The radiographic assessments of spino-pelvic compensation ...
Upload
independentCategory
view
0download
0
Trends in Pelvic Lymphadenectomy at the Time of RadicalCystectomy: 1988 to 2004
Nicholas J. Hellenthal,* Michelle L. Ramírez, Christopher P. Evans,Ralph W. deVere White and Theresa M. KoppieFrom the Department of Urology, University of California, Davis Medical Center, Sacramento, California
Abbreviations
and Acronyms
LND � lymph node dissection
SEER � Surveillance,Epidemiology and End Results
Submitted for publication October 21, 2008.* Correspondence and requests for reprints:
Department of Urology, UC Davis MedicalCenter, 4860 Y St., Suite 3500, Sacramento,California 95817 (telephone: 916-734-2893;FAX: 916-734-8094; e-mail: [email protected]).
See Editorial on page 2412.
Purpose: Studies suggest that patients who undergo thorough lymphadenec-tomy for bladder cancer benefit from improved survival. We evaluated the inci-dence of and trends in lymphadenectomy in conjunction with radical cystectomyfor bladder cancer.Materials and Methods: Using the Surveillance, Epidemiology and End Resultsregistry we identified 8,072 eligible patients with bladder cancer who underwentradical cystectomy with or without lymphadenectomy from 1988 to 2004. Afterstratification by age group, race, stage, grade and year of diagnosis we performedlogistic and linear regression to correlate variables to the mean number of lymphnodes sampled and the likelihood of undergoing lymphadenectomy (classified as1 or more, 5 or more and 10 or more nodes removed).Results: In the final cohort 1,660 patients (21%) did not have any lymph nodessampled at radical cystectomy. This number decreased from 37% in 1988 to 16% in2004. During this period the mean number of lymph nodes removed increased by 2.6nodes over all definitions of lymphadenectomy and the percentage of patients un-dergoing any form of lymph node dissection increased by an average of 19%. Year ofdiagnosis was most strongly predictive of the likelihood of undergoing lymphadenec-tomy and most correlative with the mean number of nodes sampled.Conclusions: Over time there has been improvement in terms of the perfor-mance of lymphadenectomy and node counts obtained during radical cystectomy.If these trends continue the incidence and quality of lymphadenectomy shouldcontinue to increase, ultimately to the benefit of the patients being treated.
Key Words: urinary bladder neoplasms, lymph node excision, cystectomy,
trends, incidence2490 www.jurology.com
REGIONAL lymphadenectomy duringradical cystectomy may not only be di-agnostic but may also be therapeutic inpatients with locally advanced bladdercancer. In the early 1980s it was dem-onstrated that standard bilateral pelviclymph node dissection at cystectomycould improve 5-year survival by up to36% in patients with limited nodal dis-ease.1 Since then numerous clinical andpopulation based analyses have sug-
gested that recurrence-free and cancer0022-5347/09/1816-2490/0THE JOURNAL OF UROLOGY®
Copyright © 2009 by AMERICAN UROLOGICAL ASSOCIATION
specific survival depend on the extentand ability to surgically remove localand regional disease regardless ofnodal status.2–4
Based on these data many urologistsperform bilateral pelvic lymphadenec-tomy at radical cystectomy. However,there is no accepted standard for theoptimal number of lymph nodes to re-move or the surgical limits of lymphnode dissection. There is a growing
body of evidence suggesting that re-Vol. 181, 2490-2495, June 2009Printed in U.S.A.
DOI:10.1016/j.juro.2009.02.031
TRENDS IN PELVIC LYMPHADENECTOMY 2491
moving more lymph nodes at cystectomy significantlyprolongs survival.4,5 These findings have also led tothe recommendation that the number of lymph nodesremoved should be a factor in measuring the overallquality of surgery.3
Using a national cancer database we identified thefrequency of pelvic node dissection at radical cystec-tomy and determined the predictors of node dissectionand the number of nodes removed. We hypothesize anincrease in the quantity and quality of lymphadenec-tomy over time as more urologists become aware of thedata supporting lymphadenectomy in the surgicaltreatment of bladder cancer.
