Transcultural Nursing
225
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Transcultural Nursing


CONTEMPORARY NURSE · APRIL 2008 · VOLUME 28 · ISSUE 1–2
Edited by
AKRAM OMERIAdjunct Associate Professor, University of Western Sydney NSW, Australia
and
MARILYN McFARLANDAssociate Professor, University of Michigan, Flint MI, USA
ISBN 978-0-9757710-5-1
ee ontent PTYLTDmanagementC
Sydney • Amsterdam • Palo Alto
SECOND EDITION
Advances in ContemporaryTranscultural Nursing
Transcultural nursing:Pathways of cultural awareness
CNJ 28_1_2_prelims.qxd 14/07/2008 12:04 PM Page i

Published in Australia by:eContent Management Pty LtdPO Box 1027, MalenyQLD 4552, Australia
Tel. +61-(0)7-5435 2900Fax: +61-(0)7-5435 2911E-mail: [email protected]
ABN 87 091 432 567 SAN 902-4964
Affiliates in: Sydney, Amsterdam, Palo Alto
A special issue of the Contemporary Nurse journal: Volume 28 Issue 1–2 (April 2008)
Advances in Contemporary Nursing – ISSN 1832-9861 – 4 volumes per annum from 2006
2008:Volume 9: Advances in Contemporary Aged Care – ISBN 978-0-9757710-1-3Volume 10: Advances in Contemporary Palliative and Supportive Care – ISBN 978-0-9757710-4-4Volume 11: Advances in Contemporary Transcultural Nursing, 2nd edn – ISBN 978-0-9757710-5-1Volume 12: Advances in Contemporary Nursing History & Midwifery in Australia – ISBN 978-0-9775742-8-5
2007:Volume 5: Advances in Contemporary Indigenous Health Care – ISBN 978-0-9750436-9-1Volume 6: Advances in Contemporary Community and Family Health Care – ISBN 978-0-9757710-2-0Volume 7: Advances in Contemporary Nurse Recruitment and Retention – ISBN 978-0-9757710-0-6Volume 8: Advances in Contemporary General Practice Nursing – ISBN 978-0-9757710-3-7
2006:Volume 1: Advances in Contemporary Transcultural Nursing – ISBN 978-0-9750436-1-5Volume 2: Advances in Contemporary Child and Family Health Care – ISBN 978-0-9750436-3-9Volume 3: Advances in Contemporary Mental Health Nursing – ISBN 978-0-9759436-8-4Volume 4: Advances in Contemporary Nursing and Interpersonal Violence – ISBN 978-0-9750436-6-0
Contact the publisher for annual subscription details (Boxed Sets): [email protected]
Advances in Contemporary Transcultural Nursing, Second Edition
BibliographyISBN 978-0-9757710-5-1
1. Transcultural nursing 2. Transcultural nursing – case studies 3. Culture care theory 4. Ethnonursing 5. Cultural competency 6. Nurse leadership 7. Faith-based health8. Muslim health 9. Indigenous health 10. Collaboration
I. Omeri, Akram II. McFarland, Marilyn
(Series: Advances in Contemporary Nursing – ISSN 1832-9861)
© 2008, eContent Management Pty Ltd
This publication is copyright. Other than for purposes of and subject to the conditions prescribed under the Copyright Act, no part of it may in any form or by any means (electronic, mechanical, microcopying, photocopying, recording or otherwise) be reproduced, stored in a retrieval system or trans-mitted without prior written permission. Inquires should be addressed to the Publisher at: [email protected]
Publisher: James H. Davidson, eContent Management Pty LtdPeer Review Coordinator: Jenny Gibson, eContent Management Pty LtdPrinted in Malaysia by Vivar Printing Sdn Bhd, Selangor D.E.
CNJ 28_1_2_prelims.qxd 14/07/2008 12:04 PM Page ii

NCCopyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: iii–v.
FOREWORD
iiiVolume 28, Issue 1–2,April 2008 CCCCNNNN
Transcultural nursing continues to expandworldwide to provide culturally congruent
care to cultures that in the past have often been overlooked, avoided, feared, neglected, or misunderstood. From the beginning of trans-cultural nursing, the goal of this new disciplinehas been to provide humanistic, safe, and mean-ingful care to people of diverse cultures in the world. Slowly, this goal is being promoted and maintained by nurses and other healthproviders who have been prepared in the field.These transcultural nurses contend that all cul-tures have a right to have their values, beliefs, andlifeways recognised, respected, and upheld for theirhealth and well-being.
It is most encouraging to have this SecondIssue come forward to move further to examinecontemporary trends and advances in transcul-tural nursing. Dr Akram Omeri and Dr MarilynMcFarland are to be commended for their lead-ership. For several decades, Dr Omeri has beenan outstanding leader in multicultural Australiato prepare nurses to provide transcultural nurs-ing care. She has been a very active leader to ini-tiate undergraduate and graduate seminars for
nurses and nursing students with field experi-ences in transcultural nursing. Dr Omeri hasconducted several noteworthy and breakthroughresearch studies on local and indigenous culturesin Australia.These enthonursing research studieswere the first of their kind in the country. As aconsequence, Dr Omeri has served as an out-standing role model for research and educationin transcultural nursing and to stimulate nursesto discover new ways to serve diverse cultures.
Dr Omeri was the first Australian nurse toobtain graduate preparation in transculturalnursing. She became the first certified transcul-tural nurse in Australia and provided a pathwayto help local (including Indigenous) nurses tobecome transcultural nurses. Dr Omeri was thefirst to create the TCN-Cooperative Society(RCNA) which has been a very influential forcenationally and internationally for transculturalnursing. She has been active in local, nationaland international transcultural programs throughthe Royal College of Australia’s dynamic pro-grams. She has been an outstanding role model,advocate and pioneer leader to open the doorsto study and practice transcultural nursing. She
MADELEINE M LEININGERPhD, LHD, DS, RN, CTN, FRCNA, FAAN
Professor Emeritus of NursingCollege of Nursing Wayne State University
Detroit MI, USA andThe University of Nebraska Medical Centre
College of NursingOmaha NE, USA and
FounderTranscultural Nursing and Human Care Research
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page iii

was also the first to be awarded the Dis-tinguished TCN Scholar Award by the Trans-cultural Nursing Society, and the prestigiousLeininger Award in 1998. Dr Omeri has beenactive in many other ways to promote, maintain,and establish transcultural nursing standards ofpractice in teaching, research, and education.Her leadership in Australia has been outstandingand appreciated. This special issue of the Con-temporary Nurse journal, Advances in ContemporaryTranscultural Nursing, 2nd edition, is truly anoth-er creative venture from Professor Omeri.
Marilyn McFarland received her doctorate innursing with a focus on transcultural nursingunder the mentorship of Dr Madeleine Leining-er at Wayne State University, Detroit MI (USA)in 1995, and is currently an associate professorof nursing at the University of Michigan-Flint,USA where she teaches at the undergraduateand graduate levels.
Dr McFarland has directed her professionalwork toward the care and study of elders fromdiverse cultures throughout the United States.She is a former editor of the Journal of Trans-cultural Nursing and is active worldwide in theTranscultural Nursing Society. Dr McFarlandalso teaches transcultural nursing courses andpresents her research findings about the culturecare of elders locally, nationally and worldwide.As a Certified Transcultural Nurse and as anAmerican Nurse Credentialing Center (ANCC)certified family nurse practitioner, Dr McFar-land integrates transcultural knowledge and careinto her primary care clinical practice.
This second edition of Advances in ContemporaryTranscultural Nursing builds upon the first edition(Volume 15 Issue 3, October 2003). However,the second goes further and focuses on contem-porary transcultural nursing practices, researchand education to provide culturally congruentcare.This is the central purpose and goal of tran-scultural nursing. Of special interest, this vol-ume will focus on human rights of immigrantsand refugees as they transition from one geo-political and ecological area to many different
places in the world.This transition is often verydifficult as cultures move from very differentenvironments in which political, economic, andcultural factors are extremely ambiguous anduncertain for immigrants. Transcultural nursesprepared through graduate education programswith guided mentoring experiences by qualifiednurse instructors are skilled in ways to respondappropriately to immigrant care needs as theyattempt to maintain their cultural beliefs andpractices as they adapt to new lifeways.
Dr Omeri and Dr McFarland, as transculturalspecialists, are keenly aware that historical andpolitical factors play a major role in health andillness conditions for refugees and immigrants.These transcultural nursing specialists can iden-tify diverse cultural forces that influence illnessand well-being.They can help immigrants adjustto complex and difficult situations in meaningfulways. It is, therefore, encouraging that this issuewill explicitly address these factors, especiallyhuman rights and cultural beliefs and values ofimmigrants and refugees.
In keeping with the philosophy and goals of transcultural nursing, specific cultural val-ues, needs and practices of different cultureswill be emphasized. In-depth studies of cultureswill be essential to advance nursing care knowl-edge to provide culturally congruent care andto identify new practices that are beneficial to cultures. Accordingly, diverse theoreticalapproaches and both qualitative and quantita-tive research methods will be encouraged. Inaddition, the search for care universals or com-monalities and diversities among and betweencultures will continue to be explored in keep-ing with the nature and unique focus of tran-scultural nursing.
This second edition is most timely to advancetranscultural nursing knowledge and to encour-age interdisciplinary dialogue. Currently, manydisciplines are just beginning to discover theimportance of culturally congruent care andtranscultural education and practice, so they willfind this publication a welcome addition to their
iv Volume 28, Issue 1–2,April 2008CCCCNNNN
Madeleine M LeiningerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page iv

endeavors. As all health disciplines realise thatglobalisation is a major focus in our world, tran-scultural education and practice will be recog-nised as essential in our world today and in thefuture. Fortunately, the knowledge and practicesof transcultural nursing established since theearly 1950s will become more fully recognisedand appreciated as globalisation increases andhealthcare becomes transformed from largely aunicultural to a multicultural focus. This issuewill show ways that transcultural nursing will be
valued as a discipline to meet the essential needsof diverse cultures. Undoubtedly, many newinsights and practices will be forthcoming fromthis edition as well as reaffirming knowledgeand practices already established in transculturalnursing.
Dr Omeri and Dr McFarland are to be ap-plauded for the issue and its special transculturalfoci. I welcome the contribution of authors tothis transcultural nursing publication in order toadvance the status of the discipline.
vVolume 28, Issue 1–2,April 2008 CCCCNNNN
Foreword CCCCNNNN
ADVANCES IN CONTEMPORARY TRANSCULTURAL NURSING 2ND EDN
Edited by Akram Omeri and Marilyn McFarland
ISBN: 978-0-9757710-5-1; xii + 212 pages; softcover
A special issue of Contemporary Nurse (Volume 28, Issue 1–2, April 2008)
Prices include airmail freight on all orders and GST (for Australian customers)North America, Europe, North East Asia & Middle East: Institutions US$148.50; Individuals US$77.00ANZ, Pacific, South & South East Asia, South America & Africa: Institutions AU$148.50; Individuals AU$77.00 incl postage. Students receive a 20% discount on the respective individual price
Number of copies: Total: US$ Total: AU$
A cheque made payable to eContent Management Pty Ltd is enclosed OR
Please charge this purchase to my Mastercard/Visa/Bankcard
My full card number is: / / / Expiry date: /
Cardholder Name: Signature:
Please send this order to the address below by airmail:
Name of Institution: Name of Individual:
Street address (or PO Box):
City: State: Zipcode: Country:
Tel. (with area code): Fax: (with area code):
Email: Your reference:
Fax the completed order form to +61-7-5435-2911 or post with cheque to:eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Email: [email protected]
www.contemporarynurse.com
O R D E R F O R M
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page v

Published byeContent Management Pty Ltd
PO Box 1027, Maleny QLD 4552, Australia
(SAN 902-4964)
Contemporary Nurse is aggregated/indexed/listed in:Thomson ISI’s Science Citation Index (SCIE) & Social
Science Index (SSCI), NLM’s Medline, EmCare, Scopus,PsycINFO, CINAHL, Meditext, Cengage, ProQuest,
EBSCO Publishing,Atypon, eBrary, MyiLibrary,NetiLibrary, Questia, eBooks Corp., EBSCOHost,
International Nursing Index, CSA Illumina, Cabell’s,Ulrich’s Periodicals and DEST Register of Refereed Journals
VOLUME 28 · ISSUE 1–2 · APRIL 2008CONTENTS
NCvi Volume 28, Issue 1–2,April 2008CCCCNNNN
iii FOREWORD — Madeleine M Leininger
ix PREFACE: Pathways of cultural awareness — Akram Omeri
SECTION 1: TRANSCULTURAL NURSING LEADERSHIP ANDEDUCATION
1 EDITORIAL: The state of transcultural nursing global leadership andeducation — Linda J Luna and June Miller
Leadership in transcultural nursing3 The role of RCNA in promoting transcultural nursing as a
discipline of study, research, practice and management in Australia— Rosemary B Bryant, Elizabeth R Foley and Elizabeth C Percival
13 COMMENTARY: Global leadership in transcultural practice, educationand research — Margaret M Andrews
Transcultural nursing education17 EXEMPLAR: Developing a new Bachelor of Nursing course
responsive to Australia’s culturally diverse community — Lynette M Raymond
23 Use of the culture care theory and ethnonursing method todiscover how nursing faculty teach culture care — Sandra J Mixer
37 Cultural competency of graduating US Bachelor of Sciencenursing students — Suzan Kardong-Edgren and Josepha Campinha-Bacote
FI
NA
LI
SS
UE
OF
TH
IS
VO
LU
ME
SECOND EDITION
Advances in ContemporaryTranscultural Nursing
CNJ 28_1_2_internal.qxd 31/07/2008 12:46 PM Page vi

viiVolume 28, Issue 1–2,April 2008 CCCCNNNN
VOLUME 28 · ISSUE 1–2 · APRIL 2008
SECTION 2: APPLICATION OF TRANSCULTURAL NURSINGTHEORY AND MODELS TO PRACTICE
45 EDITORIAL: Transcultural nursing theory and models:The challenges of application — Irena Papadopoulos and Akram Omeri
48 Culture care theory: A proposed practice theory guide for nursepractitioners in primary care settings — Marilyn M McFarland andMarilyn K Eipperle
64 A partnership of a Catholic faith-based health system, nursing andtraditional American Indian medicine practitioners — Ann O Hubbert
74 Lebanese cancer patients: Communication and truth-tellingpreferences — Myrna Abi Abdallah Doumit and Huda Huijer Abu-Saad
83 Bridging generic and professional care practices for Muslimpatients through use of Leininger’s culture care modes — Hiba Wehbe-Alamah
SECTION 3: TRANSCULTURAL NURSING RESEARCH:WHERE IS THE EVIDENCE?
98 EDITORIAL: Towards a culturally competent nurse workforce —Rhonda Griffiths AM and John Daly
101 Expectations and experiences of recently recruited overseasqualified nurses in Australia — Scott Brunero, Julie Smith and Emma Bates
111 A reflection on culture over time by Baccalaureate nursingstudents — Hendrika J Maltby
119 Integrative simulation: A novel approach to educating culturallycompetent nurses — Carolyn M Rutledge, Phyllis Barham, Lynn Wiles,Richardean S Benjamin, Phyllis Eaton and Kay Palmer
129 Cultural competence in action for CAMHS: Development of acultural competence assessment tool and training programme —Irena Papadopoulos, Mary Tilki and Savita Ayling
141 Cultural desire: ‘Caught’ or ‘taught’? — Josepha Campinha-Bacote
CONTENTS
Continues ...
FI
NA
LI
SS
UE
OF
TH
IS
VO
LU
ME
SECOND EDITION
Advances in ContemporaryTranscultural Nursing
CNJ 28_1_2_internal.qxd 30/07/2008 9:45 PM Page vii

viii Volume 28, Issue 1–2,April 2008CCCCNNNN
149 Perception of nursing care: Views of Saudi Arabian female nurses— Jette Mebrouk
SECTION 4: GLOBAL AGENDA IN TRANSCULTURAL NURSING162 EDITORIAL: Transcultural nursing: The global agenda —
Marilyn (Marty) Douglas and Juliene G Lipson165 Culture-specific care for Indigenous people: A primary health
care perspective — Anne McMurray and Rani Param173 The significance of a culturally appropriate health service for
Indigenous Ma-ori women — Denise Wilson189 Nursing care of vulnerable populations using a framework of
cultural competence, social justice and human rights — Dula F Pacquiao
198 Nurses on the move: Diversity and the work environment — Mireille Kingma
207 EPILOGUE: Advancing transcultural nursing through collaboration— Akram Omeri
BOOK REVIEWS211 Culture Care Diversity and Universality:A Worldwide Nursing Theory,
2nd edition, by Leininger MM and McFarland MR (Eds) — Rick Zoucha
212 Transcultural Concepts in Nursing Care, 5th edition, by Andrews Mand Boyle J — Sandra J MixerF
IN
AL
IS
SU
EO
FT
HI
SV
OL
UM
E
F I N A L I S S U E O F T H I S V O L U M E
VOLUME 28 · ISSUE 1–2 · APRIL 2008CONTENTS
SECOND EDITION
Advances in ContemporaryTranscultural Nursing
This Contemporary Nurse special issue is available for sale independently under its ISBN (978-0-9757710-5-1), or as part of the
Advances in Contemporary Nursing series, ISSN 1832-9861, Volume 11
C O U R S E R E A D E R
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page viii

NCCopyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: ix–xi.
PREFACE
ixVolume 28, Issue 1–2,April 2008 CCCCNNNN
Transcultural nursing anticipates similaritiesand differences in health care and health
care systems and nursing practices withindiverse cultural contexts and societies. Globaldevelopment of the discipline of transculturalnursing is dependent upon international collab-orative research efforts and the dissemination ofknowledge worldwide.
This Contemporary Nurse special issue on transcultural nursing, Advances in ContemporaryTranscultural Nursing, 2nd edition, is a major col-laborative endeavour that aims to share evi-dence-based transcultural nursing knowledgetoward advancing and improving care in cultur-ally meaningful ways to clients, families andcommunities. It is intended to make a majorcontribution to the dissemination of transcultur-al nursing knowledge locally and internationally.
The diverse content is structured aroundfour major themes encompassing: leadershipand education; the application of models andtheories to practice; research evidence for prac-tice and transcultural nursing research incorpo-rating principles of social justice, human rights,
compassion, and human dignity. The four sec-tions of this special issue provide a broad viewof the discipline of transcultural nursing, thescope of its interests and the application ofresearch based transcultural nursing knowledgein education, research and practice.
Section 1: Transcultural nursingleadership and educationOn transcultural nursing leadership, RosemaryBryant, Elizabeth Foley and Elizabeth Percivalpresent a historical perspective of how transcul-tural nursing emerged as a discipline of study,practice and research and the national leader-ship of a national organisation in promotingtranscultural nursing in Australia. MargaretAndrews, highlights the global leadership oftranscultural nursing(TCN) by the founder ofthe discipline, Madeleine Leininger, and discuss-es the leadership of Australian nurses in globaltranscultural nursing. These two papers high-light the significance of both national and globalleadership in TCN.
On transcultural nursing education, LynnetteRaymond highlights issues surrounding thedevelopment of a Bachelor of Nursing courseresponsive to cultural diversity. She discussesfactors that influenced the development oflearning outcomes that would enable studentnurses the opportunity to develop the knowl-edge, skills, and attitudes needed to advancepersonal and professional cultural awareness ofself and others appropriate to the Australiancontext and delivery of culturally congruent
Pathways of cultural awareness
DR AKRAM OMERIPhD, RN, CTN, FRCNA
Guest EditorAdvances in ContemporaryTranscultural NursingAdjunct Associate ProfessorUniversity of Western SydneySchool of NursingSydney NSW, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page ix

and safe nursing care for practice. Sandra Mixer,reflects upon a detailed literature reviewdemonstrating how faculties use culture-caretheory and the ethnonursing method to teachculture care.The literature revealed that despite50 years of transcultural nursing knowledgedevelopment through theory, research, andpractice; there remains a lack of formal, inte-grated cultural education in nursing. Culturalcompetencies of graduating US BSN students isrevealed in a joint research article by SuzanKarding-Edgren and Josepha Campinha-Bacote.
Section 2: Application oftranscultural nursing theory and models to practiceMcFarland and Eipperle propose Leininger’sTheory of Culture Care Diversity and Univer-sality as a basis for the educational preparation,primary care contextual practice, and outcome-focused research endeavors of advanced practicenursing. Ann Hubbert presents a historical part-nership between an American Catholic faith-based, urban hospital and a program sponsoredby a Comanche medicine man on the spirituali-ty of American Indian Traditional Indian. Cul-ture care theory is applied in discussion of thesepast experiences to explore the relationshipsamong and between the participating cultures.
Myrna Doumit and Huda Abu-Saad Huijerreport on a study of the lived experiences ofLebanese cancer patients. Using the UtrechtSchool of Phenomenology, semi-structured in-terviews with ten cancer patients and subse-quent analysis and synthesis of raw data revealedthat cancer patients expressed the need for aclear and truthful communication with healthcare professionals and family members. HibaWehbe-Alamah shares knowledge of traditionalMuslim generic (folk) care beliefs, expressions,and practices derived from research and des-criptive sources in order to assist nurses andother health care professionals to integrategeneric care practices into professional carepractices.
Section 3: Transcultural nursingresearch: Where is the evidence?A number of studies in this section are used asevidence-base for practice. Brunero, Smith andBates examined the experiences and needs of agroup of Overseas Qualified Nurses’(OQN’s) ata major metropolitan tertiary referral hospitalin Australia.The study reports an organisationaland personal approach undertaken to assist inthe process of adjustment of the participatingONQ’s into the nursing workforce in the con-text of the tertiary institution where the studytook place. In a retrospective descriptive study,Henrietta Maltby reports on reflective res-ponses by 85 junior nursing students to 126questions on culture over time. Analysis of ver-batim descriptors by participants revealed thatcultural competency although not yet fullyoperationalised in the nursing profession is adevelopmental process that goes across time andis more than learning about cultures.
Rutledge et al examine a new approach ineducating culturally competent nurses. ‘Integra-tive simulation’ is used to provide culturallydiverse learning opportunities for both univer-sity and distance mode students. Cases aredeveloped using focus groups and individualinterviews. Papadopoulos, Tilki and Aylingdetail the development of a tool to measure cul-tural competence of individuals working withinthe Children and Adolescent Mental Health Ser-vices (CAMHS).
Jospha Campinha-Bacote explores the con-struct of cultural desire in an attempt to identi-fy meaningful ways that cultural desire cannotonly be ‘caught’ by faculty who model this construct, but also be ‘taught’ within nursingcurricula as a functional component of culturalcompetence. Cultural desire is one construct ofCampinha-Bacote’s model of cultural compe-tence.
Jette Mebrouk reports the findings from aphenomenological research study on percep-tions of nursing care by Saudi Arabian femalenurses practicing in the context of Saudi Arabia.
x Volume 28, Issue 1–2,April 2008CCCCNNNN
Akram OmeriCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page x

Using in-depth semi-structured interviews withfive nurses participating in the study revealedthat perception of care is closely linked toIslamic values.
Section 4: Global agenda intranscultural nursing Papers included in this section illustrate thenature and scope of transcultural nursing as aglobal endeavour. By incorporating the princi-ples of social justice, human rights, compassion,and human dignity, transcultural nurses aim toprovide culturally competent care to fellowworld citizens, irrespective of their cultural ori-gins, human condition or social situation.
Ann McMurray and Rani Param describehow structural, historical and political factorshave contributed to the negative health statusand health outcomes of Australia’s Indigenouspeoples. The authors recommend strategies for overcoming barriers and biases relating toindigenous health. Denise Wilson describesresearch exploring the health perceptions ofMaori women and their interaction with ‘main-stream’ health care services. Findings of theresearch provide guidance for her recommenda-tions for culturally competent practice for theseMaori women.
Dula Pacquiao presents a picture of vulnera-ble populations using a framework of culturalcompetence, social justice and human rights.She states that transcultural nursing mandatesthat the principles of social justice, human rightsand cultural competence extend as much to
our professional colleagues as they do to ourpatients and clients. Mireille Kingma raises con-sciousness of the scope and magnitude of theinternational nurse recruitment efforts andidentifies the types of abuse, discrimination andexploitation reported by migrant nurses andadvocates for the development of strategies toprevent and deal with such matters in the nameof saving nursing and the profession.
Being mindful of the diverse views and ap-proaches in papers submitted, and based uponreviewed evidence-based literature above, weadopted an open mind, taking into account two major constructs essential in transculturalnursing namely ‘Culture and Care’ and howsubmitted papers could appropriately informpractice toward culturally competent nursingcare.
This special issue, on Advances in ContemporaryTranscultural Nursing builds upon the enormouswealth of evidence-based transcultural nursingknowledge from many parts of the world.
AcknowledgmentsWe are grateful to all those who made submis-sions to this issue. We also acknowledge thecontributions of all who in one way or anotherhave participated in promoting the discipline oftranscultural nursing in Australia and globally.
We extend our special acknowledgement toSandy Lovering for her contributions during ini-tial planning of this special issue and to HelenHamilton, Consulting Editor, for her kind andgenerous editing upon request.
xiVolume 28, Issue 1–2,April 2008 CCCCNNNN
Preface: Pathways of cultural awareness CCCCNNNN
Indigenous Education and theAdventure of Insight: Learning andteaching in indigenous classroomsby Neil HarrisonISBN 1-876682-59-0; $55.00 + p&h
Rethinking Indigenous Education:Culturalism, Colonialism and thePolitics of Knowingby Cathryn McConaghyISBN 1-876682-02-7; $59.50 + p&h
Reflecting on Racial Attitudes: After 24 years revisitingStudent Teachers’ attitudes towards Aboriginesby Clarence Alfred DiefenbachISBN 1-876682-48-5; $24.50 + p&h
Patrons & Riders: Conflicting Roles & HiddenObjectives in an Aboriginal Development Programmeby Peter WillisISBN 1-876682-40-X; $55.00 + p&h ee ontent PTY
LTDmanagementC
POST PRESSED Academic T i t les f rom eCONTENT
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page xi

A d v a n c e s i n C o n t e m p o r a r y N u r s i n g S e r i e s ISSN 1832-9861
A d v a n c e s i n C o n t e m p o r a r y N u r s i n g S e r i e sISSN 1832-9861 – 4 volumes per annum from 2006
xii Volume 28, Issue 1–2,April 2008CCCCNNNN
ADVANCES IN CONTEMPORARY NURSE EDUCATION
A special issue of Contemporary Nurse, Volume 32 Issue 1–2, publishing April 2009Edited by: Debra Jackson and Michael Clinton
Deadline for manuscripts: 30 September 2008Information: www.contemporarynurse.com/archives/vol/32/issue/1-2/call/
ADVANCES IN CONTEMPORARY NURSING AND GENDER
A special issue of Contemporary Nurse, Volume 33 Issue 2, publishing October 2009Edited by: Paula McGee and Kim Walker
Deadline for manuscripts: 15 December 2008Information: www.contemporarynurse.com/archives/vol/33/issue/2/call/
ADVANCES IN CONTEMPORARY MENTAL HEALTH NURSING, SECOND EDITION
A special issue of Contemporary Nurse, Volume 34 Issue 1, publishing December 2009Edited by: Nicholas Procter and Angela Frederick Amar
Deadline for manuscripts: 2 March 2009Information: www.contemporarynurse.com/archives/vol/34/issue/1/call/
ADVANCES IN CONTEMPORARY MODELING OF CLINICAL NURSING CARE
A special issue of Contemporary Nurse, Volume 35 Issue 1, publishing April 2010Edited by: Mary Chiarella and Judith Lathlean
Deadline for manuscripts: 30 April 2009Information: www.contemporarynurse.com/archives/vol/35/issue/1/call/
Author Guidelines are available from www.contemporarynurse.com
C A L L F O R P A P E R S : 2 0 0 9 & 2 0 1 0
ee ontent PTYLTDmanagementC
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911; [email protected] www.e-contentmanagement.com
B O X E D S E T S A V A I L A B L E
2009:
• Volume 13: Advances in ContemporaryNurse Education
• Volume 14: Advances in ContemporaryNursing and Gender
• Volume 15: Advances in ContemporaryMental Health Nursing, 2nd edn
• Volume 16: Advances in ContemporaryModeling of Clinical Nursing Care
2008:
• Volume 9: Advances in Contemporary Aged Care – ISBN 978-0-9757710-1-3
• Volume 10: Advances in ContemporaryPalliative and Supportive Care – ISBN 978-0-9757710-4-4
• Volume 11: Advances in ContemporaryTranscultural Nursing, 2nd edn – ISBN 978-0-9757710-5-1
• Volume 12: Advances in ContemporaryNursing History & Midwifery in Australia– ISBN 978-0-9775742-8-5
2007:
• Volume 5: Advances in Contemporary IndigenousHealth Care – ISBN 978-0-9750436-9-1
• Volume 6: Advances in Contemporary Communityand Family Health Care – ISBN 978-0-9757710-2-0
• Volume 7: Advances in Contemporary NurseRecruitment and Retention – ISBN 978-0-9757710-0-6
• Volume 8: Advances in Contemporary GeneralPractice Nursing – ISBN 978-0-9757710-3-7
2006:
• Volume 1: Advances in ContemporaryTranscultural Nursing – ISBN 978-0-9750436-1-5
• Volume 2: Advances in Contemporary Child andFamily Health Care – ISBN 978-0-9750436-3-9
• Volume 3: Advances in Contemporary MentalHealth Nursing – ISBN 978-0-9759436-8-4
• Volume 4: Advances in Contemporary Nursing andInterpersonal Violence – ISBN 978-0-9750436-6-0
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page xii

1Volume 28, Issue 1–2,April 2008 CCCCNNNN
The scholarly articles presented in this sec-tion reflect the current state of global tran-
scultural nursing leadership, as well as theprogress made in fostering cultural competencethrough transcultural nursing education.Trans-cultural nursing can be traced back to the earlyyears, over a half century ago, when Dr Madel-eine Leininger first began exploring the rela-tionship between nursing and anthropology(Leininger 1970).Through her pioneering theo-retical work, we first started using the term‘transcultural’, to mean ‘across all world nations’.We have since developed into our own disciplineof transcultural nursing, boasting of our uniqueknowledge base within the discipline of nursing.Leadership has emerged through the years, withthe establishment of the Transcultural NursingSociety in the United States in 1975, and the1994 establishment of the Transcultural NursingSociety in Australia through the Royal College ofNursing, Australia. Both organisations, throughcollaboration and individual efforts, have provid-ed leadership for the expanding discipline, toinclude the hosting of annual international con-ferences, the development of policy and positionstatements, and the encouragement and show-
casing of important research focusing on uniqueculture care perspectives.
Bryant and colleagues (2008) provide anexcellent evolutionary perspective of the rolethe Royal College of Nursing, Australia (RCNA)has played in supporting the growth and devel-opment of transcultural nursing in Australia.The official recognition of transcultural nursingas a distinct society in 1994 firmly establishedthe importance of discovering care from a cul-tural perspective in a multicultural society suchas Australia.
The article by Andrews (2008) highlights theglobal nature of transcultural nursing and identifies many Australian nurse leaders whohave been visionaries in establishing culturallyrelevant nursing practice. As a result of thescholarly work by Australian transcultural nurseleaders, there is now a significant body ofknowledge in nursing that is useful in practice,education and research around the globe.
As much as we would like to think all of thisprogress translates into effective education pro-grams for practicing nurses and faculty, read thecontemporary articles before you say otherwise.We are still only beginning to understand how
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 1–2.
NC EDITORIAL
The state of transcultural nursing globalleadership and education
LINDA J LUNAInternational NurseConsultantSchool of NursingUniversity of PhoenixNashville TN, USA
JUNE MILLERPresidentSchool of NursingJohns HopkinsUniversity Baltimore MD, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page 1

we can provide the critical learning environ-ment for students to grasp the key componentsof transcultural nursing, and to then evaluatethe effectiveness of our programs. Lynette Ray-mond, of the University of Notre Dame, SydneyAustralia (2008), shares with us a detailed BNcurriculum approach, including several requiredcourses in TCN, and the introduction of a variety of conceptual models.This very specificcurriculum focus, designed from extensive lit-erature review of research relevant to Australia,includes plans for evaluation one year aftergraduation.We look forward to the results.
On the other hand, we are faced with tworesearch studies that declare we are not findingpositive results in many of our attempts to evaluate cultural competency in undergraduate programs in the United States. Mixer (2008)describes a gap in faculty knowledge, and there-fore limited ability to provide the context ofculture care for student learning. Kardong-Edgren and Camphina-Bacote (2008) present astudy indicating that regardless of approach, bygraduation many students are not scoringbeyond cultural awareness in scales measuringcultural competence. These findings are remi-niscent of the situation with measuring criticalthinking as an outcome measure of baccalaure-ate schools of nursing. Like critical thinking, weknow that cultural competence is an importantoutcome of baccalaureate education, but howdo we measure it?
It seems that many of us who have madetranscultural nursing our life’s work, especiallyexploring theory and research, need now re-focus our leadership skills to direct our atten-tion to insuring that students and clinicians arenurtured in culture care principles.We must becreative in designing clinical cultural immersionexperiences, faculty workshops, and evaluationtools, both qualitative and quantitative to meas-ure the effectiveness of our cultural competenceprograms.
The discipline of transcultural nursing is well grounded in our scholarly theoretical
work and our extensive worldwide research.Our leaders share important findings with eachother through international conferences andscholarly journals.We talk and write extensivelyabout cultural competence for health care pro-fessionals. However, the question is whether we are actually successful at disseminating thatknowledge into clinical practice. Should wenow direct our focus away from the macroworldwide, theoretical stance and toward amicro focus on each individual student nurse, toinsure they are provided with opportunities forlearning the process of cultural competence?
TCNS International is in the final stages of launching its new certification process, toinclude an extensive curriculum which will be available to nurses worldwide. Perhaps,combined with intensive cultural immersionexperiences and more faculty opportunity forin-depth learning about teaching concepts ofTCN, we can move forward.We need to contin-ue our pioneering efforts to expand our leader-ship in creative ways to answer the importantquestions raised in the writings of these wellknown scholars of transcultural nursing. Thefuture of health care depends on the work ofthose at the bedside in every cultural context.
ReferencesAndrews MM (2008) Commentary: Global leadership in trans-
cultural practice, education and research, Advances in Contem-porary Transcultural Nursing, 2nd edn, Contemporary Nursespecial issue 28(1–2): 13–16.
Bryant RB, Foley ER and Percival EC (2008) The role of RCNAin promoting transcultural nursing as a discipline of study,research, practice and management in Australia, Advances inContemporary Transcultural Nursing, 2nd edn, Contemporary Nursespecial issue 28(1–2): 3–11.
Kardong-Edgren S and Campinha-Bacote J (2008) Culturalcompetency of graduating US Bachelor of Science nursingstudents, Advances in Contemporary Transcultural Nursing, 2ndedn, Contemporary Nurse special issue 28(1–2): 37–44.
Leininger M (1970). Nursing and Anthropology:Two worlds to blend.John Wiley & Sons: New York.
Mixer SJ (2008) Use of the culture care theory and ethnonursingmethod to discover how nursing faculty teach culture care,Advances in Contemporary Transcultural Nursing, 2nd edn,Contemporary Nurse special issue 28(1–2): 23–36.
Raymond LM (2008) Exemplar: Developing a new Bachelor ofNursing course responsive to Australia’s culturally diversecommunity, Advances in Contemporary Transcultural Nursing, 2ndedn, Contemporary Nurse special issue 28(1–2): 17–22.
2 Volume 28, Issue 1–2,April 2008CCCCNNNN
Linda J Luna and June MillerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:22 PM Page 2

3Volume 28, Issue 1–2,April 2008 CCCCNNNN
Key WordsRoyal College ofNursing,Australia;transculturalnursing; nationalnetwork;TransculturalNursing Society;multicultural;Indigenous;positionstatements;culturally diverse;care needs
CN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 3–11.
The role of RCNA in promotingtranscultural nursing as a discipline
of study, research, practice andmanagement in Australia
ABSTRACT Royal College of Nursing,Australia has supported the development and growthof transcultural nursing in Australia for well over a decade.The College’s leader-ship role has been evident on a number of fronts with events, publications andnational networking opportunities for nurses who share a passion for furtheringthe principles and practice of transcultural nursing. This paper traces thejourney of transcultural nursing in Australia from the perspective of the College,beginning with its role in forming the Transcultural Nursing Society in the1990s.Achievements are highlighted, as well as continuing work over the inter-vening years, demonstrating the involvement and leadership of the College inAustralia, in this important area of nursing practice.With increasing complexityin the ethnic profile of Australia’s society, it is of ongoing relevance for theCollege to promote transcultural nursing as a discipline of study, research,practice and management in this country.
Received 15 July 2007 Accepted 16 October 2007
ROSEMARY B BRYANTExecutive Director
Royal College of Nursing,Australia
Canberra, Australia
ELIZABETH R FOLEYDirector Policy
Royal College of Nursing,Australia
Canberra, Australia
ELIZABETH C PERCIVAL AM
Previous Executive DirectorRoyal College of Nursing,
AustraliaCanberra, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 3

4 Volume 28, Issue 1–2,April 2008CCCCNNNN
Rosemary B Bryant, Elizabeth R Foley and Elizabeth C PercivalCCCCNNNN
BACKGROUND
In 1994, Royal College of Nursing, Australia,with support from members, established a
Transcultural Nursing Society. This move wasindicative of nursing trends at the time relatingto the growing interest in, and commitment totranscultural nursing education, research, man-agement and practice.The Society reflected theCollege’s preparedness to take a leadership rolein forming a national group of nurses interestedin fostering and promoting culturally relevantnursing care practice. In welcoming transcul-tural nursing, the College was the first nursingorganisation to embrace this concept of careand give transcultural nursing a firm place as adiscipline within the profession. Indeed the Col-lege remains the only national nursing organ-isation in Australia to support transculturalnursing with a Transcultural National Networkfor its members.
This paper will trace the journey of transcul-tural nursing in Australia from the perspectiveof the College, beginning with the formation ofthe Transcultural Nursing Society, highlightingachievements and continuing work over morethan a decade of involvement and leadership inthis important area of nursing practice.
DEVELOPMENT OF TRANS-CULTURAL NURSING IN AUSTRALIAIn the early 1990s the College was creating specialty network groups for members – calledSocieties – to facilitate sharing of ideas,research, innovations in practice and educationmodels, across a range of interest areas.The aimof the Societies was also to provide a structure of programs which would ‘foster professionaldevelopment of members, individuals and theprofession’ (RCNA Archive File 863a 1994–96).Importantly the Societies would be ‘a mecha-nism for identifying and drawing upon the spe-cific interests and expertise of members throughwhom the work of the College could be fur-thered’. These Societies included: Research,Education, Gerontology, Clinical Practice, Legal
Issues, Ethics, and Transcultural Nursing. Overtime there were changes in the nature and pur-pose of these groups with some rolling intoother groups and new groupings being formed.Today there are fourteen such groups, which arenow termed National Networks.
Having formed in April 1994, the Transcul-tural Nursing Society was one of the initial Soci-eties, and resulted from strong representationfrom members. Dr Akram Omeri FRCNA was aprime instigator of the Society and the firstChair of the initial management group, and hasremained the staunchest advocate for this groupover the years. In addition, Dr Omeri has beenan advisor to the College on issues relating totranscultural nursing, and continues in this roleto the present time.
Initial canvassing of the College membershipelicited overwhelming support for the establish-ment of a Transcultural Nursing Society. Thecomments from members were reflected in aletter from Olga Kanitsaki FRCNA of 5 October1994 (RCNA Archive File 863b 1994–96)where she says of the College that ‘It clearlyillustrates its professional leadership, and res-ponsibility to its members, and society at large’.An interim Management Committee was es-tablished in early 1995, with elections for theongoing Management Committee in May of thatyear. In an interview at the time Dr Omericlaimed that ‘The College’s support was officialrecognition of the significance of transculturalnursing’ (Omeri 1995). In the same article DrOmeri described transcultural nursing as ‘thecomparative study of cultures and their caringpractices’. Referring to Dr Leininger’s work,she also said that ‘transcultural nursing movedbeyond ethnicity, examining issues relating torace, class, gender, religion, sexuality and age,identifying differences and similarities withincultures – the goal being to provide culturallyspecific nursing care’ (Leininger 1989, 1997).
With these views forming a shared under-standing within the new Society for transcultur-al nursing in Australia, the group aimed: to act
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 4

5Volume 28, Issue 1–2,April 2008 CCCCNNNN
The role of RCNA in promoting transcultural nursing as a discipline CCCCNNNN
in an advisory capacity on matters relating totranscultural nursing primarily to the Collegebut also to external policy, education and healthcare groups; to facilitate the dissemination oftranscultural nursing information to stimulateinterest and effective nursing care practices; andto promote a positive image of transculturalnursing to the profession and governments; andenrich the knowledge and practice of Australiannurses in transcultural nursing.
Benefits of membership to the Society wereidentified as:• Support to foster your interest in transcul-
tural nursing;• A part to play in the development of national
awareness about the nursing profession andits contribution to society;
• Networking opportunities to share your inter-est with like-minded colleagues;
• The chance to take an active role in theorganisation of Society activities.
(RCNA Archive File 863c 1994–96)
Over the next couple of years, the Society setabout determining strategies for achieving thearticulated aims, through a variety of formats at national and state/territory level via the Col-lege Chapters. In addition to input from themembers of the Society, advice was also soughtfrom a range of nurse leaders, especially thosewithin the Australian Indigenous community.The latter group of leaders included Dr SallyGoold OAM FRCNA (now Chair of the Congressof Aboriginal and Torres Strait Islander Nurses),Lowitja O’Donoghue Hon FRCNA (former Chairof the Aboriginal and Torres Strait IslanderCommission), and Dr Gracelyn Smallwood (ad-viser on Indigenous Health).Their engagementwas requested to provide advice on specific con-tributions from Aboriginal and Torres StraitIslander nurses to the Transcultural NursingSociety. Dr Goold continues as an advisor to theCollege on Indigenous matters, particularlyrelating to health care practices and services andnursing education.
WORK OF THE SOCIETY(NOW NETWORK)In order not to lose the momentum of thenewly formed Society, a number of actions weretaken over the first year of operation resultingin publications, meetings, and conferences. Allof these aimed to further the work of the Col-lege in strengthening the concept of transcul-tural nursing within the profession. These areoutlined below and have formed the basis forongoing work.
Newsletter/bulletinA quarterly newsletter titled Transcultural Nurs-ing Society Bulletin was commenced to shareinformation on transcultural nursing issuesrelating to education, research, managementand clinical practice. Members from each Stateand Territory were identified as key people forgathering relevant material on the practice oftranscultural nursing ideologies as these wereimplemented in their local areas.
In the first edition of the Transcultural NursingSociety Bulletin (published in October 1995) thethen Executive Director of the College, Eliza-beth Percival AM FRCNA, greeted the societymembers on the front page with the followingmessage:
I am delighted that Royal College of Nursing,Australia has been able to facilitate the estab-lishment of the Transcultural Nursing Soci-ety.Within our health system nurses are themain point of contact for all who find them-selves in hospital or are consumers of healthcare in other ways. Nurses bring scientificand technical skills and a caring dimension totheir practice. These, however, would cometo nothing if they operated without an under-standing of the cultural frameworks and cul-tural dimensions of our society.
Australia’s population is made up of manycultures.There are cultures of our oldest in-habitants; cultures of those who migratedfrom English speaking countries in the first
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 5

century or so after colonisation, and culturesof the innumerable groups who have arrivedon our shores in the last half century. In allthese cultures, socioeconomic status, class,occupational status, age, gender and ethnicityare related.
When nurses interact with patients theirvalues, their expectations, their perceptions,and their communication skills are central tothe healing process. Acquiring knowledgeabout cultures, knowing how they impact onindividuals’ health care outcomes is essentialfor nurses.
Through the work of the College’s Tran-scultural Nursing Society cultural issues willbe firmly placed on the nursing agenda, andpatient care can only be strengthened andhealth outcomes improved as a consequenceof the Society’s activities.
I welcome the establishment of this Soci-ety and wish you well for meeting the chal-lenges of the tasks ahead. (Percival 1995)
This first edition newsletter also carried a story of the dissolution of the TransculturalHealth Care Council (THCC) Inc which hadbeen founded ten years previously in the Stateof Victoria. In a demonstration of faith in thenewly establishing Transcultural Nursing Soci-ety, the THCC decided to disband, with manyof its members moving into membership of theCollege (some of course were already Collegemembers).
While levels of enthusiasm have waxed andwaned over the years, the now titled Transcul-tural National Network continues a newslettertoday, within the College’s publication for Net-works and Chapters – Connections.Through thisnewsletter, College members of the Transcul-tural National Network are encouraged to con-tinue the important foundation work of theTranscultural Nursing Society by ‘promotingtolerance towards equality of practice of ourculturally and linguistically diverse society, pro-moting the health and well-being of all, includ-
ing marginalised populations and refugees’(Omeri 2004 ). Members share experiences inclinical practice and management working withculturally diverse health care groups, as well asdisseminate research work which they are cur-rently involved in or have undertaken.
Professional development seriesIn the mid to late 1990s the College was pro-ducing a series of books called the ProfessionalDevelopment Series. While these had a price tag attached the cost was largely underwrittenby the College in fulfilling its objectives to contribute to nurses continuing professionaldevelopment. A significant demonstration of theCollege’s leadership in the area of transculturalnursing was the commissioning of a book in thisseries titled Transcultural Nursing in MulticulturalAustralia.The significance of the book was thatthis was the first collection of writings in tran-scultural nursing edited and authored by Aus-tralian nurses in the context of Australia. Thecontent of the book addressed the significanceof transcultural nursing in nursing educationand research; community and mental healthnursing; primary health care nursing; and exam-ined transcultural nursing from the consumerperspective including those of Aborigines.
In her ‘Foreword’ remarks in TransculturalNursing in Multicultural Australia, Elizabeth Perci-val AM FRCNA outlines the importance of thistext to Australian nurses:
This volume comes at a time in Australia’shistory when all members of our communityare reassessing their understanding and ac-ceptance of different cultures. More thanforty percent of Australia’s population arepeople who are post-war immigrants or chil-dren of post-war immigrants. As a result ofthis population structure nurses have beenpresented with practice challenges. In manyinstances they have not been adequately pro-vided with the opportunity to learn about
6 Volume 28, Issue 1–2,April 2008CCCCNNNN
Rosemary B Bryant, Elizabeth R Foley and Elizabeth C PercivalCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 6

7Volume 28, Issue 1–2,April 2008 CCCCNNNN
The role of RCNA in promoting transcultural nursing as a discipline CCCCNNNN
other cultures and this has left deficits in thedelivery of comprehensive nursing care.
(Omeri & Cameron-Traub 1996: 7–8)
The book has proven immensely popular withAustralian nurses and remains available to bedownloaded and printed (at no cost) for mem-bers and other nurses, from the College’s web-site: www.rcna.org.au.While now having beenwritten over a decade ago the material in thisbook is of continuing relevance to nurses inAustralia today.
Position statementsThe College’s position statement on Nursing in a Culturally Diverse Australia (RCNA 2000a)reflects its commitment to raising awarenessamongst the membership and the nursing com-munity in general, of the need for transculturalknowledge and understanding to enhance nurs-ing practice. The statement highlights the factthat cultural differences can become barriers toequal access to health care services particularlyif these differences are seen as being inferior tothe dominant (Anglo-Saxon-Celtic) culture inAustralia.The statement declares the College’sbelief that ‘Nursing practice should be culturallyinclusive, appropriate and meaningful to specificcultures to meet the diverse and different needsof the Australian community’ (RCNA 2000a).Of critical importance is the rationale statementwhich reads: ‘In a culturally diverse community,such as Australia’s, the aim of providing cultur-ally congruent and empowering health care forits citizens, requires a shift from a monoculturalfocus to a critical transcultural focus in nursingpractice and the provision of nursing services’.The College’s statement, originally released in1998, is an integral document in its ongoingwork to embed concepts of transcultural nurs-ing into nursing practice.
Two College position statements addressissues of importance to Indigenous Australian’s,namely: Health Services for Aboriginal and TorresStrait Islander Peoples (RCNA 2003a) and Nursing
Education for Aboriginal and Torres Strait IslanderPeoples (RCNA 2003b).These statements wereoriginally developed in 1998, and serve asongoing guidance documents to members andother nurses, as well as being advocacy tools inworking with policy makers in the health andeducation arenas.
In the statement on health services the Col-lege maintains that ‘in order to provide primaryhealth care, that is acceptable and meaningful to Indigenous peoples, the provision of cul-turally safe health services is necessary’ (RCNA2003a). The College has needed to reinforcethis principle when dealing with agencies whohave wanted to import nurses from entirely dif-ferent cultures, to immediately work in Indige-nous communities, without any knowledge ofthe Australian health care system let alone spe-cific cultural issues.
The College’s statement on nursing educa-tion contends that ‘the recruitment and reten-tion of Aboriginal and Torres Strait Islanderpeoples as both registered and enrolled nursesis essential to provide an increased level ofhealth care to Aboriginal and Torres StraitIslander peoples’ (RCNA 2003b).The Collegehas put the principles espoused in this statementinto action by successfully tendering for, andadministering the Australian Government PuggyHunter Memorial Scholarships for IndigenousAustralians intending to undertake studies inmedicine, nursing, dental, Aboriginal HealthWorker, management and mental health disci-plines.This funding provides essential supportfor Indigenous people to achieve qualificationsin health disciplines so that they in turn caninfluence more culturally aware health care fortheir communities.They may either practice inspecific Indigenous health services or in main-stream services accessed by Indigenous peoples.Indigenous students in receipt of any of the Australian Government nursing scholarshipsadministered by the College are also assistedthroughout their studies through a range of sup-port measures, including a mentor program.
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 7

The foregoing three identified position state-ments reflect the College’s commitment totranscultural nursing by demonstrating how it has been proactive in promoting culturallyappropriate nursing and health care to Indige-nous people, as well as to the over 200 cul-turally diverse groups who have made Australiahome. An examination of the statements willalso reveal the College’s commitment to pro-moting the inclusion of studies on Indigenousand transcultural care issues within undergradu-ate and postgraduate programs for nurses.
These position statements are available on theCollege website and form valuable guides toCollege members and other nurses relating totheir practice in a multicultural environment.The statements are equally pertinent to nursesin metropolitan, regional, rural and remoteareas of Australia.They are also used to articu-late the College’s position when making policysubmissions to governments.
In addition to the articulation of its own posi-tion, the College also provides input to thedevelopment of statements by other organ-isations, such as the International Council ofNurses’ statement on cultural and linguisticcompetence, and the Australian Nursing andMidwifery Council’s statement on the inclusionof health and cultural issues for Aboriginal andTorres Strait Islander People in programs inAustralia leading to registration or enrolment asnurses.
Conferences/collaboration withTranscultural Nursing SocietyGlobalIn 1997 the College through its TransculturalNursing Society, collaborated within Australiawith Sydney University, University of Tech-nology, Sydney and with support from Univer-sity of Western Sydney, and internationally withlead members of the Transcultural Nursing(TCN) Society Global, to host the TransculturalNursing: New Pathways, New Ventures educationworkshop and conference.The conference pro-
vided a forum for scholarly debate of transcul-tural nursing issues through:• Exploration of contemporary issues, myths
and forces that have facilitated or impededthe development of transcultural nursing inAustralia and worldwide;
• Consideration of the future of transculturalnursing in the 21st Century in advancingeducation, research and practice in Australiaand worldwide;
• Providing an overview of strategies utilised inteaching transcultural nursing in undergradu-ate and graduate programs;
• Exchange on the development of innovativepolicy, education, research and practice strate-gies in respect to transcultural nursing; and
• An opportunity to promote the College’sTranscultural Nursing Society. (RCNA 1997)
Professor Madeleine Leininger (founder of thefield of transcultural nursing) and Dr MarilynMcFarland, both from the United States ofAmerica (USA) TCN Society Global, took leadroles in the event, conducting a pre-conferenceworkshop and then addressing the conferencedelegates through the keynote paper and otherpresentations. Other speakers came from allstates and territories of Australia, New Zealand,Saudi Arabia, and the USA.
A couple of participants wrote to the Collegesaying that the conference had stimulated a ‘cat-alyst for change’ and was the ‘impetus for manyof us to realise that perhaps we are close to thetime when Australian nursing will name foritself what is relevant in this important field ofnursing. They said the conference ‘created anopportunity for ongoing debate to be informedby four decades of pioneering work by Profes-sor Madeleine Leininger in transcultural nurs-ing’.They also felt that the New Zealanders hadgiven examples of how they had developedpathways for nurses practising in colonisednations and that Australian nurses should learnfrom these innovations. Essentially these dele-gates considered that ‘together, in partnership
8 Volume 28, Issue 1–2,April 2008CCCCNNNN
Rosemary B Bryant, Elizabeth R Foley and Elizabeth C PercivalCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 8

9Volume 28, Issue 1–2,April 2008 CCCCNNNN
The role of RCNA in promoting transcultural nursing as a discipline CCCCNNNN
with those from culturally diverse groups, weshould be raising the questions and issues thatneed to be asked to arrive at a unique Australianperspective on cross cultural nursing’ (RCNAArchive File 760 1997–99).
During the late 1990s links were being forgedwith the TCN Society Global which was keen todevelop a collaborative partnership.Thus it wasthat three years after the first conference a sec-ond conference was held in 2000, jointly hostedby the TCN Society Global, the College and itsTranscultural Nursing Society.Titled Internation-al Transcultural Nursing: Leading into the new millen-nium (RCNA 2000b), this event was also aresounding success, with keynote speakers beingEmeritus Professor Madeleine Leininger, USA,Ms Irihapeti Ramsden, New Zealand and DrSally Goold OAM FRCNA, Australia. In whatshould be interpreted as a recognition of theCollege’s leading role in nursing in Australia, andspecifically in transcultural nursing, the confer-ence was opened by Senator The HonourableJohn Herron, then Federal Minister for Aborigi-nal and Torres Strait Islander Affairs.
The conference attracted speakers and dele-gates from the USA, New Zealand, SouthAfrica, the United Kingdom, Sweden, Botswanaand across Australia.This international audienceenabled Australian nurses to showcase workbeing undertaken across clinical, education,management, research and education spheres,in relation to transcultural nursing in our coun-try. It also gave an opportunity to highlight dif-ferences in our cultural profile from theircountries, which impacted on the approachesneeded to provide culturally safe nursing careand challenges faced by Australian nurses.
In recognition of the support and advicegiven by Dr Madeleine Leininger over the earli-er years of the development of the TransculturalNursing Society, in addition to her work inter-nationally, the College presented her at thisconference with our prestigious InternationalAchievement Award.
The College has taken seriously over the
years its lead role in hosting major events suchas those described above, through which net-working on transcultural nursing has been facili-tated, as well as forums that occur around the country to assist nurses on a local level toengage in similar discussions. The College’sannual conference, no matter the central theme,always promotes and contains papers pertainingto some aspect of care in a multicultural society.Most recently the College’s annual conferencein Sydney (11–14 July 2007), Illuminating Nurs-ing, provided an opportunity for speakers fromall States and Territories as well as overseas visi-tors, to give papers on nursing care in culturallydiverse environments. In particular, three of thekeynote speakers presented thought provokingpapers on issues relating to culturally diversecare: preparedness of nurses across the globe indisaster situations – Dr Hiroko Minami (Japan);critical mental health care needs in the PacificIslands – Dr Frances Hughes (New Zealand);and the appalling inequality of health care serv-ices in Indigenous communities in Australia –Dr Sally Goold OAM FRCNA (Australia).
Policy workThe College’s policy development and analysisprogram has covered over the years an extensivearray of issues relating to health and aged care in general and professional nursing issues.Theprogram includes (but is not limited to) thedevelopment of position statements, submis-sions and responses to draft government policy,representation on committees, advocacy for the profession and health and aged care, and collab-orative work with other nursing or health pro-fessional groups. Across any of these activitiesthere are opportunities for raising matters relat-ing to transcultural care.While some aspects ofthis policy work have been referred to in theforegoing paper, a perusal of the policy workundertaken since the start of this decade alone,reveals input to specific issues.The following isa snapshot of some of these: Aboriginal and Tor-res Strait Islander health workforce strategic
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 9

framework; Aboriginal and Torres Strait Islanderhealth worker training; guidelines for healthrelated research amongst Aboriginal and TorresStrait Islander peoples; development of a nation-al policy on multicultural mental health; thehealth of children in immigration detention; andhealth services for migrants, refugees, displacedand detained persons.
The latest census data of Australia’s citizens,published by the Australian Bureau of Statistics(2006) states that around thirty per cent of thepopulation of almost twenty million people,were born overseas.While there are some pre-dominant countries of origin for Australiansborn overseas (or their parents) such as theUnited Kingdom, Europe, Mediterranean coun-tries and Asia, there is an increasing number ofpeople from a wider range of countries.This hasoccurred over recent years with Australia’s poli-cies on bringing in refugees through its Human-itarian Program (DI&C 2007), which brings inmany thousands of people in need to Australiaeach year.The past decade has seen an increas-ing number of people from Middle Easterncountries and African countries.The health vul-nerabilities of some of these newer arrivals tothis country are presenting the nursing profes-sion in Australia with new and different culturalchallenges.
There are obvious implications which theCollege sees of the multicultural nature of oursociety for nursing practice, research and devel-opment. It forces us to institute systems whichfacilitate different models of care (and indeedactively explore different models rather thanjust a more passive adoption of same) and givemore than lip service to individualised care. Insome cases the research undertaken by nursesmay actually lead to new physical structuresneeding to be considered for health care facili-ties and aged care residences, as well as carepractices. Despite years now of having largepopulations of different ethnic groups withinAustralia, the mainstream health care system isstill largely geared to an homogenous, Anglo-
Saxon consumer base.The College works with-in its membership, and in collaboration withother nursing groups, to promote inclusion oftranscultural aspects in education programs;development and implementation of health andaged care policies which include attention toculturally sensitive practices and infrastructure;and encouragement of research which willdemonstrate the benefits to health outcomes ofculturally competent and respectful care.
CONCLUDING COMMENTSRoyal College of Nursing, Australia has beenprivileged to have been involved with thegrowth of transcultural nursing in Australiasince the inception of the College’s Transcul-tural Nursing Society in the early 1990s, topresent day. With members’ support the Col-lege took the initiative in providing a vehiclethrough which nurses who shared a passion fortranscultural nursing could foster and promoteculturally relevant nursing care practice. A con-tinuing record of work undertaken over theyears to further the concepts of transculturalnursing can be seen in the publications, positionstatements and policy work of the College.TheCollege’s National Network for TransculturalNursing perpetuates the values of the originalSociety and continues to make transculturalnursing a positive reality as a discipline in study,research, practice and management in Australia.The College salutes those members whoseefforts and dedication have contributed to itsability to be the lead organisation in promotingtranscultural nursing in this country. The Col-lege is continuing its commitment to assistnurses in their ability to respond effectively toall new citizens to our country and to bettermeet the health and nursing care needs of allpeople in our multicultural society.
AcknowledgementsThese go to Karen Dansey for assistance withlocating material from RCNAs archival collec-tion; and Monique Brouwer – both RCNA staff.
10 Volume 28, Issue 1–2,April 2008CCCCNNNN
Rosemary B Bryant, Elizabeth R Foley and Elizabeth C PercivalCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 10

11Volume 28, Issue 1–2,April 2008 CCCCNNNN
The role of RCNA in promoting transcultural nursing as a discipline CCCCNNNNReferencesAustralian Bureau of Statistics Census Data (2006)
accessed at http://www.abs.gov.au/websitedbs/d3310114.nsf/home/Census+data on 14 June2007.
Department of Immigration and Citizenship (DI&C)(2007) accessed at www.immi.gov.au/immigration.htm on 14 June 2007.
Leininger MM (1989) CLASSIC-TransculturalNursing: Quo Vadis (Where Goeth the Field).Journal of Transcultural Nursing 1: 33–45.
Leininger MM (1997) Transcultural nursing:Ascientific and humanistic care discipline. Journal of Transcultural Nursing 8: 54–55.
Omeri A (1995) A bedside manner to transcendborders. University of Sydney News 27(9) 26 April.
Omeri A (1996) Transcultural nursing care values,and beliefs of Iranian immigrants in NSWAustralia. Unpublished doctoral thesis,TheUniversity of Sydney Australia.
Omeri A and Cameron-Traub E (Eds) (1996)Transcultural Nursing in Multicultural Australia.Royal College of Nursing,Australia.Accessed atwww.rcna.org.au on 21 May 2008.
Omeri A (1998) Course charts cultural shift. NursingReview: 23.
Omeri A (1998) Nursing lecturer wins top interna-tional award. The University of Sydney News 12(November): 5.
Omeri A (2004) Transcultural nursing:Where fromhere! Connections 7: 35.
Omeri A (2005) Omeri wins transcultural nursingscholar award. Nursing Review December 2005.
Percival E (1995) Royal College of Nursing,Australia,Transcultural Nursing Society Bulletin 1 (October).RCNA Resources, Canberra.
Royal College of Nursing,Australia (2000a) PositionStatement: Nursing in a Culturally Diverse Australiaaccessed at www.rcna.org.au on 6 June 2007.
Royal College of Nursing,Australia (2003a) PositionStatement: Health Services for Aboriginal and TorresStrait Islander Peoples accessed at www.rcna.org.auon 8 June 2007.
Royal College of Nursing,Australia (2003b) PositionStatement: Nursing Education for Aboriginal and TorresStrait Islander Peoples accessed at www.rcna.org.auon 8 June 2007.
Royal College of Nursing,Australia (1997) Transcul-tural Nursing: New Pathways, New Ventures con-ference abstract. RCNA Resources, Canberra.
Royal College of Nursing,Australia (2000b) Interna-tional Transcultural Nursing: Leading into the NewMillennium. RCNA Resources, Canberra.
Royal College of Nursing,Australia (RCNA) ArchiveFile 760 (1997–99). Fax 17/12/97 from ToniDowd, RCNA Archive, Canberra.
Royal College of Nursing,Australia (RCNA) ArchiveFile 863a (1994–96). Societies Brochure, RCNAArchive, Canberra.
Royal College of Nursing,Australia (RCNA) ArchiveFile 863b (1994–96). Letter from Dr OlgaKanitsaki 5 October 1994, RCNA Archive,Canberra.
Royal College of Nursing,Australia (RCNA) ArchiveFile 863c (1994–96).Transcultural NursingSociety Brochure, RCNA Archive, Canberra.
IN OUR OWN RIGHT: BLACK AUSTRALIAN NURSES’ STORIES
Edited by Sally Goold OAM (Senior Australian of the Year 2006)and Kerrynne Liddle
ISBN 978-0-9757422-2-8; viii +120 pages; s/c; 2005
‘This book provides a powerful catalyst for questioning and calling into question the taken-for-granted humanity in us all.’ — Olga Kanitsaki AM
‘This book is a celebration of Indigenous Australian nurses and the difficulties they haveovercome. It is not about directing blame or guilt, but rather a commemoration of theirachievements and an inspiration for all Indigenous peoples.’ — Sally Goold OAM
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911;[email protected]; www.e-contentmanagement.com
N O W A V A I L A B L E
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 11

12 Volume 28, Issue 1–2,April 2008CCCCNNNN
IN T E R N AT I O N A L JO U R N A L O F
MULTIPLE RESEARCH APPROACHESISSN 1834 0806 www. i jmra.com
Editor-in-Chief: Professor Carol Grbich, Flinders University School of Medicine
TEACHING MIXED METHODOLOGIES
Special issue of the International Journal of Multiple Research Approaches, volume 3 issue 3, November 2009Guest editors: Nancy L Leech (Colorado), Anthony Onwuegbuzie (Texas),
Thomas Hansson (Denmark) and Priscilla Robinson (Australia)Deadline for manuscripts: 15 December 2008
Information: http://mra.e-contentmanagement.com/archives/vol/3/issue/3/call/
USING VIDEO IN SOCIAL SCIENCES AND HEALTH RESEARCH
Special issue of International Journal of Multiple Research Approaches, volume 3 issue 2, June 2009Advisory Editors: Rick Iedema, University of Technology, Sydney; Christian Heath, Kings College, London;
and Alexandra Juhasz, Pitzer College, Claremont CA, USA Guest Editors: Rowena Forsyth, University of New South Wales; Katherine Carroll, University of Technology,
Sydney; and Paul Reitano, University of New England, Australia Deadline for manuscripts: 15 September 2008
Information: http://mra.e-contentmanagement.com/archives/vol/3/issue/2/call/
MULTIPLE METHODS FOR NOVICE RESEARCHERS
Special issue of International Journal of Multiple Research Approaches, volume 3 issue 1, 2008Edited by Elizabeth Waters (Melbourne), David Este (Calgary), Alicia O’Cathain (Sheffield) and
Kathleen MT Collins (Arkansas) Deadline for manuscripts: Closed
Information: http://mra.e-contentmanagement.com/archives/vol/3/issue/1/call/
Submissions following Author Guidelines on the journal website may be addressed to:[email protected]
USING QUALITATIVE AND QUANTITATIVE METHODS IN DEVELOPMENT POLICY: Q-SQUARED DECISION MAKING IN THE CASE OF POVERTY ANALYSIS
A special issue of International Journal of Multiple Research Approaches, volume 2 issue 2ISBN 978-1-9213482-6-6; iv + 92 pages; s/c; October 2008
Edited by Paul Shaffer (University of Toronto), Ravi Kanbur (Cornell University), Ellen Bortei-DokuAryeetey (University of Ghana) and Nguyen Thang (Vietnam Academy of Social Sciences)
COMPUTER ASSISTED MULTIPLE AND BLENDED RESEARCH METHODS
A special issue of International Journal of Multiple Research Approaches, volume 2 issue 1ISBN 978-1-921348-04-4; ii + 126 pages; s/c; June 2008
Edited by Eugenio De Gregorio (Sapienza University of Rome) and Francesco Arcidiacono (University of Neuchâtel) with an epilogue by Pat Bazeley (Research Support P/L and ACU)
CONDUCTING LONGITUDINAL RESEARCH: PRACTICAL LESSONS FROMTHE AUSTRALIAN LONGITUDINAL STUDY ON WOMEN’S HEALTH
A special issue of International Journal of Multiple Research Approaches, volume 1 issue 2ISBN 978-0-9775742-9-2; ii + 134 pages; s/c; December 2007
Edited by Deborah Loxton, Julie Byles, Annette Dobson and Wendy Brown
C A L L S F O R P A P E R S : 2 0 0 9 & 2 0 1 0
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911; [email protected] www.e-contentmanagement.com
R E C E N T S P E C I A L I S S U E S
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 30/07/2008 9:46 PM Page 12

It is amazing what some women and men dare to dowith their ideas in many places in the world. Cre-
ative thinking and actions are what the world needsmost.Transcultural nursing has been an example ofthese attributes.While taking new actions may betroublesome to some people, yet new actions and newideas can lead to a wealth of new knowledge and newways to serve people.Transcultural nurses have takensuch actions and are transforming nursing and healthcare in many places in the world.
Leininger (2007: 1)
Derived from Latin roots leadership refers to theact of guiding the course or direction; precedingor introducing something by going first. Duringthe past six decades, transcultural nursing’sfoundress, United States-born nurse-anthropol-ogist Dr Madeleine M. Leininger and othertranscultural nursing leaders from Australia andelsewhere in the world have provided leadershipin establishing transcultural nursing as a formalarea of academic study and practice around theworld. Since its initial conception in the 1950sto its formal creation as a specialty and new dis-cipline within the nursing profession in subse-
quent years, a substantial and important body oftranscultural knowledge, theory, and researchhas been generated by nurse scholars not onlyfrom Australia but on every continent.
The term transcultural nursing is sometimesused interchangeably with cross-cultural, inter-cultural, or multicultural nursing. Some haveused the terms ethnic nursing care, culturalsafety, or care for people of color as they haveendeavoured to provide sensitive, meaningful,relevant, congruent, safe, and competent nurs-ing and health care for individuals, families,groups, and communities from diverse back-grounds. It should be noted that Leininger is theonly nursing leader who has developed, imple-mented, and evaluated a theory, the Theory ofCulture Care Diversity and Universality, and aresearch method, ethnonursing, to facilitate thestudy of phenomena of interest in transculturalnursing. A qualitative research method, eth-nonursing is the only research method devel-oped by a nurse for nurses and others to usewhen studying about topics such as culture,care, caring, and related subjects.
From its inception transcultural nursing was
CN
13Volume 28, Issue 1–2,April 2008 CCCCNNNN
MARGARET M ANDREWSDirector/Professor of NursingUniversity of MichiganFlint MI, USA
Key Wordsnurse leadership; transculturalnursing; nursing history; cultural care diversity and universality theory;Leininger; cultural competence
Received 20 February 2008Accepted 20 March 2008
Global leadership in transcultural practice, educationand research
C O M M E N T A R Y
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 13–16. CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 13

conceptualised by Leininger (1966, 1969, 1970,1978, 1995; Leininger & McFarland 2002,2006) as global in nature.The concept of global-isation fits the broad scope and nature of tran-scultural nursing, and Australia has been a keyleader in the global paradigm focus for morethan two decades (Andrews 2006; Omeri 1998,2003, 2004; Omeri & Cameron-Traub 1996;Percival 1995, 1996).
Leininger (1995, 2007) has identified keyhistorical periods or phases in the developmentof transcultural nursing. During the First Era(1955 to 1975): Establishing the Field of Tran-scultural Nursing, Leininger recognised therelationships between nursing and anthropolo-gy, but kept a focus on nursing and the benefitsof having a theory. From 1975 to 1983, a periodthat Leininger has identified as the Second Era:Program and Research Expansion for Transcul-tural Nursing, growing numbers of nursesbecame interested in the valuable contributionof transcultural nursing around the world.TheThird Era: Establishing Transcultural NursingWorldwide (1983 to present) is the period dur-ing which transcultural nursing’s global agendahas been the primary focus. As Dr Leininger hasrecently reflected on the evolution of transcul-tural nursing, she has added a phase that sherefers to as Breakthroughs in TransculturalNursing to Make the Discipline a Reality, andshe comments on some decisions and strategiesto support transcultural nursing as a discipline(Leininger 2007).
Establishing transcultural nursing world widehas required transcultural nurse leaders who arecreative, innovative, and visionary. Australia isamong the most multicultural nations in theworld and many key transcultural nursing lead-ers are Australian (Omeri 1998, 2003, 2004,2005; Omeri & Cameron-Traub 1996; Percival1996; Royal College of Nursing, Australia2000). Increasing numbers of nurses have beentravelling and working in different countries,and interacting with people from many differentcultures electronically and face-to-face. Nurses
and members of other health-related disciplineshave been using transcultural nursing concepts,principles, and research in their practice, teach-ing, and scholarly investigations, and many haveformally studied transcultural nursing and healthcare in degree and/or certificate programs. Aus-tralia has been a leader in the globalisation oftranscultural nursing. In 1994, the Royal Collegeof Nursing, Australia (RCNA) established a Tran-scultural Nursing Society, thus providing nation-al leadership by creating a forum for nursesinterested in culturally relevant nursing carepractice, and it continues to be the only nationalnursing organisation in Australia to support tran-scultural nursing with a Transcultural NationalNetwork for its members.
On an international level, RCNA is activelyinvolved in encouraging international affiliationwith other nursing groups and individual mem-bership of nurses in the Asia–Pacific region. Inaddition to RCNA’s membership in the Interna-tional Council of Nurses (ICN) and leadershipin promoting ICN-related activities in theregion, it also sponsored an international tran-scultural nursing conference in collaborationwith transcultural nursing leaders from the US,New Zealand and elsewhere in the world, thusfirmly establishing Australia as a Regional andInternational leader in transcultural nursing byattracting nurses worldwide. In 2000, the 26thAnnual Transcultural Nursing Research Con-ference was held on the Gold Coast, an eventthat also marked the 40th anniversary of DrLeininger’s first visit to Australia. During eachof her 15 visits to Australia, Dr Leininger hasnoted that many immigrant and non-immigrantnurses in Australia have become leaders in transcultural nursing practice, education, andresearch both within the country and the largerPacific region.
Australian transcultural nurses have beeninfluential leaders through their shared scholar-ship in a wide variety of professional publi-cations, including Contemporary Nurse, whichdedicated the entire October 2003 issue to Dr
14 Volume 28, Issue 1–2,April 2008CCCCNNNN
Margaret M AndrewsCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 14

Leininger and advances in contemporary tran-scultural nursing. Australian nurses also haveshared their expertise in transcultural nursingpractice, education and research in the Journal ofTranscultural Nursing. Established in 1988 by DrMadeleine Leininger, the purpose of this publi-cation is to share scholarly work among tran-scultural nurses and others with an interest todisseminate transcultural nursing knowledge. Inrecent years the focus of articles in this journalhas increasingly reflected the transnationalexpansion of transcultural nursing. There alsohave been transnational comparative analysesthat contribute to transcultural nursing’s devel-opment thus contributing significantly and sub-stantively to the globalisation of TCN theoryand research.The composition of the EditorialBoard for the Journal of Transcultural Nursingincludes representatives from Australia andother nations around the world.
CONCLUDING REMARKSThere is currently an extensive body of TCNknowledge generated by transcultural nursesaround the world, many of whom have usedLeininger’s Theory of Culture Care Diversityand Universality and the ethnonursing researchmethod to study culture care and caringtransnationally. Australian transcultural nurseshave contributed significantly to the globalisa-tion of TCN theory and research, and many areresponsible for breakthroughs in research, edu-cation, and practice that have significantlyadvanced TCN knowledge about culture careand related topics of relevance and interest intranscultural nursing from a global perspective(Leininger 2005). Davidson et al (2003) defineand discuss globalisation as a force for improv-ing health care for all and critically analyse theneed to go from cultural competency to socialadvocacy, noting the long history of social advo-cacy by the nursing profession.
There is now rigorous, theoretically solid,and research-based knowledge in transculturalnursing that needs to be applied to clinical prac-
tice, education, research, administration, andconsultations transnationally in the form of evi-dence-based, best practices in transculturalnursing. Opportunities for transcultural collab-oration among nurses and health care profes-sionals from other disciplines has steadilyincreased each year. Transcultural nursing hasbecome global in its focus, interests, and prac-tices, and Australian nurses have been – andcontinue to be – leaders in the globalisation oftranscultural nursing.
REFERENCESAndrews MM (2006) Globalization of trans-
cultural nursing theory and research, inLeininger MM and McFarland MR (eds)Culture Care Diversity and Universality:AWorldwide Theory of Nursing, 2nd edn, pp83–114. Jones Bartlett, Sudbury MA.
Davidson PM, Meleis A, Daly J and Douglas M(2003) Globalisation as we enter the 21stcentury: Reflections and directions fornursing education, science, research, andclinical practice. Contemporary Nurse 15(3):162–174.
Leininger MM (1966) Convergence and divergenceof human behavior:An ethnopsychologicalcomparative study of two Gadsup villages in theEastern Highlands of New Guinea. Doctoraldissertation,The University of Washington,Seattle WA.
Leininger MM (1969) Ethnoscience:A promis-ing research approach to improve nursingpractice. Image: The Journal of Nursing Scholar-ship 3: 22–28.
Leininger MM (1969) Ethnoscience:A new andpromising research approach for the healthsciences. Image: The Journal of Nursing Scholar-ship 3: 2–8.
Leininger MM (1970) Nursing and Anthropology:Two Worlds to Blend.Wiley, New York.
Leininger MM (1978) Transcultural Nursing: Con-cepts,Theories, and Practices.Wiley, New York.
Leininger MM (1985) Qualitative Research Methodsin Nursing. Grune Stratton, Orlando FL.
Leininger MM (Ed) (1989) Editorial: InauguralIssue of Journal of Transcultural Nursing.Journal of Transcultural Nursing 1: 1–2.
15Volume 28, Issue 1–2,April 2008 CCCCNNNN
Commentary: Global leadership in transcultural practice, education and research CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 15

Leininger MM (1990) The significance of cul-tural concepts in nursing. Journal of Transcul-tural Nursing 2(1): 52–59.
Leininger MM (1995) Transcultural Nursing: Con-cepts,Theories, Research & Practices. McGraw-Hill, New York.
Leininger MM (1997) Overview of the theory ofculture care with the ethnonursing researchmethod. Journal of Transcultural Nursing 8:32–52.
Leininger MM (2001) Founder’s focus:Australia:The global Transcultural Nursing Society’s26th Annual Meeting Place for 2000. Journalof Transcultural Nursing 12: 158.
Leininger MM (2005) Founder’s address:Trans-cultural nursing: Meeting the challenges ofglobal health care.Transcultural NursingSociety 31st Annual Conference, 19–22October 2003, New York.
Leininger MM (2007) The evolution of trans-cultural nursing with breakthroughs todiscipline status.Accessed at www.madeleine-leininger.com on 10 February 2008.
Leininger MM and McFarland MR (Eds) (2002)Transcultural Nursing: Concepts,Theories, Research& Practices, 3rd edn. McGraw-Hill, New York.
Leininger MM and McFarland MR (Eds) (2006),Culture Care Diversity and Universality:A World-wide Theory of Nursing, 2nd edn. Jones & Bart-lett, Sudbury MA.
Omeri A (1995) A bedside manner to transcendborders, University of Sydney News 27(9), 26April.
Omeri A (1996) Transcultural nursing carevalues and beliefs of Iranian immigrants inNSW Australia. Unpublished doctoral thesis,The University of Sydney,Australia.
Omeri A (1998) Course charts cultural shift.Nursing Review: 23.
Omeri A (1998) Nursing lecturer wins topinternational award. The University of SydneyNews 12 (November): 5.
Omeri A (2003) Meeting diversity challenges:Pathway of ‘advanced’ transcultural nursingpractice in Australia. Contemporary Nurse 15(3):175–187.
Omeri A (2004) Transcultural nursing:Wherefrom here!,Australia. Connections 7: 35.
Omeri A (2005) Omeri wins transculturalnursing scholar award. Nursing Review 2005.
Omeri A and Cameron-Traub E (Eds) (1996)Transcultural Nursing in Multicultural Australia.Royal College of Nursing, Canberra, accessedat www.rcna.org.au on 21 May 2008.
Percival E (1995) Australia Transcultural NursingSociety Bulletin 1. RCNA Resources, Canberra.
Percival E (1996) Foreward, in Omeri A andCameron-Traub E (Eds) Transcultural Nursingin Multicultural Australia. Royal College ofNursing, Canberra, accessed at www.rcna.org.au on 21 May 2008.
Royal College of Nursing,Australia (2000)Position Statement: Nursing in a Culturally DiverseAustralia, accessed at www.rcna.org.au on 8February 2008.
16 Volume 28, Issue 1–2,April 2008CCCCNNNN
Margaret M AndrewsCCCCNNNN
ORPHANED BY THE COLOUR OF MY SKIN: A STOLEN GENERATION STORY
by Mary Terszak; ISBN 978-1-921348-08-2; vi + 156 pages; 2007
Told from the heart, this book is a rare autobiographical ethnography on the impact of forced institutionalisation on an Aboriginal Australian. In the raw voice of a grandmother, the book journals the author’s maternal separation, her search for family, identity and community, broken marriage, psychological breakdown and emotional reconstruction. It provides an in-depth account of the experience of a ‘Stolen Generation’ Australian and the struggle of these vulnerable members of our society.
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911;[email protected]; www.e-contentmanagement.com
N O W AVA I L A B L E
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 16

Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 17–22.
17Volume 28, Issue 1–2,April 2008 CCCCNNNN
INTRODUCTION
The purpose of this article is to discuss issuessurrounding the development of a new
Bachelor of Nursing course for the Universityof Notre Dame, Sydney, Australia. In particular,the focus of the discussion is on the factors thatinfluenced the development of learning out-comes that would enable student nurses theopportunity to develop the knowledge, skills,and attitudes needed to advance both personallyand professionally a cultural awareness of selfand others appropriate for the Australian con-text and delivery of culturally congruent andsafe nursing care.
BACKGROUNDOver the past several decades, I have worked asa lecturer in nursing at several New South Walesuniversities and colleges. During that time, Ihave observed a diversity of teaching and learn-ing approaches utilised by staff to develop cul-tural self-awareness and cultural competenceamong undergraduate and postgraduate studentnurses. I have also observed a growing trendtowards implementing learning outcomes that
focused only on one or a limited number of theevidenced-based cultural theoretical or concep-tual approaches currently available to healthprofessionals.1 This approach to teaching stu-dent nurses about the role culture plays in in-fluencing the health and well-being of allindividuals, I believe does not encourage stu-dents to become critical thinkers, nor does itdemonstrate a sustained scholarship culture.Learning outcomes that limit the examinationof the evidenced-based research and health carepolicies available to inform practice is not con-gruent with the goals of higher education inAustralia, nor the role of universities to utiliseresearch to advance knowledge and understand-ing (MCEETYA, 2007). Therefore, the aim ofthe new Bachelor of Nursing course was todevelop a curriculum that reflected both stake-holders’ views and a diverse range of evidenced-based research on culture care and culturalsafety relevant to nursing practice for the Aus-tralian context.
The Bachelor of Nursing (BN) is a compre-hensive three-year course, which prepares stu-dent nurses to meet the Australian Nursing and
Key WordsAustralia; cultural competence;curriculum development;cultural safety; nurse education;transcultural nursing
Received 11 July 2007Accepted 26 March 2008
Developing a new Bachelor of Nursing courseresponsive to Australia’s culturally diverse community
E X E M P L A R
LYNETTE M RAYMONDClinical Coordinator/Senior LecturerThe University of Notre DameSydney NSW, Australia
CCCCNNNN
CN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 17

Midwifery Council (ANMC) National Com-petency Standards for the Registered Nurse(2006) that are currently required for registra-tion by the Nurses and Midwives Board in eachstate and territory of Australia. A transfer ofstate and territory registration to national regis-tration in Australia is anticipated during 2008 to2010.The new University of Notre Dame, Aus-tralia Bachelor of Nursing course (Sydney Cam-pus) aims to provide the student with essentialknowledge, skills, attitudes and experientiallearning that will prepare the student for therole of a professional nurse in order to providesafe care across various clinical settings andsocio-cultural contexts. Graduates will be ableto practise at a beginning level in a variety ofhealth agencies and settings, under the directionof or with access to, experienced registerednurses (RNs), until a level of independent prac-tice is achieved. The BN course also extendsattitudes and skills of the professional nurse,through researching contemporary health care/nursing issues, exploring the impact of healthpolicy and socio-cultural issues on health andthe modes used in bringing about change inhealth care delivery.
CURRICULUM DEVELOPMENTPROCESSIt became apparent early in the curriculumdevelopment process that in order to meet the diverse cultural health needs of the Aus-tralian community, a diverse range of profession-al stakeholders’ views needed to be sought.Thecurriculum developers needed to identify whatculturally relevant content needed to be inc-luded in the course units of study and learningoutcomes. The developers of the course alsoneeded to know how the Bachelor of Nursingcurricula could provide teaching and learningopportunities for the student nurse so that theycould further develop their levels of culturalawareness, knowledge, skills, and attitudes thatcould lead to culturally safe and competent prac-tice (NSWNMB 2005a, 2005b;ANMC 2006).
A wide range of professional and communityrepresentative opinions were obtained duringthe early stages of the curriculum development.Initially, the School of Nursing’s External Advi-sory Committee (EAC) was formed. The EACcomprised of representatives from the universitysector, clinical experts from the health care serv-ice sector and consumers of professional nursingcare. Representatives from a diverse range ofclinical areas included: Rural and Remote HealthNursing, Aboriginal and Torres Strait IslanderHealth, Mental Health, Aged Care, Communityand Primary Health Care Nursing and registerednurse members from other medical and surgicalspecialty areas currently working in hospitals.Other resources included clinicians and con-sultants with experience and expertise in the delivery of multicultural, transcultural, primaryhealth, and representatives from community andculture-specific health care services (Wass 2000;O’Connor-Flemming Parker 2001). In additionto these resources, current evidenced-basedresearch, Australia’s health strategic plans andpolicy requirements were identified and used asa guide (RCNA 1998; DEST 2002; Common-wealth of Australia 2006; NSW Department of Health 2007). Furthermore, the providers ofAboriginal and Torres Strait Islander health care services opinions were also investigated(Commonwealth of Australia 2004; Goold 2004;Eckerman et al 2005; S. Goold, personal com-munication, 13 December 2005 and 23 March2006; Couzos & Murray 2008).
The review of the literature revealed adiverse range of culture care theories and con-ceptual models of cultural safety and com-petence are currently available and in use by nurses and midwives globally (Campinha-Bacote 2002; Leininger & McFarland 2002;Andrews & Boyle 2003; Purnell & Paulanka2003; Giger & Davidhizar 2004; Spector 2004;Papps 2005; Wepa 2005;Jirwe Gerrish Emami2006).The literature also indicated the culturecare theories and conceptual models are utilisedby researchers and clinicians in a diverse range
18 Volume 28, Issue 1–2,April 2008CCCCNNNN
Lynette M RaymondCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 18

of specialty nursing and midwifery domainsboth in Australia and overseas (Omeri 1996;Nahas & Amasheh 1999; Raphael & Malak 2001;Leininger & McFarland 2002; Andrews & Boyle2003; Omeri, Lennings & Raymond 2005; Ray-mond 2003). Nevertheless, in some instancesspecific cultural groups were found to identifymore readily with one particular theoreticalcultural approach over and above others. Forinstance, the conceptual model of cultural safetyoriginally developed in New Zealand by Rams-den (2005) for Maori nurses and the Maoripopulation, has been adopted by Australia’sAboriginal and Torres Strait Islander peoples(Goold 2004; Papps 2005 & Wepa 2005). Theconceptual model of cultural safety togetherwith primary health care model are utilised byAboriginal Health Workers and nurses workingwith Indigenous communities, as a preferredmethod of achieving cultural self-awareness,sensitivity and culturally safe nursing and mid-wifery practice (O’Donoghue 1999; NSWDepartment of Health 2001, 2003, 2005;Thom-son 2003; Commonwealth of Australia 2004;Eckerman et al 2005; Richardson & Carryer2005; Kelly 2006; Couzos & Murray 2008).
Conversely, the ‘transcultural nursing theoryof culture care diversity and universality’devised by Leininger (1978; 2002) was found tobe both suitable and fitting for the Australiancontext (Liamputtong 1994; Omeri 1996;Nahas & Amasheh 1999; Kanitsaki 2003; Ray-mond 2003).The culture care theory enables thediscovery of culture specific care knowledge,skills, and attitudes that can utilised by nursesand midwives to guide practice in a diverserange of clinical contexts. The culture care theory and accompanying ethnonursing researchfindings also enhances the growth of professionalknowledge and understanding, thus contributingto scholarship and goals of higher education inAustralia.The culture care theory was also foundto be congruent with the principles under-pinning Australia’s Multiculturalism Agenda, aswell as the Australian Governments views and
policies on cultural diversity, health promotion,and illness prevention (Omeri & Cameron-Traub1996; Omeri 2002, 2003; Commonwealth ofAustralia 2003, 2006; NSW Department ofHealth 2007).
The principles of Australia’s MulticulturalismAgenda emphasise the importance of valuing dif-ferences, access and equity, and utilising the cul-tural knowledge and skill contributions ofpeople from different backgrounds, experiencesand perspectives to generate new ideas andways of doing things in all sectors of society(Commonwealth of Australia1999, 2003). Simi-larly, the health aims of federal, state and terri-tory governments primarily focus their healthand ageing health policies on the principles ofprimary health care, promotion of healthylifestyles, early intervention and prevention ofillness from within a social model of healthframework (Germov 2004; Daly, Speedy, Jack-son 2005; Grbich 2005; Gray 2006; Common-wealth of Australia 2007; McMurray 2007;NSWDepartment of Health 2007).
REFLECTIONSThe findings from the EAC inquiry and reviewof the literature indicated that it would betherefore, both scholarly and culturally prudentto include and teach the diverse range of culturecare theories and the conceptual model of cul-tural safety in the new Notre Dame Bachelor ofNursing course curriculum.To achieve this aim,it was decided that the general course objectivesand specific unit learning outcomes relating tocultural diversity and culturally safe nursingpractice needed to be embedded in all thecourse units, in addition to the development oftwo discrete units of study. The two specificnon-elective units of study are titled Aboriginaland Torres Strait Islander Health Care and Transcul-tural Nursing, and are included in the final yearof the course. Other supportive units of studydesigned to enhance a student’s growth towardscultural self-awareness and cultural competenceinclude units of study such as: an introduction
19Volume 28, Issue 1–2,April 2008 CCCCNNNN
Exemplar: Developing a new Bachelor of Nursing course CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 19

to nursing in the Australian context; psycholo-gy; sociology; maternal and child health; family;aged and community primary health care; ethicsand legal studies; professional role of the nurse;in addition to core nursing care units offeredthroughout the three years of the course.
The decision to be inclusive rather than ex-clusive was based on the need for student nurses to be offered teaching and learningopportunities that encouraged critical thinking,scholarship and informed clinical decision-mak-ing that is specific to the social and cultural con-text in which the nurse or midwife practises. Aneducation curriculum that encourages reflectionand critical analyses of the diverse range of evi-denced-based culture care theories is also morelikely to enhance the student’s life long journeyof acquiring cultural awareness (self and oth-ers), knowledge, skills, and attitudes requiredfor the delivery of culturally congruent, safe,sensitive, and competent nursing care.
During 2008, the University’s first cohort ofstudent nurses will be undertaking their finalyear of study and the two specific non-electiveunits of study Aboriginal and Torres Strait IslanderHealth Care and Transcultural Nursing. The stu-dents undertaking these units will be taught andassessed for cultural self-awareness and culturalcompetence utilising a diverse range of culturalself-awareness assessment tools that were intro-duced in their first year units of study (Lein-inger & McFarland 2002; Purnell & Paulanka2003; Giger & Davidhizar 2004; Wepa 2005;Munoz & Luckmann 2008). It is envisaged that,following completion of the BN course, thegraduate nurses will be culturally safe and com-petent to enter the role of registered nurse – asthe graduate nurse will be expected to have thenecessary knowledge, skills, and attitudes need-ed for working safely in a culturally and linguis-tically diverse country such as Australia. It isplanned that one year post graduation, the grad-uates will be invited to participate in a studythat evaluates their views on the suitability andvalue of their course preparation for advancing
their personal and professional cultural self-awareness and cultural competency capabilityfor working with culturally and linguisticallydiverse patients and other health care workers.
Endnote1 A group of scholars from the Transcultural
Nursing Society (Global) is currently in theprocess of compiling a resource book forthose nurses seeking TCN certification.Thisresource, a collection of nine to ten chapterswill include a comprehensive section on all the current theories and models availablein transcultural nursing to date.This publi-cation will be available late 2008 (Omeri2008).
ReferencesAndrews M and Boyle J (2003) Transcultural
Concepts in Nursing Care, 4th edn, LippincottWilliams and Wilkins, Philadelphia, USA.
ANMC (2006) National Competency Standards forthe Registered Nurse, 4th edn,ANMC,Canberra,ACT. Retrieved 26 February 2006from http://www.anmc.org.au/professional_standards/index.php.
Campinha-Bacote J (2002) The process ofcultural competence in the delivery ofhealthcare services:A model of care, Journalof Transcultural Nursing 13: 181–184.
Commonwealth of Australia (2006) CorporatePlan 2006–09: Better health, better care, betterlife, Department of Health and Ageing,Canberra,ACT. Retrieved 26 March 2007from http://www.health.gov.au/internet/wcms/publishing.nsf/content/corporateplan
Commonwealth of Australia (2004) A NationalStrategic Framework for Aboriginal and TorresStrait Islander Mental Health and Social andEmotional Well-being 2004–2009, SocialHealth Reference Group for NationalAboriginal and Torres Strait Islander HealthCouncil and National Mental Health WorkingGroup, Canberra,ACT.
Commonwealth of Australia (2003) Multicultural
20 Volume 28, Issue 1–2,April 2008CCCCNNNN
Lynette M RaymondCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:23 PM Page 20

