The Response of the Sialkot Surgical Instrument Cluster to ...
22
Collective Eciency and Collective Failure: The Response of the Sialkot Surgical Instrument Cluster to Global Quality Pressures KHALID NADVI * Institute of Development Studies, Brighton, UK Summary. — One of Pakistan’s rare examples of consistent export success has been the Sialkot stainless steel surgical instrument cluster. This cluster, consisting mainly of small and medium enterprises (SMEs), has as its main markets the United States and Western Europe. In recent years, access to these markets has become contingent on meeting international quality assurance standards. The hypothesis explored in this paper is that meeting such standards requires greater local cooperation, both among producers as well as between producers and their suppliers and subcontractors. The study draws on quantitative and qualitative data to examine how inter-firm ties, both vertical and horizontal, have changed. The evidence suggests that joint action has increased, but that there remain significant areas of collective failure. Thus, the quality assurance pressures mark a possible turning point for the cluster, raising questions as to whether local sources of competitiveness, captured in the collective eciency concept, can continue to provide the basis for export success. It also leads directly to an evaluation of the cluster’s growth trajectory. Ó 1999 Elsevier Science Ltd. All rights reserved. 1. INTRODUCTION The one truth about global competition is that it is constantly changing. As Kaplinsky (1998) has noted, competing in ever-more demanding world markets requires producers to run just in order to keep up. The criteria that define best practice in manufacturing are con- tinually developing, reflecting the constant pace of upgrading in both product and process technologies. In recent years, international standards that verify compliance on a range of issues, including quality assurance, environ- mental standards, labor norms and even social ethics, have gained importance in global com- petition. 1 Standards provide consumers with a basis for making informed consumption decisions, and manufacturers with a benchmark of best prac- tice. For many producers and service providers, from the North and the South, compliance with international standards can add a competitive edge. It may also be necessary to retain access in key niche markets. There is now a growing literature which examines standards as non- tari barriers to trade (Stephenson, 1997; EC, 1997), especially with regards to labor (Sengenberger and Campbell, 1994; OECD, 1996, 1995; Krueger, 1996; Maskus, 1997; White, 1996; ILO, 1997; Grootaert and Kanbur, 1995) and environmental standards (Dion, Lanoie and Laplante, 1997; Anderson, 1996). This paper examines how clustered producers have responded to the new standards of quality assurance, focusing in particular on inter-firm World Development Vol. 27, No. 9, pp. 1605–1626, 1999 Ó 1999 Elsevier Science Ltd. All rights reserved Printed in Great Britain 0305-750X/99/$ - see front matter PII: S0305-750X(99)00078-9 www.elsevier.com/locate/worlddev * Financial support from the Department for Interna- tional Development, London is gratefully acknowl- edged. The author thanks the Surgical Instrument Manufacturers Association in Sialkot, Pakistan for its support, and the various respondents interviewed in Sialkot for their valuable time. The excellent research assistance provided by Waheed Murad in Sialkot is highly appreciated. The author benefited from discus- sions and comments on earlier drafts provided by Tilman Altenburg, John Humphrey, Peter Knorringa, Roberta Rabellotti and Hubert Schmitz. The author is solely responsible for the views expressed in this paper. 1605
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The Response of the Sialkot Surgical Instrument Cluster to ...

Collective E�ciency and Collective Failure: The
Response of the Sialkot Surgical Instrument Cluster to
Global Quality Pressures
KHALID NADVI *
Institute of Development Studies, Brighton, UK
Summary. Ð One of Pakistan's rare examples of consistent export success has been theSialkot stainless steel surgical instrument cluster. This cluster, consisting mainly of smalland medium enterprises (SMEs), has as its main markets the United States and WesternEurope. In recent years, access to these markets has become contingent on meetinginternational quality assurance standards. The hypothesis explored in this paper is thatmeeting such standards requires greater local cooperation, both among producers aswell as between producers and their suppliers and subcontractors. The study draws onquantitative and qualitative data to examine how inter-®rm ties, both vertical andhorizontal, have changed. The evidence suggests that joint action has increased, but thatthere remain signi®cant areas of collective failure. Thus, the quality assurance pressuresmark a possible turning point for the cluster, raising questions as to whether localsources of competitiveness, captured in the collective e�ciency concept, can continue toprovide the basis for export success. It also leads directly to an evaluation of the cluster'sgrowth trajectory. Ó 1999 Elsevier Science Ltd. All rights reserved.
1. INTRODUCTION
The one truth about global competition isthat it is constantly changing. As Kaplinsky(1998) has noted, competing in ever-moredemanding world markets requires producersto run just in order to keep up. The criteria thatde®ne best practice in manufacturing are con-tinually developing, re¯ecting the constant paceof upgrading in both product and processtechnologies. In recent years, internationalstandards that verify compliance on a range ofissues, including quality assurance, environ-mental standards, labor norms and even socialethics, have gained importance in global com-petition.1
Standards provide consumers with a basis formaking informed consumption decisions, andmanufacturers with a benchmark of best prac-tice. For many producers and service providers,from the North and the South, compliance withinternational standards can add a competitiveedge. It may also be necessary to retain accessin key niche markets. There is now a growingliterature which examines standards as non-
tari� barriers to trade (Stephenson, 1997; EC,1997), especially with regards to labor(Sengenberger and Campbell, 1994; OECD,1996, 1995; Krueger, 1996; Maskus, 1997;White, 1996; ILO, 1997; Grootaert andKanbur, 1995) and environmental standards(Dion, Lanoie and Laplante, 1997; Anderson,1996).
This paper examines how clustered producershave responded to the new standards of qualityassurance, focusing in particular on inter-®rm
World Development Vol. 27, No. 9, pp. 1605±1626, 1999Ó 1999 Elsevier Science Ltd. All rights reserved
Printed in Great Britain0305-750X/99/$ - see front matter
PII: S0305-750X(99)00078-9www.elsevier.com/locate/worlddev
* Financial support from the Department for Interna-
tional Development, London is gratefully acknowl-
edged. The author thanks the Surgical Instrument
Manufacturers Association in Sialkot, Pakistan for its
support, and the various respondents interviewed in
Sialkot for their valuable time. The excellent research
assistance provided by Waheed Murad in Sialkot is
highly appreciated. The author bene®ted from discus-
sions and comments on earlier drafts provided by
Tilman Altenburg, John Humphrey, Peter Knorringa,
Roberta Rabellotti and Hubert Schmitz. The author is
solely responsible for the views expressed in this paper.
1605

relations and production organization in thecluster of surgical instrument producers inSialkot, Pakistan. This cluster is an establishedplayer in its global market but struggling tomeet the international quality assurance stan-dards.
Small and medium enterprises (SMEs) havemade Sialkot Pakistan's leading center in percapita terms for manufactured exports. Sial-kot's SMEs are organized around sector speci®cclusters producing sports goods, leather gar-ments and stainless steel surgical instruments.The latter is the largest in employment terms.The 300 or so family-run manufacturingenterprises that form the core of the Sialkotsurgical instrument cluster together exportedover US$100 million worth of instruments in1992-93. The cluster's main market is theUnited States with 60% of total export sales.During the mid-1990s the Sialkot cluster faceda major crisis of quality assurance. This crisisprovides a possible `turning point' that couldwell determine the cluster's future growth pathand its ability to remain globally competitive.2
In May 1994 the Food and Drug Adminis-tration (FDA) of the United States, the keyregulatory body in the US health sector,restricted imports of Pakistani-made surgicalinstruments for failing to meet the interna-tionally accepted quality assurance standardsof Good Manufacturing Practices (GMP). Thisaction had serious consequences for Sialkot'sproducers, especially those exporting predomi-nantly to the United States. Consignments werestranded midway, orders cancelled, many ®rmsand subcontractors ceased operation, and alarge number of workers were laid o�.
GMP standards are one measure of qualityassurance. They are closely related to otherinternationally recognized quality assurancecerti®cations, such as the ISO 9000 series,which certify that standardized and account-able quality control processes are used at eachstage in a product's design, development,manufacture and distribution. In line with theemphasis on total quality-management (TQM),they provide a system of traceability, involvingdetailed veri®cation of quality-dependent pro-cedures through internal and independentaudits, quality training of personnel and con-stant monitoring of quality performance mea-sures. Implementing such standards requireschanges in production organization and man-agement practices. This has implications for therelationship producers have with suppliers andwith other ®rms. The upgrading required
necessitates a capacity to learn both at the levelof the individual ®rm and in the relationsbetween ®rms. In the cluster context, know-ledge spillovers can facilitate such learning(Audretsch and Feldman, 1996). Moreover,cluster-wide bodies and real services centers canaccelerate the dissemination of know-howamong local producers (Brusco, 1992). Finally,compliance by local producers can enhance acluster's overall quality standards, providing itwith a highly marketable `quality label'.
Conforming to international quality assur-ance standards can be a costly process, not onlyin terms of certi®cation expenses but also inacquiring the know-how to implement therequired changes. Furthermore, pressures tomeet standards in one area can also be a pre-cursor to complying with international stan-dards requirements in other ®elds. For Sialkot'ssurgical instruments sector, continued access topremium markets in Western Europe andJapan is becoming conditional on achieving theISO 9000 series of quality assurance standards.In addition, there are growing demands on thecluster to meet global concerns on child labor.Thus, the crisis of 1994 provided an indicationof the new competitive challenges the Sialkotcluster would face in global markets.
The response to these pressures has beenimpressive. By late 1997 sales of surgicalinstruments from Sialkot were above the pre-crisis levels. Overall quality had also improved,with over 130 of the 300 manufacturers in thecluster certi®ed by the FDA as conforming toGMP standards and two ®rms havingobtained the coveted ISO 9002 quality assur-ance certi®cate. The evidence from the ®eldwas equally strong. Of the 60 ®rms surveyed inNovember 1997, 68% reported rising saleslevels since the crises. Over half the samplestated that employment levels had also goneup. Two-thirds were already GMP certi®edand 37% of the sample had begun the processof obtaining ISO 9002 certi®cation. This is, byany measure, a remarkable and rapid turn-around. This paper seeks to explain how theturnaround was achieved. In particular, itexplores whether collective e�ciency advan-tages arising from clustering, especially jointaction gains, were signi®cant in the process ofupgrading and learning required to meet suchstandards.
Elsewhere I have shown how the concept ofcollective e�ciency can take us further inunderstanding the cluster's relative success as aglobal player in a niche product line (Nadvi,
1606 WORLD DEVELOPMENT

