, the
respondents are asked how often they have been exposed to the
specific behavior during the last 6 months. The response
categories are “never”, “now and then”, “about monthly”, “about
weekly”, and “about daily”.
The questionnaire was in three sections. The first part of the
questionnaire aimed to identify the degree of bullying and
harassment using the revised NAQ scale which mentioned above.
The aim of the second part was to find out the reaction to
bullying incidents, effects of bullying on occupational health
and actions taken to escape from the bullying. The third part
consists of students’ demographic information such as gender,
year at school, marital status, age, and student’s
accommodation.
Data Analysis
Data analysis was performed using the Statistical Package
Program for the Social Sciences (SPSS version 11.5). The
frequency and percentage distributions and Pearson chi-square
analysis were used to accomplish our objectives stated in the
first section of the study.
Findings
The findings on demographic characteristics of the study group
are as follows; of 370 nursing students in the sample, the
majority were females (77.8 %), and nearly all of them were
single (97.02%), more than half of the respondents were aged 21
to 23 years (66.7 %). The majority of respondents did not have
any nursing experiences at all (95.4 %). More than half of the
nursing students’ place of birth and place where lived so far
were rural area (village and little town). Most students’
accommodation were dormitory and staying with friends (N=284,
76.6%). The distribution of the nursing schools was as
follows: 21.3 % students from Aydin Nursing School, 20.5 %
students from Canakkale Nursing School, 24.8 % students from
Balikesir Nursing School, and 33.2 % students from Bandirma
Nursing School.
A total of 222 respondents (60%) reported that they had
experienced at least one of the thirteen bullying behaviors at
daily and weekly frequencies during the last six months. As we
mentioned before NAQ scale consists of 5-likert type rating but
in our analysis, the five response categories were subsequently
combined into three categories: never, now and then/monthly,
and weekly/daily. According to the definition of bullying and
harassment which was clarified in Section 2, responses listed
as weekly/daily may best express bullying and harassment, while
now and then/monthly may express isolated incidences of
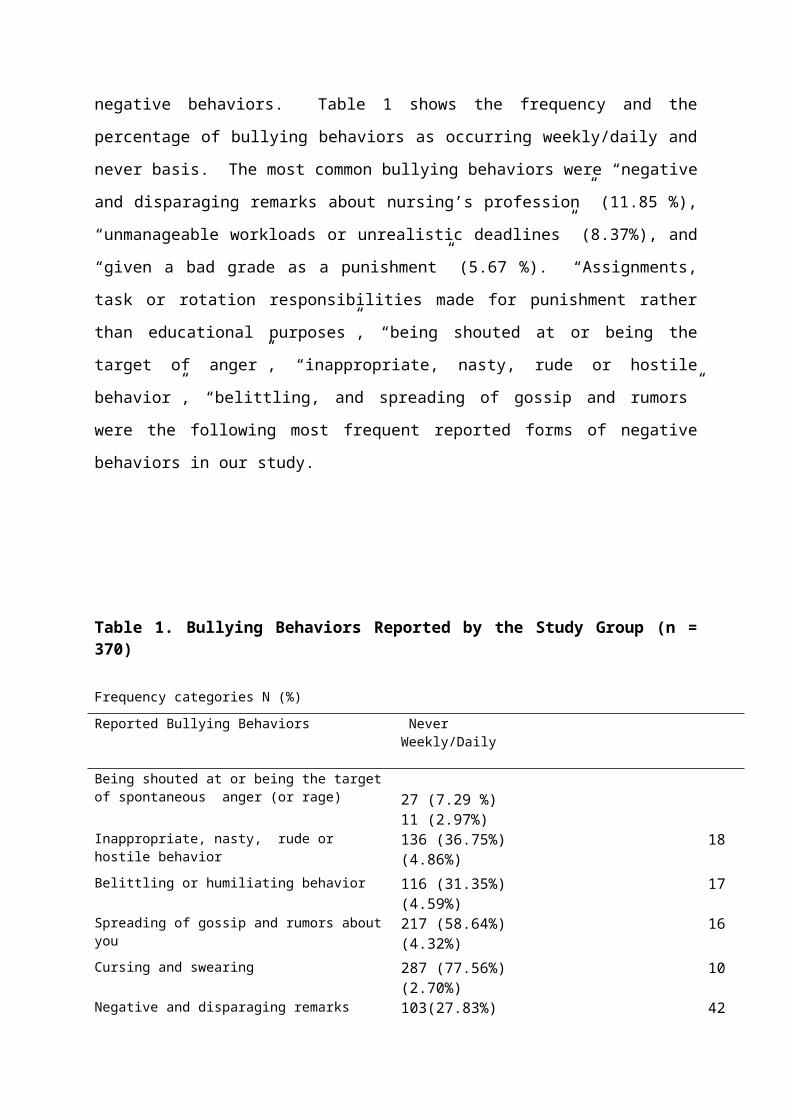
negative behaviors. Table 1 shows the frequency and the
percentage of bullying behaviors as occurring weekly/daily and
never basis. The most common bullying behaviors were “negative
and disparaging remarks about nursing’s profession” (11.85 %),
“unmanageable workloads or unrealistic deadlines” (8.37%), and
“given a bad grade as a punishment” (5.67 %). “Assignments,
task or rotation responsibilities made for punishment rather
than educational purposes”, “being shouted at or being the
target of anger”, “inappropriate, nasty, rude or hostile
behavior”, “belittling, and spreading of gossip and rumors”
were the following most frequent reported forms of negative
behaviors in our study.