Australia: United in diversity. Updating the 1999new agenda for multicultural Australia: Strategicdirections for 2003–2006, Canberra,ACT.
Commonwealth of Australia (1999) AustralianMulticulturalism for a New Century: Towardsinclusiveness, National Multicultural AdvisoryCouncil, Canberra,ACT.
Couzos S and Murray R (eds) (2008) AboriginalPrimary Health Care.An evidenced-basedapproach, 3rd edn, Oxford University Press,South Melbourne,Victoria.
Daly J, Speedy S and Jackson D (eds) (2005)Contexts of Nursing, 2nd edn, MacLennan andPetty, Sydney.
Department of Education Science and Training(2002) National Review of Nursing Education,Department of Education, Science andTraining (DEST), Canberra,ACT. RetrievedApril 24, 2003, from www.dest.au/higherednursing/pubs/multi-cultural
Eckermann A, Dowd T, Martin M, Nixon L,Gray R and Chong E (2005) Binanj Goonj:Bridging cultures in Aboriginal health, 2nd edn,University of New England Press,Armidale,NSW.
Germov J (ed) (2005) Second Opinion.AnIntroduction to Health Sociology, 3rd edn,Oxford University Press, Melbourne.
Goold S (2004) The future is now – live it,ACORN 17: 9–11.
Gray D (2006) Health Sociology:An Australianperspective, Pearson Prentice Hall,Australia.
Grbich C (ed) (2005) Health in Australia:Sociological concepts and issues, 3rd edn,Pearson Longman, Sydney.
Giger J N and Davidhizar R (2004) TransculturalNursing Assessment and Intervention, 4th edn,Mosby, St Louis, Missouri.
Jirwe M, Gerrish K and Enami A (2006) Thetheoretical framework of culturalcompetence, The Journal of MulticulturalNursing and Health 12: 6–16.
Kanitsaki O (2003) Transcultural nursing andchallenging the status quo, Contemporary Nurse15(3): v–x.
Kelly J (2006) Is it Aboriginal friendly?Searching for ways of working in researchand practice that support Aboriginal women,Contemporary Nurse 22(2): 317–326.
Liamputtong R (ed) (1994) Asian mother,Aust-ralian birth, pregnancy, childbirth and childrearing.The Asian experience in an English speakingcountry,Ausmed Publications, Melbourne.
Leininger M (ed) (1978) Transcultural NursingConcepts,Theories and Practices, Greyden Press,Columbus, Ohio.
Leininger M and McFarland M (eds) (2002)Transcultural Nursing Concepts,Theories, Researchand Practice, 3rd edn, McGraw-Hill, NewYork.
Leininger M (2002) The theory of culture careand ethnonursing research method. In MLeininger and M McFarland (eds) (2002)Transcultural Nursing Concepts Theories, Researchand Practice, 3rd edn, McGraw-Hill, NewYork.
McMurray A (2007) Community Health andWellness.A socioecological approach, 3rd edn,Elsevier,Australia.
Ministerial Council on Education, Employment,Training and Youth Affairs (2007) NationalProtocols for Higher Education Approval Processes.
MCEETYA, Canberra,ACT. Retrieved 28March 2008 from http://www.mceetya.edu.au/mceetya/national-protocols-for-higher-education-mainpage,15212.html
Munoz C and Luckmann J (2008)TransculturalCommunication in Nursing, 2nd edn,ThomsonDelmar Learning,Australia.
Nahas V and Amasheh N (1999) Culture caremeanings and experiences of postpartumdepression among Jordian Australian women:A transcultural study, Journal of TransculturalNursing 10: 37–45.
NSW Department of Health (2007) FutureDirections for Health in NSW – Towards 2025: Fitfor the future, NSW Department of Health,North Sydney, NSW. Retrieved 26 March2007 from http://www.health.nsw.gov.au/pubs/2007/pdf/future_directions.pdf.
21Volume 28, Issue 1–2,April 2008 CCCCNNNN
Exemplar: Developing a new Bachelor of Nursing course CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 21

NSW Department of Health (2005) NSWAboriginal Maternal and Infant Health StrategyEvaluation Final Report 2005, NSW Depart-ment of Health, North Sydney, NSW.
NSW Department of Health (2003) NSW HealthAboriginal Health Impact Statement andGuidelines, NSW Department of Health,North Sydney, NSW.
NSW Health Department and the AboriginalHealth and Medical Research Council ofNSW (2001) NSW Aboriginal Health PromotionProgram: Directions paper. Gladesville,NSW: Better Health Centre PublicationsWarehouse.
Nurses and Midwives Board of New SouthWales (2005a) NMB Update 2: 14–18.
Nurses and Midwives Board of New SouthWales (2005b) Retrieved 7/28/2005 http://www.nmb.nsw.gov.au/ne_inspections.htm
O’Donoghue L (1999) Towards a culture ofimproving Indigenous health in Australia,Australian Journal of Rural Health 7: 64–69.
O’Connor-Flemming M and Parker E (2001)Health Promotion: Principles and Practice in theAustralian Context,Allen and Unwin, NSW.
Omeri A, Lennings C and Raymond L (2005)Beyond asylum: Implications for nursing andhealth care delivery for Afghan refugees inAustralia, Journal of Transcultural Nursing 17:1–31.
Omeri A (2003) Meeting diversity challenges:Pathway of ‘advanced’ transcultural nursingpractice in Australia, Contemporary Nurse15(3): 175–187.
Omeri A (2002) Reflections on Australia andtranscultural nursing in the new millennium,in Leininger M and McFarland M (eds) (2002)Transcultural Nursing Concepts,Theories,Researchand Practice, 3rd edn, McGraw-Hill, New York.
Omeri A and Cameron-Traub E (eds) (1996)Transcultural Nursing Care in Multicultural Australia, Royal College of Nursing,Australia,ACT.
Omeri A (1996) Transcultural nursing carevalues, beliefs and practices of Iranian
immigrants in New South Wales Australia.PhD (Nursing), Faculty of Nursing,TheUniversity of Sydney,Australia.
Papps E (2005) Cultural safety: daring to bedifferent, In Wepa D (ed) Cultural safety inAotearoa New Zealand, Pearson Education,New Zealand.
Purnell L and Paulanka B (2003) TransculturalHealth Care.A culturally competent approach,2nd edn, F.A. Davis Company, Philadelphia,USA.
Raphael B and Malak A (eds) (2001) Diversityand Mental Health in Challenging Times,Transcultural Mental Health Centre,Parramatta, NSW.
Ramsden I (2005) Towards cultural safety, inWepa D (ed) Cultural Safety in Aotearoa, NewZealand, Pearson Education, New Zealand.
Raymond L (2003) An ethnonursing study ofthe culture care meanings of health and well-being for Mauritian immigrant childbearingfamilies living in New South Wales Australia.Unpublished doctoral thesis. Faculty ofNursing, Department of Family and Com-munity Nursing,The University of Sydney.
Richardson F and Carryer J (2005) TeachingCultural Safety in a New Zealand NursingEducation Program, Journal of NursingEducation 44: 201–208.
Royal College of Nursing,Australia (1998)Position Statement: Nursing practice in aculturally diverse Australian society. Council ofRoyal College of Nursing,Australia,Canberra,ACT.
Spector R (2000) Cultural Diversity in Health andIllness, 5th edn, Prentice Hall Health,Uppersaddle River, NJ.
Thomson N (ed) (2003) The Health of IndigenousAustralians, Oxford University Press. SouthMelbourne,Victoria.
Wass A (2000) Promoting Health.The primaryhealth care approach, 2nd edn, HarcourtSaunders, Sydney.
Wepa D (2005) Cultural Safety in Aotearoa, NewZealand, Pearson Education, New Zealand.
22 Volume 28, Issue 1–2,April 2008CCCCNNNN
Lynette M RaymondCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 22

As the world becomes increasingly multicul-tural, transcultural nursing education, prac-
tice, research and administration are imperativeto respond to the global health needs of people,communities and nations.Within the profession
of nursing, there is a need and dictum toincrease cultural sensitivity and competence innursing students (AACN 2004; McFarland &Leininger 2002; Sullivan 2004; US Departmentof Health and Human Services 1996). Nursingeducators worldwide are challenged to preparea culturally competent nursing workforce (Mc-Farland & Leininger 2002).
The culture of the nursing profession em-braces the shared value of preparing students toprovide culturally competent nursing care forpeople in an increasingly multicultural world(AACN 2004; US Department of Health andHuman Services 1996;Wilson et al 2003).Theincreasing diversity in the population in the
Key Wordsculture caretheory;ethnonursingresearchmethod;teaching culturecare; research;nursingeducation;culturallycongruent care CN
23Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 23–36.
Use of the culture care theory andethnonursing method to discover how
nursing faculty teach culture care
ABSTRACT As the world becomes increasingly multicultural, transcultural nursingeducation is critical to ensuring a culturally competent workforce.This paperpresents a comprehensive review of literature and results of an ethnonursingpilot study using the Culture Care Theory (CCT) to discover how nursingfaculty teach culture care.The literature revealed that despite 50 years oftranscultural nursing knowledge development through theory, research andpractice, there remains a lack of formal, integrated culture education innursing.The importance of faculty providing generic and professional care tonursing students and using an organising framework to teach culture care wasdiscovered.Additionally, care was essential for faculty health and well-being toenable faculty to teach culture care.This unique use of the theory and methoddemonstrates its usefulness in discovering and describing the complex nature ofteaching culture care. Larger scale studies are predicted to further substantiatethe CCT, building the discipline of nursing.Received 16 July 2007 Accepted 26 February 2008
SANDRA J MIXERAssistant Professor of NursingMiddle TennesseeState UniversityMurfreesboro TN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 23
United States and in countries throughout theworld compels nurses to examine cultural char-acteristics of persons and caring practices ofnurses (Hegyvary 2006). According to estimatesby the US Census Bureau (2005), 33% of theAmerican population in 2005 was made up ofpersons from ethnic, non-white backgrounds asrepresented by: 14.4% Hispanic/Latino, 12.8%African American, 4.3% Asian, 1% AmericanIndian/Alaskan Native and 0.2% Native Hawai-ian/Pacific Islander. Nursing faculty have theresponsibility to effectively disseminate tran-scultural nursing knowledge to ensure a cultur-ally competent workforce prepared to deliversatisfying, safe and beneficial nursing care.
As this researcher contemplated nursing stu-dents learning to provide culturally congruentcare, curiosity about faculty culture care com-petence and knowledge, skills and values neces-sary to effectively teach culture care emerged.Therefore, a pilot study was developed to dis-cover nursing faculty care expressions, patternsand practices related to teaching culture care.This article presents the review of literature andpilot study findings. A comprehensive review ofliterature was informative and essential fordeveloping the domain of inquiry and researchquestions. Discoveries from this pilot study areuseful for nursing faculty as they prepare stu-dents to provide culturally congruent care in amulticultural world.
LITERATURE REVIEW
Introduction
Culture care education in nursing focusesbroadly on nurses, nursing students and facultydeveloping transcultural expertise; the ability toprovide culturally congruent care for peoplefrom similar and diverse cultures (Leininger2006a). Developing this expertise is multifac-eted and is described in the literature as involv-ing cultural awareness and sensitivity, culturalcompetence, cultural skills, cultural content,teaching strategies, culturally diverse clinical
sites, cultural immersion experiences and insti-tutional cultures. Focus has been placed on whatis taught, how it is taught and personal and pro-fessional reflection of the nursing professional.Following is a critical discussion of the literatureincluding research studies that address culturecare education in nursing.
Cultural competence developmentCultural competence development has beendescribed as a process or journey rather than adestination. One does not become culturallycompetent; rather one works toward culturalcompetence throughout one’s professional nurs-ing career (Campinha-Bacote 2005).
The Cultural Self-Efficacy Scale (CSES) wasdeveloped by Bernal and Froman to address anurse’s knowledge about ‘cultural concepts, cul-tural patterns and skills in performing transcul-tural nursing functions’ (Coffman et al 2004:181). Early studies using the CSES were con-ducted to measure the cultural competence ofsenior nursing students. Alpers and Zoucha(1996) found that introducing cultural conceptsand care of diverse people into a course wasinsufficient in raising students’ perception ofcultural competence; and Kulwicki and Boloink(1996) found that students had little or no confidence in caring for people representingAfrican Americans, Latino-Hispanics, MiddleEasterners/Arabics, Asian/Pacific Islanders andNative American minority groups. Researcherssuggested comprehensive transcultural nursingeducation needs to be incorporated into cur-ricula. Strategies included teaching lifeways of various cultures, cultural assessment, facilitatingstudents in exploring their values and beliefsrelated to cultural differences and similarities(Alpers & Zoucha 1996), purposefully selectingclinical sites that allow students to care fordiverse people and clinical faculty role model-ing (Kulwicki & Boloink 1996). Interestingly,when Coffman, Shellman and Bernal (2004)reviewed 26 known uses of the CSES ‘findingsshowed that ethnicity, previous coursework and
24 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 24

educational experiences can increase nurses’self-efficacy in delivering culturally competentcare’ (Coffman et al 2004: 185).
After conducting an exhaustive review of literature, Rew et al (2003) proposed that cul-tural competence can be conceptualised as con-sisting of cultural awareness, cultural sensitivity,cultural knowledge and cultural skills. Theseauthors developed and tested a cultural aware-ness scale (CAS) which was found to be a reli-able and valid instrument for measuring culturalawareness in nursing students. Additionally,researchers concluded that data ‘support themultidimensional nature of cultural awareness’and the importance of faculty modeling sensi-tivity to cultural diversity (Rew et al 2003:225).
Jeffreys and Smodlaka (1999) found transcul-tural self-efficacy to be higher for senior versusbeginning nursing students. Both groups weremost confident about their transcultural attitu-dinal self-evaluations and were least confident intheir transcultural nursing knowledge. Studentsparticipating in the study represented diversityin terms of age, gender, ethnicity, income,previous health care experience and language.Results substantiated that simply belonging to aminority group does make one culturally com-petent.The researchers concluded that formal,transcultural nursing education, including cul-tural immersion experiences, are required toprepare nurses to provide culturally congruentcare (Jeffreys & Smodlaka 1999).
In determining the effectiveness of a curricu-lum to teach students cultural competence, Sar-gent et al (2005) found that fourth year nursingstudents were more culturally competent thanfirst year students. Researchers concluded thatcultural competence can be effectively taughtwhen purposefully integrated throughout the curriculum using active teaching strategies.Examples of these strategies are completing acultural self-assessment, comparing and con-trasting one’s culture to a person from a differ-ent culture through interview and review of
literature and caring for people from diversebackgrounds.The authors suggested that cultur-al desire [described by Campina-Bacote (2003)as motivation to become culturally competent]of students and faculty alike may be the mostsignificant factor in developing cultural compe-tence (Sargent et al 2005).
Teaching strategiesA descriptive survey was conducted by Ryan,Carlton and Ali (2000) to ascertain trends inteaching transcultural nursing concepts andlearning experiences in baccalaureate and mas-ter’s programs in the United States. Facultyfrom 217 National League for Nursing accredit-ed programs responded, equating to a 36%response rate. Researchers found great diversityamong schools about what was taught related toculture and transcultural nursing (TCN) andhow these concepts were taught. TCN contentwas found in most nursing curricula; howeversubstantive content and integration throughoutthe curriculum were missing. Although formalprograms of transcultural nursing study at themasters’ and doctoral level are available at sev-eral universities, the survey found insufficientnumbers of faculty with expertise in TCN avail-able to teach and some schools reported noqualified faculty were available. Researcherssuggested that more substantive content relatedto transcultural nursing be integrated through-out curricula rather than simply offering mod-ules or an elective course. Additionally, Ryan etal (2000) recommended greater support forfaculty development in transcultural nursing atthe department and university levels to fosterfaculty expertise.
Majumdar et al (2004) administered six in-struments to health care providers and patientsrandomly divided into experimental and controlgroups over one and one half years to deter-mine the effectiveness of cultural sensitivitytraining on health care providers’ knowledgeand attitudes and how this training affectedpatient care satisfaction in home care and hos-
25Volume 28, Issue 1–2,April 2008 CCCCNNNN
How nursing faculty teach culture care CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 25

pital settings. Providers in the experimentalgroup received 36 hours of cultural sensitivitytraining at the beginning of the study with base-line instrument assessment and then had in-struments administered to them and theirpatients at three, six and 12 months. Health careproviders in the control group received trainingjust before the last data collection phase. Thestudy began with 114 health care providers and133 patient volunteers. At each phase of thestudy, patients dropped out due to illness ordeath and providers due to relocation resultingin approximately 75 providers and 47 patientscompleting all phases of the study. Despite thestudy being conducted in an urban settingwhere one quarter of the population was for-eign born, demographics of the health careproviders and patients were similar with partici-pants being from predominately Europeandescent and the Roman Catholic and Protestantfaiths (Majumdar et al 2004).
The findings showed that health careproviders who had received the cultural sensi-tivity training earlier conducted more thoroughcultural assessments and rated culture as moreimportant than those in the control group.Once providers in the control group receivedtraining, they responded similarly. Qualitativeand quantitative data revealed providers whohad received training demonstrated improvedcommunication with minority patients as wellas more open-mindedness and insight towardcaring for people different than themselves.Thehealth care expenditures among long term com-munity patients were reduced by $7,000 over1.5 years of the study. Researchers concludedthat cultural sensitivity training improves cul-ture care (Majumdar et al 2004).
Baldonado et al (1998) surveyed 767 regis-tered nurses and baccalaureate nursing (BSN)students from the east coast, west coast andmidwest of the US using the Transcultural andInternational Nursing Knowledge Inventory(TINKI).This questionnaire included closed andopen-ended questions related to participants’
experiences in providing culture care.The regis-tered nurses and BSN students reported littleconfidence in caring for culturally diverse peo-ple and they learned about how to care fordiverse people most often from experience incaring for them. Few participants had receivedany formal transcultural nursing education fromtheir professional preparation, continuing edu-cation, or reading; and thus, did not describecare actions and decisions based on a conceptualframework.
Researchers assessed that these participantswere at the first stage of transcultural nursingknowledge as described by Leininger – culturalawareness. Themes identified in the researchreflected that nurses and students overwhelm-ingly perceived a need for transcultural nursingand they modified care to meet their client’sculture care needs. Recommendations were thattranscultural nursing concepts and clinicalexperiences in caring for people from diversecultures be integrated in all levels of curricula(associate degree through doctoral level) and incontinuing education programs for practicingnurses (Baldonado et al 1998).
Canales and Bower (2001) conducted agrounded theory research study of ten doctoralprepared, Latino nurse educators. It was dis-covered that these educators viewed cultureand culturally competent practice very broadly.They teach students how to care for anyonewho is ‘different’ from them using strategies ofconnecting directly through communities andimmersion in the lives of those they care for. Researchers suggested the need to expand how cultural competence is conceptualised innursing research, education and practice to car-ing for anyone who is different from oneself(Canales & Bower 2001).
At St. Luke’s College in Kansas City, Mis-souri transcultural nursing principles were pur-posefully integrated throughout the nursingcurriculum. Students were taught to examinetheir own cultural backgrounds, values andbeliefs.They were taught transcultural nursing
26 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 26

theory, Leininger’s Culture Care Theory, theethnonursing research method and culturalassessment using the Giger-Davidhizar Transcul-tural Assessment Model. Students learned aboutracial and ethnic groups in the local communityand the US and biological variations in labora-tory and clinical settings. Groups conducted in-depth studies of cultural groups and usedposters to present their learning to one another,at professional meetings, in the school of nurs-ing and in staff lounges in hospitals (Hughes &Hood 2007).
The Cross-Cultural Evaluation Tool devel-oped by Freeman (as cited in Hughes & Hood2007) is a five-point Likert-type scale whichwas used to measure student ability to makeculturally sensitive choices. The tool was usedwith students as a pretest-posttest instrument.Hughes and Hood (2007) found that nursingstudents became more culturally sensitive afterengaging in these specific strategies to teachtranscultural nursing.
A variety of additional teaching strategieswere identified in the literature as effective forteaching culture care. A sampling of the strate-gies discovered is shared here. Brennan andSchulze (2004) assigned students to analyse oneof seven randomly chosen ethnographies usingteacher-set criteria that addressed cultural fac-tors. Students then gathered in groups to dis-cuss, share and seek clarification of meanings inthe ethnographies.This teaching/learning activ-ity resulted in students examining their ethno-centrism and broadened their understanding ofcultural diversity.The need to engage students’affective and cognitive domains of learningthrough experiential learning was identified byCarpio and Majumdar (1993) as necessary foreffective culture care education. In addition,they purported that the teacher was responsibleto create a learning environment where culturaldiversity was viewed positively rather than negatively or as a threat. Finally, Evans and Severtsen (2001) taught novice nursing studentsto use story telling for cultural assessment.
Through practice with peers and then clients ina long-term care clinical setting, studentslearned to ‘listen in a nonjudgmental, contextu-al way to the values and beliefs of the story-teller’ (Evans & Severtsen 2001: 180).
Cultural immersionIn a study using a triangulated research design,St. Clair and McKenry (1999) explored therelationship between short term internationalnursing clinical immersion experiences, culturalself-efficacy and cultural competence.Two hun-dred senior and graduate nursing students par-ticipated over a two year time frame. Eightystudents chose international immersion experi-ences while the remaining 120 students caredfor culturally diverse populations in the UnitedStates.While both groups of students exhibiteda statistically significant increase in cultural self-efficacy as measured by the CSES, students whoparticipated in a two to three week interna-tional clinical immersion reported a greaterincrease than those who remained in the US.Analysis of qualitative data further revealed thatthe international immersion experience facili-tated students in recognizing their ethnocen-trism and need to develop cultural sensitivityand awareness (St Clair & McKenry 1999).
Integrating cultural content in an undergrad-uate nursing program was found to producesmall to moderate gains in students’ perceivedcultural competence. However, for studentsparticipating in a five-week international cultur-al immersion experience, perceived culturalcompetence gains were large. Authors discussedthe importance of students’ values and attitudesin motivating their commitment to provide cul-turally competent care. Opportunities to carefor persons very different from oneself werefound to be critical in developing confidenceand practice expertise (Caffery et al 2005).
Hern et al (2005) discussed a strategy todevelop cultural sensitivity, a global communityperspective and cultural competence throughcollaboration. Exchanges were arranged among
27Volume 28, Issue 1–2,April 2008 CCCCNNNN
How nursing faculty teach culture care CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 27

practicing nurses in the US and Scotland andamong faculty in the US and in Korea. Studentnurses and faculty traveled to Honduras for atwo week cultural immersion experience in thecommunity. Faculty concluded at least twoweeks or more was required to travel andassimilate to a new culture and nursing environ-ment.They pointed out, ‘a week long exchangeis not sufficient to gain sensitivity to the otherculture’ (Hern et al 2005: 41).
The authors developed a workplace modelfor practice and education partnering whichincluded: beginning with a shared vision; devel-oping infrastructure; securing funding; iden-tifying outcomes for practice, education andresearch; marketing these programs; and focus-ing on future collaboration.The importance ofinstitutional support was stressed. Authors iden-tified more similarities than differences existedamong cultural groups involved (Hern et al2005).
A collaborative partnership between the Uni-versity of Pittsburgh and Miami Children’s Hos-pital was created for senior nursing students’final, practice-intensive semester.The purposewas to cultivate undergraduate nursing stu-dents’ cultural competence through exposure topeople from different cultures. Clinical nursespecialists in Miami coordinated the clinicalexperience of students with preceptors thereand with faculty in Pittsburgh. Extensive com-munication among all participants facilitated theprocess. Technology such as video conferencecalls, e-mail and a course web-page were used.Students received scholarships to fund the expe-rience. Authors shared examples of studentlearning gained from caring for patients andfamilies from Jamaican, Hispanic and Haitianbackgrounds (Hoffman et al 2005).
Ryan,Twibell, Brigham and Bennett (2000)conducted a qualitative study of nine practicingregistered nurses who had participated in a cultural immersion experience while earningtheir baccalaureate degrees in nursing. Gradu-ates stressed that while classroom activities and
content were important, their immersion expe-rience was critical to facilitating ‘learning tocare’. Participants provided vivid examples ofhow these immersion experiences influencedthem to provide culturally competent care.Rather than offering an elective course, sugges-tions were made for transcultural care to beviewed as ‘essential’ and integrated throughoutthe curriculum (Ryan et al 2000). Additionally,Ryan and Twibell (2002) found that personalgrowth, increased sensitivity to the needs ofothers and a general expansion of one’s world-view were outcomes of participating in a cultur-al immersion experience.
Based on this review of literature, clinicalcultural immersion experiences are transforma-tive resulting in nursing students’ growth inproviding culturally competent nursing care,addressing the holistic perspective of ethno-centrism and cultivating cultural sensitivity and awareness. Some researchers wonderedwhether national immersion experiences mightbe equally as effective as international experi-ences in challenging students’ ethnocentrismand growth in cultural competence (St. Clair &McKenry 1999). In our world of internationalinstability and students with limited financialresources, national immersion experiences maybe an appropriate option for students and war-rants further study.
Institutional cultureTeaching culture care requires institutional sup-port and a cultural climate where people andexperiences which are different and similar arevalued and embraced. Yearwood et al (2002)held one focus group with seven student vol-unteers representing diverse races, religions,nationalities and genders to explore diversity.Topics included what diversity is, the role of theschool of nursing and university and ideas aboutincorporating diversity in courses and clinicalexperiences. Data gathered has application tonursing education and teaching culture care.Students defined diversity as ‘differences bet-
28 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 28

ween people including biological, religious, sex-ual orientation, life and family style’ and thatdiversity was ‘mostly about color’ (Yearwood etal 2002: 238). Students were confused by theuniversity focus on embracing diversity whileencouraging cultural events and ethnic organisa-tions that focused on differences that separatedgroups of students. Students offered the follow-ing suggestions for faculty interested in facilitat-ing development of cultural sensitivity: smallgroup activities to encourage the opportunity towork with people different from oneself; pro-moting discussion and tolerance; focus on expe-riential learning versus lecture; and a course oncultural diversity incorporated into the curricu-lum (Yearwood et al 2002).
From the educational literature, Marchesaniand Adams (1992) tackled the increasing diver-sity in the student population in higher educa-tion in America and proposed a four-part modelfor teaching and learning in a multicultural con-text. Dimensions were directly related to facili-tating a teaching/learning environment whichvalues diversity and fosters exploration andachievement of cultural competence. Compo-nents of the model speak to knowing oneself,knowing one’s students, developing courseworkwhere diverse perspectives are presented andteaching with a variety of strategies to promotesuccess in students from varied backgrounds.
Schmitz et al (1992) provided an in-depthdescription of implementing the ‘ClassroomClimate Project’ in their university.The purposewas to develop classrooms with an effectivemulticultural context for learning.The goal wasfor faculty to create a warm and inviting, inclu-sive environment where students were valuedand respected.The framework used for facultydevelopment was Palmer’s model for learningand behavioral change which involves fourstages necessary to create lasting change in theclassroom; discovering, formulating new behav-iors, producing new behaviors and generalisa-tion to the real world. Authors identified thecritical ingredient for creating this environment
is ‘a teacher who appropriately recognises andvalues different cultural styles and perspectivesand effectively engages students in the learningprocess’ (Schmit et al 1992: 75). In addition,the authors pointed out efforts for multiculturallearning must involve system wide changes.
Similarly, Grossman et al (1998) illuminatedincongruence between stated philosophical val-ues related to multicultural learning and actualpractice. In a survey of Deans and Directors ofnursing programs in Florida, programs sharedtheir mission and philosophy statements andconceptual frameworks which supported cul-tural diversity and reported that cultural content was either integrated throughout thecurriculum or taught in a specific transculturalnursing course.Yet, lack of cultural knowledge,sensitivity and awareness was most frequentlyidentified by participants as a critical issue related to cultural diversity in their nursing programs (Grossman et al 1998).
Institutional commitment to cultural diversityand creating a climate for teaching culture careshould be demonstrated in the institution’s mis-sion statement, by financial resources for faculty,staff and student development and through faculty and students valuing diversity and mul-ticulturalism (Schmitz et al 1992). Creatingmulticultural learning environments in the uni-versity setting is dependent on a ‘large-scale,complex, sustained organisational and culturaltransformation’ (Marchesani & Adams 1992: 10).
Review of literature conclusionTeaching culture care in nursing education is critical to ensuring a culturally competentworkforce. The literature indicates faculty arenot adequately prepared to teach culture care ormentor students in cultural sensitivity.The liter-ature suggests culture care and cultural compe-tence are complex phenomena requiring broad,holistic approaches and teaching strategies topromote student understanding and applicationin their nursing practice.There is ambiguity andlack of consensus in the literature about the
29Volume 28, Issue 1–2,April 2008 CCCCNNNN
How nursing faculty teach culture care CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 29

meaning and use of the terms ‘cultural compe-tence’ and ‘culturally congruent care’. Thisresearcher referred to these terms as they wereused by authors in their articles. Overwhelm-ingly, researchers recommend that formal tran-scultural nursing be integrated throughout thecurriculum (Alpers & Zoucha 1996; Baldonadoet al 1998; Hughes & Hood 2007; Ryan, Carl-ton & Ali 2000; Ryan, Twibell et al 2000; Sar-gent et al 2005) and that cultural immersionexperiences are essential for learning to provideculturally congruent care (Bosworth et al 2006;Caffery et al 2005; Ryan,Twibell et al 2000; Ryan& Twibell 2002; St Clair & McKenry 1999).
While nursing programs and institutions ofhigher learning may have mission and philoso-phy statements supporting diversity and culturalcontent incorporated in curricula, the literaturereflects there is incongruence between what isstated and the practices of faculty and studentsin classroom and clinical settings (Canales &Bowers 2001; Cook & Cullen 2000; Evans 2004;Gardner 2005; Grossman et al 1998). Learningto embrace the diverse and similar needs ofnursing students and the individuals, familiesand communities cared for requires a deep levelof personal, faculty, college and university com-mitment (Campinha-Bacote 2005; Cook & Cullen2000; Edwards 2003; Newman & Williams 2003).Cultural diversity must be valued and respectedby institutional culture and integrated through-out nursing curricula to move beyond culturalawareness and cultural sensitivity to culturalcompetence.
There are gaps in the quantitative and quali-tative research literature about the preparationfaculty have had in transcultural nursing and inteaching about culture care, cultural diversityand culturally congruent and competent care.Few studies were found which used nursing the-ory as a framework for nursing research andpractice related to teaching culture care. Manystudies have been conducted using a variety ofquantitative measurement tools to measure stu-dent learning about culture and related con-
cepts. In conclusion, there have been no studiesconducted to discover nursing faculty careexpressions, patterns and practices related toteaching culture care nor have there been anyethnonursing research studies conducted usingthe Culture Care Theory in this context. Resultsof the following pilot study provide preliminaryresearch in preparation for a major study to fillthis gap.
PILOT STUDY: PURPOSE, GOALAND DOMAIN OF INQUIRYThe domain of inquiry for this transculturalnursing pilot study was nursing faculty teachingculture care within the environmental contextof an urban baccalaureate nursing program in apublic university in the southeastern UnitedStates.This domain of inquiry is a major interestin nursing because of the growing diversity ofthe population in the United States, concernsabout the provision of global health care and thecall for more nurses prepared in transculturalnursing.The researcher predicted that nursingfaculty epistemology (knowing how to teachculture care) and ontology (faculty modelingculturally congruent care) are essential to teachstudents to provide culturally congruent care.The purpose of this study was to discover,describe and systematically analyse the careexpressions, patterns and practices of nursingfaculty related to teaching culture care.The goalof this study was to discover faculty care thatfacilitates teaching baccalaureate nursing stu-dents learning how to provide culture care.
Research questionsIn studying the domain of faculty teaching cul-ture care within the environmental context ofundergraduate baccalaureate programs in nurs-ing, two broad questions were used within theethnonursing research method to guide theresearcher.These research questions were:
1. In what ways do nursing faculty care exp-ressions, patterns and practices influenceteaching culture care?
30 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 30

2. In what ways do worldview, culture andsocial structure and environmental contextinfluence nursing faculty teaching culturecare?
Theoretical frameworkThe Culture Care Theory (CCT) together withthe Sunrise Enabler (which depicts an inte-grated holistic view of the influencing dimen-
sions and major concepts of the theory)(Leininger 2006a) provided the framework forthis research study (Figure 1).This nursing the-ory was chosen because of the researcher’sinterest in using the theory in the context ofnursing education and its relevance to thedomain of inquiry. The Culture Care Theoryprovides a holistic means to understand therange of factors that influence nursing faculty
31Volume 28, Issue 1–2,April 2008 CCCCNNNN
How nursing faculty teach culture care CCCCNNNN
FIGURE 1: LEININGER’S SUNRISE ENABLER TO DISCOVER CULTURE CARE
Source: Copyright M Leininger 2004. Reprinted with permission from Dr Leininger.
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 31

teaching culture care. McFarland & Leininger(2002) proposed that nursing education in the21st century must become ‘transculturallygrounded’ (McFarland & Leininger 2002: 528)by considering the phenomena of student, facul-ty and client culture care values, beliefs andpractices. Previously, there have been no studiesconducted to discover these phenomena relatedto teaching culture care and no ethnonursingresearch studies conducted using the CultureCare Theory in this context.
Ethnonursing research methodLeininger developed the ethnonursing researchmethod to study transcultural human care phenomena using her theory of Culture CareDiversity and Universality (Leininger 2006a).The method uses an open, largely inductiveprocess of discovery to document, describe,understand and interpret peoples’ care mean-ings and experiences (Leininger 2006b) andtherefore is useful to understand the realities offaculty teaching culture care.The ethnonursingmethod embraces the importance of discoveryfrom the people’s (emic) ways of knowing andgives credence to the professional nurse’s (etic)way of knowing (Leininger 2006b). Key in-formants are those people holding the mostknowledge about the domain of inquiry whilegeneral informants provide reflective data aboutteaching culture care, stimulating the researcherto focus on care similarities and differencesamong informants. Nursing faculty as knowerswere purposefully selected for participation inthis research study. Key informants were fulltime tenure-track nursing faculty while generalinformants were full time, non-tenure track andadjunct faculty.
Three key informants (who held doctoraldegrees) and three general informants (ad-vanced practice nurses) participated in this pilotstudy. All informants were female, ranging inage from 27 to 55 years old and had between1.5 and 27 years of teaching experience. Fourwere African American, two were Anglo-Ameri-
can (German/English-American [n = 1] andEnglish/French American [n = 1]who furtheridentified herself as a ‘liberal southerner’) andtwo spoke some Spanish. None of the inform-ants had ever had a course in transcultural nurs-ing. Four participants continued to participatein direct client care and three had psychiatricnursing backgrounds.
Approval was received from the University ofNorthern Colorado Institutional Review Boardand written consent was obtained from all par-ticipants. Data was gathered using unstructured,open-ended interviews, participant observationand extensive field notes. Data were analyzedusing Leininger’s four phases of ethnonursinganalysis for qualitative data and application ofthe qualitative criteria of credibility, confirma-bility, meaning-in-context, recurrent patterningand saturation (Leininger 2006b).
PILOT STUDY FINDINGSBased on data analysis, three major themes werediscovered by the researcher. The first themewas Faculty provided generic and professional care tonursing students to maintain and promote healthyand beneficial lifeways within the environmental con-text of a baccalaureate nursing program. Facultyexpressed they learned to care from their fami-lies, friends and mentors, ‘I learned how to careby people caring for me.’ Caring was learnedand taught to students through mentoring androle modeling; ‘listening’, ‘being approachable’,‘checking in’. Care was reciprocal and multidi-mensional.
The second theme discovered was Facultytaught students culture care with major differencesamong classroom, on-line and clinical contexts butwithout an organising conceptual framework. Somefaculty taught culture care in classroom and on-line contexts, generally within a course moduleor reading assignment. All faculty explicitlytaught culture care during clinical experienceswhich occurred in community and acute carecontexts. Faculty spoke about the diversity ofthe client population in the urban setting, ‘just
32 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 32

by the nature of being in our clinic they had to address all those cultural issues.’ Facultydescribed their nursing students had manyopportunities to care for Asian, Hispanic,African American and African patients and fami-lies. Most faculty taught culture care without anorganising conceptual framework. Culture carewas taught at the cultural diversity level as fac-ulty only discussed cultural competence relatedto race/ethnicity rather than from a broaderperspective.
The third theme discovered was care is essen-tial for faculty health and well-being and to enablefaculty to teach culture care to baccalaureate nursingstudents. Faculty expressed the importance ofmutuality as caring and mentoring. Mentoringoccurred related to teaching coursework, schol-arly work and how to ‘be’ as a faculty member.Mentors impressed the importance of caring foroneself to be enabled to care about others andbalancing the tripartite faculty roles of teaching,scholarship and service. Caring was expressedas providing leadership to create a healthy caring community for faculty. Some facultytook responsibility for their part in creating thiscommunity ‘I think everybody has to take theirresponsibility for the school; it’s not just oneperson, but it’s a collective effort’; while othersfelt administrators were responsible.
Diversity within this theme was discovered.Non-care was expressed as not assisting new fac-ulty, faculty not being on time for meetings andovert and covert racism. ‘There is still the greatdivide (in the city)… the great racial divide.’Another informant expressed that within theschool of nursing the ‘racial environment ischarged from both sides.’ A third informant dis-cussed difficulty in trusting colleagues; there-fore, she sought mentoring and encouragingrelationships within a minority professionalnursing organisation.
Discoveries for teaching culture careThe Culture Care Theory includes application
of research discoveries in nursing care using thethree modes of culture care actions and deci-sions. These modes are derived from synthesisand analysis of qualitative study data and thenconfirmed with informants for accurate mean-ings. Culture Care Preservation/Maintenance refersto those assistive, supporting, facilitative, orenabling professional actions and decisions thathelp nursing faculty retain and preserve relevantcare expressions, patterns and practices to teachculture care and contribute to the health of faculty, students and clients (derived fromLeininger 2006a: 8). Discoveries from this studysuggest nursing faculty should maintain effortsto assist students to care for culturally diverseclients in the clinical setting. For example, nurs-ing faculty discussed working hard to ensureeach nursing student had the opportunity tocare for patients and families from different eth-nic cultural groups. Faculty expressed theimportance of being mentored in learning howto care and in turn provided extensive mentor-ing and role modeling for students as theylearned to provide care.
Culture Care Accommodation/Negotiation refersto those assistive, supporting, facilitative, orenabling professional actions and decisions thathelp nursing faculty adapt to or negotiate withothers relevant care expressions, patterns andpractices to teach culture care and contribute to the health of faculty, students and clients(derived from Leininger 2006a: 8). Findingsfrom this study suggest nursing faculty maywish to negotiate integrating culture care con-tent into established nursing courses throughoutthe curriculum and introduce required andelective courses on culture care. While allinformants valued teaching culture care, therewas limited formal transcultural nursing con-cepts taught. No formal courses existed toteach culture care and there was no integrationof culture care content across the curriculum.
Culture Care Repatterning/Restructuring refersto those assistive, supporting, facilitative, orenabling professional actions and decisions that
33Volume 28, Issue 1–2,April 2008 CCCCNNNN
How nursing faculty teach culture care CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 33

help nursing faculty reorder, change, or greatlymodify relevant care expressions, patterns andpractices to teach culture care and contribute to the health of faculty, students and clients(derived from Leininger 2006a: 8).
An important finding from this study wasculture care repatterning/restructuring may beused with nursing faculty to establish the cul-ture care theory as an organising framework forteaching culture care in the classroom, on-lineand clinical contexts. The use of a theoreticalbasis for teaching culture care is necessary toassist faculty and students in moving beyond aview of culture as race/ethnicity to a broader,holistic view. Such an expanded worldviewfacilitates students and faculty respecting andunderstanding patients’ and families’ culturalvalues, beliefs and lifeways resulting in benefi-cial and satisfying care (derived from Leininger2006a: 4).
CONCLUSIONDespite 50 years of transcultural nursing knowl-edge development through theory, research andpractice, there remains a lack of formal, inte-grated culture education in nursing (Baldonado1998; Hughes & Hood 2007).This review of lit-erature and pilot study offer nursing educatorsinsight into factors influencing teaching culturecare in nursing programs. Findings are usefulfor nurse educators in university settings as they seek to prepare nursing students to providemeaningful, satisfying and beneficial care forpeople who are similar to and different fromthem resulting in nurses prepared to provideculturally congruent care in a multiculturalworld. Culturally diverse and similar studentsmay be recruited and thrive in nursing pro-grams where teaching culture care is embraced(McFarland et al 2006; Pacquiao 2007).
The Culture Care Theory with the SunriseEnabler and ethnonursing research method pro-vided a useful framework and method for thispilot study. This unique use of the theory andmethod demonstrates its usefulness in dis-
covering and describing the complex nature ofteaching culture care within the environmentalcontext of university schools of nursing. Con-ducting a larger scale research study is predictedto further support and substantiate the CultureCare Theory; thus contributing to buildingknowledge for the discipline of nursing andspecifically the practice of nursing in the areasof nursing education and the provision of cul-turally congruent and competent care.
AcknowledgementsFunding for this research was received fromMiddle Tennessee State University, FacultyResearch and Creative Projects Committee andXi Alpha Chapter of Sigma Theta Tau, Interna-tional Honor Society of Nursing. The authorwishes to acknowledge expertise and supportfrom the University of Northern Colorado fac-ulty and my dissertation committee members:Dr Debra Leners, Dr Marilyn McFarland, DrMargaret Andrews and Dr Linda Lohr.
ReferencesAlpers RR and Zoucha R (1996) Comparison of
cultural competence and cultural confidenceof senior nursing students in a private south-ern university, Journal of Cultural Diversity 3:9–15.
American Association of Colleges of Nursing(2004) Online FY05-06 Strategic Plan.Accessedat http:www.aacn.nche./edu/ContactUs/Strtplan.htm on 1 October 2004.
Baldonado A, Ludwig Beymer P, Barnes K,Starsiak D, Nemivant EB and Anonas-TernateA (1998) Transcultural nursing practicedescribed by registered nurses and bacca-laureate nursing students, Journal ofTranscultural Nursing 9: 15–25.
Bosworth TL, Halburdo EP, Hetrick C, PatchettK,Thompson MA and Welch M (2006)International partnerships to promote qualitycare: Faculty groundwork, student projectsand outcomes, The Journal of ContinuingEducation in Nursing 37: 32–38.
34 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 34
Brennan SJ and Schulze MW (2004) Culturalimmersion through ethnography:The livedexperience and group process, Journal ofNursing Education 43: 285–288.
Caffrey RA, Neander W, Markle D and Stewart B(2005) Improving the cultural competence ofnursing students: Results of integratingcultural content in the curriculum and aninternational immersion experience, Journal ofNursing Education 44: 234–240.
Campinha-Bacote J (2005) A Biblically BasedModel of Cultural Competence in the Delivery ofHealthcare Services,Transcultural CAREAssociates, Cincinnati, OH.
Campinha-Bacote J (2003) The Process of CulturalCompetence in the Delivery of Healthcare Services:A culturally competent model of care,Trans-cultural CARE Associates, Cincinnati, OH.
Canales MK and Bowers BJ (2001) Expandingconceptualizations of culturally competentcare, Journal of Advanced Nursing 36: 102–111.
Carpio BA and Majumdar B (1993) Experientiallearning:An approach to transculturaleducation for nursing, Journal of TransculturalNursing 4: 4–11.
Coffman MJ, Shellman J and Bernal H (2004) Anintegrative review of American nurses’perceived cultural self-efficacy, Journal ofNursing Scholarship 36: 180–185.
Cook PR and Cullen JA (2000) Diversity as avalue in undergraduate nursing education[Electronic version], Nursing and Health CarePerspectives 21: 178.
Edwards K (2003) Increasing culturalcompetence and decreasing disparities inhealth [Electronic version], Journal of CulturalDiversity 10(4): 111–12.
Evans BC (2004) Application of the caringcurriculum to education of Hispanic/Latinoand American Indian nursing students, Journalof Nursing Education 43: 219–228.
Evans BC and Severtsen BM (2001) Storytellingas cultural assessment, Nursing and Health CarePerspectives 22: 180–183.
Gardner J (2005) Barriers influencing the
success of racial and ethnic minority studentsin nursing programs, Journal of TransculturalNursing 16: 155–162.
Grossman D, Massey P, Blais K, Geiger E, LoweJ, Pereira O, Stewart A,Taylor R, Filer V,Nembhard J and Tally-Ross N (1998) Culturaldiversity in Florida nursing programs:Asurvey of deans and directors, Journal ofNursing Education 37: 22–26.
Hegyvary ST (2006) Health disparities related torace and ethnicity, Journal of NursingScholarship,Third Quarter: 205.
Hern MJ,Vaugh G, Mason D and Wietkamp T(2005) Creating an international nursingpractice and education workplace, Journal ofPediatric Nursing 20: 34–44.
Hoffman RL, Messmer PR, Hill-Rodriguez DLand Vazquez D (2005) A collaborativeapproach to expand clinical experiences andcultural awareness among undergraduatenursing students, Journal of Professional Nursing21: 240–243.
Hughes KH and Hood LJ (2007) Teachingmethods and an outcome tool for measuringcultural sensitivity in undergraduate nursingstudents, Journal of Transcultural Nursing 18:57–62.
Jefferies MR and Smodlaka I (1999) Constructvalidation of the transcultural self-efficacytool [Electronic version], Journal of NursingEducation 38: 222–227.
Kulwicki A and Boloink BJ (1996) Assessment oflevel of comfort in providing multiculturalnursing car by baccalaureate nursing students,Journal of Cultural Diversity 3: 40–45.
Leininger M (2006a) Culture care diversity anduniversality theory and evolution of theethnonursing method, in Leininger M andMcFarland MR (eds) Culture Care Diversity &Universality:A worldwide nursing theory, 2ndedn, Ch 1, Jones & Bartlett, New York.
Leininger M (2006b) Ethnonursing researchmethod and enablers [Revised reprint] inLeininger M and McFarland MR (Eds) CultureCare Diversity & Universality:A worldwide nursing
35Volume 28, Issue 1–2,April 2008 CCCCNNNN
How nursing faculty teach culture care CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 35

theory, 2nd edn, Ch 2, Jones & Bartlett, NewYork.
Majumdar B, Browne G, Roberts J and Carpio B(2004) Effects of cultural sensitivity trainingon health care provider attitudes and patientoutcomes, Journal of Nursing Scholarship 36:161–166.
Marchesani LS and Adams M (1992) Dynamicsof diversity in the teaching-learning process:A faculty development model for analysis andaction, New Directions in Teaching and Learning52: 9–20.
McFarland MR and Leininger M (2002)Transcultural nursing: Curricular concepts,principles and teaching and learning activitiesfor the 21st century, in Leininger M andMcFarland MR (Eds) Culture Care Diversity &Universality:A worldwide nursing theory, 2ndedn, Ch 34, McGraw-Hill, USA.
McFarland MM, Mixer SJ, Lewis AE and EasleyCE (2006) Use of the Culture Care Theory as aframework for the recruitment, engagementand retention of culturally diverse students in atraditionally European American baccalaureatenursing program, in Leininger M andMcFarland MR (Eds) Culture Care Diversity &Universality:A worldwide nursing theory, 2nd edn,Ch 8, Jones & Bartlett, New York.
Newman M and Williams J (2003) Educatingnurses in Rhode Island:A lot of diversity in alittle place [Electronic version], Journal ofCultural Diversity 10: 91–95.
Pacquiao D (2007) The relationship between cul-tural competence education and increasing div-ersity in nursing schools and practice settings,Journal of Transcultural Nursing 18: 28S–37S.
Rew L, Becker H, Cookston J, Khosropur S andMartinez S (2003) Measuring culturalawareness in nursing students, Journal ofNursing Education 42: 249–257.
Ryan M, Carlton K and Ali N (2000) Transcul-tural nursing concepts and experiences innursing curricula, Journal of TransculturalNursing 11: 300–307.
Ryan M and Twibell RS (2002) Outcomes of a
transcultural nursing immersion experience:Confirmation of a dimensional matrix, Journalof Transcultural Nursing 13: 30–39.
Ryan M,Twibell R, Brigham C and Bennett P(2000) Learning to care for clients in theirworld, not mine [Electronic version], Journalof Nursing Education 39: 402–408.
Sargent SE, Sedlack CA and Martsolf DS (2005)Cultural competence among nursing studentsand faculty, Nurse Education Today 25: 214–221.
Schmitz B, Paul S P and Greenberg J D (1992)Creating multicultural classrooms:Anexperience-derived faculty developmentprogram, New Directions for Teaching andLearning 42: 75–87.
St Clair A and McKenry L (1999) Preparing cul-turally competent practitioners [electronicversion], Journal of Nursing Education 38:228–234.
The Sullivan Commission: Kellogg Foundation(2004) Missing persons: Minorities in the healthprofessions.A report of the Sullivan Com-mission on diversity in the healthcareworkforce, Battle Creek MI, accessed athttp://admissions.duhs.duke.edu/sullivancommission/index.cfm on 14 November 2006.
US Census Bureau (2005) USA Quick Facts fromthe US Census Bureau, accessed at http://quickfacts.census.gov/qfd/states/00000.html on 9April 2007.
US Department of Health and Human Services(1996) National Advisory Council on NurseEducation and Practice: Report to the Secretary ofHealth and Human Services on the Basic RegisteredNurse Work Force, US Government PrintingOffice,Washington DC.
Wilson AH, Sanner SJ and McAlliter LE(November 2003) The Honor Society of Nursing,Sigma Theta Tau International DiversityResource Paper, accessed at http://www/nursingsociety.org/about/Diversity-paper.pdf.on 9 April 2007.
Yearwood EL, Brown DL and Karlik EC (2002)Cultural diversity: Student’s perspectives,Journal of Transcultural Nursing 13: 237–240.
36 Volume 28, Issue 1–2,April 2008CCCCNNNN
Sandra J MixerCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 36

Most US schools of nursing include somereference to a culturally competent grad-
uate in their program mission and/or outcomestatement. Cultural competence in the deliveryof nursing care is an expectation of accredita-
tion and approval boards for nursing (AmericanAssociation of Colleges of Nursing [AACN]1997; American Nurses Association 1986; NLN2003). However to date, no studies are found inthe literature evaluating which curricula are the
Key Wordsnursing; culturalcompetency;BSN students;curriculum;nursing students CN
37Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 37–44.
Cultural competency of graduatingUS Bachelor of Science
nursing students
ABSTRACT Cultural competence in the delivery of nursing care is an expectation ofaccreditation and approval boards for nursing in the United States.This studyevaluated the effectiveness of four different nursing program curricula indeveloping culturally competent new graduates. Four methodologically andgeographically diverse groups of graduating BSN students in the United Stateswere given the Inventory for Assessing the Process of Cultural CompetencyAmong Healthcare Professionals-Revised (IAPCCC-R®) prior to graduationand after completion of course work.A variety of curricular methods for achiev-ing cultural competency were included.Two programs utilise a theory or amodel developed by recognised transcultural expert nurses, Madeline Leiningerand Josepha Campinha-Bacote. One program utilised an integrated approachemploying no specific model. One program utilised a free-standing two creditculture course within the curriculum, taught by nursing faculty with strongcultural preparation. Results indicate that these 212 graduating nursing stu-dents scored only in the culturally aware range, as measured by the IAPCC-R©,regardless of what program model they attended.
Received 29 January 2008 Accepted 22 March 2008
SUZAN
KARDONG-EDGRENAssistant ProfessorIntercollegiateCollege of NursingWashington StateUniversitySpokane WA, USA
JOSEPHA
CAMPINHA-BACOTEPresidentTranscultural CAREAssociatesCase WesternReserve UniversityCincinnati OH, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 37

most successful in developing culturally compe-tent graduates (Bond 2004; Grant & Letzring2003; Jones & Bond 2000).This study evaluatedthe effectiveness of four different nursing pro-gram curricula in developing culturally compe-tent new graduates.
A universally agreed-upon definition of whatcultural competency is, is still lacking althoughdefinitions are more alike than dissimilar.‘Specific content is not defined in detail andthere is a dearth of evidence based educationstudies on what to teach in a culturally compe-tent curriculum’ (Bond 2004: 2). Multiple cur-ricular strategies are employed by nursingprograms to teach cultural competence and mayinclude free-standing cultural courses, immer-sion and international experiences of varyinglengths. Two outstanding curricula guides forteaching cultural competency, sponsored by theUnited State Department of Health and HumanServices (USDHHS), recently became availableto all online – USDHHS Office of MinorityHealth’s Culturally Competent Nursing Modules(CCNM) and USDHSS Health Resources andServices Administration’s document, Transform-ing the Face of Health Professions Through Culturaland Linguistic Competence Education: The Role of the HRSA Centers of Excellence (Campinha-Bacote2006).
Integration across the curriculum is the mostfrequently cited method for teaching culturalmaterial (Grant & Letzring 2003; Grossman etal 1998; Kardong-Edgren et al 2005; Lipson &DeSantis 2007). The integration model mayallow programs to skirt the problems associatedwith the addition of cultural content, seen bymany as soft science in a biomedically laden cur-riculum (Betancourt 2007). In addition, use ofthe integrated approach may mean cultural con-tent is ‘implemented ad hoc by a committedfew’ (Boyle 2007: 21S).The ability of faculty tointegrate culture into a curriculum remains aquestion, although a recent study suggests fac-ulty are increasingly culturally competent (Kar-dong-Edgren 2007). Some argue that the basic
definition of nursing as the diagnosis and treat-ment of human response to illness should pre-clude the need for teaching cultural competencyas a topic at all (Dreher & McNaughton 2002).However, this approach discounts ‘the macro-level sociological and economic factors in whichthis (health) encounter occurs and health deci-sions are made’ (Lipson & DeSantis 2007: 19S).
While the debate continues about the bestway to teach cultural content, ‘without ade-quate evaluation, we cannot know which is the most effective method to develop culturalcompetency’ (Lipson & DeSantis: 18S). Thereare no articles in the literature specifically eval-uating cultural competency of graduating nurs-ing students.
The purpose of this study was to evaluate thecultural competency of graduating nursing stu-dents from programs using different kinds ofcurricular approaches. If one approach provedmore efficacious, it might serve as a model forother programs struggling with best practicesfor teaching cultural content in their programs.This descriptive study used a post-test onlydesign to measure the cultural competency ofgraduating BSN students from four geographi-cally diverse nursing programs.
Cultural competency is defined as ‘theprocess in which the healthcare provider con-tinuously strives to achieve the ability to workeffectively within the cultural context of aclient, individual, family or community’ (Camp-inha-Bacote 2003: 54) for the purposes of thisstudy. Five model constructs include: culturaldesire, cultural awareness, cultural skill, cul-tural knowledge, and cultural encounters.Campinha-Bacote argues that the key to culturalcompetency is cultural desire, wanting to,rather than having to, learn and interact withother cultures.
LITERATURE REVIEWMany studies reported in the USA have evaluat-ed the cultural competency of nursing students,using a variety of instruments (Bond, Kardong-
38 Volume 28, Issue 1–2,April 2008CCCCNNNN
Suzan Kardong-Edgren and Josepha Campinha-BacoteCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 38

Edgren & Jones 2001; Felder 1990; Pope et al1994; Napholz 1999; Schlosser et al 2004;Zorn, Ponick & Peck 1995). Results have beenmixed. Senior nursing students experiencedincreased self confidence with internationalstudy abroad experiences (St. Clair & McKenry1999; Zorn et al 1995) and when receiving cul-tural content in a senior level community healthclass (Alpers & Zoucha 1996). However, othergraduating senior students expressed little self-confidence in their ability to care for ethnicallydiverse patients (Kulwicki & Bolonik 1996).
The most frequently-cited method for teach-ing culture is integration across the curriculum(Grant & Letzring 2003; Kardong-Edgren et al2005).This methodology might be consideredsuspect considering the oft-cited lack of facultyprepared to teach cultural material (Bond 2004;Leininger & McFarland 2002; Ryan et al 2000).The use of integration may have been a usefulstrategy to meet accreditation requirements,allowing those faculty who knew somethingabout culture to address it and allowing thosefaculty who did not, to catch up. Kardong-Edgren (2007) found that nursing faculty wereculturally competent, although this is contraryto recent findings (Kardong-Edgren et al 2005;Ryan et al 2000).
Evaluating cultural competency in students isdifficult because of a lack of appropriate instru-mentation for this group. Most cultural compe-tency tools have been normed on practicingnurses; students may lack ‘the experience need-ed to be aware of what they do not know’(Coffman, Shellman & Bernal 2004: 184). Coff-man et al recently advised against using the Cul-tural Self Efficacy Scale (CSES) with students.The CSES is the most frequently used tool formeasuring cultural competency.
METHODOLOGYCampinha-Bacote’s (2003) Process of CulturalCompetence in the Delivery of Healthcare Services model provided the conceptual frame-work for this study. The model constructs
were measured using a version of Campinha-Bacote’s Inventory for Assessing the Process of Cultural Competency Among HealthcareProfessionals-Revised (IAPCC-R©).The IAPCC-R© is designed to measure the level of culturalcompetence among healthcare professionals andconsists of 25 items that measure the five cul-tural constructs of desire, awareness, knowl-edge, skill and encounters. Five items addresseach construct.The IAPCC-R© uses a four-pointLikert scale reflecting the response categories ofstrongly agree, agree, disagree, strongly dis-agree; very aware, aware, somewhat aware, notaware; very knowledgeable, knowledgeable,somewhat knowledgeable, not knowledgeable;very comfortable, comfortable, somewhat com-fortable, not comfortable; and very involved,involved, somewhat involved, not involved.Completion time is approximately 10–15 min-utes. Scores range from 25–100 and indicatewhether a healthcare professional is operating ata level of cultural proficiency, cultural compe-tence, cultural awareness or cultural incom-petence. Higher scores depict a higher level ofcultural competence.The IAPCC-R© has beenused extensively with an average reliability coef-ficient Cronbach’s alpha of 0.83. Descriptivestatistics about the sample population were col-lected including age, gender, previous experi-ence in a foreign country and ability to speak aforeign language.
This study compared scored on the IAPCC-R© of graduating students from four schools ofnursing. Schools were chosen in a snowball sam-ple and after email conversations with represen-tatives at each school. A variety of curricularmethods for achieving cultural competency wereincluded. Two programs utilise a theory or amodel developed by recognised transculturalexpert nurses, Madeline Leininger and JosephaCampinha-Bacote. One program utilised an inte-grated approach employing no specific model.One program utilised a free-standing two creditculture course within the curriculum, taught bynursing faculty with strong cultural preparation.
39Volume 28, Issue 1–2,April 2008 CCCCNNNN
Cultural competency of graduating US Bachelor of Science nursing students CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 39

Graduating seniors in the fall semester of2006 in all participating schools of nursing wereasked to participate in the study. Each site coor-dinator gained institutional review board (IRB)approval from their respective school. Studysurveys were given out at each institution, inNovember or December, before fall graduation,depending on the program and after all pro-gram content had been completed. Table 1shows return rates by program. Seventy-five percent of students eligible for the study chose toparticipate.
Each student survey was coded with a num-ber corresponding to the school name. As par-ticipating students handed in their surveys, theywere invited to sign their name on a slip ofpaper that was put in a bag for a drawing for aUSD 50 incentive prize, after all surveys werecollected. Site coordinators mailed all studyforms to a central location for statistical analy-sis. Data was analyzed using ANOVA.
RESULTSCompetency scores for 218 students from fourprograms, as measured by the IAPCC-R©, werecomputed and reported as aggregate data byschool. All program means were scored in the culturally aware range, as measured by the
IAPCC-R©. No curricular strategy appeared tobe better than another.Tables 1 and 2 show theparticipant numbers, program response rates,program mean scores and descriptive statistics.The Cronbach’s alpha for the total sample wascomputed at 0.82. Post-test means of studentsfrom the four different programs were com-pared using a one-way ANOVA. Statistics byprogram are reported in Table 2. No significantdifference between programs was found (F,3214 = 1.24, P > 0.05). Extensive demograph-ic data including ethnicity, gender, age, interna-tional student status, experience abroad, andprior educational degrees are reported.
DISCUSSIONResults indicate that graduating nursing stu-dents scored only in the culturally aware range,as measured by the IAPCC-R©, regardless ofwhat program model they attended. One mighttend to think that the free-standing coursewould foster better results as students are con-centrating efforts and thought for a specificperiod of time on culture, yet there was no dif-ference. Programs with the most diverse stu-dent bodies, most international students, oldestand youngest student bodies, also did not farebetter than any other program.
40 Volume 28, Issue 1–2,April 2008CCCCNNNN
Suzan Kardong-Edgren and Josepha Campinha-BacoteCCCCNNNN
TABLE 1: PARTICIPANT SCHOOLS, METHOD OF TEACHING CULTURE, AND PERCENTAGE RETURN
School Potential participants Actual participants Percentage return
Large eastern integrated curriculum(Campinha-Bacote) 65 38 58Large western free standing cultural course 100 83 83Small western integrated (Leininger) 36 31 86Large southwestern curriculum integrated 92 66 72Total 293 218 75
TABLE 2: PROGRAM MEAN SCORES
N Mean Std deviation Cronbach’s alpha
Large eastern integrated (Campinha-Bacote) 38 73.95 8.298 0.87Large western free standing cultural course 83 70.46 11.238 0.81Small western integrated (Leininger) 31 70.97 12.758 0.85Large southwestern integrated 66 70.70 6.187 0.79
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 40

41Volume 28, Issue 1–2,April 2008 CCCCNNNN
Cultural competency of graduating US Bachelor of Science nursing students CCCCNNNN
TABLE 3: STUDENT ETHNICITY, GENDER, AGE, INTERNATIONAL STATUS BY PROGRAM
Large eastern Small western Large Largeintegrated integrated southwestern western
Campinha-Bacote Leininger integrated freestanding Total
Ethnicity/school n % n % n % n % n %
Asian 5 13.2 1 3.2 14 21.2 4 4.8 24 11Black 2 5.3 0 0 9 13.6 2 2.4 13 6Native American/
Alaskan 0 0 0 0 1 1.5 0 0 1 0.5Pacific Islander 1 2.6 1 3.2 1 1.5 3 3.6 6 2.8White 29 76.3 28 90.3 32 48.5 72 86.7 161 73.9Other 1 2.6 1 3.2 8 12.1 3 3.6 13 6.0Black and white 0 0 1 3.2 0 0 1 .5Hispanic 1 2.6 0 0 7 10.6 1 1.2 8 3.7Hispanic/white 0 0 0 0 1 .5Mex. American 0 0 1 1.5 0 1 .5Italian American 0 0 0 1 1.2 1 .5Spanish, Italian,
French, Irish 0 0 0 1 1.2 1 .5Total 38 31 66 83 218 100
Gender
Male 4 10.5 3 9.7 4 6.1 9 10.8 20 9.2Female 34 89.5 28 90.3 60 90.9 74 89.2 196 89.9Total 38 31 64 83 216 99.1
Age
Mean 26.03 32.16 26.37 24.54 26.44Median 25 29 24 23 24Min 21 23 21 20 20Max 42 52 53 52 53
International status
Yes 0 0 8 4 12 5.5Bangladesh 1 1.5Burma 1 1.5Hong Kong 1 1.5Iran 1 1.5Japan 1 1.5Nepal 1 1.5Nigeria 1 1.5Japan 2 2.4South Korea 1 1.2Ukraine 1 1.2Total 0 0 8 12.5 4 4.8 12 5.5
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 41
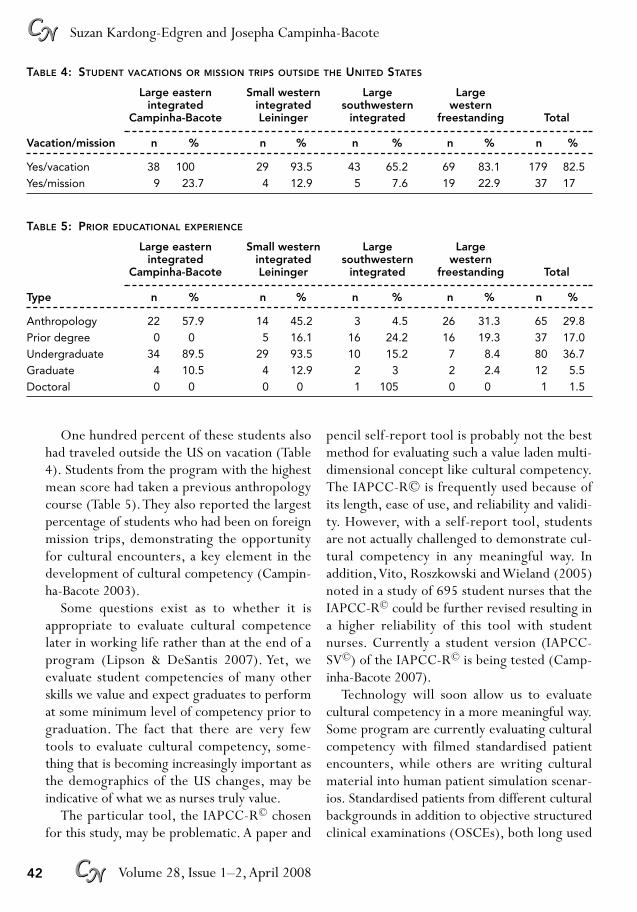
One hundred percent of these students alsohad traveled outside the US on vacation (Table4). Students from the program with the highestmean score had taken a previous anthropologycourse (Table 5).They also reported the largestpercentage of students who had been on foreignmission trips, demonstrating the opportunityfor cultural encounters, a key element in thedevelopment of cultural competency (Campin-ha-Bacote 2003).
Some questions exist as to whether it isappropriate to evaluate cultural competencelater in working life rather than at the end of aprogram (Lipson & DeSantis 2007). Yet, weevaluate student competencies of many otherskills we value and expect graduates to performat some minimum level of competency prior tograduation. The fact that there are very fewtools to evaluate cultural competency, some-thing that is becoming increasingly important asthe demographics of the US changes, may beindicative of what we as nurses truly value.
The particular tool, the IAPCC-R© chosenfor this study, may be problematic. A paper and
pencil self-report tool is probably not the bestmethod for evaluating such a value laden multi-dimensional concept like cultural competency.The IAPCC-R© is frequently used because ofits length, ease of use, and reliability and validi-ty. However, with a self-report tool, studentsare not actually challenged to demonstrate cul-tural competency in any meaningful way. Inaddition,Vito, Roszkowski and Wieland (2005)noted in a study of 695 student nurses that theIAPCC-R© could be further revised resulting ina higher reliability of this tool with studentnurses. Currently a student version (IAPCC-SV©) of the IAPCC-R© is being tested (Camp-inha-Bacote 2007).
Technology will soon allow us to evaluate cultural competency in a more meaningful way.Some program are currently evaluating culturalcompetency with filmed standardised patientencounters, while others are writing culturalmaterial into human patient simulation scenar-ios. Standardised patients from different culturalbackgrounds in addition to objective structuredclinical examinations (OSCEs), both long used
42 Volume 28, Issue 1–2,April 2008CCCCNNNN
Suzan Kardong-Edgren and Josepha Campinha-BacoteCCCCNNNN
TABLE 4: STUDENT VACATIONS OR MISSION TRIPS OUTSIDE THE UNITED STATES
Large eastern Small western Large Largeintegrated integrated southwestern western
Campinha-Bacote Leininger integrated freestanding Total
Vacation/mission n % n % n % n % n %
Yes/vacation 38 100 29 93.5 43 65.2 69 83.1 179 82.5Yes/mission 9 23.7 4 12.9 5 7.6 19 22.9 37 17
TABLE 5: PRIOR EDUCATIONAL EXPERIENCE
Large eastern Small western Large Largeintegrated integrated southwestern western
Campinha-Bacote Leininger integrated freestanding Total
Type n % n % n % n % n %
Anthropology 22 57.9 14 45.2 3 4.5 26 31.3 65 29.8Prior degree 0 0 5 16.1 16 24.2 16 19.3 37 17.0Undergraduate 34 89.5 29 93.5 10 15.2 7 8.4 80 36.7Graduate 4 10.5 4 12.9 2 3 2 2.4 12 5.5Doctoral 0 0 0 0 1 105 0 0 1 1.5
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 42

in medicine, are becoming more common innursing programs as evaluation tools.
CONCLUSIONThe findings of this study raise more questionsthan answers. In an attempt to study the effec-tiveness of four different nursing program cur-ricula in developing culturally competent newgraduates, we found that there was no statis-tically significant difference of the level of cul-tural competence (all received a level of culturalawareness) of the students regardless of the typeof cultural content and educational strategiesemployed at their respective school.This raisesthe following questions. ‘Is cultural awareness amore realistic goal for graduating nursing stu-dents?’ Cultural competence is a process and itmay be more appropriate for faculty to expect alevel of cultural competence to occur aftergraduation. Another question that can be raisedis ‘What are the qualifications of faculty cur-rently teaching cultural competence?’The Tran-scultural Nursing Society offers internationalcertification in transcultural nursing; however,fewer than 75 nurses are currently certified intranscultural nursing (Campinha-Bacote 2006).Currently, there is one nurse in Australia certi-fied by the Transcultural Nursing Society. Thefindings of this study do not reflect the qualita-tive aspect of teaching cultural content, thusone cannot attest to the quality of the teaching.Perhaps an even more fundamental question is‘How committed are accrediting bodies to actu-ally considering the question of cultural compe-tency?’ How have the members of accreditingboards been prepared in cultural competency?And lastly, ‘Is a self-report evaluation tool thebest way to assess cultural competence?’
The American Nurses Association issued itsfirst position statement on cultural diversity innursing curricula in 1986 and since then, therehas been ongoing discussion as to what is thetheoretical underpinning of cultural trainingwithin nurse education should be. Over 20years later, nurse educators continue to ask,
‘How do we effectively teach cultural compe-tence in nursing education?’
Voltaire states, ‘Judge others by their ques-tions; rather than by their answers.’ The ques-tions that studies such as this study raise willprovide nurse educators with focused researchquestions to explore as they continue the jour-ney towards cultural competence in nursingeducation.
We shall not cease from explorations;and the end of all our exploring;will be to arrive where we started;and know the place for the first time.
—TS Eliot, Four Quartets
AcknowledgementThis study was funded by a grant from the USNational League for Nursing.
ReferencesAlpers RR and Zoucha R (1996) Comparison of
cultural competence and cultural confidence ofsenior nursing students in a private southernuniversity. Journal of Cultural Diversity 3: 9–15.
American Association of Colleges of Nursing(1997) A Vision of Baccalaureate and GraduateNursing Education:The Next Decade (PositionPaper).Washington DC:Author.
American Nurses Association, Council onCultural Diversity in Nursing Practice (1986)Cultural diversity in the nursing educationcurriculum:A guide for implementation.AmericanNurses Association.
Betancourt J (2007) Commentary on ‘Currentapproaches to integrating elements of culturalcompetence in nursing education’. Journal ofTranscultural Nursing 18: 25S–27S.
Bond ML (2004) Testimony to the SullivanCommission: Diversity in the Healthcare Workforce.Washington DC.
Bond ML, Kardong-Edgren S and Jones ME(2001) Assessment of professional nursingstudents knowledge and attitudes aboutpatients of diverse cultures. Journal ofProfessional Nursing 17: 305–312.
Boyle J (2007) Commentary on ‘Current
43Volume 28, Issue 1–2,April 2008 CCCCNNNN
Cultural competency of graduating US Bachelor of Science nursing students CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 43

approaches to integrating elements of culturalcompetence in nursing education’. Journal ofTranscultural Nursing 21: 20S–22S.
Campinha-Bacote J (2003)The Process of CulturalCompetency in the Delivery of Healthcare Services:A Culturally Competent Model of Care. OH:Transcultural C.A.R.E.Associates.
Campinha-Bacote J (2006) Cultural competencein nursing curricula: How are we doing 20years later? Journal of Nursing Education 45:243–244.
Campinha-Bacote J (2007) Inventory for Assessing theProcess of Cultural Competence Among HealthcareProfessionals – Student Version.TransculturalC.A.R.E.Associates.Accessed 21 May 2007from http://www.transculturalcare.net/iapcc-sv.htm.
Coffman M, Shellman J and Bernal H (2004) Anintegrative review of American nurses’perceived cultural self-efficacy. Journal ofNursing Scholarship 36: 180–185.
Felder EJ (1990) Baccalaureate and associatedegree student nurse’s cultural knowledge ofand attitudes toward Black American clients.Journal of Nursing Education 29: 276–282.
Dreher M and McNaughton N (2002) Culturalcompetency in nursing: Foundation or fallacy?Nursing Outlook 50: 182–186.
Grant LF and Lentzring TD (2003) Status ofcultural competence in nursing education:Aliterature review. The Journal of MulticulturalNursing and Health 9: 6–13.
Grossman D, Massey P, Blais K, Geiger E, Lowe J,Pereira O, Stewart A,Taylor R, Filer V andNembhard J (1998) Cultural diversity in Floridanursing programs:A survey of deans anddirectors. Journal of Nursing Education 37: 22–26.
Jones ME and Bond ML (2000) Personaladjustment, language acquisition and culturelearning in short-term cultural immersion.International Review 2: 33–47.
Kardong-Edgren S, Bond ML, Schlosser S, CasonC, Jones ME,Warr R and Strunk P (2005) Cul-tural attitudes, knowledge and skills of nursingfaculty toward patients of four diverse cultures.Journal of Professional Nursing 21: 175–182.
Kardong-Edgren S (2007) Cultural competency ofnursing faculty. Journal of Nursing Education 46,360–366.
Kulwicki A and Bolonik BJ (1996) Assessmentlevel of comfort in providing multiculturalnursing care by baccalaureate nursing students.Journal of Cultural Diversity 3: 40–45.
Leininger M and McFarland M (2002) TransculturalNursing: Concepts,Theories, Research and Practice,3rd edn. San Francisco: McGraw-Hill.
Lipson J and DeSantis L (2007) Currentapproaches to integrating elements of culturalcompetence in nursing education. Journal ofTranscultural Nursing 18: 10S–20S.
National League for Nursing (2003) Innovation inNursing Education:A Call to Reform. NationalLeague for Nursing New York.
Napholz L (1999) A comparison of self-reportedcultural competency skills among two groupsof nursing students: Implications for nursingeducation. Journal of Nursing Education 38:81–83.
Pope-Davis D, Eliason M and Ottavi T (1994) Arenursing students multiculturally competent? An exploratory investigation. Journal of NursingEducation 33: 31–33.
Ryan M, Carlton K and Ali N (2000) Transculturalnursing concepts and experiences in nursingcurricula. Journal of Transcultural Nursing 11:300–307.
Schlosser S, Bourrand J,Warr S and Lowe M(2004) The Lived Academic Experience ofAfrican-American School of Nursing GraduatesWhile Enrolled in a Private Religious-affiliatedMajority University, 29th Annual TransculturalNursing Society Conference, San Antonio.
St. Clair A and McKenry L (1999) Preparingculturally competent practitioners. Journal ofNursing Education 38: 228–234.
Vito K, Roszkowski M and Wieland D (2005)Measuring cultural competence as acurriculum outcome:What we learned fromour experiences with two instruments,National League for Nursing EducationSummit, Baltimore.
Zorn C, Ponick D and Peck S (1995) An analysisof the impact of participation in an interna-tional study program on the cognitive develop-ment of senior baccalaureate nursing students.Journal of Nursing Education 34: 67–70.
44 Volume 28, Issue 1–2,April 2008CCCCNNNN
Suzan Kardong-Edgren and Josepha Campinha-BacoteCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 44

NCCopyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 45–47.
EDITORIAL
45Volume 28, Issue 1–2,April 2008 CCCCNNNN
The European Union has declared 2008 theEuropean Year of Intercultural Dialogue.
This is in recognition that Europe is becomingmore culturally diverse. Globalisation has inc-reased the multicultural character of manycountries, adding to the number of languages,religions, ethnic and cultural backgroundsfound in Europe and other continents.
In Australia, in contrast to many other coun-tries, the diversity of the population was wellestablished and recognised before multicultural-ism was first coined in the late 1970s (OMA1989). However, the response was in the mainrelated to the diversity of the immigrant popu-lation minimising significant aspects of diversitysuch as class, gender and culture and carebeyond multiculturalism.This has had enormousimplications for nursing and health care (Milner1993).
Today, in addition to 20 surviving Aboriginaldialects, more than one hundred other lan-guages are spoken by people from culturally andlinguistically diverse backgrounds (Departmentof Immigration & Citizenship 2008; Omeri &
Ahern 1999). Communication between culturesremains a critical issue for the cultural under-standing necessary for transcultural nursingpractice to be effective.
The social and cultural determinants of healthis emphasised by Leininger’s Culture Care Theo-ry (Leininger and McFarland, 2002). In morerecent years, equal emphasis has been placed onthe impact that social and organisational struc-tures have on our health (Papadopoulos 2006).
In a diverse world, transcultural nurses striveto make a difference to the health and wellbeing of people, irrespective of their culturalbackgrounds transcultural nurse researchersacross the world have been and continue to beengaged in the production of knowledge, whichhas the potential to make a difference for peopleat whatever point of the health/illness continu-um they may be (Omeri 2008; 2002).
In order to foster excellence in transculturalnursing practice, the development and wideapplication of transcultural nursing standards isof paramount importance to advancing excel-lence in transcultural nursing practice.Work has
Transcultural nursing theory and models:The challenges of application
IRENA PAPADOPOULOSProfessorTranscultural Health and Nursing, andHeadResearch Centre forTranscultural Studies in HealthMiddlesex UniversityLondon UK
AKRAM OMERIAdjunct AssociateProfessorUniversity of WesternSydneySchool of NursingSydney NSW, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 45

already been undertaken in this area.The certi-fication of designated transcultural nurses isbased upon eight standards developed usingLeininger’s Theory of Culture Care Diversityand Universality and Campinha-Bacote’s Modelof Cultural Competence (Leininger 1991, 1998,2006; Campinha-Bacote 2002). Standards pro-vide agreed criteria by which practice may beevaluated and teaching and learning progressed(Andrews & Boyle 2008: 10).
It can be argued that transcultural nursingtheory and models are the most appropriate forthe 21st century, as they cogently address thedeficits of the bio-medical model which domi-nated both medicine and nursing in the 20thcentury.
As the articles in this section demonstrate,transcultural nurses have the knowledge andtools to help them transform nursing and healthcare in many places in the world.
User friendly theoretical frameworks facili-tate both the production of knowledge and itsapplication. Marilyn McFarland and Marilyn KEipperle in their article ‘Culture Care Theory: Aproposed theory guide for nurse practitionerpractice in primary care settings’ (2008), pro-pose just that. Utilising Leininger’s Theory ofCulture Care Diversity and Universality as afoundation, they put forward a guide for educa-tional preparation for advanced practice nursesworking in primary care.They demonstrate howthrough the application of this theory, education,research and practice are connected as essentialcomponents toward the provision of culturallycongruent care to meet the healthcare needs ofdiverse individuals, families, groups, and com-munities by family nurse practitioners.This willgo some way towards eliminating the healthinequalities experienced by many marginalisedcommunities and individuals.
In her article, ‘A partnership of a Catholicfaith-based Health system, Nursing and AmericanIndian traditional Indian medicine practitioners’,Ann O Hubbert (2008) uses Leininger’s theoryto discuss how the creative thinking and actions
of a group of people resulted in a cultural part-nership which bridged the gap between the pro-fessionals and the lay people to bring about muchneeded improvements to the services provided toan American Indian community. We learn thattwo of the key foundations of the traditional Indi-an medicine philosophy are, the seven aspects of life and the essence of a holistic individual.Knowing these, helps us understand the person-hoods of the people of this community. Amaz-ingly, even though differences exist in humanbehaviours and actions among cultures, the sevenvalues of the sacred life discussed in this article,are also similar among cultures and different reli-gions.These are respect, honesty, truth, humility,compassion, wisdom and unconditional love.
These values are evident in the article ‘Bridg-ing Generic and Professional Care Practices forMuslim Patients Through the use of Leininger’sCulture Care Modes’ by Hiba Webbe-Alamah(2008). Although the five tenets of Islam pro-vide a strong practical framework for everydayliving, they too, promote the values of respect,honesty, truth, humility, compassion, wisdomand unconditional love.These values come alivein the descriptions of the many Muslim genericcare beliefs and practices provided in this article. Wise use of such information can helpnurses provide sensitive and appropriate care.
Myrna AA Doumit and Huda Abu-Saad Hui-jer’ (2008) address the importance of com-munication and truth telling in their article‘Lebanese cancer patients: Communication andtruth telling’. Notwithstanding the dangers ofgeneralising, it has been the practice in the indi-vidualistic ‘West’ to tell the patient their cancerdiagnosis. On the other hand much has beenpublished on how families in collectivist soci-eties, such as the Lebanese, prefer to managesuch information and request that any suchdiagnosis is not given to the patient direct.Thisarticle challenges that stereotype by providingevidence that the Lebanese patients who partici-pated in this study consider it their right toknow their diagnosis and that being more open
46 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos and Akram OmeriCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 46

about this will improve the levels of communi-cation they have with their families and profes-sional carers.
Despite the improvements in people’s healthin many countries due to biomedical and bio-technological advancements, huge health in-equalities continue to persist both betweencountries and within countries.The continueddevelopment and application of research basedTranscultural nursing insights has still a greatercontribution to make to the peoples of theworld as it realises its potential to contribute tothe elimination of health inequalities.
ReferencesAndrews M and Boyle J S (2008)Transcultural
Concepts in Nursing Care, 5th edn, Lippincott:Philadelphia.
Camphina-Bacote J (2002) The process of culturalcompetence in the delivery of healthcareservices:A model of care, Journal of TransculturalNursing 13: 181–184.
Department of Immigration and Citizenship (2008)Australian Government, National Agenda for aMulticultural Australia accessed at http://www.immi.gov.au/media/publications/multicultural/agenda/agenda89/executive.htm on April 2008.
Department of Immigration & Citizenship (2008)Australian Government, National Agenda for aMulticultural Australia accessed at http://www.immi.gov.au/media/publications/multicultural/agenda/agenda89/language.htm on April 2008.
Doumit MAA and Abu-Saad HH (2008) Lebanesecancer patients: Communication and truth-tellingpreferences, Advances in Contemporary TransculturalNursing, 2nd edn, Contemporary Nurse special issue28(1–2): 74–82.
Hubbert AO (2008) A partnership of a Catholicfaith-based health system, nursing and traditionalAmerican Indian medicine practitioners, Advancesin Contemporary Transcultural Nursing, 2nd edn,Contemporary Nurse special issue 28(1–2): 64–72.
Leininger MM (1991) Culture Care Diversity andUniversality:A theory of nursing, National Leaguefor Nursing Press: New York.
Leininger MM (1998) Twenty-five years of knowl-edge and practice development transcultural
nursing society annual research conferences,Journal of Transcultural Nursing 9: 72–74.
Leininger MM and McFarland MR (eds) (2002)Transcultural Nursing:Concepts,Theories,Research andPractice, 3rd edn, McGraw-Hill: New York.
Leininger MM and McFarland MR (2006) CareDiversity and Universality:A worldwide theory fornursing, 2nd edn, Jones & Bartlett: Sudbury.
McFarland MM and Eipperle MK (2008) Culturecare theory:A proposed practice theory guide fornurse practitioners in primary care settings,Advances in Contemporary Transcultural Nursing, 2ndedn, Contemporary Nurse special issue 28(1–2):48–63.
Milner A (1993) Beyond culture, beyond multi-culturalism, in Clark C, Forbes D and Francis R(eds) Multiculturalism, Difference and PostModernism, pp 126–139, Longman Cheshire:Melbourne.
Office of Multicultural Affairs (1989) NationalAgenda for a Multicultural Australia,AGPS:Canberra.
Omeri A and Ahern M (1999) Utilizing culturallycongruent strategies to enhance recruitment andrecognition of Australian Indigenous nursingstudents, Journal of Transcultural Nursing 10:150–155.
Omeri A (2002) Reflections on Australia andtranscultural nursing in the new millennium, inLeininger M McFarland M (eds) TransculturalNursing Concepts,Theories, Research & Practice, 3rdedn, McGraw-Hill: New York.
Omeri A (2006) Transcultural nursing: the way toprepare culturally competent practitioners inAustralia, in Papadopoulos I (ed), TransculturalHealth and Social Care: Development of CulturallyCompetent Practitioners, Ch 18, ChurchillLivingstone Elsevier: Edinburgh.
Omeri A (2008) Epilogue:Advancing transculturalnursing through collaboration, Advances inContemporary Transcultural Nursing, 2nd edn, Con-temporary Nurse special issue 28(1–2): 207–210.
Papadopoulos I (Ed) (2006) Transcultural Health andSocial Care: Development of culturally competentpractitioners, Churchill Livingstone Elsevier:Edinburgh.
Wehbe-Alamah H (2008) Bridging generic andprofessional care practices for Muslim patientsthrough use of Leininger’s culture care modes,Advances in Contemporary Transcultural Nursing, 2ndedn, Contemporary Nurse special issue 28(1–2):83–97.
47Volume 28, Issue 1–2,April 2008 CCCCNNNN
Editorial: Transcultural nursing theory and models CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 47
‘The fate of nursing conceptual models andtheories in the contemporary climate of
advanced practice nursing’ is a question we havepondered since reading an article by Fawcett,Newman, and McAllister (2004: 136). In theirscholarly dialogue, Fawcett et al explored thedevelopment and function of advanced practicenursing within the current health care system ofthe United States and discussed nursing theoryin relation to the preparation for and applicationwithin the advanced practice role. It is our pro-
posal that Leininger’s Theory of Culture CareDiversity and Universality addresses this ques-tion by providing an appropriate and useful theoretical framework/conceptual model ofnursing for nurse practitioners that informsadvanced practice nursing, particularly thenurse practitioner role, to provide culturallycongruent care to diverse and similar clients inprimary care practice contexts. ‘A framework of advanced practice nursing could guide thedevelopment of advanced practice curriculums,
Key Wordsadvancedpractice nursing;Leininger’sculture caretheory;culturallycongruent careethnonursingmethod CN
48 Volume 28, Issue 1–2,April 2008CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 48–63.
Culture care theory: A proposedpractice theory guide for nurse
practitioners in primary care settings
ABSTRACT Leininger’s Theory of Culture Care Diversity and Universality is presented as afoundational basis for the educational preparation, primary care contextualpractice, and outcomes-focused research endeavours of advanced practice nursing.Discussion emphasises the value of care and caring as the essence of advancedpractice nursing through the use of three modes of care, use of the Sunrise andother enablers, and the ethnonursing method. Education, research, practice, andkey concepts of the theory are connected as essential components toward theprovision of culturally congruent care to meet the healthcare needs of diverseindividuals, families, groups, and communities by family nurse practitioners.
Received 3 October 2007 Accepted 14 February 2008
MARILYN MMCFARLANDSchool of NursingUniversity ofMichiganFlint MI, USA
MARILYN KEIPPERLEFamily NursePractitionerKaleva MI, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 48

shape role descriptions and practice agree-ments, inform policy development related toprovider roles in healthcare, and provide direc-tion for research agendas’ (Brown 1998: 157).More specifically, as discussed by Newman andMcAllister as above, we are offering the specialcontributions this theory has been making tothe collective knowledge base of advanced prac-tice nursing theory. As Anderson (1987: 7) hasstated,‘We need to use a framework for nursingcare that allows us to examine the multipledeterminants which shape people’s experiences.’Advanced practice nursing, as defined by Han-son & Hamric (2003: 205) is ‘the application of an expanded range of practical, theoretical,and research-based therapeutics to phenomenaexperienced by [clients] within a specialisedclinical area of the larger discipline of nursing’with further clarification that the core com-petency of each role is ‘direct clinical practice’and that a nurse practitioner is therefore anadvanced practice nurse.
The focus of this article is to address whathas been done toward integrating Leininger’sTheory of Culture Care Diversity and Univer-sality into the practice of advanced practice nurs-ing in the role of the family nurse practitioner(FNP) in primary care contexts; and what, inour view, needs to be done now and in thefuture to expand the potential role of this theo-ry in nurse practitioner practice. Given that cul-ture care is a core competency domain for familynurse practitioners (United States DepartmentHealth and Human Services [DHHS] 2002), it isour view that nurse practitioners need to recog-nise the need, validity, and missing component ofculture care in nursing. Leininger (2006a: 16)refers to culturally congruent care as ‘knowl-edge, acts, and decisions used in sensitive andknowledgeable ways to appropriately and mean-ingfully fit the cultural values, beliefs, and life-ways of clients for their health and well-being,or to prevent illness, disabilities, or death … Toprovide culturally congruent care and safe carehas been the major goal of the Culture Care
Theory.’The major premise of the Culture CareTheory is that there are differences (diversities)and universalities (commonalities or similari-ties) in transcultural care knowledge and prac-tices that have awaited discovery (and have beendiscovered) to establish a growing body of rele-vant transcultural nursing knowledge as the newguide to nursing practices (Leininger 2002b:79; Omeri 2003: 181). Culture is the history orlearned symbolic human and structural organ-isation and action that make humans human(Keesing 1981 cited in Ray 1999: 178); culture‘refers to patterned lifeways, values, beliefs,norms, symbols, and practices of individuals,groups, or institutions that are learned, shared,and usually transmitted intergenerationally overtime’ (Leininger 2002b: 83).
Leininger (2006a: 12) has defined care as‘those assistive, supportive, and enabling expe-riences or ideas towards others with evident oranticipated needs to ameliorate or improve ahuman condition or lifeway ... care has culturaland symbolic meanings such as care as protection,care as respect, and care as presence’ and that caringentails ‘actions, attitudes, and practices to assistor help others toward healing and well-being.’Culturally congruent care, then, refers to ‘cultural-ly-based care knowledge, acts, and decisionsused in sensitive and knowledgeable ways toappropriately and meaningfully to the culturalvalues, beliefs, and lifeways of clients for theirhealth and well-being, or to prevent illness, dis-abilities, or death’ (Leininger 2006a: 15).
The nurse practitioner needs to be able tosensitively and competently integrate culturecare into contextual routines, clinical ways, andapproaches to primary care practice throughrole modeling, policy making, procedural per-formance and performance evaluation, and theuse of the advance practice nursing process.By using Leininger’s Sunrise Enabler (Leininger& McFarland 2006: 25) and the three caremodes to guide nursing actions and decisions,we predict the nurse practitioner would be ableto provide culturally congruent, safe, meaning-
49Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 49

ful, and beneficial care to clients in primary carecontexts (see Appendix I).
The six criteria for theory application inadvanced practice nursing posited by Newmanin Fawcett et al (2004: 136) were that nursingtheories applied in advanced practice nursingshould: be inclusive rather than exclusive; fostera focus on the whole person rather than the disease or illness; include consideration of thepatient’s/family’s/significant other’s perceptionof the situation; be holistic in nature which ishelpful to both practice and documentation;facilitate autonomous nursing practice (aspectof professionalism along with knowledge andservice); and, encourage diverse ways of know-ing, including empirics, ethics, aesthetics, per-sonal knowing, and sociopolitical knowing(Carper 1978 and White 1995, cited by Fawcettet al 2004: 136). As advanced practice nurseswho are highly skilled and educated, nurse prac-titioners have a moral duty and obligation to usetheir knowledge and skills in creative waysthrough nursing actions and decisions to pro-vide culturally competent care in clinical andnonclinical contexts to meet or assist with thediverse needs of all people. ‘[Advanced PracticeNurses] represent the majority of our profes-sion’s most highly educated nurses. It is theirresponsibility to do more than just render highquality care on a one to one basis with theirclients. Rather, they are also accountable formaintaining the systems within which that careoccurs’ (Germain 2004: 433). Through themany and various roles that nurse practitionersexpress their leadership and skills, their nursingperspective influences the actions and decisionsof the larger body (group, committee, organisa-tion, institution) in which they are a participant.Thus, culturally congruent care as provided byadvanced practice nurses/nurse practitionersshould become integrated into the collectiveworldview of that body and thereby be reflectedin their vision, mission, goals and objectives,and ultimately its functionality, actions, anddecisions for meeting the needs of the people
for whom it offers assistance. ‘Healthcareorganisations should be committed, willing, andsupportive of their staff to ensure the attain-ment of a culturally competent work environ-ment’ (Ndiwane et al 2004).
INCLUSIVE VERSUS EXCLUSIVELeininger’s Theory of Culture Care Diversityand Universality encompasses all cultures,racial, ethnic, or minority groups and is applica-ble to subgroups within the dominant societalculture. The focal application of the theory isupon individuals, families, groups, communi-ties, and institutions in diverse health contexts(Leininger 2002b: 80). ‘Culturally based caringis essential to curing and healing, for there canbe no curing without caring, but caring canexist without curing … Care is the essence of nursing and a distinct, dominant, central, andunifying focus’ (Leininger 2002b: 79). Lein-inger extrapolates this further by stating: ‘Careis an essential human need; caring is nursing;caring is the heart and soul of nursing; caring ispower; caring is healing; and caring is the dis-tinctive feature that makes nursing what it is orshould be as a profession and discipline’ (Lein-inger & McFarland 2002: 11).This perspectivehas gained widespread acceptance throughoutnursing as shown by the following:‘the develop-ment of specific theories focusing on caring innursing is indicative of the increasing recognitionbeing given to caring as a central concept withinthe discipline’ [emphasis added] (McCance,McKenna, & Boore 1999: 1394). It is essentialfor the nurse practitioner in a primary care con-text to establish a trusting relationship withclients to assist them in their endeavours to pre-vent and treat disease and move toward healthand wellness. Care and caring are cornerstonesfor developing that trusting relationship. Care,as defined by Leininger (2002a: 11), are those‘assistive, supportive, enabling, and facilitativeculturally-based ways to help people in a com-passionate, respectful, and appropriate way toimprove a human condition or lifeway or to
50 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 50

help people face illnesses, death, or disability.’The nurse practitioner needs to be sensitive tothe unique cultural expressions of each individ-ual and family while becoming knowledgeableabout the worldview, values, social structurefactors, and lifeways of clients and while devel-oping a mutual trust that will facilitate obtainingclinical and nonclinical information that is accurate, congruent, and beneficial throughadvanced nursing observation and assessment.‘The culturally competent [Advanced PracticeRegistered Nurse] is knowledgeable and res-pectful of diverse cultural beliefs and practices,and partners with the client to develop a careregimen that produces the desired health out-comes within the context of the client’s culturalvalues’ (Germain 2004: 435). It is imperativethat accurate as well as cultural specific infor-mation is used to develop the client’s therapeu-tic regimen through selected methods that arebeneficial and acceptable to the client who willimplement them. ‘In general, cultural caringrituals of clients and nurses are powerful forcesto know, understand, assess, and respectfullyuse. … Nurses will be expected to incorporategeneric rituals into client care for congruentand beneficial care’ (Leininger 2002c: 132).Therefore, care and caring are essential skills fornurse practitioners to develop, express, and sus-tain with clients throughout each healthcareencounter. ‘Culturally congruent and therapeu-tic care occurs when culture care values,beliefs, expressions, and patterns are explicitlyknown and used appropriately, sensitively, andmeaningfully with people of diverse or similarcultures’ (Leininger 2006a: 19).
The Culture Care Theory provides nurses/nursing with three modes to assist them in mak-ing care regimens meaningful and helpful toclients and through which culturally congruentnursing care actions and decisions to clients canbe made. Leininger (2006a: 8) developed thethree modes of care, defined and described as:
1. Culture care preservation and-or maintenance:those assistive, supportive, facilitative, or
enabling professional acts or decisions thathelp cultures retain, preserve, or maintain ben-eficial care beliefs and values, or to facehandicaps or death.
2. Culture care accommodation and-or negotiation:those assistive, supportive, facilitative, orenabling professional acts or decisions thathelp cultures adapt to or negotiate with othersfor culturally congruent, safe, and effectivecare for their health, well-being, or to dealwith illness or dying.
3. Culture care restructuring and-or repatterning:those assistive, supportive, facilitative, orenabling professional acts or decisions thathelp people reorder, change, modify, or restruc-ture their lifeways and institutions for better(or beneficial) healthcare patterns, prac-tices, or outcomes.
These modes allow for individualised approach-es to care actions and decisions as well as incor-porating into nursing practice the diverse waysof knowing within cultures, individuals, groups,communities, or institutions. ‘Inherent in eachof these modalities are three of the core valuesthat underlie advanced practice nursing: res-pect; advocacy; and partnership’ (Germain 2004:435). Primary care ‘deals with awareness andassessment of the connection between biologicand behavioral life experiences and health andillness. Its major features include the delivery of‘first contact’ healthcare, comprehensibility,longitudinality, prevention of disease, healthpromotion, and coordination of care services’(Starfield 1991 cited by Ray 1999: 177). It ismost essential for the nurse practitioner to usethe three modes of care and caring with respectfor the client’s beliefs, values, and expressionsregarding health and well-being and to advocatefor the client based on the client’s worldview,and to do so in partnership with the client toensure that safe, beneficial, and appropriate aswell as culturally congruent care actions anddecisions are mutually chosen.The nurse practi-tioner is accountable to the client to reflect
51Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 30/07/2008 9:47 PM Page 51

back with the client in a continual and confir-matory manner to ensure the client understandsand agrees with the chosen care modalities andis willing and able to use them.We (the authors)have used the Culture Care Theory in our ownnurse practitioner practices through the use ofthe three modes of care when establishing aclient relationship with individuals, families,groups, or institutions; when considering themanner of assessment to be performed; and,by integrating generic care approaches whenmutually establishing plans of care actions anddecisions with clients. Using open-ended ques-tions, active listening techniques, and appropri-ate language and touch are definitive ways todemonstrate caring and facilitate client trustand sharing during the assessment process aswell as throughout all phases of the nursingprocess.
WHOLE PERSON VERSUS DISEASEOR ILLNESSFawcett et al (2004: 137) state that the:
Gestalt that guides NP practice is the abilityto see the [client] as a whole and to appreci-ate that the [client] represents a complexconstellation of physical, emotional, psycho-logical, spiritual, social, environmental, andeconomic life factors that interact and con-tribute to the person’s unique wholeness andinfluence their ability to participate in healthpromotion, health maintenance, and diseasemodifying actions.
The Culture Care Theory factors influencingculture care values, practices, and beliefs andwhich are embedded in worldview include (butare not limited to) language, philosophy, religionand spirituality, kinship, social, political, legal,educational, economic, technological, ethno-historical, and environmental context (Leininger2002b: 79) as is represented by the SunriseEnabler. ‘The Sunrise Enabler helps nurses to discover and reflect on their decisions and
actions [using the three modes of care action anddecision] … and to arrive at the goal of the the-ory, namely culturally congruent care’ (Hubbert2006 cited in Leininger & McFarland 2006:355), and can be more expansively used bynurse practitioners in primary care contexts ‘toshow and predict relationships among world-view, sociocultural dimensions, environmentalcontext, language and ethnohistory, diversehealth systems and principles, and to guide[advanced practice] nursing actions and deci-sions’ (Wenger 2006 cited in Leininger & Mc-Farland 2006: 330).The Sunrise Enabler is usedby the nurse practitioner in a primary care con-text to reflect upon the client situation and todevelop care actions and decisions when assistingclients toward health and wellness. Client situa-tions may include chronic illnesses such as diabetes, pulmonary disease, dyslipidemia, orhypertension; lifestyle concerns such as alcohol,substance, or tobacco abuse, weight manage-ment, growth and development or issues relat-ing to adult stages of life, domestic violence orchild abuse, elder care planning or difficulties;family planning; immunizations; and, psycholog-ical-mental health matters.
The culture care theory guides nurses to usegeneric or folk care, nursing care, and profes-sional care-cure practices to provide culturallycongruent care for well-being, health, growth,and survival and to face handicaps or death(Leininger 2002b: 79). ‘Every human culturehas generic (lay, folk, or indigenous) careknowledge and practices and usually profes-sional care knowledge and practices, which vary transculturally and individually’ (Leininger2002b: 79). Integrating generic and professionalcare concepts into advanced practice nursingwithin the nurse practitioner role is essential toachieving beneficial care outcomes for theclient. ‘Beneficial, healthy, and satisfying cul-turally-based care influences the health andwell-being of individuals, families, groups, andcommunities within their environmental con-text’ (Leininger 2002b: 79).
52 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:24 PM Page 52

PERCEPTION OF THE SITUATION‘Cultural conflicts, cultural imposition prac-tices, cultural stresses, and cultural pain reflectthe lack of culture care knowledge to provideculturally congruent, responsible, safe, and sen-sitive care’ (Leininger 2002b: 79).Therefore, itis essential for nurse practitioners to use threemodes of care and caring through the perspec-tive of the emic (insider) lens of the client aswell as the etic (outsider) lens of the profession-al clinician/nurse practitioner. According toLeininger (2006a: 14) generic or emic care‘refers to the learned and transmitted lay,indigenous, traditional, or local folk (emic)knowledge and practices’ and professional oretic care ‘refers to formal and explicit cogni-tively learned professional care knowledge andpractices generally obtained through education-al institutions’ and experiences.
Some better known generic care practicesinclude ‘low tech’, ‘over the counter’ or ‘homeremedy’ approaches used to promote comfortand healing for musculoskeletal aches or minorinjuries, sore throats, nasal congestion, earache,or skin rashes. Traditional measures for emo-tional or psychosocial comfort include spiritualrituals using candles, incense, tobacco, or aro-matic oils. Professional acceptance of emic caremodes in complement with or in place of orwith professional care modes (where safe andappropriate) assist the client in building a trustrelationship with the nurse practitioner andhelps to promote acceptance of professionalcare practices. Cultural competence requires:
a change in mindset from viewing howclients can fit into the nurses’ world and wayof doing things because nurses’ know best(ethnocentrism) to examining how nursesmay understand and fit into the patientsworld, [thus] changing the nurses’ practicerecommendations to include those beliefs,traditions, and practices that have worked forthe patients (ethnorelativism).
(St Clair 1999: 1)
Other factors influencing clients’ views or per-ceptions in the healthcare encounter includeworldview and environmental context. Worldviewrefers to ‘the way people tend to look out uponthe world or their universe to form a picture orvalue stance about life or the world aroundthem’ (Leininger 2006a: 15).Worldview is theperception of the client. In the healthcare con-text, worldview influences the client’s under-standing of information shared by the nursepractitioner, acceptance of professional carepractices, and the client’s willingness and abilityto use the methods mutually selected as the‘plan of care’ (eg ‘fatalism’ may influence theclient not to use health promotion or diseaseprevention practices suggested by the nursepractitioner).
Environmental context also has significantinfluence upon the client’s healthcare practices.Environmental context ‘refers to the totality ofan event, situation, or particular experience thatgives meaning to people’s expressions, interpre-tations, and social interactions, and technologicfactors in specific cultural settings’ (Leininger2006a: 15). This holds significance for nursepractitioners in primary care contexts.The ‘set-ting’ of the office (eg art; literature; ambience/décor; client flow design/user friendliness;type/content of magazines and teaching litera-ture), languaging of forms, staff composition/posture/language/tone, and means of meetingand greeting all lend to ‘the totality’ of the pri-mary care experience of the client. The nursepractitioner’s body language, listening skills,approach to assessment and sharing of informa-tion, flexibility toward modifying professionalpractices advised, and attention to privacy andconfidentiality during the encounter contributeto the ‘particular experience’ of the client withinthe environmental context of the primary caresetting.These contributing factors in interactivetotality influence the client’s perspective of thenurse practitioner, the healthcare encounter, andindeed, the healthcare system, and significantly
53Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 53

affect the individual’s willingness and ability touse the modalities of care mutually chosen as the‘plan of care’.
Transcultural nurses focus more on humancaring, health, and well-being from an inte-grative and holistic perspective … Some-times in helping clients, there needs to be more emphasis on generic care than on professional care modes … such decisionsrequire knowledge of both generic and pro-fessional practices along with consumerinput. Most importantly, professional nurseshave a societal and legal mandate to alwaysinform and share relevant professional knowl-edge with clients and not neglect generic careknowledge to arrive at sound decisions.Tran-scultural nursing promotes and practicesintegrative care so that the client gets thebetter of the two worlds of knowing andtherapies. (Leininger 2002d: 148)
HOLISTIC IN NATUREFawcett et al state that nurse practitionersshould have an ‘awareness of the person’s lifefactors’ as guides to formulate a holistic plan ofcare to assist the person ‘to maintain or regainhealth by means of comprehensive health main-tenance, disease prevention, or health restora-tion.’ Through the use of the Culture CareTheory and the Sunrise Enabler, the totality ofan individual or group is approached, and servesas ‘a cognitive guide to tease out culture carephenomena from a holistic perspective of multi-ple factors that can potentially influence careand the well-being of people’ (Leininger 2002b:79). The Acculturation Healthcare and Assess-ment Guide can be readily incorporated intothe initial as well as maintenance health assess-ment processes by the family nurse practitionerin the primary care context to assess ‘whethercultural clients are more traditionally or non-traditionally oriented to their cultures indiverse areas’ (Leininger 2006a: 26, 2006b: 64,2006c: 134). These areas include worldview;
ethnohistory; kinship and social factors; culturalvalues, beliefs, and lifeways; religious, spiritual,and philosophical factors; technological factors;economic factors; political and legal factors;educational factors; language and communica-tion factors; professional and generic (folk, lay)care beliefs and practices; and general and spe-cific nursing care factors (Leininger 2006:137).The strength of this enabler is that the nursepractitioner can obtain holistic assessments todetermine the dominant patterns of caring andhealth practices as this influences advancedpractice nursing decision making and actionplanning (Leininger 2006c: 134).
‘The transcultural nurse is often asked to pro-tect clients of non-Western cultures who are unfa-miliar with Western medicines and treatmentsfrom being demeaned or shunned when usingtheir folk remedies. Establishing mutual and genuine relationships between the healthcareprovider and the client or family is critical topromote beneficial integrative care’ (Leininger2002d: 151).Therefore, it is imperative for thenurse practitioner to embrace the desired attrib-utes for integrative care so that culturally con-gruent, safe, meaningful and beneficial care canbe provided in primary care contexts. Theseattributes include trust and mutual respect incaring, healing, curing, and well-being; collabo-rative decision making using the best of emic andetic practices; seeking etic and emic care-curepractices that are congruent, safe, and meaning-ful; seeking holistic care perspectives to ensuresafe and congruent generic practices; seekingbeneficial care or healing practices that incor-porate the client’s values, beliefs, and lifewayswithin their living environments; and seekingcompetent, creative, and compassionate practi-tioners (Leininger 2002d: 150).
FACILITATE AUTONOMOUSNURSINGAutonomous nursing practice in the nurse prac-titioner role herein means ‘independent, collab-orative or consultative practice’ but not isolated
54 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 54

or insular practice.There are many studies in theliterature to support the value and contributionof primary care nurse practitioners in providingquality primary care practices to clients (Avron1991; Birkholtz & Viens 1999, 2001; Brown &Grimes 1995; Capan, Beard, & Mashburn 1993;Hall 1990; Moody, Smith, & Glenn 1999; Mund-inger et al 2000; Salkever 1992 cited in Fiandt etal 2002: 14). Nurse practitioners in the UnitedStates perform a large percentage of the ‘servic-es’ provided by family practice physicians. Basedon outcome studies, nurse practitioners outper-form physician providers in the area of healthpromotion and were more likely to provide careand support for ‘lifestyle management’ throughteaching and counseling for concerns such asnutrition, exercise, weight reduction, smokingcessation, growth and development, familyplanning, and psychosocial needs (Brown &Grimes 1995; Moody, Smith, & Glenn 1999).Through means of the three modes of care aspreviously described, the family nurse practi-tioner is able to apply the core competenciesand specialty-specific domains of advanced prac-tice in primary care contexts to meet the needsof clients. The Culture Care Theory is a usefulframework to guide autonomous advancednursing practice by guiding assessment oflifestyle, traditional and nontraditional genericcare practices, and the non-care practices ofindividuals, families, groups, or institutions.
In 2002, the American Association of Col-leges of Nursing (AACN) and the NationalOrganization of Nurse Practitioner Faculties(NONPF) established that ‘All nurse practition-ers [are] able to demonstrate these core compe-tencies [upon] graduation’ (DHHS 2002). TheDomains and Core Competencies of NursePractitioner Practice are presented in AppendixII. Each set of specialty competencies buildsupon this set of core competencies and through-out the competencies, client is defined as theindividual, family, group, and-or community.Family nurse practitioner competencies includeall six of the core competencies with the addi-
tion of the seventh domain of cultural competenceas core for the FNP specialty. Similarly, the Australian Nursing and Midwifery CouncilIncorporated (ANMC) co-commissioned withthe Nursing Council of New Zealand in 2004 areview of the scope and role of nurse practition-ers.Their efforts resulted in national standardsfor nurse practitioner practice with supportingperformance indicators. In this Nurse Practi-tioner Competency Framework (refer to Appen-dix III) it is stated that the nurse practitioner‘establishes therapeutic links with the patient/client/community that recognise and respectcultural identity and lifestyle choices’ with oneof the three performance indicators being‘[demonstrating] cultural competence by incor-porating cultural beliefs and practices into allinteractions and plans for direct and referredcare’ (ANMC 2004: 4).
Cultural competence, however, is not an areathat the family nurse practitioner addresses sep-arately with clients, but rather it is incorporatedinto the advanced practice approaches taken for each of the core competencies. In otherwords, cultural competence is integrated intonurse practitioner practice nursing assessmentand care actions and decisions in the primarycare context through the situationally approp-riate use of the three care action modes previ-ously described and discussed. Being culturallycompetent, for example, is vital for establishingthe nurse practitioner–client relationship, foreffectiveness in the teaching–coaching role, orwhen assisting clients to manage or negotiatethe healthcare delivery system.
DIVERSE WAYS OF KNOWINGCulturally congruent care incorporates diverseways of knowing which are derived from theperspective or worldview of the individual, fam-ily, group, community, or institution. ‘Theassumption that the theory only focuses on theculture of the ‘other’… is inaccurate. Imple-menting the theory into practice stimulatesnurses, as carers and researchers, to reflect upon
55Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 55

their own cultural values and beliefs and howthey may influence the provision of care’(Leininger & McFarland 2002 and Omeri 1996,1997 cited in Omeri 2003: 181). In their study,Fiandt et al (2002) explored three aspects ofnurse practitioner practice when viewed as com-plementary to physician practice: use of thenursing model; identification of the vulnerablecharacteristics of clients; and health promotionactivities. For our purposes, we will focus on thefirst and third parameters.‘Although nurse prac-titioner education is embedded in a nursingmodel, research data describing nurse practi-tioner practice have been insufficient to clearlycharacterise and differentiate nurse practitionerpractice from that of primary care physicians andphysician assistants.The complementary natureof nurse practitioner practice, although addres-sed in theory in education literature, is notreflected in the research describing nurse practi-tioner practice. Research detailing the comple-mentary aspects of nurse practitioner nursingbased on a nursing model [such as the CultureCare Theory] is needed to support nurse practi-tioner theory and education and to influencehealthcare policy’ (Fiandt et al 2002: 14). Glob-ally, national nursing accreditation bodies havecalled for the integration of cultural learning innursing education. The (Australian) NationalReview of Nursing Education MulticulturalNursing Education (Eisenbruch 2002) recom-mended the following strategies for the en-hancement of nursing cultural competence,stating that the profession needed to address thefollowing concerns: the need for a multiculturalframework in nursing education; the impact of multicultural nursing practice in a diversenation; the increasing lifelong awareness of thesociopolitical and economic context of cultureand health in developing culturally competentcare; the appropriate representation of culture ineducation and practice to suit the community;partnerships between education and practice;systematic investigation into the cultural needsof students, staff, and clients; recruitment and
retention of both Indigenous nurses and nursesfrom culturally and linguistically diverse back-grounds; attention to the employment of over-seas-qualified nurses; and, questions relating tomultidisciplinary research (Omeri 2003: 180).
In the United States, the AACN document ofOctober 2006 presents eight Essentials of Doc-toral Education for Advanced Nursing Practice.These essentials of Doctorate of Nursing Prac-tice (DNP) education are to focus the educatorand student toward meeting three goals inpreparing them as graduates for practice. Oneof the three goals is to use science-based theo-ries and concepts to determine the nature andsignificance of health and healthcare deliveryphenomena; describe the actions and advancedstrategies to enhance, alleviate, and amelioratehealth and healthcare delivery phenomena asappropriate; and evaluate outcomes. Research isa key component in developing nursing knowl-edge and thereby a key component of diverseways of knowing.
The broad scope of the Culture Care Theoryis reflected in Leininger’s definition of nursingwhich presents nursing as a ‘learned humanisticand scientific profession and discipline which isfocused on human care phenomena and activitiesin order to assist, support, facilitate, or enableindividuals or groups to maintain or regain theirwell-being (or health), in culturally meaningfuland beneficial ways or to help people face handi-caps or death (Leininger 1991 cited by Leininger2006a in Leininger & McFarland 2006: 7).Theethnonursing method was developed to studyspecific nursing care phenomena as well as theCulture Care Theory.The central purpose of theethnonursing method is to tease out complex,elusive, and largely unknown nursing dimen-sions [of care] from the people’s focal viewpointsregarding human care, well-being, health, andenvironmental influences. The ethnonursingmethod assists in discovering differences bet-ween generic or naturalistic care and profes-sional nursing care. Discovering generic ornaturalistic or folk care is essential to know and
56 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 56

use to provide professional nursing care andespecially to providing advanced practice nursingcare offered by nurse practitioners. WhenLeininger studied the Gadsup of New Guinea inthe 1960s, she found the use of the terms emicand etic useful (as previously defined herein) instudying care and other nursing phenomena.Theuse of these terms assisted Leininger to discoverthe diverse meanings and ideas of the peopleregarding the values, beliefs, and nursing ritualsand symbols of care, health and illness. In thisfirst ethnonursing study, Leininger began todevelop several enabling guides, such as the Sun-rise Enabler and the Observation-Participation-Reflection (OPR) Enabler to help her study thelifeways of the people of the Eastern Highlandsof New Guinea (Leininger 2006a: 26). Leiningerrealised that the ethnonursing method wasimportant to discover caring modes such as thecare and feeding of infants, dealing with pain andanxiety, supporting people in lifecycle eventsand crises, and finding different ways to teachpeople about how to maintain health, and hassuggested that many techniques and enablingguides developed for use with the ethnonursingmethod can be used by the clinician (Leininger& McFarland 2006: 51). For instance, theStranger to Trusted Friend Enabler can assist theclinician to move from a Distrusted Stranger to aTrusted Friend to establish favorable relation-ships with clients (Leininger 2006a: 26). Weoffer that this enabler can be used by the nursepractitioner to gauge whether the client ‘trusts’the nurse practitioner and is working ‘with’ thenurse practitioner to share essential health infor-mation regarding the his/her lifeways includingculturally sensitive health practices such as com-plementary therapies or folk remedies, nutri-tional regimes and supplementation, spirituallybased rituals, and sensitive information regard-ing sexual practices or non-therapeutic activities(such as illicit drug use or abuse of prescribednarcotics, for example).
The OPR guides researchers and clinicians todevote a period of time making observations
before becoming an active participant in theresearch or clinical process.The reflective phaseprovides an opportunity to obtain importantand confirmatory data from the people. Theguide can be adapted for use to assist the nursepractitioner in client encounters in direct clini-cal practice contexts. Leininger (2006b: 60)implies such use of this enabler when she states,‘These phases were expressly conceptualizedand developed to fit with the people centerednursing ways that professional nurses areexpected to work within their daily experi-ences.’ For example, the nurse practitionerobserving the client sitting in the waiting roomand walking down the hall to the examinationroom presents a valuable opportunity to assessgeneral appearance, gait, pain expressions,tobacco or alcohol use, cultural or non-contem-porary forms of dress, use of language, and indi-vidual means of contextualising the reason orpurpose of the healthcare visit. A period ofmeeting, greeting, and visiting with the client inthe examination room is essential to allow thenurse practitioner sufficient time for furtherobservation while assisting the client to becomemore comfortable with the situation, thus enab-ling the nurse practitioner to obtain a moreaccurate health history and physical assessment.Reflection is also a valuable part of the nursingprocess as the nurse practitioner clarifies valu-able information in reflecting findings back withthe client and confirming acceptability andunderstanding of the diagnostic findings andplan of care with the client.
CONCLUSIONSThe Theory of Culture Care Diversity and Uni-versality is inherently structured to provide theadvanced practice nurse with a sound theoreti-cal basis for doctoral education, evidence-basedresearch, and primary care practice in the nursepractitioner role. The key components of theCulture Care Theory can be readily linked tothe eight Essentials of Doctoral Education forDNP as posited by AACN in their October
57Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 57

2006 document which are: Scientific Underpin-nings for Practice; Organizational and SystemsLeadership for Quality Improvement and Sys-tems Thinking; Clinical Scholarship and Ana-lytical Methods for Evidence Based Practice;Information Systems/Technology and PatientCare Technology for the Improvement andTransformation of Healthcare; Healthcare Poli-cy and Advocacy for Healthcare; Interprofes-sional Collaboration for Improving Patient andPopulation Health Outcomes; Clinical Preven-tion and Population Health for Improving theNation’s Health; and Advanced Nursing Prac-tice.These essentials of DNP education will becritical to guiding the process of meeting thethree primary goals toward preparing graduatesfor advanced nursing practice, which are to:
1. Integrate nursing science with knowledgefrom ethics, biophysical, psychosocial, ana-lytical, and organizational sciences as thebasis for the highest level of nursing prac-tice;
2. Use science-based theories and concepts[such as culture care] to determine thenature and significance of health and health-care delivery phenomena; describe theactions and advanced strategies [such as thethree care modes] to enhance, alleviate, andameliorate health and healthcare deliveryphenomena as appropriate; and, evaluateoutcomes; and
3. Develop and evaluate new practice ap-proaches based on nursing theories [such asthe Culture Care Theory] and theories fromother disciplines. (AACN 2006: 9)
Doctorate of Nursing Practice (DNP) evidence-based projects will create new nursing knowl-edge for both the discipline and practice of theprofession of advanced practice nursing as wellas provide a basis for advancement of the nursepractitioner role. DNP degree programs willfoster and accelerate practice focused/out-comes implementation projects that involvecritical appraisal and use of existing nursing
knowledge to formulate or reformulate practiceguidelines for implementation into practice.Implementation of such practice focusedresearch projects within a nursing conceptualframework such as the Culture Care Theorywith the ethnonursing method facilitates build-ing a body of nursing knowledge and ‘practiceguided by the concepts of a conceptual model of nursing [which] is more appropriate foradvanced practice nursing than a disease treat-ment model’ (Fawcett et al 2004: 137).
Nurse practitioners are endeavoring to com-prehend and integrate culture care precepts into practice, but they need more educationabout culture care and their education needs to be integral to their generic (ASN, BSN)(early professional education and clinical) learn-ing processes because change is easiest when itstarts at the beginning. In a recent unpublishedpilot study by Mixer (2006), the researcherfound that while nursing faculty valued culturaldiversity, provided and encouraged clinicalexperiences with opportunities for students tocare for culturally diverse clients, and role mod-eled culturally sensitive awareness behaviors,the faculty did not use any formal conceptualnursing model or theory (such as the CultureCare Theory) as a basis for their teachings.
Family nurse practitioners practicing in primarycare contexts need to broaden their practice byalso demonstrating leadership in the communityas a means toward developing a wider system ofcaring and healing locally, nationally, and global-ly. The Theory of Culture Care Diversity andUniversality provides a sound basis upon whichthe nurse practitioner can develop information-al systems, bridge cultural gaps, and developcommunity/group/family consensus. Commu-nity leadership can be exercised by participationin school health programs and teaching, and bybecoming a member of the local school board,or by offering community-based health edu-cation presentations either independently orthrough other local healthcare agencies such ashospitals, senior living centres or senior com-
58 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 58

munity/day care centres, or nursing agencies;by offering to assist or present health programsto adult education programs; by participation inliteracy programs as a mentor (as literacy is adirect indicator of community health); throughlocal government participation or activism; bybecoming involved in eldercare and-or parishhealth programs, community mental health pro-grams or governing boards; and assisting in thepromotion of lay participation in healthcare(such as migrant, community mental health,library, hospital, and district health departmentboards or lay care services), and lay-professionaljointly presented health education events (healthfairs or screenings, blood drives), health pro-grams (teen pregnancy, doula, drug or STI prevention) or culturally-based community oreducation programs or events (eg, tribal pow-wow, Cinco de Mayo celebrations, AfricanAmerican Heritage events); and community-based culture care research projects. Partici-pation in professional organisations is alsoimportant to foster the development of the pro-fession. Organisations such as the TransculturalNursing Society, American Nurses’ Association,National Organization of Nurse PractitionerFaculties, Michigan Council of Nurse Practi-tioners, Michigan Nurses’ Association, Ameri-can College of Nurse Practitioners, and theAmerican Association of Nurse Practitioners,and other state, regional, national, and interna-tional nursing groups have ongoing projects andprograms directed toward fostering improvedclient care as well as the betterment of thenursing profession through education, politicalor government activism, or policy enactmentefforts.
We (the authors) propose these outcomescan be achieved through clinical, educational,and research applications of the theory of Culture Care Diversity and Universality withthe use of three modes of care and the SunriseEnabler and the ethnonursing research method.Many theories guide nursing education andresearch but we propose that the Culture Care
Theory can guide advanced nursing practice andeducation as well as practice/outcomes basedresearch that is focused on implementing evi-dence-based research findings to achieve themost safe, beneficial, and satisfying healthcareoutcomes. Putting theory into practice entails theelement of the theory, in addition to an infor-mation gathering process; knowledge of cultureand care practices; planning of healthcare; as-sessment; research; and establishing a caringhealing system (Germain 2004: 441–442).Thus, the Theory of Culture Care Universalityand Diversity guides advanced nursing practiceby:• framing knowledge and predicting similari-
ties and differences among and between cul-tures;
• providing a means to learn and gather careinformation about cultures essential for holis-tic assessment and sound nursing conclusions;
• discovery of caring and healing values, beliefs,and practices used by individuals, families,groups;
• collaboratively using Leininger’s three modesof care; using ethical reasoning, analysis, skill,and decision making relevant to culture;
• evaluation through reflective and informedpractice which is critical to determine out-come impact and establish accountability,responsibility, and demonstrated practicestewardship; research which is foundationalto the nursing discipline’s body of knowledge,core values, and to facilitate contributions tothe greater good of society and community,and to advance the art and science of nursingprofession; and
• establishing and maintaining a system of car-ing and healing system which is essential forholistic assessment, sound nursing conclu-sions, and appropriate and integrated care.
AcknowledgementsThe authors wish to gratefully acknowledge thetheoretical contributions of Dr Madeleine Lein-inger with appreciation for her ongoing support.
59Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 59

ReferencesAmerican Association of Colleges of Nursing
(2006) The Essentials of Doctoral Education forAdvanced Nursing Practice,AACN,Washington,DC.
Anderson JM (1987) The cultural context ofcaring, Canadian Critical Care Nursing Journal4: 7–13.
Australian Nursing and Midwifery Council(ANMC) and Nursing Council of NewZealand (2004) National Competency Standardsfor the Nurse Practitioner, accessed at www.anmc.org.au on October 4, 2007.
Avron J (1991) The neglected history andtherapeutic choices for abdominal pain:Anationwide survey of 799 physicians andnurses, Archives of Internal Medicine 151:694–698.
Birkholtz G and Viens D (1999) Medicaid claimsdata comparisons for nurse practitioners,physicians assistants, and primary care physi-cians in New Mexico, Journal of the AmericanAcademy of Nurse Practitioners 11: 3–10.
Birkholtz G and Viens D (2001) Developingresearch methodologies to compare primarycare nurse practitioners and physician prac-tices, The American Journal for Nurse Practition-ers: 9–10, 13–14, 17–18, 27–28, 31–32.
Brown S (1998) A framework for advancedpractice nursing, Journal of Professional Nursing14: 157–164.
Brown S and Grimes D (1995) A meta-analysisof nurse practitioners and nurse midwives inprimary care, Nursing Research 44: 332–339.
Carper BA (1978) Fundamental patterns ofknowing in nursing, Advances in NursingScience 1: 13–23.
Capan P, Beard M and Mashburn M (1993)Nurse managed clinics provide access andimprove care, Nurse Practitioner 18: 50–55.
Eisenbruch M, Rotem A,Waters D, Snodgrass Rand Creegan R (2002) Nursing Education in aMulticultural Context. CommonwealthDepartment of Education, Science, andTraining, Canberra,Australia, online ISBN 0-
642-777246-0, accessed at www.dest.gov.au/archive/highered/nursing/pubs/multi_cultural/1.htm on 06 March 2008.
Fawcett J, Newman DML and McAllister D(2004) Advanced practice nursing andconceptual models of nursing, Nursing ScienceQuarterly 17: 135–138.
Fiandt K, Laux CA, Sarver NL and Sayer RJ(2002) Finding the nurse in nursepractitioner practice:A pilot study of ruralfamily nurse practitioner practice, ClinicalExcellence for Nurse Practitioners 5: 13–21.
Germain M (2004) A cultural variable in prac-tice, cited in Joel LA (ed) Advanced NursingPractice: Essentials of Role Development, pp 430–453. FA Davis & Company, Philadelphia, PA.
Hall J (1990) Performance quality, gender, andprofessional role:A study of physicians andnonphysicians in 16 ambulatory practices,Medical Practice 28: 489–501.
Hanson CM and Hamric AB (2003) Reflectionson the continuing evolution of advancedpractice nursing, Nursing Outlook 51: 203–211.
Hubbert A O (2006) Application of the culturecare theory for clinical nurse administratorsand managers, cited in Leininger MM andMcFarland MR (eds) Culture Care Diversity andUniversality:A Worldwide Theory of Nursing, 2ndedn, pp 355, Jones and Bartlett, Sudbury,MA.
Keesing R (1981) Cultural Anthropology, Holt,Rinehart & Winston, New York, NY.
Leininger M (1991) Culture Care Diversity andUniversality:Theory of nursing, National Leaguefor Nursing, New York.
Leininger M (2002a) Transcultural nursing andglobalization of healthcare: Importance,focus, and historical aspects, cited inLeininger M and McFarland MR (eds)Transcultural Nursing: Concepts, theories, researchand practice, 3rd edn, pp 3–43, McGraw-HillMedical Publishing Division, New York.
Leininger M (2002b) Part I:The theory ofculture care and the ethnonursing researchmethod, cited in Leininger M and McFarland
60 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 60

M R (eds)Transcultural Nursing: Concepts,theories, research and practice, 3rd edn, pp71–98, McGraw-Hill Medical PublishingDivision, New York.
Leininger M (2002c) Culture care practices forcongruent competency practices, cited inLeininger M and McFarland MR (eds)Transcultural Nursing: Concepts, theories, researchand practice, 3rd edn, pp 117–143, McGraw-Hill Medical Publishing Division, New York.
Leininger M (2002d) Part 1:Toward integrativegeneric and professional healthcare, cited inLeininger M and McFarland M R (eds) Trans-cultural Nursing: Concepts, theories, research andpractice, 3rd edn, pp 145–154, McGraw-HillMedical Publishing Division, New York.
Leininger MM (2006a) Culture care diversityand universality theory and evolution of theethnonursing method, in Leininger MM andMcFarland MR (eds) Culture Care Diversity andUniversality:A Worldwide Theory of Nursing, 2ndedn, pp 1–41, Jones and Bartlett, Sudbury,MA.
Leininger MM (2006b) Ethnonursing researchmethod and enablers, in Leininger M M andMcFarland MR (eds) Culture Care Diversity andUniversality:A Worldwide Theory of Nursing, 2ndedn, pp 43–81, Jones and Bartlett, Sudbury,MA.
Leininger MM (2006c) Culture care of theGadsup Akuna of the Eastern highlands ofNew Guinea: First transcultural nursingstudy (revised reprint), in Leininger MM andMcFarland MR (eds) Culture Care Diversity andUniversality:A Worldwide Theory of Nursing, 2ndedn, pp 115–157, Jones and Bartlett,Sudbury, MA.
Leininger MM and McFarland MR (eds) (2002)Transcultural Nursing: Concepts,Theories, Researchand Practice, 3rd edn, McGraw-Hill MedicalPublishing Division, New York, NY.
Leininger MM and McFarland MR (eds) (2006)Culture Care Diversity and Universality:AWorldwide Theory of Nursing, 2nd edn, Jonesand Bartlett, Sudbury, MA.
McCance TV, McKenna HP and Boore JRP(1999) Caring:Theoretical perspectives ofrelevance to nursing, Journal of AdvancedNursing 30: 1388–1395.
Mixer S (2006) Faculty expressions, patterns,and practices related to teaching culturecare. Unpublished pilot study, DuquesneUniversity, Pittsburgh, PA.
Moody N, Smith P and Glenn L (1999) Clientcharacteristics and practice patterns of nursepractitioners and physicians, Nurse Practitioner24: 94–96, 99–100, 102–103.
Mundinger MO, Kane RL, Lenz ER,Totten AM,Tsai WY, Cleary PD, Friedwald WT, Siu ALand Shelanski ML (2000) Primary careoutcomes in patients treated by nursepractitioners or physicians, Journal of theAmerican Medical Association 283: 59–68.
Ndiwane A, Miller KH, Bonner A, Imperio K,Matzo M, McNeal G,Amertil N and FeldmanZ (2004) Enhancing cultural competenciesof advanced practice nurses: Healthcarechallenges in the twenty first century, Journalof Cultural Diversity 11: 118.
Omeri A (2003) Meeting diversity challenges:Pathway of ‘advanced’ transcultural nursingpractice in Australia, Advances in ContemporaryTranscultural Nursing 15: 175–186.
Ray M (1999) Transcultural nursing in primaryhealth care, National Academies of PracticeForum 1: 177–182.
St Clair A (1999) Preparing culturallycompetent practitioners, Journal of NursingEducation 38: 228–234.
Salkever DS (1992) Episode based efficiencycomparisons between physicians and nursepractitioners, Medical Care 20: 145–153.
Starfield B (1991) Innovative ways to studyprimary care using traditional methods citedin Norton P, Stewart M,Tudiver F, Bass Mand Dunn E (eds), Primary Care Research, pp26–39, Sage, Newbury Park, CA.
United States Department of Health andHuman Services (2002) Nurse practitionerprimary care competencies in specialty areas:
61Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 61

Adult, family, gerontological, pediatric, andwomen’s health. Health Resources and ServicesAdminstration, Bureau of Health ProfessionsDivision of Nursing, submitted by TheNational Organization of Nurse PractitionerFaculties (NONPF) in partnership with TheAmerican Association of Colleges of Nursing(AACN).
Wenger AFZ (2006) Culture care and health of
Russian and Vietnamese refugee communitiesin the United States, cited in Leininger Mand McFarland M (eds) Culture Care Diversityand Universality:A Worldwide Theory of Nursing,2nd edn, pp 355. Jones and Bartlett,Sudbury, MA.
White J (1995) Patterns of knowing: Review,critique, and update, Advances in NursingScience 17(4): 73–86.
62 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn M McFarland and Marilyn K EipperleCCCCNNNN
APPENDIX I: LEININGER’S SUNRISE ENABLER TO DISCOVER CULTURE CARE
Source: Sunrise Enabler © Used by permission of M Leininger.
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 62

63Volume 28, Issue 1–2,April 2008 CCCCNNNN
Practice theory guide for nurse practitioners in primary care settings CCCCNNNN
APPENDIX II: NURSE PRACTITIONER COMPETENCIES
Domain 1. Management of Patient Health/Illness StatusA. Health Promotion/Health Protection
and Disease Prevention i. Assessment of Health Statusii. Diagnosis of Health Statusiii. Plan of Care and Implementation
of TreatmentB. Management of Patient Illness
APPENDIX III: NURSE PRACTITIONER COMPETENCY FRAMEWORK
Standard I: Dynamic practice that incorporates application of high level knowledge and skills in extended practice across stable, unpredictable, and complex situations.
Standard II: Professional efficacy whereby practice is structured in a nursing model and enhanced by autonomy and accountability.Competency 2.2: Establishes therapeutic links with the patient/client/community that
recognise and respect cultural identity and lifestyle choices.Standard III: Clinical leadership that influences and progresses clinical care, policy, and collaboration
through all levels of health service.
Source: Australian Nursing and Midwifery Council (ANMC), Nursing Council of New Zealand 2004.
Domain 2. The Nurse Practitioner–Patient Relationship
Domain 3. The Teaching–Coaching Function Domain 4. Professional RoleDomain 5. Managing and Negotiating
Health Care Delivery Systems Domain 6. Monitoring and Ensuring the
Quality of Health Care Practice Domain 7. Cultural Competence
Source: United States Department of Health and Human Services 2002.
SOCIAL EQUITY AND HEALTHEdited by Toni Schofield (University of Sydney) and
Olle Lundberg (Centre for Health Equity Studies, Karolinska Institute, Stockholm)
A special issue of Health Sociology Review (ISSN 1446-1242) volume 16 issue 2 (2007)
This issue focuses on one of the most pressing issues of global health governance – health inequitiesor inequalities – explored from diverse methodological perspectives and national settings in
Australia, Bulgaria, Canada, India, Norway and the USA. Entrenched social divisions and differences and the local, contingent character of health inequity demand close social
investigation to underpin effective intervention through public policy.
Course Coordinators are invited to contact the Publisher for an adoption evaluation copy.
* * N O W A V A I L A B L E * *
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. [email protected]; www.e-contentmanagement.com
• Editorial — Toni Schofield
• Gender, equity and tobacco control — Lorraine Greaves
• On the inequitable impact of universal healthinsurance: The experience of Bulgaria intransition — Stephanie D. Short, ValentinDimitrov Hadjiev, Zdravka Dimitrova Toneva
• Educational inequalities in avoidable deaths inNorway: A population based study — Espen Dahl, Dag Hofoss, Jon Ivar Elstad
• Health inequity and women’s self-help groups inIndia: The role of caste and class — Anant Kumar
• Social capital, health and electronic communityin public high-rise estates: An Australian case-study — Liza Hopkins
• The impact of household type on adolescentwomen’s well-being in Kenya — Anne M.Dannerbeck, Andrew Muriuki
• Health inequity and its social determinants: A sociological commentary — Toni Schofield
• Book Reviews
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 63
Healthcare systems are increasingly adaptingtheir services and programs to comply
with global trends toward providing culturalcare accommodation for culturally diverseclient populations and professionals. The pur-pose of this paper is to present a historical dis-
cussion of the past experiences from oneCatholic faith-based urban hospital in the Amer-ican Southwest regarding the accommodation ofthe spiritual beliefs and practices of AmericanIndian (Native American/Alaska Native) clientsand staff who were practicing traditional Indianmedicine (TIM). These experiences may holdpossible applications for other healthcare sys-tems in the United States and-or Australiawhich are both facing current challenges to pro-vide culturally sensitive care for increasinglydiverse patient populations. In Australia, nurseshave been encouraged to learn about providingculturally appropriate and safe nursing care forthe Australian Indigenous peoples, Aboriginesand Torres Strait Islanders, with an open minded
Key Wordstransculturalnursing; CultureCare Theory;Traditional IndianMedicine;American Indian;spirituality inhealthcare CN
64 Volume 28, Issue 1–2,April 2008CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 64–72.
A partnership of a Catholic faith-basedhealth system, nursing and traditional
American Indian medicine practitioners
ABSTRACT The paper presents a historically unique partnership between an AmericanSouthwestern, Catholic faith-based, urban hospital and a program it sponsoredon the spirituality of American Indian Traditional Indian Medicine (TIM) by aComanche medicine man.A discussion is offered on the cultural partnerships,experiences and benefits achieved through the cultural accommodations of thesespiritual beliefs and practices within this healthcare system. The theory ofCulture Care Diversity and Universality (Culture Care Theory), including theSunrise Enabler, is applied in discussion of these past experiences to explore the relationships among and between the participating cultures.The intent ofthe partnerships within this program was not to ‘learn Indian healingceremonies’ but to share the philosophy of TIM with all people (clients andprofessionals) as a means to enhance their own way of living. Examples of actualnursing decisions and actions are provided including outcomes from the programwithin the healthcare system and globally.Received 16 July 2007 Accepted 25 March 2008
ANN O HUBBERTAssociate ProfessorUniversity of NevadaReno NV, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 64

approach (Goold 2001). In both the UnitedStates and Australia, nurses are urged to exam-ine their own beliefs and philosophy of life as abasis for understanding and practicing culturallysensitive care. In addition, the foundation ofLeininger’s (1988; 2006) theory of CultureCare Diversity and Universality (Culture CareTheory) is applied as a framework for the dis-cussion of these experiences and the partner-ships created among and between the culturesof the TIM practitioners (referred to as tradi-tional Indian medicine people), the Southwest-ern American Indian clients, nursing and otherhealthcare providers, and the Catholic faith-based healthcare system which was the mainsource of hospital and professional healthcareservices in the region.
BACKGROUNDThe United States (USA) population is becomingprogressively more diverse (Office of MinorityHealth 2001; US Census Bureau 2000a); by2010, minority cultures (non-EuroAmerican lin-eage) will represent 32% of the national popula-tion, increasing to 50% by the year 2050. In the2000 Census, 4.3 million people (or 1.5 % ofthe total US population) self identified as Ameri-can Indian or Alaska Native (United States Cen-sus 2000b). This number included 2.4 millionpeople (or 1%) who reported American Indianor Alaska Native as their sole race.
Therefore, healthcare systems and profession-als are being challenged to provide diverse popu-lations with culturally competent nursing andhealth skills as part of their healthcare services.Federal healthcare regulatory standards underthe Department of Health and Human Services,Office of Minority Health (2001), designatedthe Nationally Culturally and LinguisticallyAppropriate Services (CLAS) standards forhealthcare in order to support a more consistentand comprehensive approach to cultural and lin-guistic competence in services and to decreasehealthcare disparities. Many healthcare systems
are addressing the standards, which are alsointerpreted to include the provision of opportu-nities for culturally specific spiritual accommo-dations. In addition, the interest among Westernhealthcare providers about traditional, Indige-nous practices among shamans or healers contin-ues to grow (Leininger 2002a: 145). As nursesare the largest group of healthcare providers,they have the opportunities to incorporate cul-turally sensitive and congruent care to meet theCLAS standards, into their daily practices.
Healthcare systems consist of a vast array ofcultures and subcultures among and betweenthe client populations, employees, professionaldisciplines, and the organisational structures,and yet they have historically functioned with‘unicultural’ views and policies (Gardenswartz& Rowe 1998; Gropper 1996; Leininger 1997).Acknowledgment of the existence of manyhealthcare systems’ unicultural perspectives,including ethnocentric views (knowing what isbest), leading to ethnocentric actions (having thebest decisions), is a positive step to include newactions that enhance culturally sensitive care(Leininger 2002b: 50–51, 2006: 53–54). Thenormal perspective within Western healthcare isthe belief that academic, scientific healthcare issuperior to cultures’ folk or traditional health-care beliefs, values, and practices (Leininger1991). As a result, various aspects of healthcarepolicies and actions are based on healthcareteams’ preconceived judgments of what will be best for clients based on diagnoses withoutconsideration of cultural beliefs, values, andpractices. The American Indians are oftenincluded in this approach, as nurses are chal-lenged to remain open-minded, non-judgmen-tal, and non-ethnocentric (Weaver 1999: 201).
American Indians have rarely divulged theirparticipation in TIM, including assistance from a traditional medicine person, when they par-ticipate in Western healthcare (Struthers, Laud-erdale, Nichols & Strickland 2005;Tom-Orme2002).Their cultural practices have been regard-ed as private and often disregarded by their
65Volume 28, Issue 1–2,April 2008 CCCCNNNN
A partnership of practitioners CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 65

Western healthcare providers. As a result, theyhave often been unable to ‘partner’ the two per-spectives of healthcare together in a beneficialholistic approach to their health and lives. TheUnited States Department of Health and HumanServices, Indian Health Service (2007), defines apractitioner of Traditional Indian Medicine as ‘a person who is trained in a Native Americancommunity, and applies culturally specificknowledge and skills in the diagnosis, treatment,or referral of patients to promote their well-being physically, mentally, socially, and spiritual-ly.’ The term ‘spiritual’ has a broad meaning inAmerican Indian culture, unlike the commonWestern allocation of a patient’s ‘spiritual pref-erence/religion.’ In Traditional Indian Medicine(Garrett & Garrett 1996; Monetathchi 1988a;Ortega 1989) spirit refers to the active flow ofenergy that connects all living things to ‘God,the Universal Energy/Source, or Great Spirit,’and spiritual refers to a way of living.
An American Indian’s cultural and spiritualbehaviors, such as dropping their eyes as a sign of respect, or a period of silence beforeresponding when asked a question (Garrett &Garrett 1996; Monetathchi 1988b;Tom-Orme2002) could also lead a healthcare provider tomake an inaccurate or inappropriate assessmentor diagnosis (Gardenswartz & Rowe 1998; Lein-inger 1997). For example, an Indian patientwho does not look directly at the nurse couldbe perceived by the nurse as ‘not listening tome’ or as ‘non-compliant.’ In turn, these cultur-al interactions and relationships may contributeto cultural impositions (Leininger 2002b: 51) inwhich the healthcare professionals are seen bypatients as being in authority and thus holding alarge amount of power, influence, and authorityover them. An example offered by Monetathchi(1988a) is in the frequent subtle language oftenused by nurses, ‘my client/patient’ or ‘the dia-betic.’ Implicit can be the ethnocentrism thatthe nurse is ‘better than the individual’ (who isthe client) or as ‘expressing ownership’ versususing the language of respect and partnership,
for example, ‘Mrs Delores, the client/patientwith whom I am working.’
One healthcare system’senvironment and process withtraditional Indian medicineA historical discussion is offered of the chal-lenges faced and the benefits gained by this indi-vidual Catholic faith-based healthcare system,nurses, and employees when they sought tooffer culturally sensitive accommodations forthe spiritual practices of American Indiansclients and employees.The goals for this questwere guided by the mission of the system toprovide for the healthcare needs of our commu-nity; to embrace the whole person, in mind,body, and spirit; and to serve all people withdignity (Carondelet Health Network 2008;Carondelet Health Services 1986).
The healthcare system and providers’ chal-lenges included the following (Hubbert 2004):
1. Acknowledgement that TIM spiritual beliefsand practices are integrated with the heal-ing process;
2. Discovering how specific spiritual practicescould be addressed in nursing assessments;
3. Negotiating for physical space accommoda-tions to be made for some spiritual practices;
4. Welcoming the presence of spiritual practi-tioners; and
5. Blending the cultural spiritual practices ofpatients with the cultures of nursing andother healthcare professionals.
The identified challenges were explored andapproached with a unique cultural program overa period of six years from 1984 to 1990. Theprogram, which was internationally attended,began because an Apache nurse recognised thatmany clients of the Southwestern American Indian nations (Tohono O’odam, Pasqua-Yaqui,Navajo/Dine’, Apache, to name a few) wereoften entering an ‘unknown culture’ as inpa-tients of a Catholic faith-based healthcare sys-tem. She requested nursing administration to
66 Volume 28, Issue 1–2,April 2008CCCCNNNN
Ann O HubbertCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 66

provide an educational workshop for the nursingand interdisciplinary staff to increase their cul-tural sensitivity of American Indian spiritualitypractices.This led to development of a guidingteam that included a nurse, a nursing adminis-trator and a nurse-member of the Catholic religious community who served as a liaison tofulfill the faith-based mission of programs.
The three members of the guiding teamacknowledged their learning process about cul-tural/spiritual practices, beliefs, and values ofIndian cultures would involve self-discoverythrough reflection and re-assessment of theirown beliefs and values.They sought a partner-ship with the Indian Health Service (IHS); aComanche medicine man responded to theirrequest for assistance. Educated at Harvard Uni-versity, Mr Edgar Monetathchi Jr was thenational traditional Indian medicine specialistfor the IHS (Monetathchi, 1982). He agreed toguide and facilitate the guiding team’s questtoward ‘accommodating increased spirituality inhealthcare and healing.
The cultural sharing among and between thecultures of these four individuals, IHS and theindividual healthcare system evolved into a program of thirty-six conferences entitled Tradi-tional Indian Medicine: Spirituality and Healing inToday’s Health System which were five to sevendays in length.The programs were attended byover 7000 international lay and professionalattendees.These conferences were coordinatedand taught by the medicine man director and ateam of traditional Indian medicine people.TheAmerican Catholic Health Association recog-nised this program with their annual achieve-ment citation for ‘bold and innovative initiativesfrom Catholic healthcare providers in service totheir communities’ (Carondelet Health Ser-vices: 1986). Creative, unique partnerships hadbeen formed that worked together to establishintegrated care relationships among and bet-ween the cultures of the American Indians andtheir traditional Indian medicine, Catholic faith-based healthcare, nursing, and other healthcare
professionals. Further recognition was given bythe chief executive officer and member of theCatholic religious community, Sister St. JoanWillert, when she acknowledged that the origi-nal intent had been purely educational to ‘learnabout’ the Indian approach to sickness and heal-ing, but the healthcare providers soon realisedthe ‘many benefits we had [gained] learning thisway of life based on respect and unconditionallove’ (Carondelet Health Services 1986). Inanother unique action, this Catholic healthcaresystem subsequently hired the Comanche medi-cine man as a full-time TIM specialist upon hisretirement from IHS.
CONTEXT OF ADDRESSINGTRADITIONAL INDIAN MEDICINEIN THIS PROGRAMUnder the guidance of Mr. Monetathchi Jr, theprogram used an approach of freely sharing andgiving to address TIM’s sharing and teaching as aphilosophy of living, and that the approach tohealth and healing is truly a holistic process(Monetathchi 1988a, 1988b). The foundationfor his partnership as a medicine man and pro-gram director with the nursing team was simple: the nurses had sought his wisdom andasked for his help.The intent of the partnershipsand education was not to ‘learn Indian healingceremonies,’ but rather to share the philosophyof TIM in a way that all people, includingpatients and healthcare professionals, couldchoose directions to enhance their own way ofliving (Monetathchi 1988b).
Among the foundational keys provided by theComanche medicine man were the Seven SacredAspects of Life and the essence of a holistic individual(Monetathchi 1987a).These two concepts wereshared to establish a basis for the discussionwhich paralleled some basic tenets of the Culture Care Theory.The Seven Sacred Aspectswere shared in the conferences as the valueswith which nurses, all healthcare providers, orany other individual could guide their daily livesand actions.The seven values offered were: (1)
67Volume 28, Issue 1–2,April 2008 CCCCNNNN
A partnership of practitioners CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 67

Respect; (2) Honesty; (3) Truth; (4) Humility;(5) Compassion; (6) Wisdom; and (7) Uncondi-tional love.
The TIM portrayal of a holistic individual asshared included the concept that ‘Health EqualsBalance’ (Monetathchi 1988b, 1988c; Mone-tathchi, Ortega & Flores 1987). The individualrepresents balance among and between theirphysical being, mental being, spiritual being,their environment, and their relationship withGod. Illness or disease (dis-ease) was shared as‘any of those components being out of balance’(Monetathchi 1988b). In addition, the Circle ofLife or Way of the Circle was shared as a guide tothe Indian way of being to achieve harmony andbalance among all aspects of life, which are allconnected, and thus find harmony within thehealing process (Garrett & Garrett 1996; Mon-etathchi 1987b).
CULTURE CARE THEORYA discussion of the theory of Culture CareDiversity and Universality (Culture Care Theo-ry) is offered to show how the theory can beapplied as a framework for these partnershipexperiences among the multiple cultures in-volved, emphasising the relationships amongand between them. Since the 1950s, MadeleineLeininger has been the global leader and devel-oper of the theory of Culture Care Diversityand Universality (Leininger 1988, 1991, 2002d,2006). The theory’s foundation is used as theframework for discovering relationships thatguide working among and between diverse cul-tures, and specifically to examine the identifiedprogram’s approach to spirituality and the heal-ing process among and between cultures. Inaddition, the Sunrise Enabler provides an in-depth view of the dimensions of the theory andthe application of the theory to the actions thatoccurred (Leininger 1991, 2002b: 80–83).TheSunrise Enabler also is a paradigm that supple-ments the ‘circle if life’ ways of living for manyAmerican Indians (Tom-Orme 2002).
Leininger (1991) conceptualised generic care as
the cultures’ folk or Indigenous practices, beliefsand values. Culturally congruent care refers to cul-turally based care used to provide sensitive, cre-ative, and meaningful nursing care to support theclient’s general values, beliefs, and lifeways for effec-tive and enriched healthcare, or to deal with ill-ness, disability, or death (Leininger, 2002c:117–118). The greatest challenges for nursesand all healthcare providers are the understand-ing and acknowledgement of culturally basedcare actions in order to provide meaningful [pro-fessional] care (Leininger 1991: 47).
Universal care constructs and care valuesTranscultural nurses have actively used the eth-nonursing research process to discover domi-nant care constructs to be used as guides fornursing and healthcare. Universal care-specificconstructs have been identified that are valuedby virtually all cultures (Leininger 1991, 2002b:219–223; McFarland 2002: 107).The first uni-versal construct is respect, and followed by otherprominent constructs which include: concernfor/about; attention to; helping/assisting acts; listen-ing; presence; being connected; filial love; and under-standing. Transcultural research specific toAmerican Indians identified the dominant careconstructs as respect; presence; among familiar kin;silence; singing special songs; humour; and, spiritualconnectedness (Tom-Orme 2002). All levels ofthis transcultural research study provide sup-ports for the seven sacred aspects of TIM whichemphasized respect as the foremost aspect ofbehavior valued by American Indians for nursesand healthcare providers to demonstratethroughout their actions and decisions (Mone-tathchi 1987a).
Transcultural nursing research also providesknowledge of the context of culture care values,or the values that give meaning, order, anddirection to actions, decisions and lifewayswithin cultures (Leininger, 1991). It is impor-tant for nurses and healthcare providers tounderstand some general American Indian care
68 Volume 28, Issue 1–2,April 2008CCCCNNNN
Ann O HubbertCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 68

values. Individual nations or tribes may havespecific values, but these general values areoffered for basic understanding (Leininger1991: 357):
1. Harmony between land, people, and all ofthe environment;
2. Reciprocity with ‘Mother Earth and FatherSky’;
3. Spiritual inspiration/guidance;4. Traditional Indian medicine;5. Cultural rituals and ceremonies;6. Rhythmicity of life with nature;7. Authority of elders;8. Pride in cultural heritage and ‘Nations’,
and;9. Respect for and value of children.
These values are demonstrated through or arefound in the following behaviors: (1) active lis-tening; (2) periods of silence to hear spiritualguidance; (3) rhythmic timing of physical carewith nature; (4) respect for medicine people;(5) preserving cultural rituals; and, (6) respect-ful behaviors.
Sunrise enablerThe Sunrise Enabler (Leininger 1991, 2002d:79–83; Leininger & McFarland 2006: 24–26)provides a crucial guide for nurses to bring thetheory into action, and to reflect on their deci-sions and actions.These three ‘care modes’ canbe incorporated by nurses as guides when work-ing between and among cultures:
1. Culture care preservation and-or maintenance:Identify the cultures involved (client, nurs-ing etc), then what client or staff care assis-tance is wanted?
2. Culture care accommodation and-or negotiation:What care beliefs or practices need to beaccommodated, or what needs to be negoti-ated with staff, clients, etc.?
3. Culture care restructuring and-or repatterning:What practices need to be restructured orrepatterned, and by whom?
APPLICATION OF THE THREE CAREMODES TO THE TIM PROGRAMThe three action and decision care modes of theCulture Care Theory are described using an in-depth actual event in order to offer further dis-cussion of the strongly similar parallelfoundations between TIM and the Culture CareTheory. The example demonstrates how thisprogram was able to apply the blended practicesof the ‘partnership cultures’ to enhance spiritu-ality and the healing process by expanding theprovision of culturally congruent care withinthe healthcare system.
A nurse on an inpatient unit presented the following cultural challenge for discussionduring the educational presentations by the tra-ditional medicine people; note that the presen-ters’ responses were parallel to the SunriseEnabler. Subsequently, this scenario has beenfrequently used as a teaching supplement for theCulture Care Theory and the Sunrise Enabler(Hubbert 2004):
Mary, a 54 year-old woman from the South-western Tohono O’odham Reservation, hasbeen admitted for the first time in her life toa hospital for newly diagnosed acute diabetes.She speaks minimal English, but the nursingstaff is pleased that she appears to understandtheir instructions so well, as she nods fre-quently, smiles, and asks no questions. Thefirst evening Mary was accompanied for sev-eral hours by a granddaughter, but she had toleave to care for her family that lived overtwo hours away from the hospital.The nextmorning, Mary smiled and nodded to Kevin,the RN who brought her medications andtold her about her new medication regime.However, she refused to take the medicationsout of his hand. She kept telling him ‘No, Icannot do this ... I need to say my prayers.’Kevin did not understand, and told her thathe would return in 15 minutes, then left heralone to pray. Later, when he returned to herroom, she gave him the same response.What
69Volume 28, Issue 1–2,April 2008 CCCCNNNN
A partnership of practitioners CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 69

is happening between these cultures? Thenurse relayed that he ‘wants to help her.’
The medicine people’s responses the nurse’sscenario focused first on respect (Monetatchi,Ortega & Flores 1987); they facilitated the program participants to identify which peopleand issues needed respect, and to identify howrespect may or may not have been demonstratedby the nurse’s actions. Participants were guidedto consider the cultural way of living for theIndian, which included: the rhythm of nature andher life actions; greeting the new day with prayers;spiritual guidance for the new way of living; being‘out of balance’ (which included disruption oftraditional spiritual practices); and the barriersand challenges of the hospital environment. Thenurses were asked to consider that possibly asmile and nod from an Indian client did not nec-essarily indicate that their own expectationsways were being regarded ‘best’ nor would theybe followed. Rather, the participants were askedto consider that instead of having their fastspeaking words being understood, acknowl-edged, and followed, is was possible they (aspersons) were being greeted and honored fortheir position of authority, and that their dir-ections would be considered when the ‘timewas right?’ Instead of the nurse leaving for aperiod of time to provide privacy to pray, therewere other considerations that needed to beaddressed. What environment was consideredappropriate for the client’s prayers? Her way topray was to face the sun rising in the East everymorning, and her room faced westward. Hernew medication had not been ‘blessed’ and shehad not been ‘prayed over’ by the medicine per-son in order to begin this new way of living (inhospital) so that she could be ‘in harmony’rather than being ‘out of balance.’ Further, herfamily was not aware of these new changes andshe would not consider following the nurse’sdirections without their support.
This example of American Indian care valuescan continue to be used for various aspects of
learning and teaching along with the CultureCare Theory which emphasises universal careconstructs through the three care modes ofaction and decision as depicted in the SunriseEnabler. Respect is the foundation for all of therelationships. Knowledge of the American Indi-an cultural values and the transcultural nursingUniversal Care Constructs would assist thenurse in making decisions and guide nursingcare actions.
The use of the Sunrise Enabler offered in-depth care applications through the use of CareMode 1, culture care preservation and/or main-tenance.This included respect and preservation forboth cultures: the client’s traditional Indian ways,and the nursing culture’s philosophies and practices(to the best extent possible).
Mode 2, culture care accommodation and-ornegotiation in this situation included shortrange accommodations which later led to longrange actions for developed with Mode 3.Immediate accommodations for Mary included:transfer to a room with a bed that faced the Eastfor her morning prayers; time for her to praywith the medications she would take throughouteach day; presence of a nurse with she and herfamily; a tape recorder to play Indian music;space near her bedside for prayer objects with aposted message to staff requesting them to nottouch the objects; and, the welcoming of a med-icine person to meet with her in private. It wasalso important that these client-focused accom-modations occur very quickly in order to alsoaccommodate the nursing culture’s policiesabout care of diabetic client-patients and thetiming of their diabetic medications.
Mode 3, culture care restructuring and/orrepatterning by the nursing staff/healthcare sys-tem to meet the needs of the Indian cultureincluded: planning/arranging for Indian clients’bed assignments in the hospital for preferredEast rooms; instituting two full-time Indiantranslator/advocacy positions; a new healthcaresystem policy welcoming any medicine personat any time with provision for staff escorts
70 Volume 28, Issue 1–2,April 2008CCCCNNNN
Ann O HubbertCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 70

through the hospital; and initiation of numerouslanguage accommodations including audio tapesfor client orientation to the hospital room,equipment operation, pain assessment scales,common questions etc.
Further culture care restructuring and/orrepatterning by the nursing and healthcare sys-tem cultures included: nurses’ and any employ-ees’ attendance at TIM workshops to expandtheir knowledge of culturally specific care; revi-sion of the mission, objectives, and numerouspolicies of the nursing department to reflecttheir enhanced cultural values; creation of anew position for an Indian professional nursecase manager; and exchange of educationalinformation with the tribal health council aboutthe experiences within the healthcare systemthat were unclear. In addition, the TIM programdirector was hired as a full-time TIM specialistwhen he retired from IHS. He was provided anoffice suite and was afforded open access to allareas of the hospital as well as to any client/patient/family or employees who requested hisservices. His was frequently requested for inter-disciplinary consultations with other healthcareprofessionals.
CONCLUSIONA historical discussion has been given from the experiences of one individual, Catholic faith-based healthcare system with an in-houseTraditional Indian Medicine program of care.The program as developed later evolved into aunique array of cultural partnerships and spiri-tual enhancements for individuals and culturegroups. The theory of Culture Care Diversityand Universality (Culture Care Theory) wasapplied in this discussion as a framework forthese endeavors emphasising the relationshipsamong and between the cultures of TIM (tradi-tional Indian medicine people), SouthwesternAmerican Indian clients/patients, nursing, otherhealthcare providers, and the Catholic faith-based healthcare system. Instead of focusing on the differences, the similarities among and
between these varied cultures were discoveredand celebrated in this program, thereby benefit-ing over 7000 people.
Although this unique program cannot bereplicated identically, opportunities do exist for future cultural partnerships for the en-hancement of ‘spirituality and healing in today’shealth system’ within the framework of the Cul-ture Care Theory, including creative and reflec-tive applications of the Sunrise Enabler.There isinspiration in this discussion for all nurses,notably the example of one Apache nurse whoacted as an advocate for enhanced culturallycongruent care, and thereby was able to initiatesignificant transcultural change not only through-out one healthcare system, but globally.
ReferencesCarondelet Health Services (1986) St. Mary’s Hos-
pital (SMH) Traditional Indian Medicine programwins highest honor, The Weekly Connection, 16 June1986, CHS Media,Tucson,Arizona.
Carondelet Health Network (2008) The CarondeletHealth Network Philosophy, Mission, and Values,accessed at http://www.carondelet.org/about/mission.aspx, 6 February 2008.
Gardenswartz L and Rowe A (1998) Managing Divers-ity in Health Care, Jossey-Bass, San Francisco, CA.
Garrett JT and Garrett M (1996) Medicine of theCherokee The Way of Right Relationship, Bear &Company Publishing, Santa Fe, New Mexico.
Goold S (2001) Transcultural nursing: Can we meetthe challenge of caring for the Australian Indig-enous person? Journal of Transcultural Nursing 12:94–99.
Gropper R (1996) Culture and the Clinical Encounter,Intercultural Press,Yarmouth, Maine.
Hubbert AO (2004) The Incorporation of CultureCare To Enhance Spirituality in Health Care andHealing. Conference Proceedings, National Associationof Catholic Nurses,August, 2004, Santa Fe, NewMexico.
Indian Health Service (2007) Provider ServicesRendered Codes, PFCE Process Manual (The BlueBook) Supplemental Section, accessed at www.ihs.gov/NonMedicalPrograms/HealthEd/PDF/Blue_Manual_Supp_Sec_PROV_SERVICES_CODES.PDF, on 21 June 2007.
Leininger M (1988) Leininger’s theory of nursing:Culture care diversity and universality, NursingScience Quarterly 2: 152–160.
71Volume 28, Issue 1–2,April 2008 CCCCNNNN
A partnership of practitioners CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 71

Leininger M (1991) Becoming aware of types ofhealth practitioners and cultural imposition,Journal of Transcultural Nursing 2: 32–39.
Leininger M (1994) Transcultural nursing education:A worldwide imperative, Nursing and Health Care6: 40–51.
Leininger M (1997) Transcultural nursing research to transform nursing education and practice: 40years, Image: Journal of Nursing Scholarship 29:341–347.
Leininger M (2002a). Part I:Toward IntegrativeGeneric and Professional Health Care, inLeininger MM and McFarland MR (Eds)Transcultural Nursing Concepts,Theories, Research,& Practice, 3rd edn, pp 145–156, McGraw-Hill,New York.
Leininger M (2002b) Essential transcultural nursingcare concepts, principles, examples, and policystatements, in Leininger MM and McFarland MR(Eds)Transcultural Nursing Concepts,Theories,Research, & Practice, 3rd edn, pp 45–70, McGraw-Hill, New York.
Leininger M (2002c) Culture care assessments forcongruent competency practices, in Leininger,MM and McFarland MR (Eds) Transcultural NursingConcepts,Theories, Research, & Practice, 3rd edn, pp117–143, McGraw-Hill, New York.
Leininger M (2002d) Part I:The theory of culturecare and the ethnonursing research method, inLeininger MM and McFarland MR (Eds) Trans-cultural Nursing Concepts,Theories, Research, &Practice, 3rd edn, pp 71–98, McGraw-Hill,New York.
Leininger M (2006) Culture care diversity and uni-versality theory and evolution of the ethnonursingmethod, in Leininger MM and McFarland MR(Eds) Culture Care Diversity and Universality: AWorldwide Nursing Theory, 2nd edn, pp 1–42,Jones and Bartlett, Sudbury, MA.
McFarland MR (2002) Part II: Selected researchfindings from the culture care theory, in LeiningerMM and McFarland MR (Eds) Transcultural NursingConcepts,Theories, Research, & Practice, 3rd edn, pp99–116, McGraw-Hill, New York.
Monetathchi E Jr (1987a) The Seven Sacred Aspects:Conference proceedings.A conference sponsoredby Carondelet St Mary’s, June 1987,Tucson,Arizona.
Monetathchi E Jr (1987b) Resurgence of The AncientWays: Conference proceedings.A conferencesponsored by Carondelet St Mary’s, March 1988,Tucson,Arizona.
Monetathchi E Jr (1988a) The Spirit Within: Confer-
ence proceedings.A conference sponsored byCarondelet St Mary’s, March 1988,Tucson,Arizona.
Monetathchi E Jr (1988b) Traditional Indian Medi-cine: Philosophy of Wholeness, Wellness, andHealing: Conference proceedings.A conferencesponsored by Carondelet St Mary’s, March 1988,Tucson,Arizona.
Monetathchi E Jr (1988c) Traditional Indian Medic-ine: Mine,Yours, or Ours: Conference proceed-ings.A conference sponsored by Carondelet StMary’s, March 1988,Tucson,Arizona.
Monetathchi E Jr (1990) Spiritual Journey: Confer-ence proceedings.A conference sponsored byCarondelet St Mary’s, May 1990,Tucson,Arizona.
Monetathchi E Jr, Ortega AP and Flores A (1987)Traditional Indian Medicine:A General Session:Conference proceedings.A conference sponsoredby Carondelet St Mary’s, November 1987,Tucson,Arizona.
Ortega AP (1989) Traditional Indian Medicine: Con-ference proceedings.A conference sponsored byCarondelet St Mary’s,August 1989,Tucson,Arizona.
Struthers R, Lauderdale J, Nichols L and StricklandCJ (2005) Respecting tribal traditions in researchand publications:Voices of five Native Americannurse scholars, Journal of Transcultural Nursing 16:193–201.
Tom-Orme L (2002) Transcultural nursing and healthamong Native American peoples in Leininger MMand McFarland MR (Eds) Transcultural NursingConcepts,Theories, Research, & Practice, 3rd edn, pp429–440, McGraw-Hill, New York.
United States Bureau of the Census (2000a),Table 1a:Projected Population of the United States, by Raceand Hispanic Origin: 2000 to 2050, accessed atwww.census.gov/ipc/www/usinterimproj/natprojtab01a.pdf on 13 May 2007.
United States Bureau of the Census (2000b) We ThePeople:America Indian and Alaska Natives in theUnited States, accessed at www.census.gov/prod/2006pubs/censr-28.pdf on 6 February 2008.
United States Department of Health & Human Serv-ices (2001) Closing the Gap: Revised CLAS Standards,Office of Minority Health Newsletter, p 3.
Weaver HN (1999) Transcultural nursing with NativeAmericans: Critical knowledge, skills, and atti-tudes, Journal of Transcultural Nursing 10: 197–202.
72 Volume 28, Issue 1–2,April 2008CCCCNNNN
Ann O HubbertCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 72

73Volume 28, Issue 1–2,April 2008 CCCCNNNN
ADVANCES IN CONTEMPORARYINDIGENOUS HEALTH CARE
Australian, New Zealand and North American Perspectives
Edited by Eileen Willis, Vicki Smye and Maria RamekaDedicated to Irihapeti Merenia Ramsden
ISBN 0-9750436-9-2; xiii + 203 pages; softcover; September 2006A special issue of Contemporary Nurse, Volume 22, Issue 2
Course Coordinators are invited to contact the Publisher for an adoption evaluation copy.
* * * * N O W A V A I L A B L E * * * *
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. [email protected]; www.e-contentmanagement.com
PreliminariesDedication: Irihapeti Merenia Ramsden — Vicki SmyeVale: Nancy de Vries RN (Auntie Nance) — John Daly, Debra JacksonVale: Nancy de Vries RN (Auntie Nance) — Jill IliffeForeword: The Practice and Politics of IndigenousHealth Nursing — Denise WilsonIntroduction• Indigenous Health Care: Advances in nursing
practice — Vicki Smye, Maria Rameka, Eileen Willis
• Critical Cultural Perspectives and Health CareInvolving Aboriginal Peoples — Annette JBrowne, Colleen Varcoe
• Issues of Language Across the Cultural [andcolonial] Divide — Eileen Willis, Maria Rameka,Vicki Smye
Nursing in the Indigenous Context• Opinion Piece: ‘It’s only a mistake if you make
it twice’ — Kim O’Donnell• Decolonisation: A critical step for improving
Aboriginal health — Tania Edwards, JuanitaSherwood
• Amorphous Practice: Nursing in a remoteIndigenous community of Australia — JenniferHelen Cramer
• Characterising Maori Nursing Practice —Victoria Simon
Indigenous Understandings of Mental andPhysical Health• Opinion Piece: Indigenous Values, Cultural
Safety and Improving Health Care: The case of Native Hawaiians — Laurie D McCubbin
• Assessing Pain Across the Cultural Gap:Central Australian Indigenous peoples’ painassessment — Claire Fenwick
• At What Cost to Health? Tlicho women’s medicaltravel for childbirth — Pertice M Moffitt, Ardene Robbinson Vollman
• Insights on Aboriginal Peoples’ Views of Cancerin Australia — Pam McGrath, Hamish Holewa,Katherine Ogilvie, Robert Rayner, Mary AnnePatton
• The Experience of Whanau Caring for MembersDisabled from the Effects of a Cerebro-VascularAccident — Andrea Corbett, Karin Francis,Ysanne Chapman
Nursing Partnerships in Indigenous Health
• Opinion Piece: Nursing Partnerships inIndigenous Health — Tzu-I Tsai
• Relationship Building for Research: The SouthernSaskatchewan/Urban Aboriginal Health Coalition— Sandra Bassendowski, Pammla Petrucka,Marlene Smadu, Chief Roger Redman, Carrie Bourassa
• A Nursing Partnership for Better Outcomes inAboriginal Mental Health, Including SubstanceUse — Charlotte de Crespigny, Inge Kowanko,Scott Wilson, Helen Murray, Jackie Ah Kit, David Mills
• Meeting the Health Needs of IndigenousPeople: How is nursing education meeting thechallenge? — Sally Goold, Kim Usher
• The Yapunyah Project: Embedding Aboriginaland Torres Strait Islander perspectives in thenursing curriculum — Robyn Nash, Beryl Meiklejohn, Sandy Sacre
• Is it Aboriginal Friendly? Searching for ways ofworking in research and practice that supportAboriginal women — Janet Kelly
Epilogue: Nursing, Indigenous Peoples and CulturalSafety: So what? Now what? — Madeleine DionStout, Bernice Downey
Book Reviews
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 73

