Lack of progress in valvular heart disease in the pre–transcatheter aortic valve replacement era:...
8
Lack of progress in valvular heart disease in the pre–transcatheter aortic valve replacement era: Increasing deaths and minimal change in mortality rate over the past three decades Sean Coffey, MB, BS, a,b Brian Cox, PhD, c and Michael J. A. Williams, MD a Dunedin, New Zealand; and Oxford, United Kingdom Background Valvular heart disease (VHD) is an increasingly common problem in clinical practice. With the development of new but expensive therapeutic options, health care systems require timely epidemiological information on VHD. We sought to determine the mortality burden of VHD and how it has changed over time. Methods Population level data from the United States (US) from 1979 to 2009 were used to examine trends in VHD mortality rates over time. Our outcome measure was death, where the primary cause of death was valvular heart disease. Results The annual number of VHD deaths increased from 15,054 in 1979 to 26,663 in 2009, an increase of on average 2.8% in the US each year (R 2 = 0.97, P b .001). The total VHD mortality rate increased with older age and male sex. There was little overall change in age- and sex-adjusted total VHD mortality rate over time (mortality rate ratio per year 0.999, 95% confidence interval 0.999 to 0.999, P b .001). Non-rheumatic aortic valve disease accounted for 45.2% of all VHD deaths. Adjusted mortality rates for aortic valve disease, mitral valve disease and endocarditis increased (P b .001), while that for rheumatic heart disease decreased (P b .001). If VHD mortality rates remain stable, deaths due to VHD are projected to double over the next 25 years. Conclusions Despite improvements in mortality rates for other major conditions and in surgical outcomes for VHD, adjusted VHD mortality rates showed minimal change over the 31 years examined. The ageing population is driving a marked increase in the number of deaths due to VHD. (Am Heart J 2014;167:562-567.e2.) Valvular heart disease (VHD) is thought to be an increasing problem in contemporary medical practice. 1 The lack of any pharmacological therapies to slow or halt the progression of any valvular disease mean that treatment is often either palliative or, in the case of surgical or percutaneous therapies, associated with significant morbidity, mortality, and expense. Despite the reduction in rheumatic heart disease (RHD), the increase in prevalence is thought to be due to the ageing population leading to an increase in so-called degenera- tive valvular disease, especially aortic stenosis (AS). 2,3 There have been previous epidemiological studies examining the point prevalence of VHD. In the largest, which pooled three population-based studies in the United States (US), VHD was found in 5.2% of participants, 4 with the most frequent lesion being mitral regurgitation. There was a wide variation between different age groups, with a prevalence of 0.7% in 18- to 44-year olds rising to 13.3% in those aged 75 years and older. Aortic stenosis becomes a more important cause of VHD when viewed in the secondary care setting, as seen in the Euro Heart Survey on Valvular Heart Disease, where it was the most frequent cause of VHD in the those surveyed. 5 There is a lack of research that quantifies the extent of the problem, and how the spectrum of VHD has changed. This study sought to determine the mortality burden of valvular heart disease in the US and its change over time. From the a Department of Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand, b OxVALVE Study, Oxford University Hospitals, Oxford, United Kingdom, and c Department of Preventive and Social Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand. Submitted April 4, 2013; accepted December 25, 2013. Reprint requests: Dr. Sean Coffey, MB, BS, OxVALVE Study, Room B15, Level 0, Cardiac Investigations Annexe, John Radcliffe Hospital, Headley Way, Oxford OX3 9DU, United Kingdom. E-mail: [email protected] 0002-8703/$ - see front matter © 2014, Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.ahj.2013.12.030
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Lack of progress in valvular heart disease in the pre–transcatheter aortic valve replacement era:...

Lack of progress in valvular heart disease in thepre–transcatheter aortic valve replacement era:Increasing deaths and minimal change in mortality rateover the past three decadesSean Coffey, MB, BS, a,b Brian Cox, PhD, c and Michael J. A. Williams, MD a Dunedin, New Zealand; and Oxford,United Kingdom
Background Valvular heart disease (VHD) is an increasingly common problem in clinical practice. With thedevelopment of new but expensive therapeutic options, health care systems require timely epidemiological information onVHD. We sought to determine the mortality burden of VHD and how it has changed over time.
Methods Population level data from the United States (US) from 1979 to 2009 were used to examine trends in VHDmortality rates over time. Our outcome measure was death, where the primary cause of death was valvular heart disease.
