Percutaneous Transarterial Aortic Valve Replacement in Selected High-Risk Patients With Aortic...
10
and Sam V. Lichtenstein Cheung Robert Moss, Ajay Sinhal, Ronald G. Carere, Brad Munt, Donald Ricci, Jian Ye, Anson John G. Webb, Sanjeevan Pasupati, Karin Humphries, Christopher Thompson, Lukas Altwegg, With Aortic Stenosis Percutaneous Transarterial Aortic Valve Replacement in Selected High-Risk Patients Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2007 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation doi: 10.1161/CIRCULATIONAHA.107.698258 2007;116:755-763; originally published online July 23, 2007; Circulation. http://circ.ahajournals.org/content/116/7/755 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Circulation in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from by guest on September 26, 2013 http://circ.ahajournals.org/ Downloaded from
Transcript of Percutaneous Transarterial Aortic Valve Replacement in Selected High-Risk Patients With Aortic...

and Sam V. LichtensteinCheungRobert Moss, Ajay Sinhal, Ronald G. Carere, Brad Munt, Donald Ricci, Jian Ye, Anson
John G. Webb, Sanjeevan Pasupati, Karin Humphries, Christopher Thompson, Lukas Altwegg,With Aortic Stenosis
Percutaneous Transarterial Aortic Valve Replacement in Selected High-Risk Patients
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2007 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.107.6982582007;116:755-763; originally published online July 23, 2007;Circulation.
http://circ.ahajournals.org/content/116/7/755World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from by guest on September 26, 2013http://circ.ahajournals.org/Downloaded from

Percutaneous Transarterial Aortic Valve Replacement inSelected High-Risk Patients With Aortic Stenosis
John G. Webb, MD; Sanjeevan Pasupati, MBChB; Karin Humphries, PhD;Christopher Thompson, MD; Lukas Altwegg, MD; Robert Moss, MD; Ajay Sinhal, MD;
Ronald G. Carere, MD; Brad Munt, MD; Donald Ricci, MD; Jian Ye, MD;Anson Cheung, MD; Sam V. Lichtenstein, MD, PhD
Background—Percutaneous aortic valve replacement represents an endovascular alternative to conventional open heartsurgery without the need for sternotomy, aortotomy, or cardiopulmonary bypass.
Methods and Results—Transcatheter implantation of a balloon-expandable stent valve using a femoral arterial approachwas attempted in 50 symptomatic patients with severe aortic stenosis in whom there was a consensus that the risks ofconventional open heart surgery were very high. Valve implantation was successful in 86% of patients. Intraproceduralmortality was 2%. Discharge home occurred at a median of 5 days (interquartile range, 4 to 13). Mortality at 30 dayswas 12% in patients in whom the logistic European System for Cardiac Operative Risk Evaluation risk score was 28%.With experience, procedural success increased from 76% in the first 25 patients to 96% in the second 25 (P�0.10), and30-day mortality fell from 16% to 8% (P�0.67). Successful valve replacement was associated with an increase inechocardiographic valve area from 0.6�0.2 to 1.7�0.4 cm2. Mild paravalvular regurgitation was common but was welltolerated. After valve insertion, there was a significant improvement in left ventricular ejection fraction (P�0.0001),mitral regurgitation (P�0.01), and functional class (P�0.0001). Improvement was maintained at 1 year. Structural valvedeterioration was not observed with a median follow-up of 359 days.
Conclusion—Percutaneous valve replacement may be an alternative to conventional open heart surgery in selectedhigh-risk patients with severe symptomatic aortic stenosis. (Circulation. 2007;116:755-763.)
Key Words: stenosis � stents � valves � valvuloplasty
When aortic stenosis progresses to the point of symp-toms, the prognosis with medical management alone
is poor.1,2 Unfortunately, many patients with severe aorticstenosis do not undergo surgical aortic valve replacement(AVR), despite the proven benefits of this therapy.2–7 Suchpatients frequently have comorbidities, in particular ad-vanced age, that increase the morbidity and mortalityassociated with sternotomy, aortotomy, and cardiopulmo-nary bypass.4,5
Clinical Perspective p 763A percutaneous alternative was first explored in an animal
model by Andersen et al.8,9 Subsequently, a number of groupspursued various approaches to transcatheter aortic valveimplantation.8–16 It was not until a decade after initiallyproposed that the feasibility of percutaneous AVR wasdemonstrated in humans by Cribier et al17,18 using a trans-venous, transseptal approach. Subsequently, we described aretrograde procedure using percutaneous femoral artery ac-cess.19 We report the early and late outcomes with thisprocedure in the initial 50 high-risk patients.
MethodsPatientsPercutaneous AVR was approved for compassionate clinical use bythe Department of Health and Welfare (Ottawa, Canada) in symp-tomatic patients not considered candidates for open heart surgery. Ateam of cardiologists and cardiac surgeons accepted patients on thebasis of a consensus that conventional surgery was excessively highrisk in terms of anticipated mortality and morbidity. Patient orphysician preference alone was not considered adequate.14 Writteninformed consent was obtained.