INTRODUCTION
Effective communication between health professionals and people with cancer is an
international aim, as evidenced in published lit-erature (Fallowfield & Jenkins 1999; Gysels,Richardson & Higginson 2004). It has long beendocumented and accepted that effective com-munication with cancer patients is a significantlyessential element in any efficient care process
(Hurney 2000;Thorne, Bultz & Baile 2005). Infact communication skills are a key to achievingimportant goals of the clinical encounter inoncology (Baile & Aaron 2005). Good informa-tion exchange can decrease psychological dis-tress, promote better levels of adherence, andintroduce realistic expectations (Mills & Sulli-van 1999). Empirical evidence has revealed thatsupportive communication can positively affect
Key Wordsnursing;communication;phenomenology;qualitativestudy; truthtelling CN
74 Volume 28, Issue 1–2,April 2008CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 74–82.
Lebanese cancer patients:Communication and
truth-telling preferences
ABSTRACT The purpose of this study was to describe and interpret the phenomenon ofcommunication as lived by Lebanese cancer patients. Phenomenology based onthe Utrecht School was chosen as an interpretive descriptive methodology toguide the processes of data collection, analysis and synthesis. In-depth semistructured interviews were carried out with a purposeful sample of ten cancerpatients. Results of this qualitative study emphasise the needs of Lebanese cancerpatients for a clear and truthful communication with healthcare professionals,and family members. Informants highlighted the influence of words used duringcommunication on their outlook and morale.They also stressed the need to movefrom the paternalistic approach in care provision to patient-centered care thatpromotes patient autonomy. Informants clearly accentuated their rights to betold the truth about their condition.Received 6 July 2007 Accepted 25 March 2008
MYRNA ABI
ABDALLAH DOUMITAssistant ProfessorSchool of NursingAmerican Universityof BeirutBeirut, Lebanon
HUDA HUIJER
ABU-SAADProfessor of NursingScienceDirector, School ofNursingAmerican Universityof BeirutBeirut, Lebanon
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 74

patients’ psychological adjustment and qualityof life. Consequently, the value of effectivecommunication skills is stressed in cancer care (Liu, Mok & Wong 2005; Maguire 1999).Regardless of the value of communication toboth patients and providers, researchers havereported that only 57% of patients are satisfiedwith their providers’ listening skills, explana-tions, and respect for their opinions (USDepartment of Health and Human Services2003). Further studies reported that patientsare often unhappy with the amount and natureof information they receive (Parker et al 2001;Veronesi et al 1999).The issue of how and howmuch to tell patients with cancer about theirdiagnosis and prognosis is still approached dif-ferently in different countries (Fujimori et al2007; Georgaki et al 2002).
In Lebanon, cancer is one of the leading caus-es of death (Daher et al 2002). It is believed tobe a protracted illness causing great disabilityand suffering that finally leads to a painfuldeath. Cancer is therefore not a preferred wordto use, and euphemisms, such as waram (as pro-nounced in Arabic) which means ‘growth’ or‘lump’ have been developed as alternatives.Regarding the provision of information aboutcancer in Lebanon, in general the primary fami-ly caregiver is usually informed by the physicianof the patient’s diagnosis and prognosis beforethe patient is told the truth. Then the familycaregiver decides whether the patient should betold the truth, usually after discussion withother family members and the physician fre-quently accepts the family’s decision. In a studyassessing knowledge, attitudes and practices ofphysicians and nurses regarding palliative care inLebanon, Abu-Saad Huijer and Dimassi (2007)reported that only 19.1% of physicians informthe patients about their diagnosis. Lebanesephysicians prefer informing and involving thefamily more than the patient. In Lebanon, it is important to note that information about cancer patients’ desire for communication andtruth telling from a patient’s perspective is
unavailable. This article is intended to con-tribute to the literature by providing descriptiveand interpretive data about the phenomenon of communication from the perspective ofLebanese patients suffering from cancer.
Purpose of the studyOur reflections on the phenomenon of commu-nication surfaced while conducting a qualitativestudy about the lived experience of Lebaneseoncology patients receiving palliative care.TheNeed to Communicate emerged from the par-ticipants’ interviews as an important element intheir lives. All participants highlighted commu-nication as an important factor for moraleboosting or as a demoralising factor dependingon the communication process followed and thewords used by others. So, further analysis wascarried out to highlight the theme of communi-cation within the Lebanese culture, which is thesubject of this article.
Research methods
Design
Phenomenology based on the Utrecht schoolwas chosen as an interpretive descriptivemethodology to guide the processes of data col-lection, analysis and synthesis, from which wegenerated findings in relation to various pat-terns and themes across the sample (Polit &Beck 2008). Phenomenology, specifically theUtrecht approach, is the best fit for this studybecause it describes the meaning of the livedexperience through the shared essences amongparticipants, and it uses the language to inter-pret the connotations of the experience of theparticipants.Thus, a comprehensive, culturallymeaningful competent understanding of thephenomenon will be provided.This approach ismost valuable when the activity at hand is tocomprehend an experience as it is identified bythose who are living it and to respond to ques-tions of meaning (Polit & Beck 2008; Speziale &Carpenter 2003).
75Volume 28, Issue 1–2,April 2008 CCCCNNNN
Lebanese cancer patients: Communication and truth-telling preferences CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 75

Selection of informantsPurposive sampling was employed. Informantswere recruited based on the following inclusioncriteria:
1. Lebanese speaking Arabic;2. Living in Lebanon;3. Age of 18 years or above;4. Confirmed diagnosis of any type of cancer;5. Low expectations for remission or cure as
reported by the informant’s oncologist;6. Receiving palliative care based on the infor-
mant’s physician confirmation;7. Informant’s knowledge of his or her pallia-
tive condition;8. Agreement to share personal experiences
and participate in the study;9. Agreement to be interviewed without the
presence of a third person in order to guar-antee freedom for the informant to com-municate his or her feelings;
10. Informant’s ability of signing his or hername on the consent form.
RecruitmentAt first the principal investigator discussed thestudy with community intermediaries (nurses,house wives) and oncologists. As the communi-ty intermediaries and the oncologists identifiedpossible informants, the PI was introduced tothe potential informant and offered an invita-tion to contribute in the study. Informantsenrolled through community intermediarieswere told that their treating physician will benotified of their involvement in the study.
Description of informantsInformants represented a variation with regardto major variables such as tumor site, patientdemographics characteristics, and treatmentmodalities. The sample comprised six womenand four men.They ranged in age from 21 to 71years with varied socioeconomic and education-al backgrounds and a diversity of tumor sitesand treatments.
SettingInterviews took place based on the informants’discretion regarding place and time. Eight inter-views took place at the informants’ homes andtwo in a hospital setting. Informants were resi-dents of both rural and urban areas of Lebanonbut receiving care in Metropolitan Beirut.
Data collectionData collection took place during summer of2005. In-depth semi structured interviews wereconducted privately between the PI researcherand informant. All informants were interviewedtwice.The reason for the second interview wasto confirm with the informant the preliminaryanalysis and to clarify previous statements in thefirst interview. Interviews were conducted inArabic and then translated to English and backtranslated to Arabic to ensure credibility of thetranslated data.Translation was done by a bilin-gual trained translator.The duration of the firstinterview varied between 50 to 60 minutes;while the length of the second interview rangedbetween 30 and 45 minutes. All interviewswere audio taped and transcribed verbatim,with digital text entered into NVivo 1.2 soft-ware for sorting and organising of raw data.Informants were guaranteed confidentiality andpseudonyms were used.
The first set of interviews was triggered bythe following grand tour question ‘Can you tellme about how you have experienced your ill-ness?’ In addition probing technique was usedfor explanatory accounts of participants’ expe-rience such as ‘Please tell more about it’, ‘Is itpossible to give an example?’ In each interview,the informant was the main narrator and the PIresearcher was mainly a listener and a facilitator(Speziale and Carpenter 2003).
Data analysisAnalysis of data was ongoing throughout datacollection, transcription, and repeated readingsof the text. Analysis was done based on theUtrecht School of Phenomenology. Data were
76 Volume 28, Issue 1–2,April 2008CCCCNNNN
Myrna Abi Abdallah Doumit and Huda Huijer Abu-SaadCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 76

examined systematically using a system of coding to identify particular phenomena andcategories of interest. Analysis was done inde-pendently by two researchers in the study team,who then compared and discussed the results of their work for similarities and differences.The same codes were kept, similar codes werecombined, and the revised codes were discussedand changed until concordance was achieved.Results of the study represent the first docu-mented data about the lived experience ofLebanese cancer patients (Doumit, Abu-SaadHuijer & Kelley 2007). For the purpose of this study analysis, we draw excerpts derivedfrom the participants’ description to reflect on the implications of the tacit assumptions thatLebanese healthcare professionals hold in rela-tion to cancer and communication.
Rigour of the studySteps recommended by Lincolin and Guba(1985) were followed to secure rigor of studymethod. Credibility was fulfilled by withinmethod triangulation for data collection, mem-ber check and peer debriefing. Transferabilitywas secured by the use of thick descriptionsfrom the interviews. Dependability and con-firmability were guaranteed by doing intercoderreliability as suggested by Polit and Beck (2008)and Marques and McCall (2005).
EthicsApprovals from Institutional Review Boardswere secured before initiating data collection.All informants were provided with informationsheet describing the study and were asked togive written consent to interviews and audiorecording.
RESEARCH FINDINGSEight core themes emerged from this study,which reveal the lived experience of Lebanesecancer patients receiving palliative care. Theemerging themes were as follows:
1. Distressed from being dependent: loss of
control, disease reminder, and burden onothers;
2. Dislike for pity: threat to self-perception;3. Worried about the family and the family’s
worry;4. Reliance on God and divinity;5. Dislike of the hospital stay: feeling trapped
in time, place, and disease;6. Dislike of being non-productive;7. Fear of pain and suffering;8. The need to communicate.
It is worth noting that these core themes werenot identified or listed in order of importance(Doumit et al 2007). Further analysis was car-ried out to highlight the themes on communi-cation which are the subject of this article.The findings on communication that emergedfrom the data consisted of two themes and sub-themes: 1) the need to communicate: par-ticipant–family communication, participant–physician communication, and type of words ormessages used or sent and 2) worried about thefamilies and the family’s worry. In this themethe idea of cancer patients not sharing or com-municating their worries with family membersprevailed.
Need to communicateAll informants without exception highlightedthe importance of communication in their dis-ease trajectory. Informant–family communica-tion and truth telling were reported as majorstressors. Houda, a 51-year-old woman withbreast cancer and metastasis to bone expressedher annoyance with her family because they hidthe truth from her. She said: ‘I prefer the truthfrom the beginning. I am not a child.’
Ghandi a 59-year-old man with colon cancerand metastasis to the bone, said:
There is lots of openness between my wife,my son and me. We talk about my condi-tion… It helps a lot. It strengthens themorale and it makes me forget my disease…
77Volume 28, Issue 1–2,April 2008 CCCCNNNN
Lebanese cancer patients: Communication and truth-telling preferences CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 77

Informant–physician communication was alsoemphasised as an important aspect of the com-munication process. Aniss, a 55-year-old manwith colon cancer and metastasis to lung, bone,and brain described the relationship that shouldexist between the treating physician and thepatients and said: ‘The physician should under-stand his patient. If the patient is ready tounderstand the truth, then he should talk tohim. I prefer the truth.’ He added: ‘Nurses andphysicians have to come and talk with thepatient, your psychology will be relaxed.’
Samer, a 21-year-old male with colon cancerand bone metastasis said:
A good day is when my sister finally told methat I have cancer, why? Because I felt it in myheart. I felt that they were hiding somethingfrom me.
Amine narrated a story to emphasise the impor-tance of tactful communication and the choiceof words in communicating and he said:
One day there was a king. One day a mancame to him and he told him you are going tobury all your parents, so the king ordered hisdeath.Then another man came to him and hetold him you are going to survive all yourparents, so he gave him lots of money. So theminister questioned his king. Sir, what did thefirst man tell you to order his death? And theking told him. Then he asked what did thesecond man tell you? And the king answered.So the minister asked him, ‘My king, what’sthe difference between the two men?’ Theking told him the results are the same, butthe way it was said made the difference. So aword can make the difference and this is howmy physician deals with me. He tells methings bit by bit.This is important because Ido not like rough words. I like the way hedeals with me. He is very sensitive with me.
The choice of words with cancer patients canimpact on their morale as mentioned by Hind, a65-year-old woman with breast cancer and
metastasis to lung, brain and bone. At the timeof the interview Hind was still upset from aconversation that she had two days prior to theinterview with her brother-in-law and his wife.Though Hind perceived them as her supportsystem and she highlighted their caring attitudestowards her, one remark from them regardingher condition made her feel upset. She said:
It hurt me because as a person who is 60years old and receiving treatment, psycho-logically you feel wounded. You are undertreatment and this might mean the end, thisis what it means to you. He is not the firstone. Maybe they are 15 for now who said,‘We were not born to stay.’ Maybe they donot mean it, but psychologically you feelwounded. He is not the only one that is talk-ing like this, but around 20 individuals said sofar,‘Do not worry.We were not born to stay.’
The impact of communication on Hind was notalways positive. Relatives, with their approach,made her feel frustrated because they remindedher of her unstable health status.
Worried about the families and the family’s worryIn this second theme, informants shared theirworries about their family members. Theyclearly stated that they opted to hide their suf-ferings and pain from their children or belovedones because they did not want them to worryabout them. Informants were protecting theirfamily members by not sharing or communicat-ing with them their worries, ideas and feelingsregarding cancer or death.
Sonia, a 65-year-old woman with breast can-cer and metastasis to bone, lungs, liver, uterusand brain said:
I wish I was able to hide it (the disease) evenfrom my family members. I do not wantthem (children) to feel afraid or worry that Iam sick. I do not show anything, I do notshow anything.
78 Volume 28, Issue 1–2,April 2008CCCCNNNN
Myrna Abi Abdallah Doumit and Huda Huijer Abu-SaadCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 78

Similarly, Houda shared her worry about herchildren’s worry about her and expressed herwishes of hiding the truth. She said:
I do not want them (her children) to worryabout me, they are still young. They thinkMama will die. I do not like it. I wish theydid not know about my condition.This is mynature.
DISCUSSIONSocial attitudes towards cancer and the societalprevailing norms regarding communication andtruth telling are all known to be profoundlyaffected by cultural beliefs and norms (Mystaki-dou et al 2004). In Lebanon, most of the timesthe patient’s family is informed about the diag-nosis of cancer before it has been discussed withthe patient. Family members keep the diagnosisand prognosis a secret in order to protect thepatient from emotional trauma.The attitude ofmany healthcare professionals and their ap-proach to communication and truth telling incancer cases mirrors that of family members(Abu-Saad Huijer & Dimassi 2007; Hamadeh &Adib 1998). It is worth noting that there was aperception among Lebanese healthcare profes-sionals that Lebanese cancer patients are notready or willing to discuss their condition oreven to participate in a qualitative study.The fearwas also that family members may constitute abarrier preventing patients from participating inan unattended, in depth interview (Adib &Hamadeh 1999). But contrary to the above, allinformants without exception expressed grati-tude to the researchers because they gave themthe opportunity to discuss their condition, wor-ries, and concerns related to their current situa-tion. Family members did not object to theinterview; on the contrary, they were facilitatorsin creating the best environment.
This is the first study to describe the viewsand needs of Lebanese cancer patients regardingcommunication. Informants of this study, incontrast to the existing ideas in the Lebanese
society regarding the impact of knowing or dis-cussing the diagnosis of cancer on patients’morale expressed the need to communicate,and highlighted their right to truth telling.Theyclearly mentioned that communication with thephysician and family members was seen as amean for relieving their stress.These statementscoming from informants living in a culturewhich favors paternalism over individualism arequite significant. However one needs to be cautious because due to the limited number ofinformants in the study, there maybe someLebanese cancer patients who still would preferthe traditional approach of non disclosure.Therefore, patients need to be asked what theywant to know about their illness before the pro-vision of information is provided or a culturaldecision is made to non-disclose. It is worthnoting that an important part of communicationis being aware to the amount and type of in-formation the patient requests, knowing thatpatients may want different types and amount ofinformation as their illnesses progress (Clayton2006). Consequently communicating withpatients on an individual basis is highly recom-mended (Fujimori et al 2007).
Informants of this study stressed the need toknow about their diagnosis and prognosis, yet,they clearly mentioned their preferences forhiding their sufferings and pain in order not todisturb their beloved ones. Findings in the liter-ature (Goldsteen et al 2006; Helseth & Ulfsaet2005;Wheeler 2005) emphasise the importanceof communication to cancer patients yet theyhighlight the patients’ preferences for hidingtheir sufferings from their beloved ones.
Informants of this study wanted the commu-nication to be tempered with considerationregarding the choice of words or ideas used byothers. In order to protect their family mem-bers from being hurt or disturbed, informantskept their concerns, ideas and fears regardingtheir condition silent. In Lebanon, it is worthnoting that in general family members prefernot to discuss cancer diagnosis and prognosis
79Volume 28, Issue 1–2,April 2008 CCCCNNNN
Lebanese cancer patients: Communication and truth-telling preferences CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 79

with patients thinking that it is a kind of protec-tion to their feelings. But, evidences from theliterature (Lin et al 2003; Mizuno et al 2002)imply that patients’ stress is possible to be supe-rior with ambiguity and doubt around their ill-ness. So, leaving the patient in the shadow doesnot serve the purpose. Moreover, the familiesmost of the time ask from the medical profes-sional not to reveal the truth about the diagnosisand prognosis of the cancer to the patient.However, all study informants reported thatdespite efforts of family members of hiding thetruth they knew of their diagnosis.
Results reported in this study are in line withprevious studies conducted on cancer patients(Clark & Volker 2003; Begley & Blackwood2000; Fujimori et al 2007; Oliffe et al 2007)regarding communication needs in cancerpatients and cultural influences. In many East-ern societies there is a tendency for physiciansto abide by the families’ decisions and wishes ondisclosure or non-disclosure and non-disclosureare more prevalent (Lin et al 2003).The choiceof not telling a patient the diagnosis of cancerhas many roots. One reason being the cultureand cultural expectations of a specific society. Inthe Eastern cultures family is very important.Harmony and balance with family relationshipsshould supersede personal need and further addto social equilibrium. In Chinese societies thereis a cultural conviction that cancer can be ac-quired by contact with a person with cancer. Itis predicted that these values and beliefs woulddirectly affect the choice of patients, familiesand health professionals to the disclosure ornon-disclosure of a diagnosis of cancer (Mizuno,Onishi & Ouishi 2002; Mok & Martinson 2000).In a cross sectional study to assess the knowl-edge, attitudes and practices of physicians andnurses towards palliative care in Lebanon Abu-Saad & Dimassi (2007) reported that the major-ity of the respondents believe terminally illpatients and their families should be informedof the diagnosis and prognosis. However, it wasreported that only 19% of physicians routinely
inform terminally ill patients about their diag-nosis.Whereas it is reported that in most West-ern societies’ disclosure is the expected norm(Baile et al 2002; Georgaki et al 2002). Baile etal (2002) in an international study which com-pared the practices of oncologists on four conti-nents reported that physicians from Westerncountries were less likely to deny the patientunfavorable information at the family’s request.
Lebanon’s geographical location between theEast and the West, and the Western medical andnursing curricula followed at different universi-ties are believed to have an influence on itshealthcare culture. The norm was to hide thetruth from patients regarding the diagnosis ofcancer; however, the trend is changing. Patients,especially young people are becoming moreassertive and knowledgeable about health issues.However, the Western culture of communicationand truth telling are still in their infancy stages.Hamadeh and Adib (1998) in a study assessingcancer truth disclosure by Lebanese doctorsreported that unless hard evidence emerges indicating that Lebanese patients are seekingempowerment and would rather be told thetruth, it is less likely that those physicians wouldchange their attitude and reveal the diagnosis.
CONCLUSIONSResults of this qualitative study emphasise theneeds of Lebanese cancer patients to have clearand truthful communication with healthcareprofessionals, and family members. Informantshighlighted the influence of words used duringcommunication on their morale. Informantsalso stressed the need to move from the pater-nalistic approach to the promotion of autono-my.They clearly accentuated their rights to betold the truth about their condition.Yet, theyhighlighted the gentle approach to communica-tion versus the blunt style. Consequently, thisstudy represents a change in expectations andcertainly of the existing norms within theLebanese culture regarding communication andtruth telling. Also, it provides preliminary evi-
80 Volume 28, Issue 1–2,April 2008CCCCNNNN
Myrna Abi Abdallah Doumit and Huda Huijer Abu-SaadCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 80

dence that the cultural and values which aim atprotecting cancer patients from knowing theirdiagnosis and prognosis is not in line with thepatients’ wishes and needs.
LimitationsThe qualitative approach followed in this studydoes not allow for generalisation of findings butdoes provide interesting insights into the con-cept of communication and cancer within theLebanese culture. It is worth noting, that gener-alisability is not a goal of phenomenology.Theexperience stays private but its connotation andsignificance become public (Ricoeur 1976).
RecommendationsWe do believe that there is much to be learnedabout communication and cancer within theLebanese culture. So, it is highly recommendedto expand on the results of this study and con-duct a national study assessing the communica-tion needs of Lebanese cancer patients. Studyingthe preference for truth telling among Lebanesenurses and physicians is highly suggested. More-over, emphasising communication as an im-portant aspect of cancer care in the LebaneseNursing and Medical curricula emerges as a keyelement that needs further follow up and study.
ReferencesAbu-Saad Huijer H and Dimassi H (2007)
Palliative care in Lebanon; knowledge,attitudes and practices of physicians andnurses. Lebanese Medical Journal 55: 121–128.
Adib SM and Hamadeh GN (1999) Attitudes ofthe Lebanese public regarding disclosures ofserious illness. Journal of Medical Ethics 25:399–403.
Baile W and Aaron J (2005) Patient-physiciancommunication in oncology: past, present,and future. Current Opinion in Oncology 17:331–335.
Baile W, Lenzi R, Parker P, Buckman R andCohen L (2002) Oncologists’ attitudestowards and practice in giving bad news: an
exploratory study. Journal of Clinical Oncology20: 2189–2196.
Begley A and Blackwood B (2000) Truth-tellingversus hope:A dilemma in practice. Interna-tional Journal of Nursing Practice 6: 26–31.
Clark A and Volker DL (2003) Truthfulness.Clinical Nurses Specialist 17: 17–18.
Clayton M (2007) Communication:Animportant part of nursing care. AmericanJournal of Nursing 106: 70–75.
Daher M,Tabari H,Ammar W,AbouNasrNabhan T, Bou Khalil T and Dakwar A (2002)Lebanon: Pain relief and palliative care.Journal of Pain and Symptom Management 24:200–204.
Doumit M,Abu-Saad Huijer H and Kelley J(2007) The lived experience of Lebaneseoncology patients receiving palliative care.European Journal of Oncology Nursing 11:309–319.
Fallowfield L and Jenkins V ( 1999) Effectivecommunication skills are the key to goodcancer care. European Journal of Cancer 35:1592–1597.
Fujimori M,Akechi T, Morita T, Inagaki M,Akisuri N, Sakano Y and Uchitomi Y (2007)Preferences of cancer patients regarding thedisclosure of bad news. Psycho-Oncology 16:573–581.
Georgaski S, Kalaidopoulou O, LiarmakopoulosI and Mystakidou K (2002) Nurses’ attitudestowards truthful communication withpatients with cancer: a Greek study. CancerNursing 25: 436–441.
Goldsteen M, Houtepen R, Proot I, Huijer Abu-Saad H, Spreeuwenberg C and Widdershoven(2006) What is a good death? Terminally illpatients dealing with normative expectationsaround death and dying. Patient Education andCounseling 64: 378–386.
Gysels M, Richardson A and Higginson I (2004)Communication training for healthprofessionals who care for patients withcancer: a systematic review of effectiveness.Supportive Care in Cancer 12: 692–700.
81Volume 28, Issue 1–2,April 2008 CCCCNNNN
Lebanese cancer patients: Communication and truth-telling preferences CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 81

Hamadeh GN and Adib SM (1998) Cancer truthdisclosure by Lebanese doctors. Social Scienceand Medicine 47: 1289–1294.
Helseth S and Ulfsæt N (2005) Parentingexperiences during cancer. Journal of AdvancedNursing 52: 38–46.
Hurney C (2000) Communicating aboutcancer: patients’ needs and caregivers’ skills.Support Care Cancer 8: 437–438.
Lincolin YS and Guba EG (1985) NaturalisticInquiry. Beverly Hills, CA: Sage Publications.
Liu J, Mok E and Wong T (2005) Perceptions ofsupportive communication in Chinesepatients with cancer: experiences andexpectations. Journal of Advanced Nursing 52:262–270.
Lin CC,Tsai H, Chiou J, Lai Y, Kao C and TsouT(2003) Changes in levels of hope afterdiagnostic disclosure among Taiwanesepatients with cancer. Cancer Nursing 26:155–160.
Maguire P (1999) Improving communicationwith patients with cancer. European journal ofCancer 35: 2058–2065.
Marques JF and McCall C (2005) The applica-tion of interrater reliability as a solidificationinstrument in a phenomenological study.TheQualitative Report 10: 439–462.
Mizuno M, Onishi C and Ouishi F ( 2002) Truthdisclosure of cancer diagnoses and itsinfluence on bereaved Japanese families.Cancer Nursing 25: 396–403.
Mills ME and Sullivan K (1999) The importanceof information giving for patients newlydiagnosed with cancer:A review of the litera-ture. Journal of Clinical Nursing 8: 631–642.
Mok E and Martinson I (2000).Empowermentof Chinese patients with cancer through self-help groups in Hong Kong. Cancer Nursing 23:206–213.
Mystakidou K, Parpa E,Tsilila E, Katsouda Eand Vlahos L (2004) Cancer informationdisclosure in different culture. Support CancerCare 12: 147–154.
Oliffe J,Thorne S, Hislope TG and ArmstrongEA (2007) Truth telling and culturalassumptions in an era of informed consent.Family Community Health 30: 5–15.
Parker PA, Baile WF, De Moor C, Lenzi R,Kudella AP and Cohen L (2001) Breaking badnews about cancer: patients’ preferences forcommunication. Journal of Clinical Oncology19: 2049–2056.
Polit DF and Beck CT (2008) Nursing Research:generating and assessing evidence for nursingresearch, 8th edn,Wolters Kluwer &Lippincott Williams & Wilkins, Philadelphia.
Ricoeur P (1976) Interpretation theory: Discourseand the surplus of meaning. Fort Worth,Texas:Christian University Press.
Speziale HJS and Carpenter DR (2003)Qualitative Research in Nursing, 3rd edn,Philadelphia: Lippincott,Williams & Wilkins.
Thorne S, Bultz B and BaileW (2005) What arethe costs of poor communication in cancercare? A critical review of the existingempirical evidence. Psycho-oncology 14:875–884.
US Department of Health and Human Services,Office of Disease Prevention and HealthPromotion (2003) Communicating health:priorities and strategies for progress.Action plansto achieve the health communication objectives inhealthy people 2010, http://odphp.osophs.dhhs.gov/projects/healthcomm.
Veronesi U,Von Kleit S, Redmond K,VeronesiS, Costa A, Delvaux N, Freilich G, Glaus A,Hudson T, McVie JG, Macnamara C, MeunierF, Pecorelli S, Serin D and the CAWAC StudyGroup:A European survey of the perspec-tives and experiences of women with femalecancers. European Journal of Cancer 35:1667–1675.
Wheeler MS (2005) Interviews with patientswho have cancer and their family membersprovide insight for clinicians. Home HealthcareNurse 23: 642–646.
82 Volume 28, Issue 1–2,April 2008CCCCNNNN
Myrna Abi Abdallah Doumit and Huda Huijer Abu-SaadCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 82

INTRODUCTION
It is well known that we live in a multiculturalera characterised by increased globalisation.
Nurses all around the world are caring forclients of diverse ethnic backgrounds with different cultural beliefs, needs and practices.According to the American Community Survey,288 378 137 individuals resided in the UnitedStates of America (USA) in 2005. Of these,
74.7% were white, 12.1% were black or AfricanAmerican, 0.8% were native Americans andAlaskan natives, 4.3% were Asians, 0.1% werenative Hawaiians and Pacific Islanders and 6%were other races (United States Census Bureau2005). Similarly, 19 855 288 persons lived inAustralia in 2006 including 2.3% IndigenousAboriginal and Torres Strait Islanders (Aus-tralian Bureau of Statistics 2007a). In addition,the 2001 ‘reported ancestry by-self’ table showsthat 38.1% of residents in Australia are descen-dants of Australian, New Zealanders, Maori,Aboriginal and Torres Strait Islander ancestors,65.8% have European origins such as English,Irish, Italian and German, 18.8% have Asianancestry namely Chinese, Indian and Viet-namese, and 2% have Middle Eastern roots,specifically Lebanese and Turkish (AustralianBureau of Statistics 2007b).
Key Wordsnursing; genericcare; professionalcare; Leininger;culture caremodes; Muslim CN
83Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 83–97.
Bridging generic and professional carepractices for Muslim patients throughuse of Leininger’s culture care modes
ABSTRACT The purpose of this article is to provide knowledge of traditional Muslimgeneric (folk) care beliefs, expressions and practices derived from research anddescriptive sources, in order to assist nurses and other health care professionalsto integrate generic (folk) into professional care practices. Muslim generic (folk)care beliefs and practices related to the caregiving process, health, illness,dietary needs, dress, privacy, modesty, touch, gender relations, eye contact,abortion, contraception, birth, death and bereavement were explored. Adiscussion involving the use of Leininger’s culture care preservation and/ormaintenance, culture care accommodation and/or negotiation and culture carerepatterning and/or restructuring action modes to bridge the gap betweengeneric (folk) and professional (etic) care practices and to consequently promoteculturally congruent care is presented.Received 22 August 2007 Accepted 15 March 2008
HIBA WEHBE-ALAMAHAssistant ProfessorDepartment of NursingSchool of HealthProfessions and StudiesThe University ofMichigan-FlintFlint MI, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 83

In the USA and possibly worldwide, nursesand other health care providers are no longercaring for patients of a predominant ancestry,but are caring for clients with diverse culturalvalues, beliefs and practices.To facilitate cultur-ally congruent care and ethical interactions withpatients of diverse cultural backgrounds, nursesand other health care providers must not ignorethe importance of culture and must recognisetheir own culture specific care interpretations,expressions and practices (Zoucha & Husted2000). Leininger (2002) has long maintainedthat it is a human right to have one’s culturalvalues, beliefs, practices and needs respected,understood and appropriately used within anycaring or curing context. Such cultural valuesinclude generic care beliefs, practices and valuesheld by individuals of diverse cultural back-grounds (Leininger & McFarland 2002).
Having recognised the increased use of com-plementary, alternative, folk and/or genericcare practices, Leininger holds that providingculturally congruent care necessitates recognis-ing and bridging the two types of caring thatexist in every culture: the generic (emic or folk)and professional (etic) caring systems (Leininger1995; Leininger & McFarland 2002). Leininger(2002) defined generic care as the learned andtransmitted lay, indigenous, traditional, or localfolk knowledge and practices aimed at providingassistive, supportive and facilitative actions thatimprove well-being and help with dying andother human conditions.The theorist referredto professional care as the formal and explicit cog-nitively learned professional care knowledgeand practices that are taught in educationalinstitutions to assist nurses in providing assis-tive, supportive and facilitative actions to imp-rove the health, prevent illness and help withdying and other human conditions (Leininger2006).
This article seeks to provide knowledge ofgeneric (folk) care beliefs, expressions and prac-tices used by conservative Muslims living in theUSA, based on research and descriptive sources,
in order to assist nurses and other health careproviders to incorporate generic care practiceswith professional care practices.This may espe-cially be important when one takes into consid-eration that Muslims currently comprise about1.5 billion people or one fifth of the world totalpopulation (Mughees 2006). Furthermore, Islamis the second largest religion in the world andhas about 15 million followers in Europe, 8 mil-lion in the USA, 145 million in Indonesia, 92million in Pakistan, 50 million in the SovietUnion and 340 392 people in Australia (Mughees2006; Rashidi & Rajaram 2001).
Contrary to popular belief, only 20% ofMuslims worldwide are of Arabic origin (Gulam2003). It is expected that by the year 2010, theMuslim community will be the largest non-Christian community in the USA and willexceed 15 million by the year 2025 (Under-wood et al 1998 as cited in Rashidi & Rajaram2001: 55). In Australia where 33% of Muslimsare native born and the others come from 67different countries, Muslims already account forthe largest religious group second to Christians.The roots of Islam in Australia date back to1650 AD, as a result of interactions betweenIndigenous Australians with Muslim Indonesianfishermen and again in the 18th and 19th cen-turies with Afghan Cameleers who helped buildthe overland telegraph line and the Ghan railwayfrom Port Augusta to Alice Springs (Gulam2003).
While Muslims in the US, Australia and othercountries share similarities in their culturalbeliefs, expressions and practices, they also havemuch diversity.The two major sects in Islam arethose of Sunni and Shi’a. In 2005, of the 1.5 bil-lion Muslims in the world, 85–90% followed theSunni branch of Islam, while 10–15% followedthe Shi’a branch.The majority of Shi’a Muslimslive in Iran, Iraq, Bahrain and Azerbaijan, withlarge concentrations found in Afghanistan,Lebanon, Kuwait, Pakistan, Saudi Arabia, Syriaand Yemen (Armanios 2004). In the UnitedStates, 80% of Muslims are Sunnis and tend to
84 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:25 PM Page 84

be concentrated in New York City, Los Angeles,Chicago, Houston, Boston, Detroit and Toledo(Hodge 2005).
Sunni and Shi’a Muslims share many com-monalities and differences in their religious andcultural beliefs, expressions and practices. Justlike with any cultural group, it is erroneous toassume that all members of the cultural groupabide by the same universal values and norms.Acculturation, assimilation and enculturationprocesses affect the level of adherence to religious and cultural principals. Muslims allaround the world range from the very liberal to the extremely fundamentalist. This articlefocuses on generic (folk) care practices com-mon among conservative and traditional Mus-lims derived from ethnonursing studies andother descriptive sources.
Knowledge of generic (folk) care practicesthat are common among Muslims is critical to providing culturally congruent care to thisgroup. According to Simpson and Carter (2008),there is a scarcity of literature that addresses cul-turally appropriate health care practices for Mus-lim immigrant women in rural areas in the USA.The influx of new Muslim immigrants into theUSA, coupled with a lack of knowledge in rela-tion to cultural, religious and healthcare needs ofunfamiliar populations, are creating new healthcare challenges for health care providers. Actualor perceived ignorance in relation to the Islamiccultural or religious beliefs and practices werefound to create a barrier and a deterrent tohealth care access on the part of Muslim womenin rural areas (Simpson & Carter 2008).
Rajaram & Rashidi (2001) pointed out thathealthcare providers’ lack of understanding andsensitivity to Muslims and their traditions havefacilitated potential or directly caused health-care conflicts. In one study, it was discoveredthat healthcare providers’ cultural insensitivityand ignorance about Islamic beliefs hinderedaccess to healthcare services in Australia (Tsi-anakas & Liamputtong 2002, cited in Simpson &Carter 2008). Rassool (2000) argued that caring
from an Islamic perspective is not representedwell in Eurocentric nursing literature and thatthere is a widespread misunderstanding in theconcept and practice of Islam within the West-ern context of healthcare and nursing practice.
The growing multiculturalism and changingdemographics in Australia and around the worldhave lead to an increased diversity of needs thatrequires accommodation by a healthcare systemthat is embedded in Western culture. As aresult, considerable cultural clashes may arisewhen Muslim patients experience hospitalisa-tion in a non-Islamic healthcare facility andreceive care from health care providers withlimited knowledge about specific Muslim needs(Mohammadi, Evans & Jones 2007). Publica-tions by pioneers in this field such as Drs AkramOmeri, Afaf Meleis and Linda Luna have estab-lished the foundations for much needed study inthis area. Moreover, understanding the basictenets and common concepts of Islam providesthe basis for learning about Muslim generic carebeliefs and practices and culturally congruenthealth care practices.
BASIC TENETS OF ISLAM ANDCOMMON ISLAMIC CONCEPTSThe word Islam in Arabic means peace, purity, sub-mission and obedience. In the religious sense ofthe world, Islam is the act of submission to theWill of Allah (God) and obedience to his Law(‘Abd al ‘Ati 1998). A Muslim is a practitionerof Islam. Muslims believe that the Qur’an is the Word of God, that it was revealed to theprophet Muhammad through the angel Gabrieland is considered as man’s best guide to God’struth and to eternal happiness (‘Abd al ‘Ati1989; Hamid 1996).The Qur’an is the highestauthority for information on Islam, followed bythe Sunnah and Hadith of the Prophet. Sunnahrefers to the actions and confirmations of theProphet in matters pertaining to the meaningand practice of Islam. Narrative accounts de-picting sayings of the prophet are referred to asAhaadith (singular: hadith) (Badawi 1999).
85Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 85

There are five basic tenets or pillars of Islam:1. The shahadah or declaration of faith, which
states that there is no God but God and that Muhammad is the messenger of God:Professing this declaration is key to joiningthe global community of Muslim believers(Hodge 2005). It is also considered a pre-cursor to entering paradise, especially if it isthe last statement uttered before death(Wehbe-Alamah 2005).
2. The Salat or prayer consists of praying fivetimes a day during specific time spans whileprostrating oneself in the direction of theholy city of Mecca (Husain 1995; Zeghidour1994). Islamic prayer is a combination ofintellectual meditation, spiritual devotion,moral elevation and physical exercise. It isusually preceded by ablution or Wudu’.There are various kinds of prayer includingthe obligatory or Fard prayer, the super-erogatory or Sunnah prayer and the optionalor Nafl prayer (‘Abd al ‘Ati 1998).
3. The Zakat or giving money to charity andthe less fortunate is a means to purifyingone’s wealth, establishing social justice andproviding guidelines for positive humanbehavior and an equitable socioeconomicsystem (Husain 1995; Rassool 2000). Theminimum rate of zakat is 2.5 % of the per-son’s estimated wealth (‘Abd al ‘Ati 1998).Zakat can be given to the poor, the way-farer, the bankrupt, the needy converts, thecaptives, the collectors of zakat, or can bespent in the cause of God (Hamid 1996).
4. The Sawm or fasting during the month ofRamadan (Husain 1995): During that Islam-ic lunar month, Muslims are required torefrain from all food, drink and sexual relations from dawn to sunset. The HolyQur’an was revealed to Prophet Muham-mad during the month of Ramadan.There-fore, Muslims intensify their salat, zakat andreading of the Qur’an during that month(Hamid 1996). Fasting is considered a phys-ical and spiritual purification act and a means
to reacquaint oneself with the physical sen-sation of hunger to foster empathy towardsthe poor. Muslims are exempt from fastingif ill or if traveling but must make up themissing days of fasting at a later date. Thisrule also applies to menstruating and post-partum women (Connelly et al 1999).
5. The Hajj or pilgrimage to the city of Meccaat least once in a person’s life span: This is considered an obligatory duty to everyresponsible Muslim, male or female, pro-vided he/she is mentally, financially andphysically able (‘Abd al ‘Ati 1998).
In addition, Islam emphasises the concepts of:(a) Halal, which refers to permitted foods and
actions considered to be lawful and permis-sible according to the tenets of Islam;
(b) Haram which describes foods and conductthat are unlawful and prohibited, such as theconsumption of pork and alcohol; and
(c) Fard, which refers to compulsory actionsthat must be done according to Islamic Lawor Shari’a such as prayer.
It also stresses the concepts of:(a) Mustahab, which refers to acts which are rec-
ommended in the Sunnah of the Prophet,such as cleaning the teeth regularly beforepraying, and;
(b) Makruh, which designates foods and actionsthat are disliked and discouraged (but notprohibited) by Islam such as divorce.
(Hamid 1996; Husain 1995; Luna 1989)
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS AND PRAC-TICES RELATED TO THE ROLE OFWOMEN IN ISLAMIslam regards that, in the sight of God, allhuman beings are equal, but not necessarilyidentical. People differ in their abilities, poten-tials, ambitions and wealth. The only distinc-tions recognised by God are that of anatomy andpiety (‘Abd al ‘Ati 1998; Wadud 1999). Islam
86 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 86

regards women as independent members ofsociety who are equal to men concerning basichuman rights, pursuit of education and knowl-edge, freedom of expression, initiating enter-prise and owning property independently (‘Abdal ‘Ati 1998). Men and women are complemen-tary and not subservient to each other. ProphetMuhammad said: ‘I command you to be kind to women … The best of you is the best to his family/wife’ (Badawi 1999: 26). He is alsoreported to have said: ‘The quest for knowledgeand science is obligatory upon every Muslimman and woman’ (Hassan 2000: 55).
The Qur’an makes it clear that both men andwomen are equally capable of virtue and weak-ness and equally meritorious. Both genders areon equal footing before God; the belief in thesuperiority of men over women is not congru-ent with the teachings of Islam, but is merely areflection of culturally-bound opinions (Badawi1999). There are many variations in Muslimcountries as far as cultural beliefs, practices, tra-ditions and attitudes about women.These rangefrom the extremely conservative to the moreliberal. Many Muslim women seek higher grad-uate level education. In Egypt, women havebeen attending universities since the 1920s. Inthe United Arab Emirates, 70% of enrollees inScience and Technology University are females.Between 1990 and 1991, female students whowere enrolled in biological science courses inBahrain accounted for 68% of the total studentpopulation, compared to 67% in Kuwait, 69%in Qatar, 48% in Lebanon and 50% in Oman(Hasan 2000).Women across the Arab and Mus-lim world are increasingly becoming empow-ered to make informed health related decisionsthrough education.
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS ANDPRACTICES RELATED TO THECAREGIVING PROCESSMany Muslims like Lebanese and Syrians classifycaregiving as a responsibility shared by individ-
ual, family and community members, regardlessof diversities in age or gender. Family membersincluding children, spouses, siblings, aunts,uncles and grandparents, as well as friends,neighbors and social acquaintances are all ex-pected to participate in the caregiving processto varying degrees (Wehbe-Alamah 1999,2005). While immediate family members andclose relatives tend to provide financial, emo-tional and physical care community membersare encouraged to do the same and to assist inthe provision of spiritual care. Consequently,visiting and praying for the sick is valued byLebanese, Syrian and other Muslims and is con-sidered a cultural, social and religious obligationas well as a source of blessing (Halligan 2006,Rashidi & Rajaram 2001;Wehbe-Alamah 2005,2006). In addition, providing financial care isregarded as secondary to safeguarding and pro-tecting people’s honor and pride and may becarried out in a confidential and/or anonymousmanner.
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS RELATED TOHEALTH AND ILLNESSMuslims believe health to be a blessing fromGod and attribute to it spiritual, physical, emo-tional and psychological dimensions that involvethe well-being of the body, mind and soul.Health is also considered to be a prerequisite togive care to others as well as a requirement forand a contributor to one’s faith.The rationale isthat illness hinders individuals from engaging in the caregiving role and from performingrequired religious activities such as fasting and the five mandatory daily prayers (Wehbe-Alamah 1999, 2005). In addition, health is promoted and enhanced by the application ofIslamic religious teachings which call for abs-taining from matters that are harmful to health(such as alcohol, illicit drugs, excessive eating,sexual promiscuity, homosexuality, pork prod-ucts and its derivatives including gelatin) andengaging in health promoting practices (such as
87Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 87

prayers, meditation, cleanliness, fasting, ablu-tion, breastfeeding) (Mughees 2006; Wehbe-Alamah 1999, 2005). Pork meat and fat areconsidered unlawful because pigs are scavengingand omnivorous animals. They have no necksand therefore cannot be slaughtered accordingto Islamic law. Historically, pigs have beenlinked to parasitic infections such as trichinosisand their fat has been associated with the devel-opment of atherosclerosis (Shamsi 1999). Thevast majority of practicing Muslims still do notconsume pork products; however, some liberalMuslims who do not strictly adhere to Islamicteachings may not necessarily abide by this reli-gious commandment.
Most Muslims believe that illness is a test ofone’s faith in God and a blessing in disguise as ameans of atonement for sins of the past.There-fore, it is considered a sign of love from Godand a physiologic and religious ‘wakeup call’that allows for self-reflection and enhanced spir-itual connections and meditation. At the sametime, Muslims believe that illness is an occasionfor engaging in Salat or prayer, charity, Zikr orremembrance of God, asking for forgiveness,reading the holy book (Qur’an) and behavingwith patience (Mughees 2006). Muslims alsobelieve that God is the ultimate healer and thatillness is God’s will.They also believe that theirbody is a gift from God and that they shouldtherefore care for it. In addition, illness is linkedto biological and physiological causes and there-fore requires medical and other professionalattention (Wehbe-Alamah 1999, 2005). Conse-quently, they are encouraged to pay attentionnot only to their own personal well-being butthe health of other individuals and the publicand as a result, most Muslims will seek modernmedicine and healthcare services (Bahar et al2005; Lawrence & Rozmus 2001).
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS AND PRAC-TICES RELATED TO DIETARY NEEDSMuslims view the body as a gift from God and
as a result abide by certain dietary principlesand restrictions aimed at keeping the body in anoptimal state of health. Substances that are con-sidered to be harmful to the intelligence orintoxicant to the body are considered to beunlawful, forbidden, or haram. This includesalcohol and alcohol-based medications (such ascough syrup) except when there is no non-alco-holic alternative, as well as mind-altering drugssuch as cocaine and marijuana (Rashidi &Rajaram 2001). Other forbidden foods includethe meat of wild animals that use their claws orteeth to kill their prey (Gulam 2003).
In addition, blood of dead animals, porkproducts such as bacon, ham and lard, as well aspork derivatives such as gelatin and insulin areconsidered to be haram foods. Many Muslimswill refuse to eat meat that is bloody or slightlycooked, consume hospital-served gelatin, ortake gelatin-encapsulated medications or vita-mins and drugs that contain gelatin as an ingre-dient unless the gelatin has been confirmed tobe derived from a lawful or halal source. How-ever, Islam does allow Muslims to consumemedications with pork-derived gelatin if thereare no halal alternatives (Lawrence & Rozmus2001; Wehbe-Alamah 2006, 2007). AlthoughIslam prohibits the consumption of the blood ofdead animals, it does not forbid the use of bloodtransfusions in hospital settings (Gulam 2003).
While Muslims are allowed to eat meatslaughtered and prepared by the People of theBook such as Jewish and Christians, some ofthem will only consume halal meats that areprepared according to the Muslim law.The con-cept of halal involves the recitation of a prayerto God (Allah) while slaughtering an animal tocommemorate that the animal is a blessed crea-ture of God that is being killed for human suste-nance (Gulam 2003). When admitted to thehospital setting, Muslims who adhere strictly tohalal principles may request to have their ownmeals brought from home or choose vegetarianor seafood alternatives from the hospital menu.
During the holy month of Ramadan, healthy
88 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 88

practicing Muslims all around the world engagein the fasting process. This practice involvesabstaining from food, water, medications, sexualactivity and smoking from the break of dawnthrough sunset. Muslim women who are preg-nant or breastfeeding during that month areexcused but are not forbidden from fasting (Ball& Haque 2003; Cassar 2006; Wehbe-Alamah1999, 2005). Sick individuals are also exemptfrom fasting. Any missed fasting days are usuallymade up at a later date. Muslims who have dia-betes and other individuals who need dailymedications require adjustments to their med-ical regimen during the month of Ramadan.Thetiming of this month changes every year as itfollows a lunar versus Gregorian calendar.
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS AND PRAC-TICES RELATED TO DRESS, PRIVACY,MODESTY, TOUCH, GENDERRELATIONS AND EYE CONTACTModesty is an important concern and value forthe vast majority of Muslims.This is particularlytrue for Muslim women. The traditional dressfor conservative practicing Muslim womeninvolves the use of loose clothing that covers theentire body with the exception of the hands andface and does not reveal its shape or curvatures.Long skirts, lengthy sleeves and head coveringsare typically used (Cassar 2006). However,diverse cultures have different ethnic displays ofwhat is considered to be an acceptable mode ofdress. In Syria and Jordan many (but not all)Muslim women choose to wear a coat or Jilbabon top of their everyday clothing. In Saudi Ara-bia and Iran, women wear a black robe knownas Abaya or Chador over their garments. Someeven cover their faces. In Pakistan, most womenwear long roomy tunics and pants sets known asShalwar Kameez. It is important to note, how-ever, that not all Muslim women adhere strictlyto the Islamic dress code. Many liberal Muslimwomen have chosen to adopt the Western dressstyle.
Regardless of which form of dress a conser-vative Muslim woman uses, there is an strongneed among them to maintain privacy and mod-esty. Many Muslim women request to be drapedas much as possible during medical or nursingprocedures to safeguard their dignity. Caps areoften asked for to cover the hair in instanceswere traditional Muslim head coverings are notallowed. There are numerous accounts thatdepict requests for signs at the hospital roomdoor prohibiting men from entering the roomof a Muslim woman without first asking permis-sion to allow adequate time for the woman tocover her hair (Wehbe-Alamah 1999, 2005).
Other generic care practices aimed at main-taining modesty and privacy include requestinga same sex healthcare provider when possible.Exceptions to this request occur when facedwith an emergency situation or in cases were nocompetent same sex healthcare providers areavailable (D’avanzo & Geissler 2003 cited inCassar 2006: 28).The rationale behind this pro-hibition is to minimise unlawful male–femaletouching and unnecessary body exposure to aperson of opposite gender.
In addition, while some Muslim men andwomen shake hands with or hug members ofthe opposite sex, many do not and as a result asimple pat on the back might make them feeluncomfortable. Nurses and other healthcareproviders caring for Muslim patients of thesame gender do not have to fear touching theirpatients as this rule applies only to members ofthe opposite sex (Lawrence & Rozmus 2001).Furthermore, Muslim men and women are pro-hibited from being alone in private except withtheir spouses, children, parents, uncles, aunts,father-in-law or mother-in-law (Rashidi & Raj-aram 2001). Hence, many Muslim patients willrequest to have a chaperone or a family memberstay with them during procedures involving ahealthcare provider of the opposite sex.
In addition, Muslim men and women whoare prohibited to be alone with each other asexplained above are discouraged from looking
89Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 89

directly into each other’s faces (eyes) for pro-longed periods of time: the holy book of Islam,the Qur’an, directs Muslims of both genders to lower their gaze (Rashidi & Rajaram 2001).What is considered to be an application of one’sreligious faith by Muslims may be misinter-preted by non-Muslim health care providers as disinterest or disrespect. Similarly, Muslimhealthcare providers who avoid direct and pro-longed eye contact with non-Muslim patients orcolleagues of the opposite sex risk being misun-derstood as well as stereotyped (Wehbe-Alamah2007).
Finally, it is important to note that it is acommon belief among traditional Muslims thatfood and drink should be consumed with theright hand which is reserved for doing cleanthings. The left hand is often reserved to per-forming unclean tasks such as cleaning the private area after bathroom use. As a result,Muslim patients will accept medications handedto them with the right hand but may refuse totake them if they were distributed to them withthe left hand.
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS AND PRAC-TICES RELATED TO ABORTION ANDCONTRACEPTIONInduced abortion after 120 days of gestation isconsidered a mortal sin unless the pregnancyposes a serious threat to the mother’s life (Baharet al 2005; Mughees 2006;Wehbe-Alamah 2005).In a study conducted by Bahar et al (2005), it wasdiscovered that many Turkish Muslim womenbelieve that women who have an induced abor-tion after being pregnant for four months willbe forced to eat their babies in the next world.The authors also reported that taking Paraceta-mol or Digitoxin pills, hitting the groin, drink-ing the juice of boiled onions and beans andplacing soap in the vagina while taking ephed-rine were generic (folk) practices used by Turk-ish women to induce abortion.
On the other hand, reversible methods of
birth control are not forbidden in Islam in con-trast to nonreversible ones such as tubal ligationand vasectomy, which are considered unlawful(Mughees 2006; Wehbe-Alamah 1999, 2005).Use of oral contraceptives and/or intrauterinedevices is popular among Lebanese, Syrian, Jor-danian and Turkish Muslim women (Bahar et al2005; Kridli & Newton 2005; Wehbe-Alamah1999, 2005). Other birth control methods usedby Muslim women and men include diaphragms,spermicides, condoms, the rhythm method andcoitus interruptus. In vitro fertilisation and arti-ficial insemination are permitted in Islam aslong as the process involves the sperm or egg ofthe married couple (Mughees 2006; Wehbe-Alamah 1999, 2005).
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS ANDPRACTICES RELATED TO BIRTHMuslims believe that a special prayer should bewhispered in both baby’s ears as soon as he/sheis born to declare faith and protect the newbornfrom evil spirits (Cassar 2006; Wehbe-Alamah2005).This role is typically assigned to fathersbut is not solely reserved for them.Additionally,anyone who handles the baby is expected toverbalise the name of God and/or expressionssuch as MashaAllah (What God wills) or Sub-hanaAllah (Glory be to God), to ward off evil.Furthermore, charms and amulets containingwords or verses from the Qur’an are usuallypinned to the clothing of newborns to shieldthem from the evil eye. Blue beads are some-times used for the same rationale althoughrecent studies have revealed that their use is becoming increasingly controversial amongLebanese and Syrian Muslims in the USA due toa lack of religious or scientific evidence relatedto the success of this practice in warding off theevil eye (Wehbe-Alamah 1999, 2005).
Circumcision is a religious requirement forall male Muslims. However, this procedure doesnot have to be performed by a religious leader.It is the norm for Lebanese and Syrian Muslims
90 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 90

in the USA to have their male babies circum-cised before they are discharged from the hospi-tal (Wehbe-Alamah 1999, 2005). On the otherhand, the holy book of Muslims, the Qur’an,does not support female circumcision, which iscommonly referred to as female genital mutila-tion or clitoridectomy. This procedure, whichranges from removing the clitoral prepuce tothe removal of the clitoris, labia minora andmost of the labia majora, is considered a contro-versial subject among Muslims from diverse cul-tural backgrounds (Lawrence & Rozmus 2001).While this practice is especially prevalent insub-Saharan Africa and in countries along theHorn of Africa, it is virtually non-existent incountries such as Lebanon and Syria.This proce-dure is prohibited under Australian law (Gulam2003). In the USA, this practice is consideredillegal for girls under the age of 18 years (Unit-ed States Department of Health & Human Ser-vices 2005).
Many Muslims around the world celebratethe birth of their newborn with a banquet cele-bration called Aqiqah following the example ofProphet Muhammad.The celebration consists ofinviting friends, relatives and neighbors to afeast preferably a week after the birth of thenewborn. Meals with lamb or goat meat aretypically served. Syrian Muslims in the USAcontinue to engage in this practice as do Mus-lims of other cultures (Wehbe-Alamah 2005).
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS ANDPRACTICES RELATED TO DEATHAND BEREAVEMENTLike illness, death is regarded by Muslims as a reflection of God’s predestined will and as atest from Allah both to the dying person, thefamily and community. Muslims are expected toreceive death with patience, prayers, readingthe Qur’an and meditation (Cheraghi, Payne &Salsali 2005; Lawrence & Rozmus 2001) as theyview death as a bridge to an eternal afterlife andas a journey towards resurrection and meeting
God (Arshad, Horsfall & Yasin 2004; Wehbe-Alamah 2005).
Proper burials are required for all dead Mus-lims including for foetuses 120 days or olderwho were miscarried or who died in utero(Gulam 2003; Mughees 2006). All children areconsidered to be innocent in Islam and theirsoul is believed to ascend directly to paradiseafter death. Muslims believe that dead childrenwait for their parents at the gates of heaven andthat a great reward in the afterlife awaits theparents of dead children especially if they facedthese deaths with Sabr or patience–self-controlin this lifetime (Arshad et al 2004).
When faced with death, Muslims tend toengage in certain generic (folk) care practices:they may request to face the direction of prayerwhich is Mecca in Saudi Arabia. In the USA,Muslim patients or their families may ask tohave the hospital bed repositioned to face the North East direction whereas in Australiathey may demand to face the West-North-Westdirection (Arshad et al 2004; Gulam 2003;Wehbe-Alamah 1999, 2005). In addition, thedying patient is reminded to deliver the Shahadaor testimony of faith either directly or indirect-ly.The Shahada consists of saying: There is no Godbut Allah (God) and Muhammad is the Messenger ofAllah (God). Casual recitation of the above men-tioned statement in front of a dying Muslimpatient serves as an indirect reminder of theneed to make this final proclamation of faith. Itis believed that death that coincides with theuttering of Shahada can facilitate one’s admit-tance to heaven (Mughees 2006;Wehbe-Alamah2007).
Reading the Qur’an and offering prayers andsupplications are additional generic (folk) carepractices surrounding death and the dyingprocess for Muslims.These actions are believedto facilitate a peaceful departure of the soul andto plead for the welfare of the dying person inthe afterlife (Arshad et al 2004; Lawrence &Rozmus 2001). In addition, religious or otherartifacts that prolong the suffering or dying
91Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 91

process of Muslims should be removed from thephysical environment of a dying patient. In astudy conducted with Syrian Muslims in theUSA, it was discovered that crosses, statues,magazines, or picture frames portraying livingcreatures were believed to keep the angel ofdeath away, which would lengthen the durationof anguish associated with the dying process. Asa result, Syrian Muslims resorted to coveringthese items or removing them from the room ofdying friends or relatives (Wehbe-Alamah 2005).
Following death, special rituals are requiredfor dead Muslims. First, the dead should only be touched by members of the same sex andpreferably by Muslims.The body should be han-dled minimally and with great gentleness andrespect as it is believed to feel pain and pressure(Komaromy 2004; Mughees 2006). Second, theeyes are closed, the lower jaw is bandaged to thehead to avoid a gaping mouth, the joints areflexed and the body is straightened. Modesty isto be preserved at all times especially during theritual washing of the body called Ghusul and itssubsequent shrouding with a white garmentresembling a sheet called Kafan (Arshad et al2004; Gulam 2003;Wehbe-Alamah 2005). It ishighly preferred to bury the dead within 24hours of death as the soul is believed to feel painuntil it is buried. This is one reason why post-mortem examinations are discouraged in Islam,unless required by law. In addition, autopsiesand body embalming are disliked because theyare perceived to be associated with disfigure-ment of the body that belongs to God (Arshadet al 2004; Komaromy 2004; Lawrence & Roz-mus 2001).
Prior to burial, the body is usually taken tothe community’s mosque for Janaza prayer, aspecial prayer ritual that precedes the burial ofdead Muslims. Following the Janaza, the body istaken for entombment in a Muslim cemetery.While Muslims prefer to bury their dead dir-ectly in the soil without a coffin, the laws in theUSA enforce the use of coffins for burial. ManyArab American Muslims such as Lebanese and
Syrians line the inside of the coffins with dirt toaccommodate this legal requirement while ful-filling their religious obligation at the same time (Arshad et al 2004;Wehbe-Alamah 1999,2005). Cremation is prohibited in Islam and isconsidered equivalent to the punishment of Hell(Komaromy 2004).
Grief expressions following death and duringthe bereavement process tend to be diverse andrange from quiet stoicism characterised by self-control and patience to loud crying and wailing.A remarkable show of reliance on God and faithare often exhibited. Offering condolences to thebereaved is considered to be a Muslim duty anda virtuous act. Sympathies are typically offeredduring (but not limited to) the first three days ofmourning. The Muslim community will oftensupport the family of the deceased followingdeath. Friends, extended family and communitymembers often visit, cook food and undertakechildcare activities for the family of the deceased(Arshad et al 2004; Lawrence & Rozmus 2001).In two different ethnonursing studies, Lebaneseand Syrian Muslims in Midwestern USA citieswere observed to organise circles for Qur’anrecitations and supplications on behalf of thedeceased, in addition the above mentioned prac-tices (Wehbe-Alamah 1999, 2005).
TRADITIONAL MUSLIM GENERIC(FOLK) CARE BELIEFS AND PRAC-TICES RELATED TO HIV AND AIDSThe religion of Islam promotes chastity and dis-courages extra-marital relations, illicit drug useand homosexuality. In most Arab and Islamiccountries, contracting HIV or AIDS is perceivedto be associated with sexual promiscuity, gay–lesbian relationships, and/or unlawful drug use.This perception has lead to the development ofa stigma associated with the disease coupledwith feelings of shame and guilt. Most Arab andIslamic leaders initially denied the existence ofHIV/AIDS related problems in their countriesand did not engage in any preventive or educa-tional programs addressing this pandemic.The
92 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 92

Joint United Nations Programme on HIV/AIDS(UNAIDS) estimated that in 2005, nearly 1 mil-lion people from North Africa, the Middle Eastand predominantly Muslim Asia were infectedwith HIV (Kelly & Eberstadt 2005).
Many countries, including but not limited to Thailand, Iran and Bangladesh have morerecently acknowledged their epidemics andtaken active steps to find ways to control andprevent HIV infections. AIDS education pro-grams have been incorporated in public schoolsand other sectors of society. In 2006, the firstHIV/AIDS training for female religious leadersin the Arab world was held in Tripoli, Libya andaddressed the rights of women and children to protect themselves from HIV infection. In2007, 300 Christian and Muslim religious lead-ers from 20 Arab countries met in Cairo andlaunched the first network focused on HIV/AIDS. The network’s goal was to promotechastity and dignity and provide support, spiri-tual counseling and care for people living withHIV/AIDS and their families. It sought to high-light the links between HIV/AIDS and develop-ment, governance, gender and human rights and addressed causes of HIV/AIDS, includingpoverty, at both the national and regional levels(Berger & Mendez 2007).While active steps arebeing taken to halt the spread of HIV/AIDSpandemics, a diagnosis with HIV/AIDS remainsa taboo and a source of shame and guilt formany Muslims.
USE OF LEININGER’S CULTURECARE MODES TO PROVIDECULTURALLY CONGRUENT CARENurses and other health care professionals canrely on their knowledge of Muslim generic carebeliefs and practices while using Leininger’s culture care modes to bridge the gap betweengeneric or folk (emic) and professional (etic) carepractices and to consequently promote cul-turally congruent care. Leininger’s culture caremodes include: Culture care preservation and/or maintenance, culture care accommodation
and/or negotiation and culture care repattern-ing and/or restructuring.
Culture care preservation and/or main-tenance is defined by Leininger as ‘… thoseassistive, supportive, facilitative, or enablingprofessional acts or decisions that help culturesretain, preserve, or maintain beneficial carebeliefs and values and to face handicaps anddeath’ (Leininger & McFarland 2006: 8). Nursesand other healthcare professionals can preservethe culture care of more traditional Muslimpatients by allowing them to consume homecooked meals in the hospital setting, especiallyif the health institution lacks the ability to prepare food according to Islamic law. They can also maintain the privacy and modesty ofthese patients through avoidance of unnecessarybody exposure, prolonged direct eye contactand unlawful male–female touching as well asthrough assigning same sex healthcare providerswhen possible. Offering medications and foodtrays with the right hand and avoiding the ini-tiation of hand shaking or hugging of patients of the opposite sex are other nursing actionsdesigned to maintain the culture care of tradi-tional Muslims. When it comes to newborncare, nurses must not interfere with the recita-tion of prayer in the baby’s ears and should notremove any pinned charms and amulets fromthe infant’s clothing without seeking priorparental permission.
Culture care accommodation and/or negoti-ation refers to ‘those assistive, accommodating,facilitative, or enabling creative provider careactions or decisions that help cultures adapt toor negotiate with others for culturally congru-ent, safe and effective care for their health,well-being, or to deal with illness or dying’(Leininger & McFarland 2006: 8). Nurses canaccommodate their Muslim patients, relativesand community members by providing themwith a private and clean area for prayer and/orQur’an recitation especially when a death isimminent.They can also negotiate with them inrelation to visitation procedures especially given
93Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 93

that visiting the sick by many relatives andfriends is considered to be a religious, culturaland social duty. In addition, accommodation canbe carried out in relation to prescribing gelatinand alcohol-free alternatives to medications andvitamins and adjustments to medication andother medical-nursing regimens can be madefor fasting Muslim patients during the holymonth of Ramadan. Nurses are also in the posi-tion to be able to negotiate with the kitchenstaff to arrange for seafood and/or vegetarianalternatives for Muslim patients who strictlyadhere to halal diets.
Additional accommodations for providingculturally congruent care to Muslim femalepatients may include posting signs at the door(upon request) and asking for men to knock onthe door and seek permission before enteringthe room to allow for time to cover the hair andsecure patient modesty. Likewise, male nurses,nurse practitioners, physicians, or other healthcare professionals may accommodate femaleMuslim patients by arranging for the presenceof a female chaperone or family member duringprocedures that breach traditional Muslims’modesty or expose their private body parts.Furthermore, nurses may change the location ofhospital beds to face the direction of prayer(Mecca in Saudi Arabia) to accommodate theneeds of Muslim patients who wish to pray inbed or who are faced with impending death.Moreover, for dying Muslim patients, nursesmay remove or cover (upon request) religiousor other artifacts that portray living creatures inthe patient’s hospital room.
Following death, nurses may assist the familyof the deceased by facilitating the dischargeprocess given that burial is preferred to takeplace within 24 hours. Handling the body ofdead Muslims should be minimized and carriedout with extreme caution and respect. Nursesnot sharing the same gender as the deceased arediscouraged from touching the body.
Culture care repatterning and/or restruc-turing include ‘… those assistive, supportive,
facilitative, or enabling professional actions andmutual decisions that would help people toreorder, change, modify, or restructure theirlifeways and institutions for better (or bene-ficial) health care patterns, practices, or out-comes’ (Leininger & McFarland 2006: 8).Nurses who discover harmful beliefs and prac-tices used by patients have a responsibility toeducate their clients about the dangers and con-sequences of such actions and may strive to col-lectively explore healthy alternatives in order toreach mutual decisions that restructure the life-ways of their patients. Consequently, nurses car-ing for Turkish or any other Muslim womenwho engage in any of the generic care practicesdepicted earlier in this paper that endangerhealth in relation to inducing abortion maycounsel these women about the potential harm-ful consequences of such actions and investigatehealthy alternatives such as the use of preventa-tive birth control methods (contraception). Inaddition, nurses may educate African and otherMuslim women (and possibly men) who engagein or advocate for female genital circumcisionabout the adverse effects and ramifications offemale genital mutilation and together exploreculturally acceptable substitutes. Finally, healthcare providers may engage in culturally sensitiveeducation in relation to spread and preventionof HIV/AIDS keeping in mind the generic carebeliefs that may be associated with this illness.
CONCLUSIONAs health care professionals, we have the duty todeliver holistic and culture-specific health careservices to our patients. Ignoring unique indi-vidual cultural interpretations, beliefs and prac-tices of diverse health related issues preventsproviding culturally congruent care. Incorpor-ating generic or folk (emic) care beliefs andpractices in a professional (etic) plan of carefacilitates the delivery of care that addressesprofessional scientific standards while attendingto culture-specific needs and expectations ofclients of diverse cultural backgrounds. Bridg-
94 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 94

ing generic or folk (emic) and professional(etic) care beliefs and practices through the useof Leininger’s culture care modes not only pro-motes culturally congruent care, but may alsolead to increased client satisfaction, a pleasanthospital stay, improved client cooperation and afaster recovery rate. Muslim patients are diversein their generic care beliefs and practices. Asnurses and professional healthcare providers,we cannot assume that all Muslim patients sharethe traditional generic care beliefs and practicesdiscussed in this paper. Performing individualcultural assessments is crucial to discoveringcultural beliefs and needs and providing cultur-ally congruent care practices.
References‘Abd al ‘Ati H (1998) Islam in Focus,Amana Publi-
cations, Beltsville, MD.Armanios F (2004) Congressional Research Service
Report for Congress, Congressional ResearchService, accessed at http://www.fas.org/irp/crs/RS21745.pdf on 12 February 2008.
Arshad M, Horsfall A and Yasin R (2004) Preg-nancy loss – the Islamic perspective, BritishJournal of Midwifery 12(8): 481–484.
Australian Bureau of Statistics (2007a) 2006 CensusQuickStats:Australia, accessed at http://www.censusdata.abs.gov.au/ABSNavigation/prenav/ProductSelect?newproducttype=QuickStats&btnSelectProduct=View+QuickStats+%3E&collection=Census&period=2006&areacode=0&geography=&method=&productlabel=&producttype=&topic=&navmapdisplayed=true&javascript=true&breadcrumb=LP&topholder=0&leftholder=0¤taction=201&action=401&textversion=false on 05 July 2007.
Australian Bureau of Statistics (2007b) Year BookAustralia 2007: Cultural Diversity, accessed athttp://www.abs.gov.au/AUSSTATS/[email protected]/bb8db737e2af84b8ca2571780015701e/7056F80A147D09D3CA25723600006532?opendocument on 5 July 2007.
Badawi J (1999) Gender Equity in Islam: Basic Princi-ples,American Trust Publications, IndianapolisIN.
Bahar Z, Okcay H, Ozbicakci S, Beser A, Ustun B and Ozturk M (2005) The effects of Islam andtraditional practices on women’s health andreproduction, Nursing Ethics 12(6): 557–570.
Ba-Yunus I and Siddiqui MM (1998) A report onMuslim population in the United States ofAmerica, Center for American Muslim Research& Information, Islamic Book Center, RichmondHill, NY, in Rashidi A and Rajaram S (2001)Culture care conflicts among Asian-Islamicimmigrant women in US hospitals, HolisticNursing Practice 16(1): 55–64.
Ball C and Haque A (2003) Diversity in religiouspractice: implications of Islamic values in thepublic workplace, Public Personnel Management32(3): 315–330.
Berger R M and Mendez J (2007) Christians andMuslims fighting AIDS, Sojourners Magazine36(3): 11.
Cassar L (2006) Cultural expectations of Muslimsand Orthodox Jews in regard to pregnancy andthe postpartum period: a study in comparisonand contrast, International Journal of ChildbirthEducation 21(2): 27.
Cheraghi M, Payne S and Salsali M (2005) Spiritualaspects of end-of-life care for Muslim patients:experiences from Iran, International Journal ofPalliative Nursing 11(9): 468–474.
Connelly M, Hammad A, Hassoun R, Kysia R andRabah R (1999) Guide to Arab culture: Health caredelivery to the Arab American community,AccessCommunity Health Center, Dearborn,Michigan.
D’avanzo CE and Geissler EM (2003) CulturalHealth Assessment, Mosby, St Louis, cited inCassar L (2006) Cultural expectations ofMuslims and Orthodox Jews in regard topregnancy and the postpartum period: a studyin comparison and contrast, InternationalJournal of Childbirth Education 21(2): 27.
Gulam H (2003) Clinical update: Care of theMuslim patient, Australian Nursing Journal11(2): 23–5.
Halligan P (2006) Transcultural care, World of IrishNursing & Midwifery 14(8): 34–34.
Hamid AW (1996) Islam Natural Way, KaziPublications, Inc, Chicago, IL.
95Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 95

Hassan F (2000) Islamic women in Science, Science290(5489): 55–56.
Hodge D (2005) Social work and the house ofIslam: Orienting practitioners to the beliefsand values of Muslims in the United States,Social Work 50(2): 162–173.
Husain S (1995) What do we know about Islam? PeterBedricks Books, NewYork.
Kelly L and Eberstadt N (2005) The Muslim faceof AIDS, Foreign Policy 149: 42–48.
Komaromy C (2004) Continuing professionaldevelopment: Cultural diversity in death anddying, Nursing Management – UK 11(8): 32–36.
Kridli S and Newton S (2005) Jordanian marriedMuslim women’s intentions to use oral contra-ceptives, International Nursing Review 52(2):109–114.
Lawrence P and Rozmus C (2001) Culturallysensitive care of the Muslim patient, Journal of Transcultural Nursing 12(3): 228–233.
Leininger MM (1995) Transcultural Nursing: Con-cepts,Theories, Research, & Practice, 2nd edn,McGraw-Hill, New York.
Leininger MM and McFarland MR (2002) Trans-cultural Nursing: Concepts,Theories, Research andPractice, 3rd edn, McGraw-Hill Medical, NewYork.
Leininger MM and McFarland MR (2006) CultureCare Diversity and Universality: A WorldwideNursing Theory, 2nd edn, Jones & Bartlett,Sudbury MA.
Luna L (1989) Care and cultural context ofLebanese Muslims in an urban U.S. com-munity:An ethnographic and ethnonursingstudy conceptualized within Leininger’s theory.Unpublished Doctoral dissertation,WayneState University, Detroit MI.
Mohammadi N, Evans D and Jones T (2007)Muslims in Australian hospitals:The clash ofcultures, International Journal of Nursing Practice1: 310–315.
Mughees A (2006) Better caring for Muslimpatients,World of Irish Nursing & Midwifery 14(7):24–25.
Rashidi A and Rajaram S (2001) Culture careconflicts among Asian-Islamic immigrant
women in US hospitals, Holistic Nursing Practice16(1): 55–64.
Rassool G (2000) The crescent and Islam: healing,nursing and the spiritual dimension. Some con-siderations towards an understanding of theIslamic perspectives on caring, Journal ofAdvanced Nursing 32(6): 1476–1484.
Shamsi R (1999) Why Islam forbids pork, TheMuslim World League Journal, accessed at http://islamic-world.net/sister/h1.htm on 13February 2008.
Simpson J and Carter K (2008) Muslim women’sexperiences with health care providers in arural area of the United States, Journal ofTranscultural Nursing 19(1): 16–23.
Tsianakas V and Liamputtong P (2002) Whatwomen from an Islamic background inAustralia say about care in pregnancy andprenatal testing, Midwifery 18: 25–34.
Underwood SM, Shaikha L and Bakr D (1999)Veiled yet vulnerable: Breast cancer screeningand the Muslim way of life, in Cancer Practitioner7(6): 285–290, cited in Rashidi A and RajaramS (2001) Culture care conflicts among Asian-Islamic immigrant women in US hospitals,Holistic Nursing Practice 16(1): 55–64.
United States Census Bureau (2005) 2005American Community Survey data profile highlights,accessed at http://factfinder.census.gov/servlet/ACSSAFFFacts?_event=&geo_id=01000US&_geoContext=01000US&_street=&_county=&_cityTown=&_state=&_zip=&_lang=en&_sse=on&ActiveGeoDiv=&_useEV=&pctxt=fph&pgsl=010&_submenuId=factsheet_1&ds_name=null&_ci_nbr=null&qr_name=null®=null%3Anull&_keyword=&_industry=on 05 July 2007.
United States Department of Health and HumanServices (2005) Female genital cutting, accessedat http://www.4women.gov/FAQ/fgc.htm on01 August 2007.
Wadud A (1999) Qur’an and woman, Oxford Uni-versity Press, New York.
Wehbe-Alamah H (1999) Generic Health CareBeliefs, Expressions and Practices of LebaneseMuslims in two Urban U.S. Communities:A
96 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hiba Wehbe-AlamahCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 96

Mini Ethnonursing Study Conceptualized with-in Leininger’s Theory. Unpublished Master’sThesis, Saginaw Valley State University, MI.
Wehbe-Alamah H (2005) Generic and Profes-sional Care Meanings, Beliefs, Expressions andPractices of Syrian Muslims living in theMidwestern United States. Doctoral disser-tation, Duquesne University, Pittsburgh, PA.Accessible at: http://etd1.library.duq.edu/theses/available/etd-11172005-122600
Wehbe-Alamah H (2007) Understanding How
Racial & Ethnic Differences Affect the Deliveryof Health Care in America – The Arab/MuslimCulture,Academic Presentation on 07 March2007, University of Michigan-Flint.
Zeghidour S (1994) I want to talk to God, CreativeEducation, Mankato MN.
Zoucha R and Husted G (2000) The ethicaldimensions of delivering culturally congruentnursing and health care, Issues in Mental HealthNursing 21(3): 325–340.
97Volume 28, Issue 1–2,April 2008 CCCCNNNN
Bridging generic and professional care practices for Muslim patients CCCCNNNN
AD VA N C E S I N CO N T E M P O R A RY NU R S I N G A N D GE N D E RGuest edited by Professors Paula McGee, University of Central England, UK
and Kim Walker, St Vincent’s Private Hospital, Australia
A peer-reviewed special issue (ISBN 978-1-921348-07-5) of Contemporary Nurse, publishing in 2009.
DEADLINE FOR MANUSCRIPT SUBMISSIONS: 15 December 2008
We invite papers on all aspects of gender and nursing, including: Research papers about any aspect ofgender and nursing care including methodological issues and topics that are under-addressed; Papersabout gender orientation concerning lesbian, gay, bisexual, transgender or heterosexuality and genderreassignment; Race, ethnicity, culture, religion and gender; Relevant practice papers that provide examples of multi-professional practice or which address the practicalities, policy or managerial aspects of delivering services and care; Debate papers that address key issues relating to gender and nursing.
Papers are invited for this special issue of Contemporary Nurse devoted to all aspects of gender andnursing, including:
The Guest Editors would be pleased to discuss your submission in advance:
Professor Paula McGee, Faculty of Health, University of Central England, Perry Barr, Birmingham B42 2SU, UK;Tel: 0121 331 53401; email [email protected]
Professor Kim Walker, Adjunct Professor, St Vincent’s Private Hospital, Darlinghurst NSW 2010, Australia;Tel: 02 8382 7442; email: [email protected]
Or send electronically to [email protected] for automated distribution to the editors,indicating in the cover email that it is for the 2009 Special Issue of Contemporary Nurse on Nursing Gender.
Instructions for Authors, past issues, and other details can be found on the website:http://www.contemporarynurse.com/author_guidelines.php
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911; [email protected]
www.e-contentmanagement.com
• • • C A L L F O R P A P E R S • • •
• Research papers about any aspect of genderand nursing care including methodologicalissues and topics that are under-addressed
• Papers about gender orientation concerninglesbian, gay, bisexual, transgender orheterosexuality and gender reassignment
• Race, ethnicity, culture, religion and gender
• Relevant practice papers that provide examplesof multi-professional practice or which addressthe practicalities, policy or managerial aspectsof delivering services and care
• Debate papers that address key issues relatingto gender and nursing
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 97

NCCopyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 98–100.
EDITORIAL
The cultural diversity of Australia is consid-ered to be a strength that will assist this
nation to take advantage of, and meet the chal-lenges that come with participating in the rapid-ly changing ‘global village’. A culturally diversesociety provides its own challenges, and overthe past 30 years state and federal Governmentshave disseminated a range of policies and initi-ated programs that provide frameworks andbenchmarks for meeting the goals of access,equity and inclusiveness (Omeri 2003) for allpeople living in Australia. Responding to andaccommodating cultural diversity poses particu-lar challenges because of the intensely personalmeaning that established cultural mores have forindividuals, and the tendency for people to clingto their cultural heritage and, in some instances,biases.
Health and education are the mainstays of anation. Success in the arts, science, humanitiesand business requires people to have access to arange of educational options and access to quali-ty health care. There is a plethora of researchfrom the social, health and education disciplinesthat demonstrates unequivocally the nexus bet-ween these social foundations.There is also an
increasing body of evidence to guide the appli-cation of that research to inform the everydayissues that arise in a diverse society.
How is that cultural diversity reflected ineducation of clinicians and translated to thehealth system they work in? There is an expan-sive body of published, peer reviewed researchthat can be used by individuals and organisationsto provide an evidence based approach to tran-scultural health care.
The Australian National Review of NursingEducation Multicultural Nursing Educationreviewed the ways in which nurses are currentlyprepared for multicultural practice (Common-wealth Department of Education, Science andTraining [DEST] 2002). In that document cul-tural competence is described as:
A set of congruent behaviours, attitudes andpolicies that come together in a system ofagency or among professionals that enableeffective interactions in a cross-cultural frame-work. (DEST 2002: 4)
The report concluded that there has been anexplosion of theories of cultural competenceand literature describing its application. Exam-
Towards a culturally competent nurseworkforce
98 Volume 28, Issue 1–2,April 2008CCCCNNNN
RHONDA GRIFFITHS AM
Professor of NursingSchool of NursingUniversity of Western SydneySydney NSW, Australia andDirectorCentre for Applied Nursing ResearchSydney South West AreaHealth ServiceSydney NSW, Australia
JOHN DALYDeanFaculty of NursingMidwifery and HealthUniversity of Technology,Sydney NSW, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 98

ples from international and local facilities were analysed and included in an extensive listof areas where theories of cultural competencehad been applied to nursing in education,research, workforce planning, care delivery ingeneral and speciality settings, and health pro-motion and community care.
Individuals and organisations have a jointresponsibility to create an environment that isconducive to and will foster cultural diversity, beprepared to commit to ongoing review, andwhen necessary initiate and support change(Omeri 2003). That joint responsibility is atheme that runs through the contemporary liter-ature and is echoed by contributors in this spe-cial issue of Contemporary Nurse. In this section ofthe publication, Carolyn Rutledge et al (2008)describes an education program that uses multimedia resources and experiential learning toassist clinicians overcome many of the barriers tocultural competence they experienced in theirworkplace.This program could be implementedor adapted to suit various situations to assist positive interactions with people from diversecultures. While clinicians generally becomeaware of the construct of cultural competencethrough modelling by colleagues, Campinha-Bacote (2008) suggests that the actions requiredto function at that level can also be learned byclinicians as part of their structured educationprograms. In a longitudinal study, Maltby andcolleagues (2008) encouraged a cohort of bac-calaureate nursing students to reflect on theirattitudes towards nursing clients from diversepopulations.The themes that emerged from thedata namely: equal treatment; commitment toserve all clients; and ‘it’s not easy’, challenge cli-nicians on a daily basis. Papadopoulos et al (2008)developed and tested a tool to measure culturalcompetence of staff working in Child and Ado-lescent Mental Health services. Promoting a cul-ture of cultural competence extends beyondclient care.The workforce shortages of trainedstaff that is now a feature of health services, hasresulted in the globalisation of the nursing work-
force.The article by Brunero et al (2008) high-lights an increasingly important issue for healthservices.The migration of the nursing workforcecreates a need for health services to implementstrategies that assist Australian trained nurses toappreciate the benefits of a culturally diverseworkforce and assists overseas qualified nurses toweather the cultural clash they experience asthey ‘rotate’ around the world.
Three policy principles that are dominant in the multicultural policy agenda – access andequity and inclusiveness (Omeri 2003) – arealso dominant in the health agenda. Best practicein health care for a multicultural society requiresconsideration of cultural as well as clinical im-peratives. The needs of people from culturallydiverse backgrounds must be taken into accountwhen developing care. In some instances thiswill mean different approaches are appropriate,and the outcome of care may also be different.
Having access to evidence is only one part ofthe formula for effective transcultural nursing.In all Western countries, the health sector consumes a large proportion of Governmentfunding; however, we have little evidence todemonstrate the effectiveness of interventions,processes and models of care. Research hasmade a major contribution to health care, par-ticularly in technology led areas for examplepharmacology, diagnostics and surgery. Someinterventions are outstandingly effective inreducing mortality and morbidity, and ‘highprofile’ interventions receive attention. How-ever, at the bedside, clinical decision makingcontinues to reflect convention and tradition(Grimshaw & Eccles 2004; Grol & Grimshaw2001; Johnson & Griffiths 2001). Why is thisthe case? A variety of reasons for the sustainedtheory/practice gap have been presented. Theculture of health care facilities has been impli-cated, as has the nursing culture, clinical priori-ties, issues of leadership and communicationand resources (Johnson & Griffiths 2001). Rea-sons for this situation have been proposed,including the task oriented nature of clinical
99Volume 28, Issue 1–2,April 2008 CCCCNNNN
Editorial: Towards a culturally competent nurse workforce CCCCNNNN
CNJ 28_1_2_internal.qxd 30/07/2008 9:48 PM Page 99

practice, the absence of guiding frameworks,and lack of detailed exploration about how toimplement research.
The notion of clinician-led research intro-duces an alternate paradigm to health servicesresearch that has challenged the traditionallydesigned and accustomed roles of researcherand clinician. Factors that militate against clini-cian led change have been proposed and include(Grol & Wensing 2004; Johnson & Griffiths2001; Rycroft-Malone et al 2004):• lack of support and lack of authority to
implement change;• lack of research training for clinicians;• the absence of organisational and research
information systems; and• the constraining nature of the nursing role.
Getting evidence into practiceEnacting strategies designed to promotesocial a responsibility at both the organisa-tional and individual level.That is, providingquality care to a diverse population requiresboth systematic responses … and the deliv-ery of care by skilled and sensitive providers.
(Grol & Wensing 2004: 3).
Despite the emphasis on evidence based careand the development of resources and supportto assist clinicians to access evidence, the gapbetween the evidence and practice has not nar-rowed (Grol & Wensing 2004).
Increasingly undergraduate and post graduatecurricular include discrete learning opportuni-ties to promote skills and knowledge to achievecultural competence and outcomes againstwhich learning can be measured. Nurses whotranslate those skills into clinical practice havethe potential to change national health policy(Boyle 2000).
Ignaz Semmelweis (1818–1865) and JosephLister (1827–1912) had the idea that infectionwas associated with poor hygiene by hospitalstaff. Although their colleagues forcefully reject-ed their hypothesis they persevered and were
vindicated.The researchers and clinicians whohave contributed to this special issue of Contem-porary Nurse have put out the challenge. Provid-ing culturally competent care is a universalstandard that, when achieved, will save andchange lives for recipients and providers ofhealth care.
ReferencesBoyle J (2000) Transcultural nursing:Where do we go from
here? Journal of Transcultural Nursing 11: 10–11.Brunero S, Smith J and Bates E (2008) Expectations and
experiences of recently recruited overseas qualifiednurses in Australia, Advances in Contemporary TransculturalNursing, 2nd edn, Contemporary Nurse special issue28(1–2): 101–110.
Campinha-Bacote J (2008) Cultural desire:‘Caught’ or‘taught’? Advances in Contemporary Transcultural Nursing,2nd edn, Contemporary Nurse special issue 28(1–2):141–148.
Commonwealth Department of Education Science andTraining (DEST) (2002) National Review of NursingEducation. Multicultural Nursing Education. DEST,Canberra.
Grimshaw J and Eccles M (2004) Is evidence-basedimplementation of evidence-based care possible? Medical Journal of Australia 180: S50–S51.
Grol R and Grimshaw J (2001) From best evidence to bestpractice: Effective implementation of change in patient’scare. Lancet 363: 1225–1230.
Grol R and Wensing M (2004) What drives change? Barriersto and incentives for achieving evidence-based practice.Medical Journal of Australia 180: S57–S60.
Johnson M and Grifiths R (2001) Developing evidence-based clinicians. International Journal of Nursing Practice7: 109–118.
Maltby HJ (2008) A reflection on culture over time byBaccalaureate nursing students, Advances in ContemporaryTranscultural Nursing, 2nd edn, Contemporary Nurse specialissue 28(1–2): 111–118.
Omeri A (2003) Meeting diversity challenges: Pathways of‘advanced’ transcultural nursing practice in Australia.Contemporary Nurse 15(3): 175–187.
Papadopoulos I, Tilki M and Ayling S (2008) Culturalcompetence in action for CAMHS: Development of acultural competence assessment tool and training pro-gramme, Advances in Contemporary Transcultural Nursing,2nd edn, Contemporary Nurse special issue 28(1–2):129–140.
Rutledge CM, Barham P,Wiles L, Benjamin RS, Eaton P and Palmer K (2008) Integrative simulation:A novelapproach to educating culturally competent nurses,Advances in Contemporary Transcultural Nursing, 2nd edn,Contemporary Nurse special issue 28(1–2): 119–128.
Rycroft-Malone J, Harvey G, Seers K, Kitson A,McCormack B and Titchen A (2004) An exploration ofthe factors that influence the implementation ofevidence into practice. Journal of Clinical Nursing 13:913–924.
100 Volume 28, Issue 1–2,April 2008CCCCNNNN
Rhonda Griffiths and John DalyCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 100

