
Dermatoglyphic and radiographic findings in a mother and daughter with pseudohypoparathyroidism
10
Clinical Genetics 1978: 13: 359-368 Dermatoglyphic and radiographic findings in a mother and daughter with pseudohypoparathyroidism BEVERLY J. WHITE AND STEPHEN J. MARX Section on Cytogenetics, Laboratory of Experimental Pathology and Metabolic Diseases Branch, National Institute of Arthritis, Metabolism, and Digestive Diseases, National Institutes of Health, Bethesda, Maryland, U.S.A. The dermatoglyphic features of a mother and daughter with pseudohypoparathyroidism were compared with those of 19 other reported PHP cases and with findings typical of 45,X Turner syndrome. Our observations included large patterns with a predominance of whorls, unusual accidental patterns on the third fingers, elevated total and absolute finger ridge counts, extralimital digital triradii, intermediately placed axial triradii, and a single complete transverse palmar crease. With barium-coated hand radiographs, the positions of the palmar digital triradii were compared with those of the underlying metacarpal and carpal bones. Normally, the fourth digital triradii (c) are superficial to the epiphyseal region of the proximal phalanx, near the fourth M-P joint. In our cases, the c triradii were distal to the M-P joint, adjacent to the diaphysis of the proximal phalanx. These findings, related to post-natal differences in growth potential of osseous structures and overlying dermal ridge tissues in this disease, may also be relevant to other syndromes with abnormal development of the hand. The need for further delineation of PHP der- matoglyphics and comparison of findings with data from Turner syndrome and normals is stressed. Received 27 Septeniber, accepted 4 October 1977 Pseudohypoparathyroidism (PHP) and pseudo-pseudohypoparathyroidism (PPHP) are variations of a recognized syndrome of short stature, obesity, mild mental retarda- tion, round facies, brachydactyly, short metacarpals and metatarsals, and soft tissue calcifications. In PHP, hypocalcemia and hyperphosphatemia unresponsive to para- thyroid hormone are present (Aurbach 1971). The disease, found in both sexes and also called Albright’s hereditary osteodys- trophy, is thought to be due to an X-linked dominant or sex-influenced autosomal dom- inant mutation (McKusick 1975). Several features of PHP resemble those of 45,X Turner syndrome, including short stature and shortened fourth and fifth metacarpals. The full spectrum of PHP skeletal changes was described and compared with those of monosomy X by Steinbach & Young (1966). While the similarities in stature and skel- etal defects have been well documented, only one comparative study of dermato- glyphics in PHP and Turner syndrome has been reported (Forbes 1964). That author found that her 19 PHP cases had an in- creased frequency of digital arches and radial loops on index fingers, mean main- line indices suggesting less transverse than normal alignment of palmar ridges, increas-
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Dermatoglyphic and radiographic findings in a mother and daughter with pseudohypoparathyroidism
Clinical Genetics 1978: 13: 359-368
Dermatog lyphic and radiographic findings in a mother and daughter with pseudohypoparathyroidism
BEVERLY J. WHITE AND STEPHEN J. MARX
Section on Cytogenetics, Laboratory of Experimental Pathology and Metabolic Diseases Branch, National Institute of Arthritis, Metabolism, and
Digestive Diseases, National Institutes of Health, Bethesda, Maryland, U.S.A.
The dermatoglyphic features of a mother and daughter with pseudohypoparathyroidism were compared with those of 19 other reported PHP cases and with findings typical of 45,X Turner syndrome. Our observations included large patterns with a predominance of whorls, unusual accidental patterns on the third fingers, elevated total and absolute finger ridge counts, extralimital digital triradii, intermediately placed axial triradii, and a single complete transverse palmar crease. With barium-coated hand radiographs, the positions of the palmar digital triradii were compared with those of the underlying metacarpal and carpal bones. Normally, the fourth digital triradii (c) are superficial to the epiphyseal region of the proximal phalanx, near the fourth M-P joint. In our cases, the c triradii were distal to the M-P joint, adjacent to the diaphysis of the proximal phalanx. These findings, related to post-natal differences in growth potential of osseous structures and overlying dermal ridge tissues in this disease, may also be relevant to other syndromes with abnormal development of the hand. The need for further delineation of PHP der- matoglyphics and comparison of findings with data from Turner syndrome and normals is stressed.
