
Treatment of Lisfranc Fracture Dislocations with an Interosseous Suture Button Technique: A Review...
9
CASE REPORT Treatment of Lisfranc Fracture Dislocations with an Interosseous Suture Button Technique: A Review of 3 Cases James M. Cottom, DPM, AACFAS, 1 Christopher F. Hyer, DPM, AACFAS, 2 and Gregory C. Berlet, MD 3 Lisfranc fracture dislocations are complex and difficult to treat. Making the correct diagnosis and achieving an anatomical reduction are important factors in regard to achieving a favorable outcome with this injury. We describe a new technique that we have found to be useful for stabilizing Lisfranc fracture dislocations. This method is relatively fast, minimally invasive, and effective, and it eliminates the need for implant removal. To date, we have achieved predictable results for stabilizing and treating these difficult injuries with the use of a suture endobutton, instead of traditional interfragmental screw fixation. In this report, we describe 3 cases in which this method was used with satisfactory short-term results. Level of Clinical Evidence: 4. ( The Journal of Foot & Ankle Surgery 47(3):250 –258, 2008) Key Words: dislocation, endobutton, fracture, Lisfranc, midfoot, suture and button, trauma I njuries involving the tarsometatarsal (TMT) and midfoot region are complex, frequently missed, and often difficult to treat. The Lisfranc injury may involve osseous fractures, tearing of the ligamentous support, or a combination of these injuries. The overall incidence of fractures of the TMT joints has been reported as 0.2% of all fractures (1). It has been documented that as many as 20% of these fractures are misdiagnosed, or not recognized, upon initial clinical exam- ination (2). The diagnosis may be missed due to complex bony anatomy that is not well visualized with standard radiographs, or the confusion that may be associated with treating a patient who has sustained polytrauma. One study found that of 72 patients with Lisfranc injuries, 81% were polytrauma patients and 32% had additional ipsilateral foot and ankle fractures (3). Ligamentous Lisfranc injuries, while being common, are also notable in that they are associated with disruption of normally very strong liga- ments, resulting in articular instability without a fracture. Pure ligamentous injuries in this area are notorious for healing more slowly than osseous injuries, and they often require prolonged non–weight bearing. One report noted that patients whose injuries were both ligamentous and osseous, as compared with patients with ligamentous inju- ries only, experienced poorer treatment outcomes despite undergoing anatomic reduction and rigid internal fixation (4). For this reason, and in those cases with severe intra- articular comminution, some surgeons advocate the use of a primary arthrodesis of the medial 2 or 3 rays (5), rather than attempt to preserve the entire Lisfranc joint complex. In this report, we present a technique of Lisfranc joint complex repair that employs the use of an interosseous suture with endobuttons, namely the Arthrex Mini Tight- Rope (Arthrex, Inc., Naples, FL), instead of traditional interfragmental screw fixation. This technique has been found to be effective, fast, and yields predictable results for stabilizing and treating these difficult injuries. In this lim- ited case series, patients were able to fully bear weight on the operated foot and return to regular activities, including athletic activities, faster than what we have experienced in Address correspondence to: James M. Cottom, DPM, AACFAS, Sara- sota Orthopedic Associates, 2750 Bahia Vista St, Ste 100, Sarasota, FL 34239. 1 Fellow, Orthopedic Foot and Ankle Center, Columbus, OH. 2 Orthopedic Foot and Ankle Center, Columbus, OH. 3 Chief, Division of Foot and Ankle, Ohio State University Orthopedics, Orthopedic Foot and Ankle Center, Columbus, OH. Financial Disclosure: None reported Conflict of Interest: None reported Copyright © 2008 by the American College of Foot and Ankle Surgeons 1067-2516/08/4703-0014$34.00/0 doi:10.1053/j.jfas.2008.01.004 250 THE JOURNAL OF FOOT & ANKLE SURGERY
Transcript of Treatment of Lisfranc Fracture Dislocations with an Interosseous Suture Button Technique: A Review...
CASE REPORT
Treatment of Lisfranc Fracture Dislocationswith an Interosseous Suture ButtonTechnique: A Review of 3 Cases
James M. Cottom, DPM, AACFAS,1 Christopher F. Hyer, DPM, AACFAS,2 andGregory C. Berlet, MD3
Lisfranc fracture dislocations are complex and difficult to treat. Making the correct diagnosis andachieving an anatomical reduction are important factors in regard to achieving a favorable outcome withthis injury. We describe a new technique that we have found to be useful for stabilizing Lisfranc fracturedislocations. This method is relatively fast, minimally invasive, and effective, and it eliminates the need forimplant removal. To date, we have achieved predictable results for stabilizing and treating these difficultinjuries with the use of a suture endobutton, instead of traditional interfragmental screw fixation. In thisreport, we describe 3 cases in which this method was used with satisfactory short-term results. Level ofClinical Evidence: 4. (The Journal of Foot & Ankle Surgery 47(3):250–258, 2008)
Key Words: dislocation, endobutton, fracture, Lisfranc, midfoot, suture and button, trauma
Injuries involving the tarsometatarsal (TMT) and midfootregion are complex, frequently missed, and often difficult totreat. The Lisfranc injury may involve osseous fractures,tearing of the ligamentous support, or a combination ofthese injuries. The overall incidence of fractures of the TMTjoints has been reported as 0.2% of all fractures (1). It hasbeen documented that as many as 20% of these fractures aremisdiagnosed, or not recognized, upon initial clinical exam-ination (2). The diagnosis may be missed due to complexbony anatomy that is not well visualized with standardradiographs, or the confusion that may be associated withtreating a patient who has sustained polytrauma. One studyfound that of 72 patients with Lisfranc injuries, 81% werepolytrauma patients and 32% had additional ipsilateral foot
Address correspondence to: James M. Cottom, DPM, AACFAS, Sara-sota Orthopedic Associates, 2750 Bahia Vista St, Ste 100, Sarasota, FL34239.
