
Natural history and serial morphology of aortic intramural hematoma: A novel variant of aortic...
13
Natural history and serial morphology of aortic intramural hematoma: A novel variant of aortic dissection Isidre Vilacosta, MD, a Jose Alberto San RomAn, MD, b Joaquin Ferreirbs, MD, c Paloma Aragoncillo, MD, d Ramiro M6ndez, MD, c Juan Antonio Castillo, MD, a Maria Jesfls Rollfin, MD, a Elena Batlle, MD, a Vicente Peral, MD, a and Luis Sfinchez-Harguindey, MD, a Madrid and Valladoli~ Spain Background Acute aortic dissection is a cardiovascular emergency that requires prompt diagnosis and treatment. Transesophageal echocardiography is the current standard diagnostic imaging modality in many medical centers. Aortic intramural hematoma is a variant of aortic dissection whose natural history and prognosis have not been well studied. We performed transesophageal echocardiography in patients with aortic intramural hematoma to determine the echocardio- graphic characteristics and echocardiographic evolution of this lesion, impact on patient management, and patient outcome. Methods and Results Twenty-one consecutive patients with aortic intramural hematoma confirmed anatomically (four patients) or with an additional diagnostic imaging technique (17 patients) underwent a transesophageal echocardiographic examination. Fifteen patients with longstanding hypertension had chest or back pain, and the intramural hematoma was visualized in the ascending aorta (n = 4), along the whole aorta (n = 4), in the descending aorta (n = 6), or in the aortic arch (n = 1). The thickening of the aortic wall was crescentic. Patients with ascending aortic intramural hematoma had the following results: two patients died suddenly, three patients underwent surgery because of increased aortic wall thickening (one patient) or secondary intimal tear (two patients), and the remaining three patients had regression of the hematoma. Patients with hematoma confined to the descending aorta and the patient with aortic arch involvement (n = 7) had a different result: one patient died from aortic rupture and the remaining six patients did well. Six patients had a traumatic aortic injury, and the intramural hematoma was located along the descending thoracic aorta. The thickening of the aortic wall was circular in five patients and crescentic in one. Three of these patients had normalized thickness of the aortic wall on follow-up transesophageal echocardiographic studies. The other three patients died from multiorgan system failure. Aortography showed a reduction of the diameter of the aortic lumen in four patients; diameter in the remaining 17 patients was normal. Conclusions Aortic intramural hematoma can be detected and monitored by transesophageal echocardiography but not by aortography. Two types of aortic intramural hematoma can be distinguished: (1) traumatic of good prognosis and (2) nontraumatic, which can be an early stage of the classic aortic dissection, with bad prognosis in cases involving the ascending aorta. (Am Heart J 1997;134:495-507.) Acute dissection of the aorta is one of the most dramatic cardiovascular emergencies. To limit the possibility of death, a detailed morphologic and functional diagnosis must be quickly obtained. From the aDepartments of Cardiology, CRadiology, and dHurnan Pathology, Hospital Universitarlo de San Cados, Madrid, and the bDepartment of Cardiology, Hospital Universitario de Valladolid. Received for publication Aug. 5, •996; accepted April 24, 199Z Reprint requests: Dn Isidre Vilacosta, Serrano 46, 28001 Madrid, Spain. Copyright ©) 1997 by Mosby- Year Book, Inc. 0002-8703/97/$5.00 + 0 4/1/83046 Most aortic dissections are characterized by a transverse and longitudinal separation of the aortic media and an intimomedial tear. 1,2 However, aortic intramural hematoma (AIH) represents a variant of dissection characterized by the absence of an intimal tear. 3 In this condition, the false channel is probably created by a hemorrhage of the aortic vasa vasorum into the aortic wall. 4 This noncommunicating form of aortic dissection has been increasingly reported with modern diagnostic imaging techniques. 3,5-7 At present, the use of
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Natural history and serial morphology of aortic intramural hematoma: A novel variant of aortic...

Natural history and serial morphology of aortic intramural hematoma: A novel variant of aortic dissection Isidre Vilacosta, MD, a Jose Alberto San RomAn, MD, b Joaquin Ferreirbs, MD, c Pa loma Aragonci l lo , MD, d Ramiro M6ndez, MD, c Juan Anton io Castillo, MD, a Maria Jesfls Rollfin, MD, a Elena Batlle, MD, a Vicente Peral, MD, a and Luis Sf inchez-Harguindey, MD, a Madrid and Valladoli~ Spain
Background Acute aortic dissection is a cardiovascular emergency that requires prompt diagnosis and treatment. Transesophageal echocardiography is the current standard diagnostic imaging modality in many medical centers. Aortic intramural hematoma is a variant of aortic dissection whose natural history and prognosis have not been well studied. We performed transesophageal echocardiography in patients with aortic intramural hematoma to determine the echocardio- graphic characteristics and echocardiographic evolution of this lesion, impact on patient management, and patient outcome.