MATERIALS AND METHODS
Subjects and DatabasesWe used the SEER database, a national prospective can-cer registry maintained by the National Cancer Institute
Table 1. Patient characteristics for each cohort
No. No LND No. LND (%
Age group:Younger than 50 80 337 (81)50–59 209 1,157 (85)60–69 502 2,058 (80)70–79 648 2,223 (77)80 or Older 221 637 (74)
TNM stage:Tis/T1N0M0 304 619 (67)T2N0M0 501 1,420 (74)T3N0M0 459 1,935 (81)T4N0M0 396 739 (65)N� 0 1,699
Grade:1 171 467 (73)2 974 3,613 (79)3 515 2,332 (82)
Race:White 1,497 5,772 (79)Black 88 343 (80)Other 75 297 (80)
Yr of diagnosis:1988 59 99 (63)1989 47 117 (71)1990 59 137 (70)1991 61 150 (71)1992 73 259 (78)1993 72 231 (76)1994 92 246 (73)1995 86 279 (76)1996 88 234 (73)1997 88 266 (75)1998 67 347 (84)1999 75 379 (83)2000 205 678 (77)2001 156 719 (82)2002 140 744 (84)2003 147 791 (84)2004 145 736 (84)
Totals 1,660 6,412 (79)
that captured approximately 26% of the United Statespopulation from 1973 to 2004 (Connecticut, Iowa, ruralGeorgia, Alaska, New Mexico, Greater California, Utah,Hawaii, Kentucky, New Jersey and Louisiana as well asthe metropolitan areas of Detroit, San Francisco-Oakland,Seattle [Puget Sound], Metropolitan Atlanta, Los Angelesand San Jose-Monterey).6 We examined data from 1988 to2004 only because SEER did not collect detailed lymphnode data from 1973 to 1987.
Lymph Node DataAll patients 40 to 99 years old who underwent radical cys-tectomy or pelvic exenteration specifically for transitionalcell carcinoma of the bladder between 1988 and 2004 wereidentified. Care was taken to exclude patients from analysiswho underwent any form of partial cystectomy. Patientswere included in study when the number of nodes examinedand the number of pathologically positive nodes were docu-mented. Patients with unknown tumor grade and stage aswell as those with metastatic disease were excluded fromanalysis. We excluded patients with documented metastases
Totals OR (95% CI) p Value
417 Reference 1.01,366 1.31 (0.98–1.75) 0.0602,560 0.97 (0.75–1.27) 0.8392,871 0.81 (0.63–1.06) 0.120
858 0.68 (0.51–0.91) 0.010
923 Reference 1.01,921 1.39 (1.17–1.65) �0.0012,394 2.07 (1.75–2.46) �0.0011,135 0.92 (0.76–1.10) 0.3521,699
638 Reference 1.04,587 1.36 (1.12–1.64) 0.0012,847 1.66 (1.36–2.02) �0.001
7,269 Reference 1.0431 1.01 (0.79–1.29) 0.930372 1.03 (0.79–1.33) 0.840
158 Reference 1.0164 1.48 (0.93–2.37) 0.098196 1.38 (0.89–2.16) 0.151211 1.47 (0.95–2.27) 0.088332 2.11 (1.40–3.20) �0.001303 1.91 (1.26–2.90) 0.002338 1.59 (1.07–2.38) 0.023365 1.93 (1.29–2.89) 0.001322 1.58 (1.06–2.37) 0.026354 1.80 (1.20–2.69) 0.004414 3.09 (2.04–4.67) �0.001454 3.01 (2.01–4.52) �0.001883 1.97 (1.38–2.82) �0.001875 2.75 (1.91–3.96) �0.001884 3.17 (2.19–4.58) �0.001938 3.21 (2.22–4.63) �0.001881 3.03 (2.09–4.37) �0.001
)
8,072
TRENDS IN PELVIC LYMPHADENECTOMY2492
on the basis that many likely underwent cystectomy forpalliative reasons and, thus, would not have had a reason forlymphadenectomy. Patients were then segregated based onthe presence of lymphadenectomy, and grouped according to1 or more, 5 or more and 10 or more nodes taken.
