
Trasplante hepático en pacientes con infección por el VIH: una realidad en el año 2004
15
Liver Transplantation In Patients With HIV Infection John Fung, 1 Bijan Eghtesad, 1 Kusum Patel-Tom, 1 Michael DeVera, 1 Holly Chapman, 1 and Margaret Ragni 2 Key Points 1. Liver transplantation for human immunodeficiency virus (HIV)-positive patients with end-stage liver disease in the era of highly active retroviral therapy has proven to be an effective treatment. The concerns of HIV progres- sion have not been borne out by the growing worldwide experience. 2. CD4 counts are stable and HIV viral load is controllable with medication following liver transplantation. 3. Hepatitis C virus (HCV) coinfection in HIV-positive recipients is universal, but the severity of recurrence does not appear to be different from that in HIV-negative patients with HCV liver disease. 4. Complex pharmacokinetic interactions between the calcineurin inhibitors used for immunosuppression along with protease inhibitors are present, but management directed at recognizing the need for monitoring levels does not appear to increase the risk of toxicity. 5. The degree of immunosuppression from iatrogenic drug therapy and HIV does not lead to increased risk of infectious complications. (Liver Transpl 2004;10: S39–S53.) Human Immunodeficiency Virus (HIV) B oth HIVs, type 1 and type 2, can infect humans and lead to progressive immune deficiency. By far the best studied and the most prevalent strain in the United States is HIV-1, and for the purpose of this overview, the term “HIV” applies to HIV-1. HIV infec- tion is associated with a spectrum of clinical conditions, from no symptomatology to acquired immunodefi- ciency syndrome (AIDS; Table 1). AIDS is a syndrome that was first recognized in 1981 and is now defined as the presence of one of more than 20 conditions, includ- ing development of one or more opportunistic infec- tions and/or CD4 count less than 200 cells/mm 3 . 1 In the United States, it is estimated that there are between 750,000 and 1.5 million individuals infected with HIV, with 40,000 new cases added each year. 2 In addi- tion, approximately 40,000 deaths from HIV occur each year, and it is the leading cause of death in men between 25 and 44 years of age. Worldwide, the statis- tics are even more staggering, with more than 40 mil- lion people infected with HIV in 2000. Given the mag- nitude of this disease, tremendous progress has been made in the understanding of the virus, the process of replication, the mechanisms of inducing immune defi- ciency, and models for projecting survival. 3–5 Until the advent of antiviral therapies targeted toward HIV, the natural progression to AIDS could be predicted based on viral load and CD4 counts. 5 Although HIV is a retrovirus belonging to the lenti- virus subfamily and is structurally relatively simple, it has a complex replication cycle. 6 The virion is com- posed of a 2 single-stranded RNA genome packaged together with virally encoded proteins, including reverse transcriptase and structural proteins, as well as elements derived from the host, including cyclophilin A and a membrane composed of elements from both virus and host. The primary target is the CD4-positive T cell, by virtue of high-specificity binding of viral glycopro- tein (gp) 120 (gp120), the HIV glycoprotein associated with the trimeric gp41 complex, to the CD4 receptor. Other cells, including monocytes and glial cells, also bear CD4 antigen and can serve as a reservoir for HIV. Fusion of the virus into the target cell also requires the presence of chemokine receptors, such as CXCR4 (lym- photropic strain) or CCR5 (monocytotrophic strain). Other chemokine receptors, such as CCR3, have been shown to function in this manner. Viral fusion is medi- ated by gp41 and results in deposition of the reverse transcription complex into the cytoplasm. In some HIV strains, cyclophilin A has been implicated as playing an important role in activating reverse transcription. Com- plementary DNA (cDNA) synthesis is followed by nuclear translocation and nuclear integration facilitated Abbreviations: HIV, human immunodeficiency virus; AIDS, acquired immunodeficiency syndrome; gp, glycoprotein; NRTI, nucleo- side transcriptase inhibitors; PI, protease inhibitor; HAART, highly active antiretroviral therapy; OI, opportunistic infection; MMF, myco- phenolate mofetil; MPA, mycophenolic acid; GTP, guanosine triphos- phate; HCV, hepatitis C virus; HBV, hepatitis B virus; ESLD, end-stage liver disease; AUC, area under the curve. From the 1 Department of Surgery, Thomas E. Starzl Transplanta- tion Institute, University of Pittsburgh; and 2 Department of Medicine, Thomas E. Starzl Transplantation Institute, University of Pittsburgh, Pittsburgh, PA. Presented at the AASLD/ILTS Transplant Course, October 29, 2004, Boston, MA. Address reprint requests to: John J. Fung, MD, PhD, Department of General Surgery, Cleveland Clinic Foundation, 9500 Euclid Avenue, A80, Cleveland, OH 44195. Telephone: 216-444-3776; Fax: 216- 444-2153; E-mail: [email protected] Copyright © 2004 by the American Association for the Study of Liver Diseases Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/lt.2004.20261 S39 Liver Transplantation, Vol 10, No 10, Suppl 2 (October), 2004: pp S39 – S53
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Trasplante hepático en pacientes con infección por el VIH: una realidad en el año 2004

Liver Transplantation In Patients With HIV InfectionJohn Fung,1 Bijan Eghtesad,1 Kusum Patel-Tom,1 Michael DeVera,1
Holly Chapman,1 and Margaret Ragni2
Key Points1. Liver transplantation for human immunodeficiencyvirus (HIV)-positive patients with end-stage liver diseasein the era of highly active retroviral therapy has proven tobe an effective treatment. The concerns of HIV progres-sion have not been borne out by the growing worldwideexperience.2. CD4 counts are stable and HIV viral load is controllablewith medication following liver transplantation.3. Hepatitis C virus (HCV) coinfection in HIV-positiverecipients is universal, but the severity of recurrence doesnot appear to be different from that in HIV-negativepatients with HCV liver disease.4. Complex pharmacokinetic interactions between thecalcineurin inhibitors used for immunosuppression alongwith protease inhibitors are present, but managementdirected at recognizing the need for monitoring levelsdoes not appear to increase the risk of toxicity.5. The degree of immunosuppression from iatrogenicdrug therapy and HIV does not lead to increased risk ofinfectious complications. (Liver Transpl 2004;10:S39–S53.)
Human Immunodeficiency Virus (HIV)
Both HIVs, type 1 and type 2, can infect humansand lead to progressive immune deficiency. By far
the best studied and the most prevalent strain in theUnited States is HIV-1, and for the purpose of thisoverview, the term “HIV” applies to HIV-1. HIV infec-tion is associated with a spectrum of clinical conditions,from no symptomatology to acquired immunodefi-ciency syndrome (AIDS; Table 1). AIDS is a syndromethat was first recognized in 1981 and is now defined asthe presence of one of more than 20 conditions, includ-ing development of one or more opportunistic infec-tions and/or CD4 count less than 200 cells/mm3.1 Inthe United States, it is estimated that there are between750,000 and 1.5 million individuals infected withHIV, with 40,000 new cases added each year.2 In addi-tion, approximately 40,000 deaths from HIV occureach year, and it is the leading cause of death in menbetween 25 and 44 years of age. Worldwide, the statis-tics are even more staggering, with more than 40 mil-lion people infected with HIV in 2000. Given the mag-nitude of this disease, tremendous progress has beenmade in the understanding of the virus, the process ofreplication, the mechanisms of inducing immune defi-ciency, and models for projecting survival.3–5 Until theadvent of antiviral therapies targeted toward HIV, the
natural progression to AIDS could be predicted basedon viral load and CD4 counts.5
Although HIV is a retrovirus belonging to the lenti-virus subfamily and is structurally relatively simple, ithas a complex replication cycle.6 The virion is com-posed of a 2 single-stranded RNA genome packagedtogether with virally encoded proteins, includingreverse transcriptase and structural proteins, as well aselements derived from the host, including cyclophilin Aand a membrane composed of elements from both virusand host. The primary target is the CD4-positive T cell,by virtue of high-specificity binding of viral glycopro-tein (gp) 120 (gp120), the HIV glycoprotein associatedwith the trimeric gp41 complex, to the CD4 receptor.Other cells, including monocytes and glial cells, alsobear CD4 antigen and can serve as a reservoir for HIV.Fusion of the virus into the target cell also requires thepresence of chemokine receptors, such as CXCR4 (lym-photropic strain) or CCR5 (monocytotrophic strain).Other chemokine receptors, such as CCR3, have beenshown to function in this manner. Viral fusion is medi-ated by gp41 and results in deposition of the reversetranscription complex into the cytoplasm. In some HIVstrains, cyclophilin A has been implicated as playing animportant role in activating reverse transcription. Com-plementary DNA (cDNA) synthesis is followed bynuclear translocation and nuclear integration facilitated
Abbreviations: HIV, human immunodeficiency virus; AIDS,acquired immunodeficiency syndrome; gp, glycoprotein; NRTI, nucleo-side transcriptase inhibitors; PI, protease inhibitor; HAART, highlyactive antiretroviral therapy; OI, opportunistic infection; MMF, myco-phenolate mofetil; MPA, mycophenolic acid; GTP, guanosine triphos-phate; HCV, hepatitis C virus; HBV, hepatitis B virus; ESLD, end-stageliver disease; AUC, area under the curve.
From the 1Department of Surgery, Thomas E. Starzl Transplanta-tion Institute, University of Pittsburgh; and 2Department of Medicine,Thomas E. Starzl Transplantation Institute, University of Pittsburgh,Pittsburgh, PA.
Presented at the AASLD/ILTS Transplant Course, October 29,2004, Boston, MA.
Address reprint requests to: John J. Fung, MD, PhD, Department ofGeneral Surgery, Cleveland Clinic Foundation, 9500 Euclid Avenue,A80, Cleveland, OH 44195. Telephone: 216-444-3776; Fax: 216-444-2153; E-mail: [email protected]
Copyright © 2004 by the American Association for the Study ofLiver Diseases
Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/lt.2004.20261
S39Liver Transplantation, Vol 10, No 10, Suppl 2 (October), 2004: pp S39–S53

by viral integrase. Viral replication is the culmination ofa complex series of steps, including synthesis of viralstructural (Gag and Env) and enzymatic (pol) polypro-tein precursor and viral RNA synthesis. Viral packagingoccurs at the plasma membrane of the infected cells; thisresults in budding of immature viral particles. Autocat-alytic activation of the protease enzyme provides furtherposttranslational processing of critical polyproteinsrequired for the final maturation and subsequent infec-tivity. Certain HIV genes, in particular those encodingthe envelope proteins and reverse transcriptase, are
error prone and explain both the presence of quasispe-cies and the development of drug-resistant mutations.