Methods and Results Twenty-one consecutive patients with aortic intramural hematoma confirmed anatomically (four patients) or with an additional diagnostic imaging technique (17 patients) underwent a transesophageal echocardiographic examination. Fifteen patients with longstanding hypertension had chest or back pain, and the intramural hematoma was visualized in the ascending aorta (n = 4), along the whole aorta (n = 4), in the descending aorta (n = 6), or in the aortic arch (n = 1 ). The thickening of the aortic wall was crescentic. Patients with ascending aortic intramural hematoma had the following results: two patients died suddenly, three patients underwent surgery because of increased aortic wall thickening (one patient) or secondary intimal tear (two patients), and the remaining three patients had regression of the hematoma. Patients with hematoma confined to the descending aorta and the patient with aortic arch involvement (n = 7) had a different result: one patient died from aortic rupture and the remaining six patients did well. Six patients had a traumatic aortic injury, and the intramural hematoma was located along the descending thoracic aorta. The thickening of the aortic wall was circular in five patients and crescentic in one. Three of these patients had normalized thickness of the aortic wall on follow-up transesophageal echocardiographic studies. The other three patients died from multiorgan system failure. Aortography showed a reduction of the diameter of the aortic lumen in four patients; diameter in the remaining 17 patients was normal.
Conclusions Aortic intramural hematoma can be detected and monitored by transesophageal echocardiography but not by aortography. Two types of aortic intramural hematoma can be distinguished: (1) traumatic of good prognosis and (2) nontraumatic, which can be an early stage of the classic aortic dissection, with bad prognosis in cases involving the ascending aorta. (Am Heart J 1997;134:495-507.)
Acute dissection of the aorta is one of the most
dramatic cardiovascular emergencies. To limit the
possibility of death, a detailed morphologic and
functional diagnosis must be quickly obtained.
From the aDepartments of Cardiology, CRadiology, and dHurnan Pathology, Hospital Universitarlo de San Cados, Madrid, and the bDepartment of Cardiology, Hospital Universitario de Valladolid. Received for publication Aug. 5, •996; accepted April 24, 199Z Reprint requests: Dn Isidre Vilacosta, Serrano 46, 28001 Madrid, Spain. Copyright ©) 1997 by Mosby- Year Book, Inc. 0002-8703/97/$5.00 + 0 4/1/83046
Most aortic dissections are characterized by a
transverse and longitudinal separat ion of the aortic
media and an int imomedial tear. 1,2 However, aortic
intramural hema toma (AIH) represents a variant of
d issec t ion character ized by the absence of an
intimal tear. 3 In this condi t ion, the false channe l is
p robab ly c r e a t e d by a hemor rhage of the aortic
vasa vasorum into the aortic wall. 4 This
noncommunica t ing form of aortic d issec t ion has
been increasingly repor ted with m o d e r n d iagnost ic
imaging techniques . 3,5-7 At present , the use of
4 9 6 Vilacosta et al.
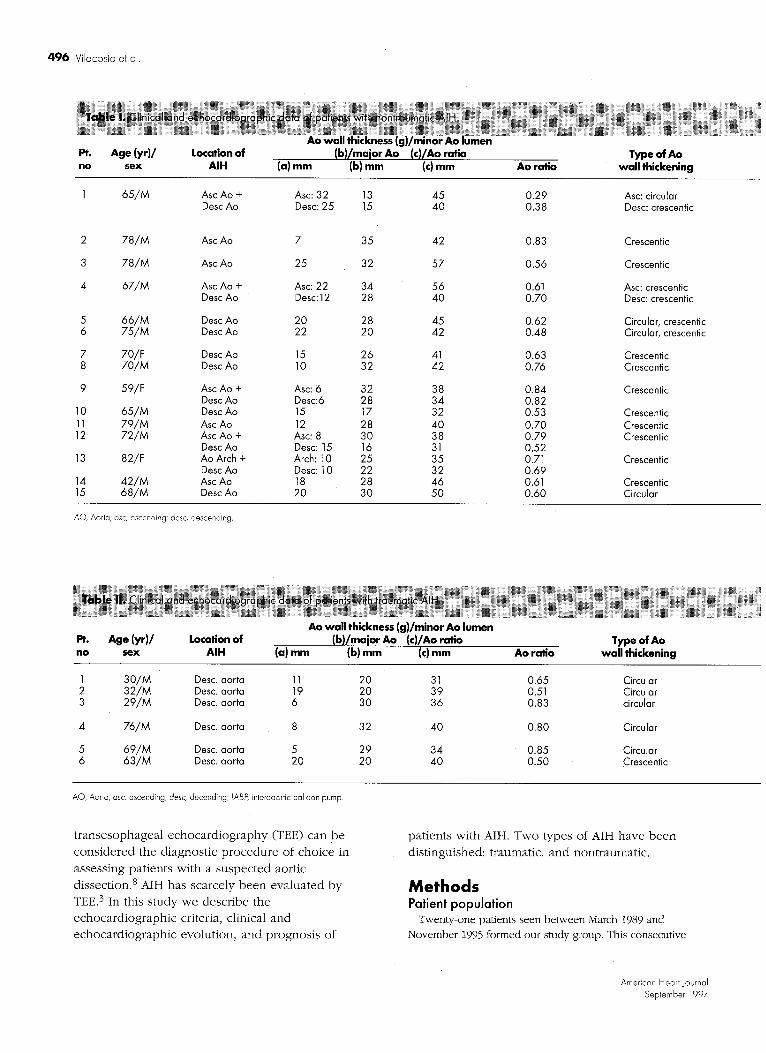
Pt. Age (yr)/ Location of no sex AIH
(b)/major Ao (a) mm (b) mm
(c)/Ao ratio (c) mm
Type of Ao Ao ratio wall thickening
1 65/M Asc Ao + Asc: 32 13 45 Desc Ao Desc: 25 15 40
2 78/M Asc Ao 7 35 42
3 78/M Asc Ao 25 32 57
4 67/M Asc Ao + Asc: 22 34 56 Desc Ao Desc: 12 28 40
5 66/M Desc Ao 20 28 45 6 75/M Desc Ae 22 20 42
7 70/F Desc Ao 15 26 41 8 70/M Desc Ao 10 32 42
9 59/F Asc Ao + Asc: 6 32 38 Desc Ao Desc:6 28 34
10 65/M Desc Ao 15 17 32 11 79/M Asc Ao 12 28 40 12 72/M Asc Ao + Asc: 8 30 38
Desc Ao Desc: 15 16 31 13 82/F Ao Arch + Arch: 10 25 35
Desc Ao Desc: 10 22 32 14 4 2 / M Asc Ae 18 28 46 15 68/M Desc Ao 20 30 50
0.29 Asc: circular 0.38 Desc: crescentic
0.83 Crescentic
0.56 Crescentic
0.61 Asc: crescentic 0.70 Desc: crescentic
0.62 Circular, crescentic 0.48 Circular, crescentic
0.63 Crescentic 0.76 Crescentic
0.84 Crescentic 0.82 0.53 Crescentic 0.70 Crescentic 0.79 Crescentic 0.52 0.71 Crescentic 0.69 0.61 Crescentic 0.60 Circular
AO, Aorta; asc, ascending; desc, descending.