1999). Local producers have bene®ted fromlocal external economies and have entered intovarious forms of joint action. Cheap labor hasundoubtedly been important, but fails toexplain why Sialkot became a leading exportcenter. In making the argument on collectivee�ciency, the main focus has been on inter®rmrelations and the basis they provide for localsources of competitiveness.
This study takes the collective e�ciencyargument further by exploring how clusteredproducers respond to an exogenous crisis. Thisparticular crisis of quality assurance raisesquestions about changes in the relationshipswithin supply chains. Do they become closer,more collaborative and obligational, or do®rms reduce the quality-related costs of mon-itoring by internalizing activities? As the crisisis cluster-wide, questions also arise on changesin horizontal collaboration and the role playedby local institutions such as the trade associ-ation. The underlying concern is with thecluster's growth trajectory. This includesunderstanding how the structure of the clus-ter, and the production relations that charac-terize it, have changed as a consequence of thecrisis.
The paper draws on qualitative and quanti-tative primary data collected in two surveyrounds.3 The pre-crisis ®eldwork, conducted in1993±94, included a survey of 57 surgicalinstrument manufacturers and 72 subcontrac-tors, alongside case studies and key informantinterviews. The post-crisis survey, conducted intwo stages, included qualitative evidence gath-ered from case study ®rms and key respondentsin January 1997, followed by a detailed surveyof 60 ®rms in November-December 1997.4
The discussion is structured as follows. Thefollowing section considers the links betweenquality assurance, upgrading and collectivee�ciency. Section 3 provides a brief overviewof the Sialkot cluster, describing the qualityassurance crisis and chronicling the events thatsubsequently took place. Section 4 shows howhorizontal relationships have changed inresponse to the crisis. Section 5 turns to verticalties, examining whether the crisis spurred jointaction with local suppliers and subcontractorsand external buyers. Section 6 tests the propo-sition that increased cooperation has had apositive impact on performance. The conclud-ing section summarizes the evidence on collec-tive e�ciency and on collective failure, anddiscusses the implications for the future devel-opment of the Sialkot cluster.
2. QUALITY ASSURANCE STANDARDSAND COLLECTIVE EFFICIENCY
Quality assurance standards move the focusaway from product to process quality. Tradi-tionally, quality standards were based onproduct characteristics such as durability, reli-ability, conformance to speci®cations andsafety. During the 1980s and 1990s however,concern began to shift toward the processesinvolved in production and a new category ofstandards began to emerge. For example, theISO 9000 series of standards (which developedfrom British Standard BS5750) concentrate onthe documentation of quality procedures, whilethe ISO14001 standard deals with the docu-mentation of environmental procedures inproduction. The motivation for quality assur-ance standards emerged as a result of the desireof component and service users for high qualityinput produced at low costs. This was directlyrelated to the changes in management practicesand the adoption of total quality control pro-cedures. Thus the issue was no longer of simplyensuring the quality of the end product, butalso of being able to verify the quality controlprocess that had been used, and the qualityvalues that had been instilled, at each and everystage of production. Among other things, thishas implications for the way production isorganized, with ``quality at source,'' ``qualityresponsibility'' and ``total quality manage-ment'' becoming key elements of a ``totalquality control'' production organization.
For the surgical instruments sector, qualityassurance is particularly signi®cant given thatthe industry manufactures what the FDA terms``critical devices.'' The consequence of instru-ment failure can be extremely costlyÐlives canbe at stake. In the West, malpractice litigationplaces a heavy penalty on failure by healthproviders. The latter require suppliers furtherdown the health provision chain to comply withquality assurance norms. The traceability ben-e®ts, o�ered by a quality assurance procedure,ensure that faults can be located and responsi-bilities for failure clearly de®ned. It also impliesthat international quality standards have beenmet. For manufacturers meeting global qualityassurance standards can potentially raise eco-nomic e�ciency, provide a basis for bench-marking, and be an important tool in a ®rm'scompetitiveness strategies. Thus, in order toraise their share of the global surgical instru-ment market, Pakistani producers have toimprove e�ciency by cutting costs and raising
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1607

productivity. They also have to raise qualityand provide documented, veri®able and inter-nationally accepted quality assurances toexisting and potential buyers.
The required upgrading calls for changes inproduction organization and managementpractices within the ®rm and in their relation-ships within the supply chain. ``Soft technolo-gies'' on organizational practices have to beabsorbed. These include: detailed record keep-ing of each production batch ¯ow through thevarious stages of production; adoption of pro-cess-speci®c quality accounting systems withsystematic testing of materials and standards atkey stages, and a restructuring of manufactur-ing to emphasize stock and quality control, aswell as health and safety standards. Thisdemands a change in management outlook andin the traditional ``ways of doing.'' Most pro-foundly, it requires the inculcation of quality-driven production values.
The FDA's actions were not directed at anindividual ®rm but to the cluster as whole. Allproducers in Sialkot were deemed to have failedto comply with international standards. Indi-vidual responses by ®rms were unlikely to resultin the compliance required. Assimilation ofquality values and upgrading of practices hadto be across the cluster.
The collective e�ciency argument is of sig-ni®cance here: it suggests that the upgradingcalled for cannot be advanced by SMEs ontheir own. A collective response is needed. Thisis likely to generate cluster-wide gains. Collec-tive e�ciency is de®ned as having two aspectsto it: external economies that clustered agentsaccrue by virtue of their location, and jointaction bene®ts that arise from deliberatecooperation between local agents. I viewexternal economies as the ``passive'' dimensionof collective e�ciency (Nadvi, 1996). The termpassive describes the nature of ties requiredbetween local agents in order to obtainexternality gains. In contrast, joint action is the``active'' dimension of collective e�ciencyrequiring deliberate and active cooperation.These two aspects can also be clearly linked;joint action by some agents can generate clus-ter-speci®c externality gains for others (Nadvi,1996). It is the combination of these bene®ts,external economies and joint action gains, thatprovide a basis for enhanced competitivenessfor clustered SMEs compared with similarlysized, yet dispersed, producers.
The collective e�ciency model relates directlyto the pressures raised by quality assurance
standards. Upgrading on quality assurancerequires upgrading of local supply chain link-ages within the cluster. While quality assurancestandards e�ectively lower transaction costs(Foss, 1996), achieving them requires thebuilding of closer ties and greater information¯ows within the supply chain. This impliesgreater cooperation in vertical relationsbetween producers and their various suppliers.Firms and suppliers both need to monitorproduction closely, keeping and sharingdetailed information on production ¯ows,source and reject rates at each and every stageof production. This suggests greater coordina-tion within the supply chain, and openness onthe part of suppliers for external monitoring byproducers. These enhanced interactions, andtheir implicit focus on quality and quality-critical stages of production, facilitate a widerset of technical discussions within the supplychain on quality and technical upgrading.Moreover, given the costs of such linkages,®rms are potentially encouraged toward moreobligational, as opposed to arms-length, ties(Sako, 1992). These changes clearly imply thatclustered ®rms can no longer rely purely on thepassive dimension of collective e�ciency inorder to compete in global markets. They needto focus increasingly on upgrading their supplychains, which requires joint action in localvertical ties.
Similarly, joint action in horizontal ties,through local multilateral institutions can assistthis process of upgrading by facilitating the ¯owof technical information on standards and byassisting in managerial training. Local institu-tions can also play a potentially key function inde®ning and regulating local product stan-dards, and thus in creating a reputational basisfor the cluster's products. This provides apowerful example of what I refer to as ``exter-nalities of joint action'' (Nadvi, 1996, 1999).
In so much as quality assurance standardsare an emerging feature of demand-drivenpressures within the new competition, theyunderline the link between market conditionsand joint action. Competing in demand-ledmarkets requires local clustered producers togo beyond the passive dimension of collectivee�ciency and engage in local cooperation bothwithin vertical supply chain linkages andthrough horizontal collaboration within localinstitutions. Furthermore, where quality assur-ance pressures raise demands for new forms ofknowledge on managerial organization andproduction best practices, upgrading requires
1608 WORLD DEVELOPMENT

learning. Learning ties, involving both interac-tion with external agents and through localfeedback and demonstration, demand greaterand more coordinated collaboration. To theextent that quality assurance standards posenew sets of questions and require new mana-gerial know-how, external buyers can becomean important conduits for such information.This clearly raises concerns of whether localsources of competitiveness within the cluster,captured in the collective e�ciency notion, aresu�cient to generate the basis for the cluster'scontinued ability to vie in global markets.
This paper puts forward the hypotheses thatupgrading to meet global standards by clus-tered producers necessitates enhanced jointaction in both vertical and horizontal ties.Moreover, it argues that such upgrading willhave positive consequences on ®rm and clustergrowth. Before turning to the empirical evalu-ation of this argument, however, the followingsection presents an overview of the cluster andthe crisis.
3. THE SIALKOT SURGICALINSTRUMENT CLUSTER AND THE
QUALITY ASSURANCE CRISIS
(a) Brief overview of the cluster
The Sialkot surgical instrument cluster con-sists of a core of 300 producers, surrounded bya range of over 1,500 process specialized sub-contractors, a further 1,000 ancillary, supplyand support units as well as a number of sup-port institutions. Among the latter are theMetal Industries Development Centre (MIDC)that provides technical services to local ®rms;the Surgical Instrument Manufacturer's Asso-ciation (SIMA) which represents local produc-ers; and, the Sialkot Dry Port Trust (SDPT)which has ``brought the port to the cluster,''providing customs handling, storage andtransportation facilities.5
Over 2000 di�erent types of surgical instru-ments are produced in Sialkot. These arethemselves di�erentiated by market segment:high quality, reusable, operation theatreinstruments and lower quality, disposable, ¯oorinstruments. The two segments are distin-guished by the type of raw material, quality ofworkmanship, and end markets. Disposableinstruments are produced from locally sourced,recycled, or scrap-based, stainless steel andexported primarily to the high volume US
market. Since the mid-1980s demand for dis-posable instruments has risen in the US fol-lowing concerns on the spread of infectiousdiseases through contaminated instruments andthe rising costs of sterilization. Reusable oper-ation theatre instruments are made from higherquality imported stainless steel, and are pre-dominantly exported to Western Europe, par-ticularly Germany where a number of theleading international surgical instrument man-ufacturers subcontract to Sialkot-based pro-ducers.
The cluster generates various agglomerationbene®ts for local producers. These include thepresence of a wide range of specialist input andservice providers who ensure competitive pricesand facilitate the ability of local producers tocompete in distant markets. Producers are notrequired to hold large stocks of input, and cancall on the wide range of export-related serviceproviders, from shipping agents to interna-tional couriers. The large presence of specialistsubcontractors generates economies of scaleand scope. The cluster also provides a concen-tration of skilled labor, the most frequentlycited locational advantage. The labor marketclears rapidly, facilitated by the easy availabil-ity of information within the cluster. In addi-tion, the ¯ow of technical and marketinginformation enhances prospects of technicaldevelopment.
In addition to these ``passive'' gains of clus-tering, which lower costs and raise e�ciency,there is evidence of local joint action. Firmscollaborate with their local suppliers and sub-contractors, particularly on issues of quality.Horizontal cooperation is less marked. Yetthere are a number of local institutions,including the trade association, the chamber ofcommerce and the dry port, which re¯ect hor-izontal inter-®rm cooperation. At the sametime local rivalry is intense. Producers competewith each other in an environment where price,quality and reliability are essential factors forexport success.
The Sialkot cluster is also highly di�erenti-ated. A small number of the cluster's originalSMEs have grown into large ®rms and havedeveloped close collaborative linkages and jointventure units with key external players, partic-ularly leading international producers. Therealso many small enterprises that struggle tosurvive. This process of increasing internaldi�erentiation, and the related intensity of thelocal competition, raises questions of the clus-ter's growth trajectory. Will price competition
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1609

