Trait-Related Decision-Making Impairment in the Three Phases of Bipolar Disorder
9
ARCHIVAL REPORT Trait-Related Decision-Making Impairment in the Three Phases of Bipolar Disorder Marc Adida, Fabrice Jollant, Luke Clark, Nathalie Besnier, Sébastien Guillaume, Arthur Kaladjian, Pascale Mazzola-Pomietto, Régine Jeanningros, Guy M. Goodwin, Jean-Michel Azorin, and Philippe Courtet Background: In bipolar disorder (BD), little is known about how deficits in neurocognitive functions such as decision-making are related to phase of illness. We predicted that manic, depressed, and euthymic bipolar patients (BPs) would display impaired decision-making, and we tested whether clinical characteristics could predict patients’ decision-making performance. Methods: Subjects (N 317; age range: 18 – 65 years) including 167 BPs (45 manic and 32 depressed inpatients, and 90 euthymic outpatients) and 150 age-, IQ-, and gender-matched healthy control (HC) participants, were included within three university psychiatric hospitals using a cross-sectional design. The relationship between predictor variables and decision-making was assessed by one-step multivariate analysis. The main outcome measures were overall decision-making ability on the Iowa Gambling Task (IGT) and an index of sensitivity to punishment frequency. Results: Manic, depressed, and euthymic BPs selected significantly more cards from the risky decks than HCs (p .001, p .01, and p .05, respectively), with no significant differences between the three BD groups. However, like HCs, BPs preferred decks that yielded infrequent penalties over those yielding frequent penalties. In multivariate analysis, decision-making impairment was significantly (p .001) predicted by low level of education, high depressive scores, family history of BD, use of benzodiazepines, and nonuse of serotonin and norepinephrine reuptake inhibitor (SNRI) antidepressants. Conclusions: BPs have a trait-related impairment in decision-making that does not vary across illness phase. However, some subtle differences between the BD groups in the individual deck analyses may point to subtle state influences on reinforcement mechanisms, in addition to a more fundamental trait impairment in risk-sensitive decision making. Key Words: Bipolar disorder, decision making, depression, euthy- mia, mania, neurocognition I t is now accepted that bipolar disorder (BD) is associated with substantial alterations in neuropsychologic function. Whereas early studies focused on attentional, mnemonic, and executive domains, recent studies have highlighted the link between simple tests of risky decision-making and the manic phase of the illness (1,2). Although trait-related cognitive impairments have been re- ported in BD patients (BPs) (3,4), the nature and extent of decision- making dysfunction across the phases of the illness remain unclear. Some studies have shown that patients have impaired decision- making in both the manic (1,2, 5–7) and depressed (8) states, whereas others have reported conflicting results in patients in re- mission (9 –13). It is also likely that other illness variables, such as number of episodes, severity of acute symptoms, type of medica- tion, and family history of BD have an impact on decision-making cognition. To our knowledge, Yechiam et al. (13) are the only group that has used the same task to assess decision-making in both the acute and remitted state of BD. However, their study was limited by small group sizes and lack of power. Decision-making occurs when the individual has to select be- tween multiple options associated with uncertain consequences. Laboratory tasks have been devised to assess competency in real- world decision-making and dissect some of cognitive processes involved. This study used the Iowa Gambling Task (IGT), a clinically sensitive tool that emulates real-world financial decision-making. Each choice leads to monetary gains or losses. Differences in IGT performance are seen in individuals with neuropsychiatric disor- ders characterized by problems in impulse control and emotional regulation (14 –17). Functional imaging (17,18) and brain lesion studies have implicated distributed neural circuitry in supporting successful decision-making on the IGT, including the ventromedial (ventromedial prefrontal cortex [VMPFC]) (19) and ventrolateral prefrontal cortex (20), and amygdala (21), areas that have been associated with BD (22). On the basis of these findings, we predict that decision-making is impaired in the acute phases but also in remission of BD. The IGT results were further analyzed in relation to sociodemographic and clinical variables in BD patients. Methods and Materials Participants The study population comprised 167 BPS (98 women and 69 men; age range: 18 – 65 years) and 150 healthy volunteers (75 women and 75 men; age range: 19 – 64 years; see power analysis in Section 1 of Supplement 1). Diagnostic assessment of the patients From the Mediterranean Institute of Cognitive Neurosciences (MA, NB, PM-P, RJ, J-MA), Department of Pharmacology and Neuropsychology of Emotions Related to Risk Taking and Reward, National Research Scien- tific Centre, and Department of Psychiatry (MA, NB, J-MA), Sainte-Mar- guerite Hospital, Mediterranean University, Marseille, France; Mental Health University Institute Douglas (FJ) and McGill Group for Suicide Studies, McGill University, Montréal, Canada; Department of Experimen- tal Psychology (LC), University of Cambridge, Cambridge, United King- dom; University Montpellier I (SG, PC), Emergency Department (SG, PC) of Academic Hospital Montpellier, and National Institute of Health and Medical Research U888 (SG, PC), Montpellier, France; University Depart- ment of Psychiatry (GMG), Warneford Hospital, Oxford, United Kingdom; and Centre Hospitalier Régional Universitaire Hôpital R. Debré (AK), Re- ims, France. Address correspondence to Marc Adida, M.D., Ph.D., Sainte-Marguerite Hos- pital, Department of Psychiatry, Mediterranean University, 270 Bd de Sainte-Marguerite, 13009 Marseille, France; E-mail: marc.adida@ap- hm.fr. Received Apr 22, 2010; revised Jan 12, 2011; accepted Jan 13, 2011. BIOL PSYCHIATRY 2011;xx:xxx 0006-3223/$36.00 doi:10.1016/j.biopsych.2011.01.018 © 2011 Society of Biological Psychiatry
Transcript of Trait-Related Decision-Making Impairment in the Three Phases of Bipolar Disorder

rpbr
Cda
dt(pmSmw
ARCHIVAL REPORT
Trait-Related Decision-Making Impairment in theThree Phases of Bipolar DisorderMarc Adida, Fabrice Jollant, Luke Clark, Nathalie Besnier, Sébastien Guillaume, Arthur Kaladjian,Pascale Mazzola-Pomietto, Régine Jeanningros, Guy M. Goodwin, Jean-Michel Azorin, andPhilippe Courtet
Background: In bipolar disorder (BD), little is known about how deficits in neurocognitive functions such as decision-making are related tophase of illness. We predicted that manic, depressed, and euthymic bipolar patients (BPs) would display impaired decision-making, and wetested whether clinical characteristics could predict patients’ decision-making performance.
Methods: Subjects (N � 317; age range: 18 – 65 years) including 167 BPs (45 manic and 32 depressed inpatients, and 90 euthymicoutpatients) and 150 age-, IQ-, and gender-matched healthy control (HC) participants, were included within three university psychiatrichospitals using a cross-sectional design. The relationship between predictor variables and decision-making was assessed by one-stepmultivariate analysis. The main outcome measures were overall decision-making ability on the Iowa Gambling Task (IGT) and an index ofsensitivity to punishment frequency.