The estimated total body pool of HIV is approxi-mately 1010 virions. The kinetics of established HIVinfection is notable for significant viral turnover: on theorder of 30% of the total body viral load is eliminatedon a daily basis and the life cycle in vivo of HIV isestimated at 1.2 days.7 Associated with this brisk viralturnover is a daily turnover of 5% of the total hostCD4� T-cell pool as part of active HIV replication.This leads to eventual depletion of the CD4� T-cellpool as the rate of destruction exceeds the ability of theprecursor pool to renew the total CD4� T-cell popula-tion.4,5 However, a small population of HIV-infectedindividuals do not follow this timeline of progression toAIDS—10% to 17% of infected individuals remainclinically free of AIDS 20 years after exposure, and asubset of these patients (less than 5% of all HIV-in-fected individuals) have stable CD4� T-cell counts—these patients are termed long-term nonprogressors.7
Immunological and virological studies of these individ-uals have failed to demonstrate a consistent pattern ofviral and host factors explaining this phenomenon.8,9
Anti-HIV Therapy
Delineation of the critical steps in viral replication andinfection has led to development of strategies and treat-ments designed to reduce viral replication. Specifically,current therapies are directed toward the defined path-ways: inhibition of viral binding and/or entry (enfu-virtide—inhibitor of gp41-mediated fusion); inhibit-ing reverse transcription (nucleoside transcriptaseinhibitors [NRTI] and non-nucleoside reverse tran-scriptase inhibitors [NNRTI]); and inhibiting proteaseactivity (protease inhibitors [PIs]). Since 1997, the vastmajority of antiretroviral therapy protocols haveincluded multiple drug therapy. Monotherapy and dualtherapies are not recommended in the treatment ofHIV-infected patients, primarily due to the high risk ofdeveloping resistance.10,11 Highly active antiretroviraltherapy (HAART) generally consists of 3 active antivi-ral agents—2 or more NRTI plus 1 PI or 1 non-nucle-oside reverse transcriptase inhibitor,11—and has beenshown to be associated with significant stabilization ofCD4 counts, reduction in the incidence of opportunis-tic infection (OI), and lower mortality. Clinical studieshave demonstrated virological, immunological, andsurvival benefits associated with the use of HAARTregimens.12–15
Other potential approaches to managing HIV infec-tion include novel observations with the use of immu-
Table 1. Revised 1993 Centers for Disease ControlClassification System of HIV Infection
Category AAsymptomatic HIV infectionPersistent generalized lymphadenopathyAcute retroviral syndrome
Category BBacillary angiomatosisOral or recurrent vaginal candidiasisCervical dysplasiaProlonged constitutional symptomsOral hairy leukoplakiaHerpes zosterIdiopathic thrombocytopenic purpuraListeriosisPelvic inflammatory diseasePeripheral neuropathy
Category CCD4 count � 200 cells/mm3
Cervical cancerChronic herpes simplexCoccidioidomycosisCryptococcosisCryptosporidiosisCytomegalovirusHistoplasmosisHIV encephalopathy/dementiaInvasive AspergillusIsosporiasisKaposi’s sarcomaLymphomaMicrosporidiosisMycobacterium aviumMycobacterium kansasiiMycobacterium tuberculosisPenicilliosisPneumocystis cariniiProgressive multifocalleukoencephalopathyPulmonary or esophageal candidiasisRecurrent pneumoniaSalmonellosisToxoplasmosis
S40 Fung et al.

nosuppressive agents. For example, it has been reportedthat HIV replication can be inhibited by cyclosporineand tacrolimus.16 Both animal17 and pilot human18,19
studies have been conducted, examining the effect ofcalcineurin inhibitors on HIV infection, presumably byinhibiting T-cell activation and thus cytokine synthesis(which can augment HIV replication), as well as inher-ent effects mediated by immunophilin receptors.Mycophenolate mofetil (MMF) is another immuno-suppressive agent that potentiates the effects of antiviralmedications. MMF is a prodrug of mycophenolic acid(MPA), which reversibly inhibits lymphocyte inosinemonophosphate dehydrogenase, thereby inhibiting denovo purine nucleotide synthesis and drasticallydecreasing intracellular guanosine triphosphate (GTP)concentrations both in vitro and in vivo. MPA has beenshown to enhance the effectiveness of purine nucleosideanalogues.20,21
Liver Disease in HIV-Infected Individuals
The irony of the diminishing mortality associated withHIV infection is the increasingly apparent impact of coin-fection with chronic viral hepatitis. HIV-positive patientsare at risk for hepatitis C virus (HCV) and hepatitis B virus(HBV) infection and the development of end-stage liverdisease (ESLD). The route for HIV acquisition is often thesame as the risk for acquisition of viral hepatitis, namely,transfusion of blood products, shared needles, and unpro-tected sexual practices. The prevalence of HCV coinfec-tion among HIV-positive patients has been reported in therange of 23% to 33%,22,23 while the prevalence of chronicHBV coinfection is approximately 9%.24 In some high-risk HIV-positive groups, such as hemophiliacs receivinglifelong serum-derived factor replacement, the incidenceof HCV coinfection has been reported to be as high as80% in HIV-positive hemophiliacs.25 It has also beenreported that the presence of HIV infection accelerates theprogression of chronic liver disease to ESLD.26–28 Thistranslates into higher mortality rates from ESLD in HIV-positive patients coinfected with viral hepatitis.26–33 In-hospital mortality was 12% in admissions for liver diseasein one study,33 and it was 4.8% in another study.32 In onestudy, the reported deaths due to ESLD has grown impres-sively, from 11.5% in 1991 to 13.9% in 1996, and to 50%in 1998–1999.31 In HCV- and HIV-coinfected hemo-philiac patients, the relative risk of developing ESLD was3.72, and death secondary to ESLD was 3.81, when com-pared to a group of non–HIV-infected hemophiliacs withHCV.25
In addition to chronic viral hepatitis, other causes ofESLD have been noted in the HIV-positive popula-
tion.34–37 Acute liver failure with lactic acidosis, hepaticsteatosis, and mitochondrial DNA injury has beenreported as a result of therapy with the “D drug” reversetranscriptase inhibitors (e.g., zalcitabine, didanosine,and stavudine).35–37 These agents are all potent inhib-itors of polymerase �, compared to other “non-Ddrugs,” such as zidovudine, lamivudine, and abacavir. Ithas also been suggested that the presence of HCV mayact in association with the use of D-drug in depletingmitochondrial DNA levels.37 Other antiviral agents, inparticular efavirenz and nevirapine, have also been asso-ciated with elevations in liver enzymes and may poten-tiate the detrimental effects of alcohol.38 HIV has alsobeen associated with an AIDS-related cholangiopathy,leading to biliary strictures. The causative agent in thesecases has been reported to include Cryptosporidium,cytomegalovirus (CMV), and Microspooridia.39,40
Lastly, there is some speculation that autoimmunityinduced by HIV and/or retroviral antigen mimicry maybe involved in primary biliary cirrhosis.41,42
HIV and Organ Transplantation
In spite of the many advances in organ transplantation, thepresence of HIV in a patient with end-stage organ failurehas been considered a relative or absolute contraindicationfor transplantation at many centers, for both medical andpsychosocial reasons.43 The conceptual conflict lies in theadministration of iatrogenic immunosuppression to the“immunocompromised” HIV-infected individual, a pro-cess that relegates organ transplantation in HIV recipientsto the status of a continued enigma. Early reports sug-gested that the course of HIV infection is accelerated intransplant patients, either due to the effect of immunosup-pression44,45 or to the role of alloantigenic stimulation oflymphocytes. However, it is difficult to separate the infec-tious complications associated with HIV from those asso-ciated with iatrogenic immunosuppression.46,47 A reviewof the relatively sparse pre-HAART experience concerningthe approach and outcome of solid organ transplantationin HIV-positive recipients is limited by the lack of abilityto discern HIV-related deaths from “normal” OI in trans-plant patients, the lack of staging information (i.e., HIVviral load or CD4� counts), and the lack of treatment forHIV based on current understanding of antiviral therapy.The use of AIDS OI terminology in the transplant popu-lation should be seriously questioned because these infec-tions can also be seen in HIV-negative organ transplantrecipients.
The first series of patients who were positive for HIVat the time of transplantation and of patients whoacquired HIV (presumably from the donor) were
S41Liver Transplantation in HIV Patients

reported by the University of Pittsburgh.47,48 In a ret-rospective serologic survey of organ donors and trans-plant recipients, 7 HIV-positive recipients had antibod-ies to HIV-1 prior to liver transplantation, while theother 8 HIV-positive recipients seroconverted afterliver transplantation. Of the 15 liver transplantpatients, 7 were alive at a mean of 2.75 years. Withfurther follow-up (12.75 years), only 2 liver transplantpatients remained alive, both on anti-HIV therapy.49
In a series of 4 hemophiliac patients at the Universityof Pittsburgh,50 performed from 1982 to 1987 (2 ofwhom were included in the analysis by Tzakis et al.48),1 patient died in the perioperative period, and 3 sur-vived for varying periods from 4 months to 44 months,before dying from a variety of OI: Pneumocystis, toxo-plasmosis, and cryptosporidiosis. These cases precededthe routine use of trimethoprim/sulfamethoxazole andthe availability of effective agents against Cryptospo-ridium. All deaths were classified as AIDS related. Inaddition, the University of Pittsburgh also reported 2additional HIV-positive liver transplants under tacroli-mus immunosuppression: 1 with chronic HBV and 1with chronic HCV.49 The HBV recipient developedHBV recurrence and died at 102 months; the HCVpatient suffered from HCV recurrence and survivedonly 7 months.
Researchers at the University of Minnesota reviewedthe overall liver transplantation experience in HIV-in-fected recipients reported in the literature from 1985 to1990.51 Twenty-two cases were identified, 10 HIV pos-itive at the time of liver transplantation and 12 devel-oping HIV perioperatively. They noted that patientsinfected pretransplant with HIV had a shorter time toprogression and a greater risk of dying from “AIDS”(defined primarily by development of posttransplantOI) or “AIDS-related complications” than those whoacquired HIV in the perioperative period. In addi-tional, the authors noted that in the HIV-positivepatients who underwent transplantation and were long-term survivors, good liver function could be demon-strated for an extended period of time. Others have alsoreported positive outcomes in isolated cases.52–54
Controversies in Liver Transplantation inHIV-Positive Patients
The following concepts summarize the current issues inoffering liver transplantation to HIV-positive candi-dates49,55,56: (1) a stable HIV-positive candidate willimmunologically decompensate with iatrogenic immu-nosuppression, (2) the viral load will increase and/or theimmunosuppression may enhance HIV mutations, (3)
the pharmacokinetics and pharmacointeractions of cur-rent antiretroviral agents and immunosuppression maylead to subtherapeutic effects or toxicity, (4) recurrentHCV infection along with HIV infection may lead toaccelerated fibrosis and graft failure, and (5) the publicperception on offering transplantation to HIV-positiverecipients will lead to diminished support for donation.Because these concerns have translated into lack ofaccess for HIV-positive patients needing liver trans-plantation and efforts by third-party payers to denycoverage,57 the remainder of this article will focus onthese issues by examining the current status of livertransplantation in the HAART era.
