
Options for glenoid labral suture anchor fixation
7
Options for Glenoid Labral Suture Anchor Fixation J.R. Rudzki, MD, MS, Derek B. Purcell, MD, and Rick W. Wright, MD Treatment of glenohumeral instability and capsulolabral pathology continues to evolve as arthroscopic techniques improve. A growing body of biomechanical and clinical research provides an enhanced perspective on results obtained with both arthroscopic and open treatment of these conditions. Labral repair and capsulolabral reconstruction can effec- tively be treated with suture anchors by both arthroscopic and open methods. Suture anchors are low-profile fixation devices that can minimize articular surface compromise and afford an anatomic reconstruction of the labrum and glenohumeral ligament complex. Although the use of suture anchors has become increasingly common to obtain stable fixation and healing at the bone-tendon interface in rotator cuff repair, critical distinctions exist between this function and their implementation in labral repair and capsulolabral reconstruction. This article examines the technical aspects of labral repair and capsulola- bral reconstruction with metallic and bioabsorbable suture anchors. The emphasis is on implant options, technical advantages, potential limitations, and relevant biomechanical considerations to better achieve an optimal outcome. Oper Tech Sports Med 12:225-231 © 2004 Elsevier Inc. All rights reserved. KEYWORDS glenoid, labrum, suture, anchor, fixation T reatment of glenohumeral instability and capsulolabral pa- thology continues to evolve as arthroscopic techniques im- prove. A growing body of biomechanical and clinical research provides an enhanced perspective on results obtained with both arthroscopic and open treatment of these conditions. This article examines the technical aspects of labral repair and capsulolabral reconstruction with metallic and bioabsorbable suture anchors. The emphasis is on implant options, technical advantages, po- tential limitations, and relevant biomechanical considerations to better achieve an optimal outcome. Labral repair and capsulolabral reconstruction can effectively be treated with suture anchors by both arthroscopic and open methods. 1-3 Suture anchors are low-profile fixation devices that can minimize articular surface compromise and afford an ana- tomic reconstruction of the labrum and glenohumeral ligament complex. Although the use of suture anchors has become in- creasingly common to obtain stable fixation and healing at the bone-tendon interface in rotator cuff repair, critical distinctions exist between this function and their implementation in labral repair and capsulolabral reconstruction. In treating the latter 2 entities, the forces and tensile stresses applied to the soft tissue– suture–anchor– bone interface are different, and, as a result, modes of failure warrant consideration from a different perspec- tive. Although numerous clinical studies have examined the relevant biomechanical forces pertaining to rotator cuff repair performed with suture anchors, 4-6 there is less biomechanical data in the literature that reflects an accurate recreation of the forces placed across a labral repair or capsulolabral reconstruc- tion with suture anchors. 7-11 Relevant Anatomy An in-depth review of the relevant anatomy for labral repair and capsulolabral reconstruction is beyond the scope of this article. Nevertheless, a brief description of the critical aspects of glenoid and labral anatomy affords an enhanced perspective in critically evaluating the strengths and weaknesses of various anchors. The average dimensions of the glenoid have been reported in the literature as 29 to 30 3 mm (anteroposterior) by 36 to 42 4 mm (superoinferior) with statistically significant gender- based differences. 12,13 The glenoid labrum adds stability by sig- nificantly increasing the depth of the glenohumeral socket by approximately 50% and increases the diameter of the glenoid surface in relation to the humeral head up to 75% vertically and up to 57% in the transverse direction. 14-16 Biomechanical Considerations in Suture Anchor Design Several factors determine the performance of a suture anchor used for labral repair and capsulolabral reconstruction. Bio- mechanical research on suture anchors continues to improve their clinical design through identifying the key issues affect- ing their performance. 8,17,18 As a result, a wide variety of Department of Orthopaedic Surgery, Washington University School of Med- icine, St Louis, MO. Address reprint requests to Rick W. Wright, MD, Division of Sports Medicine, Department of Orthopaedic Surgery, Washington University School of Medicine, Barnes-Jewish Hospital, Suite 11300, West Pavilion, One Barnes- Jewish Hospital Plaza, St Louis, MO 63110. E-mail: [email protected] 225 1060-1872/04/$-see front matter © 2004 Elsevier Inc. All rights reserved. doi:10.1053/j.otsm.2004.07.006
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Options for glenoid labral suture anchor fixation
OJ
TppaerTtb
bmctccberesmt
D
A
1d
ptions for Glenoid Labral Suture Anchor Fixation.R. Rudzki, MD, MS, Derek B. Purcell, MD, and Rick W. Wright, MD
Treatment of glenohumeral instability and capsulolabral pathology continues to evolve asarthroscopic techniques improve. A growing body of biomechanical and clinical researchprovides an enhanced perspective on results obtained with both arthroscopic and opentreatment of these conditions. Labral repair and capsulolabral reconstruction can effec-tively be treated with suture anchors by both arthroscopic and open methods. Sutureanchors are low-profile fixation devices that can minimize articular surface compromise andafford an anatomic reconstruction of the labrum and glenohumeral ligament complex.Although the use of suture anchors has become increasingly common to obtain stablefixation and healing at the bone-tendon interface in rotator cuff repair, critical distinctionsexist between this function and their implementation in labral repair and capsulolabralreconstruction. This article examines the technical aspects of labral repair and capsulola-bral reconstruction with metallic and bioabsorbable suture anchors. The emphasis is onimplant options, technical advantages, potential limitations, and relevant biomechanicalconsiderations to better achieve an optimal outcome.Oper Tech Sports Med 12:225-231 © 2004 Elsevier Inc. All rights reserved.