Results: Manic, depressed, and euthymic BPs selected significantly more cards from the risky decks than HCs (p � .001, p � .01, and p � .05,espectively), with no significant differences between the three BD groups. However, like HCs, BPs preferred decks that yielded infrequentenalties over those yielding frequent penalties. In multivariate analysis, decision-making impairment was significantly (p � .001) predictedy low level of education, high depressive scores, family history of BD, use of benzodiazepines, and nonuse of serotonin and norepinephrine
euptake inhibitor (SNRI) antidepressants.
onclusions: BPs have a trait-related impairment in decision-making that does not vary across illness phase. However, some subtleifferences between the BD groups in the individual deck analyses may point to subtle state influences on reinforcement mechanisms, in
ddition to a more fundamental trait impairment in risk-sensitive decision making.mntctas
tLwisEpdrss(pa
irc
M
P
mw
Key Words: Bipolar disorder, decision making, depression, euthy-mia, mania, neurocognition
I t is now accepted that bipolar disorder (BD) is associated withsubstantial alterations in neuropsychologic function. Whereasearly studies focused on attentional, mnemonic, and executive
omains, recent studies have highlighted the link between simpleests of risky decision-making and the manic phase of the illness1,2). Although trait-related cognitive impairments have been re-orted in BD patients (BPs) (3,4), the nature and extent of decision-aking dysfunction across the phases of the illness remain unclear.
ome studies have shown that patients have impaired decision-aking in both the manic (1,2, 5–7) and depressed (8) states,hereas others have reported conflicting results in patients in re-
From the Mediterranean Institute of Cognitive Neurosciences (MA, NB,PM-P, RJ, J-MA), Department of Pharmacology and Neuropsychology ofEmotions Related to Risk Taking and Reward, National Research Scien-tific Centre, and Department of Psychiatry (MA, NB, J-MA), Sainte-Mar-guerite Hospital, Mediterranean University, Marseille, France; MentalHealth University Institute Douglas (FJ) and McGill Group for SuicideStudies, McGill University, Montréal, Canada; Department of Experimen-tal Psychology (LC), University of Cambridge, Cambridge, United King-dom; University Montpellier I (SG, PC), Emergency Department (SG, PC)of Academic Hospital Montpellier, and National Institute of Health andMedical Research U888 (SG, PC), Montpellier, France; University Depart-ment of Psychiatry (GMG), Warneford Hospital, Oxford, United Kingdom;and Centre Hospitalier Régional Universitaire Hôpital R. Debré (AK), Re-ims, France.
Address correspondence to Marc Adida, M.D., Ph.D., Sainte-Marguerite Hos-pital, Department of Psychiatry, Mediterranean University, 270 Bd deSainte-Marguerite, 13009 Marseille, France; E-mail: [email protected].
SReceived Apr 22, 2010; revised Jan 12, 2011; accepted Jan 13, 2011.
0006-3223/$36.00doi:10.1016/j.biopsych.2011.01.018
ission (9 –13). It is also likely that other illness variables, such asumber of episodes, severity of acute symptoms, type of medica-
ion, and family history of BD have an impact on decision-makingognition. To our knowledge, Yechiam et al. (13) are the only grouphat has used the same task to assess decision-making in both thecute and remitted state of BD. However, their study was limited bymall group sizes and lack of power.
Decision-making occurs when the individual has to select be-ween multiple options associated with uncertain consequences.aboratory tasks have been devised to assess competency in real-orld decision-making and dissect some of cognitive processes
nvolved. This study used the Iowa Gambling Task (IGT), a clinicallyensitive tool that emulates real-world financial decision-making.ach choice leads to monetary gains or losses. Differences in IGTerformance are seen in individuals with neuropsychiatric disor-ers characterized by problems in impulse control and emotional
egulation (14 –17). Functional imaging (17,18) and brain lesiontudies have implicated distributed neural circuitry in supportinguccessful decision-making on the IGT, including the ventromedialventromedial prefrontal cortex [VMPFC]) (19) and ventrolateralrefrontal cortex (20), and amygdala (21), areas that have beenssociated with BD (22).
On the basis of these findings, we predict that decision-makings impaired in the acute phases but also in remission of BD. The IGTesults were further analyzed in relation to sociodemographic andlinical variables in BD patients.
ethods and Materials
articipantsThe study population comprised 167 BPS (98 women and 69
en; age range: 18 – 65 years) and 150 healthy volunteers (75omen and 75 men; age range: 19 – 64 years; see power analysis in
ection 1 of Supplement 1). Diagnostic assessment of the patients
BIOL PSYCHIATRY 2011;xx:xxx© 2011 Society of Biological Psychiatry

atibapae
C
sshw
P
H(tstrseo
I
prlbdtlP
ct(c
aimiBD
S
Dagddvt3
2 BIOL PSYCHIATRY 2011;xx:xxx M. Adida et al.
was initially performed by an experienced psychiatrist and wasconfirmed using the Structural Clinical Interview for DSM-IV (23).Exclusion criteria included a history of head injury or neurologicdisease. All subjects had normal thyroid function. No patient hadreceived electroconvulsive therapy or had a history of substanceabuse within the previous 6 months. Control subjects had no psy-chiatric history, no first-degree relatives with BD, and were nottaking any drugs that might affect cognition. The study was ap-proved by the local ethics committees. After complete descriptionof the study to the subjects, written informed consent was ob-tained.
Manic GroupForty-five inpatients suffering from mania were included (30
from Marseille University Department of Psychiatry and 15 fromOxford University Department of Psychiatry). All patients met theDSM-IV criteria for bipolar I disorder, manic episode, with a scoregreater than 12 on the Young Mania Rating Scale (YMRS) (24) andless than 7 on the Hamilton Depression Rating Scale (HDRS, 17items) (25). The manic group comprised 22 women and 23 men(age range: 18 – 65 years). Thirty-two of the 45 patients were receiv-ing antipsychotic drugs at the time of testing. No patients werereceiving D2-agonist antipsychotics. Fifteen patients were receiv-ing typical antipsychotics. Seventeen patients were receiving theatypical antipsychotics risperidone (n � 1), clozapine (n � 1), andolanzapine (n � 15). Fourteen of these patients were also receivinglithium, valproate, carbamazepine, or a combination of these drugs.Eleven patients were receiving lithium, valproate, carbamazepine,or a combination of these drugs without a neuroleptic. Twenty-three patients were receiving a benzodiazepine, typically diazepamor lorazepam.
Depressed GroupThirty-two inpatients suffering from bipolar depression were
included (16 from Marseille University Department of Psychiatryand 16 from Montpellier University Department of Psychiatry). Allpatients met the DSM-IV criteria for bipolar I disorder, depressedepisode, with a score of greater than 12 on the HDRS) (25) and lessthan 7 on the YMRS (24). The depressed group comprised 18women and 14 men (age range: 22– 63 years). Sixteen of the 32patients were receiving antipsychotic drugs at the time of testing.No patients were receiving typical antipsychotics. Sixteen patientswere receiving the atypical antipsychotics aripiprazole (n � 3), olan-zapine (n � 7), risperidone (n � 4), amisulpride (n � 1), and cloza-pine (n � 1). Fourteen were also receiving lithium, valproate, carba-mazepine, or a combination of these drugs. Thirteen patients werereceiving lithium, valproate, carbamazepine, or a combination ofthese drugs without a neuroleptic. Sixteen patients were receivinglithium, valproate, carbamazepine, or a combination of these drugswith an antidepressant. Sixteen patients were receiving a benzodi-azepine.
Euthymic GroupNinety bipolar patients in clinical remission were included (60
from Montpellier University Department of Psychiatry and 30 fromOxford University Department of Psychiatry). All patients were eu-thymic at the time of testing, as defined by a score of less than 8 onthe HDRS (25) and less than 8 on the YMRS (24), and met the DSM-IVcriteria for bipolar I disorder, euthymic state. The euthymic groupcomprised 58 women and 32 men (age range: 18 – 65 years). Fifty-two of the 90 patients were receiving lithium, valproate, carbamaz-epine, or a combination of these drugs. Twenty-two patients were
also receiving antipsychotics. Six patients were receiving typical twww.sobp.org/journal
ntipsychotics. Seventeen patients were receiving the atypical an-ipsychotics aripiprazole (n � 1), risperidone (n � 5), and olanzap-ne (n � 11). Thirty patients were receiving lithium, valproate, car-amazepine, or a combination of these drugs without anntipsychotic. Thirty-eight patients were receiving lithium, val-roate, carbamazepine, or a combination of these drugs with anntidepressant. Twenty-three patients were receiving a benzodiaz-pine.
ontrol GroupOne hundred fifty healthy volunteers were recruited as control
ubjects by advertisements in the three communities (15 from Mar-eille, 30 from Oxford, and 105 from Montpellier). Control subjectsad no psychiatric or neurological history, no first-degree relativesith BD, and were not taking any drugs that might affect cognition.
rocedure
Patients’ mood was formally assessed using the YMRS andDRS. Level of education and National Adult Reading Test (NART)
26) were used indirectly to assess premorbid intelligence level inhe four groups (Table 1). NART Z scores were defined as the Ztandardization scores of NART and fNART (French language adap-ation of the NART) (27) scores, for English and French participants,espectively. Descriptive data for the 30 manic patients from Mar-eille, 15 manic and 30 euthymic patients from Oxford, and 60uthymic patients from Montpellier have been published previ-usly (1,5,12,14).
owa Gambling Task
The computerized version of the IGT (19) was used in which thearticipant plays for a pretend monetary reward. The participant is
equired to make a series of 100 choices from four decks of cards,abeled A, B, C, and D. Each card choice results in a monetary win,ut occasional choices also result in monetary loss, and the fourecks differ in the profile of wins and losses. At the start of the task,
he participant has no information about the four decks and mustearn to choose advantageously based on trial-by-trial feedback.enalties begin after 15 picks of cards.
