
Treatment of Clostridium difficile-Associated Disease
14
Treatment of Clostridium difficile-Associated Disease Daniel A. Leffler J. Thomas Lamont Division of Gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts Clostridium difficile infection is an increasing burden to the health care system, totaling more than $1 bil- lion/year in the United States. Treatment of patients with C difficile infection with metronidazole or vanco- mycin reduces morbidity and mortality, although the number of patients that do not respond to metroni- dazole is increasing. Despite initial response rates of greater than 90%, 15%–30% of patients have a relapse in symptoms after successful initial therapy, usually in the first few weeks after treatment is discontinued. Failure to develop specific antibody response has re- cently been identified as a critical factor in recur- rence. The review discusses the different management strategies for initial and recurrent symptomatic C difficile infections. C lostridium difficile is an anaerobic, gram-positive, spore-forming, toxin-producing bacillus transmit- ted between human beings by the fecal– oral route. This pathogen infects 20% of hospitalized patients taking antibiotics 1 and is an increasing burden to the health care system. Nosocomial C difficile infection has been estimated to more than quadruple the cost of otherwise matched hospitalizations, 2 totaling $1 billion/year in the United States. 3,4 The most important control mea- sures are proper hand hygiene with the use of soap, water, and disposable gloves; isolation of infected patients; and limitation of unnecessary antibiotic use. Specific treatment of C difficile infection with metronida- zole or vancomycin reduces morbidity and mortality. In general, metronidazole’s high level of efficacy and low cost make it the initial treatment choice for nonpregnant adults. Vancomycin is reserved for individuals with severe infection and those who have failed or cannot take metronidazole therapy. C difficile is highly sensitive to both antibiotics in vitro, but treatment failures with metronidazole appear to be increasing. Despite initial response rates of 90%, 15%– 30% of patients will experience a relapse in symptoms after successful initial therapy, usually in the first few weeks after treatment is discontinued. Recurrence may involve reinfec- tion with the initial strain or a new strain. Failure to develop specific antibody response has recently been identified as a critical factor in recurrence. Management strategies for ini- tial and recurrent symptomatic C difficile infection are de- scribed in detail below. Epidemiology and Pathogenesis Infection occurs when a susceptible host ingests C difficile spores, which then colonize the large bowel (Fig- ure 1) and release 2 protein exotoxins that cause colitis and diarrhea. Healthy adults are protected from C difficile colonization and disease by normal bacterial flora and by antibody to toxin A. 1 Antibiotic therapy, bowel surgery, and rarely cancer chemotherapy change the indigenous colonic microflora, allowing C difficile to colonize in some patients. C difficile infection is most common in elderly hospitalized adults receiving either antibiotics or cancer chemotherapy. C difficile also colonizes 60%–70% of healthy newborns and infants up to 12–18 months of age who lack the adult microflora. 5,6 However, infants rarely develop colitis even with large amounts of toxins in their stool. The infantile carrier state disappears at 18 –24 months of age, at about the same time that the normal adult flora becomes established. The lack of clinical re- sponse to toxin A in newborn animals was attributed to the lack of toxin-binding receptors. 7 The actual incidence of clinical C difficile infection in hospitalized patients varies widely with time and between locations; one recent study estimated an incidence of 1.5% in adults receiving perioperative antibiotic prophylaxis from 2003 to 2005. 8 In the external environment, C difficile survives as heat-, acid-, and antibiotic-resistant spores. After ingestion and Abbreviations used in this paper: Ig, immunoglobulin; IVIG, intrave- nous immunoglobulin; MIC, minimal inhibitory concentration; VRE, vancomycin-resistant enterococci. © 2009 by the AGA Institute 0016-5085/09/$36.00 doi:10.1053/j.gastro.2008.12.070 GASTROENTEROLOGY 2009;136:1899 –1912
-
Upload
hms-harvard -
Category
Documents
-
view
0 -
download
0
Transcript of Treatment of Clostridium difficile-Associated Disease

T
D
CtlwmndgiiFcrsd
Ctpacemtsal
zgmVatvb3s
GASTROENTEROLOGY 2009;136:1899–1912
reatment of Clostridium difficile-Associated Disease
Daniel A. Leffler J. Thomas Lamont
ivision of Gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts
ttscts
duacaacphchwdsmastovsp
a
nv
lostridium difficile infection is an increasing burdeno the health care system, totaling more than $1 bil-ion/year in the United States. Treatment of patientsith C difficile infection with metronidazole or vanco-ycin reduces morbidity and mortality, although the
umber of patients that do not respond to metroni-azole is increasing. Despite initial response rates ofreater than 90%, 15%–30% of patients have a relapsen symptoms after successful initial therapy, usuallyn the first few weeks after treatment is discontinued.ailure to develop specific antibody response has re-ently been identified as a critical factor in recur-ence. The review discusses the different managementtrategies for initial and recurrent symptomatic Cifficile infections.
lostridium difficile is an anaerobic, gram-positive,spore-forming, toxin-producing bacillus transmit-
ed between human beings by the fecal– oral route. Thisathogen infects �20% of hospitalized patients takingntibiotics1 and is an increasing burden to the healthare system. Nosocomial C difficile infection has beenstimated to more than quadruple the cost of otherwiseatched hospitalizations,2 totaling �$1 billion/year in
he United States.3,4 The most important control mea-ures are proper hand hygiene with the use of soap, water,nd disposable gloves; isolation of infected patients; andimitation of unnecessary antibiotic use.
Specific treatment of C difficile infection with metronida-ole or vancomycin reduces morbidity and mortality. Ineneral, metronidazole’s high level of efficacy and low costake it the initial treatment choice for nonpregnant adults.
ancomycin is reserved for individuals with severe infectionnd those who have failed or cannot take metronidazoleherapy. C difficile is highly sensitive to both antibiotics initro, but treatment failures with metronidazole appear toe increasing. Despite initial response rates of �90%, 15%–0% of patients will experience a relapse in symptoms after
uccessful initial therapy, usually in the first few weeks afterreatment is discontinued. Recurrence may involve reinfec-ion with the initial strain or a new strain. Failure to developpecific antibody response has recently been identified as aritical factor in recurrence. Management strategies for ini-ial and recurrent symptomatic C difficile infection are de-cribed in detail below.
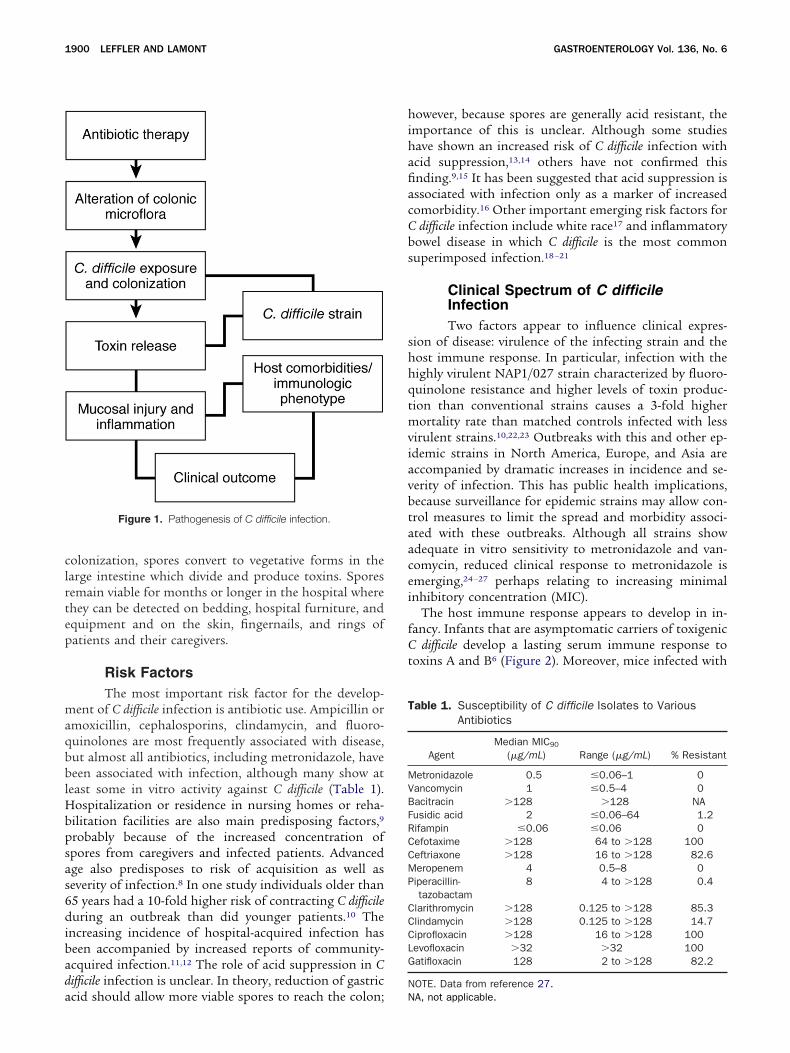
Epidemiology and PathogenesisInfection occurs when a susceptible host ingests C
ifficile spores, which then colonize the large bowel (Fig-re 1) and release 2 protein exotoxins that cause colitisnd diarrhea. Healthy adults are protected from C difficileolonization and disease by normal bacterial flora and byntibody to toxin A.1 Antibiotic therapy, bowel surgery,nd rarely cancer chemotherapy change the indigenousolonic microflora, allowing C difficile to colonize in someatients. C difficile infection is most common in elderlyospitalized adults receiving either antibiotics or cancerhemotherapy. C difficile also colonizes 60%–70% ofealthy newborns and infants up to 12–18 months of ageho lack the adult microflora.5,6 However, infants rarelyevelop colitis even with large amounts of toxins in theirtool. The infantile carrier state disappears at 18 –24
onths of age, at about the same time that the normaldult flora becomes established. The lack of clinical re-ponse to toxin A in newborn animals was attributed tohe lack of toxin-binding receptors.7 The actual incidencef clinical C difficile infection in hospitalized patientsaries widely with time and between locations; one recenttudy estimated an incidence of 1.5% in adults receivingerioperative antibiotic prophylaxis from 2003 to 2005.8
In the external environment, C difficile survives as heat-,cid-, and antibiotic-resistant spores. After ingestion and
Abbreviations used in this paper: Ig, immunoglobulin; IVIG, intrave-ous immunoglobulin; MIC, minimal inhibitory concentration; VRE,ancomycin-resistant enterococci.
