THE PSYCHOLOGY OF COSMETIC SURGERY:A REVIEW AND RECONCEPTUALIZATION
22
@ Pergamon Clinical Psychology Review, Vol. 18, No. 1, pp. 1-22, 1998 Copyright @ 1998 Elsevier Science Ltd Printed in the USA. AU rights reserved 0272-7358/98 $19.00 + .00 PII s0272-7358(97)00047-0 THE PSYCHOLOGY OF COSMETIC SURGERY:A REVIEW AND RECONCEPTUALIZATION David B. Sarweq Thomas A. Wadden, Michael]. Pertschuk, and linton A. Whitaker University of PennsylvaniaSchool of Medicine ABSTRACT. This article discussesthepsychologyof cosmeticsurgery.A review of the research on thepsycholagicalcharacteristicsof individualswhoseekcosmeticsurgmyyieldedcontradictory findings. Interview-based investigations revealed high levels of psychopathohgy in cosmetic surgerypatients, whereasstudies that used standardiud measurementsreportedfar less distur- bance. [t is dtjj$culttofuliy resolve the discrepant betweenthesetwo sets of$ndings. We believe that investigatingthe constructof bodyimage in cosmeticsurgerypatients willyield more useful findings. Thus, we propose a model of the relationshipbetweenbody image dissatisfactionand cosmeticsurgeryand outlinea researchagendabasedupon the model.Suchresearchwillgenerate infwmation that is useful to the medical and mental health communitiesand, ultimately,the patients themselves.O 1998 Elsevier ScienceLtd EACH YEAR tens of thousands of persons undergo elective, cosmetic surgery to alter their physical appearance. In 1994, for example, the American Society of Plastic and Reconstructive Surgeon8 (ASPRS) reported its membership performed more than 390,000 cosmetic procedures, the most common including liposuction (fat removal from various body regions), breast augmentation, rhinoplasty (nose alteration), and rhytidectomy (face lift) (ASPRS, 1994). This is an underestimation of the actual number performed, as general surgeons and physicians from other specialities also perform cosmetic procedures. Ultimately, these procedures were undertaken to im- prove individuals’ satisfaction with their appearance, and presumably, in many cases, their self-esteem. In this regard, cosmetic surgery can be considered a psychological intervention or, at a minimum, a surgical procedure with psychological consequences. Remarkably little is known about either the psychological statusof persons who seek cosmetic surgery or potential psychological changes following surgery. For example, Correspondence should be addressed to David B. Sarwer,PhD, Universityof Pennsylvania Medical Center, The Edwin and Fannie Gray Hall Center for Human Appearance, 10 Penn Tower,3400 Spruce Street,Philadelphia,PA 19104. 1
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of THE PSYCHOLOGY OF COSMETIC SURGERY:A REVIEW AND RECONCEPTUALIZATION
@Pergamon
Clinical Psychology Review, Vol. 18, No. 1, pp. 1-22, 1998Copyright @ 1998 Elsevier Science LtdPrinted in the USA. AU rights reserved
0272-7358/98 $19.00 + .00
PII s0272-7358(97)00047-0
THE PSYCHOLOGY OF COSMETICSURGERY:A REVIEW ANDRECONCEPTUALIZATION
David B. Sarweq Thomas A. Wadden, Michael]. Pertschuk,and linton A. Whitaker
University of PennsylvaniaSchool of Medicine
ABSTRACT. This article discussesthepsychologyof cosmeticsurgery.A review of theresearchon thepsycholagicalcharacteristicsof individualswhoseekcosmeticsurgmyyieldedcontradictoryfindings. Interview-based investigations revealed high levels of psychopathohgy in cosmeticsurgerypatients, whereasstudies that used standardiud measurementsreportedfar less distur-bance. [t is dtjj$culttofuliy resolve the discrepant betweenthesetwo sets of$ndings. We believethat investigatingthe constructof bodyimagein cosmeticsurgerypatients willyield moreusefulfindings. Thus, we propose a modelof the relationshipbetweenbody image dissatisfactionandcosmeticsurgeryand outlinea researchagendabasedupon themodel.Suchresearchwillgenerateinfwmation that is useful to the medicaland mental health communitiesand, ultimately,thepatients themselves.O 1998 ElsevierScienceLtd
EACH YEAR tens of thousands of persons undergo elective, cosmetic surgery to altertheir physical appearance. In 1994, for example, the American Society of Plastic andReconstructive Surgeon8 (ASPRS) reported its membership performed more than390,000 cosmetic procedures, the most common including liposuction (fat removalfrom various body regions), breast augmentation, rhinoplasty (nose alteration), andrhytidectomy (face lift) (ASPRS, 1994). This is an underestimation of the actualnumber performed, as general surgeons and physicians from other specialities alsoperform cosmetic procedures. Ultimately, these procedures were undertaken to im-prove individuals’ satisfaction with their appearance, and presumably, in many cases,their self-esteem. In this regard, cosmetic surgery can be considered a psychologicalintervention or, at a minimum, a surgical procedure with psychological consequences.
Remarkably little is known about either the psychological statusof persons who seekcosmetic surgery or potential psychological changes following surgery. For example,
Correspondence should be addressed to David B. Sarwer,PhD, Universityof PennsylvaniaMedical Center,The Edwin and Fannie GrayHall Center for Human Appearance, 10 PennTower,3400 Spruce Street,Philadelphia,PA 19104.
1
2 D. B. Sarweret al,
do such individuals suffer from some degree of body image dissatisfaction, includingthe clinically significant Body Dysmorphic Disorder? Alternatively, are such individualspsychologically healthy and seek surgery to enhance an already favorable self-image?Perhaps such persons intuitively grasp what social scientists have learned over the lastthree decades — that people associate physical attractiveness with numerous highlyfavorable personality traits including intelligence, competence, and social desirability(e.g., Hatfield & Sprecher, 1986).
This article discusses the psychology of cosmetic surgery. It begins by reviewing thepsychological research on cosmetic surgery patients and then discusses recent ad-vances in the psychology of body image. Most contemporary theorists believe thatbody image concerns are central to understanding cosmetic surgery patients. How-ever, there has been little formal study of this relationship. Thus, we propose a modelof the relationship between body image dissatisfaction and cosmetic surgery, andprovide recommendations for empirical research on this relationship. We note at theoutset that research on the psychology of cosmetic surgery patients is generally oflimited scope and quality, consisting largely of clinical reports. In light of the highnumber of procedures performed annually, and given the potential for psychologicalharm as well as benefit from a surgical alteration of appearance, advances in theoryand research are urgently needed.
THE PSYCHOLOGY OF COSMETIC SURGERY
In his historical review, Gifford (1972) traced interest in the psychology of cosmeticsurgery patients to Freud’s (1918) Wolf-Man, whose obsessive concern with a trivialscar from a cyst removal became a focus of one of the most famous cases in psychiatricannals. Soon after, surgical advances following World War I were accompanied byenthusiastic reports of the emotional relief experienced by disfigured individuals whounderwent reconstructive surgery. These positive reports fueled the growth of plasticsurgery as an elective procedure for nondisfigured individuals.
Formal psychiatric evaluations of persons seeking elective cosmetic surgery firstappeared in the literature during the 1940s and 1950s. Typically, these reportsreflected the dominance of psychoanalytic thinking in American psychiatry andgenerally characterized patients as highly neurotic and/or narcissistic (e.g., Hill &Silver, 1950; Linn & Goldman, 1949). Patients’ appearance complaints frequently wereconceptualized in terms of intrapsychic conflicts displaced onto somatic concerns.Surgeons were cautioned of the psychopathology of the male patient, as well as of the“insatiable” surgery patient who sought out numerous cosmetic procedures in pursuitof the perfect face. Although patients of the era were thought to be psychologicallydisturbed, surgery rarely was ruled out, and the psychiatric outcomes typically weredescribed as positive (Gifford, 19’72).
The m~ority of the psychological literature on cosmetic surgery patients has beenpublished from 1960 to the present. T~ically, these investigations have been theproduct of collaborations between plastic surgeons and psychiatrists or psychologists.They have reflected surgeons’ interest in identifying patients who are psychologicallyinappropriate for surgery, as well as psychiatrists’ interest in relating psychopathologyto specific cosmetic procedures. Plastic surgeons also perform reconstructive proce-dures to correct congenital defects or those resulting from traumatic injury. Whilethese latter procedures may involve a significant psychological component, thepresent review is limited to cosmetic procedures.
—.——-
The Psychologyof CosmeticSurgery 3
We have organized the existing research into two categories. The first includespreoperative psychological assessments of patients. The second category concernspostoperative psychological assessments and examines patients’ psychological re-sponses to the resulting change in appearance.
PREOPERATIVE PSYCHOLOGICAL INVESTIGATIONS
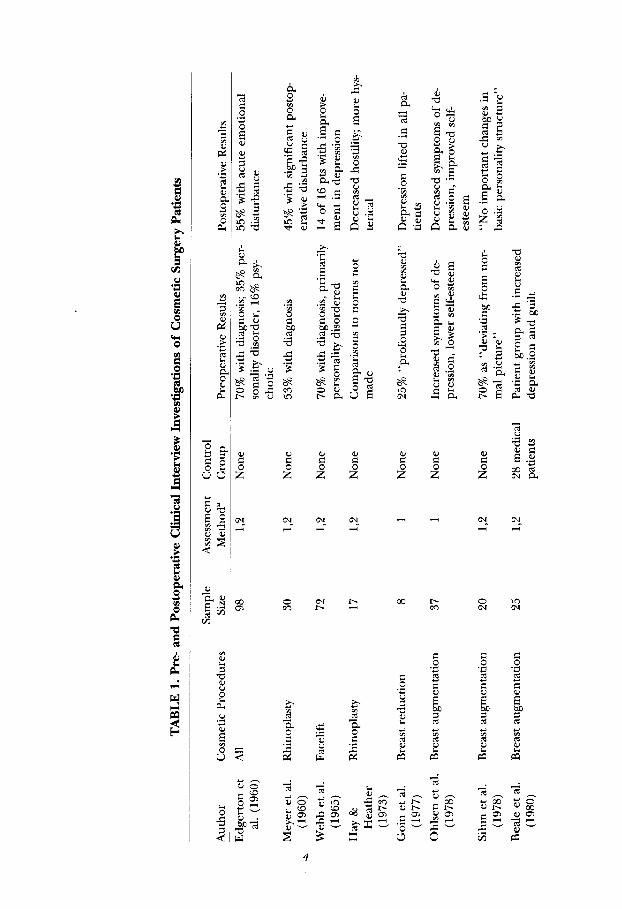
Numerous studies have assessed the preoperative psychological status of cosmeticsurgery patients. These reports, summarized in Tables 1 and 2, can be divided intothose that relied primarily on clinical interview (see Table 1) versus those that usedpsychometric measures to assess psychopathology (see Table 2).
