
Time perspective and perceived risk as related to mammography screening
17
This article was downloaded by: [Hellenic Open University] On: 12 November 2013, At: 10:08 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Women & Health Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wwah20 Time Perspective and Perceived Risk as Related to Mammography Screening Fay Griva PhD a , Fotios Anagnostopoulos PhD a & Gregory Potamianos PhD a a Department of Psychology , Panteion University of Social and Political Sciences , Athens , Greece Accepted author version posted online: 10 Sep 2013.Published online: 11 Nov 2013. To cite this article: Fay Griva PhD , Fotios Anagnostopoulos PhD & Gregory Potamianos PhD (2013) Time Perspective and Perceived Risk as Related to Mammography Screening, Women & Health, 53:8, 761-776, DOI: 10.1080/03630242.2013.836140 To link to this article: http://dx.doi.org/10.1080/03630242.2013.836140 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms- and-conditions
Transcript of Time perspective and perceived risk as related to mammography screening
This article was downloaded by: [Hellenic Open University]On: 12 November 2013, At: 10:08Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Women & HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wwah20
Time Perspective and Perceived Risk asRelated to Mammography ScreeningFay Griva PhD a , Fotios Anagnostopoulos PhD a & GregoryPotamianos PhD aa Department of Psychology , Panteion University of Social andPolitical Sciences , Athens , GreeceAccepted author version posted online: 10 Sep 2013.Publishedonline: 11 Nov 2013.
To cite this article: Fay Griva PhD , Fotios Anagnostopoulos PhD & Gregory Potamianos PhD (2013)Time Perspective and Perceived Risk as Related to Mammography Screening, Women & Health, 53:8,761-776, DOI: 10.1080/03630242.2013.836140
To link to this article: http://dx.doi.org/10.1080/03630242.2013.836140
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Women & Health, 53:761–776, 2013Copyright © Taylor & Francis Group, LLCISSN: 0363-0242 print/1541-0331 onlineDOI: 10.1080/03630242.2013.836140
Time Perspective and Perceived Risk as Relatedto Mammography Screening
FAY GRIVA, PhD, FOTIOS ANAGNOSTOPOULOS, PhD,and GREGORY POTAMIANOS, PhD
Department of Psychology, Panteion University of Social and Political Sciences,Athens, Greece
The present study explored the relation of time perspective toperceived risk for breast cancer and mammography screen-ing. Women free from breast cancer (N = 194), eligible formammography screening in terms of age, completed the ZimbardoTime Perspective Inventory (Zimbardo & Boyd, 1999) and mea-sures of perceived risk, attitude toward performing mammographyscreening, intention to get a mammogram, and mammographyscreening behavior. Hierarchical multiple regression analysisrevealed that perceived risk of breast cancer (β= .18, p < .01) andintention to be screened (β = .35, p < .01) were significantlyassociated with mammography screening, after controlling forthe effects of sociodemographic (e.g., age, education, and eco-nomic level) and health-related variables (e.g., family history ofbreast cancer and previous benign breast disease). Path analysesincluding the main psychological variables indicated that per-ceived risk was indirectly related to intention via attitude (β = .17,p < .01), and to mammography screening through attitude andintention (β = .06, p < .01). Attitude was indirectly related tomammography screening via intention (β = .20, p < .01). Also, asignificant indirect association was observed between future orien-tation and mammography screening, via perceived risk (β = .10,p < .01). Theoretical implications of study findings and suggestionsfor future research on use of mammography are presented.
Received December 8, 2012; revised July 16, 2013; accepted August 15, 2013.Address correspondence to Fay Griva, PhD, Panteion University of Social and
Political Sciences, Department of Psychology, 136 Syngrou Avenue, Athens, Greece.E-mail: [email protected]
761
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

762 F. Griva et al.
KEYWORDS mammography screening, time perspective, risk per-ception, breast cancer
INTRODUCTION
Mammography screening is probably the most effective way to detectbreast cancer early, and it has been related to reduced rates of mortal-ity (Anderson, Jatoi, & Devesa, 2006; Klemi et al., 2003). In the EuropeanUnion, the Advisory Committee on Cancer Prevention (2000) has recom-mended a mammography screening periodicity of two years for womenaged 50–69 years. However, a discrepancy is often observed between rec-ommended and actual use of mammography (Botha et al., 2003). In manyEuropean countries, women aged 50–69 years have demonstrated relativelylow mammography screening rates: France (54.5%), Italy (59.2%), Germany(54.3%), Switzerland (44.8%; Organization for Economic Co-operation andDevelopment [OECD], 2012). In a recent national survey in Greece, only53.8% of women aged 50–69 years reported having a mammogram in theprevious three years (Dimitrakaki et al., 2009). Thus, Greece, like otherEuropean countries, has relatively low mammography use rates, and Greekwomen do not adhere to the guidelines or do not follow them regularly.The issue of identifying the factors that are related to a woman’s decisionto engage in mammography screening is a critical one for designing inter-ventions that effectively promote mammography screening and increase thelikelihood of early detection of breast cancer.