© 2009 by the AGA Institute0016-5085/09/$36.00
doi:10.1053/j.gastro.2008.12.070
clrtep
maqbblHbpsas6dibada
hihafiacCbs
shhqtmviavbtaacei
fCt
T
MVBFRCCMP
CCCLG
N
1900 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
olonization, spores convert to vegetative forms in thearge intestine which divide and produce toxins. Sporesemain viable for months or longer in the hospital wherehey can be detected on bedding, hospital furniture, andquipment and on the skin, fingernails, and rings ofatients and their caregivers.
Risk FactorsThe most important risk factor for the develop-
ent of C difficile infection is antibiotic use. Ampicillin ormoxicillin, cephalosporins, clindamycin, and fluoro-uinolones are most frequently associated with disease,ut almost all antibiotics, including metronidazole, haveeen associated with infection, although many show at
east some in vitro activity against C difficile (Table 1).ospitalization or residence in nursing homes or reha-
ilitation facilities are also main predisposing factors,9
robably because of the increased concentration ofpores from caregivers and infected patients. Advancedge also predisposes to risk of acquisition as well aseverity of infection.8 In one study individuals older than5 years had a 10-fold higher risk of contracting C difficileuring an outbreak than did younger patients.10 The
ncreasing incidence of hospital-acquired infection haseen accompanied by increased reports of community-cquired infection.11,12 The role of acid suppression in Cifficile infection is unclear. In theory, reduction of gastric
Figure 1. Pathogenesis of C difficile infection.
cid should allow more viable spores to reach the colon; N
owever, because spores are generally acid resistant, themportance of this is unclear. Although some studiesave shown an increased risk of C difficile infection withcid suppression,13,14 others have not confirmed thisnding.9,15 It has been suggested that acid suppression isssociated with infection only as a marker of increasedomorbidity.16 Other important emerging risk factors for
difficile infection include white race17 and inflammatoryowel disease in which C difficile is the most commonuperimposed infection.18 –21
Clinical Spectrum of C difficileInfectionTwo factors appear to influence clinical expres-
ion of disease: virulence of the infecting strain and theost immune response. In particular, infection with theighly virulent NAP1/027 strain characterized by fluoro-uinolone resistance and higher levels of toxin produc-ion than conventional strains causes a 3-fold higher
ortality rate than matched controls infected with lessirulent strains.10,22,23 Outbreaks with this and other ep-demic strains in North America, Europe, and Asia areccompanied by dramatic increases in incidence and se-erity of infection. This has public health implications,ecause surveillance for epidemic strains may allow con-rol measures to limit the spread and morbidity associ-ted with these outbreaks. Although all strains showdequate in vitro sensitivity to metronidazole and van-omycin, reduced clinical response to metronidazole ismerging,24 –27 perhaps relating to increasing minimalnhibitory concentration (MIC).
The host immune response appears to develop in in-ancy. Infants that are asymptomatic carriers of toxigenic
difficile develop a lasting serum immune response tooxins A and B6 (Figure 2). Moreover, mice infected with
able 1. Susceptibility of C difficile Isolates to VariousAntibiotics
AgentMedian MIC90
(�g/mL) Range (�g/mL) % Resistant
etronidazole 0.5 �0.06–1 0ancomycin 1 �0.5–4 0acitracin �128 �128 NAusidic acid 2 �0.06–64 1.2ifampin �0.06 �0.06 0efotaxime �128 64 to �128 100eftriaxone �128 16 to �128 82.6eropenem 4 0.5–8 0iperacillin-tazobactam
8 4 to �128 0.4
larithromycin �128 0.125 to �128 85.3lindamycin �128 0.125 to �128 14.7iprofloxacin �128 16 to �128 100evofloxacin �32 �32 100atifloxacin 128 2 to �128 82.2
OTE. Data from reference 27.
A, not applicable.
CahtrcsAd
nComtopcstt
idtcnopwi0atiaw
idmCb
edtgtsbr
avfsaq
martcs
clcmatdcrwhpCdcapidsi
FB
May 2009 TREATMENT OF CLOSTRIDIUM DIFFICILE INFECTION 1901
difficile or vaccinated against the toxins are protectedgainst subsequent infection.28 In adult human beings,igher titers of serum immunoglobulin (Ig) G againstoxin A appear to protect against C difficile–induced diar-hea and promote the development of the asymptomaticarrier state.1 Conversely, low levels of toxin A antibody,pecifically, antitoxin A IgM and posttreatment antitoxin
IgG2 and IgG3, increase the risk of symptomatic Cifficile recurrence.29 –31
Overview of TherapyPermanent cure of C difficile requires restoration of
ormal colonic microflora, resulting in the elimination ofdifficile. Therefore, patients with mild symptoms can
ccasionally be managed conservatively by stopping ad-inistration of the inciting antibiotic and following
hem to confirm clinical improvement. In one early studyf clindamycin-associated colitis, which in retrospect wasrobably C difficile colitis, all patients recovered afteressation of clindamycin administration, followed byupportive care.32 Antibiotic treatment of C difficile aimso ameliorate symptoms while allowing gradual restora-ion of the normal gut flora (Table 2).
It is also important to note that symptoms of C difficilenfection are not specific and that confirmation of theiagnosis should be made with the use of assays for fecaloxin before specific therapy. Nonspecific antibiotic-asso-iated diarrhea, postinfectious irritable bowel syndrome,ew onset celiac disease or inflammatory bowel disease,r other infections, including Klebsiella oxytoca, Clostridiumerfringens, and Staphylococcus aureus33 all may be confusedith C difficile–associated disease.34 The reported sensitiv-
ty and specificity of C difficile toxin assays varies from.83 to 0.95 and from 0.93 to 1.00, respectively.35 Incutely ill patients with probable C difficile infection,reatment should be initiated while test results are pend-ng and, in select cases, continued despite negative toxinssays. Sigmoidoscopy or colonoscopy may be helpful
igure 2. Age-related prevalence of antibody to C difficile toxin A and. Modified from Viscidi et al.6
hen another cause such as inflammatory bowel disease p
s suspected. However, they are not recommended foriagnosis because perforation may occur, and pseudo-embranes may occur in only half of infected patients.36
olonoscopy is recommended because pseudomem-ranes may be limited to the right colon only.37
Antibiotic Treatment of Initial C difficileInfectionMost patients with acute C difficile–associated dis-
ase require antibiotic therapy and, whenever possible,iscontinuation of the predisposing antibiotics. It is vitalo assess disease severity based on clinical and demo-raphic information, to determine the most appropriatereatment for each individual. Markers of severity includeevere diarrhea, pseudomembranous colitis, ileus, feverecause of C difficile, age older than 60 years, and acuteenal failure (Table 2).
In younger patients with mild symptoms, a reasonablepproach is to stop the predisposing antibiotic and pro-ide supportive care with hydration and close monitoringor deterioration. This approach is supported by datahowing faster elimination of spores in carriers not givenntibiotics, a finding that could have important conse-uences in limiting spread and recurrence.38
For individuals with comorbidities and those withoderate-to-severe infection, specific antibiotic therapy
imed at C difficile is warranted. Although toxin-bindingesins and probiotics are currently being studied, the onlyherapies confirmed to be effective are antibiotics andolectomy for patients with fulminant disease not re-ponding to antibiotic therapy.
Primarily because of its low cost, metronidazole isurrently recommended as first-line therapy. The value ofimiting vancomycin use to slow the emergence of van-omycin-resistant enterococci (VRE) is unclear becauseetronidazole has also been shown to select for VRE,39,40
nd VRE colonization rates appear similar in patientsreated with vancomycin and metronidazole.41 The stan-ard initial therapy is 500 mg orally (7.5–15 mg/kg inhildren) 3 times daily for 14 days, which successfullyesolves symptoms in �90% of patients within 1eek.42,43 Oral vancomycin is preferred if metronidazoleas failed or is contraindicated. This approach is sup-orted by professional society guidelines44 and a recentochrane review.45 However, metronidazole’s apparentecreasing efficacy46,47 (Figure 3) and slower response,ompared with vancomycin,43 has led to controversybout this recommendation. Moreover, recent data sup-ort the use of vancomycin as a first-line treatment in
ndividuals with severe C difficile infection.48,49 Althoughata are lacking, antidiarrheal agents and narcoticshould be avoided in patients with symptomatic C difficilenfection because of concerns about toxin retention and
ossible precipitation of toxic megacolon.
fiaot
at
adssahl
w
T
CM
S
F
B
1902 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
MetronidazoleMetronidazole is generally recommended as the
rst-line treatment of C difficile. Parenteral, oral, or rectaldministration can be used in patients unable to takeral doses and leads to similar systemic and colonicissue drug levels.