Table 1. Bullying Behaviors Reported by the Study Group (n =370) Frequency categories N (%)Reported Bullying Behaviors Never
Weekly/Daily
Being shouted at or being the targetof spontaneous anger (or rage) 27 (7.29 %)
11 (2.97%)Inappropriate, nasty, rude or hostile behavior
136 (36.75%) 18 (4.86%)
Belittling or humiliating behavior 116 (31.35%) 17 (4.59%)
Spreading of gossip and rumors aboutyou
217 (58.64%) 16 (4.32%)
Cursing and swearing 287 (77.56%) 10 (2.70%)
Negative and disparaging remarks 103(27.83%) 42
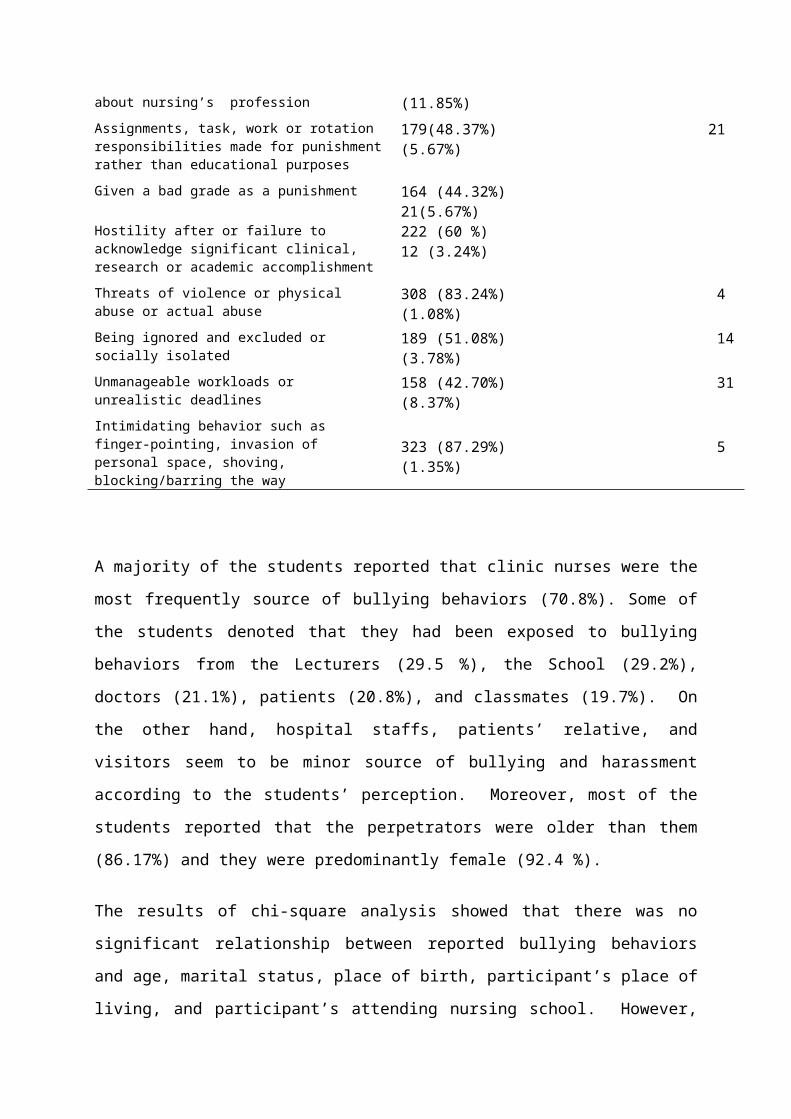
about nursing’s profession (11.85%)Assignments, task, work or rotation responsibilities made for punishmentrather than educational purposes
179(48.37%) 21 (5.67%)
Given a bad grade as a punishment 164 (44.32%) 21(5.67%)
Hostility after or failure to acknowledge significant clinical, research or academic accomplishment
222 (60 %) 12 (3.24%)
Threats of violence or physical abuse or actual abuse
308 (83.24%) 4 (1.08%)
Being ignored and excluded or socially isolated
189 (51.08%) 14(3.78%)
Unmanageable workloads or unrealistic deadlines
158 (42.70%) 31(8.37%)
Intimidating behavior such as finger-pointing, invasion of personal space, shoving, blocking/barring the way
323 (87.29%) 5 (1.35%)
A majority of the students reported that clinic nurses were the
most frequently source of bullying behaviors (70.8%). Some of
the students denoted that they had been exposed to bullying
behaviors from the Lecturers (29.5 %), the School (29.2%),
doctors (21.1%), patients (20.8%), and classmates (19.7%). On
the other hand, hospital staffs, patients’ relative, and
visitors seem to be minor source of bullying and harassment
according to the students’ perception. Moreover, most of the
students reported that the perpetrators were older than them
(86.17%) and they were predominantly female (92.4 %).