One of the most frequently examined factors in mammography screen-ing is perceived risk for breast cancer. Meta-analyses (Katapodi et al., 2004;McCaul et al., 1996) and systematic reviews (Magai et al., 2007; Schueler, Chu,& Smith-Bindman, 2008) have suggested that perceived risk is positively andsignificantly related to mammography screening. Moreover, perceptions ofrisk during the process of decision-making to adopt or maintain a healthbehavior seem to be associated with individual differences in temporal per-spectives (Apostolidis et al., 2006; Robbins & Bryan, 2004). People may tendto weigh either the immediate or the distant outcomes of a behavior in termsof costs and benefits, based on the value they assign to future rewards inrelation to more immediate rewards (Orbell & Hagger, 2006; Orbell, Perugini,& Rakow, 2004). Research has recently focused on the concept of time per-spective (TP), which refers to the nonconscious process by which individualsfilter their experiences through the temporal categories of past, present andfuture. This process affects information processing, decision-making, goalsetting and ultimately influences behavior. Zimbardo and Boyd (1999) con-ceived TP as comprising five factors: (1) past positive (PP), which is relatedto a nostalgic, positive attitude toward the past, (2) past negative (PN), which
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
Mammography Screening 763
reflects a generally negative aversive view of the past, (3) present hedonistic(PH), which suggests an orientation toward present pleasures and excite-ment, with little concern for future consequences, (4) present fatalistic (PF),which is characterized by a fatalistic, helpless, and hopeless attitude towardlife, and (5) future orientation, which is associated with planning and a striv-ing for future goals and rewards. “Present-oriented” individuals tend to relyon the immediate, salient aspects of the stimulus when making a decisionto act, whereas “past-oriented” individuals tend to rely on recall of recon-structed past scenarios that refer to analogous situations. “Future-oriented”individuals tend to rely on anticipated consequences and expectations ofimagined future scenarios. Future-oriented people seem to show greaterconcern about the consequences of their actions (perceived as risks), are self-responsible and therefore have a tendency to look after their health, becausethey are more likely to develop an increasing awareness of the contingencybetween current actions and their future outcomes. Present-time orientation,which reflects a preference for behaviors with immediate rewards, is associ-ated with risky behaviors, such as careless driving, substance use, and riskysexual behavior (Apostolidis, Fieulaine, & Soulé, 2006; Keough, Zimbardo, &Boyd, 1999; Rothspan & Read, 1996; Wills, Sandy, & Yaeger, 2001; Zimbardo,Keough, & Boyd, 1997). In contrast, a future orientation, which reflects a per-son’s tendency to sacrifice immediate rewards for the sake of future gains, isassociated with health protective behaviors, such as exercise, condom use,healthy eating habits, and smoking cessation (Adams, 2009; Henson et al.,2006; Mahon, Yarcheski, & Yarcheski, 1997).
Considering that TP may affect perceptions and actions, it is impor-tant to explore the role of individual temporal profiles with regard toperceptions of risk and actual health behaviors. Therefore, in relation tomammography screening it was hypothesized that a woman who believesthat a person’s day should be planned ahead and takes under considerationthe future consequences of a behavior (future TP) would be more likelyto use mammography screening, through heightened consideration of anyrisks regarding her health (perceived risk), as well as through positive atti-tudes toward mammography screening and a strong intention to participatein mammography screening. Thus, future orientation was expected to beassociated with perceptions of risk regarding breast cancer in the sense thata future orientation might influence perceptions of vulnerability to a serioushealth threat. This may also be the case with a woman who believes that herlife path is controlled by forces she cannot influence (present-fatalistic per-spective), and cancer is beyond her control; thus, intention to be screenedwould be weak, given that screening would be of little or no avail. In par-ticular, the notion of fatalism has been applied to cancer screening behavior(Chavez et al., 1997; Perez-Stable et al., 1992; Powe, 1995; Sugarek, Deyo, &Holmes, 1988). Moreover, a positive reconstruction of past events (PP) maybe related to screening behavior by protecting, maintaining, and enhancing
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

764 F. Griva et al.
positive self-regard, and self-esteem (Zimbardo & Boyd, 1999), serving asa repository of positive affect and strengthening a woman’s positive atti-tudes toward mammography screening. TP dimensions were hypothesizedto be associated with intention and behavior not directly, but indirectlythrough more proximal variables (i.e., attitudes; Fieulaine & Martinez, 2011).Perceived risk was hypothesized to be associated with health behaviors bothdirectly and indirectly through attitudes (Schmiege, Bryan, & Klein, 2009).We examined the relation between mammography screening and TP, asconceptualized by Zimbardo and Boyd (1999) using a reliable and validmeasure, as well as the relation of TP with other constructs already found tobe associated with mammography screening, such as perceived risk.
METHOD
Participants
The sample consisted of 194 women recruited as a convenience sampleof women attending the outpatient clinics of a general hospital in Athens,Greece, from January–June 2011. Women were included in the study ifthey were aged 40 years or older (i.e., eligible for attending mammographyscreening according to the official guidelines of most European countries[Hakama et al., 2008] and the guidelines of the Senologic Hellenic Society[Soldatos, 2006]), had a good knowledge of the Greek language, and hadnot been diagnosed with breast cancer in the past. A total of 350 womenwere approached while waiting to be referred to a general practitioner andwere briefly informed of the purpose of the study. A list with the day’sappointments was provided by the head nurse of the outpatient clinic. Whenwomen had confirmed their appointments, they were approached by theresearcher and informed about the study. They were then asked about theirage, breast cancer history, and country of origin. Women who were bornin another country and relocated to Greece were only included if they hadeither attended courses in Greek or their level of comprehending Greekwas sufficient enough to read newspapers. Of the women approached, 242(69%) were found eligible to participate in the study based on the inclusioncriteria. Ultimately, 215 (88%) women agreed to complete and return thequestionnaires. Nonparticipation was mainly due to time constraints. Thenumber of participants was further reduced to 194, after removing fromthe sample those with incomplete questionnaires. The study protocol wasapproved by the ethical and research committee of the hospital. Participantswere informed orally and in writing about the purpose of the study, abouttheir ensured anonymity, and their right to withdraw at any point from thestudy by not completing or returning the questionnaires and without detri-ment to their care. It was assumed that accepting to complete and return thequestionnaires equated with assent to participate in the study.
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

Mammography Screening 765
Data Collection Measures
TP was measured using the Zimbardo Time Perspective Inventory (ZTPI;Zimbardo & Boyd, 1999) in its validated Greek version (Anagnostopoulos& Griva, 2012). It is a 56-item measure, consisting of five subscales eachmeasuring the distinct dimensions of positive past, negative past, hedonisticpresent, and fatalistic present and future. PP was composed of 9 items (e.g.,“It gives me pleasure to think about my past”); PN was composed of 10 items(e.g., “I think about the bad things that have happened to me in the past”);PH included 15 items (e.g., “I try to live my life as fully as possible, oneday at a time”); PF included nine items (e.g., “My life path is controlled byforces I cannot influence”); and future orientation was composed of 13 items(e.g., “I believe that a person’s day should be planned ahead each morn-ing”). Subscales used a 5-point Likert-type response format ranging from 1(very uncharacteristic) to 5 (very characteristic). The internal consistencyestimates (Cronbach’s alpha) appeared to be satisfactory, ranging from .71 to.84 for the five subscales.