Metronidazole, a nitroimidazole-class antibiotic andntiprotozoal, is administered and taken up in an inac-ive state by anaerobic organisms then reduced to its
able 2. Classification and Treatment of Initial C difficile Infe
Severity Clinical manifestations
arrier ● No discernible clinical symptoms or sigild to moderate ● Mild diarrhea � 12 stools/day
● Afebrile● Mild-to-moderate abdominal discomfort
tenderness● Nausea with rare or absent vomiting● With or with hospitalization● Not in intensive care unit● Dehydration● Leukocytosis �20,000● BUN or creatinine above baseline
evere ● Severe or bloody diarrhea � 12 stools/● Pseudomembranous colitis● Severe abdominal pain● Nausea or vomiting● Ileus● Temperature �38.9°C● Age � 60 years● in intensive care unit● Leukocytosis � 20,000● Albumin � 2.5mg/dL● Renal failure
ulminant ● Toxic megacolon● Peritonitis● Albumin � 2.5mg/dL● Renal failure● Respiratory distress● Hemodynamic instability
UN, blood urea nitrogen.
ctive form. It induces microbial cell death by DNAisruption and subsequent inhibition of nucleic acidynthesis. Metronidazole is most effective in anaerobicites such as the human colonic lumen. In addition to itsntimicrobial properties, metronidazole also appears toave anti-inflammatory, antioxidant, and immunomodu-
atory effects.50,51
Oral absorption of metronidazole is highly efficient,ith a serum half-life of 8 hours and bioavailability of
Figure 3. Recent increase in re-ported treatment failures for met-ronidazole. Modified from Aslamet al.46
Treatment
● No treatment is indicated● Discontinuation of predisposing antibiotics● Hydration● Monitor clinical status● Isolation● Consider probiotics● Oral metronidazole 500 mg 3 times daily or intravenous
metronidazole 500 mg 3 times daily if not toleratingoral intake
● Oral vancomycin 125 mg 4 times daily if intolerant ofmetronidazole
● As above plus:● Oral vancomycin 125 mg 4 times daily● Consider addition of intravenous metronidazole 500 mg
3 times daily
● As above plus:● Surgical consultation● Oral vancomycin 125 mg 3 times daily and intravenous
metronidazole 500 mg 3 times daily● Consider IVIG
ction
ns
or
day

�ostmqlaafflidts
essttnramubic
mpsvirdac
bggamivctpptd
mcc
nriMnmccp
srrci
fidpdadwd
F(
May 2009 TREATMENT OF CLOSTRIDIUM DIFFICILE INFECTION 1903
90%. Food may slow the rate, but not the overall extent,f absorption. Intravenous and oral administration re-ults in distribution to all tissues and fluids, includinghe placenta and breast milk. Sixty to eighty percent of
etronidazole is metabolized by the liver and subse-uently cleared by the kidneys; the remaining unmetabo-
ized metronidazole is excreted in feces, with similarmounts reaching the colon after oral and parenteraldministration. Metronidazole preferentially diffusesrom the serum and interstitial compartment of the in-amed colon into the lumen, a property that can increase
ts efficacy against C difficile.52 Impaired renal functionoes not alter metronidazole pharmacokinetics, al-hough the dose should be reduced in patients withevere liver disease.
Side effects and toxicity. The most common sideffects of metronidazole are metallic taste, headache, nau-ea, and a disulfiram-like effect with alcohol, although theseymptoms rarely require cessation of treatment. The neuro-oxic effects of metronidazole include peripheral neuropa-hy, vertigo, and, rarely, ataxia or encephalopathy. Fortu-ately, neuropathy is seldom observed in patients whoeceive �2 weeks of therapy, and most cases have occurredfter exposure to standard doses for �1 month.53–55 Treat-ent with metronidazole should be immediately discontin-
ed if there is concern about neurotoxicity, which may note reversible. Metronidazole is rated pregnancy class B, but
t should not be given in the first trimester, because ofoncerns of teratogenicity based on animal data.
Activity. Metronidazole is highly active againstost strains of pathogenic C difficile with only rare re-
orts of antibiotic resistance.56 –58 Although MIC washown to differ between strains, MIC remains below inivo therapeutic levels in nearly all isolates.26,59,60 Increas-ng evidence suggests, that prolonged exposure to met-onidazole can lead to resistance61 and that susceptibilityecreases over time.48,62,63 For this reason, surveillance ofntibiotic resistance in C difficile is ongoing and resistanceould limit the use of this antibiotic in the future.
VancomycinVancomycin, a tricyclic glycopeptide that inhibits
acterial cell wall synthesis,64 has broad activity againstram-positive bacteria, but it essentially has no effect onram-negative bacteria or fungi. Vancomycin is orallydministered in its active form and, because o f its largeolecular weight, is not absorbed and reaches the colon
ntact, an advantage for the treatment of C difficile. Con-ersely, parenteral vancomycin is not excreted into theolonic lumen and, for this reason, is not effective forreatment of C difficile. However, ileus may result in un-redictable delivery of vancomycin to the colon. In theseatients the drug may be delivered by rectal or colonicube or by enemas. Although the initially recommended
ose used to treat C difficile was 500 mg 4 times daily, 125 og 4 times daily also results in concentrations in theolon well above the MIC for C difficile, with identicallinical outcomes (Figure 4).42
Side effects and toxicity. Because vancomycin isot absorbed systemically from the gastrointestinal tract,eported side effects observed during parenteral admin-stration, including ototoxicity, nephrotoxicity, and Red-
an syndrome, are avoided.64 Mild upset stomach andausea are the most common side effects of oral vanco-ycin and rarely limit treatment. Although systemic van-
omycin is classified as pregnancy class C, oral vancomy-in is the agent of choice for C difficile infection duringregnancy.
Activity. Vancomycin is highly active against alltrains of pathogenic C difficile, and resistance has beeneported in only a single study65 (Table 1). Vancomycin isecommended as first-line therapy in pregnant women, inhildren younger than 10 years of age, and for severenfections.
Regimen. Initial treatment and treatment of arst recurrence should be for 10 –14 days. Although thereoes not appear to be any benefit of vancomycin com-ared with metronidazole in treating mild-to-moderate Cifficile infection, some evidence suggests that outcomesre improved with the use of vancomycin for severeisease48 (Figure 5). Vancomycin enemas can be givenhen oral administration is not possible; colonoscopicecompression with vancomycin lavage was described in
igure 4. Equivalent response of low and high dose vancomycin.Modified with permission from Fekety et al.42)
ne report.66

moCt
ropAbsbd
ttmsirwatz
ftsveat
wccv
ipf
mocUcttm
dorra
Co�ifhacshtcUmw�
bd
sever
1904 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
Other TreatmentsAlthough metronidazole and vancomycin are the
ainstays of therapy for symptomatic infection, severalther agents (Table 4) are used or under investigation for
difficile, either as stand-alone treatments or as adjunc-ive agents.
Alternative AntibioticsRifaximin is a nonabsorbed antibiotic similar to
ifampin that inhibits bacterial RNA synthesis. The lackf systemic absorption gives rifaximin a favorable safetyrofile, especially in cases requiring prolonged treatment.nimal data67 and human studies68 –71 suggest efficacy inoth initial and recurrent C difficile infection, but wide-pread use of this agent for C difficile is likely to be limitedy the appearance of resistant strains.68,72 Rifaximin isesignated pregnancy class C.Nitazoxanide is a synthetic antiparasitic and antibiotic
hat appears to interfere with enzyme-dependent electronransfer and has activity against many anaerobic and
icroaerophilic bacteria. Side effects are mild and areimilar to placebo. Studies have shown in vitro and clin-cal efficacy of nitazoxanide against C difficile,25,73–76 andecent studies have reported non-inferiority comparedith both metronidazole74 and vancomycin.77 Nitazox-nide is currently approved only for use in Giardia intes-inalis and cryptosporidium infection in children. Nita-oxanide is designated pregnancy class B.
Bacitracin is an inhibitor of cell wall synthesis derivedrom Bacillus subtilis. In general, this agent is less effectivehan vancomycin, and clearance of viable spores from thetool occurs in a significantly lower percentage of indi-iduals treated with bacitracin.78 – 81 Bacitracin is morexpensive than metronidazole and currently only avail-ble in topical formulations; it is not recommended forreatment of C difficile infections.
Ramoplanin is a novel glycolipodepsipeptide antibioticith broad activity against C difficile, S. aureus, and van-
omycin-resistant enterococci, by inhibiting peptidogly-an synthesis. A phase 2 study reported similar efficacy to
Figure 5. Vancomycin is more effective than metronidazole for
ancomycin in patients with mild-to-moderate C difficile b
nfection.82 Ramoplanin is currently being tested inhase 3 trials for VRE, and further studies are plannedor C difficile.
Teicoplanin is similar to vancomycin in structure,ode of action, and antibacterial activity. Small studies
f teicoplanin report a benefit compared with vancomy-in,45 although it is not yet approved for use in thenited States. Oritavancin is another vancomycin analog
urrently under review by the Food and Drug Adminis-ration. Early data suggest that, unlike vancomycin, ori-avancin has activity against C difficile spores, a trait which
ay be important in preventing relapse.83
Rifampin has also been studied for treatment of Cifficile infection either alone or with metronidazole. Usef rifampin has fallen from favor after a recent studyeported increased mortality in patients treated with met-onidazole and rifampin compared with metronidazolelone.84
Treatment of Acute Fulminant InfectionDespite the efficacy of antibiotic treatment, acute
difficile infection remains a disease that has a high ratef morbidity with an estimated case–fatality rate of2%.85 Severe C difficile colitis tends to occur during the
nitial infection or first recurrence. Patients with riskactors such as advanced age, significant comorbidities,igh peak white blood cell count, and lactate acidemiare at increased risk of death and should be followedlosely. Importantly, diarrhea may be absent in cases ofevere C difficile infection with toxic megacolon, and aigh index of suspicion must be kept in these situationso prevent delay in therapy. Hemodynamic instability isonsistently associated with high rates of mortality.86,87
nfortunately, the interval between presentation and he-odynamic collapse can be short and unpredictable,ith a mean of 9 days in one study88 but a range of 0 to30 days.Patients with fulminant disease should be treated with
oth oral vancomycin and intravenous metronidazoleespite a lack of evidence from clinical trials about com-
e C difficile infection. Modified with permission from Zar et al.48
ination therapy. If oral administration of medications is

ncmwrttgms
tspRgaitto
3dterdmrmiotccc(rdmpat
trosttrc
tomvantroPtabftmaimm
hastofis
i
T
May 2009 TREATMENT OF CLOSTRIDIUM DIFFICILE INFECTION 1905
ot possible because of ileus, parenteral metronidazolean be supplemented with vancomycin enemas. Closeonitoring of clinical status is vital, and, for patientsho fail to respond to antibiotics or who have deterio-
ating hemodynamics, respiratory status or renal func-ion, urgent surgical intervention may be required. Pa-ients who are not good candidates for surgery can beiven doses of pooled human immunoglobulin (200 –500g/kg/day) until they improve, although evidence to
upport efficacy of this therapy is anecdotal.For patients with fulminant disease and severe ileus,
oxic megacolon, or localizing peritoneal signs, emergentubtotal colectomy and ileostomy is generally required;ostoperative mortality rates range from 35% to 80%.andomized trials evaluating the timing or type of sur-ical procedure for severe C difficile infection are unavail-ble; however, observational studies suggest that survivals improved with prompt surgical intervention in pa-ients with severe or fulminant infection.86,87,89 –93 Subto-al colectomy is the procedure of choice because reportsf hemicolectomy suggest increased mortality.91
Treatment of Recurrent C difficileInfectionAfter successful initial therapy, approximately 15%–
0% of patients experience a symptomatic recurrence afteriscontinuation of antibiotics.30,94–100 Older patients andhose with a history of prior C difficile recurrence are at anven higher risk (�50%) for recurrent disease.47,101 Mostecurrences happen within 2 weeks of stopping therapy, butelayed recurrences have been documented.95,100 Approxi-ately half of recurrent C difficile infections are caused by
epeated ingestion of bacteria (reinfection) before the nor-al intestinal flora recovers, and half are attributed to
ncomplete eradication of the original strain during antibi-tic treatment (relapse).101–104 The first recurrence can bereated with the same antibiotic, for example a 14-dayourse of metronidazole (if tolerated) or with supportiveare alone, if symptoms are mild. Unfortunately, a signifi-ant rate of further episodes follows a first recurrence�65%, in one study96). Management strategies for recur-ent C difficile infection include repeat courses of metroni-azole or vancomycin, tapered and pulsed dosing of vanco-ycin, toxin-binding agents such as cholestyramine,
robiotics such as Saccharomyces boulardii, and immunother-py, but none are supported by randomized large clinicalrials4,34,95,96,100,105–115 (Tables 3 and 4).