Received 27 Septeniber, accepted 4 October 1977
Pseudohypoparathyroidism (PHP) and pseudo-pseudohypoparathyroidism (PPHP) are variations of a recognized syndrome of short stature, obesity, mild mental retarda- tion, round facies, brachydactyly, short metacarpals and metatarsals, and soft tissue calcifications. In PHP, hypocalcemia and hyperphosphatemia unresponsive to para- thyroid hormone are present (Aurbach 1971). The disease, found in both sexes and also called Albright’s hereditary osteodys- trophy, is thought to be due t o a n X-linked dominant or sex-influenced autosomal dom- inant mutation (McKusick 1975). Several features of PHP resemble those of 45,X
Turner syndrome, including short stature and shortened fourth and fifth metacarpals. T h e full spectrum of PHP skeletal changes was described and compared with those of monosomy X by Steinbach & Young (1966).
While the similarities in stature and skel- etal defects have been well documented, only one comparative study of dermato- glyphics in PHP and Turner syndrome has been reported (Forbes 1964). That author found that her 19 PHP cases had a n in- creased frequency of digital arches and radial loops on index fingers, mean main- line indices suggesting less transverse than normal alignment of palmar ridges, increas-

360 W H I T E A N D M A R X
ed frequency of hypothenar patterns, and increased atd angles (mean 55"). Some of these characteristics were similar to those of her Turner syndrome cases. Measure- ments known to be increased in Turner syndrome such as a-b and total finger ridge counts (TFRC) were not reported, although TFRC was estimated to be increased in the PHP cases. There was also no additional in- formation in the literature about the meta- carpal shortening, characteristic of PHP and Turner syndrome, in relation to its effect on position of overlying dermal ridge landmarks. Therefore, it was felt that cor- relation of dermatoglyphic and radiographic analyses from additional PHP cases, and comparison of our findings with those in Turner syndrome, might better establish the clinical or diagnostic value of such analyses in PHP.
Case Reports
Both the mother (P.S.) and her affected daughter (J.S.) were previously documented as having clinical, X-ray, and laboratory findings typical of PHP, as described in a report of their endocrine status at ages 31 and 11 years, respectively (Marx et al. 1971). Pertinent findings in the mother were short stature, obesity, round facies, short- ened digits, IQ of 80, and variable calcium levels (7.8 to 9.6 mg/100 ml, N = 8.8 to 10.6). Her X-rays showed obvious shorten- ing of the fourth and fifth metacarpals bila- terally, and short right third through fifth metatarsals and left fourth metatarsal. The daughter's physical and laboratory findings were similar except for consistently normal calcium levels. Her skeletal survey revealed bilaterally shortened fourth metacarpals, bowing of both fifth metacarpals, and a short left fourth metatarsal. In both pa- tients, analysis of urinary 3'5' cyclic adeno- sine monophosphate excretion rate showed a blunted response to parathyroid hormone.
Materials and Methods
Dermatoglyphic analysis: Prints of fingers, palms, and soles were obtained with the Faurot inkless method (Walker 1957). Po- sition of the palmar axial triradii was deter- mined from atd angle measurements and percentage of palmar length (distance be- tween the most distal wrist crease and prox- imal crease of the fourth digit (Schaumann & Alter 1976)).
Radiographic analysis: Position of the pal- mar digital triradii relative to osseous struc- tures was evaluated using barium-coated hand radiographs. This type of analysis was first described in detail for normals by Val- sik in 1933. In our variation of the tech- nique, the palm is smeared with a thin film of barium as prepared for G-I studies. Excess barium is wiped off to outline der- mal ridges with a small amount of radio- opaque material. The hand is placed on an unexposed, developed X-ray film, the soft tissues outlined with a marking pen and simultaneously, an X-ray to visualize both soft tissues and bones is taken. The film with the dried barium palm print is saved for comparison with the simultaneous hand X-ray and the palmar inkless method prints. An X-ray positive is made to enhance ap- pearance of the ridges, so that both bones and ridges appear dark against a clear back- ground. In some areas where the X-ray was not definitive, the dried barium or inkless print was superimposed on the hand X-ray and the missing point located by extrapola- tion. A similar method has been used to study Turner syndrome dermatoglyphics (Dallapiccola et al. 1972). In the original technique (Valsik 1933), lead pellets were glued to the palmar triradii and a standard X-ray was taken.