KEYWORDS glenoid, labrum, suture, anchor, fixation
rpdft
RAcNae
t�bnasu
BiSumt
reatment of glenohumeral instability and capsulolabral pa-thology continues to evolve as arthroscopic techniques im-
rove. A growing body of biomechanical and clinical researchrovides an enhanced perspective on results obtained with bothrthroscopic and open treatment of these conditions. This articlexamines the technical aspects of labral repair and capsulolabraleconstruction with metallic and bioabsorbable suture anchors.he emphasis is on implant options, technical advantages, po-
ential limitations, and relevant biomechanical considerations toetter achieve an optimal outcome.Labral repair and capsulolabral reconstruction can effectively
e treated with suture anchors by both arthroscopic and openethods.1-3 Suture anchors are low-profile fixation devices that
an minimize articular surface compromise and afford an ana-omic reconstruction of the labrum and glenohumeral ligamentomplex. Although the use of suture anchors has become in-reasingly common to obtain stable fixation and healing at theone-tendon interface in rotator cuff repair, critical distinctionsxist between this function and their implementation in labralepair and capsulolabral reconstruction. In treating the latter 2ntities, the forces and tensile stresses applied to the soft tissue–uture–anchor–bone interface are different, and, as a result,odes of failure warrant consideration from a different perspec-
ive. Although numerous clinical studies have examined the
epartment of Orthopaedic Surgery, Washington University School of Med-icine, St Louis, MO.
ddress reprint requests to Rick W. Wright, MD, Division of Sports Medicine,Department of Orthopaedic Surgery, Washington University School ofMedicine, Barnes-Jewish Hospital, Suite 11300, West Pavilion, One Barnes-
iJewish Hospital Plaza, St Louis, MO 63110. E-mail: [email protected]
060-1872/04/$-see front matter © 2004 Elsevier Inc. All rights reserved.oi:10.1053/j.otsm.2004.07.006
elevant biomechanical forces pertaining to rotator cuff repairerformed with suture anchors,4-6 there is less biomechanicalata in the literature that reflects an accurate recreation of theorces placed across a labral repair or capsulolabral reconstruc-ion with suture anchors.7-11
elevant Anatomyn in-depth review of the relevant anatomy for labral repair andapsulolabral reconstruction is beyond the scope of this article.evertheless, a brief description of the critical aspects of glenoid
nd labral anatomy affords an enhanced perspective in criticallyvaluating the strengths and weaknesses of various anchors.
The average dimensions of the glenoid have been reported inhe literature as 29 to 30 � 3 mm (anteroposterior) by 36 to 42
4 mm (superoinferior) with statistically significant gender-ased differences.12,13 The glenoid labrum adds stability by sig-ificantly increasing the depth of the glenohumeral socket bypproximately 50% and increases the diameter of the glenoidurface in relation to the humeral head up to 75% vertically andp to 57% in the transverse direction.14-16
iomechanical Considerationsn Suture Anchor Designeveral factors determine the performance of a suture anchorsed for labral repair and capsulolabral reconstruction. Bio-echanical research on suture anchors continues to improve
heir clinical design through identifying the key issues affect-
ng their performance.8,17,18 As a result, a wide variety of225

odsnpmbsiiaa
PBBmsolabitbcms
AAAfcfbiaoposbthtt
ITjaawesi
fsstp
ISosmuamvbmreaac
sttsr
SAeut&ntstsmptotstfscpaNomltb
226 J.R. Rudzki, D.B. Purcell, and R.W. Wright
ptions are available to the surgeon performing these proce-ures, and a knowledge of the relevant issues aids not only inelection of the appropriate implant when preoperative plan-ing but also in identification of an appropriate salvage im-lant when an intraoperative complication arises. Of theany important design characteristics, 3 key factors have
een identified in the literature8,17: (1) anchor pullouttrength, (2) suture tensile strength, and (3) anchor-suturenterface. Attention to these 3 primary factors when design-ng, selecting, implanting, and critically evaluating suturenchors will afford greater clinical success in treating labralnd capsulolabral pathology.
otential Benefits ofioabsorbable Suture Anchors
ioabsorbable suture anchors have several properties thatake them a potentially attractive alternative to their nonab-
orbable equivalents.1,2,18 These include greater ease of post-perative imaging without the artifact associated with metal-ic devices as well as the potential restoration of bone stockfter resorption. The resorption of suture anchors is a criticalenefit, although not free of potential complications, because
t may ease revision surgery, which is not uncommon whenreating complex capsulolabral pathology. Should suturereakage or poor implant purchase compromise anchor effi-acy, a bioabsorbable anchor may either potentially be re-oved or overdrilled for placement of a salvage anchor of
imilar or slightly larger diameter.
ssessing Suturenchor Pullout Strength
ssessment of suture anchor pullout strength may be per-ormed though an examination of maximal load-to-failure oryclic loading. Although each technique offers valuable in-ormation in evaluating suture anchors, cyclic loading haseen described as a more accurate reproduction of the repet-
tive loads applied to tissue during the early phases of healingnd postoperative rehabilitation.21 Similarly, a broad varietyf testing models have been used to assess suture anchorullout strength, and this is a critical factor for the practicingrthopaedic surgeon to consider when comparing reportedtrengths of available anchors. These models include foamlocks, porcine tibiae and femora, sheep tibiae, polyurethaneest bone, and cadaveric glenoids. Biomechanical studiesave clearly shown distinctions between these models andheir applicability with other methods of soft-tissue fixa-ion.19
mplant Size Considerationshe dimensions of the glenoid and overlying labrum in con-
unction with the aforementioned technical aspects of idealnchor placement make implant size an important consider-tion in selection and implementation. Repair constructsith multiple points of fixation have been shown in the lit-
rature as an important determinant of capsulolabral recon-truction success.9 We believe a 3.5-mm to 4.1-mm diameter
s the maximum size for an optimal suture anchor to be used ior labral repair and capsulolabral reconstruction. Ideally, themallest implant of sufficient strength to obtain the mosttable fixation for soft-tissue healing will allow not only mul-iple fixation points but also minimize articular surface com-romise and maximize restoration of the normal anatomy.
mplant Design Considerationsuture anchor design continues to develop as a growing bodyf research identifies factors relevant to anchor pullouttrength, suture-anchor interface (eyelet) design, and anchoraterial composition. A detailed description of materialssed in suture anchor design is beyond the scope of thisrticle and addressed in other articles of this issue. A funda-ental principle in this regard is to use a material that pro-
ides the greatest strength of fixation with the least distur-ance of the native environment. With bioabsorbableaterials, a balance is sought between the induction of a
esponse to resorb or degrade the anchor and the time nec-ssary for the repaired soft tissues to achieve stability. Inddition, as discussed in the complications section later,voidance of an aggressive inflammatory response and con-omitant synovitis is clearly important.