Decks A and B are associated with high immediate wins ($100/hoice) but occasionally larger penalties that result in a net loss overime. Decks C and D are associated with smaller immediate wins$50/choice) but lower long-term losses, such that participants ac-umulate gradual profit from choosing these decks.
Decks B and D provide low-frequency but high-magnitude pen-lties (with a ratio of total wins to total losses higher in deck D than
n deck B, whereas decks A and C provide high-frequency but low-agnitude penalties (with a ratio of total wins to total losses higher
n deck C than deck A). Thus, profitability of the decks (C � D vs. A �) is orthogonalized from punishment frequency/magnitude (B �vs. A � C).
tatistical Analysis
Choices in the IGT were analyzed for individual decks A, B, C, and(Section 2 of Supplement 1), over five blocks of 20 trials (Figure 1)
nd over 100 picks of cards (Figure 2), and classified as advanta-eous (“safe”) for decks C and D and disadvantageous (“risky”) forecks A and B. The overall net score or decision-making ability is theifference between the total number of advantageous and disad-antageous choices. Net scores were calculated for each block of 20rials (Figure 1), for the first 40 and the last 60 trials (Figure 3, Sectionof Supplement 1). Data were also analyzed in terms of sensitivity
o punishment frequency by calculating a difference score [(B � D) –

C
ALN
S
M
D
n
M. Adida et al. BIOL PSYCHIATRY 2011;xx:xxx 3
Table 1. Demographic and Clinical Characteristics of Manic, Depressed, and Euthymic Bipolar Patients, and Healthy Control Subjects
Manic(n � 45)
Depressed(n � 32)
Euthymic(n � 90)
Control(n � 150) Analysis
haracteristic Mean SD Mean SD Mean SD Mean SD F df p
ge (years) 37.8 12.7 43.8 10.1 39.3 12 38.8 10.6 2.00 3,313 .11evel of Education (years) 14.0 3.1 14.6 3.2 14.0 3.5 14.3 3.0 .48 3,313 .70ART (Z score)a –.1 1.2 .1 .9 –.2 1.1 .0 .9 .89 3,313 .45
Number of Manic Episodes 4.2 3.1 3.7 2.4 3.3 3.0Number of Depressive
Episodes3.8 2.7 5.6 3.2 4.1 3.8
Age at Onset of BipolarDisorder (Years)
23.7 6.6 25.1 7.4 24.7 7
YMRS Score 21.6 5.5 1.44 1.8 3.9 2.8HDRS Score 6.16 3.7 18.6 4.8 2.3 2.5
N % N % N % N % �2 df p
ex 2.53 3,313 .12Male 23 51.1 14 43.8 32 35.6 75 50.0Female 22 48.9 18 56.3 58 64.4 75 50.0edicationAntipsychotic (D1/D2/D3/D4/
D5 Ki values)b,c32 71.1 16 50 22 24.4 47.04 2,164 �.001
D2 Antagonist 32 71.1 13 40.6 22 24.4 6.51 2,164 �.05Typical: Haloperidol (83/2/12/
3.9/147)15 33.3 0 .0 6 6.7 51.06 2,164 �.001
Atypical 17 37.8 13 40.6 16 17.8 8.88 2,164 �.05Risperidone (60/4.9/12.2/18.
6/16)1 2.2 4 13.3 5 5.6 3.01 2,164 .22
Amisulpride (� 104/1.3/2.4/�103 � 104)
0 .0 1 3.3 0 .0 4.39 2,164 .11
Clozapine (189/431/646/39/235)
1 2.2 1 3.3 0 .0 2.68 2,164 .26
Olanzapine (58/72/63/17.1/90)
15 33.3 7 21.9 11 12.2 9.91 2,164 �.01
2 AgonistAripiprazole (387/0.95/4.9/
514/� 103)0 .0 3 10 1 1.1 8.74 2,164 �.05
Lithium 9 20.0 10 31.3 28 31.1 28.43 2,164 �.05Anticonvulsant 17 40.5 27 84.4 40 44.4 17.67 2,164 �.001Antidepressant 0 .0 15 46.9 39 43.3 29.57 2,164 �.001SSRI 0 .0 7 24.1 25 27.8 15.22 2,164 �.001SNRI 0 .0 3 10.3 9 10.0 4.90 2,164 .09Tricyclic 0 .0 1 3.4 4 4.4 2.02 2,164 .36Other AD 0 .0 2 2.2 2 6.9 3.56 2,164 .17Benzodiazepine 23 54.8 16 50.0 27 30.0 9.74 2,164 �.01Anticholinergic 4 10 4 12.5 2 2.2 6.23 2,164 �.05
AD, antidepressant; D2, dopamine receptor subtype 2; HDRS, Hamilton Depression Rating Scale; Ki, inhibitor dissociation constant; NART, National AdultReading Test; SSRI, selective serotonin reuptake inhibitor; SNRI, serotonin and norepinephrine reuptake inhibitor; Euthymic; YMRS, Young Mania Rating Scale.
aNART score assesses premorbid IQ. NART Z scores were defined as the Z standardization scores of NART and fNART (French language adaptation of theNART) scores, for English and French participants, respectively.
bThe Dj-inhibitor constant Ki of an antipsychotic is the concentration of that antipsychotic needed to inhibit Dj receptor (j � 1–5). Ki values are reported inanomolar units. Classically, the potency of an antipsychotic is indicated by the D2 Ki. The higher is the Ki, the lower is the potency. An antipsychotic is said to
be D2 specific when D2 Ki is higher than D1, D3, D4, and D5 Ki. For example, we may infer from the values between brackets, that amisulpride is D2- andD3-specific.
cKi values determined by the National Institute of Mental Health (NIMH) Psychoactive Drug Screening Program. Ki values selected were those listed asNIMH Psychoactive Drug Screening Program (PDSP) assay– certified data, determined from assays using the cloned human receptors with drug of interest as
test ligands. For Ki values for which PDSP certified assay data were not listed, the average Ki value from assay data compiled on the PDSP website using thecloned human receptors with drug of interest as the test ligand was used.www.sobp.org/journal

oltrwngm
R
D
pwl
Hefm(1
mr5o
me3
esAfA
tndc2dna
t). B ater 10
4 BIOL PSYCHIATRY 2011;xx:xxx M. Adida et al.
(A � C)], where a positive score indicates a preference for low-frequency/high-magnitude penalties and a negative score a prefer-ence for high-frequency/low-magnitude penalties. The differencescore [(B � D) – (A � C)] were calculated for the first 40 and the last60 trials (Figure 4, Section 3 of Supplement 1).
The demographic, clinical, and cognitive variables were nor-mally distributed (as assessed by the Kolmogorov–Smirnov test andvisual inspection) and were analyzed with parametric statisticaltests with a threshold of p � .05 (two-tailed). Age, level of educa-tion, and NART Z score for the manic, depressed, and euthymicpatients and for control subjects were compared by one-wayANOVA, while gender and medication received were comparedusing chi-squared tests.
