
Nonsynostotic Occipital Plagiocephaly: Radiographic Diagnosis of the ???Sticky Suture
10
Nonsynostotic Occipital Plagiocephaly: Radiographic Diagnosis of the “Sticky Suture” Joseph E. Losee, M.D., Evan Feldman, B.S., Manoj Ketkar, M.D., Davinder Singh, M.D., Richard E. Kirschner, M.D., Per-Lennart Westesson, D.D.S., Ph.D., M.D., Greg Cooper, B.S., Mark P. Mooney, Ph.D., and Scott P. Bartlett, M.D. Pittsburgh, Pa.; Rochester, N.Y.; and Philadelphia, Pa. Background: While the clinical differ- ences between nonsynostotic occipital pla- giocephaly and lambdoid craniosynostosis have been described, the radiographic dif- ferentiation between the two remains ob- scure. The aim of this study was to charac- terize morphological differences in the lambdoid suture between nonsynostotic oc- cipital plagiocephaly and lambdoid cranio- synostosis. Methods: Computed tomography scans of children clinically diagnosed with nonsyn- ostotic occipital plagiocephaly (n 26) were compared with computed tomogra- phy scans from children diagnosed with lambdoid craniosynostosis (n 7). Suture and cranial morphology, ear position, and endocranial base angles were qualitatively and quantitatively compared. Results: Nonsynostotic occipital plagio- cephaly sutures demonstrated areas of focal fusion (25 percent), endocranial ridg-ing (78 percent), narrowing (59 percent), sclerosis (19 percent), and changes from overlapping to end-to-end orientation (100 percent). No sutures demonstrated ectocranial ridging. All cases of nonsynostotic occipital plagioceph- aly presented with ipsilateral occipital flatten- ing, 85 percent with ipsilateral frontal, and 95 percent with contralateral occipital bossing producing parallelogram morphology. In contrast, a greater frequency of sutures in lambdoid craniosynostosis patients demon- strated nearly complete obliteration (p 0.001) with ectocranial ridging (p 0.001); significantly more of these patients presented with ipsilateral occipital flattening with com- pensatory ipsilateral mastoid (p 0.001) and contralateral parietal (p 0.01) bossing, pro- ducing a trapezoid morphology. Sutures from nonsynostotic occipital plagiocephaly patients showed endocranial ridging, focal fusions, and narrowing, previously reported as lambdoid craniosynostosis. Conclusions: In contradiction to previous reports, lambdoid craniosynostosis is not ra- diographically unique among suture fusions. This work establishes the radiographic diag- nosis of nonsynostotic occipital plagioceph- aly. (Plast. Reconstr. Surg. 116: 1860, 2005.) It is now well understood that occipital pla- giocephaly results from either nonsynostotic occipital plagiocephaly, commonly known as deformational plagiocephaly, or synostosis of the lamboid suture, commonly referred to as lambdoid craniosynostosis. Historically, there has been difficulty in clinically differentiating between the two and this ambiguity has re- sulted in many children with nonsynostotic oc- cipital plagiocephaly incorrectly diagnosed From The Children’s Hospital of Pittsburgh, Division of Pediatric Plastic Surgery, University of Pittsburgh; The Children’s Hospital at Strong, Division of Neuroradiology, University of Rochester; The Children’s Hospital of Philadelphia, Division of Pediatric Plastic Surgery, University of Pennsylvania; and the Departments of Oral Medicine and Pathology, Anthropology, Orthodontics, and Surgery-Plastics, University of Pittsburgh. Received for publication October 5, 2004; revised November 26, 2004. Presented at the 60th Anniversary Meeting of the American Cleft Palate Craniofacial Association, Asheville, North Carolina, on April 12, 2003. DOI: 10.1097/01.prs.0000191176.62532.5e 1860
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Nonsynostotic Occipital Plagiocephaly: Radiographic Diagnosis of the ???Sticky Suture

Nonsynostotic Occipital Plagiocephaly:Radiographic Diagnosis of the “Sticky Suture”Joseph E. Losee, M.D., Evan Feldman, B.S., Manoj Ketkar, M.D., Davinder Singh, M.D.,Richard E. Kirschner, M.D., Per-Lennart Westesson, D.D.S., Ph.D., M.D., Greg Cooper, B.S.,Mark P. Mooney, Ph.D., and Scott P. Bartlett, M.D.Pittsburgh, Pa.; Rochester, N.Y.; and Philadelphia, Pa.
Background: While the clinical differ-ences between nonsynostotic occipital pla-giocephaly and lambdoid craniosynostosishave been described, the radiographic dif-ferentiation between the two remains ob-scure. The aim of this study was to charac-terize morphological differences in thelambdoid suture between nonsynostotic oc-cipital plagiocephaly and lambdoid cranio-synostosis.Methods: Computed tomography scans ofchildren clinically diagnosed with nonsyn-ostotic occipital plagiocephaly (n � 26)were compared with computed tomogra-phy scans from children diagnosed withlambdoid craniosynostosis (n � 7). Sutureand cranial morphology, ear position, andendocranial base angles were qualitativelyand quantitatively compared.Results: Nonsynostotic occipital plagio-cephaly sutures demonstrated areas of focalfusion (25 percent), endocranial ridg-ing (78percent), narrowing (59 percent), sclerosis(19 percent), and changes from overlappingto end-to-end orientation (100 percent). Nosutures demonstrated ectocranial ridging. Allcases of nonsynostotic occipital plagioceph-aly presented with ipsilateral occipital flatten-ing, 85 percent with ipsilateral frontal, and 95percent with contralateral occipital bossingproducing parallelogram morphology. In
contrast, a greater frequency of sutures inlambdoid craniosynostosis patients demon-strated nearly complete obliteration (p �0.001) with ectocranial ridging (p � 0.001);significantly more of these patients presentedwith ipsilateral occipital flattening with com-pensatory ipsilateral mastoid (p � 0.001) andcontralateral parietal (p � 0.01) bossing, pro-ducing a trapezoid morphology. Suturesfrom nonsynostotic occipital plagiocephalypatients showed endocranial ridging, focalfusions, and narrowing, previously reportedas lambdoid craniosynostosis.Conclusions: In contradiction to previousreports, lambdoid craniosynostosis is not ra-diographically unique among suture fusions.This work establishes the radiographic diag-nosis of nonsynostotic occipital plagioceph-aly. (Plast. Reconstr. Surg. 116: 1860, 2005.)
