
Thrombocytopenia: a practial approach - SGH-SSH
35
Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Thrombocytopenia: a practial approach
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Thrombocytopenia: a practial approach - SGH-SSH

Dr. med. Jeroen Goede
FMH Innere Medizin, Medizinische Onkologie, Hämatologie
FAMH Hämatologie
Chefarzt Hämatologie
Kantonsspital Winterthur
Thrombocytopenia: a practial approach

2
Outline
• Introduction and Definitions
• Diagnostic steps differential diagnosis
• Thrombocytopenia during pregnancy
• Immune thrombocytopenia
• Conclusions
3
Introduction
Thrombocytes are formed by fragmentation of the cytoplasm of
megakaryocytes
Under physiological circumstances thrombocytes then circulate in
the blood for 7-10 days and play a critical role in haemostasis
In case of significant quantitative or qualitative platelet
dysfunction:
Patients present typically with mucocutaneous bleeding
Typically no soft tissue or joint bleeding
Presence should raise suspicion of additional plasmatic
coagulation problems
4
Introduction
In most laboratories: normal platelet count between 150-450 G/l
(+/- 2 standard deviations)
By definition 2.5% of the “normal” range will be below 150 G/l
NCI-definition of grading for thrombocytopenia (for cancer
patients receiving treatment):
Grade 1 : 75-150 G/l
Grade 2 : 50-75 G/l
Grade 3 : 25-50 G/l
Grade 4 : <25 G/l
5
Introduction
In otherwise healthy conditions
Bleeding time is generally not prolonged until platelet count is
below 100 G/l
As long as platelet counts are above 20 G/l clinical
manifestations are mild
Below 10 G/l the risk for spontaneous bleeding increases
rapidly
Several factors such as functional defects modify the bleeding
risk

6
Diagnostic steps
Main laboratory questions in newly diagnosed thrombocytopenia:
Exclude pre-analytic reasons for thrombocytopenia
Concomitant anemia and/or neutropenia?
Degree of thrombocytopenia?
Tc 75-150 G/l vs. 50-75 G/l vs. 25-50 G/l vs. <25 G/l

7
Diagnostic steps
Main clinical questions in newly diagnosed thrombocytopenia:
Recent and actual medication?
History of previous thrombocytopenia?
Family history?
Pregnancy?