We used these classifications of lymphadenectomy forseveral reasons. The SEER database does not have aformal categorization for lymph node dissection but doesreport the number of nodes pathologically examined. Nu-merous studies have shown that the number of lymphnodes examined at radical cystectomy varies widely evenwhen a complete lymph node dissection is performed.Therefore, we first looked at patients who had any lymphnodes (1 or more) examined. Bochner et al demonstratedthat standard lymphadenectomy yields a mean of 2.4nodes per side if submitted en bloc and 8.5 nodes if sub-mitted in packets.7 Thus, we also looked at patients with5 or more lymph nodes examined because they more likelyrepresent patients who underwent standard LND ratherthan those in whom a few suspicious nodes were removedand those in whom nodes were inadvertently removedwith the bladder specimen. Finally we chose a cutoff of 10or more lymph nodes to represent a more contemporarylymph node dissection because this number has beenreadily cited as relevant to survival outcomes.4,8
Statistical AnalysisOur primary outcome measures were the incidence oflymphadenectomy and the mean number of lymph nodesexamined per year of diagnosis. Logistic regression analysiswas used to examine the relationship between the year ofdiagnosis and the likelihood of undergoing lymphadenec-tomy. Dummy variables were used when appropriate to cal-culate odds ratios within cohorts. Linear regression analysiswas used to examine the relationship between the year ofdiagnosis and the mean number of lymph nodes sampled.The cohort was adjusted for age group (younger than 50, 50to 59, 60 to 69, 70 to 79 and 80 years or older), race (white,black and other), tumor stage (Tis/T1N0, T2N0, T3N0, T4N0and N�) and tumor grade (1, 2 and 3). We evaluated thetimes (before 1992, 1992 to 1999, 2000 or after) on univariateanalysis to account for potential bias from the addition ofnew registries to SEER in 1992 and 2000. However, thisvariable was dropped on multivariate analysis due to itsstrong correlation (92%) to year of diagnosis. All statisticalanalysis was performed using STATA® statistical softwareversion 10.0 and all testing was 2-sided.
RESULTS
Between January 1988 and December 2004 we iden-tified 8,072 patients with transitional cell carcinomaof the bladder who underwent radical cystectomy orpelvic exenteration. In the final cohort 1,660 pa-tients (21%) had no lymph nodes examined at cys-tectomy. A total of 6,554 patients (79%) had 1 ormore lymph nodes sampled at cystectomy, while4,859 and 3,075 (60% and 38%) had 5 or more and 10or more lymph nodes examined at cystectomy, re-spectively. Table 1 illustrates the number of pa-
tients in each cohort and the relative likelihood ofundergoing lymphadenectomy (defined as 1 or morelymph nodes examined). When taken cumulativelythe year of diagnosis demonstrated the strongestassociation with lymphadenectomy.