Liver Transplantation in HIV-Positive ESLDin the HAART Era
As shown in Table 2, there is an accelerating experience inproviding liver transplantation for HIV-positive patientsin the HAART era. According to the literature, the totalnumber of liver transplants performed in HIV-positiverecipients in the HAART era is now 50: the US experiencecomprises 21 patients, the European experience comprises27 patients, and the Asian experience comprises 2 patients.HCV was the primary indication, accounting for 68% ofcauses of liver disease. With varying periods of follow-up,80% of patients were reported alive.
Roland and Stock queried the United Network forOrgan Sharing (UNOS) registry for HIV-positive livertransplants performed during the HAART era andfound 19 patients.76 The overall patient survival was79%, with a median follow-up of 314 days; this wassimilar to non–HIV-positive liver transplant recipientswith a 1-year survival of 88%.
The largest single-center series comes from the Univer-sity of Pittsburgh. A total of 29 HIV-positive ESLDpatients have been recipients of liver allografts alone since1997 (1 patient received both a liver and kidney). Theindications for liver transplantation are shown in Table 3.Overall, 89% were for HCV, 7% were for HBV, and 4%were for fulminant liver failure. Twenty-six percent werehemophiliacs that acquired viral hepatitis from coagula-tion factor replacement. Two patients also had concomi-tant hepatocellular carcinoma. The average Model forEnd-Stage Liver Disease score was 21 (range, 8-46). Thevast majority (89%) of patients were male, and the averageage at transplantation was 46.6 years (range, 34-66).
Overall, all but 1 patient received some antiretroviraltherapy at some point before transplantation; however,only 16 (55%) of recipients were taking HAART at thetime of liver transplant. Twelve patients had been dis-continued from HAART for varying periods before
S42 Fung et al.

transplantation, resulting in 12 patients who had HIVviral loads in the detectable range. In patients with liverfailure, there can be significant difficulties in dosingHAART, given the added hepatoxicity of NRTI andthe altered pharmacokinetics of PI metabolism. Wehave taken the position of allowing ESLD HIV-positivepatients to have detectable HIV loads prior to trans-plantation, as long as the pattern of drug history anddemonstrated HAART resistance pattern can predictsuppression of HIV replication following reinstitutionof HAART once normal liver function returns afterliver transplantation.
Nine patients died during the follow-up period,which averaged 18 months (range, 1-68). Perioperativecomplications not related to HIV (accelerated humoralrejection with a strongly positive crossmatch [1] andsepsis [2]) contributed to 3 deaths within 30 days. Onelate death was related directly to an infectious cause (acentral nervous system fungal infection at 58 monthsafter liver transplantation). One patient succumbed torecurrent hepatocellular carcinoma. Recurrent HCVwas the principal cause of or was a contributing factor in4 deaths (in one, treatment for acute and chronic rejec-tion exacerbated HCV, and both complications wereequal culprits in worsening liver failure). Although the1-year survival of all patients was 76% and the overallsurvival was 69%, of those that survived more than 30
days posttransplant, the 1-year patient survival was89% and the overall survival was 77%. In all cases, livertransplantation reversed the stigmata of acute andchronic liver failure, including ascites, encephalopathy,muscle wasting, fatigue, hypersplenism, and jaundice.
Due to the skewed nature of liver disease in the HIVpopulation—i.e., higher incidence of viral hepatitis—thesurvival outcomes would be more appropriately comparedto a group of viral hepatitis, non–HIV-positive liver trans-plant recipients. HIV-positive patients with HBV infec-tion, for which effective prophylaxis against recurrenceexists using hepatitis B immune globulin (HBIG) andlamivudine,77 do not appear to suffer recurrence and haveexcellent short- and long-term survival rates. However,analysis of the subset of HCV- and HIV-coinfectedpatients points to a potential concern of HCV recurrenceon long-term survival. Although it is important to note thepoor outcomes in HCV- and HIV-coinfected patientsfrom the King’s College group (in which recurrence led todecreased survival), it should be noted that their experi-ence was in the very early period, before the complexity ofHAART and immunosuppression was appreciated.65 Thecombined experience of the Universities of Miami andPittsburgh points to a more optimistic outcome, with a1-year survival rate no different from that for HCV-posi-tive, HIV-negative patients.65 At the University of Pitts-burgh, HCV recurrence was treated with ribavirin and
Table 2. Worldwide Experience with Liver Transplantation in HIV Patients in the HAART Era
Center Year Reference Number % HCV % Surviving
King’s College, UK 1996 58 1 100% 100%Milan 1998 59 1 0% 100%Pittsburgh 1999 60 1 100% 100%New York 1999 61 1 100% 100%Sweden 2000 62 1 100% 100%Bonn 2000 63 1 0% 100%King’s College, UK 2001 64,65 5 60% 40%Birmingham, UK 2001 66 1 100% 100%Leeds, UK 2001 67 1 100% 0%Japan 2002 68 1 100% 100%Barcelona 2002 69 1 NA NAMiami 2003 70 6 50% 100%Pittsburgh 2003 65,70 10 80% 80%UCSF 2003 65,71 4 25% 75%Madrid 2003 72 1 100% 100%Sweden 2003 73 3 100% 67%Taiwan 2003 74 1 0% 100%Clichy/Rome 2004 75 10 70% 80%Rome 2004 76 1 100% 100%Total 51 68% 80%
Abbreviations: NA, not applicable; UCSF, University of California, San Francisco; HIV, human immunodeficiency virus; HCV,hepatitis C virus.
S43Liver Transplantation in HIV Patients
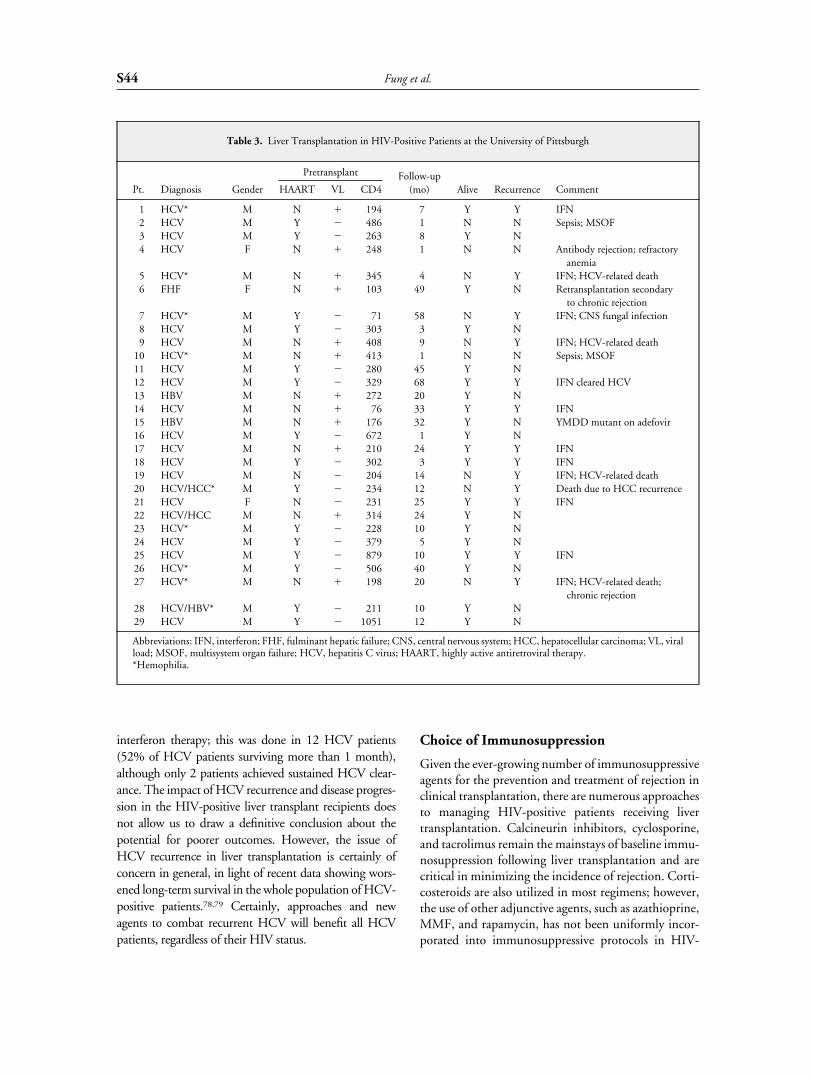
interferon therapy; this was done in 12 HCV patients(52% of HCV patients surviving more than 1 month),although only 2 patients achieved sustained HCV clear-ance. The impact of HCV recurrence and disease progres-sion in the HIV-positive liver transplant recipients doesnot allow us to draw a definitive conclusion about thepotential for poorer outcomes. However, the issue ofHCV recurrence in liver transplantation is certainly ofconcern in general, in light of recent data showing wors-ened long-term survival in the whole population of HCV-positive patients.78,79 Certainly, approaches and newagents to combat recurrent HCV will benefit all HCVpatients, regardless of their HIV status.