Individual deck (Section 2 of Supplement 1) and IGT summarymeasures were analyzed using analysis of variance (ANOVA) withgroup (manic, depressed, euthymic, control) as a between-subjectsfactor and block (1–20, 21– 40, 41– 60, 61– 80, and 81–100) as awithin-subjects factor. Sensitivity to punishment frequency scoreswere also compared with the value zero using single sample t tests.Post hoc Tukey tests of honestly significant differences (HSD) wereperformed to determine significant group differences and to con-trol for Type I error (28).
Univariate analysis with Pearson’s correlations was performed totest for associations between IGT net score for the 165 bipolarpatients and demographic and clinical variables (gender, age, levelof education, NART Z score, number of manic episodes, number ofdepressive episodes, total number of admissions, age at onset,family history of BD, HDRS score, YMRS score, alcohol misuse his-tory, drug misuse history, suicide attempt history, use of selectiveserotonin reuptake inhibitor (SSRI) antidepressant, use of serotoninand norepinephrine reuptake inhibitor (SNRI) antidepressant, useof tricyclic antidepressant, use of other antidepressant, use of arip-
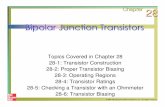
Figure 1. Number of cards selected in individual deck A, B, C, and D and decisuthymic bipolar patients (BPs), and healthy controls (HCs), graphed as aignificantly over the course of the task in deck A (one-way analysis of varianNOVA for repeated measures F � 7.40, df � 4, p � .001), deck C (one-way A
or repeated measures F � 4.77, df � 4, p � .01). (B) In euthymic BPs, the nu(one-way ANOVA for repeated measures F � 3.42, df � 4, p � .05), deck B (o
ANOVA for repeated measures F � 6.94, df � 4, p � .001), and deck D (one-whe number of cards selected changed significantly over the course of the taot in deck A (one-way ANOVA for repeated measures F � 1.70, df � 4, p � .1eck D (one-way ANOVA for repeated measures F � 1.31, df � 4, p � .27). (Dourse of the task in deck D (one-way ANOVA for repeated measures F � 4.0.08, df � 4, p � .16), deck B (one-way ANOVA for repeated measures F � 2.f � 4, p � .6). (E) Net scores changed significantly over the course of the taskot in the manic (one-way ANOVA for repeated measures F � 4.8, df � 4, p �nd euthymic BPs (one-way ANOVA for repeated measures F � 1.4, df � 4, p
over 100 picks of cards and for each block of 20 trials and classified as disadvawins but occasionally larger penalties that result in a net loss over time) andimmediate wins but negligible long-term losses that results in gradual profiare decks with high-frequency/low-magnitude penalties. Penalties begin af
iprazole, use of haloperidol, use of olanzapine, use of clozapine, use 2
www.sobp.org/journal
f amisulpride, use of risperidone, use of anticonvulsant, use ofithium, use of anticholinergic, and use of benzodiazepine). Ahreshold of p � .2 (29) was set to select variables for multivariateegression analysis. One-step multivariate linear regression analysisas then carried out to determine how much of the variation in IGTet score for bipolar patients could be explained and which demo-raphic and clinical variables might predict variations in decision-aking ability in BPs.
esults
emographic and Clinical CharacteristicsThe demographic and clinical characteristics of the manic, de-
ressed, euthymic, and control groups are shown in Table 1. Thereas no significant between-group difference with respect to age,
evel of education, NART Z score, and sex ratio.For manic patients, mean YMRS score was 21.6 � 5.5 and mean
DRS score was 6.16 � 3.7. Nine patients were experiencing a firstpisode of mania, and 22 had a manic episode with psychoticeatures. The manic group had experienced an average of 4.2 � 3.1
anic episodes (range: 1–12) and 3.8 � 2.7 depressive episodesrange: 0�9), with a mean age at onset of 23.7 � 6.6 years (range:5–38).
For depressed patients, mean YMRS score was 1.44 � 1.8 andean HDRS score was 18.6 � 4.8. The depressed group had expe-
ienced an average of 3.7 � 2.4 manic episodes (range: 1–10) and.6 � 3.2 depressive episodes (range: 0 –13), with a mean age atnset of 25.1 � 7.4 years (range: 15– 45).
For euthymic patients, mean YMRS score was 3.9 � 2.8 andean HDRS score was 2.3 � 2.5. The euthymic group had experi-
nced an average of 3.3 � 3.0 manic episodes (range: 0�9) and 4.1 �.8 depressive episodes (range: 1–9), with a mean age at onset of
aking ability on the Iowa Gambling Task (IGT), in the manic, depressed, andtion of trial block.a,b (A) In HCs, the number of cards selected changed
NOVA] for repeated measures F � 18.17, df � 4, p � .001), deck B (one-wayfor repeated measures F � 10.95, df � 4, p � .001), and D (one-way ANOVAof cards selected changed significantly over the course of the task in decky ANOVA for repeated measures F � 7.57, df � 4, p � .001), deck C (one-wayNOVA for repeated measures F � 13.69, df � 4, p � .001). (C) In manic BPs,eck C (one-way ANOVA for repeated measures F � 2.46, df � 4, p � .05) butck B (one-way ANOVA for repeated measures F � 1.19, df � 4, p � .32), andepressed BPs, the number of cards selected changed significantly over the
4, p � .01) but not in deck A (one-way ANOVA for repeated measures F �� 4, p � .06), and deck C (one-way ANOVA for repeated measures F � .27,HCs (one-way ANOVA for repeated measures F � 38.3, df � 4, p � .001) but
depressed (one-way ANOVA for repeated measures F � 3.1, df � 4, p � .13),). a Choices in the IGT were analyzed for each individual deck A, B, C, and Dous for decks A and B (the “risky” decks are associated with high immediatevantageous for decks C and D (the “safe” decks are associated with smaller
nd D are decks with low-frequency/high-magnitude penalties, and A and Cpicks of cards. b *p � .05, **p � .01, and ***p � .001.
ion-mfunc
ce [ANOVAmber
ne-waay A
sk in d5), de) In d
0, df �50, dfin the.24),� .06ntageas ad
4.7 � 7.0 years (range: 16 – 45).

ip(m
me8(efce2m
mc
S
plp
(m
A
wd(asasai
.(–tb
D
Bpdlemvcsac
dr
ddbds
cowac
with hgood
M. Adida et al. BIOL PSYCHIATRY 2011;xx:xxx 5
IGT PerformanceDecision-Making Ability. Net score changed significantly
over the course of the task in the healthy control group (one-wayANOVA for repeated measures F � 38.3, df � 4, p � 10–3) but notn the manic (F � 4.8, df � 4, p � .24), depressed (F � 3.1, df � 4,� .13), and euthymic groups (F � 1.4, df � 4, p � .06; Figure 1E)
Figure 1A, 1B, 1C, and 1D, see comments in Section 2 of Supple-ent 1).
When IGT performance was analyzed according to the decision-aking ability, one-way ANOVA revealed highly significant differ-
nces in decision-making ability between the four groups ([F (3,313) �.1, p � .001], and post hoc Tukey tests of HSD revealed that manic
p � .001; effect size [d] � .68), depressed (p � .01; d � .59), anduthymic (p � .05; d � .35) BPs selected significantly more cardsrom the risky decks than healthy control subjects, with no signifi-ant differences between manic and depressed (p � .97), manic anduthymic (p � .23), or depressed and euthymic (p � .62) BPs (FigureE) (Figure 2A, 2B, 2C and 2D, see comments in Section 2 of Supple-ent 1).