Perceived risk for breast cancer was measured as a composite variableconsisting of two items: “How likely do you think it is that you will developbreast cancer” and “Compared to other women your age, how likely areyou to develop breast cancer,” both answered on a scale ranging from 1(very unlikely) to 5 (very likely). Most studies measure perceptions of riskusing a single item. However according to Van der Pligt (1996), this mightresult in omitting the dimension of comparative perceived risk that refers toan individual’s tendency to underestimate a health risk in relation to otherpeople. Therefore, in our study a second item, one that reflected comparativerisk, was included. In addition, the Likert response scale was preferred overthe percentage (0–100%) method, because the latter may often be misleadingand may result in participants overestimating their risk for a health problem(Katapodi et al., 2004).
Attitudes toward mammography screening were measured as a compos-ite variable consisting of three items. The first item, “Getting a mammogramevery two years would be good,” was selected to reflect an overall evaluationof the behavior. The second item, “Getting a mammogram every two yearswould be useful,” was selected to reflect an instrumental dimension (i.e.,whether the behavior would achieve something) and the third item, “Gettinga mammogram every two years would be safe,” was selected to reflect anexperiential dimension (i.e., how the participant felt about the behavior).All items were answered on a scale ranging from 1 (strongly disagree) to 5(strongly agree). The selection of the items was in line with Ajzen’s (2002)suggestions on measuring attitudes in the context of the theory of plannedbehavior.
Intention to participate in mammography screening was measured usingthree items: “I plan to get a mammogram every two years,” “I want to get amammogram every two years,” and “I will try to get a mammogram every
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

766 F. Griva et al.
two years,” all answered on a scale ranging from 1 (strongly disagree) to 5(strongly agree). The items were selected to reflect generalized intention asmeasured in the context of the theory of planned behavior (Ajzen 2002).Mammography screening behavior was measured using the self-reportednumber of life-time mammograms obtained, ranging from 1 (none) to 5(more than 10).
Basic demographic and health-related information included: age, parity,economic status, educational level, family history of breast cancer, and aprevious benign breast disease. Similar variables have been measured inprevious studies on mammography screening in medical settings (e.g., Tolmaet al., 2003).
Statistical Analysis
Initial examination of the data was performed using Statistical Package forthe Social Sciences (SPSS) 17.0. Descriptive statistics, such as means andfrequencies, were used to assess the demographic characteristics of thesample. Further examination of the data involved an analysis of the cor-relations between continuous variables and frequency of mammographyscreening. Also, analysis of variance was used for the categorical vari-ables. Hierarchical multiple regression analyses were conducted to assessand control confounding variables including participants’ demographicand health-related characteristics, given their significant associations withmammography screening use found in previous studies (Griesch et al., 2009;Finney Rutten, & Iannotti, 2003; Schueler et al., 2008). The practice of clinicalbreast examination was excluded from the analyses because it was routinelypracticed in the hospital setting just before mammography screening. Modelswere assessed through inspection of change in R2 for each additional blockof variables (signifying the contribution to the explanation of the variance inthe dependent variable) and the associated F -test values. Multicollinearitywas assessed through examination of the tolerance values for all of theindependent variables (< .10). Outliers were detected by computing thestandardized residuals for all cases (> 3 in absolute value). Path analyseswere then performed using Analysis of Moment Structures 20.0 to examinefurther the existence of indirect relationships among the variables included inthe proposed model. Direct and indirect associations among variables wereestimated, and mediation was examined. A number of indices were used toassess the goodness of fit of the models. A satisfactory fit was obtained whenthe chi-square test, calculated using the Satorra- Bentler robust estimationprocedure, was nonsignificant. Apart from the χ2, the fit of the models wasalso evaluated with the root-mean-square error of approximation (RMSEA; avalue close to .06 or less indicated a good fit), the Bentler-Bonett normed fitindex (NFI; a value close to or greater than .90 indicated a good fit), and thegoodness of fit index (GFI) and the comparative fit index (CFI), for whichvalues close to .95 or greater indicated an adequate fit of the model (Hu &
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

Mammography Screening 767
Bentler, 1999). The Akaike Information Criterion (AIC) was used as an indi-cator of parsimony in model fit, with a lower value of AIC indicating a moreparsimonious model (Raykov & Marcoulides, 2000).
RESULTS
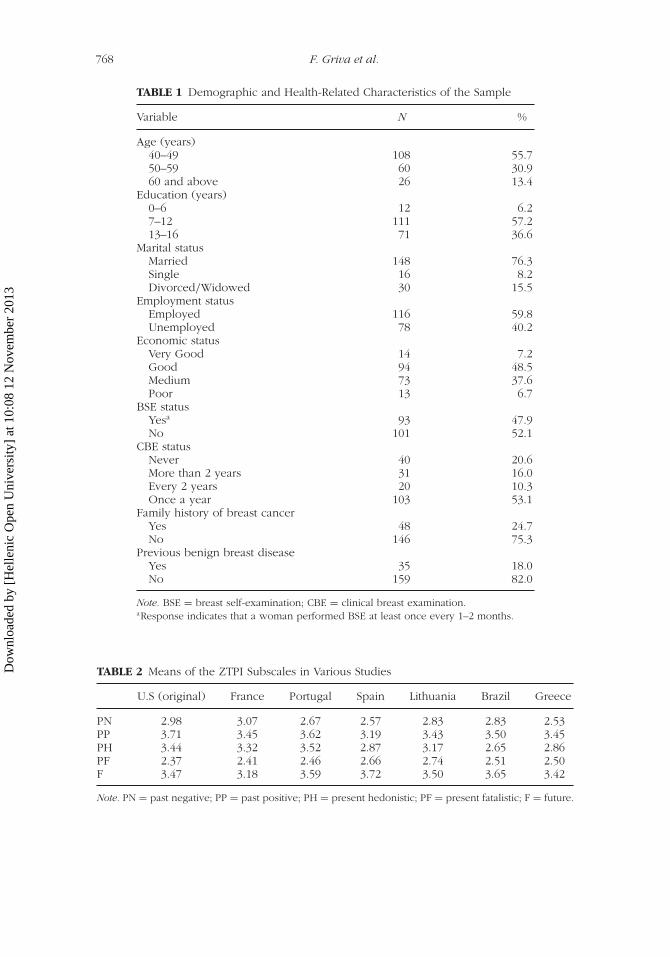
The mean age of the participants was 50.9 years (SD = 7.7), ranging from40–75 years (Table 1). Most of the respondents were married (76.3%), hada full time occupation (59.8%), and the majority had either completed highschool (57.2%) or had attended university (36.6%). Most of the respondentswere not practicing breast self-examination (52.1%), though the majority hadreceived annual clinical breast examination (53.1%).
