The effect of lateral opening wedge distal femoral osteotomy on leg length

J Physiol 593.17 (2015) pp 3917–3928 3917
The
Jou
rnal
of
Phys
iolo
gy
The role of nitric oxide in passive leg movement-inducedvasodilatation with age: insight from alterationsin femoral perfusion pressure
H. Jonathan Groot1,2, Joel D. Trinity1,3, Gwenael Layec1,3, Matthew J. Rossman1,2, Stephen J. Ives4,David E. Morgan5, Amber Bledsoe5 and Russell S. Richardson1,2,3
1Geriatric Research, Education, and Clinical Centre, VAMC, Salt Lake City, UT, USA2Department of Exercise and Sport Science, University of Utah, Salt Lake City, UT, USA3Department of Internal Medicine, University of Utah, Salt Lake City, UT, USA4Health and Exercise Sciences Department, Skidmore College, Saratoga Springs, NY, USA5Department of Anesthesia, University of Utah, Salt Lake City, UT, USA
Key points
� The passive leg movement (PLM) model is a novel approach to assess vascular function.� Increasing femoral perfusion pressure (FPP) by moving from the supine to the upright-seated
posture augments the vasodilatory response to PLM in the young, with no effect in the old,but whether this augmented vasodilatation is nitric oxide (NO) dependent is unknown.
� Using an intra-arterial infusion of NG-monomethyl-L-arginine (L-NMMA) to inhibit nitricoxide synthase (NOS), the posture-induced increases in the PLM responses in the young werenearly ablated, with no effect of NOS inhibition in the old.
� Therefore, PLM in combination with alterations in posture can be used to determine changesin NO-mediated vasodilatation with age, and thus, may be a clinically useful tool for assessingNO bioavailability across the human lifespan.
Abstract We sought to better understand the contribution of nitric oxide (NO) to passiveleg movement (PLM)-induced vasodilatation with age, with and without a posture-inducedincrease in femoral perfusion pressure (FPP). PLM was performed in eight young (24 ± 1 years)and eight old (74 ± 3 years) healthy males, with and without NO synthase inhibition viaintra-arterial infusion of NG-monomethyl-L-arginine (L-NMMA) into the common femoralartery in both the supine and upright-seated posture. Central and peripheral haemodynamicresponses were determined second-by-second with finger photoplethysmography and Dopplerultrasound, respectively. PLM-induced increases in heart rate, stroke volume, cardiac outputand reductions in mean arterial pressure were similar between age groups and conditions. Inthe young, L-NMMA attenuated the peak change in leg vascular conductance (�LVCpeak) inboth the supine (control: 7.4 ± 0.9; L-NMMA: 5.2 ± 1.1 ml min−1 mmHg−1, P < 0.05) andupright-seated (control: 12.3 ± 2.0; L-NMMA: 6.4 ± 1.0 ml min−1 mmHg−1, P < 0.05) posture,with no significant change in the old (supine control: 4.2 ± 1.3; supine L-NMMA: 3.4 ± 0.8;upright-seated control: 4.5 ± 0.8; upright-seated L-NMMA: 3.4 ± 0.8 ml min−1 mmHg−1,P > 0.05). Increased FPP augmented the �LVCpeak in the young control condition only (P < 0.05).In the upright-seated posture, NOS inhibition attenuated the FPP-induced augmentation of rapidvasodilatation in the young (control: 1.25 ± 0.23; L-NMMA: 0.74 ± 0.11 ml min−1 mmHg−1 s−1;P < 0.05), but not the old (control: 0.37 ± 0.07; L-NMMA: 0.25 ± 0.07 ml ml min−1 mmHg−1 s−1;
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society DOI: 10.1113/JP270195

3918 J. H. Groot and others J Physiol 593.17
P > 0.05). These data reveal that greater FPP increases the role of NO in PLM-induced vaso-dilatation in the young, but not the old, due to reduced NO bioavailability with age. Therefore,PLM involving alterations in posture may be useful to determine changes in NO bioavailabilitywith age.
(Received 20 January 2015; accepted after revision 9 June 2015; first published online 24 June 2015)Corresponding author R. S. Richardson: VA Medical Centre, Bldg 2, Rm 1D25, 500 Foothill Drive, Salt Lake City, UT84148, USA. Email: [email protected]
Abbreviations AUC, area under the curve; CFA, common femoral artery; CO, cardiac output; ECG, electrocardiogram;FMD, flow-mediated dilatation; FPP, femoral perfusion pressure; HR, heart rate; LBF, leg blood flow; L-NMMA,NG-monomethyl-L-arginine; LVC, leg vascular conductance; MAP, mean arterial pressure; NO, nitric oxide; PLM,passive leg movement; SV, stroke volume.
Introduction
Vascular function declines with advancing age and hasbeen linked to the pathogenesis of cardiovascular disease(Moncada et al. 1991; Lloyd-Jones & Bloch, 1996;Taddei et al. 1997; Ross, 1999; Kawashima, 2004). Theendothelium-derived vasodilator nitric oxide (NO) hasbeen demonstrated to be cardio-protective (Moncadaet al. 1991; Lloyd-Jones & Bloch, 1996), and is animportant marker of vascular function (Anderson et al.1995). Therefore, the ability to measure NO bioavailabilityacross the lifespan has important clinical implications.Recently, the validity of the most widely utilized method ofnon-invasively assessing NO-mediated vascular function,brachial artery flow-mediated dilatation (FMD), has beencalled into question (Tschakovsky & Pyke, 2005; Pyke et al.2010; Parker et al. 2011; Wray et al. 2013). Additionally,evidence that limb-specific vascular ageing leads to greaterdysfunction in the arteries of the lower limbs suggests thatbrachial artery FMD may not be an appropriate measureof systemic vascular health (Newcomer et al. 2005; Donatoet al. 2006; Wray et al. 2010). Thus, there is a growing inter-est in examining alternative methods with which to assesscardiovascular health.
Passive leg movement (PLM) transiently increases legblood flow (LBF) and leg vascular conductance (LVC)(McDaniel et al. 2010; Groot et al. 2013). Previously,in the young, although the initial rapid PLM-inducedvasodilatation was documented to be NO independent,the majority (�80–90%) of the hyperaemic response toPLM reflects NO-dependent vasodilatation (Mortensenet al. 2012; Trinity et al. 2012). In the old, boththe rapid and the overall vasodilatory responses wereattenuated compared to the young, suggesting bothimpaired non-NO-dependent and NO-dependent vaso-dilatation with age (Groot et al. 2013; Trinity et al. 2015).Due to the dominant role of NO in the PLM-inducedvasodilatation in the young, and the recognized fall inNO bioavailability with age, the attenuated PLM-inducedvasodilatation in the old has been suggested to be due,
primarily, to NO-mediated vascular dysfunction (Grootet al. 2013; Trinity et al. 2015).