and cost cutting force the cluster down a ``lowroad'' (Sengenberger and Pyke, 1991)? Or isthere the possibility of a ``high road'' wherequality led developments encourage innova-tion, growth and rising real incomes?
(b) The quality assurance crisis
In the context of these questions, the qualityassurance crisis of 1994 provides a potentialturning point for the Sialkot surgical instru-ment cluster. Before turning to the discussionon how the cluster responded it is useful to mapthe events associated with the crisis.
Concerns regarding the quality of Sialkot'ssurgical instruments had begun to emergeduring the latter half of the 1980s (Wiegersma,1989; GEMCO, 1990). In 1989 the FDA tem-porarily restricted imports of Sialkot-madeinstruments on the grounds of unacceptablemetal composition standards. Random testsrevealed that the chromium content and hard-ness of recycled Pakistani stainless steel wasbelow par, leading to a higher risk of rust andbreakage. The concerns expressed by the FDAin 1989 were largely allayed by the early 1990s.A technical dialogue ensued between Sialkot'ssurgical instrument producers and the localsteel re-rolling sector, resulting in gradualimprovements in the quality of the locallyproduced scrap-based stainless steel.
The FDA's action of May 1994 was moreserious in character to that of 1989. It wentbeyond simply quality control and metal test-ing. The critical nature of quality assurance wasbrought into sharp focus. Prior to this, know-ledge of international quality assurance require-ments was limited to large ®rms in Sialkot.While three-quarters of the large ®rms surveyedin 1993±94 were aware of the ISO 9000 stan-dards, only 31% of SMEs sampled had heard ofit. At the time, neither the local technologycenter, the MIDC, nor the cluster's trade body,SIMA, had disseminated information or pro-vided technical training on the subject.
The continued competitiveness of the clusterdepended on its ability to respond rapidly tothe demands posed by the quality assurancepressures. Incorporating the changes necessaryto conform to the new requirements, however,was not easy. In an industry reliant on tradi-tional knowledge and metalworking expertise,the adoption of new ``hard'' technologies wasrelatively simple in that the logic of newequipment could be easily understood, oftenaided by reverse engineering. Local producers
dismantled new machinery to learn how itfunctioned and then rebuilt it. As a result, anumber of formerly imported technologies weremade locally. Absorbing the ``soft technolo-gies'' associated with quality-driven productionorganization was potentially more di�cult. Anattitudinal shift was required, wherein localproducers recognized that traditional practicescould be improved upon and were aware of theurgency to do so. For the Sialkot cluster, wheremany of these changes were perceived as goingagainst the grain of locally embedded practices,such reorganization was unlikely to be smooth.
In the months following the FDA ``ban''sales to the United States were suspended, most®rms reduced production levels, some smallerunits closed down while others entered newproduct lines (such as, for example, barber'sscissors or beautician's equipment) or soughtnew markets in Europe, Asia and SouthernAfrica. A number of manufacturers tried to®nd alternative channels into the US market inorder to circumvent the FDA's barriers.Among the hardest hit segments of the clusterwere process-specialized subcontractors andsuppliers of locally manufactured scrap steel(the main raw material used for disposableinstruments produced for the US market).
The awareness of the necessity to upgradewas rapid even if the process of upgrading itselfwas gradual. Discussions on the means toacquire the requisite know-how for upgradinglocal practices began almost immediately,especially within the forum of the trade asso-ciation (investigated in depth below). ByDecember 1994, one large ®rm in Sialkot hadmanaged to become GMP certi®ed by theFDA. It did so by hiring the services of a for-eign consultant. In April 1995, 11 months afterthe FDA's action, SIMA, with ®nancial aidfrom the government, negotiated a contractwith a US quality assurance consultancy toprovide technical training for local producersto upgrade to GMP standards.
By January 1997, as a result of the trainingprovided by the consultant, 75 producers hadbeen certi®ed by the FDA as conforming tocurrent GMP standards, and were thus able toexport to the United States.6 Ten months laterthis ®gure had risen to 133 ®rms, with a further153 producers either undergoing training onquality assurance techniques or awaiting certi-®cation by the FDA. Moreover, two local ®rmshad become ISO 9002 certi®ed while at least 10other producers were con®dently expecting tobe certi®ed in the course of the next year.
1610 WORLD DEVELOPMENT

Export sales from the cluster stood at approx-imately US$125 million in 1995-96, comparedwith US$109 million in 1993±94.7 The numbersof exporting ®rms in the cluster had increased(to close to 400), as had physical productionlevels, while quality levels were generallyacknowledged as having improved. Althoughthe cluster has not yet fully extricated itselffrom the crisis there is evidence to suggest thatit has managed to upgrade. In this sense, theFDA crisis may well have been a de®ningmoment and a turning point for the cluster.
The question remains how has it done so?Moreover, what implications arise for individ-ual ®rms, and for the ways in which they areorganized? How have ties with local suppliersand subcontractors, and forward ties withexternal buyers, changed? Has horizontalcooperation that local ®rms have with eachother, and through their trade association,become more pronounced? These questions areaddressed below in Section 4 and Section 5.
4. CHANGING HORIZONTAL TIES
A key aspect of the response by the Sialkotsurgical instrument cluster to the FDA hasbeen the role played by the trade association,SIMA. In particular, the trade body mobilizedthe state to adopt a more supportive andinterventionist program for the cluster. Thissection reviews how horizontal joint actiongenerated cluster-wide gains.
Evidence of greater horizontal cooperation inthe cluster began to emerge soon after theFDA's action in May 1994. As mentionedearlier, local producers quickly began to discusshow to face the challenge posed by qualityassurance standards. Exchange of informationwas the one arena where the majority of ®rmssampled reported an increase in cooperationwith other producers. Much of this discussiontook place within the trade association. As aresult, SIMA began formulating a collectiveresponse within a month of the import ``ban''being imposed. It put together a delegation,composed predominantly of owners of large®rms, to visit the United States and negotiatedirectly with the FDA. On failing to convincethe United States regulators to accede to aphased process of GMP certi®cation, SIMAturned to the Pakistani government for ®nan-cial support to hire foreign consultants to helplocal producers upgrade quality managementprocedures. The federal government also
agreed to ®nance, at a cost of US 1.6 million,the development of a new, internationally rec-ognized, metal testing laboratory and a tech-nical training facility in Sialkot, both to bemanaged in partnership with SIMA.8 Finally,SIMA acquired approval from the governmentfor a revolving credit line, of approximatelyUS$2.5 million, to provide soft term loans tolocal manufacturers.
The growing importance of SIMA can begauged from the survey data that show that ofthe 60 ®rms sampled 61.6% reported using theservices of the association more now than theydid before the crisis. This pattern was similaracross di�erent size categories of ®rms.Although the overall package took time to takeshape, SIMA's response was seen by manylocal enterprises as the best way to address thecrisis. SMEs considered the predominance ofrepresentatives of large enterprises in SIMA'sdelegation an advantage to the cluster. As oneentrepreneur who ran a medium-sized ®rmexplained:
Owners of large ®rms have better contacts, they haveclout. Ministers in Islamabad will listen to them; theywouldn't give small ®rm owners like me even anappointment. Also, large ®rms have good contactsabroad, they can speak better English, they can nego-tiate far better on our behalf than we could (P.Ahmed, July 14, 1994).
The relatively proactive stance adopted bythe association contrasts sharply with how itwas perceived prior to the crisis. While SIMAhas a long history, having been set up almost®ve decades ago, and all manufacturing andexporting ®rms in the cluster are members, ithas traditionally been seen as relatively inef-fectual. It is meant to provide information onmarkets, trade policy, technology and otherrelevant issues to its members. It is supposed toassist them in resolving technical di�culties andin dealing with the state and other regulatorybodies. It is also mandated to regulate businesspractices within the cluster. The 1993±94 surveyfound, however, a widespread consensus in thecluster that the Association was ill-informedwith regards to technical and marketing infor-mation, was unable to provide technical guid-ance to its members and was not alwayse�ective as a `leader' or `voice' of the cluster'scollective interests. Its most common activitywas its occasional e�orts at lobbying govern-ment and representing the interests of member®rms with local state agencies, especially thecustoms and tax departments.
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1611