The results of chi-square analysis showed that there was no
significant relationship between reported bullying behaviors
and age, marital status, place of birth, participant’s place of
living, and participant’s attending nursing school. However,
there were statistically significant differences between gender
and being exposed to the target of spontaneous anger (χ2=
13.14, p=.001), belittling or humiliating behavior (χ2= 9.29,
p=.010), given a bad grade as a punishment (χ2= 17.82, p=.000),
unmanageable workloads (χ2=6.52, p=.038), and threats of
violence (χ2= 10.11 p=.006). Likewise, when the experiencing
of bullying behaviors with regard to the year at school
examined, it is found that second and third grade of students
were exposed to following bullying behaviors more than fourth
grade students; the target of spontaneous anger (χ2= 13.8,
p=.015), belittling or humiliating behavior (χ2= 21.2, p=.002),
and threats of violence and physical abuse (χ2= 13.15 p=.041).
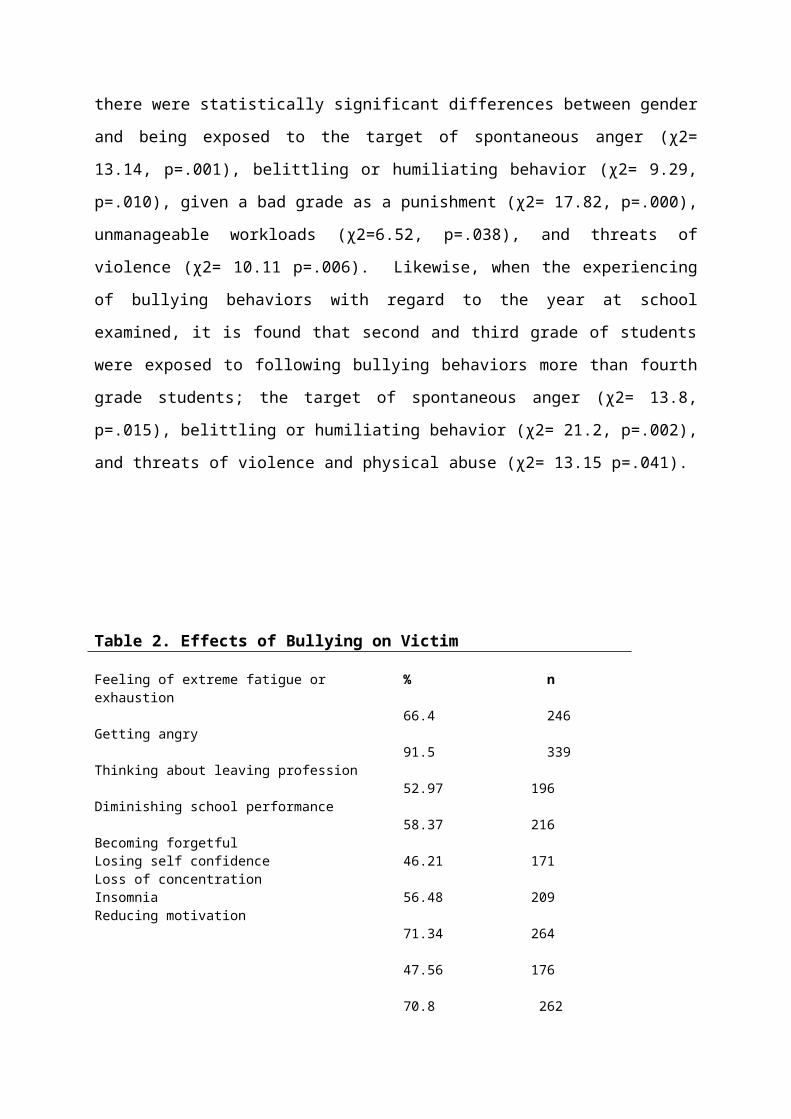
Table 2. Effects of Bullying on Victim
Feeling of extreme fatigue or exhaustion
% n 66.4 246
Getting angry 91.5 339
Thinking about leaving profession 52.97 196
Diminishing school performance 58.37 216
Becoming forgetful Losing self confidenceLoss of concentration InsomniaReducing motivation
46.21 171 56.48 209 71.34 264 47.56 176 70.8 262
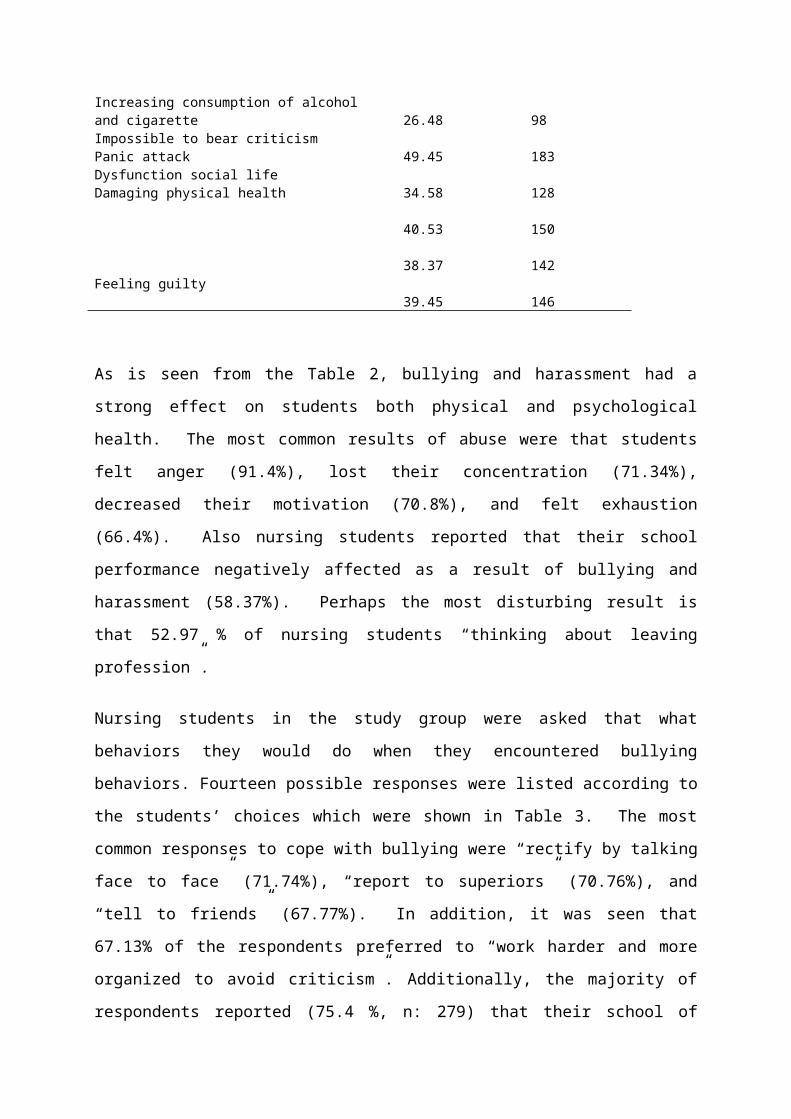
Increasing consumption of alcohol and cigarette
26.48 98