It is now well understood that occipital pla-giocephaly results from either nonsynostoticoccipital plagiocephaly, commonly known asdeformational plagiocephaly, or synostosis ofthe lamboid suture, commonly referred to aslambdoid craniosynostosis. Historically, therehas been difficulty in clinically differentiatingbetween the two and this ambiguity has re-sulted in many children with nonsynostotic oc-cipital plagiocephaly incorrectly diagnosed
From The Children’s Hospital of Pittsburgh, Division of Pediatric Plastic Surgery, University of Pittsburgh; The Children’s Hospital at Strong,Division of Neuroradiology, University of Rochester; The Children’s Hospital of Philadelphia, Division of Pediatric Plastic Surgery, Universityof Pennsylvania; and the Departments of Oral Medicine and Pathology, Anthropology, Orthodontics, and Surgery-Plastics, University ofPittsburgh. Received for publication October 5, 2004; revised November 26, 2004.
Presented at the 60th Anniversary Meeting of the American Cleft Palate Craniofacial Association, Asheville, North Carolina, on April 12, 2003.
DOI: 10.1097/01.prs.0000191176.62532.5e
1860

with lambdoid craniosynostosis and undergo-ing potentially unnecessary cranial vault re-modeling.
It has been well understood that lambdoidcraniosynostosis is the rarest form of single-suture synostosis,1–5 representing 1 to 5 percentof the cases of simple craniosynostosis. In theyears surrounding the “back-to-sleep” initiative,unusual reports emerged claiming that the in-cidence of lambdoid craniosynostosis had in-creased to new levels, and this apparent in-crease was attributed to improved clinicalrecognition, among other things.3,6,7
This lack of a complete understanding oflambdoid craniosynostosis and nonsynostoticoccipital plagiocephaly lead to the develop-ment of an entire body of literature, includingradiographic and histologic evaluations, at-tempting to demonstrate that lambdoid cranio-synostosis was unique among other forms ofcraniosynostosis8 and did not require the usualclinical and radiographic findings consistentwith classic sutural fusion. It was said that non-synostotic occipital plagiocephaly would alwaysself improve and was never progressive3,4; whilelambdoid craniosynostosis, considered to beon a continuum with nonsynostotic occipitalplagiocephaly, progressed and would not selfcorrect with the conservative treatment of re-positioning the infant.3,6 Lambdoid craniosyn-ostosis was thus considered to be a “functionalsynostosis” rather than a true synostosis, andthe sutures of lambdoid craniosynostosis weredescribed as “sticky.”9 Often, the decision toproceed with surgical correction was based onthe degree of asymmetry and its progression3,6
rather than the standard criteria for craniosyn-ostosis.
Subsequently, clinical work by Huang et al.has shown that lambdoid craniosynostosis andnonsynostotic occipital plagiocephaly are twodistinct and separate conditions.10 They estab-lished the clinical diagnostic criteria for bothconditions and convincingly demonstratedthat lambdoid craniosynostosis is not uniqueamong sutural fusions, following the classicpatterns of craniosynostosis. Despite this clini-cal work, the radiographic diagnosis of nonsyn-ostotic occipital plagiocephaly has hardly beenaddressed,11 and the controversy in the litera-ture today regarding the radiographic featuresof nonsynostotic occipital plagiocephaly stillremains.2–4,6,8 The aim of this study was to crit-ically investigate the radiographic findings of
nonsynostotic occipital plagiocephaly and pro-pose objective criteria for its diagnosis.
METHODS
Patient Demographics
Pretreatment, three-dimensional computed-tomographic scans from 33 patients were usedin the present study. Twenty-six patients wereclinically diagnosed with nonsynostotic occipi-tal plagiocephaly based on the morphologiccriteria emphasized by Huang et al.10 and in-cluded 18 boys and eight girls ranging in agefrom 2.7 to 25.4 months (average, 7.8 months).Twelve patients had nonsynostotic occipitalplagiocephaly on the right side, eight on theleft, and six bilaterally. Seven patients (fiveboys and two girls), ranging in age from 3 to 15months (average, 7.8 months) had nonsyn-dromic lambdoid craniosynostosis, diagnosedby physical exam and computed tomographyscan. Four patients had lambdoid craniosynos-tosis on the right side and three patients on theleft. All patients with nonsynostotic occipitalplagiocephaly were seen for treatment at theChildren’s Hospital at Strong, while all lamb-doid craniosynostosis patients were seen fortreatment at The Children’s Hospital of Phila-delphia.
Data Collection
The computed tomography scans were eval-uated and compared by a craniofacial surgeonand neuroradiologist. Suture morphology wasexamined on two-dimensional axial raw data.All of the three-dimensional “surface render-ings” were evaluated and endocranial-base an-gle calculations were performed on a GeneralElectric Advantage Windows Workstation run-ning 4.0 software.