Results The annual number of VHD deaths increased from 15,054 in 1979 to 26,663 in 2009, an increase of onaverage 2.8% in the US each year (R2 = 0.97, P b .001). The total VHD mortality rate increased with older age and male sex.There was little overall change in age- and sex-adjusted total VHD mortality rate over time (mortality rate ratio per year 0.999,95% confidence interval 0.999 to 0.999, P b .001). Non-rheumatic aortic valve disease accounted for 45.2% of all VHDdeaths. Adjusted mortality rates for aortic valve disease, mitral valve disease and endocarditis increased (P b .001), while thatfor rheumatic heart disease decreased (P b .001). If VHD mortality rates remain stable, deaths due to VHD are projected todouble over the next 25 years.
Conclusions Despite improvements in mortality rates for other major conditions and in surgical outcomes for VHD,adjusted VHD mortality rates showed minimal change over the 31 years examined. The ageing population is driving a markedincrease in the number of deaths due to VHD. (Am Heart J 2014;167:562-567.e2.)
Valvular heart disease (VHD) is thought to be anincreasing problem in contemporary medical practice.1
The lack of any pharmacological therapies to slow or haltthe progression of any valvular disease mean thattreatment is often either palliative or, in the case ofsurgical or percutaneous therapies, associated withsignificant morbidity, mortality, and expense. Despite
From the aDepartment of Medicine, Dunedin School of Medicine, University of Otago,Dunedin, New Zealand, bOxVALVE Study, Oxford University Hospitals, Oxford, UnitedKingdom, and cDepartment of Preventive and Social Medicine, Dunedin School ofMedicine, University of Otago, Dunedin, New Zealand.Submitted April 4, 2013; accepted December 25, 2013.Reprint requests: Dr. Sean Coffey, MB, BS, OxVALVE Study, Room B15, Level 0, CardiacInvestigations Annexe, John Radcliffe Hospital, Headley Way, Oxford OX3 9DU, UnitedKingdom.E-mail: [email protected]/$ - see front matter© 2014, Mosby, Inc. All rights reserved.http://dx.doi.org/10.1016/j.ahj.2013.12.030
the reduction in rheumatic heart disease (RHD), theincrease in prevalence is thought to be due to the ageingpopulation leading to an increase in so-called degenera-tive valvular disease, especially aortic stenosis (AS).2,3
There have been previous epidemiological studiesexamining the point prevalence of VHD. In the largest,which pooled three population-based studies in theUnited States (US), VHD was found in 5.2% ofparticipants,4 with the most frequent lesion beingmitral regurgitation. There was a wide variationbetween different age groups, with a prevalence of0.7% in 18- to 44-year olds rising to 13.3% in those aged75 years and older. Aortic stenosis becomes a moreimportant cause of VHD when viewed in the secondarycare setting, as seen in the Euro Heart Survey onValvular Heart Disease, where it was the most frequentcause of VHD in the those surveyed.5
There is a lack of research that quantifies the extent ofthe problem, and how the spectrum of VHD has changed.This study sought to determine the mortality burden ofvalvular heart disease in the US and its change over time.

Table I. Number of deaths due to valvular heart disease in the United States of America from 1979 to 2009 by age group and by cause
15-54 55-64 65-74 75-84 ≥ 85 Total (%)
All causes of valvular heart disease 59948 (9.0%) 59475 (9.0%) 118038 (17.8%) 205633 (31.0%) 221275 (33.3%) 664369 (100%)Non-rheumatic aortic valve disease 12641 15687 39449 96273 136205 300255 (45.2%)Non-rheumatic mitral valve disease 5563 5033 11680 21681 21352 65309 (9.8%)Mixed valve disease 2694 3161 6095 8874 6823 27647 (4.2%)Rheumatic heart disease 19015 21078 35978 38562 18668 133301 (20.1%)Endocarditis 19054 14347 24650 40069 38103 136223 (20.5%)Right-sided valve disease 981 169 186 174 124 1634 (0.2%)
Coffey, Cox, and Williams 563American Heart JournalVolume 167, Number 4
MethodsData sourceWe used population level data from the US, which were
available from Compressed Mortality Files providing cause ofdeath information coded using the International Classificationof Diseases (ICD).6 Data was coded using the ninth revision ofthe ICD (ICD-9) from 1979 to 1998 and using the tenth revision(ICD-10) from 1999 to 2009. For population projections, giventhe stability of total VHD mortality rates, the 2009 DetailedMortality File in combination with the 2008 populationestimates from 2010 to 2050 was used.7
Classification of cause of deathOnly those deaths where the primary cause of death was
recorded as valvular heart disease were included in the analysis.Given the much wider spectrum of disease and associatedcomorbidities in children dying of VHD, the analysis wasconfined to those aged 15 years or older, this age rather than 18being chosen to allow standard 5-year age groups to beconstructed. To allow comparison of cause of death acrosstwo different ICD coding eras six disease groups were chosen,namely non-rheumatic aortic valve disorders, non-rheumaticmitral valve disorders, endocarditis, mixed valve disease,rheumatic heart disease, and non-rheumatic right-sided valvedisease. The corresponding ICD-9 and ICD-10 codes are listed inthe online Appendix Supplementary Table I.As the mixed valve disease code (396 in ICD-9, I08 in ICD-10)
included both rheumatic and unspecified valve disease, thiscode was included for the analysis of total VHD, but excludedfor analysis of rheumatic VHD. The rheumatic heart diseaseanalysis is therefore a conservative figure, but has been used toexamine changes in RHD over time.