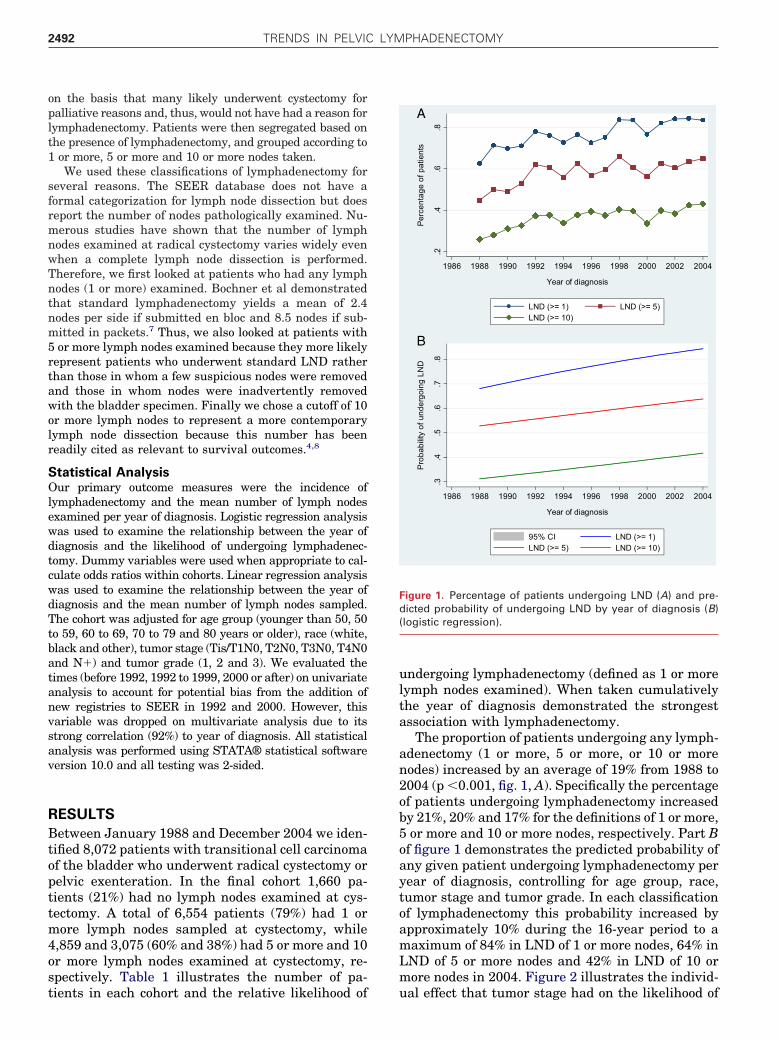
The proportion of patients undergoing any lymph-adenectomy (1 or more, 5 or more, or 10 or morenodes) increased by an average of 19% from 1988 to2004 (p �0.001, fig. 1, A). Specifically the percentageof patients undergoing lymphadenectomy increasedby 21%, 20% and 17% for the definitions of 1 or more,5 or more and 10 or more nodes, respectively. Part Bof figure 1 demonstrates the predicted probability ofany given patient undergoing lymphadenectomy peryear of diagnosis, controlling for age group, race,tumor stage and tumor grade. In each classificationof lymphadenectomy this probability increased byapproximately 10% during the 16-year period to amaximum of 84% in LND of 1 or more nodes, 64% inLND of 5 or more nodes and 42% in LND of 10 ormore nodes in 2004. Figure 2 illustrates the individ-
.2.4
.6.8
Pe
rce
nta
ge
of
pa
tien
ts
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
Year of diagnosis
LND (>= 1) LND (>= 5)LND (>= 10)
.3.4
.5.6
.7.8
Pro
ba
bili
ty o
f u
nd
erg
oin
g L
ND
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
Year of diagnosis
95% CI LND (>= 1)LND (>= 5) LND (>= 10)
A
B
Figure 1. Percentage of patients undergoing LND (A) and pre-dicted probability of undergoing LND by year of diagnosis (B)(logistic regression).
ual effect that tumor stage had on the likelihood of

TRENDS IN PELVIC LYMPHADENECTOMY 2493
undergoing LND. While higher stage disease (exceptT4N0M0) conferred an increased likelihood of LNDin all categories, the rates of increase over time weregreatest in low stage disease (Tis/T1N0M0) whichincreased from 48% to 69% (LND of 1 or morenodes), 34% to 56% (LND of 5 or more nodes) and17% to 32% (LND of 10 or more nodes).
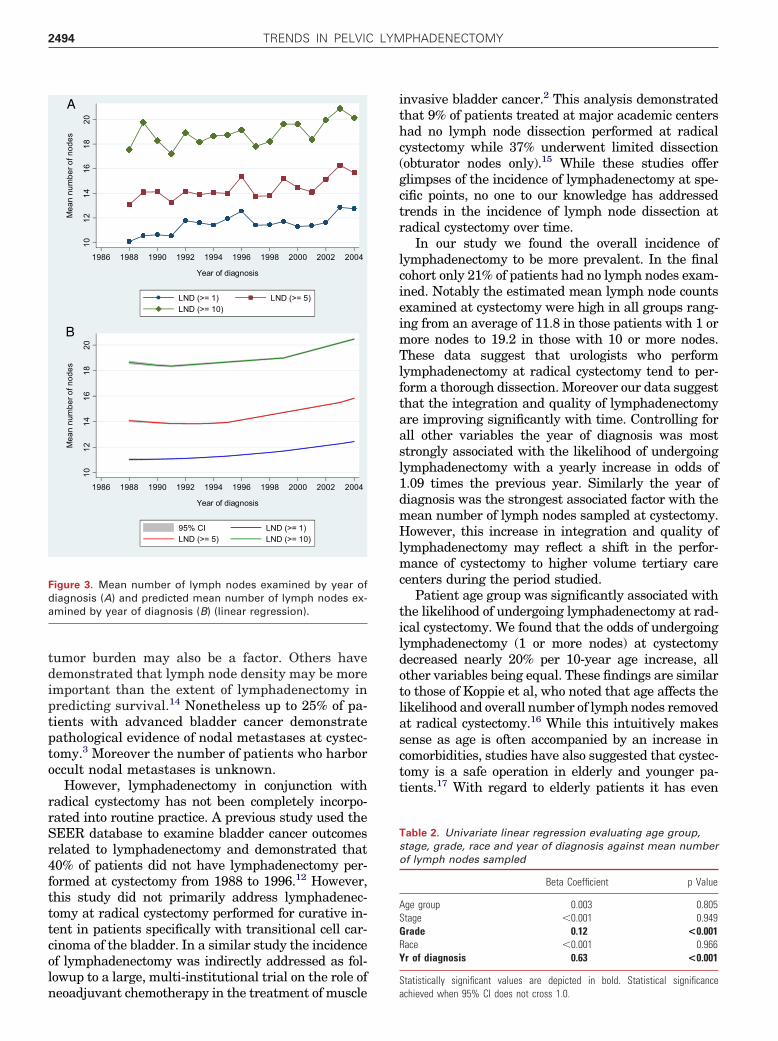
The mean number of lymph nodes examined atcystectomy also increased by a factor of 2.6 nodes ineach classification of lymphadenectomy from 1988 to2004 (p �0.001, fig. 3, A). Tumor grade and year ofdiagnosis were significantly associated with themean number of lymph nodes sampled after univar-iate linear regression (table 2). Year of diagnosisdemonstrated the strongest association. Part B offigure 3 shows the predicted mean number of lymph
.2.4
.6.8
Per
cent
age
of p
atie
nts
1986 1988 1990 1992 1994 1996 1998 2000 2002 200
Year of diagnosis
Tis/T1N0M0 T2N0M0
T3N0M0 T4N0M0
.2.4
.6.8
Per
cent
age
of p
atie
nts
1986 1988 1990 199
Tis/
T3N
A
C
Figure 2. Percentage of patients undergoing LND (1 or more nod(stratified by tumor stage).
nodes examined based on year of diagnosis control-
ling for age group, race, tumor stage and tumorgrade. This figure illustrates that the mean numberof nodes predicted to be examined for any givenpatient at cystectomy increased by approximately 2during the 16-year period to a maximum of 13 inLND of 1 or more nodes, 16 in LND of 5 or morenodes and 20 in LND of 10 or more nodes in 2004.