Impossible to bear criticismPanic attackDysfunction social lifeDamaging physical health
49.45 183 34.58 128 40.53 150 38.37 142
Feeling guilty 39.45 146
As is seen from the Table 2, bullying and harassment had a
strong effect on students both physical and psychological
health. The most common results of abuse were that students
felt anger (91.4%), lost their concentration (71.34%),
decreased their motivation (70.8%), and felt exhaustion
(66.4%). Also nursing students reported that their school
performance negatively affected as a result of bullying and
harassment (58.37%). Perhaps the most disturbing result is
that 52.97 % of nursing students “thinking about leaving
profession”.
Nursing students in the study group were asked that what
behaviors they would do when they encountered bullying
behaviors. Fourteen possible responses were listed according to
the students’ choices which were shown in Table 3. The most
common responses to cope with bullying were “rectify by talking
face to face” (71.74%), “report to superiors” (70.76%), and
“tell to friends” (67.77%). In addition, it was seen that
67.13% of the respondents preferred to “work harder and more
organized to avoid criticism”. Additionally, the majority of
respondents reported (75.4 %, n: 279) that their school of
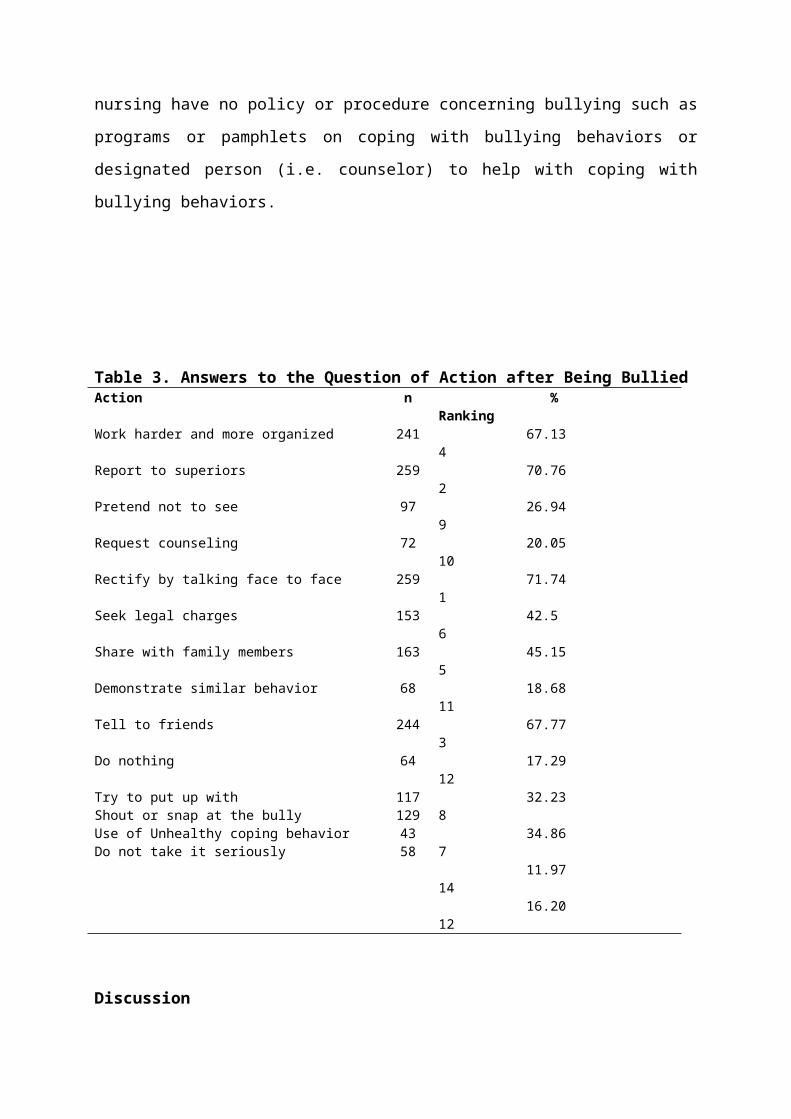
nursing have no policy or procedure concerning bullying such as
programs or pamphlets on coping with bullying behaviors or
designated person (i.e. counselor) to help with coping with
bullying behaviors.