What made SIMA a more vocal and e�ectivechampion of cluster-wide interests followingthe quality assurance crisis? In part, the expla-nation lies in changes that have taken placewithin SIMA since 1994. In 1994 there was awidespread view, especially among SMEs, thatlarge ®rms dominated SIMA's managementand that their interests determined the associ-ation's activities. While this perceived bias isdi�cult to substantiate, the majority of theannually elected chairmen of SIMA over theprevious decade and a half had been owners oflarge ®rms. The Chairman has an importantfunction within SIMA, providing executiveday-to-day management and closely in¯uencingthe level of activity displayed by the associationat any given time.
The continuing dominance of larger pro-ducers in the working of the trade body wasbrought into question by the FDA action.Representatives of large ®rms organizedSIMA's initial reaction, the formation of thedelegation. It was in their immediate interest tonegotiate with the FDA and thus ease theshipment of ongoing consignments. SMEs alsostood to bene®t from this initiative; neverthe-less large ®rms had the most at stake in terms ofproportion of exports from Sialkot. SIMA'ssubsequent e�ort in getting state support for aconsultant to provide GMP training to 200®rms within the cluster, however, provided abene®t that was particularly critical to SMEs.Large ®rms could have obtained GMP certi®-cation by acquiring know-how and trainingfrom consultants directly although at a price (assome did). Alternatively, they could turn totheir foreign buyers for assistance on upgrading(one leading US buyer had begun to providesuch aid to the large manufacturers it dealt within Sialkot in 1994). In contrast, small ®rms werein a weaker position. They were less likely tohave either the connections, or the large salesvolume, with more quality-conscious foreignbuyers to obtain the latter's support. Moreover,they lacked the resources to seek individualsolutions of hiring foreign consultants toacquire the required know-how to upgrade.The cluster-wide consultancy service, ®nancedby the state and organized through SIMA,made such know-how more widely accessible,thus making it possible for many of the smallerproducers to obtain GMP certi®cation andcontinue competing with their larger localrivals.
How did this happen? In e�ect, there appearsto have been a discernible shift in power within
SIMA since 1994. At the time of the crisis, theassociation was led by a chairman whoseinterests were said to be closely tied to those ofthe leading large ®rms in the cluster. In 1995,only ®ve ®rms (all large units) had managed toget through the GMP hurdles set by the FDA.Moreover, it had taken the association a fullyear to get an agreement with a foreign con-sultant to obtain quality management trainingfor the cluster. In the annual elections held in1995, the frustration felt by the SMEs in thecluster at the slow pace of progress came to ahead. The sense of being marginalized withinSIMA led to a process of mobilization bySMEs. Some of the more dynamic SMEs built aloose coalition with a few of the leading large®rms in the cluster and a new panel of o�cebearers was voted in the 1995 elections forSIMA's executive committee. This panel, whichwas re-elected in 1996, has as its Chairman anowner of a large enterprise. He is respectedwidely within the cluster and much credited forhis e�orts in accelerating the introduction ofconsultancy services on a cluster-wide basis.Thus, as one SME owner reports
SIMA is now more active as a consequence of theGMP and FDA issue. Before the big ®rms would hin-der the activity of SIMA and of smaller ®rms. Now,through SIMA, all ®rms in the cluster, big and small,can get the help they need to get through this [qualityassurance] problem (Rashid, January 21, 1997).
While individual agency mattered, the broadcoalition of interests and the mobilization ofcollective concerns of SMEs made such pro-gress feasible.
Of the steps initiated by SIMA, the mostimportant was clearly seeking external technicalknowledge on quality management. Acquiringthe know-how, via international consultants, toadopt the record keeping and documentationprocedures necessary for quality assurancecerti®cation became the critical element inbecoming GMP certi®ed.
As mentioned earlier, implementing qualitymanagement procedures, including reorganiz-ing production to conform to quality assurancerequirements at each stage of production is inmany ways more di�cult than the acquisitionof hard technologies. It requires quality train-ing, new management practices and the incul-cation of quality-driven values. A number ofexternal service providers, both Pakistani andforeign, began o�ering training and consult-ancy services to local producers soon after theMay 1994 FDA action. The ®rst ®rm to be
1612 WORLD DEVELOPMENT

GMP certi®ed obtained its certi®cate by hiring,at a substantial cost, such a consultant. Theresponse of this large ®rm was a clear sign ofindividual action in response to the FDA crisis.It bought the technical services and know-howit needed to get it through the FDA barrier. Itscosts were recuperated through its ability to sellagain in the US market.
While this ®rm pointed the way out of thecrisis, SIMA's action, in bringing in a qualityconsultant for the cluster as a whole, trans-formed the situation making such soft tech-nologies available to most ®rms in the cluster.The mandate for the consultant was to providetraining to 200 local producers on the man-agement, documentation, and record keepingpractices required for GMP certi®cation. Bylate 1997, the US consultant ®rm had beenoperating in Sialkot for over a year, using thepremises of the trade association as its base.Among the 133 ®rms that it helped through theFDA's certi®cation process were small, medi-um and large enterprises. Most, although notall, large ®rms became GMP certi®ed. Amongsmaller enterprises, the fact that the consult-ancy services were heavily subsidized meantthat they were able to acquire the technicalexpertise that would otherwise have beenbeyond their reach. As the consultant's repre-sentative observed ``our project in Sialkot isoperating on a level playing ®eldÐwe provideservices to everyone irrespective of their size''(D. Narejo, January 28, 1994).
Horizontal joint action, especially throughthe cluster's trade body, has played an impor-tant part in making it possible for many local®rms to cross the GMP certi®cation barrier.What does this certi®cation process, and thequality assurance problem in general, imply forvertical ties that Sialkot's manufacturers havewith their suppliers, subcontractors and buy-ers? Is there greater cooperation in these rela-tionships as a consequence of the qualityassurance crisis?
5. CHANGING VERTICAL TIES
The hypothesis put forward in this paper isthat the upgrading required to conform toquality assurance standards necessitates greaterinter-®rm cooperation, both in horizontal andvertical linkages. The latter is particularlyimportant. Quality assurance, to be e�ective,has to be ensured at all levels of the supplychain. This requires upgrading of suppliers,
implying a need for greater, quality-intensive,information ¯ows within the supply chain,potentially closer monitoring and e�ectively agreater degree of reliance that suppliers meetnew standards. In the new competitive scenar-io, failure by suppliers to conform to qualityassurance standards is potentially more harm-ful to local producers. By the same token, oncesuppliers are themselves certi®ed as meetingquality assurance standards, the transactioncosts in vertical ties would decline, providingan incentive to move to ``arms-length'' con-tracts (Foss, 1996). This section draws onsample and case study evidence to examine ifproducers in the Sialkot cluster increased ver-tical cooperation with their local suppliers andsubcontractors and their external buyers. Indoing so, it also explores how vertical ties arechanging as a consequence of the qualityassurance crisis.
One of the main ®ndings of the earlier studyon Sialkot (Nadvi, 1996) was the importanceof vertical linkages. Almost all of the 57 ®rmssurveyed in 1993±94 used subcontractors forparticular process activities, and relied on localsuppliers for stainless steel and other inputs,raw material and machinery. Similarly, most®rms dealt directly with foreign buyers. Tieswith local subcontractors and foreign buyerswere often close. The majority of producersreported assisting subcontractors in productionorganization (cited by 56% of ®rms surveyed in1993±94), and engaging in technical discus-sions on issues relating to product quality.Similarly, manufacturers often sought andobtained help from their buyers. Buyers wereone of the more frequently cited sources (re-ported by 85% of sampled respondents) fortechnical and marketing information, andaccording to 46% of the sample had assistedthem in raising quality standards. Such tieswere especially close for ®rms engaged insubcontracting, or in joint venture partner-ships, with foreign producers.
The FDA crisis of 1994 could result in twodistinct ways of reorganizing ties with subcon-tractors. The ®rst response was of producersinternalizing quality-critical stages in produc-tion, where transaction costs of monitoring andensuring that quality assurance requirementshad been met outweighed the bene®ts of sub-contracting. The second response was of ®rmscontinuing, possibly even extending, the prac-tice of subcontracting and engaging in greatercooperation in vertical linkages as the preferredpath for upgrading.
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1613

There was some evidence for both types ofresponses. Most large ®rms had already inter-nalized a number of the more quality-criticalstages in production. There were also signsthat, in response to the FDA crisis, large ®rmsplanned to further internalize production. Thiswas most clearly seen in the case of ®rmsentering into joint venture partnerships. Forexample, one large ®rm, that had signed a jointventure agreement with a German partner,stated that the planned joint venture unit wouldbe a fully integrated plant with no subcon-tracting-out. Another large ®rm proposed tobring key subcontractors into its newly con-structed facility to ensure that they workedexclusively for the ®rm and were regularlysupervised and monitored.
The second response, of closer collaborationin ties with subcontractors, however was morecommon. This is not entirely surprising becausequality concerns were already a key element ofvertical ties prior to the FDA's action. Main-taining quality standards and ensuring thatproduct speci®cations were met was the centralaspect of interaction between manufacturersand subcontractors. Assistance and evensupervision was regularly provided to subcon-tractors to ensure quality levels especiallywhere problems occurred (reported by 58% of®rms sampled in 1993±94). The new qualityassurance standards, however, require moresystematic and formalized inspection and doc-umentation. The remainder of this sectionanalyzes how vertical ties changed in responseto the new quality assurance principles imposedby the FDA.
(a) Backward ties
Take ®rst the ties with local input and rawmaterial suppliers. No respondent reported a
decline in the degree of cooperation in ties withsuppliers following the FDA crisis. While manyaspects of these relationships, such as negotia-tions over payment and delivery, remain asbefore, in other areas there has been someincrease in cooperation. As Table 1 indicates,over half the sample had increased the exchangeof information and experience with their sup-pliers. This was especially so on issues of qual-ity. Thirty percent of ®rms sampled stated thatcooperation with suppliers over qualityimprovement had risen since the 1994 crisis.There was no signi®cant pattern across ®rm size.
A key aspect of the quality assurance crisisrelates to the quality of stainless steel. It iswidely reported in the cluster that pressurefrom local producers and from the trade asso-ciation has resulted in improvements in thestandards and manufacturing processesemployed by the scrap-based steel re-rollingsector in nearby Gujranwala. Local respon-dents now consider local scrap-based stainlesssteel to be on par, in quality terms, with someimported stainless steel. Due to the FDA'spressure, and in line with the GMP require-ments, all steel bought locally is metal testedbefore it is forged, and has the required trace-ability records. This ensures for manufacturers(and their buyers) that, unlike before, the metalcomposition of the steel conforms to require-ments, that these quality standards are uniformacross the whole sheet of metal, and that thesteel producer can be held accountable. Theimprovement in local stainless steel has broughtwith it an increase in steel prices (by up to50%), much of which has been absorbed byproducers thanks to the devaluation of theRupee over this period. The key point to note isthat, in some respects cooperation with sup-pliers has increased and generated cluster-widebene®ts.
Table 1. Improvements in cooperation with suppliers a
All ®rmsN� 60 (%)
Small ®rmsN� 21 (%)
Medium ®rmsN� 22 (%)
Large ®rmsN� 17 (%)
Kendall svalue
Increase in exchange of informationand experiences
55.0 61.9 50.0 53.0 ÿ0.028
Increase in cooperation to improvequality
30.0 23.8 31.8 35.3 0.089
Change suppliers less often thanbefore FDA crisis
16.7 23.8 0 23.5 ÿ0.064
a Source: Author Survey (1997).
1614 WORLD DEVELOPMENT

