
Antithrombotic treatment in patients undergoing transcatheter aortic valve implantation (TAVI)
Upload
independentCategory
view
2download
0
Transseptal Antegrade Transcatheter Aortic Valve Replacement for Patients With No
Other Access Approach – A Contemporary Experience
Mauricio G. Cohen¶ M.D, Vikas Singh¶ M.D, Claudia A. Martinez M.D, Brian P. O'Neill M.D,
Carlos E. Alfonso M.D, Pedro O. Martinezclark M.D, Alan W. Heldman M.D,
William W. O'Neill M.D.
From the Cardiovascular Division, Department of Medicine, and the Elaine and Sydney
Sussman Cardiac Catheterization Laboratory, University of Miami Hospital, Miller School of
Medicine, Miami, Florida
Short title: Cohen at al. Transseptal Antegrade TAVR
Key Words: Aortic stenosis, Transcatheter Aortic Valve Replacement, Transseptal approach.
¶Drs Cohen and Singh contributed equally to this manuscript and share 1st authorship.
Word count: 3,611 (all inclusive)
Disclosure: Drs. Cohen and W. O’Neill have received consulting fees from Edwards
Lifesciences. Drs. Martinezclark and W. O’Neill have received consulting fees from Medtronic.
Drs. Heldman and Cohen have received research funding from Edwards Lifesciences. All other
authors do not have any conflicts of interest to disclose.
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article asdoi: 10.1002/ccd.25036
2
Correspondence: Mauricio G. Cohen, MD, University of Miami Hospital, 1400 NW 12th
Avenue, Suite 1179 Miami, Florida 33136. tel: (305) 243-5050; fax: (305) 243-5578; e-mail:
Abstract:
Objective: To assess the feasibility and outcomes in patients undergoing transvenous transseptal
(TS) transcatheter aortic valve replacement (TAVR).
Background: TS approach for TAVR was abandoned in favor of retrograde transfemoral,
transaortic or transapical approaches. TS TAVR may still be warranted in patients for whom no
other approach is feasible.
Methods: Observational consecutive case series at a single center, to evaluate technical
outcomes in inoperable patients with aortic stenosis who had contraindications for other
approaches and who underwent TAVR via a transvenous TS antegrade approach using the
Edwards-Sapien (ES) valve.
Results: Over a 4-month period, 9 patients underwent TS TAVR with 26mm (n=4) and 23mm
(n=5) ES valves. Mean age was 84.5±6.6 years and Society of Thoracic Surgeons predicted risk
of mortality was 7.8 ± 2.8%. Specific contraindications for other access included iliofemoral
arterial diameter < 7mm in 9 (100%), porcelain aorta in 6 (66%) patients, multiple (≥2)
sternotomies in 2 (22%) patients, severe pulmonary disease in 3 (33%), extreme frailty in 1
(11%), spinal stenosis with impaired ability to rehabilitate post-surgery in 1 (11%) and apical left
ventricular thrombus in 1 (11%) patient. Antegrade deployment of the ES prosthetic valve was
technically feasible in 8 patients. Major bleeding occurred in 4 patients, two patients suffered
3
acute kidney injury without need for dialysis and one patient required a permanent pacemaker.
The median (25th, 75th percentiles) fluoroscopy time was 49 (34, 81) minutes and contrast
volume was 150 (120, 225) ml. No patient had hemodynamically significant post-TAVR aortic
insufficiency nor damage to the mitral valve. At 6 months follow-up, there were no
cerebrovascular events or rehospitalizations and mean NYHA Class improved from 3.4 to 1.7.
Conclusions: The antegrade TS approach to TAVR is a technically feasible option for “no-
access" patients. Prospective assessment of the safety and efficacy of this approach in the current
era warrants further study.