1Fellow, Orthopedic Foot and Ankle Center, Columbus, OH.2Orthopedic Foot and Ankle Center, Columbus, OH.3Chief, Division of Foot and Ankle, Ohio State University Orthopedics,
Orthopedic Foot and Ankle Center, Columbus, OH.Financial Disclosure: None reportedConflict of Interest: None reportedCopyright © 2008 by the American College of Foot and Ankle Surgeons
1067-2516/08/4703-0014$34.00/0doi:10.1053/j.jfas.2008.01.004250 THE JOURNAL OF FOOT & ANKLE SURGERY
and ankle fractures (3). Ligamentous Lisfranc injuries,while being common, are also notable in that they areassociated with disruption of normally very strong liga-ments, resulting in articular instability without a fracture.Pure ligamentous injuries in this area are notorious forhealing more slowly than osseous injuries, and they oftenrequire prolonged non–weight bearing. One report notedthat patients whose injuries were both ligamentous andosseous, as compared with patients with ligamentous inju-ries only, experienced poorer treatment outcomes despiteundergoing anatomic reduction and rigid internal fixation(4). For this reason, and in those cases with severe intra-articular comminution, some surgeons advocate the use of aprimary arthrodesis of the medial 2 or 3 rays (5), rather thanattempt to preserve the entire Lisfranc joint complex.
In this report, we present a technique of Lisfranc jointcomplex repair that employs the use of an interosseoussuture with endobuttons, namely the Arthrex Mini Tight-Rope (Arthrex, Inc., Naples, FL), instead of traditionalinterfragmental screw fixation. This technique has beenfound to be effective, fast, and yields predictable results forstabilizing and treating these difficult injuries. In this lim-ited case series, patients were able to fully bear weight onthe operated foot and return to regular activities, including
athletic activities, faster than what we have experienced in
the past with patients who have undergone repair of thisinjury using traditional interfragmental screw fixation meth-ods. In addition, use of the interosseous suture with en-dobuttons obviated the need for subsequent hardware re-moval.
Case Reports
Case 1
A 39-year-old female was referred to the office afterhaving left midfoot pain for a period of approximately 6months. She had sustained a fall off a weight bench with herfoot in a plantarflexed position and fell forward over thefoot. The injury was associated with the feeling of several“pops” in her foot with severe pain localized to the mid-portion of her left foot. The patient did not follow-up withher physician for 2 months after the injury, hoping the painwould resolve on its own. At that point she was instructedto ice and rest the foot. Several months of this treatmentfailed to afford relief of her symptoms, which she describedas persistent soreness that was aggravated by weight bear-ing, especially when she attempted to rise onto the forefoot,a maneuver that she was no longer able to do.
Upon presentation to our office, the physical examinationdemonstrated excellent range of motion of the ankle jointwith no malalignment of the rearfoot or forefoot. Her mus-cle strength and neurovascular status were normal. Sheexperienced pain on palpation to the medial aspect of thesecond TMT joint and the pain was increased with abduc-tion stress of the patient’s forefoot while stabilizing therearfoot. Bilateral foot radiographs revealed an increasedspace between the first and second metatarsal bases as wellas between the medial and intermediate cuneiforms, on theleft foot. In addition a “fleck” sign was noted proximally inthe first interspace (Figure 1). Magnetic resonance imageswere evaluated, and these revealed increased signal inten-sity localized to Lisfranc’s ligament (Figure 2). In an effortto minimize the risk of future arthrosis and because thepatient was young and very active physically, it was decidedto take the patient to surgery for open reduction and internalfixation.
Surgical repair was undertaken by means of regionalanesthesia and the use of a pneumatic tourniquet placed onthe left thigh. A 5-cm linear incision located dorsally overthe proximal portion of the first intermetatarsal space wasused to debride, by means of a rongeur, the fibrotic tissueoccupying the proximal aspect of the interspace. Thereafter,the second metatarsal base was accurately repositioned intothe intercuneiform “keystone” recess, using a large bonereduction forceps. Satisfactory reduction was confirmed bymeans of fluoroscopic image intensification. However, upon
stressing the midfoot under fluoroscopic guidance, instabil-ity was noted at the medial and intermediate cuneiformlevel. It was decided to place a partially threaded cannulated4.0-mm screw across this joint in an effort to increase the
FIGURE 1 Anteroposterior radiograph demonstrating diastasis ofthe second metatarsal base with a fleck sign present.
