The PDF version of the Atlas of Genetics and Cytogenetics in INIST-CNRS OPEN ACCESS JOURNAL Atlas of...
76
The PDF version of the Atlas of Genetics and Cytogenetics in Oncology and Haematology is a reissue of the original articles published in collaboration with the Institute for Scientific and Technical Information (INstitut de l’Information Scientifique et Technique - INIST) of the French National Center for Scientific Research (CNRS) on its electronic publishing platform I-Revues. Online and PDF versions of the Atlas of Genetics and Cytogenetics in Oncology and Haematology are hosted by INIST-CNRS. INIST-CNRS OPEN ACCESS JOURNAL Atlas of Genetics and Cytogenetics in Oncology and Haematology Volume 17 - Number 5 May 2013
Transcript of The PDF version of the Atlas of Genetics and Cytogenetics in INIST-CNRS OPEN ACCESS JOURNAL Atlas of...

The PDF version of the Atlas of Genetics and Cytogenetics in Oncology and Haematology is a reissue of the original articles published in collaboration with the Institute for Scientific and Technical Information (INstitut de l’Information Scientifique et Technique - INIST) of the French National Center for Scientific Research (CNRS) on its electronic publishing platform I-Revues. Online and PDF versions of the Atlas of Genetics and Cytogenetics in Oncology and Haematology are hosted by INIST-CNRS.
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Volume 17 - Number 5 May 2013

The PDF version of the Atlas of Genetics and Cytogenetics in Oncology and Haematology is a reissue of the original articles published in collaboration with the Institute for Scientific and Technical Information (INstitut de l’Information Scientifique et Technique - INIST) of the French National Center for Scientific Research (CNRS) on its electronic publishing platform I-Revues. Online and PDF versions of the Atlas of Genetics and Cytogenetics in Oncology and Haematology are hosted by INIST-CNRS.
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Scope
The Atlas of Genetics and Cytogenetics in Oncology and Haematology is a peer reviewed on-line journal in open access, devoted to genes, cytogenetics, and clinical entities in cancer, and cancer-prone diseases. It presents structured review articles ("cards") on genes, leukaemias, solid tumours, cancer-prone diseases, more traditional review articles on these and also on surrounding topics ("deep insights"), case reports in hematology, and educational items in the various related topics for students in Medicine and in Sciences.
Editorial correspondance
Jean-Loup Huret Genetics, Department of Medical Information, University Hospital F-86021 Poitiers, France tel +33 5 49 44 45 46 or +33 5 49 45 47 67 [email protected] or [email protected]
Staff Mohammad Ahmad, Mélanie Arsaban, Marie-Christine Jacquemot-Perbal, Vanessa Le Berre, Anne Malo, Carol Moreau, Catherine Morel-Pair, Laurent Rassinoux, Alain Zasadzinski. Philippe Dessen is the Database Director, and Alain Bernheim the Chairman of the on-line version (Gustave Roussy Institute – Villejuif – France).
The Atlas of Genetics and Cytogenetics in Oncology and Haematology (ISSN 1768-3262) is published 12 times a year by ARMGHM, a non profit organisation, and by the INstitute for Scientific and Technical Information of the French National Center for Scientific Research (INIST-CNRS) since 2008. The Atlas is hosted by INIST-CNRS (http://www.inist.fr)
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5)
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Editor Jean-Loup Huret (Poitiers, France)
Editorial Board Sreeparna Banerjee (Ankara, Turkey) Solid Tumours Section Alessandro Beghini (Milan, Italy) Genes Section Anne von Bergh (Rotterdam, The Netherlands) Genes / Leukaemia Sections Judith Bovée (Leiden, The Netherlands) Solid Tumours Section Vasantha Brito-Babapulle (London, UK) Leukaemia Section Charles Buys (Groningen, The Netherlands) Deep Insights Section Anne Marie Capodano (Marseille, France) Solid Tumours Section Fei Chen (Morgantown, West Virginia) Genes / Deep Insights Sections Antonio Cuneo (Ferrara, Italy) Leukaemia Section Paola Dal Cin (Boston, Massachussetts) Genes / Solid Tumours Section Brigitte Debuire (Villejuif, France) Deep Insights Section François Desangles (Paris, France) Leukaemia / Solid Tumours Sections Enric Domingo-Villanueva (London, UK) Solid Tumours Section Ayse Erson (Ankara, Turkey) Solid Tumours Section Richard Gatti (Los Angeles, California) Cancer-Prone Diseases / Deep Insights Sections Ad Geurts van Kessel (Nijmegen, The Netherlands) Cancer-Prone Diseases Section Oskar Haas (Vienna, Austria) Genes / Leukaemia Sections Anne Hagemeijer (Leuven, Belgium) Deep Insights Section Nyla Heerema (Colombus, Ohio) Leukaemia Section Jim Heighway (Liverpool, UK) Genes / Deep Insights Sections Sakari Knuutila (Helsinki, Finland) Deep Insights Section Lidia Larizza (Milano, Italy) Solid Tumours Section Lisa Lee-Jones (Newcastle, UK) Solid Tumours Section Edmond Ma (Hong Kong, China) Leukaemia Section Roderick McLeod (Braunschweig, Germany) Deep Insights / Education Sections Cristina Mecucci (Perugia, Italy) Genes / Leukaemia Sections Yasmin Mehraein (Homburg, Germany) Cancer-Prone Diseases Section Fredrik Mertens (Lund, Sweden) Solid Tumours Section Konstantin Miller (Hannover, Germany) Education Section Felix Mitelman (Lund, Sweden) Deep Insights Section Hossain Mossafa (Cergy Pontoise, France) Leukaemia Section Stefan Nagel (Braunschweig, Germany) Deep Insights / Education Sections Florence Pedeutour (Nice, France) Genes / Solid Tumours Sections Elizabeth Petty (Ann Harbor, Michigan) Deep Insights Section Susana Raimondi (Memphis, Tennesse) Genes / Leukaemia Section Mariano Rocchi (Bari, Italy) Genes Section Alain Sarasin (Villejuif, France) Cancer-Prone Diseases Section Albert Schinzel (Schwerzenbach, Switzerland) Education Section Clelia Storlazzi (Bari, Italy) Genes Section Sabine Strehl (Vienna, Austria) Genes / Leukaemia Sections Nancy Uhrhammer (Clermont Ferrand, France) Genes / Cancer-Prone Diseases Sections Dan Van Dyke (Rochester, Minnesota) Education Section Roberta Vanni (Montserrato, Italy) Solid Tumours Section Franck Viguié (Paris, France) Leukaemia Section José Luis Vizmanos (Pamplona, Spain) Leukaemia Section Thomas Wan (Hong Kong, China) Genes / Leukaemia Sections

Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5)
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Volume 17, Number 5, May 2013
Table of contents
Gene Section
AIP (aryl hydrocarbon receptor interacting protein) 297 Sayka Barry, Márta Korbonits
DPP4 (dipeptidyl-peptidase 4) 301 Kei Ohnuma, Chikao Morimoto
FOSL1 (FOS-like antigen 1) 313 Senthilkumar B Rajamohan, Sekhar P Reddy
FOXC1 (forkhead box C1) 319 Shakila Jabeen, Vessela N Kristensen
PTPN6 (protein tyrosine phosphatase, non-receptor type 6) 327 Alessandro Beghini, Francesca Lazzaroni
HACE1 (HECT domain and ankyrin repeat containing E3 ubiquitin protein ligase 1) 333 Feng Cui, Yanzhuang Wang
MIR146B (microRNA 146b) 337 Amandine Garcia, Sylvie Mazoyer
Leukaemia Section
t(20;21)(q13.2;q22.12) ZFP64/RUNX1 341 Nathalie Douet-Guilbert, Etienne De Braekeleer, Audrey Basinko, Marie-Josée Le Bris, Frédéric Morel, Marc De Braekeleer
t(2;19)(p23;p13) TPM4/ALK 344 Jean-Loup Huret
t(3;14)(q27;q32) HSP90AA1/BCL6 346 Jean-Loup Huret
Solid Tumour Section
Colon: Colorectal adenocarcinoma 348 Viktor H Koelzer, Heather Dawson, Inti Zlobec, Alessandro Lugli
Cancer Prone Disease Section
Chediak-Higashi Syndrome 364 Xinjie Xu, Wei Shen

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 297
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
AIP (aryl hydrocarbon receptor interacting protein) Sayka Barry, Márta Korbonits
Molecular Oncology Centre, Barts Cancer Institute, Queen Mary University of London, London, United Kingdom (SB), Department of Endocrinology, Barts and the London School of Medicine, Queen Mary University of London, London, United Kingdom (MK)
Published in Atlas Database: November 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/AIPID604ch11q13.html DOI: 10.4267/2042/49696
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: ARA9, FKBP16, FKBP37, SMTPHN, XAP-2, XAP2
HGNC (Hugo): AIP
Location: 11q13.2
DNA/RNA Description The AIP gene is located on Chromosome 11 at 67250505-67258579 (GRCh37/hg19). The AIP gene is composed of 6 exons and spans approximately 8.07 kb of genomic DNA.
Transcription AIP gene encodes a 1250bp mRNA transcript. No splice variants have been identified.
Pseudogene No pseudogene reported.
Protein Description AIP protein consists of 330 amino acids with a molecular weight of 37 kDa. AIP belongs to the family of tetratricopeptide repeat (TPR) domain-containing proteins. It has three TPR-domains which are important for protein-protein interactions and an α helix at the C-terminal region and a PPIase-like domain (FKBP-type) in the N-terminus.
Expression AIP is expressed ubiquitously and found in various human tissues such as: heart, brain, lung, placenta, kidney, skeletal muscle, mouth mucosa, exocrine
pancreas, salivary gland, stomach, parathyroid, tonsil, nerve, ovary, connective adipose tissue, spleen, thymus, prostate, testis, colon, leucocytes and pituitary (Kuzhandaivelu et al., 1996; Leontiou et al., 2008).
Localisation Cytoplasm and nucleus.
Function To date, several AIP interacting partners have been identified including HBV-X, EBNA-3, AhR, Hsp90, Hsc70, PDE4A5, PDE2A3, PPARα, TRβ1, Gα13, Gαq, TOMM20, RET, survivin and ERα, which may indicate that AIP is involved in various cellular pathways, however, the consequenses ot these interactions are not fully understood (Cai et al., 2011; Trivellin and Korbonits, 2011). Clinical and functional data supports its role as a tumour suppressor gene. Loss of heterozygosity (LOH) is found in AIP mutation positive tumours. Our lab has previously shown that over-expression of wild-type AIP in human fibroblast and pituitary cell lines reduced cell proliferation compared with the empty vector control in vitro whereas the mutant AIP loses this ability compared to the wild-type AIP (Leontiou et al., 2008). AIP knockdown with siRNA also supports the tumour-suppressor role for AIP as it results in increased cell proliferation in GH3 cells (Heliovaara et al., 2009; Leontiou et al., 2008). Homozygous deletion of AIP is embryonically lethal due to cardiovascular developmental abnormalities and erythropoietic failure (Kang et al., 2011; Lin et al., 2007), suggesting that AIP has a crucial role for cardiac development and for maintaining erythropoiesis in mice. Heterozygote deletion of the AIP gene lead to the development of growth hormone- and prolactin-secreting pituitary adenomas (Raitila et al., 2010).

AIP (aryl hydrocarbon receptor interacting protein) Barry S, Korbonits M
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 298
AIP is a molecular co-chaperone protein. The most studied partner is the nuclear xenobiotic receptor AhR (aryl hydrocarbon receptor). AIP regulates its sub-cellular localization and degradation. AhR, also known as dioxin receptor is a ligand activated transcription factor found in the cytoplasm as part of a multiprotein complex with Hsp90 (Perdew, 1988), AIP (Carver and Bradfield, 1997; Meyer et al., 1998) and p23 (Kazlauskas et al., 1999). After binding to its ligand it is transported to the nucleus where it heterodimerizes with aryl hydrocarbon receptor nuclear translocator (ARNT). This complex then binds to DNA recognition sequences known as xenobiotic inducible response elements (XREs/DREs/AHREs) within the promoter region of specific genes, leading to the transcription of xenobiotic-metabolizing enzymes. However, there is conflicting data regarding the role of AIP on AhR function. Some findings suggested that AIP has a role in stabilising unliganded AhR in the cytoplasm (LaPres et al., 2000; Meyer and Perdew, 1999; Nukaya et al., 2010), therefore AIP may play a positive role in AhR-mediated signalling. In contrast, other studies have suggested that AIP has a negative effect on AhR transcriptional activity (Hollingshead et al., 2004; Pollenz et al., 2006; Pollenz and Dougherty, 2005). AIP has other functions related to the other interacting partners but it is currently not known how lack of AIP leads to pituitary tumorigenesis.
Homology AIP shares 94% and 93% sequence identity with mouse and rat AIP respectively.
Mutations Germinal Germline mutations of AIP are associated with familial isolated pituitary adenoma (FIPA). Approximately 20% of FIPA families and 13% of sporadic young (<30 years) onset have somatotroph or lactotroph adenomas (Cazabat et al., 2007; Cazabat et al., 2012; Chahal et al., 2010; Daly et al., 2007; Leontiou et al., 2008; Tichomirowa et al., 2011; Vierimaa et al., 2006). Over 50 pathogenic mutations have been identified including deletions, insertions, segmental duplications, nonsense, missense, splice-site and promoter mutations, as well as large deletions of whole exons or the entire AIP gene. Mutations are present throughout the whole length of the gene and disrupt the protein. Sixty five percent of known AIP variants result in a truncated protein. The majority of the missense mutations are typically clustered around the C-terminal part of the protein, appeared to be crucial for its biological function (Ozfirat and Korbonits, 2010). The most common mutation is found at residue 304, a mutational 'hotspot' CpG site. Informations regarding AIP mutations and polymorphisms are available in a locus-specific mutation database, available at: http://aip.fipapatients.org/.
Somatic Somatic mutations in AIP have not been found to date in sporadic pituitary adenomas. Somatic mutations in AIP have been investigated in colorectal cancers, breast cancers, prostate tumours (Georgitsi et al., 2007) as well as endocrine tumours (thyroid lesions, adrenal lesions, carcinoids, parathyroid lesions, paragangliomas, pancreatic endocrine tumours and adenocarcinoids) but no somatic mutations were found (Raitila et al., 2007; Tichomirowa et al., 2011).
Implicated in Familial isolated pituitary adenoma (FIPA) and simplex pituitary adenoma cases with germline AIP mutation Note Familial isolated pituitary adenoma (FIPA) is an autosomal dominant disease with incomplete penetrance. Heterozygote germline mutations have been identified in the aryl hydrocarbon receptor interacting protein (AIP) gene in 20% of FIPA families. FIPA has been characterised in >200 families. Most of the FIPA families with AIP mutations presented somatotropinomas or somatomammotropinomas followed by prolactinomas as well as non-functioning adenomas and very rarely corticotroph or thyrotropinomas. Approximately, eighty five percent of AIP mutation positive FIPA patients have acromegaly and around fifty percent with AIP mutation positive somatotropinomas are associated with gigantism (Daly et al., 2010). Pituitary tumours in AIP mutation positive patients have larger, more aggressive, invasive tumours, most commonly sparsely granulated subtype which show a poor response to somatostatin analogues (Daly et al., 2010) and also have a younger age at disease onset (18-24 years) (Korbonits and Kumar, 2012).
Prognosis AIP mutation positive patients show younger mean age at diagnosis than sporadic pituitary cases. Decreased level of AIP has been correlated with tumour invasiveness in somatotropinomas (Kasuki Jomori de Pinho et al., 2011). Genetic screening is now able to stratify carrier subjects and help to diagnose the presymptomatic patients (Chahal et al., 2011).
References Perdew GH. Association of the Ah receptor with the 90-kDa heat shock protein. J Biol Chem. 1988 Sep 25;263(27):13802-5
Kuzhandaivelu N, Cong YS, Inouye C, Yang WM, Seto E. XAP2, a novel hepatitis B virus X-associated protein that inhibits X transactivation. Nucleic Acids Res. 1996 Dec 1;24(23):4741-50
Carver LA, Bradfield CA. Ligand-dependent interaction of the aryl hydrocarbon receptor with a novel immunophilin homolog in vivo. J Biol Chem. 1997 Apr 25;272(17):11452-6

AIP (aryl hydrocarbon receptor interacting protein) Barry S, Korbonits M
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 299
Meyer BK, Pray-Grant MG, Vanden Heuvel JP, Perdew GH. Hepatitis B virus X-associated protein 2 is a subunit of the unliganded aryl hydrocarbon receptor core complex and exhibits transcriptional enhancer activity. Mol Cell Biol. 1998 Feb;18(2):978-88
Kazlauskas A, Poellinger L, Pongratz I. Evidence that the co-chaperone p23 regulates ligand responsiveness of the dioxin (Aryl hydrocarbon) receptor. J Biol Chem. 1999 May 7;274(19):13519-24
Meyer BK, Perdew GH. Characterization of the AhR-hsp90-XAP2 core complex and the role of the immunophilin-related protein XAP2 in AhR stabilization. Biochemistry. 1999 Jul 13;38(28):8907-17
LaPres JJ, Glover E, Dunham EE, Bunger MK, Bradfield CA. ARA9 modifies agonist signaling through an increase in cytosolic aryl hydrocarbon receptor. J Biol Chem. 2000 Mar 3;275(9):6153-9
Hollingshead BD, Petrulis JR, Perdew GH. The aryl hydrocarbon (Ah) receptor transcriptional regulator hepatitis B virus X-associated protein 2 antagonizes p23 binding to Ah receptor-Hsp90 complexes and is dispensable for receptor function. J Biol Chem. 2004 Oct 29;279(44):45652-61
Pollenz RS, Dougherty EJ. Redefining the role of the endogenous XAP2 and C-terminal hsp70-interacting protein on the endogenous Ah receptors expressed in mouse and rat cell lines. J Biol Chem. 2005 Sep 30;280(39):33346-56
Pollenz RS, Wilson SE, Dougherty EJ. Role of endogenous XAP2 protein on the localization and nucleocytoplasmic shuttling of the endogenous mouse Ahb-1 receptor in the presence and absence of ligand. Mol Pharmacol. 2006 Oct;70(4):1369-79
Vierimaa O, Georgitsi M, Lehtonen R, Vahteristo P, Kokko A, Raitila A, Tuppurainen K, Ebeling TM, Salmela PI, Paschke R, Gündogdu S, De Menis E, Mäkinen MJ, Launonen V, Karhu A, Aaltonen LA. Pituitary adenoma predisposition caused by germline mutations in the AIP gene. Science. 2006 May 26;312(5777):1228-30
Cazabat L, Libè R, Perlemoine K, René-Corail F, Burnichon N, Gimenez-Roqueplo AP, Dupasquier-Fediaevsky L, Bertagna X, Clauser E, Chanson P, Bertherat J, Raffin-Sanson ML. Germline inactivating mutations of the aryl hydrocarbon receptor-interacting protein gene in a large cohort of sporadic acromegaly: mutations are found in a subset of young patients with macroadenomas. Eur J Endocrinol. 2007 Jul;157(1):1-8
Daly AF, Vanbellinghen JF, Khoo SK, Jaffrain-Rea ML, Naves LA, Guitelman MA, Murat A, Emy P, Gimenez-Roqueplo AP, Tamburrano G, Raverot G, Barlier A, De Herder W, Penfornis A, Ciccarelli E, Estour B, Lecomte P, Gatta B, Chabre O, Sabaté MI, Bertagna X, Garcia Basavilbaso N, Stalldecker G, Colao A, Ferolla P, Wémeau JL, Caron P, Sadoul JL, Oneto A, Archambeaud F, Calender A, Sinilnikova O, Montañana CF, Cavagnini F, Hana V, Solano A, Delettieres D, Luccio-Camelo DC, Basso A, Rohmer V, Brue T, Bours V, Teh BT, Beckers A. Aryl hydrocarbon receptor-interacting protein gene mutations in familial isolated pituitary adenomas: analysis in 73 families. J Clin Endocrinol Metab. 2007 May;92(5):1891-6
Georgitsi M, Karhu A, Winqvist R, Visakorpi T, Waltering K, Vahteristo P, Launonen V, Aaltonen LA. Mutation analysis of aryl hydrocarbon receptor interacting protein (AIP) gene in colorectal, breast, and prostate cancers. Br J Cancer. 2007 Jan 29;96(2):352-6
Lin BC, Sullivan R, Lee Y, Moran S, Glover E, Bradfield CA. Deletion of the aryl hydrocarbon receptor-associated protein 9 leads to cardiac malformation and embryonic lethality. J Biol Chem. 2007 Dec 7;282(49):35924-32
Raitila A, Georgitsi M, Karhu A, Tuppurainen K, Mäkinen MJ, Birkenkamp-Demtröder K, Salmenkivi K, Orntoft TF, Arola J, Launonen V, Vahteristo P, Aaltonen LA. No evidence of somatic aryl hydrocarbon receptor interacting protein mutations in sporadic endocrine neoplasia. Endocr Relat Cancer. 2007 Sep;14(3):901-6
Leontiou CA, Gueorguiev M, van der Spuy J, Quinton R, Lolli F, Hassan S, Chahal HS, Igreja SC, Jordan S, Rowe J, Stolbrink M, Christian HC, Wray J, Bishop-Bailey D, Berney DM, Wass JA, Popovic V, Ribeiro-Oliveira A Jr, Gadelha MR, Monson JP, Akker SA, Davis JR, Clayton RN, Yoshimoto K, Iwata T, Matsuno A, Eguchi K, Musat M, Flanagan D, Peters G, Bolger GB, Chapple JP, Frohman LA, Grossman AB, Korbonits M. The role of the aryl hydrocarbon receptor-interacting protein gene in familial and sporadic pituitary adenomas. J Clin Endocrinol Metab. 2008 Jun;93(6):2390-401
Heliövaara E, Raitila A, Launonen V, Paetau A, Arola J, Lehtonen H, Sane T, Weil RJ, Vierimaa O, Salmela P, Tuppurainen K, Mäkinen M, Aaltonen LA, Karhu A. The expression of AIP-related molecules in elucidation of cellular pathways in pituitary adenomas. Am J Pathol. 2009 Dec;175(6):2501-7
Chahal HS, Chapple JP, Frohman LA, Grossman AB, Korbonits M. Clinical, genetic and molecular characterization of patients with familial isolated pituitary adenomas (FIPA). Trends Endocrinol Metab. 2010 Jul;21(7):419-27
Daly AF, Tichomirowa MA, Petrossians P, Heliövaara E, Jaffrain-Rea ML, Barlier A, Naves LA, Ebeling T, Karhu A, Raappana A, Cazabat L, De Menis E, Montañana CF, Raverot G, Weil RJ, Sane T, Maiter D, Neggers S, Yaneva M, Tabarin A, Verrua E, Eloranta E, Murat A, Vierimaa O, Salmela PI, Emy P, Toledo RA, Sabaté MI, Villa C, Popelier M, Salvatori R, Jennings J, Longás AF, Labarta Aizpún JI, Georgitsi M, Paschke R, Ronchi C, Valimaki M, Saloranta C, De Herder W, Cozzi R, Guitelman M, Magri F, Lagonigro MS, Halaby G, Corman V, Hagelstein MT, Vanbellinghen JF, Barra GB, Gimenez-Roqueplo AP, Cameron FJ, Borson-Chazot F, Holdaway I, Toledo SP, Stalla GK, Spada A, Zacharieva S, Bertherat J, Brue T, Bours V, Chanson P, Aaltonen LA, Beckers A. Clinical characteristics and therapeutic responses in patients with germ-line AIP mutations and pituitary adenomas: an international collaborative study. J Clin Endocrinol Metab. 2010 Nov;95(11):E373-83
Nukaya M, Lin BC, Glover E, Moran SM, Kennedy GD, Bradfield CA. The aryl hydrocarbon receptor-interacting protein (AIP) is required for dioxin-induced hepatotoxicity but not for the induction of the Cyp1a1 and Cyp1a2 genes. J Biol Chem. 2010 Nov 12;285(46):35599-605
Ozfirat Z, Korbonits M. AIP gene and familial isolated pituitary adenomas. Mol Cell Endocrinol. 2010 Sep 15;326(1-2):71-9
Raitila A, Lehtonen HJ, Arola J, Heliövaara E, Ahlsten M, Georgitsi M, Jalanko A, Paetau A, Aaltonen LA, Karhu A. Mice with inactivation of aryl hydrocarbon receptor-interacting protein (Aip) display complete penetrance of pituitary adenomas with aberrant ARNT expression. Am J Pathol. 2010 Oct;177(4):1969-76
Cai W, Kramarova TV, Berg P, Korbonits M, Pongratz I. The immunophilin-like protein XAP2 is a negative regulator of estrogen signaling through interaction with estrogen receptor α. PLoS One. 2011;6(10):e25201
Chahal HS, Stals K, Unterländer M, Balding DJ, Thomas MG, Kumar AV, Besser GM, Atkinson AB, Morrison PJ, Howlett TA, Levy MJ, Orme SM, Akker SA, Abel RL, Grossman AB, Burger J, Ellard S, Korbonits M. AIP mutation in pituitary adenomas in the 18th century and today. N Engl J Med. 2011 Jan 6;364(1):43-50

AIP (aryl hydrocarbon receptor interacting protein) Barry S, Korbonits M
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 300
Kang BH, Xia F, Pop R, Dohi T, Socolovsky M, Altieri DC. Developmental control of apoptosis by the immunophilin aryl hydrocarbon receptor-interacting protein (AIP) involves mitochondrial import of the survivin protein. J Biol Chem. 2011 May 13;286(19):16758-67
Kasuki Jomori de Pinho L, Vieira Neto L, Armondi Wildemberg LE, Gasparetto EL, Marcondes J, de Almeida Nunes B, Takiya CM, Gadelha MR. Low aryl hydrocarbon receptor-interacting protein expression is a better marker of invasiveness in somatotropinomas than Ki-67 and p53. Neuroendocrinology. 2011;94(1):39-48
Tichomirowa MA, Barlier A, Daly AF, Jaffrain-Rea ML, Ronchi C, Yaneva M, Urban JD, Petrossians P, Elenkova A, Tabarin A, Desailloud R, Maiter D, Schürmeyer T, Cozzi R, Theodoropoulou M, Sievers C, Bernabeu I, Naves LA, Chabre O, Montañana CF, Hana V, Halaby G, Delemer B, Aizpún JI, Sonnet E, Longás AF, Hagelstein MT, Caron P, Stalla GK, Bours V, Zacharieva S, Spada A, Brue T, Beckers A. High prevalence of AIP gene mutations following focused screening
in young patients with sporadic pituitary macroadenomas. Eur J Endocrinol. 2011 Oct;165(4):509-15
Trivellin G, Korbonits M. AIP and its interacting partners. J Endocrinol. 2011 Aug;210(2):137-55
Cazabat L, Bouligand J, Salenave S, Bernier M, Gaillard S, Parker F, Young J, Guiochon-Mantel A, Chanson P. Germline AIP mutations in apparently sporadic pituitary adenomas: prevalence in a prospective single-center cohort of 443 patients. J Clin Endocrinol Metab. 2012 Apr;97(4):E663-70
Korbonits M, Kumar AV. AIP-Related Familial Isolated Pituitary Adenomas GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle. 1993; 2012 Jun 21.
This article should be referenced as such:
Barry S, Korbonits M. AIP (aryl hydrocarbon receptor interacting protein). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):297-300.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 301
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
DPP4 (dipeptidyl-peptidase 4) Kei Ohnuma, Chikao Morimoto
Department of Therapy Development and Innovation for Immune disorders and Cancers, Graduate School of Medicine, Juntendo University, 2-1-1, Hongo, Bunkyo-ku, Tokyo 113-8421, Japan (KO, CM)
Published in Atlas Database: November 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/DPP4ID40360ch2q24.html DOI: 10.4267/2042/49697
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: ADABP, ADCP2, CD26, DPPIV, TP103
HGNC (Hugo): DPP4
Location: 2q24.2
DNA/RNA Note In 1979, a large molecular weight complex composed of adenosine deaminase (ADA) were reported to be found as an adenosine deaminase-binding protein (ADBP), also known as adenosine deaminase complexing protein-2 (ADCP2). In 1993, this adenosine deaminase-binding protein is determined to be identical to CD26, a T-cell activation molecule and a 110-kD glycoprotein that is present also on epithelial cells of various tissues including the liver, kidney, and intestine. The CD26 cDNA contains a 3465 bp open reading frame that encodes a 766 amino acid protein. The CD26 amino acid sequence has 85% amino acid identity with the
mouse and rat CD26 genes and 37% amino acid identity with D. melanogaster. Two CD26 transcripts (4,2 and 2,8 kb) were found, both of which were expressed at high levels in the placenta and kidney and at moderate levels in the lung and liver. However, only the 4,2 kb mRNA was expressed at low levels in skeletal muscle, heart, brain, and pancreas.
Transcription The 5'-flanking region does not contain a TATA box or CAAT box, commonly found in housekeeping genes. CD26 does contain a 300 base-pair G-C rich region with potential binding sites for NF-κB, AP2, or Sp1. CD26 expression is activated by interferons (IFNs) and retinoic acid in chronic lymphocytic leukemia (CLL) via Stat1α and the GAS response element (TTCnnnGAA located at bp -35 to -27) in the CD26 promoter. A hepatocyte nuclear factor 1 binding site at position -150 to -131 of the CD26 gene regulates CD26 expression in human intestinal (Caco-2) and hepatic epithelial (HepG2) cell lines.
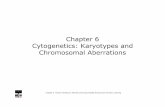
Location of DPP4 gene on chromosome 2q24.3. DPP4 spans 82,301 kbp of chromosome 2 from 162848751 to 162931052. The gene contains 26 exons (indicated in orange squares), ranging from 45 to 1,4 kb in length on the reverse strand. The Ser recognition site (G-W-S-Y-G) is split between exons 21 and 22.

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 302
The schematic diagrams of the amino acids of DPP4. The cDNA of DPP4 is composed of 2301 base pairs, translated to 766 amino acid protein. CD26/DPP4 is a ubiquitous, membrane-bound enzyme that has roles in nutrition, metabolism, the immune and endocrine systems, bone marrow mobilization, cancer growth and cell adhesion. DDPIV catalyzes the hydrolysis of N-terminal dipeptides from polypeptides with proline or alanine in the penultimate position. Note: residues 1-6: cytoplasmic domain (MKTPWK); residues 7-29: transmembrane domain (VLLGLLGAAALVTI ITVPVVLLN); residues 30-48: flexible stalk (KGTDDATADSRKTYTLTDY); residues 201-211 and Ser603: caveolin-1 binding site (WVYEEEVFSAY); residues 340-343: ADA binding site (LVAR); residues 469-479: fibronectin binding site (QLRCSGPGLPL); red *: essential for DPPIV activity (Glu205,Glu206 and Tyr547); green underlined GWSYG: serine recognition site; black *: Ser630, Asp708, His740 active site triad; red boxes: odd numbered exons; green boxes: glycosylation sites; yellow box (His750): required for homodimer formation; white square at residue 492: non-synonymous cSNP (Arg492Lys); white triangle at residues 633: mutation results in retention and degradation of mutant protein in the endoplasmic reticulum (Gly633Arg).
Protein Note CD26 is a multifunctional type II transmembrane serine peptidase that has an extracellular domain with DPPIV enzymatic activity and a short cytoplasmic domain. It interacts with extracellular molecules and is also involved in intracellular signal transduction cascades. CD26 is important in immunology, autoimmunity, HIV, diabetes, and cancer. Interacting directly with various other cell surface and intracellular molecules, CD26 can regulate receptor specificity via its DPPIV
activity and the function of various chemokines and cytokines. CD26 is expressed at low density on resting T cells, but is upregulated with T cell activation. Therefore, CD26 may have an important functional role in T-cells and overall immune function. CD26 associates with other important immunologic cell surface receptors such as CD45, CD9 and CXCR4. The multifunctional activities of CD26 are dependent on cell type and intracellular or extracellular conditions that influence its role as a proteolytic enzyme, cell surface receptor, costimulatory interacting protein and signal transduction mediator; as well as its role in adhesion and apoptosis.

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 303
Schematic representation of CD26/DPPIV. Human CD26 is composed of 766 amino acids, including a short cytoplasmic domain of 6 amino acids, a transmembrane region of 24 amino acids, and an extracellular domain with dipeptidyl peptidase activity which selectively removes the N-terminal dipeptide from peptides with proline or alanine at the penultimate position. Single amino acid point mutation in the β-propeller motif identified Glu205 and Glu206 as essential for DPPIV enzyme activity, and the central tunnel and α/β-hydrolase domains both participate in DPPIV inhibitor binding. Single amino acid point mutation at His750 residue is responsible for dimerization.
Description Originally characterized as a T cell differentiation antigen, CD26 is preferentially expressed on a specific population of T lymphocytes, the subset of CD4+CD45RO+ memory T cells, and is upregulated following T cell activation. Besides being a marker of T cell activation, CD26 is also associated with T cell signal transduction processes as a costimulatory molecule. Recent work also suggests that CD26 has a significant role in tumor biology, being both a marker of disease behavior clinically as well as playing an important role in tumor pathogenesis and development. For instance, the association of CD26/DPPIV with such key molecules as topoisomerase IIα, p38 MAPK, and integrin β1, has important clinical implications, including its potential ability to regulate tumor sensitivity to selected chemotherapies and to influence tumor migration/metastases and tumorigenesis. DPPIV inhibitors enhance the effects of incretin hormones (glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP)), increasing glucose-mediated insulin secretion and suppressing
glucagon secretion. Therefore, DPPIV inhibitors, which act by inhibiting DPPIV, the enzyme that inactivates GLP-1 and GIP have been available as a new class of antidiabetes drugs.
Expression CD26 is expressed in many tissues. Two CD26 transcripts (4,2 and 2,8 kb) are reported to be found, both of which were expressed at high levels in the placenta and kidney and at moderate levels in the lung and liver. The 4,2 kb transcript was expressed at low levels in skeletal muscle, heart, brain, and pancreas. Other organs expressing CD26 include: brain, endothelium, heart, intestine (colon adenocarcinoma, fetal colon expression disappears at birth), kidney, liver, lung, skeletal muscle, pancreas, and placenta. In the hematopoietic system CD26 is found on CD4+ T memory cells, CD8+ effector/memory T cells. It has been reported that 0-5% of freshly isolated CD20+ B cells do express the CD26 antigen. Following stimulation with PMA (phorbol 12-Myristate 13-acetate) or Streptococcus aureus protein, the fraction of CD26-positive cells increased to 51%.

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 304
3-D structure of CD26/DPPIV. CD26/DPPIV forms a homodimer in the cell surface membrane. The residues 7-28 constitute the membrane spanning region. Each subunit consists of two domains, that is, an α/β-hydrolase domain and a β-propeller domain. The N-terminal β-propeller domain of CD26/DPPIV (residues 55-497) consists of 8 blades. β-strand 2 of blade 4 of the propeller extends into a small domain (residues 234-260) that includes an antiparallel two-stranded β-sheet. The function of this arm is to stabilize the dimeric structure. The catalytic site (Ser630-Asp708-His740) is located in a large cavity (also called a central tunnel), formed between the α/β-hydrolase domain and 8-bladed β-propeller domain, which contains the consensus sequence (DW(V/L)YEEE), that is common to S9b proteases. The central tunnel and α/β-hydrolase domains both participate in inhibitor binding. This figure is reproduced from Ralf Thoma et al., Structural Basis of Proline-Specific Exopeptidase Activity as Observed in Human Dipeptidyl Peptidase-IV, Structure 2003;8:947-959, with permission by Elsevier Limited.
Meanwhile, CD26 is not expressed or is found only at low levels on monocytes of healthy adult. Flow cytometric analysis of dendritic antigen-presenting cells (DC) generated from peripheral blood of normal donors in the presence of granulocyte/macrophage colony-stimulating factor and revealed intermediate levels of CD26 expression during a 2-week culture period. Only a small fraction of peripheral NK cells was found to express CD26.
Localisation CD26 physically binds with ADA, an enzyme that plays a key role in the development and function of lymphoid tissues. ADA is essential for purine metabolism, with the loss of ADA leading to a clinical syndrome characterized by severe immunodeficiency. When the ADA inhibitor pentostatin was used in the treatment of recurrent T cell lymphomas, a significant reduction in circulating CD26+ T cells was observed in treated patients. This finding is consistent with the fact that there is a physical association between CD26 and ADA on the surface of T lymphocytes. CD26 also interacts with CD45RO, a tyrosine phosphatase with a critical role in T cell signal transduction, at lipid rafts in peripheral blood T lymphocytes to modify cellular signaling events. A lipid raft is a cholesterol-rich microdomain in cell membrane, which plays an important role in signal transduction in T-cell regulation. CD26 interaction with lipid rafts in
peripheral blood T-cells influences key cellular signaling events. Non-activated peripheral blood T-cells treated with the anti-CD26 mAb 1F7 increased CD26 recruitment to lipid rafts, resulting in increased tyrosine phosphorylation of c-Cbl, Zap70, Erk1/Erk2, p56lck, and TCR-ζ. Interestingly, CD26 is associated with CD45 RA outside of lipid rafts in cord blood T cells, and the strong physical linkage of CD26 and CD45 RA may be responsible for the attenuation of cord blood T-cell activation signaling through CD26. In addition to cell surface expression, nuclear localization of CD26 has been reported in malignant mesothelioma and malignant T cell lines, and in human thyroid carcinomas, although little is known on the functional relevance of nuclear CD26. In addition to membrane bound CD26, soluble form of CD26 (sCD26) is also detected in the sera, urine, thoracic fluid and seminal fluid. sCD26 in the sera appears to be functioned as immune enhancing protein in antigen-presenting cell (APC).
Function CD26 is a co-stimulatory molecule for T-cell signal transduction. While CD26 expression is enhanced following activation of resting T cells, CD4+CD26high T cells respond maximally to recall antigens such as tetanus toxoid. Moreover, we have previously reproted that effector CD26-mediated costimulatory activity is exerted via its DPPIV enzymatic activity.