A great deal of biomechanical information has been pre-ented in the peer-reviewed literature regarding the impor-ance of eyelet design and orientation. The interface betweenhe suture and the suture anchor eyelet is a source of greattrain on the suture and potential site of suture breakage andepair failure.20-22
uture Material Considerationsdvances in suture fabrication technology and surgeon pref-rence have led to the expansion of options available in these of suture anchors. Products such as FiberWire from Ar-hrex (Naples, FL) and DuraBraid and UltraBraid from Smith
Nephew Endoscopy (Andover, MA) are examples of alter-atives to traditional braided polyester with initial manufac-urer reports of higher tensile strength and clinically ob-erved decreased incidence of suture breakage during knotying. DuraBraid is a silicone-coated no. 2 polyester sutureimilar to Ethibond and Tevdek. UltraBraid is an ultra-higholecular weight polyethylene suture that has a unique androprietary braid configuration designed to confer greaterensile strength. FiberWire is a no. 2 composite suture madef a solid long-chain polyethylene core with a woven polyes-er jacket on the outside that has substantially greatertrength when compared with a braided polyester suture ofhe same diameter. These are valuable characteristics thatacilitate technically challenging procedures by minimizinguture failure during knot-tying and thereby limiting anchorompromise. Anchor compromise can further complicate arocedure through prolonging its length during attemptednchor removal or the compromise of bone stock as a result.evertheless, it is important for orthopedic surgeons to rec-gnize that long-term clinical follow-up data for these neweraterials has not yet been presented in the peer-reviewed
iterature, and we are as yet unaware of potential complica-ions from their intra-articular use. In addition, a growingody of research is beginning to evaluate the balance struck
n suture design between the following: strength and ease of
sp
BAptBpa3n
faeaSuSnta1BG
T
M
A
A
A
L
M
S
WZ
A
Glenoid labral suture 227
liding for knot tying, knot durability related to suture slip-age (unraveling), and suture cutout through repaired tissue.
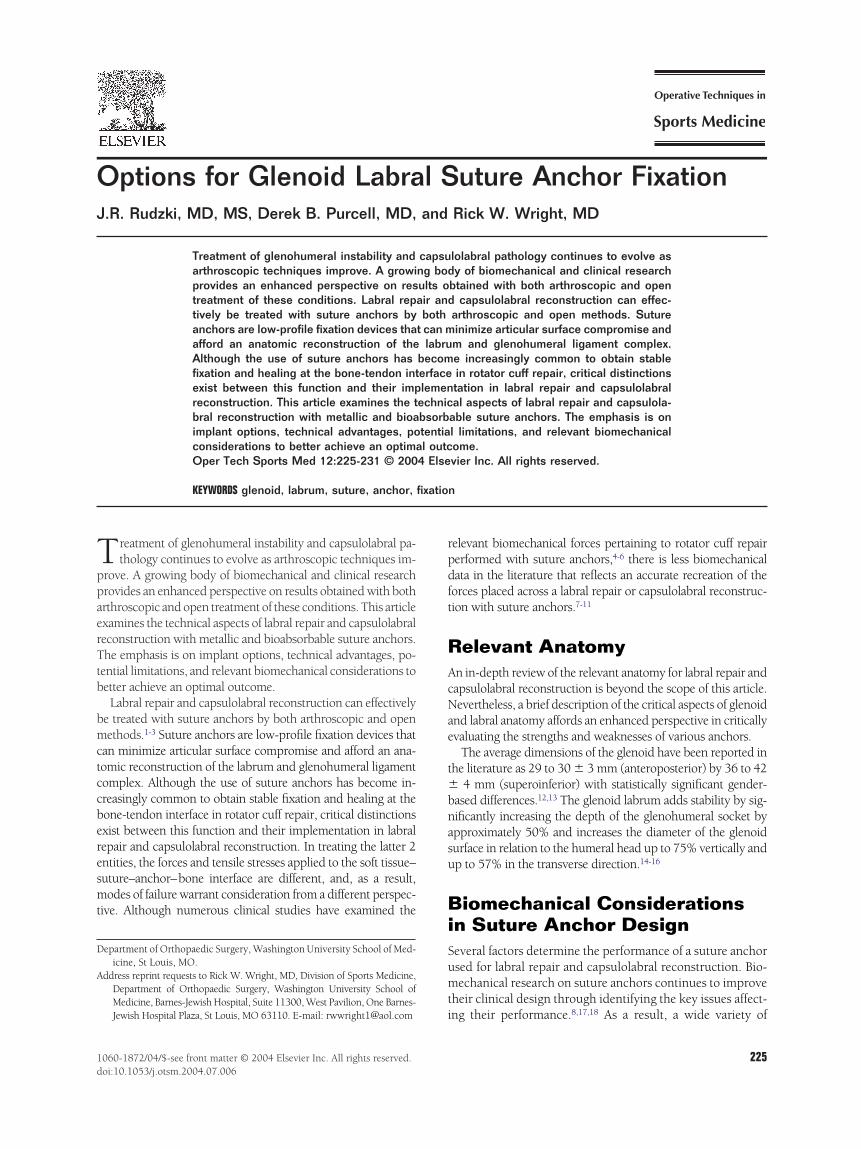
ioabsorbable Suture Anchorsrthrex makes 3 bioabsorbable suture anchors for labral re-air and capsulolabral reconstruction: the Bio-SutureTak,he Bio-FASTak, and the Bio-Corkscrew (Fig. 1; Table 1). Theio-SutureTak is a 3.0-mm diameter � 14-mm nontaperedush-in poly L-Lactide-co-D, L-Lactide (PLDLA) anchor withmolded suture eyelet of no. 2 braided polyester suture. A.7-mm version of the Bio-SutureTak is also available. Theoncrystalline PLDLA copolymer is reported by the manu-
Figure 1 Arthrex Bio-FASTak and Bio-SutureTak, Arthroand Smith & Nephew/Acufex Bio-Raptor.