4
Introduction
Transcatheter aortic valve replacement (TAVR) has gained worldwide acceptance and
emerged as a novel alternative therapeutic option for patients with aortic stenosis (AS).1, 2 The
initial TAVR approach described by Cribier et al in 2002 was antegrade transvenous transseptal
3. But the procedural complexity and technical complications with this approach led to its
replacement by the transfemoral (TF) arterial retrograde approach. Currently, there are two
TAVR systems with wide clinical experience: the balloon expandable Edwards-Sapien (ES)
valve (Edwards Lifesciences,Irvine, CA), which can be implanted retrograde via the femoral
artery (TF) or the ascending aorta (transaortic - TAo), or antegrade via the left ventricular apex
(transapical - TA); and the self-expandable Medtronic-CoreValve ReValving system (Medtronic,
Minneapolis, MN) which can only be implanted retrograde via TF, TAo or subclavian/axillary
artery approaches4, 5. Despite the availability of these options, a subgroup of patients with
symptomatic severe aortic stenosis has anatomic or physiologic features making none of these
approaches feasible.
In the United States, the TA and TF approaches are approved by the Food and Drug
Administration (FDA). In regards to the TF approach, the 23 mm and 26 mm ES valves, with
their 22F (outer diameter 25 Fr, 8.4 mm) and 24F (outer diameter 28 Fr, 9.2 mm) femoral artery
sheaths are available for clinical use. However, approximately one third of screened patients are
technically suited for the TF approach with this technology 6. Of those who cannot be treated TF,
many also have a combination of clinical features precluding the other commonly used
approaches. For example, peripheral vascular disease with iliofemoral vessels smaller than 7
mm in diameter precluding the retrograde TF approach may coexist with “porcelain” aorta with
heavy circumferential calcification of the ascending aorta and arch, precluding the TAo

5
approach, and chest wall disease or severe pulmonary disease precluding the TA approach. We
report a contemporaneous first US experience with the antegrade transvenous transseptal (TS)
approach in patients with severe AS who were not candidates for valve surgery and who had no
other access option for TAVR.
Methods:
We conducted an observational analysis of a case series to evaluate technical outcomes of TAVR
with the Edwards-Sapien (ES) valve via an antegrade transvenous TS approach. All patients had
severe aortic stenosis (AS) and were deemed inoperable by two cardiac surgeons because
surgical aortic valve replacement (SAVR) would be associated with a predicted probability of ≥
50% of death within 30 days after surgery or development of a serious irreversible complication.
All patients had an iliofemoral arterial diameter < 7 mm and contraindications for both TAo and
TA access. Severe aortic stenosis was defined as an aortic valve area < 0.8 cm2, with a mean
aortic-valve gradient ≥ 40 mm Hg or peak Doppler aortic jet velocity ≥ 4.0 m/sec. All patients
had congestive heart failure with New York Heart Association (NYHA) class III or IV
symptoms. All underwent pre-procedural coronary angiography to assess the need of
revascularization. The aortic annulus was measured by transthoracic (TTE) or transesophageal
(TEE) echocardiography, and immediately prior to the procedure by TEE and by rotational
aortography with computerized tomographic reconstruction (DynaCT, Siemens AG, Forchheim,
Germany). Patients with annular dimensions 1.8 to 2.5 cm were eligible for TAVR.
The primary outcome measure of this study was the combined occurrence of death from any
cause or repeat hospitalization within 30 days, 3 months and 6 months after the index procedure
due to valve-related or procedure related clinical deterioration. Secondary outcome measures

6
were procedural success (defined as 1 valve implanted, with less than moderate aortic
regurgitation (AR), and the patient left the procedure room alive); NYHA functional class; repeat
hospitalization due to valve-related or procedure related clinical deterioration; new pacemaker
implantation; and the rates of myocardial infarction, stroke, acute kidney injury, vascular
complications, and bleeding. Prosthetic valve performance was assessed as prosthetic aortic
valve area, gradient and severity of paravalvular regurgitation. All endpoints were defined per
Valve Academic Research Consortium criteria 7.
Technique
All procedures were performed under general anesthesia. Vascular access in both right and left
femoral arteries and veins was established; fluoroscopic and real-time ultrasound imaging
guidance were used for vascular puncture. Root aortography was performed during rapid
ventricular pacing, with rotational imaging and computerized tomographic reconstruction.