Clinical Assessments
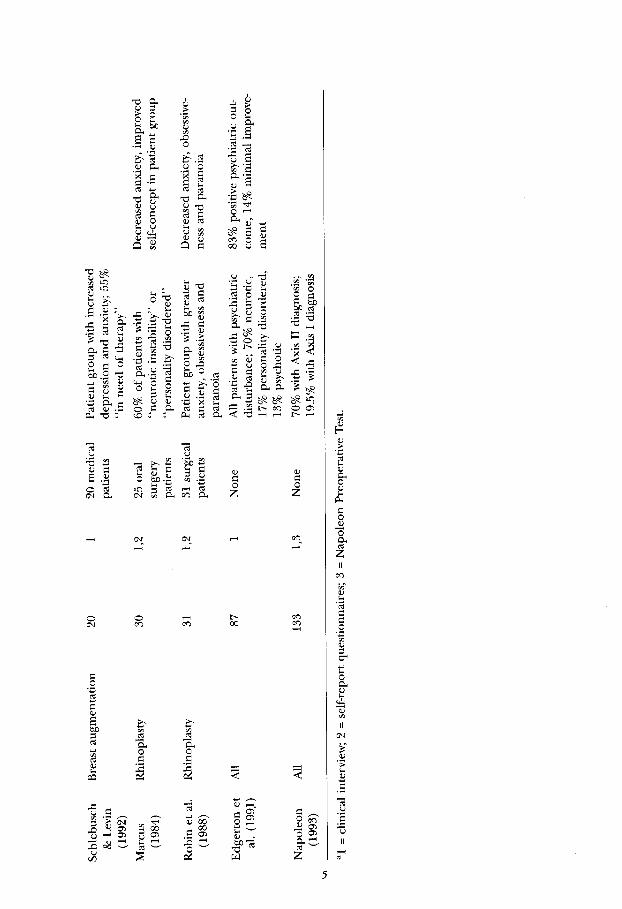
Most studies that relied on clinical interview reported significant psychopathology incosmetic surgery patients (see Table 1). In one of the earliest investigations, 70$Z0of aseries of 98 patients were diagnosed with a psychiatric disturbance, the most common ofwhich were described as neurotic depression and passivedependent personality (Edger-ton, Jacobson, & Meyer, 1960). Similar descriptions of psychopathology were reported ina series of facelift patients (Webb, Slaughter, Meyer, & Edgerton, 1965), three investiga-tions of rhinoplasty patients (Marcus, 1984; Meyer,Jacobson, Edgerton, & Canter, 1960;Robin, Copas, Jack, Kaeser,& Thomas, 1988), and four investigationsof breast augmen-tation patients (Beale, Lisper, & Palm, 1980; Ohlsen, Ponten, & Hambert, 1978; Schle-busch & Levin, 1983; Sihm,Jagd, & Pers, 1978).
Methodological shortcomings limit the confidence that can be placed in the abovefindings. First, these studies did not use standardized assessment procedures. In mostcases, the nature of the clinical interview was not described and uniform diagnosticcriteria were not used. Patient categorizations found in these papers, such as “markedpsychological disturbance,” “ deviating from the normal picture,” and “in need oftherapy” are so vague as to make replication impossible.
Some investigations augmented the interview with self-report measures, but it is notclear how these data were used in formulating the descriptions or diagnoses. Inaddition, a majority of investigations did not include a control or comparison group.As a result, it is impossible to determine if the reported level of psychologicaldisturbance was greater than that of patients who underwent other medical or surgicalprocedures, or of control subjects matched on appropriate comparison variables.Finally, the high levels of psychopathology may have been a reflection of the biases ofthe primarily psychoanalytically-trained psychiatrist investigators.
Such methodological limitations can be found even in recent interview studies.Napoleon (1993) reported that 70% of patients in a cosmetic surgery practice had anAxis II personality disorder and 19.5% of patients had an Axis I disorder. AlthoughNapoleon’s study improved upon earlier investigations by using widely accepteddiagnostic criteria (Diagnostic and StatisticalManual of Mental Disordms, third edition,muised [DSM-111-R];American Psychiatric Association [APA], 1987), the use of anunspecified clinical interview and an absence of interrater reliability of diagnosescould account for the high prevalence of Axis 11disorders in this sample.
In summary, clinical reports of psychopathology in cosmetic surgery patients mustbe viewed with caution. Given the shortcomings noted, it is impossible to determinewhether patients truly were psychologically disturbed. The above studies also did not
TA
BL
E1.
Pre
-an
dP
osto
pera
tive
Cli
nic
alIn
terv
iew
Inve
stig
atio
ns
ofC
osm
etic
Su
rger
yP
atie
nts
Au
thor
Cos
met
icP
roce
dure
s. Edg
erto
net
al.(
1960
)
Mey
eret
al.
A(1
960)
Web
bet
al.
(196
5)
Hay
&H
eath
er(1
973)
Goi
net
al.
(197
7)
Oh
lsen
etal
.(1
978)
Sih
met
al.
(197
8)
Bea
leet
al.
(198
0)
All
Rh
inop
last
y
Fac
elif
t
Rh
inop
last
y
Bre
astr
edu
ctio
n
Bre
asta
ugm
enta
tion
Bre
asta
ugm
enta
tion
Bre
asta
ugm
enta
tion
Sam
ple
Siz
e
98 30 72 17 8 37 20 25
Ass
essm
ent
Met
hod
’
1,2
1,2
1,2
1,2 1 1
1,2
1,2
Con
trol
Gro
up
Pre
oper
ativ
eRes
ult
s
Non
e
Non
e
Non
e
Non
e
Non
e
Non
e
Non
e
28m
edic
alpa
tien
ts
70%
wit
hdi
agn
osis
;35%
per-
son
alit
ydis
orde
r,16
~0p
sy-
chot
ic
53%
wit
hdi
agn
osis
70%
wit
hdi
agn
osis
,pri
mar
ily
pers
onal
ityd
isor
dere
d
Com
pari
son
sto
nor
ms
not
mad
e
25%
“pro
fou
ndl
yde
pres
sed”
Incr
ease
dsy
mpt
omso
fde
-pr
essi
on,l
ower
self
-est
eem
70%
as“d
evia
tin
gfr
omn
or-
mal
pict
ure
”
Pat
ien
tgro
up
wit
hin
crea
sed
depr
essi
onan
dgu
ilt
Pos
tope
rati
veR
esu
lts
55%
wit
hac
ute
emot
ion
aldi
stu
rban
ce
45%
wit
hsi
gnif
ican
tpos
top-
erat
ived
istu
rban
ce
14of
16pt
sw
ith
impr
ove-
men
tin
depr
essi
on
Dec
reas
edh
osti
lity
;mor
eh
ys-
teri
cal
Dep
ress
ion
lift
edin
allp
a-ti
ents
Dec
reas
edsy
mpt
omso
fde
-pr
essi
on,i
mpr
oved
self
--e
stee
m
“NO
impo
rtan
tch
ange
sin
basi
cpe
rson
alit
ystr
uctu
re”
Sch
lebu
sch
&L
evin
(199
2)
Mar
cus
(198
4)
Rob
inet
al.
(198
8)
Edg
erto
net
al.(
199.
1)
Nap
oleo
n(1
993)
Bre
asta
ugm
enta
tion
Rh
inop
last
y
Rh
inop
last
y
All
20 30 31 87
120
med
ical
pati
ents
1,2
25or
alsu
rger
ypa
tien
ts
1,2
31su
rgic
alpa
tien
ts
1N
one
All
133
1,3
Non
e
Pat
ien
tgro
up
wit
hin
crea
sed
depr
essi
onan
dan
xiet
y;55
%<
‘inn
eed
ofth
erap
y”
60%
ofpa
tien
tsw
ith
“neu
roti
cin
stab
ilit
y”or
“per
son
alit
ydi
sord
ered
”
Pat
ien
tgro
up
wit
hgr
eate
ran
xiet
y,ob
sess
iven
essa
nd
para
noi
a
All
pati
ents
wit
hps
ych
iatr
icdi
stu
rban
ce;7
0%n
euro
tic,
17%
pers
onal
ityd
isor
dere
d,13
%ps
ych
otic
70%
wit
hA
xis
IIdi
agn
osis
;19
.5%
wit
hA
xis
Idi
agn
osis
Dec
reas
edan
xiet
y,im
prov
edse
lf-c
once
ptin
pati
entg
rou
p
Dec
reas
edan
xiet
y,ob
sess
ive-
nes
san
dpa
ran
oia
83%
posi
tive
psyc
hia
tric
out-
com
e,14
%m
inim
alim
prov
e-IU
eIlt
al=
clin
ical
inte
rvie
w;2
=se
lf-r
epor
tqu
esti
onn
aire
s;3=
Nap
oleo
nP
reop
erat
iveT
est.
I I
TA
BL
E2.
Pre
-an
dP
osto
pera
tive
Psy
chom
etri
cA
sses
smen
tIn
vest
igat
ion
sof
Cos
met
icS
urg
ery
Pat
ien
ts
Ass
essm
ent
Con
trol
~A
uth
orC
osm
etic
Pro
cedu
reS
ampl
eSiz
eM
eth
od’
Gro
up
Hay
(197
0)R
hin
opla
sty
451,
2,3
45N
urs
es
Bak
eret
al.
Bre
asta
ugm
enta
tion
10(1
974)
Wri
ght
&R
hin
opla
sty
25W
righ
t(1
975)
Sh
iple
yet
al.