Statistical analysisLinear regression was used to analyze changes in unadjusted
mortality rates over time. Poisson regression was used to analyzetrends over time for mortality rates. Mortality rates weremodeled by year, with age group and sex as indicator variables.Poisson regression for each age group and separately for eachcause group was conducted, excluding right-sided VHD due tolow numbers of deaths. The average percentage change inmortality rate was calculated by (mortality rate ratio – 1) × 100%.Statistical tests were performed using Stata version 12.1
(Statacorp, College Station, TX). To look for nonlinearity inthe regression model, we used Stata’s “nl” command to look fora change in trend in the linear regression model overall and foreach age group over time. We then used these knots to
construct linear splines and performed two piecewise negativebinomial regressions for each age, the first to determine thestatistical significance of the change in trend (using the“marginal” option) and the second to determine the trendbefore and after the knot. As there were minimal changes intrends outside of the 75 to 84 years and the 85 years and over agegroups, we present only the results from these.For mortality projections, given the minimal change in age-
adjusted mortality rates over time and the uncertaintiesregarding changes in this rate due to new therapies, we electedto apply a constant mortality rate based on 2009 data. As several,but related, analyses were conducted, P b .01 was taken torepresent statistically significant trends.
FundingDr Coffey is supported by the Tony Hocken Scholarship from
the Department of Medicine, Dunedin School of Medicine,University of Otago, New Zealand. Associate Professor Cox issupported by the Director’s Cancer Research Trust.
The authors are solely responsible for the design and conductof this study, all study analyses, the drafting and editing of thepaper and its final contents.
ResultsUnadjusted mortalityThere were 664,369 deaths due to VHD in the US from
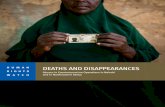
1979 to 2009, with aortic valve disease (AVD) accountingfor 45.2% of these (Table I and Figure 1). The totalnumber of deaths per year increased from 15,054 in 1979to 26,663 in 2009. Unadjusted linear regression showedan overall increase of 426 deaths, or 2.8%, per year in the1979 to 2009 time period (R2 = 0.97, P b .001).There were changes in the US population over the time
period studied, with a yearly increase in the totalpopulation and a move towards a more elderly popula-tion (online Appendix Supplementary Figure 1). Forexample, the very elderly aged 85 years and olderincreased from 2.2 million in 1979 to 5.6 million in2009, and as a proportion of the population aged 15 yearsand over increased from 1.3% in 1979 to 2.3% in 2009, a77% increase (online Appendix Supplementary Figure 2).There was a small change in the gender distribution overthe time period studied, with 52.1% of those aged 15years and over being female in 1979, compared to 51.1%

Figure 1
Number of deaths in the United States due to valvular heart diseaseper year, with underlying category of VHD. AVD, non-rheumaticaortic valve disease; MVD: non-rheumatic mitral valve disease;Mixed: mixed valve disease; Rheumatic: rheumatic heart disease.
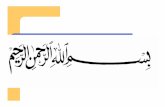
Figure 2
hanges in age-specific total VHD related mortality rate in the Unitedtates. Rates are shown per 100,000 population, by age group.
564 Coffey, Cox, and WilliamsAmerican Heart Journal
April 2014
in 2009, a 2% relative decrease. In the Poisson regressionmodel, the age-adjusted female mortality rate was 5.3%lower than the male mortality rate (95% CI, 4.8% to 5.7%,P b .001) and there was an increase in mortality withincreasing age (P b .001 for every age group compared to15-19 years old).ICD-10 coding from 1999 allows a more detailed
examination of the AVD category. There were 146,304deaths in this category from 1999 to 2009. Of these,82.7% were due to aortic stenosis, 4.0% due to aorticinsufficiency, 0.6% due to aortic stenosis with insuffi-ciency, 11.9% were unspecified or coded as due to otheraortic valve disease, and 0.7% due to congenital aorticvalve disease, which can be assumed to be predominantlybicuspid aortic valve disease.