Due to the effects of gravity, the upright-seatedposture, compared to the supine posture, generatesa hydrostatic column that differentially increases bothvenous and arterial pressure in the legs (Rowell, 1993).The greater absolute increase in arterial pressure withthe upright-seated posture results in increased femoralperfusion pressure (FPP = arterial pressure – venouspressure), the driving force for blood across thevascular bed of the leg. In the young, the change inposture augments the hyperaemic response to PLM,with no effect in the old (Groot et al. 2013). Thedifference in PLM-induced hyperaemia from the supine toupright-seated posture (upright-seated �LVCpeak minussupine �LVCpeak) has been suggested to represent a vaso-dilatory reserve in the young that is not present in theelderly (Groot et al. 2013). However, whether this vaso-dilatory reserve represents NO bioavailability or someother vasoactive factor is unknown.
Consequently, with the goal of further advancingthe clinical relevance of PLM by providing mechanisticinsight, the purpose of this study was to elucidate therole of NO, with and without increases in FPP, in thevasodilatation induced by PLM with age. We hypothesizedthat (1) the initial rapid vasodilatation, which is reducedin both the supine and upright-seated posture in the old,and augmented by increased FPP in the young only, willbe unaffected by NOS blockade across both groups andconditions, suggesting a reduced non-NO-dependentcontribution to PLM-induced vasodilatation with age;and (2) the greater vasodilatory reserve revealed duringPLM with increased FPP in the young is the resultof NO-dependent vasodilatation and, therefore, NOSblockade will ablate the vasodilatory reserve. In contrast,due to a general decrease in NO bioavailability with age,the PLM-induced hyperaemic response in the elderly willremain unchanged despite alterations in FPP or NOSblockade, indicating that the lack of a PLM-inducedvasodilatory reserve with age is due to attenuated
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

J Physiol 593.17 Nitric oxide and PLM-induced vasodilatation with age 3919
NO-dependent vascular function. If proven to be correct,these finding will support the assessment of vasodilatoryreserve as a method to assess NO-bioavailability acrossthe lifespan.
Methods
Subjects
Sixteen healthy men (8 young, 8 old) participated in thisstudy. Subjects were included based on an absence of overtcardiovascular or metabolic disease, and aged 18–30 yearsfor the young, and greater than 65 years for the old. TheInstitutional Review Boards of the University of Utahand the Salt Lake City VA Medical Centre approved allprocedures, and the study conformed to the standards setby the Declaration of Helsinki. Written informed consentwas obtained from each participant prior to inclusion inthe study.
Experimental protocol
Prior to the experimental protocol, all subjects reportedto the laboratory for a PLM familiarization trial. Duringthis trial the participants were acquainted with theexperimental procedures and a fasting blood draw andanthropometric measurements were taken.
Subjects arrived for the experimental trial fasted, andhaving refrained from vigorous exercise for 24 h. Theright common femoral artery (CFA) was catheterizedunder sterile conditions using the Seldinger technique.Following instrumentation, subjects were positioned ineither the supine or upright-seated posture. The orderingof body posture for all four passive movement trials wasassigned using a counterbalanced design. Due to thepotential long lasting effects of L-NMMA, the control(saline infusion) trials were always performed in advanceof the L-NMMA infusion. Following catheter placement,subjects rested for at least 20 min before commencementof the experimental protocol to ensure that centraland peripheral haemodynamic measures returned toresting values. An automated occlusion cuff (Hokansen,Bellevue, WA, USA) was placed on the proximal crusjust distal to the knee and inflated to 250 mmHg priorto the initiation of the L-NMMA or saline infusion, andthroughout the PLM, to ensure that the infusate remainedin the thigh. Haemodynamic measurements were thenperformed during 60 s of resting baseline with the legheld at a 180 deg knee joint angle, followed by 2 min ofpassive knee flexion–extension through a 90 degree rangeof motion (180–90°) at 1 Hz. For the duration of the trial,the contralateral control leg remained motionless withthe knee joint supported and extended at a 180 deg kneejoint angle. A member of the research team performed
PLM with real-time feedback provided by a goniometer(Vishay Intertechnology Inc., Malvern, PA, USA) anddigital display to ensure full range of motion. Cadence wasmaintained utilizing a metronome initiated prior to thestart of baseline data collection. Subjects were instructedto remain relaxed and to resist the urge to kick duringthe PLM protocol. The protocol was performed a totalof four times in each subject such that both supine andupright-seated PLM was performed under control andL-NMMA conditions, with a rest period of at least 20 minbetween trials.
L-NMMA infusion. L-NMMA (Bachem, Bubendorf,Switzerland) was diluted in normal saline from 250 mglyophilized powder to a concentration of 5 mg ml−1.Anthropometrically determined thigh volume was usedto calculate drug dosing. Prior to baseline measures,the L-NMMA was infused at a loading dose of0.48 mg dl−1 min−1 for 5 min. During the 60 s baseline,and throughout the 2 min of PLM, L-NMMA was infusedat a maintenance dose of 0.24 mg dl−1 min−1. L-NMMAdosing was based on previous research demonstratinga significant reduction in PLM-induced hyperaemia inyoung males at 0.24 mg dl−1 min−1 (Trinity et al. 2012).During control trials, normal saline was infused at anidentical rate and duration as the L-NMMA. The infusionprotocol, including the loading and maintenance doses,was identical for each PLM trial, with cessation of theL-NMMA/saline infusion during the 20 min between eachtrial.
Measurements
Central haemodynamic variables. Mean arterial pressure(MAP) was determined by finger photoplethysmographywith a Finometer (Finapres Medical Systems, Amsterdam,The Netherlands) positioned at heart level. The Modelflowmethod was used to calculate stroke volume (SV;Beatscope, version 1.1, Amsterdam; Finapres MedicalSystems), heart rate (HR) was determined using anelectrocardiogram (ECG), and cardiac output (CO) wascalculated as SV multiplied by HR.
Peripheral haemodynamic variables. Measurements ofvessel diameter and blood velocity in the CFA wereperformed in the passively moved leg distal to theinguinal ligament and proximal to the bifurcation ofthe superficial and deep femoral artery using a Logic7 ultrasound system (General Electric Medical Systems,Milwaukee, WI, USA). The Logic 7 was equipped with alinear array transducer operating at an imaging frequencyof 14 MHz, which was properly situated to sustainan insonation angle of � 60 deg. Based on real-timeultrasound visualization, the sample volume was centred
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

3920 J. H. Groot and others J Physiol 593.17
within the vessel and maximized according to vessel size.CFA diameter was determined at a perpendicular anglealong the central axis of the scanned area, and bloodvelocity was measured using the same transducer witha frequency of 5 MHz. The catheter was inserted intothe superficial femoral artery and fed proximally into theCFA, passing through the Doppler ultrasound field ofview in the CFA. The catheter was advanced at least 3 cmproximal to the Doppler ultrasound transducer locationto allow adequate infusate mixing prior to entering thescanned area and minimize the potential direct impact ofthe infusate exiting the catheter on velocity measurements.Blood flow in millilitres per minute was automaticallycalculated by commercially available software (Logic 7)using CFA diameter and mean blood velocity (Vmean;angle corrected, and intensity weighted), as Vmeanπ (vesseldiameter/2)2 × 60. LVC was calculated as LBF divided byMAP, and LBF and LVC area under the curve (LBFAUC andLVCAUC) were calculated after normalizing for baseline.�LBFpeak and �LVCpeak were calculated as the peak minusthe baseline, and the vasodilatory reserve was calculated asupright-seated �LVCpeak minus supine �LVCpeak. Initial,rapid vasodilatation was assessed as the slope of the LVCincrease over time (first 7 s).