INTRODUCTION
Over the past decade a deficit of Australiannurses has prompted active policies of
international recruitment. In Australia a shortfallof 40 000 nurses by 2010 is predicted (Jeon &
Chenoworth 2007). In consequence, the over-seas’ qualified nurse (OQN) has become anincreasingly vital component of the Australiannursing workforce (Hawthorne 2001). Invest-ment in providing appropriate support to enable
Key Wordsoverseasqualified nurse;nursing; cultureand linguisticdiversity;retention;recruitment CN
101Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 101–110.
Expectations and experiences of recently recruited overseas
qualified nurses in Australia
ABSTRACT The overseas qualified nurse (OQN) has become an important part of theAustralian nursing workforce. Efforts to enhance their adjustment to work andlife in Australia have been recommended in the literature.This study examinesthe experiences and needs of a group of OQNs at a major metropolitan tertiaryreferral hospital in Australia. Using a descriptive survey, 56 nurses reportedtheir experiences with three major themes emerging, career and lifestyle oppor-tunities, differences in practice and homesickness. Nurses from culturally andlinguistically diverse backgrounds reported not being employed in their chosenspeciality and rating the utility of ward and hospital orientations more posi-tively when compared to English speaking background nurses. From the studyresults an organisational and a personal approach has been undertaken to aidin the adjustment of OQNs into the nursing workforce.
Received 30 March 2007 Accepted 19 March 2008
SCOTT BRUNERODepartment of Liaison Mental
Health NursingPrince of Wales HospitalRandwick NSW, Australia
JULIE SMITHDepartment of Liaison Mental
Health NursingPrince of Wales HospitalRandwick NSW, Australia
EMMA BATESDepartment of Liaison Mental
Health NursingPrince of Wales HospitalRandwick NSW, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 101

overseas nurses to adapt to working in a differ-ent health care system and settling in to life in Australia is regarded as essential (Jeon &Chenoworth 2007; Gerrish & Griffith 2004).
In a recent systematic review of the literatureKonno (2006) found 64 papers on the topic ofOQNs in Australia. Two core themes emergefrom this meta-synthesis. Firstly, overseas nurs-es found entry into Australian culture very diffi-cult; and secondly they felt lonely and isolated,and experienced difficulty in settling in to nurs-ing in Australia. Konno (2006) contends that theclash of cultures between OQNs and the domi-nant Australian culture should be addressed indedicated transition programmes.
Daniel, Chamberlain and Gordon (2001) inthe United Kingdom (UK) explored the expec-tations and experiences of newly recruited Fil-ipino nurses. Key factors that influenced theirdecision to work in the UK were improvedprospects and better wages. Differences werealso noted in their expectations of their newnursing role and their actual experience. Strate-gies reported as being helpful during this adjust-ment phase were: support services, culturallyappropriate orientation programmes, trainingand opportunities for promotion.The literaturesuggests that problems in adjustment for OQNsmay include: culture shock, homesickness, com-munication difficulties, social isolation, anxietyand accommodation issues (Daniel et al 2001).Similarly, Pilette (1989) reports that interna-tional nurses undergo a process of adjustmentthat frequently leads to cultural, professionaland psychological dissonance. Pilette (1989)recommends that health care managers seek to understand this process of adjustment, andimplement assimilation programmes to supportinternational nurses, and ultimately retain themwithin the workforce.
At an international level the Internationalcouncil of Nurses (ICN 2007), has set out aposition statement on the ethical recruitment ofnurses.The ICN recognises the right of nursesto migrate and notes the benefit to nursing out-
comes of the multicultural and learning oppor-tunities gained by the process of migration.TheICN equally denounces where countries havefailed to adequately plan for human resourcesgaps and also countries that haven’t addressedreasons why nurses leave the profession. TheICN makes it clear in this position statementthat nurses have the right to proper orientationand ongoing constructive supervision/mentor-ing within the work environment (ICN 2007).
CULTURE-CARE STRATEGIES TOPROMOTE RETENTION OF OQNSIdeas that aim to strengthen retention rates and reduce the pressure on the continuousrecruitment effort warrant consideration. Avariety of interventions have been described inthe literature and they include: employment of an international support nurse, mentorship programmes, country-specific orientation pro-grammes, social programmes, intercultural com-munication courses and clinical supervision.
Oxtoby (2003) explores the role of an ‘Inter-national Support Nurse’ in the UK. The roleoffers support and guidance to the new recruitto help them understand and deal with any cul-ture shock they may experience.The education-al component of the role involves the deliveryof assertiveness training, rehearsing clinical sce-narios and improving communication betweendifferent cultural groups. Ryan (2003) reportson a North American buddy programme des-cribing the following as necessary for the OQNsadjustment.These are socialisation to the pro-fessional nursing role, acquisition of languageand other communication skills, development of clinical and organisational workplace com-petence, availability of support systems andresources within the organisation. Gerrish andGriffith (2004) report on an evaluation of anadaptation programme.They delineated that thesuccess of the programme was associated withthe OQNs gaining professional registration,their fitness for practice, reducing the nurse
102 Volume 28, Issue 1–2,April 2008CCCCNNNN
Scott Brunero, Julie Smith and Emma BatesCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 102

vacancy factor, equality of opportunity, and pro-moting a culture of valuing diversity.
ORGANISATIONAL APPROACHESAlexis and Chambers (2003) discuss the impor-tance of the culturally competent environment,where its systems, agents and stakeholders allrespond to the needs of the OQN, particularlywhen their needs are different from the domi-nant culture. In support of this view, Bruhn(1996) argues the case for creating organisationsthat have a climate of multiculturalism inhealthcare. Bruhn (1996) suggests that multi-culturalism begins with creating a climate ofopen participation, the encouragement of feed-back and allowing control to be exercised atlower organisational levels. Davidhizar, Dowdand Newman Giger (1999) sees the role of thehealth care manager, as helping a diverse work-force to understand the differences betweenindividuals and to facilitate their workingtogether in a smooth and complimentary way.Davidhizar et al (1999) propose a transculturalmodel for evaluation of a new job culture,including items such as; communication, space,social organisation, time, environmental con-trol, biological variations and a self assessmentchecklist as a strategy for adjusting to a neworganisational culture.
Senior nursing staff at the study site becameincreasingly aware of the challenges faced byrecently arrived overseas nurses, when manysought out support due to adjustment prob-lems.This prompted a discussion around whatwere the expectations, experiences, concernsand needs of the newly recruited overseasnurse. Furthermore could the organisation dobetter to facilitate the transition into a new cul-ture, and a different health care system?
STUDY AIMSThe aims of the study were to determine thecare-related culture specific expectations andexperiences of the overseas’ qualified nurse andto both recommend and implement local tar-
geted care-related interventions, to assist intheir adjustment.
METHODA descriptive survey was developed containingopen and closed questions and was constructedfrom an examination of the literature.The sur-vey was mailed to 150 nurses who had arrived atthe hospital in the past 18 months.The study siteis a major tertiary referral teaching hospital inSydney, Australia, with approximately 550 beds.The survey contained three primary sections:1. Demographic questions; age, country of
origin, English speaking background status,country of origin, locality, nursing speciali-ty, sex, length of time in Australia.
2. Participants were asked to rate on a 10-point Likert scale the hospital, and wardorientation and overall satisfaction with theservices provided.
3. Four open-ended questions were adaptedfrom a study by Daniel and Chamberlain(2001) of Filipino nurses in the UK. Theywere:(a) Why did you decide to come and work
at this hospital?(b) Before you left for Australia what were
your expectations about living andworking in Australia?
(c) When you compare your experience ofworking at this hospital with hospitalsoutside of Australia, what are the maindifferences?
(d) What do you regard as a barrier to stay-ing longer at the hospital?
South Eastern Sydney Illawarra Area Health Service, Human Research Ethics Committee,granted ethics approval. Demographic variableshave been summarised using descriptive statis-tics. All dichotomous and continuous variableswere compared by English speaking background(ESB) and non-English speaking background(NESB) status, non-parametric chi square testsand Kruskal-Wallis tests were used for the analy-
103Volume 28, Issue 1–2,April 2008 CCCCNNNN
Expectations and experiences of recently recruited overseas qualified nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 103

sis. A content analysis was undertaken to identifythe major themes of the open ended questions.Following the analysis process, the authors metto compare their coding of the themes for eachof the questions. The minor differences wereidentified, discussed and negotiated until a con-sensus was achieved (DeSantis & Ugarriza 2000).SPSS 14.0 was used to report the descriptive sta-tistics and aid in the coding processes.
RESULTSA total sample of 56 surveys was returned froman initial survey of 150 overseas nurses (areturn rate of 37.3%). The mean age of thegroup was 24 years with an age range from 21to 48 years, of these 12.3% were males and87.7% were female.This sample is significantlyyounger than the average age of all nurses inNSW, in 2004 it was 39 years (Dorian & Jones2004). The average length of experience as anRN was reported as 6 years.The average lengthof time spent in Australia was 9.6 months andtypically 6.2 months represent time employedhere at the study site.
People travelled to Australia from many dif-ferent countries, England (n = 27), Canada (n= 6), Scotland (n = 3), Ireland (n = 3), Sweden(n = 3), the United States (n = 2), Zimbabwe(n = 2), China (n = 1), Italy (n = 1), Philip-pines (n = 1), Fiji (n = 1), Singapore (n = 1),New Zealand (n = 1), Finland (n = 2), SouthAfrica (n = 2). OQNs who spoke English as afirst language account for 77.2% (n = 44) ofthe sample, and 21.1% (n = 12) speak Englishas a second language. The majority of peoplelive locally (within three kilometres of the hos-pital) (52%, n = 29), the rest (48%, n = 27)live in other Sydney suburbs. Table 1 containssample characteristics comparing nurses with anEnglish and Non English speaking background.Nurses with an ESB were more likely to secureemployment in their chosen speciality com-pared with NESB nurses, NESB nurses rated theward and hospital orientations more positivelythan nurses with an ESB. Three major themesemerged from the analysis of the open endedquestions; career and lifestyle opportunities,differences in practice and homesickness.
104 Volume 28, Issue 1–2,April 2008CCCCNNNN
Scott Brunero, Julie Smith and Emma BatesCCCCNNNN
TABLE 1: SAMPLE CHARACTERISTICS SEPARATED BY ENGLISH SPEAKING BACKGROUND (ESB) VERSUSNON-ENGLISH SPEAKING BACKGROUND (NESB)
ESB NESBn = 44 n = 12n (%) n (%) P*
Males 5 (11.4) 2 (16.7) 0.470Females 39 (88.6) 10 (83.3)Employed in speciality 30 (68) 3 (25) 0.026Not employed in speciality 14 (32) 9 (75)Live Locally 21 (47.7) 8 (66.7) 0.202Live elsewhere 23 (52.3) 4 (33.3)
Mean (SD) Mean (SD)
Age (years) 24.7 (12.4) 22.7 (14.17) 0.000Ward orientation# 5.6 (2.16) 8.1 (1.74) 0.000Hospital orientation# 3.9 (2.44) 6 (2.37) 0.000Overall support# 5.3 (2.19) 5.9 (2.74) 0.000Length of time in Australia (months) 8.7 (11.3) 12.7 (10.1) 0.000Length of time as registered nurse (years) 6.1 (6.03) 5.3 (3.26) 0.000Length of time at hospital (months) 6.1 (4.69) 6.8 (4.34) 0.000
*P value < 0.05 considered as significant.# Rated on a 10-point Likert scale 1 = not helpful to 10 = most helpful.
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 104

Career and lifestyle opportunitiesOQNs responses showed that they focused oncareer and lifestyle opportunities when makingdecisions about nursing overseas.The teachinghospital status of the study site was an attractionto several nurses. One the comments regardingthe importance of having a career focus were:
I would want to gain more knowledge and dopost-graduate courses because I had read thatit is a training/teaching hospital. I was toldby my lecturers at University that experiencein another country would help me go a longway in my nursing career.
Many of the participants were attracted by thehospital’s proximity to both the inner city andthe beach, stating that this was the main reasonfor their choice of hospital. Many nurses antici-pate a vibrant cosmopolitan city, complete witha busy and exciting social life. Others are morecaptivated by the prospects of warm weather,relaxed beachside living and friendly people.Some respondents believed that the hospitalwould be similar to those they had worked inNew Zealand, Canada or the United Kingdom.Many expected a large teaching hospital, offer-ing good educational opportunities, progressivenursing practice, modern facilities and friendly,relaxed and less hierarchical hospital atmos-phere. Others look forward to having positivenew experiences and embracing fresh chal-lenges and change in their lives.
Differences in practiceWhen comparing differences between OQNshospital of origin and the hospital study site,nurses made comparisons by describing the dif-ference they experienced in work practices.
At home, taking bloods and cannulationcomes with the work. Feels ridiculous thatyou have to be assessed to do something youdo every day at home.The medication namesare different, the system is different, and itcan be frustrating at times.
What many perceive as major differences inpractice, are reported as some of the most diffi-cult aspects of work for an OQN. Daniel et al(2001) found that having to be reassessed fortheir professional competencies created signifi-cant frustration and anxiety for OQNs. Dowd,Davidhizar and Newman Giger (1999) arguethe idea of developing tolerance to differencesand practising flexibility, as a means of workingthrough the differences in practice.
HomesicknessHomesickness was noted as a problem by anumber of OQNs.The word ‘homesickness’ andphrases such as ‘missing my family’ and ‘beingaway from family and friends’ appeared fre-quently in the text. One nurse stated:
A feeling of home sickness, It is such a long distance travel required to see family/friends. Not having the support of my imme-diate family members is hard, it gives you afeeling of despair at times, worry.
The idea of homesickness has been reported inthe literature as a major source of stress formigrant workers (Verschur, Eurelings-Bontekoe& Spinhoven 2004; Stroebe,Van Vilet; Hewstone& Willis 2002). Symptoms of homesickness mayinclude symptoms such as: physical (sleep dis-turbance, headache, fatigue, gastrointestinalcomplaints), cognitive (negative thoughts abouthome, environment, absent mindedness), behav-ioural (apathy, listlessness, lack of initiative, littleinterest in new environment) and emotional(depressive mood, insecurity, loss of control,nervousness, loneliness) (Van Tilburg, Vinger-hoets & Van Heck 1996).
DISCUSSIONThe majority of OQNs arrived from the UK.The ease of the nurse registration processbetween Australia and the UK, shared language,culture and history may aid in the adjustmentprocess for UK OQNs. Difficulties in adjustingto new cultures due to language barriers have
105Volume 28, Issue 1–2,April 2008 CCCCNNNN
Expectations and experiences of recently recruited overseas qualified nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 105

been articulated consistently in the OQN nurs-ing literature (Omeri 2006; Omeri & Atkins2002; Alexis 2002). Two previously publishedstudies of OQNs (Omeri & Atkins 2002; Jack-son 1996) both in New South Wales, Australia,report similar findings to our study. Jackson(1996) reports of being a woman, being stres-sed, being a stranger, being lonely and being a nurse, Jackson (1996) goes onto report howOQNs sought comfort and a need to establishthemselves during their adjustment phase intoAustralia. Omeri and Atkins (2002) reports onthe lived experience of five immigrant nurses in New South Wales. Omeri and Atkins (2002)through naturalistic open ended interviews,found the following emergent themes; pro-fessional negation, lack of support, otherness,cultural separateness, silencing, language andcommunication difficulties in the OQN’s expe-riences. Omeri and Atkins (2002) demonstratethe distance between people from dominant andnon dominant cultures, similar to the reportedfindings in our study.
Nurses from a NESB were less likely to beemployed in their chosen speciality than ESBnurses.Whilst we did not ask for direct reasonswhy this may have occurred, the ability of theindividual nurse to communicate their wishes in this area may be a factor. Communicationproblems for NESB nurses have been noted byseveral authors (Jeon & Chatterworth 2007;Omeri 2006; Omeri & Atkins 2002; Alexis2002). Hawthorne (2001) postulates that NESBnurses because of communication problems,have more difficulty with registration proce-dures and qualification recognition leading to a more lengthy migration process. Communi-cation problems have been further highlightedby Brown (2005) who describes the ‘Yes Syn-drome’ in a study of NESB student nurses.Brown (2005) suggests that many culturalgroups use the ‘Yes Syndrome’ when peopletypically answer ‘yes’ to a question, but meansomething different. By saying ‘yes’ to ques-tions, the person is able to avoid the embarrass-
ment of not being understood and having torepeat himself or herself in front of people fromthe dominant culture.
As mentioned previously, our study showedthat NESB nurses rated more positively theirlevel of satisfaction with the general hospitaland ward orientation, compared to ESB nurses.The specific ward orientation was described as amore rewarding experience.These are generallyconducted as one on one session with a nurseeducator. It may be that these occasions providegreater opportunities for NESB nurses to clarifymeaning and to feel less intimidated about ask-ing questions.The fear of making language andcultural mistakes may also be lessened.
The first theme identified was career andlifestyle opportunities. OQNs described careerand lifestyle goals as the main motivating factorfor immigrating. Kline (2003) examines the rea-sons why nurses migrate, concluding that nursesmigrate because they are seeking better con-ditions and wages. Daniel et al (2001) reportssimilar reasons for nurses migrating from the Philippines to the UK, they were careerprospects and financial security. Much of the lit-erature focuses on the OQN migrating fromdeveloping countries to developed countries.There is less exploration around the reason formigration from developed to developed coun-tries.Where as OQNs from developing nationshave financial motives for migrating to devel-oped countries (Hawthorne 2001; Daniels et al2001). Some evidence for this perception issupported by Connell and Brown’s (2004) studyof Tongan and Samoan nurses. Connell andBrown (2004) found that Tongan and Samoannurses were significantly more involved in send-ing remittances to their home countries in com-parison with other migrant nurse groups. Theeffects of the pressure and obligation of sendingmoney earned in Australia back to family over-seas were not explored in this study. Exploringreasons for OQNs migration may impact on thedevelopment of adaptation programmes.
Differences in practice were noted by most
106 Volume 28, Issue 1–2,April 2008CCCCNNNN
Scott Brunero, Julie Smith and Emma BatesCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 106

OQNs. OQNs gave a range of clear descrip-tions of differences in nursing practice. Thenotion of examining differences in practice hasbeen captured by Pillette (1989). Pilette (1989)describes a phase of adjustment called the‘Indignation Phase’.This period is characterisedby cultural, professional and psychological dis-sonance. It is described as an intense period ofemotion and ambiguity and typically occurs sixand nine months post arrival.The OQNs in thisstudy had been here on average 6.2 months,their comments provide a measure of supportfor the notion of ‘professional dissonance’ as anadjustment issue. Organisations that can articu-late the observed differences in practice may beable to design better assimilation programmes.The effect of not observing differences in prac-tice may lead to negative outcomes for theOQN and patient. In support of this, Blackfordand Street (2000) study of 26 nurses found that NESB nurses learned to ignore their owntraditions and practices in the dominant Anglo-Australian culture.
Homesickness was reported by many of the OQNs. Whilst not described as a formalpsychiatric disorder, homesickness is reportedas being a potential distressing state of anxietyand depressive type symptoms (Van Tilburg et al 1996). Personality types and environmentalcharacteristics play an important part in the roleand onset of homesickness. The severity andconsequences of prolonged homesickness isunclear in the literature, but there are argu-ments for its management and monitoring, as ithas been anecdotally linked to depression andanxiety symptoms in migrants (Van Tilburg et al1996).
Using the literature and the study resultsinterventions have been designed to address thedifficult issues faced by OQNs during theiradjustment phase. An organisational and a per-sonal approach have been utilised.
Organisational interventionsIt has been argued that the development of an
organisation that values diversity is key in assist-ing the OQN through their adjustment phase(Bruhn 1996). Alexis and Chambers (2003)make a case for the need of an organisationalapproach in helping with the adjustment ofOQNs. Key elements include the notion ofopen participation, the encouragement of feed-back and existence of control at lower levels ofthe organisation. At the study site these atti-tudes and behaviours are reflected in the devel-opment of transformational leaders, personcenteredness and the growth of a practice devel-opment model of nursing care, which en-compasses the central philosophies of sharedgovernance, open participation, participatoryevaluation and emancipation or developing ofthe self (McCormack 2005). These practicechanges reflect well with recommendationsfrom Bruhn (1996), Alexis and Chambers (2003)and Davidhizar et al (1999) valuing diversity,sharing beliefs and decision-making.
To further create and encourage the valuingof diversity, an electronic book style orientationmanual for OQNs has been developed and pro-duced as a web-based resource named ‘Sign-post’. After careful review of the literature andthe data from this study, Signpost was created.Key principles in writing the manual were easeof reading and accessibility. Due to the agegroup of the nurses, it was decided to presentthe information primarily in an electronic basedformat, to allow for widespread accessibility inAustralia.The study population were primarilyY generation nurses who are broadly describedfrom a western perspective as the Internet gen-eration (Martin 2001).The suggestion from thisauthor is that this generation responds to imme-diate feedback, clear expectations from employ-ers and have clear career goals. For this reasonan electronic format has been chosen for theorientation manual. In a review of health infor-mation on the Internet, Berland, Elliot andMorales (2001) found that the information waseasily accessible and reasonable, although theydid report the readability level as too high.
107Volume 28, Issue 1–2,April 2008 CCCCNNNN
Expectations and experiences of recently recruited overseas qualified nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 107

Bridges and Thede (1996) explain that for nurs-es who use the Internet, it offers a rich sourceof accessible material, with the challenge beingin the critiquing of the contents. In a series of virtual focus groups with nurses, Dickersonand Feitshans (2003) found that nurses see theInternet as a source of communication, and aresource that’s appealing and entertaining, theyalso report that nurses found it frustrating attimes, having to learn new rules and systems.Readability level is a key issue in presentinginformation and for the orientation manual itwas kept between 11th and 14th grade usingFlesch readability statistics (Davis et al 1990).
Signpost was divided into the following sec-tions: an introduction to the electronic book,background, orientation and settling in infor-mation, nursing practice model, nursing regis-tration, role definitions, professional nursingorganisation, general living, schools, transport,accommodation, staying connected, support,how to phone home, and a frequently askedquestions section.
The creation of an organisation that respectscultural and linguistically diverse groups is essential in helping the OQN to successfullyadjust to their new working environment. In aneffort to educate the dominant culture at thestudy site the hospitals newsletter is being usedto tell an OQN narrative, using the transcultur-al assessment model as described by Dowd et al(1999). The narrative will contain the expec-tations, experiences, communication, environ-mental and social issues of the OQNsexperience. The aim of these narratives is toinfluence the dominant culture and developtheir understanding of the OQN workforce atthe hospital.
Personal approachesDowd et al (1999) describes a transculturalmodel of assessment that could be used byOQNs to assist them on their arrival to theirdestination country. At the study site this isoffered in a group or individual setting, OQNs
are given a brief overview of the model and arethen taken through the self-assessment check-list, as provided by Dowd et al (1999). OQNsthat are identified as being distressed, sufferingwith the physical, cognitive, behavioural oremotional symptoms of homesickness, are givenmore information on how best to manage thesesymptoms. Interventions used for homesicknessfall within the stress management literature.VanTilburg et al (1996) review the use of a range oftherapies, from expression of feelings, cognitivebehavioural therapy (CBT), regular telephonecalls home, and assertiveness training. At thestudy site the use of CBT interventions (forexample, challenging negative thoughts thatlead to high levels of anxiety and depression) isoffered, (Ellis 1957; Ellis & Grieger 1986),through one to one sessions or via a self direct-ed reading booklet (Brunero et al 2006).
Using a CBT framework the authors havefocused on working with the expectationsOQNs have of their destination workplace.Theuse of this approach has been linked to futurereports of job satisfaction (Wanous et al 1992).Capturing a sense of the dichotomy betweenpeople’s expectations and actual experiencemay help individuals in the adjustment process.A process of assessing the accuracy of individ-ual’s expectations before they engage in theactual experience may help shape the views ontheir work satisfaction levels. At a practical levelthis may simply mean asking new recruits to listtheir expectations, how they view their workand lifestyle, and what it’s like being in the des-tination workplace. Individuals then engagewith someone from the destination (eg recruit-ment officer) who can affirm the accuracy oftheir expectations, and alleviate any misconcep-tion and emotional distress (such as anxiety,depression and anger) that a person may havedeveloped before or during their employment.This process has been named as ‘expectationaffirmation’ and has been developed into a ques-tionnaire style template (available from theauthors).
108 Volume 28, Issue 1–2,April 2008CCCCNNNN
Scott Brunero, Julie Smith and Emma BatesCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 108

CONCLUSIONSThe organisational and personal interventionswill require ongoing evaluations. A proposal tohave a OQNs support role is being developed.The intention of the role would be to broadenthe delivery and evaluation of the interventions.Offering the ‘missing’ information and inter-ventions at the recruitment and arrival stages,may encourage nurses to feel more confidentand better equipped to settle into Australianlife. Interventions designed to provide OQNs awarm welcome and an introduction to livingand working in this locale may also help themfeel that they are an essential and importantpart of this organisation.
AcknowledgmentThis study was partly funded by a NSW Department of Health Nursing InnovationsScholarship.
ReferencesAlexis O (2002) Diversity and equality recruit-
ing and retaining overseas ethnic minoritynurses in the NHS, Nursing Management 9:22–26.
Alexis O and Chambers C (2003) ExploringAlexis’ model: Part two valuing resources,Nursing Management 10: 22–25.
Berland G, Elliot M, and Morales L (2001)Health information on the Internet, TheJournal of the American Medical Association 285:2615–2621.
Blackford J and Street A (2000) Nurses of NESBworking in a multicultural community, Con-temporary Nurse 9(1): 89–98.
Bridges A and Thede L (1996) Nursing educationon the world wide web, Nurse Educator 21:11–15.
Brown V (2005) Culturally and LinguisticallyDiverse Nursing Student Education:AGrounded Theory Study. PhD Thesis, CurtinUniversity of Technology,Western Australia.
Bruhn J (1996) Creating an organisationalclimate for multiculturalism,The Health CareSupervisor 14: 11–18.
Brunero S, Cowan D, Grochulski A and GarveyA (2006) Stress Management for Nurses, accessedat http://www.nswnurses.asn.au/infopages/5696.html on 22nd November 2007.
Connell J and Brown R (2004) The remittancesof migrant Tongan and Samoan nurses fromAustralia, Human Resources for Health 2: 1–21.
Daniel P and Chamberlain G (2001) Expecta-tions and experiences of newly recruitedFilipino nurses, British Journal of Nursing 10:254–265.
Davidhizar R, Dowd S and Newman Giger J(1999) Managing diversity in the health careworkplace, The Health Care Supervisor 17:51–62.
Davis T, Crouch M,Wills G, Miller S andAbdehou D (1990) The gap between patientreading comprehension and the readability ofpatient education materials, Journal of FamilyPractice 31: 533–538.
DeSantis L and Ugarriza D (2000) The conceptof theme as used in qualitative nursingresearch, Western Journal of Nursing Research22: 351–372.
Dickerson S and Feitshans L (2003) Internetusers becoming immersed in the virtualworld: implications for nurses, Computers,Informatics, Nursing 21: 300–308.
Dowd S, Davidhizar R and Newman Giger J(1999) Will you fit if you move to a job inanother culture, The Health Care Manager 18:20–27.
Dorian D and Jones G (2004) Nurses retentionand hospital characteristics in New SouthWales, accessed at www.econ.mq.edu.au/seminars/ER.pdf on 22 January 2007.
Ellis A (1957) Rational psychotherapy andIndividual psychology, Journal of IndividualPsychology 13: 38–44.
Ellis A and Grieger R (1986) Handbook of RationalEmotive Therapy,Vol 2, Springer, New York.
Gerrish K and Griffith V (2003) Integration ofoverseas Registered Nurses: evaluation of anadaptation programme, Nursing and HealthCare Management and Policy 45: 579–587.
Hawthorne L (2001) The globalisation of thenursing workforce: barriers confronting
109Volume 28, Issue 1–2,April 2008 CCCCNNNN
Expectations and experiences of recently recruited overseas qualified nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 109

overseas qualified nurses in Australia, NursingInquiry 8: 213–229.
Hawthorne L,Toth J and Hawthorne G (2000)Patient demand for bilingual bicultural nursesin australia, Journal of Intercultural Studies 21:193–224.
ICN (2007) International Council of Nurses.Ethical Nurse Recruitment position state-ment.Accessed at http://www.icn.ch/psrecruit01.htm#_ftn1 on 22 November 2007.
Jackson D (1996) The multicultural workplace:comfort, safety and migrant nurses, Contem-porary Nurse 5: 120–126.
Jeon Y and Chenoweth L (2007) Working withculturally and linguistically diverse (CALD)group of nurses, Collegian 14: 16–23.
Kline D (2003) Push and Pull factors in Interna-tional Nurse Migration, Journal of NursingScholarship 35: 107–111.
Konno R (2006) Support for overseas qualifiednurses in adjusting to Australian nursingpractice: a systematic review, InternationalJournal of Evidence Based Healthcare 4: 83–100.
Martin C (2001) Managing Generation Y, HRDpress, Massachusetts.
McCormak B, Manley, K and Garbett R (2004)Practice Development in Nursing, 3rd edn, Black-well, London.
Omeri A and Atkins K (2002) Lived experiencesof immigrant nurses in New South Wales,
Australia: Searching for meaning, InternationalJournal of Nursing Studies 39: 495–505.
Omeri A (2006) Workplace practices withmental health implications on recruitmentand retention and retention of overseas nursesin the context of nursing shortages, Contem-porary Nurse 21(1): 50–61.
Oxtoby K (2003) The Overseas Nurses Champ-ion, Nursing Times 99: 42–43.
Pilette P (1989) Recruitment and retention ofinternational nurses aided by recognition ofphases of the adjustment process, The Journal ofContinuing Education in Nursing 20: 277–281.
Ryan M (2003) A buddy program for interna-tional nurses, JONA 33: 350–352.
Stroebe M,Van Vilet T, Hewstone M and Willis H(2002) Homesickness among students in twocultures: antecedents and consequences,British Journal of Psychology 93: 147–168.
Van Tilburg M,Vingerhoets A and Van Heck G(1996) Homesickness:A review of theliterature, Psychological Medicine 26: 899–912.
Verschuur M, Eurelings-Bontekoe E and Spin-hoven P (2004) Associations among home-sickness, anger, anxiety, and depression,Psychological Reports 94: 1155–1170.
Wanous J, Poland T, Premack S and Davis K(1992) The effects of met expectations onnewcomer attitudes and behaviours: a reviewand meta-analysis, Journal of Applied Psychology77: 288–297.
110 Volume 28, Issue 1–2,April 2008CCCCNNNN
Scott Brunero, Julie Smith and Emma BatesCCCCNNNN
SECOND LANGUAGE WRITING STRATEGIES
By Congjun Mu
ISBN: 978-1921214-06-6; 360 pages; 2007; imprint: Post Pressed
That many overseas university students whose first language is not English lack adequate proficiency in formal academic English has become an issue of growing concern. This timely study examines the writing strategies used by three Chinese post-graduate students while writing academic papers in English. Similarities and differences between the L2 and L1 writing processes are explored and a major hindrance to acculturating into the target academic discourse community is found to be a background of reader-responsibility which is regarded as a crucial feature in Eastern rhetoric and is distinguished from writer-responsibility in English rhetoric.
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911;[email protected]; www.e-contentmanagement.com
P O S T P R E S S E D A C A D E M I C
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 110

In the global environment of today’s world,nurses must be educationally prepared to
meet the needs of people from culturally andlinguistically diverse backgrounds in order toprovide high quality care. DeSantis and Lipson(2007) outline the history of the inclusion ofcultural content in nursing education, datingfrom the influences of Florence Nightingale.They summarise the impetus to include culturalcontent, and outline recent reaffirmations to doso by various jurisdictions such as the AmericanAssociation of Colleges of Nursing, the Ameri-
can Nurses Association,The Joint Commission,and the National League of Nurses to name afew. The impetus, past and present, includesglobalisation, growing diversity in the popula-tion, bioethical issues, health disparities, and theneed to increase diversity in the nursing work-force.
In the United States, the Essentials for Baccalaureate Education (American Association of Colleges of Nursing [AACN] 1998) stipulatethat graduates of baccalaureate nursing pro-grams must have the knowledge and skills tocare for a diverse population.This entails know-ing and understanding how culture, race, socio-economic status, age, gender, religious, andlifestyle factors affect health and the provisionof care (AACN 1998). The Essentials dovetailinto the National Standards for Culturally andLinguistically Appropriate Services (CLAS) inHealth Care (US Department of Health andHuman Services, Office of Minority Health[USDHHS, OMH] 2001) which are to provide
Key Wordsculturallycompetency;nursingstudents;reflection CN
111Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 111–118.
A reflection on culture over time by Baccalaureate nursing students
ABSTRACT The aim of this retrospective descriptive study was to compare students’reflective responses to a set question 18 months apart to determine if theirunderstanding of nurses’ commitment to serve all clients regardless of age,gender, religious affiliation, or racial origin changed. One hundred and twenty-six reflections (63 pairs) were thematically analysed.Three themes were devel-oped: equal treatment; commitment to serve all clients; and ‘it’s not easy’.Cultural competency, although not yet fully operationalized in the nursingprofession, is a developmental process that goes across time. It is also more thanlearning about other cultures.Received 15 July 2007 Accepted 8 April 2008
HENDRIKA J MALTBYAssociate ProfessorDepartment of NursingUniversity of VermontBurlington VT, USA andAdjunct AssociateProfessorEdith Cowan UniversityJoondalup WA, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 111

care compatible with cultural beliefs and practices in a preferred language.1 The JointCommission (the accrediting body for health-care organisations) (2007) uses CLAS to assesswhether organisations provide culturally appro-priate care in the interest of patient safety andquality of care. The definition used by USD-HHS, OMH (2001) for cultural and linguisticcompetence is:
… a set of congruent behaviors, attitudes,and policies that come together in a system,agency, or among professionals that enableseffective work in cross-cultural situations.‘Culture’ refers to integrated patterns ofhuman behavior that include the language,thoughts, communications, actions, customs,beliefs, values, and institutions of racial, eth-nic, religious, or social groups.‘Competence’implies having the capacity to function effec-tively as an individual and an organizationwithin the context of the cultural beliefs,behaviors, and needs presented by consumersand their communities.
(USDHHS, OMH 2001: 4)
This definition is how culture was understoodthroughout this project and what had beentaught in the health promotion course duringthe junior fall semester.
Despite the stipulation to incorporate cul-tural knowledge and skills to care for a diversepopulation in nursing education, Ryan, Carltonand Ali (2000) in their survey of baccalaureatenursing programs, discovered that transculturalnursing concepts were incorporated into mostof the curricula, but that ‘wide variation existsas to content, depth, and level of integration’(Ryan, Carlton & Ali 2000: 300). Only 2.3%(89 of 205 reporting) of these programs hadformal courses in transcultural nursing. Boyle(2000), Campinha-Bacote (2006), and Lipsonand DeSantis (2007) also questioned the depthof cultural content in nursing curricula.Theseresearchers cite a lack of consensus on what
should be taught, lack of standards, limited for-mal evaluation, unstated outcome standards,lack of linguistic skill, and the need for facultyqualifications and preparation. Of concern isthat integrating cultural concepts into eachcourse tends to be very dependent on interestedfaculty members related to crowded curriculaand preparation to pass the NCLEX-RN (TheNational Council Licensure Examination, forregistered nurses).
OUR PROGRAMOur program is located in a small city in a very Caucasian rural state in Northern NewEngland.There are approximately 375 studentsin the undergraduate program. Students enter-ing the nursing program spend the first threesemesters (one-and-a-half years) completingrequired courses such as the sciences, psycholo-gy/sociology, philosophy, and electives.They arealso required to take a three credit Americanrace and racism course (focusing on race, cul-ture and gender relationships in America) duringtheir program (a university wide requirement);most nursing students take this course in theirfirst three semesters. Beginning in the secondsemester second year (sophomore Spring), stu-dents begin the nursing courses which are com-posed of theory and clinical practice.They mustalso complete their elective requirements. Facul-ty ensure that transcultural nursing concepts areintegrated throughout the curriculum. This isiterated in our strategic plan as one of the firstaction steps is to ‘develop, strengthen, and sup-port international and multicultural opportuni-ties for education and research for faculty andstudents: (e) enhance faculty sensitivity and cul-tural competencies’. There has been, however,no further discussion on what this might meanor how to measure competencies.
AIMThe current study arose out of my need todetermine if integrating cultural content (asdetermined by individual faculty) in nursing
112 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hendrika J MaltbyCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 112
courses affected students’ understanding of cul-turally appropriate care.Therefore, the aim ofthis retrospective, descriptive study was to the-matically analyse and compare students’ reflec-tive responses between two points in time todetermine if their understanding of professionalnurses’ commitment to serve all clients (clientis defined as individuals, families, groups, com-munities) regardless of age, gender, religiousaffiliation, or racial origin changed between thejunior fall (first semester third year) and seniorspring (second semester fourth year). Did theirunderstanding of cultural aspects of care changeover the length of the nursing program? Werethey able to provide examples of how cultureaffected nursing care.
METHODOLOGYUsing a convenience sample, 85 junior nursingstudents were given an in-class reflection question to complete during an October classperiod (Time 1, T-1) as part of their courserequirements.The same reflection question wasanswered by the same students 18 months laterprior to graduation (Time 2, T-2). Submissionduring their final semester was not required topass the course. Although names were attachedto the responses, once the responses werematched, the names were deleted.The two setsof responses were matched and those studentswho had completed just one reflection at eithertime period were deleted. A total of 126 reflec-tions were analysed (63 pairs). InstitutionalReview Board approval was obtained for thestudy. Students could indicate that they did notwant their responses included in the studyalthough no-one chose this option.The questionwas:
Nurses’ commitment to serve all clientsregardless of age, gender, religious affiliation,or racial origin is an essential component ofthe ANA Code of Ethics.Why is this commit-ment essential in nursing practice? How
would/did you implement it in your nursingpractice?
Responses were thematically analysed by theauthor using the steps outlined by Colaizzi(1978): reading all the descriptive data, extract-ing significant themes, formulating meanings,clustering meanings, writing an exhaustive des-cription, and identifying the basic structure ofthe concepts.The final step, seeking validationby returning to the participants, could not be implemented as students had graduated andwere lost to follow-up. A second nursing col-league audited the themes and, in her experi-ence, found them credible and based on thecollected data.
LIMITATIONSThis was a small study at one school, however ithad the advantage of assessing students overtime.The reflection question itself may have ledstudents to answer in a particular manner. Aswell, validation by the students was not possible.
RESULTSA total of 63 out of a possible 85 student res-ponses (126 reflections) were included in thestudy.The final response rate was 74%.The par-ticipants in this study are overwhelmingly white(non-Hispanic) (100%) and female (95%).Thisis similar to the American registered nurse pop-ulation where 82% are estimated to be white(non-Hispanic) and 5.7% were men (HealthResources & Services Administration 2004).Ages ranged from 20 to 47 years. Three mainthemes emerged from the data: ‘equal treat-ment’, ‘commitment to serve all clients’, and‘it’s not easy’.
Equal treatmentOne of the main themes from the analysis of theresponses is that students would treat patientsequally. Comments included: ‘Implementingequal care to all is essential in my practice’ (5,T-2); ‘I implemented this in my practice by treat-
113Volume 28, Issue 1–2,April 2008 CCCCNNNN
A reflection on culture over time by Baccalaureate nursing students CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 113

ing all patients equally and not letting my per-sonal opinions and beliefs get in the way ofpatient care’ (17, T-2); ‘Regardless of gender,orientation, race, or religion they are humansand deserve equal treatment’ (19,T-1); ‘I wouldtreat all my patients equally’ (30, T-1); ‘allclients deserve to be treated equally regardlessof their gender, age, racial origin, or religiousaffiliation’ (62,T-2); and ‘I implemented this inmy practice by treating all patients equally andnot letting my personal opinions and beliefs getin the way of patient care’ (18,T-2). Students atboth time periods were very aware that bias innursing care was unacceptable and could lead topoor quality care.This was even more evident atT-2 after students had been in several clinicalrotations: ‘I make it a point to spend the neededamount of time with each of my patients andnot neglect one, just because they are ‘not thesame as me’. I prioritise based on the neededevents not the patient’s beliefs or background’(33, T-2). A few students did state that ‘everyindividual deserves equal respect’, which is fun-damental, but added ‘and treatment’ (35,T-2).The following student stated that patient char-acteristics did not affect the care but did try toprovide culturally competent care, indicatingsome confusion between equal and equality:
I cared for patients of various ages, both maleand female, from many religious affiliationsand many different racial origins. These characteristics did not affect my care of mypatients at all. I did however try to give cul-turally competent care and ask my patients ifthere were any cultural or religious beliefsthat would change their care. (58,T-2)
Treating clients/patients ‘equally’, while a noble sentiment, seems at odds with imple-menting care that is culturally appropriate asone would not treat each patient equally butaccording to needs.The concept of equal treat-ment versus equitable treatment needs furtherdiscussion in the classroom as does the meaning
of culturally sensitive and competent care. Simi-larly, Browne et al (2002) found that nurses intheir study would make an effort to treat allpatients equally, which ‘assumes that treatingpeople the same way results in equality of care’(p. 26).As Browne and Varcoe (2006) point out,cultural sensitivity is an important concept andmust be viewed from a broad perspective thattakes into account the power relationships innurse/patient interactions. Becoming aware ofour own power, knowledge, and privilege asnurses needs to be encouraged (Browne et al2002) and may lead to care that is equitable forpatients.
Commitment to serve all clientsAnother theme was that the commitment toserve all clients was essential as it is part ofbeing a nurse and led to quality care. Student 4stated ‘If you have personal biases against a cer-tain client then you may jeopardise their qualityof care’ (T-1). Another student stated ‘Whenyou choose to be a part of the [nursing] profes-sion you are accepting the challenge of provid-ing care regardless of their religious affiliation,race, etc.’ (13,T-2). Other students commentswere in a similar vein: ‘It’s up to the nurse toput their biases aside and recognise the value ofmulticultural experiences in their practice’ (59,T-1); ‘I can’t imagine wanting to be a nurse andnot being willing to care for any patient regard-less of age, gender, religious affiliation, or racialorigin’ (43, T-2); ‘Even though I may disagree[with different life situations and differentbeliefs], I wouldn’t show that or voice my ownopinion’ (14,T-1); and ‘Nursing and health careshould be completely blind to biases’ (23,T-1).Students at T-1 were more willing to state thatthey needed more knowledge about cultures inorder to understand the patients and theirneeds. As well, they were more willing to askthe patients the questions to find out the infor-mation. The increase time in clinical practicewas evident at T-2 as students could speak from some experience about putting culturally
114 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hendrika J MaltbyCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 114

appropriate care into action but very few gavespecific examples.
The commitment to serve all clients is veryclear for these students at T-1 and T-2.They arealso in the process of becoming ‘nurses’ and,despite the hours in clinical, have little experi-ence of testing this commitment. Similar to astudy by Chalmers, Sequire and Brown (2003:9) who stated ‘nursing students also believedpractitioners must be nonjudgmental in all situ-ations’, the students in our program espousedthe belief that being nonjudgmental and non-biased was an essential trait for nurses.
It’s not easyA final theme that came from the students’responses was that it is not always easy to accepta patient’s viewpoint. Most of these are from T-2 after they had clinical experiences and wereno longer speaking hypothetically. Students pro-vided the following statements: ‘I would ques-tion why a 49-year-old woman would want togo through a pregnancy because of the compli-cations associated with their age’ (14, T-2);‘Even though I may have thought to myself,‘Wow, this person is a waste of my time!’, Iwasn’t completely deterred [from educatingthem about quit smoking]’ (28, T-2); ‘When Iwas in clinical I realised how I felt about youngmoms and moms who smoke. I did not changemy practice of care towards them’ (48,T-1); and‘A nurse may find him or herself passing judg-ments about a teenage girl that is in the hospitalfor prenatal care who is still smoking cigarettes’(53,T-2).
Students were quite honest in their feelingsabout certain patients.This particular theme fitvery closely with the previous one on commit-ment and not being judgemental. Students werefinding out that not being judgemental was noteasy. Campinha-Bacote’s (1999, 2002a, 2002b)model, The Process of Cultural Competence in theDelivery of Health Care Services, can be used as a framework for exploration and reflection in practice. She defines cultural competence as
‘the ongoing process in which the health careprovider continuously strives to achieve the ability to effectively work within the culturalcontext of the client (individual, family, commu-nity)’ (2002a: 181). There are five constructsthat comprise the model. Cultural awareness isexamining one’s own biases and culture; culturalknowledge seeks to learn about different culturaland ethnic groups; cultural skill is the ability toconduct a cultural assessment; cultural encounterencourages face-to-face interactions with cul-turally diverse clients; and cultural desire is themotivation to engage in the process of culturalcompetence. Campinha-Bacote (2002b) has depic-ted her model as a volcano: when cultural desireerupts, the health care provider will genuinelyseek cultural encounters, obtain cultural knowl-edge, conduct culturally sensitive assessments,and be humble to the process of cultural aware-ness. Use of cultural awareness assessment tools(Flowers 2004) may also be useful to begin dis-cussions about biases and judgments that canlead to discriminatory practices.
DISCUSSIONThe definition of culture and cultural compe-tence has been examined and deconstructed byvarious authors including Kirkham et al (2002)and Browne and Varcoe (2006). These authorsdescribe culture as complex and provide a his-torical context of the meaning of culture.Theyfocus on previous views of culture as being‘fixed or static’ (2006: 158). As well, those thatare considered different from ‘us’, are consid-ered as ‘other’. While the definition provided by USDHHS, OMH is not explicit regarding the ‘fixed’ nature of culture, it does have theelement of ‘other’, rather than the inclusivenessthat is necessary. American Institutes forResearch report (2002: 8) build on the defini-tion of culture that encompasses the complexityof the concept: ‘ethnicity and social status areinextricably linked, and social issues such asstereotyping, institutionalised racism, and dom-inant-group privilege are as real in the examin-
115Volume 28, Issue 1–2,April 2008 CCCCNNNN
A reflection on culture over time by Baccalaureate nursing students CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 115

ing room as they are in society at large’.Kirkham and Anderson (2002: 4) state that ‘cul-ture is commonly understood as a template orblueprint for human behavior, grounded in thevalues, beliefs, norms, and practices of a partic-ular group that are learned and shared’. It must,however, be seen in context within ‘historical,social, economic, and political relationships andprocesses’ (Anderson & Kirkham 1999, cited byBrowne & Varcoe 2006: 162).
Beal (2005: 7) suggests that the ‘specificcompetencies for delivering culturally com-petent care have not yet been fully articulated’but feels that it does contribute to patient out-comes. There are a variety of teaching tech-niques that can be used to engage students inthe process of becoming culturally competentsuch as role play (Shearer & Davidhiza 2003),using exemplars from literary journalism (An-derson 2004), and using web-based interactions(Kennell, Nyback & Ingalsbe 2005). Also, dif-ferent experiences such as with the homeless(Hunt & Swiggum 2007), immigrant groups(Moch et al 1999;Warner 2002), and rural pop-ulations (Thomas et al 2003) can be included inthe curriculum. Exchanges, faculty led pro-grams abroad, and immersion experiences arealso invaluable in helping students expand theirknowledge and cultural competency (Duffy2001; Hoffmann et al 2005; Ryan & Twibell2002). Barnes (2004) provides a very detailedlist and explanation of various strategies thatcan be implemented to influence cultural en-gagement of students and practicing nurses.
CONCLUSIONIt would be impossible for nurses to have aworking knowledge of all cultures. They can,however, be aware of the role of culture (in itsbroadest sense) in providing care. Cultural com-petency, although not yet fully operationalisedin the nursing education, is a developmentalprocess that goes across time.There also needsto be a focus on outcome criteria (Boyle 2000;Campinha-Bacote 2006; Gilbert 2002) for grad-
uating students related to the provision of culturally competent nursing care. Culturalcompetency needs to be implicit and explicit inour nursing education programs not only toenhance quality client care but also to advancenursing as a profession.
The more time that I have spent in clinicalrotations, the more interactions I have hadwith clients and I realize now the importanceof religion, culture and other practices on aclient’s wellbeing. Nursing is not only aboutgiving medications and getting clients readyfor procedures; it is about building interac-tions and relationships with clients. Relation-ships cannot be formed if there are hiddenjudgments or ignorance from the nurse abouta particular client. (25,T-2)
AcknowledgmentsThank you to the students who were involved inthis study.You have taught me as well.
Endnote1 All 14 CLAS Standards are listed at: http:
//www.omhrc.gov/templates/browse.aspx?lvl=2&lvlID=15
ReferencesAmerican Association of Colleges of Nursing
(1998) The essentials of baccalaureate education.Washington, DC.
American Institutes for Research (2002) TeachingCultural Competence in Health Care:A review ofcurrent concepts, policies and practices. Reportprepared for the Office of Minority Health,Washington, DC.
Anderson KL (2004) Teaching cultural compe-tence using an exemplar from literary journal-ism. Journal of Nursing Education 43: 253–259.
Barnes LL (2004) Concept Paper: Culturallycompetent care. Commissioned for the ConsensusBuilding Meeting for the Culturally competentNursing Modules project, Office of MinorityHealth.Washington, DC:American Institutesfor Research.
Beal G (2005) Knowledge and action: Developing
116 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hendrika J MaltbyCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:27 PM Page 116
cultural competence. Journal of PsychosocialNursing and Mental Health Services 43: 7.
Bloomberg School of Public Health, Center forCommunication Programs (2002) Questionnairefor Values Clarification. Johns Hopkins.
Boyle JS (2000) Transcultural nursing:Where dowe go from here? Journal of Transcultural Nursing11: 10–11.
Browne AJ and Varcoe C (2006) Critical culturalperspectives and health care involving Aborig-inal peoples. Contemporary Nurse 22: 155–167.
Browne AJ, Johnson JL, Bottorff JL, Grewal S andHilton BA (2002) Recognizing discriminationin nursing practice. Canadian Nurse 98: 24–27.
Campinha-Bacote J (1999) A model and instru-ment for addressing cultural competence inhealth care. Journal of Nursing Education 38:203–207.
Campinha-Bacote J (2002a) The process of cul-tural competence in the delivery of healthcareservices:A model of care. Journal of TransculturalNursing 13: 181–184.
Campinha-Bacote J (2002b) A culturally con-sciously model of care, accessed at http://www.transculturalcare.net/Cultural_Competence_Model.htm
Campinha-Bacote J (2006) Cultural competencein nursing curricula: How are we doing 20years later? Journal of Nursing Education 45:243–244.
Chalmers K, Sequire M and Brown J (2003)Health promotion and tobacco control: Studentnurses’ perspectives. Journal of NursingEducation 42: 106–112.
Colaizzi P (1978) Psychological research as thephenomenologists view it, in Valle R & King M(Eds) Existential-Phenomenological Alternatives forPsychology, Oxford University Press, New York.
DeSantis LA and Lipson JG (2007. Brief history of inclusion of content on culture in nursingeducation. Journal of Transcultural Nursing 18:7S–9S.
Duffy ME (2001) A critique of cultural educationin nursing. Journal of Advanced Nursing 36:487–495.
Flowers DL (2004) Culturally competent nursingcare:A challenge for the 21st century. CriticalCare Nurse 24: 48–52.
Gilbert MJ (Ed.) (2002) Principles and Recom-mended Standards for Cultural Competence Educa-
tion of Health Care Professionals.The CaliforniaEndowment, Los Angeles CA.
Health Resources & Services Administration(2004) Preliminary Findings: 2004 NationalSample Survey of Registered Nurses.Washington,DC: US Department of Health and HumanServices, accessed at http://bhpr.hrsa.gov/healthworkforce/reports/rnpopulation/preliminaryfindings.htm
Hoffmann RL, Mesmer PR, Hill-Rodriguez DL andVazquez D (2005) A collaborative approach toexpand clinical experiences and cultural aware-ness among undergraduate nursing students.Journal of Professional Nursing 21: 240–243.
Hunt RJ and Swiggum P (2007) Being in anotherworld:Transcultural student experiences usingservice learning with families who are homeless.Journal of Transcultural Nursing 18: 167–174.
Jeffreys MR (2000) Development and psycho-metric evaluation of the transcultural self-efficacy tool:A synthesis of findings. Journal ofTranscultural Nursing 11: 127–136.
Joint Commission (2007) Hospital, language andculture, accessed at http://www.jointcommission.org/PatientSafety/HLC/
Kennell LS, Nyback MH and Ingalsbe KS (2005)Increasing cultural competence throughasynchronous web-based interactions betweentwo nursing programs. Journal of NursingEducation 44: 244.
Kirkham SR and Anderson JM (2002) Postcolonialnursing scholarship: From epistemology tomethod. Advances in Nursing Science 25: 1–17.
Kirkham SR, Smye V,Tang S,Anderson J, Blue Cand Browne A (2002) Rethinking culturalsafety while waiting to do fieldwork: Methodo-logical implications for nursing research.Research in Nursing and Health 25: 222–232.
Lipson JG and Desanti, LA (2007) Current ap-proaches to integrating elements of culturalcompetence in nursing education. Journal ofTranscultural Nursing Supp 18: 10S–20S.
Moch SD, Long GL, Jones JW, Shadick K andSolheim K (1999) Faculty and student cross-cultural learning through teaching healthpromotion in the community. Journal of NursingEducation 38: 238–240.
Office of Minority Health, US Department ofHealth and Human Services (2000) NationalStandards for Culturally and Linguistically Appropriate Services (CLAS) in Health Care.
117Volume 28, Issue 1–2,April 2008 CCCCNNNN
A reflection on culture over time by Baccalaureate nursing students CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 117

Federal Register, 65(247): 80865–80879.Rockville, MD.
Preacher KJ (2001) Calculation for the chi-squaretest:An interactive calculation tool for chi-square tests of goodness of fit and indepen-dence, accessed at http://www.psych.ku.edu/preacher/chisq/chisq.htm
Rew L, Becker H, Cookston J, Khosropour S andMartinez S (2003) Measuring cultural aware-ness in nursing students. Journal of NursingEducation 42: 249–257.
Ryan M & Twibell RS (2002) Outcomes of atranscultural nursing immersion experience.Journal of Transcultural Nursing 13: 30–39.
Ryan M, Carlton K and Ali N (2000) Transculturalnursing concepts and experiences in nursingcurricula. Journal of Transcultural Nursing 11:300–307.
Shearer R and Davidhizar R (2003) Using roleplay to develop cultural competence. Journal ofNursing Education 42: 273–276.
Thomas MD, Olivares SA, Kim HJ & Beilke C(2003) An intensive cultural experience in arural area. Journal of Professional Nursing19:126–133.
US Department of Health and Human Services,Office of Minority Health (2001) NationalStandards for Culturally and Linguistically Ap-propriate Services in Health Care: Final Report.Rockville MD:Author.Available from: http://www.omhrc.gov/assets/pdf/checked/finalreport.pdf
Warner JR (2002) Cultural competenceimmersion experiences. Public health amongthe Navajo. Nurse Educator 27: 187–190.
118 Volume 28, Issue 1–2,April 2008CCCCNNNN
Hendrika J MaltbyCCCCNNNN
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. [email protected]; www.e-contentmanagement.com
• Editorial — Ravi Kanbur, Paul Shaffer,Nguyen Thang, Ellen Bortei-Doku Aryeetey
• Combining Survey and EthnographicMethods to Improve Evaluation ofConditional Cash Transfer — Michelle Adato
• Poverty Dynamics and Life Trajectories inRural Bangladesh — Bob Baulch, Peter Davis
• On Trying to be Q2: Merging Methods for aTechnical Minded Client — Nilakshi de Silva,Gunetilleke Neranjana
• Resolving Conflicting Evidence on ‘GMOs’ in Rural India: The Warangal Method — Ronald J Herring
• Trade Liberalisation and Childhood Povertyin Vietnam: A Q2 Social Impact Analysis —Nicola Jones, Ngoc Anh Nguyen, Thu HangNguyen
• The Balance of All Things: ExplainingHousehold Poverty Dynamics in 50 Villages of Gujarat, India — Anirudh Krishna, J Daniel Lecy
• Combining Quantitative and QualitativeResearch to Further Our Understanding of Poverty Dynamics: Some MethodologicalConsiderations — David Lawson, David Hulme, James Muwonge
• Combined Methods in Poverty Analysis:Experiences from Namibia — Sebastian Levine, Benjamin Roberts
• Community-based Change Ranking toAssess the Impact of a Programme for theUltra Poor — Munshi Sulaiman, Imran Matin
ee ontent PTYLTDmanagementC
USING QUALITATIVE AND QUANTITATIVEMETHODS IN DEVELOPMENT POLICY
Q-squared Decision Making in the Case of Poverty AnalysisEdited by Paul Shaffer (University of Toronto), Ravi Kanbur (Cornell University), Ellen Bortei-Doku
Aryeetey (University of Ghana) and Nguyen Thang (Vietnam Academy of Social Sciences)
A special issue of International Journal of Multiple Research Approaches, volume 2 issue 2ISBN 978-1-9213482-6-6; iv + 92 pages; s/c; October 2008
Course Coordinators are invited to contact the Publisher for an adoption evaluation copy.
* * N O W A V A I L A B L E * *
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 118

Key Wordstransculturalnursing; culture;culturalcompetency;simulation;cultural diversity;nursing education CN
119Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 119–128.
Integrative simulation: A novelapproach to educating culturally
competent nurses
ABSTRACT Nursing education faces many challenges as a result of the population’sincreased cultural diversification. Of primary importance is the need to prepareculturally competent nurses to provide care in both urban and remote ruralareas.This paper presents a HRSA funded program that utilises simulations toprovide culturally diverse learning opportunities for both university-based anddistance learning students. Cases are developed using focus groups and individ-ual interviews.The information is used with standardised patients to developvignettes that are loaded into a web-based virtual hospital where studentsconduct interviews with culturally diverse patients.The information obtainedduring the interview is then used to provide hands-on care to a highperformance simulator (simulated mannequin).The encounters are videotapedfor use in debriefing sessions with the students, for educational programs in theclassroom, and for video-streaming to web-based distance students. Students inthe debriefing sessions and classroom participate in a review of the videotapeusing the Personal Response System to respond to question. Through theculturally enhanced integrated simulation, students have an opportunity toaddress clinical situations and the impact of culture in a relatively safe non-threatening environment where the impact of their biases can be explored.
Received 14 July 2007 Accepted 9 April 2008
Authors continued/ ...
CAROLYN M RUTLEDGESchool of Nursing
Old Dominion UniversityNorfolk VA, USA
PHYLLIS BARHAMSchool of Nursing
Old Dominion UniversityNorfolk VA, USA
LYNN WILESSchool of Nursing
Old Dominion UniversityNorfolk VA, USA
RICHARDEAN S BENJAMINSchool of Nursing
Old Dominion UniversityNorfolk VA, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 119

INTRODUCTION
Healthcare is facing a number of challenges.First and foremost is the need to provide
care to culturally diverse individuals in bothurban and remote rural areas (Paterson,Osborne & Gregory 2004). Nursing educationprograms have sought to develop strategies that could provide students with cost-effectivelearning opportunities that would increase theircultural competency while increasing the num-ber of nurses providing care in remote areas(Nairn et al 2004; Paterson, Osborne & Grego-ry 2004; Rutledge et al 2004). Strategies thathave been instituted include computer-basedprograms, high performance simulators, stan-dardised patients, and culturally oriented cur-ricula (Nairn et al 2004; Paterson, Osborne &Gregory 2004; Rutledge et al 2004). Manyschools provide some of these components;however, very few have linked them together.
BACKGROUNDDue to globalisation, many countries have ex-perienced a significant shift in the racial andethnic composition of their populations. Aprime example of this is in the United Stateswhere it is projected that by the year 2025about 40 percent of adults and 48 percent ofchildren in the United States will be from racialand ethnic minority groups (Department ofHealth and Human Services [DHHS] 1999). Bythe year 2050, people of color will represent onein three Americans (US Census Bureau 2000).
Minority Americans are poorer (incomesbelow 200% of poverty) than white Americans(Kaiser Family Foundation 2007). Approxi-mately 70 percent of elderly Hispanics and two-thirds of elderly African Americans are poor or
near poor (Kaiser Family Foundation 2007). In2005, five million more Americans were un-insured than in 2001. People of color from low-income families are at greater risk of beinguninsured, and therefore more likely to experi-ence disparities in access and quality of health-care (Kaiser Family Foundation 2007).
The National Healthcare Disparities Report[NHDR] (2005) stated that disparities in theAmerican healthcare system still do exist inrelationship to race, ethnicity, and socioeco-nomic status. According to the NHDR (2005),Hispanics and the poor are experiencing moredisparities in quality of care than any other pop-ulation. Minority populations rate their overallhealth worse than non-Hispanic whites and thepoor of all races report worse health than high-er income populations (Kaiser Family Founda-tion 2007).
There is a definite relationship between lifespan and mortality in minority populations.African Americans have a higher death rate frombreast, lung, and colorectal cancer than any ofthe other ethnic group (Kaiser Family Founda-tion 2007). Hispanics, African Americans andAmerican Indians/Alaskan Natives are morelikely to develop and die from diabetes than anyother ethnic group (DHHS 2005). The rate ofnew AIDS cases among African Americans wasover three times higher than the rate of amongwhites in 2003 (DHHS 2005). HIV is one of thefive leading causes of death for African Ameri-cans and Hispanics between the ages of 25 and44 years (Kaiser Family Foundation 2007).
In order to achieve and maintain health, in-dividuals need a source of health information,screening, and treatment that is accessible andculturally sensitive (Council on Collegiate Edu-
120 Volume 28, Issue 1–2,April 2008CCCCNNNN
Carolyn M Rutledge et alCCCCNNNN
PHYLLIS EATONSchool of Nursing
Old Dominion UniversityNorfolk VA, USA
KAY PALMERSchool of Nursing
Old Dominion UniversityNorfolk VA, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 120

cation for Nursing [CCEN] 2003).The ability ofindividuals to obtain the most effective andappropriate care is affected by the ability of thepatient to seek care and share concerns with theprovider honestly and without fear. Healthcareproviders should have an awareness and under-standing of their patient’s culture in order toprovide appropriate, quality healthcare (CCEN2003). It is imperative that health professionalsrecognise their own biases and preconceivedassumptions in order to overcome their impacton the provider–patient relationship (Nairn et al2004; Rutledge et al 2004;Varcoe & McCromick2006).
A model that can assist the healthcare profes-sional in becoming culturally competent is theProcess of Cultural Competence in the Deliveryof Healthcare Services model by Campinha-Bacote (2003). According to this model, culturalcompetence is a process and not an event. Theprocess of cultural competence consists of fiveinter-related constructs: cultural desire, culturalawareness, cultural knowledge, cultural skill,and cultural encounters.This model stresses thatthere is a direct relationship between the healthcare professional’s level of cultural competenceand their ability to provide culturally responsivecare. Utilisation of this model can enhance thecultural competence of the healthcare profes-sional, and thus improve the access to healthcareand quality of care to all populations.
The purpose of this paper is to present anintegrative program that utilises simulation toprovide baccalaureate nursing students withexperiences needed to become culturally com-petent. This program was funded by a HealthResources and Services Administration (HRSA)grant from the United States Department ofHealth and Human Services. The InstitutionalReview Board at the University reviewed andapproved the proposal for the protection ofhuman subjects. All data was presented inaggregate form and no names or other identi-fiers were included with any of the data. TheCampinha-Bacote Model of Cultural Compe-
tency (2003) was used as the framework for thedevelopment of this program. Data indicatesthat the program has been well-received by the students, standardised patients, and faculty.Students are now able to address cultural issuesthrough relatively safe and non-threateningencounters with cultures they may not other-wise be exposed.
OVERVIEW OF PROGRAMThis nursing curriculum offers pre-licensure(university-based) and post-licensure (distanceweb-based) students a unique, pragmatic learn-ing environment utilising a combination of a virtual web-based hospital, video-taped highperformance simulator (HPS) experiences andthe use of a personal response system (PRS) toenhance learning through meaningful prepara-tion, simulated cases, feedback and debriefing.The cases presented through this virtual formathave been enhanced to include cultural issuesthat may significantly impact the care of thepatient presented. Faculty has been trained to provide the cultural content through threeHRSA funded workshops with Campinha-Bacote (2003), and two other in-house work-shops. In addition, Campinha-Bacote serves as aconsultant to the project. Cultural diversity isdefined in a broad context based on ethnicity,age, gender, religion, sexual orientation, and/orspecial concerns such as disability. Simulationcases are developed from findings obtained dur-ing focus group meeting with various culturalgroups. By using videotaped simulation encoun-ters and the virtual web-based hospital, bothuniversity-based and distance learning studentsare able to participate in similar learning expe-riences.The program is outlined in Figure 1.
FOCUS GROUPSFocus groups are utilised to develop the virtualscenarios so that the students are provided withrealistic virtual encounters that are based on thepatient rather than educator perspectives. Focusgroups, originally called focused interviews,
121Volume 28, Issue 1–2,April 2008 CCCCNNNN
Integrative simulation:A novel approach to educating culturally competent nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 121

have been commonly used in social scienceresearch to collect information about the per-ceptions of individuals on a defined area ofinterest in a permissive, non-threatening envi-ronment (Morgan & Krueger 1998). Using adiscussion format, focus group sessions areguided by a skilled facilitator who encouragesparticipants to share their ideas and percep-tions. They are seen as an ideal way to collectinformation about cultural diversity perspec-tives for this program. The information ob-tained through the focus groups is being used to develop the clinical scenarios and train thestandardised patient for the virtual hospitalencounters.
Specific emphases of the focus group sessionsare on culture-specific barriers to care andeffective methods of overcoming the barriers.The focus group members are encouraged toshare their experiences, desires, and recom-mendations regarding healthcare. A semi-struc-
tured discussion guide focusing on barriers andfacilitators to access, quality of care, interactionwith healthcare providers and other factorsassociated with inpatient and outpatient settingsis used by the facilitator to direct the discussion.Topics included in the guide include:
1. What barriers have you encountered as a( ) in seeking health care?
2. What positive encounters have you hadwith health care providers?
3. Where do you prefer to receive your health-care and why? and
4. What could providers do to make yourhealthcare encounters more relevant oruseful?
Each focus group meets one time and consistsof 5–10 (average of 8) volunteers from the cultures that are prevalent in our region or atthe distance sites.The participants are recruited
122 Volume 28, Issue 1–2,April 2008CCCCNNNN
Carolyn M Rutledge et alCCCCNNNN
FIGURE 1: INTEGRATED CULTURAL COMPETENCY SIMULATION PROGRAM
Focus Group
Monarch General Hospital
(Virtual Hospital)
High Performance Simulator (Simulated
Mannequin)
Video Taping
Personal Response System (PRS)
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 122

from cultural groups, church programs, andcommunity organizations through word ofmouth or flyers. Each participant completes a consent form prior to participating in thegroup. Participants have consisted of AfricanAmerican women and then men, Filipino Amer-icans, abused women, lesbians, gays, NativeAmericans, the military, and the elderly. A facil-itator leads each group while a secretary takesnotes as well as records the encounter on anaudiotape. Once the encounter is over, the sec-retary reviews the audiotape and transcribes thenotes for use in developing the virtual scenar-ios. No names or other identifiers are used inconjunction with the data. The focus grouptranscripts are systematically analyzed forthemes and patterns using methods describedby Miles and Huberman (1994).
Monarch General Hospital (virtual hospital)Monarch General Hospital (MGH), a full-serv-ice computer generated virtual learning plat-form developed by the undergraduate faculty inthis program, is used to provide students withany-time/any-place practice options via theweb.This interactive learning venue allows forrepetitive practice opportunities and the inte-gration of culturally focused cases. Develop-ment of patient ‘full-motion video clips’ thatrespond to typed questions allows students toquery patients and receive a response includingverbal and body language cues mimicking actualencounters. A culturally diverse virtual patientpopulation is limited only by the imagination ofthe creator/writers of the program.The use ofMonarch General Hospital peopled with a cul-turally diverse patient population provides stu-dents access and exposure to virtual patientsdeveloped to expand cultural horizons. Studentsare able to practice obtaining a health history or communicating professionally with virtualpatients. The virtual patient format not onlyprovides access to culturally diverse encountersthat may not be available in the student’s com-
munity, it allows for repetition of encountersenhancing both competency and confidence.
Each virtual patient scenario is developedbased on the information obtained during the focus groups, individual interviews, and areview of literature focusing on various cultures(Base-Smith & Campinha-Bacote 2003; Brooks1992: Purnell & Paulanka 2008).The faculty isthen able to tailor each scenario to meet thelearning needs of the students in their particularclasses.The faculty works closely with the stan-dardised patient program at a local medicalschool in training standardised patients (livepatient actors) to present the cases. The stan-dardised patient provides both verbal and non-verbal responses to a set of questions whilebeing videotaped.Written consent is obtainedfrom all standardised patients prior to taping.The videotapes are edited and vignettes are cre-ated that are linked to a lexicon based on termsthat should be used by students during an inter-view.The vignettes are then loaded onto a com-puter program for access as part of MGH.
At the current time, only faculty and stu-dents in the program have access to MGH.Both pre-licensure university-based and post-licensure distance students access the virtualpatients in the Ambulatory Clinic of MGHthrough an internet address, using their univer-sity student e-mail name. Once in the virtualhospital, students access a patient based on the course in which they are enrolled. A photo-graph of the patient along with the ‘chief complaint’ appears on the student’s computerscreen.The student then types questions for thepatient. The patient’s video-taped response istriggered by the key word/s in the question.Students collect health history data by success-fully interviewing the patient. Repetition ofinterviewing patients throughout the semesterallows students to become adept at history tak-ing/data gathering and allows the faculty todetermine student accuracy and competencewhile providing feedback and corrections. Bothpre-licensure university-based and post-licen-
123Volume 28, Issue 1–2,April 2008 CCCCNNNN
Integrative simulation:A novel approach to educating culturally competent nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 123

sure distance students use the data gatheredduring the web-based interview to develop aconcise, yet thorough report of the patient’sinformation as they would in a patient’s chart.The university-based students prepare a careplan or concept map to plan appropriate nurs-ing and intra-disciplinary actions. Using thenursing care plan/concept map, the studentsthen provide hands on care to the High Perfor-mance Simulator (simulated mannequin) duringtheir in-school lab experience.This enables thestudents to address the physical needs of thepatient while considering the cultural impact.Meaningful preparation prior to the simulationexperience is a key to success in the lab, just asit is a key to success in the hospital.
High performance simulator(simulation mannequin)In order to prepare students for diverse clinicalpatient situations, the students spend time ineach course practicing their skills and demon-strating their competencies on high perform-ance simulators (HPS). The clinical laboratorysetting consists of two high performance simu-lators, three Vita-Sim Annies, one Sim kid, and avirtual intravenous (IV) trainer.This high fideli-ty equipment is housed in a newly remodeledskills laboratory that includes medical-surgical,critical care, pediatric, and women’s health/OBareas.
When the students arrive in the HPS lab,they are ‘introduced’ to the patient for whomthey should be prepared to provide care. Next,students are assigned a character for the simu-lation role play including but not limited to primary nurse, physician, health care teammember, or family member. The scenario co-ordinator gives report to the students to set the stage and the simulation scenario begins.The scenario is based on the interview the stu-dent had with the patient during the MGHencounter. Students are expected to providecare to the patient, and respond to the patientand family’s physical, psychosocial, and cultural
needs. A patient chart including a patient histo-ry, physician orders, laboratory and diagnosticdata is available to the student. Additionally, thesupplies needed to care for the patient are in thesimulation room or simulation lab store room.Students are expected to discern what equip-ment will be required as well as demonstratepsychomotor competence in completing proce-dures.A faculty member has the ability to moni-tor the simulation experience and alter theprogrammed response to the scenario based onthe student’s response, or lack thereof, to cues.
Ceiling mounted video cameras are strategi-cally located to record the students as theyinteract as a team with the simulated patient. Asthe students get involved in the case, they havestated that they quickly forget the video is run-ning. The interactions may be simultaneouslybroadcast to fellow students participating in thesame class for real time peer review or viewedby faculty on the office computer. Upon com-pletion of the scenario, the students may moveto the classroom setting to review the video anddebrief their performance. Students are provid-ed a DVD copy of their own interaction and areable to reflect on their performance duringdebriefing with faculty or peers. Prior to usingthe scenarios outside of the actual classroom, allstudents involved provide written permission.
Personal response system (PRS)The Personal Response System (PRS) is used toenhance the students’ learning related to theHPS activities. Students gather in a room andwatch the videotaped encounter with the patientsimulator.These videotaped encounters can beused with the students that just participated inthe experience or as a learning experience withother students in the class. Faculty members caninterject written questions about the scenario orstudent response on the screen. Questions canbe prepared ahead of time on PowerPoint©
slides or added during the class. Students thenuse their PRS system to log in and answer thequestion.This system enhances instruction and
124 Volume 28, Issue 1–2,April 2008CCCCNNNN
Carolyn M Rutledge et alCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 124

critical thinking by engaging the student in anactive learning process and stimulating discus-sion when there are divergent responses.
The Personal Response System (PRS) is aremote with buttons that are pressed by stu-dents in order to answer questions posed inclass. This format encourages all students toactively participate in the classroom discussionas well as provides the faculty with an assess-ment of the students’ knowledge.The PRS usesinfrared wireless transmitters to allow studentsto respond to multiple choice, true/false, ornumerical questions using the click of a button.At the end of the faculty pre-set response time,the distribution of student responses is dis-played in color on the screen.The distribution isvisible to both the faculty and the participants;however individual scores are not displayed onthe screen.This enables the faculty to determinewhether key points are being grasped thusassisting to direct the flow of the session. Addi-tionally, the item analysis provides students withimmediate feedback about their response whilemaintaining student anonymity. Upon the com-pletion of the assessment, student grades can beimported directly into a variety of course man-agement systems such as Blackboard.
Example of virtual encounterOne of the cases developed for the programfocuses on an overweight, elderly,African Amer-ican woman who works at a job that does notprovide her with health insurance. She suffersfrom diabetes, hypertension and joint pain.Thiscase was chosen because of its many culturalimplications, its prevalence, and its managementdifficulties (Base-Smith & Campinha-Bacote2003). In order to obtain patient oriented infor-mation for the development of the scenario, afocus group and individual interviews were con-ducted. During the focus group and interview,several themes emerged.These included feelingsthat their care might be negatively affected dueto their ethnicity and lack of insurance; thatproviders often did not tailor their recommen-
dations to meet their cultural needs; that manyproviders were not attentive; and that someproviders did not treat them with the respectthey felt they deserved. Specific concerns forthe focus group members included the impactthat financial constraints, dietary preferences,safety, their role in the family, and cultural viewsregarding weight could have on their health andability to make needed behavioral changes. Posi-tive factors were associated with providers thattook the time to find out what lifestyle changeswould work in their lives and providers whoseemed truly interested in helping them. Partic-ipants in the focus group stated that they wouldseek providers who demonstrated competenceand caring over the provider’s ethnicity.
The information from the focus group wasthen utilised to develop the scenario for MGH.An African American woman was hired fromthe standardised patient program at the localmedical school. The standardised patient (SP)was trained in the scenario came to the video-taping dressed in clean but plain attire. Hercharacter represented an individual with dia-betes, hypertension, and joint disease. A facultymember cued the SP by asking the questionsthat a student should ask during an interview.The SP responded using terms and expressionsthat would be culturally appropriate. For ins-tance, the SP stated that she couldn’t pay for allher medications due to having no insurance.Thefoods that were recommended were not whather family tended to eat. She also brought upsafety issues impacting walking. At the end ofthe scenario, the SP stepped out of her charac-ter role and presented information to the stu-dents regarding cultural issues they needed toconsider when caring for a patient with the cul-tural background that was presented.
The students then develop a concept mapbased on the information they obtained duringthe interview. The concept map includes therole of different disciplines as well as familymembers in the care of the patient once hos-pitalized. The students use this information as
125Volume 28, Issue 1–2,April 2008 CCCCNNNN
Integrative simulation:A novel approach to educating culturally competent nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 125

they provide care to the high performance sim-ulator (HPS). The HPS has been programmedwith different responses prior to the studentencounter. Physical conditions can be presentedsuch as attaching a leg that has an abscess as aresult of her diabetes or giving the patientCheyne-Stokes breathing.The lab values that arepresented can represent problems such ashyperglycemia, hyperlipidemia, or kidney fail-ure. The students are expected to respond tothe patient and family needs considering theinformation they obtained during the interviewthey had with the patient during the MGHencounter.
The encounter with the HPS is videotaped.This videotape can be used with the PersonalResponse System (PRS) to debrief the studentsthat participated in the case, to educate a groupof students in the classroom, or to provide educational opportunities to distance learningstudents participating in the same class. Duringthe debriefing and classroom encounters, thevideotape is shown.The instructor can stop thevideotape and asks questions that are typed ontothe screen.The students can respond using thePRS. The instructor can then provide infor-mation and stimulate discussion based on thestudents’ responses. For instance, the instructormay ask the student if the nurses in the videoaddressed the diabetic patient’s need to loseweight in a culturally sensitive manner.The stu-dent can select a yes/no response using thePRS. Once those scores are tallied, the ins-tructor can give the student a choice of fourresponses that might have been more culturallysensitive. Based on the tallies of the scores, theinstructor can then stimulate discussion onwhich item would be most appropriate andwhy.
In order to provide similar information topost-licensure distance students, the encountercan be video-streamed onto the web. The stu-dents can review the videotape and respond toquestions regarding the encounter. The ques-tions can either be responded to during a chat
room encounter, through the discussion boardon Blackboard, or through written assignments
EvaluationInitial data suggests that the integrative simula-tion program has been well received.The indi-viduals that participated in the focus groupsexpressed how much they appreciated havinghealth care professionals interested in hearingtheir ‘story.’ They believed that the healthcarethey received would be substantially better iftheir views were taken into consideration.Thefocus group leader felt that the participantswere very open with their views on health care.They found that the information obtained waseasily utilised for the development of the patientscenarios for Monarch General Hospital.
The scenarios for Monarch General Hospitalare in the pilot phase.The standardised patientsused to depict each scenario have felt that thescenarios accurately depict their culture andissues they have encountered in healthcare. Areview of the scenarios by experts in the fieldhas supported the accuracy of the scenarios.Students are able to have encounters withpatients representing cultures they may notreadily see in the clinical setting.The encountersare standardised so that the faculty is able toassess performance through various classroomassignments. Many of the assignments now con-tain a cultural emphasis that was not present inthe past. Faculty has found the development ofthe cases to be relatively easy. The cases haveallowed them to explore the students’ aware-ness and knowledge related to the provision of healthcare to members of various culturalgroups. Students have found that they needassistance in initially navigating through theMonarch General format. Plans are in place tosimplify the use of MGH and provide the stu-dents with additional training.
The high performance simulators (HPS) havebeen well received by the patients and faculty.The students have stated that they feel the HPSexperience prepares them for clinical encoun-
126 Volume 28, Issue 1–2,April 2008CCCCNNNN
Carolyn M Rutledge et alCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 126

ters. For instance, several students were in-volved in a code shortly after practicing a codeon the simulator. They felt that the code wentmore smoothly than in the past as a result of the practice sessions with the HPS. They evenrequested to see their previous video and havefuture sessions with the HPS. Faculty have beenpleased that the students have practiced variouspatient encounters prior to working with realpatients. This has resulted in better preparedstudents in the clinical setting. In addition, fac-ulty can request that students review proce-dures with the HPS when they demonstratedifficulty.
Both faculty and students have given positivefeedback about the personal response system(PRS). Faculty commented that the InterwritePRS software is easy to learn and use, the pro-gram allows for a variety of question formats,and faculty can choose whether to display quizquestions all at once or interspersed throughoutthe content. Faculty are pleased that assign-ments are graded by the PRS program and fac-ulty only need to generate a quiz report. Theability to receive immediate feedback about stu-dent knowledge was cited as a helpful teachingtool since it allows the faculty to decide theamount of time that needs to be dedicated toeach aspect of the course content being evaluat-ed. Qualitative student comments include posi-tive feedback at being able to have immediatefeedback about an assignment score.They alsosaw the PRS as a ‘safe’ way to participate in classby answering questions without ‘risking’ statinga wrong answer in front of their peers.The stu-dents commented that the use of PRS through-out the class session requires them to pay moreattention in class since they never know when aquiz question will pop up which resulted inimproved test scores.
Students are currently involved in complet-ing assessment tools to assess their level of cul-tural competency prior to participating in theprograms, at set intervals during the program,and at the completion of the program. These
include surveys on general cultural competencyand focus areas such as disability, alternativelifestyles, obesity, and the elderly.The culturalcompetency of the students is also assessedthrough course assignments, clinical logs, andthe Clinical Performance Appraisal (a final paperwhere students explore their strengths andweaknesses as a nurse).
CONCLUSIONThe simulated patient program provides anexcellent format for overcoming many of thebarriers encountered in nursing education.First, the simulated experience enables studentsto experience diverse situations in a controlledenvironment prior to working with actualpatients. Students are able to make mistakeswithout compromising the safety of theirpatients. Through the debriefing, the studentsare able to learn from the encounters and devel-op strategies to overcome their weaknesses.Once weaknesses are identified, the studentsare able to practice their newly acquired skillsusing the MGH scenarios or the HPS.The stu-dents can also review their videos as often asthey deem necessary.
Through simulation, all students are able toparticipate with culturally-oriented patient situ-ations that are deemed important for nursingstudents. It is not left up to chance in the real-life hospital environment where certain patientencounters may not be readily available to stu-dents. Furthermore, the students are able tofocus on cultural issues and address the impactof their biases on patient care. The MGHencounters enable students to learn how cultureimpacts health and develop strategies to assistdiverse patients in maximising their health.
One of the difficulties often faced in provid-ing web-based distance education is the abilityto assess the clinical skills of students.Throughon-line encounters with the patients in MGHhospital, the distance students can interviewpatients from diverse groups with various healthconcerns.This enables the faculty to assess their
127Volume 28, Issue 1–2,April 2008 CCCCNNNN
Integrative simulation:A novel approach to educating culturally competent nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 127

interviewing skills and provide needed feed-back.The video-streamed HPS encounters pro-vide the distance students with the opportunityto address clinical care by discussing peer per-formance and responding to questions on thecase that is presented.
Finally, in an environment where clinical sitesare at a premium and may be costly, the simulat-ed environment can provide a cost-effectivemethod for educating nursing students in clini-cal care. Furthermore, once developed, theclinical scenarios can be used year after year aswell as with different educational programs.
ReferencesBase-Smith V and Campinha-Bacote J (2003) The culture
of obesity, Journal of National Black Nurses Association14: 52–56.
Brooks TR (1992) Pitfalls in communication withHispanic and African American patients: Do trans-lators help or harm? Journal of the National MedicalAssociation 84: 941–947.
Campinha-Bacote J (2003)The Process of Cultural Compe-tence in the Delivery of Healthcare Services,TransculturalCARE Associates, Cincinnati OH.
Council on Collegiate Education for Nursing, SouthernRegional Board (2003) Preparing graduates to meet theneeds of diverse populations, accessed at http://www.sreb.org on 19 January 2005.
Department of Health and Human Services (1999)Mental Health:A report of the Surgeon General, USPublic Health Service,Washington DC.
Department of Health and Human Services (2005)National Healthcare Disparities Report,Agency forHealthcare Research and Quality, Rockville MD,
accessed at http://www.ahrq.gov/qual/nhdr05/nhdr05.pdf on 8 June 2007.
Kaiser Family Foundation (2007) Key facts: Race, ethnicityand medical care, accessed at http://www.census.gov/PressRelease/www/releases/archives/population/010048. html on 7 June 2007.
Miles MB and Huberman AM (1994) Quantitative DataAnalysis, 2nd edn, Sage,Thousand Oaks CA.
Morgan DL and Krueger RA (1998) The Focus Group Kit,Sage,Thousand Oaks CA.
Nairn S, Hardy C, Parumal L and Williams GA (2004)Multicultural or anti-racist teaching in nurse educa-tion:A critical appraisal, Nurse Education Today 24:188–195.
Paterson BL, Osborne M and Gregory D (2004) How dif-ferent can you be and still survive? Homogeneity anddifference in clinical nursing education, InternationalJournal of Nursing Education Scholarship 1:Article 2.
Purnell LD and Paulanka BJ (2008) Transcultural HealthCare:A Culturally Competent Approach, 3rd edn, FADavis, Philadelphia, PA.
Rutledge CM, Garzon L, Scott M and Karlowicz K(2004) Using standardised patients to teach andevaluate nurse practitioner students on culturalcompetency, International Journal of Nursing EducationScholarship 1:Article 17.
US Census Bureau (2007) Minority Population Tops 100Million, accessed at http://www.census.gov/PressRelease/www/releases/archives/population/010048.html on 8 June 2007.
Varcoe C and McCormick J (2007) Racing around theclassroom margins: Race, racism and teaching nurs-ing, in Young L and Paterson B (Eds) Learning Nursing:Developing a Student-Centered Learning Environment, pp439–468, Lippincott,Williams & Wilkins, Philadel-phia PA.
128 Volume 28, Issue 1–2,April 2008CCCCNNNN
Carolyn M Rutledge et alCCCCNNNN
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. [email protected]; www.e-contentmanagement.com
COMPUTER ASSISTED MULTIPLE AND BLENDED RESEARCH METHODS
A special issue of International Journal of Multiple Research Approaches, volume 2 issue 1
ISBN 978-1-921348-04-4; ii + 126 pages; s/c; June 2008
Edited by Eugenio De Gregorio (Sapienza University of Rome) and Francesco Arcidiacono(University of Neuchâtel) with an epilogue by Pat Bazeley (Research Support P/L and ACU)
Information: http://mra.e-contentmanagement.com/archives/vol/2/issue/1
* * N O W A V A I L A B L E * *
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 128

INTRODUCTION
This article describes a national projectaimed at developing and delivering a team-
based, practice-focused model of continuousprofessional development to promote cultural
competence for individuals working withinchild and adolescent mental health services(CAMHS) in England, UK. Participating regionsincluded East Midlands,Yorkshire and Humber,West Midlands, Greater Manchester, South West,
Key WordsCAMHS; culturalcompetence;Delphi method;measuring tool;Papadopoulos,Tilki and Taylorculturalcompetencemodel; nursing
CN
129Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 129–140.
Cultural competence in action for CAMHS: Development of a
cultural competence assessment tool and training programme
ABSTRACT This article details the development of a tool to measure the cultural com-petence of individuals working within the Children and Adolescent MentalHealth Services (CAMHS).The CAMHS Cultural Competence in Action Tool –known as the CAMHS ‘CCATool’ – was one of the components of a nationalproject which aimed at promoting cultural competence within CAMHS.Theother component was a two day training programme. Both components werebased on the Papadopoulos, Tilki and Taylor model of cultural competencedevelopment.The article also outlines the educational principles and learningstrategies used in the training.
Received 26 July 2007 Accepted 13 May 2008
IRENA PAPADOPOULOSProfessor
Transcultural Health and Nursing Head, Research Centre for
Transcultural Studies in HealthMiddlesex University
London UK
MARY TILKIPrincipal Lecturer
MemberResearch Centre for
Transcultural Studies in HealthMiddlesex University
London UK
SAVITA AYLINGNational Black and Minority Ethnic Lead
National CAMHS Support ServiceCare Services Improvement Partnership
Department of HealthLondon UK
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 129