Pt. Age (yr)/ Location of no sex AIH (a)
Ao wall thickness (g)/minor Ao lumen (b)/major Ao (c)/Ao ratio
mm (b) mm (c) mm Type of Ao
Ao ratio wall thickening
1 30 /M Desc. aorta 2 32 /M Desc. aorta 3 29 /M Desc. aorta
4 76 /M Desc. aorta
5 6 9 / M Desc. aorta 6 6 3 / M Desc. aorta
11 20 31 0.65 Circular 19 20 39 0.51 Circular 6 30 36 0.83 circular
8 32 40 0.80 Circular
5 29 34 20 20 40
0.85 Circular 0.50 Crescentic
AO, Aorta; asc, ascending; desc, decending; IABP, interaaortic balloon pump.
t r ansesophagea l echoca rd iography (TEE) can be
cons idered the diagnost ic p rocedure of choice in
assessing pat ients with a suspec ted aortic
dissection. 8 AIH has scarcely been evalua ted by
TEE. 3 In this s tudy we descr ibe the echocard iographic criteria, clinical and echocard iographic evolut ion, and prognos is of
pat ients with AIH. Two types of AIH have been
dist inguished: traumatic, and nontraumatic .
M e t h o d s Patient population
Twenty-one patients seen between March 1989 and November 1995 formed our study group. This consecutive
American Heart Journal September 1997

Vilacosta et al. 497
Echo-free Flow spaces within AIH Confirmation
Clinical presentation
Clinical and Outcome/ echocardiographic follow-up
evolution time
Yes No MRI
Yes No CT, autopsy
Yes No CT, surgery
Yes No CT
Yes No CT + MRI Yes Yes CT + MRI
Yes No CT + MRI No No CT, surgery
Yes No CT + MRI
Yes Yes CT + MRI No No CT Yes Yes CT
No No MRI
No No MRI No No CT
Chest pain, paraplegia
Chest pain
Chest pain, syncope Chest pain
Chest pain Back pain,
Chest pain Chest pain
Chest pain, syncope Back pain Back pain Back pain
Chest pain
Chest pain Chest pain
Early partial regression, Alive/3 yr late intimal disruption (type II Ao dissection); no surgery
Adventitial rupture; Death/t6 hr sudden death
Progression of AIH; Alive/2 yr shock (surgery)
Late intimal disruption Death/20 d (Type I Ao dissection); syncope (surgery) No change Alive/8 mo Partial regression Alive/8 mo syncope No change Alive/2 yr Adventitial rupture Death/48 hr
(surgery) Complete regression Alive/8 mo
Partial regression Alive/10 mo Partial regression Alive/6 mo No change Death/24 hr Sudden death Complete regression Alive/4 mo
Complete regression Alive/11 mo Complete regression Alive/2 yr
Echo-free Flow spaces within AIH Confirmation
Clinical presentation
Clinical and Outcome/ echocardiographic follow-up
evolution time
No No CT Yes No CT No No CT, autopsy
No No CT
No No CT Yes Yes CT
Trauma Trauma Trauma failure (No change) Trauma (No change) Trauma IABP
Complete regression Alive/2 yr, 8 mo Complete regression Alive/2 yr, 6 mo Multiorgan system Death/36 hr
Renal failure and sepsis Death/24 d
Complete regression Alive/1 yr, 2 mo late intimal disruption Death/12 d (type III Ao dissection)
group of patients is a composite of two subgroups, a
subgroup of 15 (17%) was selected from a group of 88
patients diagnosed by TEE with aortic dissection from
nontraumatic sources. These 15 patients had signs and
symptoms consistent with acute aortic dissection; the classic
mobile dissection flap was not visualized and a thickened
aortic wall without an intimal tear in the TEE study was
detected. Consequently, they were categorized as having a
noncommunicating aortic dissection (group 1). In the same
period 22 patients admitted to our institutions with severe
blunt chest trauma with a widened mediastinal silhouette
were studied with TEE. Five patients (22%) had increased
aortic wall thickness. A dissection flap and an entrance tear
were not detected; and they were diagnosed as having an
American Heart journal Volume 134, Number 3

498 Vilacosta et al.
Left, Cross-sectional TEE view of AIH (asterisk) confined to descending thoracic aorta (,40). Right, Schematic depicting echocardiographic aortic measurements, a, Aortic wall thickness; b, minor aortic lumen diameter; c, major aortic diameter.