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 305
Table 1. In addition, CD4+ T cells with in vitro transendothelial migratory capacity appear to express high CD26, indicating a role for CD26 in the migration of T cells, and patients with autoimmune diseases such as multiple sclerosis, Grave's disease, and rheumatoid arthritis (RA) have been found to have increased numbers of CD4+CD26+ T cells in inflamed tissues as well as in their peripheral blood, with enhancement of CD26 expression in these autoimmune diseases correlating with disease severity. Moreover, CD26highCD8+ T cells in humans belong to early effector memory T cells, and CD26highCD8+ T cells increase expression of granzyme B, TNF-α (tumor necrosis factor-α), IFN-γ and Fas ligand, and exert cytotoxic effect with CD26-mediated costimulation. CD26 binds to caveolin-1 on APC, and residues 201 to 211 of CD26 along with the serine catalytic site at residue 630, which constitute a pocket structure of CD26/DPPIV, contribute to binding to the caveolin-1 scaffolding domain. This region in CD26 contains a caveolin-binding domain (ΦΧΦΧΧΧΧΦΧΧΦ; Φ and Χ depict aromatic residue and any amino acid, respectively), specifically WVYEEEVFSAY in CD26. These observations strongly support the notion that DPPIV enzyme activity
is necessary to exert T-cell costimulatory activation via CD26 as demonstrated in our previous report using CD26 specific mAbs. The cytoplasmic tail of CD26 is responsible for T-cell costimulation induced by anti-CD3 plus caveolin-1. It has been identified that CARMA1 binds to the cytoplasmic tail of dimeric CD26, and that a PDZ domain in CARMA1 is necessary for binding to CD26. Following its phosphorylation, CARMA1 functions as a signaling intermediate downstream of PKCθ and upstream of IKK in the TCR signaling transduction pathway leading to NF-κB activation. Dimeric CD26, but not monomeric CD26, binds to CARMA1. The enzymatic pocket structure of the DPPIV catalytic site is necessary for binding of CD26 to caveolin-1, leading to the upregulation of CD86 expression on APC. Therefore, dimerization of CD26 is not only necessary for binding to caveolin-1, but also serves as a scaffolding structure for the cytoplasmic signaling molecule CARMA1. Overall, CD26 ligation by caveolin-1 on APC recruits CD26-interacting CARMA1 to lipid rafts, resulting in the formation of a CARMA1-Bcl10-MALT1-IKK complex, and this

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 306
membrane-associated Bcl10 complex then activates IKK through ubiquitination of NEMO. DPPIV inactivates incretin hormone (glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP)). Therfore, DPPIV inhibitors enhance the effects of GLP-1 and GIP, increasing glucose-mediated insulin secretion and suppressing glucagon secretion. In this regard, DPPIV inhibitors are now avalilable worldwide for use of an antidiabetic drug. Moreover, DPPIV cleaves many cytokines and chemokines, which are summerized in Table 1. Morimoto et al. showed that proinflammatory cytokines such as TNF-α or IL-1β reduce expression of CD26 in microvascular endothelial cells, and that genetical or pharmacological inhibition of CD26/DPPIV enhances endothelial growth both in vitro and in vivo. These data strongly suggest that this effect of DPP-4 inhibition on endothelial growth may be of potential use in treating diabetic vascular complications, as well as diabetes itself.
Homology CD26/DPPIV molecure is involved in DPPIV activity and/or structure homologues (DASH), comprising seprase, fibroblast activation protein α (FAP-α), DPP6, DPP8, DPP9, attractin, N-acetylated-α-linked-acidic dipeptidase I, N-acetylated- α-linked-acidic dipeptidase II and N-acetylated-α-linked-acidic dipeptidase L, quiescent cell proline dipeptidase, thymus-specific serine protease and DPPIV-β.
Mutations Note Several polymorphisms in the CD26/DPPIV gene coding region have been deposited in the National Center for Biotechnology Information single nucleotide polymorphism (SNP) database (NCBI). The functional significance of coding region SNPs (cSNPs), non-cSNPs, or other polymorphisms has not been determined. Synonymous (non-amino acid changing) polymorphisms include the following (N.D. indicates not determined): Leu8 (T->C, exon 2, frequency: N.D.), Ile405 (C->T, exon 14, frequency: heterozygosity 0.056), Gly645 (C->T, exon 22, frequency: N.D.), Tyr661 (C->T, exon 22, frequency: N.D.). The non-synonymous cSNP Arg492Lys (G->A, exon 18, frequency: N.D.) functional significance has not yet been determined. CD26 experimental mutations include: - Glu205 and Glu206 mutants (DPPIV negative activity) - Leu294, Leu340, Val341, Ala342, Arg343, Thr440, and Lys441 mutants (ADA binding) - Ser630Ala (DPPIV negative activity)
- Gly633Arg (retention and degradation of mutant protein in the endoplasmic reticulum) - His750Glu (stable dimerization).
Implicated in Adult T-cell leukemia/lymphoma Note A study of the human T-lymphotropic virus 1 (HTLV-1) related cancer adult T-cell leukemia/lymphoma (ATLL) showed a reduction of surface CD26 expression in the peripheral blood mononuclear cells. Additionally, CD26 mRNA was undetectable in 7 of 8 ATLL patients. Quantification of HTLV-1 viral DNA by PCR in cells from subjects with CD26-, CD26+, and 17 HTLV-1 carriers showed that the CD26- cells had a higher HTLV-1 copy number than CD26+ cells. This suggests that HTLV-1 has tropism for CD26- cells in vivo. In a study of 49 patients with ATLL, 10 subjects that were carriers of HTLV-1, and 4 HTLV-1 infected cell lines, ATLL HTLV-I-infected cell had reduced or absent the CD26/DPPIV expression. CD26 expression decreased with the advancement of ATLL stage. This appeared to be due to progressive aberrant methylation of CpG islands in the CD26 promoter proportional to increasing ATLL stage. This was confirmed with rescue experiments with the demethylating agent, 5-azacytidine.
Non-Hodgkin's lymphoma Note In Non-Hodgkin's lymphoma (NHL), CD26 expression is found mainly in aggressive subtypes, such as T-lymphoblastic lymphoma (LBL)/T-acute lymphoblastic leukemia (ALL) and T-cell CD30+ anaplastic large cell lymphoma (ALCL). CD26 and CD40L (CD154) expression was mutually exclusive, with CD40L expressed on cells from more indolent diseases. CD26 expression in T-cell LBL/ALL was associated with a worse survival. The majority of patients with T-ALL express CD26 on the leukemic cell surface. There appears to be high CD26/DPPIV expression on T-lymphoblasts but only moderate DPPIV activity. Aldinucci et al. showed that CD26 is a marker of poor prognosis in T-cell cancer and is a predictive marker of poor response to 2'-deoxycoformycin, pentostatin. This effect was seen in vitro in CD26/ADA positive leukemia/lymphoma T-cell lines, primary CD26+ T-cell cancers, and normal T-cells (CD26+). Loss of CD26 appears to be characteristic of cutaneous T-cell lymphoma (CTCL) and has been suggested as a useful diagnostic marker.
Sezary syndrome/mycosis fungoides Note CD26 expression is absent or weak in other T-cell lymphomas such as mycosis fungoides (MF) and Sezary syndrome (SS).

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 307
SS is a form of CTCL involving the blood and skin. Loss of CD26 appears to be characteristic of CTCL and has been suggested as a useful diagnostic marker. Chemokines and their receptors are involved in recruitment and homing of cancer cells to tissues of several tumors including non-Hodgkin's T-cell lymphomas. SS cells express CXCR4 and the skin generates its ligand, SDF-1, which may represent a target for the main destination of SS cells metastasizing to the skin. SDF-1 (CXCL12) is normally cleaved and inactivated by DPPIV mediated activity. An abnormal CD26-negative/dim T-cell population was found in a study of 66 of 69 samples from 28 SS/MF patients. These CD26negative/dim T-cells were CD26 negative in 23 patients and CD26-weakly positive in 5 patients. Sokolowska-Wojdylo and colleagues found that absence of CD26 on CLA (cutaneous lymphocyte-associated antigen)+ CD4+ T-cells was 100% sensitive for SS in 7 patients. Also, the number of CD26-negative T-cells correlated with treatments in 2 patients for over 1 year in a longitudinal study. SS patients have decreased plasma DPPIV activity. Soluble CD26 reduces the SDF-1 mediated SS cell migratory response. Inhibition of DPPIV activity in the CD26+ CTCL cell line Hut78 increases SDF-1-induced migration of SS cells. The SDF-1-CXCR4 interactions may mediate SS cell affinity for skin as a metastatic site via the regulatory activity of CD26.
T-large granular lymphocyte lymphoproliferative disorder Note CD26 expression is associated with a more aggressive clinical course in T-cell large granular lymphocyte leukemia (T-LGLL). T-LGLL patients with low expression of CD26 on T-LGLL cells had a more indolent course, while patients with high expression developed recurrent infections due to neutropenia. LGLL patients often have autoimmune diseases. CD26 expression on T-LGLL is associated with inhibition of myeloid progenitors, possibly explaining the neutropenia seen in these patients with higher levels of CD26 expression. CD26 on T-LGLL cells is unable to transmit antibody-mediated activation signals, unlike CD26 on normal T-cells, so CD26-related signaling may be aberrant in T-LGLL. In a recent report of a single institution long-term follow-up of 21 T-LGLL patients, 0 of 21 had CD26 expression.
Breast cancer Note Cheng et al. found that CD26 expressed on rat lung capillary endothelium mediated lung metastases of breast cancer cells by association with fibronectin. They studied the Fischer 344/CRJ rats, which have a CD26 Gly633Arg substitution, that leads to retention and degradation of the mutant protein in the endoplasmic reticulum, as a "protein knock-out" model
to characterize the previously established role of CD26 in metastasis. They found that lung metastases from the highly metastatic MTF7 rat breast cancer cell line were reduced by only 33% relative to normal Fischer 344 rats. Detailed immunohistochemical experiments revealed low levels of mutant enzymatically inactive CD26 on lung endothelial cells. When the mutant CD26 was purified, it had identical adhesion qualities for breast cancer cells as wild type DPPIV. The CD26/fibronectin-mediated adhesion and metastasis are effectively competed by soluble CD26, anti-CD26 mAb 6A3, and anti-fibronectin antiserum. Furthermore, peptides containing the fibronectin CD26-binding domain blocked the CD26-fibronectin interaction and significantly decreased pulmonary metastasis of breast cancer and melanoma cell lines. The utilization of fibronectin by cancer cells and fibronectin self-association in the blood suggests that CD26/fibronectin binding may be a mechanism for lung metastasis. CD26 is associated with increased topoisomerase IIa levels and tumor sensitivity to the topoisomerase II inhibitors, such as doxorubicin and etoposide. Recent studies suggest that topoisomerase IIα level is a prognostic factor in breast cancer that is independent of stage, Her-2/neu status, and histological grading. Furthermore, anthracycline treatment did not reverse the negative prognostic effect of topoisomerase IIα expression. Others have found, in retrospective studies that topoisomerase IIα overexpression confers a higher probability of response to doxorubicin. Topoisomerase IIα is currently being evaluated prospectively as a breast cancer predictive marker. The role of CD26 in breast cancer and the interaction of CD26 with topoisomerase IIα is an area for future research.
Colon cancer Note CD26 is found on the cell surface and its level correlates with disease status and tumor biology for certain cancers. In colorectal cancer, soluble CD26 (sCD26) in the sera was not related to colon cancer grade, stage, or location. The DPPIV inhibitor PT-100 (Val-boro-Pro) improved the activity of trastuzumab in human Her2+ colon cancer in xenograft models. However, the anti-cancer activity of PT-100 was not changed in CD26-/- mice, suggesting non-CD26 mediated activity. Cordero et al. found that the sCD26 concentration is diminished in serum of colorectal cancer patients compared to healthy donors, suggesting the potential utility of a sCD26 immunochemical detection test for early diagnosis. Pang et al. have identified a subpopulation of CD26+ cells uniformly present in both the primary and metastatic tumors in colorectal cancer patients with liver metastasis. Furthermore, in patients without distant metastasis at the time of presentation, the presence of CD26+ cells in their primary tumors predicted distant metastasis on follow-up.

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 308
Lung cancer Note CD26 is expressed in lung adenocarcinoma but not other subtypes of lung cancer. CD26 expression and DPPIV activity are present in normal bronchial and alveolar epithelium, but non-adenocarcinoma lung cancers lose CD26 expression. CD26 downregulation may contribute to the loss of growth control in non-small cell lung carcinoma (NSCLC) cells. NSCLC cells transfected with CD26 develop morphologic changes, altered contact inhibition, and reduced ability for anchorage-independent growth. An increased percentage of cells in G0-G1 was noted in CD26 expressing cells, indicating CD26 may promote cell cycle arrest. Amatya and colleagues assessed the diagnostic utility of caveolin-1 (Cav-1), a ligand for CD26, which is expressed in endothelial cells, alveolar type I pneumocytes and mesothelial cells, as a novel positive marker of mesothelioma. Immunohistochemical study of 80 cases of epithelioid mesothelioma and 80 cases of lung adenocarcinoma was performed for the analysis of the expression of Cav-1 and other markers. Cav-1 expression with a membranous and/or cytoplasmic pattern was found in all of the epithelioid mesothelioma. Of these, 42 cases (52,5%) showed Cav-1 expression in >50% of tumour cells, 34 cases (42,5%) in 6-50% of tumour cells, and four cases (5,0%) in <5% of tumour cells. In contrast, only six cases (7,5%) of lung adenocarcinoma showed focal Cav-1 expression in the cytoplasm of the tumour cells. They concluded that Cav-1 is a novel immunohistochemical marker for the differentiation of epithelioid mesothelioma from lung adenocarcinoma.
Hepatocellular carcinoma Note In normal liver as well as cirrhotic and steatotic liver, CD26 is expressed in the bile canalicular domains of hepatocellular membranes. In hepatocellular carcinoma (HCC), CD26/DPPIV activity was lost (2/25 cases) or had altered distribution (23/25 cases). Gaetaniello and colleagues found Tyr phosphorylation of several proteins after antibody binding to CD26 in HCC cell lines. This effect was inhibited by CD45 Tyr phosphatase. They found that a protein or proteins with kinase activity were associated with CD26. CD26 protects against apoptosis in Jurkat T-cells, while in the human hepatoma PLC/PRF/5 cells CD26 antibody binding is pro-apoptotic. CD26 expression is also pro-apoptotic in HepG2 cells.
Glioma Note Low CD26/DPPIV activity is found in poorly differentiated gliomas and high activity is found in differentiated gliomas. Differentiated gliomas have higher levels of membrane-associated isoforms of CD26/DPPIV. Sedo and colleagues studied "DPPIV activity and or structure homologs" (DASH) in 5
glioma cell lines of varying grade. They concluded that there was "no simple correlation with the degree of malignancy of the original donor tumor or morphologic phenotype...". They did note that changes in DASH composition as detected by non-denaturing polyacrylamide gel electrophoresis may reflect changes in substrate specificity and regulate changes in glioma activity.
Prostate cancer Note CD26/DPPIV biochemical activity was twice as high in prostate cancer compared to benign prostate hyperplasia (BPH) tissues. CD26/DPPIV activity was also increased in BPH adjacent to cancerous prostate tissue. DPPIV activity was present in epithelial but not stromal BPH and cancer tissues. This suggests that paracrine factors produced by prostate cancer cells may modulate the local microenvironment to increase cancer growth. Johnson et al. found that lung endothelial cells with metastatic prostate cancer cells were enriched for CD26 compared to non-metastatic prostate cancer cells. However, Wesley et al. suggested that CD26 inhibits the "malignant phenotype" of prostate cancer cells by inhibiting the FGF signaling pathway. Wilson et al. examined DPPIV activities in different prostatic tissue zones and in prostatic expressed secretions in relation to the presence of cancer. They found that expressed prostate secretions in patients with cancer were higher than in men without cancer. DPPIV activities in the transitional and especially the peripheral zone biopsies were higher in cancer patients. They concluded that secreted DPPIV originates in the transitional and peripheral zones. Measuring DPPIV levels in prostate secretion or in post-digital rectal prostate examination urine may be a useful for tumor marker for prostate cancer. Gonzalez-Gronow et al. found that in addition to its ability to inhibit tumor vascularization, angiostatin 2ε may also directly block prostate cancer metastasis by binding to CD26 on the surface of the 1-LN prostate cancer cell line. CD26/DPPIV association with plasminogen may lead to signal transduction that regulates expression of MMP-9 in prostate cancer cells. CD26 inhibitors may inhibit prostate cancer by blocking a CD26/DPPIV mediated signal transduction pathway that regulates MMP-9 expression by prostate cancer cells.
Renal cancer Note CD26 expression has previously been noted in renal cell carcinoma, with unclear significance. CD26 has a high level of surface expression on the renal cell carcinoma cell lines Caki-1, Caki-2, VRMRC-RCW, and ACHN. Inamoto and colleagues showed that anti-CD26 monoclonal antibody inhibition of the Caki-2 cell line was associated with G1/S cell cycle arrest, enhanced kip1 ID: 116> expression, down regulation of cyclin-dependent kinase 2 (CDK2) and

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 309
dephosphorylation of retinoblastoma substrate (Rb). They also found that anti-CD26 monoclonal antibody therapy attenuated Akt activity and internalized cell surface CD26 leading to decreased CD26 binding to collagen and fibronectin. More importantly, they showed that anti-CD26 monoclonal antibodies inhibited human renal cell carcinoma cell growth in a mouse xenograft model, with prolongation of survival. These results suggest that CD26 is a good target for renal cell carcinoma.
Thyroid cancer Note Benign thyroid tissue is usually negative for CD26 expression, but CD26 expression has been observed in thyroid cancer. This difference has been exploited as a diagnostic marker for the differential diagnosis of benign thyroid disease versus thyroid cancer. Kholová et al. suggest that CD26 positivity is limited to well-differentiated thyroid carcinomas including papillary carcinoma and is of limited value for diagnosing follicular and oncocytic thyroid malignancies.
Melanoma Note CD26 is highly expressed in normal melanocytes, but not in melanoma cells, suggesting CD26 expression is lost in malignant transformation. Loss of CD26 was also associated with development of specific chromosome abnormalities. When CD26/DPPIV is expressed in melanoma cells using a tetracycline-inducible expression system, melanoma growth was suppressed in the clones of cell line expressing higher levels of CD26. CD26 expression also decreased the melanoma growth in soft agar - indicating a CD26 association with anchorage-independent growth. Also, CD26 can induce MMP-9 expression in cancer cells, which may facilitate metastasis. Pethiyagoda et al. confirmed that CD26/DPPIV inhibits invasion of malignant melanoma cell lines by transfecting CD26 into melanoma cell lines. Invasion in Matrigel was decreased by 75%. This was also true for CD26 mutant transfectants that either lacked the extracellular protease activity (Ser630Ala) or the six amino acid cytoplasmic domain - demonstrating that neither DPPIV activity or the six amino acid C-terminal domain were necessary to inhibit invasiveness. Expression of either wild-type CD26 (DPPIV positive) or mutant CD26 (DPPIV negative) rescued expression of the cell surface Ser protease FAP-α. FAP-α can form a heterodimer with CD26 and may play a role in regulating melanocyte/melanoma growth. CD26 can inactivate circulating growth hormone-releasing factor (GHRF), so decreased CD26 may result in cancer growth by increased GHRF. A recent study found no effect of IFN-α on DPPIV activity in 18 patients with high-risk melanoma.
Ovarian cancer Note Expression of CD26 varies in ovarian cancer cell lines. CD26 is negatively correlated with ovarian cancer invasive potential. Specifically, overexpression of CD26 in ovarian cancer leads to increased E-cadherin and tissue inhibitors of MMPs, resulting in decreased invasive potential. CD26 transfection in ovarian cancer cell lines decreased intraperitoneal dissemination and prolonged survival in vivo in mice.
Malignant mesothelioma Note Malignant pleural mesothelioma (MPM) is an aggressive cancer arising from the mesothelial cells lining the pleura. Morimoto et al. showed that CD26 is preferentially expressed on malignant mesothelioma cells but not on normal mesothelial cells, and suggested that membranous expression of CD26 indicates an importance in treatment of patients with MPM. More importantly, humanized anti-CD26 antibody inhibited growth of malignant mesothelioma cells and induced long term survival of tumor-transplanted SCID mice. In addtion, it has been shown that cells from certain CD26-positive mesothelioma cell lines appeared to include the cancer stem cell characteristics for malignant mesothelioma in addition to CD24 and CD9-positive cells. Furthermore, Morimoto et al. showed that the CD26 molecule is expressed on the cell membrane of the epithelial and biphasic, but not the sarcomatoid, type of mesothelioma. Importantly, treatment outcome prediction study showed that CD26 membrane expression on MPM was closely correlated with disease responsiveness to chemotherapy. Meanwhile, in vitro studies showed that mesothelioma cells expressing high level of CD26 displayed high proliferative activity, and microarray analysis of CD26 knockdown and CD26-transfected mesothelioma cells showed that CD26 expression was closely linked to expression of genes contributing to cell proliferation, cell cycle regulation, drug-induced apoptotic action, and chemotherapy resistance. These data therefore strongly suggest that the CD26 molecule is a good therapeutic target for MPM and a clinically significant biomarker for the prediction of response to chemotherapy for MPM.
Gastric gastrointestinal stromal tumors Note In an immunohistochemical analysis of 152 patients with gastric gastrointestinal stromal tumors (GIST), CD26 expression was found to be associated with a poorer overall survival.
Rheumatoid arthritis Note Rheumatoid arthritis (RA) is a chronic, inflammatory autoimmune disease and is characterized by

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 310
progressive invasion of synovial fibroblasts into the articular cartilage and erosion of the undelying bone, followed by joint destruction. In antigen-induced arthritis mouse model, DPPIV-/- mice showed more severe arthritis, and enzymatic activity levels of DPPIV in the plasma were significantly decreased in RA patients. Morever, other investigators reported that inhibition of DPPIV and FAP increases cartilage invasion by RA synovial fibroblasts. However, CD26/DPPIV regulates biologic processes that are unrelated to its peptidase activity, e.g., cellular adhesion, cell differentiation, and activation via downstream signaling cascade. CD26+ T cells induce the inflammation and tissue destruction characteristic of RA by migrating to and being active in the rheumatoid synovium. Cordero et al. studied IL-12, IL-15, soluble CD26, and ADA serum levels from 35 patients with active and inactive RA as well as those of controls. Patients' sera had higher IL-12 and IL-15 levels, and the level of soluble CD26 was inversely correlated with the number of swollen joints. These findings suggest that these cytokines and CD26 are associated with the inflammation and immune activity in RA. Mavropoulos et al. found that anti-TNF-α therapy increases DPPIV activity and decreases autoantibodies to the chaperone protein Bip (GRP78) and phosphoglucose isomerase in 15 patients with RA. DPPIV inhibitors inhibit a rat model of rheumatoid arthritis in a dose-dependent manner. Ohnuma et al. described CD26+ T cells infiltrating the rheumatoid synovium using immunohistochemical studies. They found high expression of caveolin-1 in the rheumatoid synovium vasculature and synoviocytes. These data suggest that the CD26-caveolin-1 upregulation of CD86 on activated monocytes leads to antigen-specific T-cell activation in rheumatoid arthritis. DPPIV inhibitors may be useful for suppressing the immune system in rheumatoid arthritis and other autoimmune diseases.
Inflammatory bowel diseases Note Crohn's disease and ulcerative colitis are categorized as inflammatory bowel disease (IBD), being characterized by chronic remittent or progressive inflammatory conditions that may affect the entire gastrointestinal tract and the colonic mucosa, respectively, and are associated with an increased risk for colon cancer. Sera from IBD patients contain lower levels of circulating DPPIV activity, while membrane expression of CD26/DPPIV on T cells isolated from IBD patients is higher than healthy controls. These clinical observations indicate that CD26/DPPIV might play a significant role in perpetuating the inflammatory response associated with IBD.
Systemic lupus erythematosus Note Serum levels of soluble CD26 and its specific DPPIV
activity were significantly decreased in patients with systemic lupus erythematosus (SLE), and were inversely correlated with SLE disease activity index score, but not with clinical variables or clinical subsets of SLE. More recently, Lam et al. reported that CD26 expression on invariant natural killer cells of SLE patients is decreased significantly than that of healthy controls.
References Houghton AN, Albino AP, Cordon-Cardo C, Davis LJ, Eisinger M. Cell surface antigens of human melanocytes and melanoma. Expression of adenosine deaminase binding protein is extinguished with melanocyte transformation. J Exp Med. 1988 Jan 1;167(1):197-212
Aratake Y, Kotani T, Tamura K, Araki Y, Kuribayashi T, Konoe K, Ohtaki S. Dipeptidyl aminopeptidase IV staining of cytologic preparations to distinguish benign from malignant thyroid diseases. Am J Clin Pathol. 1991 Sep;96(3):306-10
Kotani T, Aratake Y, Ogata Y, Umeki K, Araki Y, Hirai K, Kuma K, Ohtaki S. Expression of dipeptidyl aminopeptidase IV activity in thyroid carcinoma. Cancer Lett. 1991 May 24;57(3):203-8
Kotani T, Asada Y, Aratake Y, Umeki K et al.. Diagnostic usefulness of dipeptidyl aminopeptidase IV monoclonal antibody in paraffin-embedded thyroid follicular tumours. J Pathol. 1992 Sep;168(1):41-5
Asada Y, Aratake Y, Kotani T, Marutsuka K, Araki Y, Ohtaki S, Sumiyoshi A. Expression of dipeptidyl aminopeptidase IV activity in human lung carcinoma. Histopathology. 1993 Sep;23(3):265-70
Johnson RC, Zhu D, Augustin-Voss HG, Pauli BU. Lung endothelial dipeptidyl peptidase IV is an adhesion molecule for lung-metastatic rat breast and prostate carcinoma cells. J Cell Biol. 1993 Jun;121(6):1423-32
Carbone A, Cozzi M, Gloghini A, Pinto A. CD26/dipeptidyl peptidase IV expression in human lymphomas is restricted to CD30-positive anaplastic large cell and a subset of T-cell non-Hodgkin's lymphomas. Hum Pathol. 1994 Dec;25(12):1360-5
Carbone A, Gloghini A, Zagonel V, Aldinucci D, Gattei V, Degan M, Improta S, Sorio R, Monfardini S, Pinto A. The expression of CD26 and CD40 ligand is mutually exclusive in human T-cell non-Hodgkin's lymphomas/leukemias. Blood. 1995 Dec 15;86(12):4617-26
Stecca BA, Nardo B, Chieco P, Mazziotti A, Bolondi L, Cavallari A. Aberrant dipeptidyl peptidase IV (DPP IV/CD26) expression in human hepatocellular carcinoma. J Hepatol. 1997 Aug;27(2):337-45
Cheng HC, Abdel-Ghany M, Elble RC, Pauli BU. Lung endothelial dipeptidyl peptidase IV promotes adhesion and metastasis of rat breast cancer cells via tumor cell surface-associated fibronectin. J Biol Chem. 1998 Sep 11;273(37):24207-15
Gaetaniello L, Fiore M, de Filippo S, Pozzi N, Tamasi S, Pignata C. Occupancy of dipeptidyl peptidase IV activates an associated tyrosine kinase and triggers an apoptotic signal in human hepatocarcinoma cells. Hepatology. 1998 Apr;27(4):934-42
Sedo A, Malík R, Krepela E. Dipeptidyl peptidase IV in C6 rat glioma cell line differentiation. Biol Chem. 1998 Jan;379(1):39-44

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 311
Wesley UV, Albino AP, Tiwari S, Houghton AN. A role for dipeptidyl peptidase IV in suppressing the malignant phenotype of melanocytic cells. J Exp Med. 1999 Aug 2;190(3):311-22
Cordero OJ, Ayude D, Nogueira M, Rodriguez-Berrocal FJ, de la Cadena MP. Preoperative serum CD26 levels: diagnostic efficiency and predictive value for colorectal cancer. Br J Cancer. 2000 Nov;83(9):1139-46
Pethiyagoda CL, Welch DR, Fleming TP. Dipeptidyl peptidase IV (DPPIV) inhibits cellular invasion of melanoma cells. Clin Exp Metastasis. 2000;18(5):391-400
Wilson MJ, Ruhland AR, Quast BJ, Reddy PK, Ewing SL, Sinha AA. Dipeptidylpeptidase IV activities are elevated in prostate cancers and adjacent benign hyperplastic glands. J Androl. 2000 Mar-Apr;21(2):220-6
Aytac U, Claret FX, Ho L, Sato K, Ohnuma K, Mills GB, Cabanillas F, Morimoto C, Dang NH. Expression of CD26 and its associated dipeptidyl peptidase IV enzyme activity enhances sensitivity to doxorubicin-induced cell cycle arrest at the G(2)/M checkpoint. Cancer Res. 2001 Oct 1;61(19):7204-10
Bernengo MG, Novelli M, Quaglino P, Lisa F, De Matteis A, Savoia P, Cappello N, Fierro MT. The relevance of the CD4+ CD26- subset in the identification of circulating Sézary cells. Br J Dermatol. 2001 Jan;144(1):125-35
Cordero OJ, Salgado FJ, Mera-Varela A, Nogueira M. Serum interleukin-12, interleukin-15, soluble CD26, and adenosine deaminase in patients with rheumatoid arthritis. Rheumatol Int. 2001 Oct;21(2):69-74
Hildebrandt M, Rose M, Rüter J, Salama A, Mönnikes H, Klapp BF. Dipeptidyl peptidase IV (DP IV, CD26) in patients with inflammatory bowel disease. Scand J Gastroenterol. 2001 Oct;36(10):1067-72
Ho L, Aytac U, Stephens LC, Ohnuma K et al.. In vitro and in vivo antitumor effect of the anti-CD26 monoclonal antibody 1F7 on human CD30+ anaplastic large cell T-cell lymphoma Karpas 299. Clin Cancer Res. 2001 Jul;7(7):2031-40
Ishii T, Ohnuma K, Murakami A, Takasawa N, Kobayashi S, Dang NH, Schlossman SF, Morimoto C. CD26-mediated signaling for T cell activation occurs in lipid rafts through its association with CD45RO. Proc Natl Acad Sci U S A. 2001 Oct 9;98(21):12138-43
Jones D, Dang NH, Duvic M, Washington LT, Huh YO. Absence of CD26 expression is a useful marker for diagnosis of T-cell lymphoma in peripheral blood. Am J Clin Pathol. 2001 Jun;115(6):885-92
Ohnuma K, Munakata Y, Ishii T, Iwata S, Kobayashi S, Hosono O, Kawasaki H, Dang NH, Morimoto C. Soluble CD26/dipeptidyl peptidase IV induces T cell proliferation through CD86 up-regulation on APCs. J Immunol. 2001 Dec 15;167(12):6745-55
Kajiyama H, Kikkawa F, Suzuki T, Shibata K, Ino K, Mizutani S. Prolonged survival and decreased invasive activity attributable to dipeptidyl peptidase IV overexpression in ovarian carcinoma. Cancer Res. 2002 May 15;62(10):2753-7
Kobayashi H, Hosono O, Mimori T, Kawasaki H, Dang NH, Tanaka H, Morimoto C. Reduction of serum soluble CD26/dipeptidyl peptidase IV enzyme activity and its correlation with disease activity in systemic lupus erythematosus. J Rheumatol. 2002 Sep;29(9):1858-66
Ohnuma K, Ishii T, Iwata S, Hosono O, Kawasaki H, Uchiyama M, Tanaka H, Yamochi T, Dang NH, Morimoto C. G1/S cell cycle arrest provoked in human T cells by antibody to CD26. Immunology. 2002 Nov;107(3):325-33
Aytac U, Sato K, Yamochi T, Yamochi T, Ohnuma K, Mills GB, Morimoto C, Dang NH. Effect of CD26/dipeptidyl peptidase IV on Jurkat sensitivity to G2/M arrest induced by topoisomerase II inhibitors. Br J Cancer. 2003 Feb 10;88(3):455-62
Cheng HC, Abdel-Ghany M, Pauli BU. A novel consensus motif in fibronectin mediates dipeptidyl peptidase IV adhesion and metastasis. J Biol Chem. 2003 Jul 4;278(27):24600-7
Dang NH, Aytac U, Sato K, O'Brien S, Melenhorst J, Morimoto C, Barrett AJ, Molldrem JJ. T-large granular lymphocyte lymphoproliferative disorder: expression of CD26 as a marker of clinically aggressive disease and characterization of marrow inhibition. Br J Haematol. 2003 Jun;121(6):857-65
Kajiyama H, Kikkawa F, Khin E, Shibata K, Ino K, Mizutani S. Dipeptidyl peptidase IV overexpression induces up-regulation of E-cadherin and tissue inhibitors of matrix metalloproteinases, resulting in decreased invasive potential in ovarian carcinoma cells. Cancer Res. 2003 May 1;63(9):2278-83
Kholová I, Ludvíková M, Ryska A, Hanzelková Z, Cap J, Pecen L, Topolcan O. Immunohistochemical detection of dipeptidyl peptidase IV (CD 26) in thyroid neoplasia using biotinylated tyramine amplification. Neoplasma. 2003;50(3):159-64
Sato K, Aytac U, Yamochi T, Yamochi T et al.. CD26/dipeptidyl peptidase IV enhances expression of topoisomerase II alpha and sensitivity to apoptosis induced by topoisomerase II inhibitors. Br J Cancer. 2003 Oct 6;89(7):1366-74
Thoma R, Löffler B, Stihle M, Huber W, Ruf A, Hennig M. Structural basis of proline-specific exopeptidase activity as observed in human dipeptidyl peptidase-IV. Structure. 2003 Aug;11(8):947-59
Aldinucci D, Poletto D, Lorenzon D, Nanni P, Degan M, Olivo K, Rapanà B, Pinto A, Gattei V. CD26 expression correlates with a reduced sensitivity to 2'-deoxycoformycin-induced growth inhibition and apoptosis in T-cell leukemia/lymphomas. Clin Cancer Res. 2004 Jan 15;10(2):508-20
Kobayashi S, Ohnuma K, Uchiyama M, Iino K, Iwata S, Dang NH, Morimoto C. Association of CD26 with CD45RA outside lipid rafts attenuates cord blood T-cell activation. Blood. 2004 Feb 1;103(3):1002-10
Ohnuma K, Yamochi T, Uchiyama M et al.. CD26 up-regulates expression of CD86 on antigen-presenting cells by means of caveolin-1. Proc Natl Acad Sci U S A. 2004 Sep 28;101(39):14186-91
Tsuji T, Sugahara K, Tsuruda K, Uemura A et al.. Clinical and oncologic implications in epigenetic down-regulation of CD26/dipeptidyl peptidase IV in adult T-cell leukemia cells. Int J Hematol. 2004 Oct;80(3):254-60
Gonzalez-Gronow M, Grenett HE, Gawdi G, Pizzo SV. Angiostatin directly inhibits human prostate tumor cell invasion by blocking plasminogen binding to its cellular receptor, CD26. Exp Cell Res. 2005 Feb 1;303(1):22-31
Mavropoulos JC, Cuchacovich M, Llanos C et al.. Anti-tumor necrosis factor-alpha therapy augments dipeptidyl peptidase IV activity and decreases autoantibodies to GRP78/BIP and phosphoglucose isomerase in patients with rheumatoid arthritis. J Rheumatol. 2005 Nov;32(11):2116-24
Ohnuma K, Yamochi T, Uchiyama M et al.. CD26 mediates dissociation of Tollip and IRAK-1 from caveolin-1 and induces upregulation of CD86 on antigen-presenting cells. Mol Cell Biol. 2005 Sep;25(17):7743-57
Sato T, Yamochi T, Yamochi T, Aytac U, Ohnuma K, McKee KS, Morimoto C, Dang NH. CD26 regulates p38 mitogen-activated protein kinase-dependent phosphorylation of integrin beta1, adhesion to extracellular matrix, and tumorigenicity of T-