Choice of Immunosuppression
Given the ever-growing number of immunosuppressiveagents for the prevention and treatment of rejection inclinical transplantation, there are numerous approachesto managing HIV-positive patients receiving livertransplantation. Calcineurin inhibitors, cyclosporine,and tacrolimus remain the mainstays of baseline immu-nosuppression following liver transplantation and arecritical in minimizing the incidence of rejection. Corti-costeroids are also utilized in most regimens; however,the use of other adjunctive agents, such as azathioprine,MMF, and rapamycin, has not been uniformly incor-porated into immunosuppressive protocols in HIV-
Table 3. Liver Transplantation in HIV-Positive Patients at the University of Pittsburgh
Pt. Diagnosis Gender
Pretransplant Follow-up(mo) Alive Recurrence CommentHAART VL CD4
1 HCV* M N � 194 7 Y Y IFN2 HCV M Y � 486 1 N N Sepsis; MSOF3 HCV M Y � 263 8 Y N4 HCV F N � 248 1 N N Antibody rejection; refractory
anemia5 HCV* M N � 345 4 N Y IFN; HCV-related death6 FHF F N � 103 49 Y N Retransplantation secondary
to chronic rejection7 HCV* M Y � 71 58 N Y IFN; CNS fungal infection8 HCV M Y � 303 3 Y N9 HCV M N � 408 9 N Y IFN; HCV-related death
10 HCV* M N � 413 1 N N Sepsis; MSOF11 HCV M Y � 280 45 Y N12 HCV M Y � 329 68 Y Y IFN cleared HCV13 HBV M N � 272 20 Y N14 HCV M N � 76 33 Y Y IFN15 HBV M N � 176 32 Y N YMDD mutant on adefovir16 HCV M Y � 672 1 Y N17 HCV M N � 210 24 Y Y IFN18 HCV M Y � 302 3 Y Y IFN19 HCV M N � 204 14 N Y IFN; HCV-related death20 HCV/HCC* M Y � 234 12 N Y Death due to HCC recurrence21 HCV F N � 231 25 Y Y IFN22 HCV/HCC M N � 314 24 Y N23 HCV* M Y � 228 10 Y N24 HCV M Y � 379 5 Y N25 HCV M Y � 879 10 Y Y IFN26 HCV* M Y � 506 40 Y N27 HCV* M N � 198 20 N Y IFN; HCV-related death;
chronic rejection28 HCV/HBV* M Y � 211 10 Y N29 HCV M Y � 1051 12 Y N
Abbreviations: IFN, interferon; FHF, fulminant hepatic failure; CNS, central nervous system; HCC, hepatocellular carcinoma; VL, viralload; MSOF, multisystem organ failure; HCV, hepatitis C virus; HAART, highly active antiretroviral therapy.*Hemophilia.
S44 Fung et al.

positive recipients. Antilymphocyte antibodies, rangingfrom panlymphocyte antibodies—e.g., antithymocyteglobulin (Thymoglobulin, ATGAM) and alemtu-zumab (Campath 1H)—to anti–T-cell antibodies(e.g., OKT3) to anti-interleukin 2-receptor antibod-ies—e.g., basiliximab (Simulect) and dacluzimab(Zenapax)—also have not found a place in immuno-suppressive protocols for HIV positive patients, therationale being based on the poorer early experienceswith OKT3 in HIV-positive patients.48
In any case, the paramount goal in the selection of agiven immunosuppressive regimen is to minimize rejec-tion, while preventing posttransplant OI. Recently,there have been intriguing reports on the potentialeffect of immunosuppressive agents in the treatment ofHIV patients. HIV utilizes cellular cyclophilin forstructural protein processing (important in the assem-bly of HIV virions) as well as for subsequent infectivi-ty.80 Cyclosporine interferes with cyclophilin activityand inhibits HIV replication in vitro through inhibitionof lymphocyte activation and specific inhibition ofcyclophilin-HIV gag polyprotein interaction.81,82
However, in a randomized, double-blind, placebo-con-trolled trial, low-dose cyclosporine (2 mg/kg) did notaffect HIV viral load or CD4� T-cell counts.83 Never-theless, the results of an earlier study showed that livertransplant patients acquiring HIV in the perioperativeperiod from contaminated blood or allografts undercyclosporine immunosuppression appeared to experi-ence a cumulative lower risk of HIV progression thanthose that were already infected.84
The possibility that corticosteroids, through inhibi-tion of lymphocyte activation and thus cytokine pro-duction, might also positively influence the impact ofHIV has also been examined. A randomized, double-blind, placebo-controlled trial examining a short courseof prednisone (0.5 mg/kg/d for 8 weeks) in patientswith CD4 counts averaging 131 cells/L showed thatthis treatment was well tolerated and reasonably safe inpatients with stable HIV disease, although no majorHIV benefit was observed.85 On the other hand, a sim-ilar study in patients with baseline CD4 counts greaterthan 200 cells/L noted an increase (�40%) in CD4� Tcells, although side effects were more notable.86
Targeting reverse transcriptase with nucleoside ana-logues provides another potential area for immunosup-pressive drug/HAART interactions. MPA, through itsinhibition of GTP synthesis, acts synergistically withguanosine analogues such as abacavir in the inhibitionof HIV replication.20 However, pilot clinical trials thatattempted to exploit this robust in vitro phenomenonfor salvage in HAART-resistant HIV-positive patients
did not demonstrate a sustained benefit, although tran-sient drops in HIV viral load were obtained.21,87 Nev-ertheless, these studies demonstrated that MMF couldbe safely administered and provide reassurance that itcan be used safely as part of a maintenance immuno-suppressive regimen.
Although modulation of host immunity withimmunosuppressive agents has yet to demonstrate aclear clinical benefit to HIV-infected patients, availabledata indicate that these maintenance immunosuppres-sive agents can be used in the context of liver transplan-tation for HIV-positive patients without dire conse-quences for safety.
Rejection
One area in which there is little scientific knowledge isthe impact of HIV on the risk of rejection and viceversa. HIV-positive patients have variable levels ofimmune deficiency, and some investigators have sug-gested that there are diminished rates of rejection inHIV positive patients and thus they may be able toreduce immunosuppression without precipitatingrejection.51 This finding has not been borne out in theearly posttransplant period, and acceptance of thisapproach may be quite harmful. Although HIV-posi-tive patients may be able to reduce the level of immu-nosuppression after transplantation, this is a commonphenomenon in non-HIV recipients. In fact, it is notsurprising that others have shown rates of rejectionequal to or even greater than non–HIV-positive trans-plant candidates.48 This is due to the fact that an esti-mated 10% of all CD4� T cells can respond to alloge-neic stimuli; thus, total CD4� T-cell counts must bemarkedly suppressed before the number of alloreactiverecipient T cells would obviate the development ofrejection. In addition, HIV-infected patients have beenshown to have dysregulated B-cell function and poly-clonal gammopathy.88,89 This has been postulated toexplain the unexpectedly high rates of rejection seen ina recent kidney transplant study.90
Early reports using cyclosporine-based immunosup-pression were associated with high rates of rejection andthe need for antilymphocyte antibody therapy, whichwas also associated with high risk of OI and death.48
Whether this increased morbidity and mortality is dueto increased risk of OI, or to the potential impact ofallogeneic stimulation of HIV-infected CD4� T cellson increasing HIV replication and thus progression ofHIV replication, has not been determined. While theoptimal approach to immunosuppression in HIV-pos-itive recipients has not been determined, it appears rea-
S45Liver Transplantation in HIV Patients

sonable to approach these patients with the same inten-sity of early immunosuppression as in non–HIV-positive patients. Nevertheless, this area will requirefurther study.
Choice of HAART Regimen
In general, the principles for HIV therapy in transplantpatients should be the same as for nontransplantpatients (Table 4). There are growing numbers ofagents and novel compounds to inhibit replication ofHIV that have been introduced into the clinical arena.Today, most treatment regimens include at least 2, andsometimes 3 different classes of antiretroviral therapy.The HIV clinician is faced with changing recommen-dations, some based on efficacy, others based on resis-tance patterns, and still others based on side effects ofantiviral agents, either alone or in combination. Theserecommendations are then overlaid on the patient’sindividual characteristics, necessitating individualizedassessment and monitoring of response to HAART.The necessity of continuous HAART after liver trans-plantation has not yet been demonstrated, although ithas been suggested that patients who cannot tolerateHAART posttransplant do poorly. Whether this is dueto the lack of HAART or the inability to tolerateHAART due to recurrent HCV has not been deter-mined.65 There is also uncertainty about the need forHAART in long-term nonprogressing HIV-positivepatients.91,92
Pharmacointeractions
Cyclosporine (CSA), tacrolimus, and rapamycin areprimarily metabolized by cytochrome P450 3A2 and3A4 isoenyzmes and are subject to pharmacokineticinteractions by other drugs that induce or inhibit thisenzyme activity. These agents are also substrates of thep-glycoprotein system, also known as the multiple drugresistance transport system. In addition, the PI agentsare similarly metabolized by this group of enzymes,some acting as inducers and others as inhibitors of these
metabolic enzyme pathways (Table 5; see also http://www.hiv-druginteractions.org and http://www.proojinf.org for additional drug interactions). Drug interactionsin hepatic metabolism between calcineurin inhibitorsand PIs have been well described in liver transplantrecipients.61,93–97
Several studies have indicated significant pharmaco-logical interactions between tacrolimus and PIs, includ-ing nelfinavir, ritonavir, and lopinavir. After liver trans-plantation and before reinstitution of HIV therapy,tacrolimus levels were adjusted to maintain therapeuticlevels. Following resumption of PIs, tacrolimus levelsrose dramatically, resulting in toxicity. Tacrolimus dos-ing was markedly reduced to minimize levels of tacroli-mus and resultant toxicity. Such interactions are fre-quent with combined tacrolimus and PI use, and theaverage maintenance dose of tacrolimus in the Univer-sity of Pittsburgh experience is 1 mg/wk.
Similar findings have been noted with cyclosporineand PI interactions. Brinkman et al. described a patientreceiving simultaneous saquinavir and cyclosporine, inwhom the addition of nelfinavir elevated cyclosporinearea–under–the curve (AUC) by 5- to 10-fold.96 Witha 50% reduction in the CSA dose, in the setting ofcontinued saquinavir use the CSA AUC was still 90%of that without the use of PIs. Like tacrolimus, whenused in combination with nelfinavir, saquinavir, orritonavir, cyclosporine levels may need to be dosed lessfrequently than once a day.
Although not a calcineurin inhibitor, rapamycinbelongs to the class of macrolide antibiotics and ismetabolized by the same cytochrome P450 pathway.Jain et al. reported significant drug interactions in aliver transplant patient on sirolimus maintenanceimmunosuppression to which nelfinavir was added.97
Therapeutic monitoring of cyclosporine, tacroli-mus, or rapamycin levels is critically important, notonly when PI use is instituted but also when it isstopped. In one case, the local physician treating HIVelected to take the patient off of HAART therapy(“drug-free holiday”). The elimination of the PI caused
Table 4. Principles Outlining Current Approaches To Treatment of HIV
Principle 1 HIV replication causes immune destruction and is always harmful.Principle 2 HIV RNA levels reflect viral replication and CD4� T-cell destruction.
Principle 3Combination antiretroviral therapy is most likely to lead to sustained suppression of HIV replication and thus limits thepotential for development of resistance.
Principle 4 Maximum achievable suppression of HIV replication is the goal of therapy.Principle 5 Given the known reservoir of HIV infected cells, “cure” is unlikely and antiviral therapy is needed to prevent reactivation.
