
PELVIC AND AORTIC LYMPHADENECTOMY
18
GYNECOLOGIC ONCOLOGY 0039-6109/01 $15.00 + .OO PELVIC AND AORTIC LYMPHADENECTOMY Pierluigi Benedetti-Panici, MD, Francesco Maneschi, MD, and Giuseppe Cutillo, MD Lymphatics are the main pathway for distant spread of gynecologic tumors. The node groups most commonly involved are located along the iliac and retroperitoneal vessels. Therefore, pelvic and aortic lymphadenectomy are per- formed for staging and therapeutic purposes. In both cases, strict indications and well-defined boundaries of dissection should be set, and a sufficient number of nodes should be removed if the best prognostic information and the maxi- mum therapeutic benefit are to be gained from the procedure (Table l).z,6,11 In this article, node nomenclature according to Benedetti-Panici et all5 is adopted. This classification includes eight pelvic and eight aortic groups (Tables 2 and 3). The pelvic groups are external iliac, superficial obturator, deep obtura- tor, common iliac, superficial internal iliac, deep internal iliac, presacral, and parametrial. The aortic groups are precaval, paracaval, superficial intercavoaor- tic, deep intercavoaortic, preaortic, paraaortic, retrocaval, and retroaortic. Adequate perioperative management and proper surgical te~hnique,'~-'~ avoidance of retroperitoneal drains; and awareness of the vascular and urinary anomalies most commonly encountered'O are all of utmost importance to de- crease perioperative complications,blood loss, operative time, and postoperative stay of patients referred for lymphadenectomy for gynecologic malignancies. Perioperative management includes mechanical bowel preparation, deep venous thrombosis prophylaxis with subcutaneous heparin, leg stockings and early mobilization, short-term antibiotic prophylaxis, and early feedingz4 In the past years, thanks to the improvements in perioperative care and advances in anes- thesia and surgical technique, a remarkable improvement has occurred in post- operative recovery after systematic lymphadenectomy. Most patients that the authors treat are now being discharged, on average, on the postoperative day 5 or 6, without significant morbidity. At the same time, having reached the plateau From the Gynecology Department, Campus Bio Medico University, Rome, Italy SURGICAL CLINICS OF NORTH AMERICA VOLUME 81 NUMBER 4 * AUGUST 2001 841
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of PELVIC AND AORTIC LYMPHADENECTOMY

GYNECOLOGIC ONCOLOGY 0039-6109/01 $15.00 + .OO
PELVIC AND AORTIC LYMPHADENECTOMY
Pierluigi Benedetti-Panici, MD, Francesco Maneschi, MD, and Giuseppe Cutillo, MD
Lymphatics are the main pathway for distant spread of gynecologic tumors. The node groups most commonly involved are located along the iliac and retroperitoneal vessels. Therefore, pelvic and aortic lymphadenectomy are per- formed for staging and therapeutic purposes. In both cases, strict indications and well-defined boundaries of dissection should be set, and a sufficient number of nodes should be removed if the best prognostic information and the maxi- mum therapeutic benefit are to be gained from the procedure (Table l).z,6,11
In this article, node nomenclature according to Benedetti-Panici et all5 is adopted. This classification includes eight pelvic and eight aortic groups (Tables 2 and 3). The pelvic groups are external iliac, superficial obturator, deep obtura- tor, common iliac, superficial internal iliac, deep internal iliac, presacral, and parametrial. The aortic groups are precaval, paracaval, superficial intercavoaor- tic, deep intercavoaortic, preaortic, paraaortic, retrocaval, and retroaortic.
Adequate perioperative management and proper surgical te~hnique,'~-'~ avoidance of retroperitoneal drains; and awareness of the vascular and urinary anomalies most commonly encountered'O are all of utmost importance to de- crease perioperative complications, blood loss, operative time, and postoperative stay of patients referred for lymphadenectomy for gynecologic malignancies. Perioperative management includes mechanical bowel preparation, deep venous thrombosis prophylaxis with subcutaneous heparin, leg stockings and early mobilization, short-term antibiotic prophylaxis, and early feedingz4 In the past years, thanks to the improvements in perioperative care and advances in anes- thesia and surgical technique, a remarkable improvement has occurred in post- operative recovery after systematic lymphadenectomy. Most patients that the authors treat are now being discharged, on average, on the postoperative day 5 or 6, without significant morbidity. At the same time, having reached the plateau
From the Gynecology Department, Campus Bio Medico University, Rome, Italy
SURGICAL CLINICS OF NORTH AMERICA
VOLUME 81 NUMBER 4 * AUGUST 2001 841

842 BENEDETTI-PANIC1 et a1
Table 1. MEDIAN NODE YIELD FROM PELVIC AND AORTIC AREAS ACCORDING TO PRIMARY TUMOR
Pelvic Nodes Aortic Nodes Primary Number of Tumor Patients Median Range Median Range
Cervix 356 47 20-107 23 7-29 Ovary 145 32 17-57 28 15-35 Endometrium 130 31 20-68 28 15-57
Table 2. NUMBER OF NODES REMOVED FROM EACH PELVIC NODE GROUP IN 631 CONSECUTIVE PATIENTS
Node Group
Common iliac Deep common iliac External iliac Obturator
Superficial Deep
Internal iliac Parametrial Presacral
Median Range
8 5-14 4 2-10
10 5-15
12 4 7 3 4
8-20 2-8 4-9 1-11 2-10
Table 3. NUMBERS OF NODES REMOVED FROM EACH AORTIC NODE GROUP IN 631 CONSECUTIVE PATIENTS
Node Group Median Range
Precaval 4 2-8 Paracaval 5 2-10 Retrocaval 4 2-16 Intercavoaortic
Superficial 6 2-12 Deep 4 2-8
Preaortic 3 2-5 Paraaortic 5 2-10 Retroaortic 4 2-8