Trends in mortality ratesChanges in age-specific VHD-related mortality rates
over time are shown in Figure 2. There was a very slightoverall reduction in age- and sex-adjusted total VHDmortality rate over time of 0.11% per year (95% CI, 0.08%-0.13%, P b .001) (Table II and online AppendixSupplementary Table II). There were differences intrends in mortality rates between different groups—anoverall increase in mortality rates for those aged 85 ormore years of 2.85% per year (95% CI, 2.80%-2.90%, P b.001), with those in younger age groups having decreas-ing mortality rates over time.The piecewise regression analysis showed that, overall,
the trend in the age- and sex-adjusted total VHD mortalityrate did not change significantly over time (P = .629 for achange after the identified knot at 1997). For age groups35 to 74 years, the trend changed slightly but continuedto show decreasing mortality rates over time, while therewas no statistically significant change in trend for those
CS
younger (online Appendix Supplementary Table III). For75- to 84-year olds, the mortality rate increased by anaverage of 2.6% per year (95% CI, 2.4%-2.8%, P b .001) upto 1991, after which it decreased by an average of 1.3%(95% CI 1.2%-1.4%, P b .001). For those aged 85 or moreyears, however, the mortality rate increased by anaverage of 6.1% per year until 1997, after which, as canbe seen in Figure 2, it reached an almost steady state, withonly a minimal average decrease of 0.6% per year (95% CI,0.2%-1.0%, P b .001).When examined by cause, there were increases in age-
adjusted mortality rates for AVD of 1.56% per year, (95%CI, 1.52%-1.61%, P b .001) and endocarditis of 1.96% peryear (95% CI, 1.90%-2.02%, P b .001), with a smallerincrease for mitral valve disease of 0.54% per year (95%CI, 0.45%-0.63%, P b .001) (Table II). Age-adjustedrheumatic heart disease mortality showed a decreaseover time of 5.34% per year (95% CI, 5.28%-5.39%, P b.001) and mixed valve disease had a smaller decrease of2.90% per year (95% CI, 2.78%-3.03%, P b .001).
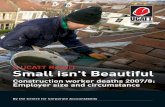
ProjectionsBased on the minimal change in the age-adjusted
mortality rate, we used 2009 age-specific mortality ratesto estimate future mortality due to VHD. Our projectionsshow that, compared to 2009 VHD deaths, total annualdeaths due to VHD will increase 63.7% to 43,653 by theyear 2030 (Figure 3), and more than double by 2036 to53,560.
DiscussionIn this study the mortality burden of VHD using
population level data from the US over 31 years wasexamined. The total number of deaths due to VHDincreased by almost 3% on average per year, driven

Figure 3
Projected absolute mortality in the US due to valvular heart disease.Mortality rates are assumed to remain stable.
Table II. Changes in annual age- and sex-adjusted mortalityrates over time
Mortality rate ratio(95% CI) P
All causes of valvular heart disease 0.9989 (0.9987-0.9992) b.001Non-rheumatic aortic valve disease 1.0156 (1.0152-1.0161) b.001Non-rheumatic mitral valve disease 1.0054 (1.0045-1.0063) b.001Mixed valve disease 0.9710 (0.9697-0.9722) b.001Rheumatic heart disease 0.9466 (0.9461-0.9472) b.001Endocarditis 1.0196 (1.0190-1.0202) b.001
CI, Confidence interval.
Coffey, Cox, and Williams 565American Heart JournalVolume 167, Number 4
mainly by deaths due to AVD, and if mortality ratesremain relatively stable, the number of deaths is expectedto double over the next 25 years. We saw a decreasingmortality rate due to RHD, as expected, but increasingmortality rates due to AVD, endocarditis, and, to a lesserextent, mitral valve disease.The prevalence of VHD markedly increases with
increasing age, and the majority of new diagnoses ofmoderate to severe VHD are in those aged over 74 years.4
In addition, older age and male sex increase the risk ofboth new calcific aortic valve disease and progression ofexisting disease.8,9 The present study shows that theseobservations translate into a higher mortality rate for theelderly, as would be expected, and for men. In addition,age- and sex-adjusted total VHD mortality rates have beenshown to change little over time, indicating that thechanging population structure is primarily responsible forthe increase in deaths due to VHD.We found that for those younger than 85 years old the
mortality rate decreased overall, while in the very elderlythe mortality rate increased until 1997, after which aminimal decrease can be seen. One possible cause for theincreased mortality rate in the 1980s and 1990s is anincreased rate of diagnosis due to the wider availability ofechocardiography, leading tomore accurate cause of deathrecording,without amajor change in case fatality rate. Casefatality rates were not examined in this study, but surgicaldatabases contain useful information about those withdisease severe enough to require intervention, but whoremain well enough to tolerate the procedure. Thesesuggest that over the past decade the case fatality rate forpatients with aortic stenosis who underwent surgeryimproved significantly.10,11 However, very elderly patients,who are at highest risk of morbidity and mortality fromVHD, are often deemed unsuitable for surgery. The EuroHeart Survey found that elderly patients aged over 85 yearsoldwere over three timesmore likely than those aged 75-80years old to be denied surgery, even after left ventricularejection fraction and comorbidity were accounted for.12
This raises the possibility that the lack of a similar degree ofimprovement in the mortality rate in the very elderlycompared to the improvement in surgical survival rate maybe due to an ongoing lack of access to cardiac surgery.