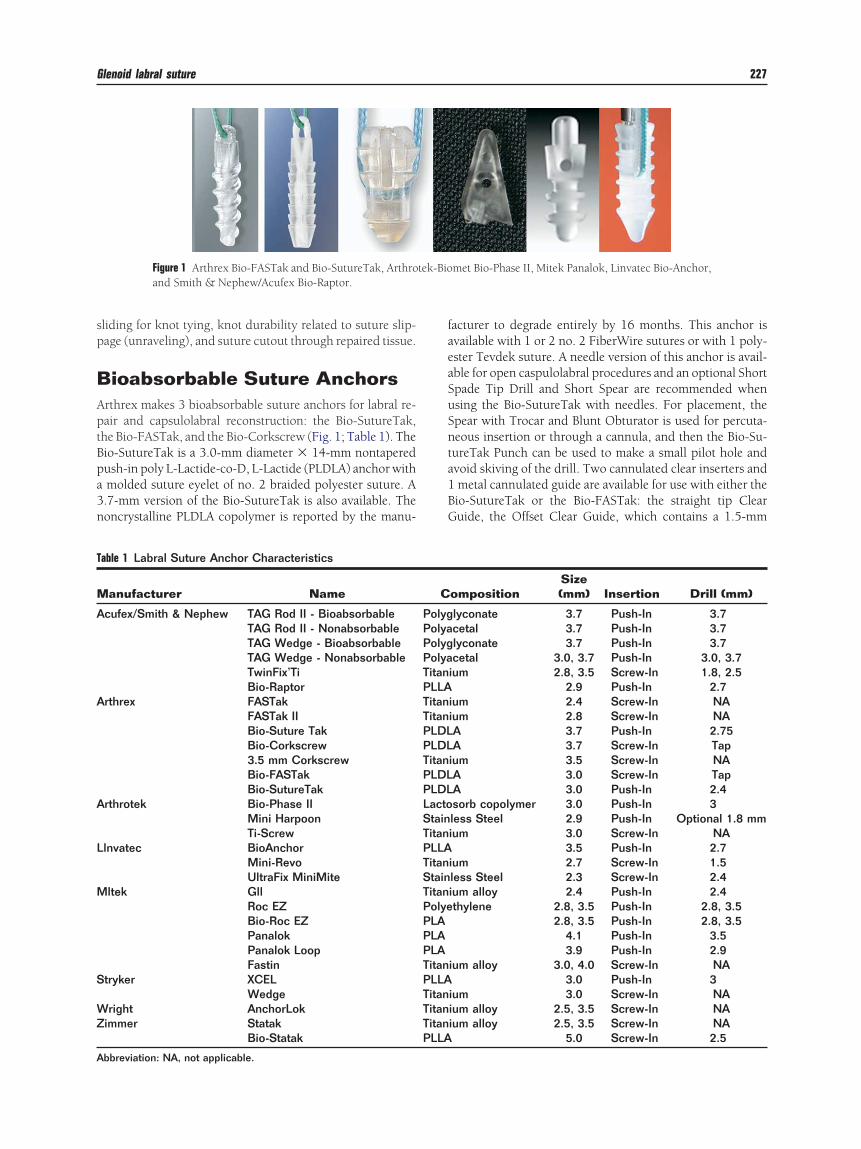
able 1 Labral Suture Anchor Characteristics
anufacturer Name
cufex/Smith & Nephew TAG Rod II - BioabsorbableTAG Rod II - NonabsorbableTAG Wedge - BioabsorbableTAG Wedge - NonabsorbableTwinFix’TiBio-Raptor
rthrex FASTakFASTak IIBio-Suture TakBio-Corkscrew3.5 mm CorkscrewBio-FASTakBio-SutureTak
rthrotek Bio-Phase IIMini HarpoonTi-Screw
lnvatec BioAnchorMini-RevoUltraFix MiniMite
ltek GllRoc EZBio-Roc EZPanalokPanalok LoopFastin
tryker XCELWedge
right AnchorLokimmer Statak
Bio-Statak
bbreviation: NA, not applicable.