Anthropometrics. Body mass and height were measuredin kilograms and metres, respectively, and used to calculatebody mass index (BMI = body mass × height2). Thighvolume was calculated as previously described (Lawrensonet al. 2003), using triplicate measurements of thigh length,thigh circumference (proximal, middle, and distal), andskinfold.
Data acquisition and statistical analysis
MAP, HR, SV, and CO signals underwent analog-to-digitalconversion and were concomitantly obtained (200 Hz)using commercially available software (AcqKnowledge,Biopac Systems Inc., Goleta, CA, USA). CFA diameter andVmean were recorded on the ultrasound Doppler (GE Logic7). Baseline for all variables was determined as the averageof the 60 s of data prior to the start of PLM. During thePLM, all variables were analysed second-by-second forthe first 60 s, and smoothed using a 3 s rolling averageprior to final data analysis, while the second minute wasanalysed using 12 s averages. A 2 × 2×2 repeated measuresANOVA was used to determine significant differences inthe absolute change from baseline to peak for HR, SV, CO,MAP, LBF and LVC, and additionally AUC for LBF andLVC. Additionally, 2 × 2×2 repeated measures ANOVAwas used to compare the slope of LVC across the first 7 s ofPLM between groups, postures, and infusion conditions.A 2 × 2 repeated measures ANOVA was used to determinesignificant differences in the vasodilatory reserve between
Table 1. Subject characteristics
Young Old
n 8 8Age (years) 24 ± 1 74 ± 3#
Height (cm) 176 ± 2 176 ± 2Weight (kg) 73 ± 2 78 ± 4BMI (kg m–2) 24 ± 1 25 ± 2Thigh volume (dl) 71 ± 4 64 ± 4CFA diameter (cm) 0.90 ± 0.03 1.05 ± 0.07#
Glucose (mg dl–1) 77 ± 4 75 ± 5Cholesterol (mg dl–1) 156 ± 11 181 ± 13Triglycerides (mg dl–1) 101 ± 19 99 ± 17HDL (mg dl–1) 46 ± 3 51 ± 4LDL (mg dl–1) 98 ± 10 117 ± 9Haemoglobin (g dl–1) 15.7 ± 0.5 15.3 ± 0.3WBC (K μl–1) 6.3 ± 0.4 5.2 ± 0.2#
Neutrophil (K μl–1) 3.4 ± 0.4 2.9 ± 0.2Lymphocyte (K μl–1) 2.2 ± 0.2 1.5 ± 0.2#
Monocyte (K μl–1) 0.52 ± 0.03 0.47 ± 0.05
Values are means ± SEM. BMI, body mass index; CFA diameter,common femoral artery diameter; HDL, high density lipoproteincholesterol; LDL, low density lipoprotein cholesterol; WBC, whiteblood cell. #P < 0.05 significantly different vs. the young.
groups and infusion conditions. Student’s t tests wereutilized for subject characteristics and post hoc analysis,where appropriate. Significance was interpreted as aP value � 0.05. Data are presented as means ± SEM.
Results
Subjects
Subject characteristics are displayed in Table 1. Youngand old subjects, despite being separated by an averageof 50 years, were well matched for height, weight, BMI,thigh volume, and the majority of blood characteristics(white blood cell and lymphocyte count were significantlylower in the old subjects, P < 0.05).
Central haemodynamics
Baseline and PLM-induced peak change data for centralhaemodynamics are displayed in Table 2.
Baseline. Infusion of L-NMMA tended to increase restingMAP in both groups and body postures, but only reachedstatistical significance in the old supine condition. COalso tended to be lower with the L-NMMA infusion,an effect that reached significance in the young supineand old upright conditions, due to decreases in HR andSV, respectively. The upright-seated posture resulted inelevated HR and CO in the young during both saline and
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

J Physiol 593.17 Nitric oxide and PLM-induced vasodilatation with age 3921
Table 2. Central and peripheral haemodynamics
Rest
Supine Upright-seated
Young Old Young Old
Saline l-NMMA Saline l-NMMA Saline l-NMMA Saline l-NMMA
MAP (mmHg) 90 ± 2 95 ± 2 90 ± 2 97 ± 2∗ 87 ± 2 93 ± 2 87 ± 3 93 ± 4CO (1 min–1) 5.6 ± 0.4 5.0 ± 0.3∗ 5.1 ± 0.8 4.2 ± 0.7 6.0 ± 0.3† 5.7 ± 0.3† 4.9 ± 0.6 3.7 ± 0.7∗#
SV (ml beat–1) 100 ± 5 99 ± 6 93 ± 17 79 ± 13 101 ± 3 97 ± 3 87 ± 11 62 ± 12#
HR (beat min–1) 56 ± 2 52 ± 2∗ 59 ± 4 60 ± 5 59 ± 2f 58 ± 3† 67 ± 5† 67 ± 7†
LBF (ml min–1) 340 ± 36 194 ± 30∗ 231 ± 55 121 ± 44∗ 305 ± 55 196 ± 31∗ 187 ± 37 150 ± 26∗
LVC (ml min–1 mmHg–1) 3.6 ± 0.6 2.1 ± 0.3∗ 2.6 ± 0.6 1.3 ± 0.4∗ 3.1 ± 0.5 2.2 ± 0.4∗ 2.2 ± 0.5 1.7 ± 0.3
Passive leg movement
Supine Upright-seated
Young Old Young Old
Saline l-NMMA Saline l-NMMA Saline l-NMMA Saline l-NMMA
�MAPpeak (mmHg) −6 ± 1 −8 ± 2 −6 ± 2 −6 ± 1 −6 ± 1 −7 ± 2 −4 ± 2 −6 ± 2�COpeak (1 min) 0.8 ± 0.2 1.0 ± 0.3 1.3 ± 0.5 0.7 ± 0.3 1.0 ± 0.3 0.6 ± 0.2 1.0 ± 0.4 0.6 ± 0.3�SVpeat (ml beat–1) 7 ± 1 4 ± 1 11 ± 4 6 ± 2 8 ± 2 7 ± 2 11 ± 3 9 ± 5�HRpeak (beat min–1) 7 ± 2 11 ± 3 9 ± 4 8 ± 2 7 ± 2 7 ± 2 8 ± 5 9 ± 4�LBFpeak (ml min–1) 620 ± 87 494 ± 98∗ 372 ± 95# 330 ± 71 967 ± 144† 563 ± 80∗ 383 ± 60# 325 ± 75#
�LBFAUC (ml) 223 ± 52 128 ± 36∗ 170 ± 62 108 ± 38 378 ± 86† 167 ± 22∗ 183 ± 42# 120 ± 47�LVCpeat (ml min–1 mmHg–1) 7.4 ± 0.9 5.2 ± 1.1∗ 4.2 ± 1.3# 3.4 ± 0.8 12.3 ± 2.0† 6.4 ± 1.0∗ 4.5 ± 0.8# 3.4 ± 0.8#
�LVCAUC (ml/mmHg–1) 2.9 ± 0.6 1.4 ± 0.4∗ 1.9 ± 0.8# 1.1 ± 0.4 4.6 ± 1.1† 1.9 ± 0.3∗ 2.0 ± 0.5# 1.2 ± 0.5
Values are means ± SEM. MAP, mean arterial pressure; CO, cardiac output; SV, stroke volume; HR, heart rate; LBF, leg blood flow; LVC,leg vascular conductance; �peak, peak change from baseline; AUC, area under the curve. ∗P < 0.05 significantly different vs. the salinecondition, #P < 0.05 significantly different vs. the young, †P < 0.05 significantly different vs. the supine posture.