North East, North London, Middlesex, SouthLondon and Eastern.
Whilst the project consisted of a culturalcompetence assessment tool and an educationalintervention, this article will primarily focus onthe former and will only briefly refer to the lat-ter, which will be the focus of a subsequent arti-cle. For brevity the project will be referred to asthe ‘CAMHS project’.
In recent years a number of events have ledto questions being asked about the ability of theUK medical, mental health and care services tomeet the needs of service users from Black andminority Ethnic (BME) communities.The death,in 1998, in a medium secure psychiatric unit ofa 38-year-old black patient, David ‘Rocky’ Ben-nett, and the publication by the National Insti-tute for Mental Health in England, of the InsideOutside (Sashidharan 2003) report contributedto the development of Delivering Race Equality inMental Health Care (DRE) (DH 2005).This is afive year action plan for ‘achieving equality andtackling discrimination in mental health servicesin England for all people of Black and minorityethnic (BME) status, including those of Irish or Mediterranean origin and east Europeanmigrants’ (DH 2005: 3).
While DRE is an age-inclusive plan, andtherefore covers the arena of Children and Ado-lescent Mental Health Services (CAMHS), thereare other imperatives impacting onto CAMHservices in England that have raised questionsabout how culturally competent the CAMHservice is. These include the Public ServiceAgreement (PSA) (DH 2002) for a Comprehen-sive CAMHS by December 2006, and the fiveoutcomes of Every Child Matters (ECM) (http://tinyurl.com/2hd2qu) as follows, of which themost relevant is ‘be healthy’:• Be healthy;• Stay safe;• Enjoy and achieve;• Make a positive contribution;• Achieve economic well-being.
Standard 9 of the National Service Framework forChildren,Young People and Maternity Services:Themental health and psychological well-being of chil-dren and young people (DH 2004: 41) definesComprehensive CAMHS thus: ‘All children andyoung people, from birth to their eighteenthbirthday, who have mental health problems and disorders have access to timely, integrated,high quality, multi-disciplinary mental healthservices to ensure effective assessment’. Theunderpinning principles to the definition go further by stating that, ‘Access to CAMHSshould be available to all children and youngpeople regardless of their age, gender, race, reli-gion, ability, class, culture, ethnicity or sexuali-ty’ (DH 2004: 48,Appendix II).
As part of its work in supporting CAMHservices in England towards achieving Com-prehensive CAMHS in line with the PSA target,the National CAMHS Support Service (NCSS)undertook to review the levels of cultural com-petence within CAMHS nationally.The reviewevidenced much of what had been suspectedanecdotally, that levels of cultural competencevaried significantly throughout CAMHS. Thiswas also borne out by the findings of the SelfAssessment Matrix (DH 2003) undertaken on a voluntary basis by CAMHS services and inwhich all London CAMH services identifiedmeeting the needs of BME service users asbeing their second most challenging problem.These reviews mirrored what was evident in theresearch literature.
NEED FOR CULTURALCOMPETENCE IN CAMHSDespite a growing body of literature on therelationship between adult mental health andethnic and cultural factors, CAMHS services inthe UK have been slow to address the ethno-cultural needs of children, adolescents and theirfamilies (Malek 2004;Timimi & Maitra 2005).The incidence of mental ill-health among youngpeople is growing as are the numbers of chil-
130 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos, Mary Tilki and Savita AylingCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:37 PM Page 130

dren and adolescents from minority ethnic andmigrant communities. There is an extensivebody of literature relating to cultural issues inadult mental health but research in the CAMHSarea is sparse. However there is an expandingcritique of mainstream practice and a call forwider debate and different ways of understand-ing the mental health of young people (Timimi& Maitra 2005).
It is argued that cultural incompetence existsamong health professionals (Maitra 2005) andthat this leads to misdiagnosis and inappropriatetreatment.There are particular concerns aboutincreasing medication to children with behav-ioural problems many of whom are childrenfrom minority ethnic groups (Timimi 2005).There are concerns about the validity of diag-nostic categories such as Attention Deficit andHyperactivity Disorder (ADHD) and childhooddepression generally but little attention is paidto differing cultural norms around childhoodbehaviour (Whitfield 2005; Maitra 2005;Timi-mi 2005).There are major concerns about access, racism and cultural competence, yet despitepolicy initiatives over the last 20 years, littleprogress has been made in addressing race equality in CAMHS (Lowe 2006). Although theRace Relations Amendment Act (2000) requirespublic authorities to address racism, the Audit Commission (2004) highlights late, sporadic and superficial compliance with legislation bypublic service providers (Lowe 2006). TheAudit Commission listed a number of barriersto progressing the equality agenda which in-clude unexplored assumptions, institutionalbehaviours, resistance from staff and confusionabout what should be achieved. Culley (2001)argues that legislation cannot tackle values andracist attitudes which persist in the hearts andminds of individuals. According to Husband(2000), inequality remains unchallenged becauseminority ethnic people are not seen by themajority community as truly equal or deserv-ing, despite liberal notions of tolerance by thepowerful.
AIMS OF THE PROJECTIn order to address the above challenges theNCSS commissioned the development of a setof learning tools that could be offered toCAMHS workers as a model to promote indi-vidual cultural competence. Having researchedwhat was already being done in mental healthservices, the NCSS commissioned the Centrefor Transcultural Studies in Health at MiddlesexUniversity, who had previously conducted asimilar project with adult mental health servic-es, to work with them in developing these toolsand delivering a national programme addressingthe cultural competence of CAMHS workers.
In this paper cultural competence is definedas ‘the process one goes through in order tocontinuously develop and refine one’s capacityto provide effective health care, taking into con-sideration people’s cultural beliefs, behavioursand needs’ (Papadopoulos 2006: 11). Thisprocess involves the amalgamation of culturalawareness, cultural knowledge, and culturalsensitivity and their application to practiceunderpinned by an anti-discrimination and peo-ple empowerment ideology.
METHODOLOGYAs stated above the CAMHS project builds on asimilar one which two of the authors (IP andMT) had generated within the adult mentalhealth services (Papadopoulos et al 2004).Thisinvolved the development and validation of a tool to measure the cultural competence of mental health workers using the Delphimethod,1 and the development of a short train-ing programme in consultation with key mem-bers of the commissioning organisation.
Both the training programme and the assess-ment tool were designed using the structureand principles of the Papadopoulos, Tilki andTaylor (1998) model for developing culturalcompetence (Figure 1). The assessment toolcontained culture-generic and culture-specificstatements.The authors posit that the culture-
131Volume 28, Issue 1–2,April 2008 CCCCNNNN
Development of a cultural competence assessment tool and training programme CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 131
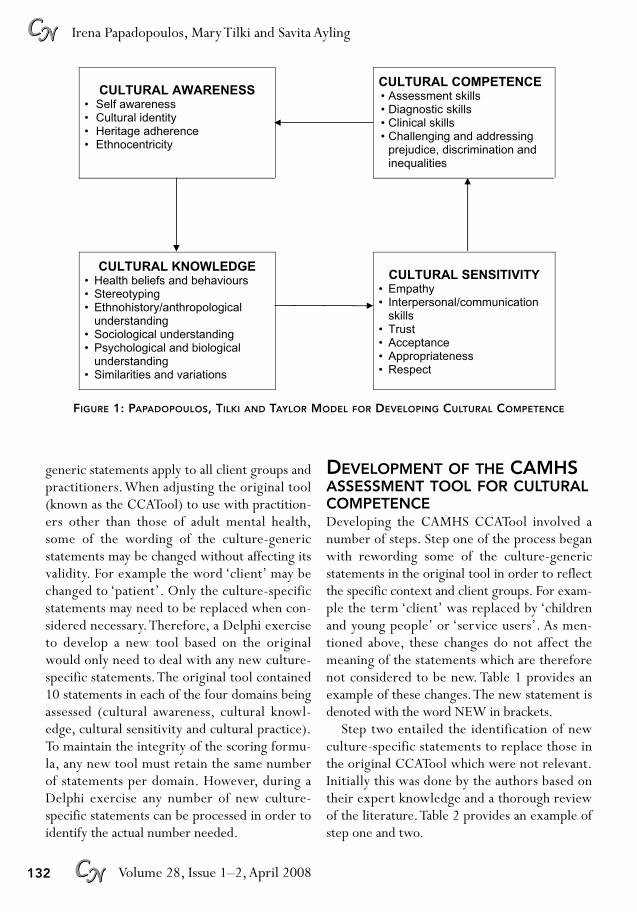
generic statements apply to all client groups andpractitioners.When adjusting the original tool(known as the CCATool) to use with practition-ers other than those of adult mental health,some of the wording of the culture-genericstatements may be changed without affecting itsvalidity. For example the word ‘client’ may bechanged to ‘patient’. Only the culture-specificstatements may need to be replaced when con-sidered necessary.Therefore, a Delphi exerciseto develop a new tool based on the originalwould only need to deal with any new culture-specific statements.The original tool contained10 statements in each of the four domains beingassessed (cultural awareness, cultural knowl-edge, cultural sensitivity and cultural practice).To maintain the integrity of the scoring formu-la, any new tool must retain the same numberof statements per domain. However, during aDelphi exercise any number of new culture-specific statements can be processed in order toidentify the actual number needed.
DEVELOPMENT OF THE CAMHSASSESSMENT TOOL FOR CULTURALCOMPETENCEDeveloping the CAMHS CCATool involved anumber of steps. Step one of the process beganwith rewording some of the culture-genericstatements in the original tool in order to reflectthe specific context and client groups. For exam-ple the term ‘client’ was replaced by ‘childrenand young people’ or ‘service users’. As men-tioned above, these changes do not affect themeaning of the statements which are thereforenot considered to be new. Table 1 provides anexample of these changes.The new statement isdenoted with the word NEW in brackets.
Step two entailed the identification of newculture-specific statements to replace those inthe original CCATool which were not relevant.Initially this was done by the authors based ontheir expert knowledge and a thorough reviewof the literature.Table 2 provides an example ofstep one and two.
132 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos, Mary Tilki and Savita AylingCCCCNNNN
FIGURE 1: PAPADOPOULOS, TILKI AND TAYLOR MODEL FOR DEVELOPING CULTURAL COMPETENCE
CULTURAL AWARENESS
• Self awareness • Cultural identity • Heritage adherence • Ethnocentricity
CULTURAL COMPETENCE • Assessment skills • Diagnostic skills • Clinical skills • Challenging and addressing
prejudice, discrimination and inequalities
CULTURAL KNOWLEDGE • Health beliefs and behaviours • Stereotyping • Ethnohistory/anthropological understanding • Sociological understanding • Psychological and biological understanding • Similarities and variations
CULTURAL SENSITIVITY
• Empathy • Interpersonal/communication
skills • Trust • Acceptance • Appropriateness • Respect
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 132

During step three the expert panel was iden-tified following intense discussion. It was agreedthat experts should meet one of the followingcriteria:• Be an experienced CAMHS practitioner/
service provider (statutory and/or voluntarysectors);
• Be a CAMHS manager;• Be a CAMHS policy maker at national level;• Be an expert on culture and mental health
(academic/researcher with relevant practicebackground).
Eight experts were selected. There are no clear directions in the literature regarding theoptimal panel size. McKenna (1994) reportsthat personal contact with experts seems toresult in a high response rate; all our expertswere spoken to either in person or on the tele-phone by one of the authors (SA). They were
subsequently informed in writing of the aimsand background of the project, that their partic-ipation would be voluntary and that their viewswould remain confidential.They were asked toindicate their consent to be involved.
Four documents were sent to the panellists.The first provided the background of the ex-ercise and instructions on what the experts had to do. The second was a brief outline of the Papadopoulos,Tilki and Taylor model (PTT)of Cultural Competence which underpinnedthe assessment tool.The third was the original(existing) tool (CCATool) with added newclient group/s specific statements, and thefourth was the ‘questionnaire’ with the new cul-ture-specific statements which they were askedto complete.They were encouraged to contactone of the authors (IP) if they had any queriesor needed further information. One of theselected experts declined the invitation to take
133Volume 28, Issue 1–2,April 2008 CCCCNNNN
Development of a cultural competence assessment tool and training programme CCCCNNNN
TABLE 1: REWORDING OF CAMHS TOOL – ASSESSING CULTURAL AWARENESS
Original statements (mental health) New statements (CAMHS)
1
2
3
4
5
6
7
8
9
10
Cultural upbringing impacts on the way in whichindividuals view other peoplePeople from different ethnic groups share manyof the same values and beliefs as people fromthe host communityThere are many differences in values and beliefswithin any single ethnic groupGender, age, class and generation are asimportant as ethnicity in forming a person’sidentityEthnic identity changes with time and theinfluence of wider social factorsSome aspects of culture are more important to aperson than othersPeople select the most relevant aspects of theirculture in different situations
People from different ethnic groups may havethe same needs but they may be expressed indifferent waysTo avoid imposing values on a client practitionersshould be aware of their own value and beliefsystemsEthnic identity is influenced by personal, socialand psychological factors
Wording unchanged
Wording unchanged
Wording unchanged
Gender, age, religion, ability and sexuality areas important as ethnicity in forming a youngperson’s identity (NEW)Wording unchanged
Some aspects of culture are more importantto a child and young person than othersChildren and young people choose the mostrelevant aspects of their culture in differentsituationsChildren and young people from differentethnic groups may have the same needs butthey may be expressed in different waysTo avoid imposing values on a service userpractitioners should be aware of their ownvalue and belief systemsWording unchanged
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 133

part as he was due to leave the country for anextensive lecture tour abroad. Another indicat-ed, soon after agreeing to take part that anexcessive workload was making it impossible torespond.This person was replaced.
The questionnaire contained only the new
CAMHS specific statements which panellistswere asked to rate on a five point Likert scaleranging from ‘not at all important’ to ‘alwaysimportant’. In addition, they were asked tocomment on the wording of the statements theyrated and to provide any statements which they
134 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos, Mary Tilki and Savita AylingCCCCNNNN
TABLE 2: REPLACEMENT CULTURE-SPECIFIC STATEMENTS IN ORIGINAL CCATOOL
Original statements (mental health) New statements (CAMHS)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
Monitoring the ethnicity of all clients can helpidentify the effectiveness of service access anddeliveryEffective care requires an adequate knowledge ofthe client’s cultureIt is not possible to have full knowledge of allculturesThere is much to be learned from the folk systemsof the clientPeople from minority ethnic groups haveparticular difficulty accessing day care services
Discrimination and harassment in everyday lifeleads people to engage in behaviours which maybe damaging to their mental healthCompulsory admission / detention rates arehigher for black peopleBlack people with mental health problems aremore likely to have contact with the criminaljustice system It is important to acknowledge particular culturalbeliefs and practices in relation to mental healthof minority ethnic groupsClients who perceive themselves to be possessedby spirits are invariably mentally disturbed
Monitoring the ethnicity of all service users can helpidentify the effectiveness of service access anddeliveryEffective care requires an adequate knowledge ofthe service users’ culture Wording unchanged
There is much to be learned from the folk systemsof the service user and of his/her familyChildren, young people and families from minorityethnic groups have particular difficulty accessingspecialist CAMHSDiscrimination and harassment in everyday life leadschildren and young people to engage in behaviourswhich may be damaging to their mental healthOmitted
Young black men with mental health problems aremore likely to have contact with the criminal justicesystem It is not important to acknowledge particular culturalbeliefs and practices in relation to mental health ofminority ethnic children and young peopleChildren and young people who are mentallydisturbed are perceived by their families andcommunities to be possessed by spiritsAdolescent African and Caribbean males are morelikely to be inappropriately referred to adult mentalhealth services (NEW)Practitioners never place too much emphasis onculture prior to exploring the complexity of themental health problem (NEW)Practitioners who dismiss the cultural background of the child and young person ignore the complexityof the mental health problem (NEW)There is a need to achieve a balance betweendismissing the culture and recognising how it con-tributes to complex mental health problems (NEW)There is a need to achieve a balance betweenattributing all mental health problems to culture,and recognising how culture contributes to complexmental health problems (NEW)Young African and Caribbean men are over-represented in tier 3 & 4 CAMHS services (NEW)
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 134

considered important for the CAMHS CCAToolbut had not been included in the questionnaire.They were asked to write their suggested state-ments as unambiguously as possible.This consti-tuted step four of the process.
Step five of the process involved the collationof the results from six of the seven experts whoreturned their questionnaires. Unfortunately twoexperts did not rate the statements as requestedbut provided suggestions on a small number ofitems they wanted to reword and comments onthe areas they wished to have included on thetool, but they did not provide any specific state-ments. By only commenting on the changes theywished to see, it appeared that they were indicat-ing an agreement with the statements they hadnot rated or commented on.
All those who rated the new statementsagreed that the new statement in the ‘culturalawareness’ domain was either ‘very important’
or ‘always important’. One of the two who didnot provide ratings suggested that statements on disability and domestic violence should beincluded in this domain. Five of the nine newstatements in the ‘cultural knowledge’ domainwere rated as ‘very important’ or ‘alwaysimportant’. Three of the nine new statements in this domain were rated as ‘important’ or‘very important’; however, one statement wasrated by one expert as ‘not at all important’whilst the other three experts rated it as‘important’ or ‘always important’. Three ex-perts offered other statements they wished toinclude whilst one compared the rated state-ments and suggested the deletion of two ofthem which were very similar to another two.This was very helpful because the intention ofthe authors was to retain only ten statements ineach domain.The two new items in the ‘culturalsensitivity’ domain (Table 3) and the three new
135Volume 28, Issue 1–2,April 2008 CCCCNNNN
Development of a cultural competence assessment tool and training programme CCCCNNNN
TABLE 3: NEW ITEMS IN CULTURAL SENSITIVITY DOMAIN
Original statements (mental health) New statements (CAMHS)
1
2
3
4
5
6
7
8
9
10
11
It is almost impossible to communicate with aclient whose first language is not EnglishGreeting family members before the service usermay be appropriate in some minority ethnic groups Clients who avoid eye contact are alwayssuspicious or withdrawnPractitioners need to be trained in the use ofinterpretersInterpreters and advocates need to be trained inorder to effectively represent the best interests ofthe child and young personService users from some minority ethnic groupscan be very demandingIt is important to discuss the impact of ethnicity onthe therapeutic relationship where the client andpractitioner are from different cultures Religion can be a source of comfort andreassurance for some clientsPeople from minority ethnic groups get littlebenefit from psychological therapies
The stigma of mental illness is greater in someminority ethnic groups than in the host community
It is almost impossible to communicate with aservice user whose first language is not EnglishWording unchanged
Children and young people who avoid eye contactare always suspicious or withdrawnPractitioners need to be trained in the use of ageappropriate interpreters and advocates (NEW)Interpreters and advocates need to be trained inorder to effectively represent the best interests ofthe child and young personService users from some minority ethnic groups canbe very demandingIt is important to discuss the impact of ethnicity onthe therapeutic relationship where the service userand practitioner are from different culturesReligion can be a source of comfort and reassurancefor some children, young people and their familiesChildren and young people from minority ethnicgroups get little benefit from psychologicaltherapiesWording unchanged
Practitioners never allow their own fears to get inthe way of developing trusting relationships withservice users (NEW)
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 135

items in the ‘cultural practice’ domain (Table 4)were rated by all as ‘very important’ to ‘alwaysimportant’. Only one expert offered additionalstatements for the ‘cultural sensitivity’ and ‘cul-tural practice’ domains.
The results of the ratings indicated a highlevel of agreement. This assured the contentvalidity of the new tool.The authors’ challengewas how to deal with the comments and sugges-tions which were offered by the experts, andwhether or not to have another round of Del-phi. After a detailed discussion it was agreedthat due to the high level of agreement and the
lack of time, the project would move to thenext stage that of piloting the new tool once thefinal statements had been agreed by the authorsas people having expertise in culture, mentalhealth and CAMHS. The following decisionswere taken regarding the qualitative data fromthe Delphi exercise:
• Cultural awareness domain: Not to take up thesuggestion by one of the experts to includestatements on disability and domestic vio-lence.The rationale for this was that notwith-standing the importance of both these areas
136 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos, Mary Tilki and Savita AylingCCCCNNNN
TABLE 4: NEW ITEMS IN CULTURAL PRACTICE DOMAIN
Original statements (mental health) New statements (CAMHS)
12
3
4
5
6
7
8
9
10
11
12
13
Subtle forms of racism are as damaging as overt formsInstitutional racism is seen in unwitting prejudice,ignorance and thoughtlessnessRecognising and challenging institutional racism is theresponsibility of each individual health practitioner
User participation is a critical component of goodpractice and should be encouraged at all levels ofservice provisionProfessionals and clients need training in userparticipationBest practice can be achieved by joint partnershipbetween statutory and voluntary sectorsThe expertise of the minority ethnic voluntary sectorshould be used more effectively to obtain advice ongood practice
Stereotypes always have an impact on how clients areassessedStereotypes may account for the high level of com-pulsory detention and treatment of people fromminority ethnic groupsThe type and route of medication should be based onsound clinical judgement of client need and thedegree of danger to self and others
Wording unchangedWording unchanged
Recognising and challenging institutional racismis the responsibility of each individual CAMHSpractitioner Wording unchanged
Professionals and service users need training inuser participationWording unchanged
The expertise of the minority ethnic voluntarysector should be used more effectively to obtainadvice on good practice in working with childrenand young peopleStereotypes always have an impact on howservice users are assessedOmitted
Omitted
Assumptions about culture never influence thediagnosis and treatment of children and youngpeople (NEW)Attention Deficit and Hyperactivity Disorder(ADHD) is less likely to be diagnosed in BMEchildren and young people (NEW)It is always easier to engage BME families in thetreatment and support of children and youngpeople with mental health problems (NEW)
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 136

the focus of the assessment of cultural aware-ness was the awareness of the impact of cul-ture and ethnicity on the self.
• Cultural knowledge domain: One of the expertssuggested that a statement should be added inthis domain which necessitated the practi-tioners to challenge, explore and negotiatebeliefs if they posed danger to the child orconflict with treatment.This expert also sug-gested a statement should be included whichacknowledged the nature of immigration inthe UK. Another expert suggested that theculture and ethnicity of a child or young per-son interconnects with other aspects of socialdisadvantage contributing to complex mentalhealth problems in children and families andthat there is a need to have an in-depthknowledge of specific and relevant culturesto work effectively in CAMHS.The authorsfelt that the latter suggestion was covered by the already validated statements No 2 andNo 3 (see Table 2) in this domain. It was feltthat statements on immigration were moregeneric in nature whilst the suggestion aboutchallenging beliefs was more suited to the‘cultural practice’ domain; proposed state-ment No 11 in the ‘cultural practice’ (seeTable 4) domain was considered a suitableresponse to this suggestion. Based on thefeedback and ratings of the panel the follow-ing ten statements were selected to beincluded in the ‘cultural knowledge’ domain:1, 2, 3, 5, 6, 8, 9, 10, 11 and 13 (Table 2).
• Cultural sensitivity domain: One expert offeredthe following two statements: ‘It is essentialfor practitioners to enable children andyoung people to define/describe their ownethnicity/culture’ and ‘It is important forusers to have someone from their own cul-ture to work with them’. It was felt that thefirst suggestion was adequately catered for inthe ‘cultural awareness’ domain as well as bystatement No 7 in this domain.With regards
to the second suggestion we acknowledgedthat it would be difficult to assess as somepeople may agree with it and some may havereservations about it. For this reason theauthors decided not to use it.
• Cultural practice domain: One expert offeredthe following statements: ‘Every practitionermust take personal responsibility for trainingin culturally sensitive practice’; ‘It is essentialfor BME children, young people and familiesto have access to a range of therapies suitableto their particular culture/ethnicity’; ‘It isessential for the practitioner to understandthe issues of professional and personal powerto work in a culturally sensitive way’.Whilstthe first and third suggestions were verynoble, it was difficult to see which of theother four new statements in this domain,which had gained a high level of agreementregarding their importance, we should exc-lude in order to have them. After much con-sideration it was agreed not to include thesestatements. Regarding the second suggestion,we felt that the issue highlighted in the state-ment was addressed by a number of otherstatements in the tool all be it from a differ-ent angle.
The authors acknowledge the difficulty in thesedecisions particularly when there is a limit tothe length of the instrument being designed. Itcould be argued that a lengthy instrument ismore likely to be comprehensive whilst othersmay argue that a well designed shorter one maystill capture the essence of that which is beingmeasured in less laborious ways. In any case theinstrument or tool being discussed here wasfirmly based on a pre-existing tried and testedmodel.
PILOTThe new CCATool for CAMHS was pilotedwith 47 individuals working within the CAMHservices.Table 5 provides a combination of their
137Volume 28, Issue 1–2,April 2008 CCCCNNNN
Development of a cultural competence assessment tool and training programme CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 137

professional backgrounds or roles.To test howwell the set of statements (or items) in the toolmeasured cultural competence, the Cronbach’salpha test was employed. If the average inter-item correlation is high the alpha will be highand vice versa.This means that if the inter-itemcorrelations are high, then the items are meas-uring the same underlying construct, in ourcase, that of ‘cultural competence’. A ‘good’reliability is achieved if an alpha of 0.70 or higher is reached. Our tests revealed that theCronbach´s alpha for the CAHMS CCATool was0.763. This was a good result particularly asthose who took part in the pilot came from avariety of professional backgrounds and occu-pied a variety of roles. Therefore no furtherchanges needed to be made to the statementsbefore administering the tool during the nation-al training programme.The only changes whichwere made to the new CAMHS CCATool wereon the demographic variables. In particular thefeedback indicated that the ‘work’ categoriesneeded to be re-worded to reflect more accu-rately the roles of people working in CAMHS.
OUTLINE OF THE TRAININGPROGRAMMEBased on the mental health project which twoof the authors (IP and MT) had undertaken pre-viously, a two day training programme wasnegotiated with the NCSS.The first day of the
programme focused on cultural awareness andcultural knowledge whilst the second dayfocused on cultural sensitivity and cultural com-petence. Prior to the beginning of each pro-gramme (see regional programme sites), theattendees were asked to complete the CAMHSCCATool. This was voluntary and individualswere told that their scores would remain confi-dential and would be fed back to them individu-ally at the end of the project by the NationalBlack and Minority Ethnic Lead (SA).With theexception of three individuals all others com-pleted the assessment tool.
The educational principles used to underpinthe training programme aimed to:• Respect and use trainees’ knowledge and
experience.• Encourage reflection on existing knowledge
and experience.• Encourage peer exchange of knowledge and
experiences.• Add to existing knowledge and cognitive
skills.• Acknowledge that a two-day course in cul-
tural competence does not necessarily andimmediately transform trainees into cultural-ly competent practitioners. It is an opportu-nity to consolidate the trainees’ levels ofcultural competence and provide the plat-form for further development and lifelonglearning in cultural competence.
• Be realistic. It is impossible to deliver a two-day course which will meet everyone’sexpectations and needs. Acknowledge thattrainees may be at different levels of culturalcompetence but aim for the middle level.
• Emphasise anti-discriminatory/antiracist ap-proaches (dealing with difficult issues).
During the two-day programme, techniqueswere applied that promoted peer learning com-munities, problem based learning, and reflectivelearning. All these techniques necessitate the useof active and interactive learning such as selfreflective activities and group discussions. How-
138 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos, Mary Tilki and Savita AylingCCCCNNNN
TABLE 5: PROFESSIONAL BACKGROUNDS/ROLES OFCAMHS PILOTS
Professional background/roles Number
Social worker 5Community development worker 7Psychologist (in various clinical roles) 6CAMHS/Mental health nurse 11Manager (with backgrounds in social work, nursing and psychology) 7Administrator 4Occupational therapist 5Psychiatrists 2TOTAL 47
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 138

ever, we also used a very small number of shortlectures which provided cultural knowledgeefficiently in the time constraints associatedwith such a short programme. One of the im-portant messages of the programme was that weare all cultural beings and therefore culturalcompetence is relevant to all aspects of every-one’s professional work. In order to help devel-op and maintain the ‘cultural competence habit’an electronic mailing list was established at theend of the project. This provides the vehiclethrough which members can exchange informa-tion, ask for or provide advice, thus continuingthe process of reflection and personal develop-ment. An information pack containing all thematerials used during the training was also dis-tributed to each participating team.
CONCLUSIONThe CAMHS project took place in 2006. Todate, it remains the most extensive and coher-ent programme of cultural competence trainingand assessment in the UK. Nearly 200 individu-als were assessed and trained.The programmecontinues to be delivered by local trainers who were trained to cascade the work of theauthors.The assessment tool has been convertedinto a user-friendly software by one of theauthors (IP) and has been licensed to allCAMHS regions in England. The programmehas been evaluated by the authors and it is cur-rently the focus of an external evaluation. Theauthors hope to publish more details on thedelivery and evaluation of the programme in thenear future. This article forms one of the out-puts aimed at disseminating the authors’ experi-ences and sharing their approaches.
Endnote1 The Delphi method has been used since the
1950s in industry (Lindeman 1975) but inthe last 20 years it has become popularamong health researchers. It is a techniqueinvolving a panel of experts in order toobtain group consensus on a particular topic
(Polit & Hungler 1999, McKenna, 1994,Keeney, Hasson, & McKenna, 2001). Theprocedure is characterised by a series ofrounds (usually two to three) of question-naires asking the panel of experts to rate orrank items on their importance or level ofagreement with them. Each round providesfeedback on the results from the previousround (Irvine, 2005) with the process con-tinuing until consensus is reached. In eachround, a summary of responses to the previ-ous round is fed back to the panellists.Therefore the Delphi method when used inthe development of an assessment tool helpsto identify the items which will compose thetool and assures the content validity of thesethrough its rigorous methodological process.
ReferencesAudit Commission (2004)The Journey to Race
Equality: Delivering improved services to localcommunities. Holbook Printers, Portsmouth.
Children’s Green Paper (2003) Every Child Matters,Cm 5860,The Stationery Office, London.Accessed at http://www.everychildmatters.gov.uk/_files/EBE7EEAC90382663E0D5BBF24C99A7AC on 23 July 2007.
Culley L (2001) A critique of multiculturalism inhealthcare: the challenge for nurse education.Journal of Advanced Nursing 23: 564–570.
Department of Health (DH) (2002) Technical Notefor the Spending Review 2002. Public ServiceAgreement. Department of Health, London.
Department of Health (DH) (2003) CAMHSAssessment Matrix. National CAMHS SupportService. Department of Health, London.
Department of Health (DH) (2004) NationalService Framework for Children,Young People andMaternity Services: The mental health and psycho-logical well-being of children and young people.Department of Health, London.Accessed athttp://tinyurl.com/32z8n4 on 23 July 2007.
Department of Health (DH) (2005) DeliveringRace Equality in Mental Health Care:An actionplan for reform inside and outside services and theGovernment’s response to the Independent inquiryinto the death of David Bennett. Department of
139Volume 28, Issue 1–2,April 2008 CCCCNNNN
Development of a cultural competence assessment tool and training programme CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 139

MURA SOLWATA KOSKER: WE SALTWATER WOMENBy Ellie Gaffney AM; ISBN 978-0-9775742-0-9; iv + 112 pages; s/c; Verdant House; 2006
Ellie Gaffney was a strong advocate both within Australia and internationally (including her address to theUnited Nations on Indigenous Rights) of the interests and welfare of Torres Strait Islanders. She has beenparticularly committed to advancing the rights of Indigenous women. As an administrator, Ellie Gaffneyplayed a significant part in the development of hostel accommodation and primary health care for all
Torres Strait Islanders. This memoir is a fitting reminder of the work and stature of a dedicated woman.
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911;[email protected]; www.e-contentmanagement.com
Health, London.Accessed at http://tinyurl.com/32z8n4 on 23 July 2007.
Husband C (2000) Recognising diversity anddeveloping skills: the proper role of trans-cultural communication. European Journal ofSocial Work 3: 225–234.
Irvine F (2005) Exploring district nursing compe-tencies in health promotion: the use of theDelphi technique. Journal of Clinical Nursing14: 965–975.
Keeney S, Hasson F and McKenna HP (2001) A critical review of the Delphi technique as aresearch methodology for nursing. InternationalJournal of Nursing Studies 38: 195–200.
Lindeman CA (1975) Delphi survey prioritising inclinical nursing research. Nursing Research 24:434–441.
Lowe F (2006) Containing persecutory anxiety:child and adolescent mental health services andBlack and minority ethnic communities. Journalof Social Work Practice 20: 5–25.
Maitra B (2004) The cultural relevance of themental health disciplines. In Malek M &Joughin C (Eds) Mental Health Services forMinority Ethnic Children and Adolescents. JessicaKingsley, London.
Maitra B (2005) Culture and the mental health ofchildren:The cutting edge of expertise. InTimimi S & Maitra B (Eds) Critical Voices in Childand Adolescent Mental Health. Free AssociationBooks, London.
Malek M (2004) Understanding ethnicity andchildren’s mental health. In Malek M & JoughinC (Eds) Mental Health Services for Minority EthnicChildren and Adolescents. Jessica Kingsley,London.
McKenna HP (1994) The Delphi technique:A
worthwhile research approach for nursing?Journal of Advanced Nursing 19: 1221–1225.
Papadopoulos I (2006) The Papadopoulos,Tilkiand Taylor model of developing CulturalCompetence. In Papadopoulos I (Ed) Trans-cultural Health and Social Care: Development ofCulturally Competent Practitioners. ChurchillLivingstone Elsevier, Edinburgh.
Papadopoulos I,Tilki M and Taylor G (1998)Transcultural Care.A guide for health care profes-sionals. Quay Publications, Dinton Wilts.
Papadopoulos I,Tilki M and Lees S (2004)Promoting cultural competence in health carethrough a research based intervention. Journalof Diversity in Health and Social Care 1: 107–115.
Polit D and Hungler B (1999) Nursing Research,Prin-ciples and Methods. Lippincott, Philadelphia PA.
Race Relations Amendment Act (2000) The StationeryOffice, London.
Sashidharan S (2003) Inside Outside: Improvingmental health services for black and minority ethniccommunities in England. National Institute forMental Health England.The Stationery Office,London.
Timimi S (2005) The politics of attention deficithyperactivity disorder (ADHD) In Timimi S &Maitra B (Eds) Critical Voices in Child and Adoles-cent Mental Health. Free Association Books,London.
Timimi S and Maitra B (2005) (Eds) Critical Voicesin Child and Adolescent Mental Health. FreeAssociation Books, London.
Whitfield C (2005) Childhood trauma as a causeof ADHD, aggressions, violence and anti-socialbehaviour. In Timimi S & Maitra B (Eds) CriticalVoices in Child and Adolescent Mental Health. FreeAssociation Books, London.
140 Volume 28, Issue 1–2,April 2008CCCCNNNN
Irena Papadopoulos, Mary Tilki and Savita AylingCCCCNNNN
N O W A V A I L A B L E
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 30/07/2008 10:06 PM Page 140

INTRODUCTION
There has been much discussion in the literature on what constitutes cultural com-
petence in nursing education and practice (Lip-son & DeSantis 2007; Campinha-Bacote 2006a;Betancourt 2007; Grant & Letzring 2003). Healthprofession literature supports a growing con-sensus that cultural competency curricular con-tent should focus on attitudes, skills andknowledge. However, affective constructs, suchas cultural desire, have received little attention
in the transcultural health care literature. Someargue that affective constructs such as desiremust be ‘caught’ rather than ‘taught,’ for howdoes one objectively measure or evaluatewhether or not a student has obtained culturaldesire? The purpose of this article is to morefully explore the construct of cultural desire inan attempt to identify meaningful ways that cul-tural desire can not only be ‘caught’ by facultywho model this construct, but also be ‘taught’within nursing curricula as a foundational com-ponent of cultural competence.
‘Caught’ or ‘taught’?It is without question that cultural desire rep-resents an affective or attitudinal construct.However, what is not clear is how it is to beincorporated into the cultural competence con-tent of nursing curricula. Leng (2002) assertsthat affective characteristics can be learnedcapabilities that affect human performances and
Key Wordsculture; nursing;healthcare;competence;transcultural;desire CN
141Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 141–148.
Cultural desire: ‘Caught’ or ‘taught’?
ABSTRACT There has been much discussion in the literature on what constitutes culturalcompetence training in nursing education and practice.The health professionliterature supports a growing consensus that cultural competency curricularcontent should focus on attitudes, skills and knowledge. However, affectiveconstructs, such as cultural desire, have received little attention in the trans-cultural health care literature. Some argue that affective constructs such asdesire must be ‘caught’ rather than ‘taught,’ for how does one objectivelymeasure or evaluate whether or not a student has obtained cultural desire? Thepurpose of this article is to explore more fully the construct of cultural desire inan attempt to identify meaningful ways that cultural desire can not only be‘caught’ by faculty who model this construct, but also be ‘taught’ withinnursing curricula as a foundational component of cultural competence.
Received 24 May 2007 Accepted 20 March 2008
JOSEPHA
CAMPINHA-BACOTEPresidentTranscultural CAREAssociatesCincinnati OH, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 141

recommends a two-prong strategy of ‘taughtand caught.’ He states that affective characteris-tics can be ‘caught’ from an informal environ-ment like peer groups and field trips, while‘more structured activities can include sharingof success stories, meeting with actual rolemodels, role playing, simulations, using videos,games, the media, case studies, current affairs,personal encounters, autobiographies, biogra-phies and testimonies from invited speakers todepict the desirable choices of affective charac-teristics’ (Leng 2002: 5). Using this approach,cultural desire can be ‘caught’ from other nurs-ing students, faculty who model cultural desire,cultural encounters and/or invited speakerswho are passionate about cultural competencein healthcare delivery. This approach can beevaluated through the use of such instrumentsas the Inventory for Assessing the Process ofCultural Competence Among Healthcare Pro-fessionals–Revised (IAPCC-R) which measuresthe construct of cultural desire along with otherconstructs of cultural competence (Campinha-Bacote 2007).
The more difficult question is ‘How can cultural desire be taught?’ The Process of Cultural Competence in the Delivery of Health-care Services (Campinha-Bacote 2007) modelof cultural competence can serve as a viableframework for teaching the construct of cultur-al desire.
Model of cultural competenceThe Process of Cultural Competence in theDelivery of Healthcare Services is a practice andeducational model of cultural competence inhealthcare delivery that defines cultural com-petence as the ongoing process in which thehealthcare professional continuously strives toachieve the ability and availability to work effec-tively within the cultural context of the patient(individual, family, community) (Campinha-Bacote 2007).This model requires nurses to seethemselves as becoming culturally competentrather than being culturally competent and
involves the integration of cultural desire, cul-tural awareness, cultural knowledge, culturalskill and cultural encounters.
Cultural competence is pictorially depictedas a volcano (see Figure 1) and symbolically,when cultural desire erupts, it gives forth thedesire to ‘want to’ enter into the process ofbecoming culturally competent by genuinelyseeking cultural encounters, obtaining culturalknowledge, possessing the skill to conduct cul-turally sensitive assessments and being humbleto the process of cultural awareness. In this con-ceptualisation of cultural competence, it is clearthat cultural desire is the foundational and piv-otal construct of cultural competence.
Cultural desireCultural desire is defined as the motivation ofthe nurse to ‘want to’ engage in the process ofbecoming culturally competent; not the ‘haveto’ (Campinha-Bacote 2003a).This motivationis genuine and authentic, with no hidden agen-das. Rogers (1951) states that genuineness, orcongruence, is the very basic ability of a personto read his own inner experience and allow the
142 Volume 28, Issue 1–2,April 2008CCCCNNNN
Josepha Campinha-BacoteCCCCNNNN
FIGURE 1: PROCESS OF CULTURAL COMPETENCEIN DELIVERY OF HEALTHCARE SERVICES
Source: © Campinha-Bacote 2002.Not to be reprinted without permission.
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 142

quality of this inner experience to be apparentin the relationship.
Cultural desire comes from one’s aspirationand not out of one’s desperation (Campinha-Bacote 2005). It includes a genuine passion andcommitment to be open and flexible with oth-ers; a respect and understanding of differences,yet a commitment to build upon similarities;a willingness to learn from patients and othersas cultural informants; and a sense of humility(Campinha-Bacote 2003a).This article puts for-ward the assertion that the building blocks ofcultural desire are caring and love, sacrifice,social justice, humility, compassion and sacredencounters.
Caring and loveThe concepts of caring and love are central tothe construct of cultural desire. Cultural desireis based on the humanistic value of caring and the spiritual aspect of loving one another(Campinha-Bacote 2005). We are all uniqueindividuals who belong to the same race – thehuman race, with similar basic human needs tobe cared for and loved. Our goal in providingculturally competent nursing care is to seek thiscommon ground.
Cultural desire mandates a genuine passionand commitment to caring. May (1975) des-cribes care as ‘a state in which something doesmatter; it is the source of human tenderness.’ Ithas been said that people do not care how muchyou know, until they first know how much youcare.This type of caring comes from the heart;not from the mouth (Campinha-Bacote 1998).The goal is not to offer comments that are pol-itically correct (words from the mouth), butrather to offer comments to the patient thatreflect true caring (words from the heart).
Caring can be viewed as a virtue. Whenapplied to the health professions, the virtue ofcaring should be seen as a practical comport-ment towards others, which has the goal ofenhancing the health-related existence of others(van Hooft 1999: 193).Van Hoof (1999) further
suggests that the motivation of caring is impor-tantly ‘other-directed’ as opposed to self.
Individuals who are primarily committed toserving others above themselves can be charac-terised as having a ‘Servant’s Heart’ (Chapman2005: 66). A Servant’s Heart symbolises love’sgreatest expression, which assumes the fullinvolvement of our best thought processes(Chapman 2005: 10). Chapman (2005: 12)adds, ‘Nurses don’t choose the nursing profes-sion to become rich. The best nurses choosecaregiving out of a passion to serve.’
Chapman (2005) supports a synergistic viewof the concepts of love and caring, which herefers to as radical loving care. Radical lovingcare is not random thoughtful gestures. Radicalloving care is defined as ‘creating a continuouschain of caring light around each patient’(Chapman 2005: 4)
SacrificeCharles Dubois (nd) said: ‘The important thingis this: To be able at any moment to sacrificewhat we are for what we could become.’Cultural desire encompasses the capacity to sac-rifice. One must be willing to sacrifice one’sprejudice and biases towards culturally differentclients in order to develop cultural desire.Howard (2003) adds that we must also sacrificeour ‘proprietary assumptions of our own right-ness and our unreflective grip on our own cer-tainty.’This type of sacrifice involves the moralcommitment to care for all patients, regardlessof their cultural values, beliefs or practices.
The task of sacrifice may be difficult whencaring for challenging patients who engage inbehaviors that may be in direct moral conflictwith the healthcare professional (eg abortion,spousal abuse, sexual addictions). How does anurse care for a patient whose political and/orreligious beliefs are in direct contrast to theirbeliefs? As healthcare professionals we do nothave to accept the patient’s belief system, how-ever, we must treat each person as a uniquehuman being worthy and deserving of our
143Volume 28, Issue 1–2,April 2008 CCCCNNNN
Cultural desire:‘Caught’ or ‘taught’? CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 143

love and care. In this sense, cultural desire isexpressed in terms of human dignity, humanrights, social justice and equity (Campinha-Bacote 2006b).
Social justiceMartin Luther King Jr once said, ‘Of all formsof inequality, injustice in health care is the mostshocking and inhumane’ (King nd). Culturalcompetence must be based on a commitment tosocial justice. Culturally competent individualshave the skills necessary to break down systemsof practice that perpetuate inequities (Ndurand). Stacks, Salgado and Holmes (2004) callsfor ‘socially just cultural competence’ and as-serts that true cultural competence necessitatesan understanding of social inequalities and howthey affect individuals and communities.
Hart, Hall and Henwood (2003) content thateducators face a difficult task in preparing students to work with patients in ways that take account of differences in background andlifestyle and which respect human rights anddignity. These authors propose an ‘InequalitiesImagination’ model to enhance equality of careto all.This model makes explicit a process thatassists nurses to move towards a greater under-standing and awareness of the way they workwith disadvantaged patients and offers strategiesto bridge the gap between the challenges theyface in day-to-day practice and what they needto achieve to aspire to provide equality care(Hart et al 2003).
Research continues to demonstrate a directcorrelation between inequality and negativehealth outcomes and it is because of this linkthat healthcare professionals must consciouslyconnect cultural competence with social justice.Stacks et al (2004) contend that when culturalcompetence partners with social justice, we canfinally achieve equality in health outcomes forall, regardless of race/ethnicity, language, gen-der, religion, or sexual orientation.
Several nursing organisations have demon-
strated a commitment to social justice. TheAmerican Nurses Association’s Position Statementon Ethics and Human Rights (1991) supports thisview, as evidenced in the following statements:• Human beings deserve respect as ends in
themselves and therefore, deserve health careservices that are equitable in terms of acces-sibility, availability, affordability and quality;
• Justice requires that the differences amongpersons and groups are to be valued.Whenthose differences contribute to the unequaldistribution of the quality and quantity ofhealth care, then remedial actions are obli-gated;
• Because nursing care is an essential but some-times limited commodity, allocation of careis a pressing issue that cannot be effectivelyaddressed when specific individuals are exc-luded or when the burdens of limited accessare borne by particular groups;
• The principle of justice applies to nurses asproviders as well as to nurses as recipients ofcare. ANA is committed to addressing theneed for racial and ethnic diversity amongnurses. Such diversity is a critical element inproviding fair and equitable care.
The Transcultural Nursing Society (TCNS) hasmade a recommitment ‘to safeguard humanrights and quality health care through the dis-covery and implementation of culturally com-petent care’ by recently developing a PositionStatement on Human Rights (Andrews et al 2007).This document serves as evidence that they are‘committed to the rights of all peoples to enjoytheir full human potential, including the highestattainable standard of health.’
The culturally competent nurse mustbecome aware and sensitised to the overt andcovert social inequities faced by others. Thisrequires a community perception of the chal-lenges of social justice for all. Therefore, amajor step toward socially just cultural compe-tence is to enter into community partnerships.‘The process of becoming culturally competent
144 Volume 28, Issue 1–2,April 2008CCCCNNNN
Josepha Campinha-BacoteCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 144

now moves outward from the individual, intothe community’ (Stacks et al 2004: 5).
HumilityHumility is a quality of seeing the greatness inothers and coming into the realisation of thedignity and worth of others. Nurses who arehumble have a genuine desire to discover howtheir patients think and feel differently fromthem. A humble person is generally thought tobe someone who does not think that he or she isbetter or more important than others. Howev-er, humility does not command us to considerourselves lower in stature. Humility is notthinking less of yourself; but thinking of your-self, less.
In integrating humility into the construct ofcultural desire, it is helpful to view it as thevirtue of serving others. Matthew 20: 26–27states, ‘but whoever wishes to become greatamong you shall be your servant and whoeverwishes to be first among you shall be your slave’(New American Standard Bible 2002). The virtueof humility, in this sense, is directed towardserving our fellow man.
However, there is said to be a paradox in pos-sessing humility, for when we become aware ofour humility and openly acknowledge it, we’velost it.This begs the question: ‘Is it possible toseek or learn humility?’ Drawing from the fieldof theology, Ells (nd) argues that there are theo-logical ways to humble oneself that are found inthe books of Proverbs, Philippians, Corinthians,Matthew, Thessalonians, Ephesians and James(New American Standard Bible 2002). His exam-ples include accepting a lowly place, receivingcorrection and feedback from others graciously,choosing to serve others, being quick to for-give, cultivating a grateful heart, purposelyspeaking well of others and acknowledging yourwrongdoings to others.
Tervalon and Murray-Garcia (1998) haveapplied the concept of humility to the processof becoming culturally competent healthcareprofessionals and coined the term, ‘cultural
humility.’ Cultural humility is defined as a life-long commitment to self-evaluation and self-critique, re-addressing the power imbalances inthe patient-healthcare professional relationshipand developing mutually beneficial partnershipswith communities on behalf of individuals anddefined populations.
CompassionCompassion is an emotion of shared sufferingand the desire to alleviate or reduce such suffer-ing as well as demonstrating kindness to thosewho suffer. It is creating a space where patientswho suffer can tell their story to someone whocan listen with real attention (Nouwen 1998).As quoted by Maya Angelou (nd), ‘There is nogreater agony than bearing an untold storyinside you.’ Compassion is difficult because it necessitates that we enter into the pain ofanother (Chapman 2005).
Ironically, conflict can provide nurses with aunique opportunity for developing compassion –the emotional task of sharing in one’s suffering.Mason Cooley (nd) reminds us that ‘compassionbrings us to a stop and for a moment we riseabove ourselves.’ Culture is always a factor inconflict, whether it plays a major role or influ-ences it subtly (LeBaron 2003). LeBaron adds‘for any conflict that touches us where it mat-ters, where we make meaning and hold ouridentities, there is always a cultural component.’When cross-cultural conflict arises, the goal is torespond with compassion. However, the obviousquestion is, ‘How does one cultivate compassionin the midst of cross-cultural conflict?’
Arai (cited in Gallaher 2007) offers the following analogy regarding the relationshipbetween conflict and compassion: ‘How arerocks polished? You put them in a tumbler, theyhit against each other, the sharp edges areknocked off resulting in mutually polished stones.The key term here is mutually.’ Cultivating com-passion requires that we understand from theother’s point of view and engage in self-reflec-tion of how our actions are affecting the other
145Volume 28, Issue 1–2,April 2008 CCCCNNNN
Cultural desire:‘Caught’ or ‘taught’? CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 145

person (Gallaher 2007). Gallaher adds that‘understanding the point of view of the othermeans you are more likely to respond withcompassion rather than judgment.’ During thisreflection process one gradually comes into theawareness that we share more similarities thandifferences. Our sharp edges have been knockedoff resulting in ‘polished hearts’ (Gallaher2007).
‘Sacred encounters’Compassion will lead nurses into a place ofmeeting in which there is ‘deep respect for dif-ferences and equally intentional openness to thepossibility of connection’ (Howard 2003).Thisconnection embodies an encounter, which Chap-man (2005) calls ‘Sacred encounters’. Sacredencounters occur ‘whenever we meet another’sdeep need with a loving response’ (Chapman2005: 58). More simply put, it is the merging oflove and need. Consider the following scenario:
A patient is crying out with unimaginablepain. His cry seems to signal not only physi-cal pain but fear, loneliness and sadness all inone. The nurses are barred from giving fur-ther relief medication because of the delicatenature of the patient’s condition. Instead,they simply stand by him and stroke his armand hold his hand and struggle to soothe himwith the soft instruments of their voices.They seem like two mothers trying to calm acrying baby – except that this is a full-grownman in exquisite pain. Still, one of them evenrefers to him as ‘baby,’ reinforcing how clear-ly she understands this patient’s deep needfor the loving comfort of a mother.
(Chapman 2005: 138)
Chapman (2005) argues that loving care doesnot require twice the time, however it doesrequire more than twice the presence. Everyencounter is a cultural counter and our goal isto make each cultural encounter a Sacredencounter.
SummaryAlthough there has been some consensus in thetranscultural health care literature on what toteach in regard to the topic of cultural compe-tence, there is no consensus on how to teach it– especially concerning affective or attitudinalconstructs such as cultural desire. Before nurseeducators can decide how to teach culturaldesire, they must acquire an in-depth knowl-edge of this concept. Unfortunately the affectiveconstruct of cultural desire has been given littleattention in the nursing literature. In order tomore fully understand cultural desire and itscomponents, this article has provided nurseeducators and students with a closer examina-tion of the construct. It is concluded that car-ing, love, sacrifice, social justice, humility,compassion and sacred encounters are salientcomponents of cultural desire that must beaddressed in the teaching of this construct.
However, it is recommended that a formalconcept analysis of cultural desire be conductedto further understand this construct. In addition,research is needed to propose the best ways toassess and measure this construct. As a certifiedtranscultural nurse, I have recently developed a self-assessment instrument, Inventory forAssessing the Process of Cultural CompetenceAmong Healthcare Professionals-Student Version(IAPCC-SV), to measure the construct of cul-tural desire of student nurses (Campinha-Bacote2007). In measuring cultural desire, it is impor-tant to pursue both quantitative and qualitativemeasures.Therefore, mixed methods of evalua-tion are needed to assure that we have capturedthe breadth of cultural desire that may not be captured by quantitative tools alone. Onerecommendation is to use the quantitative meas-urement of the IAPCC-SV alongside of suchqualitative measures as journaling, role playing,and field notes.
Napoleon Hill (nd) remarks that, ‘The start-ing point of all achievement is desire. He addsthat ‘weak desires bring weak results’ (Hill nd).It is desire that creates our future and if nursing
146 Volume 28, Issue 1–2,April 2008CCCCNNNN
Josepha Campinha-BacoteCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 146

wants to create a future of rendering culturallycompetent care, it will have to be driven bydesire. Cultural desire is the fuel necessary todraw us into a personal journey towards cul-tural competence (Campinha-Bacote 2003a).
ReferencesAmerican Nurses Association (1991) Position
Statement on Ethics and Human Rights, accessedat http://nursingworld.org/ readroom/position/ethics/etethr.htm on 19 March2007.
Andrews M, Leininger M, Leuning C, Ludwig-Beymer P, Miller J, Pacquiao D and Papadop-oulos R (2007) Transcultural Nursing SocietyPosition Statement on Human Rights, accessed athttp://.www.tcns.org on 10 April 2007.
Angelo M (n.d.) Maya Angelou Quotes, accessedat http://www.brainyquote.com/quotes/authors/m/maya_angelou.html on 21 May2007.
Betancourt J (2007) Commentary on ‘Currentapproaches to integrating elements ofcultural competence in nursing education,Journal of Transcultural Nursing 18: 25S–27S.
Campinha-Bacote J (2007)The Process of CulturalCompetence in the Delivery of Healthcare Services:The Journey Continues, 5th edn,TransculturalC.A.R.E.Associates, Ohio.
Campinha-Bacote J (2006a) Cultural compe-tence in nursing curricula: How are we doing20 years later? Journal of Nursing Education 45:243–244.
Campinha-Bacote J (2006b) Enhancing CAREThrough Transcultural Nursing:‘Can youpaint with all the colors of the wind?’Presentation at the 32nd Annual Conferenceof the Transcultural Nursing Society,Annapolis, MD.
Campinha-Bacote J (2005) A Biblically BasedModel of Cultural Competence in the Delivery of Healthcare Services,Transcultural CAREAssociates, Ohio.
Campinha-Bacote J (2003a) Cultural desire:The development of a spiritual construct of
cultural competence, Journal of ChristianNursing 20: 20–22.
Campinha-Bacote J (2003b) Cultural desire:The key to unlocking cultural Competence,Journal of Nursing Education 42: 239–240.
Campinha-Bacote J (1998)The Process of CulturalCompetence in the Delivery of Healthcare Services:A Culturally Competent Model of Care, 3rd edn,Transcultural C.A.R.E.Associates, Ohio.
Chapman E (2005) Radical Loving Care, BaptistHealing Hospital,TN.
Cooley M (nd) Mason Cooley Quotes, accessedat http://www.brainyquote.com/quotes/authors/m/mason_cooley.html on 21 May2007.
Dubois C (nd) Wisdom Quotes, accessed athttp://www.wisdomquotes.com/cat_sacrifice.html on 22 May 2007.
Ells A (nd) What does the Bible say about ...Humility?, Bible.com, accessed at fromhttp://www.bible.com/bibleanswers_result.php?id=120 on 15 April 2007.
Gallaher D (2007) Polishing the heart, Journal of Scared Work, accessed at http://journalofsacredwork.typepad.com/journal_of_sacred_work/ 2007/04/ polishing_the_h.htm on13 April 2007.
Grant L and Letzring T (2003) Status of culturalcompetence in nursing education:A litera-ture review, Journal of Multicultural Nursing &Health 9: 6–13.
Hart A, Hal V and Henwood F (2003) Helpinghealth and social care professionals developan ‘inequalities imagination’:A model for usein education and practice, Journal of AdvancedNursing 41: 480–489.
Hill N (n.d.) Napoleon Hill quotes, BrainyQuotes, accessed at http://www.brainyquote.com/quotes/authors/n/napoleon_hill.html on 22 May 2007.
Howard G (2003) Speaking of difference:Reflections on the possibility of culturallycompetent conversation, New Horizons forLearning Online Journal 9(2), accessed at
147Volume 28, Issue 1–2,April 2008 CCCCNNNN
Cultural desire:‘Caught’ or ‘taught’? CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 147

http://www.newhorizons.org/strategies/multicultural/howard.htm on 15 April 2007.
Jeffreys M (2006) Teaching Cultural Competence inNursing and Health Care: Inquiry,Action andInnovation, Springer Publishing Company, NY.
King M (nd) Cited in Molly Rush’s article,‘Making universal healthcare a reality.’TheThomas Merton Center, accessed at http://www.thomasmertoncenter.org/The_New_People/Nov2004/making_universal_healthcare_a_re.htm on 29 April 2007.
LeBaron M (2003) Communication tools forunderstanding cultural differences:Beyondintractability, in Burgess G and Burgess H(Eds) Conflict Research Consortium, University ofColorado, Boulder, accessed at http://www.beyondintractability.org/essay/communication_tools/ on 10 April 2007.
Leng Y (2002) Learner analysis in instructionaldesign:The affective domain, CDTLink 6:14–15, accessed at http://www.cdtl.nus.edu.sg/link/pdf/nov2002.pdf on 22 May 2007.
Lipson J and DeSantis L (2007) Currentapproaches to integrating elements ofcultural competence in nursing education,Journal of Transcultural Nursing 18: 10S–20S.
May R (1975) The Courage to Create, Bantam, NY.Ndura E (nd) The role of cultural competence
in the creation of a culture of Nonviolence,Culture of Peace Online Journal 2: 39–48,accessed at http://www.copoj.ca/pdfs/Elavie.pdf on 15 April 2007.
New American Standard Bible (2002) Zondervan,MI.
Nouwen H (1998) Reaching Out, Zondervan, MI.Rogers C (1951) Client-Centered Therapy,
Houghton Mifflin, MA.Stacks J, Salgado M and Holmes S (2004)
Cultural competence and social justice:Apartnership for change, Transitions 15: 4–5,accessed at http://www.advocatesforyouth.org/PUBLICATIONS/transitions/transitions1503.pdf on 10 April 2007.
Tervalon M and Murray-Garcia J (1998)Cultural humility versus culturalcompetence:A critical distinction in definingphysician-training outcomes in multiculturaleducation, Journal of Health Care for the Poorand Underserved 9: 117–125.
van Hooft S (1999) Acting from the virtue ofcaring in nursing, Nursing Ethics 6: 189–201.
148 Volume 28, Issue 1–2,April 2008CCCCNNNN
Josepha Campinha-BacoteCCCCNNNN
S O U L W O R K : FINDING THE WORK YOU LOVE, LOVING THE WORK YOU HAVE
(Revised edition; January 2007; ISBN 978-0-9775742-3-0)Deborah P Bloch PhD, Professor, Department of Leadership Studies, University of San Francisco
Lee J Richmond PhD, Professor, Loyola College in MarylandWhat programs address career development in an holistic way, including issues of meaning and purpose,
spirituality, and ‘work within a life’? Written for career planners, executive coaches, life change counsellors,HR and human services managers and all those interested in employee development, workplace values,
life-career assessment and personal transformation, this book helps to connect your career to the spiritualvalues that give your life meaning. SoulWork: Finding the Work you Love, Loving the Work You Have
relates your career to spiritual themes, and aims to provide advice and support to people in working through their personal choices. Updated from 1998, the revised edition places career choices in the
context of holistic, personal, spiritual development and internal change. A spiritual approach to integrating work/career with all life issues.
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911
[email protected]; www.e-contentmanagement.com
* * N O W A V A I L A B L E * *
CNJ 28_1_2_internal.qxd 14/07/2008 12:38 PM Page 148

INTRODUCTION
Research setting/context
The Kingdom of Saudi Arabia wasfounded in 1932 by King AbdulAziz Al
Saud.The population of Saudi Arabia con-sists of approximately 17,000,000 of whichSaudi nationals represent 72.7%, whileexpatriates of various origins comprise therest (Ballal, Hafiz & Sebiany 2002). Withthe discovery of oil in the 1930s, a tremen-
Key Wordsnursing;perception ofcare; values;Saudi Arabia;female Muslimnurses; Islam CN
149Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 149–161.
Perception of nursing care: Views of Saudi Arabian
female nurses
ABSTRACT ‘Values are principles and standards that have meaning and worth to anindividual, family, group, or community’ (Purnell & Paulanka 1998: 3).Valuesare central to the care provided by nurses.The provision of nursing care withinthe context of value clarification, has been explored from various perspectives,however, as values vary within cultures, there is a limited range of studies ref-lecting on Saudi Arabian nurses’ perspectives of nursing care.
Through a Heideggerian phenomenological research design, six nurses wereenrolled through purposive sampling. Semi-structured, in-depth interviews,which were audio tape-recorded, were chosen as the methods of data collection.A seven stage framework approach was applied to analyse and organise theresearch findings in three conceptual themes: values in context of Islam, thenurse-patient relationship, and identity’s influence on being in the world ofnursing.The findings of the research indicate that values in nursing and theperception of care are closely linked to the Islamic values of the informants.However, one of the most challenging aspects emerging from this study isrelated to these nurses’ experiences related to the public’s negative perception ofnursing as a profession for Saudi Arabian women.
Received 6 July 2007 Accepted 26 April 2008
JETTE MEBROUKProgram DirectorNursing Education and ResearchNursing AffairsKing Faisal Specialist Hospital & Research CenterJeddah, Saudi Arabia
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 149

dous development commenced. The develop-ment of industry, education and healthcare serv-ices quickly brought the country towards thestandard of other industrialised countries (Ballalet al 2002).Today the Kingdom of Saudi Arabiahas a population who has embraced the modernworld while at the same time having held on totheir cultural traditions and values.
Islamic worldviewIslam, which connotes submission, surrenderand obedience to Allah (Mawdudi 1985) is thefundamental religion of the society in Saudi Ara-bia, with the whole of the national populationbeing Muslim. Qur’an is the holy script, andthere are five pillars of Islam. Prophet Muham-mad [PBUH1] said that Islam is based on fivepillars: to testify that there is no god but Allah and that Muhammad is Allah’s apostle,to perform prayers, to pay obligatory charity,to perform pilgrimage, and to fast Ramadan(Alkhuli 2000: 46). While these aspects aremandatory in Islam, Sunnah, denoting the wayProphet Muhammad (PBUH) lived his life, isfollowed voluntarily by Muslims (Sunnah 2008).
Muslims believe in the creation of man andwoman, Adam and Eve, both coming from a sin-gle soul, whereby neither is better than theother, and every human being counts, as the lifeof each individual is sanctified (Elnaggar 2005).Muslims believe that humans have been givenfree will, but also that Allah knows their destiny(Hameed 2002). Actions that are permissibleare termed Halal while prohibited actions arecalled Haram, and both these concepts areessential in practice of Islam. Rassool (2000)explains how the worldview of Muslim patientsincludes perception of illness, suffering anddeath as being part of life and a test from Allah,and that these aspects of life are to be addressedwith patience, meditation and prayers.
Women’s status within an Islamic orientedsociety has always been a controversial issue(Hassan 1999). Women have, based on Islamicvalues, essential roles as caregivers and home-
makers. It is difficult to separate Islamic and tra-ditional values, but in general a woman is con-sidered to possess qualities such as being gentle,caring and self-sacrificing. Men are complemen-tarily considered to be protectors of women(Hassan 1999). Family is an essential factor in aMuslim’s life, and Islamic ethical values involvestandards of behaviours that control relationshipamongst family members, such as honesty, res-pect, obedience, decency, loyalty, mercy, sym-pathy, and truth-telling (Alkhuli 2000).
Nursing in the Islamic context has roots backto the time of Prophet Muhammad (PBUH).Rufaidah bint Saad was known as the first Mus-lim nurse. She learned medical care by workingtogether with her father who was a physician.In war times, Rufaidah cared with other vol-unteers for the wounded soldiers, and in timesof peace she provided nursing care for sickpatients in a tent outside the Prophet’s mosquein Madina (Kasule 2008).
Education in Saudi ArabiaFormal education of females in Saudi Arabiadeveloped radically in the beginning of the1960s. At that time, women gained the oppor-tunity to join formal education and universities,and become employed within a few sectorswhile being able to maintain the traditions andrespect for the moral code of Islam (Megalli2002; Doumato 1999). Nursing was one of theprofessions that opened to Saudi females. In col-laboration with the World Health Organization(WHO), the Saudi Arabian Ministry of Health(MOH) opened the first nursing schools with a one-year program for men in the late 50s. Afew years later similar programs for womenwere opened in Riyadh and Jeddah. In 1981 theadmission criteria were raised from fifth andsixth grade to ninth grade entry level, and thecurriculum was increased to a three-year pro-gram (Al-Osimy 1994).The Bachelor of Sciencein Nursing (BSN) was introduced in Saudi Arabia in 1976, followed by establishment ofMasters Programs in 1987. A minimum of 12
150 Volume 28, Issue 1–2,April 2008CCCCNNNN
Jette MebroukCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 150

years of elementary and secondary educationwas required for entry to the BSN program(Tumulty 2001; Aldossary, White & Barriball2008). Up until recently, all BSN programs havebeen exclusively for females. The first male BSN program was reported in 2006 to have 307 Saudi male students enrolled and distrib-uted over the four years of academic program(MOH 1427H report). Although nursing educa-tion has undergone a tremendous developmentand the profession of nursing for females hasIslamic roots, it is still a profession with societalstigma attached (Miller-Rosser, Chapman &Francis 2006).
Values and nursing careLeininger (1997) describes the premises of theCultural Care Theory, where care is interlinkedwith cultural values, beliefs and practices thatare influenced by and often embedded in theworldview, namely: language, philosophy, reli-gion, kinship, social, political, legal, education-al, economic, technological, ethno-historical,and environmental context of culture.
‘Values are principles and standards that havemeaning and worth to an individual, family,group, or community’ (Purnell & Paulanka 1998:3).Values are also a personal perception of whatis ‘good and useful and contribute to self-evalu-ation and development of one’s identity.Withina specific culture, values refer to the persistent,powerful, and directive forces that give meaningand direction to the individual’s, group’s, fami-ly’s, or community’s actions, decisions and life-ways (Andrew & Boyle 1995).
Culturally sensitive care based on patient andfamily’s values is fundamental to nursing. As val-ues, culture and caring are core concepts withinnursing, extensive literature and research havebeen published, with a focus on values and perspectives of the Muslim patient being carefor by nurses of diverse cultural backgrounds(McKennis 1999; Lawrence & Rozmos 2001;Hammoud, White & Fetters 2005; Miklancie2007). On the other hand, limited attention has
been given to the caring relationship betweenthe Muslim patient and Muslim nurse, particu-larly within the Saudi Arabian context.
Research questionsThe research focussed on exploration of Saudifemale nurses’ experiences, seeking to answerthe following questions: What are commonaspects of their experiences in provision of care?Which values do Saudi Arabian female nursesperceive to be central to nursing care of SaudiArabian patients? How does nursing influenceeveryday life of Saudi Arabian female nurses?And how does nursing give meaning to theSaudi Arabian female existence?
RESEARCH DESIGN
Methodology
Although philosophical understanding guides all research, and the choices of methodologydepends on the project’s intent and the researchproblem (Wellard 1999), the great challenge tothe researcher was to provide meaningfulnessby applying the findings to nursing practice.Qualitative research methodology was selected,as it focuses on exploration of everyday lives ofpeople and their experiences as seen from theirperspective (Turner & Emden 2002).While var-ious approaches exist within the qualitativeresearch paradigm, the topic under investigationin this research was highly appropriate for aphenomenological research approach.
Phenomenology is appealing to nursingresearch because it reflects upon values andbeliefs. As phenomenology seeks to illuminatephenomena by uncovering unnoticed or over-looked aspects, it allows inquiry and discoveryof unknown phenomena that are important tonursing, and it is through exploration of suchquestions that description of experiences fur-ther understanding of a phenomenon (O’Brian2003). The process to discovery describes andanalyses raw data in search of phenomena im-portant to nursing care.
151Volume 28, Issue 1–2,April 2008 CCCCNNNN
Views of Saudi Arabian female nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 151

Selection of informantsThe researcher used purposive sampling, as thissampling method was thought to provide therichness of experience and perspectives on theconcepts of caring, values, beliefs and how theseare integrated in provision of nursing care.Inclusion criteria were set to ensure enrolmentof appropriate informants. Saudi Arabian femalenurses who graduated from a Saudi ArabianSchool of Nursing, with a minimum of one yearof clinical nursing experience, the ability tospeak English, and who were employed at thespecific tertiary hospital in Saudi Arabia wherethe research took place, were selected.
To prevent coercion, nurses in student rolesundertaking one of the post-graduate nursingDiploma courses, and nurses working in thesame department as the researcher were ex-cluded from participation in the study.
Adequate sample size in qualitative research isnot dependent on the numbers of informants,but rather in the richness of data collected. Inqualitative research the aim is to reach a stage ofsaturation of data, which refers to the stagewhere no new or controversial information isuncovered (Burns & Grove 2007). Initially sixinformants were included, but one withdrewfrom the study when she left the hospital, and nolonger could take part in the research.The agesof the remaining five informants ranged from 23to 26 years. All informants were born and raisedin Saudi Arabia, were unmarried at the time ofthe study and had between one and three yearsof nursing experience after graduation.
Data collectionIn Hermeneutic research, such as Heideggerphenomenology there is an interactive involve-ment of the researcher with the informants withthe researcher becoming actively involved in the research, rather than a ‘passive onlooker’(O’Brian 2003). This study used naturalisticinterviewing as the data collection tool. Theinterviews were semi-structured, in-depth in-terviews, with open-ended questions. In the tra-
dition of phenomenology, the questions focussedon experiences of the informants with the intentof uncovering the informants’ perception ofnursing care. Each informant met twice with the researcher for interviews, each averaging 45minutes. Interviews were audio taped, and tran-scribed verbatim.
Data analysisData analysis in qualitative research is distinctlydifferent from data analysis in quantitative stud-ies. One of the challenges faced by a researcherin a qualitative study with a large amount of narrative data, is how to apply a systematicapproach when analysing the data (Taylor, Ker-mode & Roberts 2007). Data collected in phen-omenological research will inevitably containmany words and phrases used by the informantsto describe their experiences.
Data analysis in this research was approachedusing Drauker’s (1999) seven stages of dataanalysis. The initial stage of the process wasreading and re-reading interview transcriptswhile listening to the tapes to enhance compre-hension of the written word and to gain recall of paralinguistic aspects of the conversation.Thereafter, an interpretive summary and manualcolour coding of the text took place, which was the initial step in theme identification. Inthe next step, informants were involved if theresearcher needed to seek clarification of am-biguous aspects. The researcher then reviewedthe coding and initial themes, followed by com-paring and contrasting of the data, whereby con-stitutive patterns that linked the themes wereidentified. The appropriateness of inter-raterreliability in qualitative research has been ques-tioned, however where the investigator’s bias isespecially likely to be perceived to be a prob-lem, it may have a valid place (Pope, Ziebland &Mays 2000). Inter-rater reliability was used toaddress potential bias and ensure credibility ofthe research. A Masters prepared nurse per-formed an independent analysis based on thetranscriptions, identifying main aspects. Dif-
152 Volume 28, Issue 1–2,April 2008CCCCNNNN
Jette MebroukCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 152

ferences between these and the researcher’sthemes were merely related to choice of words,which made no significant difference to themeaning of the themes.
Ethical considerationsEthical approval for the research was obtainedthrough the Institutional Review Board (IRB) ofthe research setting and Deakin UniversityHuman Research Ethics Committee (DUHREC),Australia, where the researcher was enrolled ina Masters of Health Science (Nursing). Invita-tions to participate in the research were sent topotential informants in English and Arabic. Eachinformant provided informed consent beforeenrolment in the research project, and wasinformed both verbally and in writing of theirright to withdraw from the study at any timewithout any repercussion. Informants wereensured confidentiality, which included securemanagement and storage of the audio tapes andthe verbatim transcriptions of the interviews ina lockable cabinet. Ethical considerations werealso addressed within the informant–researcherrelationship. Although the research was not an-ticipated to be of potential risk for the inform-ants, Saudi Arabian female nurses are a minoritygroup, and the researcher did consider this inplanning the interviews ensuring proper use ofthe Islamic code of communication.
Validity of the researchValidity in qualitative research should not beabout strict adherence to a set of rules, butrather about the faithfulness to the essence and notion of the research approach (Wellard1999). Lincoln and Cuba’s (1984) criteria ofcredibility, transferability, dependability andconformability were sought as measures forvalidity in this study. Credibility can be ad-dressed by field notes and research journalentries providing a research trail (Koch 1994).The researcher’s personal experience of work-ing and living in Saudi Arabia also enabled her with in-depth insight in the cultural context
to build on a trust relationship with the in-formants.
Data saturation, referring to the stage whereno new information is uncovered (Burns &Grove 2007) was achieved by undertaking twointerviews with each of the five informants.Theresearch methodology was not selected with adesire to provide a total representation of allSaudi Arabian female nurses. The informantswere perceived by the researcher to representthemselves, with the acknowledgment that eachindividual person is unique.The study popula-tion was, however, to some extent, consideredto represent perception of care of Saudi Arabianfemale nurses.
RESEARCH FINDINGSLack of discussion or definition of the termstheme and pattern seem to challenge readers ofqualitative research, when searching for thefindings of the research (Sandelowski & Barroso2002).The themes identified in this research aredefined as conceptual headlines within the Hei-deggerian philosophy.The goal with this inter-pretive study was to generate understanding,rather than to make generalisations, and thevalue of each individual informant’s experienceand perception were therefore of great impor-tance to the study. Data included under eachtheme may for this reason have originated fromall of the informants or only from some ofthem.To give the reader insight into how com-mon the aspect was, the researcher has includedthe number of informants who provided datafor each topic analysed.The data analysis gener-ated could be group into three themes, namely:• Values in context of Islam;• The nurse–patient relationship; and• Identity’s influence on being in the world of
nursing.
Theme 1: Values in context of IslamValues in context of Islam emerged clearly withcontribution from all informants. The themewas constructed based on informants narratives
153Volume 28, Issue 1–2,April 2008 CCCCNNNN
Views of Saudi Arabian female nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 153

related to Qur’an,2 Sunnah,3 prayers, Zamzam,honey, end-of-life-care, and gender segregation.
Holy Qur’an and SunnahThree of the informants described how theyused their Islamic belief consciously in theirnursing care, by providing the patients withexplanations for specific care interventions.Their explanations were based on two aspects;the Holy Qur’an and Sunnah that together formthe base for the Saudi Arabian population’s wayof existence (Daar & Al Khitamy 2001). One ofthese informants explained that she uses the tra-dition of Sunnah in her patient teaching. Anexample she used was regarding the importanceof cleaning the skin before an injection, whereshe compared the Prophet’s (PBUH) emphasison cleanliness to the reason for why it is neces-sary to clean skin before an injection.
Another informant described how she con-sciously uses the Qur’an in combination withconventional interventions to help her patients:
... give him the antiemetic and I am herebeside him, and I am reading the holy Qur’anfor him, so it will make it much of a differ-ence, because we all believe in the Qur’anand the role of it, the spiritual feeling.
An informant also described how she continu-ously uses Islam to comfort palliative patients,by encouraging them to listen to recitations ofthe holy Qur’an or watch Islamic lessons on thetelevision.
PrayersUsing prayers as part of nursing care wasdescribed by two of the informants. Praying wasconnected to distorted psychological well-being, and was not replacing conventional treat-ment, but used complementarily. One of theinformants explained how she respects the situ-ation by avoiding interruption or walking infront of or in close proximity to the patient dur-ing prayer. She also explained how she would
offer to pray with the patient, as prayers in theIslamic faith are known to improve well-beingand the ability to deal with illness.
ZamzamZamzam, the holy water from the spring inMecca, was mentioned by two of the informantsas being important to Muslim patients and theirtreatment.The Zamzam was explained to have acurative role. At the same time, Zamzam wasdescribed as being used in addition to conven-tional treatment, such as using it instead of reg-ular water when a patient takes his or her oralmedication. One of the informants highlightedhow she would ensure that the use of Zamzamwould not compromise a patient’s health, byexplaining that the Zamzam has to be boiled forpatients with neutropoenia to reduce the intakeof microorganisms. In this way she combinedIslamic values and scientific reasoning to pro-vide the best care for her patient.
HoneyThe use of honey was discussed by two inform-ants, who mentioned that honey is considered,based on the holy Qur’an, to have a place incurative interventions.The two informants weregiving patients advice on how to use honeyappropriately. One of the informants advisedher patients to avoid honey while being neu-tropoenic, and the other informant discussedthe problem when diabetic patients want to eathoney. She explained how she would teach adiabetic patient that honey can be used in differ-ent ways, such as topically on wounds.
End-of-life careIt was highlighted by two of the informants thatthey incorporate religious considerations in the end-of-life care.While dying or soon afterdeath, they would turn the patient to faceQuibla, which is the direction of Mecca that allMuslims turn to for prayer. Specific ceremonialcleansing of the deceased was also mentioned byone of the informants.
154 Volume 28, Issue 1–2,April 2008CCCCNNNN
Jette MebroukCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 154

Gender segregationAll informants mentioned the importance ofgender segregation, and described specific con-siderations to both male and female privacy.Theinformants would ensure that Saudi Arabianfemale patients remained appropriately coveredat all times, even when unconscious. In spite ofthe societal value of gender segregation thethree informants, who discussed the issue oftaking care of male patients, did not report hav-ing major concerns if their patient assignmentwould involve care for a male patient. It was,however, mentioned that physical assessmentsthat involved inspection of genital area wereimpossible, and that the nurse would be able toidentify potential problems through conversa-tion – an actual physical assessment would haveto be performed by a male health care profes-sional.
Theme: Nurse–patient relationshipTwo subcategories, ‘communication’ and ‘quali-ties of the nurse’ were used to organise andpresent the findings for this theme.The topic ofcommunication included verbal as well as non-verbal communication, while qualities of thenurse involved discussion on, helping and caringabout others.
CommunicationVerbal communication was first and foremostdiscussed in relation to language. It was high-lighted that mastering of the Arabic languagewould affect patients’ satisfaction and outcome.One of the informants also described how shesaw value in both the patient and nurse speakingwith the same Arabic dialect. Language seemedfor this informant to bond her and patienttogether while sharing common ground.Verbalcommunication with medical focus was oftenapproached with a personal focused conversa-tion. Jokes and humour in the verbal communi-cation were mentioned as being ways to relaxpatients by two of the informants.
Eye contact was considered valuable for com-
munication. Descriptions of eye contact didhowever include concerns in relation to situa-tions with male patients. Eye contact with malepatients was not considered to be totally elimi-nated, and one of the informants referred to eyecontact with a male relative as being inappropri-ate. She explained that she was cautious becausemen would not accept it and they would thinkshe would be impolite if looking directly intotheir eyes.
Touch was also considered an importantaspect of communication when providing nurs-ing care.This aspect was also incorporated withconsideration to the gender of the patient. Oneof the informants described the touch of a malepatient as:‘The professional touch.’
Smiling was mentioned as valuable in nursingcare, and smiling did not appear to need specialconsideration for male patients. Smiling waseven considered possible to use for nurses wear-ing face veil,4 as the eyes look different whensmiling. One of the informants mentioned thatpatients can detect smiles in ways other than byseeing the actual smile, saying: ‘It will appear inmy eyes and in my voice.’
Qualities of the nurseThe informants used a variety of characteristicsand values to describe a nurse and nursing care.These characteristics and values primarily ad-dressed the nurse–patient relationship. All in-formants described, in various ways, theirdesire to help people. These were referring toexperiences of helping in restoration of health,ensuring optimal treatment, patient’s accept-ance of the disease and situation, voicing ques-tions and concerns, and achieve quality of life.One specific way of helping was emphasised as:‘Trying to see things from patients’ pers-pective’, which the nurse described as leadingto personal and emotional involvement. Todescribe characteristics of a good nurse theinformants included re-telling of experiencesthat described themselves or other nurses asshowing empathy, patience, and respect; being
155Volume 28, Issue 1–2,April 2008 CCCCNNNN
Views of Saudi Arabian female nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 155

honest and trustworthy; and while being anactive listener also being able to control emo-tions.
Discussion about respect was approachedfrom various angles.While the informants sawquality of a nurse to include respect, it was alsostressed that they expected mutual respect fromtheir patients and families.
Theme 3: Identity’s influence onbeing in the world of nursingThree categories, career choice, external fac-tors, and internal factors, emerged during thedata analysis and led to the theme identity’sinfluence of being in the world of nursing.
Career choiceMedicine versus nursing as a profession was oneof the topics that came up during the interviews.The informants unanimously expressed thattheir career choice had involved, at one time oranother, a decision about whether to enrol in themedical school or the nursing school.
There were different motivational factorsinvolved in their choice to enrol and continuewith their nursing studies.The informants wereguided into the health care sector by their desireto help people.Two informants explained howthey admired their mothers who were nurses,and how their choice of selecting nursing ascareer path was influenced by the way they sawtheir mothers caring for people. One of themexplained: ‘In fact, inside me, I like to help peo-ple and that’s what I like my mother for, becauseshe is caring about us and she is caring aboutpeople.’ Another informant described how shewas motivated by the TV programs such as ERand 911.
External factorsOther factors that were found to influence theidentity of the nurses were presented in discus-sions focused on experiences of the society’sview of nursing, the family’s acceptance andsupport, and teamwork in the workplace.These
factors were grouped under the category exter-nal factors.
Society’s view of nursingThe society’s view of nursing directly influ-enced their identity.The informants described,in various terms, their experiences as challeng-ing, in relation to the view of the society. Oneinformant explained the comments that oftenwere made by her patients: ‘The most commonhere in Saudi Arabia, if the patient really likeyou, and see that you are very good, they alwaysask: “Why are you in nursing?” “Why didn’t youstudy medicine?” ’
Another informant described how shethought the reason for the societal disapprovalof women working as nurses is due to lack ofgender segregation:
They are looking at us like somebody strange… They are thinking that we are doing some-thing wrong … They are rejecting us as nurs-es. They are refusing that we are workingwith males in the same area … they do notbelieve that this is the right job for a woman.
While some TV programs had a positive effecton how society views nursing, other programswere seen as having a negative influence on thesociety’s perception. It was highlighted that it isnot uncommon that nurses in Egyptian moviesare portrayed as promiscuous or alcoholic, sup-porting the idea that female nurses engage inimmoral behaviour.This view was also found tobe promoted in a public debate within thenewspapers, although the informants thoughtthat recently this has changed and other per-spectives are voiced.
Importance of the family’sacceptance and supportThe importance of the family’s acceptance andsupport was unanimously described.They gen-erally expressed that their nursing career wouldnot have been possible if they had not had the
156 Volume 28, Issue 1–2,April 2008CCCCNNNN
Jette MebroukCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 156

support of their families. Both parents’ opinionswere found to be important to the informants;however, the fathers were often mentioned asplaying a special role. One of the informantsexplained how she had modified her uniform inorder to comply with the hospital’s policy ofwearing pants, while meeting her father’s wishof having her wear a long dress. Another nurseexplained how her father had supported herwhen she would come tired home from work.She reported that he would usually say to her:‘It will be good for you and good for yourpatient, and as I know … that if you do anythinggood, God will reward you.’
Teamwork in the workplaceTeamwork in nursing seemed to take an essen-tial role in the development of identity. Theinformants saw themselves as part of a nursingteam. One of the informants described how shesaw it to be valuable that nurses would do aquick assessment and emergency interventionbefore calling the physician. Care was consid-ered easily achievable through collaborationwithin the members of the team. One inform-ant described the team’s work as placing piecesin a jigsaw puzzle, where everyone contributedand continued from where the previous nursehad let off.The desire for teamwork seemed tobe strengthened during stressful situations.Theimportance of presence of team work and theinformant’s ability to work within the team,helped creating a meaning of being in the worldof nursing. At the same time teamwork createdrelationships between colleagues who collec-tively demonstrate concern for the patients andconcern for each other.Teamwork is in this wayclosely linked to a caring relationship betweencolleagues.
Internal factorsFactors such as self-realisation, self-concept andreligious identity were subcategories of the cat-egory internal factors.
Self-realisationDiscovering one’s self is essential to one’s iden-tity, and self-discovery takes place throughoutthe lifespan. Lived experiences may make onecome to self-realisation (Benner & Wruble1989).The informants shared some of their self-discovery during the interviews. One of theinformants explained how she had gone througha process: ‘I’m happy now in nursing. I knowthat life is not fair and it does not give me allthat I want, but I am trying to find a way toadjust and be right with myself … I don’t wantto live in conflict.’
Self-conceptAll of the informants explained their wish tocontinue their education with Masters degreesafter they had gained more clinical experience.One of the informants explained that she wouldlike to take a Masters degree and continue towork as a nurse, hoping to become a role modelfor other Saudi Arabian nurses. In this way, herself-concept became a link in an identity devel-opment, both for herself and potentially for theSaudi Arabian female nurses that she wanted tobecome a role model for.
Religious identityIslam being fundamental to values in nursingcare came so clearly through in the data analysisthat a whole theme was dedicated to this aspect,at the same time Islam also came through as sig-nificant in exploration of identity.The inform-ants unanimously reflected that they would notbe nurses if it was not supported within Islam.
Questions during the interview that from theresearcher’s perspective had cultural focus wereoften answered with religious content. At times,the informants deliberately tried to separate theconcept of culture and that of religion, but oftenthe informants answered as if culture and reli-gion are synonymous. One of the informantsexpressed the essence of this inquiry as,‘our cul-ture depends on our religion, which is Islam.’
157Volume 28, Issue 1–2,April 2008 CCCCNNNN
Views of Saudi Arabian female nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 157