acturer to degrade entirely by 16 months. This anchor isvailable with 1 or 2 no. 2 FiberWire sutures or with 1 poly-ster Tevdek suture. A needle version of this anchor is avail-ble for open caspulolabral procedures and an optional Shortpade Tip Drill and Short Spear are recommended whensing the Bio-SutureTak with needles. For placement, thepear with Trocar and Blunt Obturator is used for percuta-eous insertion or through a cannula, and then the Bio-Su-ureTak Punch can be used to make a small pilot hole andvoid skiving of the drill. Two cannulated clear inserters andmetal cannulated guide are available for use with either theio-SutureTak or the Bio-FASTak: the straight tip Clearuide, the Offset Clear Guide, which contains a 1.5-mm
met Bio-Phase II, Mitek Panalok, Linvatec Bio-Anchor,
ompositionSize(mm) Insertion Drill (mm)
lyconate 3.7 Push-In 3.7cetal 3.7 Push-In 3.7lyconate 3.7 Push-In 3.7cetal 3.0, 3.7 Push-In 3.0, 3.7
ium 2.8, 3.5 Screw-In 1.8, 2.52.9 Push-In 2.7
ium 2.4 Screw-In NAium 2.8 Screw-In NAA 3.7 Push-In 2.75A 3.7 Screw-In Tap
ium 3.5 Screw-In NAA 3.0 Screw-In TapA 3.0 Push-In 2.4sorb copolymer 3.0 Push-In 3less Steel 2.9 Push-In Optional 1.8 mmium 3.0 Screw-In NA
3.5 Push-In 2.7ium 2.7 Screw-In 1.5less Steel 2.3 Screw-In 2.4ium alloy 2.4 Push-In 2.4thylene 2.8, 3.5 Push-In 2.8, 3.5
2.8, 3.5 Push-In 2.8, 3.54.1 Push-In 3.53.9 Push-In 2.9
ium alloy 3.0, 4.0 Screw-In NA3.0 Push-In 3
ium 3.0 Screw-In NAium alloy 2.5, 3.5 Screw-In NAium alloy 2.5, 3.5 Screw-In NA
5.0 Screw-In 2.5
tek-Bio
C
PolygPolyaPolygPolyaTitanPLLATitanTitanPLDLPLDLTitanPLDLPLDLLactoStainTitanPLLATitanStainTitanPolyePLAPLAPLATitanPLLATitanTitanTitanPLLA

mCed
assoawTnsupPS
sswmwa
slt(htt
swytaipuif
fRB24iddtlbcucWtmtt
mbw
228 J.R. Rudzki, D.B. Purcell, and R.W. Wright
edial offset position relative to the glenoid rim; and theannulated Guide, which has a stiff metal wall that can tol-rate bending forces applied to leveraging soft tissue withoutamaging the anchor insertion instrumentation.The Bio-FASTak is a 3.0-mm � 14-mm threaded PLDLA
nchor with a molded suture eyelet of no. 2 braided polyesteruture. This anchor is available with 1 or 2 no. 2 FiberWireutures or with 1 polyester Tevdek suture. A needle versionf this anchor is available for open caspulolabral procedures,nd an optional Short Tap and Short Drill are recommendedhen using the Bio-FASTak with needles. The Spear withrocar is used for percutaneous insertion or through a can-ula and then the Conical Point Obturator is used to make amall pilot hole and avoid skiving of the tap, which is alwayssed. An optional pin from the Portal Dilation Set may belaced through a percutaneous approach followed by theortal Dilator for Bio-FASTak, and then by the Bio-FASTakpear.
The 3.7-mm Bio-Corkscrew is a screw-in, threaded PLDLAuture anchor that comes prethreaded with 1 no. 2 FiberWireuture. Insertion is performed after predrilling a pilot holeith a punch and using a tap in harder bone. This anchoray prove to be a useful salvage option for situations inhich the 3.0-mm Bio-SutureTak or Bio-FASTak do not have
dequate purchase.Arthrotek-Biomet (Warsaw, IN) makes a 3.0-mm bioab-
orbable push-in suture anchor for labral repair and capsu-olabral reconstruction called the Bio-Phase II made of Lac-oSorb copolymer reported to degrade within 9 to 15 monthsFig. 1). Insertion is performed through creation of a pilotole with a 3.0-mm drill or awl. The Bio-Phase II anchor ishen tapped into place and the sutures are pulled to engagehe anchor within the bone.
Linvatec (Largo, FL) makes a 3.5-mm � 10.5-mm bioab-
Figure 2 Smith & Nephew/Acufex TwinFix Ti, Linvatecand Stryker XCEL.
Figure 3 Arthrex FASTak, Mitek GII, Smith & Nephew/A
Medical Anchorlok.orbable Bio-Anchor of molded poly-L-lactic acid (PLLA)ith a manufacturer reported total absorption time of 3 to 5ears that maintains 80% of its original tensile strength at 10o 14 months (Fig 1). The ribbed press-fit Bio-Anchor isvailable with a single strand of no. 2 polyester suture. Fornsertion, a locator alignment tool with teeth and short slots islaced on the prepared glenoid rim and a 2.7-mm drill issed to create a pilot hole. The push-in anchor is then tapped
nto place. Meyer and coworkers19 reported a mean load toailure for this anchor of 213 N.
Mitek (Westwood, MA) produces 3 bioabsorbable anchorsor labral repair and capsulolabral reconstruction, the Bio-OC EZ, the Panalok, and the Panalok Loop. The push-inioROC EZ is made of polylactic acid (PLA) and comes in.8-mm and 3.5-mm sizes that expand to 3.3-mm and.3-mm diameters when deployed. The anchors obtain an
nterference fit via radial osteo-compression. The glenoid isrilled with a 2.8-mm or 3.5-mm drill to the appropriateepth. Drilling 1 to 2 mm beyond the mark may be necessaryo confirm no anchor protrusion from the bone surface. Dril-ing along a single appropriate axis is critical to prevent drillreakage and limit the risk of radial osteo compression fitompromise. The BioROC EZ is then advanced into the holentil the deployment tip contacts the bone surface, which ishecked by lifting the drill guide for visual confirmation.hen satisfactory positioning of the anchor is confirmed, the
rigger is squeezed to deploy the device. Careful attention toaintaining suture freedom during deployment is necessary
o avoid incomplete deployment before passage of the suturehrough the tissue to be repaired.