FIGURE 2 T2-weighted MRI demonstrating increased signal in-tensity within Lisfranc’s ligament.
stability of the reduction. The inherent design of the screw
VOLUME 47, NUMBER 3, MAY/JUNE 2008 251

FIGURE 6 Proper placement of the guidewire.
FIGURE 3 The Arthrex Mini TightRope, wherein the Keith needlecomes attached to the Fiberwire for ease of passage through the bone tunnel (at the bottom of the picture).FIGURE 4 Close-up view of the endobuttons and nonabsorbablesuture for interosseous (and transarticular) placement. Note that theoblong button (on the right side) is the leading button that gets
passed through the medial cuneiform.removed.
FIGURE 5 Bone reduction forceps maintaining the reduction.Note that the guidewire is passed from the base of the secondmetatarsal to the medial cuneiform, and the position of the wireshould be checked by means of image intensification before
drilling.252 THE JOURNAL OF FOOT & ANKLE SURGERY
FIGURE 7 The 2.7-mm cannulated drill is placed over the guide-wire. It is necessary to drill through the medial cortex of the medialcuneiform. Note the hemostat placed medially on the guidewire inorder to prevent the wire from backing out laterally when the drill is
FIGURE 8 Passing the interosseous suture through the bone tun-nel. It is helpful to have an assistant slowly back the guidewire outmedially while the surgeon advances the Keith needle through the
tunnel.
provided interfragmental compression. Next, the ArthrexMini TightRope was used to stabilize the Lisfranc complex(Figures 3 and 4). This was done by positioning a guidewiredirected from the base of the second metatarsal into themedial cuneiform, under fluoroscopic guidance (Figures 5and 6). After confirming the position of the guidewire, a2.7-mm cannulated drill was used to create a tunnel forpassage of the interosseous suture over the guidewire (Fig-ure 7). The guidewire was then removed and the interosse-ous suture endobutton with the leading oblong button,which was attached to a Keith needle, was passed from thelateral aspect of the second metatarsal base to the medialcuneiform through the bone tunnel, after which the Keithneedle was passed through the skin (Figure 8). The oblongbutton, upon exiting the medial cuneiform subcutaneously,was then flipped by applying proximal and medial tension tothe suture as it exited the skin medially (Figures 9 and 10).
FIGURE 9 The Keith needle penetrating the skin on the medialside of the foot.
FIGURE 10 The oblong button is toggled upon exiting the medialcuneiform subcutaneously, by applying proximal and medial tensionto the suture as it exits the medial skin, in order to have the buttonlie flush with the medial cortex of the medial cuneiform.
Next, the trailing button was seated into proper position at
the base of the second metatarsal by applying laterallydirected tension to the lateral suture. The lateral suture wasthen cut and the bone reduction forceps removed. Reductionwas noted both with static and stress fluoroscopic images.The incision was then closed in a routine fashion and theextremity placed in a well-padded posterior splint.
The patient was seen in the office 10 days after theprocedure, at which time the skin sutures were removedand the left lower extremity was placed into a below-the-knee cast, and the patient was instructed to remain non-weight bearing for 6 weeks. At 6 weeks postoperative,the patient began partial weight bearing in a below-the-knee, fixed immobilizing brace (cam walker), and at 8weeks full weight bearing in an athletic shoe was al-lowed. At 10 months postoperative, the clinical exami-nation revealed no evidence of pain at the operative site,and the patient had resumed all of her regular activitiesincluding sports without complications. Furthermore, ra-diographs at that time revealed satisfactory bone andjoint healing (Figure 11).
Case 2
An 18-year-old male high school basketball player pre-sented to the office for a second opinion after sustaining aleft midfoot injury, initially diagnosed as a Lisfranc frac-ture, 1 day prior to the visit. He had been told that he wouldneed to be in a cast for 12 weeks, non–weight bearing. Sincethis particular patient was a highly competitive athlete, onewho was being recruited by a number of National CollegiateAthletic Association Division I schools for basketball, aprolonged period of cast immobilization was consideredparticularly undesirable.
Upon physical examination, edema was noted about themidfoot region and there was pain upon palpation to the firstand second TMT joints. Radiographs demonstrated a Lis-franc fracture that was subluxated with widening of the jointbetween the medial and intermediate cuneiforms (Figure12). The lateral TMT joints were in anatomic position andthere was no dorsal subluxation of any of the metatarsals onthe tarsal bones. A computerized tomogram (CT) demon-strated a second metatarsal base fracture. The patient wasplaced in a Jones compressive dressing and scheduled forsurgery the next day.