PELVIC AND AORTIC LYMPHADENECTOMY 843
of the learning curve, a substantial reduction of operating time has been achieved, with the procedure lasting less than 1 hour in most patients.
PELVIC LYMPHADENECTOMY
Indications
Lymphadenectomy for gynecologic tumors generally is considered a staging procedure aimed to sample the lymph nodes most commonly involved by the primary tumor. Given that pelvic nodes are the most common sites of occult metastases of cervical and uterine tumors: 11, 23 it has been suggested that systematic lymphadenectomy may have a therapeutic role in selected clinical conditions. Number and site of lymph node removed differentiate sampling from systematic lymphadenectomy.
Systematic pelvic lymphadenectomy is the first step of the surgical treatment of patients with early (International Federation of Gynecologic Oncology [FIGO] stages IA2, IB1, and IIA)39 and locally advanced (FIGO stages IB2, IIB, and 111) cervical cancer undergoing surgery after neoadjuvant ~hemotherapy.~ Thorough dissection of pelvic nodes includes the removal of all the lymphatic tissue surrounding the pelvic vessels. Parametrectomy is considered a part of this lymphadene~tomy.~~ With such a dissection, 40 to 60 lymph nodes can be collected." Pathologic study on patterns of lymphatic spread has shown that the nodes primarily draining the uterine cervix are those located at the iliac bifurca- tion, over the obturator nerve. In approximately 1% of patients, the primary nodes can be located over the external iliac artery or at the level of the common iliac vessels.", l8 This information can be used to perform a selective sampling lymphadenectomy and intraoperative frozen section to assess nodal status dur- ing surgery. The sensitivity and specificity of intraoperative frozen section of these nodes have been reported to be 96% and loo%, respectively.8 It has been suggested that node-negative patients may undergo a modified radical hysterectomy, either abdominals or whereas node-positive patients can be shifted to radiotherapy or treated with radical hysterectomy and systematic pelvic and aortic lymphadenectomy8, 25 In patients with pelvic bulky nodes, it has been shown that surgical debulking significantly improves survival of these patients, with an acceptable morbidity rate.22, 26, 31
In the case of endometrial cancer, pelvic lymphadenectomy is considered a staging procedure. Nevertheless, recent data have suggested a therapeutic Retroperitoneal dissection is indicated in patients having moderate to high risk for lymph node metastasis (grades 2 and 3 tumor, myoinvasion > 50%, serous papillary and clear cell tumors).23 In patients with low risk for node metastasis (myornetrial invasion absent or < 50% with grades 1 and 2 tumors) lymphade- nectomy is questionable. Thus, to select patients who are candidates for lym- phadenectomy, intraoperative assessment of myoinvasion with frozen section is indicated. This makes lymphadenectomy the second step of endometrial cancer surgery. Patterns of lymphatic spread indicate that lymphadenectomy should include superficial obturator, external iliac, and common iliac nodes6 With such a dissection, 20 to 70 lymph nodes can be removed, and the procedure can be considered adequate if 20 to 25 lymph nodes are removed.6,30 Internal iliac, deep obturator, deep common iliac, and presacral nodes should be removed only from patients having node metastases at frozen section. A thorough staging lymphadenectomy provides more accurate information to select patients who are candidates for adjuvant treatment. It has been shown that, among patients with deep myometrial infiltration without node metastases after systematic

844 BENEDETTI-PANIC1 et a1
staging lymphadenectomy, the 5-year survival rate is 90% without adjuvant
In the case of epithelial ovarian cancer, given the patterns of lymphatic drainage of the ovary, lymphadenectomy must include the removal of the pelvic and aortic nodes.2 The pelvic groups primarily involved by the tumor are the superficial obturator, external iliac, and common iliac.2 Pelvic node dissection can be considered adequate if the number of nodes removed from these groups is more than 20. In patients with retroperitoneal metastases and a frozen pelvis, node dissection also should remove the deep obturator, deep common iliac, internal iliac, and presacral nodes, when cytoreductive intent is pursued.
41
Surgical Technique
Transperitoneal Approach
The patient is placed in lithotomy position, with moderate Trendelenburg. The abdomen is opened through a median or a transversal incision. The choice of the incision is based on the need to extend the lymphadenectomy toward the aortic area. This can be easily accomplished with the median incision, but not with the transversal one. The abdomen is kept open by a self-retaining retractor, and the bowel is kept in place with warm, wet pads.