The Panalok anchor is a bioabsorbale PLA push-in anchoreasuring 4.1 mm � 6 mm designed to lock into cancellous
one (Fig. 1). It is reported to retain 80% strength through 6eeks. Several suture options are available for the Panalok
ix MiniMite and Mini-Revo, Mitek Fastin and Roc EZ,
edge and TAG Rod II, Arthrotek TiScrew, and Wright
UltraF
cufex W

awnFaa(belfiEepotTao
2Ihn
USPpaTliisdTtatpmhts
asd2apgmddb
NAl(F1fwTnnmcant3
2t1itisipcn
tccsaNwl
swTadccMlbwtappm
r2b
Glenoid labral suture 229
nchor including no. 2 Panacryl (braided absorbable sutureith reported absorption time of 1.5-2.5 years), PDS II, ando. 2 Ethibond (Ethicon, Somerville, NJ) in green or white.or implantation, a 3.5-mm drill bit is used to create a hole todepth of 18 mm. The anchor is placed into the pilot hole onsheathed inserter without tapping, and its triangular design
Fig. 1) causes the insertion pin to bend and fit the holeefore pin memory forces the leading edge of the anchor tongage cancellous bone. Withdrawal of the inserter uses theeading edge of the anchor as a fulcrum and spins the anchoror engagement. After removing the inserter, nominal tensions applied to the suture lengths to completely set the anchor.xcessive tension or overloading the suture is avoided asither could lead to bone breakage and subsequent deviceullout or suture breakage. The Panalok Loop is a variationn this design, which measures 3.9 mm � 9 mm and con-ains a no. 1 braided suture eyelet to facilitate suture sliding.his anchor is available with no. 2 Ethibond or no. 2 Panacrylnd is inserted with a 2.9-mm � 17.8-mm drill bit as previ-usly described.Smith & Nephew recently introduced the Bio-Raptor
.9-mm push-in bioabsorbable PLLA suture anchor (Fig. 1).t is inserted with a 2.7-mm spade tip drill to create a pilotole. It will be available with 2 no. 2 DuraBraid sutures or 1o. 2.
ltraBraid Suturetryker (San Jose, CA) produces the 3.0-mm bioabsorbableLLA XCEL anchor, which comes preloaded with braidedolyester no. 2 suture. A unique feature of this anchor is rigidttachment of the anchor to the inserter until deployment.his is accomplished with a barb that catches on the cancel-
ous bone during insertion to rotate off and break free of thenserter (Fig. 2). A rigid connection between the anchor andnsertion device can potentially facilitate capsulolabral recon-truction and labral repairs when portal placement dictatesifficult access to portions of the glenoid rim (eg, 6 o’clock).his anchor obtains a wedge-type fit on the undersurface of
he subchondral bone that is somewhat similar to thatchieved with the Mitek Panalok described earlier. For inser-ion, a 3-mm drill is used to create a pilot hole to an appro-riate depth and the anchor is inserted to a horizontal laserark on the inserter. An additional vertical laser mark iselpful to the surgeon in confirming suture eyelet orientationo assure an optimal deployment with minimal suture abra-ion characteristics.
Finally, Zimmer (Warsaw, IN) offers a 5.0-mm bioabsorb-ble fully threaded PLLA Bio-Statak anchor that comes in aingle-piece assembly with attached needles and a disposableriver. For insertion, the Bio-Statak is predrilled with a.5-mm drill at a recommended angle of 20° to 40° to therticular surface. The pilot hole is then tapped with a taplaced through the drill guide, and depth is confirmed with arooved line on the tap barrel. The manufacturer recom-ends partial-depth tapping in situations of limited boneensity. The anchor is then inserted until it deploys off of theriver tip or the grooved depth line on the driver tip sits
elow the bone surface. conabsorbable Suture Anchorsrthrex has 3 nonabsorbable suture anchors available for
abral repair and capsulolabral reconstruction: the FASTakFig. 3), the FASTak II, and the 3.5-mm Corkscrew. TheASTak is 2.4 mm � 11.7 mm, the FASTak II is 2.8 mm �1.7 mm, and the Corkscrew is 3.5 mm � 15 mm. All 3 areully threaded titanium anchors inserted directly into boneithout predrilling on a powered drill or manually with theear Drop Handle and Keyless Chuck. Each is available witho. 2 FiberWire or Tevdek (braided polyester). These tita-ium anchors may be inserted quickly, however, surgeonsust be aware that the tapered or conical design requires
aution during final tightening as backing an anchor out forny reason will compromise its osseous purchase. The 3 can-ulated inserters previously described are available for bothhe FASTak and FASTak II. A guide is not available for the.5-mm Corkscrew.The Arthrotek-Biomet (Warsaw, IN) Mini-Harpoon is a
.9-mm stainless steel push-in anchor, which obtains an in-erference fit without required predrilling (an optional.8-mm drill is available). To implant the device, the anchor
s placed with its limited reusable handle perpendicular tohe glenoid rim face and gently tapped until the driver collars seated on cortical bone. The handle is then disassembled byeparating the upper and lower sections, and the foam inserts removed from the driver handle and the driver handle isulled straight out. Gentle tension is applied to the sutures toonfirm the anchor is appropriately seated within the gle-oid.Arthrotek also offers the Ti Screw 3.0-mm titanium
hreaded screw-in suture anchor (Fig. 3). The Ti Screwomes preloaded with 1 no. 2 braided polyester suture butan easily be reloaded with alternate preferred suture if de-ired. For insertion, the anchor inserter is gently tapped withmallet until the leading thread engages the cortical bone.ext, the anchor is screwed in until flush with the bone athich point the handle is removed and the sutures are re-
eased.Linvatec offers the Mini-Revo 2.7-mm � 8.5-mm nonab-
orbable fully-threaded titanium suture anchor preloadedith no. 2 nonabsorbable braided polyester suture (Fig. 2).he anchor is inserted into a predrilled 1.5-mm pilot holend may potentially be removed by reattaching the insertionriver, although, as with other nonabsorbable suture an-hors, stripping of the insertion driver may require a moreomplicated extrication. Linvatec also produces the UltraFixiniMite 2.3-mm � 6.5-mm nonabsorbable push-in stain-
ess steel suture anchor that may be loaded with 2 no. 2raided polyester sutures (Fig. 2). The anchor is insertedith a 2.4-mm drill to create a 14-mm long pilot hole and
hen an insertion gun for deployment, which expands thenchor to a 4.7-mm postdeployed arc range. This 4.7-mmostdeployment size is an important consideration and mayotentially be a limiting factor of the anchors utility whenultiple fixation points are desired.Mitek produces 4 nonabsorbable suture anchors for labral
epair and capsulolabral reconstruction. The Mitek GII is a.4-mm � 8.8-mm push-in titanium alloy anchor, which haseen used for several types of soft-tissue reconstruction pro-
edures and is available with either no. 2 Ethibond or no. 2
P2
t4paa
e34tB
uahansaUbNbsct
dwM2Z
ncaenidpaptacdtalb
a21cts
ACPfiiaisioaap
PoAusapabttvtcthpwc
asrlipimcsitcptabctpp
230 J.R. Rudzki, D.B. Purcell, and R.W. Wright
anacryl (Fig. 3). It is inserted after creation of a predrilled.4-mm � 14.2-mm pilot hole.The Mitek FASTIN is a threaded, self-drilling, self-tapping
itanium alloy anchor available in 3.0-mm � 8.4-mm and.0-mm � 9.7-mm sizes with no. 2 Ethibond (Fig. 2). Forlacement, the anchor is placed onto a drill chuck or manu-lly inserted into the prepared glenoid without the need fordditional instrumentation.