DPP4 (dipeptidyl-peptidase 4) Ohnuma K, Morimoto C
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 312
anaplastic large cell lymphoma Karpas 299. Cancer Res. 2005 Aug 1;65(15):6950-6
Sokolowska-Wojdylo M, Wenzel J, Gaffal E et al.. Absence of CD26 expression on skin-homing CLA+ CD4+ T lymphocytes in peripheral blood is a highly sensitive marker for early diagnosis and therapeutic monitoring of patients with Sézary syndrome. Clin Exp Dermatol. 2005 Nov;30(6):702-6
Yamochi T, Yamochi T, Aytac U, Sato T, Sato K, Ohnuma K, McKee KS, Morimoto C, Dang NH. Regulation of p38 phosphorylation and topoisomerase IIalpha expression in the B-cell lymphoma line Jiyoye by CD26/dipeptidyl peptidase IV is associated with enhanced in vitro and in vivo sensitivity to doxorubicin. Cancer Res. 2005 Mar 1;65(5):1973-83
Wilson MJ, Haller R, Li SY, Slaton JW, Sinha AA, Wasserman NF. Elevation of dipeptidylpeptidase iv activities in the prostate peripheral zone and prostatic secretions of men with prostate cancer: possible prostate cancer disease marker. J Urol. 2005 Sep;174(3):1124-8
Inamoto T, Yamochi T, Ohnuma K, Iwata S, Kina S, Inamoto S, Tachibana M, Katsuoka Y, Dang NH, Morimoto C. Anti-CD26 monoclonal antibody-mediated G1-S arrest of human renal clear cell carcinoma Caki-2 is associated with retinoblastoma substrate dephosphorylation, cyclin-dependent kinase 2 reduction, p27(kip1) enhancement, and disruption of binding to the extracellular matrix. Clin Cancer Res. 2006 Jun 1;12(11 Pt 1):3470-7
Ohnuma K, Inoue H, Uchiyama M, Yamochi T, Hosono O, Dang NH, Morimoto C. T-cell activation via CD26 and caveolin-1 in rheumatoid synovium. Mod Rheumatol. 2006;16(1):3-13
Inamoto T, Yamada T, Ohnuma K, Kina S et al.. Humanized anti-CD26 monoclonal antibody as a treatment for malignant mesothelioma tumors. Clin Cancer Res. 2007 Jul 15;13(14):4191-200
Ohnuma K, Uchiyama M, Yamochi T, Nishibashi K, Hosono O, Takahashi N, Kina S, Tanaka H, Lin X, Dang NH, Morimoto C. Caveolin-1 triggers T-cell activation via CD26 in association with CARMA1. J Biol Chem. 2007 Mar 30;282(13):10117-31
Thompson MA, Ohnuma K, Abe M, Morimoto C, Dang NH. CD26/dipeptidyl peptidase IV as a novel therapeutic target for cancer and immune disorders. Mini Rev Med Chem. 2007 Mar;7(3):253-73
Havre PA, Abe M, Urasaki Y, Ohnuma K, Morimoto C, Dang NH. The role of CD26/dipeptidyl peptidase IV in cancer. Front Biosci. 2008 Jan 1;13:1634-45
Ohnuma K, Dang NH, Morimoto C. Revisiting an old acquaintance: CD26 and its molecular mechanisms in T cell function. Trends Immunol. 2008 Jun;29(6):295-301
Ohnuma K, Takahashi N, Yamochi T, Hosono O, Dang NH, Morimoto C. Role of CD26/dipeptidyl peptidase IV in human T cell activation and function. Front Biosci. 2008 Jan 1;13:2299-310
Amatya VJ, Takeshima Y, Kohno H, Kushitani K, Yamada T, Morimoto C, Inai K. Caveolin-1 is a novel immunohistochemical marker to differentiate epithelioid mesothelioma from lung adenocarcinoma. Histopathology. 2009 Jul;55(1):10-9
Havre PA, Abe M, Urasaki Y, Ohnuma K, Morimoto C, Dang NH. CD26 expression on T cell lines increases SDF-1-alpha-mediated invasion. Br J Cancer. 2009 Sep 15;101(6):983-91
Ohnuma K, Uchiyama M, Hatano R, Takasawa W, Endo Y, Dang NH, Morimoto C. Blockade of CD26-mediated T cell costimulation with soluble caveolin-1-Ig fusion protein induces anergy in CD4+T cells. Biochem Biophys Res Commun. 2009 Aug 21;386(2):327-32
Wong PT, Wong CK, Tam LS, Li EK, Chen DP, Lam CW. Decreased expression of T lymphocyte co-stimulatory molecule CD26 on invariant natural killer T cells in systemic lupus erythematosus. Immunol Invest. 2009;38(5):350-64
Yamada K, Hayashi M, Du W, Ohnuma K, Sakamoto M, Morimoto C, Yamada T. Localization of CD26/DPPIV in nucleus and its nuclear translocation enhanced by anti-CD26 monoclonal antibody with anti-tumor effect. Cancer Cell Int. 2009 Jun 26;9:17
Pang R, Law WL, Chu AC, Poon JT, Lam CS et al.. A subpopulation of CD26+ cancer stem cells with metastatic capacity in human colorectal cancer. Cell Stem Cell. 2010 Jun 4;6(6):603-15
Takasawa W, Ohnuma K, Hatano R, Endo Y, Dang NH, Morimoto C. Inhibition of dipeptidyl peptidase 4 regulates microvascular endothelial growth induced by inflammatory cytokines. Biochem Biophys Res Commun. 2010 Oct 8;401(1):7-12
Abe M, Havre PA, Urasaki Y, Ohnuma K, Morimoto C, Dang LH, Dang NH. Mechanisms of confluence-dependent expression of CD26 in colon cancer cell lines. BMC Cancer. 2011 Feb 1;11:51
Ohnuma K, Hosono O, Dang NH, Morimoto C. Dipeptidyl peptidase in autoimmune pathophysiology. Adv Clin Chem. 2011;53:51-84
Aoe K, Amatya VJ, Fujimoto N, Ohnuma K et al.. CD26 overexpression is associated with prolonged survival and enhanced chemosensitivity in malignant pleural mesothelioma. Clin Cancer Res. 2012 Mar 1;18(5):1447-56
Hatano R, Ohnuma K, Yamamoto J, Dang NH, Morimoto C. CD26-mediated co-stimulation in human CD8(+) T cells provokes effector function via pro-inflammatory cytokine production. Immunology. 2013 Feb;138(2):165-72
This article should be referenced as such:
Ohnuma K, Morimoto C. DPP4 (dipeptidyl-peptidase 4). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):301-312.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 313
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
FOSL1 (FOS-like antigen 1) Senthilkumar B Rajamohan, Sekhar P Reddy
Department of Medicine, Institute for Integrative Physiology, University of Chicago, Chicago, Illinois, USA (SBR), Department of Pediatrics, University of Illinois, Chicago, Illinois, USA (SPR)
Published in Atlas Database: November 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/FOSL1ID40622ch11q13.html DOI: 10.4267/2042/49698
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: FRA, FRA1, fra-1
HGNC (Hugo): FOSL1
Location: 11q13.1
DNA/RNA Description Fra-1 (Fosl-1) is a basic leucine zipper (bZIP) transcription factor and a member of Fos family of proteins (Cohen and Curran, 1988). The Fra-1 gene spans about 8.31 kb including four exons and is located on chromosome 11q13. It contains two regulatory elements, an upstream 5'-flanking region and an intragenic sequence, that are known to regulate its transcriptional induction (Verde et al., 2007). Two critical elements of the promoter, the upstream TPA response element (TRE) and the serum response element (SRE), are required for Fra-1 transcriptional induction in response to external stimuli, such as mitogens and cytokines (Adiseshaiah et al., 2003; Adiseshaiah et al., 2005). The intragenic regulatory element containing the TRE/TRE-like elements also contribute to Fra-1 induction (Bergers et al., 2005).
Transcription Fra-1 transcription is strongly inducible by mitogens and inflammatory cytokines as well by a wide variety of environmental toxicants,
carcinogens, and pathogens. In contrast to the early activation of c-Jun and c-Fos (which peaks at 15-30 min), the induction of Fra-1 by various mitogenic and stressful stimuli peaks at 90-180 min, and this delayed induction is postulated to play important role in modulating the transcriptional response initiated by the AP-1 complex composed of Jun/c-Fos dimers. The Fra-1 promoter region contains a c-Fos-like serum response element (SRE), which is constitutively occupied by the serum response factor (SRF) and the ternary complex factor, Elk1. Recruitment of c-Jun to the upstream TRE and the presence of downstream SRE as well as the activating transcription factor (ATF) site are essential for Fra-1 induction by mitogenic and cytokine stimuli (Adiseshaiah et al., 2007). Sp1 family members also regulate Fra-1 transcription (Adiseshaiah et al., 2005). Other studies have shown that cis-elements, such as TRE and E boxes, located in the intragenic region also contribute to Fra-1 transcription (Bergers et al., 1995, Casalino et al., 2003,). Histone modifications, such as the phosphorylation of Histone 3 by PIM1 on the nucleasome at the MYC binding sites, regulate the transcriptional activation of Fra-1 (Zippo et al., 2007). In addition to transcriptional induction, ERK- dependent phosphorylation has been shown to play a key role in the protein stability and DNA binding activity of Fra-1 (Basbous et al., 2007, Young et al., 2002).

FOSL1 (FOS-like antigen 1) Rajamohan SB, Reddy SP
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 314
Transcriptional regulation of Fra-1 (Fosl-1): MAPK signaling activates transcriptional factors binding at the human Fra-1 promoter. Binding of Fra-1 and c-Jun to TRE sites of first intron regulates Fra-1 transcription. TRE - TPA response element, SRE - Serum response element, SRF - serum response factor, ATF - activating transcription factor binding site.
A schematic diagram showing the modular structure of Fra-1 (1-271 AA). DBD -DNA binding domain, LZD - leucine-zipper domain, N - amino terminus, C - carboxyl terminus. P1 - Thr 231, P2 - Ser252, P3 - Ser265. In this, ERK mediated phosphorylation of serine residues 252 and 265 requires for the stabilization of Fra-1 in certain tumor cell lines (Basbous et al., 2007). Pseudogene One pseudo gene is identified, the FOS-like antigen pseudogene, FOSL1P1 (NCBI, HGNC ID: 44055).
Protein Description Fra-1 (Fosl-1) protein encodes for 271 amino acids with an expected molecular weight of 29.4 kDa. However, in immunoblot analysis of cellular extracts isolated from cells stimulated with growth factors or from cancer cells, Fra-1 exhibits multiple forms ranging from 30-40 kDa. The appearance of these multiple forms is mainly attributed to post-translational modification (e.g., phosphorylation) of this protein. Human and mouse Fra-1 exhibits 6 and 1 splice variants, respectively, and both exhibit one unspliced form. These different transcripts encode proteins with different functional domains. The functional significance of these alternatively spliced variants of Fra-1 for both in physiology and pathological processes remains unclear.
Expression The expression of Fra-1 is high in smooth muscle cells, bronchial epithelial cells (trachea), and the pancreas, but its expression is low in other tissues, such as the brain and prostate.
Localisation Fra-1 (Fosl-1) contains a nuclear localization signal and is predominantly found in the nucleus. However, Fra-1 antigen is observed in the cytoplasm under certain conditions, such as elevated levels of oxidative stress (Burch et al., 2004) and in cancerous tissues (Song et al., 2006). Furthermore, a distinct cytoplasmic location of Fra-1 has been noted in non-small-cell lung cancer (Ma et al., 2009). Nuclear and cytoplasmic expression of Fra-1 is markedly elevated in human adenomas, adenocarcinomas and neuroendocrine carcinomas (Zhang et al., 2005).
Function After dimerization, mainly with the Jun or ATF family of proteins, Fra-1 binds to the TPA response element (TRE, or AP-1 site) and regulates gene expression in a context-dependent manner (Cohen et al., 1989). Fra-1 plays important roles in various biological processes, including inflammation, transformation, proliferation, and metastasis. Increased expression levels of Fra-1 is detectable in breast, lung, brain, colon and prostate cancers and its knockdown affects cancer cell progression (see below).
Homology The Fra-1 gene is conserved in chimpanzee, dog, cow, mouse, rat, and Zebra fish.
FOSL1 (FOS-like antigen 1) Rajamohan SB, Reddy SP
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 315
Mutations Note No genetic mutations leading to activation or inactivation of this transcription factor in human disease development and in malignancies have been yet documented. Recently, the presence of SNPs was demonstrated in human Fra-1 (FOSL-1) gene, and these SNPs were shown to be associated with a decreased rate of lung function (Sandford et al., 2012).
Implicated in Thyroid cancer Note Analysis of samples from thyroid cancer patients has shown an increase in Fra-1 protein expression in thyroid nodules (Chiappetta et al., 2000). Induction of Fra-1 expression has also been observed in human thyroid cancer cell lines (Battista et al., 1998). Inhibition of Fra-1 prevents the retrovirally induced neoplastic transformation of rat thyroid cells (Vallone et al., 1997). In thyroid cancer cells, Fra-1 binds to the cyclin A promoter and regulates its expression during cell-cycle progression (Casalino et al., 2007).
Non-small-cell lung cancer (NSCLC) Note Expression of AP-1 family proteins, and particularly Fra-1 has been detected in NSCLC cell lines (Risse-Hackl et al., 1998). Decreased levels of Fra-1 protein expression have been noted in the tumor tissue of non small cell lung cancer patients (Ma et al., 2009), and these decreased levels have been positively correlated with progression of tumor stage and worsening prognosis. Ectopic expression of Fra-1 in lung adenocarcinoma cells induces cancer. Interestingly, it has been reported that a DNA vaccine specific to Fra-1 prevents pulmonary cancer metastasis in syngeneic mice (Luo et al., 2005).
Breast cancer Note Increased expression of Fra-1 was observed in human breast cancer cells (Philips et al., 1998). Several studies have shown its involvement in cancer cell proliferation, motility and invasiveness (Bamberger et al., 1999; Belguise et al., 2005; Logullo et al., 2011). An increase in nuclear or cytoplasmic localization of Fra-1 has been considered as a marker of progression of breast cancer (Song et al., 2006, Chiappetta et al., 2007). Knockdown of Fra-1 in tumor associated macrophages with small interfering RNA has been found to significantly suppress the invasion, angiogenesis and metastasis of breast cancer tumor cells (Luo et al., 2010). Likewise, knockdown of Fra-1 in estrogen- resistant MCF-7 cells significantly affected their growth and enhanced their susceptibility to cell death in response to estrogen treatment (Pennanen et al., 2011). An increased
accumulation of Fra-1 protein in estrogen-negative breast cancer cells is mediated through PKCθ pathway (Belguise et al., 2012). A mouse Fra-1 targeted DNA vaccine has been found to be effective in protection against breast cancer in mice (Luo et al., 2003). Low level of miRNA-34 has been correlated with an elevated level of Fra-1 expression in breast cancer tissues and cell lines, but ectopic miRNA-34 expression causes a down-regulation of Fra-1 levels and inhibits breast cancer cell progression (Yang et al., 2012). In a different study, Fra-1 overexpression was shown to increase the chemosensitive of breast cancer stem cells, suggesting Fra-1 can be considered as a prognostic responsive marker in breast cancer therapy (Lu et al., 2012).
Bladder cancer Note An increased level of Fra-1 expression is found in bladder tumor and cancer cell lines. Fra-1, via the transcriptional induction of the receptor tyrosine kinase AXL, promotes bladder cancer cell motility (Sayan et al., 2012).
Colon cancer Note Fra-1 and its dimeric partner, c-Jun, are up-regulated in human colorectal tumors (Zhang et al., 2005; Wang et al., 2002). In colon carcinoma cells, the basal induction and stabilization of Fra-1 has been shown to be regulated by ERK activity, and knockdown of Fra-1 suppresses colon cancer cell polarization and progression (Vial and Marshall, 2003). A potential role for Fra-1 in the regulation of vimentin during Ha-RAS-induced epithelial-to- mesenchymal transition and migration has been documented (Andreolas et al., 2008). By upregulating miR-34a, p53 indirectly down regulates Fra-1 mRNA and protein expression in colon cancer cells and inhibits cell migration and invasion (Wu et al., 2012).
Prostate cancer Note Akt signaling contributes to Fra-1 induction in the prostate cancer cells, mainly at the transcription level (Tiwari et al., 2003). An abnormal activation of Fra-1 has been linked to elevated expression levels of IL-6, which promote prostate cancer cell progression and resistance to chemotherapeutic agents (Zerbini et al., 2003).
Esophageal squamous cell carcinoma (ESCC) Note Immunoreactive analysis of two different ESCC cell lines (HKESC-1 and HKESC-2) derived from ESCC patients has demonstrated Fra-1 expression in these cell line (Hu et al., 2001). An elevated level of Fra-1 expression is associated with poor prognosis of ESCC.

FOSL1 (FOS-like antigen 1) Rajamohan SB, Reddy SP
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 316
Furthermore, Fra-1 knockdown in ESCC cell lines decreases tumor cell progression and invasion (Usui et al., 2012).
Nasopharyngeal carcinoma (NPC) Note Expression profiling of nasopharyngeal carcinoma and normal cells has revealed elevated expression levels of Fra-1 in NPC cancer cells (Fung et al., 2000). Fra-1 has been shown to play an important role in controlling latent membrane protein 2A (LMP2A)-induced NPC epithelial cell motility and invasiveness (Lan et al., 2012). Either inhibition of Fra-1 induction or suppression of ERK1 and ERK2 activation will block the LMP2A-induced MMP-9 expression required for cancer cell progression.
Glioma Note Ectopic Fra-1 expression in malignant glioma cells leads to phenotypic changes associated with invasiveness and tumorigenicity (Debinski and Gibo, 2005). In contrast, knock down of Fra-1 in high-grade glioma (HGG) cells alters the morphology, reduces both anchorage-independence and tumorigenic potential (Debinski and Gibo, 2011). In rat C6 glioma cells, Fra-1 overexpression suppresses their proliferation rate and tumorogenic potential and promotes cellular apoptosis (Shirsat and Shaikh, 2003).
Head and neck squamous cell carcinoma (HNSCC) Note Analysis of the tumor samples from patients with head and neck squamous cell carcinomas (HNSCC) has shown an increase in Fra-1 mRNA expression when compared to matched adjacent mucosa samples. Furthermore, tumor tissue staining for Fra-1 in tumor tissues is intensely more reactive immunoreactive than that of adjacent normal tissue (Mangone et al., 2005).
Fibrosis Note Fra-1 transgenic mice have been shown to be prone to developing biliary hepatic fibrosis, and Fra-1 has been associated with ductular proliferation and infiltration of inflammatory cells (Kireva et al., 2011). On the other hand, it negatively regulates pulmonary fibrosis (Rajasekaran et al., 2012). Genetic disruption of Fra-1 causes increased levels of inflammation, collagen accumulation, and profibrotic and fibrotic gene expression following bleomycin treatment when compared to wild-type Fra-1.
Osteopetrosis Note Genetic disruption of Fos leads to osteopetrosis in mice (Matsuo et al., 2000). However, over expression of Fra-1 rescues this phenotype in c-Fos mutant mice. Rankl,
an osteoclast differentiation factor, has been reported to induce Fra-1 expression in a c-Fos-dependent manner, suggesting the involvement of c-Fos-RANKL-Fra-1 signaling in osteoclast differentiation. It has also been reported that overexpression of Fra-1 in mice increases bone mass up to 5-fold compared to wild-type mice (Roschger et al., 2004).
Acute lung injury and Sepsis Note Increased expression of Fra-1 has been reported in lung epithelial cell of acute respiratory syndrome patients (Fudala et al., 2011). Mice lacking Fra-1 show decreased levels of acute lung injury and inflammation as well as increased survival following endotoxin (LPS) treatment when compared to their wild-type counterparts (Vaz et al., 2012); this improvement was associated with diminished and increased levels of NF-kB and c-Jun/AP-1 binding, respectively. In agreement with this result, mice overexpressing Fra-1 were shown in another study to have enhanced susceptibility to endotoxin-induced death (Takada et al., 2011).
References Cohen DR, Curran T. fra-1: a serum-inducible, cellular immediate-early gene that encodes a fos-related antigen. Mol Cell Biol. 1988 May;8(5):2063-9
Cohen DR, Ferreira PC, Gentz R, Franza BR Jr, Curran T. The product of a fos-related gene, fra-1, binds cooperatively to the AP-1 site with Jun: transcription factor AP-1 is comprised of multiple protein complexes. Genes Dev. 1989 Feb;3(2):173-84
Bergers G, Graninger P, Braselmann S, Wrighton C, Busslinger M. Transcriptional activation of the fra-1 gene by AP-1 is mediated by regulatory sequences in the first intron. Mol Cell Biol. 1995 Jul;15(7):3748-58
Vallone D, Battista S, Pierantoni GM, Fedele M, Casalino L, Santoro M, Viglietto G, Fusco A, Verde P. Neoplastic transformation of rat thyroid cells requires the junB and fra-1 gene induction which is dependent on the HMGI-C gene product. EMBO J. 1997 Sep 1;16(17):5310-21
Battista S, de Nigris F, Fedele M, Chiappetta G, Scala S, Vallone D, Pierantoni GM, Mega T, Santoro M, Viglietto G, Verde P, Fusco A. Increase in AP-1 activity is a general event in thyroid cell transformation in vitro and in vivo. Oncogene. 1998 Jul 23;17(3):377-85
Philips A, Teyssier C, Galtier F, Rivier-Covas C, Rey JM, Rochefort H, Chalbos D. FRA-1 expression level modulates regulation of activator protein-1 activity by estradiol in breast cancer cells. Mol Endocrinol. 1998 Jul;12(7):973-85
Bamberger AM, Methner C, Lisboa BW, Städtler C, Schulte HM, Löning T, Milde-Langosch K. Expression pattern of the AP-1 family in breast cancer: association of fosB expression with a well-differentiated, receptor-positive tumor phenotype. Int J Cancer. 1999 Oct 22;84(5):533-8
Chiappetta G, Tallini G, De Biasio MC, Pentimalli F, de Nigris F, Losito S, Fedele M, Battista S, Verde P, Santoro M, Fusco A. FRA-1 expression in hyperplastic and neoplastic thyroid diseases. Clin Cancer Res. 2000 Nov;6(11):4300-6

FOSL1 (FOS-like antigen 1) Rajamohan SB, Reddy SP
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 317
Fung LF, Lo AK, Yuen PW, Liu Y, Wang XH, Tsao SW. Differential gene expression in nasopharyngeal carcinoma cells. Life Sci. 2000 Jul 14;67(8):923-36
Matsuo K, Owens JM, Tonko M, Elliott C, Chambers TJ, Wagner EF. Fosl1 is a transcriptional target of c-Fos during osteoclast differentiation. Nat Genet. 2000 Feb;24(2):184-7
Hu YC, Lam KY, Law S, Wong J, Srivastava G. Identification of differentially expressed genes in esophageal squamous cell carcinoma (ESCC) by cDNA expression array: overexpression of Fra-1, Neogenin, Id-1, and CDC25B genes in ESCC. Clin Cancer Res. 2001 Aug;7(8):2213-21
Wang HL, Wang J, Xiao SY, Haydon R, Stoiber D, He TC, Bissonnette M, Hart J. Elevated protein expression of cyclin D1 and Fra-1 but decreased expression of c-Myc in human colorectal adenocarcinomas overexpressing beta-catenin. Int J Cancer. 2002 Oct 1;101(4):301-10
Young MR, Nair R, Bucheimer N, Tulsian P, Brown N, Chapp C, Hsu TC, Colburn NH. Transactivation of Fra-1 and consequent activation of AP-1 occur extracellular signal-regulated kinase dependently. Mol Cell Biol. 2002 Jan;22(2):587-98
Adiseshaiah P, Papaiahgari SR, Vuong H, Kalvakolanu DV, Reddy SP. Multiple cis-elements mediate the transcriptional activation of human fra-1 by 12-O-tetradecanoylphorbol-13-acetate in bronchial epithelial cells. J Biol Chem. 2003 Nov 28;278(48):47423-33
Casalino L, De Cesare D, Verde P. Accumulation of Fra-1 in ras-transformed cells depends on both transcriptional autoregulation and MEK-dependent posttranslational stabilization. Mol Cell Biol. 2003 Jun;23(12):4401-15
Luo Y, Zhou H, Mizutani M, Mizutani N, Reisfeld RA, Xiang R. Transcription factor Fos-related antigen 1 is an effective target for a breast cancer vaccine. Proc Natl Acad Sci U S A. 2003 Jul 22;100(15):8850-5
Shirsat NV, Shaikh SA. Overexpression of the immediate early gene fra-1 inhibits proliferation, induces apoptosis, and reduces tumourigenicity of c6 glioma cells. Exp Cell Res. 2003 Nov 15;291(1):91-100
Tiwari G, Sakaue H, Pollack JR, Roth RA. Gene expression profiling in prostate cancer cells with Akt activation reveals Fra-1 as an Akt-inducible gene. Mol Cancer Res. 2003 Apr;1(6):475-84
Vial E, Marshall CJ. Elevated ERK-MAP kinase activity protects the FOS family member FRA-1 against proteasomal degradation in colon carcinoma cells. J Cell Sci. 2003 Dec 15;116(Pt 24):4957-63
Zerbini LF, Wang Y, Cho JY, Libermann TA. Constitutive activation of nuclear factor kappaB p50/p65 and Fra-1 and JunD is essential for deregulated interleukin 6 expression in prostate cancer. Cancer Res. 2003 May 1;63(9):2206-15
Burch PM, Yuan Z, Loonen A, Heintz NH. An extracellular signal-regulated kinase 1- and 2-dependent program of chromatin trafficking of c-Fos and Fra-1 is required for cyclin D1 expression during cell cycle reentry. Mol Cell Biol. 2004 Jun;24(11):4696-709
Roschger P, Matsuo K, Misof BM, Tesch W, Jochum W, Wagner EF, Fratzl P, Klaushofer K. Normal mineralization and nanostructure of sclerotic bone in mice overexpressing Fra-1. Bone. 2004 May;34(5):776-82
Adiseshaiah P, Peddakama S, Zhang Q, Kalvakolanu DV, Reddy SP. Mitogen regulated induction of FRA-1 proto-oncogene is controlled by the transcription factors binding to both serum and TPA response elements. Oncogene. 2005 Jun 16;24(26):4193-205
Belguise K, Kersual N, Galtier F, Chalbos D. FRA-1 expression level regulates proliferation and invasiveness of breast cancer cells. Oncogene. 2005 Feb 17;24(8):1434-44
Debinski W, Gibo DM. Fos-related antigen 1 modulates malignant features of glioma cells. Mol Cancer Res. 2005 Apr;3(4):237-49
Luo Y, Zhou H, Mizutani M, Mizutani N, Liu C, Xiang R, Reisfeld RA. A DNA vaccine targeting Fos-related antigen 1 enhanced by IL-18 induces long-lived T-cell memory against tumor recurrence. Cancer Res. 2005 Apr 15;65(8):3419-27
Mangone FR, Brentani MM, Nonogaki S, Begnami MD, Campos AH, Walder F, Carvalho MB, Soares FA, Torloni H, Kowalski LP, Federico MH. Overexpression of Fos-related antigen-1 in head and neck squamous cell carcinoma. Int J Exp Pathol. 2005 Aug;86(4):205-12
Zhang W, Hart J, McLeod HL, Wang HL. Differential expression of the AP-1 transcription factor family members in human colorectal epithelial and neuroendocrine neoplasms. Am J Clin Pathol. 2005 Jul;124(1):11-9
Song Y, Song S, Zhang D, Zhang Y, Chen L, Qian L, Shi M, Zhao H, Jiang Z, Guo N. An association of a simultaneous nuclear and cytoplasmic localization of Fra-1 with breast malignancy. BMC Cancer. 2006 Dec 28;6:298
Adiseshaiah P, Lindner DJ, Kalvakolanu DV, Reddy SP. FRA-1 proto-oncogene induces lung epithelial cell invasion and anchorage-independent growth in vitro, but is insufficient to promote tumor growth in vivo. Cancer Res. 2007 Jul 1;67(13):6204-11
Basbous J, Chalbos D, Hipskind R, Jariel-Encontre I, Piechaczyk M. Ubiquitin-independent proteasomal degradation of Fra-1 is antagonized by Erk1/2 pathway-mediated phosphorylation of a unique C-terminal destabilizer. Mol Cell Biol. 2007 Jun;27(11):3936-50
Casalino L, Bakiri L, Talotta F, Weitzman JB, Fusco A, Yaniv M, Verde P. Fra-1 promotes growth and survival in RAS-transformed thyroid cells by controlling cyclin A transcription. EMBO J. 2007 Apr 4;26(7):1878-90
Chiappetta G, Ferraro A, Botti G, Monaco M, Pasquinelli R, Vuttariello E, Arnaldi L, Di Bonito M, D'Aiuto G, Pierantoni GM, Fusco A. FRA-1 protein overexpression is a feature of hyperplastic and neoplastic breast disorders. BMC Cancer. 2007 Jan 25;7:17
Verde P, Casalino L, Talotta F, Yaniv M, Weitzman JB. Deciphering AP-1 function in tumorigenesis: fra-ternizing on target promoters. Cell Cycle. 2007 Nov 1;6(21):2633-9
Zippo A, De Robertis A, Serafini R, Oliviero S. PIM1-dependent phosphorylation of histone H3 at serine 10 is required for MYC-dependent transcriptional activation and oncogenic transformation. Nat Cell Biol. 2007 Aug;9(8):932-44
Andreolas C, Kalogeropoulou M, Voulgari A, Pintzas A. Fra-1 regulates vimentin during Ha-RAS-induced epithelial mesenchymal transition in human colon carcinoma cells. Int J Cancer. 2008 Apr 15;122(8):1745-56
Ma K, Chang D, Gong M, Ding F, Luo A, Tian F, Liu Z, Wang T. Expression and significance of FRA-1 in non-small-cell lung cancer. Cancer Invest. 2009 Mar;27(3):353-9
Luo YP, Zhou H, Krueger J, Kaplan C, Liao D, Markowitz D, Liu C, Chen T, Chuang TH, Xiang R, Reisfeld RA. The role of proto-oncogene Fra-1 in remodeling the tumor microenvironment in support of breast tumor cell invasion and progression. Oncogene. 2010 Feb 4;29(5):662-73
Debinski W, Gibo DM. Fos-related antigen 1 (Fra-1) pairing with and transactivation of JunB in GBM cells. Cancer Biol Ther. 2011 Jan 15;11(2):254-62

FOSL1 (FOS-like antigen 1) Rajamohan SB, Reddy SP
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 318
Fudala R, Allen TC, Krupa A, Cagle PT, Nash S, Gryczynski Z, Gryczynski I, Kurdowska AK. Increased levels of nuclear factor κB and Fos-related antigen 1 in lung tissues from patients with acute respiratory distress syndrome. Arch Pathol Lab Med. 2011 May;135(5):647-54
Kireva T, Erhardt A, Tiegs G, Tilg H, Denk H, Haybaeck J, Aigner E, Moschen A, Distler JH, Schett G, Zwerina J. Transcription factor Fra-1 induces cholangitis and liver fibrosis. Hepatology. 2011 Apr;53(4):1259-69
Logullo AF, Stiepcich MM, Osório CA, Nonogaki S, Pasini FS, Rocha RM, Soares FA, Brentani MM. Role of Fos-related antigen 1 in the progression and prognosis of ductal breast carcinoma. Histopathology. 2011 Mar;58(4):617-25
Pennanen PT, Sarvilinna NS, Toimela T, Ylikomi TJ. Inhibition of FOSL1 overexpression in antiestrogen-resistant MCF-7 cells decreases cell growth and increases vacuolization and cell death. Steroids. 2011 Sep-Oct;76(10-11):1063-8
Takada Y, Gresh L, Bozec A, Ikeda E, Kamiya K, Watanabe M, Kobayashi K, Asano K, Toyama Y, Wagner EF, Matsuo K. Interstitial lung disease induced by gefitinib and toll-like receptor ligands is mediated by Fra-1. Oncogene. 2011 Sep 8;30(36):3821-32
Belguise K, Milord S, Galtier F, Moquet-Torcy G, Piechaczyk M, Chalbos D. The PKCθ pathway participates in the aberrant accumulation of Fra-1 protein in invasive ER-negative breast cancer cells. Oncogene. 2012 Nov 22;31(47):4889-97
Lan YY, Hsiao JR, Chang KC, Chang JS, Chen CW, Lai HC, Wu SY, Yeh TH, Chang FH, Lin WH, Su IJ, Chang Y. Epstein-Barr virus latent membrane protein 2A promotes invasion of nasopharyngeal carcinoma cells through ERK/Fra-1-mediated induction of matrix metalloproteinase 9. J Virol. 2012 Jun;86(12):6656-67
Lu D, Chen S, Tan X, Li N, Liu C, Li Z, Liu Z, Stupack DG, Reisfeld RA, Xiang R. Fra-1 promotes breast cancer chemosensitivity by driving cancer stem cells from dormancy. Cancer Res. 2012 Jul 15;72(14):3451-6
Rajasekaran S, Vaz M, Reddy SP. Fra-1/AP-1 transcription factor negatively regulates pulmonary fibrosis in vivo. PLoS One. 2012;7(7):e41611
Sandford AJ, Malhotra D, Boezen HM, Siedlinski M, Postma DS, Wong V, Akhabir L, He JQ, Connett JE, Anthonisen NR, Paré PD, Biswal S. NFE2L2 pathway polymorphisms and lung function decline in chronic obstructive pulmonary disease. Physiol Genomics. 2012 Aug 1;44(15):754-63
Sayan AE, Stanford R, Vickery R, Grigorenko E, Diesch J, Kulbicki K, Edwards R, Pal R, Greaves P, Jariel-Encontre I, Piechaczyk M, Kriajevska M, Mellon JK, Dhillon AS, Tulchinsky E. Fra-1 controls motility of bladder cancer cells via transcriptional upregulation of the receptor tyrosine kinase AXL. Oncogene. 2012 Mar 22;31(12):1493-503
Usui A, Hoshino I, Akutsu Y, Sakata H, Nishimori T, Murakami K, Kano M, Shuto K, Matsubara H. The molecular role of Fra-1 and its prognostic significance in human esophageal squamous cell carcinoma. Cancer. 2012 Jul 1;118(13):3387-96
Vaz M, Reddy NM, Rajasekaran S, Reddy SP. Genetic disruption of Fra-1 decreases susceptibility to endotoxin-induced acute lung injury and mortality in mice. Am J Respir Cell Mol Biol. 2012 Jan;46(1):55-62
Wu J, Wu G, Lv L, Ren YF, Zhang XJ, Xue YF, Li G, Lu X, Sun Z, Tang KF. MicroRNA-34a inhibits migration and invasion of colon cancer cells via targeting to Fra-1. Carcinogenesis. 2012 Mar;33(3):519-28
Yang S, Li Y, Gao J, Zhang T, Li S, Luo A, Chen H, Ding F, Wang X, Liu Z. MicroRNA-34 suppresses breast cancer invasion and metastasis by directly targeting Fra-1. Oncogene. 2012 Sep 24;
This article should be referenced as such:
Rajamohan SB, Reddy SP. FOSL1 (FOS-like antigen 1). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):313-318.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 319
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
FOXC1 (forkhead box C1) Shakila Jabeen, Vessela N Kristensen
Department of Clinical Molecular Biology and Laboratory Sciences (EpiGen), Division of Medicine, Akershus University Hospital, Lorenskog, Norway (SJ, VNK)
Published in Atlas Database: November 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/FOXC1ID40624ch6p25.html DOI: 10.4267/2042/49699
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: ARA, FKHL7, FREAC-3, FREAC3, IGDA, IHG1, IRID1, RIEG3
HGNC (Hugo): FOXC1
Location: 6p25.3
DNA/RNA Description Orientation: Plus strand. Genomic Size: 3447 bases. Exon Count: 1. Coding Exon Count: 1. RefSeq DNA sequence: NC_000006.11- NT_007592.15 contains Fork Head domain (FHD).
Basal Isoelectric point: 8.7.
Transcription Gene is transcribed into 3454 bps mRNA, containing one exon.
Protein Description Sequence length: 553 amino acids, mass: 56789 Dalton. It contains one Fork Head DNA binding domain, consists approximately of 110 amino acids. FHD is a conservative sequence shared by all FOX proteins.
Figure1: Gene sequence (grey) and transcriptional product of FOXC1. Forkhead DNA binding domain (FH Domain) contains 4 alpha helices (H1, H2, H4 and H3), 2 beta sheets (B2 and B3) and two wings (W1 and W2).