S46 Fung et al.

drastic reduction in tacrolimus levels, precipitatingacute rejection that evolved into chronic rejection.95
This case also highlights the critical need for those man-aging transplant immunosuppression and those manag-ing HIV medications to communicate before makingadjustments in either medication. Unfortunately, thedrug interactions are sufficiently complex that drugdosing must be determined empirically for each patient.Although HIV PI levels are not routinely measured,there is reason to consider studying the utility of mon-itoring of PI levels in patients receiving tacrolimus,cyclosporine, or rapamycin. In one report in whichsaquinavir levels were measured, the AUC was 4 to 11times higher than in patients receiving saquinavir butnot cyclosporine.96
Drug interactions between anti-HIV and antire-jection and transplant medications are not only lim-ited to calcineurin inhibitor and PI use. As notedearlier, MPA is a potent, selective, noncompetitive,and reversible inhibitor of inosine monophosphatedehydrogenase, an enzyme involved in the synthesisof deoxyguanosine triphosphate (dGTP). Reductionin intracellular dGTP concentrations induced byMPA is expected to increase the antiretroviral activ-ity of abacavir, a guanosine analogue. In vitro studiesshow that MPA synergistically increases the antiviraleffect of abacavir, didanosine, and tenofovir againstmulti – NRTI-resistant HIV strains.20 Antagonismdue to inhibition of thymidine kinase has been notedwith MPA (and MMF) plus the thymidine analogues
Table 5. Drug Interactions Between Commonly Used Transplant Medications and HAART
Agent Toxicity Interactions
Nucleoside ReverseTranscriptase Inhibitors
Didanosine (ddI) GI, neuropathy Ganciclovir, azoles, MMF, Bactrim, allopurinol,pentamidine, ribavirin
Lamivudine (3TC) GI, neuropathy BactrimStavudine (d4T) Neuropathy, leukopenia,
hepatotoxicityGanciclovir, ribavirin, pentamidine
Zalcitabine (ddC) Neuropathy, rash, pancreatitis Aminoglycoside, bactrim, Flagyl, ribavirin,dapsone, amphotericin, foscarnet, phenytoin
Zidovudine (AZT) Anemia, neutropenia, GI, myopathy Azathioprine, Bactrim, dapsone, azoles,ganciclovir, amphotericin, ribavirin,pentamidine, foscarnet, �-interferon
Non-Nucleoside ReverseTranscriptase Inhibitors
Delaviridine (Rescriptor) Rash, GI, hepatotoxicity Azoles, cyclosporine, tacrolimus, rapamycin,phenytoin, phenobarbital, tenofovir, calciumchannel blockers, sildenafil, cisapride, Prozac,statins, glipizide, midazolam, caspofungin, ddI,corticosteroids
Efavirenz (Sustiva) Dizziness, GI, hepatotoxicity, rash Same as Delaviridine (Rescriptor)Nevirapine (Viramune) GI, rash, hepatotoxicity, fever Same as Delaviridine (Rescriptor)
Protease InhibitorsIndinavir (Invirase,Criixivan)
GI, nephrolithiasis Azoles, cyclosporine, tacrolimus, rapamycin,phenytoin, phenobarbital, tenofovir, calciumchannel blockers, sildenafil, cisapride, Prozac,statins, glipizide, midazolam, caspofungin, ddI,corticosteroids
Nelfinavir (Viracept) GI, fatigue Same as Indinavir (Invirase, criixivan)Ritonavir (Norvir) GI, asthenia, lipid abnormalities,
hepatotoxicity, paresthesiasSame Indinavir (Invirase, criixivan)
Saquinavir (Fortovaase) GI, mouth sores Same Indinavir (Invirase, criixivan)Amprenavir (Agenerase)Atazanavir (Reyataz)Lopinavir
Abbreviation: GI, gastrointestinal.
S47Liver Transplantation in HIV Patients

zidovudine and stavudine (Table 6). This also raisesthe important concern of whether the mitochondrialtoxicity of NRTI will be potentially augmented bythe effect of MPA. Mitochondrial toxicity and lacticacidosis has been linked to the use of D drugs such asdidanosine, stavudine, and zalcitabine and is attrib-uted to the damage of mitochondrial polymerase �by these agents. Patients with this syndrome canpresent with lethargy, malaise, hepatitis, peripheralneuropathy, pancreatitis, and other end-organ dam-age. Failure to identify this syndrome may result indeath from hypoxia and lactic acidosis. This has alsobeen suggested to be a potential area for enhancedtoxicity.76
Ribavirin used in combination for HCV therapy hasbeen shown to inhibit phosphorylation of zidovudine,stavudine, and zalcitabine. Ribavirin may also increasethe potency of didanosine and improve anitviral activ-ity. Since ribavirin is also a known inhibitor of inosinemonophosphate dehydrogenase, this would addanother level of potential interaction with MPA andNRTI and could account for enhanced toxicity. In areport of an HCV-coinfected HIV patient on HAART,MMF, and ribavirin, with lactic acidosis and a liverbiopsy revealing 80% microsteatosis, electron micros-copy revealed abnormalities in mitochondrial structureconsistent with NRTI toxicity.98
Opportunistic Infections
OI refers to the development of infectious disease inindividuals with significant defects in host defenses.The pathogens responsible for this infection often lackintrinsic virulence and therefore require an immune orinflammatory defect to establish infection.
Probably the single most important achievement in
the management of the immunocompromised patientare the improvements in the strategies for detection,prevention, and treatment of OI. For prophylaxis, theroutine addition of trimethoprim/sulfamethoxazole hasreduced the incidence of Pneumocystis jiroveci (formerlyPneumocystis carinii), Toxoplasmosis gondii, and Listeriamonocytogenes. The development of assays to detect OIwhen the infection is subclinical or at the earliest onsetof disease allows for targeted preemptive therapy. Suchis the case in CMV, in which pp65 antigenemia orCMV polymerase chain reaction monitoring allows forearlier detection and better assessment of efficacy oftreatment.99 However, the utility of early detectionwould not be of benefit if effective agents were notavailable for treatment. The development of ganciclo-vir, first intravenously and now orally, has reduced themorbidity and mortality of CMV infection.100 Whilesimilar assays are being developed for fungal infectionsand Epstein-Barr viral infections, these tests remain inthe developmental phase.
The risk of OI in immunosuppressed HIV-positivetransplant patients does not appear to be above andbeyond the risk of immunosuppressed HIV-negativetransplant recipients using current-day prophylaxis,monitoring, and treatment. The ability to attain rou-tine suppression of HIV viral loads on HAART is asso-ciated with stabilization or improvement in CD4counts, which has been shown to decrease OI in HIV-positive patients.101
Current Recommendations for LiverTransplantation in HIV-Positive Patients
HIV-infected ESLD patients should be considered forliver transplantation if they meet standard medical cri-teria for inclusion/exclusion as currently practiced by amultidisciplinary transplant team and meet UNOS cri-teria for listing. Added institutional requirementsinclude expertise in HIV management, a transplantpharmacologist with expertise in drug interactions, atransplant infectious diseases specialist, and a fiscaladministrator knowledgeable in the area of insurancecoverage. In addition to the standard transplant evalu-ation process, CD4� T-cell counts, quantitative HIVloads, and current/prior responsiveness to antiviraltherapy must be obtained. Patients who demonstratedrug resistance can be considered if an effective antiret-roviral drug regimen can be devised; drug-resistancepattern determinations may be required if a clear his-tory of antiviral therapy cannot be obtained in the pres-ence of detectable HIV viral load. Clinical responsive-ness to antiretroviral therapy is defined as suppression
Table 6. Effect of Mycophenolate Mofetil (MMF) onNucleoside Reverse Transcriptase Inhibitors (NRTI)
NRTI Mechanism Effect of MMF
Zidovudine(AZT; Retrovir)
Thymidine analogue Antagonist
Stavudine(d4T; Zerit)
Thymidine analogue Antagonist
Zalcitabine(ddC; HIVID)
Cytidine analogue
Lamivudine(3TC; Epivir)
Cytidine analogue
Didanosine(ddI, Videx)
Inosine analogue Enhances
Abacavir (Ziagen) Guanosine analogue Enhances
S48 Fung et al.

of HIV RNA to less than 0.4 � 103 copies/mL (usingthe Chiron assay). Individuals with severe liver dysfunc-tion preventing tolerance of antiretroviral therapyshould be considered if they have shown prior respon-siveness to, or are naive to HAART. It has been sug-gested that HAART be stopped before transplantationin order to allow “wild type virus [to] rebound”; how-ever, this approach has not been proven.102 These sameauthors have suggested that lamivudine-resistant hepa-titis B may pose a problem in patients with HIV andHBV. However, the options of using high-dose hepati-tis B immune globulin and/or the promising experiencewith adefovir and tenofovir disoproxil for lamivudine-resistant HBV appear to effectively suppress HBVrecurrence.
Exclusion criteria are continuing to evolve as moreexperience is gleaned. Those conditions known to neg-atively affect survival after liver transplantation, such asrenal failure, requirement for life support, andadvanced malnutrition are risk factors that haveexcluded patients from active consideration. The crite-ria for OI exclusions include a previous OI within theprevious 6 to12 months; previous Kaposi’s sarcoma(given the high rate of recurrence103,104); and patientswith evidence of JC polyoma viral infection. In the 29cases of liver transplant at the University of Pittsburgh,6 patients had a remote history of Pneumocystis cariniipneumonia with posttransplant prophylaxis, and noneof them experienced PCP recurrence. While most cen-ters that are performing kidney transplantation in HIV-positive candidates have used a CD4 cutoff of 200cells/mm3 as being the lower threshold for consider-ation, liver transplant patients have hypersplenism thatmay render the CD4 count artifactually low and maynot actually reflect the overall status of the patient.Thus, lower CD4 counts for these patients can beaccepted based on a relative comparison of the CD4count with the absolute neutrophil count. Lastly, giventhe complexity of posttransplant monitoring and com-plex drug regimens, a strong history of noncomplianceshould be considered a contraindication; however, itshould be recognized that due consideration should begiven on an individual basis to extenuating circum-stances, e.g., long-term nonprogressors.
Because of a relatively high rate of acute cellularrejection in HIV-positive patients, calcineurin-basedimmunosuppression should be used, with or withoutsteroids and with or without other adjunctive agents,such as MMF. Although we have avoided using anti-lymphocyte induction, use of induction antibodies hasbeen used in HIV-positive kidney transplant recipientswithout any apparent detrimental effects on HIV or
increased risk of OI (Dr. Henke Tan, University ofPittsburgh, personal communication, July 2004).