Patients underwent coronary and aortofemoral angiography. Thediameter of the aortic annulus was measured from the echocardio-graphic parasternal long-axis view at the level of the leaflet attach-ments. Patients were excluded if the aortic annulus diameter was�18 or �26 mm, if there was severe iliofemoral arterial disease, orif a reasonable quality or duration of life was considered unlikelydespite valve replacement because of comorbidities.
Prosthetic Valve ImplantationProcedures were performed in a catheterization laboratory, usuallyunder general anesthetic with endotracheal intubation. Patients werepremedicated with aspirin, clopidogrel, and vancomycin. Heparinwas used to maintain activated clotting time �250 seconds. Vaso-
Received February 22, 2007; accepted June 1, 2007.From the Divisions of Cardiology and Cardiac Surgery, St Paul’s Hospital and the Centre for Health Evaluation and Outcome Sciences, University of
British Columbia, Vancouver, British Columbia, Canada.Correspondence to John Webb, MD, Director, Cardiac Catheterization, St. Paul’s Hospital, 1081 Burrard St, Vancouver, BC, Canada V6Z 1Y6. E-mail
[email protected]© 2007 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.107.698258
755
Valvular Heart Disease
constrictor agents were used to maintain coronary perfusion pressureduring periods of hemodynamic instability. Cardiopulmonary bypasswas not used. A percutaneous sheath (22F or 24F) was placed in thefemoral artery.
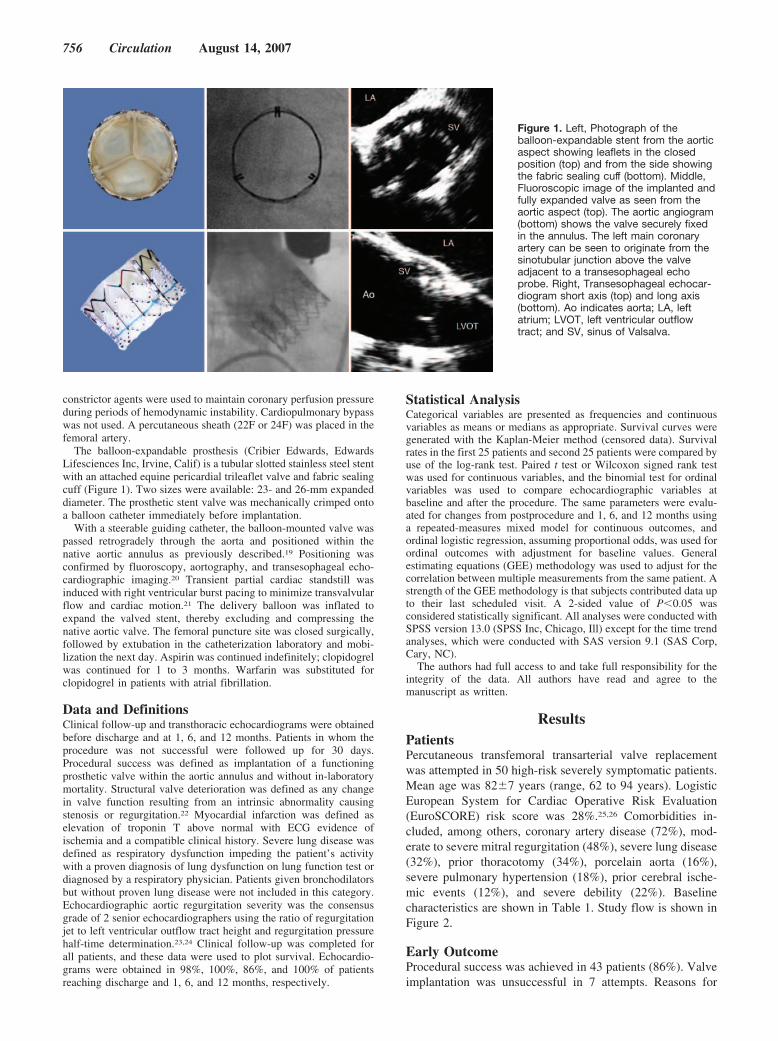
The balloon-expandable prosthesis (Cribier Edwards, EdwardsLifesciences Inc, Irvine, Calif) is a tubular slotted stainless steel stentwith an attached equine pericardial trileaflet valve and fabric sealingcuff (Figure 1). Two sizes were available: 23- and 26-mm expandeddiameter. The prosthetic stent valve was mechanically crimped ontoa balloon catheter immediately before implantation.
With a steerable guiding catheter, the balloon-mounted valve waspassed retrogradely through the aorta and positioned within thenative aortic annulus as previously described.19 Positioning wasconfirmed by fluoroscopy, aortography, and transesophageal echo-cardiographic imaging.20 Transient partial cardiac standstill wasinduced with right ventricular burst pacing to minimize transvalvularflow and cardiac motion.21 The delivery balloon was inflated toexpand the valved stent, thereby excluding and compressing thenative aortic valve. The femoral puncture site was closed surgically,followed by extubation in the catheterization laboratory and mobi-lization the next day. Aspirin was continued indefinitely; clopidogrelwas continued for 1 to 3 months. Warfarin was substituted forclopidogrel in patients with atrial fibrillation.