Bre
asta
ugm
enta
tion
28(1
977)
1,2,
3,4
Non
e
425
surg
e~pa
tien
ts
2,6
28sm
all-
brea
sted
wom
enan
d28
aver
age-
brea
sted
wom
en
Pre
o~er
ativ
eRes
ult
sP
osto
pera
tive
Res
ult
s
Pat
ien
tgro
up
mor
en
euro
tic
and
obse
ssiv
e;18
diag
nos
edw
ith
pers
onal
ityd
isor
der
Nor
mal
com
posi
tepr
ofil
e
Pd
scal
esi
gnif
ican
tly>
inN
osi
gnif
ican
tdif
fere
nce
inrh
inop
last
ygro
up,
no
path
o-pr
e/po
stsc
ores
logi
cals
core
sin
rhin
opla
sty
grou
p
Pat
ien
tssc
ored
low
eron
ach
ieve
men
tan
dfe
min
ity;
all
scor
esw
ith
1S
Dof
nor
mat
ive
sam
ple
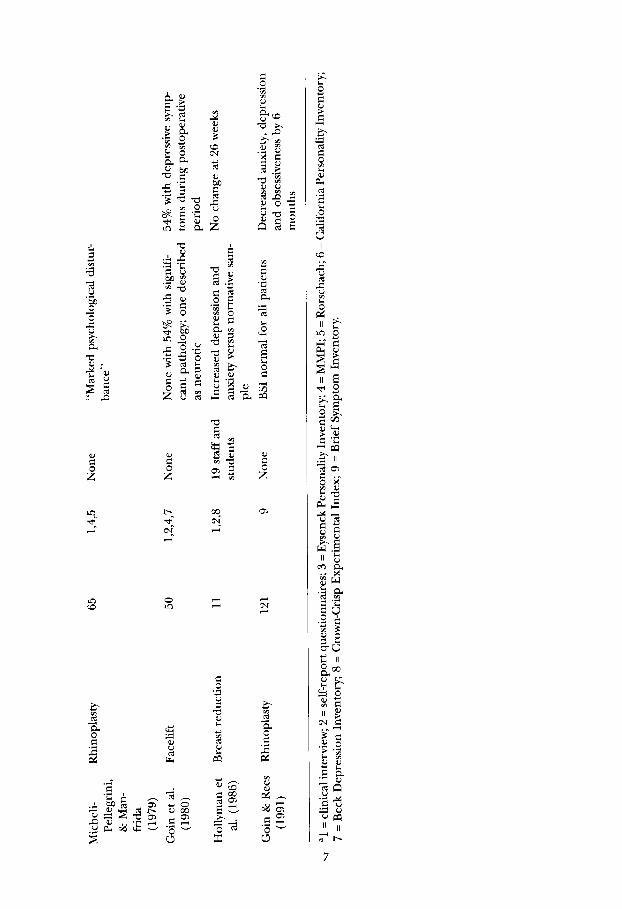
Mic
hel
i-P
elle
grin
i,&
Man
-fi
-ida
(197
9)
Goi
net
al.
(198
0)
Hol
lym
anet
al.(
1986
)
Goi
n&
Ree
s(1
991)
Rh
inop
last
y
Fac
elif
t
Bre
astr
edu
ctio
n
Rh
inop
last
y
65 50 11 121
1,4,
5N
one
“Mar
ked
psyc
hol
ogic
aldi
stu
r-ba
nce
”
1,2,
4,7
Non
eN
one
wit
h54
%w
ith
sign
ifi-
can
tpat
hol
ogy;
one
desc
ribe
das
neu
roti
c
1,2,
819
staf
fan
dIn
crea
sed
depr
essi
onan
dst
ude
nts
anxi
etyv
ersu
snor
mat
ives
am-
ple
9N
one
BS
Inor
mal
for
allp
atie
nts
54%
wit
hde
pres
sive
sym
pto
ms
duri
ng
post
oper
ativ
epe
riod
No
chan
geat
26w
eeks
Dec
reas
edan
xiet
y,de
pres
sion
and
obse
ssiv
enes
sby
6m
onth
s
val
=cl
inic
alin
terv
iew
;2=
self
-rep
ortq
ues
tion
nai
res;3
=E
ysen
ckP
erso
nal
ityI
nve
nto
ry;4
=M
MP
I;5
=R
orsc
hac
h;6
=C
alif
orn
iaP
erso
nal
ityI
nve
nto
ry;
7=
Bec
kD
epre
ssio
nIn
ven
tory
;8=
Cro
wn
-Gri
spE
xper
imen
talI
nde
x;9
=B
rief
Sym
ptom
Inve
nto
ry.

8 D. B. Sarweret al.
determine whether patients who sought the same cosmetic procedure, such as a“type-changing” rhinoplasty (in which the nose is altered to a new appearance),shared specific psychological problems that differed from those of persons whounderwent a different procedure, such as a “restorative” face lift (in which the faceis returned to a younger, former state). Rather, the clinical literature reviewed aboveconcluded, perhaps prematurely, that a majority of cosmetic surgery patients werepsychologically disturbed.
Psychometric Assessments
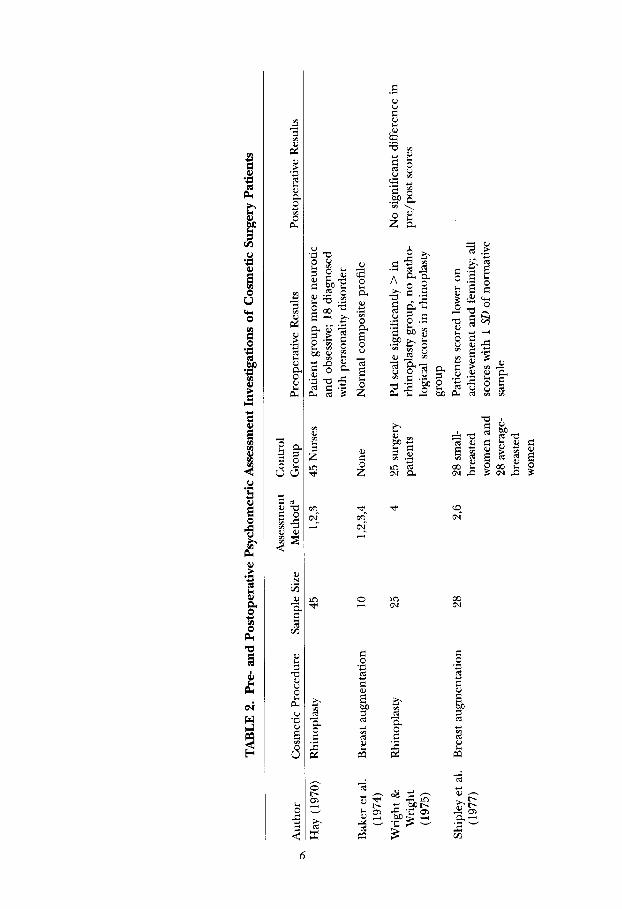
Studies that used standardized tests to assesspsychopathology generally have reportedless disturbance, as compared with the results of clinical interview investigations (seeTable 2). The most frequently used measure of psychopathology has been the Min-nesota Multiphasic Personality Inventory (MMPI). No significant psychopathology wasreported for 50 facelift patients who completed the MMPI preoperatively (Goin,Burgoyne, Goin, & Staples, 1980).
Similarly, normal MMPI profiles were found in a series of 10 breast augmentationpatients (Baker, Kolin, & Bartlett, 1974), and in two separate investigations of rhino-plasty patients (Micheli-Pellegrini & Manfrida, 1979; Wright & Wright, 1975).
Investigations that used other measures also found mild or no psychopathology.Twenty-eight breast augmentation patienfi only differed from small- and average-breast-size control group women on variables of “Achievement via Independence”and “Flexibility,” as measured by the California Personality Inventory (Shipley,O’Donnell, & Bader, 1977). Similarly,a series of 121 rhinoplasty patients scored in thenormal range on the Brief Symptom Inventory (Goin & Rees, 1991). Mild psychopa-thology was observed in two other studies. Using a battery of tests that included theEysenck Personality Inventory, rhinoplasty patients were found to be more neuroticand obsessive than a control group of hospital nurses (Hay, 1970). A sample of 11breast-reduction patients also was found to have mild psychopathology, includingincreased depression and anxiety, as compared to normative values of the Crown-CrispExperimental Index (Hollyman, Lacey, Whitfield, & Wilson, 1986).
While these results suggest far less psychopathology in cosmetic surgery patients ascompared with the interview investigations, these studies also have limitations. In mostcases, the measures used were not designed to tap the types of psychopathologyspecific to these patients. While a measure such as the MMPI psychasthenia scale mayprovide a “global” measure of worry and obsessiveness, it may not be sensitive to typesof disturbances associated with appearance concerns. In addition, several investiga-tions failed to use control or comparison groups. Finally,investigations that comparedpatients to normative samples frequently failed to describe similarities or differenceson descriptive characteristics between the two groups. As such, the appropriateness ofsuch comparisons is unknown.
Conclusions from the Preoperative Assessments
We believe that the results of the objective, paper-and-pencil tests generally are morereliable and valid than those derived from clinical interview. We tentatively conclude,based on an admittedly small number of studies, that a majority of cosmetic surgerypatients do not suffer from serious psychological disturbance. Moreover, there ap-pears to be no clear relationship between a given cosmetic procedures and specificforms of psychopathology.

The Psychologyof CosmeticSurgery 9
Two alternative interpretations, however, of the disparity between the interview- andpsychometric-based findings warrant consideration. First, the nature of the cosmeticsurgery population has changed over time. Prior to the 1970s, when investigatorsreported higher rates of psychopathology, cosmetic surgery was far less common.Today, not only are more individuals seeking cosmetic surgery than ever before, butthese women and men come from a wider range of age and socioeconomic-economicgroups (ASPRS, 1994). Perhaps one had to be more psychologically disturbed to seekout cosmetic surgery when it was not the highly marketed service that it is today. Asecond possibility, as noted above, is that earlier investigators, many of whom wereskilled clinicians, uncovered more subtle psychological features in their interviewsthat may have been missed by standardized measures. Unfortunately, the nature ofthese traitsmay have been inadequately described and, therefore, lost as a result of thecomparatively vague psychiatric nomenclature of the time.