Chromosome analysis: Standard cytogenetic studies were previously reported as normal
D E R M A T O G L Y P H I C S I N P H P 361
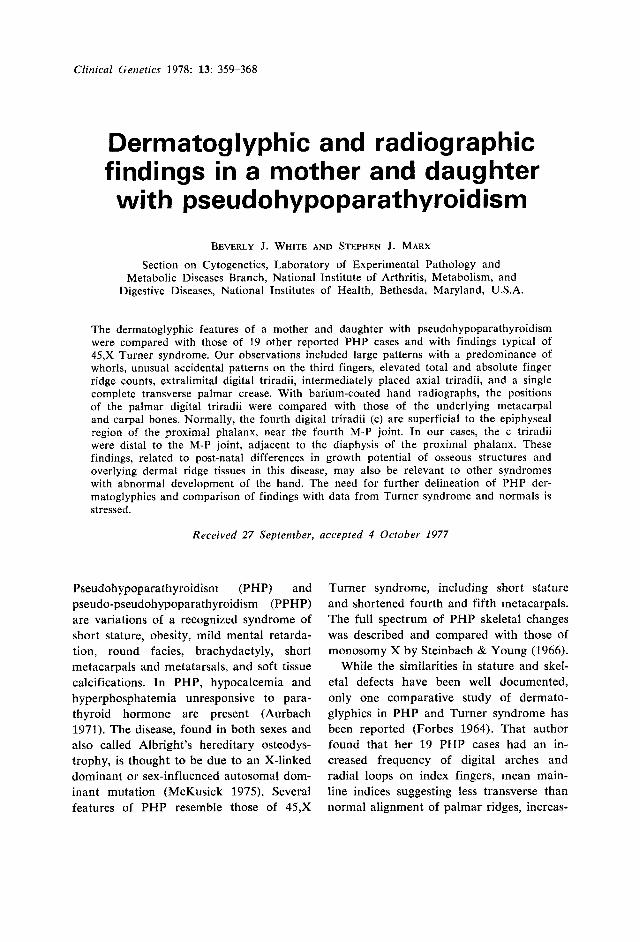
Table 1
Finger pattern types and quantitative measurements
Mother Daughter
Left hand 5 Wd' 19/-.,18' L" -27 4 W 21/&?2 W 28/25 3 Acc(W/Ld) -2512315 Acc(Wd11L") 1 911 913 2 W -27123 WdI 19113 1 W"' 20130 W 19/22 a-b count 42 37 atd angle axial triradius absent 49O, 54" (t't')t Qh palmar length axial triradius absent 16.1 %, 37.8 O I o (t't') main-line index 10 9 hallucal loop count 24 20
Right hand 1 2 3 4 5 a-b count atd angle % palmar length main-line index hallucal loop count
AFRC TFRC Summed a-b count Summed atd angles
Wd' 26137 LU 33 Acc(W/Ld) -2112216 W -221-25 W 11/17
40 48" (t')
18.3 @lo (t') 10 30
453 257
82 -
20121 s W 1 3 -1 8137
29/32 18
39 46" (t')
17.1 O/o (t') 6
10
404 245 76
1oo"t
* Approximate counts (-), due to extralimital triradii. t Includes wider atd angle of triradius near ulnar margin left palm (t").
in our patients; these were repeated using two banding techniques. For Giemsa-band- ing, the trypsin technique (Seabright 1971) was used and for quinacrine, the method of Caspersson (1970). Fifty peripheral blood metaphases were analyzed in the mother and 100 in the daughter. All studies de- scribed here were done during readmission to the National Institutes of Health, when the patients were 34 and 13 years old, re- spectively.
Results
Both mother and daughter had short, broad palms and short fingers and toes. Their fourth and fifth fingers were dispropor- tionately shortened, a finding more pro-
nounced in the mother. There was no clino- dactyly, and both patients had normal fin- ger creases. The mother had a right com- plete transverse palmar crease (so-called simian line).