Table 3. Answers to the Question of Action after Being BulliedAction n %
RankingWork harder and more organized 241 67.13
4 Report to superiors 259 70.76
2Pretend not to see 97 26.94
9Request counseling 72 20.05
10Rectify by talking face to face 259 71.74
1Seek legal charges 153 42.5
6Share with family members 163 45.15
5Demonstrate similar behavior 68 18.68
11Tell to friends 244 67.77
3Do nothing 64 17.29
12Try to put up withShout or snap at the bully Use of Unhealthy coping behavior Do not take it seriously
1171294358
32.23 8 34.86 7 11.97 14 16.20 12
Discussion
This study was carried out in four Nursing School which located
western part of the country and discussed the nature, severity,
frequency and sources of bullying experienced by students
gaining both academic education and clinical experience. More
than half of the respondents were exposed to bullying during
their education (60%). These results are consistent with
previous studies involving nursing students which found that
bullying and harassment at nursing education is an important
problem and that such bullying behaviors have detrimental
effects (Magnussen & Amundson, 2003; Longo, 2007; Ferns &
Meerabeau, 2007; Curtis, Bowen, & Reid, 2007; Hinchberger,
2009; Cooper et al, 2009; 2011; Celebioglu et al, 2010;
Magnavita & Heponiemi, 2011).
The result of present study supports the findings of previous
Turkish study which found that 50.3% of the students were
subjected to violence in the clinical settings. Verbal
violence (91.6%) was the most frequently encountered type of
abuse, followed by physical violence (4.2%), and sexual abuse
(4.2%) (Celebioglu et al, 2010: 689). In addition, another
study which was undertaken by Celik and Bayraktar (2004)
investigated the abuse experiences of nursing students found
that verbal abuse was the most frequently reported type of
abuse with all participants reported being behaved toward in an
inappropriate, nasty, rude, or hostile way, being yelled at,
and being humiliated or belittled.
We found that work related bullying (e.g., negative and
disparaging remarks about nursing’s profession, unmanageable
workloads, assignments, task or rotation responsibilities made
for punishment rather than educational purposes) were the most
frequently encountered type of bullying behaviors, 34.80% in
total, followed by personal related bullying (e.g., being
shouted, spreading gossip, socially isolated), 23.22 % in
total. On the other hand, only very small amount of
respondents, only 2.43 % reported physical intimidating forms
of bullying (e.g., threats of violence or physical abuse,
intimidating behavior such as finger pointing). Nursing
students reported that work related bullying was the most
annoying problem for them but this finding need to be read
carefully because it is possible that students in general do
not understand assignments, workload and deadlines as a part of
the learning environment. Responses were only based on student
perceptions and therefore it is unknown whether the behaviors
are actually occurring or whether grades and workloads which
are fairly given are perceived by students as being punishing.
In any case, student perceptions of being exposed to bullying
and harassment are of concern given the potential negative
impact on student health and academic performance (Cooper et
al, 2011: 12).
An interesting result from this study that most students
reported clinic nurses as their bully, indicating that the
perpetrators were mostly females and older than them. In
previous Turkish studies of nursing students’ abuse, the
abusive behaviors considered were mainly those committed by
patients and their relatives, and classmates (Celebioglu et al,
2010; Celik & Bayraktar ; 2004). In present study, nursing
students rarely reported bullying and harassment on the part of
patients and their relatives and classmates. The reasons might
account for using different sample from different part of the
country, with different characteristics of participants. For
instance, the study of Celebioglu et al (2010) was carried out
in a nursing school where located in the eastern part of the
country, and the sample in the study of Celik and Bayraktar
(2004) included nursing students from Ankara where is in the
middle of the country. Turkey is a large country and there are
huge cultural differences between western and eastern side of
the country, therefore, a nationwide survey of the students of
different nursing schools will be needed for investigating the
nature and sources of bullying phenomenon to be further
developed.
On the other hand, in consistent with the present study that
nurse-on-nurse bullying is a significant workplace problem that
depends on the flow of power within workplace. Bullying within
nursing is primarily intra-professional (i.e. between nurse and
nurse) and horizontal violence is common in nursing and the
victims are especially the younger and student nurses (Stevens,
2002; Lewis, 2006; Curtis et al, 2007; Longo, 2007;
Hinchberger, 2009; Efe & Ayaz, 2010). It is proposed that
external pressures are often held responsible, such as health
care workers’ need to find a scapegoat for errors as a reason
for the existence of bullying behavior towards nursing students
(Stevens, 2002). Recent change in health sector in Turkey
which involves adaptation requirements for the issue of
accreditation and patient rights and the financing of hospitals
on output-based formula which leads to greater levels of
alertness in the hospital patient population increased
workloads for nurses. Therefore, increased stress and pressure
on clinical nurses might cause increased tendency of bullying
student nurses in the clinical settings.