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 320
Figure 2: Amino acid sequence of the FHD of FOXC1, spanning from 69 to 178, H3 (alpha helix) mainly contribute to binding of the domain to DNA. FHD, a helix-turn-helix DNA binding motif, is composed of three alpha helices and two large "wing-like" loops. FHD contains nuclear localization signals at the N- and C- termini of the forkhead box, required to translocate the protein into cell nuclei. Alpha helix no.3 is responsible for DNA specific binding (Carlsson et al., 2002).
Expression Fork head protein is expressed in all tissues and cell lines examined (Hormas et al., 1993). FOXC1 in human is expressed in cornea, eye, heart, kidney, liver, lung and muscles (Wang et al., 2001).
Localisation FOXC1 protein localizes in nucleus (Berry et al., 2002).
Function FOXC1 plays a major role in embryonic and ocular development as a transcriptional factor and transcription regulator. Function of FOXC1 is related to several hundred genes, change in expression pattern of FOXC1 may cause change in the expression pattern of hundreds of the genes (Berry et al., 2008; Huang et al., 2008). Function of FOXC1 protein involves DNA binding and bending (Pierrou et al., 1994). Binding of the fork head proteins to their cognate sites, results in bending of the DNA at an angle of 80-90 degrees, thus, enhancing transcriptional activity of certain genes (Saleem et al., 2001). Malfunction related to various Glaucoma phenotypes including congenital glaucoma, iridogoniodysgenesis anomaly, REG3, iris hyperplasia and Peter anomaly. During ocular development, it interacts and regulates expression of FOXO1A. The promoter region of FOXO1A contains consensus FOXC1 binding site (GTAAACAAA). FOXO1A is responsible for regulation of cellular homeostasis and cell survival during ocular development, its functioning depends on function of FOXC1. Other targets of FOXC1 in transcriptional regulation in the eye include NOTCH2, RAB3GAP and CSPG5 (Berry et al., 2008). Function of FOXC1 protein in ocular cells is regulated by p32, a cytoplasmic protein which has a binding site at FHD of FOXC1 and can be colocalized in nucleus. It regulates FOXC1-mediated transcription activation in a dose-dependent manner but does not affect FOXC1
DNA-binding ability. Malfunction of p32 or mutation in FHD of FOXC1, effecting binding ability of p32 might result in Axenfeild-Reiger malformations (Huang et al., 2008). FOXC1 along with FOXC2 regulates the establishment of paraxial versus intermediate mesoderm cell fates in the vertebrate embryos (Wilm et al., 2004). FOXC1 and FOXC2 are required in kidney, urinary tract and early heart development processes, especially acting upstream of the Tbx1-FGF cascade during morphogenesis of the OFT (outflow tract) (Soe and Kume, 2006; Kume et al., 2000). Kume et al. (2001) proposed that FOXC1 and FOXC2 interact with the Notch signalling pathway and are required for prepatterning of anterior and posterior domains in the presumptive somites through a putative Notch/Delta/Mesp regulatory loop. Savage et al. (2010) found out that expression of FOXC1 along with FOXC2 is dependent on a complex interplay from Wnt and Shh pathways during early stages of in vitro skeletal myogenesis.
Homology Fork head domain (FHD), an approximately 110 amino acid segment is a common element shared by FOX proteins. Human Forkhead-box (FOX) gene family consists of at least 43 members, including FOXA1, FOXA2, FOXA3, FOXB1, FOXC1, FOXC2, FOXD1, FOXD2, FOXD3, FOXD4, FOXD5 (FOXD4L1), FOXD6 (FOXD4L3), FOXE1, FOXE2, FOXE3, FOXF1, FOXF2, FOXG1 (FOXG1B), FOXH1, FOXI1, FOXJ1, FOXJ2, FOXJ3, FOXK1, FOXK2, FOXL1, FOXL2, FOXM1, FOXN1, FOXN2 (HTLF), FOXN3 (CHES1), FOXN4, FOXN5 (FOXR1), FOXN6 (FOXR2), FOXO1 (FOXO1A), FOXO2 (FOXO6), FOXO3 (FOXO3A), FOXO4 (MLLT7), FOXP1, FOXP2, FOXP3, FOXP4, and FOXQ1. FOXE3-FOXD2 (1p33), FOXQ1-FOXF2-FOXC1 (6p25.3), and FOXF1-FOXC2-FOXL1 (16q24.1) loci are FOX gene clusters within the human genome. FOXC1, FOXC2, FOXE1, FOXE3, FOXL2, FOXN1, FOXP2 and FOXP3 genes are mutated in human congenital disorders (Katoh and Katoh, 2004). The forkhead box (Fox) family of transcription factors, which originated in unicellular eukaryotes, has expanded over time through multiple duplication events, and sometimes through gene loss, to over 40 members in mammals (Hannenhalli and Kaestner,

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 321
2009) found out that Fox genes have evolved to acquire a specialized function in many key biological processes. Mutations in Fox genes have a profound effect on human disease, causing phenotypes as varied as cancer, glaucoma and language disorders.
Mutations Germinal Deletion of distal 6p is associated with a distinctive clinical phenotype including Axenfeld-Rieger malformation, hearing loss, congenital heart disease, dental anomalies, developmental delay, and a characteristic facial appearance. By DNA sequencing of FOXC1 in 5 families and 16 sporadic patients a 6p microdeletion resulted from a de novo 6:18 translocation was recognized. The same translocation was reported in a child with specific ocular and facial phenotype (Maclean et al., 2005). Detailed analysis confirmed deletion of the FOXC1, FOXF2 and FOXQ1 forkhead gene cluster at 6p25. It showed central nervous system (CNS) anomalies, including hydrocephalus and hypoplasia of the cerebellum, brainstem, and corpus callosum with mild to moderate developmental delay. The mouse gene Mf1 is homolog of FOXC1. Homozygous null Mf1-lacZ mice die at birth with hydrocephalus, eye defects, and multiple skeletal abnormalities identical to those of the classic mutant, congenital hydrocephalus. Kume et al. (1998) showed that congenital hydrocephalus involves a point mutation in Mf1, generating a truncated protein lacking the DNA-binding domain. Mesenchyme cells from Mf1-lacZ embryos differentiated poorly into cartilage in micro-mass culture and did not respond to added BMP2 and TGF-beta-1. The differentiation of arachnoid cells in the mutant meninges was also abnormal.
Somatic Using genotyping and FISH as method of investigations, Lehmann et al. (2002) studied a 9-generation Scottish family segregating autosomal dominant iridogoniodysgenesis. The team found an interstitial duplication of chromosome 6p25 which encompassed the FOXC1 gene. Nishimura et al. (2001) analyzed the coding region of the FOXC1 gene in 70 probands with congenital anterior chamber defects and detected 9 mutations, 8 of which were novel. Affected members from 2 families, one with iris-hypoplasia and the other with Peters anomaly, had 2 different partial duplications of 6p25, respectively, both encompassing the FOXC1 gene. These data suggested that both FOXC1 haploinsufficiency and increased gene dosage may cause anterior-chamber defects of the eye. Fetterman et al. (2009) identified a heterozygous FOXC1 missense mutation outside of the forkhead
domain, and in the inhibitory domain, in 2 unrelated patients with iridogoniodysgenesis. Iridogoniodysgenesis phenotype is more commonly associated with FOXC1 duplications than point mutation. Honkanen et al. (2003) identified the F112S (a point) mutation in the FOXC1 gene in 5 affected members of a 4-generation family segregating autosomal dominant anterior segment defects, including a patient who also had Peters anomaly. Saleem et al. (2001) investigated 5 missense mutations of the FOXC1 transcription factor found in patients with Axenfeld-Rieger malformations to determine their effects on FOXC1 structure and function. Molecular modelling of the FOXC1 fork head domain predicted that the missense mutations did not alter FOXC1 structure. Biochemical analyses indicated that whereas all mutant proteins correctly localized to the cell nucleus, the I87M mutation reduced FOXC1 protein levels. DNA-binding experiments revealed that although the S82T and S131L mutations decreased DNA binding, the F112S and I126M mutations did not. However, the F112S and I126M mutations decreased the transactivation ability of FOXC1. Saleem et al. (2003) studied an additional 5 missense mutations in the FOXC1 gene. Biological analyses indicated that all missense mutations studied caused various FOXC1 perturbations, including nuclear localization defects, reduced or abolished DNA binding capacity, and a reduction in the transactivation capacity of FOXC1.
Implicated in Breast cancer Note Methylation status of FOXC1 promoter can be related to invasiveness of breast cancer and patient survival. Higher methylation means lower expression and more invasiveness of tumour, in advanced breast tumors as concluded by Dejeux et al. (2010) and Muggerud et al. (2010) methylation levels of FOXC1 were higher in oestrogen receptor (ER) positive vs. ER negative tumours; whereas methylation levels lower in tumours with a TP53 mutation. FOXC1 showed a significant increase in the methylation frequency in invasive tumours. Low FOXC1 gene expression in both methylated and unmethylated DCIS (ductal carcinoma in situ) and IDCs (invasive ductal carcinomas) indicates that the loss of expression of FOXC1 happens at earlier stage during the progression of breast cancer.
Prognosis Recently FOXC1 has been reported as potential prognostic biomarker with functional significance in basal like breast cancer by Ray et al. (2010) and Dejeux et al. (2010).

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 322
Invasive carcinoma Oncogenesis Zhou et al. (2002) showed that TGF-beta1 up regulated transcription of FOXC1 in a number of human cancer cell lines. In FOXC1 homozygous knockdown (-foxc1/-foxc1) HeLa cell line, ectopic expression of FOXC1 cDNA restored the potential of TGF-beta1 to inhibit cell growth by arresting cells in the G0/G1 phase. Which reveals the FOXC1 having a tumour suppressive function. Furthermore, screens of primary endometrial and ovarian cancers revealed that FOXC1 was deleted in 6.7% out of 11.7% transcriptional silenced primary cancers. It suggests that FOXC1 functions as a tumour suppressor through TGF-beta1 mediated signals. Van der Heul-Nieuwenhuijsen et al. (2009) analysed a set of 12 different FOX genes, including FOXC1, by quantitative reverse transcription-polymerase chain reaction in prostate zones, prostate cancer, lymph node metastases, benign prostatic hyperplasia (BPH), xenografts and several prostate cell lines. Various members of the FOX family were differentially expressed in the zones of the normal prostate and in benign and malignant out-growths. The expression profiles of FOXF1 and FOXF2 suggest a role in epithelial to mesenchymal transition, while FOXA1 and FOXC1 expression is linked to androgen-associated growth status of cancer. FOXC1 contribute to microvascular invasion in primary hepatocellular carcinoma, making FOXC1 a candidate predictive marker of microvascular invasion. Inhibition of FOXC1 may reduce tumour metastasis in hepatocellular carcinoma (liver cancer) (Xu et al., 2012).
Axenfield-Reiger Syndrome (ARS) or Axenfield-Reiger syndrome type 3 (RIEG3) also known as Axenfield syndrome or Axenfield Anomaly Note Phenotype may show posterior corneal embryotoxon, prominent Schwalbe line and iris adhesion to the Schwalbe line. It may also show hypertelorism, hypoplasia of the malar bones, congenital absence of some teeth and mental retardation. Tooth anomalies are associated with Reiger syndrome. Glaucoma may occur in almost fifty percent of the patients with Axenfield-Reiger malformations (Ito et al., 2007).
Cytogenetics As results of different studies of ARS/ RIEG3 cases: Nishimura et al. (1998) found an 11-bp deletion upstream of the FOXC1 forkhead domain. The team also identified a C-to-T transition within the forkhead domain, causing a ser131-to-leu (S131L) amino acid substitution. The Nishimura team found a C-to-G transversion within the forkhead domain. This change resulted in an ile126-to-met (I126M) amino acid
substitution. They also identified a T-to-C transition in the FOXC1 gene that resulted in a phe112-to-ser (F112S) transition within the forkhead domain. Mirzayans et al. (2000) found that Axenfeld-Rieger syndrome (RIEG3) was associated with a 67C-T transition in the FOXC1 gene, predicted to cause a gln23-to-ter (E23X) substitution upstream of the forkhead domain. Nishimura et al. (2001) found a 22-bp insertion from position 26 through 47 in the cDNA of theFOXC1 gene. Mears et al. (1998) identified heterozygosity for a 245G-C transversion in the FOXC1 gene, predicted to result in a ser82-to-thr (S82T) substitution at the start of helix 1 of the forkhead domain. They also identified a 261C-G transversion in the FOXC1 gene, resulting in an ile87-to-met (I87M) substitution in helix 1 of the forkhead domain. Ito et al. (2007) identified a heterozygous 388C-T transi-tion in the FOXC1 gene, resulting in a leu130-to-phe (L130F) substitution in helix 3, the so-called 'recognition helix' of the forkhead domain. Weisschuh et al. (2008) identified heterozygosity for a 358C-T transition in the FOXC1 gene, resulting in a gln120-to-ter (Q120X) substitution causing truncation of part of the forkhead domain.
Peters anomaly (PA) and Iridogoniodysgenesis anomaly (IGDA) Note IGDA is an autosomal dominant phenotype characterized by iris hypoplasia, goniodysgenesis, and juvenile glaucoma. Peters anomaly consists of a central corneal leukoma, absence of the posterior corneal storma and Descemet membrane, and a variable degree of iris and lenticular attachments to the central aspect of the posterior cornea (Honkanen et al., 2003).
Cytogenetics As results of different studies of PA and IGDA cases: Lehmann et al. (2000) found by genotyping of FOXC1, with microsatellite repeat markers, the presence of a chromosomal duplication. Nishimura et al. (2001) identified a partial duplication of chromosome 6p25, which encompassed the FOXC1 gene. Fetterman et al. (2009) identified heterozygosity for an 889C-T transition in the FOXC1 gene, resulting in a pro297-to-ser (P297S) substitution in the inhibitory domain.
References Hromas R, Moore J, Johnston T, Socha C, Klemsz M. Drosophila forkhead homologues are expressed in a lineage-restricted manner in human hematopoietic cells. Blood. 1993 Jun 1;81(11):2854-9
Pierrou S, Hellqvist M, Samuelsson L, Enerbäck S, Carlsson P. Cloning and characterization of seven human forkhead

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 323
proteins: binding site specificity and DNA bending. EMBO J. 1994 Oct 17;13(20):5002-12
Kume T, Deng KY, Winfrey V, Gould DB, Walter MA, Hogan BL. The forkhead/winged helix gene Mf1 is disrupted in the pleiotropic mouse mutation congenital hydrocephalus. Cell. 1998 Jun 12;93(6):985-96
Mears AJ, Jordan T, Mirzayans F, Dubois S, Kume T, Parlee M, Ritch R, Koop B, Kuo WL, Collins C, Marshall J, Gould DB, Pearce W, Carlsson P, Enerbäck S, Morissette J, Bhattacharya S, Hogan B, Raymond V, Walter MA. Mutations of the forkhead/winged-helix gene, FKHL7, in patients with Axenfeld-Rieger anomaly. Am J Hum Genet. 1998 Nov;63(5):1316-28
Nishimura DY, Swiderski RE, Alward WL, Searby CC, Patil SR, Bennet SR, Kanis AB, Gastier JM, Stone EM, Sheffield VC. The forkhead transcription factor gene FKHL7 is responsible for glaucoma phenotypes which map to 6p25. Nat Genet. 1998 Jun;19(2):140-7
Kume T, Deng K, Hogan BL. Murine forkhead/winged helix genes Foxc1 (Mf1) and Foxc2 (Mfh1) are required for the early organogenesis of the kidney and urinary tract. Development. 2000 Apr;127(7):1387-95
Lehmann OJ, Ebenezer ND, Jordan T, Fox M, Ocaka L, Payne A, Leroy BP, Clark BJ, Hitchings RA, Povey S, Khaw PT, Bhattacharya SS. Chromosomal duplication involving the forkhead transcription factor gene FOXC1 causes iris hypoplasia and glaucoma. Am J Hum Genet. 2000 Nov;67(5):1129-35
Mirzayans F, Gould DB, Héon E, Billingsley GD, Cheung JC, Mears AJ, Walter MA. Axenfeld-Rieger syndrome resulting from mutation of the FKHL7 gene on chromosome 6p25. Eur J Hum Genet. 2000 Jan;8(1):71-4
Kawase C, Kawase K, Taniguchi T, Sugiyama K, Yamamoto T, Kitazawa Y, Alward WL, Stone EM, Nishimura DY, Sheffield VC. Screening for mutations of Axenfeld-Rieger syndrome caused by FOXC1 gene in Japanese patients. J Glaucoma. 2001 Dec;10(6):477-82
Kume T, Jiang H, Topczewska JM, Hogan BL. The murine winged helix transcription factors, Foxc1 and Foxc2, are both required for cardiovascular development and somitogenesis. Genes Dev. 2001 Sep 15;15(18):2470-82
Nishimura DY, Searby CC, Alward WL, Walton D, Craig JE, Mackey DA, Kawase K, Kanis AB, Patil SR, Stone EM, Sheffield VC. A spectrum of FOXC1 mutations suggests gene dosage as a mechanism for developmental defects of the anterior chamber of the eye. Am J Hum Genet. 2001 Feb;68(2):364-72
Saleem RA, Banerjee-Basu S, Berry FB, Baxevanis AD, Walter MA. Analyses of the effects that disease-causing missense mutations have on the structure and function of the winged-helix protein FOXC1. Am J Hum Genet. 2001 Mar;68(3):627-41
Wang WH, McNatt LG, Shepard AR, Jacobson N, Nishimura DY, Stone EM, Sheffield VC, Clark AF. Optimal procedure for extracting RNA from human ocular tissues and expression profiling of the congenital glaucoma gene FOXC1 using quantitative RT-PCR. Mol Vis. 2001 Apr 17;7:89-94
Berry FB, Saleem RA, Walter MA. FOXC1 transcriptional regulation is mediated by N- and C-terminal activation domains and contains a phosphorylated transcriptional inhibitory domain. J Biol Chem. 2002 Mar 22;277(12):10292-7
Borges AS, Susanna R Jr, Carani JC, Betinjane AJ, Alward WL, Stone EM, Sheffield VC, Nishimura DY. Genetic analysis of PITX2 and FOXC1 in Rieger Syndrome patients from Brazil. J Glaucoma. 2002 Feb;11(1):51-6
Dintilhac A, Bernués J. HMGB1 interacts with many apparently unrelated proteins by recognizing short amino acid sequences. J Biol Chem. 2002 Mar 1;277(9):7021-8
Lehmann OJ, Ebenezer ND, Ekong R, Ocaka L, Mungall AJ, Fraser S, McGill JI, Hitchings RA, Khaw PT, Sowden JC, Povey S, Walter MA, Bhattacharya SS, Jordan T. Ocular developmental abnormalities and glaucoma associated with interstitial 6p25 duplications and deletions. Invest Ophthalmol Vis Sci. 2002 Jun;43(6):1843-9
Panicker SG, Sampath S, Mandal AK, Reddy AB, Ahmed N, Hasnain SE. Novel mutation in FOXC1 wing region causing Axenfeld-Rieger anomaly. Invest Ophthalmol Vis Sci. 2002 Dec;43(12):3613-6
Zhou Y, Kato H, Asanoma K, Kondo H, Arima T, Kato K, Matsuda T, Wake N. Identification of FOXC1 as a TGF-beta1 responsive gene and its involvement in negative regulation of cell growth. Genomics. 2002 Nov;80(5):465-72
Honkanen RA, Nishimura DY, Swiderski RE, Bennett SR, Hong S, Kwon YH, Stone EM, Sheffield VC, Alward WL. A family with Axenfeld-Rieger syndrome and Peters Anomaly caused by a point mutation (Phe112Ser) in the FOXC1 gene. Am J Ophthalmol. 2003 Mar;135(3):368-75
Komatireddy S, Chakrabarti S, Mandal AK, Reddy AB, Sampath S, Panicker SG, Balasubramanian D. Mutation spectrum of FOXC1 and clinical genetic heterogeneity of Axenfeld-Rieger anomaly in India. Mol Vis. 2003 Feb 18;9:43-8
Rice R, Rice DP, Olsen BR, Thesleff I. Progression of calvarial bone development requires Foxc1 regulation of Msx2 and Alx4. Dev Biol. 2003 Oct 1;262(1):75-87
Saleem RA, Banerjee-Basu S, Berry FB, Baxevanis AD, Walter MA. Structural and functional analyses of disease-causing missense mutations in the forkhead domain of FOXC1. Hum Mol Genet. 2003 Nov 15;12(22):2993-3005
Saleem RA, Murphy TC, Liebmann JM, Walter MA. Identification and analysis of a novel mutation in the FOXC1 forkhead domain. Invest Ophthalmol Vis Sci. 2003 Nov;44(11):4608-12
Katoh M, Katoh M. Human FOX gene family (Review). Int J Oncol. 2004 Nov;25(5):1495-500
Mortemousque B, Amati-Bonneau P, Couture F, Graffan R, Dubois S, Colin J, Bonneau D, Morissette J, Lacombe D, Raymond V. Axenfeld-Rieger anomaly: a novel mutation in the forkhead box C1 (FOXC1) gene in a 4-generation family. Arch Ophthalmol. 2004 Oct;122(10):1527-33
Saleem RA, Banerjee-Basu S, Murphy TC, Baxevanis A, Walter MA. Essential structural and functional determinants within the forkhead domain of FOXC1. Nucleic Acids Res. 2004;32(14):4182-93
Wilm B, James RG, Schultheiss TM, Hogan BL. The forkhead genes, Foxc1 and Foxc2, regulate paraxial versus intermediate mesoderm cell fate. Dev Biol. 2004 Jul 1;271(1):176-89
Maclean K, Smith J, St Heaps L, Chia N, Williams R, Peters GB, Onikul E, McCrossin T, Lehmann OJ, Adès LC. Axenfeld-Rieger malformation and distinctive facial features: Clues to a recognizable 6p25 microdeletion syndrome. Am J Med Genet A. 2005 Feb 1;132(4):381-5
Rice R, Rice DP, Thesleff I. Foxc1 integrates Fgf and Bmp signalling independently of twist or noggin during calvarial bone development. Dev Dyn. 2005 Jul;233(3):847-52
Berry FB, Lines MA, Oas JM, Footz T, Underhill DA, Gage PJ, Walter MA. Functional interactions between FOXC1 and PITX2 underlie the sensitivity to FOXC1 gene dose in Axenfeld-

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 324
Rieger syndrome and anterior segment dysgenesis. Hum Mol Genet. 2006 Mar 15;15(6):905-19
Berry FB, Mirzayans F, Walter MA. Regulation of FOXC1 stability and transcriptional activity by an epidermal growth factor-activated mitogen-activated protein kinase signaling cascade. J Biol Chem. 2006 Apr 14;281(15):10098-104
Cella W, de Vasconcellos JP, de Melo MB, Kneipp B, Costa FF, Longui CA, Costa VP. Structural assessment of PITX2, FOXC1, CYP1B1, and GJA1 genes in patients with Axenfeld-Rieger syndrome with developmental glaucoma. Invest Ophthalmol Vis Sci. 2006 May;47(5):1803-9
Hannenhalli S, Putt ME, Gilmore JM, Wang J, Parmacek MS, Epstein JA, Morrisey EE, Margulies KB, Cappola TP. Transcriptional genomics associates FOX transcription factors with human heart failure. Circulation. 2006 Sep 19;114(12):1269-76
Mattiske D, Kume T, Hogan BL. The mouse forkhead gene Foxc1 is required for primordial germ cell migration and antral follicle development. Dev Biol. 2006 Feb 15;290(2):447-58
Mattiske D, Sommer P, Kidson SH, Hogan BL. The role of the forkhead transcription factor, Foxc1, in the development of the mouse lacrimal gland. Dev Dyn. 2006 Apr;235(4):1074-80
Seo S, Fujita H, Nakano A, Kang M, Duarte A, Kume T. The forkhead transcription factors, Foxc1 and Foxc2, are required for arterial specification and lymphatic sprouting during vascular development. Dev Biol. 2006 Jun 15;294(2):458-70
Seo S, Kume T. Forkhead transcription factors, Foxc1 and Foxc2, are required for the morphogenesis of the cardiac outflow tract. Dev Biol. 2006 Aug 15;296(2):421-36
Sommer P, Napier HR, Hogan BL, Kidson SH. Identification of Tgf beta1i4 as a downstream target of Foxc1. Dev Growth Differ. 2006 Jun;48(5):297-308
Tamimi Y, Skarie JM, Footz T, Berry FB, Link BA, Walter MA. FGF19 is a target for FOXC1 regulation in ciliary body-derived cells. Hum Mol Genet. 2006 Nov 1;15(21):3229-40
Weisschuh N, Dressler P, Schuettauf F, Wolf C, Wissinger B, Gramer E. Novel mutations of FOXC1 and PITX2 in patients with Axenfeld-Rieger malformations. Invest Ophthalmol Vis Sci. 2006 Sep;47(9):3846-52
Aldave AJ, Sonmez B, Bourla N, Schultz G, Papp JC, Salem AK, Rayner SA, Yellore VS. Autosomal dominant cornea plana is not associated with pathogenic mutations in DCN, DSPG3, FOXC1, KERA, LUM, or PITX2. Ophthalmic Genet. 2007 Jun;28(2):57-67
Fuse N, Takahashi K, Yokokura S, Nishida K. Novel mutations in the FOXC1 gene in Japanese patients with Axenfeld-Rieger syndrome. Mol Vis. 2007 Jun 27;13:1005-9
Ito YA, Footz TK, Murphy TC, Courtens W, Walter MA. Analyses of a novel L130F missense mutation in FOXC1. Arch Ophthalmol. 2007 Jan;125(1):128-35
Lowry RB, Gould DB, Walter MA, Savage PR. Absence of PITX2, BARX1, and FOXC1 mutations in De Hauwere syndrome (Axenfeld-Rieger anomaly, hydrocephaly, hearing loss): a 25-year follow up. Am J Med Genet A. 2007 Jun 1;143A(11):1227-30
Martinez-Glez V, Lorda-Sanchez I, Ramirez JM, Ruiz-Barnes P, Rodriguez de Alba M, Diego-Alvarez D, Ramos C, Searby CC, Nishimura DY, Ayuso C. Clinical presentation of a variant of Axenfeld-Rieger syndrome associated with subtelomeric 6p deletion. Eur J Med Genet. 2007 Mar-Apr;50(2):120-7
Strungaru MH, Dinu I, Walter MA. Genotype-phenotype correlations in Axenfeld-Rieger malformation and glaucoma
patients with FOXC1 and PITX2 mutations. Invest Ophthalmol Vis Sci. 2007 Jan;48(1):228-37
Zarbalis K, Siegenthaler JA, Choe Y, May SR, Peterson AS, Pleasure SJ. Cortical dysplasia and skull defects in mice with a Foxc1 allele reveal the role of meningeal differentiation in regulating cortical development. Proc Natl Acad Sci U S A. 2007 Aug 28;104(35):14002-7
Berry FB, Skarie JM, Mirzayans F, Fortin Y, Hudson TJ, Raymond V, Link BA, Walter MA. FOXC1 is required for cell viability and resistance to oxidative stress in the eye through the transcriptional regulation of FOXO1A. Hum Mol Genet. 2008 Feb 15;17(4):490-505
Ferrell RE, Kimak MA, Lawrence EC, Finegold DN. Candidate gene analysis in primary lymphedema. Lymphat Res Biol. 2008;6(2):69-76
Hayashi H, Kume T. Forkhead transcription factors regulate expression of the chemokine receptor CXCR4 in endothelial cells and CXCL12-induced cell migration. Biochem Biophys Res Commun. 2008 Mar 14;367(3):584-9
Hosgood HD 3rd, Menashe I, Shen M, Yeager M, Yuenger J, Rajaraman P, He X, Chatterjee N, Caporaso NE, Zhu Y, Chanock SJ, Zheng T, Lan Q. Pathway-based evaluation of 380 candidate genes and lung cancer susceptibility suggests the importance of the cell cycle pathway. Carcinogenesis. 2008 Oct;29(10):1938-43
Huang L, Chi J, Berry FB, Footz TK, Sharp MW, Walter MA. Human p32 is a novel FOXC1-interacting protein that regulates FOXC1 transcriptional activity in ocular cells. Invest Ophthalmol Vis Sci. 2008 Dec;49(12):5243-9
Khan AO, Aldahmesh MA, Al-Amri A. Heterozygous FOXC1 mutation (M161K) associated with congenital glaucoma and aniridia in an infant and a milder phenotype in her mother. Ophthalmic Genet. 2008 Jun;29(2):67-71
Weisschuh N, Wolf C, Wissinger B, Gramer E. A novel mutation in the FOXC1 gene in a family with Axenfeld-Rieger syndrome and Peters' anomaly. Clin Genet. 2008 Nov;74(5):476-80
Abdelmohsen K, Srikantan S, Yang X, Lal A, Kim HH, Kuwano Y, Galban S, Becker KG, Kamara D, de Cabo R, Gorospe M. Ubiquitin-mediated proteolysis of HuR by heat shock. EMBO J. 2009 May 6;28(9):1271-82
Aldinger KA, Lehmann OJ, Hudgins L, Chizhikov VV, Bassuk AG, Ades LC, Krantz ID, Dobyns WB, Millen KJ. FOXC1 is required for normal cerebellar development and is a major contributor to chromosome 6p25.3 Dandy-Walker malformation. Nat Genet. 2009 Sep;41(9):1037-42
Berker N, Alanay Y, Elgin U, Volkan-Salanci B, Simsek T, Akarsu N, Alikasifoglu M. A new autosomal dominant Peters' anomaly phenotype expanding the anterior segment dysgenesis spectrum. Acta Ophthalmol. 2009 Feb;87(1):52-7
Chakrabarti S, Kaur K, Rao KN, Mandal AK, Kaur I, Parikh RS, Thomas R. The transcription factor gene FOXC1 exhibits a limited role in primary congenital glaucoma. Invest Ophthalmol Vis Sci. 2009 Jan;50(1):75-83
Fetterman CD, Mirzayans F, Walter MA. Characterization of a novel FOXC1 mutation, P297S, identified in two individuals with anterior segment dysgenesis. Clin Genet. 2009 Sep;76(3):296-9
Golebiowski F, Matic I, Tatham MH, Cole C, Yin Y, Nakamura A, Cox J, Barton GJ, Mann M, Hay RT. System-wide changes to SUMO modifications in response to heat shock. Sci Signal. 2009 May 26;2(72):ra24

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 325
Hannenhalli S, Kaestner KH. The evolution of Fox genes and their role in development and disease. Nat Rev Genet. 2009 Apr;10(4):233-40
Hosgood HD 3rd, Menashe I, He X, Chanock S, Lan Q. PTEN identified as important risk factor of chronic obstructive pulmonary disease. Respir Med. 2009 Dec;103(12):1866-70
Ito YA, Footz TK, Berry FB, Mirzayans F, Yu M, Khan AO, Walter MA. Severe molecular defects of a novel FOXC1 W152G mutation result in aniridia. Invest Ophthalmol Vis Sci. 2009 Aug;50(8):3573-9
Kaur K, Ragge NK, Ragoussis J. Molecular analysis of FOXC1 in subjects presenting with severe developmental eye anomalies. Mol Vis. 2009 Jul 13;15:1366-73
Talmud PJ, Drenos F, Shah S, Shah T, Palmen J, Verzilli C, Gaunt TR, Pallas J, Lovering R, Li K, Casas JP, Sofat R, Kumari M, Rodriguez S, Johnson T, Newhouse SJ, Dominiczak A, Samani NJ, Caulfield M, Sever P, Stanton A, Shields DC, Padmanabhan S, Melander O, Hastie C, Delles C, Ebrahim S, Marmot MG, Smith GD, Lawlor DA, Munroe PB, Day IN, Kivimaki M, Whittaker J, Humphries SE, Hingorani AD. Gene-centric association signals for lipids and apolipoproteins identified via the HumanCVD BeadChip. Am J Hum Genet. 2009 Nov;85(5):628-42
Shen M, Vermeulen R, Rajaraman P, Menashe I, He X, Chapman RS, Yeager M, Thomas G, Burdett L, Hutchinson A, Yuenger J, Chanock S, Lan Q. Polymorphisms in innate immunity genes and lung cancer risk in Xuanwei, China. Environ Mol Mutagen. 2009 May;50(4):285-90
Tümer Z, Bach-Holm D. Axenfeld-Rieger syndrome and spectrum of PITX2 and FOXC1 mutations. Eur J Hum Genet. 2009 Dec;17(12):1527-39
van der Heul-Nieuwenhuijsen L, Dits NF, Jenster G. Gene expression of forkhead transcription factors in the normal and diseased human prostate. BJU Int. 2009 Jun;103(11):1574-80
Bailey SD, Xie C, Do R, Montpetit A, Diaz R, Mohan V, Keavney B, Yusuf S, Gerstein HC, Engert JC, Anand S. Variation at the NFATC2 locus increases the risk of thiazolidinedione-induced edema in the Diabetes REduction Assessment with ramipril and rosiglitazone Medication (DREAM) study. Diabetes Care. 2010 Oct;33(10):2250-3
Dejeux E, Rønneberg JA, Solvang H, Bukholm I, Geisler S, Aas T, Gut IG, Børresen-Dale AL, Lønning PE, Kristensen VN, Tost J. DNA methylation profiling in doxorubicin treated primary locally advanced breast tumours identifies novel genes associated with survival and treatment response. Mol Cancer. 2010 Mar 25;9:68
Guey LT, García-Closas M, Murta-Nascimento C, Lloreta J, Palencia L, Kogevinas M, Rothman N, Vellalta G, Calle ML, Marenne G, Tardón A, Carrato A, García-Closas R, Serra C, Silverman DT, Chanock S, Real FX, Malats N. Genetic susceptibility to distinct bladder cancer subphenotypes. Eur Urol. 2010 Feb;57(2):283-92
Hecht JH, Siegenthaler JA, Patterson KP, Pleasure SJ. Primary cellular meningeal defects cause neocortical dysplasia and dyslamination. Ann Neurol. 2010 Oct;68(4):454-64
Liu CY, Wu MC, Chen F, Ter-Minassian M, Asomaning K, Zhai R, Wang Z, Su L, Heist RS, Kulke MH, Lin X, Liu G, Christiani DC. A Large-scale genetic association study of esophageal adenocarcinoma risk. Carcinogenesis. 2010 Jul;31(7):1259-63
Muggerud AA, Rønneberg JA, Wärnberg F, Botling J, Busato F, Jovanovic J, Solvang H, Bukholm I, Børresen-Dale AL, Kristensen VN, Sørlie T, Tost J. Frequent aberrant DNA methylation of ABCB1, FOXC1, PPP2R2B and PTEN in ductal
carcinoma in situ and early invasive breast cancer. Breast Cancer Res. 2010;12(1):R3
Ray PS, Wang J, Qu Y, Sim MS, Shamonki J, Bagaria SP, Ye X, Liu B, Elashoff D, Hoon DS, Walter MA, Martens JW, Richardson AL, Giuliano AE, Cui X. FOXC1 is a potential prognostic biomarker with functional significance in basal-like breast cancer. Cancer Res. 2010 May 15;70(10):3870-6
Savage J, Voronova A, Mehta V, Sendi-Mukasa F, Skerjanc IS. Canonical Wnt signaling regulates Foxc1/2 expression in P19 cells. Differentiation. 2010 Jan;79(1):31-40
Tanwar M, Kumar M, Dada T, Sihota R, Dada R. MYOC and FOXC1 gene analysis in primary congenital glaucoma. Mol Vis. 2010 Oct 8;16:1996-2006
Balikova I, de Ravel T, Ayuso C, Thienpont B, Casteels I, Villaverde C, Devriendt K, Fryns JP, Vermeesch JR. High frequency of submicroscopic chromosomal deletions in patients with idiopathic congenital eye malformations. Am J Ophthalmol. 2011 Jun;151(6):1087-1094.e45
Danielsen JM, Sylvestersen KB, Bekker-Jensen S, Szklarczyk D, Poulsen JW, Horn H, Jensen LJ, Mailand N, Nielsen ML. Mass spectrometric analysis of lysine ubiquitylation reveals promiscuity at site level. Mol Cell Proteomics. 2011 Mar;10(3):M110.003590
D'haene B, Meire F, Claerhout I, Kroes HY, Plomp A, Arens YH, de Ravel T, Casteels I, De Jaegere S, Hooghe S, Wuyts W, van den Ende J, Roulez F, Veenstra-Knol HE, Oldenburg RA, Giltay J, Verheij JB, de Faber JT, Menten B, De Paepe A, Kestelyn P, Leroy BP, De Baere E. Expanding the spectrum of FOXC1 and PITX2 mutations and copy number changes in patients with anterior segment malformations. Invest Ophthalmol Vis Sci. 2011 Jan 21;52(1):324-33
Kelberman D, Islam L, Holder SE, Jacques TS, Calvas P, Hennekam RC, Nischal KK, Sowden JC. Digenic inheritance of mutations in FOXC1 and PITX2 : correlating transcription factor function and Axenfeld-Rieger disease severity. Hum Mutat. 2011 Oct;32(10):1144-52
Ma J, Zhong Y, Zhao C, Zhang X, Sui R, Chu P, Zhao J. Axenfeld-Rieger syndrome in monozygotic twins. J Glaucoma. 2011 Dec;20(9):584-6
McKeone R, Vieira H, Gregory-Evans K, Gregory-Evans CY, Denny P. Foxf2: a novel locus for anterior segment dysgenesis adjacent to the Foxc1 gene. PLoS One. 2011;6(10):e25489
Ray PS, Bagaria SP, Wang J, Shamonki JM, Ye X, Sim MS, Steen S, Qu Y, Cui X, Giuliano AE. Basal-like breast cancer defined by FOXC1 expression offers superior prognostic value: a retrospective immunohistochemical study. Ann Surg Oncol. 2011 Dec;18(13):3839-47
Tatham MH, Matic I, Mann M, Hay RT. Comparative proteomic analysis identifies a role for SUMO in protein quality control. Sci Signal. 2011 Jun 21;4(178):rs4
Chung TK, Lau TS, Cheung TH, Yim SF, Lo KW, Siu NS, Chan LK, Yu MY, Kwong J, Doran G, Barroilhet LM, Ng AS, Wong RR, Wang VW, Mok SC, Smith DI, Berkowitz RS, Wong YF. Dysregulation of microRNA-204 mediates migration and invasion of endometrial cancer by regulating FOXC1. Int J Cancer. 2012 Mar 1;130(5):1036-45
Seo S, Singh HP, Lacal PM, Sasman A, Fatima A, Liu T, Schultz KM, Losordo DW, Lehmann OJ, Kume T. Forkhead box transcription factor FoxC1 preserves corneal transparency by regulating vascular growth. Proc Natl Acad Sci U S A. 2012 Feb 7;109(6):2015-20
Xu ZY, Ding SM, Zhou L, Xie HY, Chen KJ, Zhang W, Xing CY, Guo HJ, Zheng SS. FOXC1 contributes to microvascular

FOXC1 (forkhead box C1) Jabeen S, Kristensen VN
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 326
invasion in primary hepatocellular carcinoma via regulating epithelial-mesenchymal transition. Int J Biol Sci. 2012;8(8):1130-41
This article should be referenced as such:
Jabeen S, Kristensen VN. FOXC1 (forkhead box C1). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):319-326.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 327
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
PTPN6 (protein tyrosine phosphatase, non-receptor type 6) Alessandro Beghini, Francesca Lazzaroni
Department of Medical Biotechnology and Translational Medicine, Universita degli Studi di Milano, Milano, Italy (AB, FL)
Published in Atlas Database: November 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/PTPN6ID41920ch12p13.html DOI: 10.4267/2042/49700
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: HCP, HCPH, HPTP1C, PTP-1C, SH-PTP1, SHP-1, SHP-1L, SHP1
HGNC (Hugo): PTPN6
Note Orientation: plus strand.
DNA/RNA Description The human PTPN6 gene is divided in 17 exons spanning a length of 14740 bp. A notable feature of the PTPN6 gene is that it has two promoter regions. Whereas the distal promoter, P1, located upstream of the very short exon 1 (also known as exon 1a) is active in epithelial cells, the proximal promoter P2 that initiates gene transcription from exon 2 (known as exon 1b), is utilized by the hematopoietic cells. The function of P1 promoter has been partially elucidated, while the structure and regulatory mechanism of the P2 promoter remain essentially unknown. Recent findings, characterized the hematopoietic cell-specific P2 promoter of PTPN6 gene as well as identified the PU.1 transcription factor as the activator of the P2 promoter.
Transcription There are three transcript variants: The variant 1 represents the predominant variant and encodes the shortest isoform. The variant 2 originates by an alternate 5' terminal exon compared to transcript variant 1, resulting in an isoform (2) with a distinct and longer (by 2 aa) N-terminus, compared to isoform 1. The variant 3 uses an alternate 5' terminal exon, and an alternate acceptor splice site at the penultimate exon, compared to transcript variant 1, resulting in a longer isoform (3, also known as 70 kDa SHP-1L protein) with distinct N and C termini, compared to isoform 1.
Protein Description PTPN6 contain two adjacent NH2 - terminal SH2 domains, two tandem Src homology (SH2) domains, a catalytic domain, and a -COOH terminal tail of 100 amino-acid residues.
Expression PTPN6 tyrosine phosphatase is encoded by the PTPN6 gene and expressed primarily in the hematopoietic and epithelial cells.