The pelvic peritoneum is opened by cutting the round ligament and ex- tending the incision cephalad toward the ipsilateral paracolic gutter. The ureter, psoas muscle, genitofemoral nerve, iliac vessels, and umbilical artery are identi- fied. The umbilical artery and the ureter are the landmarks for developing the paravesical and pararectal spaces. Exposure of this area is maintained by using two Deaver retractors, one inserted in the paravesical and the other in the pararectal fossa.
Extraperitoneal Approach
The extraperitoneal approach can be used for staging and nodal debulking in patients with advanced uterine and vulvar cancer, and for therapeutic pur- poses in conjunction with radical hysterectomy. The abdomen can be opened through a median or a transversal incision according to the patient and tumor characteristics. Below the arcuate line, either a vertical or transverse incision of the fascia provides easy access to the pelvic retroperitoneal spaces. The perito- neum can be detached easily from the fascia transversalis entering the space of Retzius and continuing the dissection laterally until the external iliac vessels and psoas muscle are encountered. Caution must be exercised to protect the inferior epigastric vessels. The extraperitoneal portion of the round ligament must be identified and divided to identify the iliac vessels, psoas muscle, ureter, and umbilical artery. The paravesical and pararectal spaces are developed as described earlier, and two Deaver retractors are placed in these spaces (Fig. 1).
Systematic Pelvic Lymphadenectomy
Node dissection is begun by separating the lymph nodes overlying the external iliac artery from the vessel. Dissection must be carried out entering the plane of dissection between the adventitia of the artery and the areolar tissue. Dissection is carried out caudally down to the inguinal ligament and proximally up to the iliac bifurcation (Fig. 2). The lymphatic pad overlying the artery is separated from the psoas muscle and sent to the pathologist as external iliac
PELVIC AND AORTIC LYMPHADENECTOMY 845
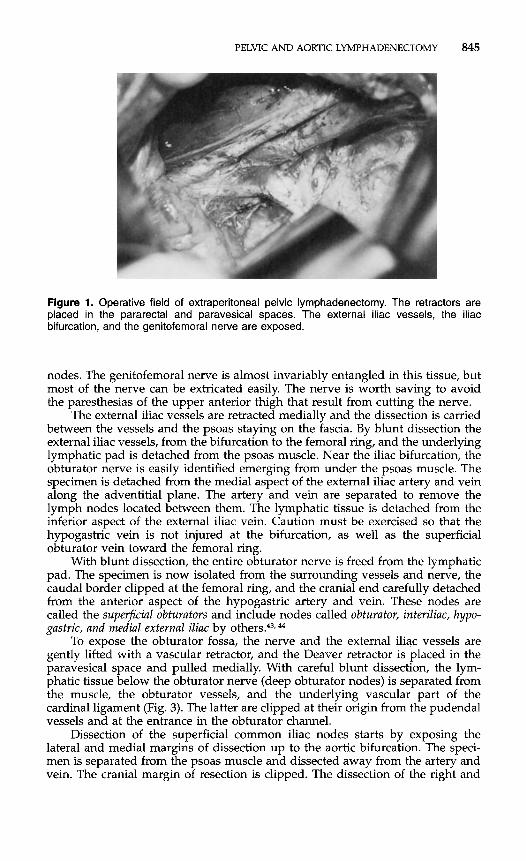
Figure 1. Operative field of extraperitoneal pelvic lymphadenectomy. The retractors are placed in the pararectal and paravesical spaces. The external iliac vessels, the iliac bifurcation, and the genitofemoral nerve are exposed.
nodes. The genitofemoral nerve is almost invariably entangled in this tissue, but most of the nerve can be extricated easily. The nerve is worth saving to avoid the paresthesias of the upper anterior thigh that result from cutting the nerve.
The external iliac vessels are retracted medially and the dissection is carried between the vessels and the psoas staying on the fascia. By blunt dissection the external iliac vessels, from the bifurcation to the femoral ring, and the underlying lymphatic pad is detached from the psoas muscle. Near the iliac bifurcation, the obturator nerve is easily identified emerging from under the psoas muscle. The specimen is detached from the medial aspect of the external iliac artery and vein along the adventitial plane. The artery and vein are separated to remove the lymph nodes located between them. The lymphatic tissue is detached from the inferior aspect of the external iliac vein. Caution must be exercised so that the hypogastric vein is not injured at the bifurcation, as well as the superficial obturator vein toward the femoral ring.
With blunt dissection, the entire obturator nerve is freed from the lymphatic pad. The specimen is now isolated from the surrounding vessels and nerve, the caudal border clipped at the femoral ring, and the cranial end carefully detached from the anterior aspect of the hypogastric artery and vein. These nodes are called the superficial obturators and include nodes called obturator, interiliac, hypo- gastric, and medial external iliac by
To expose the obturator fossa, the nerve and the external iliac vessels are gently lifted with a vascular retractor, and the Deaver retractor is placed in the paravesical space and pulled medially. With careful blunt dissection, the lym- phatic tissue below the obturator nerve (deep obturator nodes) is separated from the muscle, the obturator vessels, and the underlying vascular part of the cardinal ligament (Fig. 3). The latter are clipped at their origin from the pudendal vessels and at the entrance in the obturator channel.
Dissection of the superficial common iliac nodes starts by exposing the lateral and medial margins of dissection up to the aortic bifurcation. The speci- men is separated from the psoas muscle and dissected away from the artery and vein. The cranial margin of resection is clipped. The dissection of the right and
44