Once adjusted for age, there was little improvement intotal VHD mortality rates over time, in contrast toremarkable improvements in mortality rates for othermajor causes of mortality such as coronary heart disease(CHD) and cancer, in the US and developed countriesworldwide. For example, CHDmortality rates fell 59% from1950 to 1999 in the Framingham study13 and continue todecline to the present day in the US population,14 withapproximately half of the decline from 1980 to 2000thought to be due to risk factor reduction and half due toimproved treatments.15 The fall in mortality rate is seeneven in the very elderly, with an average reduction inannual mortality rate between the years 1980 and 2002 forwomen andmen aged 85 years and older of 2.5% and 2.6%,respectively.16 Similarly, cancer mortality rates started todecrease in the early 1990s in the US, and declined 13.7%from 1999 to 2009, with a 10.3% decrease in the 85 yearsand older age group.17 That such an improvement is notevident in VHD related mortality rates indicates the lack ofprogress made in treatments for those most affected byVHD over the three decades examined. The advent ofsurgical treatments for VHD in the 1950’s and 1960’s, priorto the time period examined in this study, almost certainlyprovided a significant mortality benefit in those fit enoughto undergo the procedures,18–21 and the small improve-ment in mortality rate seen after 1997 may reflect theimproved survival seen after surgical aortic valve replace-ment (SAVR). Unfortunately, pharmacotherapy for valvedisease has not lived up to expectation,22–24 whiletranscatheter aortic valve replacement (TAVR), with itsdemonstrated reduction in mortality in those not suitablefor SAVR,25 was not widely available over the time periodexamined.

566 Coffey, Cox, and WilliamsAmerican Heart Journal
April 2014
Our projections of future VHD deaths assume that age-adjusted mortality rates continue to remain stable into thefuture, an approach we chose rather than speculate onthe relative influence of competing effects on mortalityrates in the future. Certainly, the reduction in mortalitywith SAVR and the introduction of TAVR as an option forpatients unable to undergo surgery supports an optimisticview that mortality rates due to AS may decrease in thefuture. However both SAVR and TAVR currently carrysignificant risk, and are not suitable for many elderlypatients. The expense associated with both SAVR andTAVR puts these treatments beyond the reach of manyindividuals and many healthcare systems. The overlap inrisk factors between CHD and AS,8,26–28 coupled with thedramatically improved mortality rate of CHD, may heralda switch from CHD deaths to AS deaths in the future.Mortality rates due to other causes of VHD may alsochange—for example, the increasing use of cardiacimplantable electronic devices, the increasing comorbid-ities of those receiving cardiac implantable electronicdevices, and the high mortality seen with device-relatedendocarditis, are all factors likely to continue to drive theincreasing mortality rate of endocarditis.29,30
This study concentrated on themortality burden of VHD,without taking account of the large impact VHD has onother aspects of a patient’s life. For example, of the 179patients allocated to standard therapy arm in the PARTNERtrial, at 12 months there was a mean of 2.2 hospitaladmissions and for every two deaths, there was a survivorin moderate to severe heart failure.25 The mean healthcarecost over one year in the standard therapy arm was US$53,621.31 Nevertheless, mortality provides a very robustmeasure of disease impact, and by concentrating only onthose deaths where VHD was the primary cause themethodology used is likely to result in a conservativeestimate of the extent of the problem. It is reasonable toinfer from these results that, just as the absolute mortalityburden of VHD is expected to continue to increase in thefuture, so too will the other aspects of the populationburden of VHD, such as increased hospital admissions,increased healthcare expense, and loss of health-relatedquality of life. Further research is needed to investigate this.There are a number of limitations to the present study,
most notably the reliance on cause of death data. Formalstudies on the validity of death certification in VHD havenot, to our knowledge, been conducted. However, the USis one of only 23 countries that have been classified by theWorld Health Organization as providing “high-quality”cause of death data,32 and has among the lowest rates of“garbage” coding in the world.33 In addition, autopsy-based studies have shown that death certificates estimaterelatively accurately34 or underestimate the number ofdeaths due to VHD.35,36 The mortality rates described hereare therefore likely to be conservative figures. Thecomparability of ICD-9 and ICD-10 codes can also beviewed as an issue. In particular the estimated compara-
bility ratio for RHD is relatively low at 82%.37 Howeverboth the decline in RHD deaths and increase in AVD deathsare seen (Figure 1 and online Appendix SupplementaryTable II) to occur through the 1980’s and 1990’s before theintroduction of ICD-10 coding. Finally, the datasets did notallow investigation of the contribution of confounderssuch as concommitant coronary artery disease or recentcardiac surgery.In conclusion, the results of this study show VHD
mortality has increased substantially over the past 30 years,driven primarily by AVD mortality. Due to the ageing ofthe population, the burden of VHD can be expected toincrease for the foreseeable future. These projectionsshould provide an urgent impetus for both the refinementof current effective invasive techniques and the develop-ment of new treatments. A sustainable health serviceresponse will be needed to control the expected increaseddemand for this important group of diseases.