With respect to the selection of HAART, very often thechoice of antiretroviral medications is dictated by the pasthistory of their use and the patient’s responsiveness tovarious regimens. In our liver transplant patients, HAARThas utilized PI combination antiretroviral therapy before(unless not tolerated because of severe liver dysfunction)and after transplantation, when the total bilirubin hasfallen to 2 mg/dL. Care should be taken in prescribingantiretroviral medications to continue already successfulcombinations used by the patient and to avoid drugs thatare associated with clinical resistance in the patient. It iscritical to modify doses of cyclosporine, tacrolimus, andrapamycin—based on pharmacokinetic interactions withHAART that includes PI)—based on their respectiveblood levels routinely monitored after transplantation. Inaddition, HAART will pose a challenge in patients withHCV due to the augmented risk of hepatotoxicity.105,106
Because HCV is the most common coinfection in theHIV-positive patient with ESLD, the issues of HCVrecurrence that plague non–HIV-positive liver transplantrecipients also apply to the HIV-positive patient.Although the guidelines for treatment of HCV recurrenceare evolving, HCV treatment should be initiated post-transplant when there is liver biopsy documentation ofrecurrent HCV infection and disease is moderate –tosevere or progressive. A liver biopsy should be obtainedprior to treatment and a HAI score greater than 8 and/orfibrosis stage greater than 2 should be considered as thethreshold for treatment with interferon and ribavirin.However, these agents are not without substantial side–effects: ribavirin is excreted by the kidney, and given thehigh incidence of renal dysfunction in liver transplantpatients, dosing should be started at low levels andincreased as tolerated. The contraindications for interferonand ribivarin use are shown in Table 7.
In addition, the added risk to medical and surgicalteams of HIV exposure is not irrelevant—this argumenthas been put forward as a reason not to perform trans-plants at all in this population. All members of thesurgical team should be made aware of risks and a treat-ment plan for prophylaxis should be determined beforeinitiating the transplant procedure.56
Future Directions
A multicenter prospective study funded by the NationalInstitutes of Health and coordinated by the Universityof California, San Francisco, was designed to evaluatevarious outstanding issues in the use of liver and kidneytransplantation in people with HIV disease.55,57 The
S49Liver Transplantation in HIV Patients

long-range goals are (1) to provide patients and clini-cians with information regarding the HIV-specific risksof transplantation, (2) to provide clinicians with infor-mation necessary to manage immunosuppressive andHAART medications together, and (3) to understandunderlying basic science mechanisms that explainpatient outcomes so that clinical management may beadjusted to maximize these outcomes. The study antic-ipates enrolling 150 kidney transplant recipients and125 liver transplant recipients over 3 years with 2 to 5years of follow-up. The primary endpoints are subjectsurvival and graft survival; secondary endpoints include(1) opportunistic complications and changes in CD4�
T-cell counts and HIV-1 RNA levels; (2) viral markersand host responses to viral copathogens, including hep-atitis B and C and herpesviruses; (3) rejection rates andmarkers of alloresponse; and (4) pharmacokinetic inter-actions between immunosuppressive agents and thehepatically metabolized antiretroviral agents.
Conclusions
We believe that while there should be further accrualand follow-up of these patients to assess long-term ben-efits and risks, there is ample evidence to support theapplication of this life-saving procedure to selectedHIV-positive patients with ESLD. The growing expe-
rience summarized here suggests that liver transplanta-tion is effective in selected HIV-positive patients.
There have been significant advances in the manage-ment of transplant patients and in the management ofHIV infection that have allowed liver and other transplantprocedures to be successful. The successful application ofother transplant procedures, such as kidney107–109 andheart,110 highlights the growing acceptance of transplan-tation in HIV-positive patients. Indeed, a recent editorialsupports broader application of all solid-organ transplantprocedures for HIV-positive patients.111
References1. 1993 Revised Classification System for HIV Infection and
Expanded Surveillance of Definition for AIDS Among Adoles-cents and Adults. MMWR Recomm Rep 1992;31:1–19.
2. Karon JM, Rosenberg PS, McQuillan G, Khare M, Gwinn M,Peterson LR. Prevalence of HIV infection in the United States.JAMA 1996;276:126–131.
3. Enger C, Graham N, Peng Y, Chmiel JS, Kingsley LA, Detels R,Munoz A. Survival from early, intermediate, and late stages ofHIV infection. JAMA 1996;275:1329–1334.
4. Fauci AS, Pantaleo G, Stanley S, Weissman D. Immunopatho-genic mechanisms of HIV infection. Ann Intern Med 1996;124:654–663.
5. Mellors JW, Munoz A, Giorgi JV, Margolick JB, Tassoni CJ,Gupta P, et al. Plasma viral load and CD4� lymphocytes asprognostic markers of HIV-1 infection. Ann Intern Med 1997;126:946–954.
6. Stevenson M. Viral genes and their products. In Merigan TC,Bartlett JG, Bolognesi D, eds. Textbook of AIDS Medicine, 2nded. pp. 13-48, Baltimore: Williams & Wilkins; 2001;13–48.
7. Wei X, Ghosh SK, Taylor ME, Johnson VA, Emini EA, DeutschP, et al. Viral dynamics in human immunodeficiency virus type 1infection. Nature 1995;373:117–122.
8. Buchbinder SP, Katz MH, Hessol, NA, O’Malley PM, Holm-berg SD. Long-term HIV-1 infection without immunologic pro-gression. AIDS 1995;8:1123–1128.
9. Pantaleo G, Menzo S, Vaccarezza M, Graziosi C, Cohen OJ,Demarest JF, et al. Studies in subjects with long-term nonpro-gressive human immunodeficiency virus infection. N Engl J Med1995;332:209–216.
10. Hammer SM, Katzenstein DA, Hughes MD, Gundacker H,Schooley RT, Haubrich RH, et al. A trial comparing nucleosidemonotherapy with combination therapy in HIV-infected adultswith CD4 cell counts from 200 to 500 per cubic millimeter.AIDS Clinical Trials Group Study 175 Study Team. N EnglJ Med 1996;335:1081–1090.
11. Tavel JA, Miller KD, Masur H. Guide to major clinical trials ofantiretroviral therapy in human immunodeficiency virus-in-fected patients: Protease inhibitors, non-nucleoside reverse tran-scriptase inhibitors, and nucleotide reverse transcriptase inhibi-tors. Clin Infect Dis 1999;28:643–676.
12. Murphy EL, Collier AC, Kalish LA, Assmann SF, Para MF,Flanigan TP, et al. Highly active antiretroviral therapy decreasesmortality and morbidity in patients with advanced HIV disease.Ann Intern Med 2001;135:17–26.
13. Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer
Table 7. Contraindications to the Use of Interferon andRibivirin in HIV-Positive Liver Transplant Recipients
Absolute Contraindications to ribavirin use1. Dialysis2. Prior serious adverse reaction to ribavirin3. Hemoglobin � 10 g/dL and inability to correct with
growth factorsRelative contraindications to ribavirin use
1. Serum creatinine � 2.0 mg/dL2. Hemolytic anemia3. Concomitant use of “D drugs” — ddI, d4T, ddC
Absolute Contraindications to interferon use1. Uncontrolled depression or other psychiatric disease2. Uncontrolled thyroid disease3. History of significant retinopathy (visual loss)
Relative contraindications to interferon use1. Autoimmune disease (e.g., lupus, ulcerative colitis,
psoriatic arthritis)2. Concomitant use of AZT3. Ongoing acute or chronic rejection4. Platelet count � 40,000 or WBC � 3,000 and
inability to correct with growth factors
Abbreviations: ddI, didanosine; d4T, stavudine; ddC, zalcit-abine; AZT, zidovudine; WBC, white blood cell count.
S50 Fung et al.
J, Satten GA, et al. Declining morbidity and mortality amongpatients with advanced human immunodeficiency virus infec-tion. HIV Outpatient Study Investigators. N Engl J Med 1998;338:853–860.
14. Hammer SM, Squires KE, Hughes MD, Grimes JM, DemeterLM, Currier JS, et al. A controlled trial of two nucleoside ana-logues plus indinavir in persons with human immunodeficiencyvirus infection and CD4 cell counts of 200 per cubic millimeteror less. AIDS Clinical Trials Group 320 Study Team. N EnglJ Med 1997;337:725–733.
15. Autran B, Carcelain G, Li TS, Blanc C, Mathez D, Tubiana R, etal. Positive effects of combined antiretroviral therapy on CD4�T cell homeostasis and function in advanced HIV disease. Sci-ence 1997;277:112–116.
16. Karpas A, Lowdell M, Jacobson SK, Hill F. Inhibition of humanimmunodeficiency virus and growth of infected T cells by theimmunosuppressive drugs cyclosporin A and FK506. Proc NatlAcad Sci U S A 1992;89:8351–8355.
17. Martin LN, Murphey-Corb M, Mack P, Baskin GB, Pantaleo G,Vaccarezza M, et al. Cyclosporin A modulation of early virologicand immunologic events during primary simian immunodefi-ciency virus infection in rhesus monkeys. J Infect Dis 1997;176:374–383.
18. Andrieu JM, Even P, Venet A, Tourani JM, Stern M, Lowen-stein W, et al. Effects of cyclosporin on T-cell subsets in humanimmunodeficiency virus disease. Clin Immunol Immunopathol1988;47:181–198.
19. Levy R, Jais JP, Tourani JM, Even P, Andrieu JM. Long-termfollow-up of HIV positive asymptomatic patients havingreceived cyclosporin A. Adv Exp Med Biol 1995;374:229–234.
20. Margolis D, Heredia A, Gaywee J, Oldach D, Drusano G, RedfieldR. Abacavir and mycophenolic acid, an inhibitor of inosine mono-phosphate dehydrogenase, have profound and synergistic anti-HIVactivity. J Acquir Immune Defic Syndr 1999;21:362–370.
21. Chapuis AG, Paolo Rizzardi G, D’Agostino C, Attinger A, Kna-benhans C, Fleury S, et al. Effects of mycophenolic acid onhuman immunodeficiency virus infection in vitro and in vivo.Nat Med 2000;6:762–768.
22. Sulkowski MS, Moore RD, Mehta SH, Chaisson RE, ThomasDL. Hepatitis C and progression of HIV disease. JAMA 2002;288:199–206.
23. Staples CT Jr, Rimland D, Dudas D. Hepatitis C in the HIV(human immunodeficiency virus) Atlanta V.A. (Veterans AffairsMedical Center) Cohort Study (HAVACS): The effect of coin-fection on survival. Clin Infect Dis 1999;29:150–154.