Diagnostic steps
Mr. S.O. 1971

9
Diagnostic steps
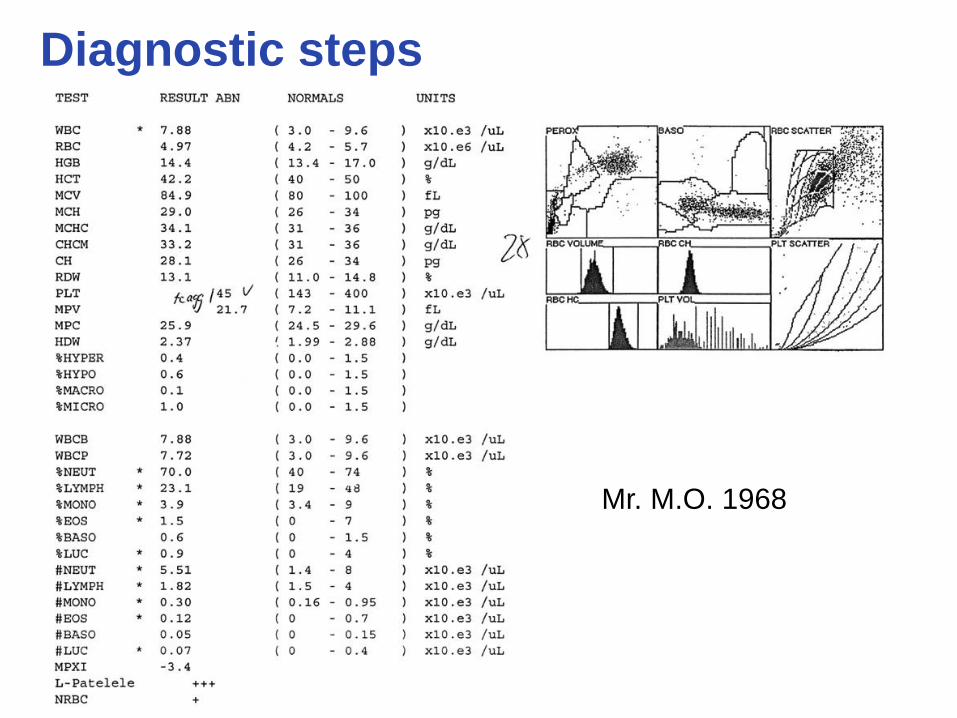
Diagnostic steps
Mr. M.O. 1968

11
Diagnostic steps

12
Diagnostic steps
Diagnosis:
Bernhard-Soulier-Syndrome
13
Diagnostic steps
Initial laboratory evaluation:
Peripheral blood smear with reticulocytes
Serum creatinine
DIC panel
LDH
Total and direct bilirubin
AST and ALT
Ev. pregnancy testing
This allows as initial determination whether thrombocytopenia is
an isolated abnormality or part of a constellation of abnormalities
Diagnostic steps
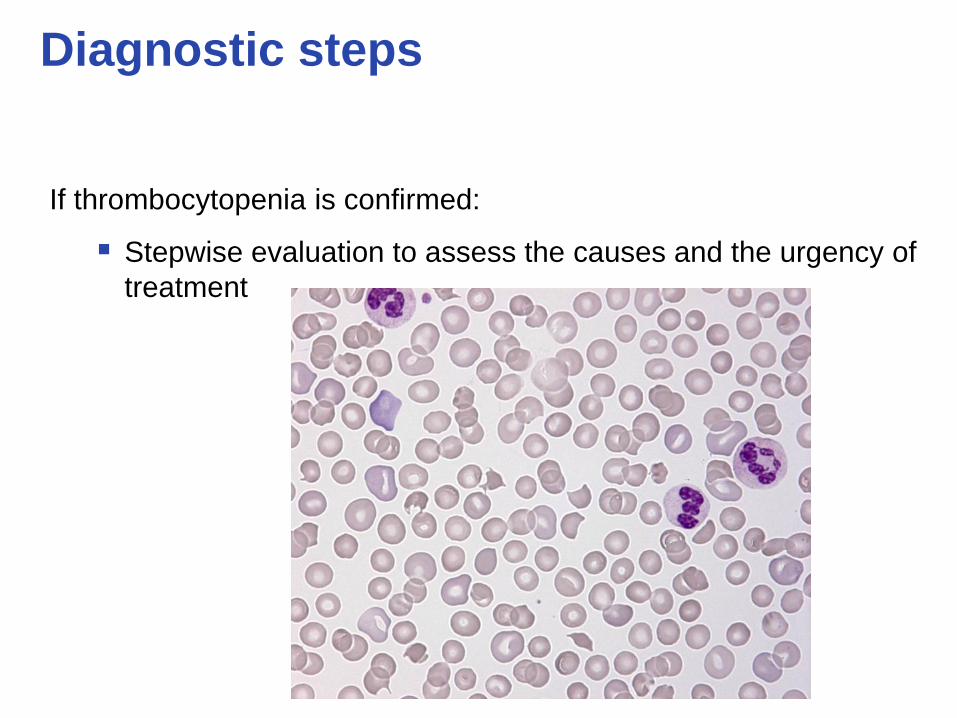
If thrombocytopenia is confirmed:
Stepwise evaluation to assess the causes and the urgency of
treatment
15
Diagnostic steps
If thrombocytopenia is confirmed:
Stepwise evaluation to assess the causes and the urgency of
treatment:
Thrombotic thrombocytopenic purpura (TTP)
Heparin-induced thrombocytopenia (HIT)
Immediate Intervention is required

16
Diagnostic steps
Isolated thrombocytopenia without specific clues on the
peripheral blood smear:
Diagnosis of immune-thrombocytopenia (ITP) is probable
Drug induced thrombocytopenia can’t be excluded
17
Diagnostic steps
The role of bone marrow exam:
Differentiation between inadequate production versus
excessive destruction/consumption as predominant cause of
thrombocytopenia
With age the incidence of primary marrow disorders is rising
(lymphoma as condition that causes ITP)

Differential diagnosis
Decreased production:
Hematologic malignancies
Aplastic anaemia
Myelodysplasia
Chemotherapy and alcohol
Radiation
HIV
Vitamin D deficiencies
Hereditary thrombocytopenia
Metastatic cancer to bone marrow
Increased destruction:
Immune:
ITP
HIT
Drug-induced antibodies
HIV
Post transfusion purpura
Connective tissue diseases
Nonimmune:
DIC
Sepsis
Cardiac valves
TTP-HUS
Splenic sequestration