For patients who experience �2 recurrences of symp-omatic C difficile infection, a change in strategy is war-anted. Before starting antibiotic therapy, the diagnosisf recurrent C difficile infection should be confirmed bytool assay, because other causes, including postinfec-ious irritable bowel syndrome, have similar presenta-ions. For confirmed recurrent C difficile infection, weecommend a 6-week pulsed-tapered course of oral van-
omycin therapy (Table 3). During continuous antibiotic nherapy C difficile persists in the bowel lumen as antibi-tic-resistant spores.106,107 Pulsed doses of antibioticsay allow spores to germinate into antibiotic-sensitive
egetative forms, which are then killed on the next day ofntibiotic therapy. Pulsing may also allow restoration oformal colonic flora while conferring adequate protec-ion against C difficile. Metronidazole is generally notecommended for long-term therapy, because of the riskf peripheral neuropathy, particularly in older patients.robiotics or toxin-binding resins107 may provide addi-ional benefit when added in the later weeks of thentibiotic taper and continued for 4 – 6 weeks after anti-iotic therapy is stopped. A more recent strategy reportedor treatment of multiply-recurrent C difficile infections ishe addition of a 2-week course of rifaximin (400 – 800
g daily) in 2 or 3 divided doses for 2 weeks, immediatelyfter 10 –14 days of vancomycin therapy while the patients still in clinical remission.68 Seven of 8 patients with a
inimum of 4 prior recurrent episodes treated in thisanner had no further recurrences.Despite these treatment strategies, some patients still
ave repeat bouts of C difficile infection, after multiplettempts at eradication. For infirm or elderly patients, weometimes recommend chronic vancomycin therapy athe lowest effective dose, usually 125 mg daily or everyther day for an indefinite period. Immunotherapy orecal bacteriotherapy, described below, are other optionsn younger patients or if recurrences are particularlyevere.
Toxin-Binding ResinsC difficile toxins in the colonic lumen lead to clin-
cal disease, but the bacteria itself is not invasive and does
able 3. Treatment of Recurrent C difficile Infection
Initial recurrence● 14-day course of oral metronidazole or vancomycin● Consider probiotics
Second Recurrence● Tapered pulse dose oral vancomycin
� 125 mg 4 times daily for 1 week� 125 mg twice daily for 1 week� 125 mg daily for 1 week� 125 mg every other day for 1 week� 125 mg every third day for 2 weeks
● Consider 1-month course of probiotics starting in the final 2weeks of antibiotic therapy
Third or subsequent recurrence● Tapered pulse dose oral vancomycin (see above)
Followed by● 14-day course of rifaximin, nitazoxanide, or toxin-binding resins● Consider 1-month course of probiotics starting in the final 2
weeks of antibiotic therapy● Consider intravenous immunoglobulin or fecal bacteriotherapy● Consider chronic low-dose suppressive therapy with oral
vancomycin for elderly patients and those with multiplecomorbidities
ot cause tissue damage. This observation prompted

rsfltarruftdCcb
otsiwiolrt
atmmbtva
r
rrwa2radirrorta
hftastad
apCarrpdcg
T
M
V
R
B
NI
P
S
1906 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
esearch into the efficacy of compounds that bind andequester C difficile toxin but do not alter the intestinalora or lead to antibiotic resistance. Unfortunately, ini-ial studies with the bile acid– binding resins colestipolnd cholestyramine were disappointing, with responseates in patients with acute infection of 36% and 68%,espectively.116 –118 These findings largely relegated these of binding resins to adjunct therapy of patients who
ail to respond to antibiotics or those with mild diseasehat do not tolerate or need antibiotics. Later studiesetermined that the binding affinity of cholestyramine to
difficile toxin was substantially greater than that ofolestipol119; these findings suggest that higher affinityinding agents might be more effective.
Tolevamer, a nonabsorbed anionic polymer, was devel-ped specifically as a high-affinity binder of C difficileoxins. Studies in animals showed that tolevamer wasuperior to metronidazole in reducing acute C difficilenfection.120 A phase 2 study reported efficacy in patientsith mild-to-moderate C difficile infections that was sim-
lar to that of vancomycin with a trend toward lower ratesf recurrence in the group given tolevamer.121 However a
arger phase 3 study suggested that tolevamer was infe-ior to vancomycin.49 Investigations into other formula-ions of tolevamer are underway.122
ImmunotherapyThe association between low serum levels of IgG
ntitoxin A and increased disease severity1,30,31 suggestshat bolstering the immune response to C difficile toxins
ight prevent or ameliorate disease in patients. Animalodels support this concept; passive immunization has
een shown to substantially improve outcome123,124 ando reduce C difficile colonization rates.125 Currently intra-enous immunoglobulin (IVIG) is the only available ther-peutic option.
Randomized clinical trials are not available, but case
able 4. Treatment Options for C difficile Infection
Treatment Regimen
etronidazole 250–500 mg 3 times daily orby mouth or intravenously
ancomycin 125–500 mg 3 times daily orby mouth
ifaximin 400–800 mg twice daily or 3 tmouth
inding resins; cholestyraminepreferred over colestipol
4 g 3 times daily or 4 times d
itazoxanide 500 mg twice daily by mouthmmunoglobulin 300–500 mg/kg daily until res
maximum of 6 dosesrobiotics Variable oral dosing
urgery Subtotal colectomy with ileost
eports suggest efficacy of IVIG in patients with either a
ecurrent or severe acute disease.113–115 Two small studieseported IVIG treatment for recurrent C difficile infectionith response rates of 100% in children114 and 60% indults.115 In the typical regimen, patients were given00 –500 mg IVIG/kg/day (1 and 5 total doses); a clinicalesponse occurred in most patients within 1 week. Innother small series, IVIG provided no benefit in acuteisease.126 In addition to issues of expense and availabil-
ty, side effects of IVIG are common and include infusioneactions, hemolytic anemia, neutropenia, anaphylaxis,enal toxicity, and aseptic meningitis. We reserve the usef IVIG for patients with multiple moderate-to-severeecurrences of C difficile who have failed vancomycin taperherapy at least twice, in combination with probioticsnd toxin-binding resins or rifaximin.
Active vaccination of animals against C difficile toxinsas been successful in preventing infection and death
rom C difficile.127,128 Phase 1 trials have shown that in-ramuscular injection of C difficile toxoid vaccine is safend immunogenic in healthy volunteers, inducing robusterum IgG antitoxin and fecal IgA antitoxin produc-ion.129,130 A small case series suggested efficacy of ther-peutic vaccination in adults with multiply recurrentisease.131
Microbiologic TherapyThe critical factor in C difficile pathogenesis is
ntibiotic-induced reduction of colonization resistance,rovided by the normal colonic microflora, which allows
difficile to have a selective advantage. For this reason,ctive reconstitution of the normal colonic flora is theo-etically attractive for prevention and treatment. Severaleports have documented the efficacy of stool trans-lants, delivered by enema or gastric tube, from a healthyonor to patients with recurrent132,133 or acute134 C diffi-
ile infection. Inadvertent spread of pathogenic microor-anisms from donor to host as well as distaste by patients
Comments
es daily First-line therapy or in combination with vancomycinin severe disease
es daily First-line therapy for severe disease
daily by Adjunctive in recurrent C difficile infection
Adjunctive with antibiotics; must be taken �2hours apart from vancomycin
Adjunctive in recurrent C difficile infectionon or Adjunctive with antibiotics in severe refractory or
recurrent C difficile infectionAdjunctive with antibiotics for treatment or
prevention of recurrent C difficile infectionEarly surgical consultation recommended in severe
disease
4 tim
4 tim
imes
aily
oluti
omy
nd physicians have limited the use of this technique.