IGT performance was also analyzed according to the decision-aking ability, over the first 40 picks and over the last 60 picks of
ards (Figure 3, see comments in Section 3 of Supplement 1).
ensitivity to Punishment FrequencyWhen IGT performance was analyzed according to sensitivity to
unishment frequency, all four groups preferred decks offeringow-frequency penalties (B � D) over those with high-frequencyenalties (A � C; t � 5.0, p � .001; t � 6.0, p � .001; t � 7.5, p � .001;
and t � 7.4, p � .001 for manic, depressed, and euthymic BPs andhealthy volunteers, respectively), with no significant differencesbetween the four groups [one-way ANOVA F (3,313) � 1.5, p � .22]Figure 4A) (Figure 4B and 4C, see comments in Section 3 of Supple-
Figure 2. Number of cards selected in individual decks A, B, C and D, and decieuthymic bipolar patients (BPs) and healthy control subjects (HCs), over 100
ifferences in deck A overall score between the four groups [F(3,313) � 3.evealed that manic BPs selected significantly more cards from the deck A th
depressed BPs and HCs (p � .99), euthymic BPs and HCs (p � .43), or deifferences in deck B overall score between the four groups [F(3,313) � 7.50epressed (p � .01; D � .79), and euthymic (p � .05; d � .44) BPs selected setween manic and depressed (p � .94), manic and euthymic (p � .58), or deifferences in deck C overall score between the four groups [F(3,313) � 2.45core between the four groups [F(3,313) � 4.42, p � .01], and post hoc Tukey
deck D than HCs (p � .01; effect size d � .53) with no significant differencedepressed and euthymic (p � .99) BPs. One-way ANOVA revealed highly sig� 8.1, p � .001]. Post hoc Tukey tests of HSD revealed that manic (p � .001;BPs selected significantly more cards from the risky decks than HCs witheuthymic (p � .23), or depressed and euthymic (p � .62) BPs.a (E) Choices in
ards and for each block of 20 trials and classified as disadvantageous forccasionally larger penalties that result in a net loss over time) and as advantins but negligible long-term losses that results in gradual profit). B and D a
re decks with high-frequency/low-magnitude penalties. Penalties begin aftalculated as the difference between each of the three patient groups an
histogram.d Budescu (59) reported that for normally distributed populationsf � m/, the square root of the ni-weighted population variance, results in
ent 1). m
ssociation Between IGT Performance and Clinical VariablesUnivariate analysis of sociodemographic and clinical variables
as carried out against IGT net score for the 167 BD patients. Gen-er (females performed worse; r � –.23, p � .01), level of education
r � .26, p � .001), NART Z score (r � .17, p � .05), total number ofdmissions (r � –.22, p � .05), HDRS score (r � –.25, p � .01), YMRScore (r � –.28, p � .01), use of benzodiazepine (r � –.29, p � .001),nd family history of BD (r � –.22, p � .05) correlated with IGT netcore at p � .05 and were subjected to multivariate analysis withge at onset and use of serotonin and norepinephrine reuptake
nhibitor antidepressants (SNRIs; p � .2).In multivariate analysis, level of education (� � .26, t � 2.79, p �
01), HDRS score (� � –.24, t � 2.46, p � .05), family history of BD� � –.23, t � -2.53, p � .05), use of benzodiazepine (� � –.19, t �1.93, p � .05), and use of SNRI antidepressant (� � .21,� 2.29, p � .05) were significant predictors of IGT net score inipolar patients (Table 2).
iscussion
Impaired decision-making was detected in all three phases ofD. Risk-taking behavior is a diagnostic feature of mania, and de-ressed patients also exhibit difficulties in decision-making in theiraily lives. The translation of these ecological observations to the
aboratory is difficult. It is therefore relevant to report that, using anxperimental paradigm to detect risky-choice preference, bothanic and depressed patients showed lower scores than healthy
olunteers. These findings in the acute phases of BD are broadlyonsistent with previous studies of decision-making deficits as-essed with the IGT (1,5–7), with the Cambridge Gamble Task (6 – 8),nd in relation to an increased sensitivity to error during a two-hoice prediction task (2). In addition, we report impaired decision-
aking ability on the Iowa Gambling Task (IGT) in the manic, depressed, andof cards.a,b,c,d (A) One-way analysis of variance (ANOVA) revealed significant� .05], and post hoc Tukey tests of honestly significant differences (HSD)d HCs (p � .05; effect size [d] � .48), with no significant differences betweened and euthymic BPs (p � .73). (B) One-way ANOVA revealed significant001] and post hoc Tukey tests of HSD revealed that manic (p � .01; d � .68),cantly more cards from the deck B than HCs with no significant differencesed and euthymic (p � .28) BPs. (C) One-way ANOVA revealed no significant071]. (D) One-way ANOVA revealed significant differences in deck D overallof HSD revealed that manic BPs selected significantly fewer cards from theeen depressed BPs and HCs (p � .40), euthymic BPs and HCs (p � .08), or
nt differences in decision-making ability between the four groups [F(3,313)t size d � .68), depressed (p � .01; d � .59), and euthymic (p � .05; D � .35)
nificant differences between manic and depressed (p � .97), manic andGT were analyzed for each individual deck (A, B, C, and D) over 100 picks ofs A and B (the “risky” decks are associated with high immediate wins but
s for decks C and D (the “safe” decks are associated with smaller immediatecks with low-frequency/high-magnitude penalties, whereas decks A and Cpicks of cards.b *p � .05, **p � .01, and ***p � .001.c Cohen’s d effect size iscontrol group. The value of d is typed at the top of each patient group’seterogeneous variances, substituting for , in the denominator of equationpower approximations.
sion-mpicks24, pan dipress, p � .ignifipress
, p � .tests
s betwnificaeffecno sig
the Ideck
ageoure deer 10
d the
aking in euthymic patients, which is also in accordance with some
www.sobp.org/journal

rusfditselfollatfsdm
mvruSmpttbdehbgoclctw
pdo
scaeihp(tomTm
afBafwaab
6 BIOL PSYCHIATRY 2011;xx:xxx M. Adida et al.
previous studies of decision-making deficits assessed with the IGT.Yechiam et al. (13) reported a similar decision-making impairmentin 14 euthymic patients assessed with the IGT. Christodoulou et al.(10) reported an IGT score close to 0 in a group of 25 euthymicsubjects. These findings suggest that decision-making alterations
Figure 3. Iowa Gambling Task (IGT) net score, in the manic, depressed, andeuthymic bipolar patients (BPs) and healthy control subjects (HCs), over thefirst 40 and the last 60 picks of cards,a,b,c (A) One-way analysis of variance(ANOVA) revealed no significant differences in IGT net score between thefour groups [F(3,313) � 1.61, p � .18] over the first 40 picks of cards. (B)One-way ANOVA revealed highly significant differences in IGT net scorebetween the four groups [F(3,313) � 7.9, p � .001] over the last 60 picks ofcards. Post hoc Tukey tests of honest significant difference revealed thatmanic (p � .001), depressed (p � .05), and euthymic (p � .01) BPs selectedsignificantly more cards from the risky decks than HCs with no significantdifferences between manic and depressed (p � .86), manic and euthymic (p �.57), or depressed and euthymic (p � .99) BPs.a Choices in the IGT were
nalyzed for each individual deck (A, B, C, and D) over 100 picks of cards andor each block of 20 trials and classified as disadvantageous for decks A and
(the “risky” decks are associated with high immediate wins but occasion-lly larger penalties that result in a net loss over time) and as advantageousor decks C and D (the “safe” decks are associated with smaller immediate
ins but negligible long-term losses that results in gradual profit). B and Dre decks with low-frequency/high-magnitude penalties, whereas decks And C are decks with high-frequency/low-magnitude penalties. Penaltiesegin after 10 picks of cards.b *p � .05, **p � .01, and ***p � .001.c Budescu
(59) reported that for normally distributed populations with heterogeneousvariances, substituting for , in the denominator of equation f � m/, thesquare root of the ni-weighted population variance, results in good powerapproximations.
could be considered as a trait abnormality in BD. l
www.sobp.org/journal
The failure of the BD patients to select from the safe decks mayeflect a classic “myopia for the future” (30), that is, the inability tose outcome information to guide an advantageous long-termtrategy, acting as a trait marker in BD. However, some subtle dif-erences were observed between the BD groups in the individualeck analyses. First, all groups preferred the two decks that yielded
nfrequent penalties over those that yielded more frequent penal-ies. This indicates that bipolar patients appear to be normally sen-itive to the impact of losses. Nevertheless, the depressed BD groupxhibited a specific punishment-sensitive pattern of choice by se-
ecting more cards in decks with low-frequency penalties (B, D) andewer cards in decks with high-frequency penalties (A, C) than didther groups; this difference was statistically significant over the
ast 60 trials of the task. In contrast, manic bipolar patients were lessikely to avoid low-magnitude/high-frequency punishments (A, C)nd more likely to avoid high-magnitude/low-frequency (B, D), as ifhey were less sensitive than other bipolar groups to the impact ofrequent and small losses. These differences may point to subtletate influences on reinforcement mechanisms that operate duringecision-making, over and above a more fundamental trait impair-ent in risk-sensitive decision-making.