Data and DefinitionsClinical follow-up and transthoracic echocardiograms were obtainedbefore discharge and at 1, 6, and 12 months. Patients in whom theprocedure was not successful were followed up for 30 days.Procedural success was defined as implantation of a functioningprosthetic valve within the aortic annulus and without in-laboratorymortality. Structural valve deterioration was defined as any changein valve function resulting from an intrinsic abnormality causingstenosis or regurgitation.22 Myocardial infarction was defined aselevation of troponin T above normal with ECG evidence ofischemia and a compatible clinical history. Severe lung disease wasdefined as respiratory dysfunction impeding the patient’s activitywith a proven diagnosis of lung dysfunction on lung function test ordiagnosed by a respiratory physician. Patients given bronchodilatorsbut without proven lung disease were not included in this category.Echocardiographic aortic regurgitation severity was the consensusgrade of 2 senior echocardiographers using the ratio of regurgitationjet to left ventricular outflow tract height and regurgitation pressurehalf-time determination.23,24 Clinical follow-up was completed forall patients, and these data were used to plot survival. Echocardio-grams were obtained in 98%, 100%, 86%, and 100% of patientsreaching discharge and 1, 6, and 12 months, respectively.
Statistical AnalysisCategorical variables are presented as frequencies and continuousvariables as means or medians as appropriate. Survival curves weregenerated with the Kaplan-Meier method (censored data). Survivalrates in the first 25 patients and second 25 patients were compared byuse of the log-rank test. Paired t test or Wilcoxon signed rank testwas used for continuous variables, and the binomial test for ordinalvariables was used to compare echocardiographic variables atbaseline and after the procedure. The same parameters were evalu-ated for changes from postprocedure and 1, 6, and 12 months usinga repeated-measures mixed model for continuous outcomes, andordinal logistic regression, assuming proportional odds, was used forordinal outcomes with adjustment for baseline values. Generalestimating equations (GEE) methodology was used to adjust for thecorrelation between multiple measurements from the same patient. Astrength of the GEE methodology is that subjects contributed data upto their last scheduled visit. A 2-sided value of P�0.05 wasconsidered statistically significant. All analyses were conducted withSPSS version 13.0 (SPSS Inc, Chicago, Ill) except for the time trendanalyses, which were conducted with SAS version 9.1 (SAS Corp,Cary, NC).
The authors had full access to and take full responsibility for theintegrity of the data. All authors have read and agree to themanuscript as written.
ResultsPatientsPercutaneous transfemoral transarterial valve replacementwas attempted in 50 high-risk severely symptomatic patients.Mean age was 82�7 years (range, 62 to 94 years). LogisticEuropean System for Cardiac Operative Risk Evaluation(EuroSCORE) risk score was 28%.25,26 Comorbidities in-cluded, among others, coronary artery disease (72%), mod-erate to severe mitral regurgitation (48%), severe lung disease(32%), prior thoracotomy (34%), porcelain aorta (16%),severe pulmonary hypertension (18%), prior cerebral ische-mic events (12%), and severe debility (22%). Baselinecharacteristics are shown in Table 1. Study flow is shown inFigure 2.
Early OutcomeProcedural success was achieved in 43 patients (86%). Valveimplantation was unsuccessful in 7 attempts. Reasons for
Figure 1. Left, Photograph of theballoon-expandable stent from the aorticaspect showing leaflets in the closedposition (top) and from the side showingthe fabric sealing cuff (bottom). Middle,Fluoroscopic image of the implanted andfully expanded valve as seen from theaortic aspect (top). The aortic angiogram(bottom) shows the valve securely fixedin the annulus. The left main coronaryartery can be seen to originate from thesinotubular junction above the valveadjacent to a transesophageal echoprobe. Right, Transesophageal echocar-diogram short axis (top) and long axis(bottom). Ao indicates aorta; LA, leftatrium; LVOT, left ventricular outflowtract; and SV, sinus of Valsalva.
756 Circulation August 14, 2007

failure included inability to pass the iliac artery in 1 patientand cross the aortic valve in 3 patients, a defective prototypedelivery catheter in 1 patient, and malpositioning in 2patients.
Malpositioning of the prosthesis occurred in 2 patients veryearly in the experience (patients 4 and 9). In both cases, theprosthesis was incorrectly expanded above the level of theaortic annulus so that it was free in the ascending aorta,although constrained by the delivery catheter. The valveswere withdrawn with the delivery catheter and further dilatedand fixed within the transverse aorta in a location wheremajor branch vessels would not be compromised. Bothprocedures were otherwise uncomplicated. One patient sub-sequently underwent elective conventional AVR at 103 days.A second patient continues on medical management for aorticstenosis. Both patients remain alive at 12 months after theirprocedures.