DISCUSSION
The role of lymphadenectomy at cystectomy hasshifted from a primarily diagnostic intervention to atherapeutic procedure.9,10 Several studies haveshown that the removal of increasing numbers oflymph nodes at radical cystectomy is associated withimproved overall survival.11–13 Although this may
.2.4
.6.8
Per
cent
age
of p
atie
nts
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
Year of diagnosis
Tis/T1N0M0 T2N0M0
T3N0M0 T4N0M0
1996 1998 2000 2002 2004
diagnosis
T2N0M0
T4N0M0
B
5 or more nodes [B], 10 or more nodes [C]) by year of diagnosis
4
2 1994
Year of
T1N0M0
0M0
es [A],
largely be due to more accurate staging, decreasing
TRENDS IN PELVIC LYMPHADENECTOMY2494
tumor burden may also be a factor. Others havedemonstrated that lymph node density may be moreimportant than the extent of lymphadenectomy inpredicting survival.14 Nonetheless up to 25% of pa-tients with advanced bladder cancer demonstratepathological evidence of nodal metastases at cystec-tomy.3 Moreover the number of patients who harboroccult nodal metastases is unknown.
However, lymphadenectomy in conjunction withradical cystectomy has not been completely incorpo-rated into routine practice. A previous study used theSEER database to examine bladder cancer outcomesrelated to lymphadenectomy and demonstrated that40% of patients did not have lymphadenectomy per-formed at cystectomy from 1988 to 1996.12 However,this study did not primarily address lymphadenec-tomy at radical cystectomy performed for curative in-tent in patients specifically with transitional cell car-cinoma of the bladder. In a similar study the incidenceof lymphadenectomy was indirectly addressed as fol-lowup to a large, multi-institutional trial on the role of
10
12
14
16
18
20
Me
an
nu
mb
er
of
no
de
s
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
Year of diagnosis
LND (>= 1) LND (>= 5)LND (>= 10)
10
12
14
16
18
20
Me
an
nu
mb
er
of
no
de
s
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004
Year of diagnosis
95% CI LND (>= 1)LND (>= 5) LND (>= 10)
A
B
Figure 3. Mean number of lymph nodes examined by year ofdiagnosis (A) and predicted mean number of lymph nodes ex-amined by year of diagnosis (B) (linear regression).
neoadjuvant chemotherapy in the treatment of muscle
invasive bladder cancer.2 This analysis demonstratedthat 9% of patients treated at major academic centershad no lymph node dissection performed at radicalcystectomy while 37% underwent limited dissection(obturator nodes only).15 While these studies offerglimpses of the incidence of lymphadenectomy at spe-cific points, no one to our knowledge has addressedtrends in the incidence of lymph node dissection atradical cystectomy over time.