PTPN6 (protein tyrosine phosphatase, non-receptor type 6) Beghini A, Lazzaroni F
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 328
Schematic representation of the human PTPN6 gene. Adapted from Wu et al., 2003.
Function PTPN6 plays a peculiar role in the maturation and functional differentiation of lymphoid and myeloid cells as underlined by the aberrant proliferation and impaired hematopoiesis in the "motheaten" (me) mice that display defects in the Shp-1 gene expression. The role of PTPN6 in hematopoiesis has been shown in motheaten and viable motheaten (meν) mice, characterized by mutations at the Shp-1 locus. The Shp-1 mRNA from me bone marrow cells have a 101 bp frameshift deletion in the coding region of the N-terminal SH2 domain, while meν bone marrow cells have an in-frame 15 bp deletion or a 69 bp in-frame insertion within the PTPase catalytic domain. Shp-1 acts in the immune and other hematopoietic cells by inhibiting signaling through receptors for cytokines, growth factors and chemokines as well as receptors involved in the immune responses and programmed cell death. Moreover, PTPN6 acts as tumor suppressor and loss of its expression has been identified in the whole spectrum of myeloid and lymphoid malignancies. According to Gilfillan, PTPN6 is found to be
constitutively associated with FcεRI, with an opponing roles in FcεRI-mediated mast cell signaling. The study demonstrated that PTPN6 caused the decreased phosphorylation of FcεRI and Syk, but, also, an enhanced phosphorylation of JNK and an increased of the TNF production is observed. This study, suggests that PTPN6 may play a negative role proximal to FcεRI. It was also demonstrated that the PTPN6 protein tyrosine phosphatase negatively modulates the glucose homeostasis and insulin activity, through a dephosphorylation of transmembrane glycoprotein Carcinoembryonic Antigen-related Cell Adhesion Molecule-1 (CEACAM-1). The data obtained from in vitro studies, suggested that the deficiency of PTPN6 was associated with the increase in insulin-evoked tyrosin phosphorylation of the insulin receptor, IRS-1 and IRS-2, as well as enhanced activation of PI3K and Akt in liver and skeletal muscle. Moreover, the activation of PTPN6, through a PKC-δ and p38α MAPK actions on PDGFRβ is involved in hyperglycemia and causes an increase vascular cell apoptosis and diabetic vascular complications.

PTPN6 (protein tyrosine phosphatase, non-receptor type 6) Beghini A, Lazzaroni F
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 329
Crystal structure of human protein tyrosine phosphatase SHP-1. The blue region represents the N-terminal of protein, while the red region represents the C-terminal of protein.
Mutations Note The absence or impaired function of PTPN6 in the homozygous state causes the development of the motheaten phenotype in mice, an autosomal recessive condition with focal skin inflammation and the absence of hair. Failure of neutrophils to undergo apoptosis results in the accumulation of these cells in the peripheral blood, skin, lung and spleen of affected mice.
Somatic A pathologically similar extensive skin infiltration by neutrophils is present in Pyoderma gangrenosum (PG) and Sweet's syndrome (SW), two uncommon neutrophilic dermatoses of unknown origin. Isoforms resulting from deletions of exons 2, 5, 11, and 15 and retention of intron 1 or 5 were identified in a patients with a familial case of SW, who had a neonatal onset of an inflammatory disorder with skin lesions and a biopsy specimen consistent with SW. These isoforms were associated with a heterozygous E441G mutation and a heterozygous 1,7-kbp deletion in the promoter region of the PTPN6 gene. The E441G mutation changes the hydrophilic, negatively charged amino acid glutamate to the hydrophobic nonpolar, aliphatic amino acid glycine, thereby potentially affecting the tertiary
structure of PTPN6. SW an acute febrile neutrophilic dermatoses appears in several clinical forms as idiopathic, tumor associated, postinfectious and drug induced (for example after an administration of granulocyte macrophage colony stimulating factor). SW and PG have strong associations with hematological tumors. Recent studies have shown that patient with leukemia and lymphoma had methylated a P2 promoter in the PTPN6 gene, causing the absence of PTPN6 protein. PTPN6 is expressed at low level in non-hematopoietic cells while higher levels of this protein are found in hematopoietic precursors. PTPN6 promoter methylation causes loss of expression in leukemias, which results in the activation of the JAK/STAT pathway. PTPN6 plays a role in chronic myelogenous leukemia transformation and progression: it seems to be physically associated with BCR-ABL being able both to block BCR-ABL-dependent transformation and to mediate PP2A induced BCR-ABL proteosome-degradation. The tyrosine phosphatase PTPN6 plays a prominent role as resistance determinant of Imatinib (IMA) treatment response in Chronic Myelogenous Leukemia cell lines (sensitive/KCL22-S and resistant/KCL22-R). The lack of PTPN6 expression is frequent in malignant T cells and results from methylation of the PTPN6 gene promoter. Loss of PTPN6 enhances JAK3/STAT3

PTPN6 (protein tyrosine phosphatase, non-receptor type 6) Beghini A, Lazzaroni F
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 330
signaling and decreases proteosome degradation of JAK3 and NPM-ALK in ALK + anaplastic large-cell lymphoma. According to Wu's research, in most human Burkitt's lymphoma cell lines, the expression of SHP-1 is decreased suggesting a role of SHP-1 in a developing of Burkitt's lymphoma, a non-Hodgkin's lymphoma, associated with EBV infection. Moreover the activity of PTPN6, is also implicated in a breast cancer, ovarian cancer, prostate cancer, and pancreatic cancer.
Implicated in T-cell lymphomas Disease Cutaneous T-cell lymphoma (CTCL) is generally classified as a type of non-Hodgkin's lymphoma, and it represents a spectrum of diseases composed of malignant clonal helper T lymphocytes of the CD4 phenotype. Widely known variants include Sezary syndrome, Woringer-Kolopp disease (Pagetoid Reticulosis), CD8+ T-cell lymphoma, granulomatous slack skin, peripheral T-cell lymphoma, angiocentric lymphoma, adult T-cell leukemia/lymphoma, large-cell or anaplastic lymphoma, and lymphomatoid granulomatosis. Poikiloderma atrophicans vasculare, small and large plaque parapsoriasis, alopecia mucinosa, and lymphomatoid papulosis likely represent early forms of CTCL, but there is a problem to whether these represent CTCL or separate premalignant entities. Accurate diagnosis of early CTCL is difficult because of the varied clinical and histologic expressions of the disease and because of a lack of uniformity regarding diagnosis and treatment.
Prognosis Treatment regimens in CTCL include skin-directed therapies with UVA irradiation, topical chemotherapy with mechlorethamine (nitrogen mustard) and carmustine, and electron beam radiation, as well as systemic therapies such as chemotherapy and interferons.
Acute myeloid leukemia Note The first hint that A-to-I RNA editing has fundamental implications in leukemic disorders derives from Beghini and co-authors, who detected altered editing events in the protein tyrosine phosphatase (PTPN6/SHP-1) transcript of patients affected by AML (Galeano et al., 2012). The analysis of PTPN6 mRNA revealed a multiple A-I editing conversion of A7866, a branch site in IVS3 of PTPN6 mRNA causing the retention of IVS1.
Disease Adult acute myeloid leukemia (AML) is a type of cancer in which the bone marrow makes abnormal myeloblasts (a type of white blood cell), red blood
cells, or platelets. Adult acute myeloid leukemia (AML) is a cancer of the blood and bone marrow. This type of cancer usually gets worse quickly if it is not treated. It is the most common type of acute leukemia in adults. AML is also called acute myelogenous leukemia, acute myeloblastic leukemia, acute granulocytic leukemia, and acute nonlymphocytic leukemia. Most AML subtypes are based on how mature (developed) the cancer cells are at the time of diagnosis and how different they are from normal cells. Acute promyelocytic leukemia (APL) is a subtype of AML that occurs when parts of two genes stick together. APL usually occurs in middle-aged adults. Symptoms of APL may include both bleeding and forming blood clots.
Prognosis Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the spinal column (intrathecal chemotherapy), an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Intrathecal chemotherapy may be used to treat adult AML that has spread, or may spread to the brain and spinal cord. Combination chemotherapy is treatment using more than one anticancer drug. Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. Stem cell transplant is a method of giving chemotherapy and replacing blood-forming cells that are abnormal or destroyed by the cancer treatment. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the chemotherapy is completed, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
Pyoderma gangrenosum (PG) Disease Pyoderma gangrenosum (PG) is a rare noninfectious neutrophilic dermatosis first described in 1930. Clinically it begins with sterile pustules that rapidly progress and turn into painful ulcers of variable depth and size with undermined violaceous borders. The legs are most commonly affected but other parts of the skin and mucous membranes may also be involved. Extracutaneous manifestations include involvement of

PTPN6 (protein tyrosine phosphatase, non-receptor type 6) Beghini A, Lazzaroni F
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 331
upper airway mucosa, eye, sterile pulmonary neutrophilic infiltrates, and neutrophilic myositis. The ulcer starts as a follicular pustule with rapid growth, tissue necrosis and enlargement of the area. The surrounding skin is erythematous with infiltration end edema. Ulcerative colitis is found in 10-15% of cases. Another associated disease is Crohn's regional enteritis with a frequency close to that of ulcerative colitis. Hepatitis C, seronegative polyarticular arthritis, spondylitis, and a broad spectrum of lymphoproliferative disorders including monoclonal gammopathies, leukemia, lymphoma, and myelodysplastic syndrome have been described in association with PG. Two main variants of PG exist: classic and atypical. Classic PG: characterized by a deep ulceration with a violaceous border that overhangs the ulcer bed. May occur anywhere on the body; but most commonly found on the legs. Atypical PG: has a vesciculopustular component only at the border, is erosive or superficially ulcerated, and most often occurs on the dorsal surface of the hands, the extensor parts of the forearms, or the face.
Prognosis Local care: debridement, intralesional injection of steroids or cyclosporin, topical agents to alter immune response (nitrogen mustard, steroids, acetic acid, 5-aminosalicylic acid) or inhibit infection. Systemic care: glucocorticoids (prednisone). These agents have anti-inflammatory properties and cause metabolic effects. In addition, these agents modify the body's immune response to diverse stimuli. Immunosuppressives agents (Cyclosporine, Azathioprine, Mycophenolate, Cyclophosphamide, Tacrolimus, Chlorambucil) have immunomodulatory effects. These agents are used to improve the clinical and immunologic aspects of the disease. They may decrease autoantibody production and increase solubilization and removal of immune complexes. Immunomodulators (Thalidomide, Clofazimine).
Sweet's syndrome (SW) Disease Sweet's syndrome (acute febrile neutrophilic dermatosis) is characterized by physical features, and pathologic findings which include fever, neutrophilia, tender erythematous skin lesions (papules, nodules, and plaques), and a diffuse infiltrate consisting predominantly of mature neutrophils that are typically located in the upper dermis. Sweet's syndrome presents in three clinical settings: Classical Sweet's syndrome (CSS) usually presents in women between the age of 30 to 50 years, it is often preceded by an upper respiratory tract infection and may be associated with inflammatory bowel disease and pregnancy. The malignancy-associated Sweet's syndrome (MASS) can occur as a paraneoplastic syndrome in patients with
an established cancer or individuals whose Sweet's syndrome-related hematologic dyscrasia or solid tumor was previously undiscovered; MASS is most commonly related to acute myelogenous leukemia. The dermatosis can precede, follow, or appear concurrent with the diagnosis of the patient's cancer. Drug-induced Sweet's syndrome (DISS) most commonly occurs in patients who have been treated with granulocyte-colony stimulating factor, however, other medications may also be associated with DISS.
Prognosis The pathogenesis of Sweet's syndrome may be multifactorial and still remains to be definitively established. Systemic corticosteroids are the therapeutic gold standard for Sweet's syndrome. Horio et al. originally described the dramatic improvement in patients with Sweet's syndrome who were treated with potassium iodide in 1980. He confirmed his earlier observations with a larger study in 1983. Subsequently, several other investigators have also observed similar improvement when using potassium iodide to treat patients with Sweet's syndrome. Vasculitis and hypothyroidism are potential drug-induced side effects of potassium iodide. Other agents are: colchicine, indomethacin, clofazimine, cyclosporin, dapsone.
References Horio T, Imamura S, Danno K, Furukawa F, Ofuji S. Treatment of acute febrile neutrophilic dermatosis (Sweet's Syndrome) with potassium iodide. Dermatologica. 1980;160(5):341-7
Yi TL, Cleveland JL, Ihle JN. Protein tyrosine phosphatase containing SH2 domains: characterization, preferential expression in hematopoietic cells, and localization to human chromosome 12p12-p13. Mol Cell Biol. 1992 Feb;12(2):836-46
Tsui HW, Siminovitch KA, de Souza L, Tsui FW. Motheaten and viable motheaten mice have mutations in the haematopoietic cell phosphatase gene. Nat Genet. 1993 Jun;4(2):124-9
Banville D, Stocco R, Shen SH. Human protein tyrosine phosphatase 1C (PTPN6) gene structure: alternate promoter usage and exon skipping generate multiple transcripts. Genomics. 1995 May 1;27(1):165-73
Yang J, Liang X, Niu T, Meng W, Zhao Z, Zhou GW. Crystal structure of the catalytic domain of protein-tyrosine phosphatase SHP-1. J Biol Chem. 1998 Oct 23;273(43):28199-207
Beghini A, Ripamonti CB, Peterlongo P, Roversi G, Cairoli R, Morra E, Larizza L. RNA hyperediting and alternative splicing of hematopoietic cell phosphatase (PTPN6) gene in acute myeloid leukemia. Hum Mol Genet. 2000 Sep 22;9(15):2297-304
Zhang J, Somani AK, Siminovitch KA. Roles of the SHP-1 tyrosine phosphatase in the negative regulation of cell signalling. Semin Immunol. 2000 Aug;12(4):361-78
Wu C, Sun M, Liu L, Zhou GW. The function of the protein tyrosine phosphatase SHP-1 in cancer. Gene. 2003 Mar 13;306:1-12
Sapienza MS, Cohen S, Dimarino AJ. Treatment of pyoderma gangrenosum with infliximab in Crohn's disease. Dig Dis Sci. 2004 Sep;49(9):1454-7

PTPN6 (protein tyrosine phosphatase, non-receptor type 6) Beghini A, Lazzaroni F
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 332
Nagaishi T, Pao L, Lin SH, Iijima H, Kaser A, Qiao SW, Chen Z, Glickman J, Najjar SM, Nakajima A, Neel BG, Blumberg RS. SHP1 phosphatase-dependent T cell inhibition by CEACAM1 adhesion molecule isoforms. Immunity. 2006 Nov;25(5):769-81
Amin HM, Hoshino K, Yang H, Lin Q, Lai R, Garcia-Manero G. Decreased expression level of SH2 domain-containing protein tyrosine phosphatase-1 (Shp1) is associated with progression of chronic myeloid leukaemia. J Pathol. 2007 Aug;212(4):402-10
Cohen PR. Sweet's syndrome--a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007 Jul 26;2:34
Wlodarski P, Zhang Q, Liu X, Kasprzycka M, Marzec M, Wasik MA. PU.1 activates transcription of SHP-1 gene in hematopoietic cells. J Biol Chem. 2007 Mar 2;282(9):6316-23
Gallo A, Galardi S. A-to-I RNA editing and cancer: from pathology to basic science. RNA Biol. 2008 Jul-Sep;5(3):135-9
Gilfillan AM, Rivera J. The tyrosine kinase network regulating mast cell activation. Immunol Rev. 2009 Mar;228(1):149-69
Iype T, Sankarshanan M, Mauldin IS, Mullins DW, Lorenz U. The protein tyrosine phosphatase SHP-1 modulates the suppressive activity of regulatory T cells. J Immunol. 2010 Nov 15;185(10):6115-27
Nouvion AL, Oubaha M, Leblanc S, Davis EC, Jastrow H, Kammerer R, Breton V, Turbide C, Ergun S, Gratton JP, Beauchemin N. CEACAM1: a key regulator of vascular permeability. J Cell Sci. 2010 Dec 15;123(Pt 24):4221-30
Xiao W, Ando T, Wang HY, Kawakami Y, Kawakami T. Lyn- and PLC-beta3-dependent regulation of SHP-1 phosphorylation controls Stat5 activity and myelomonocytic leukemia-like disease. Blood. 2010 Dec 23;116(26):6003-13
Croker BA, Lewis RS, Babon JJ, Mintern JD, Jenne DE, Metcalf D, Zhang JG, Cengia LH, O'Donnell JA, Roberts AW. Neutrophils require SHP1 to regulate IL-1β production and prevent inflammatory skin disease. J Immunol. 2011 Jan 15;186(2):1131-9
Lodeiro M, Alén BO, Mosteiro CS, Beiroa D, Nogueiras R, Theodoropoulou M, Pardo M, Gallego R, Pazos Y, Casanueva FF, Camiña JP. The SHP-1 protein tyrosine phosphatase negatively modulates Akt signaling in the ghrelin/GHSR1a system. Mol Biol Cell. 2011 Nov;22(21):4182-91
Nesterovitch AB, Gyorfy Z, Hoffman MD, Moore EC, Elbuluk N, Tryniszewska B, Rauch TA, Simon M, Kang S, Fisher GJ, Mikecz K, Tharp MD, Glant TT. Alteration in the gene encoding protein tyrosine phosphatase nonreceptor type 6 (PTPN6/SHP1) may contribute to neutrophilic dermatoses. Am J Pathol. 2011 Apr;178(4):1434-41
Galeano F, Tomaselli S, Locatelli F, Gallo A. A-to-I RNA editing: the "ADAR" side of human cancer. Semin Cell Dev Biol. 2012 May;23(3):244-50
This article should be referenced as such:
Beghini A, Lazzaroni F. PTPN6 (protein tyrosine phosphatase, non-receptor type 6). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):327-332.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 333
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
HACE1 (HECT domain and ankyrin repeat containing E3 ubiquitin protein ligase 1) Feng Cui, Yanzhuang Wang
Department of Molecular, Cellular and Developmental Biology, University of Michigan, Ann Arbor, MI 48109-1048, USA (FC, YW)
Published in Atlas Database: December 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/HACE1ID44285ch6q16.html DOI: 10.4267/2042/49701
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity HGNC (Hugo): HACE1
Location: 6q16.3
DNA/RNA Note HACE1 was first cloned by sequencing clones obtained from a fetal brain cDNA library, and was designated as KIAA1320 (Nagase et al., 2000). The cDNA encodes a 909 amino acid protein (GenBank: NM_020771.3).
Description The HACE1 gene is located on chromosome 6 (105175968-105307794); 24 exons.
Protein Description Human HACE1 encodes HACE1 protein, which containing 909 amino acid residues (size ~103 kDa) (Anglesio et al., 2004). HACE1 possesses six N-
terminal ankyrin repeats (amino acid: 64-93; 97-126; 130-159; 163-192; 196-227; 228-257) and a C-terminal HECT domain (amino acid: 572-909; active cysteine residue at position 876).
Expression Anglesio et al. showed that a 4,6-kb transcript of HACE1 with strong expression in heart, brain, placenta, pancreas, as well as adult and fetal kidney. HACE1 expression is virtually undetectable in the SK-NEP-1 Wilms' tumor cell line and in four of five additional primary Wilms' tumor cases compared with patient-matched normal kidney (Anglesio et al., 2004). Zhang et al. showed that HACE1 mRNA transcripts are ubiquitously expressed in normal human tissues; but the mRNA expression of HACE1 decreases markedly in breast, renal, thyroid, vulva and liver tumors compared to the organ-matched normal tissue samples from the same individuals. The transcripts are downregulated in almost all lines from the NCI-60 panel of human cancer cell lines compared to control HEK293 cells.
Schematic structure of the HACE1 protein. HACE1 contains six ankyrin repeats at the N terminus and a HECT domain at the C terminus. A cysteine residue essential for the ubiquitin ligase activity is at position 876.

HACE1 (HECT domain and ankyrin repeat containing E3 ubiquitin protein ligase 1) Cui F, Wang Y
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 334
Lower expression is strongly associated with hypermethylation of two CpG islands located upstream of the HACE1 locus (Zhang et al., 2007). HACE1 is also downregulated in natural killer/T-cell lymphoma of the nasal type (NKTCL) (Huang et al., 2010), colorectal cancer (Hibi et al., 2008) and gastric cancer (Sakata et al., 2009). However, the expression of HACE1 varies in different breast cancer cell lines (Kao et al., 2009). In neuroblastomas, low HACE1 expression is associated with worse overall survival, suggesting that HACE1 may function as a tumor suppressor (Diskin et al., 2012).
Localisation Anglesio et al. indicated that the subcellular localization of HACE1 is predominantly in the endoplasmic reticulum (ER) and cytosol, and a small amount of endogenous protein is also present in other fractions of NIH3T3 cells (Anglesio et al., 2004). Tang et al. showed that a fraction of HACE1 colocalizes with Golgi markers in HeLa and normal rat kidney (NRK) cells; the association of HACE1 with Golgi membranes is through interaction with Golgi Rab GTPases, in particular Rab1 (Tang et al., 2011).
Function Tumor suppressor Anglesio et al. showed that HACE1 possesses intrinsic ubiquitin ligase activity, utilizing UBCH7 as a candidate partner E2 enzyme (Anglesio et al., 2004). Zhang et al. demonstrated that HACE1 is frequently downregulated in human tumors and maps to a region of chromosome 6q21 implicated in multiple human cancers. Genetic inactivation of HACE1 in mice resulted in the development of spontaneous, late-onset cancer. Their data suggested that HACE1 is involved in phosphorylation dependent degradation of cyclin D1, indicating a role for HACE1 in inhibiting cell cycle progression (Zhang et al., 2007). HACE1 deficient mice are spontaneously prone to developing multiple malignant tumors in various organs (Zhang et al., 2007). Degradation of Rac1 In 2011, Torrino et al. reported that HACE1 binds preferentially GTP-bound Rac1 and catalyzes its polyubiquitination. HACE1 expression increases the ubiquitination of Rac1 when the GTPase is activated. HACE1 is required for cytotoxic necrosis factor 1 (CNSF1)-mediated depletion of Rac1 and efficient invasion of endothelial cell monolayer by bacteria, suggesting that HACE1 plays a major role in host defense against pathogens (Torrino et al., 2011). Castillo-Lluva et al. further showed that HACE1 catalyzes polyubiquitination of Rac1 at lysine 147 following its activation by a migration stimulus, such as hepatocyte growth factor (HGF), resulting in Rac1 degradation by the proteasome. HACE1-depletion is accompanied by an increased total Rac1 level and accumulation of Rac1 in membrane ruffles.
Furthermore, HACE1-depletion leads to enhanced cell migration, which may be significant for malignant conversion (Castillo-Lluva et al., 2012). Golgi biogenesis Tang et al. reported that HACE1 is targeted to the Golgi membrane through interactions with Rab proteins. The ubiquitin ligase activity of HACE1 in mitotic Golgi disassembly is required for subsequent post-mitotic Golgi membrane fusion. Depletion of HACE1 using small hairpin RNAs or expression of an inactive HACE1 mutant protein in cells impairs post-mitotic Golgi membrane fusion. The identification of HACE1 as a Golgi-localized ubiquitin ligase provides evidence that ubiquitin has a critical role in Golgi biogenesis during the cell cycle (Tang et al., 2011). Repression of the RAR (retinoic acid receptor)-regulated transcription HACE1 was isolated as a RARβ3 AB region interacting protein. HACE1 functionally represses the transcriptional activity of RARα1 and RARβ isoforms 1, 2 and 3, but not RARγ1 in luciferase reporter assays. In addition, HACE1 represses several endogenous RAR-regulated genes. The E3 ubiquitin ligase activity is not required for the repression effect of HACE1 on the transcriptional activity of RARβ3. HACE1 also inhibits the retinoic acid-dependent degradation of RARβ3. The repression of RAR-regulated transcription by HACE1 is possibly due to its ability to inhibit RA-induced degradation of RARs (Zhao et al., 2009). Determinant of the equol-producing phenotype HACE1 was identified in a genome-wide association study (GWAS) designed to find genetic factors associated with the equol-producing phenotype in Korean population. The authors identified 5 single-nucleotide polymorphisms in HACE1. Individuals with a minor allele of the most significant SNP rs6927608 did not produce equol. The interaction between equol production and the rs6927608 HACE1 SNP was significantly associated with systolic blood pressure. Finally, the authors concluded that equol production is linked to blood pressure, and HACE1 might be a determinant of the equol-producing phenotype (Hong et al., 2012).
Homology The HACE1 gene is conserved in chimpanzee, dog, cow, mouse, rat, chicken, and zebrafish.
Implicated in Sporadic Wilms' tumor Note In 2004, Anglesio et al. analyzed the chromosome 6q21 breakpoint of a non-constitutional t(6;15)(q21;q21) rearrangement in sporadic Wilms' tumor. They showed that although the HACE1 locus was not directly interrupted by the translocation in the index Wilms' case, its expression was markedly lower in tumor

HACE1 (HECT domain and ankyrin repeat containing E3 ubiquitin protein ligase 1) Cui F, Wang Y
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 335
tissues compared with adjacent normal kidney. Moreover, HACE1 expression is virtually undetectable in the SK-NEP-1 Wilms' tumor cell line and in four of five additional primary Wilms' tumor cases compared with patient-matched normal kidney. Their data implicated that low expression of HACE1 was associated with sporadic Wilms' tumor (Anglesio et al., 2004). In 2010, Slade et al. indentified a t(5;6)(q21;q21) translocation in a child with bilateral, young-onset Wilms' tumor. The 6q21 breakpoint transects and truncates HACE1, which has been implicated as a somatically inactivated target in Wilms tumorigenesis. To evaluate the contribution of HACE1 to Wilms' tumor predisposition, the gene was screened in 450 individuals with Wilms' tumor. One child with unilateral Wilms' tumor and a truncated HACE1 mutation was identified. It was concluded that constitutional disruption of HACE1 likely predisposes Wilms' tumor. However, HACE1 mutations are rare and therefore can only make a small contribution to Wilms' tumor incidence (Slade et al., 2010).
Lymphoma Note HACE1 is downregulated in natural killer/T-cell lymphoma of the nasal type (NKTCL) in both gene expression profiling and array-base comparative genomic hybridization analyses. Since HACE1 is the target of epigenetic inactivation in Wilms' tumor and has been proposed as a tumor suppressor gene in multiple human cancers, it is tempting to speculate that HACE1 might be involved in the pathogenesis of NKTCL (Huang et al., 2010).
Colorectal carcinomas and gastric cancer Note The methylation status of the HACE1 gene was examined in primary carcinomas and the corresponding normal tissues derived from 32 patients with colorectal cancer using quantitative methylation-specific PCR (qMSP), and the correlation between the methylation status and the clinic pathological findings was evaluated. The aberrant methylation of HACE1 was frequently observed in colorectal cancer. Thus HACE1 might act as a tumor suppressor in colorectal carcinomas and HACE1 methylation might present a malignant potential in colorectal cancer (Hibi et al., 2008). Similar research was performed in primary gastric carcinomas, and HACE1 was found frequently methylated in gastric carcinoma derived from male patients (Sakata et al., 2009).
Breast cancer Note Kao et al. utilized the whole-genome DNA microarrays to profile gene expression and DNA copy number alterations (CANs) in a collection of 52 widely used
breast cancer cell lines, and comparisons were made to existing profiles of primary breast tumors. The expression level of HACE1 varies between different breast cancer cell lines. The contribution of HACE1 breast cancer biogenesis is still unclear (Kao et al., 2009).
Neuroblastomas Note In a genome-wide association study of 2817 neuroblastoma cases and 7473 controls, HACE1 and LIN28B were identified as two new associations at 6q16. Low HACE1 and high LIN28B expression in diagnostic primary neuroblastomas are associated with worse overall survival. These data suggested that HACE1 might function as a tumor suppressor and LIN28B as an oncogene in advanced neuroblastomas (Diskin et al., 2012).
References Nagase T, Kikuno R, Ishikawa KI, Hirosawa M, Ohara O. Prediction of the coding sequences of unidentified human genes. XVI. The complete sequences of 150 new cDNA clones from brain which code for large proteins in vitro. DNA Res. 2000 Feb 28;7(1):65-73
Anglesio MS, Evdokimova V, Melnyk N, Zhang L, Fernandez CV, Grundy PE, Leach S, Marra MA, Brooks-Wilson AR, Penninger J, Sorensen PH. Differential expression of a novel ankyrin containing E3 ubiquitin-protein ligase, Hace1, in sporadic Wilms' tumor versus normal kidney. Hum Mol Genet. 2004 Sep 15;13(18):2061-74
Zhang L, Anglesio MS, O'Sullivan M, Zhang F, Yang G, Sarao R, Mai PN, Cronin S, Hara H, Melnyk N, Li L, Wada T, Liu PP, Farrar J, Arceci RJ, Sorensen PH, Penninger JM. The E3 ligase HACE1 is a critical chromosome 6q21 tumor suppressor involved in multiple cancers. Nat Med. 2007 Sep;13(9):1060-9
Hibi K, Sakata M, Sakuraba K, Shirahata A, Goto T, Mizukami H, Saito M, Ishibashi K, Kigawa G, Nemoto H, Sanada Y. Aberrant methylation of the HACE1 gene is frequently detected in advanced colorectal cancer. Anticancer Res. 2008 May-Jun;28(3A):1581-4
Kao J, Salari K, Bocanegra M, Choi YL, Girard L, Gandhi J, Kwei KA, Hernandez-Boussard T, Wang P, Gazdar AF, Minna JD, Pollack JR. Molecular profiling of breast cancer cell lines defines relevant tumor models and provides a resource for cancer gene discovery. PLoS One. 2009 Jul 3;4(7):e6146
Sakata M, Kitamura YH, Sakuraba K, Goto T, Mizukami H, Saito M, Ishibashi K, Kigawa G, Nemoto H, Sanada Y, Hibi K. Methylation of HACE1 in gastric carcinoma. Anticancer Res. 2009 Jun;29(6):2231-3
Zhao J, Zhang Z, Vucetic Z, Soprano KJ, Soprano DR. HACE1: A novel repressor of RAR transcriptional activity. J Cell Biochem. 2009 Jun 1;107(3):482-93
Huang Y, de Reyniès A, de Leval L, Ghazi B, Martin-Garcia N, Travert M, Bosq J, Brière J, Petit B, Thomas E, Coppo P, Marafioti T, Emile JF, Delfau-Larue MH, Schmitt C, Gaulard P. Gene expression profiling identifies emerging oncogenic pathways operating in extranodal NK/T-cell lymphoma, nasal type. Blood. 2010 Feb 11;115(6):1226-37
Slade I, Stephens P, Douglas J, Barker K, Stebbings L, Abbaszadeh F, Pritchard-Jones K, Cole R, Pizer B, Stiller C,

HACE1 (HECT domain and ankyrin repeat containing E3 ubiquitin protein ligase 1) Cui F, Wang Y
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 336
Vujanic G, Scott RH, Stratton MR, Rahman N. Constitutional translocation breakpoint mapping by genome-wide paired-end sequencing identifies HACE1 as a putative Wilms tumour susceptibility gene. J Med Genet. 2010 May;47(5):342-7
Tang D, Xiang Y, De Renzis S, Rink J, Zheng G, Zerial M, Wang Y. The ubiquitin ligase HACE1 regulates Golgi membrane dynamics during the cell cycle. Nat Commun. 2011 Oct 11;2:501
Torrino S, Visvikis O, Doye A, Boyer L, Stefani C, Munro P, Bertoglio J, Gacon G, Mettouchi A, Lemichez E. The E3 ubiquitin-ligase HACE1 catalyzes the ubiquitylation of active Rac1. Dev Cell. 2011 Nov 15;21(5):959-65
Castillo-Lluva S, Tan CT, Daugaard M, Sorensen PH, Malliri A. The tumour suppressor HACE1 controls cell migration by regulating Rac1 degradation. Oncogene. 2012 May 21;
Diskin SJ, Capasso M, Schnepp RW, Cole KA, Attiyeh EF, Hou C, Diamond M, Carpenter EL, Winter C, Lee H, Jagannathan J, Latorre V, Iolascon A, Hakonarson H, Devoto M, Maris JM. Common variation at 6q16 within HACE1 and LIN28B influences susceptibility to neuroblastoma. Nat Genet. 2012 Oct;44(10):1126-30
Hong KW, Ko KP, Ahn Y, Kim CS, Park SJ, Park JK, Kim SS, Kim Y. Epidemiological profiles between equol producers and nonproducers: a genomewide association study of the equol-producing phenotype. Genes Nutr. 2012 Oct;7(4):567-74
This article should be referenced as such:
Cui F, Wang Y. HACE1 (HECT domain and ankyrin repeat containing E3 ubiquitin protein ligase 1). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):333-336.