Sudhir S. et al. SMJ, 2006

Thrombocytopenia during pregnancy:
21
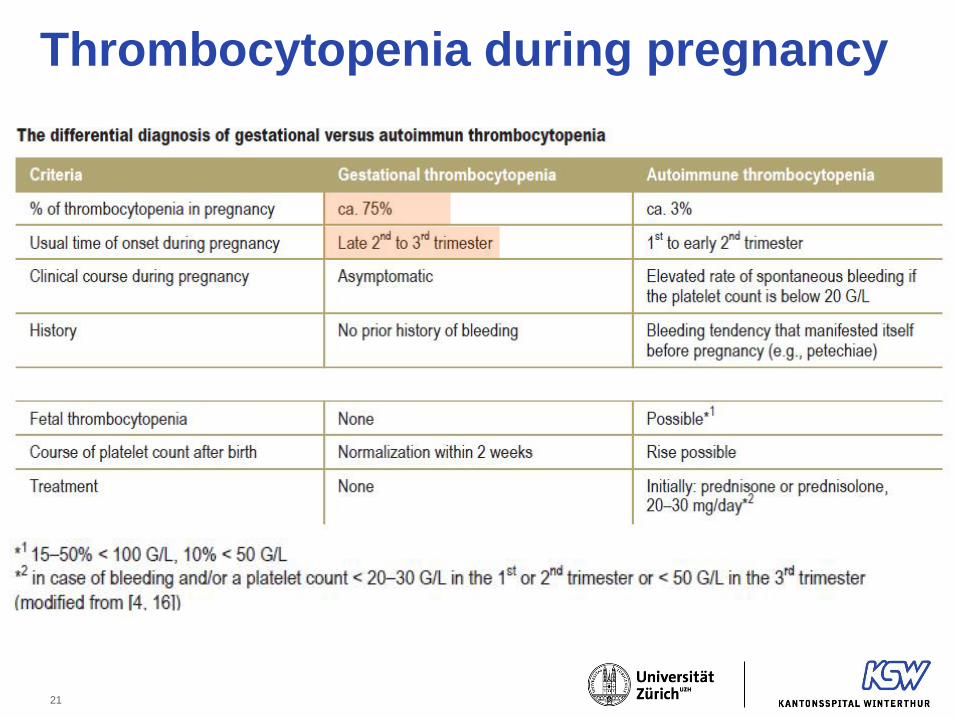
Thrombocytopenia during pregnancy

22
Immune thrombocytopenia (ITP)
Immune thrombocytopenia of the adult:
• Outcome 5 years after diagnosis (Sailer, Haematologica 2006, McMillan,
Blood 2004):
• 40% of the patients have a platelet count lower than 100 G/l
• 15% of the patients have a platelet count lower than 30 G/l
• 60% of the patients are in remission
• ITP is becoming more and more a disease of elderly people
(median of age around 50 years)

23
Schoonen, BJH 2009
Immune thrombocytopenia (ITP)
24
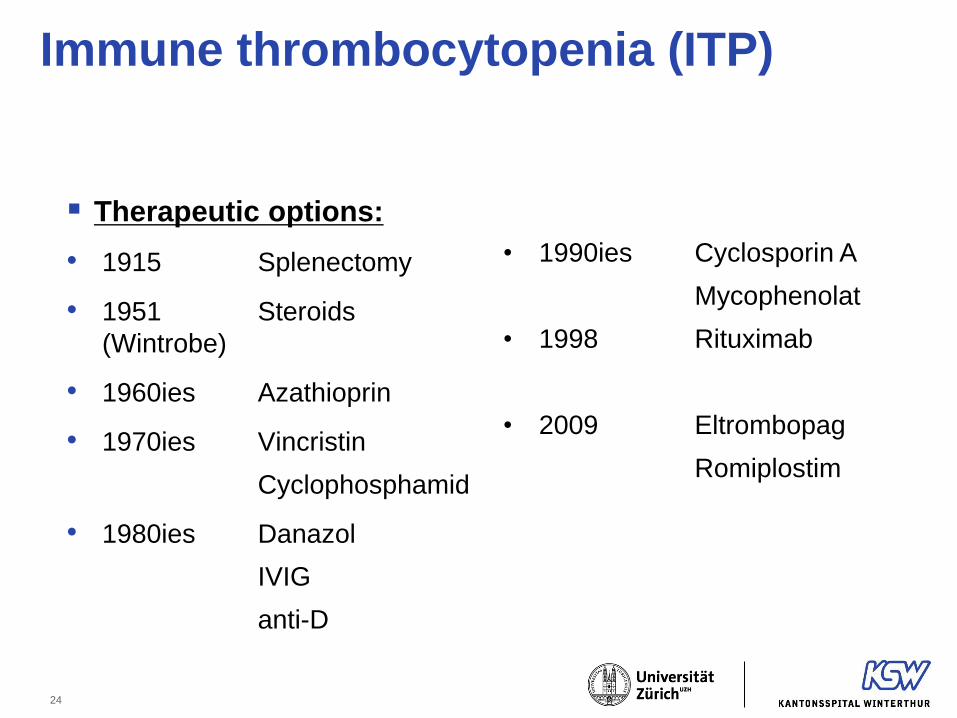
Therapeutic options:
• 1915 Splenectomy
• 1951 Steroids
(Wintrobe)
• 1960ies Azathioprin
• 1970ies Vincristin
Cyclophosphamid
• 1980ies Danazol
IVIG
anti-D
• 1990ies Cyclosporin A
Mycophenolat
• 1998 Rituximab
• 2009 Eltrombopag
Romiplostim
Immune thrombocytopenia (ITP)