AIH. Four patients had a classic aortic dissection, and the
remaining 13 patients with chest trauma had a normal aorta
by TEE. During the study period, one patient had a
barotraumatic aortic injury from an intraaortic balloon pump
that was studied by TEE and diagnosed as AIH. These six
patients with AIH formed group 2.
Overall, 21 patients were considered to have an AIH: 15
nontraumatic (group 1) and six traumatic (group 2).
Confirmation of this echocardiographic diagnosis was
performed by surgery or necropsy (four patients) or with a n
additional imaging technique---computed tomography (CT)
or magnetic resonance imaging (MRI)--and on the basis of
clear follow-up TEE changes (17 patients). Conventional
aortography was done in all patients. Meticulous clinical and
echocardiographic follow-up was performed in all patients.
Group 1 was composed of 12 men and three women (aged
48 to 82 years). Group 2 was composed of six men (aged 29
to 76 years). Tables I and II describe clinical presentation
and patient demographics.
Echocardiographic evaluation All TEE examinations were performed with commercially
available 5 MHz monoplane, biplane, and multiplane
transducers (Toshiba SSH 160A, Toshiba SSH 140 A, and
ATL, Ultramark 9). Before the transesophageal examination,
patients were sedated with an intravenous short-acting
benzodiazepine w-ith the addition of meperidine (25 to 50
mg). Local anesthesia of the pharynx was achieved with
benzocaine 20% spray to suppress the gag reflex. TEE studies were safely completed within 15 + 6 minutes. The
TEE study included standard views of the heart followed by
a complete two-dimensional and color-flow mapping examination of the ascending, arch, and descending
MRI. Sagittal section shows AIH (arrows) extending throughout extent of descending thoracic aorta. There was no flow in thickened aortic wall.
thoracic aorta. The ascending part of the aortic arch could
not routinely be visualized because of interposition of the
left bronchus.
Classic aortic dissection was diagnosed when a consistent
mobile linear echo indicative of a dissection flap and an
intimomedial tear were seen within the aortic lumen. 8 Two
specific echocardiographic criteria were used to differentiate
AIH from classic aortic dissection in these patients with
clinically suspected acute aortic dissection: (1) circular or
crescentic thickening (>5 ram) of the aortic wall (this
thickened aorta had a thrombuslike echo pattern), and (2)
absence of an intimomedial tear. 3 Measurements of the aortic
diameter and wall thickness were performed at the level of
the maxi/nal thickness of the AIH from the intima to the
adventitia (Fig. 1). The longitudinal extension of the AIH was
evaluated by scanning the whole aorta from the aortic valve
to below the diaphragm. Several other echocardiographic
findings were also assessed: central displacement of intimal
calcification, a layered appearance of the thickened aortic
wall, and presence of echo-free spaces and color Doppler
flow signals within the AIH. All but three patients who died
within 48 hours from admission had between three and
seven TEE studies. During the echocardiographic follow-up studies six types of evolution of the AIH were expected: (1)
no change in wall thickness, (2) increase of wall thickness
(progression of AIH), (3) decrease of wall thickness (partial regression of AIH), (4) normalization of the thickened aortic
American Heart ,Journal September 1997

Vilacosta et al. 4 9 9
Autopsy specimen of AIH (asterisk) in ascending aorta. Aortic intima is intact. A, Transverse section; B, longitudinal section.
wall (total regression of AIH), (5) development of a typical
dissection (visualization of an entrance tear), and (6) rupture
of the adventitia of AIH. If the development of a classic
dissection occurred in the follow-up studies, the location and
extent of the dissection flap were used to determine the type
of aortic dissection according to DeBakey classification: type
I if the flap was seen in the ascending and descending
thoracic aorta, type II if the flap was confined to the
ascending aorta, and type III if the flap was seen only in the descending thoracic aorta.
To establish TEE criteria that would distinguish AIH from type III chronic aortic dissection with thrombosed false
lumen or from a descending aortic aneurysm with mural
thrombosis, six consecutive patients with a chronic aortic
American Heart JournaJ Volume 134, Number 3

500 Vilacosta et a].
Transesophageal longitudinal (left) and transverse (right) views of AIH (asterisk) located in ascending aorta (,40). AI, Left atrium.
dissection and a clotted false lumen and six patients with a
surgically proven aortic aneurysm with mural thrombus were
also enrolled into the study.
CT CT scans were obtained in 11 of the 15 patients in group 1
and in all patients in group 2. Intravenous boluses of 80 to
150 ml of nonionic contrast medium were used for radio-
graphic CT. Transverse CT slices of 10 mm were obtained
from the arch to the aortic bifurcation. AIH was defined by
cT as a nonenhancing circular or crescentic thickening of the
aortic wail without evidence of the typical intimal flap. 5
Central displacement of intimal calcification was specifically
sought. 5 The presence of mediastinal hemorrhage and
pleural effusion was also evaluated. CT studies were
reviewed independent of the TEE findings for the presence
and longitudinal extension of AIH.