Nonmetric Data Collection
The affected lambdoid sutures in nonsynos-totic occipital plagiocephaly and lambdoid cra-niosynostosis, as well as their contralateral, un-affected, “control” sutures, were subjectivelyexamined for the presence or absence of cer-tain characteristics. Lambdoid sutures weremorphologically reviewed for patency and fo-cal fusions, endocranial and ectocranial ridg-ing, sutural narrowing, perisutural thickeningand thinning, sclerosis (increased bone den-sity), and changes in orientation from the nor-mal overlapping to end-to-end morphology.The affected lambdoid craniosynostosis sutures
Vol. 116, No. 7 / NONSYNOSTOTIC PLAGIOCEPHALY 1861
(n � 7) were compared with the affected non-synostotic occipital plagiocephaly sutures (n �32; 20 unilateral and six bilateral cases), andthen the affected nonsynostotic occipital pla-giocephaly sutures, in unilateral cases, werecompared against their contralateral, nonaf-fected “control” sutures (n � 20).
The three-dimensional surface renderingsalso were subjectively analyzed for overall cra-nial shape, presence or absence of compensa-tory bossing, ear position, and presence of in-creased frontal or occipital subarachnoidspacing.
Metric Data Collection
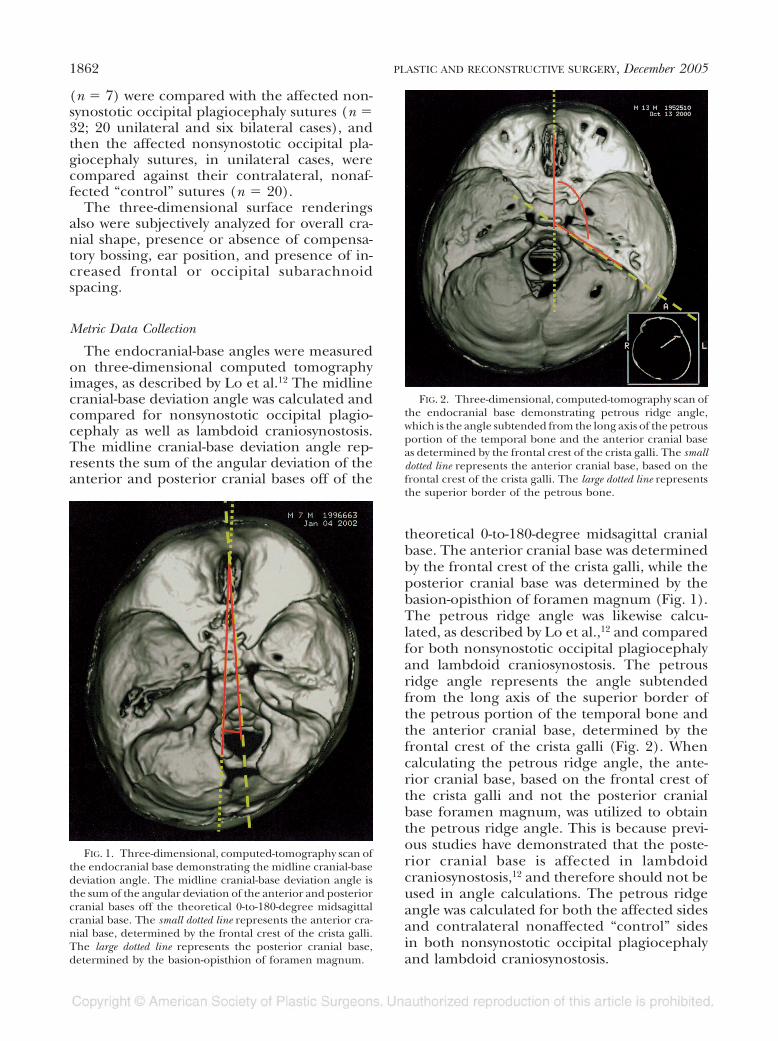
The endocranial-base angles were measuredon three-dimensional computed tomographyimages, as described by Lo et al.12 The midlinecranial-base deviation angle was calculated andcompared for nonsynostotic occipital plagio-cephaly as well as lambdoid craniosynostosis.The midline cranial-base deviation angle rep-resents the sum of the angular deviation of theanterior and posterior cranial bases off of the
theoretical 0-to-180-degree midsagittal cranialbase. The anterior cranial base was determinedby the frontal crest of the crista galli, while theposterior cranial base was determined by thebasion-opisthion of foramen magnum (Fig. 1).The petrous ridge angle was likewise calcu-lated, as described by Lo et al.,12 and comparedfor both nonsynostotic occipital plagiocephalyand lambdoid craniosynostosis. The petrousridge angle represents the angle subtendedfrom the long axis of the superior border ofthe petrous portion of the temporal bone andthe anterior cranial base, determined by thefrontal crest of the crista galli (Fig. 2). Whencalculating the petrous ridge angle, the ante-rior cranial base, based on the frontal crest ofthe crista galli and not the posterior cranialbase foramen magnum, was utilized to obtainthe petrous ridge angle. This is because previ-ous studies have demonstrated that the poste-rior cranial base is affected in lambdoidcraniosynostosis,12 and therefore should not beused in angle calculations. The petrous ridgeangle was calculated for both the affected sidesand contralateral nonaffected “control” sidesin both nonsynostotic occipital plagiocephalyand lambdoid craniosynostosis.
FIG. 1. Three-dimensional, computed-tomography scan ofthe endocranial base demonstrating the midline cranial-basedeviation angle. The midline cranial-base deviation angle isthe sum of the angular deviation of the anterior and posteriorcranial bases off the theoretical 0-to-180-degree midsagittalcranial base. The small dotted line represents the anterior cra-nial base, determined by the frontal crest of the crista galli.The large dotted line represents the posterior cranial base,determined by the basion-opisthion of foramen magnum.
FIG. 2. Three-dimensional, computed-tomography scan ofthe endocranial base demonstrating petrous ridge angle,which is the angle subtended from the long axis of the petrousportion of the temporal bone and the anterior cranial baseas determined by the frontal crest of the crista galli. The smalldotted line represents the anterior cranial base, based on thefrontal crest of the crista galli. The large dotted line representsthe superior border of the petrous bone.