The initial 2 patients in the series (patients 1 and 2)suffered iliac injury requiring major vascular repair, withsubsequent mortality in 1 patient. In a third patient, perfora-tion of the abdominal aorta resulting in mortality occurred asa consequence of difficulty in advancing the bulky prosthesisacross the stenotic aortic valve. A fourth patient with retro-
peritoneal bleeding from an iliac artery perforation wassuccessfully treated with a covered stent. Two patientsreceived antibiotics for access site infections after complexvascular closure. During the course of this experience, vas-cular access techniques, equipment, and screening evolvedwith a reduction in vascular complications.
Periprocedural stroke occurred in 2 patients, with completerecovery in 1 patient and mortality at day 29 in the second.Median hospital stay was 5 days (interquartile range, 4 to 13).By 30 days after successful valve replacement, 50% ofpatients had improved by �1 New York Heart Associationfunctional classes (P�0.0001). Outcome events are listed inTable 2.
Mortality at 30 days was 12% in patients in whom thelogistic EuroSCORE risk score was 28%.25,26 There was 1intraprocedural death caused by aortic injury (2%). Theadditional 5 postprocedural deaths occurring within 30 daysof the procedure were a consequence of ventricular arrhyth-mia, left main occlusion, iliac injury, stroke, and multiorganfailure (each in 1 patient). No patient underwent conversionto open heart surgery within the initial 30-day follow upperiod.
Late OutcomeAll procedures were done �6 months and 30 were done �1year before last follow-up contact. There were 3 deathsoccurring after 30 days (days 56, 71, and 98 as a result ofrespiratory failure, myocardial infarction, and renal failure,respectively) but no subsequent deaths. Of the successfullyimplanted patients, 35 and 17 patients were alive at 6 and 12months, respectively (Figure 2). At a median follow-up of359 days (interquartile range, 60 to 371 days), 35 of 43patients undergoing successful transcatheter AVR (81%)remained alive. Figure 3A illustrates the Kaplan-Meier sur-vival after percutaneous valve implantation.
Subsequent valve procedures were performed in 3 patients.In each case, the reason was ongoing symptomatic aorticstenosis after an unsuccessful transcatheter procedure. Repeatvalve procedures consisted of transcatheter AVR using directleft ventricular apical puncture at day 11, conventionalsurgical AVR at day 103 (as discussed above), and reat-tempted transfemoral transcatheter AVR at day 466. All 3procedures were successful with all 3 patients remaining aliveat the 30-day follow-up.
Structural valve deterioration was not observed duringfollow-up. The early improvement in functional classachieved after valve insertion was maintained at 6 monthsand 1 year (P�0.59, GEE for time trend) (Figure 4E).
Learning CurveCharacteristics and outcomes in the initial 25 patients andsubsequent 25 patients were compared. Baseline characteris-tics were not significantly different with respective mean agesof 82�7 versus 82�8 years. However, rates of proceduralsuccess, malposition, and intraprocedural and periproceduralmortality were more favorable in the later group. Proceduralsuccess increased from 76% to 96% (P�0.10), malpositionfell from 8% to 0%, and intraprocedural mortality fell from4% to 0%. Logistic EuroSCORE25,26 operative mortality
TABLE 1. Baseline Characteristics of 50 High-Risk PatientsUndergoing Percutaneous AVR
Characteristic
Age, y, mean�SD 82�7
Female sex 20 (40)
New York Heart Association class
I 0 (0)
II 5 (10)
III 32 (64)
IV 13 (26)
Body mass index
�20 kg/m2 4 (8)
20–24.9 kg/m2 19 (38)
25–29.9 kg/m2 16 (32)
�30 kg/m2 11 (22)
Hypertension 31 (62)
Diabetes 12 (24)
Coronary artery disease 36 (72)
Severe lung disease 16 (32)
Cerebral ischemic event 6 (12)
Peripheral vascular disease 10 (20)
Prior thoracotomy 17 (34)
Glomerular filtration rate �60 mL/min 26 (52)
Ejection fraction �50% 12 (24)
Mitral regurgitation (moderate or severe) 24 (48)
Pulmonary hypertension �60 mm Hg 9 (18)
Porcelain aorta 8 (16)
Frail and poor mobility 11 (22)
Predicted 30-d surgical mortality, mean %* 28
Values are expressed as n (%) unless otherwise noted.*Logistic EuroSCORE
Webb et al Percutaneous AVR 757

estimation was 26% in the initial cohort and 30% in the latercohort. Actual 30-day mortality was 16% in the initial cohort,falling to 8% in the later cohort (P�0.39). Survival at 0, 1,and 6 months in the early and late cohorts was 96%, 84%, and70% in the initial cohort and 100%, 92%, and 88% in the latercohort as illustrated in Figure 3B (P�0.09). There were nodeaths between 6 and 12 months.
Echocardiographic EvaluationTransthoracic echocardiography documented an immediatereduction in transaortic mean gradient from 46�17 to11�5 mm Hg (P�0.001) and an increase in estimated aorticvalve area from 0.6�0.2 to 1.7�0.4 cm2 (P�0.0001). Timetrend using the multiple linear regression models showed thisimprovement to be maintained up to 1 year (Figure 4A).Echocardiography documented prosthetic valve durabilitywith no structural or significant hemodynamic deteriorationat a median follow-up of 359 days extending to a maximumfollow-up of 734 days.