MRI MRI scanning has the capability to estimate the age of
a thrombus by assessing methemoglobin versus oxyhemo-
globin spin-echo signals. By using the fat-suppression
technique, AIH was defined as a circular or crescentic high-
intensity thickening of the aortic wall without evidence of
the classic intimal flap (Fig. 2) and absence of blood flow
within the thickened aortic wall during cine MRI. 7
Transverse, coronal, and oblique sagittal planes were
obtained in all patients. Cine MRI was performed in all patients to assess flowing blood in the thickened aortic wall
segments. MRI studies were done in 8 of the 15 patient in
Transesophageal longitudinal views of AIH in ascending aorta (top arrows). Bottom, echo-free areas (arrows) located immediately beneath dissection flap can be seen. AI, Left atrium; AO, aorta; AP, pulmonary artery.
group 1. No patient from group 2 had an MRI study. All
MRI studies were reviewed independently.
Aortography Aortograms were performed in the standard manner in all
patients in both groups, and all were reviewed by
experienced angiographers who were unaware of the
echocardiographic findings. An angiographic diagnosis of
aortic dissection was established with the identification of an
intimal flap or a double lumen. Reduction of the diameter of
the aortic lumen and rectification of the aortic contour were
specifically sought.
Results Nontraumatic AIH
Table I p resen t s clinical character is t ics of the s tudy
pat ients . All pa t ien ts h a d a long h is tory of hype r t ens ion .
American Heart Journal September 1997

Vilacosla et al. SO1
A, Admission CT scan of patient 4, who was seen with acute chest pain. Mild crescentic thickening of descending thoracic aortic wall was seen. Severe paricardial effusion is also shown. B, Seventeen days later new CT scan displayed classic type I aortic dissection.
Eleven patients had chest pain and four had back pain
on admission and were clinically indistinguishable from
patients with classic aortic dissection. In addition to the
chest or back pain, three patients had syncope and one
had paraplegia at the time of admission. Renal function
was acutely compromised in two cases in whom AIH
involved the descending aorta (one from compromise
of the left renal artery). Chest radiograph on admission
revealed a widened mediastinum caused by a
prominent aortic silhouette in seven patients and
A, Cross-sectional TEE view of patient 1. Huge AIH (arrows) can be observed. Regression of aortic hematoma is demonstrated in B. Secondary intimal tear and formation of false channel (asterisk) is seen in C. AI, Atrium; AO, aorta.
pleural effusion in six. Aortic regurgitation was found in
three patients, and all had an AIH in the ascending
aorta. Diagnosis of AIH was confirmed by anatomy
(three patients) (Fig. 3), CT (four patients), MRI (three
American Heart journal Volume 134, Number 3

502 Vilacosta et al.
MRI scan of patient 14. Large intramural hematoma involving ascending aorta is present (asterisk) on admission (A). Three months later hematoma regressed (B).
patients), or CT and MRI (five patients). Aortography showed a reduction of the aortic lumen in two patients and rectification of the aortic contour in one patient; in the remaining 12 patients the aortogram was normal.
Echocardiography Table I summarizes echocardiographic findings. The
AIH was visualized in the ascending aorta in four
patients (Fig. 4), along the whole aorta in four
patients, in the descending aorta in six patients, and in /
the aortic arch in one patient. The maximal aortic wall
thickness at the site of t/he AIH ranged from 6 to 32 mm (mean 20 mm), the mean minor aortic lumen
diameter at the site of the AIH was 34 mm (range 13
to 35 mm), the maximal diameter of the aorta at the
level of AIH varied between 31.and 57 mm (mean 55
mm), and the mean aortic ratio (minor aortic lumen diameter divided by major aortic diameter) at the level
of AIH was 0.84 (range 0.29 to 0.84). In 11 patients the hematoma led to a crescentic aortic wall
thickening; in three patients the thickening was
crescentic in some aortic segments and circular in
others, and one patient had an asymmetrical circular
thickening of the aortic wall. In 10 of these 15 patients echo-free spaces within the AIH were present, and in
only three patients a very slow flow with color
Doppler flow mapping could be visualized within the
echolucent areas. In the remaining patients no flow could be detected within the AIH. In three patients
these echolucent areas were located immediately
beneath the intimomedial dissection flap, permitting
the visualization of the dissection flap (Fig. 5). Three
patients with involvement of the ascending aorta had pericardial effusion.
Clinical and echocardiographic evolution Medical therapy and close clinical and
echocardiographic follow-up was judged to be the
adequate treatment of choice for ail patients at the
time of admission. In eight patients the AIH affected
the ascending aorta (Table I). Two patients died suddenly in the first 24 hours after initial diagnosis (in
one patient AIH and adventitial rupture were
documented at necropsy), one patient underwent surgery because of an increase of the aortic wall thickening (progression of AIt-I) and hypotension, and
in one patient the initial AIH evolved into a type I classic dissection and required surgery (Fig. 6).
Another patient came to the emergency room with a
huge AIH (Fig. 7, A) and moderate aortic regurgitation; 36 hours later the AIH regressed
dramatically (Fig 7, B) and there was no aortic regurgitation. A routine TEE study several months later revealed an asymptomatic secondary intimal tear (Fig 7, C). In the remaining three patients with AIH
affecting the ascending aorta, regression of the intramural hematoma, partial (n = 1) and complete (n = 2), was documented (Fig. 8).