DisclosuresConflicts of interest: None.
References1. d’Arcy JL, Prendergast BD, Chambers JB, et al. Valvular heart disease:
the next cardiac epidemic. Heart 2011;97:91-3.2. Iung B, Vahanian A. Valvular heart diseases in elderly people. Lancet
2006;368:969-71.3. Iung B, Vahanian A. Degenerative calcific aortic stenosis: a natural
history. Heart 2012;98(Suppl 4):iv7-13.4. Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart
diseases: a population-based study. Lancet 2006;368:1005-11.5. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients
with valvular heart disease in Europe: The Euro Heart Survey onValvular Heart Disease. Eur Heart J 2003;24:1231-43.
6. Centers for Disease Control and Prevention. CDC Wonder. http://wonder.cdc.gov/2012. [Accessed 16th July 2013].
7. United States Census Bureau. Population Projections—2008 NationalPopulation Projections. http://www.census.gov/population/projections/2009. [Accessed 16th July 2013].
8. Owens DS, Katz R, Takasu J, et al. Incidence and progression ofaortic valve calcium in the Multi-ethnic Study of Atherosclerosis(MESA). Am J Cardiol 2010;105:701-8.
9. NovaroGM, Katz R, Aviles RJ, et al. Clinical factors, but not C-reactiveprotein, predict progression of calcific aortic-valve disease: theCardiovascular Health Study. J Am Coll Cardiol 2007;50:1992-8.
10. Dunning J, Gao H, Chambers J, et al. Aortic valve surgery: Markedincreases in volume and significant decreases in mechanical valveuse-an analysis of 41,227 patients over 5 years from the Society forCardiothoracic Surgery in Great Britain and Ireland Nationaldatabase. J Thorac Cardiovasc Surg 2011;142:776-82.
11. Brown JM, O’Brien SM, Wu C, et al. Isolated aortic valvereplacement in North America comprising 108,687 patients in 10years: changes in risks, valve types, and outcomes in the Society ofThoracic Surgeons National Database. J Thorac Cardiovasc Surg2009;137:82-90.
12. Iung B, Cachier A, Baron G, et al. Decision-making in elderly patientswith severe aortic stenosis: why are so many denied surgery? EurHeart J 2005;26:2714-20.

Coffey, Cox, and Williams 567American Heart JournalVolume 167, Number 4
13. Fox CS, Evans JC, Larson MG, et al. Temporal trends in coronaryheart disease mortality and sudden cardiac death from 1950 to1999: the Framingham Heart Study. Circulation 2004;110:522-7.
14. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and strokestatistics–2013 update: a report from the American Heart Associa-tion. Circulation 2013;127:e6-245.
15. Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S.deaths from coronary disease, 1980-2000. N Engl J Med 2007;356:2388-98.
16. Ford ES, Capewell S. Coronary heart disease mortality among youngadults in the U.S. from 1980 through 2002: concealed leveling ofmortality rates. J Am Coll Cardiol 2007;50:2128-32.
17. Kochanek KD, Xu J, Murphy SL, et al. Deaths: Final Data for 2009.Natl Vital Stat Rep 2011;60:1-166.
18. Hufnagel CA, Harvey WP, Rabil PJ, et al. Surgical correction of aorticinsufficiency. Surgery 1954;35:673-83.
19. Braunwald NS, Cooper T, Morrow AG. Complete replacement of themitral valve. Successful clinical application of a flexible polyurethaneprosthesis. J Thorac Cardiovasc Surg 1960;40:1-11.