Left ventricular ejection fraction increased after AVR froma mean of 53�15% to 57�13% (P�0.0001) within days.This improvement in ejection fraction was sustained up to 1
year (P�0.80, GEE for time trend). For the most part, thisincrease was due to an improvement in patients with moder-ate to severe left ventricular dysfunction. A left ventricularejection fraction �40% at baseline was documented in 21%of patients before successful valve implantation, falling to12%, 13%, 0%, and 6% at discharge and 1, 6, and 12 months,respectively (Figure 4B). Figure 5A shows the time trend inleft ventricular ejection fraction in the 30 patients in whomleft ventricular function was assessed at 6 months. This showsa trend to further improvement in ejection fraction after thetime of discharge not resulting from patient selection, al-though this trend was not significant on the basis of GEEevaluation for time trend.
Mitral regurgitation grade decreased from a median grade2 (moderate) to grade 1 (mild) at discharge (P�0.01).Moderate to severe mitral regurgitation at baseline waspresent in 53% of successfully implanted patients, falling to33%, 31%, 25%, and 24% at discharge and 1, 6, and 12months, respectively (Figure 4C). The improvement in mitralregurgitation after valve insertion was maintained up to 1year (P�0.52, GEE for time trend). Figure 5B examines the29 patients who had mitral regurgitation assessed at 6 months.
Figure 2. Diagram illustrating study flow.BEAV indicates balloon-expandable aorticvalve; SVD, structural valve deterioration.
758 Circulation August 14, 2007

There was a trend toward ongoing improvement in mitralregurgitation up to 6 months. Most of this improvementoccurred in patients with moderate or severe mitralregurgitation.
Most patients had some degree of aortic insufficiency atbaseline (Figure 4D). After AVR, aortic regurgitation in-creased from a median grade 0 (none/trivial) to grade 1 (mild)(P�0.57) as determined by transthoracic echocardiography.Aortic regurgitation grade after valve implantation was un-changed in 24%, worsened in 44%, and improved in 32%.Postprocedural aortic insufficiency was determined by trans-esophageal echocardiography to be valvular (through thevalve) or paravalvular (around the valve). In no patient wasprosthetic valvular insufficiency more than mild. Most pa-tients did have some degree of paravalvular insufficiency.
When paravalvular insufficiency was judged excessive bytransesophageal echocardiography, the prosthesis was some-times redilated at the discretion of the operator, often with theaddition of a very small amount of fluid to the semicompliantvalvuloplasty balloon to achieve more complete and symmet-rical expansion of the valve. Cautious redilation was notobserved to result in leaflet damage or displacement of theprosthetic valve. No patient was left with severe paravalvularinsufficiency. Moderate paravalvular insufficiency was ob-served in 3 patients, all of whom remained stable at follow-up. Clinical hemolysis was not observed.
DiscussionMortality RiskPrognosis in patients with symptomatic aortic stenosis ispoor,2,27 and surgical AVR can be performed in good candi-dates at very low risk.7 However, large surgical series reporta 5% to 15% operative mortality for isolated AVR in patients�70 years of age,27 and benchmark Medicare data documentan operative mortality of 8.8% for patients �65 years ofage.28 Surgical mortality rates escalate in the presence ofcomorbidities or the need for additional cardiac proce-dures.27,29–34 The factors that have a major impact on the riskof thoracotomy, aortotomy, or cardiopulmonary bypass (suchas porcelain aorta, lung disease, or debility) may differ fromthose factors that determine the risk associated with atransarterial procedure such as iliofemoral disease. Betterunderstanding of the risks associated with transcatheter pro-cedures may allow improved patient selection.
Our experience suggests that percutaneous AVR can beperformed with a mortality that compares favorably with thatof open heart surgery in selected high-risk patients. Intrapro-cedural mortality was 2%, and 30-day mortality was 12%. Inthe latter half of this first-in-man percutaneous retrogradetransarterial balloon-expandable valve experience, 30-day
TABLE 2. Outcome After Percutaneous AVR in 50High-Risk Patients
Characteristic
Procedural success 43 (86)
Stroke 2 (4)
Myocardial infarction 1 (2)
Ventricular fibrillation 2 (4)
Heart block, new and sustained 2 (4)
Tamponade* 1 (2)
Transfusion �3 U 9 (18)
Emergent cardiac surgery 0 (0)
Endocarditis 0 (0)
Death, intraprocedural 1 (2)
Death, 30 d 6 (12)
Death, stroke, or myocardial infarction at 30 d 8 (16)
Values are expressed as n (%).*Complication of postprocedural implantation of a permanent pacemaker.
Figure 3. Kaplan-Meier survival. A, First consecutive 50 transarterial AVR patients. Logistic EuroSCORE mortality estimate was 28%. B,First 25 patients vs second 25 patients. Logistic EuroSCORE estimates were 26% and 30%, respectively.
Webb et al Percutaneous AVR 759

Figure 4. Follow-up of functional class and echocardiographic parameters. A, Time trends in aortic valve area and aortic valve meangradient (error bars indicate �1 SD). B, Time trend in left ventricular ejection fraction (EF). C, Time trend in mitral regurgitation. D, Timetrend in aortic regurgitation. E, New York Heart Association functional class in patients who reached the 1-month follow-up.