L-NMMA, but only an elevation in HR in the old (duringboth saline and L-NMMA), without an increase in CO. COand SV were significantly lower in the old upright-seatedL-NMMA condition compared to the young in the samecondition, with no other age-related differences.
Passive leg movement. PLM resulted in significantincreases in HR, SV, and CO, and a significant reductionin MAP in both groups and across all conditions, asevidenced by the peak change from rest in these centralhaemodynamic factors. However, there was no significantdifference between age groups, body postures, or infusiontype.
Peripheral haemodynamics
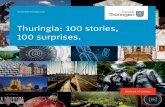
Baseline, PLM-induced peak change and area under thecurve data for peripheral haemodynamics are displayed inTable 2. Tracings for LVC, as well as �LVCpeak, and LVCAUC
are displayed in Fig. 1.
Baseline. Infusion of L-NMMA significantly reducedresting LBF and LVC in both groups, and across all
conditions, with the exception of LVC in the oldupright-seated posture, which was unaltered.
Passive leg movement. Due to the tendency for MAPto be elevated with NOS inhibition (Table 2), and thefocus of this study on vasodilatory capacity, the results anddiscussion of peripheral haemodynamics will be restrictedto LVC as an indication of vasodilatation. However, itshould be noted that the LBF response to PLM wassimilar to that for LVC. The older subjects demonstratedan attenuated PLM-induced �LVCpeak compared to theyoung in both the supine and upright-seated posturesduring saline infusion (Fig. 1B). Furthermore, increasedFPP elicited via the upright-seated posture augmentedthe PLM-induced �LVCpeak in the young, with noeffect in the old (Fig. 1B). Thus, the elderly lacked asignificant posture-induced vasodilatory reserve (Fig. 2).In the young, infusion of L-NMMA in both the supineand upright-seated posture reduced the PLM-induced�LVCpeak, with no change in the old (Fig. 1B, Fig. 3).Additionally, the magnitude of the reduction in �LVCpeak
during NOS inhibition in the young was greater in theupright-seated posture compared to supine (reduction
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

3922 J. H. Groot and others J Physiol 593.17
due to L-NMMA supine: 2.2 ± 0.7 ml min−1 mmHg−1,�30%; upright-seated: 6.0 ± 1.2 ml min−1 mmHg−1,�50%; P < 0.05, Fig. 3), resulting in a significantattenuation (�80%) in vasodilatory reserve capacity inthe young in the L-NMMA condition (Fig. 2). DuringL-NMMA infusion in the supine posture, �LVCpeak wasno longer different between young and old (Fig. 1B). A
similar pattern was observed when the data were expressedas area under the curve (Fig. 1C).
L-NMMA infusion had no significant effect on the rapidvasodilatation (first 7 s) in either the young (control:0.78 ± 0.10 ml ml min−1 mmHg−1 s−1; L-NMMA:0.71 ± 0.16 ml ml min−1 mmHg−1 s−1; P > 0.05) orthe old (control: 0.22 ± 0.12 ml ml min−1 mmHg−1 s−1;
SupineA
Time (s)
0 30 60 90 120
Leg V
asc
ula
r C
onduct
ance
(ml/m
in/m
mH
g)
Leg V
asc
ula
r C
onduct
ance
(ml/m
in/m
mH
g)
0
2
4
6
8
10
12
14
16
18Young SalineYoung L-NMMAOld SalineOld L-NMMA
BL
B
Pea
k C
ha
ng
e in
Leg
Va
scula
r C
onduct
ance
(m
l/min
/mm
Hg)
Pea
k C
ha
ng
e in
Leg V
asc
ula
r C
onduct
ance
(m
l/min
/mm
Hg)
Young Old0
2
4
6
8
10
12
14
16
SalineL-NMMA
#
C
Leg
Va
scula
r C
onduct
ance
AU
C(m
l/mm
Hg)
Leg
Va
scula
r C
onduct
ance
AU
C(m
l/mm
Hg)
0
1
2
3
4
5
6
7
Upright-seated
Time (s)
0 30 60 90 1200
2
4
6
8
10
12
14
16
18
BL
Young Old
Young Old Young Old
0
2
4
6
8
10
12
14
16
##
0
1
2
3
4
5
6
7
#
Figure 1. PLM-induced leg vascular conductance peak change and area under the curveA, leg vascular conductance (LVC, ml min−1 mmHg−1) in both the supine (left) and upright-seated (right) posturein the young (n = 8) and old (n = 8). Baseline (BL) indicates the average of the 60 s just prior to initiation of passiveleg movement (PLM). Dashed line at 0 s indicates the start of 2 min of PLM. B, peak change (�) in LVC. C, areaunder the curve (AUC) for LVC. ∗P < 0.05 significantly different vs. the saline condition, #P < 0.05 significantlydifferent vs. the young, †P < 0.05 significantly different vs. the supine posture. Data illustrated as means ± SEM.
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

J Physiol 593.17 Nitric oxide and PLM-induced vasodilatation with age 3923
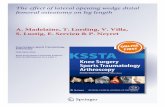
L-NMMA: 0.31 ± 0.09 ml ml min−1 mmHg−1 s−1;P > 0.05) in the supine posture (Fig. 4). However, inthe upright-seated posture, NOS inhibition significantlyattenuated the rapid vasodilatation in the young(control: 1.25 ± 0.23 ml ml min−1 mmHg−1 s−1;L-NMMA: 0.74 ± 0.11 ml ml min−1 mmHg−1 s−1;P < 0.05), with no such change in the old (control:0.37 ± 0.07 ml ml min−1 mmHg−1 s−1; L-NMMA:0.25 ± 0.07 ml ml min−1 mmHg−1 s−1; P > 0.05).