POSTOPERATIVE PSYCHOLOGICAL INVESTIGATIONS
Investigations of the psychological outcome of cosmetic surgery have not yieldeddefinitive results. As shown in Table 1, 6 of 10 studies that used clinical interviewsreported generally favorable psychological outcome (Edgerton et al., 1991; Goin et al.,1977; Marcus, 1984; Ohlsen et al., 1978; Robin et al., 1988; Webb et al., 1965), whiletwo observed negative consequences (Edgerton et al., 1960; Meyer et al., 1960), andtwo others noted no change or mixed results (Hay& Heather, 1973; Sihm et al., 19’78).In addition to the criticisms of the preoperative interview assessments describedpreviously, pre- and postoperative interviews frequently were conducted by the sameinterviewer, a practice that increases the potential for interviewer bias. Thus, althoughthe reports of positive psychological change following cosmetic surgery are encour-aging, they should be viewed cautiously.
Table 2 shows that only four studies used standardized tests to assesspsychologicaloutcome. One study showed favorable change (Goin & Rees, 1991) and two observedno change (Hollyman et al., 1986; Wright & Wright, 1975). One described an increasein depressive symptoms in facelift patients during the postoperative period, althoughBDI scores, in fact, had decreased from preoperative levels (Goin et al., 1980).
As noted previously, one of the principal reasons that practitioners assessed pa-tients’ psychological status was to identi~ those at risk of an adverse emotionalresponse to surgery. While clinical experience suggested the potential role of twovariables — the patient’s motivation for surgery and the patient’s gender — neitherhas been empirically investigated. Moreover, there have been no studies that system-atically examined the relationship between baseline measures of psychopathology andeither patient satisfaction with surgery or changes in psychosocial status postopera-tively. Therefore, given the limited number of studies and the absence of method-ologically sound investigations, we believe that it is premature to conclude thatcosmetic surgery produces psychological benefit in a majority of patients.
COSMETIC SURGERY AND BODY IMAGE
Clearly, physical appearance is a common concern of cosmetic surgery patients.Research on the psychology of physical appearance has grown rapidly in the last twodecades, but this topic has been sparsely investigated in cosmetic surgery patients.Some investigators contend that these patients obtain much of their self%steem fromtheir appearance (Napoleon & Lewis, 1989) and that when their self-esteem declines,
10 D. B. Sarweret al.
LReality of
Physical
Appearance
‘exceptions of
Appearance
developmental
Influences
Sociocultural
Influences
Self-Esteem
{CosmeticSurgety?
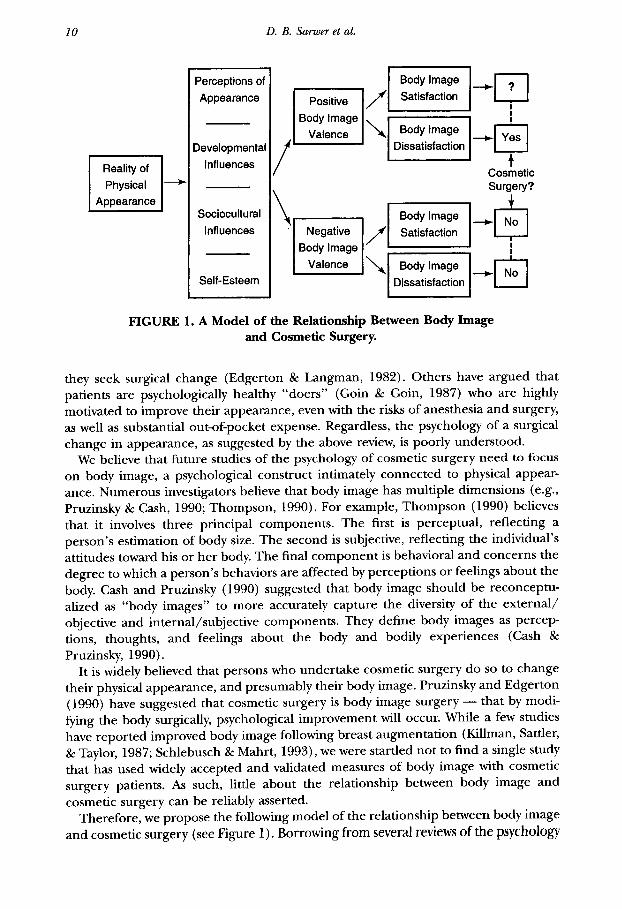
FIGURE 1. A Model of the Relationship Between Body Imageand Cosmetic Surgery.
they seek surgical change (Edgerton & Langman, 1982). Others have argued thatpatients are ~sychologi~ally he~lthy “doers”- (Goin & Goin, 1987) who are highlymotivated to improve their appearance, even with the risks of anesthesia and surgery,as well as substantial out-of-pocket expense. Regardless, the psychology of a surgicalchange in appearance, as suggested by the above review, is poorly understood.
We believe that future studies of the psychology of cosmetic surgery need to focuson body image, a psychological construct intimately connected to physical appear-ance. Numerous investigators believe that body image has multiple dimensions (e.g.,Pruzinsky & Cash, 1990; Thompson, 1990). For example, Thompson (1990) believesthat it involves three principal components. The first is perceptual, reflecting aperson’s estimation of body size. The second is subjective, reflecting the individual’sattitudes toward his or her body. The final component is behavioral and concerns thedegree to which a person’s behaviors are affected by perceptions or feelings about thebody. Cash and Pruzinsky (1990) suggested that body image should be reconceptu-alized as “body images” to more accurately capture the diversity of the external/objective and internal/subjective components. They define body images as perceptions, thoughts, and feelings about the body and bodily experiences (Cash &Pruzinsky, 1990).
It is widely believed that persons who undertake cosmetic surgery do so to changetheir physical appearance, and presumably their body image. Pruzinsky and Edgerton(1990) have suggested that cosmetic surgery is body image surgery — that by modi-
@ng the body surgically, psychological improvement will occur. while a few studieshave reported improved body image following breast augmentation (Killman, Sattler,& Taylor, 1987; Schlebusch & Mahrt, 1993), we were startled not to find a single studythat has used widely accepted and validated measures of body image with cosmeticsurgery patients. As such, little about the relationship between body image andcosmetic surgery can be reliably asserted.
Therefore, we propose the following model of the relationship between body imageand cosmetic surgery (see Figure 1). Borrowing from several reviews of the psychology
———. —.-————-.
The Psychologyof CosmeticSurgery 11
of body image (e.g., Cash & Pruzinsky, 1990; Thompson, 1990, 1996),1 the modelconsiders both physical and psychological influences on the development of bodyimage. The model expands upon this knowledge by specifically discussing howthoughts and feelings about appearance may influence the decision to seek cosmeticsurgery.
A MODEL OF THE RELATIONSHIP BETWEEN BODY IMAGEAND COSMETIC SURGERY
Physical Reality of Appearance
While body image often is seen as a “psychological” phenomenon, the physical realityofappearance lays the foundation for an individual’s body image. Physicalappearance is apotent determinant of person perception, as it is typically among the first sources ofinformation availableto others to guide social interaction (Alley, 1988). Persons consid-ered physically attractivereceive preferential social treatment in virtuallyevery situationstudied, including education, employment, medical care, and partner selection (Bull &Rumsey 1988; Hatfield & Sprecher, 1986). In contrast, those seen as ugly or disfigured,whether by “bad genes”, congenital deformity, or traumatic accident are thought to be atincreased riskfor social and psychological problems (Bull & Rumsey, 1988). Furthermore,one’s physicalappearance ismaUeablein response to stimuliboth within (such as changesin muscle and fat mass) and beyond our control (such as physical insults and aging)(Alley, 1988). Thus, the physical realityof appearance at any given point in time “sets thestage” for the psychological influences on body image.
Psychological/Influences on Body Image
Several investigators have outlined the potential psychological influences on bodyimage (Gash, 1996; Heinberg, 1996). For example, Heinberg (1996) has divided thetheories of body image disturbance into three categories — perceptual, developmen-tal, and sociocultural. At present, these theories have been applied primarily toindividuals who suffer from eating disorders and/or with excessive weight and shapeconcerns (Heinberg, 1996). However, they also may be useful in understanding therelationship between body image and cosmetic surgery. In addition, we believe therelationship between self-esteem and body image is important in understanding thepursuit of cosmetic surgery.
Pmeptual injlwnce s. Heinberg (1996) described three perceptual theories of bodyimage — the cortical deficit theory, the adaptive failure theory, and perceptual artifacttheory. The cortical defect theory suggests that body size overestimation results froman interaction between visual spatial defects and both cognitive and affective influ-ences (Dolce, Thompson, Register, & Spana, 1987; Thompson & Spana, 1991). Theadaptive failure theory suggests that individuals’ perceptions of body size do notchange at the same rate as their actual size changes as a result of weight gain or loss(Heinberg, 1996). Similarly, the perceptual artifact theory suggests that the tendencyto overestimate one’s body size is related to one’s actual body size (Penner, Thomp-son, & Coovert, 1991).
1The reader interestedin a more detaileddiscussionof body image and body image development than is possible here is referred to these reviews.
-..—
12 D. B. Sarweret al.
The perceptual theories of body image appear to have little empirical supportbeyond the studies cited. Furthermore, they are most frequently used to explaindissatisfaction with one’s overall body size or shape (Heinberg, 1996). Thus, theirapplicability to cosmetic surgery patients, who more frequently have concerns with adiscrete feature of their appearance, is unknown.
Nevertheless, we believe perceptual influences on body image are relevant incosmetic surgery patients. These patients often report to their surgeon that anappearance feature is different in size, shape, or appearance from the objective realityof the feature. These anecdotal reports are consistent with the ecological psychologyliterature that suggests that the ability to perceive changes in physical appearance israther imprecise (Alley, 1988). However, such perceptual inaccuracies have yet to beformally studied in cosmetic surgery populations.
Developmental influences. Developmental theories of body image disturbance focus onthe contribution of childhood and adolescent experiences to adult body image. Thetheory of puberty and maturational timing suggests that girls who have early me-narche are more likely to have a negative body image (Heinberg, 1996), as evidencedby body size overestimation (Fabian & Thompson, 1989) and their reports of bodyimage dissatisfaction (Brooks-C;unn & Warren, 1985). However, this relationship mayonly exist in normal weight individuals, as it was not observed in obese women(Sarwer, Wadden, & Foster, 1997). Disparagement and teasing in childhood alsoappear to predispose females to weight and shape dissatisfaction (Cash, Winstead, &Janda, 1986). Such a relationship has been identified in adolescent and adult popu-lations, as well as in obese and nonobese individuals (e.g., Fabian & Thompson, 1989;Grilo, Wilfley, Brownell, & Rodin, 1994).