The results of the fingerprint analysis and other dermatoglyphic measurements are indicated in Table 1. Both patients had pre- dominantly large whorl patterns. The mother had 21 digital triradii, including 7 which were extralimital, or extended beyond the ridged surface of the finger. Four of the daughter's 19 digital triradii were extra- limital. There were complex or accidental patterns on both the mother's third digits and on the daughter's left third finger. This is an infrequent pattern type, comprising 0.13 % of all prints in one large series
362 WHITE A N D M A R X
i / P.
1. s.
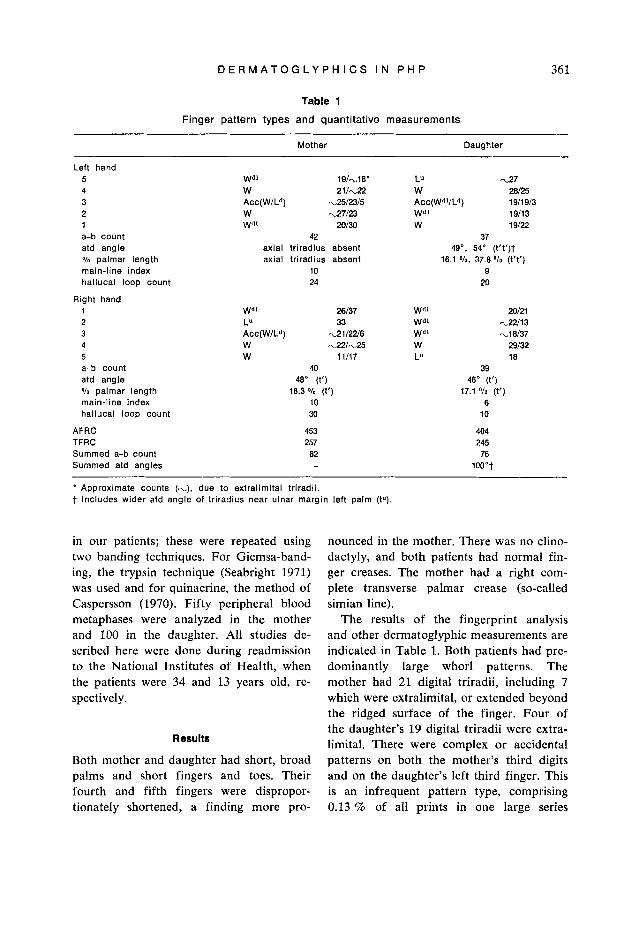
Fig. 1. Pattern types and position of palrnar and plantar triradii and major flexion creases of mother (P.S.) and daughter (J.S.).
(Cummins & Midlo 1961). The total finger ridge counts (TFRC) of both patients were increased well above the mean value for the
North American population of phenotypic- ally normal females (120.4 * 52.3 (Schau- mann & Alter 1976)). The absolute finger ridge counts (AFRC) of both were also in- creased, indicating high pattern intensity as well as increased pattern size. However, their summed a-b ridge counts were not elevated in relation to normal female values (N = 81.4 t 10.6). The main-line indices of the mother’s palms (both = 10) indicated predominantly transverse orientation of pal- mar ridges. The daughter’s right palmar ridge orientation was more vertical (right index = 6, left = 9). Neither patient had thenar termination of the A main-lines, a characteristic frequent in Turner syndrome. Both had left hypothenar loops radial (Lr); the triradius of the mother’s loop was extra- limital. Hypothenar “S” patterns, reported to be more frequent in monosomy X, were not present. Bilateral hallucal loops distal (Ld) were present in both patients. The mother’s were large, with higher ridge counts (right = 30, left = 24) than the daughter’s (right = 10, left = 20).