Turning to ties with subcontractors, the pic-ture is more complex. A core requirement ofinternational quality assurance systems is thedocumentation of each lot and batch of pro-duction at each and every stage in production.This implies that all batches have to carryrecord cards for each process, listing whoundertook the task, the defects that occurred atthat stage, the amount that was rejected as aconsequence, and the results of each stage-wisequality inspection. Where processes are put-outby manufacturers to subcontractors, the latterare required to complete these documents,referred to locally as ``travel cards,'' for eachbatch and each stage of the process that theyundertake. The ®rm is responsible for the sub-contractor ful®lling these requirements. In thissituation the cost to the ®rm of the subcon-tractor failing to keep to the quality assurancestipulations are high.
With one exception, manufacturers reportedthat subcontractors had di�culty in furnishingthe correct documentation. Unlike most man-ufacturers subcontractors are often illiterate,rarely maintain appropriate records, and usu-ally lack the management training to meetquality assurance assessment and documenta-tion needs. Consequently, some ®rms ``®ll-in''their subcontractor's record cards themselves, apractice which raises doubts on the legitimacyof overall standards certi®cation within thecluster. Others carry out regular inspectionsand monitoring of subcontractors for eachbatch lot. A few ®rms, recognizing the highertransactions costs of monitoring, have begun tolower their extent of subcontracting. Othershave brought some of their key subcontractorsinto their premises in order to ensure moni-toring and appropriate stage-wise documenta-tion.
The extent to which subcontracting declinedas a consequence of the FDA crisis is re¯ected
in Table 2 below. As this shows, while theinternalization of most key processes hasincreased, this has not, with the exception ofthe ®ling stage, taken place on a large scale.The variation in this pattern by ®rm size is alsonot signi®cant. At the same time, it has to benoted that subcontracting did not appear toincrease in the cluster. Only three out of the 60®rms surveyed reported increasing subcon-tracting in any given process.
The aggregated data would imply that theincreased transactions costs associated withquality assurance monitoring and documenta-tion in any given process, with the possibleexception of the ®ling process, do not sub-stantively outweigh the gains that ®rms accruefrom subcontracting. This, however, veilsimportant di�erences within the cluster. Casestudy evidence suggests that the process ofinternalization was signi®cant for some large®rms.
Take the example of Amir Surgicals, a large®rm which in 1994 had 125 employees and salesin excess of US$1 million, the bulk of which(90%) was to the US market. Prior to the FDAaction, the ®rm subcontracted all of its ®lingtasks to some 30 subcontractors as well as halfof its polishing work to another 25 subcon-tractors. It has now internalized some of theseactivities and foresees reducing its reliance onexternal subcontractors even further. Since1994 sales have increased and the ®rm isexpanding. As part of its expansion plan, a newunit is being built on Sialkot's outskirts. In thisfacility the ®rm plans to internalize all pro-cesses. It will continue to use some of its currentsubcontractors, especially for labor-intensive®ling tasks. They will, however, have to workfrom within the new premises.
It costs us a lot of time and e�ort to monitor that thesubcontractors follow the correct quality assurance
Table 2. Decline in extent of subcontracting in key process activities a
Reduction in extent of subcontractingsince FDA crisis
All ®rmsN� 60 (%)
Small ®rmsN� 21 (%)
Medium ®rmsN� 22 (%)
Large ®rmsN� 17 (%)
Kendall svalue
Key processesForging 8.3 4.8 9.1 11.8 0.082Milling & Grinding 11.7 4.8 13.6 17.7 0.055Filing 23.3 14.3 27.3 29.4 0.139Polishing 10.0 14.3 4.5 5.9 ÿ0.040Heat Treatment 3.4 4.8 0 5.9 ÿ0.081
a Source: Author Survey (1997).
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1615

procedures. By having these subcontractors locatedwithin our larger compound we will be able to ensurethat they prioritize our work and that they are fol-lowing the correct quality procedures. Also it be-comes easier for us to do the documentation whichwill come with the ISO 9000 (S. Amir, January 21,1997).
Amir Surgicals gains in that its quality-re-lated monitoring costs are lowered while thelabor ¯exibility that comes with subcontractingis retained.
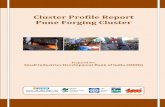
In 1994 the extent of subcontracting wasalready inversely related to ®rm size. AsFigure 1 makes clear, most medium and alllarge ®rms internalize some intermediate pro-cesses (such as polishing) and all ®nishingtasks. The pattern of production emerging insome large ®rms, as illustrated in the case ofAmir Surgicals above, indicates a desire toretain aspects of subcontracting while mini-mizing monitoring costs by ``bringing subcon-tractors into the ®rm.'' Supervision andmonitoring costs associated with qualityassurance are kept low and core subcontrac-tors are available on an assured basis. Forsubcontractors, this practice is consideredadvantageous in that they obtain rent-freespace, their search costs for new work aremuch reduced as they can expect a regularstream of work, and they get access to newforms of knowledge (and potentially training)from outside the cluster. Subcontractorsremain responsible for their own labor, itstraining and for some machinery, and theycontinue to be paid on a piece-rated job basis.Firms that have adopted this practice haveidenti®ed a core group of ®rst-tier subcon-tractors with whom ties are closer. Subcon-tractors left outside this ®rst-tier are in a more
precarious position, with poorer access toexternal knowledge and to a guaranteed ¯owof work.
This trend also has consequences for smalland medium-sized ®rms. Take the case ofUnimed, a medium-sized ®rm with a workforceof 31 persons (six of whom were family mem-bers) in 1994, and sales of US$350,000 pri-marily to the German market. Whatdistinguished Unimed from other SMEs was itsadherence to high quality standards and thefact that it had acquired the technology tomanufacture higher value-added instruments.It relied extensively on process specializedsubcontractors with whom it had particularlyclose ties. A number of its subcontractorsreported in 1994 that they had gained more intechnical feedback through their relationshipwith Unimed than with many large ®rms. Withrising quality standards in the cluster, andincreasing numbers of GMP certi®ed SMEs,Unimed lost its quality-based competitive edge.Unable to retain key buyers, it has seen a dropin sales. As a result, the volume of work sub-contracted out has also declined. Many ofUnimed's more dynamic subcontracting unitsare now seeking closer ties with large ®rmswhich are more likely to provide them with acontinued ¯ow, and potentially larger volume,of work. Consequently, the intensity and depthof the technical dialogue that the Unimed for-merly enjoyed with its subcontractors hasdiminished.
Despite the somewhat uneven patterns ofchange in subcontracting, it appears thatcooperation with subcontractors has increasedfollowing the quality assurance pressures. AsTable 3 shows, three-quarters of sampled ®rmsreported an increase in cooperation with sub-
Figure 1. Subcontracting in key process activities by ®rm size. (Kendall s signi®cant at 95% for grinding and ®lingprocesses and at 90% for forging.)
1616 WORLD DEVELOPMENT

contractors on quality improvement. Almosttwo-thirds of the sample stated that there was agreater exchange of information and experiencein these ties. Moreover, a third of the totalsample noted that subcontractors were changedless frequently than before, indicating moreconsistent arrangements. In none of these areasof increased cooperation was ®rm size signi®-cant.
No ®rm reported a decline in cooperationwith subcontractors as a consequence of thequality assurance pressures. Yet, there are cleargaps where increased cooperation did notoccur. Thus, 88% of respondents report noincrease in cooperation with subcontractors onthe issue of technical upgrading of equipment.Some 77% report no change in cooperation onlabor training (where the onus continues to restwith the subcontractor), while 65% state nochange in cooperation with subcontractors onimproving production organization. Coopera-tion with suppliers, and more so with subcon-tractors, has focused on information exchangeand on discussions aimed at raising qualitystandards. While not denying the importance ofsuch exchanges, further collaboration in supplychains on issues of labor training, productionorganization and technical upgrading, have yetto take place.
These ®ndings suggest that the demands ofquality assurance are changing the pattern ofsubcontracting in the cluster, with greater dif-ferentiation between producers and amongsubcontractors. At the same time, cooperationwith subcontractors has tended to increase.
(b) Forward ties
Forward linkages with external buyers wereseen in 1994 as a key source for the soft tech-nology necessary to pass the new qualityassurance standards, and thus a critical link forlocal producers to upgrade. As the manager ofone ®rm suggested: ``With these new require-ments on quality control, we need to have tieswith foreign buyers to get us through the newstandards'' (S. Tariq, July 16, 1994). In 1994,some buyers had begun to take the initiative,assisting local ®rms by providing qualityassurance training manuals and developingmanagement processes and software packagesfor quality assurance documentation.
Since then, ties with buyers have altered inseveral ways. Although the overall qualitystandards of Sialkot's instruments hasimproved, and a number of local producers arenow GMP certi®ed, unit prices of instrumentsmanufactured in Sialkot have fallen in theworld market. According to local respondents,this decline in price is a direct outcome of thecompetition prevalent in the US market, par-ticularly among US-based Pakistani marketagents. More established and larger US buyershave gained. The fact that a signi®cant numberof Sialkot's producers, both large and small®rms, are now GMP certi®ed has also had animpact. Thus, while there is evidence that thecrisis led to the forging of closer relationshipsbetween some buyers and producers, manybuyers moved to more transient, market-ori-ented ties in order to bene®t from the overall
Table 3. Improvements in cooperation with subcontractors a
All ®rmsN� 57 (%)
Small ®rmsN� 21 (%)
Medium ®rmsN� 21 (%)
Large ®rmsN� 15 (%)
Kendall svalue
Increase in exchange of information& experiences
64.9 57.1 66.7 73.3 0.140
Increase in cooperation to improvequality
75.5 71.4 80.9 73.3 0.172
Increase in cooperation in technicalupgrading
12.3 4.8 9.5 26.7 0.238 �
Increase in cooperation in productionorganization
35.1 23.8 42.9 40.0 0.180
Increase in cooperation in labortraining
22.8 14.3 23.8 33.3 0.186
Change subcontractors less oftenthan before FDA crisis
36.9 23.8 47.6 40.0 0.164
� Kendall s signi®cant at 90%.a Source: Author Survey (1997).
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1617