25
Definition of response to treatment
• Complete response:
• increase in platelet count above 100 G/l
• Clinically relevant response:
• platelet increase above 30 G/l with at least a twofold
increase of the baseline count and the absence of bleeding
26
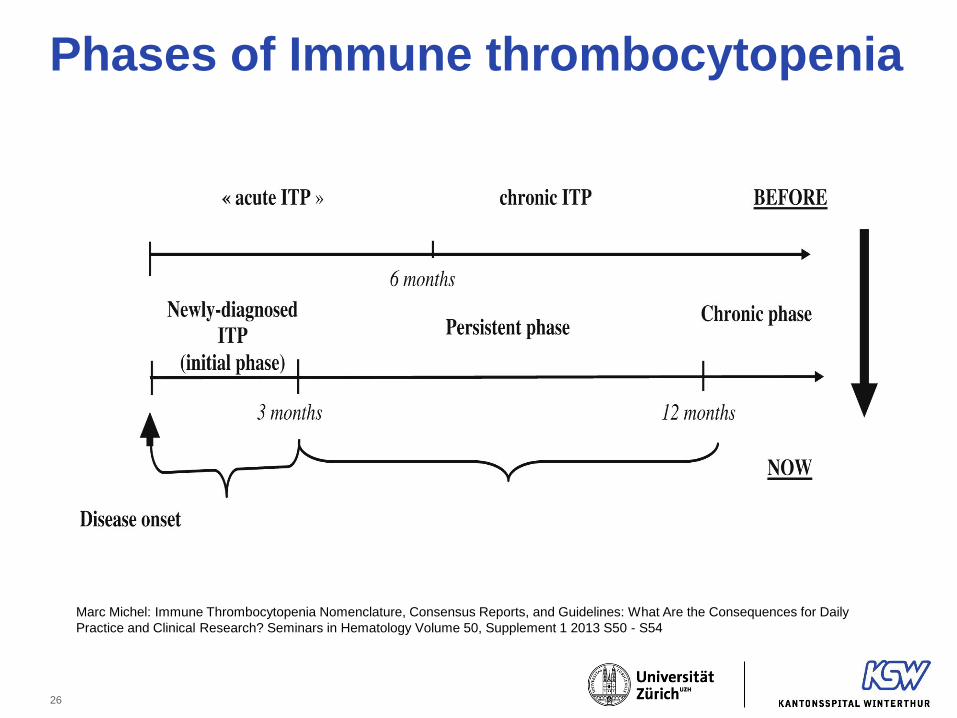
Marc Michel: Immune Thrombocytopenia Nomenclature, Consensus Reports, and Guidelines: What Are the Consequences for Daily
Practice and Clinical Research? Seminars in Hematology Volume 50, Supplement 1 2013 S50 - S54
Phases of Immune thrombocytopenia
27
TPO agonists
Very good clinical data with a high proporiton of responders
Good tollerability
Chronic treatment
Chronic costs