DISCUSSIONReligion is involved at various levels in differentsocieties. In Western countries religion is oftena private matter, where the individual might feelviolated if they were addressed with religiousexpectation, particularly from persons that arestranger to them (Benn & Hyder 2002). Islam,for the Saudi Arabian population is, on the otherhand, a public affair. Saudi Arabian nurses have atacit understanding of the meaning of Islam.
People in end-of-life situations frequentlyexpress belief that God has priority over life and can do more for patients than health care professionals can (Kagawa-Singer & Blackhall2001). Similar perspectives were found incor-porated in the experiences of the informants,who described how they respectfully would takecare of the patient and the family by helpingwith the Islamic ritual during end-of-life.The informants’ familiarity with the culture,its population and the Islamic religion is mergedin taken-for-granted practice, based on tacitunderstanding and actions.
Gender segregation takes place in most soci-eties. Public toilets are generally assigned bygender. Most hospitals, if not all, throughout theworld, assign patients to shared rooms accordingto gender. However, gender segregation in SaudiArabia is more strict, and is based on Islamicmoral and ethical principles. It should not beunderestimated that gender segregation is wide-ly accepted in Saudi Arabia, and even thoughsome of the informants in this study expressedthat they do take care of male patients, manyagreed that they would prefer gender segrega-tion to greater extent. The informants in thisresearch clearly perceived value in gender segre-gation, which reflects that stereotypical views ofgender segregation being male dominance aremisunderstandings or ethnocentric perspectives.
The informants entered a relationship withtheir patients based on shared humanity. Ex-periences seemed to include combinations ofuniversal human values and values based on theIslamic foundation. Values significant to the
Islamic society include principles of justice,brotherhood and a dynamic balance of right andobligations. The informants’ professional andpersonal identity appeared intertwined, andinseparable from Islamic values, and signifieshow Islamic values penetrate the daily lives ofall members of the society.
Worldwide, communication is acknowledgedto play a central role in the provision of nursingcare, and while verbal and non-verbal commu-nication in this research was identified to havesimilar importance for the Saudi Arabian femalenurses, approach to such communication maybe shaped differently. The issue of non-verbalcommunication for Saudi Arabian female nursesmay be surrounded with some degree of pre-conceived ideas or bias due to the tradition ofwearing face veil.The researcher had thereforeprepared questions to explore the informants’experiences in this regards. The informantsreflected that non-verbal communication is notthreatened due to application of a face veil,and it was found that there exists a taken-for-granted situation in this aspect as well. Verbalcommunication was often approached using ice-breaking questions that were considered to cre-ate a bond between the patient and the nurse,and it was thought to be ideal to lead the con-versation naturally over on the patient’s ownconcerns.
Being and belonging in the world seemed tobe extended through shared language. Commu-nication is inherent in the nurse–patient rela-tionship, although communication is approachdifferently depending on the gender of thepatient and relative. The informants have dis-covered ways for them to practice nursing that incorporates the values of communication,while respecting fundamental principles andvalues of Islam.
A large amount of the generated data seemedto be rooted in subjects related to the conceptof identity. Nursing literature discusses twokinds of identity: personal identity and profes-sional identity. Personal identity includes norms
158 Volume 28, Issue 1–2,April 2008CCCCNNNN
Jette MebroukCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 158

and values shaped by family, schooling, religion,and friends. Feelings, expectations, life experi-ences, body image, knowledge, and sense ofself-worth are also aspects of personal identity.Professional identity encompasses characteris-tics in relation to the profession of nursing.These characteristics are common beliefs aboutnursing and are shared with other nurses(Bradley & Edinberg 1990). Professional identi-ty, referred to as nursing identity, is a processthat develops throughout professional nurses’career (Cook, Glimer & Bess 2003).
Career choices by Saudi Arabian womentakes place within a complex interplay of familydynamics, Islamic values and the society’s in-fluence (Lovering 1996). Complexity arises forSaudi Arabian women, as nursing is associatedwith the low status of nursing in Saudi Arabia(Littlewood & Yousuf 2000). Unlike teaching,nursing is not considered to be a traditionaloccupation for women (Marrone 1999).
There was no description of an experiencethat led to exploration of professional autonomyexcept for one of the informants who describedhow she saw it to be valuable to do a quickassessment and emergency intervention beforecalling the physician.This may be linked to theIslamic values where honesty, respect, obedi-ence, decency, loyalty, mercy, sympathy, andtruth-telling are of central importance (Alkhuli2000). It is though important to bear in mindthat there were no questions that directly askedthe informants to reflect upon autonomy. It mayalso be an effect of the fact that the Saudi Arabi-an society is of collectivist orientation, whichmay influence the individual to value autonomydifferently than perhaps a nurse from an individ-ualistic oriented society (Aboul-Enein 2002).
Image of nursing is a challenge that faces thenursing profession throughout the world, butdifferent factors may be at play in the context ofthe Islamic society of Saudi Arabia. It is a con-cern that was highlighted by the informants, andit is a topic that needs in-depth exploration inorder to address it further.
IMPLICATIONS FOR NURSINGIN SAUDI ARABIAThis phenomenological research project hastaken interest in a minority group that hasexperienced limited attention in regards toperception of care. While exploring values,the problem of nursing for Saudi Arabianfemale was related to in terms of low image ofnursing.
Value of gender segregation of the population,including situations of health care is potentiallygoing to be a much bigger problem that merelyrelated to whether female nurses can providecare for male patients. While nursing still lackacknowledgement as a suitable profession forSaudi Arabian females, there is an increasing riskthat Saudi Arabian females will become morereluctant to enter nursing schools, and this willbecome a conflicting situation that eventuallywill lead to significant problems in provision ofcare to the Saudi Arabian female population asthe nursing shortage will increase.This researchhas demonstrated that Saudi Arabian femalenurses are able to form caring relationships withtheir patients while maintaining their lifestylebased on Islamic values.
CONCLUSIONThis research has identified common aspects of nursing care experiences of Saudi Arabianfemale nurses, of which the significant impor-tance of Islam was evident.Values were closelyrelated to Islamic values, and signified theimportance of Islam not only as an apparentreligion in relation to faith, but a religion thatsaturate the entire lifestyle of the Saudi Arabianfemale nurses. The informants in this researchhave clarified how they practice nursing fromsuch basis, while at the same time reflecting thepredicament of the low image nursing in theSaudi Arabian society where nursing shortage ispredicted to become worse as for the rest of theworld. Recommendations of this researchincludes further investigation in the challengesSaudi Arabian nurses experience, and an exten-
159Volume 28, Issue 1–2,April 2008 CCCCNNNN
Views of Saudi Arabian female nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 159

sive exploration of the image of nursing in theSaudi Arabian cultural context.
Endnotes1 PBUH stands for Peace Be Upon Him. It is
said by Muslims after each time ProphetMuhammad (PBUH) is mentioned in writ-ing as well as spoken communication. It isused in this article to signify the researcher’srespect of values of the informants and theIslamic society.
2 Qur’an meaning Koran is written in this way as the pronunciation of the word is best reflected as such, it also signifies theresearcher’s sincere respect to the Saudi Ara-bian culture and the Islamic religion.
3 Sunnah is the term used for the traditionalportion of Muslim law, based on the wordsand acts of Muhammad (PBUH).
4 Face veiling in Saudi Arabia is practised withseveral variations. While women who useface veil may choose in general to covertheir eyes, this is not practised indoors in thehealth care setting.
ReferencesAboul-Enein FH (2002) Personal contemporary
observations of nursing care in Saudi Arabia.International Journal of Nursing Practice 8:228–230.
Aldossary A,While A and Barriball L (2008)Health care and nursing in Saudi Arabia.International Nursing Review 55: 125–128.
Alkhuli MA (2000) Morality in Islam, 1st edn,Dar Alfalah, Jordan.
Al Osimy MH (1994) Nursing in Saudi Arabia.Saudi Arabia: King Fahad National LibraryCataloging-in-Publication.
Andrews MM and Boyle JS (1995) TransculturalConcepts In Nursing Care, 2nd edn, JBLippincott: Philadelphia.
Ballal SG, Hafiz AO and Sebiany AM (2002)Occupational health in Saudi Arabia.Occupational Medicine 17: 491–507.
Benn C and Hyder AA (2002) Equity and
resource allocation in health care: Dialoguebetween Islam and Christianity. Medicine,Health Care and Philosophy 5: 181–189.
Benner P and Wrubel J (1989) A phenomeno-logical view of the person:The self-interpreting being, in The Primacy of Caring:Stress and Coping in Health and Illness, pp41–51,Addison-Wesley Publishing: MenloPark, USA.
Bradley JC and Edinberg MA (1990) Communi-cation in the Nursing Context, 3rd edn,Northwalk: Connecticut, USA.
Burns N and Grove SK (2007) UnderstandingNursing Research. Building on Evidence-BasedPractice, 4th edn, Elsevier: St Louis, Missouri.
Cook TH, Gilmer MJ and Bess CJ (2003)Beginning students’ definitions of nursing: aninductive framework of professional identity.Journal of Nursing Education 42: 311–317.
Daar SA and Al Khitamy AB (2001) Islamicbioethics. Canadian Medical Association Journal164: 60–67.
Doumato EA (1999) Women and work in SaudiArabia: How flexible are Islamic margins?The Middle East Journal 53: 568–583.
Draucker CB (1999).The critique of Heideg-gerian hermeneutical nursing research.Journal of Advanced Nursing 30: 360–373.
Elnaggar M (2005) Islam and the Human Being,http://www.islamonline.net/english/introducingislam/Individual/article07.shtmlretrieved on16/04/2008.
Hameed S (2002) Fate and Free Will, http://www.readingislam.com/servlet/Satellite?cid=1123996015716&pagename=IslamOnline-English-AAbout_Islam/AskAboutIslamE/AskAboutIslamE last retrieved on16/04/2008.
Hammoud MM,White CB and Fetters MD(2005) Opening cultural doors: Providingculturally sensitive healthcare to Arab Ameri-can and Arab Muslim patients. American Journalof Obstetrics & Gynecology 193: 1307–1311.
Hassan AG (1999) The Rights and Duties of Womenin Islam. Riyadh, Saudi Arabia: Darussalam.
160 Volume 28, Issue 1–2,April 2008CCCCNNNN
Jette MebroukCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 160

Kagawa-Singer M and Blackhall LJ (2001)Negotiating cross-cultural issues at the end oflife ‘You got to go where he lives’. JAMA 286:2993–3001.
Kasule OH (2008) Rufaidah bint Saad, http://www.crescentlife.com/thisthat/feminist%20muslims/rufaida_bint_saad.htm lastretrieved on 16/04/2008.
Koch T (1994) Establishing rigour in qualitativeresearch: the decision trail. Journal of AdvancedNursing 19: 976–986.
Lawrence P and Rozmus C (2001) Culturallysensitive care of the Muslim patient. Journalof Transcultural Nursing 12: 228–233.
Leininger M (1997) Overview of the theory ofculture care with the ethnonursing researchmethod. Journal of Trancultural Nursing 8:32–52.
Lincoln YS and Guba EG (1985) NaturalisticInquiry. Sage,Thousand Oaks CA.
Littlewood J and Yousuf S (2000) Primary healthcare in Saudi Arabia:Applying global aspectsof health for all locally. Journal of AdvancedNursing 32: 675–681.
Lovering S (1996) Saudi Nurse Leaders: CareerChoices and Experiences. UnpublishedMasters thesis, Massey University, NewZealand.
Marrone SR (1999) Nursing in Saudi Arabialeadership development of a multiculturalstaff. JONA 29: 9–11.
Mawdudi A (1985) Towards Understanding Islam,2nd edn, Gassim: Saudi Arabia
McKennis AT (1999) Caring for the Islamicpatient. Association of Operating Room NursesJournal 69: 1185–1202.
Megalli M (2002) Saudi women face complexchoices. Arab News. Retrieved through on-lineservice of Arab News, October 2003.
Miklancie MA (2007) Caring for patients ofdiverse religious traditions: Islam a way oflife for Muslims. Home Healthcare Nurse 25:413–417.
Miller-Rosser K, Chapman Y and Francis K(2006) Historical, cultural, and contem-
porary influences on the status of women innursing in Saudi Arabia. Online Journal of Issuesin Nursing 11: 3.
Ministry of Health (2006) Annual Report. www.moh.gov.sa/en. Retrieved 12 April 2008.
O’Brian L (2003) Phenomenology. In SchneiderZ, Elliott D, Beanland C, LoBiondo-Wood Gand Haber J (Eds) Nursing Research Methods,Critical Appraisal and Utilization, 2nd edn, pp193–204. Mosby, St Louis MO.
Pope C, Ziebland S and Mays N (2000) Qualita-tive research in health care:Analysing quali-tative data. British Medical Journal 320:114–116.
Purnell LD and Paulanka BJ (1998). TransculturalHealth Care A Culturally Competent Approach. FADavis Company: Philadelphia PA.
Rassool GH (2000) The crescent and Islam:Healing, nursing and the spiritual dimension.Some considerations towards an under-standing of the Islamic perspectives on caring.Journal of Advanced Nursing 32: 1476–1484.
Sandelowski M and Barroso J (2002) Findingthe finding in quantitative studies. Journal ofNursing Scholarship 34: 213–222.
Sunnah (2008) Sunnah and Adherence, http://www.unbsj.ca/clubs/msa/sunnah.html lastretrieved on 16 April 2008.
Taylor B, Kermode S and Roberts K (2007)Research in Nursing and Health Care: Evidence forPractice, 3rd edn, Melbourne,Australia.
Tumulty G (2001) Professional development ofnursing in Saudi Arabia. Journal of NursingScholarship 33: 285–292.
Turner DS and Emden C (Eds) (2002) Inter-pretive Research Practices and Challenges.Monograph for module HNN722, ResearchMethodologies in Nursing. Deakin University,School of Nursing: Geelong,Australia.
Wellard S (1999) ‘Research:Ventures in Know-ing’, and ‘Issues of Validity in Research’.Research Methodologies in Nursing Study Guidefor Module HNN 728. Geelong,Australia:Deakin University.
161Volume 28, Issue 1–2,April 2008 CCCCNNNN
Views of Saudi Arabian female nurses CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 161

Transcultural nursing must be more thancaring for the patients or clients who come
through our doors. It is not and cannot be solelyabout those we serve in our small corner of theworld. Just as the fluttering of butterfly wingson one side of the world can contribute to theformation of hurricanes half way around theglobe, social, political and economic events inone hemisphere affect the lives of people in theother half. This reality is becoming more evi-dent with each passing day as globalisationbecomes more firmly rooted and the internetreaches the farthest corners of our planet. Weare becoming global citizens, tied inextricablyto each other.What affects one group of citizenshas an impact on the lives of every other group.This interdependence, along with a sense ofobligation and our common humanity, underliesthe imperative for social justice when address-ing the health care needs of our fellow worldcitizens.
In the paper by Pacquiao (2008) that followsin this section, the author outlines the skillsneeded for world citizenship and describes howthese skills form the basis for providing cultur-ally competent care for vulnerable populations,
particularly those who have migrated because ofpolitical, economic or environmental dangers.Within this framework, she explains the con-cepts of social justice, human rights and com-passion in relation to cultural competence. Sheoffers a number of strategies for teaching theseabstract concepts and skills to health care stu-dents and practitioners.
Perhaps the timing of a new millennium hasmade the desire for change almost palpable inthe air we breathe. Old political administrationsare being defeated by electorates or parties whowant to overturn that which has been, even ifthe new younger voices have not yet been test-ed.The mood is one of wanting something dif-ferent from the old way of doing things,whether it is in Australia or the United States,Kenya, Russia, or the Middle East. But changecan also cause chaos if it is not accomplishedwith care, especially when this change occurswithin an unstable social or political context.
In the world today there are many examplesof change, chaos, unrest and increasing socialinequality, which have resulted in many peopleon the move. Motion and chaos seem to definethis current historical period. Whether from
162 Volume 28, Issue 1–2,April 2008CCCCNNNN
NCCopyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 162–164.
EDITORIAL
Transcultural nursing: The global agenda
MARILYN (MARTY)DOUGLASAssociate ClinicalProfessorSchool of NursingUniversity of CaliforniaSan Francisco CA, USA
JULIENE G LIPSONProfessor EmeritaSchool of NursingUniversity of CaliforniaSan Francisco CA, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 162

war that shifts populations to refugee camps,or the hopelessness of poverty that drives theable-bodied to seek work in more promisingeconomies, many become refugees, pawns inhuman trade, asylum seekers, or voluntary mig-rants. Large numbers of nurses are among theseresettled migrants, many recruited from thedeveloping countries by the western indus-trialised countries whose aging populationsneed increased nursing care.These nurses facetremendous challenges, potential exploitation,and numerous barriers to the optimal use oftheir professional skills. Transcultural nursingmandates that the principles of social justice,human rights and cultural competence extendas much to our professional colleagues as theydo to our patients and clients.
In the paper by Mireille Kingma (2008) theauthor summarizes the scope and magnitude ofthe international nurse recruitment efforts andidentifies the types of abuse, discrimination andexploitation reported by migrant nurses. Theposition of the International Council of Nurses(ICN) is presented along with its key principlesfor ethical recruitment and employment prac-tices. In addition, ICN’s educational standardsfor assisting internationally-recruited nurses toadapt to their new environment are cited, aswell as strategies for integrating these nursesinto the host country’s organisational structure.Culturally competent nurses can help make thetransition easier for their international col-leagues by encouraging their education andprofessional growth through mentorship, com-passion, patience and support. Ultimately, thelearning becomes bidirectional; the mentorgains new insights about health care beliefs andpractices from the mentee and vice versa.
Vulnerable populations, whether on anotherside of the globe or indigenous to our owncountry, are a particular focus in transculturalnursing.The health care values, beliefs and prac-tices of these populations may be as differentfrom our own as those from another continent.Yet we may be blind to our own biases and prej-
udices because of the prolonged exposure of liv-ing within a dominant society that has isolatedand stigmatised these populations. One of thefirst steps in the process of gaining culturalcompetence entails self-reflection. One aspectis examining our own practice for evidence ofracial discrimination that can lead to disparitiesin health outcomes due to the inherent biases ofhealth care professionals.
In Section 4 of this issue, the authors of two papers address culturally competent care ofindigenous populations. McMurray and Param(2008) describe how structural, historical andpolitical factors have contributed to the negativehealth status and health outcomes of Australia’sAboriginal and Torres Strait Islander peoples.Included in these structural factors are barriersto health care access as well as biases of healthcare professionals themselves, especially whenassessing and analysing health problems. Strate-gies for overcoming these barriers and biasesare recommended by indigenous health profes-sionals and organisations of professional healthcare providers in Australia. In the second paper,Wilson (2008) describes her research thatexplores the health perceptions of Ma-oriwomen and their interaction with ‘mainstream’health care services. Results of her study provide guidance for her recommendations for culturally competent practice for these Ma-ori women.
Finally, these two papers also illustrate theneed for using culturally-appropriate researchmethods when investigating health problems ofvulnerable populations. Sensitivity to the cultur-al norms of the group is necessary throughoutthe research process.To give an example fromthe US, permission of the tribal chief of an Indian population is required by institutionalresearch review boards before initiation of anyresearch with a tribe. However, obtaining thispermission may be accompanied by difficultiesin conducting the research. In some tribes, butnot others, health care practices are consideredthe secret purview of the tribal healer and can-
163Volume 28, Issue 1–2,April 2008 CCCCNNNN
Editorial: Transcultural nursing:The global agenda CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 163

not be shared outside the tribe (Struthers et al2005).Therefore the research may be limited bythe questions that can be asked and the findingsthat may be published. Sensitivity to these issuescan prevent a violation of trust, which couldinterfere with cross cultural communication andlead to misleading findings and irrelevant rec-ommendations for practice.
The papers in this section illustrate thenature and scope of transcultural nursing as aglobal endeavor. By incorporating the principlesof social justice, human rights, compassion, andhuman dignity, transcultural nurses aim to pro-vide culturally competent care to fellow worldcitizens, irrespective of their cultural origins,human condition or social situation. By inte-grating our clients’ cultural practices into theirhealth care plan, we improve the probability ofachieving positive health outcomes and meetingthe primary objective of the World HealthOrganization (WHO), that of ‘attainment by allpeoples of the highest possible level of health’.
ReferencesKingma M (2008) Nurses on the move: Divers-
ity and the work environment, Advances inContemporary Transcultural Nursing, 2nd edn, Con-temporary Nurse special issue 28(1–2): 198–206.
McMurray A and Param R (2008) Culture-specific care for Indigenous people:Aprimary health care perspective, Advances inContemporary Transcultural Nursing, 2nd edn, Con-temporary Nurse special issue 28(1–2): 165–172.
Pacquiao DF (2008) Nursing care of vulnerablepopulations using a framework of culturalcompetence, social justice and human rights,Advances in Contemporary Transcultural Nursing, 2ndedn, Contemporary Nurse special issue 28(1–2):189–197.
Struthers R, Lauderdale J, Nichols LE,Tom-Orme L and Strickland CJ (2005) Respectingtribal traditions in research and publications,Journal of Transcultural Nursing 16: 193–201.
Wilson D (2008) The significance of a culturallyappropriate health service for Indigenous Ma-ori women, Advances in Contemporary TransculturalNursing, 2nd edn, Contemporary Nurse special issue28(1–2): 173–188.
World Health Organization WHO (2006)Constitution of the World Health Organization.Basic Documents, 44th edn,WHO: Geneva,accessed at http://www.who.int/governance/eb/who_constitution_en.pdf on 29 Febru-ary 2008.
164 Volume 28, Issue 1–2,April 2008CCCCNNNN
Marilyn (Marty) Douglas and Juliene G LipsonCCCCNNNN
PLEASE KNOCK BEFORE YOU ENTER: ABORIGINAL REGULATION
OF OUTSIDERS AND THE IMPLICATIONS FOR RESEARCHERS
By Karen L Martin; ISBN 978-1-921214-37-0; 170 pp; Post Pressed; 2008
Karen Martin’s thesis was highly praised by two internationally renowned scholars. Professor Norman Denzin, (University of Illinois) remarked, ‘this is a brilliant and stunning dissertation, original in conception and bold in execution ... Relatedness theory is a major contribution to this literature.’
Professor Manulani Meyer, (University of Hawaii) celebrated this work for its cultural truth and integrity and wrote, ‘Her research showed flair, originality, depth and significant independent scholarship within an Aboriginal community. It has brought us new insights into a people and Nation that will help our own knowledge systems evolve ... Her work is timely.’
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911;[email protected]; www.e-contentmanagement.com
N E W T I T L E A V A I L A B I L I T Y
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 164

INTRODUCTION
Primary health care provides an ideal frame-work for conceptualising the issues and inf-
luences related to culturally appropriate carefor Indigenous people. A primary health careapproach is strategic, focusing on equity, access,
empowerment and intersectoral partnerships as essential elements for maintaining health.Contemporary thinking in health and healthcare underlines the convergence of these centraltenets of primary health care around inequali-ties embedded in the social conditions of peo-
Key WordsIndigenousculture; culturecare; socialinequality;Aboriginalhealth; primaryhealth care CN
165Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 165–172.
Culture-specific care for Indigenous people: A primary
health care perspective
ABSTRACT This article argues that a primary health care approach is an appropriateconceptual framework for addressing the health needs of Indigenous people.Primary health care is strategic, focusing on equity, access, empowerment andintersectoral partnerships as essential elements for maintaining health. Stereo-typical notions of Indigenous ill health as being embedded in a general view of‘culture’ can mitigate against achieving equity, access to health care andultimately self-determinism. Because health is embedded in the social condi-tions of people’s lives, the emphasis in Indigenous health care should firstaddress Indigenous social disadvantage and ways of working in partnershipwith various groups of Indigenous people to achieve their health goals. Acritical multicultural approach situates cultural differences within the widernexus of power relations, and helps overcome the negative stereotyping thatoften prevents inclusive, self-determined care. Recommendations are suggestedfor change at the societal, professional and individual level.
Received 25 June 2007 Accepted 18 March 2008
ANNE MCMURRAYChair in NursingPeel Health Campus Murdoch UniversityPerth WA, Australia
RANI PARAMLecturer
Centre for Aboriginal Medical and Dental Health (CAMDH)
The University of Western AustraliaPerth WA, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 165

ple’s lives. These social conditions determinewhere and how people live, and what opportu-nities exist for their education, employment andtheir capacity as parents and citizens (White-head 2007;World Health Organization [WHO]2005).This is not to imply that a person’s socialenvironment at one point in time predeter-mines health status and health outcomes acrossthe life course. Circumstances can change, andinequities can be countered in numerous waysat different stages. However, a position of rela-tive disadvantage from birth combined withexposure to adverse circumstances can create asystematic life exposure trajectory that playsout in both overt and subtle ways to constrainthe capacity for a healthy and satisfying life(Hertzman & Power 2006). Unfortunately, thisis the inequitable life situation for many In-digenous people. For nurses and other health professionals it poses a critical question as towhether and to what extent culture-specificcare can redress health at birth and throughoutthe life course.
INDIGENOUS DISADVANTAGEReports of disadvantage among the world’s 350 million Indigenous people are indisputable(Smith 2003). In Australia alone, a proliferationof data illustrates the extent to which our half amillion Aboriginal and Torres Strait Islanderpeople live in disadvantaged social conditionsrelative to other Australians (Australian Instituteof Health and Welfare [AIHW] 2004; AustralianMedical Association [AMA] 2007; Trewin &Madden 2005). The level of disadvantage hasleft Indigenous Australians with a 17 year dis-parity in life expectancy, and a mortality rate4.6 times higher than the overall population(Trewin & Madden 2005). A comprehensiveanalysis of the plight of Aboriginal people, whorepresent 90% of Australian Indigenous people,show that they are at least twice as likely to havea profound or severe activity limitation, oftenfrom an earlier age (Trewin & Madden 2005).
Aboriginal Australians experience earlier onsetof most chronic diseases, are three times morelikely to have a major coronary event than non-Aboriginal Australians (AMA 2007) and experi-ence a disease prevalence of diabetes mellitusfour times greater than non-Aboriginal people,resulting in five times the hospitalisation ratefor this disease (Trewin & Madden 2005). Hos-pitalisation rates for respiratory diseases andinjury among Aboriginal people is twice that ofnon-Aboriginal people and Aboriginal peoplehave 12 times the rate of dialysis treatment forkidney disease (Trewin & Madden 2005).
In terms of a healthy start to life, the infantmortality rate, prevalence of low birth weight,hospitalisation, malnutrition, and infection ratesare substantially higher than among the generalAustralian community (AIHW 2004;Trewin &Madden 2005). In subsequent years, especiallyin remote areas, issues of transport, economiccommunity and management issues related tofood, education and other resources contributeto disadvantage by denying Aboriginal com-munities access to the fundamental elements of good health, education and social support.Social problems in some Aboriginal families canalso compromise the health of children, includ-ing hazardous consumption of alcohol, familyviolence and poor parental mental health(Trewin & Madden 2005; Zubrick et al 2005).Poor family functioning is also rooted in socio-economic disadvantage.
The AMA (2007) describes the health dispar-ities between Indigenous and non-Indigenouspeople as a national tragedy that shows our fail-ings as a community. Despite recognition thatIndigenous people have numerous financial,geographic, and personal barriers to accessingcare, health professionals and social commenta-tors alike are often inclined to attribute thepoor health of Aboriginal people to culture,rather than structural, historical or political fac-tors.The efficacy and feasibility of this assump-tion can only be logically challenged once wedispel the notion that Indigenous people repre-
166 Volume 28, Issue 1–2,April 2008CCCCNNNN
Anne McMurray and Rani ParamCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 166

sent a monolithic society (Toussaint 2003). Ifthis were the case, knowledge of Indigenousculture would afford health planners a set ofculturally appropriate guidelines from which to develop culture-specific care. Since there isconsiderable diversity among Indigenous Aus-tralians a more realistic view can be illustratedthrough a critical multicultural approach,wherein health professionals develop alternativeways of thinking about Indigenous values andworldviews which don’t entail the reification ofIndigenous culture as a set of fixed culturalproperties (Culley 2006).
Critical multiculturalism is reflexive, situat-ing cultural differences within the wider nexusof power relations (Culley 2006). It is anti-essentialist in that culture is not used to denotedifference or to engender negative stereotyping.Instead, it should be seen as a movable socialprocess, which does not limit professional prac-tice to a deficit model, but rather, celebratesdiversity and adopts inclusive strategies in allcare planning (Culley 2006).The role of healthprofessionals in this type of approach is basedon close engagement with the group and anunderstanding that initiatives to improve healthoutcomes must emanate from within the group.Health professionals act as resource persons ingenuine, authentic partnerships to seek politicaland structural solutions to health problems.Thisapproach is congruent with primary health care,which also mandates that the health of thegroup is embedded in a broad, intersectoralapproach that unravels the various interactionsbetween culture, societal structures and socialinequalities that create disadvantage for the par-ticular Indigenous group.These interactions canreveal where barriers exist to accessing healthcare, or where they impede members of thegroup from becoming sufficiently health literateto make empowered decisions for better health.
Before this level of empowerment is achieved,strategies to overcome historical disempower-ment must be implemented.These focus on theconditions that promote awareness of vulner-
ability, and that include representation membersof the group at the tables where decisions aremade, in equal standing with all parties. This is the key to achieving substantive freedom, whatNobel Prize winner Amartya Sen describes ashaving the capabilities to choose a life that a per-son has reason to value (Sen 1999). According toPearson (2005) the end point of developing thesecapabilities is the development of a civil society;networks of families, communities and business-es that do not emerge from bureaucratic power,but from public order and safety and the motiva-tion to develop skill, self-confidence and person-al responsibility.
AUSTRALIAN INDIGENOUSSOCIETIES: COMMONALITIESAND DIFFERENCESDespite the commonalities that bind membersof a cultural group, some behaviours, culturaltraits and predispositions are often tacit aspectsof behaviour; unconscious, shared predisposi-tions that are not always expressed in the sameway by all who claim membership in the group.Individual expressions of attitudes, beliefs andbehaviours vary according to age, gender, per-sonal histories, and situational factors, and theseare, in turn, influenced by family, group andcommunity influences. However, irrespective ofthe heterogeneity of Aboriginality (Toussaint2003), as health professionals it is crucial tohave some understanding of cultural norms andtraditions. This knowledge helps health careproviders understand different ways of thinkingabout health, life, and different perspectives ofwell-being. For example, cultural knowledgeoften prescribes diet and eating habits, child-rearing practices, reactions to pain, stress anddeath, a sense of past, present and future,community and economic structures, responses to health care services and practitioners, andwhich behaviours are considered a violation ofsocial norms (McMurray 2007).
The most recognisable feature shared by many
167Volume 28, Issue 1–2,April 2008 CCCCNNNN
Culture-specific care for Indigenous people:A primary health care perspective CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 167

Indigenous cultures is a holistic, ecological, spir-itual view of health and well-being.This encom-passes physical, mental, cultural, and spiritualdimensions of health, and the harmonised inter-relationships between these and environmental,ideological, political, social and economic condi-tions (Eckermann et al 2006; Mignone & O’Neil2005; Swan & Raphael cited in Zubrick et al2005;Toussaint 2003). At the centre of Aborigi-nal people’s relationship with each dimension ofhealth is a fundamental spiritual connection withland, symbolising the ecological connectionbetween health and place.This is a metaphysicalconnection, wherein the spiritual element gov-erns all other inter-relationships. Historical fac-tors are also significant in these relationships.Colonisation by non-Indigenous people and thepolitical decisions that have ensued from col-onisation have disrupted Indigenous people’s connection between health and place, leavinggenerations of Indigenous Australians feeling dis-possessed of their place, both symbolically andgeographically (Adelson 2005; Eckermann et al2006; Pomaika’i Cook,Tarallo-Jensen,Withy &Berry 2005; Shore & Spicer 2004).
Dispossession, as a marker of inequity and disadvantage, is therefore one of the most im-portant issues that must be dealt with meaning-fully if Indigenous people are to develop andenhance their capacity for health. Recognisingand articulating the influence and impact of dis-possession should therefore be the central organ-ising principle in planning culturally sensitivecare for any specific Indigenous group.This alsolies at the forefront of the Australian Council forAboriginal Reconciliation Commission’s (ACAR)goals, to try to bring to voice Indigenous history,the misunderstandings between Indigenous andnon-Indigenous people, and the need to addressdisadvantage and disempowerment so that In-digenous Australians can achieve genuine self-determination (ACAR 1994). Achieving thisbegins by peeling back the layers of socialinequality perpetrated by both historical factorsand contemporary Australian social life.
SOCIAL INEQUALITIESUnravelling the various dimensions of inequalitymust begin with the recognition that a problemexists between Indigenous and non-Indigenoussocial life (Whitehead 2007). Failing to under-stand the persistence and multidimensionalnature of health inequalities can lead to prema-ture closure in defining the problem(s), and atendency to dismiss health outcomes as beingattributed to ‘culture’ when they need to beframed within structural features of politicaland social life, especially socioeconomic status(Whitehead 2007). For example, Indigenouswomen rarely have health problems examinedin relation to gender issues.Yet gender relationsare a significant part of the life of many Indigenous women, whose health problems may also vary considerably between geographic,socioeconomic and family situations.Timidity ingrappling with issues of family violence, preven-tative care or the need for women’s educationand empowerment can occur because of a lackof understanding or the inclination to assumethat it is unwise to challenge the group’s genderrelations and norms of behaviour. This line oflogic is paradoxical in light of national televisioncampaigns to illustrate appropriate norms ofgendered behaviour in relation to violenceagainst women, and by the legal system’s in-tolerance of minority groups using so-calledcultural defence to justify sexual assault, as evi-denced by the judicial conclusion of the notori-ous 2002 gang-rape of adolescent girls by fourPakistani-Muslim brothers (Adelman, Erez &Shalhoub-Kevorkian 2003). Among Aboriginalcommunities, increasing social inequality andthe continuing effects of colonisation have de-stabilised traditional systems governing conflictresolution and gendered behaviours, leading torisky patterns of substance use, intergenera-tional stress and trauma, and physical and psychological abuse (Astbury et al 2000).Attributing high rates of family violence to ‘cultural factors’ or to how Indigenous Aus-tralians lived traditionally not only is blatantly
168 Volume 28, Issue 1–2,April 2008CCCCNNNN
Anne McMurray and Rani ParamCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 168

ill-informed and simplistic, but further hindersAboriginal communities’ and health care provi-ders’ collective efforts to address the problem,thereby reinforcing inappropriate stereotypes.
Whether intentional or not, subtle and overtforms of racism exist in contemporary media.These include depictions that stereotype Indige-nous Australians as living in discrete remotecommunities (Scrimgeour 2007; Johns 2006),the framing and reporting of news (Bannerjee &Osuri 2000), and in inappropriate comparisonswith unrelated minority groups in other coun-tries (Shaw 2000). We assert that this type ofstereotyping is racist.
In general, mainstream nurse researchershave failed to confront racism as an issue thathas become conflated with culture (Anderson etal 2003; Barnes et al 2003; Culley 2006; Gustaf-son 2005; O’Brien 2006). Racism in any formdenotes certain groups as being uncivilised,inferior, and having cultural traits that are linkedto their physical appearance. It postulates prac-tices that differentiate, exclude, alienate anddominate (Culley 2006). In the health care sys-tem this can include direct psychological orphysical violence, exclusionary practices, un-healthy symptoms or institutional practices thatdeny access to adequate or appropriate care(Culley 2006). The cause of this type of biasoften lies in health professionals’ approach toassessing and analysing health problems. Usingexisting inventories to assess problems can leadto defining Indigenous people according tonorms established in the non-Indigenous popu-lation (Puzan 2003;Ten Fingers 2005). It is alsoillustrated when health professionals mistakesocial and health problems for cultural charac-teristics, or ignore inequities in the health caresystem that lead to under-servicing in the hos-pital system compared with equally ill non-Indigenous patients (AMA 2007; Browne 2005).This runs the risk of disempowerment, wherepredominant discourses and the way non-Indigenous health professionals approach Indige-nous health create a feeling of powerlessness and
disengagement from cultural life as well as healthcare (Durie 2004; Eckermann et al 2006).
Many Indigenous people are also disadvan-taged in Australia’s health system through theconflict between efficiency and equity. Thisoccurs when medical doctors or administratorstry to prioritise care or inclusion in treatmentschedules on the basis of low-risk interventionsor stereotypical expectations, especially forIndigenous people who have multiple risks thatexclude them from treatments (AMA 2007).Another problem occurs when Indigenous peo-ple refuse treatment, which may be dismissedby health professionals as cultural. In fact, manyrefusals are due to a lack of appropriate com-munication or language barriers (AMA 2007).Indigenous people may also be discriminatedagainst because of homelessness, or becausefamily structures are not recognised by the system that allocates payments or co-paymentson the Medical or Pharmaceutical BenefitsSchemes (AMA 2007). For example, consentfor the treatment of minors often does notallow for Indigenous kinship structures wherecare, responsibility and decision-making forchildren can rest with extended family, in ad-dition to that of biological parents or legalguardians, particularly when parents might beill or not able to care for their children.Thesekinship systems are important to maintainingsocial organisation in many Indigenous com-munities, which further illustrate the need for flexible, culturally-inclusive approaches toIndigenous health.
The Australian Indigenous Doctors Associa-tion (AIDA) (2007), the AMA (2007) and theCouncil of Aboriginal and Torres Strait IslanderNurses (CATSIN) (2007) have recently launch-ed attempts at moving the institutionalisedracism of Australia’s health care system to theforefront of public discussion.They, along witha small number of nurse researchers (Andersonet al 2003; Barnes et al 2000), advocate the needto make explicit the interactions between cul-ture and other aspects of care in the clinical
169Volume 28, Issue 1–2,April 2008 CCCCNNNN
Culture-specific care for Indigenous people:A primary health care perspective CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 169

context (AIDA 2007). AIDA (2007) recom-mends a five-pronged approach for the healthcare system in terms of attitudes, structures,policies and services.These include:• valuing diversity;• developing a capacity for cultural self-assess-
ment;• maintaining awareness of the dynamics inher-
ent in the interactions between cultures;• institutionalising cultural knowledge;• adapting service delivery to reflect the under-
standing of diversity between and within cul-tures.
The AMA and CATSIN also recommend includ-ing sensitivity to Indigenous cultures in medicaland nursing education programs and accredita-tion of providers, and both groups have lobbiedthe Commonwealth government for additionalresources to improve Indigenous health out-comes (AIDA 2007;AMA 2007).
IS CULTURE-SPECIFICCARE POSSIBLE?The question of culture-specific care is con-tentious with respect to Indigenous Australians,especially in the absence of a single, uniformIndigenous Australian culture. Instead the focusshould be on cultural relativism and breakingdown the power relations that pervade clinicalinteractions. Cultural relativism is a reflectionof the local partnership approach to care,which, within the tenets of primary health careis the most salient strategy for developing cultural competence. In this context, healthproviders are not always the dominant group,making decisions for rather than with anothergroup (Gustafson 2005).Working as partners,while responding to identified needs for inter-vention, reflects an egalitarian approach to thehealth care situation. A partnership approachhelps ensure that the diagnosis and plan fortreatment includes culturally embedded inputand decision-making in relation to how peoplemaintain their health in the context of relation-
ships with the social and natural environmentand the social order (Fisher 2006).This positiondisputes the contention that health care pro-fessionals provide culture-specific care. Rather,through egalitarian partnerships health profes-sionals work with Indigenous people to planculturally appropriate care.
CONCLUSIONClearly, there are a number of areas for changein both health care and Australian society.Theseinclude the following recommendations forchange:• Create public recognition of the unique
needs and sensitivities of Indigenous Aus-tralians.
• Develop national policies to support thedevelopment of economic, social and culturalcapital to foster self-determinism, includingand strategies for culturally appropriate,sufficiently resourced education and skilldevelopment.
• Identify culturally appropriate needs such as infrastructure and housing, to supportIndigenous families within which childrencan grow safely, within their cultural, familyand community groups.
• Address inequities in service provision interms of partnerships to help develop indi-vidual capacity and greater access and equityin health services.
• Promote greater connectivity between Indige-nous people and their advocates in health andsocial interactions, and cultural sensitivity inall health care practices.
• Build Indigenous workforce capacity throughnational training plans, culturally safe emp-loyment strategies including interview andselection procedures, and ongoing skills andcapacity development (Adelson 2005; Bram-ley et al 2005; CATSIN 2007; Pearson 2005;Ring & Brown 2003; Zubrick et al 2005).
• Provide cultural awareness training in thetreatment and management of specific condi-
170 Volume 28, Issue 1–2,April 2008CCCCNNNN
Anne McMurray and Rani ParamCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:41 PM Page 170

tions among Indigenous people, includingcancer and chronic diseases (NHRA 2007).
• Ensure health promotion programs and theresearch that informs them includes authen-tic case studies of Indigenous people that illu-minate the unique Indigenous experiences oflife and of health care (Reimer-Kirkham 2002;CATSIN 2007).These measures can help pro-vide a basis for strength-based approaches to health promotion that validate culturalidentities and capacities (Brough Bond & Hunt2004; Reading, Ritchie, Victor & Wilson2005).
ReferencesAdelman M, Erez E and Shalhoub-Kevorkian N
(2003) Policing against minority women inmulticultural societies:‘Community’ and thepolitics of exclusion, Police and Society 7:105–133.
Adelson N (2005) The embodiment of inequity:Health disparities of Aboriginal Canada. Canad-ian Journal of Public Health 96(S2): S45–S61.
Anderson J, Perry J, Blue C, Browne A, Hender-son A, Koushambbi B, Reimer Kirkham S,Lynam J, Semiuk P and Smye V (2003) ‘Re-writing’ cultural safety within the postcolonialand postnational feminist project. Advances inNursing Science 26(3): 196–214.
Astbury J,Atkinson, J, Duke, JE, Easteal, PL,Kurrie, SE,Tait, PR,Turner, J (2000) Theimpact of domestic violence on individuals.Medical Journal of Australia 173: 427–731.
Australian Council for Aboriginal Reconciliation(1994) Walking together: the first steps. Report ofthe Australian Council for Reconciliation.Canberra:AGPS.
Australian Indigenous Doctors Association(2007) An introduction to cultural competency.Royal Australasian College of Physicians.Accessed at http://www.racp.edu.au/hpu/policy/indig_cultural_competence.htm on23 January 2007.
Australian Institute of Health and Welfare (2004)
Australia’s Health 2004. Cat No AUS 44.Canberra:AGPS.
Australian Medical Association (2007) Aboriginaland Torres Strait Islander Health: InstitutionalisedInequity Not Just a Matter of Money. Report CardSeries 2007. Canberra:AMA.
Bannerjee SB and Osuri G (2000) Silences of themedia: whiting out Aboriginality in makingnews and making history. Media, Culture andSociety 22(3): 263–284.
Barnes D, Craig K and Chambers K (2000) Areview of the concept of culture in the holisticnursing literature. Journal of Holistic Nursing18(3): 207–221.
Browne A (2005) The sociopolitical context ofnurses’ encounters with First Nations womenin a Canadian health care setting. InternationalConference on innovations in Nursing.Keynote Presentation. Fremantle WesternAustralia 12 November.
Brough M, Bond C and Hunt J (2004) Strong inthe City: towards a strength-based approach inIndigenous health promotion. Health PromotionJournal of Australia 15(3): 215–220.
Council of Aboriginal and Torres Strait IslanderNurses (2007). Professional issues.Accessed on13 June 2007 at www.indiginet.cm.au/catsin/professional_issues.html.
Culley L (2006) Transcending transculturalism?Race, ethnicity and health-care. Nursing Inquiry13(2): 144–153.
Durie M (2004) An Indigenous model of healthpromotion. Health Promotion Journal of Australia15(30): 181–185.
Eckermann A, Dowd T, Chong E, Nixon L, GrayR and Johnson S (2006) Binan Goonj: BridgingCultures in Aboriginal Health, 2nd edn. Sydney:Elsevier.
Fisher R (2006) Congruence and functions ofpersonal and cultural values: Do my valuesreflect my culture’s values. Personality andSocial Psychology 32(11): 1419–1431.
Gustafson D (2005) Transcultural nursing theoryfrom a critical cultural perspective. Advances inNursing Science 28(1): 2–16.
171Volume 28, Issue 1–2,April 2008 CCCCNNNN
Culture-specific care for Indigenous people:A primary health care perspective CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 171

Hertzman C and Power C (2006) A life courseapproach to health and human development.In Heymann J, Hertzman C, Barer M andEvans R (Eds) Healthier societies: From analysis toaction, pp 83–106. Oxford: Oxford UniversityPress.
Johns G (2006) Social Stability and StructuralAdjustment, Bennelong Society 6th AnnualConference – Leaving Remote Communities.Accessed at www.bennelong.com.au/conferences/pdf/Johns2006.pdf on 1 June 2007.
McMurray A (2006) Community Health andWellness:A Socio-ecological Approach, 3rd edn.Sydney: Elsevier.
Mignone J and O’Neil J (2005) Social capital andyouth suicide risk factors in First NationsCommunities. Canadian Journal of Public Health96 (S1): S51–S54.
National Rural Health Alliance (2007). After fortyyears it’s time, Media Release, accessed on 26May 2007 online at www.ruralhealth.org.au.
O’Brien A (2006) Moving toward culturallysensitive services for Indigenous people:Anon-Indigenous mental health nursing pers-pective. Contemporary Nurse 21(1): 22–31.
Pearson N (2005)The Cape York Agenda.Address tothe National Press Club. Canberra, Nov. 30.
Pomaika’I Cook B,Tarallo-Jensen L,Withy K andBerry S (2005) Changes in Kanaka maoliMen’s Roles and Health: Healing the WarriorSelf. International Journal of Men’s Health 4(2):115–130.
Puzan E (2003) The unbearable whiteness of being(in nursing). Nursing Inquiry 10(3): 193–200.
Reading J, Ritchie A,Victor C and Wilson E(2005) Implementing empowering healthpromotion programs for Aboriginal youth intwo distinct communities in British Columbia,Canada. Promotion and Education X11(2):62–65.
Reimer Kirkham S and Anderson J (2002)Postcolonial nursing scholarship: Fromepistemology to method. Advances in NursingScience 25(1): 1–17.
Sen A (1999) Development as freedom. New York:Alfred A. Knopf.
Scrimgeour D (2007) Town or country: which isbest for Australia’s Indigenous peoples? MedicalJournal of Australia 186(10): 532–533.
Shaw W (2000) Ways of Whiteness: HarlemisingSydney’s Aboriginal Redfern. AustralianGeographical Studies 38(3): 291–305.
Shore J and Spicer P (2004) A model for alcohol-mediated violence in an Australian Aboriginalcommunity. Social Science and Medicine 58:2509–2521.
Smith R (2003) Learning from Indigenouspeople. Editorial, British Medical Journal 327: 1.
Ten Fingers K (2005) Rejecting, revitalizing, andreclaiming. Canadian Journal of Public Health96(Suppl 1): S60–S63.
Toussaint S (2003) ‘Our shame, blacks live poor,die young’. Indigenous health practice andethical possibilities for reform. In Liam-puttong P and Gardner H (Eds) Health, SocialChange and Communities, pp 241–56.Melbourne: Oxford University Press.
Trewin D and Madden R (2005) The Health andWelfare of Australia’s Aboriginal and Torres StraitIslander Peoples. Canberra:ABS Cat No 4704.0AIHW Cat No IHW14.
Whitehead M (2007) A typology of actions totackle social inequalities in health. Journal ofEpidemiology Community Health 61: 473–478.
World Health Organization (2005) Action on thesocial determinants of health: Learning fromprevious experiences.A background paperprepared for the Commission on SocialDeterminants of Health, March. Geneva:WHO accessed on 6 June 2006 at http://www.who/int/social_determinants/en/.
Zubrick S, Silburn S, Lawrence D, Mitrou F,Dalby R, Blair E, Griffin J, Milroy H, de MaioJ, Cox A and Li J (2005) The Western AustralianAboriginal Child Health Survey.The Social andEmotional well-being of Aboriginal Children andYoung People. Perth: Curtin University ofTechnology and The Telethon Institute forChild Health Research.
172 Volume 28, Issue 1–2,April 2008CCCCNNNN
Anne McMurray and Rani ParamCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 172

INTRODUCTION
Accessing culturally appropriate and accept-able health services is vital for engendering
the trust of clients who are Indigenous peoples,and extends beyond the establishment of rela-tionships to respecting their worldviews andcultural preferences. Failure to identify key cul-tural beliefs and practices, or the worldview ofhealth, well-being, and illness risks providinghealth care that lacks relevance and compromis-es its efficacy.When interventions ‘go wrong’ oroutcomes are not achieved, it is not unusual forclients to be blamed and labelled ‘non-compli-ant’.This is a phenomena experienced by manyMa-ori women (Indigenous to Aotearoa NewZealand) who are often subjected to victim
Key WordsMa-ori health;indigenoushealth; culturalsafety; culturalcompetence;worldview;nursing CN
173Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 173–188.
The significance of a culturallyappropriate health service for
Indigenous Ma-ori women
ABSTRACT A culturally appropriate health service is contingent on the inclusion of client’s cultural beliefs and practices into intervention plans. Not establishing key cultural beliefs and practices risks providing a health service that lacksrelevance and compromises its efficacy for its recipients. Anecdotally, culturalappropriateness and acceptability of health services is often lacking for Ma-ori women (Indigenous to Aotearoa New Zealand), hindering positive healthexperiences and outcomes.This paper explores an aspect of findings of researchundertaken with Ma-ori women to discover what was important for their healthand well-being, and their interactions with mainstream health services. Datafrom semi-structured interviews with 38 Ma-ori women was used to generate aGlaserian grounded theory informed by a Ma-ori-centred approach to explainthe weaving of their health and well-being. It explains, in part, the importanceof determining Ma-ori women’s cultural worldviews and practices when assessingand planning effective interventions. Cultural safety and cultural competencewill be explored as vehicles to improve culturally appropriate and acceptablehealth care for Indigenous women.Received 6 August 2007 Accepted 19 March 2008
DENISE WILSONSenior Lecturer in Nursing(Ma-ori Health)Massey UniversityAuckland, New ZealandandFellow of the College ofNursesAotearoa, New Zealand
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 173

blaming, negative labels and racism, mistakenlyreinforced by their under-utilisation of, and latepresentation to, health services when they areunwell.This situation is similar to other Indige-nous women in countries where they have beensubject to colonisation (Baker & Daigle 2000;Browne & Fiske 2001; Dodgson & Struthers2005), and is an approach that denies who theyare and their unique health needs.
Anecdotally, the cultural appropriateness andacceptability of health services and health care providers, such as nurses, is often foundlacking by Ma-ori (Indigenous to Aotearoa NewZealand), compromising their access and use of health services (Reid and Robson 2006).Theimportance of culture and health is well est-ablished as a concept in nursing (Campicha-Biacote 2002; Giger & Davidhizar 1999; Lein-inger 1985; Ramsden 1990; Wepa 2005), andMcCloskey and Diers’ (2005) research into theNew Zealand health reforms demonstrates thatnursing is linked to the quality of client out-comes. In response to the importance of cul-ture, safety and Indigenous concerns about the negative health experiences of Ma-ori, NewZealand nurses have been required to undergocultural safety education, and demonstrate cul-turally safe practice since the early 1990s(Ramsden 1990). More recently, with the in-troduction of competency based practising certificates, they are required to demonstratecompetency in culturally safe practice.This situ-ation raises the question: How, when nurses,along with other health professionals, are edu-cated in the importance of culture in health, andrequired to demonstrate competency in cultur-ally safe practice do claims of culturally in-appropriate and unacceptable experiences inmainstream health services still exist more than15 years later?
This paper will focus on an aspect of Glas-erian grounded theory about the weaving ofhealth and well-being by Ma-ori women. Tobegin, Ma-ori women’s health, and the place ofculture in nursing, will be described as a back-
ground. This will be followed by a descriptionof the research and an overview of the ground-ed theory generated. An analysis will be under-taken of the importance of nurses recognisingand integrating important cultural beliefs andpractices of Indigenous Ma-ori women into theirhealth experiences to increase the likelihood ofpositive health outcomes.The value and efficacyof cultural safety will be critically exploredwithin the contexts of first, the professionalenvironment and then the regulated environ-ment within Aotearoa New Zealand requiringnurses to demonstrate competency in culturallysafe practice, using the research findings. Thenotion of cultural competence will be exploredas a foundation for improving the delivery ofculturally appropriate health care for Indigenouswomen, such as Ma-ori.
BACKGROUNDMa-ori women, like many other women, holdimportant roles in maintaining the health oftheir children and wha-nau (immediate andextended family). They are referred to as thekaitiaki (guardians) of wha-nau health and well-being (Public Health Group 1997). However,Ma-ori experience inequalities in health statusand health outcomes when compared to othergroups within Aotearoa New Zealand.This is asimilar situation for the Indigenous peoples ofAustralia, Canada, America and Hawaii (Ander-son et al 2006), and is related to histories ofcolonisation that have contributed to their con-temporary socioeconomic disadvantage, un-helpful stereotypes, and racism, all negativelyimpacting on the health of individuals and com-munities. Health determinants extend beyondgenetics and disease processes to include factorssuch as socioeconomic deprivation, ethnicityand race, colonisation, and racism, all reasonsfor differential access and use of health servicesby Indigenous peoples (Ibrahim,Thomas & Fine2003; Reid & Robson 2006).
Socioeconomically, Ma-ori women are morelikely to experience deprivation and have life
174 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 174

circumstances that reflect this.The level of dep-rivation they experience highlights significantinequalities that exist between Ma-ori and otherpeoples living in Aotearoa New Zealand, despitegradually declining mortality rates between1980 and 1999 (Blakely et al 2004). Ma-oriwomen have a life expectancy of 73 years, nineyears less than the 82 years experienced by non-Ma-ori (Ministry of Health 2006).The five majorcauses of mortality (by numbers) for Ma-oriwomen are ischaemic heart disease, lung cancer,chronic obstructive pulmonary disease, cere-brovascular disease, and diabetes. Breast canceris added to this list when years of life lost areconsidered, with Ma-ori women 1.3 times morelikely than non-Ma-ori women to be diagnosedwith, and twice as likely to die from breast cancer. Ma-ori women also experience adversehealth effects of violence with an assault andhomicide hospitalisation rate that is greater thanfive times than non-Ma-ori women. Despite atargeted campaign to improve access to screen-ing and early intervention for cervical cancer,Ma-ori women are twice as likely to be diagnosedwith cervical cancer, and four times as likely to die from it (Ministry of Health 2006).Theseexamples are indicative of issues relating to theiraccess and use of primary and secondary healthservices. Ma-ori, health care provider, and gov-ernment concerns regarding these inequalitiesresulted in the identification of Ma-ori health as anational health priority in 2000 (King 2000).
The 2002–2003 New Zealand Health Survey(Ministry of Health 2006) found that being un-able to contact the doctor, having no transport,cost, time, difficulty with scheduling timely andsuitable appointments, and either not wanting tomake a fuss or being bothered were reasonscited for not seeing a general practitioner whenneeded. Indeed, the avoidable and amenable(relates to deaths from conditions responsive tohealth care) mortality rates and avoidable andambulatory sensitive (conditions responsive totimely access to primary care services, prevent-ing hospitalisation) hospitalisation rates are 2.5
times and 1.5 times higher than non-Ma-ori,respectively (Ministry of Health 2006).
Globally, Indigenous women with histories ofcolonisation have comparable experiences ofmainstream health services, despite concepts ofcultural safety, transcultural nursing care, andcultural competence being part of the nursingbody of knowledge. The notion of culture incontemporary nursing practice has been evidentsince the introduction of transcultural nursingby Madeleine Leininger in the 1950s. Culturalsafety was instigated in the 1990s in AotearoaNew Zealand in response to Indigenous Ma-oriconcerns about the inequalities in their healthstatus and the negative health service experi-ences they encountered in health care prov-iders. A Ma-ori nursing student described this,within the context of safety in nursing, as a lackof ‘cultural safety’ to explain Ma-ori experienceswhere their cultural beliefs, practices and needswere neither acknowledged nor respected (Rams-den 2002).
Culture is defined by Wepa (2005: 31) as:
Our way of living is our culture. It is ourtaken-for-grantedness that determines anddefines our culture. The way we brush ourteeth, the way we bury people, the way weexpress ourselves through art, religion, eat-ing habits, rituals, humour, science, law andsport; the way we celebrate occasions … isour culture. All these actions we carry outconsciously and unconsciously.
Simply, culture refers to the beliefs and prac-tices people undertake daily, contributing to theway they view the world, and providing a pointof reference for comprehending health, illness,life and death (Giger & Davidhizar 1999; Lein-inger 1978, 1685, 1988, 1996, 2001, 2006).Culture is dynamic, varies between and withingroups, and changes in response to time andsocietal changes, and is evident in language.
Leininger’s Culture Care Diversity and Uni-versality theory requires nurses to deliver
175Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 175

culturally congruent nursing care to peoplethrough helpful acts toward, or for, them guidedby the Sunrise Model (Leininger 1985). Anunderlying premise of transcultural nursing(informed by an anthropological perspective) isthat cultural knowledge can be acquired about arange of different cultures.Transcultural nurs-ing aims to improve client care, and offers a the-ory to predict and explain cultural information,through the formal education of nurses. A num-ber of cultural competence frameworks arisingout of transcultural nursing care exist to assessnurse’s practice.While transcultural nursing hasbeen used internationally, nurses in AotearoaNew Zealand adopted the conceptual frame-work of cultural safety. Ramsden (1990) arguedthat the reality of gathering culturally specificknowledge about groups was problematic dueto the variability that is present among andwithin groups.
The evolution of cultural safety in AotearoaNew Zealand has been fraught and marked bypublic and political interference. Originally cul-tural safety was grounded in the Treaty of Waitangi and biculturalism, but over time hasexpanded to include cultural groups beyondethnicity (Nursing Council of New Zealand2005;Wepa 2005). Briefly, the Treaty of Wait-angi is an agreement between Ma-ori and theBritish Crown that outlined their relationship,and guaranteed Ma-ori the right to self-determi-nation, equal rights as British citizens, and pro-tection. Ramsden (1990, 2002) argues that theworldviews of nurses and health services con-trast with Ma-ori, thus requiring nurses to iden-tify the key beliefs and practices for health andwell-being of Ma-ori clients.To prepare nurses,cultural safety education requires nurses to initially examine their own cultural realities and attitudes, and how these and the power thatthey hold as nurses, can impact on those thatthey work with, and the development of rela-tionships.
One of the underlying premises of culturalsafety is the recognition that diversity exists not
only between cultural groups but within them.Thus, the development of specific beliefs andpractices for nurses to learn is resisted. Theestablishment of relationships with clients toelicit the cultural beliefs and practices that need to be respected and integrated into theirhealth experience is essential. Consequently, itis the recipient of nursing care who determineswhether a nurse’s practice is safe, not nurses(Nursing Council 2005). This is a weakness ofcultural safety as it is generally nurses whomake a judgement about whether a nurse’spractice is culturally safe or not.There is anec-dotally a difficulty in freely ascertaining aclient’s perspective of the care they receivedrelated to nurse–client power imbalances, theirpotential vulnerable status, and the likelihood ofthem needing to reuse a health service. Regis-tered nurses in Aotearoa New Zealand, how-ever, have been required to undergo educationin cultural safety since the early 1990s, anddemonstrate their competency.
Registered nurses in Aotearoa New Zealand,however, have been required to undergo educa-tion in cultural safety since the early 1990s, anddemonstrate their competence in this area. Morerecently, registered nurses along with other registered health professionals are required todemonstrate ongoing ‘cultural competence’ inaccordance with section 118(iv) of the HealthPractitioners Competence Assurance (HPCA)Act 2003 – legislation designed to protect thehealth and safety of members of the public.Therequirements for demonstrating competence area combination of meeting a prescribed minimumof practice and professional development hours,and demonstrating the Council’s competenciesin the registered nurse’s area or context of prac-tice. This process involves providing evidencegenerated from a combination of self-assess-ment, peer assessment or review, and assessmentby a senior nurse. Guiding this process is theNursing Council’s definition of cultural compe-tence: ‘the combination of skills, knowledge,attitudes, values and abilities that underpin effec-
176 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 176

tive performance as a nurse’ (Nursing Council2008). However, competency 1.5 requires nurs-es to ‘practise nursing in a manner that the clientdetermines as culturally safe’, which by defini-tion requires a judgement to be made by therecipients of care (Nursing Council 2005).
Both transcultural nursing and cultural safetyaim to ensure that nurses consider people’s cultural needs and that these are integrated into their nursing practice.The body literatureand research demonstrating the efficacy of cul-tural safety, however, is limited with the majori-ty of research focused on the efficacy of facetsof cultural safety education (McEldowney et al 2006,Wepa 2003). Johnstone and Kanitsaki(2007), who researched its appropriateness forAustralia by establishing Australian health careproviders’ level of understanding, rightfullycriticise the lack of research into the efficacy ofcultural safety practice. However, Johnstone andKanitsaki’s (2007) report has limitations, with acovert agenda to reinforce the inappropriate-ness of cultural safety for Australia apparent,along with a lack of key information on aspectsof the research design and in the reporting offindings. Notably the importance of an educa-tive process in the development of culturallysafe practice was not acknowledged.
The role of culture in health and well-being,and its significance for nurses and other healthcare providers is well established. Culturallyappropriate services are fundamental for imp-roving the access and use of services by Ma-oriwomen (Wilson 2004). But the notion of beingknowledgeable about Maori culture is fraughtand not always possible – Ma-ori were not ahomogenous group pre-colonisation, and greatdiversity in beliefs and practice is evident in con-temporary Ma-ori.The development of meaning-ful relationships with Ma-ori women that respectand value their cultural beliefs and practices iscrucial to meeting their health needs. Such anapproach minimises the impact of Ma-ori womenbeing caught between health care providersdelivering services informed by a biomedical
worldview, and their own unique worldview andlife circumstances. A paucity of research into Ma-ori women’s interactions with mainstreamhealth services exists. Given the key role Ma-oriwomen have in caring for their wha-nau and inthe transmission of health information it is im-portant to gain an insight and understanding oftheir perspectives on health and illness, and theinfluences of their culture on their health behav-iours. Such information can then provide insightand inform the practices of nurses and otherhealth care providers.
RESEARCHThe research aimed to explore Ma-ori womens’understanding of health, and their interactionswith mainstream health services guided by thequestion, What is happening for Ma-ori women,their health, and their interactions with ‘mainstream’health services? Ethical approval for the researchwas obtained from the Massey University HumanEthics Committee and the Bay of Plenty EthicsCommittee.
MethodologyMa-ori have a history of being subjected to negative research processes and outcomes (notdissimilar to other Indigenous peoples) (Sporle2003). Therefore, it was imperative that theresearch methodology and approach selectedenabled the values, beliefs and traditions of Ma-ori women to be respected. This decisionwas guided by Smith’s (1999) assertion thatthere is little benefit in perpetuating disrespect-ful research processes and negative stereotypes,and interpreting findings through the prevailingdominant cultural lens, or romanticising ‘desir-able’ aspects of Ma-ori culture. A Ma-ori centredapproach described by Durie (1997) provided a blueprint to develop a research process toensure Ma-ori values and processes informed it,beginning with initial consultation and formingthe question to align the research with Ma-oriaspirations, to disseminating the findings throughconsultation processes.The underlying assump-
177Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 177

tions of the Ma-ori-centred approach used were,that:
1. The research should be beneficial to Ma-oriwomen.
2. Many Ma-ori women integrate a holisticworldview into their everyday lives.
3. The lives of Ma-ori women involve multipleand complex interactions, reflective of thevarious roles they hold within a biculturalsociety.
4. Ma-ori should have the opportunity to main-tain control through processes of consul-tation and participation throughout theresearch process in order to protect theircultural interests.
The Ma-ori centred principles of whakapiki tangata (enablement), whakatuia (integration),and mana Ma-ori (control) described by Durie(1997) informed the research process. Pragmat-ically, this translated into Ma-ori women beingactively involved in advising the development ofthe research question, and the process of meet-ing and working with participants was based on Ma-ori values and practices, such as sharing foodand establishing mutual connections with placesand people. A Ma-ori-centred approach ensuredthe research was culturally responsive and ap-propriate, and crucial in gaining ethical approvalfor research with Ma-ori.
To explicate the research, the inductive natureof Glaserian grounded theory both philosophi-cally and practically lent itself to being inform-ed by a Ma-ori centred approach. Eliciting theinterpretations and experiences Ma-ori womenhad about their health and interactions withmainstream health services was essential, andthe inductive nature of Glaserian grounded theory enabled discovering the main concerns for Ma-ori women about health and mainstreamservice use. As Glaser (1999: 840) claims,‘Grounded theory is what is [sic], not whatshould, could, or ought to be’.
METHOD
Participants
Thirty-eight women who identified as Ma-oriaged between 24 to 61 years were initiallyrecruited using a purposeful network samplingstrategy (Polit & Hungler 1991), and as thestudy progressed theoretically sampling wasused. Participant selection was a collaborativeendeavour with two Ma-ori women advisors,known within the Ma-ori community, activelyinvolved in the development of the researchdesign. Aided by a sound understanding of theselection criteria and the processes of theoreticalsampling, these women also assisted in ap-proaching potential participants, and negotiatingthe nature of their involvement in the study andtheir availability for an interview.Their strengthwas in being known within the community andbeing able to determine, what Morse (1991)terms as,‘insiders’ and ‘outsiders’.
The Ma-ori women participating in the studycame from mixed backgrounds.They lived in avariety of relationships (permanent, non-per-manent and alone) and the majority had chil-dren, with many living in homes with morethan one family or generation.Their educationalbackgrounds varied considerably along a con-tinuum with some having no school qualifica-tions to those who had completed tertiary levelstudy. While most of the women were in paidwork, the majority were in part-time employ-ment, with some unemployed receiving state-funded income support. Not all women hadaccess to telephones or private transport. Ifunwell, the women generally sought advicefrom either a medical practitioner or Ma-orihealth provider (a health service delivered with-in a Ma-ori philosophy and provided by Ma-orihealth professionals, such as nurses).
Data collection and analysisSemi-structured interviews with individuals andgroups (dependent upon their choice and con-gruent with a Ma-ori centred approach) were
178 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 178

undertaken with the Ma-ori women. To elicittheir understanding and experiences and tominimise researcher bias, Schreiber (2001) sug-gested the interviews be guided by broad ques-tions, such as:• Tell me what does health mean to you?• What are the things that are important for
your health?• Tell me about your experience with health
services and the people working in them.
The interview questions were designed toenable issues to be explored as they arose, andareas for theoretical sampling to be identified.Data was collected with detailed field notes anda reflective journal (Glaser 1998).
Data collection occurred simultaneously withdata analysis (Glaser & Strauss 1967) using con-stant comparative analysis to generate codes,emerging concepts and categories.These wereverified and refined until saturation was reached– that is, when no new information could beadded to a concept or category (Glaser 1978).Theoretical sampling purposefully guided datacollection, including the exploration, clarifica-tion, verification, and saturation of the emergingcodes, concepts and categories (Glaser 1998). Asproperties emerged and codes were refined intoconcepts and categories, these were sorted andre-sorted. Coding was confined to the substan-tive area under study to promote the relevance,fit and work of emerging categories.The devel-opment of the ideas and emerging meaningwere captured by recording of memos that alsoassisted in tracking the conceptualisation ofcodes, concepts, categories and their relation-ships and the basic social psychological process(BSPP) of weaving.
Glaser’s (1978) criteria of fit, relevance,work and modifiability were used to establishthe rigour of the study.The ‘fit’ was establishedthrough a systematic reviewing of the processesfor generating codes, categories, and conceptu-alisation of the data to confirm that these andthe BSPP of weaving were the concerns of the
Ma-ori women.The ‘relevance’ and ‘work’ of thegrounded theory (Glaser 1978) was confirmedits ability to explain, predict and interpret thesubstantive area of Ma-ori womens’ health andtheir interaction with health services.This wasdemonstrated by a Ma-ori woman saying the fol-lowing about the grounded theory produced:
Your observations are truly accurate and I amblown away by what I consider to be deeplyinsightful comments … I just wanted toshare how moved I’ve been reading yourpaper! (E-mail correspondence JM)
The grounded theory generated is dynamic andresponsive to the societal and environmentalchanges impacting on Ma-ori women, and hasthe potential to be ‘modifiable’. It is expectedthat the BSPP of weaving would remain withoutvariation.
NGA- KAIRARANGA ORANGA –THE WEAVERS OF HEALTH ANDWELL-BEING‘Nga- Kairaranga Oranga – The Weavers of Healthand Well-being’ is the substantive grounded theory that explains the health and well-being of Ma-ori women. It provides a conceptualinsight into what Ma-ori women had about theirhealth and well-being, and their interactionswith ‘mainstream’ health services and healthcare providers. ‘The Weavers of Health andWell-being’ comprises three core categories:‘Mana Wa-hine’ (the prestige and status of Ma-oriwomen), ‘The Way It Is’, and ‘Engaging withHealth Services’ and the basic social psychologi-cal process (BSPP) of weaving that integrates thenumerous dimensions that determines healthand well-being.The position a Ma-ori woman hasin the world, along with influences such as age,wisdom, resources and life circumstances allaffect the weaving of their health and well-being.The process of weaving health and well-being is aunique lifelong process for each Ma-ori woman,and illustrates how the core categories and their
179Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 179

dimensions are complexly and diversely woventogether.The outcome of the weaving of healthand well-being, that is optimal or less than opti-mal is dependent upon the strength, the con-tinuity and the endurance of the weaving ofhealth and well-being.
Mana Wa-hineThe first core category, ‘Mana Wa-hine’, explainsthe important components for the health andwell-being of Ma-ori women, such as wha-nau(family), spirituality, traditional and contem-porary knowledge, and self-care behaviours.This category outlines areas that health careproviders should explore by eliciting their viewof health and well-being to ensure the culturalintegrity of a Ma-ori woman is maintained whatis important for their health and well-being.
Way it is‘The Way It Is’, is the second core category that explains the challenges and barriers Ma-oriwomen have to experience positive health out-comes.These challenges and barriers may eitheroriginate from the women themselves or pastexperiences of health services they have in-teracted with directly or vicariously through wha-nau and friends. Challenges and barriersinvolve a strong socialisation to put others first,fears and past health experiences, particularlyrelating to deaths of wha-nau members, and neg-ative encounters with health care providers.This category provides an indication as to whatprevents Ma-ori women from accessing healthservices in a timely manner.
Engaging with health servicesThe final core category, ‘Engaging with HealthServices’, explains the needs of Ma-ori women,based on both positive and negative experi-ences, when they interact with health servicesand health care providers.The ability of Ma-oriwomen to develop positive relationships withhealth care providers either promotes or im-pedes connecting and relating, enabling the
access and use of relevant health services.Influencing access to services, connecting withan appropriate service and forming effectiverelationships, weave together to determine thenature of engagement a Ma-ori woman has witha health service, and its health care providers.The quality of information shared, feelings ofcomfort and interpersonal relationships areindicative of effective relationships, but theseare counteracted by Ma-ori women’s hypersensi-tivity to negative and judgmental attitudes ofhealth care providers.
IMPORTANCE OF CULTURALLYAPPROPRIATE HEALTH SERVICESOf note, the Ma-ori women in this research con-sistently encountered health services and healthcare providers that were problem-focused, whocompartmentalized their health issues or prob-lems that resulted in their needs not beingrecognised and planned interventions beinginappropriate. Adopting a predominately prob-lem-based, biomedical focus neglects not onlythe specific needs of each Ma-ori woman, butalso the socio-cultural dimensions that impacton health and well-being. This can increase the likelihood of being recipients of victimblaming or deficit explanations when healthcare providers determine outcomes that are notachieved, the responsibility being placed onindividual Ma-ori women and their wha-nau.
This research reinforces the need for cultur-ally appropriate and acceptable interventionsand health care providers, such as nurses, arevital for improving access, use, and ongoing use by Ma-ori women, especially for long-termhealth issues. However, without meaningfulrelationships with Ma-ori women their specificneeds or factors necessary to achieve positivehealth outcomes will be overlooked, or recog-nising some are beyond their immediate con-trol, such as socioeconomic circumstances.Continued access and use of health services isdependent upon, and optimized by the develop-ment of effective relationships with nurses and
180 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:42 PM Page 180

other health care providers – a powerful indica-tor of the nature of future access and use ofhealth services.
Understanding how Ma-ori women ‘weave’their health and well-being can positivelyinform the practise of ‘mainstream’ health careproviders, such as nurses. ‘The Weavers ofHealth and Well-being’ illustrates the importantaspects for Ma-ori womens’ health and well-being, along with the barriers and challenges to,and factors that facilitate, accessing and usinghealth services. Acknowledging cultural beliefs,and practices are a crucial link to facilitatingoptimal health outcomes, even for those womenwho had not been raised in ‘traditional’ Ma-oriways, illustrated by the following:
Not all Ma-ori women have been taught the‘old ways’ and Ma-ori culture had been sup-pressed, but it was knowing you were Ma-ori– it was who one was. (Interview 4)
Fundamental to a culturally appropriate healthservice is the determination of a Ma-ori woman’skey beliefs and practices for her health and well-being that need to be recognised, respected andintegrated into her health experience, especiallyplans for interventions. Diversity exists bet-ween and within cultural groups leading to mul-tiple and diverse worldviews – while there maybe similarities, there are important differencesfor each woman.Thus, meaningful and genuinedialogue with Ma-ori women is crucial, alongwith a respect of their beliefs and practices,and a willingness to include important culturalpractices that vary from those promoted by the ‘mainstream’ health services. Determining a Ma-ori woman’s beliefs and worldview ispremised by the notion that different pathwaysthat can be taken to reach an intended outcome.
There needs to be a flexible approach to-gether with a wider scope of who and how aservice is provided to achieve the right per-son and right service. In other words there
needs to be flexibility to do things outside ofthe traditional way in which health servicesare provided. (Interview 2)
It is the cultural component that makes it dif-ferent for Ma-ori women. (Interview 5)
Ma-ori women are no strangers to walking in two worlds (Ihimaera 1998), but personalworldviews should not be automatically sub-jugated when they move from the world of Ma-ori to that of mainstream health services.Sibthrope, Anderson and Cunningham (2001)stress the domination of one worldview overothers is problematic, especially when the roleof culture is not considered in the developmentof health behaviours. For example, while anindividual Ma-ori woman may be the focus of theattention of a nurse, her identity and possiblyhealth issues may well be constructed within acollective context that includes wha-nau or hap?(a group of wha-nau with a common ancestor).Often when their health beliefs and practiceschallenge those of ‘mainstream’ health services,poor health outcomes are attributed to somedeficit in the Ma-ori woman, as previously men-tioned. Such explanations ignore health systemdeficits related to the delivery of services arenot being addressed, such as not identifying cul-tural beliefs and practices.
Acknowledging cultural beliefs and practicesenables the holistic and spiritual dimensionsmany Ma-ori women have to be recognised, thatusually contrast with western middle-class val-ues and the biomedical view of health and ill-ness (Mizrachi, Shuval and Gross 2005; Samson1999). The beliefs and worldviews of Ma-oriwomen may contrast with those of nurses creat-ing tension and conflict, compounded by a lackof understanding the historical and socio-politi-cal context for Ma-ori.The diverse experiencesand influences Ma-ori are exposed to, highlightsthe need for nurses to reject adopting a univer-sal approach to service delivery, outside of acuteinterventions needed for acute lifesaving inter-
181Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 181

ventions. Universal approaches to health caredelivery are based on the notion that all users ofhealth services, including Ma-ori, are treated thesame, have similar health needs and can be gen-erally approached in similar ways. Such prac-tices are no longer acceptable or appropriate,although some Ma-ori women noted how achange toward universal approaches missedtheir culturally related needs:
Nurses used to do ‘things’, but they do notdo these now.The ‘things’, such as old valuesand practices, contribute to spiritual well-being. (Interview 4)
DISCUSSIONIdentifying and respecting the beliefs and world-views of Ma-ori women is essential to improvetimely access and use health services. Paraha(cited in Moir 1994:9) highlights the impor-tance of acknowledging and respecting the real-ities of Ma-ori women, stating:‘At the bottom ofeach social pile I met Indigenous women, mar-ginalised by a colonising power, who were fight-ing for their identity.’ The non-recognition ofMa-ori womens’ health needs, constructed with-in their socio-cultural reality denies their identi-ty. Participants reported culturally based healthneeds were generally overlooked, and indicatedthe existence of cultural dissonance.
Ma-ori persist in calling for culturally appro-priate services (Durie 1998d; Reid et al 2000)maintaining issues underlying Ma-ori health sta-tus (in addition to factors such as socioecon-omic determinants of health) are reflective ofculturally unacceptable and inappropriate serv-ices.A growing body of literature (Bophal 2001;Browne & Fiske 2001; Eliason 1999; Jones 1999;Karlsen & Nazroo 2002; Kirchheimer 2003;McKenzie 2003; Reid et al 2000; Reid & Rob-son, 2006) points to a detrimental connectionbetween health disparities and personal andinstitutional racism, and associated discrimin-ating practices. Bophal (2001:1504) maintainsthat: ‘Racism is the most disturbing of the
potential explanations for … [health] inequali-ties.’ As racism is communicated through atti-tudes, behaviours and language, it necessitatesnurses to undertake the process of self reflec-tion and explore the negative impact attitudesand behaviours may have on Ma-ori women.Karlsen and Nazroo (2002), Kirchheimer (2003)and McKenzie (2003) all suggest racism is apublic health issue. Failure to address personaland institutional racism within a health serviceperpetuates the complicity by health careproviders in maintaining racism. Contemporarylanguage and behaviours shrouded in politicalcorrectness that serves to make contentiousissues more palatable, negates the realities that‘others’, like Ma-ori women, may experience.Not acknowledging and addressing the negativeeffects of racism could be considered a failure inthe duty to care and does little to facilitate theengagement of Ma-ori women in health services.
VALUE AND EFFICACYOF CULTURAL SAFETYGiven that registered nurses have been edu-cationally prepared in cultural safety since theearly 1990s, it is somewhat concerning that Ma-ori women participating in this researchreport their cultural beliefs and practices areroutinely not ascertained by nurses. Culturallysafe practice requires nurses to:(a) Examine their personal cultural beliefs and
values and how these may impact on theirpractice with people from an different cul-ture, along with the power differentials thatmay exist; and
(b) Recognise and respect of the beliefs andpractices of health consumers, and incorpo-rate these into intervention and treatmentplans.
(Nursing Council of NZ 2005; Ramsden 2002)
If improvements are to be made in the healthstatus of Ma-ori women, nurses must continueto engage in a process of reflection on theirpractice that aims to increase their effectiveness
182 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 182

in delivering culturally appropriate and accept-able health services – a strength of cultural safe-ty. Such a process would involve reflecting onthe interactions they have with Ma-ori womenand how well their needs are determined andmet in order to evaluate the efficacy of theinteraction(s). Part of this process should alsoinclude a critique of the degree the nurse’ per-sonal and professional cultural values and beliefshave facilitated or impeded the achievement of outcomes for a Ma-ori woman. Developinginsight about the efficacy of one’s nursing prac-tice is an important step in delivering culturallyappropriate and acceptable health services.
Since the implementation of legislation, reg-istered health professionals are required todemonstrate competency to practice, culturalsafety being one area the Nursing Council ofNew Zealand (The Nursing Council) requiresregistered nurse to demonstrate competency.Therein lies a fundamental problem in assessingnurses’ practise is culturally safe, as it is therecipient of nursing practice not the NursingCouncil who determines whether a nurse’spractice is culturally safe or not (Nursing Coun-cil 2005). Despite the Nursing Council (2005)guidelines for cultural safety providing meas-ures to assess practice none of these involveobtaining direct client feedback. Obtainingaccurate client feedback is potentially problem-atic and at risk of the Hawthorne effect (Burnsand Grove 1993), especially when Ma-ori womenare reticent to create problems that may nega-tively affect any future health experiences bymaking a negative judgment about a nurse’spractice. But as ‘outsiders’, nurses are unable tomake accurate judgements about whether a col-league’s practice is culturally safe. Nonetheless,nurses frequently judge their own and their colleague’s practice as ‘culturally’ safe while the recipients of the care, such as the Ma-oriwomen, may have differing perceptions but feelunable to articulate feelings of dissatisfaction.Often they endure a negative experience not to return again. Speaking out was generally not
considered an option for Ma-ori women, withparticipants stating simply:
The attitudes of health care providers arebad. (Interview 1)
Complaining is not an option as things mayget worse. (Interview 6)
This situation lends weight to Johnstone andKanitsaki’s (2007) views on the limitations ofcultural safety.
In addition to clinical expertise, the credi-bility of health care providers is a reflection oftheir efficacy and can influence the success ofinterventions and possibly health outcomes for Ma-ori women accessing and using health ser-vices. Attitudes and behaviours, in addition tothe beliefs and stereotypes held by nurses, influ-ence the nature of the relationships with Ma-oriwomen. Positive health experiences stem frommeaningful partnerships established betweennurses and clients, and influence the efficacy ofhealth care providers. In such partnerships,nurses bring health and illness expertise, whileMa-ori women bring the knowledge about theirhealth beliefs and practices, and life circum-stances. Christensen (1990) asserts the notionof client as ‘expert’ is crucial to nurses’ prac-tice, and for engendering trust and credibility.Table 1 outlines questions nurses can use tooptimise culturally appropriate practice.
Papps (2002) maintains that cultural safetyeducation aims to address issues, such as racism,by increasing insight into stereotyped beliefsand assumptions held about Ma-ori seekinghealth services, and the impact these have onthe delivery of services.The intention of cultur-al safety education is to improve outcomes bydeveloping the efficacy of nurses working withMa-ori, and other cultural groups (Ramsden1990, 2002), nevertheless the reality that allclients have a culturally safe experience ques-tionable. Universal approaches to practice denyclients their identity, and as Reid and Robson
183Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 183

184 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNNTABLE 1: QUESTIONS TO OPTIMISE CULTURALLY APPROPRIATE PRACTICE
Maintaining the Mana (status) and integrity of Ma-ori women
• How are the key beliefs and practices (worldview) of Ma-ori women determined?• How are the principles of partnership, participation, and protection implemented when working with
Ma-ori women?• What opportunities are enabled to undertake cultural practices that are important for a Ma-ori woman’s
well-being?• How are life-circumstances relevant to health, identified and incorporated into the assessment and
intervention plans?• How are barriers to the (a) access, and (b) use of a health service identified?• What barriers to the access and use of health services can nurses either minimise or remove?
Promoting trust in the service
• What are the beliefs that I, as a nurse, personally hold about Ma-ori (Indigenous) women and their health?• How can these beliefs potentially, or actually, impact on those I work with?• What knowledge or practice frameworks guide working ‘with’ Ma-ori women?• What knowledge and skills are required to develop my practice for working with Ma-ori women?• Are my attitudes and behaviours toward Ma-ori women genuine and non-judgmental? If not, why?• Does the health service have policies and processes that aim to improve the delivery of services to
Ma-ori, and include the implementation of beliefs and practices of Ma-ori?• Are Ma-ori frameworks of health and services evident in the delivery of my nursing practice, or the health
service?
Facilitating access and use of a health service
• What mode of communication is used to contact Ma-ori women about appointments, admissions, etc? Are there more effective ways that could be used?
• Is the language used, ‘user-friendly’ and contain minimal or no jargon?• How are Ma-ori women greeted and welcomed to the service?• What Ma-ori images, language, etc are present in the physical environment of the health service to make
it more inviting?• What choices do Ma-ori women have about how and when they access and use a health service? How are
these choices communicated to Ma-ori women?
Building on existing strengths
• What existing knowledge does a Ma-ori woman have about her current health status?• What self-care and health promoting behaviours does this Ma-ori woman undertake?• Has this Ma-ori woman undertaken any recent changes in lifestyle or self-care activities?• What support systems does this Ma-ori woman have? How are these accessed?• What additional knowledge and skills does this Ma-ori woman require to support her self-care activities?
Converging worldviews
• How are the beliefs and practices of Ma-ori women, integrated into treatment and intervention plans?• How are the needs, outcomes, or goals of Ma-ori women identified? What support is required to achieve
the outcomes for each Ma-ori woman?• What processes exist to include the wha-nau (immediate and extended family) of Ma-ori women in their
health experiences, if they so wish?
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 184