1862 PLASTIC AND RECONSTRUCTIVE SURGERY, December 2005
Statistical Analysis
Group differences in nonmetric data wereanalyzed using nonparametric Fisher exact andMcNemar’s tests. Mean differences in metric(angle) data were analyzed using paired andunpaired t tests.13 Differences were consideredsignificant if p � 0.05. For measurement reli-ability, the subjective data were obtained bysimultaneous consensus of the craniofacial sur-geon and neuroradiologist.
RESULTS
Nonmetric Data
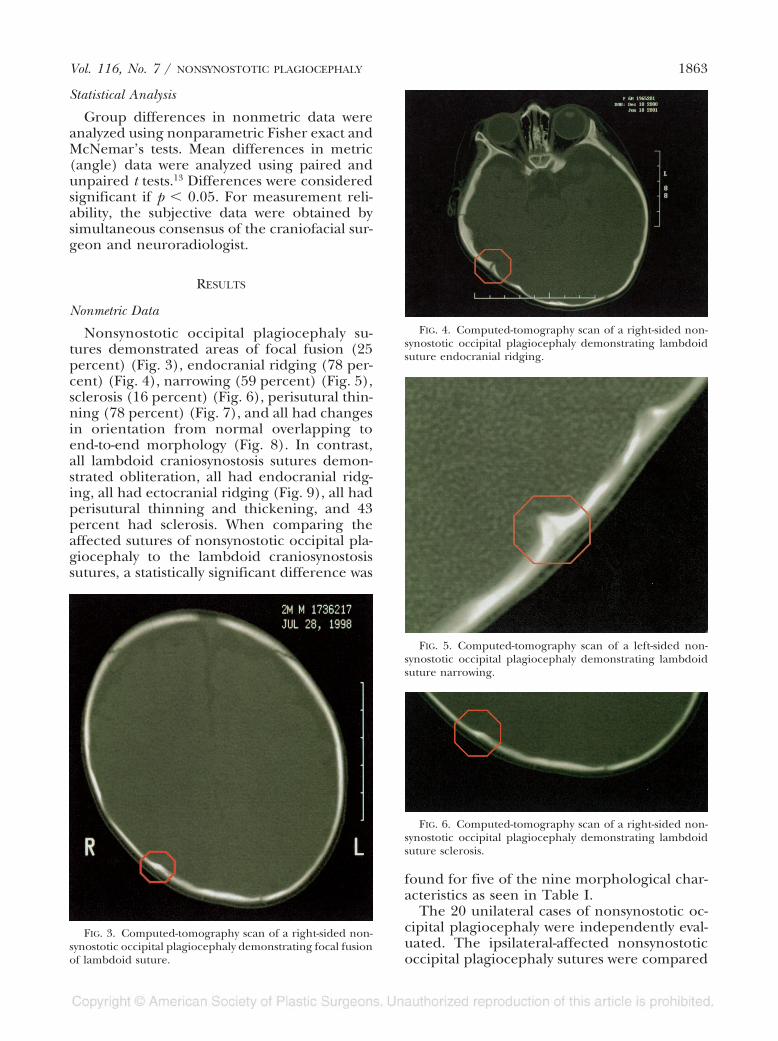
Nonsynostotic occipital plagiocephaly su-tures demonstrated areas of focal fusion (25percent) (Fig. 3), endocranial ridging (78 per-cent) (Fig. 4), narrowing (59 percent) (Fig. 5),sclerosis (16 percent) (Fig. 6), perisutural thin-ning (78 percent) (Fig. 7), and all had changesin orientation from normal overlapping toend-to-end morphology (Fig. 8). In contrast,all lambdoid craniosynostosis sutures demon-strated obliteration, all had endocranial ridg-ing, all had ectocranial ridging (Fig. 9), all hadperisutural thinning and thickening, and 43percent had sclerosis. When comparing theaffected sutures of nonsynostotic occipital pla-giocephaly to the lambdoid craniosynostosissutures, a statistically significant difference was
found for five of the nine morphological char-acteristics as seen in Table I.
The 20 unilateral cases of nonsynostotic oc-cipital plagiocephaly were independently eval-uated. The ipsilateral-affected nonsynostoticoccipital plagiocephaly sutures were compared
FIG. 3. Computed-tomography scan of a right-sided non-synostotic occipital plagiocephaly demonstrating focal fusionof lambdoid suture.
FIG. 4. Computed-tomography scan of a right-sided non-synostotic occipital plagiocephaly demonstrating lambdoidsuture endocranial ridging.
FIG. 5. Computed-tomography scan of a left-sided non-synostotic occipital plagiocephaly demonstrating lambdoidsuture narrowing.
FIG. 6. Computed-tomography scan of a right-sided non-synostotic occipital plagiocephaly demonstrating lambdoidsuture sclerosis.
Vol. 116, No. 7 / NONSYNOSTOTIC PLAGIOCEPHALY 1863

with their contralateral, nonaffected, “control”sutures. Statistically significant differences, be-tween the affected and nonaffected sutures, inthe unilateral cases, were found for overlap-ping suture orientation (p � 0.05), endocra-nial ridging (p � 0.001), and perisutural bonethinning (p � 0.001). While no statistical sig-nificance was established (p � 0.06), a differ-ence in sutural patency, focal fusions, and achange in suture orientation to end-to-endmorphology, were observed.