760 Circulation August 14, 2007

mortality fell further to 8% compared with a logistic Euro-SCORE of 30%. Admittedly, the accuracy of this and otheravailable objective predictors of surgical mortality is contro-versial, sometimes underestimating risk but perhaps morecommonly overestimating risk.14,25,35,36 However, patients inthe present series also were considered excessively high riskfor surgery according to a consensus of senior surgeons andcardiologists representative of clinical practice in a high-volume center. It seems likely that with further incrementalimprovements in patient selection, techniques, and equip-ment, mortality rates with transcatheter valve implantationcan decline further.
MorbidityAs important as mortality risk may be, procedural morbiditymay weigh as heavily in the decisions made by elderlypatients and their physicians.37 Hospital stay in this percuta-neous high-risk group of largely elderly patients was rela-tively short at a median of 5 days and as little as 2 days.Although morbidity is difficult to further quantify, a proce-dural stroke rate of 4% and a sustained improvement infunctional class are encouraging.
Learning CurveFemoral transarterial valve implantation shares much incommon with other percutaneous cardiac procedures.19 Nev-ertheless, a learning curve was apparent, likely attributable toincremental improvements in technique, equipment, and pa-tient selection. Procedural success increased from 76% in thefirst half of this experience to 96% in the latter half.Malposition occurred very early in the experience and did notrecur later in this experience as a consequence of improve-ments in understanding of the requirements of accuratepositioning at the time of deployment and improvements inimaging. Major arterial complications declined with improve-ments in sheaths, angiographic screening, and technique. Left
main occlusion, which occurred early in the experience, hasnot recurred after the application of routine fluoroscopic,angiographic, and echocardiographic screening for the pres-ence of excessively bulky aortic valve leaflets, although thepotential for it requires further study.
Valve and Cardiac FunctionA prosthetic valve area of 1.7 cm2 compares favorably withcurrently available surgical valves. Neither structural valvedeterioration nor inadequate fixation of the prosthesis wasobserved at a mean follow-up of almost 1 year or inindividual patients out to 2 years. Paravalvular insufficiencywas common but generally mild, stable, and less of a concernthan anticipated.18 However, paravalvular insufficiency doesremain a concern, and further evaluation, including thepotential for low-grade hemolysis and other hematologicalabnormalities, is required.38,39
In the present series, 48% of patients had moderate tosevere mitral regurgitation, and 72% had coronary diseasepossibly sufficient to warrant the additional potential in-creased mortality risk with mitral valve replacement orcoronary bypass had these patients undergone conventionalAVR.27,29–33 Mitral regurgitation and coronary disease weregenerally well tolerated in these mostly elderly patients onceaortic stenosis was relieved. Successful percutaneous aorticvalve implantation was associated with a significant improve-ment in left ventricular function, mitral regurgitation, andfunctional class. Improvements were sustained at 1 year.Importantly, lack of late valve failure during clinical andserial echocardiographic with a median follow-up of almost 1year suggests durability sufficient to offer significant benefit.
Study LimitationsContraindications specific to transcatheter aortic valve im-plantation include an annulus too small or too large toaccommodate the currently available prostheses or a partic-
Figure 5. Left ventricular ejection fraction (EF) and mitral regurgitation trends in patients who completed the 6-month echocardiograph-ic assessment.
Webb et al Percutaneous AVR 761

ularly bulky aortic valve so that the prosthetic valve mightdisplace an enlarged leaflet and obstruct a coronary ostium.Left ventricular dysfunction with nonrevascularized coronarydisease and the potential for global ischemia during theprocedure are relative contraindications. Arterial diseasesevere enough to prevent safe introduction of the prosthesis isa contraindication to a transarterial procedure. Vascularaccess injury, atheroembolism, and paravalvular insuffi-ciency remain concerns and require further improvements inequipment and technique. In vivo durability of transcathetervalves equivalent to conventional surgical valves remains tobe demonstrated. The presence of a learning curve requirescareful dissemination of knowledge gained during develop-ment of this procedure. Early favorable experience withpercutaneous AVR will need to be cautiously replicated inother centers, with larger numbers of patients, longer follow-up, and randomized evaluation.
ConclusionsConventional open heart surgery remains first-line therapyfor symptomatic aortic stenosis. However, percutaneousvalve replacement is a viable alternative to conventional openheart surgery in selected high-risk patients with severesymptomatic aortic stenosis.
DisclosuresDrs Munt and Webb are consultants to Edwards Lifesciences Inc.The remaining authors report no conflicts.
References1. Vahanian A, Baumgartner H, Bax J, Butchart E, Dion RFG, Flachskampf
F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A,Priori SG, Blanc JJ, Budaj A, Camm J, Dean V, Deckers J, Dickstein K,Lekakis J, McGregor K, Metra M, Morais J, Ostersprey A, Tamargo J,Zamorano JL, Angelini A, Antunes M, Fernandez MA, Gohlke-BaerwolfC, Habib G, McMurray J, Otto C, Pierard L, Pomar JL, Prendergast B,Rosenhek R, Uva MS, Tamargo J. Guidelines on the management ofvalvular heart disease: the Task Force on the Management of ValvularDisease of the European Society of Cardiology. Circulation. 1998;28:230–268.