The Mitek ROC EZ is a push-in nonabsorbable polyethyl-ne suture anchor, which comes in 2.8-mm � 13.0-mm and.5-mm � 13.0-mm sizes, which expand to 3.3-mm and.3-mm diameters when deployed (Fig. 2). The anchors ob-ain an interference fit similar to that described earlier for theioROC EZ and are inserted in similar fashion.The Smith & Nephew TwinFix suture anchor line has a
nique and patented double-helix “Hi-Lo” thread designvailable in 2.8-mm and 3.5-mm sizes (Fig. 2). In areas ofard bone, predrilling with the available 3.5-mm drill guidend 1.8-mm drill bit is suggested. These are available witheedles and dual-armed sutures packaged in an anchor in-erter and needle delivery system. Various suture options arevailable with these anchors including the newly developedHMW braided polyethylene UltraBraid suture and theraided polyester Durabraid suture produced by Smith &ephew. The 2.8-mm anchor comes with either a no. 1raided polyester or no. 2 Durabraid suture or a highertrength alternative no. 2 UltraBraid suture. The 3.5-mm an-hor comes with 2 no. 2 Durabraid or no. 2 UltraBraid su-ures with or without needles.
Stryker makes the 3.0-mm fully threaded titanium self-rilling and self-tapping Wedge suture anchor, which comesith a single preloaded suture. In addition, Stryker offers theainstay ZIP fully threaded titanium suture anchor in
.7-mm and 3.5-mm sizes. Available sutures for the MainstayIP include no. 0, no. 2, and no. 5 braided polyester.Wright Medical Technology (Arlington, TN) produces the
onabsorbable self-drilling, self-tapping titanium alloy An-horLok anchors in 2.5-mm and 3.5-mm sizes (Fig. 3). Thesenchors come preloaded with nonabsorbable braided poly-ster no. 2 or no. 0 suture. A semicircular reverse cuttingeedle is attached to each end of the preloaded suture. For
mplantation, the anchor is manually inserted with an anchorriver that must be kept perpendicular to bone at all times torevent premature dissociation (this may be difficult to reli-bly perform in capsulolabral reconstruction where portallacement dictates an angle other than 90° for anchor inser-ion; however, the difficulty with this issue is not unique tony one type of anchor). A theoretical advantage of the An-horLok system is the chamfering portion on the insertionriver designed to remove sharp bone edges from the inser-ion site that have the potential to cause premature suturebrasion and breakage. In addition, the insertion device al-ows for anchor removal without destruction of adjacentone.Zimmer (Warsaw, IN) offers a fully threaded nonabsorb-
ble self-drilling, self-tapping titanium alloy Statak anchor in.5-mm and 3.5-mm sizes. The 2.5-mm version comes withno. 0 braided polyester suture, and the 3.5-mm version
omes with a no. 2 braided polyester suture. For insertion,he Statak anchor and driver is connected to a drill via a
tandard Jacob’s chuck and drilled directly into the bone. puthors’ Preferredharacteristics
eer-reviewed literature has clearly established that multiplexation points provide a biomechanically sounder construct
n Bankart repair. The size of the glenoid and its rim makenchor size a critical consideration in implant selection andmplementation. Our preferred characteristics for anchor de-ign are as follows: a bioabsorbable anchor less than 5.0 mmn diameter with a guide system that allows for visualizationf the depth of deployment, suture eyelets that minimizebrasion and limit deleterious effects of anchor orientation,nd a rigid insertion device for deployment that allows forercutaneous insertion through accessory portals.
otential Complicationsf Suture Anchors
s with any orthopedic implant or technique, suture anchorsage for labral repair and capsulolabral reconstruction haseveral potential complications of which the surgeon must beware. Infection may occur whenever a surgical procedure iserformed and has been reported with the use of suturenchors in the shoulder 23. Although suture anchors haveeen shown to provide equivalent or superior results for thereatment of labral and capsulolabral pathology, some au-hors have found greater rates of failure and continue to ad-ocate transosseous suture fixation techniques.24,25 Prepara-ion of the glenoid surface and mobilization of theapsulolabral structures is critical with these procedures forhe generation of a healthy bleeding bony bed to maximizeealing potential.26 In preparing the glenoid rim for anchorlacement, however, the surgeon must exercise cautionhen decorticating so as not to compromise anchor pur-
hase.Inflammatory responses to various bioabsorbable materi-
ls including polyglycolic acid and PLLA have been de-cribed, and this potential must be recognized.27 A relativelyare potential complication of either bioabsorbable or metal-ic suture anchors that has been reported with the latter ismplant material failure with intraarticular migration andossible joint destruction.28,29 Suture breakage at any point
n the operative procedure will render an implant useless anday require extrication. This process has the potential to
ompromise articular cartilage and bone stock. Failure at theuture-tissue interface may result in repair or reconstructionncompetence as well; however, if this occurs intraopera-ively, salvage options exist. As described earlier, those an-hors with 2 sutures available prevent complete loss of im-lant utility, and, with bioabsorbable anchors, overdrillinghe anchor may allow placement of a similar size or largernchor in the same pilot hole. The latter technique may alsoe used should the complication of inadequate anchor pur-hase in subchondral and cortical bone occur. Finally, addi-ional theoretical complications of osteolysis around im-lants and chondrolysis related to drilling or glenoidreparation may develop and compromise the efficacy of the
rocedure.