The study participants did not seem to differ in their time orientationcompared to samples from the United States (Zimbardo & Boyd, 1999),which was the country of origin of the ZTPI, and to other samples fromFrance (Apostolidis & Fieulaine, 2004), Spain (Diaz-Morales, 2006), Brazil(Milfont et al., 2008), Portugal (Ortuño & Gamboa, 2009), or Lithuania(Liniauskaite & Kairys, 2009; Table 2).
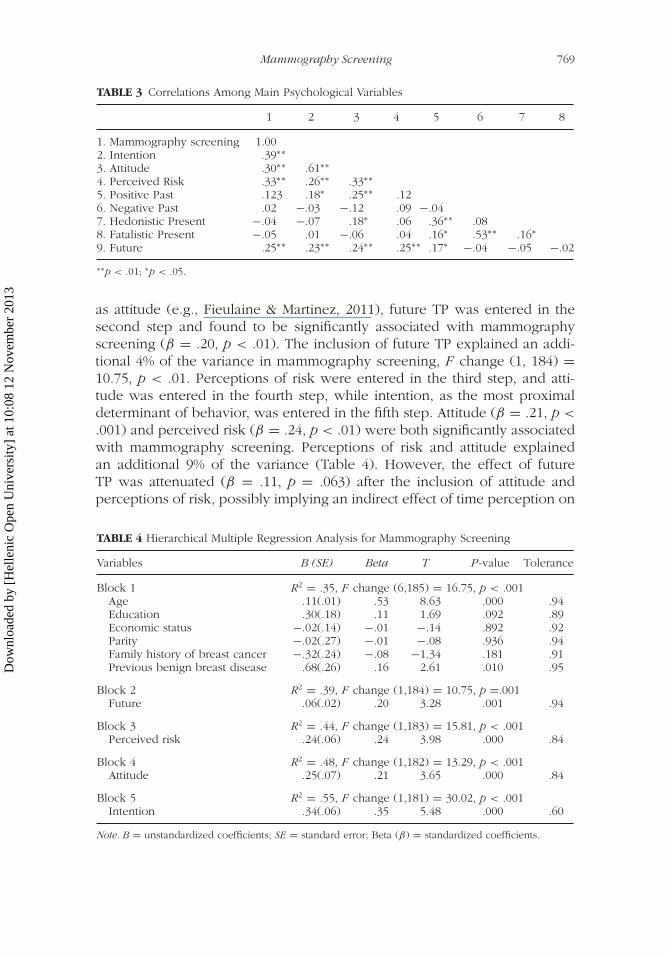
One-way analysis of variance revealed that none of the demographicvariables was associated with intention to use mammography screening.Moreover, only two of the health-related variables, namely having a clin-ical breast examination (F = 9.24, p = .001) and family history of breastcancer (F = 4.19, p = .017), were significantly associated with intention.Correlational analyses revealed that two of the five TP dimensions were sig-nificantly related to intention and mammography screening behavior. Futureorientation was associated with both intention (r = .23, p < .01) andmammography screening (r = .25, p < .01), and positive past was asso-ciated with intention (r = .18, p < .05). Perceived risk of breast cancer wasassociated with both intention (r = .26, p < .01) and screening behavior (r =.33, p < .01). Intention was associated with screening behavior as expected(r = .39, p < .01). Significant and conceptually justifiable correlations wereobserved among the five TP dimensions (Table 3).
Regression analyses were then conducted to determine whether themain psychological variables were related to mammography screening aftercontrolling for demographic and health-related characteristics. Age, parity,economic status, educational level, family history of breast cancer, and a pre-vious benign breast disease were included as control variables in the first stepof the analyses, due to their associations with mammography use in previousresearch. Of the above mentioned variables. Only age (β = .53, p < .001) anda previous benign breast disease (β = .16, p = .01) were significantly asso-ciated with mammography screening. These control variables explained 35%of the variance in mammography screening, F change (6, 185) = 16.75,p < .001. Based on previous research that highlighted the effect of TP onhealth behavior, through its impact on proximal predictors of behavior such
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
768 F. Griva et al.
TABLE 1 Demographic and Health-Related Characteristics of the Sample
Variable N %
Age (years)40–49 108 55.750–59 60 30.960 and above 26 13.4
Education (years)0–6 12 6.27–12 111 57.213–16 71 36.6
Marital statusMarried 148 76.3Single 16 8.2Divorced/Widowed 30 15.5
Employment statusEmployed 116 59.8Unemployed 78 40.2
Economic statusVery Good 14 7.2Good 94 48.5Medium 73 37.6Poor 13 6.7
BSE statusYesa 93 47.9No 101 52.1
CBE statusNever 40 20.6More than 2 years 31 16.0Every 2 years 20 10.3Once a year 103 53.1
Family history of breast cancerYes 48 24.7No 146 75.3
Previous benign breast diseaseYes 35 18.0No 159 82.0
Note. BSE = breast self-examination; CBE = clinical breast examination.aResponse indicates that a woman performed BSE at least once every 1–2 months.
TABLE 2 Means of the ZTPI Subscales in Various Studies
U.S (original) France Portugal Spain Lithuania Brazil Greece
PN 2.98 3.07 2.67 2.57 2.83 2.83 2.53PP 3.71 3.45 3.62 3.19 3.43 3.50 3.45PH 3.44 3.32 3.52 2.87 3.17 2.65 2.86PF 2.37 2.41 2.46 2.66 2.74 2.51 2.50F 3.47 3.18 3.59 3.72 3.50 3.65 3.42
Note. PN = past negative; PP = past positive; PH = present hedonistic; PF = present fatalistic; F = future.