Early messages in childhood and adolescence, whether negative (“You’re funnylooking”) or positive (“What a beautiful girl/handsome boy”), appear to influencethe adult body image. While previous investigations have identified a relationshipbetween childhood teasing and overall body image dissatisfaction, we have witnesseda similar relationship between teasing and dissatisfaction with specific body features incosmetic surgery patients. These individuals frequently describe how they first becameaware of their prominent nose or lack of breast development as a result of thederogatory comments of others. As with the perceptual influences, developmentalinfluences have yet to be formally studied in these individuals.
Sociocultural in.uences. Sociocultural theories have stressed the influence of socialnorms and expectations on both the etiology and maintenance of body imagedisturbance (Heinberg, 1996). As a whole, these theories emphasize the interaction ofthe mass media and cultural ideals of appearance (which frequently portray unreal-istic, exaggerated, or unattainable body image models) with tenants of both self-idealdiscrepancy (Thompson, 1992) and social comparison theory (Festinger, 1954). Ac-cording to this theory, people compare their appearance to that of fashion models,Hollywood celebrities, or superstar athletes, and find that they come up short bycomparison, resulting in increased body image dissatisfaction (Heinberg, 1996). Thiscollection of theories has wide intuitive appeal and has received some correlationalsupport (e.g., Heinberg, Thompson, & Stormer, 1995; Mazur, 1986).
Not surprisingly, the social and cultural standards of beauty portrayed in the massmedia are thought to directly influence the increasing demand for cosmetic surgery(Pruzinsky, 1993). In recent years, cosmetic surgery has become highly publicized and
———————-—

The Psycholo@ of CosmeticSurgery 13
marketed. Both the print and electronic media routinely report on the latest cosmeticprocedure or the celebrity most recently suspected of having cosmetic surgery. Often,cosmetic surgery is portrayed as the pathway to having a face and body just like thatof the models in magazine advertisements and television commercials, and thereforethe only way to directly address dissatisfaction with appearance. AS such, we believethat the sociocultural influences on body image may be the most relevant to under-standing the role of body image in cosmetic surgery.
Se~%teem. The physical body, in both structure and function, has long been consid-ered a critical part of one’s sense of self (Fisher, 1986, 1990).2 Early psychoanalytictheorists, such as Freud, Jung, and Adler, as well as more contemporary writers havepostulated that the physical body is actually a representation of the self (Fisher, 1990).In one of the first empirical investigations of body-self relationship, Jourard andSecord (1955) identified a modest correlation between satisfaction with the body andsatisfaction with the self. More recent investigations have replicated this relationshipbetween body image and self-esteem (e.g., Cash et al., 1986; Fabian & Thompson,1989; Foster, Wadden, & Vogt, 1997; Sarwer et al., 1997).
Cash has proposed a cognitive-behavioral model of the relationship between bodyimage and self<steem (Cash, 1996; Cash & Labarge, 1996). Cognitive-schema theory,or more specifically self-schema theory, suggests that people have schemas or cognitivestructures, derived from past experience, which organize and guide informationabout current experience (Beck, Freeman and Associates, 1990; Markus, 1977). Suchschemas may exist for a variety of domains, including physical appearance or bodyimage (Cash & Labarge, 1996). Environmental stimuli about appearance from anynumber of sources could activate this appearance-related or body image schema,which then, in turn, influence affect and behavior (Cash & Labarge, 1996). Accordingto Cash and Labarge (1996), in persons with such a schema, self-esteem is closely tiedto feelings about physical appearance.
This theoretical description of the relationship between body image and self--esteem is intuitively pleasing, and recently has begun to be empirically investigated.From Cash and Labarge’s (1996) explanation, however, it appears that only certainindividuals have an appearance-related or body image schema. Alternatively, it maybethat we all have a body image schema, but that it has a differential valence thatdetermines its relative importance to overall self-esteem. At present, such schemaappear to be more salient to the self-image of women than men, as evidenced byincreased body image dissatisfaction in women (Cash et al., 1986). This differenceperhaps is best understood as a result of the differential socialization of women andmen about appearance-related issues (Hatfield & Sprecher, 1986).
Body Image: Valence and Value
Cash and colleagues have further suggested that the attitudinal component of bodyimage itself is two-dimensional, consisting of an orientation component (representingthe importance or attention given to the body) and an evaluative component (rep-resenting the affective elements of body image) (Brown, Cash, & Mikulka, 1990). Thistheory of the two-dimensional attitudinal component of body image has been sup-
2Thereader interestedin a detailed discussionof the theoreticalrelationshipof the body andthe self is referred to thiswork.
14 D. B. Sarweret al.
ported by factor analysisof the Multidimensional Body-Self Relations Questionnaire ina nationwide sample (Brown et al., 1990).
As the relationship between body image and cosmetic surgery is considered, we alsobelieve that attitudes about the body are two-dimensional, consisting of both a valence(i.e., a measure of importance to one’s self-esteem) and a value (i.e., the actual degreeof satisfaction or dissatisfaction with one’s body). Body image valence and value aresimilar to the orientation and evaluative dimensions of body image, respectively(Brown et al., 1990; Cash et al., 1986). For example, individuals with a high bodyimage valence may derive much of their self-esteem from their body image. As such,they may be more attentive to information about their appearance, similar to indi-viduals with an appearance-related schema (Cash & Labarge, 1996). In contrast,persons with a low body image valence are not as dependent upon their physicalappearance to support their self%steem. These individuals may be unconcerned oreven oblivious to issues of appearance. Similarly, body image valence may vary de-pending upon the body part in question. For example, the number of women whoreport dissatisfaction with their body weight and shape suggests that a “body shapeschema” may have a relatively high valence as compared to a “height schema, ” anappearance feature with which women show far less dissatisfaction (Cash et al., 1986).
In addition, body image also has a value. Body image dissatisfactionis so prevalent thatit has been described as a “normative discontent” (Rodin, Silberstein, & Striegel-Moore,1985). However, it is difllcult to determine the point atwhich an individual’s perceptions,attitudes, and behaviors regarding his or her body become problematic or psychopatlmlogical. At present, there isno accepted cutoff point between “normative discontent” and“pathological dissatisfaction.” Nevertheless, we believe the degree of body image dissat-isfaction serves as a motivational component to cosmetic surgery.
Continuum of Body Image Dissatisfaction
In the absence of widely accepted criteria for body image dissatisfaction, we believethat it should be considered on a continuum. Such a continuum could be anchoredon one end by persons with body image satisfaction and on the other by persons withextreme body image dissatisfaction.
Body image sati@action. Individuals with body image satisfaction would be thought tohave an overall positive body image. Although they may dislike an aspect of theirappearance, they are not greatly distressed by it. While they might, on occasion, wishto change an aspect of their appearance, they would be unlikely to seek out cosmeticsurgery, as their overall body image is favorable.
Body image dissatisjhdion. Potentially, there are several degrees of body image dissat-isfaction, the first of which may be a dislike of an aspect of appearance. Such dislikemay lead to relatively frequent distress or concern and be associated with maladaptivebehavioral change. Similarly, an individual may be dissatisfied with one aspect of hisor her appearance, but may be satisfied with other features. At present, it is not clearat what point such dissatisfaction, whether specific to one appearance feature or moreglobal, leads to cosmetic surgery.
Body image disturbance. The next level of dissatisfaction is body image disturbance(Thompson, 1990), or what also has been referred to as body image disorder (Rosen,
The Psychologyof CosmeticSurgery 15
1992, 1996; Thompson, 1992). Such individuals experience greater affective distressand exhibit more profound behavior change, including “camouflaging” the offend-ing body part or refusing to allow others to view it. Others may exhibit cognitive orperceptual distortions of their appearance, resulting from a combination of irrationalthoughts and unrealistic expectations about the body (Freedman, 1990). At present,the relationship between body image disturbance and more severe forms of bodyimage psychopathology is not well established.
Body dysmorphic disotrk Body dysmorphic disorder (BDD) is the only diagnostic termin DSM-IV (American Psychiatric Association, 1994) directly addressing body imageconcerns. BDD is defined as a preoccupation with a defect in appearance that is eitherimagined, or if slight, leads to markedly excessive concern. The preoccupation mustcause significant distress or impairment in social, occupational, or other importantareas of functioning (APA, 1994). The preoccupation is difficult to resist or control(Hollander & Phillips, 1993), and is thought to become more intense in socialsituations in which the person feels self-conscious (Rosen, 1996). Most patients engagein repetitive behaviors involving checking, examining, hiding, or improving thedefect. Although any area of the body maybe affected, the most common areas are theskin, face, and nose (Phillips, McElroy, Keck, Pope, & Hudson, 1993).
The diagnosis of BDD is relatively new to American psychiatry, first appearing inDSM-111-RIt was initially described in the European psychiatric literature over 100years ago as dysmorphophobia — a subjective feeling of ugliness in a person of normalappearance (Morselli, 1886). More contemporary reports have described the primarysymptom of dysmorphophobia as an excessive and distressing belief that one isunattractive (Andreasen & Bardach, 1977), frequently coupled with depression andextreme body image dissatisfaction (Hardy, 1982). However, there are several prob-lems with previous descriptions of dysmorphophobia. First, given the sizable minorityof individuals who report dissatisfaction with their appearance (e.g., Cash et al., 1986),the definition is far too broad. Second, dysmorphophobia does not meet the criteriaof a phobia, as there is no fear of physical abnormality and no avoidance of theugliness of others (Pruzinsky, 1990). Finally, persons with body image disturbancetypically do not recognize their concern as excessive or unreasonable, as do phobicindividuals.
BDD is classified as a somatoform disorder in DSM-lV It is most often compared toobsessive-compulsive disorder (OCD), an anxiety disorder. Hollander (1993) hassuggested that BDD is an obsessive-compulsive spectrum disorder based on thesimilarity of symptoms, etiology, comorbidity, age of onset, course of illness, andtreatment response. Differential and comorbid diagnoses of BDD typically includeOCD, social phobia, depression, hypochondriasis, eating disorders, and numerouspersonality disorders (Neziroght, McKay, Todaro, & Yaryura-Tobias, 1996; Rosen,1996; Veale et al., 1996).