846 BENEDETTI-PANIC1 et a1
Figure 2. The external iliac nodes are separated from the artery.
left side is quite different because, on the right, the common iliac artery is medial to the vein and, on the left side, is lateral to the vein. Caution must be exercised regarding the small vein entering the lymphatic pad: a small tear may create a severe hemorrhage from the common iliac vein. By retracting medially the common iliac vessels, the lymph nodes lying between these vessels and the psoas muscle can be exposed (deep common iliac nodes). These nodes can be gently removed, and the sciatic nerve roots are exposed (Fig. 4). The dissection of this area may be hazardous because of several iliolumbar veins entering the iliac vein. For this reason, the iliac vessels must be mobilized very gently, and dissection must be blunt and delicate.
By mobilizing the sigmoid-rectum anteriorly the presacral space is opened. The lymphofatty tissue located at the aortocaval bifurcation and above the lumbosacral junction can be dissected away from the right common iliac artery, anterior aspect of the fifth lumbar vertebra, sacrum, and left common iliac vein.
Figure 3. Operating field showing the external and internal iliac vessels cleared from the lymphatic tissue. The nodes located below the obturator nerve were completely removed.

PELVIC AND AORTIC LYMPHADENECTOMY 847
Figure 4. The nodes located between the common iliac vein and the psoas muscle were entirely removed. The sciatic root and the obturator netve are visible, and also a large iliolumbar vein.
Caution must be exercised to avoid injury to the left common iliac vein. Follow- ing the medial aspect of the common iliac vessels caudally, the node covering the medial surface of the hypogastric vein can be gently dissected and removed. At the end of the procedure, the pelvic peritoneum is left open:* and no drains are used?
Parametrectomy
Parametrectomy is a part of systematic pelvic lymphadenectomy with thera- peutic purposes.29 It has been reported recently that nodal status is a reliable predictor of parametrial status, thus suggesting that parametrectomy could be tailored according to the pelvic nodal r tat us.^
Following systematic pelvic lymphadenectomy, the parametrectomy is be- gun with the identification of the uterine artery, which originates in almost all patients from the umbilical artery. The artery is ligated and cut and the proximal end is maintained. The vascular part of the cardinal ligament is approached. The parametrial vessels, usually four to six, are exposed by pulling on the retractors placed in the fossae and by elevating the obturator nerve and the external iliac vessels with the vascular retractor. Each vessel is identified, double- clipped, and cut, proceeding ca~dally.'~ The lymphofatty tissue remaining after this step, over the pudendal vessels, is removed and sent to the pathologist as the distal part of the lateral parametrium.
The ureter is separated from the posterior leaf of the large (broad) ligament until the entrance in the cardinal ligament tunnel. The peritoneum of the recto- uterine fold is opened, and the rectovaginal space is developed for approxi- mately 4 cm. By pulling the uterus upward and the rectum posteriorly, the rectovaginal and the uterosacral ligaments are well stretched. The closed scissors are introduced between the ligament and the rectum, then are opened parallel to the ligaments, thus isolatings the ligament, which are coagulated and cut. The level of section toward the sacrum and the pelvic floor can be tailored according to the tumor characteristics and the vaginal involvement.
The medial stump of the uterine artery is lifted, and the ureter is freed from
848 BENEDETTI-PANIC1 et a1
the surrounding tissue at the entrance of the tunnel. The uterus is pulled cranially, a Deaver retractor is inserted in the vesicovaginal space, and a Babcock clamp is used to lift the bladder. The entire cervicovesical ligament is stretched and exposed. Dissection is begun near the umbilical artery. With blunt dissection, the small vessels running in the ligament are isolated, coagulated, and cut layer by layer. The dissection is carried medially toward the vagina and deeply until the ureter is unroofed. The ureter is displaced upward and laterally. The space between the vagina and the vaginovesical ligament is entered by blunt dissec- tion. The ligament is stretched by lifting the bladder and is clamped and cut at the bladder insertion.
AORTIC LYMPHADENECTOMY
Indications
Systematic aortic lymphadenectomy includes the removal of all the lympho- fatty tissue located around and between the cava and the aorta. The cranial border of dissection is located at the level of renal veins in the case of ovarian and endometrial cancer and at the level of the inferior mesenteric artery in the case of cervical cancer.
In patients with cervical cancer, metastases to the aortic nodes are secondary to the pelvic ones, with the risk for aortic node metastasis being 5% in FIGO stage IB1, increasing to 30% in FIGO stage III.lS Because of the suboptimal sensitivity of CT scanning and MR imaging in detecting small nodal aortic lymphadenectomy is considered a staging procedure. It has been reported that the removal of paraaortic, superficial intercavoaortic, and paracaval nodes is adequate to evaluate the aortic node status." The median number of nodes to be removed for an accurate staging has been suggested to be 13." In the early invasive disease aortic dissection is indicated at time of laparotomy for radical hysterectomy when common iliac node metastasis is diagnosed.39 Aortic lymph- adenectomy is a part of the surgical staging of patients with locally advanced disease because the knowledge of aortic nodal status can be useful for planning the extension of radi~therapy.~~ In patients who are candidates for radiation treatment, it has been reported that the removal of aortic bulky nodes found at staging improved survival compared with patients with unresected bulky nodes.22, 26 In patients with locally advanced cervical cancer treated with neoadju- vant chemotherapy, the 10% to 15% risk for aortic node metastases is less than expected, probably because of a therapeutic effect of chemotherapy on lymphatic disease." Given the poor prognosis of patients with aortic node metastasis after neoadjuvant chemotherapy, the intraoperative finding of aortic node metastasis may lead to aborted radical surgery.
In patients with endometrial cancer, despite the fact that anatomic stud- ies19,43.44 and autopsy series32 indicate aortic and pelvic nodes as primary stations for disease from the uterine corpus, data from surgical series6, 23, 40 have shown that endometrial cancer spreads primarily to the pelvic nodes. The prevalence of isolated aortic metastasis is less than 2%. The risk for aortic node metastasis is less than 5% for patients with myometrial invasion of less than 50% and is more than 20% for patients with myometrial invasion of more than 50%. Aortic node metastases are significantly increased with the intraoperative finding of pelvic node and adnexal rnetastask6, 23 For these reasons, aortic lymphadenec- tomy is indicated in patients with high risk for aortic metastasis, including myoinvasion of more than 50%, pelvic node metastasis found on frozen-section analysis, and adnexal metastasis. It has been reported that aortic lymphadenec-

PELVIC AND AORTIC LYMPHADENECTOMY 849
tomy may have a therapeutic role in these patient^.^^,^^ According to the studies reporting the patterns of aortic spread, lymphadenectomy should include the removal of paracaval, paraaortic, and intercavoaortic nodes, with a yield of approximately 15 to 20 lymph nodes6
In patients with ovarian cancer, indications for lymphadenectomy are still debated in early stage and advanced disease. Currently, lymphadenectomy is considered a part of intensive surgical staging when the disease is confined to the p e l ~ i s . ~ In patients with disease apparently confined to the ovary, the low rate of lymphatic metastasis leads the authors to reconsider that subset of patients as candidates for aortic lymphadenectomy. It has been shown that G1-2 tumors confined to the ovary have less than a 10% risk for lymphatic spread compared with the more than 30% risk for patients with G3 tumor (Table 4).16,27,34 For this reason, lymphadenectomy is indicated in G3 tumor but is questionable in G1-2 tumors.16 Patterns of retroperitoneal spread suggest that lymph node dissection may be limited to the aortic and pelvic nodes ipsilateral to the site of primary disease6, if no bulky nodes are found. Nevertheless, because available data are still limited, systematic aortic and pelvic lymphade- nectomy should be considered a part of intensive surgical staging in all patients with early stage disease.
In cases in which the disease has spread in the abdomen, knowledge of nodal status is of little or no value to stage the disease. Thus, lymphadenectomy for staging purposes could be omitted. The larger the extent of retroperitoneal spread in patients with advanced ovarian cancer? 27 the poorer the prognosis of patients with lymphatic metastasi~.'~ The common finding of positive nodes at second look1 suggests that systematic pelvic and aortic lymphadenectomy may have a role in the treatment of these patients when optimal cytoreduction (abdominal residual tumor < 1 cm) is a~hieved.~ When cytoreductive intent is pursued, the patterns of aortic spread indicate that node dissection should be systematic by removing all aortic and pelvic nodes as potential sites of metasta- sis; with a nodal yield of 20 to 25 aortic nodes. Preliminary results of a randomized study aimed to evaluate the therapeutic role of lymphadenectomy in optimally debulked patients4 showed that patients with bulky nodes who underwent lymphadenectomy had a longer median survival time than did similar patients not referred for lymphadenectomy.
Surgical Technique
Optimal exposure of the aorta and the cava from the bifurcation to the renal vessels is the key to a safe and successful aortic lymphadenectomy. This requires meticulous preparation of the surgical field and a strict standardization of each surgical step.
Table 4. OVARIAN CARCINOMA: NODE METASTASIS BY GRADE IN WOMEN WITH TUMOR APPARENTLY CONFINED TO THE OVARY
FIG0 Grade
Study G1 N+ 6 2 N+ G3 N+
Knipscheer (1982)" 4 7 5
Benedetti-Panici (1997) 14 1 16 1 34 9
- 9 - Di Re (1989)26 37 4 43 4 22 6
Total 55 5 (9%) 68 5 (7%) 63 20 (32%)