24. Rusti V, Hoofnagle J, Gerin J. Hepatitis B virus infection in theacquired immunodeficiency syndrome. Ann Intern Med 1984;101:795–797.
25. Ragni MV, Belle SH. Impact of human immunodeficiency virusinfection on progression to end-stage liver disease in individualswith hemophilia and hepatitis C virus infection. J Infect Dis2001;183:1112–1115.
26. Eyster ME, Sherman KE, Goedert JJ, Katsoulidou A, Hatzakis A.Natural history of hepatitis C virus infection in multitransfusedhemophiliacs: Effect of coinfection with human immunodefi-ciency virus. The Multicenter Hemophilia Cohort Study. JAcquir Immune Defic Syndr 1993;6:602–610.
27. Ockenga J, Tillmann HL, Trautwein C, Stoll M, Manns MP,Schmidt RE. Hepatitis B and C in HIV infected patients. Prev-alence and prognostic value. J Hepatol 1997;27:18–24.
28. Soto B, Sanchez-Quijano A, Rodrigo L, del Olmo JA, Garcia-Bengoechea M, Hernandez-Quero J, et al. Human immunode-
ficiency virus infection modifies the natural history of chronicparenterally-acquired hepatitis C with an unusually rapid pro-gression to cirrhosis. J Hepatol 1997;26:1–5.
29. Monga HK, Rodriguez-Barradas MC, Breaux K, Khattak K,Troisi CL, Velez M,Yoffe B. Hepatitis C virus infection-relatedmorbidity and mortality among patients with human immuno-deficiency virus infection. Clin Infect Dis 2001;33:240–247.
30. Soriano V, Garcia-Samaniego J, Rodriguez-Rosado R, GonzalezJ, Pedreira J. Hepatitis C and HIV infection: Biological, clinical,and therapeutic implications. J Hepatol 1999;31(suppl 1):119–123.
31. Bica I, McGovern B, Dhar R, Stone D, McGowan K, Scheib R,Snydman DR. Increasing mortality due to end-stage liver diseasein patients with human immunodeficiency virus infection. ClinInfect Dis 2001;32:492-497.
32. Soriano V, Garcia-Samaniego J, Valencia E, Rodriguez-RosadoR, Munoz F, Gonzalez-Lahoz J. Impact of chronic liver diseasedue to hepatitis viruses as cause of hospital admission and deathin HIV-infected drug users. Eur J Epidemiol 1999;15:1–4.
33. Puoti M, Spinetti A, Ghezzi A, Donato F, Zaltron S, Putzolu V,et al. Mortality from liver disease in patients with HIV infection:A cohort study. J Acquir Immune Defic Syndr 2000;24:211–217.
34. Gordon S, Reddy R, Gould E. The spectrum of liver disease inthe acquired immunodeficiency syndrome. J Hepatol 1986;2:475–484.
35. Carr A, Morey A, Mallon P, Williams D, Thorburn DR. Fatalportal hypertension, liver failure, and mitochondrial dysfunctionafter HIV-1 nucleoside analogue-induced hepatitis and lacticacidaemia. Lancet 2001;357:1412–1414.
36. Chariot P, Drogou I, de Lacroix-Szmania I, Eliezer-VanerotMC, Chazaud B, Lombes A, et al. Zidovudine-induced mito-chondrial disorder with massive liver steatosis, myopathy, lacticacidosis, and mitochondrial DNA depletion. J Hepatol 1999;30:156–160.
37. Walker UA, Bauerle J, Laguno M, Murillas J, Mauss S, SchmutzG, et al. Depletion of mitochondrial DNA in liver under anti-retroviral therapy with didanosine, stavudine, or zalcitabine.Hepatology 2004;39:311–317.
38. Ena J, Amador C, Benito C, Fenoll V, Pasquau F. Risk anddeterminants of developing severe liver toxicity during therapywith nevirapine- and efavirenz-containing regimens in HIV-in-fected patients. Int J STD AIDS 2003;14:776–781.
39. Bouche H, Housset C, Dumont JL, Carnot F, Menu Y, AvelineB, et al. AIDS-related cholangitis: Diagnostic features and coursein 15 patients. J Hepatol 1993;17:34–39.
40. Pol S, Romana CA, Richard S, Amouyal P, Desportes-Livage I,Carnot F, et al. Microsporidia infection in patients with thehuman immunodeficiency virus and unexplained cholangitis.N Engl J Med 1993;328:95–99.
41. Zandman-Goddard G, Shoenfeld Y. HIV and autoimmunity.Autoimmun Rev 2002;1:329–337.
42. Mason AL, Xu L, Guo I, Munoz S, Jaspan JB, Bryer-Ash M, et al.Detection of retroviral antibodies in primary biliary cirrhosis andother idiopathic biliary disorders. Lancet 1998;351:1620–1624.
43. Spital A. Should all human immunodeficiency virus-infectedpatients with end-stage renal disease be excluded from transplan-tation? Transplantation 1998;65:1187–1191.
44. Phillips A, Wainberg MA, Coates R, Klein M, Rachlis A, Read S,et al. Cyclosporine-induced deterioration in patients with AIDS.Can Med Assoc J 1989;140:1456–1460.
S51Liver Transplantation in HIV Patients

45. Baum KF. Immunosuppression in HIV-infected transplantrecipients. Clin Infect Dis 1992;14:622–623.
46. Schwarz A., Offermann G, Keller F, Bennhold I, L’age-Stehr J,Krause PH, Mihatsch MJ: The effect of cyclosporine on theprogression of human immunodeficiency virus type 1 infectiontransmitted by transplantation—data on four cases and review ofthe literature. Transplantation 1993;55:95–103.
47. Dummer JS, Erb S, Breinig MK, Ho M, Rinaldo CR Jr, Gupta P, etal. Infection with human immunodeficiency virus in the Pittsburghtransplant population. A study of 583 donors and 1043 recipients,1981-1986. Transplantation 1989;47:134–140.
48. Tzakis AG, Cooper MH, Dummer JS, Ragni M, Ward JW,Starzl TE. Transplantation in HIV� patients. Transplantation1990;49:354–358.
49. Fung JJ. Transplantation in HIV-positive patients? MedscapeAsk the Experts. Available at www.medscape.com/medscape/transplantation/AskExperts/2000/02/TRAN-ae09.html.Accessed February 29, 2000.
50. Ragni MV, Bontempo FA, Lewis JH. Organ transplantation inHIV-positive patients with hemophilia. N Engl J Med 1990;322:1886–1887.
51. Erice A, Rhame FS, Heussner RC, Dunn DL, Balfour HH Jr.Human immunodeficiency virus infection in patients with solid-organ transplants: Report of five cases and review. Rev Infect Dis1991;13:537–547.
52. Jacobson SK, Calne RY, Wreghitt TG. Outcome of HIV infec-tion in transplant patient on cyclosporin [letter]. Lancet 1991;337:794.
53. Gordon FH, Mistry PK, Sabin CA, Lee CA. Outcome of ortho-topic liver transplantation in patients with haemophilia. Gut1998;42:744–749.
54. Vanhems P, Bresson-Hadni S, Vuitton DA, Miguet JP, Gillet M,Lab M, Brechot C. Long-term survival without immunosuppres-sion in HIV-positive liver-graft recipients. Lancet 1991;337:126.
55. Kuo PC, Stock PG. Transplantation in the HIV� patient. Am JTransplant 2001;1:13–17.
56. Samuel D, Duclos Vallee JC, Teicher E, Vittecoq D. Liver trans-plantation in patients with HIV infection. J Hepatol 2003;39:3–6.
57. Roland M, Lo B, Braff B, Stock PG. Key clinical, ethical, andpolicy issues in the evaluation of the safety and efficacy of solidorgan transplantation in HIV-infected patients. Arch InternMed 2003;163:1773–1778.
58. McCarthy M, Gane E, Pereira S, Tibbs CJ, Heaton N, Rela M,et al. Liver transplantation for haemophiliacs with hepatitis Ccirrhosis. Gut 1996;39:870–875.
59. Caccamo L, Colledan M, Rossi G, Gridelli B, Maggi U, VannelliA, et al. Post-transplant primary disease does not influence 6-yearsurvival after liver transplantation beyond 1 year. Transpl Int1998;11(suppl 1):S212–S220.
60. Ragni MV, Dodson SF, Hunt SC, Bontempo FA, Fung JJ. Livertransplantation in a hemophilia patient with acquired immuno-deficiency syndrome. Blood 1999;93:1113–1114.
61. Sheikh AM, Wolf DC, Lebovics E, Goldberg R, Horowitz HW.Concomitant human immunodeficiency virus protease inhibitortherapy markedly reduces tacrolimus metabolism and increasesblood levels. Transplantation 1999;68:307–309.
62. Schvarcz R, Rudbeck G, Soderdahl G, Stahle L. Interactionbetween nelfinavir and tacrolimus after orthotopic liver trans-plantation in a patient coinfected with HIV and Hepatiitis Cvirus (HCV). Transplantation 2000;69:2194–2195.
63. Schliefer K, Paar WD, Aydemir G, Wolff M, Rockstroh JK,
Spengler U, Sauderbruch T. Orthotopic liver transplantation ina 33-year-old patient with fulminant hepatitis B and HIV infec-tion. Dtsch Med Wochenschr 2000;125:523–526.
64. Prachalias A, Anton P, Taylor C, Srinivasan P, Muiesan P, Wen-don J, et al. Liver transplantation in adults coinfected with HIV.Transplantation 2001;72:1684–1688.
65. Ragni M, Belle SH, Im KA, Neff G, Roland M, Stock P, et al.Survival of human immunodeficiency virus-infected liver trans-plant recipients. J Infect Dis 2003;188:1412–1420.
66. Gow PJ, Mutimer D. Liver transplantation for an HIV-positivepatient in the era of highly active antiretroviral therapy. AIDS2001;15:291–292.
67. Tolan DJ, Davies MH, Millson CE. Fibrosing cholestatic hepa-titis after liver transplantation in a patient with Hepatitis C andHIV infection [letter]. N Engl J Med 2001;345:1781.
68. Sugawara Y, Ohkubo T, Makuuchi M, Kimura S, Morisawa Y,Tachikawa N, Oka S. Living donor liver transplantation in anHIV-positive patient with hemophilia. Transplantation 2002;74:1655–1656.
69. Rafecas A, Rufi G, Fabregat J, Xiol X. Liver transplantation in apatient infected by human immunodeficiency virus. Med Clin(Barc) 2002;119:596.