The percentage of cosmetic surgery patients who meet criteria for BDD is un-known. Andreasen and Bardach (1977) estimated from their clinical experience that2% of patients who requested cosmetic surgery suffered from the disorder. Unfortu-nately, no formal prevalence studies have been completed, and previous work hasbeen based on case reports and small case series that lacked clearly operationalizeddefinitions (Phillips, 1991).
The typical presentation of BDD patients for cosmetic surgery also is unknown.Pruzinsky (1993, 1996) has suggested that patients with “minimal deformity” maybe
——
16 D. B. Sarweret al.
the most likely to meet the diagnosis of BDD. However, the “insatiable” patient, whoreturns for multiple surgical procedures, also may be a candidate for the diagnosis,using the successive surgeries (in an almost ritualistic fashion) to seek relief fromprofound body image dissatisfaction. Support for this contention comes from theobservation that BDD patients typically use appearance remedies just as hypochon-driacal patients overuse medical services (Rosen, 1996).
The Decision to Have Cosmetic Surgery
We believe that it is the interaction between body image valence and body image valuethat leads to the decision to pursue cosmetic surgery. Persons with a lower body imagevalence, whose self-esteem is not dependent on their appearance, would seem unlikelyto pursue cosmetic surgery. Regardless of whether such individuals are satisfied ordissatisfied with their body image, the valence of body image in self-esteem is not greatenough to motivate a surgical change in appearance.
In contrast, individuals with a higher body image valence may be more likely topursue cosmetic surgery. Individuals with a high body image valence, for whom bodyimage is an important part of self-esteem, and who have a significant degree of bodyimage dissatisfaction, may well comprise the majority of cosmetic surgery patients.These individuals place a high degree of importance on their appearance and aredissatisfied with a feature of it..As noted above, while some degree of dissatisfactionmay be identified in most patients, extreme dissatisfaction or preoccupation may berepresentative of body image disturbance or BDD. Individuals with both high bodyimage valence and high satisfaction with their appearance also may seek cosmeticsurgery. These individuals may represent the healthy “doers” who wish to enhancetheir appearance and an already favorable self-esteem (Goin & Goin, 1987).
FUTURE RESEARCHPRIORITIES
The proposed model of the relationship between body image and cosmetic surgerycan be used to guide empirical research. Initial research efforts should investigate thedegree of body image dissatisfaction in cosmetic surgery populations. While ourmodel depicts body image dissatisfaction as the motivational component to a surgicalchange in appearance, this has yet to be empirically demonstrated. We believe this isan important first step in understanding the relationship between body image andcosmetic surgery.
Assessmentof Body Image Dissatisfaction and BDD
Several measures of body image dissatisfaction could be used with cosmetic surgerypopulations. The Multidimensional Body-Self Relations Questionnaire (MBSRQBrown et al., 1990; Cash et al., 1986) and the Body Dysmorphic Disorder Examination(BDDE; Rosen& Reiter, 1996) maybe the most appropriate. The MBSRQis a 69-itemself-report inventory for the assessment of patients’ attitudes toward their bodies. Its10 subscales allow for the measurement of the multidimensional characteristics ofbody image. The measure has acceptable validity and 1 month test-retest reliabilitiesranging from .89 to .71 for the subscales (Brown et al., 1990). It frequently has beenused as a measure of body image dissatisfaction in nonclinical populations. Morespecifically, the Appearance Orientation and Appearance Evaluation subscales of the
————
The Psycholo~ of CosmeticSurgery 17
MBSRQ (Brown et al., 1990; Cash et al., 1986) maybe appropriate measures of boththe body image valence and the degree of body image dissatisfaction, respectively.
As a more specific measure of BDD, Rosen and Reiter (1996) developed the BDDE.It can be used as a semi-structured interview or self-report measure of BDD symptomsexperienced within the last 4 weeks. In addition to yielding a total score for BDDseverity, there are recommended criteria for the diagnosis of BDD. The measure hasadequate internal consistency (Cronbach’s alphas ranging from .81 to .93) andinterrater reliability (r= .98) and shows promise in the assessment of BDD (Rosen &Reiter, 1996). The BDDE may serve as a useful tool in establishing the prevalence ofBDD in cosmetic surgery populations.
For individuals with more profound body image dissatisfaction, such as BDD, thepotential benefits of cosmetic surgery are unclear. Early data suggest that some BDDpatients have an exacerbation of symptoms after surgery, while others find a newdefect to correct surgically (Phillips et al., 1993). Several writers suggest that the moreappropriate treatment for such patients is psychiatric, not surgical (Andreasen &Bardach, 197’7; Birtchnell, 1988). Studies assessing changes in body image dissatisfac-tion postoperatively are needed to further assess the potential for psychologicalbenefit for these individuals following cosmetic surgery.
Development of Body Image Disturbance
Future research should assess the role of the developmental, sociocultural, andperceptual influences on body image. For example, for some women early onset ofphysical maturation accompanied by negative verbal comments about breast develop-ment may result in body image clissatisfaction that leads to breast reduction surgery.Such a relationship can be empirically explored through the use of the PhysicalAppearance Related Teasing Scale (PARTS; Thompson, Fabian, Moulton, Dunn, &Altabe, 1991) to assess a history of appearance-related teasing. The PARTS has twosubscales that assess both weight and body size teasing, as well as more generalappearance-related teasing. These subscales have internal consistencies of .91 and .71,and 2-week test-retest reliabilities of .86 and .87, respectively. Potentially useful forboth breast reduction and augmentation patients, the Breast/Chest Rating Scale(Thompson & Tantleff, 1992) assesses satisfaction with current breast size. Using fiveschematic figures of the female torso ranging in size from small to large, subjectsindicate their current breast size, ideal size, the size preferred by men and women, andthe breast size associated with a collection of personality characteristics. Test-retestreliability ranges from .69 (for ideal breast size) to .85 (current breast size), suggestingmoderate to good reliability. This scale also may be an appropriate measure forevaluating postoperative changes in breast satisfaction.
Similarly,sociocultural theories have described how the thinness of female mass mediaimages are thought to contribute to the prevalence of weight and eating disorders(Heinberg, 1996). At present, the impact of such images on the selection of cosmeticprocedures, such as liposuction, is unknown. However, a measure such as the Sociocul-tural Attitudes Towards Appearance Questionnaire (SATAQ Heinberg, Thompson, &Stormer, 1995) may serve as a useful tool in the assessmentof the effects of socioculturalinfluences on the pursuit of cosmetic surgery. The SATAQ is a 14item scale that assessesrecognition and acceptance of societal standardsof appearance. Itssubscalesof Awareness(which assessesthe pressures on women to appear attractive) and Internalization (whichassessesthe acceptance or rejection of these sociocuh-al messages) have internal con-
18 D. B. Sarweret al.
sistencycoefficients of .71 and .88, respectively.As discussed above, while clinical reportssuggest that cosmetic surgery patients frequently display perceptual inaccuracies in esti-mating the size and shape of bodily features, these reports have not been empiricallyevaluated. Newer technology, such as visualimaging systems,which allow for the comput-erized modification of facial and bodily features, can be used in fiture studies to assesstheperceptual component of body image.
Future studies also should clari~ the relationship between body image and self--esteem. General measures of self-esteem, such as the Rosenberg Self-Esteem Scale(Rosenberg, 1979), may be helpful, but newer measures that provide a multidimen-sional assessment of self-esteem probably will be more useful. Developed from Cash’s(1996) cognitive-schema model of body image and body image dissatisfaction, theAppearance Schemas Inventory (ASI; Cash & Labarge, 1996) maybe a useful tool forthe assessment of the relationship between body image and self-esteem. The ASIassesses core beliefs about the importance, meaning, and effects of appearance inone’s life. It has acceptable reliability (Cronbach’s alpha = .84) and demonstratedconvergent and discriminant validity with several other measures of the cognitive,affective, and behavioral components of body image.
Changes in Body Image Following Surgery
Although patients typically report high levels of satisfaction with their surgical result(Wengle, 1986), long-term satisfaction has not been well investigated. Given theproposed relationship between sociocultural influences and body image, it may bethat cosmetic surgery patients only report satisfaction during the period immediatelyfollowing surgery, while they are receiving positive reinforcement about their appear-ance from family and friends. Future research that uses standardized measures of bodyimage can assess if improvements are maintained over longer periods of time, as therate of external reinforcement presumably decreases. Pre- and postoperative investi-gations of body image dissatisfaction may provide the most useful evidence to date forthe utility of cosmetic surgery as a body image therapy.
Nonsurgical Treatment of Body Image Dissatisfaction
Nonsurgical treatments for body image problems are relatively new. Cognitive-behavioral treatment has been used effectively to treat women dissatisfied with theirbody image (Butters & Cash, 1987; Dworkin & Kerr, 1987; Fisher& Thompson, 1994;Grant & Cash, 1995; Rosen, Cado, Silberg, Srebnik, & Wendt, 1990; Rosen, Saltzberg,& Srebnik, 1989). More recently, the same treatment has been used successfully withwomen with BDD (Rosen, Reiter, & Orosan, 1995). There are several reports ofsuccessful treatment of BDD with behavioral interventions, such as exposure andresponse prevention (Marks & Mishan, 1988; Munjack, 1978; Neziroglu et al., 1996;Neziroglu & Yaryura-Tobias, 1993). There also is evidence for successful pharmaco-logic treatment of BDD with selective (SSRIS) and nonselective serotonin reuptakeinhibitors (SRIS) such as fluoxetine and clomipramine, respectively (Hollander, Co-hen, Simeon, Rosen, DeCaria, & Stein, 1994; Hollander, Liebowitz, Winchel, Klumker& Klein, 1989; PhilIips et al., 1993). However, these treatments have yet to be usedspecifically with cosmetic surgery populations.