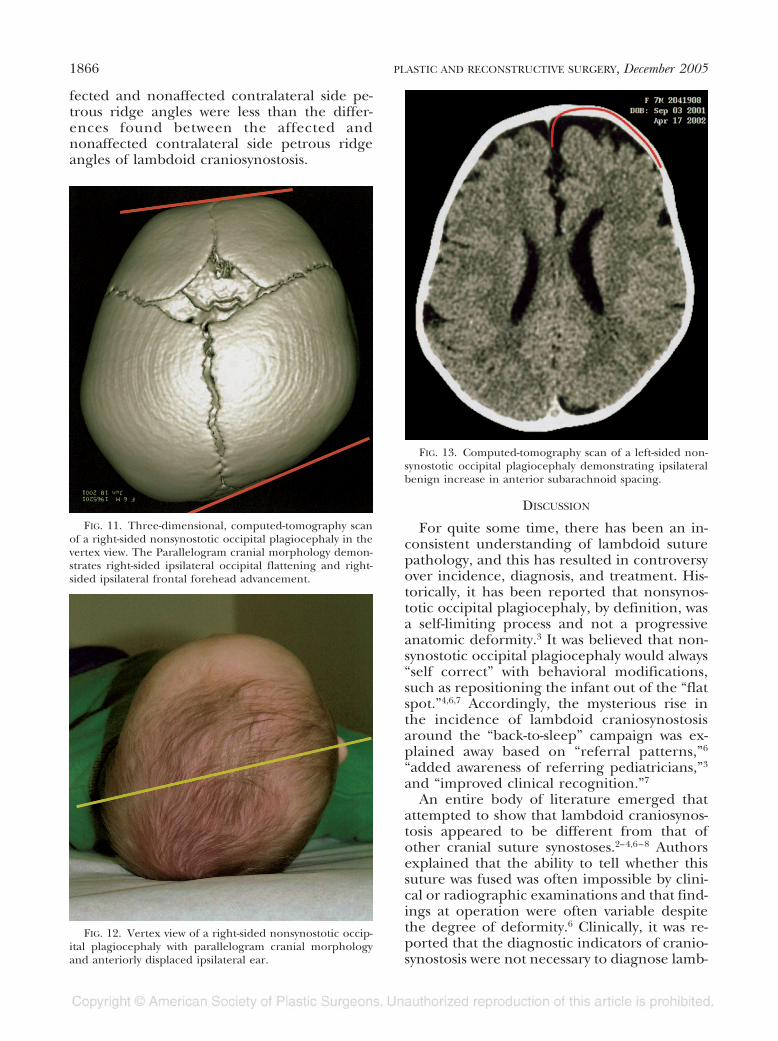
Overall three-dimensional, computed-to-mography scan cranial morphology was alsoevaluated. In all seven of the lambdoid cranio-synostosis patients, ipsilateral occipital flatten-ing, ipsilateral mastoid bossing, and contralat-eral parietal eminence bossing were found(Fig. 10). In none of the lambdoid craniosyn-ostosis patients was ipsilateral frontal bossingor contralateral occipital bossing found. Fromthe vertex view in lambdoid craniosynostosis,an overall trapezoid shape to the cranial vaultwas observed. From the posterior view in lamb-doid craniosynostosis, a parallelogram-shapedcranial morphology was observed. In all 26 ofthe nonsynostotic occipital plagiocephaly pa-tients, ipsilateral occipital flattening was evi-dent, and in no cases of nonsynostotic occipitalplagiocephaly was ipsilateral mastoid bossingobserved. Contralateral occipital bossing wasseen in 63 percent of the 26 patients (n � 16)with nonsynostotic occipital plagiocephaly, ip-silateral frontal bossing was seen in 53 percent(n �14), and contralateral parietal bossing wasseen in 38 percent (n � 10). From the vertexview, more than 50 percent of the 26 nonsyn-ostotic occipital plagiocephaly patients exhib-ited clear-cut parallelogram cranial morphol-ogy (Fig. 11). From the posterior view, allnonsynostotic occipital plagiocephaly patientspresented with symmetric skull-base morphol-
ogy. Significantly more nonsynostotic occipitalplagiocephaly patients had ipsilateral frontalbossing (p � 0.01) and contralateral occipitalbossing (p � 0.01), compared with lambdoidcraniosynostosis patients. In contrast, signifi-cantly more lambdoid craniosynostosis patientshad contralateral parietal eminence bossing (p� 0.01) and ipsilateral mastoid bossing (p �0.001) compared with nonsynostotic occipitalplagiocephaly patients.
Ear position was also evaluated from the ver-tex view. In six of seven cases (84 percent) oflambdoid craniosynostosis patients, the ear onthe ipsilateral side was found to be symmetricalwith the nonaffected side, while in one case (14percent), the ear was found displaced anteri-orly on the affected side. In contrast, whenlooking at the 20 cases of unilateral nonsynos-totic occipital plagiocephaly, 17 children (85
FIG. 8. Computed-tomography scan of a right-sided non-synostotic occipital plagiocephaly demonstrating end-to-endsuture orientation and left-sided normal lambdoid sutureoverlapping morphology.
FIG. 9. Computed-tomography scan of a left-sided lamb-doid craniosynostosis demonstrating ectocranial ridging.
FIG. 7. Computed-tomography scan of a right-sided non-synostotic occipital plagiocephaly. The oval demonstrateslambdoid perisutural thinning.
1864 PLASTIC AND RECONSTRUCTIVE SURGERY, December 2005

percent) presented with an anteriorly dis-placed ear on the affected side (Fig. 12) andthree children (15 percent) had symmetricears. All six cases of bilateral nonsynostoticoccipital plagiocephaly had symmetric ears. Anipsilateral increase in the anterior subarach-noid spacing was also noted in 47 percent ofthe nonsynostotic occipital plagiocephaly cases(Fig. 13) and in none of the lambdoid cranio-synostosis cases.
Metric Data
The mean midline cranial-base deviation an-gle (Fig. 1) for nonsynostotic occipital plagio-
cephaly patients was 4.1 degrees (�/– 2.1;range, 0 to 9 degrees) and 10.3 degrees (�/–5.0; range, 0 to 15 degrees) for lambdoid cra-niosynostosis patients. Patients with lambdoidcraniosynostosis had a significantly greater (t �3.77; p � 0.01) midline cranial-base deviationangle than nonsynostotic occipital plagioceph-aly patients, representing greater cranial-basescoliosis (Table II).