On the following day, the patient was brought to theoperating room where regional anesthesia and a thigh tour-niquet were used. Attention was directed to the medialaspect of the medial cuneiform where, under fluoroscopicguidance, a guidewire for a 4.0-mm cannulated screw wasinserted from medial to lateral into the intermediate cunei-form. A 2.9-mm drill was inserted over the guidewire andthe hole drilled and measured, after which the appropriate
length screw was inserted and reduction of the intercunei-VOLUME 47, NUMBER 3, MAY/JUNE 2008 253

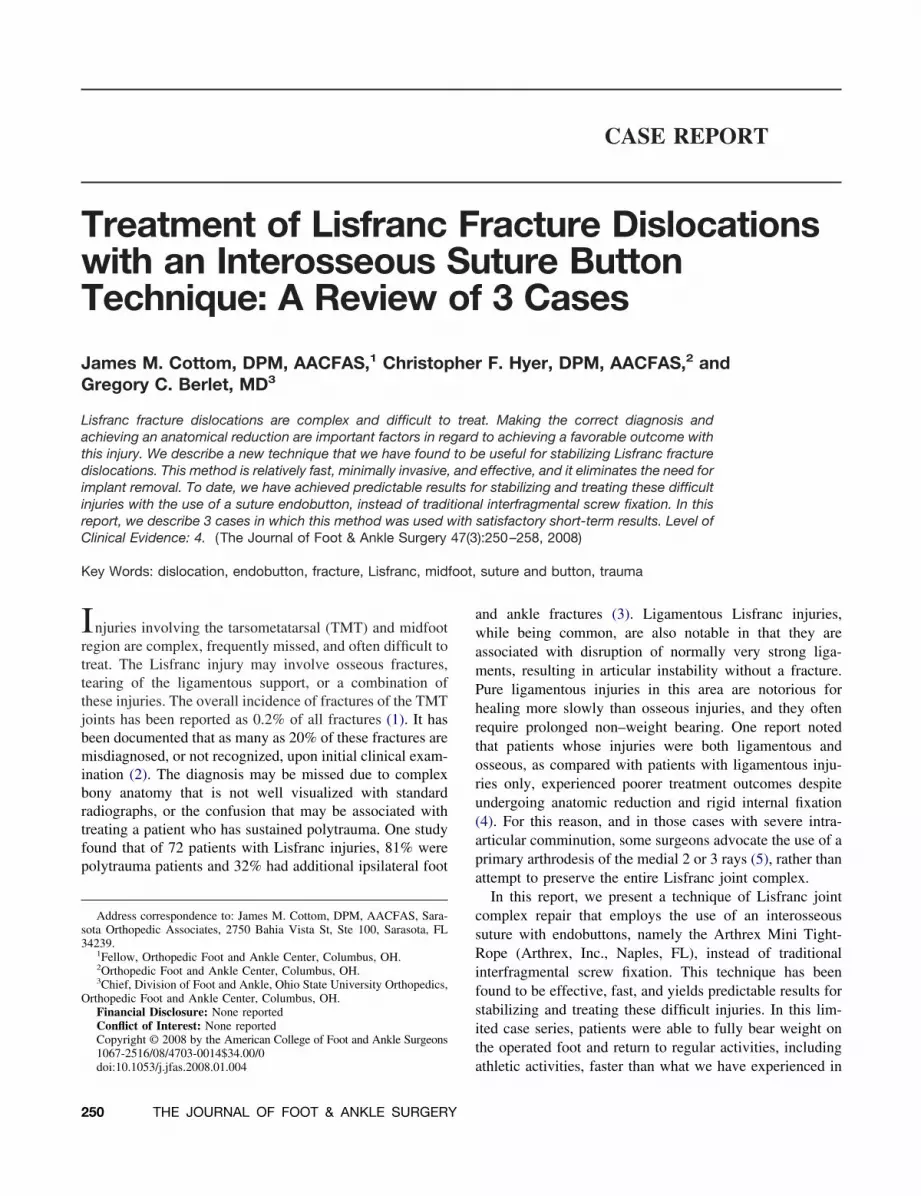
form joint was observed. Thereafter, a bone reduction for-ceps was positioned from the lateral border of the base ofthe second metatarsal to the medial aspect of the medialcuneiform (Figure 13). The second metatarsal base wasreduced back to its “keystone position.” Next, the interosse-ous suture with endobuttons was used to stabilize the Lis-franc complex in a fashion similar to that described in case1, above. Fluoroscopy confirmed correct anatomic reductionafter removal of the bone reduction forceps (Figure 14), andthe reduction held up under stress manipulation. After rou-tine wound closure, the extremity was placed into a poste-rior splint for 10 days. Ten days after the procedure, skinsutures were removed and the patient was placed into abelow the knee non–weight bearing cast. At 4 weeks post-operative, the patient began gradual weight bearing on hisoperated foot with a below the knee boot walker. Physicaltherapy was initiated at 6 weeks after the procedure and, at8 weeks, the patient was in an athletic shoe playing basket-
FIGURE 11 Anteroposterior radiograph 10 months postoperative.The reduction is maintained and there is no sign of hardware loos-ening or failure.
ball. At 10 months after the procedure, the patient denied
254 THE JOURNAL OF FOOT & ANKLE SURGERY
having any midfoot pain, the reduction was maintained andthere is no sign of hardware loosening or complication
FIGURE 12 Anteroposterior radiograph demonstrating diastasisof the second metatarsal base with a fleck sign. Also note diastasisof the intercuneiform joint.