drop in price and the rising quality standardsprevalent in the cluster.
This, for example, was the most importantfactor behind the decline in the fortune ofUnimed, the medium-sized ®rm discussedabove. Despite the fact that it did not sell to theUS market, Unimed was one of the earliestSMEs to seek GMP certi®cation. According tothe owner, ``the GMP certi®cation was free, sowe thought it was worthwhile going through it,and we hoped it might impress some of ourEuropean parties [buyers] as well'' (Rashid,January 22, 1997). Yet, it has had to competewith a larger number of local producers tryingto sell in the relatively more quality-drivenEuropean market, following the initial FDAban. Unimed lost orders with some of its long-standing buyers who could now source morecheaply from other quality assured suppliers inthe cluster.
While the decline in prices was a generalexperience, the relationships with buyers didnot always deteriorate. In fact, Table 4 showsincreases in cooperation with buyers followingthe quality assurance crisis: 62% of ®rms sam-pled reported an increase in exchange ofinformation, while 65% reported greater coop-eration with buyers over quality control andquality improvement issues. In contrast, only aminority of ®rms experienced increased coop-eration with buyers in developing qualityassurance systems and reorganizing produc-tion. Finally, a quarter of the sample (andalmost half the large ®rms interviewed) statedthat buyers were changed less often than beforethe FDA crisis, indicating that these ties had
become more consistent and long standing.Unlike backward linkages, ®rm size appearedto be more signi®cant a factor in upgrading offorward ties. Large ®rms tended to haveincreased cooperation with buyers more sothan small and medium enterprises.
Case study evidence again helps bring outmore sharply how the nature of forward ties arechanging. Take again the example of AmirSurgicals. Unlike Unimed, which saw its closelinks with its European buyers weaken, AmirSurgicals has become more closely tied to itsleading buyer. In 1994, the ®rm owner hadstated his preference for a diversi®ed set ofbuyers within and across his leading exportmarkets. At that time he pointed out that
we have one very big buyer in the US who takes about60% of our total output. He would like to purchasemore from us. In fact to satisfy his demand we wouldhave to more than double our capacity. But we don'twant to get too tied and dependent on him, althoughthis American client has been very good for our busi-ness. Instead we try to ensure that at least 40% of ourproduction is sold to other buyers, not only in the US,but also in Europe and the Far East. It is good to bediversi®ed this way (S. Amir, Febuary 22, 1994).
This diversi®cation proved di�cult to main-tain. Following the FDA's action, Amir Sur-gical was faced with the prospect of having toshut down its operation given that the bulk ofits production was destined for the US market.The ®rm sought alternative end markets, inEurope and especially in Japan. To some extentthis was achieved, nevertheless the dependence
Table 4. Improvements in cooperation with buyers a
Ties with buyers All ®rmsN� 60 (%)
Small ®rmsN� 21 (%)
Medium ®rmsN� 22 (%)
Large ®rmsN� 17 (%)
Kendall svalue
Increase in exchange of information& experiences
61.7 47.6 63.6 76.5 0.214 �
Increase in cooperation to improvequality
65.0 61.9 81.8 47.1 ÿ0.050
Increase in cooperation in technicalupgrading
16.6 4.8 18.2 29.4 0.251 ��
Increase in cooperation in produc-tion organization
3.4 0 9.1 0 0.021
Increase in cooperation in develop-ing quality assurance system
29.3 (n� 57) 30.0 (n� 20) 27.2 31.3 (n� 15) 0.021
Change buyers less often thanbefore FDA crisis
26.7 9.5 27.3 47.0 0.370 ��
� Kendall s signi®cant at 90%.�� Kendall s signi®cant at 95%.a Source: Author Survey (1997).
1618 WORLD DEVELOPMENT

on the US market remained. Its leading USbuyer o�ered to assist, by selling Amir's outputunder its own brand name and providing itsown quality guarantees.
They [the US buyer] were willing to put their qualityreputation on the line for us. This enables us to getaround the FDA barriers and to continue productionat a time when most of the industry in Sialkot werebarred from the US market (S. Amir, January 21,1997).
There was however a cost to this arrange-ment. The buyer placed a condition that AmirSurgical would not market its product in theUnited States through any other agent. Thisbuyer now takes three-quarters of the ®rm'soutput. In addition to this dependence, furtherdisadvantages are emerging from this agree-ment.
My US buyer sells a smaller and more standardizedrange of instruments than I used to manufacture be-fore. So there are a number of items that were verypro®table which I am no longer producing. In termsof prices I am also tied (S. Amir, January 21, 1997).
The ®rm's predicament is not unique. Anumber of local producers report a growingreliance on key foreign buyers since the FDAcrisis. Buyers have also begun to adjust theirrelationships with Sialkot's manufacturers andin doing so have tried to improve their positionvis-�a-vis the cluster. There are two ways inwhich this has happened. The ®rst is, theexperience observed in Amir Surgicals, wherethe weak position of the producer has allowedthe buyer to negotiate better terms. The rela-tionship between speci®c buyers and producersis sustained, but the terms of trade are shiftingin the former's favor. Second, buyers havebegun to shop around much more than before.Thus, as with Unimed, long-standing buyershave sought out cheaper alternative sources inSialkot.
In fact, as a consequence of the fact that asigni®cant number of local producers havebecome GMP certi®ed and that prices havefallen, technical ties that buyers had withSialkoti producers have in some cases weak-ened. Take, for example, the case of a leadingUS buyer of disposable instrumentsÐAmeri-trade. Prior to the FDA crisis of 1994Ameritrade directly monitored the productionquality of its dozen large suppliers in Sialkot.Frequent and regular on-site inspections werecarried out and, where needed, technical
assistance was provided directly at the shop¯oor to resolve quality related problems. Inthis process, Ameritrade's Sialkot representa-tive became a technical knowledge bank for itslocal suppliers. Many local producers consid-ered this a key relationship and Ameritradeitself also bene®ted: reject rates declined sub-stantially.
In keeping with the importance thatAmeritrade attached to its technical assistancerole within the cluster, Ameritrade's Sialkoto�ce began to assist its local suppliers soonafter the FDA crisis. It helped them developstatistical process control packages and designdocumentation for quality assurance systems.At the same time, Ameritrade's representativewas clear that Sialkot's producers had toadopt rapidly the quality assurance require-ments or lose key buyers. Since 1994 thenature of Ameritrade's relationship with thecluster has radically changed. It continues topurchase large quantities of Sialkot-made sur-gical instruments, almost at the same level asin 1994, but it no longer maintains closetechnical ties with its local suppliers and hasdownsized its Sialkot operation. The localrepresentative in Sialkot provides Ameritradewith intelligence on the cluster as a whole, onlocal ®rms from whom purchases are beingmade and on the progress these ®rms havemade on quality assurance. Given that allinstruments now being sold in the US areGMP certi®ed, however, the quality-relatedtransaction costs that Ameritrade previouslyhad to bear are now much reduced. Moreover,this reduction in quality-related transactioncosts has been achieved without Ameritrade'sintervention.
Ameritrade, and other buyers like it, realized thatonce the Pakistani government got interested intothe quality assurance issue and were keen to provideassistance to the cluster, the FDA problem could besolved without them [the buyer] having to invest fur-ther in raising quality standards. That is why we havealmost stopped our earlier quality control programmehere (N. Rahim, January 21, 1997).
In summary, both the quantitative and thequalitative data help bring out the ways inwhich vertical ties are changing in the Sialkotcluster. Although at times apparently contra-dictory, case study and survey ®ndings togetherprovide a more nuanced understanding of howvertical ties have evolved as a consequence ofpressures to meet international quality assur-ance standards. Ties with local steel suppliers
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1619

have improved, resulting in a higher qualityraw material base. As far as ties with subcon-tractors are concerned, the higher costs ofmonitoring quality have led to some large ®rmsinternalizing more activities and ``bringingsubcontractors into the premises.'' The surveyevidence suggests however that internalizationis not a universal trend, not even among large®rms. SMEs, in particular, continue to rely onsubcontractors for a wide range of tasks.Nevertheless, subcontractors are also becomingmore di�erentiated as large ®rms seek todevelop ®rst-tier suppliers. This has conse-quences for SMEs who formerly had close, andoften technically rich, ties with their subcon-tractors. Forward ties to foreign buyers havealso become weaker in some cases, and inothers closer and often more dependent. Buy-ers have been able to bring about a shift intheir favor in the terms of trade as price com-petition has forced down unit prices for Sialk-ot's instruments. Is this a long-term responseon the part of buyers, or are they likely to(re)build technical ties with Sialkot's producersas prices stabilize? Again the evidence from thequantitative survey suggests that greatercooperation in vertical ties is most pronouncedin links with buyers, especially for larger ®rms.But such increases in cooperation were limitedto exchange of information and qualityimprovement and did not extend to broaderconcerns of technological and organizationalchange.
6. COOPERATION AND PERFORMANCE:IS THERE A RELATIONSHIP?
This section statistically evaluates the rela-tionship between ®rm performance and coop-eration, both vertical and horizontal. To recap,our contention has been that Sialkot's ®rmsmust engage in greater joint action to face the
challenges posed by the new quality assurancestandards. Section 4 and Section 5 indicatethat, while uneven, increasing collaboration hasbeen observed in both horizontal and verticallinkages. This section examines whether ®rmsthat have increased cooperation have per-formed better. Evaluating the relationshipbetween changes in levels of cooperation and®rm growth allows for an assessment of thecluster's growth trajectory. In addition, disag-gregating this relationship facilitates anappraisal of the types of inter®rm relationships,both local and external, that are becomingmore critical for growth. The discussion belowis structured as follows. First, using the surveydata, indices of performance and cooperationare generated, and the correlation betweenthese various indices analyzed. Second, regres-sion analysis is carried out to assess if there is asigni®cant association between cooperationand performance.
Cooperation indices were developed for tieswith suppliers (COPSUPL2), with subcontrac-tors (COPSUBC2), with buyers (COPBUYR2),with other ®rms (COPFIRM2) and with thetrade association (COPSIMA2).9 Table 5 pro-vides the frequency distribution for these indi-ces of cooperation.
The majority of ®rms sampled stated therehad been a small increase in cooperation in allthe cooperation indices. The index for cooper-ation with other ®rms was dropped from sub-sequent analysis as none of the sampled ®rmsreported an index value of greater than 0.5.The extent of such horizontal collaborationwas limited and had not changed since theFDA crisis. The only area where there was asigni®cant increase in such horizontal cooper-ation was in exchange of information andexperience with other ®rms (55% of the samplereporting an increase), much of which tookplace at the time of the crisis and had sincediminished.
Table 5. Changes in cooperation indices since the FDA crisis
Big increase>1.0(%)
Small increase0±1.0(%)
No change0
(%)
Small decreaseÿ1.0 to 0
(%)
Big decrease>ÿ1.0
(%)
COPSIMA2 11.7 61.7 25.0 1.7 0 N� 60COPFIRM2 0 53.3 46.7 0 0 N� 60COPSUPL2 0.7 54.9 41.7 1.7 0 N� 60COPSUBC2 11.7 70.0 18.3 0 0 N� 60COPBUYR2 5.1 72.4 17.2 5.1 0 N� 58
1620 WORLD DEVELOPMENT