Transseptal puncture was made from the right femoral vein using a Brockenbrough needle and
Mullins sheath, under fluoroscopic and TEE guidance. Either a 7F balloon tipped catheter, or 6F
AL1 angiographic catheter was advanced through the Mullins sheath, looped in the LV and used
to direct the passage of a 0.035” floppy tipped Wholey guidewire antegrade across the aortic
valve into the ascending aorta and arch. If needed, this wire was snared in the descending aorta
from the left femoral artery using a 12-20 mm three-lobed vascular snare (Atrieve, Angiotech),
to permit the introduction of a 6F 125 cm long multipurpose angiographic catheter through the
TS sheath and around the aortic arch. Through catheter, a 400 cm flexible shaft 0.035” nitinol
wire (Nitrex, EV3) was advanced into the descending aorta, snared, and externalized through the
left femoral artery. A 6 French MPA1 guiding catheter was advanced retrograde over the
externalized wire and to the aortic root, to maintain control of the wire loop in the left ventricle.
7
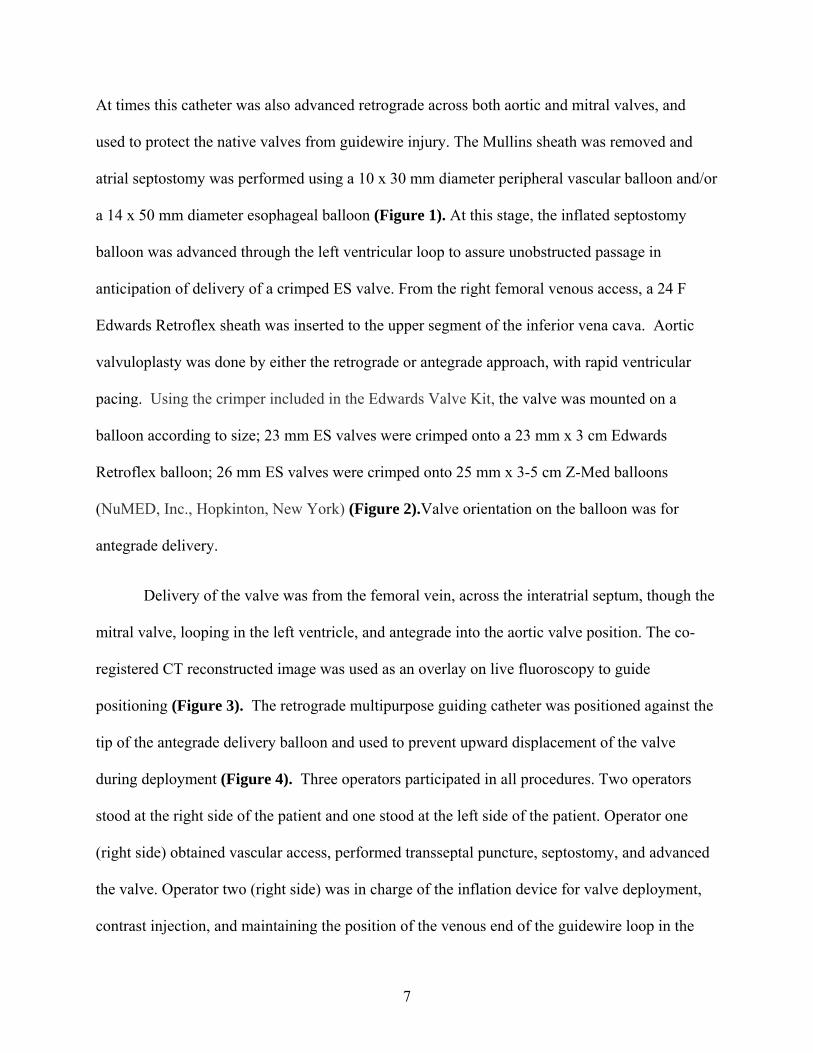
At times this catheter was also advanced retrograde across both aortic and mitral valves, and
used to protect the native valves from guidewire injury. The Mullins sheath was removed and
atrial septostomy was performed using a 10 x 30 mm diameter peripheral vascular balloon and/or
a 14 x 50 mm diameter esophageal balloon (Figure 1). At this stage, the inflated septostomy
balloon was advanced through the left ventricular loop to assure unobstructed passage in
anticipation of delivery of a crimped ES valve. From the right femoral venous access, a 24 F
Edwards Retroflex sheath was inserted to the upper segment of the inferior vena cava. Aortic
valvuloplasty was done by either the retrograde or antegrade approach, with rapid ventricular
pacing. Using the crimper included in the Edwards Valve Kit, the valve was mounted on a
balloon according to size; 23 mm ES valves were crimped onto a 23 mm x 3 cm Edwards
Retroflex balloon; 26 mm ES valves were crimped onto 25 mm x 3-5 cm Z-Med balloons
(NuMED, Inc., Hopkinton, New York) (Figure 2).Valve orientation on the balloon was for
antegrade delivery.