Young Old
Vaso
dila
tory
Rese
rve
(ml/m
in/m
mH
g)
0
1
2
3
4
5
6
7
SalineL-NMMA
#
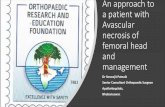
Figure 2. Contribution of nitric oxide to vasodilatory reservecapacity with ageThe difference in the PLM-induced peak change in leg vascularconductance (�LVCpeak, ml min−1 mmHg−1) between the supineand upright-seated posture (vasodilatory reserve) in the young(n = 8) compared to the old (n = 8) during infusion of saline orL-NMMA. ∗P < 0.05 significantly different vs. the saline condition,#P < 0.05 significantly different vs. the young. Data illustrated asmeans ± SEM.
Supine Upright-seated
-8
-7
-6
-5
-4
-3
-2
-1
0
YoungOld
Dru
g-I
nd
uce
d R
ed
uct
ion
inL
eg
Va
scu
lar
Co
nd
uct
an
ce P
ea
k C
ha
ng
e(m
l/min
/mm
Hg
)
# #
Figure 3. Reductions in the PLM-induced peak change in legvascular conductance during nitric oxide synthase inhibitionThe reduction in the PLM-induced peak change in leg vascularconductance (�LVCpeak, ml min−1 mmHg−1) due to intra-arterialinfusion of L-NMMA during the supine and upright-seated posturesin old (n = 8) and young (n = 8) subjects. †P < 0.05 significantlydifferent vs. the supine posture, #P < 0.05 significantly different vs.the young. Data illustrated as means ± SEM.
Additionally, the rapid vasodilatation in the older sub-jects was attenuated compared to the young in both bodypostures and drug conditions (Fig. 4, P < 0.05).
Discussion
With the goal of further advancing the clinical relevanceof PLM as an assessment of vascular function by providingmechanistic insight, this study sought to elucidate thecontribution of NO to PLM-induced vasodilatation withage, both with and without posture-induced increasesin FPP. Findings novel to this investigation include:(1) in young subjects, increased FPP augments the roleof NO in the PLM-induced vasodilatation; (2) NO playsa greater role in the rapid vasodilatory response withincreased FPP only in the young; and (3) a deficit inNO bioavailability is primarily responsible for the lackof upright posture-induced vasodilatory reserve capacityin the old. These findings, in combination with theobservation that the central haemodynamic responsesto PLM were not different between age groups orconditions, indicate that PLM-induced vasodilatation hasa significant NO-dependent component, and can be usedto discern age-related reductions in vascular function.This is particularly the case in the upright-seated post-ure. Furthermore, PLM incorporating an assessment ofthe vasodilatory reserve may be a useful tool to morecompletely characterize changes in NO bioavailabilityacross the lifespan.
The role of NO in PLM-induced vasodilatationwith age
Advancing age has a deleterious effect on NObioavailability and therefore NO-mediated vasodilatation(Egashira et al. 1993; DeSouza et al. 2000; Taddei et al. 2001;Newcomer et al. 2005; Al-Shaer et al. 2006). Utilizing thePLM model, our group has been able to identify differencesin the movement-induced vasodilatation between youngand old subjects (McDaniel et al. 2010; Groot et al. 2013)that appear to be mediated primarily by NO (Trinity et al.2012; Trinity et al. 2015).
Leg vascular conductance peak change and AUC. Inthe current investigation, we augmented FPP via theupright-seated posture in order to increase the stimulusto vasodilate, and subsequently attempted to block theNO-mediated portion of the resulting vasodilatation. Asa result of NOS inhibition achieved by intra-arterialinfusion of L-NMMA, in the young the �LVCpeak in thesupine posture was reduced by �30%. Interestingly, witha posture-induced increase in FPP in the young, NOSinhibition caused a significantly greater reduction in the�LVCpeak of �50% (Table 2, Fig. 1B, Fig. 3). This suggests
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

3924 J. H. Groot and others J Physiol 593.17
that the increase in FPP with the upright-seated postureaugments the endothelial shear stimulus during the PLM,and due to greater NO bioavailability, results in a greaterrelease of NO that explains the subsequently augmented�LVCpeak in the young. Therefore, while it is clear that NOplays a significant role during PLM-induced vasodilatationin the supine posture in the young, these data reveal amuch greater reliance on NO-mediated vasodilatation inthe upright-seated posture.
In the old, �LVCpeak and LVCAUC were significantlylower compared to the young in both the supineand upright-seated posture during the saline infusion,indicating a reduced PLM-induced vasodilatory response,as previously reported (Groot et al. 2013). In contrast tothe young, NOS inhibition in the old had no significanteffect on PLM-induced �LVCpeak in either body post-ure. LVCAUC tended to be reduced in both the supine(P=0.12) and upright-seated (P=0.08) posture (Fig. 1C),but the magnitude of these effects were much attenuatedcompared to the young. Taken together these data suggestthat, while some relatively small contribution of NOto PLM-induced vasodilatation remains with age, thedifferences in PLM-induced LVC between young and oldare largely due to reduced NO bioavailability with age.
Vasodilatory reserve capacity. The ability for the�LVCpeak to increase when moving from the supineto upright-seated posture has been postulated torepresent a vasodilatory reserve capacity (Groot et al.2013). Previously, our group has demonstrated that theupright-seated posture elicits a �7 mmHg increase inFPP in both young and old subjects, as measured directlyin the common femoral artery and vein. IncreasingFPP has the potential to augment endothelial shearstimulus at the onset of PLM, leading to a greater
release of NO. In the young, greater FPP did indeedresult in a more rapid and sustained NO-mediatedvasodilatation that ultimately increased the peak hyper-aemic response to PLM, revealing a significant vaso-dilatory reserve (4.9 ± 1.4 ml min−1 mmHg−1, P < 0.05,Fig. 2). In contrast, increased FPP had no effect onany of the central or peripheral haemodynamic factorsduring PLM in the old, and therefore, there was noevidence of a significant vasodilatory reserve, furtherdifferentiating PLM-induced vascular responses in theyoung and old. Additionally, NOS inhibition reducedthe vasodilatory reserve in the young nearly fivefold(saline: 4.9 ± 1.4 ml min−1 mmHg−1; L-NMMA:1.1 ± 0.9 ml min−1 mmHg−1, P < 0.05), so that youngsubjects’ vasodilatory responses were no longer differentfrom the old during saline (0.3 ± 0.6 ml min−1 mmHg−1,P = 0.57), or L-NMMA (0.1 ± 0.7 ml min−1 mmHg−1,P=0.27) conditions. Finally, due to the lack of a significantvasodilatory reserve under saline conditions in the old,the infusion of L-NMMA had no effect on their vaso-dilatory reserve (P = 0.77). The contribution of NO tothe vasodilatory reserve is clear, and provides furtherevidence that old subjects have reduced NO bioavailability,as assessed by the PLM model with alterations inposture.