FIGURE 13 Percutaneous technique useful in some acute cases.The bone reduction clamp maintains reduction of Lisfranc’s jointwhile the interosseous suture is passed through the lateral stabincision.
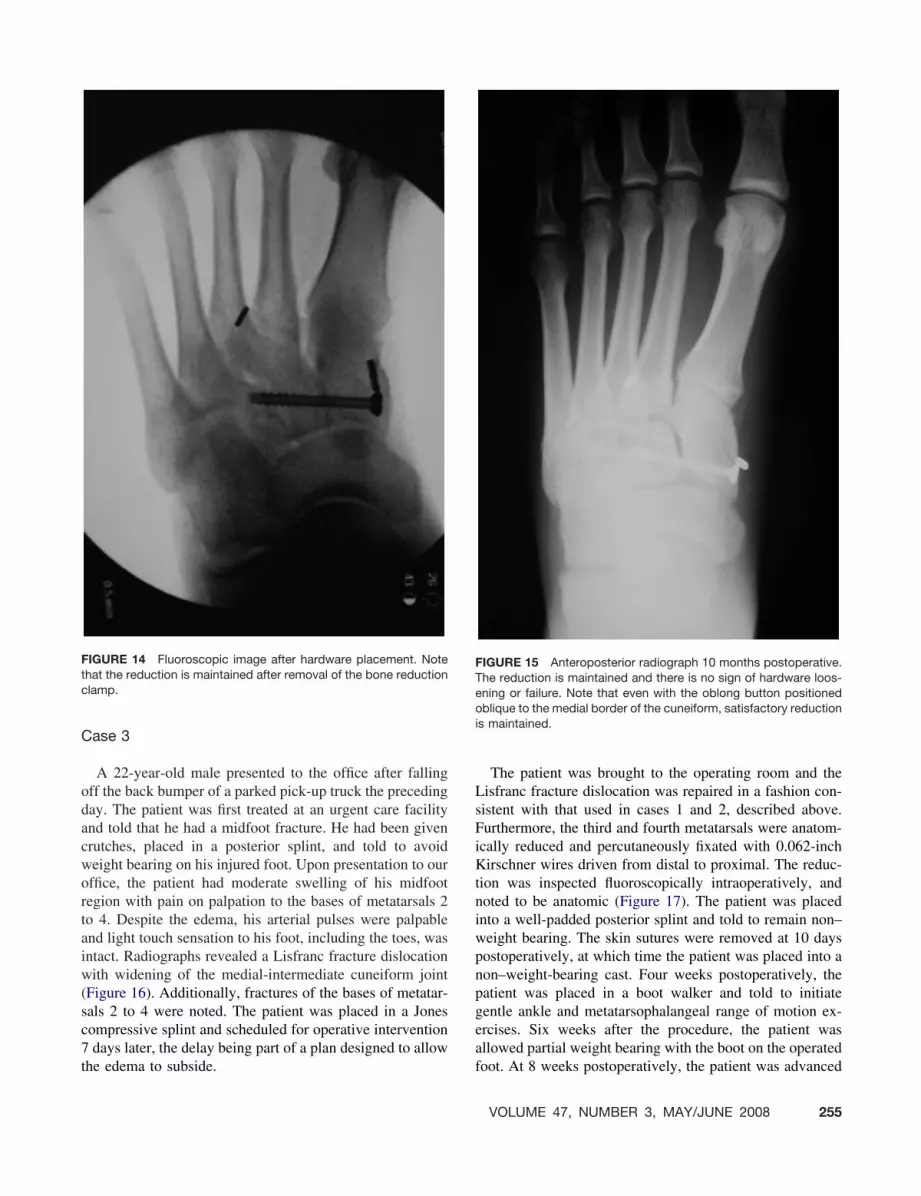
(Figure 15).