Delivery of the valve was from the femoral vein, across the interatrial septum, though the
mitral valve, looping in the left ventricle, and antegrade into the aortic valve position. The co-
registered CT reconstructed image was used as an overlay on live fluoroscopy to guide
positioning (Figure 3). The retrograde multipurpose guiding catheter was positioned against the
tip of the antegrade delivery balloon and used to prevent upward displacement of the valve
during deployment (Figure 4). Three operators participated in all procedures. Two operators
stood at the right side of the patient and one stood at the left side of the patient. Operator one
(right side) obtained vascular access, performed transseptal puncture, septostomy, and advanced
the valve. Operator two (right side) was in charge of the inflation device for valve deployment,
contrast injection, and maintaining the position of the venous end of the guidewire loop in the

8
LV. Operator three snared and externalized the guidewire from the left femoral artery to
maintain the position of the arterial end of the guidewire loop in the LV and applied retrograde
pressure with a multipurpose catheter against the delivery balloon to prevent movement of the
prosthesis into the aorta during deployment.
After valve implantation, hemodynamics were recorded in the LV and aorta (Figure 5). The
guidewire was withdrawn, with care to maintain a catheter positioned to protect the valves from
guidewire laceration. The Retroflex delivery sheath was removed from the right femoral vein and
hemostasis achieved with manual pressure and a topical hemostatic patch. Arterial hemostasis
was achieved using either manual pressure or a vascular closure device.
Analysis
Data were collected using a prospectively designed database approved by the University of
Miami Human Subjects Research Office. Numeric variables are presented as means ± SD or as
median (25th, 75th quartiles). Categorical data are presented as frequencies with their respective
percentages.
Results
From March 2012 to June 2012, 9 patients (5 men and 4 women) considered inoperable
with severe symptomatic AS underwent antegrade TS TAVR with ES valves (Table 1). Mean
age was 84.5±6.6 years; Society of Thoracic Surgeons predicted risk of mortality (STS PROM)
was 7.8 ± 2.8%; hemoglobin 11.2±1.6 g/dL; and serum creatinine 1.1± 0.6 mg/dL. Diabetes was
present in 4 (44%) patients, and atrial fibrillation in 2 (22%). All patients had severe congestive
heart failure ≥ NYHA class 3. Previous cardiac procedures included percutaneous coronary
interventions in 5 (55%) patients and coronary bypass surgery in 3 (33%). Transthoracic

9
echocardiography demonstrated aortic valve area 0.61±0.23 cm2, mean gradient 39.9±8.0
mmHg, and Doppler aortic velocity 4.16±0.35 m/sec. The aortic annulus diameter was 2±0.2 cm,
and left ventricular ejection fraction 51.7 ± 11.6 %.
All patients had inadequate iliac and femoral arteries for TF TAVR. Specific features
preventing SAVR, TA TAVR, or TAo TAVR included “porcelain” aorta in 6 (66%) patients,
multiple (≥2) sternotomies in 2 (22%) patients, severe pulmonary disease in 3 (33%), extreme
frailty in 1 (11%), spinal stenosis with impaired ability to rehabilitate post-surgery in 1 (11%)
and apical LV thrombus in 1 (11%) patient. Additional comorbidities included coronary artery
disease (n=8), peripheral arterial disease (n=7), and cerebrovascular disease (n=9). Table 1
depicts individual baseline characteristics.