Splenectomy
• Splenectomy is an option with a high rate of durable and
complete remissions
• Mortality of the intervention: 0.5-1%
• Gonzalez-Porras JR et al. Eur J Haematol. 2013 Sep;91:
• Comparison of 57 patients ≥65 years of age with 162
patients below the age of 65 years with splenectomy due
to ITP:
• Favorable response in 72% of elderly patients and 92% of younger patients (P=0.005)
• Probability of maintaining response for 14 years after
splenectomy was 56%
• In elderly patients mortality is higher (1.8% vs. 0.6%)

29
Splenectomy
30
Rituximab
• First report at ASH 1998:
Perotta, ASH Annual Meeting 1998
• Since then many case reports and phase II studies, but only
two phase III studies in first line treatment:
Zaja, Blood 2010
Gudbrandsdottir, Blood 2013
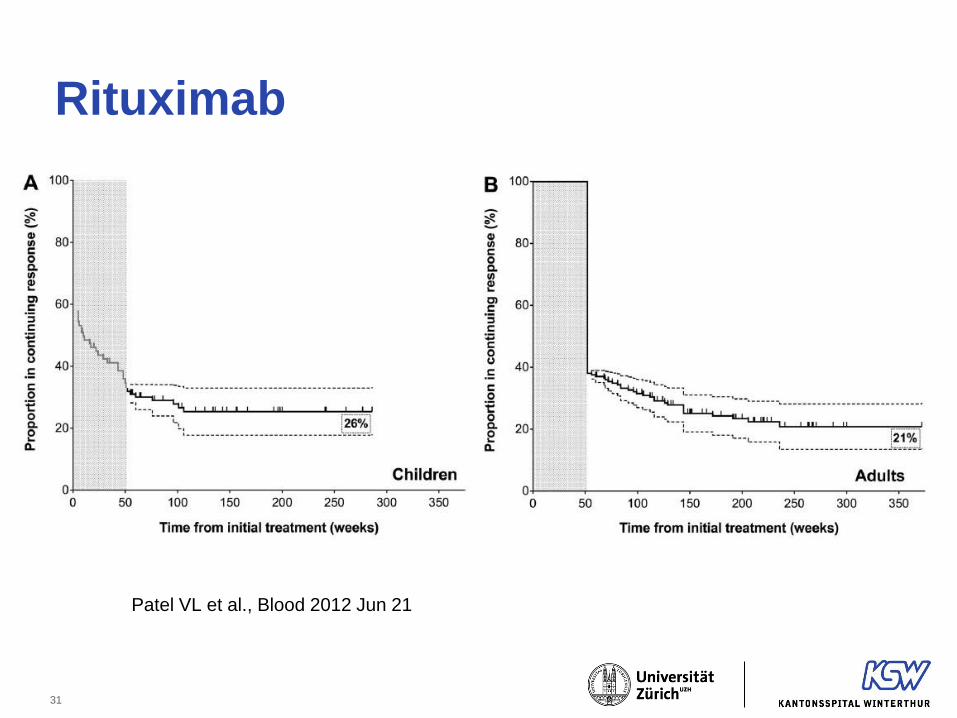
• With rituximab we can expect 21% of adult patients to be
without ITP-treatment after 5 years
Patel VL et al., Blood 2012 Jun 21
31
Rituximab
Patel VL et al., Blood 2012 Jun 21

32
Marc Michel: Immune Thrombocytopenia Nomenclature, Consensus Reports, and Guidelines: What Are the Consequences for Daily
Practice and Clinical Research? Seminars in Hematology Volume 50, Supplement 1 2013 S50 - S54
Which treatment in which phase of the disease?

33
• Newly diagnosed ITP (during the first 3 months):
• Be sure that steroids don’t work
• Personally I prefer dexamethason (4 days every 14-28 days)
• In clinically severe cases I give IVIg and wait for the action of
steroids (I don’t give up to early)
• In general: I avoid second line treatment
• Persistent and chronic ITP (3 – 12 months and later)
• Now I know that steroids did not work !
• I start with a TPO receptor agonist the patient gets stabilized.
• After stabilization I discuss the option of rituximab
• Splenectomy can be discussed in chronic phase
My approach in ITP

34
Conclusion
• At first diagnosis of thrombocytopenia:
• Combined evaluation of laboratory and clinical data
• Laboratory and clinical data determine further investigations
• Diagnostic algorithms can be helpful
• Thrombocytopenia during pregnancy
• In most cases not therapy is indicated or very low doses of
prednisone resolve the problem
• Immune thrombocytopenia
• Despite the number of treatment options: some cases still
stay very challenging!

35




