The research outlined in this section has two ultimate goals. First, it should be usedto assess the relationship between body image dissatisfaction and cosmetic surgery, interms of both the pre-existing degree of body image dissatisfaction, aswell as the utility
The Psychologyof CosmeticSurgery 19
of surgery as body image therapy. Second, the research should be used to identifi bothpatients for whom surgery may be beneficial, as well as those for whom it is contrain-dicated. Through the use of body image construct, we will begin to better understandthe psychology of this unique population.
Acknowledgements— This researchwassupported by a Fellowshipfrom the Edwinand FannieGrayHallCenterfor HumanAppearance (to Dr.Sarwer)and by a NationalInstituteof MentalHealthResearchScientistDevelopmentAward (to Dr.Wadden).
REFERENCES
Atley,T. R (1988).Socialanda~liedaspectsof-”vingfme.s. Hillsckde,NJ:LawenceErlbaumAssociates.AmericanPsychiatricAssociation.(1987).fi”agnosticand stali.sticatmanualof mentaldisorders(3rdcd., rev.).
Washington,DC:Author.AmericanPsychiatricAssociation.(1994).Diagnosticandstatisticalrnunualof mentaldisordas(4thcd.).Washing-
ton, DC:Author.AmericanSocietyof PlasticandReconstructiveSurgeons(ASPRS).(1994). 1994pksticswgnypmceduralstatistics.
ArlingtonHeights,IL:Author.Audreasen,N. C., & Bardach,J. (1977). Dysmorphophobia:Symptomor disease.AnwicanJawnaZofPsychiatry,
134,673-676.Baker,J. L., Kolin, I. S., & Bartlett,E. S. (1974). Psychosexualdynamicsof patientsundergoing mammary
augmentation.PlasticandReconstructiveSurgvry,53, 652–659.Beale,S.,Lisper,H., & Palm,B. (1980).A psychologicalstudyof patientsseekingaugmentationmammaplasty
&“tishJmmnaZofPsychiatsy,136,133-138.Beck,A. T., Freemau,A., & Associates(1990).Cognitivetkerapyfwpenonali~disordets.NewYork:GuilfordPress.Birtchnell,S.A. (1988).Dysmorphophobia—A centenarydiscussion.BritishJournalofPsychiat~,153,41-43.Brooks-Gunn,J.,&WarrenM.P.(1985).Effectsofdelayedmenarcheindifferentcontexts:Danceandnondauce
students.Journalof YouthandAdolescence,14,285-300.Brown,T.A., Cash,T.F.,& Mikulka,P.J. (1990).Attitudinalbodyimageassessment:Factoranalysisof theBody
SelfRelationsQuestionnaire.JournalqfPsrsonali~Assessmt, 55, 135-144.Bull,R., & RumseyN. (1988). T?szsocialpsychologyofftil a/@ararue.NewYork:Springer-Verlag.Buttem,J.W.,&Cash,T.F.(1987).Cognitive-behavioraltreatmentofwomen’s bodyimagedissatisfaction.JoumaZ
of c~ulting andG!inica~Psychokgy,553889+397.Cash,T. F. (1996). The treatmentof body-imagedisturbances.In J. K Thompson (Ed.), Bodyima~, eating
disoroh,andobesi~(pp. 83-107). Washington,DC:AmericanPsychologicalAmociation.Cash,T. F., & Labarge,A. S. (1996). Developmentof the AppearanceSchemasInventory:A new cognitive
body-imageassessment.CognitiveThera@andReseanh,20, 37-50.Cash,T. F.,& Pruzinsky,T. (1990). Bodyinuge.s:Devel@ment,deviance,andchangz.NewYork:GuilfordPress.Cash,T. F.,Winstead,B. A., &Jauda,L. H. (1986). The greatAmericanshape-up:Body imagesurveyreport.
Psycholo@Today> 20,30-37.Dolce, J. J., Thompson, J. K, Register,A., & Spana,R E. (1987). Generalizationof body size distortion.
InternatwrudJoumal@EatingDisordem8,401-408.Dworkin,S. H., & Kerr,B. A. (1987).Comparisonof interventionsfor womenexperiencingbody image
problems.Journalof GnmsetingPychotogv,34, 136-140.Edgerton,M. T.,Jacobson,W. E.,& Meyer,E. (1960).Surgical-psychiatricstudyof patientsseekingplastic
(cosmetic)surgery:Ninety-eightconsecutivepatientswithminimaldeformity.BritishJournalofPtuXtiSuqyry,13, 136-145.
Edgerton,M. T. & Langman,M. W. (1982). Psychiatricconsiderations.In E. H. Courtiss(Ed.), Maleoesthzticswgzry(pp. 17–38).St.Louis,MO: C.V.Mosby.
Edgerton,M.T.,Langrnau,M.W., &Pruzinsky,T. (1991).Plasticsurgeryand psychotherapyin the treatmentof100psychologicallydisturbedpatients.PlusticandRecmstnsztiueSurgw-y,88,594-608.
Fabian,L.J., & Thompson,J. K (1989). Body image and eatingdisturbancein young females.InternationalJw~al ofEatingDisorders,8,6.3-74.
Festinger,L. (1954). A theoryof socialcomparisonprocesses.HumanRekztions,7, 117-140.Fisher,S. (1986). Developmentand structureof the body image (Vols.1 and 2). HiBsdale,PJJ:Erlbaum.

20 D. B. Sarweret al.
Fisher,S. (1990). The evolutionof psychologicalconceptsabout the body. In T.F.Cash&T. Pruzinsky(Eds.).Development,devianceand change (pp. 3-20). NewYork:GuilfordPress.
Fisher,E., & Thompson,J. K (1994). A comparativeevaluationof cognitive-behavioralthecapy(CBT) versusexercisetherapy(ET) for the treatmentof body-imagedisturbance:Preliminaryfindings.BehaviorA40dtfica-tion,18, 171–185.
Foster,G. D., Wadden,T. A., & Vogt, R.A. (1997). Body image before, during,and afterweightloss. HealthPsychology,16,226-229.
Freedman,R. (1990). Cognitive-behavioralperspectiveon body-imagechange. In T. F. Cash& T. Pruzinsky(Eds.),Bodyimagvs:Develupmerct,dzwiance,andchange(pp. 272-295). NewYork:GuilfordPress.
Freud.S. (1918). Fromthehistoryof au infantileneurosis(1918). InJ. Strachey(Ed.), Thestandardeditionof thxcompletepsychobgicalwoksofSigmundFreud(pp. 3-122). London: Hogarthand Instituteof Psychoanalysis.
Gifford,S. (1972). Cosmeticsurgeryand pemonalitychange:A reviewand some clinicalobservations.In R. M.Goldwyn(Ed.), l-heunfawrablz resultin plasticsurgzry:Avoidanceand treatrrwrct(pp. 11–33). Boston: Little,Brown.
Goin,M. K, Burgoyne,R.W.,Goin,J.hf.,& Staples,F.R (1980).A prospectivepsychologicalstudyof 50 femalefact+liftpatients.PlasticandReconstructiveSurgery,65,436-442.
Goin,J. M., & Goin, M. K (1987). Psychologicalunderstandingand managementof theplasticsurgerypatient.In N. G. Georgiade,G. S.Georgiade,R. Riefkohl,&W.J. BarWick(Eds.),Essentialsofpkmtic,maxillofacial,andreconstructivesurgery(pp. 1127–1143).Baltimore,MD:Williams& Wilkens.
Coin, M.K.,Goin,J.M.,&Gianini,M. H. (1977).The psychicconsequencesof a reductionmammaplasty.Pc’asticandReconstructiveSurpy, 59, 530-534.
Goin, M. R., & Rees,T.D. (1991).A prospectivestudyof patients’psychologicalreactionsto rhinoplasty.Annalsofp~t~ Surgv>27, 210-215.
Grant,J., & Cash,T. F. (1995). Cognilive-behavioralbody-imagetherapy:Comparativeefficacyof group andmodest<ontacttreatments.BehaviorTherapy,26, 69-84.
Grilo,C. M.,Wikley,D. E.,Brownell,K.D.,&Rodin,J. (1994).Teasing,body image,and self-esteemin a clinicalsampleof obese women.AddictiveBehaviom,19,443-450.
Hardy G. E. (1982). Bodyimagedisturbancein dysmorphophobia.BritishJmcrnaZofPsychiatry,141,181-185.Hatfield,E.,& Sprecher,S. (1986). Miww mim.. Tk importanceof looksineoaydaylije.Albany,NY:SUNYPress.Hay,G. G. (1970). Psychiatricaspectsof cosmeticnasaloperations.BritishJournalofPsychiatry,116,85-97.Hay,G. G., & Heather,B. B. (1973). Changesin psychometrictestresultsfollowingcosmeticnasaloperations.
BritishJournalofPsychiatry,122,89–90.Heinberg,L.J. (1996).Theoriesof bodyimagedisturbance.InJ.K Thompson (Ed.), Bodyimage,eatingdisorder,
andobesi~(pp. 27-47). Washington,DC:AmericanPsychologicalAssociation.Heinberg, L. J., Thompson,J. K, & Stormer,S. (1995). Developmentand validationof the Sociocultural
AttitudesTowardsAppearanceQuestionnaire(SATAQ).InternatiorcalJourcccdofEatingDi.sorok,17,81-89.Hill,G.,& Silver,A. G. (1950).Psychodynamicandestheticmotivationsfor plasticsurgery.PsychosornuticMedicine,
12,345-352.Hollander,E. (1993). Obsessive-cmrcpulsil)erekzteddi.scmkn.Washington,DC:AmericanPsychiatricPress.Hollander,E., Cohen, L., Simeon,D., Rosen,J., DeCaria,C., & Stein,D.J. (1994). Fluvoxaminetreatmentof
body dysmorphicdisorder.Journalof ClinicalPharmacology,14,75-77.Hollander,E.,Liebowitz,M. R.,Winchcl,R.,Klumker,A., & Rlein,D. F. (1989). Treatmentof bodydysmorphic
disorderwithserotoninreuptakeblockers.Am”canJournalofPsychiatry,146,768-770.Hollander,E.,& Phillips,K A. (1993). Bodyimageand experientialdisordemIn E. Hollander(Ed.), Obsessive
compulsiverebteddisorcitm(pp. 17-48). Washington,DC:AmericanPsychiatricPress.Hollyman,J.A., Lacey,J.H.,Whitfield,I’.J.,&Wilson,J.S.P.(1986).Surgeryfor thepsyche:A longitudinalstudy
of women undergoingreductionmammoplasty.BritishJournalofPlasticSurgery,39, 222–224.Jourard,S. M., & SecordP.F. (1955). Bodycathexisand the idealfemalefigure.JourruzZofAbnormalandSocial
Psycholqj,50, 243-246.Killman,P.R., Sattler,J. L, & Taylor,J. (1987). The impactof augmentationmammaplasty:A follow-upstudy.