Antegrade deployment of the ES prosthetic valve was technically feasible in 8 patients.
Valve sizes were 26 mm in 4 cases and 23 mm in 5 cases. In one case the ES valve could not be
antegrade across the mitral valve, because of severe mitral annular calcification. The prosthesis
was withdrawn to the femoral vein, where its removal caused venous laceration requiring
vascular repair. This patient left the hospital without consequences and died of congestive heart
failure after 135 days of follow-up.
Post-procedural TEE did not show significant aortic regurgitation or damage to the mitral
valve. Femoral artery complications occurred in 2 patients, related to retrograde balloon aortic
valvuloplasty. One patient suffered transient complete heart block and hemodynamic collapse
requiring pacing and balloon counterpulsation. VARC major bleeding occurred in 4 patients,
minor bleeding in one patient, and 7 patients received blood transfusion. One patient required a
permanent pacemaker and two patients suffered acute kidney injury without need for dialysis.

10
The median (25th, 75th percentiles) fluoroscopy time was 49 (34, 81) minutes and contrast
volume was 150 (120, 225) ml. The median length of intensive care unit stay was 3 (2, 3) days
and total length of hospital stay was 5 (5, 11) days. The total number of deaths were 0, 1 (11%)
and 2 (22%) at 30days, 3 months and 6 months follow-up. There were no cerebrovascular events
or re-hospitalizations and mean NYHA Class improved from 3.4 to 1.7. Table 2 displays a
detailed individual outcome analysis.
Discussion:
Our case series demonstrates the feasibility of TS TAVR using contemporary equipment,
with 89% (8/9) technical success in patients who had contraindications to SAVR, TF, TA and
TAo TAVR approaches. At 6 months follow up 7/9 patients were free of re-hospitalization and
noted a significant improvement in functional capacity.
ES TAVR is now commercially available and an increasing number of high risk patients
with AS are undergoing this procedure. The current challenge in TAVR technology is to improve
the deliverability of the device minimizing patient’s morbidity and mortality through device
development and patient selection.
The initial reports of successful TAVR using a transvenous, transseptal approach in
patients with severe symptomatic AS were accepted world-wide with enthusiasm. From 2002-
2005, valve placement was primarily done via the antegrade transseptal approach with a
procedural success rate of over 75% 8. The femoral vein was accessed and the valve delivered in
the aortic position by traversing the atrial septum and the mitral valve. This technique had
several advantages. It was easier to cross the smooth aspect of the native valve in the antegrade
rather than the retrograde direction, especially in case of excessive aortic valve calcification. In
11
addition, the distensible veins could accommodate the large catheter sheath and avoid any
aortofemoral arterial complications. This approach, however, was technically more demanding
with a more circuitous path to deploy the prosthetic valve and required more experience. The
major disadvantage of this approach was the need to externalize a long stiff guide wire through
the left femoral artery in order to provide support to track the prosthetic valve. It was difficult to
maintain a generous loop in the left ventricle, and straightening of the stiff guide wire loop
caused tethering of the anterior mitral valve leaflet, hence leading to severe mitral regurgitation
and hemodynamic collapse 9. These problems limited the expansion of this approach and induced
future improvements in the delivery system, and led to development of the retrograde approach.
We report our contemporaneous experience and demonstrate intraprocedural safety with
the TS approach for a subgroup of inoperable patients with severe AS and concomitant severe
peripheral vascular disease, pulmonary dysfunction, porcelain aorta, history of multiple
sternotomies or radiation exposure. One of our patients had an LV thrombus, which is of
particular concern because wire and device manipulation within the LV can increase the risk of
stroke and thromboembolic events. Patients with any intracardiac thrombus were excluded in
major pivotal randomized clinical trials. One of our patients had an apical aneurysm with an
organized and calcified mural thrombus. We made a conscious effort to avoid the apical area of
the ventricle during the procedure. The decision to proceed with TS TAVR was driven by the
lack of other viable treatment options. The patient did not suffer a stroke or any other
thromboembolic complication after the procedure.