Gene Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 337
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
MIR146B (microRNA 146b) Amandine Garcia, Sylvie Mazoyer
CNRS UMR5286 Inserm U1052, Universite Lyon 1, Cancer Research Centre of Lyon, Centre Leon Berard, Lyon, France (AG, SM)
Published in Atlas Database: December 2012
Online updated version : http://AtlasGeneticsOncology.org/Genes/MIR146BID50855ch10q24.html DOI: 10.4267/2042/49702
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: MIRN146B, miRNA146B
HGNC (Hugo): MIR146B
Location: 10q24.32
Local order: Based on Mapviewer, gene flanking MIR146B oriented from centromere to telomere on 10q24.32 are: - NFKB2: Nuclear factor of kappa light polypeptide gene enhancer in B-cell 2 - PSD: pleckstrin and Sec7 domain containing - FBXL15: F-box and leucine-rich repeat protein 15 - CUEDC2: CUE domain containing 2 - MIR146B: microRNA 146b - LOC100505761: hypothetical LOC100505761 - TMEM180: transmembrane protein 180 - ACTR1A: ARP1 actin-related protein 1 homolog A
DNA/RNA Note The MIR146B gene is transcribed into a precursor that produces two mature microRNAs, miR-146b-5p and miR-146b-3p. These microRNAs belong to the miR-146 family, which comprises 2 other members, miR-146a-5p and miR-146a* (recently renamed miR-146a-3p) produced from a gene, MIR146A, localized on chromosome 5.
Description MIR146B is located in an intergenic region.
Transcription RNA Polymerase II is suggested to be the most likely enzyme involved in microRNA transcription, leading to the production of a ~1000 nucleotide primary microRNA, in this case pri-miR-146b. The beginning and the end of the pri-miR-146b sequence are unknown. pre-miR-146b miRBase accession number: MI0003129. Length: 73 nucleotides. Sequence: 5'-CCUGGCACUGAGAACUGAAUUCCAUAGGCUGUGAGCUCUAGCAAUGCCCUGUGGACUCAGUUCUGGUGCCCGG-3' mature miR-146b-5p miRBase accession number: MIMAT0002809. Length: 22 nucleotides. Sequence: 5'-UGAGAACUGAAUUCCAUAGGCU-3' mature miR-146b-3p miRBase accession number: MIMAT0004766. Length: 22 nucleotides. Sequence: 5'-UGCCCUGUGGACUCAGUUCUGG-3'
Pseudogene No reported pseudogenes.

MIR146B (microRNA 146b) Garcia A, Mazoyer S
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 338
A. Homo sapiens stem-loop structure of pre-miR-146b. This figure represents the sequence and structure of the miR-146b precursor (pre-miR-146b). Two different mature miRNAs are produced from this precursor: miR-146b-5p (sequence in blue) and miR-146b-3p (sequence in pink). The orientations 5' to 3' are indicated by the direction of the arrows. B. The miR-146 family members. Identities between the sequences of miR-146a-5p and miR-146b-5p are shown in orange and those between the sequences of miR-146a-3p and miR-146b-3p are shown in green. MiR-146a-5p and miR-146b-5p differ by only two nucleotides located outside the seed region, while miR-146a-3p and miR-146b-3p are much more divergent, especially in the seed region.
Protein Note microRNAs aren't translated into amino acids.
Mutations Note The 1000 Genome project identified a SNV (single nucleotide variation) in one West African individual, a C>T variation at position 104196269 (according to hg19-Feb_2009) in the first nucleotide of pre-miR-146b. The minor allele frequency is 0.059 in 118 individual samples of a West Africa population. This variation is reported in the NCBI SNP database and referenced with the number rs76149940 (submission in March 2010).
Implicated in Breast cancer Prognosis mir-146b-5p along with other microRNAs may permit to differentiate breast tumour sub-types. However,
conflicting results have been obtained. One study, where miR-146b has been analysed in 167 breast cancer cases, showed an elevated expression in triple negative breast tumours. This study comprised analyses of several different tumour mammary cell lines and miR-146b-5p was found to be the most expressed in basal-like tumour cell lines (Garcia et al., 2011). A second study, based on 20 samples only, identified specific expression of a set of seven microRNAs (including miR-146b-5p) in normal basal cells but not in basal-like breast cancers, which are close to triple negative breast cancers. miR-146b-5p may have an elevated expression in malignant myoepithelioma of the breast (Bockmeyer et al., 2011).
Oncogenesis Two studies described a biological role for miR-146b in breast tumour progression. The BRMS1 (Breast cancer Metastasis Suppressor 1) protein up-regulated the expression of miR-146b in MDA-MB-435, a tumour mammary cell line. Moreover, the overexpression of this microRNA down-regulated the expression of EGFR (Epidermal Growth Factor Receptor) in another tumour cell line, MDA-MB-231. This study showed an impact, in vitro, of

MIR146B (microRNA 146b) Garcia A, Mazoyer S
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 339
miR-146b on invasion and migration of cells and on the suppression of metastasis (Bockmeyer et al., 2011). The second study depicted a direct target of miR-146b-5p, BRCA1 (BReast CAncer 1), one of the two major breast cancer predisposition genes. The binding of miR-146-5p to the BRCA1 3'UTR decreased the expression of BRCA1, induced cellular proliferation and reduced the homologous recombination rate. miR-146b seemed to have an important role in tumour progression via BRCA1 (Garcia et al., 2011).
Thyroid cancer Disease Three studies showed that miR-146b, along with a set of other microRNAs, are overexpressed in tumours versus hyperplasic nodules or versus uncertain malignant potential tumours (Nikiforova et al., 2008; Lassalle et al., 2011; Chen et al., 2008). miR-146b is consistently overexpressed in both papillary and follicular thyroid carcinomas (Chen et al., 2008) and is associated with extrathyroidal invasion (Chou et al., 2010) and with aggressive papillary thyroid carcinoma (Yip et al., 2011). Of note, in these two studies, miR-146b overexpression seems correlated with BRAF mutations.
Prognosis The expression of miR-146b and of a set of six other microRNAs was able to predict malignancy of thyroid fine needle aspiration specimens (Shen et al., 2012; Agretti et al., 2012).
Oncogenesis In thyroid follicular cells, miR-146b-5p was shown to bind directly the 3'UTR of SMAD4, an important member of the TGF-β signalling pathway. This modulation of the TGF-β signal confirmed the oncogenic role of miR-146b-5p in thyroid cancers (Geraldo et al., 2012).
Lung cancer Prognosis A microarray analysis of 61 squamous cell carcinoma samples versus 10 normal lung samples showed that miR-146b had the strongest prediction accuracy for stratifying Non-Small Cell Lung Cancer (NSCLC) in prognostic groups (Raponi et al., 2009). Another study completed this observation and found a significant reduction of a set of seven microRNAs (including miR-146b) in serum of NSCLC patients (Heegaard et al., 2012).
Oncogenesis A study analysed the effect of miR-146b overexpression in A549 lung cancer cells. A 3-8-fold increase in the expression of pre-miR-146b did not alter the major cellular functions classically involved in oncogenesis, such as proliferation, migration or invasiveness. This overexpression only impacted the
ability to form colonies, perhaps because miR-146b-5p and miR-146b-3p may have opposing effects (Patnaik et al., 2011).
Other cancers Note (like prostate, pancreas, kidney, colorectal)
Disease microRNA profiling by microarrays has shown that miR-146b is overexpressed in many cancer types, such as glioma (Xia et al., 2009), melanoma (Jukic et al., 2010), oesophageal cancer (Zhao et al., 2012), bladder cancer (Pignot et al., 2012), colorectal cancer (Ragusa et al., 2010) or oral cancers (Scapoli et al., 2010). miR-146b seems to be also overexpressed in some prostate and colorectal cancers (Kanaan et al., 2012).
Immunity Note Innate immunity and inflammation play an important role in cancer development and it is therefore noteworthy to mention that the miR-146 family is involved in these mechanisms of cell protection. Even if more evidence has been gathered in the case of the former, both miR-146a and miR-146b control Toll-like receptor and cytokine signaling pathways. miR-146b is predicted to bind the 3'UTR of the IL-1 receptor-associated kinase 1 and TNF receptor-associated factor 6 transcripts. The expression of MIR146B is regulated by NF-κB (Taganov et al., 2006).
References Taganov KD, Boldin MP, Chang KJ, Baltimore D. NF-kappaB-dependent induction of microRNA miR-146, an inhibitor targeted to signaling proteins of innate immune responses. Proc Natl Acad Sci U S A. 2006 Aug 15;103(33):12481-6
Chen YT, Kitabayashi N, Zhou XK, Fahey TJ 3rd, Scognamiglio T. MicroRNA analysis as a potential diagnostic tool for papillary thyroid carcinoma. Mod Pathol. 2008 Sep;21(9):1139-46
Nikiforova MN, Tseng GC, Steward D, Diorio D, Nikiforov YE. MicroRNA expression profiling of thyroid tumors: biological significance and diagnostic utility. J Clin Endocrinol Metab. 2008 May;93(5):1600-8
Raponi M, Dossey L, Jatkoe T, Wu X, Chen G, Fan H, Beer DG. MicroRNA classifiers for predicting prognosis of squamous cell lung cancer. Cancer Res. 2009 Jul 15;69(14):5776-83
Xia H, Qi Y, Ng SS, Chen X, Li D, Chen S, Ge R, Jiang S, Li G, Chen Y, He ML, Kung HF, Lai L, Lin MC. microRNA-146b inhibits glioma cell migration and invasion by targeting MMPs. Brain Res. 2009 May 7;1269:158-65
Chou CK, Chen RF, Chou FF, Chang HW, Chen YJ, Lee YF, Yang KD, Cheng JT, Huang CC, Liu RT. miR-146b is highly expressed in adult papillary thyroid carcinomas with high risk features including extrathyroidal invasion and the BRAF(V600E) mutation. Thyroid. 2010 May;20(5):489-94
Jukic DM, Rao UN, Kelly L, Skaf JS, Drogowski LM, Kirkwood JM, Panelli MC. Microrna profiling analysis of differences between the melanoma of young adults and older adults. J Transl Med. 2010 Mar 19;8:27

MIR146B (microRNA 146b) Garcia A, Mazoyer S
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 340
Ragusa M, Majorana A, Statello L, Maugeri M, Salito L, Barbagallo D, Guglielmino MR, Duro LR, Angelica R, Caltabiano R, Biondi A, Di Vita M, Privitera G, Scalia M, Cappellani A, Vasquez E, Lanzafame S, Basile F, Di Pietro C, Purrello M. Specific alterations of microRNA transcriptome and global network structure in colorectal carcinoma after cetuximab treatment. Mol Cancer Ther. 2010 Dec;9(12):3396-409
Scapoli L, Palmieri A, Lo Muzio L, Pezzetti F, Rubini C, Girardi A, Farinella F, Mazzotta M, Carinci F. MicroRNA expression profiling of oral carcinoma identifies new markers of tumor progression. Int J Immunopathol Pharmacol. 2010 Oct-Dec;23(4):1229-34
Bockmeyer CL, Christgen M, Müller M, Fischer S, Ahrens P, Länger F, Kreipe H, Lehmann U. MicroRNA profiles of healthy basal and luminal mammary epithelial cells are distinct and reflected in different breast cancer subtypes. Breast Cancer Res Treat. 2011 Dec;130(3):735-45
Garcia AI, Buisson M, Bertrand P, Rimokh R, Rouleau E, Lopez BS, Lidereau R, Mikaélian I, Mazoyer S. Down-regulation of BRCA1 expression by miR-146a and miR-146b-5p in triple negative sporadic breast cancers. EMBO Mol Med. 2011 May;3(5):279-90
Lassalle S, Hofman V, Ilie M, Bonnetaud C, Puisségur MP, Brest P, Loubatier C, Guevara N, Bordone O, Cardinaud B, Lebrigand K, Rios G, Santini J, Franc B, Mari B, Al Ghuzlan A, Vielh P, Barbry P, Hofman P. Can the microRNA signature distinguish between thyroid tumors of uncertain malignant potential and other well-differentiated tumors of the thyroid gland? Endocr Relat Cancer. 2011 Oct;18(5):579-94
Patnaik SK, Kannisto E, Mallick R, Yendamuri S. Overexpression of the lung cancer-prognostic miR-146b microRNAs has a minimal and negative effect on the malignant phenotype of A549 lung cancer cells. PLoS One. 2011;6(7):e22379
Yip L, Kelly L, Shuai Y, Armstrong MJ, Nikiforov YE, Carty SE, Nikiforova MN. MicroRNA signature distinguishes the degree of aggressiveness of papillary thyroid carcinoma. Ann Surg Oncol. 2011 Jul;18(7):2035-41
Agretti P, Ferrarini E, Rago T, Candelieri A, De Marco G, Dimida A, Niccolai F, Molinaro A, Di Coscio G, Pinchera A, Vitti
P, Tonacchera M. MicroRNA expression profile helps to distinguish benign nodules from papillary thyroid carcinomas starting from cells of fine-needle aspiration. Eur J Endocrinol. 2012 Sep;167(3):393-400
Geraldo MV, Yamashita AS, Kimura ET. MicroRNA miR-146b-5p regulates signal transduction of TGF-β by repressing SMAD4 in thyroid cancer. Oncogene. 2012 Apr 12;31(15):1910-22
Heegaard NH, Schetter AJ, Welsh JA, Yoneda M, Bowman ED, Harris CC. Circulating micro-RNA expression profiles in early stage nonsmall cell lung cancer. Int J Cancer. 2012 Mar 15;130(6):1378-86
Kanaan Z, Rai SN, Eichenberger MR, Barnes C, Dworkin AM, Weller C, Cohen E, Roberts H, Keskey B, Petras RE, Crawford NP, Galandiuk S. Differential microRNA expression tracks neoplastic progression in inflammatory bowel disease-associated colorectal cancer. Hum Mutat. 2012 Mar;33(3):551-60
Pignot G, Cizeron-Clairac G, Vacher S, Susini A, Tozlu S, Vieillefond A, Zerbib M, Lidereau R, Debre B, Amsellem-Ouazana D, Bieche I. microRNA expression profile in a large series of bladder tumors: Identification of a 3-miRNA signature associated with aggressiveness of muscle-invasive bladder cancer. Int J Cancer. 2012 Nov 20;
Shen R, Liyanarachchi S, Li W, Wakely PE Jr, Saji M, Huang J, Nagy R, Farrell T, Ringel MD, de la Chapelle A, Kloos RT, He H. MicroRNA signature in thyroid fine needle aspiration cytology applied to "atypia of undetermined significance" cases. Thyroid. 2012 Jan;22(1):9-16
Zhao Y, Schetter AJ, Yang GB, Nguyen G, Mathé EA, Li P, Cai H, Yu L, Liu F, Hang D, Yang H, Wang XW, Ke Y, Harris CC. microRNA and inflammatory gene expression as prognostic marker for overall survival in esophageal squamous cell carcinoma. Int J Cancer. 2012 Nov 23;
This article should be referenced as such:
Garcia A, Mazoyer S. MIR146B (microRNA 146b). Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):337-340.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 341
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
t(20;21)(q13.2;q22.12) ZFP64/RUNX1 Nathalie Douet-Guilbert, Etienne De Braekeleer, Audrey Basinko, Marie-Josée Le Bris, Frédéric Morel, Marc De Braekeleer
Cytogenetics Laboratory, Faculty of Medicine, University of Brest, France (NDG, ED, AB, MJL, FM, MD)
Published in Atlas Database: December 2012
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t2021q13q22ID1590.html DOI: 10.4267/2042/49703
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Chronic myelomonocytic leukemia (CMML)
Epidemiology This is a rare chromosomal rearrangement, only reported twice in myeloid hemopathies, without molecular characterization but for the case reported by Richkind et al. (2000) who showed rearrangement of RUNX1 (Secker-Walker et al., 1995; Richkind et al., 2000).
Clinics A 91-year old woman seen for fever and thrombopenia.
Cytogenetics Note The t(20;21)(q13.2;q22.12) involves the RUNX1 (alias AML1) gene that acts as an activator or repressor of target gene expression depending upon the large number of transcription factors, coactivators and corepressors that interact with it. RUNX1 functions as an organizing protein that facilitates assembly of transcriptional activation or repression complexes. All the translocations that retain Runt homology
domain but remove the transcription activation domain have a leukemogenic effect by acting as dominant negative inhibitors of wild-type RUNX1 in transcription activation (De Braekeleer et al., 2011).
RHG banding showing chromosomes 20 and 21 and the derivatives der(20) and der(21).
Cytogenetics morphological t(20;21)(q13.2;q22.12) identified by FISH in a clone having a trisomy 8 (cryptic rearrangement).
Cytogenetics molecular FISH showed that the breakpoint on 21q22 was located in RUNX1. To confirm the position of the breakpoint on chromosome 20, BACs located at 20q13 were used as probes in FISH experiments. Analysis with RP11-184L6 showed that one signal hybridized to the normal chromosome 20, and the other splitted and hybridized to both der(20) and der(21). Co-hybridization with the RP11-184L6 clone and a RUNX1 probe (RP11-77G18) showed two fusion signals. RP11-184L6 contains the ZFP64 gene.

t(20;21)(q13.2;q22.12) ZFP64/RUNX1 Douet-Guilbert N, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 342
FISH with BACs RP11-77G18 (spectrum green, located in 21q22.12 and containing RUNX1) and RP11-184L6 (spectrum orange, located in 20q13.2 and containing ZFP64) showing co-hybridization of both derivative chromosomes.
Genes involved and proteins RUNX1 Location 21q22.12
Note RUNX1 belongs to a family of genes that share a 128 amino acid region of high sequence homology, known as the 'Runt domain', first identified in the Drosophila runt gene. This 'Runt homology domain' is responsible for heterodimerization with the core-binding factor-b (CBF-b or PEBP2b) to form a transcription factor and for DNA binding. RUNX1 acts as a key regulator of hematopoiesis through the regulation of various hematopoietic genes, including growth factors (GM-CSF, MPO and IL-3), surface receptors (TCRA, TCRB, M-CSF receptor and FLT3), signaling molecules (CDKN1A, BLK and BCL2) and transcription activators (STAT3 and MYB).
DNA/RNA The RUNX1 gene spans 260 kb and consists of 12 exons with two distinct promoters.
At least 12 different RUNX1 mRNAs differing in their types of 5' and 3' untranslated regions (UTRs) and their coding regions are generated.
Protein The RUNX1 protein contains a 'Runt homology domain' as well as transcription activation and inhibition domains. It acts as an activator or repressor of target gene expression depending upon the large number of transcription factors, coactivators and corepressors that interact with it. RUNX1 functions as an organizing protein that facilitates assembly of transcriptional activation or repression complexes. By recruitment of non-DNA binding proteins as p300/CBP and histone acetyltransferase, it contributes to the activation of transcription of target genes. Upon recruitment of non-DNA binding repressors such as mSin3A, Groucho/TLE and histone deacetylase, it represses transcription of target genes.
ZFP64 Location 20q13.2

t(20;21)(q13.2;q22.12) ZFP64/RUNX1 Douet-Guilbert N, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 343
DNA/RNA The ZFP64 gene contains 6 exons spanning 41 kb. Twelwe transcripts are known, of which 9 are protein coding.
Protein ZFP64 protein belongs to the krueppel C2H2-type zinc-finger protein family and contains 9 C2H2-type zinc fingers. It may be involved in transcriptional regulation. It interacts with the intracellular domain of Notch1, and acts as a coactivator of the Notch intracellular domain (Sakamoto et al., 2008).
References Secker-Walker LM, Mehta A, Bain B. Abnormalities of 3q21 and 3q26 in myeloid malignancy: a United Kingdom Cancer Cytogenetic Group study. Br J Haematol. 1995 Oct;91(2):490-501
Richkind K, Hromas R, Lytle C, Crenshaw D, Velasco J, Roherty S, Srinivasiah J, Varella-Garcia M. Identification of two new translocations that disrupt the AML1 gene. Cancer Genet Cytogenet. 2000 Oct 15;122(2):141-3
Sakamoto K, Tamamura Y, Katsube K, Yamaguchi A. Zfp64 participates in Notch signaling and regulates differentiation in mesenchymal cells. J Cell Sci. 2008 May 15;121(Pt 10):1613-23
De Braekeleer E, Douet-Guilbert N, Morel F, Le Bris MJ, Férec C, De Braekeleer M. RUNX1 translocations and fusion genes in malignant hemopathies. Future Oncol. 2011 Jan;7(1):77-91
This article should be referenced as such:
Douet-Guilbert N, De Braekeleer E, Basinko A, Le Bris MJ, Morel F, De Braekeleer M. t(20;21)(q13.2;q22.12) ZFP64/RUNX1. Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):341-343.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 344
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
t(2;19)(p23;p13) TPM4/ALK Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH)
Published in Atlas Database: January 2013
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t0219p23p13ID1549.html DOI: 10.4267/2042/49704
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Anaplastic large cell lymphoma (ALCL)
Clinics Only one case to date, an 18-month-old boy with a null-ALCL (Meech et al., 2001).
Cytology Cells expressed both myeloid (CD13, CD33, HLA-DR) and natural killer (CD3-/CD56+, germline TCR genes, CD25+/CD122+/granzyme B+) cell antigens.
Evolution The patient was in remission 14 months after completion of therapy.
Cytogenetics Cytogenetics morphological To be noted is that an identical t(2;19)(p23;p13), also involving TPM4 and ALK, has been found in a case of inflammatory myofibroblastic tumor (Lawrence et al., 2000). A pre-B cell acute leukemia was described with a t(9;12)(q22;p13) and ETV6 rearrangement, and also a t(2;19)(p23;p13) (Pérez-Vera et al., 2005). It is likely that this translocation t(2;19)(p23;p13) is different at the molecular level.
Genes involved and proteins ALK Location 2p23.2
Protein 1620 amino acids; ALK is a membrane associated tyrosine kinase receptor of the insulin receptor superfamily.
TPM4 Location 19p13.12
Protein 248 amino acids; tropomyosins are actin-binding proteins; component of cytoskeletal microfilaments; role in the calcium dependent regulation of striated muscle.
Result of the chromosomal anomaly Hybrid gene Description 5'TPM4-3'ALK. Fusion between TPM4 nucleotide 714 and ALK nucleotide 4084.

t(2;19)(p23;p13) TPM4/ALK Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 345
References Lawrence B, Perez-Atayde A, Hibbard MK, Rubin BP, Dal Cin P, Pinkus JL, Pinkus GS, Xiao S, Yi ES, Fletcher CD, Fletcher JA. TPM3-ALK and TPM4-ALK oncogenes in inflammatory myofibroblastic tumors. Am J Pathol. 2000 Aug;157(2):377-84
Meech SJ, McGavran L, Odom LF, Liang X, Meltesen L, Gump J, Wei Q, Carlsen S, Hunger SP. Unusual childhood extramedullary hematologic malignancy with natural killer cell properties that contains tropomyosin 4--anaplastic lymphoma kinase gene fusion. Blood. 2001 Aug 15;98(4):1209-16
Pérez-Vera P, Montero-Ruiz O, Frías S, Ulloa-Avilés V, Cárdenas-Cardós R, Paredes-Aguilera R, Rivera-Luna R, Carnevale A. Detection of ETV6 and RUNX1 gene rearrangements using fluorescence in situ hybridization in Mexican patients with acute lymphoblastic leukemia: experience at a single institution. Cancer Genet Cytogenet. 2005 Oct 15;162(2):140-5
This article should be referenced as such:
Huret JL. t(2;19)(p23;p13) TPM4/ALK. Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):344-345.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 346
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
t(3;14)(q27;q32) HSP90AA1/BCL6 Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH)
Published in Atlas Database: January 2013
Online updated version : http://AtlasGeneticsOncology.org/Anomalies/t0314q27q32ID1356.html DOI: 10.4267/2042/49705
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Note Most of the t(3;14)(q27;q32) where molecular genetics studies were performed showed the involvement of IGH@ and BCL6. It is unknown if the prognoses are different.
Clinics and pathology Disease Non Hodgkin lymphoma
Clinics Four cases available to date: a case of primary gastric lymphoma (Xu et al., 2000); a gastric diffuse large B-cell lymphoma with residual MALT lymphoma (DLCLML) case (Chen et al., 2006), a case of primary central nervous system lymphoma (PCNSL, a diffuse large B cell lymphoma confined to the brain) (Montesinos-Rongen et al., 2003), and another lymphoma case (Akasaka et al., 2000).
Genes involved and proteins BCL6 Location 3q27.3
Protein 706 amino acids; composed of a NH2-term BTB/POZ domain (amino acids 1-130 (32-99 according to Swiss-Prot) which mediates homodimerization and protein-protein interactions with other corepressors (including HDAC1 and NCOR2/SMRT to constitute a large repressing complex, another transcription repression domain (191-386), PEST sequences (300-417) with a
KKYK motif (375-379), and six zinc finger at the C-term (518-541, 546-568, 574-596, 602-624, 630-652, 658-681), responsible for sequence specific DNA binding. Transcription repressor; recognizes the consensus sequence: TTCCT(A/C)GAA (Albagli-Curiel, 2003). Role in germinal centers of lymphoid follicles. BCL6 prevents ATM and TP53 to induce apoptosis in response to DNA rearrangements such as somatic hypermutation and class switch recombination. Therefore essential for normal B cell development.
HSP90AA1 Location 14q32.31
Protein HSP90AA1 is also known as HSP90. Molecular chaperone. Possesses an ATP binding site with intrinsic ATPase activity that regulates its conformation. Promotes the maturation, structural maintenance and regulation of specific target proteins called 'client' proteins. Maintains protein homeostasis. HSP90AA1/HSP90 interacts with regions of client proteins where protein folding clefts merge. Folding clefts are a general topological feature of proteins in native conformation, and many of these hydrophobic clefts, must open to permit access of ligands. HSP90AA1/HSP90 stabilizes the open cleft, impeding further unfolding and Hsp70-dependent ubiquitination (Pratt et al., 2010). HSP90AA1/HSP90 and its associated co-chaperones facilitate a precise and efficient working environment beneficial for telomere function (DeZwaan and Freeman, 2010). HSP90AA1/HSP90 is exploited by cancer cells to support the activated and/or metastable forms of oncoproteins, and to buffer cellular stresses induced by the malignancy. Hsp90 is often overexpressed in cancer cells (Neckers and Workman, 2012).

t(3;14)(q27;q32) HSP90AA1/BCL6 Huret JL
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 347
Result of the chromosomal anomaly Hybrid gene Description The break occurs in HSP90AA1 intron 1, resulting in the exchange of the first non-coding exons of HSP90AA1 and BCL6.
References Akasaka H, Akasaka T, Kurata M, Ueda C, Shimizu A, Uchiyama T, Ohno H. Molecular anatomy of BCL6 translocations revealed by long-distance polymerase chain reaction-based assays. Cancer Res. 2000 May 1;60(9):2335-41
Xu WS, Liang RH, Srivastava G. Identification and characterization of BCL6 translocation partner genes in primary gastric high-grade B-cell lymphoma: heat shock protein 89 alpha is a novel fusion partner gene of BCL6. Genes Chromosomes Cancer. 2000 Jan;27(1):69-75
Albagli-Curiel O. Ambivalent role of BCL6 in cell survival and transformation. Oncogene. 2003 Jan 30;22(4):507-16
Montesinos-Rongen M, Akasaka T, Zühlke-Jenisch R, Schaller C, Van Roost D, Wiestler OD, Siebert R, Deckert M. Molecular characterization of BCL6 breakpoints in primary diffuse large B-cell lymphomas of the central nervous system identifies GAPD as novel translocation partner. Brain Pathol. 2003 Oct;13(4):534-8
Chen YW, Hu XT, Liang AC, Au WY, So CC, Wong ML, Shen L, Tao Q, Chu KM, Kwong YL, Liang RH, Srivastava G. High BCL6 expression predicts better prognosis, independent of BCL6 translocation status, translocation partner, or BCL6-deregulating mutations, in gastric lymphoma. Blood. 2006 Oct 1;108(7):2373-83
DeZwaan DC, Freeman BC. HSP90 manages the ends. Trends Biochem Sci. 2010 Jul;35(7):384-91
Pratt WB, Morishima Y, Peng HM, Osawa Y. Proposal for a role of the Hsp90/Hsp70-based chaperone machinery in making triage decisions when proteins undergo oxidative and toxic damage. Exp Biol Med (Maywood). 2010 Mar;235(3):278-89
Neckers L, Workman P. Hsp90 molecular chaperone inhibitors: are we there yet? Clin Cancer Res. 2012 Jan 1;18(1):64-76
This article should be referenced as such:
Huret JL. t(3;14)(q27;q32) HSP90AA1/BCL6. Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):346-347.

Solid Tumour Section Review
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 348
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Colon: Colorectal adenocarcinoma Viktor H Koelzer, Heather Dawson, Inti Zlobec, Alessandro Lugli
Clinical Pathology Division and Translational Research Unit, Institute of Pathology, University of Bern, Murtenstrasse 31, CH-3010 Bern, Switzerland (VHK, HD, IZ, AL)
Published in Atlas Database: December 2012
Online updated version : http://AtlasGeneticsOncology.org/Tumors/colon5006.html DOI: 10.4267/2042/49706
This article is an update of : Sayar N, Banerjee S. Colon: Colorectal adenocarcinoma. Atlas Genet Cytogenet Oncol Haematol 2008;12(1):62-67. Hamelin R. Colon: Colorectal adenocarcinoma. Atlas Genet Cytogenet Oncol Haematol 1998;2(4):144-145. This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Classification Colorectal Cancer (CRC) can be classified from the molecular or etiological point of view:
Molecular pathway - Chromosome instability (CIN) -- 85% of all CRCs -- Somatic inactivation of APC, p53; - Microsatellite instability (MSI) -- 15% of all CRCs -- Hypermethylation or somatic inactivation of DNA repair enzymes;
Etiology - Sporadic CRC -- 84% microsatellite stable (MSS) CRC -- 10% microsatellite instable (MSI) CRC; - Hereditary CRC -- 1% Familial Adenomatous Polyposis (FAP) (MSS CRC) -- 5% Hereditary Non-Polyposis Colorectal Cancer (HNPCC) (MSI CRC).
In the last years, downstream molecules of different pathways such as KRAS and BRAF are included in proposals for a more differentiated molecular classification of CRC.
The CpG Methylator Phenotype (CIMP) status also seems to play an important role in the pathogenesis of CRC.
Clinics and pathology Etiology According to the WHO Classification of Tumors of the Digestive System the following factors may play an etiological role in the development of CRC: - Diet (high caloric food, meat consumption) - Obesity - Sedentary lifestyle - Smoking - Alcohol consumption - Inflammatory Bowel Disease (IBD) -- Cohn's disease -- Ulcerative colitis.
Epidemiology The following epidemiologic data are based on the WHO Classification of Tumors of the Digestive System: - In 2008, 1.23 million new CRC cases occurred worldwide (9.7% of all new cancers). - CRC is the 4th most frequent cancer in men and 3rd in women. - Higher rates occur in industrialized, high-resource countries (40-60 per 100000). - Incidence increases with age. - Rates of colon cancer are about 20% higher and rectal cancer about 50% higher in men than in women. - Worldwide mortality rate is about 50% of the incidence rate.

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 349
Clinics - Change bowel habits including constipation and diarrhea - Melena - Abdominal pain - Anemia due to chronic low-grade bleeding - Weight loss - Fever
- Malaise.
Pathology The histological diagnosis of CRC is based on the invasion through the muscularis mucosae into the submucosa. The different histological subtypes include: - Adenocarcinoma -- Mucinous adenocarcinoma

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 350
-- Signet ring cell carcinoma -- Medullary carcinoma -- Serrated adenocarcinoma -- Cribriform comedo-type adenocarcinoma -- Micropapillary adenocarcinoma - Adenosquamous carcinoma - Spindle cell carcinoma - Squamous cell carcinoma - Undifferentiated carcinoma. The gold standard for staging is the TNM classification proposed by the UICC/AJCC. Important parameters included in the TNM classification are: - T : Primary Tumor - N: Regional Lymph Nodes - M: Distant Metastasis - G: Histopathological grading - L: Lymphatic invasion - V: Venous invasion - Pn: Perineural invasion. Molecular features in Pathology that can be important in the daily diagnostic practice are: - Microsatellite status: Determined by immunohistochemistry and/or PCR - KRAS status: Determined by PCR - BRAF status: Determined by PCR.
Treatment Surgery is the primary therapy of CRC. Adjuvant therapy: - Colon Cancer: Chemotherapy - Rectal Cancer: Chemo- and radiotherapy - Anti-EGFR therapy: dependent on the KRAS mutational status.
Prognosis The prognosis is mainly based on the TNM staging system (see Pathology section). Additional prognostic factors can be: - Tumor border configuration - Tumor budding - Tumor regression grade - Bowel perforation - Intra- and peritumoral inflammation - Circumferential resection margin - Microsatellite status - BRAF - EGFR - VEGF - Loss of heterozygosity - CEA level - miRNA - CIMP status.
Cytogenetics Cytogenetics Morphological There are two types of colorectal cancers, according to the ploidy:
Aneuploid tumors showing numerous allelic losses; Aneuploidy, loss and rearrangements of chromosome 1p (about 70%), 5q (55%, loss of APC), 15q, 18q (65%, loss of DCC), 17p (80%, TP53), and 17q (30%); and abnormalities in 7q (25%) and 8p (55%). Reciprocal translocation t(5;10)(q22;q25), inv(5)(q22q31.3). Diploid tumours without frequent allelic losses.
Genes involved and proteins Note Extensive data on the genetic background of tumor progression in colorectal cancer (CRC) is available based on molecular pathology methods including genome wide sequencing. Alterations in oncogenes and tumor suppressor genes are intricately involved in the development and progression of CRC, some of which are strong predictors of treatment response to targeted therapies and chemotherapeutics. In the following, a comprehensive overview of both hereditary and somatic genetic changes in CRC is provided including genetic changes causing DNA mismatch repair deficiency as well as genomic alterations leading to deregulation of the WNT, RTK/Ras/MAPK, PI3K, TGF-Beta and P53 signaling pathways.
Mismatch repair MLH1 (mutL homolog 1, colon cancer, nonpolyposis type 2 (E. coli)) Location 3p22.3
DNA / RNA 19 exons, 2524 bp mRNA.
Protein Involved in mismatch repair (MMR) process after DNA replication. Forms heterodimer with PMS2 (also known as MutLα). This heterodimer is responsible for downstream MMR events such as strand discrimination, recruiting proteins needed for excision and resynthesis.
Germinal mutations Most frequent cause of Lynch syndrome (also known as HNPCC). Over 300 mutations have been described (nucleotide substitutions or insertions/substitutions) resulting in a truncated protein. Hereditable germline epimutations have also recently been reported. The full penetrance of Lynch syndrome requires the biallelic "double hit" inactivation of the responsible MMR gene (see also MSH2, MSH6 and PMS2) for tumor development.
Somatic mutations Mutation is rare; usually epigenetic modification due to methylation which results in MSI-H status. Methylation of MLH1 is by far the most frequent cause of sporadic MSI-H in CRC.