PLM-induced rapid vasodilatation. The initial, rapidhyperaemic response to PLM in the supine posture haspreviously been suggested to represent NO-independentvasodilatation. Indeed, alterations in thigh muscle length,causing mechanical deformation of the vascular beds,may initiate this predominantly NO-independent cascadeof events (Clifford et al. 2006; McDaniel et al. 2010; Kirbyet al. 2012) that ultimately results in NO-dependentvasodilatation (Trinity et al. 2012). Furthermore, in the
Supine Upright-seated
Time (s)0 1 2 3 4 5 6 7
Leg V
asc
ula
r C
onduct
ance
(ml/m
in/m
mH
g)
0
1
2
3
4
5
6
7
8
9Young SalineYoung L-NMMAOld SalineOld L-NMMA
#
#
Time (s)0 1 2 3 4 5 6 7
0
1
2
3
4
5
6
7
8
9
#
#
Figure 4. Effects of altered femoral perfusion pressureand age on the contribution of nitric oxide (NO) toPLM-induced rapid vasodilatationThe slopes calculated for the increase in the leg vascularconductance (LVC, ml min−1 mmHg−1) over time (7 s) reveala reduced NO-independent contribution to rapidvasodilatation with age in the supine posture (left). Increasedfemoral perfusion pressure (FPP) (upright-seated) resulted ina more rapid onset of NO-mediated vasodilatation in theyoung (n = 8), with no effect in the old (n = 8). ∗P < 0.05significantly different vs. the saline condition, #P < 0.05significantly different vs. the young, †P < 0.05 significantlydifferent vs. the supine posture. Data illustrated asmeans ± SEM.
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

J Physiol 593.17 Nitric oxide and PLM-induced vasodilatation with age 3925
old, this rapid vasodilatory response to PLM is reducedcompared to the young (Groot et al. 2013). The currentinvestigation again revealed an attenuated PLM-inducedrapid vasodilatation in the old while in the supine posture,with no effect of NOS inhibition in either age group(Fig. 4), supporting the notion that the rapid vasodilatoryresponse in the supine posture is NO independent andreduced with age. Similar to these findings, Carlson et al.(2008) demonstrated that rapid vasodilatation followinga single forearm muscle contraction was reduced with ageat 10, 20, and 40% of maximal voluntary contraction, andthis was evident within one cardiac cycle post contraction.Current evidence suggests that increased α-adrenergictone, as well as reduced potassium-mediated smoothmuscle hyperpolarization and prostaglandin-mediatedvasorelaxation, may contribute to this age-associatedreduction in NO-independent rapid vasodilatation in theold (Brock et al. 1998; Casey & Joyner, 2012; Crecelius et al.2013).
Novel to this investigation is the assessment ofthe contribution of NO to PLM-induced rapid vaso-dilatation during increased FPP. Indeed, contrary toour expectations, NOS inhibition during PLM in theupright-seated posture significantly reduced the rapidvasodilatory response in the young, and resulted in aslope similar to that of the young in the supine post-ure (Fig. 4). This increase in the rate of PLM-inducedrapid vasodilatation when moving from the supine tothe upright-seated posture, which can be ablated byNOS blockade, implies an earlier onset of NO-mediatedvasodilatation in the young driven by an increase inFPP. The old, however, were not affected by either theincrease in FPP, or the inhibition of NOS, as evidencedby the unaltered rate of change in LVC, indicating that,unlike the young, increasing FPP does not invoke anNO-dependent rapid vasodilatory response in the old.In support of a role for NO in rapid vasodilatationin certain circumstances, it was previously documentedthat NOS inhibition significantly attenuated the increasein vascular conductance following a single forearmcontraction (Brock et al. 1998; Crecelius et al. 2013), aswell as the slope of forearm vascular conductance overtime from baseline to peak hyperaemia during continuousforearm contraction in young subjects (Casey et al. 2013).These prior studies set a precedent for NO as an importantfactor in rapid vasodilatation; however, to the best ofour knowledge, the current investigation is the first toelucidate the contribution of NO to the rapid vaso-dilatation following mechanical deformation of vascularbeds in the leg.
Taken together, these data demonstrate the diminishedrole for NO, particularly with increased FPP, inPLM-induced vasodilatation with age. While the rapidvasodilatory response suggests that NO-independentmechanisms are also reduced with age, the increasing
role of NO in this movement-induced vasodilatation withgreater FFP is clearly attenuated in healthy older subjectscompared to their young counterparts.
Passive leg movement as a clinically relevantassessment of NO-mediated vasodilatation
Due to the antiatherogenic properties of NO, theassessment of NO bioavailability is an important clinicaloutcome. Specifically, NO is associated with the inhibitionof platelet aggregation, leukocyte adhesion, and smoothmuscle cell migration and proliferation (Lloyd-Jones& Bloch, 1996). NO-mediated vasodilatation has beenquantified in both human and animal models bystimulating the NO pathway utilizing the predominantlyNO-mediated vasodilator acetylcholine (ACh) or bluntingNO production with a NOS inhibitor, such as L-NMMA.In aged rats, the vasodilatory response to ACh is reducedcompared to their young counterparts (Trott et al. 2009;Donato et al. 2013). In humans, intra-arterial infusion ofACh into the brachial (DeSouza et al. 2000; Taddei et al.2001; Newcomer et al. 2005; Al-Shaer et al. 2006) andcoronary (Vita et al. 1990; Egashira et al. 1993) arteries, aswell as NOS inhibition during concomitant ACh infusionin the brachial artery (Taddei et al. 2001), have revealedan attenuated NO-mediated vasodilatation in the old.However, due to the invasive nature of these experimentaltechniques, it remains impractical to perform these testsclinically.
The flow-mediated vasodilatation (FMD) test followingischaemic cuff occlusion, typically performed in thebrachial artery, has been used as a non-invasive methodof assessing vascular function. The FMD test does notrequire invasive arterial catheters or the infusion ofvasoactive drugs. However, even when following pre-viously established guidelines for performing the FMD test(Harris et al. 2010), results depend on the ability of thesonographer to accurately image both the superficial anddeep walls of the brachial artery in order to obtain precisemeasurement of small changes in diameter. The long livedpopularity for the FMD test has been largely based onearly studies revealing a correlation between brachial FMDand presence of coronary artery dysfunction (Andersonet al. 1995), but the validity of brachial artery FMD as anindicator of NO bioavailability has recently been calledinto question (Tschakovsky & Pyke, 2005; Parker et al.2011; Wray et al. 2013). Therefore, there is a growing inter-est in developing an alternative measure of NO-mediatedvascular function.
Previously, the PLM model has been used todifferentiate the movement-induced hyperaemia, andtherefore vasodilatation, between young and old sub-jects (McDaniel et al. 2010; Groot et al. 2013). In thecurrent study, the acute reduction in NO bioavailability,achieved by NOS inhibition, greatly attenuated the overall
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

3926 J. H. Groot and others J Physiol 593.17
hyperaemic response to PLM (60–80%, Figs 1 and 3), therapid vasodilatory response in the upright-seated posture(Fig. 4), and the vasodilatory reserve in the young (Fig. 2),with little to no effect in the old. Furthermore, in clinicalpopulations known to have vascular dysfunction, suchas heart transplant (Hayman et al. 2010), and peripheralartery disease patients (Mortensen et al. 2012), PLM hasbeen able to detect significantly attenuated vasodilatoryresponses compared to healthy controls. Therefore, thePLM model may be a useful clinical tool for detectingchanges in NO bioavailability with age or pathology.