The average petrous ridge angle (Fig. 2) onthe affected side in nonsynostotic occipital pla-giocephaly patients, was 121.5 degrees (�/–3.6; range, 117 to 127 degrees), and the aver-age petrous ridge angle on the contralateralnonaffected side in nonsynostotic occipital pla-giocephaly patients was 126.7 degrees (�/–4.5; range, 120 to 134 degrees). The averagepetrous ridge angle on the affected side inlambdoid craniosynostosis patients was 115.7degrees (�/– 3.6; range, 112 to 120 degrees),and the average petrous ridge angle on thecontralateral nonaffected side in lambdoid cra-niosynostosis patients was 132 degrees (�/–3.8; range 128 to 140 degrees). Lambdoid cra-niosynostosis patients were found to have asignificantly greater petrous ridge angle on theaffected side (t � 3.58; p � 0.01), comparedwith nonsynostotic occipital plagiocephaly pa-tients. Both lambdoid craniosynostosis (t �7.71; p � 0.01) and nonsynostotic occipitalplagiocephaly (t � 3.99; p � 0.01) patients hadsignificantly greater petrous ridge angles onthe affected sides compared with the unaf-fected sides (Table III). The data demonstratethat the affected petrous ridge angles in non-synostotic occipital plagiocephaly are less de-formed than those affected angles of lambdoidcraniosynostosis. For nonsynostotic occipitalplagiocephaly, the differences between the af-
FIG. 10. Three-dimensional, computed-tomography scan ofa left-sided lambdoid craniosynostosis in posterior view. The ovalmarking represents ipsilateral mastoid bossing, the wavy line rep-resents the synostosed lambdoid suture, and the curved line rep-resents contralateral parietal eminence bossing.
TABLE INSOP and LC Suture Characteristics
Suture CharacteristicNSOP Sutures(%) (n � 32)
LC Sutures(%) (n � 7) p
Focal fusion 25 0 NSEndocranial ridging 78 100 NSEctocranial ridging 0 100 �0.001Narrowing 59 0 �0.01Sclerosis 18.8 42.9 NSPerisutural thinning 78.1 100 NSPerisutural thickening 6.3 100 �0.001Overlapping 62.5 0 �0.01End-to-end 100 0 �0.001Obliteration 0 100 �0.001
NSOP, nonsynostotic occipital plagiocephaly; LC, lambdoid craniosynostosis.
Vol. 116, No. 7 / NONSYNOSTOTIC PLAGIOCEPHALY 1865
fected and nonaffected contralateral side pe-trous ridge angles were less than the differ-ences found between the affected andnonaffected contralateral side petrous ridgeangles of lambdoid craniosynostosis.
DISCUSSION
For quite some time, there has been an in-consistent understanding of lambdoid suturepathology, and this has resulted in controversyover incidence, diagnosis, and treatment. His-torically, it has been reported that nonsynos-totic occipital plagiocephaly, by definition, wasa self-limiting process and not a progressiveanatomic deformity.3 It was believed that non-synostotic occipital plagiocephaly would always“self correct” with behavioral modifications,such as repositioning the infant out of the “flatspot.”4,6,7 Accordingly, the mysterious rise inthe incidence of lambdoid craniosynostosisaround the “back-to-sleep” campaign was ex-plained away based on “referral patterns,”6
“added awareness of referring pediatricians,”3
and “improved clinical recognition.”7
An entire body of literature emerged thatattempted to show that lambdoid craniosynos-tosis appeared to be different from that ofother cranial suture synostoses.2–4,6–8 Authorsexplained that the ability to tell whether thissuture was fused was often impossible by clini-cal or radiographic examinations and that find-ings at operation were often variable despitethe degree of deformity.6 Clinically, it was re-ported that the diagnostic indicators of cranio-synostosis were not necessary to diagnose lamb-
FIG. 11. Three-dimensional, computed-tomography scanof a right-sided nonsynostotic occipital plagiocephaly in thevertex view. The Parallelogram cranial morphology demon-strates right-sided ipsilateral occipital flattening and right-sided ipsilateral frontal forehead advancement.
FIG. 12. Vertex view of a right-sided nonsynostotic occip-ital plagiocephaly with parallelogram cranial morphologyand anteriorly displaced ipsilateral ear.
FIG. 13. Computed-tomography scan of a left-sided non-synostotic occipital plagiocephaly demonstrating ipsilateralbenign increase in anterior subarachnoid spacing.