70. Neff GW, Bonham A, Tzakis AG, Ragni M, Jayaweera D, SchiffER, et al. Orthotopic liver transplantation in patients withhuman immunodeficiency virus and end-stage liver disease. LiverTranspl 2003;9:239–247.
71. Stock PG, Roland ME, Carlson L, Freise CE, Roberts JP, HiroseR, et al. Kidney and liver transplantation in human immunode-ficiency virus-infected patients: A pilot safety and efficacy study.Transplantation 2003;76:370–375.
72. Gonzalez Alonso R, Barcena R, Blesa C, Garcia M, Moreno A,Fortun J, et al. Liver transplantation in a patient coinfected withhuman immunodeficiency virus and hepatitis C virus. Trans-plant Proc 2003;35:1846–1847.
73. Nowak P, Schvarcz R, Ericzon BG, Flamhole L, Sonnerborg A.Follow-up of a antiretroviral treatment in liver transplant recip-ients with primary and chronic HIV type 1 infection. AIDS ResHum Retroviruses 2003;19:13–19.
74. Jeng LB, Lee WC, Hung CM, Yu MC, Kuo LM, Chen MF.Liver transplantation in a patient with human immunodefi-ciency virus infection: A case report. Transplant Proc 2003;35:361.
75. Boschetto A, Ettorre GM, Durand F, Dondero F, Francoz C,Soommacale D, et al. Is anti-retroviral treatment after transplan-tation in HIV positive patients always necessary? [abstract no.14]. 10th Congress of the International Liver TransplantationSociety, Kyoto, Japan, 10 June 2004. Liver Transpl 2004;10:C6.
76. Roland M, Stock PG. Review of solid-organ transplantation inHIV-infected patients. Transplantation 2003;75:425–429.
77. Yoshida EM, Erb SR, Partovi N, Scudamore CH, Chung SW,Frighetto L, et al. Liver transplantation for chronic hepatitis Binfection with the use of combination lamivudine and low-dosehepatitis B immune globulin. Liver Transpl Surg 1999;5:520–525.
78. Berenger M, Forman LM, Lewis JD, Berlin HA, Feldman HI,Lucey MR. The association between hepatitis C infection andsurvival after orthotopic liver transplantation. Gastroenterology2002;122:889–896.
79. Berenguer M, Ferrell L, Watson J, Prieto M, Kim M, Rayon M,et al. HCV-related fibrosis progression following liver transplan-tation: Increase in recent years. J Hepatol 2000;32:673–684.
80. Luban J, Bossolt KL, Franke EK, Kalpana GV, Goff SP. Human
S52 Fung et al.

immunodeficiency virus type 1 Gag protein binds to cyclophilinsA and B. Cell 1993;73:1067–1078.
81. Bartz SR, Hohenwalter E, Hu MK, Rich DH, Malkovsky M.Inhibition of human immunodeficiency virus replication bynonimmunosuppressive analogs of cyclosporin A. Proc NatlAcad Sci U S A 1995;92:5381–5385.
82. Mlynar E, Bevec D, Billich A, Rosenwirth B, Steinkasserer A. Thenon-immunosuppressive cyclosporin A analogue SDZ NIM 811inhibits cyclophilin A incorporation into virions and virus replica-tion in human immunodeficiency virus type 1-infected primary andgrowth-arrested T cells. J Gen Virol 1997;78:825–835.
83. Calabrese LH, Lederman MM, Spritzler J, Coombs RW, Rox L,Schock B, et al. Placebo-controlled trial of cyclosporin-A inHIV-1 disease: Implications for solid organ transplantation. JAcquir Immune Defic Syndr 2002;29:356–362.
84. Bouscarat F, Samuel D, Simon F, Debat P, Bismuth H, SaimotAG. An observational study of 11 French liver transplant recip-ients infected with human immunodeficiency virus type 1. ClinInfect Dis 1994;19:854–859.
85. McComsey GA, Whalen CC, Mawhorter SD, Asaad R, ValdezH, Patki AH, et al. Placebo-controlled trial of prednisone inadvanced HIV-1 infection. AIDS 2001;15:321–327.
86. Wallis RS, Kalayjian R, Jacobson JM, Fox L, Purdue L, ShikumaCM, et al. A study of the immunology, virology, and safety ofprednisone in HIV-1-infected subjects with CD4 cell counts of 200to 700 mm3. J Acquir Immune Defic Syndr 2003;32:281–286.
87. Coull JJ, Turner D, Melby T, Betts MR, Lanier R, MargolisDM. A pilot study of the use of mycophenolate mofetil as acomponent of therapy for multidrug-resistant HIV-1 infection. JAcquir Immune Defic Syndr 2001;26:423–434.
88. Lane HC, Masur H, Edgar LC, Whalen G, Rook AH, Fauci AS.Abnormalities of B-cell activation and immunoregulation inpatients with the acquired immunodeficiency syndrome. N EnglJ Med 1983;309:453–458.
89. Shirai A, Cosentino M, Leiitman-Klinman SF, Klinman DM.Human immunodeficiency virus infection induces both poly-clonal and virus-specific B cell activation. J Clin Invest 1992;89:561–566.
90. Hirose K, Baxter-Lowe LA, Carlson L, Freise CE, Hirose R,Cunniffe K, et al. Unexpectedly high rejection rates in HIV-positive recipients of renal transplants [abstract no. 481]. 2004American Transplant Congress, Boston, MA, 16 May 2004.Am J Transplant 2004;4(suppl 8):290.
91. Toso C, Berney T, Oberholzer J, Chave JP, Martin PPY,Zeender E, et al. Kidney-pancreas transplantation in a long-termnon-progressor HIV-infected recipient. Am J Transplant 2003;3:631–633.
92. Purgus R, Tamalet C, Poignard P, Spire B, George F, Robert A,Olmer M. Long-term nonprogressive human immunodeficiencyvirus-1 infection in a kidney allograft recipient. Transplantation1998;66:1384–1386.
93. Jain AB, Venkataramanan R, Shapiro R, Scantlebury V, PotdarS, Bonham A, et al. The interaction between antiretroviral agentsand tacrolimus in liver and kidney transplant patients. LiverTranspl 2002;8:841–845.
94. Jain AB, Venkataramanan R, Eghtesad B, Marcos A, Ragni M,Shapiro R, et al. Effect of coadministered lopinavir and ritonavir(Kaletra) on tacrolimus blood concentration in liver transplanta-tion patients. Liver Transpl 2003;9:954–960.
95. Antonini M, Ettorre GM, Vennarecci G, D’Offizi G, Narciso P,
Del Non F, et al. Anti-retrovirals and immunosuppressive druginteractions in a HIV-positive patient after liver transplantation.Hepatogastroenterology 2004;51:646–648.
96. Brinkman K, Huysmans F, Burger DM. Pharmacokinetic inter-action between saquinavir and cyclosporine [letter]. Ann InternMed 1998;129:914–915.
97. Jain AK, Venkataramanan R, Fridell JA, Gadomski M, ShawLM, Ragni M, et al. Nelfinavir, a protease inhibitor, increasessirolimus levels in a liver transplantation patient: A case report.Liver Transpl 2002;8:838–840.
98. Antoniades C, Macdonald C, Knisely A, Taylor C, Norris S.Mitochondrial toxicity associated with HAART following livertransplantation in an HIV-infected recipient. Liver Transpl2004;10:699–702.
99. Kusne S, Shapiro R, Fung J. Prevention and treatment of cyto-megalovirus infection in organ transplant recipients. TransplInfect Dis 1999;1:187–203.
100. McGavin JK, Goa KL. Ganciclovir: An update of its use in theprevention of cytomegalovirus infection and disease in trans-plant recipients. Drugs 2001;61:1153–1183.
101. Price P, Mathiot N, Krueger R, Stone S, Keane NM, FrenchMA. Immune dysfunction and immune restoration disease inHIV patients given highly active antiretroviral therapy. J ClinVirol 2001;22:279–287, 2001.
102. Gow PJ, Pillay D, Mutimer D. Solid organ transplantation inpatients with HIV infection. Transplantation 2001;72:177–181.
103. Gomez E, Aguado S, Rodriguez M, Alvarez-Grande J. Kaposi’ssarcoma after renal transplantation—disappearance afterreduction of immunosuppression and reappearance 7 yearslater after start of mycophenolate mofetil treatment. NephrolDial Transplant 1998;13:3279–3280.
104. Doutrelepont JM, De Pauw L, Gruber SA, Dunn DL, QunibiW, Kinnaert P, et al. Renal transplantation exposes patientswith previous Kaposi’s sarcoma to a high risk of recurrence.Transplantation 1996;62:463–466.
105. den Brinker M, Wit FW, Wertheim-van Dillen PM, Jurriaans S,Weel J, van Leeuwen R, et al. Hepatitis B and C virus co-infectionand the risk for hepatotoxicity of highly active antiretroviral ther-apy in HIV-1 infection. AIDS 2000;14:2895–2902.
106. McGovern B, Bica I. Risk of HAART therapy in hepatitis C.Hepatology 2002;35:730.
107. Abbott KC, Swanson SJ, Agodoa LY, Kimmel PL. Humanimmunodeficiency virus infection and kidney transplantationin the era of highly active antiretroviral therapy and modernimmunosuppression. J Am Soc Nephrol 2004;5:1633–1639.
108. Ahuja TS, Zingman B, Glicklich D. Long-term survival in anHIV-infected renal transplant recipient. Am J Nephrol 1997;17:480–482.
109. Swanson SJ, Kirk AD, Ko CW, Jones CA, Agodoa LY, AbbottKC. Impact of HIV seropositivity on graft and patient survivalafter cadaveric renal transplantation in the United States in thepre highly active antiretroviral therapy (HAART) era: An his-torical cohort analysis of the United States Renal Data System.Transpl Infect Dis 2002;4:144–147.
110. Calabrese LH, Albrecht M, Young J, McCarthy P, Haug M,Jarcho J, Zackin R. Successful cardiac transplantation in anHIV-1-infected patient with advanced disease. N Engl J Med2003;348:2323–2328.
111. Halpern SD, Ubel PA, Caplan AL. Solid-organ transplantationin HIV-infected patients. N Engl J Med 2002;347:284–287.
S53Liver Transplantation in HIV Patients















![[Chapitre] Résonances individuelles et sociales des nouveaux traitements de l'infection à VIH](https://static.fdokumen.com/doc/165x107/6323b25b3c19cb2bd106a2f7/chapitre-resonances-individuelles-et-sociales-des-nouveaux-traitements-de-linfection.jpg)