850 BENEDETTI-PANIC1 et a1
The patient is placed in lithotomy position, and the abdomen is entered through a xyphopubic incision. The peritoneum is opened and, when necessary, a complete adhesiolysis is performed to displace the bowel. Afterward, the omentum, the transverse colon, and the small bowel are packed into a plastic bag and exteriorized on the chest wall. A large Deaver retractor is positioned to hold the small bowel. Access to the right and median retroperitoneum is ob- tained through two separate peritoneal incisions: the first along the right para- colic gutter up to the hepatocolic ligament, the second along the ileal mesenteric route up to the ligament of Treitz. Access to the left retroperitoneum is obtained through the incision of the left paracolic gutter up to the splenocolic ligament. For left-sided tumor apparently localized to the ovary and without bulky nodes at palpation, this may be the only peritoneal incision necessary to perform an ipsilateral aortic lymphadenectomy.lz
To obtain adequate mobilization of the ascending and descending colon with their mesenteries avoiding bowel lesions and minimizing blood loss, the avascular plane located between Gerota’s and Toldt’s fasciae must be entered. Following the right plane of dissection, the ureters and the ovarian pedicles are left on the plane of the great abdominal vessels. Before starting nodal dissection, the ureter is identified at pelvic brim, separated from the ovarian pedicle and the surrounding connective tissue up to the renal pelvis, and laterally displaced with a Deaver retractor.
Node dissection is begun at aortic bifurcation by removing the preaortic nodal groups. Lymphofatty tissue over the aorta is grasped with a DeBakey forceps and separated from the artery using a scissors-spreading technique that makes it easier to identify the adventitial plane, which is the cleavage plane. The preaortic lymphatic tissue is separated from the tissue lying laterally and medially by sharp dissection. This step is carried out up to the cranial border of dissection. The left ovarian artery is coagulated or clipped. In this field of dissection, caution must be exercised to avoid injury to the inferior mesenteric artery.
Dissection of the precaval nodes is performed in the same way. The scissors enter the adventitial plane at the level of bifurcation, and the lymphatic pad is separated from the anterior aspect of the vena cava, up to the right ovarian vein in the case of cervical cancer, and to the right renal vein in the case of endome- trial and ovarian cancer. Moving up the nodal dissection, the insertion of the right ovarian vein into the cava and the origin of the right ovarian artery are identified. The ovarian vein is ligated with absorbable suture or hemoclips while the ovarian artery is coagulated. Separation of the tissue lying lateral to the cava is done by sharp dissection. To prevent severe venous bleeding, caution must be exercised with the lymphovascular anastomosis entering the inferior cava on its front side, which must be preventively clipped or coagulated and then cut.
When dissecting the nodes from the anterior aspect of the aorta and cava, the possibility of encountering accessory vessels to the lower renal pole (polar veins and arteries) should never be overlooked. Accidental resection of these vessels may determine important postoperative complications.1°
The lymphatic tissue located between the aorta and the cava is separated from the medial wall of the great vessels by blunt and sharp dissection. Caution must be exercised to avoid injury to the lumbar vein and arteries. By displacing the aorta and the vena cava with a small pledget mounted on ring forceps, all the lymphofatty tissue behind the lumbar vessels (deep intercavoaortic group) is resected (Fig. 5) .
The lymphatic tissue located lateral to the vena cava is separated from the lateral aspect of the vena entering the adventitial plane (Fig. 6). This step is carried out up to the cranial border of resection. The specimen is detached from

PELVIC AND AORTIC LYMPHADENECTOMY 851
Figure 5. Operating field of systematic aortic lymphadenectomy for ovarian cancer. The left renal vein that is the cranial border of dissection is exposed. The vena cava and also the anterior aspect of the aorta are cleared. The superficial intercavoaortic nodes were removed. The caudal deep intercavoaortic nodes were removed exposing the prevertebral fascia. The cranial deep intercavoaortic nodes are still in place.
the psoas muscle and from the lateral attachment by blunt dissection. The cranial margin of section is clipped and cut. By displacing the cava medially with a small pledget, the lymphofatty tissue lying posteriorly can be dissected gently and removed along the entire cava.
Removal of lymph nodes located below the left renal vein is the most challenging part of aortic lymphadenectomy (Fig. 7) because of the common finding in this area of anomalous veins, which can be inadvertently injured, leading to massive bleeding that is very difficult to handle if the exposure of the surgical field is less than optimal. To prevent such a complication, caution must be exercised when isolating and cutting the left ovarian vein. During this step, it must be always kept in mind that there is a variable course and insertion of the second lumbar vein. Moreover, the possible finding of a circumaortic left renal vein should not be overlooked.
To achieve an adequate surgical field, medial mobilization of the left colon is recommended. The left paracolic gutter is incised from up to the splenocolic ligament, which can be resected when needed. The posterior aspect of the colon is detached from Gerota's fascia; thus the left colon is displaced medially until the aorta and the left renal vein are exposed. In this way, a beautiful exposure of the left retroperitoneum is obtained.
The left ovarian vein is identified and separated from the ureter by blunt and sharp dissection. The latter is displaced laterally with a Deaver retractor. The lymphatics overlying the left renal vein are lifted with atraumatic forceps,

852 BENEDETTI-PANIC1 et a1
Figure 6. Dissection of the paracaval nodes. The right ureter is displaced by the retractor. The vena cava is mobilized medially with small pledgets. The right ovarian vein is visible.
Figure 7. Operating field of dissection of cranial precaval, preaortic, and paraaortic nodes. The vena cava, the left renal vein, and the aorta were cleared. The left ovarian vein was ligated and cut. The suprarenal vein is visible.