The aggregated performance variable(PERF2) was developed through principalcomponent analysis, using the SPSS package.PERF2 consisted of the three performancevariables that had the highest factor loadingsfor the main factor (which was seen to accountfor 39.6% of the total variation). These are:growth over the past ®ve years in sales(Q2ASALES), improvements in product qual-ity (Q2FQUAL), and in employment(Q2GWRKRS).
As a ®rst step in assessing the relationshipbetween the aggregate measure of performance(PERF2) and the cooperation indices, KendallCorrelation Coe�cients were generated. AsTable 6 shows, the performance measure issigni®cantly and positively correlated (at the1% level) with the cooperation with buyersindex (COPBUYR2), and with the cooperationwith subcontractors index (COPSUBC2). Thecoe�cient is particularly high with cooperationwith buyers suggesting that overall perfor-mance and ®rm growth is most closely associ-ated with collaborative ties with buyers (0.436),followed by ties with subcontractors (0.286).Ties with suppliers also has a positive associa-tion on performance, however, this is onlysigni®cant at the 10% level. Interestingly, col-laboration through the trade association SIMAappears not to be associated with performance.This result, while appearing to diverge fromwhat the qualitative ®ndings suggests, supportsthe notion that sequencing and timing of sup-port is important. SIMA played a critical roleat the time of the crisis through a number ofstrategic interventions. Once the required pathto address the FDA's concerns had beenadopted, its in¯uence diminished.
It is also apparent that (at the 1% level ofsigni®cance) there is a positive correlationbetween cooperation with suppliers and coop-eration with subcontractors. This suggests that®rms which cooperate more closely with sub-contractors do the same with input suppliers.There is no signi®cant relationship howeverbetween cooperation in backward ties andcooperation with buyers. This is an importantresult, suggesting that while performance ismost closely related to improved ties withbuyers, greater cooperation with buyers is notcorrelated with improved ties with suppliersand subcontractors. Clearly, this indicates aweakness in the vertical chain relationship.Firms appear to address concerns of improvingtheir ties with external buyers independently oftheir relationships with local suppliers andsubcontractors.
It is important to consider whether there is acausal relationship between increasing cooper-ation and improved performance. To explorethis, simultaneous and step-wise regressionmethods were used to estimate the followingequation:
PERF2 � b1 � b2COPSIMA2
� b3COPSUPL2� b4COPSUBC2
� b5COPBUYR2:
The simultaneous multiple regression led tothe coe�cients for the independent variablesshown in Table 7.
While the R2 value is relatively low, there is aclear positive and signi®cant coe�cient for thecooperation with buyers and cooperation withsubcontractors indices. As can be expected this
Table 6. Correlation of performance and cooperation (Kendall coe�cients)
COPSUPL2 0.1768N(60)
Sig 0.090COPSUBC2 0.2235 0.3739
N(57) N(57)Sig 0.029 Sig 0.000
COPBUYR2 0.0846 0.0878 0.1225N(58) N(58) N(55)
Sig 0.403 Sig 0.406 Sig 0.238PERF2 0.0759 0.2011 0.2861 0.4358
N(60) N(60) N(60) N(58)Sig 0.440 Sig 0.051 Sig 0.005 Sig 0.000
COPSIMA2 COPSUPL2 COPSUBC2 COPBUYR2
a (Coe�cient/(Cases)/2-tailed Signi®cance).
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1621

is further borne out by the step-wise regressionmethod (where the variables COPSIMA2 andCOPSUPL2 were dropped). This results in aslightly better ®t, and a higher level of signi®-cance for the variable COPSUBC2 (seeTable 8).
These ®ndings substantiate the earlier resultsthat performance (and thus growth) over theprevious ®ve years has been associated withincreasing cooperation in ties that local ®rmshad with their buyers and their subcontractors.Cooperation in forward and backward tiesin¯uence performance. There is no evidence tosuggest, however, that this is the case for hor-izontal cooperation, nor is it clear that coop-eration in forward ties is necessarily associatedwith cooperation further down the supplychain.
To further strengthen this ®nding, it wouldbe important to see how the performance isin¯uenced by other factors not directly relatedto cooperation. This requires conducting aregression analysis for the same equation abovebut with a further independent variable for ®rmsize (SIZE). This is reported below using asimultaneous equation method (see Table 9).
Introducing ®rm size into the picture clearlyhas some in¯uence on the speci®cations of theequation and on the relationship with perfor-mance. Firm size is positively and signi®cantlycorrelated with performance. It is also appar-ent however, that cooperation with buyers(COPBUYR2) remains the variable most
closely associated with growth. None of theother variables are signi®cant. Carrying outthis exercise using a step-wise regressionmethod reveals similar results. What thisimplies is that if ®rm size is taken into con-sideration, greater cooperation in forward tiesstill has a positive and signi®cant in¯uence onperformance.
7. CONCLUSION
The evidence above shows that, in responseto the pressures posed by the quality assurancecrisis, there has been upgrading in manufac-turing practices in the Sialkot surgical instru-ment cluster. Furthermore, such upgrading hasinvolved greater joint action, both in verticaland horizontal ties. Joint action has also beenpositively associated with improved ®rm per-formance. This suggests not only that the col-lective e�ciency model continues to be valuablein explaining the competitive advantages thatlocal producers gain by virtue of being locatedin a sector specialized cluster, but also thatsustained competitiveness demands local jointaction.
In terms of backward ties it appears thatlinks with suppliers have led to signi®cantimprovements in the quality of stainless steelused. With regard to the widespread practice ofsubcontracting within the cluster, the trend onjoint action is less clear. There is evidence tosuggest that some large ®rms are movingtoward greater internalization of production asa way to reduce quality-related transactioncosts. This practice has involved ``in-house''subcontracting and has resulted in the emer-gence of ®rst-tier suppliers with whom large®rms have closer ties, not only for purposes ofmonitoring but also for quality upgrading. Itremains to be seen how widespread this practice
Table 8. Step-wise regression
CONSTANT ÿ0.039COPSUBC2 0.581 �
COPBUYR2 1.085 ��
Multiple R: 0.603 R2: 0.364, Adjusted R2: 0.340
� T-value signi®cant at 5%.�� T-value signi®cant at 1%.
Table 9. Simultaneous equation regression with ®rm size
CONSTANT ÿ0.506 �
COPSIMA2 0.076COPSUPL2 0.390COPSUBC2 0.264COPBUYR2 0.926 ���
SIZE 0.285��
Multiple R: 0.654 R2: 0.428, Adjusted R2: 0.370
� T-value signi®cant at 10%.�� T-value signi®cant at 5%.��� T-value signi®cant at 1%.
Table 7. Simultaneous multiple regression
CONSTANT ÿ0.033COPSIMA2 ÿ0.053COPSUPL2 0.291COPSUBC2 0.513 �
COPBUYR2 1.043 ���
Multiple R: 0.611 R2: 0.374, Adjusted R2: 0.323
� T-value signi®cant at 10%.��� T-value signi®cant at 1%.
1622 WORLD DEVELOPMENT

will become and the consequences it will haveon subcontracting more widely within thecluster. For most medium and small ®rms,subcontracting remains a signi®cant element ofproduction organization. There are signs ofgreater cooperation in ties that SMEs have withtheir subcontractors. It is also apparent, how-ever, that with the exception of the use of`travel cards', there is little to suggest that suchties have technically improved. Quality con-cerns were an important feature of these rela-tionships before the FDA's actions, yet thereare no apparent signs to show a qualitativeupgrading within such production linkages as aconsequence of the new competition.
Greater cooperation with buyers emerges asstatistically the most signi®cant factor associ-ated with ®rm growth, even when accountingfor ®rm size. In some cases it is apparent thatforward ties have weakened, due to pricecompetition and reduction in unit prices thathave been seen in the leading export markets,and as a consequence of certi®cation itself. Onthe whole though, ties with external buyershave grown in importance in the cluster, par-ticularly as conduits of information and newknow-how. It is also apparent that they haveled to a shift in the terms of trade in favor ofbuyers. Meanwhile horizontal joint action,particularly through the trade association, hasbeen a key arena for strategic local cooperationand has generated cluster-wide advantages. Theassociation helped connect local producers toexternal technical know-how at a critical junc-ture in the crisis, allowing SMEs to accessknowledge that was prohibitively costly. Theassociation also mobilized the state to interveneat this point.
Has the joint action that has occurred beenwholly bene®cial for the cluster or not? Sialk-ot's response to the FDA crisis provides clearsigns of greater collective action as well as ele-ments of what I term collective failureÐthat isto say, where collective action failed to takeplace, or where the actions of local agents led toa deterioration of their collective position.
The previous sections provide an account ofhow vertical and horizontal production andtrade ties have changed since 1994. In somecases these developments have also led to theemergence of further problems for the cluster,and there are other areas where the lack ofjoint action has meant that existing problemsremain unresolved. These areas of collectivefailure include the inability of the cluster toaddress a number of collective problems that
were present before the FDA crisis and whichremain an issue: poor infrastructure, and san-itation, low safety and health standards andthe continued use of child labor. Sialkot'sother leading export cluster, the sports goodindustry, has seen the damaging e�ect the useof child labor can have on its global reputa-tion and on its exports (Marcus and Harper,1996; Save the Children Fund, 1997). Childlabor is less of a problem in the surgicalinstrument sector but it does exist. SIMA hasbegun to work with its members to ensure thatthey do not use child labor. It has not, how-ever, been able to change practices amongsubcontractors where some child labor can befound.
Another area where there remains a collec-tive failure within the cluster is environmentalcosts of surgical instrument manufacturing.The GMP and ISO 9000 quality assurancerequirements are only the ®rst stage in anincreasingly more stringent and quality-drivenmarket environment. ISO 14000 requirementsare likely to follow hard on the heels of thecurrent quality-assurance demands. This willbecome another important area for the Sialkotcluster where joint action could lead to signi-®cant improvements in working conditions,health and safety standards, pollution controland overall improvement of the physicalenvironment in which manufacturing takesplace.
Similarly, the poor condition of local infra-structureÐespecially power supply, roads, andsewerageÐact as an inhibiting factor on thecluster's potential growth. Again, local pro-ducers have not yet explored the possibility ofjoint action. All of these are issues that thecluster will have to address if it is to raise itsproductive e�ciency and continue to meet theincreasingly stringent standards that Westernmarkets demand.
A particularly important aspect of collectivefailure, highlighted by the survey data onchanges in horizontal and vertical ties, is thelimited increase in inter-®rm cooperation aimedat bringing about improvements in labortraining. The cluster's skill base is traditional,and to some extent artisanal. It has been a keyfactor in generating the cluster's competitive-ness. As the quality assurance crisis has indi-cated, however, the nature of markets arerapidly changing, calling for new skills andundermining the basis of traditional practices.In this rapidly changing environment, a failureto improve labor skills and to build the cluster's
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1623