This is also the first report of any associations between decision-aking impairment in BD and clinical variables. Five independent
ariables were found to be associated with IGT overall score in theegression analysis: high depression ratings, low level of education,se of benzodiazepines, nonuse of SNRIs, and family history of BD.everal additional factors that were associated with IGT perfor-ance in the univariate, but not the multivariate, analysis, were
robably intercorrelated with one or more of those predictors. In-erestingly, a relationship was previously reported in BD betweenhe number of episodes and the severity of depression, which coulde explained by the presence of residual symptoms from priorepressive episodes (31). Moreover, women with BD may experi-nce more depressive episodes than men (32). Thus, in our study,igh levels of depression (HDRS score) might be correlated withoth total number of admissions and gender. In support of this, ourroup of depressed patients exhibited a greater number of previ-us depressive episodes and a higher proportion of females inomparison with the manic group. Similarly, the association with
evel of education is consistent with previous reports of a positiveorrelation between performance in cognitive and executive func-ion tests and level of education in BD (33). However, its associationith decision-making is disputed (34).
The association between the use of benzodiazepine and im-aired decision-making is consistent with previous reports of theserugs to have an adverse effect on psychomotor ability and mem-ry (35).
The positive correlation between the use of SNRI antidepres-ants and decision-making ability in BD is consistent with the psy-hopharmacology of SNRI antidepressant action. Although SNRIntidepressants are commonly called dual-action serotonin-nor-pinephrine agents, they actually have a third action on dopamine
n the prefrontal cortex, but not elsewhere in the brain: they en-ance dopamine levels and increase dopamine’s diffusion radius,robably enhancing the ability of dopamine to regulate cognition
36). Furthermore, a large increase of dopamine release may facili-ate learning in corticostriatal systems (37) when salient stimuliccurred. This salience may be produced by unexpected or high-agnitude rewarding or punishing events or by novelty (38,39).
hus, boosting dopamine with SNRIs may improve IGT perfor-ance; however, we assume that excessive tonic dopamine might
ead to reduced punishment sensitivity.

elg
dacpomtiae
pViarhbdmi
rwrBcapcbao
a“Dl withc
b
sf
M. Adida et al. BIOL PSYCHIATRY 2011;xx:xxx 7
The association between family history of BD and impaired de-cision-making observed here also parallels the genetics of mooddisorders in which bipolar patients with a family history of BD ex-hibit enrichment of genetic effects compared with bipolar patientswithout a family history of BD (40). One target for future researchwill be to determine whether impaired decision-making impair-ment might be a candidate endophenotype to BD. This is sug-gested by Lovallo et al. (41) in alcoholic patients. According toHasler et al. (42), a dysmodulation of motivation and reward mightbe a candidate endophenotype to BD. Thus, we would recommendthat future studies test for other criteria for the identification of
Figure 4. Difference score [(B � D) – (A � C)] on the Iowa Gambling Taskcontrols (HCs) over 100 picks of cards (sensitivity to punishment frequency),decks offering low-frequency/high-magnitude penalties (decks B and D) over.001; t � 6.0, p � .001; t � 7.5, p � .001; and t � 7.4, p � .001 for manic, depbetween the four groups [one-way analysis of variance (ANOVA) F(3,313) �(A�C)] score between the four groups [F(3,313) � .53, p � .66] over the first 4– (A � C)] score between the four groups [F(3,313) � 2.75, p � .05] over the laa significant difference between depressed (p � .05) but not manic (p �depressed and euthymic (p � .05) but not between manic and depressed (p
nalyzed for each individual deck (A, B, C, and D) over 100 picks of cards andrisky” decks are associated with high immediate wins but occasionally large
(the “safe” decks are associated with smaller immediate wins but neglow-frequency/high-magnitude penalties, whereas decks A and C are decksards. b *p � .05.
Table 2. Multivariate Linear Regression Analysis of Demographic andClinical Variables Associated with Decision-Making Ability in Patients withBipolar Disordera
Analysis
Variable � t p
Constant 1.09 .28Sex .03 .28 .78Level of Education (years) .26 2.79 �.01b
NART (Z score)c –.14 –1.56 .12YMRS Score –.18 –1.77 .08HDRS Score –.24 –2.46 �.05b
Total No. Hospital Admissions –.10 –1.06 .29Age at Onset of BD (years) .06 .64 .53Familial History of BD –.23 –2.53 �.05b
Medication ReceivedSNRI AD .21 2.29 �.05b
Benzodiazepine –.19 –1.93 �.05b
AD, antidepressant; BD, bipolar disorder; HDRS, Hamilton DepressionRating Scale; NART, National Adult Reading Test; SNRI, serotonin and nor-epinephrine reuptake inhibitor; YMRS, Young Mania Rating Scale.
aThe significance of the explained amount of variance (R2) was assessedy analysis of variance [F(7,92) � 6.37; p � .001].
bR2 � .41; adjusted R2 � .35.cNART score assesses premorbid IQ. NART Z scores were defined as the Z
otandardization scores of NART and fNART (French language version) scores,or English and French participants, respectively.
ndophenotype: heritability, cosegregation with BD within fami-ies, and presence in unaffected relatives at a higher rate than in theeneral population (43).
Previous studies on decision-making in patients with psychiatricisorders suggest that age (44), female sex (45), drug misuse (46),nd suicide attempt (14) are associated with disadvantageous de-ision-making. In this study, these variables were not related to IGTerformance. Age may be a critical factor in adolescent (47) and inld-age individuals (48) who are not represented in our study. Fe-ale sex was associated with a lower IGT net score in bipolar pa-
ients and control subjects, but the effect did not survive multivar-ate analysis. The lack of replication in drug misuse and suicidettempt may be related to a strong effect of BD leading to a groundffect in these patients.
Brain lesion studies implicate distributed neural circuitry in sup-orting successful decision-making on the IGT, including theMPFC (20,49) and amygdala (21). Several functional imaging stud-
es of manic (22), depressed (22), and euthymic (22) patients havelso implicated VMPFC dysfunction. Thus, VMPFC attenuation mayepresent a trait feature of the disorder (22). In support of thisypothesis, Stanfield et al. (50) reported gray matter deficits in theilateral VMPFC in 66 bipolar patients in different phases of theisorder. Our findings are consistent with a model of VMPFC abnor-alities in mania, bipolar depression, and euthymia, leading to
mpaired decision-making.This study has several limitations. First, all bipolar patients were
eceiving some type of medication. Although univariate analysisas unable to detect any differences between patients who were
eceiving (71% of manic, 50% of depressed and 24% of euthymicPs) or not receiving antipsychotic medication, there is a strongase for reinforcement learning performance and decision-makingbility to be sensitive to dopaminergic agents (51–53). Thus, com-arison of decision-making ability between BD subgroups might beonfounded by this point. In addition, we detected differencesetween BD patients who were receiving or not receiving benzodi-zepines. These drugs have been reported to have an adverse effectn psychomotor ability and memory (35) and for anticonvulsants
in the manic, depressed, and euthymic bipolar patients (BPs) and healthyhe first 40, and over the last 60 picks of cards.a,b (A) All four groups preferred
with high-frequency/low-magnitude penalties (decks A and C; t � 5.0, p �d, and euthymic BPs and HCs, respectively), with no significant differences� .22]. (B) One-way ANOVA revealed no significant differences in [(B�D) -
ks of cards. (C) One-way ANOVA revealed a significant difference in [(B � D)picks of cards. Post hoc Tukey tests of honest significant difference revealedr euthymic (p � .99) BPs and HCs, with a significant difference between9) or between manic and euthymic (p � .98) BPs. a Choices in the IGT werech block of 20 trials and classified as disadvantageous for decks A and B (thelties that result in a net loss over time) and as advantageous for decks C andlong-term losses that results in gradual profit). B and D are decks with
high-frequency/low-magnitude penalties. Penalties begin after 10 picks of
(IGT)over t
thoseresse1.5, p0 picst 60.98) o� .1
for ear penaigible
n general cognitive functioning (54), although the importance of
www.sobp.org/journal