Figure 1 illustrates the palmar and plantar patterns of both patients and indicates
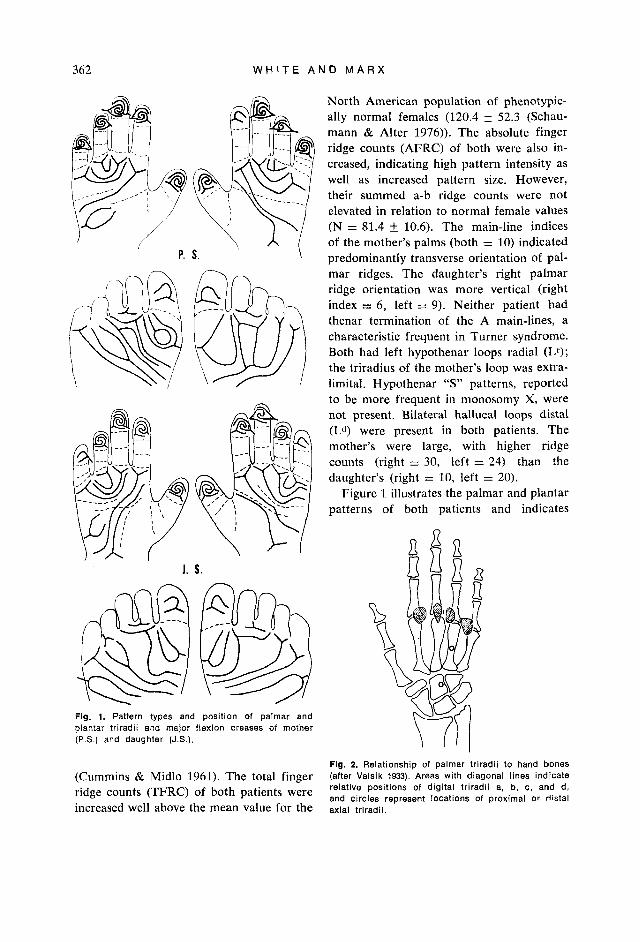
Fig. 2. Relationship of palrnar triradii to hand bones (after Valsik 1933). Areas with diagonal lines indicate relative positions of digital triradii a, b, c, and d, and circles represent locations of proximal or distal axial triradii.

D E R M A T O G L Y P H I C S I N P H P 363
positions of triradii, main-lines, and major flexion creases. The mother’s left axial tri- radius was not well-defined; her right axial triradius was intermediately placed (t’) ac- cording to atd angle measurement; accord- ing to percentage of palmar length, it was also intermediate (18.3 %, over 149” = t’). The daughter’s axial triradii were also intermediate according to both methods of measurement.
Figure 2 illustrates the regions where the palmar digital and axial triradii are nor- mally located in relation to the bony struc- tures (Valsik 1933). The four digital triradii are superficial to the epiphyseal region at the proximal end of the proximal phalanges, near the metacarpal-phalangeal (M-P) joints; proximal axial triradii are adjacent to the capitate bone. When distally displaced, axial triradii are distributed along the fourth metacarpal axis. Figure 3a and b shows barium-coated hand radiograph positives of the mother indicating locations of her dig- ital and axial triradii. Barium determina- tions made for both patients were trans- ferred to standard hand X-rays (Fig. 3c-f). Location of the mother’s left axial triradius was omitted, since it was either atrophic or not clearly developed. The fourth digital triradii (c) of both patients were medial and superficial to the diaphyses, rather than the epiphyseal regions of the proximal fourth phalanges. It was also apparent that the c triradii were more distal to the fourth M-P joint in the mother than in the daughter. The relationships of the remaining digital triradii (a, b, and d) did not appear unusual, even though the mother’s fifth metacarpals were also shortened. Their three centrally placed axial triradii, all intermediate (t’) ac- cording to atd angle and palmar length measurements, were not distal in relation to the carpal bones. All were superficial to
the capitate, a location typical of proximally placed axial triradii.
Quinacrine- and Giernsa-banded chromo- some analyses of both patients were normal 46,XX with no evidence of X chromosomal deletion or 45,X mosaicism.
Discussion
Some of the findings of Forbes (1964) and of our own cases suggest that there may be some overlap in the dermatoglyphics of PHP and Turner syndrome. However, the lack of quantitative measurements, such as TFRC and summed a-b ridge counts, in the 19 other reported PHP cases makes exact comparison difficult. Since various radiographic and dermatoglyphic features of Turner syndrome have been well de- scribed and together are diagnostically useful (Dallapiccola et al. 1972), a com- parison between dermatoglyphics of our cases and general characteristics considered typical of Turner syndrome (Schaumann & Alter 1976) is of interest. The following are associated with Turner syndrome according to the latter authors’ review: 1) no altera- tion in frequency of pattern types; 2) in- creased mean TFRC (154.4) or increased pattern size; 3) increased mean summed a-b ridge count (89.5); 4) increased frequency of patterns, often large, in the third and fourth palmar interdigital areas; 5 ) a frequently large hypothenar pattern in 51.1 % of palms; 6) distally displaced axial triradii in 55.9 % of palms (mean summed atd angle 100.5”); 7) frequent (27.7 70 of palms) full or transitional single transverse palmar crease; 8) missing c palmar digital triradius; 9) main-line A terminating in the thenar area; 10) large hallucal whorl or loop distal; and 11) decreased frequency of plantar p triradii.