Case 3
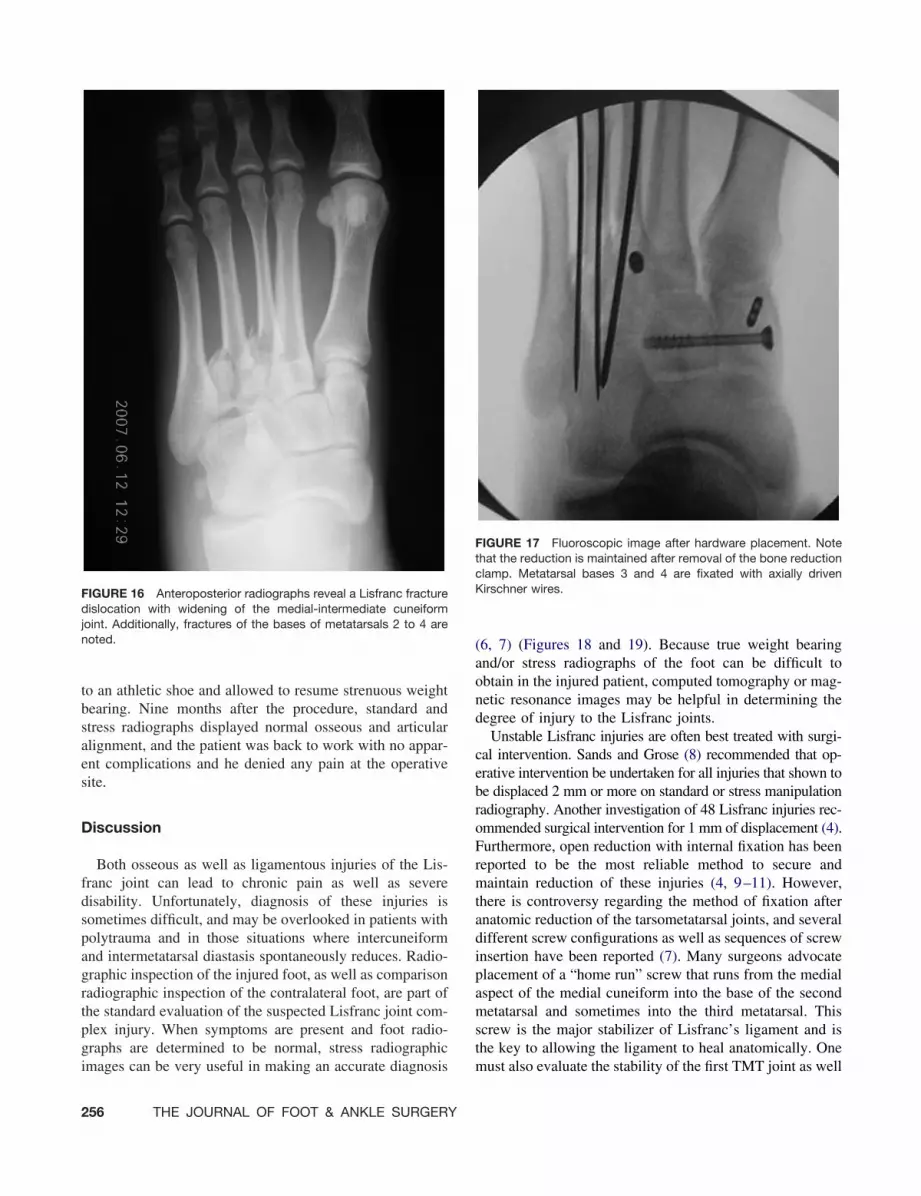
A 22-year-old male presented to the office after fallingoff the back bumper of a parked pick-up truck the precedingday. The patient was first treated at an urgent care facilityand told that he had a midfoot fracture. He had been givencrutches, placed in a posterior splint, and told to avoidweight bearing on his injured foot. Upon presentation to ouroffice, the patient had moderate swelling of his midfootregion with pain on palpation to the bases of metatarsals 2to 4. Despite the edema, his arterial pulses were palpableand light touch sensation to his foot, including the toes, wasintact. Radiographs revealed a Lisfranc fracture dislocationwith widening of the medial-intermediate cuneiform joint(Figure 16). Additionally, fractures of the bases of metatar-sals 2 to 4 were noted. The patient was placed in a Jonescompressive splint and scheduled for operative intervention7 days later, the delay being part of a plan designed to allow
FIGURE 14 Fluoroscopic image after hardware placement. Notethat the reduction is maintained after removal of the bone reductionclamp.
the edema to subside.
The patient was brought to the operating room and theLisfranc fracture dislocation was repaired in a fashion con-sistent with that used in cases 1 and 2, described above.Furthermore, the third and fourth metatarsals were anatom-ically reduced and percutaneously fixated with 0.062-inchKirschner wires driven from distal to proximal. The reduc-tion was inspected fluoroscopically intraoperatively, andnoted to be anatomic (Figure 17). The patient was placedinto a well-padded posterior splint and told to remain non–weight bearing. The skin sutures were removed at 10 dayspostoperatively, at which time the patient was placed into anon–weight-bearing cast. Four weeks postoperatively, thepatient was placed in a boot walker and told to initiategentle ankle and metatarsophalangeal range of motion ex-ercises. Six weeks after the procedure, the patient wasallowed partial weight bearing with the boot on the operated
FIGURE 15 Anteroposterior radiograph 10 months postoperative.The reduction is maintained and there is no sign of hardware loos-ening or failure. Note that even with the oblong button positionedoblique to the medial border of the cuneiform, satisfactory reductionis maintained.
foot. At 8 weeks postoperatively, the patient was advanced
VOLUME 47, NUMBER 3, MAY/JUNE 2008 255
to an athletic shoe and allowed to resume strenuous weightbearing. Nine months after the procedure, standard andstress radiographs displayed normal osseous and articularalignment, and the patient was back to work with no appar-ent complications and he denied any pain at the operativesite.