2. Bonow RO, Carabello BA, Kanu C, de Leon AC Jr, Faxon DP, FreedMD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA,Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK, Adams CD,Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL, HiratzkaLF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA2006 guidelines for the management of patients with valvular heartdisease: a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines. Circulation. 2006;114:e84–e231.
3. Varadarajan P, Kapoor N, Bansal R, Pai R. Clinical profile and naturalhistory of 453 nonsurgically managed patients with severe aortic stenosis.Ann Thorac Surg. 2006;82:2111–2115.
4. Bramstedt KA. Aortic valve replacement in the elderly: frequentlyindicated yet frequently denied. Gerontology. 2003;49:46–49.
5. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Barwolf C, LevangOW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P,Vahanian A. A prospective survey of patients with valvular heart diseasein Europe: the Euro Heart Valve Survey on Valvular Disease. EurHeart J. 2003;24:1231–1243.
6. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study.Lancet. 2006;368:1005–1011.
7. Charlson E, Legedza ATR, Hamel MB. Decision-making and outcomesin severe symptomatic aortic stenosis. J Heart Valve Dis. 2006;15:312–321.
8. Andersen HR, Knudsen LL, Hasenkam JM. Transluminal implantation ofartificial heart valves: description of a new expandable aortic valve and
initial results with implantation by catheter technique in closed chest pigs.Eur Heart J. 1992;13:704–708.
9. Andersen HR. Transluminal catheter implanted prosthetic heart valves.Int J Angio. 1998;7:102–106.
10. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F,Derumeaux G, Anselme F, Laborde F, MB L. Trans-catheter implantationof balloon-expandable prosthetic heart valves: early results in an animalmodel. Circulation. 2001;104(suppl II):I-552.
11. Sochman J, Peregrin JH, Pavcnik D, Timmermans H, Rosch J. Percuta-neous transcatheter aortic disc valve prosthesis implantation: a feasibilitystudy. Cardiovasc Intervent Radiol. 2000;23:384–388.
12. Lutter G, Kuklinski D, Berg G, Von Samson P, Martin J, Handke M,Uhrmeister P, Beyersdorf F. Percutaneous aortic valve replacement: anexperimental study. J Thorac Cardiovasc Surg. 2002;123:768–776.
13. Bonhoeffer P, Boudjemline Y, Qureshi SA, Le Bidois J, Iserin L, Acar P,Merckx J, Kachaner J, Sidi D. Percutaneous insertion of the pulmonaryvalve. J Am Coll Cardiol. 2002;39:1664–1669.
14. Vassiliades TA Jr, Block PC, Cohn LH, Adams DH, Borer JS, FeldmanT, Holmes DR, Laskey WK, Lytle BW, Mack MJ, Williams DO. Theclinical development of percutaneous heart valve technology: a positionstatement of the Society of Thoracic Surgeons (STS), the AmericanAssociation for Thoracic Surgery (AATS), and the Society for Cardio-vascular Angiography and Interventions (SCAI) endorsed by theAmerican College of Cardiology Foundation (ACCF) and the AmericanHeart Association (AHA). J Am Coll Cardiol. 2005;45:1554–1560.
15. Boudjemline Y, Bonhoeffer P. Steps toward percutaneous aortic valvereplacement. Circulation. 2002;105:775–778.
16. Webb JG, Munt B, Makkar RR, Naqvi TZ, Dang N. Percutaneous stent-mounted valve for treatment of aortic or pulmonary valve disease.Catheter Cardiovasc Interv. 2004;63:89–93.
17. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F,Derumeaux G, Anselme F, Laborde F, Leon MB. Percutaneous transcath-eter implantation of an aortic valve prosthesis for calcific aortic stenosis:first human case description. Circulation. 2002;106:3006–3008.
18. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Sebagh L, BashA, Nusimovici D, Litzler PY, Bessou JP, Leon MR. Early experience withpercutaneous transcatheter implantation of heart valve prosthesis for thetreatment of end-stage inoperable patients with calcific aortic stenosis.J Am Coll Cardiol. 2004;43:698–703.
19. Webb JG, Chandavimol M, Thompson CR, Ricci DR, Carere RG, MuntBI, Buller CE, Pasupati S, Lichtenstein S. Percutaneous aortic valveimplantation retrograde from the femoral artery. Circulation. 2006;113:842–850.
20. Munt B, Webb J. Percutaneous valve repair and replacement techniques.Heart. Oct 2006;92:1369–1372.
21. Webb JG, Pasupati S, Achtem L, Thompson CR. Rapid pacing tofacilitate transcatheter prosthetic heart valve implantation. Catheter Car-diovasc Interv. 2006;68:199–204.
22. Edmunds LH, Clark RE, Cohn LH, Miller C, Weisel RD. Guidelines forreporting morbidity and mortality after cardiac valvular operations. AnnThorac Surg. 1988;46:257–259.