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
8 BIOL PSYCHIATRY 2011;xx:xxx M. Adida et al.
these effects is disputed (35). Second, we did not use any comple-mentary neuropsychological test with the IGT to characterize BDpatients in this study. Fellows et al. (55) showed that deficit inreversal learning was an important mechanism underlying the dif-ficulties in the IGT. Maia et al. (53) reported that IGT might assess notonly pure implicit decision-making, on the basis of somatic markersinaccessible to consciousness, but both conscious and noncon-scious knowledge. Thus, impaired decision-making in BPs may beassociated with defects in reversal learning or explicit memory.From this study, we cannot determine whether deficits reported inBPs are specific abnormalities in decision-making (and what sub-processes may be implicated) or refer to a more global impairmentin cognitive control processes. Thus, further research should in-clude additional investigations. Third, the multicenter nature of thestudy might have introduced potential site differences in clinicalcharacteristics and IGT performance of bipolar and control partici-pants. The only difference detected here between IGT net scoreswas for the 30 British euthymic subjects compared with the 60French euthymic patients but was explained by level of education.Fourth, the study did not assess smoking status, which should beconsidered in further studies. Fifth, there is a strong case for anecologically valid support for a link between cognitive and psycho-social functioning in BD (56,57). Further research should test for anassociation between decision-making ability and psychosocialfunctioning in BD (58).
In conclusion, manic, depressed, and euthymic BD patientsshowed poor performance in a laboratory test (IGT) of decision-making. Impaired decision-making was correlated with high de-pression scores, low level of education, use of benzodiazepines,nonuse of SNRIs, and family history of BD. Thus, the decision-mak-ing capacity of patients with BD is modulated by state, education/IQ, and medication. The observation that trait-related deficits in BDare characterized by an objective failure to weigh costs versus ben-efit in a simple game is of clinical interest and may represent afuture therapeutic target.
This work was supported by National Research Scientific Centre(CNRS), Marseille, France; National Institute of Health and MedicalResearch, Montpellier, France; Academic Hospital (CHU) Lapeyronie,CHU Sainte-Marguerite, and Oxford University. We thank Professors C.Lançon and J. Naudin for their collaboration; Dr. Adéla Ionita and Mrs.Nadia Corréard, Nathalie Viglianese-Salmon, and Sara-Nora Elissaldefor their help in assessment; Anderson Loundou from the Public HealthDepartment, University of Marseille, for his help concerning statistics;and Professors A. Bechara and A. Damasio for the use of the IowaGambling Task.
Philippe Courtet has accepted reimbursement for advice or partici-pation in industry-supported symposia from most pharmaceuticalcompanies with an interest in bipolar disorder or suicide in the past 5years. Jean-Michel Azorin has accepted reimbursement for advice orparticipation in industry-supported symposia from most pharmaceu-tical companies with an interest in bipolar disorder in the past 5 yearsand holds grants from Lilly and Sanofi-Aventis. Luke Clark is a consul-tant for Cambridge Cognition. Guy M. Goodwin has accepted reim-bursement for advice or participation in industry-supported symposiafrom most pharmaceutical companies with an interest in bipolar dis-order in the past 5 years and holds grants from Sanofi-Aventis for thebalance trial and from Servier. Marc Adida received grants from Lilly(Bourse Lilly en Santé Mentale 2008) and Servier (Bourses de l’InstitutServier 2008 et 2009) for his postdoctoral years in United Kingdom.Fabrice Jollant, Nathalie Besnier, Sébastien Guillaume, Arthur Kalad-jian, Pascale Mazzola-Pomietto, and Régine Jeanningros report no
biomedical financial interests or potential conflicts of interest.2
www.sobp.org/journal
Supplementary material cited in this article is available online.
1. Adida M, Clark L, Pomietto P, Kaladjian A, Besnier N, Azorin JM, et al.(2008): Lack of insight may predict impaired decision making in manicpatients. Bipolar Disord 10:829.
2. Minassian A, Paulus MP, Perry W (2004): Increased sensitivity to errorduring decision-making in bipolar disorder patients with acute mania. JAffect Disord 82:203–208.
3. Wingo AP, Harvey PD, Baldessarini RJ (2009): Neurocognitive impair-ment in bipolar disorder patients: Functional implications. Bipolar Dis-ord 11:113–125.
4. Torres IJ, Boudreau VG, Yatham LN (2007): Neuropsychological func-tioning in euthymic bipolar disorder: A meta-analysis. Acta PsychiatrScand Suppl:17–26.
5. Clark L, Iversen SD, Goodwin GM (2001): A neuropsychological investi-gation of prefrontal cortex involvement in acute mania. Am J Psychiatry158:1605–1611.
6. Murphy FC, Rubinsztein JS, Michael A, Rogers RD, Robbins TW, Paykel ES,Sahakian BJ (2001): Decision-making cognition in mania and depres-sion. Psychol Med 31:679 – 693.
7. Rubinsztein JS, Fletcher PC, Rogers RD, Ho LW, Aigbirhio FI, Paykel ES, etal. (2001): Decision-making in mania: A PET study. Brain 124:2550 –2563.
8. Rubinsztein JS, Michael A, Underwood BR, Tempest M, Sahakian BJ(2006): Impaired cognition and decision-making in bipolar depressionbut no “affective bias” evident. Psychol Med 36:629 – 639.
9. Jollant F, Guillaume S, Jaussent I, Bellivier F, Leboyer M, Castelnau D, etal. (2007): Psychiatric diagnoses and personality traits associated withdisadvantageous decision-making. Eur Psychiatry 22:455– 461.
0. Christodoulou T, Lewis M, Ploubidis GB, Frangou S (2006): The relation-ship of impulsivity to response inhibition and decision-making in remit-ted patients with bipolar disorder. Eur Psychiatry 21:270 –273.
1. Rubinsztein JS, Michael A, Paykel ES, Sahakian BJ (2000): Cognitive im-pairment in remission in bipolar affective disorder. Psychol Med 30:1025–1036.
2. Clark L, Iversen SD, Goodwin GM (2002): Sustained attention deficit inbipolar disorder. Br J Psychiatry 180:313–319.
3. Yechiam E, Hayden EP, Bodkins M, O’Donnell BF, Hetrick WP (2008):Decision making in bipolar disorder: A cognitive modeling approach.Psychiatry Res 161:142–152.
4. Jollant F, Bellivier F, Leboyer M, Astruc B, Torres S, Verdier R, et al. (2005):Impaired decision making in suicide attempters. Am J Psychiatry 162:304 –310.
5. Bar-On R, Tranel D, Denburg NL, Bechara A (2003): Exploring the neuro-logical substrate of emotional and social intelligence. Brain. 126: (1790 –1800).
6. Bolla KI, Eldreth DA, Matochik JA, Cadet JL (2005): Neural substrates offaulty decision-making in abstinent marijuana users. Neuroimage 26:480 – 492.
7. Ernst M, Bolla K, Mouratidis M, Contoreggi C, Matochik JA, Kurian V, et al.(2002): Decision-making in a risk-taking task: A PET study. Neuropsycho-pharmacology 26:682– 691.
8. Fukui H, Murai T, Fukuyama H, Hayashi T, Hanakawa T (2005): Functionalactivity related to risk anticipation during performance of the IowaGambling Task. Neuroimage 24:253–259.
9. Bechara A, Damasio H, Tranel D, Damasio AR (1997): Deciding advanta-geously before knowing the advantageous strategy. Science 275:1293–1295.