Otsdwt
tildhdrdydr
oprbIsmttpCtopObficofua
pasddhC
b
dVeatwcfgctcsoTetmsrc
phi
usptowiiot
T
May 2009 TREATMENT OF CLOSTRIDIUM DIFFICILE INFECTION 1907
ral administration of nontoxigenic strains of C difficileo compete with and limit the growth of toxin-producingtrains was reported to lead to remission of recurrent Cifficile infection in 2 patients,135 and studies are under-ay to characterize a strain that is suitable for larger
rials.136
Probiotic TherapyProbiotics are commonly used for prevention and
reatment of infectious diarrhea.137,138 Organisms stud-ed in C difficile include Saccharomyces boulardii, Lactobacil-us rhamnosus GG, Lactobacillus plantarum, Lactobacillus aci-ophilus, and Bifidobacterium bifidum. Most studies to dateave focused on the prevention of antibiotic-associatediarrhea and C difficile infection. A recent meta-analysiseviewed 31 studies of various probiotics for C difficileiarrhea (25 studied prevention of disease).139 This anal-sis found that prophylactic probiotics significantly re-uced the subsequent incidence of acute C difficile diar-hea (relative risk [RR], 0.43; P � .001).
A smaller number of studies have evaluated the efficacyf probiotics for treatment of C difficile diarrhea andrevention of recurrence. Although no individual studyeduced recurrence, in aggregate, a significant therapeuticenefit of probiotics was reported (RR, 0.59; P � .005).139
n contrast, a recent Cochrane Review found only 4tudies of sufficient quality for inclusion and suggested a
odest benefit of Saccharomyces boulardii in both preven-ion of recurrence and cessation of diarrhea as an adjuncto antibiotics. Lactobacillus rhamnosus GG and Lactobacilluslantarum did not appear to provide any benefit. Thisochrane Review concluded that evidence is insufficient
o recommend probiotic therapy as an adjunct to antibi-tic therapy and that no evidence supports the use ofrobiotics alone in the treatment of C difficile diarrhea.140
ther studies not included in this meta-analysis haveeen published,141,142 with some studies reporting bene-t, while others found no difference. Despite these dis-repant results, probiotics remain a safe and reasonableption for prevention of initial infections and possiblyor treatment of recurrent infections. Animal studies arenderway to optimize the type and dose of organismsnd to explore the mechanisms of action.136,143–148
PreventionAs with any disease, C difficile is better managed by
revention than by cure (Table 5). Appropriate use ofntibiotics, especially broad-spectrum agents and thosehown to have a particular predisposition to cause Cifficile infections, will continue to be the cornerstone ofisease control for the foreseeable future. Several studiesave shown that antibiotic prescription guidelines reducedifficile infection rates by approximately 50%.149 –152
Although community-acquired C difficile infection has
een increasingly reported,11,153 the main nidus of Cifficile remains hospitals and nursing facilities.34,154 –160
iable C difficile spores are widespread in the hospitalnvironment155,156,161–163 and are spread by asymptom-tic carriers and hospital personnel, giving rise to hospi-al outbreaks and geographic clustering in specificards.155,156,161 The use of alcohol wipes or solutions to
lean hands and equipment after patient contact is inef-ective against C difficile spores. Only the use of disposableloves, gowns, and hand washing with chlorhexidine glu-onate– containing soap have been documented to reducehe spread of C difficile by health care workers.164,165 De-ontamination of rooms and equipment with the use ofporicidal agents such as sodium hypochlorite, ethylenexide, and alkaline glutaraldehyde is recommended.34
reatment of known carriers with vancomycin is notffective.38 Combination of tactics that include educa-ion, increased case finding, expanded infection-control
easures, a C difficile infection management team, andtringent antimicrobial guidelines has been shown toeduce the spread of C difficile and to improve out-omes.166
ConclusionsC difficile prevention requires avoidance of inap-
ropriate antibiotic use, combined with proper handygiene by medical staff and surveillance and prompt
solation of new cases of C difficile infection.For infected individuals, treatment should be individ-
alized and based on severity of symptoms and whetherymptomatic disease is primary or recurrent. For mostatients with active symptoms, metronidazole is thereatment of choice for initial infection and first or sec-nd recurrence, because of cost concerns. For patientsith severe disease or multiple recurrences, vancomycin
s recommended. Surgical consultation is warranted earlyn the course of suspected fulminant disease. The roles ofther antibiotics, probiotics, binding resins, and vaccina-ion hold great promise for future management.
References
1. Kyne L, Warny M, Qamar A, Kelly CP. Asymptomatic carriage ofClostridium difficile and serum levels of IgG antibody against
able 5. Guidelines for the Prevention of C difficile Infection
Individual patient● Limit antibiotics
Institution● Hand washing after all patient contact● Isolation for patients known to be infected with C difficile● Use of gloves and gowns when in contact with patients known
or suspected to be infected with C difficile● Disinfect contaminated objects with appropriate agents, including
sodium hypochlorite, glutaraldehyde, or ethylene oxideRegional
● Educate medical staff and at-risk populations about C difficile
toxin A. N Engl J Med 2000;342:390–397.

1908 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
2. Vonberg RP, Reichardt C, Behnke M, Schwab F, Zindler S,Gastmeier P. Costs of nosocomial Clostridium difficile-associ-ated diarrhoea. J Hosp Infect 2008;70:15–20.
3. Kyne L, Hamel MB, Polavaram R, Kelly CP. Health care costs andmortality associated with nosocomial diarrhea due to Clostrid-ium difficile. Clin Infect Dis 2002;34:346–353.
4. Kelly CP, Pothoulakis C, LaMont JT. Clostridium difficile colitis.N Engl J Med 1994;330:257–262.
5. Larson HE, Barclay FE, Honour P, Hill ID. Epidemiology of Clos-tridium difficile in infants. J Infect Dis 1982;146:727–733.
6. Viscidi R, Laughon BE, Yolken R, et al. Serum antibody responseto toxins A and B of Clostridium difficile. J Infect Dis 1983;148:93–100.
7. Eglow R, Pothoulakis C, Itzkowitz S, et al. Diminished Clostridiumdifficile toxin A sensitivity in newborn rabbit ileum is associated withdecreased toxin A receptor. J Clin Invest 1992;90:822–829.
8. Carignan A, Allard C, Pepin J, Cossette B, Nault V, Valiquette L.Risk of Clostridium difficile infection after perioperative antibac-terial prophylaxis before and during an outbreak of infection dueto a hypervirulent strain. Clin Infect Dis 2008;46:1838–1843.
9. Pepin J, Saheb N, Coulombe MA, et al. Emergence of fluoro-quinolones as the predominant risk factor for Clostridium diffi-cile-associated diarrhea: a cohort study during an epidemic inQuebeC Clin Infect Dis 2005;41:1254–1260.
10. Pepin J, Valiquette L, Cossette B. Mortality attributable to nos-ocomial Clostridium difficile-associated disease during an epi-demic caused by a hypervirulent strain in QuebeC CMAJ 2005;173:1037–1042.
11. Wilcox MH, Mooney L, Bendall R, Settle CD, Fawley WN. Acase-control study of community-associated Clostridium difficileinfection. J Antimicrob Chemother 2008;62:388–396.
12. Surveillance for community-associated Clostridium difficile—Connecticut, 2006. MMWR Morb Mortal Wkly Rep 2008;57:340–343.
13. Dial S, Delaney JA, Schneider V, Suissa S. Proton pump inhibitoruse and risk of community-acquired Clostridium difficile-associ-ated disease defined by prescription for oral vancomycin ther-apy. CMAJ 2006;175:745–748.
14. Dial S, Delaney JA, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostrid-ium difficile-associated disease. JAMA 2005;294:2989–2995.
15. Kyne L, Sougioultzis S, McFarland LV, Kelly CP. Underlyingdisease severity as a major risk factor for nosocomial Clostrid-ium difficile diarrhea. Infect Control Hosp Epidemiol 2002;23:653–659.
16. Leffler D, Cloud JW, Kelly CP. Gastric acid-suppressive agentsand risk of Clostridium difficile-associated disease [letter].JAMA 2006;295:2599–2600; author reply 2600–2601.
17. Redelings MD, Sorvillo F, Mascola L. Increase in Clostridiumdifficile-related mortality rates, United States, 1999–2004.Emerg Infect Dis 2007;13:1417–1419.
18. DuPont HL, Garey K, Caeiro JP, Jiang ZD. New advances inClostridium difficile infection: changing epidemiology, diagno-sis, treatment and control. Curr Opin Infect Dis 2008;21:500–507.
19. Issa M, Ananthakrishnan AN, Binion DG. Clostridium difficileand inflammatory bowel disease. Inflamm Bowel Dis 2008;14:1432–1442.
20. Rodemann JF, Dubberke ER, Reske KA, Seo da H, Stone CD.Incidence of Clostridium difficile infection in inflammatory boweldisease. Clin Gastroenterol Hepatol 2007;5:339–344.
21. Mylonaki M, Langmead L, Pantes A, Johnson F, Rampton DS.Enteric infection in relapse of inflammatory bowel disease: im-portance of microbiological examination of stool. Eur J Gastro-enterol Hepatol 2004;16:775–778.
22. Loo VG, Poirier L, Miller MA, et al. A predominantly clonal
multi-institutional outbreak of Clostridium difficile-associated di-arrhea with high morbidity and mortality. N Engl J Med 2005;353:2442–2449.
23. Warny M, Pepin J, Fang A, et al. Toxin production by an emergingstrain of Clostridium difficile associated with outbreaks of se-vere disease in North America and Europe. Lancet 2005;366:1079–1084.
24. Freeman J, Baines SD, Saxton K, Wilcox MH. Effect of metroni-dazole on growth and toxin production by epidemic Clostridiumdifficile PCR ribotypes 001 and 027 in a human gut model. JAntimicrob Chemother 2007;60:83–91.
25. Hecht DW, Galang MA, Sambol SP, Osmolski JR, Johnson S,Gerding DN. In vitro activities of 15 antimicrobial agents against110 toxigenic clostridium difficile clinical isolates collected from1983 to 2004. Antimicrob Agents Chemother 2007;51:2716–2719.
26. Odenholt I, Walder M, Wullt M. Pharmacodynamic studies ofvancomycin, metronidazole and fusidic acid against Clostridiumdifficile. Chemotherapy 2007;53:267–274.
27. Bourgault AM, Lamothe F, Loo VG, Poirier L. In vitro susceptibil-ity of Clostridium difficile clinical isolates from a multi-institu-tional outbreak in Southern Quebec, Canada. Antimicrob AgentsChemother 2006;50:3473–3475.