With the recent advances in the field of percutaneous valve technology and the use of
contemporary equipment such as Edwards sheath, DynaCT, and nitinol wires, the procedure can
now be reconsidered as an alternative approach when no other access option is available. The use

12
of a Nitinol wire appeared to be instrumental in maintaining a wide ventricular loop to avoid
severe mitral regurgitation or mitral valve damage. In addition, to create a wide LV loop it is
necessary to perform the transseptal puncture under transesophageal or intracardiac
echocardiographic guidance to assure a posterior septostomy.
Operators should be mindful of TS approach especially for this subgroup of patients with
no arterial access. We continued to find tethering of the mitral valve a very challenging part of
the procedure, requiring careful coordination between all operators involved in the cases. Due to
the complexity and infrequent use of this procedure in the current era, it should be reserved for
operators who are experienced in transseptal catheterization and antegrade BAV. Operators naïve
to this procedure should perform a number of antegrade BAV procedures to become familiar
with the technical aspects of the procedure. Difficulties and complications were initially
encountered while conducting the procedures however; the learning curve became evident after
each case.
Conclusion:
Antegrade transvenous TS approach using currently available equipment is a technically feasible
option and still has a place in the current TAVR era for patients with no other access approach.
This approach should be revisited and studied in the current era with prospective clinical trials.
Our preliminary study suggests that antegrade transvenous TS TAVR can be incorporated to the
therapeutic armamentarium at high-volume and experienced sites.

13
Figures and tables legends:
Figure 1: Septostomy: Flouroscopic image depicting atrial septostomy using a 14 x 50 mm
diameter esophageal balloon.
Figure 2: Mounting and Crimping: Series of images demonstrating the sequence of mounting
and crimping of the ES valve using the Edwards Valve Kit. Valve orientation on the balloon was
for antegrade delivery.
Figure 3: DynaCT: The DynaCT reconstructed image as an overlay on live fluoroscopy to
guide positioning of the valve.
Figure 4: Deployment: Flouroscopic image showing the antegrade deployment of the ES valve.
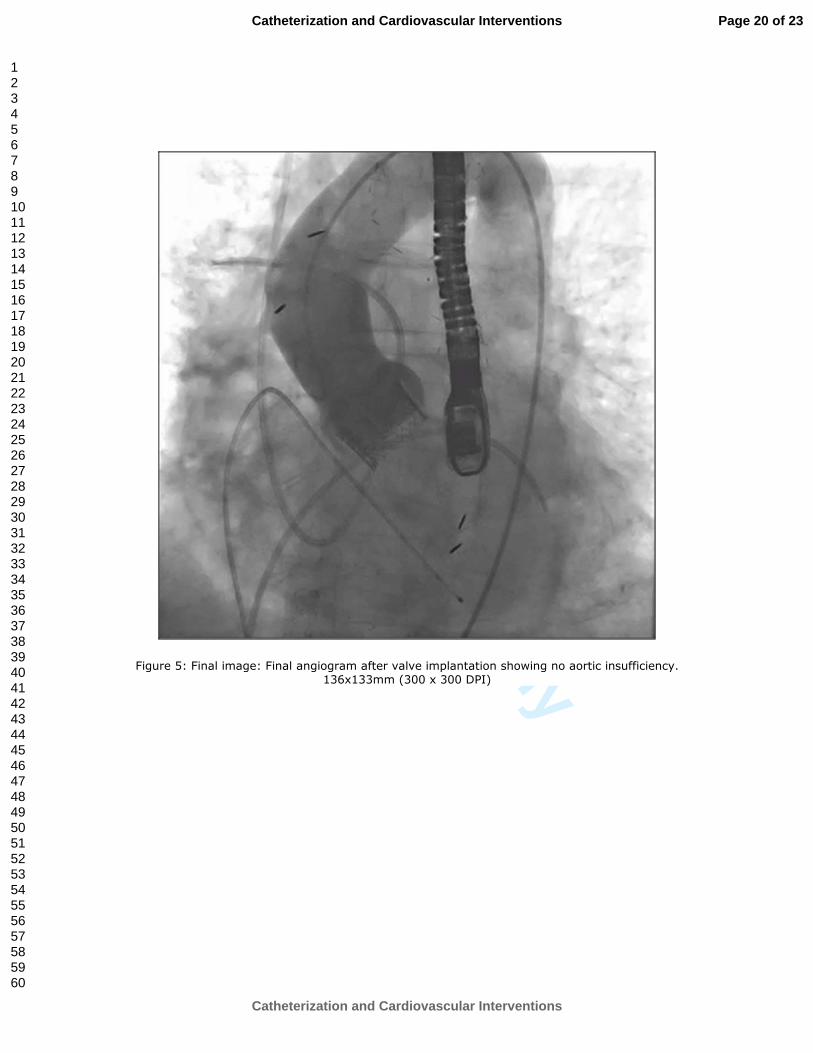
Figure 5: Final image: Final angiogram after valve implantation showing no aortic
insufficiency.