Additionally, as is well explained in the study of Curtis et al
(2007: 157) nursing as a profession is considered to be
oppressed; in this context, a hierarchical system has arisen in
which nurses, in order to succeed, must accept that their roles
is defined by those with power and authority. Such a system
supports the occurrence of horizontal violence, and in many
case, perpetrators are usually themselves past or current
victims and most are convinced that their experiences have
strengthen them for their nursing role. It is suggested that
the cycle of horizontal violence actually begins during nursing
education. The findings of this study support this suggestion
as lecturer and the faculty was reported being responsible for
bullying followed by clinical nurses.
Longo (2007:177) states that when nursing students in a
practice setting encounter horizontal bullying and harassment,
their approach to practice, as well as their intent to become a
nurse, can be influenced. In same manner, Bartholomew (2006)
claims that in a study of nurse-to-nurse hostility that 60 per
cent of new graduates leave their first position within the
first 6 months because of horizontal hostility. Moreover,
Curtis et al (2006) indicate that over half of the students in
their study had experienced or witnessed horizontal violence
during their education and all of those students revealed that
those experiences of violence from clinical nurse would
influence their future employment choices. Likewise, the
findings of the present study shows that nursing students who
experienced bullying behaviors felt anger, lost their
concentration, their social life affected badly, and they even
thought of leaving profession as a consequences. The nursing
shortage is considered to be world-wide problem and in many
countries, including Turkey, facing a shortage of nurses.
According to the OECD report, Turkey takes the last place among
51 countries in European region in terms of the number of
nurses per 1000 individuals. In other words, Turkey had the
fewest nurses having fewer than five nurses per 1000 in the
Europe (OECD, 2010). This alarming fact suggests that further
research is needed to clarify the extent of nursing students’
experiences of bullying and the practical effects on their
choices.
In contrast to previous studies on bullying in nursing
education, this study shows that students preferred active
responses to cope with bullying instead of using unhealthy and
passive coping behaviors which were found in other studies
(Celik & Bayraktar , 2004; Celebioglu et al, 2010; Cooper et
al; 2009; 2011 ). When coping responses of nursing students
considered in four categories; the most frequently reported
responses to bullying were active responses, such as rectify
by talking face to face (71.74%), report to superiors (70.76%),
tell to friends (67.77%), seek legal charges (42.5%), and share
with family members (45.15 %). Additionally, passive responses
were used by some of students such as work harder and more
organized to avoid criticism (67.13%), pretend not to see it
(26.94 %), do not take it seriously (16.20%), and did nothing
(17.29 %). Some of the respondent preferred aggressive
responses; shout or snap at the bully (34.86 %), and
demonstrated similar behaviors (18.68%). However, unhealthy
responses were reported rarely such as use of unhealthy coping
behavior such as drinking or taking medications (11.97%). As
is noticed from the Table 4, the respondents reported
discussing the bullying incidents more frequently with friends
and family members rather than with their nursing instructors
or counselors. This result shows that instructors or lecturers
at nursing school need to create open atmosphere in which
students are willing to share their stories and seek guidance
in dealing with the situation as suggested by Longo (2007:
178).
These findings are similar to Einarsen’s study (2000) which was
found that bullying victims actively use a problem-solving
process and when they cannot solve the problem they leave the
institution. The result indicates that latest studies and some
court case have a good effect on people comprehension of
bullying as a work life problem. The respondents in this study
seem to be aware of bullying, but as is mentioned in previous
section, the nursing schools have no policy or procedure about
the bullying phenomenon therefore, nursing students try to cope
with bullying and harassment paddling theirs own canoe. This
study suggests that nursing schools should provide anti-
bullying policies and procedures to allow students to cope with
bullying properly.
Study limitations
Some methodological limitations of the present study need to be
mentioned. Firstly, the data reported are based on self-
reports which suggest problems with both common method variance
and issues of validity in the classification of victims as is
presented by Einarsen (1996). This type of research enables
measuring only perceptions, not the actual behaviors and this
study is subject to single-rater bias as only the students’
responses have been considered. The present study does not
include any information from the nursing school’s staff and the
hospital’s staff or independent observers confirming the
victimization reported. Therefore, it would be beneficial if
multiple data collection methods and multiple raters are used
in the future study.
Secondly, the number of people participated into the study
located in one certain part of the country and although they
were representative of the total population of nursing students
in this area the obtained results could not be generalized.
Future research could focus on larger samples from different
nursing schools in all over the country. In addition, students
in the western part of the country where the present research
took place may not be more likely to experience aggressive
incidents than those in some parts of the Turkey which are more
rural and have less educated population. In the future, a
cross cultural study can be more instrumental in investigating
bullying and harassment at nursing school.
Finally, as is mentioned in the study of Ferns and Meerabeau
(2007) questionnaire approaches may be accused of bias due to
an unrepresentative sample because people who do not return
questionnaires frequently differ from those who do. But, in
this study the response rate is quite high (92 %) this may
offer confidence in the findings.
Conclusion
The findings of the study have found that nursing students
experience high levels of bullying and harassment during their
education. Work related bullying were the most frequently
encountered type of bullying behaviors followed by personal
related bullying behaviors. It is seen that bullying in
nursing education is detrimental to the health and well-being
of students, and to the provision of quality nursing care.
Moreover, our analyses have shown that there was no significant
relationship between reported bullying behaviors and age,
marital status, place of birth, participant’s place of living,
and participant’s attending nursing school. This may suggest
that bullying can happen to anyone, regardless of their age,
gender or education etc.