28. Chen X, Katchar K, Goldsmith JD, et al. A mouse model ofClostridium difficile-associated disease. Gastroenterology 2008;135:1984–1992.
29. Katchar K, Taylor CP, Tummala S, Chen X, Sheikh J, Kelly CP.Association between IgG2 and IgG3 subclass responses totoxin A and recurrent Clostridium difficile-associated disease.Clin Gastroenterol Hepatol 2007;5:707–713.
30. Kyne L, Warny M, Qamar A, Kelly CP. Association betweenantibody response to toxin A and protection against recurrentClostridium difficile diarrhoea. Lancet 2001;357:189–193.
31. Bacon AE III, Fekety R. Immunoglobulin G directed against toxinsA and B of Clostridium difficile in the general population andpatients with antibiotic-associated diarrhea. Diagn Microbiol In-fect Dis 1994;18:205–209.
32. Tedesco FJ, Barton RW, Alpers DH. Clindamycin-associated co-litis. A prospective study. Ann Intern Med 1974;81:429–433.
33. Dalal A U C. Enterocolitis caused by methicillin-resistant Staph-ylococcus aureus. Infect Dis Clin Pract 2008;16:222–223.
34. Fekety R. Guidelines for the diagnosis and management ofClostridium difficile-associated diarrhea and colitis. AmericanCollege of Gastroenterology, Practice Parameters Committee.Am J Gastroenterol 1997;92:739–750.
35. Planche T, Aghaizu A, Holliman R, et al. Diagnosis of Clostridiumdifficile infection by toxin detection kits: a systematic review.Lancet Infect Dis 2008;8:777–784.
36. Bartlett JG, Gerding DN. Clinical recognition and diagnosis ofClostridium difficile infection. Clin Infect Dis 2008;46(Suppl1):S12–S18.
37. Tedesco FJ, Corless JK, Brownstein RE. Rectal sparing in anti-biotic-associated pseudomembranous colitis: a prospectivestudy. Gastroenterology 1982;83:1259–1260.
38. Johnson S, Homann SR, Bettin KM, et al. Treatment of asymp-tomatic Clostridium difficile carriers (fecal excretors) with van-comycin or metronidazole. A randomized, placebo-controlledtrial. Ann Intern Med 1992;117:297–302.
39. Donskey CJ, Chowdhry TK, Hecker MT, et al. Effect of antibiotictherapy on the density of vancomycin-resistant enterococci inthe stool of colonized patients. N Engl J Med 2000;343:1925–1932.
40. Carmeli Y, Eliopoulos GM, Samore MH. Antecedent treatmentwith different antibiotic agents as a risk factor for vancomycin-resistant Enterococcus. Emerg Infect Dis 2002;8:802–807.
41. Al-Nassir WN, Sethi AK, Li Y, Pultz MJ, Riggs MM, Donskey CJ.Both oral metronidazole and oral vancomycin promote persis-
tent overgrowth of vancomycin-resistant enterococci during
May 2009 TREATMENT OF CLOSTRIDIUM DIFFICILE INFECTION 1909
treatment of Clostridium difficile-associated disease. Antimi-crob Agents Chemother 2008;52:2403–2406.
42. Fekety R, Silva J, Kauffman C, Buggy B, Deery HG. Treatment ofantibiotic-associated Clostridium difficile colitis with oral vanco-mycin: comparison of two dosage regimens. Am J Med 1989;86:15–19.
43. Wilcox MH, Howe R. Diarrhoea caused by Clostridium difficile:response time for treatment with metronidazole and vancomy-cin. J Antimicrob Chemother 1995;36:673–679.
44. Gerding DN, Johnson S, Peterson LR, Mulligan ME, Silva J Jr.Clostridium difficile-associated diarrhea and colitis. Infect Con-trol Hosp Epidemiol 1995;16:459–477.
45. Nelson R. Antibiotic treatment for Clostridium difficile-associ-ated diarrhea in adults. Cochrane Database Syst Rev 2007:CD004610.
46. Aslam S, Hamill RJ, Musher DM. Treatment of Clostridium diffi-cile-associated disease: old therapies and new strategies. Lan-cet Infect Dis 2005;5:549–557.
47. Pepin J, Alary ME, Valiquette L, et al. Increasing risk of relapseafter treatment of Clostridium difficile colitis in Quebec, Canada.Clin Infect Dis 2005;40:1591–1597.
48. Zar FA, Bakkanagari SR, Moorthi KM, Davis MB. A comparisonof vancomycin and metronidazole for the treatment of Clostrid-ium difficile-associated diarrhea, stratified by disease severity.Clin Infect Dis 2007;45:302–307.
49. Louie T, G M, Grimard D, Johnson S, et al. Results of a PhaseIII trial comparing tolevamer, vancomycin and metronidazole inpatients with Clostridium difficile-associated diarrhea (CDI) [ab-stract]. Presented at the 47th annual meeting of ICAAC, 2007.
50. Krehmeier U, Bardenheuer M, Voggenreiter G, Obertacke U,Schade FU, Majetschak M. Effects of antimicrobial agents onspontaneous and endotoxin-induced cytokine release of humanperipheral blood mononuclear cells. J Infect Chemother 2002;8:194–197.
51. Miyachi Y, Imamura S, Niwa Y. Anti-oxidant action of metronida-zole: a possible mechanism of action in rosacea. Br J Dermatol1986;114:231–234.
52. Bolton RP, Culshaw MA. Faecal metronidazole concentrationsduring oral and intravenous therapy for antibiotic associatedcolitis due to Clostridium difficile. Gut 1986;27:1169–1172.
53. Stahlberg D, Barany F, Einarsson K, Ursing B, Elmqvist D,Persson A. Neurophysiologic studies of patients with Crohn’sdisease on long-term treatment with metronidazole. Scand JGastroenterol 1991;26:219–224.
54. Boyce EG, Cookson ET, Bond WS. Persistent metronidazole-induced peripheral neuropathy. DICP 1990;24:19–21.
55. Duffy LF, Daum F, Fisher SE, et al. Peripheral neuropathy inCrohn’s disease patients treated with metronidazole. Gastroen-terology 1985;88:681–684.
56. Johnson S, Sanchez JL, Gerding DN. Metronidazole resistancein Clostridium difficile. Clin Infect Dis 2000;31:625–626.
57. Wong SS, Woo PC, Luk WK, Yuen KY. Susceptibility testing ofClostridium difficile against metronidazole and vancomycin bydisk diffusion and Etest. Diagn Microbiol Infect Dis 1999;34:1–6.
58. Barbut F, Decre D, Burghoffer B, et al. Antimicrobial suscepti-bilities and serogroups of clinical strains of Clostridium difficileisolated in France in 1991 and 1997. Antimicrob Agents Che-mother 1999;43:2607–2611.
59. Gerber M, Walch C, Loffler B, Tischendorf K, Reischl U, Acker-mann G. Effect of sub-MIC concentrations of metronidazole,vancomycin, clindamycin and linezolid on toxin gene transcrip-tion and production in Clostridium difficile. J Med Microbiol2008;57:776–783.
60. Drummond LJ, McCoubrey J, Smith DG, Starr JM, Poxton IR.
Changes in sensitivity patterns to selected antibiotics in Clos-tridium difficile in geriatric in-patients over an 18-month period.J Med Microbiol 2003;52:259–263.
61. Pelaez T, Cercenado E, Alcala L, et al. Metronidazole resistancein Clostridium difficile is heterogeneous. J Clin Microbiol 2008;46:3028–3032.
62. Baines SD, O’Connor R, Freeman J, et al. Emergence of reducedsusceptibility to metronidazole in Clostridium difficile. J Antimi-crob Chemother 2008;62:1046–1052.
63. Pepin J, Valiquette L, Gagnon S, Routhier S, Brazeau I. Out-comes of Clostridium difficile-associated disease treated withmetronidazole or vancomycin before and after the emergence ofNAP1/027. Am J Gastroenterol 2007;102:2781–2788.
64. Moellering RC Jr. Vancomycin: a 50-year reassessment. ClinInfect Dis 2006;42(Suppl 1):S3–S4.
65. Dworczynski A, Sokol B, Meisel-Mikolajczyk F. Antibiotic resis-tance of Clostridium difficile isolates. Cytobios 1991;65:149–153.
66. Shetler K, Nieuwenhuis R, Wren SM, Triadafilopoulos G. Decom-pressive colonoscopy with intracolonic vancomycin administra-tion for the treatment of severe pseudomembranous colitis.Surg Endosc 2001;15:653–659.
67. Kokkotou E, Moss AC, Michos A, et al. Comparative efficacies ofrifaximin and vancomycin for treatment of Clostridium difficile-associated diarrhea and prevention of disease recurrence inhamsters. Antimicrob Agents Chemother 2008;52:1121–1126.
68. Johnson S, Schriever C, Galang M, Kelly CP, Gerding DN. Inter-ruption of recurrent Clostridium difficile-associated diarrhea ep-isodes by serial therapy with vancomycin and rifaximin. ClinInfect Dis 2007;44:846–848.
69. Garey KW, Salazar M, Shah D, Rodrigue R, DuPont HL. Rifamy-cin antibiotics for treatment of Clostridium difficile-associateddiarrhea. Ann Pharmacother 2008;42:827–835.
70. Garey KW, Jiang ZD, Bellard A, Dupont HL. Rifaximin in treat-ment of recurrent Clostridium difficile-associated diarrhea: anuncontrolled pilot study. J Clin Gastroenterol [published onlineahead of print April 1, 2008].
71. Berman AL. Efficacy of rifaximin and vancomycin combinationtherapy in a patient with refractory Clostridium difficile-associ-ated diarrhea. J Clin Gastroenterol 2007;41:932–933.
72. O’Connor JR, Galang MA, Sambol SP, et al. Rifampin and rifaxi-min resistance in clinical isolates of clostridium difficile. Antimi-crob Agents Chemother 2008;52:2813–2817.