In our study we found the overall incidence oflymphadenectomy to be more prevalent. In the finalcohort only 21% of patients had no lymph nodes exam-ined. Notably the estimated mean lymph node countsexamined at cystectomy were high in all groups rang-ing from an average of 11.8 in those patients with 1 ormore nodes to 19.2 in those with 10 or more nodes.These data suggest that urologists who performlymphadenectomy at radical cystectomy tend to per-form a thorough dissection. Moreover our data suggestthat the integration and quality of lymphadenectomyare improving significantly with time. Controlling forall other variables the year of diagnosis was moststrongly associated with the likelihood of undergoinglymphadenectomy with a yearly increase in odds of1.09 times the previous year. Similarly the year ofdiagnosis was the strongest associated factor with themean number of lymph nodes sampled at cystectomy.However, this increase in integration and quality oflymphadenectomy may reflect a shift in the perfor-mance of cystectomy to higher volume tertiary carecenters during the period studied.
Patient age group was significantly associated withthe likelihood of undergoing lymphadenectomy at rad-ical cystectomy. We found that the odds of undergoinglymphadenectomy (1 or more nodes) at cystectomydecreased nearly 20% per 10-year age increase, allother variables being equal. These findings are similarto those of Koppie et al, who noted that age affects thelikelihood and overall number of lymph nodes removedat radical cystectomy.16 While this intuitively makessense as age is often accompanied by an increase incomorbidities, studies have also suggested that cystec-tomy is a safe operation in elderly and younger pa-tients.17 With regard to elderly patients it has even
Table 2. Univariate linear regression evaluating age group,stage, grade, race and year of diagnosis against mean numberof lymph nodes sampled
Beta Coefficient p Value
Age group 0.003 0.805Stage �0.001 0.949Grade 0.12 <0.001Race �0.001 0.966Yr of diagnosis 0.63 <0.001
Statistically significant values are depicted in bold. Statistical significance
achieved when 95% CI does not cross 1.0.
TRENDS IN PELVIC LYMPHADENECTOMY 2495
been shown that the true survival benefit seen withcystectomy may lie in the lymphadenectomy itself.18
Tumor stage was also significantly associatedwith the likelihood of undergoing lymphadenectomy(1 or more nodes) in our analysis. We found that foreach increase in stage from TisN0M0 to T3N0M0the odds of undergoing lymphadenectomy increasedby a factor of 1.5. However, the likelihood of under-going LND decreased once T4N0M0 status wasreached. While we were unable to determine surgi-cal intent from this retrospective data set, this maybe because a number of these cystectomies wereperformed with palliative intent. Interestingly wealso found the highest rate of change in the proba-bility of LND was in patients with Tis/T1N0M0 dis-ease, demonstrating a clear trend toward LND forpatients with lower risk disease.
This study does have limitations. The SEER data-base does not include specific data on comorbidities,prior radiation or grossly palpable lymph nodes, whichmay factor into the decision to perform lymphadenec-tomy. Moreover while the SEER database does pro-vide the number of nodes pathologically examined itprovides little information on the dissection itself suchas the anatomical boundaries of dissection, or whether
nodes were submitted en bloc or in separate packets.REFERENCES
(www.seer.cancer.gov) Limited-Use Data (1973– J Urol 2003; 169: 946.
Even in surgically controlled studies the number oflymph nodes removed during radical cystectomy var-ies widely due to a number of factors which cannot beaddressed in this retrospective data set. Finally aswith any large database analysis there is the possibil-ity of data entry miscoding or pathological miscount-ing of nodes examined. However, this potential errorshould be nonselective over the cohort analyzed and,in effect, cancel out any overt bias.
CONCLUSIONS
Urologists have continued to improve in terms of theperformance of lymphadenectomy and node counts ob-tained at radical cystectomy. As of 2004, 84% of pa-tients had at least 1 lymph node (and a mean of 13nodes) examined at cystectomy. If these trends con-tinue the incidence and quality of lymphadenectomyshould continue to increase, ultimately to the benefit ofthe patients being treated.