Discussion
Both osseous as well as ligamentous injuries of the Lis-franc joint can lead to chronic pain as well as severedisability. Unfortunately, diagnosis of these injuries issometimes difficult, and may be overlooked in patients withpolytrauma and in those situations where intercuneiformand intermetatarsal diastasis spontaneously reduces. Radio-graphic inspection of the injured foot, as well as comparisonradiographic inspection of the contralateral foot, are part ofthe standard evaluation of the suspected Lisfranc joint com-plex injury. When symptoms are present and foot radio-graphs are determined to be normal, stress radiographic
FIGURE 16 Anteroposterior radiographs reveal a Lisfranc fracturedislocation with widening of the medial-intermediate cuneiformjoint. Additionally, fractures of the bases of metatarsals 2 to 4 arenoted.
images can be very useful in making an accurate diagnosis
256 THE JOURNAL OF FOOT & ANKLE SURGERY
(6, 7) (Figures 18 and 19). Because true weight bearingand/or stress radiographs of the foot can be difficult toobtain in the injured patient, computed tomography or mag-netic resonance images may be helpful in determining thedegree of injury to the Lisfranc joints.
Unstable Lisfranc injuries are often best treated with surgi-cal intervention. Sands and Grose (8) recommended that op-erative intervention be undertaken for all injuries that shown tobe displaced 2 mm or more on standard or stress manipulationradiography. Another investigation of 48 Lisfranc injuries rec-ommended surgical intervention for 1 mm of displacement (4).Furthermore, open reduction with internal fixation has beenreported to be the most reliable method to secure andmaintain reduction of these injuries (4, 9–11). However,there is controversy regarding the method of fixation afteranatomic reduction of the tarsometatarsal joints, and severaldifferent screw configurations as well as sequences of screwinsertion have been reported (7). Many surgeons advocateplacement of a “home run” screw that runs from the medialaspect of the medial cuneiform into the base of the secondmetatarsal and sometimes into the third metatarsal. Thisscrew is the major stabilizer of Lisfranc’s ligament and isthe key to allowing the ligament to heal anatomically. One
FIGURE 17 Fluoroscopic image after hardware placement. Notethat the reduction is maintained after removal of the bone reductionclamp. Metatarsal bases 3 and 4 are fixated with axially drivenKirschner wires.
must also evaluate the stability of the first TMT joint as well

more prominent, upon stress manipulation.
as the medial and intermediate cuneiform joint and, if thereis excessive motion noted with fluoroscopic guidance, thenthese articulations should also be stabilized. Traditionally,placing a screw across these joints is the preferred methodof stabilization, however in cases involving severe commi-nution, primary arthrodesis may be the procedure of choice(Figure 20). Unfortunately, one of the problems with openreduction and internal fixation of Lisfranc joint injuries isthat the “home run” screw usually is not tolerated by thepatient and subsequently must be removed several monthsafter implantation. There has been debate that this screw isanalogous to the syndesmotic screw in ankle fracture repair.It is theorized that even subtle motion between the first andsecond rays stresses this “home run” screw causing boneirritation, loosening and sometimes breakage. We havefound that the intercunieform screw is tolerated well andneed not be removed, but the screw placed from the medialcuneiform into the base of the second metatarsal should be
FIGURE 18 Anteroposterior radiograph demonstrates a smallamount of diastasis at Lisfranc’s joint with a fleck sign.
removed at a minimum of 3 months. This course of treat-
FIGURE 19 Same foot depicted in Figure 18, upon stress manip-ulation. The hind-foot is held in the neutral subtalar joint positionwith one hand, and the forefoot is stressed into abduction with theother hand. Note that the diastasis increased, and the fleck sign is
FIGURE 20 Primary arthrodesis of the first and second tarsometataral
joints for the treatment of extensive comminuted fractures of the midfoot.VOLUME 47, NUMBER 3, MAY/JUNE 2008 257

ment imparts another surgery and the associated potentialrisks and costs.