73. Musher DM, Logan N, Mehendiratta V, Melgarejo NA, Garud S,Hamill RJ. Clostridium difficile colitis that fails conventionalmetronidazole therapy: response to nitazoxanide. J AntimicrobChemother 2007;59:705–710.
74. Musher DM, Logan N, Hamill RJ, et al. Nitazoxanide for thetreatment of Clostridium difficile colitis. Clin Infect Dis 2006;43:421–427.
75. Cohen SA. Use of nitazoxanide as a new therapeutic option forpersistent diarrhea: a pediatric perspective. Curr Med Res Opin2005;21:999–1004.
76. McVay CS, Rolfe RD. In vitro and in vivo activities of nitazoxanideagainst Clostridium difficile. Antimicrob Agents Chemother2000;44:2254–2258.
77. Musher D L N, Bressler A, Johnson D, R JF. Nitazoxanide vs.vancomycin to treat Clostridium difficile disease. Presented atthe 48th Interscience Conference on Antimicrobial Agents andChemotherapy, Washington DC, 2008.
78. Dudley MN, McLaughlin JC, Carrington G, Frick J, NightingaleCH, Quintiliani R. Oral bacitracin vs vancomycin therapy forClostridium difficile-induced diarrhea. A randomized double-blindtrial. Arch Intern Med 1986;146:1101–1104.
79. Young GP, Ward PB, Bayley N, et al. Antibiotic-associated colitisdue to Clostridium difficile: double-blind comparison of vanco-
mycin with bacitracin. Gastroenterology 1985;89:1038–1045.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1910 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
80. Tedesco FJ. Bacitracin therapy in antibiotic-associatedpseudomembranous colitis. Dig Dis Sci 1980;25:783–784.
81. Chang TW, Gorbach SL, Bartlett JG, Saginur R. Bacitracin treat-ment of antibiotic-associated colitis and diarrhea caused by Clos-tridium difficile toxin. Gastroenterology 1980;78:1584–1586.
82. Clinical studies of ramoplanin in CDAD: ramoplanin vs. vanco-mycin in the treatment of Clostridium difficile diarrhea: a phase2 study. Presented in poster form at the 44th meeting of ICAAC.
83. Baines S, OC R, Saxton K, Freeman J, Wilcox M. Comparison oforitavancin versus vancomycin as treatment for clindamycin-induced C difficile ribotype 027 infection in a human gut model[abstract 540]. Presented at the 18th European Congress ofClinical Microbiology and Infectious Diseases 2008.
84. Lagrotteria D, Holmes S, Smieja M, Smaill F, Lee C. Prospective,randomized inpatient study of oral metronidazole versus oralmetronidazole and rifampin for treatment of primary episode ofClostridium difficile-associated diarrhea. Clin Infect Dis 2006;43:547–552.
85. Zilberberg MD, Shorr AF, Kollef MH. Increase in adult Clostrid-ium difficile-related hospitalizations and case-fatality rate,United States, 2000–2005. Emerg Infect Dis 2008;14:929–931.
86. Ali SO, Welch JP, Dring RJ. Early surgical intervention for fulmi-nant pseudomembranous colitis. Am Surg 2008;74:20–26.
87. Hall JF, Berger D. Outcome of colectomy for Clostridium difficilecolitis: a plea for early surgical management. Am J Surg 2008;196:384–388.
88. Dallal RM, Harbrecht BG, Boujoukas AJ, et al. Fulminant Clos-tridium difficile: an underappreciated and increasing cause ofdeath and complications. Ann Surg 2002;235:363–372.
89. Synnott K, Mealy K, Merry C, Kyne L, Keane C, Quill R. Timing ofsurgery for fulminating pseudomembranous colitis. Br J Surg1998;85:229–231.
90. Lamontagne F, Labbe AC, Haeck O, et al. Impact of emergencycolectomy on survival of patients with fulminant Clostridiumdifficile colitis during an epidemic caused by a hypervirulentstrain. Ann Surg 2007;245:267–272.
91. Koss K, Clark MA, Sanders DS, Morton D, Keighley MR, Goh J.The outcome of surgery in fulminant Clostridium difficile colitis.Colorectal Dis 2006;8:149–154.
92. Longo WE, Mazuski JE, Virgo KS, Lee P, Bahadursingh AN,Johnson FE. Outcome after colectomy for Clostridium difficilecolitis. Dis Colon Rectum 2004;47:1620–1626.
93. Rubin MS, Bodenstein LE, Kent KC. Severe Clostridium difficilecolitis. Dis Colon Rectum 1995;38:350–354.
94. Gerding DN, Muto CA, Owens RC Jr. Treatment of Clostridiumdifficile infection. Clin Infect Dis 2008;46(Suppl 1):S32–S42.
95. Maroo S, Lamont JT. Recurrent clostridium difficile. Gastroen-terology 2006;130:1311–1316.
96. McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle:treatment strategies for 163 cases of recurrent Clostridiumdifficile disease. Am J Gastroenterol 2002;97:1769–1775.
97. Kyne L, Kelly CP. Recurrent Clostridium difficile diarrhoea. Gut2001;49:152–153.
98. McFarland LV, Surawicz CM, Rubin M, Fekety R, Elmer GW,Greenberg RN. Recurrent Clostridium difficile disease: epidemi-ology and clinical characteristics. Infect Control Hosp Epidemiol1999;20:43–50.
99. Do AN, Fridkin SK, Yechouron A, et al. Risk factors for earlyrecurrent Clostridium difficile-associated diarrhea. Clin InfectDis 1998;26:954–959.
00. Fekety R, McFarland LV, Surawicz CM, Greenberg RN, ElmerGW, Mulligan ME. Recurrent Clostridium difficile diarrhea: char-acteristics of and risk factors for patients enrolled in a prospec-tive, randomized, double-blinded trial. Clin Infect Dis 1997;24:
324–333.01. Young GP, Bayley N, Ward P, St John DJ, McDonald MI. Antibi-otic-associated colitis caused by Clostridium difficile: relapseand risk factors. Med J Aust 1986;144:303–306.
02. Walters BA, Roberts R, Stafford R, Seneviratne E. Relapse ofantibiotic associated colitis: endogenous persistence of Clos-tridium difficile during vancomycin therapy. Gut 1983;24:206–212.
03. Young G, McDonald M. Antibiotic-associated colitis: why dopatients relapse? Gastroenterology 1986;90:1098–1099.
04. Wilcox MH, Fawley WN, Settle CD, Davidson A. Recurrence ofsymptoms in Clostridium difficile infection—relapse or reinfec-tion? J Hosp Infect 1998;38:93–100.
05. McFarland LV, Surawicz CM, Greenberg RN, et al. A randomizedplacebo-controlled trial of Saccharomyces boulardii in combina-tion with standard antibiotics for Clostridium difficile disease.JAMA 1994;271:1913–1918.
06. Tedesco FJ, Gordon D, Fortson WC. Approach to patients withmultiple relapses of antibiotic-associated pseudomembranouscolitis. Am J Gastroenterol 1985;80:867–868.
07. Tedesco FJ. Treatment of recurrent antibiotic-associatedpseudomembranous colitis. Am J Gastroenterol 1982;77:220–221.
08. Stepan C, Surawicz CM. Treatment strategies for C difficileassociated diarrhea. Acta Gastroenterol Latinoam 2007;37:183–191.
09. Surawicz CM, McFarland LV, Greenberg RN, et al. The search fora better treatment for recurrent Clostridium difficile disease:use of high-dose vancomycin combined with Saccharomycesboulardii. Clin Infect Dis 2000;31:1012–1017.
10. Kimmey MB, Elmer GW, Surawicz CM, McFarland LV. Preventionof further recurrences of Clostridium difficile colitis with Saccha-romyces boulardii. Dig Dis Sci 1990;35:897–901.
11. Surawicz CM, McFarland LV, Elmer G, Chinn J. Treatment of recur-rent Clostridium difficile colitis with vancomycin and Saccharomy-ces boulardii. Am J Gastroenterol 1989;84:1285–1287.
12. Surawicz CM, Elmer GW, Speelman P, McFarland LV, Chinn J,van Belle G. Prevention of antibiotic-associated diarrhea bySaccharomyces boulardii: a prospective study. Gastroenterol-ogy 1989;96:981–988.
13. Salcedo J, Keates S, Pothoulakis C, et al. Intravenous immu-noglobulin therapy for severe Clostridium difficile colitis. Gut1997;41:366–370.
14. Leung DY, Kelly CP, Boguniewicz M, Pothoulakis C, LaMont JT,Flores A. Treatment with intravenously administered gammaglobulin of chronic relapsing colitis induced by Clostridium dif-ficile toxin. J Pediatr 1991;118:633–637.
15. Wilcox MH. Descriptive study of intravenous immunoglobulin forthe treatment of recurrent Clostridium difficile diarrhoea. J An-timicrob Chemother 2004;53:882–884.
16. Mogg GA, Arabi Y, Youngs D, et al. Therapeutic trials of antibi-otic associated colitis. Scand J Infect Dis Suppl 1980;(Suppl22):41–5.
17. Kreutzer EW, Milligan FD. Treatment of antibiotic-associatedpseudomembranous colitis with cholestyramine resin. JohnsHopkins Med J 1978;143:67–72.
18. Sinatra F, Buntain WL, Mitchell CH, Sunshine P. Cholestyraminetreatment of pseudomembranous colitis. J Pediatr 1976;88:304–306.
19. Taylor NS, Bartlett JG. Binding of Clostridium difficile cytotoxinand vancomycin by anion-exchange resins. J Infect Dis 1980;141:92–97.
20. Kurtz CB, Cannon EP, Brezzani A, et al. GT160-246, a toxinbinding polymer for treatment of Clostridium difficile colitis.Antimicrob Agents Chemother 2001;45:2340–2347.
21. Louie TJ, Peppe J, Watt CK, et al. Tolevamer, a novel nonantibi-
otic polymer, compared with vancomycin in the treatment of
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
May 2009 TREATMENT OF CLOSTRIDIUM DIFFICILE INFECTION 1911
mild to moderately severe Clostridium difficile-associated diar-rhea. Clin Infect Dis 2006;43:411–420.