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 351
MLH3 (mutL homolog 3 (E. coli)) Location 14q24.3
DNA / RNA 12 exons, 2 major mRNA transcripts: 7911 and 7839 bp.
Protein Involved in mismatch repair process after DNA replication. Competes against PMS2 to form heterodimer with MLH1 (MutLγ) which assists MutLα.
Germinal mutations Only few MLH3 germline mutations have been described in Lynch syndrome, by far most of which amino acid substitutions. Implications are still unclear. To date, there is no evidence that these germline mutations cause the full Lynch syndrome phenotype.
Somatic mutations Shows insertions/deletions usually in A(8) repeats in MSH-H tumors. Considered to be a secondary mutation which is believed to further increase genetic instability.
MSH2 (mutS homolog 2, colon cancer, nonpolyposis type 1 (E. coli)) Location 2p21
DNA / RNA 16 exons, mRNA transcript 3145 bp.
Protein Involved in mismatch repair process after DNA replication. Binds to MSH6 or MSH3 to form the MutSα or MutSβ complex. The MutS complex associates with the MutL complex composed of MLH and PMS2.
Germinal mutations Frequent cause of Lynch syndrome. Over 300 mutations have been described (nucleotide substitutions or insertions/substitutions) resulted in a truncated protein. Hereditable germline epimutations have also recently been reported.
Somatic mutations Rare; sporadic MSH2 mutations have been described in sporadic MSI-H cases. Somatic methylation usually occurs as a "second hit" of the wild-type allele in cases with germline mutation.
MSH3 (mutS homolog 3 (E. coli)) Location 5q14.1
DNA / RNA 24 exons with 2 mRNA transcripts of 5 and 3.8 kb.
Protein Involved in post-replicative DNA mismatch repair. Binds with MSH2 to form the MutSβ heterodimer, which recognizes large insertion-deletion loops. Forms
a ternary complex with MutLα after mismatch binding.
Germinal mutations Mostly LOH and missense variants, seen in MSI-L tumors.
Somatic mutations Hypermethylation has been described in other tumors such as endometrial carcinoma. Functional impairment of MSH3 is probably not required for the formation of MMR-deficient tumors but is selected for during tumor progression.
MSH6 (mutS homolog 6 (E. coli)) Location 2p16
DNA / RNA 10 exons, mRNA transcript 4435 bp.
Protein Involved in post-replicational DNA mismatch repair. Forms heterodimer with MSH2 (MutSα).
Germinal mutations A less frequent cause of Lynch syndrome with variable penetration. Deletion and frameshift mutation result in a truncated protein. Can be associated with so-called early-onset CRC or Lynch syndrome with atypical features, such as endometrial cancer.
Somatic mutations Mutation or epigenetic activation is rare in CRC.
PMS2 (PMS2 postmeiotic segregation increased 2 (S. cerevisiae)) Location 7p22.1
DNA / RNA 15 exons, mRNA transcript 2851bp.
Protein Involved in post-replicational DNA mismatch repair. Forms the MutLα complex together with MLH1.
Germinal mutations Mostly deletions, some missense variants, most mutations are unique. Mutation gives rise to Lynch syndrome, probably of lower penetrance than in germline MLH1 and MSH2 mutations. Previously thought to be very rare in Lynch syndrome primarily due to technical difficulties in analysis. Mutations have recently been found to occur frequently using newly developed detection methods.
Somatic mutations Probably very rare, putative somatic mutation reported. Supposedly last mismatch repair gene to undergo methylation.
POLE (polymerase (DNA directed), epsilon, catalytic subunit) Location 12q24.3

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 352
DNA / RNA 19 exons.
Protein Member of the Family B DNA polymerases consisting of 4 subunits. Participates in chromosomal DNA replication, recombination as well as DNA repair via base excision and nuclear excision.
Germinal mutations Sequence alterations, mainly in the catalytic subunit including the proofreading domain have been found in MLH1-mutant CRC. It has been suggested that defective polymerase proofreading can contribute to the mutator phenotype as a "booster" in CRC.
WNT-Signaling APC (adenomatous polyposis coli) Location 5q21-q22
DNA / RNA 16 exons, 10702 bp mRNA.
Protein Tumor suppressor protein composed of 2843 amino acids; the APC gene product interacts with the adherens junction proteins α- and β-catenin suggesting involvement in cell adhesion. APC may also inhibit the pathway regulated by the beta-catenin/Tcf complex. Other functions include anterior-posterior pattern formation, axis specification, cell cycle, cell migration, apoptosis, chromosome segregation and spindle assembly.
Germinal mutations Point mutations in APC gene results in the generation of stop codons, small deletions, LOH, 1-2 bp insertions. Most mutations result in a truncated protein, mostly in the first half. Results in FAP and AFAP.
Somatic mutations The APC gene is mutated in about 50% of sporadic colorectal tumors. Most mutations are frameshifts or nonsense mutations resulting in premature stop codons. Some mutations in beta-catenin have been described in tumors and cell lines without mutations in the APC gene. APC loss may also be due to interstitial deletion or mitotic recombination, LOH, and nonsense mutations. Most of the somatic mutations are clustered in the exon 15 in mutation cluster region (MCR). About 20% of APC mutations are observed with mutation of TP53. Methylation of the promoter may be related.
DKK1 (dickkopf 1 homolog (Xenopus laevis)) Location 10q11.2
DNA / RNA 12 exons, 3762 bp mRNA.
Protein Human DKK1 is a potent inhibitor of WNT signaling over interaction with LRP5 and LRP6.
Somatic mutations Genomic alterations (inactivation) are found in up to 33% of hypermutated CRC and 4% of non-hypermutated CRC cases.
LRP5 (low density lipoprotein receptor-related protein 5) Location 11q13.4
DNA / RNA 23 exons, 5161 bp mRNA.
Protein LRP5 encodes a transmembrane low density lipoprotein receptor (1615 amino acids). It acts as a co-receptor with FZD10 on the cell surface, forming a Wnt-LRP5-LRP6-FZD10 complex for signal transduction of Wnt proteins. Signal transduction is mediated by an intracellular PPP(S/T)P motif, which is phosphorylated following WNT activation. The phosphorylated intracellular PPP(S/T)P motif then serves as a docking site for AXIN2.
Somatic mutations Genomic alterations (inactivation) are infrequent in CRC and are found in <1% of hypermutated CRC and up to 10% of non-hypermutated cases.
FZD10 (frizzled family receptor 10) Location 12q24.33
DNA / RNA 1 exon, intronless, 3282 bp mRNA.
Protein Encodes a 581 amino acid protein; member of the frizzled gene family seven-transmembrane-type WNT protein receptors. Acts as part of the Wnt-LRP5-LRP6-FZD10 receptor complex for signal transduction of WNT proteins. Upregulation leads to increased WNT signaling activity, inhibition of β-catenin degradation and accumulation of β-catenin in the cytoplasm.
Somatic mutations Genomic alterations (activation) are found in 19% of non-hypermutated CRC and 13% of hypermutated CRC cases. Frequent events include overexpression of FZD10, in one series in up to 17% of cases.
AXIN1 (axin 1) Location 16p13.3
DNA / RNA 10 exons, 3675 bp mRNA.
Protein Encodes an 862 amino acid protein. AXIN1 is an
Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 353
important component of the beta-catenin destruction complex binding GSK3B, FAM123B and CTNNB1 (β-catenin). AXIN stabilizes this complex, which supports the hyperphosphorylation of β-catenin by GSK3B, followed by ubiquitination and degradation. AXIN thereby negatively regulates Wnt signaling; consequently loss of AXIN expression would be predicted to lead to decreased phosphorylation and degradation of β-catenin, causing increased WNT-signaling.
Somatic mutations Limited data available. AXIN1 mutations (frequently missense mutations) have been described in up to 11% of colorectal cancer cases.
AXIN2 (axin 2) Location 17q23-q24
DNA / RNA 10 exons, 4259 bp mRNA.
Protein Encodes an 843 amino acid protein. Part of the axin protein family; Substitutes for AXIN1 as an important component of the beta-catenin destruction complex binding GSK3B, FAM123B and CTNNB1 (β-catenin).
Germinal mutations Limited evidence suggests that germline mutations in AXIN2 may increase the risk for development of CRC.
Somatic mutations Axin2 is frequently mutated in MMR deficient CRC cells. The mutations result in the stabilization of beta catenin. Genomic alterations are infrequent in non-hypermutated CRC. In hypermutated CRC up to 23% of cases show inactivation of the AXIN2 locus.
FAM123B (family with sequence similarity 123B) Location Xq11.2
DNA / RNA 2 exons, 7500 bp mRNA.
Protein Encodes an 1135 amino acid protein. Forms the β-catenin destruction complex together with CTNNB1, GSK3B, AXIN1/AXIN2. Mutation is thought to contribute to the stabilization of β-catenin in CRC. Interacts with WT1.
Somatic mutations The FAM123B gene contains a T6-microsatellite in the N-terminal coding region and is infrequently mutated in the setting of mismatch repair deficiency due to frame shift mutations (described in 5% of MSI cases in one series). More recent studies by the Cancer Genome Atlas Network have indicated genomic alterations (inactivation) in approximately 7% of non-hypermutated CRC and 37% of hypermutated CRC
cases. Further, FAM123B shows inactivating mutations in approximately 30% of Wilms tumors.
CTNNB1 (catenin (cadherin-associated protein), beta 1, 88kDa) Location 3p21
DNA / RNA 16 exons, 3362 bp mRNA.
Protein Encodes the 781 amino acid protein β-catenin. β-catenin functions as partner of E-cadherin in the formation of adherens junctions. Further, it is a central target of Wnt-signaling: In absence of Wnt-signaling, b-catenin forms a complex with APC, GSK-3 and Axin; Complex formation leads to phosphorylation of β-catenin through the action of GSK-3, which leads to degradation of the protein through the ubiquitin system. In case of APC mutation, β-catenin accumulates in the cell cytoplasm and translocates into the nucleus, where it has been shown to associate with transcription factors of the T cell factor-lymphoid enhancer factor (Tcf-Lef) family. This is assumed to lead to activation of genes involved in the positive regulation of epithelial to mesenchymal transition, proliferation and inhibition of apoptosis.
Germinal mutations Germline inactivating mutations of the APC gene lead to the FAP syndrome.
Somatic mutations Inactivating mutations in the APC gene represent early events in the chromosomal instability pathway of CRC. APC mutation leads to dissociation of the β-catenin- APC-GSK-3-Axin complex, and reduced phosphorylation and degradation of β-catenin. Genomic alterations (inactivation) are frequent in CRC, and are mostly due to biallelic inactivation of the APC gene, found in approximately 80% of non-hypermutated CRC and 50% of hypermutated CRC cases.
TCF7L2 (transcription factor 7-like 2 (T-cell specific, HMG-box)) Location 10q25.2
DNA / RNA 17 exons, predicted mRNA: 1490 bp.
Protein Encodes a 619 amino acid transcription factor containing a high mobility group box; Interacts with CTNNB1 in the Wnt signaling pathway; Acts on numerous Wnt targeted genes containing a TCF7L2 binding domain.
Somatic mutations In colorectal cancer cell lines, VTI1A-TCF7L2 fusions have been identified, supporting anchorage independent tumor growth. In CRC, genomic alterations

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 354
(inactivation) are found in approximately 12% of non-hypermutated CRC and 30% of hypermutated CRC cases.
FBXW7 (F-box and WD repeat domain containing 7, E3 ubiquitin protein ligase) Location 4q31.3
DNA / RNA 10 exons, 3927 bp mRNA.
Protein Encodes a 707 amino acid protein representing the variable F-box subunit of the SCF (SKP1-cullin-F-box) complex which functions as an ubiquitin ligase. FBXW7 acts as a tumor suppressor and is involved in the ubiquitination and degradation of the cell cycle regulators Cyclin E and c-Myc; further targets include notch intracellular domain (NICD), c-Myb, NOTCH1 and presenilin 1. Experimentally, loss of FBXW7 leads to accumulation of β-catenin; Further, mutation of FBXW7 has been suggested to increase cell proliferation.
Germinal mutations Somatic mutations of FBXW7 in HNPCC and FAP patients have been described. The frequency of FBXW7 mutations in FAP and HNPCC corresponded to patients with sporadic carcinomas.
Somatic mutations Somatic mutations have been described in ovarian and breast cancer cell lines. In CRC, genomic alterations (inactivation) are found in approximately 10% of non-hypermutated CRC and 43% of hypermutated CRC cases.
SOX9 (SRY (sex determining region Y)-box 9) Location 17q23
DNA / RNA 3 exons, 3963 bp mRNA.
Protein Encodes a 509 amino acid protein which contains a high-mobility-group (HMG) domain; Acts as a transcription factor and inhibits CTNNB1 (β-catenin) activity; In particular, the SOX9 product has been shown to interfere with the activation of β-catenin dependent gene targets and acts as a promoter beta-catenin ubiquitinylation and degradation; important in skeletal development.
Somatic mutations In CRC, genomic alterations of SOX9 are infrequently described. Genomic alterations are found in
approximately 4% of non-hypermutated CRC and 7% of hypermutated CRC cases.
TGFβ-Signaling
TGFBR1 (transforming growth factor, beta receptor 1) Location 9q22
DNA / RNA 9 exons, complex locus; transcription produces 11 different mRNAs.
Protein The 503 amino acid TGFBR1 proteins form a homodimer and associate with TGFBR2 homodimers to form the TGF-beta receptor; Both subunits of the TGF-beta receptor, TGFBR1 and TGFBR2, act as transmembrane serine/threonine kinases. After binding of the TGF-beta cytokine dimers TGFB1, TGFB2 or TGFB3, the TGFBR2 and TGFBR1 form a stable receptor complex; TGFBR2 is a constitually active type II transmembrane serine/threonine kinase and phosphorylates TGFBR1 (a type I receptor) upon ligand binding. The TGFBR1 serine/threonine kinase binds and phosphorylates SMAD2, a receptor-associated signaling molecule. SMAD2 dissociates from the receptor and interacts with SMAD4; the SMAD2/SMAD4 complex then translocates into the nucleus and modifies the transcription of TGF-beta regulated genes. TGF-beta mediated signaling has been shown to have anti-proliferative effects on epithelia, mesenchymal and hematopoietic cells and to modulate cell-stroma interactions. Physiologic TGF-beta signaling promotes cell differentiation and can induce apoptosis. In cancer cells, TGF-beta signaling is frequently disrupted by mutations in the receptor or downstream mediators turning off the signaling pathway; In the tumor microenvironment, TGF-beta modulates tumor-host interaction by increasing angiogenesis and converting T-effector cells into immunosuppressive Regulatory T-cells, thereby supporting tumor progression and inhibiting the anti-tumoral immune defense. In conjunction with IL-6, TGF-beta has been shown to induce the differentiation of Th17 cells.
Germinal mutations An increased prevalence of SNPs in the TGFBR1 locus resulting in decreased TGFBR1 allelic expression (up to 9.3% of cases) have been shown in patients with colorectal cancer.
Somatic mutations In CRC, genomic alterations (inactivation) of TGFBR1 are frequent in patients with hypermutated CRC (17%). Genomic alterations of the TGFBR1 locus are infrequently observed in patients with non-hypermutated CRC (<1%).

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 355
TGFBR2 (transforming growth factor, beta receptor II (70/80kDa)) Location 3p22
DNA / RNA 8 exons, 2094 bp mRNA.
Protein Encodes a 567 amino acid protein which forms a homodimer and associates with TGFBR1 to form the TGF-beta type II receptor. Possesses serine/threonine kinase function and activates SMAD2 and SMAD3 by phosphorylation. Activated SMAD2 forms a heterodimer with SMAD4 to form a complex which translocates into the nucleus and modulates the transcription of TGF-beta regulated genes.
Somatic mutations The TGFBR2 gene locus contains a poly A mononucleotide tract in the coding region, which is frequently mutated in MSI-high CRC (up to 74%), leading to inactivation of the gene. TGFBR2 mononucleotide mutations have not shown an impact on outcome in initial studies. Inactivation of TGFBR2 by point mutation has been demonstrated in up to 15% of MSS CRC cases in initial studies. More recent studies by the Cancer Genome Atlas Network have indicated genomic alterations (inactivation) in approximately 2% of non-hypermutated CRC and 43% of hypermutated CRC cases.
SMAD2 (SMAD family member 2) Location 18q21.1
DNA / RNA 12 exons, 10384 bp mRNA.
Protein Encodes a 467 amino acid protein; Downstream signaling molecule of TGF-Beta signaling. SMAD2 is phosphorylated by the heteromeric TGF-beta type II receptor serine/threonine kinase domain. SMAD2 forms a dimer with SMAD4 followed by translocation into the nucleus; the SMAD2/SMAD4 dimer then modifies the transcription of TGF-Beta target genes by forming a transcription repressor complex.
Somatic mutations Somatic mutations of SMAD2 have been described in 3.4% of sporadic CRC, mostly causing missense changes in the protein which reduces SMAD2/SMAD4 complex formation. Joint biallelic hits are common. Recent studies by the Cancer Genome Atlas Network indicate inactivating genomic alterations in 6% of non-hypermutated CRC and 13% in hypermutated cases.
SMAD3 (SMAD family member 3) Location 15q22.33
DNA / RNA 9 exons, 5808 bp mRNA.
Protein Encodes a 425 amino acid protein; Downstream signaling molecule of TGF-Beta and activin signaling. Phosphorylated by the heteromeric TGF-beta type II receptor serine/threonine kinase and the activin type 1 receptor kinase domain. SMAD3 forms a dimer with SMAD4 followed by translocation into the nucleus; the SMAD3/SMAD4 dimer then modifies the transcription of TGF-Beta target genes.
Somatic mutations Somatic mutations of SMAD3 have been described in 4.3% of sporadic CRC. Missense changes in the protein lead to reduced association with SMAD4 by alteration of the phosphorylation regulated Ser-Ser-X-Ser motifs within SMAD3. Further, mutations cause reduced SMAD3 transcriptional activity. Joint biallelic hits are common. Recent data from the Cancer Genome Atlas Network indicate infrequent genomic alterations in 2% of non-hypermutated CRC. Inactivating genomic alterations are described in up to 17% of hypermutated cases.
SMAD4 (SMAD family member 4) Location 18q21.1
DNA / RNA 13 exons, 3202 bp mRNA.
Protein The SMAD4 protein is coded from 11 exons and contains 552 amino acids. SMAD4 forms a heterodimer with phosphorylated SMAD2 or SMAD3 and translocates into the nucleus. The SMAD2/SMAD3-SMAD4 complex then forms a transcription repressor complex and modifies transcription of TGF-Beta target genes.
Germinal mutations Results in juvenile polyposis with an approximate lifetime risk of 40% for development of CRC.
Somatic mutations Somatic mutations of SMAD4 have been described in 8.6% of sporadic CRC. Missense changes in the protein structure reducing the association with SMAD2 in the SMAD2/4 complex. Joint biallelic hits are common. Recent studies by the Cancer Genome Atlas Network indicate inactivating genomic alterations in 15% of non-hypermutated CRC and 20% in hypermutated cases.

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 356
ACVR2A (activin A receptor, type IIA) Location 2q22.3
DNA / RNA 11 exons, 5217 bp mRNA.
Protein The 513 amino acid ACVR2A proteins forms a homodimer (type IIa receptor subunit) and associate with ACVR1B homodimers (type IB receptor subunit) to form the Activin receptor; Both ACVR2A and ACVR1B act as transmembrane serine/threonine kinases. After binding of activin A, activin B or inhibin A, which belong to the TGF-Beta protein superfamily, ACVR2A and ACVR1B form a stable receptor complex; ACVR2A is a type II transmembrane serine/threonine kinase and phosphorylates ACVR1B (a type I receptor) upon ligand binding. The ACVR1B serine/threonine kinase binds and phosphorylates receptor-associated signaling molecule from the SMAD family (SMAD2, SMAD3). SMAD2 dissociates from the receptor and interacts with SMAD4; the SMAD2/SMAD4 complex then translocates into the nucleus and modifies the transcription of TGF-beta regulated genes.
Somatic mutations Somatic mutations in ACVR2A are particularly common in MSI-high CRC. The ACVR2A locus encompasses two poly A repeats within the coding sequence of exon 3s and 10 which have been shown to be mutated in up to 83% of MSI-high CRC leading to loss of protein expression in up to 62% of the cases with mutations. Further studies have identified methylation and LOH of the ACVR2A locus in association with loss of protein expression.
ACVR1B (activin A receptor, type IB) Location 12q13
DNA / RNA 7 exons, 2375 bp mRNA.
Protein The 505 amino acid ACVR1B proteins (type IB receptor subunit) form the activin receptor complex in association with ACVR2A or ACVR2B homodimers (type IIa receptor subunit) to form the Activin receptor; Act as transmembrane serine/threonine kinases and activate receptor-associated signaling molecule from the SMAD family (SMAD2, SMAD3).
Somatic mutations Data on genomic alterations in CRC are scarce. Recent studies by the Cancer Genome Atlas Network indicate frequent inactivating genomic alterations in 20% of hypermutated cases. Genomic alterations of the ACVR1B locus are infrequently observed in patients
with non-hypermutated CRC (4%). Frequent somatic mutations have been described in pancreatic cancer (up to 30%).
RTK-RAS-Signaling ERBB2 (v-erb-b2 erythroblastic leukemia viral oncogene homolog 2, neuro/glioblastoma derived oncogene homolog (avian)) Location 17q12
DNA / RNA 30 exons, 4478 bp.
Protein The Epidermal Growth Factor Receptor (EGFR) family consists of 4 receptor tyrosine kinases, EGFR (ERBB1/ HER1), ERBB2 (HER2), ERBB3 (HER3) and ERBB4 (HER4). ERBB2 encodes a 1255 aa protein that has no ligand binding domain of its own and therefore cannot bind growth factors. However, it does bind tightly to other ligand-bound EGFR family members to form a heterodimer, stabilizing ligand binding and enhancing kinase-mediated activation of downstream signaling pathways.
Somatic mutations Mutations and focal amplifications of ERBB2 in colorectal cancers are rare (<5%). As potentially drug-targetable, the predictive value of ERBB2 amplifications in these patients remains to be determined.
ERBB3 (v-erb-b2 erythroblastic leukemia viral oncogene homolog 3 (avian)) Location 12q13
DNA / RNA 28 exons, 5511 bp.
Protein 1342 aa. ERBB3 possesses an extracellular ligand-binding domain, a transmembrane domain and a tyrosine kinase domain. However, the kinase domain has no tyrosine kinase activity. Erbb3 therefore can bind ligand but cannot convey the signal into the cell through protein phosphorylation. It however does dimerize with other EGF receptor family members.
Somatic mutations Mutations in ERBB3 appear only as rare events in colorectal cancers.
KRAS (v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog) Location 12p12.1

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 357
DNA / RNA 6 exons, 5436 bp.
Protein 189 aa. KRAS belongs to the ras gene family containing also HRAS and NRAS. The KRAS protein is a GTPase that plays a central role in several different signal transduction pathways. In colorectal cancer, ligand binding and heterodimerization of the EGFR leads to activation of the oncogenic Ras-Raf-MEK-ERK signaling pathway acting on cell proliferation, cell survival and tumor angiogenesis.
Somatic mutations Activating point mutations in KRAS occur in approximately 30-40% of all patients with colorectal cancer and are frequent in exon 2 codons 12 and 13 as well as in exon 3 codon 61. These mutations are no longer considered to be of prognostic value. Evidence suggests that metastatic patients with KRAS mutated colorectal cancers undergoing anti-EGFR based therapies have a significantly reduced treatment response rate compared to patients with wild-type tumors. Nonetheless, recent retrospective analyses indicate that specific KRAS gene mutations, for example, G13D, may confer a degree of responsiveness in these patients.
NRAS (neuroblastoma RAS viral (v-ras) oncogene homolog) Location 1p13.2
DNA / RNA 7 exons, 4461 bp.
Protein 189 aa. N-ras belongs to the ras gene family containing also KRAS and HRAS. NRAS is an oncogene that encodes a membrane protein with GTPase activity that is activated by a guanine nucleotide-exchange factor and inactivated by a GTPase activating protein.
Somatic mutations Substitution missense mutations occurring predominantly in codons 12, 13 and 61 have been reported in <5% of patients with colorectal cancer. These mutations may have predictive value as biomarkers of non-response in patients treated with anti-EGFR based therapies.
BRAF (v-raf murine sarcoma viral oncogene homolog B1) Location 7q34
DNA / RNA 18 exons, 2949 bp.
Protein 766 aa. Braf is an oncogenic protein and one of three Raf kinases that play a role in the Ras-Raf-MEK-ERK signaling pathway by phosphorylating MEK.
Germinal mutations BRAF mutations generally do not occur in patients with Lynch syndrome associated colorectal cancers (HNPCC) and are often used as an exclusion criterion for detection of these patients.
Somatic mutations BRAF point mutations in colorectal cancers occur in 9-12% of all patients. They are commonest in exon 15 codon 600 (p.V600E). BRAF gene mutations are frequently detected in patients with microsatellite instability-high (MSI-H) colorectal cancers as well as in tumors displaying high-level CpG Island Methylator Phenotype (CIMP). BRAF mutations have been linked to more unfavorable survival, often independently of the MSI status; they are not predictive of response in patients treated with anti-EGFR based therapies.
PI3K-Signaling IGF2 (insulin-like growth factor 2 (somatomedin A)) Location 11p15.5
DNA / RNA 5 exons, 1354 bp mRNA.
Protein Encodes a 180 amino acid protein; member of the family of insulin-like polypeptide growth factors recognized by the Insulin like growth-factor 1 receptor (IGF1R). Activation of IGF1R (a receptor tyrosine kinase) leads to phosphorylation of insulin-receptor substrates 1 and 2 (IRS1/IRS2), which contribute to the activation of both the PI3K-AKT/PKB pathway and the Ras-MAPK pathway. PI3K-AKT/PKB regulates cell survival and sensitivity to apoptosis; Ras-MAPK signaling controls cell proliferation, cell survival and tumor angiogenesis. Both pathways play important roles for malignant transformation and tumor progression in CRC.
Somatic mutations 15-22% of colorectal cancers show overexpression of IGF2, which is particularly common in non hypermutated, MSS CRC. IGF2 overexpression has not been described as a pathogenetic feature of MSI-high CRC.
PIK3CA (phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit alpha) Location 3q26.3
DNA / RNA 21 exons, 3207 bp mRNA.
Protein Encodes a protein predicted with 1068 amino acids,

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 358
representing the catalytic subunit alpha of class I PI 3-kinases (PI3K). PI3K are a group of enzymes that play a central function for intracellular signal transduction by the generation of phosphatidylinositol 3,4,5-trisphosphate at the plasma membrane. PI3K generates PI3 by phosphorylating phosphatidylinositol 4,5-diphosphates (PI2) in the plasma membrane which then serve as docking sites for proteins containing a phosphoinositide-binding domains (e.g. pleckstrin homology domains). This includes protein kinase B (Akt), thereby triggering the Akt/mTOR pathway. The Akt pathway has a central regulatory role and pleiotropic effects on cell growth, differentiation and proliferation, cell motility and migration as well as the regulation of angiogenesis and apoptosis.
Somatic mutations In CRC, activating mutations are frequently observed in exon 9 and exon 20 of the PIK3CA locus. Frequency of genomic alterations ranges from approximately 15% in non-hypermutated CRC to 37% in hypermutated cases. PIK3CA exon 20 mutations have been correlated to a reduced response rate of CRC patients to anti-epidermal growth factor receptor (EGFR) monoclonal antibodies. Further, concomitant exon 9 and exon 20 mutations have been shown to predict significantly worse disease-specific survival while isolated mutations in either exon 9 or 20 did not impact survival outcome.
PTEN (phosphatase and tensin homolog) Location 10q23.3
DNA / RNA 9 exons, 3147 bp mRNA.
Protein Tumor suppressor protein, which negatively regulates AKT/PKB signaling. The protein is a dual specificity phosphatidylinositol-3,4,5-trisphosphate 3-phosphatase, removing phosphates from serine, tyrosine and threonine; Further, PTEN acts as a lipid phosphatase, removing phosphate groups from phosphatidylinositol 3,4,5-trisphosphate, thereby antagonizing PI 3-kinase function and negatively regulating the Akt/mTOR pathway; PTEN thereby assumes tumor-suppressor functions, inhibiting cell growth, proliferation, motility and migration and supporting apoptosis in many different cancer subtypes.
Germinal mutations Germinal mutations in PTEN are associated with the hereditary Cowden Syndrome which is characterized by development of multiple hamartomas in skin and gastrointestinal tract (intestinal hamartomatous polyps), gangliocytoma of the cerebellum and a severely increased risk for the development of breast carcinoma, non-medullary carcinoma of the thyroid, endometrial
carcinoma, colorectal cancer, kidney cancer and melanoma. Further, germinal mutations in PTEN are associated with rare hereditary syndromes including Bannayan-Riley-Ruvalcaba Syndrome, Proteus syndrome and Proteus-like syndrome.
Somatic mutations Somatic mutations of PTEN are more frequently observed in MSI-high CRC (18% of cases) than MSS CRC. Somatic mutations (inactivation) in MSI-high CRC are the consequence of frameshift mutations, nonsense, missense, and splice-site mutations.
P53-Signaling TP53 (tumor protein p53) Location 17p13
DNA / RNA 11 exons, 1179 bp mRNA.
Protein Encodes a 393 amino acid protein. P53, the "master watchman of the genome" has central tumor suppressor function and an essential role in cell cycle regulation, particularly at the G1 DNA damage checkpoint. The five highly-conserved gene regions contain a transactivation domain, a DNA-binding domain, nuclear localization signals and a tetramerization domain. Intracellular P53 levels are low in cellular homeostasis, but are quickly upregulated in response to cellular and oncogenic stress, in particular DNA damage. P53 targets genes involved in the cell cycle, stopping the progression of the G1 phase (through activation of p21) if DNA damage or other stress signals are present.
Germinal mutations Results in the autosomal dominant Li-Fraumeni Syndrome, which leads to a severely increased risk for the development of soft tissue tumors (sarcomas, osteosarcomas), brain tumors (glioblastoma) as well as hematologic malignancies (leukemia) and epithelial malignancy (breast cancer, adrenal cortical carcinoma). An increased risk for colorectal carcinomas has been described in initial studies, mostly in association with missense or nonsense mutations between exons 4-10.
Somatic mutations Mutations of P53 are most frequent in non-hypermutated cancers (59%), and are mostly located in exons 4 to 8 with hotspots at codons 175, 245, 248, 273 and 282. Both deletions and insertions as well as missense, non-sense and splicing mutations have been described resulting in a truncated p53 protein. 80% of mutations result from deamination of methylated cytosine in CpG region of the gene (codons 175, 248 and 273). Mutant p53 is found to be overexpressed in primary colon cancer. p53 mutation is observed in 40-50% of

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 359
colorectal carcinomas, and is associated with aggressive carcinomas. p53 mutation or LOH of chromosome 17p is observed mostly in carcinoma rather than adenoma, in both familial and non-familial patients.
Others ARID1A (AT rich interactive domain 1A (SWI-like)) Location 1p35.3
DNA / RNA 20 exons, 8585 bp mRNA.
Protein Encodes the 2285 amino acid AT-rich interactive domain-containing protein 1A (ARID1A); member of the SWI/SNF family; ARID1A possesses helicase and ATPase function and regulates transcriptional activation and repression of target genes through modification of the chromatin structure, including the MYC-oncogene (repression).
Somatic mutations Somatic (truncating) mutations have been described in up to 10% of colorectal cancers, with more than half of these cases found to be associated with microsatellite instability (out-of-frame insertions or deletions at mononucleotide repeats). Recurrent inactivating genomic alterations have been confirmed in up to 37% of hypermutated cases in recent studies by the Cancer Genome Atlas Network; genomic alterations non-hypermutated CRC were infrequent (5%).
STK11 (serine/threonine kinase 11) Location 19p13.3
DNA / RNA 10 exons, 3276 bp mRNA.
Protein Encodes a 433 amino acid protein. Tumor suppressor serine-threonine kinase, with important functions in the activation of adenine monophosphate-activated protein kinase (AMP)-activated protein kinase kinases in the setting of energy deprivation; Activation of AMP kinases contributes to the maintenance of cell polarity and negatively regulates cell cycle progression and cell growth.
Germinal mutations Mutations (Nonsense, missense, frameshift), result in the autosomal dominant Peutz-Jeghers syndrome, which results in the formation of benign hamartomatous polyps in the gastrointestinal tract; other characteristics include pigmented macules on the oral mucosa and lips.
Patients with Peutz-Jeghers syndrome carry a severely increased risk for the development of CRC estimated at about 39%.
Somatic mutations Somatic mutations in STK11 are rare in sporadic colorectal cancer outside inherited hamartomatous syndromes.
BMPR1A (bone morphogenetic protein receptor, type IA) Location 10q22.3
DNA / RNA 13 exons, 3616 bp mRNA.
Protein Encodes a 532 amino acid protein; Transmembrane serine-threonine kinase, type1 receptor, closely related to the ACVR1 and ACVR2 activin receptors; ligands include bone morphogenetic protein 2 and 4 (BMP-2 and BMP-4) from the TGF-Beta superfamily.
Germinal mutations Nonsense, missense, frameshift and splice-site mutations. Associated with Juvenile polyposis, which carries an approximate lifetime risk of 40% for development of CRC.
MUTYH (mutY homolog (E. coli)) Location 1p34.1
DNA / RNA 16 exons, 1839 bp mRNA.
Protein DNA glycosylase. Functions in oxidative DNA damage repair (base excision repair), nicks A-G mismatches, as well as A-8oxoG and A-C mismatches.
Germinal mutations Tyr82-Cys and Gly253 -Asp transitions affect glycosylase activity, resulting in APC mutations in somatic cells. Nonsense mutations, missense and truncated protein mutations. Mutations cause 93-fold increase in colorectal cancer risk.
DCC (deleted in colorectal carcinoma) Location 18q21.3
DNA / RNA 29 exons, 4609 bp mRNA.
Protein DCC is thought to be receptor for neptin-1 (axonal chemoattractant). In absence of ligand, it induces apoptosis but when neptin-1 is bound, it prevents apoptosis.