The data presented here further our understandingof the role of NO in PLM-induced vasodilatation bydemonstrating the importance of increased FPP, not onlyin augmenting the temporal and peak NO release in theyoung, but also in detecting reductions in NO-mediatedvasodilatation in the old. As the common femoral arterydoes not dilate, the PLM test, in contrast to brachialartery FMD, does not rely upon the measurement ofsmall changes in diameter, but rather the relativelysimple measurement of blood velocity in the easilyimaged common femoral artery for the calculation ofblood flow and, in combination with blood pressure,vascular conductance. This eliminates the need for morechallenging high-resolution imaging and subsequentlyspecific image analysis software, making the PLM testrelatively easy to perform. Furthermore, PLM is anon-invasive test that could be used on a wide range ofclinical populations. Finally, limb-specific vascular agingleads to greater vascular dysfunction in the lower limbs(Nishiyama et al. 2008; Wray et al. 2010), possibly makingan assessment of vascular function in the legs, such asPLM, more clinically relevant than brachial artery FMDfor the assessment of vascular health. Taken together, ourfindings support examination of the vasodilatory responseduring the PLM test as a clinically relevant assessment ofNO bioavailability and vascular function with age.
Experimental considerations
This study measured arterial pressure at heart level inboth the supine and upright-seated posture instead ofdirectly measuring common femoral arterial and venouspressures, as we did previously (Groot et al. 2013).Interestingly, the measurement of heart level arterialpressure is unaffected by posture, while femoral pre-ssures are differentially effected by moving from thesupine to the upright-seated posture, such that femoralperfusion pressure increases by �7 mmHg (Groot et al.2013). Due to these concomitant differential effects ofpostural change, measuring arterial pressure at heartlevel overestimates leg vascular conductance in theupright-seated posture. However, the overestimation isrelatively minimal (�6%) and does not alter the inter-pretation of the results. Furthermore, as our previous
measurements of femoral perfusion pressure indicateda similar effect of postural change in both young andold subjects, the calculation of leg vascular conductancewould be equally overestimated in both groups, havingno qualitative impact on the findings of this study. Thishaving been said, it must be acknowledged that the mostaccurate assessment of perfusion pressure would entailthe simultaneous measurement of pressure in the arteryand vein immediately entering and exiting, respectively,the region being assessed (prior to any venous valves thatmay alter distal pressure assessments) and currently, inhumans, this is not possible. This is a limitation of thecurrent study and all other studies that have relied uponpressures assessed in the common femoral artery and veinto imply leg perfusion pressure.
Although the ordering of body posture for all fourpassive movement trials was assigned using a counter-balanced design, due to the potential long lasting effects ofL-NMMA, the control (saline infusion) trials were alwaysperformed in advance of the L-NMMA infusion. Thus,the potential for an ordering effect cannot be ruled out;however, due to the otherwise balanced design and theclarity of the results, this is unlikely to have had an impacton the current findings.
Conclusions
Alterations in FPP during PLM in the young and old havefurther elucidated the role of NO in movement-inducedvasodilatation with age. Specifically, in the young, greaterFPP increased the contribution of NO during PLM,leading to a more rapid onset of NO-mediated vaso-dilatation and a subsequently augmented peak changeand overall hyperaemic response. This implicates NO asprimarily responsible for the vasodilatory reserve in theyoung. However, due to reduced NO bioavailability withage, the old were unable to take advantage of the increasedFPP-induced stimulus to vasodilate. Therefore, PLM incombination with alterations in posture can be used todetermine changes in NO-mediated vasodilatation withage, and thus, may be a clinically useful tool for assessingNO bioavailability.
References
Al-Shaer MH, Choueiri NE, Correia ML, Sinkey CA, Barenz TA& Haynes WG (2006). Effects of aging and atherosclerosis onendothelial and vascular smooth muscle function inhumans. Int J Cardiol 109, 201–206.
Anderson TJ, Uehata A, Gerhard MD, Meredith IT, Knab S,Delagrange D, Lieberman EH, Ganz P, Creager MA, YeungAC et al. (1995). Close relation of endothelial function in thehuman coronary and peripheral circulations. J Am CollCardiol 26, 1235–1241.
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

J Physiol 593.17 Nitric oxide and PLM-induced vasodilatation with age 3927
Brock RW, Tschakovsky ME, Shoemaker JK, Halliwill JR, JoynerMJ & Hughson RL (1998). Effects of acetylcholine and nitricoxide on forearm blood flow at rest and after a single musclecontraction. J Appl Physiol (1985) 85, 2249–2254.
Carlson RE, Kirby BS, Voyles WF & Dinenno FA (2008).Evidence for impaired skeletal muscle contraction-inducedrapid vasodilation in aging humans. Am J Physiol Heart CircPhysiol 294, H1963–H1970.
Casey DP & Joyner MJ (2012). Influence of alpha-adrenergicvasoconstriction on the blunted skeletal musclecontraction-induced rapid vasodilation with aging. J ApplPhysiol (1985) 113, 1201–1212.
Casey DP, Mohamed EA & Joyner MJ (2013). Role of nitricoxide and adenosine in the onset of vasodilation duringdynamic forearm exercise. Eur J Appl Physiol 113, 295–303.
Clifford PS, Kluess HA, Hamann JJ, Buckwalter JB & JasperseJL (2006). Mechanical compression elicits vasodilatation inrat skeletal muscle feed arteries. J Physiol 572, 561–567.
Crecelius AR, Kirby BS, Luckasen GJ, Larson DG & DinennoFA (2013). Mechanisms of rapid vasodilation after a briefcontraction in human skeletal muscle. Am J Physiol HeartCirc Physiol 305, H29–H40.
DeSouza CA, Shapiro LF, Clevenger CM, Dinenno FA,Monahan KD, Tanaka H & Seals DR (2000). Regular aerobicexercise prevents and restores age-related declines inendothelium-dependent vasodilation in healthy men.Circulation 102, 1351–1357.
Donato AJ, Uberoi A, Wray DW, Nishiyama S, Lawrenson L &Richardson RS (2006). Differential effects of aging on limbblood flow in humans. Am J Physiol Heart Circ Physiol 290,H272–H278.
Donato AJ, Walker AE, Magerko K, Bramwell RC, Black AD,Henson GD, Lawson BR, Lesniewski LA & Seals DR (2013).Life-long caloric restriction reduces oxidative stress andpreserves nitric oxide bioavailability and function in arteriesof old mice. Aging Cell 12, 772–783.
Egashira K, Inou T, Hirooka Y, Kai H, Sugimachi M, Suzuki S,Kuga T, Urabe Y & Takeshita A (1993). Effects of age onendothelium-dependent vasodilation of resistance coronaryartery by acetylcholine in humans. Circulation 88, 77–81.