20. Harken DE, Soroff HS, Taylor WJ, et al. Partial and completeprostheses in aortic insufficiency. J Thorac Cardiovasc Surg 1960;40:744-62.
21. Starr A, Edwards ML, McCord CW, et al. Aortic replacement: clinicalexperience with a semirigid ball-valve prosthesis. Circulation 1963;27:779-83.
22. Cowell SJ, Newby DE, Prescott RJ, et al. A randomized trial ofintensive lipid-lowering therapy in calcific aortic stenosis. N Engl JMed 2005;352:2389-97.
23. Rossebø AB, Pedersen TR, Boman K, et al. Intensive lipid loweringwith simvastatin and ezetimibe in aortic stenosis. N Engl J Med 2008;359:1343-56.
24. Chan KL, Teo K, Dumesnil JG, et al. Effect of Lipid lowering withrosuvastatin on progression of aortic stenosis: results of the aorticstenosis progression observation: measuring effects of rosuvastatin(ASTRONOMER) trial. Circulation 2010;121:306-14.
25. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valveimplantation for aortic stenosis in patients who cannot undergosurgery. N Engl J Med 2010;363:1597-607.
26. Thanassoulis G, Massaro JM, Cury R, et al. Associations of long-termand early adult atherosclerosis risk factors with aortic and mitral valvecalcium. J Am Coll Cardiol 2010;55:2491-8.
27. Stewart BF, Siscovick D, Lind BK, et al. Clinical factors associated withcalcific aortic valve disease. Cardiovascular Health Study. J Am CollCardiol 1997;29:630-4.
28. Völzke H, Haring R, Lorbeer R, et al. Heart valve sclerosis predicts all-cause and cardiovascular mortality. Atherosclerosis 2010;209:606-10.
29. Athan E, Chu VH, Tattevin P, et al. Clinical characteristics andoutcome of infective endocarditis involving implantable cardiacdevices. JAMA 2012;307:1727-35.
30. Greenspon AJ, Patel JD, Lau E, et al. 16-year trends in the infectionburden for pacemakers and implantable cardioverter-defibrillators inthe United States 1993 to 2008. J Am Coll Cardiol 2011;58:1001-6.
31. Reynolds MR, Magnuson EA, Wang K, et al. Cost-effectiveness oftranscatheter aortic valve replacement compared with standard careamong inoperable patients with severe aortic stenosis: results from theplacement of aortic transcatheter valves (PARTNER) trial (Cohort B).Circulation 2012;125:1102-9.
32. Mathers CD, Fat DM, Inoue M, et al. Counting the dead and whatthey died from: an assessment of the global status of cause of deathdata. Bull World Health Organ 2005;83:171-7.
33. Naghavi M, Makela S, Foreman K, et al. Algorithms for enhancingpublic health utility of national causes-of-death data. Popul HealthMetr 2010;8:9.
34. Saad R, Yamada AT, Pereira da Rosa FHF, et al. Comparisonbetween clinical and autopsy diagnoses in a cardiology hospital.Heart 2007;93:1414-9.
35. Anderson RE, Hill RB, Key CR. The sensitivity and specificity of clinicaldiagnostics during five decades. Toward an understanding ofnecessary fallibility. JAMA 1989;261:1610-7.
36. Sington JD, Cottrell BJ. Analysis of the sensitivity of death certificatesin 440 hospital deaths: a comparison with necropsy findings. J ClinPathol 2002;55:499-502.
37. Anderson RN, Miniño AM, Hoyert DL, et al. Comparability of causeof death between ICD-9 and ICD-10: preliminary estimates. Natl VitalStat Rep 2001;49:1-32.

Coffey, Cox, and Williams 567.e1American Heart JournalVolume 167, Number 4
Appendix
Supplementary Table I. Cause of death by group, with corresponding ICD-9 and ICD-10 codes
ICD-9 codes ICD-10 codes
Non-rheumatic aortic valve disorders, including bicuspid aortic valve 424.1, 746.4 I35, Q23.0, Q23.1,Non-rheumatic mitral valve disorders 424.0 I34, Q23.3Endocarditis 421, 424.9 I33, I38, I39Mixed valve disease, rheumatic or unspecified 396 I08Rheumatic heart disease 391, 392, 393, 394, 395, 397, 398 I01, I02.0, I05, I06, I07, I09Non-rheumatic right sided disease 424.2, 424.3, 746.0, 746.1, 746.2 Q22, I36, I37
Supplementary Figure 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1979 1984 1989 1994 1999 2004 2009
85+
75-84
65-74
55-64
15-54
Change in the structure of the adult population of the United Statesover the time period examined in the study. Although small, there is aclear increase in the percentage of the very elderly.