0. Lawrence NS, Jollant F, O’Daly O, Zelaya F, Phillips ML (2009): Distinctroles of prefrontal cortical subregions in the Iowa Gambling Task. CerebCortex 19:1134 –1143.
1. Bechara A, Damasio H, Damasio AR, Lee GP (1999): Different contribu-tions of the human amygdala and ventromedial prefrontal cortex todecision-making. J Neurosci 19:5473–5481.
2. Blumberg HP, Leung HC, Skudlarski P, Lacadie CM, Fredericks CA, HarrisBC, et al. (2003): A functional magnetic resonance imaging study ofbipolar disorder: State- and trait-related dysfunction in ventral prefron-tal cortices. Arch Gen Psychiatry 60:601– 609.
3. Spitzer RL, Williams JBW, Gibbon M, First MB (1996): SCID I, version 2.0for DSM-IV. Indianapolis, IN: Lilly Research Laboratories.
4. Young RC, Biggs JT, Ziegler VE, Meyer DA (1978): A rating scale formania: Reliability, validity and sensitivity. Br J Psychiatry 133:429 – 435.
5. Hamilton M (1960): A rating scale for depression. J Neurol Neurosurg,Psychiatry 23:56 – 62.

3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
M. Adida et al. BIOL PSYCHIATRY 2011;xx:xxx 9
26. Nelson HE (1982): National Adult Reading Test (NART) Test Manual. Berk-shire, UK: NFER-Nelson.
27. MacKinnon A, Ritchie K, Mulligan R (1999): The measurement propertiesof a French language adaptation of the National Adult Reading Test. IntJ Methods Psychiatr Res 8:27–38.
28. Tukey JW, Brillinger DR (1994): The Collected Works of John W Tukey.Monterrey, CA: Wadsworth Advanced Books & Software.
29. Cohen J, Cohen P (2003): Applied Multiple Regression/Correlation Analysisfor the Behavioural Sciences, 3rd ed. Mahwah, NJ: Erlbaum.
0. Bechara A, Damasio AR, Damasio H, Anderson SW (1994): Insensitivity tofuture consequences following damage to human prefrontal cortex.Cognition 50:7–15.
1. Tohen M, Vieta E, Gonzalez-Pinto A, Reed C, Lin D (2010): Baselinecharacteristics and outcomes in patients with first episode or multipleepisodes of acute mania. J Clin Psychiatry 71:255–261.
2. Angst J, Felder W, Frey R, Stassen HH (1978): The course of affectivedisorders. I. Change of diagnosis of monopolar, unipolar, and bipolarillness. Arch Psychiatr Nervenkr 226:57– 64.
3. Martinez-Aran A, Vieta E, Reinares M, Colom F, Torrent C, Sanchez-Moreno J, et al. (2004): Cognitive function across manic or hypomanic,depressed, and euthymic states in bipolar disorder. Am J Psychiatry161:262–270.
4. Evans CE, Kemish K, Turnbull OH (2004): Paradoxical effects of educationon the Iowa Gambling Task. Brain Cogn 54:240 –244.
5. Stein RA, Strickland TL (1998): A review of the neuropsychological ef-fects of commonly used prescription medications. Arch Clin Neuropsy-chol 13:259 –284.
6. Stahl SM (2008): Stahl’s Essential Psychopharmacology NeuroscientificBasis and Practical Application, 3rd ed. New York: Cambridge UniversityPress.
7. Reynolds JN, Wickens JR (2002): Dopamine-dependent plasticity of cor-ticostriatal synapses. Neural Netw 15:507–521.
8. Seamans JK, Yang CR (2004): The principal features and mechanisms ofdopamine modulation in the prefrontal cortex. Prog Neurobiol 74:1–58.
9. Shizgal P, Arvanitogiannis A (2003): Neuroscience. Gambling on dopa-mine. Science 299:1856 –1858.
0. Craddock N, Forty L (2006): Genetics of affective (mood) disorders. Eur JHum Genet 14:660 – 668.
1. Lovallo WR, Yechiam E, Sorocco KH, Vincent AS, Collins FL (2006): Work-ing memory and decision-making biases in young adults with a familyhistory of alcoholism: Studies from the Oklahoma family health patternsproject. Alcohol Clin Exp Res 30:763–773.
2. Hasler G, Drevets WC, Gould TD, Gottesman MHK II (2006): Towardconstructing an endophenotype strategy for bipolar disorders. Biol Psy-chiatry 60:93–105.
3. Gottesman GTD II (2003): The endophenotype concept in psychiatry:
Etymology and strategic intentions. Am J Psychiatry 160:636 – 645.4. Denburg NL, Tranel D, Bechara A (2005): The ability to decide advanta-geously declines prematurely in some normal older persons. Neuropsy-chologia 43:1099 –1106.
5. Bolla KI, Eldreth DA, Matochik JA, Cadet JL (2004): Sex-Related Differ-ences in a Gambling Task and its Neurological Correlates. Cereb Cortex14:1226 –1232.
6. Dom G, De Wilde B, Hulstijn W, van den Brink W, Sabbe B (2006): Deci-sion-making deficits in alcohol-dependent patients with and withoutcomorbid personality disorder. Alcohol Clin Exp Res 30:1670 –1677.
7. Hooper CJ, Luciana M, Conklin HM, Yarger RS (2004): Adolescents’ per-formance on the Iowa Gambling Task: Implications for the developmentof decision making and ventromedial prefrontal cortex. Dev Psychol40:1148 –1158.
8. Denburg NL, Cole CA, Hernandez M, Yamada TH, Tranel D, Bechara A,Wallace RB (2007): The orbitofrontal cortex, real-world decision-making,and normal aging. Ann N Y Acad Sci 1121:480 –98.
9. Clark L, Manes F, Antoun N, Sahakian BJ, Robbins TW (2003): The contri-butions of lesion laterality and lesion volume to decision-making im-pairment following frontal lobe damage. Neuropsychologia 41:1474 –1483.
0. Stanfield AC, Moorhead TW, Job DE, McKirdy J, Sussmann JE, Hall J, et al.(2009): Structural abnormalities of ventrolateral and orbitofrontal cor-tex in patients with familial bipolar disorder. Bipolar Disord 11:135–144.
1. Sevy S, Hassoun Y, Bechara A, Yechiam E, Napolitano B, Burdick K, et al.(2006): Emotion-based decision-making in healthy subjects: Short-termeffects of reducing dopamine levels. Psychopharmacology Berl 188:228 –235.
2. Beninger RJ, Wasserman J, Zanibbi K, Charbonneau D, Mangels J, Beni-nger BV (2003): Typical and atypical antipsychotic medications differen-tially affect two nondeclarative memory tasks in schizophrenic patients:A double dissociation. Schizophr Res 61:281–292.
3. Maia TV, McClelland JL (2004): A reexamination of the evidence for thesomatic marker hypothesis: What participants really know in the Iowagambling task. Proc Natl Acad Sci U S A 101:16075–16080.
4. Devinsky O (1995): Cognitive and behavioral effects of antiepilepticdrugs. Epilepsia 36(suppl 2):S46 –S65.
5. Fellows LK (2007): The role of orbitofrontal cortex in decision making: Acomponent process account. Ann N Y Acad Sci 1121:421–30.
6. Burdick KE, Goldberg JF, Harrow M (2010): Neurocognitive dysfunctionand psychosocial outcome in patients with bipolar I disorder at 15-yearfollow-up. Acta Psychiatr Scand 122:499 –506.
7. Rosa AR, Reinares M, Michalak EE, Bonnin CM, Sole B, Franco C, et al.(2010): Functional impairment and disability across mood states in bi-polar disorder. Value Health 13:984 –988.
8. Goldberg JF, McLeod LD, Fehnel SE, Williams VS, Hamm LR, Gilchrist K(2010): Development and psychometric evaluation of the Bipolar Func-tional Status Questionnaire (BFSQ). Bipolar Disord 12:32– 44.
9. Budescu DV (1982): The power of the F test in normal populations with
heterogeneous variances. Educ Psychol Meas 42:409-416.www.sobp.org/journal