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
Mammography Screening 769
TABLE 3 Correlations Among Main Psychological Variables
1 2 3 4 5 6 7 8
1. Mammography screening 1.002. Intention .39∗∗3. Attitude .30∗∗ .61∗∗4. Perceived Risk .33∗∗ .26∗∗ .33∗∗5. Positive Past .123 .18∗ .25∗∗ .126. Negative Past .02 −.03 −.12 .09 −.047. Hedonistic Present −.04 −.07 .18∗ .06 .36∗∗ .088. Fatalistic Present −.05 .01 −.06 .04 .16∗ .53∗∗ .16∗9. Future .25∗∗ .23∗∗ .24∗∗ .25∗∗ .17∗ −.04 −.05 −.02
∗∗p < .01; ∗p < .05.
as attitude (e.g., Fieulaine & Martinez, 2011), future TP was entered in thesecond step and found to be significantly associated with mammographyscreening (β = .20, p < .01). The inclusion of future TP explained an addi-tional 4% of the variance in mammography screening, F change (1, 184) =10.75, p < .01. Perceptions of risk were entered in the third step, and atti-tude was entered in the fourth step, while intention, as the most proximaldeterminant of behavior, was entered in the fifth step. Attitude (β = .21, p <
.001) and perceived risk (β = .24, p < .01) were both significantly associatedwith mammography screening. Perceptions of risk and attitude explainedan additional 9% of the variance (Table 4). However, the effect of futureTP was attenuated (β = .11, p = .063) after the inclusion of attitude andperceptions of risk, possibly implying an indirect effect of time perception on
TABLE 4 Hierarchical Multiple Regression Analysis for Mammography Screening
Variables B (SE) Beta T P-value Tolerance
Block 1 R2 = .35, F change (6,185) = 16.75, p < .001Age .11(.01) .53 8.63 .000 .94Education .30(.18) .11 1.69 .092 .89Economic status −.02(.14) −.01 −.14 .892 .92Parity −.02(.27) −.01 −.08 .936 .94Family history of breast cancer −.32(.24) −.08 −1.34 .181 .91Previous benign breast disease .68(.26) .16 2.61 .010 .95
Block 2 R2 = .39, F change (1,184) = 10.75, p =.001Future .06(.02) .20 3.28 .001 .94
Block 3 R2 = .44, F change (1,183) = 15.81, p < .001Perceived risk .24(.06) .24 3.98 .000 .84
Block 4 R2 = .48, F change (1,182) = 13.29, p < .001Attitude .25(.07) .21 3.65 .000 .84
Block 5 R2 = .55, F change (1,181) = 30.02, p < .001Intention .34(.06) .35 5.48 .000 .60
Note. B = unstandardized coefficients; SE = standard error; Beta (β) = standardized coefficients.
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
770 F. Griva et al.
mammography screening through perceptions of risk, attitude, and intention.The inclusion of intention in the fifth step explained an additional 7% of thevariance, F change (1,181) = 30.02, p < .001 and resulted in the attenua-tion of the effect of attitude (β = .01, p = .829), implying a mediated effectof intention in the relationship between attitude and mammography screen-ing. Perceived risk of breast cancer (β = .18, p < .01), and intention (β =.35, p < .01) were significantly associated with mammography screening,after controlling for the effects of demographic and health-related variables.Altogether, 55% of the variability in mammography screening behavior wasexplained by the variables included in the regression model, F(10, 181) =22.08, p < .001.
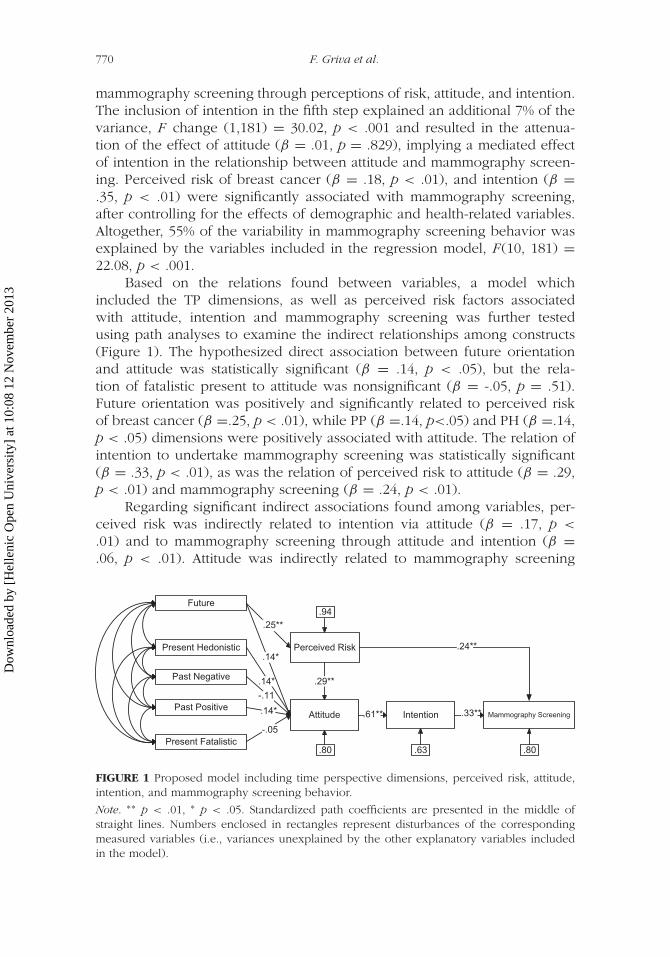
Based on the relations found between variables, a model whichincluded the TP dimensions, as well as perceived risk factors associatedwith attitude, intention and mammography screening was further testedusing path analyses to examine the indirect relationships among constructs(Figure 1). The hypothesized direct association between future orientationand attitude was statistically significant (β = .14, p < .05), but the rela-tion of fatalistic present to attitude was nonsignificant (β = -.05, p = .51).Future orientation was positively and significantly related to perceived riskof breast cancer (β =.25, p < .01), while PP (β =.14, p<.05) and PH (β =.14,p < .05) dimensions were positively associated with attitude. The relation ofintention to undertake mammography screening was statistically significant(β = .33, p < .01), as was the relation of perceived risk to attitude (β = .29,p < .01) and mammography screening (β = .24, p < .01).
Regarding significant indirect associations found among variables, per-ceived risk was indirectly related to intention via attitude (β = .17, p <
.01) and to mammography screening through attitude and intention (β =
.06, p < .01). Attitude was indirectly related to mammography screening
Perceived Risk
Intention
Future
Past PositiveMammography Screening.14*
.94
Past Negative
Present Fatalistic
Present Hedonistic
-.05
Attitude
.29**.14*
.14*
.25**
-.11
.24**
.61** .33**
.80.63.80
FIGURE 1 Proposed model including time perspective dimensions, perceived risk, attitude,intention, and mammography screening behavior.