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 360
Germinal mutations Chromosome 18 sequences are frequently (74%) lost in colorectal carcinoma. Loss of DCC is mostly observed in metastatic cancers.
To be noted Note The RER+ sporadic colon cancers are mostly diploid, without LOH, with few mutations of p53 and APC and right-sided; they contain mutations in repetitive coding sequences of a number of genes such as the TGFbeta type II receptor, the receptor of the Insulin-like growth factor and the BAX gene implicated in apoptosis. The RER- are polyploid, with LOH (5q, 17p, 18q), mutations in p53, and more often left-sided, they have a worse prognosis.
References Rodenhuis S, van de Wetering ML, Mooi WJ, Evers SG, van Zandwijk N, Bos JL. Mutational activation of the K-ras oncogene. A possible pathogenetic factor in adenocarcinoma of the lung. N Engl J Med. 1987 Oct 8;317(15):929-35
Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990 Jun 1;61(5):759-67
Rodrigues NR, Rowan A, Smith ME, Kerr IB, Bodmer WF, Gannon JV, Lane DP. p53 mutations in colorectal cancer. Proc Natl Acad Sci U S A. 1990 Oct;87(19):7555-9
Joslyn G, Carlson M, Thliveris A, Albertsen H, Gelbert L, Samowitz W, Groden J, Stevens J, Spirio L, Robertson M. Identification of deletion mutations and three new genes at the familial polyposis locus. Cell. 1991 Aug 9;66(3):601-13
Cottrell S, Bicknell D, Kaklamanis L, Bodmer WF. Molecular analysis of APC mutations in familial adenomatous polyposis and sporadic colon carcinomas. Lancet. 1992 Sep 12;340(8820):626-30
Grimmond SM, Raghavan D, Russell PJ. Detection of a rare point mutation in Ki-ras of a human bladder cancer xenograft by polymerase chain reaction and direct sequencing. Urol Res. 1992;20(2):121-6
Kikuchi-Yanoshita R, Konishi M, Ito S, Seki M, Tanaka K, Maeda Y, Iino H, Fukayama M, Koike M, Mori T. Genetic changes of both p53 alleles associated with the conversion from colorectal adenoma to early carcinoma in familial adenomatous polyposis and non-familial adenomatous polyposis patients. Cancer Res. 1992 Jul 15;52(14):3965-71
Lane DP. Cancer. p53, guardian of the genome. Nature. 1992 Jul 2;358(6381):15-6
Miyoshi Y, Nagase H, Ando H, Horii A, Ichii S, Nakatsuru S, Aoki T, Miki Y, Mori T, Nakamura Y. Somatic mutations of the APC gene in colorectal tumors: mutation cluster region in the APC gene. Hum Mol Genet. 1992 Jul;1(4):229-33
Powell SM, Zilz N, Beazer-Barclay Y, Bryan TM, Hamilton SR, Thibodeau SN, Vogelstein B, Kinzler KW. APC mutations occur early during colorectal tumorigenesis. Nature. 1992 Sep 17;359(6392):235-7
Thibodeau SN, Bren G, Schaid D. Microsatellite instability in cancer of the proximal colon. Science. 1993 May 7;260(5109):816-9
Bronner CE, Baker SM, Morrison PT, Warren G, Smith LG, Lescoe MK, Kane M, Earabino C, Lipford J, Lindblom A.
Mutation in the DNA mismatch repair gene homologue hMLH1 is associated with hereditary non-polyposis colon cancer. Nature. 1994 Mar 17;368(6468):258-61
Cho KR, Oliner JD, Simons JW, Hedrick L, Fearon ER, Preisinger AC, Hedge P, Silverman GA, Vogelstein B. The DCC gene: structural analysis and mutations in colorectal carcinomas. Genomics. 1994 Feb;19(3):525-31
Nicolaides NC, Papadopoulos N, Liu B, Wei YF, Carter KC, Ruben SM, Rosen CA, Haseltine WA, Fleischmann RD, Fraser CM. Mutations of two PMS homologues in hereditary nonpolyposis colon cancer. Nature. 1994 Sep 1;371(6492):75-80
Papadopoulos N, Nicolaides NC, Wei YF, Ruben SM, Carter KC, Rosen CA, Haseltine WA, Fleischmann RD, Fraser CM, Adams MD. Mutation of a mutL homolog in hereditary colon cancer. Science. 1994 Mar 18;263(5153):1625-9
Lynch HT, Smyrk T, McGinn T, Lanspa S, Cavalieri J, Lynch J, Slominski-Castor S, Cayouette MC, Priluck I, Luce MC. Attenuated familial adenomatous polyposis (AFAP). A phenotypically and genotypically distinctive variant of FAP. Cancer. 1995 Dec 15;76(12):2427-33
Papadopoulos N, Nicolaides NC, Liu B, Parsons R, Lengauer C, Palombo F, D'Arrigo A, Markowitz S, Willson JK, Kinzler KW. Mutations of GTBP in genetically unstable cells. Science. 1995 Jun 30;268(5219):1915-7
van der Luijt RB, Tops CM, Khan PM, van der Klift HM, Breukel C, van Leeuwen-Cornelisse IS, Dauwerse HG, Beverstock GC, van Noort E, Snel P. Molecular, cytogenetic, and phenotypic studies of a constitutional reciprocal translocation t(5;10)(q22;q25) responsible for familial adenomatous polyposis in a Dutch pedigree. Genes Chromosomes Cancer. 1995 Jul;13(3):192-202
Liu B, Parsons R, Papadopoulos N, Nicolaides NC, Lynch HT, Watson P, Jass JR, Dunlop M, Wyllie A, Peltomäki P, de la Chapelle A, Hamilton SR, Vogelstein B, Kinzler KW. Analysis of mismatch repair genes in hereditary non-polyposis colorectal cancer patients. Nat Med. 1996 Feb;2(2):169-74
Thiagalingam S, Lengauer C, Leach FS, Schutte M, Hahn SA, Overhauser J, Willson JK, Markowitz S, Hamilton SR, Kern SE, Kinzler KW, Vogelstein B. Evaluation of candidate tumour suppressor genes on chromosome 18 in colorectal cancers. Nat Genet. 1996 Jul;13(3):343-6
Hamelin R, Laurent-Puig P. [p53 and colorectal cancer]. Pathol Biol (Paris). 1997 Dec;45(10):876-81
Hemminki A, Tomlinson I, Markie D, Järvinen H, Sistonen P, Björkqvist AM, Knuutila S, Salovaara R, Bodmer W, Shibata D, de la Chapelle A, Aaltonen LA. Localization of a susceptibility locus for Peutz-Jeghers syndrome to 19p using comparative genomic hybridization and targeted linkage analysis. Nat Genet. 1997 Jan;15(1):87-90
Olschwang S, Hamelin R, Laurent-Puig P, Thuille B, De Rycke Y, Li YJ, Muzeau F, Girodet J, Salmon RJ, Thomas G. Alternative genetic pathways in colorectal carcinogenesis. Proc Natl Acad Sci U S A. 1997 Oct 28;94(22):12122-7
Howe JR, Ringold JC, Summers RW, Mitros FA, Nishimura DY, Stone EM. A gene for familial juvenile polyposis maps to chromosome 18q21.1. Am J Hum Genet. 1998 May;62(5):1129-36
Howe JR, Roth S, Ringold JC, Summers RW, Järvinen HJ, Sistonen P, Tomlinson IP, Houlston RS, Bevan S, Mitros FA, Stone EM, Aaltonen LA. Mutations in the SMAD4/DPC4 gene in juvenile polyposis. Science. 1998 May 15;280(5366):1086-8
Jenne DE, Reimann H, Nezu J, Friedel W, Loff S, Jeschke R, Müller O, Back W, Zimmer M. Peutz-Jeghers syndrome is

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 361
caused by mutations in a novel serine threonine kinase. Nat Genet. 1998 Jan;18(1):38-43
Kinzler KW, Vogelstein B. Landscaping the cancer terrain. Science. 1998 May 15;280(5366):1036-7
Lengauer C, Kinzler KW, Vogelstein B. Genetic instabilities in human cancers. Nature. 1998 Dec 17;396(6712):643-9
Mehlen P, Rabizadeh S, Snipas SJ, Assa-Munt N, Salvesen GS, Bredesen DE. The DCC gene product induces apoptosis by a mechanism requiring receptor proteolysis. Nature. 1998 Oct 22;395(6704):801-4
Sedlacek Z, Kodet R, Poustka A, Goetz P. A database of germline p53 mutations in cancer-prone families. Nucleic Acids Res. 1998 Jan 1;26(1):214-5
Takenoshita S, Mogi A, Nagashima M, Yang K, Yagi K, Hanyu A, Nagamachi Y, Miyazono K, Hagiwara K. Characterization of the MADH2/Smad2 gene, a human Mad homolog responsible for the transforming growth factor-beta and activin signal transduction pathway. Genomics. 1998 Feb 15;48(1):1-11
Dihlmann S, Gebert J, Siermann A, Herfarth C, von Knebel Doeberitz M. Dominant negative effect of the APC1309 mutation: a possible explanation for genotype-phenotype correlations in familial adenomatous polyposis. Cancer Res. 1999 Apr 15;59(8):1857-60
Grady WM, Myeroff LL, Swinler SE, Rajput A, Thiagalingam S, Lutterbaugh JD, Neumann A, Brattain MG, Chang J, Kim SJ, Kinzler KW, Vogelstein B, Willson JK, Markowitz S. Mutational inactivation of transforming growth factor beta receptor type II in microsatellite stable colon cancers. Cancer Res. 1999 Jan 15;59(2):320-4
Gerdes H, Elahi A, Chen Q, Jhanwar SC.. Characterization of newly established colorectal cancer cell lines: correlation between cytogenetic abnormalities and allelic deletions associated with multistep tumorigenesis. Journal of Genetics. 2000;79:113-23.
Liu W, Dong X, Mai M, Seelan RS, Taniguchi K, Krishnadath KK, Halling KC, Cunningham JM, Boardman LA, Qian C, Christensen E, Schmidt SS, Roche PC, Smith DI, Thibodeau SN.. Mutations in AXIN2 cause colorectal cancer with defective mismatch repair by activating beta-catenin/TCF signalling. Nat Genet. 2000 Oct;26(2):146-7.
Ma AH, Xia L, Littman SJ, Swinler S, Lader G, Polinkovsky A, Olechnowicz J, Kasturi L, Lutterbaugh J, Modrich P, Veigl ML, Markowitz SD, Sedwick WD.. Somatic mutation of hPMS2 as a possible cause of sporadic human colon cancer with microsatellite instability. Oncogene. 2000 Apr 27;19(18):2249-56.
Yan H, Papadopoulos N, Marra G, Perrera C, Jiricny J, Boland CR, Lynch HT, Chadwick RB, de la Chapelle A, Berg K, Eshleman JR, Yuan W, Markowitz S, Laken SJ, Lengauer C, Kinzler KW, Vogelstein B.. Conversion of diploidy to haploidy. Nature. 2000 Feb 17;403(6771):723-4.
Huang J, Kuismanen SA, Liu T, Chadwick RB, Johnson CK, Stevens MW, Richards SK, Meek JE, Gao X, Wright FA, Mecklin JP, Jarvinen HJ, Gronberg H, Bisgaard ML, Lindblom A, Peltomaki P.. MSH6 and MSH3 are rarely involved in genetic predisposition to nonpolypotic colon cancer. Cancer Res. 2001 Feb 15;61(4):1619-23.
Lindblom A.. Different mechanisms in the tumorigenesis of proximal and distal colon cancers. Curr Opin Oncol. 2001 Jan;13(1):63-9. (REVIEW)
Su GH, Bansal R, Murphy KM, Montgomery E, Yeo CJ, Hruban RH, Kern SE.. ACVR1B (ALK4, activin receptor type 1B) gene mutations in pancreatic carcinoma. Proc Natl Acad Sci U S A. 2001 Mar 13;98(6):3254-7.
Al-Tassan N, Chmiel NH, Maynard J, Fleming N, Livingston AL, Williams GT, Hodges AK, Davies DR, David SS, Sampson JR, Cheadle JP.. Inherited variants of MYH associated with somatic G:C-->T:A mutations in colorectal tumors. Nat Genet. 2002 Feb;30(2):227-32. Epub 2002 Jan 30.
de Chadarevian JP, Dunn S, Malatack JJ, Ganguly A, Blecker U, Punnett HH.. Chromosome rearrangement with no apparent gene mutation in familial adenomatous polyposis and hepatocellular neoplasia. Pediatr Dev Pathol. 2002 Jan-Feb;5(1):69-75.
Smith G, Carey FA, Beattie J, Wilkie MJ, Lightfoot TJ, Coxhead J, Garner RC, Steele RJ, Wolf CR.. Mutations in APC, Kirsten-ras, and p53--alternative genetic pathways to colorectal cancer. Proc Natl Acad Sci U S A. 2002 Jul 9;99(14):9433-8. Epub 2002 Jul 1.
Zhou XP, Kuismanen S, Nystrom-Lahti M, Peltomaki P, Eng C.. Distinct PTEN mutational spectra in hereditary non-polyposis colon cancer syndrome-related endometrial carcinomas compared to sporadic microsatellite unstable tumors. Hum Mol Genet. 2002 Feb 15;11(4):445-50.
Sieber OM, Lipton L, Crabtree M, Heinimann K, Fidalgo P, Phillips RK, Bisgaard ML, Orntoft TF, Aaltonen LA, Hodgson SV, Thomas HJ, Tomlinson IP.. Multiple colorectal adenomas, classic adenomatous polyposis, and germ-line mutations in MYH. N Engl J Med. 2003 Feb 27;348(9):791-9.
Akiyama H, Lyons JP, Mori-Akiyama Y, Yang X, Zhang R, Zhang Z, Deng JM, Taketo MM, Nakamura T, Behringer RR, McCrea PD, de Crombrugghe B.. Interactions between Sox9 and beta-catenin control chondrocyte differentiation. Genes Dev. 2004 May 1;18(9):1072-87.
Jung B, Doctolero RT, Tajima A, Nguyen AK, Keku T, Sandler RS, Carethers JM.. Loss of activin receptor type 2 protein expression in microsatellite unstable colon cancers. Gastroenterology. 2004 Mar;126(3):654-9.
Lammi L, Arte S, Somer M, Jarvinen H, Lahermo P, Thesleff I, Pirinen S, Nieminen P.. Mutations in AXIN2 cause familial tooth agenesis and predispose to colorectal cancer. Am J Hum Genet. 2004 May;74(5):1043-50. Epub 2004 Mar 23.
Nassif NT, Lobo GP, Wu X, Henderson CJ, Morrison CD, Eng C, Jalaludin B, Segelov E.. PTEN mutations are common in sporadic microsatellite stable colorectal cancer. Oncogene. 2004 Jan 15;23(2):617-28.
Oliveira C, Westra JL, Arango D, Ollikainen M, Domingo E, Ferreira A, Velho S, Niessen R, Lagerstedt K, Alhopuro P, Laiho P, Veiga I, Teixeira MR, Ligtenberg M, Kleibeuker JH, Sijmons RH, Plukker JT, Imai K, Lage P, Hamelin R, Albuquerque C, Schwartz S Jr, Lindblom A, Peltomaki P, Yamamoto H, Aaltonen LA, Seruca R, Hofstra RM.. Distinct patterns of KRAS mutations in colorectal carcinomas according to germline mismatch repair defects and hMLH1 methylation status. Hum Mol Genet. 2004 Oct 1;13(19):2303-11. Epub 2004 Aug 4.
Plaschke J, Kruger S, Jeske B, Theissig F, Kreuz FR, Pistorius S, Saeger HD, Iaccarino I, Marra G, Schackert HK.. Loss of MSH3 protein expression is frequent in MLH1-deficient colorectal cancer and is associated with disease progression. Cancer Res. 2004 Feb 1;64(3):864-70.
Vogelstein B, Kinzler KW.. Cancer genes and the pathways they control. Nat Med. 2004 Aug;10(8):789-99. (REVIEW)
Farrington SM, Tenesa A, Barnetson R, Wiltshire A, Prendergast J, Porteous M, Campbell H, Dunlop MG.. Germline susceptibility to colorectal cancer due to base-excision repair gene defects. Am J Hum Genet. 2005 Jul;77(1):112-9. Epub 2005 May 3.

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 362
Floch MH, Floch NR, Kowdley KV, Pitchumoni CS, Rosenthal RJ, Scolapio JS.. Netter's Gastroenterology. Icon Learning Systems, 1st ed., Carlstadt NJ. 2005.
Hanson CA, Miller JR.. Non-traditional roles for the Adenomatous Polyposis Coli (APC) tumor suppressor protein. Gene. 2005 Nov 21;361:1-12. Epub 2005 Sep 26. (REVIEW)
Worthley DL, Walsh MD, Barker M, Ruszkiewicz A, Bennett G, Phillips K, Suthers G.. Familial mutations in PMS2 can cause autosomal dominant hereditary nonpolyposis colorectal cancer. Gastroenterology. 2005 May;128(5):1431-6.
Cao X, Eu KW, Kumarasinghe MP, Li HH, Loi C, Cheah PY.. Mapping of hereditary mixed polyposis syndrome (HMPS) to chromosome 10q23 by genomewide high-density single nucleotide polymorphism (SNP) scan and identification of BMPR1A loss of function. J Med Genet. 2006 Mar;43(3):e13.
Hendriks YM, Jagmohan-Changur S, van der Klift HM, Morreau H, van Puijenbroek M, Tops C, van Os T, Wagner A, Ausems MG, Gomez E, Breuning MH, Brocker-Vriends AH, Vasen HF, Wijnen JT.. Heterozygous mutations in PMS2 cause hereditary nonpolyposis colorectal carcinoma (Lynch syndrome). Gastroenterology. 2006 Feb;130(2):312-22.
Segditsas S, Tomlinson I.. Colorectal cancer and genetic alterations in the Wnt pathway. Oncogene. 2006 Dec 4;25(57):7531-7. (REVIEW)
Wong P, Verselis SJ, Garber JE, Schneider K, DiGianni L, Stockwell DH, Li FP, Syngal S.. Prevalence of early onset colorectal cancer in 397 patients with classic Li-Fraumeni syndrome. Gastroenterology. 2006 Jan;130(1):73-9.
Yang J, Zhang W, Evans PM, Chen X, He X, Liu C.. Adenomatous polyposis coli (APC) differentially regulates beta-catenin phosphorylation and ubiquitination in colon cancer cells. J Biol Chem. 2006 Jun 30;281(26):17751-7. Epub 2006 May 3.
Huang J, Zhao YL, Li Y, Fletcher JA, Xiao S.. Genomic and functional evidence for an ARID1A tumor suppressor role. Genes Chromosomes Cancer. 2007 Aug;46(8):745-50.
Korhonen MK, Raevaara TE, Lohi H, Nystrom M.. Conditional nuclear localization of hMLH3 suggests a minor activity in mismatch repair and supports its role as a low-risk gene in HNPCC. Oncol Rep. 2007 Feb;17(2):351-4.
Zenker M, Lehmann K, Schulz AL, Barth H, Hansmann D, Koenig R, Korinthenberg R, Kreiss-Nachtsheim M, Meinecke P, Morlot S, Mundlos S, Quante AS, Raskin S, Schnabel D, Wehner LE, Kratz CP, Horn D, Kutsche K.. Expansion of the genotypic and phenotypic spectrum in patients with KRAS germline mutations. J Med Genet. 2007 Feb;44(2):131-5. Epub 2006 Oct 20.
Imai K, Yamamoto H.. Carcinogenesis and microsatellite instability: the interrelationship between genetics and epigenetics. Carcinogenesis. 2008 Apr;29(4):673-80. Epub 2007 Oct 17. (REVIEW)
Kelsen DP, Daly JM, Kern SE, Levin B, Tepper JE, Van Cutsem E.. Principles and Practice of Gastrointestinal Oncology. Lippincott Williams and Wilkins, a Wolters Kluwers business: Philadelphia. 2nd ed. 2008.
Pico AR, Kelder T, van Iersel MP, Hanspers K, Conklin BR, Evelo C.. WikiPathways: pathway editing for the people. PLoS Biol. 2008 Jul 22;6(7):e184. doi: 10.1371/journal.pbio.0060184.
Senter L, Clendenning M, Sotamaa K, Hampel H, Green J, Potter JD, Lindblom A, Lagerstedt K, Thibodeau SN, Lindor NM, Young J, Winship I, Dowty JG, White DM, Hopper JL, Baglietto L, Jenkins MA, de la Chapelle A.. The clinical phenotype of Lynch syndrome due to germ-line PMS2
mutations. Gastroenterology. 2008 Aug;135(2):419-28. doi: 10.1053/j.gastro.2008.04.026. Epub 2008 May 2.
Dai F, Lin X, Chang C, Feng XH.. Nuclear export of Smad2 and Smad3 by RanBP3 facilitates termination of TGF-beta signaling. Dev Cell. 2009 Mar;16(3):345-57. doi: 10.1016/j.devcel.2009.01.022.
Jung B, Gomez J, Chau E, Cabral J, Lee JK, Anselm A, Slowik P, Ream-Robinson D, Messer K, Sporn J, Shin SK, Boland CR, Goel A, Carethers JM.. Activin signaling in microsatellite stable colon cancers is disrupted by a combination of genetic and epigenetic mechanisms. PLoS One. 2009 Dec 14;4(12):e8308. doi: 10.1371/journal.pone.0008308.
Miyaki M, Yamaguchi T, Iijima T, Takahashi K, Matsumoto H, Mori T.. Somatic mutations of the CDC4 (FBXW7) gene in hereditary colorectal tumors. Oncology. 2009;76(6):430-4. doi: 10.1159/000217811. Epub 2009 May 6.
Nagayama S, Yamada E, Kohno Y, Aoyama T, Fukukawa C, Kubo H, Watanabe G, Katagiri T, Nakamura Y, Sakai Y, Toguchida J.. Inverse correlation of the up-regulation of FZD10 expression and the activation of beta-catenin in synchronous colorectal tumors. Cancer Sci. 2009 Mar;100(3):405-12. doi: 10.1111/j.1349-7006.2008.01052.x. Epub 2008 Dec 24.
Bosman FT, Carneiro F, Hruban RH, Theise ND.. WHO Classification of Tumours of the Digestive System. IARC: Lyon. 2010.
Cheng YW, Idrees K, Shattock R, Khan SA, Zeng Z, Brennan CW, Paty P, Barany F.. Loss of imprinting and marked gene elevation are 2 forms of aberrant IGF2 expression in colorectal cancer. Int J Cancer. 2010 Aug 1;127(3):568-77. doi: 10.1002/ijc.25086.
De Roock W, Claes B, Bernasconi D, De Schutter J, Biesmans B, Fountzilas G, Kalogeras KT, Kotoula V, Papamichael D, Laurent-Puig P, Penault-Llorca F, Rougier P, Vincenzi B, Santini D, Tonini G, Cappuzzo F, Frattini M, Molinari F, Saletti P, De Dosso S, Martini M, Bardelli A, Siena S, Sartore-Bianchi A, Tabernero J, Macarulla T, Di Fiore F, Gangloff AO, Ciardiello F, Pfeiffer P, Qvortrup C, Hansen TP, Van Cutsem E, Piessevaux H, Lambrechts D, Delorenzi M, Tejpar S.. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol. 2010 Aug;11(8):753-62. doi: 10.1016/S1470-2045(10)70130-3. Epub 2010 Jul 8.
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti IIIA.. AJCC Cancer Staging Handbook. 7th ed. Springer: New York. 2010.
Greenson JK.. Diagnostic Pathology Gastrointestinal. 1st ed. Amirsys. Salt Lake City. 2010.
Geer LY, Marchler-Bauer A, Geer RC, Han L, He J, He S, Liu C, Shi W, Bryant SH.. The NCBI BioSystems database. Nucleic Acids Res. 2010 Jan;38(Database issue):D492-6. doi: 10.1093/nar/gkp858. Epub 2009 Oct 23.
Giraldez MD, Balaguer F, Bujanda L, Cuatrecasas M, Munoz J, Alonso-Espinaco V, Larzabal M, Petit A, Gonzalo V, Ocana T, Moreira L, Enriquez-Navascues JM, Boland CR, Goel A, Castells A, Castellvi-Bel S.. MSH6 and MUTYH deficiency is a frequent event in early-onset colorectal cancer. Clin Cancer Res. 2010 Nov 15;16(22):5402-13. doi: 10.1158/1078-0432.CCR-10-1491. Epub 2010 Oct 5.
Nagasaka T, Rhees J, Kloor M, Gebert J, Naomoto Y, Boland CR, Goel A.. Somatic hypermethylation of MSH2 is a frequent event in Lynch Syndrome colorectal cancers. Cancer Res. 2010 Apr 15;70(8):3098-108. doi: 10.1158/0008-5472.CAN-09-3290. Epub 2010 Apr 13.

Colon: Colorectal adenocarcinoma Koelzer VH, et al.
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 363
Pasche B, Wisinski KB, Sadim M, Kaklamani V, Pennison MJ, Zeng Q, Bellam N, Zimmerman J, Yi N, Zhang K, Baron J, Stram DO, Hayes MG.. Constitutively decreased TGFBR1 allelic expression is a common finding in colorectal cancer and is associated with three TGFBR1 SNPs. J Exp Clin Cancer Res. 2010 May 25;29:57. doi: 10.1186/1756-9966-29-57.
Scheel SK, Porzner M, Pfeiffer S, Ormanns S, Kirchner T, Jung A.. Mutations in the WTX-gene are found in some high-grade microsatellite instable (MSI-H) colorectal cancers. BMC Cancer. 2010 Aug 9;10:413. doi: 10.1186/1471-2407-10-413.
Sobin LH, Gospodarowicz MK, Wittekind C.. TNM classification of malignant tumours. UICC, 7th ed. Wiley-Blackwell: Oxford. 2010.
Babaei-Jadidi R, Li N, Saadeddin A, Spencer-Dene B, Jandke A, Muhammad B, Ibrahim EE, Muraleedharan R, Abuzinadah M, Davis H, Lewis A, Watson S, Behrens A, Tomlinson I, Nateri AS.. FBXW7 influences murine intestinal homeostasis and cancer, targeting Notch, Jun, and DEK for degradation. J Exp Med. 2011 Feb 14;208(2):295-312. doi: 10.1084/jem.20100830. Epub 2011 Jan 31.
Bass AJ, Lawrence MS, Brace LE, Ramos AH et al.. Genomic sequencing of colorectal adenocarcinomas identifies a recurrent VTI1A-TCF7L2 fusion. Nat Genet. 2011 Sep 4;43(10):964-8. doi: 10.1038/ng.936.
Kastrinos F, Syngal S.. Inherited colorectal cancer syndromes. Cancer J. 2011 Nov-Dec;17(6):405-15. doi: 10.1097/PPO.0b013e318237e408. (REVIEW)
Shima K, Morikawa T, Yamauchi M, Kuchiba A, Imamura Y, Liao X, Meyerhardt JA, Fuchs CS, Ogino S.. TGFBR2 and BAX mononucleotide tract mutations, microsatellite instability, and prognosis in 1072 colorectal cancers. PLoS One. 2011;6(9):e25062. doi: 10.1371/journal.pone.0025062. Epub 2011 Sep 20.
van Lier MG, Westerman AM, Wagner A, Looman CW, Wilson JH, de Rooij FW, Lemmens VE, Kuipers EJ, Mathus-Vliegen EM, van Leerdam ME.. High cancer risk and increased mortality in patients with Peutz-Jeghers syndrome. Gut. 2011 Feb;60(2):141-7. doi: 10.1136/gut.2010.223750.
Yoshida R, Miyashita K, Inoue M, Shimamoto A, Yan Z, Egashira A, Oki E, Kakeji Y, Oda S, Maehara Y.. Concurrent genetic alterations in DNA polymerase proofreading and mismatch repair in human colorectal cancer. Eur J Hum Genet. 2011 Mar;19(3):320-5. doi: 10.1038/ejhg.2010.216. Epub 2010 Dec 15.
No authors available.. GeneTests Medical Genetics Information Resource (database online). Copyright, University of Washington, Seattle. 1993-2012. Available at http://www.genetests.org.
Apweiler R, Jesus Martin M, O'onovan C, Magrane M, Alam-Faruque Y, Antunes R, Barrera Casanova E, Bely B, Bingley M, Bower L, Bursteinas B, Mun Chan W, Chavali G, Da Silva A, Dimmer E, Eberhardt R, Fazzini F, Fedotov A, et al.. Reorganizing the protein space at the Universal Protein Resource (UniProt). Nucleic Acids Res. 2012 Jan;40(Database issue):D71-5. doi: 10.1093/nar/gkr981. Epub 2011 Nov 18.
Compton CC.. Pathology and prognostic determinants of colorectal cancer. In: UpToDate, Tanabe KK (Ed), UpToDate, Waltham, MA, 2012.
Jones S, Li M, Parsons DW, Zhang X, Wesseling J, Kristel P, Schmidt MK, Markowitz S, Yan H, Bigner D, Hruban RH, Eshleman JR, Iacobuzio-Donahue CA, Goggins M, Maitra A, Malek SN, Powell S, Vogelstein B, Kinzler KW, Velculescu VE, Papadopoulos N.. Somatic mutations in the chromatin remodeling gene ARID1A occur in several tumor types. Hum Mutat. 2012 Jan;33(1):100-3. doi: 10.1002/humu.21633. Epub 2011 Nov 23.
Kolben T, Perobner I, Fernsebner K, Lechner F, Geissler C, Ruiz-Heinrich L, Capovilla S, Jochum M, Neth P.. Dissecting the impact of Frizzled receptors in Wnt/?-catenin signaling of human mesenchymal stem cells. Biol Chem. 2012 Dec 1;393(12):1433-47. doi: 10.1515/hsz-2012-0186.
Liao X, Morikawa T, Lochhead P, Imamura Y, Kuchiba A, Yamauchi M, Nosho K, Qian ZR, Nishihara R, Meyerhardt JA, Fuchs CS, Ogino S.. Prognostic role of PIK3CA mutation in colorectal cancer: cohort study and literature review. Clin Cancer Res. 2012 Apr 15;18(8):2257-68. doi: 10.1158/1078-0432.CCR-11-2410. Epub 2012 Feb 22.
Tan MH, Mester JL, Ngeow J, Rybicki LA, Orloff MS, Eng C.. Lifetime cancer risks in individuals with germline PTEN mutations. Clin Cancer Res. 2012 Jan 15;18(2):400-7. doi: 10.1158/1078-0432.CCR-11-2283.
Fleming NI, Jorissen RN, Mouradov Det al.. SMAD2, SMAD3 and SMAD4 Mutations in Colorectal Cancer. Cancer Res. 2013 Jan 15;73(2):725-735. Epub 2012 Nov 8.
This article should be referenced as such:
Koelzer VH, Dawson H, Zlobec I, Lugli A. Colon: Colorectal adenocarcinoma. Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):348-363.

Cancer Prone Disease Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 364
INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Chediak-Higashi Syndrome Xinjie Xu, Wei Shen
Cytogenetics Laboratory, Center for Human Genetics, Inc, Cambridge, MA, USA (XX), Waisman Center, University of Wisconsin-Madison, Madison, WI, USA (WS)
Published in Atlas Database: December 2012
Online updated version : http://AtlasGeneticsOncology.org/Kprones/ChediakHigashiID10128.html DOI: 10.4267/2042/49707
This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2013 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names CHS
Note Chediak-Higashi Syndrome is a rare genetic disease. The clinical features include oculocutaneous albinism, immunodeficiency, neurological manifestations, mild coagulation defects and a predisposition to lymphoma-like cancer.
Inheritance Autosome Recessive.
Clinics Phenotype and clinics The symptoms of CHS patients are variable. They have highly variable hypopigmentation of the skin, eye and hair (oculocutaneus albinism). The Neurological manifestations are also variable, including cognitive impairment, peripheral neuropathy, ataxia, and parkinsonism. In addition, the CHS patients have frequent infections, particularly bacterial infections of the skin and respiratory tract. Symptoms can appear anytime from childhood to early adulthood. Generally speaking, CHS patients have mild coagulation defects including epistaxis, gum/mucosal bleeding, and easy bruising. The accelerated phase, which occurs in 85% of individuals with CHS, can take place at any age. Clinical manifestations include fever, lymphadenopathy, hepatosplenomegaly, anemia, neutropenia, and sometimes thrombocytopenia.
Originally thought to be a malignancy resembling lymphoma, the accelerated phase is now known to be a hemophagocytic lymphohistiocytosis characterized by multiorgan inflammation. The accelerated phase and its complications are the most common causes of mortality in CHS patients. Most CHS patients present in early childhood and die unless treated by bone marrow transplantation. About 10-15% of patients exhibit a much milder clinical symptoms and survive to adulthood, but develop progressive and often fatal neurological dysfunction. Very rare patients exhibit an intermediate adolescent CHS phenotype, with severe infections in early childhood, but a milder course by adolescence, and no accelerated phase.
Treatment Infections are treated with antibiotics. Antiviral drugs such as acyclovir and chemotherapy drugs are often used in the accelerated phase of the disease. Surgery may be needed to drain abscesses in some cases. Patients in the accelerated phase are treated with chemoimmunotherapy followed by transition to continuation therapy. Allogenic HSCT is the only treatment to cure hematologic and immunologic defects. Platelet transfusions are needed for serious bleeding. Corrective lenses help to improve visual acuity. Treatment by rehabilitation specialists are used for neurologic complications.
Prognosis CHS patients usually die in their first decade of life, from chronic infections or accelerated disease. However, some mildly affected children have survived longer.

Chediak-Higashi Syndrome Xu X, Shen W
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 365
Figure 1. The structure and mutations of the human LYST gene. Filled box indicate coding sequences. Hatched box indicate 5' and 3' untranslated sequences. Left-hatched indicates 5' untranslated sequences in mRNA containing exons 1 and 3, right-hatched indicates 5' untranslated sequences in mRNAs containing exon 2, and double- hatched indicates common 5' and 3' untranslated sequences. E1 and E2 represent mutually exclusive 5' terminal exons, and corresponding alternative promoters are indicated by right-facing arrows. Filled
diamonds denote frameshifts, filled triangles denote nonsense mutations, and filled circles denote missense substitutions. (Katrim et al., 2002).
Genes involved and proteins LYST Location 1q42.3
DNA/RNA
Description 55 exons spanning 205.9 kb of genomic DNA.
Transcription Two alternative transcriptions. The large transcript (12.0 kb) produces functional protein. The function of the small transcript (5.8 kb) is unknown.
Protein
Figure 2. A schematic representation of motifs found in CHS protein. (Ward et al., 2000).
Description The CHS protein is composed of 3801 amino acids. The molecular weight of the CHS protein is 430 kDa. The N-terminus of the protein has a large stretch of alpha-helices termed HEAT repeats (Figure 2). HEAT repeats are important to mediate membrane associations and are associated with vesicle transport. The C-terminus of the protein has two domains that are conserved between the human and mouse homologues.

Chediak-Higashi Syndrome Xu X, Shen W
Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 366
The first of these domains has been referred to as the BEACH domain. The BEACH domain contains a consensus 'WIDL' amino acid stretch as well as several other conserved amino acids that define members of the CHS protein family. The second domain contains a WD-40 repeat region, indicative of a protein-protein interaction domain.
Expression LYST is expressed in all cells.
Localisation Cytosolic.
Function Lysosome trafficking regulator.
Homology There are 82% identity and 88% homology between the human and mouse proteins. Similar degrees of identity are seen among human, rat and cow CHS genes.
Mutations
Note More than 50 mutations have been identified, most of which are nonsense mutations that result in premature stop codons and thus a truncated protein. Figure 1 shows the distribution of the mutations.
References Nagle DL, Karim MA, Woolf EA, Holmgren L, Bork P, Misumi DJ, McGrail SH, Dussault BJ Jr, Perou CM, Boissy RE, Duyk GM, Spritz RA, Moore KJ. Identification and mutation analysis
of the complete gene for Chediak-Higashi syndrome. Nat Genet. 1996 Nov;14(3):307-11
Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chediak-Higashi syndrome. Mol Genet Metab. 1999 Oct;68(2):283-303
Ward DM, Griffiths GM, Stinchcombe JC, Kaplan J. Analysis of the lysosomal storage disease Chediak-Higashi syndrome. Traffic. 2000 Nov;1(11):816-22
Huizing M, Anikster Y, Gahl WA. Hermansky-Pudlak syndrome and Chediak-Higashi syndrome: disorders of vesicle formation and trafficking. Thromb Haemost. 2001 Jul;86(1):233-45
Karim MA, Suzuki K, Fukai K, Oh J, Nagle DL, Moore KJ, Barbosa E, Falik-Borenstein T, Filipovich A, Ishida Y, Kivrikko S, Klein C, Kreuz F, Levin A, Miyajima H, Regueiro J, Russo C, Uyama E, Vierimaa O, Spritz RA. Apparent genotype-phenotype correlation in childhood, adolescent, and adult Chediak-Higashi syndrome. Am J Med Genet. 2002 Feb 15;108(1):16-22
Eapen M, DeLaat CA, Baker KS, Cairo MS, Cowan MJ, Kurtzberg J, Steward CG, Veys PA, Filipovich AH. Hematopoietic cell transplantation for Chediak-Higashi syndrome. Bone Marrow Transplant. 2007 Apr;39(7):411-5
Introne WJ, Westbroek W, Golas GA, Adams D. Chediak-Higashi Syndrome In: Pagon RA, Bird TD, Dolan CR, Stephens K, Adam MP, editors. Source GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-. 2009 Mar 03 [updated 2012 Feb 16].
This article should be referenced as such:
Xu X, Shen W. Chediak-Higashi Syndrome. Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5):364-366.

INIST-CNRS
OPEN ACCESS JOURNAL
Atlas of Genetics and Cytogenetics in Oncology and Haematology
Instructions to Authors Manuscripts submitted to the Atlas must be submitted solely to the Atlas. Iconography is most welcome: there is no space restriction. The Atlas publishes "cards", "deep insights", "case reports", and "educational items". Cards are structured review articles. Detailed instructions for these structured reviews can be found at: http://AtlasGeneticsOncology.org/Forms/Gene_Form.html for reviews on genes, http://AtlasGeneticsOncology.org/Forms/Leukaemia_Form.html for reviews on leukaemias, http://AtlasGeneticsOncology.org/Forms/SolidTumour_Form.html for reviews on solid tumours, http://AtlasGeneticsOncology.org/Forms/CancerProne_Form.html for reviews on cancer-prone diseases. According to the length of the paper, cards are divided, into "reviews" (texts exceeding 2000 words), "mini reviews" (between), and "short communications" (texts below 400 words). The latter category may not be accepted for indexing by bibliographic databases. Deep Insights are written as traditional papers, made of paragraphs with headings, at the author's convenience. No length restriction. Case Reports in haematological malignancies are dedicated to recurrent -but rare- chromosomes abnormalities in leukaemias/lymphomas. Cases of interest shall be: 1- recurrent (i.e. the chromosome anomaly has already been described in at least 1 case), 2- rare (previously described in less than 20 cases), 3- with well documented clinics and laboratory findings, and 4- with iconography of chromosomes. It is mandatory to use the specific "Submission form for Case reports": see http://AtlasGeneticsOncology.org/Reports/Case_Report_Submission.html. Educational Items must be didactic, give full information and be accompanied with iconography. Translations into French, German, Italian, and Spanish are welcome.
Subscription: The Atlas is FREE!
Corporate patronage, sponsorship and advertising Enquiries should be addressed to [email protected].
Rules, Copyright Notice and Disclaimer Conflicts of Interest: Authors must state explicitly whether potential conflicts do or do not exist. Reviewers must disclose to editors any conflicts of interest that could bias their opinions of the manuscript. The editor and the editorial board members must disclose any potential conflict. Privacy and Confidentiality – Iconography: Patients have a right to privacy. Identifying details should be omitted. If complete anonymity is difficult to achieve, informed consent should be obtained. Property: As "cards" are to evolve with further improvements and updates from various contributors, the property of the cards belongs to the editor, and modifications will be made without authorization from the previous contributor (who may, nonetheless, be asked for refereeing); contributors are listed in an edit history manner. Authors keep the rights to use further the content of their papers published in the Atlas, provided that the source is cited. Copyright: The information in the Atlas of Genetics and Cytogenetics in Oncology and Haematology is issued for general distribution. All rights are reserved. The information presented is protected under international conventions and under national laws on copyright and neighbouring rights. Commercial use is totally forbidden. Information extracted from the Atlas may be reviewed, reproduced or translated for research or private study but not for sale or for use in conjunction with commercial purposes. Any use of information from the Atlas should be accompanied by an acknowledgment of the Atlas as the source, citing the uniform resource locator (URL) of the article and/or the article reference, according to the Vancouver convention. Reference to any specific commercial products, process, or service by trade name, trademark, manufacturer, or otherwise, does not necessarily constitute or imply its endorsement, recommendation, or favouring. The views and opinions of contributors and authors expressed herein do not necessarily state or reflect those of the Atlas editorial staff or of the web site holder, and shall not be used for advertising or product endorsement purposes. The Atlas does not make any warranty, express or implied, including the warranties of merchantability and fitness for a particular purpose, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of any information, and shall not be liable whatsoever for any damages incurred as a result of its use. In particular, information presented in the Atlas is only for research purpose, and shall not be used for diagnosis or treatment purposes. No responsibility is assumed for any injury and/or damage to persons or property for any use or operation of any methods products, instructions or ideas contained in the material herein. See also: "Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publication - Updated October 2004": http://www.icmje.org.
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

Atlas Genet Cytogenet Oncol Haematol. 2013; 17(5) 368