Table 1 demonstrates baseline characteristics of the patients:
Table 2 demonstrates procedural outcomes:

14
References:
1. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb
JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria
JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S.
Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo
surgery. N Engl J Med.363(17):1597-1607.
2. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb
JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani
VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D,
Pocock SJ. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N
Engl J Med.364(23):2187-2198.
3. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, Derumeaux G,
Anselme F, Laborde F, Leon MB. Percutaneous transcatheter implantation of an aortic
valve prosthesis for calcific aortic stenosis: first human case description. Circulation.
2002;106(24):3006-3008.
4. Piazza N, Grube E, Gerckens U, den Heijer P, Linke A, Luha O, Ramondo A, Ussia G,
Wenaweser P, Windecker S, Laborde JC, de Jaegere P, Serruys PW. Procedural and 30-
day outcomes following transcatheter aortic valve implantation using the third generation
(18 Fr) corevalve revalving system: results from the multicentre, expanded evaluation
registry 1-year following CE mark approval. EuroIntervention. 2008;4(2):242-249.
5. Webb JG, Pasupati S, Humphries K, Thompson C, Altwegg L, Moss R, Sinhal A, Carere
RG, Munt B, Ricci D, Ye J, Cheung A, Lichtenstein SV. Percutaneous transarterial aortic

15
valve replacement in selected high-risk patients with aortic stenosis. Circulation.
2007;116(7):755-763.
6. Jilaihawi H, Bonan R, Asgar A, Ibrahim R, Spyt T, Chin D, Kovac J. Anatomic
suitability for present and next generation transcatheter aortic valve prostheses: evidence
for a complementary multidevice approach to treatment. JACC Cardiovasc
Interv.3(8):859-866.
7. Leon MB, Piazza N, Nikolsky E, Blackstone EH, Cutlip DE, Kappetein AP, Krucoff
MW, Mack M, Mehran R, Miller C, Morel MA, Petersen J, Popma JJ, Takkenberg JJ,
Vahanian A, van Es GA, Vranckx P, Webb JG, Windecker S, Serruys PW. Standardized
endpoint definitions for Transcatheter Aortic Valve Implantation clinical trials: a
consensus report from the Valve Academic Research Consortium. J Am Coll
Cardiol.57(3):253-269.
8. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Sebagh L, Bash A, Nusimovici
D, Litzler PY, Bessou JP, Leon MB. Early experience with percutaneous transcatheter
implantation of heart valve prosthesis for the treatment of end-stage inoperable patients
with calcific aortic stenosis. J Am Coll Cardiol. 2004;43(4):698-703.
9. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Nercolini D, Tapiero S, Litzler
PY, Bessou JP, Babaliaros V. Treatment of calcific aortic stenosis with the percutaneous
heart valve: mid-term follow-up from the initial feasibility studies: the French experience.
J Am Coll Cardiol. 2006;47(6):1214-1223.

For Review O
nly
Figure 1: Septostomy: Flouroscopic image depicting atrial septostomy using a 14 x 50 mm diameter
esophageal balloon.
139x139mm (300 x 300 DPI)
Page 16 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
Figure 2: Mounting and Crimping: Series of images demonstrating the sequence of mounting and crimping of the ES valve using the Edwards Valve Kit. Valve orientation on the balloon was for antegrade delivery.