Fig. 3. Barium-coated radiograph positives of (a) left and (b) right hand of mother; pen marks indicate tri- radii. Position of triradii superimposed on standard X-rays of mother (c, d) and daughter (e, f).

364 W H I T E A N D M A R X

D E R M A T O G L Y P H I C S I N P H P 365
Our cases of PHP have some findings which are more frequent in Turner syn- drome than normals: 1) increased TFRC, 2) patterns in third or fourth interdigital areas (see Fig. l ) , 3) hypothenar patterns, 4) increased mean summed atd angle (daughter), 5) single transverse palmar crease (mother), 6) large hallucal loops (mother), and 7) absent p triradius (daughter). In our cases it was not possible to assess the significance of the excess of digital whorls by doing a family study, since the mother was adopted and had only a single affected daughter. The father of her child was not available for study.
Both Forbes (1964) and Preus (1976) noted that whorls are very infrequent on the thumbs of Turner syndrome cases. Since such patterns were present bilaterally on the thumbs of both of our cases and on 29 % of all first digits of the 19 PHP cases of Forbes, a difference between PHP and Turner syndrome with respect to this char- acteristic is suggested. The observation of Forbes that digital arches were increased in PHP in comparison to both Turner syn- drome and normals also suggests another difference in pattern type between PHP and Turner syndrome. However, the latter author also estimated that total finger ridge counts in PHP were increased, a finding usually associated with large loops or whorls rather than increased arches. Analysis of more PHP families is necessary in order to determine if certain pattern types are more frequent in this disease, particularly arches or the unusual accidental patterns found on the third fingers of both of our cases.
Preus (1976) has developed a quantita- tive index utilizing eight dermatoglyphic features (digital pattern types, number of digits with a high ridge count, thenar exit of A-line, a-b ridge count, presence and type of hypothenar pattern, simian line, type of hallucal pattern and ridge count, absent p triradius), as well as five pheno-
typic traits, in order to discriminate between individuals with Turner syndrome and the normal female population. Individuals with a high positive score possess more of the traits selected as most frequently associated with Turner syndrome; those with fewer of the traits have near-zero or negative scores. Certain findings considered most frequent in the syndrome are weighted more heavily in the numerical scoring system. Examples are whorls on digit one (if present, a relatively large minus score) and five or more digits with a high ridge count (if present, a relatively large plus score). Characteristics of palmar axial tri- radii were not included in the index. A final diagnostic score cannot be determined for our two cases, since measurements neces- sary to score the five phenotypic traits are not available. However, total negative scores for both mother (-0.10) and daughter (- 1.21) are obtained when the derrnato- glyphic portion of the index alone is used. The results of the comparison, although in- complete, suggest that use of the Preus scoring system might allow discrimination between PHP and Turner syndrome der- matoglyphics; the mother’s score falls with- in, and her daughter’s score just below, the area of overlap in distribution of the Preus normal and Turner syndrome log index scores. It therefore appears worthwhile to apply this index to larger numbers of PHP cases and relatives to determine further if PHP dermatoglyphics can be definitively separated from those of the normal or Turner syndrome populations on the basis of mean scores. Although devised to aid in the diagnosis of Turner syndrome, the index is of interest in PHP, since both our study and that of Forbes indicate overlap of cer- tain dermatoglyphic traits in both syn- dromes.