1866 PLASTIC AND RECONSTRUCTIVE SURGERY, December 2005

doid synostosis, and specifically that suturalridging and prominence was not routinelyfound. It was further discussed that, quite of-ten, the pathologic lambdoid suture was openor had less prominent interdigitations.4 There-fore, many clinicians, unable to truly differen-tiate between lambdoid craniosynostosis andnonsynostotic occipital plagiocephaly, came tothe conclusion that it was logical to refer to thecondition of lambdoid craniosynostosis as“functional lambdoid synostosis,” rather than“typical synostosis,” and to make the decisionof surgical intervention based on the degree ofasymmetry and its progression.3,6 These pa-tients with “functional lambdoid synostosis,” or“sticky sutures,”9 had plain skull films oftendemonstrating perisutural sclerosis (increasedbone density), believed to represent impend-ing synostosis, as well as sutural indistinctness.9Computed-tomography scans often demon-strated abnormalities of the lambdoid sutures,consistent with sclerosis, indistinctness, andeven “spot welding”2 or focal fusions. A notedchange in suture orientation, from the normaloverlapping pattern to end-to-end morphol-ogy, as well as perisutural thickening or thin-ning, was reported.3 However, in many cases,such findings were absent, and the degree ofabnormal radiographic findings were neverable to be correlated to the degree of clinicaldeformity, or even obvious sutural changes atthe time of surgical intervention. Histologicand gross evaluations of the affected lambdoidsutures, believed to be synostosed, often dem-onstrated inconsistent thickening andsclerosis,3 as well as incomplete interdigitations
and endocranial ridging.6 Microscopic exami-nation often revealed patent sutures with noovert fusion. Occasionally, narrowing of thesuture with active bone growth, spot welding,or areas of bony bridging and micro-spiculeformation across the suture with associated fi-brosis, and fibrous union was believed toclearly establish the diagnosis of synostosis, atleast on a local level.2,3,14 It has been said thatthe radiographic diagnosis of the affectedlambdoid suture is more difficult and less clearcompared with other synostotic sutures.4 Con-clusions were reached that computed tomog-raphy evidence of complete bone fusion wasnot necessary to diagnose lambdoid synostosis,and that fibrous union can cause the clinicalsequelae of craniosynostosis.8
In multiple historic publications, variousphysical exam descriptions,2,3,7 photographs,7cartoons,6 and computed-tomography scans,3all used to previously describe the “functional”synostosis of lambdoid craniosynostosis, arenow understood to be nonsynostotic occipitalplagiocephaly. This is largely because of theclinical work of Huang et al.10 In their land-mark article, they firmly established the clinicaldiagnosis of nonsynostotic occipital plagio-cephaly and lambdoid craniosynostosis. Theirconclusions confirmed that lambdoid cranio-synostosis was a specific rare entity whose clin-ical features, including imaging, operative, andhistologic characteristics, were consistent withthose of other craniosynostoses.10
Based on Huang’s clinically accepted diag-nostic criteria, our study focused on the radio-graphic diagnosis of the lambdoid sutures ofchildren clinically diagnosed with nonsynos-totic occipital plagiocephaly. Our findings in-dicate that the lambdoid sutures demonstrateareas of focal fusion, endocranial ridging, nar-rowing, sclerosis, and changes from the normaloverlapping morphology to an end-to-end ori-entation. In addition, our data confirmed thecranial morphology as described for nonsynos-
TABLE IIMidline Cranial-Base Deviation Angle in Degrees
Mean SD Range t p
NSOP 4.1 �/–2.1 0–9 3.77 �0.01LC 10.3 �/–5.0 0–15
NSOP, nonsynostotic occipital plagiocephaly; LC, lambdoid craniosynos-tosis.
TABLE IIIPetrous Ridge Angle in Degrees
Mean SD Range t p
NSOP: ipsilateral affected side 121.5 �/–3.6 117–127 3.99 �0.01NSOP: contralateral nonaffected side 126.7 �/–4.5 120–134LC: ipsilateral affected side 115.7 �/–3.6 112–120 7.71 �0.01LC: contralateral nonaffected side 132 �/–3.8 128–140
NSOP, nonsynostotic occipital plagiocephaly; LC, lambdoid craniosynostosis.When comparing NSOP and LC ipsilateral affected sides: t � 3.58; p � 0.01.
Vol. 116, No. 7 / NONSYNOSTOTIC PLAGIOCEPHALY 1867

totic occipital plagiocephaly and lambdoid cra-niosynostosis by Huang et al. These radio-graphic findings of nonsynostotic occipitalplagiocephaly are consistent with those previ-ous reports of the “functional” fusion of lamb-doid craniosynostosis. The endocranial-baseangle findings are consistent with those of Loet al.12 The midline cranial-base deviation an-gle was significantly more deviated in lambdoidcraniosynostosis than in nonsynostotic occipi-tal plagiocephaly, and this represents a greatercranial-base scoliosis in lambdoid craniosynos-tosis. In addition, when comparing the petrousridge angles in nonsynostotic occipital plagio-cephaly and lambdoid craniosynostosis, analy-sis of the data demonstrate significantly lesscranial-base deviation in nonsynostotic occipi-tal plagiocephaly.
It is now clear that the sutures of nonsynos-totic occipital plagiocephaly are not entirelynormal and in this article the radiographiccriteria for their diagnosis has been delineated.In 1984, in an article discussing the normaldevelopment of the lambdoid suture as well asits pathologic “synostosis,” the authors re-ported that histologically “synostosed” lamb-doid sutures (which we know today by theirdescriptions to likely represent specimens ofnonsynostotic occipital plagiocephaly) weresimilar in appearance to that of the 60-year-oldcontrol specimens, with accentuated but nor-mal histology for the subject’s age. They pos-tulated that factors such as increased tension,ischemia, or anoxia may play a role in theincreased proliferative activity.15,16 This pro-posed etiology may very well account for thefindings in the sutures of nonsynostotic occip-ital plagiocephaly where a persistent sleep po-sition might result in greater tension and de-formational forces.5 It is interesting to notethat experimental immobilization of normalrabbit sutures using cyanoacrylate also showedvery similar morphologic and histologic find-ings to those found in infants with “sticky”sutures,16 thus supporting a functional etiologyof nonsynostotic occipital plagiocephaly.
Along with many today,10,12 we believe thatnonsynostotic occipital plagiocephaly andlambdoid craniosynostosis are separate enti-ties, and do not lie along a continuum of thesame diagnosis as historically postulated.4,6,7
Given these advances in both the clinical andradiographic differentiation between nonsyn-ostotic occipital plagiocephaly and lambdoidcraniosynostosis, it is our suggestion that, for
clinical purposes, sutures be described accord-ingly: “open” as found in normal infants,“closed” as found in normal adults, “fused” or“obliterated” in true craniosynostosis, and “de-formed” as in nonsynostotic occipital plagio-cephaly. The vast majority of “deformed” su-tures, found in patients with nonsynostoticoccipital plagiocephaly, can be effectivelytreated with repositioning the infant and “un-loading” the affected suture, thereby allowingnormal head growth to correct the deformity.In cases of nonsynostotic occipital plagioceph-aly where repositioning has failed, cranial-molding-helmet therapy has been extremelysuccessful in correcting the deformity. Infre-quently, because of the severity of the defor-mity and/or late presentation for therapy, cra-nial-molding-helmet-therapy may notadequately treat this craniofacial deformity,and the surgical option of cranial-vault remod-eling can be explored.