Supplementary Figure 2
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
0
1
2
3
4
5
6
7
1979 1984 1989 1994 1999 2004 2009
A
B
Changes in the numbers and percentages of the very elderly in theUnited States over time. An almost identical increase can be seen inthe two graphs. IIA. The very elderly aged 85 years and over as apercentage of the adult population aged 15 years and over in theUnited States over the time period examined in the study. IIB. Absolutenumbers in millions of the very elderly aged 85 years and over in theUnited States over the time period examined in the study.

Supplementary Table II. Crude mortality rate due to valvular heart disease per 100,000 population from 1979 to 2009, with age- and sex-adjusted mortality rate ratio
AVD MVD Mixed Rheumatic Endocarditis All VHD
1979 2.5 0.6 0.6 3.9 1.1 8.71980 2.7 0.7 0.6 3.9 1.1 9.01981 2.7 0.7 0.6 3.6 1.2 8.71982 2.8 0.7 0.5 3.4 1.2 8.71983 3.0 0.7 0.5 3.2 1.3 8.81984 3.1 0.7 0.5 3.2 1.4 9.01985 3.3 0.8 0.5 3.0 1.5 9.11986 3.4 0.9 0.5 2.9 1.5 9.31987 3.6 0.9 0.5 2.8 1.6 9.61988 3.8 0.9 0.5 2.8 1.8 10.01989 4.0 1.0 0.5 2.6 1.8 9.91990 4.1 1.0 0.6 2.5 2.0 10.21991 4.3 1.1 0.5 2.5 2.0 10.41992 4.5 1.1 0.5 2.3 2.1 10.51993 4.7 1.1 0.5 2.3 2.1 10.81994 4.7 1.1 0.4 2.2 2.1 10.51995 5.0 1.1 0.4 2.0 2.2 10.81996 5.2 1.1 0.4 1.9 2.3 10.91997 5.2 1.2 0.4 1.9 2.3 11.11998 5.4 1.2 0.4 1.8 2.5 11.31999 5.6 1.3 0.2 1.5 2.6 11.22000 5.6 1.3 0.2 1.4 2.5 11.12001 5.5 1.2 0.2 1.3 2.6 10.82002 5.5 1.2 0.3 1.3 2.6 10.92003 5.5 1.1 0.4 1.2 2.7 10.92004 5.5 1.1 0.4 1.0 2.7 10.62005 5.6 1.1 0.4 1.0 2.7 10.82006 5.8 1.1 0.4 1.0 2.6 10.92007 6.4 1.1 0.3 1.0 2.8 11.62008 5.9 1.0 0.4 0.9 2.6 10.82009 6.0 0.9 0.4 0.9 2.6 10.9Mortality rate ratio per year 1.0156 1.0054 0.9710 0.9466 1.0196 0.998995% CI 1.0152-1.0161 1.0045-1.0063 0.9697-0.9722 0.9461-0.9472 1.0190-1.0202 0.9987-0.9992
MVD, Non-rheumatic mitral valve disease; Mixed, mixed valve disease; Rheumatic, rheumatic heart disease.
Supplementary Table III. Results of piecewise regression analysis
Age group Initial mortality rate ratio (95% CI) Knot Subsequent mortality rate ratio (95% CI) P for change in trend
15-19 No knot identified on linear regression20-24 0.9560 (0.9419-0.9702) 1991 0.9798 (0.9692-0.9904) .03625-34 0.9748 (0.9707-0.9789) 2001 0.9812 (0.9666-1.000) .4735-44 0.9800 (0.9771-0.9829) 2002 0.9596 (0.9477-0.9717) .00445-54 0.9481 (0.9415-0.9548) 1990 0.9843 (0.9806-0.9880) b .00155-64 0.9641 (0.9614-0.9668) 1995 0.9736 (0.9704-0.9769) b .00165-74 0.9802 (0.9790-0.9814) 2000 0.9684 (0.9651-0.9717) b .00175-84 1.0258 (1.0237-1.0279) 1991 0.9872 (0.9861-0.9884) b .00185 years and older 1.0614 (1.0582-1.0645) 1997 0.9944 (0.9901-0.9988) b .001
The sex-adjusted mortality rate ratio (derived from negative binomial regression) is shown before and after the knot identified during a linear regression analysis for each age group.Note that the p-value is reported for a change in trend, rather than for the subsequent mortality rate ratio itself.Abbreviation: 95% CI, 95% confidence interval.
567.e2 Coffey, Cox, and WilliamsAmerican Heart Journal
April 2014