The presence of two disorders in patients with suspected PHP and dermatoglyphic traits frequent in Turner syndrome should

366 W H I T E A N D M A R X
be considered in certain instances, since 45,X gonadal dysgenesis with PHP has been reported (Miller et al. 1965). While our cases were karyotypically normal and lacked evidence of gonadal dysgenesis, patients with PHP and evidence of gonadal dys- function should have chromosomal anal- ysis, and these findings should be correlated with dermatoglyphics to evaluate further the resemblance of this possibly X-linked, domi- nant disease to monosomy X. The existence of a common biochemical defect has been suggested by Zisman et al. (1970), who found that some cases of Turner syndrome were similar to PHP cases in their resist- ance to the effects of parathyroid extract upon the kidneys. These same investigators also noted that their patients with both syndromes had decreased olfactory acuity, not corrected by hormonal (Turner) or calcium and vitamin D (PHP) therapy. Thyroid dysfunction is also noted in some patients with both disorders (Zisman et al. 1969, McHardy-Young et al. 1970, Marx et al. 1971). The possibility that the der- matoglyphics in both syndromes may be influenced by similar or common biochem- ical defects or genetic mechanisms must also be considered.
We have detected radiographically in PHP, an alteration of the normal develop- mental relationship of the c triradius and fourth M-P joint. This observation is con- sistent with the normal sequence of devel- opment of bones and epidermal ridges: Studies of human fetuses indicate that the ridges are formed from the third to the sixth months of gestation (Schaumann & Alter 1976), and dermatoglyphic analysis of individuals with congenital hand and foot defects suggests that growth distur- bance during the period of ridge formation causes corresponding dermal ridge distor- tion (Cummins & Midlo 1961). Factors thought to influence ridge alignment, pat- tern type, and location of landmarks such
as triradii include stress on the skin induced by differential growth in various regions of the palm or sole, amount of tissue fluid, presence of neurovascular complexes, and contour of volar pads. In the case of tri- radii, final location may represent intersec- tion of lines of force generated by differ- ential growth of adjacent structures, includ- ing developing tendons, muscles, vessels, nerves, and bones.
In human embryos, cartilaginous precur- sors of the carpal, metacarpal, and proximal phalangeal bones are present by 8 weeks of gestation; by 9 weeks, ossification centers have appeared at the mid-diaphyses of the metacarpals (Patten 1968). At 10 weeks, ossification of the metacarpal diaphyses is nearly complete. The adjacent epiphyses of the metacarpals and proximal phalanges are usually represented by cartilaginous growth centers a t birth (Crelin 1969), which ossify post-natally. Therefore, the cartilaginous precursors of the bones of the hand are all established prior to completion of palmar ridge formation. Their presence may in- fluence ridge orientation, since they con- tinue to enlarge and some begin to ossify during the period of ridge development. Our finding in PHP that the palmar c triradii have their usual superficial relationship to the other palmar dermatoglyphic landmarks (see Fig. 1) but are not in close proximity to the fourth M-P joint (see Fig. 3), suggests that during fetal development all of the metacarpal primordia were normal in size and location, playing a role in inducing for- mation of adjacent triradii. According to this interpretation, no abnormalities would be detectable at the end of the period of fetal ridge differentiation. The proximity of the triradius to the fourth M-P joint would be altered post-natally, as the fourth meta- carpals fail to elongate and the soft tissue structures continue to grow more normally. This explanation is consistent with clinical and X-ray observations of the syndrome,

D E R M A T O G L Y P H I C S I N P H P 367
which indicate that the typical skeletal changes may not become detectable until after early infancy (Steinbach 6r Young 1966, Monn et al. 1976).
The barium-coated hand radiograph alone ;nay not provide a practical means of earlier diagnosis in suspected cases of PHP. Rather, it has provided evidence about the time of appearance of an abnormal relation- ship between specific osseous and dermal structures. Such a technique may also be of value in other syndromes with hand defects, in order to study the sequence of develop- ment of abnormal bony structures and their associated dermal ridge landmarks. While some of the dermatoglyphic characteristics observed in this study and that of Forbes (1964) suggest that PHP patients may have a higher frequency of traits considered to be of diagnostic value in Turner syndrome than does the normal female population, the actual value of including dermatogly- phic studies in the initial evaluation of sus- pected PHP cases is not yet established. It is hoped that the results of this case study will stimulate interest in systematic der- matoglyphic analysis of PHP cases and families, particularly those quantitative traits (Preus 1976, Schaumann & Alter 1976) considered t o be of greatest diag- nostic value in Turner syndrome.