American Heart journal September 1997

Vilacosta et al. 503
AIH (n = 6)
Classic chronic Ao dissection with thrombosed
false lumen (n = 6)
M u r a l thrombosis in aortic
aneurysm (n = 6)
Presence of spontaneous contrast 1 {17%} Maximum thickness of aortic echodensity 17 mm Presence of dissection flap 0 Type of aortic echodensity (circular/crescentic) I /3 * Echo-free spaces 4 (67%) Presence of flow within the aortic echodensity 2 (33%) Minor aortic lumen diameter 28 mm Major aortic diameter 42 mm Aortic ratio: (aortic lumen/aortic diameter) 0.60 Presence of distinct echogenic wall layers 1 (16%) Central displacement of Ca++ 4 (66%)
2 (33%) 5 (83%) 27 mm 13 mm
5 (83%) 0 0/6 2/4
4 (67%) 1 (16%) 2 (33%) 0 25 mm 48 mm 40 mm 65 mm 0.66 0.76
2 (33%) 1 (16%) 4 (66%) 0
Ao, Aortic. *Two patients hod both types of thickening (circular and crescentic) along the descending aorta.
Cross-sectional TEE views of patient with AIH confined to descending thoracic aorta (left). One month later (right) regression of AIH is shown.
Cross-sectional TEE view of patient with traumatic AIH. Existence of different echogenic wall layers (arrows) can be observed. AO, aorta.
Six patients in w h o m AIH exclusively involved the descending aorta and in one patient in which the aortic arch was the main aortic segment affected had a different result (Table I). One patient died from aortic rupture, whereas the remaining six patients did well during their follow-up. Two patients' aortic wall thickness did not change, whereas in four patients
the thickened aortic wall normalized totally (two patients) or partially (two patients) (Fig. 9). The patient with aortic arch involvement (patient !3) had normalized aortic wall thickness during follow-up.
Six patients with a classic type III chronic aortic dissection with a clotted false lumen and six patients with a descending thoracic aortic aneurysm with mural thrombosis were enrolled into this study to be
American Heart Journal Volume ]34, Number 3

504 Vilacosta et a].
Transesophageal longitudinal (left) and transverse (right) views of AIH located in descending thoracic aorta. Central displacement of intimal calcification can be observed (arrows).
Top, Cross-sectional TEE view of patient with traumatic AIH (asterisk). Bottom, Normalization of aortic wall thickness was demonstrated several days later. AO, Aorta; DPL and PE, pleural effusion.
Traumatic A IH
Six patients had a traumatic aortic injury, five had had
a traffic accident and a widened mediastinal silhouette
on chest radiograph, and one patient had a barotrau-
matic aortic injury from an intraaortic bal loon pump
(Table I!). Diagnosis of AIH was confirmed by anatomy
in one patient and by CT in all patients. Aortography
was normal in four patients; in patient 2 a reduction of
the diameter of the aortic lumen could be recognized.
In patient 6 aortography was performed on follow-up.
echocardiographical ly compared with the six patients
with AIH confined to the descending aorta because
these three aortic pathologic conditions share a similar
echocardiographic image. Table III summarizes the
echocardiographic characteristics of these patients. The
classic dissection flap was seen in five patients (83%) with chronic aortic dissection; in this group four
patients had echo-free spaces and central displacement
of calcium. Five patients with a descending aortic
aneurysm had spontaneous contrast within the aortic
lumen; in this subgroup of patients the presence of a
dissection flap, visualization of flow within the aortic echodensity, and central displacement of calcium could not be detected.
Echocardiography
Table II summarizes echocardiographic findings. The
AIH was localized along the descending aorta with a
variable longitudinal extension. The maximal aortic wall
thickness at the site of AIH ranged from 5 to 22 mm
(mean 1i mm), the mean minor aortic lumen diameter
at the site of the MH was 25 mm (range 20 to 32 mm),
the maximal diameter of the aorta at the level of AIH
varied between 31 and 40 mm (mean 36 mm), and the
mean aortic ratio at the level of AIH was 0.69 (range
0.50 to 0.85). In five patients the AIH led to a circular
aortic wall thickening; the patient with an intraaortic
balloon pump had a crescentic type of wall thickening.
Echo-free spaces within the AIH could be visualized in
two patients. The dissection flap was seen in one
patient. Blood flow within the aortic wall thickening
American Heart Journal September 1997

Vilacosia et al. $05
could be only detected in the patient with a
barotraumatic aortic injury. In two patients shearing of
different echogenic wall layers during the cardiac cycle
could be observed (Fig. 10).
Clinical and echocardiographic evolution As for the nontraumatic group, a conservative
medical approach was chosen. Three patients had
normalized aortic wall thickness (complete regression,
Fig. 11) during follow-up and did well. Two patients
died early in their follow-up, one from a multiorgan
system failure and the other fi'om septicemia and
renal failure. In these two patients changes in aortic
wall thickness could not be demonstrated. The pat ient
with a barotraumatic aortic injury that resulted in a
classic type III aortic dissection confirmed by an
aortography eventually died from septicemia and
multiorganic failure. 9
Discussion Most aortic dissections are characterized by a key
finding: an intimomedial tear. 1 This inner wall laceration
is considered to be the beginning of the dissection and
has been called the entrance tear.: Thereafter blood
under pressure dissects the media longitudinally, and as
a consequence a double-channel aorta is formed. The
partition between the true and false channels is the so-
called intimomedial flap. 2 Necropsy data have showed
that in <5% of patients with dissection it is not possible
to locate an entry tear. :° In the clinical setting, some
authors have also noted the absence of an entrance tear
in a small[ proportion of patients with dissection studied
with noninvasive imaging techniques (TEE, CT, and MRI).3'5-7'11-13 This variant of dissection (noncom-
municating aortic dissection) has been denominated
MH. 3 In these cases, the false lumen is created by a
hemorrhage into the aortic media, most likely after
rhexis of the vasa vasorum that penetrate the outer half
of the media from the adventitia and arborize at this
level. 4 The natural history, treatment, and prognosis of
MH have not been well delineated. TEE has excellent
sensitivity in diagnosing aortic dissection, can be
quickly performed at the patient's bedside, and is
readily available in most hospitals. Therefore many
authors maintain that TEE should be considered the first
diagnostic technique of choice in cases of suspected
aortic dissection. 8 In this study, we have shown the
echocardiographic evolution, natural history, and
prognosis of two types of MH (traumatic and
Schematic drawing of evolution of patient 1. Hematoma formation, regression, and late intimal disruption. AI, Left atrium; AO, aorta; VI, left ventricle.
nontraumatic), with TEE as the first-line imaging modality for diagnosing aortic dissection.