CAptocctasa
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
22
2
2
2
Glenoid labral suture 231
onclusionrthroscopic and open treatment of labral and capsulolabralathology has been greatly facilitated through the use of su-ure anchors. With a broad variety of options available to therthopedic surgeon and an everexpanding volume of biome-hanical and clinical outcomes research regarding suture an-hor performance, a knowledge of the strengths and limita-ions of these implants is critical for optimal patient care. Inddition, this knowledge will afford the treating orthopaedicurgeon to critically evaluate future implants as they becomevailable.
eferences1. Warme WJ, Arciero RA, Savoie FH 3rd, et al: Nonabsorbable versus
absorbable suture anchors for open Bankart repair. A prospective, ran-domized comparison. Am J Sports Med 27:742-746, 1999
2. Cole BJ, Romeo AA: Arthroscopic shoulder stabilization with sutureanchors: technique, technology, and pitfalls. Clin Orthop 390:17-30,2001
3. Kim SH, Ha KL, Cho YB, et al: Arthroscopic anterior stabilization of theshoulder: Two to six year follow-up. J Bone Joint Surg Am 85:1511-1518, 2003
4. Lo IK, Burkhart SS: Spotlight on surgical techniques. Current conceptsin arthroscopic rotator cuff repair. Am J Sports Med 31:308-324, 2003
5. Halder AM, O’Driscoll SW, Heers G, et al: Biomechanical comparisonof effects of supraspinatus tendon detachments, tendon defects, andmuscle retractions. J Bone Joint Surg Am 84:780-785, 2002
6. Burkhart SS, Diaz Pagan JL, Wirth MA, et al: Cyclic loading of anchor-based rotator cuff repairs: Confirmation of the tension overload phe-nomenon and comparison of suture anchor fixation with transosseousfixation. Arthroscopy 13:720-724, 1997
7. Hecker AT, Shea M, Hayhurst JO, et al: Pull-out strength of sutureanchors for rotator cuff and Bankart lesion repairs. Am J Sports Med21:874-879, 1993
8. Roth CA, Bartolozzi AR, Ciccotti MG, et al: Failure properties of sutureanchors in the glenoid and the effects of cortical thickness. Arthroscopy14:186-191, 1998
9. Black KP, Schneider DJ, Yu JR, et al: Biomechanics of the Bankartrepair: The relationship between glenohumeral translation and labralfixation site. Am J Sports Med 27:339-344, 1999
0. Burkart A, Debski RE, Musahl V, et al: Glenohumeral translations areonly partially restored after repair of a simulated type II superior labrallesion. Am J Sports Med 31:56-63, 2003
1. DiRaimondo CA, Alexander JW, Noble PC, et al: A biomechanical
comparison of repair techniques for type II SLAP lesions. Am J SportsMed 32:727-733, 2004
2. von Shroeder HP, Kuiper SD, Botte MJ: Osseous anatomy of the scap-ula. Clin Orthop 383:131-139, 2001
3. Lehtinen JT, Tingart MJ, Apreleva M, et al: Anatomy of the superiorglenoid rim. Repair of superior labral anterior to posterior tears. Am JSports Med 31:257-260, 2003
4. Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology, andvascularity of the glenoid labrum. An anatomical study. J Bone JointSurg Am 74:46-52, 1992
5. Howell SM, Galinat BJ: The glenoid-labral socket. A constrained artic-ular surface. Clin Orthop 243:122-125, 1989
6. Nam EK, Snyder SJ: Clinical sports medicine update. The diagnosis andtreatment of superior labrum, anterior and posterior (SLAP) lesions.Am J Sports Med 31:798-810, 2003
7. Barber FA, Herbert MA, Click JN: Internal fixation strength of sutureanchors—Update 1997. Am J Sports Med 13:355-362, 1997
8. Wetzler MJ, Bartolozzi AR, Gillespie MJ, et al: Fatigue properties ofsuture anchors in anterior shoulder reconstructions: Mitek GII. Am JSports Med 12:687-693, 1996
9. Meyer DC, Fucentese SF, Ruffieux K, et al: Mechanical testing of ab-sorbable suture anchors. Arthroscopy 19:188-193, 2003
0. Bailey SB, Grover DM, Howell SM, et al: Foam-reinforced elderly hu-man tibia approximates young human tibia better than porcine tibia: Astudy of the structural properties of three soft tissue fixation devices.Am J Sports Med 32:755-764, 2004
1. Meyer DC, Nyffeler RW, Fucentese SF, et al: Failure of suture materialat suture anchor eyelets. Arthroscopy 18:1013-1019, 2002
2. Bardana DD, Burks RT, West JR, et al: The effect of suture anchordesign and orientation on suture abrasion: An in vitro sudy. Arthros-copy 19:274-281, 2003
3. Ticker JB, Lippe RJ, Barkin DE, et al: Infected suture anchors in theshoulder. Arthroscopy 12:613-615, 1996
4. Tamai K, Higashi A, Tanabe T, et al: Recurrences after the open Bankartrepair: A potential risk with use of suture anchors. Jour Should ElbowSurg 8:37-41, 1999
5. Zarins B: Letter to the editor. Am J Sports Med 31:636, 20036. Morgan CD, Bartolozzi AR: Arthroscopic Bankart suture repair: Tech-
nique and early results. Arthroscopy 3:111-122, 19877. Freehill MQ, Harms DJ, Huber SM, et al: Poly-L-lactic acid tack syno-
vitis after arthroscopic stabilization of the shoulder. Am J Sports Med31:643-647, 2003
8. Silver DJ: Symptomatic interarticular migration of glenoid suture an-chors. Arthroscopy 16:102-105, 2000
9. Kaar TK, Schenck RC Jr, Wirth MA, et al: Complications of metallicsuture anchors in shoulder surgery: A report of 8 cases. Arthroscopy
17:31-37, 2001



