Note. ∗∗ p < .01, ∗ p < .05. Standardized path coefficients are presented in the middle ofstraight lines. Numbers enclosed in rectangles represent disturbances of the correspondingmeasured variables (i.e., variances unexplained by the other explanatory variables includedin the model).
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

Mammography Screening 771
via intention (β = .20, p < .01). Also, a significant indirect association wasobserved between future orientation and mammography screening, throughperceived risk (β = .10, p < .01). The proposed model exhibited good fit tothe data, Satorra- Bentler χ2 (21) = 26.14, p = .20, confirmed by the otherfit indices (RMSEA = .036; NFI = .93; CFI = .98; GFI = .97; AIC= 74.14).
DISCUSSION
The goal of the present study was to examine the relation between TP andmammography screening, and the association of TP with the well-establishedfactor of perceived risk of breast cancer. The demographic and health-relatedcharacteristics of the sample were comparable to those reported in otherregional studies about mammography screening (e.g., Anagnostopouloset al., 2012), and a recent nationwide survey on mammography screening(Dimitrakaki et al., 2009), as well as in surveys about breast screen-ing practices in the European Union (e.g., Special Eurobarometer, 2007).Consequently the sample of the study was considered to be representativeof the population of women undergoing mammography screening. Age andprevious benign breast disease were associated with mammography screen-ing. This finding is consistent with evidence drawn from previous researchshowing an association of sociodemographic characteristics or health-relatedvariables with increased mammography use (Rakowski et al., 2004, 2006).The psychological variables of TP, risk perceptions, attitude, and intentionexplained an additional 20% of the variance in undertaking mammographyscreening after controlling for the sociodemographic and health-related vari-ables. The results confirmed the role of perceived risk in mammographyscreening as hypothesized. This finding was in line with that of previousmeta-analyses and reviews (Katapodi et al., 2004; Magai et al., 2007; Schueleret al., 2008). The positive and significant relation of perceived risk to attitude,and the direct association of perceived risk with mammography screening,were also consistent with previous research (Aiken et al., 1994; Katapodiet al., 2004; McQueen et al., 2006). Thus, perceived risk seems to affectmammography screening both directly and indirectly, through the formationof a positive attitude towards the probable advantages of mammographyscreening. Consequently, a positive attitude toward screening can result intoa strong intention to get a mammogram. The finding that attitude was indi-rectly associated with mammography screening through intention, was alsoconsistent with previous research on mammography screening (Drosaert,Boer, & Seydel, 2003; Rutter, 2000; Tolma et al., 2003). Furthermore, the anal-yses revealed that the future TP dimension was associated with perceptionsof risk. It is reasonable to suggest that women who take under consider-ation the future consequences of their actions are inclined to take underconsideration any risks regarding their health. Regarding attitude towardmammography screening, women with a positive reconstruction of their past
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
772 F. Griva et al.
exhibited positive attitudes, presumably because they viewed themselves asvalued individuals who sought to preserve good health status.
The significant indirect association of future TP with mammographyscreening was in line with findings from previous research on health pro-tective behaviors (Adams, 2009; Henson et al., 2006; Mahon et al., 1997).The finding that the fatalistic present dimension of TP was not associatedindirectly with mammography screening was not consistent with previousresearch that had suggested a close association between screening for breastcancer and fatalistic perceptions (Chavez et al., 1997; Powe, 1995; Sugareket al., 1988). However, all of the previously mentioned studies had beenconducted with either minority populations, or with non-western popula-tions, and findings might have been influenced by cultural or other societaldifferences, such as lack of knowledge related to breast cancer. Researchon women of different cultural backgrounds, such as Hispanic, AfricanAmerican, and Muslim Arab, has revealed fatalistic attitudes about breast can-cer, such as the belief that cancer is God’s punishment for immoral behavior(Austin et al., 2002; Soskolne, Marie, & Manor, 2007; Terán et al., 2007).
The importance of TP in the context of health behaviors has been estab-lished through research on interventions to promote health behaviors andhealth preventive communication. Hall and Fong (2003) studied TP for anintervention to increase physical activity among adolescents and concludedthat strengthening the future orientation of adolescents led to a concomitantincrease in physical activity, while the results of the intervention were main-tained up to 6 months after the initial evaluation. Additionally, TP has beenrelated to decisions to adopt behaviors that promote health in studies con-ducted in the context of communication of health preventive behavior. Morespecifically, in research examining the effect of tailored messages to partic-ipate in colorectal cancer and type 2 diabetes screening programs, peoplelow on future orientation appeared to become more convinced when theprompting messages were framed to emphasize the short-term positive con-sequences of screening instead of the long-term negative consequences ofnot screening, whereas the reverse was true for people that scored high onfuture orientation (Orbell & Hagger, 2006; Orbell et al., 2004).
This study had some limitations. First, due to the cross-sectional design,it was not possible to determine the temporal directions and, thus, causal-ity among study variables. Potentially, the frequency of mammographyscreening uptake may have enhanced a woman’s future TP or it may haveinfluenced, in the long-run, a woman’s perception of risk for breast can-cer, reassuring her that her current health status was good. Second, thesmall sample size of the study provided limited statistical power to detectsome meaningful differences as statistically significant. Third, although thesample appeared to be representative of screened women, some possibleshortcomings in the setting of the study (e.g., hospital) or the self-reportedmethod of collecting data may have resulted in response biases, including
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13

Mammography Screening 773
recall bias or social desirability bias, that could hinder the generalizabilityand/or accuracy of the findings. However, it should be noted that previousresearch on mammography screening has shown considerable congruencebetween self-reported behavior and objective measures of behavior, suchas medical records (e.g., King et al., 1990). Finally, other variables relatedto mammography screening, such as knowledge about breast cancer andbreast cancer screening benefits, or emotional responses to screening, werenot examined in the present study, which could have resulted in residualuncontrolled confounding. Along with cognitive and emotional variables,future research should examine a number of health care system factors asso-ciated with the use of mammography screening, including patient reminders,physician recommendation, insurance status or lack of adequate health carefacilities, which were not examined in this study.