technical capacity does not bode well for itsability to upgrade in a sustained fashion.
On the speci®c and immediate issue ofquality assurance, however, there was a signi-®cant increase in inter®rm cooperation. Thisconclusion needs to be quali®ed. Once agents(and more broadly the cluster as a whole) arecerti®ed as meeting regulatory standards,transaction costs for external buyers engagingwith local producers are e�ectively lowered.Standard certi®cation assures that ®rms con-form to international quality assurancerequirements. Standards, therefore, provide abasis for what Zucker (1986) refers to as insti-tutional trust. This can potentially allow for theexistence of arms-length contracts betweenagents within the supply chain. The institu-tional trust encapsulated in GMP certi®cationhas for some buyers meant a return to arms-length contracts with local producers. Suchbuyers could loosen their longstanding ties withlocal producers and search out cheaper alter-native suppliers.
Nevertheless, ensuring that the cluster as awhole complies, and that local ®rms thereforeobtain the bene®ts of this reputation e�ect,requires e�ective local governance and regula-tion. Cooperation of private actors is not suf-®cient and the state has a role to play here. Insubsidizing the costs for local ®rms to obtainthe know-how to get through the GMP hur-dles, the state in coordination with the tradeassociation provided the cluster's producers,particularly SMEs, with a way through thecrisis.
Thus this study indicates a mixed story onthe response of the Sialkot surgical instrument
cluster to the crisis in quality assurance. Therehas been extensive local cooperation especiallythrough a more invigorated trade body. Jointaction in vertical ties is apparent, but uneven.Alongside examples of collective action thereremains collective failure. The evidence sug-gests that a process of di�erentiation hasresulted, with SMEs being squeezed whilelarger producers are better positioned to switchgears and become internationally certi®ed inquality assurance. At the same time the moreproactive stance of the trade body and its rolein facilitating the provisioning of quality-relat-ed services to the cluster as whole has allowedmany SMEs to upgrade and comply with GMPstandards. What is of importance and at issue,however, is not so much the demise of smaller®rms but the survival and continuing growth ofthe cluster as whole. Here there may be evi-dence that Sialkot's surgical instrument clustermay manage to rise to the challenge. Clearly theability of the cluster to do so will rest in largemeasure on the issue of local governance. Thetype of governance determines the nature ofinter-®rm relations within vertical supplychains that link local suppliers and manufac-turers to external markets, as well as thestrength of horizontal relations that provide thebasis for collective joint action within thecluster. The challenge for the Sialkot cluster isto address the collective failures pointed outabove. The increasing di�erentiation makes itdi�cult to rely entirely on the cooperation ofprivate actors to solve these problems. Publicintervention in partnership with private initia-tive is required to sustain the cluster's compet-itiveness.
NOTES
1. On labor standards see, for example, Sengenberger
and Campbell (1994), ILO (1997) and Lee (1997). On
standards and global ``value chains,'' see Brown et al.
(1993). On ethical standards, see Zadek and Ti�en
(1996) on fair trade initiatives, Hilowitz (1997) on social
labeling and van Liemt (1998) and Murray (1997) on
corporate codes of conduct.
2. The paper is based on research undertaken prior to
the ®nancial crisis that Pakistan faced in 1998 following
the explosion of nuclear devices and, therefore, does not
take into account the impact of these events on the
cluster.
3. For reasons of con®dentiality all ®rm and respon-
dent names, where reported, have been altered.
4. The survey instrument was based on one developed
jointly with Peter Knorringa, Roberta Rabellotti and
Hubert Schmitz.
5. On the cluster's history see Nadvi (1996).
6. The consultant does not do the actual GMP
certi®cation. That is left to the FDA. Its task is simply
to train management on GMP and TQM issues. This is
done through day-long seminars, the dissemination of
1624 WORLD DEVELOPMENT

quality related literature, on-site training and pre-certi-
®cation inspections.
7. Source: SIMA and Federal Bureau of Statistics.
8. It should be noted, however, that by December 1997
neither facility had been set up.
9. The index was generated by attaching equal weights
to each of the speci®c relevant variables in each category
of backward, forward and horizontal relationships. The
®ve possible responses for each variable, from ``big
increase'' to ``big decrease'' were coded on a range of +2
to ÿ2, with no change being coded as 0. Variables that
were seen to have been insigni®cant for this particular
case study (such as speeding up delivery) were dropped
from the analysis, while others that were unique to the
Sialkot cluster (such as help in developing quality
assurance systems) were included in the respective
indices.
REFERENCES
Anderson, K. (1996) Environmental standards andinternational trade. Proceedings of the World BankAnnual Conference on Development Economics, 317±338.
Audretsch, D. and Feldman, M. (1996) R & D spilloversand the geography of innovation and production.American Economic Review (June), 630±640.
Brown, H. S., Derr, P., Renn, O. and White, A. L.(1993) Corporate Environmentalism in a GlobalEconomy. Quorum, Westport, CT.
Brusco, S. (1992) Small ®rms and the provision ofreal services. In Industrial Districts and Local Eco-nomic Regeneration, ed. F. Pyke and W. Sengenber-ger. International Institute of Labour Studies,Geneva.
Dion, C., Lanoie, P. and Laplante, B. (1997) Monitoringenvironmental standards: Do local conditions mat-ter? World Bank Development Research Group PolicyResearch Working Paper No. 1701. World Bank,Washinton, DC, January.
Foss, N. J. (1996) Higher-order industrial capabilitiesand competitive advantage. Journal of IndustryStudies 3(1), 1±20.
GEMCO Industrial Development (1990) Technologyneeds assessment (Draft). MIDC project, Unpub-lished manuscript, Sialkot, Pakistan.
Grootaert, C. and Kanbur, R. (1995) Child labour: Aneconomic perspective. International Labour Review134, 187±203.
Hilowitz, J. (1997) Social labeling to combat childlabour: Some considerations. International LabourReview 136(2), 215±232.
ILO (1997) Child labour: How the challenge is being metprepared by Mark Lansky. International LabourReview 136(2), 233±257.
Kaplinsky, R. (1998) Globalisation, industrialisationand sustainable growth: The pursuit of the Nth rent.Discussion Paper No. 365, Institute of DevelopmentStudies, University of Sussex, Brighton.
Krueger, A. B. (1996) International labor standards andtrade. Proceedings of the World Bank Annual Con-ference on Development Economics, 281±315.
Lee, E. (1997) Globalisation and labour standards: Areview of issues. International Labour Review 136(2),173±189.
van Liemt, G. (1998) The social policy implications ofcodes of conduct, with particular reference to the
relations between companies adopting such codesand their suppliers and subcontractors. Paper pre-sented at International workshop on Global Produc-tion and Local Jobs: New Perspectives on EnterpriseNetworks, Employment and Local DevelopmentPolicy, International Institute of Labour Studies,Geneva, March 9±10.
Marcus, R. and Harper, C. (1996) Small hands: Childrenin the working world. Working Paper No. 16, Savethe Children Fund, London.
Maskus, K. E. (1997) Should core labor standards beimposed through international trade policy? WorldBank Development Research Group Policy ResearchWorking Paper No. 1817, World Bank, Washington,DC, August.
Murray, J. (1997) Corporate codes of conduct and fairlabour standards. Paper presented at Internationalworkshop on Global Production Systems andLabour Markets, International Institute of LabourStudies, Geneva, May 22±23.
Nadvi, K. M. (1996) Small Firm Industrial Districts inPakistan. DPhil Thesis. University of Sussex.
Nadvi, K. (1999) The cutting edge: Collective e�ciencyand international competitiveness in Pakistan. Ox-ford Development Studies 27(1), 81±107.
OECD (1996) Trade, Employment and Labour Stan-dards: A Study of Core Workers' Rights and Inter-national Trade. OECD, Paris.
OECD (1995) Trade and Labour Standards: A Review ofthe Issues. Prepared by Gary Fields, OECD, Paris.
Sako, M. (1992) Prices, Quality and Trust. CambridgeUniversity Press, Cambridge.
Save the Children Fund, (1997) Stitching Football:Voices of Children. Save the Children Fund, London.
Sengenberger, W. and D. Campbell, eds. (1994) Inter-national Labour Standards and Economic Interdepen-dence. International Institute for Labour Studies,ILO, Geneva.
Sengenberger, W. and Pyke, R. (1991) Small ®rmindustrial districts and local economic regenera-tion: Research and Policy issues. Lobour and Society16(1).
Stephenson, S.M. (1997) Standards and conformityassessment as non-tari� barriers to trade. WorldBank Development Research Group Policy ResearchWorking Paper No. 1826, World Bank, Washington,DC, September.
COLLECTIVE EFFICIENCY AND COLLECTIVE FAILURE 1625

Wiegersma, S. (1989) Analysis of the quality scene in thePakistan surgical instruments industry. MissionReport, Dutch Technical Aid Program, Islamabad.
White, B. (1996) Globalisation and the child labourproblem. Journal of International Development 8(6),829±839.
Zadek, S. and Ti�en, P. (1996) ``Fair trade'': Business orcampaign? Development 3.
Zucker, L. G. (1986) Production of trust: Institutionalsources of economic structure, 1840±1920. Researchin Organisational Behaviour 8, 53±111.
1626 WORLD DEVELOPMENT