This study supports previous reports of bullying against
Turkish student nurses (Celebioglu et al, 2010; Celik &
Bayraktar ; 2004) and adds to the scant body of literature
showing that nursing students often experience bullying and
harassment from clinical nurses (Horizontal bullying), and
importantly, this may influence their future employment
choices. Moreover, although educators need to be sensitive to
its occurrence and assist students to deal with it, but our
findings show that the school and lecturer also considerable
source of the bullying behaviors. Nursing students were exposed
to bullying and harassment in both the practice settings and
the educational settings, as suggested by Randle (2003) there
is concern that students may begin to assimilate this conduct
into their practice, perpetuating the behavior. For this
reason, the aspect of bullying in nursing education need to be
crucially taken into consideration in order to stop this
vicious cycle of bullying in nursing profession.
As is recommended by the American Association of Colleges of
Nursing Position Statement, all faculties (schools of nursing)
prepare nurses to recognize and prevent all form of violence in
the workplace. Nursing students also should be treated fairly
and consistently, and with respect and dignity, wherever they
study or undertake practice placements (AACN, 2011). Therefore
strategies to increase students’ awareness of this problem and
its potential consequences are indicated. Reliable procedures,
education, follow up and organizational policies and clear
statement of a “Zero Tolerance” approach are needed to diminish
workplace bullying and to prevent its negative consequences.

REFERENCES
American Association of College of Nursing (AACN). (2011).
Hallmarks of the Professional Nursing Practice Environment, Retrieved
from
http://www.aacn.nche.edu/publications/positions/hallmarks.ht
m
Aquino, K., & Thau, S. (2009). Workplace victimization:
Aggression from the target`s perspective. Annual Review of
Psychology. 60, 717-741.
Bartholomew, K. (2006). Ending Nurse-to-Nurse Hostility: Why Nurses Eat
Their Young and Each Other. HCPro: Marblehead, MA
Brodsky, C. (1976). The harassed worker. Toronto: LexingtonBooks, DC Heath Company.
Celebioglu A., Akpinar R.B., Kucukoglu, & Engin R. (2010).
Violence experienced by Turkish nursing students in clinical
settings: their emotions and behaviors. Nurse Education Today,
30, 687-691.
Celik, S.S., & Bayraktar, N. (2004). A study of nursing student
abuse in Turkey. Journal of Nursing Education, 43(7), 330-336.
Celik, S.S., Celik, Y. Agirbas, & Ugurluoglu O. (2007). Verbal
and physical abuse against nurses in Turkey, International
Nursing Review, 54, 359-366.
Cooper, J.R.M., Walker, J.T., Askew, R., Robinson J.C., &
McNair M. (2011). Students` perceptions of bullying
behaviors by nursing faculty. Issues in Educational Research,
21(1), 1-21.
Cooper, J.R.M., Walker, J.T., Winters K., Williams R.P., Askew
R., & Robinson J.C. (2009). Nursing students` perceptions of
bullying behaviors by classmates. Issues in Educational Research,
19(3), 1-13.
Cox, H.C. (1987). Verbal abuse in nursing: Report of a study.
Nursing Management, 18 (11), 47-50.
Curtis, J. Bowen I., & Reid A. (2007). You have no credibility:
Nursing students` experiences of horizontal violence. Nurse
Education in Practice, 7, 156-163.
Efe, S.Y. & Ayaz, S. (2010). Mobbing against nurses in the
workplace in Turkey. International Nursing Review, 57, 328-334.
Einarsen, S., Hoel H., Z., & Cooper C.L. (2011). Bullying and
Harassment in the Workplace: developments in theory, research, and practice,
Second Edition, New York: Taylor and Francis.
Einarsen, S., Hoel H., Zapf D., & Cooper, C.L. (2003). The
concept of bullying at work: the European tradition. In S.
Einarsen, H. Hoel, D. Zapf, & C.L. Cooper (Eds.), Bullying and
Emotional Abuse in the Workplace International Perspectives in Research and
Practice, (pp. 3-30). London: Taylor and Francis.
Einarsen, S., Matthiesen, S.B., & Skogstad A. (1998). Bullying,
burnout and well-being among assistant nurses. Journal of
Health Safety, 14(6)563–568.
Einarsen, S., & Raknes. B.I. (1997). Harassment at work and the
vicimization of men. Victims and Violence, 12, 3; 247-263.
Einarsen, S. (2000). Harassment and bullying at work: A review
of the Scandinavian approach. Aggression and Violent Behavior, 5,
379-401.
Einarsen, S. (1999). The nature and causes of bullying at work.
International Journal of Manpower, 20(1/2), 16-27.
Ferns, T., & Meerabeau, L. (2007). Verbal abuse experienced by
nursing students. Journal of Advanced Nursing, 61( 4), 436-444.
Ferns, T. (2006), Under-reporting of violent incidents against
nursing staff. Nursing Standard, 20(40), 41-45.
Gok, A. U., & Kocaman G. (2011). Reason for leaving nursing: A
study among Turkish Nurses. Contemporary Nurse, 39(1): 75-84.
Hinchberger, P.A. (2009). Violence against female student
nurses in the workplace. Nursing Forum, 44(1), 37-46.
Hodgkinson, P.E., Mclvor, L., & Phillips M. (1985). Patient
assaults on staff in a psychiatric hospital: a two year
retrospective study. Medicine, Science and Law, 11(1), 5-11.