ACKNOWLEDGMENTS
Garrett R. Hellenthal, PhD, Department of Statis-tics, University of Oxford, Oxford, United Kingdomevaluated and validated the statistical methodology
used in this study.1. Skinner DG: Management of invasive bladdercancer: a meticulous pelvic node dissection canmake a difference. J Urol 1982; 128: 34.
2. Grossman HB, Natale RB, Tangen CM, SpeightsVO, Vogelzang NJ, Trump DL et al: Neoadjuvantchemotherapy plus cystectomy compared withcystectomy alone for locally advanced bladdercancer. N Engl J Med 2003; 349: 859.
3. Bochner BH, Cho D, Herr HW, Donat M, KattanMW and Dalbagni G: Prospectively packagedlymph node dissections with radical cystectomy:evaluation of node count variability and nodemapping. J Urol 2004; 172: 1286.
4. Herr HW, Bochner BH, Dalbagni G, Donat SM,Reuter VE and Bajorin DF: Impact of the numberof lymph nodes retrieved on outcome in patientswith muscle invasive bladder cancer. J Urol 2002;167: 1295.
5. Wright JL, Lin DW and Porter MP: The associa-tion between extent of lymphadenectomy andsurvival among patients with lymph node metas-tases undergoing radical cystectomy. Cancer2008; 112: 2401.
6. National Cancer Institute, Surveillance ResearchProgram, Cancer Statistics Branch: Surveillance,Epidemiology and End Results (SEER) Program
2004). Released April 2007 (revised September2007), based on the November 2006 submission.
7. Bochner BH, Herr HW and Reuter VE: Impact ofseparate versus en bloc pelvic lymph node dis-section on the number of lymph nodes retrievedin cystectomy specimens. J Urol 2001; 166: 2295.
8. Herr HW, Smith JA and Montie JE: Standardiza-tion of radical cystectomy: time to count and becounted. BJU Int 2004; 94: 481.
9. Leissner J, Hohenfellner R, Thuroff JW and WolfHK: Lymphadenectomy in patients with transitionalcell carcinoma of the urinary bladder; significancefor staging and prognosis. BJU Int 2000; 85: 817.
10. Stein JP, Cai J, Groshen S and Skinner DG: Riskfactors for patients with pelvic lymph node me-tastases following radical cystectomy with enbloc pelvic lymphadenectomy: concept of lymphnode density. J Urol 2003; 170: 35.
11. Dhar NB, Klein EA, Reuther AM, Thalmann GN,Madersbacher S and Studer UE: Outcome afterradical cystectomy with limited or extended pel-vic lymph node dissection. J Urol 2008; 179: 873.
12. Konety BR, Joslyn SA and O’Donnell MA: Extentof pelvic lymphadenectomy and its impact onoutcome in patients diagnosed with bladder can-cer: analysis of data from the Surveillance, Epi-demiology and End Results Program data base.
13. Stein JP, Lieskovsky G, Cote R, Groshen S, FengAC, Boyd S et al: Radical cystectomy in thetreatment of invasive bladder cancer: long-termresults in 1,054 patients. J Clin Oncol 2001; 19:666.
14. Steven K and Poulsen AL: Radical cystectomy andextended pelvic lymphadenectomy: survival of pa-tients with lymph node metastasis above thebifurcation of the common iliac vessels treatedwith surgery only. J Urol 2007; 178: 1218.
15. Herr HW, Faulkner JR, Grossman HB, Natale RB,DeVere White R, Sarosdy MF et al: Surgical factorsinfluence bladder cancer outcomes: a cooperativegroup report. J Clin Oncol 2004; 22: 2781.
16. Koppie TM, Vickers AJ, Vora K, Dalbagni G andBochner BH: Standardization of pelvic lymphade-nectomy performed at radical cystectomy: can weestablish a minimum number of lymph nodes thatshould be removed? Cancer 2006; 107: 2368.
17. Clark PE, Stein JP, Groshen SG, Cai J, Miranda G,Lieskovsky G et al: Radical cystectomy in theelderly: comparison of clinical outcomes betweenyounger and older patients. Cancer 2005; 104: 36.
18. Chamie K, Hu B, Devere White RW and EllisonLM: Cystectomy in the elderly: does the survivalbenefit in younger patients translate to the octo-
genarians? BJU Int 2008; 102: 284.Copyright © 2022 FDOKUMEN