(2006:22) contend: ‘This obsession with “treat-ing everyone the same” comes without acknowl-edgement of the need to treat people differentlyto achieve equal outcomes.’Yet, ‘The Weavers ofHealth and Well-being’ highlight negative expe-riences where Ma-ori women consistently felttheir needs were not identified, and meaningfulrelationships not established.
CULTURAL COMPETENCECampinha-Bacote (2002) and Rosenjack Burch-um (2002) both stress that cultural competenceis a lifelong process rather than a definitive end-point, and while cultural safety is also a constantprocess, it polarises each nursing interaction intosafe or unsafe according to Polaschek (1998).Cooper Braithwaite’s (2005) evaluative studylinks cultural competence with the achievementof improved outcomes and found that educationimproves competency. However, the differingunderstandings of cultural competence presentchallenges in terms of accurately and reliablycapturing its meaning, making its measurementproblematic (Geron 2002; Rosenjack Burchum2002). Geron (2002) also questioned the ac-curacy of measuring cultural competence based on health care providers self-report withoutclient input, and based on self-report is open to manipulation to accomplish a favourable outcome.
Measuring practice competency is more than assessing technical or psychomotor compe-tency, and includes the nurse’s attitudinal andbehavioural capability to incorporate knowledgeand skills to ensure a client’s cultural dimensionis integrated into their health experience.Rosenjack Burchum (2002) found that the notionof cultural competence frequently includes the delivery of culturally specific information.However, the acquirement of culturally specificinformation does not acknowledge that diver-sity that exists between, and within culturalgroups, such as Ma-ori, and is the antithesis ofculturally safe practice within the Aotearoa NewZealand context.
Durie (2001) maintains that cultural compe-tency is less about behaving correctly, and moreabout practising in a sound manner. He goesfurther, citing the need to develop the conceptof cultural safety (that focuses on the recipient’sexperience) and proposes cultural competenceto shift the focus on assessment onto the healthcare provider’s capability to deliver culturallysafe practice.
While attempts to measure cultural safetycompetency are generally devoid of client input,the notion of cultural competence proposed byDurie (2001) provides other dimensions that can be used for assessment. Based on Durie’s(2001b) work, the crux of cultural competencycomprises:
1. The nurse (knowledge, beliefs, attitudes,power dimensions);
2. The nurse’s actions that improve a client’shealth status; and
3. The ability to integrate a client’s cultureinto clinical practice.
Cultural competence, therefore, is defined as the capability of nurse to articulate anddemonstrate culturally appropriate and accept-able health services where clients feel culturallysafe, and that reflecting the nurse’s reflexivity,knowledge, and skills, and an ability to workmeaningfully with clients to meet their uniquehealth and cultural needs during their healthexperience. ‘The Weavers of Health and Well-being’ informs criteria to measure a nurse’scompetence through education and the capa-bility to deliver a culturally appropriate andacceptable health service when working withMa-ori women. Table 2 outlines criteria underthe headings the nurse, actions aimed to im-prove health status, and integrating culturalbeliefs and practices into clinical practice,demonstrating culturally competent practice.Effective preparation of nurses in these areascontributes to their making a difference in thehealth status of Ma-ori women. The culturalcompetency model proposed provides a plat-
185Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 185

form for reflecting upon previous interactionswith Ma-ori women, and how such interactionscould be improved and managed more effec-tively.
CONCLUSIONMa-ori women using ‘mainstream’ health ser-vices should rightfully expect that their culturalbeliefs and practices will be respected, at a minimum.The importance of culture has beenprofessionally recognised for several decades innursing, and in Aotearoa New Zealand has beena regulated feature of nurses’ practice since the1990s. When this expectation is not met, theexperience can be unpleasant, and difficult, andrisks compromising access and use of healthservices. The Ma-ori women in this researchreported feeling that their beliefs and practices
were frequently not recognised and devalued by‘mainstream’ health care providers, and gener-ally not included as part of their health careexperience.While preparation of nurses in cul-tural safety and competence is essential in termsof its reflexive nature, its measurement is prob-lematic. The evolution of cultural safety toinclude a framework to develop and assess cul-tural competency is timely. It offers a way ofreducing the dissonance between nurses’ andMa-ori womens’ perceptions of a nurse’s prac-tice, and their practice to be better assessed.
ReferencesAnderson I, Crengle S, Leialoha Kamaka M, Chen
T, Palafax N and Jackson-Pulver L (2006)Indigenous health in Australia, New Zealandand the Pacific, The Lancet 367: 1775–1785.
Baker C and Daigle MC (2000) Cross-culturalhospital care as experienced by Mi’kmaq
186 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
TABLE 2: COMPETENCE OF A HEALTH CARE PROVIDER’S CAPABILITY TO DELIVER A CULTURALLY APPROPRIATEAND ACCEPTABLE SERVICE
FOCUS AREA OF COMPETENCE COMPETENT ACTION
1. The nurse
2. Actions of nurseaimed to improvethe client’s healthstatus
3. Nurse’s ability to integrate aclient’s cultureinto clinicalpractice
• Articulates knowledge, and an analysis of Ma-ori women’s health, and the historical, socioeconomic, and political influences on their health status.
• Identifies beliefs and attitudes held about Ma-ori women, and how these may impact on practice through a reflexive process.
• Identifies the power the nurse holds and its potential impact on the health experience and health outcomes of Ma-ori women.
• Demonstrates sound interpersonal communication skills necessary to establish meaningful relationships based on respect with Ma-ori women.
• Discusses the significance of the Treaty of Waitangi and its application to health.
• Assesses and communicates in a manner that is respectful, clear, and direct.• Involves the Ma-ori woman in the assessment, planning and decision making phases
of her health experience.• Determines necessary support person(s) and/or advocate.• Determines the understanding a Ma-ori woman has of:
(a) Health, wellness, ill-health, and illness.(b) Why she is accessing and/or using the health service.
• Identifies cultural beliefs and practices that a Ma-ori woman needs observed while interacting with the health service.
• Explains why information about key (cultural) beliefs and practices is being collected.• Integrates cultural beliefs and practices into the Ma-ori woman’s health experience,
as appropriate.• Incorporates beliefs and practices into the Ma-ori woman’s intervention plan.• Evaluates the appropriateness and effectiveness of interventions with a Ma-ori woman.
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 186

clients, Western Journal of Nursing Research 22:8–28.
Blakely T,Ajwani S, Robson B,Tobias M andBonne M (2004) Decades of disparity:Widen-ing ethnic mortality gaps from 1980 to 1999,New Zealand Medial Journal 117: 995–1015.
Bophal R (2001) Racism in medicine, BritishMedical Journal 322: 1503–1504.
Browne AJ and Fiske J (2001) First Nationswomen’s encounters with mainstream healthcare services, Western Journal of Nursing Research23: 126–147.
Burns N and Grove SK (1993) The Practice ofNursing Research: Conduct, Critique & Utilization,2nd edn,WB Saunders, Philapdelphia PA.
Campinha-Bacote J (2002) The process of culturalcompetence in the delivery of healthcare ser-vices:A model of care, Journal of TransculturalNursing 13: 181–184.
Christensen J (1990) Nursing Partnership:A Modelfor Nursing Practice. Daphne Brassell Associates,Wellington, NZ.
Dodgson JE and Struthers R (2005) Indigenouswomen’s voices: Marginalization and health,Journal of Transcultural Nursing 16: 339–346.
Durie M (1998) Whaiora: Maori Health Develop-ment, 2nd edn, Oxford University Press,Auckland, New Zealand.
Durie M (2001) Cultural competence andmedical practice in New Zealand. Paperpresented to the Australian and New ZealandBoards and Council Conference,Wellington,New Zealand.
Durie MH (1997) Identity, access and Maoriadvancement: in The Indigenous Future: EditedProceedings of the New Zealand EducationalAdministration Society Research Conference, pp1–15.Auckland Institute of Technology,Auckland, New Zealand.
Eliason MJ (1999) Nursing’s role in racism andAfrican American women’s health. Health Carefor Women International 20: 209–219.
Geron SM (2002) Cultural competency: How is it measured? Does it make a difference?Generations 26: 39–45.
Giger JN and Davidhizar RE (1999) TransculturalNursing:Assessment and Intervention, 3rd edn, CVMosby, St Louis MO.
Glaser BG (1978) Theoretical Sensitivity, SociologyPress, Mill Valley CA.
Glaser BG (1998) Doing Grounded Theory: Issues andDiscussions, Sociology Press, Mill Valley, CA.
Glaser BG (1999) The future of grounded theory,Qualitative Health Research 9: 836–845.
Glaser BG and Straus AL (1967) The Discovery ofGrounded Theory: Strategies for Qualitative ResearchAldine Publishing, New York.
Ibrahim SA,Thomas SB and Fine MJ (2003)Achieving health equity:An incrementaljourney, American Journal of Public Health 92:1619–1621.
Ihimaera W (ed) (1998) Growing up Ma-ori,TandemPress,Auckland, New Zealand.
Johnstone M-J and Kanitsaki O (2007) Anexploration of the notion and nature of theconstruct of cultural safety and its applicabilityto the Australian health care context, Journal ofTranscultural Nursing 18: 247–256.
Jones C (2000) Levels of racism:A theoreticframework and a gardener’s tale, AmericanJournal of Public Health 90: 1212–1215.
Karlsen S and Nazroo J (2002) Relation betweenracial discrimination, social class and healthamong ethnic minority groups, American Journalof Public Health 92: 624–631.
King (2000) The New Zealand Health Strategy,Ministry of Health,Wellington, New Zealand.
Kirchheimer S (2003) Racism should be a publichealth issue, British Medical Journal 326: 65–66.
Leininger M (1978) Transcultural nursing: Concepts,theories and practices, John Wiley, New York.
Leininger MM (1985) Transcultural care diversityand universality:A theory of nursing, Nursingand Health Care 6: 209–212.
Leininger MM (1988) Leininger’s theory ofnursing: Cultural care diversity and univers-ality, Nursing Science Quarterly 1: 152–160.
Leininger MM (1996) Culture care theory,research and practice, Nursing Science Quarterly9(2): 71–78.
Leininger MM (2001) Cultural Care Diversity andUniversality:A theory of nursing, National Leaguefor Nursing Press, New York.
Leininger MM and McFarland MR (2006) Culture Care Diversity and Universality: Aworldwide nursing theory, 2nd edn, Jones &Bartlett, Sudbury, MA.
McCloskey B and Diers D (2005) Effects of NewZealand’s health reengineering on nursing andpatient outcomes, Medical Care 43: 1140–1146.
187Volume 28, Issue 1–2,April 2008 CCCCNNNN
The significance of a culturally appropriate health service for Indigenous Ma-ori women CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 187

McEldowney R, McDonald S, Richardson F,TuriaD, Laracy K and Scott W (2006) Opening OurEyes – Shifting our Thinking,Victory Universityof Wellington,Wellington, New Zealand.
McKenzie K (2003) Racism and health:Anti-racism is an important health issue, BritishMedical Journal 326: 65–55.
Ministry of Health (2006)Tatau Kahukura: Ma-oriHealth Chart Book, Public Health IntelligenceMonitoring Report No. 5, Ministry of Health,Wellington, New Zealand.
Mizrachi N, Shuval JT and Gross S (2005) Bound-ary at work:Alternative medicine in bio-medical settings, Sociology of Health & Illness27:20–43.
Moir M (1994) Mataahua Wa-hine: Images of Ma-oriWomen.Tandem Press,Auckland, New Zealand.
Morse JM (1991) Strategies for sampling, in JMMorse (ed), Qualitative Nursing Research: AContemporary Dialogue, pp 1127–1145, SagePublications, Newbury Park CA.
Nursing Council of NZ (2005) Guidelines forCultural Safety, the Treaty of Waitangi, and Ma-oriHealth in Nursing Education and Practice, NursingCouncil of NZ,Wellington, New Zealand.
Nursing Council of NZ (2008) ContinuingCompetence Framework, accessed at http://www.nursingcouncil.org.nz/contcomp.html on 28March 2008.
Papps E (2002) Cultural safety:What is the ques-tion, in E Papps (Ed), Nursing in New Zealand:Critical Issues Different Perspectives, pp 95–107,Pearson Education,Auckland, New Zealand.
Polaschek NR (1998) Cultural safety:A newconcept in nursing people of differentethnicities, Journal of Advanced Nursing 27:427–457.
Polit DF and Hungler BP (1991) Nursing Research:Principles and Methods, 4th edn, J.B. Lippincott,Philadelphia PA.
Public Health Group (1997) Whaia Te Whanau-kataka: Oraka Whanau – The Wellbeing Of MaoriWhanau:A Discussion Document, Ministry ofHealth,Wellington, New Zealand.
Ramsden I (1990) Kawa Whakaruruhau: CulturalSafety in Nursing Education, Ministry of Health,Wellington, New Zealand.
Ramsden I (1992) Teaching cultural safety, NZNursing Journal, June: 21–28.
Ramsden IM (2002) Cultural Safety and Nursing
Education in Aotearoa and Te Pounamu.Unpublished Doctoral Thesis.VictoriaUniversity of Wellington, New Zealand,accessed at http://culturalsafety.massey.ac.nz/on 6 August 2007.
Reid P and Robson B (2006) The state of Ma-orihealth, in M Mulholland (ed), State of the Ma-oriNation:Twenty-First-Century Issues in Aotearoa, pp17–32, Reed Publishing,Auckland, NewZealand.
Reid P, Robson B and Jones CP (2000) Disparitiesin health: Common myths and uncommontruths, Pacific Health Dialog 7: 38–47.
Rosenjack Burchum JL (2002) Cultural compe-tence:An evolutionary perspective, NursingForum 37: 5–15.
Samson C (1999) Biomedicine and the body, in C Samson (Ed), Health Studies, pp 3–21,Blackwell, Oxford.
Schreiber RS (2001) The ‘how to’ of groundedtheory:Avoiding the pitfalls, in RS Schreiberand PN Stern (eds), Using Grounded Theory inNursing, pp 55–58, Springer, New York.
Sibthorpe B,Anderson I and Cunningham J(2001) Self-assessed health among IndigenousAustralians: How valid is a global question?American Journal of Public Health 91:1660–1663.
Smith LT (1999) Decolonising Methodologies:Research and Indigenous Peoples, University ofOtago Press, Dunedin, New Zealand.
Sporle A (2003) ‘So Ma-ori fits in how?’ – Therealities of attempting to implement kaupapaMa-ori practice evaluation in a contractualsituation, in N Lunt, C Davidson and KMcKegg (Eds), Evaluating Policy And Practice:ANew Zealand Reader, pp 64–67, PearsonEducation New Zealand,Auckland, NewZealand.
Wepa D (2003) An exploration of the experiencesof cultural safety educators in New Zealand:Anaction research approach, Journal of TransculturalNursing 14: 339–348.
Wepa D (2005) Cultural Safety in Aotearoa NewZealand, Pearson Education,Auckland NZ.
Wilson DL (2004) Nga- kairaranga oranga – Theweavers of health and well-being:A groundedtheory study. Unpublished PhD Thesis, MasseyUniversity, New Zealand.
188 Volume 28, Issue 1–2,April 2008CCCCNNNN
Denise WilsonCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 188
Globalisation has intensified worldwide rela-tions and interdependence resulting from
complex economic and social ties that link coun-tries and people around the world (Giddens2001). A major component of globalisation ismigration of great numbers of people from one
region to another across the globe.The twenti-eth and twenty-first centuries are termed theAge of Diasporas (Helman 2007) as all countrieshave large numbers of their citizens living inother countries. Migration may be voluntary or involuntary. Involuntary migrants include
Key Wordshuman rights;ethics; socialjustice; culturalcompetence;nursing care of vulnerablepopulations/refugees/asylumseekers CN
189Volume 28, Issue 1–2,April 2008 CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 189–197.
Nursing care of vulnerable populationsusing a framework of cultural compe-tence, social justice and human rights
ABSTRACT The article attempts to present a model linking cultural competence withadvocacy for social justice and protection of human rights in caring forvulnerable groups such as refugees and asylum seekers. Using the human rightsprinciple focuses the moral obligation to address social inequities and sufferingof vulnerable populations. Cultural competent care and culturally-congruentactions place the universal principles of social justice and protection of humanrights within the cultural contexts of people’s lives and the environment inwhich they are situated.
Compassion is identified as the key component for culturally-competentadvocacy for social justice and human rights protection. Compassion compelsactions advocating social justice and protection of human rights formarginalised and powerless groups. Educational strategies for developingcompassion are centered on collaboration, partnership and advocacy. Inte-gration of experiential and didactic learning relevant to cultural competentcare for refugees and asylum seekers are recommended.Received 29 July 2007 Accepted 25 March 2008
DULA F PACQUIAOAssociate Professor and DirectorCenter for Multicultural Education, ResearchUniversity of Medicine and Dentistry of New JerseyNewark NJ, USA, andPractice CoordinatorPhD in Urban Health SystemsSchool of NursingUniversity of Medicine and Dentistry of New JerseyNewark NJ, USA
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 189

refugees, asylum seekers, internally displacedpersons, returnees, and stateless persons.Thesegroups have fled their homes because of wars,political upheavals, economic disasters or naturaldisasters. As a result of their marginal existenceand experience with oppression, violence, dep-rivation or loss, they have multiple physical, psy-chological, and sociocultural vulnerabilities.Thisarticle specifically addresses refugees and asylumseekers as one group of vulnerable populations.
Vulnerable population groups are those whoare not only particularly sensitive to risk factorsbut also possess multiple cumulative risk fac-tors.They are more likely than others to devel-op health problems as a result of exposure torisk or have worse outcomes from these healthproblems than the rest of the population (Aday2001). An influx of refugees and asylum seekersnecessitates allocation of resources that may tax or overwhelm the receiving country. Com-peting with other groups for these resources,refugees and asylees may face discrimination,isolation and deprivation. Migration is not limit-ed to movement of people, it also involvesmovement of ideologies and life ways that maybe in conflict with those of the receiving socie-ty. Migration for these groups can mean pro-longed displacement and traumatic experiencesthat perpetuate a state of liminality.
Vulnerable migrants’ experience with health-care services and professionals can significantlyinfluence their transition to the new society.Healthcare needs are at the forefront of theirmultiple and complex needs that bring them in early and direct contact with professionalsfrom the host society and different countries.Although the explicit purpose is humanitarian,this contact can be riddled with cultural con-flicts between the migrant and the healthcareproviders.
MAGNITUDE OF THE PROBLEMIn 2005, the UN High Commissioner for Refu-gees (UNHCR) estimated approximately 8.4million refugees worldwide who sought safety
in a neighboring country to escape persecutionin their homeland.The United States, Australiaand Canada were the top countries hostingrefugees. In early 2006, there were about773 500 asylum seekers or people who fledtheir country and seek sanctuary in anothercountry by applying for asylum which grants theright to be recognised as bona fide refugees,receive legal protection and material assistance.About 7.1 million internally displaced person(IDPs) exist worldwide. These persons are insimilar situations as refugees, but remain intheir own countries rather than cross interna-tional borders. There are roughly 2.3 millionstateless persons worldwide and 1.1 millionreturnees who return home as soon as circum-stances permit but continue to need protectionand assistance (UNHCR 2006).
GLOBAL ETHIC OF CAREGlobalisation has heightened the need for healthprofessionals to have a world wide perspectiveand assume an ethical-moral obligation to enterand function in a worldwide community (Lein-inger 2002). In her book, Cultivating Humanity,Nussbaum (1997) has proposed the need tohave world citizenship skills. One of these skills is the ability to critically evaluate one’s self and one’s own cultural traditions. Critical self-reflection examines one’s own beliefs and practices to determine reasonable support forpersonal beliefs rather than accept them asabsolute truths. Another skill is the ability to seethe equality of humanity in order to develop agenuine concern and commitment to the wel-fare of all persons. Lastly, one needs to have theability to see the world from the point of viewof the other. Understanding and feeling the dis-tress of another provides the impetus for thedesire to help.
The concept of world citizenship is embodiedin the literature on cultural competence. Cul-tural competence implies having the capacity to function effectively as an individual and anorganisation within the context of the cultural
190 Volume 28, Issue 1–2,April 2008CCCCNNNN
Dula F PacquiaoCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 190

beliefs, behaviors, and needs presented by indi-viduals [consumers] and [their] communities(Cross et al 1989). Self-awareness and self-reflection are essential to cultural competencedevelopment (Campinha-Bacote 2007). Cultur-al humility is openness to actively engage inmeaningful interactions with others to learnfrom them by assuming the stance of a learnerrather than expert (Tervalon and Murray-Garcia1998). Appreciation of the equality in culturesis embedded in the need to switch one’s frameof understanding to see the validity of other’sways of being and take actions that respect and accommodate cultural differences (Pacquiao2008). Understanding the deepest layer or emicperspective of the other ensures culturally-con-gruent, supportive and meaningful care (Lein-inger 2006).
Cultural competence has a moral agenda thatadvances patient/group autonomy and justice.In the US, cultural competent care is identifiedas the pathway to remove barriers to access tohealth care and eliminate health disparities. Cul-tural competence is predicated on a profoundunderstanding of culture and its significantinfluence in people’s lives. Such understandingpromotes respect for cultural differences. Cul-tural competent caregivers function to min-imise the negative consequences of culturaldifferences (Paasche-Orlow 2004).
GLOBAL ETHIC VERSUSETHICAL PLURALISMEthical fundamentalism views ethical principlesas universally applicable. Moral truths are viewedas timeless and rooted in human nature inde-pendent of societal conventions. By contrast,multiculturalism holds that ethical principles areculturally bound and context dependent (Crig-ger et al 2001; Harper 2006). Leininger (2006)has advocated for the primacy of examining bothsimilarities and differences across cultures as fundamental to culturally-congruent care. Car-ing according to Leininger is culturally con-stituted that needs to be explicated from the
people in order to be meaningful and support-ive. Moral assumptions are culture-bound and asociety’s moral philosophy is embedded in itshealthcare system and actions of health care pro-fessionals are often congruent with these premis-es. Health care in a particular society reflects thedominant cultural norms that transcend profes-sional behaviors and health services (Pacquiao2008).
Culturally competent advocacy is rooted inthe commitment to preserve and protect funda-mental human rights. A human rights frame-work compels a healthcare provider to act tofacilitate access to services that promote therefugees’ survival, decrease their suffering, pre-vent injury and death, and promote their securi-ty as well as those of their loved ones. Advocacyfor social justice is inherent in cultural compe-tent care for vulnerable groups. Social justiceimplies a shift of emphasis from beneficent andcompassionate act to moral obligation.
COMPASSION AND CARING FORVULNERABLE POPULATIONSThe challenge is how to move healthcare profes-sionals to culturally competent advocacy forsocial justice and human rights protection forpopulations who are powerless and dependenton others to address their complex vulner-abilities. The key antecedent to action is the development of compassionate health care professionals who can transform others, organi-sations and communities towards cultural com-petence. Campinha-Bacote (2007) has positedcultural desire as the central motivation towardsongoing cultural competence development togain critical knowledge of one’s self and others,acquire cultural skills in dealing with culturaldifferences and actively engage with diversegroups to promote care effectiveness.
Compassion has been identified by severalauthors (Nussbaum 1997; Crigger, Brannigan &Baird 2006) as the motivation that compels oneto act on behalf of others. Compassion is thedesire to help which is intimately linked with an
191Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nursing care of vulnerable populations CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 191
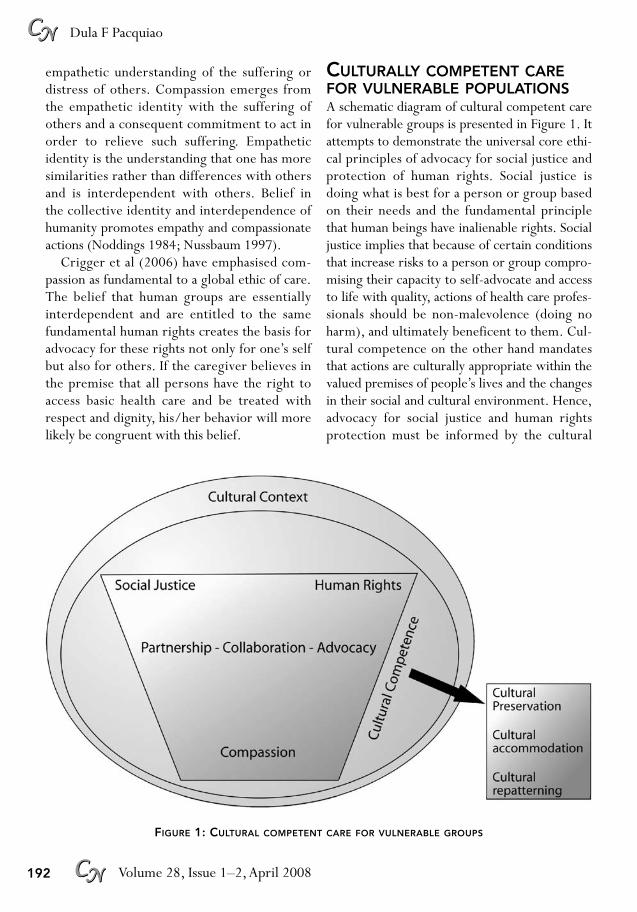
empathetic understanding of the suffering ordistress of others. Compassion emerges fromthe empathetic identity with the suffering ofothers and a consequent commitment to act inorder to relieve such suffering. Empatheticidentity is the understanding that one has moresimilarities rather than differences with othersand is interdependent with others. Belief in the collective identity and interdependence ofhumanity promotes empathy and compassionateactions (Noddings 1984; Nussbaum 1997).
Crigger et al (2006) have emphasised com-passion as fundamental to a global ethic of care.The belief that human groups are essentiallyinterdependent and are entitled to the samefundamental human rights creates the basis foradvocacy for these rights not only for one’s selfbut also for others. If the caregiver believes inthe premise that all persons have the right toaccess basic health care and be treated withrespect and dignity, his/her behavior will morelikely be congruent with this belief.
CULTURALLY COMPETENT CAREFOR VULNERABLE POPULATIONSA schematic diagram of cultural competent carefor vulnerable groups is presented in Figure 1. Itattempts to demonstrate the universal core ethi-cal principles of advocacy for social justice andprotection of human rights. Social justice isdoing what is best for a person or group basedon their needs and the fundamental principlethat human beings have inalienable rights. Socialjustice implies that because of certain conditionsthat increase risks to a person or group compro-mising their capacity to self-advocate and accessto life with quality, actions of health care profes-sionals should be non-malevolence (doing noharm), and ultimately beneficent to them. Cul-tural competence on the other hand mandatesthat actions are culturally appropriate within thevalued premises of people’s lives and the changesin their social and cultural environment. Hence,advocacy for social justice and human rights protection must be informed by the cultural
192 Volume 28, Issue 1–2,April 2008CCCCNNNN
Dula F PacquiaoCCCCNNNN
FIGURE 1: CULTURAL COMPETENT CARE FOR VULNERABLE GROUPS
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 192

context of the people and their situated environ-ment. Although the principle of social justiceand human rights are universal, these conceptsevolve from human conditions in specific con-texts. Hence, there is need to apply these con-cepts in a culturally competent fashion.
Social justice is central to advocating forelimination of health disparities by ensuring thebasic human right to access to quality healthcare. Social justice and human rights principlesare necessary conditions for each other thus,fundamentally complementary. Cultural compe-tent care for vulnerable populations is achievedby commitment to both principles.
The universal impetus for individuals andgroups to move towards advocacy for social jus-tice and human rights protection is compassion.Compassion is the critical motivation that com-pels people to act on behalf of others whichemerges from an affective and cognitive under-standing and identification with others’ experi-ences. It is the fire that ignites the energy totake on actions on problems involving enor-mous risks, complexities and resources. Com-passion requires the ability to distinguish theoppressed from the oppressor, victims fromperpetuators, and the disadvantaged from thepowerful. Compassion is the commitment to gobeyond the purview of one’s own perspectivesand affiliations. It is beyond cultural desire(Campinha-Bacote 2007) as it moves the personto action.
Compassionate actions need to be culturallycongruent and competent otherwise advocatingsocial justice for one group may bring conse-quent disenfranchisement of others. Culturallycompetent compassion is immersed in balancingthe rights of the vulnerable with those of others. Culturally competent action modes ac-cording to Leininger (2006) are embedded incultural preservation, accommodation and re-patterning. One or all there modes of actionmay be used simultaneously or in a continuumof actions. Cultural preservation maintains thecore values, beliefs and practices significant to
the individual or group. Cultural accommoda-tion negotiates with existing cultural differencesin order to find a meaningful existence of one’scultural life ways with those of others. Culturalrepatterning attempts to help individuals andgroups change their way of life to achieve ahealthy, safe and meaningful existence.
CASE EXAMPLESHelsel and Mochel (2002) identified the needby Hmong refugees to take home their placentabecause of their belief that one’s soul may notrest in peace if one is not united with one’safterbirth in death. The practice may not be preserved without accommodating the publichealth policy of disease prevention and control.Some hospitals have developed policies afterconsultation with public health officials andpathologists. In the absence of infectious dis-eases and public health risk to the community, apatient or family can take the placenta home.Disposing the placenta within public healthguidelines while accommodating their practicesuses cultural accommodation and repatterning.
Refugees from the Muslim countries of EastAfrica have a common need for shelter, food,protection from violence, and basic health serv-ices. In working with these communities oneneeds to address violence and oppression offemales and children which may be perpetuatedby members of their own group. Culturallycompetent approaches need to use the threemodes of action to advocate for intra and inter-group rights within the context of the culturalorganisation of patriarchy and Islamic traditions.While cultural repatterning of societal expec-tations of women and children may be a longrange goal, there is need for an immediate focuson negotiating the security and protection ofthese women and children. Health care providersneed to work with the established social hier-archy and the women to accomplish this goal.
In dealing with refugees from third worldcountries, the hosting country may have legiti-mate concerns regarding potential spread of
193Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nursing care of vulnerable populations CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 193

resistant strains of tuberculosis to the generalpopulation. This concern however should beaccompanied by an equal concern for uninfect-ed refugees who need immediate protectionfrom the disease. Prompt detection and isola-tion of infected individuals needs to be donewhile working with the refugee community todevelop an understanding of the need for thisaction (cultural repatterning). With isolationcomes the ethical obligation to provide the rightof infected refugees’ to treatment. Collabora-tion with both governmental and non-govern-mental agencies as well as private donors canhelp address the lack of resources for controland treatment of the disease in the refugee com-munity.
FOSTERING DEVELOPMENTOF COMPASSIONResearch has found key educational strategies infacilitating the transformation of the individual’scompassion to action.The core strategies pro-posed in the model are centered on collabora-tion, partnership and advocacy. Collaborativepartnership with refugees and asylum seekers isbuilt on mutual understanding and empathy.Listening to the stories of refugees and asyleessensitise caregivers to the subjective and highlypersonal reconstruction of their experiences.This encounter develops empathy for the per-son’s suffering and facilitates a full under-standing of the person as a human being. Theprofessional gains knowledge of the unique con-text of the person’s life experiences. Giving avoice to their personal narratives provides affir-mation of their suffering and existence. Objecti-fication and reduction of the person (Foucault1994) are prevented by unfolding the storyusing the individual’s system of meanings rep-lete with biophysical, psychological, spiritualand sociocultural dimensions.
Repeated cultural encounters enhances thehealth care professionals’ ability in demonstrat-ing attentiveness, genuine concern, presence,warmth and empathy. Clinical encounters with
diversity are found to be significant in develop-ing cultural proficiency and effectiveness (Pac-quiao 2007). Similarly, by listening to theunabridged stories of others, the healthcareprovider learns important lessons in culturalsimilarities and differences in specific contexts.Keeping a journal of one’s thoughts, feelingsand behaviors during the encounter promotesinsight into one’s personal biases and reactions.Reflexivity is promoted by analysing one’s ownreactions within the context of the purpose andoutcome of the encounter.
Use of video presentations, case studies orethnographies of experiences of refugees andasylees can increase’ sensitivity and empatheticunderstanding of their plight. Fadiman’s (1999)powerful story of the experience of a Hmongrefugee family in California is an example ofsuch stories. Fadiman’s book provides insight onhow good intentions of healthcare providerscreated undue suffering on the family because ofcultural inappropriateness of their assumptions.It is apropos for learning differential outcomesof caring decisions based on different contextsused by participants. Rigoberta Menchu’s (Bur-gos-Debray 1994) autobiography is a grippingportrayal of a group of people’s continuingstruggle with oppression and violence. It docu-ments the ripple effects of discrimination on the lives of generations of Quiche Indians in Guatemala. These two ethnographies give scenarios of microsocial (Hmong family) andmacrosocial (Quiche Indian people) contextsand consequences of professional and organiza-tional cultural imposition and social oppression.
Developing collaborative partnerships withrefugees and migrant communities promotecontextual understanding of their needs.This inturn promotes effectiveness and responsivenessof health services. Omeri, Lennings and Ray-mond (2006) found that among Afghan refugeesin Australia, health care providers’ lack ofknowledge of gender and family roles, Islamicreligion, language, and health beliefs and prac-tices of the group resulted in stereotypes, in-
194 Volume 28, Issue 1–2,April 2008CCCCNNNN
Dula F PacquiaoCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 194

appropriate care and mistrust.The authors rec-ommended the significant value of collaboratingwith the refugee community in structuringhealth care delivery that is responsive to theirneeds.This process enables the refugees to gainmore control of their lives.
Healthcare providers need experience in car-ing for vulnerable populations locally or abroad.Experience with organisations and advocacygroups serving refugees and asylees may includelocal churches, the Red Cross, homeless shel-ters, Doctors without Borders, the UnitedNations and others. Awareness of resourceslocally, nationally and globally promote accessto and development of more comprehensiveservices. Building collaborative partnershipswith organisations and communities is im-portant as refugees and asylees have complex,multiple needs that are both simultaneous and evolving. Partnerships allow sharing ofresources, services and best practices acrosslocal, national and global contexts. Servicelearning is an excellent opportunity for nursingstudents to learn about organisations and thecommunities they serve. Strengthening thecommunity health nursing component in thecurriculum sensitises students to public healthissues, social inequities affecting health andcommunity resources.
Cultural competence development requiresexperiential learning over a sustained period.Integration of concepts and learning experi-ences throughout the curriculum promotescontinuity and progression of students’ learn-ing. Progression in clinical learning should beguided by the correlation between the students’previous and concurrent learning. Curricularintegration gives students the opportunity torefine their skills and see progress in caring forpeople with multiple vulnerabilities which canotherwise be traumatic and overwhelming.
IMPLICATIONS FOR EDUCATIONEducation of health professionals must includeculturally competent care for transnationals,
asylum seekers, refugees and resettled migrants.They need to critically evaluate state, nationaland global policies affecting these populations.They also need the skill to examine practices ofother health practitioners for vulnerable popu-lations (Koehn 2006). Knowledge of popula-tion-based health risks of refugees and asylumseekers pre and post migration can facilitateearly diagnosis, treatment and surveillance. Useof specialty services and access to relevant edu-cational health programs specific to the prob-lems can be facilitated (Carlsten 2003; Cook etal 2006).
Health professionals need to have the abilityto elicit the complex problems of refugees andmigrants. In addition to physical examination,the immigration history, mental illness, anxietyand depression should be assessed. Understand-ing the cultural support systems within theircultures is important in facilitating a network ofsupport for the refugee. Cultural healers can beof assistance in assisting the refugee in accessinghealth care in a culturally acceptable and mean-ingful way (Carlsten 2003).
Health professionals need training in workingwith non-English speakers and using interpreterseffectively. Proficiency in the dominant languageof the host country is not a requirement forhumanitarian entrants (Lamb and Smith 2002)hence, language barriers often result in miscom-munication, misdiagnosis and lack of appropriatefollow-up (Moreno et al 2001). Selecting inter-preters appropriate to the refugee’s dialect, gen-der and age preferences is based on adequateknowledge of the refugee’s indigenous culture.Bicultural navigators or brokers are recom-mended to promote use of health services andtrust between providers and refugees.
CONCLUSIONCultural competence is the bridge between eth-ical fundamentalism and pluralism as it requiresadapting initiatives within the life context of the refugees and the new environment wherethey are situated. Cultural competent care for
195Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nursing care of vulnerable populations CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 195

refugees and asylum seekers who have multipleand complex needs and rendered powerless bytheir marginalised status and prolonged experi-ence with vulnerabilities requires commitmentto social justice and human rights protection.Leininger’s culturally congruent action modesof cultural preservation, accommodation andrepatterning are applicable in advocating forrefugees and asylum seekers.
Ideals of advocacy for social justice, humanrights protection and cultural competent careremain abstract ideologies without the collec-tive identification with the suffering and distressof others. Compassion is the necessary sparkthat prompts action and enactment of these ideologies. Compassion is rooted in the beliefthat cultural competent advocacy for social jus-tice and protection of human rights is a moralobligation, not merely an act of good will andnon-malevolence. It enables achievement ofbeneficent outcomes for individuals and groupsby minimising the negative consequences of vul-nerabilities and cultural differences.
With globalisation, health care professionalsneed to have world citizenship skills by develop-ing a profound understanding of their own lifeways and those of others. Health professionalsneed to develop a sense of collective identitywith others which brings a consequent appreci-ation of the influence of culture in all aspects oflife, and respect for cultural differences andhuman rights across humanity.This compassion-ate understanding and identity with others isthe key ingredient for taking action to reducesocial inequities resulting in unfair burden of ill-ness and disparate access to quality health serv-ices in vulnerable groups.
ReferencesAday L (2001) At Risk in America: The health and health care
needs of vulnerable populations in the United States, 2ndedn, Jossey-Bass: San Francisco.
Burgos-Debray E (ed) (1994) I,Rigobertya Menchu an Indianwoman in Guatemala,Verso: USA.
Campinha-Bacote J (2007) The Process of Cultural Compe-tence in the Delivery of Healthcare Services, 5th ed, Ohio,Transcultural CARE Associates Press, http://www.
transculturalcare.net/Resources.htm.Accessed July 22 2007.
Carlsten C (2003) Refugee and immigrant health care,Ethnomed http:www.ethnomed.org.Accessed July 292007.
Crigger NJ, Holcomb L and Weiss J (2001) Fundamental-ism, multiculturalism and problems of conductingresearch with populations in developing nations,Nursing Ethics 8: 459–468.
Crigger NJ, Brannigan M and Baird M (2006) Compas-sionate nursing professionals as good citizens of theworld, Advances in Nursing Science 29: 15–26.
Cook PA, Downing J, Rimmer P, Syed Q and Bellis MA(2006) Treatment and care of HIV positive asylumseekers, Journal of Epidemiology and Community Health60: 836–838.
Cross T, Bazron B Dennis K and Isaacs M (1989) Towards aCulturally Competent System of Care,Volume I. George-town University Child Development Center, CASSPTechnical Assistance Center:Washington DC.
Fadiman A (1999) The Spirit CatchesYou andYou Fall Down.Farrar Strauss and Giroux, NY.
Foucault M (1994) The Birth of the Clinic:An archeology ofmedical perception.Vintage Books, NY.
Giddens A (2001) Sociology. Polity: Cambridge.Harper MG (2006) Ethical multiculturalism an evolution-
ary analysis, Advances in Nursing Science 29: 110–124.Helman C (2007) Culture, Health and Illness, 5th edn,
Oxford University Press: NY.Helsel DG and Moche M (2002) Afterbirths in the after-
life: Cultural meaning of placental disposal in a HmongAmerican community, Journal of Transcultural Nursing13: 282–286.
Koehn PH (2006) Transnational migration, state policyand local clinician treatment of Asylum seekers andresettled migrants, Global Social Policy 6: 21–26.
Lamb CF and Smith M (2002). Problems refugees facewhen accessing health services, NSW Public HealthBulletin 13: 161–163.
Leininger M (2002) Transcultural nursing and globalisa-tion of healthcare: Importance, focus and historicalaspects. In Leininger M and McFarland M, TransculturalNursing Concepts,Theories, Research and Practice, 3rd edn,pp 3–44, McGraw Hill: New York.
Leininger M (2006) Culture Care Diversity and Universality aWorldwide Nursing Theory, 2nd edn, Jones & Bartlett:Massachussetts.
Moreno A, Piwowarczyk L and Grodin MA (2001).Human rights violations and refugee health, Journal ofthe American Medical Association 285: 1215.
Nodding N (1984) Caring, University of California Press:Berkeley.
Nussbaum M (1997) Cultivating Humanity, Harvard Univ-ersity Press: London.
Omeri A, Lennings C and Raymond L (2006) Beyondasylum implications for nursing and health caredelivery for Afghan refugees in Australia, Journal ofTranscultural Nursing 17: 30–39.
196 Volume 28, Issue 1–2,April 2008CCCCNNNN
Dula F PacquiaoCCCCNNNN
CNJ 28_1_2_internal.qxd 30/07/2008 9:49 PM Page 196

Pacquiao DF (2007) The relationship between culturalcompetence education and increasing diversity innursing schools and practice settings, Journal ofTranscultural Nursing 18: 28S–37S.
Pacquiao DF (2008) Culturally-competent ethical decisionmaking. In Andrews M and Boyle J, TransculturalConcepts in Nursing Care, 5th edn, pp 408–423.Lippincott Williams & Wilkins: Philadelphia.
Paasche-Orlow M (2004) The ethics of cultural-competence, Academic Medicine 79: 347–350.
Tervalon M and Murray-Garcia J (1998). Cultural hum-ility versus cultural competence:A critical distinctionin defining physician-training outcomes in multi-cultural education, Journal of Health Care for the Poor and Underserved 9: 117–125.
United Nations High Commissioner for Refugees(UNHCR) (2006) Refugees by Numbers 2006 edn, http://www.unhcr.org/basics/BASICS/3b028097c.html,Accessed July 22 2007.
197Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nursing care of vulnerable populations CCCCNNNN
* * * F O R T H C O M I N G 2 0 0 8 * * *
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. [email protected]; www.e-contentmanagement.com
ee ontent PTYLTDmanagementC
INNOVATIVE APPROACHES TO FAMILY VIOLENCESpecial DOUBLE ISSUE of the Journal of Family Studies (ISSN 1322-9400)
ISBN 978-1-921348-05-1 softcover iv + 172 pages October 2008
Edited by Margot Schofield and Rae Walker (La Trobe University, Melbourne)
Course co-ordinators are invited to contact the Publisher for an adoption evaluation copy.
• Editorial – Lawrie Moloney• Guest editorial – Margot J Schofield, Rae Walker• Intimate partner violence in Vietnam and among
Vietnamese diaspora communities in Westernsocieties: A comprehensive review – Angela JTaft, Rhonda Small, Kim A Hoang
• Violence against women in Papua New Guinea –Iona Lewis, Bessie Maruia, Sharon Walker
• Changed forever: Friends reflect on the impact ofa woman’s death through intimate partnerhomicide – Patricia McNamara
• Silent parental conflict: Parents’ perspective –Magdalena M Kielpikowski, Jan E Pryor
• Problems in the system of mandatory reporting ofchildren living with domestic violence – CathyHumphreys
• Indigenous family violence and sexual abuse:Considering pathways forward – Kylie Cripps,Hannah McGlade
• Violence allegations in parenting disputes: Reflec-tions on court-based decision making before andafter the 2006 Australian family law reforms –Lawrie Moloney
• An historical perspective on family violence andchild abuse: Comment on Moloney et al, Allega-tions of Family Violence, 12 June 2007 – NicholasBala
• Family violence in children’s cases under theFamily Law Act 1975 (Cth): Past practice andfuture challenges – Rae Kaspiew
• The idealized post-separation family in Australianfamily law: A dangerous paradigm in cases ofdomestic violence – Amanda Shea Hart, DaleBagshaw
• The rhetoric and reality of preventing familyviolence at the local governance level in Victoria,Australia – Carolyn Whitzman, Tracy Castelino
• The invisibility of gendered power relations indomestic violence policy – Karen Vincent, Joan Eveline
• Baby lead the way: Mental health group work forinfants, children and mothers affected by familyviolence – Wendy Bunston
• Understanding the impact of abuse and neglecton children and young people: Analysis of referraland assessment data from a therapeuticintervention program – Margarita Frederico,Annette Jackson, Carlina M Black
• Intrafamilial adolescent sex offenders: Familyfunctioning and treatment – Jennifer A Thornton,Gillian Stevens, Jan Grant, David Indermaur,Christabel Chamarette, Andrea Halse
• A brief counseling intervention by health profes-sionals utilising the ‘readiness to change’ conceptfor women experiencing intimate partner abuse:The weave project – Kelsey L Hegarty, Lorna J O’Doherty, Jane Gunn, David Pierce, Angela J Taft
CNJ 28_1_2_internal.qxd 30/07/2008 9:49 PM Page 197

INTRODUCTION
According to the International Organizationfor Migration, women migrants have become
agents of economic change as they enter theinternational labour market and participate in anew distribution of global wealth (IOM 2003).This article looks at current nurse migrationflows, the impact migration has on nurses andthe value of positive practice environments forthe full integration of international nurses.The
following scenarios reflects on some of theexperiences of migrating nurses with implica-tions for nurse shortages.
I feel safe. I am happy here and can now planmy life.
Fatima Ansari,*1 born in the Middle East and amember of an ethnic minority, dreamed ofbeing a nurse. Making the wish a reality was a continuing challenge and in spite of the pow-erful social pressures, Ansari persevered andreceived her diploma with the promise of awonderful future. However, victimised daily bythe harmful and discriminatory practices of hercolleagues and employers, she was offered onlysporadic temporary work contracts and earnedvery little money. Given no hope of a better lifein her home country, Ansari finally decided tojoin her sister and brother in Sweden. Recallingher years in Sweden, Ansari insists they have
Key Wordsnurse; nursing;migration; equalopportunity;workenvironment;discrimination;recruitment;ethics CN
198 Volume 28, Issue 1–2,April 2008CCCCNNNN
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 198–206.
Nurses on the move: Diversity and the work environment
ABSTRACT Over 191 million people make up the international migrant population oftoday.Their numbers have doubled since 1970, with women now accounting for almost half.The migrant population has been transformed and is changingthe very nature of society in both source and destination countries. Greaterdifferences in culture, language, work relationships, and coping mechanisms – inshort, greater diversity in society and the workplace – offer many opportunitiesfor excellence in transcultural nursing but also provides fertile ground fordiscrimination, victimisation, harassment and isolation.This article explores and describes current nurse migration flows, the impact migration has on nursesand the value of positive practice environment for the full integration ofinternational nurses.Received 17 July 2007 Accepted 31 March 2008
MIREILLE KINGMAConsultantNursing and Health PolicyInternational Council of NursesGeneva, Switzerland
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 198

been positive. ‘I have been treated well – betterthan in my home country.The decision to movewas mine and I would do it again’ (Kingma2006: 1).
Vicki Bigambo* also faced serious profes-sional and personal problems in her home coun-try of Tanzania. Proposed a job in a Glasgownursing home, she signed the contract that wasto offer her a new life in the United Kingdom.Upon arrival, the recruitment agency took herpassport and attempted to force her into signinga new contract for a lower salary, longer hoursand a new location far from the city. Bigambowas warned that if she spoke to anyone abouther situation she would be deported (Kingma2006).
Fatima Ansari and Vicki Bigambo are part ofthe growing phenomenon of global mobility.Today, over 191 million people live in countriesother than where they were born. This popu-lation has doubled since 1970, with women now accounting for almost half, many migratingwithout their families and alone (IOM 2005;Timur 2000; UN 2006). The migrant popula-tion has been transformed and is changing thevery nature of society in both source and desti-nation countries.
LITERATURE REVIEWNursing has always been a mobile profession.Thousands of nurses every year migrate insearch of better pay and working conditions,career mobility, professional development, abetter quality of life, personal safety, or some-times just novelty and adventure (Kingma 2006).Already in the 1970s, more Filipino nurses wereregistered in the United States and Canada thanin the Philippines (Martineau, Decker & Bun-dred 2002). Today, however, a wider range ofsupplier countries is satisfying the growinglabour needs of an increasing number of desti-nation countries, developing as well as indus-trialised. For example, the number of countriessending international nurse recruits to the Unit-ed Kingdom is known to have increased from
seventy-one in 1990 to ninety-five in 2001(Buchan & Sochalski 2004). Factors facilitatingthe flow between source and destination coun-tries include long-standing trade and economicties, a history of colonial relationships, the exis-tence of established transnational communitiesor diaspora (see the case of Fatima Ansari) aswell as a shared culture, religion or language.Traditional flows in South–North migration are, however, subject to change over time.For example, the Philippines, once the leadingsource of nurse migrants to Ireland and theUnited Kingdom, was outranked by India in2005 (Kingma 2007).
The percentage of foreign-educated physi-cians working in Australia, Canada, the UnitedKingdom (UK) and the United States (US) iscurrently reported to be between 21% and33%, while foreign-educated nurses represent5–10% of these countries’ nurse workforce.New Zealand reports that 21% of its nurses aretrained abroad, a significant increase in the lastdecade (WHO 2006). In 2005–2006, registerednurses were the largest group of workersrecruited by Australian organisations (ANMC2007). In Switzerland, 30% of employed regis-tered nurses are foreign-educated and in at leastone university hospital 70% of new recruits arefrom abroad (Artigot 2003). In 2005, 84% ofthe new entrants to the Irish nursing registerwere foreign-educated; a total of 60% if Euro-pean Union source countries are excluded (An Bord Altranais 2005). In 2002, the number of foreign-educated nurse entrants to the UK Nursing and Midwifery Council Registerexceeded the number of newly qualified nurseseducated in the UK (Ball and Pike 2004).Whilethe percentage of new foreign-educated nurseregistrations in the UK has decreased in recentyears (approximately 35% in 2004–2005)(NMC 2005), there is a reported bottleneck of 37 000 foreign nurses in the country waitingfor clinical placements in order to fulfill ac-creditation requirements (Parrish & Pickersgill2005).
199Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nurses on the move: Diversity and the work environment CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 199

MIGRATION FLOWSTraditionally, the flow of migrant nurses tendedto be North–North or South–South. It is therapid growth in international recruitment fromdeveloping countries to industrialised countriesthat has gained most media and policy attentionin recent years (Dugger 2006). The WorldHealth Organization estimates that 30,000nurses and midwives educated in sub-SaharanAfrica are now employed in seven OECD coun-tries2 (WHO 2006). There is evidence thatnurses often duplicate the ‘carousel’ movementof physicians – using stops in various destinationcountries to build up their skills and credentials(Martineau et al 2002). A nurse may move fromGhana to the United Kingdom, then head toCanada only to leave one or two years later forwhat is often the ultimate destination, the Unit-ed States. Or the route may be even more cir-cuitous, starting in India with stops in SaudiArabia, the United Kingdom, and then NorthAmerica. For example, 40% of the surveyed Fil-ipino nurses employed in the United Kingdomhad previously worked in Southeast Asia and theMiddle East (Opiniano 2002).
Although migration flows have been based onlong-standing political, economic, and socialties, new sources feeding the international skillpool are being sought as the nursing shortage isaffecting an increasing number of countries. Asmentioned, a common language has often beena critical factor in establishing migration flowsin the past.Yet, industrialised countries are nowconsidering the 1.2 million Chinese nurses anuntapped source of nursing human resources.In spite of language differences, countries likeSaudi Arabia, the United States, the UnitedKingdom, Ireland and Australia, have alreadyrecruited Chinese nurses. Greater differences inculture, language, work relationships and copingmechanisms – in short, greater diversity in soci-ety and the workplace – offer many opportuni-ties for excellence in transcultural nursing butalso provide fertile ground for discrimination,victimisation, harassment and isolation.
RISKSCareer moves often enable nurses to achievepersonal career goals, professional developmentand improve their quality of life. This in turnpromotes job satisfaction and excellence in nurs-ing practice while supporting nurse retention aswell as recruitment.The dangers must, however,also be acknowledged. Nurses may be employedunder false pretences or misled as to the condi-tions of work and possible remuneration andbenefits. International nurses may be particularlyvulnerable as the terms of a work contract areharder to verify when distance and languagepresent significant barriers (ICN 2002).
ABUSE AND EXPLOITATIONAbuse may begin with the recruitment processitself. According to the International Council ofNurses, examples include:
• Hidden charges (eg agency fee);• Double charges (eg agency and employer
recruitment fee);• False/misleading information (eg accommo-
dation, orientation);• Inappropriate accommodation charges;• Non-payment or non-compliance with the
terms of the contracted agreement (eg returnflight);
• Implied but refused access to grievance pro-cedures;
• Imposed non-paid orientation period;• Unspecified conditions of work (eg hours,
leave, duration of contract, insurance);• Unspecified work assignment (eg contagious
ward with no barrier equipment);• Abusive treatment (eg retention of travel
documents, forced re-negotiation of contractupon arrival);
• Hidden or unclear penalty clauses (eg pay-ment of fine if employment period not res-pected);
• Absent termination clause.(International Council of Nurses 2001: 7–8)
200 Volume 28, Issue 1–2,April 2008CCCCNNNN
Mireille KingmaCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 200

A wide range of abusive practices exists allalong the recruitment process. Bogus agencieshave charged nurses for services that they willnever provide. In the Philippines, Ghana andIndia, nurses have reported registering withemployment agencies only to find when theyreturn for a progress report, that the businessesno longer exist and their money has disap-peared.
Accommodation charges have also been avehicle for exploitation.Taking one case in Scot-land, four nurses were obliged to live in a two-bedroom apartment, each charged an exorbitantprice. While the usual rent for a similar apart-ment was £395, the nurses together were paying£1,100 per month, three times the going rate.Accommodation abuses have also been reportedin the United States. To give but one example,eight migrant nurses were allocated a four-bedroom in a hospital dormitory.The nurses werethen rostered or scheduled to work differentshifts so that the beds were in constant use(Kingma 2006).
In a letter to the Joint Standing Committeeon Migration Department of the House of Representatives, the Australian Nursing Councilconfirms the existence of exploitation of over-seas nurses by recruiters in the country.Whilethe number of such complaints was small, theANC recognised that migrants are loath to com-plain in fear of losing their visa (ANC 2003).For further examples of abuse and exploitation,see Omeri (2006).
The lack of regard for international nurses’expertise and past work experience negatestheir sense of professional worth and under-mines their confidence (Omeri & Atkins 2002),making them more vulnerable to exploitationand discrimination, and contributes to the dete-rioration of a much-needed skill pool. Nurses,who in the past may have run hospitals or provided expert clinical care, may be obliged todo domestic chores in order to keep their workpermit, eg putting out rubbish, ironing bedlinen, mopping floors or washing the emp-
loyer’s car. One 31-year-old Kenyan nurse nowworking in the United Kingdom expresses hergrief and anguish: ‘Some of the skills I had –they’re dead because I don’t have a chance touse them’ (Allan and Larsen 2003: 6). De-skilling – the loss of skills due to lack of regularpractice or active use – constitutes a type of discrimination that is both an emotional andprofessional insult. In the light of the criticalnursing shortage, it is an unacceptable waste ofprecious resources.
DISCRIMINATION: IMPACT AND OUTCOMEMigrant nurses are frequent victims of poorlyenforced equal-opportunity policies and perva-sive double standards. Colleagues may purpose-fully pretend to misunderstand them, try toundermine their professional skills, refuse tohelp, and sometimes even bully them, all ofwhich increases the nurses’ sense of isolation.Alice Winston,* a Jamaican nurse, remembersthe prevalent racism in her US hospital perpe-trated not only by native-born nurses but byother migrant groups:
There was bias in the assignments and roster-ing. Colleagues would set me up to makemistakes.They would leave out vital informa-tion in the reports between shifts. The Fil-ipino nurses would talk together in theirlanguage.They created a clique – I felt mar-ginalised, an outcast.The other nurses intimi-dated me. Racism is scary.You get attackedbecause of your ethnic origins.
(Kingma 2006: 70–71)
The terrible psychological impact of such treat-ment is obvious.The threat to patient safety isof serious concern.
Recent Australian research documents thediscrimination practised against foreign-educat-ed nurses.The complexity of the phenomenonis highlighted, as different groups of migrantnurses are reserved special treatment. Race,
201Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nurses on the move: Diversity and the work environment CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 201

gender and religion are not the only basis fordiscrimination. The various national groupswere found to be treated differently on the basis of their language background (Hawthorne2001). Analysing the career paths of English-speaking background (ESB) and non-English-speaking background (NESB) migrant nurses,Hawthorne (2001) concluded that discrimina-tion is indisputable.While both groups of nursesfound employment after registration, significantand persistent labour market segmentation wasevident over time. NESB nurses proved to bemuch less likely to be promoted despite theirqualifications and relative seniority. A dispro-portionate concentration of foreign nurses withnon-English-speaking backgrounds was dep-loyed in the ‘least prestigious’ nursing homesector – a sector in the process of redefinitionas ‘foreign labour’ (Hawthorne 2001: 226).Thereality of such high proportions of migrant pro-fessionals in this sector has dramatically modi-fied its image (Kingma 2006). These jobs maybecome doubly stigmatised – first because theyare too difficult, too remote, or too low tech,and then again because it is work only foreign-ers will do.
Employers, supervisors, and colleagues arenot the only ones who discriminate againstmigrant nurses. The Royal College of Nursing(UK) declared that two-thirds of black and eth-nic minority nurses report having been raciallyharassed by patients. In some cases, patientshave refused the care given by nurses from cer-tain ethnic groups or nationalities (Ball & Pike2004).
For decades, the pay and benefits of foreignnurses contracted to work in the Middle Eastdepended on where they had been educated.Although employed as professional nurses underthe same working conditions and often with thesame responsibilities, those coming from themore industrialised counties, like the UnitedStates, the United Kingdom, and Australia, werepaid higher salaries than those emigrating fromthe Philippines, China, or India. This practice
goes for the most part unchallenged by the nurs-es from developing countries, who accept thelower pay as a condition of employment (King-ma 2006).
Paradoxically, with the aggressive recruitmentof international nurses and multiple employmentincentives, many domestic-educated nurses feeltheir employers are exercising reverse discrimi-nation against loyal staff.They see sign-on bonus-es, housing and travel subsidies, educationalgrants, and promises of good schedules beinggiven to international recruits while they areneglected. Recruitment incentives have tendedto be more easily introduced than retentionmeasures. National nurses may sometimes per-ceive the support given to international nurses aspreferential treatment and a form of discrimina-tion against them (Payne 2003).
Discrimination, in any shape or form, is highly destructive. It undermines the person butalso society and its health system as a whole(Adams & Kennedy 2006). De-skilling, discrim-ination and marginalisation of the internationalnurse threatens patient safety and disrupts thehealth team cooperation dynamic required toadvance the delivery of care.
RECOGNISING STRENGTHS:VALUING DIVERSITYThe examples previously discussed illustratevarious forms of discrimination, exploitationand abuse present in the recruitment processitself – before the international nurse physicallyenters the workplace. Increasingly, there havebeen calls for an ethical framework for nurserecruitment.The International Council of Nurs-es (ICN) in its Position Statement on EthicalNurse Recruitment ‘denounces unethical re-cruitment practices that exploit nurses or mis-lead them into accepting job responsibilities andworking conditions that are incompatible withtheir qualifications, skills and experience. ICNand its member national nurses’ associations callfor a regulated recruitment process based onethical principles that guide informed decision-
202 Volume 28, Issue 1–2,April 2008CCCCNNNN
Mireille KingmaCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 202

making and reinforce sound employment poli-cies on the part of governments, employers andnurses’ (2007a: 1).These key principles include:• Effective human resources planning, manage-
ment and development, leading to nationalself-sustainability;
• Credible nursing regulation;• Access to full employment;• Freedom of movement;• Freedom from discrimination;• Good faith contracting;• Equal pay for work of equal value;• Access to grievance procedures;• Safe work environment;• Effective orientation/mentoring/supervision;• Employment trial periods;• Freedom of association;• Regulation of recruitment.
The principles above, while particularly impor-tant for vulnerable migrant populations, shouldalso be applied to the recruitment of domesti-cally-educated nurses. They provide a frame-work that supports excellence in the delivery ofservices, effective human resources manage-ment and high productivity of health systems.
The Australian Nursing and Midwifery Coun-cil in its Position Statement on the EthicalRecruitment of Internationally Qualified andRegistered Nurses and Midwives supports theprinciples and practice of ethical recruitment,consistent with the ICN and International Con-federation of Midwives positions (see www.anmc.org.au).
CRITICAL QUESTIONSThe potential perils of exploitation and abuseexist when making career moves that involvechanging countries as well as workplaces. Toooften, this may result in a decreased income,lower professional status and/or threatenedpersonal safety. Well-informed decisions arepart of the solution. Access to informationneeds to be ensured and facilitated by nurses’professional and trade union organisations.
Career moves must be decided on the groundsof reliable information on the key stakeholdersinvolved, the contract process, conditions ofemployment, benefits, imposed fees and theimpact on nurses’ present and future quality oflife. The basic questions that need to be posedbefore making an international career move are:• What are the credentials of the recruit-
ment/employment agency?• What are the credentials of the employer?• What are the conditions of employment?• What is the job description?• What is the impact of this career move?
(ICN 2002: 16)Similar precautionary evidence-gathering is recommended by the Australian Nursing Fed-eration in their policy statement on NursesWorking Overseas (see www.anf.org.au). Oncethese questions have been answered to satisfac-tion and the decision to accept employmentabroad has been taken, workplace strategiesmust be in place to make the most of inter-national nurses’ skills and their potential forprofessional growth. For further useful infor-mation, see Omeri (2006).
POSITIVE PRACTICEENVIRONMENTSThe beneficial effects of positive practice envi-ronments on health service delivery, healthworker performance, patient outcomes andinnovation are well documented (ICN 2007b).A workplace that promotes workers’ safety,provides opportunities for life-long learning,encourages professional advancement and sup-ports employees’ participation in decision-mak-ing tends to have a highly motivated, committedand productive staff, as demonstrated by theaccredited Magnet hospitals (Aiken et al 2002).These factors translate into lower burnoutrates, higher job satisfaction and better patientoutcomes.
According to TS Kristensen (1999), the fol-lowing factors are required for optimal socialand psychological well-being in the workplace:
203Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nurses on the move: Diversity and the work environment CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 203

• Demands that fit the resources of the person(absence of work pressures);
• A high level of predictability (job securityand workplace safety);
• Good social support from colleagues andmanagers and access to education and pro-fessional development opportunities (teamwork, study leave);
• Meaningful work (professional identity);• A high level of influence (autonomy, control
over scheduling, leadership); and• A balance between effort and reward (remu-
neration, recognition, rewards).(Kristensen 1999 cited in ICN 2007b).
The link between the above factors (or rathertheir absence) and the cases of internationalnurse exploitation described previously is easilydrawn. It comes as no surprise that the full utili-sation of the knowledge and skills of interna-tional nurses will depend to a large extent ontheir integration into the health care team.Thisin turn will depend on the quality of the prac-tice environment. Treating people fairly, withrespect and dignity, is the foundation and guid-ing principle of positive practice environments.Environment issues need to be addressed if theworking conditions and work performance ofthe international nurse are to be improved.
There are many positive practice initiativesdeveloped for the integration of internationalnurses globally (Adams & Kennedy 2006, seecase studies at http://www.intlnursemigration.org/uk-event.shtml).They are often guided orinfluenced by equality legislation, mutual agree-ments, ethical recruitment practices, educa-tional standards and the proactive work ofnumerous national nurses associations. Emp-loyers are developing good human resourcesmanagement practices with comprehensive ori-entation programmes, language preparation,mentoring, education support and career pro-gression. The value of such an approach isrecognised by professional regulatory bodies,including the Australian Nursing and Midwifery
Council (ANMC 2007), as well as professionalunions such as the Australian Nursing Federa-tion (see their policy on Recruitment of Nursesfrom Overseas www.anf.org.au). Cultural aware-ness programmes, both for the ‘home nurses’ andthe international nurses, are increasingly beingdeveloped and implemented, making a differencefor nurses, their patients and families.
WHERE DO WE GO FROM HERE?In order to support long-term integration andretention of international nurses, it is necessaryto have credible and strong human resourcemanagement systems that are capable of adapt-ing to multiple and changing contexts. Tradi-tionally, human health resources managementhas ranked low on the policy agenda. This hasmost certainly contributed to the historicallyhigh turnover rates in nursing, that destabilisethe health work environment and seriouslythreaten health systems’ ability to care effective-ly for patients, ie loss of continuity of care,increased workloads and staff stress levels,disrupted communication channels, reducedefficiency and higher costs (WHO 2006).Human resource practices that support ade-quate staffing, investment in education, team-work, employee autonomy and empowermentare associated with high levels of retention andenhanced organisational outcomes and perform-ance (The European Observatory on HealthSystems and Policies 2006, cited in Adams &Kennedy 2006).
A multi-prong approach is required to effec-tively recruit and retain international nurses.The process must screen and inform interna-tional recruits prior to employment, prepareexisting staff before the arrival of the interna-tional nurse and, finally, provide on-going sup-port through fair human resource managementpractices.
Prior to developing an integration strategy atthe organisational level, each employer, in con-sultation with nurse representatives, shouldidentify the key issues and challenges facing
204 Volume 28, Issue 1–2,April 2008CCCCNNNN
Mireille KingmaCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 204

international nurses in their organisation(Adams & Kennedy 2006). This will require agood communication system, a clear under-standing of the issues to be addressed, a trans-parent problem-solving approach and effectivegrievance procedures.
Evidence suggests there are four major areasto be addressed when attempting to retain andeducate international nurses once employed intheir new destination countries:• Socialisation to the professional nursing role;• Acquisition of language and other communi-
cation skills;• Development of workplace competence, both
clinical and organisation;• Availability of support systems and resources
within the organisation.(Ryan 2003 cited in Adams & Kennedy 2006)
Building positive practice environments willassist the integration of international nurses,support nurses in the host environments andcontribute to creating a dynamic team by valu-ing and using the skills and abilities of all nurses.The enriched cultural backgrounds internation-al nurses bring to the workplace should facili-tate the exchange of information with regard toa wide range of health beliefs and cultural prac-tices. A more comprehensive understanding in this area will facilitate the development ofculturally competent care practices that arerequired of all nurses.These interventions mustbe integrated in curricula at the basic and post-basic levels if services to a diverse patient popu-lation are to be effective. At the same time,international nurses will need to develop a cul-tural understanding of the new country, itshealth care environment, practice settings andclinical expectations (ANMC 2007). This canmost easily be done through targeted and well-supported orientation programmes.
IMPROVING QUALITYPATIENT CAREThe evidence demonstrates that quality health
care workplaces are critical if quality patientcare is to be ensured.The delivery of safe, effec-tive and efficient health services depends on thecompetence of health workers and a work envi-ronment that supports performance excellence.The on-going underinvestment in the healthsector in many countries has resulted in a dete-rioration of working conditions.This has had aserious negative impact on the recruitment andretention of health personnel, the productivityand performance of health facilities, and ulti-mately on patient outcomes (ICN 2006;WHO2006). ICN has launched a global call to addressand improve the serious deficiencies currentlyexisting in the health work environment in allregions.‘We believe patients and the public havethe right to the highest performance from nurs-es and other health care professionals.This canonly be achieved in a workplace that enables andsustains a motivated, well-prepared workforce,’declared Hiroko Minami, ICN President (ICN2007c). In the light of the multi-cultural andmulti-national workforce that presently exists inmany health systems of the world, the full inte-gration of international nurses is a mandatorystep in meeting national and international healthtargets.The fair treatment of international nurs-es remains the key to respecting universallyaccepted human and workers’ rights.
Endnotes1 An asterisk following a name indicates a
pseudonym.2 Canada, Denmark, Finland, Ireland, Portu-
gal, United Kingdom, United States
ReferencesAdams E and Kennedy A (2006) Positive Practice
Environments: Key Considerations for the Developmentof a Framework to Support the Integration ofInternational Nurses, International Council ofNurses, Geneva.
Aiken L, Clarke S, Sloane D, Sochalski J and Silber J(2002) Hospital nurse staffing and patient mortal-ity, nurse burnout, and job dissatisfaction, Journalof the American Medical Association 288: 1987–1993.
205Volume 28, Issue 1–2,April 2008 CCCCNNNN
Nurses on the move: Diversity and the work environment CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 205

Allan H and Larsen J (2003) We Need Respect:Experiences of Internationally Recruited Nurses in theUK, Royal College of Nursing, London.
An Bord Altranis (2005) Registration Information2005.Accessed at http://www.nursingboard.ie on July 10, 2006.
Artigot F (2003) Les hôpitaux canadiens battent lerappel des infirmières québécoises exilées inSuisse, Le Temps October 17.
Australian Nursing Council (2003) Letter to the JointStanding Committee on Migration Department ofHouse of Representatives.Accessed at www.aph.gov.au/house/committee/mig/skillmig/subs/sub15a.pdf on 18 October 2007.
Australian Nursing and Midwifery Council (2007)Position Statement Orientation of InternationallyQualified and Registered Nurses and Midwives to theAustralian Healthcare Context.Accessed at www.anmc.org.au/position_statement_guidelines/index.php on 18 October 2007.
Ball J and Pike G (2004) Stepping Stones: Careers ofNurses in 2003, Royal College of Nursing,London.
Buchan J and Sochalski J (2004) Nurse Migration:Trends and the Policy Context, Unpublished.
Dugger C (2006) U.S. Plan to Lure Nurses MayHurt Poor Nations, New York Times May 24.
Hawthorne L (2001) The globalisation of the nursingworkforce: barriers confronting overseasqualified nurses in Australia, Nursing Inquiry 8:213–229.
ICN (2002) Career Moves and Migration: Critical Ques-tions, International Council of Nurses, Geneva.
ICN (2006) The Global Nursing Shortage: Priority Areasfor Intervention, International Council of Nurses,Geneva.
ICN (2007a) Position Statement: Ethical Nurse Recruit-ment, International Council of Nurses, Geneva.
ICN (2007b) Positive Practice Environments, Interna-tional Council of Nurses, Geneva.
ICN (2007c) ICN Calls for Positive Practice Environmentsto Ensure Quality Patient Care, InternationalCouncil of Nurses, Geneva.
IOM (2003) World Migration 2003 – ManagingMigration – Challenges and Responses for People on theMove, International Organization for Migration,Geneva.
IOM (2005) World Migration 2005: Costs and Benefits
of International Migration, InternationalOrganization for Migration, Geneva.
Kingma M (2006) Nurses on the Move: Migration andthe Global Health Care Economy, Cornell UniversityPress, Ithaca NY.
Kingma M (2007) Nurses on the move:A globaloverview, Health Services Research 42: 1281–1298.
Kristensen TS (1999). Challenges for research andprevention in relation to work and cardiovasculardisease. Scandinavian Journal of Work, Environmentand Health 25: 550–557.
Martineau T, Decker K and Bundred P (2002)Briefing note on international migration of healthprofessionals: Leveling the playing field for developingcountry health systems, Liverpool School of TropicalMedicine, Liverpool.
NMC (2005) Statistical analysis of the register. 1 April2004 to 31 March 2005. Report August 2005.London: Nursing and Midwifery Council.Accessed at http://www.nmcuk.org/aFrameDisplay.aspx?DocumentID=856 on 10 July 2006.
Omeri A (2006) Workplace practices with mentalhealth implications impacts on recruitment andretention of overseas nurses in the context ofnursing shortages. Contemporary Nurse 21: 50–61
Omeri A and Atkins K (2002) Lived experiences ofimmigrant nurses in New South Wales,Australia:Searching for meaning. International Journal ofNursing Studies 39: 495–505.
Opiniano J (2002) Over 100 Pinoy nurses exploited inUK private nursing homes.Accessed at http://cyberdyaryo.com/features/f2002_0325_04.htmon 5 January 2004.
Parrish C and Pickersgill F (2005) Home officeconsiders special visa to support overseas nurses,Nursing Standard 19: 12.
Payne L (2003) Differing viewpoints on the issue ofoverseas nurses, Nursing Times 99: 15.
Timur S (2000) Changing Trends and major issues ininternational migration:An overview of theUNESCO programmes. International Migration165: 255–269.
UN (2006) International migration facts and figures.Accessed at http://www.un.org/esa/population/hldmigration/Text/Migration_factsheet.pdfon 18 July 2006.
WHO (2006) The World Health Report 2006 – Workingtogether for health,World Health Organization,Geneva.
206 Volume 28, Issue 1–2,April 2008CCCCNNNN
Mireille KingmaCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 206

NCCopyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 207–210.
EPILOGUE
207Volume 28, Issue 1–2,April 2008 CCCCNNNN
Collaboration is evident in today’s organisa-tional, government and business life (Hux-
ham & Vangen 2000) and skills to work acrossboundaries and to form alliances and partner-ships are sought in today’s leaders.The health-care arena is no different and the concept ofboundaries to be crossed is implicit in the verynature of transcultural nursing. Successfullynegotiated partnerships, coalitions and collabo-rations between participating healthcare groupsare at the heart of advancing transcultural nurs-ing knowledge.
Extending the healthcare research capacityand capability beyond national borders andacross professions through global collaborativeendeavours spreads the work load and accel-erates the production of knowledge (Pearson2007) for nursing and other disciplines. Suchdesirable outcomes can result from effectivecollaborative efforts.
Most countries in today’s world require qual-ity health care interventions and practices thatcan be justified or based on research evidence ofsuperior efficacy and efficiency. Responsibility
for providing such interventions and practiceslies with the health care professionals who arelooked to for the development of such interven-tions and the provision of guidance for bestpractices. Most countries also have difficulty inreconciling the increasing demand for the healthcare influenced by the speedy internationalknowledge exchange via the World Wide Weband the imperative of doing more with less asresources become scarcer. These factors com-bined with the understanding that most ‘nationsand cultures are more alike than they are dif-ferent’ (Pearson 2007: 69) suggest that greatercollaboration on a global level would be pro-ductive and beneficial to all partners in a collab-orative effort.
Essentials of a successfulcollaborative effortEffective collaboration is premised upon settingworthwhile goals of mutual benefit to con-sumers, service providers and other stake hold-ers. It means achieving the desired outcomes byreducing or removing boundaries that impedethe realisation of goals that benefit consumersand others. Collaboration involves joint effortand implies joint ownership (Linden 2002) forall partners and means the commitment of eachto the goals of an enterprise/project to gainworthwhile benefits.
Essential to a collaborative endeavour is aclear expression, understood and agreed by allparties in the alliance, of the joint purpose ofthe collaborative effort, its goals and objectives
Advancing transcultural nursing throughcollaboration
AKRAM OMERIPhD, RN, CTN, FRCNA
Guest EditorAdvances in ContemporaryTranscultural NursingAdjunct Associate ProfessorUniversity of Western SydneySchool of NursingSydney NSW, Australia
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 207

(Clegg et al 2005 cited in Brown et al 2006)and the development of a strong sense of com-mon purpose. In our joint collaboration, asguest editors, we adopted the goal of transcul-tural nursing in order ‘to prepare a new genera-tion of nurses who would be knowledgeable,sensitive, competent and safe to care for peoplewith different and similar lifeways, values,beliefs, and practices in meaningful, explicit,and beneficial ways’ (Leininger & McFarland2002: 6).
A sense of common purpose underpins thedevelopment of strong, balanced relationships,based on trust and respect, between the part-ners. A key element in collaborative endeavoursis effective communication and the develop-ment of strategies to ensure shared decisionmaking (Kantar 1994). Successful developmentof an alliance also depends upon engaging thebest possible people in the task with the author-ity and autonomy to speak (Huxham & Vangen2000). It also requires time and sufficientresources to establish a project and to sustain it(Huxham 1996a, 1996b; Linden 2002).
Collaborative challengeTranscultural nurses recognise that we live in amulticultural world and that ‘all health caremust be transculturally based to serve peopleappropriately from different cultures in theworld’ (Leininger 1995: 681).The challenge isto provide research based transcultural knowl-edge to guide practice and to be effective inhelping others and for the development of tran-scultural education of clinicians and faculty.
As Leininger (Leininger & McFarland 2002:578) has identified that it is the coming genera-tion of nurses, who experience cultural diversi-ty in their daily interactions that see the needfor transcultural nursing knowledge; they turnto their educators for knowledge to assist themin their practice. As Leininger (Leininger &McFarland 2002: 7) has stated: ‘Nursing stu-dents expect their faculty to be knowledgeableand competent in transcultural nursing so they
will be effectively guided in their practice.’Leininger has also identified that the challenge isto prepare students who are ‘knowledgeable,sensitive, competent, and safe to care for peoplewith different or similar lifeways, values,beliefs, and practices in meaningful, explicit,and beneficial ways.’ This challenge can only be met if faculty are themselves transculturallyqualified and prepared to contribute, on the one hand, to the development of transculturalknowledge and, on the other, to teach it to theirstudents to assist them to meet the pressingdemands for care that is culturally safe, mean-ingful and effective. Leininger predicted that ‘bythe year 2020 more nurses will be prepared ingraduate transcultural nursing studies whichwill facilitate meeting consumer expectationsand transcultural nursing education and practicegoals’ (Leininger & McFarland 2002: 578).
Nursing in Australia in recent years has muchto be proud of given the immense changes innursing practice and education it has embracedand sustained, and the developing and growingbody of nursing knowledge through researchconcomitant with the higher education of nurs-es (Halcomb, Patterson & Davidson 2006).Thefuture development of nursing still has numer-ous challenges ahead.These challenges are theglobalisation of health care, and the contempo-rary demands on health care (Pearson 2007). Inresponse to these challenges transcultural col-laborative effort is called for from the nursingprofession.
As Pearson (2007) has noted internationalcollaboration is not well established in nursing.Much of nursing research is small in scale andlocal in application which severely limits itscapacity to make a substantive contribution toadvancing nursing science. A much greater con-tribution could be made to global health prob-lems by nursing science through the medium oftranscultural concepts. It remains for us in thecoming decade to become more global andstrategic in our thinking and research efforts,to seek and nurture research across national
208 Volume 28, Issue 1–2,April 2008CCCCNNNN
Akram OmeriCCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 208

boundaries in collaborative partnerships, notonly with other nurses but also with other pro-fessions.
Our commitmentAs transcultural nurses our pursuit of excellencecontinues as a major objective in the transcultur-al nursing journey by our continued leadershipin research and education informing practice atthe highest levels and sharing such worldwideknowledge across boundaries. It is our commit-ment to continue, and grow, as key participantsin contributing to the profession of nursing, andto advocate for the culturally meaningful andcongruent/competent health care needs of the sick and well, to promote social justice andhuman rights of people towards equality ofaccess to health and welfare services, and healthas a right not privilege of all.
This Contemporary Nurse special issue on transcultural nursing, Advances in Contemporary Transcultural Nursing, 2nd edition (ISBN 978-0-9757710-5-1) is one major collaborativeendeavour aiming to advance shared and evi-dence-based transcultural nursing knowledgetoward improving care in culturally meaningfulways to clients and nurses. It has taken twoyears of planning, and organisation to bring thiscollection of research-based transcultural nurs-ing knowledge in the volume of ContemporaryNurse in two issues which could be shared glob-ally.This volume provides a collection of freshideas and research in transcultural nursing edu-cation, research and practice in diverse con-texts.
We, as guest editors, are both certified tran-scultural nurse specialist and scholars, mentoredby the Founder of the discipline of transculturalnursing, Madeleine Leininger, from culturallydiverse backgrounds, worlds apart. Having hadprevious joint partnership in a number of collab-orative projects in Australia, USA and othercountries, our collaboration in this major projectwas well advanced. From the early planningstages, we were assured to possess qualities of
strong, balanced relationships, based on trustand respect, good and effective communication,and a shared decision-making as stated by (Kan-tar 1994) essential in the success of this collabo-rative plan.
Our association dates back to the early1990s, two decades ago, when we met duringthe first joint venture, attending the first tran-scultural nursing theory conference at MadonnaUniversity, Livonia, Michigan. At the time wewere both pursuing graduate studies in trans-cultural nursing with mentorship from DrMadeleine Leininger. Since then, our mutualinterests in transcultural nursing have continuedto grow.We have continued working collabora-tively to strengthen and advance transculturalnursing knowledge through education, researchand leadership.
As part of our collaboration, we have trav-eled to joint transcultural nursing conferencesand educational activities in Australia and USAas well as other countries, on numerous occa-sions. We have also been actively involved asmembers of committees of the TransculturalNursing Society including Leininger AwardCommittee, Certifications Committee and theNomination Committee of the TransculturalNursing Society.
In addition to conferencing, we have consult-ed and collaborated in the design and teachingstrategies for the development and delivery of courses in transcultural nursing. We haveexchanged ideas, philosophies, pathways of howbest to deliver the message of transculturalnursing for students and faculty in BN, MN,PhD as well as in continuing education pro-grams, in diverse contexts and in culturally andeducationally meaningful ways.
We have sought ways of advancing transcul-tural nursing through research, conferencepresentation and joint projects. Joint guest edit-ing for this Contemporary Nurse special issue intranscultural nursing, Advances in ContemporaryAdvances in Transcultural Nursing, 2nd edition, hasbeen a major joint commitment in collaboration
209Volume 28, Issue 1–2,April 2008 CCCCNNNN
Epilogue:Advancing transcultural nursing through collaboration CCCCNNNN
CNJ 28_1_2_internal.qxd 14/07/2008 12:50 PM Page 209

across borders, reflecting our latest interna-tional collaboration.We have consulted onlinevia email and telephone in order to compareour views on editing and suitability of manu-scripts for this special issue.
We guest editors, are well advanced in ourcollaborative endeavours. Plans are in place fortwo joint projects including; Collaboration insupervision of post-graduate nursing students onlineand Nurse practitioners and their roles in rural–remote areas. Nurses are realising that what weteach and how we care for people necessitateshaving transcultural nursing knowledge andskills to be effective and helpful to others. Liv-ing in a multicultural world challenges nurses tounderstand trends and cultural realities. Meet-ing the challenge will be greatly facilitated bycollaborative effort and shared endeavour in thediscovery of transcultural knowledge.
Leininger has stated that by 2020: ‘all healthcare must be transculturally based to serve peo-ple appropriately from different cultures in theworld’ (Leininger 1995 cited in Leininger &McFarland 2002: 577). In a multicultural worldthe challenge for the health professions and thesystems that support them, is to ensure enoughhealth professionals are available with the skills,knowledge and attitudes to provide culturally
meaningful and safe care. When this comes topass, Leininger’s prediction that: ‘Transculturalnursing will continue to soar to many places in the world in the 21st century to servehumanity’ (Leininger 1960 cited in Leininger &McFarland, 2002: 577) will be realised.
ReferencesBrown D,White J and Leibbrandt L (2006) Collaborative part-
nership for nursing faculties and health service providers:what can nursing learn from business literature? Journal ofNursing Management 14: 170–179.
Clegg S, Kronberger M and Pitsis T (2005) Managing and Organ-izations:An introduction to theory and practice. Sage Publications,London.
Halcomb E, Patterson E and Davidson P (2006) Evolution ofpractice nursing in Australia, Journal of Advanced Nursing 55:376–388.
Huxham C (Ed) (1996a) Creating Collaborative Advantage, SagePublications, London.
Huxham C (1996b) Collaboration and collaborative advantage.In Huxham C (Ed) Creating Collaborative Advantage, pp 1–18,Sage, London, UK.
Huxham C and Vangan S (2000) Ambiguity, complexity anddynamics in the membership of collaboration. Human Rela-tions 53: 771–809.
Kantar R (1994) Collaborative advantage:The art of alliances.Harvard Business Review 72: 142–149.
Leininger MM and McFarland M (2002) Transcultural NursingConcepts,Theories, Research & Practice, 3rd edn, McGraw Hill,New York.
Leininger MM (1990) Ethical and Moral Dimensions of Care,WayneState Press: Detroit MI.
Linden R (2002) A framework for collaborating, Public Manager31: 3–7.
Pearson A (2007) Editorial: Exploiting the potential of interna-tional collaboration in nursing, International Journal of NursingPractice 13: 69.
210 Volume 28, Issue 1–2,April 2008CCCCNNNN
Akram OmeriCCCCNNNN
INTERNATIONAL JOURNAL OF MULTIPLE RESEARCH APPROACHES
Indigenous Research MethodsVolume 4 Issue 1 • April 2010 • Special Issue
DEADLINE FOR MANUSCRIPT SUBMISSIONS: 30 Apr i l 2009
Submissions are welcome from indigenous and non-indigenous researchers and students working onapproaches to Indigenous research methodologies across all the disciplines represented by the journal,
including (but not limited to) Education, Health, Management, Psychology, Sociology, Social Work,Development Policy and Political Science. Authors are invited to send their abstract in advance ofsubmission to co-Guest Editor, Dr Karen Martin: [email protected]; tel. +61-2-66203610
Submissions following Author Guidelines on the journal website (www.ijmra.com) may be addressed to:[email protected]
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. +61-7-5435-2911; [email protected]
www.e-contentmanagement.com
• • • C A L L F O R P A P E R S • • •
CNJ 28_1_2_internal.qxd 30/07/2008 9:50 PM Page 210

Culture Care Diversity andUniversality: A Worldwide Nursing Theory, 2nd EditionLeininger MM and McFarland MR (eds) (2006)Jones and Bartlett, Sudbury; ISBN 0-7637-3437-3;PB; xviii + 413 pp;AUD 71.00
This book is the second edition based on a life-time of work and the continued development
of the 1991 edition. It is appropriate for beginningnursing students, graduate students and experi-enced nurse researchers interested in theorydevelopment and transcultural nursing research.
The 16 chapters include a very in-depth intro-duction and description of culture care diversityand universality theory, along with the evolutionof the theory and ethnonursing research method.The first three chapters and last chapter in thebook deal with the theory, research method, glob-alisation of transcultural nursing theory andresearch, and predictions for the future. Eightchapters deal directly with the utilisation of theethnonursing research method as findings andfour chapters discuss the use of the theory in
nursing administration, clinical application, andindirectly nursing education. The book uses res-pected scholars in the field to present the applica-tion of the theory and findings using the researchmethod.
The authors do a good job of articulating thescope of the book through the foundational chap-ters related to the theory and research methodthat is unique to nursing and specifically devel-oped to understand and discover phenomena ofinterest to nursing. Overall, the chapters that fol-low the foundational chapters assist the reader inunderstanding the relationship to the theory inpractice, administration and education, as well asthe rigor involved in the research process specificto the theory and research method. The authorsalso make a very clear connection to the theoryand research method for use in discovery of cul-ture care phenomena in nursing globally.
The book could have been laid out differentlyby grouping the chapters using the theory in nurs-ing, followed by the research chapters. There isrelevance in using classic work to articulate theuse of the theory and research method; however,presenting contemporary work could advance thecontinued development of the theory and researchmethod. Presenting studies using the researchmethod with large immigrant populations acrossthe globe such as Mexican, or sub-cultures such asgays and lesbians, would be beneficial for futureeditions.
211Volume 28, Issue 1–2,April 2008 CCCCNNNN
R E V I E W E RRICK ZOUCHA
Associate Professor, School of Nursing Duquesne University
Pittsburgh, Pennsylvania
CCCCNNNN
BOOK REVIEWS
Copyright © eContent Management Pty Ltd. Contemporary Nurse (2008) 28: 211–212.
If you have a book for review, or would like to submit a review, please contact:
Dr Merri PaechBook Reviews Editor, Contemporary Nurse
Division of Health Sciences, University of South Australia, North Terrace SA 5000
E-mail: [email protected]
CNJ 28_1_2_internal.qxd 30/07/2008 9:50 PM Page 211

Transcultural Concepts in NursingCare, 5th EditionAndrews M and Boyle J (2008)Wolters Kluwer Health/Lippincott Williams &Wilkins, Philadelphia; ISBN 9780 7817 9037 6;PB; xx + 487 pp;AUD 82.50
As the world becomes increasingly multicultur-al, the fifth edition of Andrews’ and Boyle’s
well-known transcultural nursing text continuesto synthesise transcultural theories, models, andresearch to facilitate culturally congruent andcompetent nursing care.This comprehensive textfocuses on application of transcultural nursingknowledge to nursing practice encompassing thecare of individuals, families, groups, communities,and institutions across the lifespan. Rather thanmemorising a laundry list of cultural groups’attributes, Andrews and Boyle purport thatthrough cultural assessment and critical thinking,nurses throughout their professional careers willbe able to meet the culture care needs of diversepeople.
The book is divided into four parts: historicaland theoretical foundations of transcultural nurs-ing; transcultural nursing across the lifespan;nursing in multicultural health care settings; andcontemporary challenges in transcultural nursing.With its focus on application to nursing practice,each chapter includes case studies and learningactivities based on each author’s actual clinicalencounters. New features in this edition are boxescontaining evidenced based practice research stud-ies to assist the reader in applying knowledge topractice.
The chapters related to creating culturallycompetent organisations and cultural diversity inthe health care workforce are especially useful forstudents and nurses who may embrace transcul-tural care of diverse patients and families and yet,may not have considered how to apply this knowl-edge to working with diverse colleagues.The textemphasises the importance of creating an organi-sational environment where cultural similaritiesand differences are embraced and may be crucialfor facilitating culturally congruent and compe-tent care.
This comprehensive text provides an excellentresource for nursing practice and is useful fornursing students, nurses, educators, researchers,and administrators. Andrews and Boyle bringtogether theory, research and practice to supportnurses in their quest to provide culturally compe-tent and congruent care.
212 Volume 28, Issue 1–2,April 2008CCCCNNNN
Book reviewsCCCCNNNN
R E V I E W E RSANDRA J MIXER
Assistant Professor of NursingMiddle Tennessee State University
Murfreesboro TN
• • • C A L L F O R P A P E R S • • • ADVANCES IN CONTEMPORARY
MENTAL HEALTH NURSING – SECOND EDITIONGuest editors: Nicholas Procter, School of Nursing and Midwifery, University of South Australia, Angela
Frederick Amar, William F. Connell School of Nursing, Boston College, Chestnut Hill MA, and Chang KamHock, Department of Nursing Faculty of Medicine and Health Sciences, University Malaysia Sarawak
DEADLINE FOR MANUSCRIPT SUBMISSIONS: 2 March 2009
A special issue of Contemporary Nurse, volume 34 issue 1, publishing December 2009ISBN 978-0-9775242-6-6; iv+124 pages; softcover
More information: http://www.contemporarynurse.com/archives/vol/34/issue/1/call/
eContent Management Pty Ltd, PO Box 1027, Maleny QLD 4552, AustraliaTel.: +61-7-5435-2900; Fax. [email protected]; www.e-contentmanagement.com
ee ontent PTYLTDmanagementC
CNJ 28_1_2_internal.qxd 30/07/2008 9:50 PM Page 212