Overall, the findings of this study suggest that TP should be takeninto account when studying factors related to health protective behaviors.Our results indicated that the proposed model provided a good fit to thedata, although the amount of variance in mammography screening behaviorexplained by the variables included in the model was modest and wouldbe improved by inclusion of appropriate variables found in prior studies tobe related to mammographic screening. Future research should test interac-tions of the TP with other identified explanatory variables, such as attitudes,knowledge or emotional responses to screening, in an attempt to developa more integrated model of mammography screening behavior that couldbe further tested to assess its utility in other health protective behaviors.The identification and exploration of these factors could lead investigators todesigning effective interventions to promote mammography screening, thusincreasing the likelihood of early detection of and reduced mortality frombreast cancer.
REFERENCES
Adams, J. M. 2009. The role of time perspective, in smoking cessation amongst olderEnglish adults. Health Psychol 28:529–34.
Advisory Committee on Cancer Prevention. 2000. Recommendations on cancerscreening in the European Union. Eur J Cancer 36:1473–78.
Aiken, L. S., S. G. West, C. K. Woodward, R. R. Reno, and K. D. Reynolds. 1994.Increasing screening mammography in asymptomatic women: Evaluation of asecond-generation, theory-based program. Health Psychol 13:526–38.
Ajzen, I. 2002. Constructing a TPB questionnaire: Conceptual and methodolog-ical considerations. Retrieved from http://www.people.umass.edu/aizen/pdf/tpb.measurement.pdf
Anagnostopoulos, F., C. Dimitrakaki, D. Fitzsimmons, G. Potamianos, D. Niakas,and Y. Tountas. 2012. Health beliefs and illness perceptions as related tomammography uptake in randomly selected women in Greece. J Clin PsycholMed Settings 19:147–64.
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
774 F. Griva et al.
Anagnostopoulos, F., and F. Griva. 2012. Exploring time perspective in Greek youngadults: Validation of the Zimbardo Time Perspective Inventory and relationshipswith mental health indicators. Soc Indic Res 106:41–59.
Anderson, W. F., I. Jatoi, and S. S. Devesa. 2006. Assessing the impact of screen-ing mammography: Breast cancer incidence and mortality rates in Connecticut(1943–2002). Breast Cancer Res Treat 99:333–40.
Apostolidis, T., and N. Fieulaine. 2004. Validation française de l’échelle deTemporalité—The Zimbardo Time Perspective Inventory (ZTPI). Rev EurPsychol Appl 54:207–17.
Apostolidis, T., N. Fieulaine, L. Simonin, and G. Rolland. 2006. Cannabis use, timeperspective and risk perception: Evidence of a moderating effect. Psychol Health21:571–92.
Apostolidis, T., N. Fieulaine, and F. Soulé. 2006. Future time perspective as predictorof cannabis use: Exploring the role of substance perception among Frenchadolescents. Addict Behav 31:2339–43.
Austin, L. T., F. Ahmad, M. J. McNally, and D. E. Stewart. 2002. Breast and cervicalcancer screening in Hispanic women: A literature review using the health beliefmodel. Womens Health Issues 12:122–8.
Botha, J. L., F. Bray, R. Sankila, and D. M. Parkin. 2003. Breast cancer incidence andmortality trends in 16 European countries. Eur J Cancer 39:1718–29.
Chavez, L. R., F. A. Hubbell, S. I. Mishra, and R. B. Valdez. 1997. The influence offatalism on self-reported use of Papanicolaou smears. Am J Prev Med 13:418–24.
Diaz-Morales, J. F. 2006. Estructura factorial y fiabilidad del inventario de pespectivatemporal de Zimbardo [Factor structure and reliability of the Zimbardo timeperspective inventory]. Psicothema 18:565–71.
Dimitrakaki, C., D. Boulamatsis, A. Mariolis, N. Kontodimopoulos, D. Niakas, and Y.Tountas. 2009. Use of cancer screening services in Greece and associated socialfactors: Results form the nationwide Hellas Health I survey. Eur J Cancer Prev18:248–57.
Drossaert, C. H. C., H. Boer, and E. R. Seydel. (2003). Prospective study on thedeterminants of repeat attendance and attendance patterns in breast cancerscreening using the theory of planned behavior. Psychology & Health 18:551–65.
Fieulaine, N., and F. Martinez. 2011. About the fuels of self-regulation: Time perspec-tive and desire for control in adolescents substance use. In The psycholologyof self-regulation, ed. Vassilis Barboukis, 102–21. New York: Nova SciencePublishers.
Finney Rutten, L. J., and R. J. Iannotti. 2003. Health beliefs, salience of breast cancerfamily history, and involvement with breast cancer issues: Adherence to annualmammography screening recommendations. Cancer Detect Prev 27:353–9.
Griesch, J. M., S. C. O’Neill, B. K. Rimer, J. T. DeFrank, J. M. Bowling, C. S. Skinner.2009. Factors associated with annual-interval mammography for women in their40s. Cancer Epidemiol 33:72–8.
Hakama, M., M. P. Coleman, D. M. Alexe, and A. Anssi. 2008. Cancer screening:Evidence and practice in Europe 2008. Eur J Cancer 44:1404–13.
Hall, P. A., and G. T. Fong. 2003. The effects of brief time perspective interventionfor increasing physical activity among young adults. Psychol Health 18:685–706.
Henson, J. M., M. P. Carey, K. B. Carey, and S. A. Maisto. 2006. Associations amonghealth behaviors and time perspective in young adults: Model testing with boot-strapping replication. J Behav Med 29:127–37.
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
Mammography Screening 775
Hu, L., and P. M. Bentler. 1999. Cut-of criteria for fit indexes in covariance struc-ture analysis: Conventional criteria versus new alternatives. Struct Equ Modeling6:1–55.
Katapodi, M. C., K. A. Lee, N. C. Facione, and M. J. Dodd. 2004. Predictors ofperceived breast cancer risk and the relation between perceived risk and breastcancer screening: A meta-analytic review. Prev Med 38:388–402.
Keough, K. A., P. G. Zimbardo, and J. N. Boyd. 1999. Who’s smoking, drinking andusing drugs? Time perspective as a predictor of substance use. Basic Appl SocPsychol 21:149–64.
King, E. S., B. K. Rimer, B. Trock, A. Balshem, and P. Engstrom. 1990. How valid aremammography self-reports? Am J Public Health 80:1386–88.