Acknowledgments
The authors wish t o acknowledge the ef- forts and interest of the N.I.H. diagnostic radiology department in preparing the barium radiographs.
References
Aurbach, G. D. (1971). Genetic disorders in- volving parathyroid hormone and calcitonin. Birth Defects: Original Article Series, Vol.
Caspersson, T., L. Zech, C. Johansson & E. J. Modest (1970). Identification of human chromosomes by DNA-binding fluorescing agents. Chromosoma 30, 215-227.
VII , NO. 6, 48-54.
Crelin, E. S. (1969). Anatomy of the Newborn. Philadelphia, Lea and Febiger.
Cummins, H. & C. Midlo (1961). Finger Prints, Palms and Soles. A n Introduction to Der- matoglyphics. New York, Dover Publica- tions, Inc.
Dallapiccola, B., B. Bagni & G. Pistocchi (1972). Dermatoglyphic and skeletal hand abnormalities in Turner’s syndrome. A ten- tative scoring method. Acta Genet. med. Genzell. 21, 69-78.
Forbes, A. P. (1964). Fingerprints and palm prints (dermatoglyphics) and palmar-flexion creases in gonadal dysgenesis, pseudohypo- parathyroidism and Klinefelter’s syndrome. New Engl. J . Med . 270, 1268-1277.
Holt, S. B. & L. S. Penrose (1968). The Gen- etics of Derninl Ridges. Springfield, C. C. Thomas.
Marx, S. J., J. M. Hershman & G. D. Aurbach (1971). Thyroid dysfunction in pseudohypo- parathyroidism. J . clin. Endocr. Metab. 33,
McHardy-Young, S., D. Doniach & P. E. Po- lani (1970). Thyroid function in Turner’s syndrome and allied conditions. Lancet ii,
McKusick, V. (1975). Mendelian Inheritance in Man. Baltimore, Johns Hopkins University Press.
Miller, J. Q., M. J. Rostafinski & M. S. Hyde (1965). Gonadal dysgenesis and brachymeta- carpal dwarfism (Pseudopseudohypoparathy- roidism). Arch. int. Med. 116, 940-943.
Mom, E., J. B. Osnes, I. Oye & C. W. Wef- ring (1976). Pseudohypoparathyroidism. A difficult diagnosis in early childhood. Acta paediat. scand. 65, 487-493.
Patten, B. M. (1968). Human Embryology. New York, McGraw-Hill.
Preus, M. (1976). A screening test for patients suspected of having Turner syndrome. Clin. Genet. 10, 145-155.
Schaumann, B. & M. Alter (1976). Dermato- glyphics in Medical Disorders. New York, Springer-Verlag.
Seabright, M. (1971). A rapid banding tech- nique for human chromosomes. Lancet ii,
Steinbach, H. L. & D. A. Young (1966). The roentgen appearance of pseudohypopara- thyroidism (PH) and pseudo-pseudohypopara- thyroidism (PPH). Amrr . J . Roentg. 97,
Valsik, J. A. (1933). X-ray skeletotopics of palmar dermatoglyphics with reference to
8 22-8 28.
1161-1 164.
971-972.
49-66.

368 W H I T E A N D M A R X
some actual problems. Biol. Listy 18, 21-62. Walker, N. F. (1957). Inkless methods of fin-
ger, palm and sole printing. J . Pediat. 50,
Zisman, E., M. Lotz, M. E. Jenkins & F. C. Bartter (1969). Studies in pseudohypopara- thyroidism. Two new cases with a probable selective deficiency of thyrotropin. Amer. J . Med. 46, 464-471.
Zisman, E., R. L. Henkin, G. T. Ross & F. C. Bartter (1970). A biochemical similarity between chromatin negative gonadal dys- genesis and pseudohypoparathyroidism: Re-
27-29.
sistance to parathyroid extract. Acta endocr. panam. 1, 49-71.
Address: Beverly J . White, M . D . Bldg. 10, Room 4 0 4 8 Section on Cytogenetics Laboratory of Experimental Pathology National Institute of Arthritis, Metabolism &
National Institutes of Health Bethesda, Maryland 20014, U.S.A.
Digestive Diseases



