22. Peppe J, Porzio A, Davidson DM. A new formulation of tole-vamer, a novel nonantibiotic polymer, is safe and well-toleratedin healthy volunteers: a randomized phase I trial. Br J ClinPharmacol 2008;66:102–109.
23. Corthier G, Muller MC, Wilkins TD, Lyerly D, L’Haridon R. Pro-tection against experimental pseudomembranous colitis in gno-tobiotic mice by use of monoclonal antibodies against Clostrid-ium difficile toxin A. Infect Immun 1991;59:1192–1195.
24. Lyerly DM, Bostwick EF, Binion SB, Wilkins TD. Passive immu-nization of hamsters against disease caused by Clostridiumdifficile by use of bovine immunoglobulin G concentrate. InfectImmun 1991;59:2215–2218.
25. Pechine S, Janoir C, Boureau H, et al. Diminished intestinalcolonization by Clostridium difficile and immune response inmice after mucosal immunization with surface proteins of Clos-tridium difficile. Vaccine 2007;25:3946–3954.
26. Juang P, Skledar SJ, Zgheib NK, et al. Clinical outcomes ofintravenous immune globulin in severe clostridium difficile-as-sociated diarrhea. Am J Infect Control 2007;35:131–137.
27. Giannasca PJ, Warny M. Active and passive immunizationagainst Clostridium difficile diarrhea and colitis. Vaccine 2004;22:848–856.
28. Kyne L, Kelly CP. Prospects for a vaccine for Clostridium diffi-cile. BioDrugs 1998;10:173–181.
29. Aboudola S, Kotloff KL, Kyne L, et al. Clostridium difficile vac-cine and serum immunoglobulin G antibody response to toxin A.Infect Immun 2003;71:1608–1610.
30. Kotloff KL, Wasserman SS, Losonsky GA, et al. Safety andimmunogenicity of increasing doses of a Clostridium difficiletoxoid vaccine administered to healthy adults. Infect Immun2001;69:988–995.
31. Sougioultzis S, Kyne L, Drudy D, et al. Clostridium difficile toxoidvaccine in recurrent C difficile-associated diarrhea. Gastroenter-ology 2005;128:764–770.
32. Tvede M, Rask-Madsen J. Bacteriotherapy for chronic relapsingClostridium difficile diarrhoea in six patients. Lancet 1989;1:1156–1160.
33. Persky SE, Brandt LJ. Treatment of recurrent Clostridium diffi-cile-associated diarrhea by administration of donated stool di-rectly through a colonoscope. Am J Gastroenterol 2000;95:3283–3285.
34. You DM, Franzos MA, Holman RP. Successful treatment offulminant Clostridium difficile infection with fecal bacterio-therapy. Ann Intern Med 2008;148:632–633.
35. Seal D, Borriello SP, Barclay F, Welch A, Piper M, BonnycastleM. Treatment of relapsing Clostridium difficile diarrhoea byadministration of a non-toxigenic strain. Eur J Clin Microbiol1987;6:51–53.
36. Sambol SP, Merrigan MM, Tang JK, Johnson S, Gerding DN.Colonization for the prevention of Clostridium difficile disease inhamsters. J Infect Dis 2002;186:1781–1789.
37. Goldin BR, Gorbach SL. Clinical indications for probiotics: anoverview. Clin Infect Dis 2008;46(Suppl 2):S96–S100; discus-sion S144–S151.
38. Huebner ES, Surawicz CM. Probiotics in the prevention andtreatment of gastrointestinal infections. Gastroenterol ClinNorth Am 2006;35:355–365.
39. McFarland LV. Meta-analysis of probiotics for the prevention ofantibiotic associated diarrhea and the treatment of Clostridiumdifficile disease. Am J Gastroenterol 2006;101:812–822.
40. Pillai A, Nelson R. Probiotics for treatment of Clostridium diffi-cile-associated colitis in adults. Cochrane Database Syst Rev2008:CD004611.
41. Thomas MR, Litin SC, Osmon DR, Corr AP, Weaver AL, Lohse
CM. Lack of effect of Lactobacillus GG on antibiotic-associateddiarrhea: a randomized, placebo-controlled trial. Mayo Clin Proc2001;76:883–889.
42. Gorbach SL, Chang TW, Goldin B. Successful treatment ofrelapsing Clostridium difficile colitis with Lactobacillus GG. Lan-cet 1987;2:1519.
43. Songer JG, Jones R, Anderson MA, Barbara AJ, Post KW, TrinhHT. Prevention of porcine Clostridium difficile-associated dis-ease by competitive exclusion with nontoxigenic organisms. VetMicrobiol 2007;124:358–361.
44. Massot J, Sanchez O, Couchy R, Astoin J, Parodi AL. Bacterio-pharmacological activity of Saccharomyces boulardii in clinda-mycin-induced colitis in the hamster. Arzneimittelforschung1984;34:794–797.
45. Toothaker RD, Elmer GW. Prevention of clindamycin-inducedmortality in hamsters by Saccharomyces boulardii. AntimicrobAgents Chemother 1984;26:552–556.
46. Segarra-Newnham M. Probiotics for Clostridium difficile-associateddiarrhea: focus on Lactobacillus rhamnosus GG and Saccharomy-ces boulardii. Ann Pharmacother 2007;41:1212–1221.
47. Castagliuolo I, LaMont JT, Nikulasson ST, Pothoulakis C. Sac-charomyces boulardii protease inhibits Clostridium difficile toxinA effects in the rat ileum. Infect Immun 1996;64:5225–5232.
48. Pothoulakis C, Kelly CP, Joshi MA, et al. Saccharomyces bou-lardii inhibits Clostridium difficile toxin A binding and enterotox-icity in rat ileum. Gastroenterology 1993;104:1108–1115.
49. Fowler S, Webber A, Cooper BS, et al. Successful use of feed-back to improve antibiotic prescribing and reduce Clostridiumdifficile infection: a controlled interrupted time series. J Antimi-crob Chemother 2007;59:990–995.
50. Mendez MN, Gibbs L, Jacobs RA, McCulloch CE, Winston L,Guglielmo BJ. Impact of a piperacillin-tazobactam shortage onantimicrobial prescribing and the rate of vancomycin-resistantenterococci and Clostridium difficile infections. Pharmacother-apy 2006;26:61–67.
51. Thomas C, Riley TV. Restriction of third generation cephalospo-rin use reduces the incidence of Clostridium difficile-associateddiarrhoea in hospitalised patients. Commun Dis Intell 2003;27(Suppl):S28–S31.
52. Ludlam H, Brown N, Sule O, Redpath C, Coni N, Owen G. Anantibiotic policy associated with reduced risk of Clostridiumdifficile-associated diarrhoea. Age Ageing 1999;28:578–580.
53. Kuijper EJ, van Dissel JT, Wilcox MH. Clostridium difficile: chang-ing epidemiology and new treatment options. Curr Opin InfectDis 2007;20:376–383.
54. McFarland LV, Surawicz CM, Stamm WE. Risk factors for Clostrid-ium difficile carriage and C difficile-associated diarrhea in a cohortof hospitalized patients. J Infect Dis 1990;162:678–684.
55. McFarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomialacquisition of Clostridium difficile infection. N Engl J Med 1989;320:204–210.
56. Johnson S, Clabots CR, Linn FV, Olson MM, Peterson LR, Ger-ding DN. Nosocomial Clostridium difficile colonisation and dis-ease. Lancet 1990;336:97–100.
57. Valiquette L, Low DE, Pepin J, McGeer A. Clostridium difficileinfection in hospitals: a brewing storm. CMAJ 2004;171:27–29.
58. Uppal B, Wadhwa V, Mittal SK. Nosocomial diarrhea. IndianJ Pediatr 2004;71:883–885.
59. Samore MH. Epidemiology of nosocomial Clostridium difficileinfection. Compr Ther 1993;19:151–156.
60. Thibault A, Miller MA, Gaese C. Risk factors for the developmentof Clostridium difficile-associated diarrhea during a hospitaloutbreak. Infect Control Hosp Epidemiol 1991;12:345–348.
61. Fekety R, Kim KH, Brown D, Batts DH, Cudmore M, Silva J Jr.Epidemiology of antibiotic-associated colitis; isolation of Clos-tridium difficile from the hospital environment. Am J Med 1981;
70:906–908.
1
1
1
1
1
R
D0
C
1912 LEFFLER AND LAMONT GASTROENTEROLOGY Vol. 136, No. 6
62. Kim KH, Fekety R, Batts DH, et al. Isolation of Clostridiumdifficile from the environment and contacts of patients withantibiotic-associated colitis. J Infect Dis 1981;143:42–50.
63. Fekety R, Kim KH, Batts DH, et al. Studies on the epidemiologyof antibiotic-associated Clostridium difficile colitis. Am J ClinNutr 1980;33:2527–2532.
64. Srinivasan A, Song X, Ross T, Merz W, Brower R, Perl TM. Aprospective study to determine whether cover gowns in additionto gloves decrease nosocomial transmission of vancomycin-resistant enterococci in an intensive care unit. Infect ControlHosp Epidemiol 2002;23:424–428.
65. Johnson S, Gerding DN, Olson MM, et al. Prospective, con-trolled study of vinyl glove use to interrupt Clostridium difficile
nosocomial transmission. Am J Med 1990;88:137–140.66. Muto CA, Blank MK, Marsh JW, et al. Control of an outbreak ofinfection with the hypervirulent Clostridium difficile BI strain in auniversity hospital using a comprehensive “bundle” approach.Clin Infect Dis 2007;45:1266–1273.
Received October 21, 2008. Accepted December 22, 2008.
eprint requestsAddress requests for reprints to: Daniel A. Leffler, MD, Beth Israel
eaconess Medical Center, 330 Brookline Avenue, Boston, MA2215. e-mail: [email protected]; fax: (617) 667-2767.
onflicts of interest
The authors disclose no conflicts.



