PELVIC AND AORTIC LYMPHADENECTOMY 853
separated from the vein, secured with clips, and divided. The lymphatic pad is separated from the lateral aspect of the aorta entering the adventitial plane down to the bifurcation. The lateral margin of dissection is delimited by separat- ing bluntly the specimen from the renal fat. The left ovarian vein is isolated up to its origin, clamped, and ligated. The left renal vein is displaced gently cranially, and all the lymphofatty tissue located around the renal vessels is dissected down to the psoas muscle and the prevertebral fascia. The specimen is completely detached from the psoas muscle and sent to the pathologist. Because the paraaortic lymphatic pad continues in that direction located laterally to the common iliac vessels, these must be exposed for a safe dissection of the caudal paraaortic nodes.
To remove the retroaortic nodes, the aorta is displaced medially, and the lymphatic pad is removed by blunt dissection along the entire aorta. At the end of the procedure the peritoneum of the mesentery root is sutured from Treitz to the cecum, and no drains are used.5
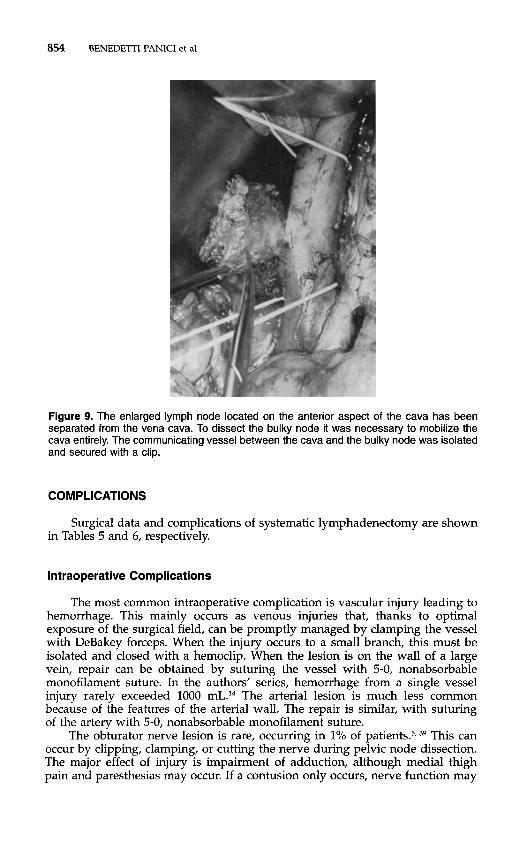
To remove aortic bulky nodes, the surgical field must be adequately pre- pared by removing the lymphatic tissue surrounding the bulky node to mobilize the vessel (aorta or cava) entirely (Fig. 8). The node can be separated from the aorta and the cava by blunt dissection, entering the adventitial plane (Fig. 9). In cases in which the node is firmly adherent to the vessel wall, dissection is not easy, and the vessel may be damaged. This occurs easily with the vena cava because of its thin wall. Nevertheless, when the surgical field is adequately prepared, the damage can be repaired.
Figure 8. An enlarged lymph node located on the anterior aspect of the cava has been isolated from the surrounding lymphatic tissue. The anterior aspect of the aorta and also the vena cava cranial and caudal to the bulky node are cleared.
854 BENEDETII-PANIC1 et a1
Figure 9. The enlarged lymph node located on the anterior aspect of the cava has been separated from the vena cava. To dissect the bulky node it was necessary to mobilize the cava entirely. The communicating vessel between the cava and the bulky node was isolated and secured with a clip.
COMPLICATIONS
Surgical data and complications of systematic lymphadenectomy are shown in Tables 5 and 6, respectively.
lntraoperative Complications
The most common intraoperative complication is vascular injury leading to hemorrhage. This mainly occurs as venous injuries that, thanks to optimal exposure of the surgical field, can be promptly managed by clamping the vessel with DeBakey forceps. When the injury occurs to a small branch, this must be isolated and closed with a hemoclip. When the lesion is on the wall of a large vein, repair can be obtained by suturing the vessel with 5-0, nonabsorbable monofilament suture. In the authors’ series, hemorrhage from a single vessel injury rarely exceeded 1000 mL.14 The arterial lesion is much less common because of the features of the arterial wall. The repair is similar, with suturing of the artery with 5-0, nonabsorbable monofilament suture.
The obturator nerve lesion is rare, occurring in 1% of patients?, 39 This can occur by clipping, clamping, or cutting the nerve during pelvic node dissection. The major effect of injury is impairment of adduction, although medial thigh pain and paresthesias may occur. If a contusion only occurs, nerve function may

PELVIC AND AORTIC LYMPHADENECTOMY 855
return within 6 weeks. The transected nerve is repaired by careful realignment of the ends using a few interrupted 8-0 monofilament nonabsorbable sutures through the epineurium only.
Postoperative Complications
Lymphocyst is a specific complication of pelvic lymphadenectomy. It occurs in approximately 10% to 25% of patients, most of whom are a s y m p t o m a t i ~ . ~ , ~ ~ , ~ ~ These cysts can be detected with clinical examination and sonography. In 5% to 10% of patients, lymphocysts become symptomatic, manifesting with fever, pain, prolonged ileus, leg edema, and deep venous thrombo~is.~, 35, 41, 42 The diagnosis is made most easily and accurately by pelvic sonography. The management of large or symptomatic lymphocysts is by percutaneous drainage with sono- graphic or CT guidance, which is effective in most cases.21 Drainage catheters must be left in situ until drained fluid collection is less than 50 mL/d. Rarely, lymphocysts require laparotomy and marsupialization.
Different from pelvic lymphocysts, aortic lymphocysts are rare complica- tions of lymphadenectomy. In the authors’ experience, only 2 of more than 500 patients developed such a complication (Table 6). Percutaneous drainage with sonographic or CT guidance is indicated for symptomatic patients.
In patients referred for systematic aortic and pelvic lymphadenectomy, if no drains are placed and the peritoneum is left open, in certain circumstances (e.g., advanced ovarian cancer or positive nodes), very intensive lymphorrhea leading to ascites develops (.!-lo% of patient^).^ Treatment is with percutaneous drainage of the abdominal fluid, colloid infusion, and diuretics for approximately 10 days.
Deep venous thrombosis occurs in 3% to 5% of patients. It is commonly associated with lymphocysts and may cause pulmonary emb~lism.~ Diagnosis is made easily with Doppler examination of the lower leg. Anticoagulant treatment is started with intravenous heparin; when the therapeutic goal is achieved, oral anticoagulation can be started. Treatment must be prolonged for 6 months to reduce the risk for venous thrombosis relapse.2o
Leg lymphedema has been reported in 4% to 20% of patients who undergo pelvic lymphadenectomy.5, 22, 37, 41 This complication occurs most commonly after systematic node dissection. Pelvic adjuvant radiotherapy may worsen lymph- edema, leading to functional impairment of the leg.37
The occurrence of external iliac artery thrombosis is rare (< 0.5%) but is a severe complication of systematic pelvic lymphadenectomy. The main symptom
Table 5. OPERATIVE DATA OF PELVIC AND AORTIC LYMPHADENECTOMY
Years
Data 1986-1 992 1993-1 999
No. patients 309 322 Mean operating time (min)
Aortic 75 (45-135) 45 (25-90) Pelvic 60 (45-90) 40 (2040)
Estimated blood loss (mL) Aortic 350 (100-2000) 200 (50-1500) Pelvic 200 (80-1200) 150 (80-1500)
Postoperative stay (d) 10 (7-55) 6 (4-105)