Hoel, H., Rayner, C., & Cooper C. L. (1999). Workplace
bullying, In C.L. Cooper, & I.T. Robertson (Eds.),
International Review of Industrial and Organizational Psychology (pp. 195-
230). Chichester: John Wiley and Sons.
Inoue, M., Tsukano, K., Muraoka, Mitsutaro, Kaneko, F., &
Okamura, H. (2006). Psychological impact of verbal abuse and
violence by patients on nurses working in psychiatric
departments. Psychiatry and Clinical Neurosciences, 60 (1), 29–36.
Keashly, L. (1998). Emotional abuse in the workplace:Conceptual and empirical issues. Journal of Emotional Abuse, 1, 85-117.
Keely, B.R. (2002). Recognition and prevention of hospital
violence. Dimensions of Critical Care Nursing, 21 (6), 236-24.
Kisa, S. (2008). Turkish nurses` experiences of verbal abuse at
work. Archives of Psychiatric Nursing, 22(4), 200-207.
Kuehn, B.M. (2010). Violence in health care settings on rise.
Journal of the American Medical Association, 304(5), 511-512.
Lewis, M. (2006). Nurse bullying: organizational considerations
in the maintenance and perpetration of health care bullying
culture. Journal of Nursing Management, 14, 52-58.
Leymann, H. (1990). Mobbing and psychological terror atworkplaces. Violence and Victims, 5, 119–126.
Longo, J. (2007). Horizontal violence among nursing students.
Archives of Psychiatric Nursing, 21(3), 177-178.
Magnavita, N., & Heponiemi, T. (2011). Workplace violence
against nursing students and nurses: an Italian experience.
Journal of Nursing Scholarship, 43(2), 203-210.
Magnussen, L., & Amundson, M. J. (2003). Undergraduate nursing
student experience. Nursing and Health Sciences, 5, 261-267.
Nielsen, M.B., Notelaers, G., & Einarsen S. (2011). Measuring
exposure to workplace bullying. In. S. Einarsen, H. Z. Hoel,
& C.L. Cooper (Eds.), Bullying and Harassment in the Workplace:
developments in theory, research, and practice, Second Edition, New
York: Taylor and Francis.
Notelaers, G., Einarsen S., DE Witte, H., & Vermunt, J. (2006).
Measuring exposure to bullying at work: Validity and
advantages of the latent class cluster approach. Work and
Stress, 20 (4), 289-302.
Notelaers, G. (2011). Workplace Bullying: A risk Control Perspective,
Dissertation for the degree of philosophies doctor (PhD),
University of Bergen, Norway.
OECD. (2010). Health at a Glance: Europe 2010, OECD Publishing.
Retrieved from http://dx.doi.org/10.1787/health_glance-2010-
en
Oztunc, G. (2006). Examination of incidents of workplace verbal
abuse against nurses. Journal of Nursing Care Quality, 21(4), 360-
365.
Ozturk, H., Sokmen, S., Yilmaz, F., & Cilingir, D. (2008).
Measuring mobbing experiences of academic nurses:
Development of a mobbing scale. Journal of the American Academy of
Nurse Practitioners, 20(9), 435-442.
Pinar, R., & Ucmak F. (2010). Verbal and physical violence in
emergency departments: a survey of nurses in Istanbul,
Turkey. Journal of Clinical Nursing, 20, 510-517.
Pranjic, N., Males-Bilic, L., Beganlic, A., & Mustajbegovic, J.
(2006). Mobbing, stress and work ability index among
physicians in Bosnia and Herzegovina: Survey Study. Croatian
Medical Journal, 47, 750-758.
Quine, L. (2001). Workplace bullying in nurses”, Journal of Health
Psychology, 6(1), 73-84.
Randle, J. (2003). Bullying in the nursing profession. Journal of
Advanced Nursing, 43(4), 395-401.
Stevens, S. (2002). Nursing Workplace Retention: Challenging A
bully Culture. Health Affairs, 21(5), 189-193.
Uzun, O. (2003). Perceptions and experiences of nurses in
Turkey, about verbal abuse in clinical settings. Journal of
Nursing Scholarship, 35(1), 81-85.
Yildirim, A., & Yildirim, D. (2007). Mobbing in the workplace
by peers and managers: Mobbing experienced by nurses working
in healthcare facilities in Turkey and its effect on nurses.
Journal of Clinical Nursing, 16(8), 1444-1453.
Zapf D., Escartin J., Einarsen S., Hoel H., & Vartia M. (2011).
Empirical findings on prevalence and risk groups of bullying
in the workplace. In S. Einarsen, H. Z. Hoel, & C.L. Cooper
(Eds.), Bullying and Harassment in the Workplace: developments in theory,
research, and practice, Second Edition, New York: Taylor and
Francis.
Serap Palaz PhD MA is an associate professor in the Departmentof Labor Economics and Industrial Relations at University ofBalikesir, Turkey. She received her doctorate degree from DeMontfort University in England in 1999. She was served as thedirector of Bandirma Health School at University of Balikesirduring the period of January, 2007 to January 2011. Herresearch priorities are labor market discrimination andbullying at workplace. Her main duties at University ofBalikesir include teaching social policy, labor economics andconducting research on various subjects relating to bullying atworkplace recently.
.





