Diagnosis of AIH Nontraumatic AIH affected patients with longstanding
hypertension who were clinically undistinguishable from patients with classic aortic dissection. In our study comprising a large number of patients, the frequency of nontraumatic AIH was 17%. In other clinical series, noninvasive imaging techniques identified AIH in 12.8% (MRI) and 23% (TEE) of patients with acute aortic dissection. 7,3 Angiographic abnormalities detected by conventional aortography were observed in four of the 21 patients (traumatic and nontraumatic) enrolled in this study. The low rate of detection of AIH by aortography is explained by the impossibility to opacify the false channel because of the absence of an entrance tear. :4 The diagnosis of AIH by TEE relies on the detection of localized increased aortic wall thickness (>5 mm). 3 This segmental thickening of the aortic wall was circular or crescentic and had a thrombuslike echocardiographic appearance (Fig. 12). In patients with nontraumatic AIH, the aortic wall thickening was usually crescentic (14 of 15), whereas in patients with traumatic AIH the thickening was generally circular (5 of 6). Fifty-seven
American Heart journal Volume 134, Number 3

5 0 6 Vilacosta et ak
percent of our patients (12 of 21) (traumatic and nontraumatic) had echo-free spaces within the intramural hematoma probably representing liquid areas. When these echolucent areas were located immediately beneath the intimomedial flap, a
nonmobile dissection flap could be seen. In our series this flap was seen in four (19°/0) patients. Therefore the visualization of the dissection flap per se should not be
an exclusion criteria for diagnosing AIH. We do not know if these echo-free spaces are a sign of active bleeding, that is, vasa vasorum hemorrhage that has not yet clotted. If so, the lack of these echolucent areas could portend a better prognosis in terms of progression because this would suggest that bleeding has stopped. In this series the presence or absence of these areas had no prognostic implications. Because of the absence of an entrance tear the presence of blood flow within the intramural hematoma is an unfrequent finding. 3 In most patients, the false channel has not
been decompressed by reentry tear formation and, therefore, there is no choice for detecting color Doppler flow signals in these patients. Nonetheless, in a few patients there are some communicating points between the hematoma and the true lumen, probably caused by the pressure generated by the intramural hematoma. These points permitted the entrance of slow blood flow into the false channel. Four (19%) patients in this series had low-velocity color-Doppler flow signals within the echo-free areas of the intramural hematoma. Most importantly, a definitive echocardiographic aspect in the diagnosis of patients with AIH is the dynamic behavior of the hematoma. 3 The thickened aortic wall tends to vary with time. Spontaneous partial regression
(resorption) and even disappearance (normalization of wall thickening) of the AIH was seen in 10 patients (47%) in this series. Progression (increased thickening) of AIH was detected in one patient. Development of a classic dissection occurred in three patients (14%). One patient (patient 1) had early AIH regression and late intimal disruption (Fig. 13). It is worthy to emphasize that aortic insufficiency and pericardial effusion can occur in AIH without an associated dissection flap. Discriminating between AIH and other aortic lesions, including classic DeBakey type III aortic dissection with thrombosed false lumen and severe atherosclerosis with segmental wall thickening, may be clinically difficult and echocardiographically confusing. Our patients always had a second diagnostic imaging technique (CT or MRI) to confirm the echocardiographic diagnosis. The high density of fresh hematoma on CT scans is
specific for AIH, and MRI permits assessment of the age
of the hematoma on the basis of the high signal
intensity exhibited by the formation of methemoglobin.
At the initial examination some echocardiographic clues
will help to differentiate AIH from the aforementioned
aortic pathologies (Table III). The chronic descending
aortic dissection with a clotted false lumen frequently
exhibits the presence of a dissection flap, central
displacement of calcium, and echo-free spaces; in
addition, the type of thickening is crescentic. The
echocardiographic appearance of a severe
atherosclerosis in the descending aorta is commonly
depicted by a dilated aorta with spontaneous contrast
and absence of signs of dissection within the thickened
aortic wall (flap, flow, central displacement of calcium
and echo-free areas). The echocardiographic
characteristics of a descending AIH have already been
commented on, but if after a thorough clinical
echocardiographic evaluation uncertainty persists one
has the recourse to appeal to the dynamic nature of this
disease, and if echocardiographic follow-up changes are
detected the diagnosis of AIH is likely.
In this study we have shown that AIH can be present
in patients who are involved in violent deceleration
accidents who are seen with a widened mediastinal
silhouette on chest radiograph. Parmley et al., 15 on the
basis of anatomic specimens obtained from patients
with traumatic injuries, observed the presence of aortic
intimal hemorrhage. By TEE, intimomedial laceration of
the aorta, false aneurysm formation, and partial or
complete aortic disruption in patients with traumatic
aortic injuries have been described. ~6 Therefore our
observation of AIH in these patients is not surprising.