856 BENEDETTI-PANIC1 et a1
Table 6. PERIOPERATIVE COMPLICATIONS OF PELVIC AND AORTIC LYMPHADENECTOMY
Years
Data 1986-1 992 1993-1 999
No. of patients Intraoperative complications
Vessel lesion Severe hemorrhage (> 1000 mL) Obturator nerve injury
Postoperative complications Deep venous thrombosis Pulmonary embolism Infectious morbidity Lymphocyst
Pelvic Aortic
Acute arterial thrombosis Symptomatic ascites
309
30 (10%)
1 (0.3%) 5 (2%)
15 (5%)
60 (19%) 3 (1%)
54 (18%) 1 (0.3%) 1 (0.3%) -
322
15 (5%) 3 (1%) 1 (0.3%)
9 (3%)
44 (15%)
16 (5%)
10 (3%)
2 (0.6%)
1 (0.3%) 2 (0.6%)
is unilateral leg pain in the early hours following surgery. The femoral and leg pulses are absent, and diagnosis is confirmed by arteriography. Treatment is with immediate embolectomy by Fogarty catheter, which in our experience leads to complete and successful resolution in all cases. Delayed diagnosis and treatment may lead to severe consequences, so routine checking of pulses in the legs for the first 24 postoperative hours is warranted.
SUMMARY
Pelvic and aortic lymphadenectomy for gynecologic malignancies has changed from a random "picking" of some pelvic and aortic lymph nodes to a well-established technique based on adequate knowledge of the patterns of spread of the primary tumor. The identification of the node groups to remove, the number of nodes to count, and the border of dissection in the different clinical situations make pelvic and aortic lymphadenectomy a reproducible sur- gical intervention. The large experience accumulated over the years has greatly improved the technique and perioperative and complication management. The improved knowledge of the natural history of gynecologic tumors has refined the indications for lymph node dissection. Today, pelvic and aortic lymphadenec- tomy is primarily a staging procedure. The therapeutic value of lymphadenec- tomy is recognized in the surgical treatment of cervical cancer, but it is still under evaluation in ovarian and endometrial tumors.
References
1. Baiocchi G, Grosso G, Di Re E, et al: Systematic pelvic and paraaortic lymphadenec-
2. Benedetti-Panici P, Greggi S, Maneschi F, et al: Anatomical and pathological study of
3. Benedetti-Panici P, Greggi S, Scambia G, et al: Long-term survival following neoadju-
tomy at second-look laparotomy for ovarian cancer. Gynecol Oncol 69:151, 1998
retroperitoneal nodes in epithelial ovarian cancer. Gynecol Oncol 51:150, 1993

PELVIC AND AORTIC LYMPHADENECTOMY 857
vant chemotherapy and radical surgery in locally advanced cervical cancer Eur J Cancer 34:341, 1998
4. Benedett-Panici P, Landoni F, Scarabelli C, et al: Systematic aortic and pelvic lymphad- enectomy versus resection of any bulky node only for optimally debulked advanced ovarian cancer: Preliminary report from an international randomized trial [abstract A1321. Presented at the 7th Biennial Meeting International Gynecologic Cancer Society, Rome, 1999. Int J Gynecol Cancer 9(suppl):44, 1999
5. Benedetti-Panici P, Maneschi F, Cutillo G, et al: A randomized study comparing retroperitoneal drainage with no drainage after lymphadenectomy in gynecologic malignancies. Gynecol Oncol 65:478, 1997
6. Benedetti-Panici P, Maneschi F, Cutillo G, et al: Anatomical and pathological study of retroperitoneal nodes in endometrial cancer. Int J Gynaecol Cancer 8322, 1998
7. Benedetti-Panici P, Maneschi F, Cutillo G, et a1 Lymphadenectomy in early epithelial ovarian cancer: when and how [abstract 58Bl. Presented at the 6th Biennal Meeting of the International Gynecologic Cancer Society. Int J Gynecol Cancer 7(suppl 2):17, 1997
8. Benedetti-Panici P, Maneschi F, Cutillo G, et a1 Staging surgery for early ovarian and tuba1 cancers. In Greer BE, Montz FJ (eds): Contemporary Clinical Management of Gynecologic Malignancies (Atlas of Clinical Gynaecology, vol 4). Philadelphia, Apple- ton & Lange, 1999, p 12.1
9. Benedetti-Panici P, Maneschi F, Cutillo G, et al: Tailored surgery in stage IAMB1 cervical cancer based on lymphadenectomy of primary pelvic groups: Preliminary results of a pilot study. Int J Gynaecol Obstet 121, 2000
10. Benedetti-Panici P, Maneschi F, D’Andrea G, et a1 Early cervical carcinoma: The natural history of lymph node involvement redefined on the basis of thorough parametrectomy and giant section study. Cancer 88:2267, 2000
11. Benedetti-Panici P, Maneschi F, Scambia G, et a1 Anatomic abnormalities of the retro- peritoneum encountered during aortic and pelvic lymphadenectomy. Am J Obstet Gynecol 170:111, 1994
12. Benedetti-Panici P, Maneschi F, Scambia G, et al: Lymphatic spread of cervical cancer: An anatomical and pathological study based on 225 radical hysterectomies with systematic pelvic and aortic lymphadenectomy. Gynecol Oncol 62:19, 1996
13. Benedetti-Panici P, Maneschi F, Scambia G, et al: A new transabdominal approach to the left retroperitoneum for systematic removal of lymph nodes left of the aorta in gynecologic malignancies. Obstet Gynecol 83:1060, 1994
14. Benedetti-Panici P, Scambia G, Baiocchi G, et al: Radical hysterectomy: a randomized study comparing two techniques for resection of the cardinal ligament. Gynecol Oncol 50:226, 1993
15. Benedetti-Panici P, Scambia G, Baiocchi G, et al: Anatomical study of para-aortic and pelvic lymph nodes in gynecologic malignancies. Obstet Gynecol 79:498, 1992
16. Benedetti-Panici P, Scambia G, Baiocchi G, et al: Technique and feasibility of radical para-aortic and pelvic lymphadenectomy for gynecologic malignancies: A prospective study. Int J Gynaecol Cancer 1:133, 1991
17. Burghardt E, Girardi F, Lahousen M, et al: Patterns of pelvic and paraaortic lymph node involvement in ovarian cancer. Gynecol Oncol40:103,1991
18. Burghardt E: Surgical treatment of cervical cancer. In Burghardt E (ed): Surgical gynecologic oncology. Stuttgart, George Thieme Verlag, 1993, p 257
19. Burke TW, Levenback C, Tomos C et al: Intraabdominal lymphatic mapping to direct selective pelvic and para-aortic lymphadenectomy in women with high risk endome- trial cancer: Results of a pilot study. Gynecol Oncol 62169, 1996
20. Clagett G, Anderson FA, Heit J, et al: Prevention of venous thromboembolism. Chest 108(suppl):312, 1995
21. Conte M, Benedetti-Panici P, Guariglia L, et al: Pelvic lymphocele following radical para-aortic and pelvic lymphadenectomy for cervical carcinoma: Incidence rate and percutaneous management. Obstet Gynecol 76:268, 1990
22. Cosin JA, Fowler JM, Chen MD, et al: Pretreatment surgical staging of patients with cervical carcinoma: the case for lymph node debulking. Cancer 822241, 1998
23. Creasman WT, Morrow CP, Bundy BN, et a1 Surgical pathological spread patterns of endometrial cancer: A Gynecologic Oncology Group study. Cancer 609035, 1987
24. Cutillo G, Maneschi F, Franchi M, et a1 Early feeding compared with nasogastric decompression in major gynaecologic oncology surgery. Obstet Gynecol 93:41, 1999