Klemi, P. J., I. Parvinen, L. Pylkkanen, L. Kauhava, P. Immonen-Raiha, O. Rasanenand H. Helenius. 2003. Significant improvement in breast cancer survivalthrough population-based mammography screening. Breast 12:308–13.
Liniauskaite A., and A. Kairys. 2009. The Lithuanian version of the Zimbardo timeperspective inventory (ZTPI). Psichologija 40:66–87.
Magai, C., N. Consedine, A. I. Neugut, and D. L. Hershman. 2007. Common psy-chosocial factors underlying breast cancer screening and breast cancer treatmentadherence: A conceptual review and synthesis. J Womens Health 16:11–23.
Mahon, N. E., T. J. Yarcheski, and A. Yarcheski. 1997. Future time perspectiveand positive health practices in young adults: An extension. Percept Mot Skills84:1299–1304.
McCaul, K. D., A. D. Branstetter, D. M. Schroeder, and R. E. Glasgow. 1996. Whatis the relationship between breast cancer risk and mammography screening? Ameta-analytic review. Health Psychol 15:423–9.
McQueen, A., S. W. Vernon, R. E. Myers, and B. C. Tilley. 2006. Examining mediatorsof perceived susceptibility on colorectal cancer screening intention and behav-ior among male autoworkers. Paper presented at the 27th annual meeting forSociety of Behavioral Medicine, San Francisco, CA.
Milfont, T. L., P. R. Andrade, R. P. Belo, and V. S. Pessoa. 2008. Testing ZimbardoTime Perspective Inventory in a Brazilian sample. Interamer J Psychol 42:49–58.
Orbell, S., and M. Hagger. 2006. Temporal framing and the decision to take part intype 2 diabetes screening: Effects of individual differences in consideration offuture consequences on persuasion. Health Psychol 25:537–48.
Orbell, S., M. Perugini, and T. Rakow. 2004. Individual differences in sensitivity tohealth communications: Consideration of future consequences. Health Psychol23:388–96.
Organization for Economic Cooperation and Development. 2012. Health at a Glance:Europe 2012. Paris: OECD Publishing.
Ortuño, V., and V. Gamboa, 2009. Estrutura factorial do Zimbardo Time PerspectiveInventory—ZTPI numa amostra de estudantes universitários portugueses.Avances en Psicologia Latinoamericana 27:21–32.
Perez-Stable E. J., F. Sabogal, R. Otero-Sabogal, R. A. Hiatt, and S. J. McPhee.1992. Misconceptions about cancer among Latinos and Anglos. J Am Med Assoc268:3219–23
Powe, B. D. 1995. Fatalism among elderly African Americans: Effects on colorectalcancer screening. Cancer Nurs 18:385–92.
Rakowski, W., N. Breen, H. Meissner, B. K. Rimer, S. W. Vernon, M. A., Clark, andA. N. Freedman. Prevalence and correlates of repeat mammography among
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13
776 F. Griva et al.
women aged 55-79 in the Year 2000 National Health Interview Survey. PrevMed 39:1–10.
Rakowski, W., H. Meissner, S. W. Vernon, B. Breen, B. Rimer, and M. A. Clark. 2006.Correlates of repeat and recent mammography for women ages 45 to 75 in the2002 to 2003 Health Information National Trends Survey (HINTS 2003). CancerEpidemiol Biomarkers Prev 15: 2093–2101.
Raykov, T., and G. A. Marcoulides. 2000. A first course in structural equationmodelling. Mahwah, NJ: Lawrence Erlbaum.
Robbins, R. N., and A. Bryan. 2004. Relationships between future orientation,impulsive sensation seeking, and risk behavior among adjudicated adolescents.J Adolescent Res 19:428–45.
Rothspan, S., and S. J. Read. 1996. Present versus future time perspective and HIVrisk among heterosexual college students. Health Psychol 15:131–4.
Rutter, D. R. 2000. Attendance and reattendance for breast cancer screening: Aprospective 3 year test of the theory of planned behavior. Br J Health Psychol5:1–13.
Schmiege, S. J., A. Bryan, and W. M. P. Klein. 2009. Distinctions between worryand perceived risk in the context of the theory of planned behavior. J App SocPsychol 39:95–119.
Schueler, K. M., P. W. Chu, and R. Smith-Bindman. 2008. Factors associated withmammography utilization: A systematic quantitative review of the literature.J Womens Health 17:1477–98.
Soldatos, T. 2006. Mammography screening guidelines. Senologic Hellenic Society.Retrieved from http://www.mastologia.gr/Article/733/
Soskolne, V., S. Marie, and O. Manor. 2007. Beliefs, recommendations and intentionsare important explanatory factors of mammography screening behavior amongMuslim Arab women in Israel. Health Educ Res 22:665–76.
Special Eurobarometer. 2007. Health in the European Union. Brussels: EuropeanCommission. Retrieved from http://ec.europa.eu/health/ph_publication/eb_health_en.pdf.
Sugarek, N. J., R. A. Deyo, and B. C. Holmes. 1988. Locus of control and beliefsabout cancer in a multi-ethnic clinic population. Oncol Nurs Forum 15:481–6.
Terán, L., L. Baezconde-Garbanati, M. Márquez, E. Castellanos, and K. Belkic. 2007.On-time mammography screening with a focus on Latinas with low income: Aproposed cultural model. Anticancer Res 27:4325–38.
Tolma, E. L., B. M. Reininger, J. Ureda, and A. Evans. 2003. Cognitive motivationsassociated with screening mammography in Cyprus. Prev Med 36:363–73.
Van der Pligt, J. 1996. Risk perception and self-protective behavior. Eur Psychol1:34–43.
Wills, T. A., J. M. Sandy, and A. M. Yaeger. 2001. Time perspective and early-onsetsubstance use: A model based on stress-coping theory. Psychol Addict Behav15:118–25.
Zimbarbo, P. G., and J. N. Boyd. 1999. Putting time in perspective: A valid, reliableindividual-differences metric. J Pers Soc Psychol 77:1271–88.
Zimbardo, P. G., K. A. Keough, and J. N. Boyd. 1997. Present time perspective as apredictor of risky driving. Pers Indiv Differ 23:1007–23.
Dow
nloa
ded
by [
Hel
leni
c O
pen
Uni
vers
ity]
at 1
0:08
12
Nov
embe
r 20
13




