Usually trauma patients undergo aortography to role out
the presence of traumatic disruption of the aorta and, as
has been demonstrated in this study, this technique will
fail in detecting the existence of an AIH. All traumatic
AIH were located in the descending thoracic aorta in
the region of the aortic isthmus. This finding is in
agreement with the results of Vignon et al. 16 and Smith
et al. 17 In this traumatic series there was no patient in
whom the aortic injury involved the ascending aorta.
Mediastinal hematomas are relatively common in
trauma patients because of associated laceration of
small mediastinal vessels. Interestingly, the most
important differential echocardiographic sign between AIH and mediastinal hematoma is that in the former
there is a decrease of the aortic lumen diameter.
American Heart Journd September 1997

ViJacosta et al. 507
Prognosis of AIH Because different pathophysiologic processes lead to
intramural hemorrhage, the prognosis of nontraumatic and traumatic AIH is different. In this series the prognosis of patients with nontraumatic AIH confined to the descending aorta was good. Only one patient of seven died; he had adventitial rupture and required surgery. The outcome of patients with nontraumatic AIH that involved the ascending aorta is much worse. Two patients died suddenly, two resulted in a classic aortic dissection, and in one patient a progression of the AIH was documented. In contrast, patients with traumatic AIH had a good echocardiographic follow-up and their prognosis depended on the patient's situation. In this subgroup only one trauma patient of six resuIted in a classic dissection, two patients died from multiorgan failure, and the remaining three patients did well. In this series the degree of aortic wall thickening had no prognostic implications.
Conclusions First, AIH is an infrequent variant of aortic dissection
that can be detected and monitored by TEE but not by conventional aortography. Second, two types of MH can be distinguished: (1) traumatic of good prognosis and (2) nontraumatic, which can be an early stage of the classic aortic dissection with bad prognosis in cases involving the ascending aorta.
References 1. Roberts WC. Aortic dissection: anatomy, consequences, and causes.
Am Heartj 1981;101:195-214. 2. Vilacosta I, Castillo JA, San Ram6n JA, Roll6n M J, Aragoncillo P,
Sdnchez-Harguindey L. New echo-anatomical correlations in aortic dissection. Eur H cart J ] 995116:126-8.
3. Mohr-I<ahaly S, Erbel R, Kearny P, Puth M, MeyerJ. Aortic intramural hemorrhage visualized by transesophageal echocardiography: findings and prognostic implications, j Am Coil Cardio[ ]994123:658 64.
4. Krukenberg E. Beitr@ge zur frage des aneurysma dissecans. 8eitr Path Anat AIIg Path 1920;67:329-51.
5. Yamada T, Tada S, Harada J. Aortic dissection without intimal rupture: diagnosis with MR imaging and CT. Radiology 1988; ]68:347-52.
6. Robbins RC, McManus RP, Mitchell RS, Latter DR, Moon MR, Qlinger GN, et al. Management of patients with intramural hematoma of the thoracic aorta. Circulation 1993; 88 suppl Ih [I-1-10.
Z Nienaber CA, van Kodolitsch Y, Petersen B, Loose R, Helmchen U, Haverich A, el ah Intramural hemorrhage of the thoracic aorta. Diagnostic and therapeutic implications. Circulation 1995;92:1465-72.
8. Erbel R, Engberding R, Daniel W, Roelandt J, Visser C, Rennollet H. Echocardiagraphy in diagnosis of aortic dissection. Lancet 198911:457-60.
9. Vilacosta I, Castillo JA, Petal V, Batlle E, Roll6n M J, S6nchez Harguindey L. Intramural aortic hematoma following intraaortic balloon counterpulsation. Documentation by transesophageal echocardiography. Eur HeartJ 1995116:20154.
10. Hirst AE, Johns Vj, Kime SW. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine 1958;37:217-79.
11. Lui RC, Menkis AH, Neil Mckenzie F. Aortic dissection without intimal rupture: diagnosis and management. Ann Thorac Surg 1992;53:886-8.
12. Stanson AW, Welch TJ, Ehman RL, Sheedy PF I]. A variant of aortic dissection: computer tomography and magnetic resonance findings. Cardiovasc Imaging 198911:55-9.
13. Vilacosta I, San Rom6n A, Peral V, CastilJo J, Dominguez L, BatHe E, et ak Imaging aortic intramural hematoma. Identification of two groups of patients [abstract]. Circulation 1995;92 suppl 1:1-307
14. Bansal RC, Chandrasekaran K, Ayala K, Smith DC. Frequency and explanation of false negative diagnosis of aortic dissection by aortography and transesophageal echocardiography. J Am Coil Cardiol 1995;25:1393-401.
15. Parmley LF, Mattingly TW, Manion WC, Jahnke Ej. Nonpenetrating traumatic injury of the aorta. Chculation 1958;17:1086-101.
16. Vignon P, Gu6ret P, Vedrinne j, Lagrange P, Cornu E, Abrieu O, et al. Role of transesophagea[ echocardiography in the diagnosis and management of traumatic aortic disruption. Circulation 1995;92:2959-68.
17 Smith MD, Cassidy JM, Souther S, Morris EJ, Sapin PM, Johnson SB, et ak Transesophageal echocardiography in the diagnosis of traumatic rupture of the aorta. N Engl J Med 1995;332:356-62.
American Heart Journal Vdume 134, Number 3




