An admitted weakness of this study rests inthe fact that the craniofacial surgeon and neu-roradiologist were not blinded to the clinicaldiagnosis previously made by morphogenic cri-teria as they reviewed the computed tomogra-phy scans. The retrospective nature of thestudy allows for observer bias as scans with aclinical diagnosis were evaluated. The readershould also be cautioned that although meandifferences in proportions were found betweenthe nonsynostotic occipital plagiocephaly andlambdoid craniosynostosis groups, no logisticregression or discriminant function analyseswere done on these data because of the smallsample size, particularly in the lambdoid cra-niosynostosis group. These analyses may sug-gest which variables are the best predictors ofnonsynostotic occipital plagiocephaly or lamb-doid craniosynostosis and are the focus of on-going study.
CONCLUSIONS
These data support criteria for the radio-graphic diagnosis of nonsynostotic occipitalplagiocephaly to include findings consistentwith: (1) sutural sclerosis and narrowing; (2)endocranial ridging; (3) focal fusions; (4)change in normal overlapping suture morphol-ogy to end-to-end orientation; (5) perisuturalthickening and thinning; and (6) increases inipsilateral frontal subarachnoid spacing.
1868 PLASTIC AND RECONSTRUCTIVE SURGERY, December 2005

Joseph E. Losee, M.D.Division Pediatric Plastic SurgeryChildren’s Hospital of Pittsburgh3705 Fifth AvenuePittsburgh, Pa. [email protected]
ACKNOWLEDGMENTS
This study was reviewed and approved by InstitutionalReview Boards at Children’s Hospital at Strong and Chil-dren’s Hospital of Philadelphia.
REFERENCES
1. Shillito, J., and Matson, D. D. Craniosynostosis: Reviewof 519 surgical patients. Pediatrics 41: 829, 1968.
2. Goodrich, J. T., and Argamaso, R. Lambdoid stenosis(posterior plagiocephaly) and craniofacial asymmetry:Long-term outcomes. Childs Nerv. Syst. 12: 720, 1996.
3. VanderKolk, C. A., and Carson, B S. Lambdoid synos-tosis. Clin. Plast. Surg. 21: 575, 1994.
4. Jimenez, D. F., Barone, C. M., Argamaso, R. V., Goodrich,J. T., and Shprintzen, R. J. Asterion region synos-tosis. Cleft Palate Craniofac. J. 31: 136, 1994.
5. Cohen, M. M., Jr. Radiographic evaluation of Cranio-synostosis. In M. M. Cohen, Jr., and R. E. MacLean(Eds.) Craniosynostosis: Diagnosis, Evaluation, and Man-agement. New York: Oxford Press, 2000. Pp. 147–157.
6. McComb, J. G. Treatment of functional lambdoid syn-ostosis. Neurosurg. Clin. North Am. 2: 665, 1991.
7. Muakkassa, K. F., Hoffman, H. J., Hinton, D., Hendrick,B., Humphreys, R. P., and Ash, J. Lambdoid synos-tosis. Part 2: Review of cases managed at the Hospitalfor Sick Children, 1972–1982. J. Neurosurg. 61:3401984.
8. Furuya, Y., Edwards, M. S., Alpers, C. E., Tress, B. M.,Norman, D., and Oursterhout, D. K. Computerizedtomography of cranial sutures. Part 2: Abnormalitiesof sutures and skull deformity in craniosynostosis. J.Neurosurg. 61: 59, 1984.
9. Rollins, N., and Sklar, F. Factitious lambdoid perisu-tural sclerosis: Does the “sticky suture” exist? Pediatr.Radiol. 26: 356, 1996.
10. Huang, M. H., Gruss, J. S., Clarren, S. K., et al. Thedifferential diagnosis of posterior plagiocephaly: Truelambdoid synostosis versus positional molding. Plast.Reconstr. Surg. 98: 765, 1996.
11. Kirschner, R. E., Hunter, J. V., Bartlett, S. P., and Whi-taker, L. A. Synostotic and nonsynostotic posteriorplagiocephaly: Distinct entities or a pathophysiologiccontinuum? In Proceedings of the Congress of the Interna-tional Society of Craniofacial Surgery, Santa Fe, N.M.,September 15–17, 1997.
12. Lo, L. J., Marsh, J. L., Pilgram, T. K., and Vannier, M. W.Plagiocephaly: Differential diagnosis based on endocra-nial morphology. Plast. Reconstr. Surg. 97: 282, 1996.
13. Der, G., and Everitt, B. S. Handbook of statistical analysesusing SAS. 2nd Ed. Boca Raton, Fla.: CRC Press. Pp.1–376.
14. Furuya, Y., Edwards, M. S., Alpers, C. E., et al. Com-puterized tomography of cranial sutures. Part 1: Com-parison of suture anatomy in children and adults. J.Neurosurg. 61: 53, 1984
15. Hinton, D. R., Becker, L. E., Muakkassa, K. F., and Hoff-man, H. J. Lambdoid synostosis. Part 1. The lamb-doid suture: Normal development and pathology of“synostosis.” J. Neurosurg. 61: 33, 1984.
16. Kokich, V. G. The biology of sutures. In M. M. Co-hen, Jr. (Ed.),Craniosynostosis: Diagnosis, Evaluation,and Management. New York: Raven Press, 1986. Pp.81–103.
Vol. 116, No. 7 / NONSYNOSTOTIC PLAGIOCEPHALY 1869




