In an effort to eliminate the need for screw stabilizationof the Lisfranc joint complex, we have used an interosseousnonabsorbable suture with endobuttons. Suture endobuttonshave been successfully used for graft fixation in distalbiceps rupture (12), syndesmosis stabilization (13, 14), an-terior cruciate reconstruction (15), and for tibiofibular sta-bilization in the Ertl (16) technique of below-the-knee am-putation (personal communication, Greg Berlet, MD, July 7,2007). The interosseous suture with endobuttons used in thepatients described in this report, is an adaptation of thelarger TightRope system. We believe that one of the advan-tages of using this technique is that implant fatigue and/orbreakage is not likely and, therefore, removal is not rou-tinely needed. In addition, the implant allows a smallamount of micro-motion to occur, much like a healthyligament allows, and is strong enough to enable early weightbearing. Therefore, the method of surgical repair describedin this report may decrease the likelihood of complicationssuch as the loss of reduction that can be observed followingremoval of traditional interfragmental fixation screws. Fur-thermore, the #2 Fiberwire (Arthrex, Naples, FL) used in asthe interosseous suture in the cases depicted in this report isnonabsorbable, very strong, and unlikely to fatigue or breakwhen used as described. Specifically, the material consistsof a braided polyester suture covering an ultra-high molec-ular weight polyethylene (UHMWPE) core. The endobut-tons are available in surgical stainless steel and titanium,and the choice of the material to be used should be made sothat the buttons are compatible with other hardware used inthe repair. Because of the features of the interosseous sutureand endobuttons used in the technique that we have de-scribed in this report, patients were able to begin physicaltherapy at a faster rate and ultimately resume weight-bear-ing activities and sports quicker in the postoperative phase,in comparison to traditional fixation methods used for Lis-franc injuries. Still further, with this method, minimal inci-sions can be used to reduce the Lisfranc injury in thosesituations that warrant such intervention. Chronic injuriesshould be opened with a formal incision and scar tissueremoved to allow anatomic reduction. One must alwaysconsider a formal incision and debridement of any looseosseous or cartilaginous fragments within the tarsometatar-sal articulations. The interosseous suture with endobuttonscan still be used in these cases, as we have shown.
In conclusion, Lisfranc injuries are complex and can bedifficult to treat. If not treated correctly with anatomicreduction, then permanent disability may ensue. Most sur-
geons would agree that displaced fractures and/or disloca-258 THE JOURNAL OF FOOT & ANKLE SURGERY
tions need anatomic reduction with internal fixation toachieve optimal results. We describe a new technique usedto stabilize Lisfranc fracture dislocations. This method isrelatively fast, minimally invasive, and effective, and iteliminates the need for subsequent implant removal. Theinterosseous suture with endobuttons simulates the role ofthe ligaments until they heal, and allows patients to bearweight on their operated foot at an earlier stage of thepostoperative period. Furthermore, diastasis is not a concernbecause very strong, nonabsorbable suture is used to restorethe strength and integrity of the articulations until the TMTligaments heal.
References
1. Buzzard BM, Briggs PJ. Surgical management of acute tarsometatarsalfracture dislocation in the adult. Clin Orthop Relat Res Aug:125–133,1998.
2. Thompson MC, Mormino MA. Injury to the tarsometatarsal jointcomplex. J Am Acad Orthop Surg 11:260–267, 2003.
3. Myerson MS, Fisher RT, Burgess AR, Kenzora JE. Fracture disloca-tions of the tarsometatarsal joints: end results correlated with pathol-ogy and treatment. Foot Ankle Int 6:225–242, 1986.
4. Kuo RS, Tejwani NC, DiGiovanni CW, Holt SK, Benirschke SK,Hansen ST, Sangeorzan BJ. Outcome after open reduction and internalfixation of Lisfranc joint injuries. J Bone Joint Surg 82-A:1609–1618,2000.
5. Coetzee CJ, Ly TV. Treatment of primarily ligamentous lisfranc jointinjuries: primary Arthrodesis compared with open reduction and in-ternal fixation. J Bone Joint Surg 89-A:122–127, 2007.
6. de Palma L, Santucci A, Sabetta SP, Rapeli S. Anatomy of the Lisfrancjoint complex. Foot Ankle Int 18:356–364, 1997.
7. Trevino S, Kodros S. Controversies in tarsometatarsal injuries. OrthopClin North Am 262:299–338, 1995.
8. Sands AK, Grose A. Lisfranc injuries. Injury 35(s):71–76, 2004.9. Myerson MS. The diagnosis and treatment of injuries to the Lisfranc
joint complex. Orthop Clin North Am 20:655–664, 1989.10. Arntz CT, Veith RG, Hansen ST. Fractures and fracture dislocations of
the tarsometatarsal joint. J Bone Joint Surg 70-A:173–181, 1988.11. Curtis MJ, Myerson M, Szura B. Tarsometatarsal joints in the athlete.
Am J Sports Med 214:497–502, 1993.12. Bain GI, Prem H, Heptinstall RJ, Verhellen R, Paix D. Repair of distal
biceps tendon rupture: a new technique using the Endobutton. J Shoul-der Elbow Surg 9:120–126, 2000.
13. Thrones B, Shannon F, Guiney AM, Hession P, Masterson E. Suture-endobutton syndesmosis fixation. Clinic Orthop Rel Research 431:207–212, 2005.
14. Thornes B, Walsh A, Hislop M, Murray P, O’Brien M. Suture-endobutton fixation of ankle tibio-fibular diastasis: a cadaver study.Foot Ankle 24:142–146, 2003.
15. Barrett GR, Papendick L, Miller C. Endobutton button endoscopicfixation technique in anterior cruciate ligament reconstruction. Arthro-scopy 11:340–343, 1995.
16. von Ertl JW. [The care of amputation stumps by osteo-myeloplastic
according to v. Ertl] [German]. Z Plast Chir 5:184–189, 1981.



