23. Perry GJ, Helmcke F, Nanda NC, Byard C, Soto B. Evaluation of aorticinsufficiency by Doppler color flow mapping. J Am Coll Cardiol. 1987;9:952–959.
24. Teague SM, Heinsimer JA, Anderson JL, Sublett K, Olson EG, VoylesWF. Quantification of aortic regurgitation utilizing continuous waveDoppler ultrasound. J Am Coll Cardiol. 1986;8:592–599.
25. Nashef SA, Roques F, Hammill BG, Peterson ED, Michel P, Grover FL,Wyse RK, Ferguson T. Validation of European System for CardiacOperative Risk Evaluation (EuroSCORE) in North American cardiacsurgery. Eur J Cardiothorac Surg. 2002;22:101–105.
26. Nilsson J, Algotsson L, Hoglund P, Luhrs C, Brandt J. Early mortality incoronary bypass surgery: the EuroSCORE versus the Society of ThoracicSurgeons risk algorithm. Ann Thorac Surg. 2004;77:1235–1239.
27. Task Force on the Management of Valvular Heart Disease of theEuropean Society of Cardiology. Guidelines on the management of val-vular heart disease. Eur Heart J. 2007;428:e1–e39.
28. Goodney PP, O’Connor GT, Wennberg DE, Birkmeyer JD. Do hospitalswith low mortality rates in coronary artery bypass also perform well invalve replacement? Ann Thorac Surg. 2003;76:1131–1136.
29. Alexander KP, Anstrom KJ, Muhlbaier LH, Grosswald RD, Smith PK,Jones RH, Peterson ED. Outcomes of cardiac surgery in patients �80years: results from the National Cardiovascular Network. J Am CollCardiol. 2000;35:731–738.
762 Circulation August 14, 2007

30. Asimakopoulos G, Edwards MB, Taylor KM. Aortic valve replacement inpatients 80 years of age and older: survival and cause of death based on1100 cases: collective results from the UK Heart Valve Registry. Circu-lation. 1997;96:3403–3408.
31. Dalrymple-Hay MJ, Alzetani A, Aboel-Nazar S, Haw M, Livesey S,Monro J. Cardiac surgery in the elderly. Eur J Cardiothorac Surg.1999;15:61–66.
32. Kolh P, Kerzmann A, Lahaye L, Gerard P, Limet R. Cardiac surgery inoctogenarians: peri-operative outcome and long-term results. Eur Heart J.2001;22:1235–1243.
33. Langanay T, De Latour B, Ligier K, Derieux T, Agnino A, Verhoye JP,Corbineau H, Chaperon J, Leguerrier A. Surgery for aortic stenosis inoctogenarians: influence of coronary disease and other comorbidities onhospital mortality. J Heart Valve Dis. 2004;13:545–552.
34. Suttie SA, Jamieson WR, Burr LH, Germann E. Elderly valve replacementwith bioprostheses and mechanical prostheses: comparison by composites ofcomplications. J Cardiovasc Surg (Torino). 2006;47:191–199.
35. Fuster V, Goldbarg SH, Hansalia RJ, Stevens GR, Tiyyagura SR. Theinoperable valvular heart disease patient: the pluses and minuses ofpercutaneous valvular replacement. Eurointervention. 2006;2:154–160.
36. Roques F, Nashef SA, Michel P, for the EuroSCORE Study Group. Riskfactors for early mortality after valve surgery in Europe in the 1990’s:lessons from the EuroSCORE pilot program. J Heart Valve Dis. 2001;10:572–578.
37. Mazur DJ, Hickam DH, Mazur MD. The role of doctor’s opinion inshared decision making: what does shared decision making really meanwhen considering invasive medical procedures? Health Expect. 2005;8:97–102.
38. Pate GE, Chandavimol M, Naiman SC, Webb JG. Heyde’s syndrome: areview. J Heart Valve Dis. 2004;13:701–712.
39. Ionescu A, Fraser AG, Butchart EG. Prevalence and clinical significanceof incidental paraprosthetic valvar regurgitation: a prospective studyusing transesophageal echocardiography. Heart. 2003;89:1316–1321.
CLINICAL PERSPECTIVETranscatheter aortic valve replacement represents an endovascular alternative to conventional open heart surgery withoutthe need for sternotomy, aortotomy, or cardiopulmonary bypass. Percutaneous implantation of a balloon-expandable stentvalve using a femoral arterial approach was attempted in 50 high-risk patients with severe symptomatic aortic stenosis.Mortality at 30 days was 12% in patients in whom the logistic European System for Cardiac Operative Risk Evaluationrisk estimate was 28%. With experience, procedural success increased from 76% in the first 25 patients to 96% in thesecond 25, and 30-day mortality fell from 16% to 8%. After valve insertion, there was a significant improvement in leftventricular ejection fraction, mitral regurgitation, and functional class. Clinical improvement and valve function weremaintained at 1 year. Percutaneous valve replacement may be an alternative to conventional open heart surgery in selectedhigh-risk patients with severe aortic stenosis.
Webb et al Percutaneous AVR 763