Groot HJ, Trinity JD, Layec G, Rossman MJ, Ives SJ &Richardson RS (2013). Perfusion pressure andmovement-induced hyperemia: evidence of limited vascularfunction and vasodilatory reserve with age. Am J PhysiolHeart Circ Physiol 304, H610–H619.
Harris RA, Nishiyama SK, Wray DW & Richardson RS (2010).Ultrasound assessment of flow-mediated dilation.Hypertension 55, 1075–1085.
Hayman MA, Nativi JN, Stehlik J, McDaniel J, Fjeldstad AS,Ives SJ, Walter Wray D, Bader F, Gilbert EM & RichardsonRS (2010). Understanding exercise-induced hyperemia:central and peripheral hemodynamic responses to passivelimb movement in heart transplant recipients.Am J Physiol Heart Circ Physiol 299, H1653–H1659.
Kawashima S (2004). Malfunction of vascular control inlifestyle-related diseases: endothelial nitric oxide (NO)synthase/NO system in atherosclerosis. J Pharmacol Sci 96,411–419.
Kirby BS, Crecelius AR, Voyles WF & Dinenno FA (2012).Impaired skeletal muscle blood flow control with advancingage in humans: attenuated ATP release and local vasodilationduring erythrocyte deoxygenation. Circ Res 111, 220–230.
Lawrenson L, Poole JG, Kim J, Brown C, Patel P & RichardsonRS (2003). Vascular and metabolic response to isolated smallmuscle mass exercise: effect of age. Am J Physiol Heart CircPhysiol 285, H1023–H1031.
Lloyd-Jones DM & Bloch KD (1996). The vascular biology ofnitric oxide and its role in atherogenesis. Ann Rev Med 47,365–375.
McDaniel J, Hayman MA, Ives S, Fjeldstad AS, Trinity JD, WrayDW & Richardson RS. (2010). Attenuated exercise inducedhyperaemia with age: mechanistic insight from passive limbmovement. J Physiol 588, 4507–4517.
Moncada S, Palmer RM & Higgs EA (1991). Nitric oxide:physiology, pathophysiology, and pharmacology. PharmacolRev 43, 109–142.
Mortensen SP, Askew CD, Walker M, Nyberg M & Hellsten Y(2012). The hyperaemic response to passive leg movement isdependent on nitric oxide; a new tool to evaluate endothelialnitric oxide function. J Physiol 590, 4391–4400.
Newcomer SC, Leuenberger UA, Hogeman CS & Proctor DN(2005). Heterogeneous vasodilator responses of humanlimbs: influence of age and habitual endurance training. AmJ Physiol Heart Circ Physiol 289, H308–H315.
Nishiyama SK, Wray DW & Richardson RS (2008). Agingaffects vascular structure and function in a limb-specificmanner. J Appl Physiol 105, 1661–1670.
Parker BA, Tschakovsky ME, Augeri AL, Polk DM, ThompsonPD & Kiernan FJ (2011). Heterogenous vasodilator pathwaysunderlie flow-mediated dilation in men and women. Am JPhysiol Heart Circ Physiol 301, H1118–H1126.
Pyke K, Green DJ, Weisbrod C, Best M, Dembo L, O’Driscoll G& Tschakovsky M (2010). Nitric oxide is not obligatory forradial artery flow-mediated dilation following release of 5 or10 min distal occlusion. Am J Physiol Heart Circ Physiol 298,H119–H126.
Ross R (1999). Atherosclerosis – an inflammatory disease. NewEng J Med 340, 115–126.
Rowell LB (1993). Human Cardiovascular Control. OxfordUniversity Press, New York.
Taddei S, Virdis A, Ghiadoni L, Salvetti G, Bernini G, MagagnaA & Salvetti A (2001). Age-related reduction of NOavailability and oxidative stress in humans. Hypertension 38,274–279.
Taddei S, Virdis A, Mattei P, Ghiadoni L, Fasolo CB, Sudano I& Salvetti A (1997). Hypertension causes premature aging ofendothelial function in humans. Hypertension 29,736–743.
Trinity JD, Groot HJ, Layec G, Rossman MJ, Ives SJ, MorganDE, Gmelch BS, Bledsoe AD & Richardson RS (2015).Passive leg movement and nitric oxide-mediated vascularfunction: The impact of age. Am J Physiol Heart Circ Physiol308, H672–H679.
Trinity JD, Groot HJ, Layec G, Rossman MJ, Ives SJ, Runnels S,Gmelch B, Bledsoe A & Richardson RS (2012). Nitric oxideand passive limb movement: a new approach to assessvascular function. J Physiol 590, 1413–1425.
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society

3928 J. H. Groot and others J Physiol 593.17
Trott DW, Gunduz F, Laughlin MH & Woodman CR (2009).Exercise training reverses age-related decrements inendothelium-dependent dilation in skeletal muscle feedarteries. J Appl Physiol (1985) 106, 1925–1934.
Tschakovsky ME & Pyke KE (2005). Counterpoint:Flow-mediated dilation does not reflect nitricoxide-mediated endothelial function. J Appl Physiol (1985)99, 1235–1237; discussion 1237–1238.
Vita JA, Treasure CB, Nabel EG, McLenachan JM, Fish RD,Yeung AC, Vekshtein VI, Selwyn AP & Ganz P (1990).Coronary vasomotor response to acetylcholine relates to riskfactors for coronary artery disease. Circulation 81, 491–497.
Wray DW, Nishiyama SK, Donato AJ & Richardson RS (2010).Human vascular aging: limb-specific lessons. Exerc Sport SciRev 38, 177–185.
Wray DW, Witman MA, Ives SJ, McDaniel J, Trinity JD,Conklin JD, Supiano MA & Richardson RS (2013). Doesbrachial artery flow-mediated vasodilation provide abioassay for NO? Hypertension 62, 345–351.
Additional information
Competing interests
None of the authors has any conflicts of interests.
Author contributions
H.J.G: Conception and design of experiments. Collection,analysis and interpretation of the data and drafting of the
manuscript. J.D.T: Conception and design of experiments.Collection, analysis and interpretation of the data. G.L:Conception and design of experiments. Collection, analysisand interpretation of the data. M.J.R: Conception and designof experiments. Collection, analysis and interpretation of thedata. S.J.I: Conception and design of experiments. Collection,analysis and interpretation of the data. D.E.M: Collection andinterpretation of the data and provided medical oversight.A.B: Collection and interpretation of the data and providedmedical oversight. R.S.R: Conception and design of experiments.Collection, analysis and interpretation of the data and draftingof the manuscript. All authors were involved in revising themanuscript, providing intellectual content, and approving thefinal version.
Funding
The work was supported by National Institutes of Health GrantP01-H1-091830 (to R.S.R.), Veterans Affairs RehabilitationResearch and Development Service Grant E6910R (to R.S.R.),and SPiRe Grant E1433-P (to R.S.R.).
Acknowledgements
We would like to express our thanks to the subjects who partookin this research. Their time and effort is much appreciated.
C© 2015 The Authors. The Journal of Physiology C© 2015 The Physiological Society
Copyright © 2022 FDOKUMEN