PlasticandRecmstncztiveSum, 80,374-378.Linn, L., & Goldman,L B. (1949). Psychiatricobservationsconcerning rhinoplasty.PsychosomattiMedicine,11,
307-315.Marcus,P. (1984). Psychologicalaspecwof cosmeticrhinoplasty.BritishJournalofPkzsticSurgery,37, 313-318.Marks,I., & Mishan,J. (1988). Dysmorphophobicavoidancewithdisturbedbodilyperception:A pilot studyof
exposuretherapy.Briti.shJourrcalofPsychiatry,152,674-678.Markus,H. (1977). Self-schemataand processinginformationabout the self.JmmrcaZof Persorcali~andSocial
Psychology,35, 63-78.

The Psycholo~ of CosmeticSurgery 21
Mazur,A. (1986).U.S.trendsin femininebeautyand overadaptation.TkeJournaZof.%xRe.seamh,22, 281-303.Meyer,E.,Jacobson, W. E., Edgerton,M. T., & Canter,A. (1960). Motivationalpatternsin patientsseeking
electiveplasticsurgery.PsychosmnatkMedicine,22, 193-202.Micheli-Pellegrini,V., & Manfiida,G. M. (1979).Rhinoplastyand itspsychologicalimplications:Applied
psychologyobsemationsinaestheticsurgery.AestheticPlasticSurgery,3, 299-319.Momelli,E. (1886). Sulladismorfofobiae sullatafefobia.NolktinnoDeL!aAcazdmntidi Geaova,6, 110-119.Munjack,D.J. (1978). The behavioraltreatmentof dysmorphophobia.Jouncedof BehaviorTkzrapyandExperi.
mtal Psychiatry,152,674-678.Napoleon,A. (1993). The presentationof personalitiesin plasticsurgery.AnnaLsrrfP/a.sticSrugq, 31, 193-208.Napoleon,A., & Lewis,C. (1989). Psychologicalconsiderationsin lipopkasty:theproblematicor “specialcare”
patient.AnnalsofPkrsttiSuVay,23,430-432.Neziroglu,F.A., & Yaryura-Tobias,J. A. ( 1993).Exposure,responseprevention,and cognitivetherapyin the
treatmentof body dysmorphicdisorder.BehauihrTkzrafi,24, 431-438.Neziroglu,F.,McKay D., Todaro,J., & Yaryura-Tobias,J. A. (1996). Effectof cognitivebehatior therapyon
personswithbody dysmorphicdisorderand comorbid axis11diagnoses.BehaviorTkzrapy,27,67-77.Ohlsen,L., Ponten,B., & Hambert,G. (1978). Augmentationmammapkisty:A surgicaland psychiatricevalu-
ationof the results.AnnalsofPlasticSurg~, 2, 42-52.Penner,L.A.,Thompson,J.K, & Coovert,D. L. (1991). Sizeestimationamonganorexics:Muchado aboutvery
little.JournalofAbnml Pqchokr@,100,90-93.Phillips,ILA. (1991).Bodydysmorphicdisorder:The distressof imaginedugliness.AnwricanJmraaLofPsychiahy,
148,1138-1149.Phillips,K A.,McElroy,S.L.,Keck,P.E.,Pope,H. G.,&Hudson,J.L (1993).Bodydysmorphicdisorder:30cases
of imaginedugliness.AmericanJournalofPsychiatq,150,302-308.Pruzinsky,T. (1993). Psychologicalfactorsin cosmeticplasticsurgery:Recentdevelopmentsin patientcare.
PlasticSurgicalNuming13,64-71.Pruzinsky,T. (1996). Cosmeticplasticsurgeryand body image:Criticalfactorsin patientassessment.InJ. IL
Thompson (Ed.), Bodyimq, eatingdismden,andobesi~(pp. 109-127). Washington,DC: AmericanPsycho-logicalAssociation.
Pruzinsky,T.,& Cash,T.F. (1990). Integrativethemesin body-imagedevelopment,deviance,and change.In T.F.Cash&T. Pruzinsky(Eds.),Bodyimagw:llweloprnent,deviance,andchan~(pp. 337–349).NewYork:GuilfordPress.
Pruzinsky,T., & Edgerton,M. T. (1990). Body image change in cosmeticplasticsurgery.In T. F. Cash& T.Pruzinsky(Eds.),Bodyimxzgr.s:Deue@mwcct,deoiance,andchange(pp. 217–236).NewYork:GuilfordPress.
Robin,A.A.,Copa.s,J.B.,Jack,A. B.,Kaeser,A. C.,&Thomas,P.J.(1988).Reshapingthepsyche:The concurrentimprovementin appearanceand mentalstateafterrhinoplasty.BritishJournalofPsychiat~,152,539-543.
Rodin,J., Silberstein,L. R., & Striegel-Moore,R. H. (1985). Women andweight:A normativediscontent.In T.B.Sonderegger(Ed.),PsychologyandgtndesNebraskasym@iumonmotivation(pp. 267–307).Lincoln:Univemityof NebraskaPress.
Rosen,J.C. (1992).Bodyimagedisorder:Definition,developmentandcontributionto eatingdisorders.InJ. H.Crowther,D. L. Tennenbaum,S.E. Hobfoll, & M.A. P.Stephens(Eds.), Theetiologyofbulimtk:Tkeindividualand,fami~cmctext(pp. 157-177). Washington,DC: HemispherePublishers.
Rosen~J.C. (1996). Bodydysmorphicdisorder:Assessmentand treatment.InJ. K.Thompson (Ed.), Bodyimage,eatingdisordem,andobesity(pp. 149-170). Washington,DC:AmericanPsychologicalAssociation.
Rosen,J. C., Cado, S., Silberg,N. T., Srebnik,D., & Wendt,S. (1990). Cognitivebehaviordrerapywithandwithoutsizeperceptiontrainingfor womenwithbody imagedisturbance.BehaviorTkerapy,21, 481+98.
Rosen,J.C.,& Reiter,J.(1996). Developmentof thebody dysmorphicdisorderexamination.BehauiourResearchandTherafi,34, 755-766.
Rosen,J. C., Reiter,J., & Orosan,P. (1995). Cognitivebehavioralbody image therapyfor Body DysmorphicDisorder.Journalof Consultingand CliniudPsycho@y,63,26>269.
Rosen,J. C., Sahzberg,E.,& Srebnik,D. (1989). Cognitivebehaviortherapyfor negativebody image.BehaviorTkerafl,20, 39?-404.
Rosenberg,M. (1979). Ccma”uingtheselfNewYork:BasicBooks.Sarwer,D.B.,Wadden,T.A., &Foster,G. D. (1997).Assessrmmtofbodyim.agedissati.sfizctioninobeseZoc?rmm:syecyicity,
WW@, andclinicalsigrczficance.Unpublishedmanuscript.Schlebusch,L., & Levin,A. (1983).A psychologicalprofileof womenselectedfor augmentationmammoplasty.
SouthAjiicanMedicalJoumcalj64,481-483.Schlebusch,L., & Mahrt,I. (1993). Long-termpsychologicalsequeleaof augmentationmammoplasty.South
A@”canh4edicalJrrurnal,83, 267-271.
22 D. B. Sarweret al.
Shipley,R H., O’Donnell,J. M., & Bader,K F. (1977). Personalitycharacteristicsof women seekingbreastaugmentation.PlasticandRmm.structiveSutgmy60,369-376.
Sihm,F.,Jagd, M., & Pers,M. (1978). Psychologicalassessmentbefore and afteraugmentationmammaplasty.ScandinavianJournulofPla.sticandReconstructiveSum, 12,295-298.
Thompson,J.K (1990).BodyimzgEdistudwuz:AssesmwntandtreatmentNewYork:PergamonPress.Thompson,J.K (1992).Bodyimage:Extentof disturbance,associatedfeatures,theoreticalmodels,assessment
methodologies,interventionstmtegies,and a proposalfor a newDSMl%’diagnosticcategory— Bodyimagedisorder.In M. Hersen,R. M. Eider,& P.M. Miller(Eds.),Ptvgw.win behauin-modt@atsbn(VOI.28, pp. 3-54).Sycamore,IL: SycamorePublishingCompany.
Thompson, J. K (1996). BodyzmugE,eatingdimrden,and &es@. Washington,DC:AmericanPsychologicalAssociation.
Thompson,J.K, Fabian,L.J.,Moulton,D. O., Dunn,M.F.,&Altabe,M.N. (1991).Developmentandvalidationof the physicalappearancerelatedteasingscale.JmwmdofPenwnaZityAsssssrrumt,56, 513-521.
Thompscm,J. K.,& Spana,R E. (1991). VkuospatiaJabilityand sizeestimationaccuracy.Pemeptu.alandMoturSkills,73,335-338.
Thompscm,J.K,& Tantleff,S.(1992).Femaleandmaleratingsof uppertorso:Actual,ideal,andstereotypicalconceptions.JourrwlofSocialBehaviorandPemnudity,7,345-354.
VealeD.,Boocock,A.,Gournay,K, Dryden,W.,Shah,F.,WilLson,R, &WalburnJ. (1996).Bodydysmorphicdisorder:A surveyof fiftycases.BtitishJ~mulofPychiaby,169,196-201.
Webb,W.L.,Slaughter,R, Meyer,E.,&Edgerton,M. (1965).Mechanismsof psychosociala@sstmentin patientsseeking“face-lift”operation.PsychosomattiMedi&se,2Z 183-192.
Wengle,H. P. (1986). The psychologyof cosmeticsurgery:A criticaloverviewof the literature1960-1982-PartI. AnnalsofPkzsttiSmgerj,16,435-443.
Wright,M. R., & Wright,W. K (1975). A psychologicalstudyof patientsundergoingcosmeticsurgery.AmhivssOfok?.kzryngvlogy101,145-151.
—