858 BENEDETTI-PANIC1 et a1
25. Dargent D Laparoscopic lymphadenectomy in the management of cervical cancer. In Benedetti-Panici P, Scambia G, Maneschi F, et a1 (eds): Wertheim’s Radical Hysterec- tomy. Rome, SEU Edizioni, 1996, p 175
26. Di Re F, Fontanelli R, Raspagliesi F, et al: Pelvic and para-aortic lymphadenectomy in cancer of the ovary. Baillieres Clin Obstet Gynaecol 3:131 1989
27. Downey GO, Potish RA, Adcock LL, et al: Pretreatment surgical staging in cervical carcinoma: Therapeutic efficacy of pelvic lymph node resection. Am J Obstet Gynecol 160:1055, 1989
28. Franchi M, Ghezzi F, Zanaboni F, et a1 Nonclosure of peritoneum at radical abdominal hysterectomy and pelvic node dissection: A randomized study. Obstet Gynecol 90:622, 1997
29. Girardi F, Lichtenegger W, Tamussino K, et al: The importance of parametrial lymph nodes in the treatment of cervical cancer. Gynecol Oncol34:206, 1989
30. Girardi F, Petru E, Heydarfadai M, et al: Pelvic lymphadenectomy in the surgical treatment of endometrial cancer. Gynecol Oncol49:177, 1993
31. Hacker NF, Wain GV, Nicklin J L Resection of bulky positive lymph nodes in patients with cervical carcinoma. Int J Gynaecol Cancer 5:250, 1995
32. Henricksen E: The lymphatic spread of carcinoma of the cervix and of the body uterus. Obstet Gynecol58924, 1949
33. Kilgore LC, Partridge EE, Alvarez RD, et a1 Adenocarcinoma of the endometrium: Survival comparisons of patients with and without pelvic node sampling. Gynecol Oncol 56:29, 1995
34. Knipscheer RJ: Paraaortal lymph nodes dissection in 20 cases of primary epithelial ovary carcinoma stage I: Influence of staging. Eur J Obstet Gynecol Reprod Biol 13:303, 1982
35. Lopes A, Hall JR, Monaghan JM: Drainage following radical hysterectomy and pelvic lymphadenectomy: Dogma or need? Obstet Gynecol 86:960, 1995
36. Mariani A, Webb MJ, Galli L, et al: Potential therapeutic role of para-aortic lymphade- nectomy in node-positive endometrial cancer. Gynecol Oncol 76:348, 2000
37. Martimbeau PW, Kjorstad KE, Kolstad P: Stage I carcinoma of the cervix, the Norwe- gian Radium Hospital, 1968-1970: Results of treatment and major complications: I. Lymphedema. Am J Obstet Gynecol 131:389,1978
38. Mohan DS, Samuels MA, Selim MA, et al: Long-term outcomes of therapeutic pelvic lymphadenectomy for stage I endometrial adenocarcinoma. Gynecol Oncol70:165,1998
39. Morrow P, Curtin J: Surgery for cervical neoplasia. In Morrow P, Curtin J (eds): Gynecological Cancer Surgery. New York, Churchill Livingstone, 1996, p 522
40. Onda T, Yoshikawa H, Mutuzani K, et a1 Treatment of node positive endometrial cancer with complete node dissection, chemotherapy and radiation therapy. Br J Cancer 75:1836, 1997
41. Orr JW, Holimon JL, Orr PF: Stage I corpus cancer: Is teletherapy necessary? Am J Obstet Gynecol 176:777, 1997
42. Petru E, Tamussino K, Lahousen M, et al: Pelvic and para-aortic lymphocysts after radical surgery because of cervical and ovarian cancer. Am J Obstet Gynecol 161:937, 1989
43. Plentl AA, Friedman EA: Lymphatic System of the Female Genitalia. Philadelphia, WB Saunders, 1971
44. Reiffensthul G: The Lymphatics of the Female Genital Organs. Philadelphia, JB Lippin- cott, 1964
45. Walsh JW, Jones CM I11 Diagnostic imaging techniques in gynecologic oncology. In Hoskins WJ, Perez CA, Young RC (eds): Principles and Practice of Gynecologic Oncol- ogy. Philadelphia, JB Lippincott, 1992, p 443
Address reprint requests to Pierluigi Benedetti-Panici, MD
Area di Ginecologia Universiti Campus Bio Medico
Via Longoni 83 00155 Roma
Italy




