84x51mm (300 x 300 DPI)
Page 17 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
Figure 3: DynaCT: The DynaCT reconstructed image as an overlay on live fluoroscopy to guide positioning of the valve.
131x124mm (300 x 300 DPI)
Page 18 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
Figure 4: Deployment: Flouroscopic image showing the antegrade deployment of the ES valve. 129x119mm (300 x 300 DPI)
Page 19 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Review O
nly
Figure 5: Final image: Final angiogram after valve implantation showing no aortic insufficiency. 136x133mm (300 x 300 DPI)
Page 20 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review Only
Table 1: Baseline characteristics of the patients:
STS PROM: Society of Thoracic Surgeons predicted risk of mortality, NYHA: New York Heart Association Functional Classification,
EF: Ejection Fraction, CAD: Coronary Artery Disease, BAV: Balloon Aortic Valvuloplasty.
Patient Age/Sex
STS
PROM
(%)
NYHA
Class
EF
(%)
AVA
(cm2)
Mean
Gradient
(mmHg)
Aortic
annulus
(cm)
Extent of
CAD (N of
vessels)
Prior BAV Creatinine (mg/dL)
1 78/F 9.9 4 55 0.93 25.8 1.9 1 Yes 1
2 86/M 4.54 3 45 0.94 35.3 2.3 3 Yes 1.1
3 87/F 5.2 3 55 0.43 49 1.8 0 Yes 1
4 89/M 7.9 4 65 0.58 41 2.3 2 Yes 1.1
5 92/M 7.9 3 60 0.64 32.8 2.2 2 Yes 0.7
6 83/F 7.3 3 55 0.78 47 2 2 Yes 1.7
7 90/M 9.4 3 25 0.32 39.1 1.9 1 Yes 2.7
8 85/F 12.96 4 55 0.4 50 1.8 2 No 1.4
9 71/M 4.7 4 50 0.44 39 2.1 3 No 1.2
Page 21 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review Only
Table 2: Procedural outcomes:
Patient
BAV
modality
Valve
Size
(mm)
AVA/Mean
gradient
Complications
AI
(Angio/ECHO)
LOS
(Total/ICU)
Peak
Creatinine
Follow-up
NYHA class
1 Retrograde 23 1.5/9 Iliac artery dissection Trace/ Trace 4/1 1.3 1
2 Antegrade 26 NA
Valve could not be
advanced past mitral valve,
retrieval of the valve
required venous cutdown
9/3 1.4 3
3 Retrograde 23 1.6/7
Unstable SVT requiring
cardioversion
Mild/ Mild 5/3 1 1
4 Retrograde 26 1.6/6.5 None Mild/ Mild 5/3 1.1 2
5 Antegrade 26 1.3/12 None Trace/Mild 3/1 0.9 1
6 Antegrade 23 1.7/9
Common iliac artery
dissection, acute on
chronic kidney injury,
Trace/ Trace 12/3 3.3 1
Page 22 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review Only
BAV: Balloon Aortic Valvuloplasty, AVA: Aortic Valve Area, AI: Aortic Insufficiency, LOS: Length of stay, NYHA: New York
Heart Association (NYHA) Functional Classification, SVT: Supraventricular Tachycardia, IABP: Intra aortic balloon pump, CPR:
Cardiopulmonary resuscitation, MR: Mitral regurgitation, ICU: Intensive care unit.
Gastrointestinal bleed
7
Not
performed
26 1.6/11
Complete heart block,
IABP-22hrs, Pacemaker,
CPR, Severe MR due to
wire impingement
Trace/Mild 11/7 3 2
8 Antegrade 23 1.6/9 None Trace/Mild 14/4 2.5 2
9 Antegrade 23 1.6/7 None Mild/ Trace 5/2 1.2 2
Page 23 of 23
Catheterization and Cardiovascular Interventions
Catheterization and Cardiovascular Interventions
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Copyright © 2022 FDOKUMEN




















